
Screening Parents During Child Evaluations: Exploring Parent and Child Psychopathology in the Same...
10
NEW RESEARCH Screening Parents During Child Evaluations: Exploring Parent and Child Psychopathology in the Same Clinic Hilary B. Vidair, Ph.D., Jazmin A. Reyes, M.S., Sa Shen, Ph.D., Maria A. Parrilla-Escobar, M.D., Charlotte M. Heleniak, B.A., Ilene L. Hollin, M.PH., Scott Woodruff, B.A., J. Blake Turner, Ph.D., Moira A. Rynn, M.D. Objective: Children of depressed and/or anxious parents are at increased risk for developing psychiatric disorders. Little research has focused on screening parents bringing their children for psychiatric evaluation, and few studies have included fathers or Hispanic children. This study had the following aims: 1) to identify current symptom rates in parents bringing their children for evaluation; and 2) to determine whether parental symptoms were associated with children’s symptoms, diagnoses, and functioning. Method: The sample included 801 moth- ers, 182 fathers, and 848 children (aged 6 through 17 years). The majority (55.66%) were Hispanic, who attended a child and adolescent psychiatric evaluation service. Parent and child symptoms were assessed via parental reports. Children’s diagnoses and functioning were determined by clinicians. Multiple regression analyses were used to determine whether severity of parental symptoms was associated with clinical child variables adjusting for child and parent demographic variables. Results: In all, 18.80% of mothers and 18.42% of fathers reported elevated internalizing symptoms. Maternal symptoms were significantly associated with problems in children’s functioning and children’s anxiety, depression, and oppositional/ conduct diagnoses; but not attention-deficit/hyperactivity disorder. Adjusting for parental and child demographics had a reduction on the effect of maternal symptoms on child depression. Paternal symptoms and functioning were positively associated with children’s diagnoses, but the associations were smaller and not significant. Both parents’ symptoms were significantly associated with children’s internalizing and externalizing symptoms. However, these significant effects were not moderated by marital status or child ethnicity. Conclusions: This study highlights the importance of screening parents when their children receive a psychiatric evaluation. The findings support the development of mental health services that address psychiatric needs of the entire family within one clinical setting. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(5):441– 450. Key Words: parent screening, child psychiatric evaluation C hildren and adolescents whose parents experience depression and anxiety are at high risk for developing their own psy- chiatric symptoms and disorders. Top-down studies assessing offspring of parents with life- time symptoms as compared to nonsymptomatic parents 1-3 and bottom-up studies comparing first-degree relatives of psychiatrically ill and non-ill children 4-6 have demonstrated signifi- cantly higher rates of psychopathology in symp- tomatic children and parents, respectively. How- ever, few studies assessing the relationship between parent and child psychopathology have specifically targeted families in which either the parent or child is experiencing current psychiatric symptoms for which they are seeking treatment. Pilowsky et al. 7 examined children of mothers currently experiencing a major depressive disor- der and found that approximately 34% of chil- dren met criteria for depressive, anxiety, or dis- ruptive behavior disorders. Beidel and Turner 8 also reported that 35% of children of parents with a current anxiety disorder and 38% of children of This article is discussed in an editorial by Dr. David Reiss on page 431. An interview with the author is available by podcast at www.jaacap.org. JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY VOLUME 50 NUMBER 5 MAY 2011 441 www.jaacap.org
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Screening Parents During Child Evaluations: Exploring Parent and Child Psychopathology in the Same...
NEW RESEARCH
Screening Parents During ChildEvaluations: Exploring Parent and Child
Psychopathology in the Same ClinicHilary B. Vidair, Ph.D., Jazmin A. Reyes, M.S., Sa Shen, Ph.D.,
Maria A. Parrilla-Escobar, M.D., Charlotte M. Heleniak, B.A., Ilene L. Hollin, M.PH.,Scott Woodruff, B.A., J. Blake Turner, Ph.D., Moira A. Rynn, M.D.
Objective: Children of depressed and/or anxious parents are at increased risk for developingpsychiatric disorders. Little research has focused on screening parents bringing their childrenfor psychiatric evaluation, and few studies have included fathers or Hispanic children. Thisstudy had the following aims: 1) to identify current symptom rates in parents bringing theirchildren for evaluation; and 2) to determine whether parental symptoms were associated withchildren’s symptoms, diagnoses, and functioning. Method: The sample included 801 moth-ers, 182 fathers, and 848 children (aged 6 through 17 years). The majority (55.66%) wereHispanic, who attended a child and adolescent psychiatric evaluation service. Parent and childsymptoms were assessed via parental reports. Children’s diagnoses and functioning weredetermined by clinicians. Multiple regression analyses were used to determine whetherseverity of parental symptoms was associated with clinical child variables adjusting for childand parent demographic variables. Results: In all, 18.80% of mothers and 18.42% of fathersreported elevated internalizing symptoms. Maternal symptoms were significantly associatedwith problems in children’s functioning and children’s anxiety, depression, and oppositional/conduct diagnoses; but not attention-deficit/hyperactivity disorder. Adjusting for parentaland child demographics had a reduction on the effect of maternal symptoms on childdepression. Paternal symptoms and functioning were positively associated with children’sdiagnoses, but the associations were smaller and not significant. Both parents’ symptoms weresignificantly associated with children’s internalizing and externalizing symptoms. However, thesesignificant effects were not moderated by marital status or child ethnicity. Conclusions: Thisstudy highlights the importance of screening parents when their children receive a psychiatricevaluation. The findings support the development of mental health services that addresspsychiatric needs of the entire family within one clinical setting. J. Am. Acad. Child Adolesc.Psychiatry, 2011;50(5):441–450. Key Words: parent screening, child psychiatric evaluation
n
cddr
C hildren and adolescents whose parentsexperience depression and anxiety are athigh risk for developing their own psy-
chiatric symptoms and disorders. Top-downstudies assessing offspring of parents with life-time symptoms as compared to nonsymptomaticparents1-3 and bottom-up studies comparingfirst-degree relatives of psychiatrically ill and
This article is discussed in an editorial by Dr. David Reiss on page431.
An interview with the author is available by podcast at
www.jaacap.org.JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
on-ill children4-6 have demonstrated signifi-cantly higher rates of psychopathology in symp-tomatic children and parents, respectively. How-ever, few studies assessing the relationshipbetween parent and child psychopathology havespecifically targeted families in which either theparent or child is experiencing current psychiatricsymptoms for which they are seeking treatment.
