Journa - California Dental Association
72
NOVEL TECHNOLOGIES AND MATERIALS IN DENTISTRY Yiming Li, DDS, MSD, Ph Yiming Li, DDS , MSD, PhD Journa CALIFORNIA DENTAL ASSOCIATION 3D Printing Resin-Based Composites Biomaterials Orthodontic External Root Resorption May 2019
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Journa - California Dental Association

NOVEL TECHNOLOGIES AND MATERIALS IN DENTISTRYYiming Li, DDS, MSD, PhYiming Li, DDS, MSD, PhD
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
3D Printing
Resin-Based Composites
Biomaterials
Orthodontic External Root Resorption
May 2019

Explore a free member benefit. Visit The Dentists Supply Company at
CDA’s Member Benefits Center, booth 1102, to browse the online catalog of supplies and
small equipment from popular brands like 3M,
Dentsply, GC America, Kerr and Crosstex.
Discover savings potential. Want to save money on supplies, but don’t have
time to comparison shop? TDSC can help. Request
a free custom price comparison, and experts
will compare tdsc.com prices to your current
invoices to find easy ways to save.
Enter to win an iPad®. When you stop by booth 1102, have your
convention badge scanned to be entered to
win TDSC’s iPad giveaway.2 Visit every
day to be entered into each daily drawing.
Get set to shop the site. Let TDSC’s experts help you set up your free
tdsc.com account and show you how easy
it is to save an average of 20%1 on dental
supplies. Join other CDA members who are
saving more on supplies than they pay in
annual tripartite dues.
Play Whack-a-Molar to win! Tap into your inner child or
competitive side by playing a
boisterous old-school arcade-style
game. Win cool gifts and bucks to shop for supplies online. Bring
your whole team and compete for the
highest score!
SAVE AND WIN. VISIT TDSC AT CDA PRESENTS, BOOTH 1102.
Join the excitement!
1 Price comparisons are made to the manufacturer’s list price. Actual savings will vary on a product-by-product basis. 2 THIS PROMOTION IS FOR THE PURPOSE OF SOLICITING SALES OF DENTAL SUPPLIES. NO PURCHASE NECESSARY. Void where prohibited and outside 50 US and DC. Begins 9:30 am PST on 5/16/19; ends 4:30 pm PST on 5/18/19, with prize drawings daily. ARV of all prizes: $1,500. Odds of winning depend on number of entries received. Visit tdsc.com/giveaway for complete Official Rules. Sponsor: The Dentists Supply Company (TDSC), 1201 K St, Sacramento, CA. TDSC operates an online marketplace for dentists, offering dental supplies from major manufacturers and distributors.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 287
Novel Technologies and Materials in Dentistry
An introduction to the issue.Yiming Li, DDS, MSD, PhD
3D Printing and Bioprinting Technology for Specific Applications in Surgical Implant Dentistry: A Review
This review article describes the application of three different uses of stereolithographic 3D printing, including diagnostic bone models, modified surgical guides and bone reduction guides.Jaime Lozada, DDS; Carolina Herrera, DMD; Brian Goodacre, DDS, MSD; Aladdin Al-Ardah, BDS, MS; and Erik Sahl, DDS, MSD
Advances in Restorative Resin-Based Composites: A Review
This article reviews the history of aesthetic composites including monomers, curing, fillers and more.H. Ralph Rawls, PhD, and Kyumin Whang, PhD
Biomaterials for the Next Generation of Dental Restoratives: Our Design and Materials Performance
This review highlights new materials including ether-based, hydrolytically and enzymatically stable monomers and the composition-controlled resin networks.Jirun Sun, PhD, and Drago Skrtic, PhD
Mechanotransduction of Orthodontic External Root Resorption (OERR)
The objective of this article is to clarify the current scientific outlook of orthodontic external root resorption.Rodrigo F. Viecilli, DDS, PhD
299
303
311
329
337
May 2019
D E PA R TM E N T S
F E AT U R E S
293
The Associate Editor/Hands Up
Letter to the Editor
Impressions
RM Matters/Depression Screening: Not a Legal Obligation, but an Ethical One
Regulatory Compliance/Ignorance Is Not Bliss — Regulatory Compliance Tips for the New Practice Owner
Tech Trends
289
291
293
345
349
354

C DA J O U R N A L , V O L 4 7 , Nº 5
288 M AY 2 01 9
Volume 47, Number 5 May 2019
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
can include photos to help buyers
see the potential.
And if you’re hiring, candidates
anywhere can apply right from
the site. Looking for a job? You can
post that, too. And the best part—
it’s free to all CDA members.
All of these features are designed to
help you get the results you need,
faster than ever. Check it out for
yourself at cda.org/classifieds.
CDA Classifieds. Free postings.Priceless results.
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
CDA Offi cersR. Del Brunner, DDSPRESIDENT
Richard J. Nagy, DDSPRESIDENT-ELECT
Judee Tippett-Whyte, DDS VICE PRESIDENT
Ariane R. Terlet, DDS SECRETARY
Steven J. Kend, DDSTREASURER
Debra S. Finney, MS, DDS, SPEAKER OF THE HOUSE
Natasha A. Lee, DDSIMMEDIATE PAST PRESIDENT
ManagementPeter A. DuBoisEXECUTIVE DIRECTOR
Carrie E. GordonCHIEF STRATEGY OFFICER
Kristine AllingtonCHIEF MARKETING OFFICER
Alicia MalabyCOMMUNICATIONS
DIRECTOR
Cris WeberCREATIVE AND UX DIRECTOR
EditorialKerry K. Carney, DDS, CDEEDITOR-IN-CHIEF
Ruchi K. Sahota, DDS, CDEASSOCIATE EDITOR
Brian K. Shue, DDS, CDEASSOCIATE EDITOR
Gayle Mathe, RDHSENIOR EDITOR
Yiming Li, DDS, MSD, PhDGUEST EDITOR
Andrea LaMattina, CDEPUBLICATIONS MANAGER
Kristi Parker JohnsonEDITORIAL AND
COMMUNICATIONS SPECIALIST
Blake EllingtonTECH TRENDS EDITOR
Jack F. Conley, DDSEDITOR EMERITUS
Robert E. Horseman, DDSHUMORIST EMERITUS
ProductionRandi TaylorSENIOR GRAPHIC DESIGNER
Upcoming Topics June/General TopicsJuly/Safety and Risk Management IAugust/Dental Phobias
AdvertisingSue Gardner ADVERTISING SALES
Permission and ReprintsAndrea LaMattina, CDEPUBLICATIONS MANAGER
Manuscript Submissionswww.editorialmanager.com/jcaldentassoc
Letters to the Editorwww.editorialmanager.com/jcaldentassoc
SubscriptionsAnnual subscriptions are available to association members at a rate of $36. To manage your printed Journal subscription online, log in to your cda.org account or email [email protected] for assistance. View the publication online at cda.org/journal.
published by the California Dental Association 1201 K St., 14th Floor Sacramento, CA 95814 800.232.7645 cda.org
Journal of the California Dental Association (ISSN 1043–2256) is published monthly by the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814, 916.554.5950. Periodicals postage paid at Sacramento, Calif. Postmaster: Send address changes to Journal of the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814.
The California Dental Association holds the copyright for all articles and artwork published herein. The Journal of the California Dental Association is published under the supervision of CDA’s editorial staff . Neither the editorial staff , the editor, nor the association are responsible for any expression of opinion or statement of fact, all of which are published solely on the authority of the author whose name is indicated. The association reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition that they are contributed solely to the Journal.
Copyright 2019 by the California Dental Association. All rights reserved.
@cdadentists
Connect to the CDA community by following and sharing on social channels

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 289
Assoc. Editor
You may have seen stories in the media that say the surfaces of smartphones, computer keyboards, gasoline pumps, elevator buttons, etc. are dirtier
than toilet seats. It may alarm you for a day or two, but then you probably move on.
But what about your dental offi ce environment? You may take that for granted, as you and your team regularly follow infection-control protocols in the operatories, which of course include proper hand hygiene. Simple, but important.
But even so, infections caused in the course of receiving care in health care settings still occur at a surprising rate. The Centers for Disease Control and Prevention (CDC) reports that U.S. hospitals every year cause more than 722,000 health care-associated infections (HCAI), which kill about 75,000 patients. The World Health Organization (WHO) states that HCAI occur in an estimated 5 million Europeans each year, along with about 135,000 deaths. And for various reasons, the risk is much higher in developing countries.
It starts with poor hand hygiene. The CDC states that hand hygiene is “considered the single most critical measure for reducing the risk of transmitting organisms to patients and health care personnel.” The WHO echoes this: “Hand hygiene is the primary measure proven to be effective in preventing HCAI and the spread of antimicrobial resistance.” And a great deal of the WHO’s infection-prevention and control guidelines focus on hand hygiene.
We all know the required proper hand hygiene as it applies in the dental practice. In 2016, the CDC restated its guidelines to use soap, water, paper towels and/or alcohol-based hand rubs for routine dental procedures and only soap and water when hands are visibly soiled with blood and
body fl uids, but recommends an antimicrobial soap and alcohol-based hand rub with persistent activity if performing surgical procedures (biopsy, periodontal surgery, apical surgery, implant surgery and surgical extractions). Cal/OSHA requires handwashing facilities or antiseptic hand cleaners with clean towels or antiseptic towelettes, but hands are to be washed with soap as soon as feasible and immediately if contacted with blood or other potentially infectious materials. The Minimum Standards for Infection Control from the Dental Board of California state that all dental health care personnel (DHCP) “shall perform hand-hygiene procedures before donning gloves and after removing and discarding gloves” and also must “thoroughly wash their hands with soap and water at the start and end of each workday.” The standards also state that all DHCP must use new gloves before treatment of each patient and hands must be “thoroughly dried before donning gloves in order to prevent promotion of bacterial growth.”
But knowledge doesn’t always transfer to action. The WHO also states that health care workers “encounter diffi culties in complying with hand-hygiene indications at different levels.” A study reported by both the CDC and the WHO listed “observed risk factors for poor adherence to recommended hand-hygiene practices,” usually in cases where there was a “higher demand for hand hygiene.” It found that hand-hygiene practices
decreased when the subject was a doctor, a male, works on weekdays, is frequently interrupted, works in highly critical hospital departments, is understaffed and wears gowns and gloves, among other factors.
Much effort has been done to fi nd out why the hand hygiene of health care workers is poor. It is diffi cult to quantitate and evaluate, given the many factors, reporting modes and observations. In spite of that, much effort continues on a worldwide level to infl uence health care workers.
Various campaigns exist to reinforce the importance of hand hygiene. This year, the WHO created the “Save Lives: Clean Your Hands” campaign for World Hand Hygiene Day on May 5, 2019, and its theme is “Clean Care for All: It’s in Your Hands.” It is also holding a global survey to focus on infection prevention and hand hygiene in health care facilities, which will concentrate on proven educational tools and improvements.
The CDC also created the “Clean Hands Count” campaign to focus on World Hand Hygiene Day. The CDC’s goal is to bring hand-hygiene awareness to health care workers, address myths and misperceptions and involve patients in their care. The CDC presents facts to promote good hand-hygiene practices, such as how alcohol-based hand sanitizers are more effective and less drying on the hands than using soap and water or that such hand sanitizers do not cause antibiotic resistance. The CDC and the WHO also encourage patients to speak up to their health care team when
Hands UpBrian K. Shue, DDS, CDE
The CDC states that hand hygiene is “considered the single most critical measure for reducing the risk of transmitting organisms to patients and health care personnel.”
C DA J O U R N A L , V O L 4 7 , Nº 5
290 M AY 2 01 9
M A Y 2 0 1 9 A S S O C . E D I T O R
necessary to remind them to clean their hands. Don’t be surprised if this happens to you. It could also give you a chance to open a discussion about this important matter.
Observe your routine. Look into your own hand-hygiene practices. Examine those of your fellow health care workers and employees. Having agencies tell you what to do is one thing, but being responsible and doing what’s right will take your own actions.
Historically, hand hygiene with soap and water has been known to be important in health care, but one of the fi rst examples of the effi cacy of antibacterial hand sanitizer came in Vienna in 1846. Dr. Ignaz
Semmelweis signifi cantly reduced puerperal fever when his hospital’s doctors cleansed their hands with a 4% sodium hypochlorite solution after leaving the autopsy room and before going to the obstetrics department.
The CDC states that “failure to perform appropriate hand hygiene is considered the leading cause of health care-associated infections and spread of multiresistant organisms and has been recognized as a substantial contributor to outbreaks.” That is a great take-home message. And if you didn’t get to celebrate World Hand Hygiene Day this year, no problem. Global Handwashing Day is just around the corner on Oct. 15. ■
RESOURCES
CDC. Infection Prevention Checklist for Dental Settings: Basic Expectations for Safe Care, March 2016.CDC. Guideline for Hand Hygiene in Health-Care Settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR Recomm Rep 2002;51(No. RR–16).WHO guidelines on hand hygiene in health care: A summary, 2009.
Brian K. Shue, DDS, CDE, is the dental director of a federally qualified health center. He is a certified dental editor, the San Diego County Dental Society editor and a fellow of the American College of Dentists and the Pierre Fauchard Academy.
SHARE THE BENEFITS OF MEMBERSHIP. Help others discover organized dentistry’s
advocacy, support, education and protection,
plus CDA’s newest benefit: big savings on
dental supplies through tdsc.com.
For every colleague you successfully refer to join
CDA, you’ll earn DOUBLE REWARDS:
$100 American Express® gift card from ADA*
plus $100 to shop tdsc.com from CDA*
* Rewards issued to referring member once referral joins and pays required dues. Total rewards possible per calendar year are limited to $500 in gift cards from ADA and $500 in value from CDA.
THE MORE NEW MEMBERS YOU REFER, THE MORE REWARDS!
Get started at cda.org/refer.
TOTOOTOT GEGEEGEOO THTHTHTHERERERWE WE WE WEWE AREAREAREARARER
LLLLIMIIMIIMIMIIM TLTLTLTLLESESESESSSSSSSSSSSSS
®
REFER AMEMBER. EARN DOUBLE REWARDS.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 291
The Journal welcomes lettersWe reserve the right to edit all
communications. Letters should discuss an item published in the Journal within the last two months or matters of general interest to our readership. Letters must be no more than 500 words and cite no more than fi ve references. No illustrations will be accepted. Letters should be submitted at editorialmanager.com/jcaldentassoc. By sending the letter, the author certifi es that neither the letter nor one with substantially similar content under the writer’s authorship has been published or is being considered for publication elsewhere, and the author acknowledges and agrees that the letter and all rights with regard to the letter become the property of CDA.
Dr. Robert J. Genco, 1938–2019
Robert J. Genco, DDS, PhD, world-renowned SUNY distinguished professor of oral biology, microbiology and immunology at the University at Buffalo (UB) and director of UB’s Periodontal Research Center, died at the age of 80 on March 6, 2019. Lauded as the “father of oral science” by the Journal of Dental Research, Dr. Genco was the world’s leading periodontal researcher and pioneer on the perio-systemic link. He was fascinated by oral health’s impact on overall health and this interest resulted in numerous insights on the bacteria that cause gum disease and the establishment of how smoking, diabetes, osteoporosis and stress infl uence the perio-systemic relationship.
Dr. Genco is fondly remembered as a scholar, educator, mentor, innovator and committed leader at UB. He began his work at the university in 1968 after receiving his dental degree from UB in 1963 and a doctorate in microbiology and immunology from the University of Pennsylvania in 1967. Dr. Genco contributed to more than 400 scientifi c articles and edited nearly 30 books and chapters. Serving in several editorial positions at 11 scientifi c journals, he is best remembered by the periodontal profession for his tenure as the editor-in-chief of the Journal of Periodontology from 1988 to 2006. At UB, Dr. Genco taught clinical periodontics and microbiology and was a mentor to more than 80 graduate and postdoctoral students, many of whom are leaders in dental academics. His innovative nature was demonstrated by the translational science activities he performed, resulting in the launch of more than 80 businesses and facilitating more than 1,300 discoveries.
Dr. Genco received numerous awards throughout his career, including the ADA Gold Medal Award for
Letter
Excellence in Dental Research, the ADA Norton M. Ross Award for Excellence in Clinical Research, the American Association for Dental Research (AADR) Distinguished Scientist Award and the SUNY Research Foundation Lifetime Achievement Award. He was a past president of the AADR and the International Association for Dental Research, vice provost at the UB Office of Science, Technology Transfer and Economic Outreach from 2002–2016, director of the UB Microbiome Center since 2016 and a member of the National Academy of Medicine.
Dr. Genco will also be remembered for his willingness to give back to both the community and his family. He served on the advisory board of the new Institute of Graduate Dental Biosciences at Thomas Jefferson University, on the board of the Buffalo Museum of Science and as a trustee at Nichols School. He was also an avid golfer at Park Country Club. Dr. Genco married Sandra Clarke in 1959 and raised two daughters and a son. Unfortunately, Mrs. Genco died in 2002. In 2006, he married Frances Doherty. He is survived by Frances, his daughters and son, his grandchildren and great-grandchildren.
“Dr. Genco was a legendary fi gure in dental research known throughout the world,” remarked Joseph J. Zambon, DDS, PhD, dean of the UB School of Dental Medicine. “He will be remembered for his towering intellect, for innovative research that transformed the scientifi c basis of dental practice and, most of all, for his exceptional humanity, which he generously shared with his many students and colleagues.”
R I C H A R D K AO, D D S
Cupertino, Calif.
(855) 886-4824 | rstrepublic.com | New York Stock Exchange symbol: FRCMEMBER FDIC AND EQUAL HOUSING LENDER
“We treat our patients with respect and great service. Th at’s exactly how First Republic treats us.”
L E E & YO U N G O RT H O D O N T I C S
Rodney Lee, D.D.S., Owner (left ); Glen Young, D.D.S., Owner (right)
CDAJour Oct_18 LeeYoung ND2017.indd 1 8/21/18 12:09 PM

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 293
Impressions
The nub:
1. Ethical issues cannot be resolved by facts or reason.
2. Deciding what you want to do and then looking for a justifi cation is easy, but it is not ethics.
3. Potential ethical issues can be avoided by ignoring others’ values.
David W. Chambers, EdM, MBA, PhD, is a professor of dental education at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry in San Francisco and the editor of the American College of Dentists.
How To Spot an Ethical ProblemDavid W. Chambers, EdM, MBA, PhD
Is the decision to prophylactically remove third molars an ethical issue? What about insurance plans that limit the frequency of periodontal treatments, a single standard of care for patients regardless of their level of cooperation, public water fl uoridation or where one locates a dental practice? Are they ethical issues? Those questions were selected because they are not addressed by the ADA or CDA codes and because multiple and confl icting principles from dentistry and others from ethics generally can be used to give different answers. So are they really ethical issues?
Strange to say, ethics experts have tended to focus more on looking for situations (often small and trivial ones) where their theories or principles apply than on clarifying the boundaries between ethical behavior and actions that can safely be taken without having to worry about the ethical dimensions. The hottest topic in professional ethics today is “trollyology.” Should you push a fat man off an overpass to slow down or stop an out-of-control trolley headed toward fi ve folks tied to the tracks ahead? If all the papers written on the topic were dropped on the tracks, they would probably stop the trolley.
Here is my take on how to spot an ethical issue. If my action affects others and the other person’s actions affect me, we might have an ethical problem. It is further required that our disagreement about what is mutually best cannot entirely be resolved by appeal to fact or by either acting alone.
Some dentists prefer aggressive and some conservative approaches to TMJ problems; some believe that early orthodontic treatment is unsound because it adds cost and does not change outcomes; some dentists are alarmed over amalgam. Holding these opinions or even writing and speaking about them occasionally under an ethical fl ag is most often attempted by talking to a friendly crowd instead of those affected. But if all those with a stake in our proposed actions are not part of the conversation, we still do not have an ethical issue.
When the others involved are patients, the ethical issue is typically one of sharing information, because there is a large overlap in the goals of dentists and patients. When informed consent is disguised as “hold-harmless” language instead of an invitation to explore joint actions, this is legal territory, not ethical. When facts are shared but differences remain to be worked out, ethics begins.
One way to cheat in ethics is to say that others’ values are wrong. If our facts are not convincing, we paint others as ignorant, stubborn or watching the wrong TV channel. Sometimes in frustration with the seeming impossibility of bringing others around to our values by telling them our side, we simply say their values do not really matter. ■
C DA J O U R N A L , V O L 4 7 , Nº 5
294 M AY 2 01 9
M A Y 2 0 1 9 I M P R E S S I O N S
DNA in the tumor fl uid, researchers also found that the presence of bacterial DNA was higher in patients who had undergone invasive pancreas endoscopy, a procedure that involves the insertion of a fl exible tube into the mouth to examine and treat pancreatic conditions and which could result in the possible transfer of oral bacteria into the pancreas.
“The results were not completely
unequivocal, so the endoscopy can’t be the whole answer to why the bacteria is there,” Dr. Sällberg said. “But maybe we can reduce the risk of transferring oral bacteria to the pancreas by rinsing the mouth with an antibacterial agent and ensuring good oral hygiene prior to examination.”
Learn more about this study in Gut (2019); dx.doi.org/10.1136/gutjnl-2018-317458.
Oral Bacteria in Pancreas Linked to Aggressive Tumors
A study by researchers at the Karolinska Institutet in Sweden found that the presence of oral bacteria in cystic pancreatic tumors is associated with the severity of the tumor, which could help to improve diagnosis and treatment of pancreatic cancer. The study was published in the journal Gut in March 2019.
Researchers examined the presence of bacterial DNA in fl uid from pancreatic cysts in 105 patients and compared the type and severity of the tumors. In doing so, they found that the fl uid from the cysts with high-grade dysplasia and cancer contained much more bacterial DNA than that from benign cysts.
To identify the bacteria, the researchers sequenced the DNA of 35 samples that had high amounts of bacterial DNA. They found large variations in the bacterial composition between different individuals, but also a greater presence of certain oral bacteria in fl uid and tissue from cysts with high-grade dysplasia and cancer.
“We fi nd most bacteria at the stage where the cysts are starting to show signs of cancer,” said corresponding author Margaret Sällberg Chen, PhD. “What we hope is that this can be used as a biomarker for the early identifi cation of the cancerous cysts that need to be surgically removed to cure cancer, which will in turn also reduce the amount of unnecessary surgery of benignant tumors.”
In studying different factors that could affect the amount of bacterial
Family Use May Infl uence Teen Opioid RiskA study published in the journal JAMA Surgery found that the presence of
one or more family members using long-term opioids before a surgical procedure was associated with a higher likelihood that adolescents prescribed opioids for the first time would continue prescriptions long after their own surgeries. The research was led by surgery and pediatric teams at the University of Michigan C.S. Mott Children’s Hospital.
The observational study used data from a commercial insurance database for about 346,000 patients aged 13 to 21 who underwent such procedures as third molar extraction, appendix removal, hernia repair and knee and shoulder surgery. The data included dependents on a family insurance plan between 2010 and 2016.
Among the 257,000 (74%) of patients who had their first-ever opioid prescription filled, about 11,000 (4.3%) had at least one family member with long-term opioid use. These included family members who had filled opioid prescriptions 120 or more days during the 12 months before the young person’s procedure or filled three or more opioid prescriptions within 90 days.
Persistent opioid use (one or more opioid prescriptions filled three or more months after surgery) occurred in 453 patients (4.1%) with a family member who was a long-term user of opioids compared with 5,940 patients (2.4%) without long-term opioid use by a family member.
Senior author Jennifer Waljee, MD, said providers should discuss with families the potential harms of continued opioid use and provide help for patients still seeking refills three or more months after a procedure.
“Surgeons and providers should heighten efforts to prevent opioid dependence among patients with any potential risk factors,” she said.
Learn more about this study in JAMA Surgery (2019); doi:10.1001/jamasurg.2018.5838.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 295
Most reptiles and fi sh have multiple sets of teeth during their lifetime, while most mammals, such as humans, have only one set of replacement teeth. And some mammals, like mice, have only a single set with no replacement. This diversity raises both evolutionary and developmental
questions that researchers from the King’s Faculty of Dentistry, Oral and Craniofacial Sciences at King’s College London sought to answer in a new study published recently in the journal Development.
The research team pinpointed why mice don’t have replacement teeth by
comparing gene expression in the dental lamina of the mouse and the mini pig, which has two sets of teeth. While Wnt signaling is known to be required for tooth replacement in other vertebrates, the researchers found that Wnt activity is absent in a rudimentary form of the dental lamina in mice. This structure forms in the mouse but then disappears, stopping the generation of another set of teeth. Using sophisticated genetic techniques, the researchers activated Wnt signaling in the mouse RSDL at E15.5 and E16 stages of development, revitalizing this structure, and additional teeth were formed as a consequence.
The researchers also report that culturing the RSDL in isolation stimulated its tooth-forming potential, suggesting that the fi rst generation of teeth might prevent replacement teeth from developing and that the previous set of teeth also infl uence the development of a next set.
These results provide a conceptual advancement in the tooth-replacement fi eld as well as providing new insights into how traits are lost during mammalian evolution and how they might be restored, according to the study.
“This is relevant to human tooth replacement, as structures similar to the RSDL have been identifi ed next to the permanent teeth during development,” said researcher Abigail Tucker, PhD. “In normal development of our teeth, therefore, the second set or permanent tooth may inhibit the generation of a third set of teeth.”
Learn more about this study in Development (2019); doi:10.1242/dev.171363.
Tooth Regeneration Activated in Mice
Mouthwash Could Raise Blood PressureNew research published in the journal Frontiers in Cellular and Infection
Microbiology shows that an antiseptic compound found in mouthwash destroys “friendly” oral bacteria that help maintain normal blood pressure levels.
The research team, led by Nathan Bryan, PhD, from the department of molecular and human genetics at Baylor College of Medicine in Houston, used 16S rRNA gene sequencing and analysis to examine whether using chlorhexidine antiseptic mouthwash twice a day for one week changed the oral bacterial communities and blood pressure levels in 26 healthy individuals. After one week, the 26 study volunteers went back to their usual oral hygiene practices.
The researchers collected samples of the participants’ saliva and tongue scrapings and measured their blood pressure at four different points throughout the study: at baseline, then seven, 10 and 14 days later. They found that twice-daily chlorhexidine usage was associated with a significant increase in systolic blood pressure after one week of use and recovery from use resulted in an enrichment in nitrate-reducing bacteria on the tongue.
A balanced oral microbiome helps maintain good cardiovascular health by helping the conversion of dietary nitrate into nitric oxide (NO) — a signaling molecule that helps maintain normal blood pressure. Because of the “ubiquitous” nature of the NO molecule, the systemic effects of orally produced bacteria may have other significant effects on human health beyond maintenance of blood pressure, according to the study.
“We know one cannot be well without an adequate amount of NO circulating throughout the body, yet the very first thing over 200 million Americans do each day is use an antiseptic mouthwash, which destroys the ‘good bacteria’ that helps to create the NO,” Dr. Bryan said. “These once thought of as good habits may be doing more harm than good.”
Learn more about this study in Frontiers in Cellular and Infection Microbiology (2019); doi.org/10.3389/fcimb.2019.00039.
Revitalized tooth gene. (Credit: Elena Poppa)

C DA J O U R N A L , V O L 4 7 , Nº 5
296 M AY 2 01 9
“These fi ndings continue to suggest that the public does not understand that combustion escalates the health risks in tobacco products that are smoked, making them more harmful than noncombusted smokeless tobacco on a continuum of risk,” said lead researcher Olivia Wackowski, PhD.
Learn more of about this study in Addictive Behaviors (2019); doi.org/10.1016/j.addbeh.2018.11.011.
risks, while about 38% perceived that snus poses less risk for lung cancer and heart disease than cigarettes but had the same oral cancer risk as cigarettes. Another 17% accurately perceived snus to have lower risks for lung cancer but perceived risks for oral cancer and heart disease to be about the same as that from smoking. Almost 40% incorrectly perceived the risk of oral cancer to be higher from snus use than smoking.
Health Risks of Snus Misunderstood by U.S. Smokers
American smokers mistakenly think that using snus, a type of moist snuff smokeless tobacco product, is as dangerous as smoking tobacco, according to a Rutgers study published in the journal Addictive Behaviors.
Snus, a product popular in Scandinavia but newer to the United States, is a moist powder tobacco that can be sold in a loose form or in small prepacked pouches that users place under the top lip. It is typically spit-free. While smokeless tobacco products are addictive, contain cancer-causing chemicals and are linked with cardiovascular and certain cancer risks, products such as snus have comparatively fewer health risks than smoking when used exclusively — not in tandem with smoking — and may serve as harm-reduction alternatives for smokers unable or unwilling to completely quit tobacco. In Sweden, snus use has been linked to a decrease in tobacco smoking and smoking-related diseases.
For the study, researchers reviewed how 256 smokers responded to questions about their perceived risk of developing lung cancer, heart disease and oral cancer from using snus versus cigarettes and whether there were subgroups of smokers with similar patterns of beliefs. More than 75% of the participants smoked daily and about 20% had tried smokeless tobacco.
Research results show that about 45% perceived snus to be as harmful as smoking overall and for all health three
M A Y 2 0 1 9 I M P R E S S I O N S
TMD Pain Best Treated With Self-Care TreatmentsWhile oral appliances are the most common treatment for facial pain
from temporomandibular disorders (TMD), patients rate them as less helpful than self-care treatments, according to new research published in the journal Clinical Oral Investigations. The study conducted by researchers at the NYU College of Dentistry suggests that self-care treatments should be the first line of treatment for muscle-related TMD (mTMD).
In the study, researchers examined what nonmedication treatments women with mTMD use to manage their pain and how effective patients perceive the treatments to be. The researchers examined and interviewed a total of 125 women with mTMD in order to determine whether treatment differed for patients with widespread pain.
The most common treatments reported were oral appliances and self-care treatments such as physical therapy and at-home jaw exercises. Less common self-care treatments included acupuncture, seeing a chiropractor, trigger-point injection, exercise or yoga and meditation or breathing. Participants often used more than one treatment.
Participants reported the most improvement in their pain from the self-care treatments, with more than 84% reporting that these activities helped them at least a little. In contrast, only 64% of those who used oral appliances reported that they helped at least a little. A small proportion of women who used oral appliances said that oral appliances made their pain worse.
“Our results support the use of self-management as the first line of treatment for mTMD before considering more expensive interventions,” said Karen Raphael, PhD, the study’s co-author.
Read more of this study in Clinical Oral Investigations (2019); doi.org/10.1007/s0078.
CDA. THIS IS WHERE STRONG
MEETS SMART.
TOTOTOTOTOTOT GEGEGEGEGEGETHTHTHTHTHHHTHERERERERRERRWEWEWEWEWEWEWEW AAAAAAAREREREEEEEE
LILILILILLLIMIMIMIMIMMIMITTTLTLLLEESESESESESESSSSSSS
®
Insights, tools and resources from
Practice Support experts to help
you navigate the business side of
dentistry. Just a few of the limitless
member benefits at cda.org.
Dedicated expertise.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 299
i n t r o d u c t i o n
surgery as it is capable of revolutionizing the process of manufacturing prostheses and devices. While digital dentistry, such as intraoral scanning and computer-aided design/computer-aided manufacturing (CAD/CAM), has become a part of dental practice, 3D printing is a relatively new technology to dentistry. With its advantages, such as highly feasible custom design and quick manufacturing process, 3D printing has become a technology of great interest to dentistry. The article written by the team led by Jaime Lozada, DDS, at Loma Linda University provides an excellent overview of stereolithographic 3D-printing technology in dental implantology and its application for producing diagnostic bone models, modifi ed surgical guides, bone reduction guides and bone scaffolds used for guided bone regeneration procedures.
The discovery of Bis-GMA resin by Rafael “Ray” Bowen, DDS, DSc, in 1962 was one of the revolutionary milestones in the advances of dentistry. Thanks to its excellent properties, Bis-GMA quickly became and has been the predominant dental resin used in daily dental practice, especially for restorative
GUEST EDITOR
Yiming Li, DDS, MSD, PhD, is a distinguished professor and the associate dean for research at the Loma Linda University School of Dentistry.Confl ict of Interest Disclosure: None reported.
Dentistry has been known as a profession of science and art. On May 15, 1923, Robert Geoffrey Keyworth, DDS, provided justifi cations for this concept
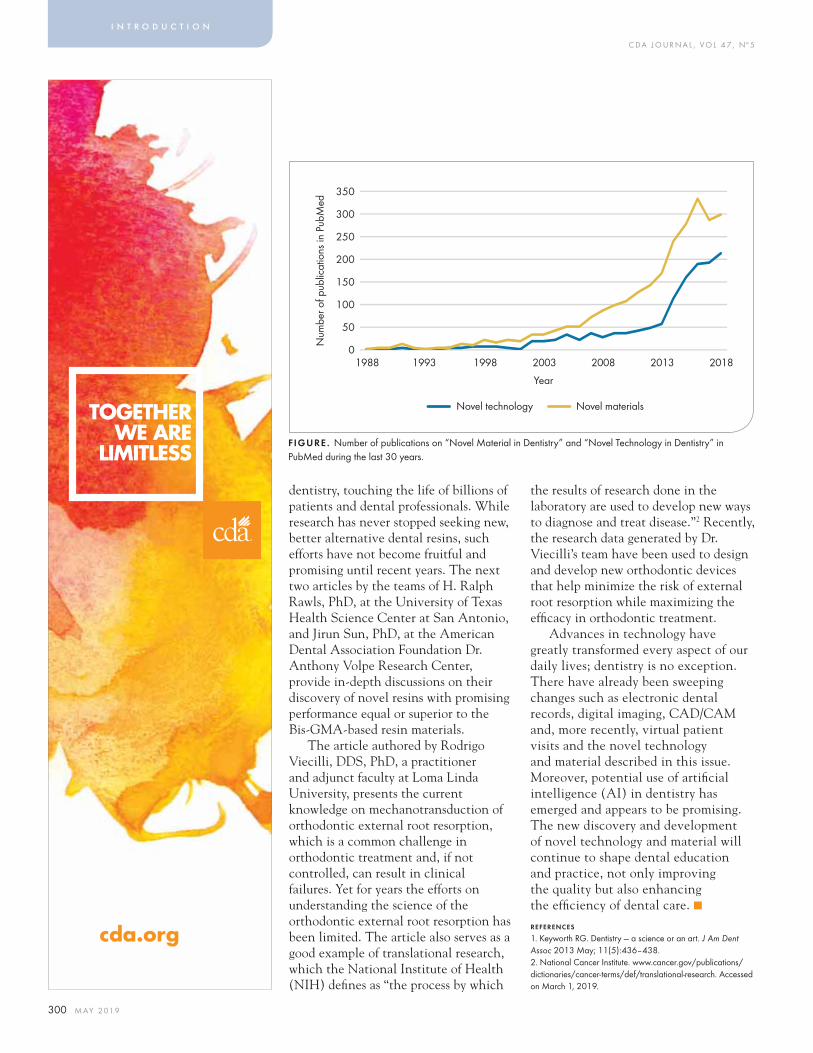
to his fellow members of the Manson Research and Clinic Club, which were subsequently published in the Journal of the American Dental Association.1 Historically, discoveries of novel materials and technology have been a major driving force in advancing the education and practice of dentistry. In recent years, accelerated advances in science and technology have also been refl ected in dentistry; publications on topics of novel materials and technology in dentistry have increased dramatically, especially in the last 10 years (FIGURE). This issue of the CDA Journal provides an insight of fundamental and practical knowledge in three important areas: 3D printing, dental resins and mechanotransduction of external root resorption in orthodontic treatment.
The 3D-printing technology was initially used in aerospace and automobile industries, armaments and art and design. It quickly attracted signifi cant interest and attention in health care fi elds, especially orthopedic
Novel Technologies and Materials in DentistryYiming Li, DDS, MSD, PhD
C DA J O U R N A L , V O L 4 7 , Nº 5
300 M AY 2 01 9
i n t r o d u c t i o n
dentistry, touching the life of billions of patients and dental professionals. While research has never stopped seeking new, better alternative dental resins, such efforts have not become fruitful and promising until recent years. The next two articles by the teams of H. Ralph Rawls, PhD, at the University of Texas Health Science Center at San Antonio, and Jirun Sun, PhD, at the American Dental Association Foundation Dr. Anthony Volpe Research Center, provide in-depth discussions on their discovery of novel resins with promising performance equal or superior to the Bis-GMA-based resin materials.
The article authored by Rodrigo Viecilli, DDS, PhD, a practitioner and adjunct faculty at Loma Linda University, presents the current knowledge on mechanotransduction of orthodontic external root resorption, which is a common challenge in orthodontic treatment and, if not controlled, can result in clinical failures. Yet for years the efforts on understanding the science of the orthodontic external root resorption has been limited. The article also serves as a good example of translational research, which the National Institute of Health (NIH) defi nes as “the process by which
the results of research done in the laboratory are used to develop new ways to diagnose and treat disease.”2 Recently, the research data generated by Dr. Viecilli’s team have been used to design and develop new orthodontic devices that help minimize the risk of external root resorption while maximizing the effi cacy in orthodontic treatment.
Advances in technology have greatly transformed every aspect of our daily lives; dentistry is no exception. There have already been sweeping changes such as electronic dental records, digital imaging, CAD/CAM and, more recently, virtual patient visits and the novel technology and material described in this issue. Moreover, potential use of artifi cial intelligence (AI) in dentistry has emerged and appears to be promising. The new discovery and development of novel technology and material will continue to shape dental education and practice, not only improving the quality but also enhancing the effi ciency of dental care. ■REFERENCES
1. Keyworth RG. Dentistry — a science or an art. J Am Dent Assoc 2013 May; 11(5):436–438.2. National Cancer Institute. www.cancer.gov/publications/dictionaries/cancer-terms/def/translational-research. Accessed on March 1, 2019.
FIGURE. Number of publications on “Novel Material in Dentistry” and “Novel Technology in Dentistry” in PubMed during the last 30 years.
350
300
250
200
150
100
50
0
Num
ber o
f pub
licat
ions
in P
ubM
ed
Year
Novel technology Novel materials
1988 1993 1998 2003 2008 2013 2018
TOGETHERWE ARE
LIMITLESS
®
cda.org
Keeping the game fair...
...so you’re not fair game.The fast-changing practice of dentistry
is getting hit from all angles.
Choose a specialized protection plan designed
to help you cover your unique California risks.
You get game-changing coverage made easy.
800.282.6242 • DentistCare.com
Professional Liability Insurance & Risk Resource Services
ProAssurance Group is rated A+ (Superior) by A.M. Best.

