
Research update for articles published in EJCI in 2009
16
Research update for articles published in EJCI in 2010 Christopher Adlbrecht 1 , Elmar Aigner 2 , Juan M. Bello ´n 3,4 , Izolde Bouloukaki 5 , Alberto Bouzas-Mosquera 6 , Alexandre J. F. Carrilho 7 , Kuo-Chu Chang 8 , Nipon Chattipakorn 9 , Siriporn C. Chattipakorn 9 , Yi-Jen Chen 10,11 , Yuan-Chiang Chung 12 , Roshan Colah 13 , Christian Datz 14 , Jens B. Frøkjær 15 , Shunji Fujimori 16 , Panagiota Georgiadou 17 , Cintia M. Grion 7 , Chih-Ping Hsu 18 , Martin Hu ¨ lsmann 1 , Ming-Jui Hung 19 , Ming-Yow Hung 20,21 , Efstathios K. Iliodromitis 22 , Irene M. Lang 1 , Ting- I. Lee 10,23 , Winfried Ma ¨ rz 24,25,26 , Sona B. Nair 13 , Gemma Pascual 3,4 , Jesu ´ s Peteiro 6 , Choitsu Sakamoto 16 , Atsushi Satomura 27 , Sophia E. Schiza 5 , Peter Sta ¨ rkel 28,29 , Tatjana Stojakovic 24 , David L. Vesely 30,31 , Darren L.Walters 32 and Yusuf Yilmaz 33,34 1 Division of Cardiology, Department of Internal Medicine II, Medical University of Vienna, Vienna, Austria, 2 First Department of Medicine, Paracelsus Medical University Salzburg, Salzburg, Austria, 3 Detartment of Medical Specialities and Surgery, University of Alcala, Alcala ´ de, Spain, 4 Networking Research Centre on Biomaterials, Bioengineering and Nanomedicine (CIBER-BBN), Madrid, Spain, 5 Sleep Disorders Unit, Department of Thoracic Medicine, Medical School, University of Crete, Heraklion, Greece, 6 Department of Cardiology, Hospital Universitario A Corun ˜ a, A Corun ˜ a, Spain, 7 Department of Internal Medicine, Londrina State University, Londrina, PR, Brazil, 8 Department of Physiology, College of Medicine, National Taiwan University, Taipei, Taiwan, 9 Cardiac Electrophysiology Research and Training Center, Chiang Mai University, Chiang Mai, Thailand, 10 Graduate Institute of Clinical Medicine, College of Medicine, Taipei, Taiwan, 11 Division of Cardiovascular Medicine, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan, 12 Department of Surgery, Cheng-Ching General Hospital, Taichung, Taiwan, 13 National Institute of Immunohematology (I.C.M.R.), K.E.M Hos- pital Campus, Parel, Mumbai, India, 14 Department of Internal Medicine, General Hospital Oberndorf, Oberndorf, Austria, 15 Mech-Sense, Department of Radiology, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark, 16 Department of Gastroenterology, Graduate School of Medicine, Nippon Medical School, Tokyo, Japan, 17 2nd Division of Interventional Cardiology, Onassis Cardiac Surgery Center, Athens, Greece, 18 Department of Medical Laboratory Science and Biotech- nology, Yuanpei University, Hsinchu, Taiwan, 19 Department of Cardiology, Chang Gung Memorial Hospital, Keelung, Chang Gung University College of Medicine, Gueishan, Taoyuan, Taiwan, 20 Department of Internal Medicine, School of Medicine, College of Medicine, Taipei, Taiwan, 21 Division of Cardiology, Department of Internal Medicine, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan, 22 2nd University Department of Cardiology, Medical School, Attikon University General Hospital, Athens, Greece, 23 Division of Endocrinology and Metabolism, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan, 24 Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University of Graz, Graz, Austria, 25 Institute of Public Health, Social and Preventive Medicine, Mannheim Medical Faculty, University of Heidelberg, Mannheim, Germany, 26 Synlab Academy, Synlab Services GmbH, Mannheim, Germany, 