Respiratory response to tobacco dust exposure among biddi binders: A follow up and bronchodilator...
7
57 Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 2 57 Respiratory response to tobacco dust exposure among biddi binders: A follow up and bronchodilator study B.P. Chattopadhyay, P.K. Gangopadhyay, Anirban Das, Sk. Jane Alam, Mubarak Hossain, Anirban Chowdhury, Amar Kundu Regional Occupational Health Centre (Eastern), (Indian Council of Medical Research), Block‑DP, Sector‑V, Salt Lake City, Kolkata, India For correspondence: Dr. B. P. Chattopadhyay, Regional Occupational Health Centre (Eastern), (Indian Council of Medical Research), Block‑ DP, Sector‑ V, Salt Lake City, Kolkata ‑ 700 091, India. E‑mail: bpc_rohc_ [email protected] INTRODUCTION Biddi making is a skilled job in which tobacco is rolled in a processed kendu leaf and tied with a cotton thread. The kendu leaves are moistened and then cut into pieces of required size and shape. Tobacco mixed with hand and then the processed tobacco is wrapped and rolled in the prepared cut piece of kendu leaf. The biddi workers work from morning (6 am) to 11 am and again from 2 pm to 10 pm. Some biddi factories were there at one time but now the factories are closed. Only a small group works together in some places. The airborne tobacco dust around the work places of biddi making units is the potential risk factors causing respiratory disorders to the biddi binders. The tobacco and the leaves were kept on the lap of the biddi binders and it is very much close to the nostrils and mouth. Besides these, different microbes and airborne fungal spores may be added into the working atmosphere from the processed kendu leaves. These are all the probable risk factors causing respiratory disorders among the workers. Keeping in mind the long‑term exposure of tobacco dust exposure on lung function test of biddi binders, a follow‑up study was conducted to verify the lung function changes after 2 years of exposure. MATERIALS AND METHODS Medical study In both male and female biddi binders, a validated questionnaire was administered and relevant information such as history of illness, was noted. Clinical examination was performed following standard procedures. This is a follow‑up study after 2 years of the initial study. A total of 86 (male, 41; female, 45) biddi binders were followed up. The parameters of importance were compared with the initial study findings and the results are discussed in the following section. Only 86 biddi binders of initial study group had been followed up. So the present reporting compared the results of the initial study group with those of their follow‑up study group. Abstract Intorduction: The tobacco dusts get air borne during biddi making and it is inhaled by the biddi binders, which affects their health. Results: In a follow‑up study, 86 biddi binders (male, 41; female, 45) were studied at a gap of 2 years. A high respiratory morbidity was observed among males than females both in the initial and follow‑up study. The main complaints such as cough, sputum, and breathlessness showed high prevalence rates in the follow‑up study. The high prevalence rates of weakness, giddiness, chronic diarrhea, and dyspepsia were noted in most of the cases the above complaints showed higher rates in the follow‑up study. Pulmonary function test (PFT) values in the follow‑up study of male and female biddi binders showed lowered compared with the initial study of same gender. In male and female biddi binders, the lung volumes SVC, FVC, FEV 1 , and the flow rates FEF 0.2–1.2 l , FEF 25%–75% , FEF 75%–85% were significantly lowered in the follow‑up study compared with the initial study. Age‑related decrement in PFT was observed in both the studies. In nonsmokers, smokers, and ex‑smokers, the PFT values are lowered. The current smokers have the lowest values in both the studies. With the administration of the bronchodilator aerosol (salbutamol) in 63 biddi binders (male, 27; female, 36), the effect of bronchodilator aerosol on the PFT parameters showed significant changes as all PFT parameters showed positive bronchodilatation. Conclusion: The pattern of bronchodilator response on PFT values of the biddi binders suggests that the obstructions in the airways are reversible in nature. Key words: Biddi binders, biddi making, bronchodilator aerosol, initial and follow‑up study, tobacco dust Access this article online Website: www.ijoem.com DOI: 10.4103/0019-5278.146891 Quick Response Code: Original Article [Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal
Transcript of Respiratory response to tobacco dust exposure among biddi binders: A follow up and bronchodilator...
57Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 2 57
Respiratory response to tobacco dust exposure among biddi binders: A follow up and bronchodilator study
B.P. Chattopadhyay, P.K. Gangopadhyay, Anirban Das, Sk. Jane Alam, Mubarak Hossain, Anirban Chowdhury, Amar KunduRegional Occupational Health Centre (Eastern), (Indian Council of Medical Research), Block‑DP, Sector‑V, Salt Lake City, Kolkata, India
For correspondence: Dr. B. P. Chattopadhyay, Regional Occupational Health Centre (Eastern), (Indian Council of Medical Research), Block‑ DP, Sector‑ V, Salt Lake City, Kolkata ‑ 700 091, India. E‑mail: [email protected]
INTRODUCTION
Biddi making is a skilled job in which tobacco is rolled in a processed kendu leaf and tied with a cotton thread. The kendu leaves are moistened and then cut into pieces of required size and shape. Tobacco mixed with hand and then the processed tobacco is wrapped and rolled in the prepared cut piece of kendu leaf. The biddi workers work from morning (6 am) to 11 am and again from 2 pm to 10 pm. Some biddi factories were there at one time but now the factories are closed. Only
a small group works together in some places.
