Send Orders for Reprints to [email protected] Liver Stem Cells: From Preface to...
12
Send Orders for Reprints to [email protected] Current Stem Cell Research & Therapy, 2014, 9, 00-00 1 1574-888X/13 $58.00+.00 © 2014 Bentham Science Publishers Liver Stem Cells: From Preface to Advancements Kanwal Rehman 1 , Muhammad Javed Iqbal 2 , Nureen Zahra 3 and Muhammad Sajid Hamid Akash 1,4,* 1 Institute of Pharmacology, Toxicology and Biochemical Pharmaceutics, College of Pharmaceutical Sciences, Zhejiang University Hangzhou, China; 2 Department of Biochemistry and Molecular Biology, University of Gujrat, Gujrat, Paki- stan; 3 Instititute of Molecular Biology and Biotechnology, The University of Lahore, Lahore, Pakistan; 4 College of Pharmacy, Government College University Faisalabad, Faisalabad, Pakistan Abstract: Liver is a major metabolic organ of the body and is known to comprise of two epithelial cell lineages, namely, hepatocytes and cholangiocytes which are known to originate from hepatoblasts during fetal developing stages. Upon acute injury, the hepatocytes and cholangiocytes undergo cellular division to compensate the loss, however, chronic dam- age may suppress this proliferative ability and as a consequence hepatic and extra-hepatic stem cells may contribute for liver regeneration. Facultative liver stem cells (oval cells) may emerge, proliferate and contribute in replacing damaged hepatic cells. Similarly, bone marrow and mesenchymal stem cells are also known for contributing in liver regeneration having their ability of self renewal and differentiation. However, a closer look is still required to bridge the existing knowledge gaps between functionality and limitations. Thereby, we have discussed the detailed mechanistic insights of both hepatic and extra-hepatic stem cells including, stem/progenitor cells, adult/fetal hepatocytes, oval cells, bone marrow and mesenchymal stem cells. We have also focused on few in vitro and in vivo studies elucidating therapeutic applications and challenges related to the liver stem cells. We believe that such conversations may provide invaluable contribution for realistic advancement in the state of therapeutic stem-cell transplantation. Keywords: Bioartificial liver, hepatocellular carcinoma, hepatocytes, oval cells, stem/progenitor cells. INTRODUCTION Stem cell research is one among the most fascinating patches of contemporary biology. More than 30 years ago, in 1981 scientists discovered different ways to isolate stem cell from early mouse embryo [1, 2]. The elaborated molecular analysis of the mouse stem cells led to the discovery of a technique to isolate and grow stem cells from human embryo in a laboratory, in 1998 [3]. In 2006, researchers achieved another milestone by enabling stem cell to be “repro- grammed” genetically. It included genetically reprogram- ming of adult cells into embryonic stem cells (ESCs) which hold miraculous power to express genes and other factors that are mandatory for normal ESCs. This new type was named as induced pluripotent stem cells (iPSCs) [4]. Such types of investigational studies provided a hope for further discovering and understanding of functional stem cells and looking them as a therapy for organ disorders. Many years ago, it was believed that some organs such as liver or brain had no or only a few stem cells that have restricted differen- tiation abilities [5]. However, during the last decade, re- searchers have revealed the fact that adult stem cells have potential to differentiate into tissues from which they have been derived. Undeniable evidences strongly indicated that stem cells derived from adult tissues have ability to repair *Address correspondence to this author at the Institute of Pharmacology, Toxicology and Biochemical Pharmaceutics, College of Pharmaceutical Sciences, Zhejiang University Hangzhou, China and College of Pharmacy, Government College University Faisalabad, Faisalabad, Pakistan; Tel: +86-15558171291; Fax: +86-571-88208416; Email: [email protected] and replace selective cell types that are already present in their neighborhood. These adult stem cells are generally con- sidered as “multipotent” [6]. The most evolutionary area of this ascertainment is the widely studied example of the abil- ity of hematopoietic stem cells (HSCs) to regenerate organs such as liver. A progenitor/stem cell compartment was rec- ognized in adult livers for its probable ability of being a tar- get for liver regeneration [7]. The therapeutic potential of such cells can prove to be a remarkable way of providing opportunity for the transplantation of cells/tissue, gene ther- apy and drug development. STEM CELLS/PROGENITOR CELLS The words, progenitor cell and stem cell are often used interchangeably. “Stem cells” have potential to replenish their own population in addition to differentiate into commit- ted daughter cells. However, the term “progenitor cell” may genetically define as “cell that can divide and has the ability to differentiate”. As a result of these progenitor cells, a prog- eny is produced which can differentiate and possess self re- newal abilities [8]. As ESCs are derived from pluripotent blastocyst, these cells progenerate somatic stem cells that possess potential to differentiate into multipotent tissue specific stem cells. Some stem cells have been shown to possess exceptional capability to differentiate into any cell type within the body. Stem cells have also been further categorized as totipotent and pluripo- tent cells and have been distinguished from the other cells [9] owing to their distinct characteristics as, i) they have mi- raculous renewal or self-maintenance potential, occasionally
-
Upload
universityofgujrat -
Category
Documents
-
view
6 -
download
0
Transcript of Send Orders for Reprints to [email protected] Liver Stem Cells: From Preface to...

Send Orders for Reprints to [email protected]
Current Stem Cell Research & Therapy, 2014, 9, 00-00 1
1574-888X/13 $58.00+.00 © 2014 Bentham Science Publishers
Liver Stem Cells: From Preface to Advancements
Kanwal Rehman1, Muhammad Javed Iqbal
2, Nureen Zahra
3 and Muhammad Sajid Hamid Akash
1,4,*
1Institute of Pharmacology, Toxicology and Biochemical Pharmaceutics, College of Pharmaceutical Sciences, Zhejiang
University Hangzhou, China; 2Department of Biochemistry and Molecular Biology, University of Gujrat, Gujrat, Paki-
stan; 3Instititute of Molecular Biology and Biotechnology, The University of Lahore, Lahore, Pakistan;
4College of
Pharmacy, Government College University Faisalabad, Faisalabad, Pakistan
Abstract: Liver is a major metabolic organ of the body and is known to comprise of two epithelial cell lineages, namely,
hepatocytes and cholangiocytes which are known to originate from hepatoblasts during fetal developing stages. Upon
acute injury, the hepatocytes and cholangiocytes undergo cellular division to compensate the loss, however, chronic dam-
age may suppress this proliferative ability and as a consequence hepatic and extra-hepatic stem cells may contribute for
liver regeneration. Facultative liver stem cells (oval cells) may emerge, proliferate and contribute in replacing damaged
hepatic cells. Similarly, bone marrow and mesenchymal stem cells are also known for contributing in liver regeneration
having their ability of self renewal and differentiation. However, a closer look is still required to bridge the existing
knowledge gaps between functionality and limitations. Thereby, we have discussed the detailed mechanistic insights of
both hepatic and extra-hepatic stem cells including, stem/progenitor cells, adult/fetal hepatocytes, oval cells, bone marrow
and mesenchymal stem cells. We have also focused on few in vitro and in vivo studies elucidating therapeutic applications
and challenges related to the liver stem cells. We believe that such conversations may provide invaluable contribution for
realistic advancement in the state of therapeutic stem-cell transplantation.
Keywords: Bioartificial liver, hepatocellular carcinoma, hepatocytes, oval cells, stem/progenitor cells.
INTRODUCTION
Stem cell research is one among the most fascinating patches of contemporary biology. More than 30 years ago, in
1981 scientists discovered different ways to isolate stem cell
from early mouse embryo [1, 2]. The elaborated molecular analysis of the mouse stem cells led to the discovery of a
technique to isolate and grow stem cells from human embryo
in a laboratory, in 1998 [3]. In 2006, researchers achieved another milestone by enabling stem cell to be “repro-
grammed” genetically. It included genetically reprogram-
ming of adult cells into embryonic stem cells (ESCs) which hold miraculous power to express genes and other factors
that are mandatory for normal ESCs. This new type was
named as induced pluripotent stem cells (iPSCs) [4]. Such types of investigational studies provided a hope for further
discovering and understanding of functional stem cells and
looking them as a therapy for organ disorders. Many years ago, it was believed that some organs such as liver or brain
had no or only a few stem cells that have restricted differen-
tiation abilities [5]. However, during the last decade, re-searchers have revealed the fact that adult stem cells have
potential to differentiate into tissues from which they have
been derived. Undeniable evidences strongly indicated that stem cells derived from adult tissues have ability to repair
*Address correspondence to this author at the Institute of Pharmacology,
Toxicology and Biochemical Pharmaceutics, College of Pharmaceutical
Sciences, Zhejiang University Hangzhou, China and College of Pharmacy,
Government College University Faisalabad, Faisalabad, Pakistan;
Tel: +86-15558171291; Fax: +86-571-88208416;
Email: [email protected]
and replace selective cell types that are already present in their neighborhood. These adult stem cells are generally con-sidered as “multipotent” [6]. The most evolutionary area of this ascertainment is the widely studied example of the abil-ity of hematopoietic stem cells (HSCs) to regenerate organs such as liver. A progenitor/stem cell compartment was rec-ognized in adult livers for its probable ability of being a tar-get for liver regeneration [7]. The therapeutic potential of such cells can prove to be a remarkable way of providing opportunity for the transplantation of cells/tissue, gene ther-apy and drug development.