27 Division of Laboratory Medicine, Department of Pathology and Microbiology, Nihon University School of Medicine, Tokyo, Japan, 28 Institut de recherche expe ´ rimentale et clinique (IREC), Universite ´ Catholique de Louvain, Brussels, Belgium, 29 Department of Gastroenterology, St. Luc University Hospital, Brussels, Belgium, 30 Departments of Internal Medicine and Molecular Pharmacology and Physiology, James A. Haley Veterans Hospital, Tampa, FL, USA, 31 University of South Florida Health Sciences Cardiac Hormone Center, Tampa, FL, USA, 32 The Prince Charles Hospital, University of Queensland, Brisbane, Qld, Australia, 33 Institute of Gastroenterology, Istanbul, Turkey, 34 Department of Gastroenterology, School of Medicine, Marmara University, Istanbul, Turkey Differential effects of fluvastatin alone or in combination with ezetimibe on lipoprotein subfractions in patients at high risk of coronary events (Tatjana Stojakovic and Winfried Ma ¨ rz) Recently [1] Winkler et al. [2] reported that total cholesterol, LDL-C and small, dense LDL (sdLDL) were significantly reduced with ezetimibe 10 mg (E10), simvastatin 20 mg (S20) and the combination of E10 ⁄ S20 in patients with type 2 dia- betes and a preponderance of sdLDL. The further decrease of sdLDL by adding ezetimibe to simvastatin was not signif- icant. Florentin et al. [3] showed that S10 plus E10 is simi- larly effective to S40 in improving sdLDL and LDL particle size in patients with primary hypercholesterolaemia. In the study of Berneis et al. [4], healthy men were treated with European Journal of Clinical Investigation Vol 42 1149 DOI: 10.1111/eci.12001 RESEARCH UPDATE
-
Upload
meduniwien -
Category
Documents
-
view
0 -
download
0
Transcript of Research update for articles published in EJCI in 2009

Research update for articles published in EJCI in2010Christopher Adlbrecht1, Elmar Aigner2, Juan M. Bellon3,4, Izolde Bouloukaki5, Alberto Bouzas-Mosquera6,Alexandre J. F. Carrilho7, Kuo-Chu Chang8, Nipon Chattipakorn9, Siriporn C. Chattipakorn9, Yi-Jen Chen10,11,Yuan-Chiang Chung12, Roshan Colah13, Christian Datz14, Jens B. Frøkjær15, Shunji Fujimori16, PanagiotaGeorgiadou17, Cintia M. Grion7, Chih-Ping Hsu18, Martin Hulsmann1, Ming-Jui Hung19, Ming-Yow Hung20,21,Efstathios K. Iliodromitis22, Irene M. Lang1, Ting- I. Lee10,23, Winfried Marz24,25,26, Sona B. Nair13, GemmaPascual3,4, Jesus Peteiro6, Choitsu Sakamoto16, Atsushi Satomura27, Sophia E. Schiza5, Peter Starkel28,29,Tatjana Stojakovic24, David L. Vesely30,31, Darren L.Walters32 and Yusuf Yilmaz33,34
1Division of Cardiology, Department of Internal Medicine II, Medical University of Vienna, Vienna, Austria, 2First Departmentof Medicine, Paracelsus Medical University Salzburg, Salzburg, Austria, 3Detartment of Medical Specialities and Surgery,University of Alcala, Alcala de, Spain, 4Networking Research Centre on Biomaterials, Bioengineering and Nanomedicine(CIBER-BBN), Madrid, Spain, 5Sleep Disorders Unit, Department of Thoracic Medicine, Medical School, University of Crete,Heraklion, Greece, 6Department of Cardiology, Hospital Universitario A Coruna, A Coruna, Spain, 7Department of InternalMedicine, Londrina State University, Londrina, PR, Brazil, 8Department of Physiology, College of Medicine, National TaiwanUniversity, Taipei, Taiwan, 9Cardiac Electrophysiology Research and Training Center, Chiang Mai University, Chiang Mai,Thailand, 10Graduate Institute of Clinical Medicine, College of