Pilowsky et al.7 examined children of mothersurrently experiencing a major depressive disor-er and found that approximately 34% of chil-ren met criteria for depressive, anxiety, or dis-uptive behavior disorders. Beidel and Turner8
also reported that 35% of children of parents with
a current anxiety disorder and 38% of children of441www.jaacap.org

VIDAIR et al.
parents with a current depressive disorder metcriteria for a current psychiatric disorder. Thispercentage increased to 45% when parents hadboth disorders. Identifying current parental symp-toms is important because parental psychopathol-ogy has been found to lead to poorer treatmentresponse in their children9-11 and increased psycho-pathology later in their lives.3,12 Recent studiessuggest that successful treatment of depressedmothers improves child outcome.13-15
Given the relationship between parent andchild psychopathology, the clinical evaluationshould include screening mothers and fathers forsymptoms of depression and anxiety at the time oftheir child’s evaluation. It gives the clinician anopportunity to engage parents in a dialogue aboutthe relationship between their symptoms and theirchild’s treatment outcomes, the potential benefits ofseeking their own treatment, and referral options.However, it is not standard practice to screenparents of children undergoing psychiatric evalua-tion. Only two studies have screened mothersbringing their children to a child mental healthclinic for evaluation. Ferro et al.16 examined psy-chiatric problems in 117 mothers bringing theirchildren for the evaluation or treatment of dep-ression. Based on a modified screener of thePRIME-MD Patient Problem Questionnaire, 31% ofthese mothers endorsed symptoms suggestingcurrent psychiatric diagnosis, whereas 43% re-ported subsyndromal symptoms. Swartz et al.17
assessed 222 mothers who brought their childrenfor evaluation and found that 61% met DSM-IVcriteria for an axis I disorder, most commonlydepressive and anxiety disorders. This was the firstpaper to assess the relationship between maternaland child psychopathology at the time of a child’spsychiatric evaluation. Children of mothers with adiagnosis were significantly more likely to presentwith a current axis I disorder and more diagnosesthan children of healthy mothers.
Although these two studies demonstrate theimportance of screening mothers who are bringingchildren for psychiatric evaluation, the samplesizes were small and did not include fathers. Fewclinical studies have assessed paternal psychopa-thology. Cassano et al.18 examined 702 articles onclinical child and adolescent research that includedparental participation to determine the frequencyof fathers’ inclusion. Overall, 55% of the studiesincluded only mothers, whereas only 1% focusedsolely on the fathers. When both parents were
included (45% of studies), researchers rarely con-JOURN
442 www.jaacap.org
ducted separate analyses for each gender, making itdifficult to draw parent-specific conclusions. Inaddition, at least 94% of studies did not includeresearch on Hispanic individuals. It is important toaddress the gap in parent–child research for His-panic families because little evidence is availableregarding effective treatment of Hispanic parentsand children, who are the largest and fastest-grow-ing minority in the United States.19
The goals of the present study were as follows:1) toidentify the current rates of parental symp-toms in families coming to the New York StatePsychiatric Institute (NYSPI)/Columbia Univer-sity (CU) Child and Adolescent Psychiatric Eval-uation Service (CAPES); 2) to determine whetherthere was a relationship between parental symp-toms and parent reports of their children’s symp-toms; and 3) to determine whether severity ofparental symptoms was associated with chil-dren’s diagnoses and functioning. This study isthe first to screen fathers bringing their childrenfor psychiatric evaluation and has the largestsample size of parents screened during childpsychiatric evaluation, more than half of whomwere Hispanic. We expected elevated rates of pa-rental depressive and anxious symptoms in thissample because children with psychopathology of-ten have parents with psychiatric disorders them-selves. We expected that parents with elevatedsymptoms of depression and anxiety would reportsignificantly more psychiatric symptoms and func-tional impairment in their children than parentswithout elevated symptoms. Children of parentswith elevated symptoms would also be signifi-cantly more likely to have psychiatric diagnoses. Inaddition, we explored whether results would differamong Hispanic and non-Hispanic and betweenmarried and single parents. Marital status wasexamined as a moderator because the literaturesuggests that single mothers of lower socioeco-nomic status are more likely to be depressedand/or to have anxiety disorders, whereas theirchildren are more likely to have symptoms andfunctional impairment.20,21
METHODStudy data come from the CAPES database. CAPESprovides free expert consultation, evaluation, and re-ferrals for children and adolescents with a range ofsocial, emotional, and behavioral difficulties. CAPESfunctions as part of the Advanced Center for Interven-tion and Services Research (ACISR) for Pediatric Psy-
chiatric Disorders at NYSPI/CU and serves as a liaisonAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011

apSfd(spitaasrfoaigdwssc[b(
Casts
SCREENING PARENTS AT CHILD EVALUATIONS
between families and various research, training, andclinical programs available.
The sample includes youth 6 through 17 years ofage who were evaluated between June 10, 2002, andMarch 27, 2008. The majority of families included inthe study were referred by pediatricians and reside inNew York City. Before evaluation, one parent (or legalguardian) completed a telephone interview assessingthe presence of the child’s psychiatric symptoms. Thisinterview was designed to exclude children with alife-threatening medical illness, active psychosis, ac-tive suicidality, mental retardation, pervasive develop-mental disorder, or physical/sexual abuse.
To be included in analysis, children needed to haveat least one parent complete the Brief Symptom Inven-tory 18 (BSI) 22 and the Child Behavior Checklist(CBCL).23 Children with a primary diagnosis of psy-chotic disorder, bipolar disorder, trichotillomania,mental retardation, or pervasive developmental disor-der were excluded because they were not typicallyincluded in CAPES.
Of 1,193 children evaluated, 345 were excluded forthe following reasons: they were younger than 6 years(n � 206); they did not have a parent who completedboth the BSI and CBCL (n � 87); or they met criteria foran excluded disorder (n � 52). Overall, 848 childrenand adolescents (mean age � 10.43 years, SD � 3.19years) met criteria for this study, and 31.49% (N � 267)were female. The sample included a total of 801 mothers(mean age � 38.87 years, SD � 7.97 years) and 182fathers (mean age � 42.95 years, SD � 8.56 years). Ofthese, 135 were couples.
MeasuresDemographic Form. The Demographic Form is a 23-item parent-report measure created by ACISR to col-lect biographical information about parents and chil-dren. Information regarding child age, gender, race,ethnicity, education, and medical history is collected.Parents also provide information concerning their age,gender, race, ethnicity, and marital, education, andoccupational status.Child Behavior Checklist for Ages 6-18 (CBCL).23 TheCBCL is a measure that allows parents to rate theirchildren’s behavior and social-emotional functioning.The CBCL is normed separately for boys and girls, andconsists of 118 items. Externalizing and internalizingfactor T scores generated from fathers’ and mothers’responses were analyzed.Brief Symptom Inventory-18 (BSI).22 The BSI is aself-report measure designed to assess psychologicaldistress in medical and community samples. The BSIconsists of 18 items that describe symptoms relatedto depression, anxiety, and somatization. A GlobalSeverity Index of distress is derived by totaling thethree subscales. For each item, parents were in-
structed to report on a five-point Likert scale howJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
much they were distressed by particular problemsduring the past 7 days (0 � not at all to 4 �extremely). Higher scores indicate higher levels ofsymptom severity.Diagnostic Interview. A clinician semistructured di-
gnostic interview administered separately to thearent and child, based on the Diagnostic Interviewchedule for Children, assessed DSM-IV TR criteriaor anxiety, mood, oppositional defiant and conductisorder, attention-deficit/hyperactivity disorder
ADHD), and eating, pervasive developmental, andubstance use disorders. Clinicians asked about eachotential symptom and circled “yes” or “no” on an
nterview form. Developmental, educational, andreatment histories were obtained. Interviews tookpproximately 90 minutes to complete with parentsnd 45 to 60 minutes with children. Often otherources of information were available (teachers, refer-ing pediatrician). Axis I diagnoses were grouped intoour categories: depression (any major depressive dis-rder without psychotic features, dysthymic disorder,nd depressive disorder not otherwise specified), anx-ety (panic disorder with or without agoraphobia,eneralized anxiety disorder, separation anxiety disor-er, social phobia, specific phobia, anxiety not other-ise specified, phobia unspecified, obsessive compul-
ive disorder, somatization disorder, post-traumatictress disorder. and selective mutism), oppositional/onduct disorder (oppositional defiant disorderODD], any conduct disorder [CD], and disruptiveehavior disorder not otherwise specified) and ADHDany type).