WE’RE HERE TO HELP.
Our smart analysts and sharp tools can help you
navigate working with dental benefit plans. And,
a streamlined process makes it more convenient to
share your challenges with claim denials, delays and
miscommunications. Once your online form is submitted,
you’ll get expert guidance on your next steps.
Learn more at cda.org/dentalbenefits.
CHALLENGES WORKING WITHBENEFIT PLANS?
800.232.7645cda.org/practicesupport
®
Practice ManagementEmployment PracticesDental Benefit PlansRegulatory Compliance
PRACTICE SUPPORT
d,
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 303
Three-dimensional printing and the rapid prototyping technology have been extensively used in the industrial, engineering and medical fi elds for many years,
enabling manufacturers to fabricate parts and medical devices.1 Furthermore, rapid prototyping has been used in various fi elds of dentistry, including prosthodontics,2–5 orthodontics6 and assisting in the fabrication of fi xed and removable maxillofacial prostheses as well as the planning of simple to complex surgeries in implant dentistry.7
Within implant dentistry, affordable desktop 3D printers along with user-friendly 3D software provide opportunities for the use of fused deposition and polymer-based, 3D-printed materials across many facets of implant dentistry.8–15
Those devices and materials enable
3 d p r i n t i n g
AUTHORS
Jaime Lozada, DDS, is a professor and the director of the Advanced Education Program in Implant Dentistry at the Loma Linda University School of Dentistry.Confl ict of Interest Disclosure: None reported.
Carolina Herrera, DMD, is a graduate student in the Advanced Education Program in Prosthodontics at the University of Illinois at Chicago College of Dentistry.Confl ict of Interest Disclosure: None reported.
Brian Goodacre, DDS, MSD, is an assistant professor in the division of general dentistry at the Loma Linda University School of Dentistry.Confl ict of Interest Disclosure: None reported.
3D Printing and Bioprinting Technology for Specifi c Applications in Surgical Implant Dentistry: A ReviewJaime Lozada, DDS; Carolina Herrera, DMD; Brian Goodacre, DDS, MSD; Aladdin Al-Ardah, BDS, MS; and Erik Sahl, DDS, MSD
A B S T R AC T Three-dimensional printing is rapidly evolving in dentistry. In the fi eld of implant dentistry, countless numbers of laboratory and clinical applications are consistently being developed. This review article describes the application of three different uses of stereolithographic 3D printing, including diagnostic bone models, modifi ed surgical guides and bone reduction guides. Furthermore, the use of 3D-bioprinting technology in printing bone scaffolds that could be used during guided bone regeneration (GBR) procedures is also presented.
Aladdin Al-Ardah, BDS, MS, is an associate professor in the Advanced Education Program in Implant Dentistry at the Loma Linda University School of Dentistry.Confl ict of Interest Disclosure: None reported.
Erik Sahl, DDS, MSD, is an associate professor and the director of the Advanced Education Program in Periodontics at the Loma Linda University School of Dentistry.Confl ict of Interest Disclosure: None reported.
the in-offi ce printing of diagnostic casts, teaching aids and surgical guides among many other applications.7–10
More recently the possibility of 3D printing bone scaffolds is becoming popular because of the ability to directly print porous scaffolds based on digitally designed shapes, controlled chemistry and interconnected porosity. Some of these inorganic scaffolds are biodegradable and have proven ideal for bone-tissue engineering and site-specifi c growth factor/drug delivery.16
Today, several affordable desktop 3D printers can permit an in-offi ce protocol to produce anatomical casts, implant drilling guides and other diagnostic and clinical devices.17–20 This review article focuses on specifi c applications of 3D-printing technology with emphasis on current stereolithography protocols for implant dentistry and the

C DA J O U R N A L , V O L 4 7 , Nº 5
304 M AY 2 01 9
3 d p r i n t i n g
early experience of the authors with bioprinting bone scaffolds based on fused deposition modeling protocols, along with an assessment of the current challenges and future directions of this technology. See TABLE 1 for a list of defi nitions commonly used in digital dentistry.
StereolithographyStereolithography (SLA or SL, also
known as stereolithography apparatus, optical fabrication, photo-solidifi cation or resin printing) is a form of 3D-printing technology used for creating models, prototypes, patterns and production of parts in a layer-by-layer fashion using photopolymerization, a process by which light causes chains of molecules to link together forming polymers.26
The fi rst part of this report presents the use of a desktop stereolithographic printer (Form 2, Formlabs Inc.) coupled with a biocompatible resin (Dental SG, Formlabs Inc.) that is certifi ed to comply with the international standards for class I biocompatibility, International Organization for Standardization (ISO) standard 10993-1 and U.S. Pharmacopoeia (USP) Class VI for specifi c applications in implant dentistry.21
This technique uses a method where a photosensitive resin bath is positioned between a build platform and light-polymerizing source of a specifi c wavelength.17,22,23 The build platform is lowered into the resin bath and the light is directed by the computer to polymerize the resin layer by layer to create the desired 3D object.17,24,25
The second part of this report briefl y describes the potential benefi t of 3D-bioprinting technology applied to the printing of bone scaffolds that could be used during guided bone regeneration (GBR) procedures.
Clinical ApplicationsThis report describes the application
of three different uses of 3D printing by the stereolithographic approach: diagnostic bone models, modifi ed surgical guides and bone reduction guides.
Diagnostic Bone ModelsIn implant dentistry, a common use
of this application is for the treatment planning of model-guided implant surgery and GBR planning. Model-guided implant surgery allows for a detailed evaluation of a 3D-printed model that, in combination with conventional diagnostic prosthodontic procedures, allows for the accurate planning of dental implants and the fabrication of a surgical guide to assist
in a simplifi ed surgical procedure. Having an exact replica of the patient’s mandible or maxilla also permits the evaluation of anatomical features, such as the exact location of the mental foramen and the fl oor of the nose or the maxillary sinus, assisting in the ideal positioning of an implant. The most common application of this type of procedure is the fabrication of bone-supported surgical guides that allow for the use of a pilot or fully guided surgical guide (FIGURES 1–3).
Additionally, the intraoperative trimming of a template/pattern can be used to outline and trim the desired size of a prefabricated membrane or mesh when undergoing a GBR procedure. This provides the desired adaptation around the defect and supports the graft materials. This particular step extends the surgical time and requires constant manipulation of the template.
A preoperative stereolithographic 3D-printed model that includes the defect to be grafted allows for the
FIGURE 1. Stereolithographic 3D model of a mandible with compromised dentition.
FIGURE 4 . 3D-printed model. Notice the defi cient posterior ridge.
FIGURE 2. Laboratory manufactured pilot drill guide for an “All-on-4” treatment modality.
FIGURE 5. 3D-printed model of an anterior defi cient ridge. The design of a template for a GBR procedure is simplifi ed with the model in hand.
FIGURE 3 . Pilot drill guide (bone supported) positioned in place after ridge (bone) reduction.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 305
prefabrication of these templates ahead of surgery with more precision and simplicity. Therefore, clinicians can intraoperatively execute all the necessary trimming and adaptation of membranes or meshes without the inconvenience previously described (FIGURES 4 and 5).
The authors have previously described a novel approach for planning and augmenting a large osseous defect utilizing a titanium mesh (TiMe).27 The required bone volume (horizontally and vertically) can be digitally augmented and
subsequently a 3D-printed bone model can be used to contour a TiMe in accordance with the augmented bone model.
With the contoured/preformed TiMe on the 3D-printed model, a positioning jig can be manufactured to aid the placement of the TiMe during surgery. Although this technique does not impact the fi nal outcome of the augmentation procedure, it allows the clinician to virtually design the augmentation, preform and contour the TiMe and create a positioning jig, reducing surgical time and error (FIGURES 6–8).27
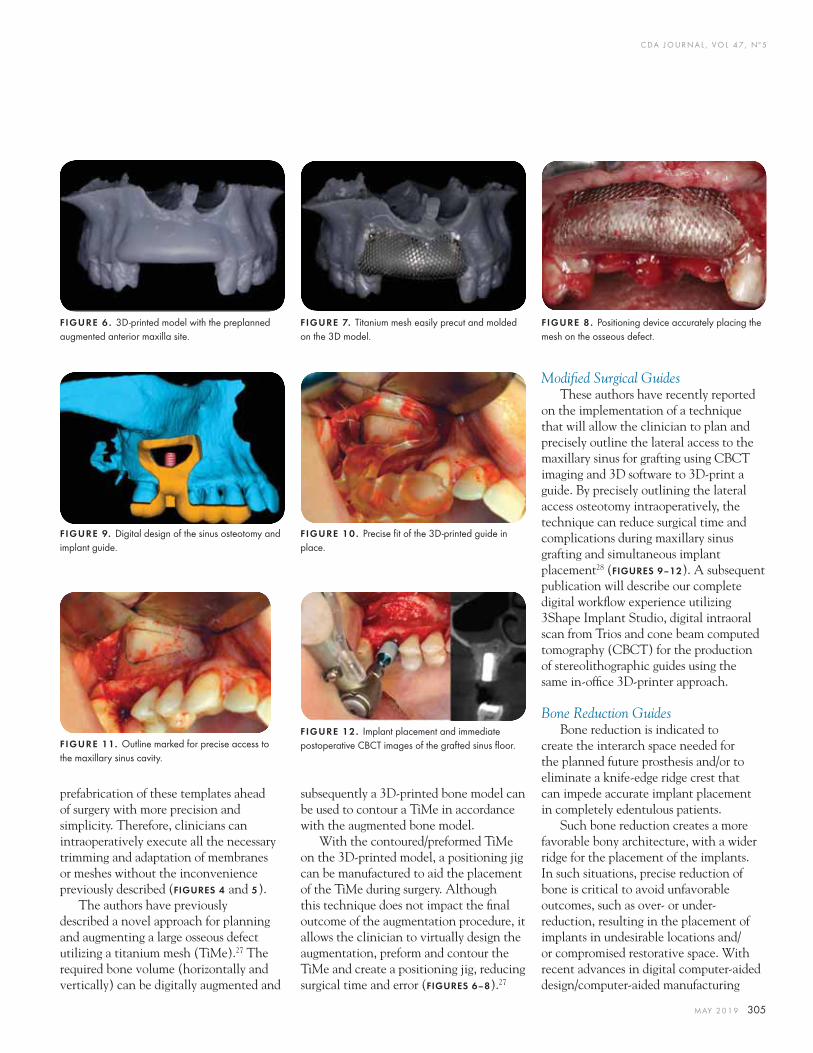
Modifi ed Surgical GuidesThese authors have recently reported
on the implementation of a technique that will allow the clinician to plan and precisely outline the lateral access to the maxillary sinus for grafting using CBCT imaging and 3D software to 3D-print a guide. By precisely outlining the lateral access osteotomy intraoperatively, the technique can reduce surgical time and complications during maxillary sinus grafting and simultaneous implant placement28 (FIGURES 9–12). A subsequent publication will describe our complete digital workfl ow experience utilizing 3Shape Implant Studio, digital intraoral scan from Trios and cone beam computed tomography (CBCT) for the production of stereolithographic guides using the same in-offi ce 3D-printer approach.
Bone Reduction GuidesBone reduction is indicated to
create the interarch space needed for the planned future prosthesis and/or to eliminate a knife-edge ridge crest that can impede accurate implant placement in completely edentulous patients.
Such bone reduction creates a more favorable bony architecture, with a wider ridge for the placement of the implants. In such situations, precise reduction of bone is critical to avoid unfavorable outcomes, such as over- or under-reduction, resulting in the placement of implants in undesirable locations and/or compromised restorative space. With recent advances in digital computer-aided design/computer-aided manufacturing
FIGURE 6 . 3D-printed model with the preplanned augmented anterior maxilla site.
FIGURE 9. Digital design of the sinus osteotomy and implant guide.
FIGURE 11. Outline marked for precise access to the maxillary sinus cavity.
FIGURE 7. Titanium mesh easily precut and molded on the 3D model.
FIGURE 10 . Precise fi t of the 3D-printed guide in place.
FIGURE 12. Implant placement and immediate postoperative CBCT images of the grafted sinus fl oor.
FIGURE 8 . Positioning device accurately placing the mesh on the osseous defect.

C DA J O U R N A L , V O L 4 7 , Nº 5
306 M AY 2 01 9
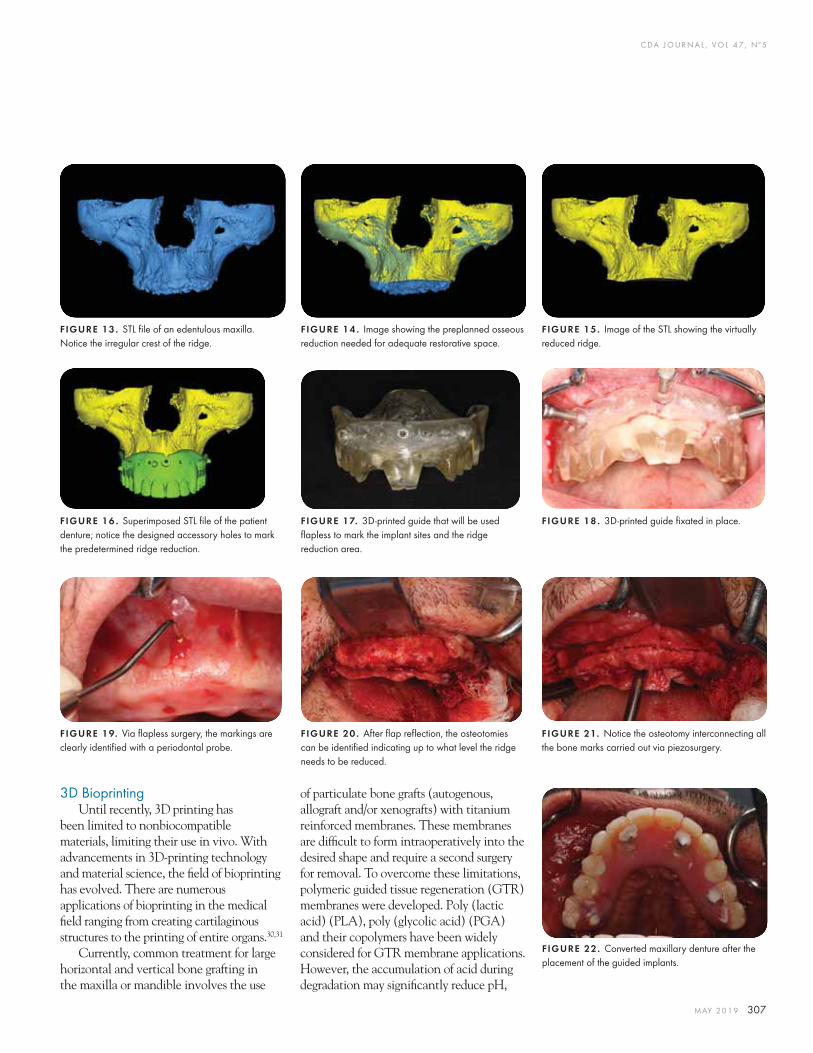
(CAD/CAM) technology, it may now be possible to provide a more accurate treatment outcome in such cases.29 Most bone reduction guides are used after fl ap refl ection and stabilized on the residual ridge to indicate the amount of bone deduction needed. A modifi ed technique developed by the authors can precisely locate the areas to perform the bone osteotomy for the bone reduction before refl ecting the fl aps. With this technique, the guide can be placed on the tissue, prior to fl ap refl ection, ensuring the accurate location for the bone reduction. For the implementation of this modifi ed technique, a “dual scan” CBCT protocol is required.
The fi rst CBCT scan involves the placement of at least six fi duciary radiopaque markers on a functionally and aesthetically verifi ed denture prior to the scanning of the denture. The second CBCT scan involves the
placement of the previously mentioned denture with radiopaque markers in the patient’s mouth and acquiring a CBCT scan. Implant planning software is then used (BlueSky Plan, BlueSkyBio LLC) to superimpose the two scans together, allowing the planning and designing of the reduction guide. The implant positions are prosthetically driven using a pilot drill guide to mark the position of the implants. The guide fi xation pins are planned along with additional accessory osteotomy holes used for the fl apless marking of the desired level of bone reduction. Once the surgical guide is printed and sterilized, it is used as follows:
■ The patient is anesthetized for the surgical placement of four implants in the maxilla.
■ The surgical guide is placed on the supporting mucosa and secured in place using the fi xation pins.
■ In this fl apless approach, the pilot drill is used to mark the implant positions, ensuring the osteotomy goes beyond the level of the planned bone reduction.
■ Utilizing the same pilot drill, bone-marking osteotomies are prepared through the accessory holes via a fl apless approach. At this point, fl apless osteotomies have been prepared for the implant insertions and fl apless osteotomies that mark the level of the bone reduction.
■ The guide is then removed and a crest of the ridge incision is made to consequently raise a fl ap beyond the buccal osteotomies.
■ The osteotomies are easily recognized; utilizing a piezoelectric handpiece instrument, a bone-reduction osteotomy is performed by connecting all the buccal bone markings.
■ After the residual bone is reduced, the osteotomies for the implant placement are still visible since the original osteotomies for the implants were prepared to the appropriate depth.
■ No additional guide is needed at this point to complete the osteotomies for the implant placement. If the protocol requires immediate provisionalization, the denture conversion is then completed (FIGURES 13–22).
3 d p r i n t i n g
TABLE 1
Commonly Used Definitions in Digital Dentistry39,40
Guided surgery A surgical procedure that uses a device (surgical guide) that was printed or milled from a digital fi le of the cone beam computed tomography (CBCT) and surface tiss ue (STL) scans.
Surgical guide A guide used to assist in proper surgical placement and angulation of dental implants.
Guided bone regeneration (GBR)
Using barrier membranes, either resorbable or nonresorbable, to exclude certain cell types, such as rapidly proliferating epithelium and connective tissue, thus promoting the maturation of slower-growing cells capable of forming bone.
Stereolithography (STL) or 3D printing
A computer numerical control (CNC) additive fabrication of an object. In dentistry, it relates to the laser initiation of light-reactive resin layering to make replicas of casts and devices; the alternative to processes of casting, injection molding and vacuum thermoforming.
Bioprinting The fabrication of tissue and/or organs through the deposition of ultrathin layers of living cells.
Bone reduction guide A guide used to assist in proper amount of bone removal before implant placement to accommodate for increased interocclusal space requirements.
TABLE 2
Pros and Cons of Digital Dentistry Workflows41
Pros Cons
Increased accuracy as compared to conventional placement
Increased cost
Reduced surgical time Longer planning time
Precision that can help avoidance of vital structures Technique sensitive
Less morbidity due to option of fl apless approach More radiation exposure due to the need for 3D scan
Higher chance of more primary stability in case of immediate implant placement
Limited access in the posterior regions namely in patients with limited mouth opening
Ability to fabricate provisional prosthesis before implant surgery
Complexity of diff erent available software
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 307
3D BioprintingUntil recently, 3D printing has
been limited to nonbiocompatible materials, limiting their use in vivo. With advancements in 3D-printing technology and material science, the fi eld of bioprinting has evolved. There are numerous applications of bioprinting in the medical fi eld ranging from creating cartilaginous structures to the printing of entire organs.30,31
Currently, common treatment for large horizontal and vertical bone grafting in the maxilla or mandible involves the use
of particulate bone grafts (autogenous, allograft and/or xenografts) with titanium reinforced membranes. These membranes are diffi cult to form intraoperatively into the desired shape and require a second surgery for removal. To overcome these limitations, polymeric guided tissue regeneration (GTR) membranes were developed. Poly (lactic acid) (PLA), poly (glycolic acid) (PGA) and their copolymers have been widely considered for GTR membrane applications. However, the accumulation of acid during degradation may signifi cantly reduce pH,
FIGURE 13. STL fi le of an edentulous maxilla. Notice the irregular crest of the ridge.
FIGURE 14 . Image showing the preplanned osseous reduction needed for adequate restorative space.
FIGURE 15. Image of the STL showing the virtually reduced ridge.
FIGURE 16 . Superimposed STL fi le of the patient denture; notice the designed accessory holes to mark the predetermined ridge reduction.
FIGURE 19. Via fl apless surgery, the markings are clearly identifi ed with a periodontal probe.
FIGURE 17. 3D-printed guide that will be used fl apless to mark the implant sites and the ridge reduction area.
FIGURE 20 . After fl ap refl ection, the osteotomies can be identifi ed indicating up to what level the ridge needs to be reduced.
FIGURE 18 . 3D-printed guide fi xated in place.
FIGURE 21. Notice the osteotomy interconnecting all the bone marks carried out via piezosurgery.
FIGURE 22. Converted maxillary denture after the placement of the guided implants.
C DA J O U R N A L , V O L 4 7 , Nº 5
308 M AY 2 01 9
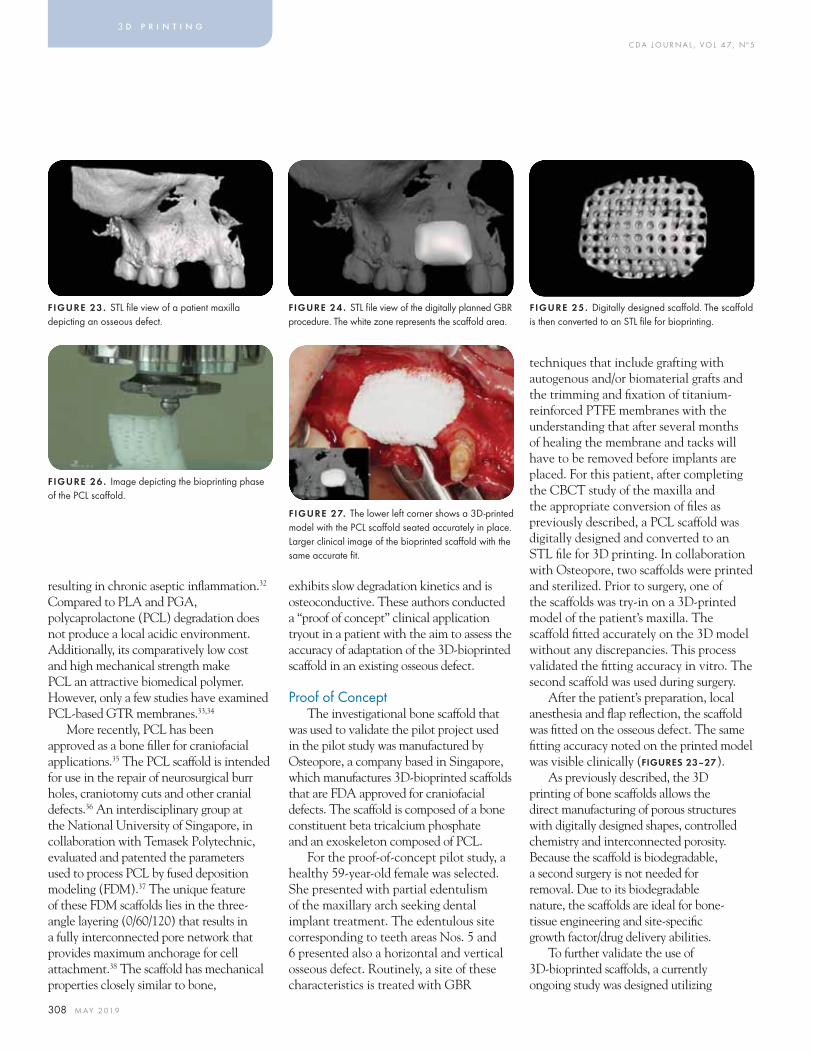
techniques that include grafting with autogenous and/or biomaterial grafts and the trimming and fi xation of titanium-reinforced PTFE membranes with the understanding that after several months of healing the membrane and tacks will have to be removed before implants are placed. For this patient, after completing the CBCT study of the maxilla and the appropriate conversion of fi les as previously described, a PCL scaffold was digitally designed and converted to an STL fi le for 3D printing. In collaboration with Osteopore, two scaffolds were printed and sterilized. Prior to surgery, one of the scaffolds was try-in on a 3D-printed model of the patient’s maxilla. The scaffold fi tted accurately on the 3D model without any discrepancies. This process validated the fi tting accuracy in vitro. The second scaffold was used during surgery.
After the patient’s preparation, local anesthesia and fl ap refl ection, the scaffold was fi tted on the osseous defect. The same fi tting accuracy noted on the printed model was visible clinically (FIGURES 23–27).
As previously described, the 3D printing of bone scaffolds allows the direct manufacturing of porous structures with digitally designed shapes, controlled chemistry and interconnected porosity. Because the scaffold is biodegradable, a second surgery is not needed for removal. Due to its biodegradable nature, the scaffolds are ideal for bone-tissue engineering and site-specifi c growth factor/drug delivery abilities.
To further validate the use of 3D-bioprinted scaffolds, a currently ongoing study was designed utilizing
exhibits slow degradation kinetics and is osteoconductive. These authors conducted a “proof of concept” clinical application tryout in a patient with the aim to assess the accuracy of adaptation of the 3D-bioprinted scaffold in an existing osseous defect.
Proof of ConceptThe investigational bone scaffold that
was used to validate the pilot project used in the pilot study was manufactured by Osteopore, a company based in Singapore, which manufactures 3D-bioprinted scaffolds that are FDA approved for craniofacial defects. The scaffold is composed of a bone constituent beta tricalcium phosphate and an exoskeleton composed of PCL.
For the proof-of-concept pilot study, a healthy 59-year-old female was selected. She presented with partial edentulism of the maxillary arch seeking dental implant treatment. The edentulous site corresponding to teeth areas Nos. 5 and 6 presented also a horizontal and vertical osseous defect. Routinely, a site of these characteristics is treated with GBR
resulting in chronic aseptic infl ammation.32 Compared to PLA and PGA, polycaprolactone (PCL) degradation does not produce a local acidic environment. Additionally, its comparatively low cost and high mechanical strength make PCL an attractive biomedical polymer. However, only a few studies have examined PCL-based GTR membranes.33,34
More recently, PCL has been approved as a bone fi ller for craniofacial applications.35 The PCL scaffold is intended for use in the repair of neurosurgical burr holes, craniotomy cuts and other cranial defects.36 An interdisciplinary group at the National University of Singapore, in collaboration with Temasek Polytechnic, evaluated and patented the parameters used to process PCL by fused deposition modeling (FDM).37 The unique feature of these FDM scaffolds lies in the three-angle layering (0/60/120) that results in a fully interconnected pore network that provides maximum anchorage for cell attachment.38 The scaffold has mechanical properties closely similar to bone,
3 d p r i n t i n g
FIGURE 23. STL fi le view of a patient maxilla depicting an osseous defect.
FIGURE 24 . STL fi le view of the digitally planned GBR procedure. The white zone represents the scaff old area.
FIGURE 25. Digitally designed scaff old. The scaff old is then converted to an STL fi le for bioprinting.
FIGURE 26 . Image depicting the bioprinting phase of the PCL scaff old.
FIGURE 27. The lower left corner shows a 3D-printed model with the PCL scaff old seated accurately in place. Larger clinical image of the bioprinted scaff old with the same accurate fi t.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 309
literature. J Dent (Shiraz) 2015;16:1–9.25. Bikas H, Stavropoulos P, Chryssolouris G. Additive manufacturing methods and modeling approaches: A critical review. Int J Adv Manuf Tech 2016;83:389–405.26. U.S. Patent 4,575,330. Apparatus for Production of Three-Dimensional Objects by Stereolithography. www.lens.org/lens/patent/022-138-245-291-118.27. Al-Ardah A, Alqahtani N, AlHelal A, Goodacre B, Swamidass R, Garbacea A, Lozada J. Using virtual ridge augmentation and 3D printing to fabricate a titanium mesh positioning device: A novel technique letter. J Oral Implantol 2018 Aug;44(4):293–299. doi: 10.1563/aaid-joi-D-17-00160. Epub 2018 May 2.28. Goodacre BJ, Swamidass RS, Lozada J, Al-Ardah A, Sahl E. A 3D-printed guide for lateral approach sinus grafting: A dental technique. J Prosthet Dent 2018 Jun;119(6):897–901. doi: 10.1016/j.prosdent.2017.07.014. Epub 2017 Nov 15.29. Alzoubi F, Massoomi N, Nattestad A. Bone Reduction To Facilitate Immediate Implant Placement and Loading Using CAD/CAM Surgical Guides for Patients With Terminal Dentition. J Oral Implantol 2016 Oct;42(5):406–410. Epub 2016 Jun 8.30. Axpe E, Oyen ML. Applications of alginate-based bioinks in 3D bioprinting. Int J Mol Sci 2016 Nov 25;17(12). pii:E1976.31. Hölzl K, Lin S, Tytgat L, Van Vlierberghe S, Gu L, Ovsianikov A. Bioink properties before, during and after 3D bioprinting. Biofabrication 2016 Sep 23;8(3):032002.32. Bergsma J, Bruijn WD, Rozema F, Bos R, Boering G. Late degradation tissue response to poly(L-lactide) bone plates and screws. Biomaterials 1995;16:25e31.33. Fujihara K, Kotaki M, Ramakrishna S. Guided bone regeneration membrane made of polycaprolactone/calcium carbonate composite nano-fi bers. Biomaterials 2005 Jul;26(19):4139–47.34. Yang F, Both SK, Yang X, Walboomers XF, Jansen JA. Development of an electrospun nano-apatite/PCL composite membrane for GTR/GBR application. Acta Biomater 2009 Nov;5(9):3295–304. doi: 10.1016/j.actbio.2009.05.023. Epub 2009 May 24.35. Osteopore. 510K FDA K051093. www.accessdata.fda.gov/cdrh_docs/pdf5/K051093.pdf.36. Chim H, Hutmacher DW, Chou AM, Oliveira AL, Reis RL, Lim TC, Schantz JT. A comparative analysis of scaff old material modifi cations for load-bearing applications in bone tissue engineering. Int J Oral Maxillofac Surg 2006 Oct;35(10):928–34.37. Zein I, Hutmacher DW, Tan KC, Teoh SH. Fused deposition modeling of novel scaff old architectures for tissue engineering applications. Biomaterials 2002 Feb;23(4):1169–85.38. Rai B, Teoh SH, Ho KH, Hutmacher DW, Cao T, Chen F, Yacob K. The eff ect of rhBMP-2 on canine osteoblasts seeded onto 3D bioactive polycaprolactone scaff olds. Biomaterials 2004 Nov;25(24):5499–506.39. The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent 2017 May;117(5S):e1–e105. doi: 10.1016/j.prosdent.2016.12.001.40. Laney WR. Glossary of Oral and Maxillofacial Implants. Int J Oral Maxillofac Implants 2017 Jul/Aug;32(4):Gi–G200. doi: 10.11607/jomi.2017.4.gomi.41. Kattadiyil MT, et al. CAD/CAM guided surgery in implant dentistry: A brief review. Alpha Omegan 2014 Spring;107(1):26–31.
THE CORRESPONDING AUTHOR, Jaime Lozada, DDS, can be reached at [email protected].
9. Scherer MD. A contemporary approach to intraoral optical scanning and in-offi ce 3-D printing. Dent Today 2015 Dec;34(12):46–7.10. Hazeveld A. Accuracy and reproducibility of dental replica models reconstructed by diff erent rapid prototyping techniques. Am J Orthod Dentofacial Orthop 2014 Jan;145(1):108–15. doi: 10.1016/j.ajodo.2013.05.011.11. Kasparova M, Grafova L, Dvorak P, Dostalova T, Prochazka A, Eliasova H, et al. Possibility of reconstruction of dental plaster cast from 3D digital study models. Biomed Eng Online 2013 May 31;12:49. doi: 10.1186/1475-925X-12-49.12. Van Noort R. The future of dental devices is digital. Dent Mater 2012 Jan;28(1):3–12. doi: 10.1016/j.dental.2011.10.014. Epub 2011 Nov 26.13. Cho SH, Chang WG. Mirror-image anterior crown fabrication with computer-aided design and rapid prototyping technology: A clinical report. J Prosthet Dent 2013 Feb;109(2):75–8. doi: 10.1016/S0022-3913(13)60018-9.14. Kattadiyil MT, Mursic Z, AlRumaih H, Goodacre CJ. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J Prosthet Dent 2014 Sep;112(3):444–8. doi: 10.1016/j.prosdent.2014.03.022. Epub 2014 May 29.15. Martelli N, Serrano C, Van Den H, Pineau J, Prognon P, Borget I, et al. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016 Jun;159(6):1485–1500. doi: 10.1016/j.surg.2015.12.017. Epub 2016 Jan 30.16. Bose S, Tarafder S, Bandyopadhyay A. Eff ect of Chemistry on Osteogenesis and Angiogenesis Towards Bone Tissue Engineering Using 3D Printed Scaff olds. Ann Biomed Eng 2017 Jan;45(1):261–272. doi: 10.1007/s10439-016-1646-y. Epub 2016 Jun 10.17. Whitley D, Bencharit S. Digital Implantology with Desktop 3D Printing. Formlabs White Paper 2015:1–15.18. Arisan V, Karabuda CZ, Mumcu E, Ozdemir T. Implant positioning errors in freehand and computer-aided placement methods: A single-blind clinical comparative study. Int J Oral Maxillofac Implants 2013 Jan–Feb;28(1):190–204. doi: 10.11607/jomi.2691.19. Flugge TV, Nelson K, Schmelzeisen R, Metzger MC. Three-dimensional plotting and printing of an implant drilling guide: Simplifying guided implant surgery. J Oral Maxillofac Surg 2013 Aug;71(8):1340–6. doi: 10.1016/j.joms.2013.04.010.20. Nickenig HJ, Eitner S, Rothamel D, Wichmann M, Zoller JE. Possibilities and limitations of implant placement by virtual planning data and surgical guide templates. Int J Comput Dent 2012;15:9–21.21. Centers for Devices and Radiological Health. Use of International Standard ISO 10993-1, “Biological evaluation of medical devices-Part 1: Evaluation and testing within a risk management process” Guidance for industry and Food and Drug Administration staff . June 16, 2016. U.S. Department of Health and Human Services, Food and Drug Administration, CDRH. Washington DC. 2016:1–68. www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm348890.pdf.22. Dada K, Pariente L, Daas M. Strategic extraction protocol: Use of an imagefusion stereolithographic guide for immediate implant placement. J Prosthet Dent 2016;116:652–6.23. Pozzi A, Polizzi G, Moy PK. Guided surgery with tooth-supported templates for single missing teeth: A critical review. Eur J Oral Implantol 2016;9(suppl 1):135–53.24. Torabi K, Farjood E, Hamedani S. Rapid prototyping technologies and their applications in prosthodontics, a review of
the New Zealand white rabbit model. One of the objectives is to determine the biodegradation rate to develop the guidelines for human clinical applications.
ConclusionThe rapid advances in 3D-printing
technology are infl uencing many aspects of implant dentistry. The in-offi ce capabilities and convenience of 3D printing in surgical implant dentistry will continue to evolve. This review article provides examples of the use of 3D printing for various applications in implant surgery as well as a review of the potential benefi t of 3D bioprinting. (See TABLE 2 for a list of pros and cons of digital dentistry.) Future research related to printed scaffolds shall be investigated to evaluate the most favorable degradation and resorption kinetics of these materials. ■
REFERENCES
1. Jindal SK, Sherriff M, Waters MG, Coward TJ. Development of a 3D printable maxillofacial silicone: Part I. Optimization of polydimethylsiloxane chains and cross-linker concentration. J Prosthet Dent 2016 Oct;116(4):617–622. doi: 10.1016/j.prosdent.2016.02.020. Epub 2016 May 4.2. Sun J, Zhang FQ. The application of rapid prototyping in prosthodontics. J Prosthodont 2012 Dec;21(8):641–4. doi: 10.1111/j.1532-849X.2012.00888.x. Epub 2012 Jul 23.3. Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet Dent 2015 Dec;114(6):818–25. doi: 10.1016/j.prosdent.2015.08.001. Epub 2015 Sep 26.4. Kurahashi K, Matsuda T, Goto T, Ishida Y, Ito T, Ichikawa T. Duplication of complete dentures using general-purpose handheld optical scanner and three-dimensional printer: Introduction and clinical considerations. J Prosthodont Res 2017 Jan;61(1):81-86. doi: 10.1016/j.jpor.2016.06.002. Epub 2016 Jun 23.5. Gracco A, Mazzoli A, Raff aeli R, Germani M. Evaluation of 3D technologies in dentistry. Prog Orthod 2008;9(1):26–37.6. Di Giacomo GA, Cury PR, de Araujo NS, Sendyk WR, Sendyk CL. Clinical application of stereolithographic surgical guides for implant placement: preliminary results. J Periodontol 2005 Apr;76(4):503–7.7. Ayoub AF, Rehab M, O’Neil M, Khambay B, Ju X, Barbenel J, et al. A novel approach for planning orthognathic surgery: The integration of dental casts into three-dimensional printed mandibular models. Int J Oral Maxillofac Surg 2014 Apr;43(4):454–9. doi: 10.1016/j.ijom.2013.08.016. Epub 2013 Oct 3.8. Soares PV, de Almeida Milito G, Pereira FA, Reis BR, Soares CJ, de Sousa Menezes M, et al. Rapid prototyping and 3D-virtual models for operative dentistry education in Brazil. J Dent Educ 2013 Mar;77(3):358–63.