The airborne tobacco dust around the work places of biddi making units is the potential risk factors causing respiratory disorders to the biddi binders. The tobacco and the leaves were kept on the lap of the biddi binders and it is very much close to the nostrils and mouth. Besides these, different microbes and airborne fungal spores may be added into the working atmosphere from the processed kendu leaves. These are all the probable risk factors causing respiratory disorders among the workers. Keeping in mind the long‑term exposure of tobacco dust exposure on lung function test of biddi binders, a follow‑up study was conducted to verify the lung function changes after 2 years of exposure.
MATERIALS AND METHODS
Medical studyIn both male and female biddi binders, a validated questionnaire was administered and relevant information such as history of illness, was noted. Clinical examination was performed following standard procedures.
This is a follow‑up study after 2 years of the initial study. A total of 86 (male, 41; female, 45) biddi binders were followed up. The parameters of importance were compared with the initial study findings and the results are discussed in the following section. Only 86 biddi binders of initial study group had been followed up. So the present reporting compared the results of the initial study group with those of their follow‑up study group.
AbstractIntorduction: The tobacco dusts get air borne during biddi making and it is inhaled by the biddi binders, which affects their health. Results: In a follow‑up study, 86 biddi binders (male, 41; female, 45) were studied at a gap of 2 years. A high respiratory morbidity was observed among males than females both in the initial and follow‑up study. The main complaints such as cough, sputum, and breathlessness showed high prevalence rates in the follow‑up study. The high prevalence rates of weakness, giddiness, chronic diarrhea, and dyspepsia were noted in most of the cases the above complaints showed higher rates in the follow‑up study. Pulmonary function test (PFT) values in the follow‑up study of male and female biddi binders showed lowered compared with the initial study of same gender. In male and female biddi binders, the lung volumes SVC, FVC, FEV1, and the flow rates FEF0.2–1.2 l, FEF25%–75%, FEF75%–85% were significantly lowered in the follow‑up study compared with the initial study. Age‑related decrement in PFT was observed in both the studies. In nonsmokers, smokers, and ex‑smokers, the PFT values are lowered. The current smokers have the lowest values in both the studies. With the administration of the bronchodilator aerosol (salbutamol) in 63 biddi binders (male, 27; female, 36), the effect of bronchodilator aerosol on the PFT parameters showed significant changes as all PFT parameters showed positive bronchodilatation. Conclusion: The pattern of bronchodilator response on PFT values of the biddi binders suggests that the obstructions in the airways are reversible in nature.
Key words: Biddi binders, biddi making, bronchodilator aerosol, initial and follow‑up study, tobacco dust
Access this article onlineWebsite: www.ijoem.comDOI: 10.4103/0019-5278.146891Quick Response Code:
Original Article[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal
Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
58 Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 258
Pulmonary Function Test: The PFT was carried out by spirometric method. A total of 89 biddi binders (male, 43; female, 46) were studied. Vital capacity (VC) and forced vital capacity (FVC) was recorded by Spirovit SP‑10 (Schiller Health Care Pvt Ltd., Switzerland) and Peak Expiratory Flow Rate by Wrights Peak Flow meter (Clement and Clarke, UK). Forced expiratory volume in the 1st s (FEV1) and the 3rd s (FEV3), Forced expiratory volume in 1st and 3rd s as the percentage of FVC (FEV1% and FEV3%), forced expiratory flow at FEF200 mL–1200 mL, FEF25%–75%, and FEF75%–85% was calculated from the tracings. The subjects were well motivated thus ensuring recording at optimum levels. The PFT measurements were made in a comfortable standing position. The body height and body weight were measured with a standard scale without footwear. All measured lung volumes obtained was expressed in body temperature pressure saturated with water vapor (BTPS).[1] Body surface area (BSA) was calculated from the Du‑Bois and Du‑Bois[2] formula. PFT values were predicted from the standard prediction equation of the Kolkata normal subjects. The criteria followed for categorization of the severity of restrictive impairment are based on the ratios between predicted and observed values of VC and obstructive impairment based on FEV1%.
