ROLE OF VIRECHANA KARMA WITH HRIDYA VIRECHANA ...
183
ROLE OF VIRECHANA KARMA WITH HRIDYA VIRECHANA LEHA IN THE MANAGEMENT OF PSORIASIS By Dr. CYRUS NEUPANE B.A.M.S. Dissertation submitted to the RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BENGALURU In partial fulfillment of the requirements for the degree of AYURVEDA VACHASPATI (Doctor of Medicine) In PANCHAKARMA Under the Guidance of Dr. NIRANJAN RAO M.D. (Ayu) Professor & H.O.D. Department of P.G. Studies in Panchakarma S.D.M. College of Ayurveda, Udupi Co-Guide Dr. POOJA B. A. M.D., PhD (Panchakarma) Assistant Professor Department of P.G. Studies in Panchakarma S.D.M. College of Ayurveda, Udupi DEPARTMENT OF POST GRADUATE STUDIES IN PANCHAKARMA S.D.M. COLLEGE OF AYURVEDA, UDUPI – 574118 2017- 2018
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ROLE OF VIRECHANA KARMA WITH HRIDYA VIRECHANA ...
ROLE OF VIRECHANA KARMA WITH HRIDYA
VIRECHANA LEHA IN THE MANAGEMENT OF PSORIASIS
By
Dr. CYRUS NEUPANE B.A.M.S.
Dissertation submitted to the
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA,
BENGALURU
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATI
(Doctor of Medicine)
In
PANCHAKARMA
Under the Guidance of
Dr. NIRANJAN RAO M.D. (Ayu)
Professor & H.O.D.
Department of P.G. Studies in Panchakarma
S.D.M. College of Ayurveda, Udupi
Co-Guide
Dr. POOJA B. A. M.D., PhD (Panchakarma)
Assistant Professor
Department of P.G. Studies in Panchakarma
S.D.M. College of Ayurveda, Udupi
DEPARTMENT OF POST GRADUATE STUDIES IN PANCHAKARMA
S.D.M. COLLEGE OF AYURVEDA, UDUPI – 574118
2017- 2018



VIII
LIST OF ABBREVIATIONS USED
Ag. Pu. - Agni Purana
As. Hr. - Ashtanga Hridaya
As. Sa. - Ashtanga Sangraha
Ath. - Atharvaveda
ATP - Adenosine Triphosphate
B. P. - Bhava Prakasha
Bh. Ra. - Bhaishajya Ratnavali
Bh.S. - Bela Samhita
C.D. - Chakra Datta
Ch. Sa. - Charaka Samhita
K.S. - Kashyapa Samhita
Ka. - Kalpasthana
M. N. - Madhava Nidana
Sh. Sa. - Sharngadhara Samhita
Su.Sa. - Susruta Samhita
Y.V. - Yajurveda

IX
LIST OF TABLES
SR.
NO. TITLE OF TABLE
PAGE
NO.
1. Indications of Virechana 6
2. Contraindications of Virechana 7
3. Dose of Virechana drugs 12
4. Dose of Virechana drugs according to Koshtha 13
5. Observation of Suddhi Lakshanas of Virechana 14
6. Samyak Yoga Lakshana of Virechana Karma 14
7. Ayoga Lakshana of Virechana Karma 15
8. Atiyoga Lakshana of Virechana Karma 16
9. List of Virechana Vyapat 17
10. Peyadi Samsarjana Karma based on Suddhi 19
11. Points to classify Kushtha under Maha and Kshudra 27
12. Classification of Kushtha according to different Acharyas 27
13. Classification of Kushtha based on dominance of the Dosha 29
14. Nidana of Kushtha related to Atisevana 30
15. Nidana of Kushtha related to Mithya Ahara 31
16. Viharaja Nidana of Kushtha 32
17. Various Acharajanya Nidana for Kushtha 32
18. Poorvaroopa of Kushtha 34
19. Sadyasadhyata of Kushtha 36
20. Rasapanchaka of ingredients of Moorchhita Tila Taila 54
21. Age wise Distribution of Patients 70
22. Showing Sex Distribution 71
23. Showing Patients’ Distribution according to Religion 72
24. Distribution of patients based on their Education 73
25. Distribution according to Marital Status 73
26. Distribution of patients according to Socio-economic Status 74
27. Distribution of patients according to Occupation 75
28. Distribution according to Desha 76
X
29. Distribution according to Age of Onset 76
30. Distribution according to Chronicity of Disease 77
31. Distribution according to Aggravating factors 78
32. Distribution according to Relieving Factors 79
33. Distribution according to Family history 80
34. Distribution according to Vegetarian/Mixed food habit 81
35. Distribution of patients based on addictions 82
36. Distribution of patients based on Involvement of Joints 82
37. Distribution of patients according to changes in nails 83
38. Distribution according to Type of Psoriasis 84
39. Distribution according to Prakriti 85
40. Distribution according to Sara 86
41. Distribution according to Samhanana 87
42. Distribution according to Satmya 87
43. Distribution according to Satva 88
44. Distribution according to Abhyavaharana Shakti 89
45. Distribution according to Jarana Shakti 90
46. Distribution according to Vyayama Shakti 90
47. Distribution according to Koshtha 91
48. Observation of Snehajiryamana Lakshana 92
49. Observation of various Snehajirna Lakshana 93
50. Showing number of days to attain Samyak Snigdha Lakshana 94
51. Samyak Snigdha Lakshana observed on last day of Snehapana 95
52. Samyak Swinna Lakshana observed 96
53. Showing Vegiki Shuddhi 97
54. Laingiki Shuddhi 98
55. Antiki Shuddhi 99
56. Showing Maniki Shuddhi 100
57. Distribution of patients based on Atiyoga, Ayoga and Samyak
Yoga of Virechana 101
58. Distribution of patients based on Samsarjana Krama days 102
59. Virechana Aushadha Karya Samaya observed in patients 102
XI
60. Result for head after Virechana 104
61. Result for head after follow up 104
62. Result for upper limb after Virechana 105
63. Result for upper limb after follow up 105
64. Result for trunk after Virechana 106
65. Result for trunk after follow up 106
66. Result for lower limb after Virechana 107
67. Result for lower limb after follow up 107
68. Result on Total PASI Score after Virechana 107
69. Result on Total PASI Score after follow up 108
70. Effect on 5D Itch Score after Virechana 108
71. Effect on 5D Itch Score after follow up 108
XII
LIST OF FIGURES
SR.
NO.
NAME OF FIGURES
PAGE
NO.
1. Figure showing Samprapti of Kushtha 36
2. Age wise Distribution of Patients 71
3. Showing Sex Distribution 71
4. Showing Patients’ Distribution according to Religion 72
5. Distribution of patients based on their Education 73
6. Distribution according to Marital Status 74
7. Distribution of patients according to Socio-economic Status 74
8. Distribution of patients according to Occupation 75
9. Distribution according to Desha 76
10. Distribution according to Age of Onset 77
11. Distribution according to Chronicity of Disease 78
12. Distribution according to Aggravating factors 79
13. Distribution according to Relieving Factors 80
14. Distribution according to Family history 80
15. Distribution according to Vegetarian/Mixed food habit 81
16. Distribution of patients based on Addictions 82
17. Distribution of patients according to Joints Involvement 83
18. Distribution of patients according to changes in nails 83
19. Distribution according to Type of Psoriasis 84
20. Distribution according to Prakriti 85
XIII
21. Distribution according to Sara 86
22. Distribution according to Samhanana 87
23. Distribution according to Satmya 88
24. Distribution according to Satva 88
25. Distribution according to Abhyavaharana Shakti 89
26. Distribution according to Jarana Shakti 90
27. Distribution according to Vyayama Shakti 91
28. Distribution according to Koshtha 92
29. Observation of Snehajiryamana Lakshana 93
30. Observation of various Snehajirna Lakshana 94
31. Showing no. of days to attain Samyak Snigdha Lakshana 95
32. Samyak Snigdha Lakshana observed on last day of Snehapana 96
33. Samyak Swinna Lakshana observed 97
34. Showing Vegiki Shuddhi 98
35. Laingiki Shuddhi 99
36. Antiki Shuddhi 99
37. Showing Maniki Shuddhi 100
38. Patients’ distribution based on Atiyoga, Ayoga and Samyak
Yoga of Virechana
101
39. Distribution of patients based on Samsarjana Krama days 102
XV
STRUCTURED ABSTRACT with Key Words:
Title:
“ROLE OF VIRECHANA KARMA WITH HRIDYA VIRECHANA LEHA IN THE
MANAGEMENT OF PSORIASIS”
Background:
Virechana is the most suitable therapy for Pitta and disorders due to Pitta Prakopa.
Shodhana therapies are unique Ayurvedic therapies, where Doshas, which are
fundamental causes for the disease, are expelled out of the body. Psoriasis is one of
the most common dermatological conditions affecting 2% of world population. It is
a chronic inflammatory skin disorder clinically characterized by erythematous,
sharply demarcated papules and rounded plaques, covered by silvery micaceous scale.
Multi-dimensional assessment of Psoriasis was done with Psoriasis area severity
index (PASI), and 5 D itch score, Auspitz sign, and Candle grease sign.
Objectives:
To evaluate the Efficacy of Virechana Karma with Hridya Virechana Leha in
Psoriasis.
Methods:
It is an open clinical study with pre-test and post- test design in which, 25 diagnosed
patients of Psoriasis and fulfilling the selection criteria in the age group of 16 – 70
years, of either sex were selected. After Deepana and Pachana, Snehapana in Arohana
Krama was started and after obtaining Samyak Snigdha Lakshana, patients were
subjected for Parisheka for 4days. On 4th
day after Parisheka, Virechana Karma was
performed in empty stomach around 9:30 am and Samsarjana Krama was advised
according to the Shuddhi. Assessment of the patient was carried out before treatment,
after Treatment and 7 days after the Samsarjana Krama (follow up).
Results:
Study showed statistically significant result in decrement in PASI Score and 5D ITCH
Score.
Interpretation and Conclusion:
Hence, Virechana Karma with Hridya Virechana Leha was found to be effective in
reducing signs and symptoms of Psoriasis.
Keywords: Virechana, Kushtha, Psoriasis, PASI, 5D Itch Score.
Introduction
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 1
INTRODUCTION
Virechana is a procedure in which the morbid Doshas are eliminated through
Adhobhaga, where Acharya Chkrapani while commenting on Adhobhaga clarifies it
as the Guda (anal route) 1
. Psoriasis is a chronic inflammatory skin disorder
clinically characterized by erythematous, sharply demarcated papules and rounded
plaques, covered by silvery micaceous scale.2 It is one of the most common
dermatological conditions, affecting around 2% of the world population, where in
about three-quarters of patients, the onset is before the age of 40 years and in about
one-third, it appears before the age of 20 years3.
In Ayurveda, almost all the skin diseases have been described under Kushtha.
Psoriasis is considered as one type of Kushtha and may resemble Ekakushta, Kitibh,
Mandala Kushta. Kushta is a Tridoshaja Vikara4
and Virechana is the best Shodhana
for Pitta predominant disorders5, meanwhile it also exerts its action on
Sleshmasamsrishta Avasta6 and also corrects the morbid Vata Dosha
7.
In Sahasrayoga, Hridya Virechana Leha is presented as one of the Vairechanik Yoga8.
It is one of the preparations of Trivrit and Trivrit is considered as the best drug
causing Rechana9. So, with this background, the study is taken to evaluate the efficacy
of Virechana Karma using Hridya Virechana Leha for the management of Psoriasis.
In the present study, patients diagnosed with Psoriasis were selected based on
selection criteria and subjected to Snehana and Swedana as Purvakarma, and
Virechana as Pradhana Karma and Samsarjana Krama as Pashchat Karma. Snehana
was achieved by internal administration of Moorchhita Tila Taila followed by Karanja
Kwatha Pariseka Swedana.
Introduction
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 2
Virechana Karma in this clinical study was administered with Hridya Virechana Leha
with hot milk as Anupana.
Depending on Shuddhi, the Pashchat Karma was decided. Dosage and duration of all
the procedures were in accordance with Dosha Bala, Rogi Bala, Agni Bala, Koshtha
etc.

Objectives
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 3
OBJECTIVES
1. To evaluate the efficacy of Virechana Karma with Hridya Virechana Leha in
Psoriasis.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 4
REVIEW OF LITERATURE
VIRECHANA KARMA
HISTORICAL REVIEW:
Veda:
References of Virechana Yoga such as Haritaki, Trivrit etc. are found.
Agnipurana:
Agnipurana has stated Virechana as a best treatment for the disease caused due to
Pitta. It is mentioned to be indicated in Urdhwaga Raktapitta, Jwara, Hridroga. But
detailed description of Virechana is not found.
Vinaya Pitaka (Buddhist Literature):
In the text of Vinaya Pitaka, which was written during Buddha Kala, description of
administration of Virechana is found, where Virechana was given to Gautam Buddha
by Vaidya Jivaka. He used Greya Yoga, i.e. making Buddha smell some powder
spread over Utpalpatra.
Samhita Kala:
Virechana has been dealt elaborately in Charak Samhita, Sushruta Samhita, Astanga
Hridaya, Astanga Sangraha etc. The details will dealt below under different headings.
In Mesopotamia, Virecahan was in practice for pain in abdomen. Drugs used for
Virechana were Svarnapatri and Indrayana. (Jacqutta Hewks and Leonard Wooley).
In Western Medicine, the cathartics are amongst the most ancient methods of internal
medication used for treatments.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 5
Etymology:
The word Virechana is composed of three components (Vachaspatyam):
Vi: Upasarga (prefix)
Rich: Rich Dhatu (root)
Lyut: Pratyaya (suffix)
Accordind to Shabdakalpadruma:
Rechana is derieved from word root – Rich dhau and Lyut pratyaya.
Virechana word is formed from the root ‗Rich‘ dhatu, ‗Vi‘ Upasarga with ‗Nich‘ and
‗Lyut‘ Pratyaya, giving the meaning ‗Virechana Rechayateeti‘.
Rechana word is commonly used for the act of evacuation. As the evacuation of
Doshas is done by both Vamana and Virechana, sometimes the word Virechana
broadly may imply the both. But in general consideration, the word Virechana denotes
the evacuation of the doshas through the ‗Guda Marga‘. (Charkrapani on Ca. Ka. 1/4)
Definition:
Virechana may be defined as a process of eliminating the vitiated Doshas through the
Adhobhaga. Here, Chakrapani has clearified the meaning of Adhobhaga as ‗Guda‘14
.
It is the procedure in which orally administered drug acts on internally vitiated Dosha
(especially Pitta), and expels them through the Guda Marga.
Synonyms of Virechana:
Sramsan, Praskandanam.15
Panchabhoutika Sangathana:
Virechana drugs have the dominancy of Prithvi and Jala Mahabhuta. Virechana drugs
have Ushna, Teekshna, Sukshma, Vyavayi and Vikasi Guna. But many drugs though
may have Prithvi and Jala Mahabhuta priedominance, still may not exhibit
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 6
Vairechanika property. This has been attributed to the Prabhava of the Virechana
drugs.16
Karyakshetra of Virechana:
Virechana has got actions on the following Dosha, Dhushya, Srotas, and Agni:
Dosha: Virechana is beneficial for Pitta Dosha predominant disorders, since
Virechana eliminates vitiated Pitta out of the body from its root. According to
Bagbhata, Virechana is helpful even in Pitta combined with Kapha, or Kapha in Pitta
Sthana.17
Also Acharya Bhela mentions Virechana in Sannipata condition also.
Dhushya: Virechana is mentioned as a Shodana procedure in Dushti of Rasa, Rakta,
Mamsa, Asthi, Majja and Shukra Dhatu. Hence, in majority of the Dhatu-Pradosaja
Vikaras, Virechana is a suitable treatment protocol.18
Srotas: Since on the above mentioned Dushya, Virechana is helpful, it can be inferred
that it is beneficial in Rasavaha, Raktavaha, Mamsavaha, Asthivaha, Majjavaha and
Shukravaha Srotodushti.
Agni: As in the Samyak Virikta Lakshana, Deeptagni is mentioned, so it can be
inferred that Virechana improves the Jatharagni and other Agni present in the body.
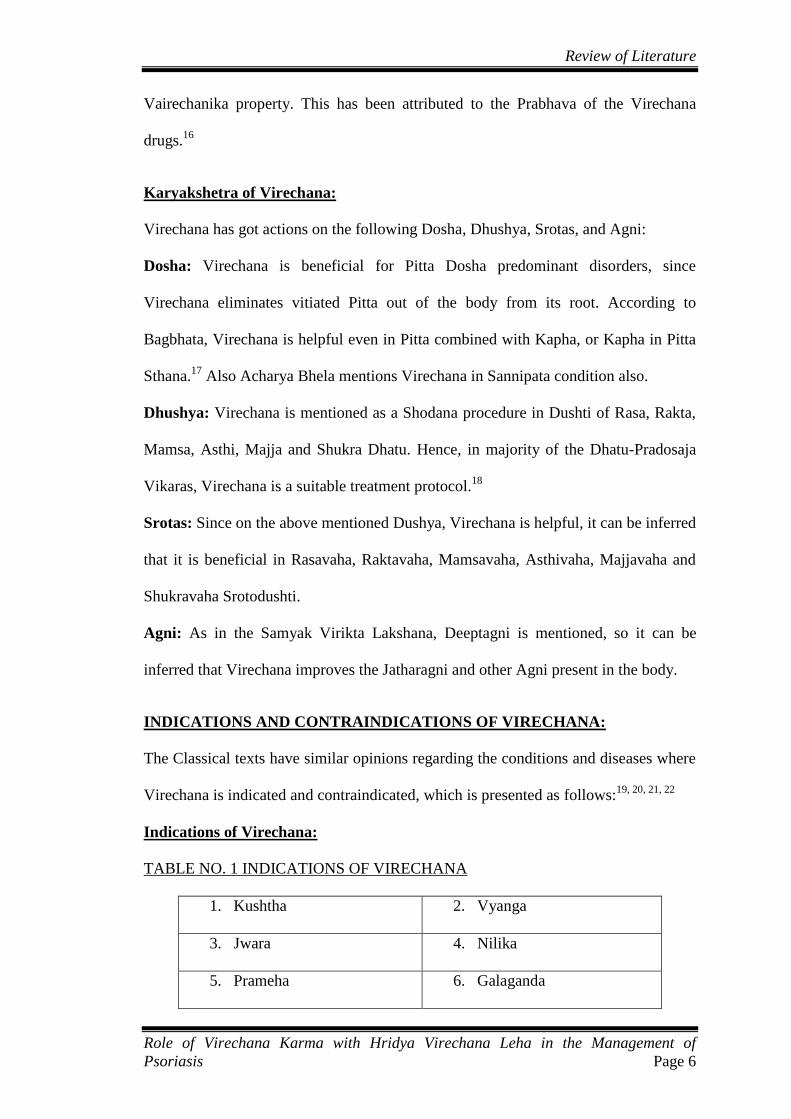
INDICATIONS AND CONTRAINDICATIONS OF VIRECHANA:
The Classical texts have similar opinions regarding the conditions and diseases where
Virechana is indicated and contraindicated, which is presented as follows:19, 20, 21, 22
Indications of Virechana:
TABLE NO. 1 INDICATIONS OF VIRECHANA
1. Kushtha 2. Vyanga
3. Jwara 4. Nilika
5. Prameha 6. Galaganda

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 7
7. Pandu 8. Visphotaka
9. Halimaka 10. Bradhna
11. Naasasrava 12. Unmada
13. Netradaha 14. Apasmara
15. Shvasa 16. Yonidosha
17. Aasyadaha 18. Arbuda
19. Kasa 20. Bhagandara
21. Paiitika vyadhi 22. Arsha
23. Shotha 24. Vidradhi
25. Pakwashaya ruja 26. Granthi
27. Netrasrava 28. Dushtavrana
29. Shirashula 30. Vriddhi
31. Visarpa 32. Apache
33. Parshvaruja 34. Timira
35. Hridroga 36. Abhisyanda
37. Gulma 38. Kacha
39. Pliha 40. Akshipaka
41. Vatarakta 42. Krimikoshtha
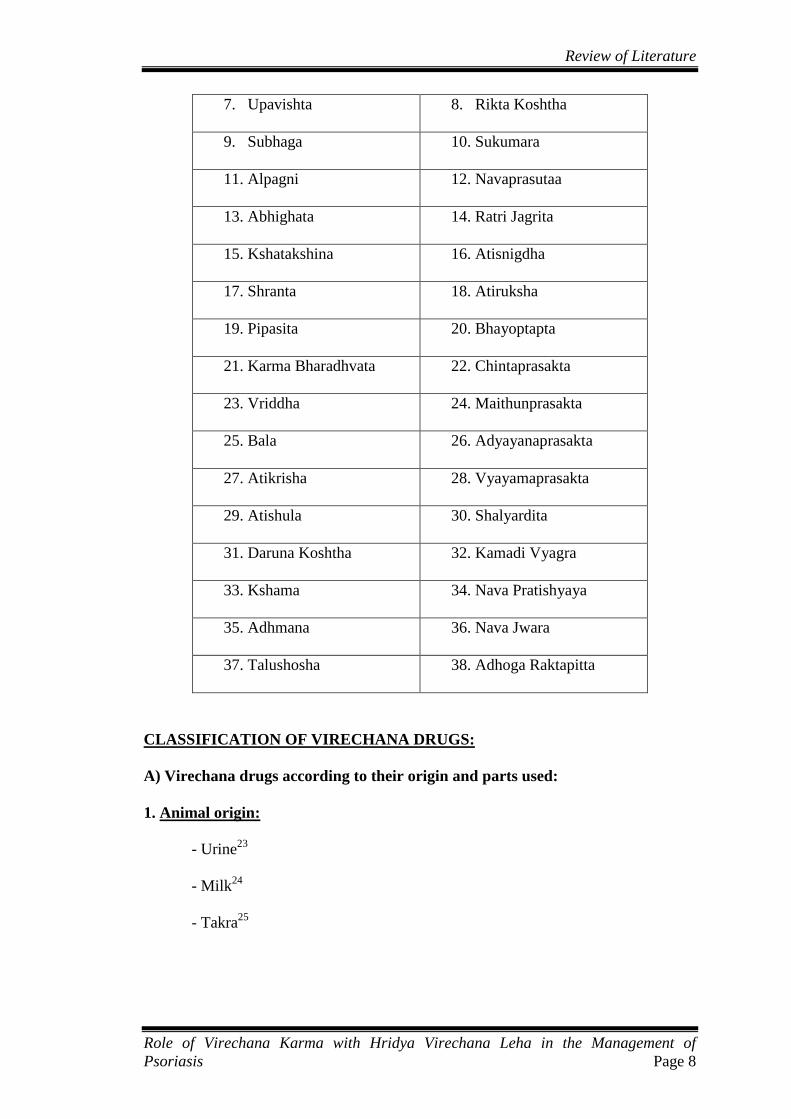
Contraindications of Virechana:
TABLE NO.2 CONTRAINDICATIONS OF VIRECHANA
1. Langhita 2. Urustambha
3. Durbala 4. Garbhini
5. Durbalendriya 6. Bhakta
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 8
7. Upavishta 8. Rikta Koshtha
9. Subhaga 10. Sukumara
11. Alpagni 12. Navaprasutaa
13. Abhighata 14. Ratri Jagrita
15. Kshatakshina 16. Atisnigdha
17. Shranta 18. Atiruksha
19. Pipasita 20. Bhayoptapta
21. Karma Bharadhvata 22. Chintaprasakta
23. Vriddha 24. Maithunprasakta
25. Bala 26. Adyayanaprasakta
27. Atikrisha 28. Vyayamaprasakta
29. Atishula 30. Shalyardita
31. Daruna Koshtha 32. Kamadi Vyagra
33. Kshama 34. Nava Pratishyaya
35. Adhmana 36. Nava Jwara
37. Talushosha 38. Adhoga Raktapitta
CLASSIFICATION OF VIRECHANA DRUGS:
A) Virechana drugs according to their origin and parts used:
1. Animal origin:
- Urine23
- Milk24
- Takra25
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 9
2. Plant origin:
Mulini Virechana Dravya: Roots that have been recommended for Virechana are
Hastidanti, Shyamatrivrit, Adhoguda (Vidhara), Saptala, Pratyakshirni (Danti),
Gavakshi (Indrayana), Jyotismati, Bimbi, Vishanika, Ajagandha, Dravanti.26
Shankhini, Snuhi, Svarnakshiri, Chitraka, Kusha, Kasha, Kihini (Apamarga).27
Shalaparni, Prishniparni, Kantakari, Gokshura, Punarnava.28
Phalini Virechana Dravya: Fruits that are considered are Shankhini, Vidanga,
Anupa Klitaja(Madhuyasti), Sthalaja Klitaja, Prakirya (Latakaranaja), Abhaya,
Antahkotarpushpi, Kampillaka and Aragvadha.29
Puga, Amalaki, Haritaki, Vibhitaki,
Nilini, Chaturangula, Eranda, Kampillaka.30
Pilu, Priyala, Kuvala, Badara, Karkandu,
Kashmarya, Parusaka, Draksha.
Here, it is noteworthy that Acharya Charaka has mentioned the use fruit for
Virechana, while Acharya Susruta has told the root.
Kshirini Dravya: Latex of Snuhi and Arka.31
Saptacchada (Saptaparna), Jyotismati.32
Twak Dravya: Bark of Putika, Tilvaka,33
Kampillaka, Ramyaka, Patola.34
B) According to intensity of Action:
Mridu Virechana: Drugs that are Manda in Virya, administered in patient with
Ruksha Shareera, that too in low dose, drugs which have been given Bhavana with
drugs of oppsite Virya cause less degree of purgation. 35
Indiction: Alpa Dosha, Mridu Koshtha, Purva Shodhita
Drugs used: Draksha, Ksheera, Eranda Taila, Ambu36
Madhyama Virechana: Drugs which are Madyama in their Guna and Karma, drugs
which are exposed to water, heat, insects, not grown in proper Desha and Kala, and
not having all the desired properties will induce Madhyama Virechana. Also if a drug

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 10
is given to a patient who is not properly Snigdha, or Swinna, then the drug givenfor
Virechana will have only Maadhyama Virechana action.37
Indication: Mdhyama Koshtha, Mdhyama Bala
Drugs used: Trivrit, Katuki, Aragvdha38
Tikshna Virechana: Drugs that have Tikshna Guna and Karma, and that cause
numerous loose stools by eliminating Doshas in large quantity without producing
Glani, pain in Guda and Hridaya Pradesha.39
Indication: Krura Koshtha, Balavana Rogi
Drugs used: Snuhi, Hemakshiri, Danti40
C) According to degree and Agrya Dravya41
:
Sukha Virechana: Trivrit (Operculina turpethum)
Mridu Virechana: Aragvadha (Cassia fistula)
Tikshna Virechana: Snuhi (Euphorbia nerifolia)
D) On the basis of mode of Action:
Sarangadhara has classified Virechana into four types depending on action, potency of
drug, onset and consistency of excretory product.
Anulomana: Drugs that do the digestion of Malas and breaks its Bandha and later
expels out through Adhobhaga are known as Anulomaka. Eg. Haritaki (Terminalia
chebula)42
. Acharya Sushruta has considered Sara as synonym of Anuloman, and
Dalhana addsthat Anulomana causes expulsion of Vata and Kapha.43
Bhavamishra
has considered undigested Doshas as Mala, and opines that drugs which expel them
are Anulomana.

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 11
Sramsana: Drugs that expel the semi-digested and sticky Malas without digestion
come under this category. Eg. Aragvadha (Cassia fistula). The difference between the
Anulomana and Samsrana is about the digestion of Mala.44
Bhedana: Drugs that break Abaddha, Baddha, and Pindita Mala and expel them
through Guda come under Bhedana. Eg. Katuki (Picorriza kurroa)45.
Rechana: Drugs that expel both digested and undigested Mala after making them
watery through Guda Marga fall under this category. Eg. Trivrit (Operculina
turpethum)46
E) According to Kalpana:
Ghrita Yoga, Taila Yoga, Ksheera Yoga, Madya Yoga, Mutra Yoga, Mamsarasa
Yoga, Bhakshana Yoga, Avaleha Yoga47
are certain Kalpanas that are prepared based
on the purpose of easy intake (palatability), for enhancing or altering the potency, for
preserving for longer duration, and also for mixing with other drugs s as to increase or
reduce the potency.
Amongst the Virechana drugs, the following have been considered as the best in their
respective area:48
Mula Virechana: ShyamaTrivrit
Phala Virechana: Haritaki
Twak Virechana: Tilwaka
Swarasa Virechana: Karavellaka
Dugdha Virechana: Snuhi
PROCEDURE OF VIRECHANA:
The whole procedure of Virechana can be dealt under three headings viz. Poorva
Karma, Pradhana Karma and Paschata Karma.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 12
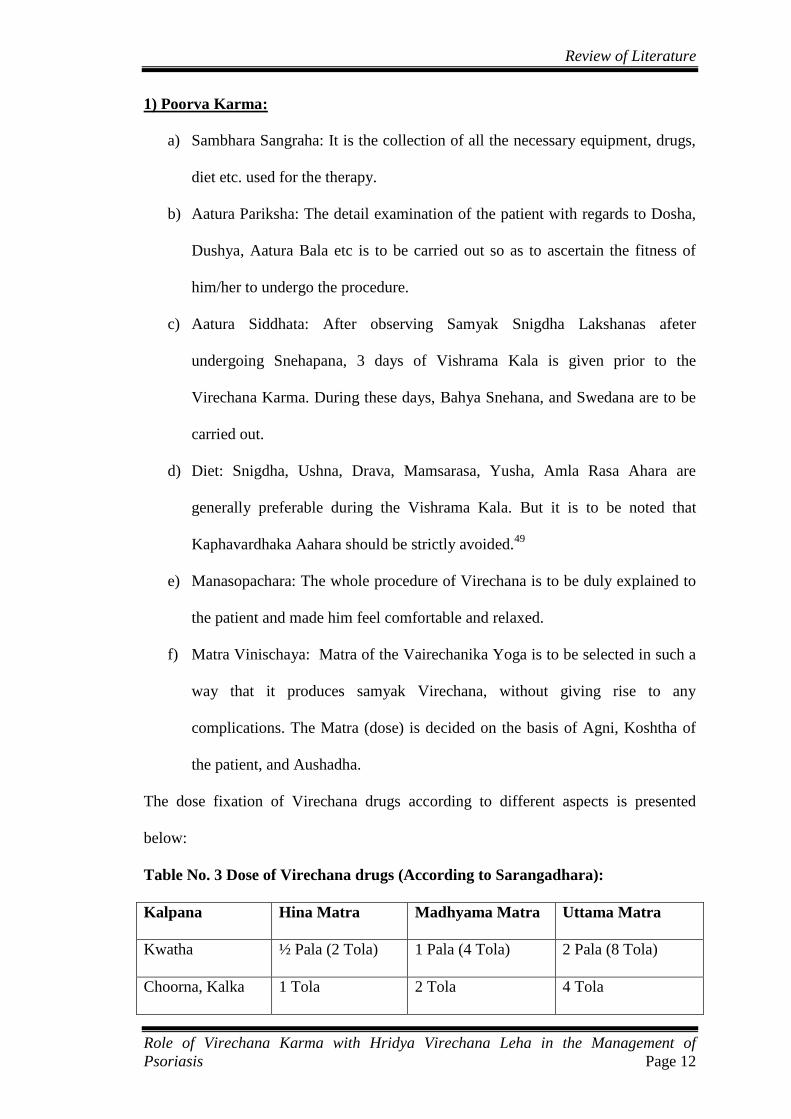
1) Poorva Karma:
a) Sambhara Sangraha: It is the collection of all the necessary equipment, drugs,
diet etc. used for the therapy.
b) Aatura Pariksha: The detail examination of the patient with regards to Dosha,
Dushya, Aatura Bala etc is to be carried out so as to ascertain the fitness of
him/her to undergo the procedure.
c) Aatura Siddhata: After observing Samyak Snigdha Lakshanas afeter
undergoing Snehapana, 3 days of Vishrama Kala is given prior to the
Virechana Karma. During these days, Bahya Snehana, and Swedana are to be
carried out.
d) Diet: Snigdha, Ushna, Drava, Mamsarasa, Yusha, Amla Rasa Ahara are
generally preferable during the Vishrama Kala. But it is to be noted that
Kaphavardhaka Aahara should be strictly avoided.49
e) Manasopachara: The whole procedure of Virechana is to be duly explained to
the patient and made him feel comfortable and relaxed.
f) Matra Vinischaya: Matra of the Vairechanika Yoga is to be selected in such a
way that it produces samyak Virechana, without giving rise to any
complications. The Matra (dose) is decided on the basis of Agni, Koshtha of
the patient, and Aushadha.
The dose fixation of Virechana drugs according to different aspects is presented
below:
Table No. 3 Dose of Virechana drugs (According to Sarangadhara):
Kalpana Hina Matra Madhyama Matra Uttama Matra
Kwatha ½ Pala (2 Tola) 1 Pala (4 Tola) 2 Pala (8 Tola)
Choorna, Kalka 1 Tola 2 Tola 4 Tola

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 13
Table No. 4 Dose of Virechana drugs according to Koshtha:
Authors Mridu Koshtha Madhyama
Koshtha
Kroora Koshtha
Sushruta (Su.
Chi.33/21)
Mridu Matra Madyama Matra Tikshna Matra
Vangasena 1 Tola 2 Tola 3 Tola
2) Pradhana Karma:
Pradhana Karma includes:
a. Administration of Virechana Yoga
b. Observation and management during Virechana Vega
c. Observation of:
- Shuddhi Lakshanas
- Virechana Vyapat (if any)
a. Administration of Virechana Yoga:
The method of administration of Virechana Karma has been elaborately dealt by
Acharya Charaka. After the completion of Bahya Snehana and Swedana, after
checking if the patient has slept well the previous night, is cheerful, has digested his
previous night‘s meal, is advised to perform auspicious rites. Then after, considering
the Vaya, bala, dosha, Bhesaja etc., and after passing the time of Kapha Prakopa in
morning, the patient should be given with the Virechana Yoga in the empty
stomach.50
After administration of the Virechana drug, cold water is sprinkeled over the face so
as to avoid vomiting sensation, andthen the patient isasked to gargle with hot water,
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 14
and to smell fragrance of flower etc. He is advised to avoid cold winds, and take rest.
He is advised not to hold the Vega, while also not to do Pravahana.51
b. Observation andmanagement during Virechana Vega:
During all the time, Vaidya should concentrate on the manifestation of Lakshanas of
Jirna/Ajirna of Aushadha, Suddhi and Vypat etc.
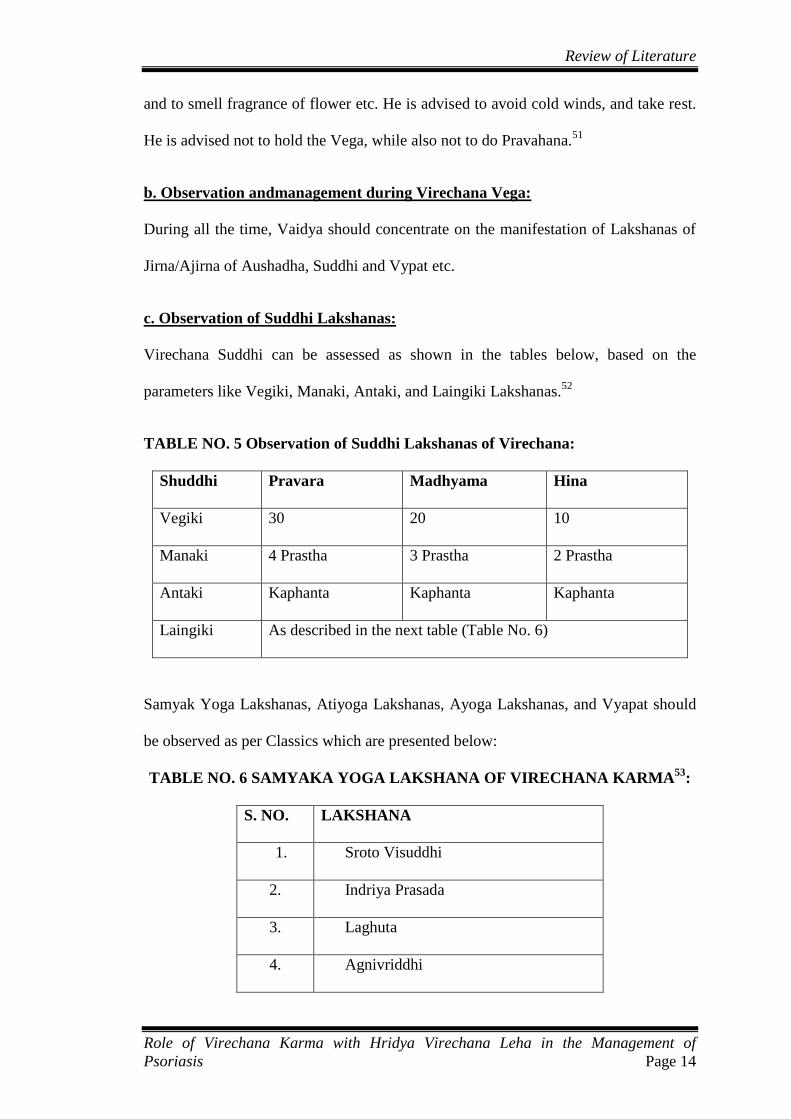
c. Observation of Suddhi Lakshanas:
Virechana Suddhi can be assessed as shown in the tables below, based on the
parameters like Vegiki, Manaki, Antaki, and Laingiki Lakshanas.52
TABLE NO. 5 Observation of Suddhi Lakshanas of Virechana:
Shuddhi Pravara Madhyama Hina
Vegiki 30 20 10
Manaki 4 Prastha 3 Prastha 2 Prastha
Antaki Kaphanta Kaphanta Kaphanta
Laingiki As described in the next table (Table No. 6)
Samyak Yoga Lakshanas, Atiyoga Lakshanas, Ayoga Lakshanas, and Vyapat should
be observed as per Classics which are presented below:
TABLE NO. 6 SAMYAKA YOGA LAKSHANA OF VIRECHANA KARMA53
:
S. NO. LAKSHANA
1. Sroto Visuddhi
2. Indriya Prasada
3. Laghuta
4. Agnivriddhi
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 15
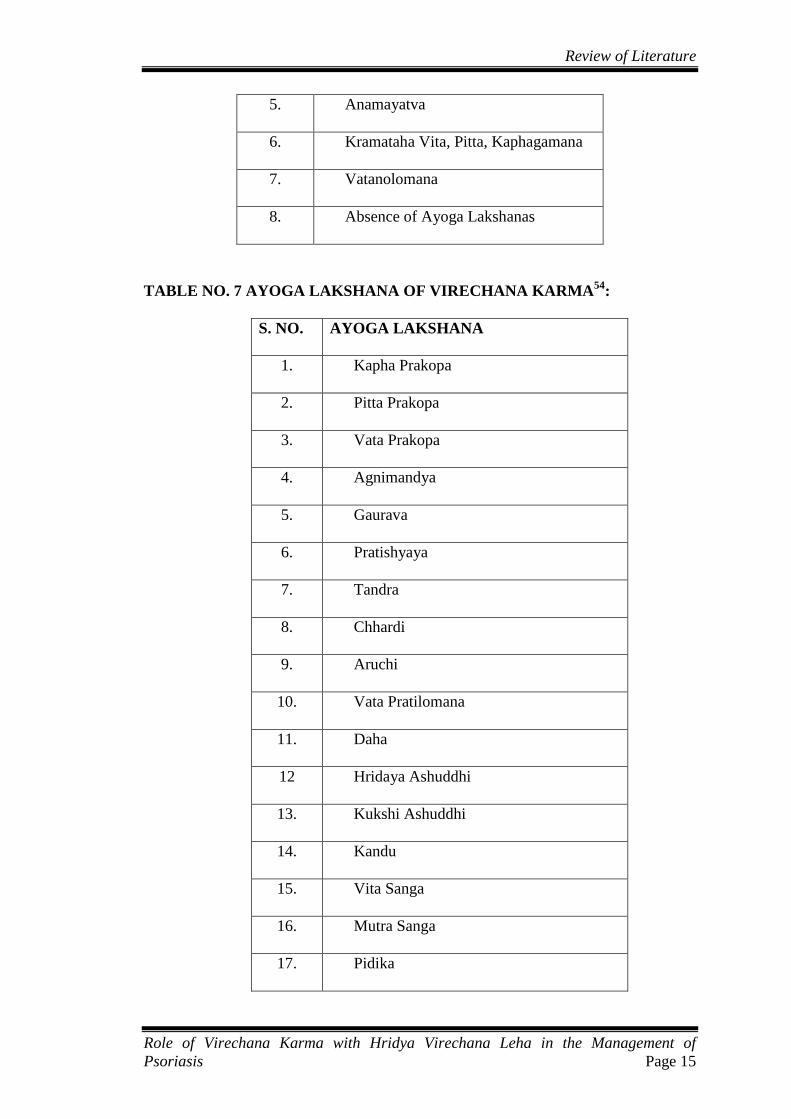
5. Anamayatva
6. Kramataha Vita, Pitta, Kaphagamana
7. Vatanolomana
8. Absence of Ayoga Lakshanas
TABLE NO. 7 AYOGA LAKSHANA OF VIRECHANA KARMA54
:
S. NO. AYOGA LAKSHANA
1. Kapha Prakopa
2. Pitta Prakopa
3. Vata Prakopa
4. Agnimandya
5. Gaurava
6. Pratishyaya
7. Tandra
8. Chhardi
9. Aruchi
10. Vata Pratilomana
11. Daha
12 Hridaya Ashuddhi
13. Kukshi Ashuddhi
14. Kandu
15. Vita Sanga
16. Mutra Sanga
17. Pidika
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 16
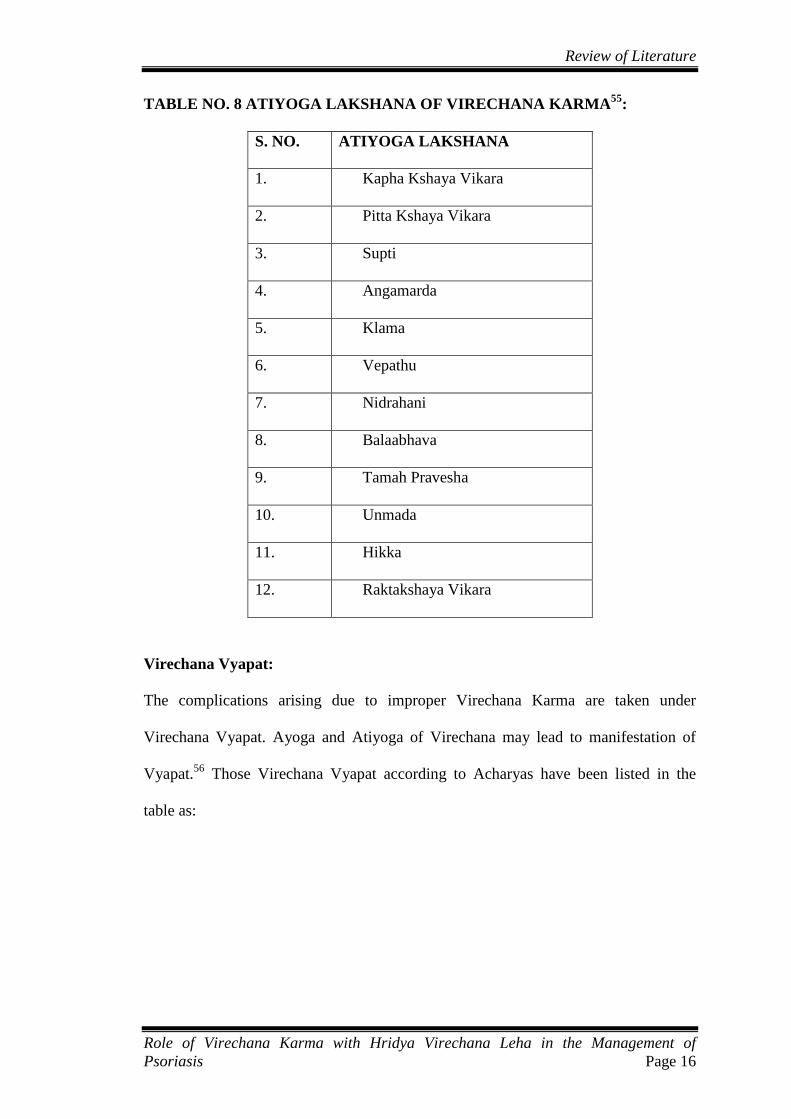
TABLE NO. 8 ATIYOGA LAKSHANA OF VIRECHANA KARMA55
:
S. NO. ATIYOGA LAKSHANA
1. Kapha Kshaya Vikara
2. Pitta Kshaya Vikara
3. Supti
4. Angamarda
5. Klama
6. Vepathu
7. Nidrahani
8. Balaabhava
9. Tamah Pravesha
10. Unmada
11. Hikka
12. Raktakshaya Vikara
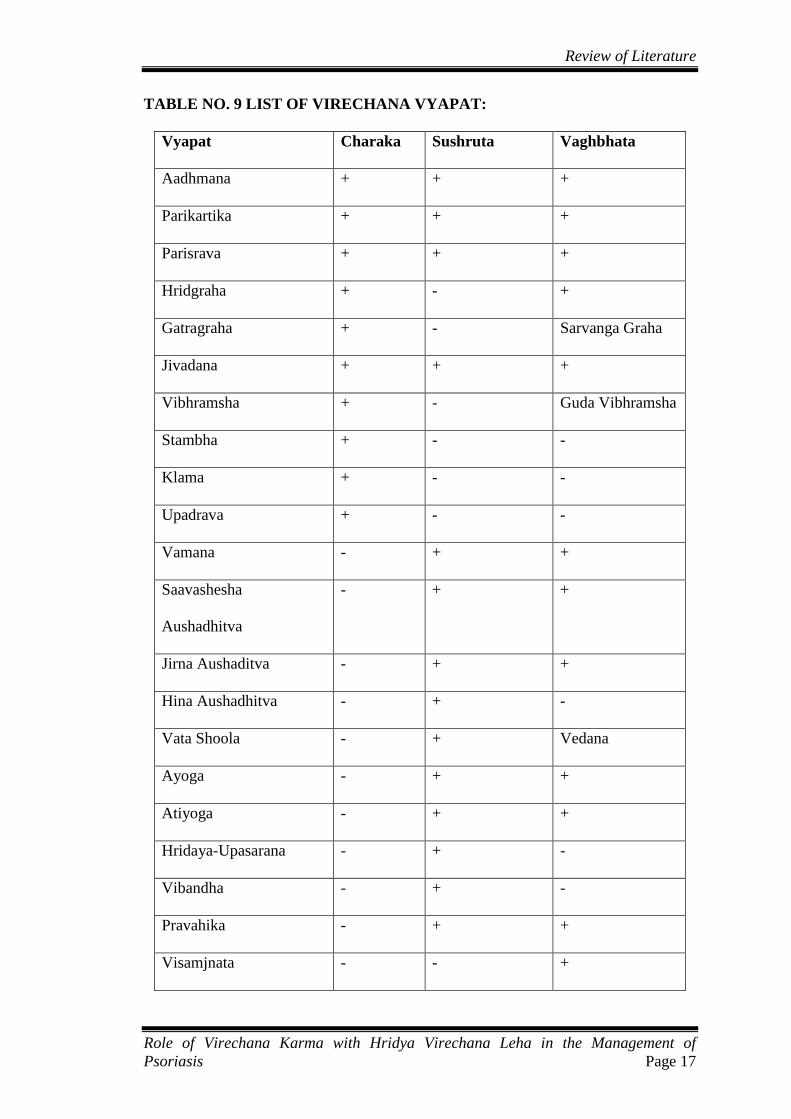
Virechana Vyapat:
The complications arising due to improper Virechana Karma are taken under
Virechana Vyapat. Ayoga and Atiyoga of Virechana may lead to manifestation of
Vyapat.56
Those Virechana Vyapat according to Acharyas have been listed in the
table as:
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 17
TABLE NO. 9 LIST OF VIRECHANA VYAPAT:
Vyapat Charaka Sushruta Vaghbhata
Aadhmana + + +
Parikartika + + +
Parisrava + + +
Hridgraha + - +
Gatragraha + - Sarvanga Graha
Jivadana + + +
Vibhramsha + - Guda Vibhramsha
Stambha + - -
Klama + - -
Upadrava + - -
Vamana - + +
Saavashesha
Aushadhitva
- + +
Jirna Aushaditva - + +
Hina Aushadhitva - + -
Vata Shoola - + Vedana
Ayoga - + +
Atiyoga - + +
Hridaya-Upasarana - + -
Vibandha - + -
Pravahika - + +
Visamjnata - - +

