Resistance of Plasmodium falciparum to antimalarial drugs in a highly endemic area of southern Viet...
11
Scandinavian Journal of Infectious Diseases, 2010; 42: 22–32 ISSN 0036-5548 print/ISSN 1651-1980 online © 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS) DOI: 10.3109/00365540903289670 Correspondence: R. Durand, Laboratoire de Parasitologie-Mycologie, AP-HP, Hôpital Avicenne, 125 rue de Stalingrad, 93009 Bobigny Cedex, France. E-mail: [email protected] (Received 25 June 2009; accepted 24 August 2009) REVIEW ARTICLE History and current status of Plasmodium falciparum antimalarial drug resistance in Madagascar VALÉRIE ANDRIANTSOANIRINA 1 , DIDIER MÉNARD 1 , LUCIANO TUSEO 2 & RÉMY DURAND 3 From the 1 Malaria Research Unit, Institut Pasteur de Madagascar, Antananarivo, Madagascar, 2 World Health Organization Office of Madagascar and La Réunion, Antananarivo, Madagascar, and 3 Laboratoire de Parasitologie-Mycologie, Hôpital Avicenne, AP-HP, Bobigny, France Abstract Malaria remains a major health problem in Madagascar. Over past decades, the burden of malarial disease has fluctuated over time, partly in line with the successes and failures of antimalarial policy. In the 1950s and 1960s, a sharp decline in malaria transmission was observed in the central highlands due to indoor spraying with DDT and to the massive use of chloroquine by the population. Following this, the discontinuation of the ‘nivaquinization’ policy was followed by devastat- ing outbreaks in the central highlands in the 1980s. Currently, the rate of in vitro chloroquine-resistant Plasmodium falci- parum isolates does not exceed 5%. This figure appears disconnected from the high level of clinical treatment failure (near 40%). pfcrt mutant isolates are found in less than 1% of isolates on the Island. Conversely, pfmdr1 mutant isolates are found in more than 60% of isolates and may be responsible for the bulk of resistance to chloroquine in Madagascar. Other anti- malarials remain generally effective in Madagascar. Recent clinical and in vitro data support the complete efficacy of the combination artesunate–amodiaquine in Madagascar. As such, this artemisinin combination therapy should play a central role in the control and possible elimination of P. falciparum malaria in Madagascar. Introduction Malaria remains a major health problem in Mada- gascar [1,2]. Together with indoor spraying of DDT (and the use of long lasting impregnated bed nets), the use of antimalarial drugs is central to the control of malaria [3]. Malaria morbidity and mortality have fluctuated over time, partly in line with the successes and failures of antimalarial policy. In the 1950s and 1960s, a sharp decline in malaria transmission was observed, mostly in the central highlands, due to indoor spraying with dichlorodiphenyltrichloroethane (DDT) and to the massive use of chloroquine by the population [4,5]. These results were obtained because of the well-organized healthcare system, which in particular allowed the implementation of parasitological diag- nosis. Subsequently, the discontinuation of the ‘niva- quinization’ policy was followed by devastating outbreaks in the central highland areas in the 1980s [6–8]. Meanwhile, Plasmodium falciparum clinical resistance emerged and spread [9]. Today, artemisinin- based combination therapy (ACT) has replaced chloroquine as the first-line treatment, whereas the sulfadoxine–pyrimethamine combination (SP) is given intermittently as preventive treatment in pregnant women. Following the global trend, the Malagasy government claims as its objective the elimination of malaria as a public health problem [10]. The aim of this review is to present the history and current status of P. falciparum antimalarial drug resistance in Madagascar and to consider its impact on malaria control programmes. Context and malaria situation in Madagascar Madagascar appears as an isolated fragment of the ancient continent ‘Gondwana’, which was separated from Africa 65–100 million y ago [11]. Human set- tlement in Madagascar occurred relatively recently, with the population originating from overseas. The first arrivals are thought to have settled during the first centuries of the Christian era, reaching the central highlands only in the 5 th –7 th centuries. Parasites and Scand J Infect Dis Downloaded from informahealthcare.com by HINARI on 02/23/15 For personal use only.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Resistance of Plasmodium falciparum to antimalarial drugs in a highly endemic area of southern Viet...

Scandinavian Journal of Infectious Diseases, 2010; 42: 22–32
ISSN 0036-5548 print/ISSN 1651-1980 online © 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS)DOI: 10.3109/00365540903289670
Correspondence: R. Durand, Laboratoire de Parasitologie-Mycologie, AP-HP, Hôpital Avicenne, 125 rue de Stalingrad, 93009 Bobigny Cedex, France. E-mail: [email protected]
(Received 25 June 2009; accepted 24 August 2009)
REVIEW ARTICLE
History and current status of Plasmodium falciparum antimalarial drug resistance in Madagascar
VALÉRIE ANDRIANTSOANIRINA 1, DIDIER MÉNARD1, LUCIANO TUSEO2 &RÉMY DURAND3
From the 1Malaria Research Unit, Institut Pasteur de Madagascar, Antananarivo, Madagascar, 2World Health Organization Offi ce of Madagascar and La Réunion, Antananarivo, Madagascar, and 3Laboratoire de Parasitologie-Mycologie, Hôpital Avicenne, AP-HP, Bobigny, France
AbstractMalaria remains a major health problem in Madagascar. Over past decades, the burden of malarial disease has fl uctuated over time, partly in line with the successes and failures of antimalarial policy. In the 1950s and 1960s, a sharp decline in malaria transmission was observed in the central highlands due to indoor spraying with DDT and to the massive use of chloroquine by the population. Following this, the discontinuation of the ‘nivaquinization’ policy was followed by devastat-ing outbreaks in the central highlands in the 1980s. Currently, the rate of in vitro chloroquine-resistant Plasmodium falci-parum isolates does not exceed 5%. This fi gure appears disconnected from the high level of clinical treatment failure (near 40%). pfcrt mutant isolates are found in less than 1% of isolates on the Island. Conversely, pfmdr1 mutant isolates are found in more than 60% of isolates and may be responsible for the bulk of resistance to chloroquine in Madagascar. Other anti-malarials remain generally effective in Madagascar. Recent clinical and in vitro data support the complete effi cacy of the combination artesunate–amodiaquine in Madagascar. As such, this artemisinin combination therapy should play a central role in the control and possible elimination of P. falciparum malaria in Madagascar.