Children’s Global Assessment Scale (CGAS).24 TheGAS, an adaptation of the Global Assessment Scale fordults, is a 100-point scale measuring psychological,ocial, and school functioning for children aged 6hrough 17 years. Scores 70 or below are associated withignificant functional impairment.
ProcedureProcedures were approved by NYSPI’s institutionalreview board. Written informed consent was obtainedfrom a parent, and informed consent or assent wasobtained from the child/adolescent during the initialvisit. Parents and children were instructed to completeself-report questionnaires. A master’s level psychologystudent or postdoctoral clinical fellow in psychologyconducted the semistructured diagnostic interview.Clinicians were supervised by a licensed psychologistand child psychiatrist. Families then received feedbackfrom the clinician and psychologist and/or psychia-trist. A bilingual translator served as an interpreter forSpanish-speaking parents during the parent interview.Spanish parent self-report measures were available.
Each evaluation lasted 3 to 4 hours and took placeover one to two visits, typically within 2 to 3 weeks.
Diagnostic consensus from a multidisciplinary team443www.jaacap.org

tt1
sil
VIDAIR et al.
was obtained for each case. After consensus wasreached, families were mailed a written report.
Data AnalysisFor descriptive purposes, demographic variables formothers, fathers, and children are presented. Preva-lence for each child diagnosis is calculated by dividingthe number of positive cases by the total number ofcases assessed and presented as a percentage. Toexamine the “accuracy” of parents’ reports based onthe frequency of their own psychiatric symptoms,relationships between parental reports of children’sinternalizing and externalizing symptoms on theCBCL and clinician’s reports of children’s internalizingand externalizing diagnoses are assessed.
The relationship of overall parental BSI scores tocontinuous child outcomes (CBCL, CGAS) are as-sessed using linear regression. When child diagnosis isused as the outcome, the effects of BSI scores areestimated using logistic regression. These models areestimated both with and without adjustments fordemographic variables (child age, gender, race/ethnic-ity; parent age, marital status, occupation). Normality istested for continuous predictors and outcomes (Shapiro–Wilk test statistics range from 0.85 to 0.99 in mothers andfrom 0.80 to 0.99 in fathers). All continuous predictorsand outcomes are standardized, and standardized coef-ficients/odd ratios are estimated.
No child demographic data are missing. Missingdata on parental demographic characteristics are han-dled through multiple imputation. Multiple imputationwith a Markov Chain Monte Carlo was used to imputemissing continuous values. Multiple imputation withoutrounding was also used to impute categorical missingdata. Five completed datasets were created using a SASprocedure PROC MI. For each individual imputed dataset,linear regressions are carried out on continuous outcomesand logistic regression on the dichotomous outcome. Re-sults of analyses across the five imputed datasets are com-bined via PROC MIANALYZE to generate final param-eter estimates and their corrected standard errors.
To test the moderation effects of parental maritalstatus on the relation of parent’s BSI scores to CBCLscores, CGAS scores, or children’s diagnoses, the in-teraction of parental marital status and BSI scores isalso included in the corresponding models. Analysesare performed on mothers and fathers, respectively.Similar analyses are used to test the moderation effectsof child ethnicity (Hispanic versus non-Hispanic).
All analyses were performed in SPSS v13.0 or SASv9.0, with two-tailed 5% significance levels.
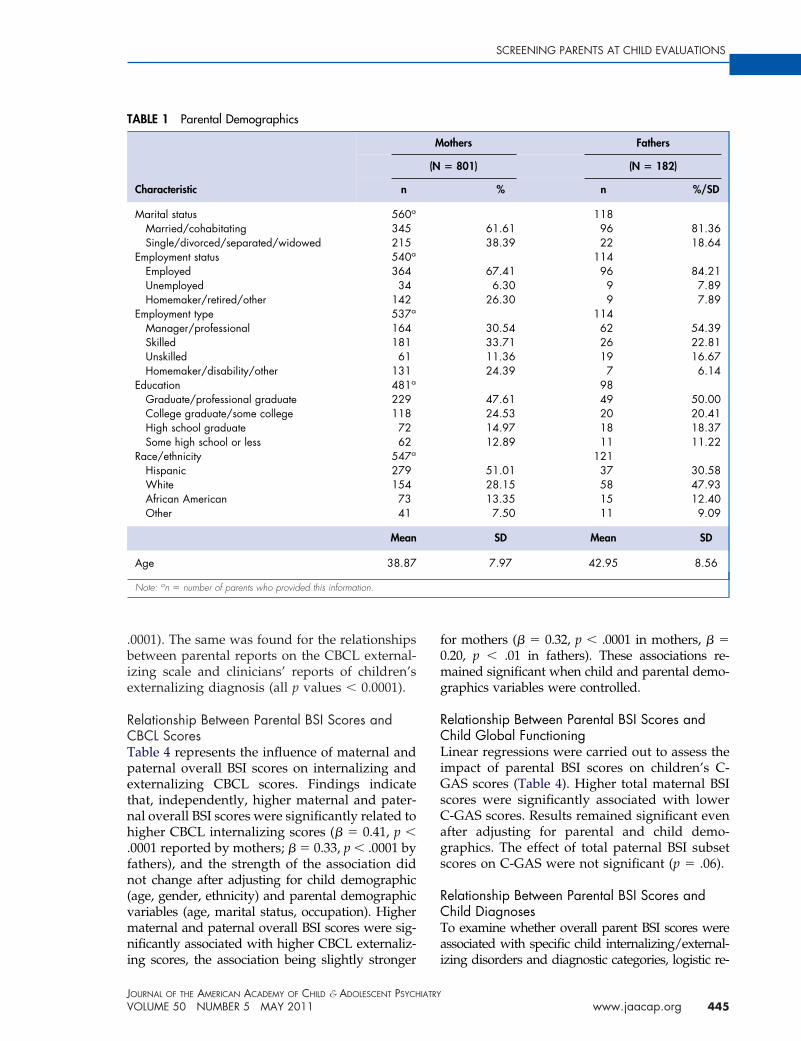
RESULTSDemographic CharacteristicsDemographic information for parents and childrenis reported in Tables 1 and 2, respectively. Of 848
children and adolescents, 55.66% were Hispanic. mJOURN