STEM CELLS/PROGENITOR CELLS
The words, progenitor cell and stem cell are often used interchangeably. “Stem cells” have potential to replenish their own population in addition to differentiate into commit-ted daughter cells. However, the term “progenitor cell” may genetically define as “cell that can divide and has the ability to differentiate”. As a result of these progenitor cells, a prog-eny is produced which can differentiate and possess self re-newal abilities [8].
As ESCs are derived from pluripotent blastocyst, these cells progenerate somatic stem cells that possess potential to differentiate into multipotent tissue specific stem cells. Some stem cells have been shown to possess exceptional capability to differentiate into any cell type within the body. Stem cells have also been further categorized as totipotent and pluripo-tent cells and have been distinguished from the other cells [9] owing to their distinct characteristics as, i) they have mi-raculous renewal or self-maintenance potential, occasionally

2 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
after long period of immobility, ii) they generate into organ or tissue specific cells with special functions under specific growth conditions, iii) they acquire serial transplantable dex-terity (plasticity/trans-differentiation). On the other hand, progenitor cells are known to have capability to divide rap-idly but have short term tissue reconstruction [9, 10]. Though, specifically derived adult stem cells are more accu-rately referred to as progenitor until they completely execute according to the characteristics of a stem cells but it is still difficult to distinguish between stem and progenitor cell be-cause of self-renewal and proliferative properties. Hence, here we will refer stem cells as stem/progenitor cells.
STEM/PROGENITOR CELLS IN LIVER REGEN-
ERATION
As far as the liver is concerned, liver transplantation has been thought to be the only convincing therapy to deal with the end stage liver disease, although it has certain disabilities including risk of rejection, which is one of the worldwide health problems [11]. This factor accounts the molecular biologists to identify and isolate exemplary source of stem cells that have attractive innumerable potential to generate large amount of hepatocytes used to repair damaged liver or to make biological artificial liver.
Mounting evidences are available that liver stem/progenitor cell (LSCs) can play regenerative role in the liver which is stimulated by specific pathological or physio-logical stimuli. Most classical demonstration of liver regen-eration was presented in 1997 by a serial transplantation of
-galactosidase marked liver cells in mouse model. This showed that the growth potential of adult mouse hepatocytes was similar to that of HSCs [12]. Recently, the cells derived from bone marrow (BM) in diseased livers of human and rodents have demonstrated that these stem cells may play critical role in the liver repair. BM cells have miraculous regenerative potential to generate several types of hepatic epithelial cells such as hepatocytes, oval cells and duct epi-thelium. It is hypothetically believed that LSCs possess po-tential deriving force to replace liver epithelial cells [13].
However, the characterization and recognition of en-dogenous LSCs and the signals that dictate their differentia-tion and proliferation to adult hepatocytes might direct this fascinating pathway of biology to the development of clini-cally feasible channels to induce liver regeneration from these endogenous cells or to allow maturation of stem/progenitor cells to hepatocytes in vitro and in vivo.
Here we have attempted to discuss in detail the mechanistic insight of liver stem/progenitor cell including their niches, stimulating factors and their derivation from resident and/or extra-hepatic cells along with therapeutic applications and limitations for utilizing LSCs in liver disease.
LIVER STEM/PROGENITOR CELLS
Liver, the essential body organ comprises of complicated structure and various cell types. The liver parenchymal cells are called hepatocytes which are about 80% of the organ and perform important liver functions. However others are non-parenchymal cells of liver like cholangiocytes (which form bile duct), kupffer and endothelial cells [14]. Many reports have defined cells as LSCs which possess the ability to pro-liferate and differentiate into two epithelial cell lineages, namely, hepatocytes and cholangiocytes which are known to originate from similar origin, hepatoblasts during fetal de-veloping stages [15]. As a matter of fact, from the fetal en-doderm foregut, hepatoblasts emerge yielding hepatocytes and cholangiocytes thereby may be known as embryonic liver stem/progenitor cells [16] (Fig. 1). Signaling pathways, TGFb/Activin and Notch have been known to initiate the differentiation of hepatoblasts into cholangiocytes [17]. Whereas at latter stages, parenchymal hepatoblasts expand with the help of mesothelial cells present on their surface [18]. Further, these mesothelial cells bring about the forma-tion of mesenchymal cells in the liver [19]. Several studies during the last decade have identified cells both outside and within the liver exhibiting the properties of hepatic stem cells that can differentiate into hepatocyte and bile duct epithelial cells in culture in addition to their transplantation [20]. Ini-tially, it was believed that adult hepatocytes have limited potential to proliferate but in the last decade ,researches in this area have demonstrated that under specialized condi-tions, hepatocytes have boundless proliferation potential [21]. Upon acute injury, the hepatocytes and cholangiocytes undergo cellular division to compensate the loss of injured cells/tissue; however, chronic damage may suppress this proliferative ability of liver cells. As a consequence, hepatic and/or extra-hepatic stem/progenitor cells may contribute for liver regeneration [14].
Though, the ESCs are totipotent but they are well-known to be tumorigenic as well. On contrary, progenitor cells might be less persuading being committed cells and can be useful for transplantation [22]. Stem cells play a dominant role in tissue homeostasis and tissue repairing after acute injury. However, in mammalian liver, turnover of normal
Fig. (1). Developmental stages of liver cells. From the fetal endoderm foregut, hepatoblasts emerge which proliferate and form two distinct
committed linage which further differentiate yielding hepatocytes and cholangiocytes.

Liver Stem Cells: From Preface to Advancements Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 3
epithelial cells is very slow but hepatocytes display rapid cell division and replacement of lost cells within few days as in case of acute liver injury [23].
Several convincing experiments conducted by diverse group of researchers have highlighted the hepatocyte poten-tial for proliferation. In FAH (fumary-lacetoacetate hydro-lase) knockout mice with inclusive and continuous liver in-jury, nearly complete liver repopulation can be achieved with reconstruction of normal function and structure by trans-planted wild type hepatocytes [12]. In another study, trans-plantation of wild type hepatocytes into transgenic mice with extensive and continuous necrosis of host hepatocyte showed 12 or more cell divisions replacing most of the host liver [24].
LIVER STEM/PROGENITOR NICHE
A stem/progenitor cell niche includes supporters in term of self-renewal property of stem/progenitor cells and may comprise of cellular and extra-cellular microenvironment [25]. The inspiring thought about stem cell niche arose from the concept that stem cells may inhabit in the “microenvi-ronment” that stimulate their differentiation. Such niches have been analyzed in BM, skin, brain and intestinal musosa [26-29], where specific signals and factors affecting their behavior of proliferation and differentiation [27]. However, the most favorable candidate for the liver stem cell niche is the “Canal of Hering”. For hepatocytes, their niche is thought to be composed of various cells including hepato-cytes and cholangiocytes themselves, inflammatory cells, kupffer cells, endothelial cells and stellate cells. For instance, a close cross-talk has been suggested to exist between LSCs and hepatic stellate cells [30]. Interestingly, LSCs have most probably thought to be supported by myofibroblasts/ hepatic stellate cells matrix [31]. This matrix is recognized to help LSCs travel for differentiation to compensate the loss of he-patocytes. Similarly, various studies have suggested the regulation of cholangiocytes proliferation to be influenced by different factors including growth factors, steroid hormones and neurotransmitters [32, 33]. In addition, cytokines and chemokines released from inflammatory cells are also known to influence the growth and differentiation of LSCs via dif-ferent signals [34]. In this regard, Jakubowski et al. have suggested that TNF-like weak apoptotic inducer expressed by T-cells may encourage proliferation of LSCs [35]. Simi-larly, according to a study on mouse cholangiocytes, it was found that their proliferation was increased in response to histamine receptor stimulation [36]. Further, the importance of hepatic cell niche have been recognized by carrying out studies involving various cellular and extra-cellular factors like non-parenchymal cells to improve the functioning of liver cells when co-cultured with them [37-39]. Thereby, LSCs niches may involve a combination of factors; however, a productive discussion might probably be helpful to build up the association among existing perceptions regarding LSCs and their niches.
INTRA-HEPATIC AND EXTRA-HEPATIC STEM CELLS AND LIVER REGENERATION
Though, the liver has remarkable regeneration ability but under certain extreme conditions like chronic liver disease, the organ has to be dependent on other sources for its re-
population for example, the intra-hepatic stem cells and ex-tra-hepatic stem cells. Intra-hepatic stem cells include mature (adult) hepatocytes and fetal hepatic progenitor cells while, extra-hepatic stem cells comprise of bone marrow stem cells, mesenchymal stem cells, and embryonic stem cells.
Adult Hepatocytes
According to the increasing literature, it has been shown that some adult hepatocytes have potential to proliferate 12-18 times to develop into functional progeny. To test their regenerative competency, researchers transplant hepatocyte (serial transplantation) from adult donors. No indication of altered liver architecture and function was detected in re-populated animals [24]. Researchers by adopting isolated hepatocyte cell transplantation model, further depicted that normal adult hepatocytes have proficiency to be serially transplanted through seven generations of mice, with indi-vidual transplanted cell undergo divisions with an average of more than 68 divisions and by applying retroviral marking, FAH+ hepatocytes can be amplified clonally and repopulate to FAH-/- mouse liver by serial passages [12, 40]. It has been reported that genetically modified hepatocytes that express seminal proliferative capability in hosts with liver injury have also been used experimentally [41]. In case of exces-sive bile duct injury, it has also been reported that hepato-cytes have potential to differentiate into cholangiocytes and form mature bile ducts, showing bipotential differentiation of hepatocytes [42].
Oval Cells
The hepatic progenitor cells in rats are termed as oval cells (OCs) which are minute proliferative cells with oval and large nuclei along the bile canaliculi. OCs possess het-erogeneous stemness potential i.e. they may differentiate into both hepatocytes and cholangiocytes [43].