RESULTS AND DISCUSSION
Medical studyThe average age of the male subjects of the initial study and the follow‑up study were 49.66 ± 9.88 and 51.54 ± 10.54 years and 36.09 ± 9.34 and 38.34 ± 9.67 years for females, respectively. The mean age of the total population male and female combined at the initial study is 42.04 ± 12.03 and the follow‑up study is 44.63 ± 12.03.
Their mean height and weight of the first study (initial study) were 155.41 ± 7.61 cm (male, 161.02 ± 6.50 cm; female, 151.29 ± 4.41 cm) and in the follow‑up study
were 155.49 ± 7.34 (male, 160.42 ± 6.81 cm and female 151.00 ± 4.34 cm); similarly the weight in the initial study was 47.71 ± 9.16 kg (male, 50.88 ± 9.78 kg; female, 44.82 ± 9.16 kg) and in the follow‑up study, the mean weight was 49.44 ± 9.31 kg (male, 52.93 ± 9.94 and female 46.26 ± 7.47).
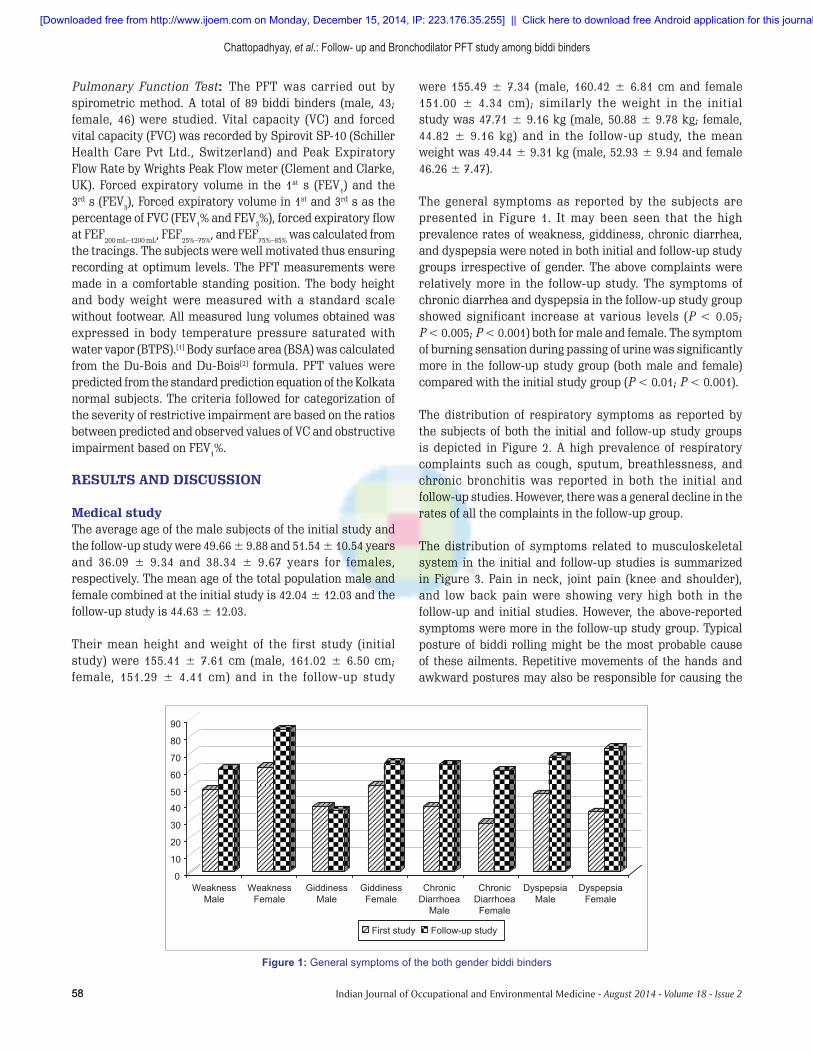
The general symptoms as reported by the subjects are presented in Figure 1. It may been seen that the high prevalence rates of weakness, giddiness, chronic diarrhea, and dyspepsia were noted in both initial and follow‑up study groups irrespective of gender. The above complaints were relatively more in the follow‑up study. The symptoms of chronic diarrhea and dyspepsia in the follow‑up study group showed significant increase at various levels (P < 0.05; P < 0.005; P < 0.001) both for male and female. The symptom of burning sensation during passing of urine was significantly more in the follow‑up study group (both male and female) compared with the initial study group (P < 0.01; P < 0.001).
The distribution of respiratory symptoms as reported by the subjects of both the initial and follow‑up study groups is depicted in Figure 2. A high prevalence of respiratory complaints such as cough, sputum, breathlessness, and chronic bronchitis was reported in both the initial and follow‑up studies. However, there was a general decline in the rates of all the complaints in the follow‑up group.