444 www.jaacap.org
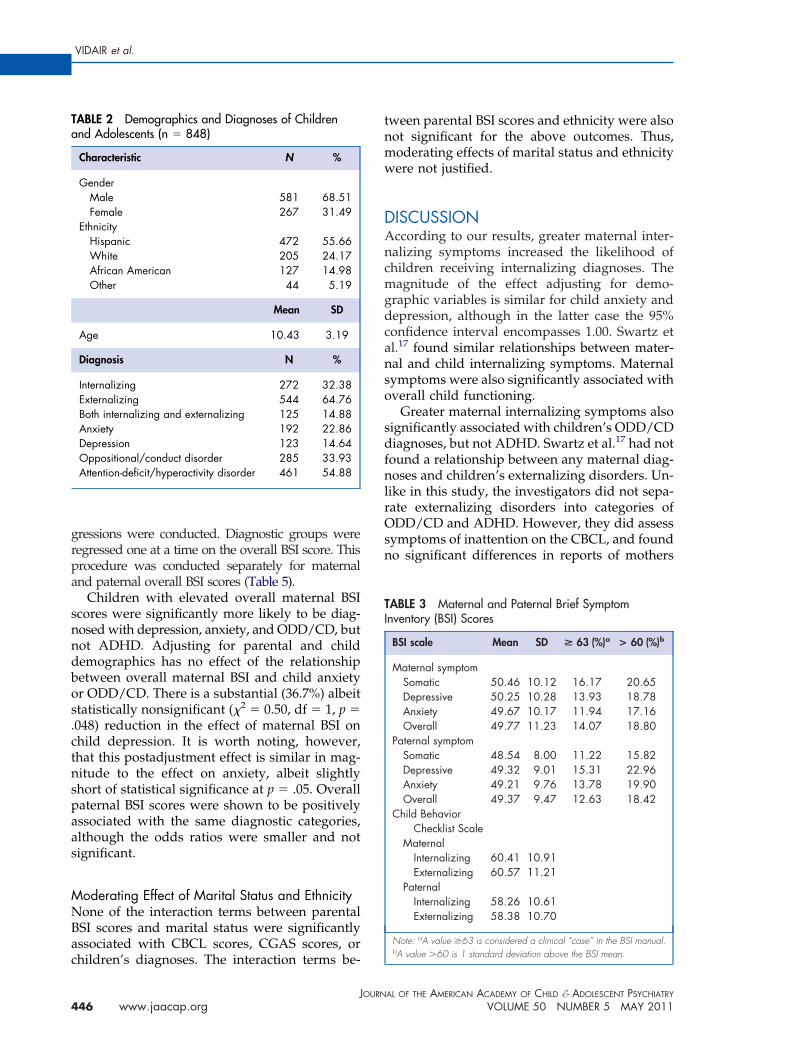
Children’s DiagnosesTable 2 describes the percentage of children whoreceived any internalizing (anxiety or depression)or externalizing diagnosis (ADHD, ODD, or CD).The percentage of children who fell into specificcategories of diagnoses (i.e., ADHD, ODD/CD,anxiety, or depression) is also reported in Table 2.As shown, the diagnostic group most commonlyrepresented in the sample was that with ADHD,followed by that with ODD/CD, anxiety, and de-pressive disorders, respectively.
Overall, 43.28% of children had diagnoses thatfell into one of these diagnostic categories (4.95%depressive disorders only, 8.73% anxiety disor-ders only, 6.01% ODD/CD only, 23.58% ADHDonly). Of those with comorbid disorders, 33.25%met criteria for two diagnostic categories (19.81%ADHD and ODD/CD, 4.48% ADHD and anxi-ety, 3.66% anxiety and depression, 2.00% anxietyand ODD/CD, 1.77% ADHD and depression,and 1.53% depression and ODD/CD); 4.49% metcriteria for three diagnostic categories (most com-monly anxiety, ODD/CD, and ADHD); and0.47% met criteria for four diagnostic categories.Because we were assessing whether severity ofparental symptoms was associated with specificchild diagnoses, we decided to include a child ina diagnostic category if that child had any diag-nosis that met that category’s criteria.
Overall, 64.76% of the children met criteria foran externalizing diagnosis, and 32.38% met criteriafor an internalizing diagnosis, whereas 14.88% metcriteria for both.
BSI and CBCL ScoresMean maternal and paternal BSI scores andCBCL scores are presented in Table 3. Overall,801 mothers and 182 fathers completed the BSI.Mothers’ mean BSI overall distress index scorewas 49.77 (SD � 11.23), whereas fathers’ was49.37 (SD � 9.47). The percentage who scored 1SD above the mean (�60) was 18.80% for moth-ers and 18.42% for fathers. Mothers’ reports ofchildren’s CBCL internalizing symptoms had amean of 60.41 (SD � 10.92). The mean for exter-nalizing symptoms was 60.56 (SD � 11.22). Fa-hers’ mean score for CBCL internalizing symp-oms was 58.18 (SD � 10.75) and 58.44 (SD �0.89) for externalizing symptoms.
Parental reports on the CBCL internalizingcales were highly correlated with children’snternalizing diagnoses when controlling forevel of symptoms found on the BSI in both
others’ and fathers’ reports (all p values �
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
SCREENING PARENTS AT CHILD EVALUATIONS
.0001). The same was found for the relationshipsbetween parental reports on the CBCL external-izing scale and clinicians’ reports of children’sexternalizing diagnosis (all p values � 0.0001).
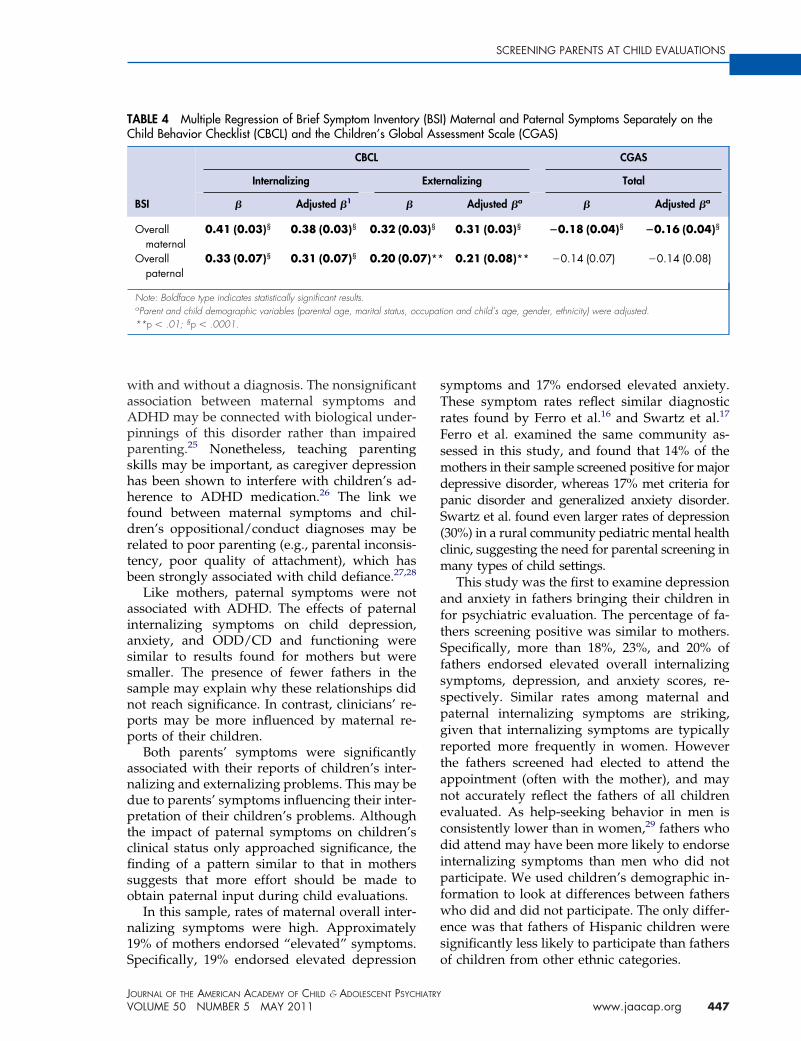
Relationship Between Parental BSI Scores andCBCL ScoresTable 4 represents the influence of maternal andpaternal overall BSI scores on internalizing andexternalizing CBCL scores. Findings indicatethat, independently, higher maternal and pater-nal overall BSI scores were significantly related tohigher CBCL internalizing scores (� � 0.41, p �.0001 reported by mothers; � � 0.33, p � .0001 byfathers), and the strength of the association didnot change after adjusting for child demographic(age, gender, ethnicity) and parental demographicvariables (age, marital status, occupation). Highermaternal and paternal overall BSI scores were sig-nificantly associated with higher CBCL externaliz-
TABLE 1 Parental Demographics
Characteristic n
Marital status 560a
Married/cohabitating 345Single/divorced/separated/widowed 215
Employment status 540a
Employed 364Unemployed 34Homemaker/retired/other 142
Employment type 537a
Manager/professional 164Skilled 181Unskilled 61Homemaker/disability/other 131
Education 481a
Graduate/professional graduate 229College graduate/some college 118High school graduate 72Some high school or less 62
Race/ethnicity 547a
Hispanic 279White 154African American 73Other 41
Mean
Age 38.87
Note: an � number of parents who provided this information.