Though OCs are particularly used for the rodent models however, in conditions of liver diseases like chronic intoxi-cation or viral infection which results in suppressed hepato-cytes proliferation, OCs-like cells emerge from peri-portal area (canal of hering, hepatocytes or cholangiocytes) and take the command to proliferate for the replacement of dam-aged hepatic cells [44, 45].
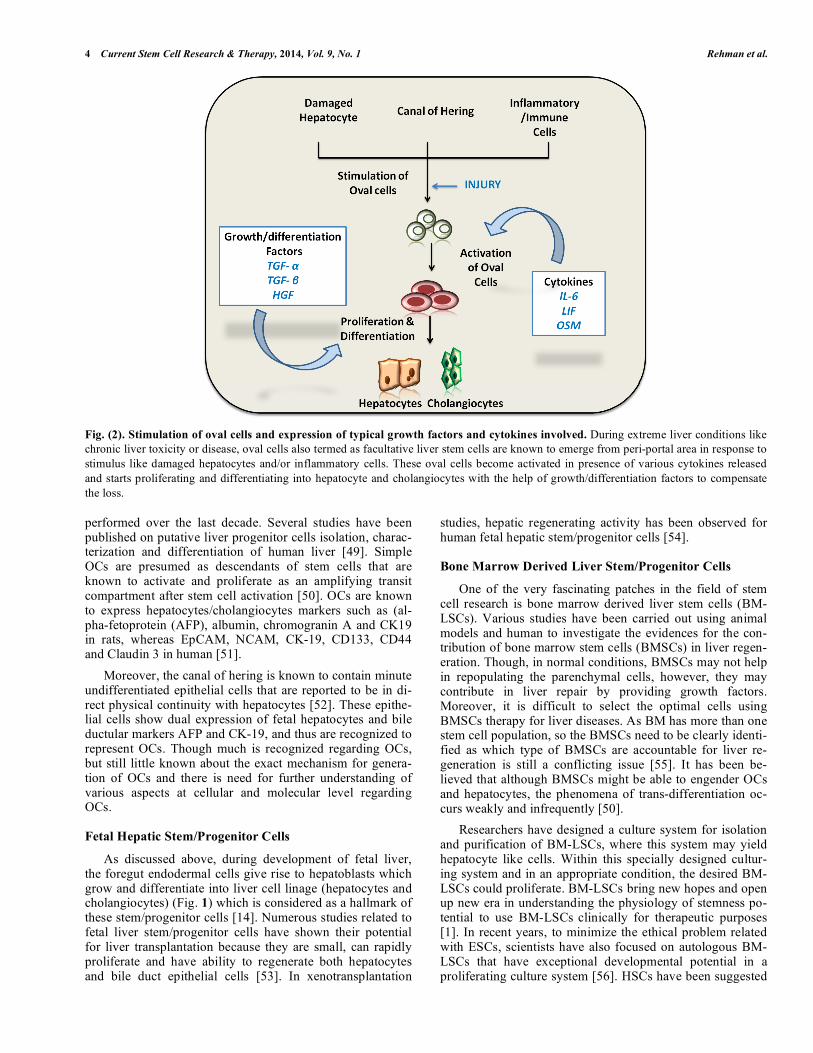
Though the exact mechanism for OCs activation is not completely understood, however, they are presumed to be activated by involvement of different cell types including, damaged hepatocytes, canal of hering, inflammatory and immune cells. Moreover, there are various factors involved in the activation of OCs [46] including cytokines like IL-6, leukemia inhibitory factor (LIF), and oncostatin M which further stimulate transcriptional pathways. After being acti-vated, different growth and/or differentiation factors have been recognized to promote the progression of OCs prolif-eration and differentiation (Fig. 2), including transforming growth factor- (TGF- ), transforming growth factor- (TGF- ) and hepatocyte growth factor (HGF) [46]. Moreo-ver, different inflammatory cytokines have been reported to modulate the OCs responses [47, 48]. Similarly, mesenchy-mal cells have been reported for signal induction in OCs by direct interaction [43]. Isolation, differentiation and in vivo transplantation of liver, OCs have been successfully
4 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
Fig. (2). Stimulation of oval cells and expression of typical growth factors and cytokines involved. During extreme liver conditions like
chronic liver toxicity or disease, oval cells also termed as facultative liver stem cells are known to emerge from peri-portal area in response to
stimulus like damaged hepatocytes and/or inflammatory cells. These oval cells become activated in presence of various cytokines released
and starts proliferating and differentiating into hepatocyte and cholangiocytes with the help of growth/differentiation factors to compensate
the loss.
performed over the last decade. Several studies have been published on putative liver progenitor cells isolation, charac-terization and differentiation of human liver [49]. Simple OCs are presumed as descendants of stem cells that are known to activate and proliferate as an amplifying transit compartment after stem cell activation [50]. OCs are known to express hepatocytes/cholangiocytes markers such as (al-pha-fetoprotein (AFP), albumin, chromogranin A and CK19 in rats, whereas EpCAM, NCAM, CK-19, CD133, CD44 and Claudin 3 in human [51].
Moreover, the canal of hering is known to contain minute undifferentiated epithelial cells that are reported to be in di-rect physical continuity with hepatocytes [52]. These epithe-lial cells show dual expression of fetal hepatocytes and bile ductular markers AFP and CK-19, and thus are recognized to represent OCs. Though much is recognized regarding OCs, but still little known about the exact mechanism for genera-tion of OCs and there is need for further understanding of various aspects at cellular and molecular level regarding OCs.
Fetal Hepatic Stem/Progenitor Cells
As discussed above, during development of fetal liver, the foregut endodermal cells give rise to hepatoblasts which grow and differentiate into liver cell linage (hepatocytes and cholangiocytes) (Fig. 1) which is considered as a hallmark of these stem/progenitor cells [14]. Numerous studies related to fetal liver stem/progenitor cells have shown their potential for liver transplantation because they are small, can rapidly proliferate and have ability to regenerate both hepatocytes and bile duct epithelial cells [53]. In xenotransplantation
studies, hepatic regenerating activity has been observed for human fetal hepatic stem/progenitor cells [54].
Bone Marrow Derived Liver Stem/Progenitor Cells
One of the very fascinating patches in the field of stem cell research is bone marrow derived liver stem cells (BM-LSCs). Various studies have been carried out using animal models and human to investigate the evidences for the con-tribution of bone marrow stem cells (BMSCs) in liver regen-eration. Though, in normal conditions, BMSCs may not help in repopulating the parenchymal cells, however, they may contribute in liver repair by providing growth factors. Moreover, it is difficult to select the optimal cells using BMSCs therapy for liver diseases. As BM has more than one stem cell population, so the BMSCs need to be clearly identi-fied as which type of BMSCs are accountable for liver re-generation is still a conflicting issue [55]. It has been be-lieved that although BMSCs might be able to engender OCs and hepatocytes, the phenomena of trans-differentiation oc-curs weakly and infrequently [50].
Researchers have designed a culture system for isolation and purification of BM-LSCs, where this system may yield hepatocyte like cells. Within this specially designed cultur-ing system and in an appropriate condition, the desired BM-LSCs could proliferate. BM-LSCs bring new hopes and open up new era in understanding the physiology of stemness po-tential to use BM-LSCs clinically for therapeutic purposes [1]. In recent years, to minimize the ethical problem related with ESCs, scientists have also focused on autologous BM-LSCs that have exceptional developmental potential in a proliferating culture system [56]. HSCs have been suggested

Liver Stem Cells: From Preface to Advancements Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 5
by Sell et al. in 2001 to be one of the probable sources for the regeneration of liver cells during liver injury [57]. How-ever, isolated hepatocyte progenitor cells from BM and liver have been known to be combination of both as they ex-pressed the common surface receptor and/or antigen (CD34, Thy-1, FLT and c-Kit) [58, 59]. Avital et al. [60] have re-ported the isolation of LSCs from BM using lack of 2
-
microglobulin ( 2m) and presence of Thymus cell antigen (Thy-1) as trackers for liver progenitor cells. However, ow-ing to the expression of hematopoietic cell antigens (e.g. Thy-1, CD34), a probable speculation for the derivation of OCs from BM also exist [61]. Unlike hepatocytes, where the derivation from BM is considered to be limited, the BMSCs are thought to contribute for liver non-parenchymal cells. The monocyte resident of liver which are known as kupffer have been recognized for their phagocytic function in dis-eased condition by releasing TNF- and IL-6 as inflamma-tory cytokines [55]. A bone marrow derived mesenchymal stem cell (BM-MSCs) population was studied that differenti-ated into hepatocyte-like cells expressing AFP, albumin markers (Fig. 3) and Cytochrome P450 activity [62]. Nu-merous investigational studies on murine transplantation have suggested BM derivation of Kupffer cells [63, 64] though few animal and patient studies have been conducted [65-67] on preliminary stages but there is still a need for wide-ranging understanding of BMSCs associated liver re-population.
Fig. (3). Bone Marrow derived-stem cells differentiation into
hepatocytes. Bone marrow has been known to comprise of two
types of major bone marrow stem cell (BMSCs) population includ-
ing hematopoietic stem cells (HSCs) and mesenchymal stem cell
(MSC). Studies have suggested HSCs and MSCs to participate in
replenishing the number of lost hepatocytes by differentiating into
hepatocyte-like cells and expressing hematopoietic cell specific
markers. However, the generation of oval cells (OCs) by bone mar-
row derived stem cell is still under debate.
