
ROLE OF PRIMARY HEALTH CARE CENTRES IN KARNATAKA
14
ROLE OF PRIMARY HEALTH CARE CENTRES IN KARNATAKA Introduction : The task of saving the lives of millions of women and children throughout the world, who die every year from easily prevented illness, is daunting. The outrage provoked by so many needless deaths however can now be tempered by hope because this demands for better health care and improved quality of health care and quality of life for women are being voiced by communities health personnel, researchers and policy makers. Keeping in view the constitutional obligations, the Government of India planned several approaches for the health care delivery. However, the basis for organization of health services in India through the primary health care in modern time, was laid by the recommendations and guidance provided by the 'Health Survey and Development Committee' (Bhore Committee) in 1946. The community development programme was launched in October 1952 as the first integrated all-round rural development programme. It was proposed to establish one primary health centre 136 (PHC) for each community development block. At that time, the operational responsibilities of the PHC were to cover medical care, control of communicable diseases, maternal and child health (MCH), nutrition, health education, school health, environmental sanitation and the collection of vital statistics. Each PHC had three sub-centres, being looked after by a trained midwife for providing MCH services. The Declaration of Alma-Ata was adopted at the international conference on Primary Health Care (Almaty, Kazakhstan, 6-12 September 1978) It expressed the need for urgent action by all governments, all health and development workers and the world
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of ROLE OF PRIMARY HEALTH CARE CENTRES IN KARNATAKA

ROLE OF PRIMARY HEALTH CARE CENTRES IN KARNATAKA
Introduction :
The task of saving the lives of millions of women and children
throughout the world, who die every year from easily prevented
illness, is daunting. The outrage provoked by so many needless
deaths however can now be tempered by hope because this demands
for better health care and improved quality of health care and
quality of life for women are being voiced by communities health
personnel, researchers and policy makers. Keeping in view the
constitutional obligations, the Government of India planned
several approaches for the health care delivery. However, the
basis for organization of health services in India through the
primary health care in modern time, was laid by the
recommendations and guidance provided by the 'Health Survey and
Development Committee' (Bhore Committee) in 1946. The community
development programme was launched in October 1952 as the first
integrated all-round rural development programme. It was proposed
to establish one primary health centre 136 (PHC) for each
community development block. At that time, the operational
responsibilities of the PHC were to cover medical care, control of
communicable diseases, maternal and child health (MCH), nutrition,
health education, school health, environmental sanitation and the
collection of vital statistics. Each PHC had three sub-centres,
being looked after by a trained midwife for providing MCH
services.
The Declaration of Alma-Ata was adopted at the international
conference on Primary Health Care (Almaty, Kazakhstan, 6-12
September 1978) It expressed the need for urgent action by all
governments, all health and development workers and the world

community to protect and promote health care approach has since
then been accepted by member countries of the World Health
organisation as the key to achieving the goal of ‘Health For All’.
CONCEPT AND DIMENSIONS OF HEALTH AND PRIMARY HEALTH CARE
Health
Health is a state of complete physical, mental and social well-
being which is essential for leading a productive life, and it is
not merely the absence of disease or infirmity. Provision for
health should be considered a fundamental human right, and
attainment of highest level of health is a most important social
goal.
Primary Health Care
An essential health care should be based on practical,
scientifically sound and socially acceptable methods and
technology. It should be made universally accessible to the
individuals and the family in the community through their full
participation. It is to be made available at a cost which the
community and the country can afford to maintain at every stage of
its development in a spirit of self-reliance and self-
determination. Primary health care is the first level of contact
of the individuals, the family and the community with the national
health system bringing health care as close as possible to where
the people live and work. It constitutes the first element of the
process of continuing health care, and this should get full
support from the rest of the health system. This support would be