Introduction
Malaria remains a major health problem in Mada-gascar [ 1,2]. Together with indoor spraying of DDT (and the use of long lasting impregnated bed nets), the use of antimalarial drugs is central to the control of malaria [ 3]. Malaria morbidity and mortality have fl uctuated over time, partly in line with the successes and failures of antimalarial policy. In the 1950s and 1960s, a sharp decline in malaria transmission was observed, mostly in the central highlands, due to indoor spraying with dichlorodiphenyltrichloroethane (DDT) and to the massive use of chloroquine by the population [4,5]. These results were obtained because of the well-organized healthcare system, which in particular allowed the implementation of parasitological diag-nosis. Subsequently, the discontinuation of the ‘niva-quinization’ policy was followed by devastating outbreaks in the central highland areas in the 1980s [6–8]. Meanwhile, Plasmodium falciparum clinical resistance emerged and spread [ 9]. Today, artemisinin-based combination therapy (ACT) has replaced
chloroquine as the fi rst-line treatment, whereas the sulfadoxine–pyrimethamine combination (SP) is given intermittently as preventive treatment in pregnant women. Following the global trend, the Malagasy government claims as its objective the elimination of malaria as a public health problem [ 10]. The aim of this review is to present the history and current status of P. falciparum antimalarial drug resistance in Madagascar and to consider its impact on malaria control programmes.
Context and malaria situation in Madagascar
Madagascar appears as an isolated fragment of the ancient continent ‘Gondwana’, which was separated from Africa 65–100 million y ago [ 11]. Human set-tlement in Madagascar occurred relatively recently, with the population originating from overseas. The fi rst arrivals are thought to have settled during the fi rst centuries of the Christian era, reaching the central highlands only in the 5 th–7th centuries. Parasites and
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

Antimalarial drug resistance in Madagascar 23
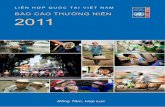
reported 1.01 million cases in 2006 [ 15]. Reported cases since 1999 are presented in Figure 1 . More than 90% of malaria cases are due to P. falciparum. The prevalence of P. vivax has been estimated to be 6.3% and of P. malariae to be 1.1% [ 16,17]. The estimated population of the whole island soared from 2.5 million in 1900 to 5.5 million in 1961, 9 million in 1980 and 18 million in 2008 [ 10]. Children aged � 5 y make up 16.7% of the population and half of the population is aged � 20 y. The Republic of Mada-gascar is one of the poorest countries in the world. Malaria is the second most important cause of mor-bidity (after acute respiratory infections) and mortal-ity (after diarrhoea). Malaria is responsible for more than 30% of outpatient attendance at health centres [ 10].
The 587,000 km 2 of Madagascar can be divided into 5 geographical regions: the east coast, the Tsar-atanana Massif, the central highlands, the west coast, and the southwest. For epidemiological studies and malaria control purposes, the country has been strat-ifi ed into 4 distinct zones (as there is no transmission in the Tsaratanana Massif): equatorial in the east, austral in the central highlands, tropical in the west, and semi-arid in the south ( Figure 2 ) [ 18]. In the east and in the west, transmission is stable – perennial in
vectors were probably introduced to the Malagasy coasts by the Indonesian, Bantou and Arab migrations of the 1 st to 14 th centuries [ 12]. Hence, all human malaria species except Plasmodium knowlesi (P. fal-ciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae) are found in Madagascar. Currently, the main vectors (Anopheles gambiae, Anopheles funestus and Anopheles arabiensis) are very similar to those of the African continent. The symptoms of ‘tazomoka’ (mosquito-borne fever), the Malagasy word for malaria, were known by the local inhabitants who treated them with traditional herbal remedies. Europeans brought with them their anti-malarial medication in the form of Cinchona bark powder (from which quinine was isolated in 1820). At the end of the 19 th century, French colonizers, lead by Gallieni, brought large quantities of quinine to Madagascar [ 10]. Chloroquine (CQ), the fi rst synthetic antimalarial compound, was introduced in 1945. Resistance to CQ (CQR) in Madagascar was suspected in 1975 [ 13] and confi rmed in 1981–1983 [9,14]. However the level of CQR remained low for many years and even today CQ is still used, though it should be replaced by other antimalarials.
Half of the population of Madagascar is at high risk of malaria. The National Malaria Control Programme
0
500000
1000000
1500000
2000000
2500000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
0
2
4
6
8
10
12
number of reported malaria cases incidence (%)
Figure 1. Malaria incidence and number of cases in the y 1999–2008 in Madagascar.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

24 V. Andriantsoanirina et al.
travel and migration may also contribute to the emer-gence of epidemics. Madagascar is located between Asia and Africa, both of which are known to have a high prevalence of antimalarial resistance. Interna-tional travel and trade between Madagascar and these 2 continents has resulted in an increase in importedmalaria cases. A high prevalence of antimalarial resis-tance is also present in the Comoros Islands, which are not far from Madagascar [ 20].
History of antimalarial use in Madagascar
CQ was the fi rst 4-aminoquinoline introduced to the Island. In 1949, the Ministry of Health launched an ambitious campaign for malaria prevention in children,
the east and more seasonal on the west coast, with a decrease in transmission in July and August. In both regions, immunity amongst adults is reported to be high and most of the severe cases affect children aged � 10 y and pregnant women. In the central highlands, malaria is stable up to 1000 m in altitude, unstable with seasonal transmission from November to May between 1000 and 1500 m, and rare above 1500 m. In the semi-desert of the south, malaria is unstable and hypoendemic, with a short seasonal transmission. In both the central highlands and in the south, immunity is limited and all age groups are vulnerable to periodic epidemics, which are often associated with high levels of morbidity and mortality. Human activity such as the cultivating of rice fi elds is of paramount importance for the proliferation of the vectors [ 19]. Transportation,
Figure 2. Map of Madagascar based on malarious epidemiological strata and 1982–2002 collection sites of isolates used in the in vitro studies. EIR: entomological inoculation rate.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

Antimalarial drug resistance in Madagascar 25
First detection of antimalarial resistance
In 1975, Goasguen et al. reported 2 cases of suspected CQR in Madagascar [ 13]. The fi rst case was a prophylactic failure and a treatment failure in a Britannic traveller. The second case was a treatment failure in a Malagasy woman. Parasitological diagnosis was performed and both cases were cured with SP, however isolates were not sent to a reference centre to validate the CQR. Five y later, Aronsson et al. observed 2 further cases of prophylactic and treat-ment failure with CQ in 2 Swedish women who had stayed several months in Andekaleka [ 14]. Correct plasma drug concentrations were found and in vitro tests showed CQR isolates. These cases showed that prophylaxis failure in travellers may lead to the earlier detection of resistance and at weaker levels than treatment failures within the local population, because the doses used are lower and because travellers are usually non-immune subjects.