Mesenchymal Stem Cells
Mesenchymal stem cells that are known as pluripotent cells are recognized to have long-term self-renewal ability deriving from cartilage, bone, other connective tissues, and nervous and adipose tissue [68]. MSCs are known to be de-rived from various tissues differentiating into a range of other cells [69]. MSCs were first isolated from BM as stro-mal cells [70]. Moreover, adipose tissue-derived mesenchy-mal stem cells (AT-MSCs) have been known to differentiate into hepatocytes [71, 72]. A sound engraftment of hepato-cyte-like cells which were resultant of AT-MSCs was ob-served in a xenogenetic transplantation model with 15 times higher serum albumin in pre-differentiated AT-MSCS trans-planted mice [73]. Several recent studies have reported nu-merous MSCs markers including CD44, CD73, CD90, CD105, and CD166 for BM-MSC. Besides BM-MSCs, markers for other MSCs are CD49e, CD51, CD54, CD59, CD71, and CD117 [74-78]. Interestingly, the extracellular matrix of umbilical cord (UC) is known to comprise of Wharton’s jelly cells (WJC) as a main component [79]. WJC has shown to secrete cytokines similar to BM-MSCs [80] and has been recognized to function for in vivo hema-topoietic stem cell engraftment [81]. WJC-MSCs have ex-pressed BM-MSCs like markers [82, 83] namely, CD10, CD13, CD29, CD44, CD49e, and CD166 [74, 84, 85]. Few have been designated WJ-MSCs as multipotent cells which can differentiate into various cell types [86]. A study showed well functioning of UCB after differentiation into hepato-cyte-like cells including AFP, albumin production and Cyto-chrome P450 activity [62]. Similarly, in an in vitro and in vivo study, authors have presented the importance of liver microenvironment on hepatic differentiation in which they observed in vivo loss of chimerical phenotype in BM-MSCs differentiated hepatocytes that was observed to be presenting in in vitro [87].
However, vigilance is still required regarding both the efficacy and side effects of the current proposed hepatic stem cell choices.
THERAPEUTIC APPLICATIONS OF LIVER
STEM/PROGENITOR CELLS
Though for the management and cure of many chronic liver diseases, liver transplant seems to be an eventual treat-ment, however, various recent investigations have paved a pathway for novel therapies of liver diseases. Such investiga-tions include progresses and challenges relating to the dis-covery, technical and clinical aspects of liver stem/progenitor cells which can provide a better alternate for liver treatment.
The major potential of these liver stem/progenitor cells is evident from their availability for cell transplantation, gene therapy, bioartificial devices and drug testing [22] as com-pared to the donor availability for organ transplant. We have already discussed it in earlier sections that ESCs, mature hepatocytes, HSCs/BM-LSCs, MSCs, fetal and/or adult liver progenitor/stem cells have the ability of self renewal and generating similar progeny with ability of self renewal and differentiation (Fig. 4). Here, we will discuss different stud-ies and investigations relating to diverse stem cells reported to be candidate for human clinical trials and their relevant challenges.

6 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
Fig. (4). Repopulation of liver cells by intra-hepatic and extra-hepatic stem cells. Normally, mature hepatocytes proliferate and divide to
balance the number of hepatocytes (top; shown in red), however in chronic liver toxicity or viral diseases, hepatocyte proliferation is sup-
pressed. In such conditions, oval cells become activated and divide to differentiate into hepatocytes (bottom; shown in green). Similarly, few
of the extra-hepatic sources are also recognized as a resource to provide stem cells including bone marrow stem cells (BSCs) and mesenchy-
mal stem cells (MSCs). These cells may differentiate into hepatocytes and participate in liver regeneration (right; shown in blue). Moreover,
according to therapeutic application, stem cell transplantation/liver assist devices can play vital role in contributing for liver regeneration as
suggested by ongoing researches using isolated adult/fetal hepatic stem/progenitor cells, embryonic stem cells and bone marrow derived-stem
cells (left; shown in yellow).
Liver Cellular Transplantation
The transplantation of liver cells has been now recog-nized as a novel and promising approach for the treatment of various liver diseases. The cells that have been considered for this type of cellular transplantation and differentiation to hepatic lineage include BM-LSCs, ESCs, and MSCs [88]. It has been suggested that the use of stem/progenitor cells de-rived hepatocytes might have more advantage over trans-plantation of mature hepatocytes [89]. The major advantages of cell therapy over organ transplant is that it can be cost effective, simply directed with efficient in vitro cellular growth and above all a solo donor liver may perhaps to be collectively utilized for the treatment of several patients with liver diseases [90]. For genetic liver defects, studies using hepatocyte transplantation have been conducted on animal models as well as on humans [91-94]. Contribution of donor hepatocytes up to 10% of total organ mass was observed when allogeneic hepatocytes were transplanted in patients with liver failure [95]. BM-LSCs have shown their efficiency by differentiating into hepatocytes in vitro and in vivo [96-98]. Recently, adult BM cells were transplanted into defi-cient in fumarylacetotate hydrolyse-deficient and type-1 ty-rosinemia mice which resulted in improved liver functioning [98]. Jang et al., have reported restoration of liver function
via conversion of HSCs into hepatocytes after a week of HSCs transplantation in liver-injured mice [99]. Clinical transplantation of hepatocytes, fetal hepatocytes, BMCs and MSCs has shown success in patients with fulminant liver failure [100-102] and liver cirrhosis [67, 103, 104]. The iso-lation of hepatic stem/progenitor cells from fetal and adult human livers has been carried out by means of human liver progenitor cell markers including Cell Adhesion Molecule (EpCAM) or Thy-1 [105, 106] and in future, the confront is still there to efficiently gain hepatocytes from non-damaged stem/progenitor cells.
There are few challenges that still have to be considered critical regarding liver cellular transplantations [107]. Though, pluripotent cells including ESCs and iPSCs have been known for their efficient replicative ability as compared to BMCs and MSCs but are also recognized to have high oncogenic potential. Similarly, while focusing over hepato-cyte derivation and differentiation from stem cells, the liver-specific functions also need to be well thought-out, i.e. the metabolic and detoxification capacity of differentiated hepa-tocytes, for example ammonia metabolism, bilirubin detoxi-fication, clotting factor synthesis. Route of liver cell trans-plantation could be another major concern to be confronted, however so far various routes of cell delivery to the livers

Liver Stem Cells: From Preface to Advancements Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 7
including catheter into the portal vein or hepatic/splenic ar-tery, have provided improved liver functioning [107]. Still there is a need to reconsider the routs for cellular transplanta-tion in a damaged liver keeping in mind the stressor factors like oxidative stress affecting the environment of diseased hepatocytes.
Liver Engineering/Liver Assist Devices
The purpose of bioengineered external devices is to en-gender biological functions within the body in the most probable similar way as the normal organ would. The bioar-
tificial liver devices have been also designed to perform the metabolic, detoxification synthetic properties of liver in an accurate manner in patients with acute or acute-on-chronic liver failure [108]. These devices are designed using hepato-
cytes and artificial supports which interface with patient’s circulation. The liver cell bioreactors either have hollow fi-ber or monolayer culture usually using porcine hepatocytes [109-111]. These bioreactors comprising of hepatocytes 10%
of liver weight allow blood to pump through them as like in dialysis [108]. As far as the standards for hepatocytes to be used in these devices is concerned, Fiegel et al. have flaw-lessly compiled criteria for the hepatocytes to accomplish the
purpose of these bioengineered devices, which include proper in vitro cell growth, genetic/immulogical handling of candidate cells, cell cryopreservation and genetic modifica-tion of recipient’s in ex vivo environment before re-
implantation [112]. These bioartificial liver assist devices have undergone various investigational and clinical studies. A bioartificial liver that was used for liver patients utilizing hepatoblastoma-derived HepG2A/C3A cell line was named
extracorporeal liver-assisted device (ELAD) system which has shown slight improvement from clinical point of view [113]. A phase I clinical trial with CellModule was also per-formed on liver patients utilizing human and porcine hepato-
cytes [114]. Another device, HepatAssist was used in a ran-domized, controlled multicenter study was conducted on patients with fulminant/subfulminant hepatic failure which showed an improved 30-day survival [115]. Recently,
adult/fetal hepatocytes were subjected to reversible immor-talization with the help of immortalization gene which helped in the growth of hepatocytes. These hepatocytes were then incorporated into bioartificial device after deleting the
immortalization genes [116]. Moreover, Kobayashi [117] proposed the abilities of human ES cell KhESC-1 cell line-differentiated hepatocytes which included albumin produc-tion (351ng / g cells), ammaonia and lidocaine metabolism
(7.8% and 23.6% respectively).
Though, as compared to the orthotopic liver transplanta-tion, the use of bioartificial liver assist devices and cellular transplantation seems to have advantage of being available preserved by cryopreservation [118] with appropriate freez-ing and thawing, however, these experimental procedures and cells used still need to undergo a lot of investigational studies to prove their ability used for surviving and maintain-ing liver functions being an external system.
Drug Screening
One of the unique application of stem cells is the drug screening by utilizing LSCs [119] though they require a
complete metabolic profile for screening of new drugs, as major drug withdrawals are expected to be correlated with liver toxicity [120].