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 18
3) Pashchat Karma:
Following points are to be considered under Pashchat Karma:
1. Tatkalika Paschat Karma:
After the stoppage of Virechana Vega, the patient is advise to wash his/her hands,
feet, face, and also s/he is consoled if s/he is somewhat distressed, and then instructed
to follow the Pathya explained in the context of Snehana and Virechana.
2. Kalantarika Pashchat Karma:
The individual is instructed to follow appropriate Samsarjana Krama, as per the
Shuddhi Lakshanas:
- Peyadi Samsarjana
- Tarpanadi Samsarjana
Samsarjana Krama is a specific dietary regimen, which is to be followed after the
Shodhana Krama. The aim of Samsarjana Krama is to augment the Agni that gets
weakened during the whole process of Shodhana Karma.
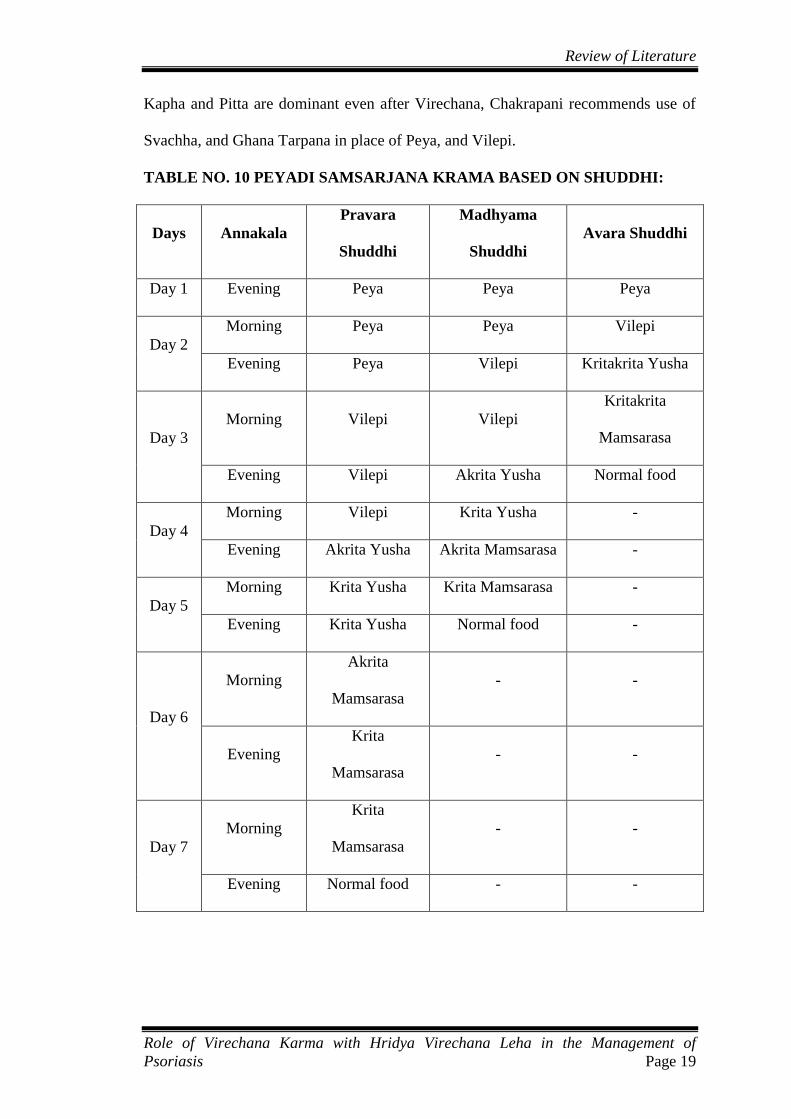
Different Acharyas have given different modality of Samsarjana Krama, though the
goal is the same. Acharya Charaka has mentioned the use of Peya, Vilepi, Akrita
Yusha, Krita Yusha, Akrita Mamsarasa, and Krita Mamsarasa, which is depicted in
the table given below (Table 10). Achrya Susruta has mentioned Yusha of Kulattha,
Adhaki, Mudga, and Mamsa Rsa for this purpose. Dalhana advises that the Peya
should be given in the conditions of Kshina Kapha, but when Vata is dominant,
Mamsa Rasa is advisable.
Instead of Peyadi Samsarjana Krama, Tarpanadi Samsarjana Krama has been
mentioned in the case where proper Virechana hasn‘t taken place. It is also mentioned
that in persons who are addicted to alcohol, having Vata Pitta Prakriti, and in whom
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 19
Kapha and Pitta are dominant even after Virechana, Chakrapani recommends use of
Svachha, and Ghana Tarpana in place of Peya, and Vilepi.
TABLE NO. 10 PEYADI SAMSARJANA KRAMA BASED ON SHUDDHI:
Days Annakala
Pravara
Shuddhi
Madhyama
Shuddhi
Avara Shuddhi
Day 1 Evening Peya Peya Peya
Day 2
Morning Peya Peya Vilepi
Evening Peya Vilepi Kritakrita Yusha
Day 3
Morning Vilepi Vilepi
Kritakrita
Mamsarasa
Evening Vilepi Akrita Yusha Normal food
Day 4
Morning Vilepi Krita Yusha -
Evening Akrita Yusha Akrita Mamsarasa -
Day 5
Morning Krita Yusha Krita Mamsarasa -
Evening Krita Yusha Normal food -
Day 6
Morning
Akrita
Mamsarasa
- -
Evening
Krita
Mamsarasa
- -
Day 7
Morning
Krita
Mamsarasa
- -
Evening Normal food - -

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 20
MODE OF ACTION OF VIRECHANA:
Acharya Charaka explains mechanism of Virechana on the basis of qualities.
Virechana drugs have properties Ushna, Tikshna, Sukshma, Vyavayi, and Vikashee.
Prithvi and Jala Mahabhuta are predominant in Vairechanika Dravya whereas they
possess Adho Bhaga Prabhava, thus they act in downward direction.
Virechana Aushadhi by virtue of their Ushna, Tikshna, Sukshma, Vyavai and
Vikashee Guna, and their Swa Virya (Swo Prabhava), reach to Hridaya and spread
through Dhamani to all the macro and micro channels in the body. Here, Acharya
Chakrapani clearfies that it is not the Aushadhi in its physical form itself that traverses
throughout the Dhamani in body, rather it is the Virya of Aushadhi that spreads to all
the Dhamani. Then, Ushan Guna causes liquefaction of Dosha Samuha in the body;
Tikshna Guna causes disintegration (Vichhinnata) of Dosha. Those disintegrated
(Vichhinna) Dosha by virtue of the Anu Pravana Bhava (property to traverse through
microchannels) move smoothly to Amashaya of Sneha Bhavita patient, without
getting adhered in the route, similar to that of moving of honey smoothly in the
properly anointed mud pot. Then being the Virechana Aushadha Dravya predominant
of Prithvi and Apa Mahabhuta and its having Adho Bhagahara Prabhava, the Dosha
that were brought to Amashaya are expelled out through the Guda Marga by the
Aushadha.
CONTEMPORARY SCIENCE VIEW:
Laxatives/Aperients and Purgatives/Cathartics:
These are the drugs that promote evacuation of bowels. A distinction is made
according to intensity of action:
a. Laxative or Aperient: milder action, elimination of soft but formed stools.
b. Purgative or Cathartic: stronger action resulting in more fluid evacuation.

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 21
Many drugs in low doses act as laxative and in larger doses as purgative.
Classification:
1. Bulk forming: Eg. Dietary fibre: Bran, Psyllium ispaghula (Plantago) etc.
2. Stool softener: Eg. Docusates, Liquid paraffin
3. Osmotic purgatives Eg. Magnesium salts, Lactulose etc.
4. Stimulant purgatives:
a. Diphenlmethanes Eg. Bisacodyl, sodium picosulphate
b. Anthraquinones Eg. Senna
c. 5-Ht4 agonist Eg. Tegaserod
d. Fixed oil Eg. Castor oil
Mechanism of action:
All purgatives increase the water content of faeces by:
a. A hydrophilic or osmotic action, retaining water and electrolytes in the
intestinal lumen- increase volume of colonic content and make it easily
propelled
b. Acting on intestinal mucosa, decrease net absorption of water and electrolyte;
intestinal transit is enhanced indirectly by the fluid bulk.
c. Increasing propulsive activity as primary action-allowing less time for
absorption of salt nand water as a secondary effect.
For some of the drugs, controversy continue as to whether they increase water
content of stools as the primary action or it is a consequence of increased motility.
However, certain purgatives do increase motility through an action on the
myenteric plexuses. Laxatives modify the fluid dynamics of the mucosal cell and
may cause fluid accumulation in gut lumen by one or more of following
mechanisms:

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 22
a. Inhibiting Na+K
+ATPase of villous cells-impairing electrolyte and water
absorption.
b. Stimulating adenylyl cyclase in crypt cells-increasing water and electrolyte
secretion
c. Enhancing prostaglandin synthesis in mucosa which increases secretion.
d. Structural injury to the absorbing intestinal mucosal cells.
Stimulant purgatives: They are powerful purgatives: often produce gripping. They
were thought to irritate the intestinal mucosa and thus stimulate motor activity.
Though some of them do primarily increase motility by acting on myenteric plexuses,
the more important mechanism of action is accumulation of water and electrolytes in
the lumen by altering absorptive and secretory activity of the mucosal cell. They
inhibit Na+K
+ATPase at the basolateral membrane of villous cells-transport of Na
+
and accompanying water into the interstitium is reduced. Secretion is enhanced by
activation of cyclic adenosine monophosphate (cAMP) in crypt cells and by increased
prostaglandin synthesis.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 23
DISEASE REVIEW: KUSHTHA
In Ayurveda, almost all the skin diseases can be taken under generalized term
‗Kushtha‘. Acharya Charaka has quoted ‗Havi Prashanmeha Kushthayoh‘57
, which
indicates that Kushtha is a Santarpanajanya Vyadhi. Considering the vast number of
skin diseases with various morphology, colour, distribution, predominance of Dosha,
Acharya Charaka has classified Kushtha as 7 types, 18 types and also said that it can
be taken as innumerable58
. The Importance of Kushtha is highlighted by mentioning it
as ‗Agrya‘ for chronic diseases.
HISTORICAL REVIEW OF KUSHTHA
A.VEDIC PERIOD:
Rigveda :
In Rigveda there is no complete description about the ‗Kushtha Roga‘. But some
description indicates that Kushtha was prevalent during that period also.
- The Charmaroga of Apala was cured by Lord Indra (R.V. 8-91-7).
- Ghosa was suffering from ‗Kushtha Roga‘. By administration of proper medication
she got cured & ultimately was accepted by her husband. (R.V. 1-1/7-7).
Yajurveda :
Shukla Yajurveda mentions various medicines having Kushthanashaka properties.
(Y.V. 1-23, 1-4, 1-24, 10 – 13/30, 8-10).
Atharvaveda :
The names of various diseases have been illustrated, and Kushtha has been described
as Kshetriya Roga. There is description of some herbs like Rama, Nili, Asuri, Shyama
etc. for the treatment of Kushtha (Ath.1/23).
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 24
B. PURANA KALA
Mahabharata:
It has been mentioned that the person suffering from ‗Tvakadosha‘ is not fit to be a
king. This reference highlights the fact that at that time people suffering from
‗Kushtha‘ were looked down by the society.
Agnipurana
Kushthaghna preparations are mentioned under the heading of ‗Nana Rogahara
Aushadhani‘ (Ag.Pu. 120/3).
C. SAMHITA KALA
Charaka Samhita :
Achrya Charaka is the one who has described Kushtha in detail for the first time. He
has described 18 types of Kushtha. Seven types of Kushtha have been described as
Mahakushtha in Nidana Sthana -5th
Chapter in detail. In the Chikitsa Sthana -7th
Chapter, eighteen types of Kushtha have been described where they are classified as
Mahakushtha 7 and Kshudrakushtha 11. Apart from the description of Kushtha in
Nidana Sthana - 5 and Chikitsa Sthana -7, there are some other references related to
Kushtha in Charaka Samhita; some of them are as follows :
(a) Kushtha is described as the Samanya Hetu of Nija Shotha59
.
(b) Use of Stambhana Dravyas in the initial stage of Raktapitta, Raktarsha &
Amatisara leads to Kushtha59
.
(c) Kushtha is mentioned in Lekhana Yogya & Prachhana Yogya Vyadhi59
.
(d) Agnikarma is contraindicated in Kushthaja Vrana59
.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 25
Sushruta Samhita :
Aacharya Sushruta for the first time clearly described the Anuvansika (hereditary) &
Krimija (infectious) Nidana as a causative factor of Kushtha60
. Kushtha has also been
included in the list of Aupasargika Roga, which may spread from one person to
another60
. Sushruta has described Chikitsa of Kushtha in two chapters i.e. Kushtha
Chikitsa and Mahakushtha Chikitsa. Guggulu, Shilajita, Shveta Bakuchi etc.
Rasayana drugs are mentioned in its Chikitsa.
Ashtanga Hridaya :
Acharya Vagbhata has followed Acharya Sushruta regarding classification of
Mahakushtha & Kshudrakushtha61
. But Ekakushtha has been mentioned under
Kshudrakushtha with same Lakshanas as described by Charaka61
.
D. SANGRAHA KALA
Madhava Nidana:
Madhava has described Nidana Panchaka of Kushtha as per Charaka & Vagbhata.
While Dhatugatatva, Sadhya-Asadhyata & Sankramakata (contagious) have been
described according to Sushruta.
Sharangadhara Samhita :
Classification of Kushtha has been described in Purvakhanda. According to
Sharngdhara, Tamra which is the fourth layer of the skin is the site of all types of
Kushtha62
.
Vangasena :
Vangasena has mentioned 7 types of special causes of Kushtha that is Tilataila,
Kulattha, Valmika, Linga Roga, Mahisha Dugdha, Mathita Dadhi & Vruntaka63
.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 26
Bhava Prakasha :
Bhava Prakasha has given detail description of Kushtha Roga. He has followed
Charaka for classification & nomenclature of Kushtha. The Dhatugatatva & Sadhya-
Asadhyata are compiled from Sushruta.
ETYMOLOGY:
The word ‗Kushtha‘ is derived from ‗Kush nishkarshane‘ + ‗Kthan‘ (कुष्नननकर्षणेहनन
+ क्थन ्)64
which implies ‗to destroy‘, ‗to scrap out‘ or to deform, by adding the suffix
‗kthan‘ which stands for firmness or certainty. Thus the word Kushtha means that
which destroys with certainty.
DEFINITION
Siddhanta Kaumudi:
कुनणानिननिःशरॆ्ेणकर्षनिविऱेखनंकरोनिअङ्गप्रत्यङ्गाननधािुउऩधािूननइनिकुनठम॥्
Kushtha is the condition in which different organs, Dhatus, Upadhatus are destroyed.
Ashtanga Hridaya:
त्िचिःकुिषष्तिििैर्ण्यदंनु्ािःकुनठमशुष्तििि।्
काऱेनोऩेक्षऺियंस्मात्सिषकुनणानिित्िऩिुः ।।65
The pathological condition of the body, in which the Dosha discolour the skin and
cause vitiation in all the Dhatu, and if untreated or neglected, destroys the entire body
is called Kushtha.
Acharya Charaka and Acharya Sushruta have mentioned that 7 Dravya Sangraha i.e.
Tridosha, Tvacha, Rakta, Mamsa and Lasika make the skin Kustsita (deformed). If it
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 27
is neglected then normal condition of whole body may be affected therefore it is
called Kushtha.
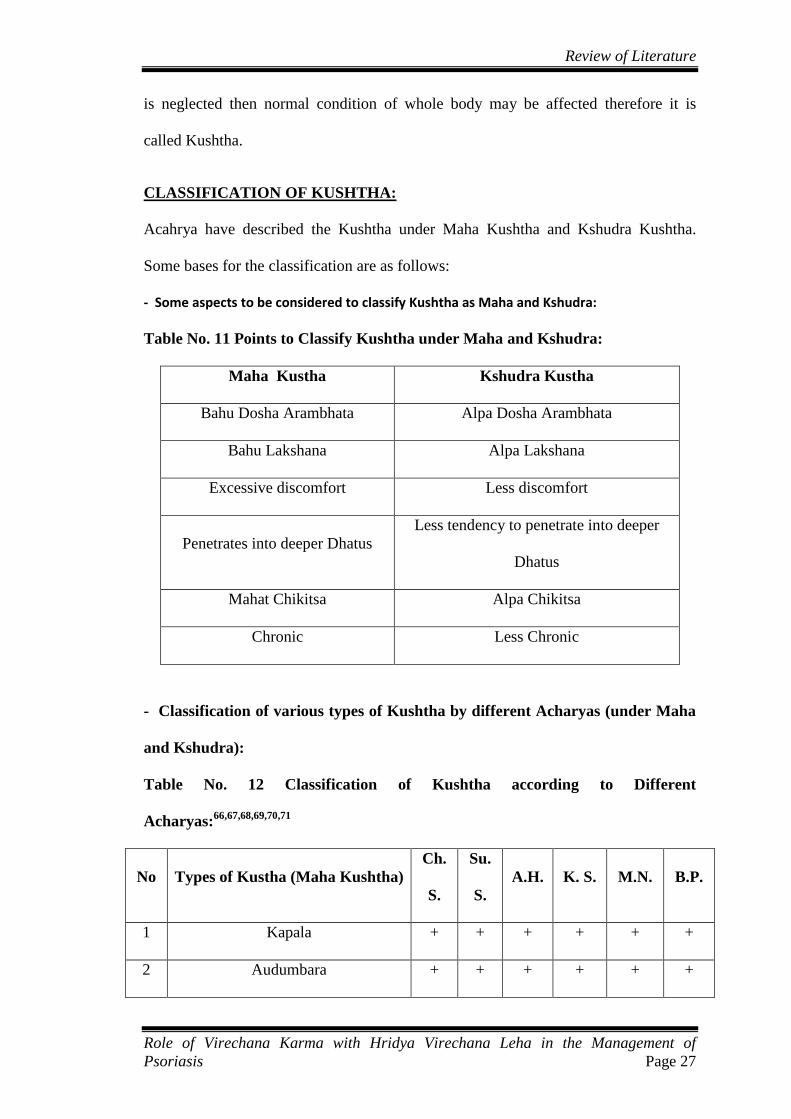
CLASSIFICATION OF KUSHTHA:
Acahrya have described the Kushtha under Maha Kushtha and Kshudra Kushtha.
Some bases for the classification are as follows:
- Some aspects to be considered to classify Kushtha as Maha and Kshudra:
Table No. 11 Points to Classify Kushtha under Maha and Kshudra:
Maha Kustha Kshudra Kustha
Bahu Dosha Arambhata Alpa Dosha Arambhata
Bahu Lakshana Alpa Lakshana
Excessive discomfort Less discomfort
Penetrates into deeper Dhatus
Less tendency to penetrate into deeper
Dhatus
Mahat Chikitsa Alpa Chikitsa
Chronic Less Chronic
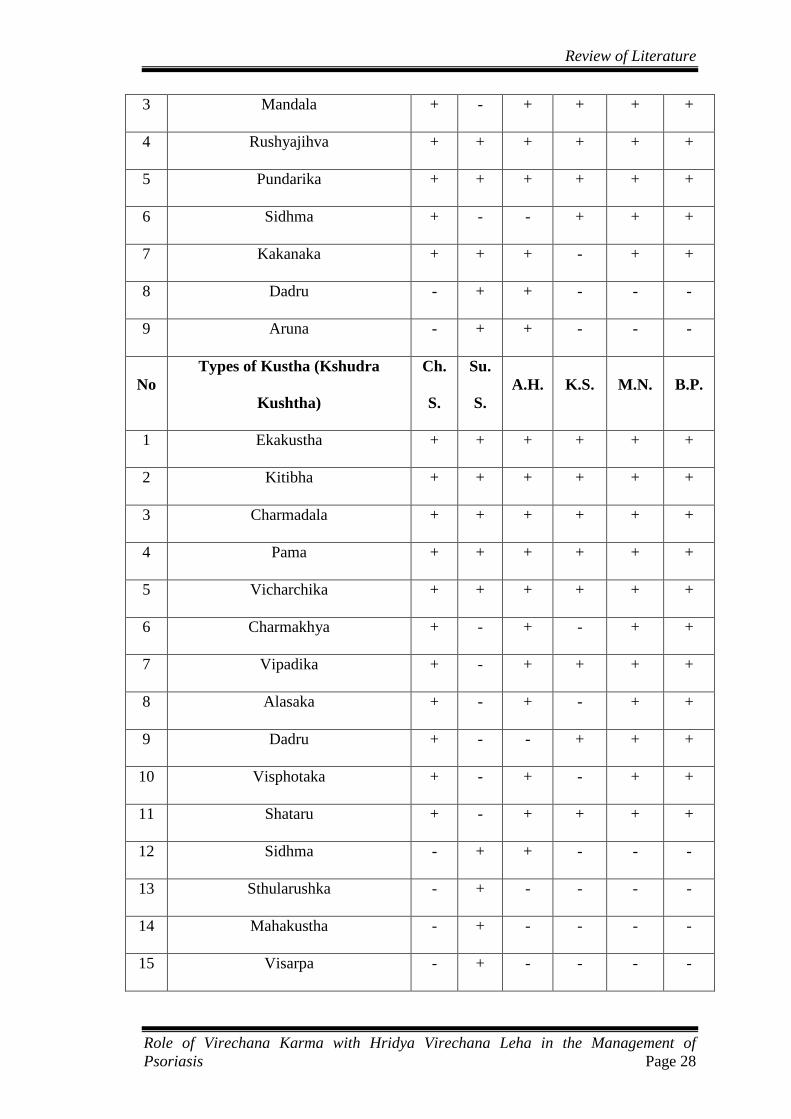
- Classification of various types of Kushtha by different Acharyas (under Maha
and Kshudra):
Table No. 12 Classification of Kushtha according to Different
Acharyas:66,67,68,69,70,71
No Types of Kustha (Maha Kushtha)
Ch.
S.
Su.
S.
A.H. K. S. M.N. B.P.
1 Kapala + + + + + +
2 Audumbara + + + + + +
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 28
3 Mandala + - + + + +
4 Rushyajihva + + + + + +
5 Pundarika + + + + + +
6 Sidhma + - - + + +
7 Kakanaka + + + - + +
8 Dadru - + + - - -
9 Aruna - + + - - -
No
Types of Kustha (Kshudra
Kushtha)
Ch.
S.
Su.
S.
A.H. K.S. M.N. B.P.
1 Ekakustha + + + + + +
2 Kitibha + + + + + +
3 Charmadala + + + + + +
4 Pama + + + + + +
5 Vicharchika + + + + + +
6 Charmakhya + - + - + +
7 Vipadika + - + + + +
8 Alasaka + - + - + +
9 Dadru + - - + + +
10 Visphotaka + - + - + +
11 Shataru + - + + + +
12 Sidhma - + + - - -
13 Sthularushka - + - - - -
14 Mahakustha - + - - - -
15 Visarpa - + - - - -

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 29
16 Parisarpa - + - - - -
17 Raksha - + - - - -
19 Vishaja - - - + - -
- Classification of Kushtha based on dominance of Dosha:
Table No. 13 Classification of Kushtha based on Dominance of Dosha72,73,74
:
Predominance of Dosha Name of Kushtha
Vata Kapala
Pitta Audumbara
Kapha Mandala, Vicharchika
Vata Kapha
Sidhma, Ekakushtha, Alasaka,
Charmakhya, Kitibha,Vipadika
Vata Pitta Rishyajihva
Kapha Pitta
Pundarika, Dadru, Charmadala,
Pama, Visphotaka, Shataru
Vata Pitta Kapha Kakanaka
NIDANA OF KUSHTHA:
Ayurvedic texts have described Samanya Nidana for all types of Kushtha instead of
specific Nidana for any particular type of Kushtha.
The Nidana can be categorized as follows:-
1. Aharaja- diet and dietetic pattern
2. Viharaja- pertaining to lifestyle
3. Acharaja- pertaining to conduct
4. Miscellaneous
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 30
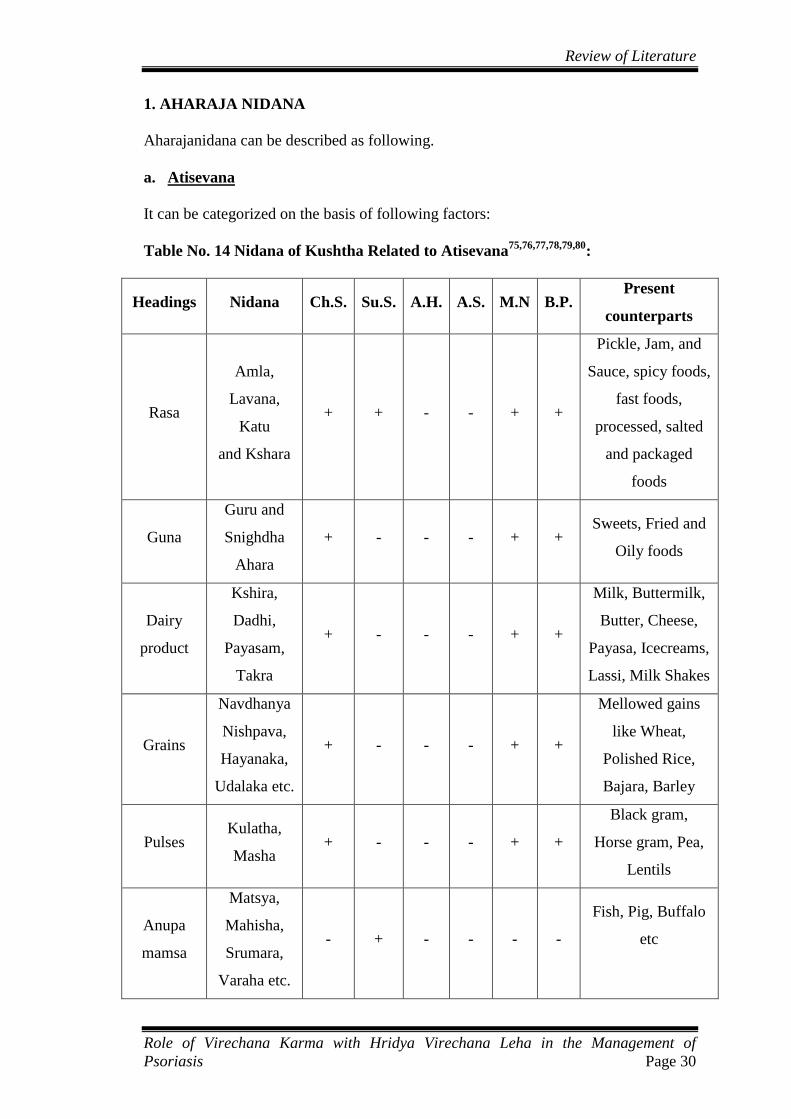
1. AHARAJA NIDANA
Aharajanidana can be described as following.
a. Atisevana
It can be categorized on the basis of following factors:
Table No. 14 Nidana of Kushtha Related to Atisevana75,76,77,78,79,80
:
Headings Nidana Ch.S. Su.S. A.H. A.S. M.N B.P. Present
counterparts
Rasa
Amla,
Lavana,
Katu
and Kshara
+ + - - + +
Pickle, Jam, and
Sauce, spicy foods,
fast foods,
processed, salted
and packaged
foods
Guna
Guru and
Snighdha
Ahara
+ - - - + + Sweets, Fried and
Oily foods
Dairy
product
Kshira,
Dadhi,
Payasam,
Takra
+ - - - + +
Milk, Buttermilk,
Butter, Cheese,
Payasa, Icecreams,
Lassi, Milk Shakes
Grains
Navdhanya
Nishpava,
Hayanaka,
Udalaka etc.
+ - - - + +
Mellowed gains
like Wheat,
Polished Rice,
Bajara, Barley
Pulses Kulatha,
Masha + - - - + +
Black gram,
Horse gram, Pea,
Lentils
Anupa
mamsa
Matsya,
Mahisha,
Srumara,
Varaha etc.
- + - - - -
Fish, Pig, Buffalo
etc

