
Risk Perception, Universal Precautions ComplianceA Descriptive Study of Nurses Who Circulate
11
JANUARY 1994, VOL 59, NO I AORN JOURNAL Risk Perception, Universal Precautions Compliance A DESCRIPTIVE STUDY OF NURSES WHO CIRCULATE Linda L. Ronk, RN; Nancy J. Girard, RN rotection for health care workers in the hospital setting is increasingly important P because of the prevalence of HIV and hepatitis B virus (HBV). According to the Centers for Disease Control and Prevention (CDC), at least 40,000 new HIV infections occur among adults and teenagers each year.' Various studies indicate that between 3% and 24% of patients admitted to health care facili- ties are HIV positive.* The CDC estimates that 300,000 people per year become HBV infected. Of these people, 25% will develop acute hep- atitis, and 6% to 10% will become carriers. The CDC also calculates that each year 12,000 health care workers become infected with HBV, and 250 of these infected health care workers will die.3 In 1987, the CDC published universal pre- cautions, a system of guidelines designed to protect health care worker^.^ The CDC updated these guidelines in 1989, and the Occupational Safety and Health Administration (OSHA) made them mandatory and enforceable for health care facilitie~.~ According to these guidelines, patients' blood and other body flu- ids (eg, semen; vaginal secretions; cere- brospinal, synovial, pericardial, amniotic fluid) are considered potentially infectious for HIV, HBV, and other bloodborne pathogens. To guard against exposure to these potentially fatal secretions, barrier precautions (ie, gloves, gowns, eye protection, leg coverings) are to be used appropriately when dealing with every patient-thus the term universal precautions. Because it is not always possible, even with testing, to verify specific patients as carriers of HIV, treating all patients as potentially infected provides maximum protection for health care workers.h Perioperative nurses are repeatedly exposed to blood and body fluids in their roles as circu- lators. These exposure-prone activities include starting TV lines, assisting with intubations, handling bloody sponges and specimens such Linda L. Ronk, RN, BSN, CNOR, is the trans- plum ream leader at the Wilford Hall Medical Center, Lackland AFB, Tex. She earned her BS degree in nursing at Indiana Wesleyan University , Marion. The opinions or assertions contained in this article are the private views of the authors and are not to he construed as official or as rejlect- ing the views of the Air Force Medical Department or the Department of Defense Nancy J. Girard, RN, PhD, CS, is an assistant professor at the University of Texas Heulth Science Center School of Nursing, Sun Antonio. She earned her diploma in nursing at the Salem City (Ohio)Hospital School of Nursing; her BS degree in nursing at the University of Nebraska School of Nursing, Omaha; her MS degree in medical-surgical nursing at the University of Texas Health Science Center School of Nursing, Sun Antonio; and her PhD in educa- tion at the University of Texas, Austin. 253
Transcript of Risk Perception, Universal Precautions ComplianceA Descriptive Study of Nurses Who Circulate
JANUARY 1994, VOL 59, NO I AORN JOURNAL
Risk Perception, Universal Precautions Compliance
A DESCRIPTIVE STUDY OF NURSES WHO CIRCULATE
Linda L. Ronk, RN; Nancy J. Girard, RN
rotection for health care workers in the hospital setting is increasingly important P because of the prevalence of HIV and
hepatitis B virus (HBV). According to the Centers for Disease Control and Prevention (CDC), at least 40,000 new HIV infections occur among adults and teenagers each year.' Various studies indicate that between 3% and 24% of patients admitted to health care facili- ties are HIV positive.* The CDC estimates that 300,000 people per year become HBV infected. Of these people, 25% will develop acute hep- atitis, and 6% to 10% will become carriers. The CDC also calculates that each year 12,000 health care workers become infected with HBV, and 250 of these infected health care workers will die.3
In 1987, the CDC published universal pre- cautions, a system of guidelines designed to protect health care worker^.^ The CDC updated these guidelines in 1989, and the Occupational Safety and Health Administration (OSHA)
made them mandatory and enforceable for health care f a c i l i t i e ~ . ~ According to these guidelines, patients' blood and other body flu- ids (eg, semen; vaginal secretions; cere- brospinal, synovial, pericardial, amniotic fluid) are considered potentially infectious for HIV, HBV, and other bloodborne pathogens. To guard against exposure to these potentially fatal secretions, barrier precautions (ie, gloves, gowns, eye protection, leg coverings) are to be used appropriately when dealing with every patient-thus the term universal precautions. Because it is not always possible, even with testing, to verify specific patients as carriers of HIV, treating all patients as potentially infected provides maximum protection for health care workers.h
Perioperative nurses are repeatedly exposed to blood and body fluids in their roles as circu- lators. These exposure-prone activities include starting TV lines, assisting with intubations, handling bloody sponges and specimens such
Linda L. Ronk, RN, BSN, CNOR, is the trans- plum ream leader at the Wilford Hall Medical Center, Lackland AFB, Tex. She earned her BS degree in nursing a t Indiana Wesleyan Un iversity , Marion.