ISOLATED LIVER STEM CELLS
In general, it is believed that liver transplantation is only
the effective treatment of end stage liver cirrhosis. However, molecular biologists proposed successful clinical trials based on the intra-hepatic liver cells transplantations that have ex-tensive potential to repopulate injured liver [121]. These
cells include hepatocytes, MSCs, OCs and iPSCs. Recently, bipotent epithelial colony-forming cells have been suggested to be isolated form mouse liver (fetal and adult) using Ep-CAM positive cells [122, 123], and by the activation of OCs,
EpCAM+
and TROP2+ cells contributed in the regeneration
of liver [123].
Isolation of Human Fetal Liver Stem Cells
Researchers have designed a system to isolate culture and identify human fetal LSCs in vitro in order to lay down the infrastructure/foundation of biological artificial liver sup-
porting system and hepatocyte transplantation [124]. They isolated fetal liver stem cells from the liver of dead human fetus and maintained the suspension in DMEM and incu-bated it. Immunohistochemistry was used to identify the
phenotypes of the cultured cells. By staining techniques, they found some cells were positive for CK19 and albumin. They concluded that in human fetal liver, stem cells exist and pos-sess potential to differentiate. Researchers have isolated,
cultured and passaged liver epithelial cells of human fetal with bipotent competency and numbers of studies have pro-claimed their consecutive differentiation into hepatocytes after transplantation into SCID mice [125]. Such studies in-
dicate that a human counterpart to the rodent fetal LSCs or progenitor cells still exists and mounting attainments paved these emerging grooves in the near future to ensure these cells will become available for liver repopulation.
Isolation of Human Adult LSCs
In 2006, an attempt was made to isolate and characterized
the population of human LSCs. They identified a pluripotent population in mature human liver that could provide a basis for clinical cell therapy strategies. Researchers isolated hu-man hepatocytes from surgical specimens of patients who
had undergone hepatectomies by collagenase dissection [126].
Mammalian Resident LSCs
Mammalian resident liver stem cell (RLSCs), a non-tumorigenic stem cell line has been obtained from fetal and neonatal murine livers. RLSCs possess potential to sponta-neously differentiate into hepatic epithelia and are reported
to derive from the murine fetal and neonatal livers. Al-though, it possesses potential to express -fetoprotein ( FP), a predominant marker for early hepatocyte but it fails to ex-press albumin. RLSCs are the useful tool that may enhance
our understandings of LSCs and might lead to a successful new therapeutic approach for liver diseases in the coming era [127].

8 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
CHALLENGES RELATED TO LSCs
Thus far, we have discussed the probable sources of LSCs, however, conversely some of these sources have been also identified as a cause of hepatocellular carcinoma [128] enlightening the fact that development of cancer might be a major challenge related to LSCs.
Tumorigenesis
Cancer stem cells (CSCs) are characterized as the cells that have self renewal, differentiation and tumor initiative characteristics [129]. Recently, it has been reported that in the cell population, tumor is inhabited and cells that acquire potential of tumor growth are known as CSCs. Worldwide, hepatocellular carcinoma (HCC) is the most abundant cancer among primary liver cancers [130]. It is believed that like other cancers, HCC develops due to 3-6 critical mutations in genes that are critical for cell renewal and cell growth. These critical mutations are vital for transformation of normal cells into cancerous cells. To date, a growing body of evidence has reported the existence of CSCs in breast cancer, brain, colon, lungs and prostate cancers [131, 132].
It is worth mentioning that oncomirs (miRNAs) have emerged as key regulators in the cellular process. Mounting evidence suggests about behaviors of miRNAs during differ-entiation of human embryonic stem cells (hESCSs) into a specialized cell type. hESCSs were induced to definitive endoderm (DE) cells and further differentiated to hepato-cytes [133]. Recently, it has been found that miR-512-3p, miR-512-5p and miR-520c-3p were enriched in hESCSs, miR-9, miR-205 and miR-375 in hESCS-derived DE cells [134]. Compelling evidence indicates that let-7 and miR-181 family members were up-regulated in HSCs. Moreover, sup-pression of let-7 enhanced the chemosensitivity of HSCs to sorafenib and doxorubicin whereas abrogation of miR-181 led to a reduction in invasive potential of HSCs [135]. It is interesting to note that miRNAs contribute in the neoplastic transformation of liver cancer stem cells (LCSCs) during hepatocarcinogenesis. In accordance with the assumption, miR-10b, miR-21, miR-470, miR-34c-3p and let-7i were identified as overexpressed in HCC cells compared to fetal liver cells [136].
On a similar note, it has lately been found that differenti-ated aggressive HBs overexpressed the miR-371-3 cluster with simultaneous down-regulation of the miR-100/let-7a-2/miR-125b-1 cluster [137]. Consistent with the same con-cept miR-193b was considerably down-regulated in most of the HCC tissues however, re-establishment of miR-193b considerably suppressed the ability of hepatoma cells to form colonies in vitro and to develop tumors in nude mice [138]. Another intriguing mechanism that has recently been dis-mantled is cell-derived microvesicles (MVs). MVs after in-ternalization within target cells may deliver genetic informa-tion. Human liver resident stem cells were shown to release MVs shuttling functional mRNAs [139].
According to increasing information, it has been ac-claimed that microRNA-23b cluster microRNAs regulate transforming growth factor-beta/bone morphogenetic trans-duction cascade and liver stem cell differentiation by target-ing SMADs [140]. The idealistic potential of regeneration in mammalian liver after intensive injury serves as an impres-
sive tool to understand the role of stem cells in tissue recon-struction as well as in tumorigenesis. There has been accu-mulating evidence supporting the fact that CD133+ stem / progenitor cells identified as part of CSCs population that are responsible for the tumor formation in brain, prostate, liver and other type of cancers [141]. CD133+ cells possess greater proliferative potential, efficient colony and tumor formation ability in vivo [61, 142].
Liver Cancer and Epigenetic Regulation of CSCs
Cancer is a genetically derived disease and is tightly regulated by number of epigenetic factors. CSCs are consid-ered as the germinal center of tumor evolution [142]. In the past few years, growing evidence also support the confirma-tion that CSCs are not only involve in the tumor initiation but also in the metastasis and relapses. Varieties of stem cell surface markers are used to identify CSCs. These markers detect surface protein and most widely used surface markers for CSCs are CD133, CD90 and EpCAM (epithelial cell ad-hesion molecule). Intensive research efforts have unraveled various molecular mechanism of hepato-tumorigenesis [51, 143, 144]. Number of molecular pathways that are linked to the stem cell self renewal, maintenance and pluripotency are identified including WNT/ -Catenin, Myc, P53, hedgehog, NOTCH, TGF- , EGF etc. Growing evidence supporting the fact that deregulation of these pathways leads to the progno-sis of liver cancer [145]. WNT signaling is found to be in-volved in the embryonic development and maintenance of proliferation, cell fate and survival. Disruption of WNT sig-naling due to genetic and epigenetic changes results in the wide range of diseases included liver and Colon cancer [146]. Proto-Oncogene “MYC” is stimulated by wide range of stimuli and involve in the regulation of 15% of all genes. Proto-Oncogene MYC play critical role in the apoptosis, proliferation, differentiation and maintenance of stem cell pluripotency. Structural modification and over-expression of MYC gene involve in wide range of cancers including hu-man and murine hepatocarcinogenesis [147].
Intensive research efforts have suggested that notch plays decisive role in apoptosis, differentiation, cell fate determi-nation and many other developmental processes. Any disrup-tion in notch signaling results in large number of cancers including liver cancer [148, 149].
CONCLUSIVE REMARKS AND FUTURE PERSPEC-
TIVES
In summary, to improve the repopulation of liver, re-searchers have focused on liver stem cell as alternative source for liver therapy along with immortalized human he-patocytes, stem cell derived hepatocytes and fetal hepato-cytes. To deal with the end stage liver complications, differ-ent alternative therapies for liver transplant have been carried out. Nowadays, scientists have focused on the concept of “regenerative medicines” that relies on the exclusive poten-tial of stem cells because of their eligibility for liver cell re-placement including embryonic and fetal stem cells, induce pluripotent cells, endogenous LSCs, annex stem cells and extra-hepatic stem cells. Primarily, it has to be figured out whether the animal studies can be practiced according to human situation. A major complication faced during human study is difficulty in isolating human LSCs and requires the
Liver Stem Cells: From Preface to Advancements Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 9
identification of suitable stem cell markers; moreover, the dilemma of immune rejection also needs to be addressed. Finally, understanding of rules for the basis of hepatic differ-entiation is critical for realistic advancement in the state of therapeutic stem-cell transplantation.
CONFLICT OF INTEREST
The authors confirm that this article content has no con-flicts of interest.
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
[1] Evans MJ, Kaufman MH. Establishment in culture of pluripotential cells from mouse embryos. Nature 1981; 292(5819): 154-6.
[2] Martin GR. Isolation of a pluripotent cell line from early mouse embryos cultured in medium conditioned by teratocarcinoma stem
cells. Proc Natl Acad Sci USA 1981; 78(12): 7634-8. [3] Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. Embryonic stem
cell lines derived from human blastocysts. Science 1998; 282(5391): 1145-7.
[4] Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors.
Cell 2006; 126(4): 663-76. [5] Weissman I. Stem cells: units of development, units of regenera-
tion, and units in evolution. Cell 2000; 100(1): 157-68. [6] Robert P, Christine M. Origin and use of embryonic and adult stem
cells in differentiation and tissue repair. Cardiovasc Res 2003; 58(2): 324-335.
[7] Libbrecht L, Roskams T. Hepatic progenitor cells in human liver diseases. Semin Cell Dev Biol 2002; 13(6): 389-96.