The distribution of symptoms related to musculoskeletal system in the initial and follow‑up studies is summarized in Figure 3. Pain in neck, joint pain (knee and shoulder), and low back pain were showing very high both in the follow‑up and initial studies. However, the above‑reported symptoms were more in the follow‑up study group. Typical posture of biddi rolling might be the most probable cause of these ailments. Repetitive movements of the hands and awkward postures may also be responsible for causing the
Figure 1: General symptoms of the both gender biddi binders
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal

Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
59Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 2 59
above‑mentioned symptoms. Similar types of observations were also noted by NIOH.[3,4] A substantial number of subjects in both the follow‑up and initial study groups complained of peripheral neuropathy. Although the prevalence rate of peripheral neuropathy (tingling, numbness, burning sensation, and weakness of limbs) in males in the follow‑up study group (68.3%) was less than that in the initial study group (82.9%), but in females the follow up study group (77.8%) showed significantly higher rates (P < 0.05) than in the initial study group (57.8%).
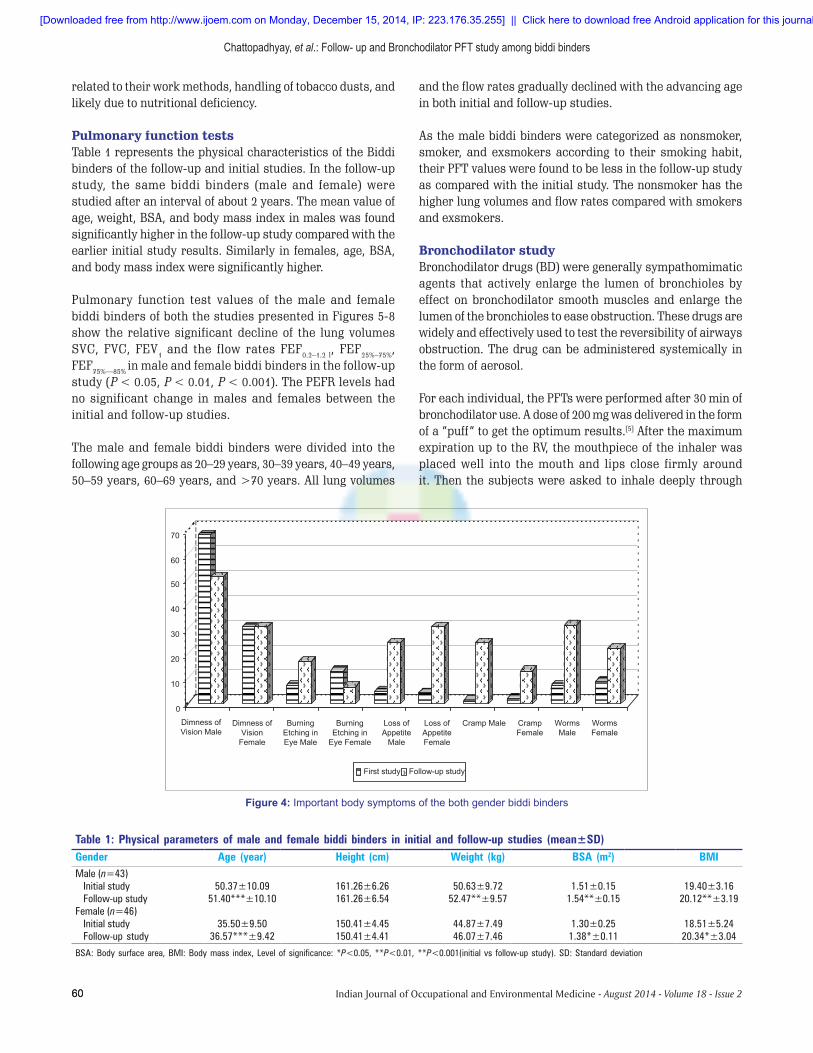
Other important symptoms, such as burning and itching of eye, dimness of vision, loss of appetite, feeling of cramps, and others, are given in Figure 4. Loss of appetite and feeling of cramps of males of follow‑up study showed significantly higher rate compared with that of male subjects of initial study (P < 0.001, P < 0.05). Similarly, significantly more number of females complained loss of appetite and feeling of cramps in the follow‑up study (P < 0.001; P < 0.05). It
is a matter of concern that the overall complaints of worm infestations has increased to 26.7% from 10.5% of the initial study. As usual thread worm/pin worm, was the main type of worms that infected them and are significantly more in the follow‑up study group compared with the initial study group (P < 0.01).
The distribution of angular stomatitis and glossitis showed lower rates in males in the follow‑up study than that of the initial study group. Females showed a higher rate of pallor and angular stomatitis.