The opinions or assertions contained in this article are the private views of the authors and are not to he construed as official or as rejlect- ing the views of the Air Force Medical Department or the Department of Defense
Nancy J . Girard, RN, PhD, CS, is an assistant professor at the University of Texas Heulth Science Center School of Nursing, Sun Antonio. She earned her diploma in nursing at the Salem City (Ohio) Hospital School of Nursing; her BS degree in nursing at the University of Nebraska School of Nursing, Omaha; her M S degree in medical-surgical nursing at the University of Texas Health Science Center School of Nursing, Sun Antonio; and her PhD in educa- tion at the University of Texas, Austin.
253

AORN JOURNAL JANUARY 1994, VOL 59, NO 1
as cultures and blood for blood gases, and pick- ing up bloody instruments that have been dropped from the operative field. Because of the many tasks centering around exposure to blood and other body fluids, nurses who circu- late are at risk for exposure to HIV, HBV, and other bloodborne pathogens. Although the data indicate that nurses who circulate are at risk because of their activities, little is known about their perception of this risk. This is extremely important because if nurses do not think they are at risk, they may not adequately protect themselves by using universal precautions. Because of the importance of this issue, this study was developed to answer the following questions: To what extent do nurses who circu- late perceive they are at risk for exposure to HIV and HBV? To what extent do nurses who circulate report compliance with universal pre- cautions?
Background
he OSHA believes that 2 million hospi- tal health care workers are at risk for T exposure to harmful bloodborne
pathogens; 60% of these health care workers are nurses. The OSHA also considers the surgi- cal suite to be among one of the highest risk areas in the hospitaL7
Exposure to bloodborne pathogens in the occupational setting occurs in two ways: cuta- neous (ie, contact with skin and mucous mem- brane) and percutaneous (ie, needle stick or other sharp instrument injury). Studies indicate that nurses who circulate encounter numerous cutaneous exposures to blood, most of which could be prevented by glove use. According to the CDC, the risk of acquiring HIV following a percutaneous exposure is 0.4%.8 Although not as prevalent, transmission by nonparenteral routes also has been do~umented.~ Hepatitis B virus is the most common infectious agent transmitted through needle stick injuries, but it also has been reported through indirect means such as blood- contaminated instruments, which is of particular importance to perioperative nurses. lo
Use of universal precautions. Comparisons
of studies show that health care workers who perceive a high risk for exposure practice a higher standard of infection control.I1 One study compares the self-reported frequencies of cutaneous exposures to blood and body sub- stances before and after implementation of uni- versal precautions. Although cutaneous expo- sure to blood and other body fluids was not eliminated, the universal precaution training significantly decreased the exposure rate. Another study reports that physicians were three times more likely to take barrier precau- tions after universal precautions implementa- tion than before.I3
Another study examines emergency depart- ment nursing staff members.I4 Although the nurses in the study underestimated their degree of risk, the use of gloves and protective eye wear increased significantly after a universal precautions inservice program. Glove use increased 21%, and eye wear increased from 0% to more than 17%. The studies’ conclusions are similar. When used, universal precautions provide effective protection against blood and other body fluids.
Although universal precautions are intended for the protection of health care workers, research shows that the actual use of universal precautions varies widely. Researchers believe that the practice of universal precautions will not be universal until health care workers develop a better understanding of the potential for any patient to be infectious.15 Many studies suggest that there is a correlation between per- ception of risk and the use of universal precau- tions.16 Although various studies address the use of universal precautions among health care workers, few studies specifically address peri- operative nurses who circulate and even fewer examine whether penoperative nurses who cir- culate believe they are at risk for exposure to potentially fatal bloodborne pathogens.
The Study, Methodology
s a result of the trend toward poor com- pliance with universal precautions and A the lack of extensive research on the
254
AORN JOURNAL JANUARY 1994, VOL 59, NO I
topic in regard to nurses who circulate, this descriptive study was designed to identify peri- operative nurses’ perception of risk for expo- sure to HIV and HBV and their perception of their use of universal precautions. Cause and effect relationships were not investigated.
Sample. The study investigators used a con- venience sample of 126 circulating periopera- tive nurses from 10 hospitals in San Antonio. These facilities were chosen solely on the basis of availability.
Znstrument. The lack of previous research on the topic as it pertains to perioperative nurses who circulate necessitated developing a suit- able instrument. The researchers developed a questionnaire to determine
how perioperative nurses who circulate perceive their risk for exposure to blood- borne pathogens during specific operative procedures, during what situations nurses are more likely to comply with universal precau- tions,
0 how nurses perceive their risk levels in comparison to the risk levels of other health care workers,
0 if nurses are familiar with universal pre- cautions, and to what extent nurses believe that using universal precautions reduces their risk for exposure.
To accomplish these objectives, the ques- tionnaire was divided into four sections: per- ception of risk, compliance with universal pre- cautions, background and demographic data (ie, AORN membership, CNOR certification, type of facility, nursing education background, length of time as an RN and a circulating nurse) (Table l ) , and open-ended (ie, short essay) questions. The questionnaire incorporated many Likert-type scale statements (ie, state- ments that require responses according to a spe- cific rating scale). Participants responded to various statements with “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”; or “always,” “usually,” “some- times,” “rarely,” and “never,” depending on the statement. The validity of the study’s question-
naire was ensured by five experts in the fields of clinical nursing and nursing research.