[8] Smith A.A glossary for stem-cell biology. Nature 2006; 441: 1060. [9] Potten C, Loeffler M. Stem cells: attributes, cycles, spirals, pitfalls
and uncertainties; lessons for and from the crypt. Development 1990; 110(4): 1101-1120.
[10] Marshman E, Booth C, Potten CS. The intestinal epithelial stem cell. BioEssays 2002; 24(1): 91-8.
[11] Belghiti J, Carr BI, Greig PD, Lencioni R, Poon RT. Treatment before Liver Transplantation for HCC. Ann Surg Oncol 2008;
15(4): 993-1000. [12] Overturf K, Al-Dhalimy M, Ou C, Finegold M, Grompe M. Serial
transplantation reveals the stem-cell-like regenerative potential of adult mouse hepatocytes. Am J Pathol 1997; 151(5): 1273-80.
[13] Grompe M. The Role of Bone Marrow Stem Cells in Liver Regen-eration. Semin Liver Dis 2003; 23(4): 363-72.
[14] Itoh T, TanakaTanaka M, Miyajima A. Liver Stem Cells. In Re-generative Medicine 2011; (pp: 327-349). Springer Netherlands.
[15] Tanaka M, Itoh T, Tanimizu N, Miyajima A. Liver stem/progenitor cells: their characteristics and regulatory mechanisms. J Biochem
2011; 149(3): 231-9. [16] Matsumoto K, Yoshitomi H, Rossant J, Zaret KS. Liver organo-
genesis promoted by endothelial cells prior to vascular function. Science 2001; 294(5542): 559-63.
[17] Antoniou A, Raynaud P, Cordi S, et al. Intrahepatic bile ducts develop according to a new mode of tubulogenesis regulated by the
transcription factor SOX9. Gastroenterology 2009; 136(7): 2325-33.
[18] Onitsuka I, Tanaka M, Miyajima A. Characterization and func-tional analyses of hepatic mesothelial cells in mouse liver devel-
opment. Gastroenterology 2010; 138(4): 1525-35. [19] Ijpenberg A, Pérez-Pomares JM, Guadix JA, et al. Wt1 and retinoic
acid signaling are essential for stellate cell development and liver morphogenesis. Dev Biol 2007; 312(1): 157-70.
[20] Shafritz DA, Oertel M, Menthena A, Nierhoff D, Dabeva MD. Liver stem cells and prospects for liver reconstitution by trans-
planted cells. Hepatology 2006; 43(2): S89-S98. [21] Oertel M, Shafritz DA. Stem cells, cell transplantation and liver
repopulation. Biochim Biophys Acta 2008; 1782(2): 61-74.
[22] Dan YY, George CY. Liver stem cells: a scientific and clinical
perspective. J Gastroenterol Hepatol 2008; 23(5): 687-98. [23] Michalopoulos G, DeFrances M. Liver regeneration. Science 1997;
276(5309): 60-6. [24] Rhim J, Sangren E, Degan J, Palmiter R, Brinster R. Replacement
of diseased mouse liver by hepatic cell transplantation. Science 1994; 263(5150): 1149-52.
[25] Moore K, Lemischka I. Stem cells and their niches. Science 2006; 311(5769): 1880-1885.
[26] Mills JC, Gordon JI. The intestinal stem cell niche: There grows the neighborhood. Proc Natl Acad Sci USA 2001; 98(22): 12334-6.
[27] Tumbar T, Guasch G, Greco V, et al. Defining the epithelial stem cell niche in skin. Science 2004; 303(5656): 359-63.
[28] Conover JC, Notti RQ. The neural stem cell niche. Cell Tissue Res 2008; 331(1): 211-24.
[29] Sugiyama T, Nagasawa T. Bone Marrow Niches for Hematopoietic Stem Cells and Immune Cells. Inflamm Allergy Drug Targets
2012; 11(3): 201-6. [30] Santoni-Rugiu E, Jelnes P, Thorgeirsson SS, Bisgaard HC. Pro-
genitor cells in liver regeneration: molecular responses controlling their activation and expansion. APMIS, 2005; 113(11-12): 876-
902. [31] Van Hul N, Abarca J, Sempoux C, Horsmans Y, Leclercq IA. Rela-
tion between liver progenitor cell expansion and extracellular ma-trix deposition in a CDE-induced murine model of chronic liver in-
jury. Hepatology 2009; 49(5): 1625-35. [32] Alvaro D, Onori P, Metalli VD, et al. Intracellular pathways medi-
ating estrogen-induced cholangiocyte proliferation in the rat. Hepa-tology, 2002; 36(2): 297-304.
[33] Alvaro D, Alpini G, Onori P, et al. Effect of ovariectomy on the proliferative capacity of intrahepatic rat cholangiocytes. Gastroen-
terology, 2002; 123(1): 336-44. [34] Alison MR, Islam S, Lim S. Stem cells in liver regeneration,
fibrosis and cancer: the good, the bad and the ugly. J Pathol 2009; 217(2): 282-98.
[35] Jakubowski A, Ambrose C, Parr M, et al. TWEAK induces liver progenitor cell proliferation. J Clin Invest 2005; 115(9): 2330-40.
[36] Francis H, Glaser S, Demorrow S, et al. Small mouse cholangio-cytes proliferate in response to H1 histamine receptor stimulation
by activation of the IP3/CaMK I/CREB pathway. Am J Physiol Cell Physiol 2008; 295(2), C499-C513.
[37] Xiong A, Austin TW, Lagasse E, et al. Isolation of human fetal liver progenitors and their enhanced proliferation by three-
dimensional coculture with endothelial cells. Tissue Eng Part A 2008; 14(6): 995-1006.
[38] Jindal R, Nahmias Y, Tilles AW, Berthiaume F, Yarmush ML. Amino acid-mediated heterotypic interaction governs performance
of a hepatic tissue model. FASEB Journal 2009; 23(7): 2288-98. [39] Krause P, Saghatolislam F, Koenig S, Unthan-Fechner K, Probst I.
Maintaining hepatocyte differentiation in vitro through co-culture with hepatic stellate cells. In vitro Cell Dev Biol Anim 2009; 45(5-
6): 205-12. [40] Overturf K, al-Dhalimy M, Finegold M, Grome M. The repopula-
tion potential of hepatocyte population differing in size and prior mitotic expansion. Am J Pathol 1999; 155(6): 2135-43.
[41] Yuan R, Ogawa A, Ogawa E, Neufeld D, Zhu L, Shafritz D. p27Kip1 inactivation provides a proliferative advantage to trans-
planted hepatocytes in DPPIV/Rag2 double knockout mice after repeated host liver injury. Cell Transplant 2003; 12(8): 907-19.
[42] Michalopoulos G, Barua L, Bowen W. Transdifferentiation of rat hepatocytes into biliary cells after bile duct ligation and toxic bil-
iary injury. Hepatology 2005; 41(3): 535-44. [43] Paku S, Schnur J, Nagy P, Thorgeirsson S. Origin and structural
evolution of the early proliferating oval cells in rat liver. Am J Pathol 2001; 158(4): 1313-23.
[44] Dabeva MD, Shafritz DA. Activation, proliferation, and differen-tiation of progenitor cells into hepatocytes in the D-galactosamine
model of liver regeneration. Am J Pathol 1993; 143(6): 1606-20. [45] Fausto, N. Liver regeneration and repair: hepatocytes, progenitor
cells, and stem cells. Hepatology 2004; 39(6): 1477-87. [46] Erker L, Grompe M. Signaling networks in hepatic oval cell activa-
tion. Stem cell Res 2008; 1(2): 90-102. [47] Knight B, Yeoh GC, Husk KL, et al. Impaired preneoplastic
changes and liver tumor formation in tumor necrosis factor receptor type 1 knockout mice. J Exp Med 2000; 192(12): 1809-18.

10 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
[48] Akhurst B, Matthews V, Husk K, Smyth MJ, Abraham LJ, Yeoh
GC. Differential lymphotoxin-beta and interferon gamma signaling during mouse liver regeneration induced by chronic and acute in-
jury. Hepatology 2005; 41(2): 327-35. [49] Duret C, Gerbal S, Ramos J, et al. Isolation, characterization, and
differentiation to hepatocyte-like cells of nonparenchymal epithe-lial cells from adult human liver. Stem Cells, 2007; 25(7): 1779-90.
[50] Fausto N, Campbell JS. The role of hepatocytes and oval cells in liver regeneration and repopulation. Mech Dev 2003; 120(1): 117-
30. [51] Duncan A, Dorrell C, Grompe M. Stem cells and liver regenera-
tion. Gastroenterology 2009; 137(2): 466-81. [52] Theise N, Saxena R, Portmann B, et al. The canals of hering and
hepatic stem cells in human. Hepatology 1999; 30(6): 1425-33. [53] Oertel M, Menthena A, Dabeva MD, Shafritz DA. Cell competition
leads to a high level of normal liver reconstitution by transplanted fetal liver stem/progenitor cells. Gastroenterology 2006; 130(2):
507-20. [54] Mahieu-Caputo D, Allain JE, Branger J, et al. Repopulation of
athymic mouse liver by cryopreserved early human fetal hepa-toblasts. Hum Gene Ther 2004; 15(12): 1219-28.
[55] Kallis YN, Alison MR, Forbes SJ. Bone marrow stem cells and liver disease. Gut 2007; 56(5): 716-24.
[56] Cai Y, Sheng C, Shu-Ying S, Zuo-Jun Z, Huan-Wei C. Passage of bone-marrow-derived liver stem cells in a proliferating culture sys-
tem. World J Gastroenterol 2009; 13(13): 1630-5. [57] Sell S. Heterogeneity and plasticity of hepatocyte lineage cells.
