
Peter Kollock Source - Social Dilemmas - Sabin Vaccine Institute

Health & Place 7 (2001) 319–331
Safety becomes danger:dilemmas of drug-use in public space
Kim Doveya,*, John Fitzgeraldb, Youngju Choia
aFaculty of Architecture, Building and Planning, University of Melbourne, Melbourne, Vic., 3010, AustraliabDepartment of Criminology, University of Melbourne, Melbourne, Australia
Abstract
This paper provides a socio-spatial analysis of injecting drug-use in public space. It focusses on one urban district in
Melbourne, Australia, which has become strongly identified with heroin sale and use in public space. Selling activitiesare camouflaged within a diverse streetlife while injecting sites are dispersed through a broad diversity of laneways,carparks and toilets. These injecting zones occupy liminal places which slide between categories of private and public,
and which mediate complex and paradoxical relations between safety and danger. Those who inject in public space arecaught in a dilemmaFneeding both privacy and exposure in the event of an overdose, safety from police becomesdanger from an overdose. This empirical work, based on interview and spatial analysis, is presented as a basis for
theorizing the socio-spatial construction of heroin use and for assessing the prospects for safe injecting.r 2001 ElsevierScience Ltd. All rights reserved.
Keywords: Drug-use; Injecting; Spatial; Urban; Safety; Privacy; Risk
Introduction
‘Smith Street’ is a shopping strip in an inner cityneighbourhood of Melbourne which has becomestrongly identified through the media as a site of heroin
sale and use. The trade is incorporated into the diversestreetlife of the retail strip; consumption mostly followsvery swiftly in a plethora of spaces within the
surrounding urban fabric. These practices have persisteddespite successive rounds of heavy policing and havecoincided with an increase in overdose figures. This
paper is a study of this intersection between injectingdrug-use and urban space. Research on the nexusbetween place and health has largely focussed on themacroscale patterns of health and disease embedded in
and sustained by spatial relations and meanings of place(Hayes et al., 1992; Kearns and Gesler, 1998; MacIntyreet al., 1993). Our focus is on the smaller scale experience
and use of urban space, on the specific mediations of
built form and spatial practice.
Study area
The study area extends for 800m along Smith Streetand about 100m on either sideFan area of about
16 hectares encompassing the major heroin trade anduse (Fig. 1). A brief excursion into the history and socialdemographics of the surrounding context is useful in
understanding why such activity has become entrenchedhere. Smith Street developed as a shopping strip duringthe second half of the 19th century (Fitzgerald et al.,1998). It was the retail heart of a working class
community which included both Fitzroy to the westand Collingwood to the east. Just beyond easy walkingdistance from the city, it was serviced with a tramline
from 1869 and remained a flourishing retail area into theearly 20th century with major department stores and avibrant streetlife.
The 1950s brought increasing waves of new migrantsto the area. Entire blocks of older housing were
*Corresponding author. Tel.: +61-3-9344-7779; fax: +61-3-
9344-5532.
E-mail address: [email protected] (K. Dovey).
1353-8292/01/$ - see front matter r 2001 Elsevier Science Ltd. All rights reserved.
PII: S 1 3 5 3 - 8 2 9 2 ( 0 1 ) 0 0 0 2 4 - 7

demolished and replaced with high-rise public housingin the 1960s. These estates of 8–10 hectares each are
located within half a kilometre east and west of SmithStreet. By the 1970s these estates were occupied byincreasing numbers of Vietnamese refugees and the
broader social mix of the area also changed with aninflux of high-income professionals. During the mid-1990s the public housing estates were publicized in the
media as ‘hot spots’ for the sale and use of heroin.Subsequent police operations ensured a displacement ofthe trade from the estates to the commercial space ofSmith Street (Fitzgerald et al., 1998).
There is a good deal of literature focussing on crime inhigh-rise public housing estates, much of it concernedwith the role of urban spatial structure in mediating
crime and socially transgressive behaviour (Newman,1972; Coleman, 1985; Franck, 1984; Greenberg andRohe, 1984; Hillier, 1988). It is not our intention to
explore this issue here except to make the point that thedisplacement which occurred in 1995 was between twoutterly different conditions of urban spatial structure.The heroin trade and use on the estates was linked to
domestic space and to the semi-public zones of
corridors, shared laundries and stairwells that charac-terize the modernist estates (Fitzgerald et al., 1998). In
Smith Street the trade moved to the streets and lanewaysof the traditional city. Whatever the connections ofspatiality to heroin use, the trade and use of heroin was
not ‘caused’ by the spatial dispositions of either theestate or the Smith Street area.This shift from semi-private to public trading has
coincided with an increase in both heroin overdose anddeath. In 1998 there were over 100 non-fatal overdoseincidents per month and deaths increased from 6 to 16 inthe 2 years to 1999 (Fitzgerald et al., 1998). Approxi-
mately 70% of these incidents occurred in public space.1
The dangers of overdose are linked to a range of factorsincluding drug quality, tolerance and multiple drug-use.
However, death from overdose generally occurs onlywhen medical assistance is not provided. Our primary
Fig. 1. Study area and context.
1Turning Point Alcohol and Drug Centre, personal commu-
nication. These figure relate to a statistical zone which is
broader than the study area . Specific figures for overdose or
death which correlate exactly to specific sites within the study
area are unavailable.