Study and follow-up of antimalarial resistance
In vivo studies
Methodologies used to monitor antimalarial drug resistance have varied over time [ 25]. Until the end of the 1980s, most in vivo studies focused on the parasitological response to a given drug, and malaria episodes were classifi ed as sensitive (S) or resistant (R) at 1 of 3 levels, R1, R2 or R3. An R1 response corresponded to an initial clearance of parasitaemia followed by recrudescence 8 or more days after treat-ment; an R2 response was the clearance or substantial reduction of parasitaemia with recrudescence of parasitaemia on day 7; and an R3 response referred to a situation in which there was no initial reduction of asexual parasitaemia or even increase in level of parasitaemia. Treated patients were assessed weekly until day 7, day 14 or day 28, depending on the dif-ferent studies. World Health Organization (WHO) protocols have been modifi ed and simplifi ed to facil-itate their use in high-transmission areas in Africa, where populations may have asymptomatic parasi-taemia. Therapeutic responses were then classifi ed as either adequate clinical response (ACR) or early or late treatment failure (ETF and LTF). The therapeutic response is classifi ed as ETF if the patient develops clinical or parasitological symptoms during the fi rst 3 days of follow-up, and as LTF if the patient develops symptoms during the follow-up period from day 4 to day 14, without previously meeting the criteria for ETF. ACR is defi ned as either the absence of parasitaemia on day 14 (irrespective of axillary temperature), or the absence of clinical symptoms on day 14 (irrespective of parasitaemia), in patients who did not meet the criteria of ETF or LTF before. In vitro protocols
on the basis of a weekly administration of CQ [ 4,5]. A sharp decline in malaria prevalence was observed at the end of the 1950s in the central highlands and on its fringes. The weekly administration of CQ was maintained at all primary schools and at the Red Cross centres on the Island until 1970. In addition, CQ was readily available in many groceries. A short-age in CQ supply then occurred, together with the end of indoor residual spraying with DDT. This was followed by a large-scale epidemic in the late 1980s, killing an estimated 30,000–100,000 people per y over the course of 3 y [ 11,18,21,22]. The outbreak was brought under control by resuming indoor residual spraying and wide-scale access to CQ treat-ment. CQ is still used, though in December 2005 the Ministry of Health recommended its replace-ment (and abandonment) as fi rst-line treatment for uncomplicated cases, with the combination artesu-nate plus amodiaquine (ASAQ), which is an ACT. The policy for the management of fever in children, launched in 2003, led to a wide-scale distribution of free pre-packaged CQ treatments, and very large quantities of CQ were ordered in 2007 by the health districts [ 23]. Thus, CQ remains easily available in Madagascar and its importation is, as yet, not for-bidden.
Amodiaquine, a 4-aminoquinoline, has been reg-istered and commercially available in Madagascar since the 1950s. It has been used without discontinuation for more than 20 y.
Sulfadoxine–pyrimethamine (SP) is an antifolate combination recommended as second-line treatment for uncomplicated malaria cases since 1997. It was already in use on the Island many years before this date. It has also been used since 2005 for the intermittent presump-tive/preventive treatment of pregnant women [ 10].
Quinine has been used for many years in Mada-gascar. It is still very effective, but should be reserved for the treatment of severe malaria and cases of failure with other antimalarial treatments.
Artemisinin is the active ingredient of an ancient Chinese medicinal beverage used to treat fevers. It is obtained from the leaves of the plant Artemisia annua and it was rediscovered in the 1970s by scientists who called this crystalline compound ‘qinghaosu’ or ‘artemisinin’. Artesunate and other compounds derived from artemisinin, such as arte-mether, appear to be very effective at killing P. fal-ciparum. Artemether was introduced to the Malagasy markets for the fi rst time in early 1990 [ 24]. ACTs are today the basis of the malaria control/elimination programme, together with the use of insecticide-impregnated bed nets and indoor spraying with DDT. However, in 2008, few of the health districts of Madagascar had adequate supplies of artesunate–amodiaquine (ASAQ).
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

26 V. Andriantsoanirina et al.
small series of uncomplicated cases collected in 2003 [40,41]. In a multi-site study performed in 2006–2007, SP showed a mean of near 97% effi cacy, with some variation depending on site (range from 0% to 12.5%) [ 37].
Amodiaquine. In 1983, on the east coast of the Island, Deloron et al. reported 10.6% R1 or R2 among uncomplicated cases ( n� 47) treated with 10 mg/kg [ 42]. In 1985–1986, on the east coast, Marchais et al. reported 24.1% of SR1 and 3.4% of R1 in uncomplicated cases ( n� 58) treated with 19 mg/kg [ 28]. Using 25 mg/kg or more, other authors obtained better results, indicating that treat-ment failure was dependent on the dose prescribed. In 1984, on the east coast and in the central highlands, Biaud et al. reported complete effi cacy on day 14 in uncomplicated cases ( n� 64) treated with 25 mg/kg [27]. Lepers et al. reported a complete effi cacy during the 14-day follow-up in their study of 25 mg/kg in uncomplicated cases ( n� 35) collected in 1988 in the central highlands [ 31]. Randriamanantena et al. reported a complete effi cacy on day 14 in uncomplicated cases (n� 25) treated with 30 mg/kg collected in 2004 on the east coast and in the central highlands [ 42]. In a multi-site study performed in 2006–2007, Ménard et al. reported near 99% effi cacy on day 14 ( n� 372)and near 98% on day 28 ( n� 356) in those treated with 30 mg/kg [ 37].
Other antimalarials. Very few in vivo studies have been performed with other antimalarials in Madagascar [ 43]. Quinine remained highly active in 2 studies performed in 1988 and 1997 [ 31,38,44]. The combination artesunate–amodiaquine showed complete effi cacy on day 14 and less than 2% of overall treatment failure on day 28 in a multi-site study performed in 2006–2007 [ 37].
In vitro studies
Various in vitro studies have been performed to monitor CQ susceptibility [ 9,24,27,28,31,33,36,43,46–53,55,57–60]. The fi rst in vitro studies performed in the 1980s reported variable rates of CQR, depend-ing on the site, ranging from 1% to 36% of CQR isolates ( Table I ). The main event in those years was the sudden increase in CQR reported in 1988 in 2 distinct areas (one located in the central highlands and the other on the east coast) [ 33]. The only study that was performed in the 1990s showed 8.3% of CQR isolates ( n� 216) [ 60]. Results from the malaria resistance surveillance network (RER) founded in September 1999 by the Ministry of Health and the Institut Pasteur de Madagascar, showed 4.6% of CQR isolates ( n� 216) in isolates collected in 2001 from different sites on the Island [ 47]. Today, the rate of in vitro CQR isolates remains surprisingly
have also varied over time and between the different laboratories involved in phenotype determination of antimalarial resistance.
Chloroquine. Various studies have been performed to follow CQ treatment effi cacy. Since 1982, stan-dard protocols have been followed. In vivo tests were performed using 25 mg/kg of CQ (10 mg/kg on day 0 and day 1 and 5 mg/kg on day 2). Thin and thick smears were performed on day 0, day 7 and day 14.