ing scores, the association being slightly stronger
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
for mothers (� � 0.32, p � .0001 in mothers, � �0.20, p � .01 in fathers). These associations re-mained significant when child and parental demo-graphics variables were controlled.
Relationship Between Parental BSI Scores andChild Global FunctioningLinear regressions were carried out to assess theimpact of parental BSI scores on children’s C-GAS scores (Table 4). Higher total maternal BSIscores were significantly associated with lowerC-GAS scores. Results remained significant evenafter adjusting for parental and child demo-graphics. The effect of total paternal BSI subsetscores on C-GAS were not significant (p � .06).
Relationship Between Parental BSI Scores andChild DiagnosesTo examine whether overall parent BSI scores wereassociated with specific child internalizing/external-
others Fathers
� 801) (N � 182)
% n %/SD
11861.61 96 81.3638.39 22 18.64
11467.41 96 84.216.30 9 7.89
26.30 9 7.89114
30.54 62 54.3933.71 26 22.8111.36 19 16.6724.39 7 6.14
9847.61 49 50.0024.53 20 20.4114.97 18 18.3712.89 11 11.22
12151.01 37 30.5828.15 58 47.9313.35 15 12.407.50 11 9.09
SD Mean SD
7.97 42.95 8.56
M
(N
izing disorders and diagnostic categories, logistic re-
445www.jaacap.org
nso
sdfnlrOsn
VIDAIR et al.
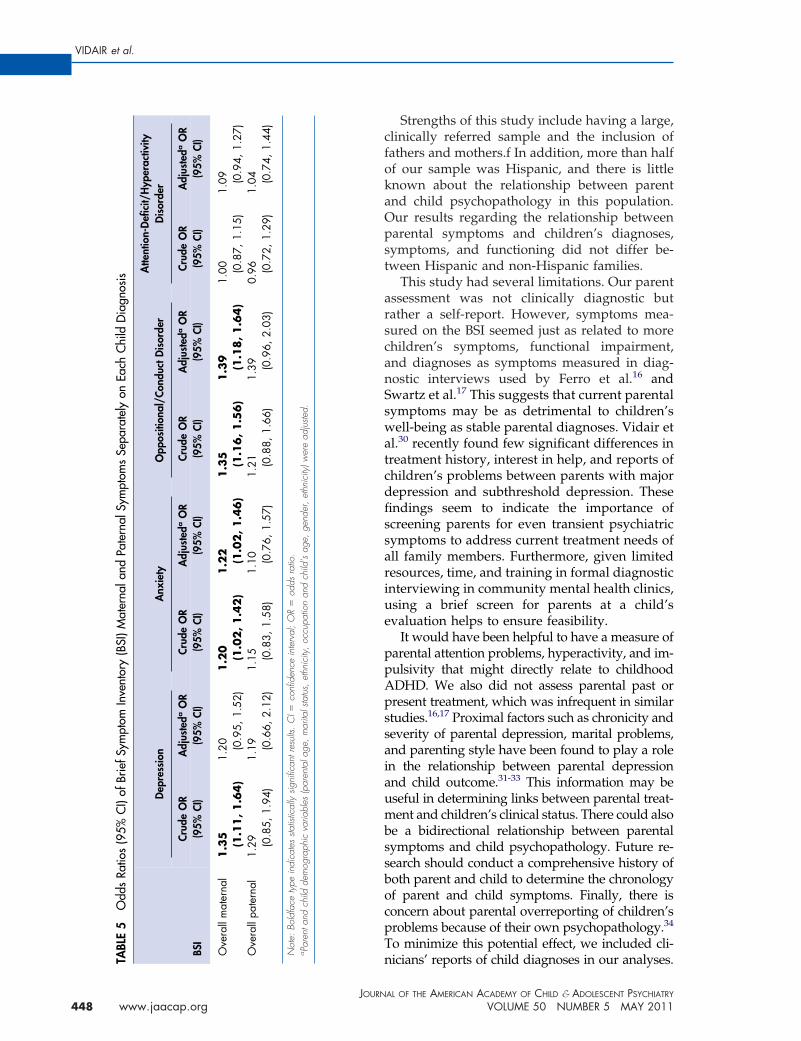
gressions were conducted. Diagnostic groups wereregressed one at a time on the overall BSI score. Thisprocedure was conducted separately for maternaland paternal overall BSI scores (Table 5).
Children with elevated overall maternal BSIscores were significantly more likely to be diag-nosed with depression, anxiety, and ODD/CD, butnot ADHD. Adjusting for parental and childdemographics has no effect of the relationshipbetween overall maternal BSI and child anxietyor ODD/CD. There is a substantial (36.7%) albeitstatistically nonsignificant (�2 � 0.50, df � 1, p �.048) reduction in the effect of maternal BSI onchild depression. It is worth noting, however,that this postadjustment effect is similar in mag-nitude to the effect on anxiety, albeit slightlyshort of statistical significance at p � .05. Overallpaternal BSI scores were shown to be positivelyassociated with the same diagnostic categories,although the odds ratios were smaller and notsignificant.
Moderating Effect of Marital Status and EthnicityNone of the interaction terms between parentalBSI scores and marital status were significantlyassociated with CBCL scores, CGAS scores, or
TABLE 2 Demographics and Diagnoses of Childrenand Adolescents (n � 848)
Characteristic N %
GenderMale 581 68.51Female 267 31.49
EthnicityHispanic 472 55.66White 205 24.17African American 127 14.98Other 44 5.19
Mean SD
Age 10.43 3.19
Diagnosis N %
Internalizing 272 32.38Externalizing 544 64.76Both internalizing and externalizing 125 14.88Anxiety 192 22.86Depression 123 14.64Oppositional/conduct disorder 285 33.93Attention-deficit/hyperactivity disorder 461 54.88
children’s diagnoses. The interaction terms be-
JOURN
446 www.jaacap.org
tween parental BSI scores and ethnicity were alsonot significant for the above outcomes. Thus,moderating effects of marital status and ethnicitywere not justified.