K. Dovey et al. / Health & Place 7 (2001) 319–331320

interest in this paper is to ask how spatial contextmediates, however indirectly, the range of competing risks
for injecting drug-usersFincluding both risks to health(overdose and the spread of blood-borne virus throughshared syringes) as well as the risks of social margin-
alization and arrest. We are also interested in findingclues for interventions in both policy and urban formwhich may help to reduce the impact of this epidemic.
Method and methodology
This paper utilizes data from a number of sources and
combines the findings of ethnographic fieldwork withspatial mapping and analysis. As an illegal behaviour,heroin use is particularly difficult to measure empiri-
cally. Many of the indicators of heroin use are secondaryindicators. Estimates of the locations and extent of streetheroin use were drawn from a number of data sources:syringe collection and distribution data; behavioural
trace analysis (drug paraphernalia in street locations);consultation with service providers and police. Narra-tives of spatial experience were derived from in-depth
tape-recorded interviews with heroin users (n ¼ 54).2
The spatial analysis consists of a series of layeredmappings of the study area including pedestrian access
networks, public/private ownership, functional mix andstreetlife volume. These layered mappings of urbanspace are derived primarily from the field of urban
design theory as those most likely to mediate behaviourand meaning in urban space (Dovey, 1999; Hillier, 1996;Jacobs, 1965). These analyses were overlaid withmappings of dealing and injecting locations. Streetlife
densities are based on global counts of people visible inpublic space; ethnographic observations involving ex-tended periods of fieldwork over an 18 month period
were also undertaken.3
While the methods of this study are empirical, themethodological and theoretical framework is more
broadly influenced by the so-called ‘spatial turn’ insocial theory which has had such an impact ongeographic theory (Dear, 2000) and has opened oppor-tunities for re-thinking the relations of health to place
(Moon, 1995; Kearns, 1994; Dorn and Laws, 1994).Through the interviews we are concerned to understandboth the phenomenology of such practices and places, as
well as discursive framings and narratives. Like Poland’s(1998) account of the stigmatization of smoking, we areinterested in the formations of identity constructed and
performed through marginalized spatial practices. While
the material presented here is primarily descriptive andthe theory is not pursued very far, we will contend that
such places and practices may be best understood interms of shifting identities, ‘nomadic’ and ‘rhizomatic’practices in the context of a Deleuzian epistemology
(Deleuze, 1993, 1985). The distinction between ‘smooth’and ‘striated’ space is suggested as one framework ofinterpretation (Deleuze and Guattari, 1987; Moon andBraun, 1998). Such theory, however, does not drive the
methods which are more traditionally empirical.
Spatial structure and streetlife
The 16 hectares of the study area have been analysed
through a series of layered mappings of the spatialstructure together with the functions and streetlife itsustains. While these mappings are empirical, ourinterest is in broad spatial patterns rather than specific
causal relations. We are interested in how the practicesof heroin trade and use insinuate themselves intoeveryday urban life. We begin by looking at the ways
in which spatial configurations operate to mediate socialrelations. Urban street networks can be seen aspedestrian movement patterns which enable and con-
strain flows of pedestrian life (Hillier, 1996).4 Fig. 2ashows the accessible pedestrian space network andpedestrian densities in and around Smith Street. Thisis a mapping of access rather than ownershipFroad-
ways are mostly excluded and some privately ownedspace is accessible.The average levels of pedestrian density during the
day (10 a.m.–6 p.m.) are linked to both the multipliereffect of retail functions (which are attracted to streetlife,then attract more of it), and to the quality of
permeability or ‘ringiness’ in the pedestrian network(since cul-de-sac streets and lanes carry only localtraffic). This ‘ringiness’ or permeabilityFthe degree to
which urban space returns upon itselfFis a key factor inany urban spatial structure since it structures socialencounter and therefore social capital (Hillier, 1996).The streetlife is highly diverse in terms of social class,
gender, age, behaviour and dress. This is linked to thedemographics of the area and the diversity of shops andfacilitiesFa mix of discount stores, supermarket, gam-
ing, video, pawn and a range of cafes and restaurantsfrom the takeaway to up-market. The diversity offunctions produces a variety of behaviour from cafes,
supermarket, houses, offices, nightclubs, and restau-rants. The study area has many of the qualities thatJacobs (1965) has long argued characterize a vital and
healthy urban fabricFpermeability, mixed use, densityand mixed building stock. It is also undergoing a decline
2Citation of interview transcripts is indicated using interview
codes.3The research was approved by the University of Melbourne
Human Research Ethics Committee and the Victoria Police
Research Committee. The area is well known to police,
including its selling and injecting locations.
4This analysis of spatial structure is loosely based in Hillier’s
spatial syntax analysis (Hillier and Hanson, 1984) as adapted by
Dovey (1999).