Medicine, Taipei, Taiwan, 11Division of CardiovascularMedicine, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan, 12Department ofSurgery, Cheng-Ching General Hospital, Taichung, Taiwan, 13National Institute of Immunohematology (I.C.M.R.), K.E.M Hos-pital Campus, Parel, Mumbai, India, 14Department of Internal Medicine, General Hospital Oberndorf, Oberndorf, Austria,15Mech-Sense, Department of Radiology, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark, 16Department ofGastroenterology, Graduate School of Medicine, Nippon Medical School, Tokyo, Japan, 172nd Division of InterventionalCardiology, Onassis Cardiac Surgery Center, Athens, Greece, 18Department of Medical Laboratory Science and Biotech-nology, Yuanpei University, Hsinchu, Taiwan, 19Department of Cardiology, Chang Gung Memorial Hospital, Keelung, ChangGung University College of Medicine, Gueishan, Taoyuan, Taiwan, 20Department of Internal Medicine, School of Medicine,College of Medicine, Taipei, Taiwan, 21Division of Cardiology, Department of Internal Medicine, Shuang Ho Hospital, TaipeiMedical University, New Taipei City, Taiwan, 222nd University Department of Cardiology, Medical School, Attikon UniversityGeneral Hospital, Athens, Greece, 23Division of Endocrinology and Metabolism, Department of Internal Medicine, Wan FangHospital, Taipei Medical University, Taipei, Taiwan, 24Clinical Institute of Medical and Chemical Laboratory Diagnostics,Medical University of Graz, Graz, Austria, 25Institute of Public Health, Social and Preventive Medicine, MannheimMedicalFaculty, University of Heidelberg, Mannheim, Germany, 26Synlab Academy, Synlab Services GmbH, Mannheim, Germany,27Division of Laboratory Medicine, Department of Pathology and Microbiology, Nihon University School of Medicine, Tokyo,Japan, 28Institut de recherche experimentale et clinique (IREC), Universite Catholique de Louvain, Brussels, Belgium,29Department of Gastroenterology, St. Luc University Hospital, Brussels, Belgium, 30Departments of Internal Medicine andMolecular Pharmacology and Physiology, James A. Haley Veterans Hospital, Tampa, FL, USA, 31University of South FloridaHealth Sciences Cardiac Hormone Center, Tampa, FL, USA, 32The Prince Charles Hospital, University of Queensland,Brisbane, Qld, Australia, 33Institute of Gastroenterology, Istanbul, Turkey, 34Department of Gastroenterology, School ofMedicine, Marmara University, Istanbul, Turkey
Differential effects of fluvastatin alone or incombinationwith ezetimibe on lipoproteinsubfractions in patients at high risk ofcoronary events (Tatjana Stojakovic andWinfried Marz)
Recently [1] Winkler et al. [2] reported that total cholesterol,
LDL-C and small, dense LDL (sdLDL) were significantly
reduced with ezetimibe 10 mg (E10), simvastatin 20 mg (S20)
and the combination of E10 ⁄ S20 in patients with type 2 dia-
betes and a preponderance of sdLDL. The further decrease
of sdLDL by adding ezetimibe to simvastatin was not signif-
icant. Florentin et al. [3] showed that S10 plus E10 is simi-
larly effective to S40 in improving sdLDL and LDL particle
size in patients with primary hypercholesterolaemia. In the
study of Berneis et al. [4], healthy men were treated with
European Journal of Clinical Investigation Vol 42 1149
DOI: 10.1111/eci.12001
RESEARCH UPDATE

E10, S40 or their combination. The authors stated that eze-
timibe alone increased sdLDL so that potentially athero-
protective effects of simvastatin are offset by ezetimibe.