DISCUSSIONAccording to our results, greater maternal inter-nalizing symptoms increased the likelihood ofchildren receiving internalizing diagnoses. Themagnitude of the effect adjusting for demo-graphic variables is similar for child anxiety anddepression, although in the latter case the 95%confidence interval encompasses 1.00. Swartz etal.17 found similar relationships between mater-
al and child internalizing symptoms. Maternalymptoms were also significantly associated withverall child functioning.
Greater maternal internalizing symptoms alsoignificantly associated with children’s ODD/CDiagnoses, but not ADHD. Swartz et al.17 had not
ound a relationship between any maternal diag-oses and children’s externalizing disorders. Un-
ike in this study, the investigators did not sepa-ate externalizing disorders into categories ofDD/CD and ADHD. However, they did assess
ymptoms of inattention on the CBCL, and foundo significant differences in reports of mothers
TABLE 3 Maternal and Paternal Brief SymptomInventory (BSI) Scores
BSI scale Mean SD > 63 (%)a > 60 (%)b
Maternal symptomSomatic 50.46 10.12 16.17 20.65Depressive 50.25 10.28 13.93 18.78Anxiety 49.67 10.17 11.94 17.16Overall 49.77 11.23 14.07 18.80
Paternal symptomSomatic 48.54 8.00 11.22 15.82Depressive 49.32 9.01 15.31 22.96Anxiety 49.21 9.76 13.78 19.90Overall 49.37 9.47 12.63 18.42
Child BehaviorChecklist Scale
MaternalInternalizing 60.41 10.91Externalizing 60.57 11.21
PaternalInternalizing 58.26 10.61Externalizing 58.38 10.70
Note: aA value �63 is considered a clinical “case” in the BSI manual.
bA value �60 is 1 standard deviation above the BSI mean.AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
SCREENING PARENTS AT CHILD EVALUATIONS
with and without a diagnosis. The nonsignificantassociation between maternal symptoms andADHD may be connected with biological under-pinnings of this disorder rather than impairedparenting.25 Nonetheless, teaching parentingskills may be important, as caregiver depressionhas been shown to interfere with children’s ad-herence to ADHD medication.26 The link wefound between maternal symptoms and chil-dren’s oppositional/conduct diagnoses may berelated to poor parenting (e.g., parental inconsis-tency, poor quality of attachment), which hasbeen strongly associated with child defiance.27,28
Like mothers, paternal symptoms were notassociated with ADHD. The effects of paternalinternalizing symptoms on child depression,anxiety, and ODD/CD and functioning weresimilar to results found for mothers but weresmaller. The presence of fewer fathers in thesample may explain why these relationships didnot reach significance. In contrast, clinicians’ re-ports may be more influenced by maternal re-ports of their children.
Both parents’ symptoms were significantlyassociated with their reports of children’s inter-nalizing and externalizing problems. This may bedue to parents’ symptoms influencing their inter-pretation of their children’s problems. Althoughthe impact of paternal symptoms on children’sclinical status only approached significance, thefinding of a pattern similar to that in motherssuggests that more effort should be made toobtain paternal input during child evaluations.
In this sample, rates of maternal overall inter-nalizing symptoms were high. Approximately19% of mothers endorsed “elevated” symptoms.
TABLE 4 Multiple Regression of Brief Symptom InventoryChild Behavior Checklist (CBCL) and the Children’s Globa
BSI
CBCL
Internalizing
� Adjusted �1 �
Overallmaternal
0.41 (0.03)§ 0.38 (0.03)§ 0.32 (0.0
Overallpaternal
0.33 (0.07)§ 0.31 (0.07)§ 0.20 (0.0
Note: Boldface type indicates statistically significant results.aParent and child demographic variables (parental age, marital status, oc**p � .01; §p � .0001.
Specifically, 19% endorsed elevated depression
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
symptoms and 17% endorsed elevated anxiety.These symptom rates reflect similar diagnosticrates found by Ferro et al.16 and Swartz et al.17
Ferro et al. examined the same community as-sessed in this study, and found that 14% of themothers in their sample screened positive for majordepressive disorder, whereas 17% met criteria forpanic disorder and generalized anxiety disorder.Swartz et al. found even larger rates of depression(30%) in a rural community pediatric mental healthclinic, suggesting the need for parental screening inmany types of child settings.
This study was the first to examine depressionand anxiety in fathers bringing their children infor psychiatric evaluation. The percentage of fa-thers screening positive was similar to mothers.Specifically, more than 18%, 23%, and 20% offathers endorsed elevated overall internalizingsymptoms, depression, and anxiety scores, re-spectively. Similar rates among maternal andpaternal internalizing symptoms are striking,given that internalizing symptoms are typicallyreported more frequently in women. Howeverthe fathers screened had elected to attend theappointment (often with the mother), and maynot accurately reflect the fathers of all childrenevaluated. As help-seeking behavior in men isconsistently lower than in women,29 fathers whodid attend may have been more likely to endorseinternalizing symptoms than men who did notparticipate. We used children’s demographic in-formation to look at differences between fatherswho did and did not participate. The only differ-ence was that fathers of Hispanic children weresignificantly less likely to participate than fathers
) Maternal and Paternal Symptoms Separately on theessment Scale (CGAS)
CGAS
rnalizing Total
Adjusted �a � Adjusted �a
0.31 (0.03)§ �0.18 (0.04)§ �0.16 (0.04)§
0.21 (0.08)** �0.14 (0.07) �0.14 (0.08)
ion and child’s age, gender, ethnicity) were adjusted.
(BSIl Ass
Exte
3)§
7)**
cupat
of children from other ethnic categories.
447www.jaacap.org
swa
saiaumbssbocp
BLE
5O
dds
Ratio
s(9
5%C
I)of
Brie
fSym
ptom
Inve
ntor
y(B
SI)M
ater
nala
ndPa
tern
alSy
mpt
oms
Sepa
rate
lyon
Each
Chi
ldD
iagn
osis
SI
Dep
ress
ion
Anx
iety
Opp
ositi
onal
/Con
duct
Dis
orde
rA
ttent
ion-
Defi
cit/
Hyp
erac
tivity
Dis
orde
r
Crud
eO
RA
djus
teda
OR
Crud
eO
RA
djus
teda
OR
Crud
eO
RA
djus
teda
OR
Crud
eO
RA
djus
teda
OR
(95%
CI)
(95%
CI)
(95%
CI)
(95%
CI)
(95%
CI)
(95%
CI)
(95%
CI)
(95%
CI)
vera
llm
ater
nal
1.3
5(1
.11
,1
.64
)1.
20 (0.9
5,1.
52)
1.2
0(1
.02
,1
.42
)1
.22
(1.0
2,1
.46
)1
.35
(1.1
6,1
.56
)1
.39
(1.1
8,1.6
4)
1.00 (0
.87,
1.15
)1.
09 (0.9
4,1.
27)
vera
llpa
tern
al1.