Hepatology 2001; 33(3): 738-50. [58] Fujio K, Evarts R, Hu Z, Marsden ER, Thorgeirsson SS. Expres-
sion of stem cell factor and its receptor, c-kit, during liver regenera-tion from putative stem cells in the adult rat. Lab Invest 1994;
70(4): 511-6. [59] Peterson B, Goff J, Greenberger J, Michalopoulos GK. Hepatic
oval cells express the hematopoietic stem cell marker Thy-1 in the rat. Hepatology 1998; 27(2): 433-45.
[60] Avital I, Inderbitzin D, Aoki T, et al. Isolation, characterization, and transplantation of bone marrow-derived hepatocyte stem cells.
Biochem Biophys Res Commun 2001; 288(1): 156-64. [61] Lee J, Thorgeirsson S. Genetic profiling of human hepatocellular
carcinoma. Semin Liver Dis 2005; 25(2): 125-32. [62] Lee KD, Kuo TK, Whang-Peng J, et al. In vitro hepatic differentia-
tion of human mesenchymal stem cells. Hepatology 2004; 40(6): 1275-84.
[63] Fujii H, Hirose T, Oe S, Yasuchika K, et al. Contribution of bone marrow cells to liver regeneration after partial hepatectomy in
mice. J Hepatol 2002; 36(5): 653-9. [64] Abe S, Lauby G, Boyer C, Rennard SI, Sharp JG. Transplanted BM
and BM side population cells contribute progeny to the lung and liver in irradiated mice. Cytotherapy 2003; 5(6): 523-33.
[65] Sakaida I, Terai S, Yamamoto N, et al. Transplantation of bone marrow cells reduces CCL4-induced fibrosis in mice. Hepatology
2004; 40(6): 1304-11. [66] Oyagi S, Hirose M, Kojima M, et al. Therapeutic effect of trans-
planting HGF-treated bone marrow mesenchymal cells into CCL4-injured rats. J Hepatol 2006; 44(4): 742-8.
[67] Terai S, Ishikawa T, Omori K, et al. Improved liver function in liver cirrhosis patients after autologous bone marrow cell infusion
therapy. Stem Cells 2006; 24(10): 2292-8. [68] Ksiazek K. A comprehensive review on mesenchymal stem cell
growth and senescence. Rejuven Res 2009; 12(2): 105-16. [69] Kung JW, Forbes SJ. Stem cells and liver repair. Curr Opin Bio-
technol 2009; 20(5): 568-74. [70] Friedenstein AJ, Gorskaja JF, Kulagina NN. Fibroblast precursors
in normal and irradiated mouse hematopoietic organs. Exp Hematol 1976 ; 4(5): 267-74 .
[71] Sgodda M, Aurich H, Kleist S, et al. Hepatocyte differentiation of mesenchymal stem cells from rat peritoneal adipose tissue in vitro
and in vivo. Exp Cell Res 2007; 313(13): 2875-86. [72] Banas A, Teratani T, Yamamoto Y, et al. Adipose tissue-derived
mesenchymal stem cells as a source of human hepatocytes. Hepa-tology 2007; 46(1): 219-28.
[73] Aurich H, Sgodda M, Kaltwasser P, et al. Hepatocyte differentia-tion of mesenchymal stem cells from human adipose tissue in vitro
promotes hepatic integration in vivo. Gut 2009; 58(4): 570-81.
[74] Hung SC, Chen NJ, Hsieh SL, et al. Isolation and characterization
of size-sieved stem cells from human bone marrow. Stem Cells 2002; 20(3): 249 -58.
[75] De Ugarte DA, Alfonso Z, Zuk PA, et al. Differential expression of stem cell mobilization-associated molecules on multi-lineage cells
from adipose tissue and bone marrow. Immunol Lett 2003; 89(2-3): 267-70.
[76] Xu W, Zhang X, Qian H, et al. Mesenchymal stem cells from adult human bone marrow differentiate into a cardiomyocyte phenotype
in vitro. Exp Biol Med 2004; 229(7): 623-31. [77] Reger RL, Tucker AH, Wolfe MR. Differentiation and characteri-
zation of human MSCs. Methods Mol Biol 2008; 449: 93-107. [78] Kuang D, Zhao X, Xiao G, et al. Stem cell factor/c-kit signaling
mediated cardiac stem cell migration via activation of p38 MAPK. Basic Res Cardiol 2008; 103(3): 265- 73.
[79] Can A, Karahuseyinoglu S. Human umbilical cord stroma with regard to the source of fetus-derived stem cells. Stem Cells 2007;
25(11): 2886-95. [80] Lu LL, Liu YJ, Yang SG, et al. Isolation and characterization of
human umbilical cord mesenchymal stem cells with hematopoietic-supportive function and other potentials. Haematologica 2006;
91(8): 1017-26. [81] Friedman R, Betancur M, Boissel L, Tuncer H, Cetrulo C,
Klingemann H. Umbilical cord mesenchymal stem cells: adjuvants for human cell transplantation. Biol Blood Marrow Transplant
2007; 13(12): 1477-86. [82] Deans RJ, Moseley AB. Mesenchymal stem cells: biology and
potential clinical uses. Exp Hematol 2000; 28(8): 875-84. [83] Bühring HJ, Battula VL, Treml S, Schewe B, Kanz L, Vogel W.
Novel markers for the prospective isolation for human MSC. Ann N Y Acad Sci 2007; 1106: 262-71.
[84] Karahuseyinoglu S, Cinar O, Kilic E, et al. Biology of stem cells in human umbilical cord stroma: in situ and in vitro surveys. Stem
Cells 2007; 25(2): 319-31. [85] Bakhshi T, Zabriskie RC, Bodie S, et al. Mesenchymal stem cells
from the Wharton's jelly of umbilical cord segments provide stro-mal support for the maintenance of cord blood hematopoietic stem
cells during long-term ex vivo culture. Transfusion 2008; 48(12): 2638-44.
[86] Anzalone R, Iacono ML, Corrao S, et al. New emerging potentials for human Wharton's jelly mesenchymal stem cells: immunological
features and hepatocyte-like differentiative capacity. Stem Cells Dev 2010; 19(4): 423-38.
[87] Lysy PA, Campard D, Smets F, et al. Persistence of a chimerical phenotype after hepatocyte differentiation of human bone marrow
mesenchymal stem cells. Cell Prolif 2008; 41(1): 36-58. [88] Jameson E. Cellular Transplantation for Liver Diseases. Gastroen-
terol Res 2008; 1(1): 8-13. [89] Sancho-Bru P, Najimi M, Caruso M, et al. Stem and progenitor
cells for liver repopulation: can we standardise the process from bench to bedside? Gut 2009; 58(4): 594-603.
[90] Braun KM, Degen JL, Sandgren EP. Hepatocyte transplantation in a model of toxin-induced liver disease: variable therapeutic effect
during replacement of damaged parenchyma by donor cells. Nat Med 2000; 6(3): 320-6.
[91] Wilson JM, Chowdhury NR, Grossman M, et al. Temporary ame-lioration of hyperlipidemia in low density lipoprotein receptor-
deficient rabbits transplanted with genetically modified hepato-cytes. Proc Natl Acad Sci USA 1990; 87(21): 8437-41.
[92] Fox IJ, Chowdhury JR, Kaufman SS, et al. Treatment of the Crigler-Najjar syndrome type I with hepatocyte transplantation. N
Engl J Med 1998; 338(20): 1422-6. [93] Chowdhury JR, Chowdhury NR, Strom SC, Kaufman SS, Horslen
S, Fox IJ. Human hepatocyte transplantation: gene therapy and more? Pediatrics 1998; 102(3): 647-8.
[94] Nguyen TH, Birraux J, Wildhaber B, et al. Ex vivo lentivirus transduction and immediate transplantation of uncultured hepato-
cytes for treating hyperbilirubinemic Gunn rat. Transplantation 2006; 82(6): 794-803.
[95] Bilir BM, Guinette D, Karrer F, et al. Hepatocyte transplantation in acute liver failure. Liver Transplantation 2000; 6(1): 32-40.
[96] Petersen BE, Bowen WC, Patrene KD, et al. Bone marrow as a potential source of hepatic oval cells. Science, 1999; 284(5417):
1168-70.

Liver Stem Cells: From Preface to Advancements Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 11
[97] Fiegel HC, Lioznov MV, Cortes-Dericks L, et al. Liver-specific
gene expression in cultured human hematopoietic stem cells. Stem Cells, 2003; 21(1): 98-104.
[98] Lagasse E, Connors H, Al-Dhalimy M, et al. Purified hema-topoietic stem cells can differentiate into hepatocytes in vivo. Nat
Med 2000; 6(11): 1229-34. [99] Jang YY, Collector MI, Baylin SB, Diehl AM, Sharkis SJ. Hema-
topoietic stem cells convert into liver cells within days without fu-sion. Nature Cell Biol 2004; 6(6): 532-9.
[100] Habibullah CM, Syed IH, Qamar A, Taher-Uz Z. Human fetal hepatocyte transplantation in patients with fulminant hepatic fail-
ure. Transplantation 1994; 58(8): 951-2. [101] Strom SC, Chowdhury JR, Fox IJ. Hepatocyte transplantation for
the treatment of human disease. Semin Liver Dis 1999; 19(1): 39-48.
[102] Cho CH, Parashurama N, Park EY, et al. Homogeneous differentia-tion of hepatocyte-like cells from embryonic stem cells: applica-
tions for the treatment of liver failure. FASEB Journal 2007; 22(3): 898-909.