However, using relative proportions of individual subfrac-
tions alone may be misleading when assessing the effects of
lipid-lowering therapy on LDL metabolism [5]. The most
balanced interpretation of the available evidence is that
ezetimibe is less effective than statins in reducing sdLDL
when administered at doses equally effective in reducing
LDL-C.
Five a-globin chain variants identified duringscreening for haemoglobinopathies (Sona B. Nairand Roshan Colah)
The evidence that has accumulated reinforces our statement
to undertake systematic investigations while screening for
b-haemoglobinopathies to identify rare a-chain variants in a
population [6]. The first case of Hb Fontainebleu
[a-21(B2)GCT fi CCT] with Hb S was identified in a new-
born and her mother along with one case each of Hb O
Indonesia [a-116(GH4) GAG fi AAG] and Hb Koya Dora
[a-142(B2) TAA fi TCA] during our newborn screening pro-
gramme for sickle cell anaemia [7]. We have identified four
new cases of Hb J Paris I [a-12(A10) GCC fi GAC] and
two of Hb O Indonesia during our routine screening for
b-haemoglobinopathies (unpublished data). There are reports
of one case each of Hb O Indonesia and Hb J Meerut [a-120(H3) GCG fi GAG], both identified in two pregnant ladies
who came for antenatal screening for b-thalassaemia ⁄A1c
estimation [8,9]. We also identified many cases of Hb Sal-
lanches [a-104(G11)TGC fi TAC] causing HbH disease
using HPLC, cellulose acetate electrophoresis (pH 8Æ9) andDNA sequencing while investigating cases with a b-thalas-saemia intermedia like presentation [10,11].
Epidermal Growth Factor’s Activation of Ras isInhibited by Four Cardiac Hormones (David L.Vesely)
The conclusions of this investigation were that (i) four cardiac
hormones specifically inhibit (up to 79%) epidermal growth fac-
tor’s activation of Ras and (ii) that these cardiac hormones’ anti-
cancer effects involve the inhibition of mitogens such as
epidermal growth factor’s ability to activate Ras (1) as well as
their inhibiting unstimulated basal activity of Ras [12–14].
There is evidence that other mitogen besides epidermal growth
factor that is insulin’s stimulation of Ras can also be blocked by
these four cardiac hormones [15]. There is very recent evidence
that there may be a negative feedback relationship of the
cardiac hormones’ inhibition of Ras as dexamethasone-induced
Ras protein 1 inhibits one of the cardiac hormones that is atrial
natriuretic peptide’s release [16]. Thus, the cardiac hormones
inhibit mitogen stimulated Ras and Ras, in turn, can inhibit
ANP’s release. There is no new evidence that weakens the
previously conclusions.
Cardiovascular Hormones Eliminate SomeSquamous Cell Carcinomas in Athymic Mice(David L. Vesely)
The conclusions of this investigation were that (i) three of the
four cardiac hormones synthesised by the atrial natriuretic pep-
tide gene (namely vessel dilator, kaliuretic peptide and atrial
natriuretic peptide) can eliminate human squamous cell lung
carcinomas in athymic mice when treated subcutaneously for
four weeks and (ii) the fourth cardiac hormones that is long-
acting natriuretic peptide, decreased the volume of one squa-
mous cell lung carcinoma to 2% of that of untreated animals,
suggesting that it, too, has beneficial effects on squamous cell
lung cancers [17]. Noteworthy, there is a much more robust
elimination of another lung cancer with these cardiac hormones
in that they eliminate up to 86% of human small-cell lung
cancers in athymic mice [18]. Both of these lung cancers, once
eliminated, never return in the lifespan of the mice [17,18].
There have been no further studies on the cardiac hormones
and lung cancers in vivo.