29 (0.8
5,1.
94)
1.19 (0
.66,
2.12
)1.
15 (0.8
3,1.
58)
1.10 (0
.76,
1.57
)1.
21 (0.8
8,1.
66)
1.39 (0
.96,
2.03
)0.
96 (0.7
2,1.
29)
1.04 (0
.74,
1.44
)
ote:
Bold
face
type
indi
cate
ssta
tistic
ally
signi
fican
tres
ults.
CI�
confi
denc
ein
terv
al;
OR
�od
dsra
tio.
Pare
ntan
dch
ildde
mog
raph
icva
riabl
es(p
aren
tala
ge,
mar
itals
tatu
s,et
hnic
ity,
occu
patio
nan
dch
ild’s
age,
gend
er,
ethn
icity
)wer
ead
juste
d.
VIDAIR et al.
448
Strengths of this study include having a large,clinically referred sample and the inclusion offathers and mothers.f In addition, more than halfof our sample was Hispanic, and there is littleknown about the relationship between parentand child psychopathology in this population.Our results regarding the relationship betweenparental symptoms and children’s diagnoses,symptoms, and functioning did not differ be-tween Hispanic and non-Hispanic families.
This study had several limitations. Our parentassessment was not clinically diagnostic butrather a self-report. However, symptoms mea-sured on the BSI seemed just as related to morechildren’s symptoms, functional impairment,and diagnoses as symptoms measured in diag-nostic interviews used by Ferro et al.16 andSwartz et al.17 This suggests that current parentalymptoms may be as detrimental to children’sell-being as stable parental diagnoses. Vidair et
l.30 recently found few significant differences intreatment history, interest in help, and reports ofchildren’s problems between parents with majordepression and subthreshold depression. Thesefindings seem to indicate the importance ofscreening parents for even transient psychiatricsymptoms to address current treatment needs ofall family members. Furthermore, given limitedresources, time, and training in formal diagnosticinterviewing in community mental health clinics,using a brief screen for parents at a child’sevaluation helps to ensure feasibility.
It would have been helpful to have a measure ofparental attention problems, hyperactivity, and im-pulsivity that might directly relate to childhoodADHD. We also did not assess parental past orpresent treatment, which was infrequent in similarstudies.16,17 Proximal factors such as chronicity andeverity of parental depression, marital problems,nd parenting style have been found to play a rolen the relationship between parental depressionnd child outcome.31-33 This information may beseful in determining links between parental treat-ent and children’s clinical status. There could also
e a bidirectional relationship between parentalymptoms and child psychopathology. Future re-earch should conduct a comprehensive history ofoth parent and child to determine the chronologyf parent and child symptoms. Finally, there isoncern about parental overreporting of children’sroblems because of their own psychopathology.34
To minimize this potential effect, we included cli-
nicians’ reports of child diagnoses in our analyses.TAB O O N a
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011www.jaacap.org

psm
SCREENING PARENTS AT CHILD EVALUATIONS
Parental reports of children’s symptoms werehighly correlated with clinicians’ reports of chil-dren’s diagnoses regardless of the level of parentalsymptomatology. However, clinician diagnosis isstill influenced by parental perception of their chil-dren’s symptoms and functioning.
Overall, this study highlights the feasibility ofscreening parents in addition to their childrenwhen they are brought in for psychiatric evalua-tion. Our results confirmed that a significant per-centage of parents presenting with their childrenfor a psychiatric evaluation are experiencing de-pressive and anxious symptoms themselves. Thisdemonstrates the importance of addressing ser-vices needs in parents with elevated clinical symp-toms. Unfortunately, the presence of parental psycho-pathology has serious implications for child treatmentoutcome. Garber et al.10 recently found that adoles-cents fared worse in treatment when a parent waspresently depressed. It has been suggested that everychild who has a parent with a serious affectivedisorder be screened. 35 Based on our findings, weadvise that all parents be assessed at their child’spsychiatric evaluation. Given limited resources anddiagnostic training in real-world clinics, a parentsymptom screen is likely to be feasible.
Given the National Institute of Mental Health’spriority to personalize treatment for individuals,36
there is also a need for development of treatmentparadigms for children whose parents have theirown psychopathology. Initial evidence indicatesthat treating parental psychopathology alone isassociated with child improvement.3,13-15 Yet fac-tors such as parental understanding of their symp-toms and its effect on their children, ways tocommunicate with their child about their mentalhealth, and improvement in parenting style are
important targets for evaluation and treat-Psychopathology in parents of depressed children and adoles-cents. J Am Acad Child Adolesc Psychiatry. 1989;28:352-357.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
ment.14,32,37 Innovative and effective programs forarents with depression have focused not only onymptom alleviation but on understanding andanaging the parent–child relationship.14,37 There
is a great need to develop mental health systemsthat will be able to provide assessments and deliverevidenced-based treatments to children, mothers,and fathers within the same clinical setting. &
Accepted January 31, 2011.
Drs. Vidair, Shen, Turner, and Rynn, and Ms. Heleniak, and Ms. Hollinare with Columbia University/New York State Psychiatric Institute. Ms.Reyes is with Rutgers University. Dr. Parrilla-Escobar is with ComplejoAsistencial de Ávila, Spain. Mr. Woodruff is with Catholic University.
Child and Adolescent Psychiatric Evaluation Service (CAPES) wassupported by Grant P30MH071478 from the National Institute ofMental Health (NIMH).
The content is solely the responsibility of the authors and does notnecessarily represent the official views of the NIMH or the NationalInstitutes of Health.
We thank clinical interviewers and supervisors, particularly Dr. KellyPosner of the New York State Psychiatric Institute and Dr. Lisa Kotler ofthe NYU Child Study Center. We also thank Drs. David Shaffer andLawrence Greenhill, founders of CAPES, and Dr. Laura Mufson ofNew York State Psychiatric Institute for manuscript review, and partic-ipating parents and children.
Disclosure: Dr. Vidair has received research support from the NationalInstitute of Mental Health. Dr. Parilla-Escobar was supported by anAlicia Koplowitz Fellowship. Dr. Turner serves as a consultant forSuicide Prevention International. He has received research supportfrom the National Institute of Mental Health. He participates inDSM-V-related research with the American Psychiatric Association.Dr. Rynn has received research support from the National Institute ofMental Health, Boehringer Ingelheim, Wyeth, and Neuropharm. Shehas served as a consultant for Wyeth and Pharmastar. She receivesroyalties from American Psychiatric Publishing Inc. Dr. Shen, Ms.Heleniak, Ms. Hollin, Ms. Reyes, and Mr. Woodruff report nobiomedical financial interests or potential conflicts of interest.
Correspondence to Dr. Hilary B. Vidair, Columbia University/NewYork State Psychiatric Institute (NYSPI), 1051 Riverside Drive, Unit 24,New York, NY 10032; e-mail: [email protected]
0890-8567/$36.00/©2011 American Academy of Child andAdolescent Psychiatry
DOI: 10.1016/j.jaac.2011.02.002
REFERENCES1. Beardslee WR, Keller MB, Lavori PW, Staley J, Sacks N. The
impact of parental affective disorder on depression in offspring: alongitudinal follow-up in a nonreferred sample. J Am Acad ChildAdolesc Psychiatry. 1993;32:723-730.