The Dentists Insurance Company was founded
by dentists, to protect only dentists, and is led
by your peers. With this collective strength and
singular focus, TDIC has been rated A (Excellent)
by AM Best for 25 consecutive years.
Rated A by AM Best
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | Insurance Lic. #0652783
25 CONSECUTIVE YEARS
@TDICinsurance
A.M. Best Company rating effective March 2019. For the latest rating, access ambest.com.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 311
AUTHORS
H. Ralph Rawls, PhD, is a professor of biomaterials in the dental school at the University of Texas Health Science Center at San Antonio and a professor in the core faculty of the joint UTSA/UTHSCSA biomedical engineering program. Confl ict of Interest Disclosure: None reported.
Advances in Restorative Resin-Based Composites: A Review H. Ralph Rawls, PhD, and Kyumin Whang, PhD
A B S T R A C T The history of aesthetic composites is reviewed, including monomers, curing, fi llers, etc. Recently introduced restoratives include fl owable, packable and bioactive materials. After a background in biocompatibility, initiatives currently in development for future clinical products to substantially improve resin composite oral durability and extend clinical service lifetime are described as are initiatives to use tissue engineering concepts and bioactive fi llers to stimulate biological repair and inhibit caries.
Kyumin Whang, PhD, is the director of the Offi ce of Sponsored Agreements and the Division of Research at the UT Health San Antonio School of Dentistry.Confl ict of Interest Disclosure: None reported.
c o m p o s i t e s
Aesthetic restorative materials have been in increasing demand since the early 20th century. The demand led to the development of
silicate restoratives, which have excellent aesthetics but deteriorate quickly and were soon displaced by powder/liquid poly(methyl methacrylate)/methyl methacrylate (PMMA/MMA). In turn, this was replaced by resin composites, which continue to form the basis of today’s modern aesthetic restorative materials (RL Bowen 1962). 1 Bowen’s original resin composites, as with most today, contained a blend of Bis-GMA (bisphenol A-glycidyl methacrylate), a high molecular weight dimethacrylate, with lower molecular weight comonomers, inorganic reinforcing fi ller particles such as quartz or glass and a silane coupling agent to bind the fi ller particles into a
cross-linked, rigid resin matrix.1 Shortly before Bowen’s introduction of dental resin composites, Michael Buonocore demonstrated that acid-etched enamel forms superior bonds with PMMA restorations.2 Together, these advances allowed cavities to be restored both easily and conservatively for the fi rst time. Since the early 1970s, resin-based composites and their dimethacrylate resins have become the material of choice for aesthetic anterior restorations and increasingly for posterior occlusal areas and other high-stress-bearing sites. They are also used in a variety of other dental applications such as pit and fi ssure sealants, bonding of ceramic veneers and cementation of fi xed prostheses. The average longevity of posterior composites (seven years) is approaching that of amalgam (10 years). 3,4 Incremental improvements since then have gradually
C DA J O U R N A L , V O L 4 7 , Nº 5
312 M AY 2 01 9
brought resin composites to a leading position in restorative dentistry, primarily through progress in fi ller technology and curing systems. However, despite these advances, dental composites continue to suffer from shrinkage stress during curing, insuffi cient wear resistance, excessive thermal expansion coeffi cient and unforgiving handling properties. Various techniques have been developed to circumvent or minimize these defi ciencies with varying degrees of success, but often are procedure sensitive and impose demanding attention to detail and require extra time. Current composites are based on blends of dimethacrylate monomers and display a variety of performance characteristics for storage stability, intra- and extraoral manipulation, curing reactivity, biocompatibility and durability after curing. These restorative materials have improved since the 1960s, mainly via the introduction of visible light curing and advances in reinforcing fi llers, plus expanded functions such as fl uoride release for caries resistance. The current emphasis is to further improve handling properties, oral durability, increased degrees of monomer-polymer conversion, increased abrasion resistance and decreased cure shrinkage and stress buildup during and following curing.5
Structural and Nonstructural Components6
There are three structural components in dental resin-based composites:
■ Matrix — A polymeric resin material that forms a continuous phase upon initiation and binds the fi ller particles.
■ Filler — Reinforcing particles and/or fi bers that are dispersed in the matrix.
■ Coupling agent — Difunctional molecules that promote adhesive bonds between fi ller and matrix.
Dental composites are highly cross-linked polymeric materials reinforced by a dispersion of inorganic or resin fi ller particles bound to the matrix by silane or other coupling agents.
Nonstructural components include an activator-initiator system, which is required to initiate the addition polymerization process and convert the resin paste from a soft, moldable cavity-fi lling material to a hard, durable restorative resin. Other components are included to enhance performance, appearance and durability. For example, pigments help to shade
match the color of teeth, UV absorbers and other additives improve color stability and polymerization inhibitors extend storage life and provide working time for chemically activated resins.
Current Aesthetic Resin CompositesAlthough resin composites
are aesthetic, they shrink during polymerization, 7,8 which can result in recurrent caries.9 Mjör reported10 that recurrent caries is the primary reason for restoration failure. Shrinkage produces stresses at the restoration interfaces, 11 which can distort and, if the cavity form used is large enough, fracture the tooth.12 Substantial cure shrinkage, less wear resistance than teeth and a coeffi cient of thermal expansion greater than tooth structure are the main reasons that resin
composites have not yet been adopted as a universal replacement for amalgam, despite substantial progress.7 The ideal restorative material would develop high early strength, produce little or no shrinkage during curing, leave no residual stresses to disrupt the marginal seal, have suffi cient rigidity (i.e., elastic modulus, E´) to support weakened tooth structure, provide abrasive wear resistance similar to enamel and be biocompatible, tooth colored and translucent.11
Monomers and Matrix
Monomers, Monomer-Polymer Conversion and Cross-Linking 6,7
Resin composites consist of a matrix-forming paste, which is a blend of large, viscous, dimethacrylate monomers such as Bis-GMA (bisphenol A glycidyl methacrylate, also bisphenol A-diglycidyl-dimethyl acrylate) and less viscous monomers such as triethylene glycol dimethacrylate (TEGDMA) and/or urethane dimethacrylate (UDMA). These or other methacrylates are combined in proportions that have a workable, less-viscous consistency, together with a free radical initiation system. Upon polymerization, a highly cross-linked, hardened structure is formed in restorative, adhesive and sealant materials.13
The degree of monomer to polymer conversion (DoC), or degree of cure, is the percentage of monomers that have reacted and form a polymeric resin. The higher the DoC, the better the cure, the strength, wear resistance, biocompatibility and other performance properties. A conversion of 50 to 60%, typical of highly cross-linked Bis-GMA-based composites, indicates that 50 to 60% of the methacrylate groups have reacted and form part of a polymer chain. This does not imply that 40 to 50% of the monomer
c o m p o s i t e s
Restorative materials have improved since the 1960s, mainly via the introduction of visible light curing and advances in reinforcing fi llers.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 313
molecules are left in the resin and are extractable. One of the two methacrylate groups per dimethacrylate monomer may have remained unreacted, while the other bonded covalently to the polymer chain, forming a pendant group. Conversion of monomer to polymer is dependent on several factors, such as resin composition, the transmission of light through the material and the concentration of sensitizer, initiator and inhibitor present. Transmission of light through the material is controlled by lamp intensity, translucency, absorption and scattering of light by fi ller particles and opacifi ers and by any tooth structure interposed between the light source and composite.
Degree of conversion does not differ between chemically activated (also known as “self-cured”) and light-activated composites containing the same monomer formulations as long as adequate light curing is employed. Room temperature conversion values of 50 to 70% are achieved for both types of curing system and volumetric shrinkage is not signifi cantly different. Shrinkage occurs as monomers are converted from a collection of free-fl owing molecules to a rigid assembly of cross-linked polymer chains. As a polymer, the mer (repeating) units are connected by covalent bonds with about 20% less volume than the unreacted monomers. The result is a substantial volume contraction (shrinkage) during curing. In light-cured materials, cure shrinkage leads to substantially greater stress buildup than in self-cured resins. This cure shrinkage produces unrelieved stresses after the point where the resin begins to harden. These stresses focus on the tissue/composite interfaces, thereby weakening the bond and eventually producing a gap at the restoration margins. This in turn leads to staining, sensitivity, recurrent (“marginal”) caries and other clinical problems.
Bis-GMA and UDMA have almost fi ve times the molecular weight of methyl methacrylate; the density of methacrylate double-bond groups is approximately one-fi fth as high in these monomers, which reduces polymerization shrinkage proportionately. The use of a dimethacrylate also results in extensive cross-linking that increases the strength and rigidity of the polymer.
While a high molecular weight of a monomer reduces curing shrinkage and improves mechanical properties, it also increases viscosity (i.e., more diffi cult to
blend, fl ow and manipulate). Bis-GMA has a particularly high viscosity (similar to honey), which makes it necessary to use lower molecular weight, highly fl uid monomers to dilute and “thin” it and similar resins to attain suffi ciently high fi ller levels (discussed below) while also producing resin pastes with consistencies suitable for clinical manipulation. These diluent monomers can be any fl uid methacrylate, but are usually dimethacrylates such as TEGDMA. The reduction in viscosity is signifi cant when TEGDMA is added to Bis-GMA. A blend of 75wt% Bis-GMA and 25wt% TEGDMA has a viscosity of 4,300 centipoise, whereas the viscosity of a 50wt% Bis-GMA /50wt% TEGDMA blend is 200 centipoise (like thin syrup or a fl owable paste for composites).
Dimethacrylate monomers also have the advantage of producing extensive cross-linking among polymer chains. This results in a rigid resin matrix that is highly resistant to softening and/or degradation by heat and solvents such as water and alcohol. Unfortunately, the trade-offs among polymerization shrinkage, fi ller loading and manipulation properties place severe limits on the ability to optimize the performance of composite materials. The need for a better balance of properties among these confl icting requirements has made the development of a “universal” composite elusive and has resulted in a proliferation of new monomers and formulations, each designed for a specialized application. Examples of these are provided in the next section.
New Monomers and Recent Variations of Dimethacrylates Monomers6,14
Low-Shrinkage, Low-Stress MonomersKalore: High-molecular-weight
urethane with a rigid central section and fl exible end groups also known as DX-511 (GC America, Alsip, Ill.). These provide a rod-like shape that facilitates self-assembly into compact molecular structures. This, together with dilution of the number of polymerizable end groups due to the high molecular weight (895 compared to 512 for Bis-GMA), reduces cure shrinkage, while the fl exible end groups promote reactivity and enhance monomer-polymer conversion.
Venus Diamond: A urethane dimethacrylate with a bulky, space-fi lling central group. 4,8-di(urethane methacryloxy)-tricyclodecane (TCD-urethane) (Heraeus Kulzer, South Bend, Ind.). The bulky three-ring tricyclodecane group provides steric hindrance, which holds the monomers apart and thus slows the rate of polymerization. This expands the time
Shrinkage occurs as monomers are converted from a collection of free-fl owing molecules to a rigid assembly of cross-linked polymer chains.

C DA J O U R N A L , V O L 4 7 , Nº 5
314 M AY 2 01 9
required to reach the point where the resin begins to harden and provides time for adjacent polymer chain segments to slip among themselves, rearrange and relieve developing stresses.
Filtek LS: “Silorane” ring-opening, tetrafunctional epoxy siloxane (3M ESPE, St. Paul, Minn.). Siloranes involve an entirely different chemistry based on epoxy, rather than acrylic, functionality. These tetrafunctional silorane monomers use ring-opening polymerization. Silorane chemistry utilizes a combination of epoxy functionality (three-unit ring with two carbons and an oxygen) combined with siloxane units (–O–Si–O–) that can be cured with low shrinkage via a cationic cross-linking mechanism. When the rings open, they lengthen and occupy more space; the resulting expansion offsets a substantial proportion of the polymerization shrinkage and residual stress while otherwise matching the restorative characteristics of the typical methacrylate resins.15 This explains the “LS” (low shrinkage) designation for the commercial product. The siloxane units also provide hydrophobicity and thereby limit water sorption, which enhances long-term intraoral clinical service.
N’Durance: A high molecular-weight phase-separating dimer dicarbamate dimethacrylate (DDCDMA) (Septodont USA, Lancaster, Pa.) that also contains a bulky central group, somewhat analogous to the TDC-dimethacrylate as discussed previously for Heraeus Kulzer’s Venus Diamond. The bulky center is comprised of a six-carbon aliphatic ring with two long hydrocarbon side chains derived from a linoleic acid dimer. The center section is connected to two methacrylate end groups via urethane groups (–NH–CO–O–, also referred to as carbamate groups). The chain length between reactive ends is very long (having a molecular weight
of 843, similar to that of Kalore DX-511), which provides double-bond dilution and hence reduced shrinkage. The bulky center section allows greater conversion during copolymerization as well as greater stress relaxation. The hydrophobic center group restricts water absorption as well as solubility with the other dimethacrylates in the formulation. This latter leads to formation of two separate phases during polymerization and produces a small expansion, which partially offsets polymerization shrinkage and the associated stresses.16
Operator Friendly — Ease of Manipulation — Monomers
A major source of defect is related to operator error, much of which is related to various factors of diffi culty in handling throughout the restoration process. A number of new products have been introduced to reduce this source of error. For example, two recently introduced novel “fl owable” composites, SureFil SDR fl ow (Dentsply, York, Pa.) and Tetric EvoFlow Bulk Fill (Ivoclar Vivadent AG, Liechtenstein), illustrate such operator-friendly materials. Both are highly translucent and offer fl owable rheologies (i.e., consistencies) and easy handling together with large depths and degrees of conversion and are marketed as bulk fi ll, universal
restorative resins with exceptional ease of placement characteristics.
Both exhibit low shrinkage and low-shrinkage stress when tested in vitro, and early clinical trial results show them to have similar early-stage wear resistance and durability as current posterior resins:
SureFil SDR Flow: Utilizes a “polymerization modulator” in the backbone of the SDR resin monomer, which is a photoactive group. When the resin is exposed to light, these groups undergo photocleavage, which relieves cure stress and generates free radicals that continue to propagate conversion and cross-linking. This urethane dimethacrylate monomer has a bulky, space-fi lling central group that prevents monomers from aligning and thus further offsets polymerization shrinkage and stress buildup. Results show that the material has fl ow and other handling characteristics, together with a high translucency that promotes a high degree and depth of cure, that place it in the category of technique insensitive. 17 Any methacrylate-based universal composite can be used to cap the restoration and provide enhanced aesthetics, wear resistance and strength.
Tetric EvoFlow Bulk Fill: This fl owable posterior resin composite is self-adapting, radiopaque and can photocure up to 4 mm in 10 seconds. The monomer/matrix composition consists of Bis-GMA, urethane dimethacrylate and 1,10-decandiol dimethacrylate, which are not novel but are combined with a nano-hybrid blend designed for high loading while remaining self-adaptable and producing a high level of wear resistance.
These highly fl owable composites also contain reinforcing fi ller in proportions approximating that of highly loaded, nonfl owable, even “packable” hybrids such as those described below as “special purpose” resins. This high
c o m p o s i t e s
Any methacrylate-based universal composite can be used to cap the restoration and provide enhanced aesthetics, wear resistance and strength.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 315
loading, together with low cure stress and a high level and depth of cure, is expected to produce high durability and a long service life. 18 Given the intensity of research and development in this area, further improvements toward the durability and forgiveness of amalgam, combined with the aesthetics of porcelain, can be expected.
Curing Mechanisms, Problems and Techniques 6,7
Activation and Initiation SystemsThe methacrylate monomers
polymerize by addition polymerization initiated by free radicals. Free radicals can be generated by chemical activation or by external energy activation (heat, light or microwave). Dental composites for direct placement use chemical activation, light activation or a combination.
Chemically activated resins. Originally, a chemically activated polymerization process was used to cure all composites. This is also referred to as cold-curing or self-curing. Chemical activation is initiated by mixing two pastes just prior to use. During mixing, it is almost impossible to avoid incorporating air into the mix, thereby forming pores that weaken the structure and contain oxygen that inhibits polymerization during curing. Another problem is that the operator has no control over the working time after mixing and both insertion and contouring must be completed quickly. One paste typically contains benzoyl peroxide, as initiator, and the other an amine activator such as N,N-dimethyl-p-toluidine. Upon mixing, the amine reacts with the benzoyl peroxide to form free radicals and addition polymerization is initiated. At present, chemical curing is mainly used in circumstances where a light source cannot be used.
Light activation. To overcome the problems of chemical activation, resins were developed that do not require mixing. This was achieved by use of a photosensitive initiator system and a light source for activation. The first light-activated systems used ultraviolet (UV) light to initiate free radicals. Today, the UV light-cured composites have been replaced by visible blue-light activated systems with greatly improved depth of cure, a controllable working time and other advantages. Due to these
advantages, visible light-activated composites are more widely used than are chemically activated composites.
In addition to avoiding the porosity of chemically activated resins, light-cured materials also allow the operator to complete both insertion and contouring before curing is initiated. Further, when curing is initiated, an exposure time of 40s or less is required to cure a 2 mm-thick layer, as compared to several minutes for chemically cured materials. Also light-cured composites are less sensitive to oxygen inhibition than are chemical-cured resins. There are, however, substantial limitations when using light-cured composites. Because of limited light penetration, incremental placement is required beyond 2–3 mm depth. Thus, light-cured composites can require more
time when placing large restorations such as Class II cavity preparations. Other disadvantages include the cost of the lamp, sensitivity to room illumination and several complicating factors associated with light sources and photocure technique. These limitations are further discussed below.
Light-cured composites are supplied as a single paste contained in a lightproof syringe. The free-radical initiating system, consisting of a photosensitizer and an amine initiator, is contained in this paste. As long as these two components are not exposed to light, they do not interact. However, exposure to light in the blue-violet region produces an excited state of the photosensitizer, e.g., camphorquinone (CQ), which interacts with an amine activator to form free radicals that in turn initiate addition polymerization. Camphorquinone is a commonly used photosensitizer that absorbs visible light in the blue-to-violet spectral range.
Depth of Cure and Exposure TimeAbsorption and scattering of light
in resin composites reduces the degree of conversion exponentially with depth of penetration. Intensity can be reduced by a factor of 10 to 100 in a 2 mm layer of composite. This reduces monomer conversion to an unacceptable level at depths greater than 2–3 mm for most products, although a few can be cured to 4–5 mm. Thus, the surface must be irradiated for a longer time to deliver suffi cient power density well below the surface. Given the limits imposed by inherent light scattering and absorption, plus other factors,19 the tradeoffs are such that increased intensity will allow either shortened curing times for a given depth of cure or increased depth of cure for a given exposure time, but there is little advantage in attempting to achieve both simultaneously. The practical consequence is that curing depth is limited to 2 to 3 mm unless excessively
Originally, a chemically activated polymerization process was used to cure all composites. This is also referred to as cold-curing or self-curing.

C DA J O U R N A L , V O L 4 7 , Nº 5
316 M AY 2 01 9
long exposure times are used, regardless of lamp intensity. Thus, solutions to this problem have come through advances in composite structures and chemistry rather than through advances in clinical technique or the technology of curing lamps. Some of these recent advances in resin materials are discussed later.
Attenuation of light is dependent on light scattering due to fi ller size and refractive index, fi ller concentration and pigment opacity and shade. For these reasons, manufacturers typically recommend curing times based on a particular curing device for each shade and type of resin. These recommended times are usually the absolute minimum. To maximize both degree of cure and long-term clinical durability, light-source intensity must be matched to exposure time and curing technique and the lamp’s intensity should be closely monitored.
Light is also absorbed and scattered when passing through tooth structure, especially dentin, thereby causing incomplete curing in such critical areas as proximal boxes. When attempting to polymerize the resin through tooth structure, the exposure time should be increased by a factor of two to three to compensate for the reduction in light intensity.
Despite the many advantages of light-cured resins, there is still a need for self-cured/chemically cured composites and resins in certain situations. For example, when used as a luting agent under metallic restorations, only chemically cured materials can be used with reliable results.
Dual-Cure Resins and Extraoral CuringOne way to overcome limits on curing
depth and some of the other problems associated with light curing is to combine self-curing/chemical-curing and light-curing components in the same resin. So-called dual-cure materials are widely available and consist of two light-curable pastes, one of
which contains benzoyl peroxide (BP) as initiator, while an aromatic tertiary amine activator is added to the other. When these two pastes are mixed and then exposed to light, light curing is promoted by the amine/CQ combination and chemical curing is promoted by the amine/BP interaction. Dual-cure materials are intended for any situation that does not allow suffi cient light penetration to produce adequate monomer conversion, for example, cementation of bulky ceramic inlays. As with the chemical-cure resins, air inhibition and porosity are problems with dual-cure resins.
In addition to intraoral chemical curing and/or light curing, extraoral heat or light can also be used to promote a higher level of cure. For example, a chemical- or light-curing composite can be used to produce an inlay on a tooth or a die. That inlay can be cured directly within the tooth or on the die and then transferred to an oven where it receives additional heat or light curing. After completion, the inlay is then cemented to the tooth with a self-cured resin composite.
Reduction of Cure-Shrinkage and Residual Stresses
The light-activated resins have overcome many of the defi ciencies of chemical-activated resins, including lack of control over working time, yellowing and porosity. However, the internal pores
in chemically cured resins act to relax residual contraction stresses that build up during curing (the pores enlarge during hardening and reduce the concentration of stresses at the margins). Also, the slower curing rate of chemical activation allows more shrinkage to be compensated by internal fl ow between the developing polymer chains prior to formation of extensive cross-linking and hardening. After this “gel” point is reached, stresses cannot be relieved, but instead continue to increase and concentrate adjacent to the bonded interfaces.
Marginal leakage. When the gingival margins of the cavity preparation are located in dentin, cementum or both and the resin is fi rmly anchored to the etched enamel at the other margins, the material tends to pull away from the gingival margins during curing due to polymerization shrinkage. This leads to residual stress at that interface and formation of a marginal gap. Subsequently, marginal leakage, with its ensuing problems, is enhanced. Undoubtedly, this is one of the greatest problems of composites used for Class II and Class V restorations. All measures should be taken to maintain the integrity of the dentin-resin or cementum-resin interfaces. The role of dentin-bonding agents in this context is not addressed here.
Two approaches have been used to overcome stress concentration and marginal failure experienced with light-activated resins: Reduction in volume contraction by altering the chemistry and/or composition of the resin system and clinical techniques designed to offset the effects. The former is the more desirable solution, and intensive research and development efforts are currently in progress to develop resins with ever-lower shrinkage and low thermal expansion. In the meantime, a variety of techniques have been investigated that can
c o m p o s i t e s
To maximize both degree of cure and long-term clinical durability, light-source intensity must be matched to exposure time and curing technique.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 317
immediately be put into practice by the clinician. These techniques are associated with incremental buildup and curing rate control, as presented later in this paper.
Incremental buildup and cavity confi guration. This technique is designed to reduce the confi guration factor (C-factor). The C-factor is the ratio of bonded to nonbonded surface areas of the cavity preparation. Residual polymerization stress increases directly with this ratio. During curing, shrinkage leaves the bonded cavity surfaces in a state of stress. At the nonbonded surfaces — those that reproduce the original external tooth anatomy — most of the stress is relaxed as the curing resin contracts toward the bulk of the material. The layering technique reduces polymerization stress buildup at the bonded surfaces by minimizing the C-factor. Thinner layers reduce bonded surface area and thus minimize the associated C-factor. Limitations on the depth of photocure dictate the use of incremental buildup as well. An incremental technique overcomes both limited depth of cure and residual stress concentration, but adds to the time and diffi culty of restoration.
Soft-start, ramped curing and delayed curing. Another approach is to follow the example of chemical initiation by providing an initial low rate of polymerization, thereby extending the time available for stress relaxation prior to hardening. This can be accomplished by using a “soft-start” technique. In this technique, curing begins with a low intensity and fi nishes with a high intensity. The approach allows for a slow initial rate of polymerization and a high level of stress relaxation during the early stages and only uses the maximum available intensity after initial hardening has occurred. This drives the curing reaction to the highest possible conversion only after most of the stress has been relieved. Several studies have shown that
varying levels of reduction in cavity-wall stress can be achieved with this technique. It does not increase total exposure time nor sacrifi ce either degree of conversion or depth of cure. Consequently, a variety of protocols have been developed and lamps have been made available that automatically provide one or more soft-start exposure sequences. 19,20
Variations on this technique include ramping and delayed cure. In ramping, the intensity is gradually increased or “ramped up” during exposure in a step-wise, linear or exponential manor.
Although effective, this technique requires more operator skill than the other variations and is less frequently used.
In delayed curing, the restoration is initially incompletely cured at low intensity. After contouring to the correct occlusion, a second exposure forms the fi nal cure. This delay allows substantial stress relaxation to take place. The longer the time period available for relaxation, the lower the residual stress. Delayed curing and exponential ramp curing appear to provide greater reductions in curing stress.
High-Intensity CuringAs discussed above, increased lamp
intensity allows for shorter exposure times for a given depth of cure in a particular shade and type of resin. Curing depths equivalent to that of a
500 mW/cm2 QTH (quartz-tungsten halogen) lamp (2 mm at 40s) have been demonstrated using an exposure time of 10s with certain PAC (plasma arc) lights and 5s with an argon laser. Thus, these high-intensity lamps could provide substantial savings in clinical time. However, high intensity plus short exposure times causes accelerated rates of curing and the possibility of substantial residual stress buildup because insuffi cient time is allowed for stress relaxation, even when used in combination with incremental buildup and soft-start curing. This aspect is currently being intensively investigated.11,19,21 Substantial evidence exists 22 that as the proportion of the total volume shrinkage taking place before initial hardening increases, the contraction taking place later decreases and the lower the uncompensated stress that develops. 23 Thus, there is a limit above which increasing radiant energy density produces neither a signifi cant increase in double-bond conversion nor improved mechanical properties yet does produce higher levels of uncompensated residual stress.24 It is this post-gel stress that sets the conditions that can lead to marginal breakdown, leakage and secondary decay. Due to the wide range of curing characteristics found among various lamps and exposure times, clinicians should consider the trade-offs before using expensive, high-intensity lamps.
Reinforcing FillersThe primary purpose of fi llers
is to reinforce a composite and to reduce the amount of matrix material. Incorporation of fi ller into a resin matrix greatly improves material properties, provided that the fi ller is well-bonded to the matrix, as discussed in the following Coupling Agent section.
An incremental technique overcomes both limited depth of cure and residual stress concentration, but adds to the time and diffi culty of restoration.
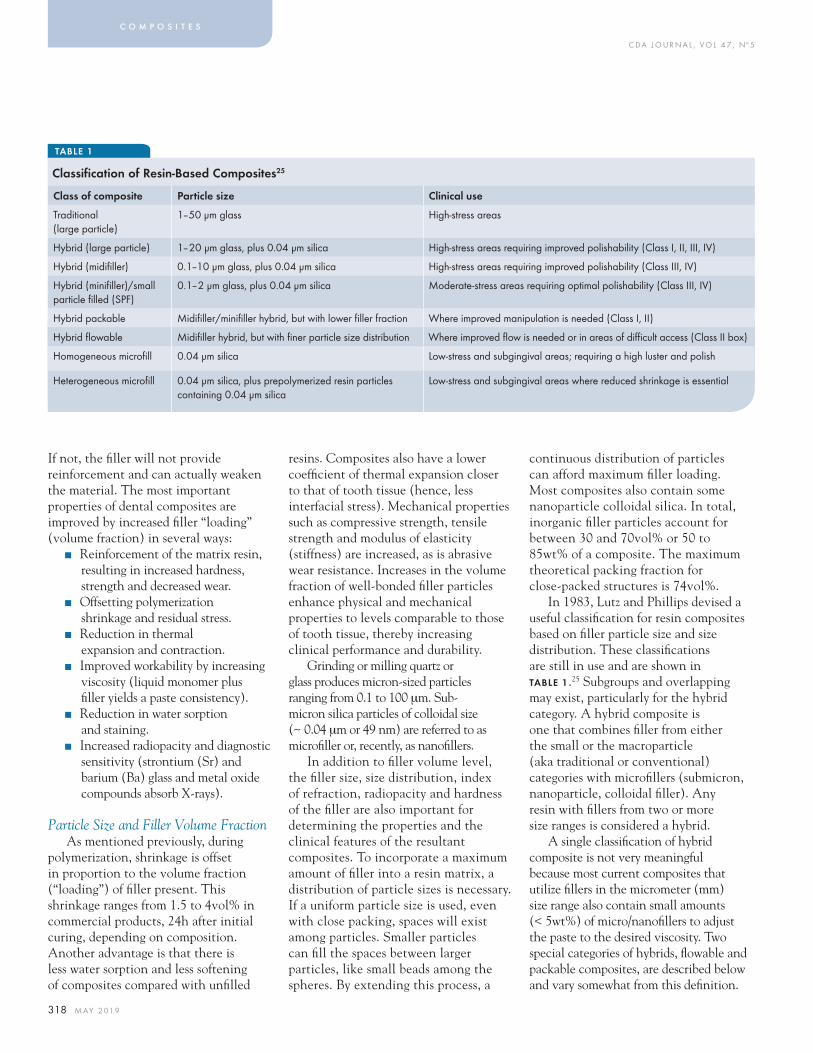
C DA J O U R N A L , V O L 4 7 , Nº 5
318 M AY 2 01 9
If not, the fi ller will not provide reinforcement and can actually weaken the material. The most important properties of dental composites are improved by increased fi ller “loading” (volume fraction) in several ways:
■ Reinforcement of the matrix resin, resulting in increased hardness, strength and decreased wear.
■ Offsetting polymerization shrinkage and residual stress.
■ Reduction in thermal expansion and contraction.
■ Improved workability by increasing viscosity (liquid monomer plus fi ller yields a paste consistency).
■ Reduction in water sorption and staining.
■ Increased radiopacity and diagnostic sensitivity (strontium (Sr) and barium (Ba) glass and metal oxide compounds absorb X-rays).
Particle Size and Filler Volume FractionAs mentioned previously, during
polymerization, shrinkage is offset in proportion to the volume fraction (“loading”) of fi ller present. This shrinkage ranges from 1.5 to 4vol% in commercial products, 24h after initial curing, depending on composition. Another advantage is that there is less water sorption and less softening of composites compared with unfi lled
resins. Composites also have a lower coeffi cient of thermal expansion closer to that of tooth tissue (hence, less interfacial stress). Mechanical properties such as compressive strength, tensile strength and modulus of elasticity (stiffness) are increased, as is abrasive wear resistance. Increases in the volume fraction of well-bonded fi ller particles enhance physical and mechanical properties to levels comparable to those of tooth tissue, thereby increasing clinical performance and durability.
Grinding or milling quartz or glass produces micron-sized particles ranging from 0.1 to 100 μm. Sub- micron silica particles of colloidal size (~ 0.04 μm or 49 nm) are referred to as microfi ller or, recently, as nanofi llers.
In addition to fi ller volume level, the fi ller size, size distribution, index of refraction, radiopacity and hardness of the fi ller are also important for determining the properties and the clinical features of the resultant composites. To incorporate a maximum amount of fi ller into a resin matrix, a distribution of particle sizes is necessary. If a uniform particle size is used, even with close packing, spaces will exist among particles. Smaller particles can fi ll the spaces between larger particles, like small beads among the spheres. By extending this process, a
continuous distribution of particles can afford maximum fi ller loading. Most composites also contain some nanoparticle colloidal silica. In total, inorganic fi ller particles account for between 30 and 70vol% or 50 to 85wt% of a composite. The maximum theoretical packing fraction for close-packed structures is 74vol%.
In 1983, Lutz and Phillips devised a useful classifi cation for resin composites based on fi ller particle size and size distribution. These classifi cations are still in use and are shown in TABLE 1.25 Subgroups and overlapping may exist, particularly for the hybrid category. A hybrid composite is one that combines fi ller from either the small or the macroparticle (aka traditional or conventional) categories with microfi llers (submicron, nanoparticle, colloidal fi ller). Any resin with fi llers from two or more size ranges is considered a hybrid.
A single classifi cation of hybrid composite is not very meaningful because most current composites that utilize fi llers in the micrometer (mm) size range also contain small amounts (< 5wt%) of micro/nanofi llers to adjust the paste to the desired viscosity. Two special categories of hybrids, fl owable and packable composites, are described below and vary somewhat from this defi nition.
c o m p o s i t e s
TABLE 1
Classification of Resin-Based Composites25
Class of composite Particle size Clinical use
Traditional (large particle)
1–50 μm glass High-stress areas
Hybrid (large particle) 1–20 μm glass, plus 0.04 μm silica High-stress areas requiring improved polishability (Class I, II, III, IV)
Hybrid (midifi ller) 0.1–10 μm glass, plus 0.04 μm silica High-stress areas requiring improved polishability (Class III, IV)
Hybrid (minifi ller)/small particle fi lled (SPF)
0.1–2 μm glass, plus 0.04 μm silica Moderate-stress areas requiring optimal polishability (Class III, IV)
Hybrid packable Midifi ller/minifi ller hybrid, but with lower fi ller fraction Where improved manipulation is needed (Class I, II)
Hybrid fl owable Midifi ller hybrid, but with fi ner particle size distribution Where improved fl ow is needed or in areas of diffi cult access (Class II box)
Homogeneous microfi ll 0.04 μm silica Low-stress and subgingival areas; requiring a high luster and polish
Heterogeneous microfi ll 0.04 μm silica, plus prepolymerized resin particles containing 0.04 μm silica
Low-stress and subgingival areas where reduced shrinkage is essential
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 319
Nanosized Particles (Microfi llers and Below)
The practical amount of fi ller that can be incorporated into a resin is greatly affected by the total fi ller surface area, which is a function of particle size with surface area increasing as size decreases for a constant volume of fi ller. Because of their extremely small size, colloidal silica particles have extremely large surface areas ranging from 50 to as much as 400 m2 per g. The silica surfaces form polar bonds with the monomer molecules, which inhibits their fl ow, drives up the viscosity and “thickens” the resin paste, even with very small amounts. Because of this effect the micro/nanofi lled composites contain colloidal silica in the 20–60vol% range. So-called “organic” fi ller (discussed further, below), with a particle size between 5 and 30 μm, constitute the remainder.
Microfi lled composites. The problems of surface roughening and low translucency associated with traditional and small particle composites can be overcome through the use of colloidal silica particles as the inorganic fi ller. The individual particles are approximately 0.04 μm (40 nm) in size. This value is one-tenth of the wavelength of visible light and 200 to 300 times smaller than the average particle in traditional composites. The concept of the microfi lled composite entails the reinforcement of the resin by means of the fi ller, yet these composites exhibit a smooth surface similar to that obtained with the unfi lled direct-fi lling acrylic resins.
These colloidal, nanometer-sized silica particles agglomerate to become microparticles in the 0.04 to 0.4 μm size range. During mixing, some, but not all, of the agglomerates are broken up.
It would be ideal if this colloidal silica fi ller could be added in large amounts directly to the resin matrix. However, this
is not practical, as explained previously, because of the large surface area that must be wetted by the matrix resin and especially because of the formation of polymer-like chains among the colloidal particles. These phenomena signifi cantly increase the viscosity and produce undue thickening, even with very small additions of microfi llers. Although several approaches may be used to increase the fi ller loading, each compromise the idealized concept of a homogeneous resin fi lled with dispersed colloidal silica. One approach is to sinter the colloidal
silica so that particles several tenths of a micrometer in size are obtained. This larger agglomerate results in a reduced surface area, allowing more fi ller to be incorporated with less compromise to the rheology of the material. The most common method for increasing fi ller loading is to make new fi ller particles from a prepolymerized composite that is highly loaded with colloidal silica particles. Particles of this highly microfi lled material are then incorporated into the resin paste to produce a fi lling material with acceptable handling characteristics.
The preparation of the prepolymerized fi ller involves adding 60 to 70wt% (about 50vol%) of silane-treated colloidal silica to the monomer at a slightly elevated temperature to lower its viscosity. When the fi ller is thoroughly mixed into the
resin, the composite paste is heat cured using benzoyl peroxide initiator. The degree of conversion of the resin is about 80%. The cured composite is then ground into particles of sizes that may be larger than the quartz particles used in traditional composites. The prepolymerized particles are often called “organic” fi llers, a term that is somewhat misleading because they contain a high percentage of inorganic fi ller. These “composite particles,” along with additional silane-treated colloidal silica, are then blended with monomer to form the composite paste.
The fi nal inorganic fi ller content may be only about 50wt%, but if the composite particles also provide reinforcement, the fi ller content is closer to 80wt% (approximately 60vol%). This is an important consideration for understanding certain properties of these materials, such as the volumetric shrinkage during polymerization. The composite particles do not shrink when the composite is cured. Thus, a microfi lled composite, despite having a much lower volume fraction of inorganic fi ller than a traditional or small particle composite, will not shrink as much as expected based on the total resin volume. A major shortcoming of these materials is that the bond between the composite particles and the clinically cured matrix is relatively weak, facilitating wear by a chipping mechanism. Because of this defi ciency, most microfi lled composites are not suitable for use as stress-bearing surfaces, with some notable exceptions.6
Microfi lled composites have physical and mechanical properties that are generally inferior to those of macrofi ller (traditional) composites. This is to be expected because 50 to 70vol% of the restorative material is made up of resin. The larger amount of resin compared with inorganic fi ller results in greater water sorption, a higher coeffi cient of
Microfi lled composites have physical and mechanical properties that are generally inferior to those of macrofi ller (traditional) composites.