Distribution of small intestinal mucosal injuriesas a result of NSAID administration (ShunjiFujimori and Choitsu Sakamoto)
In our study [19], many small intestinal mucosal breaks were
detected after dicrofenac and omeprazole concomitant treat-
ment. Recently, Wallace et al. [20] reported that proton pump
inhibitors (PPIs) exacerbate nonsteroidal anti-inflammatory
drug (NSAID)-induced small intestinal injury in rat. The study
shows that omeprazole and lansoprazole impair the ability to
disinfect by PPI-induced low acid gastric environment and
resulted in transubstantiation of intestinal flora exacerbated
NSAID-induced small intestinal injury. If PPI exacerbating
small intestinal injury is true, our study might have over-evalu-
ated the frequency of NSAID-induced small intestinal injury.
However, our results partially supported the new idea because
the severe small intestinal lesions such as ulcers were predomi-
nantly located in the distal small intestine in our study. The dis-
tal small intestine maintains a more diverse microflora and a
higher bacterial population [21]. Microflora must have an
important role in NSAID-induced small intestinal injury in the
studies.
1150 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com

Long-term outcome after thrombectomy in acutemyocardial infarction (Christopher Adlbrecht andIreneM. Lang)
Acute myocardial infarction (AMI) is caused by thrombotic
coronary occlusion. In our publication, we documented long-
term risk reduction for death or cardiac rehospitalisation for
patients with AMI randomised to thrombectomy prior to per-
cutaneous coronary intervention (PCI), compared to PCI
without thrombectomy [22]. Few studies have evaluated
long-term outcome in patients with AMI after thrombectomy
[23], however, one-year cardiac mortality was recently shown
to be reduced in large-scale randomised controlled trials [24],
and thrombectomy prior to PCI is now recommended in
practice guidelines [25]. A new challenge comes from more
recent trials where administration of glycoprotein IIb ⁄ IIIaantibodies via a perfusion balloon during PCI significantly
reduced infarct size [26]. Ongoing thrombectomy trials
(e.g. TOTAL) will contribute to a better understanding of the
role of this strategy in contemporary AMI treatment algo-
rithms and of its impact on long-term outcomes.
Osteopontin as a novel prognostic marker instable ischaemic heart disease: a 3-year follow-upstudy (Panagiota Georgiadou and Efstathios KIliodromitis)
Baseline levels of osteopontin (OPN) were reported to be asso-
ciated with rapid coronary plaque progression and in-stent
restenosis at 6-month follow-up [27,28]. High levels of OPN in
carotid and femoral atherosclerotic plaques independently pre-
dicted the risk of new cardiovascular events and interventions
at 3-year follow-up; the predictive value of serum OPN levels
was less strong but still significant in these patients [29]. A posi-
tive association of OPN with arterial stiffness and the extent of
coronary artery disease (CAD) have been demonstrated in
patients with CAD [30]. Similarly, OPN levels correlated with
the severities of both coronary and aortic atherosclerosis but on
multivariate analysis, only aortic atherosclerosis remained sig-
nificant [31]. An independent association was also found
between OPN levels and the presence and severity of nephro-
pathy and CAD in diabetic patients [32]. Hence, OPN levels are
more likely to reflect not only coronary atherosclerosis but also
atherosclerosis in other vascular beds.
Lipoproteins and CETP levels as risk factors forsevere sepsis in hospitalised patients (AlexandreJ. F. Carrilho and Cintia M. Grion)
More recent studies have investigated [33] the anti-inflammatory
role of HDL particles in innate immunity. Hara et al. [34] dem-
onstrated that HDL obtained from knockout mice for endothe-
lial lipase, a member of the lipase gene family that promote
HDL catabolism, was more potent in neutralising microorgan-
ism endotoxin than control HDL in vivo and in vitro. This effect
was related to increase in phospholipid rather than protein con-
tent in HDL particles. In another study, Henning et al. [35] sug-
gest that the C-terminal half of apoA1 is the main domain
responsible for the endotoxin neutralisation of this protein.