2. Biederman J, Petty C, Faraone SV, et al. Parental predictors ofpediatric panic disorder/agoraphobia: a controlled study in high-risk offspring. Depress Anxiety. 2005;22:114-120.
3. Weissman MM, Wickramaratne P, Nomura Y, Warner V, Pi-lowsky D, Verdeli H. Offspring of depressed parents: 20 yearslater. Am J Psychiatry. 2006;163:1001-1008.
4. Last CG, Hersen M, Kazdin A, Orvaschel H, Perrin S. Anxietydisorders in children and their families. Arch Gen Psychiatry.1991;48:928-934.
5. Kovacs M, Devlin B, Pollock M, Richards C, Mukerji P. Acontrolled family history study of childhood-onset depressivedisorder. Arch Gen Psychiatry. 1997;54:613-623.
6. Mitchell J, McCauley E, Burke P, Calderon R, Schloredt K.
7. Pilowsky DJ, Wickramaratne PJ, Rush AJ, et al. Children ofcurrently depressed mothers: a STAR*D ancillary study. J ClinPsychiatry. 2006;67:126-136.
8. Beidel DC, Turner SM. At risk for anxiety: I. Psychopathology inthe offspring of anxious parents. J Am Acad Child AdolescPsychiatry. 1997;36:918-924.
9. Cobham VE, Dadds MR, Spence SH. The role of parental anxietyin the treatment of childhood anxiety. J Consult Clin Psychol.1998;66:893-905.
10. Garber J, Clarke GN, Weersing VR, et al. Prevention of depressionin at-risk adolescents: a randomized controlled trial. JAMA.2009;301:2215-2224.
11. Owens EB, Hinshaw SP, Kraemer HC, et al. Which treatment forwhom for ADHD? Moderators of treatment response in the MTA.J Consult Clin Psychol. 2003;71:540-552.
12. Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk forearly-adulthood anxiety and depressive disorders in adolescents
with anxiety and depressive disorders. Arch Gen Psychiatry. Jan1998;55:56-64.449www.jaacap.org
VIDAIR et al.
13. Gunlicks ML, Weissman MM. Change in child psychopathologywith improvement in parental depression: a systematic review. JAm Acad Child Adolesc Psychiatry. 2008;47:379-389.
14. Swartz HA, Frank E, Zuckoff A, et al. Brief interpersonal psycho-therapy for depressed mothers whose children are receivingpsychiatric treatment. Am J Psychiatry. 2008;165:1155-1162.
15. Pilowsky DJ, Wickramaratne P, Talati A, et al. Children ofdepressed mothers 1 year after the initiation of maternal treat-ment: findings from the STAR*D-Child Study. Am J Psychiatry.2008;165:1136-1147.
16. Ferro T, Verdeli H, Pierre F, Weissman MM. Screening fordepression in mothers bringing their offspring for evaluation ortreatment of depression. Am J Psychiatry. 2000;157:375-379.
17. Swartz HA, Shear MK, Wren FJ, et al. Depression and anxietyamong mothers who bring their children to a pediatric mentalhealth clinic. Psychiatr Serv. 2005;56:1077-1083.
18. Cassano M, Adrian M, Veits G, Zeman J. The inclusion of fathersin the empirical investigation of child psychopathology: an up-date. J Clin Child Adolesc Psychol. 2006;35:583-589.
19. Rodriguez N. Theoretical and methodological issues of Latina/oresearch. In: Rodriguez H, Saenz R, Menjivar C, ed. Latinas/os inthe United States: Changing the Face of America. New York, NY:Springer; 2008:2-15.
20. Cairney J, Boyle M, Offord DR, Racine Y. Stress, social supportand depression in single and married mothers. Soc PsychiatryPsychiatr Epidemiol. 2003;38:442-449.
21. Talati A, Wickramaratne PJ, Pilowsky DJ, et al. Remission ofmaternal depression and child symptoms among single mothers:a STAR*D-Child report. Soc Psychiatry Psychiatr Epidemiol.2007;42:962-971.
22. Derogatis L, Savitz K. The SCL-90-R and Brief Symptom Inven-tory (BSI) in primary care. In: Maruish ME, ed. Handbook ofPsychological Assessment in Primary Care Settings. Mahwah, NJ:Erlbaum; 2000:297-334.
23. Achenbach TR, L. Manual for the ASEBA School-Age Forms andProfiles. Burlington, VT: University of Vermont, Research Centerfor Children, Youth, and Families; 2001.
24. Shaffer D, Gould MS, Brasic J, et al. A Children’s Global Assess-ment scale (CGAS). Arch Gen Psychiatry. 1983;40:1228-1231.
JOURN
450 www.jaacap.org
25. Lifford KJ, Harold GT, Thapar A. Parent-child hostility and childADHD symptoms: a genetically sensitive and longitudinal anal-ysis. J Child Psychol Psychiatry. 2009;50:1468-1476.
26. Leslie LK, Aarons GA, Haine RA, Hough RL. Caregiver depres-sion and medication use by youths with ADHD who receiveservices in the public sector. Psychiatr Serv. 2007;58:131-134.
27. Reid MJ, Webster-Stratton C, Hammond M. Follow-up of chil-dren who received the Incredible Years Intervention for Opposi-tional-Defiant Disorder: maintenance and prediction of 2-yearoutcome. Behav Ther. 2003;34:471-491.
28. Patterson GR. Coercive Family Processes. Eugene, OR: Castalia;1982.
29. Moller-Leimkuhler AM. Barriers to help-seeking by men: a re-view of sociocultural and clinical literature with particular refer-ence to depression. J Affect Disord. 2002;71:1-9.
30. Vidair H, Boccia A, Johnson J, Verdeli H, Wickramaratne P, KlinkK. Parental Depression: treatment needs and children’s problemsin an urban family medicine practice. Psychiatr Serv. 2011;62:317-321.
31. Beardslee WR, Versage EM, Gladstone TR. Children of affectivelyill parents: a review of the past 10 years. J Am Acad Child AdolescPsychiatry. 1998;37:1134-1141.
32. Oyserman D, Bybee D, Mowbray C. Influences of maternalmental illness on psychological outcomes for adolescent children.J Adolesc. 2002;25:587-602.
33. Shelton KH, Harold GT. Interparental conflict, negative parent-ing, and children’s adjustment: bridging links between parents’depression and children’s psychological distress. J Fam Psychol.2008;22:712-724.
34. Najman JM, Williams GM, Nikles J, et al. Bias influencing mater-nal reports of child behaviour and emotional state. Soc PsychiatryPsychiatr Epidemiol. 2001;36:186-194.
35. Jellinek MS, Bishop SJ, Murphy JM, Biederman J, Rosenbaum JF.Screening for dysfunction in the children of outpatients at apsychopharmacology clinic. Am J Psychiatry. 1991;148:1031-1036.
36. Insel TR. Translating scientific opportunity into public healthimpact: a strategic plan for research on mental illness. Arch GenPsychiatry. 2009;66:128-133.
37. Beardslee WR, Wright EJ, Gladstone TR, Forbes P. Long-term effects
from a randomized trial of two public health preventive interven-tions for parental depression. J Fam Psychol. 2007;21:703-713.AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011




