Hypertension [blood pressure (BP) >140/90 mmHg] was observed in 5.8% subjects in the follow‑up study (male, 4.9%; female, 6.7%). Only systolic hypertension (systolic BP >140 mmHg) was noted in male –12.2% and female – 8.9% compared with initial study male –2.4% and female –4.4%. Diastolic hypertension (BP >90 mmHg) was observed only in the follow‑up study. Most of the signs and symptoms may be
Figure 2: Respiratory symptoms of the both gender biddi binders
Figure 3: Musculo ‑ skeletal system of the both gender biddi binders
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal
Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
60 Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 260
related to their work methods, handling of tobacco dusts, and likely due to nutritional deficiency.
Pulmonary function testsTable 1 represents the physical characteristics of the Biddi binders of the follow‑up and initial studies. In the follow‑up study, the same biddi binders (male and female) were studied after an interval of about 2 years. The mean value of age, weight, BSA, and body mass index in males was found significantly higher in the follow‑up study compared with the earlier initial study results. Similarly in females, age, BSA, and body mass index were significantly higher.
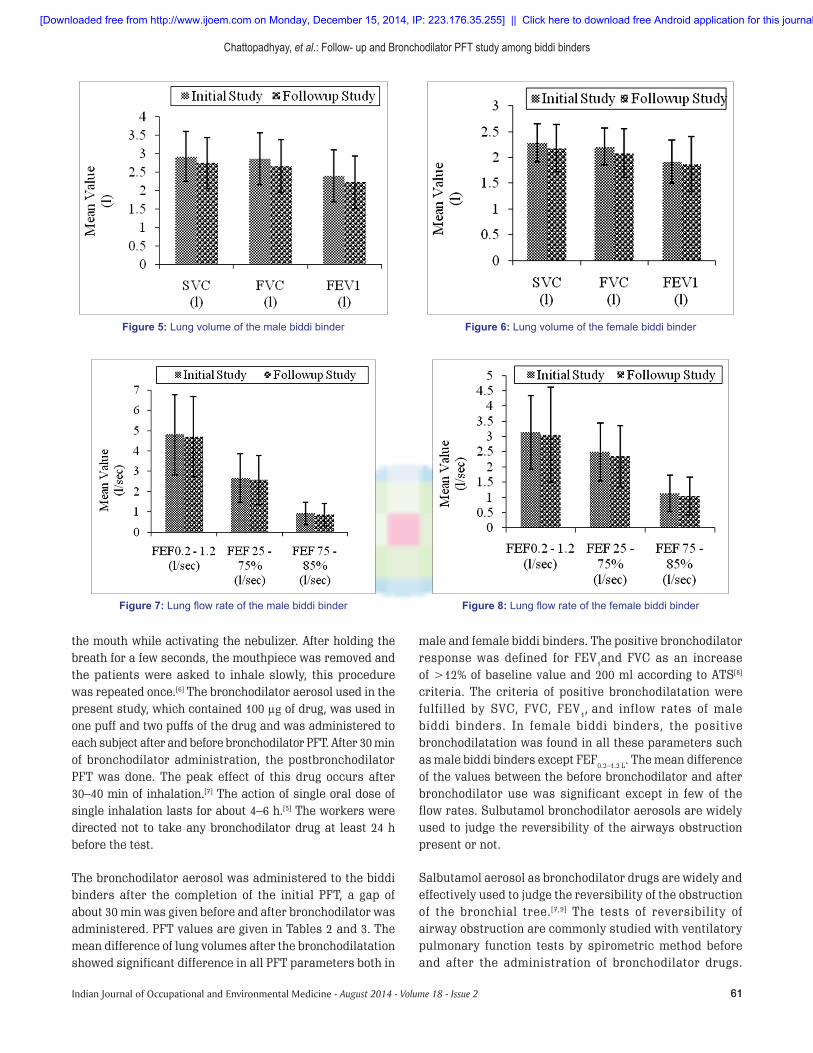
Pulmonary function test values of the male and female biddi binders of both the studies presented in Figures 5‑8 show the relative significant decline of the lung volumes SVC, FVC, FEV1 and the flow rates FEF0.2–1.2 l, FEF25%–75%, FEF75%—85% in male and female biddi binders in the follow‑up study (P < 0.05, P < 0.01, P < 0.001). The PEFR levels had no significant change in males and females between the initial and follow‑up studies.
The male and female biddi binders were divided into the following age groups as 20–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, and >70 years. All lung volumes
and the flow rates gradually declined with the advancing age in both initial and follow‑up studies.
As the male biddi binders were categorized as nonsmoker, smoker, and exsmokers according to their smoking habit, their PFT values were found to be less in the follow‑up study as compared with the initial study. The nonsmoker has the higher lung volumes and flow rates compared with smokers and exsmokers.