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 31
Prasaha
Mamsa
Marjara,
Go, Khara,
Mushika
etc.
- + - - - -
Chicken, Mutton,
Peacock,
Cow,
Rat and Mice
Sweet
substances Madhu + - - - - - Honey
Guda + - - - + + Jaggery
Oil Tila, Atasi
Kusumbha + - - - + +
Gingily Oil,
Flax Seed Oil,
Saf-Flower Oil
Vegetables
Mulaka,
Lakucha,
Kakmachi
+ - - - + +
Raddish,
Monkey Jack,
Black Night Shade
Missellane
ous
Pishtaanna,
Tila, Kola + - - - - -
Noodles made out
of refined flour,
Tiila, Laddu etc
b. Mithya Ahara:
Table No. 15 Nidana of Kushtha Related to Mithya Ahara81,82,83,84,85,86
:
Headings Nidana Ch. S. Su. S. A.H. A. S. M. N. B. P. Present
counterparts
Foods
Vidahi,
Vidagdha,
Upaklinna,
Putianna
+ - - - - -
Too Spicy and
chilly foods,
Grilled foods,
Frozen foods,
Old Foods
Food
pattern
Viruddhashana + + + + + + Prakati, Karana,
Samyoga, Rashi etc.
Ajirnabhojana
+ - - - - -
Taking food
without digestion
of previous food
Asatmyabhoja - + - - - - Taking food which
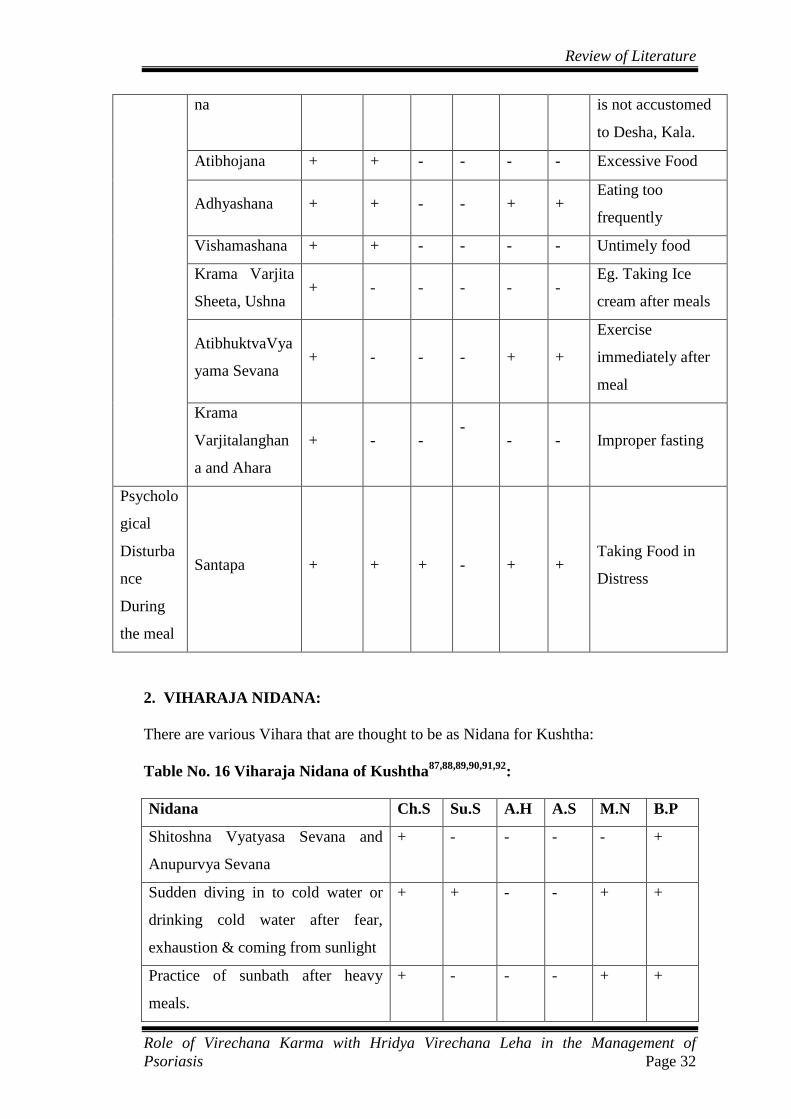
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 32
na
is not accustomed
to Desha, Kala.
Atibhojana + + - - - - Excessive Food
Adhyashana + + - - + + Eating too
frequently
Vishamashana + + - - - - Untimely food
Krama Varjita
Sheeta, Ushna + - - - - -
Eg. Taking Ice
cream after meals
AtibhuktvaVya
yama Sevana + - - - + +
Exercise
immediately after
meal
Krama
Varjitalanghan
a and Ahara
+ - - -
- - Improper fasting
Psycholo
gical
Disturba
nce
During
the meal
Santapa + + + - + + Taking Food in
Distress
2. VIHARAJA NIDANA:
There are various Vihara that are thought to be as Nidana for Kushtha:
Table No. 16 Viharaja Nidana of Kushtha87,88,89,90,91,92
:
Nidana Ch.S Su.S A.H A.S M.N B.P
Shitoshna Vyatyasa Sevana and
Anupurvya Sevana
+ - - - - +
Sudden diving in to cold water or
drinking cold water after fear,
exhaustion & coming from sunlight
+ + - - + +
Practice of sunbath after heavy
meals.
+ - - - + +
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 33
Sex indulgence in Ajirna + - - - + +
Suppression of Chhardi, Mutra,
Purisha like Vegas
+ + - - + +
Kupathya in Panchakarma + + - - + -
Divasvapna after lunch + - - - - -
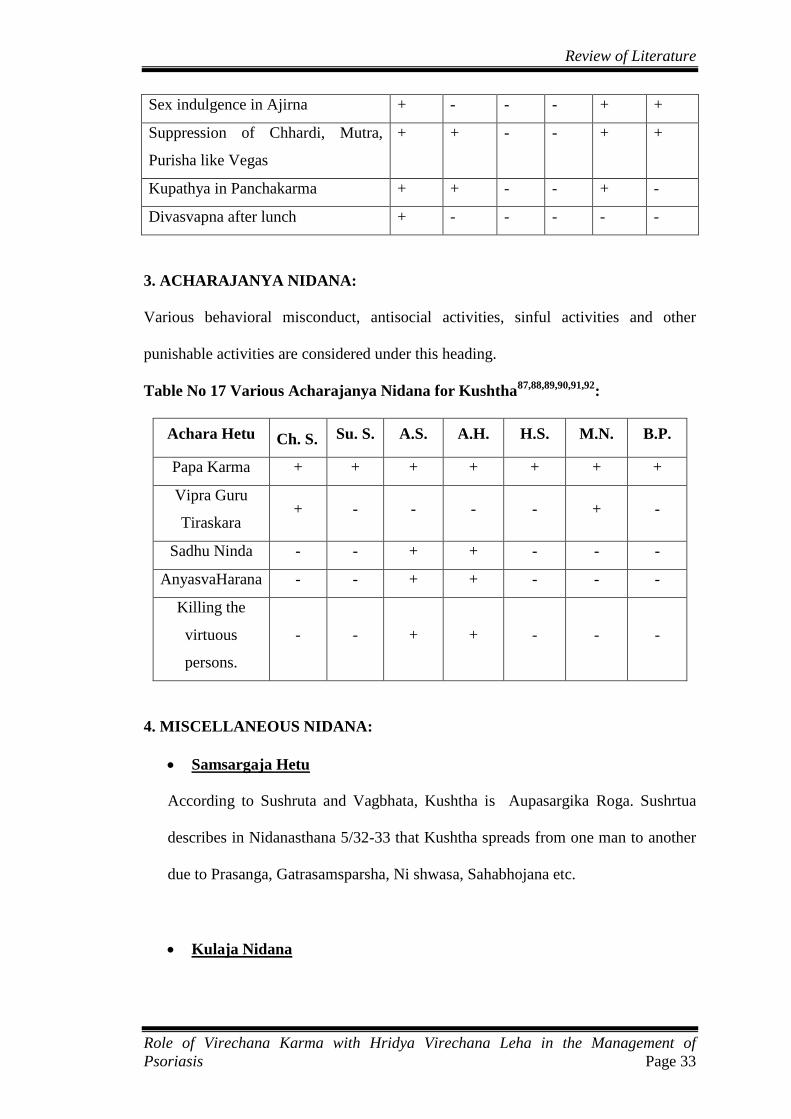
3. ACHARAJANYA NIDANA:
Various behavioral misconduct, antisocial activities, sinful activities and other
punishable activities are considered under this heading.
Table No 17 Various Acharajanya Nidana for Kushtha87,88,89,90,91,92
:
Achara Hetu Ch. S. Su. S. A.S. A.H. H.S. M.N. B.P.
Papa Karma + + + + + + +
Vipra Guru
Tiraskara + - - - - + -
Sadhu Ninda - - + + - - -
AnyasvaHarana - - + + - - -
Killing the
virtuous
persons.
- - + + - - -
4. MISCELLANEOUS NIDANA:
Samsargaja Hetu
According to Sushruta and Vagbhata, Kushtha is Aupasargika Roga. Sushrtua
describes in Nidanasthana 5/32-33 that Kushtha spreads from one man to another
due to Prasanga, Gatrasamsparsha, Ni shwasa, Sahabhojana etc.
Kulaja Nidana
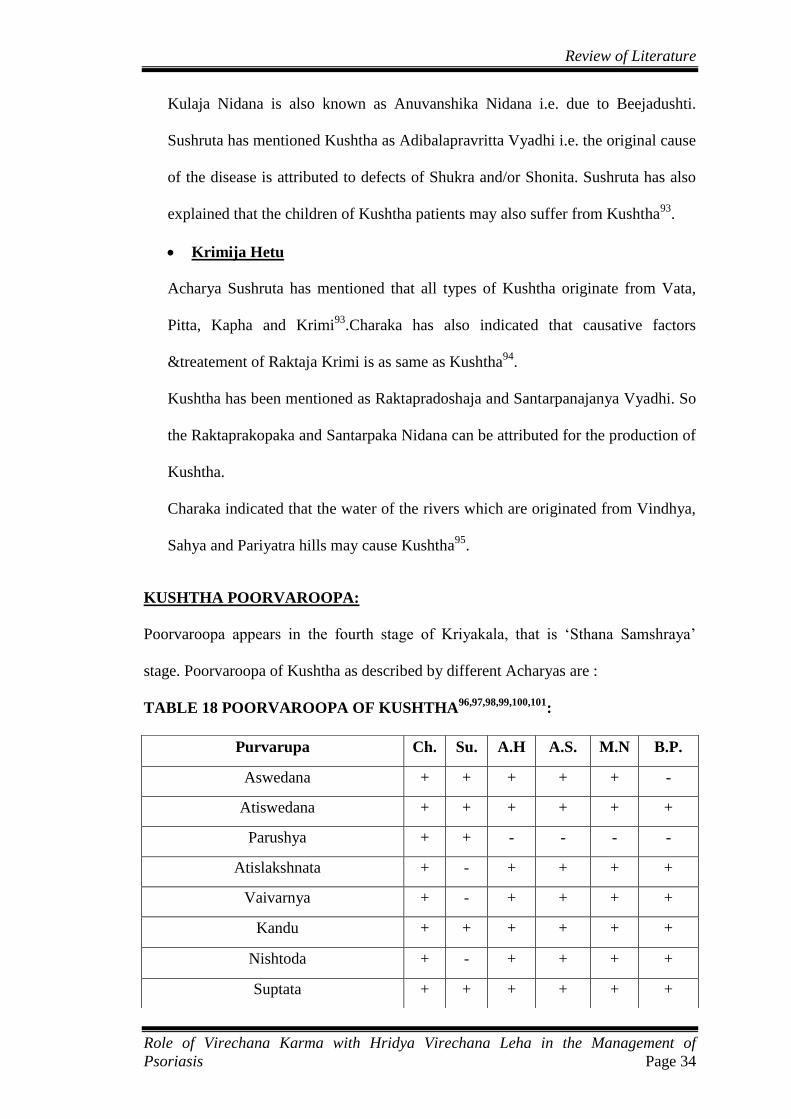
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 34
Kulaja Nidana is also known as Anuvanshika Nidana i.e. due to Beejadushti.
Sushruta has mentioned Kushtha as Adibalapravritta Vyadhi i.e. the original cause
of the disease is attributed to defects of Shukra and/or Shonita. Sushruta has also
explained that the children of Kushtha patients may also suffer from Kushtha93
.
Krimija Hetu
Acharya Sushruta has mentioned that all types of Kushtha originate from Vata,
Pitta, Kapha and Krimi93
.Charaka has also indicated that causative factors
&treatement of Raktaja Krimi is as same as Kushtha94
.
Kushtha has been mentioned as Raktapradoshaja and Santarpanajanya Vyadhi. So
the Raktaprakopaka and Santarpaka Nidana can be attributed for the production of
Kushtha.
Charaka indicated that the water of the rivers which are originated from Vindhya,
Sahya and Pariyatra hills may cause Kushtha95
.
KUSHTHA POORVAROOPA:
Poorvaroopa appears in the fourth stage of Kriyakala, that is ‗Sthana Samshraya‘
stage. Poorvaroopa of Kushtha as described by different Acharyas are :
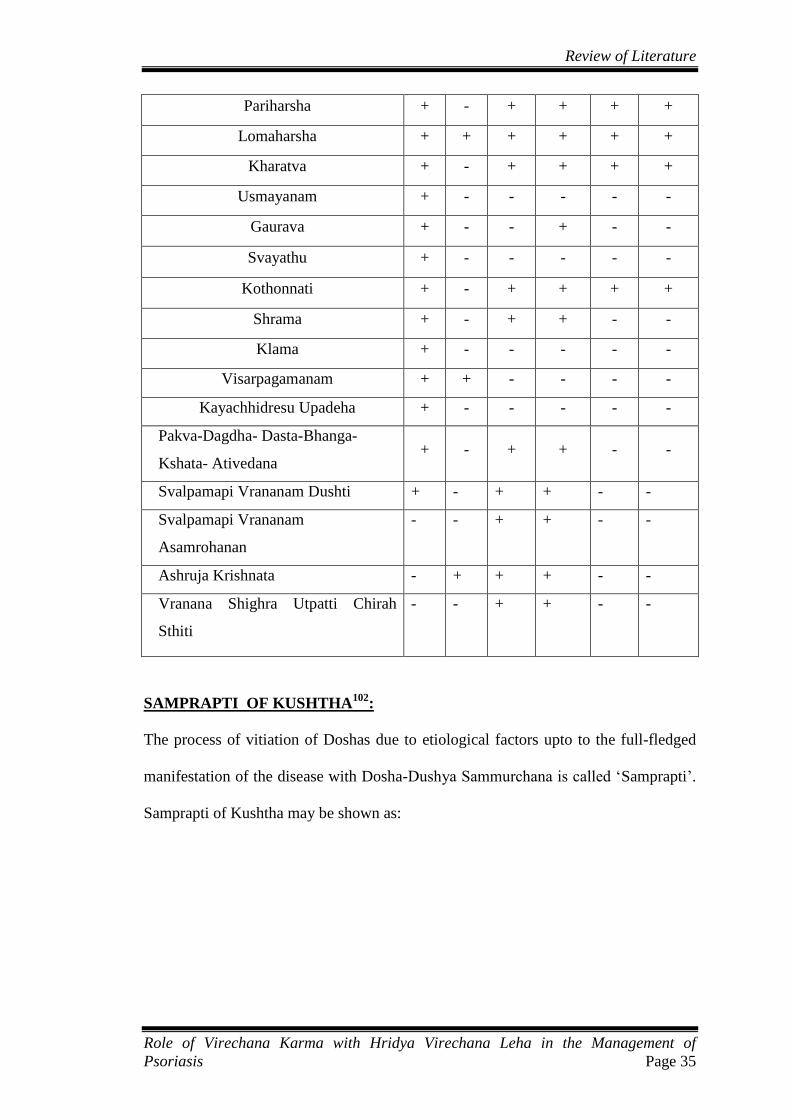
TABLE 18 POORVAROOPA OF KUSHTHA96,97,98,99,100,101
:
Purvarupa Ch. Su. A.H A.S. M.N B.P.
Aswedana + + + + + -
Atiswedana + + + + + +
Parushya + + - - - -
Atislakshnata + - + + + +
Vaivarnya + - + + + +
Kandu + + + + + +
Nishtoda + - + + + +
Suptata + + + + + +
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 35
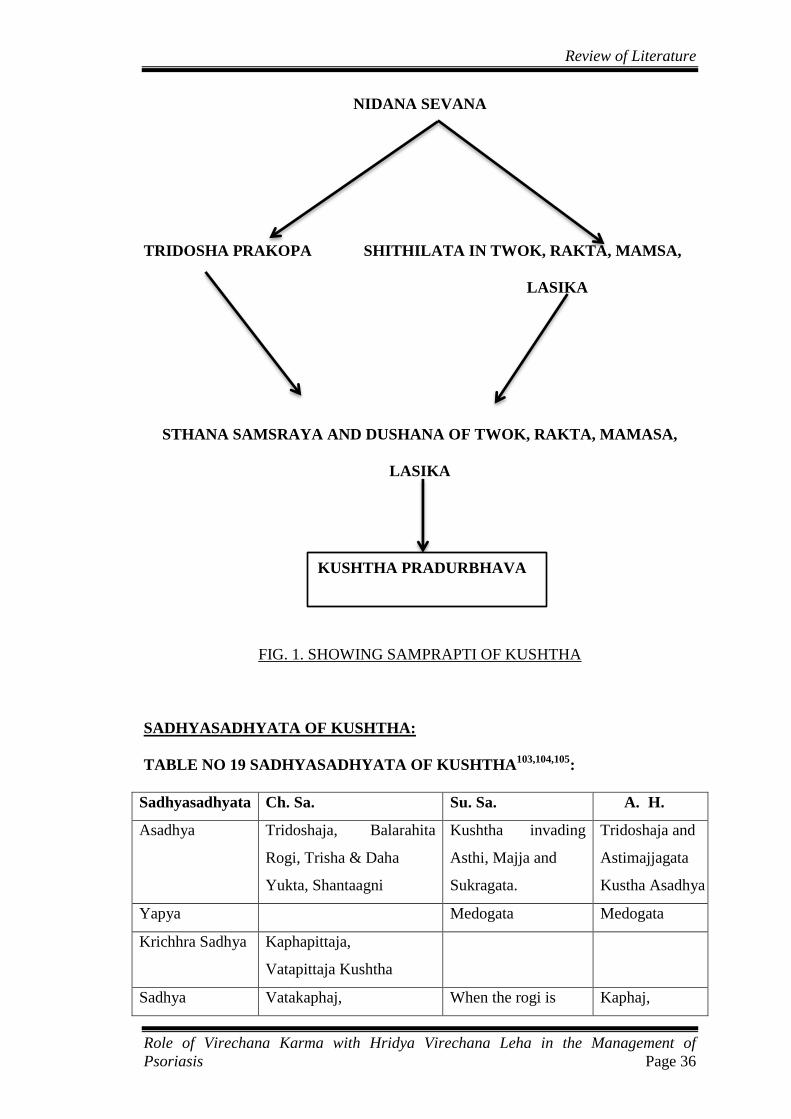
SAMPRAPTI OF KUSHTHA102
:
The process of vitiation of Doshas due to etiological factors upto to the full-fledged
manifestation of the disease with Dosha-Dushya Sammurchana is called ‗Samprapti‘.
Samprapti of Kushtha may be shown as:
Pariharsha + - + + + +
Lomaharsha + + + + + +
Kharatva + - + + + +
Usmayanam + - - - - -
Gaurava + - - + - -
Svayathu + - - - - -
Kothonnati + - + + + +
Shrama + - + + - -
Klama + - - - - -
Visarpagamanam + + - - - -
Kayachhidresu Upadeha + - - - - -
Pakva-Dagdha- Dasta-Bhanga-
Kshata- Ativedana + - + + - -
Svalpamapi Vrananam Dushti + - + + - -
Svalpamapi Vrananam
Asamrohanan
- - + + - -
Ashruja Krishnata - + + + - -
Vranana Shighra Utpatti Chirah
Sthiti
- - + + - -
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 36
NIDANA SEVANA
TRIDOSHA PRAKOPA SHITHILATA IN TWOK, RAKTA, MAMSA,
LASIKA
STHANA SAMSRAYA AND DUSHANA OF TWOK, RAKTA, MAMASA,
LASIKA
FIG. 1. SHOWING SAMPRAPTI OF KUSHTHA
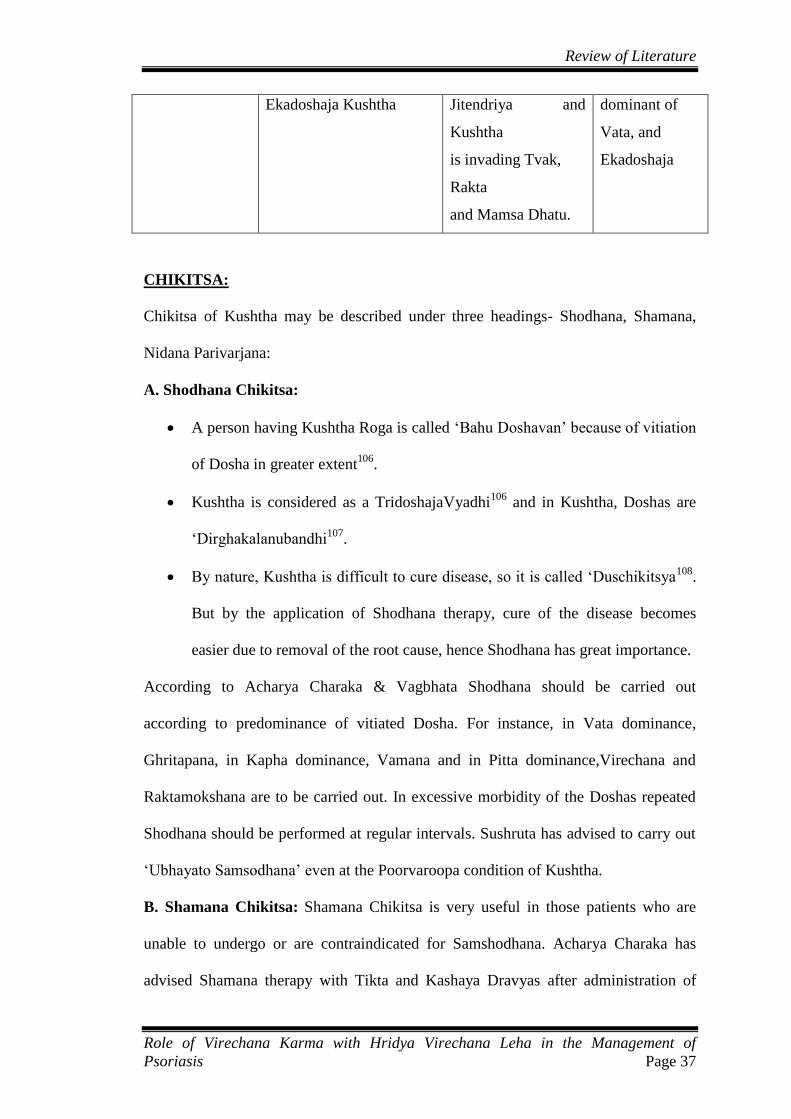
SADHYASADHYATA OF KUSHTHA:
TABLE NO 19 SADHYASADHYATA OF KUSHTHA103,104,105
:
Sadhyasadhyata Ch. Sa. Su. Sa. A. H.
Asadhya Tridoshaja, Balarahita
Rogi, Trisha & Daha
Yukta, Shantaagni
Kushtha invading
Asthi, Majja and
Sukragata.
Tridoshaja and
Astimajjagata
Kustha Asadhya
Yapya Medogata Medogata
Krichhra Sadhya Kaphapittaja,
Vatapittaja Kushtha
Sadhya Vatakaphaj, When the rogi is Kaphaj,
KUSHTHA PRADURBHAVA
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 37
Ekadoshaja Kushtha Jitendriya and
Kushtha
is invading Tvak,
Rakta
and Mamsa Dhatu.
dominant of
Vata, and
Ekadoshaja
CHIKITSA:
Chikitsa of Kushtha may be described under three headings- Shodhana, Shamana,
Nidana Parivarjana:
A. Shodhana Chikitsa:
A person having Kushtha Roga is called ‗Bahu Doshavan‘ because of vitiation
of Dosha in greater extent106
.
Kushtha is considered as a TridoshajaVyadhi106
and in Kushtha, Doshas are
‗Dirghakalanubandhi107
.
By nature, Kushtha is difficult to cure disease, so it is called ‗Duschikitsya108
.
But by the application of Shodhana therapy, cure of the disease becomes
easier due to removal of the root cause, hence Shodhana has great importance.
According to Acharya Charaka & Vagbhata Shodhana should be carried out
according to predominance of vitiated Dosha. For instance, in Vata dominance,
Ghritapana, in Kapha dominance, Vamana and in Pitta dominance,Virechana and
Raktamokshana are to be carried out. In excessive morbidity of the Doshas repeated
Shodhana should be performed at regular intervals. Sushruta has advised to carry out
‗Ubhayato Samsodhana‘ even at the Poorvaroopa condition of Kushtha.
B. Shamana Chikitsa: Shamana Chikitsa is very useful in those patients who are
unable to undergo or are contraindicated for Samshodhana. Acharya Charaka has
advised Shamana therapy with Tikta and Kashaya Dravyas after administration of
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 38
proper Shodhana. Charaka has also indicated several other drugs & formulation of
Shamana therapy in 7th
chapter of Chikitsa Sthana109
.
- External application :
Kushtha, being exhibited through the skin, external application are also advocated.
For the external application drug should be applied after elimination of the Doshas
from the body by Shodhana Karma andRaktamokshana. Various forms of local
application are prescribed likeUdvartana, Pralepa, Parisheka, Abhyanga, etc. Kshara
Karma and Agadaprayoga are also prescribed in special condition of Kushtha.
C. Nidana Parivarjana: NidanaParivarjana stops the further progression of the
disease, by restricting vitiation of Doshas. Main etiological factors of Kushtha are
MithyaAhara-Vihara & Viruddha Ahara so they should be avoided.
PATHYAPATHYA:
PATHYA110
:
Ahara
Laghu Anna, TiktaShaka, PuranaDhanya, JangalaMamsa, MudgaPatola, Food
and Ghee prepared by Bhallataka, Triphala& Nimba, PuranaShali, Shashtika,
Yava, Godhuma, Kordusha, Shyamaka, Udaalaka: Mandukaparni, Bakuchi,
Atarushaka, Siddha Ghrita.
Vihara
Abhyanga with Karanja Taila, Utsadanam with AaragvadhadiKashaya, Pana,
Parisheka, Avagaha etc. with KhadiraKashaya.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 39
APATHYA110
:
Ahara
Guru Anna, Amla Rasa, Dugdha, Dadhi, Anupa Matsya, Guda, Tila, Mamsa,
Taila, Kulattha, Masha, Nishpava, Ikshupishta, Pishta-Vikara,
VirudhaBhojana, Adhyasana, Ajirnasana, Vidahi-AbhishyandiAhara.
Vihara
Divasvapna, Maithuna, Vegadharana, Paapkarma, Tapa Sevana, Svedana etc.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 40
PSORIASIS
ETYMOLOGY:
The word psoriasis is derived from the Greek word ‗Psora‘ and ‗iasis‘. ‗Psora‘ means
itch or scale and ‗iasis‘ means condition.
DEFINITION:
Psoriasis is a chronic inflammatory skin disorder clinically characterized by
erythematous, sharply demarcated papules and rounded plaques, covered by silvery
micaceous scale.
They vary in size from pinpoint to large plaques. At times, it may manifest as
localized or generalized pustular eruption111
.
EPIDEMIOLOGY:
Incidence and prevalence
In most reviews, the prevalence of psoriasis is said to be 2% of the world‘s
population112
. However, its prevalence in different populations varies from 0.1
percent to 11.8 percent, according to published reports. The incidence of the
disease has been estimated to be 60 individuals per 1, 00,000 per year. This study
also provided support for seasonal variation, with 68% of cases first diagnosed in
winter and spring months. The prevalence rate is estimated to be around 0.44% to
2.8% in India113
.
Racial and ethnic variation112
There are considerable racial variations with populations having a lower
prevalence of disease. In China, psoriasis is estimated to affect 0.3% of the
population, while the disease is very rare or nonexistent in Inuits, Latin American

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 41
Indians or Samoans. Climate also appears to affect psoriasis prevalence, with
higher rates recorded in single countries at greater latitudes from the Equator.
Age of onset114
Psoriasis may begin at any age, but it is uncommon under the age of 10 years. It is
most likely to appear between the ages of 15 and 30 years.
Sex ratio115
Psoriasis is equally common in males and females.
ETIOLOGY:
A) Genetic predisposition: Studies have shown evidence that psoriasis has an
important genetic component. According to studies, about one out of three
people with psoriasis report having a relative with psoriasis116
. If one parent
has psoriasis, a child has about a 10% chance of having psoriasis, while if
both parents have psoriasis, a child has approximately 50% chance of
developing the disease116
.
B) Environmental / External risk factors117
: Many environmental factors
otherwise called ‗External triggers‘ have been linked to psoriasis, and have
been implicated in, for example, initiation of the disease process and
exacerbation of pre-existing disease. However, conclusive evidence is so far
lacking. External triggers are as follows:
1) Trauma
Psoriasis at the site of an injury is well known (Koebner phenomenon).
Koebner phenomenon is observed in approximately 25% of patients
with psoriasis. A wide range of injurious local stimuli, including
physical, chemical, electrical, surgical, and infective and inflammatory
insults, have been recognized to elicit psoriatic lesions.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 42
2) Infection
Acute guttate psoriasis is strongly associated with preceding or
concurrent streptococcal infection, particularly of the throat. As
mentioned earlier, guttate and chronic plaque psoriasis share strong
HLA associations, particularly with HLA-Cw6. HIV infection has also
been associated with psoriasis.
3) Drugs
There are many drugs reported to be responsible for the onset or
exacerbation of psoriasis. Chief amongst these are lithium salts,
antimalarials, beta-adrenergic blocking agents, non-steroidal anti
inflammatory drugs (NSAIDs), angiotensin-converting enzyme (ACE)
inhibitors and the withdrawal of corticosteroids.
4) Climate
Most of the psoriasis patients state either first incidence of the disease
in winter or aggravation of disease in winter.
5) Light
Although sunlight is generally beneficial, in a small minority of
patients, psoriasis may be provoked by strong sunlight and cause
summer exacerbations in exposed skin. Rarely ultraviolet radiation
from the sun or from artificial source can worsen the condition. This
occurs in approximately 10% of cases.
6) Alcohol and Smoking
It has long been suspected that both cigarettes and alcohol have a
detrimental effect on psoriasis. Studies suggest that alcohol may
exacerbate pre-existing disease but does not appear to induce psoriasis.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 43
Excess drinking is undoubtedly also a consequence of the disease and
leads to treatment resistance and reduced therapeutic compliance.
C) Systemic triggering factors:
1) Endocrine factors117
:
Hypocalcemia has been reported to be a triggering factor for generalized pustular
psoriasis. Although active vitamin D3 analogues improve psoriasis, abnormal vitamin
D3 levels have not been shown to induce psoriasis. The early onset of psoriasis in
women, with a peak around puberty, changes during pregnancy and provocation of
psoriasis by high dose oestrogen therapy potentially indicates a role for hormonal
factors in the disease.
2) Metabolic factors:
Incomplete protein digestion and bowel toxaemia disturb the formation of cAMP and
therefore increasing the rate of cell proliferation.In patients with hypoparathyroidism
low serum calcium levels have been shown to exacerbate psoriasis.
3) Psychogenic Factors118
:
Psychogenic stress is a well-established systemic triggering factor in Psoriasis. It has
been associated with initial presentations of the disease as well as flares of pre-
existing psoriasis.
PATHOGENESIS OF PSORIASIS119,120
:
Components of Psoriatic Pathogenesis
Epidermal proliferation
A variety of techniques have demonstrated that the increased keratinocyte
proliferation observed in psoriasis is a consequence of an increase in the proliferating
cell compartment in the basal and supra basal levels of the epidermis, and not due to
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 44
shortened cell cycle time. The number of cycling cells is increased approximately
sevenfold. Multiple growth factors, cytokines, which experimentally have been shown
to modulate keratinocyte proliferation, are present in lesional skin.
Vascular changes
Vertical dermal capillary loops in lesional skin are dilated, elongated and twisted.
Using various in vivo models of angiogenesis, it has been demonstrated that
epidermal keratinocytes are the primary source of angiogenicactivity. These cells
produce an array of soluble mediators with angiogenic activity including vascular
endothelial growth factor (VEGF). It is over-expressed in psoriatic epidermis as are
its receptors on lesional psoriatic microvasculature.
Immunology and inflammation
There is considerable evidence that T lymphocytes play an important role in
development of plaques of psoriasis. This includes:
(i) Early influx of T cells into expanding lesions
(ii) Strong association with the MHC, particularly HLA-Cw6
(iii) Ablative effect of anti-T-cell therapy
(iv) Increased antigen presentation in psoriatic plaques
(v) Anecdotal evidence of development of psoriasis after syngeneic bone
marrow transplant
(vi) Change in phenotype to lesional psoriatic skin in non-lesional psoriatic
skin transplanted on to severe combined immunodeficient mice and
injected with autologous T cells
Those T cells involved in psoriasis pathogenesis express markers of memory,
activation and skin homing (CLA).However, it is increasingly clear that the innate
immune system, which provides an early response.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 45
CLINICAL FEATURES OF PSORIASIS121,122
:
The classic lesion of psoriasis is a well-demarcated, raised, red plaque with a
white scaly surface. Lesions can vary in size from pinpoint papules to plaques that
cover large areas of the body. Under the scale, the skin has a glossy homogeneous
erythema, and bleeding points appear when the scale is removed, traumatizing the
dilated capillaries below (the Auspitz sign).
Koebner phenomenon (also known as the isomorphic response) is the traumatic
induction of psoriasis on nonlesional skin; it occurs more frequently during flares
of disease and is an all-or-none phenomenon (i.e., if psoriasis occurs at one site of
injury it will occur at all sites of injury). The Koebner phenomenon is not specific
for psoriasis but can be helpful in making the diagnosis when present.
CLINICAL PATTERNS OF SKIN PRESENTATION
1. Psoriasis vulgaris, chronic stationary psoriasis, plaque-type psoriasis
Psoriasis vulgaris is the most common form of psoriasis, seen in approximately 90
percent of patients. Red, scaly, symmetrically distributed plaques are
characteristically localized to the extensor aspects of the extremities, particularly the
elbows and knees, along with scalp, lower lumbosacral, buttocks, and genital
involvement. Other sites of predilection include the umbilicus and the intergluteal
cleft. Single small lesions may become confluent, forming plaques in which the
borders resemble a land map (psoriasis geographica). Lesions may extend laterally
and become circinate because of the confluence of several plaques (psoriasis gyrata).
Occasionally, there is partial central clearing, resulting in ring-like lesions (annular
psoriasis).

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 46
2. Guttate (eruptive) psoriasis
Guttate psoriasis (from the Latin gutta, meaning ‗a drop‘) is characterized by eruption
of small (0.5 to 1.5 cm in diameter) papules over the upper trunk and proximal
extremities. It typically manifests at an early age and as such is found frequently in
young adults. This form of psoriasis has the strongest association to HLA-Cw6, and
streptococcal throat infection frequently precedes or is concomitant with the onset or
flare of guttate psoriasis. Patients with a history of chronic plaque psoriasis may
develop guttate lesions, with or without worsening of their chronic plaques.
3. Erythrodermic psoriasis
Psoriatic erythroderma represents the generalized form of the disease that affects all
body sites, including the face, hands, feet, nails, trunk, and extremities. Although all
the symptoms of psoriasis are present, erythema is the most prominent feature, and
scaling is different compared with chronic stationary psoriasis. Instead of thick,
adherent, white scale there is superficial scaling. Patients with erythrodermic psoriasis
lose excessive heat because of generalized vasodilatation, and this may cause
hypothermia. Patients may shiver in an attempt to raise their body temperature.
Psoriatic erythroderma has a variable presentation, but two forms are thought to exist.
In the first form, chronic plaque psoriasis may worsen to involve most or the entire
skin surface, and patients remain relative responsive to therapy. In the second form,
generalized erythroderma may present suddenly and unexpectedly or result from non-
tolerated external treatment (e.g., UVB, anthralin), thus representing a generalized
Koebner reaction.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 47
4. Pustular psoriasis
Several clinical variants of pustular psoriasis exist: generalized pustular psoriasis (von
Zumbusch type), annular pustular psoriasis, impetigo herpetiformis, and two variants
of localized pustular psoriasis—pustulosispalmarisetplantaris and acrodermatitis
continua. In children, pustular psoriasis can be complicated by sterile, lytic lesions of
bones and can be a manifestation of the SAPHO syndrome (synovitis, acne,
pustulosis, hyperostosis, osteitis).
A. Generalized pustular psoriasis (Von Zumbusch)
Generalized pustular psoriasis (Von Zumbusch) is a distinctive acute variant of
psoriasis. It is usually preceded by other forms of the disease. Attacks are
characterized by fever that lasts several days and a sudden generalized eruption
of sterile pustules 2 to 3 mm in diameter. The pustules are disseminated over the
trunk and extremities, including the nail beds, palms, and soles. The pustules
usually arise on highly erythematous skin, first as patches and then becoming
confluent as the disease becomes more severe. Characteristically, the disease
occurs in waves of fevers and pustules. Cases of acute respiratory distress
syndrome associated with generalized pustular psoriasis have been reported.
B. Exanthematic Pustular Psoriasis
Exanthematic pustular psoriasis tends to occur after a viral infection and consists
of widespread pustules with generalized plaque psoriasis. However, unlike the
von Zumbusch pattern, there are no constitutional symptoms, and the disorder
tends not to recur.
C. Annular Pustular Psoriasis.
Annular pustular psoriasis is a rare variant of pustular psoriasis. It usually
presents in an annular or circinate form. Lesions may appear at the onset of

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 48
pustular psoriasis, with a tendency to spread and form enlarged rings, or they
may develop during the course of generalized pustular psoriasis. There is
usually no personal or family history of psoriasis.
5. Inverse psoriasis
Psoriasis lesions may be localized in the major skin folds, such as the axillae, the
genito-crural region, and the neck. Scaling is usually minimal or absent, and the
lesions show a glossy sharply demarcated erythema, which is often localized to areas
of skin-to-skin contact. Sweating is impaired in affected areas.
6. Sebo psoriasis
A common clinical entity, sebopsoriasis presents with erythematous plaques with
greasy scales localized to seborrheic areas (scalp, glabella, nasolabial folds, perioral
and presternal areas, and intertriginous areas). In the absence of typical findings of
psoriasis elsewhere, distinction from seborrheic dermatitis is difficult. Sebopsoriasis
may represent a modification of seborrheic dermatitis by the genetic background of
psoriasis and is relatively resistant to treatment.
7. Psoriasis of the scalp
The scalp is a favored site for psoriasis and may be the only site affected. Plaques are
similar to those of the skin except that the scale is more readily retained; it is anchored
by hair. Extension of the plaques onto the forehead is relatively common. A dense,
tight-feeling scale can cover the entire scalp. Even in the most severe cases, the hair is
not permanently lost.
8. Psoriasis of the palms and soles
The palms and soles may be involved as part of a generalized eruption, or they may
be the only locations involved in the manifestation of the disease. There are several
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 49
presentations. Superficial red plaques with thick brown scale may be indistinguishable
from chronic eczema. Smooth, deep red plaques are similar to those found in the
flexural area.
9. Psoriasis of the nails
Nail changes are characteristic of psoriasis offer supporting evidence for the diagnosis
of psoriasis when skin changes are equivocal or absent.
Onycholysis.
Psoriasis of the nail bed causes separation of the nail from the nail bed. Unlike the
uniform separation caused by pressure on the tips of long nails, the nail detaches in an
irregular manner. The nail plate turns yellow, simulating a fungal infection.
Pitting.
Nail pitting is the best known and possibly the most frequent psoriatic nail
abnormality. Nail plate cells are shed in much the same way as psoriatic scale is shed,
leaving a variable number of tiny, punched-out depressions on the nail plate surface.
Nail deformity
Extensive involvement of the nail matrix results in a nail losing its structural integrity,
resulting in fragmentation and crumbling.
PSORIATIC ARTHRITIS123
Psoriatic arthritis (PsA) is a chronic inflammatory arthropathy of the peripheral joints,
spine, and enthuses. It may precede, accompany, or, more often, follow the skin
manifestations. Onset may occur at any age, but peak occurrence is between ages 20
and 40; women and men are equally affected. Symmetric polyarthritis with joint pain
and joint swelling often indicates erosive progressive disease. Unlike in rheumatoid

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 50
arthritis, the distal interphalangeal joints are regularly involved. The presence of
inflammatory arthritis in patients with psoriasis varies between 5% and 42%.
Approximately 15% of patients with PsA have an onset of arthritis before the onset of
psoriasis. The prevalence of psoriatic arthritis is higher among patients with more
severe cutaneous disease.
Despite active treatment and a reduction in joint inflammation and the rate of damage,
psoriatic arthritis may be a progressively deforming arthritis.
Clinical features.
The most common pattern is an asymmetric arthritis involving one or more joints of
the fingers and toes. Usually one or more proximal interphalangeal (PIP), distal
interphalangeal (DIP), metatarsophalangeal, or metacarpophalangeal joints are
involved. During the acute phase, the joint is red, warm, and painful. Continued
inflammation promotes soft tissue swelling on either side of the joint (―sausage
finger‖) and restricts mobility. HLA-DR7 is significantly increased in this group with
peripheral arthritis.
COMPLICATIONS OF PSORIASIS124
Patients with psoriasis have an increased morbidity and mortality from
cardiovascular events, particularly those with severe and long duration of
psoriasis. Risk of myocardial infarction is particularly elevated in younger
patients with severe psoriasis.
Psoriasis patients have also been shown to have increased relative risk of
lymphoma, particularly in patients with more severe disease.
Psoriasis is emotionally disabling, carrying with it significant psychosocial
difficulties. Emotional difficulties arise from concerns about appearance,

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 51
resulting in lowered self-esteem, social rejection, guilt, embarrassment,
emptiness, sexual problems, and impairment of professional ability. The
presence of pruritus and pain can aggravate these symptoms. Psychological
aspects can modify the course of illness; in particular, feeling stigmatized can
lead to treatment noncompliance and worsening of psoriasis. Likewise,
psychological stress can also lead to depression and anxiety. According to a
recent survey, 79 percent of patients with severe psoriasis reported a negative
impact on their lives.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 52
DRUG REVIEW
Drug has an important role amongst Chikitsa Chatushpada, so, it is placed next to the
part of physician. The selection of a proper drug in the management of a disease is
very important. Because, without proper planning of the drugs, Chikitsa is not going
to yield proper results. In Ayurvedic classics specific formulations are advocated for
particular disease.
Drugs used for present study
1) Drugs for Pachana Deepana
2) Drugs used for Snehapana
3) Drugs used for Swedana Karma
4) Drug used for Virechana Karma- Hridya Virechana Leha
DRUG USED FOR PACHANA-DEEPANA:
Shunthi Qwatha
SHUNTHI125
:
Botanical Name: Zingiber officinale
Family: Zingiberaceae
Gana: Triptighna, Arshoghna, Deeepaneeya, Shoolaprashamana,Trishnanigrahana (A.
Charaka); Pippalyadi Gana, Trikatu (A. Susruta)
Chemical composition: water 10.9%, protein 15.4%, Starch 5.3%, Total Ash 6.6%,
Volatile oil1-2.7%; Zingiberine, Zingiberol, Oleoresin-Gingerin, Gingerol, Shogaol,
Zingerone
Guna: Laghu, Snigdha; (Guru, Ruksha, Tikshna-Ardaka)
Rasa: Katu
Vipaka: Madhura; (Katu-Ardraka)
Virya: Ushna
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 53
Dhoshaghnata: Kapha Vata Samaka
Action on Digestive System: Triptighna, Rochana, Deepana, Pachana, Vatanulomana,
Shoolaprashamana, Arshoghna
Action on Cardiovascular System: Shothahara, Raktashodhaka
Satmikarana: Aamapachana, Srotoshodhaka
Parts used: Rizome (Kanda)
ABHYANTARA SNEHANA:
MoorchhitaTila Taila
Preparation of Moorchhita Tila Taila has been described in Jwara chapter in Bhaisajya
Ratnavali126
.
Ingredients:
Tila Taila : 1 part (400 ml)
Manjishta : 1/16 part (25 gm)
Haridra : 1/64 part (6.25gm)
Lodhra : 1/64 part (6.25gm)
Musta : 1/64 part (6.25gm)
Nalika : 1/64 part (6.25gm)
Amalaki : 1/64 part (6.25gm)
Haritaki : 1/64 part (6.25gm)
Vibhitaki : 1/64 part (6.25gm)
Suchipushpa : 1/64 part (6.25gm)
Vatankura : 1/64 part (6.25gm)
Hribera : 1/64 part (6.25gm)
Water : 4 parts(1600ml)

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 54
Procedure:
Tila Taila is taken in a clean wide mouthed iron vessel. It is heated until frothing
subsides. Then it is taken out of fire and allowed to self-cool. Then fine powder of the
herbal ingredients is taken and prepared fine paste adding little water. This paste is
added to the oil. Water is added, and started heating, until the oil part only remains.
The final product obtained is the Moorchhita Tila Taila.
Table No. 20. Rasapanchaka of ingredients of Moorchhita Tila Taila:
Drug Latin
name Rasa Guna Virya Vipaka
Doshagh-
nata Karma
Tila Sesamum
indicum
Madhura,
Kashaya,
Tikta
Guru
Snigdha Ushna
Madhu
ra Vatahara
Twachya
Balya
Shukrala
Manjishta Rubia
cordifolia
Madhura,
Tikta
Guru
Ruksha Ushna Katu
Kaphapitt
ahara
Varnya
Vishaghna
Lodhra Symplocos
racemosa
Kashaya,
Tikta
Laghu,
Ruksha Sheeta Katu
Kaphapitt
ahara
Grahi
Chakshushya
Musta Cyperus
rotundus
Tikta,
Katu
Laghu,
Ruksha Sheeta Katu
Kapha
Pitta
Shamaka
Pachaka
Amalaki Emblica
officinalis
Lavana-
Rahita-
Pancha-
Rasa
Snigha,
Laghu Sheeta
Madhu
ra
Tridosha
ghna Rasayana
Haritaki Terminalia
chebula
Lavana-
Rahita-
Pancha-
Rasa
Ruksha,
Laghu,
Ushna
Ushna Madhu
ra
Tridosha
ghna Rasayana
Bibhitaki Terminalia
belerica Kashaya
Laghu,
Ruksha
Ushna Madhu
ra
Kapha
pittaghna Rasayana

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 55
Suchee
pushpa
Pandanus
odorotissimus
Tikta,
Madhura,
Katu
Laghu,
Snigdha Ushna Katu
Tridosha
Samaka
Katu
Paushtika
Vatankura Ficus
bengalensis Kashaya
Guru,
Ruksha Sheeta Katu
Kapha
pittahara
Varnya
sthambhana
Hribera Coleus
zeylanicus Tikta
Laghu,
Ruksha Sheeta
Madhu
ara
Kapha
Pitta
Shamaka
Balya,
Shukrala,
Pachaka
After Moorchana, Aamadosha of Tila Taila will be alleviated, and the Taila becomes
orange-tinged yellow, clear, and devoid of unpleasant smell126
. Tila Taila is
Yogavahi, after Dravyantara by Samyoga and Samskara, it becomes
Tridoshasamaka127
; and since it has Snigdha Guna predominance, and is indicated in
Twachagata Vikara127
, it can be used as a suitable Snaihika Dravya for Snehapana in
Twakgata Vikara, ie. Kushtha. Acharya Charaka has told one of the Guna of Tila as
Twachya128
, while Acarya Susruta also has mentioned Twachya as one of the
properties of Tila129
.
DRUG USED FOR SWEDANA:
Karanja Qwatha Pariseka
Karanja has been mentioned almost by every Acharya in the use of Kushtha. It is also
indicated in Raktavikara, Shotha, Aamavata etc. Kushtha, being a disease where
Rakta is invariably involved and Pitta is also involved (as Kushtha is Tridoshaja
Vyadhi, though Pitta may be in different Doshic proportionas per type of Kushtha), in
such Vyadhis, where Rakta and Pitta are involved, Achrya Susruta has advised to go
for Drava variety of Sweda, which is again of two variety- Pariseka and Avagaha.
Here, Pariseka with Karanja Qwatha is selected.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 56
Karanja130
:
Botanical Name: Pongamia pinnata
Family: Leguminaceae
Gana: Kandughna, Virechana, Katuskandha, Tiktaskandha (A. Charaka);
Aaragvadhadi Gana, Varunadi, Shyamadi, Shirovirechana, Kaphasamshamana (A.
Susruta)
Guna: Laghu, Tikshana
Rasa: Tikta, Katu, Kashaya
Vipaka: Katu
Virya: Ushna
Doshaghnata: Kaphavata Samaka
Parts used: Twak, Patra, Beeja (For Pariseka, Patra generally used)
Chemical composition: Karanjin, Pongamin, Pongamia oil, Pongamol
Systemic action (External): Bark and Leaves- Jantughna, Kandughna, and Shothahara
Integumentary System: Kushthaghna
Cardiovascular System: Raktashodhaka, Shothahara
DRUG USED FOR VIRECHANA:
Hridya Virechana Leha
―Hridya‖ means palatable or that is favorable for a person to take. Hridya Virechana
Leha is a preparation in which Trivrit is predominant, and Trivrit is considered as one
among the Shrestha Dravyas to cause Rechana. Hridya Virechana Leha is described
as one of the favourable preparations for Virechana.
Ingredients of Hridya Virechana Leha131
:
a. Trivrit
b. Sita
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 57
c. Trijata (Twok, Ela, Patra)
d. Madhu
a. Trivrit:
Botanical Name : Operculina turpethum
Family : Convolvulaceae
Pharmacodynamics
Rasa : Tikta, Katu
Guna : Laghu, Ruksha, Tikshna
Virya : Ushna
Vipaka : Katu
Parts used : Moolatwak
Doshaghnata : KaphaPitta Samshodhana
Karma: It does Bhedana and Rechana. It is one of the best drugs for Sukha
Virechana. It has uses in Aanaha, Vibandha, Arsha, Kamala, Shotharoga, Udara Roga,
Vatarakta etc. Acharya Charaka has considered Trivrit as a Shreshtha Virechana
dravya (Cha. Ka. 6/3).
Chemical Composition: Root bark has glycoside up to 10%, and it is odorless, bitter,
and pungent; it contains Turpethin- a glucoside, which is the main component to
cause Rechana. Similarly, it also contains 2 more glycosides, and volatile oil.
b. Sita132
:
- Sumadhura
- Roochyaa
- Vata Piita Daha Shmaka
- Raktavikara Shamaka
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 58
- Alleviates Moorchha, Chhardi, Jwara, Sheeta
- Shukrakara
c. Trijata (Twak, Ela, Patra)
Trijata is a mixture of Twak, Ela and Patra in equal quantity. It is also called as
Trisugandhi. It is Hridya, Rochana, Rooksha, Tikshna, Ushna,
Mookhadoorgandhahrita, Laghu, Agnivardhaka, and mitigates Kapha Vata and
alleviates poison133
.
1. Twok:
Botanical Name : Cinnamomuma verum
Family : Lauraceae
Pharmacodynamics
Rasa : Katu, Tikta, Madhura
Guna : Laghu, Ruksha, Tikshna
Virya : Ushna
Vipaka : Katu
Parts used : Twok, Taila, Patra
Doshaghnata : Vatakapha Shamaka
Karma:-
Gastrointestinal System: Deepana, Pachana, Vatanulomana, Yakrttottejaka, Grahi,
Jantughna
Cardiovascular System: Hridayottejaka, Ojovardhaka, Raktashodhaka
Respiratory System: Shlesmahara and Yakshmanashaka
Urinary System: Mutrajanana

Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 59
Chemical Composition: Bark has an oil1/2-1%, which contains Cinnamaldehyde 50-
65% and Eugenol 60-75%. Leaf contains oil thathasEugenol 70-95%. Rootbark has
3% colourless oil; Seed has 33% fixed oil.
2. Ela:
Botanical Name : Elettaria cardamomum
Family : Zingiberaceae
Pharmacodynamics
Rasa : Katu, Madhura
Guna : Laghu, Rooksha
Virya : Sheeta
Vipaka : Madhura
Parts used : Veeja
Doshaghnata : Tridoshahara (Guna and Rasa- Kaphahara, Vipaka-Vata Shamaka,
Virya-Pitta Samaka)
Karma:-
Gastrointestinal System: Mukhashodhana, DUrgandhanashana, Chhardinigrahana,
Trishnanigrahana, Rochana, Deepana, Pachana, Anulomana
Cardiovascular System: Hridya
Satmikarana: Balya
Chemical Composition: Seeds have : volatile oil 2-8%, Potassium salt 3%, Starch
3%, Slimy substance 2%, Ash 6-10%, which contains Manganese. Oil has Cineol,
Terpineol, Terpinene, Limonene and Sabinene.
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 60
3. Patra:
Botanical Name : Cinnamomum tamala
Family : Lauraceae
Pharmacodynamics
Rasa : Katu, Tikta, Madhura
Guna : Laghu, Ruksha, Tikshna
Virya : Ushna
Vipaka : Katu
Parts used : Twok, Taila, Patra
Doshaghnata : Vatakapha Shamaka
Karma:-
Gastrointestinal System: Deepana, Pachana, Vatanulomana, Yakrttottejaka, Grahi,
Jantughna
Cardiovascular System: Hridayottejaka, Ojovardhaka, Raktashodhaka
Respiratory System: Shlesmahara and Yakshmanashaka
Urinary System: Mutrajanana
Chemical Composition: Leaves contain dark brown coloured odourous 1% oil,
which contains Eugenol-70-95%. Rootbark has 3% odourous oil, while seeds contain
33% fixed oil.
d. Madhu :
As told by Acharya Charaka134
:
Rasa : Kashaya, Madhura
Guna : Rooksha, Guru
Virya : Sheeta
Review of Literature
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 61
Karma : Vatala, Raktapittahara, Kaphahara, Sandhaneeya, Chedana
According to Acharya Susruta, Madhu is Tridhosha Shamaka135
. Nava Madhu is
Brimhaneeya, Ishat Kaphaghna, and Sara, while Purana Madhu is Atilekhana, Grahi,
Medohara, and Sthoulyanashaka. Madhu is Uttama Yogavahi, so is useful in different
preparations, in different diseases.
Chemical Composition: It is a viscous fluid with specific gravity 1.359-1.361. Is
97% sweet when compared to Sucrose. Contains moisture 12-24%, Dextrose 26-36%,
Laevulose 30-44%, Sucrose 0.4-6%, Dextrin and gum 0.7%. Contains Vitamin B and
C.
Method of preparation:
One Tula (400 Tola) of Trivrit Churna is taken, and added to 1 Vaha Jala (4096 Tola
or 49.152 litre), and boiled and reduced to 12.288 liter. And then filtered. To it, added
40 Pala (160 Tola) of Sita or Sugar candy, and heated until semisolid consistency is
obtained. Then 2 Kudava (16 Tola or 192 gm) each of Twok, Ela, and Patra should be
added along with 80 Tola of Madhu.136
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 62
METHODOLOGY
Kushtha is a Tridoshaja Vyadhi137
, in which Virechana Karma is presented as a prime
modality of treatment. And, Hridya Virechana Leha is a preparation of Trivrit, which
itself is considered as the best Virechana Dravya. This clinical Study was under taken
to assess the efficacy of Virechana performed with Hridya Virechana Leha in the
management of Psoriasis.
Objective of study
To evaluate the efficacy of Virechana Karma with Hridya Virechana Leha in
Psoriasis.
Source of data
Minimum of 20 patients diagnosed as Psoriasis will be selected for study from
IPD/OPD of S.D.M. Ayurveda Hospital Kuthpady, Udupi.
Diagnostic Criteria
1. The clinical signs and symptoms of Psoriasis like Itching, Scaling and
Erythema.
2. Positive Auspitz Sign, and Candle Grease Sign
a. Auspitz Sign
This sign occurs in psoriasis. There is a classical silvery white scaling and when
hyperkeratosis scales are mechanically removed from a psoriatic plaque by
scratching, within a few minutes, small blood droplets appear on erythematous
surface. This phenomenon is called Auspitz Sign.
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 63
b. Candle Grease Sign
When a psoriatic lesion is scratched with the point of a dissecting forceps, a
candle- grease-like scale can be repeatedly produced even from the non-scaling
lesions. This is called the Candle Grease Sign.
Inclusion Criteria:
1. Patients with signs and symptoms of Psoriasis.
2. Patients of either sex of age group between 16-70 years.
3. Patients fit for Virechana Karma.
Exclusion Criteria:
1. Patients suffering from other Systemic disorders.
2. Severely ill patients with weight loss
Assessment Criteria
1. PASI (Psoriasis area and severity index)
2. 5 D ITCH SCORE
Investigations
To evaluate the other pathologies and to avoid possible complications during
Virechana, the following laboratory investigations are carried out.
Hematological examination :
- Hb%, TLC, DLC, ESR, Blood Sugar
Skin Biopsy if required
Study design:
It is an open clinical study with pre-test and post-test design; where in minimum
of 20 patients diagnosed with Psoriasis of either sex with the age group between 16-

Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 64
70 years will be selected. All patients fulfilling the inclusion criteria will be subjected
to Virechana Karma.
INTERVENTION
1. POORVA KARMA
A. Deepana Pachana with Shunthi Qwatha.
20 ml thrice in a day is given to the patient until Agnivriddhi and Ama
Pachana take place.
B. Snehapana with Moorchhita Tila Taila
I. Method of Snehapana:
The patients were given with Arohanakrama Snehapana starting with 25 ml
around 6.30 am (immediately after sun rise) with Ushnajala as Anupana.
It was gradually increased according to the symptoms present in the patient
(time taken to digest Sneha).
Maximum emphasis was given for attainment of Samyaksnigdha Lakshanas
and was recorded accordingly.
Patients were advised to avoid excessive wind, sunlight, emotional
exacerbations, heavy work, day sleep, sitting in the same posture, excessive
talking, standing.
Patients were advised to take the rice gruel when they would feel strong
sensation of hunger in the afternoon and in the evening.
Patients were advised to take lukewarm water frequently (whenever they felt
thirsty).
On the achievement of Samyaksnigdha symptoms, administration of ghee was
stopped.
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 65
I. Duration of Snehapana:
Snehapana was advised till patient exhibited Samyaksnigdha Lakshanas.
(Minimum 3 days – Maximum 7 days).
II. Assessment of Snehana attainment (by Snehapana):
1. Dose and Duration (for Snehajeernata):
Snehamatra
Time of Sneha administration
Time of onset and duration of Snehajeeryamana lakshnas
Time of appearance of Snehajeerna lakshanas.
2. Samyaksnigdha Lakshana:
Vatanulomana- Assessed by the normal expulsion of the flatus, faeces and
urine.
Deeptagni- Based on the time of feeling of hunger, and Matra of Sneha
Asamhata Varchas- Based on the loose consistency of the faeces.
Snigdha Varchas- Confirmed by greasy/ sticky/ pasted-like stool, floating
of faeces over water.
Twaka snigdhata- Assessed by comparing the touch, texture and also
luster of the skin before, during and after Snehapana.
Glani- It was assessed by presence of exhaustion / fatigue / debility.
Anga Laghava- By enquiring with the patient.
Snehodhvega- Confirmed by the presence of aversion towards Sneha.
Overall assessment of Samyaksnigdha Lakshana was done based on the
percentage of manifestation of Samyaksnigdha Lakshanas.
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 66
C. Pariseka with Karanja Qwatha
a. Pariseka Method
The patient was subjected to Pariseka with Karanja Qwatha for 4 days, ie. in 3
gap days after stoppage of Snehapana, and on the day of Virechana, at
morning time.
b. Duration of Parisheka
Pariseka was administered to the patient until s/he got Samyak Swinna
Lakshanas, but care was taken so as not to give for more time.
c. Assessment of Swedana
Swedana was assessed based upon Samyak Swinna Lakshana viz
Sheetovyuparama, Shoolovyuparama, Stambhanigraha, Gauravanigraha,
Mardavata, Swedapradurbhava, Viratirmataha, and Laghuta.
Importance of 3 Days Gap: After completion of Snehapana, 3 days gap was given
before the administration of Virechana, in order to bring Kapha to Manda stage.
Because since Sneha and Kapha have similar Gunas, Sneha administered as Purva
Karma increases Kapha. And in state of increased Kapha, if Virechana is
administered, there is possibility that Kapha covers the Grahani, and conditions like
Pravahika, Gaurava and Grahani may develop and even Vamana may happen instead
of Virechana, since there is Kapha Utkleshavastha. Hence, for Kapha Shamana, three
days’ time gap is helpful. Thereafter, the process of Virechana can be carried out.
Virechana Aushadhi also should be administered after passing of Kapha Kala.138
2. PRADHANA KARMA
After the Karanja Qwatha Pariseka followed by Ushna Jala Snana in the morning,
the patient was administered with Hridya Virechana Leha at around 9.30 am, with
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 67
Anupana of milk. Dose was decided on the basis of Koshtha, Agni of the patient
as well as Rga Bala and Rogi Bala. Based upon the Shuddhi, Samsarjana Krama
was advised.
ASSESSMENT CRITERIA FOR VIRECHANA
Criteria for assessment:
1. Number of Vegas: Number of Vegas of each patient was recorded. (Calculation of
Vegas was done leaving first 2 Mala Vegas).
2. Time of administration of drug and time of onset of first Virechana Vega were
noted. Latency was calculated by subtracting time of onset of first Vega from the
time of administration of drug.
3. Time of last Vega was noted and duration of Virechana was calculated by
subtracting the time of last Vega from the time of onset of Vega.
4. Laingiki Shuddhi:
The main 8 Laingiki subjective and objective Lakshanas were observed, viz. Vit
Pitta Kapha Kramatha, Vatanulomana, Anamayatva, Sharira Laghuta, Indriya
Prasada, Sroto Shuddhi, absence of Ayoga Lakshanas, and Agni Dipti.
5. Antiki Lakshanas :
Antiki Lakshanas were assessed based on the features exhibited at the last Vega
i.e. Malanta, Pittanta and Kaphanta.
6. Maniki Lakshanas :
In the present study, during each time of defecation, urine and stool was collected
and then measured separately. This was performed excluding first and second Vega.
Then finally the value of total quantity of stool and urine added to obtain total
amount of output. Apart from this total amount of water consumed by patient after
passing each Vega was documented and it was consider as total amount of input.

Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 68
Afterwards difference between total amount of output and input was calculated and
documented as Maniki feature in terms of mililitres.
Criteria for the assessment of Psoriasis
(a) Itching
Itching was assessed with 5 D itch score.
5 d itch score.
5 d itch score is a measure of pruritus. The 5-D itch scale was developed as a
brief but multidimensional questionnaire designed to be useful as an outcome
measure in clinical trials. The five dimensions are degree, duration, direction,
disability and distribution.
Scoring
There will be 1 question covering one domain with the scoring from 1 to 5. So 5-D
scores can potentially range between 5 (no pruritus) and 25(most severe pruritus).
Single-item domain scores (duration, degree and direction) are equal to the value
indicated below the response choice (range 1–5).The disability domain includes
four items that assess the impact of itching on daily activities: sleep, leisure/social
activities, housework and work/school. The score for the disability domain is
achieved by taking the highest score on any of the four items. For the distribution
domain, the number of affected body parts is tallied (potential sum 0–16) and the
sum is sorted into five scoring bins: sum of 0–2 = score of 1, sum of 3–5 = score of
2, sum of 6–10 = score of 3, sum of 11–13 = score of 4, and sum of 14–16 = score
of 5. In present study, 5 d itch score was taken before Snehapana begins, after
Virechana and after 7th
day of Samsarjana Krama.
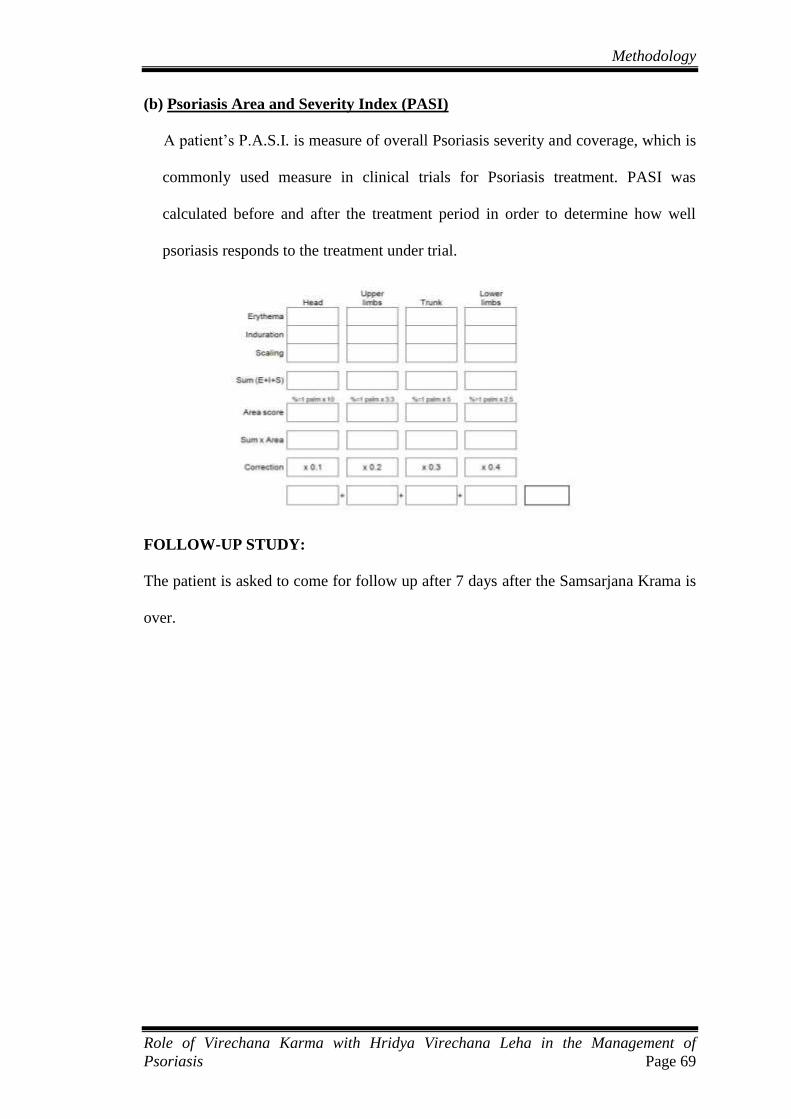
Methodology
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 69
(b) Psoriasis Area and Severity Index (PASI)
A patient’s P.A.S.I. is measure of overall Psoriasis severity and coverage, which is
commonly used measure in clinical trials for Psoriasis treatment. PASI was
calculated before and after the treatment period in order to determine how well
psoriasis responds to the treatment under trial.
FOLLOW-UP STUDY:
The patient is asked to come for follow up after 7 days after the Samsarjana Krama is
over.

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 70
OBSERVATIONS AND RESULTS
In this clinical study, 25 patients of psoriasis were registered and subjected to
Virechana Karma. Observations were made before and after the treatment.
Total Number of Patients Registered for the clinical study: 25
Total Number of Patients that completed the clinical study: 25
Number of dropouts: 0
A. EPIDEMIOLOGICAL OBSERVATIONS:
1. Age:
In this study, maximum number of patients belonged to the age group 51-60 years, i.e.
36% (9), followed by 28% (7) to age group 31-40 years. It was followed by 24% (6)
to age group 41-50, while there were 8% (2) in age group 21-30 and one patient (4%)
was of age group 61-70. The details are presented below in Table No. 21 and Figure
No. 2.
Table No. 21. Age wise Distribution of Patients
Age (in years) No. of Patients Percentage
21-30 2 8
31-40 7 28
41-50 6 24
51-60 9 36
61-70 1 4
Total 25 100