C DA J O U R N A L , V O L 4 7 , Nº 5
320 M AY 2 01 9
thermal expansion and decreased elastic modulus. In addition, the weak bond of the prepolymerized particles to the clinically cured resin matrix results in decreased tensile strength similar to that of composites with nonsilanized fi ller particles. Nevertheless, micro-/nanofi lled composites remain remarkably wear resistant for several years, with rates of wear comparable to those of the highly fi ller-loaded composites designed for posterior occlusal surfaces. In the longer term, however, if microfi lled composites are placed in wear-prone areas, they eventually begin to break down and wear at a rate too high for acceptable clinical performance. If placed in areas of proximal contact, anterior tooth “drifting” may occur. The wear process has been found to be due to fracture propagation around the poorly bonded organic fi ller particles.6
Of course, compared with unfi lled acrylic resins, microfi lled composites have signifi cantly improved properties and they provide the smoothest surface fi nish available among aesthetic composite restorations. Thus, they are often preferred for restoring teeth with carious lesions on smooth surfaces (Classes III and V). The inorganic fi ller particles are smaller than the abrasive particles used for fi nishing the restoration. Thus, the silica fi ller is removed along with the resin in which it is embedded.
Optical Properties and RadiopacityTo ensure acceptable aesthetics, the
translucency of a composite restoration is important. Therefore, the index of refraction of the fi ller must closely match that of the resin. For Bis-GMA and TEGDMA, the refractive indices are about 1.55 and 1.46, respectively, and a mixture of the two components in equal proportions by weight yields a refractive index of about 1.50. The glasses and quartz fi llers have refractive
indices ranging from 1.52 to 1.55, which is a close enough match to achieve a translucency similar to that of enamel.
Radiopacity.26 Resins are inherently radiolucent. However, leaking margins, secondary caries, poor proximal contacts, wear of proximal surfaces, etc., cannot be detected unless there is adequate radiographic contrast. Radiopacity is imparted by certain glass fi ller particles containing heavy metal atoms. Although not all composite resins are radiopaque, most demonstrate suffi cient radiopacity so this seldom poses a problem. For
optimum diagnostic contrast, the restoration should have a radiopacity approximately equal to that of enamel, which is about twice that of dentin. A wide range of radiopacity values have been considered to be adequate, but exceeding the radiopacity of enamel by a large degree will have the effect of obscuring radiolucent areas caused by gap formation or secondary caries.
The radiopacity of composites is provided by a number of glasses, ceramics that contain heavy metals such as barium (Ba) and strontium (Sr). The glasses have indices of refraction of about 1.50 to match that of the resin matrix. The most commonly used glass fi ller is barium glass. While glass fi llers with high atomic number metals provide radiopacity, they are not as inert as quartz and
amorphous silica and are slowly leached and weakened in oral fl uids. Thus, there is the possibility that radiopaque, glass-fi lled composites may gradually become more susceptible to abrasive wear and hence have a shorter functional lifetime compared with silica-reinforced resins.
Coupling AgentsIt is essential that fi ller particles
are bonded to the resin matrix. This allows the more fl exible polymer matrix to transfer stresses to the more rigid fi ller particles. A coupling agent provides the fi ller/matrix bond in composites. A properly applied coupling agent can impart improved physical and mechanical properties and inhibit leaching by preventing water from penetrating along the fi ller-resin interface.27
Although titanates and zirconates can be used as coupling agents, organosilanes such as γ– methacryloxypropyltrimethoxysilane are most often utilized. In the presence of water, the silane methoxy groups (–SiOCH3) are hydrolyzed to silanol (–Si–OH) groups that can bond with other silanols on the fi ller surfaces by formation of a siloxane bond (–Si–O–Si). The organosilane methacrylate groups form covalent bonds with the resin when it is polymerized, thereby completing the coupling process. Proper coupling by means of organosilanes is extremely important to the clinical performance of resin-based composite restorative materials.
Special-Purpose Restorative Resins
Flowable CompositesA modifi cation of the small particle and
hybrid composites results in the so-called fl owable composites (see Operator Friendly — Ease of Manipulation —Monomers in previous section). Such composites have
c o m p o s i t e s
For optimum diagnostic contrast, the restoration should have a radiopacity approximately equal to that of enamel, which is about twice that of dentin.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 321
reduced fi ller loading so as to provide a consistency that enables the material to fl ow readily, spread and intimately adapt to a cavity form and produce a desired dental anatomy.17 The reduced fi ller makes them more susceptible to wear, but improves the clinician’s ability to form a well-adapted cavity base or liner, especially in Class II posterior preparations and other situations where access is diffi cult. In Class I restorations, these are useful in gingival areas because of their greater ease of adaptation and greater fl exibility as a cured material. Another application is in minimal Class I restorations to prevent caries, when used in a manner similar to the use of fi ssure sealants. Applications where there is poor accessibility and little or no exposure to wear and/or when excellent adaptation is needed are indicated for fl owable composites.28
Direct Posterior CompositesAmalgam has long been the direct
fi lling material of choice for restoration of posterior teeth. Its attributes are ease of placement, good mechanical properties, excellent wear resistance and the unique characteristic of reducing leakage within marginal gaps as the restoration ages. However, with the demand for aesthetics and the concern for mercury toxicity, composites are the material of choice for Class I and Class II restorations.
Condensable/packable composites.29 Compared with amalgam, composite placement is very time consuming and demanding. Because of its paste-like consistency, most composite categories cannot be condensed into a cavity such that there is intimate contact with the cavity walls and a matrix band must be used for proximal contacts. Such composites are somewhat analogous in their handling characteristics to spherical particles amalgams. Resin composites with fi ller characteristics
that increase the strength and stiffness of the uncured material and that provide a consistency analogous to lathe-cut amalgams offer a solution to this problem
Fibers and other high-aspect ratio fi llers. Packable, or condensable, resins form a special category of hybrid composite. These materials provide resin composites with characteristics that allow techniques similar to those used for amalgam restorations. The packable/condensable characteristic derives from inclusion of elongated, fi brous, fi ller particles and/or textured surfaces such that they can
interlock and resist fl ow. This causes the uncured resin to be stiff and resistant to slumping, yet moldable under the force of condensing instruments. Blends of fi brous and particulate fi llers with rough surfaces produce a packable consistency and enable other properties to be optimized for clinical performance. Although this is a useful approach, many of the limitations of resin composites prevail and about twice the time for amalgam placement is required. Also, an increased contraction stress occurs with packable resins compared to nonpackable resins with similar fi ller loadings. This is considered to be due to the comparably higher modulus (stiffness) of the packable resi ns.30 Other than being somewhat similar to amalgam in their placement technique, these materials have been
found to have several disadvantages but no advantageous properties or characteristics over the hybrid resins. Thus, at present, packable composites have not proved to be a solution to the general need for highly wear-resistant, low-cure-shrinkage, reliably placed posterior resins with a depth of cure greater than 2 mm, despite the claims of some manufacturers.18
Another type of packable composite, ormocers, appears to have overcome these problems.
Ormocer (hybrid composites with an organic-ceramic matrix). To overcome some of the limitations of the glass-reinforced resins, ormocer-packable restorative materials were introduced.31 ORMOCER is a trade name of the Fraunhofer Institute and an acronym for organically modifi ed ceramics. Ormocers are molecule-sized hybrid fi ller-reinforced inorganic-organic copolymer resins. Reactive monomers are bound to a silicate (–Si–O–Si–) polysiloxane network. Thus, the ormocer matrix is a polymer prior to curing, which produces lower shrinkage than the dimethacrylate matrix found in other composites. Polymerizable side chains are added to the polysiloxane chains, which react during curing and form the set matrix. These molecular hybrids consist of, for example, methacrylate-terminated chains grafted onto 2 to 3 nm silica particles that are homogenously dispersed on a molecular scale. The result is a high molecular weight, fl exible, relatively low-viscosity, cross-linkable “oligomer” molecule. This provides wider spacing between cross-links, which minimizes polymerization shrinkage and stress. The silicate network also provides high abrasive-wear resistance because of its glasslike structure,32 and its hydrophobicity produces low water sorption and enhanced degradation resistance.33
These hybrid composites are also highly translucent with good stain resistance34 and therefore have excellent
With the demand for aesthetics and the concern for mercury toxicity, composites are the material of choice for Class I and Class II restorations.
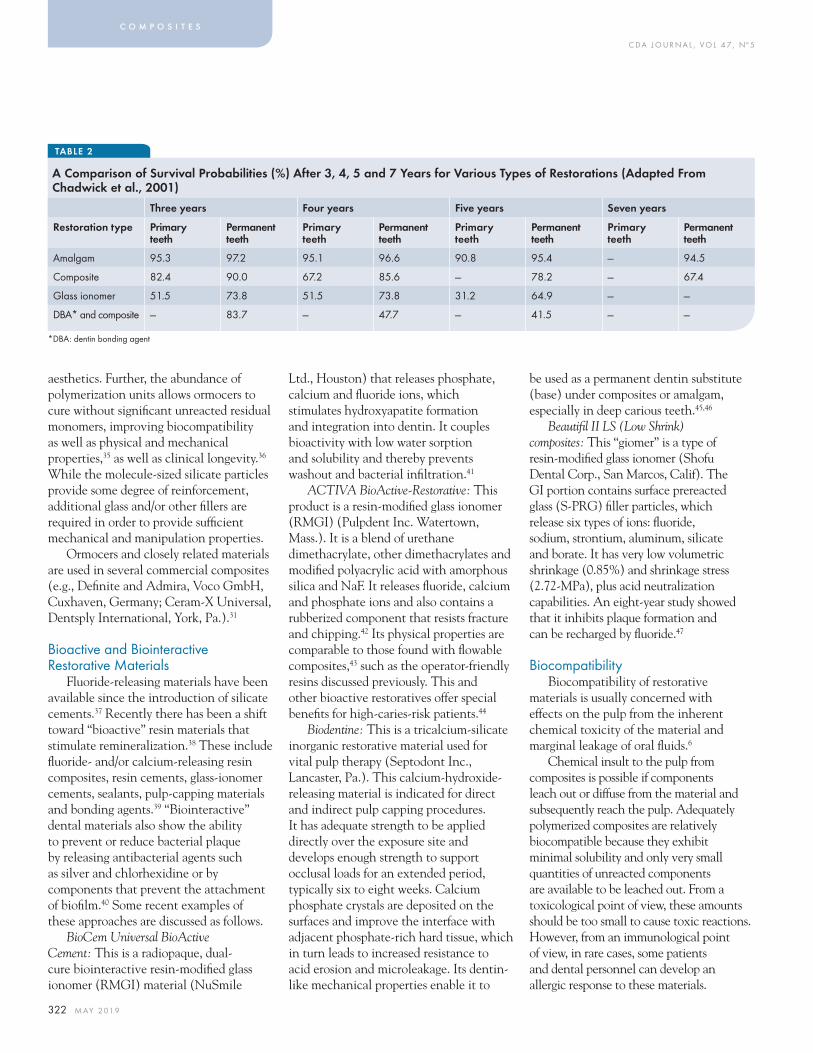
C DA J O U R N A L , V O L 4 7 , Nº 5
322 M AY 2 01 9
aesthetics. Further, the abundance of polymerization units allows ormocers to cure without signifi cant unreacted residual monomers, improving biocompatibility as well as physical and mechanical properti es,35 as well as clinical longevity.36 While the molecule-sized silicate particles provide some degree of reinforcement, additional glass and/or other fi llers are required in order to provide suffi cient mechanical and manipulation properties.
Ormocers and closely related materials are used in several commercial composites (e.g., Defi nite and Admira, Voco GmbH, Cuxhaven, Germany; Ceram-X Universal, Dentsply International, York, Pa.).31
Bioactive and Biointeractive Restorative Materials
Fluoride-releasing materials have been available since the introduction of silicate cements.37 Recently there has been a shift toward “bioactive” resin materials that stimulate remineralization.38 These include fl uoride- and/or calcium-releasing resin composites, resin cements, glass-ionomer cements, sealants, pulp-capping materials and bonding agents.39 “Biointeractive” dental materials also show the ability to prevent or reduce bacterial plaque by releasing antibacterial agents such as silver and chlorhexidine or by components that prevent the attachment of biofi lm.40 Some recent examples of these approaches are discussed as follows.
BioCem Universal BioActive Cement: This is a radiopaque, dual-cure biointeractive resin-modifi ed glass ionomer (RMGI) material (NuSmile
Ltd., Houston) that releases phosphate, calcium and fl uoride ions, which stimulates hydroxyapatite formation and integration into dentin. It couples bioactivity with low water sorption and solubility and thereby prevents washout and bacterial infi ltration.41
ACTIVA BioActive-Restorative: This product is a resin-modifi ed glass ionomer (RMGI) (Pulpdent Inc. Watertown, Mass.). It is a blend of urethane dimethacrylate, other dimethacrylates and modifi ed polyacrylic acid with amorphous silica and NaF. It releases fl uoride, calcium and phosphate ions and also contains a rubberized component that resists fracture and chipping.42 Its physical properties are comparable to those found with fl owable composites,43 such as the operator-friendly resins discussed previously. This and other bioactive restoratives offer special benefi ts for high-caries-risk patients.44
Biodentine: This is a tricalcium-silicate inorganic restorative material used for vital pulp therapy (Septodont Inc., Lancaster, Pa.). This calcium-hydroxide-releasing material is indicated for direct and indirect pulp capping procedures. It has adequate strength to be applied directly over the exposure site and develops enough strength to support occlusal loads for an extended period, typically six to eight weeks. Calcium phosphate crystals are deposited on the surfaces and improve the interface with adjacent phosphate-rich hard tissue, which in turn leads to increased resistance to acid erosion and microleakage. Its dentin-like mechanical properties enable it to
be used as a permanent dentin substitute (base) under composites or amalgam, especially in deep carious teeth.45,46
Beautifi l II LS (Low Shrink) composites: This “giomer” is a type of resin-modifi ed glass ionomer (Shofu Dental Corp., San Marcos, Calif). The GI portion contains surface prereacted glass (S-PRG) fi ller particles, which release six types of ions: fl uoride, sodium, strontium, aluminum, silicate and borate. It has very low volumetric shrinkage (0.85%) and shrinkage stress (2.72-MPa), plus acid neutralization capabilities. An eight-year study showed that it inhibits plaque formation and can be recharged by fl uoride.47
BiocompatibilityBiocompatibility of restorative
materials is usually concerned with effects on the pulp from the inherent chemical toxicity of the material and marginal leakage of oral fl uids.6
Chemical insult to the pulp from composites is possible if components leach out or diffuse from the material and subsequently reach the pulp. Adequately polymerized composites are relatively biocompatible because they exhibit minimal solubility and only very small quantities of unreacted components are available to be leached out. From a toxicological point of view, these amounts should be too small to cause toxic reactions. However, from an immunological point of view, in rare cases, some patients and dental personnel can develop an allergic response to these materials.
c o m p o s i t e s
TABLE 2
A Comparison of Survival Probabilities (%) After 3, 4, 5 and 7 Years for Various Types of Restorations (Adapted From Chadwick et al., 2001)
*DBA: dentin bonding agent
Three years Four years Five years Seven years
Restoration type Primary teeth
Permanent teeth
Primary teeth
Permanent teeth
Primary teeth
Permanent teeth
Primary teeth
Permanent teeth
Amalgam 95.3 97.2 95.1 96.6 90.8 95.4 — 94.5
Composite 82.4 90.0 67.2 85.6 — 78.2 — 67.4
Glass ionomer 51.5 73.8 51.5 73.8 31.2 64.9 — —
DBA* and composite — 83.7 — 47.7 — 41.5 — —

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 323
Inadequately cured composite materials at the fl oor of a cavity can serve as a reservoir of diffusible components that can induce long-term pulp infl ammation. This situation is of particular concern for light-activated materials.26 If a clinician attempts to cure too thick a layer of resin or if the exposure time to the light is inadequate, the uncured or incompletely polymerized resin can release leachable constituents that can diffuse into the pulp.
A second biological concern derives from the shrinkage stresses that a composite develops during curing11 and the resultant marginal leakage. Marginal leakage leads to bacterial ingrowth and may cause secondary caries and/or pulp reactions. Therefore, the restorative procedure must be designed to minimize polymerization shrinkage and marginal leakage.
A precursor of Bis-GMA, bisphenol A (BPA), is a xenoestrogen — a synthetic compound that mimics the effects of estrogen due to its affi nity for estrogen receptor sites. Such endocrine disrupting chemicals (EDCs) have been shown to cause reproductive anomalies and other biological problems. BPA has also been shown to exhibit antiandrogenic activities, which may prove to be detrimental in organ development. The estrogenicity of compounds that may leach from resins is associated primarily with BPA and its dimethacrylate derivative (BPA-DM). In vitro reports have confi rmed that BPA and BPA-DM applied to cancer cells signifi cantly increase cell proliferation and DNA synthesis similar to the effect of estrogen. In vivo studies with mammals have revealed numerous effects such as delayed and sustained hyperprolactinemia changes in estrogen receptors in the hypothalamus and pituitary glands.
It is unclear how much BPA or BPA-DM is released to the oral cavity and what dosage is enough to affect human health. A clinical study48 revealed that BPA collected in saliva after one hour of sealant placement, leading the authors to conclude that sealant application led to xenoestrogen exposure in children. Recent studies showed that BPA-DM should be restricted for use in sealants and resin composites because of its very potent estrogenic effect and high levels found in the body, but that the effect of BPA is negligible.49
Future Directions
Restoration LongevityAn evidence-based review of the
longevity of composite and amalgam restorations in permanent teeth was reported by Chadwick et al. for a 10-year period.3
The survival probability for restorations showed that amalgams have the most consistent survival levels. As summarized in TABLE 2, the overall survival rate found for composites in permanent teeth after seven years was 67.4% compared with 94.5% for amalgams. More than 90% of amalgam restorations were found to have survived over nine years. In comparison, only 64% of glass ionomer restorations survived after fi ve years. In contrast, only 41% of
Class V composites placed with dentin bonding agents survived after fi ve years.
Amalgam remains in use because of its ease of manipulation, relatively low cost, wear resistance, freedom from excessive setting shrinkage and high survival rate. Even though there are controversies about its biocompatibility, amalgam continues to display superior clinical characteristics compared with many currently available resin composites.
In 2013, a new initiative to at least double the service life of resin composite restorations was funded by the NIH, National Institute for Dental and Craniofacial Research.50 This resulted in fi ve awards, each of which is designed to explore various polymer chemistries and formulations that have promise of meeting the objecti ve.51 Each uses rationales and technical approaches designed to fi nd an improved balance among mechanical properties, shrinkage stress, resistance to enzymatic and hydrolytic degradation and abrasive wear, translucency and color stability, biocompatibility, ability to be scaled up for manufacture, ease of manipulation and cost. These initiatives have shown the way to a variety of attractive possibilities for product development47 and are briefl y described as follows:
Self-healing divinyl ether composites with antimicrobial titania nanorods. This investigation utilizes an ether-based resin network, which is enzymatically and hydrolytically stable.52 This is combined with a photopolymerization approach that avoids composition shift caused by diffusion limitation during the forming of cross-linking resins. These novel resin composites are signifi cantly stronger and tougher than a Bis-GMA/TEGDMA control. A self-healing fi ller system is also incorporated and increases fatigue life up to fi ve times compared to the control.53 Lastly, pH-controlled,
The overall survival rate found for composites in permanent teeth after seven years was 67.4% compared with 94.5% for amalgams.

C DA J O U R N A L , V O L 4 7 , Nº 5
324 M AY 2 01 9
reversible switching, antimicrobial titania nanorods are incorporated for inhibition of acid-producing bacteria.
These unique features are signifi cant improvements that are promising for development of resin composites with superior performance and extending clinical lifetime.54
Tough, durable, tertiary methacrylamide/thiourethane composites.14 Tertiary methacrylamide polymers are resistant to hydrolysis and enzymatic attack and can be photoactivated with the same type of photosensitizers as current dimethacrylate resins such as Bis-GMA/TEGDMA. In addition, methacrylamide-functionalized thiourethane oligomeric additives provide more homogeneous networks with substantially lower residual stress and thus enhanced toughness as well as greater depth of cure via better match of refractive index between resin matrix and reinforcing fi llers.
These features indicate that the tertiary methacrylamide/thiourethane restorative composites will have signifi cantly reduced oral degradation, reduced polymerization shrinkage and stress and enhanced toughness and therefore will have substantially greater clinical longevity.
“Smart” addition-fragmentation, thiol-ene resins with fl uorapatite fi ller.55 Concurrent thiol-ene polymerization and allyl sulfi de addition-fragmentation chain transfer produce cross-linked resins that develop both low shrinkage and low shrinkage stress. Incorporation of polymerizable mechanically activated chromophores shows the presence of raised stresses. This material is labeled as “smart” because when the shrinkage stress of the composite is greater than a preselected threshold, a visual signal is produced that allows practitioners to assess restoration success.
The addition of enamel-like fl uorapatite nanocrystals to these glass-fi lled composites produces decreased biofi lm formation at low cytotoxicity, while a remineralizing level of fl uoride is released and also stimulates pulp stem cells to mineralize and aid in protecting the pulp in deep cavities. The overall balance of mechanical properties is in the range of the Bis-GMA/TEGMA control. These features indicate that composites formulated with addition-fragmentation/thiol-ene resins with fl uorapatite fi ller will substantially enhance clinical lifetime.
Copper-catalyzed azide-alkyne cycloaddition composites.56 This approach uses amide-alkyne “click” polymerization as a very effi cient, copper-catalyzed photocure reaction that produces polymer networks with triazole ring structures that impart noncovalent bond formation, which increases toughness, Tg (glass transition/softening) temperature and modulus (stiffness) of the cross-linked resin matrix.
Compared with methacrylate controls, these materials have somewhat reduced mechanical properties but produce higher degrees of cure with lower polymerization stress and are resistant to chemical and mechanical degradation in the oral environment.14 Despite the copper catalyst, they can be formulated to have low toxicity
and are not subject to discoloration. This approach has shown substantial promise of yielding a dental composite system that will substantially enhance the clinical service life of restorations.
Photoinitiated thiol-vinyl sulfone composites. Thiol-vinyl sulfone polymerization is a highly effi cient, rapid reaction that can produce cross-linked networks with a very high degree of cure (monomer-polymer conversion approaching 80%) but with low levels of shrinkage and residual stress as well as minimal extractable components. This is partly due to the development of effi cient photobase generator initiators, together with a high glass transition temperature (Tg as high as 100 degrees Celsius). The high Tg allows longer lasting monomer mobility, thus retaining reactivity throughout most of the cure process and resulting in increased conversion and reduced toxic potential.
Monomer structures for these materials have been designed to eliminate degradable esters and produce networks that resist swelling. All together, these features provide the capability of at least a twofold increase in clinical lifetime.57
Epoxy and acrylic interpenetrating polymer network composites. This approach combines two resin-forming monomer systems that cure independently and form two intertwined, noncross-linked, polymer networks.58 Such a resin is called an interpenetrating polymer network (IPN) and offers inherent advantageous characteristics such as resistance to residual stress buildup during curing due to minimal cross-linking, the ability to have one monomer system cure at a slower rate than the other, which also reduces stress buildup and promotes development of a higher level of cure, and resistance to enzymatic and hydrolytic degradation.59
c o m p o s i t e s
Monomer structures for these materials have been designed to eliminate degradable esters and produce networks that resist swelling.
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 325
Two prototype formulations have been developed that have performance properties that make them attractive candidates for commercial development for the dental market. These are currently undergoing fi nal testing for oral durability and biocompatibility.
Natural Replacement of Lost Tissue — Tissue Engineering
Synthetically produced dentin, enamel and whole teeth have been shown to be capable of repairing and/or replacing hard tissues lost due to accident or disease.60
A similar tissue-engineering approach using amelogenin-derived peptide enables in vitro remineralization of human enamel. This approach resulted in remineralization of fairly thick (10 μm) dense mineralized layers containing hydroxyapatite mineral, as in healthy enamel. The newly formed mineralized layer exhibited integration with the underlying enamel as evidenced by cross-sectional imaging. The peptide-guided remineralization approach sets the foundation for future development of biomimetic products and treatments for dental health care.61
Bioactive Glass Fillers Reduce Bacterial Penetration Into Gaps
Bioactive glass (BAG) is known to possess antimicrobial and remineralizing properties (similar to S-PRG,43 discussed previously). However, the use of BAG as a fi ller for resin-based composite restorations to slow recurrent caries has not been studied until now.62
A bioreactor system was used for in vitro cyclic loading of tooth-fi lling samples on which biofi lms were grown on simulated restorations that contained either 15wt% bioactive glass or control composites with 0wt% bioactive glass.
The average depth of bacterial penetration into the marginal gap for the 15wt% bioactive glass samples was signifi cantly smaller (∼ 61%) in comparison to the control composites, in which 100% penetration was observed with biofi lm penetrating underneath some restorations.
These results suggest that composites containing bioactive glass have the potential to slow the development and propagation of secondary tooth decay at restoration margins. ■
REFERENCES
1. Bowen RL. Dental filling material comprising vinyl-silane treated fused silica and a binder consisting of the reaction product of bisphenol and glycidyl methacrylate. U.S. Patent 3,006,112, 1962.2. Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res 14:849–53, 1955.3. Chadwick BL, Dummer PMH, Dunstan F, Gilmour ASM, Jones RJ, Phillips CJ, Rees J, Richmond S, Stevens J, Treasure ET. The longevity of dental restorations: A systematic review. National Health Service Centre for Reviews and Dissemination, University of York, 2001. See also review by Goldstein G. J Evid Base Dent Pract 2010;10:30–31. 4. Soncini JA, Maserejian NM, Trachtenberg GH, Tavares M, Hayes C. The longevity of amalgam versus compomer/composite restorations in posterior primary and permanent teeth. J Am Dent Assoc 2007 Jun;138(6):763-72. doi: 10.14219/jada.archive.2007.0264.5. Moszner N, Salz U. Recent developments of new components for dental adhesives and composites. Macromol Mater Eng 2007 292:245–271.6. Restorative Resins. In: Anusavice K, Shen C, Rawls HR, eds. Phillips’ Science of Dental Materials. 12th ed. New York: Elsevier/Saunders; 2013.7. Cramer NB, Stansbury JW, Bowman CN. Developments in Composite Dental Restorative Materials. J Dent Res 2011 90(4):402–416. doi: 10.1177/0022034510381263.8. Carvalho RM, Pereira JC, Yoshiyama M, Pashley DH. A review of polymerization contraction: The infl uence of stress development versus stress relief. Oper Dent 1996 Jan–Feb;21(1):17–24.9. Hickel R, Manhart J, Garcia-Godoy F. Clinical results and new developments of direct posterior restorations. Am J Dent 2000 Nov;13(Spec No):41D–54D.10. Mjör IA, Toffenetti O. Secondary caries: A literature review with case reports. Quintessence Int 2000 Mar;31:165–179. PMID: 11203922.11. Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater 2005 Jan;21(1):36–42.12. Donly KJ, Jensen ME, Reinhardt J, et al. Posterior Composite Polymerization Shrinkage in Primary Teeth: An In Vivo Comparison of Three Restorative Techniques. Pediatr Dent 1987 Mar;9(1):22–25.
13. Vasudeva G. Monomer systems for dental composites and their future: A review. J Calif Dent Assoc 2009 Jun;37(6):389–98.14. Fugolin APP, Pfeifer CS. New Resins for Dental Composites. J Dent Res 2017 Sep;96(10):1085–1091. doi: 10.1177/0022034517720658. Epub 2017 Jul 21.15. Weinmann W, Thalacker C and Guggenberger R. Siloranes in dental composites. Dent Materials 2005 Jan;21(1):68–74.16. Stansbury JW. Article on a high-molecular-weight, phase-separating dicarbamate with hydrophobic side chains. J Polym Sci Part A: Polym Chem 2006 44:3921–3929.17. Xiaoming J, Louis B, Qizhou D, O’Connor MT, Hammesfahr PD, Koltisko B. Inventors. Low-stress flowable dental composition. U.S. Patent US2011315928, 2015.18. Gupta R, Tomer AK, Kumari A, Mullick S, Dubey S. Bulk fill flowable composite resins – A review. Int J Appl Dent Sci 2017 3(2):38–40.19. Leprincea JG, Levequec P, Nysten B, et al. New insight into the “depth of cure” of dimethacrylate-based dental composites. Dent Mater 2012 May;28(5):512-20. doi: 10.1016/j.dental.2011.12.004. Epub 2012 Jan 2.20. Atria PJ, Sampaio CS, Cáceres E, Fernández J, Reis AF, Giannini M, Coelho PG, Hirata R. Micro-computed tomography evaluation of volumetric polymerization shrinkage and degree of conversion of composites cured by various light power outputs. Dent Mater J 2018 Jan 30;37(1):33–39. doi: 10.4012/dmj.2016-430. Epub 2017 Oct 27.21. Ilie N, Bauer H, Draenert M, Hickel R. Resin-based Composite Light-Cured Properties Assessed by Laboratory Standards and Simulated Clinical Conditions. Oper Dent 2013 Mar–Apr;38(2):159–67. doi: 10.2341/12-084-L. Epub 2012 Jul 11.22. Watts DC, Al Hindi A. Photo-polymerization shrinkage-kinetics in an acrylate-based resin composite. Dent Mater 1999 15:39–45.23. Sakaguchi RL, Berge HX. Reduced light energy density decreases post-gel contraction while maintaining degree of conversion in composites. J Dent 1998 Nov;26(8):695–700.24. Suh BI. Controlling and understanding the polymerization shrinkage induced stresses in light-cured composites. Compend Contin Educ Dent Suppl 1999;(25):S34–41.25. Lutz F, Phillips RW. A classification and evaluation of composite resin systems. J Prosthet Dent 1983 Oct;50:480–8.26. Montes-Fariza R, Monterde-Hernández M, Cabanillas-Casabella C, Pallares-Sabater A. Comparative study of the radiopacity of resin cements used in aesthetic dentistry. J Adv Prosthodont 2016 Jun;8(3):201–206. doi: 10.4047/jap.2016.8.3.201.27. Nihei T. Dental applications for silane coupling agents. J Oral Sci 2016;58(2):151–5. doi: 10.2334/josnusd.16-0035.28. Baroudi K, Rodrigues JC. Flowable Resin Composites: A Systematic Review and Clinical Considerations. J Clin Diagn Res 9(6):ZE18–ZE24. 2015 doi: 10.7860/JCDR/2015/12294.6129 PMID: 26266238.29. Gupta R, Tomer AK, Kumari A, Mullick S, Dubey S. Bulk fill flowable composite resins — A review. Int J Appl Dent Sci 2017 3(2):38–40.