K. Dovey et al. / Health & Place 7 (2001) 319–331 321

in diversity through gentrification as everyday goodssuch as grocers, butchers and furniture are beingdisplaced by cafes, restaurants and hairdressers (Fitz-
gerald et al., 1998).Fig. 2b maps selling and injecting practices. When
compared with Fig. 2a it shows the way in which the
drug selling zones co-locate with the density of streetlife.The selling of heroin is concentrated into the mostdiverse and down-market part of Smith Street, an area
which extends for about 300–400m on both sides of thestreet. Minor selling zones extend into all adjacent sidestreets since the sale often takes place across time andspace. A drug sale may be agreed in Smith Street (or on
the telephone) and then concluded in the side street. Thesale is not so much an event as a trajectory which flowswith and in the streetlife. The structures and meanings of
a prevailing urban order are utilized as camouflage, theavailable identities of the prevailing urban order areused like masks in order to pass through (Massumi,
1993, p. 105).The selling zone is also marked and anchored by some
key facilities and functions, primarily the public toilets,public telephones and pharmacies. The telephones are
used by potential buyers and sellers for pre-sale contact
and they are located on the east side of Smith Street ateach end and the middle of the selling zone. The publictoilets mark the ends of the selling zone and the two
pharmacies are located within 50m of each toilet. Thusthere is a constellation of facilities distributed across theselling zone and anchoring its ends. There is also a
broader range of facilities which we have categorized as‘quick-fix’ functionsFprimarily fast cash (automaticteller machines, pawn shops), fast food and gaming/
gambling. It is notable that the selling zone is integratedwith the permeable network of side streets and alleysthat characterize the central section.Fig. 2b shows the selling zones juxtaposed with the
full range of documented injecting zones shown as smallstars. These zones are often difficult to see in thesubsequent figures where they are juxtaposed against a
series of other layers of information. While we willultimately attempt to clarify the micro-spatiality of suchzones, at this scale the unclarity reflects the sense of
camouflage which pervades the place and may be moreaccurate than highlighting each injecting zone throughanother graphic language.Fig. 3 maps the selling and injecting patterns against
the functional patterns of landuse. We have analysed
Fig. 2. Pedestrian networks and IV drug-use.
K. Dovey et al. / Health & Place 7 (2001) 319–331322
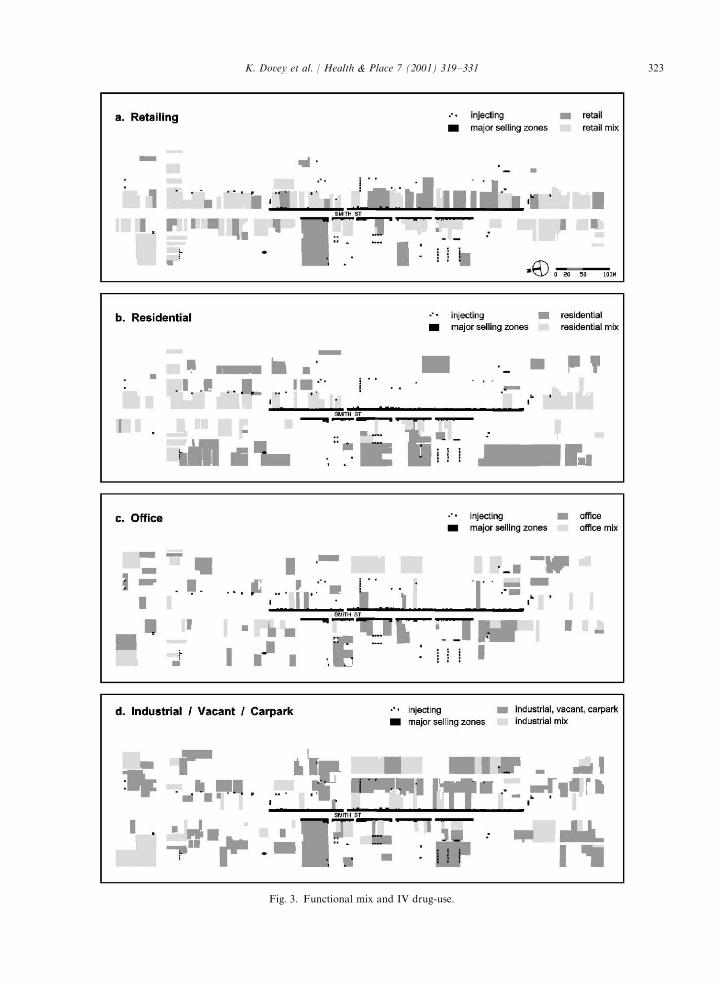
Fig. 3. Functional mix and IV drug-use.
K. Dovey et al. / Health & Place 7 (2001) 319–331 323

building functions into four primary categories of office,residential, retail and industrial. Since different functions
are often mixed on the same site we have added suchmixed uses to each map. Fig. 3 shows each of thesefunctions including mixed sites. Fig. 3a shows that
retailing activities are concentrated along Smith streetfrontages where they occupy nearly all buildings, mostlymixed with office or residential. Only one zone of thestreet is exclusively retail (unmixed) and this zone
coincides with the major selling zone. Residentialfunctions (Fig. 3b) tend to be exclusive uses alongsecondary streets or above shops on Smith Street.
Neither selling nor injecting tends to occur nearexclusively residential frontages. Office functions(Fig. 3c) are distributed throughout the site and appear
to have no clear co-location with selling or injectingzones. Industrial uses which we have grouped withvacant lots and carparks (Fig. 3d) are located almost
exclusively off Smith Street and primarily line thelaneways and small streets one block back. There is astrong co-location of such functions with injectingzones.