Deloron et al. reported 20% of late treatment failure among standard treatments ( n� 40) per-formed in 1983 [ 26]. Biaud et al. reported 4.3% of R1 treatment failure among standard treatments (n� 70) in 1986 by day 28 of follow up [ 27]. Mar-chais et al. reported 12.3% of R2 and 45.6% of R1 treatment failure among standard treatments by day 28 of follow up ( n� 57) in 1987 and concluded that CQ was ‘perfectly active’ in the 2 studied sites of Madagascar, because CQ retained its clinical effi cacy [ 28]. Until 1987, the rates of CQR studied in various points of the Island were always below 10%, with some rare cases of R2 [ 29]. In 1989, Lepers et al. reported a ‘serious degradation’ of the effi cacy of CQ, with 10% of R1, 19% of R2 and 32% of SR1 (parasitaemia recurring between days 7 and 14, corresponding to late recrudescence or reinfection) among standard treatments ( n� 41) performed on the island of Sainte-Marie (northeast coast of Madagascar) [ 30]. Comparable results were found in 1988 ( n� 91) and in 1989 ( n� 123) in the central highlands by the same team [ 31,32]. However Lepers et al. continued to recommend CQ as fi rst-line treatment of malaria in Madagascar for “economical reasons and for its good tolerance and ease of use” and because of the lack of reported R3 resistance [ 32–34]. These authors also sug-gested the close monitoring of CQ effi cacy to detect the emergence of R3 in the future. Ringwald et al. reported a stability of CQR in the central highlands in the y 1990–1991 [ 35]. R3 resistance was fi rst evidenced by Randrianarivelojosia et al. in 1997 [36]. A study performed in 2001 in Ankazobe reported 23.5% of treatment failure ( n� 46), including 2 R3 resistance cases [ 1]. In the most recent studies, treatment failure of the standard regimen (25 mg/kg over 3 days) evaluated by day 28 of follow-up exceeded 40% ( n� 300), but early treatment failure remained below 5% [ 37].
Sulfadoxine–pyrimethamine. A fi rst survey of SP effi cacy showed parasitaemia for 2 patients out of 26 on day 7 [ 38]. Another study performed in 1997 showed R1 or R2 resistance for 2 patients out of 46 [ 36]. A lack of pyrimethamine resistance was reported in 2002 by Randrianarivelojosia et al. [ 39]. Randrianasolo et al. showed the complete effi cacy of SP in a relatively
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

Antimalarial drug resistance in Madagascar 27
Table 1: In vitro susceptibilities and prevalence of resistant P. falciparum isolates to anti-malarial drugs, Madagascar, 1982-2002.
Years Collection sitesNo. ofisolates
Resistantisolates (%)
Geometric mean of IC50% (nM)
IIC50%range (nM) Ref.
Chloroquine
1982 Antananarivo, Moramanga, Toamasina 34 20.6 - - 591983 Ifanadiana, Andekaleka, Ankazobe 23 4.3 - - 57
Manakara, Foulpointe 24 8.3 - - 26Morondava, Nosy-Be 19 26.3 - - 58Morondava, Nosy-Be, Manakara, Foulpointe, Tamatave, Ankazobe
78 35.9 - - 9
1984 Alatsinainy 91 16.0 - - 33Antananarivo, Nosy-Be, Andekaleka 91 1.1 - - 27Morondava, Nosy-Be, Manakara 91 16.5 - - 9
1985 Central Highlands 91 16.5 - - 331985–1986 Foulpointe 40 5.0 35 - 28
Toamasina 16 0 17 -Foulpointe, Ankazobe 30 6.7 - - 9East 56 8.9 - - 33
1987 Manarintsoa 139 5.8 - - 55, 33- 84 9.0 - - 43
1988 Central Highlands 104 27.9 - - 33Manarintsoa 104 29.8 78 10–364 31
1987–1989 Manarintsoa 243 15.6 - - 601990–1991 Ankazobe 42 9.5 39 - 351990–1993 Ankazobe 216 8.3 - - 601997 Marovoay, Nosy-Be, Sainte-Marie,
Toamasina90 4.4 161.7
43.7--
36
1998–1999 Ankazobe, Saharevo 46 11.0 171 109–245 2418 0.4–79
Ankazobe, Saharevo, Toamasina, Tolagnaro 205 5.8 9.4 - 501999–2000 Ankazobe, Moramanga, Tolagnaro 190 7.9 52.6 0.2–283.4 482000 Ankazobe, Saharevo, Mahakary, Sainte-Marie,
Toamasina, Marovoay, Nosy-Be, Tolagnaro255 4.8 - - 53
Sainte-Marie 27 14.8 34.9 - 512001 Toamasina 18 16.6 66.3 42.6–90 52
Mahajanga 25 0 22.6 16.8–28.7East 96 5.2 39.7 4.1–206.6 49West 31 3.2 31.6 0.2–152.1Centre 19 4.5 33.3 0.2–292.8
2000–2001 17 sites of the RER 432 5.7 - - 472001–2002 Tsiroanomandidy, Sainte-Marie, Saharevo 74 1.3 29.9 - 46
Amodiaquine
1983 Ifanadiana, Andekaleka, Ankazobe 23 0 - - 58Manakara, Foulpointe 27 0 - - 26
18 5.5 - - 581984 - 84 0 - Max range 76 571985–1986 Foulpointe 26 0 18 - 28
Toamasina 11 0 42 -Foulpointe 25 0 19 -Toamasina 5 0 59 -
1999–2000 Ankazobe, Moramanga, Tolagnaro 118 0 15.3 0.2–52.5 482000 Sainte-Marie 13 0 9.4 - 92001 Toamasina 17 0 17.8 10.4–25.3 52
Mahajanga 24 0 7.9 5.5–10.4East 96 0 12.7 0.4–57.9 49West 31 0 9.3 0.01–27.5Centre 86 0 9.9 1.4–64.2
2001–2002 Tsiroanomandidy, Sainte-Marie, Saharevo 71 0 10.8 9.2–12.4 45
(Continued)
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

28 V. Andriantsoanirina et al.
Table I. (Continued)
Years Collection sitesNo. ofisolates
Resistantisolates (%)
Geometric mean of IC50% (nM)
IC50%range (nM Ref.