Data collection. The study investigators con- tacted the operating room directors at San Antonio hospitals to obtain permission to administer the questionnaire to their periopera- tive nurses. The principle investigator visited each facility when most of the nurses were on duty. If possible, the investigator explained the study to the nurses. Otherwise, the investigator gave the questionnaires with detailed instruc- tions on data collection methods to the educa- tion coordinators, who administered the ques- tionnaires at a more convenient time. Participation in the study was voluntary, and anonymity was guaranteed. Completion of the questionnaire indicated consent to participate. Because respondents could not be identified and there was no risk to respondents, the study was exempt from the institutional review board review.
Results
he study investigators collected the questionnaires and analyzed the data. T Because the nurses occasionally did not
answer all the questions, some totals do not equal 100%.
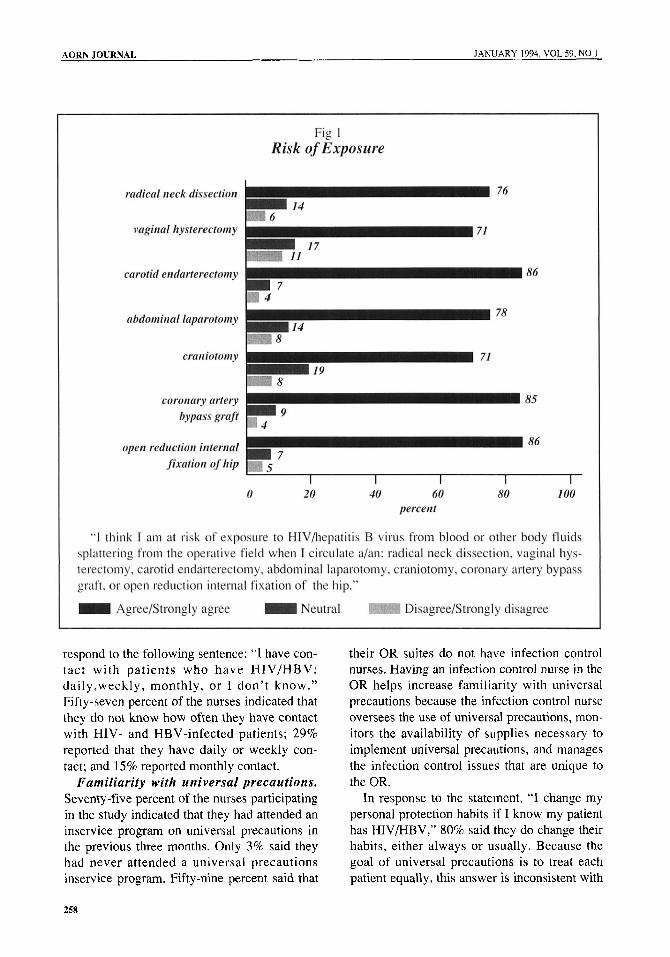
Risk perception. For the risk perception sec- tion of the questionnaire, the study participants considered the statement: “I think I am at risk for exposure to HIV/HBV from blood or other body fluids splattering from the operative field when I circulate a/an: radical neck dissection, vaginal hysterectomy, carotid endarterectomy, abdominal laparatomy, craniotomy, coronary artery bypass graft, or open reduction internal fixation of the hip.” Most of the respondents agree or strongly agree that they are at risk dur- ing these procedures (Fig 1). Those who had been nurses for more than 20 years were much less likely to think that they were at risk than were those who had been nurses for a shorter length of time.