C DA J O U R N A L , V O L 4 7 , Nº 5
326 M AY 2 01 9
30. Chen HY, Manhart J, Hickel R, Kunzelmann KH. Polymerization contraction stress in light-cured packable composite resins. Dent Mater 2001 May;17(3):253–259.31. Hickel R, Dasch W, Janda R, Tyas M, Anusavice K. New direct restorative materials. Int Dent J 1998 Feb;48(1):3–16.32. Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties and wear behavior of light-cured packable composite resins. Dent Mater 2000 Jan;16(1):33–40.33. Kalra S, Singh A, Gupta M, Chadha V. Ormocer: An aesthetic direct restorative material; An in vitro study comparing the marginal sealing ability of organically modified ceramics and a hybrid composite using an ormocer-based bonding agent and a conventional fifth-generation bonding agent. Contemp Clin Dent 2012 Jan;3(1):48–53. doi: 10.4103/0976-237X.94546.34. Llena C, Fernández S, Forner L. Color stability of nanohybrid resin-based composites, ormocers and compomers. Clin Oral Investig 2017 May;21(4):1071–1077. doi: 10.1007/s00784-016-1850-z. Epub 2016 May 16.35. Admira Fusion (2018 Preferred Product). Dental Advisor 35 (1):2018.36. van Dijken JW, Pallesen U. Eight-year randomized clinical evaluation of Class II nanohybrid resin composite restorations bonded with a one-step self-etch or a two-step etch-and-rinse adhesive. Clin Oral Investig 2015 Jul;19(6):1371–9. doi: 10.1007/s00784-014-1345-8. Epub 2014 Oct 31.37. Cao W, Hench LL. Bioactive materials. Ceram Int 1996 22(6):493–507.38. Jeffries SR. Bioactive and biomimetic restorative materials: A comprehensive review. Part II. J Esthet Restor Dent 2014 Jan–Feb;26(1):27–39. doi: 10.1111/jerd.12066. Epub 2013 Dec 17.39. Goldstep F. Proactive intervention dentistry: A model for oral care through life. Compend Contin Educ Dent 2012 Jun;33(6):394–6, 398-402; quiz 404, 416.40. Cheng L, Zhang K, Zhang N, Melo MAS, Weir MD, Zhou XD, Bai YX, Reynolds MA, Xu HHK. Developing a New Generation of Antimicrobial and Bioactive Dental Resins. J Dent Res 2017 Jul;96(8):855–863. doi: 10.1177/0022034517709739. Epub 2017 May 22.41. Abdulhadi BS, Abdullah MM, Alaki SM, Alamoudi NM, Attar MH. Clinical evaluation between zirconia crowns and stainless steel crowns in primary molars teeth. J Pediatr Dent 2017 5:21–7.42. Chen L, Shen H, Suh BI. Bioactive dental restorative materials: A review. Am J Dent 2013 Aug;26(4):219–27.43. Pameijer CH, Garcia-Godoy F, Morrow BR. Jefferies S. Flexural strength and flexural fatigue properties of resin-modified glass ionomers. J Clin Dent 2015;26(1):23–27.44. ACTIVA Bioactive-Restorative (two year). Dental Advisor 35(01):5, Jan/Feb 2018.45. Burgess J, et al. Mechanical and Physical Properties of Vital Pulp Materials. Poster, AADR, Tampa 2012.46. Rajasekharan S, Martens LC, Cauwels RGEC, Verbeeck RMH. Biodentine material characteristics and clinical applications: A review of the literature. Eur Arch Paediatr Dent 2014 Jun;15(3):147–58. doi: 10.1007/s40368-014-0114-3. Epub 2014 Mar 11.
47. Gordan VV, Mondragon E, Watson RE, Garvan C, Mjör IA. A clinical evaluation of a self-etching primer and giomer restorative. J Am Dent Assoc 2007 May;138(5):621–7.48. Olea N, Pulgar R, Perez P, et al. Estrogenicity of resin-based composites and sealants used in dentistry. Environ Health Perspect 1996 104:298–305. 49. Naciff JM, Jump ML, Torontalli SM, et al. Gene expression profile induced by 17 alpha-ethynyl estradiol, bisphenol A and genistein in the developing female reproductive system of the rat. Toxicol Sci 2002 Jul;68(1):184–199. 50. National Institute of Dental and Craniofacial Research, Design and Development of Novel Dental Composite Restorative Systems (U01). The focus of this opportunity is to support the design and development of novel dental composite restorative systems that demonstrate superiority in material properties and endurance in the oral environment. RFA-DE-13-001, Sept. 2013.51. Symposium, Moving Dental Composites Beyond Methacrylate-based Resins. AADR/IADR Annual Meeting, Session 21 (Fort Lauderdale, Fla.) March 21, 2018. 52. Wang X, Huyang G, Palagummi SV, Liu X, Skrtic D, Beauchamp C, Bowen R, Sun J. High Performance Dental Resin Composites with Hydrolytically Stable Monomers. Dent Mater 2018 Feb;34(2):228–237. doi: 10.1016/j.dental.2017.10.007. Epub 2017 Nov 4.53. Yahyazadehfar M, Huyang G, Wang X, Fan Y, Arola D, Sun J. Durability of self-healing dental composites: A comparison of performance under monotonic and cyclic loading. Mater Sci Eng C, 2018 (accepted). Mater Sci Eng C Mater Biol Appl 2018 Dec 1;93:1020–1026. doi: 10.1016/j.msec.2018.08.057. Epub 2018 Aug 30.54. Wang X, Song S, Chen L, Stafford C, Sun J. Short-time dental resin biostability and kinetics of enzymatic degradation. Acta Biomater 2018 Jul 1;74:326–333. doi: 10.1016/j.actbio.2018.05.009. Epub 2018 May 9.55. Clarkson BH, Scott TF. Boactive “Smart” Dental Composite Materials. U.S. Patent 2017/0172854A1, Jun.22, 2017. 56. Song HB, Sowan N, Shah PK, Baranek A, Flores A, Stansbury JW, Bowman CN. Reduced shrinkage stress via photo-initiated copper(I)-catalyzed cycloaddition polymerizations of azide-alkyne resins. Dent Mater 2016 Nov;32(11):1332–1342. doi: 10.1016/j.dental.2016.07.014. Epub 2016 Aug 11.57. Podgórski M, Becka E, Chatani S, Claudino M, Bowman CN. Ester-free thiol-X resins: New materials with enhanced mechanical behavior and solvent resistance. Polym Chem 2015 6(12):2234–2240.58. Danso R, Milman A. Whang K, Wendt S, Li Y, Zhang W, Rawls HR. Oxarane-Acrylate System to Double the Clinical Service Life of Restorative Resins. AADR abst. 1013 (Fort Lauderdale, Fla.) March 23, 2018.59. Danso R, Hoedebecke B, Whang K, Sarrami S, Johnston A, Flipse S, Wong N, Rawls HR. Development of an Oxirane/Acrylate Interpenetrating Polymer Network Resin System. Dent Mater 2018 Oct;34(10):1459–1465. doi: 10.1016/j.dental.2018.06.013. Epub 2018 Aug 1.60. Yamagishi K, Onuma K, Suzuki T, Okada F, Tagami J, Otsuki M, Senawangse P. A synthetic enamel for rapid tooth repair. Nature 2005 Feb 24;433(7028):819.
61. Dogan S, Fong H, Yucesoy DT, et al. Biomimetic tooth repair: Amelogenin-derived peptide enables in vitro remineralization of human enamel. ACS Biomater Sci Eng 2018 4(5):1788–1796. doi: 10.1021/acsbiomaterials.7b00959.62. Khvostenko D, Hilton TJ, Ferracane JL, Mitchell JC, Kruzic JJ. Bioactive glass fillers reduce bacterial penetration into marginal gaps for composite restorations. Dent Mater 2016 Jan;32(1):73–81. doi: 10.1016/j.dental.2015.10.007. Epub 2015 Nov 24.
THE CORRESPONDING AUTHOR, H. Ralph Rawls, PhD, can be reached at [email protected].
c o m p o s i t e s
SELL YOUR PRACTICE . . . . .. . . . to the right buyer!Knowing how, means doing all of the following - with precision:1. Valid practice appraisal.
2. Contract preparation and negotiations, including critical tax allocation consideration.
3. Bank financing or Seller financing, with proper agreements to adequately protect the Seller and make the deal close - realistically and expeditiously.
4. Performance of “due diligence” requirements, to prevent later problems.
5. Preparation of all documentation for stock sale, when applicable.
6. Lease negotiations.
Lee Skarin & Associates has scores of Buyers in their database. The Buyers’ profiles personal desires and financial ability have been categorized to expertly select the right Buyer for your practice. Expert Buyer selection solidifies a deal. Lee Skarin & Associates services all of Southern California.
Your calls are invited. Put our thirty years of experience to work for you!Visit our website for current listings: www.LeeSkarinandAssociates.com
All six of these services costs no more.
Maybe even less!Lee Skarin & Associates is Cali-fornia’s leading Dental Practice Broker. Their in-house attor-ney, Kurt Skarin, PhD., J.D., specializes in these matters. He does all of the above, and more. He is the catalytic agent that makes the sale happen - quick-ly and smoothly.
Dental Practice BrokersCA DRE #00863149 805.777.7707
818.991.6552 800.752.7461
LEE S
KARI
N&
ASSO
CIAT
ES IN
C.
®
ENDORSEDPROGRAMS
CDA has leveraged the strength of our large membership
to deliver even more value, including resources to support
you in the business side of practice. Endorsed Programs provide money-saving solutions from vendors that have
been vetted by CDA.
cda.org/endorsedprograms
STRENGTH.SAVINGS.CONFIDENCE.
Flex cash flow and fuel growth. When you need financing for your practice, it’s important to work with someone who understands your profession. For more than 20 years, Bank of America Practice Solutions has helped dentists across the nation reach their goals through smart financial solutions* and expert guidance. Whether you own your practice or are just getting started, benefit from financial services that are customized to meet your short-term needs and long-term aspirations.
As a CDA member, you enjoy a 50% reduction in loan administration fees.** Explore Endorsed Program offers online or call a Bank of America Practice Solutions specialist at 800.497.6076.
* All programs are subject to credit approval and loan amounts are subject to credit worthiness. Some restrictions may apply. **To be eligible for this reduction, applicants must provide association name and membership number at time of approval.
F E AT U R E D E N D O R S E D P R O G R A M
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 329
Biomaterials for the Next Generation of Dental Restoratives: Our Design and Materials Performance Jirun Sun, PhD, and Drago Skrtic, PhD
A B S T R AC T We present recently developed dental resin composites with novel functions incorporated into major components of the polymeric composite restoratives, i.e., resin networks, fi llers and additives. Properties critical for the overall performance of the next-generation dental resin composites, e.g., resin biostability against enzymatic challenges, low polymerization stress, self-healing ability and stimuli-responsive antimicrobial effi cacy, are specifi cally emphasized.
AUTHORS
Jirun Sun, PhD, is a biomaterial scientist with a Master and a Doctor of Polymer Science and completed postdoctoral work in tissue engineering and dental materials at the National Institute of Standards and Technology. He is a senior project leader at the Volpe Research Center/ADA Foundation and a National Institutes of Health-funded principal investigator.Confl ict of Interest Disclosure: None reported.
Resin composite restorations have gained and continue gaining popularity for their tooth-color matching aesthetic advantages and clinical practicality.1–4 The
contemporary dental restoratives generally contain three key components: A resin network typically entailing bisphenol A glycidyl dimethacrylate/triethylene glycol dimethacrylate (Bis-GMA/TEGDMA; see TABLE 1 for list of abbreviations) and/or urethane dimethacrylate (UDMA); reinforcing fi ller particles treated with coupling agents to improve the binding at the resin/fi ller interface; and additives to provide unique functions such as antimicrobial and/or remineralization capabilities. Bis-GMA/TEGDMA-based composites, invented a half-century ago by Rafael “Ray” Bowen, DDS, DSc, who retired from the American Dental Association in December 2018 after 62
Drago Skrtic, PhD, is a material scientist with a Master of Science of Analytical Chemistry and a Doctor of Medicinal Chemistry. He has long funding history from the National Institute of Dental and Craniofacial Research and is the director of research at the Volpe Research Center/ADA Foundation.Confl ict of Interest Disclosure: None reported.
years with the organization,1,5,6 remain a gold standard for the resin-based composite materials to date. In these formulations, Bis-GMA serves as a base monomer and TEGDMA as a diluent monomer. They provide mechanically strong networks and the color of their composites typically matches dentin. However, Bis-GMA’s and TEGDMA’s intramolecular ester groups undergo irreversible hydrolysis when challenged by acid, enzymes and/or cariogenic bacteria. Consequently, the resins decompose and restorations are prone to fracturing and secondary caries and they eventually fail.7,8 In addition, polymerization stress developed upon curing may cause microleakage and, in severe cases, restored teeth fracturing. While resin composite restorations are still the top choice in replacing amalgam, their relatively short service life evinces a need for the longer-lasting dental restoratives.
b i o m a t e r i a l s
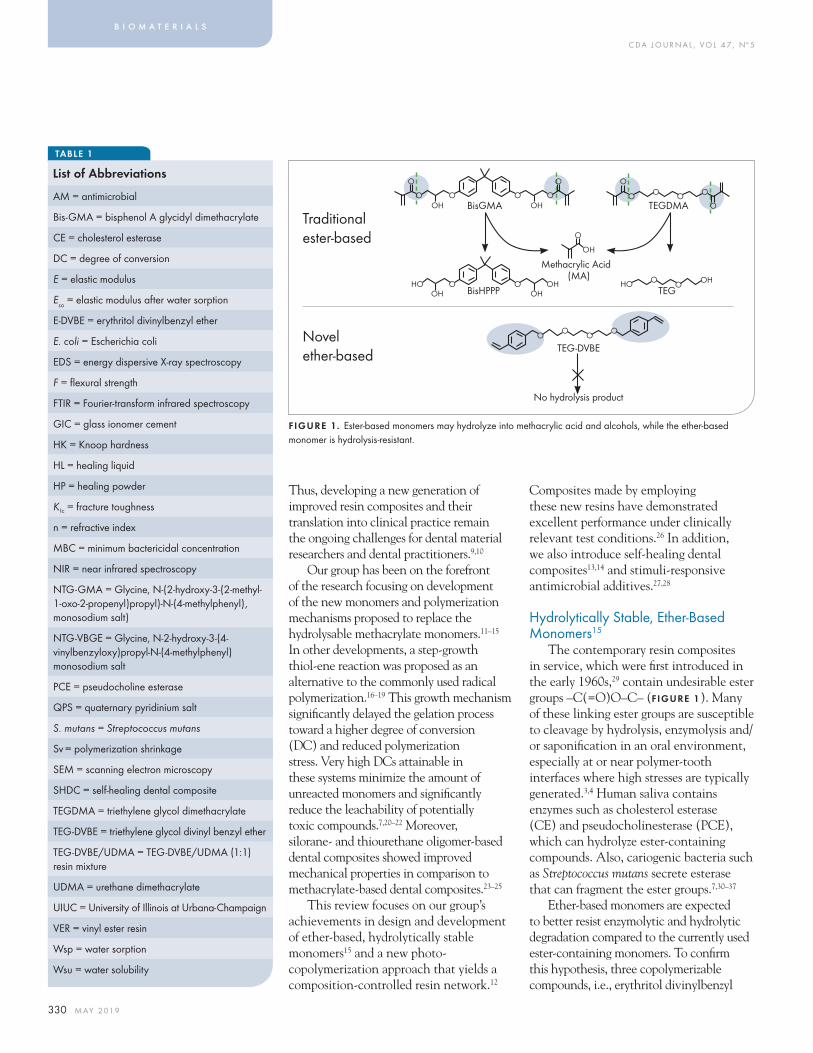
C DA J O U R N A L , V O L 4 7 , Nº 5
330 M AY 2 01 9
Composites made by employing these new resins have demonstrated excellent performance under clinically relevant test conditions.26 In addition, we also introduce self-healing dental composites13,14 and stimuli-responsive antimicrobial additives.27,28
Hydrolytically Stable, Ether-Based Monomers15
The contemporary resin composites in service, which were fi rst introduced in the early 1960s,29 contain undesirable ester groups –C(=O)O–C– (FIGURE 1). Many of these linking ester groups are susceptible to cleavage by hydrolysis, enzymolysis and/or saponifi cation in an oral environment, especially at or near polymer-tooth interfaces where high stresses are typically generated.3,4 Human saliva contains enzymes such as cholesterol esterase (CE) and pseudocholinesterase (PCE), which can hydrolyze ester-containing compounds. Also, cariogenic bacteria such as Streptococcus mutans secrete esterase that can fragment the ester groups.7,30–37
Ether-based monomers are expected to better resist enzymolytic and hydrolytic degradation compared to the currently used ester-containing monomers. To confi rm this hypothesis, three copolymerizable compounds, i.e., erythritol divinylbenzyl
Thus, developing a new generation of improved resin composites and their translation into clinical practice remain the ongoing challenges for dental material researchers and dental practitioners.9,10
Our group has been on the forefront of the research focusing on development of the new monomers and polymerization mechanisms proposed to replace the hydrolysable methacrylate monomers.11–15 In other developments, a step-growth thiol-ene reaction was proposed as an alternative to the commonly used radical polymerization.16–19 This growth mechanism signifi cantly delayed the gelation process toward a higher degree of conversion (DC) and reduced polymerization stress. Very high DCs attainable in these systems minimize the amount of unreacted monomers and signifi cantly reduce the leachability of potentially toxic compounds.7,20–22 Moreover, silorane- and thiourethane oligomer-based dental composites showed improved mechanical properties in comparison to methacrylate-based dental composites.23–25
This review focuses on our group’s achievements in design and development of ether-based, hydrolytically stable monomers15 and a new photo-copolymerization approach that yields a composition-controlled resin network.12
b i o m a t e r i a l s
TABLE 1
List of Abbreviations
AM = antimicrobial
Bis-GMA = bisphenol A glycidyl dimethacrylate
CE = cholesterol esterase
DC = degree of conversion
E = elastic modulus
Eso = elastic modulus after water sorption
E-DVBE = erythritol divinylbenzyl ether
E. coli = Escherichia coli
EDS = energy dispersive X-ray spectroscopy
F = fl exural strength
FTIR = Fourier-transform infrared spectroscopy
GIC = glass ionomer cement
HK = Knoop hardness
HL = healing liquid
HP = healing powder
K Ic = fracture toughness
n = refractive index
MBC = minimum bactericidal concentration
NIR = near infrared spectroscopy
NTG-GMA = Glycine, N-(2-hydroxy-3-(2-methyl-1-oxo-2-propenyl)propyl)-N-(4-methylphenyl), monosodium salt)
NTG-VBGE = Glycine, N-2-hydroxy-3-(4-vinylbenzyloxy)propyl-N-(4-methylphenyl) monosodium salt
PCE = pseudocholine esterase
QPS = quaternary pyridinium salt
S. mutans = Streptococcus mutans
Sv = polymerization shrinkage
SEM = scanning electron microscopy
SHDC = self-healing dental composite
TEGDMA = triethylene glycol dimethacrylate
TEG-DVBE = triethylene glycol divinyl benzyl ether
TEG-DVBE/UDMA = TEG-DVBE/UDMA (1:1) resin mixture
UDMA = urethane dimethacrylate
UIUC = University of Illinois at Urbana-Champaign
VER = vinyl ester resin
Wsp = water sorption
Wsu = water solubility
FIGURE 1. Ester-based monomers may hydrolyze into methacrylic acid and alcohols, while the ether-based monomer is hydrolysis-resistant.
O O OO
TEG-DVBE
No hydrolysis product
O O OHHO
O
O OO O
OTEGDMA
O
O O OOH BisGMA OH
O
O
O OOH OH
OHHOBisHPPP TEG
O
OH
Methacrylic Acid(MA)
Traditional ester-based
Novel ether-based
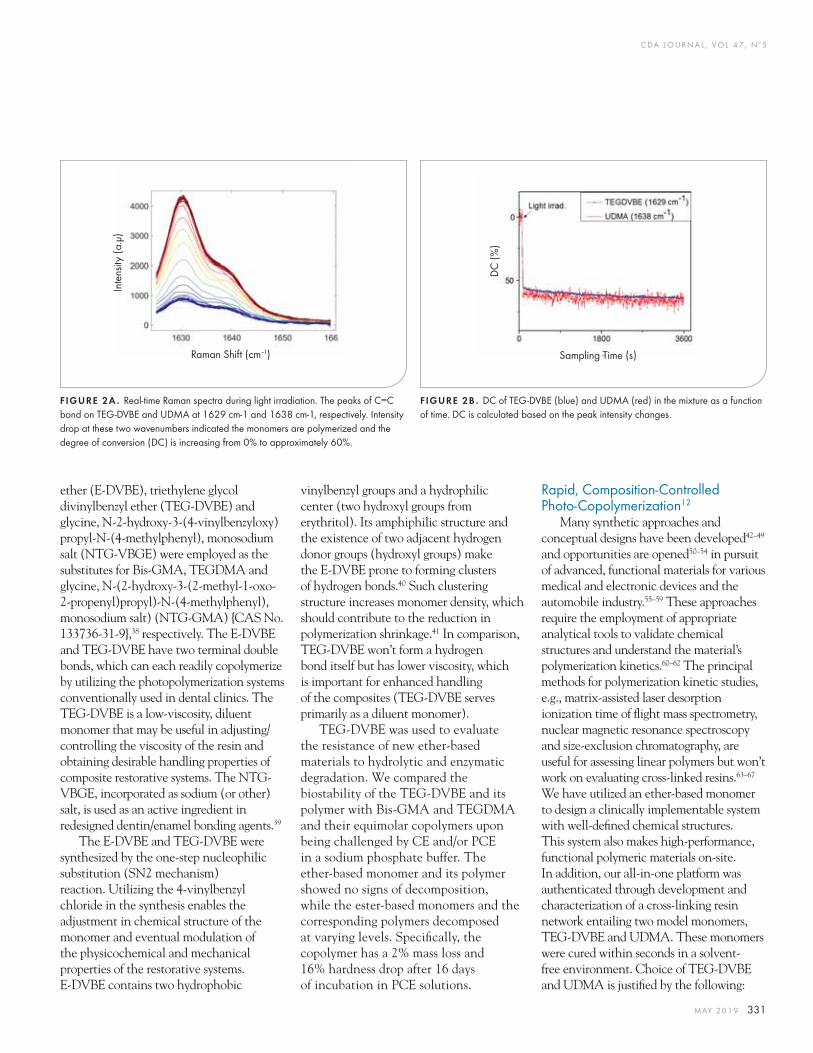
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 331
Rapid, Composition-Controlled Photo-Copolymerization12
Many synthetic approaches and conceptual designs have been developed42–49
and opportunities are opened50–54 in pursuit of advanced, functional materials for various medical and electronic devices and the automobile industry.55–59 These approaches require the employment of appropriate analytical tools to validate chemical structures and understand the material’s polymerization kinetics.60–62 The principal methods for polymerization kinetic studies, e.g., matrix-assisted laser desorption ionization time of fl ight mass spectrometry, nuclear magnetic resonance spectroscopy and size-exclusion chromatography, are useful for assessing linear polymers but won’t work on evaluating cross-linked resins.63–67
We have utilized an ether-based monomer to design a clinically implementable system with well-defi ned chemical structures. This system also makes high-performance, functional polymeric materials on-site. In addition, our all-in-one platform was authenticated through development and characterization of a cross-linking resin network entailing two model monomers, TEG-DVBE and UDMA. These monomers were cured within seconds in a solvent-free environment. Choice of TEG-DVBE and UDMA is justifi ed by the following:
vinylbenzyl groups and a hydrophilic center (two hydroxyl groups from erythritol). Its amphiphilic structure and the existence of two adjacent hydrogen donor groups (hydroxyl groups) make the E-DVBE prone to forming clusters of hydrogen bonds.40 Such clustering structure increases monomer density, which should contribute to the reduction in polymerization shrinkage.41 In comparison, TEG-DVBE won’t form a hydrogen bond itself but has lower viscosity, which is important for enhanced handling of the composites (TEG-DVBE serves primarily as a diluent monomer).
TEG-DVBE was used to evaluate the resistance of new ether-based materials to hydrolytic and enzymatic degradation. We compared the biostability of the TEG-DVBE and its polymer with Bis-GMA and TEGDMA and their equimolar copolymers upon being challenged by CE and/or PCE in a sodium phosphate buffer. The ether-based monomer and its polymer showed no signs of decomposition, while the ester-based monomers and the corresponding polymers decomposed at varying levels. Specifi cally, the copolymer has a 2% mass loss and 16% hardness drop after 16 days of incubation in PCE solutions.
ether (E-DVBE), triethylene glycol divinylbenzyl ether (TEG-DVBE) and glycine, N-2-hydroxy-3-(4-vinylbenzyloxy)propyl-N-(4-methylphenyl), monosodium salt (NTG-VBGE) were employed as the substitutes for Bis-GMA, TEGDMA and glycine, N-(2-hydroxy-3-(2-methyl-1-oxo-2-propenyl)propyl)-N-(4-methylphenyl), monosodium salt) (NTG-GMA) {CAS No. 133736-31-9},38 respectively. The E-DVBE and TEG-DVBE have two terminal double bonds, which can each readily copolymerize by utilizing the photopolymerization systems conventionally used in dental clinics. The TEG-DVBE is a low-viscosity, diluent monomer that may be useful in adjusting/controlling the viscosity of the resin and obtaining desirable handling properties of composite restorative systems. The NTG-VBGE, incorporated as sodium (or other) salt, is used as an active ingredient in redesigned dentin/enamel bonding agents.39
The E-DVBE and TEG-DVBE were synthesized by the one-step nucleophilic substitution (SN2 mechanism) reaction. Utilizing the 4-vinylbenzyl chloride in the synthesis enables the adjustment in chemical structure of the monomer and eventual modulation of the physicochemical and mechanical properties of the restorative systems. E-DVBE contains two hydrophobic
FIGURE 2A . Real-time Raman spectra during light irradiation. The peaks of C=C bond on TEG-DVBE and UDMA at 1629 cm-1 and 1638 cm-1, respectively. Intensity drop at these two wavenumbers indicated the monomers are polymerized and the degree of conversion (DC) is increasing from 0% to approximately 60%.
Inte
nsity
(a.μ
)
Raman Shift (cm–1)
DC
(%)
Sampling Time (s)
FIGURE 2B . DC of TEG-DVBE (blue) and UDMA (red) in the mixture as a function of time. DC is calculated based on the peak intensity changes.
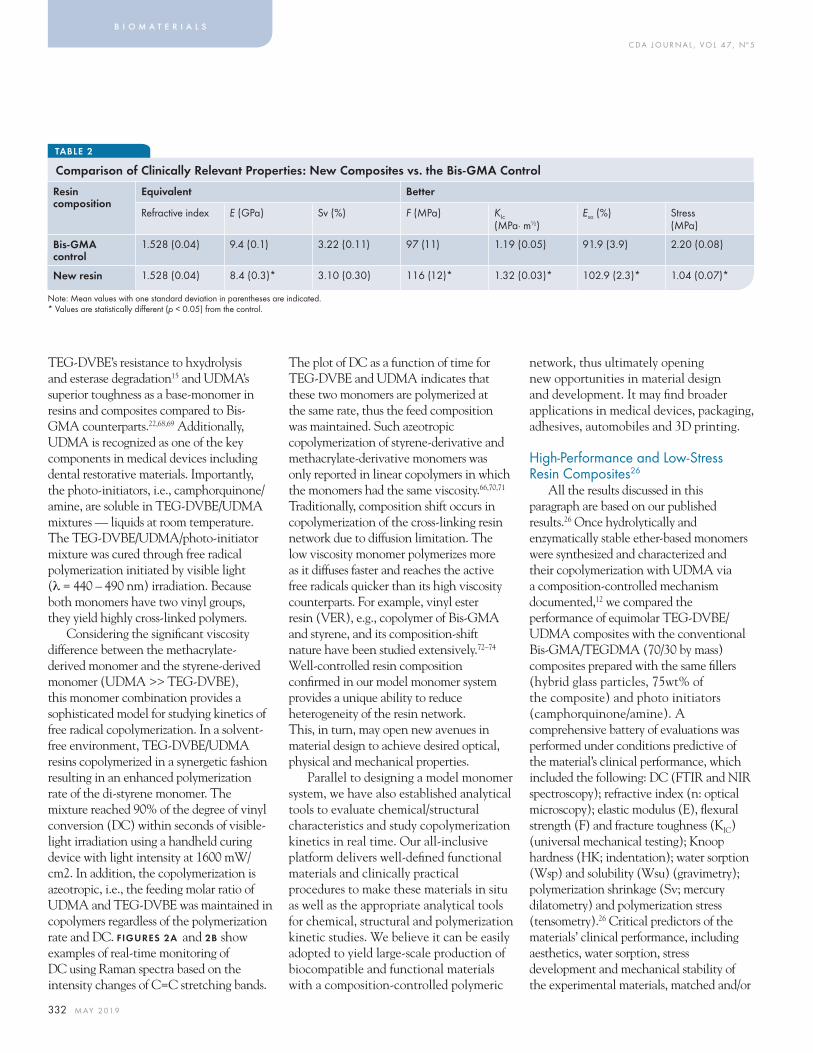
C DA J O U R N A L , V O L 4 7 , Nº 5
332 M AY 2 01 9
TABLE 2
network, thus ultimately opening new opportunities in material design and development. It may fi nd broader applications in medical devices, packaging, adhesives, automobiles and 3D printing.
High-Performance and Low-Stress Resin Composites26
All the results discussed in this paragraph are based on our published results.26 Once hydrolytically and enzymatically stable ether-based monomers were synthesized and characterized and their copolymerization with UDMA via a composition-controlled mechanism documented,12 we compared the performance of equimolar TEG-DVBE/UDMA composites with the conventional Bis-GMA/TEGDMA (70/30 by mass) composites prepared with the same fi llers (hybrid glass particles, 75wt% of the composite) and photo initiators (camphorquinone/amine). A comprehensive battery of evaluations was performed under conditions predictive of the material’s clinical performance, which included the following: DC (FTIR and NIR spectroscopy); refractive index (n: optical microscopy); elastic modulus (E), fl exural strength (F) and fracture toughness (KIC) (universal mechanical testing); Knoop hardness (HK; indentation); water sorption (Wsp) and solubility (Wsu) (gravimetry); polymerization shrinkage (Sv; mercury dilatometry) and polymerization stress (tensometry).26 Critical predictors of the materials’ clinical performance, including aesthetics, water sorption, stress development and mechanical stability of the experimental materials, matched and/or
The plot of DC as a function of time for TEG-DVBE and UDMA indicates that these two monomers are polymerized at the same rate, thus the feed composition was maintained. Such azeotropic copolymerization of styrene-derivative and methacrylate-derivative monomers was only reported in linear copolymers in which the monomers had the same viscosity.66,70,71 Traditionally, composition shift occurs in copolymerization of the cross-linking resin network due to diffusion limitation. The low viscosity monomer polymerizes more as it diffuses faster and reaches the active free radicals quicker than its high viscosity counterparts. For example, vinyl ester resin (VER), e.g., copolymer of Bis-GMA and styrene, and its composition-shift nature have been studied extensively.72–74 Well-controlled resin composition confi rmed in our model monomer system provides a unique ability to reduce heterogeneity of the resin network. This, in turn, may open new avenues in material design to achieve desired optical, physical and mechanical properties.
Parallel to designing a model monomer system, we have also established analytical tools to evaluate chemical/structural characteristics and study copolymerization kinetics in real time. Our all-inclusive platform delivers well-defi ned functional materials and clinically practical procedures to make these materials in situ as well as the appropriate analytical tools for chemical, structural and polymerization kinetic studies. We believe it can be easily adopted to yield large-scale production of biocompatible and functional materials with a composition-controlled polymeric
TEG-DVBE’s resistance to hxydrolysis and esterase degradation15 and UDMA’s superior toughness as a base-monomer in resins and composites compared to Bis-GMA counterparts.22,68,69 Additionally, UDMA is recognized as one of the key components in medical devices including dental restorative materials. Importantly, the photo-initiators, i.e., camphorquinone/amine, are soluble in TEG-DVBE/UDMA mixtures — liquids at room temperature. The TEG-DVBE/UDMA/photo-initiator mixture was cured through free radical polymerization initiated by visible light (λ = 440 – 490 nm) irradiation. Because both monomers have two vinyl groups, they yield highly cross-linked polymers.
Considering the signifi cant viscosity difference between the methacrylate-derived monomer and the styrene-derived monomer (UDMA >> TEG-DVBE), this monomer combination provides a sophisticated model for studying kinetics of free radical copolymerization. In a solvent-free environment, TEG-DVBE/UDMA resins copolymerized in a synergetic fashion resulting in an enhanced polymerization rate of the di-styrene monomer. The mixture reached 90% of the degree of vinyl conversion (DC) within seconds of visible-light irradiation using a handheld curing device with light intensity at 1600 mW/cm2. In addition, the copolymerization is azeotropic, i.e., the feeding molar ratio of UDMA and TEG-DVBE was maintained in copolymers regardless of the polymerization rate and DC. FIGURES 2A and 2B show examples of real-time monitoring of DC using Raman spectra based on the intensity changes of C=C stretching bands.
b i o m a t e r i a l s
Comparison of Clinically Relevant Properties: New Composites vs. the B is-GMA Control
Resin composition
Equivalent Better
Refractive index E (GPa) Sv (%) F (MPa) KIc
(MPa· m½ )Eso (%) Stress
(MPa)
Bis-GMA control
1.528 (0.04) 9.4 (0.1) 3.22 (0.11) 97 (11) 1.19 (0.05) 91.9 (3.9) 2.20 (0.08)
New resin 1.528 (0.04) 8.4 (0.3)* 3.10 (0.30) 116 (12)* 1.32 (0.03)* 102.9 (2.3)* 1.04 (0.07)*
Note: Mean values with one standard deviation in parentheses are indicated.* Values are statistically diff erent (p < 0.05) from the control.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 333
the potentially toxic and expensive healing agents utilized in the UIUC model with the clinically acceptable GICs. Compared to the conventional resin composites, the SHDCs have two additional components: (1) healing powder (HP), e.g., strontium fl uoro-aluminosilicate particles; and (2) healing liquid (HL), e.g., aqueous solutions of polyacrylic acids encapsulated in silica microcapsules. The microcapsules protect the HL from the premature release during composite preparation. Upon cracking, the HL is released from microcapsules and reacts with the HP upon contact to form a reparative GIC within the crack. The three distinctive self-healing steps are illustrated in FIGURE 3 . Initially, crack formation is accompanied by water diffusion (A). The second step involves breaking of the microcapsule and release of the HL (B). In the third step, as a result of HL and HP reaction, the GIC that repairs the defect is formed (C).
Based on this model, we formulated and prepared a series of SHDCs with different mass percentages of silica microcapsules containing HL. We demonstrated the autonomic crack repairing of SHDCs in simulated oral environments based on mechanical, chemical and morphological evidence. FIGURES 4 illustrate the morphological
signifi cantly exceeded those of the controls.26 TABLE 2 highlights some of these properties. Most signifi cantly, the new composites showed up to 52.7% reduction in polymerization stress formation in comparison with the Bis-GMA/TEGDMA control. These high-performance, low-stress composites formed by composition-controlled copolymerization have a strong potential as a new generation of dental restoratives with improved service life.
Self-Healing Dental Restorations13,14
Micro-cracks in dental composites are very diffi cult to detect and almost impossible to repair manually. Since the self-healing concept has been introduced by researchers from the University of Illinois at Urbana-Champaign (UIUC),3,11,48,75–79 autonomic self-healing composites have shown signifi cant enhancement in extending the service life of polymeric materials.80,81 The progress has opened a new era of intelligent materials.48,82–84 We have recently designed and developed a clinically applicable self-healing dental composite (SHDC) that may repair micro-cracks autonomously.13,14
Our SHDC was achieved by combining the fracture-release-healing proposed by the UIUC model48 and the chemistry of glass ionomer cements (GICs).85–87 For the enhanced clinical appeal, we have replaced
and chemical changes before and after healing. Specifi cally, FIGURES 4A and4B are scanning electron microscopy (SEM) images that show a fractured microcapsule before and after healing. The colors in these images highlight the presence of aluminum (light blue) and silicon (red) as determined by energy dispersive X-ray spectroscopy (EDS). Complete surface elemental analyses are provided in FIGURES 4C and 4D, respectively. In addition, the transition in aluminum-silicon-strontium ratios (table in FIGURES 4) confi rms that GIC forms. The formation of GIC (a representative chemical structure of cross-links in GIC is also listed in FIGURES 4) draws more strontium and aluminum to the healing area due to the reaction of HP with HL. In comparison, the mechanical performance of the SHDC in terms of E and KIc was equivalent to the controls containing no microcapsules.13,14 The success of the healing, i.e., healing effi ciency, expressed as the percent recovery of the SHDC’s fracture toughness reached up to 25%, thus confi rming the SHDC’s repairing ability.13,14,88
Additionally, study employing compact tension and cyclic loading indicated that at 25% healing effi ciency, the fatigue life increased more than fi ve times.88
FIGURES 4 . Morphological and chemical confi rmation of the successful healing as the result of GIC formation. SEM-EDS images of (A) nonhealed SHDC surface; (B) the healed SHDC surface, artifi cially colored to match the signal count of Al and Si; and the elemental analysis by EDS on sections of the (C) nonhealed and (D) healed regions of the SHDC. Table shows the transition in aluminum-silicon-strontium ratios. Scheme shows a representative cross-link of GIC.
FIGURE 3. Self-healing steps of SHDC: (A) A crack forms and water comes in; (B) a microcapsule is broken due to crack propagation and HL is released; (C) the HL reacts with HP and the product is GIC with an ionic cross-linking network.
A
C
B
D
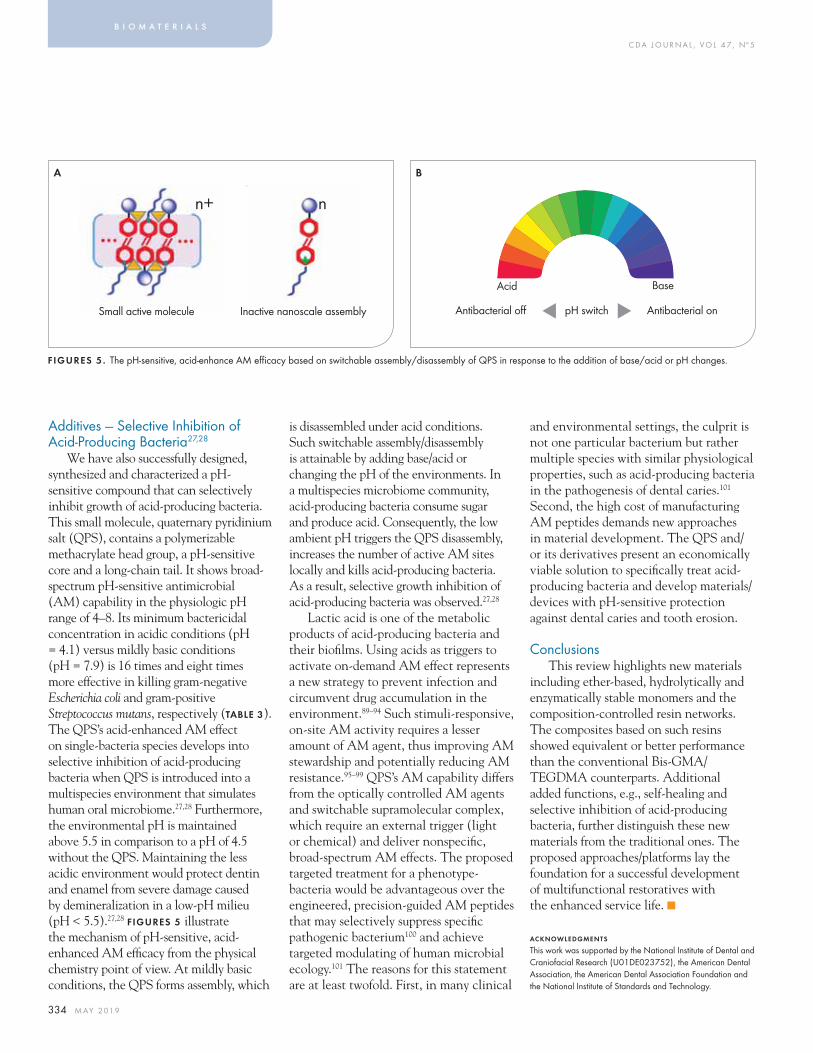
C DA J O U R N A L , V O L 4 7 , Nº 5
334 M AY 2 01 9
Additives — Selective Inhibition of Acid-Producing Bacteria27,28
We have also successfully designed, synthesized and characterized a pH-sensitive compound that can selectively inhibit growth of acid-producing bacteria. This small molecule, quaternary pyridinium salt (QPS), contains a polymerizable methacrylate head group, a pH-sensitive core and a long-chain tail. It shows broad-spectrum pH-sensitive antimicrobial (AM) capability in the physiologic pH range of 4–8. Its minimum bactericidal concentration in acidic conditions (pH = 4.1) versus mildly basic conditions (pH = 7.9) is 16 times and eight times more effective in killing gram-negative Escherichia coli and gram-positive Streptococcus mutans, respectively (TABLE 3). The QPS’s acid-enhanced AM effect on single-bacteria species develops into selective inhibition of acid-producing bacteria when QPS is introduced into a multispecies environment that simulates human oral microbiome.27,28 Furthermore, the environmental pH is maintained above 5.5 in comparison to a pH of 4.5 without the QPS. Maintaining the less acidic environment would protect dentin and enamel from severe damage caused by demineralization in a low-pH milieu (pH < 5.5).27,28 FIGURES 5 illustrate the mechanism of pH-sensitive, acid-enhanced AM effi cacy from the physical chemistry point of view. At mildly basic conditions, the QPS forms assembly, which
is disassembled under acid conditions. Such switchable assembly/disassembly is attainable by adding base/acid or changing the pH of the environments. In a multispecies microbiome community, acid-producing bacteria consume sugar and produce acid. Consequently, the low ambient pH triggers the QPS disassembly, increases the number of active AM sites locally and kills acid-producing bacteria. As a result, selective growth inhibition of acid-producing bacteria was observed.27,28
Lactic acid is one of the metabolic products of acid-producing bacteria and their biofi lms. Using acids as triggers to activate on-demand AM effect represents a new strategy to prevent infection and circumvent drug accumulation in the environment.89–94 Such stimuli-responsive, on-site AM activity requires a lesser amount of AM agent, thus improving AM stewardship and potentially reducing AM resistance.95–99 QPS’s AM capability differs from the optically controlled AM agents and switchable supramolecular complex, which require an external trigger (light or chemical) and deliver nonspecifi c, broad-spectrum AM effects. The proposed targeted treatment for a phenotype-bacteria would be advantageous over the engineered, precision-guided AM peptides that may selectively suppress specifi c pathogenic bacterium100 and achieve targeted modulating of human microbial ecology.101 The reasons for this statement are at least twofold. First, in many clinical
and environmental settings, the culprit is not one particular bacterium but rather multiple species with similar physiological properties, such as acid-producing bacteria in the pathogenesis of dental caries.101 Second, the high cost of manufacturing AM peptides demands new approaches in material development. The QPS and/or its derivatives present an economically viable solution to specifi cally treat acid-producing bacteria and develop materials/devices with pH-sensitive protection against dental caries and tooth erosion.
ConclusionsThis review highlights new materials
including ether-based, hydrolytically and enzymatically stable monomers and the composition-controlled resin networks. The composites based on such resins showed equivalent or better performance than the conventional Bis-GMA/TEGDMA counterparts. Additional added functions, e.g., self-healing and selective inhibition of acid-producing bacteria, further distinguish these new materials from the traditional ones. The proposed approaches/platforms lay the foundation for a successful development of multifunctional restoratives with the enhanced service life. ■
ACKNOWLEDGMENTS
This work was supported by the National Institute of Dental and Craniofacial Research (U01DE023752), the American Dental Association, the American Dental Association Foundation and the National Institute of Standards and Technology.
b i o m a t e r i a l s
Small active molecule
n+
Inactive nanoscale assembly
n
Acid Base
pH switch Antibacterial onAntibacterial off ▲ ▲
FIGURES 5. The pH-sensitive, acid-enhance AM effi cacy based on switchable assembly/disassembly of QPS in response to the addition of base/acid or pH changes.
A B

