ResearchSpace@Auckland ...
249
http://researchspace.auckland.ac.nz ResearchSpace@Auckland Copyright Statement The digital copy of this thesis is protected by the Copyright Act 1994 (New Zealand). This thesis may be consulted by you, provided you comply with the provisions of the Act and the following conditions of use: • Any use you make of these documents or images must be for research or private study purposes only, and you may not make them available to any other person. • Authors control the copyright of their thesis. You will recognise the author's right to be identified as the author of this thesis, and due acknowledgement will be made to the author where appropriate. • You will obtain the author's permission before publishing any material from their thesis. To request permissions please use the Feedback form on our webpage. http://researchspace.auckland.ac.nz/feedback General copyright and disclaimer In addition to the above conditions, authors give their consent for the digital copy of their work to be used subject to the conditions specified on the Library Thesis Consent Form.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ResearchSpace@Auckland ...

http://researchspace.auckland.ac.nz
ResearchSpace@Auckland
Copyright Statement The digital copy of this thesis is protected by the Copyright Act 1994 (New Zealand). This thesis may be consulted by you, provided you comply with the provisions of the Act and the following conditions of use:
• Any use you make of these documents or images must be for research or private study purposes only, and you may not make them available to any other person.
• Authors control the copyright of their thesis. You will recognise the author's right to be identified as the author of this thesis, and due acknowledgement will be made to the author where appropriate.
• You will obtain the author's permission before publishing any material from their thesis.
To request permissions please use the Feedback form on our webpage. http://researchspace.auckland.ac.nz/feedback
General copyright and disclaimer In addition to the above conditions, authors give their consent for the digital copy of their work to be used subject to the conditions specified on the Library Thesis Consent Form.

TEE EPIDEUTOLOGY OF I.TOTOR NEURON DrSEASE rN ScoTI.AIID 1989-90.
A PROSPECTTVE STUDY OF TNCTDENCE, CrrrNrcAL FEATURES AlrD PROGNOSrS
aND TNCORPORATTNG A CASE cotfTRorr gruDy oF allrEcEDENa
EITVTRONI,TENTAIJ FACTORS .
A thesis subuitted toTbs Faculty of ttedicine, university of Auckland, New zealand
forThe Degree of Doctor of l,tedicine, LggZ.
by
Andrew [artin Chancellor BHB, ttBChB, FRACP

To
Patricia and Blaine

"somehow in the race for success in sciencet ve areI??yi"g behind the patient. There is no inhereit conpe-titiveness or recip-rocity between the ;;I;;;;- "il"'Lrtof medicine- without a knowredge of ""i"n-"",-;;;;p;r-sionate wish to. improve the neinn of mankind is mean-ingress - - .The incieased comprexity oi technology-inadiagnostie and treatment optiont
^ix"L- even more criti-""+ the physician's skirt- in managing irrness "ni-in"art of communicating with patieits- and their lovedones. There but for the grace of God go yre arr, fora77 ot us and our fanirfes are or witt event|ailybecome patients.',
Louis R.Caplanl

IABI,E OF COIITETI!8
List of chapter contentsList of appendicesList of tablesList of figuresList of commonly used abbreviationsThesis synopsisList of publications arising from this thesisPreface: Statement of the authorrs contributionto this thesisAcknowledgrmentsDeclarationBody of thesisAppendicesReferences
5781011L218
192L2324159224

OutlineI,I8T OF CEAPTER CONTENTS
CEAPTER 1: TNTRODUCTTON TO THE THESTS. A BTSTORY OF THEEJART,Y DESCRTPTTONS OF UOTOR NEURON DISEA8E
The contributions by Edinburgh graduates to thefirst descriptions of MNDFormulation of the nodern concept of MNDTerninology relating to MNDWhy measure the incidence of MND?
CEAPTER 2: FORLDWfDE UORTALITY, INCfDENCE AIIDDISTRIBUTION OF ADULT ONSET I,TOTOR NEURON DISEJASESrncE 1950
IntroductionMethods of data retrieval for reviewAnalysis of existing studies
Mortality studiesfncidence studiesCrude ratesAge and_?ex specific incidence rates,standardised ratesCLustersWestern pacific forms of MND
Summary and criteria for the ideal studyof MND incidence
IntroductionMethods
Morbidity data retrievalMortality data retrieval
ResultsMorbidity dataMortality data
DiscussionMorbidity dataMortality data
21
25303337
38
39404L4L4444
454748
51
CEAPTER 3: THE SCOTTTSE UOTOR NEURON DISEASE REGISTER:uElrEoDoLocy, rNcrDEDrcE, DEttocRApHy AND crrrNrcArr FEATuRESOF PATIENT8 DIAGNOSED 1989-1990 55
IntroductionMe'LhodslrirlilliTli*r* *oClinicatly probable MNDResults
Discussion
CEAPTER l: TnE urrLrry oF EosprrArJ ttoRBrDrry DATA AlrDDEATE cERTrFrcATEs coDED Ag litoroR NEURON DrgEAsE(ICD 335) Itf ScoTLAlfD 1989-90
675770707L7477
97
989999101101101LO2103103105

OutlineCEAPTER 5 3 A CASE-CoNTRoIJ STUDy To EXAITINE PRIoREYPOTEESES CONCERNTNG TEE POS8IBLE ROLE OF CERTAINEITVIRONIIENTAL FACTORS ANTECEDENT TO TUE DBYELOPITENTOF IiIOTOR NEURON DrSEASE
fntroductionPreceding traunaoccupation, environmental toxins andxenobioticsSocial class and the environmentin childhood
MethodsPatientsControlsData collection
ResultsPatient characteristicsTraumaoccupation, environmental toxins andxenobioticsSocial class and the environmentin childhood
DiscussionSources of biasRisk factors
TraumaOccupation, environnental toxins andxenobioticsSocial class and the environmentin childhood
CEAPTER 6: TtrE PRoGNosTS oF IIIoToR NEuRoNDTsE]A8E
fntroductionMethods
PatientsStatistical methods
ResultsDiscussion
CIIAPTER 7: CONcLugIoNs.I(AXING UsE OF THE WORK FROt,t THrS THESTS
113
LL4tL4
115
115119119119L20L23L23L24
L25
L25L26L26L28L28
130
131
1t6
L47148148L49150151
161

OutlineI,T8T OF APPEIIDICES
APPENDIX A:
ST'I.{MARY OF THE CLINTCAL FEATT'RES OF28 PATIENTS EXCLUDED FROM THE MATN ANALYSES ].69
APPENDTX B:
DETATLS OF FAMILY MEMBERS TN 11 PEDTGREES WHERE AGENETIC BASTS FOR MOTOR NETIRON DISEASESEEI,TS LTKELY 19O
APPEIVDIX C:
SUI{MARY OF THE PATHOLOGICAL FEATURES OF15 PATIENTS TNCLUDED TN THE MAIN ANALYSES WHOI'NDERWENT AUTOPSY 2O3
APPENDIX Ds
QUESTIONNAIRE USED IN THE CASE_CONTROLSTUDY zuo
APPENDIX E3
TNFORMATION FOR MEDICAL PRACTITTONERS CONCERNINGTHE SCOTTTSH MOTOR NETIRON DISEASE REGTSTER 2L8
RBFERENCESS 224

2-Lz
2-2a2,
2-2b:
2-3a:
2-3b:
2-3cz
OutlineIJTST OF TABLEg
syndromes which nay mimic or resemble idiopathicII{ND
Studies of adult onset MND based only on- nortality (death certificate) dataA conparison of age specific rnortality ratesper lOOrOO0 between countriesRetrospective incidence studies of adult onset
MND most likely to have conplete or nearcomplete case ascertainnentRetrospective incidence studies of adult onset
MND where case ascertainment is likely to beincompleteRetrospective incidence studies of adurt onset
MND which rely exclusively or principally ontertiary referraL centres for Laseascertainment2-3d: A comparison of age and sex specific incidenceand age standardised incideirce, 4S_74 years,by country
3-1: SMNDR Registration form details3-22 physical signs by regio. ..="a-in theclassification of patients with MND3-3: Sunmary of diagnostil categories usea Uy theSMNDR
3-4: Arternatives for the distribution of crinicarsigns in the limbs and trunk for diagnosis ofdifferent categories of MND by the sfir.lpn3-5: summary of patients registered ,itn tne -br.ltlpn
but excluded from the main analyses3-6: Descriptive statistics comparinq tn" differencesbetween the means for seiected variabres3-72 First source of referrar to the sMNDR in 19g9-9o3-8: Clinical classification of MND subtypes atdisease onset and by January 1st. Lgg23-9: Anatomical site of onset of muscre weakness3-10: Relative.risks (RR) and 95t confidence rinitsfor clini"?l.subtypes of MND according to sex3-11: Age-sex specific inliaence rates for MND inScotland (1989_90)3-r2: standardised incidence ratios for the ninescottish regions and three island areas 19g9-90
56
57
58
59
62
83
83
8687
8889
82
84
85
60
61
90
92
91
8

4-1:
4-2 t4-3:
4-4:
4-5:
4-6 z
5-1:5-2 z
5-3a:5-3b:
5-3c:
5-3d:
5-4:
5-5:
5-6:5-7:5-8:
5-9a:
5-9b:
5-10:
6-1:
OutlineList of tables (cont)
fnternational classification of diseases_9(L979); 335, anterior horn ceII disordersSunmary of SHIPS in relation to the SMNDRsensitivity and positive predictive varue of a__ di3gngsis of l0lo as detirmined by snipsclassification of LL2 patients rnisioded as MNDby SHIpSSummary statistics relating to 1989-90 deathcertificates coded as ICD 335Errors in nortality data with respect to MND
Published case control studies of MNDPatients included in the case control studyFractures by case, control, sex and numberMatched case-control analysis, alI subjectslifetirne history of fralturesMatched case-control analysis of fractureswithin five years of syirptorn onsetDetails of patients with-r'tr.rp who sustained afracture within five years of symptom onsetDistribution of injurie3 by case, controland number of injuriesDistribution of op-rations by case, controland number of operationsElectric shocksBlood transfusionMatched case control analysis of occupation(nanual vs non-manual)Matched case-control analysis of
environrnental /occupatioial toxinsDetails of 19 patienls with MND in whom leadexposure hras reported over a period of morethan L2 monthsMatched case-control analysis of domesticanenities in the first :_O years of life
Studies of prognosis in MND
LO7108
109
110
111LL2
133135136
L37
L37
138
139
139139139
140
140
L4L
]-42
L54

2-Lz
2-Lz
2-2:
3-1:
3-2 z
3-3:
3-4:
5-1a-5-1d:
5-2 z
5-3:
5-15-8:
Appendix B:pedigrees of farnilial cases
OutlineLIST OF FIGURE8
Mean annual death rates per lOO,OOO populationfor MND in NorwayAge specific incidence of adult onset MNDin three countriescorrelation of age standardised incidence of
MND with degrees north latitude
Diagram to illustrate the organisation of theSII{NDR
Age specific incidence (959 cI) for 22gpatients with MND in dcotland 1989_90Age and sex specific incidence for 132 ma1es,97 females witn mtO in Scotland 1989_90Age adjusted standardised incidenc"-ritio= "rMND by region in Scotland 1989_90
Age standardised. mortarity ratios for rung cancerand MND in Scotland by deprivation-"it"goryDistribution of fractur6 frlquency by intervalbefore onset of symptons due to motor neuronqlseaseOdds ratio for a fracture occurring at variousintervals before the onset of ttttO iynptoms
Actuariar anarysis of survivar for 229 patientswith MND in Scotland 1989-90
64
63
65
95
96
93
143
L44
145
156-163
L92-202
10

OutlineIJIST OF COUIIO}IIJY USED ABBREVIETIONS
MND
ALS
PBP
PMA
PLS
NCS
EMG
CT
I{RI
Motor neuron disease
Anyotrophic lateral sclerosisProgressive bulbar palsy
Progressive muscular atrophy
Prinary lateral sclerosisNerve condution studies
Electromyography
Conputed tonographic scan
Magnetic resonance imaging
OPCS Office of population Censuses and SurveysSHIPS Scottish hospital in patient surveyrsD rnformation and statistics division of the
Common Services Agency for the ScottishHealth Service
SMNDA scottish Motor Neuron Disease AssociationSMNDR Scottish Motor Neuron Disease Register
Relative riskOdds ratioConfidence interval
RR
OR
CI
11

Outline
Outlineplaces is complicated by non standardised nethods of case-ascer-tainrnent and diagnosis but evidence is presented which challengesthe traditional concept that the distribution of MND in deve-Ioped countries is uniform and static. rt remains uncertain,from the evidence available, if age specific incidence continuesto rise into o1d age and the apparent ,'peak,t in late-niddle 1ifeis due to ascertainment bias. This is an important considerationon which to base aetiological hypotheses. In the northern hemi-sphere there is a weak positive correlation between standardised,age specific incidence and distance from the equator. There is a
high prevarence focus of an atypical MND/ALS on Guam, and whirean environmentar factor is probably responsible, its nature isuncertain. The relevance of other reported clusters of MND isdiscussed and the reguirements for the ideal study of MND inci-dence are outlined, which acted as the inpetus for the scottishMotor Neuron Disease Register (SMNDR).
chapt€r 3
The methodorogy of the SI{NDR is described. This is thefirst collaborative, popuration based, prospective, epidemiologi-cal study of MND and illustrates the feasibility of such a studyand the way in which scotland is suited (in terms of size andNational Health service structure) to such a project. Diagnosticcriteria are outlined for application to this and other largescale studies.
Of 257 patients registered with the SMNDR as possible MND
diagnosed in 1989 and 1990 in scotrand, 22g with proven (byautopsy), clinically definite or probable, sporadic or farnilialII{ND' form the basis of the description of incidence, distribu-
13

Outlinetion, clinical features and natural history contained in thischapter. The crude incidence was 2.24/loorooo/year and agespecific incidence continued to rise steepry with age into thevery elderly age bands. No evidence for clustering on the basisof scottish regions was found. 5t of patients had a family his-tory of MND; the clinicar pattern varied according to sex and&9€, with erderry women most rikery to present with, oF develop,progressive bulbar palsy.
Chapter IThe utility of the 1989-90 Scottish Hospital In-patient
statistics (sHrps) and i-989-90 death certificate coding (Reqi-strar General for scotland) by rnternational classification ofDiseases (rcD)-g, 335 (I.{ND) are anarysed as a tool for epidernio-logicar studies and heath care planning. coded hospital dis-charge data were an inaccurate record of a diagnosis of MND witha positive predictive value of a diagnosis of MND as determinedby sHrPS of 7oz- such data cannot, in their present form, beused as a reliabre rneasure of incidence in scotrand.
Greater care is required in the preparation ofsummaries and coding if these data are to be usefulcare pranning and epideniol0gicar research. However,as an irnportant source of case notification for theachieve a comprete sampre of patients. There was arsonatic farse positive rate (r.og) for nortarity datasource more closely approximated true incidence.
discharge
for health
SHfPS acted
SMNDR toa proble-
but this
L4

OutlineChapter s
A review of previous case control studies of environmentalrisks for MND is presented. rn order to test the hypothesis thatcertain environrnentar factors may play a rore in the aetiorogy ofMND, a case contror study of 103 incident patients (diagnosisdate May 1990-october 1991 i s7 from the above cohort (as de-scribed in chapter 3) and 46 diagnosed in 1991, a9e and sexmatched with conmunity contrors was conducted and is <lescribed.Measures htere taken to minimise potential sources of bias andthese are discussed.
Fractures were more common in patients than controls especi-ally in the in the five years prior to syrnptom onset (odds ratio= 15 (95t cr, 2.3-654). Manual workers srere over represented anda number of environmentar exposures of potential toxicity in_cruding exposure to lead (oR = 5.3 ,gst cr,1.5-11) and sorventsor chemicals (oR = 3.8, 958 cr 1.5-i.1) vrere found. The linritedextent of these associations favours a rnultifactoriar aetiologyfor MND' No rerationship to sociar class, poliovirus infectionor to factors which rnight increase the risk of enteroviral infec-tion in chirdhood (home space and domestic anenities) was found.
Cbapter 6
A comprehensive review of previous prognostic studies in MND
is presented. An actuarial anarysis of the survivar of thecohort of 229 incident patients (57 seen in person) in scotlandin 1989-90, with comprete forrow up for a mean of two years frorndiagnosis, is calcurated on the basis of the SMNDR crinicalclassification system.
The overarr 5ot survivar from diagnosis v/as L.2 years (95t
1_5

Outlinecr, 1-0-1-4) and from sympton onset, 2.5 years (95* cr, 2.2-3.oyears). There hrere significant differences in survival with a
poorer prognosis for: progressive bulbar parsy (pBp), femalesex and age > 65 years. The presence of pBp and ord age were thestrongest predictors of outcorne, the difference in survivalbetween the sexes was due to the higher frequency of pBp infernales. The overall five year survival frorn symptorn onset Iras
27-7* (95* cr, 19.9-36.0*) but for patients with pBp as thepresenting feature was onry 3.5t (95g cr, o.o-15t). These resurtssuggest that, in welr defined cohorts, survival can be predictedwith some confidence and are useful for the planning of treatrnenttrials.
Chapter Z
In this concluding chapter f consider thethe work contained in this thesis.
applications of
Appendix L
This appendix describes the clinical details of 2g patientsregistered with the sMNDR and diagnosed in 1989-90 but excludedfrom the analysis of incidence because of failure to fulfil SMNDR
diagnostic criteria (eg coexisting neurological disease or revi-sion of diagnosis with forrow up). This group represents part ofthe differentiar diagnosis of MND and highlights some of thedifficulties in rnaking the diagnosis when the disease is incom-pletely developed.
L6

OutlineAppendir B
A summary of the pathorogicar findings of those patientsincluded in the incidence analysis who underwent autopsy isrecorded. "By definition, alr patients had typical findings ofMND' including some with the recently described ubiquinatedinclusion bodies.
Appendix C
The resurts of pedigree searches of 11 families (5t ofincident patients) with a probabre genetic basis for !{ND arepresented. These families demonstrate that autosornal doninantinheritance is usual and illustrate clinical heterogeneity ofage and disease pattern.
Appendix D
Details of the questionnaire administered to subjects inthe case-control study.
Appendix E
Sarnple letter of explanation toafter patient registration with theRegister.
General Practitioners, sent
Scottish Motor Neuron Disease
L7

Outl,ine
I,I8T OF PUBLICATIONS ARISING FROI,! NORX
ASSOCTATED WTTH TIIrS THE8r8
(Excludes publications in abstract form)
chancellor AM, carstairs v, Erton RA, swingler RJ, !{arlow cp.Affruence, age and motor neuron disease Iretter]. J Epide-miol Community Health L9g2 ; t6zL72-L73.
Mitchell JD, Chancellor AM. Amyotrophic Tateral sclerosis-Aran'sEdinburgh_ inspiration? T'izproCeedings ot the third Europeanmeeting for the history of the neurosciences Lgg2
Chancellor Al'1, Mitchell JD, Swingler RJ. The first description ofidiopathic progressive bulbar paIsy. J IVeuroJ, n6urosurgPsych L9921In press.
chancellor AM, warlow cp. Adult onset motor neuron disease:I{orldwide mortality, incidence and distribution since 1950.J Neurol lfeurosurg psychiatry L992;ID press.
chancellor AM, swingler RJ, Fraser H, warrow cp. The scottishmotor neuron disease register: A prospective study of adultonset rnotor neuron disease in Scotland. Methodology, demo-graphy and clinical features of incident cases in-fgeg. .7Neurol Neurosurg psychiatry L992;fn press.
chancelror AM, Fraser H, swingrer RJ, clarke JA, warlow cp. Theutility of Scottish rnorbidity and rnortality data for epide-nriological studies of motor neuron disease. Suhnitted to JEpidenioT Community HeaTth Lgg2.
de Belleroche J, chancelror AM, King A, Hardy J, Lane R, HourdenH. Absence of linkage between chromosome 2L loci and fami-Iial amyotrophic lateral sclerosis Iletter]. Submitted toThe New EngTand Journal of l4edicine Lgg2.
chancelror AIu, Fraser H, srattery J, swingrer RJ, warrow cp. Theclinical features and prognosis of rnotor neuron disease: Aprospective population based study. rn preparation Lgg2.
chancellor AM, swingrer RJ, Fraser H, srattery J, warlow cp.Motor neuron disease and the environrnent: A case-controlstudy In preparation L992.
wirlison HJ, chancellor AM, whiteraw JW, warlow cp. The frequencyof anti-GM1 antibodies and paraproteins in rnotor nLurondisease: A population based case-control study. rn prepara-tion L992.
18

OutlinePREFACE! STATEI,IENT OF THE AUTHORIS CONTRIBUTION TO TETS
TEE8T8
My work for this thesis spanned two years and began on a
part time basis in June 1990, when working as Clinical NeurologyRegistrar for the Lothian Health Board. fn November 1990 I began
a full time Research Fellowship in the University of Edinburghbased in the Departnent of Clinical Neurosciences, Western Gen-
erar Hospitar. The thesis was conpleted in May Lg92.
The observations concerning the early descriptions of MotorNeuron Disease by Edinburgh graduates were ny own, based on
reading in the Royal College of Physiciansr of Edinburgh libraryand information from the British Librdry, London. The identifica-tion and compilation of the references to previous work essentialfor background reading including the review of the worldwideepiderniology of MND and the entry and organisation of all refer-ences within a medical reference database (Research Informationsysterns rrReference Managerrr) vras my own work. AII referencesquoted in this thesis have been viewed in the original except forparts of foreign language references, some of which hrere nottranslated in their entirety.
r vtas responsible for: the supervision and organisation ofpatient infornation conpiled by the Scottish Motor Neuron Regis-terr' ongoing adaptation of the patient database to the needs ofthe project; keeping collaborators with the project informed ofdevelopments by monthly newsletter; devising diagnostic criteriasuitabre for use by the project; classification of patientsaccording to these criteria; negotiating retrieval of Scottishhospital rnorbidity and mortality data for rnternational Classi-fication of diseases code 335 (Motor Neuron Disease) for 19g9-90
19

Outline
and the inspection of alr medical records (hospital, generalpractice and autopsy records) relating to the patients describedincluding the detairs of pedigrees :ior farniriar MND.
I approached the specialists and GPrs for pernission to see
all (n=103) patients in the case control study and interviewedthese patients with 103 control subjects at their homes in allregions of Scotland as necessary. The questionnaire for the case
control study was devised personally and all data entered into a
computerised database (dbase lV-registered trade rnark) myself. Isahr and exanined six patients from four of the pedigrees withfanilial UND and undertook correspondence to establish featuresof fanily members in other pedigrees. r collected and arrangedfor the storage and transportation of all blood samples includingthose for linkage analysis (not reported here).
The statistical analysis of demographic variables, inci-dence, distribution, and descriptive statistics relating to theclinical features of alt patients described herein was my own
work.
20
OutlineACKNOWLEDGI{ENT8
Many people have contributed to this thesis without whose
help it would never have reached fruition. The Scottish MotorNeuron Disease Register (SMNDR), funded by The scottish MotorNeurone Disease Association (SMNDA) was established in January1989' largely through the work of Dr.R.J.Swingler and I was rnost
fortunate to have the opportunity to build upon his work. The
SMNDR is a collaborative project and r am grateful to the neuro-logists, neurophysiologists and others in Scotland for theirregistrations and the permission to see their patients withoutwhose help this thesis would not have been possible. They inclu-ded:
Dr J.E.C. Hern, Dr. R. Knight (Aberdeen)i Dr. D.
Davidson, Dr. A. Forster, Dr. R. Roberts (Dundee) i Dr.
B. Ashworth, Dr. R.E. CuII, DE. E.H. Jellinek, Dr. A.
Mcrnnes, Dr. B. pentland, Dr. p.A.G. sandercock, pro-fessor c.p. Warlow, Dr. R. will (Edinburgh), Dr. J.p.Ballantyn€, professor p.O. Behan, Dr. f. Bone, pro-fessor F.I.Caird, Dr. f. Draper, Dr. W.F. Durward, Dr.
G. Jamal, Professor p. Kennedy, Dr. R. Metcalfe, Dr.M. Thomas, Dr. A.I. Weir (Glasgow); Dr. L.R. Fisher(Inverness) .
r am especially grateful to Mrs. Hazer Fraser, with whom rworked closely, and who rnanaged the large amount of secretarialwork associated with running the SMNDR database and helped in theretrieval of patient records. I would like to thank Miss Shona
Henderson and Mrs. Rita walker, SMNDA faniry care officers, for
2t

Outline
informing patients about the SMNDR and for their helpful liaisonwhen approaching patients. Dr. susan Holloway, Clinical Geneti-cist, helped with the description of pedigrees of fanilial MND
(Appendix B) by tracing the death certificates of affected and
unaffected reratives in Register House, Edinburgh i r haveappried measures of deprivation (chapter 5) to a cohort ofdeaths frorn MND based on work by Dr. Vera carstairs (EdinburghHealth Services Research Network). Much of the statisticalcomputation relating to the case contror study and to the progn-osis of Ir{ND vras done by Mr.J.slattery, Medical statistician.Dr. Jan BeII, neuropathologist at the Western General Hospital,Edinburgh, performed most of the autopsies described in Appendixc. susan McHugh, medical artist, was responsible for some ofthe graphical illustrations; Huub t{irrians, Dutch Medicarstudent, helped in translation of papers in German and Rosemarie
Bland, those in French. Dr. J.D.Mitchelr introduced me to thewritings of charles Bell. r wourd rike to thank The Davidcunmings Trust, based in Brenheirn, New Zearand for monetaryassistance with the purchase of items.of computer hardware.
Finarly, r am immensely gratefur to professor charles p.
Warlow for allowing me to join his Department to undertake thiswork, for his tireless instruction in the science of clinicalnedicine and his continuing guidance, support and encouragement,
both in personal and professional rnatters.
22

Outline
DECI,ARATTON
No work contained in this thesis has ever been presented fora degree or diplona at the University of Auckland or any otheruniversity, neither is it presentry being subnitted for a degreeor diploma, except to the university of Auckland.
23

CNAPTER 1
TNTRODUCTTON TO TEE TEE8Is.
A EISTORI Of TEE EARITI DESCRIPIIONS OF I|OTOR XEURON DISEASB
24
Chapter l-
t0. - -Life itself is a whoLe process of rediscovery otwhat our forebears have known-pain and preasure, ec-sta-sy and despair, beauty and ugliness. ana for even themost modest of those who have had the privirege ofworking in biomedicai science there has bebn the iedis-covery:,ot something that we can share even with Gali-7eo-the excitement of making a discovery.Sir C.C.Booth2.
" Now and again there is a man whose rife and wor? makean.enduring inpressjon and who, escaping the thralrs ofnationalism becomes a teacher and a lealCler.,,
From sir william oslerrs obituary on Jean-MartinCharcotJ.
THE CONTRIBUTIONS BY EDTNBURGH GRADUATES TO TEE
FIRST DE8CRIPTTONS OF I{OTOR NEURON DTSEASE
It difficult to disentangle the precise sequence of eventsin the rnid 19th century surrounding the early descriptions ofidiopathic motor neuron disease (MND) and its principal clinicalpresentations: amyotrophic laterar sclerosis (ALs), progressiveburbar palsy (PBP), progressive muscular atrophy (pMA) andprinary raterar sclerosis (pl,s). Virtuarly no disease subsequ-ently eponymousry endowed has been described by only one personand the process of rediscovery is a particular feature of theclinical practice of medicine2. Nowhere is this more truethan for MND, for while there is no doubt that the definitivesynthesis of the clinical and pathological features was crystal-lised in the writings of charcot4, whose name is associatedwith ilclassicalr' MND, many other physicians contributed to theearriest descriptions. of these there are four who, to a greateror lesser extent, b/ere associated with the rGolden Agerr of Edin-burgh medicine.
25

Chapter t-
A letter by R.vf.R.Robinson (L777-L966,, of preston, Engrand
dated JuIy 2l-st. L825, is quoted by the Edinburgh neuroanatomistand surgeon sir charles Belr (L274-18 42) , in his book on thenervous systems and is probably the first documented case of MND.
This contribution by Robinson and BeII to the early descriptionsof MND has not previously been recognised. Robinson was born inLancashire and graduated doctor of rnedicine at Edinburgh on 12thseptenber, 1800. He was president of Edinburgh,s Royal MedicarSociety, founded in L734 by a group of medical students after theacquisition of a fresh body for dissection and meeting initiallyin taverns
't -. -with the intention that a dissertation in Englishor _Lati\ pn some medicar subject...shou-Ld be conlposedand readt,o -
Robinsonrs doctorate was not, howeverr oD a neurologicarsubject (Disputatio medica inauguraTis de vesicea, urethraequenorbis); he became a Licentiate of the college of physicians(London) in 1807 and practised in Lancashire where he sras an
important influence in the board of.management of the prestonDispensdry, founded in L8o97. He wrote to charres Berr foradvice about a previously welr hronan of nearry 70 years.
" From the tirst of her complaint to the presentmoment she has been free from headaeh lsic) ind trompain, numbness, or debility ot the linbs. 'The visionand hearing are natural; tie appetite good; the bowersregular, and th9.2lgep naturar- ....sonb tew nonths agoshe had sone ctitticilty in using the tongue and inexpressing. particuTar -words. frnis ditticuTty hasgraduaTTy increased, and now she cannot protrude thetonguet ot even move it. she has rosi her speechartogether. ,.The tongue itself is soft and puTpf; butit retains its sense of taste and feeling. Tnt'd'egru-tination is inpaired and occasionaTly sni is distressedwith a sense of suftocation, in at€enpting to swarlowtood, which she is now obliged to ao iitn great care.
26

Chapter 1
she cannot hack up any thing from the throat, nor draw?!y thing trom the posterior nares by a baci< draught.The features of the face are quite-naturar, and'theskin retains its feeling. rie sariva occasionarlyflows from the mouth.',
No follow up is available to teII if the disease became
more widespread, neither is information available about theexamination of deep tendon reflexes which was not introduced intoclinical practice until 18758. BeII noticed the sinrilaritybetween this patientrs condition and the syndrome observed in a
dog after section of the lower cranial nerves and concluded thatthe patient was suffering from
00...a paralytic affection of the ninth nerve.',and noted that the0t...function of the titth nerve was entire.,'
He recommended nauseating rnedicines and Ieeches under thenastoid amongst other remedies. This syndrome cornbining anar-thria, impaired degrutition, ptyalism and impaired tongue move-ment, probably with mixed upper (slow clumsy tongue) and rower(soft, possibly wasted tongue) notor neuron signs, is undoubtedlydue to PBP and was published 30 years before that usualry quo-ted9 ' 10 as the first descriptions of pBp by Duchenne deBoulongne in 186011 and Leyd"r12 in 1870.
The Edinburgh contribution to early descriptions of l{ND isalso evident in the writings of Berl himserfS. charres Belrhras born in Edinburgh where he trained in anatomy and surgery.His contributions to neurorogy are numerou=13, incruding theformulation of the concept of a different function for the post-erior and anterior spinal roots; he is remembered by every
27

Chapter 1
medical student for Bellts palsy and for the long thoracic nerveof Bell but he also nade other, less well known, original clini-cal descriptions in neuroloqyL{r15. He was a surgeon in theNapoleonic htars; an author of beautifully illustrated books on
neuroanatorny and a medical artist (his paintings of opisthotonusin tetanus and gun shot wounds adorn the Edinburgh CoIIege ofSurgeonrs museum). fn the book which contains Robertsonfs let-ter5 he described a woman of 4L,
0t - -.apparentry in good hearth with weakness of theTeft toot, and tive weeks aftenrards, with weakness otth? right to.o!, .graduarry she w-as artogether de-prived of motion in her regs-... jt was remarkabre thats!9 experienced no dininution of the sensibirity of theskin of the affected parts...a tlea bite diitressedhe_r, yet she could not hove to scratch hersert. . .A yearafter the commencement of the compraint, the weaknessextended to the arms, and she Eegan-to experiencedifficuTly in her breathing. The accessory muscres ofrespiration in the neck and chest were thei seen to actwith remarkable force...and died in six weeks,'.
John Abercrornbie (L780-1844) r^/as born in Aberdeen and gra-duated MD from Edinburgh in 1803. He became physician to theKing in Scotland in 1828 but failed in his bid to become profes-sor of medicine; oxford awarded him the degree of Doctor ofMedicine and it was remarked of him by Dr. James Gregory,
"...that wee feLLow will some day be Edinburgh, s mostsought atter consuTtant',.
His portrait can be seen today in the Royal corlege ofPhysiciaD's, Edinburgh, as can the copy of his book on the brainand spinal cord which he donated to the libraryl6 and whichwas translated into French and quoted by Aran. He describes a
patient who had a scapulo-humerar syndrome, probabry a spinarrnuscular atrophy:
28

Chapter L
0t...a,young man, aged 14, who had nearly lost themuscul.ar.power of the upper part of aoti his arms,accompanied by a most renar*iole dininution of sub-stance of the principal muscres. The dertoid andbic_eps are reduced to Lhe appearance of mere membranesand the sarne affection exteicls in rather a Less degreeto the rnus-cl.es upon the scapular- the muscres upon'theforearm, however are turf and vigorous....i; otherrespects he is in perfect hearth. The affection hascome on gradually.
He speculates as to the lesion involved:nrt is inpossibre, r think, to expTain such cases asthese, except upon the principTe of rocar affections ofthe nerves, which are at fresent invorved in muchobscurity" .
six "cases of a peculiar species of pararys!snL7 areoutrined by the fourth Edinburgh graduate, John Darwarr (L7g6-1833). Darwall graduated MD from Edinburgh in 1821 with histhesis entitled "Diseases of Artisans with particular referenceto the inhabitants of Birmingham,' - where he was born and spentmuch of his 1ife18. His cases are heterogeneous and some may
have had brachial neuritis as the disease responsible for thepatchy linb weakness beginning in proximal arm muscles and spar-ing the burbar region, however, some may have had MND. Darwalldied of septicaemia forrowing a post mortem room accidentlg.
unfortunately it is unrikery that these four Edinburghgraduates ever exchanged ideas in person because a review of thechronology shows that they were never all residing simultaneouslyin Edinburgh2o.
29

Chapter 1
FORIIUIJATION oF TtrE ttoDERN coNcEPT oF l,toToR NEURON DrgEAgE
F-M- Aran (1817-1861), and his teacher c.M.A. Duchenne de
Boulogne (1805-1895) were responsible for the more definitivedescriptions of pIr{A, particularry the j uveni le, inheritedf orrns2L ' 22 although, to begin with, there was conf usionover the difference between the amyotrophies and muscular dys-trophies23. A patient with arnyotrophy and coric, thought tobe due to lead poisoning, prornpted Aran to wonder if lead rnight
be responsible for other, apparently idiopathic cases of ltpo21.
Duchenne noted the palatal weakness in pgpll.
" The patient courd not produce a large enough breath,not even to extinguish a candre. But lt we pinched thepatient's nose the breath emanating from tha mouth wassufficient...pronunciation of the tetters p and b wasmuch clearer when the nose was pinched shutj"
In Goldblattrs account of the history of motor neuron dis-
""="24 the descriptions of pMA by Aran and Duchenne in 1g4B-
50 were said to predate those of ALs. However, a review by
veltena25 of the case of prosper Lecompte, a French circusowner and patient of J. Cruveilheir (1791-1874), who was adnittedin 1850 and died in 1853, shows that descriptions of ALS hrere
documented about the same time as discussions of pMA. The de-scription of Lecompters illness leaves no doubt that he had a
combination of lower motor neuron (LMN) and upper motor neuron(uMN) signs, although there is no information on deep tendonreflexes. Intellect, sensation and sphincter function wereunaffected and the anterior roots were shrunken at autopsy.
Duchenne was a close and trusted friend of the great J-M
charcot (L825-1893). rn t-869 charcot described, in detail, boththe clinical and pathological features of ALS in two cases at the
30

Salp€triEre26.
Chapter 1
It is to Charcot that most of the credit isdue for setting down the definitive descriptions of ALS in lec-tures given in L874 and subsequently, based on 20 clinical casesand 5 autopsies4,27 . charcot recognised medulrary invor-vement and the UMN signs described as "spasmodic" and ',contrac-ture" as welr as the previously ernphasised atrophy of muscres.His preponderance of females is an early example of selectionbias, given the Salp€triErers use for
"...the con{inement of beggars, unwanted womanhood andthe intirm"J.
charcot also described a patient with isorated spasticquadraparesis due to degenerative disease of the pyramidaltract2S and w.H. Erb (1840-192r-) was also one of the earliestto draw attention to a chronic form of spastic spinal paral-ysis29 in L875, the year of the account of the tendon reflexes.rn his account of 16 cases, translated by saundby, Erb acknow-Iedged Charcotrs case report but felt that
" -. -not a singre_ exampre of the rear prinary rateralscTerosis existed in the Titerature'and
" .. -the disease approached the ,scl6rose rat4-rareamyotrophic', exceTTentry described by charcot, but theabsence of muscurar atrobny, of which no trace was everpresent, distinguishes it tron that...the anterior glreymatter cannot be naterially inplicated...the diseasemust be distinquished tron tie tortowing: chronictransverse nyelili", tabes dorsaris...murtiple screr-osis .and paralysis of the cauda equina, alsd the hemi-pLegic form from cerebral heniplegia...',
In nine of Erbrs patients the spasticity hras isolated butnearly half had disturbances of sensation (but not anaesthesia),
3l_

Chapter 1
two had "bladder feebleness as a temporaty condition". one had
bulbar involvement but non had sexual dysfunction, cognitivedisturbances, pain or bedsores.
Sir I{.R. Gowers (1845-1915) also entertained the possibil-ity of a "Pute" primary lateral sclerosis. spillane refers toGowerrs ttl{anual of diseases of the nervous system as the ,rnet)to-
Togical bibrs"1o. rn this authoritative text (viewed in theNationar Hospital ribrary, eueenrs square, London) Gowers expan-
ded the concept of PLS as a disease due to "sclerosis" of pyrarni-dal tracts manifesting only UMN signs while sparing sensation and
sphincter function. He separated this from nultiple sclerosisand the ataxias although some of his patients may have had here-ditary spastic paraparesis3O. The debate about whether pLS repre-sents a discrete entity has continued but recent clinicaL3L,32and pathologicar33r34 evidence supports the concept of an isora-ted UMN (corticospinal) degeneration as one of the subgroups ofmotor neuron disease. Gos/ers entertained the possible relation-ship of traurna to MND and also coined the terrn rrabiotrophytr todescribe the selective premature decay of a functionally relatedpopulation of n"uror,=35.
By the end of the nineteenth century, ds the anatony ofupper and lower motor neurons as separate anatomical structuresbecame acknowledged, the clinical descriptions of MND in itsvarious forms h/ere well docurnented in standard textbooks of theday, arthough the rerationship of pathorogy to clinical signsremained a matter of debat"36.
32

Chapter 1
TERllrNoLocY RETTATTNG To ttoroR NEuRoN DrgEegB
Charcot coined the term "sc76rose Tatlrale anyotrophiqus"3Tto emphasiq$ the pronounced degeneration of lateral corticospinaltracts principally in the cervical cord and noted the atrophy ofhypoglossar nucrei and the anterior but not dorsar roots."charcot's Disease,, is sometimes appried to "classicart, ALs as
well as to other diseases for which the founder of modern neuro-logy is nohr remembered. However, rnotor infornation is conveyedfrom higher centres to the brainstem in the cerebral pedunclesand pyranids, not by raterar corumns, so that the term ALs, ifriterally apptied, impries disease confined to the spinar cord(arthough this sras not as originally intended by charcot). rnaddition, gliosis is the najor histological finding in Mlru not"sc7erosis", derived from a Greek word for hard38, usualry ap-plied to overgrowth of fibrous tissue.
From the start there hras a confusion over when to use theterrns ALs, PMA and PBP. Charcot had included cases of pBp withhis list of earlier descriptions of ALs. Leydenl2 allottedthe syndrome of ALS to the category of either pMA or pBp dispen-sing with the former. Gowersr pathological illustrations in hisManual of Diseases of the Nervous systern3o show the sirnilar-ity of lesions in cases with clinically defined pLS, plrlA and ALS
he stated:
u r have not met with a singre case of progressivemuscuTar atrophy in which tie pyranidar -tra-cts wereunaf fected', (p373 ) .
He did not think Charcotrs introduction of the terrn ALS veryherpfur, with its irnprication that the primary lesion was the
33

Chapter L
degeneration of the pyramidal tracts, and that the atrophy of theanterior horn cerls was secondary or "deuteropathic,,.
" charcot's distinction js in effect givinq a nevr nameto an ord disease....a division i-nto -two c-l,asses[meaning PMA and ALs] (into which the same case mayfa77 at difterent periods) js J.ess in harmony with th;facts ot the disease than is a recognitibn of thevarying extent of the resion and the correspondingvariation of clinical character and cou,rse,,3o.
A unifying concept of diseases of the notor system hras
evolved by Brain and the terrn t'motor neurone disease,, introducedto apply to a spectrum of clinicar subtypes39, reaving authors todescribe more precisely to which clinical pattern they refer.This approach has influenced much British writing when discuss-ing this group of disorders and is a useful generic term whichhas withstood the ephemeral fashions of classification systems.
Today, the terms used today by authors under the rubric ofI'{ND often vary in their meaning4o. ALS in the North Americanliterature is usuaJ.ty applied to mean MND, with both uMN and LMN
involvement, either confined to spinal levels or with bulbarfeatures. However, even recent North American studies use ALs
to describe patients with onry LMN signs4L,42 and some
authors even separate MND and ALS as different disorder"43.The term PMA may be used to mean late onset chronic forms of
spinal muscular atrophy. However the evidence, based on clinicaland genetic studies, suggests a real subdivision between spinalmuscular atrophy and PMA. The latter being a disease of adultlife which blends clinically and pathologically into the othersubtypes of adult onset MND, while spinal rnuscular atrophy isprincipally an infantile and childhood disease usually of proxi-
an autosomal recessive
34
maI distribution with

Chapter 1
inheritanc,e44 ,45 .
A patient with both a combination of PBp and pMA nay arbi-trarily be classified by some as pBp46. whether pBp everrenains isolated to the brainstem, as the name irnplies, withoutspread to other levels is uncertain. There is increasing evi-dence, with the widespread use of rnagnetic resonance irnaging thatPLS, a numericalry small group, and much debated entity, is partof the spectrum of MND but with exclusively upper motor neuron(UlO[) signs32 '34.
The distribution of pathological changes does not necessari-Iy correlate with clinical features even in well st,udiedcases4T '48 and ALs, pBp, pMA and pLS, the usuarry acceptedprincipat clinical subtypes in adults, are almost certainlyvarieties of a single disease with the common pathological fea-ture of anterior horn cells loss and variable pyramidal tractinvolvement.
"Lou Gehrig's disease,, is the euphemism often used by rayArnericants, after the most famous first baseman in rnajor 1eaguehistory. Gehrig died in L94L but his declining batting averageand cinemagraphic evidence has been used as an indirect measure
of his muscular strength pointing to the onset of his illness in193849. "creeping parary.sis,,, a particurarry vivid descriptionof its effect, is sornetimes used to describe ltNo5o.
The most famous Britons to be affected are David Niven,actor, and Professor s. Hawking, present Lucasian professor ofmathematics at Cambridge University, who has been described as
the greatest theoretical physicist since AIbert Einstein5l.As described both in a recent television documentary of his lifeand work and in his book52, Hawking was tord, in 1963, that
35

Chapter 1
he had MND and courd expect to rive for two ye.r=52. His illnessdemonstrates a striking dichotomy between his great disabilityand his handicap, which is slight, dt reast as far as theoreticalphysics is concerned. His ilrness also raises irnportantquestions about predicting prognosis in MND.
The spelling of the word rrneuronrf in MND is also a source ofsome disagreement. Gourd nedical dictionary3S gives bothrrneuronerr and ,neuronrr as acceptabre. The word is derived fromthe Greek for sinew, string, nerve, related to the Latin mnervusrl
and to the Engrish 'sinewr. rt refers to the comprete nervecel1, including the cerr body, axon, and dendrites. wartonrsauthorit,ative textbook on neuromuscurar disorders53 usesrrneuronerr but in most medicar journals and in particurar, neuro-Iogical journals, the spelling rrneuronr is in most widespread andbecoming preferred although the Lancet uses rmotoneuronr orff motorneuronerr or rmotorneuronr. rn North America the ,e, inrrneuronrr is uniforrnry deleted although American authors publish-ing in British Journals may include the rrsrr54. rNeuronr is usedthroughout this thesis except when quoting a different sperringused by other authors.
36

Chapter 1
WHY TIEASURE TBE INCIDENCE OF IIOTOR NEURON DISEASE?
Despite recent advances in the understanding of those formsof MND which have a genetic basis45,55'56 and arthough condi-tions have been, and continue to be, described which may rnirnicMND (table 2-L), for the vast najority of patients with sporadicadurt onset disease the cause is unknown, the subject of much
speculation and a wide variety of diverse hypotheses of aetiopa-thogenesis5T-59 .
The possibility that environmental factors play a role inMND, particularly in the light of studies from the western paci-ric6o (chapter 2), is an appealing and recurring theme61.However, this hypothesis is not supported by the traditionarteaching that the distribution of MND in developed countries isuniform and static62-66. A recent editori aL67 has challengedthis view, suggtesting that the distribution of MND in tine andprace may not be as uniforrn as previously berieved. clearly anynon-randon distribution in place and tirne is important to identi-fy as a crue to potentiar environmentar risks.
As welr as studying ternporal and geographic trends, inci-dence studies offer an opportunity to collect population baseddata to help clarify some of the issues alluded to above anddiscussed in more detail in the subsequent chapters, ie accuratedemographic features, crinicar description, appropriate classi-fication and prognosis. Finally, and importantly, reliabrymeasuring the size of a problem allows the appropriate pranningand allocation of health care resources.
37

CHAPTER 23
roRrrDrrDE ltoRrAr,rrY, rNcrDENcE, AND DrgrRIBurIox
OF ADUI,T ONsEr UOIOR NEI'RON DrSEASE SrNCE 1950
38

Chapter 2
INTRODUCTION
"ft is from we77-arranged medico-statisticalgraphical inquiries that we are ultinately tovast inctease to our knowledge of the renotedisease . . .The vaTue of these t_'esearches. . .canbe estimated too highly.',Streeten creen, written in 1g4058.
and topo-expect a
causes ofscarceTy
The last published review of the epiderniology of MND was 10
years ago66 arthough the preparation of this thesis coinci-ded with a further analysis by KurtzkeS9. A thorough reap-praisal of previous research is appropriate as the backgroundto the incidence study which forrns the basis of this thesis.The aims of this chapter are therefore to:
(1) Critically review all publications concerned with themortality and incidence of adurt (>15 years) onset MND in de-fined populations. Publications were specifically reviewed forany evidence of a non-random distribution in place both betweenstudies and within populations. Sorne incidence studies alsocalculate, or include, a prevalence survey but studies exclusive-Iy of MND prevalence are not incorporated in this analysis as
they do not add further to aetiorogical considerations.(2) Review secular trends in this disease.(3) Examine the reports of clusters of MND which night
provide clues to environrnental influences.(4) Compare the epiderniology of sporadic MND with the West-
ern Pacific forms and summarise the results of the intensivesearch for the cause of this MND variant.
(5) Identify standards for future epidemiological studiesposs ible
39
of MND and research directions.