required in the following areas: (a) consultation on health
problems; (b) referral of patients to local or other specialized
institutions; (c) supportive supervision and guidance; and (d)
logistic support and supplies.
For achieving success in HFA development, at least eight essential
components of primary health care need to be properly implemented.
For this the cooperation and support of other social and economic
development sectors, such as education, social and women's
welfare, food and agriculture, animal husbandry, water resources,
housing, rural development, energy, environmental protection,
industry, communication, etc. would be vital. It would be well to
recognize that planning, organization and operation of primary
health care is a long process, and total population coverage may
be achieved progressively in stages, both in terms of geographical
coverage and the contents.
Today, Primary Health Centres are State owned health care
facilities in India. They are essentially single-doctor clinics
usually with facilities for minor surgeries too. They are a part
of the government funded public health system in India, and are in
fact the most basic units of this system. The 6th Five Year Plan
(1983-88) proposed reorganisation of PHCs which covers population
of 30,000 in plain areas and 20,000 in hilly and tribal areas.
Community Health Centres are upgraded from PHCs to cover primary
and curative services. They also act as first referral units to
the surrounding PHCs. For many in rural areas PHCs stresses on
preventions rather than cure. It relies on home self-help,
community participation and technology that the people find
acceptable, appropriate and affordable. It combines modern,
scientific knowledge and feasible health technology with
acceptable, effective traditional healing practices of special

importance for women is that the effectiveness of PHCs depends
very much upon community acceptance of primary health care
workers, most of who are women and who in most cases are recruited
form and selected with the participation of the community.
There are 23,673 PHCs functioning in the country as on March 2010
as per Rural Health Statistics Bulletin, 2010. The number of PHCs
functioning on 24/7 basis are 9107 and number of PHCs where three
staff nurses have been posted are 7629(2011). PHCs are referral
units for 6 sub-centres and refer out cases to CHC and higher
order public hospitals at sub-district and district hospitals. It
has 4-6 indoor beds for patients.
Essential components of PHC
In the Alma Ata Declaration, it is stated that at least the following
components should be included in primary health care which are
also the objectives of PHC :
1. Educate people about prevailing health problems and methodsof preventing and controlling them.
2. Promotion of food supply and proper nutrition.
3. Adequate supply of safe water and basic sanitation.
4. Maternal and child health care and family planning.
5. Immunization against major infectious diseases.
6. Prevention and control of locally endemic diseases.
7. Appropriate treatment of common diseases and injuries.
8. Provision of essential drugs.

Areas of medical treatments by PHCs
Infant immunisation programmes
Anti-epidemic programmes
Birth control programmes
Pregnancy and related care
Emergencies – Anti-venoms, anti-rabies etc.
By strengthening PHCs a health care delivery activity in the
areas as per government of India pattern is adopted. PHCs
provide primary health care in the areas through the network
of Sub-centres and other Para medical staff. PHCs include
preventive services, curative services, environmental
sanitation, health education, family welfare services and
recording of health statistics of various National Health
Programmes which are in force from time to time and also
implementing through a network of PHCs.
IPHS guidelines for PHCs
Directorate General of Health Services, Ministry of Health
and Family Welfare Government of India, under Indian Public
Health Standards (IPHS) guidelines for PHC frames certain
rules for all the PHCs in its functioning. The rules are with
regard to:
Infrastructure
Manpower- Number of doctors required (both male and female)
Staff nurses, Para medical staff and others.
Transport facilities with assured referral linkages
Laundry services – for maintenance of hygiene

Dietary facilities for indoor patients – mother, new born
infants and other patients
Waste management at PHC level
Quality assurance at PHCs
Monitoring of PHC functioning
Accountability of PHC
Statutory and regulatory compliance
PRIMARY HEALTH CARE IN KARNATAKA
Karnataka is one of the pioneer States in the country in providing
comprehensive public services to people. Even before the concept
of PHCs were conceived by the Government of India, the State had
already made a beginning in establishing a number of PHCs for
proving comprehensive health care and a delivery system consisting
of curative preventive and rehabilitative health care to its
people. Primary Health Care in Karnataka has a better public
service with respect to child care and health care. The State has
a birth rate of 0.7%, 2.2 % death rate and 5.5% of infant
mortality rate. As of 2004 State’s health and family welfare
services , Karnataka had 8,143 sub-centres, doctor population
ration 1:10, 581 primary health units, 1,679 PHCs at village
level, 17 urban PHCs and 110 community health centres . The
responsibility for maternal health care is mainly at the sub-
centre and PHC which provides pre-natal, childbirth and post-natal
services through the auxiliary nurse mid wives(ANMs) .