[103] Mito M, Kusano M, Kawaura Y. Hepatocyte transplantation in man. Transplant Proc 1992; 24(6): 3052-3.
[104] Lyra AC, Soares MB, da Silva LF, et al. Feasibility and safety of autologous bone mar-row mononuclear cell transplantation in pa-
tients with advanced chronic liver disease. World J Gastroenterol 2007; 13(7): 1067-73.
[105] Schmelzer E, Zhang L, Bruce A, et al. Human hepatic stem cells from fetal and postnatal donors. J Exp Med 2007; 204(3): 1973-
1987. [106] Weiss TS, Lichtenauer M, Kirchner S, et al. Hepatic progenitor
cells from adult human livers for cell transplantation. Gut 2008; 57(8): 1129-38.
[107] Dan YY. Clinical Uses of Liver Stem Cells. In Liver Stem Cells 2012; (pp. 11-23). Springer New York.
[108] Streetz KL. Bio-artificial liver devices-tentative, but promising progress. J Hepatol 2008; 48(2): 189-91.
[109] Pearse MJ, Witort E, Mottram P, et al. Anti-gal antibody-mediated allograft rejection in alpha1,3-galactosyltrans-ferase gene knockout
mice: a model of delayed xenograft rejection. Transplantation 1998; 66(6): 748-54.
[110] Obermayer N, Busse B, Grünwald A, et al. Biochemical charac-terization of bioreactors for hybrid liver support: serum-free liver
cell coculture of nonparenchymal and parenchymal cells. Trans-plant Proc 2001; 33(1-2): 1930-1.
[111] Bartolo LD, Bader A. Flat membrane bioreactor for the replace-ment of liver functions. Ernst Schering Res Found Workshop 2002;
(35): 89-104. [112] Fiegel HC, Kaufmann PM, Bruns H, Kluth D, Horch RE, Vacanti
JP, Kneser U. Hepatic tissue engineering: from transplantation to customized cell-based liver directed therapies from the laboratory.
J Cell Mol Med 2007; 12(1): 56-66 [113] Ellis AJ, Hughes RD, Wendon JA, et al. Pilot-controlled trial of the
extracorporeal liver assist device in acute liver failure. Hepatology 1996; 24(6): 1446-51.
[114] Sauer IM, Kardassis D, Zeillinger K, et al. Clinical extracorporeal hybrid liver support – phase I study with primary porcine liver
cells. Xenotransplantation 2003; 10(5): 460-9. [115] Demetriou AA, Brown RS, Busuttil RW, et al. Prospective, ran-
domized, multicenter, controlled trial of a bioartificial liver in treat-ing acute liver failure. Ann Surg 2004; 239(5): 660-7.
[116] Poyck PP, van Wijk AC, van der Hoeven TV, et al. Evaluation of a new immortalized human fetal liver cell line (cBAL111) for appli-
cation in bioartifi cial liver. J Hepatol 2008; 48(2): 266-75. [117] Kobayashi N. Life support of artificial liver: development of a
bioartificial liver to treat liver failure. J Hepatobiliary Pancreat Surg 2009; 16(2): 113-7.
[118] Schneider A, Attaran M, Meier PN, et al. Hepatocyte transplanta-tion in an acute liver failure due to mushroom poisoning. Trans-
plantation 2006; 82(2): 1115-6. [119] Choi SM, Kim Y, Shim JS, et al. Efficient drug screening and gene
correction for treating liver disease using patient-specific stem cells. Hepatology 2013; 57(6): 2458-68.
[120] Lee WM. Acute liver failure in the United States. Semin Liver Dis 2003; 23(3): 217-26.
[121] Piscaglia AC, Campanale M, Gasbarrini A, Gasbarrini G. Stem cell-based therapies for liver diseases: state of the art and new per-
spectives. Stem Cells Int 2010; 2010: 259461.
[122] Tanaka M, Okabe M, Suzuki K, et al. Mouse hepatoblasts at dis-
tinct developmental stages are characterized by expression of Ep-CAM and DLK1: drastic change of EpCAM expression during
liver development. Mech Dev 2009; 126(8-9): 665-76. [123] Okabe M, Tsukahara Y, Tanaka M, et al. Potential hepatic stem
cells reside in EpCAM+ cells of normal and injured mouse liver. Development 2009; 136(11): 1951-60.
[124] Mao H, Yao-Kai C, Yu-Ming W, Lei Z,Guo-Dong L. Isolation, culture and identification of human fetal liver stem cells in vitro.
World Chin J Digestol 2005; 15(4): 452-5. [125] Ma S, Chan KW, Hu L, et al. Identification and Characterization of
Tumorigenic Liver Cancer Stem/Progenitor Cells. Gastroenterol-ogy 2007; 132(7): 2542-56.
[126] Dan Y, Riehle K, Lazaro C, et al. Isolation of multipotent progeni-tor cells from human fetal liver capable of differentiating into liver
and mesenchymal lineages. Proc Natl Acad Sci USA 2006; 103(26): 9912-7.
[127] Conigliaro1 A, Colletti M, Cicchini1 C, et al. Isolation and charac-terization of a murine resident liver stem cell. Cell Death Different
2008; 15(1): 123-33. [128] Knight B, Matthews VB, Olynyk JK, Yeoh GC. Jekyll and Hyde:
evolving perspectives on the function and potential of the adult liver progenitor (oval) cell. Bioessays 2005; 27(11): 1192-202.
[129] Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells. Nature 2007; 414(6859): 105-11.
[130] El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiol-ogy and molecular carcinogenesis. Gastroenterology 2007; 132(7):
2557-76. [131] Dick JE. Breast cancer stem cells revealed. Proc Natl Acad Sci
USA 2003; 100(7): 3547-3549. [132] Visvader JE, Lindeman GJ. Cancer stem cells in solid tumours:
accumulating evidence and unresolved questions. Nat Rev Cancer 2008; 8(10): 755-768.
[133] Agarwal S, Holton KL, Lanza R. Efficient Differentiation of Func-tional Hepatocytes from Human Embryonic Stem Cells. Stem Cells
2008; 26(5): 1117-27. [134] Kim N, Kim H, Jung I, Kim Y, Kim D, Han YM. Expression pro-
files of miRNAs in human embryonic stem cells during hepatocyte differentiation. Hepatol Res 2011; 41(2): 170-83.
[135] Meng F, Glaser SS, Francis H, et al. Functional Analysis of mi-croRNAs in HumanHepatocellular Cancer Stem Cells. J Cell Mol
Med 2012; 16(1): 160-73. [136] Li R, Qian N, Tao K, You N, Wang X, Dou K. MicroRNAs in-
volved in neoplastic transformation of liver cancer stem cells. J Exp Clin Cancer Res 2010; 29: 169.
[137] Cairo S, Wang Y, de Reyniès A, et al. Stem cell-like micro-RNA signature driven by Myc in aggressive liver cancer. Proc Natl Acad
Sci USA 2010; 107(47): 20471-20476. [138] Xu C, Liu S, Fu H, et al. MicroRNA-193b regulates proliferation,
migration and invasion in human hepatocellular carcinoma cells. Eur J Cancer 2010; 46(15): 2828-36.
[139] Collino F, Deregibus MC, Bruno S, et al. Microvesicles derived from adult human bone marrow and tissue specific mesenchymal
stem cells shuttle selected pattern of miRNAs. PloS One 2010; 5(7): e11803.
[140] Rogler CE, Levoci L, Ader T, et al. MicroRNA-23b cluster mi-croRNAs regulate transforming growth factor-beta/bone morpho-
genetic protein signaling and liver stem cell differentiation by tar-geting Smads. Hepatology 2009; 50(2): 575-84.
[141] Ma S, Chan KW, Hu L, et al. Identification and characterization of tumorigenic liver cancer stem/progenitor cells. Gastroenterology
2007; 132(7): 2542-56. [142] Feinberg AP, Tycko B. The history of cancer epigenetics. Nat Rev
Cancer 2004; 4(2): 143-153. [143] Villanueva A, Newell P, Chiang D, Friedman S and Llovet J. Ge-
nomics and signaling pathways in hepatocellular carcinoma. Semin Liver Dis 2007; 27(1): 55-76.
[144] Marquardt J, Thorgeirsson S. Stem cells in hepatocarcinogenesis: evidence from genomic data. Semin Liver Dis 2010; 30(1): 26-34.
[145] Moon R, Kohn A, De Ferrari G, Kaykas A. WNT and beta-catenin signalling: diseases and therapies. Nat Rev Genet 2004; 5(9): 691-
701. [146] Barker N, Clevers H. Mining the Wnt pathway for cancer therapeu-
tics. Nat Rev Drug Discov 2006; 5(12): 997-1014.

12 Current Stem Cell Research & Therapy, 2014, Vol. 9, No. 1 Rehman et al.
[147] Shachaf C, Kopelman A, Arvanitis C, et al. MYC inactivation
uncovers pluripotent differentiation and tumour dormancy in hepa-tocellular cancer. Nature 2004; 431(7012): 1112-1117.
[148] Bolos V, Grego J, Pompa J. Notch signaling in development and cancer. Endocr Rev 2007; 28(3): 339-63.
[149] Tan J, Hytiroglou P, Wieczorek R, Park Y, Thung S, Arias B. Im-
munohistochemical evidence for hepatic progenitor cells in liver diseases. Liver 2002; 22(5): 365-73.
Received: July 30, 2013 Revised: September 27, 2013 Accepted: September 28, 2013