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 335
TABLE 3
Minimum Bactericidal Concentration (MBC) Against E. coli and S. mutans in Media With Different pH
REFERENCES
1. Bowen RL. Properties of a silica-reinforced polymer for dental restorations. J Am Dent Assoc 1963;66:57–64.2. Bowen RL, Marjenhoff WA. Dental composites glass ionomers: The materials. Adv Dent Res 1992 Sep;6:44–9.3. Ferracane JL. Resin composite — state of the art. Dent Mater 2011 Jan;27(1):29-38. doi: 10.1016/j.dental.2010.10.020. Epub 2010 Nov 18.4 Ferracane JL. Resin-based composite performance: Are there some things we can’t predict? Dent Mater 2013 Jan;29(1):51–8. doi: 10.1016/j.dental.2012.06.013. Epub 2012 Jul 17.5. Bowen RL. Eff ect of particle shape and size distribution in a reinforced polymer. J Am Dent Assoc 1964;69:481–95.6. Cramer NB, Stansbury JW, Bowman CN. Recent Advances and Developments in Composite Dental Restorative Materials. J Dent Res 2011 Apr; 90(4): 402–416. doi: 10.1177/0022034510381263.7. Delaviz Y, Finer Y, Santerre JP. Biodegradation of resin composites and adhesives by oral bacteria and saliva: A rationale for new material designs that consider the clinical environment and treatment challenges. Dent Mater 2014 Jan;30(1):16–32. doi: 10.1016/j.dental.2013.08.201. Epub 2013 Oct 7.8. Jaff er F, Finer Y, Santerre JP. Interactions between resin monomers and commercial composite resins with human saliva derived esterases. Biomaterials 2002 Apr;23(7):1707–19.9. Rekow ED, Fox CH, Watson T, Petersen PE. Future Innovation and Research in Dental Restorative Materials. Adv Dent Res 2013 Nov;25(1):2–7. doi: 10.1177/0022034513502205.10. Pitts NB, Drummond J, Guggenberger R, Ferrillo P, Johnston S. Incorporating New Materials and Techniques into Clinical Practice. Adv Dent Res 2013 Nov;25(1):33–40. doi: 10.1177/0022034513502209.11. Jandt KD, Sigusch BW. Future perspectives of resin-based dental materials. Dent Mater 2009 Aug;25(8):1001–6. doi: 10.1016/j.dental.2009.02.009. Epub 2009 Mar 29.12. Yang Y, Urbas A, Gonzalez-Bonet A, Sheridan RJ, Seppala JE, Beers KL, et al. A composition-controlled cross-linking resin network through rapid visible-light photo-copolymerization. Polym Chem 2016;7:5023–30. doi: 10.1039/C6PY00606J.13. Huyang G, Sun J. Clinically Applicable Self-Healing Dental Resin Composites. MRS Advances 2016;1:547–52. doi.org/10.1557/adv.2016.86. Published online: Feb. 5, 2016.14. Huyang G, Debertin AE, Sun J. Design and development of self-healing dental composites. Mater Des 2016;94:295–302. doi.org/10.1016/j.matdes.2016.01.046.15. Gonzalez-Bonet A, Kaufman G, Yang Y, Wong C, Jackson A, Huyang G, et al. Preparation of dental resins resistant to enzymatic and hydrolytic degradation in oral environments. Biomacromolecules 2015 Oct 12;16(10):3381–8. doi: 10.1021/acs.biomac.5b01069. Epub 2015 Sep 23.16. Xi WX, Scott TF, Kloxin CJ, Bowman CN. Click chemistry in
materials science. Adv Funct Mater 2014;24:2572–90. doi.org/10.1002/adfm.201302847.17. Kloxin CJ, Bowman CN. Covalent adaptable networks: Smart, reconfi gurable and responsive network systems. Chem Soc Rev 2013 Sep 7;42(17):7161–73. doi: 10.1039/c3cs60046g. Epub 2013 Apr 12.18. Boulden JE, Cramer NB, Schreck KM, Couch CL, Bracho-Troconis C, Stansbury JW, et al. Thiol-ene-methacrylate composites as dental restorative materials. Dent Mater 2011;27(3):267–72. doi: 10.1016/j.dental.2010.11.001.19. Cramer NB, Couch CL, Schreck KM, Carioscia JA, Boulden JE, Stansbury JW, et al. Investigation of thiol-ene and thiol-ene-methacrylate based resins as dental restorative materials. Dent Mater 2010 Jan;26(1):21–8. doi: 10.1016/j.dental.2009.08.004.20. Van Landuyt KL, Nawrot T, Geebelen B, De Munck J, Snauwaert J, Yoshihara K, et al. How much do resin-based dental materials release? A meta-analytical approach. Dent Mater 2011 Aug;27(8):723–47. doi: 10.1016/j.dental.2011.05.001. Epub 2011 Jun 12.21. Simon CG, Antonucci JM, Liu DW, Skptic D. In vitro cytotoxicity of amorphous calcium phosphate composites. J Bioact Compat Polym 2005;20:279–95. doi.org/10.1177/0883911505051854.22. Floyd CJE, Dickens SH. Network structure of bis-GMA- and UDMA-based resin systems. Dent Mater 2006 Dec;22(12):1143–9. Epub 2006 Jan 10.23. Bacchi A, Pfeifer CS. Rheological and mechanical properties and interfacial stress development of composite cements modifi ed with thio-urethane oligomers. Dent Mater 2016 Aug;32(8):978–86. doi: 10.1016/j.dental.2016.05.003. Epub 2016 May 30.24. Palin WM, Fleming GJP, Nathwani H, Burke FJT, Randall RC. In vitro cuspal defl ection and microleakage of maxillary premolars restored with novel low-shrink dental composites. Dent Mater 2005 Apr;21(4):324–35.25. Weinmann W, Thalacker C, Guggenberger R. Siloranes in dental composites. Dent Mater 2005 Jan;21(1):68–74.26. Wang XH, Huyang G, Palagummi SV, Liu XH, Skrtic D, Beauchamp C, et al. High performance dental resin composites with hydrolytically stable monomers. Dent Mater 2018 Feb;34(2):228–237. doi: 10.1016/j.dental.2017.10.007. Epub 2017 Nov 4.27. Zhang K, Wang S, Zhou C, Cheng L, Gao X, Xie X, et al. Advanced smart biomaterials and constructs for hard tissue engineering and regeneration. Bone Res 2018; 6:31. doi: 10.1038/s41413-018-0032-9-.28. Yang Y, Reipa V, Liu G, Meng Y, Wang XH, Mineart KP, et al. pH-Sensitive Compounds for Selective Inhibition of Acid-Producing Bacteria. ACS Appl Mater Interfaces 2018, 10 (10):8566–8573. doi: 10.1021/acsami.8b01089.29. Bowen RL. Dental fi lling material. U.S. Dept. of Commerce. 1962. p. US 3,066,112.30. Lee YK, Powers JM. Infl uence of salivary organic substances on the discoloration of esthetic dental materials — a review. J Biomed Mater Res B Appl Biomater 2006 Feb;76(2):397–402. doi: 10.1002/jbm.b.30380.31. Lin BA, Jaff er F, Duff MD, Tang YW, Santerre JP. Identifying enzyme activities within human saliva which are relevant to dental resin composite biodegradation. Biomaterials 2005 Jul;26(20):4259–64. doi.org/10.1016/j.biomaterials.2004.11.001.32. Munksgaard EC, Freund M. Enzymatic-hydrolysis of (di)
methacrylates and their polymers. Scand J Dent Res 1990 Jun;98(3):261–7. doi: 10.1111/j.1600-0722.1990.tb00971.x.33. Santerre JP, Shajii L, Leung BW. Relation of dental composite formulations to their degradation and the release of hydrolyzed polymeric-resin-derived products. Crit Rev Oral Biol Med 2001;12(2):136–51. doi.org/10.1177/10454411010120020401.34. Santerre JP, Shajii L, Tsang H. Biodegradation of commercial dental composites by cholesterol esterase. J Dent Res 1999 Aug;78(8):1459–68. doi.org/10.1177/00220345990780081201.35. Finer Y, Santerre JP. Salivary esterase activity and its association with the biodegradation of dental composites.J Dent Res 2004 Jan;83(1):22–6. doi org/10.1177/ 154405910408300105.36. Finer Y, Santerre JP. Infl uence of silanated fi ller content on the biodegradation of bisGMA/TEGDMA dental composite resins. J Biomed Mater Res A 2007 Apr;81(1):75–84. doi.org/10.1002/jbm.a.31004.37. Bourbia M, Ma D, Cvitkovitch DG, Santerre JP, Finer Y. Cariogenic bacteria degrade dental resin composites and adhesives. J Dent Res 2013 Nov;92(11):989–94. doi: 10.1177/0022034513504436. Epub 2013 Sep 11.38. Bowen RL. Multistep method for obtaining strong adhesive bonding of composites to dentin, enamel and other substrates. American Dental Association Health Foundation. 1986. p. 16 pp. Cont.-in-part of U.S. 4,521,50. US4588756A.39. Bowen RL, Cobb EN, Rapson JE. Adhesive bonding of various materials to hard tooth tissues — improvement in bond strength to dentin. J Dent Res 1982 Sep;61(9):1070–6. doi.org/10.1177/00220345820610090901.40. Sun J, Yu KH, Russo PS, Pople J, Henry A, Lyles B, et al. Some structural observations of self-assembled, fi brillar gels composed of two-directional bolaform arborols. Polymeric Nanofi bers 2006;918:370-83. doi: 10.1021/bk-2006-0918.ch026.41. Moraes RR, Garcia JW, Barros MD, Lewis SH, Pfeifer CS, Liu JC, et al. Control of polymerization shrinkage and stress in nanogel-modifi ed monomer and composite materials. Dent Mater 2011 Jun;27(6):509–19. doi: 10.1016/j.dental.2011.01.006. Epub 2011 Mar 8.42. Barnes JC, Ehrlich DJC, Gao AX, Leibfarth FA, Jiang YV, Zhou E, et al. Iterative exponential growth of stereo- and sequence-controlled polymers. Nat Chem 2015;7:810–5. doi: 10.1038/nchem.2346.43. Chen W, Schuster GB. Precise sequence control in linear and cyclic copolymers of 2,5-bis(2-thienyl)pyrrole and aniline by DNA-programmed assembly. J Am Chem Soc 2013 Mar 20;135(11):4438–49. doi: 10.1021/ja312507z. Epub 2013 Mar 8.44. Coluzza I, van Oostrum PDJ, Capone B, Reimhult E, Dellago C. Sequence controlled self-knotting colloidal patchy polymers. Phys Rev Lett 2013 Feb 15;110(7):075501. Epub 2013 Feb 11. doi: 10.1103/PhysRevLett.110.075501.45. Ghosh B, Urban MW. Self-Repairing Oxetane-Substituted Chitosan Polyurethane Networks. Science 2009 Mar 13;323(5920):1458–60. doi: 10.1126/science.1167391.46. Kramer JW, Treitler DS, Dunn EW, Castro PM, Roisnel T, Thomas CM, et al. Polymerization of enantiopure monomers using syndiospecifi c catalysts: A new approach to sequence control in polymer synthesis. J Am Chem Soc 2009 Nov 11;131(44):16042–4. doi: 10.1021/ja9075327.
pH MBC against E. coli (μg/mL)
MBC against S. mutans (μg/mL)
4.1 2.5 1.25
5.8 10 5
7.9 40 10
C DA J O U R N A L , V O L 4 7 , Nº 5
336 M AY 2 01 9
47. Solleder SC, Meier MAR. Sequence control in polymer chemistry through the passerini three-component reaction. Angew Chem Int Ed Engl 2014 Jan 13;53(3):711–4. doi: 10.1002/anie.201308960. Epub 2013 Dec 4.48. White SR, Sottos NR, Geubelle PH, Moore JS, Kessler MR, Sriram SR, et al. Autonomic healing of polymer composites. Nature 2001 Feb 15;409(6822):794–7. doi: 10.1038/35057232.49. Anastasaki A, Nikolaou V, Pappas GS, Zhang Q, Wan C, Wilson P, et al. Photoinduced sequence-control via one pot living radical polymerization of acrylates. Chem Sci 2014;5:3536–42.50. Baradel N, Fort S, Halila S, Badi N, Lutz JF. Synthesis of single-chain sugar arrays. Angew Chem Int Ed Engl 2013 Feb 18;52(8):2335–9. doi: 10.1002/anie.201209052. Epub 2013 Jan 23.51. Braunecker WA, Matyjaszewski K. Controlled/living radical polymerization: Features, developments and perspectives. Prog Polym Sci 2007;32:93–146.52. Hawker CJ, Wooley KL. The convergence of synthetic organic and polymer chemistries. Science 2005;309:1200–5.53. Lutz JF, Ouchi M, Liu DR, Sawamoto M. Sequence-controlled polymers. Science 2013;341:628–36.54. Xu JT, Jung K, Atme A, Shanmugam S, Boyer C. A Robust and Versatile Photoinduced Living Polymerization of Conjugated and Unconjugated Monomers and Its Oxygen Tolerance. J Am Chem Soc 2014 Apr 9;136(14):5508–19. doi: 10.1021/ja501745g. Epub 2014 Apr 1.55. Gody G, Maschmeyer T, Zetterlund PB, Perrier S. Rapid and quantitative one-pot synthesis of sequence-controlled polymers by radical polymerization. Nat Commun 2013;4:2505. doi: 10.1038/ncomms3505.56. Gutekunst WR, Hawker CJ. A general approach to sequence-controlled polymers using macrocyclic ring opening metathesis polymerization. J Am Chem Soc 2015 Jul 1;137(25):8038–41. doi: 10.1021/jacs.5b04940. Epub 2015 Jun 23.57. Leibfarth FA, Johnson JA, Jamison TF. Scalable synthesis of sequence-defi ned, unimolecular macromolecules by Flow-IEG. PNAS Aug. 25, 2015 112 (34) 10617–10622. published ahead of print Aug. 12, 2015. doi.org/10.1073/pnas.1508599112.58. Nakatani K, Ogura Y, Koda Y, Terashima T, Sawamoto M. Sequence-regulated copolymers via tandem catalysis of living radical polymerization and in situ transesterifi cation. J Am Chem Soc 2012 Mar 7;134(9):4373–83. doi: 10.1021/ja211436n. Epub 2012 Feb 24.59. Zhang Z, You YZ, Wu DC, Hong CY. Syntheses of sequence-controlled polymers via consecutive multicomponent reactions. Macromolecules 2015;48:3414–21.60. Patton DL, Page KA, Hoff EA, Fasolka MJ, Beers KL. A robust and high-throughput measurement platform for monomer reactivity ratios from surface-initiated polymerization. Polym Chem 2012;3:1174–81.61. Srichan S, Kayunkid N, Oswald L, Lotz B, Lutz JF. Synthesis and characterization of sequence-controlled semicrystalline comb copolymers: Infl uence of primary structure on materials properties. Macromolecules 2014;47:1570–7.62. Willemse RXE, van Herk AM. Copolymerization kinetics of methyl methacrylate-styrene obtained by PLP-MALDI-ToF-MS. J Am Chem Soc 2006;128:4471–80.63. Andrzejewska E. Photopolymerization kinetics of multifunctional monomers. Prog Polym Sci 2001;26:605–65.
64. Anseth KS, Wang CM, Bowman CN. Kinetic evidence of reaction-diff usion during the polymerization of multi(meth)acrylate monomers. Macromolecules 1994;27:650–5.65. Cook WD. Photopolymerization kinetics of dimethacrylates using the camphorquinone amine initiator system. Polymer 1992;33:600–9.66. Coote ML, Johnston LPM, Davis TP. Copolymerization propagation kinetics of styrene and methyl methacrylate-revisited. 2. Kinetic analysis. Macromolecules 1997;30:8191–204.67. Roy RK, Lutz JF. Compartmentalization of single polymer chains by stepwise intramolecular cross-linking of sequence-controlled macromolecules. J Am Chem Soc 2014;136:12888–91.68. Papakonstantinou AE, Eliades T, Cellesi F, Watts DC, Silikas N. Evaluation of UDMA’s potential as a substitute for Bis-GMA in orthodontic adhesives. Dent Mater 2013 Aug;29(8):898–905. doi: 10.1016/j.dental.2013.05.007. Epub 2013 Jun 17.69. Sideridou I, Tserki V, Papanastasiou G. Eff ect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials 2002;23:1819–29.70. Denizli BK, Lutz JF, Okrasa L, Pakula T, Guner A, Matyjaszewski K. Properties of well-defi ned alternating and random copolymers of methacrylates and styrene prepared by controlled/living radical polymerization. J Polym Sci Pol Chem 2005;43:3440–6.71. Kuo JF, Chen CY. Studies on the radical chain copolymerizaiton of mehtyl-methacrylate and styrene at their azeotropic composition. Macromolecules 1981;14:335–9.72. Schroeder WF, Aranguren MI, Borrajo J. Reactivity Ratios and Copolymer Composition Evolution During Styrene/Dimethacrylate Free-Radical Crosslinking Copolymerization. J Appl Polym Sci 2010;115:3081–91.73. Scott TF, Cook WD, Forsythe JS. Eff ect of the degree of cure on the viscoelastic properties of vinyl ester resins. Eur Polym J 2008;44:3200–12.74. Scott TF, Cook WD, Forsythe JS, Bowman CN, Berchtold KA. FTIR and ESR spectroscopic studies of the photopolymerization of vinyl ester resins. Macromolecules 2003;36:6066–74.75. Dry C. Procedures developed for self-repair of polymer matrix composite materials. Compos Struct 1996;35:263–9.76. Hillewaere XKD, Du Prez FE. Fifteen chemistries for autonomous external self-healing polymers and composites. Prog Polym Sci 2015;49-50:121–53.77. Zhu DY, Rong MZ, Zhang MQ. Self-healing polymeric materials based on microencapsulated healing agents: From design to preparation. Prog Polym Sci 2015;49-50:175–220.78. Lehn JM. Perspectives in Chemistry-Aspects of Adaptive Chemistry and Materials. Angew Chem Int Ed Engl 2015 Mar 9;54(11):3276–89. doi: 10.1002/anie.201409399. Epub 2015 Jan 12.79. Van Tittelboom K, De Belie N. Self-Healing in Cementitious Materials — A Review. Materials (Basel) 2013 May 27;6(6):2182–2217. doi: 10.3390/ma6062182.80. Jones AS, Rule JD, Moore JS, Sottos NR, White SR. Life extension of self-healing polymers with rapidly growing fatigue cracks. J R Soc Interface 2007;4:395–403.81. Jones AS, Rule JD, Moore JS, White SR, Sottos NR. Catalyst morphology and dissolution kinetics of self-healing polymers. Chem Mat 2006;18:1312–7.82. Aissa B, Therriault D, Haddad E, Jamroz W. Self-Healing Materials Systems: Overview of Major Approaches and Recent
Developed Technologies. Adv Mater Sci Eng 2012.83. Mauldin TC, Kessler MR. Self-healing polymers and composites. Int Mater Rev 2010;55:317–46.84. Olugebefola SC, Aragon AM, Hansen CJ, Hamilton AR, Kozola BD, Wu W, et al. Polymer Microvascular Network Composites. J Compos Mater 2010;44:2587–603.85. Lohbauer U. Dental glass ionomer cements as permanent fi lling materials? Properties, limitations and future trends. Materials (Basel) 2010;3:76–96.86. Wilson AD, Kent BE. New translucent cement for dentistry-glass ionomer cement. Br Dent J 1972;132:133–5.87. Wilson AD, Nicholson JW. Polyalkenoate cements. Chem Solid State Mater 1993;3:90–196.88. Yahyazadehfar M, Huyang G, Wang X, Fan Y, Arola D, Sun J. Durability of self-healing dental composites: A comparison of performance under monotonic and cyclic loading. Mater Sci Eng C 2018;93:1020–6.89. Levin-Reisman I, Ronin I, Gefen O, Braniss I, Shoresh N, Balaban NQ. Antibiotic tolerance facilitates the evolution of resistance. Science 2017;355:826–30.90. Harms A, Maisonneuve E, Gerdes K. Mechanisms of bacterial persistence during stress and antibiotic exposure. Science 2016;354:9.91. Hurdle JG, O’Neill AJ, Chopra I, Lee RE. Targeting bacterial membrane function: An underexploited mechanism for treating persistent infections. Nat Rev Microbiol 2011;9:62–75.92. Clatworthy AE, Pierson E, Hung DT. Targeting virulence: A new paradigm for antimicrobial therapy. Nat Chem Biol 2007;3:541–8.93. Buffi e CG, Bucci V, Stein RR, McKenney PT, Ling LL, Gobourne A, et al. Precision microbiome reconstitution restores bile acid mediated resistance to Clostridium diffi cile. Nature 2015;517:4.94. Hancock REW, Sahl HG. Antimicrobial and host-defense peptides as new anti-infective therapeutic strategies. Nat Biotechnol 2006;24:1551–7.95. Velema WA, van der Berg JP, Szymanski W, Driessen AJM, Feringa B. Orthogonal Control of Antibacterial Activity with Light. ACS Chem Biol 2014;9:1969–74.96. Velema WA, van der Berg JP, Hansen MJ, Szymanski W, Driessen AJM, Feringa BL. Optical control of antibacterial activity. Nat Chem 2013;5:924–8.97. Velema WA, Szymanski W, Feringa BL. Photopharmacology: Beyond Proof of Principle. J Am Chem Soc 2014 Feb 12;136(6):2178–91. doi: 10.1021/ja413063e. Epub 2014 Feb 4.98. Bai HT, Yuan HX, Nie CY, Wang B, Lv FT, Liu LB, et al. A Supramolecular Antibiotic Switch for Antibacterial Regulation. Angew Chem Int Ed Engl 2015 Nov 2;54(45):13208–13. doi: 10.1002/anie.201504566. Epub 2015 Aug 26.99. Qian WJ, Texter J, Yan F. Frontiers in poly(ionic liquid)s: syntheses and applications. Chem Soc Rev 2017;46:1124-59.100. Li L, He J, Eckert R, Yarbrough D, Lux R, Anderson M, et al. Design and characterization of an acid-activated antimicrobial peptide. Chem Biol Drug Des 2010;75:127–32.101. Guo LH, McLean JS, Yang Y, Eckert R, Kaplan CW, Kyme P, et al. Precision-guided antimicrobial peptide as a targeted modulator of human microbial ecology. Proc Natl Acad Sci U S A 2015 Jun 16;112(24):7569-74. doi: 10.1073/pnas.1506207112. Epub 2015 Jun 1.
THE CORRESPONDING AUTHOR, Jurin Sun, PhD, can be reached at [email protected].
b i o m a t e r i a l s

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 337
r o o t r e s o r p t i o n
AUTHOR
Rodrigo F. Viecilli, DDS, PhD, is an adjunct associate professor in the department of orthodontics and the director of the Craniofacial Biomechanics Laboratory at the Loma Linda University School of Dentistry. He also maintains a private practice in Fort Worth, Texas.Confl ict of Interest Disclosure: None reported.
Mechanotransduction of Orthodontic External Root Resorption (OERR)Rodrigo F. Viecilli, DDS, PhD
ABSTR ACT The objective of this article is to clarify the current scientifi c outlook of orthodontic external root resorption. Although it is known that hormonal and traumatic factors can infl uence root resorption independently of orthodontic treatment, our focus is on the role of mechanical factors and subsequent infl ammation and how the latter varies with individual genetic background.
What we discuss here pertains to the following clinical scenario: An orthodontic patient
comes to your offi ce and you observe exaggerated root resorption on a few teeth being moved. What is the scientifi c rationale necessary to understand this phenomenon? Is this an idiopathic fi nding? Could anything related to current treatment be attributed as cause? Is it simply a genetic predisposition?
Moderate root length loss due to orthodontic external root resorption (OERR) (> 3 mm) occurs in more than 25% of individuals.1 It can result in compromised prosthetic support, mobility, a reduced tooth lifespan, low tolerance of mechanical trauma and even tooth loss.2–5 Around 5% of orthodontic patients undergo severe OERR of over 5 mm during treatment.6,7 Histology shows that periodontal ligament (PDL) necrosis occurs near areas of high damage.8,9 Most
of these studies underestimate OERR due to 2D radiographic limitations.10
Therefore, the problem is likely more severe than reported. OERR is the most important iatrogenic and legal concern in orthodontic treatment.6,7,11–15 This is evidenced by both scientifi c literature and online attorney advertisements directed at patients. OERR produces 6% of dental malpractice claims, according to a recent survey. Of those claims, 70% include general dentists and 30% include orthodontists.11 Although dentists and orthodontists have argued that scientifi c evidence to support OERR prevention is lacking,16 this has not prevented payment of up to $1 million in damages.17
Although it is generally accepted that “high forces” should be avoided, there is no scientifi c evidence defi ning which load is considered “high,” in part because the biomechanical environment that leads to OERR is unclear.18–20 Unfortunately, there is no established protocol to prevent severe OERR in susceptible
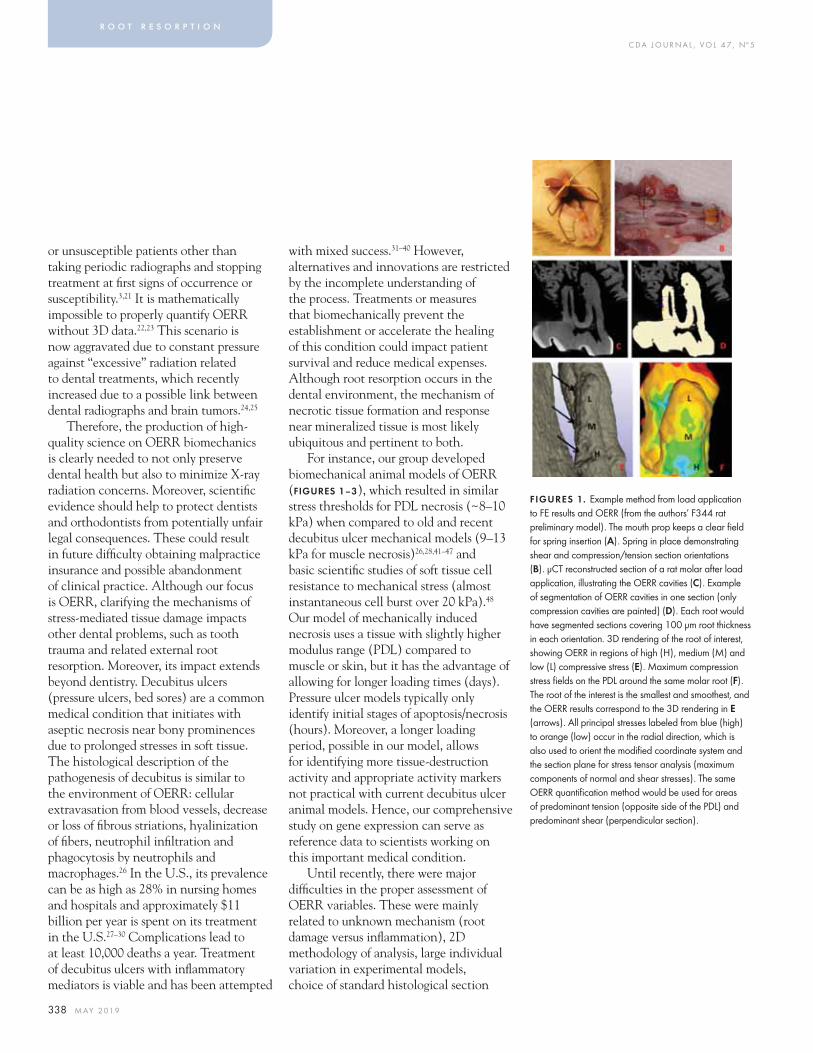
C DA J O U R N A L , V O L 4 7 , Nº 5
338 M AY 2 01 9
or unsusceptible patients other than taking periodic radiographs and stopping treatment at fi rst signs of occurrence or susceptibility.3,21 It is mathematically impossible to properly quantify OERR without 3D data.22,23 This scenario is now aggravated due to constant pressure against “excessive” radiation related to dental treatments, which recently increased due to a possible link between dental radiographs and brain tumors.24,25
Therefore, the production of high-quality science on OERR biomechanics is clearly needed to not only preserve dental health but also to minimize X-ray radiation concerns. Moreover, scientifi c evidence should help to protect dentists and orthodontists from potentially unfair legal consequences. These could result in future diffi culty obtaining malpractice insurance and possible abandonment of clinical practice. Although our focus is OERR, clarifying the mechanisms of stress-mediated tissue damage impacts other dental problems, such as tooth trauma and related external root resorption. Moreover, its impact extends beyond dentistry. Decubitus ulcers (pressure ulcers, bed sores) are a common medical condition that initiates with aseptic necrosis near bony prominences due to prolonged stresses in soft tissue. The histological description of the pathogenesis of decubitus is similar to the environment of OERR: cellular extravasation from blood vessels, decrease or loss of fi brous striations, hyalinization of fi bers, neutrophil infi ltration and phagocytosis by neutrophils and macrophages.26 In the U.S., its prevalence can be as high as 28% in nursing homes and hospitals and approximately $11 billion per year is spent on its treatment in the U.S.27–30 Complications lead to at least 10,000 deaths a year. Treatment of decubitus ulcers with infl ammatory mediators is viable and has been attempted
with mixed success.31–40 However, alternatives and innovations are restricted by the incomplete understanding of the process. Treatments or measures that biomechanically prevent the establishment or accelerate the healing of this condition could impact patient survival and reduce medical expenses. Although root resorption occurs in the dental environment, the mechanism of necrotic tissue formation and response near mineralized tissue is most likely ubiquitous and pertinent to both.
For instance, our group developed biomechanical animal models of OERR (FIGURES 1–3), which resulted in similar stress thresholds for PDL necrosis (~8–10 kPa) when compared to old and recent decubitus ulcer mechanical models (9–13 kPa for muscle necrosis)26,28,41–47 and basic scientifi c studies of soft tissue cell resistance to mechanical stress (almost instantaneous cell burst over 20 kPa).48 Our model of mechanically induced necrosis uses a tissue with slightly higher modulus range (PDL) compared to muscle or skin, but it has the advantage of allowing for longer loading times (days). Pressure ulcer models typically only identify initial stages of apoptosis/necrosis (hours). Moreover, a longer loading period, possible in our model, allows for identifying more tissue-destruction activity and appropriate activity markers not practical with current decubitus ulcer animal models. Hence, our comprehensive study on gene expression can serve as reference data to scientists working on this important medical condition.
Until recently, there were major diffi culties in the proper assessment of OERR variables. These were mainly related to unknown mechanism (root damage versus infl ammation), 2D methodology of analysis, large individual variation in experimental models, choice of standard histological section
r o o t r e s o r p t i o n
FIGURES 1. Example method from load application to FE results and OERR (from the authors’ F344 rat preliminary model). The mouth prop keeps a clear fi eld for spring insertion (A). Spring in place demonstrating shear and compression/tension section orientations (B). μCT reconstructed section of a rat molar after load application, illustrating the OERR cavities (C). Example of segmentation of OERR cavities in one section (only compression cavities are painted) (D). Each root would have segmented sections covering 100 μm root thickness in each orientation. 3D rendering of the root of interest, showing OERR in regions of high (H), medium (M) and low (L) compressive stress (E). Maximum compression stress fi elds on the PDL around the same molar root (F). The root of the interest is the smallest and smoothest, and the OERR results correspond to the 3D rendering in E (arrows). All principal stresses labeled from blue (high) to orange (low) occur in the radial direction, which is also used to orient the modifi ed coordinate system and the section plane for stress tensor analysis (maximum components of normal and shear stresses). The same OERR quantifi cation method would be used for areas of predominant tension (opposite side of the PDL) and predominant shear (perpendicular section).
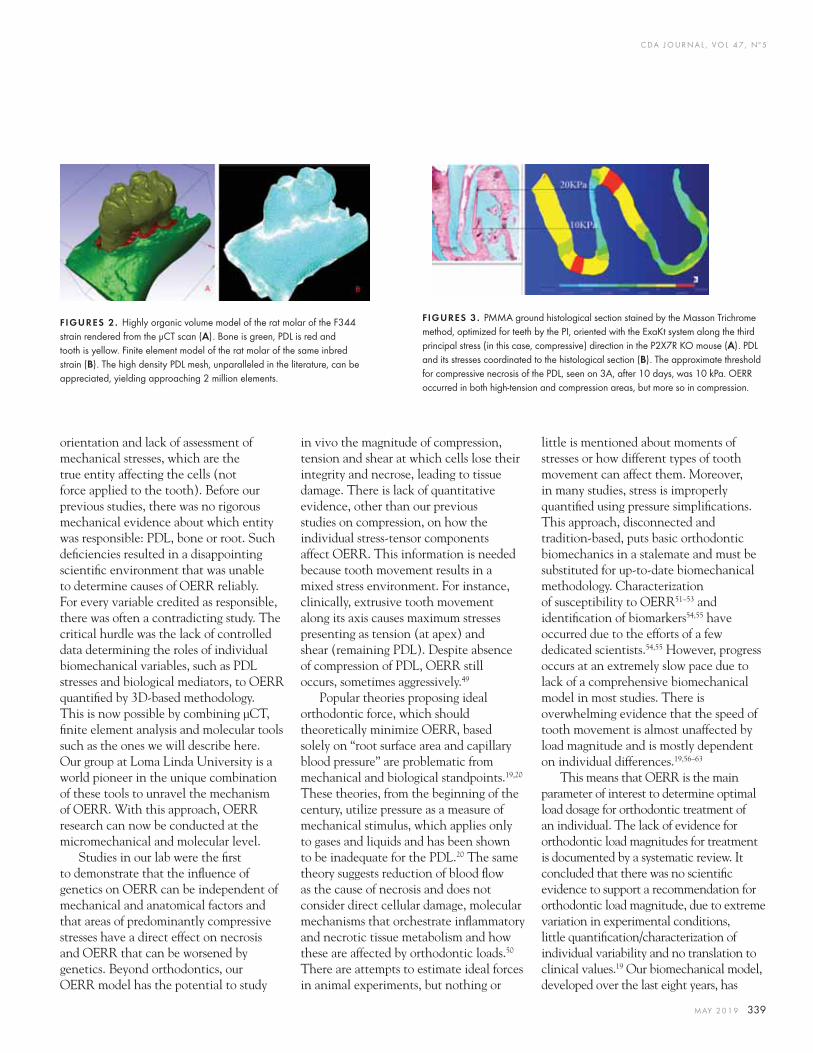
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 339
orientation and lack of assessment of mechanical stresses, which are the true entity affecting the cells (not force applied to the tooth). Before our previous studies, there was no rigorous mechanical evidence about which entity was responsible: PDL, bone or root. Such defi ciencies resulted in a disappointing scientifi c environment that was unable to determine causes of OERR reliably. For every variable credited as responsible, there was often a contradicting study. The critical hurdle was the lack of controlled data determining the roles of individual biomechanical variables, such as PDL stresses and biological mediators, to OERR quantifi ed by 3D-based methodology. This is now possible by combining μCT, fi nite element analysis and molecular tools such as the ones we will describe here. Our group at Loma Linda University is a world pioneer in the unique combination of these tools to unravel the mechanism of OERR. With this approach, OERR research can now be conducted at the micromechanical and molecular level.
Studies in our lab were the fi rst to demonstrate that the infl uence of genetics on OERR can be independent of mechanical and anatomical factors and that areas of predominantly compressive stresses have a direct effect on necrosis and OERR that can be worsened by genetics. Beyond orthodontics, our OERR model has the potential to study
in vivo the magnitude of compression, tension and shear at which cells lose their integrity and necrose, leading to tissue damage. There is lack of quantitative evidence, other than our previous studies on compression, on how the individual stress-tensor components affect OERR. This information is needed because tooth movement results in a mixed stress environment. For instance, clinically, extrusive tooth movement along its axis causes maximum stresses presenting as tension (at apex) and shear (remaining PDL). Despite absence of compression of PDL, OERR still occurs, sometimes aggressively.49
Popular theories proposing ideal orthodontic force, which should theoretically minimize OERR, based solely on “root surface area and capillary blood pressure” are problematic from mechanical and biological standpoints.19,20 These theories, from the beginning of the century, utilize pressure as a measure of mechanical stimulus, which applies only to gases and liquids and has been shown to be inadequate for the PDL.20 The same theory suggests reduction of blood fl ow as the cause of necrosis and does not consider direct cellular damage, molecular mechanisms that orchestrate infl ammatory and necrotic tissue metabolism and how these are affected by orthodontic loads.50 There are attempts to estimate ideal forces in animal experiments, but nothing or
little is mentioned about moments of stresses or how different types of tooth movement can affect them. Moreover, in many studies, stress is improperly quantifi ed using pressure simplifi cations. This approach, disconnected and tradition-based, puts basic orthodontic biomechanics in a stalemate and must be substituted for up-to-date biomechanical methodology. Characterization of susceptibility to OERR51–53 and identifi cation of biomarkers54,55 have occurred due to the efforts of a few dedicated scientists.54,55 However, progress occurs at an extremely slow pace due to lack of a comprehensive biomechanical model in most studies. There is overwhelming evidence that the speed of tooth movement is almost unaffected by load magnitude and is mostly dependent on individual differences.19,56–63
This means that OERR is the main parameter of interest to determine optimal load dosage for orthodontic treatment of an individual. The lack of evidence for orthodontic load magnitudes for treatment is documented by a systematic review. It concluded that there was no scientifi c evidence to support a recommendation for orthodontic load magnitude, due to extreme variation in experimental conditions, little quantifi cation/characterization of individual variability and no translation to clinical values.19 Our biomechanical model, developed over the last eight years, has
FIGURES 2. Highly organic volume model of the rat molar of the F344 strain rendered from the μCT scan (A). Bone is green, PDL is red and tooth is yellow. Finite element model of the rat molar of the same inbred strain (B). The high density PDL mesh, unparalleled in the literature, can be appreciated, yielding approaching 2 million elements.
FIGURES 3. PMMA ground histological section stained by the Masson Trichrome method, optimized for teeth by the PI, oriented with the ExaKt system along the third principal stress (in this case, compressive) direction in the P2X7R KO mouse (A). PDL and its stresses coordinated to the histological section (B). The approximate threshold for compressive necrosis of the PDL, seen on 3A, after 10 days, was 10 kPa. OERR occurred in both high-tension and compression areas, but more so in compression.
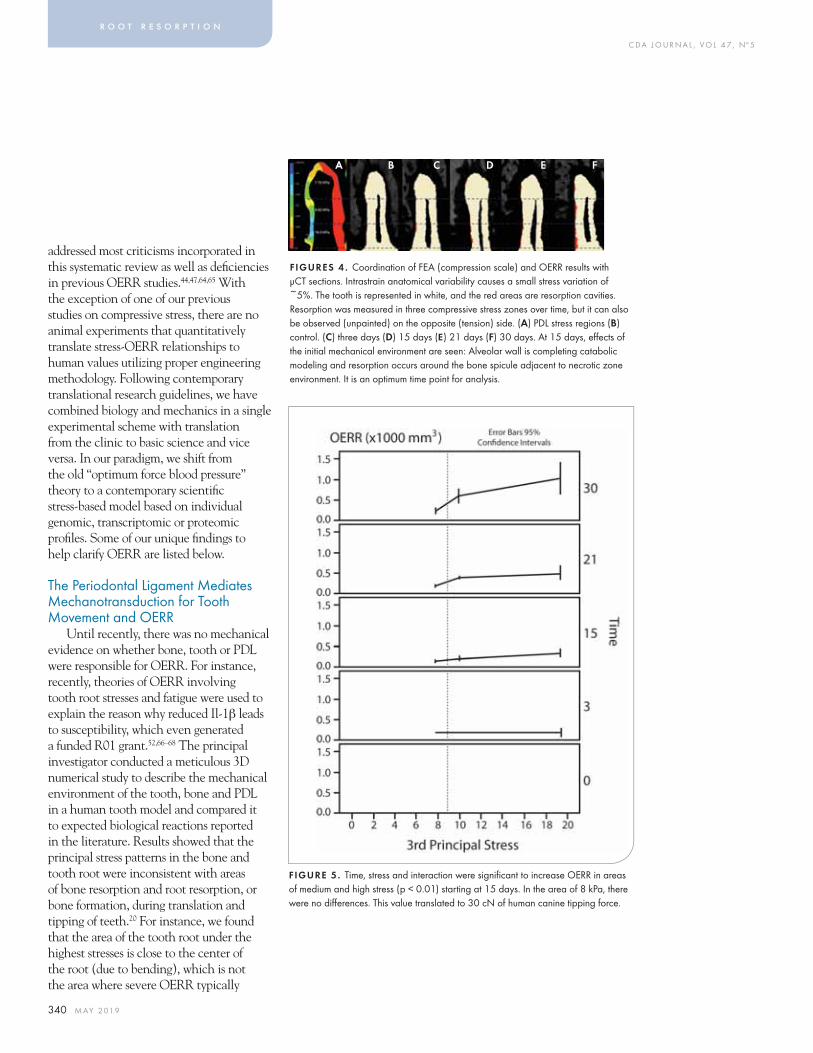
C DA J O U R N A L , V O L 4 7 , Nº 5
340 M AY 2 01 9
addressed most criticisms incorporated in this systematic review as well as defi ciencies in previous OERR studies.44,47,64,65 With the exception of one of our previous studies on compressive stress, there are no animal experiments that quantitatively translate stress-OERR relationships to human values utilizing proper engineering methodology. Following contemporary translational research guidelines, we have combined biology and mechanics in a single experimental scheme with translation from the clinic to basic science and vice versa. In our paradigm, we shift from the old “optimum force blood pressure” theory to a contemporary scientifi c stress-based model based on individual genomic, transcriptomic or proteomic profi les. Some of our unique fi ndings to help clarify OERR are listed below.
The Periodontal Ligament Mediates Mechanotransduction for Tooth Movement and OERR
Until recently, there was no mechanical evidence on whether bone, tooth or PDL were responsible for OERR. For instance, recently, theories of OERR involving tooth root stresses and fatigue were used to explain the reason why reduced Il-1β leads to susceptibility, which even generated a funded R01 grant.52,66–68 The principal investigator conducted a meticulous 3D numerical study to describe the mechanical environment of the tooth, bone and PDL in a human tooth model and compared it to expected biological reactions reported in the literature. Results showed that the principal stress patterns in the bone and tooth root were inconsistent with areas of bone resorption and root resorption, or bone formation, during translation and tipping of teeth.20 For instance, we found that the area of the tooth root under the highest stresses is close to the center of the root (due to bending), which is not the area where severe OERR typically
r o o t r e s o r p t i o n
FIGURES 4 . Coordination of FEA (compression scale) and OERR results with μCT sections. Intrastrain anatomical variability causes a small stress variation of ~5%. The tooth is represented in white, and the red areas are resorption cavities. Resorption was measured in three compressive stress zones over time, but it can also be observed (unpainted) on the opposite (tension) side. (A) PDL stress regions (B) control. (C) three days (D) 15 days (E) 21 days (F) 30 days. At 15 days, eff ects of the initial mechanical environment are seen: Alveolar wall is completing catabolic modeling and resorption occurs around the bone spicule adjacent to necrotic zone environment. It is an optimum time point for analysis.
FIGURE 5. Time, stress and interaction were signifi cant to increase OERR in areas of medium and high stress (p < 0.01) starting at 15 days. In the area of 8 kPa, there were no diff erences. This value translated to 30 cN of human canine tipping force.
A B C D E F