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 71
Fig. No. 2 Age wise Distribution of patients
2. Sex:
Among 25 patients in this study, 88% (22) were male while 12% (3) were female. The
same is presented below in Table No. 22 and Fig. No. 3:
Table No. 22 Showing Sex Distribution
Sex No. of Patients Percentage
Male 22 88
Female 3 12
Total 25 100
Fig. No. 3 Showing Sex Distribution
0
5
10
15
20
25
30
35
40
21-30 31-40 41-50 51-60 61-70
No. of Patients
Percentage
0
10
20
30
40
50
60
70
80
90
Male Female
No. of Patients
Percentage
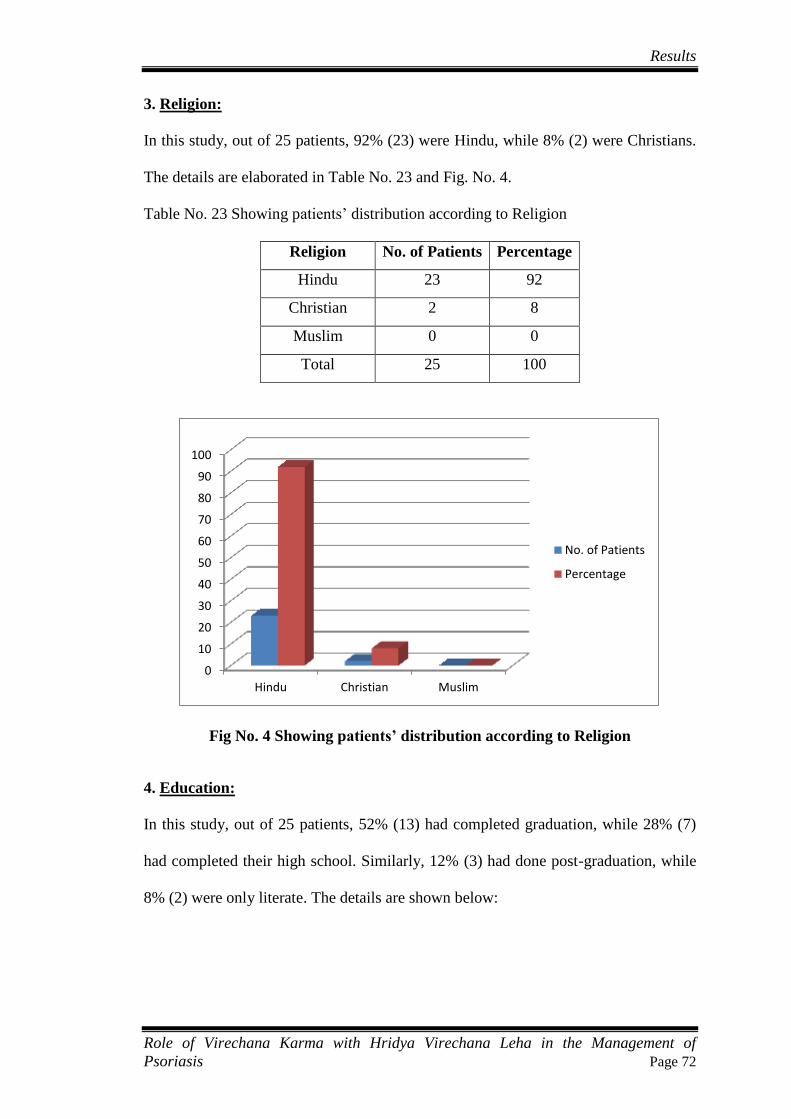
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 72
3. Religion:
In this study, out of 25 patients, 92% (23) were Hindu, while 8% (2) were Christians.
The details are elaborated in Table No. 23 and Fig. No. 4.
Table No. 23 Showing patients’ distribution according to Religion
Religion No. of Patients Percentage
Hindu 23 92
Christian 2 8
Muslim 0 0
Total 25 100
Fig No. 4 Showing patients’ distribution according to Religion
4. Education:
In this study, out of 25 patients, 52% (13) had completed graduation, while 28% (7)
had completed their high school. Similarly, 12% (3) had done post-graduation, while
8% (2) were only literate. The details are shown below:
0
10
20
30
40
50
60
70
80
90
100
Hindu Christian Muslim
No. of Patients
Percentage
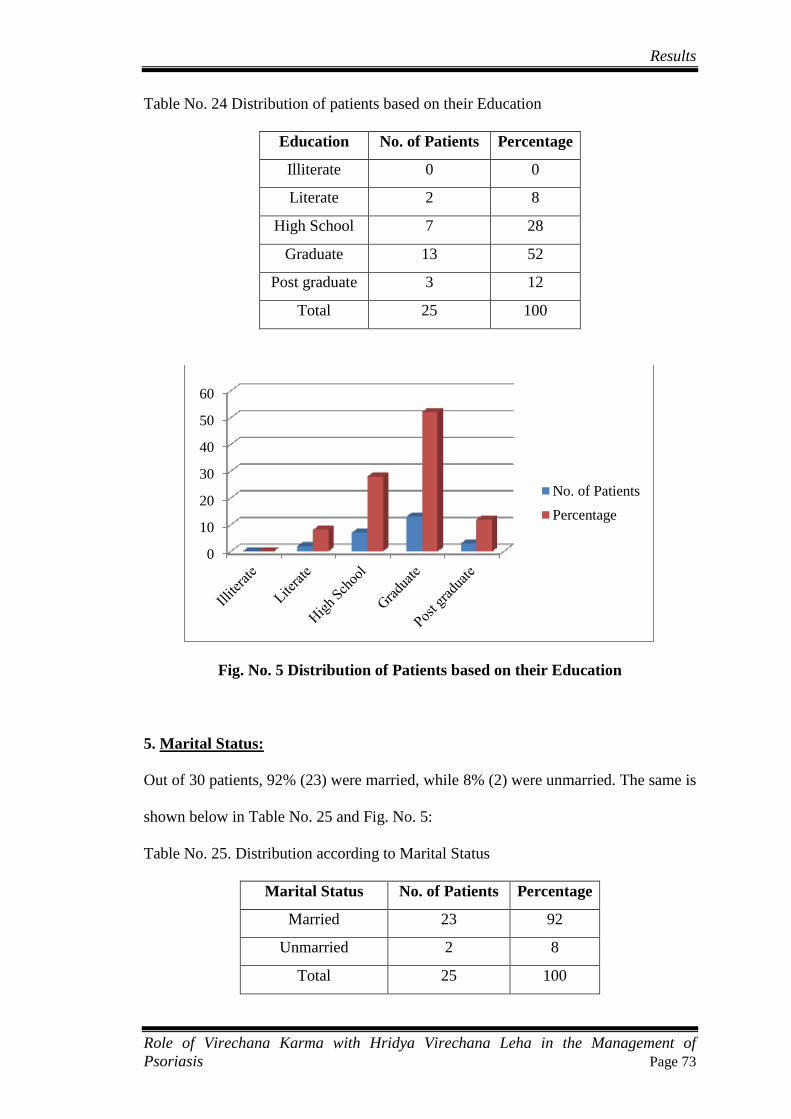
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 73
Table No. 24 Distribution of patients based on their Education
Education No. of Patients Percentage
Illiterate 0 0
Literate 2 8
High School 7 28
Graduate 13 52
Post graduate 3 12
Total 25 100
Fig. No. 5 Distribution of Patients based on their Education
5. Marital Status:
Out of 30 patients, 92% (23) were married, while 8% (2) were unmarried. The same is
shown below in Table No. 25 and Fig. No. 5:
Table No. 25. Distribution according to Marital Status
Marital Status No. of Patients Percentage
Married 23 92
Unmarried 2 8
Total 25 100
0
10
20
30
40
50
60
No. of Patients
Percentage
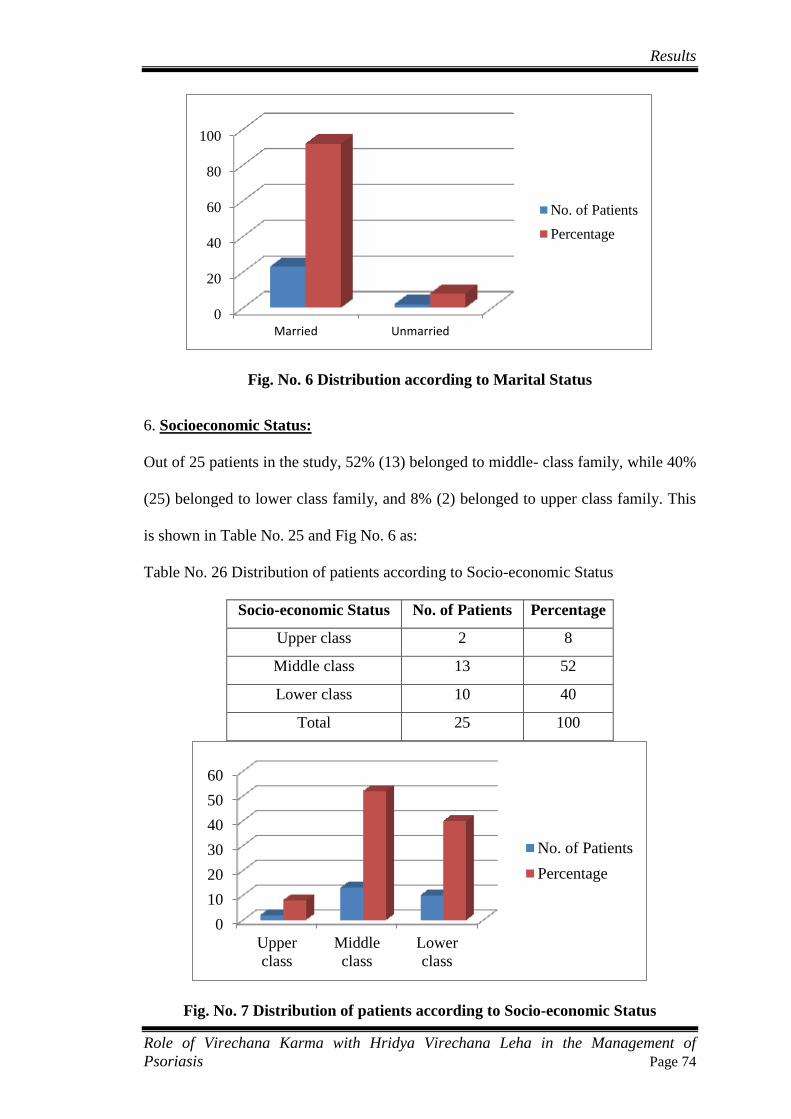
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 74
Fig. No. 6 Distribution according to Marital Status
6. Socioeconomic Status:
Out of 25 patients in the study, 52% (13) belonged to middle- class family, while 40%
(25) belonged to lower class family, and 8% (2) belonged to upper class family. This
is shown in Table No. 25 and Fig No. 6 as:
Table No. 26 Distribution of patients according to Socio-economic Status
Socio-economic Status No. of Patients Percentage
Upper class 2 8
Middle class 13 52
Lower class 10 40
Total 25 100
Fig. No. 7 Distribution of patients according to Socio-economic Status
0
20
40
60
80
100
Married Unmarried
No. of Patients
Percentage
0
10
20
30
40
50
60
Upper
class
Middle
class
Lower
class
No. of Patients
Percentage
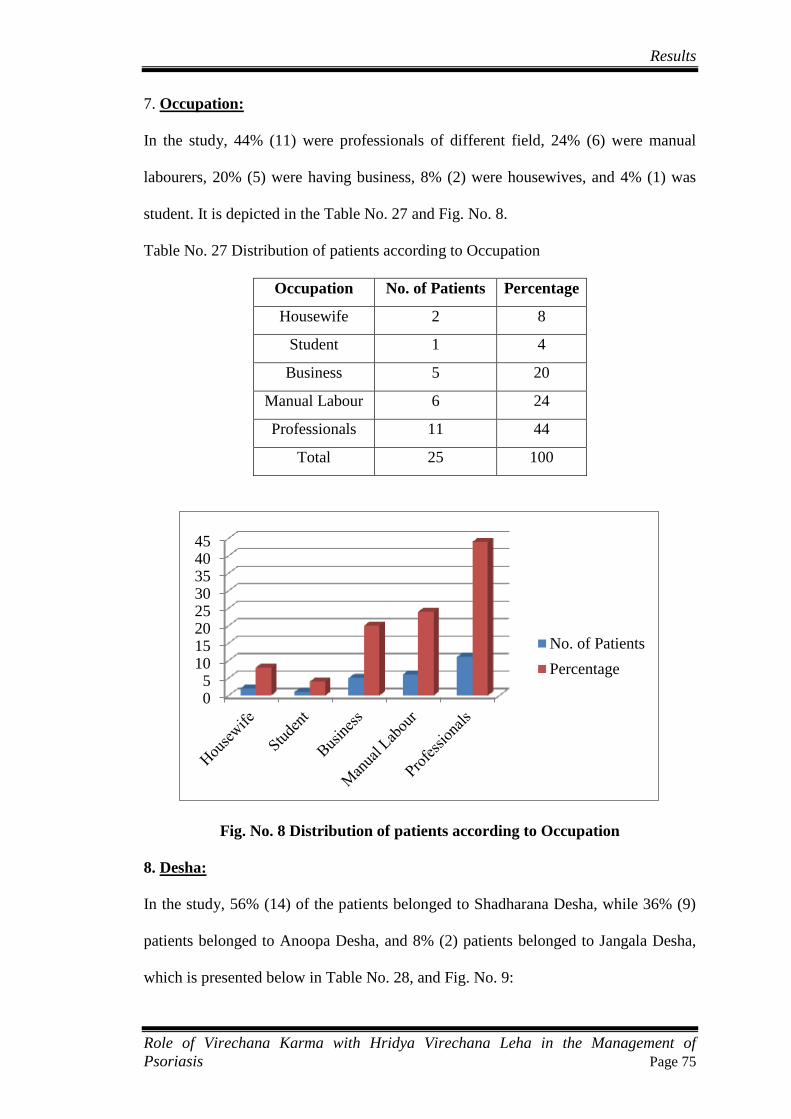
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 75
7. Occupation:
In the study, 44% (11) were professionals of different field, 24% (6) were manual
labourers, 20% (5) were having business, 8% (2) were housewives, and 4% (1) was
student. It is depicted in the Table No. 27 and Fig. No. 8.
Table No. 27 Distribution of patients according to Occupation
Occupation No. of Patients Percentage
Housewife 2 8
Student 1 4
Business 5 20
Manual Labour 6 24
Professionals 11 44
Total 25 100
Fig. No. 8 Distribution of patients according to Occupation
8. Desha:
In the study, 56% (14) of the patients belonged to Shadharana Desha, while 36% (9)
patients belonged to Anoopa Desha, and 8% (2) patients belonged to Jangala Desha,
which is presented below in Table No. 28, and Fig. No. 9:
05
1015202530354045
No. of Patients
Percentage
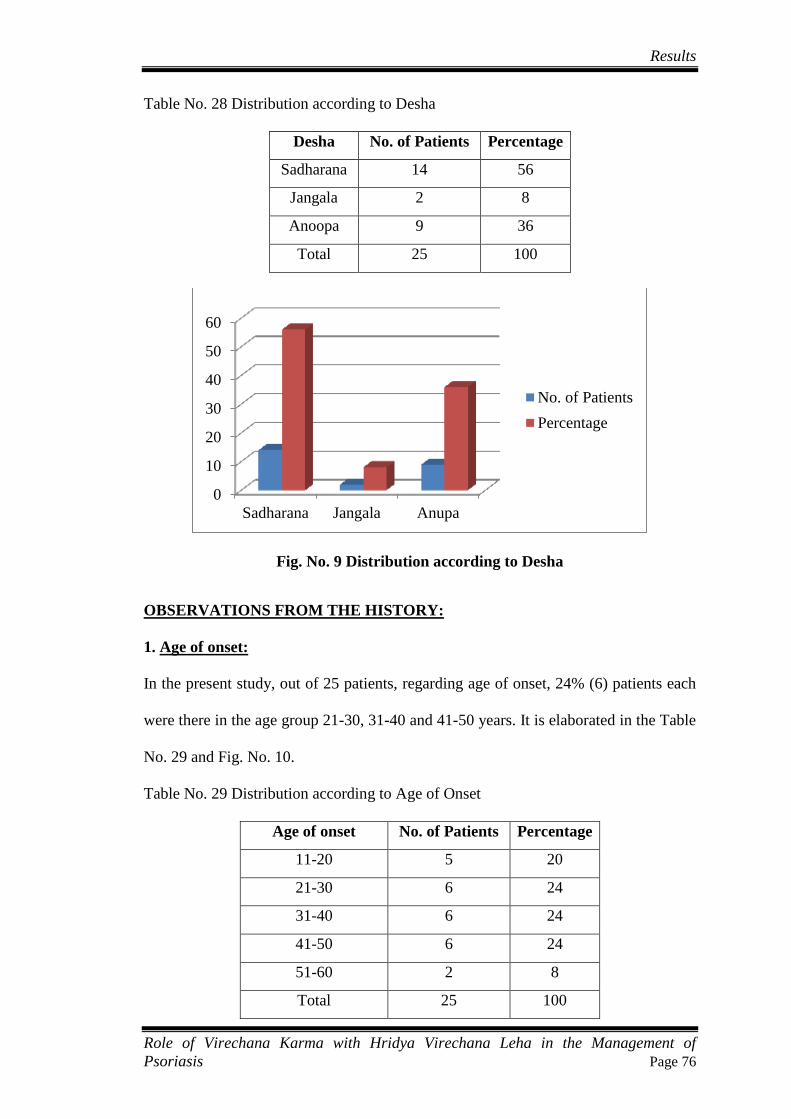
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 76
Table No. 28 Distribution according to Desha
Desha No. of Patients Percentage
Sadharana 14 56
Jangala 2 8
Anoopa 9 36
Total 25 100
Fig. No. 9 Distribution according to Desha
OBSERVATIONS FROM THE HISTORY:
1. Age of onset:
In the present study, out of 25 patients, regarding age of onset, 24% (6) patients each
were there in the age group 21-30, 31-40 and 41-50 years. It is elaborated in the Table
No. 29 and Fig. No. 10.
Table No. 29 Distribution according to Age of Onset
Age of onset No. of Patients Percentage
11-20 5 20
21-30 6 24
31-40 6 24
41-50 6 24
51-60 2 8
Total 25 100
0
10
20
30
40
50
60
Sadharana Jangala Anupa
No. of Patients
Percentage
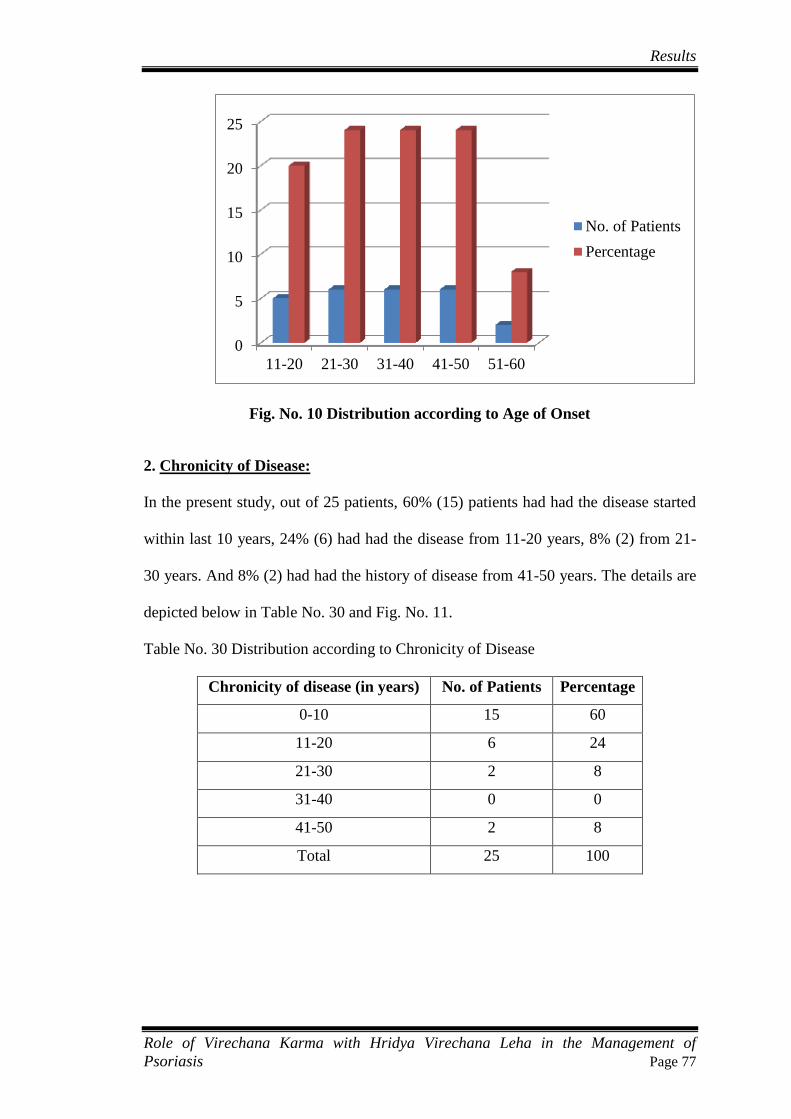
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 77
Fig. No. 10 Distribution according to Age of Onset
2. Chronicity of Disease:
In the present study, out of 25 patients, 60% (15) patients had had the disease started
within last 10 years, 24% (6) had had the disease from 11-20 years, 8% (2) from 21-
30 years. And 8% (2) had had the history of disease from 41-50 years. The details are
depicted below in Table No. 30 and Fig. No. 11.
Table No. 30 Distribution according to Chronicity of Disease
Chronicity of disease (in years) No. of Patients Percentage
0-10 15 60
11-20 6 24
21-30 2 8
31-40 0 0
41-50 2 8
Total 25 100
0
5
10
15
20
25
11-20 21-30 31-40 41-50 51-60
No. of Patients
Percentage
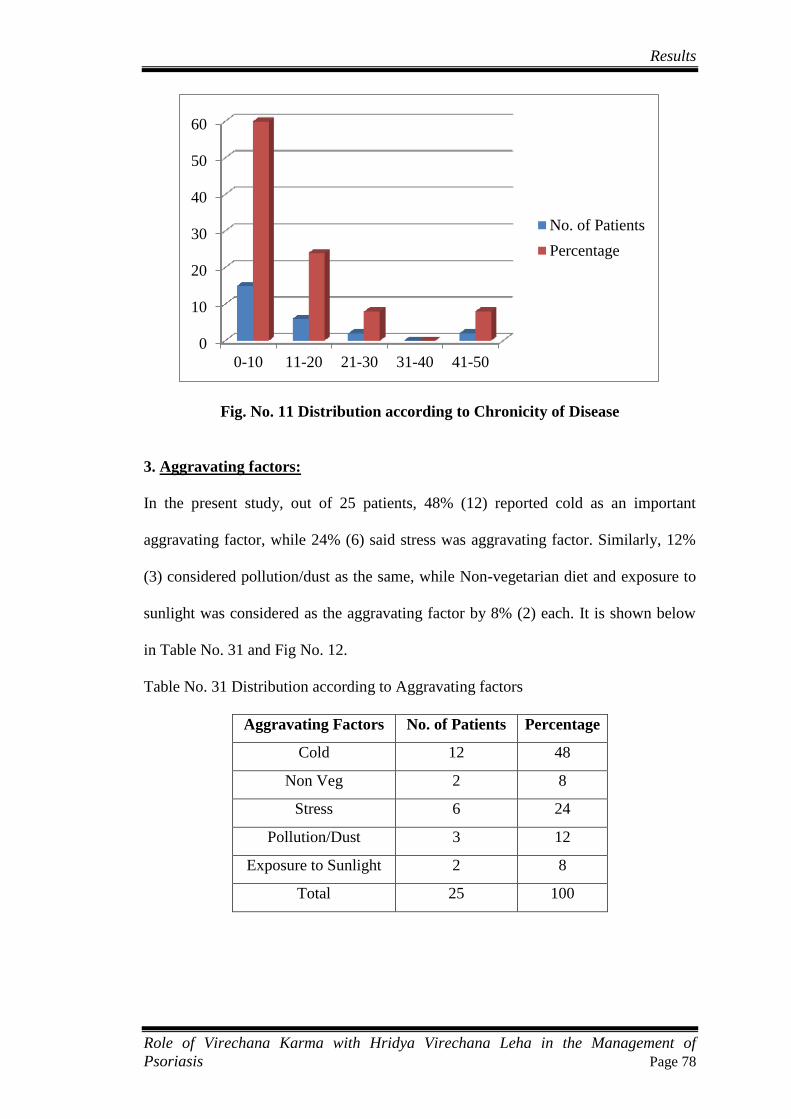
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 78
Fig. No. 11 Distribution according to Chronicity of Disease
3. Aggravating factors:
In the present study, out of 25 patients, 48% (12) reported cold as an important
aggravating factor, while 24% (6) said stress was aggravating factor. Similarly, 12%
(3) considered pollution/dust as the same, while Non-vegetarian diet and exposure to
sunlight was considered as the aggravating factor by 8% (2) each. It is shown below
in Table No. 31 and Fig No. 12.
Table No. 31 Distribution according to Aggravating factors
Aggravating Factors No. of Patients Percentage
Cold 12 48
Non Veg 2 8
Stress 6 24
Pollution/Dust 3 12
Exposure to Sunlight 2 8
Total 25 100
0
10
20
30
40
50
60
0-10 11-20 21-30 31-40 41-50
No. of Patients
Percentage
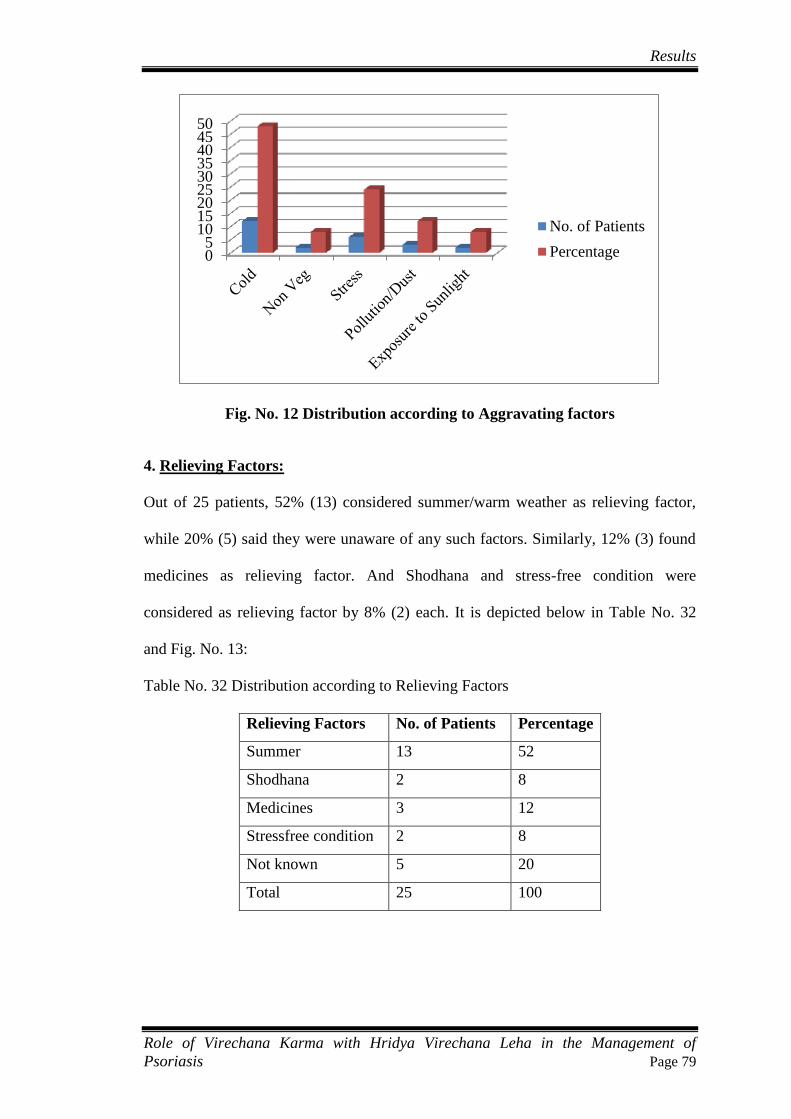
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 79
Fig. No. 12 Distribution according to Aggravating factors
4. Relieving Factors:
Out of 25 patients, 52% (13) considered summer/warm weather as relieving factor,
while 20% (5) said they were unaware of any such factors. Similarly, 12% (3) found
medicines as relieving factor. And Shodhana and stress-free condition were
considered as relieving factor by 8% (2) each. It is depicted below in Table No. 32
and Fig. No. 13:
Table No. 32 Distribution according to Relieving Factors
Relieving Factors No. of Patients Percentage
Summer 13 52
Shodhana 2 8
Medicines 3 12
Stressfree condition 2 8
Not known 5 20
Total 25 100
05
101520253035404550
No. of Patients
Percentage
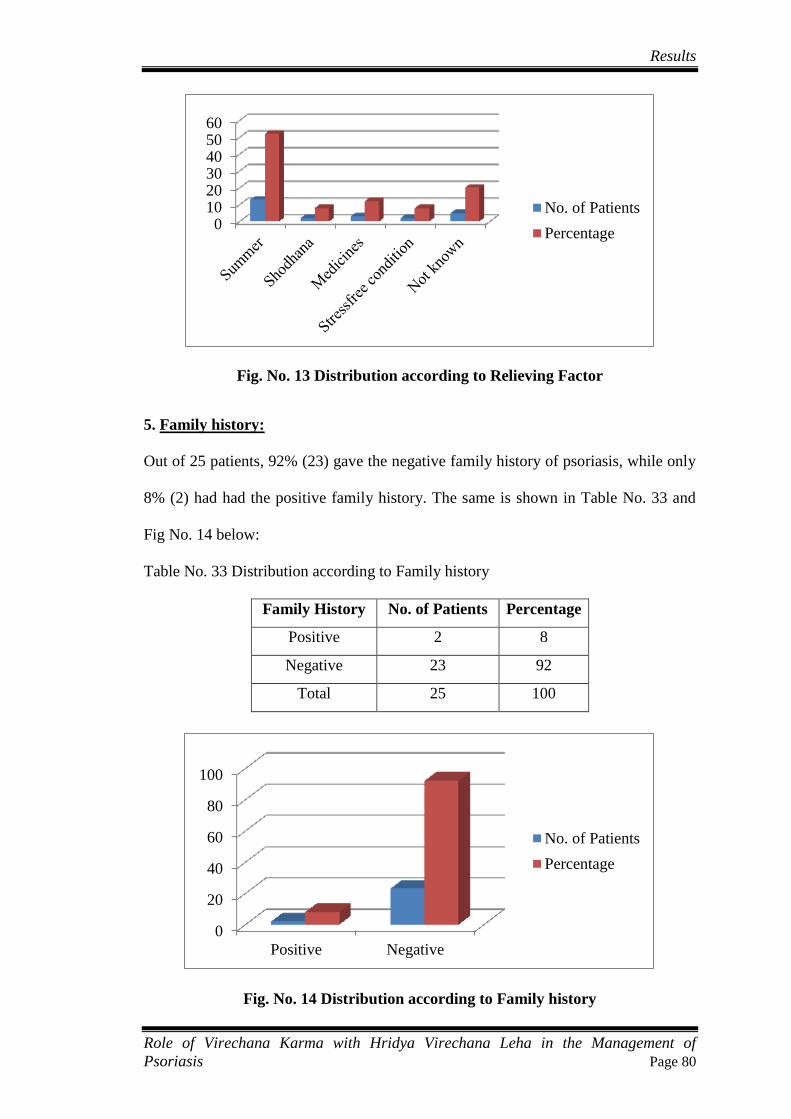
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 80
Fig. No. 13 Distribution according to Relieving Factor
5. Family history:
Out of 25 patients, 92% (23) gave the negative family history of psoriasis, while only
8% (2) had had the positive family history. The same is shown in Table No. 33 and
Fig No. 14 below:
Table No. 33 Distribution according to Family history
Family History No. of Patients Percentage
Positive 2 8
Negative 23 92
Total 25 100
Fig. No. 14 Distribution according to Family history
0102030405060
No. of Patients
Percentage
0
20
40
60
80
100
Positive Negative
No. of Patients
Percentage
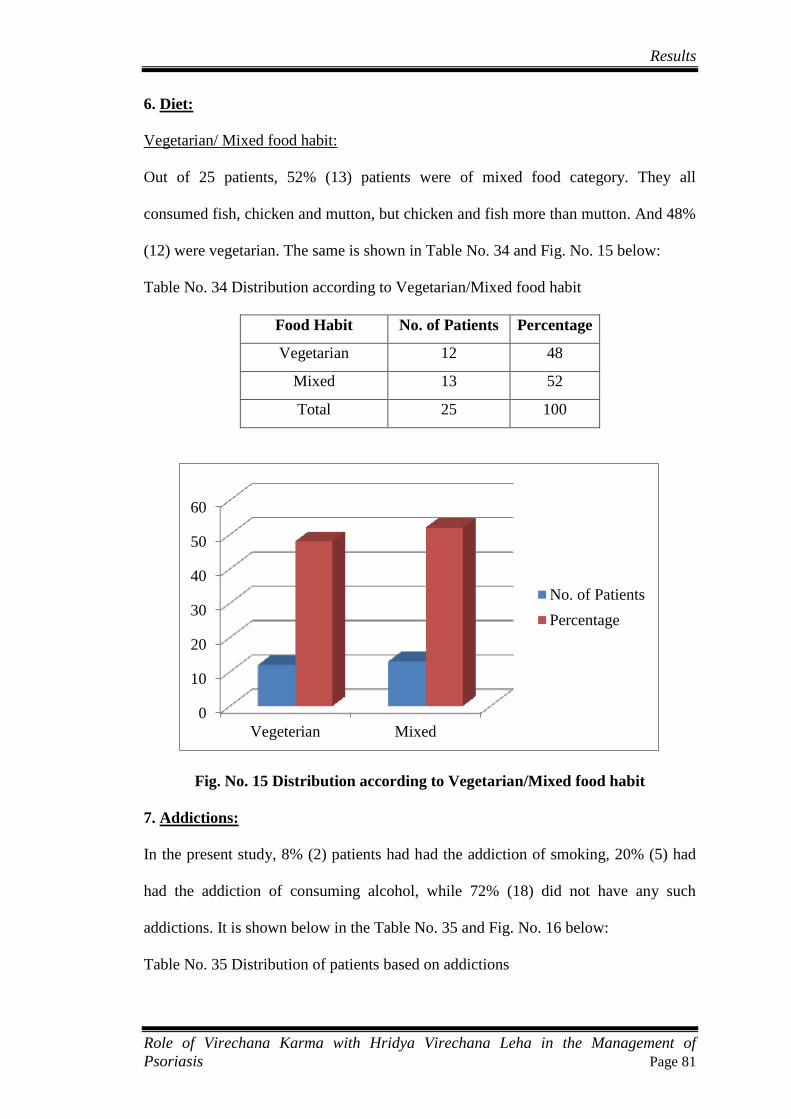
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 81
6. Diet:
Vegetarian/ Mixed food habit:
Out of 25 patients, 52% (13) patients were of mixed food category. They all
consumed fish, chicken and mutton, but chicken and fish more than mutton. And 48%
(12) were vegetarian. The same is shown in Table No. 34 and Fig. No. 15 below:
Table No. 34 Distribution according to Vegetarian/Mixed food habit
Food Habit No. of Patients Percentage
Vegetarian 12 48
Mixed 13 52
Total 25 100
Fig. No. 15 Distribution according to Vegetarian/Mixed food habit
7. Addictions:
In the present study, 8% (2) patients had had the addiction of smoking, 20% (5) had
had the addiction of consuming alcohol, while 72% (18) did not have any such
addictions. It is shown below in the Table No. 35 and Fig. No. 16 below:
Table No. 35 Distribution of patients based on addictions
0
10
20
30
40
50
60
Vegeterian Mixed
No. of Patients
Percentage
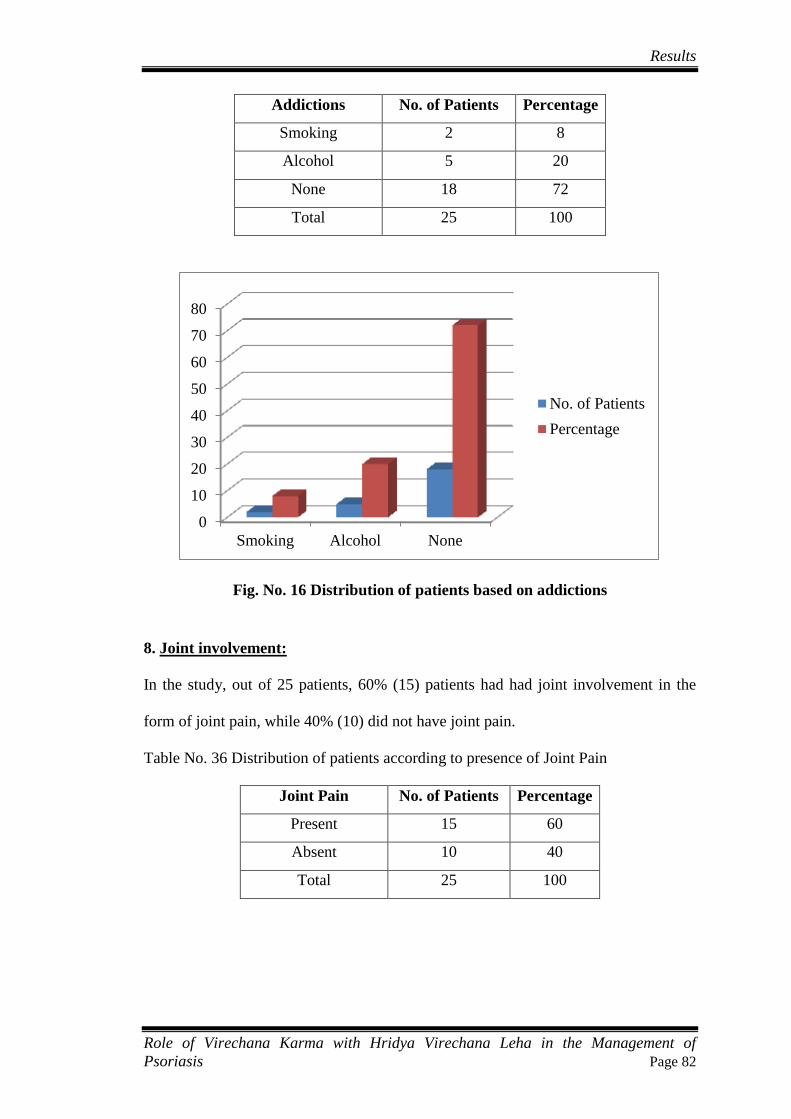
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 82
Addictions No. of Patients Percentage
Smoking 2 8
Alcohol 5 20
None 18 72
Total 25 100
Fig. No. 16 Distribution of patients based on addictions
8. Joint involvement:
In the study, out of 25 patients, 60% (15) patients had had joint involvement in the
form of joint pain, while 40% (10) did not have joint pain.
Table No. 36 Distribution of patients according to presence of Joint Pain
Joint Pain No. of Patients Percentage
Present 15 60
Absent 10 40
Total 25 100
0
10
20
30
40
50
60
70
80
Smoking Alcohol None
No. of Patients
Percentage
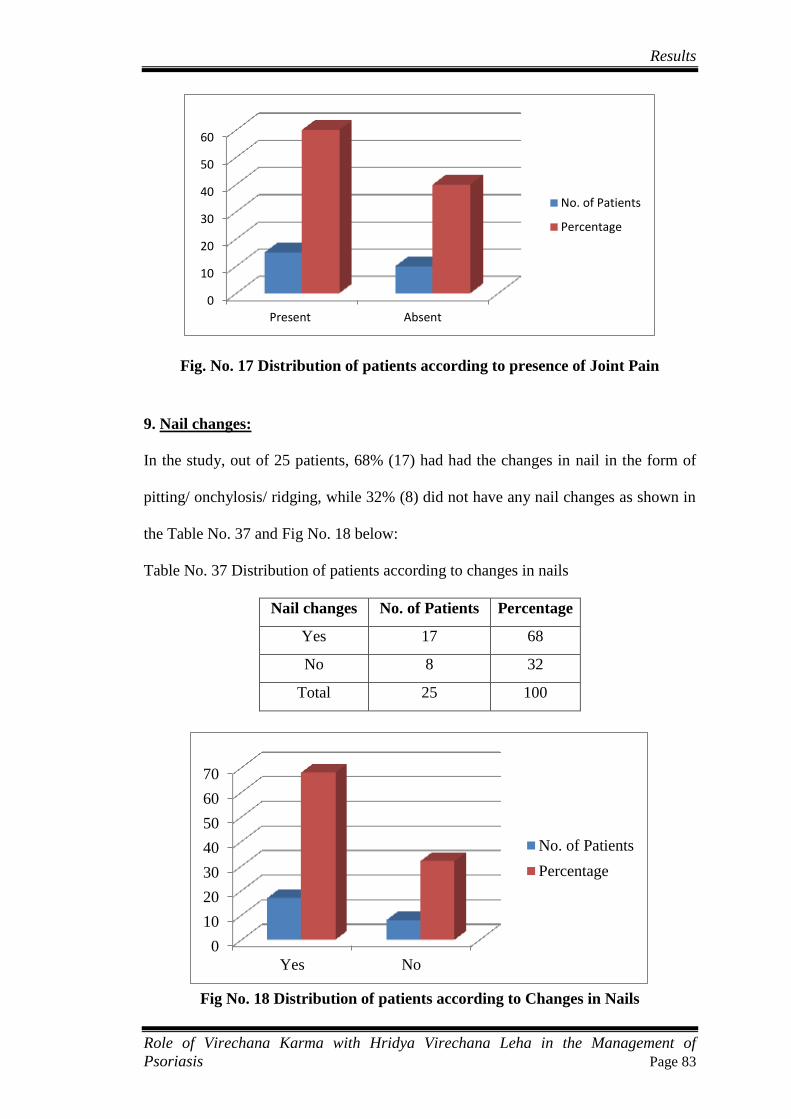
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 83
Fig. No. 17 Distribution of patients according to presence of Joint Pain
9. Nail changes:
In the study, out of 25 patients, 68% (17) had had the changes in nail in the form of
pitting/ onchylosis/ ridging, while 32% (8) did not have any nail changes as shown in
the Table No. 37 and Fig No. 18 below:
Table No. 37 Distribution of patients according to changes in nails
Nail changes No. of Patients Percentage
Yes 17 68
No 8 32
Total 25 100
Fig No. 18 Distribution of patients according to Changes in Nails
0
10
20
30
40
50
60
Present Absent
No. of Patients
Percentage
0
10
20
30
40
50
60
70
Yes No
No. of Patients
Percentage
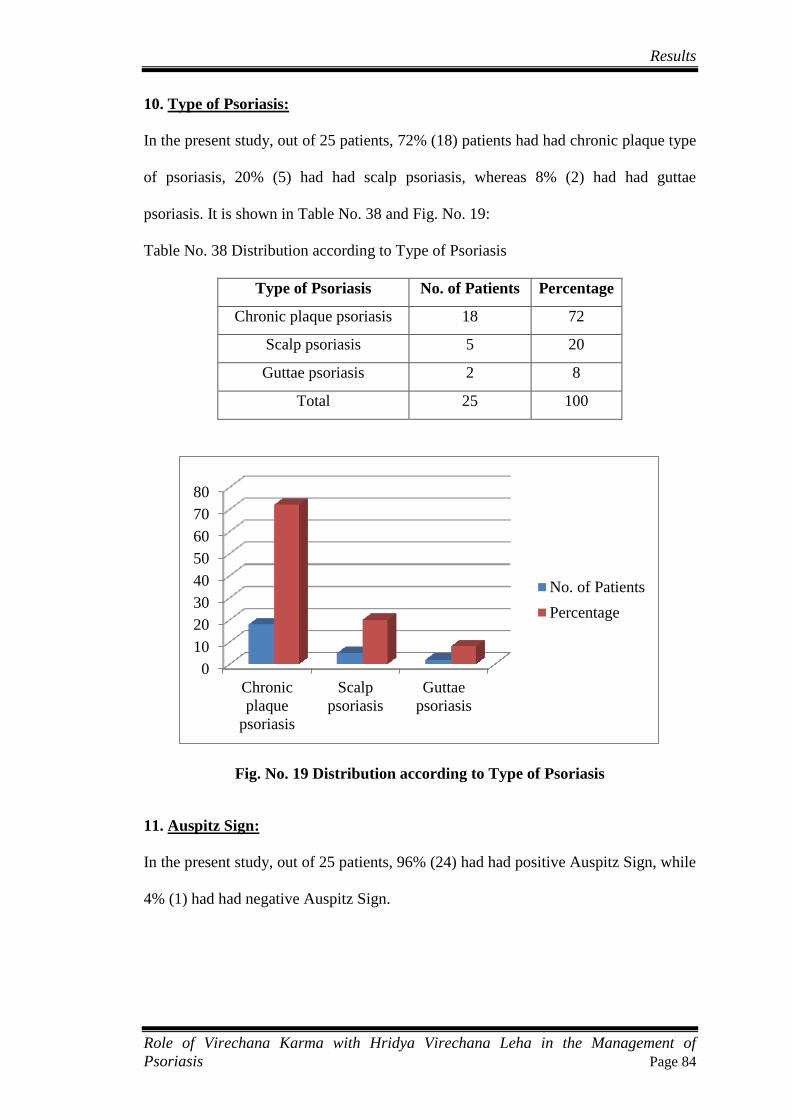
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 84
10. Type of Psoriasis:
In the present study, out of 25 patients, 72% (18) patients had had chronic plaque type
of psoriasis, 20% (5) had had scalp psoriasis, whereas 8% (2) had had guttae
psoriasis. It is shown in Table No. 38 and Fig. No. 19:
Table No. 38 Distribution according to Type of Psoriasis
Type of Psoriasis No. of Patients Percentage
Chronic plaque psoriasis 18 72
Scalp psoriasis 5 20
Guttae psoriasis 2 8
Total 25 100
Fig. No. 19 Distribution according to Type of Psoriasis
11. Auspitz Sign:
In the present study, out of 25 patients, 96% (24) had had positive Auspitz Sign, while
4% (1) had had negative Auspitz Sign.
0
10
20
30
40
50
60
70
80
Chronic
plaque
psoriasis
Scalp
psoriasis
Guttae
psoriasis
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 85
12. Candle Grease Sign:
In the study, out of 25patients, in 88% (22) patients, Candle Grease Sign was found to
be positive, while in 12% (3) patients, the Sign was found to be negative.
13. Shareerika Prakriti:
Among 25 patients, 36% (9) patients’ Prakriti was found to be of Vata Pitta, 28% (7)
patients’ was assessed to be as Pitta Kapha, while that of 20% (5) patients’ of Vata
Kapha. Similarly the Prakriti was assessed to be of Kapha in 12% (3) patients, while it
was found to be of Pitta in 4% (1) patient. It is depicted in Table No. 39 and Fig. No.
20.
Table No. 39 Distribution according to Prakriti
Sharirika Prakriti No. of Patients Percentage
Pitta 1 4
Kapha 3 12
Vata Pitta 9 36
Pitta Kapha 7 28
Vata Kapha 5 20
Total 25 100
Fig. No. 20 Distribution aacording to Prakriti
0
5
10
15
20
25
30
35
40
Pitta Kapha Vata
Pitta
Pitta
Kapha
Vata
Kapha
No. of Patients
Percentage
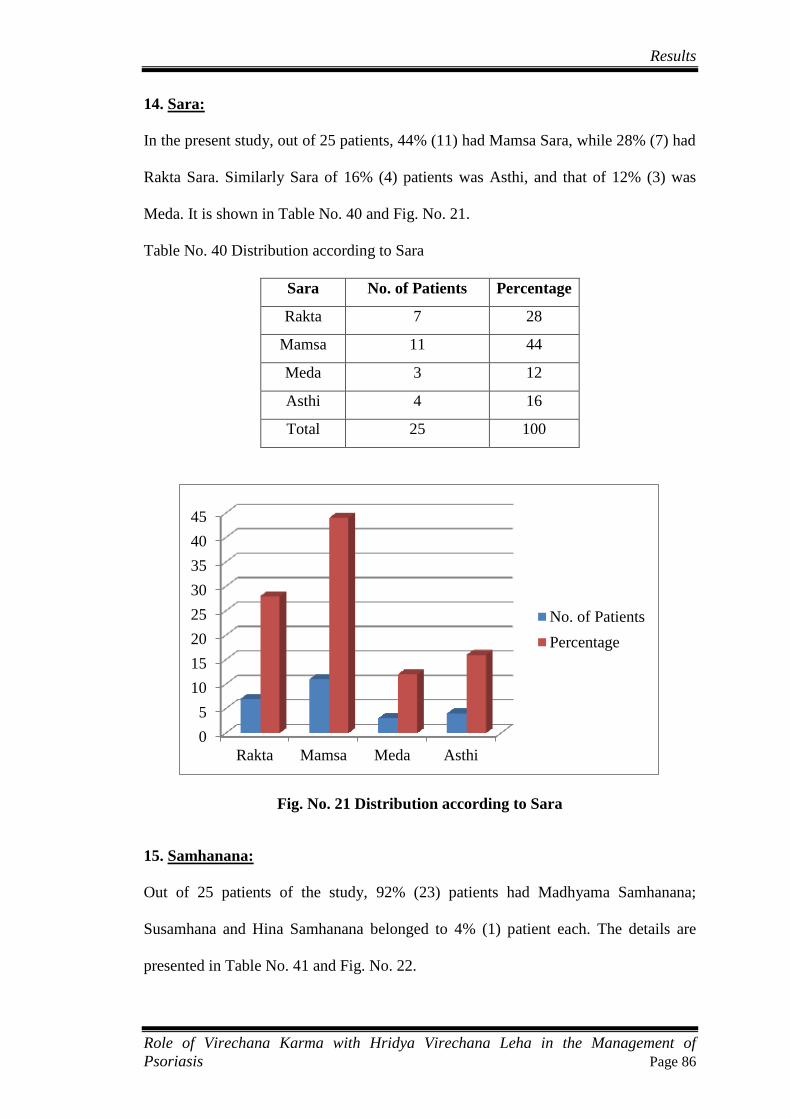
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 86
14. Sara:
In the present study, out of 25 patients, 44% (11) had Mamsa Sara, while 28% (7) had
Rakta Sara. Similarly Sara of 16% (4) patients was Asthi, and that of 12% (3) was
Meda. It is shown in Table No. 40 and Fig. No. 21.
Table No. 40 Distribution according to Sara
Sara No. of Patients Percentage
Rakta 7 28
Mamsa 11 44
Meda 3 12
Asthi 4 16
Total 25 100
Fig. No. 21 Distribution according to Sara
15. Samhanana:
Out of 25 patients of the study, 92% (23) patients had Madhyama Samhanana;
Susamhana and Hina Samhanana belonged to 4% (1) patient each. The details are
presented in Table No. 41 and Fig. No. 22.
0
5
10
15
20
25
30
35
40
45
Rakta Mamsa Meda Asthi
No. of Patients
Percentage
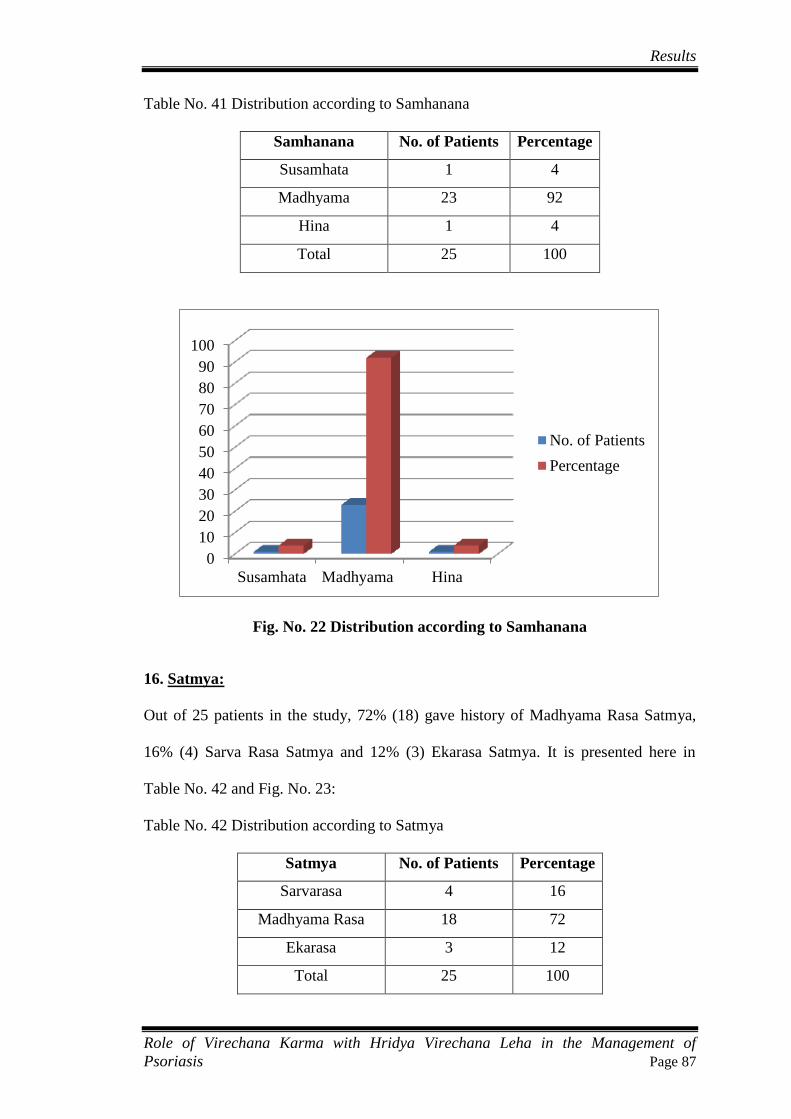
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 87
Table No. 41 Distribution according to Samhanana
Samhanana No. of Patients Percentage
Susamhata 1 4
Madhyama 23 92
Hina 1 4
Total 25 100
Fig. No. 22 Distribution according to Samhanana
16. Satmya:
Out of 25 patients in the study, 72% (18) gave history of Madhyama Rasa Satmya,
16% (4) Sarva Rasa Satmya and 12% (3) Ekarasa Satmya. It is presented here in
Table No. 42 and Fig. No. 23:
Table No. 42 Distribution according to Satmya
Satmya No. of Patients Percentage
Sarvarasa 4 16
Madhyama Rasa 18 72
Ekarasa 3 12
Total 25 100
0
10
20
30
40
50
60
70
80
90
100
Susamhata Madhyama Hina
No. of Patients
Percentage
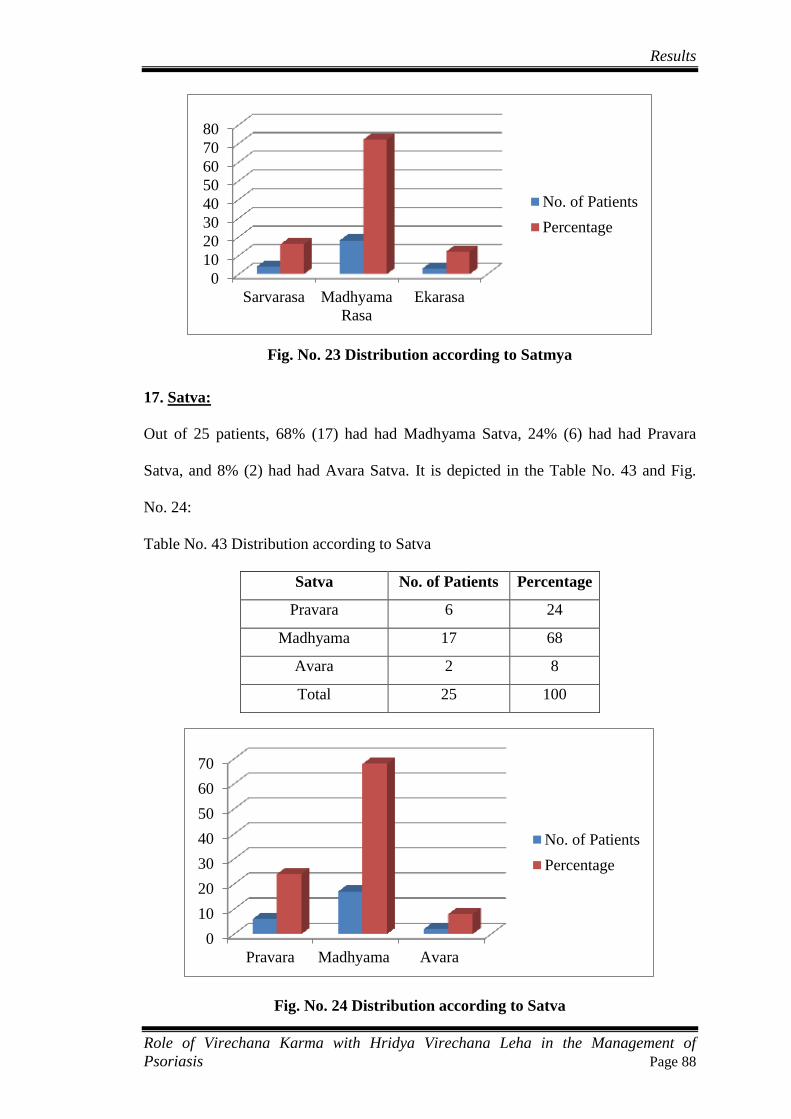
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 88
Fig. No. 23 Distribution according to Satmya
17. Satva:
Out of 25 patients, 68% (17) had had Madhyama Satva, 24% (6) had had Pravara
Satva, and 8% (2) had had Avara Satva. It is depicted in the Table No. 43 and Fig.
No. 24:
Table No. 43 Distribution according to Satva
Satva No. of Patients Percentage
Pravara 6 24
Madhyama 17 68
Avara 2 8
Total 25 100
Fig. No. 24 Distribution according to Satva
0
10
20
30
40
50
60
70
80
Sarvarasa Madhyama
Rasa
Ekarasa
No. of Patients
Percentage
0
10
20
30
40
50
60
70
Pravara Madhyama Avara
No. of Patients
Percentage
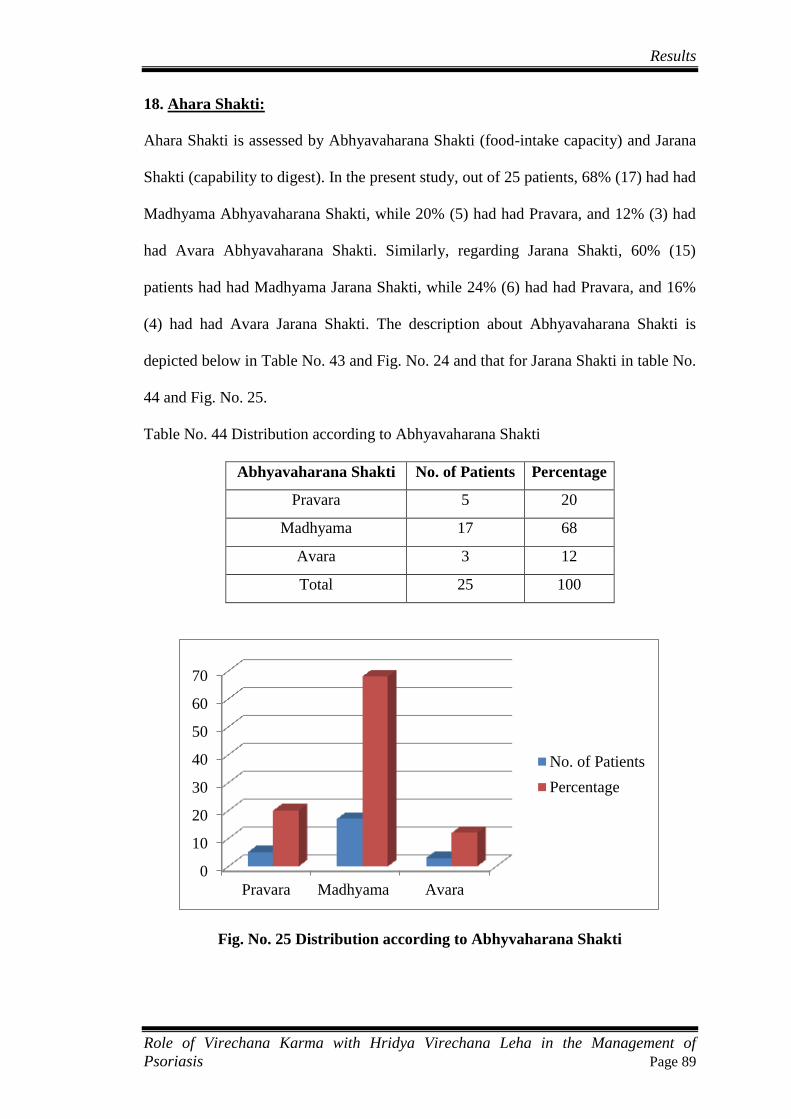
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 89
18. Ahara Shakti:
Ahara Shakti is assessed by Abhyavaharana Shakti (food-intake capacity) and Jarana
Shakti (capability to digest). In the present study, out of 25 patients, 68% (17) had had
Madhyama Abhyavaharana Shakti, while 20% (5) had had Pravara, and 12% (3) had
had Avara Abhyavaharana Shakti. Similarly, regarding Jarana Shakti, 60% (15)
patients had had Madhyama Jarana Shakti, while 24% (6) had had Pravara, and 16%
(4) had had Avara Jarana Shakti. The description about Abhyavaharana Shakti is
depicted below in Table No. 43 and Fig. No. 24 and that for Jarana Shakti in table No.
44 and Fig. No. 25.
Table No. 44 Distribution according to Abhyavaharana Shakti
Abhyavaharana Shakti No. of Patients Percentage
Pravara 5 20
Madhyama 17 68
Avara 3 12
Total 25 100
Fig. No. 25 Distribution according to Abhyvaharana Shakti
0
10
20
30
40
50
60
70
Pravara Madhyama Avara
No. of Patients
Percentage
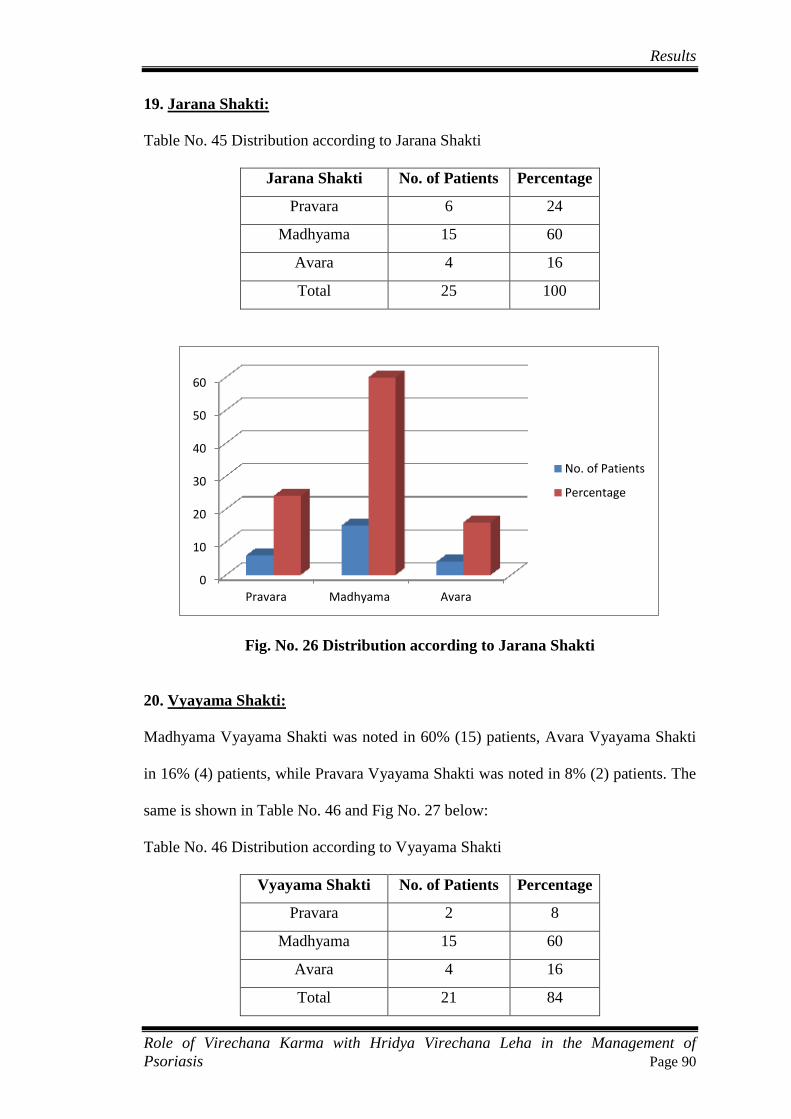
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 90
19. Jarana Shakti:
Table No. 45 Distribution according to Jarana Shakti
Jarana Shakti No. of Patients Percentage
Pravara 6 24
Madhyama 15 60
Avara 4 16
Total 25 100
Fig. No. 26 Distribution according to Jarana Shakti
20. Vyayama Shakti:
Madhyama Vyayama Shakti was noted in 60% (15) patients, Avara Vyayama Shakti
in 16% (4) patients, while Pravara Vyayama Shakti was noted in 8% (2) patients. The
same is shown in Table No. 46 and Fig No. 27 below:
Table No. 46 Distribution according to Vyayama Shakti
Vyayama Shakti No. of Patients Percentage
Pravara 2 8
Madhyama 15 60
Avara 4 16
Total 21 84
0
10
20
30
40
50
60
Pravara Madhyama Avara
No. of Patients
Percentage
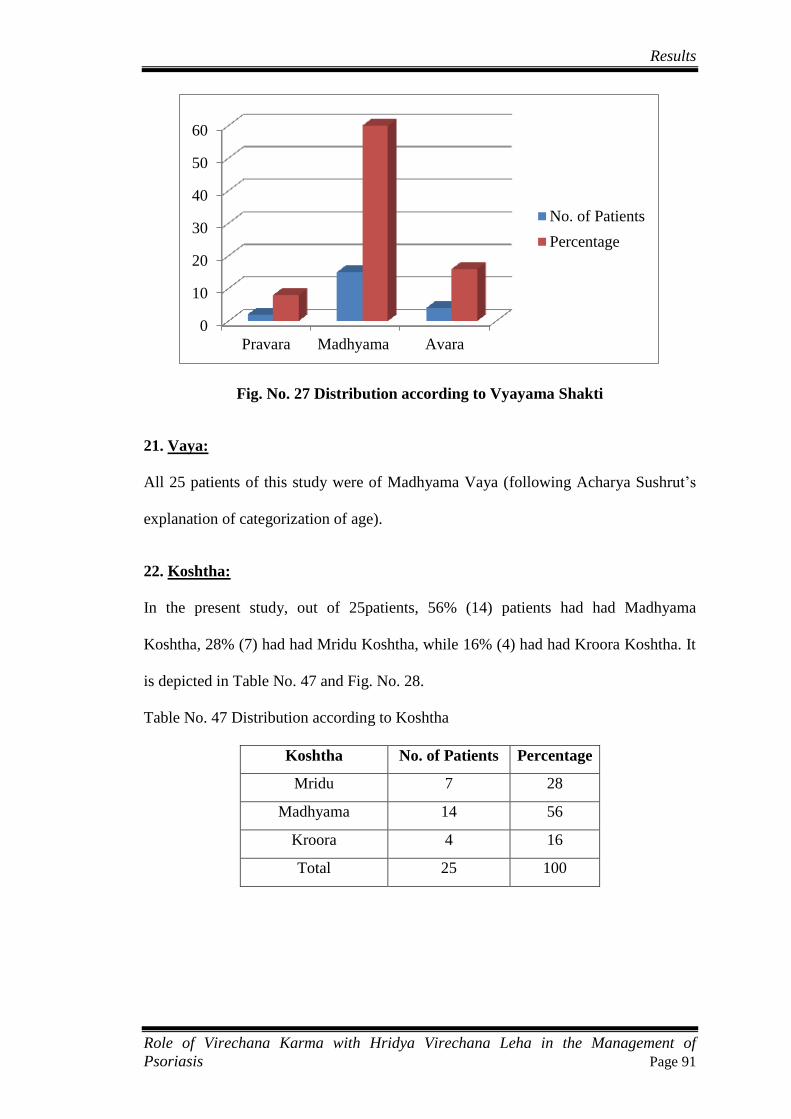
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 91
Fig. No. 27 Distribution according to Vyayama Shakti
21. Vaya:
All 25 patients of this study were of Madhyama Vaya (following Acharya Sushrut’s
explanation of categorization of age).
22. Koshtha:
In the present study, out of 25patients, 56% (14) patients had had Madhyama
Koshtha, 28% (7) had had Mridu Koshtha, while 16% (4) had had Kroora Koshtha. It
is depicted in Table No. 47 and Fig. No. 28.
Table No. 47 Distribution according to Koshtha
Koshtha No. of Patients Percentage
Mridu 7 28
Madhyama 14 56
Kroora 4 16
Total 25 100
0
10
20
30
40
50
60
Pravara Madhyama Avara
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 92
Fig. No. 28 Distribution according to Koshtha
OBSERVATIONS DURING THE TREATMENT
1. Observations of Sneha Jiryamana Lakshana:
Out of 25 patients, after Snehapana, Shiroruja was felt by 92% (23) patients, while
Bhrama and Murchha did not happen in any of the patients. Lalasrava was
experienced by 88% (22) patients, Angasada by 52% (13), Klama by 36% (9), Trishna
by all 100% (25) patients, Daha by 64% (16) patients, while Arati was felt by 76%
(19) patients. The details are given below in Table No. 48 and Fig. No. 29.
Table No. 48 Observation of Snehajiryamana Lakshana
Sneha Jiryamana Lakshana No. of Patients Percentage
Shiroruja 23 92
Bhrama 0 0
Lalashrava 22 88
Angasada 13 52
Murchha 0 0
Klama 9 36
Trishna 25 100
Daha 16 64
Arati 19 76
0
10
20
30
40
50
60
Mridu Madhyama Kroora
No. of Patients
Percentage
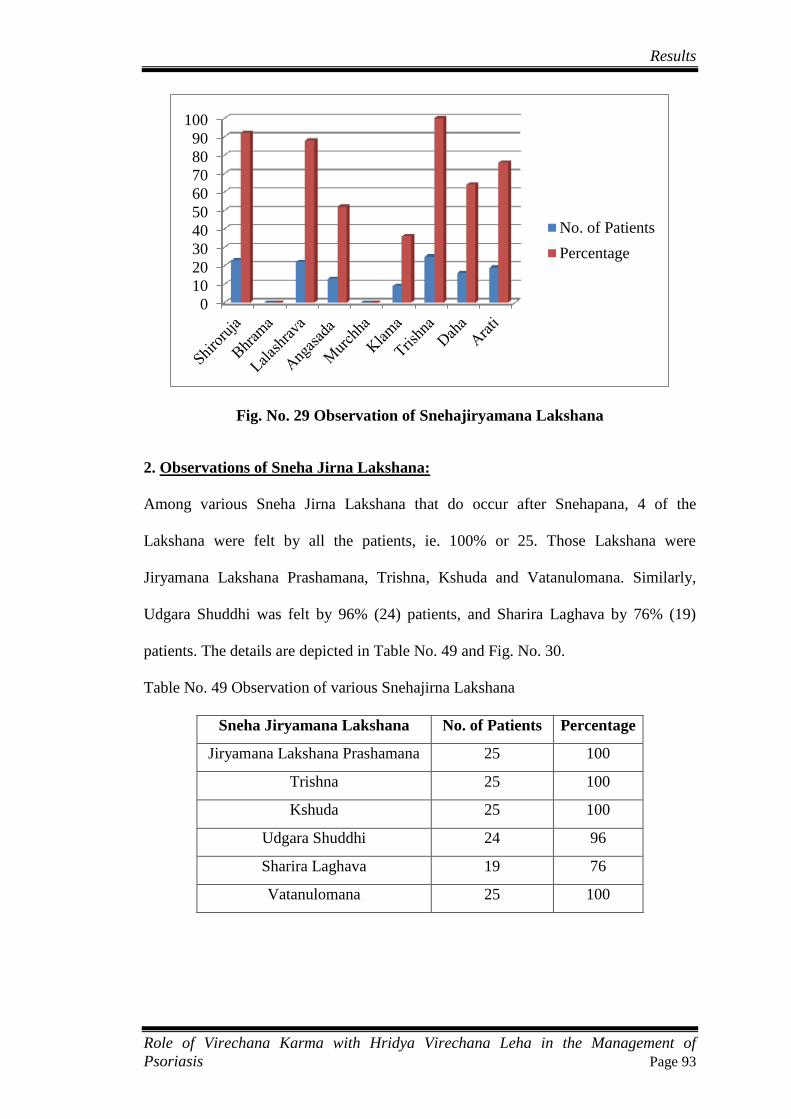
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 93
Fig. No. 29 Observation of Snehajiryamana Lakshana
2. Observations of Sneha Jirna Lakshana:
Among various Sneha Jirna Lakshana that do occur after Snehapana, 4 of the
Lakshana were felt by all the patients, ie. 100% or 25. Those Lakshana were
Jiryamana Lakshana Prashamana, Trishna, Kshuda and Vatanulomana. Similarly,
Udgara Shuddhi was felt by 96% (24) patients, and Sharira Laghava by 76% (19)
patients. The details are depicted in Table No. 49 and Fig. No. 30.
Table No. 49 Observation of various Snehajirna Lakshana
Sneha Jiryamana Lakshana No. of Patients Percentage
Jiryamana Lakshana Prashamana 25 100
Trishna 25 100
Kshuda 25 100
Udgara Shuddhi 24 96
Sharira Laghava 19 76
Vatanulomana 25 100
0
10
20
30
40
50
60
70
80
90
100
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 94
Fig. No. 30 Observation of various Snehajirna Lakshana
3. Day of attainment of Samyak Snigdha Lakshana:
In the present study, Samyak Snigdha Lakshana were seen in the 3rd
day of Snehapana
in 32% (8) patients, in 4th
day of Snehapana in 40% (10) patients. 16% (4) patients
took 5 days to show Samyak Snigdha Lakshana, while 8% (2) patients took 6 days to
show the same. 4% (1) patient took 7 days to attain Samyak Snigdha Lakshana. It is
shown below in Table No. 50 and Fig. no. 31.
Table No. 50 Showing no. of days to attain Samyak Snigdha Lakshana
Days to Attain Samyak Snigdha Lakshana No. of Patients Percentage
3 days 8 32
4 days 10 40
5 days 4 16
6 days 2 8
7 days 1 4
Total 25 100
0102030405060708090
100
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 95
Fig. No. 31 Showing No. of Days to Attain Samyak Snigdha Lakshana
4. Total number of Samyak Snigdha Lakshana observed on the last day of
Snehapana:
Regarding the Samyak Snigdha Lakshana that were exixibited by/in the patients on
the last day of Snehapana, the observation was as described ahead. Vatanulomana was
present in 84% (21) patients; Agnideepti was felt by 88% (22) patients. Snigdha
Varcha was seen in all the 25 patients. Asamhat Varcha was seen in 96% (24)
patients, while Snehodvega was felt by 92% (23) patients. Gatramardavata was seen
in 92% (23) patients, while Twok Snigdhata was seen in 88% (22) patients. The same
is depicted in Table No. 50 and Fig. No. 31:
Table No. 51 Samyak Snigdha Lakshana observed on last day of Snehapana
Samyak Snigdha Lakshana No. of Patients Percentage
Vatanulomana 21 84
Agnideepti 22 88
Snigdha Varcha 25 100
Asamhat Varcha 24 96
Snehodvega 23 92
Gatramardavata 23 92
Twok Snigdhata 22 88
0
5
10
15
20
25
30
35
40
3 days 4 days 5 days 6 days 7 days
No. of Patients
Percentage
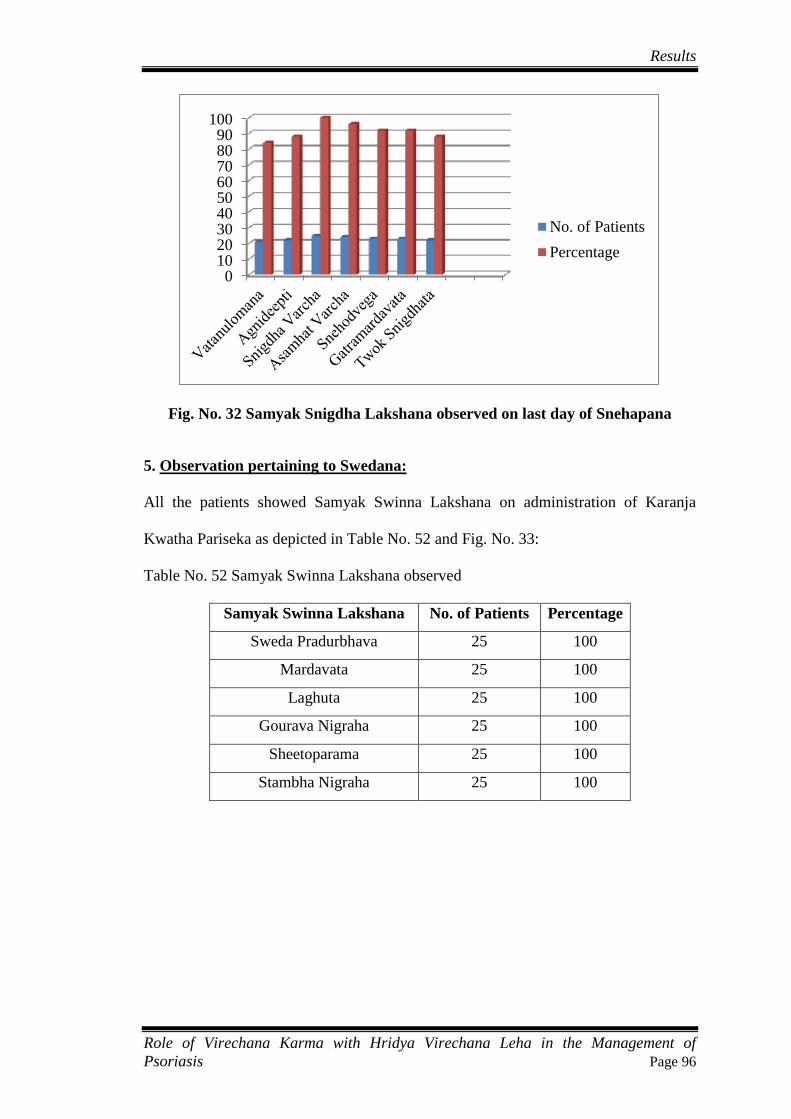
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 96
Fig. No. 32 Samyak Snigdha Lakshana observed on last day of Snehapana
5. Observation pertaining to Swedana:
All the patients showed Samyak Swinna Lakshana on administration of Karanja
Kwatha Pariseka as depicted in Table No. 52 and Fig. No. 33:
Table No. 52 Samyak Swinna Lakshana observed
Samyak Swinna Lakshana No. of Patients Percentage
Sweda Pradurbhava 25 100
Mardavata 25 100
Laghuta 25 100
Gourava Nigraha 25 100
Sheetoparama 25 100
Stambha Nigraha 25 100
0102030405060708090
100
No. of Patients
Percentage
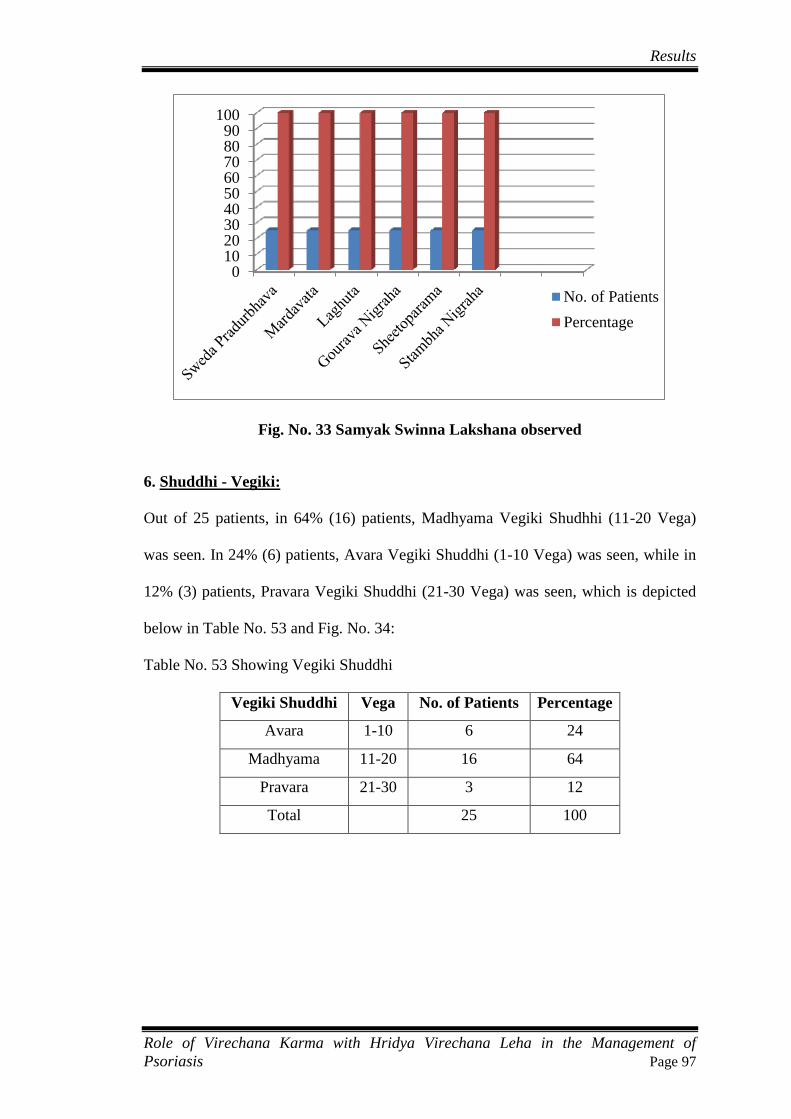
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 97
Fig. No. 33 Samyak Swinna Lakshana observed
6. Shuddhi - Vegiki:
Out of 25 patients, in 64% (16) patients, Madhyama Vegiki Shudhhi (11-20 Vega)
was seen. In 24% (6) patients, Avara Vegiki Shuddhi (1-10 Vega) was seen, while in
12% (3) patients, Pravara Vegiki Shuddhi (21-30 Vega) was seen, which is depicted
below in Table No. 53 and Fig. No. 34:
Table No. 53 Showing Vegiki Shuddhi
Vegiki Shuddhi Vega No. of Patients Percentage
Avara 1-10 6 24
Madhyama 11-20 16 64
Pravara 21-30 3 12
Total
25 100
0102030405060708090
100
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 98
Fig. No. 34 Showing Vegiki Shuddhi
7. Laingiki Shuddhi:
Out of 25 patients, among Laingiki Shuddhi, Srotovishuddhi was seen in 84% (21)
patients, Indriyaprasada in 96% (24) patients. In 92% (23) patients, Laghuta and
Agnivriddhi each were seen. In 88% (22) patients, Anamaytva was seen, while in
84% (21) patients, Vatanulomana and Vitpittakapaha Kramataha Nissarana each were
seen. In 12% (3) patients, Ayogabhava of Virechana Karma was seen. The same is
depicted in Table No. 54 and Fig. No 35.
Table No 54 Laingiki Shuddhi
Laingiki Shuddhi No. of Patients Percentage
Srotovishuddhi 21 84
Indriyaprasada 24 96
Laghuta 23 92
Agnivriddhi 23 92
Anamayatva 22 88
Vatanulomana 21 84
Vitpittakapha Kramataha Nissarana 21 84
Ayogabhava 3 12
0
10
20
30
40
50
60
70
1-10 11-20 21-30
Avara Madhyama Pravara
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 99
Fig. No. 35 Laingiki Shuddhi
8. Antiki:
In the present study, out of 25 patients, 84% (21) had had Kaphanta at the end of
Virechana, while 12% (3) had had Pittanta, and 4% (1) patient had had Malanta. It is
shown in Table No. 55 and Fig. No. 36:
Table No. 55 Antiki Shuddhi
Antiki No. of Patients Percentage
Kaphanta 21 84
Pittanta 3 12
Malanta 1 4
Total 25 100
Fig. No. 36 Antiki Shuddhi
0
20
40
60
80
100
No. of Patients
Percentage
0
10
20
30
40
50
60
70
80
90
Kaphanta Pittanta Malanta
No. of Patients
Percentage