Chapter 2
T{ETHODS OI' DATA RETRTEVAI.I FOR REVIEW
This review was conducted according to recent guidelinesfor medical revier=7o,71. A comprehensive search by indi_vidual year using cambridge compact Disc Medline from January1965-June 1991 was used to identify all publications in English,or with English abstracts, dealing with the frequency (rnortalityor incidence) of adult onset MND in defined populations world-wide' The references in these pubrications v/ere used to crosscheck the thoroughness of this search and to locate papers pub-lished from 1950-1965. rn addition any papers dearing withsurvival or prognosis, which may contain incidence data andreports of crusters, were specifically sought. Alr papers werereviewed in the original.
Many population-based studies of MND have been publishedwhich vary widely in their quality. For the purposes of sys-tematic analysis these were divided into mortality studies, basedonry on death certificate data 72-86, and incidence studiesdivided according to their methodorogy. Varid comparisons be-tween studies can only be made if sinilar rnethodological stan-dards and diagnostic criteria are applied. while most epidernio-logical studies included the syndromes of amyotrophic lateralscrerosis (ALS), restricted progressive burbar palsy (pBp) andprogressive muscular atrophy (PMA) some studies were confined toALs. The best incidence studies used multiple sources'of caseascertainment, and/or were based on recognised systematic rnedicaldocumentation systemsST-97. The second group of incidence stu-dies were based on more than just tertiary referral records butthere was some doubt about the completeness of case findinggS-106. The third group were those in which incidence had been
40

Chapter 2
calculated using singre hospitar records, usuarly neurologydepartmentsr oF where data hrere inconplete in review, or wherethe diagnosis was based on unverified hospital discharge dataloT-LL7. There are a large number of published series of patientswith MND but these were not included if not specifically dealingwith incidence or the population denominator was unclearllS-L23. sorne syndromes may rnimic or resemble idiopathic MND butsuch studies of motor neuronopathy or neuropathy with recognisedcause were excluded (table 2-L,) .
AIIAIJYSIS OF EXTSTING STUDTES
l{ortality studies (Tables 2-Za,b)
According to the rules for selection of cause of death forprinary mortality tabulation by the world Health organisation,MND shourd be coded as the underrying cause even if it appears asa contributing fac1'or72. However, this may not be forlowed instandard practice and some studies have used rates for MND clas-sif ied as the trunderlying causerr and .excluded patients with l,lND
whose deaths were certified as due to another ".rr="73 whireothers have separated the two gro.,p"78 or used rates based onwherever the diagnosis appears on the death certificateTg.comparison of rates for subgroups of MND (ie ALs,pBprpMA) basedon death certificate data are cornplicated by changes in theInternational classification of Diseases (IcD) and non-standar-dised methods of diagnosis. rcD-9, introduced in Lg79, was afurther change from rcD-B with respect to MND56 (see chapter4) ' ALs had previously been recorded as a distinct entity (code
348-0, rcD-8), although some studies use ALs to refer to arr
Unir,,ersity of Aunklancl '
Pl ltL$cf'l l..i :1R.r.''
SC'r !rJCL OF I'i;:ii, -
FAI ili $tt;i]- &uui'' - -
4L

Chapter z
types of MND80. rn rcD-9 a new code, rcD-335, riras created forall anterior horn cell diseases with 335.2 for rmotor neuronediseaseff , which contains ,ALs; MND (burbar) (mixed type), and plrlA
(pure) r' (Tab1e 4-1) . A further ICD is planned for 1993. Deathcertificate data alone are therefore unlikely to be reliableenough for comparing rates of MND subgroups or even for conparingrates between different countries, particularly when these over-Iap rCD chang€s, and because of the confusion which exists overdiagnostic criteria (see below).
Age specific nortality rates, where given, usuarly rise toa peak between 60 and 75 years, followed by a sharp decline, butthis simply rnay reflect difficulties with diagnosis in the veryelderly. rn England and Wales, for birth cohorts after 19oofollowed up separately over time, mortality increases contin-uousry with age (c.Martyn, personar comrnunication), the same
finding has been reported from sweden75. Rates in males areconsistently higher than femares, usuarry around r-.5:1.
when international- rnortality figures srere last reviewed indeta !L72 , a rise from rgs2 to 1960. forrowed by a sharp farruntir L97L was observed in Japan whire in contrast, a rise inEuropean and Australasian rates and stationary figures for theusA were noted. There is more recent evidence from the uKz3,swed"n75' :JSA76'77, Fran."79, Norr.y82 (Fig 2-L)and most recently, scotland (Dr.R.J.swingler, personar communica-tion, paper in preparation) that nortality rates are continuingto rise with tirne (tabre 2-La), Fig 2-L gives the typical scareof the increase which has been observed in these studies.
rn the usA overalt ALs rnortality increased 462 for men and
492 for women between 1-977 and L986; the greatest increases in
42

Chapter z
age specific mortarity have occurred in the order agegroup=77 but increases are arso apparent in rniddre agegroups76. The question arises if this trend is artefactual,a result of improvement in diagnostic accuracy and increased caseascertainment (particurarry in the elderly where age specificrates are high), or due to changes in rcD coding. Hovrever,nortarity from MND does not correlate with the nurnber of neurolo-gists in the uK73 or the physician/popuration ratio in theusa81; there has been much less of a parallel increase in thenurnber of neurorogists in the uK than usA; technologicaladvances such as nucrear magnetic resonance inaging and theidentification of syndromes which rnirnic MND are rilcery to re-duce, rather than inflate rates and the disease is distinctiveand of such high lethality that significant changes in reportingseem unlikely. on this basis it seems rikely that the death rateincrease is real and the apparent decline in age specific nortal-ity is probably a measurement artifact. Mortality statistics may
be adequate for following trends in total MND rates within coun-tries
The interpretation of variation in mortality with place iscomplicated by changes over time, the use of different age bandsfor age specific rates, and variabre methods in the extraction ofdeath certificate information. A cornparison of standardisednortality rates for the age bands between 60 and 74 years (whererandom error and diagnostic bias are probably least) is presentedin table 2-2b; these data are extracted from those nortalitystudies in tabre 2-2a where this was possible. Higher rates areobserved in the uK compared with Finland and the usA.
whether the incidence of MND (as opposed to trends) can be
43

Chapter 2
studied adequately on the basis of mortarity data alone isuncertainTS. Arthough 7o-9og of patients diagnosed with MND
have this recorded on their death certificate72,73,L24,L2s,only one study from Japan has examined the false positive rateof death certificate coding (in i-965) by an extensive attempt toverify the diagnosis from other sources. As many as one thirdof males hrere coded as dying of MND without having it, but theaccuracy was better for females72.
Incidence studies (Table 2-3arbrcrd)1. crud€ rates The best incidence studies are presented in
table 2-3a together with the rnethods, crude incidence with calcu-lated 952 confidence interva L=L26 , prevalence rates (wherestated) and notes. Although crude incidence may differ betweenpopulations because of differences in age structure, when thestudies hrere divided according to the quality of their nethodo-Iogy, in general, the crude rates tended to reflect, the likelydegree of case ascertaj-nnent. There $/as a significant differencebetween the mean crude rate of those, studies in table 2-3a when
compared with all other studies (table 2-3b and 2-3c) (difference= 0.64/Loo,oOo/year 952 cr 0.L5-1.13) and when studies in table2-3a were compared with those which relied on single hospitalcase ascertainment (tabre 2-3c) (difference o.75/Loo,o00/year,95t cr 0.21-r-.3). However, there v/ere exceptionsr. for exarnpr€, a
row crude rate was seen in rsraer, based on a comprehensivesurvey of Jews as part of a national neurological disease regis-ter, and in sardinia, which used five separate sources of casefinding. The clairn of a low incidence in MexicolOo was basedon individuals with access to a government health programme and
44

Chapter 2
while medical facilities may have been excellent for those withaccess, it is not certain that all affected individuals with MND
were identified. A lower mortality in Mexico than any other of33 countries, incruding others in the deveroping third worrd,was observed in a rarge comparative anarysis of average ageadjusted rates, €rt least around 195086. rf this observationis not artefactual then it nay be evidence of an ethnic rrresis-tancerr r ot a resurt of environmentar factors.
2' Age and sex specific incidence rates, standardised ratesAge and sex specific rates in arr incidence studies, exceptRochester, show a steady rise to a peak, usually between 60 and75 years with a sharp decline after this (Fig 2-2). rn Rochesterthe rate appears to continue to rise with d9€, arthough thenumbers are snall and confidence intervals for the older agegroups are so wide that a decline cannot be excluded. This isof considerable interest from an aetiologicar viewpoint; if atrue decline occurs in the elderry then the disease is perhapsmore likery to refrect an environmental infruence rather thansinply a result of age related neuronal attrition. The nrajor-ity of reports show a nale predominance with a range betweenL-2zL to 2.ozr, but some show no sex differer,""99 or even a
femare predomin.n""8o. rncidence rates with time, arthoughreported as increasing, are unretiable in studies with snallnurnbersS8. rn rsraet this increase was considered to be dueto causes other than irnproved case ascertainmentSg.
Meaningful direct, statistical cornparisons of age and sexspecific rates between studies are complicated by methodologicaldifferences, the use of different age bands and because overrap
45

Chapter 2
with the same years of study are necessary to minimise possibledifferences due to changing incidence over tine. The age speci-fic rates for males and females combined frorn three of the bestincidence studies88,89t94 are protted in figure 2-2 todemonstrate the range. rt can be seen that there are differencesin incidence between the studies from Rochester and Israel and
the 958 confidence intervals for these two studies (not shown)
suggest the difference is rear. when the rates for the age
bands 45-74 years (like1y to be the rnost reliable for comparativepurposes) for males and females are standardised to the Scottishpopulation (table 2-3d), the differences between populations arealso apparent. when age standardised rates (over 4s-74 years)for nales and fenales conbined from those studies in tabl- 2-3a(excluding NW England where insufficient data for this calcula-tion are provided) are plotted against their degrees north lati-tude (Fig 2-3), there is a positive correration (p varue for theslope 0.05) with a factor of around three times higher in north-ern ratitudes. rt could be argued that this observationstrengthens the case for differences,in the distribution of MND
for, while this correlation may stirl be due to better caseascertainment, only the best incidence studies, which used multi-ple resources, are included. rf rear it rnay be due to genetic orenvironmental factors and is akin to the nuch debated correlationof murtiple screrosis prevalence with 1atitude127.
46

Chapter 2
3. clusters There are reports of conjugarL28,L29 andother non-consanguineous clusters of MND outside the WesternPacific, with rates much higher than would be expected by chance.Examples incrude peopre who work13o,L31 or rivel.32-L34in crose proximity; pray in the same sports team135; have beenv/ar evacueesT36 ' share an environrnental peculiarity such as highsoil sereniunL3T; or a common occupational exposure such asleatherl38 or texti1.L39 workers. Toxins from freshrycaught fish were irnplicated in a cluster in Wisconsinl40. rn oneexampre, al1 those affected were of Ashkenazi Jewishextractionl33. rt is not crear if the high incidence in Filipi-no men in Hawaii is because of a geneticalry susceptible poolwith a high predisposition to develop MND or whether otherfactors are responsible98,14L. other studies show a
significantl42 or non-significant73,8o,8L'97 uneven distributionbut most studies that have examined distribution within a popula-tion have dernonstrated geographical uniforrnity. It is difficultto know whether smarl clusters are purery due to chance, particu-larly when the overall poputation incidence is not known143. Arecent publication from north west Englandg6 atternpted to providefurther data in this regard by analysing the distribution of L73
cases according to postar areas and alrocated through a gridreference to 338 electoral wards. several wards had a signific-antry higher than expected rate but, as the authors point out,the actual number of wards showing this non random distributionmay not have been greater than the expected nornal variation.
one intriguing attenpt to demonstrate clustering of MND inrelation to an infectious aetiology has examined the correlationsbetween infectious disease notification rates in 1931-39 with
47

Chapter 2
nortality from MND in 1968 -7g. There was a specific positivecorrelation for polionyelitis but not for other infectious dis-easesi nor did polionyelitis correlate with other leading causes
of death144. The suggestion has been made that the risingrate of poliornyelitis during the early decades of this centuryaccounts for the present increasing trend in MND mortality (due
to subclinical infection). There is, howeverr no such correla-tion in scotland and no support for viral infection from labora-tory studiesr45. Although rate neurorogicar deteriorationafter poriornyeritis may resembre MND146, the rerationshipbetween previous poliornyelitis and sporadic MND remains a matterof debate.
l. llestern pacif ic f orns of l,tND The western pacif iccrusters are found in: (i) Guam, the southernmost and largest ofthe Mariana isrands, where the charnorro rndians areaffectedL4T-L49; (ii) the Kii peninsura of Japanl5o and (3)the Auyu and Jakai people of west New cuineal51. rn Guam, themost extensively studied of these endemic variates, the clinicalfeatures resemble sporadic MND/ALS, but in the same popurationthere is arso a high incidence of a parkinsonism/denentia comprex(PDc) and some patients have a combination of ALs and pDC. Thepathology of these Guamanian diseases includes extensive neuro-fibrilrary tangles in the cerebrum and brainstem of rnost pa-tients, and in the spinar cord of a minority, €rs well as ante-rior horn cerl ross in those with ALs152,L53. This differencesuggests that the sporadic and Western Pacific forms may have a
different aetiology but should the cause of these high incidencefoci be clarified then widespread repercussions for the under-
48

Chapter 2
standing of sporadic MND are possible.
As a result of systenatic surveys carried out in the early1950rs prevalence rates 5o-1oo times greater than in developedcountries hlere established. Since then it was thought that theserates were decriningl54-l-58, however, the accur-acy of some later reports has been questioned and the nostrecent prevalence survey of three vilIages, based on small nun-bers' suggests that rates are still as high as in the mid decades
of this centurylsg. Disease duration is thought to be sinilarto that in deveroped countries while the age of onset may be
increasingl53 ' l-59.
An environmental cause, or at least a genetically determinedhost response to an exogenous factor seemslikeIyla 1, 16 o-L62
. The disease is confined to a
particular area of the Mariana islands despite a shared origi-nal migration patternl63' there is no evidence for MendelianinheritancelSO and the disease is of no higher incidence inoffspring of affected than non affected Guamanians. MND
does not develop amongst those who have had a brief exposureto the irnplicated environmentl64 and the ratency for the deve-lopnent of MND, dS judged by studies of chamorro migrants tothe United States, is long165'156 inplying that an early expo-sure may be crucialr oF any proposed environmental factor must be
slowly actingr or ageing is interacting with an earlier environ-rnental f actor.failed167.
Attempts to transrnit the disease have
The putative environmental cause is unknown. The suggested
declining incidence coincided with adoption of a lifestyle closerto Western standards so factors associated with a prirnitive
49

Chapter zlifestyle may be important. Neurotoxins in the seeds of the nutcycad circinalis (farse sago palrn), and used by the natives ofGuam for the production of frour, are thought by some to beresponsibrel6S. A degenerative motor system disease withsinilarities to MND has been produced in primates by feedingthe cycad derived toxin BMAA (a-amino-B-rnethylaminoproprionicacid) L69 'L7o but motor neuron pathorogy can arso be inducedby other experirnental methodsLTL. Doses required for theseexperirnents are high and washing of the seeds, €rs is the custon,removes alr but minute traces of gy,Lg172, probabry to such lowrevels that toxicity is unrikelylTr. cadjusek and otherssuggest an alternative mechanismls8,L74'L75. In New GuineaIow concentrations of calcium and magnesium and high levels ofaluninium, silicon, titanium, chromium, iron and manganese arepresent in the well and spring water of those villages in whichMND is found and not in those which rie on the rnajor rargerivers which originate in the central highrands. Thebiochemical abnormarities in the water or diet in Guarn are resscertain but intraneuronal deposits of calcium and aluminiunsuggest that basic defects in mineral metabotisn rnight irnpairtransport of neurofiLarnent proteins, leading to neurofibrillarytangle forrnationLT6. The interested reader is referred else-where for details of the extensive debatel,77,L78.
50

Chapter 2
SulllilARy AllD CRITERIA FoR THE rDEAr, gTuDy oF ttND INCIDENCE
Mortality statistics in MND may be sufficient for studyingtrends with tirne, and possibry variation in prace, but arelikely to underestimate rates in the erderry, particularly innedically deprived areas, where age specific rates may be higherthan reported (see chapter 5 for discussion of deprivation and
MND). Death certificate data are subject to changes in codingpractice and there is little information on the frequency offalse positive coding. Nonetheless recent studies of mortalitydo show rising rates with tirne, particurarly in order agegroups. This is a consistent finding in a number of countries,and it nay be real rather than due to ascertainment bias but, ifso, its cause is uncertain. Kurtzke also concluded that therewas rr...evidence to support a real increase in the frequency ofALs'f69. rf rates realry are increasing, then this conplicatescomparisons between studies in different places conducted overdifferent periods.
There are certainly variations in reported incidence ratesin place, most of which can be explained on the basis of differ-ences in case ascertainment with higher rates tending to be frommore complete studies. However, there may be real differencesof two to four fold between well studied populations in developedcountries, suggesting a non random distribution of II{ND. The
evidence for an environmentar factor in the aetiorogy of thewestern Pacific forms is now very strong. The precise factorsresponsibre are unknown but rdy, if discovered, have irnportantinplications for research into the cause of sporadic MND. Areasof interest for future epiderniological research include studies
5t_

Chapter 2
of MND incidence in racial rninorities in developed countrieslthe developnent of sensitive rnethods for studying the distribu-tion of MND within populations, such as the computer assistedgeographicar rnapping techniques by grid referen".96i pro-spectively designed studies; and attention to Iife events andenvironnental exposures which may be remote frorn the developmentof MND.
criteria for the idear study of MND incidenceFrom this review the standards for studies of MND incidence
should be:
Standardised diagnostic criteria: The reader must be ableto understand clearly what is meant by MND. There are no uni-versally accepted criteria for the diagnosis and there is lackof agreement between neurologists in different countries presen-ted with the same case summaries, particularry when the diseaseis ctinically less fully developed, but pathologically provenl79.
A practical consensus statement for clinical and epidemiolo-gical studies is required which deals'with the problems of defin-ing the crinicar rirnits of MND (see chapter 1), reducing interobserver error in the interpretation of physicar signs (forexample when is a retained reflex in a wasted correspondingmyotome an UMN sign?) and to define the subgroups of MND whichmay have a different prognosis. A subcommittee of the WorldFederation of Neurology has recentry drafted proposals for a
system of classification of ALS, but this is so extraordinarilycomplex, and dependent on detaited electrophysiological evalua-tion, that it is quite unsuitable for application in large scaleepiderniological studies. rn chapter 3 diagnostic criteria which
52

Chapter 2
can be applied to large epideniological studies of patients who
will have been investigated by different centres, to differentdegrees with varying investigations, is presented in furl.
comprete case ascertainment.. A study design ensuring com-
plete case ascertainment is of overwhelrning importance when
studying variation of incidence in time and prace, seeking puta-tive environmental factorsr or when studying prognosis. rndeveloped countries most patients are likely to have attendedregional neurological services but conplete case ascertainmentcannot be guaranteed by studies which rely exclusively on datafrorn such sources. In particular, studies from specialised cen-
tres180'181 are rikery to be biased in favour of youngerpatients and possibly unusuar forms of MND. The erderry, where
age specific rates are high, but where diagnosis may be more
difficult, are particularly like1y to be missed without searchesusing multiple sources of case ascertainment. However, specialcare is required in the etderly as the diagnosis may be particu-larly difficult due to frairty, coexisting disease, or death fronother causes before the passage of time has ctarified the dia-gnosr-s. Multipre sources of case ascertainment should incrudeneurologists; a review of hospitar discharge datai an approach
to prirnary care physicians for identification of patients who
may not reach tertiary care centres, and finally, death certifi-cate rnonitoring. Patient organisations or farnily care workersmay provide useful information but cannot be used as the solesource as this is likeIy to lead to an underestirnate of the trueincidence and contamination by other diseases.
53

Chapter 2
WelT defined denominator and standard presentation of ratesby age, sex and race.' Accurate demographic information of thepopulation at risk must be available so that appropriate denomi-nators can be used. This may be a problem in deveroping coun-tries. The denominator in open upper age bands is sensitive tochanges in the overall population alte structure and becausenumbers are smalr in this age group, changes in age specificincidence within populations over tirne, ot differences betweenpopulations' may be misleading and result from the different age
structure of open upper age bands. Results of incidence studiesmay be interpreted differently by the use of variabre upper age
bands, this is illustrated in figure 3-2. Therefore, informationshourd be provided in five year age bands for the totar p:pula-tion to allow comparison over tirne and between studies for a
given age bandr oE combination of age bands.
Ptospective design and Targe population base.. Retrospectivestudies allow the passage of time to clarify diagnostic problemsbut are disadvantaged in other ways. ,prospective data collectionallows the application of standardised diagnostic criteria in-cluding electrodiagnostic tests. The low incidence of MND means
such studies require a large population base and hence widecorraboration and rigorous case nonitoring and folrow up.
No incidence studies are available which fulfil all thesecriteria and it is on this basis that The Scottish Motor Neuron
Disease Register (SMNDR) was established with a view to conduct-ing a prospective, population based, colraborative study of MND
incidence, distribution and prognosis and providing a resource
54

Chapter 2
for research activity into MND in Scotland. This is the firstsuch study of MND with this design.
55

rable 2-l: syn&ores rhich ray riric or reserble illD ard are irportantto distingrrish fror idiopatlic iltD
Ebysical factors:Cervical spndylotic ryeloradiculopaQylS2Radiation iyelipathy/piexopatxylS3:1es'Cranial inadiation and iniratirecal cherotheraovlS6Folloring severe electric shock43, 187, 188
lletabolic/Endocrinerlisorderss -
Eexosarinadase def iciencyl89, 190
Adrenoleukodystrophy ([yperinsulin
Phosphate def iciency/hyperparatiyroi6ir.l9l, 195
Related to raligancy or distrrbed immity:f{eningeal retastasis riti radiculopathy/cranial neurgp4eyhrltif ocal neuropat!1, and antibodiirs to' qangliosideslgS-2mGanglioside tierapyzur-- _--Plasra cell dyscrii iu2o2,2o3Subacute rotoi neuronopattry ?ilS, nitX tnplgra?9{0ther paraneoplastic {ru.i cell carcino;a2ls '206Foraren mgnur tutourszu/
Infestions:Post-Plio sYndrorel{6' 208-2LI
[uan irnmodef iciency vins : rononeruitis/ryelopasyphilitic ar11|ronhii reningoryelisir2l5,216Cysticercosisz
lorins/Itsrre:' kt;d2l},2I9, rercury220, ranganese22l, 222, selenirul 37, alup!4iur2238-ll-oralylarino-L-alanine ( lfeurolatlyrisr, Mric a I Isial 2rrc-arino-B-rethylarinoproprionic acid- in Cycad sds on' 61612158Doroic acid ingeslign^g;6r contarinated russels in canada225Solvent poisoningrrd, zzo
Pesticide exposure (pyrglhrin and chlordan e bass61227,228Aritriptyline overdose?rze
- floigre's syndrore (pseudoallergic reaction) with penici11in230Vascular:
Rbernatoid arthritis niti arteritis and neuropathy23lIschaeria of the anterior horns of tie spinal corAn2htulti-infarct state uiti bulbar palsy
0tber prirarily narorogicar diseases or^tp esociated rith otber disease:Benig fasciolations and crarpszrrSyringoryelia (rittrout sensory siEs123{Peroneal nscular atrophy riti pyiariE4l^f9atures235'236spastic paraparesis lviriors^gqil 61237,238Cyst of the conus redullariszrylryotrophy in rultisyster disease gg {q$eph disease2{OlllfD uitlr derentia of various typ$r0,2flSpinal ronorelic aryotrophy,
^fii:q]-cervical poliopati y212-215
X-linked bulbospinal atrophyz{o,4 /r
) lel
Uy2I2'2Lt
lfotes: A differential diagosis of tie idiopatxic anterior horn ceIIdisorders is not included. * ilay be classified niti adult onset HtfD.
56

|rl@
I
@(Aqt.E+,v,
?t)!:t
5a.d >..=E€+,ern
o(H E3oolnEqr€.A.eB-ag.eeoo,+, at'()'-gg-t !.88E.U.dd.o tD€(D
I
tse!. qlEg>. a6-+)lAEL.E.4 aet(H
G'(HE:Eo.60!{ Er+,ot c! .6
€l{<)!a .4ort Ei
F:EE!4t<)E:=(D<) (D .our.E e.U+, OE*n'-'9 8.A.!.'689'sE g
cr!.r F! tt)O.4(l) ]-o oE=E*
G-6-\Fs g g g gE E* F
9>.q g -:-. E !Ea E .iE a g;q -sR; €E i e 3-tE'e 8E'- ofi q € 'i F??o 'i-r iE $ ; g E;EE e'5'€ oH -E* 4 4 .n E'- E i6 >.or.6E€# ffitEH ;g*; a siEqo: xE€ '.<' Eo ; E .n .g.F EIE= 8Ls HF.3 f;S t s : i.A H.id'i'ic, >.EE evjt €- : 6 E Ft€rF'=Es E=;
=gEEBS EEe EeE AF g.,g- i sf; a;:6E 1;; 'Frrrr (,>r g'IE S :€ :Eg*J s.EH '=€g €E;:Fi f;E: ;g; 1€ ; F; ; g€ €.FE*€ HE': g;E ;''E 'H ;e g es 5'E€€'€ Eg$ .,=.8€ E:s. g g.; F .Fe An'*=
aae 9 n IE ,., d E'E-E { E tc i o, o\ i iic; -j J Fg -; d : -.t j-.:
IEig.ttrHr
EE
e,ctooG'H
agqtEb
oa2>.g8attt8.9-.q.ECt {r
@E|'tE: CtgBa'II:x
EZo
Is
5atG'
ct+tIC-a
{J
I
.1da!|ott>.+t
aEC:oF..1E:oaoEe-+to!aE:o+t
=.E'at.tac,o(DB.Jv,
a;a'itI(\ro4€
S$Sco\.'rT gI I? ?!E EE EE $
Ev)FA€s(t) '6 €_rrEASFEE=aFzfi€E5fi',i5ge
r.('l@
I
r.OCA
E:oEBalt
,.c)@ct\
IOrtr!or
IAo!UsttE.t'EllE
hl
FI
cqr')Or
Ei(6aoa-

?able 2-2b: t coparison of age specific rortality rates per 1m,000 betreo cuntrieefrol studies in table 2a rlere tlis infonation can be derived.
Country
hgland and nalesT3
flale Femle
fge and ser specific rates:
5.8 1.57,7 5.58.5 5.8
Itnibd Statusz
llale Femle
ridandso
lale Felale
fge Band
60-5{years55-69years70-7{years
1.9 3.56.1 {.1?.6 t,7
{.5 3.56.0 6.12,8 3.5
Itortality rates standardised to th t9s9 scottish ppulatioa (age eo-zr years):
7.5 5.3 6.{ 1.1 1,2 t.{
58

+)E.u<)
EE^u,egilta=iIA.teq,(,t^
(ol{q,.E
(,-4,o.ol-+,oFll .?t) eA.no!POE-+tI=-o lh
ga'.
+)at.g
EiOE+,tEE
dtl-{-8-.tt >.+t -c.EAE0
H(tsa +,o€!a t{E5>r
=tC)i9l..Erxoou!tE(D L.€EnbeA.Er ltEE.-a -€AE38rvl rA.U -aE8.
''{8.8+) F{ar, =.d.Q
tagC) .a.4 V)EE+,'-.Fut cLq,u€g-tu
AFFFF.A
Ei +,(De.rJ o,(D .d.4, +) (\. EEo 8. ."B Eaoq I - e - e
-o .=E €E 6g.H l{ El Ul <) -O .4(DOOk^'(t <-) (D tn O Q.ad g C
'r V, .-€ c} t
"'e g-8 I 9- .5.9
XE €E € iE E^-H
E-A >r =
.a E2(DE &= EE '6ts 5g9.1' (lll 9 +r+t adE UD-g 5 e'i go' fl." E,a!>. ota &d .!b -.95a EF EE EE ealr)!t(
"d.,;di
€o@cn
SSFF]A,-g *a3€ v, 8ET'6
=.$: F EE =ts'- .= E +' vtEE e -'99 .U:
od € E'E dgB.E 'd €.5- +,(D'*- .= $'.E Fig= ."r .3.9; .9F?E .= €.9E e!'HE.a n Ei -E Fo€= H ,En*'F:BE E E€E ;i
rfi
(\1 1I, F) 6l OrF)da/)GrdrrttldGtFtcro
a\lddd
rct !l. tt ct\ r<t(\IH6IHH
FQ)tsq!oo+.5.Adoct
eFr.gN€e'
--
->
>.
\O r.(, F) CqtF)FFlHdH
Orn-tcilctN@}Fodo
\4, @ ct\.v) . -..do6td
c'r@
q,!t
ec\l
I!td
F
o(\
rf'tr.lto
==
'.
$sa (\t
>. >.
>.t
>. >.
|.ao,a6 +)+) aAraO .d
+r € ttl'-q,E gg 'E€ +,
'r{ Cr+).u
''{ .tt rtl 16o .6E2 qt.! c).d 9.c) o, ().d(H C) Ut +t .H.d tt.d O !x.4+, .E' C! +' +'l{ >. (D|t{I 8t i'd8
-{+r P oE O.d .a arr -c+),-O.A+,.! FO O?t2Oq, o o od (Dtr -,E lE€a
qrqt@6dtttttlo
FTFFtsct\ or cn c orddd
>l+) <tEC=eiOd<)EEO
'4 Ei '4€f-..Ek=--G.UE l{ (D En +).6E€ g d 6 5EHP 6 E - -F>u) o - = 7)(J
sss,A d, ,AsEadd
'..*,r3aHg.s86.=EgEae3
>
tx
-->r
>{
t
->.
>.
rq,q) u! .AEqr.!.d +, -clo.6.d c) .dE.4+)s e'F € s(D q.k .U5 0g a €
O Ut Vt .-{ (l)_ ol ()E O EtQ'€ .i.J aA liPQE3.9O.!|C) .d (1, E aA .E(rjt.d 4E (D C)
Hq o E.a q,.d.d s c,+, .d
58 p.'i b8 igD ! d9-q .d aE
=Gl .4urP =.1 Q. aeE sg 5E g
.AE:I5'l{a(D€
IA>.k +)ET(D E
€.8 El{ +, L.=.4 d(D +' O.E<)Ot,a'E at(.)CL!x'5-, Atn at.d L{ Ct+r(D'-.t'E3=u8 I
oco4'aH
Eq,ttErt)E+,l{o=
8g6SC.98 € .E+) q, +)g: .s q.g#g s
;€ E E.drH d !.d o E.E .so 6 .9.3 'e-{ tt +, |5lr aAs.= gg €
EL.o.}a FOC:3Eu
l6taleI
I
I
I
lselEi--l-a ctl.tc,l>.{lE-ItstelGtlGtlcro-IC)C'AlEir{Hl€ bsI6EfitE:l{orlH <i, sIts-t.E t!l"-l5at36l.!-a
-l Fl
=.<I O..{8sfA.R3-
€5s
EI
E.J
il
.jC:g.3tao<)aatIoaJ{tcr.
Er{tE'LoactAUoaE!
a>.oJ'
{a6IA
=.JI6
{-td€alt
qact
o+t(,R6I+tE-ld
;oTI.Ju,
I6€(tE'
6FtI(\l.D
AGF.