Map showing PHC’s in Karnataka
At the first level the duties of ANMs are important. These
auxiliary nurses and midwives are the paramedical staff trained in
reproductive health care and are based in sub centres or at the
PHC itself. They have multiple responsibilities. They maintain
health department records, document information related to
fertility, pregnancies, child birth details and immunization. They
enrol pregnant women are expected to provide postnatal care.
At the second level of service which is at PHC , a medical doctor
and nurse are available for consultation and child birth. However,
not all PHCs have complete facilities for maternal care. There are
1700 PHCs in Karnataka, and the status and quality services
provided by them are important indicators of the quality of
reproductive health services.

The next level of services is the community health centres (CHCs)
and referral hospitals at the sub-district level and General
hospitals and maternity hospitals at the district level.
According to the statistics provided by 11th FP (2007-2012) the
status of PHCs in Karnataka can be clearly understood.
Sub Centres PHCs CHCs0
10002000300040005000600070008000900010000
Shortfall of Health infrastructure as per 2011 , Population of
India
Required Provided Shortage0
100020003000400050006000700080009000
Sub CentresPHCsCHCs

Graph showing availability of Doctors and Health workers (female)
010002000300040005000600070008000900010000
DoctorsHealth workers
Graph indicating Every single PHC with doctors/without doctors
4 Doctors 3 Doctors 2 Doctors 1 Doctor Without Doctor
0
500
1000
1500
2000
2500

Nursing staff at PHCs and CHCs
Registered Available0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
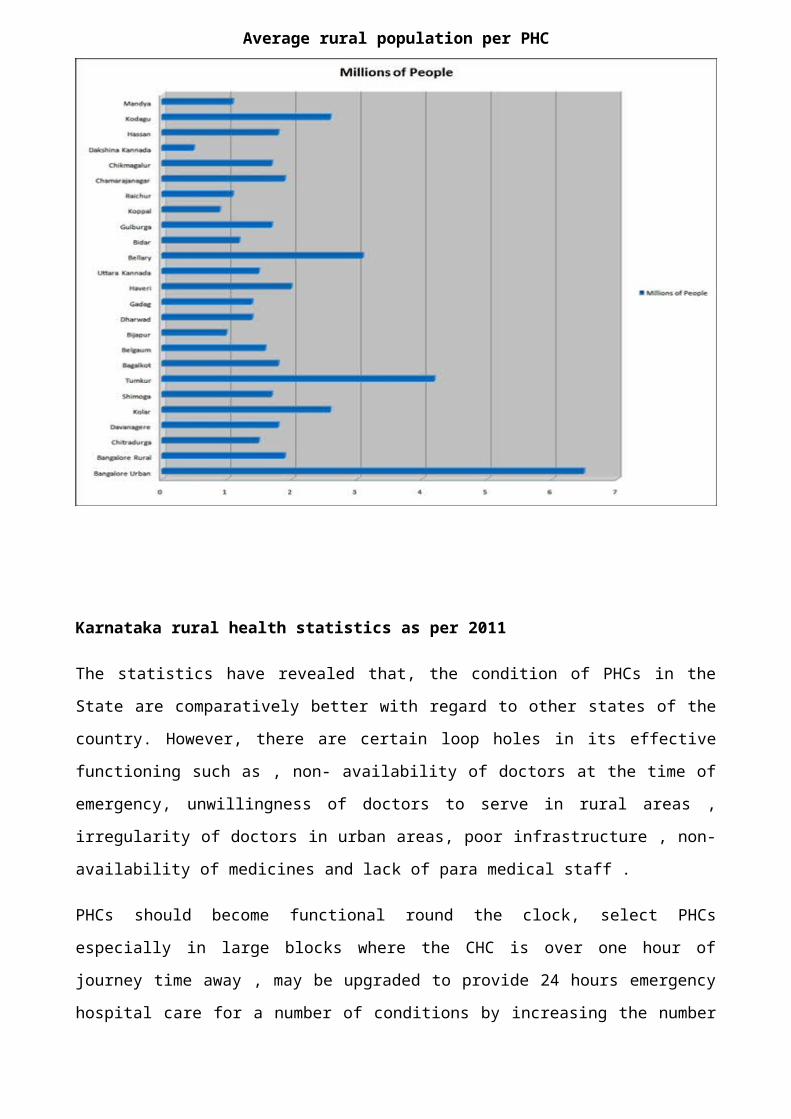
Average rural population per PHC
Karnataka rural health statistics as per 2011
The statistics have revealed that, the condition of PHCs in the
State are comparatively better with regard to other states of the
country. However, there are certain loop holes in its effective
functioning such as , non- availability of doctors at the time of
emergency, unwillingness of doctors to serve in rural areas ,
irregularity of doctors in urban areas, poor infrastructure , non-
availability of medicines and lack of para medical staff .
PHCs should become functional round the clock, select PHCs
especially in large blocks where the CHC is over one hour of
journey time away , may be upgraded to provide 24 hours emergency
hospital care for a number of conditions by increasing the number