These studies reinforce the known HDL role as immune modu-
lator; however, regarding to HDL cholesterol protection against
severe sepsis in hospitalised patients, there are not new data
confirming or refuting this hypothesis. We think that a multi-
centre study could shed light on this important question.
High-dose tirofiban with enoxaparin andinflammatory markers in high-risk percutaneousintervention (Darren L. Walters)
Since the publication of our article [36], we have continued to
work in the area of optimal anticoagulation in patients with
acute coronary syndromes and study the link between inflam-
matory markers and cardiac events. As a follow-up to our
study, we found that inflammatory markers continue to be
present long after the index event with increased expression of
monocyte tissue factor and soluble CD40 ligand at mid-term
follow-up following percutaneous coronary intervention [37].
In a related study, we also found that preoperative platelet acti-
vation as evidenced by platelet-bound CD40 ligand was associ-
ated with cardiac events [38]. In terms of optimal
anticoagulation in percutaneous intervention (PCI), there has
been an increasing recognition that heparin and routine use of
glycoprotein IIbIIIa inhibitors is associated with increased
bleeding events. These bleeding events are strongly associated
with an increased risk of subsequent mortality in patients
undergoing PCI [39]. Therapy is now more tailored and used in
a selective fashion. A number of studies have now demon-
strated the benefit of novel antiplatelet agents that exhibit both
a faster onset of action and a superior level of platelet inhibition
compared with clopidogrel [40,41]. Many new clinical chal-
lenges have been posed with the arrival of these more potent
agents. Therapies must balance bleeding risk against the throm-
botic complications of the disease and invasive treatments.
Increased serum FGF21 levels in patients withnonalcoholic fatty liver disease (Yusuf Yilmaz)
Recent clinical [42] studies have largely confirmed the associa-
tion between increased FGF21 levels and the presence of nonal-
coholic fatty liver disease (NAFLD). In addition, the evidence
that FGF21 chiefly mirrors the extent of hepatic steatosis has
reinforced. In this regard, Li et al. [43] reported that serum
European Journal of Clinical Investigation Vol 42 1151
RESEARCH UPDATE

FGF21 levels were significantly higher in patients with NAFLD
compared with the controls and had a high positive correlation
with intrahepatic triglyceride content. In addition, Yan et al.
[44] have shown that serum FGF21 increased progressively
with the increase of hepatic fat content as measured by proton
magnetic resonance spectroscopy, but when hepatic fat content
increased in the fourth quartile, FGF21 tended to decline. Taken
together, the data concordantly show that serum FGF21 may
serve as a potential biomarker to reflect the hepatic fat content
in patients with mild or moderate NAFLD.
Electrical optimisation of cardiacresynchronisation in chronic heart failure – still acontroversially discussed issue (ChristopherAdlbrecht andMartin Hulsmann)
Electrical optimisation of cardiac resynchronisation therapy
(CRT) in patients with chronic heart failure is recommended
by the manufacturers and by the study investigators of large
RCTs [45]. Similar to optimal medical background therapy
[46] in this setting evidence is still lacking. In 2010, we pub-
lished a retrospective analysis demonstrating a positive influ-
ence [45]. A randomised, patient and observer blinded study
compared a fixed AV-interval set at 120 ms, AV-delay pro-
grammed with the echocardiography-determined mitral
inflow method or by an algorithm. The authors found no dif-
ferences in outcome in 980 patients randomised and con-
cluded that routine use of echocardiographic optimisation as
well as algorithm-based AV-interval optimisation is not
clinically warranted [47].
While our data [45] are limited by the retrospective design,
other investigators stated that the study of Ellenbogen [47] was
underpowered and that one should not exclude patients from
electrical optimisation of the AV-interval [48].