The responses to the next statement, “As a circulator, I think my risk for exposure to HIV/HBV is greater than that of a/an: floor
256
JANUARY 1994, VOL 5Y, NO 1 AORN JOURNAL
less than 1 1 to 5 years 6 to 10 years 11 to 15 years 16 to 20 years 2 1 to 25 years 26 to 40 years
ADN Diploma BSN MSN
6 to 10 OR suites I 1 to 15 OR suites 16 to 20 OR suites
CNOR certification
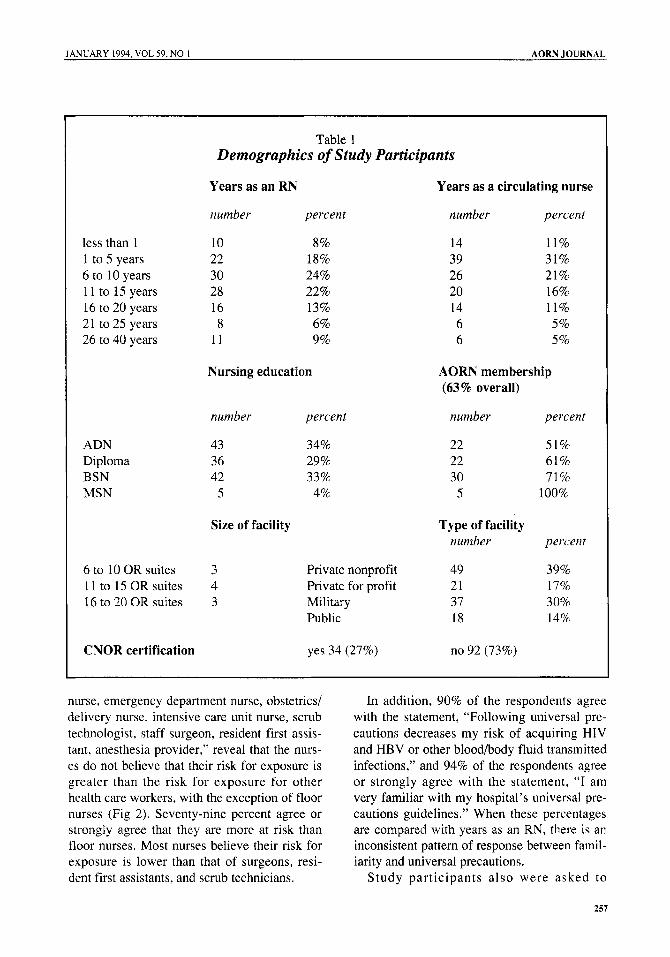
Table 1 Demographics of Study Participants
Years as an RN Years as a circulating nurse
number percent number percent
10 8% 22 18% 30 24% 28 22% 16 13% 8 6%
11 9%
Nursing education
14 11% 39 31% 26 21% 20 16% 14 11% 6 5% 6 5%
AORN membership (63 96 overall)
number percent number percent
43 34% 36 29% 42 33%
5 4%
Size of facility
3 4 3
22 51% 22 61% 30 71%
5 100%
Type of facility number percent
Private nonprofit 49 39% Private for profit 21 17% Military 37 30% Public 18 14%
yes 34 (27%) no 92 (73%)
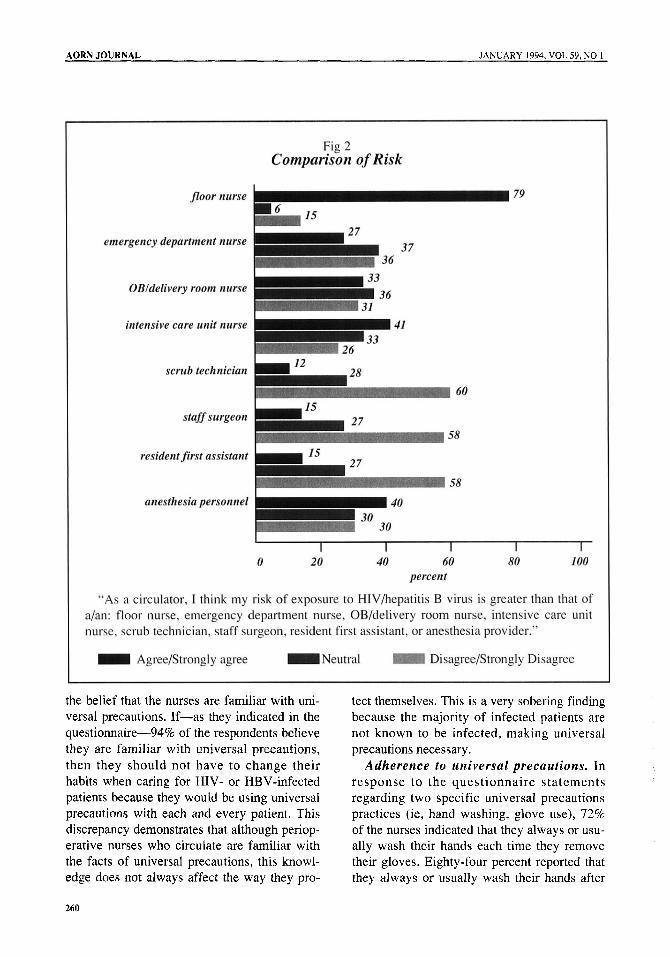
nurse, emergency department nurse, obstetrics/ delivery nurse, intensive care unit nurse, scrub technologist, staff surgeon, resident first assis- tant, anesthesia provider,” reveal that the nurs- es do not believe that their risk for exposure is greater than the risk for exposure for other health care workers, with the exception of floor nurses (Fig 2). Seventy-nine percent agree or strongly agree that they are more at risk than floor nurses. Most nurses believe their risk for exposure is lower than that of surgeons, resi- dent first assistants, and scrub technicians.
In addition, 90% of the respondents agree with the statement, “Following universal pre- cautions decreases my risk of acquiring HIV and HBV or other blood/body fluid transmitted infections,” and 94% of the respondents agree or strongly agree with the statement, “I am very familiar with my hospital’s universal pre- cautions guidelines.” When these percentages are compared with years as an RN, there is an inconsistent pattern of response between famil- iarity and universal precautions.
Study participants a lso were asked to
251
AORN JOURNAL JANUARY 1994, VOL 59, NO 1
respond to the following sentence: “I have con- tact w i t h patients who have HIV/HBV: daily,weekly, monthly, or I don’t know.” Fifty-seven percent of the nurses indicated that they do not know how often they have contact with HIV- and HBV-infected patients; 29% reported that they have daily or weekly con- tact; and 15% reported monthly contact.