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 341
occurs. A similar contradiction was found in bone. The PDL was the only tissue where the highest stresses were perfectly related to bone and root resorption. With animal experiments, we later demonstrated with certainty that OERR mechanotransduction starts in the PDL.
PDL Necrosis and OERR Are Related and the PDL Compressive Stress Magnitudes
An animal model was used to validate our numerical fi ndings and pursue causes for individual differences. The method was to coordinate histology, μCT and FEA. This allowed for relating the mechanical environment directly to the biological response. Histology at this time was required to confi rm data due to a limited resolution of the μCT. This is no longer an issue with the newer generation of μCTs. We showed that aggressive OERR occurs near highly compressive zones. There were strong (p < 0.001) signifi cant differences, up to fourfold, in the incidence of OERR in the higher compressive PDL stress regions compared to low-stress regions. Interestingly, OERR was not different from baseline in areas of low stress, independently of mouse genetic background. From the histology, we approximated the stress threshold for
necrosis at ~10 kPa. These values are within 3 kPa of the medical literature relating stress to necrosis in decubitus ulcer models and to cell viability in vitro studies.26,41,44,46–48,69 Using our human FE model, we determined that PDL stresses < 10 kPa are produced by < 40cN of MD tipping or < 120cN MD translation. Innovatively, these data provided quantitative and translatable evidence on how “high” PDL stresses and force must be to cause substantial OERR.
Impairment of the ATP-P2X7-Il-1β Pathway Conditionally Increases OERR According to Compressive Stress
Clinical studies demonstrated that a polymorphism in the Il-1β gene that leads to its reduced gene expression increases OERR.52 This result was confi rmed with an Il1-β knockout mouse.66 We were able to test the mechanism by reducing Il-1β activation (NALP3 infl ammasome pathway) inactivating the P2X7R gene (P2X7R KO mouse). The P2X7R is a calcium channel ATP (DAMP) receptor that promotes a pathway for Il1-β activation and is important for apoptotic/necrotic tissue resorption. An ineffi cient acute response to eliminate dying cells early can lead to massive macrophage infi ltration and generalized tissue damage.50,64,65,70,71 The KO had a much slower rate of hyalinized tissue resorption and increased OERR. OERR was increased by at least ~20%, measured by 3D μCT. With histology and section orientations coordinated with our FE model, we determined that there was a signifi cant difference only in the region of the highest PDL stress, with 27% more (P < 0.02) root resorption craters in the KO mice.53 Ten days after the force was applied, the KO mice had about eight times more (p < 0.001) necrotic PDL than the WT mice. For the WT force group, ERR was 1.8 times higher (P < 0.002) and 3.7 times
higher (p < 0.001) in the area of high stress compared with medium and low stress, respectively. A similar pattern was noted for the KO force group: respective scores were 4.7 times (P < 0.001) and 3.5 times (p < 0.002) higher. Histopathological analysis of the trichrome-stained specimens revealed strong chronic infl ammatory cell accumulation near severe OERR zones, especially in the P2X7R KO.
Stress and Time Eff ects on Bone and OERR in the Rat Model
A preliminary study on 42 rats was conducted to determine the best time point to perform our experiments. We used the F344 as a “reference” strain for this purpose (FIGURES 4–6), applying a 10cN load from three to 30 days to study changes in bone and root resorption with μCT and TRAP immunohistochemistry. At 15 days, the resorption of the initial necrotic tissue was nearing completion (evidenced by bone spiculae near the alveolar crest) with presence of active OERR. After 21 days, a new hyalinization zone formed near the middle portion of the root due to a change in the mechanical environment caused by a change in alveolar height.
ConclusionsCurrent science suggests that when
encountering a patient with isolated root resorption during orthodontic treatment, possible mechanical causes of overloading should be investigated and minimized. When these are not substantiated, the dentist should inform the patient of possible susceptibility and provide the patient the choice to continue treatment under careful minimization of loads and periodical radiographic monitoring. It is already possible to test patients for susceptibility before treatment is started, but only a few genes have so far been determined to be signifi cant and testing negative doesn’t imply the patient is safe. ■
FIGURES 6 . MB root PDL sections with compression near the apex and high compression near the alveolar crest. R = root, B = bone, H = hyalinization, UR = undermining resorption, DR = direct resorption. (A) TRAP IHC revealed OERR mostly in the high-stress zone. The alveolar crest was resorbed by 30% (B) and (C). Consecutive sections of a 15-day specimen showing active resorption of mineralized and necrotic tissue (H). Osteoclasts (OC) perform direct resorption at the low-stress zone with no root resorption. Necrosis is present in the high-stress zone at three days, but at 15 days, its resorption is close to completion. There is presence of chronic infl ammatory infi ltrate and active root resorption.
A B C
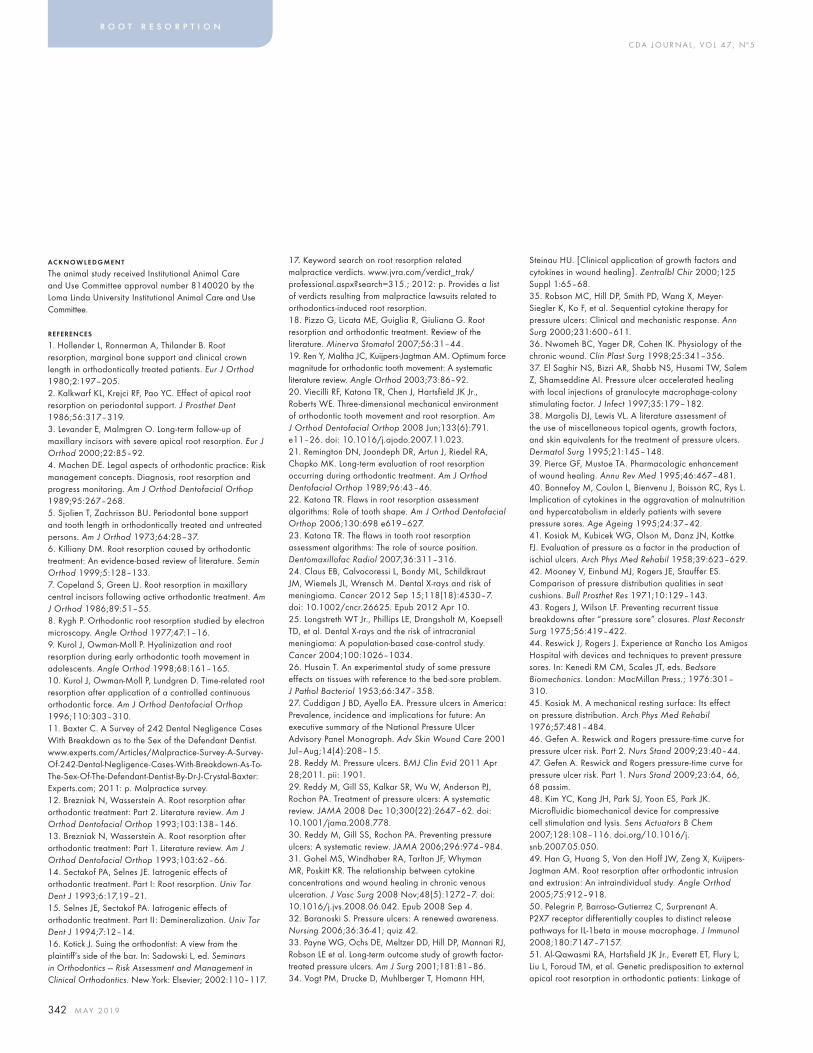
C DA J O U R N A L , V O L 4 7 , Nº 5
342 M AY 2 01 9
AC KNOWLEDGMENT
The animal study received Institutional Animal Care and Use Committee approval number 8140020 by the Loma Linda University Institutional Animal Care and Use Committee.
REFERENCES
1. Hollender L, Ronnerman A, Thilander B. Root resorption, marginal bone support and clinical crown length in orthodontically treated patients. Eur J Orthod 1980;2:197–205.2. Kalkwarf KL, Krejci RF, Pao YC. Effect of apical root resorption on periodontal support. J Prosthet Dent 1986;56:317–319.3. Levander E, Malmgren O. Long-term follow-up of maxillary incisors with severe apical root resorption. Eur J Orthod 2000;22:85–92.4. Machen DE. Legal aspects of orthodontic practice: Risk management concepts. Diagnosis, root resorption and progress monitoring. Am J Orthod Dentofacial Orthop 1989;95:267–268.5. Sjolien T, Zachrisson BU. Periodontal bone support and tooth length in orthodontically treated and untreated persons. Am J Orthod 1973;64:28–37.6. Killiany DM. Root resorption caused by orthodontic treatment: An evidence-based review of literature. Semin Orthod 1999;5:128–133.7. Copeland S, Green LJ. Root resorption in maxillary central incisors following active orthodontic treatment. Am J Orthod 1986;89:51–55.8. Rygh P. Orthodontic root resorption studied by electron microscopy. Angle Orthod 1977;47:1–16.9. Kurol J, Owman-Moll P. Hyalinization and root resorption during early orthodontic tooth movement in adolescents. Angle Orthod 1998;68:161–165.10. Kurol J, Owman-Moll P, Lundgren D. Time-related root resorption after application of a controlled continuous orthodontic force. Am J Orthod Dentofacial Orthop 1996;110:303–310.11. Baxter C. A Survey of 242 Dental Negligence Cases With Breakdown as to the Sex of the Defendant Dentist. www.experts.com/Articles/Malpractice-Survey-A-Survey-Of-242-Dental-Negligence-Cases-With-Breakdown-As-To-The-Sex-Of-The-Defendant-Dentist-By-Dr-J-Crystal-Baxter: Experts.com; 2011: p. Malpractice survey.12. Brezniak N, Wasserstein A. Root resorption after orthodontic treatment: Part 2. Literature review. Am J Orthod Dentofacial Orthop 1993;103:138–146.13. Brezniak N, Wasserstein A. Root resorption after orthodontic treatment: Part 1. Literature review. Am J Orthod Dentofacial Orthop 1993;103:62–66.14. Sectakof PA, Selnes JE. Iatrogenic effects of orthodontic treatment. Part I: Root resorption. Univ Tor Dent J 1993;6:17,19–21.15. Selnes JE, Sectakof PA. Iatrogenic effects of orthodontic treatment. Part II: Demineralization. Univ Tor Dent J 1994;7:12–14.16. Kotick J. Suing the orthodontist: A view from the plaintiff ’s side of the bar. In: Sadowski L, ed. Seminars in Orthodontics — Risk Assessment and Management in Clinical Orthodontics. New York: Elsevier; 2002:110–117.
17. Keyword search on root resorption related malpractice verdicts. www.jvra.com/verdict_trak/professional.aspx?search=315.; 2012: p. Provides a list of verdicts resulting from malpractice lawsuits related to orthodontics-induced root resorption.18. Pizzo G, Licata ME, Guiglia R, Giuliana G. Root resorption and orthodontic treatment. Review of the literature. Minerva Stomatol 2007;56:31–44.19. Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: A systematic literature review. Angle Orthod 2003;73:86–92.20. Viecilli RF, Katona TR, Chen J, Hartsfield JK Jr., Roberts WE. Three-dimensional mechanical environment of orthodontic tooth movement and root resorption. Am J Orthod Dentofacial Orthop 2008 Jun;133(6):791.e11–26. doi: 10.1016/j.ajodo.2007.11.023.21. Remington DN, Joondeph DR, Artun J, Riedel RA, Chapko MK. Long-term evaluation of root resorption occurring during orthodontic treatment. Am J Orthod Dentofacial Orthop 1989;96:43–46.22. Katona TR. Flaws in root resorption assessment algorithms: Role of tooth shape. Am J Orthod Dentofacial Orthop 2006;130:698 e619–627.23. Katona TR. The flaws in tooth root resorption assessment algorithms: The role of source position. Dentomaxillofac Radiol 2007;36:311–316.24. Claus EB, Calvocoressi L, Bondy ML, Schildkraut JM, Wiemels JL, Wrensch M. Dental X-rays and risk of meningioma. Cancer 2012 Sep 15;118(18):4530–7. doi: 10.1002/cncr.26625. Epub 2012 Apr 10.25. Longstreth WT Jr., Phillips LE, Drangsholt M, Koepsell TD, et al. Dental X-rays and the risk of intracranial meningioma: A population-based case-control study. Cancer 2004;100:1026–1034.26. Husain T. An experimental study of some pressure effects on tissues with reference to the bed-sore problem. J Pathol Bacteriol 1953;66:347–358.27. Cuddigan J BD, Ayello EA. Pressure ulcers in America: Prevalence, incidence and implications for future: An executive summary of the National Pressure Ulcer Advisory Panel Monograph. Adv Skin Wound Care 2001 Jul–Aug;14(4):208–15.28. Reddy M. Pressure ulcers. BMJ Clin Evid 2011 Apr 28;2011. pii: 1901.29. Reddy M, Gill SS, Kalkar SR, Wu W, Anderson PJ, Rochon PA. Treatment of pressure ulcers: A systematic review. JAMA 2008 Dec 10;300(22):2647–62. doi: 10.1001/jama.2008.778.30. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: A systematic review. JAMA 2006;296:974–984.31. Gohel MS, Windhaber RA, Tarlton JF, Whyman MR, Poskitt KR. The relationship between cytokine concentrations and wound healing in chronic venous ulceration. J Vasc Surg 2008 Nov;48(5):1272–7. doi: 10.1016/j.jvs.2008.06.042. Epub 2008 Sep 4.32. Baranoski S. Pressure ulcers: A renewed awareness. Nursing 2006;36:36-41; quiz 42.33. Payne WG, Ochs DE, Meltzer DD, Hill DP, Mannari RJ, Robson LE et al. Long-term outcome study of growth factor-treated pressure ulcers. Am J Surg 2001;181:81–86.34. Vogt PM, Drucke D, Muhlberger T, Homann HH,
Steinau HU. [Clinical application of growth factors and cytokines in wound healing]. Zentralbl Chir 2000;125 Suppl 1:65–68.35. Robson MC, Hill DP, Smith PD, Wang X, Meyer-Siegler K, Ko F, et al. Sequential cytokine therapy for pressure ulcers: Clinical and mechanistic response. Ann Surg 2000;231:600–611.36. Nwomeh BC, Yager DR, Cohen IK. Physiology of the chronic wound. Clin Plast Surg 1998;25:341–356.37. El Saghir NS, Bizri AR, Shabb NS, Husami TW, Salem Z, Shamseddine AI. Pressure ulcer accelerated healing with local injections of granulocyte macrophage-colony stimulating factor. J Infect 1997;35:179–182.38. Margolis DJ, Lewis VL. A literature assessment of the use of miscellaneous topical agents, growth factors, and skin equivalents for the treatment of pressure ulcers. Dermatol Surg 1995;21:145–148.39. Pierce GF, Mustoe TA. Pharmacologic enhancement of wound healing. Annu Rev Med 1995;46:467–481.40. Bonnefoy M, Coulon L, Bienvenu J, Boisson RC, Rys L. Implication of cytokines in the aggravation of malnutrition and hypercatabolism in elderly patients with severe pressure sores. Age Ageing 1995;24:37–42.41. Kosiak M, Kubicek WG, Olson M, Danz JN, Kottke FJ. Evaluation of pressure as a factor in the production of ischial ulcers. Arch Phys Med Rehabil 1958;39:623–629.42. Mooney V, Einbund MJ, Rogers JE, Stauffer ES. Comparison of pressure distribution qualities in seat cushions. Bull Prosthet Res 1971;10:129–143.43. Rogers J, Wilson LF. Preventing recurrent tissue breakdowns after “pressure sore” closures. Plast Reconstr Surg 1975;56:419–422.44. Reswick J, Rogers J. Experience at Rancho Los Amigos Hospital with devices and techniques to prevent pressure sores. In: Kenedi RM CM, Scales JT, eds. Bedsore Biomechanics. London: MacMillan Press.; 1976:301–310.45. Kosiak M. A mechanical resting surface: Its effect on pressure distribution. Arch Phys Med Rehabil 1976;57:481–484.46. Gefen A. Reswick and Rogers pressure-time curve for pressure ulcer risk. Part 2. Nurs Stand 2009;23:40–44.47. Gefen A. Reswick and Rogers pressure-time curve for pressure ulcer risk. Part 1. Nurs Stand 2009;23:64, 66, 68 passim.48. Kim YC, Kang JH, Park SJ, Yoon ES, Park JK. Microfluidic biomechanical device for compressive cell stimulation and lysis. Sens Actuators B Chem 2007;128:108–116. doi.org/10.1016/j.snb.2007.05.050.49. Han G, Huang S, Von den Hoff JW, Zeng X, Kuijpers-Jagtman AM. Root resorption after orthodontic intrusion and extrusion: An intraindividual study. Angle Orthod 2005;75:912–918.50. Pelegrin P, Barroso-Gutierrez C, Surprenant A. P2X7 receptor differentially couples to distinct release pathways for IL-1beta in mouse macrophage. J Immunol 2008;180:7147–7157.51. Al-Qawasmi RA, Hartsfield JK Jr., Everett ET, Flury L, Liu L, Foroud TM, et al. Genetic predisposition to external apical root resorption in orthodontic patients: Linkage of
r o o t r e s o r p t i o n

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 343
66. Al-Qawasmi RA, Hartsfi eld JK, Hartsfi eld JK Jr., Everett ET, Weaver MR, Foroud TM, et al. Root resorption associated with orthodontic force in IL-1Beta knockout mouse. J Musculoskelet Neuronal Interact 2004;4:383–385.67. Al-Qawasmi RA, Hartsfield JK Jr., Everett ET, Weaver MR, Foroud TM, Faust DM et al. Root resorption associated with orthodontic force in inbred mice: Genetic contributions. Eur J Orthod 2006;28:13–19.68. Abass SK, Hartsfield JK Jr., Al-Qawasmi RA, Everett ET, Foroud TM, Roberts WE. Inheritance of susceptibility to root resorption associated with orthodontic force in mice. Am J Orthod Dentofacial Orthop 2008 Dec;134(6):742–50. doi: 10.1016/j.ajodo.2007.04.035.69. Kosiak M. Etiology of decubitus ulcers. Arch Phys Med Rehabil 1961;42:19–29.70. Barbera-Cremades M, Baroja-Mazo A, Gomez AI, Machado F, Di Virgilio F, Pelegrin P. P2X7 receptor-stimulation causes fever via PGE2 and IL-1beta release. FASEB J 2012 Jul;26(7):2951–62. doi: 10.1096/fj.12-205765. Epub 2012 Apr 6.
71. Pelegrin P. Targeting interleukin-1 signaling in chronic inflammation: Focus on P2X(7) receptor and Pannexin-1. Drug News Perspect 2008 Oct;21(8):424–33. doi: 10.1358/dnp.2008.21.8.1265800.
THE AUTHOR, Rodrigo F. Viecilli, DDS, PhD, can be reached at [email protected].
chromosome-18 marker. J Dent Res 2003;82:356–360.52. Al-Qawasmi RA, Hartsfield JK Jr., Everett ET, Flury L, Liu L, Foroud TM, et al. Genetic predisposition to external apical root resorption. Am J Orthod Dentofacial Orthop 2003;123:242-252.53. Viecilli RF, Katona TR, Chen J, Hartsfield JK Jr., Roberts WE. Orthodontic mechanotransduction and the role of the P2X7 receptor. Am J Orthod Dentofacial Orthop 2009 Jun;135(6):694.e1–16; discussion 694-5. doi: 10.1016/j.ajodo.2008.10.018.54. George A, Evans CA. Detection of root resorption using dentin and bone markers. Orthod Craniofac Res 2009 Aug;12(3):229–35. doi: 10.1111/j.1601-6343.2009.01457.x.55. Balducci L, Ramachandran A, Hao J, Narayanan K, Evans C, George A. Biological markers for evaluation of root resorption. Arch Oral Biol 2007 Mar;52(3):203–8. Epub 2006 Nov 13.56. Van Leeuwen EJ, Kuijpers-Jagtman AM, Von den Hoff JW, Wagener FA, Maltha JC. Rate of orthodontic tooth movement after changing the force magnitude: An experimental study in beagle dogs. Orthod Craniofac Res 2010;13:238–245. doi.org/10.1111/j.1601-6343.2010.01500.x.57. Von Bohl M, Maltha J, Von den Hoff H, Kuijpers-Jagtman AM. Changes in the periodontal ligament after experimental tooth movement using high and low continuous forces in beagle dogs. Angle Orthod 2004;74:16–25.58. van Leeuwen EJ, Maltha JC, Kuijpers-Jagtman AM. Tooth movement with light continuous and discontinuous forces in beagle dogs. Eur J Oral Sci 1999;107:468–474.59. Pilon JJ, Kuijpers-Jagtman AM, Maltha JC. Magnitude of orthodontic forces and rate of bodily tooth movement. An experimental study. Am J Orthod Dentofacial Orthop 1996;110:16–23.60. Iwasaki LR, Chandler JR, Marx DB, Pandey JP, Nickel JC. IL-1 gene polymorphisms, secretion in gingival crevicular fluid and speed of human orthodontic tooth movement. Orthod Craniofac Res 2009 May;12(2):129–40. doi: 10.1111/j.1601-6343.2009.01446.x.61. Iwasaki LR, Gibson CS, Crouch LD, Marx DB, Pandey JP, Nickel JC. Speed of tooth movement is related to stress and IL-1 gene polymorphisms. Am J Orthod Dentofacial Orthop 2006;130:698 e691–699.62. Iwasaki LR, Crouch LD, Tutor A, Gibson S, Hukmani N, Marx DB, et al. Tooth movement and cytokines in gingival crevicular fluid and whole blood in growing and adult subjects. Am J Orthod Dentofacial Orthop 2005;128:483–491.63. Iwasaki LR, Haack JE, Nickel JC, Morton J. Human tooth movement in response to continuous stress of low magnitude. Am J Orthod Dentofacial Orthop 2000;117:175–183.64. Lister MF, Sharkey J, Sawatzky DA, Hodgkiss JP, Davidson DJ, Rossi AG, et al. The role of the purinergic P2X7 receptor in inflammation. J Inflamm (Lond) 2007;4:5.65. Chen L, Brosnan CF. Regulation of immune response by P2X7 receptor. Crit Rev Immunol 2006;26:499–513.
Specializing in selling and appraising dental practices for over 40 years!
CONTACT US FOR A FREE CONSULTATION Phone: (800) 697-5656
WWW.CALPRACTICESALES.COM CA BRE #00283209
youtube.com/mycpsteam faceboook.com/mycpsteam
Come Visit Us at the 2019 CDA Conven on in Anaheim - May 16-18 Booth #317
LOS ANGELES COUNTY
CENTURY CITY—GP in 11 story prof med bldg. Has 5 eq in a 1,955 sq . Grossed approx. $715K. Buyer’s net of $149K. Property ID 4509.
DIAMOND BAR— COMING SOON!
DUARTE—COMING SOON!
ENCINO— GP with 40 years of goodwill in pres gious 12 story med/prof. building. Has 4 eq ops and 1 plumbed not eq. Grossed ap-prox. $309K in 2018. Property ID #5263.
LANCASTER—GP + Real Estate! Long estab-lished prac ce w/ 4 eq ops in a single standing bldg. On a major downtown street. Net $239K. Property ID #5222.
LA PUENTE - Established in 1961 in single free standing building with 4 eq ops and 1 plumbd not eq. Grossed approx. $300K in 2018. Prop-erty ID # 5269.
LOS ANGELES— Beau ful office with a great built out. Has 5 eq ops and 1 plmbd not eq . Has Easy 2000 so ware. Grossed approx. $420K in 2018. Property ID # 4489.
LYNWOOD— GP in single story busy shopping center. Absentee owner. Grossed approx. $610K in 2018. Property ID #5264.
ROWLAND HEIGHTS—COMING SOON!
ORANGE COUNTY
ANAHEIM— GP located in 2 story building w/ heavy traffic flow. Has 8 eq ops. Grossed ap-prox. $754K in 2018. Property ID #5255.
IRVINE (GP / Specialty) In premier shopping center. Established in 2012. Spacious opera-tories. Grossed approx. $847K in 2018. Proper-ty ID #5230.
LADERA RANCH— Beau ful GP in premier shopping center. Has 11 eq ops. Grossed $1.9M in 2018. Property ID 5262.
ORANGE— Turn-Key GP in small shopping center on a major heavy traffic street. Has 3 eq ops in a 1,800 sq suite. Proj. approx. $164K for 2018. Property ID # 5253.
ORANGE—(Turn-Key) General prac ce located in med/dent building. Has 4 eq operatories. Reasonable rent. Grossed approx. $165K IN 2018. Great opportunity for a full me den st. Property ID 5277.
SANTA ANA— GP W/ 3 eq ops and 1 plmb not eq in 4 story med bldg. Property ID 5113.
STANTON— Turn-Key GP in a single story corner strip mall. PPO and Cash only! Has 2 eq ops in 797 sq suite. Grossed approx. $237K in 2018. Property # 5267.
STANTON—GP in shopping plaza. On busy intersec on. Has 5 eq operatories with Camsight so ware. Grossed approx. $461K in 2018. Extremely well laid out office. Property ID #5268
YORBA LINDA— GP established in 1987 con-sists of 4 eq ops in a 1,150 sq suite. PPO & Cash Only. Grossed approx. $658K in 2018. Property # 5258.
EL CAJON - GP + Real State. Consists of 5 eq ops and equipped with 3D Sirona CBCT Digital X-ray. Grossing over $1M in the past 10 years. Property ID # 5265.
ESCONDIDO— Turn-Key GP in single free standing building w/ 8 parking spaces. Seller is the landlord. Has 4 eq ops in an approx. 2,400 sq office. Grossed approx. $312K in 2018. Property ID #5275.
LA JOLLA—Beau ful GP with 17 yrs of goodwill near the beach. Has 4 eq ops in 1,100 sq condo suite. Grossed approx. $335K in 2018. State of the art prac ce. Property ID #5271.
OCEANSIDE— Established in 1990 with 4 eq ops in a one story busy shopping center. PPO and Cash Only. Grossed approx. $560K in 2018. Property ID #5267.
RANCHO BERNARDO—COMING SOON!
SAN DIEGO— Beau ful GP in a 2 story profes-sional bldg w / 6 eq ops and 2 plmd not eq in a 2,250 sq suite. Grossed approximately $1.2M in 2018. Property ID #5251.
SAN DIEGO—Turn key prac ce with 3 eq ops and 1 plumbed not eq on an approx. 1,815 sq
suite. PPO and Cash only. Grossed approx. $325K in 2018. Property ID # 5274.
SORRENTO VALLEY– Located in premier shop-ping place with convenient freeway access. Established in 1992. Has 3 eq ops and 3 plumbed not eq ops room for expansion on an approximate 2,400 sq suites (2). Grossed approx. $486K in 2018. Property ID #5272.
RIVERSIDE &
SAN BERNARDINO COUNTIES
TEMECULA—Absentee owner GP with 2 GP Associates. Has 4 eq ops in busy shopping center. Grossed approx. $327K in 2018. Prop-erty ID 5259.
PRACTICES RECENTLY SOLD IN
Woodland Hills, Oceanside, Goleta, Irvine, Glendale, Tus n & Diamond Bar
SAN DIEGO COUNTY
CARLSBAD— This beau ful prac ce has over 22 yrs of goodwill. Has 4 eq ops in a 1,800 sq suite. Fee for service office. Projec ng approx. $440K for 2018. Property ID # 5256.
CHULA VISTA (Turn-Key) —Well laid out prac-ce in a 2 story med/dent building. Has 3 eq
operatories and 1 plumbed not eq. On a ap-prox. 1,400 sq suite. Grossed approximately $588K in 2018. Great poten al for a full me den st. Property ID #5273.

C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 345
RM Matters
In a perfect world, all patients would receive the care they need to improve their health. But too often patients hesitate to seek the care they need, especially
when it comes to mental health. It is an unfortunate reality that there is still a stigma associated with mental illness, and those in need of treatment don’t always ask for help.
The Dentists Insurance Company’s Risk Management Advice Line has recently received calls from concerned practice owners who became aware of patients or employees suffering from depression or suicidal thoughts. In some cases, a patient mentioned feeling despondent or hopeless. In others, employees threatened suicide or self-harm. While mental health is out of a dental professional’s clinical scope of practice, they have an ethical obligation to help individuals who exhibit distress to access services or support.
Patients: A Cry for HelpTDIC Risk Management Analyst
Trina Cervantes recalls a case in which a patient, whose depression and suicidal thoughts were noted in her medical history, came in for an appointment and mentioned to staff that she “just wanted to end it.” The dental staff asked her if she would accept a referral to an advice line, which she agreed to. They asked for permission to reach out to her family, which she declined. They chose not to report the situation to the authorities, but followed up with a phone call that evening to check on her and asked if there was anything they could do. She informed them that she planned to call her medical doctor.
Depression Screening: Not a Legal Obligation, but an Ethical OneTDIC Risk Management Staff
Cervantes said the offi ce staff did everything they could in this case, both legally and ethically, to help the patient, as her comment did not appear to be an immediate threat. Had she said “I’m going to end it all tonight” or “I’m going to kill myself today,” staff would have reconsidered contacting the authorities.
“It is crucial that every dental offi ce take inventory of what they are presented with,” Cervantes said. “As much as we’d like to guarantee
From one-on-one risk management advice by phone
to informed consent forms to expert-led seminars,
we’re here to help you practice with confidence.
We are The Dentists Insurance Company.
Learn more at tdicinsurance.com/rm
answers
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | Insurance Lic. #0652783
While mental health is out of a dental professional’s clinical scope of practice, they have an ethical obligation to help individuals who exhibit distress to access services or support.