Exposure and seclusion
While the selling of heroin may hide in the glare ofpublicity and in the diversity and anonymity of publicspace, once the purchase is made users seek a level ofprivacy away from the public gaze. The opposition
between public and private space can be mapped in avariety of ways. The legal division of space betweenpublic and private ownership denoted by lot lines marks
the boundaries of potential governance and legalsanction. Yet public access through the accessiblepedestrian network often extends into legally private
space. Of interest here are the ways in which these twolayers intersect and overlap into zones of public accessto legally private space. In the back lanes where the legal
boundary is not enforced by walls or fences, wherepublic access flows into carparking bays and openbackyards we find many injecting spots in the liminalzones of publicly accessible yet legally private space.
However the users’ concern is primarily that of beingout of the public gaze:
yif you are looking for a place to go and have a
shot, you usually find other people have been using ittoo, a secluded spot that the police aren’t likely todrive pastylike it’s out of sight from the street where
the police might be driving up and down(I11)
A threshold of streetlife which is crucial in this regardis what Hillier (1996) terms ‘continuous co-presence’
Fthose public spaces with a continuous presence ofmore than two people within each field of view. Hillier
suggests that people are alert to this condition of co-presence (linked to ‘passive surveillance’) and adjust
their perceptions and behaviour accordingly. The con-dition of continuous co-presence throughout the day islinked to streets which are lined with front entrances,
with all their comings and goings. The white areas ofFig. 4 show these areas of continuous co-presencethroughout the day, while the degrees of grey show thedegree of seclusion or separation from these areas of co-
presence, coded according to the number of spatial turnsor 10m segments deep into laneways.Fig. 4 also shows the injecting zonesFthis time as
white stars which they show most clearly against thedeeper and darker sections of public space. A proportionof them (primarily toilets and public carparks) are lost in
the zones of co-presence. It is notable that many of thedeepest (darkest) segments of laneway are not used forinjecting.
The degree to which injecting behaviour is under (orpotentially under) the gaze of others involves theconfluence of several dimensions. First is the way sightlines are mediated by the spatial disposition of buildings,
fences, trees and cars. The second involves the waywindows and doors (coupled with traces of use) operateas signifiers of potential surveillance because someone
could be watching or open the door. Exposure is alsomediated by distanceFbeyond about 20–30m exposurecan protect privacy since intruders will become visible
before they get close. Finally, contrasts of sun and shadeenable the possibility of hiding in the glare.When approaching such issues from the point of view
of an injecting drug-user, what is most interesting is the
potential for the public location of drug-use to shape thesocial identity of the user. The quest for privacy is adialectic process which mediates the spatial construction
of social identity (Altman, 1975). The risk of disclosureis more than simply a risk of prosecution, exposurewhile injecting in public entails being labelled with the
abject social identity of the ‘junkie’ which many usersregard with some shame:
yit makes me feel like I’m a, I’m a scumbag to be
shooting up on the street(I5)
It is not only the act of injecting but also the locationwhich constructs this identity through its connections of
derelict space to derelict identity, homelessness andsocial marginality.
Injecting zones
Fig. 4 shows that primary injecting zones in the studyarea range from about 10–100m from the Smith Street
selling zones. Injecting zones range in size from abouthalf a square metre to larger lineal strips. They are
K. Dovey et al. / Health & Place 7 (2001) 319–331324

termed ‘zones’ because they are often neither centred norbounded. The only thing that they all have in common isminimal degrees of seclusion. They are also prone to
cycles of use and displacement as resident or policeaction is taken to stop them being used and as the streettrade rises and falls with supply, media publicity and
police operations. The following accounts are based onpatterns of use over a period of time in early 1999.Figs. 5a–d show parts of the study area in more detail.
Areas of continuous co-presence are again shown inwhite, grading to dark grey with degrees of seclusion.The injecting zones are shown as white spots andoutlined where they appear in the areas of co-presence.
One of the key findings is that there is no dominant type
of injecting place, however the zones can be looselycategorized as follows.
Public toilets
These are perhaps the most popular injecting zones,
accessible within a few metres of the selling zone onSmith Street (Figs. 5a and b). Users remain within thezone of urban encounter, yet quite secure from the
public gaze. The toilets cross categories of space,meshing public access with private control, publicidentity with private behaviour. So long as the general
public continue to use the toilets then they act ascamouflage for heroin use. The toilets, however, are not
Fig. 4. Exposure, seclusion and IV drug-use.
K. Dovey et al. / Health & Place 7 (2001) 319–331 325

Fig. 5. Detailed zones of IV drug-use.
K. Dovey et al. / Health & Place 7 (2001) 319–331326

safe in the event of an overdose, as is recognized byusers:
ypeople are going into the cubicles and use, and ifthey’re gonna OD they’re gonna sit down, and noone’s there to help themyand that’s a real big risk I
suppose, they could be there for a long time beforesomeone noticesy(I40)
Since the door is locked from the inside and the drugs
can be flushed, the toilets are quite safe from police. Yetthis ‘safety’ becomes acute danger in the event of anoverdoseFthe door locks have been smashed in theattempt to save lives.