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 100
9. Maniki Shuddhi:
In the present study, out of 25 patients, in 72% (18) of patients, the output was
between 1000ml-2000ml, while in 20% (5) patients, the output was below 1000ml,
and in 8% (2) patients, it was between 2000ml-3000ml. it is depicted in Table No. 56
and Fig. No. 37.
Table No. 56 Showing Maniki Shuddhi
Maniki Shuddhi No. of Patients Percentage
0-1000 ml 5 20
1000-2000 ml 18 72
2000-3000 ml 2 8
Total 25 100
Fig. No. 37 Showing Maniki Shuddhi
10. Samyak-Asamyak Yoga:
In the present study, out of 25 patients, 88% (22) patients exhibited Samyak Yoga
features, while 12% (3) patients exhibited Ayoga features. The details are given in
Table No. 57 and Fig. No. 38:
0
10
20
30
40
50
60
70
80
0-1000 ml 1000-2000 ml 2000-3000 ml
No. of Patients
Percentage
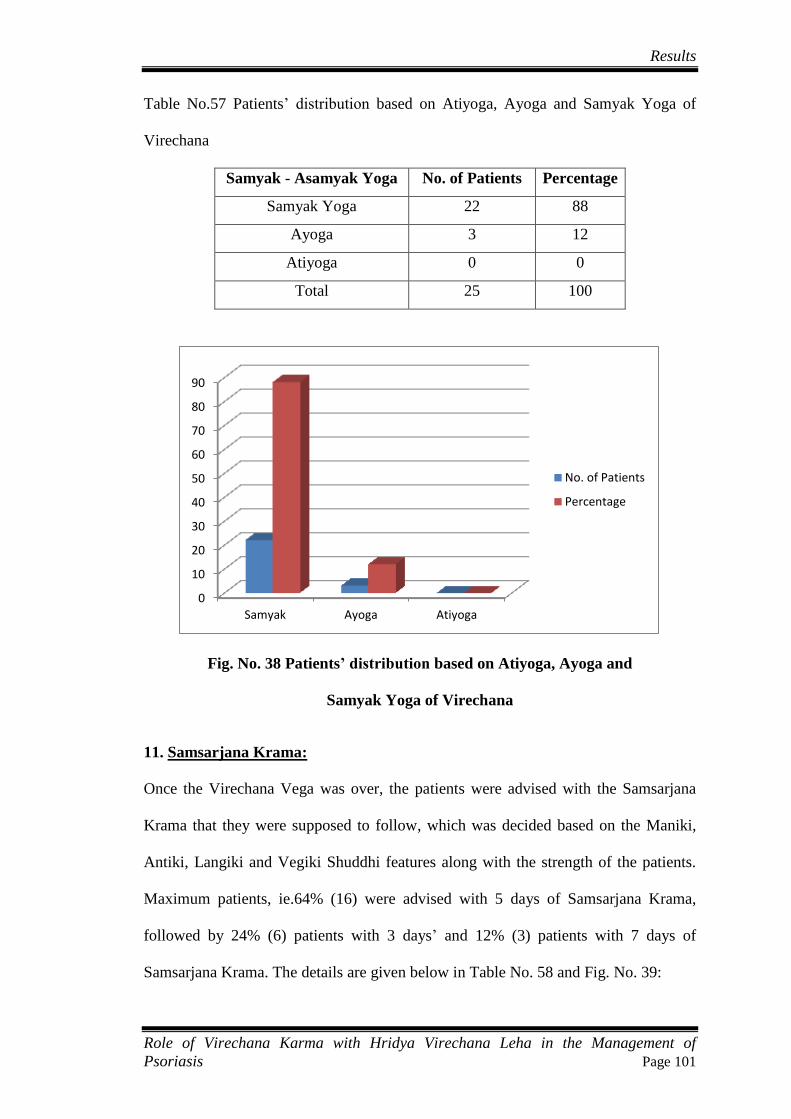
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 101
Table No.57 Patients’ distribution based on Atiyoga, Ayoga and Samyak Yoga of
Virechana
Samyak - Asamyak Yoga No. of Patients Percentage
Samyak Yoga 22 88
Ayoga 3 12
Atiyoga 0 0
Total 25 100
Fig. No. 38 Patients’ distribution based on Atiyoga, Ayoga and
Samyak Yoga of Virechana
11. Samsarjana Krama:
Once the Virechana Vega was over, the patients were advised with the Samsarjana
Krama that they were supposed to follow, which was decided based on the Maniki,
Antiki, Langiki and Vegiki Shuddhi features along with the strength of the patients.
Maximum patients, ie.64% (16) were advised with 5 days of Samsarjana Krama,
followed by 24% (6) patients with 3 days’ and 12% (3) patients with 7 days of
Samsarjana Krama. The details are given below in Table No. 58 and Fig. No. 39:
0
10
20
30
40
50
60
70
80
90
Samyak Ayoga Atiyoga
No. of Patients
Percentage
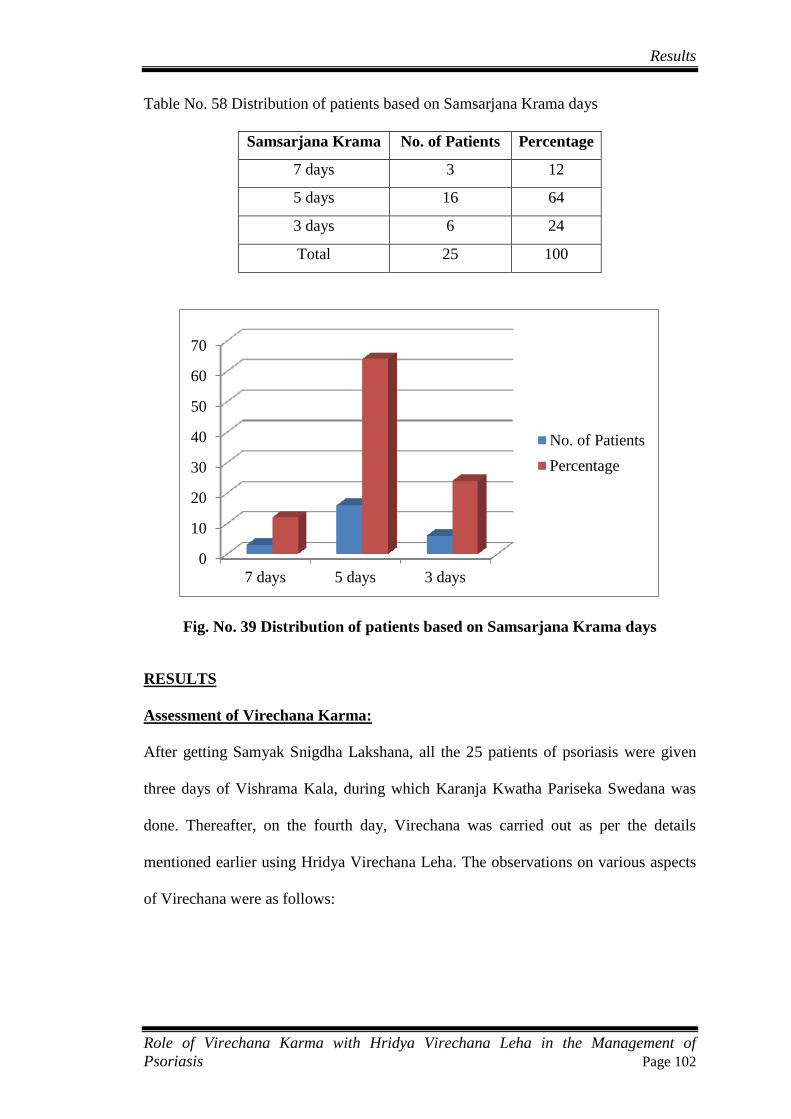
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 102
Table No. 58 Distribution of patients based on Samsarjana Krama days
Samsarjana Krama No. of Patients Percentage
7 days 3 12
5 days 16 64
3 days 6 24
Total 25 100
Fig. No. 39 Distribution of patients based on Samsarjana Krama days
RESULTS
Assessment of Virechana Karma:
After getting Samyak Snigdha Lakshana, all the 25 patients of psoriasis were given
three days of Vishrama Kala, during which Karanja Kwatha Pariseka Swedana was
done. Thereafter, on the fourth day, Virechana was carried out as per the details
mentioned earlier using Hridya Virechana Leha. The observations on various aspects
of Virechana were as follows:
0
10
20
30
40
50
60
70
7 days 5 days 3 days
No. of Patients
Percentage
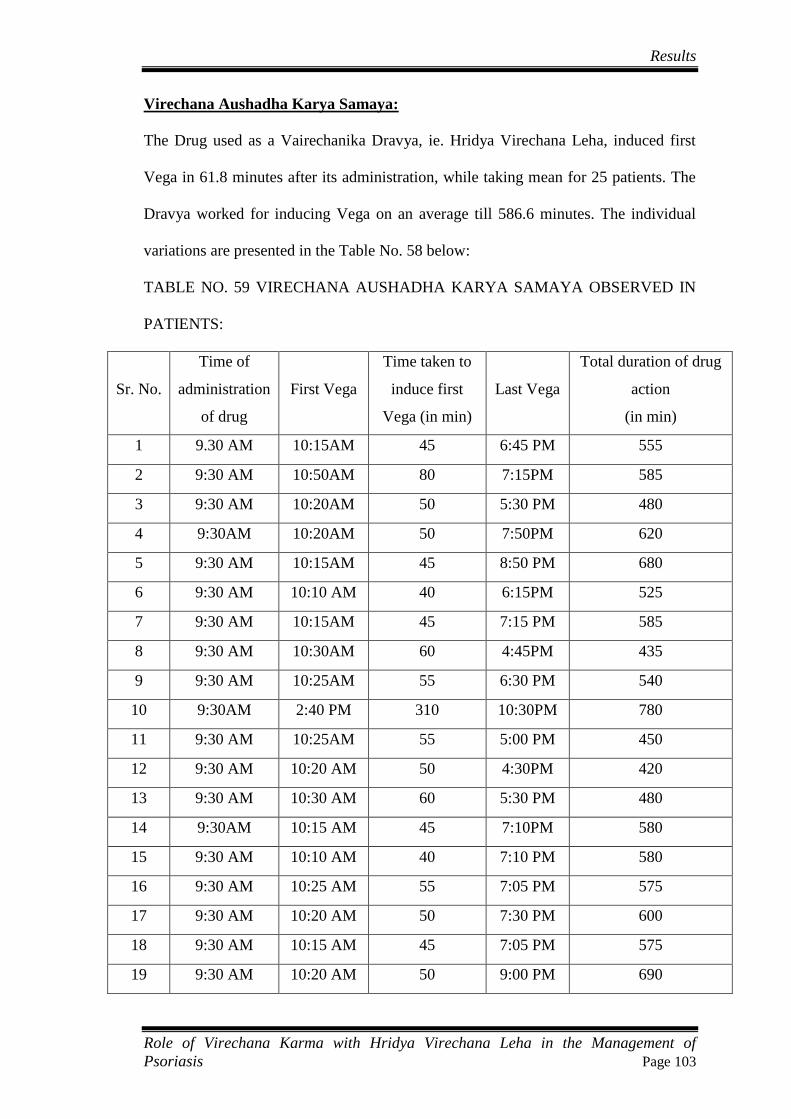
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 103
Virechana Aushadha Karya Samaya:
The Drug used as a Vairechanika Dravya, ie. Hridya Virechana Leha, induced first
Vega in 61.8 minutes after its administration, while taking mean for 25 patients. The
Dravya worked for inducing Vega on an average till 586.6 minutes. The individual
variations are presented in the Table No. 58 below:
TABLE NO. 59 VIRECHANA AUSHADHA KARYA SAMAYA OBSERVED IN
PATIENTS:
Sr. No.
Time of
administration
of drug
First Vega
Time taken to
induce first
Vega (in min)
Last Vega
Total duration of drug
action
(in min)
1 9.30 AM 10:15AM 45 6:45 PM 555
2 9:30 AM 10:50AM 80 7:15PM 585
3 9:30 AM 10:20AM 50 5:30 PM 480
4 9:30AM 10:20AM 50 7:50PM 620
5 9:30 AM 10:15AM 45 8:50 PM 680
6 9:30 AM 10:10 AM 40 6:15PM 525
7 9:30 AM 10:15AM 45 7:15 PM 585
8 9:30 AM 10:30AM 60 4:45PM 435
9 9:30 AM 10:25AM 55 6:30 PM 540
10 9:30AM 2:40 PM 310 10:30PM 780
11 9:30 AM 10:25AM 55 5:00 PM 450
12 9:30 AM 10:20 AM 50 4:30PM 420
13 9:30 AM 10:30 AM 60 5:30 PM 480
14 9:30AM 10:15 AM 45 7:10PM 580
15 9:30 AM 10:10 AM 40 7:10 PM 580
16 9:30 AM 10:25 AM 55 7:05 PM 575
17 9:30 AM 10:20 AM 50 7:30 PM 600
18 9:30 AM 10:15 AM 45 7:05 PM 575
19 9:30 AM 10:20 AM 50 9:00 PM 690
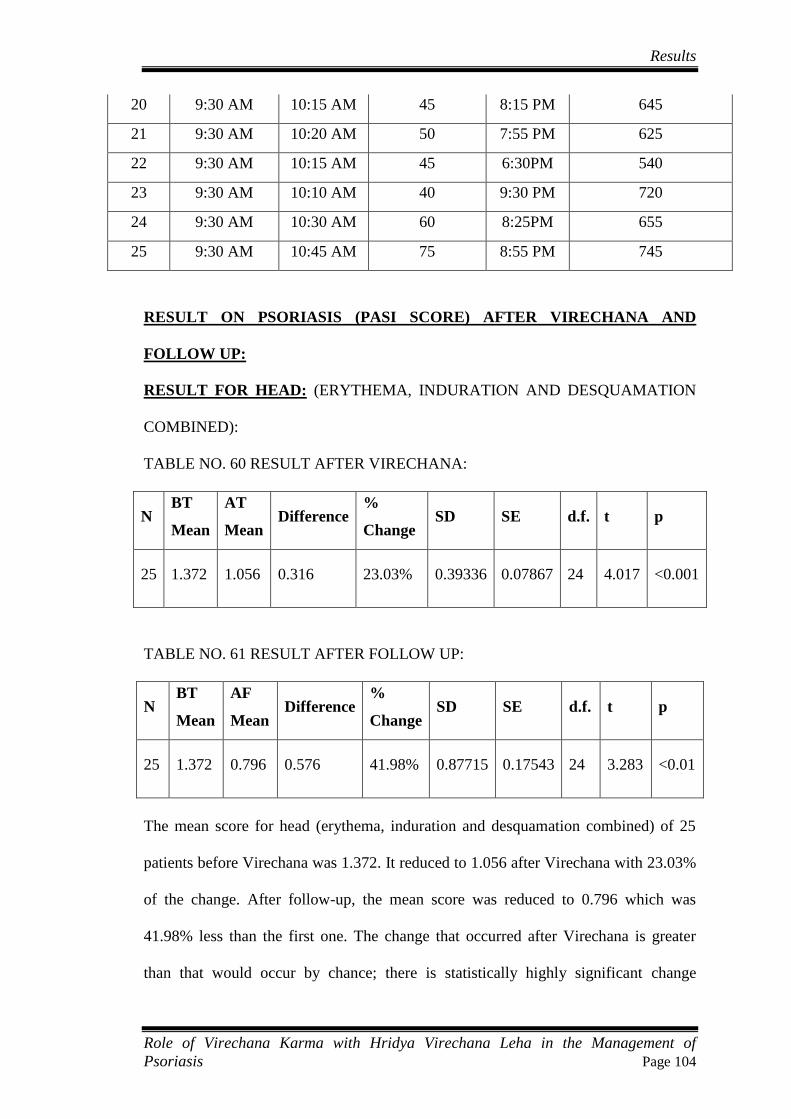
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 104
20 9:30 AM 10:15 AM 45 8:15 PM 645
21 9:30 AM 10:20 AM 50 7:55 PM 625
22 9:30 AM 10:15 AM 45 6:30PM 540
23 9:30 AM 10:10 AM 40 9:30 PM 720
24 9:30 AM 10:30 AM 60 8:25PM 655
25 9:30 AM 10:45 AM 75 8:55 PM 745
RESULT ON PSORIASIS (PASI SCORE) AFTER VIRECHANA AND
FOLLOW UP:
RESULT FOR HEAD: (ERYTHEMA, INDURATION AND DESQUAMATION
COMBINED):
TABLE NO. 60 RESULT AFTER VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 1.372 1.056 0.316 23.03% 0.39336 0.07867 24 4.017 <0.001
TABLE NO. 61 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 1.372 0.796 0.576 41.98% 0.87715 0.17543 24 3.283 <0.01
The mean score for head (erythema, induration and desquamation combined) of 25
patients before Virechana was 1.372. It reduced to 1.056 after Virechana with 23.03%
of the change. After follow-up, the mean score was reduced to 0.796 which was
41.98% less than the first one. The change that occurred after Virechana is greater
than that would occur by chance; there is statistically highly significant change
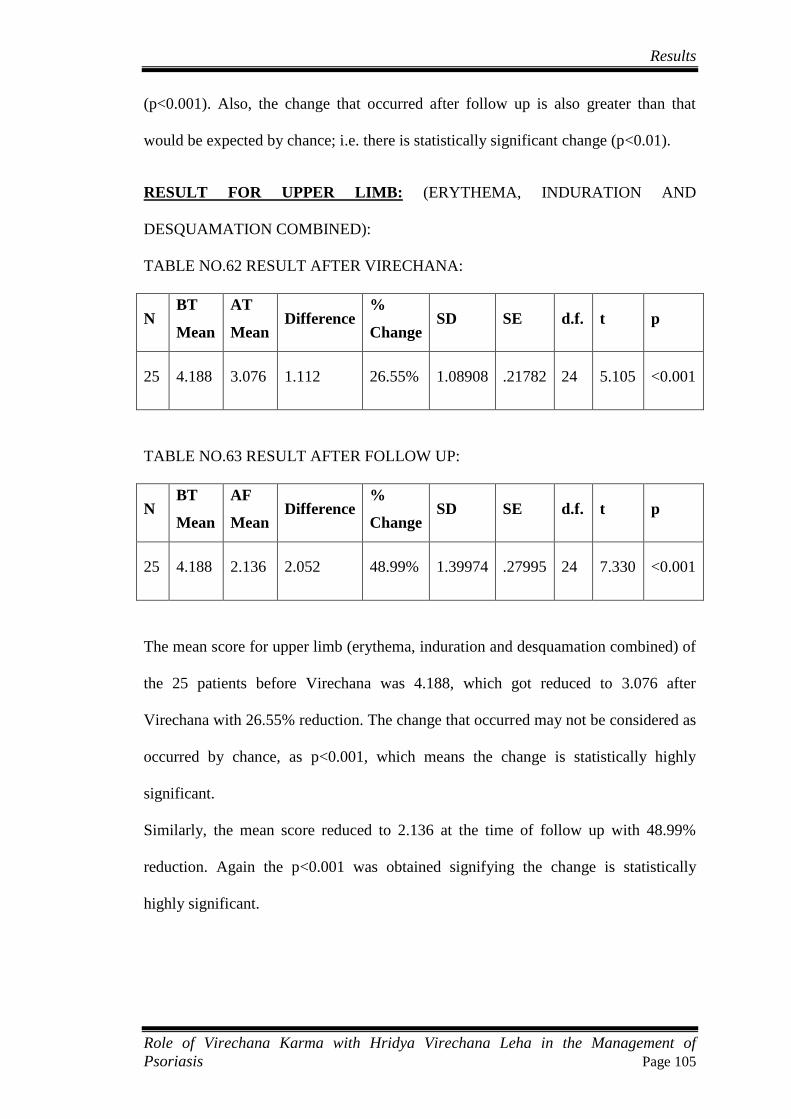
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 105
(p<0.001). Also, the change that occurred after follow up is also greater than that
would be expected by chance; i.e. there is statistically significant change (p<0.01).
RESULT FOR UPPER LIMB: (ERYTHEMA, INDURATION AND
DESQUAMATION COMBINED):
TABLE NO.62 RESULT AFTER VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 4.188 3.076 1.112 26.55% 1.08908 .21782 24 5.105 <0.001
TABLE NO.63 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 4.188 2.136 2.052 48.99% 1.39974 .27995 24 7.330 <0.001
The mean score for upper limb (erythema, induration and desquamation combined) of
the 25 patients before Virechana was 4.188, which got reduced to 3.076 after
Virechana with 26.55% reduction. The change that occurred may not be considered as
occurred by chance, as p<0.001, which means the change is statistically highly
significant.
Similarly, the mean score reduced to 2.136 at the time of follow up with 48.99%
reduction. Again the p<0.001 was obtained signifying the change is statistically
highly significant.

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 106
RESULT FOR TRUNK: (ERYTHEMA, INDURATION AND DESQUAMATION
COMBINED):
TABLE NO. 64 RESULT AFTER VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 4.964 3.792 1.172 23.61% 1.15525 .23105 24 5.073 <0.001
TABLE NO.65 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 4.964 2.644 2.32 46.74% 1.28517 .25703 24 9.026 <0.001
The mean score for trunk (erythema, induration and desquamation combined) of 25
patients before Virechana was 4.964. It reduced to 3.076 after Virechana with 23.61%
of the change. After follow-up, the mean score was reduced to 2.644 which was
46.74% less than the before treatment value. The change that occurred after Virechana
is greater than that would occur by chance; there is statistically highly significant
change (p<0.001). Also, the change that occurred after follow up is also greater than
that would be expected by chance; ie. there is statistically highly significant change
(p<0.001).

Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 107
RESULT FOR LOWER LIMB: (ERYTHEMA, INDURATION AND
DESQUAMATION COMBINED):
TABLE NO. 66 RESULT AFTER VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 7.776 6.176 1.6 20.58% 2.02649 .40530 24 3.948 <0.001
TABLE NO. 67 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 7.776 3.904 3.872 49.79% 2.43508 .48702 24 7.950 <0.001
The mean score for lower limb (with erythema, induration and desquamation
combined) of the 25 patients was 7.776 before Virechana. It reduced to 6.176 after
Virechana which was 20.58% reduction. Again after follow up, the mean score was
reduced to 3.904, which was 49.79% reduction. Here, the change that occurred both
the times were not merely co-incidental as the value of p<0.001 both the times,
signifying that the changes that occurred were statistically highly significant.
EFFECT ON TOTAL PASI SCORE:
TABLE NO.68 RESULT AFTER VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 18.364 14.208 4.156 22.63% 2.45103 .49021 24 8.478 <0.001
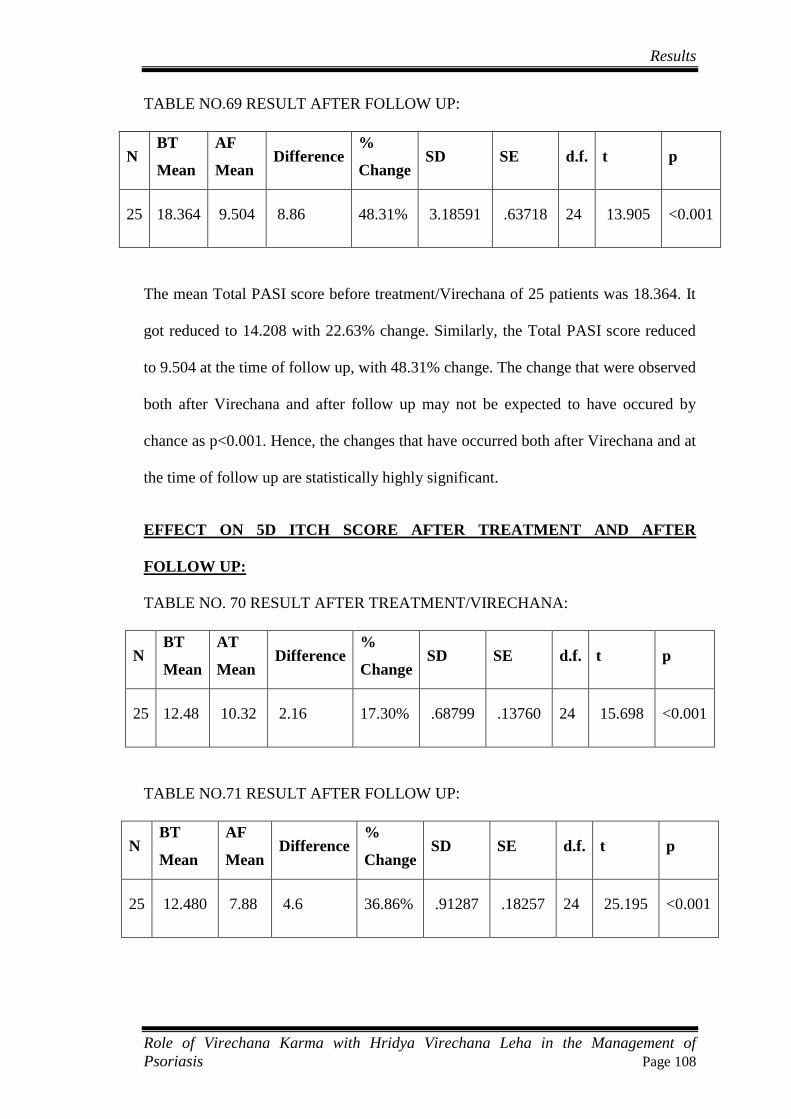
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 108
TABLE NO.69 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 18.364 9.504 8.86 48.31% 3.18591 .63718 24 13.905 <0.001
The mean Total PASI score before treatment/Virechana of 25 patients was 18.364. It
got reduced to 14.208 with 22.63% change. Similarly, the Total PASI score reduced
to 9.504 at the time of follow up, with 48.31% change. The change that were observed
both after Virechana and after follow up may not be expected to have occured by
chance as p<0.001. Hence, the changes that have occurred both after Virechana and at
the time of follow up are statistically highly significant.
EFFECT ON 5D ITCH SCORE AFTER TREATMENT AND AFTER
FOLLOW UP:
TABLE NO. 70 RESULT AFTER TREATMENT/VIRECHANA:
N BT
Mean
AT
Mean Difference
%
Change SD SE d.f. t p
25 12.48 10.32 2.16 17.30% .68799 .13760 24 15.698 <0.001
TABLE NO.71 RESULT AFTER FOLLOW UP:
N BT
Mean
AF
Mean Difference
%
Change SD SE d.f. t p
25 12.480 7.88 4.6 36.86% .91287 .18257 24 25.195 <0.001
Results
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 109
Regarding 5D Itch Score, the mean score of 25 patients was 12.48, which was
reduced to 10.32 after Virechana. It was 17.30% change. Similarly, the mean Score of
5D Itch was found to be 7.88 at the time of follow up with 36.86% change. The t
value was calculated as 15.698 and 25.195 respectively for after Virechana and after
follow up, so the p value was found to be p<0.001 which signifies the change that
occurred after Virechaa and after follow up are both statistically highly significant.
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 110
DISCUSSION
Virechana is the procedure in which orally administered drug acts on internally
vitiated Dosha (especially Pitta), and expels them through the Guda Marga. Virechana
is considered as Shrestha procedure for Pitta Harana. Also it is indicated in Kapha
Samsrishta condition. Similarly, it is also advocated in Vatasyopakrama. Hence, it
can be inferred that Virechana can help correct all three morbid Doshas.
Psoriasis is a non-infectious, chronic inflammatory disease of the skin, characterized
by well-defined erythematous plaques with silvery scale, with a predilection for the
extensor surfaces and scalp, and a chronic fluctuating course. It is one of the most
common dermatologic diseases, affecting up to 2.5% of the world‟s population.
Studies have shown that major fractions of people with psoriasis consider their
disease to be a large problem in their everyday life. It is found that the disease affects
the quality of life, which again varies depending upon different factors.
Kushtha is a term in Ayurveda with much broad spectrum, and under which much of
the skin diseases can be put. Kushtha is basically a Tridoshaja Vyadhi as has been
said “Kushthanam Saptadravyako Sangrahah”. Samsodhana has been highlighted in
the management of Kushtha. Virechana has been quoted to perform as a
Samshodhana in Kushtha Chapter. As Kushtha is a Tridoshaja Vyadhi, with
involvement of Rakta Dhatu as well, Virechana on the other hand, is a measure that
may have its effect on all the three Doshas, along with its action in Raktaja Dhatu,
Virechana may act as one of the suitable treatment protocol in Kushtha disease.
In the present study, Virechana was performed in the patients of Psoriasis; psoriasis
being a condition that may be correlated with Ekakushtha, Mandala or Kitibha
according to different presentations. Prior to Virechana Karma, Deepana Pachana and
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 111
Snehapana were carried out as expected. Shunthi Qwatha was selected as Deepana-
Pachana Drug, which was given to enhance the Agni and also to digest Ama if any.
Moorchhita Tila Taila was used as Snehana Dravya for Snehapana. It was
administered in Arohana Matra depending upon the changes seen in patient until
Samyak Snigdha Lakshana were acheieved. Virechana was administerd with Hridya
Virechana Leha, which contains Trivrit as a main ingredient and Trivrit is considered
as one of best Sukha Virechana Dravya as well as Virechana Dravya. The individual
dose was fixed depending upon the Agni, Koshtha, Roga Bala, Rogi Bala etc. of the
individual.
Significant findings of the research work are discussed below with the following
headings:
Age:
In this study, maximum number of patients, i.e. 36% belonged to age group 51-60,
followed by 28% to age group 31-40 years, 24% to age group 41-50 years, 8% to age
group 21-30 years and 4 % to age group 61-70 years. The age wise distribution shows
the disease was found more in middle aged people and adults; the possible reason that
may be seen here is this age group is involved in some sort of income generating
works and it causes them to undergo mental stress, bear environmental extremities
like outdoor cold and heat, lack of rest, improper food, untimely food, familial
responsibilities etc.
Sex:
In this present study, out of 25 patients, 88 % (22) were male and 12% (3) were
female. Though in some studies, incidence and prevalence rate is shown to be slightly
more in males than in females, but most of the literatures do not accept any gender
variation as such. In one study published in 2010, with title „Psoriasis in India:
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 112
Prevalence and Pattern ‟, the researchers concluded that in their study psoriasis was
found to be twice more common in males than in females.139
But the question may
arise how much credibility may be given to the study. In this study, it may be co-
incidental, or some causes such as financial, social, familial aspects may have played
a role.
Religion:
In this study, out of 25 patients, 92% (23) were Hindu, while 8% (2) were Christians.
As this could be a result of demographical factors, no specific relation can be
established from this observation.
Education:
In the present study, 52% were graduates, 28% had completed high school, 12% were
post graduates, and 8% were literate. From the educational status, it may be difficult
to draw any direct relationship or conclusion but if there does exist any indirect or
slight relationship, it is beyond the scope of this study because of the small sample
size of this study.
Marital Status:
Out of 25 patients, 92% were married whereas 8% were unmarried. From the scope of
present study, there may not be found any obvious relationship between marriage and
Psoriasis.
Socioeconomic Status:
Out of 25 patients, 52% belonged to middle- class family, while 40% belonged to
lower class family, and 8% belonged to upper class family. Majority of people in
India belong to middle class and the same is seen in the study. No obvious or direct

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 113
relation may be thought of between these two variables, but if there does exist any, it
is difficult to say anything due to the small sample size of the present study.
Occupation:
Maximum numbers of patients were professionals, i.e. 44% (11) while 20% (5) were
businessmen. Generally, people of these professional background do have a lot of
mental stress, with hectic work schedule, as well majority of them are exposed to air
conditioner for much more time, contributing to increased incidence of Psoriasis.
Similarly, 24% (6) were manual labourers, and they too have to get themselves
undergo heavy physical works under extreme weather conditions as well which may
again contribute to the disease. Similarly, 8% (2) were housewives, 4% (1) was
student.
Desha:
In the study, 56% (14) of the patients belonged to Shadharana Desha, while 36% (9)
patients belonged to Anoopa Desha, and 8% (2) patients belonged to Jangala Desha.
Desha may have some role to play as in Anoopa Desha excessive Kledata is found,
while in Sadharana Desha in cold season, excessive cold is found which may
correlated with the above observation.
Age of onset:
There were 24% (6) patients each for 21-30, 31-50, and 41-50 years age group as
onset age group. Similarly, there were 20% (5) patients for 11-20 years. And there
were 8% (2) for 51-60. So this observation roughly matches with the idea that
psoriasis may start at any age but is unusual before age of 5, and also goes along the
idea that two epidemiological pattern may be found for psorisis i.e. early onset
(teenage or early adult years) and late onset (fifties or sixties).
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 114
Chronicity of Disease:
Out of 25 patients, 60% (15) patients had had history of psoriasis since last 10 years
or below, 24% (6) had had history of 11-20 years, and 8% (2) had had for each 21-30
years and 41-50 years. It shows the chronicity of the disease along with fluctuating
nature.
Aggravating factors:
48% (12) found cold weather or climate as the most sensitive aggravating factor, 24%
(6) found mental stress, 12% (3) found pollution or dust, and 8% (2) found each non-
vegetarian food and exposure to sunlight as most sensitive aggravating factor. This
observation shows cold as the important aggravating factor, which actually dries up
the skin and causes flare up of the disease.
Relieving Factors:
52% (13) patients opined summer/warm weather as relieving factor, 12% (3)
Samanaga Aushadhi, 8% (2) each stress free environment and Shodhana as relieving
factor. 20% (5) said they did not realize any such factor.
Family history:
92% (23) patients had had negative family history, while 8% (2) had had positive
family history. In medical literature it is said that Psoriasis has got genetic
predisposition, which is seen in this study as well but the figure may not have
matched due to small sample size of this study.
Diet:
Vegetarian/ Mixed food habit:
In the study, 52% (13) patients had had mixed food habit while 48% (12) were
vegetarians. The patients with mixed food habit generally consumed fish, chicken and

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 115
mutton. This data may indicate psoriasis is more common in non-vegetarians than in
vegetarians.
Addictions:
20 % (5) patients had had habit of consuming alcohol, while 8% (2) patients used to
smoke. And 72% (18) patients had had no addictions as such. Various addictions may
act as a Hetu for Kushtha due to Dosha Kopana but from this datal, no conclusion
may be drawn as sample size is small.
Joints Involvement:
60% (15) patients had had joint involvement in the form of pain in various joints,
while 40% (10) did not have any joint involvement. As the disease psoriasis
progresses, in considerable fraction of patients, joints involvement is found especially
form of joint/s pain, joint/s deformity. The same has been seen here that more than
half of the patients had had joints pain; it may be noteworthy that most of the patients
enrolled in this study had had quite long time history of the disease.
Nail changes:
Out of 25 patients, 68% (17) had had the changes in nail in the form of pitting/
onchylosis/ ridging, while 32% (8) did not have any nail changes. As the disease
psoriasis progresses, the changes in nail is also a feature, which is seen in this study.
Type of Psoriasis:
Out of 25 patients, 72% (18) had had chronic plaque type of psoriasis, 20% (5) had
had scalp psoriasis, and 8% (2) had had guttae psoriasis. It can be found in agreement
that chronic plaque type of psoriasis is the most common variety of psoriasis in the
world followed by others.
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 116
Auspitz Sign:
Out of 25 patients, 96% (24) had had positive Auspitz Sign, while 4% (1) had had
negative Auspitz Sign. Auspitz Sign is a classical finding in psoriasis but Auspitz
Sign may not be absolutely sensitive and specific to psoriasis. Here, most of the
patients had had positive Auspitz Sign.
Candle Grease Sign:
Out of 25patients, in 88% (22) patients, Candle Grease Sign was found to be positive,
while in 12% (3) patients, it was negative. It is a diagnostic sign of psoriasis but it is
not mandatory that all psoriasis patients have positive Candle Grease Sign.
Prakriti:
Among the 25 patients, maximum number of patients, i.e.36% (9) possessed Vata
Pitta Prakriti, followed by Pitta Kapha Prakriti by 28% (7) patients, Vata Kapha by
20% (5) patients, Kapha by 12% (3) patients and Pitta by 4% (1) patient.
Sara:
Study showed the maximum number of patients, i.e. 44% (11) were of Mamsa Sara,
followed by 28% (7) patients of Rakta Sara, 16% (4) patients of Asthi Sara and 12%
(3) patients of Meda Sara.
Samhanana:
Out of 25 patients in the study, 92% (23) patients possessed Madhyama Samhanana,
while Susamhana and Hina Samhanana each were possessed by 4% (1) patient.
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 117
Satmya:
Out of 25 patients in the study, Madhyama Rasa Satmya was possessed by 72% (18)
patients, Sarva Rasa Satmya by 16% (4) patients and Ekarasa Satmya by 12% (3)
patients.
Satva:
68% (17) patients were of Madhyama Satva, while 24% (6) of Pravara Satva and 8%
(2) of Avara Satva. Satva may have role in planning treatment, at least in terms of
preparing patient for the treatment.
Ahara Shakti:
Ahara Shakti is assessed by Abhyavaharana Shakti and Jarana Shakti. In the present
study, out of 25 patients, 68% (17) had had Madhyama Abhyavaharana Shakti, while
20% (5) had had Pravara, and 12% (3) had had Avara Abhyavaharana Shakti.
Similarly, regarding Jarana Shakti, 60% (15) patients had had Madhyama Jarana
Shakti, while 24% (6) had had Pravara, and 16% (4) had had Avara Jarana Shakti.
Vyayama Shakti:
In the study, out of 25 patients, 60 % (15) had had madhyama Vyama Shakti, while
16% (4) had had Avara Vyayama Shakti and 8 % (2) had had Pravara Vyayama
Shakti.
Vaya:
All the patients in this study belonged to Madhyama Vaya.
Koshtha:
Maximum number of patients, i.e. 56% (14) patients possessed Madhyama Koshtha,
28% (7) patients Mridu Koshtha while 16% (4) patients possessed Kroora Koshtha.