Familiarity with universal precautions. Seventy -five percent of the nurses participating in the study indicated that they had attended an inservice program on universal precautions in the previous three months. Only 3% said they had never attended a universal precautions inservice program, Fifty-nine percent said that
their OR suites do not have infection control nurses. Having an infection control nurse in the OR helps increase familiarity with universal precautions because the infection control nurse oversees the use of universal precautions, mon- itors the availability of supplies necessary to implement universal precautions, and manages the infection control issues that are unique to the OR.
In response to the statement, “I change my personal protection habits if I know my patient has HIV/HBV,” 80% said they do change their habits, either always or usually. Because the goal of universal precautions is to treat each patient equally, this answer is inconsistent with
258
AORN JOURNAL JANUARY 1994, VOL 59, NO 1
the belief that the nurses are familiar with uni- versal precautions. If-as they indicated in the questionnaire-94% of the respondents believe they are familiar with universal precautions, then they should not have to change their habits when caring for HIV- or HBV-infected patients because they would be using universal precautions with each and every patient. This discrepancy demonstrates that although periop- erative nurses who circulate are familiar with the facts of universal precautions, this knowl- edge does not always affect the way they pro-
tect themselves. This is a very sobering finding because the majority of infected patients are not known to be infected, making universal precautions necessary.
Adherence to universal precautions. In response to the questionnaire statements regarding two specific universal precautions practices (ie, hand washing, glove use), 72% of the nurses indicated that they always or usu- ally wash their hands each time they remove their gloves. Eighty-four percent reported that they always or usually wash their hands after
260
AORN JOURNAL JANUARY 1994, VOL 59, NO 1
every patient contact. Past observational stud- ies of hand washing practices of unit staff nurses, however, indicate only a 41% compli- ance rate. The reported hand washing frequen- cy was three times the observed frequency.lg If this premise holds true for this study, actual hand washing rates might be much less than reported.
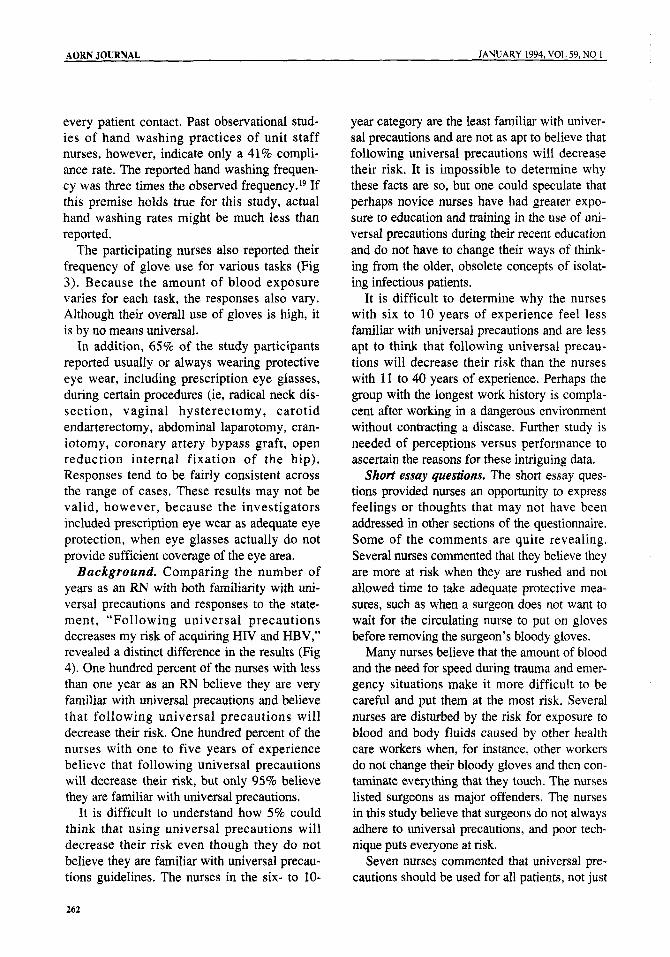
The participating nurses also reported their frequency of glove use for various tasks (Fig 3). Because the amount of blood exposure varies for each task, the responses also vary. Although their overall use of gloves is high, it is by no means universal.
In addition, 65% of the study participants reported usually or always wearing protective eye wear, including prescription eye glasses, during certain procedures (ie, radical neck dis- section, vaginal hysterectomy, carotid endarterectomy, abdominal laparotomy, cran- iotomy, coronary artery bypass graft, open reduction internal fixation of the hip). Responses tend to be fairly consistent across the range of cases. These results may not be valid, however, because the investigators included prescription eye wear as adequate eye protection, when eye glasses actually do not provide sufficient coverage of the eye area.