Laneways and alcoves
The deepest of injecting zones are located no more
than about 100m from the Smith Street selling zone.They saturate all sites within this area which satisfyminimal conditions of seclusion. They are often adjacentto rear entrances with low levels of use and where the
potential for encounter or overlooking is minimal. Theyoccupy both public and private land in the legal sense.But they are zones where neither private nor public
usage has appropriated the space for regular or specificfunctions, or where such functions are intermittentor time dependent (like storage, garbage, or private
carparking). Often this is a section of unenclosed pri-vate space at the rear of a property. If it is public landthen, similarly, it has not been fully appropriated for
public use and tends to be used intermittently as accessfor a few private properties. Thus these injecting zonesare ‘derelict’ in the sense that they are less ordered,appropriated and controlled than the fully private or
public space. They are liminal zones which oftenstraddle the legal and social boundaries betweenpublic and private space. They often occupy the
zone where legally public space comes to ‘seem’ privatesince the public have no reason to be there. Thisliminality or fluidity of spatial identity seems to be a key
attribute of many injecting zones. Yet injecting does notoccur in many of the deepest spaces in the urban fabric.It is as if some spaces are just too deep, too secluded,
with no routes of escape from police, no excuse to bethere and little chance of being discovered after anoverdose.Fig. 5d shows a short dead-end laneway off Webb
StreetFa rear entry to a building which looks a bitlike a factory but is in fact an office. Notices taped tothe windows say: ‘‘this lane is under video surveillance’’,
but there are no cameras. A fictional panoptic regimehas been established by the occupants of the officeswho have a good view of the lane and found it
distressing to see people injecting. This is a relativelysafe place to inject since an overdose during the day
is highly likely to be reported, yet those who make itsafer are acting to eradicate its use. A key point is that
it is the ambiguous identity of the adjacent building,sliding between office/factory, which makes it safer.The illusion of privacy makes it safer from overdose but
it is used because it seems private and not because itseems safe. The realization, or even the illusion, ofsurveillance may displace the injecting to a moredangerous location.
Many of the injecting sites are quite close to the zonesof co-presence. On the Peel Street corner of a laneway inFig. 5b is a small garage with an open entrance. This
alcove is very close to the zone of co-presence yet hiddenfrom overlooking by both walls and darkness. This siteis also inscribed with the desire to eradicate drug-use
through surveillance; a slogan is written in chalk both onoutside and interior walls: ‘‘Junkies we are watchingyouFResidents’’. Here two identities are affirmedFthe
legitimate, stable ‘resident’ and the transgressive, noma-dic ‘junkie’. The message on the walls carries multipleand conflicting meanings. If it were true that residentswere watching it may render the location safer in the
event of an overdose (if they call the ambulance) or moredangerous (if they call the police).Fig. 5a shows an area where Bedford Street almost
becomes a dead-end and then jogs twice through a smallgap to connect with a laneway lined with industrial uses.The three small corners created through the zig-zag are
injecting zones. This is an interstitial zone whichconnects the street to the laneFit is almost, but notquite, possible to see from street to lane and vice versa.This space has the dual quality of being both deep
and yet permeable; it is a fluid space from whereone can easily disappear into the opposite street/lane ifanyone comes. However, the degree of visual control
over the approach is not high. The chances of beingdisturbed during injection or discovered after an over-dose are high since the injecting zone is used as a
through path.Some injecting sites are relatively exposed to view
from the zones of co-presence yet protected by distance.
Fig. 5d shows an injecting zone in the middle of astraight lane connecting Charles and Webb Streets. Thissite is fully visible from both streets but gains privacy asa site which offers the chance to detect intruders from a
considerable distance. It is safe from sudden interrup-tion with an escape route, and any overdose is likely tobe quickly detected.
Public carparks
There are two large public carparks used for injecting,highly visible from public streets and often used as ashortcut by pedestrians (Figs. 5b and d). They are
generally not overlooked from adjacent entries orwindows except at a distance. Their use for injecting is
K. Dovey et al. / Health & Place 7 (2001) 319–331 327

based on the camouflage offered by pedestrian presence,the permeable or ‘ringy’ spatial structure, the visual
cover offered by the cars, and the cover offered by theshade of trees in a context of glarey sunlight. The spatialstructure shifts from completely open in the early
morning to a highly ringy structure as it fills up withcars. The cars create a shifting visual field where thefluidity of movement camouflages individual behaviour.The injecting spots in the public carparks tend to be
located along the edges and under the trees; the patternof drug-use varies with the disposition of cars. Carinteriors are also used as injecting locations along many
of the side streets and in carparks.
Private carparks
Private carparks tend to have a stronger sense ofenclosure than the public carparks and often produce
enclosed corners hidden from the street. Many are gatedduring the evening. The interior carpark on the corner ofGore and Moor Streets (Fig. 5c) has injecting spots intwo of its four cornersFexcluding the deepest and the
shallowest. The injecting sites are secluded when thereare cars in the car park. Each offers a place to seewithout being seen coupled with the prospect of escape.
The street corner does not have this seclusion and thedeep corner does not have easy exit. The space is inprivate ownership but with full public access during the
day.
Safety/danger
Smooth and striated space
We want to conclude with some preliminary con-ceptualizing of this material and as a prelude we sketchan outline of the distinction between smooth and
striated space suggested by Deleuze and Guattari(1987, Chapter 14). The term ‘striated’ captures theetymological links to the ‘strict’ and ‘stringent’ con-
trasted with the ‘smooth’ which implies a slipperinessand movement where one slides seamlessly from one site(place, meaning, image, identity) to another. Striated
space is where identity has become stabilized withterritorial roots based in tree-like hierarchies. Smoothspace is identified with ‘rhizomatic’ forms which thrivewithin and migrate across the cracks and interstices of a
larger order; the smooth is associated with the refugeeand with nomadic movement across surfaces. Thephenomenology of striated space involves the dom-
inance of the visual over other senses with a focus onoptical perspective and the gaze. The phenomenology ofthe smooth involves the haptic and multi-sensory
micropractices of the body. Smooth space is the spaceof resistance; it utilizes the potential power of camou-
flage and guerrilla action within the striations ofauthority which serve it as masks (Massumi, 1993).