Quinine
1988 Manarintsoa 64 0 157 25–440 3184 0 - Max range 560 43
1998–1999 Ankazobe, Saharevo, Toamasina, Tolagnaro 199 0 26.8 501999–2000 Ankazobe, Moramanga, Tolagnaro 212 0 107.7 11.1–630.7 482000 Sainte-Marie 26 0 93.1 48.1–138.1 512001 Toamasina 17 0 194.2 125.6–262.9 52
Mahajanga 25 0 88.8 69–108.6Antsiranana, Mahajanga, Ranohira, Morondava, Toliary, Antananarivo, Saharevo, Sambava, Sainte-Marie, Toamasina, Esana
215 0 133.7 - 46
East 96 0 108.1 4.2–584.2 49West 31 0 109.9 32.5–214.7Centre 87 0 85.1 8.5–280.4
2001–2002 Tsiroanomandidy, Sainte-Marie, Saharevo 71 0 70.6 59.2–82 453 sites 153 0 - - 54
Halofantrine
1984 Antananarivo, Nosy-Be, Andekaleka 91 0 � 12 - 2784 0 - - 44
3 sites 153 0 - - 541998–1999 Ankazobe, Saharevo, Toamasina, Tolagnaro 56 0 0.3 - 50
Mefl oquine
1988 Manarintsoa 23 0 12.5 2.1–33 31- 84 0 - - 43
1998–1999 Ankazobe, Saharevo 46 0 10.5 - 24Ankazobe, Saharevo, Toamasina, Tolagnaro 199 2 3.8 - 50
1999–2000 Ankazobe, Moramanga, Tolagnaro 139 0.71 11.57 2.9–124.6 482000 Ankazobe, Saharevo, Mahakary, Sainte-Marie 254 8.6 - - 53
Toamasina, Marovoay, Nosy-Be, Tolagnaro, Sainte-Marie
25 4.0 12.3 3.1–21.5 51
2001 Toamasina 12 0 12.9 8.1–17.8 53Mahajanga 15 0 11.5 7.2–15.9East 46 2.17 12.1 1.7–53.2 49West 18 0 10.2 3.4–20.4Centre 46 0 8.8 1.3–24.1Antsiranana, Mahajanga, Ranohira, Morondava, Toliary, Antananarivo, Saharevo, Sambava, Sainte-Marie, Toamasina, Esana
110 0.9 18.3 - 46
2001–2002 Tsiroanomandidy, Sainte-Marie, Saharevo 59 1.7 - - 45
Cycloguanil
1999–2000 Ankazobe, Moramanga, Tolagnaro 79 0 12.4 0.1–275.9 482001 17 sites RER 56 0 - - 49
Toamasina 10 0 9.8 2.7–16.8 52Mahajanga 7 0 6.2 0.4–12.2Antsiranana, Mahajanga, Ranohira, Morondava, Toliary, Antananarivo, Saharevo, Sambava, Sainte-Marie, Toamasina, Esana
56 0 � 50 46
Pyrimethamine
1997 Marovoay, Nosy-Be, Sainte-Marie, Toamasina 46 2.17 - - 361999–2000 - 58 0 30.5 - 39
Ankazobe, Moramanga, Tolagnaro 86 0 46.7 0.1–679.6 482001 Toamasina 12 0 - - 52
Mahajanga 9 0 - -17 RER sites 98 0 - - 49
RER, malaria resistance surveillance network (Réseau d’Etude de la Résistance).
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

Antimalarial drug resistance in Madagascar 29
thresholds for in vitro resistance interpretation accord-ing to the study have been noted. For this reason, the implementation of regional (RER) or global (Obser-vatoire de la Resistance aux Antipaludiques, ORA, www.oranet.fr or World Antimalarial Resistance Net-work, WARN) networks of surveillance for antima-larial resistance, using comparable methodologies, represents major progress in the control of malaria.
Though CQR was reported early in Madagascar in comparison with other African countries, and despite an important and continuous drug pressure, the level of CQR remained low for many years on the Island, and even today the level of CQR is lower than that encountered in African countries. This CQR most often leads to late treatment failure; early treatment failure is rare. This is in sharp contrast to reports from mainland Africa and the Comoros Islands, where early CQ treatment failure occurs at a high rate, particularly in children [ 62]. Currently, the rate of in vitro CQR isolates does not exceed 5%. This fi gure appears disconnected from the level of CQ clinical failure (near 40%). It appears that CQR in Madagascar differs from other areas of the world in that pfcrt mutant isolates are very uncommon. Conversely, pfmdr1 mutant isolates are frequently found and may be responsible for the bulk of CQR in Madagascar. This may also be in relation to the fact that most clinical CQ treatment failures in Mad-agascar are late clinical failures.
CQ treatment failure reached an intolerable rate around 2004, which promoted the Ministry of Health to recommend that the fi rst-line treatment for uncom-plicated malaria be changed to a drug with better effi -cacy. CQ is no longer recommended for the treatment of P. falciparum, except at the community level, in the home management of fever until ACTs are available. The problem is, that though often ineffective, treat-ment with CQ may be perceived as successful by the population [ 66]. Indeed, most acute fevers are treated with antimalarials without laboratory diagnosis. Two-thirds of these fevers are not malarial in origin and generally resolve spontaneously in a few days. In addi-tion, a proportion of malaria attacks resolve spontane-ously due to the immunity of the subject. Moreover, as treatment failure with CQ is most often late treat-ment failure in Madagascar, the recrudescence of fever 3 weeks later or more may not be perceived as a failure of the treatment. This misperception by the consumer could delay the replacement of CQ by ACTs.
The clinical effi cacy of SP remains high in Mad-agascar, but with variations according to site, and in vitro data show reassuring results. However, the tri-ple mutant DHFR allele and DHPS G 437 mutant alleles are present in a high proportion. The triple mutant DHFR allele is probably the same as that originating from Southeast Asia, which has invaded
low – near 5%. In vitro resistance to other antima-larials is anecdotal [ 9,24,27,28,31,36,39,43,45,46,48–54,56–58]. Most recent data on the sentinel sites from the RER did not show any in vitro resistance to pyrimethamine, cycloguanil, quinine or dihydroartemisinin. Rates of in vitro resistance to amodiaquine and mefl oquine were below 1%.
Molecular markers
It has previously been shown that a single pfcrt mutant allele (T 76) associated with CQR emerged in South-east Asia and invaded the African continent in the 1970s [ 61]. Molecular studies did not report the presence of this pfcrt mutant allele in Madagascar until 2001–2002, when it was found in 3.3% of isolates ( n� 183) collected from 2 sites (one in the central highlands and the other on the northeast coast) [ 62,63]. A recent study has shown that para-sites having the pfcrt mutant allele were introduced into Madagascar by travellers coming from the Comoros Islands [ 20]. However, the rate of isolates harbouring this mutant allele remained low in comparison to the rate of CQ clinical treatment failure. Conversely, the pfmdr1 Y 86 mutation, which has been associated elsewhere with in vitro CQR [ 64 ], was present in 67.5% of isolates ( n� 117) collected at 3 sites in Madagascar [ 45]. In addition, pfmdr1mutant genotypes, including Y 86, F 184 and Y 1246mutations, have frequently been found on the Island (Andriantsoanirina et al., submitted). Randrianariv-elojosia et al. reported a lack of mutant dihydrofolate reductase (DHFR) N 108 allele in isolates ( n� 58) col-lected in 1999–2000 at 1 site in the central highlands and at another site on the east coast [ 39]. However, parasites carrying DHFR mutant alleles are imported from the Comoros Islands. Recent data show that the triple DHFR I 51R59N108 mutant allele has spread widely in Madagascar (Andriantsoanirina et al., sub-mitted). In addition, unusual DHFR haplotypes, including the L 164 mutation, have recently been reported in Madagascar [ 65]. However, the quadru-ple mutant DHFR I 51R59N108L164 associated with high levels of resistance to antifolates and resulting in a complete ineffi cacy of SP, has not been reported in Madagascar so far. A recent longitudinal and multi-site study has shown that the dihydropteroate syn-thase (DHPS) G 437 mutant allele is increasingly being reported (Andriantsoanirina et al., submitted).