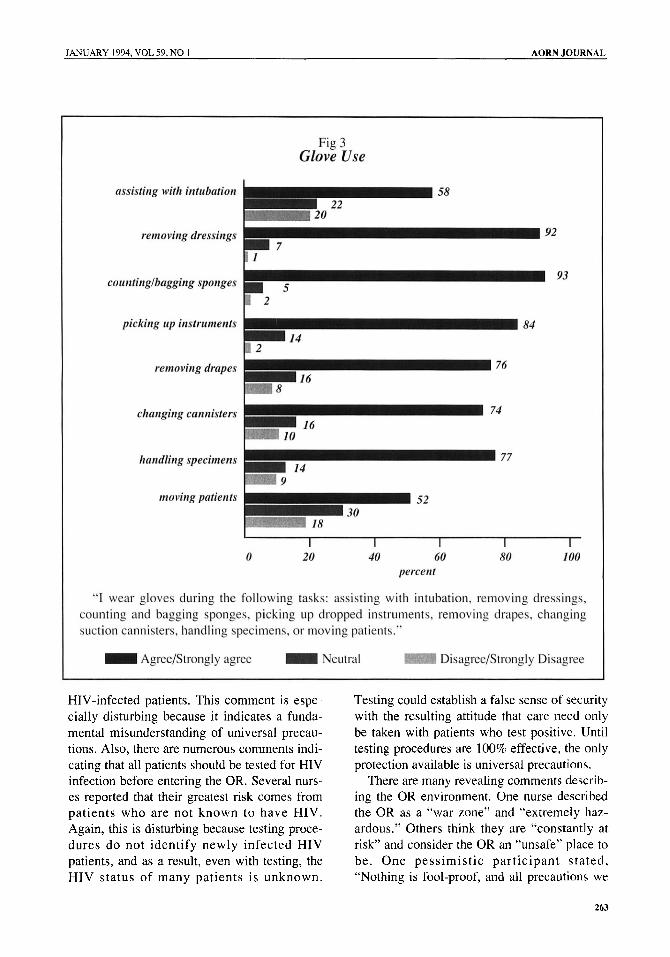
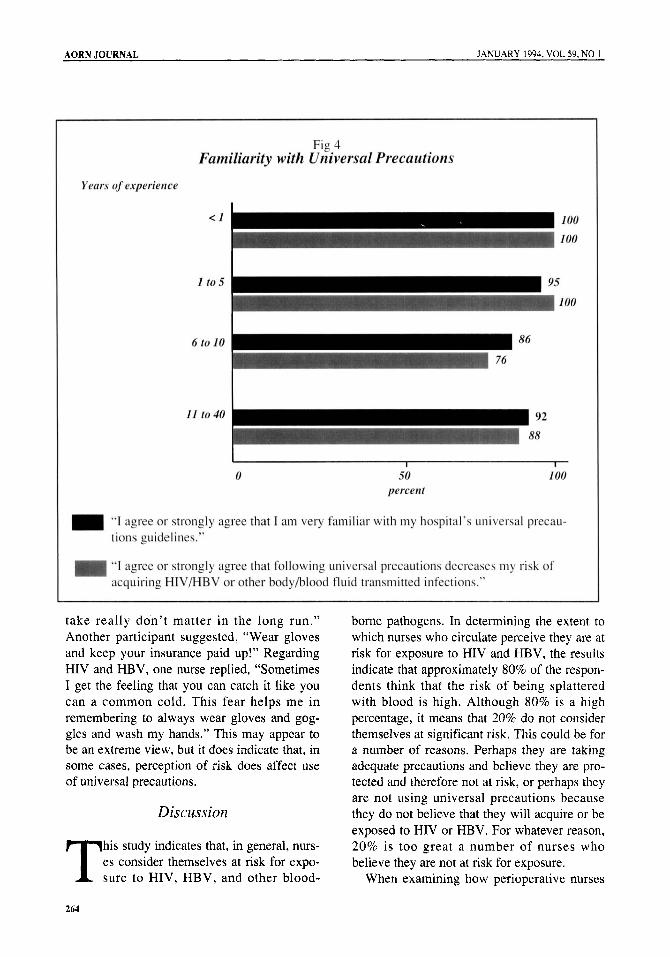
Background. Comparing the number of years as an RN with both familiarity with uni- versal precautions and responses to the state- ment, “Following universal precautions decreases my risk of acquiring HIV and HBV,” revealed a distinct difference in the results (Fig 4). One hundred percent of the nurses with less than one year as an RN believe they are very familiar with universal precautions and believe that following universal precautions will decrease their risk. One hundred percent of the nurses with one to five years of experience believe that following universal precautions will decrease their risk, but only 95% believe they are familiar with universal precautions.
It is difficult to understand how 5% could think that using universal precautions will decrease their risk even though they do not believe they are familiar with universal precau- tions guidelines. The nurses in the six- to 10-
year category are the least familiar with univer- sal precautions and are not as apt to believe that following universal precautions will decrease their risk. It is impossible to determine why these facts are so, but one could speculate that perhaps novice nurses have had greater expo- sure to education and training in the use of uni- versal precautions during their recent education and do not have to change their ways of think- ing from the older, obsolete concepts of isolat- ing infectious patients.
It is difficult to determine why the nurses with six to 10 years of experience feel less familiar with universal precautions and are less apt to think that following universal precau- tions will decrease their risk than the nurses with 11 to 40 years of experience. Perhaps the group with the longest work history is compla- cent after working in a dangerous environment without contracting a disease. Further study is needed of perceptions versus performance to ascertain the reasons for these intriguing data.