of medical officers preferably such PHCs should have the same IPHS
norms as for CHC.
Challenges for PHCs
Non availability of doctors is a major problem faced by PHCs.
Lack of education among people about health matters
Malnutrition among nursing mothers, infants and children.
Non availability of safer drinking water and basic sanitation
facilities.
High rate of maternal mortality(4to5 per 1000 live births) due
to anaemia , illegal abortion and malnutrition during
pregnancy.
High infant mortality (105/1000 births) due to poor maternal
health, inadequate care of mothers, lack of infrastructure in
hospitals and low birth weight
Malnutrition among children in the age group of 0-5 years.
Lack of awareness among people about family planning
Suggestions to improve the working of PHCs in Karnataka
People and the community need to be convinced and satisfied
with the services being provided at the primary and secondary
contact levels
Bypassing the local facilities which causes overcrowding at
referral centres/urban centres needs to be regulated as a
result of which the quality of care at referral hospitals can
be improved
Physical facilities, back-up support and supervision, mobility
of health personnel, communication between government and PHCs
needs to be improved.
Transport during emergency cases and effective logistic and
supply system should be given importance.

Priority should be given to the referred cases by the
consultants of the Urban/referral centres
Conclusion
While poor infrastructure and staff shortage are leading to loss
of lives in government hospitals, people going to Community Health
centres and Primary Health Centres have to turn to pharmacies with
empty shelves. Over 3000 health institutions have not received
drug supplies during 2007-12, according to the Controller and
Audit General of India audit. The Karnataka State Drug Logistics
and Warehousing society is responsible for ensuring the drug
supply to health centres. The CAG audit found that KDLWS does not
have evidence to show that 3,093 health institutions in the state
received drug supplies during 2007-12.
Its scrutiny also revealed that 2,360 PHCs and CHCs with sub-
centres , 277PHcs and three CHCs were denied drug supplies in this
period due to ineffective monitoring by the society . The report
said ‘This evidently affected delivery of healthcare services to
the needy public’. Karnataka has been the IT hub and this has been
India’s pride. .When the state has earned such laurels, why should
the most basic facilities of health be denied to the rural areas?
With this regard the PHCs and CHCs needs to be given highest
priority in order to streamline the rural and urban health .
Bibliography
Agarwal, A.N. Varma, and Gupta R.C, Nutrition Health andEducation. Social Science Press, New Delhi, Economic InformationYear Book 1992-93 . National Publishing House.
Abhay Bang, M.H., Reddy, M.D.and Desh Muki, Child Mortality inMaharashtra.

Economic and Political Weekly, 2002
Dr. Eshwar Naik, Schemes for involving private organisations in
the management of PHCs , Government of Karnataka, Department of
health and family welfare, 2008
Deodhar N.S., Primary Health Care in India Journal , Public Health
Policy, 1982
Government of India, PHc in India, Ministry of Health and Family
Welfare, 2012
Seetha Prabhu and Sudarshan R. (ed). Poverty, Nutrition Health andEducation.Social Science Press, New Delhi.productive Health, 1992
Indian public health standards (IPHS) guidelines for PH centres,revised ,2012
Whose public action? Analysing inter- sectorial collaboration forservice delivery, Economic and social research council, 2008
WHO, Alma-ata, Primary Health Care:Health for all, 1978




