>..=o.I+,ao
!ao
=o9e(D
.a
.AI
fAtla-O.
>rv,
6A+t'-|8-8-a=8.a
(D.u>tat v,E.actaLL
:FEff>.4rl+,4at
.d at7
v,tsg!{gq, <)o.A'-O-{
a6EN L.E(D.o(!=i -l8.tVl.d.oEA.to.d
''r+)€oq) >.iE.d tl-l v)
.lut4qt
BC+, llvt zE
6E+t !xOll-,>
oEF;-:-6'6-ES=======eIEoeo.'e .Eg >. 6e oE ': 5
Ul C) (Ha Eo- s oI F>r l-tl) L.E gE gH € ?E .4P - c) E c\t.U .n -€ .4e Er '9'6 g o 5ts 8g -..5 o, g g 9 =€ 'do o-
= o n € A .S'd 'E8 8," E +') g 'd E t.= .96 ts= F E g .= E e€ @E 8.9 I A E E = €9 Eio af.
'| E Ur .E -'E 2.= An 5 A 2 E A .5
(vt @ d <t \o u-t(\I O 6t r<t 6l d.r
6l\cr@d@ocaF.:adetoGtoc.td(\t-t- I | | | | | | 't-@Fcil-to(o6\bicrG'erod€dod
oor<f\c, lrlFHC<\ldoo€Ho6ICr6t
\9Fddcal<rt<t6tFd
Q9odrtoo\1l.lGrr€|€Oo(5OGloOG.
--=G.
= (\.
>
'.
@ @F
->.>.
='.!x
>'-
t:.d .U
.AG' ()+r€ .dv,d.d >. Ot8f; 8"dt €L{ +) +J=L. L.Rq :-€8 st.5 ggH q
A>rCr AP9'eE gtA.a -€H. I
>>. ggX 3:.9 A8 v,.E .u-> {- - otd .(, <D .E -C +f
sl' 'a crl' 5 e= IE 8 EE .5 EE 8EE.a E .Et A .DE F5AF =,a t 'i, 1 = .3A lbe'd I 'e €s 'E 6.9 aoE'A B E ,A'.2 -E E2 E 5=E I E EA g 8..i qEE* .u 'o 86 E -rE Aq:t
= I g * e .6 r:+' <.) .d .n E 'E tg €.oE.n q .d FE ><v, !{ Er qr+,gR I A 8o Ai E.= ?8E6 0' 6 6€ 6.: d.2 -g',igH
= E 3.= 3A +,." g'dag f I eH. jg€ 2.='69
oaBSPRAgA"\A"\+$.t+AATEEEFsAAdddidHt
-r d*rC2.dr-lda'daE.s€.d.9.F.-log3.-lAEr:rE E ': g 2 = s F €EAE,g8e2ge
EELo
aFa FOC:raH
ooG'cto
t{l>.ctooct Facr c,.{orrlrE ('r
C.'
c,
dlo
4EI
ctae
IElc!tctl-l
IEIo.
Il8t6l€tdt<)
l:t8t:IC'tdl+tl.dtatal-l*ft3a
EJE
nI:x
5g
d+,{t-{rr.Ec:
.tC'
.J
>.-lo.t4.1o+t-a
E.3l|gatIg{tfE+tt6aJertaA
a}lC'
o{J<,8.o15g.<a!
;t.J1A
8E'ct€(,E
-clFII
c\a
o4€

>r.1Ae+)r!|t{C'
=o9Eq,
u,]AgrL'All4-A>.IA
-l8.l-.8=Ao.aahgbS.ctllAoAvt.Agqt
F{()rh
g(D+,ct
C)
Eo.e+,o>EIa!tl3Io-tl-.Ao>.tl
;o+,()o
8aQ|I.Utt
9aoH.tto,>+,9,
(}a
aHoL{q,G','{oEiEi€EiIv,.!E
E+,.tl
.AoErt)
IAo+,o-
ts @ (tr o .1 q -t tt u-)' rcr- i--aoo-!;aJdddd€HHd:aJddd
IEtgl(}. F
le€II
II
I
II
I
IIlrotaleIl-lPotarol-l ot.!l>otg=lA.-leI GtaI ctFrI e(,locrrall<)octlc:dvt@\l=t ol6ElnElatE^l3€I C:-to6td E:r+' CDl.!dtd=lgsI
lFIAlR3E
Eg
gI
C!(tdg
{Jt:gF!.U
+D
Eeo6
E8LorFlq
EE
ffdE>.5
{Jto5>r
&<,F:
etc)>.o
3<,tao>.-lg€.C:-tl
=a-rt6
{J
e€Ga.|oo+t<,toIi'ga!
;ct
E+r6
EtonE
(,E:
(tCDI
6{o-lAoF.
ts?tsE e H E; HE Hsq€u €E i[ ;E E € E E =
f ; E EE E E g ; e g E s E sE:€g E: T:g€E E
e 'E E E e F E g g; E
|rt(liodF6tlfrc)Fc{eidc.;-.ld"iJ;
d9 o t<t -: @ ts' -,fr- (\t q, qr::HHOIqErq Ei 3i3i i5;-;-;3-;-jddd:-.;o9;; q :; ;;;; ;d.;e;S-;:d.iddi
@r}NdnF@\od
ca rJ)@(\t F(\ld!tr) to rt tft
oao
>
Eg+,k8.o
@>..a=te,
@coI@F
O1
>.g,.o-Eo+ttno-
q) |r.l ctrqF|fl
e;d-id
>>.>.>i
>.
-c)
qE E'.e ts '*E -g --hE <) tEE ts E8g 'i E $e.F f H EEil E g .gg
>. .9 >. €.ga a a ?sE E E Eg|r)tftoHtstt@€s,Al-Laaaaddd
f; E 5EgE.s€E E;3.Ed:E.E6FEs8I A .9
oEatgr' *- +, P
E ga f; € E*6 iig g. HF FF'g F a Fcvt d.6 >{ s .g €€t ir g F E Fg'E Es e E E E.g: ;.E F : e :EE *.E g F g FE'a €g 2 'a E 'aa
\on=rf|6|frtF@€@€+44+.A{aahBSs+-=(DE 5 A5 H
=.s.A-sgo-€*l .g-:nH E E.H E Egibs'dEhqa1e88EAASS=

E>.oorI]A€.clrrg
E.a>r (D\cno.!|oo ttrr-iCl .der!(\ldot\gNtn *.O, .d (Dt," !E.L En
C) 'dAC'5E I= .tt -l+ro,6t.8o,€oE! 3A tn5E*En FlEEiq,
=EE.c-L. O. C/)o(U9.L{Eatr kt:O)
.g E€-*9+) .Eo(DrlE+r6t
.ttA)4.g 9.6sgE(, xca.d O,
.d O) >.<.) 'r+t8.'6 E- E8q,P
Er att Gt.!,-Ca6(t
-a.!.d Eca.H LI'd.66r <.)>qt &rr-a anA.o.!@+, En o)aE|48.oE!-a O) qta6 .i .taoE rro, +r (H?tt aA
E H€eEg
F
<t!O
oo|r)6t <f |rt\\\
9.()|f)o\Er)lrrcn
a!ttaE:F.! Or<J
st@(3o\
@.{f
Hd.HO
6\\\OFGa ro
\.€OE
!tE:6F tfld (trE
o
N
@lf)ood)|r)\\\.!a d (\l Gt\E61 |r)'.o
ItafagE!tag
(\t lrlE i i {.8:EE'!:'F6;E.doi:n;I>.<tI3
dcog.
-E : i e.s-;EE'.'.d g E-: J = g;adcr.8.€at -{Eqn,':3acl€rHd'lslEE :SsFI56d
9$
arc\r€lrEqd A -.i -.: -.;q o'-o@\E-H E (\r Ft ait € o(rs5g.a
('gd-,!l(}.dE9EE A * : i rE:
bEbgs5&l 3=.E'd6i3FJgo(-,
vrooL{L.'.EEE>.
'.. >.
|rl\Otsrtlrtlrrl.()rrlf)\o
EcogEEg
>.t+tE8>.tl
Eg.!tFIrft=sg,€oE'
EEG'E'aaoottt.U<,C:a!
E6€(,E:
(tr}r
E.otaf<tE!att
o,ttr-e.C)
OtaI.<ttart!(riloFlJIg

Fig 2-1: Mean annual age-adjusted death rates /100 0OOpopulation for Motor Neuron Disease in Nonlray,standardised to total 1gg0 Norwegian populatidn.(Flaten t9S9)
1969-71 1922-74 1gz*lrt 192&Bo rrigr-sg

Fig 2-2: Age specific(total male &
incidence of adult onset MNDfemale for 3 population based studies)
16
14
12
10
I
6
4
2
0
Rochester 1925-84(>7s)(u
o
-a3EiEcroo'F
=cuOO9EbgPoc (>70)
lsrael1959-74
Denmark 1974-86
(>80)
30 35 40 4520-49
30-49
55 60 65 7050-59 60-69
50-59 60-69
55-64 65-74
Age group
80 85 9075
70-79lsrael
Denmark
Rochester

Fig 2-3: Correlation of age standardised incidence of MND with meandegrees north latitude in 8 populatlon based studles
6S 4455056
Degrees North Lailtude
10G,3; e
ES IECtoogo- 7gt:5 6XEDditr' E€EE; 4cfif g
toOlt AED.
1

CITAPTER 3
rTB SCOTTISE IToToR NEURoN DISEA8B REGISTER3
l'iETEoDoLocy, INCTDENCE, DEldocRAPEy AttD cIrINIceL FEATUREB oF
PATTBNTS DIEGNOSED 1989-1990
66

Chapter 3
INTRODUCTION
u rt is sometimes said that crinicar observation hasTittre more to otter neurorogry, yet crinicar observa-tion continues to discover new syndromes and to rein-terpret oLd symptoms and I foresee great scope for itsti77 . "
Lord grain248
scotrand is in the north of the united Kingdorn (uK) and
covers an area of 30,414 square rniles between 54 3gr and Go 51t
3off north ratitude and between r Asr and 6 L4t west rongitude249.The population estimate for L989 was 5,OgO,7OO of whon 1Bt were
over 65 years2so. The country is divided into g regions, 3
island areas, 53 districts and L2LL postcode sectors and isserved by 3041 general practitioners. Neuromedical services are
provided by 19 consultant neurologists and 4 consurtantclinical neurophysiologists who are likely to see most but notaII patients with MND.
rn January L9g9 the SMNDR was launched with the aim ofprospectively achieving complete case ascertainment in order toreriabry study the incidence, denography, clinicar features and
prognosis of MND in scotrand and to provide a resource for re-search into this disease.
ITETBODS OF THE SCOTTTSH UOTOR NEURON DISEASE RECTSTER
1. All Scottish consultant neurologists and neurophysiolo-gists agreed to collaborate and acted as the principal source ofcase notification. They were requested to complete a sirnpleregistration form (table 3-1) which hras forwarded to the study
67

Chapter 3
coordinators based at the Western General Hospital, Edinburgh forinclusion on a centralised database. Collaborators were encour-
aged to register patients when the diagnosis of t{ND was firstentertained so that suspected, as well as definite cases, courd
be followed up, although the threshold of individuat collabora-tors with respect to the registration of suspected cases varied.
2. The two fanily care officers ernployed by the ScottishMotor Neurone Disease Association (SMNDA) offered patients theoption of self-referral to the register.
3. rn 1990 and 1991 a retter was sent to arl Gprs in scot-land, asking for detairs of any patients with MND in theirpractice diagnosed after January lst. 1989.
4. The Information and Statistics Division of the common
Service Agency for the Scottish Health Service provided a list ofaII patients discharged frorn Scottish hospitals in 1989 and 1990
coded by International Classification of Diseases (ICD) 9 as
code 335 (anterior horn celr disease). The records of all pa-
tients older than 15 years, not arready included on the regis-ter, vrere obtained and reviewed before inclusion.
5. A request was made to neuropathology departments for any
patients diagnosed at post mortern.
6. AII death certificates for 1989-90 identified fron theGeneral Register office for Scotland h/ere examined when fCD-9 335
lras recorded as the underlying cause of death or as a contribu-ting factor. GP practice records with their letters and surunaries
from hospital consultations were then requested from Hea1th
Boards.
7. Pedigrees were traced in farnilies where a genetic cause
seemed likely or possible. Information of personal details of
68

Chapter 3
unaffected or affected reratives (parents, chirdren, siblings,aunts, uncles and cousins) were obtained frorn the proband wher-ever possible to allow tracing of death certificate coding and insome cases, clinical notes.
After registration, clinical details included in dischargesummaries or outpatient correspondence and the reports of neuro-physiological investigations, hrere obtained to allow classifica-tion of MND subtypes based on clinicar features (see berow).After the patientts death the complete hospital and Gp recordswere scrutinised and pathology reports obtained when available.Figure 3-1 shows the structure of the SMNDR.
Patients were included on the register, ie considered inci-dent, if the diagnosis of MND had been made or suggested for thefirst tirne after December 31st 1998. At registration, the pa-
tient's GP was inforned of the aims of the study. Forlow up ofall patients $tas achieved principally through Gprs with a sixnonthly questionnaire concerning any revision of the diagnosis,any change of GP (to arlow transfer of folrow up) and simplecrinicar features, such as difficulty speaking or swarlowing,Iirnb weakness the date and place of death and if other fanilymembers were affected. Collaborators, who were informed of thestudyrs progress by a monthly newsletter, vrere also encouraged tosend copies of follow up correspondence from hospital clinics. A
paper file was maintained for each patient and the Dbase rvmanagement system for microcomputers was used to construct a
computerised database for compiling features of key interest and
to permit organised retrieval of data. Hospital ethical approvalwas obtained.
The 1989 population estimate for scotland and its
69

Chapter 3
regions250 (derived from the last population census in 1981)
was used for the calculation of rates and standardised incidence
ratios. A census in 1991 has not yet published population
figures. Age specific incidence was calculated using age at
diagnosis, usually in relation to the first hospital admission
for investigations. The significance of differences between the
means for ages according to sex was exanined using the Studentrs
t-test. Age adjusted standardised incidence ratios (of observed
to expected cases) were calculated for each of the 9 regions and
3 island areas using the indirect method2SL. confidence
intervals (CI) were calculated using the Confidence Intervals
Analysis Programme2S2 .
Diagnostie criteria
A set of sirnple but specific criteria suitable for applica-
tion to this, and other large scale studies !{as devised, using
aspects of the World Federation of Neurology Subcommittee on
Neuromuscular Diseases approach253. The criteria for dia-
gnosis are as follows:
The terrn rrmotor neuron diseasetr is used to encompass any
adult (>15 years) onset progressive motor system disorder (spora-
dic or fanilial) with the following categories:
1. Clinically definite ttND: A combination of lower motor
neuron (LmI) signs, clinically or by electrornyography (EMG) , and
upper motor neuron (UMN) signs (table 3-2), not due to longstand-
ing neurological disease, (eg previous stroke or recognised com-
pressive mononeuropathy), involving the brainstern and implica-
ting involvernent of one or more spinal regions. Three spinal re-
gions were used for classification of physical signs, they were:
70

Chapter 3
Cl-Tl (cervical region; neck and upper linb), T2-LL (thoracicregion) , L2-sacral segments (lurnbosacral region). If signs
were lirnited to the brainstem and only 1 spinal region (eg only
upper linbosigns as the sole nanifestation of involvement outside
the brainstem) then both UMN and LMN signs $rere required in thatregion, otherwise it htas not considered necessary for both IJMN
and LMN signs to be present in each of the involved regions.
Normal or brisk deep tendon reflexes in the presence of a clearlywasted corresponding myotome, €g triceps jerk in wasted tricepsmuscle, were used as evidence of UMN involvement.
Qualitications: fn addition the following were mandatory:
a progressively deteriorating course; the absence of sensory
signs (including visual abnormalities) apart from rnild vibrationsense loss in the elderlyp absence of sphincteric disturbance,parkinsonism, dementia and causes of syndrornes which may rninic
MND (table 2-L'), after appropriate investigations and follohr up.
Patients in this group vrere assigned a category which gave
an indication of the clinical pattern of the MND as follows:(1-1) ALS/PBP. CIinicaIIy definite MND which began with
Iinb synptoms but later developed bulbar features.(L-2) PBP/ALS. Clinically definite MND which began with
bulbar symptoms and later developed limb symptoms or began with
bulbar and Iinb synptorns sinultaneously.
2. Clinically probable ltNDs (2-L) PBP: A syndrorne inwhich dysarthria and dysphagia of UMN or LMN origin are thepredominant features (but which may be accompanied by sterno-nastoid weakness as the only [potentially] extrabulbar LMN sign)
in the absence of LMN limb signs but which nay be accompanied by
7L

Chapter 3
t[r{N linb signs (eg extensor plantar response) but not syrnptoms
(e9 difficulty walking) .
(2-2) Spinal ALs (2 regions) and (2-3) Spinal ALS (3
regions): Two and three regions (cervical, thoracic and lumbosa-
cral) involved respectively, with a combination of ttMN and LMN
signs, not necessarily both in the same region, but without
bulbar features and given the above qualifications, in particular
exclusion of cervical spondylotic nyelopathy. Patients regis-
tered with monomelic atrophy were not included in the calculation
of incidence data.
(2-4) PMA: An exclusively LMN motor disorder, including
absent deep tendon reflexes in affected myotomes, involving at
Ieast two regions with a clearly progressive course supported by
consistent neurophysiological investigations (see below) .
(2-5) PLS: An exclusively UMN motor system disorder (after
at least two EMG examinations separated by at least six months)
affecting aII four lirnbs with or without involvernent of the
brainstem, in the absence of a farnily history of gait distur-
bance and with no evidence of multiple sclerosis or MND mirnic
syndrornes after CSF immunological studies, visual evoked re-
sponses and magnetic resonance inaging of the brain or cervical
cord. Patients with unspecified spastic paraparesis were expli-
citly excluded. Diagnostic categories are summarised in table 3-
3 and the alternatives for the distribution of clinical signs
are shown in table 3-4.
The above classification was applied (i) at registration
(initial diagnosis) based on the documented features of the iII-
ness when patients first came to medical attention, oEr if
patients were identified through hospital discharge or nortality
72

Chapter 3
data, retrospectively, again based on the features at presenta-
tion and supported by hospital consultation documentation. (ii)
When the fuII extent of the disease htas established after follow
up, or aII available data (hospital notes, GP records and patho-
Iogy reports) had been reviewed after death, whichever came first
(tina7 diagnosisl.
Additional notes: Criteria for neurophysiological diagnosis
were not established prospectively and are difficult to appty
rigorously given the variation in clinical practice between
neurophysiologists. When available, particular attention was
paid to the results of nerve conduction studies and EMG:
1. To exclude other causes of LMN disease, in particular,
po lyneuropath ies , compres s ive neuropath ies / rad icu Iopathies ,
multifocal motor neuropathy196,L97 and myopathies.
2. To identify LMN involvement which was not evident on
ctinical examination and which could therefore be used to assist
subgroup classification. Equal weight was given to the finding
of dennervation potentials on EMG as to the clinical LMN signs
(table 3-2, when determining the extent of regional involvernent.
3. As a means of docurnenting spread of LMN abnormalities
and therefore the progressive nature of the disease, if this was
in doubt.
Myelography was usually performed when MND was incompletely
developed and confined to spinal segrments. An acellular cerebro-
spinal fluid (CSF) result was required before a clinically prob-
able diagnosis was attached but CSF examination was not consid-
ered mandatory for the diagnosis if clinically definite, as
defined above. In some instances support for the diagnosis was
obtained with swallowing tests (Bariun cine swallow) and muscle
73

Chapter 3
biopsy. Anti-ganglioside antibodies vtere not routinely per-
formed.
The diagnosis was considered proven by autopsy if this
showed LMN and t l,IN neuronal loss in the brainstem or spinal cord
and neuronal atrophy with loss of Nissl substance, corticospinal
tract degeneration and the absence of extensive central chromato-
Iysis, active neuronophagia, neurofibrillary tangles, abnormal
storage material, spongiform change and extensive inflammation.
REgUL,Tg
A total of 257 patients hrere registered with the SMNDR in
1989-90 but 28 patients were excluded from the main analyses
because an MND like syndrome coexisted with other neurological
disease; the diagnosis was subsequently shown not to be MND or
did not fulfil the criteria above (Table 3-5). The details of
these patients are presented in Appendix A. Unless otherwise
stated, ages refer to those at diagnosis.
Of the 229 patients with proven, clinically definite or
probable MND L32 (57.62) were men (mean age at diagnosis 63.1
years, SD L2.2 years, range L9.5-84.2 years) and 97 (42.42) were
women (nean age at diagnosis 67.4 years; SD 1L.0 yearsi range
30.4-9O.7 years), giving a male to female ratio of 1.4:1.
There was a significant difference in mean age between the sexes
of 5.4 years (95e" CI 2.3-8.6). For patients older than 65 years
the sex ratio was 1.1:l- compared to 1.9:1 for those younger than
55 years, a significant difference. A summary of the descriptive
statistics is presented in table 3-5.
Many patients were notified from rnultiple sources. However,
74

Chapter 3
the first source of referral is shown in table 3-7. 190 patients
(83t) were seen at some time by a neurologist and 188 (822) had
an EMG. Patients who had not seen a neurologist (n:37, 16t) were
older than the remainder with a difference in the means of 7.6
years (958 cI 0.4-14.9).
Table 3-8 shows the clinical pattern of MND based on infor-mation at the presentation to nedical attention (initial dia-gnosis) and the final classification with follow up (final dia-gnosis), after all records were reviewed, at the tirne of data
censoring on January 1st. t992 (this date also used for survivalestimates in Chapter 6). Table 3-8 documents the natural pro-
gression of MND with most patients who presented with PBP deve-
loping spinal involvement (PBP/ALS) and many patients with only
spinal disease (ALS), as the initial diagnosis, developing PBP
(ALS/PBP). Patients with PMA and PLS were in the ninority.The site of onset of MND (table 3-9) shows an approximately
one third division into those patients whose weakness began inthe upper linb, lower linb and bulbar region. Men were more
Iikety than women to present with weakness of the hand, a re-flection to some extent of the sex differences in clinical sub-
types (see below). However, onset in the lower linb showed no
difference between the sexes. Women were significantly more
likely to present with PBP and to have PBP as a component of MND
at any stage of the illness, whereas males were more likety tohave exclusively spinal disease (table 3-10). This hras particu-Iarly true of women over 65 years where there was a relative riskof 4 .5 (952 CI 2 . L-9 .6 years ) conpared to men ,over 55 years.
Three patients presented with shortness of breath as the princi-pal complaint and in one 60 year old male with PMA this was due
75

Chapter 3
to a highly selective diaphragmatic palsy with EMG evidence of
more widespread dennervation.
Eleven patients (5 8) had a fanily history of MND but none
were related to each other, the pedigree details are contained in
Appendix B. This group riras younger than the sporadic cases;
difference in means $ras 9.6 years (958 Cl, 5.5-13.6). The pat-
tern of fanilial disease suggested a probable or definite autoso-
mal doninant inheritance in aII but one fanily where X-linkage
appears likely (a diagnosis of x-linked bulbospinal
neuronopatny2aTl. In some families (SF,RP-appendix B) premature
death, or young age of unaffected members make interpretation of
inheritance more difficult. These families formed a heterogen-
eous sample of different clinical subtypes both within and be-
tween pedigrees.
In 15 (68) the diagnosis was proven by autopsy, the patho-
logical details of these patients are included in Appendix C.
The crude incidence for Scotland was 2.25/100,000/year (95t
CI L.96-2.541 lOO,OOO/year). Age and sex specific incidence rates
are presented in table 3-11 and figure 3-2 and continued to risesteeply to a peak between 75-84 years for women and 65-74 years
for men (fiq 3-3). There is then an apparent decline in rates
over 85 years. The age adjusted standardised incidence ratios
for individual regions showed some variation (table 3-L2; fig 3-
4'). However, 952 confidence linits overlapped with unity, indi-cating none were significantly different from the expected at the
p<0.05 level, although lower standardised ratios were observed
in the north east and island areas.
76

Chapter 3
DI8CUSSION
The epiderniological method may provide inportant clues tothe causes of MND by demonstrating temporal and geographical
trends in distribution. Difficulties arise in delineating the
optinun size for such a study: under-ascertainment and error indiagnosis wiII bias nortality studies based on very large popula-
tions, whereas random variation wilI lead to imprecise estimates
if too small a sample is used. In this project size has not
compromised diagnostic accuracy because data can be sought pro-
spectively and studied over several years.
Some studies of incidence and/or clinical features in MND
have relied on data collected from tertiary referral centres but,
in general, such studies give a lower incidence than those which
make a more concerted effort in case finding (Chapter 2). OnIy
two other countries, both frorn Scandinavia93 '95, reporteda higher crude incidence higher than Scotland but denorninators
were not provided in these papers so it is difficult to be sure
that this is not due to differences in age structure. The
previous study of MND incidence in Seotlandll2, based on unver-
ified hospital discharge data (L968-77), and therefore likely tobe contaminated with diseases other than MND, gave a high crude
average first discharge rate of 4.7 and 3.OL/IOO,OOO/year for men
and women respectively. Mortality statistics collected over the
same period gave average rates of L.57 and L.18/LOO,OOO/year (see
Chapter 4 for analysis and discussion of this source of data). A
further incidence study confined to the Lothian regionllo hras
inconplete in tracing case records and reported a range of
incidence over L968-75 of 1.0-1.9/LOO,OOO/year. The female to
male ratio is within linits previously described (between 1:1 and
77

Chapter 3
1:1.5).
A finding of aII studies that have examined age specificincidence, except that from Rochester, is a decline in rates inthe nost elderly age groups. Our data show that the highest age
specific incidence of 9.9/ lOO,OOO/year for nales and fernales
combined in the 65-74 year group !/as maintained into the 75-84
year group, given the confidence limits of this estinate (Table
3-11). Caution is needed in the interpretation of the apparent
decline in age specific incidence in the most elderly. Presenta-
tion of the data with an upper age band of >75, years rather than
>85 years (Fig 3-21, suggests that a true decline may not actual-fy occur, given the confidence limits. Proper comparison with
other studies needs careful attention to open ended upper age
bands (see page 54). The decline in rates over 85 years is
difficult to interpret, particularly because of the small nurn-
bers (n=2) and may be due to failure to diagnose the illness in
this age group (see also chapter 51, rather than poor ascertain-
ment of diagnosed patients. If rates really do continue to rise
into old age rather than decline, as .is generally reported, then
senescence must make a najor contribution to the development of
MND.
The age pattern of this population based cohort is older
than series which have been described based on referred samples,
particularly neurology departnental recordslSL'254'255 (table 2-
3c) and is the result of an unbiased patient group. The age dif-
ferences between patients who were, oF t/ere not seen, by a neuro-
Iogist (table 3-6) also inplies that studies based only on neuro-
logy departmental records are unlikely to reflect the true
demographic features of the disease. The diagnosis date (and
78

Chapter 3
therefore the decision about whether a patient was incident or
not) was standardised to the tirne when the diagnosis hras firstsuggested as possible.
The registration of patients by different collaboratorsvaried with respect to how far advanced the disease process was,
hence some neurologists preferred to register patients when the
diagnosis was first entertained and some preferred to aIlow the
passage of time to remove diagnostic doubt. Delay in registra-tion and the lower than anticipated rate of first registration by
neurologists was largely due to this factor. Those patients who
were eventually excluded (Table 3-5 and Appendix A), are a biased
group but represent a sample for which the diagnosis MND was
entertained and therefore form part of the differential dia-gnosis of this disease. Of particular note are patients who were
eventually diagnosed as cervical spondylotic nyelopathy. The
absence of bulbar involvernent (ie clinically probable MND)
should be a cautionary sign and prompt appropriate investiga-tion of the cervical spine.
The interpretation of the figures relating to the clinicalsubtypes is highly dependent on the way physicat signs are used
for the classification of patients. In this study, preserved
reflexes in the presence of a corresponding wasted myotome were
used as evidence of UMN involvement and therefore such patients
were classified as having ALS included in their subtype (ALS;
ALS/PBP; PBP/ALS). There rnay be little pathological basis fordividing sporadic MND into subgroups given the poor correlationbetween clinical pattern and pathological distribution of the
Iesions4T. However, appropriate classification is irnportant
to standardise patients who wiII be included in clinical trials
79

Chapter 3
and for prognostic reasons (see Chapter 6).
Differences in the sex ratio, d9€ (wonen older) and the
clinical patterns have been observed by others, including thepredilection of women, especially those in the older age groups,
to present with or develop PBP more commonly than,".94, 181 ,256 .
The 5? rate of familial MND is in accordance with other
studies which range from 2.7-10t65,257. patients with a
fanily history were younger than sporadic cases and formed aheterogeneous group of disease pattern with examples of most
subtypes represented, dS reported by others258,259 (see Appen-
dix B for details). The likely dominant inheritance seen in most
of the farnilies has been reported as the most common pattern inadult onset MND258'260,26L but inheritance was anbiguous inone of our kindreds (RP) and occasional recessive inheritance ofMND may o..ur262. X-linkage appears to be the inheritancepattern in one farnily (JH) with a presentation of bulbospinalneuronopathy (Kennedy syndrome55, 247 l. Although some farni-Iial MND is linked to chromosome 2L, this disease is geneticallyheterog"rr"orr=4 1 . The low frequency of farnilial MND and the
decreasing likelihood that as age increases a patient who pre-
sents with MND has a fanity history25T suggests that inheri-ted, as opposed to somatic, mutations make only a small contribu-tion to adult onset MND.
The distribution of patients within Scotland gives no cl.ear
evidence of non-random distribution and therefore in itselfprovides no evidence for an environmental etiology. Failure todemonstrate non uniformity rnay be due to the inadequate statisti-
cal pohrer of this sample so far and in the futurer ds SMNDR
80

Chapter 3
registrations accrue, distribution can be analysed by other means
such as by postcode.
81

Table 3-1: glfDR Registration fon details.(respnses 16, F, ucertain)
@neral:
llrscular yeakness
Progressive history
lisence of smsory sigs
Seen by a neurologist
Distrihtion of sip:
etlbar sigs
tlllX bulbar sigs
Illlf butbar sigs
tirb sigs
Ulll{ lirb siqs
IXll Iirb sigs
EG perforred?
Is tiere any suggestion of an alternative diagosis?
Is ttrere any associated disorder?
Is tie patient arare of ttre diagosis?
Date of onset
Date of diagosis
Is ttre diagosis def inite/probable/suspected?
82

lable 3-2: Itysical sigs by region rsed in tie classification of patiots rittr ttD
Region llpper rotor mron sigs Inuer rotor neuron sigs
Bulbar Dysarthria (ray be ml)r flasted tonge or cranial nsolatureDysphagia (ray Ue uU1* Fasciculation of the tongeSpastic,chusy tongue Dysphonia/reak cougb
Exaggerated jan jerk/facial jerks Palatal reakness/nasal escapSpastic tetraparesis tiasting/neahress/fasciculation ofExtensor plantar respnse(s) sternorastoid
Cervical Reflexes present in a rasted upper lirb Hasting/fasciculation C2-Tl
Iinger jerks Paradoxical breathing/diaphragatic palsy
Spastic tetraparesis/extensor lbsent upper lirb reflexesplantar(s),uitlout bulbar sigs
Ihoracic Spastic paraparesis Puaspinal/aMorinal fasciculationReflexes in rasted lorer lirb Paraspinal rastittg, truncal realoessExtensor plantar respnse(s) Intercostal ueakness/reduced vital capacity
Lrubo/sacral fasting/fasciolation t2-S2
ADsent lorer lirb reflexes
In deciding if bulbar involverent uas or was not present, no atterpt ras rade to distingish syrptorsdue to tlll{ as opposed to tllllf lesion(s).
Iable 3-3: Smary of tie diagostic categrie used by tbe Smln
r.Clinically definite lllD1-1 ArS/PBP
L-2 PBP/ArS
2. Clinically probable fD2-T PBP
2-2 ilS (2 rEions)2-t ilS (3 rEions)2-l H{A
2.5 PH
3. |0t nD3-1 Spasticparaparesis (unspecified)3-2 !tultisyster diseases3-3 l.liscellaneors
AIS= Aryotrophic lateral sclerosis; PBF Progressive bulbar palsy;tA= Progressive rrscular atrophy; PLS= Prirary lateral sclerosis;
83

lable 3-l: tlternatives for tDe distrihrtion of clinical sigs inthe lirbs and trud( for tb diaqosis of differentcategories of lltD by tXe $m (see tert for qulifications)
l.Clinically definite:
lhe least extent penissible for diagnosis:
Bulbar Ullll
or Bulbar Lml
and Ut (C) or trunk (I) or tt (t/S) tlllland llllll signs in tie sare spinal rEion
2-2. Clidcally probable XID (N, 2 regiom):
lfo bulbar sigms, 2 spinal regions corbining tllllf and ttltl signs E:
n ufi (r/s)U UHlf (T or C)
ttut
Hrf (r/s)uffi (c)
tt Ulllf (T or C)
ilil (r/s)w m{ (c)
fnnk tllll (I)nr m (c)
tt Ullf (T or C)
uril (T)
m (r/s)uor (c)
z-3.Clfuically probable nfD (ilS 3 regions):
lfo bulbar sigs, 3 spinal regions corbining tltlll and ulll sigs eg
tt
ut
tote: If Ut (C) UIX signs are present tben cannot be certaintiat tt ttlllt sigs are drre to disease of tie sare (C) regionor (T) region. lllll= Upper rotor neuron; Ullf= [,orer rotorneuron; U[= Upper lirb; [L= Iouer lirb.C= Cervicali I= ftoracici [= lurbosasral.
84

Iable 3-5: $mary of patients registered ritn tbe $m but ercludedfror the rain analyses (for rletails see fppendir f.)
f. Ohical featrre of lilD hrt ottrer narological featuresooeristed (n=8).
llllD associated niti derentia or atypical patiological features I
lll{D nitlt extrapyraridal sigs 2
Corbined neuonopatXy and neuopatXy witi plycytieria 1
tongtanding neurological disease raking diagosis uncertain I
B. Diagosis subseqmtty sbcn to be otler thar nD rittr follorq (n=15).
Cervical spndylotic ryelo ( radiculo )pathy
Cerebrovascular disease
llotor neuronopathy associated witi lyrpbora (paraneoplastic)
Polyryositis
Retropbyrangal turour
lfeuropathy and bydrocepablus
Deryelinating disease, probably late onset rultiple sclerosis
l{etabolic derangerents and debility
C. Diagosis ucertain hrt fail to fulfil Sl[D[ criteria for ttrediagosis of clinically rtefinite or probable nD (n=5).
tlonorelic siErs
Spastic paraparesis not otienise specified
Possible PIS, pssible rultiple sclerosis
ilrrestedt llllD/ non-progressive
Brainster lesion, non progressive
85

ch ll,F) a.)HdtlF|fl|rl rrt
oc\o -tlrf €.
o
rct <t or@@u1ttlfr)(N@(\t6to
F (\t -l'Foilc !t'oo@ coortttli.<l Gt tcl (l
ttF ct\odu'l Hrrl
cil r) Fr.0dr u.) o i.oOF C Ftrtl€N @gtt d cti citd<1. d!'
!t (\t (\t F lf'l FF Ctr .to !te,@@ @ot @c6d, .5+ +A3F Cno dCndc\t do <tF)
@c
d(D eF(\tF (\tts
d
6ad @!l6lcit F dlr<, F TI' F
r}t.C, Fd!tlfr |r)@t<t |rl r.o |rt
r.(to H-l ttodF ./)O FOr<t t<, t.C, r<, \4, F
6lr (\F 6lo\lav}( F)C Fts
!Efa -&r -Er
@d @ddH Ftdail oil
aFi a.Fiu)tu ct)h
oor
c{t ts cil Fctr c.) ctt FtHd
+r+l=z --
F
EO
rOF
<tlrl
(v)
lt,!r.ct
GI
H(J
frr|('i
elIE
B
6'CD
E:a9eag5
o\O €(v)nr(\l dF)Hd dd
c\lN 6lo Fts6tH 6td orodd dd d
aaEa-{Jao8-toE=oa6at{ dala ta-a .trE>
TEEBEa.1-aoErOgt8e'!a 6'c) +t
a5{Js866o .ctt' -a
.J E:g8l{C)f6 rfttsa;!
6'D
o,na
I=aAE8 n 5'+r +, E .tteE 5 '8
b€ H F^La e .4+rort32 t €51 s st'l.Cl E -E
ar;
rrt
'-.uq,u, >r!at'od).4
t,a5 +' P?tth Q urvt aE
e.dC)-a O E4QfEd+,P4.1 .!| (t'
R5 s g?t Y. 14 -q
C,;
tnl-E.6 q)Vt >. V,
OL.L?JE.tEE>r.i>.ovtEO +, E .=,glool+)Et .d (to9E- gDg.! .at .!o
ac qr cn En-.E-EaE.j

Iable 3-7: First sorce of refenal to ttre Scottish totor laron Disease fegister in 198990
?otal nrnber of incident Patiots
Collaborating rnruologists/neuropbysiologists
[ospital discbarge data
General Practitioners
gcottish llllD tssociation farily care officers
llortality data (deattr certificates)
Pattrology recnrG
Seeu by a narologist
fCs/Erc perforred
?n
12e (56.st)
{{ (letl
27 (Lztl
23 (10t)
5 (2t)
I (0.5t)
188 (82t)
leo (83t1
87

tctctd
Oi6lc\t
aoG'd
o'r.\r6a
a€*#d€*\o (\l:o<t6tGl(\lFoa--l
6P**d)q?*RaO.rC)dJSai-i
dP dPotF
ar) (\l
(vr to\olrt|f)d
ao(rddnro
o<fH
R=SS-
9..,RoirH
(t@ARoit
*aPH-(tr)61 6l
-)
F-t
g(\I
dGT
g Eg -E d=- 6'9 9A s,4 etu-r!. U,e -8 a@a
=e 4 5 E
E E E g 9c,;; eagaE'='= V qeao.-.=ctql 44I E" F i F'E 'a t n-H-dAActav'
Eii Eiiiir
qt
",. IABda!
E€d4=aE: EI6a]? &.
.1a!
.JC'='o
-8c) F3
-t ctraJ at-.d E
.J !E
ECEi^E.JH-,- -
6lOr.'td
*;6r{rgE6"?>.JI<te6+r6{JatgA+td6t'..+teoa
=.HcteC'
.JEt{
Iat4oIci(,@!
F'
oAA5F.

6re.;
Iqcit
ttCA
|r|tlEE2GI.E
+,c+Jq,taEioE|i--gog.!lHoJ43r,
l-Q'
+,.E
dg-.,;
Erl.!a4=€c>.
PI
9IEi.tt+)-l=e.At{o
.41
=A=Pc,TA
5f,
AAAE raPaF a?dfte
- -6 FFe 6rOOr !!| 9i.cn€d CIGIF {'oe, ! -:Fa 6" (\ldd c'l cild d N
||srE R aRg RaR 6" .., N
oag 5 5+- gRS o d S
oo.r3 R fiRs +RP cD ."t E
:.tttt-gF
'i.E.. €*€ € g
EAE=EE'ugFct4FE-tse€ g Hsg
EI-eTo4oEC>
g6
IHc,o+to.<IgaEdi!
art(DA.clate.

Table 3-10: Relative risks (nn) aDd 95t confirlence lirits for ttreclinical srrbtypes of llD according to ser
tR of a felale having lop as tle initiaf feature (PSP; ttP/ilS as initial diaEosis)
Ferales = l7 of. 97
lfales = 25 of. L32 RR= 2.5 (1.7-3.7)
tR of a ferate having EP at any stage of lllDFerales = 81 of 97
lfales = 73 of. I32 RR= 1.5 (1.3-1.8)
tR of a feHle over 65 years having PBP as tle initiaf featrre (PBP; ffP/fIS) as initial diagosis
ferales = 3l of 65
l{ales = 1{ of ?1 RR= {.5 (2.1-9.6)
tR of a Hle presenting ritl spinaf disease (ilS as initial diaEosis)
llales = 81 of 132
Ferales = 17 of 97 RR= 1.3 (1.0-1.7)
xf, of a Hle having only spinal disease (il,!i as finaf diaEcis)tlales = 91 of 132
Ferales = 17 ot 97 RR=1.1 (1.1-1.8)
tf of a Hle presenting rith HI (Hf as initial'diagosis)Itales = 20 of 132
Ferales = 2 of 97 RR= 7.1 (1.8-30)
lR of a rale rittr Plll only (as finaf diaEosis)Hales = 1{ of 132
Ferales = 2 of.97 RR= 5.1 (1.2-221
90

Ll -t!o@lrlH<IAIdtlrrororo ot grrooH
6r, ]oGl rfl 6lC'l Fa Gl
G)6lIG'
@
OroCr
|rlcil!o
aOr.al
d<tttt
F'c"
Ia".ftH
.flc!
G'
(\lo
Oraat
ct
(trttoIrflct
o
C'rd
o
ctF'oIoct
oioG'G'
rflroctH. 6'! 6l
?{dro(\lr!llflrnF
<t 6rl !trfl Gt H
{r ('r !trat cr d)OOG{d
roFI
oiIraltt{|It@ro
1r|o.alI
or
F'G'<r
ct(\lIoo
eF'ral
Ct!etutoo
C'r6to
(\l10oIoo
oFIdct
GOFDoIG'o
o
aa a;' aa ^ 6;' - e!6td
-vF vvQ) i-r.r(\l vvafi vv(D
-v<f Gr 6t
cte ^(\1 <.e' i!_
= gg- 99". S!so. :ggFi 3gS g:9R (\. B
A^ F= 6R- ?- c!cqo 6qtt iisor a\i-F (..'a\iol d|r)or d!
d vv<\l vvrO i-ri--a i;-ci .jiJa(i vvd G) H
C rt{ -tt?? r.r A|f|o|.t oO _9F@F F.
c" <tost ct\Fro F@tft -toF |rf Fif (\ld!? FH *FR *sN Eg6 *eG E6E EsE E E6 criirib 16rrrii ..clirn rrrsf at trlot- QE{o ql orF =g= gHE RRH RRn R=a 5=s a a
OFF @dor \ar\o6l dFQ QOiGI c/td.t -.F (\!q, rrir.Ofu 6;;,i ;.H6 9C+id roc\rs -t.f $3 !9 A6 -6ali eiFaa oeF Gtoc-t Oro(\l F€H =*F Es= 5se $=S +8T EFa € qcr (\td.,, aad ;;dt iiF ;=(i 6\Fd .al Crl
F,e \9o1r4 oqrlt ,o4b dq3! S.oB c Fio o. EF ( roto -l 1.o0r o@Ge edb i-=5 dt'n6 oa6 N-,!: S=A g8ie! B AF og+ Fmo qtltreb
=@d (oi{e rtoQ d!(t6 acrO qq{d c <l
!t 6tdo aari i-i- aFi-<ri dF- u1 .'lOr H 6l
{' C !t!t o'r:tt c'rs{ q== O}sCdr -rt.t -++ stoln !Q\9rP \9q-q'$ ngs S+S +*+ *lg* tbRs
rfld .O<rrat.dFl CtIFaGDratlltsC'6!.ct6l
!(l ONrt+cto'.o!OG'Fa Gt 6l
tfl
dI
deto.{<t(trF'd
ctoI
GItO
oor!tIrOo
H
oG'D
a"
d
6tI
oOcrlct
@ooet
oooI!t
oo
Flralo
oralG'Ioe
ct
a\a
ct
H(JiltalOrt{'..O\-oo
-! GtoGt€Ga ct(roC: Fl
g
t-l(J;t(l(t!L>rE>E: G'oGt
-l€d-lGt+r <, ct8€<.
6
gB"
HC'tralOrtF'.at\(, Gt
E: G'oettG. GIoGtEFI
5g
EF-
ortCN E:6A
do=tIorE<tEE:
T{J2o<tE:Aottra!aaF..oHhaEaO
B.<IH(J
^rato('r<'rAEER€38
Ei.EoEa <,g6{Jt81tt, q<tEi Ei'8E|o-qra!c,te.88>raJ |rl6htEcC:Oo>tt -a6uictr.
E:c)oa{ aJ€eCL.l{OCD
-ooLo@l4l615a,-jidIF'@Aa

Iable 3-12: Standadised incidence ratios for tle nine Scottish regions and
tiree island areas 1989-90 (0rkney and Sheilam corbined)
tegion Fopulation
(lotaf)
0bserved
n
Upected
n
Standardisedincidenoe ratio(e5t cI)
Borders
Central
Durfries/GaIIonay
fife
Grarpian
Eigbland
Iottrian
Stratlclyde
Tayside
Orkney/Shetland
Hestern Isles
Scotlad
102,700
27r,lN
1t7,500
34{,800
503,500
201,900
712,9N
2,3rL,2W
392,500
{,1570
3,0630
5,ogor7oo
I
10
{
1l
19
l0
12
110
13
2
0
229
5.36
12.05
6.85
15.60
2I.61
8.98
33.06
103.00
L8.62
L.92
1.5{
2n
1.19 (0.61-2.e{)
o.s3 (0.3e-1.52)
0.58 (0.15-1.{e)
0.71 (0.35-1.26)
0.88 (0.53-1.37)
1.11 (0.53-2.0s)
1.27 (0.92-1.721
1.07 (0.88-1.29)
o.12 (0.12-1.10)
1.0{ (0.13-3.76}
o.0o (0.00-{.e2)
1.00
92

=IFol.|.i5oo
zl!
E=o, P!EE;;gEEooaa6FO6o;E+E;.ep=oEEE4roo+E
'69eetcrio6
coxo6
=sI Ert =b"g$Eb->t-> eP+?E E€e9$gEEEEE'J
PE
Loo'AtoEov,oooocoL3ozl-oo=Eoo(,ooGfrFoc.9-(UIc6EtLoI
crtCDlr
E=o,otolIl-c
3E P<f g?l- O=3EE
o6o=