The smooth and the striated are not types of spacesince every real place is a mixture of the two in areciprocal relation where they are constantly ‘enfolded’
into each other (Deleuze and Guattari, 1987, p. 486).Folding is movement through a liminal conditionwhereby one thing ‘folds’ into another. A spatiallabyrinth is a multiplicity of spatial folds where the
twists and turns of lanes and alleys disorients andproduces a mix of desire/danger (Deleuze, 1993, p. 3).The ‘folds’ of the ‘labyrinth’ are its ‘labia’ where a
dominant order folds into sites of slippage and danger;where one loses the controlling gaze over spatial order.Smooth spaces are derelict spaces; ‘cracks’ in the
instumentalized habitat (Massumi, 1993, p. 104–105);holes in the socially structured habitus (Bourdieu, 2000);paradoxical places/spaces of desire and danger.
Safety becomes danger
There are multiple dimensions of safety and dangerwith regard to the practices outlined above and in thefollowing section we will explore several of them. Whatare the range of dangers and their priorities as perceived
by drug-users in relation to spatial forms and practices?How does the perception of safety and danger becomeinscribed in urban space through drug-use practices?
There is clearly a ‘dis-ease’ associated with injecting inthe public gaze and the safer users feel from the policeand the public gaze, the more relaxed they will be. This
seclusion can be achieved, as we have seen, in a numberof ways: with distance and warning of approachingpassersby; with the enclosure of laneways and stairwells;with the camouflage of carparks and sunshading; and
with the lockable doors of the toilets. The danger ofbeing suddenly interrupted by police or passersby ispronounced in some zones but none of the public
injecting zones are completely safe from overlookingand/or interruption.Fig. 6 is a preliminary and abstract mapping of some
of the spatial practices and dilemmas outlined herewithin in the context of a Deleuzian epistemology. Whilethe diagram depicts what appear to be binary pairs of
safety/danger and exposure/seclusion, the spaces, prac-tices and meanings we have described all focus on thezones between categories and the various vectors andtrajectories across them. Each end of the exposure/
seclusion trajectory has its dilemma: more exposedmeans safer in the event of an overdose yet more dangerfrom police; more secluded means safer from police yet
more danger from an overdose. The retreat to one kindof safety (in privacy) leads to another kind of danger.The meaning of ‘safety’ slips across contexts: the ‘safe’
strength of the drug, ‘safe’ from police and the publicgaze; ‘safe’ in the event of an overdose. The interviews
K. Dovey et al. / Health & Place 7 (2001) 319–331328

with users reveal some of the nuances of theseexperiences. Some engage in an illusion of safety and
invisibility:
yusers, young people full stop, are indestructible,invisible and indestructible you know, it’s like the
dog who rolls in dog shit and thinks you can’t seethem because they’ve covered up their scent.(I35)
Such an illusion of invisibility may be protectivein overdose terms since it may lead to a belief insafety from surveillance coupled with the reality of
help in an emergency. Safety is also perceived withina context of speed and urgency: ‘‘yout on the street,you know, it’s just a big rush, and you don’t really
take care of everythingy’’ (cited in Fitzgerald andO’Brien, 1999, p. 46). This ‘rush’ is at once the rush ofscoring and injecting, the rush to be rid of the evidenceand the rush of the drug experience. Scoring and
injecting are not separate acts so much as differentphases of a single trajectory which encompasseseconomic, symbolic, chemical, spatial and experiential
consumption. The rush associated with using in publicspace can lead to unsafe practices including the sharingof needles:
ythere have been times when I shared (needles) inpublic because it’s been, like you just want to get itdone as quickly as possible you know.(I5)
The speed of this trajectory needs to be understoodboth as a whole and as a cluster of issues. It begins
with the speedy nature of the deal, the glance whichinitiates it and the exchange which concludes it. Therisk of being seen by police ensures that the period
of possession between scoring and injection is a time oflegal vulnerability which increases the urgency toinject. The hurry to inject is also driven by the need
to ease the sickness experienced by those who havedeveloped a habit. Using in public when they would
prefer to use at home is one indication of a habit onecannot control:
yyou’ll go and use in public places because you need
a shot now, coz usually like you’re sick you knowyitbecomes a necessity more than anything.(I52)
Yet at the same time scoring and using in public is
also seen as an exciting urban experience which isenmeshed in social constructions of identity:
yI don’t know a junkie who doesn’t love scoring offthe street, they all bitch and moan about it you know
what I mean, but they all fucken love it. I love scoringoff the streetythere’s always this bit of a thrill ofanticipation, like you know you’re doing thisyex-change in front of people who, you believe anyway,
aren’t really hip to what’s going on at allyyou feelsort of like separated from the mainstream, you feellike you’re part ofya club sort of tripy(I52)
This desirable risk is linked to changes in the socialmeaning of heroin use and the social identity of drug-users. Some users see public injecting in terms of a formof performance, framed within the mainstream media’s
portrayal of Smith Street as ‘Smack Street’:
I shot up on the stairwell of a carpark which wasgreat, I loved it, it was like I was a character in amovie.(I50)
For many younger users the narrative is one ofnavigating a terrain of risk and pleasure in a difficultworld of socially constructed ‘performances’ in thepublic gaze:
I can go without heroin entirely and then I’ll walkdown the street and I’ll think to myself no I’d ratherbe on heroin and enjoying my life than trying to do
the right thing by the public eye because the publiceye really is, um, a blind eye anyway ah, and toperform for the public eye I might as well just beperforming for yourself because the public eye is not
ever going to see what’s really going down in theworld anywayythe public eye don’t care about kidson heroin(I42)
The dilemma for drug-users lies in having to play off
competing risks and desires when they inject in a publicspace. However, there are also dilemmas for thecommunity and for public policy. Attempts to control
public injecting have important implications for urbandesign, public expenditure and the vision we have forcivil life in public space. The identity of the ‘street
junkie’ has a very low social status as a stereotypeconstructed by a larger community in order to identifyand thereby stabilize a perceived threat. The spatial shift
of injecting from relative privacy to the publicity of thestreet would appear to be permanent, even if the
Fig. 6. Dilemmas of public injecting.