Short essay questions. The short essay ques- tions provided nurses an opportunity to express feelings or thoughts that may not have been addressed in other sections of the questionnaire. Some of the comments are quite revealing. Several nurses commented that they believe they are more at risk when they are rushed and not allowed time to take adequate protective mea- sures, such as when a surgeon does not want to wait for the circulating nurse to put on gloves before removing the surgeon’s bloody gloves.
Many nurses believe that the amount of blood and the need for speed during trauma and emer- gency situations make it more difficult to be careful and put them at the most risk. Several nurses are disturbed by the risk for exposure to blood and body fluids caused by other health care workers when, for instance, other workers do not change their bloody gloves and then con- taminate everything that they touch. The nurses listed surgeons as major offenders. The nurses in this study believe that surgeons do not always adhere to universal precautions, and poor tech- nique puts everyone at risk.
Seven nurses commented that universal pre- cautions should be used for all patients, not just
262
JANUARY 1994, VOL 59, NO 1 AORN JOURNAL
HIV-infected patients. This comment is espe- cially disturbing because it indicates a funda- mental misunderstanding of universal precau- tions. Also, there are numerous comments indi- cating that all patients should be tested for HIV infection before entering the OR. Several nurs- es reported that their greatest risk comes from patients who are not known to have HIV. Again, this is disturbing because testing proce- dures do not identify newly infected HIV patients, and as a result, even with testing, the HIV status of many patients is unknown.
Testing could establish a false sense of security with the resulting attitude that care need only be taken with patients who test positive. Until testing procedures are 100% effective, the only protection available is universal precautions.
There are many revealing comments describ- ing the OR environment. One nurse described the OR as a “war zone” and “extremely haz- ardous.” Others think they are “constantly at risk” and consider the OR an “unsafe” place to be. One pessimistic participant stated, “Nothing is fool-proof, and all precautions we
263
AORN JOURNAL JANUARY 1994, VOL 59, NO 1
take really don’t matter in the long run.” Another participant suggested, “Wear gloves and keep your insurance paid up!” Regarding HIV and HBV, one nurse replied, “Sometimes I get the feeling that you can catch it like you can a common cold. This fear helps me in remembering to always wear gloves and gog- gles and wash my hands.” This may appear to be an extreme view, but it does indicate that, in some cases, perception of risk does affect use of universal precautions.
Discussion
his study indicates that, in general, nurs- es consider themselves at risk for expo- T sure to HIV, HBV, and other blood-
borne pathogens. In determining the extent to which nurses who circulate perceive they are at risk for exposure to HIV and HBV, the results indicate that approximately 80% of the respon- dents think that the risk of being splattered with blood is high. Although 80% is a high percentage, it means that 20% do not consider themselves at significant risk. This could be for a number of reasons. Perhaps they are taking adequate precautions and believe they are pro- tected and therefore not at risk, or perhaps they are not using universal precautions because they do not believe that they will acquire or be exposed to HIV or HBV. For whatever reason, 20% is too great a number of nurses who believe they are not at risk for exposure.
When examining how perioperative nurses
264
JANUARY 1994, VOL 59, NO I AORN JOURNAL
preceive their risk for exposure to HIV and HBV compared to other health care workers, they appear to believe they are much less at risk than other OR personnel. Again, this could be because they believe they are taking adequate precautions or because they think surgeons, res- idents, and scrub technicians are more at risk due to their proximity to the operative field.
The fact that 80% of the nurses change their habits when they know that their patients are HIV or HBV infected is alarming. This could mean they are careful all the time and extra careful when dealing with infected patients, or it could mean that they are careful only when dealing with known infected patients, which is dangerous practice.
Although the use of universal precautions is now mandatory for health care workers in exposure-prone settings, perioperative nurses who circulate still need to exercise discretion and nursing judgment in the use of universal precautions. The question then is, are these nurses exercising judgment or are they being lax? According to AORN recommended prac- tices for universal precautions, “appropriate protective measures can be selected when exposure to blood or other potentially infec- tious materials is reasonably anticipated.”’* The type of protection used depends on “the task and the degree of exposure anticipated.” Therefore, the nurse must decide what methods of protection to use and when.
The size and sample of this study, the use of only one city for data collection, and the non- experimental design suggest that the findings from this study might not be applicable to a larger population. The information obtained, however, is clinically significant and provides a good starting point for future examination.
Suggestions for Further Research
he information obtained from this study indicates a need for further research in T several areas. It is imperative that we
discover what-if not perception of risk-will motivate perioperative nurses to adhere to uni- versal precautions. Observational research of
perioperative nursing activities could be very important in identifying the relationship between the actual use of universal precautions and the reported frequency of use. The relation- ship between knowledge and compliance also should be investigated further. A test of univer- sal precautions knowledge also would be important because there appears to be a funda- mental misunderstanding of the basics of uni- versal precautions among many of the nurses who participated in this study.
Personal interviews of perioperative nurses who circulate may prove helpful in determining why universal precautions are not used more often. Determining how nurses use nursing judgment and discretionary skills in dealing with situations that are not clearly defined as mandatory also would be beneficial. Research investigating the relationship between locus of control (ie, external, internal) and consistent use of universal precautions also could be helpful.