Fig 3-2: The Scottish Motor Neuron Disease Reglster 1989-90- Age specific incidence rates (n=229)
1*24 25-34 3+44 4$s4 5$64 6974
Age groups
r-oo
E1o-oooC)CopC'E
L(go
810q.ooo(,co5E'Ec
15-24 25-34 3*44 4$54 55-64 65-74 75-84 85+
Age groups

Fig 3-3: The Scottish Motor Neurone Disease Reglster 1989'90Age and Sex Specific Incidence Rates
* Men (n=132)
* Women (n=97)
Age
L(Eo
ooqoC'
o(,co3(,tr
15-24 25-34 35-44 45-il 55-64 65-74 75-U 85+

;F4EO5a?
E6E
o6E(,
l_J
!l
6oo
EoEo6o
I
oIL
-€-E9F:FCt
F9aaFCIE;Oci
o{ACIqC)
Iool!Eooo
=
a!?Fq=ctOFi;
R
E}gE:sotoEg rC'rc ;^E8 FF8E FifrB E:Ei8EE
EH6sE.E1aE.E
=P8gf#TctctrlJ.
tat
cgo(oo
€ogE3o
dt
dC'
lo
+oaoo
6coo
'j.ec...-

CEAPTER I
Tf,E UTITJITY OF EOSPITAI' }TORBIDITY DATA AITD DEATE CERrIFICATES
coDED Ag ttOTOR ltEURoN DISEA8E (ICD 33s) Itt SCOIIIIAND 1989-90
97

Chapter 4
INTRODUCTION
" Physicians of the Utmost FameWere -ca77ed at once; but when they cameThey answered as they took their Fees,"There is no cure tor this Disease."
From rrHenry Kingrr, Hilaire BeIloc263
National Health Service manalters, adrninistrators and public
health specialists use norbidity and mortality data to plan the
appropriate allocation of health care resources. Therefore, it is
important that this infornation is as accurate as possible.
Sorne investigators, using unverified hospital discharge
rates, have reported an incidence of MND approximately two to
three times that measured by other ne.ns112. This discrepancy
suggests that a Iarge but unknovtn number of patients coded as
MND following hospital discharge do not actually have this dis-
ease.
More comrnonly, mortality statistics are used both to follow
trends and as an indirect measure of incidence of MND73 'L24
(see chapter 2), with the belief that such data have a hiqh
degree of a accuracy, given the generally fatal outcome of this
disease within a year or two of diagnosis. In L979 the ninth
revision of the IcD264 introduced an amended classification of
anterior horn cell disease and the clinical subtypes of MND were
included under the rubric 335.2 (table 4-1).
The accuracy of such routinely collected statistics depends
on: (1) The proportion of incident patients admitted to hospital
or dying from the disease (21 The precision of diagnosis at
discharge from hospital or at the tirne of death (3) The satis-
factory cornpletion of Scottish Morbidity Record (SMR 1) forms and
98

Chapter 4
death certificates (4) The appropriateness of IcD coding (5)
The accuracy of transcription of inforrnation to the Scottish
Hospitat In-Patient Statistics (SHIPS) and Registrar Generalrs
computer file and (6) The efficiency of the linkage programme
which retrieves first, rather than aII, discharges and the satis-
factory retrieval of death certificates for the relevant year'
There have been no formal studies to compare the accuracy of
hospital discharge data with other case finding rnethods, oE the
extent to which these data wilr identify all patients who develop
l{ND, yet this is an irnportant requirement f or studies which
require an unbiased and complete sample of cases- some inforna-
tion is available concerning the false negative rate of death
certificatesT3 'L24,L25 but much less is available concerning
the false positive ra1':e72. In this chapter I have cornpared
the accuracy of hospital discharge data and mortatity statis-
tics with the SMNDR.
uElrBoD8
The SMNDR Was considered as the rrgold standardrr for the
purpose of this study, although 2Lz of SMNDR registrations in
1989-90 had been ascertained for the first time from sHIPs and
2* fron nortalitY returns.
Uorbidity data retrieval
The inpatient and day case records summary sheet of hospital
morbidity in Scotland (SMR1) collects biographic, adninistrative
and clinical information relating to every hospital death, dis-
charge or transfer and includes a section pertaining to diagnosis
which should rrbe completed by the doctor on discharge of pa-
99

Chapter 4
tientn265. Clerical staff conplete the remaining details and
code the assigned diagnoses according to the ICD-9' This form is
the basis for data transferred to the SHIPS computer, although it
has novr been replaced by a computerised patient adrninistration
system in a nurnber of hosPitals.
A request was rnade to the Information and Statistics Divi-
sion of the common services Agency for the scottish Health ser-
vice for det,ails of all patients coded as ICD-9 335 in any part
of their discharge form for L989 and 1990, and which, through a
record linkage systen, was restricted to first discharge with
this diagnosis. This was available in the August following the
year of interest. The hospital records of aII such patients in
scotland who vrere not already registered with the SMNDR were
requested, with the permission of the consultant in charge of the
patient, through the relevant medical records officer (see chap-
ter 3). Patients who fulfilled the criteria for probable or
definite MND, htho were not already included on the SMNDR' and
who had been diagnosed on or after January 1st 1989 (incident) 'were therefore eligible for inclusion in the SMNDR and accord-
ingly registered. Other patients had been coded correctly but
were discovered to be prevalent to the SMNDR (diagnosis made
before January lst 1989), despite first adnission in that year'
The diagnoses of aII patients coded as ICD-335 who did not have
MND s/ere recorded and the records examined to try and determine
the reason for the error. The SMNDR was also used to identify
all patients diagnosed as definite MND and first discharged from
hospital in 1989 and 1990 who did not appear in the sHIPS'
r_00

Chapter 4
l{ortalitY data retrieval
A list of all deaths older than L5 years, coded as ICD 335
in position 1 or 2 on the death certificate, Itas retrieved by the
Registrar General I s Office for Scotland approxinately 1 year
after the end of the year of interest (see chapter 3) ' This
information enabled the retrieval of General Practice records'
which contain a copy of aII hospital correspondence, through the
relevant Health Board. This information liras treated along the
same lines as that derived from SHIPS (see above), SMNDR records
were searched to deternine the false negative rate of retrieval
for rnortality statistics.
RESULTg
ttorbidity data
A summary of the SHIPS data in relation to the SMNDR is
displayed in table 4-2. Of a total of 379 patients older than 15
years discharged for the first time in 1989-90, LAL hlere already
registered with SMNDR and 27 were known to be prevalent from
other sources, Ieaving 2LL for whom hospital records were re-
viewed for diagnostic details. LLz did not have MND, ie the
false positive rate was 303. 52 MND patients included on the
SMNDR (232 of incident cases) did not appear on SHIPS in the two
years examined. SHIPS overestirnated the incidence of MND by a
factor of L.6. Table 4-3 displays the utility of SHIPS in terms
of sensitivity (84?) and positive predictive value (7Ot) of a
diagnosis of MND as determined by ICD 335. If it is assumed that
alI patients discharged from hospitals in Scotland who did not
have MND were not coded as IcD-335 then, given this very large
true negative rate, dD hypothetical specificity would be close
Lo1

Chapter 4
to 1OO?.
Table 4-4 gives the diagnosis in the LL2 patients miscoded
as MND. The largest group were patients with a pseudobulbar palsy
due to cerebrovascular disease (38t). In 18t the coding accura-
tely reflected the medical summary but the diagnosis was incor-
rect, either because of a failure to meet standard criteria for
diagnosis, or because a rrprobablerr or rrpossiblerr diagnosis of MND
was disproven at follow up. L2* of miscoding appeared to be due
to a transcription error, dS no possible Source of confusion for
IcD 335 could be determined from the records'
trtortality data
Summary statistics relating the death certificates coded as
ICD 335 in relation to the SMNDR are displayed in table 4-5'
27 l28L deaths, (1Ot) contained false positive errors giving a
positive predictive value for mortality returns of 908' Again,
niscoding of patients with pseudobulbar/bulbar palsy was the rnost
common source of error. 12 (44*l of these errors htere due to
misdiagnosis although coding stas correct, 15 (558) were due to
rniscoding of other conditions (Table 4-6)'
seven of 95 SMNDR patients who died with MND were not
retrieved by the Registrar General, giving a false negative rate
of 62. However, inspection of these returns revealed that MND
$ras recorded as a cause of death in 3 cases, So presumably there
was a transcription error at some point in retrieval. As the
death rate of patients on the SMNDR wiII continue to rise, 8t
Ieast until LggL-z, when a steady state of rnortality will re-
flect incidence more closely, it is not possible to calculate
the sensitivity of a death certified as MND'
LO2

Chapter 4
DISCUSSION
l,torbidity data
This audit demonstrates that SHIPS is inaccurate. 308 of
patients coded with ICD 335 did not have MND and therefore these
data cannot, in their crude form, be used as a reliable guide to
the incidence of MND in Scotland which would have overestimated
the rate for 1989-90 by a factor of 1.6. This figure will faII
slightly if the same audit is repeated at a later date as the
number cases prevalent witn respect to the SMNDR wiII be less
however the problem of false positive coding will persist unless
measures are taken to correct its cause. 49 of 229 (2L*) of
incident patients were identified by SHIPS as the first source
of referral for the SMNDR and therefore this resource was neces-
sary to accurately deternine the incidence of MND in Scotland.
There are three major reasons for these errors. Firstly,
while the importance of accurate codinq may be appreciated by
many doctors, this task seems to receive a low priority. AI-
though medical staff make the diagnosis, they do not take
primary responsibility for the supervision of diagnostic coding,
which is delegated to clerical staff who may not be able to
interpret adequately the nuances of anbiguous nedical termino-
Iogy. In some cases records staff are left extracting informa-
tion from poorly worded letters rather than specifically listed
discharge diagnoses and hence take nedical conditions out of
context eg for rrpseudobulbar palsy due to cerebrovascular dis-
easerr some patients were assigned to the $tronq ICD or to both
ICD-335.2 and 437.9.
Secondly, the ICD classification does not allow practitio-
ners to indicate whether a diagnosis is firrnly established'
103

Chapter 4
requiring further infornation, or largely speculative' This is
in contrast to clinical practice lirhere revision is often re-
quired and the passage of tirne clarifies a diagnostic problen
(for example the differential diagnosis of spondylotic cervical
myelopathy and MND). It is this flaw, when the diagnosis did not
meet generally accepted minimal criteria for probable or definite
m{D266 (Chapter 3), which accounted for 18t of the diagnostic
inaccuracY (Table 4-4).
Finally, some of the errors arose because coding with the
ICD-9 can be ambiguous, for example the alphabetical listing
directs rbulbar (progressive) (chronic) tt and rrbulbar-pseudo (not
elsewhereclassified)||tolcD.335.2,whichrnaybeinappropriate.Although the accuracy of a general sample of mo'bidity
informagiorr26T and for a nurnber of other specific diseases in
ScotIand26S-27 L has previously been examined, and
while many epidemiological studies of MND have collected hospi-
tal discharge data as part of a case finding
exercise9L,92,94,95, some of whom have cornmented on their
inaccuracY95, none have forrnally evaluated their utility for
this disease. Neither have previous studies been able to compare
accuracy with a more or less independent case finding rnethod such
as the SMNDR.
The results indicate that more diligent efforts to ensure
correct coding are required. The nature and uses of SHIPS should
be made clear to the medical staff responsible for discharge
documents. Doctors should be encouraged to use clear and unam-
biguous terminology, preferably within a standardised discharge
format. Guidelines issued to area medical committees in 1990
have emphasised that a senior member of the clinical tearn should
l-04

Chapter 4
be responsible for .;od,ingz12. Regular audit of case records
is irnportant in this regard and quality assurance within the
Information and Statistics Division has noht been established
whereby experienced staff wilt blindly recode a randon sample of
SMR records to quantitate the accuracy of existing coding' As a
result of this review sources of error will be discussed with
coding staff and the SMNDR will continue to rnonitor SHIPS returns
to see if accuracy imProves.
Mortality data
Interpretation of variations in tirne and place which night
be used to generate aetiological hypotheses depends on an under-
standing of the accuracy of the data on which such comparisons
are based. In this study, mortality data were much more accurate
than sHIPsr 6s rnight be predicted. However, some of the problems
relating to discharge data also apply to death certificate co-
ding, in particular the miscoding due to other neurological
conditions, rnainly bulbar palsy of various causes, in turn due to
the difficulties with the ICD coding system.
Whether the incidence of MND can be studied adequately with
mortality data alone is controversialTS (see Chapter 2l '
Other studies of the accuracy of mortality data have shown that
70-90* of patients diagnosed with MND have this condition recor-
ded on their death certif icat e72 '-13 'L24 tL25. In Scotland
mortality data also have a low false negative rate. OnIy one
other study frorn Japan has examined the false positive rate of
death certificate coding (in 1965); an extensive attenpt to
verify the diagnosis frorn other sources showed that aS many as
one third of men were coded as dying of MND without having the
105

Chapter 4
disease, but the accuracy htas better for ton1"rr72' SMNDR
mortality statistics were much more accurate than this'
These findings have important implications for epideniolo-
gists interpreting trends in MND frequency. There is evidence
from a number of countries that the mortality from MND has in-
creased stead i 1y over the past 3 0
years73,75-77,79,82 and this is also the case in
Scotlandz73. This increase may be real, rather than due to
ascertainment bias or inproved diagnostic skills, but it would be
helpful to confirm this with other sources, e9 incidence data'
Frorn this analysis, it can be inferred that changes in the
ICD coding system, or alterations in coding practice, are likely
to have an effect on both morbidity and rnortality rates which
could be mistaken for a real variation in disease incidence'
Whether these results are applicable to other countries is
uncertain but the anomalies in ICD-9 will apply ever)rwhere.
L06

Iable l-1: International Classification of Disases-9(1979); 335, anterior lorn oell disorders.
335.0 ler&ig[offrann disease
Infurtile spinal nscular atroPbY
335.1 Siml tlsatlar atroPhY
Kugelberg{elander
Adult spinal ruscular atrophY
335.2 llotor leuron Disse
Aryotrophic lateral sclerosis
llotor neuron disease (bufbar) (dxed type)
Progressive nrscular atrophy (pure)
335.8 Other
LO7

*,cotr,.Uo
I
=oca6
.a(U
o€tgcl
=r|aov,U'oeEr.gaI
l.;o.n
aE$lEat
oEioH(D
=l{aIE.A+,+,8u)Eo=-?t
RS* @oS = A eqF d(\t -t-td-l 6l Gl :d
or(\1 6lral Gl
@oroo6oco -to(\t o - (\l - |r| F!-i6= Jlirii.daF - t-)<-t F
FadCDFd <t\oo H (\lFa(lC F)NU)dd
dF.{Fa Fa
OF
a6'€'E t.=a a g-6 urqT E E E
=E e ; b eE'sqfe^ EB E: E: :38^ = E ;E 3e E:o; g E..{ o8 x 5 tsS gE EE;E E i *A Es AE e3aa ; E zz zg <tE'l JSJg E .E oo'- 5gg3'c e.E.E.s E. = E=E .E.
giEE iE€iE. : E EEF E
€g':3 E;Ee*t F e *eE s
EEA; EA;EEE * E;E*q EgEIE :g. neg F IHt€s &
gEgg Eg BgE; E BEffiE E
.E+ta
aa!<toulearti ota! FaE€<lk6oor.fgil
l9 to'-r+ O@:r- d (t!E clH(Do-6a-iIHILo
.Jga+J+t<taCDaC'+,
6.JsgE:
w,o.H
aI+,o{-tattt+taaJaI-iH
gc!.agI6+ta,8ttsa}ac,>.L
-l6(i;I<t@
FIAg

oo
o+r(Dvto()>.(.)
a+a
ot*aao F.!
tlo,gB
dd
l-xo. q,€F{ d€'d
=!t+,?-.dottg+ro660(D
'rd u:4(D)<|!
.d qt€>+8'[email protected]>t Er.4
Ct +'* ='d588.€.rg 3.dX-t! + 3r\€qrc,qr>>Lr .d 'd'PPar.A.A(,rA.ng &&=EE+r'-l{5F.F.
' abtt8.i .aE.i EE8EL. CLCL
-8o€HEr|lct
.uDItr A. Otc:H >.d ?E.AE^R.d9.dE o8€5eLa .do>q,(J.i i>O) +' 'd!.d P
A2 .-l-68-.?t tu
,rA
c7) |
6lddlt
5€
(tro (\lNlrl
FdFI
g6
Eet{rileEgeL.aIE{JgE
GDC'r
.r d.E gs+t atE iaec,tF{4r-cl'Aigea{5AoC'EE-c! d3D {Jdoa+rd.J +J8Svr 4t
dot&ooC!ig,ae
a= f{ootg:g
*.I ao5Itad Od CLdg 8c,EiE 6g€ H- i:2I6 eO, V, rP^
es=E.afEeEP AA().d
?ESo.ggE sea$ aEEa'sgHi:;HgF;;+on€

df 6Po6rd
Gt u'r odd\od(\l
@-)-)tfd
oGT
Nd6t ro
(t) rt <t
AIOHd <l' Fa
etr)$ |rl
6lrtt
(!d
f;.n.82.AEE 'E E -qrEiEi e o tggg F=-. ts 'r{&to EE '.d Eo'98 o& b Al- AE .a O .1 -tCl .4 r f{ +, do=E ==6 b ts P a-.1 J-a O El .!. d q,g;E EE E g E E:: - o EL F€ ?q)E sEe =F E E E E
H 'i'd;' t - g .J B +,8 r''H -- 7=u, E 5 E P5 Eo'S 5E o € 6 : e
3sH EgiEEe€E:7.E ee.3 'ilFE dF : E ; :; ;gE LrH Et€ He € '5 E EE *'E5 €E€ E3g .2= >r 'd i =H 8^€ *8- -.=^ :E E E H Fs €.9
€ gE* 5:E €: ; E E Eg gFe .eer a'+€ 9* H a F gg -q'eE €ii Eag E; E= g :g EE E- tA ttlA 7 >.Fa o.gv OA,t:t
I
qt.JoF.
ctC'r('rFa
('roG'rFa
,;(,a,o{Jat.Jv,+ta
{'t
Le
sFgE!a+,
83r,gF.>rn
-o.Eao6ET
o{J
6.J
E
6ldd
SaoEctaJIt}ao!oa!4(-,
!tI<to-lng

+)rH(DO>.,'r +,eeL.Qt vt .t,
au .da'! 6ag'E e'd8a9d oCr.d -q4998b-.-g.o+, >.tt+, q,,d .d ttrE?EP.-Hl' ov,eEato+rO(D.d9
e.? sctEe >+,'-oE. C, >Gtl'+,.ds 86 g
v, .4 .a .-l.l .H.Et€F5 g'dE L OO
s 3.9 isO+t+, La.d.9 E'd -.=o'.8-giE8;* H,.d*(rlrssgtE|| cl Er lta=.9^59-835E:
=EE+JP.UO{dB 6f <8c, .d4€ 6R -ll tL.E I O
9dd
E E gR?Et-.-o.a- Eii-. . .r. O, a.t (1,
.€:'E:e9. ggfi
*ct dedio
-f CfrF|rrlAlrn6!GttsGlol
qt{JdAR
o('r -lctr c.)d
S@Cr rt
Folo grH@ @ (v)
rC, <f a.t<t<, 6t o
3"Fa
d,dCn|rtdro
dFa tI,\r, Gt \at o !tdd<tc\l d oil
Eo *t6d c=
iEieE Egt Eg eiaEEg€;ffis3flEEYE EA : 8 8;E t.s: as E g ;EB R Hg ; €
s; EE E e gEE € =g
g €E-E Era a ; E€; E EE E A:fi EE g * ;sE I #s s ;Es Qs E e EgE g EE E e
rala'DG"EI<.'H
a=o6EoI
{J8
laa
t84{JIiE'
oOrICt@ct!do
{J
bDE:aJsggD^C)Hda{a,6f.dOaJatH.JoEit{ aJddEOF8.31, v
aflI!to.1.cle

lable l-6: Brrors in rortality data (n=2?) rit! repct to adult onset m. Diagosis
sDom is based on reiien of redical recorG atd deat! certificates.
1. hfbar or pseudobulbar palsy due to cerebrovascrrlar disease,
rultiple silerosis or rrnspcified (non-progressive)
2. tlotor nergopatiies, radiolopattries, ilorer rotor neuron nealgessi
3. tlultisyster neurological disease
l. Probable cervical spndylosis
5. Diagosis unlooutr or uncertain but insufficient evidence for lltD
tote: t5 rlirt not have ltilD in tie body of tie deatl certificate ht rere cuded IO 335t
12 had lllD on tie deattr certificate ie coding correst but t[lD risdiagnosed.
11
5
2
I
8
LL2

CITAPTER 5
A CA8E-CONTROIJ 8TUDY TO EXAITINE PRIOR EYPOTEESES CONCERNINC AEE
POSSIBI,E ROI,E OF CERTAIN EM/IRONT{ENTAI, FACTORS ANTECEDENtr IIO TEE
DEVEITOPUENT OF IiOTOR NEURON DISEASE.
113

Chapter 5
INTRODUCTION
" To restore the human subject at the centte thesuttering, affTicted, tighting, human subject - we mustdeepen ^- cate history to a narrative or taTe; onTy thendo ie have a ttwhl,' as we77 as a ttwhatt', a real petsan,i patient in relation to disease in relation to thephysical."
oliver sacks274
One framework for research into the aetiology of MND, is to
consider the potential interaction of ageing with environmental
factors which might be ternporally remote from the onset of
clinical disease275. Support for this hypothesis is derived
from the study of the Western Pacific forms of MND276, the low
concordance observed in twin studies277, and reports of MND
or MND-tike diseases in relation to a variety of exogenous tox-
ins2 L8,22O,22L '226,278 . Case-control studies have also
suggested that a number of environmental factors may be of
potential importance in increasinq risk for subsequent MND (see
table 5-1). This case-control study hras planned to examine the
following hypotheses relating to 'controversial issues:
1. Preceding trauma
,,... trauma-and particulatTy najor trauma to the limbs,is in fact a risk factor for anyottophic Tatetal scler-osis...it seerns a lead worth puVsuing in this othentisehopeTess disorder"
J.F.Kurtzke46
This statement is based on evidence from the close temporal
relationship of physical trauma to the development of MND in
nunerous anecdotal case reports2T9-286, in uncontrolled series of
patients published as recently as LggL43 and evidence from case-
114

Chapter 5
control studies, some of which have suggested a possible link
between blunt trauma, electric shock, surgical procedures or hard
physical labour/manual worklo1 '287-292 (Table 5-1). The interpre-
tation of fiany studies is Iirnited by rnethodological problems
which risk introducing important sources of bias, particularly
when pat,ients are a selected 9roup290'29L, orr as is often the
case, the investigators cannot avoid the recall bias inherent in
asking patients who have a vested interest in explaining their
disease. Furthermore, case-control studies based on a diagnosis
included on death certificates may result in associations which
are the consequence of the disease itself e9 superficial
injury78. The potential relationship of MND hrith trauma is
important, not only for aetiological considerations, but for
medico-legal proceedings. Therefore, this case-control study
sought to further examine this putative association.
2. Occupation, environmental toxins and xenobiotics
Exposure to single large doses of a neurotoxic substance, or
more prolonged cumulative exposure to low doses, could produce
motor neuron ceII loss. Occupational groups rnight provide clues
to such possible environmental risks; for example, it has been
suggested that 11 138I eather'J t L'
, textiIel39,
agricultural91,LL2,293 and manual workers292 may be at in-
creased risk. occupational exposure to a variety of minerals and
metals is also a potential mechanism of neuronal
attritio,,22O, 223, 294 .
Willians et dl, observed a patient who developed MND fol-
Iowing intoxication by the insecticide pyrethr,,t2 2 7 ' 228 ,
which is metabolised quickly to safer substances in rnammals but
115

Chapter 5
not insects, whom it paralyses and kills. This observation
suggests that some toxic substances may have the capacity toproduce MND directly or, that a genetically deternined biocheni-
cal aberration, conbined with the rrwrongrr environmental factors
might predispose to the development of disease (ecogenetic/xeno-
biotic hypothesis2gs). Patients with MND nay have a defect of
sulphur oxidation and rnethylation which results in a high
cysteine to sulphate ratio296 '297 . Therefore, an individualwith poor S-oxidation capacity on a genetic basis who acquires a
second insult, for example by the consumption of large anounts of
sulphur containing cornpounds (eg the brassicae group of veget-
ables) rnight then be prone to develop t*ttlo295.
Accordingly information was sought about all occupationsl
the subjectrs perceived toxic environmental exposure; the con-
surnption of brassicae (cabbage, cauliflower or brussel sprouts)
and an interest in the cultivation of vegetables.
3.Socia1 class and the environnent in childhood
The risk for MND could be related to factors associated with
socio-economic deprivation, or affluence. Measurement of social
class is fraught with difficulty, particularly for women employed
in the home. To avoid some of these difficulties, Carstairs has
devised a measure of socio-economic deprivation in Scot1and293
using information available from the last (1981) census which
allocates a numerical score to individual postcode sectors (which
contain an average of 6000 persons). Using the z-score technique
to give a single score, the percentage values are combined for
each postcode sector based on the four variables of car owner-
ship, degree of overcrowding, unemployment and social class. The
scores are distributed into seven categories within 0.3, 0.8, 1.5
116

Chapter 5
and >1.5 standard deviations (sd) either side of the mean
(+0.3sd to -0.3sd as the niddre category). one important advant-
age of this rnethod is that it can be applied to males and fe-males, regardless of occupation, whether working or not. When
standardised mortality ratios (SMRs) based on this scale are
calculated, a number of common causes of death (eg cancer of the
Iung) show a highly significant trend (Fig 5-1a), with higherratios from deprived areas.
In contrast fig 5-1b also shows the SMRs based on the 533
deaths from MND (ICD 335), in Scotland 1980-85, male and female.
This demonstrates the reverse trend, that is, higher SMRs inindividuals who live in areas of greater affluence. Confidence
Iirnits overlap with unity, and the Chi squared value for the
Poisson regression is 2.2L (ns) , but the graph does follow a
rrdose responsett relationship. Because of concern about accurate
diagnosis of the cause of death in the elderly, particularly fora rare neurological disease, the total group has been dividedinto those aged 20-74 years (fig 5-Lc) and aged >'75 years (fig5-1d). It is then apparent that elderly people largely account
for the overall trend in SMR with the Chi squared for the regres-
sion being 3.2 (p
may reflect a failure to diagnose MND in elderly patients from
deprived areas which probably are not so well supplied withrnedical services as affluent areas. Alternatively, if environ-
mental factors associated with affluence do predispose to MND,
the reason for the difference in the two age groups may be thatthe elderly have benefited less than younger people from impro-
vements in the standard of living since the second world war.
This observation argues strongly against factors associated with
LL7

Chapter 5
deprivation increasing the risk for subsequent MND but this issue
can also be addressed by the case control study'
A related question is the is;sue of the childhood environ-
ment and the risk of infection, particularly with poliovirus'
Although late deterioration after polionyelitis is weII recog-
nisedl46'2O8-2LL'299, the rnajority of case-control studies which
have examined the frequency of preceding poliomyelitis in pa-
tients or fanily do not support a causal association2SS-2go'
AIso the vast rnajority of patients with MND cannot recall an
episode of polionyelitis. The hypothesis Iinking the two dis-
eases, expounded by Uartyn74, hinges on the concept that a sub-
clinical infection depletes motor neurons and renders the indi-
vidual susceptible to age related neuronal depletion, or a second
insult. Unfortunately past exposure to polionyelitis cannot be
distinguished serologically from antibody due to immunisation,
introduced in the earlY 195Ors.
In an attempt to look for indirect evidence of a link be-
tween the two diseases Martyn noted a specific positive correla-
tion of MND nortality 1968-1978 with'poliomyelitis notification
rates 1931-39 in England and Wales; poliomyelitis did not corre-
Iate with other leading causes of death144. In addition, the
suggestion has been rnade that the rising rate of poliornyelitis
during the early decades of this century accounts for the present
increasing trend in MND rnortality. Population based epidemiolo-
gical investigations in the 195O's identified the major determi-
nants of Seroconversion as absence of domestic amenities, domes-
tic overcrowding and large sibship size3OO'301. With impro-
vements in hygiene the proportion of children who escaped infec-
tion in the relatively rrsaferr period (fron a clinical disease
l-18

Chapter 5
point of view) increased and paralytic poliornyelitis becane a
disease of areas well supplied in terms of standard of
housingT4.
Two possible predictions with respect to patients with MND
can be made iro. this information: either, (1) If conditions are
of a high standard of hygiene in childhood then later exposure
to poliovirus rnight result in greater, albeit subclinical' ner-
vous system damage because of greater vulnerability of motor
neurons at this age and therefore childhood affluence should
correlate with risk of UHO74, ds suggested by the recent observa-
tion in Scotland described above302, or (2) If childhood was
spent in circumstances of poor donestic hygiene then the nurnber
of individuals exposed to poliovirus infection would be greater
and thereby increase subsequent risk of MND, if the two are
related144.
Therefore this case control study design sought to seek any
difference in the childhood environment with respect to standard
of housing, domestic arnenities, overcrowding and social class of
the patientrs father
IIETHODS
Throughout, r|case|| or l|patient|l refers to a person affected
with MND, rrcontrolrr refers to an unaffected person and ttsubjectrl
refers to either case or control.
Patients
Incident patients in Scotland with MND vtere identified from
the Scottish Motor Neuron Disease Register (SMNDR) (Chapter 3) '
L1-9

Chapter 5
The nethod of identification of the 103 patients included in the
case-control study is described in table 5-2. Onty patient,s with
a nixture of upper and lower motor neuron signs vtere included
(SMNDR classification = ALS; ALS/PBP; PBP/ALS). In each case the
permission of the consultant neurologist or physician concerned
and the patient I s GP was sought before inclusion in the
study.
Controls
After discussion of the nature of the study with each pa-
tient t s Gp, an age and sex matched comrnunity control vtas identi-
fied from the practice age and sex reqister, usually computer-
ised, ds the person with the date of birth nearest to that of the
patient. In this way selection bias in obtaining controls was
avoided as the GPrs age and sex register constitutes a conplete
list of patients registered with a given practice (ie no records
are rnissing because the patient is unwell). One control was
identified for each patient. In two instances, after repeated
attempts, the first control could tt:t be located and then the
next subject in the age and sex register hras approached. One
control refused to cooperate and in this instance the GP also
declined further help, so a neighbouring practice assisted. The
only potential reasons for exclusion of a control was dementia
or psychological disturbance of such an extent to prevent ade-
quate cooperation with a questionnaire; in fact, in no instance
did this happen.
Data collection
I visited the case and then the corresponding control,
atl regions of Scotland, in their respective homes, usually
in
on
L20

Chapter 5
the same day, after arrangements had been made in advance of the
visit. For patients, details of the history and clinical fea-
tures as obtained by the SMNDR htere verified and updated if
discrepancies existed. A neurological examination was perforrned
particularly to confirm the distribution of physical signs,
which may have changed since registration with the SMNDR' Very
particular care was taken in the establishment of dates of symp-
torn onset. case and control were treated in an identical fashion
as far as the quest,ions pertaining to antecedent factors were
concerned. An equivaient date was assigned to controls corre-
sponding to the onset of symptoms due to MND in the patients and
only events prior to this date were recorded. Some prior indica-
tion of the nature of the questions was given in advance of the
visit and information was collected by standardised question-
naire. The spouse of the case was invited to contribute to the
answers and then, whenever possible the controlrs Spouse was
also used for help in ascertaining an accurate response' If no
Spouse was available for the case then the controlrs spouse htas
also excluded
The standardised questionnaire (Appendix D) recorded the
dates, anatomical location and nature of a77 trauma tequiting
medical consultation, including fracturesl blunt trauma; opera-
t,ions requiring a general anaesthetic; and any electric shocks
resulting in loss of consciousness, injury or post shock residual
syrnptoms. Trauma which rnay have been associated with the onset
of weakness was excluded by taking the history of the illness at
the outset of the patientrs interview. If the subject reported a
fracture or injury near the tine of the patientrs sympton onset
and there was any question of a weak limb predisposing to a
T2L

Chapter 5
fracture eg a foot drop resulting in upper lirnb fracture, then
the trauma hras excluded from analysis. FoIlowing the interviews
aII the GP practice records, which included reports fron accident
and emergency departments and results of x-rays, for the case and
control, lrere scrutinised to ascertain any injuries or operations
requiring medical consultation which may have been ornitted during
the subjectrs interview. Systematic GP records began with the
introduction of the National Health Service around 1948 and are
transferred to the nevr cP when a patient moves to a different
area and so represent a valuable source of unbiased information
prior to the development of MND. In one pair access to the notes
was denied by the cP but information regarding trauma was provi-
ded in letter form. In this way an account was obtained of the
subjectsr recaII of traumatic events (fractures, blunt trauma
requiring rnedical consultation and operations) i trauma according
to the GP records and this information could be analysed
separately or on the basis of best information frorn both sources.
A detailed Iifetirne employment history lvas obtained and
classified according to the Office .of Population and Censuses
and Surveys (OPCS) 303. Details of toxic exposures (solvents,
lead, minerals and ores) with regular contact over a period of
L2 months or more hrere recorded. Structured questions about
cigarette snoking and a history of atherosclerotic disease were
also included.
A lifetine residential history was recorded of residences
of more than 2 yearrs duration (limited to a maximum of the six
of greatest duration if there were more than this number but
always including residential details for the first 10 years of
childhood). For each residence information was collected on its
L22

Chapter 5
rocation whether urban (city or town), or rurar (village or
isolated house); the availability of domestic amenities (a
garden, separate bathroom with a fixed bath, running hot water,
and flush Iavatory); and residence size, (nurnber of occupants
per room and Per bedroom).
Data were entered, ds they were collected, intO a microcom-
puter using dbase IV (Borland Inc. ), for subsequent analysis by
The Statisticat Package for the Social Sciences (SPSS-X and SPSS-
pc) using chi square for categorical data and rank test for
continuous data. Confidence intervals lfere calculated using a
computerised analysis programme, applying a matched case control
rnethodl2 6 '252 .
REgUL,Tg
Patient Characteristics
The age and sex distribution of the patient group were
representative of the total population of incident patients with
MND, 1989-90. There were 51 males (mean age 63.4, range 35-85
years) and 42 females (mean age 67.L' range 28-86 years). HoW-
ever, not surprisingly, the mean survival from symptorn onset of
patients who died before I could include them, $/as shorter than
the 49 patients involved in the case-control study who had died
by January lst Lgg2, with a difference in the means of 6'4 months
(958 CI -O.L-Lz.gr. AII patients had a mixture of upper and
lower motor neuron signs in the tirnbs i 7L (692) also had a bul-
bar/pseudobulbar palsy (ALS /PBP; PBP;ALS), the remainder had
multilevel spinal disease without bulbar signs (ALS) ' The age of
controls was identical to that of patients, a result of the
matching Process.
L23

Chapter 5
l.Trauma
Tables 5-3a shows the total number of fractures by case or
control and sex. There was no significant difference in the
distribution of fracture frequency by case or control for men or
the total group, although the Chi square for females ltas just
significant (pcO.05). With matched case-control analysis there
was an overall non-significant excess of fractures in patients
(table 5-3b) and a significant excess of fractures (with a very
wide confidence interval) occurring within the prior five years
before symptorn onset, this remained significant when only those
fractures docurnented by the GPrs records hrere included (table
5- 3c) . Table 5-3d shows the details of patients' fractures
within 5 years of synpton onset. For the 4 patients with frac-
tures within one month of symptom onset lirnb weakness could not
have been responsible for the fracture, after this the increas-
ing intervar between fracture and slrmpton onset makes error even
Iess like1y. Figure 5-2 shows the distribution of fractures in
case and control by interval before first MND symptoms (or equi-
valent in control) and figure 5-3 the'odds ratios for a fracture
at variable intervals before symptom onset.
There was no significant difference in the number of non-
bony traumatic events requiring rnedical attention, nurnber of
operations, electric shocks or blood transfusions (Tables 5-4 to
5-71. There was no correlation between the site of fracture or
injury and the anatomical area in which the weakness began'
Patients were as good as controls (kappa:o.8) in recalling the
true number of events when GP records were conbined with sub-
jectrs recall and analysis of the results based on the patientsl
account only produced no further positive associations'
L24

Chapter 5
2. Occupation, environmental toxins and xenobiotics
No single occupational group was significantly over repre-
sented, although the numbers in each of the L6 categories defined
by the oPcs were small. The highest odds ratio (oR) of 3.0 (95t
CI, 0.5-30) vJas in unskilled and labouring occupations. OveraII
and for men, patients were significantly more likely to have
engaged in manual work than controls (table 5-8)'
There was an excess of patients who perceived they had been
exposed to some agents of potential toxicity (Table 5-9a) with an
odds ratio for lead exposure of 5.3 (958 CI, 1.5-11.0). Table 5-
9b details the nature of lead exposure in cases.
No difference was found in the number of tirnes per week that
patients ate members of the brassicae or in the frequency with
which they undertook vegetable gardening.
3.s0cial class and the environment in childbood
There was a non-significant trencl for patients to have had
no hot water or a fitted bath (Table 5-10). However, this htas
not supported by any difference in the availability of a flush
toilet; home space, ds judged by the presence of a garden or the
number of individuals per room in the house or rural versus
urban living. No patients gave a history of paralytic poliornyel+-
tis although 4 patients and 6 controls had contact with a fanily
member with polionyelitis (OR 0.7; O.L-2.8). The frequency of the
common chitdhood infections was the same in patient and control
groups. The social class of patientsr and the patientsr fathers
social class did not differ from that of controls. There were no
associations with pet ownership, vascular disease, hypertension
or tobacco use.
L25

Chapter 5
DISCUSsION
Sources of bias
The case-control method as a technique for establishing
aetiology is relatively weak, subject to many potential sources
of bias, rarely proves cause and effect, and rather than explain
alr cases, sirnpry identifies risk factors304-306'
In this study clinical homogeneity was achieved with prede-
termined specific diagnostic criteria for inclusion, ie a mixture
of nultilevel spinal involvement with or without bulbar palsy'
selection bias vras rninimised by using incident, rather than
prevalent, population based patients. Despite attempts to in-
clude aII incident patients in a given time period and achieving
a representative group in terms of demographic variables, there
was a non significant trend towards longer survival in those
included in the case-control study. There were practical diffi-
culties in timing appropriately involvement of patients at a
stage when the diagnosis was secure but distress was not caused
by approaching moribund patients. However, it seems unlikely that
factors associated with a Ionger survival are systematically
related to the issues examined.
Reca77 bias is a major source of systenatic case-control
study bias. This was reduced by not giving specific information
to subjects about the hypothesis under examination and, in addi-
tion, ds far as trauma htas concerned, I htas able to verify
events by the use of General Practice records. These are un-
biased for the knowledge of subsequent developrnent of MND, and
are a complete nedical history, dt least for events after L948
when the National Health Service was introduced. Recall bias did
L26

Chapter 5
not, however, appear to be influencing the account of injuries
obtained from patientsr as aII subjects, whether case or control,
approximated the true trauma rate (ie best information combining
both sources) equally weII, and when the results were analysed on
the basis of subject recall only, ro false positive associations
were made.
Unlike trauma, where this could be checked, recall bias may
have been contributing to the findings related to environmental
toxinsr ds there sras no reliable way of verification of this
information by independent means. On the other hand, the pro-
blem of over-matching rnay be spuriously nasking an association
between occupational related factors and MND dSr for example,
certain large employers in small towns engaged both patient and
control t ot a rural residence for the patient (and thereby a
Iikely association with agricultural occupation) was also likely
to apply to the control. However, overmatching wiII not have
resulted in spurious fatse-positive associations. Controls
were identified in an unbiased fashion from the comrnunity in
which the patients lived, .
Non-res pondent bias, for example that resulting from a
mailed questionnaire29L'3O7, was avoided by rny personal approach
as was membership bias by not identifying cases prirnarily from
charitable bodies (in Scotland, The Scottish MND Association) as
in some studies29o '3o7 .
Exposure suspicion (interviewer) bias hras possible but a
standardised questionnaire hras used; pre-specified hypotheses
were tested, every effort was taken to avoid eliciting a biased
account from patients and results were analysed after data
By only recording events beforecollection were comPlete.
L27

Chapter 5
symptom onset any associations ltere more Iikely to represent
prinary rather than secondary phenomena'
Any study has constraints in terms of tine and resources.
Wrong sample bias may have resulted from the numbers it was
possible to include (103 cases matched one to one), thereby
reducing statistical pohter of the analysis, particularly when
some factors are observed in only a few individuals.
FinaIIy, jnsensjtive measure bias may be operating if the
questions asked are not a good reflection of the putative expo-
sure or mechanism under examination. Taking a dietary history to
estimate the ingestion of sulphur containing compounds is a very
crude guide to this and questions about the absence domestic
amenities may be too indirect to neasure risk of enteroviral
infection.
Discussion of risk factors
1. Trauma
This study lends some further support to the cumulative
evidence which clairns an association of physical trauma' particu-
larly fractures, with MND. An overall non-significant trend was
mainly due to the much higher fracture rate in the five years
before synptorn onset. However, these findings are not supported
by any relationship of MND to non-fracture or operative trauma.
One of the Largest case-control studieszSS ' in two parts,
identified patients from (i) death certificates (with inforrnation
fron the spouse) and (ii) cases known to the ALS research group
(selected collaborating neurologists) versus a mixture of hospi-
tal and neighbourhood controls. This study was vulnerable to
selection bias, recall bias, and potential non-standardised data
L28