K. Dovey et al. / Health & Place 7 (2001) 319–331 329

particular streetscapes upon which these practices focusmay change. Rose (1993) and Butler (1990) have
suggested that social identities are produced andreproduced through the repetition of performative actsin public. This has the capacity to lend legitimacy to
such acts, but also to destabilize social identities such asthe stereotypic ‘junkie’ (Nelson, 1999). Regardless of thespeculation, there may be opportunities to intervene in amanner that re-shapes the social meaning and the health
outcomes of heroin use.Our analysis suggests that there are no safe places for
injecting in public. There are many interventions which
could be made to displace dangerous behaviour fromsome of these places. These include fences, cameras,lights and other design interventions. One of the
laneways in this study has since been fenced. However,it is not at all clear that such displacement would be tosafer locations and difficult to predict where it might be
displaced to. Many of the urban design practices whichoccur under the slogan of ‘designing out crime’ could bebetter termed ‘redistributing danger’, the displacementof unwanted behaviour and perceived threat into some-
one else’s neighbourhood (Dovey, 2000).
Supervised injecting
While public injecting practices cannot be renderedsafe, supervised injecting facilities (SIFs) offer the best
short-term prospect for alleviating the dangers. Mel-bourne is currently in the midst of a fierce public debateover the establishment of SIFs, one of which will be
located in the study area if approved. The effectivenessof SIFs in saving lives is well established and based onthe fact that death from overdose is very rare whentreatment is administered. With this in mind, there may
be lessons from this study to help with the programmingand design of such facilities. The challenge in terms ofboth policy and design is to avoid responses which
construct or reproduce negative social stereotypes. Aswe have argued, the spatial transition from selling toinjecting is a fluid trajectory of experience and behaviour
which moves from the camouflage of publicity to theseclusion of privacy. For Deleuze this is a ‘line offlight’Fan experience of tension, thrill, rush and
danger; a time (and place) when users run the risks ofbeing arrested, of being identified as a ‘street junkie’ andof death through overdose.What lessons might we take from this study to help
with the programming and design of such facilities? Theinjecting zones are transition spaces of flow and move-ment rather than places of stabilized identityFwe
suggest that any supervised injecting facilities shouldembody similar qualities. Yet the task of supervisedinjecting is specifically to attract the injecting practices
into the panoptic gaze of medical supervisionFaparadigm case of ‘striated’ space. The traditional role
of architecture has been to create and stabilize identitiesin urban space. Can there be a set of tactics for SIFs
which mirrors the patterns of injecting drug-use outlinedhere? The challenge for architectural thinking runscounter to the traditional role of architecture. Archi-
tecture inevitably involves a stabilization of spatialrelations and built forms. In doing so it stabilizes and‘grounds’ our sense of being. Architecture stabilizes thespatial practices of what Bourdieu (2000) terms the
‘habitus’; our spatial ‘habit’ geared to ‘habitat’. Indeedstabilizing and controlling ‘habit’ is precisely whatsupervised injecting is designed to achieve. How can
this be done without also reinforcing a negative identityof the ‘street junkie’? And a further dilemma here is thatthe public gaze of the media and police on such facilities
may drive users away as they become subject to bothmedical and public supervision.If SIFS are to mirror the existing practices of drug-use
in public space then we suggest some approaches to theirlocation and design. First, they should be liminal placeswhich attempt to overcome the binary logic (in/out;either/or) of spatial thinking; the excessive segmentation
of space which infuses most facility programming,embodied in the very language of supervised injecting‘rooms’. SIFs could be located in a manner that parallels
the liminal locations of existing injection zonesFoccu-pying zones between functions and categories; betweendead-ends and shallow shopfronts, between inside and
outside, between public and private. The facilities couldbe designed with diffuse boundaries in urban space,avoiding thresholds, portals or doorways at which theidentity of the place, and therefore the user, is signified.