Comments and concluding remarks
The evolution of in vivo protocols over time and a relative lack of standardization between the different in vitro studies have rendered the comparison of results somewhat unreliable. In particular, variable
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

30 V. Andriantsoanirina et al.
Joncour G. The fi ght against malaria in Madagascar. Bull[5]World Health Organ. 1956;15:711–23.Blanchy S, Rakotonjanabelo A, Ranaivoson G, Rajaonarivelo [6]E. Epidémiologie du paludisme sur les hautes terres mal-gaches depuis 1878. Santé. 1993;3:155–61.Lepers JP, Deloron P, Fontenille D, Coulanges P. Reappear-[7]ance of falciparum malaria in central highland plateaux of Madagascar. Lancet. 1988;1:586. Mouchet J, Laventure S, Blanchy S, Fioramonti R, Rakoton-[8]janabelo A, Rabarison P, et al. The reconquest of the Mada-gascar highlands by malaria. Bull Soc Pathol Exot. 1997;90:162–8.Coulanges P, Le Bras J, Deloron P, Ramanamirija JA, [9]Biaud JM, Marchais H. In vivo and in vitro study of the chemosensitivity of Plasmodium falciparum in Madagascar, 1982–1986. Arch Inst Pasteur Madagascar. 1987;53:63–76. Ministère de la Santé, du Planning Familial et de la Protec-[10]tion Sociale . Plan stratégique de lutte contre le paludisme, du contrôle vers l’élimination du paludisme à Madagascar. Madagascar : Ministry of Health ; 2007. p. 54. Mouchet J, Carnevale P, Coosemans M, Julvez J, Manguin[11]S, Richard-Lenoble D, et al. Iles du sud-ouest de l’océan Indien. In: Libbey J, editor. Biodiversité du paludisme dans le monde. Paris : Eurotext; 2004. pp. 167–74.Hewitt R, Krause A, Goldman A, Campbell G, Jenkins [12]T. b -Globin haplotype analysis suggests that a major source of Malagasy ancestry is derived from Bantu-speaking negroids. Am J Hum Genet. 1996;58:1303–8.Goasguen J, Gentelet B, Moreau J, Fouquet R, Coulanges P. [13]Plasmodium falciparum chloroquino-résistant? A propos des deux premiers cas malgaches. Arch Inst Pasteur Madagascar 1975;44:143–5.Aronsson B, Bengtsson E, Bjorkman A, Pehrson PO, Rombo[14]L, Wahlgren M. Chloroquine-resistant falciparum malaria in Madagascar and Kenya. Ann Trop Med Parasitol. 1981;75: 367–73.World Health Organization. World malaria report. Geneva: [15]WHO; 2008. Available at: http://malaria.who.int/wmr2008/MAL2008-CountryProfi les/MAL2008-Madagascar-EN.pdf (accessed September 2009). Barnadas C, Tichit M, Bouchier C, Ratsimbasoa A, Randria-[16]nasolo L, Raherinjafy R, et al. Plasmodium vivax dhfr and dhpsmutations in isolates from Madagascar and therapeutic response to sulfadoxine–pyrimethamine. Malar J. 2008;7:35. Barnadas C, Ratsimbasoa A, Ranaivosoa H, Ralaizandry D, [17]Raveloariseheno D, Rabekotonorina V, et al. Short report: prevalence and chloroquine sensitivity of Plasmodium malar-iae in Madagascar. Am J Trop Med Hyg. 2007;77:1039–42.Mouchet J, Blanchy S, Rakotonjabelo A, Ranaivoson G, [18]Rajaonarivelo E, Laventure S, et al. Epidemiological stratifi -cation of malaria in Madagascar. Arch Inst Pasteur Mada-gascar. 1993;60:50–9.Blanchy S, Rakotonjanabelo A, Ranaivoson G. Surveillance [19]épidémiologique du paludisme instable. Santé. 1993;3:247–55. Ménard D, Randrianarivo-Solofoniaina AE, Ahmed BS, [20]Jahevitra M, Andriantsoanirina V, Rasolofomanana JR, et al. Drug-resistant malaria parasites introduced into Madagas-car from Comoros Islands. Emerg Infect Dis. 2007;13: 1759–62.Razanamparany MS, Randriamiharisoa FA, Razanamparany [21]NJ, Ramialimanana V. The malaria epidemic in Antananarivo from 1983 to 1994 as seen through the Pediatric Service A in the Befelatanana General Hospital. Santé. 1995;5:382–5. Razanamparany M, Bosman A, Ravelomanana N, Randriami-[22]harisoa F, Razafi mantsoa L. The malaria epidemic in Antan-anarivo observed from Pediatric Service ‘A’ of the Befelatanana General Hospital. Parassitologia. 1989;31:89–99.
the African continent [ 61], but this has to be assessed by microsatellite genotyping studies. The SP drug pressure has increased since the adoption of inter-mittent preventive treatment for pregnant women. A survey of its effi cacy is required in order to continue recommending SP for this indication.
Recent clinical and in vitro data support the com-plete effi cacy of the ASAQ combination in Madagascar. As such, this ACT should play a central role in the control of P. falciparum malaria. In the current efforts towards the elimination of P. falciparum from the Island, ASAQ could play a role as important as CQ did in the 1950–1970s. It is important to note that the re-emer-gence of malaria in the central highlands in the 1980s and the major outbreaks that followed were not due to CQR, which was moderate at that time, but to a short-age of CQ treatment following the deterioration of the public health system. These past events highlight the necessity to durably sustain the purchase of ACTs at subsidized or preferential prices and to distribute them to populations for an indefi nite period [ 67]. One can only hope that the current global fi nancial crisis will not result in drastic cuts in the funding dedicated to the fi ght against malaria in developing countries and that ACTs will preserve their good effi cacy in the future.
Acknowledgements
The authors thank the staff of the Ministry of Health of Madagascar. This work was supported by grants from Natixis/Impact Malaria through the ‘Observa-toire de la Résistance aux Antipaludiques’ project. Valérie Andriantsoanirina is a graduate PhD student funded by the Institut Pasteur de Madagascar (Bourse ‘Girard’) and the Direction des Affaires Internation-ales (Institut Pasteur).
Declaration of interest: None declared.