Chapter 5
collection. However, the two different methodological approa-
ches of this study were consistent in their conclusion, that
mechanical injuries were two to three tines more frequent in both
sexes heralding MND. A further study claiming a relationship of
MND to trauma was lirnited to males, cases were ascertained from
death certificates and used rnilitary records collected prior to
the development of MND as the source of information on trauma'
thereby avoided the major problem of recall bias' Lifetime
operations, injuries and fractures were more than twice as comnon
in ""="=287. A recent study which made a concerted effort to
achieve patient homogeneity, used a selection of control groups'
tested specific hypotheses and attenpted to minimise recall bias'
failed to dernonstrate any such relationsnip3oS'
when considering the cause of, or associations with, dis-
ease, the judgnent of the relevence of any association should be
based on a nurnber of factors3o9. Case-control studies are gener-
ally less persuasive than cohort studjes but follow up of a
group of patients with fractures to the development of MND would
require such enormous numbers and such a long tirne and as to make
it irnpracticable. How specific is the association? Trauma has a
potential role in parkinsonts disease3lo, Alzheinerrs disease3ll
and dystonia3l2 and so this may weaken the argument with respect
to MND. However, the association of MND and trauma is consis-
tent- almost aII comparisons of this relationship in MND have
been positive, whether or not statistically significant6g (table
s-1). was the association hypothesis testing or is it hypoth-
esjs generating? In this case-control study I ventured to test
prespecified nu1I hypotheses (the najor issues outlined above) '
Given the number of questions, however, some ttsignificantrr asso-
L29

Chapter 5
ciations could have occurred by chance (1 in 20 at the p:0'05
Ievel). There does not appear to be a clear bioTogical plaus-
ibiTity, unless tissue damage in sone way influences motor neuron
functi-on, perhaps mediated by trophic factors. It has not been
possible to demonstrate a dose-r€sprf,fl5;s relationship (eg in those
patients with fractures, that MND developed earlier); the asso-
ciation is not strong (ie not a common ocurrence in patients); on
the other hand, it could be argu.ed that there is a temporaT
relationship, of fractures with MND (clustered in the years
before syrnPtom onset) .
2. Occupation, environmental toxins and xenobiotics
AII the potential environmental toxins for which inforrna-
tj,on was sought resulted in an OR of more than 1'0 and 95t CIs
did not overlap with unity for exposure to lead and
solvent/chemicals (ie significant at p<0.05 level) ' Cornbining
aII the factors increased the statistical power of an association
between environmental toxins and MND, in a non-specific vtay
(Table 5-9a). However, this result must be interpreted with
great caution as there was no $'ay to avoid recall bias (see
above).
The major nervous systen effects of lead intoxication are
encephalopathy and motor neuropattry. The descriptions of selec-
tive motor involvement and amyotrophy date from Aran2l but
upper rnotor neuron signs have also been described in patients
with lead poisoning3ll. Lead is widespread in the environment'
with large increases in deposits (for example in quiescent
Greenland ice caps) which correspond to the onset of industriali-
sation in the mid eighteenth century and have accelerated since
Univorsity of A';:rl:!rrd l.:] : :Fl-i :, :.,''.i I 'ii;- | a,'
$Cl''l{:'i-i,t t}ir tr,'"1 }ii)'1,FAru(if t.-&,i'j,!Ci(U.*-*.,L,,
130

Chapter 5
the use of leaded petrol2l9. Individuals are likely to have
quite variable exposures314, for example due to occupation or
dietary habits315. The evidence for an association of lead and
!IND2L8,ztr -9.U the possibility of interactions of lead and other
minerals in MND is controversial294 '3L6'3L7 . A role for lead has
been suggested based on findings of increased levels in spinal
cord, muscle, plasma or CSF in patients with l{ND318-321. How-
ever these measurements are likely to be a crude reflection of
the direct motor neuron exposure. other case control studies
have also suggested that lead exposure may be important in the
aetiology of MND322 t323 (table 5-1) with the most recent study
frorn the Mayo grorrp3oS reporting a significant exposure in men,
OR= 5.5 (958 CI, L.44-21.0).
Some solvents are neurotoxic, usually producing a peri-
pheral neuropathy, toxic encephalopathy324 or extrapyramidal
syndrome226. The case reports of MND associated with insecti-
cide u=e227 '228 and a possible association with tolulene
use in Sweden325 and with textiIel39 and Ieather
workersl3S make it conceivable that occupational exposures are
important in increasing the risk for MND. There is no support
from this study to suggest that the consumption of brassicae is
greater in MND patients than controls295 '
3. 80cia1 class and the environnent in childhood
No correlation was found with highest social class of the
patient or the patientrs father. An occupational history which
included manual work had an OR = 2.6 (958 CI, 1.1-6'3)' thus
there is no further support, from this study, fot the possible
correlation of MND mortality with affluence302 '
131

Chapter 5
Although some factors related to socio-econornic deprivation
in early childhood (the absence of hot water or a bath) showed a
trend towards patients being relativety deprived, the evidence
based on this study is weak and does not favour a role of factors
related to deprivation, particularly communicable diseases,
including poliornyelitisr ds playing a part in the aetiology of
MND. These findings are consistent with others who have also
failed to show any relationship to home =p.""288, or polionrye-
litis288-29O '326.
It has been suggested that MND rnay not have a single etio-
logy, but rather, a vulnerable motor neuron cell population is
depleted by a variety of environmental or other factors acting
with age to produce MND as the final common pathway3oS'327 '
The finding that some factors examined in this study have a
Iinited association with MND favours the hypothesis that the
aetiolgy of MND is rnultifactorial and that the environment may be
important in increasing an individualrs risk for the subsequent
development of MND.
L32

gE.E'E E"E'cn 6l -rr-FF6"(\l Firj N a= 6r dt qq
Fi'i-i-oircrl.
E vrat9 E€:s g.Eec*aigt i ia*B- xg,E at Z" EE uE fiHE E: EE aE Es EEegE ea cE 3E ,E E E Eifis gH aE ae EE EeEle Ea g3 iE
.eg rE 9i
Ei Ag $B sg fiE iE$ge fia a$ aA EF Ee Ei
ffiE,e E E
g€ Ei € fis 'EE E
e Ea .E g E
FE f:i gf {gF3i 3fi Ei- psEEE EE ss ssa
c{ ra,C'F
ia,tl
lft FH
d u'ltfF
.E 6€ v,s EE s 6 si,; s. g g €
.99 -.'i o a e
AE.3s; F s =
ogeoe,F 8 A seY F E q EaA*E ; E Es g;5oE 2€-q P = S.1 .1ssn EE E = Es ,=f;&
r.O@
aott|rloo
lfl
F)C F lod :Gt@ roc'r -1ttttlodt 6lo Fde, .{d
^;^6f r.(, FFF
<st ts)\Ocilttttl Fu:IF!dd i6ld
d<. rr|doi6t (\l (\t rt '{
AO i.Clq..i .r;trl d r.)ttltf O d
.< d G. (\l
O\!t trt 6(\it .rt d o
+,<)ct
aTA
(D
Ctrau,
ad
=.ot{F.
<f+
tCr!t FO.{ 6l Gl .v)
o<.co ttF
CtrF
olrt!to|rr
Foto \o o<tCNo
(tre,
6lr{Fcttt\r,
sfC'!olr)6lr
EEat
& -'r.
o
EgeC'
Ea,e
{J-,8adEC: +,Er6o8I8a- qrv
AOE2 3to E:--or*qEvcr-|E5Eoa?(DqE utP8s5
ots68dda!9add tl)B8^d@rEtr 6-
lFl
6 9agt+tv
EatEi
>.BP6C'LoEo-lIac,-,EtEi
afo€.:HC'rILla
d
-2ra.1EIEci
oot6
q
€aIaEil-C'
{Jg9-aC'qloEaJo
I+t-!8oo6(,<tctE6
eO.
Irrlo4JI6e.

o,al,
Evt€oPg(DeotaEHo,-AEI-?d
q)
rftCtr
|'agstla.
g>rA
E+,ao
=C)
Il1oao,
E|i]na
?
t{(-,d.PrttCA
,'ESll*
@et*388Xi-6r;J
os66'El.d fu F .v)oolr6l
.9 e---: EB les E E .a- sgE 2F E'A?afi EE g E:=e; gE € € iE3 _fls siEt i E.€ Ea: E B[+EE-E ;g le E x€9 ii E E= qF= /-Ebt*E E;s6 EEE gaE.^;frE==Eelea. ;;E: EE; ii€f;gEEaa;.FEEE€e:EgE EHg Fs;:E;;E€EsaaEAfiEEEF:geE EEEi$6E:AZEg
an>r€+, E3dr (D
OHO.H3A-sE|<.HElno<+roC)LC) +,-tEE8
Es .eE ts E
E$ Ei e, E* EAg
E$ Ef 3E HE EEE
ag€ E E €=g €.ee * E- .F6i sE
H 1 f;EBEEEE
otE€a.!€Eq,
r5o.A58a5
6lI<t
H
|rl|rl
F(\tt
Fd
.cloA.- Ci
= -:.3.E g
:EEi E *.gE€e E I.1'34'E E 4 E 4E'.g,gE E E a E
C'.4e>i
EEoe6
=gr-(D.9 -B..64
E E .98.rq PP!. + '4 atlr .ag E6
e E'g 83 '4
rJl3(\r(N
|rlavr
\1,(\l
@rOa.t
(vtCtrr(ld
a
@|c,
-^-.:FNe\lt @O a.t !t (w)trtll
NOdd F)ddFad d
ct!<r
I@
o -^-. Cti <f rC,
dCti6lFllll
-lOG)ddHdd
d@(\lo <!6t d cq .\l 6r
€tt6t
@@\oF(v) 6l d (\l
(D
ett&-(DE
-BO'El.d
o6l
!tF
eoro@
rf) oo
G'.9aL.ad-YgE€5 9.9 I* E€ E.€€frggE
aEictiJoFa rJ'l
.Ao.q@g6 rrl
eild
FcitF
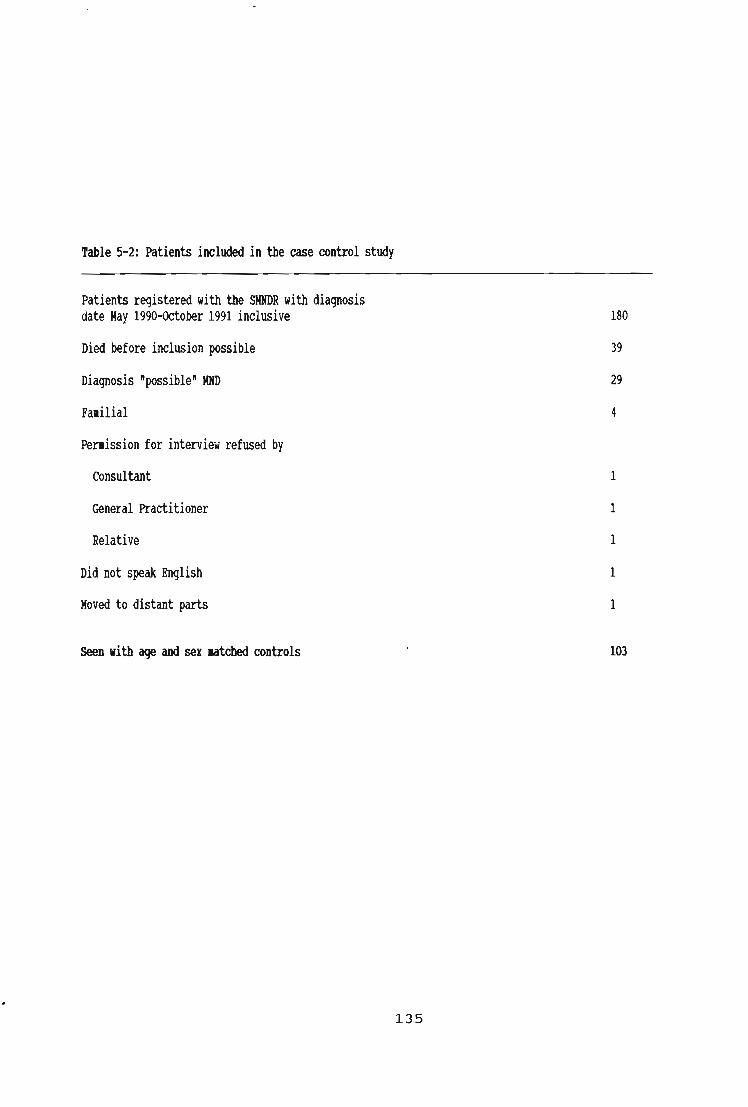
Iable 5-2: Patients inchded in ttre case oontrol sttdy
Patients registered nitl tXe S|IXDR nitl diaEosisdate lhy 1990-0ctober 1991 inclrsive
Died before inclrsion Pssible
Diagosis ipssiblei llltD
Farilial
Penission for inteniiel refused by
Consultant
General Practitioner
Relative
Did not spalr Brylish
loved to distant Parts
Seen rit! age and ser ratded oontrols
180
39
29
4
135

|r'c;
aa ttc2eC|.
r.o \4, c41riltlBtsB9?e':rt oit @|lllllo
'g.H B.€-E-EgD
-lsg g.d .! q,E EIHL.,-l{ooog r|a i|a
s€
EIt.E<-l
ft
.!
A-
(\t <\lt'-t
\l, rO
B.
ts-
E4
ro-
E
!t:E
E
G.l -
E
o{-
eo
(\td
o(3
dF
cro
d(\l
(=t
Fa c"
(tr F)
-tattrC:
Ec,3d!oga.JC)g(l{GaCD
L
E=c,
dF
odoit Gt
odc|t c.t
c'\ r{tNoit
eEtsato<-' C..'
aE8gAclt!tE:.E
.<8g
36
d{Jettrct
dti.966
-l{J
HC'l)aE
d
+,oaI35Eoagci=t.Eo.!gx
€r-L4r!. goaJ
;5.dt€8 ag(,
taqt 4ldsE
a€-6C'6rL.A &.d'a"oI c'Dr.t .A8oA.<-ct .cle€

Iable 5-3b: [atc1ed case-control analysis, all subjects lifetire history of fractue,yes or m (r). nnbers in parentnesis are based on GP records only **
Case and control
Case only
Control only
lleither
lhle
2L
11
15
1{
Ierale
5
L7
6
14
rlI
26 (r2l
28 (261
2L (2Ll
28 ({{)
Odds ratio (CI) 0.7(0.3-1.7) 2.S(1.1-8.8) 1.3 (0.7-2.s)
* Based on best infonation corbining patient,s recall and GP recorG.** pre lg{8/chilrtbood fractures nhich are not recorded in GP notes account for ttredifferences ritb tnre rate. 0R for only GP recorded fractures = L,2 (0.7-2,31
lable 5-3c: XatcDed casffitrol analysis of fractures rithin five years of syrytol omet.
nders in parentlesis are based on @ recods only
Case and control
Case only
Control only
lleitXer
llale
0
7
0
5{
toale'
0
8
I
33
lotal
0 (0)
15 (1lr)
I (1)
87 (88)
Odds ratio o (1.87 - o)
rFracture occurred overseas
0dds ratio based on GP records only = 11 (2'1-506)
8 (1.1-348) 15 (2.3-65{)
L37

Iable 5-3d: Iletails of patiots rittr lil) rbo srstained a fractue rit[in five years of syrytor onset
tge of hacture rechanisromet
69 reII (triP)
35 rell (drunk)
73 Assaulted
79 reII (?trip)
67 rett (?trip)
58 FelI fror roof
73 reII (trip)
{8 Road traffic accidmt
?l Uncertain
5s reII (triP)
27 tssaulted
72 rell (triP)
60 FeII fror roof
70 Road traffic accident
56 FeII fror roof
Practrre site
Bilateral Colles
Right CoIIes
hrltiple ribs,Rigbt rctacarpal
lfasal bones
Rigbt first retacarPal(corpund)
Right lateral ralleolus
Icft distal radius
Ieft Tibia and fibula
12tX tXoracic vertebra
Left Colles
llandible
teft CoIIs
3 ribs
Icft tibia and fibula*
Right tibia
Site of llID omet
Dysartiria
Riqbt band
Uysphagia
Dysartiria
Rigbt footdrop
teft band
Inft band
Right footdrop
Ri$t band
Dysartnria
Right footthop
Ieft leg
Right hand
night footlrop
Rigtt leg
Intewaluntil lltD
I ronti
I ronth
I ronttr
I rontl
3 rontis
6 ronttrs
10 rontis
11 rontls
25 rontis
30 rontis
3{ ronttrs
39 rontis
{8'rontb
50 rontXs
54 rontb
* All fractures above recorded in GP records, except tlis (occtrred overseas)
138

table 5-t: Distrihrtion of iniuries reqrriring dicaf attention, by case, control and nrnber of injuies'CoDines inforration bued on patient's recall and GP recorG.
nLber of iniuries
--j 0 1 2 3 | 5 7 8 lotal
Case272919910720103
Control 33 28 2L 13 6 I I 0 103
Chi sguare value 1.4, DF= 7 (ns)
rable 5-5: Distrihrtion of operations requiring gneraf anaetbetic, by case, control and nrnDer of operations.
&Sines inforration based ol patient's recall ard Gp reorG
nder of operations
0123158lotal
Case 15 35 20 19 5 5 0 103
Control 13 35 22 19 9 2 2 103
Chi sEnre value 5.7, DF= 7 (ns)
Iable 5-5: Blectric sbocfs (patient recall)
Ies Io
Case 8 95
Control { 99
Chi sErare l.{, DF=l (ns)
lable 5-7: Blood transfrsion (patient recalf)
Ies no lotal
11 92 103
15 88 103
Chi sErare 0.7, DF= I (ns)
L39

o"
Iro
6t
I@et
!t
.A
@
ooilIqI
rfl
CA
I@et
c)!t
H(.)J?|f)CA
ogthEa
oo6tcta"NO
c)@F(llPE
=tEcrSS
EE6618
sIG'lxe
tqE
(ta,6a
bgtsEc€55 ic, R ..' I
EE '..eE E E EggEE
F)rloI
rat6t
4gP$RcR
oC2
EagaE
5E
EE+.C'6
->.A
eFI
E5IEIEo{JTi.Aon€
etCA
I(tetct6l
lr!olo
e
H(J6Pratcn
o+)gqA<ta
ga9."r@!tR
isP...'
€>.8>..EEEEE$$E.E

table 5-gb: Details of 19 patients rit! tilD in sor lead erpoore ras reported over a perid of rore than 12 rontB'
Age Ser Details of lead erycure
65 [ale Plurber and labor[er. Jointing and relding of lead pipes.
17 llale labourer and driver. [andling lead in roof nork'
17 llale Drain layer and labotger. Reroving old lead pipes and fitting new'
55 tlale Electrician. Stripping and handting cables often rith lead.
59 llale Driver. Unloading and loading of lead cased containers and barrels'
50 llale Plruber. Reroving old lead pipes and fitting ner'
57 llale Roofer. ortting and fitting of roof flashing.
76 ltale Painter. Stripping and application of lead paints over several years.
{0 tlale Sbipni$t. fitting of lead sheeting in boats'
59 ltale thintenance engineer in a gas uorks. Jointing, uelding lead pipes'
62 tale Etestrician. [andling of lead cables.
55 lhle laDourer. Rooving of old lead pipes for ner'
65 llale Scrap retal dealer. [andlittg of sctap lead'
67 llale Roofer. ortting and fitting of lead flasbings'
60 llale tlecbanic. Soldering and bandling lead raterials, car fure erposure'
73 Ferale Fonn&y and retal rorker. florking riti lead Hterials.
56 lhle Glazier. Icad strip rrsed over rany years to supprt glass during fittittg'
75 llale lypesetter. Inad rat*ials.
63 llale flire rope raler. used rolten lead in galvanising shop.
llotes: Reported erposure in six controls of a sirilar nature to ttre above (see table 5-9a)'
L4L

@
I
ct
Cfr
e
t-
o10d
|r|N
I
o
\rt
Iu1ocnct
c,o?|rlc
o+,g.A€a
?EI-{E = = E E
kg*a,€CDlf)FFrt-€.N
',:? ':
Fact ctr rfl ctr ct={cit
6Eactt
2 S R R S
E>.8 >.E€-lF 6E,E(DQr+r+,sss E
o.L
at{C'or{g.G'd
{J
E9.
s-,
tc-(taJotcd
+aC'oF.FIde4e+t6*IEEaJsct,Ao€€

C)
llcaagtoAo-=!
ao
$tlcaogIttRcl-=(,
TESRSTEFF
uuls
altC'roIIc
rof,ctclC)
o-=I
ro
t,ifc(\|(o
oooE6olc5
6
toct6€(tt'.LoctfG)uo()trof6LCLoIt.ClItc6-o(,a.Eoo(EL
=.B ai- !t=arC'=LLncLxoxtt.tsllEF'6.jttcco63OEosFti tt.Z?
;jI
u)Etlr
o6|

o==
?PoctroY
9no9!
fi*
€*
fte
;€
fie
€3
roT
ci,ct(o!t
EtroC)
I
c,otou,6C'
r//AW
olHootrogoolt6l-o=oEO -AHHh6EEs 9eg sF?Jps
?,tu 6E9 EE9 ;,T IF L
=- 6Ee sEgg!t.9oEE5c,:lF
E9-AE6Act6CD
lr

Fig 5-3: Odds ratio for a fracture occurring at variousintervals before the onset of MND symptoms
16
14
12
10
8
6
4
2
0<5 <10 <15 40 <25 <30 <35 <& <45 >45
Interval (years)
.9(UEottIto

CIIAPTER 6
THE PROGNOSIS OF I{OTOR NEURON DISEASE
L46

Chapter 6
INTRODUCTION
,, Two years before [in 1953) I had been diagnosed assuffszring from ALS comnonly known as Lou Gehrig'salZ]it" "t motor neurone diiease and given to- under-stand that I onTy had one or two more yeats to live"',
Stephen W.Hawking, Lucasian profess^og of Mathenatics'Canbridge University, written in L988-"
There have been many retrospective studies of prognosis
in MND, usually in conjunction with incidence studies, and some
are population based. Two prospective studies are based on
patients referred to tertiary care facilities (table 6-1) ' De-
spite agreement on a generally poor prognosis for this disease
the conclusions of individual studies differ in a number of
inportant respects. Survival predictions can be hazardous, as
illustrated by the opening quote and several questions remain
unresolved or in doubt concerning the prognosis of MND:
(i) can reliable predictions of outcome be made based on
clinical features at presentation or during the course of the
illness? Reference is still made to the rrvariable outconerr of
this disease and while it is generally agreed that PMA has a
more benign "orrr="335 and that the presence of PBP is a poor
prognostic signloL,256,336,337, some studies have failed to
demonstrate any clear prognostic variables and estimates of
median survival, even for patients with a combination of upper
and lower motor neuron signs, vary frorn 48 months338 to L2
nonths256 from diagnosis (table 6-1).
(ii) Is old age a poor prognostic variable and is age an
independent risk factor, or does the increased frequency of PBP
in older patients account for the suggested poorer prognosis with
L47

Chapter 6
increasing ug.339? Some studies of selected patients255 '340
contradict the more widely held view that increasing age is a
poor prognostic factor.
(iii) Is their evidence for a subgroup of patients with MND
who have a prolonged survival? Estinates of 5 year survival vary
from 4-4O293 '34L and observations of rrresistancerr to progres-
sion for some patients have been made48.
Un1ike acute medical iLlness such as stroke, there are
difficulties in obtaining precise estimates of a time of onset
for a disease of insidious progression, while prognosis based on
date of diagnosis may vary with local practice. Predicting
outcome related to the clinical pattern of MND is also hindered
by a lack of internationally accepted diagnostic criteria, confu-
sion in terminology, or by too srnall numbers in some studies to
show any difference, should this exist88. These factors can
be improved by a prospective, population based study of weII
defined patients and aIlow reliable predictions based on present-
ing features and progress. There are no such studies to date
which fulfil aII these requirenents342 lcnapter 2l '
IIETHODs
Patients
This analysis of survival relates to all 229 patients inclu-
ded in chapter 3. Follow up was complete for a mean of 2 years
(range 1-3 years) . 57 patients (252) had been seen in person, as
part of the case control study, and 842 by a SMNDR collaborator'
At the tine of data censoring (January 1st L992) there had been
L44 deaths (72 rnales and 72 females) '
148

Chapter 6
statistical netbods
Data were collected and surnmarised using Dbase IV, a data-
base nanagement system for microcomputers (Borland Inc. ) for
subsequent analysis with The Statistical and Epideniological
Research Corporation (EGRET) package for survival analysis using
the Kaplan Meier techniq.r"343 arrd Coxrs proportional hazards
model. Calculations $tere based on day zero of follow up as
either (a) the date of onset or (b) the date when the diagnosis
had first been suggested as likely or probable. Patient groups
were analysed overall and according to d1e, sex, and clinical
subtypes as defined in Chapter 3.
Except for time zeto, the numbers at risk, included below
the survival curves (figures), for any given tine of follow (eg
I year, 1.5 years etc), are an approximate for that interval'
This is because the Kap1an-Meir statistic generates survival
intervals in fractions of years after each ttfailed[ individual.
Hence the quoted figures at risk represent the number at the
nearest tirne interval generated in the calculation before that
which I have plotted on the x axis and, at longer periods of
follow up, are over-estinates. For examPle, for survival by sex,
the number of nales at risk 4.8 years from synpton onset was 11
and at 5.2 years was 8. The number plotted corresponding to 5
years of follow up is 11.
L49

Chapter 6
REgULTg
FoIIow up was complete and survival curves are included at
the end of this chapter. The numbers at risk for any given tirne
of foltow up are included below the curves to further allow
comparisons of numbers on which individual curves are based (see
above). The numbers in each group at tirne zeto are also included
in table 3-8.
The overall 50? survival from onset was 2.5 years (95t Cf,
2.2-3.O years) and from diagnosis L.2 years (95t CI, 1.0-1.4).
There are no differences in the overall conclusions of survival
curve comparisons according to clinical and denographic vari-
ables whether curves are calculated from the time of onset or
from the tine of diagnosis.
There were significant differences in survival with poor
prognostic factors for: age (>55 years, P<o.oo1); gender (female
sex, pco.O1) and clinical pattern (PBP, P(O.OO1). PBP remained
a poor prognostic sign, whether considered as the presenting
feature (initial diagnosis PBP; PBP/ALS), or as a component of
the illness at any tirne (final diagnosis PBP; PBP/ALS; ALS/PBP) '
This conclusion is not altered by comparing patients htith PBP
with those $tith purely spinal disease (ALS) ie removing patients
nith PMA, who have an overall good prognosis (p<.005). cox|s
proportional hazards model showed that the difference in survival
between the sexes was accounted for by the greater proportion of
females with PBP, although age rernained a significant variable
(pco. os) .
Five year survival estimates can only be based on time from
s)rmpton onset at this stage of follow up. Overall 5 year survi-
L50

Chapter 6
val fron onset hras 27.7* but the small numbers at this tine of
follow up result in a large degree of uncertainty with 958 CI for
this estimate = 19.98-35.0*. Five year survival htas considerably
Iess for patients with PBP as the presenting feature (PBP;
PBP/ALS) = 3.5? (95? CI, O.O-15t) or for patients with PBP as a
component of the initial diagnosis (PBP; PBP/ALS; ALS/PBP) :
10.6? (95? Cr, 3.8*-21.48).
There were 15 patients on the SMNDR with survival for rnore
than five years from synptorn onset. Five had PMA subtype, 10 had
ALS as the initial diagnosis and in only two did PBP develop,
both in the few months before their death shortly after the
censoring date.
DISCUSgION
The interpretation of the figures relating to the clinical
subtypes is highly dependent on the way physical signs are used
in the classification of patients. In this study, preserved
reflexes in the presence of a corresponding wasted myotome were
used as evidence of UMN involvement and therefore such patients
were classified as having ALS included in their subtype (ALS;
ALS/PBP; PBP/ALS). In any event, there may be little pathologi-
cal basis for dividing sporadic MND into subgroups given the poor
correlation between clinical pattern and pathological distribu-
tion of the lesions47,48. However, appropriate classification is
important to standardise patients for prognostic studies and
planning treatment trials344.
Fanilial cases (n=11-) were not excluded from the survival
analysis as previous studies have Suggested, and this sample
r.51

ChaPter 6
confirrned, that their survival does not differ significantly
frorn sporadic adult onset MND and demographic and clinical fea-
tures are stronger predictors of outcome than whether the disease
appears to be inherited345. It is possible that patients who
are older at diagnosis were identified at a later stage of their
disease and hence have an apparently shortened survival but the
difference in survival according to age is also observed based
on time frorn onset so this observation is likely to be real'
studies which use retrospective approaches, or are based on
referral centres, are more likely to be biased towards younger
patients and produce much longer estinates of survival338'34L' A
study design ensuring complete case ascertainment is of major
importance when estirnating prognosis in MND'
My findings are similar to another population based, but
retrospective study in Denmarkg4 '256. Christensen et al de-
scribed 186 patients identified from hospital discharg€sr
including geriatric units. 1l't were from outside neurology
departments and the mean age of this cohort (65.9 years for rnen
and 62.4 years for women) makes significant ascertainment bias
unlikely. The nedian survival of this group vtas 12 months (95t
cI 1O-t-4 months) from diagnosis (23 nonths from onset), the 3
year survival L2z,5 year survival 4*. Otd age and a bulbar
onset were poor prognostic factors'
with respect to the questions posed in the introduction,
these results suggest that: (i) In weII defined cohorts survival
can be predicted with a high degree of confidence, that (ii) the
higher rnortality rate in females is largely related to the in-
creased frequency of PBP, but oId age rernains a significant
independent poor prognostic variable. (iii) As far as longevity
L52

Chapter 6
with tt{ND is concerned, aII survivors beyond f ive years from
symptom onset presented with PMA or ALS, without PBP, and in
only 2 did PBP develop, Iate in the course of the illness'
Reports of patient rrresistancerr to progression in ALs48
with 5 year survival of 2OZ are likely to be because the dis-
ease remains confined to spinal segments (numerically a much
smaller group) or to referral bias of atypical cases' Three of
the four patients surviving for more than 5 years in the study by
Christensen256 did not have bulbar symptoms until the fifth year
after diagnosis.
Clearly the clinical pattern of disease is of major inpor-
tance in predicting outcome from MND and needs to be considered
when making decisions about patient management, advising those
affected with this disease and planning treatrnent trials344 '
153

FctF-(D'q\rt-(-'<'=E=3=gasEFro_ t-l
rOtf
gB.E<DE
'E3 Ee €g ",E i 5 r 5 6- c)
EF EEBse: sae.EE^E;EE: EE;HA.E€E:EEsFe. E s
;H gB;EeFHsEeaAaFaErs
.9vt91T Ea fr* -a.Age E.E ee <' cr-'!
!. L. = a. 'd'4 e t=rtrtr a v, 6o;; ;; F X* s a s s€ a R ss Rc.t Kl
o4
5ts-B.EE E=8.- Ig 8€ AS'ilE $ =9 a
*lfr6t
o Ctr6l arn
*cf€d9@AI@GI
1Ac,> a
rA tnot q)t- sgs v,c,
Fc2
FA aasa
I 99 e299
Ctr@
;' a= e66dde e e 2 2 g I I g g e
Egg s
ooH
aho>e2ee
e
orte:g3oR=a6o.rFld
GIororr|I =E
o{JttEa,viHsI o.H
a l.+,
5Ee
g
to g3
g--! rao5-rt
a
iEI,>.
tasE
46
i2o
G-gl
F.43c,3
+tE6ata
tIF.rat
eT
gH
{J
a
oEraB
T
L9EECr. O
3cE
;o+tI-leCL
aHctra3lx
ataobEctA
{Jo.1
Or,AagooBooCtiIctre.1eFIttra€ecr.
-t
dil€c2
ctC'taga!a
E-,Fo.
.HC'oo
Evtt
FaItoct4.cltEC{

q;
gao,.HO1l +rA.H (\I
tro(Do
-t .-. Pt6.d O.F-EEts-dgE- e3t2-.dg
=,3 rn+,,-(D.dCrq)'8E>r.! Ov,8E-,g3gC'e.(DP .b>. F{ L{rh Gt>>r.E' .d L{
E B.g= =P(,tkuto.a ClpEr^a6 E:UIL.Oor(DE EEa6 Ei .l'E-g-+, llr{a6+rorO Ot-4Ci=A(H (D
P(D= r-teR g.:98!=QJ .4c2-,!.9 d5 9..8'ii I-F??tt.J Fa 6lE.E-
Ul .d O,.9E6E HA-rnoB+t C)
E Ctr >r,tt E: dE.d L;E E*8-..<,Ld66Og a,3=t = attsgE8-,8rarS rr.E€^od=rkv
to rfl F|f!lftttH-) oil (Yt d
c40c u.)Hd-)d
ctit:(t@@F-Ft@(l(v)o a.)o(\1 ts)d
9Eg = -") $b x; t e 2 q-^ E E: Ei= E € € gE I sd rt 'i A ."' -g --rj,-. HF ; ;E gEE s F s-. e. H 5E: EE E 6i,:g; e E E Es FE B E6'E Hur e ';'= a
Ea; aEEg: iEiE€EEE$ =E*EET E E}E ;E ;fi g ESEA Ff g; AE FE5 ! = d g E& o,dr ta ?>€g.€ -e H E E Eg E$ g gli f;a eE gH .€t h
rf)6l
-t6l €6l
d€a
d9d€dPe|rl*arldHOFIV
o (\to(rit
!f6l 6l
(vt(\I
ano>.
((\r
<. tt q, rt@Gl6t 6t + st<tF avt
ut.4aaoE13.U
.d€IslL
\Cl F (H(v) v
a3*4.4 A
lho,E>.
ltto-.Ao>.
r.(, @
EEEE:x s sg
\atrlrl SGBBB
o= e e I e e eSe o-
3-Ad?l) s;.| .f E >'Fl
=+a dq-i=,rlr .- E .-!^A^ E3 O -!E ,+. E !p s.d
tr c Fcqf -, = SE G!d f! tr.tro+H \.o rtt
3..dr ^o A.t' {) dd E&i 6 dg 2 egE= g E c e
o-o=
dcl6V, ]dE9gezE
t'@
ct!<tl<,@rr|
rtFct\ c.)@
Frr)rfttrl .t F ct! 6l
<'6IOFcoFl

The Scottish Motor Neuron Disease Register 1989'90Suruival from diagnosis, all patients
Survlval from diagnosls by sex
No. at rlsk(See text)
y2 .7.7 p<lo.Ol
F-----------------+-----------------{------------------}-----------------+---------------'l9767482417e
No. at rlsk

The Scottlsh Motor Neuron Dtsease Register 1989-90
Suruival from diagnosis bY age
No. at rlgk
Suruival from diagnosis, progresslve muscular atrophy
72 .12.8 F0.001
F-----------------+-------------t------.---------.1----.-'...-+'----'--'--1pq i7 56 it 18 7a
'72.9.4 50.005
Years
l-----------------+-----------------{------------------}-----..--""""+"""..""-'4zig tit tis io 35 21
No. at rlsk

The Scottlsh Motor Neuron Dlsease Reglster 1989'90Surulval from dlagnosls, bulbar palsy at any stage
No. st dsk
F-----------------{------------------f ----------------}1----------'-+----'----------{rfu titg is .l 24 15
ts----------------+-----------------t----------------'-l---'-'----------r'+-------'-'-_--''ric rirs ig it 24 16
PBP Or PBP/ALS OT
ALSPBP (Flnal dlagnoell)
Years
No. at rlsk

The Scottish Motor Neuron Disease Reglster 1989'90Surulval from dlagnosls, bulbar palsy at presentatlon
E.:?fo*
No.atrlsk rss rio uig dt 36 25
l---------------+-----------{--------------}--------------+---"----'{ig,isie12s5
72 t 15.3 p<0.001
ALS olALS/PBP
(lnltlsl dllgnodt)
a2 .8.9 p<O.OOi
Years
Years
F-----------------+-----------------{------------------}--------------+------------1Tg,is28 1255
No. at risk

The Scottish Motor Neuron Disease Register 1g8g-90Suruival from symptom onset, all patients
tlo. at dsk(see lexl)
Surulval from symptom onset by sex
X2 r 7.6 p<0.01
-t---------+-----------------r------------------l---------------+-------------{e7 86 {e 2s iz iz
No. at rlsk

The scottish Motor Neuron Disease Register lggg-g0Suruival from symptom onset by age
EEtJo
"{
No.8t rlsk
sullval from symptom onset, progresstve muscular atrophy
72.f.2 p<0.OOl
No. at rlsk

The scottish Motor Neuron Disease Reglster lggg-g0survival from symptom onset, burbar parsy at any stage
ru-.:E:ta
"{PBP or P8P/ALS orALVPBP (Ftnat dlagrrcetr)
No. at rlsk ?
E.:EJ1r,
}s
PBP or PBP/ALSor AL9FBP (Flnel dlagnorle)
r$i------------lir-------#------3?-----T;-------iNo. at rlsk

The scotfish Motor Neuron Disease Register lggg-gosuruival from symptom onset, bulbar patsy at presentation
o
EJos
l.lo. at rlsk
72 o24.8 p<O.OOl
ALS orALS/PBP
st"l---, PBP o. P8P/ALSt1 (lnlrtrl dtagnodr)*----L_
72.35.7 FO.OOI
z5.------S-------S-------ii-*---*i------------{No. at rlsk

CEAPTER 7
collctJugroNs- uArrNG ugE oF TrE roRK rNcrruDED rN rErg TIIEgrg
L64

;" Chapter 7
" The best test of a physician's suita.bi rity for thepractice of neu_rorogy- i; not his "iiiity-i; ^Z^ori.""inprobabre syndrom66 nut whether i"-""n continue tosupport a case of motor neurone disease and keep thepatient' his reratives and hin"Ji-i" a reasonabrycheerful frame of mind.',
Professor w. B.Mathew s352
" r tealised that a man's interrigence is not the surnof what he knows but the soundnes i of his iu-ageieit ofpnopre and his po*er to understand ""a
-Lo nLq- ii;;. "
Yevgeny yevtushenko353
r have highlighted the need for standardised diagnosticcriteria for l{ND. Arthough there is no rear difficulty inrecognising the disease at an advanced stage, there may be con_siderable diagnostic uncertainty at presentation to nedicalattention and there is confusion over the terninorogy used todescribe MND' Accurate diagnosis is essential if patients are tobe advised appropriatery, epidemiorogicar studies are to becompared usefully and well defined patients are to be recruitedin treatment trials. This study outlines simpre but conprehen_sive diagnostic crj-teria (chapter 2) which take account of varia-tion in clinical pattern at presentation and it is hoped thatthese criteria, which do have prognostic significance (chapter6), can be applied in future studies of MND.
This thesis has examined the traditionar concept of a uni-form worrdwide distribution of MND (chapter 2), highlighted thedifficurties in comparing popurations and thus rnight provide ani-mpetus to further studies of MND distribution, for exampre inirnrnigrant populations frorn deveroped countries or a search forclusters based on rarge numbers anarysed using snall geographicalareas.
155

Chapter 7
rnportantry, the SMNDR has developed a nover approach tostudies in MND by, for the first tine in this disease, prospect-ively recruiting population basec patients and enabling studiesof incident patients during rife (chapter 3). There hrere practi-cal difficulties experienced, particularly in tirning appropria-tely the invorvement of patients in studies, other than sirnpleregistration, such as the case-control study, dt a stage whenthe diagnosis was secure but that distress was not caused byapproaching moribund patients. The often aggressively deter_iorating course of MND also means that it is difficurt to includesome patients from distant regions in studies during rife.However, with an inforned corlaborative group, it was possibreto conduct this study of MND, in a relativery short space oftirner orl a scale which would be difficult for individual orsnall groups of neurorogists. This irnportant property of the
'MNDR may be usefur when considering treatnent triars.
The measurement of incidence afforded by this study isnecessary in placing in perspective the importanee of a particu-lar disease for delivery of health eare and to enable charities,such as the scottish Motor Neuron Disease Association, to promoteits interests and those of its members.
Traditionalry, studies of MND have reri-ed on statisticswhich are not rfpurpose built" for this disease ie retrospectivelyexamined norbidity and mortality data. This informatiori is proneto error due to nisdiagnosis, false positive coding and changesbrought about by the periodic alterations to the rnternationalclassification of Diseases used for coding. r have been abre toanalyse in detail the utirity of these data sources so thatbetter use and interpretation of studies based on this inforna-
L66
Chapter 7
tion is possible (chapter 41. However, such results must beinterpreted in the light of rocal practices which rnight differfrom systems enployed in Scotland.
rt comes as no surprise that in many patients there is noapparent cause for the disease. The case-control study (chapter5) identified a number of factors of potential inportance in thepathogenesis of MND, which crearly cannot exprain the totatityof MND' but which rnake a contribution to the weight of evidenceaccumurating from other epiderniological studies and may shape theapproach for basic neuroscience research.
Patients expect an honest but sensitive expranation of thenature of their irlness and what to expect frorn it354. r wasable to provide useful prognostic data (chapter 6) based on thediagnostic crassification system and so the contents of thisthesis have direct clinical application for the practising neuro-logist who is pranning patient management. r have arso been ableto review part of the differential diagnosis of MND as itarises in routine clinicar practice (tabre z-L and appendix A).
Not included in this thesis, but mentioned in the pubrica_tions list, hrere two laboratory based projects which were insti-gated or supported by the SMNDR and my work.. Firstly, a study ofantigangrioside antibodies in conjunction with workers in theneuroimmunorogrical laboratory at the rnstitute of Neurologicalsciences, Grasgow, examined the potential rore of anti-GMl anti_bodies and paraproteins in the pathogenesis of MND. secondly, rcorlected blood from some pedigrees (appendix c) to assist in thesearch for a genetic marker in famirial MND.
on a personal level this study has been important, not onlyfor learning methods in observationar epidemiology but for
1,67