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 118
Koshtha assessment has crucial role to play especially during Snehapana so as to
make patient attain Samyak Snigdha Avastha.
EFFECT OF THE THERAPY:
Effect of Deepana and Pachana:
Nirama Avastha was achieved by Deepana Pachana with Shunthi Kwatha 20 ml thrice
a day prior to Snehapana. It is Laghu and Ushna and helps in Deepana Pachana.
Observation of Sneha Jiryamana Lakshana:
Out of 25 patients, after Snehapana, Shiroruja was felt by 92% (23) patients,
Lalasrava was experienced by 88% (22) patients, Angasada by 52% (13) patients,
Klama by 36% (9) patients, Trishna by all 100% (25) patients, Daha by 64% (16)
patients, and Arati was felt by 76% (19) patients.
Observation of Sneha Jirna Lakshana:
After Snehapana, various Sneha Jirna Lakshana are felt by patients. Among them,
four Lakshanas, viz. Jiryamana Lakshana Prashamana, Trishna, Kshuda and
Vatanulomana were experienced by all 25 patients, i.e. 100% patients. Similarly,
Udgara Shuddhi was felt by 96% (24) patients, and Sharira Laghava by 76% (19)
patients.
Days required for attainment of Samyak Snigdha Lakshana by patient:
In the present study, 40% (10) patients attained Samyak Snigdha Lakshana in 4th
day
of Snehapana, while 32% (8) patients in 3rd
day, 16% (4) patients in 5th
day, 8% (2) in
6th
day and 4% (1) patient took 7 days to attain the same. This shows the various types
of Koshtha of patients.
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 119
Total number of Samyak Snigdha Lakshana observed on the last day of
Snehapana:
Regarding Samyak Snigdha Lakshana, Vatanulomana was present in 84% (21)
patients; Agnideepti was felt by 88% (22) patients. Snigdha Varcha was seen in all the
25 patients. Asamhat Varcha was seen in 96% (24) patients, Snehodvega in 92% (23)
patients, Gatramardavata in 92% (23) patients and Twok Snigdhata in 88% (22)
patients. Most of the Samyak Snigdha Lakshana were exhibited by most of the
patients.
Observation of Swedana:
The study showed that 100% of the patients attained Samyak Swinna Lakshana on
administration of Karanja Kwatha Pariseka.
Observation pertaining to Virechana Karma:-
Virechana Aushadha Karya Samaya:
The Drug used as a Vairechanika Dravya, ie. Hridya Virechana Leha, induced first
Vega in 61.8 minutes at an average for 25 patients after its administration. The
Dravya worked for inducing Vega till 586.6 minutes on an average. Total time
required for first to last Vega suggests action of Hridya Viechana Leha depending on
Koshtha of the patient and also the quantum of Dosha vitiation. Major ingredient in
Hridya Virechana Leha that induces Virechana is Trivrit.
Vegiki Shuddhi:
Out of 25 patients, 64% (16) patients had had the number of bowels between 11-20,
i.e. in them Madhyama Shuddhi occurred, in 24% (6) patients, the bowel number was
1-10, i.e. Avara Shuddhi occurred and in 12% (3) patients it was between 21-30
indicating Pravara Shuddhi.

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 120
Antiki Shuddhi:
In 84% (21) patients, Virechana ended with Kaphanta, in 12% (3) Virechana ended
with Pittanta, while in 4% (1) patient, it ended in Malanta.
Maniki Shuddhi:
Among 25 patients, 72% (18) patients had had the output between 1000-2000 ml,
while in 20% (5) patients, it was below 1000ml and in 8% (2) patients, it was between
2000-3000ml.
Laingiki Shuddhi:
In the study, 96% (24) patients experienced Indriyaprasada after the Virechana,
Laghuta and Agnivriddhi each were felt by 92 % (23) patients, 88% (22) patients
developed Anamayatva, while Srotovishuddhi, Vatanulomana and Vitpittakapha
Kramataha Nissarana each were experienced by 84% (21) patients, and 12% (3)
patients experienced Ayoga Bhava. Hridya Virechana Leha produced Samyak Virikta
Lakshana in maximum number of patients.
Samyak-Asamyak Yoga:
It was observed in the clinical study that 88% (22) patients had had Samyak Yoga
features of Virechana, while 12% (3) patients had had developed more of Ayoga
features of Virechana.
Samsarjana Krama:
After the completion of Virechana, Samsarjana Krama was advised to the patients and
explained the importance of it and instructed to strictly adhere to it. The Samsarjana
Krama was decided on factors such as Maniki, Antiki, Langiki and Vegiki Shuddhi
features along with the strength of the patients. Maximum patients, ie.64% (16) were
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 121
advised with 5 days of Samsarjana Krama, 24% (6) patients with 3 days‟ and 12% (3)
patients with 7 days of Samsarjana Krama.
RESULTS:
Paired t-test was used for comparing the results and IBM SPSS Statistics was used for
data analysis.
a. PASI:- Erythema, induration and desquamation were taken into account
combined first for head, upper limb, trunk and lower limb separately. Then overall
PASI was calculated for after Virechana and after follow up.
Result for head (Erythema, Induration and Desquamation):
Erythema, induration and desquamation were taken into account combined first for
head, upper limb, trunk and lower limb separately. Then overall PASI was calculated
for after Virechana and after follow up.
For head, the mean of 25 patients was 1.372 before treatment and it reduced to 1.056
after treatment, with 23.03% change. It was reduced to 0.796 after follow up from
1.372 before treatment, with 41.98% change. In first result, i.e. after treatment, the p
value was less than 0.001, indicating the change that occurred was statistically highly
significant, or the result that occurred was highly unlikely that it occurred merely
because of chance. Similarly for after follow up result, the p<0.01 indicating that it is
statistically significant and may not be considered as occurred by chance alone.
Result for upper limb (Erythema, Induration and Desquamation):
The mean before treatment was 4.188 and it got reduced to 3.076 after treatment
which is 25.66% change. Similarly, after follow up the mean was reduced to 2.136,
with 48.99% change.

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 122
In both the incidences, the p<0.001 indicating the changes that have occurred are
statistically highly significant and not because of merely chance.
Result for trunk (Erythema, Induration and Desquamation):
The mean score before treatment was 4.964 which reduced to 3.792 after treatment,
with 23.61% change and t-value being 5.073. Similarly, after follow up the mean was
2.644 with 46.74% change and t-value being 9.026. In both the cases, the p<0.001
signifying the changes that occurred were statistically highly significant.
Result for lower limb (Erythema, Induration and Desquamation):
The mean score before treatment for lower limb was 7.776 and after treatment, it was
6.176, with 20. 58 % change. The mean score after follow up was 3.904 with 49.79%
change from the before treatment value. In both the cases p<0.001 signifying the
changes were statistically highly significant.
Total PASI Score:
The mean PASI score before treatment was 18.364 which got reduced to 14.208 after
treatment, with 22.63% change. Similarly the mean PASI score after follow up was
reduced to 9.504, with 48.31% change. The p value was less than 0.001 in both the
cases, so signifying the changes occurred at both the times were statistically highly
significant.
b. 5 D Itch Score:-
It is a score used to calculate overall aspects of itching. The mean score prior to
treatment was 12.48 which got reduced to 10.32, with 17.30% decrement. The mean 5
D Itch score after follow up was found to be 7.88, which was 12.48 before treatment,
and the change observed here was 36.86%. In both the cases, the p value was less than
Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 123
0.001, which indicates that the change that occurred was statistically highly
significant and may not be considered to have occurred merely due to chance.
Probable Mode of Action of Virechana Drug:
Virechana drugs have properties Ushna, Tikshna, Sukshma, Vyavayi, Vikashee. They
have predominance of Prithvi and Jala Mahabhuta. They have Prabhava Adhobhaga
Doshaharatwa. Virechana Aushadhi by virtue of their Ushna, Tikshna, Sukshma,
Vyavai and Vikashee Guna, and their Swa Virya (Swo Prabhava), reach to Hridaya
and spread through Dhamani to all the macro and micro channels in the body. Here,
Acharya Chakrapani clearfies that it is not the Aushadhi in its physical form itself that
traverses throughout the Dhamani in body, rather it is the Virya of Aushadhi that
spreads to all the Dhamani. Then, Ushan Guna causes liquefaction of Dosha Samuha
in the body; Tikshna Guna causes disintegration (Vichhinnata) of Dosha. Those
disintegrated (Vichhinna) Dosha by virtue of the Anu Pravana Bhava (property to
traverse through microchannels) move smoothly to Amashaya of Sneha Bhavita
patient, without getting adhered in the route, similar to that of moving of honey
smoothly in the properly anointed mud pot. Then being the Virechana Aushadha
Dravya predominant of Prithvi and Apa Mahabhuta and its having Adho Bhagahara
Prabhava, the Dosha that were brought to Amashaya are expelled out through the
Guda Marga by the Aushadha.
Laxatives probably induce limited low-grade inflammation in the small and larger
bowel to promote accumulation of water and electrolytes, and also stimulate intestinal
motility. From the above view, we may assume that Virechana Dravya (Shodhana
Variety) are mild irritant to the stomach and the intestinal mucosa, and cause
inflammation to them. Due to this, the permeability of the membrane changes and
those substances are facilitated to come out, which cannot come out in normal

Discussion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 124
condition. This medically produced mild inflammation initially facilitates quick
absorption of the active principles (Virya) of the drug. Later on, it facilitates the
excretion of morbid matters that are usually not excreted out under normal
circumstances.
Conclusion
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 125
CONCLUSION
Virechana is a procedure in which orally administered drug acts on morbid Doshas,
especially Pitta, and expels them out through the Guda Marga (rectal route).
Psoriasis is a non-infectious, chronic inflammatory disease of the skin, characterized
by well-defined erythematous plaques with silvery scale, with a predilection for the
extensor surfaces and scalp, and having a chronic fluctuating course.
In Ayurveda, almost all the skin diseases have been described under the heading
‘Kushtha’. Psoriasis can be considered as one type of Kushtha and may resemble
Ekakushtha, Kitibha or Mandala Kushtha based upon its presentation.
Kushtha is a Tridoshaja Vyadhi and Virechana is best Shodhana therapy for Pitta
predominant disorders, meanwhile it also exerts its action on Shleshmasamsrishta
Avastha and also corrects the morbid Vata Dosha.
In this clinical study, Hridya Virechana Leha has been administered as Vairechanika
Yoga in the management of psoriasis. Trivrit is the chief component of Hridya
Virechana Leha, and Trivrit is considered as the best Virechana Dravya.
The results were found to be statistically significant. The results dealt with decrement
in the signs and symptoms of psoriasis viz. erythema, thickness, scaling and itching.
Summary
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 126
SUMMARY
The dissertation entitled “ROLE OF VIRECHANA KARMA WITH HRIDYA
VIRECHANA LEHA IN THE MANAGEMENT OF PSORIASIS” consists of 8
Chapters namely Introduction, Objective, Review of Literature, Methodology,
Results, Discussion, Conclusion and Summary.
1. Chapter-1 Introduction: A brief introduction which gives concise idea about the
disease in Ayurvedic perspective as well as contemporary science perspective and
utility of Samshodhana and Virechana in treating psoriasis.
2. Chapter-2 Objectives: Gives idea about aims and objectives of the study.
3. Chapter-3 Review of Literature: Consists of 4 parts:
Part-1 Virechana Karma is described under the following headings:
Etymology of Virechana and its definition, Synonyms, Historical review of
Virechana, Indications and Contraindications of Virechana, Classification of
Virechana drugs, Procedure of Virechana - Poorvakarma, Pradhana Karma
and Paschat Karma, Samyak Yoga of Virechana, Virechana Vyapat, Mode of
action of Virechana.
Part-2 Kushtha is dealt in following headings: Etymology, Definition,
Historical review, Classification, Nidana, Poorvaroopa, Samprapti,
Sadhyasadhyata, Chikitsa, Pathyapathya
Part-3 Psoriasis is described under following headings: Etymology,
Definition, Epidemiology, Etiology, Pathogenesis, Clinical features, Types of
Psoriasis, Complications.
Part-4 Drug Review explains the properties of the drugs used in Deepana-
Pachana, Snehapana, Pariseka, Virechana Karma.

Summary
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 127
4. Chapter-4 Methodology: Deals with the overall aspect of the Clinical Study, i.e.
materials and methods including selection of the patients for the study, study design,
interventions, criteria for assessment of results.
5. Chapter-5 Results: All the Observations regarding Epidemiology, history, clinical
examination, intervention were obtained and analyzed, and graphically presented.
Results of Assessment Criteria scorings obtained were analyzed statistically and
presented.
6. Chapter-6 Discussion: Deals with interpretation of the Review of Literature and
its subheadings, Methodology, results, i.e. change in PASI and 5 D Itch scores. Also
describes the logical interpretation of observation obtained in the clinical study.
7. Chapter-7 Conclusion: Conclusion of the various sections of the work are given
here.
8. Chapter-8 Summary: Summarizes the entire work.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 128
REFERENCES:
1. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-651
2. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL ,Jameson JL ,
Loscalzo, Editors. Harrison’s Principle of Internal Medicine, Volume-1 17th
Edition MC Graw - Hill Medical Publishing division, Pp-1364 Page no-315
3. Apps.who.int/gb/ebwha/B133_5-en.pdf
4. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-216
5. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-132
6. Vagbhatacharya, Ashtanga Sangraha with Vidhyotini Vyakhya. Kaviraj
Aatridev Gupta. Krishnadas academy, 1993 Varanasi, Pp-407, p-197
7. Kashyapa, Kashyapa Samhita, Revised by Vatsya, Hindi commentary and
translation by Satyapala Bhishagacharya, 5th
edition. Varanasi, Chaukamba
Sanskrit Samstana, 1998, Siddisthana, 2nd
chapter. Pp- 364, p- 150
8. Dr. D B Panditrao, Hindi Translation of Sahasrayoga, Chapter 4, Verse 348,
New Delhi, Central Council for Research in Ayurveda and Sidda, 1990, 245
9. Sharangdhara Samhita; Translated into English by Dr. P. Himsagara Chandra
Murthy; Chowkhamba Orientilia , Varanasi ; Edition: 2010 Pp- 454 Pg-34
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 129
10. Devarushi V. Praveen ; “Role of Virechana karma in the management of
Psoriasis- A clinical study” [Department of P.G. Studies in Panchakarma,
S.D.M. College of Ayurveda , Kuthpady, Udupi, RGUHS, Karnataka, 2009 ]
11. M.N. Girija ; “ Role of virechana karma in the management of the psoriasis –
A clinical study” [Department of P.G. Studies in Panchakarma , S.D.M.
College of Ayurveda , Kuthpady, Udupi, RGUHS, Karnataka, 2011]
12. Rao Srinivas ; “To evaluate the efficacy of Virechana with Karvellaka patra
and Abhyadi modaka in Ekakushta w.s.r. Psoriasis – A comparative study”;
[Government Ayurvedic Medical College Bangalore, Karnataka , 2011]
13. Thakur Avantika; “Role of Virechana Karma with Kalyanaka Guda in the
management of Psoriasis”; SDM College of Ayurveda, Udupi, Karnataka,
2016]
14. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-649
15. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-86
16. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-649
17. Vagbhata; Ashanga Samgraha with Sasilekha Commentary Choukambha
Krishnadas academy, Varanasi 2006. Indu, Sutrasthana 27/4
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 130
18. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-180
19. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-688
20. Sushruta, Sushruta Samhita with Nibandha Sangraha Commentary
Choukhamba Sanskrit series 2002.Chikitsa Sthana 33/25-32 page no 518-519
21. Vagbhata; Astanga Hridaya with Sarvaga Sundara Commentary, Krishnadas
academy, Varanasi 1995.Sutrasthana 27/8-9 page no 327
22. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Uttara
Khanda, 4/7-11 page no 313
23. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-21
24. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-22
25. Vagbhata; Ashanga Samgraha with Sasilekha Commentary Choukambha
Krishnadas academy, Varanasi 2006. Indu, Sutrasthana 14/4
26. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series. Varanasi.1994.Sutra Sthana 1/78-80 page no 20
27. Sushruta, Sushruta Samhita with Nibandha Sangraha Commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 39/4 page no 170.

References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 131
28. Vagbhata; Ashanga Samgraha with Sasilekha Commentary Choukambha
Krishnadas academy, Varanasi 2006. Indu, Sutrasthana 14/4
29. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Sutra Sthana 1/82-87 page no 21.
30. Sushruta, Sushruta Samhita with Nibandha Sangraha Commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 39/4 page no 170.
31. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Sutra Sthana 1/115-116 page no
22.
32. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 39/4 page no 170.
33. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Sutra Sthana 1/117-118
page no 22.
34. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 39/4 page no 170
35. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Kalpa Sthana 12/56 page no 673.
36. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Uttara
Khanda, 4/13 page no 313
37. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Kalpa Sthana 12/56 page no 673.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 132
38. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Uttara
Khanda, 4/14 page no 314
39. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994.Kalpa Sthana 12/51-53 page no
672-673
40. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Uttara
Khanda, 4/14 page no 314
41. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Purva
Khanda, 4/3 page no 35
42. Sushruta, Sushruta Samhita with Nibandha Sangraha Commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 46/329 page no 237
43. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Purva
Khanda, 4/4 page no 35
44. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Purva
Khanda, 4/5 page no 35
45. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Purva
Khanda, 4/6 page no 36

References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 133
46. Sharangadhara, Sharangadhara Samhita with Commentaries Adhamallas
Dipika and Kasiramas Gudhartha Dipika, Published by, Varanasi. Purva
Khanda, 4/6 page no 36
47. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 44/90-91page
48. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002.Sutra Sthana 44/3 page no188
49. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002. Sutra chikitsa 33/20 page no 518
50. Agnivesa, Charaka Samhita with Ayurveda Dipika Commentary,
Choukhamba Sanskrit series .Varanasi.1994. Sutra Sthana 15/17 page no 95
51. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002.Chikitsa Sthana 33/2 page no 519
52. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002. Chikitsa Sthana 33/24 page no 520
53. Sushruta, Sushruta Samhita with Nibandha Sangraha commentary
Choukhamba Sanskrit series 2002. Chikitsa Sthana 33/23 page no 519
54. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-680
55. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-680
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 134
56. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-70
57. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-227.
58. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No 216.
59. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No.513,458,616,600.
60. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika samskruta tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba samskruta samsthana, Varanasi, edition:
Reprint 2010, Pp:824, Page no.82,167
61. Vagbhatacharya, Astanga Hrudaya, Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskrita Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp: 956, Page no 244.
62. Sharngadhara, Sharngadhara Samhita, Deepika by Adhamalla, Gudhartha
Deepika by Kashirama,Edited by Pandit Parushurama Shastri, Edition: Printed
1931, Nirnaya Sagara Press, Mumbai, Pp:398, Page No144.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 135
63. Vangasena, Vanga Samhita, Hindi Commentary by Kaviraj Sri Saligramaji
Vaidya, Samshodhan Karta Sri Vaidya Shankarlala Jain Khemaraja; Sri
Krishnadas Prakashana, Varanasi
64. Agnivesha, Charakasamhita, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
, Page No 227
65. Vagbhatacharya, Astanga Hrudaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp:956, Page no143
66. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-451.
67. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrita Tika by
Dalhana, Nyayachandrika Samskrita Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskrita Samsthana, Varanasi, Edition:
Reprint 2010, Pp:824, Page no :230
68. Vagbhatacharya, Astanga Hrudaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp:956, Page no524.
69. Maharshi Kashyapa or Vridhajivaka, Kashyapa Samhita or Vridha Jivaka
Tantra revised by M Narayanan Vaydyar Edakkad, Danwantari Publishers
1995 Pp 656 Page No: 437
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 136
70. Madhava, Madhava Nidana, Edited by Yadavji Trikamji, Edition – 1st 1920,
Nirnaya Sagara Press, Mumbai, Pp:495, Page No: 334.
71. Bhavamishra, Bhavaprakasha Part 2, Edited by and Vidyotini Hindi
commentary by Brahmashankara Mishra, Edition: 1st Edition, 1941,
Choukhamba samskruta series, Varanasi, Pp:755, Page No: 561
72. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-654.
73. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrita Tika by
Dalhana, Nyayachandrika Samskrita Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskrita Samsthana, Varanasi, Edition:
Reprint 2010, Pp:824, Page no 283
74. Vagbhatacharya, Astanga Hrudaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp:956, Page no524
75. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-450.
76. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrita Tika by
Dalhana, Nyayachandrika Samskrita Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskrita Samsthana, Varanasi, Edition:
Reprint 2010, Pp: 824, Page no: 230
77. Vagbhatacharya, Astanga Hrudaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 137
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp:956, Page no524.
78. Vagbhatacharya, Astanga Samgraha, Shashilekha Samskrita Commentry by
Indu, Edited by Dr. Shivaprasada Sharma, Edition: reprint 2010, Choukhamba
Samskrita Samsthana, Varanasi, Pp:964, Page no :408.
79. Madhava, Madhava Nidana, Edited by Yadavji Trikamji, Edition1st
1920,
Nirnaya Sagara Press, Mumbai, Pp:495, Page No: 330.
80. Bhavamishra, Bhavaprakasha Part 2, Edited by and Vidyotini Hindi
Commentary by Brahmashankara Mishra, Edition: 1st Edition, 1941,
Choukhamba Samskrita Series, Varanasi , Pp:755, Page No: 561
81. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-450.
82. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrita Tika by
Dalhana, Nyayachandrika Samskrita Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskrita Samsthana, Varanasi, Edition:
Reprint 2010, Pp: 824, Page no:230
83. Vagbhatacharya, Astanga Hrudaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp: 956, Page no 524.
84. Vagbhatacharya, Astanga Samgraha, Shashilekha Samskrita Commentry by
Indu, Edited by Dr. Shivaprasada Sharma, Edition: reprint 2010, Choukhamba
Samskrita Samsthana, Varanasi, Pp: 964, Page no: 408.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 138
85. Madhava, Madhava Nidana, Edited by Yadavji Trikamji, Edition1st
1920,
Nirnaya Sagara Press, Mumbai, Pp:495, Page No: 330.
86. Bhavamishra, Bhavaprakasha Part 2, Edited by and Vidyotini Hindi
Commentary by Brahmashankara Mishra, Edition: 1st Edition, 1941,
Choukhamba Samskrita Series, Varanasi, Pp: 755, Page No: 561
87. Chakrapanidatta, Caraka Samhitha of Agnivesha with Ayurveda Dipika
Commentary Edited by Acharya Jadavji Trikamji. Edition: reprint, 2013.
Varanasi, U.P.: Chaukhamba Prakashan; Pp-738 Page no-450.
88. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrita Tika by
Dalhana, Nyayachandrika Samskrita Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskrita Samsthana, Varanasi, Edition:
Reprint 2010, Pp: 824, Page no: 230
89. Vagbhatacharya, Astanga Hridaya Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri Samskruta Commentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskrita Samsthana, Varanasi, Pp: 956, Page no 524.
90. Vagbhatacharya, Astanga Samgraha, Shashilekha Samskrita Commentry by
Indu, Edited by Dr. Shivaprasada Sharma, Edition: reprint 2010, Choukhamba
Samskrita Samsthana, Varanasi, Pp: 964, Page no:408.
91. Madhava, Madhava Nidana, Edited by Yadavji Trikamji, Edition1st
1920,
Nirnaya Sagara Press, Mumbai, Pp: 495, Page No 330.
92. Bhavamishra, Bhavaprakasha Part 2, Edited by and Vidyotini Hindi
Commentary by Brahmashankara Mishra, Edition: 1st Edition, 1941,
Choukhamba Samskrita Series, Varanasi, Pp: 755, Page No: 561
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 139
93. Maharshi Sushruta, Sushruta Samhita, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika samskruta tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba samskruta samsthana, Varanasi, edition:
Reprint 2010, Pp:824, Page no. 230
94. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No.235
95. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No177.
96. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No 450.
97. Maharshi Sushruta, “Sushruta Samhita”, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika samskruta tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba samskruta samsthana, Varanasi, edition:
Reprint 2010, Pp:824, Page no :230
98. Vagbhatacharya, “Astanga Hrudaya” Sarvangasundara by Arunadatta and
Ayurveda rasayana by Hemadri SamskrutaCommentry ,edited by Dr Anna
Moreshvara Kunte and Dr Krishna shastry navare, Edition: reprint 2010,
Choukhamba samskruta samsthana, Varanasi, Pp:956, Page no :524.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 140
99. Vagbhatacharya, “Astanga Samgraha” ShashilekhaSamskruta Commentry by
Indu, edited by Dr. Shivaprasada Sharma, Edition: reprint 2010, Choukhamba
samskruta samsthana, Varanasi, Pp:964, Page no :408.
100. Madhava, “Madhava Nidana” edited by Yadavji Trikamji, Edition1st1920,
Nirnaya Sagara Press, Mumbai, Pp:495, Page No: 334.
101. Bhavamishra, “Bhavaprakasha Part 2” Edited by and vidyotini Hindi
commentary by Brahmashankara Mishra, Edition: 1st Edition, 1941,
Choukhamba samskruta series, Varanasi , Pp:755, Page No: 556
102. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No 217.
103. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No 452.
104. Maharshi Sushruta, “Sushruta samhita”, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika samskruta tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba samskruta samsthana, Varanasi, edition:
Reprint 2010, Pp:824, Page no :232
105. Vagbhatacharya, “Astanga Hrudaya” Sarvangasundara by Arunadatta and
Ayurveda rasayana by Hemadri SamskrutaCommentry ,edited by Dr Anna
Moreshvara Kunte and Dr Krishna shastry navare, Edition: reprint 2010,
Choukhamba samskruta samsthana, Varanasi, Pp:956, Page no :527.

References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 141
106. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No 259.
107. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No.176.
108. Maharshi Sushruta, “Sushruta Samhita”, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika samskruta tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba samskruta samsthana, Varanasi, edition:
Reprint 2010, Pp:824, Page no :232,357
109. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp : 738
:Page No.262
110. Vagbhatacharya,”Astanga Samgraha” ShashilekhaSamskruta Commentry by
Indu, edited by Dr. Shivaprasada Sharma, Edition: reprint 2010, Choukhamba
samskruta samsthana, Varanasi, Pp:964, Page no :550.
111. Tony burns, Stephen breathnach, Neil cox, Christopher Griffiths, “Rook’s
Textbook of Dermatology, 8th
edition, 2010, Wilie-Blackwell Publication,
Volume 1, Chapter No 20, Page no 20.
112. Jean L Bolognia, Joseph L Jorizzo,Julie V Schaffer, Jeffrey P Callen,
George J Hruza, James W Patterson, Lorenzo Cerroni, Anthony J Mancini,

References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 142
Martin Röcken, Warren R Heymann, Thomas Schwarz, ”Dermatology”, 3rd
edition 2012, Elsevier Saunders, Pp:2572, Page no:135
113. Dogra S, Yadav S. Psoriasis in India: Prevalence and Pattern. Indian J
Dermatol Venerol Ceprol.2010;76:595-601
114. Klaus wolffs, Lowella A. Goldsmith, Stephen I. Katz, Barbara A. Gilchrest,
Amy S. Paller, David J. Leffel,” Fitzpatrick’s Dermatology in general
medicine”, 7th
edition, 2008, The Mcgraw-Hill Companies, Inc, Volume 1,
Chapter No 18, Pp: 1190, Page no 170.
115. Tony burns, Stephen breathnach, Neil cox, Christopher Griffiths, “Rook’s
Textbook of Dermatology, 8th
edition, 2010, Wilie-Blackwell Publication,
Volume 1, Chapter No 20, Page no 20.1
116. www.mg217.com/your-psoriasis/statistics
117. Jean L Bolognia, Joseph L Jorizzo, Julie V Schaffer, Jeffrey P Callen,
George J Hruza, James W Patterson, Lorenzo Cerroni, Anthony J Mancini,
Martin Röcken, Warren R Heymann, Thomas Schwarz, ”Dermatology”, 3rd
edition 2012, Elsevier Saunders,Pp:2572, Page no:139
118. Tony burns, Stephen breathnach, Neil cox, Christopher Griffiths, “Rook’s
Textbook of Dermatology, 8th
edition, 2010, Wilie-Blackwell Publication,
Volume 1, Chapter No 20, Page no 20.7.
119. Tony burns, Stephen breathnach, Neil cox, Christopher Griffiths, “Rook’s
Textbook of Dermatology, 8th
edition, 2010, Wilie-Blackwell Publication,
Volume 1, Chapter No 20, Page no 20.7.
120. Jean L Bolognia, Joseph L Jorizzo, Julie V Schaffer, Jeffrey P Callen,
George J Hruza, James W Patterson, Lorenzo Cerroni, Anthony J Mancini,
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 143
Martin Röcken, Warren R Heymann, Thomas Schwarz, ”Dermatology”, 3rd
edition 2012, Elsevier Saunders,Pp:2572, Page no:137.
121. Klaus Wolffs, Lowella A. Goldsmith, Stephen I. Katz, Barbara A. Gilchrest,
Amy S. Paller, David J. Leffel,” Fitzpatrick’s Dermatology in general
medicine”, 7th
edition, 2008, The Mcgraw-Hill Companies, Inc, Volume 1,
Chapter No 18, Pp: 1190, Page no 178.
122. Thomas P Habif, “Clinical Dermatology; A color guide to diagnosis and
therapy” Fifth edition, 2010, Mosby Publications, Pp: 1028 Page no 267
123. Thomas P Habif, “Clinical Dermatology; A color guide to diagnosis and
therapy” Fifth edition, 2010, Mosby Publications, Pp: 1028 Page no 276.
124. Klaus wolffs, Lowella A. Goldsmith, Stephen I. Katz, Barbara A. Gilchrest,
Amy S. Paller, David J. Leffel,” Fitzpatrick’s Dermatology in general
medicine”, 7th
edition, 2008, The Mcgraw-Hill Companies, Inc, Volume 1,
Chapter No 18, Pp: 1190, Page no 183
125. Sharma Priyavrat, Dravyaguna Vigyana, Vol 2, Reprinted 2013, Chokhamba
Bharati Akadami, Varanasi, Pp: 873, Page no 331-334
126. Bhaisajya Ratnavali, Edited by Acharya Siddhinandan Mishra, Chaukhamba
Surabharati Prakashana, Varanasi, Pp 1194, Page no 206
127. Sharma Priyavrat, Dravyaguna Vigyana, Vol 2, Reprinted 2013, Chokhamba
Bharati Akadami, Varanasi, Pp: 873, Page no 122
128. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, Edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp: 738,
Page no155
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 144
129. Maharshi Sushruta, “Sushruta Samhita”, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika Samskruta Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskruta Samsthana, Varanasi, Edition:
Reprint 2010, Pp: 824, Page no 217
130. Sharma Priyavrat, Dravyaguna Vigyana, Vol 2, Reprinted 2013, Chokhamba
Bharati Akadami, Varanasi, Pp: 873, Page no 145
131. Dr. D B Panditrao, Hindi Translation of Sahasrayoga, Chapter 4, Verse348,
New Delhi, Central Council for Research in Ayurveda and Sidda, 1990, Pp:
621, Page no-245
132. Bhavaprakasha, Commentry by Bulusu Sitaram, Vol. 1 , Chaukhamba
Orientalia, Varanasi, Pp: 738, page no 538
133. Bhavaprakasha, translated by K. R. Shrikantha Murthy, Vol. 1, Reprint
2008, Choukhamba Krishnadas Academy, Varanasi, Pp: 738, Page no 217
134. Agnivesha, “Charaka Samhita”, redacted by Charaka and Dridhabala,
Ayurvedadipika commentary of Chakrapanidatta, Edited by Yadavji Trikamji,
Reprint edition 2011, Chaukhambha Orientalia, Varanasi, U.P. 2008. Pp: 738,
Page no167
135. Maharshi Sushruta, “Sushruta Samhita”, Nibandhasangraha Samsrutatika by
Dalhana, Nyayachandrika Samskruta Tika by Gayadasa, Edited by Yadavji
Trikamji Acharya, Choukhamba Samskruta Samsthana, Varanasi, Edition:
Reprint 2010, Pp: 824, Page no 207-8
136. Vagbhatacharya, “Astanga Hrudaya” Sarvangasundara by Arunadatta and
Ayurveda Rasayana by Hemadri SamskrutaCommentry, Edited by Dr Anna
Moreshvara Kunte and Dr Krishna Shastry Navare, Edition: reprint 2010,
Choukhamba Samskruta Samsthana, Varanasi, Pp: 956, Page no 742.
References
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis Page 145
137. Chakrapanidatta, Charaka Samhita of Agnivesha with Ayurveda Dipika
commentary edited by Acharya Jadavji Trikamji edition: reprint, 2013
Chaukhamba Prakashan, Varanasi U.P. Pp-738, page no-216.
138. Chakrapanidatta, Charaka Samhita of Agnivesha with Ayurveda Dipika
commentary edited by Acharya Jadavji Trikamji edition: reprint, 2013
Chaukhamba Prakashan, Varanasi U.P. Pp-738, page no-649
139. Dogra S, Yadav S. Psoriasis in India: Prevalence and Pattern. Indian J
Dermatol Venerol Ceprol. 2010; 76:595-601
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 146
FORMAT OF CONSENT FORM
I, ……………………………………, declare that I have been briefed and here by
consent to be included as a subject in the following dissertation, “Role of Hridya
Virechana Leha in the management of Psoriasis”.
I have been informed to my satisfaction by the attending Dr. Cyrus Neupane, the
purpose of work done and laboratory investigations required and other investigations
that may be required in management of my case.
This has been explained to me in the language I understand and fully consent for
the same.
Signature of the doctor: Signature of patient:
Name of doctor: Date:
Date:

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 159

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 147
PROFORMA FORMAT
DEPARTMENT OF PG STUDIES IN PANCHKARMA
S.D.M. COLLEGE OF AYURVEDA,
KUTHPADY, UDUPI
RESEARCH PROFORMA FOR STUDY ON
ROLE OF VIRECHANA KARMA WITH HRIDYA VIRECHANA LEHA IN
THE MANAGEMENT OF PSORIASIS
Guide: Dr. Niranjan Rao Co-guide: Dr. Pooja B A
Scholar: Dr. Cyrus Neupane
Name: Serial No.:
Age: OPD No.:
Sex: IPD No.:
Education: DOA:
Occupation: DOD:
Social status: Address:
Marital status: Phone No.:
Religion: Desha:
Chief Complaints: Duration:
Associated Complaints:
Any joint complaints: Yes/ No
Any nail changes: Onchylosis/ Ridging/
Pitting
HISTORY OF PRESENT ILLNESS:
1. Onset of lesion: Sudden/ Gradual/
Insidious
2. Site of onset:
3. Character of lesion: Continuous/ Intermittent/ Progressive/ Waxing and
waning
4. Aggravating factor:
5. Relieving factor (if any):
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 148
HISTORY OF PAST ILLNESS:
H/o similar complaints earlier as well: Yes/ No
H/o Systemic illness:
H/o Others :
FAMILY HISTORY:
TREATMENT HISTORY:
Ayurvedic: Duration
Allopathic: Duration
Others: Duration
PERSONAL HISTORY:
1. Ahara Veg/ Mixed
Veg- Yava/ Shali/ Snigdha/ Madhura/ Amla/ Lavana/Katu rasa
pradhana Ahara/ Ksheera/Dadhi/Udada/Avalaki/Moolaka/
Vruntaka/Any Kanda Saka Ahara
Non-veg: Matsya/ Aja Mamsa etc
2. Emotional
status
Normal/ Anxiety/ Depression/Anger/ Irritation/Fear/Jovial
3. Vyasana Beedi/Cigarettes Yes/No
If yes, _ (No.)/day/week Duration
Alcohol Yes/No
If yes, _ (Quantinty)/ day/ week/month Duration
Tobacco chewing Yes/No
If yes, _ (No. of times/ Quantity)/ day/ week/month Duration
Tea/ Coffee Yes/ No
If yes, number of cups _ /day Duration
4. Vyayama Work Nature of work: both physical
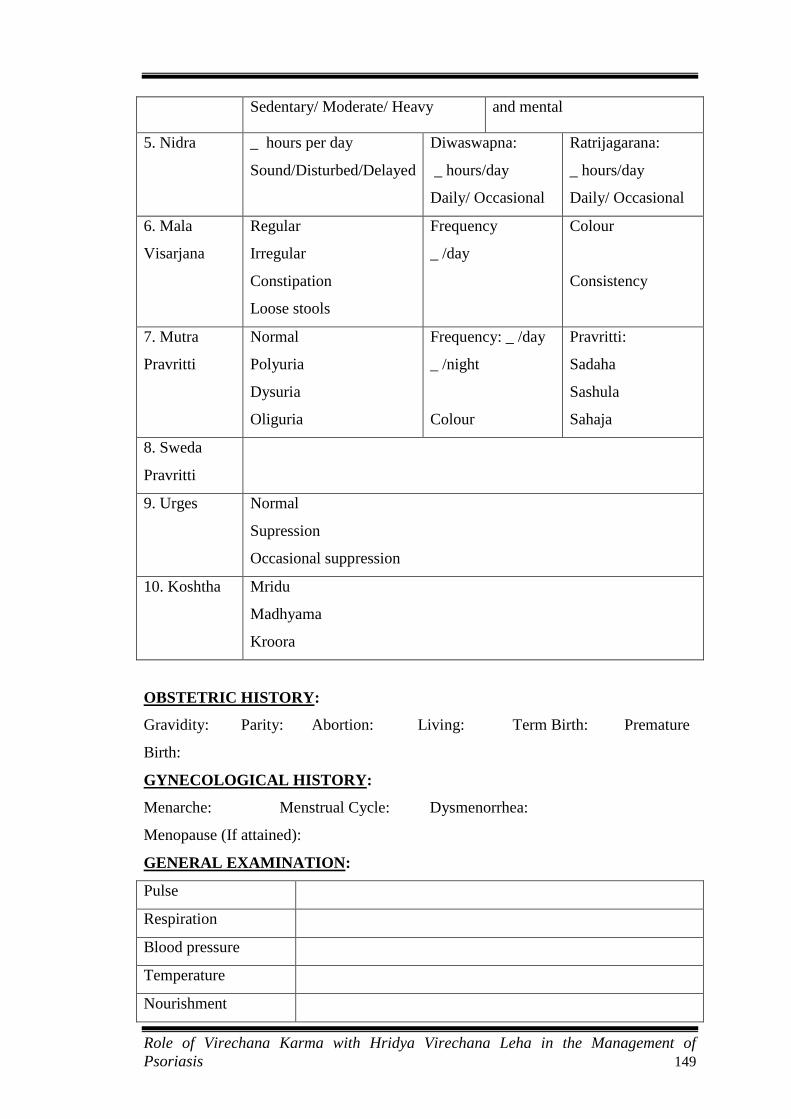
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 149
Sedentary/ Moderate/ Heavy and mental
5. Nidra _ hours per day
Sound/Disturbed/Delayed
Diwaswapna:
_ hours/day
Daily/ Occasional
Ratrijagarana:
_ hours/day
Daily/ Occasional
6. Mala
Visarjana
Regular
Irregular
Constipation
Loose stools
Frequency
_ /day
Colour
Consistency
7. Mutra
Pravritti
Normal
Polyuria
Dysuria
Oliguria
Frequency: _ /day
_ /night
Colour
Pravritti:
Sadaha
Sashula
Sahaja
8. Sweda
Pravritti
9. Urges Normal
Supression
Occasional suppression
10. Koshtha Mridu
Madhyama
Kroora
OBSTETRIC HISTORY:
Gravidity: Parity: Abortion: Living: Term Birth: Premature
Birth:
GYNECOLOGICAL HISTORY:
Menarche: Menstrual Cycle: Dysmenorrhea:
Menopause (If attained):
GENERAL EXAMINATION:
Pulse
Respiration
Blood pressure
Temperature
Nourishment

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 150
Built
Pallor
Icterus
Cyanosis
Clubbing
Lymphadenopathy
Oedema
Deformities
Contractures
Others
DASHAVIDHA PAREEKSHA:
Prakriti
Vikriti
Sara
Samhanana
Prammana
Satmya
Satva
Ahara Shakti
Vyayama Shakti
Vaya
SYSTEMIC EXAMINATION:
RS
CVS
PA
CNS
EXAMINATION OF THE SKIN:
1. Colour of the skin Normal, Black, White, Other
2. Shape of the lesion Round/ Oval/ Polygonal/ Irregular
3. Type of lesion Macule/ Papule/ Maculo palpular/ Plaque/