References
[1] Willcox ML, Rakotondrazafy E, Andriamanalimanana R, Andrianasolo D, Rasoanaivo P. Decreasing clinical effi cacy of chloroquine in Ankazobe, Central Highlands of Madagas-car. Trans R Soc Trop Med Hyg 2004;98:311–4.Robert V, Le Goff G, Andrianaivolambo L, Randimby FM, [2]Domarle O, Randrianarivelojosia M, et al. Moderate trans-mission but high prevalence of malaria in Madagascar. Int J Parasitol 2006;36:1273–81.Romi R, Razaiarimanga MC, Raharimanga R, Rakotond-[3]raibe EM, Ranaivo LH, Pietra V, et al. Impact of the malaria control campaign (1993–1998) in the highlands of Madagas-car: parasitological and entomological data. Am J Trop Med Hyg. 2002;66:2–6.Bernard PM. Trois ans de lutte antipaludique à Madagascar [4](1950–1951–1952). Bull Madagascar. 1954;96:415–20.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

Antimalarial drug resistance in Madagascar 31
Rakoto SA, Raharimalala L, Jambou R. Etude de la [38]chimiosensibilité de Plasmodium falciparum à Madagascar: 1 – situation des médicaments de seconde ligne à Taolagnaro (quinine, sulfadoxine–pyrimeéthamine). Arch Inst Pasteur Madagascar. 1998;64:51–5.Randrianarivelojosia M, Ariey F, Raharimalala LA, Parzy D, [39]Rogier C, Jambou R. Current absence of pyrimethamine resistance of Plasmodium falciparum in Madagascar. Trans R Soc Trop Med Hyg. 2002;96:557–9.Randrianasolo L, Randriamanantena A, Ratsimbasoa A, [40]Rakotoson JD, Randriambelosoa J, Raveloson A, et al. Surveil-lance de l’effi cacité de sulfadoxine–pyriméthamine (Fansidar®,Paludar®) pour le traitement de l’accés palustre à Madagascar : proposition d’un protocole simplifi é. Arch Inst Pasteur Madagascar. 2003;69:52–6.Randrianasolo L, Randriamanantena A, Ranarivelo L, [41]Ratsimbasoa A, Domarle O, Randrianarivelojosia M. Monitor-ing susceptibility to sulfadoxine–pyrimethamine among cases of uncomplicated Plasmodium falciparum malaria in Saharevo, Madagascar. Ann Trop Med Parasitol. 2004;98:551–4.Randriamanantena A, Randrianasolo L, Vonimpaisomihanta [42]JA, Tafangy PB, Bayant Z, Randrianarivelojosia M. Thera-peutic effi cacy of amodiaquine against uncomplicated malaria in Madagascar. Santé. 2007;17:75–8.Deloron P, Le Bras J, Ramanamirija JA, Coulanges P. Plas-[43]modium falciparum in Madagascar: in vivo and in vitro sen-sitivity to seven drugs. Ann Trop Med Parasitol. 1985;79: 357–65.Deloron P, Lepers JP, Verdier F, Chougnet C, Remanamirija [44]JA, Andriamangatiana-Rason MD, et al. Effi cacy of a 3-day oral regimen of a quinine–quinidine–cinchonine association (Quinimax) for treatment of falciparum malaria in Madagas-car. Trans R Soc Trop Med Hyg. 1989;83:751–4.Rason MA, Andrianantenaina HB, Ariey F, Raveloson A, [45]Domarle O, Randrianarivelojosia M. Prevalent pfmdr1 N86Y mutant Plasmodium falciparum in Madagascar despite absence of pfcrt mutant strains. Am J Trop Med Hyg. 2007;76:1079–83. Randrianarivelojosia M, Randrianasolo L, Randremanana[46]RV, Randriamanantena A, Ratsimbasoa A, Rakotoson JD. Susceptibility of Plasmodium falciparum to the drugs used to treat severe malaria (quinine) and to prevent malaria (mefl oquine, cycloguanil) in Comoros Union and Madagas-car. S Afr Med J. 2004;94:47–51.Randrianarivelojosia M, Sahondra-Harisoa JL, Raharimalala [47]LA, Raveloson A, Mauclère P, Ariey F. A network RER rooted on in vitro readout assays of Plasmodium falciparum sensitivity to chloroquine in the Indian Ocean region. Santé. 2003;13:95–100.Randrianarivelojosia M, Harisoa JL, Rabarijaona LP, Raha-[48]rimalala LA, Ranaivo L, Pietra V, et al. In vitro sensitivity of Plasmodium falciparum to amodiaquine compared with other major antimalarials in Madagascar. Parassitologia. 2002;44: 141–7.Randrianarivelojosia M, Rakotonjanabelo LA, Mauclère P, [49]Ratsimbasoa A, Raharimalala LA, Ariey F. National network study to perpetuate the surveillance of Plasmodium falci-parum sensitivity to antimalarials in Madagascar. Arch Inst Pasteur Madagascar. 2002;68:73–8.Randrianarivelojosia M, Ratsimbasoa A, Randrianasolo L, [50]Randrianarijaona A, Jambou R. In-vitro sensitivity of Plasmo-dium falciparum to chloroquine, halofantrine, mefl oquine and quinine in Madagascar. East Afr Med J. 2002;79:237–41.Raharimalala AL, Randrianarivelojosia M, Randriamanan-[51]tena A, Ranarivelo LA, Jaureguiberry S, Rason MA, et al. Chemosensitivity of Plasmodium falciparum in Sainte Marie island, east coast of Madagascar: in vivo and in vitro studies. Arch Inst Pasteur Madagascar. 2000;66:26–31.