Bronchodilator studyBronchodilator drugs (BD) were generally sympathomimatic agents that actively enlarge the lumen of bronchioles by effect on bronchodilator smooth muscles and enlarge the lumen of the bronchioles to ease obstruction. These drugs are widely and effectively used to test the reversibility of airways obstruction. The drug can be administered systemically in the form of aerosol.
For each individual, the PFTs were performed after 30 min of bronchodilator use. A dose of 200 mg was delivered in the form of a “puff” to get the optimum results.[5] After the maximum expiration up to the RV, the mouthpiece of the inhaler was placed well into the mouth and lips close firmly around it. Then the subjects were asked to inhale deeply through
Figure 4: Important body symptoms of the both gender biddi binders
Table 1: Physical parameters of male and female biddi binders in initial and follow‑up studies (mean±SD)Gender Age (year) Height (cm) Weight (kg) BSA (m2) BMIMale (n=43)
Initial study 50.37±10.09 161.26±6.26 50.63±9.72 1.51±0.15 19.40±3.16Follow‑up study 51.40***±10.10 161.26±6.54 52.47**±9.57 1.54**±0.15 20.12**±3.19
Female (n=46)Initial study 35.50±9.50 150.41±4.45 44.87±7.49 1.30±0.25 18.51±5.24Follow‑up study 36.57***±9.42 150.41±4.41 46.07±7.46 1.38*±0.11 20.34*±3.04
BSA: Body surface area, BMI: Body mass index, Level of significance: *P<0.05, **P<0.01, **P<0.001(initial vs follow‑up study). SD: Standard deviation
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal
Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
61Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 2 61
the mouth while activating the nebulizer. After holding the breath for a few seconds, the mouthpiece was removed and the patients were asked to inhale slowly, this procedure was repeated once.[6] The bronchodilator aerosol used in the present study, which contained 100 µg of drug, was used in one puff and two puffs of the drug and was administered to each subject after and before bronchodilator PFT. After 30 min of bronchodilator administration, the postbronchodilator PFT was done. The peak effect of this drug occurs after 30–40 min of inhalation.[7] The action of single oral dose of single inhalation lasts for about 4–6 h.[5] The workers were directed not to take any bronchodilator drug at least 24 h before the test.
The bronchodilator aerosol was administered to the biddi binders after the completion of the initial PFT, a gap of about 30 min was given before and after bronchodilator was administered. PFT values are given in Tables 2 and 3. The mean difference of lung volumes after the bronchodilatation showed significant difference in all PFT parameters both in
male and female biddi binders. The positive bronchodilator response was defined for FEV1and FVC as an increase of >12% of baseline value and 200 ml according to ATS[8] criteria. The criteria of positive bronchodilatation were fulfilled by SVC, FVC, FEV1, and inflow rates of male biddi binders. In female biddi binders, the positive bronchodilatation was found in all these parameters such as male biddi binders except FEF0.2–1.2 L. The mean difference of the values between the before bronchodilator and after bronchodilator use was significant except in few of the flow rates. Sulbutamol bronchodilator aerosols are widely used to judge the reversibility of the airways obstruction present or not.
Salbutamol aerosol as bronchodilator drugs are widely and effectively used to judge the reversibility of the obstruction of the bronchial tree.[7,9] The tests of reversibility of airway obstruction are commonly studied with ventilatory pulmonary function tests by spirometric method before and after the administration of bronchodilator drugs.