Chapter 7
future clinical practice. This thesis has not discussed thehuman suffering to which r have been witness. Motor neurondisease is a tragic affliction which combines many of the mostdespairing features of irrness. rt can affect young adults withdependents; it is an inexorabry progressive terminar disease forthe majority; there is loss of independence and regression to anexistence which requires herp with feeding, toireting, washing,and the most sirnple of tasks, such as relief frorn an itch or anuncomfortable position. rt is frightening, especiarry when dys-phagia or respiratory failure develop and many patients becomelonely, bored, frustrated, angry or depressed. Despite theseobstacres, r have been struck with the rernarkable emotionarresirience of many sufferers in the face of such terribre circum-stances.
Arthough it is possibre to read about the feeri-ngrs ofsuffere"=355, who vividly portray the isolationSor356 andnihilistic approach of many doctors3iT, there can be no sub-stitute for the experience of patient contact and the ressonsinherent therein. This work has taught me much that is not con-tained in the preceding pages, particurarry about the probremsand nanagement of neurologicar disability ?nd that synptornatictreatruent, often rerativery sirnple in nature, combined with humancontact and support, can go a long way to easing the burden ofthis incurable, but not untreatable, disease.
168

APPENDTX A
SUlrUARv OF TEE CLINfCAIJ FEATURE8 OF 28 PATIENT8 REcTSTERED rfTETtrE SCOTTISH I.TOTOR NEURON DTSEASE REGISTER BUT EXCI,UDED FROTI TEE
UErDr ANAIJYSES
L69

Appendix A
A. PATIENTS WITH CLINICAL FEATURES OF
COEXTSTING ilEUROLOGICAL DISEASE (n=8).:.i
Hlf, fenale age 78, SMNDR No: ?.
rnitiaT diagnosis: pBp/ALS
Twelve nonth illness to death with mixed pseudobulbar andbulbar palsy' generalised wasting and fasciculation and patholo-gicalry brisk reflexes- There was an asyrnmetric intention tremorin both upper rinbs. Ncs/Evrc: compatibre with MND; cr scannormar apart from prominence of the ventricars and calcificationof the basar ganglia. Progressive deterioration in both motorsystem disease and her tremor. No autopsy.
FinaT diagnosis: MND with cerebelrar signs. possible roultisystem degeneration.
EE, nale age 93, srtNDR No: Lz. Referrar: corraboratorInitial diagnosis : ALS/pBp
sustained a rnild right henisphere stroke which recovered andhad a long-standing weakness of the I'eft arrn which appeared non-progressive. Then a 5 year history of difficurty walking andswarrowing with nasar regurgitation of fruids. past history ofcarcinoma of the colon. Examination showed dysarthria and bovj-necough, deafness, but no fascicuration of the tongue. He had adropped left shoulder with marked wasting of scapurar and pector-ar muscres on that side from c5 TL. Fasciculation in deltoidand small hand muscres, normar tone throughout and norrnal po!,rerin the rower limbs. Absent biceps and supinator reflex, brisktriceps and preserved lower Iimb reflexes, absent vibrationsensation at the ankle, sensation otherwise normal. Ncs/EMG:
I,IND BUT IIIIO EAVE OTEER
Refeual: Collaborator
L70

Appendix Anormal nerve conduction studies but notor unit potentiarin the left biceps, brachioradialis and right first dorsalosseous (FDI). Since then a very gradual deterioration insymptoms and in rinb weakness. Forrow-up continues.
Finar diagnosis: uncertain, excruded because of ronging neurological signs making diagnosis uncertain.
changes
inter-bulbar
stand-
rA, fenale age 56, SMNDR No: 51. Referrar: collaboratorfnitial diagnosis : pBp/ALS
27 months ilrness to death. presented with progressivedysphagia and dysarthria due to a mixed pseudoburbar and bulbarpalsy with normar rirnbs apart from brisk refrexes. A cr scan,EMG and csF were normal at this stage but cK was elevated at 3o7.26 nonths after the onset she was anarthric and disinterested,withdrawn, inappropriately euphoric and thought to be demented,creutzferdt-Jakob disease was considered. she continued to deter-iorate, rower motor neuron signs appeared in the upper rirnbs andshe became breathless.
At autopsy the cerebral hemisphere showed mild to moderateglobal cortical atrophy with accompanying ventricular dilatation.There were no focar abnormarities identified. sections of thefrontal cortex showed focal degenerative changes in the outerIayers of the grey natter with slight gliosis. The central whitematter was also gliotic and showed perivascular accumurations ofpigment laden rnacrophages. The white matter in the frontal lobestas pare consistent with a slight degree of corticar degenera_tion- These changes s/ere not apparent in sections frorn theoccipitar and tenporal lobes which were virtuarly normar inappearance and showed no spongy change. There were no Alzheimer
L7L

Appendix Adisease changes and no Lewy bodies identified. The medullashowed degenerative changes in the motor nuclei of the floor ofthe 4th ventricre confirmed by the presence of ubiquitinatedinclusions in these neurones. The cereberrum was normar. Thespinal cord showed a variety of degenerative changes in anteriorhorn ceIIs, including chromatolysis. some of these cells con-tained intensery ubiquitin-positive incrusions. Anterior rootswere somewhat shrunken and there was pallor of nyelin. peripheralmuscle and tongue showed denervation atrophy.
Final diagnosis: Motor neuron disease and dementia of front-aI lobe type with non-specific frontal lobe degenerative changes.
ET fenale, age 91, SlrNDR No: ?8. Referral: corraboratorInitial diagnosis: pBp
23 months ilrness to death. presented with progressivedysarthria and dysphagia with choking and drooting. past historyof gastric carcinoma. Exanination showed paralysis of tongue andpalate with only occasional monosylrabic words possible. No
wasting or fascicuration. Jaw jerk present and rinb tendonreflexes brisk and syrnmetricar but with no motor or sensorydeficit in the 1inbs. cr scan showed atrophic changes particu_larly in the posterior fossa; csF protein rnirdry erevated ato.88 g/r; Ncs/EMG: widespread neurogenic abnormality. progres-sive course, mentar function difficult to assess in view ofcommunication difficulties but not clearly demented. Developedwasting in both hands and quadriceps with weakness and patholo-gically brisk reflexes.
Autopsy showed rnild cortical atrophy and ventricular dilata-tion with anterior spinal nerve root thinning. Microscopical
L72

Appendix Aexamination showed a generalised loss of nerve cells accompaniedby reactive griosis, numerous senile praques and neurofibrilrarytangles. There vras pronounced rc,ss of rarger neurones in theregion of the motor cortex but nerve celr loss in the bulbarnucrei was less pronounced. Numerous Lewy bodies were identifiedwithin pignnented neurones. A small focus of lymphocytic infil_tration was noted within one of the fifth nerve roots, accompa-nied by focal denyelination but no evidence of inflanrmation else-where in the cNs or peripherar nerves. sections of the spinarcord showed patchy ross of anterior horn cells with negativestaining with ubiquitin. The gastric neoprasm showed an infir-trating moderately differentiated adenocarcinoma without rynrphnode metastases.
FinaL diagnosis:Lewy body disease and
disease?).
MND syndrome with pathological evidence ofAlzhej-rner disease changes (rnulti_system
EP, fenare age 52, gurIDR No: L2z. Referrar: corraboratorfnitial diagnosis: ALS (2 regions)Presented with a 6 month history of slowry progressive
difficutty walking and widespread rirnb cramps without sensory orbulbar slnnptoms. on examination there was a slight tremor of thehead and a rest tremor in the right hand which was ar.so presentin the outstretched position. she rooked a little bradykinetic.No burbar signsr Do wasting. scanty fasciculations in the quadri-ceps, weakness of the entire right leg except the quadriceps,particutarly affecting distal muscres and brisk reflexes through-out although the right ankle jerk depressed cornpared to the left.Normal sensation. EMG: cornpatibre with a diffuse disorder of
L73

Appendix Aanterior horn ceII origin. rn addition there was an abnormalityin the right peronear nerve, suggesting a co-existing lesion atthe right fiburar head. Normal myerogram, csF and protein elec-trophoresis. Probably slow1y worsening and appearance of burbarsYmPtoms.
Final diagnosis: MND with extrapyramidal disorder/parkin-sonism.
ar[c, male age 6L, StOlDR No: 161. Referral: collaboratorfnitial diagnosis : Multisystem atrophy13 month illness to death. commenced with slurred speech and
clumsiness of the reft side with unsteadiness of walking. Exarni-nation showed gait ataxia, dysarthria, reft upper motor neuronfacj'ar weakness and striking left sided ataxia with a rnild leftheniparesis and brisk reflexes with increased tone on the reft.rnitiarty thought to have a posterior fossa mass resion lying onthe reft side within the cereberrun perhaps with hydrocephalus,however cr scan normar. He deteriorated with the appearance ofwasting and fasciculation particularry on the left as well as hisprogressive pseudobulbar palsy. There !,ras no evidence of demen-tia. cr and MRr hrere normal as were EEG, csF, extensive broodtests and neuropsychology. EMG: typical of MND. Trial of sine-met was unhelpful. His disease progressed inexorabry and naso-gastric tube feeding was considered.
Final diaqnosis: Multi-system degeneration combining predo_ninant rnotor system disorder, extra-pyrarnidal and cerebelrarfeatures.
L74

Appendix A8C, nale ag€ 66, SUNDR No: 2O{.. Referral: gf,Ipg
Initial diagnosis: ALS (3 regions)L3 month illness to death. Presented with a 5 nonth history
of dragging of the left leg with a tendency for it to give hray
and then a progressive deterioration in gait with wasting of bothhand muscles progressing to generarised weakness but no cramps.on exarnination he warked with a spastic circumducted reft leg,had a mild birateral spastic paraparesis and fasciculation wasplentiful over the upper arms and the right EDB. There was grosswasting of the left side of arr intrinsic hand nuscles, the peri-scapurar and forearm muscres and both quadriceps. sternomastoidweak, brisk asymnetric refrexes. He had a recognised, rongstanding pigrnentary retinopathy (pR) and poor dark adaptation.rnvestigation revealed a high haematocrit which proved to be truepolycythaenia and a marrow trephine had features consistentwith, though not compretely diagnostic of, prirnary porycythemia,he underwent venesections. csF was normar as were biochernicaltests. He had an enrarged spreen but no evidence of a hyperne-phroma' Ncs/EMG: prolonged F v/ave latencies and srowed motorconduction in the right peronear nerve (37 m/sec) with smarrcompound muscre action potentiars but normal sensory studies.widespread denervation was observed affecting upper and rowerrimbs but the overall eLectrophysiorogicar diagnosis was of anixed axonal and dernyelinating neuropathy. An electroretinogranshowed a normal lrtave form with only rnildly reduced anptitudes andtherefore his pR was thought to be atypicar or possibly due tothe carrier state. His motor system disease progressed, no autop_sy hras perforned.
Final diagnosis: uncertain, conbined features of a neuono-
L75

pathy hrith clear UUN signsscribed in association with
Appendix A
and neuropathy (not that usually de_
polycythernia) .
88, female age 5{, SMNDR No: 333. Referral: Gp nailsbotInitial diagnosis: ALS
ssrs mother was armost certainly affected by MND with pro-gressive loss of rnobility, falls and difficurty swallowing andspeaking' ss had an illness of 21 rnonths to death. she presentedwith a one year history of behavioural and cognitive disturbancewith confusion and disorientation. she becarne vacant and disin-terested and her behaviour odd. 4 months later she was noted tobe quiet and withdrawn but otherwise normal, she then developedcramps' she resigned her teacherrs job and became distressed atthe prospect of developing her motherrs illness. she forlowedher relatives around to distraction, she was unable to firl informs, had no responsibility towards money and her memory deter-iorated- she was unabre to place jigsaw puzzres correctry. shedid not appear to understand her reading nateriar. A year afteronset she fell and broke her arm. Forlowing this, she had diffi_culty in hording up her head and wourd support it with her handeven when standing. Her walking deteriorated. she had a fewchoking attacks and lost the strength in her upper arms. Hermemory continued to deteriorate. she became withdrawn, stoopedand crooned constantry to herself answering every guestion with arrNorr. Her back muscre rost its tone and she was unabr_e to sup_port her trunk- Examination showed emotionar 1abi1ity, cogni-tive disturbance, foot drop, scoriosis, bent knees, widespreadfascicuration with normal tone and sensation. A neuropsychologi_car evaruation showed that she courd write quite comprex words
L76

Appendix Afrom dictation and read arone comprex passalres of script. rncontrast she made errors indicatin!, named body parts and naningindicated body parts. she hras easily distractable. csF wasnormal, €rD EMG showed a widespread neurogenic disturbance withdenervation potentials. Her cognitive function continued todeteriorate together with her rnotor systen disease and she beganto aspirate' At autopsy macroscopic appearances hrere normar.scattered senire plaques were seen in the parahippocampal cortex,but neurofibritlary tangles were scanty. No plagues or tangles inthe hippocampus or cortex samples. pyramidal tract nerve fibredepletion in the rnedulla and spinal cord. Anterior horns shrunkenand hyperchromatic. ubiquitin positive cytoplasm in a few ante_rior horn celIs.
Final diagnosis: MND with dementia and organic psychosis,although no neuropathologicar basis for the cognitive changres.
B. REGISTERED WITIT THE SITNDR BUT DTAGNOSTS REVTSED WTTEFoLLOw Up OR AUTOpgy (n=15).
FC, nale age 6?, SttNDR No: 13.
fnitial diagnosis: pMA
Referral: Collaborator
Presented with a 3 year history of rnild progressive asym-netric, principarty proximal muscle weakness without burbarinvorvement or uMN signs. cK 355 242. The possibirity of MND
was raised on NCS/EMG which showed normal nerve conduction stu-dies apart frorn an absent superficial peroneal sAp and there hrerewidespread motor unit potential abnormalities without spontaneousactivity. Because of a rarge number of polyphasic units heproceeded to a muscre biopsy which showed features of a pri.mary
L77

Appendix Atuyopathic process with inflarnrnatory changes, focar chronic in-flammation, atrophy and no fibre type grouping.
Final diagnosis: Chronic pollrrnyositis.
AB, nale age 4L, suNDR No: 25. Referrar! corraboratorIndiagnosjs.. ALS (2 regions).2 year history of progressive weakness particurarly in the
left leg without sensory or sphincter disturbance. on examina-tion he had fascicurations in some of the muscre groups of hisupper arms but no wasting. There was a nird asymmetric spasticparaparesis with reflexes generally brisk incruding his jaw jerk.cervicar spine X-rays showed some narrowing of the c5, c6, c7discs with snarr osteophytes in the posterior disc margins en-croaching on the spinar canar. There was indentation of thecontrast corumn at c5-6 and cG-7 with some compression of thecervical cord without evidence of nerve root inpingement. csFnormar' Ncs/EMG showed nild but definite LMN degeneration in awide spread distribution, MND was thought likely, but a furtherEI.{G 9 months rater showed no progression. rf anything, hisclinical situation irnproved and MRr showed nixed disc and osteo-phyte protrusion just touching the cord c5-6.
Finar diagnosis: cervicar spondyrosis causing rnyeropathy.Surgery is being considered.
J.78

Appendix AVcrfsmale age ?rl, gttllDR No: 31. Referral: Gp
Initiat diagnosis: ALS (3 regions)Presented with a 2-3 year history of difficurty warking
resulting in falrs. Examination showed wasting of her thighsand hand muscres and ross of power in the rower rimbs but nofasciculation or sensory signs. The reflexes $rere brisk with upgoing prantars. The possibility of MND was raised (GeriatricMedicine). Motor conduction studies showed mild reduction incompound muscre action potential arnpritude, variable F wavelatency, absent sural potentials and needle EMG occasional fi-brillations and positive sharp hraves in the regs with notor unitpotentiar abnormalities principalry in distar muscres. Thefindings hrere thought to suggest a chronic neuropathy but becauseof her brisk reflexes further investigations were undertaken anda diagnosis of normal pressure hydocephalus was made on the basisof the cr scan- Her verbal re was L2s, perfornance re, gg. sheunderwent ventricular pressure rnonitoring and right ventricularperitoneal shunt insertion.
Final diagnosis: chronic peripheral neuropathy of uncertaincause and normal pressure hydocephalus.
88, male age 6s, gIrtNDR No: 35. Referral! collaboratorInitial diagnosis: pBp
Presented with dysarthria and dysphagia over a 6 rnonthperiod' Examination showed evidence of palatal and larangealmuscle weakness. NMR scanning did not show a brain stem lesion.Ncs/EMG: normal nerve conduction studies, denervation potentialsin extensor digitorurn brevis and widespread motor unit potentialchanges with increased polyphasia and inpaired recruitment.
L79

Appendix AHowever, there was no change in these abnorrnalities over 2 se-quential examinations. subsequent review showed a hard swerlingin the right sub-mandibular region and he hras found to have somefurlness in the right tonsil and tongue base and cr scannin!, onthis occasion showed a non vascurar parapharyngeal space tumoursuspected to be an adenocystic carcinoma of the deep lobe of thesub-mandiburar gtand and his management was transferred to theENT surgeons.
Final diagnosis : Retro-pharyngeal tumour.
AE, fenale age: g3, SI{NDR No: 75. Referral: collaboratorfnitial diagnosis: ALS (2 regions)Presented with 7 month history of progressive weakness of
the left hand' on exarnination the craniar nerves hrere normar,there was wasting and weakness without fasciculation of the smalIrnuscres of the left hand and the forearm extensors but nowasting or fascicuration elsewhere. possibly slightly increasedtone in the reft arm and refrexes very brisk generarry with a fewbeats of clonus at the ankres. possibre urnar sensory ross inthe left hand- Ncs/EMG abnormatities srere confined to the leftupper linb without denervation potentiars. cervicar spine X-rayshowed gross spondylosis but in view of her age a cervical rnyero_gram was not thought appropriate. with folrow-up the initialsuggestion of MND was thought ress rikery as there was no pro_gression over J-g months.
FinaT diagnosis : Cervical rnyeloradiculopathy.
L80

Appendix A
nE, nare age 65, gttNDR No: 92. Referrar: corraboratorfnitial diagnosis: pMA
Two month history of weakness of the left arrn and wasting ofthe reft biceps muscre without pain. vague tingring over theleft shoulder. Examination showed wasting and weakness of theleft deltoid, biceps, brachoradialis and pectoralis rnuscle withpreservation of triceps bulk and widespread fasciculation of theshoulder girdle bilaterally and involving the quadriceps. Dirni-nished reflex at the left biceps and supinator but preserved inthe triceps, ho burbar involvement or crear upper motor neuronesigns. ltildry raised cK at zL7. rmmunogloburins normar, EMG
showed abnormalities in left deltoid biceps and triceps withmotor unit potential changes and positive sharp hraves. Nerveconduction studies normal. The findings were thought to suggesta c5-6 lesion. Myelogram not performed but no change with fol_low-up.
FinaT diagnosis: ?cervicar spondyrotic radicuropathy.
JFr nale age zg, gl.rNDR Nos 1{9. Referrar3 colraboratorInitial diagnosis: pMA
Presented with weakness to the extent that he was unableto open his left hand associated with some mild neck discomfort.Mode of onset was uncertain. There was some numbness over the cgarea on the lef t which was interrnittent. There sras wasting andweakness confined to the left upper lirnb particularly distallyaffecting the hypothenar and thenar eminences and wrist exten-sion' Reflexes vtere depressed in the upper lirnbs and absent atthe biceps, supinator and ankles. NCs lEvIe examination showeddelayed F wavesr Do denervation potentials and motor unit poten-
L81

Appendix Atial changes in both upper rimbs and the right leg and sterno-nastoid' cervical spine x-ray showed considerabre degenerativechanges in the lower and rnid cervicar spine. csF was normalapart from a mildly erevated protein at 0.69 glL. Forrow-up over13 rnonths showed no crinical deterioration.
Final diagnosis: polyradiculopathy due to cervicar spondylo-tic disease.
JB, male age 56, gtofDR No3 150. Referral: colraboratorInitial diagnosis: ALS (2 regions)Presented with pain and weakness of the reft upper rimb,
particurarly the left hand. The pain had a radicular quality andthere were occasionar paraesthesia but these were not impressive.There was wasting of the left FDr and weakness of 1B/TL in theleft hand and guestionable pyramidal distribution of weakness inthe remainder of the left upper linb. The refrexes hrere briskthroughout. There hrere no sensory signs. EMG examinationshowed motor unit potentiar changes confined to the reft arm,nyelograrn with cr scanning failed a: show any evidence of com_pression of cervical roots. However, with forrow-up there was nochange in his syrnptoms or signs.
FinaT diagnosis : uncertain, non-progressive cervical lesion.
RB, nale age 29, gIrrNDR No: 160. Referrar: corraboratorInitial diagnosis: ALS (3 regions)Presented with an 8 month history of progressive reft hand
and arrn weakness without pain or paraesthesia. Diabetes mellituscontrolled by diet. The abnormal signs v/ere confined to the leftupper linb with marked wasting of biceps but weakness affected
L82

Appendix Aall nuscle groups in the same limb. The deep tendon reflexeswere exaggerated throughout and there was no sensory ross.Ncs/EMG: the upper lirnbs were norrnal apart from an absent ulnarsensory action potential. There vtas some denervation in EDB and
TA and in addition motor unit potential abnornalities in all fourlirnbs and sternornastoid. A diagnosis of MND was revised when amyelogram showed considerable spondylotic change in the cervicalspine with obliteration of CG root pockets.
Final diagnosis: Spondylotic myeloradiculopathy.
rD, mare age 51, gttNDR No: 1?5. Referrals colraboratorf nitial dj_agnosis: pLS
Presented with a 2 year history of a very srowry progtres-sive irrness dominated by upper motor neuron symptoms and signsaffecting arl 4 rinbs in an asymmetric fashion worse on theright. However, this was accompanied by wasting of the right legof uncertain duration. There was also rnild bilateral wasting andweakness at the first dorsal interosseous but no definite bulbarfeatures. He had interrnittent tingling of the hands and feet.An MRI including the cervical cord and csF studies hrere normalbut he did not have EI.{G. with forrow-up he deveroped a leftoptic neuropathy but compressive causes $/ere excluded with ap-propniate irnaging.
Final diagnosis: Dernylinating disease of undetermined cause,possibly late onset rnultiple sclerosis.
PC, nare age 46, gllltDR No: 1g3. Referral: collaboratorfnitial diagnosis: ALS (2 regions)rnprecise history of clumsiness of the hands and difficurty
183

Appendix Awalking over several months. There was a history of arcoholabuse. oistal wasting and weakness of his limbs without fasci-culation- Brisk symmetrical refrexes, no sensory loss. serumproteins and erectrophoresis were normal. Neurophysiologicalstudies showed evidence of motor unit abnormalities in musclesinnervated by cg on either side, suggesting a lesion of cg notorroots. He had birateral rudinentary cervical ribs, and mj.nordegrees of root irnpingernent at c6-7 on the left and c5-6 on theright and the cervical cord appeared marginarly widened althoughthere hras no evidence of tonsilar prorapse. csF normar. Atfolrow-up 4 months later there had been no progression clinicallyor electrophysiorogicary. He deveroped a broncho-pneumonia anddied.
At autopsy the spreen was enrarged as were the rnajority ofthe rymph nodes in the chest and abdomen. Historogy showed theinternal architecture repraced by masses of tumour into whichthere were many Reed-sternberg-rike giant ceIls, the appearanceswere those of Hodgkins or T-cell lynphorna. Detaired historogicarexamination of the nervous system revealed extensive neuronalloss, astrocytosis and proliferation of microglia in both thala-mae but outwith these areas no abnormalities in the cortex,cerebral or cerebelrar hemispheres or brain stern. rn the spinalcord at c8 there was no evidence of tumour either within themeninges or within the spinal cord but there was some ross ofmotor neurons within the ventrar horn with an associated astro-cytosis and hyperplasia of microglia. A sample of other spinalIevels was normal, the right deltoid showed focal clustering of asmall number of contracted muscre fibres suggestive of neurogenicatrophy. The right nedian nerve rnras normal and the right ulnar
184

Appendix Anerve hras norrnal being both welr rnyerinated and popurated bynormar axons, there was no evidence of infiltration by tumour.
FinaL diagnosis: Motor neuronopathy associated with T-celllymphoma.
AR nale age 80, SUNDR No: Lg2. Referral: Gp
fnitial diagnsosis: pMA
Presented with unsteadiness of warking, possibry dysarthriaand dirninished refrexes of uncertain duration and was suspectedof having MND by a consultant physician. Also sustained black-outs thought to be due to transient ischaernic attacks. No rowermotor neuron signs or progression of neurorogical signs.
Final diagnosis: uncertain, possible cerebrovascurar dis-ease.
Jlfa nale, age ZS, gl,0{DR No: 2Lg. Referrals gHlpg
Initial diagnosis: ALS (extent?)The diagnosis was suggested by a consurtant neurorogist
during admission for diuretic induced.hyponatraernia' (sodiun 118) .
He stas noted to have wasting of the muscles of both hands withfascicuration and generally brisk refrexes but the remainingdetails at registration are scanty. No Ncs/EMG examination.subsequent forrow-up from the cP indicated that this diagnosishad not been substantiated and there $/as no change in his neuro-logical condition.
Finar diagnsosis; Hand wasting of uncertain cause, hypona-traemia.
L85

Appendix Aill'l male age Go, SUNDR No: 24o. Referral3 gHrpg
Initial diagnosis: pBp
Presented with a one year history of a burbar parsy withdysarthriac'and marked swallowing difficulties, mode of onsetuncertain' Examination showed a rnild upper motor neuron facialweaknessr rlo tongue fasciculation and a pseudobulbar palsy. Lirnbrefrexes hrere brisk without sensory disturbance. Ncs/El{c showeda mild motor neuropathy with no denervation potentiars. A dia-gnosis of MND l/as made (neurologist) but 10 months later thereappeared to have been little change in his bulbar parsy and anisolated vascular lesion in the rnedurra was suspected. An ![Rr ofthe head showed murtiple bilateral focal resions concentratedaround the inferior thalanus and internal capsule-basar ganglianregions. There was no change in erectrophysiorogicar appear-ances.
Final diagnosis: pseudobulbar palsy due to ischaenic leu-coencephalopathy.
JK, nale age 23. 8INDR No: 2gL. Referral: cp ]railshotInitial diagnosis: ALS (2 regions)Presented with a 3 month history of weakness and aching in
both legs without sensory synptorns. Examination showed smallrnuscl.e wasting in the hand, a tremor of uncertain type and a nildspastic paraparesis. An MRr scan showed straightening of thenormal cervical curvature with rnultiple offsets. The cord was
sonewhat atrophic at c3 where there was evidence of impingementand at c5-5 where impingenent was associated with oedema of thecord' Nerve conduction studies showed evidence of bilateralurnar entrapment at the elbow and an upper motor neuron pattern
186

Appendix Ain the lower Limbs but no other lower motor
FinaT diagnosis: Cervical rnyelopathytions for tardy ulnar palsy.
neuron signs.
and previous opera-
C.DIAGNO8I8 UNCERTAIN
FOR CI/TI|ICALLY DEFINTTE OR
OR FAILS TO FULFfIJ THE Sl,tNDR CRITERfA
PROBABLE II|ND (n=5)
lf8, female age l{, gtrtNDR No: 53. Referral3 collaboratorInitial diagnosis: ALS (2 regions)Presented with a 10 month history of weakness of the left
arm and pains around the erbow. Aware of occasionar fascicula-tion in the intrinsic muscres of the reft hand and a tendacy todrop objects. some neck discomfort. Examination showed fascicu-lation of the intrinsic muscres as well as the forearm muscresand wasting of the intrinsic muscles of the left hand with a norewidespread weakness of pectorars, rhomboids, triceps and intrin_sic muscurature. Triceps jerk absent, rimb reflexes otherwisebrisk and plantars equivocal. Ncs/EMG: normar nerve conductionstudies and possible fasciculation potentials in the rower lirnbsas werl as the affected rinb. Myerogram and csF normar. Thepatient was informed of the diagnosis of probable MND but hersituation remained entirery stabre with folrow-up.
FinaT diagnosis: Monornelic MND, non progressive.
LB' femare age s?, sMNDR No: 66. Referrar: corraboratorfnitial diagnosis: ALS (2 regions)Four month history of progressive weakness of the reft
ankle leading to a foot drop. Examination showed normar craniarnerves, brisk upper rinb refrexes and an asymmetric spastic
L87

Appendix Aparaparesis vtorse on the left without sensory abnormalities.Fasciculation was observed in the left quadriceps on one examina-tion. Lumbar radiculogram (orthopaedic service) and then a totalmyerogram did not show a compressive resion. Routine bloodtests, BL2 and folate, cr scan, EMG normar. Mildry raised csFprotein (o-53 g/L') but no oligocronar bands, vERrs normar. Atreview her signs were stabre, she complained of cramp but on thisoccasion no fasciculation was evident.
Final diagnosis: spastic paraparesis, cause uncertain,follow up continues.
irB, female age 6?, gIrtNDR No: o7t. Referral: colraboratorInitial diagnosis: pLS
Presented with a 2z year history of progressive dysarthriaand gait difficulty due to pseudobulbar palsy and asynmetricspastic quadraparesis without definite LMN or sensory signs. csF(including immunologicar studies), uRr, EMG normar. Excruded onthe basis of a history of a previous episode of possibre trans-verse myelitis 15 years previousry :ttd abnormal visual evokedresponses' although diagnosis is unclear and follow up continues.
Finar diagnosis: uncertain, possible pLS, possibre rnultipresclerosis.
w8, nare age 69, sMl{DR No: 188. Refenal: corraboratorfnitial diagnosis: ALS
Presented with an 18 month history of stiffness and weaknessof the left teg. A little weakness in the left hand. No otherabnormalities apart from a sright hesitancy of urine. No cramp.Exanination showed normal craniar nerves, cg-T1 weakness in the
L88

Appendix A
hands but no upper limb fascicuration. wasting of the reftquadriceps and fasciculation in several lower lirnb rnuscles withbirateral increase in leg tone anrl a mild spastic paraparesis.Normal upper lirnb reflexes. uild vibration sense irnpairrnent atthe toes. Ncs/EMG: delayed F vraves in both upper and lowerlimbs, absent sural sAp and sone motor unj-t potential changesaffecting the left lower lirnb onry. Normal cr scan, myelograrnand csF. Follohr-up 6 months rater showed no definite change.
FinaT diagnosis: possibry arrested MND, forrow up conti-nues.
Rr, nale age 66, SMNDR No: 3{{. Referrar corraboratorInitial diagnosis: pBp
Presented with srurring of speech which seemed to be pro-gressive but since a tentative diagnosis of MND in e/89 remainedrargery static. signs rather equivocal with crumsy tongue butnormal faciat jerks and no lower motor neuron involvement or lirnbsigns. Thrornbocythemia of uncertain cause. Awaiting MRr.
Finar diagnosis: Brainstem resion not yet diagnosed ?ar-rested UND, follow up continues
189

APPBNDIX B
DETArIJ8 OF TAUrTY ITEIIBER8 IN PEDIGRESS IIEERB A cENETIc cAUgB FoR
UOTOR NEURON DISEASE gEEUg LftrELy. (n=111.
190
Appendix B
Xey to pedigrees
rn all pedigrees a circre indicates a femare, square a mare.shading indicates affected with MND. A diagonal line indicates adeceased individuar and age at death is incruded (where known).If unshaded, cause of death was not I,{ND.
The proband on the sMNDR is indicated by initials. No faurilyhas more than one member on the sMNDR at this stage. != born.
Roman numerals are used for separate generations and indi_viduals numbered from right to reft for reference berow thefanily tree. The source of information is incruded.
191

tr
Itr
Appendix B
DD, fenale age G?, SMI{DR tfo: 60
2-22 ALs with burbar invorvement as for proband. Duration L7months (death certificate and farnily histo;tt. -
3'2'- (DD): SMNDR. 26 month ilrness. ALs with burbar invorve-ment.
L92

tr
Appendix B
DG, uale age lL, gttNDR No3 68
1'1: Progressive wasting disorder affecting the left arm but notelsewhere. Died 6 months later witti p"""tn""i" which wascertif ied cause of death (history frorn rarnily) . -
ALS and PBP.
2.22 Typical ALS with pBp
2.Lz (DG) SMNDR. Rapid (<L2 months) illness to death. Typical
(neurologist's report to SMNDR).
Details of earlier generation uncertain, birth and death certifi-cates of parents not in Register House (Edinburgh), nay have, died in England.
193

tr
m
Appendix B
GG, nale age 50, gltNDR No: SO
1.1: -Fiy" year h.istory of pro_gressive paralysis of arr tinbs. Nobulbar symptoms. -confined'to bed f-or fi-nar 6-L2 months, diedwith. pneurnbnia (nistory from farniry, death certif icates ofprevious generation not- in n"gi=["r House, Edinburgh).
2'L: (cG) SMNDR. 14 month illness. ALs pBp, autopsy (appendixC): typical pathologicat findings-of mlO.
b.1964
L94

tr
m
Appendix B
iIL, nale age 69, gl,tNDR No3 2Zg(Bulbospinal neuronopathy/Kennedy syndrone)Lz2z carrier? Detairs of her two brothers unknown.
2'22 Long duration of rrmotor neuron diseaser, similar illness toproband (history from family).2.3: (JL) suNDR. L2 yea{ history of progressive generarisedmuscular atrophy, faciar weakriess, -uut5ar parary-sis, tt;;;:comastia (seen in person 1991).
2'42 23 year his-tory of qeneralised progressive rnuscular atrophy,i:::l:iln face and burbar muscf"s. strikins shourder sirdretnvolvement (seen in person 1990).
b 1949 b 1956
195

tr
m
ry
Appendix B
iIB, male age tL, gltNDR No: L22
2.2: rrDystrophica myotonicail . (death certificate) . rrregitimate,father unkown, mother alive3'1: (JB) sl{NDR. Rapidry progressive muscurar atrophy withbreathlessness lseLn in p^ersLn-iiTgol3 '22 Died after 3 year irrness of progressive muscurar atrophywith bulbar ana respirai"d l"J"r""ment (seen in person
3 /9L')
4.L-4.9: AII children are younger than 25 years.
196

tr
Appendix B
m
IV
iIO, male age 66, gIr0fDR No: 2
1.1: Bulbar paralysis (death certificate). Rcords of parentscannot be traced.2-42 Progressive generalised weakness of muscres (died in theUsA, age uncertain, history frorn iarnify)2.6: Died at sea in world war II.3-2: one year his_tory of progressive muscurar atrophy with re_spiratory and truiuar symptorns. Autopsy: spi1al cord anteriorhorn cell loss and pirror of anterior and dorsar roots.Myelophages
. in- poster-ior corurnn nlcreii. lleurogenic atrophyof muscle. (Medical records)3'3: (Jo) sIr{NDR. 11 rnonth history of ALS. Autopsy: Anterior rootatrophy, spinar cord anteri6r noin cerr rbsls and posteriorcorurnn nyelophages. Astrocyti- gri"=l= -=-or-" -perivascular
lymphocytic cuffs.3'42 <L2 nonth history of progressive muscular weakness of ar1limbs. some parasrhesial. -i;;;;;yl
nypogrossal nucrei neuronloss, anterior horn cerr ross.-'N"urogenic atrophy of mus_cres- some posterior root ganglia cetr loss (rnedicar re-cords).
L97

tr
Appendix B
m
rv
Kll, nale age 52, Bl.llfDR No: 62
L.2z Died of pulnonary tuberculosis2'Lz Died of .lrr.tress.suggesting a progressive burbar pararysis(probandfs descripti6nl ' -)
3 '22 (KM) 'MNDR-
srowry progressive wasting and weakness oflinbs. principally irns. pIr{A.
b.1967
198

tr
Appendix B
m
TV
v
ttD, male age SG, gl.tNDR No! 2A3
L'22 Died of heart disease, mother not affected, father no record(death certificate).2'2i Died in canada of a neurological illness which involveddefinite wasting ?nd weakness bf muscres but detairs ="i"iv(history from fimily member).
2.3: -seven yea{ hi_story of wasting and weakness of the limbs,b-ecoming wheelchair bound, sp-eech disturbance in terminalphase only. Proband reports tfris illness closely resenbledhis own.
3 . 1: (MD) SMNDR. rrrness be.gan 3 /g7, diagnosis LL/go. rnexorablyprogressive, _ asymmetrit, generatis6a wastini and weaknesswith fasciculation. useieJs right arm, droopy head, birat-eral foot drop, needs assistanie for most iitivities. pMA
(Seen in person 3/92).
b 1950'r
199

Appendix B
RP, nals age ?6, g[ttDR t{o3 ga
2-L: Parkinsonisn and dementia (history from family).2.22 Motor neuron disease (death certificate).2.32 (RP) SMNDR. L4 rnonth illness. ALS with pBp.
RPrs father wa: illegitinate, therefore no information on pro-band.rs- paternar grandfather. MND not included on d6athcertificates of probandrs maternar grandparents.
tr
200

tr
Appendix B
8F, fenale age ?1, SultDR lfo: 31a
m
IV
L.2l
2.2r
4. 1:
rrLupus of the face and nose and exhaustioh,,of MND (Death certificate).(sr) SMNDR. Typical pBp/ALs.
Juvenile MND with pathological confirnationtailed report denied Uy pattrologistf.
but no mention
(access to de-
20L

Appendix B
tr
m
ry
plt nale age s6, B*ilDR tlo: 3oz
2.22 spastic parapregia (death certificate) and creeping paral-ysis (history from family)
3.42 wasted regs, wheer chair dependent, died of pneunonia(history from farnity) .
4.22 Died L2 months after diagnosis of MND. Generalised muscleweakness, . respiratory dis€ress and upper motor neuron signs(ALS). (Discussion with Gp).
4.42 10 year history of a progressive muscular atrophy (neurolo-gistrs diagnosis).
4.62 (tfi{) sl{NDR. Tive year. history, notr fully dependent for aIIactivities. progressive nusiurar atrop-hy biegining in theshoulders and later rnild bulbar invotveineit lJeen i; personLLIeL).
202

APPENDTX C
8UullARy oF aEE PATf,oLoGIclD FEATUREB oF TaogE pATIEttTs rNcr,UItED
rN THE l'tArN ANArrygEg wHo IINDERWENT Auropgy (l{=15t
203

Appendix C
JO, nale age 66, SMNDR No: oo2.
Diagnosis : ALS (Familial)Macroscopic appearance: Anterior root atrophy in the spinal
cord.
Microscopic apPearance: cerebral hernispheres normal andhypoglossar nucleus normar. striking depretion of anterior horncerls and pare roots. Myerophages present most obviousry in thedorsal column nuclei.
E8, female age ?2, sIrlNDR No: o23.
Diagnosis: pBp/ALS
I4acroscopic aPPearance: Thin cauda equina but otherwisenormal.
I{icroscopic appeatance: Neuronal depletion in the anteriorhorns of the spinar cord, degrenerative changes in survivingneurons' Associated increase of astrocytes and microglial cells,no ubiquinated incrusions identified. Myerin parror unequar oneither side in the crossed and uncrossed pyramidal tracts. Mirdpalror in the medurlary pyranids and depletion of neurons in thehypoglossal nuclei accompanied by gliosis.
GG, nale age:60, gl.tNDR No: OSO.
Diagnosis : ALS/pBp (familial)I4acroseopic appearance: parietal atrophy. Mild ventricurar
dilatation otherwise normal.
Iticroscopic appearance: cortex normarr. parlor of the centrarwhite matter; flea bite infarcts; focar atrophy of the folia inthe cerebellum. cortico-spinal tract nyelin depletion and accu_
204

Appendix C
mulation of rnyerinophages. Demyelination of the anterior rootsof the spinar cord with tract degeneration and rnyerin ross in theraterar and anterior cortico-spinar tracts. Depleti_on of ante_rior horn celr neurons, occasionar ubiquitin-positive inclusions.severe degeneration of anterior roots of the cauda-equina.Denervation atrophy of peripheral muscles. Terminal bronchopneu-monia.
l{G, female age 62 years, glrll{DR No: 06Z.Diagnosis: ALS/pBp
Macroscopie appearance: smalr pons and flattened pyramids,shrunken anterior roots of the spinar cord and arr regionsr pdF_ticularly at the cauda equina.
I[icroscopic examination.. cortex and hemispheres normar.sworlen neurons and depreted Nissl substance in the froor of thefourth ventricar. Demyerination of the pyranids, depretion ofanterior horn cerrs in the spinar cord, poorry myelinated corti_co-spinal tracts and shrunken anterior spinar roots. At thecauda equina the anterior roots contrasted rnarkedly with theposterior roots showing ross of myerin and increased corragenisa-tion. Hashimoto's dj-sease in the thyroid, nicroadenoma of thepituitary, terminal bronchopneumonia..
AII, feuale age 69, SI{NDR Nos 081.
Diagnosis: ALS/pBp
I{acroscopic aPPearance: Normal brain, cerebellum and brainstem' obvious atrophy of ventral roots of cervicar region in thecauda equina.
Microscopic examination: Loss of neurons in the ventral horn
205