Spatial screening could ensure that entrance transitionoccurs over a distance or through several spatial turns.Multiple entries could be used so there is no single
threshold. The facility could be construed as a ‘field’where the gaze of supervision extends beyond a medicalcore, perhaps with decreasing levels of supervision/
safety. The SIF could be co-located or nested with otherfacilities and functions such that its identity becomesblurred. There could be a diversity of types of facility
mixed with a variety of functions: chemist shops,medical facilities, vacant buildings, gaming arcades,carparks and train stations. The signage may deploycodings whereby it is labelled as one thing yet under-
stood (by some) to be another. Finally, the location anddesign of SIFs may need to be ephemeral or mobileFeven the best designed and located facilities may have
a short-lived success if the market moves or the locationis exposed in the tabloid media.Having said all this, consider a further dilemma in this
‘politics of visibility’. If supervised injection facilities aredesigned to mirror existing marginalized practices ofinjecting drug use, do we run the risk of institutionaliz-
ing this marginality through the very tactics ofliminality, diffusion, multiplicity and ephemerality
K. Dovey et al. / Health & Place 7 (2001) 319–331330

outlined above? Is it not in the user’s interest tonormalize injecting practices under clear forms of
governance, deploying a stabilizing architecture? Such‘mainstreaming’ and normalization of injecting drug-usewill at once render such practices more safe and less
thrilling. But then will it meet its market? The furtherone explores these issues, the more the dilemmasmultiply. We do not claim to have resolved them, butrather to have exposed them a little. Our sense, and our
hope, is that these are not just dilemmas for the injectingdrug-user, but may have some ripples of consequencefor the broader debates about health and place.
Acknowledgements
This study was made possible by a research grantfrom the National Health and Medical Research
Council of Australia. We also thank Sandra Gifford,Mary O’Brien and two anonymous reviewers for help inrefining the ideas.
References
Altman, I., 1975. The Environment and Social Behavior.
Brooks Cole, Monterey.
Bourdieu, P., 2000. Pascalian Meditations. Polity Press, Cam-
bridge.
Butler, J., 1990. Gender Trouble. Routledge, New York.
Coleman, A., 1985. Utopia on Trial. Hilary Shipman, London.
Dear, M., 2000. The Postmodern Urban Condition. Blackwell,
Oxford.
Deleuze, G., 1985. Nomad thought. In: Alison, D. (Ed.), The
New Nietzsche. MIT Press, Cambridge, MA.
Deleuze, G., 1993. The Fold. University of Minnesota Press,
Minneapolis.
Deleuze, G., Guattari, F., 1987. A Thousand Plateaus. Athlone,
London.
Dorn, M., Laws, G., 1994. Social theory, medical geography
and body politics. The Professional Geographer 46,
106–110.
Dovey, K., 1999. Framing Places: Mediating Power in Built
Form. Routledge, London.
Dovey, K., 2000. Redistributing danger. The Australian
Planner 37 (1), 10–13.
Fitzgerald, J., O’Brien, M., 1999. Health in larger terms.
Research Report, Department of Criminology, University
of Melbourne.
Fitzgerald, J., Broad, S., Dare, A., 1998. Regulating the street
heroin market in Fitzroy/Collingwood. Research Report,
VicHealth, Melbourne.
Franck, K., 1984. Exorcising the ghost of environ-
mental determinism. Environment and Behavior 16 (4),
413–435.
Greenberg, S., Rohe, W., 1984. Neighborhood design and
crime. Journal of the American Planning Association 50 (1),
48–61.
Hayes, M., Foster, L., Foster, H. (Eds.), 1992. Community,
Environment and Health. University of Victoria, Victoria,
BC, pp. 213–229.
Hillier, B., 1988. Against enclosure. In: Teymur, N., Markus,
T., Wooley, T. (Eds.), Rehumanising Housing. Butter-
worths, London.
Hillier, B., 1996. Space is the Machine. Cambridge UP,
Cambridge.
Hillier, B., Hanson, J., 1984. The Social Logic of Space.
Cambridge UP, Cambridge.
Jacobs, J., 1965. The Death and Life of Great American Cities.
Penguin, Harmondsworth.
Kearns, R., 1994. Putting health and health care into place. The
Professional Geographer 46, 111–115.
Kearns, R., Gesler, W. (Eds.), 1998. Putting Health into Place.
Syracuse UP, Syracuse, 1998.
MacIntyre, S., MacIvor, S., Sooman, A., 1993. Area, class and
health. Journal of Social Policy 22 (2), 213–234.
Massumi, B., 1993. A User’s Guide to Capitalism and
Schizophrenia. MIT Press, Cambridge.
Moon, G., 1995. (Re)placing research on health and health
care. Health and Place 1, 1–4.
Moon, G., Braun, T., 1998. Place, space and health service
reform. In: Kearns, R., Gesler, W. (Eds.), Putting Health
into Place. Syracuse UP, Syracuse, pp. 270–288.
Nelson, L., 1999. Bodies (and spaces) do matter. Gender, Place
and Culture 6 (4), 331–353.
Newman, O., 1972. Defensible Space. Macmillan, New York.
Poland, B., 1998. Smoking, stigma and the purification of
public space. In: Kearns, R., Gesler, W. (Eds.), Putting
Health into Place. Syracuse UP, Syracuse, pp. 208–225.
Rose, G., 1993. Feminism and Geography. University of
Minnesota Press, Minneapolis.
K. Dovey et al. / Health & Place 7 (2001) 319–331 331
Copyright © 2022 FDOKUMEN




