Ratsimbasoa A, Randrianarivelojosia M, Millet P, Soarès JL, [23]Rabarijaona L, Rakotoson B, et al. Use of pre-packaged chlo-roquine for the home management of presumed malaria in Malagasy children. Malar J. 2006;5:79. Randrianarivelojosia M, Raharimalala LA, Randrianasolo L, [24]Ratsimbasoa A, Rason MA, Ariey F, et al. Madagascan isolates of Plasmodium falciparum showing low sensitivity to arte-mether in vitro. Ann Trop Med Parasitol. 2001;95:237–43. Talisuna AO, Bloland P, D’Alessandro U. History, dynamics, [25]and public health importance of malaria parasite resistance. Clin Microbiol Rev. 2004;17:235–54.Deloron P, Ramanamirija JA, Verdíer F, Coulanges P. [26]4-Aminoquinoline-sensitivity of Plasmodium falciparum in Madagascar. II. Study in two regions of the east coast. Arch Inst Pasteur Madagascar 1984;51:43–55.Biaud JM, Ramanamirija JA, Ramiliarisoa O, Verdier F, Cou-[27]langes P, Le Bras J. Drug sensitivity of malaria in Madagascar. Comparison in vivo and in vitro of the effects of chloroquine and amodiaquine on Pfalciparum in 1984. Arch Inst Pasteur Madagascar. 1985;52:73–84.Marchais H, Ramanamirija JA, Le Bras J, Coulanges P. In[28]vivo and in vitro sensitivity to 4-aminoquinolines of Plasmo-dium falciparum in Madagascar: results of a study conducted on the east coast (July 1985–July 1986). Arch Inst Pasteur Madagascar. 1987;53:43–62.Coulanges P, Le Bras J, Deloron P, Ramanamirija JA. Resist-[29]ance of Plasmodium falciparum to 4-aminoquinolines. Areview based on the Madagascar experience. Arch Inst Pas-teur Madagascar. 1987;53:77–103.Lepers JP, Ramanamirija JA, Randriasamimanana JR, Ram-[30]anandraibe LM, Rahelimalala RS, Rene JP, et al. Malaria in Ile de Sainte Marie in 1988. Epidemiological approach Chlo-roquine sensitivity of Plasmodium falciparum. Arch Inst Pas-teur Madagascar. 1989;56:131–42.Lepers JP, Deloron P, Andriamangatiana-Rason MD, Ram-[31]anamirija JA, Coulanges P. Sensitivity of Plasmodium falci-parum to different antimalarials. A study in 1988 in a village in the Hauts-Plateaux of Madagascar. Bull Soc Pathol Exot. 1989;82:650–7.Andriamangatiana-Rason MD, Lepers JP, Raharimalala [32]Andrianavalona L, Verdier F, Coulanges P. Aspects of in vivo chemosensitivity of Plasmodium falciparum to chloroquine in a village of the highland plateaux of Madagascar in 1989. Arch Inst Pasteur Madagascar. 1990;57:93–104.Lepers JP, Deloron P, Mouden JC, Le Bras J, Coulanges P. [33]Sudden increase in number of isolates of Plasmodium falci-parum resistant to chloroquine in Madagascar. Trans R Soc Trop Med Hyg. 1989;83:491–2.Blanchy S, Rakotonjanabelo A, Ranaivoson G. Evolution of [34]Plasmodium falciparum drug sensitivity in Madagascar from 1982 to 1993 and operational consequences. Bull Soc Pathol Exot. 1993;86:254–9.Ringwald P, Rabarison P, Raharimalala L, Rason MD, Lep-[35]ers JP, Le Bras J, et al. Stability and chemosensitivity of Plas-modium falciparum to chloroquine in 1990 and 1991 in Ankazobe, a village in high plateau Madagascar. Bull Soc Pathol Exot. 1992;85:219–22.Randrianarivelojosia M, Raharimalala L, Randriamanan-[36]tena A, Jambou R. Drug resistance of Plasmodium falci-parum in coastal regions of Madagascar. Med Trop. 2000; 60:243–9.Ménard D, Ratsimbasoa A, Randrianarivelojosia M, Rabari-[37]jaona LP, Raharimalala L, Domarle O, et al. Assessment of the effi cacy of antimalarial drugs recommended by the National Malaria Control Programme in Madagascar: up-dated baseline data from randomized and multi-site clinical trials. Malar J. 2008;7:55.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.

32 V. Andriantsoanirina et al.
Rason MA, Ariey F, Rafi dimanantsoa L, Andrianantenaina BH, [52]Sahondra Harisoa JL, Randrianarivelojosia M. Monitoring the drug-sensitivity of Plasmodium falciparum in coastal towns in Madagascar by use of in vitro chemosensitivity and mutation detection tests. Parasite. 2002;9:247–53.Milijaona R, Jambou R, Raharimalala L, Ranaivo L, Rason[53]MA, Roux J. Mefl oquine-resistant strains of Plasmodium falciparum in Madagascar: impact on tourists and public health. Ann Trop Med Parasitol. 2000;94:313–7.Milijaona R, Raharimalala L, Ramambanirina L, Ranaivo [54]LH, Jambou R. Drug resistance of Plasmodium falciparum along the borders of the highlands in Madagascar: outlook for a national control program. Med Trop. 1998;58:261–5.Lepers JP, Ramanamirija JA, Rason MD, Coulanges P. In[55]vitro sensitivity of Plasmodium falciparum to chloroquine in the highland region of Madagascar in 1987. Bull Soc Pathol Exot. 1988;81:338–44.Ramanamirija JA, Deloron P, Biaud JM, Le Bras J, Cou-[56]langes P. In vivo and in vitro sensitivity to 4-aminoquinolines of Plasmodium falciparum in Madagascar: results of 2 years’ study. Bull Soc Pathol Exot. 1985;78:606–14.Deloron P, Ramanamirija JA, Le Bras J, Coulanges P. 4-Ami-[57]noquinoline-sensitivity of Plasmodium falciparum in Mada-gascar III Studies in three regions of the interior. Arch Inst Pasteur Madagascar. 1984;51:57–68.Deloron P, Ramanamirija JA, Le Bras J, Verdier P, Coulanges[58]P. 4-Aminoquinoline-sensitivity of Plasmodium falciparum in Madagascar. I. Study in two regions of the west coast. ArchInst Pasteur Madagascar. 1984;51:29–42.Le Bras J, Dulat C, Coulanges P, Ralamboson D, Rakotoniri-[59]na-Randriambeloma PJ, Deloron P. Preliminary in vitro study of drug sensitivity of Plasmodium falciparum in Mada-gascar. Arch Inst Pasteur Madagascar. 1982;50:15–22.
Raharimalala L, Lepers JP, Lepers-Rason MD, Rabarison [60]P, Ramambanirina L, Roux J. Aspects of Plasmodium falci-parum sensitivity to chloroquine in Madagascar from 1982 to 1993. Arch Inst Pasteur Madagascar. 1993;60:60–4.Ariey F, Fandeur T, Durand R, Randrianarivelojosia M, [61]Jambou R, Legrand E, et al. Invasion of Africa by a single pfcrt allele of South East Asian type. Malar J. 2006;5:34. Ariey F, Randrianarivelojosia M, Duchemin JB, Rakotondra-[62]marina D, Ouledi A, Robert V, et al. Mapping of a Plasmo-dium falciparum pfcrt K76T mutation: a useful strategy for controlling chloroquine resistance in Madagascar. J Infect Dis. 2002;185:710–2.Randrianarivelojosia M, Fidock DA, Belmonte O, Valderra-[63]mos SG, Mercereau-Puijalon O, Ariey F. First evidence of pfcrt mutant Plasmodium falciparum in Madagascar. Trans R Soc Trop Med Hyg. 2006;100:826–30.Picot S, Olliaro P, de Monbrison F, Bienvenu AL, Price RN, [64]Ringwald P. A systematic review and meta-analysis of evi-dence for correlation between molecular markers of parasite resistance and treatment outcome in falciparum malaria Malar J. 2009;8:89. Ménard D, Andriantsoanirina V, Jahevitra M, Barnadas C, [65]Tichit M, Bouchier C, et al. Dihydrofolate reductase I164L mutation in Plasmodium falciparum, Madagascar. EmergInfect Dis. 2008;14:1166–7.Hastings IM, Korenromp EL, Bloland PB. The anatomy[66]of a malaria disaster: drug policy choice and mortalityin African children. Lancet Infect Dis. 2007;7:739–48.Randrianarivelojosia M, Raveloson A, Randriamanantena A, [67]Juliano JJ, Andrianjafy T, Raharimalala LA, et al. Lessonslearnt from the six decades of chloroquine use (1945–2005) to control malaria in Madagascar. Trans R Soc Trop Med Hyg. 2009;103:3–10.
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
on 0
2/23
/15
For
pers
onal
use
onl
y.