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 151
Lichenification/
Nodule/ Patch/ Other
4. Distribution Exposed area/ Closed area/ Exposed+Closed
area/ Flexor/ Extensor/ Medial Lateral/
Anterior/ Posterior
5. Pattern Localised/ Generalised/ Symmetrical/
Asymmetrical
6. Border Well demarcated/ diffused
7. Itching Present/ Absent
8. Type of scale Dry/ Moist/ Greasy
9. Discharge Present/ Absent
10. Vedana Supti/ Shoola/ Daha/ Kandu
11. Sparsha Rooksha/ Khara/ Kathina/ Shootha
Kushtha Dosha Taratamatva:
Vataja Lakshana-
Roukshya Shosha Sankocha Ayama
Parushya Kharabhava Harsha Shyavaarunatva
Pittaja Lakshana-
Raga Prisrava Paka Visragandanda
Kleda Daha Angapatana
Kaphaja Lakshana-
Shveitya Shaitya Sneha Kleda
Sthairya Gaurava Kandu Utsedha
CONFIRMATORY SIGNS
Auspitz Sign
Candle grease Sign
INVESTIGATIONS
Hb%
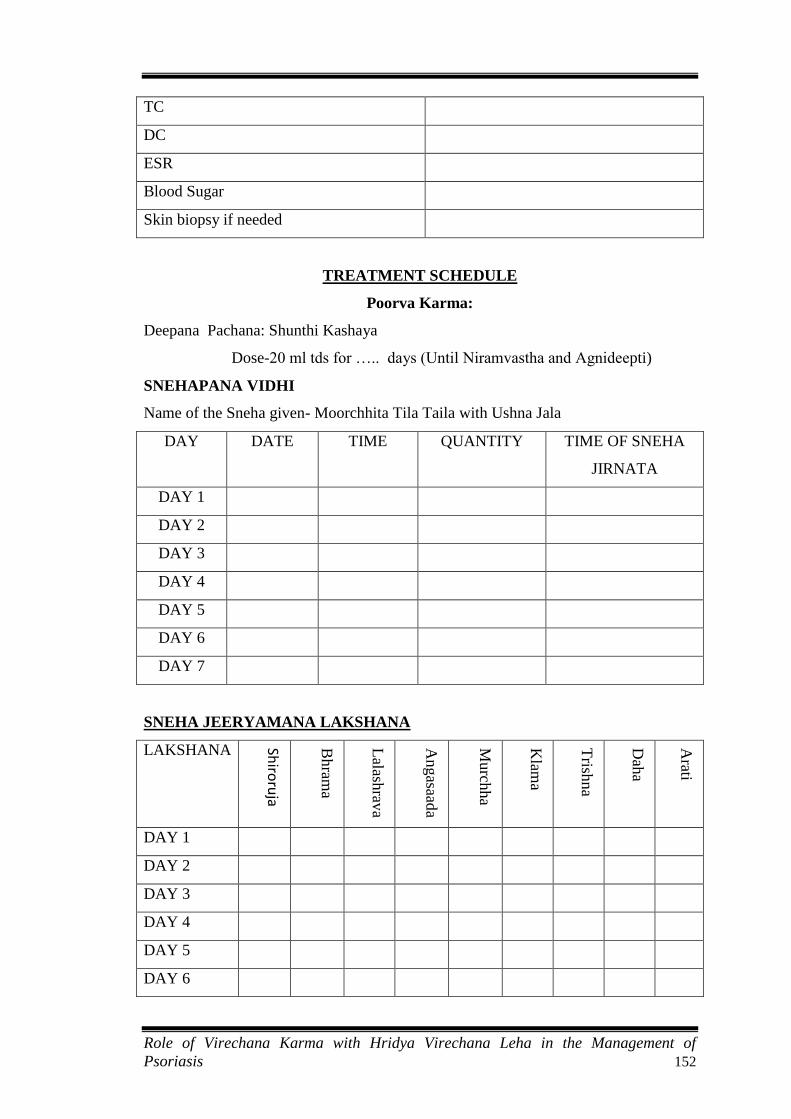
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 152
TC
DC
ESR
Blood Sugar
Skin biopsy if needed
TREATMENT SCHEDULE
Poorva Karma:
Deepana Pachana: Shunthi Kashaya
Dose-20 ml tds for ….. days (Until Niramvastha and Agnideepti)
SNEHAPANA VIDHI
Name of the Sneha given- Moorchhita Tila Taila with Ushna Jala
DAY DATE TIME QUANTITY TIME OF SNEHA
JIRNATA
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
DAY 6
DAY 7
SNEHA JEERYAMANA LAKSHANA
LAKSHANA Shiro
ruja
Bh
rama
Lalash
rava
Angasaad
a
Murch
ha
Klam
a
Trish
na
Dah
a
Arati
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
DAY 6
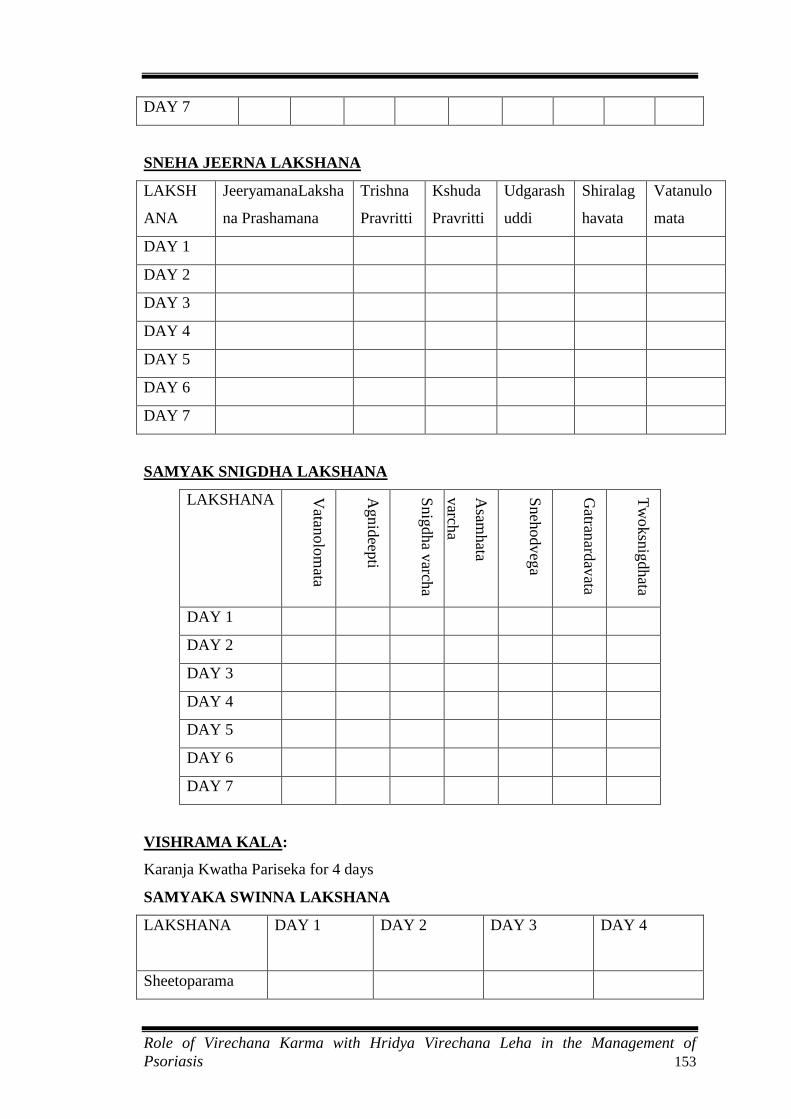
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 153
DAY 7
SNEHA JEERNA LAKSHANA
LAKSH
ANA
JeeryamanaLaksha
na Prashamana
Trishna
Pravritti
Kshuda
Pravritti
Udgarash
uddi
Shiralag
havata
Vatanulo
mata
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
DAY 6
DAY 7
SAMYAK SNIGDHA LAKSHANA
LAKSHANA Vatan
olo
mata
Agnid
eepti
Snig
dha v
archa
Asam
hata
varch
a
Sneh
odveg
a
Gatran
ardav
ata
Tw
oksn
igd
hata
DAY 1
DAY 2
DAY 3
DAY 4
DAY 5
DAY 6
DAY 7
VISHRAMA KALA:
Karanja Kwatha Pariseka for 4 days
SAMYAKA SWINNA LAKSHANA
LAKSHANA
DAY 1 DAY 2 DAY 3 DAY 4
Sheetoparama
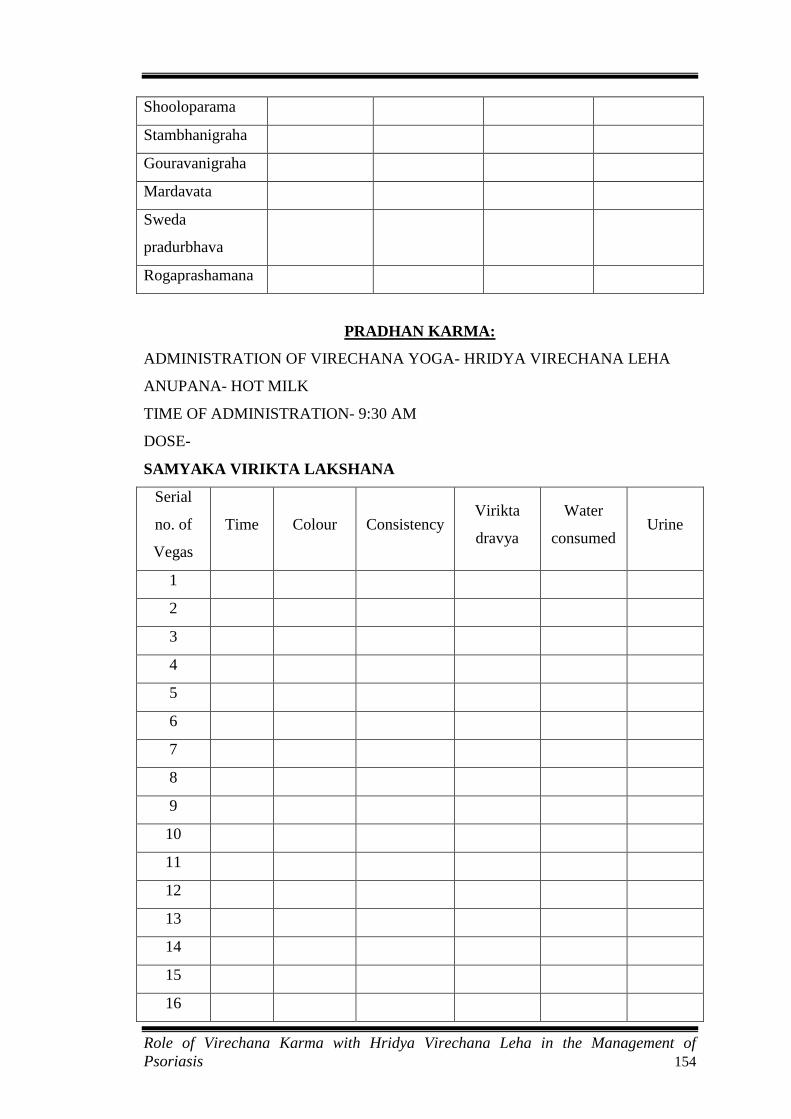
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 154
Shooloparama
Stambhanigraha
Gouravanigraha
Mardavata
Sweda
pradurbhava
Rogaprashamana
PRADHAN KARMA:
ADMINISTRATION OF VIRECHANA YOGA- HRIDYA VIRECHANA LEHA
ANUPANA- HOT MILK
TIME OF ADMINISTRATION- 9:30 AM
DOSE-
SAMYAKA VIRIKTA LAKSHANA
Serial
no. of
Vegas
Time Colour Consistency Virikta
dravya
Water
consumed Urine
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
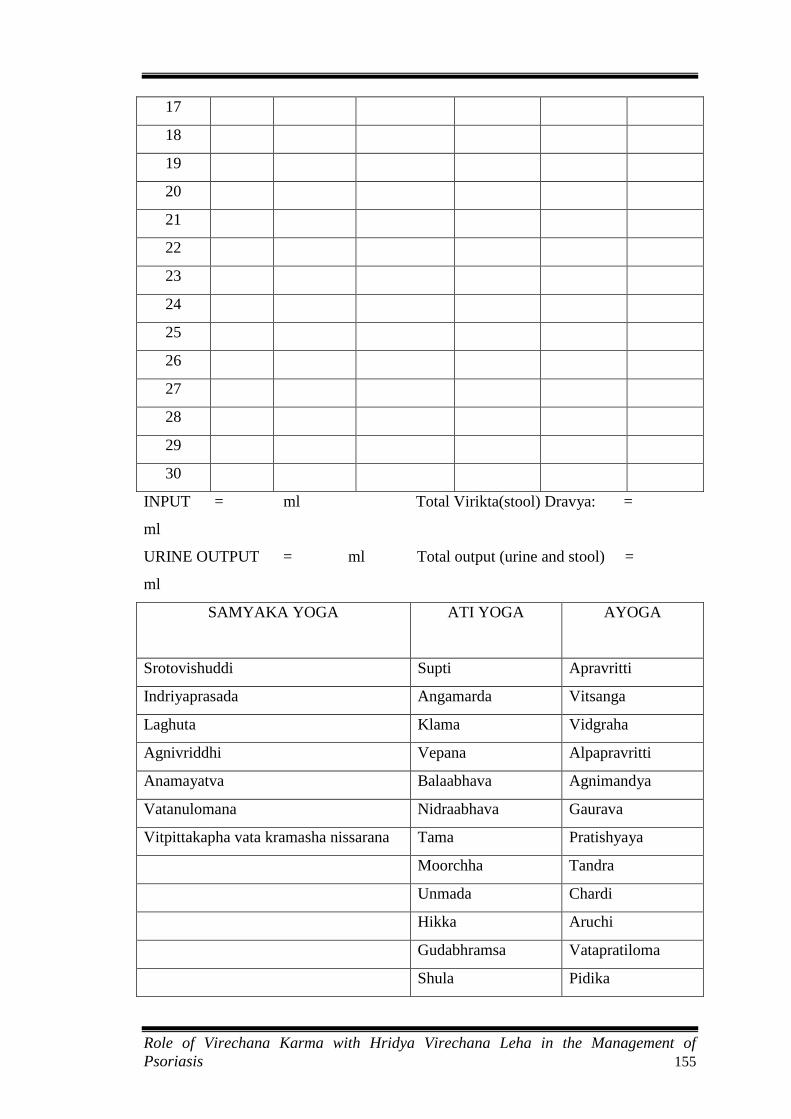
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 155
17
18
19
20
21
22
23
24
25
26
27
28
29
30
INPUT = ml Total Virikta(stool) Dravya: =
ml
URINE OUTPUT = ml Total output (urine and stool) =
ml
SAMYAKA YOGA ATI YOGA AYOGA
Srotovishuddi Supti Apravritti
Indriyaprasada Angamarda Vitsanga
Laghuta Klama Vidgraha
Agnivriddhi Vepana Alpapravritti
Anamayatva Balaabhava Agnimandya
Vatanulomana Nidraabhava Gaurava
Vitpittakapha vata kramasha nissarana Tama Pratishyaya
Moorchha Tandra
Unmada Chardi
Hikka Aruchi
Gudabhramsa Vatapratiloma
Shula Pidika
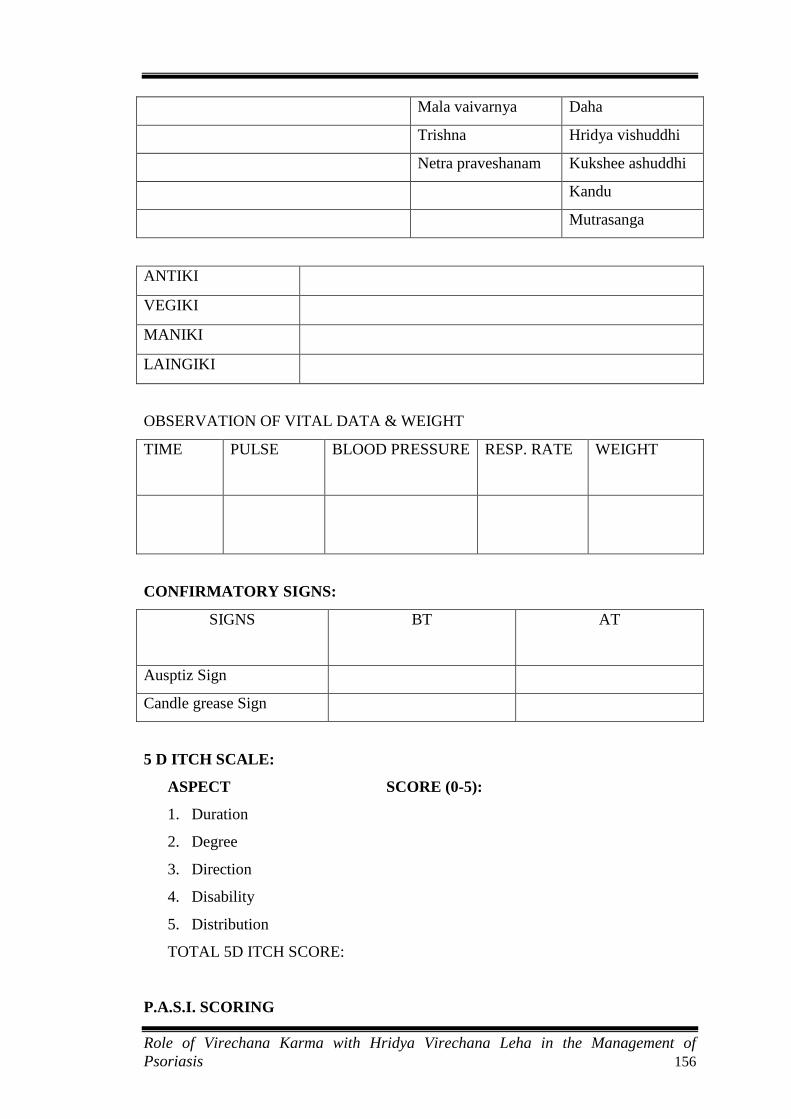
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 156
Mala vaivarnya Daha
Trishna Hridya vishuddhi
Netra praveshanam Kukshee ashuddhi
Kandu
Mutrasanga
ANTIKI
VEGIKI
MANIKI
LAINGIKI
OBSERVATION OF VITAL DATA & WEIGHT
TIME
PULSE BLOOD PRESSURE RESP. RATE WEIGHT
CONFIRMATORY SIGNS:
SIGNS
BT AT
Ausptiz Sign
Candle grease Sign
5 D ITCH SCALE:
ASPECT SCORE (0-5):
1. Duration
2. Degree
3. Direction
4. Disability
5. Distribution
TOTAL 5D ITCH SCORE:
P.A.S.I. SCORING
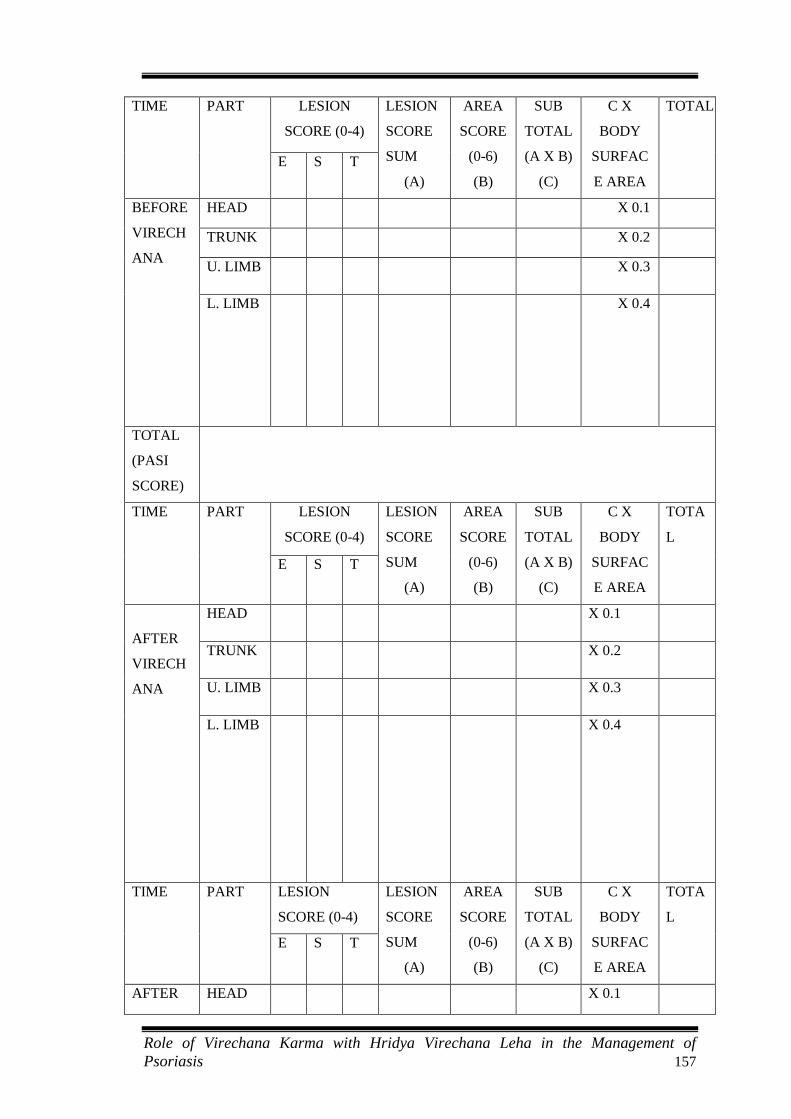
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 157
TIME
PART LESION
SCORE (0-4)
LESION
SCORE
SUM
(A)
AREA
SCORE
(0-6)
(B)
SUB
TOTAL
(A X B)
(C)
C X
BODY
SURFAC
E AREA
TOTAL
E S T
BEFORE
VIRECH
ANA
HEAD X 0.1
TRUNK X 0.2
U. LIMB X 0.3
L. LIMB X 0.4
TOTAL
(PASI
SCORE)
TIME
PART LESION
SCORE (0-4)
LESION
SCORE
SUM
(A)
AREA
SCORE
(0-6)
(B)
SUB
TOTAL
(A X B)
(C)
C X
BODY
SURFAC
E AREA
TOTA
L
E S T
AFTER
VIRECH
ANA
HEAD X 0.1
TRUNK X 0.2
U. LIMB X 0.3
L. LIMB X 0.4
TIME
PART LESION
SCORE (0-4)
LESION
SCORE
SUM
(A)
AREA
SCORE
(0-6)
(B)
SUB
TOTAL
(A X B)
(C)
C X
BODY
SURFAC
E AREA
TOTA
L
E S T
AFTER HEAD X 0.1

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 158
FOLLO
W UP
TRUNK X 0.2
U. LIMB X 0.3
L. LIMB X 0.4
I= ITCHING E= ERYTHEMA S= SCALING T= THICKNESS
Signature of the candidate
Signature of the guide
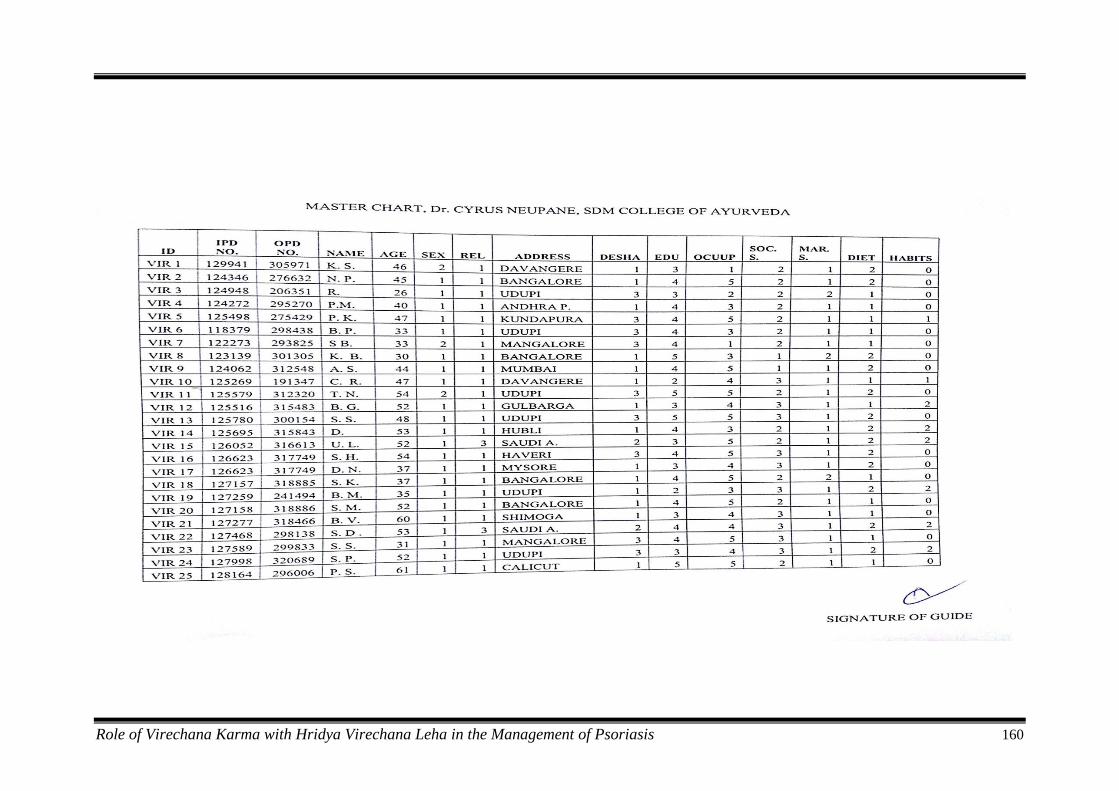
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 160
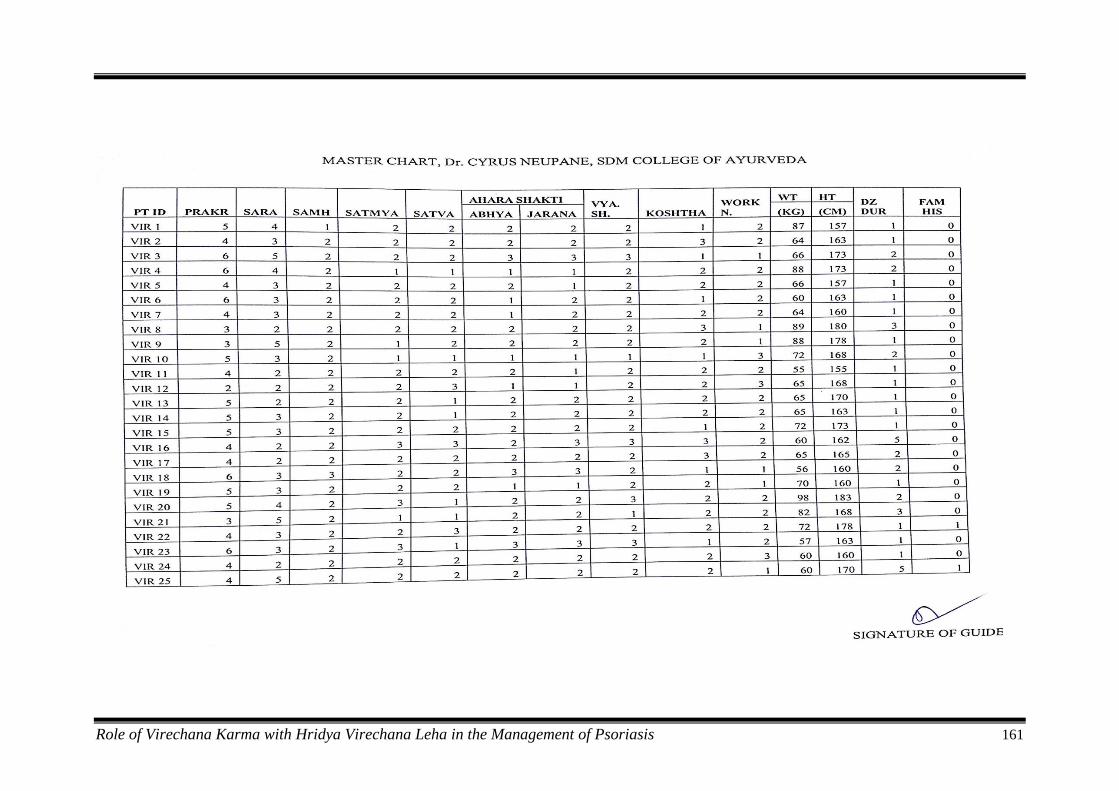
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 161
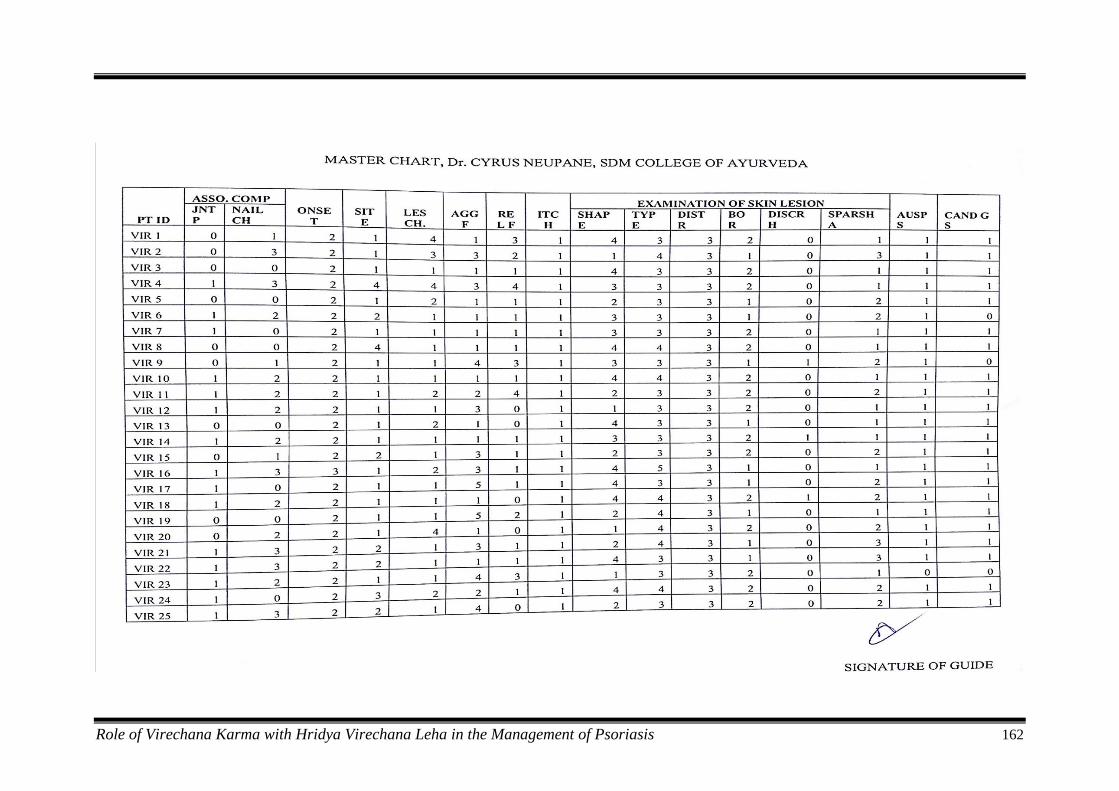
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 162
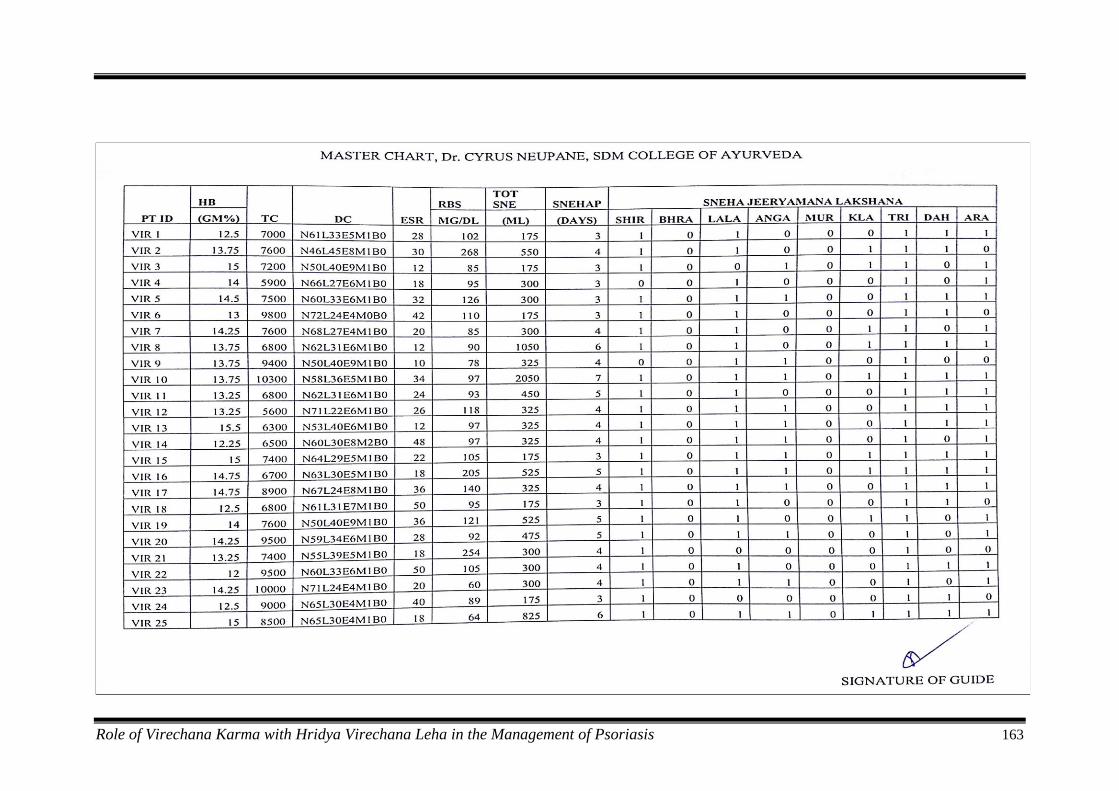
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 163
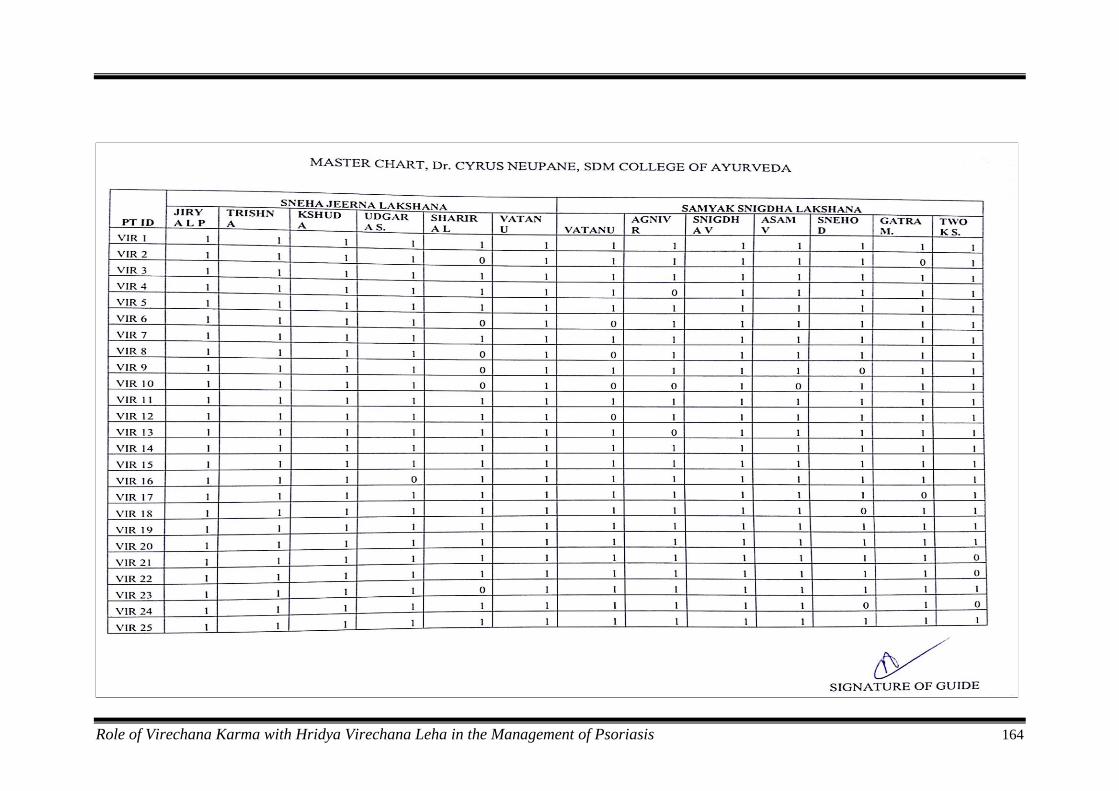
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 164

Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 165

Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 166
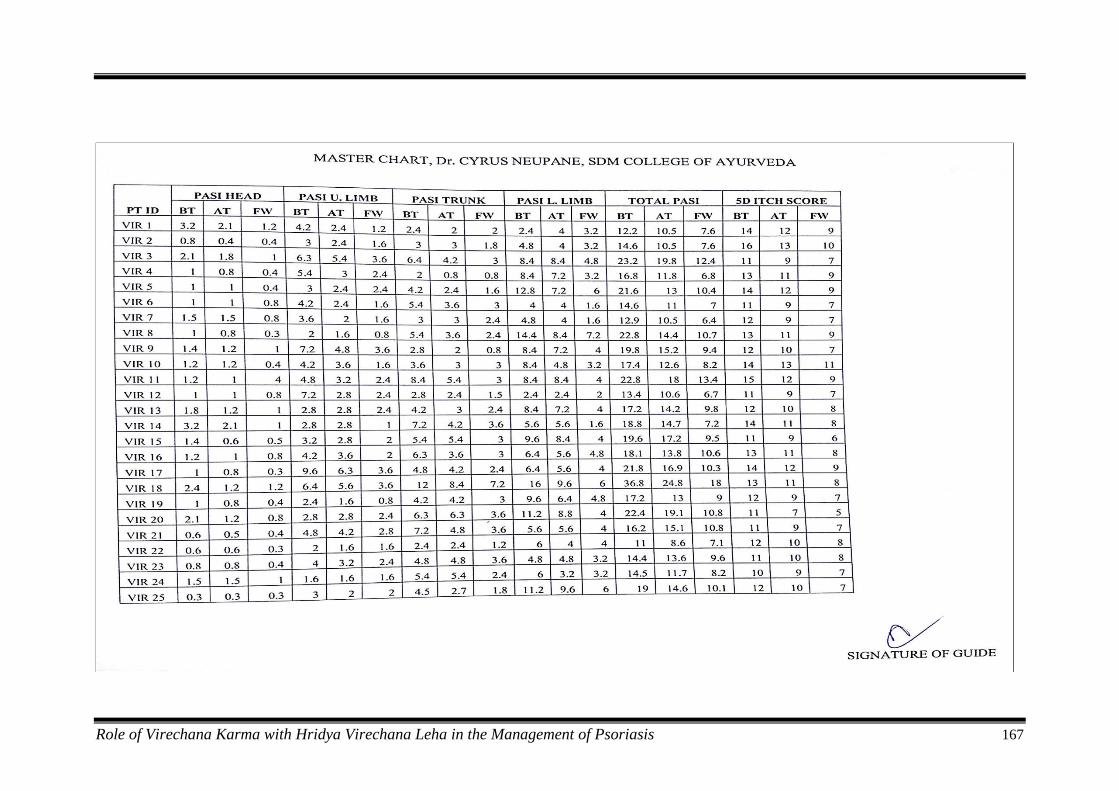
Role of Virechana Karma with Hridya Virechana Leha in the Management of Psoriasis 167
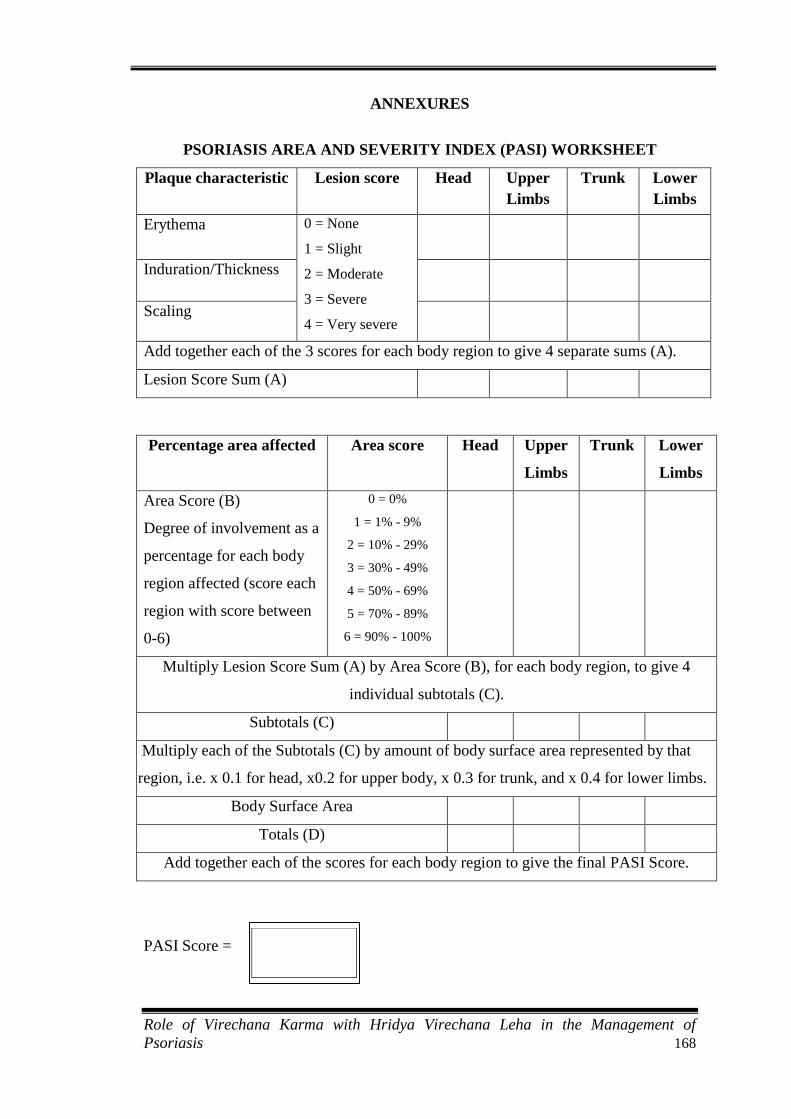
Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 168
ANNEXURES
PSORIASIS AREA AND SEVERITY INDEX (PASI) WORKSHEET
Plaque characteristic Lesion score Head Upper
Limbs
Trunk Lower
Limbs
Erythema 0 = None
1 = Slight
2 = Moderate
3 = Severe
4 = Very severe
Induration/Thickness
Scaling
Add together each of the 3 scores for each body region to give 4 separate sums (A).
Lesion Score Sum (A)
Percentage area affected Area score Head Upper
Limbs
Trunk Lower
Limbs
Area Score (B)
Degree of involvement as a
percentage for each body
region affected (score each
region with score between
0-6)
0 = 0%
1 = 1% - 9%
2 = 10% - 29%
3 = 30% - 49%
4 = 50% - 69%
5 = 70% - 89%
6 = 90% - 100%
Multiply Lesion Score Sum (A) by Area Score (B), for each body region, to give 4
individual subtotals (C).
Subtotals (C)
Multiply each of the Subtotals (C) by amount of body surface area represented by that
region, i.e. x 0.1 for head, x0.2 for upper body, x 0.3 for trunk, and x 0.4 for lower limbs.
Body Surface Area
Totals (D)
Add together each of the scores for each body region to give the final PASI Score.
PASI Score =

Role of Virechana Karma with Hridya Virechana Leha in the Management of
Psoriasis 169