C DA J O U R N A L , V O L 4 7 , Nº 5
346 M AY 2 01 9
M A Y 2 0 1 9 R M M A T T E R S
the perfect outcome, it simply isn’t possible. But it is possible to empower a dental offi ce to analyze the facts of each situation and make an informed decision on what steps to take.”
According to the National Institute of Mental Health, an estimated 16.2 million people in the United States suffer from depression. Even more people are undiagnosed. Patients may talk about or display mental health issues in the dental practice. Some patients don’t know where else to turn or don’t have insurance coverage for mental health care. Others feel there is less stigma attached to seeking help in the dental setting than going to a designated mental health care practitioner.
Signs of depression include lack of concentration, poor appetite, weight changes, fatigue, insomnia, mood swings and lack of energy. But dental professionals should be wary of making comments that could be construed as making a diagnosis. For example, rather than saying, “It sounds like you are suffering from depression. I’ll refer you to an outside provider,” dentists could say, “You may benefi t from talking to someone who can help you.”
If a patient has indicated a history of depression or suicidal thoughts on his or her intake form or if the patient’s record shows the use of antidepressants or other medications for mental illness, it’s a good idea to be alert for comments that may suggest their condition is not under control.
“Sometimes it’s just important to listen to your patient,” Cervantes said. “If they have a history of mental illness, keep your eyes and ears open for signs that they may need help. If you are faced with a patient who mentions depression, suicidal
thoughts, severe anxiety or any other conditions, ask if the patient will provide consent for you to reach out to their medical doctor or trusted family member on their behalf. View these cases no differently than if a patient exhibits any other type of medical concern, such as high blood pressure, which would warrant a referral to an outside provider.
Also, be sure the patient has signed a notice of privacy practices. If you provide a referral to a medical provider, it should be charted. If the patient is a minor, his or her parent or guardian must sign a notice of privacy practices and be informed of any referrals.
When patients decline consent, you can still offer information about community resources that they can access on their own. The National Suicide Prevention Lifeline is a good place to start: suicidepreventionlifeline.org or 800.273.TALK (8255).
Another benefi cial resource is the Suicide Prevention Resource Center, online at sprc.org, which provides a suicide prevention toolkit designed for primary care providers that can also be used in the dental setting. The toolkit offers an offi ce protocol to defi ne roles and responsibilities, a learning module on risk assessment and intervention approaches according to the level of risk.
Implementing specifi c protocols and procedures is especially helpful in areas where the risk of depression or suicide is high and the likelihood of a patient seeking mental health care is low. Some community dental clinics have chosen to implement formal screening procedures and hire on-site mental health counselors to better serve the unique needs of their patient bases.
EmployeesShould an employee inform
you or a co-worker of thoughts of suicide, encourage him or her to seek professional help and to enlist the help of a trusted family member. Provide the same resources you would provide to patients, such as referral to outreach programs and community services.
The fi rst priority should be keeping your patients and employees safe, so if you hear secondhand that an employee may be planning to take action at work, notify the authorities. It is your responsibility as an employer to keep the workplace safe and to act on any potential security risks.
Dental professionals often fi nd themselves on the front lines with individuals suffering from mental health issues. While formal mental health screenings aren’t common in dental practices, taking a proactive approach when you do encounter at-risk patients can be the fi rst step in helping them obtain the help they need. It is natural to be confused, concerned or anxious about what to do. A dentist can feel compelled to take some kind of action. Be confi dent that there are resources available to provide to others in their times of need. If you are ever in doubt about your options, TDIC’s Risk Management Advice Line can help you take inventory of the situation or give you guidance to shape your practice’s protocols. ■
TDIC’s Risk Management Advice Line is a benefi t of CDA membership. If you need to schedule a confi dential consultation with an experienced risk management analyst, visit tdicinsurance.com/RMconsult or call 800.733.0633.
4338 PENINSULA PROSTHODONTIC PRACTICE Preeminent 45year Prosthodontic practice located in mid peninsula neighborhood.State-of-the-art 1,242 square foot facility with 5 operatories. Sellerwilling to help in the transition. Outstanding referral sources. AverageGross Receipts $1.3M with 4 doctor-days per week. Asking $884K.
4256 SANTA CRUZ COUNTY GP Seller moving out-of-state andoffering 33 years of goodwill. Wonderful location on major thoroughfarein a charming beach community close to wineries and the water.Tranquil and modern, beautifully appointed, 5 op facility. Approx. 1,300active patients (all fee-for-service). Seller will help for smooth transition.Asking $180K.
4343 CAPITOLA GP Ample 3,000 sq.ft. faciltiy w/5 fully-equippedoperatories,. Terrific opportunity to own the facility and well-establishedcommunity practice with quality and seasoned staff. Average GrossReceipts $870K+. Asking $643K.
4261 CAPITOLA GP Retiring doctor offering an established practice inprofessional office complex built around a garden setting. Beautiful andmodern 1,465 square foot facility with 4 fully-equipped operatories.Average gross $743K+ with 3 doctor days and 6 hygiene days perweek. Approximately 1,800 active patients. Asking $562K.
4349 CONTRA COSTA COUNTY PEDIATRIC Practice in a brightand relaxing atmosphere in an ample 1,600 sq. ft. 3 op facility withlarge private office that can be upgraded to include a fourth op.Surrounded by referral sources in a class A medical center. 3 doctordays per week. Scan X with Visix software fully-integrated with OpenDental. Seller retiring. Great upside potential. Asking $141K.
4172 NAPA GP Amazing opportunity to own the practice of yourdreams in one of the world’s premier wine destinations! Situated in aprime neighborhood close to many amenities. 1,200 square foot officewith 4 fully-equipped and updated operatories. Over 1,000 activepatients. Average annual gross receipts over $700K. Asking price forpractice $484K. Building available for purchase.
4233 SF GP Seller offering 26+ year general practice in SF Financialdistrict. Ground floor office with high volume foot traffic. Approx. 1,200sq. ft. facility with 4 fully-equipped ops. $930K+ avg. annual GR. Sellerwilling to help for a smooth transition. Asking $640K.
4331 SF GP Downtown SF practice in gorgeous, remodeled 1,300office with panoramic views. Suite includes 4 fully equipped ops,reception area, business office, private office, staff lounge, lab area,and sterilization area. Beautiful, modern cabinetry and equipment.1,600 active patients with 15-20 new patients/mo. Owner/doctorworks 3 days/wk with 5 hygiene days/wk. Average gross receipts$738K with average adj. net of $305K. Asking $495K.
4344 SF GP Prime & convenient location in Laurel Heightsneighborhood. 9 year practice averageing $500K+ with approx. 50%overhead in fully-equipped 2 op. modern faciltiy. Motivated sellerrelocating out-of area. Asking $110K.
4336 SAN BRUNO GP Legacy practice centrally located in acombined commercial & residential neighborhood, convenient tohighways 101, 280, and 380 and close to the BART station. Elegant,remodeled 1,463 sq. ft. office with 5 fully-equipped ops. & digitalradiography. 5 year average Gross Receipts $922K+. 1,000 activepatients with an average of 10 new patients per month. Asking $661K.
4316 SARATOGA GP Vibrant and active practice located in beautiful4 op, fully-equipped, facility at upscale residential, professional, andcommercial neighborhood. 10 new pts./month. 4 doctor days & 4hygiene days per week. $464 avg. Gross Receipts. Asking $357K.
4216 SIERRA NEVADA FOOTHILLS 23 year practice located in theheart of the Sierra Nevada foothills in modern building close todowntown area. 1,024 square foot office with 4 fully- equipped ops.,upgraded major equipment and digital radiography. Average GrossReceipts $890K+ with 56% average overhead. Asking price for practice$604K. Seller is offering real estate for sale to the buyer of his practice.
4262 MOUNTAIN VIEW GP Desirable 1,700 square foot MountainView location. 5 fully equipped operatories. Average Gross Receipts$886K+ with 4 doctor days and 6 hygiene days. Practice with anemphasis on Restorative and Preventative care. Seller retiring. Greatopportunity for a skilled dentist to take over a 35 year practice withseasoned staff and loyal patient base. Asking $619K.
4352 PETALUMA GP Seller retiring, offering 20+ years of goodwill.Beautifully appointed office in the heart of vibrant downtown Petaluma.Walking distance to restaurants, park square, shopping and more. 4ops in 1,440 sq. ft. Equipment is in pristine condition (most of it is 2-12years old). Office is truly fee-for-service as Seller is not contracted withany Insurance/PPO carriers. Average GR $599K, with adjustedaverage net $236K. Seller will help for smooth transition. Asking price$394K. Long term lease is available, or Buyer can purchase thecommercial Real Estate.
COMING SOON: SF GP, Santa Clara GP, Napa County GP &Monterey County GP
carroll.company [email protected] (650) 362-7004 (650) 362-7007
CARROLL& C O M P A N YV “Matching the Right Dentist to the Right Practice”
Mike Carroll Pamela Carroll-Gardiner Mary McEvoy Carroll
Carroll & Company2055 Woodside Road, Suite 160Redwood City, CA 94061BRE #00777682
PENDING
SOLD
SOLD
SOLD
SOLD
PENDING
SOLD
PENDING
PENDING

Making your transition a reality.
www.henryscheinppt.com1.800.519.3458
• • • ••
1.888.685.8100
C DA J O U R N A L , V O L 4 7 , Nº 5
MAY 2 0 1 9 349
A new practice owner has much to do prior to opening doors to the public. The following regulatory compliance tips are based
on questions asked of CDA Practice Support by dentists opening new practices. More information is available on the CDA Practice Support website.
Review “Starting a Dental Practice Checklist”
This resource is an overview of the steps a dentist should complete when opening a new practice. It can be found on the CDA Practice Support website.
Decide whether to incorporate and whether to use a fi ctitious name
A dentist who incorporates does not need to notify the California Dental Board of that action. California state law excludes dentists from the ability to form limited liability corporations or another limited liability entity. If contracts, leases and registrations have been signed under a dentist’s name and later that dentist decides to incorporate, the dentist may need to have contracts, leases and registrations revised to include the corporate name.
A dentist who incorporates and wants to operate under a fi ctitious name must apply to the board for a fi ctitious name permit as well as register the fi ctitious name with the county. Any dentist who operates under a fi ctitious name must have a board permit. Fictitious name permits are address specifi c.
Ignorance Is Not Bliss — Regulatory Compliance Tips for the New Practice OwnerCDA Practice Support
Regulatory Compliance
Have required written policies and procedures in place before seeing patients
When an employee is injured by a contaminated sharp is not the time to fi gure out a postexposure protocol. Having to respond to an enforcement agency’s demand for required documentation also is not the ideal time to put together those documents.
Take the time to learn what policies and procedures are required and utilize CDA templates and ADA resources to create them. It takes time to become familiar with regulations but knowledge of them can help a dentist evaluate the value of using a regulatory compliance consultant and of various products promoted as being “required” – in other words, knowledge of regulatory requirements could save a dentist from unnecessary expenses.
If hiring an employee before the practice opens, consider having the employee assist in putting these documents together. The documents do not need to be perfect the fi rst time, but they should be periodically reviewed and revised as needed. Hiring a regulatory compliance consultant to create the documents is another option.
A dental practice is required to have these documents with information specifi c to the practice:
■ Radiation safety plan. ■ Cal/OSHA plans – exposure
control, hazard communication, injury and illness prevention.
■ HIPAA policies and procedures. ■ Regulated waste management plans.
■ Written protocols for instrument processing, operatory cleanliness and injury management, as required by the dental board’s infection-control regulations.
Conduct and document a HIPAA risk analysis and develop a risk management plan
In order to protect patient information and to ensure its access to that information, a dental practice must identify the risks and vulnerabilities to its electronic information systems and develop a risk management plan. Cyber security is a significant threat to a practice’s ability to provide care. The risk analysis process is not complicated but it must be comprehensive. Review the HIPAA Security Rule and discuss with a professional information technology consultant what safeguards can be implemented to both comply with the rule and secure patient information.
Obtain and read the required employment posters
The employment posters can answer a practice owner’s questions on overtime rules, how to implement an alternative workweek schedule, what an unlicensed dental assistant with an orthodontic permit is allowed to do, and more. CDA distributes to practice owners every other year a set of the required posters and also includes a list of the required posters as an appendix to the Regulatory Compliance Manual.
C DA J O U R N A L , V O L 4 7 , Nº 5
350 M AY 2 01 9
Obtain or create required patient notifi cations
These notices must be posted and/or made available to patients:
■ HIPAA notice of privacy practices. ■ Dental board’s notice of
licensure/ dental hygiene board’s notice of licensure.
■ Dental board’s dental material fact sheet.
■ Business license. ■ Proposition 65 notice. ■ Notice of nondiscrimination
(Section 1557) (only by practices that receive certain types of
M A Y 2 0 1 9 REGUL ATORY COMPL IANCE
government programs such as Denti-Cal).
■ Dental licenses (if name tags are not worn) and radiation safety certifi cates of unlicensed dental assistants.
■ Radiation warning sign.
Obtain or create informed consent forms
The Dental Practice Act requires informed consent forms in these circumstances:
■ To administer general anesthesia. ■ To administer conscious sedation.
■ To prescribe an opioid to a minor.These and other informed-
consent forms are available on the CDA Practice Support website.
Register radiographic equipmentThe owner of radiographic
equipment is responsible for registering it with the California Department of Public Health. Manufacturers and distributors of the equipment have separate reporting requirements. The acquisition, sale, transfer or disposal of radiographic equipment must be reported to CDPH by the equipment owner. Dental practices in Los Angeles and San Diego counties are also required to submit plan checks to the respective county radiological programs. ■
Regulatory Compliance appears monthly and features resources about laws that impact dental practices. Visit cda.org/practicesupport for more than 600 practice support resources, including practice management, employment practices, dental benefi ts plans and regulatory compliance.
6163 CLEAR LAKE Long established and highly respected. 4-days of Hygiene. Revenues of $950,000 with $400,000+ in Profits. Beautiful office. Great staff. 6162 REDDING 2018 collected $700,000 on Owner’s 3.5 day week with 8-weeks off. 8-days of ygiene. 5-ops. River views. Full Price $235,000.6160 SAN FRANCISCO’S 450 SUTTER 12th floor with unencumbered views of Downtown. Upgraded office, technology and delivery systems.PPO practice collected $270,000 part-time due to Owner’s East Bay practice.6159 WOODLAND 3-day practice perfect for first practice, or acquisition by nearby DDS as can be relocated. Collections in 2018 totaled $518,000. 3-days of Hygiene. 4-ops in well-designed office. Quality patients. Full Price $250,000.6158 FORTUNA Relaxed lifestyle in Humboldt County’s Banana Belt. Adjacent to Ferndale. Perfect for Dentist seeking small town living. Collects $390,000. 6-weeks off. Lots of work referred. Full Price $75,000.6157 SACRAMENTO’S ELK GROVE AREA 2018 collected $909,000 on Owner’s 3-day week. Successor can immediately increase to 4-days as practice is rich in patients. 25+ new patients per month. 5-ops, digital Pan, strong Recall, great staff. Want to be busy and make a “no-risk” acquisition? Then investigate this opportunity.6156 SANTA ROSA Sited on Sonoma Highway near Oakmont. Strong foundation evidenced by 4-days of Hygiene. Well-designed 5-op office.2018 collected $730,000. Over $200,000 invested in equipment and technology. Full Price $325,000.6155 LAKEPORT - “SOLD” 5-days of Hygiene. 2018 collected $825,000. Lakeside location and nicely equipped. Seller happily looks forward to retirement.6152 SAN RAFAEL - “SOLD” Across the street from Marin Academy. 2018 collected $520,000. Stand-alone building optional purchase. Nearby DDS who desires their own building should vertically integrate their practice here and have an instant $1+ Million practice in a superior location.6151 MODESTO - “SOLD” Located on north end of Coffee Road where new development is occurring. Attractive 3-op office. 2018 collected $408,000 on 2-day week. Did $700,000+ in 2016 when Owner was full time with $240,000 in Profits. 6150 HAYWARD - “SOLD” Strong Dental DNA. Well-designed 5-op office. Digital radiography and computers. 2018 trending $850,000+.of ygiene. 6149 NOVATO - PERFECT START-UP OPPORTUNITY – BUILDING + 3-YEAR OLD OFFICE Stand-alone building at busy stop light intersection off Highway 101. 4-ops, paperless at cost of $180,000. Doorway to Hamilton with 100s of homes. No competition. Perfect for Dentist seeking perfect location. Scott McDonald from Doctor Demographics states: “Well, I have to say that you were right, Ray. This is an interesting and viable location.”6147 SAN FRANCISCO BAY AREA - “OUT-OF-NETWORK” - “SOLD” 2018 collected $2.2 Million. Hygiene produced $1+ Million.$700,000+ in profits. Unique in so many ways! Seller available for long transition.6143 BERKELEY’S ALTA BATES VILLAGE - “SOLD” 3-day week collected $540,000 in 2018. 4-days of Hygiene. Housed in its own building on Webster Street.
AR LAKE Long established and highly respected
NORTHERN CALIFORNIA(415) 899-8580 – (800) 422-2818
Raymond and Edna [email protected]
California DRE License 1422122
SOUTHERN CALIFORNIA(714) 832-0230 – (800) 695-2732Thomas Fitterer and Dean George
California DRE License 324962
UNIQUE OPPORTUNITIES – Call Tom Fitterer at 714-832-0230 or 714-345-9659 Cell
PRACTICE #1 Unique opportunity for Ambitious Successor. Roll upsleeves and improve performance in absentee-owned practice. 30,000 charts,100 new patients/month. Work four 10-hour days. Net $800,000.PRACTICE #2 Grossing $1,500,000 and Nets $500,000. Great location.Take to $2,000,000.
ALTA LOMA Great Shopping Center, 5-Ops ill do $1 Million.BAKERSFIELD with building. Grosses $650,000.BAKERSFIELD AREA Grosses $40,000 month. 1,800 sq.ft. building
$330,000.CAPISTRANO BEACH Low overhead. Grosses $200,000 16 hoursweek. k Denti-Cal increase to $500,000. net $250,000 with Denti-Cal. Full Price $165,000.DIAMOND BAR Fantastic Shopping Center Location. 5- ps. Full Price$150,000GLENDALE / BURBANK Absentee owned. Absolutely gorgeous freestanding building. Real estate also available. Grosses $840,000. 5 ps.$300,000 in recent upgrades. Full Price $750,000HEMET Super Bargain. Assume mortgage. 3,500 sq.ft. building. 5-ops.Absentee owned. Full price $65,000.INLAND EMPIRE can do $1,000,000. Averages 50 newpatients per month. Low rent.INLAND EMPIRE Alongside freeway, high identity location.$10,000/month HMO income. 7-ops, low rent. Grosses $500,000. Should bedoing $1,000,000. Full Price $485,000.IRVINE GP with small children will sell and work back or share withDentist. Grosses $1 Million.LA HABRA Large mall. 6-ops. Female D does not to own, willwork back. Needs marketing. 1,600 sq.ft. Full Price $270,000.ORANGE COUNTY BEACH CITY Buyer will do $1.5 Million first year.Special circumstances makes this a Super Purchase. 1,800 sq.ft., 4-ops, ConeBeam. Rent only $3,600. Seller will work back 1+ year. HMO checks shallpay rent. This is a fantastic buy! Full Price $850,000.ORANGE COUNTY – THREE PRACTICES All High Identity, allgrossing near or over $1,000,000 – all First Cabin.PALM SPRINGS AREA 8-Ops, Gross $1,000,000+ with Specialists.Bargain.REDLANDS Established 25-years, 5-Ops. Did $600,000 in past. Needshands on Owner.SAN GABRIEL / PASADENA Seller lost Lease. Grossing $1,400,000.Seller will work back 2+ years. 10 days of Hygiene/Week.SAN GABRIEL PEDO Losing Lease. 35-years. 3,500-to-5,000 families.SANTA CLARITA Location, Location, Location. 2,600 sq.ft., 10-Ops. 3Tenant Dentist will pay rent free to Buyer. 50-to-70,000 auto pass per day$250,000SANTA CLARITA Shopping center. Share 5-ops. Full Price $50,000VENTURA Established 20-years. $10,000 month HMO . Grossing $1WEST COVINA Absentee owned. Grosses $650,000. Beautiful 3-op office.
PracticesWanted
NORT RN CALIFORNIA SOUTHERN CALIF
Specialists in the Sale and Appraisal of Dental PracticesServing California Dentists since 1966
How much is your practice worth??
Visit PPS at CDA Anaheim Booth 1157
Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database
Allows Us To Offer You
Better Exposure
Better Fit
Better Price
BAY AREA CONTINUED CC-963 SANTA ROSA: Dream Prac ce in Free Standing Building on major thoroughfare. 1765 sf w/ 5 ops $$550k CG-616 NAPA COUNTY: State-of-the-Art office! ~850 sf w/ 2 Ops. PPrice Reduced – Seller Motivated $250k CG-859 SONOMA: Priced below market value at only $395k! 2000 sf w/ 4 ops highly esteemed FFS Prac-tice $$395k CN-911 SANTA ROSA: “Quality Care & Pa ent well-being FIRST”. 2250 sf w/4 ops + 1add’l. $$545k CN-951 VALLEJO Facility: Move In Ready! 2000 sf w/ 4 fully equipped ops. Nego ate your new lease! Only $50K DC-930 FREMONT (Facility): 1846 sf w/5 ops! In-cludes some dental equipment! FFREE – JUST TAKE OVER LEASE! DC-984 SUNNYVALE: Invest yourself in this li le gem! Near Apple, Google & Microso . 965 sf & 3 ops $$185k DG-862 MID-PENINSULA: Rare gem with up to 7 operatories in the Bay Area!! 2274 sf w/ 6ops + 1 add’l. $475k DG-936 SUNNYVALE: Hesitate and you may lose out on this opportunity of a life me! ~1000 sf w/ 3 ops. Call for Details! DG-978 PALO ALTO: Imagine the possibili es with the newly opened Amazon corporate office near-by! $$455k DG-986 CAMPBELL: The ideal opportunity to prac-
ce in this community! 988 sf w/ 3 ops SSeller Mo vated $325k DN-898 SAN JOSE: Built-out 2015 w/ loca on, visi-bility, convenience in mind! 2,204 sf w/4ops + 2 add’l. $500k DN-937 SAN JOSE: This opportunity is wai ng for your talent & skills! 2210 sf w/ 4 Ops + 2 add’l. $500k DN-938 SUNNYVALE: The ideal opportunity to prac-
ce in this community! 2000 sf w/ 4 Ops + 2 add’l. $500k DN-928 CASTRO VALLEY: Con nue the tradi on of delivering quality dental care! 883 sf w/ 3 Ops. $275k
NORTHERN CALIFORNIA EN-664 SACRAMENTO Facility: Corner loca on w/ excellent visibility 2300 sf w/ 4 ops. ! FFREE – JUST TAKE OVER LEASE!
BAY AREA AC-886 SAN FRANCISCO (Facility): Unsurpassed visibility & loca on! Poten al here is limitless! 850 sf w/ 3 ops $85k AC-989 SAN FRANCISCO (Facility): Busy Retail Shop-ping Plaza w/ major anchor tenants! 3 ops $$150k AG-871 SAN FRANCISCO: Seller Mo vated! 600 sf w/ 2 ops PPrice Reduced $65k AG-944 SAN FRANCISCO: An opportunity like this does not come along very o en! 980 sf w/ 3 ops $595k AG-945 SOUTH SAN FRANCISCO: Be a part of this vibrant, diverse popula on. 1800 sf w/ 4 ops $$495k AG-990 SAN FRANCISCO: Build the prac ce of your dreams! 850 sf w/ 3 ops $$228k AG-993 SAN FRANCISCO: Desirable area w/ easy commute to downtown. 1000sf w/ 3 ops $450k AG-994 SAN FRANCISCO: Highly profitable with net profit over $400k! 850 sf w/ 3 Ops $$825K AN-939 REDWOOD CITY: 1165sf w/ 4 op + 2 add’l. $295k AN-947 DALY CITY: 1500sf w/ 4 ops. $$375k BC-741 DANVILLE (FACILITY): Move in Ready! ~ 1600 sf w/ 3 ops. PPRICED TO SELL! $10k BC-926 ANTIOCH: Long established, well respect-ed office. 1866 sf w/ 5 ops $$495k BC-949 ALBANY: Desirable commercial/residen al area. Medical Prof Bldg w/ good frontage. 3200sf w/ 4 ops $$695k Real Estate: $1.8 BG-925 HAYWARD: Profits close to $900K per year! ~ 1930 sf w/ 6 ops $$1.15M BG-981 BERKELEY: Long established, family-oriented practice. 1100 sf w/ 3 Ops $$345k/ Real Estate Available $499k BN-891 PINOLE: This seller is ready to re re, & looking for someone to con nue the legacy! 1300 sf w/3 ops. $$350k BN-943 MARTINEZ: Opportuni es like this only comes along every great once in a while. 1520sf w/ 4 ops +1 add’l.. $450k BN-952 BERKELEY: Step into this quality prac ce and you’ll know you belong here! ~ 835 sf w/ 3 Ops. $450k CC-846 SAN RAFAEL: Prof/Retail Building Complex. 3 ops 640 sf Collections $433k in 2017 $275k CC-927 SAN RAFAEL: Build the practice of your dreams by increasing this 2-day work week! 800 sf w/ 3 ops $$225k CC-960 SONOMA: Great location in one-of-a-kind setting! 950 sf w/ 3 ops. $$385k/ Real Estate Availa-ble $350k
NORTHERN CALIFORNIA CONTINUED EG-910 MIDTOWN SACRAMENTO:
$210k/ Real Estate $395k EG-965 SOUTH AUBURN VICINITY:
. $350k EG-968 SACRAMENTO:
$550kEG-972 ELK GROVE:
$599k EG-996 SACRAMENTO:
. $250k EN-836 CITRUS HEIGHTS:
$188k EN-885 ROSEVILLE Facility:
Reduced: $45k EN-977 MIDTOWN SACRAMENTO: Grossed over $1.4M in 2018!
$950k EN-976 SACRAMENTO:
$595kFC-650 FORT BRAGG: 350k for the Prac ce & $400k for the Real Estate FC-962 HEALDSBURG:
$180kFG-841 ARCATA:
Reduced Price: $250k/ Real Estate Available FN-961 EUREKA: $395k/ Real Estate Available $395k!FN-855 NO. HUMBOLDT:
$275k GN-953 CHICO:
$315k GN-924 TEHAMA COUNTY:
Prac ce $495k / Real Estate $455k GN-988 YUBA CITY: Excellent Merger Opportunity!
. $100k HG-815 TRUCKEE AREA:
$165k/ Real Estate $437k HG-827 SO. LAKE TAHOE:
$310k HG-851 SO LAKE TAHOE:
$425kHG-983 GRASS VALLEY:
Call For Details!HN-618 SIERRA FOOTHILLS:
$65k HN-740 SHASTA CO:
$475k/ Real Estate $350k HN-773 SUTTER CREEK:
Only $95k!
NORTHERN CALIFORNIA CONTINUED HN-879 SONORA:
Reduced Price: $265k HG-934 GRASS VALLEY:
$225k/Real Estate $190k HN-941 GOLD COUNTRY/CALAVERAS CO:
$175k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IC-975 MODESTO: $225kIG-832 OAKHURST: $235k/ Real Estate 375kIG-881 TURLOCK: $360kIN-764 STOCKTON: $220k IN-917 MERCED AREA:
Reduced! $295k JC-811 FRESNO COUNTY:
$350kJC-823 LOS BANOS: $80kKL-909 SAN DIEGO:
REDUCED! NOW ONLY $910k KG-921 SANTA MARIA:
Seller Mo vated $285k KL-955 SAN DIEGO:
$225k
SPECIALTY PRACTICES BC-784 CENTRAL CONTRA COSTA CO Perio:
$395k BG-843 WALNUT CREEK Perio
Reduced Price: $595kDC-835 TRI-VALLEY Perio: $800k DG-912 SUNNYVALE Ortho:
$925kDN-908 SAN JOSE Pedo:
$175kDN-959 APTOS Perio:
$750k / Real Estate Available $650k EG-903 CARMICHAEL Oral Surgery:
Amazingly Priced: $450k GG-940 NORTH OF SACRAMENTO Pedo:
Reduced $650k JG-757 VISALIA Perio:
Steal at $335k
800.641.4179 [email protected] “ASK THE BROKER” WWW.WESTERNPRACTICESALES.COM

Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database
Allows Us To Offer You
Better Exposure
Better Fit
Better Price
BAY AREA CONTINUED CC-963 SANTA ROSA:
$550k CG-616 NAPA COUNTY:
Price Reduced – Seller Motivated $250kCG-859 SONOMA:
$395kCN-911 SANTA ROSA:
$545kCN-951 VALLEJO Facility:
Only $50K DC-930 FREMONT (Facility):
FREE – JUST TAKE OVER LEASE!DC-984 SUNNYVALE:
$185kDG-862 MID-PENINSULA:
$475k DG-936 SUNNYVALE:
Call for Details!DG-978 PALO ALTO:
$455k DG-986 CAMPBELL:
Seller Mo vated $325k DN-898 SAN JOSE:
$500k DN-937 SAN JOSE:
$500k DN-938 SUNNYVALE:
$500k DN-928 CASTRO VALLEY:
$275k NORTHERN CALIFORNIA
EN-664 SACRAMENTO Facility:
FREE – JUST TAKE OVER LEASE!
BAY AREA AC-886 SAN FRANCISCO (Facility):
$85k AC-989 SAN FRANCISCO (Facility):
$150kAG-871 SAN FRANCISCO:
Price Reduced $65k AG-944 SAN FRANCISCO:
$595k AG-945 SOUTH SAN FRANCISCO:
$495k AG-990 SAN FRANCISCO:
$228k AG-993 SAN FRANCISCO:
$450k AG-994 SAN FRANCISCO:
$825K AN-939 REDWOOD CITY: $295k AN-947 DALY CITY: $375k BC-741 DANVILLE (FACILITY):
PRICED TO SELL! $10kBC-926 ANTIOCH:
$495kBC-949 ALBANY:
$695k Real Estate: $1.8BG-925 HAYWARD:
$1.15M BG-981 BERKELEY:
$345k/ Real Estate Available $499kBN-891 PINOLE:
$350k BN-943 MARTINEZ:
. $450k BN-952 BERKELEY:
$450k CC-846 SAN RAFAEL:
$275kCC-927 SAN RAFAEL:
$225k CC-960 SONOMA:
$385k/ Real Estate Availa-ble $350k
Jon B. Noble, MBA Mona Chang, DDS John M. Cahill, MBA
NORTHERN CALIFORNIA CONTINUED EG-910 MIDTOWN SACRAMENTO: Unlimited Poten al! ~ 1107 sf w/ 2 ops + 1 add’l. $210k/ Real Estate $395k EG-965 SOUTH AUBURN VICINITY: The ideal opportunity to prac ce in this community! ~1100 sf w/ 4 Ops.. $350k EG-968 SACRAMENTO: Desirable, mid-town neighborhood, w/ ample parking in garage! ~1527 sf w/ 5 Ops. $$550k EG-972 ELK GROVE: Prime loca on & spacious office! ~3500 sf w/8 ops +add’l. $$599k EG-996 SACRAMENTO: Beau ful office that you must see first-hand! ~1100 sf w/ 3 Ops.. $250k EN-836 CITRUS HEIGHTS: Well-established, quality prac ce. 30+ years of goodwill. 1300 sf w/3 ops + 2 add’l. $$188k EN-885 ROSEVILLE Facility: Ideal loca on w/ visibility & close to about any-thing! 1000 sf w/3 ops. RReduced: $$45k EN-977 MIDTOWN SACRAMENTO: Grossed over $1.4M in 2018! State-of-the-art equipped, 1800sf w/5 ops. $$950k EN-976 SACRAMENTO: Philosophy to treat pa ents like family & listen to their needs. 1750sf w/5ops. $$595k
FC-650 FORT BRAGG: Family-oriented prac ce. 5 ops in 2000 sf $3350k for the Prac ce & $400k for the Real Estate FC-962 HEALDSBURG: Known as 1 of top 10 small cities in the US! Amazing practice w/ 1200 sf & 3 ops. Beautifully landscaped professional plaza $$180k FG-841 ARCATA: Great demographics w/ very little competition! 1114 sf w/3 ops RReduced Price: $250k/ Real Estate Available FN-961 EUREKA: Where the quality of life can’t be beat! 1400sf w. 4 ops. $395k/ Real Estate Available $395k! FN-855 NO. HUMBOLDT: Seller reloca ng! Long-established, 100% FFS prac ce! 1600 sf w/ 3ops + 1 add’l. $$275k GN-953 CHICO: Established for 55 years and the seller is passing their good-will on to you! 1067sf w/ 3ops. $$315k GN-924 TEHAMA COUNTY: Don’t miss this ideal opportunity! 3000 sf w/ 6 ops. PPrac ce $495k / Real Estate $455k GN-988 YUBA CITY: Excellent Merger Opportunity! Loca on and Lifestyle! 1,600 sf w/ 3 ops.. $100k HG-815 TRUCKEE AREA: Busy, productive practice with 3 days of hygiene! 1000 sf w/ 3 ops $165k/ Real Estate $437k HG-827 SO. LAKE TAHOE: Ski, live, play and prac ce here where your lifestyle can’t be beat! 1200 sf w/4 ops. $310k HG-851 SO LAKE TAHOE: Projected Revenue on track to do just under $700k this year! 2100 sf w/ 5 ops $$425k HG-983 GRASS VALLEY: Newly remodeled office in highly desirable neigh-borhood! ~1250 sf w/ 3 ops. CCall For Details! HN-618 SIERRA FOOTHILLS: Seller Retiring! Huge opportunity for growth by increasing office hours! 750 sf w/ 2 ops $$65k HN-740 SHASTA CO: Beau ful mountain community, well-established prac ce, excep onal long-term staff. 2400 sf w/5 ops + 1 add’l. $$475k/ Real Estate $350k HN-773 SUTTER CREEK: Qualified & creden aled Seller willing to show you how! 1536 sf w/4 ops + 1 add’l Only $95k!
NORTHERN CALIFORNIA CONTINUED HN-879 SONORA: Great Cash-Flow for Only 3 Days a Week! 2950 sf w/ 3 ops Reduced Price: $265k HG-934 GRASS VALLEY: Just imagine living and prac cing here! ~1200 sf w/ 3 Ops $$225k/Real Estate $190k HN-941 GOLD COUNTRY/CALAVERAS CO: This is the right prac ce for you! 2,300sf w/2 ops + 3 add’l. $$175k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IC-975 MODESTO: Established 33 years. 1,100 sf w/ 3 ops $$225k IG-832 OAKHURST: 2048 sf w/3 ops + 1 add’l. $$235k/ Real Estate 375k IG-881 TURLOCK: ~3500 sf w/ 10 Ops (shared). $$360k IN-764 STOCKTON: 5,000 sf w/10 ops. $$220k IN-917 MERCED AREA: Well established prac ce with a stable, loyal pa-
ent base! 1300 sf w/ 3 Ops. RReduced! $$295k JC-811 FRESNO COUNTY: Amazing Opportunity! Considerable Goodwill in Community! 3,000 sf w/ 6 ops $$350k JC-823 LOS BANOS: Heavy emphasis on hygiene. 1000 sf w/ 3 ops $$80k KL-909 SAN DIEGO: Remarkable Opportunity. Long established in vi-brant North Park. 2400 sf w/ 5 ops & 2 Pedo chairs RREDUCED! NOW ONLY $910k KG-921 SANTA MARIA: Live and prac ce in this desirable collegiate coastal community! 930 sf w/ 3 ops SSeller Mo vated $285k KL-955 SAN DIEGO: Just Listed! Well established & centrally located in 1st floor suite w/easy freeway access. Adjacent vacant suite available for expansion. $$225k
SPECIALTY PRACTICES BC-784 CENTRAL CONTRA COSTA CO Perio: Seasoned Staff. Office runs like well-oiled machine! 3 ops $$395k BG-843 WALNUT CREEK Perio: Collec ons over $1M! Great gross and profit for only 2 ½ days per week! 1085 sf w/ 4 ops RReduced Price: $595k DC-835 TRI-VALLEY Perio: Collections over $1.2M. 2,100 sf $800k DG-912 SUNNYVALE Ortho: Premier ORTHO practice opportunity in the Silicon Valley today! ~2030 sf w/ 5 chairs in open bay $$925k DN-908 SAN JOSE Pedo: Amazing Location! Providing affordable pediatric den stry to families! 3600 sf w/ 4ops + 3 add’l. $$175k DN-959 APTOS Perio: Highly successful at this proven loca on! 1350sf w/ 4op. $$750k / Real Estate Available $650k EG-903 CARMICHAEL Oral Surgery: Gross receipts were over $1.1 million in 2017! Stable pa ent base won’t be affected by transi on! 2282 sf w/ 5 ops Amazingly Priced: $450k GG-940 NORTH OF SACRAMENTO Pedo: Prac ce is on track to collect more than $1M in revenues this year! 4300 sf w/ 5 ops. RReduced $$650k JG-757 VISALIA Perio: 9 Hygiene days per week, this practice is a rare gem! ~ 2,000 sf w/ 5 ops Steal at $335k
Edmond P. Cahill, JD Timothy Giroux, DDS
800.641.4179 [email protected] “ASK THE BROKER” can now be found at WWW.WESTERNPRACTICESALES.COM

C DA J O U R N A L , V O L 4 7 , Nº 5
354 M AY 2 01 9
A look into the latest dental and general technology on the market
Tech Trends
BUBM Universal Double Layer Travel Organizer ($15, BUBM)
The world relies on mobile technology. Whether intraoffi ce communication, patient management or direct clinical care, chances are that a laptop, smartphone or tablet facilitates some facet of any given practice operation. A forgotten consequence of mobile technology is the tsunami of extras that follow: power supplies, credit card readers, styli, mice and attachments just to connect to other attachments. These peripheral gadgets for our gadgets take space, are easy to lose and easily cripple systems when they are lost. Founded in 2012 in Shenzhen, China, BUBM specializes in the design and manufacturing of fabric bags for all electronics, from digital cameras to virtual reality headsets. This review focuses specifi cally on its “Universal Double Layer” travel organizer.
Measuring 8 inches by 10 inches by 2 inches, this padded storage organizer has two large external compartments that open like a book. The external zippers can be connected to a sewn-in metal ring, which can be used to secure the zippers and prevent the bag itself from opening. BUBM calls this a security feature, though the level of security attained from using this feature is superfi cial at best as the organizer can be easily pocketed and cut open. The fi rst compartment has a wealth of straps, mesh pouches and one zippered pocket, ideal for storing cables, USB fl ash drives, card readers and wall chargers. Of note is the quality of the mesh pouches: Unlike other products that tend to fray with repeated use, these pouches retain their integrity and elasticity even after a year of frequent daily use. The padding in this compartment is thin and clearly intended for things that can take a light beating. The second compartment — intended for large gadgets like external hard drives, tablets and other handheld objects — off ers two large pouches and one Velcro pocket. This compartment is slightly more padded than its counterpart, but off ers only minimal drop protection; bear in mind, this is an organizer, not a device protector. Overall, the BUBM Universal Double Layer organizer is a durable and aff ordable product that helps tame mobile peripherals.
— Alexander Lee, DMD
Duolingo (Free, Duolingo)
There are numerous educational resources available to learn new foreign languages, from traditional courses to online programs. The success of these programs is heavily dependent on how much time is spent interacting with the content and its relevance to the learner. People with busy lives may not have the appropriate time or motivation to devote extended amounts of time for this endeavor. Duolingo is an engaging modern cross-platform online experience that gives users a fun and addictive way to pick up a new language at their own pace and level of learning for free.
Duolingo is language learning through adaptive gamifi cation. Each language is divided into subjects, which are then subdivided into levels. Lessons in a level are short, bite-sized and customized appropriately for the skill level of the learner. Learners can unlock next levels by completing all the lessons within the current level for a subject. Points are earned for every lesson accomplished. Gems are earned for every level accomplished. A streak counter records how many consecutive days were spent learning a language. Hearts represent life, which allows the learner to continue taking lessons. Hearts are lost when the learner answers incorrectly within lessons. When hearts are depleted, no more lessons can be taken, but learners can gain more hearts by practicing, purchasing gems or waiting until the next day when hearts automatically replenish. Achievement badges are attained through completion of various activities. Learners can add Duolingo friends to compare and compete for achievements.
There are 32 language courses available for English speakers. Each lesson is broken down into separate reading, listening and speaking skill components short enough to accomplish within minutes. Immediate feedback is given with every answer in a lesson. While there is no minimum amount of time learners are required to engage with the course, seemingly endless amounts of rewards are given based on points earned, longest streaks and time of day spent taking lessons. Learners can set daily point goals that comfortably match their pace.
— Hubert Chan, DDS

Learn more at cdapresents.com
Explore dental innovations at CDA Presents. Visit the exhibit hall to shop, network and drop in on free lectures. Check out 550+ exhibitors and save with convention-only deals.
®
The Art and Science of Dentistry
THE NEXT GENERATION of the Ultrapro Tx Prophylaxis Equipment Familyaxis Equipment Family
Our next generation Ultrapro Tx prophylaxis equipment family creates a powerful,
comfortable, and effective solution to all your polishing needs.
ULTRADENT. COM800.552.5512
Learn more at ultradent.com/ultraprotx