Appendix C
and the cervical and lumbar regions, Do obvious abnormafity in
rnyelination. Carcinoma of the sigmoid colon.
IB, female age 67, SUNDR No: 09{.
Diagnosis: ALS/PBP
l{acroscopic appeatance: SIight general cortical atrophy,
dilated ventricles, brain stern and cerebellum normal. Shrinkage
of the anterior spinal roots in the cervical region and to a
lesser extent in the cauda equina.
ILicroscopic examination: Normal cortex. Focal abnormalities
of the neurons in the floor of the fourth ventricle and the
presence of rnyelinophages in cortico-spinal tract on both sides
at various levels in the brainstem. Myelin loss in the cortico-
spinal tracts and the pyramids. Depletion of Purkinje cells in
the cerebellum. Anterior horn cells of the spinal cord focally
swollen and loss of Nissl substance. Demyelination of the corti-
co-spinal tracts and the cauda equina. Denervation atrophy in
rnuscle.
Tl{, DaIe, age 80, SI{NDR No! 096.
Diagnosis: PBP/ALS
Samples of the nervous system deteriorated during transport-
ing and examination not possible.
JM, nale age 77, SUNDR Nos LO7.
Diagnosis: ALS/PBP
Irlacroscopic appearance: Moderate degree of cortical atrophy.
I,Iicroscopic appearance: Pyramids reduced in size with loss
of rnyelinated axons. Depletion of motor cells from the hypoglos-
206

Appendix C
sal nucrei and occasionar cytoprasmic incrusions on ubiquitinimmunocytochernistry. parror of nyerin in the spinar cord pyrarni-dar tracts and anterior horn cerr population reduced. peripheralnerves showed large axonal loss and secondary demyelination.Focal group atrophy in muscle.
COr, female age ?ST SIT|NDR No:1?6.
Diagnosis: pBp/ALs
I4acroscopic appearance: Cauda equina atrophy.Itlicroscopic appearance: Loss of neurones in the hypoglossal
nucrei and demylination in the lateral and anterior white columnsbut spinal cord structure well rnaintained.
l,tR, fenale age 61 , SMNDR No: 2OO.
Diagnosis: ALS/pBp
Macroscopic appearance.' Gaping central sulcus, otherwisenormal.
Microscopic appearance: Typicar spinal cord changes withloss of neurons in the central horn and palror of rnyelin stainingin the laterar and ventrar corumns, ross of neurons in the hypo_glossar nucrei, estabrished neurogenic atrophy of muscre.
SC, female age ?4, SMNDR No: ZOS.
Diagnosis: ALS/pBp.
I4acroscopic aPpearance: No external abnormality of the brainor spinal cord.
Microscopic appearance: Marked neuronar ross in the hypo-glossal nuclei and some ventrar horns in the spinal cord.shrinkage of the ventral nerve groups. parror of staining of
207

Appendix C
raterar and ventrar white corumns. Atrophy of ventral nerveroots and the spinal cord and cauda equina.
PT, nale age 66, SttNDR Nos zLg.
Diagnosis: ALS
I{acroscopic appearance: Normal.
Microscopic appeatance: Depletion of anterior horn celI neu-rons particularly in the lunbo-sacral region with associatedincrease of neurogliar cerls. pyramidar tract normar. Brainstem normal. Neurogenic atrophy without inflammation in muscle.
MC, female age 66, gItlNDR No: 232.
Diagnosis: pBp/ALS
Macroscopic appearance: Normar apart from an unconpricatedone centirnetre vascurar marformation in the cerebelrum.
Microscopic appearance: Mild spongiosis of the outermostlayers of the cerebrar cortex unaccompanied by praques, neurofi-brillary tangres or inframmation. Depletion of hypogrossalneurons, neyrinophages in the cortico-spinar tract. widespreaddegeneration and atrophy of skeletal muscles fibres includingsternomastoid, tongue and quadriceps.
rP, male age 74, SUNDR Nos 256.
Diagnosis: ALS/pBp
Awaiting report from the procurator Fiscal, Grasgohr. un-available as of 15.5.91.
208

Appendix C
AF, nale age 69, stltNDR No: 290.
Diagnosis: ALS/pBp
Itlacroscopic appearance: sright to moderate symmetricardilation of the ventricurar system and atrophy of the ventrarroots particularly in the cauda equina.
ttlicroscopic appearance: Loss of motor neurons in arl spinalsegments exanined. partiar atrophy of the nucrei of the l0wercraniar nerves, particurarry grosso-pharyngeal and hypogrossal.Clusters of nicroglial ceIIs tuithin the fifth nerve nuclei.Dennervation atrophy of muscre with normar peripheral(nedian, femoral) nerve.
209

APPENDTX D
QUESTTONNATRE usED rN THE cASE-coNTRorr gTUDv
21,O

Appendix D
Contents
1. Patient Details2. Clinical Features3. Past Medical History4. Trauma -prior to MND5. Toxin Exposure6. Fanily History7. Educational and Occupational History8. Residential History
1. Patient DetailsCCS Identification number:(odd numbers=case, even nunbers=corresponding controrRegister Study No:
Name:
Address:
Telephone No:
General Pratitionerrs name, address and terephone nurnber:
Neurologist or physician:
Patientfs date of birth (day/month/year):
Age:
Sex:
Date of fnterview (day/month/year) :
Throughout coding 1 for yes, 2 for no, 3 for canrt recarr.
2LL

Appendix D
2. Clinical features
Eistory
when did your symptoms rerating to MND begin? (rnonth/year)Total duration of slrrnptorns relating to MND (rnonths)
First Slznpton
1. Muscle cranps,2. Muscle twitching,3 ' Hand weakness or wasting or difficurty writing,4. other UL weakness or waiting,5. Footdrop,6' other LL weakness or wasting or difficurty warking,7. Difficulty swallowing,8. Difficulty speaking, -'9. Other (e.9. pain, iweating specify)Present Slmptons (code as above)
Signs at visitUMN bulbar signsLMN bulbar signsIIMN signs (arrns)ttMN signs (legs)LMN signs (arrns)LMN signs (legs)SMNDR CLassification:
Examine eye movement/ocular nobility(analysis not in this thesis)1. voluntary or saccadic movements (horizontal and verticar)Restricted excursionInability to naintain eccentri. qazeSlow saccadesHyponetric saccadesProlonged reaction tine2. Snooth pursuit (horizontal and vertical)Restricted excursionSaccadic pursuit3. Convergence
4. Optokinetic nyastagmus.Failure to generite slow phase velocities5. .Suppression of vestibulo-ocualar reflex.Failure to suppress
Date of Diagnosis of MND (fron records)
2L2
Appendix D
3. Past medical history(Record response from patient and rater as from Gp Notes)Have you ever suffered from:
Angina or a heart attack?(central chest pain related to exertion, relieved by rest and/orresulting in adrnission with a diagnosis of angina oi r.try
Strokes or TIAs?(sudden onset of a focal neurological/ocular cNS disturbance withno other explanation at fo1low up)
Leg Claudication?(Pain in the calf or buttock related to exertion and relieved byrest with absent foot pulses)
Slpertension(Higlt BP requiring treatment, record Bp before diagnosis of MNDin GPrs notes)
Previous fnfectionsMeasles
Chickenpox
Scarlet fever
Diptheria
Munps
Glandular feverPoliomyelitis
Yes/No/Canrt rememberIf Yes, how old?Yes/No/Canrt rememberIf Yes, how old?Yes/No/Canft rememberff Yes, how old?Yes/No/Canrt rememberIf Yes, how old?Yes/No/Canrt rememberff Yes, how old?Yes/No/Cantt rememberIf Yes, how old?Yes/No/Can I t remernberIf Yes, how old?
Did any of your farnily ever have polio?Yes/No/Canrt remember
If yes, hrere you living in the same houseas them? Yes/No/Canrt rernember
If yes, how old were you at the tirne?Record details of person
Have you received polio vaccination?
2L3

Appendix D
l. Trauma prior to MND
Recording the same information from the patient and the Gprecords.
Date Gp records began
How many fractures have you had? (nurnber)
How old? (age of first, age of last)Date of most recent fractureDetails of fractureLocation of most recent fracture?l=UL, 2=LL, 3=Head, 4=Spine, S=Ribs
Have you ever sustained another injury requiring rnedicalconsurtation, including severe erectric stiocks? (n)How old hrere you?
Date of most recent injuryDetails of injuryLocation of most recent injury (code as above)
Have you had a tonsillectony?Have you ever had a blood transfusion?Have you ever had an operation requiring a GA?
List all prior to onset of MND (excr. ,tonsirrectomy)oPeration Age (not coded)
Date of onset of MND
21,4

Appendix D
5. Toxin exposure
If response yes, specify detailsHave you ever worked in extraction of minerals or ores, manufac-ture of rnetals?
Have you vrorked with read as part of your occupation?Have you ever had an occupation with known exposure to solventsor chemicals (eg shoemakers, tanners, houje painters, rubberproduct .makers, compositors, typesetters, iaundry worker,petrol station attendants) ?
Have you ever bgen exposed to pesticides or herbicides, domesticor conmercial?
Have you ever been a pOW?
Snoking (Rol1 your own Loz=28 cigarettes)Current smoker?If Yes, n per dayEx smoker?When stopped (age)Max n/day when smoking
Are you vegetarian?
Do you keep or have you kept (for 2 ormore seasons) a vegetable garden?
Do you eat garlic?Do you eat cabbdg€, caulifloweror sprouts: 1
2 L-3lweek3 < l/week
6. Fanily bistoryHas anyone in your farnily had MND? yes=L, No=2Details:
{.= anyone in your faniry had any neurorogicar disorderincluding pD or ATD?Yes=l-, No=2
Draw a family tree for families with MND/PD/ATD
For deceased relatives:1=Fu11 name 2=Date of birth 3=year of death4=Town of residence at death S:cause of death if known
2L5

Appendix D
?. Educational and oceupational historyHow old hrere you when you left school?
Did you obtain any qualifications afterthe age of 18?
lnlt were your 4 principar jobs (begin with rnost recent)code according to opcs reeoll-1G, iicruae Military-i"r.ri"".Occupation Address Dates
what is the main occupation of your wife/husband?
what was the main occupation of your father when you hrere born?code patientts and father's social class (opcs 19go)L Professional (1)2 fnternediate occupations e,)3N Skilled occupations - non manual iti3M Skilled occupations - manual ei4 Partly skilled5 unskirred (s)
(6)
01' Professionat & retated supporting management, senior nationat & Local, goverrment managers02. Professionat and rel.ated in education, relfare and hea(th03. Literary, artistic, sports04. Professional and retated in science, engineering technotogy and simil,ar fietds05. l{anageriat06. Cterical,07. Sel. t ing08. Security09. Catering, cteaning, hairdressing. personat service10. Farming, fishing and retated11. llateriat processing, making and repairing (exclr.rding netat and etectricat)12. Processing, making, repairing (metat and etectricat)13. Painting, repetative assernbting, product inspecting, packaging and retated14. Construction, mining and retated not identified elserhere15. Transport operating, materiats moving and storing16. l,lisc. inclrding tabourers and unski l. [ed
2t6

Appendix D
8. Residential history(Each house of more that 1 year residence)House Number (1-6)
where was the 1st house you rived in after you were born?Address:
Was this your residence when you developed MND?(equivalent for controls)l=Large town 2=smarr town 3=Virrage 4=rsolated house
During which years? Fron/ToDid the house have a garden? yes/No/canrt remember
Did the house have a separatebathroom? yes/No/Canrt remember
Did the house have a runninghot water systern? yes/No/Canrt remernber
Did the house have a flushlavatorY? yes/No/canrt remember
How many bedrooms did the house have?
Who lived in the house?(include anyone staying for more than 5 rnonths)
Total adults:Total children (under 18):Total number of rooms:
Pet Exposure
Did dogs sleep in the house?Did cats sleep in the house?
Did you have regular contact with farm animals?
2L7

APPENDIX E
TEE sCOI[TI8E IIOTOR NEURON DISEJASE REGISTER3 IITFoRITA.IIIor roR
UEDICEL PRACTTrIONERS
2L8

Appendix E
Copy of the information sentregistration of a patient with theRegister. -:
to General practionioners upon
Scottish I[otor Neuron Disease
trhat is the Scottish UND register?A national register of patients with motor neuron disease is
being co-ordinated from the Department of clinical Neurosciences,western General Hospitar, Edinburgh, with financial support fromthe scottish Motor Neurone Disease Association. Ar1 the consul-tant neurologists and clinical neurophysiorogists in scotrand arecollaborating. The register has been approved by the hospitalethical committee and the Data Protection officer for the LothianHearth Board' we are ascertaining cases frorn arl of the cc.,nsul-tant neurologists and clinicar neurophysiologists in scotrand.Additional information is being obtained from the membershiplists of the scottish Motor Neurone Disease Association andcomputerised records of Hospital discharges and deaths held bythe common services Agency and the Registrar Generar for scot_Iand.
My do we need a Scottish Register?There are no rearry good epidemiorogicar studies of motor
neuron disease, most series consisting onry of a hundred or sopatients. what we want to do is estabrish prospectively aregister of all the cases presenting to medicar attention inscotrand, which wirr be about 70 a year. scotrand is an idealplace to do this si-nce it is geographicalry welr defined, veryfew patients in scotrand are unrikely to get health care outside
2L9

Appendix E
the country, and the number of cases coming to attention everyyear is reasonable. As the years go by, we wilr therefore,progressively build up an irnpressive series of patients. we areregistering the patients and then asking if we could have aphotocopy of the rerevant medical summary. This arrows us tocrassify the nature of the motor neuron disease. Arso, rir€ arecontacting the patients I general practitioners so that we canfind out some sirnpre follow up infornation and when the patientdies' From these very sinple data vre can look at incidence,geographical clustering, and natural history.
Eow will the register be constructed?
unrike many other surveys in which everyone is sent a ques-tionnaire at exactly the same time, the Register wirr have to bebuilt on a rrollingr basis so that doctors will be asked forinformation as their patients are registered, and subsequentrequests for help will follow at regular intervals from thatinitiar contact. we rearise that the progression of the condi-tion may mean that this could be problematic, although we believethat we have to work this way to ensure that the infornation we
obtain is properly gathered and organised for research use.Two separate, but related, computing systems are being used
one which wilI assist the administratj-on of the co-ordj-natingcentre in Edinburgh by charting contacts with those aiding theunitrs work, and the other on which the main research informationwirr be held- These systems wirr be modified and developed asnecessary to enable smooth operation of the work of the Co-ordi-nating Centre.
220

Appendix E
Who should be registered?
Because we wish to study the natural history of the diseasehre are trying to register patients as soon as possible, even whenthe diagnosis is onry suspected. rt wilr then be possible, dt a
later date, to reclassify patients after collating infornationfrom aII sources to produce a register of patients that conformto more rigorous diagnostic criteria. we have registeredpatients since January 1989 and if this rate of ascertainmentcontinues it seems likery that incidence will be eguar to orhigher than we predicted (50-1OO patients /year).
will the patients be inforned that they are registered?rf patients subrnit a request for disclosure of information
held on computer the Data Protection officer wiII inforrn us. we
have discussed this legal issue with the Data protection officerof the Lothian Health Board whose interpretation of the law isthat the release of such information is at the discretion of theconsurtant responsibre for the care of the patient and may bewitheTd it it is rikeTy to be danaging. There is no regarobrigation to telr people that they are on a cornputerised regis-ter- However we would not object if patients were told by thereferring doctor that sirnple data about them are being correctedin Edinburgh so that we can learn more about the disease (whetherthey are told the diagnosis precisery at this stage is entirelyup to the referring doctor).
self-referred patients, or those contacted through thesIt{NDA' will be asked to give written consent for their participa-tion (if necessary through a proxy), and for obtaining confirma-tion of their medicar diagnosis. Data on patients wirr be com-
22t

Appendix E
pletely confidential, both under the terms of the Data protectionAct and following normal medical conventions. patients will be
continuously recruited to the register, but can withdraw fron theregister at any tirne.
Hho silt be contacted?
At present there are no prans for approaching patientsdirectly but a case-control study of environmental factors ante-cedent to the development of motor neuron disease is planned and
contact will be made under a seperate cover concerning this. We
hope to set up a systen of systematic blood collection as part ofa study of the genetic contribution to sporadic motor neurondisease in conjunction with the MRc Hurnan Genetics Unit at thewestern General Hospitar, Edinburgh. Details of this wirl beposted at a later date after registration.
IIow sill patients be followed up?
we intend to folrow the patients' progress by writing totheir generar practitioners in the finst instance. Because we donot want to produce too much paper work for those registeringcasesr'any one GP is extraordinarily unlikely to have more thanone case at a time so that any extra work for him/her is minimal.
collaboration with other clinical and Medical ResearchThe Register is arso intended to be a research resource for
clinicians and scientists who may wish to pursue projects inrelation to motor neuron disease, subject to satisfactory scien-tific and ethical criteria being futfilled.
222

Appendix E
Eow to obtain Dore infornation.we hope that you wirl be reassured that this project is
scientificatry and ethicalry sound. rf you personarry have anyworries about registering patients wourd you prease let us knowas soon as possibre. Further information about the project isavailabre on request (see below) and we plan to send regurarnewsletters to doctors who have registered patients.
For further infornation write to:
Professor cp warlow, Dr AM chancerror or Mrs Hazel Fraser,Scottish Motor Neurone Disease Register,Neurosciences Trials UnitDepartment of Clinical Neurosciences,
Western General Hospital,Crewe Road,
Edinburgh EH4 2XU.
o31 332 43A7
223

1 caplan LR- The effective clinical neuroTogist, oxford: Black-well Scientific publications , LggO.
2 Booth cc- Rediscoveries. BMJ r99o;301:753-768.3 capildeo R. charcot in the B\s. rn: Historical aspects of theneutosciences, eds Rose FC, Bynum wF. New york: -Raven press,
1991:383-39G.
4 charcot JM. De ra scl6rose rat6rale amyotrophique. Le progrdsI{€dical LB74;2 (3 parts) :325_455.
5 Berl c. The nervou,s system of the human body: As exprained ina series of pape.rs iead before the Royal 'society of rondon.with an appendix of cases and consurtations on nervousdjseases, London: LongTman, 1g36: 390_391.
6 Hormes JD. Early years of the medical society of Edinburgh.Univ Edin J L9G8;ZZzt33-340.
7 wilkinson J. preston's Royar rnfirmary, preston: carnegiepress, L997.
8 Lanska DJ. The history of ref rex hammers. Iveuro rogy1989 i392L542-1549.
9 Morton LT. A medical bibliography. Nr annotated checklist ottext iTTustrating the his'tory -ot iedicine, iotraotr: Butlerand Tanner, 1983: 4th Ed. 603:646.
10 spiltane JD. The tiowering ot neurology. rn: The doctrine ofthe nerves - chapters in' the ' lii-ot neurorogy, oxford:Oxford University press, 1981: ZZZ_qgg.
l-1 Duchenne de_ Bourogne G. paralysie musculaire progressive deIa langue,du voile du palais'et aes l€vres. Archives G6n6r-ales de l"I6dicine 1g60 ;)2283_2gG.
L2 Leyden E. Vorliiufige nittheilung tiber progressive bulbiirpara-Iyse. Arch psychiat 1870;2:A22.
Gordon-Taylor G, walls Ew. sir charles Berr. His life andtimes, Edinburgh: Livingstone, 1958.
Furukawa T. charres Berils description of the phantom pheno-menon in 1830. NeuroJ.ogy L99O;loiraro.Furukawa T. charles Belrrs description of numb chin syndrone.NeuroTogy L988; 38 : 3 31_ .
Abercronbie J. pathologicar and practicar researches ondiseases of the brain aia spinar c6rd, Edinburgh, ieze.Darwall J. ca.s.es of a peculiar species of pararysis. LondonMedicaT Gazette 1g3j- ;Z:ZO1-203.
13
L4
l_5
16
REFERENCES
L7
224

18 Anonymous. obituary for John Darwarl. Lancet i_833 ;74o.19 Meiklejohn A. John Darwar-l, MD (L796-1833) and diseases ofartisans. Br J Ind Med J,956;13:laZ_LIL.20 Mitchell JD, chancellor AM. Anyotrophic laterar sclerosis-Aran's Edinbulvh inspiration?'rn: iroceedings of the thirdEuropean neeting for-the history of the n"ur6t"iences, lggL.2L Aran FA' Recherches sur une maladie non encore d6crite dusystEme rnuscuraire (atrophie muscuraire p;;;;;=sivei. -
ri"Goldbatt 1959). Archives c6n6rales de lq6,diain; 1850;21:5-35.22 Duchenne de-Bourogne G. 6tuae cornpar6e des l6sions anatomi-ques dans ilatrophie- musculaire- paralysie progressive etdans ra pararysie g6n6rale. L,unioi aca iasr ;zizoz.23 charcot JM. IVosographical revision of the amyotrophies. rn:clinicar rectuies on diseases of the nerv6us system, edssavirl T. London: The New sydenham society, iaSg z L64-L82.24 Goldbratt D. I{otor neu.ron disease: historical introduction.rn: Itlotor neuron djseases: Research on "^yoiro-phic Lateralsclerosis and rerated disorders, eds Horri's rnr' x.rrrand LT.New York and London: Grune and stratton, Lg6g: '2-LL.
25 veltema AN. The case of the saltirnbanque prosper Lecomte. Acontribution to the study of the histo;t-oi-progressivernuscular a.trophy (Ara-n-Duchenne) and .rny6trophic lateralsclerosis (charcot) . crin lVeuror il"utoturg Lg75;7822o4-2o9.26 charcot JM, Joffroy A. Deux cas dratrophie muscuraire pro-gressive avec l6sions de Ia substance giise et des faisceauxant6ro-latEraux de ra moelle 6pini6re. Arch physior norm etpathoT (transrated in Lynan,R 3 crassics in'nLirorogy, pubSpringtield, f lLinois, pTsB-J_6o 1869 i2:354,629.27 charcot JM. Appendix. Anyotrophlc,Tateral sclerosis. Autonomyand spasmodic character of Lnis affection. rn: Lectures onthe TocaTisation of cerebrar and spin"l- ii""""" deliveredat the faculty of medicine ot parii, eds Hadden wB. London:The new Sydenharn Society, 18g3: 317_336.
28 charcot J-M. scl6rose des cordons rat6raux de ra moelle6piniEre chez une femme hyst6rique atteinte de contracturepermanente des quatre mernbres . aitl soc lred Hop paris ;.easli(suppl 2l :24-42.
29 Erb wA. uber einen wenig bekannten spinaren symptomencompLex.BerTiner Kiinische wocienschritt re?s ; L2 2357 -359.30 Gowers wR. _Degenerations of the cord. rn: A manuar of dis-eases of the_nervous system, phiradelphia: Brakiston,son andCo, 1888: 323-391.
31 sotanierni KA, Myllyra w. prirnary lateral screrosisl a deba-ted entity. Acta Neuror scand 1995;7L:334-33G.
225

32 Gastaut JL, Micher B, Figarerra-Branger D, sornma-Mauvais H.chronic progressive spiioburbar -paJticiiv. a-,"r" forn ofprimary lateral screrolis. ar:ci- tl,Eirot rged; 15: 509_513 .
33 Bear MF, Richardson Ep,Jr. prirnary lateral screrosis: a casereport. Arch Neurol 1981;38:630_Sgg.
34 Younger DS, Chou S, Hay: ll, Lange DJ, Emerson R, Brin M,Thompson -tl,JF., nowland r,p. nririary rateral screrosis. Aclinical diagnosis reemerges. Arch NeuroT 1988;t5:1304-1307.35 Gowers I{R. A Lecture on Abiotrophy. Lancet Lgo2;1:1oo3_1007.35 Beevor cE. Amyotrophic raterar screrosis. rn: A system otmedicine, eds Arrtutt Tc. r,ondon: MacMirran and co Ltd,1899 z L7 G-] 85.
37 charcot JM. De 1a scr6rose rat6rare amyotrophique (in Gold-blatt 1969) . Le progrls M6dical J€Z+;22325 t34L,453.38 Brakistonrs. Gourd nedicaj dictionary, New york: Mccrahr Hilt,L984: 4th Ed. L228.
39 Brain wR- Diseases of the nervous system, oxford: oxforduniversity press, 1962: 6th Ed. 532.40 Rowland Lp. Ten central themes in a decade of ALs research.Adv Neurol 1991 ;56:3-23.4L siddiqu€ T, Figrewicz DA, pericak-vance MAr Haines JL, Rou-leau G, J-effers AJ, sa.pp p, Hung wu-yen, Bebout J,IrtcKenna-Yasek D, Deng G, Horvitz- HR, cuslrra JF, Brown RH, Roses AD,and corlaborators Linga.ge of a gene causing farniriaramyotrophic lateral sclerosii to chromosone 2L and evidenceof genetic-rocus heterogeneity. w nnil J Med 1991;324:1381_1384.
42 Correction. N EngT J IIed 1991 ;32527L.43 Gallagher JP, Talbert oR. Motor neuron disease after electricshock. Acta Neurol Scand L99O;83:79_82.
44 Bundey s, Loverace RE. A crinicar and genetic study of chro_nic proxirnar spinar muscurar atropny. 'ar"ii tgli;gSz4ss-472.45 Mylsllt.Tl,, skerry L, Korf B, pober B, schapira y, Gascon GG,Al-Rajeh sM, Dubowitz v, Davies K, Brzust-owicz ilM, penchas-
zadeh GK, Gilriam Tc. phenotypic heterogeneity of spinirmuscurar atrophy mapping to chiornosome 5q11 .z-nls (sMA 5g) .NeuroTogy 1990; rlO: J_831-183 6.
46 Kurtzke JF - Motor neuron (e) disease I editoriat ] . BI,IJ1982 ;284 z L4L-I42 .
47 Brownell B, oppenheimer DR, Hughes JT. The central nervoussystem in motor neurone disease-. J Neurol Neurosurg psychia-try L97O;33:338-357.
226

48 Mulder DW, Howard FMJr. Patient resistance and prognosis inamyotrophic lateral sclerosis. Llayo clin proc tgza;51:532-541 .
49 Kasarskis EJ, winsrow M. when did Lou Gehrigfs personalillness begin? Neurology L9B9 ;39:L243-L245.50 Rabin Ft. credo for creeping pararysis. cogito ergo sum. JAIIAl-983 i249i2G49-2650.
51 France M. Metaphysical education. scotsman Lggz;Jan 5th:29.52 Hawking sw. A brief history of tine. From the big bang tohlack holes, London: Bantam books, 1988: 53.
53 Walton J. CLinical examination,difterential diagnosis andclassifieation. rn: Disorders of voluntary niscte, edswarton J. Edinburgh: churchill Livingston, tga-g: 482-518.54 Noffis FH, Smith RA, Denys EH. Motor neurone disease: towardsbetter care. BILJ 1985 i29L2259-262.55 conneally PM. A first step toward a molecurar genetic anary-sis of amyotrophic riterar screrosis. f Engr J ||ed
1991 ;32ttzL43O-L432.
56 La spada A, wilson EM, Lubahn DB, Harding AE, Fischber-k KH.Androgen receptor gene mutations in xltinicea spinal .ttaburbar muscurar atrophy. IVature 199r i3s2.77-7g.57 Tandan R, Bradrey wG. Amyotrophic rateral sclerosis: part 2.Etiopathogenesis . Ann feurol. 1985;18:419-431.
58 Rowland LP- Motor neuron diseases and amyotrophic 1ateralscrerosis: research progress . TrNs LTBT;ro:ggs-igz.59 Williarns DB, Windebank AJ. Motor neuron disease (amyotrophiclaterar sclerosis). Iqayo crin proc 1991 ;66:54-g2.60 Gajdusek DC. Foci of ltlotor Neuron Disease in High Incidencein Isolated PopuTations of East Asia and the w'estern paci-
tic. rn: Human Motor Neuron Diseases, eds Rowrand Lp. NewYork: Raven press , Lgg2: 353-393.
51 Eisen AAr Hudson AJ. Anyotrophic lateral sclerosis: conceptsin pathogenesis and etiorogy. can J Neuror sci L}BTiLlzsis-652.
62 Kurland LT, choi Nw, sayre cp. rnplications of incidence andgeographic patterns on the cTaisification of amyotrophiclateral scJ.erosis. rn: Motor neuron diseases:Researci onamyotrophic IateraT sclerosis and rel-ated disordets, edsNorris F,H.. New york and London: Grune and stratton, .L9692
29-49.
63 Kurrand LT. Epiderniorogic investigations of amyotrophicLateral sclerosis III A genetic int6rpretation of-incidlenceand geographic distribution. trlayo cLi; proc L}ST;322449-462.
227

64 Anonlnnous. Motor Neurone Disease. Int J198.
Epideniol L972;LtL97-
65 Bobowick AR, Brody JA. Epidemiology of motor-neuron diseases.N EngI J IIed L973;288:1047-1055.
56 Kurtzke JF. EpidenioTogy of anyotrophic lateral sclerosjs.rn: Human ttlotor lVeuron-Diseas6s, eds Rowrand p. New york:Raven press, L9g2: 2gL-3O2
67 Anonymous. what causes motoneuron disease? Lancet1990;336:1033-1035.
58 Green streeten. Introductory address. provincial l[ed Surg1840;1:1.
69 Kurtzke JF. Risk factors in amyotrophic lateral sclerosis.Adv Neurol 1991 ;552245-27O.70 MuIrohI cD. The rnedical review article: state of the science.Ann Int Med L9B7;106:485-488.
7L sackett DL, Haynes RB, Guyatt GH, Tugwerl p. How to readreviews and economic anaryzis. rn i ctiiicai epideniotogy-.-ibasic science tor cLinicAL medicine, Boston: Little Brownand Compdny, 19912 379-391.8d. 2nd
72 Kondo K, Tsubaki T. changing mortarity patterns of motorneuron disease in Japan. J Neuror sci tgzi;32241L-424.73 Buckley J, warrow c, smith. p, Hilton-Jones D, rrvine s, TewJR. Motor neuron disease in Engrand and wales Lg59-Lg7g. ;INeurol Neurosurg psychiatry Lgga ; 162L97_2O5.
74 Martyn cN,. Barker DJp, osmond c. Motoneuron disease and pastpoliornyelitis in nngiand and trlales. Lancet 1988;1:L3 Lg-L322.75 Gunnarsson L-G, Lindberg e, s6derfert B, Axelson o. Themortality of motor neuron disease in Sweden. erch Neurol
1990 ;12 :42-46.
76 Lilienfeld DE, chan 8,. Ehrand J, Godbord J, Landrigan pJ,Marsh G, PerI DP. Rising mortality from rnotoneuron diseasein the USA Lg62-94. nancet 1989 ij-zito-ttz.
77 Riggs JE. Longitudinar Gompertzian anal_ysis of amyotrophiclaterar screrosis rnortality in the u.s. , Lg77-L986: evidencefor an inherently susceptiUfe population subset. |Iech ageingdev 1990;53z2O7-22O.
78 Leone ML, chantlra V, schoenberg Bs. Motor neuron disease inthe united states,rgTL and Lgi3-Lg7B:patterns of mortalityand associated conditions at the tine of a""tn. r"uro rog?L987;32 2L339-L343.
79 Durrleman 9, Alperovitch A. Increasing trend of ALS in Franceand elsewhere: are the changes realf Neurorogy 1999-3gt76g-773.
228

80 Jokelainen.M. The epidemiology of anyotrophic lateral scler-osis in Finland. A study based on the aeltn certificates of421 patients. J Neurol Scj lg76i2g.55-63.
81 Bharucha NE, schoenberg BS, Raven RH, pickle LW, Byar Dp,Mason TJ. Geographic distribution of motor neuron -diseaseand correlation with possible etiologic factors. Neurology1983 ;33:911-915.
82 Flaten TP. Rising mortality from motoneuron disease. Lancet1989; i: 1018-1019.
83 Buncher cR, White M, Moomaw CJ. Anyotrophic Tateral sc1erosjstates in ohio,l-960-L986. In: enyotropLic Tateral sclerosis.New advances in toxicorogy and epidbniorogy, eds Rose FC,Norris FH. London: srnith-cordon an-d cornpany ita, 19902 7-Lo.
84 vemireddi NK, Crevoiserat CAJr. Arnyotrophic lateral sclerosisin Cancer (error in published titiershould read rfKansasr notcancer) . J Miss state rfied Assoc LgTg;L9:2oL-2o4.
85 BaIe GS. Anyotrophic lateral sclerosis in rowa. J Chronic DisL97 5 ;2a z 3 05-3 10 .
86 Go.rdberg rD, Kurland LT. Mortarity in 33 countries fromdiseases of the nervous system. Worfd neuroT 1963 ;3:444-465.87 Juergens sM, Kurrand LT, okazaki H, Mulder DW. ALs in Roches-ter, Minnesota, L925-L977 . NeuroT0gy 1980;30:463-470.88 Yoshida s, Mulder DW, Kurrand LT, chu cp, okazaki H. Follow-up study on amyotrophic lateral sclerosis in Rochester,Minn., L925 through 1984 . Neuroepideniology L986isz6L-to.89 Kahana E' Zilber N. changes in the incidence of anyotrophicrateral sclerosis in rsraer. Arch Neuror 1984;t:152-160.90 Kahana E, Arter M, Ferdman s. Arnyotrophic laterar screrosis:a population study. J Neurol Lg76i2L2t2O5-2L3.
91 Rosali G, Pinna L, Granieri E, Aiello r, Tola R, Agnetti v,Pirisi A, de Bastiani p. studies on epideniorogicai, clinilcal, and _etiorogicar aspects of ALS disease in sardinia,southern rtary. Acta Neuror scand Lg77;ssz23l-244.92 Forsgren L, Arnay BG, Holmgren c, Irlarr s. Epidemiorogy ofmotor neuron disease in northern Sweden. ecfa Neurol sbana
1983 i68:20-29.
93 Gunnarsson LG, PaIm R. Motor neuron disease and heavy manuallabour: an ep_ideniorogic survey of varmrand countylsweden.NeuroepidenioTogy L984 ;3 z L95-2O6 .
94 Hojer-Pedersen E, christensen pB, Jensen NB. rncidence andprevalence of motor neuron disease in two Danish counties,IVeuroepidemiology L9B9;8 : 151-J_59 .
229

95 Murros K, Fogerholm l. Anyotrophic rateral screrosis inMiddle-Finrand: an epidemidrogiclr study. A,cta Neuror scand1983;6Zz4I-47.
96 Mitchell JD, Gibson HN, Gatrell A. Arnyotrophic lateral scler-osis in Lancashire and south <-.unbriJ, nrriii"a, 1sze-t9g6. Ageographicar study. Arch NeuroT 1990 i47 r815-88b.97 Hudson AJ, Davenport A, Hader wJ. The incidence of amyotro-phic raterar sclerosis in southwestern ontario, |i;;a;.Neurology L9B6 ; 36 : L524-LS2B .
98 Matsumoto N, worth RM., Ku_rland LT, okazaki H. Epiderniorogicstudy of amyotrophic lateral sclerosis in Hawaii rden-tificatio_n of high incidence among Firipino ,*n . NeurorogyL972 i222934-940.
99 Juvarra G, _ Bettoni Lt Bortone E, Garavelri A, Montanari E,Rocca M. Anyotrophic raterar screrosis in the province ;hParma, rtary: a crinicar, and epideniorogicii-sluay in th"period 1e6o-1980. rtar J Neuroi'sci 1983;iriii-ate.
10o olivares L, Esteban ES, Alter M. Mexican lrresistancer toamyotrophic lateral sclerosis. Arch Neurol LgT2izz 23g7-4o2.101 Granieri E, carreras M, Tola R, paorino E, Trarli G, EreopraR, Serra G. Motor neuron disease in the province of Ferrara,rtary, in L964-L982. NeuroT0gy 1988 i 3s: r.ao4-1608.Lo2 zack MM, Levitt Lp, schoenberg B. Motor neuron disease inLehigh coylty,pennsylvania:an dpideniorogi" =t,ray . J chronicDis L9Z7;30:813-S1g:
103 Leone Mr.chio A, Mortara p, Rosso MG, schiffer D. Motorneuron disease in the province of rurih, ra;it, L971-1980.Acta Neurol Scand 1983;68: 3L6_327 .
104 Murray TJr_ cameron J, Heffernan .Lp, MacDonald HN, King DB,Bedwell -Sl, Scott M, patil J, Shears A, Malik HG, et aIAmyotrophic lateral sclerosis in Nova scotia. Adv Exp l{edBiol L9B7 i2og z345-349.
105 Radhakrish-naD K, Ashok pp, sridharatr R, Mousa ME. Descriptiveepideniology of motor neuron disease in n"r.,!irazi, l,iuva.Neuroepidemiology L9g6 ; S : 47 -54 .
106 Qizilbash N, Bates D. rncidence of notor neurone disease inthe northern region. J EpidenioT coniunitf- niiliiL987;41: 18-20.
Lo7 Kristens"l o, MergaardrB. Motor neuron disease. prognosis andepiderniology. Acta Neuror scand L977;s6 2gg-3o8.108 cendrowski I, wen_der M, owsianowski M. Analyse 6pid6nirogiquede Ia scl6rose lat6rale anyotrophique sur Ie €erritoife -de
ra Grande-Polongne lrngliih auitrictl. Acta IVeuro-L scandL97O;t6:609-6L7.
230

109 Giagheddy {, Puggioni G, Masala c, Biancu F, pirari c, pirasMR, Rachele M_G. _Epi.demiologic study of amyotrophic iateiiisclerosis in sardinia, rtaly. Acta NeuroJ, scand 1gg3 ;6az3g4-404.
1l-o Holloway sM, Mitchell JD. Motor neurone disease in the Lo-thian Region of scotland 1961-81. J zpiaeniol conmunityHealth 1986 ; 40 : 344-350.
111 Bracco L, Antuono p, Amaducci L. study of epiderniorogicar andetiological factors of amyotrophic taterai sclerosis in theprovince of Florence, Italy. icta Neurol Scand Lg79;6OzLL2-L24.
LLz H-o.lloway.sMr Elery AEH. The epideniology of motor neurondisease in scotlan-a. Muscre wefve LgB2;5:131-133.113 salemi G, .Fierro B' Arcara A, cassata M, castigrione MG,savettieri G. .A-nyotrophic raterar screrosis i; r.i"rr",rtary: an epidemiologicar study . rtar J Neuro-r, scil_989;10: 505-509.
114 L6pez-Vega JM, calleja J, combarros o, polo JM, Berciano J.Motor neuron disease in Cantabria. Acta tieurol Scand1988 ;72 zL-5.
115 De Domenico p, Marara cE, Marabelro L, pugrisi RM, MeneghiniF, serra f , Giuseppe c, Musorino R. Arnyotrophic raterarsclerosis:An epiderniological study in the ir""iii"e of Messi-na, rtary , L97 5-198 5 . weuroepidenioiogy 1988; 7 : L52-L58 .
116 chazot F ' V_al1at. JM, Hugon J , Lubeau M, Durnas M. Arnyotrophiclateral sclerosis in tilnousin (Lirnoges area, France). Neuro-epidemiology 1996 ; S 2 39-46.
LL7 Tysnes o-8, _volrset.sE, Aa_rli JA. Epiderniorogy of arnyotrophiclateral screrosis in Hordarand cou-nty, west-6rn Norway. ActaNeurol Scand 1991;83:2gO-295.
L18 sahadevan MG. Motor neurone disease: a crinicar study. JAssoc Physicians India L969;Lt ({):255_260.
119 Norris FH, Denys EH, sang K, Mukai E. The naturar history ofALS in a specified popritation, with comments on risk iac-tors, prognosis and syhptornatic treatrnents. Rjnsho Shinkei-gaku 1989 ;29 : t48S-L492.
L2O Marco R, Rivera-Reyes L. Motor neuronA study of Z6 cases. BoI Asoc Iiled pdisease in Puerto Rico:
R 1983 i75z4OO-4O2.L2L Bharucha NE. Motor neurone disease. J postgrad ltled
L973 ; L9 z SL-62 .
L22 Wa1l DW, Gelfand M. Motor neuron disease in Rhodesian Afri-cans. Brain L972;93z5L7-52O.
23L

L23 Lawyer T, Netsky MG. Anyotrophic lateral sclerosis - a clini-coanato-mi-c study of 5 3 cases . Arch rveurol, psychiat1953;G9zL7I-L92.
L24 Hoffman pM, Brody JA. The reliability of death certifi-cate reporting for arnyotrophic raterai-="rerosis. JChronic Dis L97L;21:5-8
L25 orMarrey _F., Dean G, Elian M. Murtiple screrosis and motorneurone disease: survival and how Certified after death. JEpideniol Community Health L9g7 ;{ L:L4_L7 .
L26 Gardner MJ, Altrnan DG. statistics with confidence-contidenceintervaTs and statisticar guiderines, London: BMJ, 1989:L27 skegg DcG. Murtiple sclerosis: nature or nuture? BMJ1991 ;3O2:247-248.
L28 Paolino E, Granieri E, Tola MR, Rosati c. conjugar amyotro-phic lateral screrosis. Ann Neuror 1983;Lrz69{.L29 chad D, Mits_unoto H, Adernan LS, Bradrey wG, Munsat TL,zieper -r. conjugal motor neuron disease. NeuroT0gy
L982 ;32:3 06-3 07 .
130 sanders M. clustering of amyotrophic lateral sclerosisIletter] . JAIIA 1980 ;zU:435.,131 Hyser cL, Kissel.JT, Mendell JR. Three cases of amyotrophiclateral sclerosis in a common occupational envir6nrneni,. ;Neurol L9B7 i234: 443-444.
L32 Hochberg FH_, Bry.an JA, wheran MA. clustering of anyotrophiclateral sclerosis I retter] . Lancet Lg7 4 ;L:3a.133 Me1ned c' Krieger c. A cluster of anyotrophic lateral scler-osis. Arch Neurol tg9z;39:595-596.
134 Norris FH- Four northern califlornia amyotrophic |ateralsc-lerosis cl.usters. rn: Anyottophic Tate'ral silerosis. Newadvances in toxicorogy and bpiaeniorogy, eds Rose FC, NorrisFH. London: snith-Gordon and company rta, 1990: Lg-2L.135 Gallagher Jp. ALS [retter]. south tled J 19gg;aL:4L7.1,36 Jokelainen M, wikstr6m J, paro J. Effect of birthprace onthe development of amyotrophic laterar sclefosis andnultiple sclerosis. A study amon-g Finnish hrar evacuees. ActaNeuroT Scand t979 ;GO:283-298
L37 Kirness AWr. Hochberg FH. Amyotrophic laterar sclerosis in ahigh serenium environrnent. ieua lgll ;23? 22843-2844.
138 Hawkes cH, Fox AJ. Motor neurone disease in leather workersIletter]. Lancet 1981;i:502.
139 Abarbanel JM, Herishanu y, Frishertextile factory workers. Isr J Med
S. Motor neuron disease inSci 1985;2L:924-92s.
232