Figure 5: Lung volume of the male biddi binder Figure 6: Lung volume of the female biddi binder
Figure 7: Lung flow rate of the male biddi binder Figure 8: Lung flow rate of the female biddi binder
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal
Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
62 Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 262
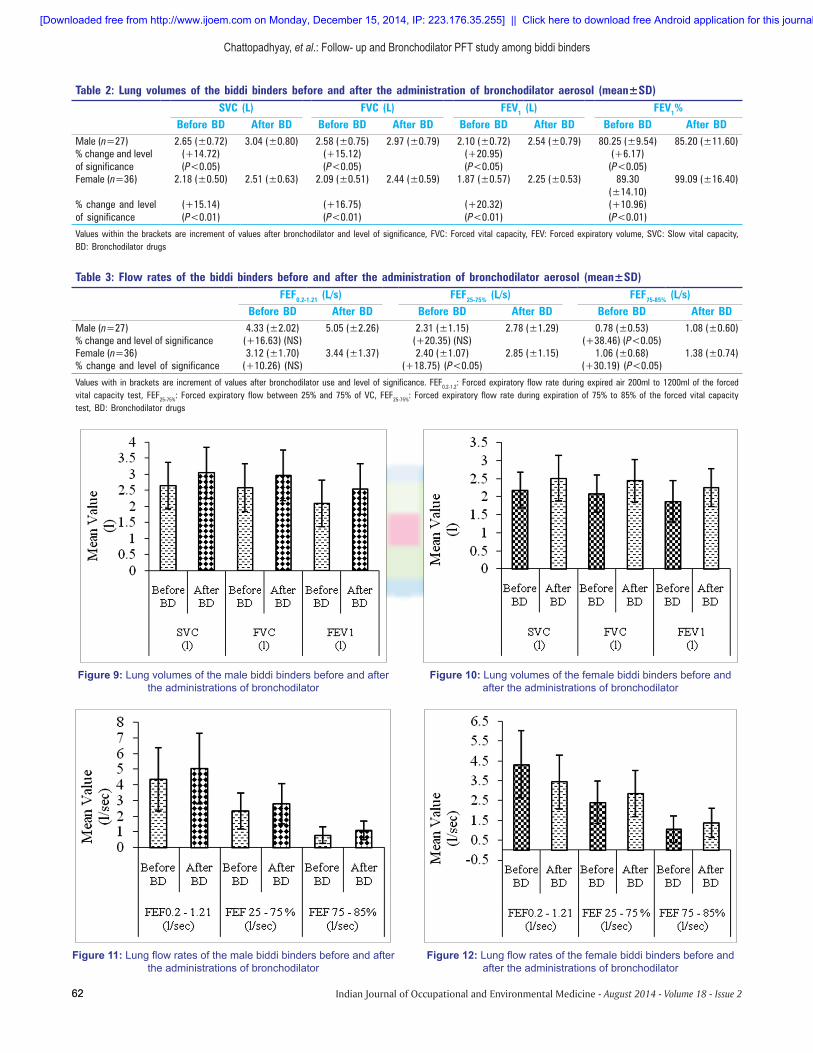
Table 2: Lung volumes of the biddi binders before and after the administration of bronchodilator aerosol (mean±SD)SVC (L) FVC (L) FEV1 (L) FEV1%
Before BD After BD Before BD After BD Before BD After BD Before BD After BDMale (n=27) 2.65 (±0.72) 3.04 (±0.80) 2.58 (±0.75) 2.97 (±0.79) 2.10 (±0.72) 2.54 (±0.79) 80.25 (±9.54) 85.20 (±11.60)% change and level of significance
(+14.72) (P<0.05)
(+15.12) (P<0.05)
(+20.95) (P<0.05)
(+6.17) (P<0.05)
Female (n=36) 2.18 (±0.50) 2.51 (±0.63) 2.09 (±0.51) 2.44 (±0.59) 1.87 (±0.57) 2.25 (±0.53) 89.30 (±14.10)
99.09 (±16.40)
% change and level of significance
(+15.14) (P<0.01)
(+16.75) (P<0.01)
(+20.32) (P<0.01)
(+10.96) (P<0.01)
Values within the brackets are increment of values after bronchodilator and level of significance, FVC: Forced vital capacity, FEV: Forced expiratory volume, SVC: Slow vital capacity, BD: Bronchodilator drugs
Table 3: Flow rates of the biddi binders before and after the administration of bronchodilator aerosol (mean±SD)FEF0.2‑1.21 (L/s) FEF25‑75% (L/s) FEF75‑85% (L/s)
Before BD After BD Before BD After BD Before BD After BDMale (n=27) 4.33 (±2.02) 5.05 (±2.26) 2.31 (±1.15) 2.78 (±1.29) 0.78 (±0.53) 1.08 (±0.60)% change and level of significance (+16.63) (NS) (+20.35) (NS) (+38.46) (P<0.05)Female (n=36) 3.12 (±1.70) 3.44 (±1.37) 2.40 (±1.07) 2.85 (±1.15) 1.06 (±0.68) 1.38 (±0.74)% change and level of significance (+10.26) (NS) (+18.75) (P<0.05) (+30.19) (P<0.05)
Values with in brackets are increment of values after bronchodilator use and level of significance. FEF0.2‑1.2: Forced expiratory flow rate during expired air 200ml to 1200ml of the forced vital capacity test, FEF25‑75%: Forced expiratory flow between 25% and 75% of VC, FEF25‑75%: Forced expiratory flow rate during expiration of 75% to 85% of the forced vital capacity test, BD: Bronchodilator drugs
Figure 9: Lung volumes of the male biddi binders before and after the administrations of bronchodilator
Figure 10: Lung volumes of the female biddi binders before and after the administrations of bronchodilator
Figure 11: Lung flow rates of the male biddi binders before and after the administrations of bronchodilator
Figure 12: Lung flow rates of the female biddi binders before and after the administrations of bronchodilator
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal

Chattopadhyay, et al.: Follow- up and Bronchodilator PFT study among biddi binders
63Indian Journal of Occupational and Environmental Medicine - August 2014 - Volume 18 - Issue 2 63
Response to bronchodilator aerosol is commonly tested by the measurement of FEV1 before and after the dose of the drug.[10] Astin[11] evidenced that the possible causes of airway resistance in these subjects are not fully known, although the possible causes might be mucous gland hypertrophy, mucosal edema, intraluminal secretion, and bronchial muscle constrictions. This might be the possible reason for the obstruction in the present study. It has been found that a significant part of these increased airway resistance are reversible in these subjects after bronchodilator aerosol administration. In the present study, there is a significant increase in SVC, FVC, FEV1, FEV1%, and FEF75%–85% after the administration of salbutamol bronchodilator aerosol reflects that there is some obstruction. In the present study, the airway obstruction of the biddi binders is reversible and it satisfies the criteria of positive bronchodilator response according to the criteria established by American Thoracic Society. A significant part of the increased airway resistance was reversed in the present subject in the bronchodilator use. This finding of positive bronchodilatation corresponds to the findings of Sobol et al.[12] The statistically significant changes of PFT values in some parameters might be due to the reversal of smooth muscle tone present as evidenced [Figures 9‑12].[13]