Conclusion
he majority of the nurses surveyed are using universal precautions; however, T the indications are that nurses may not
be as familiar with universal precautions as they think they are. To be effective, universal precautions must be just that-universal. Although specific situations involve the use of nursing judgment and discretion, every patient needs to be treated as potentially infectious. There is no room for discretion in this area. The only way universal precautions will become universal is through better education and train- ing. Although correct responses to questions on a universal precautions test are essential, “head knowledge” is not enough. The use of universal precautions needs to become a habit. It has to be automatic. As professionals, perioperative nurses need to use their knowledge and skills in the care they take of themselves as well as in the patient care that they provide. n Notes
1. Centers for Disease Control, “HIV prevalence estimates and AIDS case projections for the United States: Reports based upon a workshop,” Morbidity
265
AORN JOURNAL JANUARY 1994, VOL 59, NO 1
and Mortality Weekly Report 39 (NOV 30, 1990) 1-30. 2. J S Hammond et al, “HIV, trauma and infec-
tion control: Universal precautions are universally ignored,” The Journal of Trauma 30 (May 1990) 555-561; F M Gordin et al, “Prevalence of the human immunodeficiency virus and hepatitis B in unselected hospital admissions: Implications for mandatory testing and universal precautions,” The Journal of Infectious Diseases 16 1 (January 1990)
3. Centers for Disease Control, Guidelines for Prevention of Transmission of Human Immunodeficiency Virus and Hepatitis B Virus to Health-Care and Public-Safety Workers: A Response to P . L. 100-607, The Health Omnibus Programs Extension Act of 1988 (Washington, DC: US Government Printing Office, 1989) 1-46.
4. Centers for Disease Control, “Recom- mendations for prevention of HIV transmission in health care settings,” Morbidity and Mortality Weekly Report 36 (Aug 21, 1987) 1s-16s.
5. I Gurevich, “Acquired immunodeficiency syndrome: Realistic concerns and appropriate pre- cautions,” Heart and Lung 18 (March 1989) 107- 112; “Regs put new legal force behind universal pre- cautions,” American Journal of Nursing 92 (January
6. Gurevich, “Acquired immunodeficiency syn- drome: Realistic concerns and appropriate precau- tions,” 107-112; M D Hagen, K B Meyer, S G Pauker, “Routine preoperative screening for HIV: Does the risk to the surgeon outweigh the risk to the patient?” Journal of the American Medical Association 259 (March 4, 1988) 1357-1359.
7. Federal Register 54 “Proposed Rule 29,” CFR 1910 (May 30,1989) 23078.
8. Centers for Disease Control, Guidelines for Prevention of Transmission of Human Immuno- deficiency Virus and Hepatitis B Virus to Health- Care and Public-Safety Workers: A Response to P. L . 100-607, The Health Omnibus Programs Extension Act of 1988, 1-46.
9. Centers for Disease Control, “Update: HIV infection in health care workers exposed to blood of infected patients,” Morbidity and Mortality Weekly Report 36 (May 22, 1987) 285-288.
10. D J Weber, W A Rutala, “Hepatitis B immu- nization update,” infection Control and Hospital Epidemiology 10 (1989) 541-546.
11. A L Panlilio et al, “Blood contacts during sur- gical procedures,” Journal of the American Medical Association 265 (March 27, 1991) 1533-1537; S L Popejoy, D F Fry, “Blood contact and exposure in the operating room,” Surgery, Gynecology and Obstetrics 172 (June 1991) 480-483; J L Gerberding et al, “Risk for exposure of surgical personnel to patients’ blood during surgery at San Francisco
14-17.
1992) 82-84.
General Hospital,” The New England Journal of Medicine 322 (June 21, 1990) 1788-1793.
12. B J Fahey et al, “Frequency of nonparenteral occupational blood and body fluids before and after universal precautions training,” The American Journal of Medicine 90 (February 1991) 145.153.
13. E S Wong et al, “Are universal precautions effective in reducing the number of occupational exposures among health care workers? A prospective study on physicians on a medical service,” Journal of the American Medical Association 265 (March 6,
14. D A Talan, L J Baraff, “Effect of education on the use of universal precautions in a university hos- pital emergency department,” Annals of Emergency Medicine 19 (November 1990) 1322-1326.
1991) 1123-1128.
15. Ibid. 16. Gerberding et al, “Risk of exposure of surgical
personnel to patients’ blood during surgery at San Francisco General Hospital,” 1788-1793; R G Kaczmarek et al, “Glove use by health care workers: Results of a tristate investigation,” American Journal oflnfection Control 19 (October 1991) 228-232.
17. K McNabb, M L Keller, “Nurses’ risk taking regarding HIV transmission in the workplace,” Western Journal of Nursing Research 13 (December 1991) 732-745.
18. “Recommended practices for universal pre- cautions in the perioperative practice setting,” in AORN Standards and Recommended Practices (Denver: Association of Operating Room Nurses, Inc, 1993) 223.
266




