140 sienko DG, Davis Jp, Tayror JA, Brooks BR. Amyotrophic rat-eral sclerosis. A case-control study toriowin'g detection ofa cluster in a snalI wisconsin cornnunity.- Arch Neurol1990 ; 17 :38-4L.
L4L Garruto RM, Gajdusek DC, chen KM. Arnyotrophic lateral scler_osis and parkinsonisn-denentia amoig FiTipi; nigrant= -i"Guam . Ann tveurol. 1981 ; 10 : 3 41-3 50 .
L42 Jokelain"l M. Anyotrophic lateral sclerosis in Finrand. r: Anepiderniologic study . Acta lVeuro-l scand rg77;56: 185-193 .L43 Armon c' Kurland LT. when is a ,tclusterr a true cluster?Apprication to neurorogy. Ann Neuror 1989;26:t4o-141.L44 Martyn cN. Poliovirus and rnotor neuron disease. J Neurol1990 ;232:336-338.
145 Kennedy PGE. on the possible role of viruses in the aetiologyof motor neurone disease: a review. ,l-ioyat soc ltled1990 ;83 z7 84-7 87 .
L46 Darakas MC, Edler G, Hallett M, Ravits J, Baker M, papadopou-los N, Arbrecht p, sever J. A rong-term follow-up study ofpatients yi-t_h post-po_liornyelitis neuronuscular symptoms. tIEngT J Med 1986;314:959-963.
L47 Brody JA, stanhope JM, Kurrand LT. patterns of arnyotrophicIateral sclerosis and parkinsonism-dementia on Guarn. contempNeurol Ser L975; L2: 45-7O.
148 Kurland LT. Geographic isorates: their role in neuroepidernio-Iogy . Adv IVeuroI Lg7 8 ; L9 z 69-82 .
L49 Gajdusek Pc. Urgent opportunistic observations: the studyof changing, transienC Lnd disappearing ptt.no."nl or medicalinterest in disrupted prinitiie human communities. cibaFound Synp L977 i 19:.G9-94.
150 Yase Y. Neurologic disease inwith a report on the focussclerosis found in the KiiI6ed Hyg L97 o;19 : 155-166 .
the western pacific islands,of amyotrophic lateralpeninsula, Japan. An J Trop
151 Gajdusek DC, Salazar AM. Amyotrophic lateral sclerosis andparkinsonian syndromes in high iicidence .rong-tn" arryq andJakai people of west New Guinea. Neurology Lggi;32zLo7-L26.L52 Brody JAr.Hirano A, scott RM. Recent neuropathorogic obser-vations in_ amyotrophic lateral sclerosis j"a p""kinsonism-denentia of Guam. IVeurol. ogy L97L;2L:528-536.
153 Rodgers-Johnson p, Garruto RM, yanagihara R, chen KM, cajdu-sek Pc, Gibbs cJ,Jr. Arnyotrophii raterar screrosis andparkinsonism-dementia on Guam: a 3O-year evaruation ofclinicat and neuropathorogic trends. Neu.rology 1986 i36,7-L3.
233

154 Reed D, r.abarthe D, chen KM, stalrones R. A cohort study ofamyotrophic lateral scerlosis and parkinsonism-dementii onGuam and Rota. Nn J Epideniol L9BT;L2S(1):92-100.
155 Reed DM, Brody. JA. Amyotrophic lateral sclerosis and parkin-sonism-dementia on Guam, I945-L972. f. Descriptive epia"ri"-logy. Nn J Epideniol_ L975,.101 r2g7-3OL.
156 Prato cc, Garruto RM, Fox KMr Gajdusek Dc. Amyotrophic lat-eral sclerosis and parkinsonism-dementia on Griarn: I zs-yearprospective case-control study. Am J npiaeiiol1986 iL24 (4) :643-656.
L57 stanhop" {M, Brody JA, Morris cE. Epideniorogic features ofamyotropic lateral sclerosis and parkinsonism-dementia inGuam, Mariana rsrands. rnt J Epidenlor Lg72;1:199-210.
158 Garruto RM, Yanagihara Rr Gajdusek DC. Disappearance of high-incidence amyotrophic lateral sclerosis lna parkinsoniJur-dementia on Guam. NeuroTogy t_995;35:193-19g.
159 Lavine L,_ steere JC, wolfe N, calne DB, orBrien pc, wilriamsDB, Kurland LTr Schoenberg Bs. Amyotrophic lateral scler-osis/parkinsonism-dementiJ conplex in sbuthern Guam: is itdisappearing? Adv Neurol 1991 iSiz271-2g5.160 Reed DM' Torres JM, Brody JA. Amyotrophic lateral scLerosisand parkinsonism-dementia on cuim, ti+s-Lg72. rI. Farnilialand genetic studies. Nn J Epidenior LgTs;101:302-310.
151 Kurland L!, Molgaard cA. Guamanian ALS: hereditary or ac-quired? Adv Neurol Lgg2;36zL6S-L7L.
L62 Hoffman PM, Robbins DS, Gibbs cJ,Jr.t Gajdusek DC, GarrutoRM, Terasaki or. Histocompatibility antigLns in amyotrophiclateral sclerosis and parkins6nism-tementia on c-uarnIletter]. Lancet L977 i2z7L1.
163 Yanagihara RT, Garruto lM, Gajdusek Dc. Epidemiorogicarsurveillance of amyotrophic lateral sclerosii and parki-nson-ism-denentia in the Commonwealth of the Northern MarianaIslands. Ann Neurol 1983 ;L3l.79-86.L64 Brody JA, Edgar AH, Girrespie MM. Amyotrophic laterarsclerosis. No increase among US construction workers incuam. JAI,|A L97g i24O:551-560.
165 Eldridge R, Ryan E, Rosario J, Brody JA. Amyotrophic laterarsclerosis and parkinsonism dementia in a frigrant populationfrom cuam. Neurology L969 ;L9zLO29-1032.
165 Garruto RM, Gajdusek c, chen KM. Amyotrophic lateral scler-osis among charnorro rnigrants from Guam. Ann IVeuro-1.1980 i8:5L2-6L9.
234

L67 Gibbs cJJr, Gajdusek Dc. Anyotrophic laterar sclerosis,Parkinsonrs disease, and the amyotrophic lateral scler-osis-Parkinsonism-dementia complex on Guam: a review andsunmary of attenpts to demonstrate infection as the aetio-logy . J CIin pathol (Suppt) L972,.6: 13 2-L4O.
158 Spencer,- Ps. Linking cycad to the etioTogy of Western pacificanyot*fophic ratdrai screrosis. rn: -inyotrophic raterarsclerosis. New advances in toxicorogy and epidZniorogy, easRose FC, Norris FH. London: snith--cbrdon alna conpaiy rtd,1990 z 29-34.
169 spencer PS, Nunn pB, Hugon J, Ludorph A, Roy DN. Motorneuronedisease on Guam: poLsibie rore of a food neurotoxinIletter] . Lancet 1986;1:955.
L7O Spencer PS, Nunn pB, Hugon J, Ludolph AC, Ross SM, Roy DN,Robertson RC. Guam amyotrophic lateral sclerosis-larkin=olnian-dementia Iinked tb a plant excitant neurotoxin-. ScienceL987 ;237:5L7-522.
L7L Garruto RM, shankar sK., yanagihara R, sarazar AM, Anyx HL,Gajdusek Dc. Low-calciurn, nign-afuminum diet-induced motorneuron pathol0gy in cynomolgus monkeys. Acta NeuropathoT(BerI) 1999 ;7Bz2LO-2L9.
L72 Duncan MW, steere JC, .Kopin rJ, Markey sp. 2-Amino-3-(.,.ethy-Ianino)-propanoic acid_ (BMAAI in cycaa flour: an "tiiif."iycause of amyotrophic lateral sclerosis and parkinsonisrnl
dementia of Guam . Neurology t-990 ; tOz767-772.
L73 Steele JC, Quinata-Guzman T. The Chamorro diet:an unlihelycause of neurofibriTTary degeneration on Guam. fn z Amyotro--ph+c raterar scr.erosjs. iew advances in toxicoloii -ZiaepidenioTogy, eds Rose FC, Norris FH. London: snith--c'ordonand company ltd, 19902 7L-78.
L74 Yanagihara R, Garruto RM, Gajdusek DC, Tomita A, uchikawa T,Konagaya Y, chen KM, sobue r, prato cc, Gibbs cirJr.. carci-um and vitarnin D metabolism in Guamanian Chamorros withamyotrophic lateral sclerosis and parkinsonism-dementia. /utnNeurol 1984;15:42-48.
L75 Yase Y. The basic process of amyotrophic lateral sclerosis asref Tected i-n Kii peninsura aia Guam. rn: fieuro logy pro-ceedings of the t-j-th world congress of Neurology-,- ed,s denHartog Jager wA, Bruyn GW, Heijstee ApJ. nxceiiia MedicaAmsterdarn, L97g: 413 -427 .
L76 Garruto RM, swyt c, yanagihara R, Fiori cE, Gajdusek Dc.Intraneuronal co-Iocalization of silicon witn cllciurn andaluminurn in. arnyotrophic lateral sclerosis and parkinsonismwith dernentia of cuarn Iletter]. N EngT J IIed f-gee ;315 |TLL-7L2.
t77 Amyotrophic Tateral scJerosis. New advances in toxicolgy andepidemioTogy . Edited by Rose, F .c . and Norris, F .H , r,6iraon:Snith-Gordon, L990.
235

L78 Duncan MW. Role of the cycad neurotoxin BMAA in the anyotro-phic lateral sclerosis-parkinsonism denentia complex of thewestern Pacific. Adv Neurol 1991;55:301-310.
L79 Li Ting-Ming, swash M, Alberman E, Day sJ. Diagnosis of motorneuron disease by neurologists: a study in three countries.J NeuroT lVeurosurg psychiatry 1991-;5zt:980-983 .
180 vejjajiva A, Foster JB, Mirler H. Motor neuron disease. Aclinical study. J Neurol Scj Ls67;42299-3L4.
181 Li Ting-Ming, Alberrnan E, swash M. crinicar features andassociations of 560 cases of motor neuron disease. J NeurolIVeurosurg Psychiatry 1990 ;53 : 1043-1045.
L82 Dorsen M, Ehni c. cervicar spondyrotic radicuropathyproducing motor manifestations rnimicking prinary rnustulaiatrophy. fieurosurgery L979 ; Sz 427 -43L.183 Sadowsky CH, Sachs E, ochoa J. Postradiation rnotor neuron
syndrome . Arch lVeuro-I. L97 6 i332786-787 .
184 Marapert D, Brugieres p, Degos JD. Motor neuron syndrome inthe arms after radiation treatment [letter]. J Neulol Neuro-surg Psychiatry L992 ;54:.LL23-LL24.185 Bradley wG, Robison sH, Tandan R, Besser D. post-radiation
motor neuron syndromes. Adv Neuror l99l-;55:341-353.
186 Tan SV, Pye fF. Postradiation motor neurone syndrome of theupper cervical region-a rnanifestation of the cbrnbined effectof cranial irradiation and intrathecal chemotherapy? JNeurol ffeurosurg psychiatry 1991 i469.L87 Farrell DF, Starr A. Delayed neurological sequelae of elec-trical injury. IVeuro-l ogy rsea;1s:601-606.
188 Saha PK, Shenoy KT, Ravindran M. Unusual sequelae of electricshock (a case report) . J Assoc Physicians -India 1981 i29277-78.
189 Argov z, Navon R. crinicar and genetic variations in thesyndrome of adult cM2 gangliosidosis resulting frorn hexosa-minadase A deficiency. Ann NeuroJ. Lg84;L6:L4-2-O.
190 Mitsumoto H, sriman RJ, schafer rA, sternick cs, wilbourn A,Horwitz sJ. Motor neuron disease and adult hexosaminadase Adeficiency in two families: evidence for multisysten dege-neration. Ann lVeurol l_995 ;L7..379-384.191 Moser HW, Naidu S. The Adrenoleukodystrophies. CRC crit revneurobiol L9g7 ; 3 : 29-88 .
L92 Mulder DW, Bastron JA, Lambert EH. Hyperinsulin neuronopathy.NeuroTogy 1956 i 6 z 627 -G35.
236

193 Fisher M, Mateer JE, ullrich r, Gutrecht JA. pyramidal tractdeficits- and. polyneuropathy in hyperthyroidisfi, combinationclinically nimicking arnyotiophic iateral sclerosis. Artt J Med1985 ;7a:LO41-1044 .
L94 Patten BM, Enger wK. phosphate and parathyroid disordersassociated with the syndrohe of amyotrophic- lateral scler-osis. Adv Neurol Lgg2;1e:tA1-200.
195 carnevare v, Minisola s, Rornagnoli E, Df Erasmo E, Bragoni 
2os Buchanan DS, Malamud N. Motor neuron disease with renal ceIIcarcinoml_ and postoperative neurologic remission. NeurologyL973;23:89 1-894.
206 Evans BK, Fagan ct Arnord T, Dropcho EJ, oh sJ. paraneoplas-tic rnotor neuron disease and renal cell carcinoma: rmprove-ment after nephrectomy. Neurology L99O;rtO:960_962.
207 Anonomyous. Missed foramen-magnum tumours. Lancet Lg73;L4g2.2og canpberr AM, wirriams ER, pearce J. Late motor neuron dege-neration following polionyelitis. tleurorogy Lg69;19:1101-
1106.
209 Murder DW, Rosenbaum RA, Layton DD,Jr.. Late progression ofpoliornyelitis or forme frusle amyotrophic tate'rat sclerosis?t4ayo CIin proc Lg72 i 4Z 1756-7 6L.
2Lo sonies BC, Dalakas MC. Dysphagia in patients with the post-porio syndrome. N Engr i iea iggti32r.LL62-LL67.2LL Dalakas M' II1a I. Post-polio syndrome: concepts in clinicaldiagnosi_s, pathogen6sis, ind etiorogy. Adv NeuroI1991;56 : 495-511 .
2L2 Dalakas MC, Pezeshkpour GH. Neuromuscular diseases associatedwith human irnrnunodef iciency virus. Ann Neurol1988 iz3 (suppll : S38-S48.
2L3 Hoffman PM, Festoff BW, Giron LT, Horrenbeck LC, Garruto RM,Ruscetti Fw. Isolation of LAV/HTLv-III from a patient wittramyotrophic lateral screrosis. N Engr J t4ed 19g5;313:324-325.
2L4 Dalakas MC, Pezeshkpour GH. Neuromuscular diseases associatedwith human imrnunodef iciency virus i.nfection. Ann IVeuro-L1988;23: 53B-S49.
215 Martin JP. Anyotrophic meningo-rnyelitis (spinal progressivemuscular atrophy of syphiritic origin) .'n'rain tbzs;le:153-L82.
2L6 Datta A, Dasadhikary c, Ghosh s. syphiritic amyotrophy, Jfndian l4ed Assoc 1966 i4?2287-2gO.
2L7 Kahn P- Cysticercosis of the central nervous system withamyotrophic lateral sclerosis: case report ana rerTiew of theliterature. J Neuror Neurosurg psychiulry Lg72;israr-az.2LB Boothby JA, Dejesus PV, Rowland LP. Reversible forms of motorneuron disease. Lead ilneuritisil. Arch Neuror Lg74;31:19-23.2L9 conradi s, Ronnevi Lo, Norris FH. Motor neuron disease andtoxic metals. Adv Neurol Lgg2;362201-23L.
220 Adans CR, Ziegler DK, Lin JT. Mercury intoxication sirnulatinganyotrophic raterar sclerosis. JAI{A 1983 i2soz642-643.
238

221 Mitchelt JD. Trace eTements, neuroTogical disease and amyo-trophic Tateral scl.erosjs. In: Cirrent trends in trZceeTements reseatch, eds chazot G. srnith-cordon, Lggg: 116-L24.
222 Mitcherr JD, Pentland B, East BW, Harris rA, Jackson MJ.Trace elements and free radicals in motor neutone disease(amyotrophic raterar sclerosis) . rn: Free Radj cals, cerlDamage and Djsease, eds Rice-Evans c. London: nichelieuPress, 1986: 263-272.
223 Patten BM, Brown s. Anyotrophic lateral sclerosis associatedwith aluminium intoxilatioi. rn t Amyotrophic lateral scLer-osis . New advances in toxicology anla epi'aeniology, eds RoseFC, Norris FH. srnith- Gordon and compariy rtd, 1991:
224 Ludolph AC, Hugon J, Dwivedi Mp, schaumburg HH, spencer ps.Studies on the aetiology and pathogenesis- of motor neurondiseases .1. Lathyrisrn:- ctini-caf findings in establishedcases . Brain L9B7; 110 : t_49-165 .
225 Teiterbaun JS, Zatorre RJ, carpenter s, Gendron D, Evans AC,Gjedde A, Cashman NR. Neurological sequelae of domoic acidintoxication due to the ingestion of co-ntaninated mussels. IVEngl J Med 1990;322:L7BL-L797.
226 voss'H. Progressive bulbiir paralyse und amyotrophische later-alskrerose nach chronisCher rnanganverlirtting- ar"n -itJtGewebepath und Gewebhyg J-939 ;9:464_476.
227 Palr HS, williarns AC, waring R, Erias E. Motorneurone diseaseas manifestation of pesticide toxicity Iretter]. LancetL987; ii: 685.
228 steventoD- _G8., waring R. Pecticide toxicity and motor neuronedisease Iretter]. i neurot lVeurosurg psy;hiatry 199o;53:621-625.
22g Leys D, Petit H. clinical signs of arnyotrophic lateral scler-osis developing after potyriaiculoneuropaltry associated withanitriptyline . Br[J 199b;:oo . GL4 .
23o Behan Po, Bakheit AM. Association of amyotrophic lateralsclerosis, Hoignets syndrome and residencd in cian. J NeurolNeurosurg Psychiatry 199L r.5rl : 90-9L.
23L Ghatak NR, Hirano A, Zimmerman HM. Rheumatoid arthritiswith arteritis and neuropathy rnasking amyotrophicraterar screrosis. Rjnsho shinkelga*u tgzz ;tz:iot-410.232 Mathe JF, FEve JR, Labat JJ, De-Kersaint Gilly-A, potagas c,Dubois c. rsch6mie de ra corne ant6rieure- d; la nberri
IEngrish abstract]. Rev Neurol (paris) 1989;1{5:60-64.
233 Shepherd Fleet w, Watson RT. From benign fasiculations andcramps to motor neuron disease. Neurology L9g6;362997-99g.
239

234 Rafalowska J, wasowicz B. syringomyeria simurating amyotro_phic laterar screrosis. por lred'J 1958 ;?:L214-1218.235 van Gent EM, Hoogrand RA, Jennekens FGr. Distal amyotrophy ofpredominantly the upper lirnbs with pyranidaf reatures in alarge kinship. J Neuror Neurosurg 'e'sychiaiiv 1985;taz266-269.
236 Harding AE, Thomas PK. Peroneal muscular atrophy with pyrarni-dar features. J Neuror Neurosurg psychi"irv Ig'a1i1.7zL6B-L72.237 Tandan R. Disotders of the upper and lower motor neurons. rn:NeuroTogy in crinicar practlce, eds eradrey wc, Daroff RB,Fenichel GM, Marsden c. Butterworth-Heinerninn, rsso, L6g7-L7L7.
238 Harding AE. Hereditary rrpurerr spastic paraplegia: a crinicarand gene-t-i_c, study or 2, famities. J Neuior-neurosurg psy-chiatry 1981 ; t4 z 87 l--893 .
239 Korosue K, shibasaki H, Kuroiwa y, Machi T, sawada K, Kita-mura K, rkeda_ J. cyst of the conus rneduliaris maniiesai;gamyotrophic raterar screrosis syndrome. rorii ;;i;ir;lNeurol Jpn l_991;35: 507-510.
240 Rosenberg.RN. Anyotrophy in lluTtisystem Genetic Diseases. rn:Human ltrotor Neuron Djseases, eds howland Lp. New york: RavenPress, L9923 L49-L57.
241 Hudson AJ. . Amyotrophic lateral sclerosis and its asso-ciation with dementia, parkinsonism and other neurologicaldisorders: a review. ariin 19g1;rol.2L7-247.
242 Gourie-Devi M, suresh TG, shanker sK. pattern of motorneurone disease in south rndia and monomeTic anyotrophy (abenign atypicaT torm). rn: I{otor neurone djsease . proceed-ings. of the international symposium on ILND (rg|4) , edsGouri-Devi M. New Delhi: oxfor-d ind rBH, Lg87: 171-189.243 oryema J, Ashby p, spiegel s. Mononelic atrophy. can J Neuro-l,sci 1990;L?2L24-l_30.
244 Hirayarnd Kr.Tomonagd M, Kitano K, yarnada T, Kojima s, Arai K.Foca} cervical poliopathy causing juvenile nrjscufar atroptryof distal upper extiemiiy: a paln6rogicar study. J NeurollVeurosurg psychiatry L9BT ; 50 : 285_2gO.
245 serratrice c. spinal monomeric amyotrophy. Adv NeuroiL991;56: 1G9-129.
246 Harding AE, Thornas pK, Baraitser M, Bradbury pG, Morgan-Hughes JA, ponsford JR. x-Linked recessiv6 uuiuospinatneuronopathy: a report of ten cases. J Neurol neurZsurgpsychiatry L982; ls : forz-1019 .
247 olney RK, Aminof_f. MJ, so yr. crinical and erectrodiagnosticfeatures of x-rinked bulbospinar neuronopathy. neirotogy1991 ;4L2823-829.
240

248 Brain WR. Some unsolved problems of cervical spondylosis. BI1J1963 iLz77L.
249 Whitaker J. llhitaker's Almanack, London: Joseph Whitaker andSons Ltd, 1989: t-21st Ed. 6L2-6L3.
25O The. Registrar General . Annual Report tot Scotland 7gyg,Edinburgh: Government Statistical bervice General negisteiOffice, 1999: 135th Ed.
251 Gardner MJ, Altman DG. Caiculating confidence intervals forrerative risks, odds ratios, and. standardjsed ratios andrates. In: Statistics with contidence-confidence intervalsand statistical guidTines, London: Br Med J, LgBg: 5o-63.252 Gardner sB, winter pD, Gardner MJ. confidence intervarsanalysis version L.o (personar computer software), London:
BMJ, 1989:
253 Parrette gfr, Bradrey wG, Brooks BR, et ar . criteria for thediagnosis of amyotrophic lateral sclerosis: preliminarydraft of the ALS/MND research foundation scientific commititee, Escorial,spain. world Neurology (in press) L992i
254 Mulder Dw. ClinicaL Linits of Anyotrophic Lateral Sc-Lerosjs.rn: Human Motor Neuron DiseaseJ, edJ nowrand Lp. New york:Raven Press, L9g2: L5-22.
255 David P, Lo-Monaco M, parieri G, scoppetta c, servidei s,Tonari P, Vaccario ML. crinical feJtures of amyotrophiiamyotrophic lateral sclerosis. rtal J Neurol scj rgier izzitl-LL7.
256 christensen pB, Hojer-pedersen E, Jensen NB. survivar ofpatients with amyotrophic lateral sclerosis in 2 Danishcounties . NeuroTogy L99O; rtO: 600-604 .
257 Emery AEH, Horloway s. Fanitiar ,I|otor Neuron Djseases. rn:Advances in Neutorogy, eds Rowrand Lp. New york: RavenPress, L9g2z 39-47.
258 chio A, Brignorio F, Meineri p, schiffer D. phenotypic andgenetic he_terogeneity of dominantly inherited ary-oirophicraterar screrosis. Acta Neuro_z scand Lg87 i?sz27z (4)--2g2.-
259 Li Ting-Ming, Alberrnan E, swash M. comparison of sporadic andfanilial disease amongst 580 cases oi motor n"ur6n disease.J Neurol Neurosurg psychiatry l_988 iSLz778-784.260 Vertema AN, Roos RA, Bruyn Gw. Autosomar dominant adultamyotrophic lateral sclerosis. A six generation Dutch fani-Iy. J Neurol Scj 1990;91:93-11_5.
261 Horton wA, Eldridge R, Brody JA. Farnirial motor neuron dis-ease. Evidence for at least three different types. IVeuro-Togy ]-976i262450-465.
24L

262 Delra sara s, Laratta F, Mazzini L. Amyotrophic raterarsclerosis: a possible example of autosomal receisive inneriltance. schweiz Arch Neuror psychiatr 1991 iL42zL39-L47.263 Belloc Hilaire. stories, essays and poems, London: J.M.Dentand Sons Ltd, 1939: 431
264 l{anuaT of the international statist ical classification otdiseases, injuries and causes of death, gth revision, WorfaHealth Authority, L977 z
265 Heasman MA. scottish hospital in-patient statistics-sourcesand uses. Health Bulletin 1968;Ze:fO-fa.
266 chancerlor AIvt, swingler RJ, Fraser H, warrow cp. The scottishrnotor neuron disease register: A prospective study of adultonset motor neuron disease in scotland. Methodology, demo-graphy and clinical features of incident cases iri-igeg. JNeuro-l lVeurosurg psychiatry LggZ i fD press.
267 Lockwood -E. Accuracy of scottish hospital morbidity data . BrJ Prev Soc tled L97L;2Szt6-83.
268 Pater AR'.9r-ay G, Lang GD, Bairrie F,c.H., Flening L, wilsonGM. scottish hospital rn_orbidity data 1. Errors itt ii"gtt-=-tic returns. Health Bulletin t5ze;34:2Ls-22o.269 Murchison J, Barton qR, Ferguson A. An anarysis of casesincorrectly coded as inflanmitory bowel diseaJe in scottishhospitar in-patient statist-ics (sHrps). scot Med J1991;36: 136-138.
27o Kohli HS, Knill-Jones RP. How accurate are SMR1 (Scottishmorbidity record 1) data? Health Burretin Lgg2;sozL4-23.27L Park RHR, Mccabe p, Russell Rr. who should rog sHrps? Theaccuracy of Scottish hospital morbidity data ior Wilsonrsdisease. Health Bultetin lggz;Soz24-28.
272 Scottish Hea1th service Common Services Agency. preciseclinical summaries: the source of high quarit! sun a.t.. rsDpublications 1990 ; 1-10.
273 Swingler RJ, Warlow cP. Polio and Motor Neurone Disease inscotrand. J Neuror Neurosurg psychiatry Lgg2lrn press.274 Sacks o. The man who mistook his wife for a hat and otherclinical tal.es, New york: Harper and Row, Lgg7.
275 calne DB, Eisen. A, McGeer E, spencer p. Arzheinerrs disease,Parkinsonrs disease and notorneurone disease: abiotropicinteraction between ageing and environment? Lancet1986; ii: 1062-1o70.
276 Steele JC, Guzman T. observations about amyotrophic lateralsclerosis and the parkinsonism-dernentia com-ptex bf Guam withregard to epidemiology and etiorogy. can J Neurol sciL987;1,1:3 58-362.
242

277 Hawkes cH, Graham AJ. what cause motoneuron disease?Itetter] . Lancet 1991 ;332: 180.
278 Livesley B' Sissons,S.E. Chronic lead intoxication nirnickingrnotor neurone disease . BIIJ 1969; { : 3g7-39g.
279 Woods AH. Trauma as a cause of amyotrophic lateral sclerosis.JAILA r'grr,.55: 1876 -L877 .
280 Jerriffe sE. The amyotrophic laterar screrosistrauma. J Nerv Ment Dis 1935;82241-5-435.
syndrome and
281 Turner AJW, Oxfd BM. Trauma and progressive muscular atrophy.Lancet 1939,- ii: 548-551.
282 Arpers BJ, Farmer RA. Role of repeated trauma by pneumaticdrill in production of amyotrophlc lateral scteioiis. ArchNeurol Psychiat L949 ; 62 z L78-L82.
283 Ask-Upnark E. Arnyotrophic Lateral Sclerosis observed in 5persons after gastric resection. GastroenteroT0gy1950 ;LSz257-259.
284 Galragher Jp, sanders M. Apparent motor neuronlowing the use of pneumati- tools . Ann IVeuro-Z695.
disease fol-1983;L.z694-
285 Milanese c, Martin L. Amyotropic lateral sclerosis and trau-ma. Acta Neurol Belg L97O;?O:482-49L.
286 Gallagher JP. Amyotrophic lateral sclerosis following armtrauma Iletter]. Arch Neurol 1,986;43t755.
287 Kurtzke JF, Beebe cw. Epiderniology of arnyotrophic laterarsclerosis: 1. A case-control comparilon 6ased on ALsdeaths . Neurology L98O;30:453-462.
288 Kondo K, Tsubaki T. case-controL studies of motor neuronedisease- Association with rnechanical injuries. Arch lfeuro-I.1981 ;38:220-226.
289 Gawel M, zaiwalla z, Rose Fc. Antecedent events in motorneuron disease. J Neurol Neurosurg Psychiatry 19g3;{6:1041-1043.
29o Deapen DM, Henderson BE. A case-control study of arnyotrophiclaterar sclerosis. Anr J Epidenior 1986;L23:zbo-zgg.
29L Gallagher Jp, sanders M. Traurna and anyotrophic laterarscrerosis: A report of 7B patients. Acta iveuroJ. scandL987 ;75:L45-l_50.
292 Provinciali _L, Giovagnoli AR. Antecedent events in amyotro-phic lateral sclerosis: do they influence clinical onset andprogression? Neuroepideniology L99O ;9 z255-262.
243

293 Gunnarsson LG, Lindberg G, soderferdt B, Axelson o. Arnyotro-phic lateral sclerosis in sweden in reiation to occupition.Acta NeuroJ. Scand 1990;83 : 394-398.
294 Mitchell JD-. Heavy metals and trace elements in amyotrophiclateral sclerosis. NeuroTogic crinics LggT is?43-60.295 williams.A. Ecogenetics, xenobiotic biochemistry and neurolo-gical disease. J Neurol. 1991 .23a:187-190.
296 tflar,inq RH, sturman sG, qnith McG, steventon GB, Heafield II{TE,Willians AC. S-Methylation in notor neuron disease .naParkinsonrs disease. Lancet 1989 iz2356-357.297 steventon GB, waring RH, wilriams AC, parr Hs. Xenobioticmetabolism in motor neuron disease. La.ncet 1998;22644-647.
298 carstairs v, Morris R. Deprivation and health, Aberdeen:Aberdeen University press, LggL.
299 Darakas Mc. Amyotrophic raterar screrosis and post-polio:differences and sirnilarities . Birth Defects L9B7;2g:Sg-gt.
3oo Backett EM. social patterns of antibody to poliovirus. LancetL957 ; L2778-783 .
301 Macleod R_c, MacGregor rG, Larrninie HE, Grist NR. serorogicarepidemiology of poliomyelitis in central Scotland. scoE LIedJ 1958;327 6-81.
3o2 chancelror AM, carstairS V, Erton RA, swingrer RJ, warlow cp.Affluence, age and motor neurone disease-. I npidemiol Com-nunity HeaLth L9g2 i 462L72-L13.
303 Government Statistical Service . classification of occupationL980, London: Her Majestyrs Stationary Office, 19gO:
304 sackett DL. Bias in analytic.research. J chronic DisL979;32251 -63.
305 Kopec JA, Esdaite JM. Bias in case-control studies. A review.J EpidenioT Community HeaTth 1990 itlizLTg-1gG.306 Kelsey JL, Thonpson wD, Evans As. case-control studjes. rn:Iilethods in observational epidemioTogy, New york: oxfordUniversity press, LgB6: l_48-t-86.
3o7 Hanisch R, Dworsky RL, Henderson BE. A search for cluesto the cause of amyotrophic lateral sclerosis Iletter].Arch Neuro-l. L97 6;33:456- 457 .
308 Armon c, Kurland LTr Daube JR, orBrien pc. Epiderniorogiccorrelates of sporadic anyotrophic lateral scleiosis. feulo-Togy 1991 ; 11,2 LO77-1084.
244

309 sackett PL-, Haynes RB, Tugwerr p. Deciding whether yourtreatment has done harm. rn: crinicar Epidenlorogy. e 6asicscienee tot clinical medicine, Toronto: Little Brown andCompany, 1985: 230.
310 stern M, Dulaney E, Gruber sB, Golbe L, Bergan M, Hurtig H,Gollomp s, Stolley P. The epiderniotogy of iarkinsonrs 6is-ease- A case-control study of young and old onset patients.Arch Neurol 1991;48 : 903-907
311 Graves AB, White E, Koepsell TD. The association between headtrauma and Alzheimerrs disease. An J Epideniol 1990i131-49L-501.
3L2 Fletcher NA_, .Ha.rding AE, Marsden cD. The relationship betweentrauma and idiopathic torsion dystonia. J Neurol ileurosurgPsychiatry L99L ; 54 :7 L3-7 L7 .
313 wirson sA5. The amyotrophy of chronic lead poisoning: Amyo-trophic lateral screroiii of toxic origin. Rev Neulor p?y-chiatry L9O7 ; S z 44L-445 .
314 Lee wR, Moore MR. Low lever exposure to lead. BMJ1090 r.301:504-5O5.
315 Graziano JH, Brum c. Lead exposure from lead crystar. LancetL991 ;337 zt4L-L42.
316 Yanagihara R. Heavy rnetals and essential minerals in motorneuron disease. Adv Neurol Lg82;362233_242.
3L7 Barber TE. fnorganic mercuryamyotrophic lateral sclerosis.
318 cavalreri A., Minoia c, ceroni M, poloni M. Lead in cerebro-spinal fluid and its relationship to plasna lead in hurnans.J AppT Toxicol 1984;4tG3-65.
319 Stober T' Ste1te w, Kunze K. Lead concentrations in blood,plasma, erythrocytes, and cerebrospinar fluid in amyotrophiclaterar screrosis. J Neurol sci 19-83 i6Lz2L-26.32o conradi s,^ Ronnevi Lo, Nise G, Vesterberg o. Abnormal distri-bution of lead in amyotrophic lateral sclerosis reestima-tion of read in tha cefebrospinal f luid. .r Neuror scj
l_980 i lai 413-4L9.
32L conradi sr. Ronnevi Lo, Vesterberg o. rncreased plasma levelsof lead in patients with amyotrophic lateril sclerosiscompared with control subjects as determined by flamelessatonic absorption spectrophotometry. J weurof NeurosurgPsychiatry L97 Bi al : 389-393 .
322 Canpbell AMG, Williarns ER, Barltrop D. Motor neurone diseaseand exposure to read. J weurol. Neurosurg psychiatryL97 O;33 z 877 -885 .
intoxication reminiscent ofJ Occup l4ed L97 8 i 20 z 662 -669 .
245

323 Roelofs-rverson RA, Murder DW, Erveback LR, Kurland LT,Morgaard cA. ALs and heavy metars: a pilot case-controrstudy. lleurol. ogy L9B4;3t: 39J-395.
324 Baker EL, smith TJ, et al. The neurotoxicity of industrialsolvents: a review of the literature. Arnerican Journal otIndustrial ltledicine 1985;8 (3 | :2O7 -2L7 .
325 Gunnarsson LG, Lindberet G. Anyotrophic lateral sclerosis insweden 1970-83 and sorvent exposure Iletter]. Lancet1989; i:958.
326 den Hartog Jager wA, Hanro pw, Ansink BJ, Vermeuren MB.Results of a questionnaire in 1oo ALS patients and 1oocontrol cases. crin Neurol, Neurosurg L9g7;ee :n-at.327 Patten BM,_ Engel wK. Phosphate and Parathyroid DisordersAssociated with the Syndrome of Anyotrophi| Lateral Scler-osis. rn: Human trotoi Neuron Diseales, eas Rowrand Lp. NewYork: Raven press, L9g2: l_gl--200.
328 Felmus MT, Patten BM, Swanke L. Antecedent events in amyotro-phic laterar sclerosis. Neurology r976;262L67-L72.
329 Kondo K. D^oes gastrectony predispose to amyotrophic lateralsclerosis? Arch NeuroJ. LgTg;36: 58 6-587 .
330 schenkmaD N, Tarras sc, Boesch RR, Mulvihirl MN, caroscio JT.Anyotrophic lateral sclerosis and pet exposure-. N EngI J qt1ed1983 i 309 2244.
331 Tarras s, schenkman N, Boesch R, Murvihilr v!, caroscio JT.ALS and pet exposure. Neurology L9B5i33z7L7-720.
332 Gresharn LS, Morgaard cA, Gorbeck AL, snith R. Anyotrophiclateral sclerosis and occupational heavy metal exposure: acase-control study. Neuroepideniorogy 1986 ;s:29-38.333 Gresham LSr Molgaard cA, Gorbeck AL, snith R. Amyotrophiclateral sclerosis and history of skeletal fracture: a case-control study. Neurology L987 ;32 zZLT-7L9.
334 Armon c, Kurland LT, o'Brien pc, Mulder Dw. Antecedent rnedi-cal diseases in patients with arnyotrophic lateral sclerosis.A population-based case-controlled study in Rochester, Minn,L925 through L997. Arch Neurol 1991;482283-296.
335 chi6 A, Brignrio F, Leone M, Mortara p, Ross MG, Triboro A,Schiffer D. A survival analysis of 155 cases of progressivemuscurar atrophy. Acta Neurol scand 1985 i72z4o7-4L3.
336 Mortara P, Bardelli D, Leone M, schiffer D. prognosis andclinical varieties of ALs disease. rtal J N-eurol sci1981;2:237-242.
337 Bornan K, Meurman T. Prognosis of amyotrophic lateral scler-osis. Acta Neurol Scand L967i432489-4gg.
246

338 caroscio JT, Murvihirl MN, sterling R, Abrams B. Arnyotrophiclateral sclerosis. rts natural history. NeuroJ,ogiS c6i,iaaL987;5: 1-8.
339 Kristensen o, Melgaard B. Motor neuron disease. prognosis andepidemiology - Acta NeuroT scand Lg77 ;56:299-308.340 Hodkinson HM. More favourable prognosis of motor neuronedisease in old age. Age Ageing tbzZ;1:182_184.
341 Rosen AD. Amyotrophic lateral sclerosis: CIinicaI featuresand prognosis. Arch Neurol L9TB;35:538-642.
342 Chancellor AM, Warlow CP. Adult onset rnotor neuron disease:Worldwide rnortality, incidence and distribution since 1950.J Neurol lleurosurg psychiatry Lgg2iIn press.343 Kaplan EL, Meier P. Nonparametric estimations from incornpleteobservations . American statis tical Association ,loirnal
1958 ;53:457-48L.344 Brooks BRr s,u.f i.t RL, Depaul R, Tan yD, sanjak M, Robbins J.Design of clinical therapetrtic trials'in aln-yotroinic lateralsclerosis. Adv Neurol 1991 ;56:521-546.345 Strong MJ., Hudson AJ, Alvord WG. Familial anyotrophic lateralsclerosis,1850-t_989: A statisticar anaryiis of the worrdliterature. Can J Neurol Scj 1991;18:45_59.
346 Boman K, Meurman T. Factors infruencing the prognosis ofamyotrophic raterar sclerosis. Acta aleurot scandL967;t3:Suppl 31:1.
347 osuntokun Bo, Adeuja Ao, Bademosi o. The prognosis ofmotor neuron disease. in Nigerian africais. A prospec-tive study of 92 patients. Braii L974;9?2385-394.
348 Gimenez-Roldan S, Esteban A. Prognosis in hereditary amyotro-phic rateral screrosis. Arch nelror Lg77;342706-708.
349 Gubbay ss, Kahana E, Zirber N, cooper G, pintov s, LeibowitzY: Anyotrophic laterar screrosis- A study of its presenta-tion and prognosis. J Neurol 1985;232:295-300.
350 Jablecki -cK, Berry c, Leach J. survival prediction in amyo-trophic laterar screrosis. truscre Nerve 19g9 iL2zg33-g41.351 scarpa M, colombo A, panzetti p, sorgato p. Epideniology ofamyotrophic lateral sclerosis in the province of uodEna,Italy. Influence of environmental exposure to lead. ActaNeurol Scand 1989 ;?? :456-460.
352 Mathews wB. practical neurology, oxford: Brackwerl, L97s: 3rdEd. ]-37.
353 Yevtushenko yevgeny (translated by AR MacAndrehr). Aprecocious autobiography, London: Collins and Harvitl press,1963: 53.
247

354 Beisecker AE, cobb AK, Ziegrer DK. patientsr perspectives ofthe role of care providers in amyotrophic latLraf sclerosis.Arch Neurol 19gB;t5 : 553-556.
355 Henke E. Motor neurone disease-a patientts view. BI4J1968;l:765-766.
356 Rabin D, Rabin pL, Rabin R. occasionar notes. compounding theordeal of ALS: rsolation from my ferlow physicians. N Eigr JI{ed L982 i3O7: 506-509.
357 carus R. Motor neurone dj.sease: a deneaning illness. BI{J1980 ;455-456.
248