CONCLUSION
Biddi binders are exposed to tobacco dust, which effects their respiratory functions. Comparison of initial and follow‑up studies provides evidence of relative increase of the prevalence of various ailments as well as PFT values, irrespective of gender and age group after continuation for 2 years of exposure in the same occupational activity. Administration of bronchodilator drug could inevitably bring positive bronchodilatation and easing of airway airway resistance of the biddi binders indicating the obstruction in the airways might be reversible in nature.
ACKNOWLEDGMENT
The investigators are grateful to the Department of Science and Technology, Govt. of West Bengal, for the sponsorship and financial
support to carry out this important project. Thanks are due to the Anchal pradhans of Mograhut Gram Panchyat south and north for their kind co‑operation in the study. Active participation by the biddi binders in the study is highly appreciated.
REFERENCES
1. Cotes JE. Lung function assessment and application in Medicine. 3rd ed. Oxford: Blackwell Scientific Publication; 1976.
2. Du‑Bois D, Du‑Bois EF. Clinical calorimetry. A formula to estimate the approximate surface area if height and weight be known. Arch Intern Med 1916;17:868‑1.
3. Annual Report 1980b, National Institute of Occupational Health, Ahmedabad,‑Occupational Health survey of Women Workers engaged in Biddi making (rolling).
4. Annual Report 1983‑84, National Institute of Occupational Health, Ahmedabad, ‑Occupational Health survey of Women Workers engaged in Bidi making (rolling:1983‑84, p. 78‑86.
5. Satoskar S, Bhandarkar SD. Pharmacology and pharmacotherapies. 7th ed. Bombay, India: Popular Prakashan; 1980. p. 210‑86.
6. Crofton J, Douglas A. Respiratory diseases. 4th ed. Blackwell: Blackwell Scientific Publications; 1997. p. 697‑8.
7. Gilmal AG, Goldman LS, Gilman A. The Pharmacological basis of Therapeutics. INC New York: Macmillan Publishing Company; 6th ed. 1982. p. 166‑8.
8. Lung function testing: Selection of reference values and interpretative strategies. American thoracic society. Am Rev Respir Dis 1991;144:1202‑18.
9. Gilman AG, Goodman LS, Gilman A. The pharmacological basis of therapeutics. 6th ed. New York: McMillan Publishing Company Inc; 1982. p. 166‑8.
10. Pierson RN Jr, Grieco MH. Isoproterenol aerosol in normal and asthmatic subjects. Am Rev Respir Dis 1969:100;533‑41.
11. Astin TW. Reversibility of airways obstruction in chronic bronchitis. Clin Sci 1972;42:725‑33.
12. Sobol BJ, Emirgil C, Waldie JR, Reed R. A response to isoproterenol in normal subjects and subjects with asthma. Am Rev Respir Dis 1974;109:290‑2.
13. Widdicombe JG. Regulation of tracheobronxhil smooth muscle. Physiol Rev 1963;43:1‑37.
Cite this article as: Chattopadhyay BP, Gangopadhyay PK, Das A, Alam SJ, Hossain M, Chowdhury A, et al. Respiratory response to tobacco dust exposure among biddi binders: A follow up and bronchodilator study. Indian J Occup Environ Med 2014;18:57‑63.
Source of Support: Nil, Conflict of Interest: None declared.
[Downloaded free from http://www.ijoem.com on Monday, December 15, 2014, IP: 223.176.35.255] || Click here to download free Android application for this journal