Therefore, and in the light of small prospective studies [49]
and larger retrospective analyses [45], the exact role of optimi-
sation of the AV-interval and interventricular delay in CRT
remains to be determined, and the latest version of guidelines
still provide no recommendation on this issue [50].
Value of exercise echocardiography for predictingmortality in elderly patients (Alberto Bouzas-Mosquera and Jesus Peteiro)
Peak treadmill exercise echocardiography – the technique
employed in our study [51] – has recently shown to be more
sensitive than bicycle stress echocardiography, at least for
detecting multivessel coronary artery disease [52]; this may be
particularly relevant in elderly patients, in whom bicycle stress
echocardiography is often inconclusive owing to premature
interruption of exercise and ⁄or problems of coordination.
In patients unable to perform an exercise stress test, dobuta-
mine stress echocardiography has shown to predict cardiac
events and death in patients ‡60 years, but only cardiac events
in those <60 years [53].
Finally, a recent meta-analysis [54] on noninvasive imaging
techniques in patients >65 years confirmed that stress echocardio-
graphy effectively stratified risk in these patients; the annua-
lised cardiac event rate for a normal stress echocardiographic
study was 1Æ9% vs. 8% after an abnormal test (P < 0Æ001), andthere were no significant differences in the event rates between
patients undergoing pharmacological and exercise stress tests.
C-reactive protein evolution in obstructive sleepapnoea patients under CPAP therapy (Sophia E.Schiza and Izolde Bouloukaki)
Previously, our team has shown that, in patients with OSA and
without preexisting cardiac disease, effective CPAP treatment
results in a significant CRP reduction after 3 months and a
steeper decline after 6 months [55]. This is consistent with the
findings of a recent meta-analysis [56] and with the results from
another published study from our team, which shows that
CPAP’s protective role in males is achieved at an earlier time
point [57]. Furthermore, in another study, effective 3 month
CPAP treatment significantly decreased CRP [58]. In contrast,
Colish et al. [59] failed to find significant changes in CRP levels
after 12 months of CPAP therapy; however, the number of
patients was small, which is prone to a false conclusion, and
the baseline levels of CRP were within normal limits. In conclu-
sion, using CRP as a marker of systemic inflammation, CPAP
reduction of CRP levels may benefit patients’ cardiovascular
health.
Effects of acetyl-L-carnitine and oxfenicine onaorta stiffness in diabetic rats (Kuo-Chu Chang)
Malondialdehyde (MDA) [60] is a highly toxic by-product
formed by lipid oxidation-derived free radicals, which can react
with collagen to form MDA-collagen cross-links. Slatter et al.
[61] proposed a pathway of MDA cross-linking of cardio-
vascular collagen in diabetes mellitus: the glucose-glycated
collagen stimulates oxidation of LDL producing MDA, which
then cross-links the collagen; the MDA-mediated cross-linking
of collagen may in turn contribute to the reduction in its already
low turnover, stiffening the aortas, thereby promoting further
glycation. In our study, treating streptozotocin-induced dia-
betic rats with acetyl-L-carnitine had diminished aortic MDA
content, which might cause a fall in cross-links of collagen and
improve aortic distensibility [60]. By contrast, without any sig-
nificant changes in MDA content, oxfenicine therapy showed
no benefits for the mechanical properties of the elastic
1152 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com

reservoirs. Thus, we suggest that MDA-mediated cross-linking
of aortic collagen may be one of the major contributing factors
for arterial stiffening in intact diabetic animals.
Relationship between oligomer and functionalserummannose-binding lectin in chronic renalfailure (Atsushi Satomura)
Our study published in EJCI in 2010 showed functional man-
nose-binding lectin (MBL) levels were significantly lower in
both pre-haemodialysis and haemodialysis patients than in
healthy subjects, and moreover, lower in pre-haemodialysis
patients than in haemodialysis patients [62]. Therefore, we
sought to determine whether functional MBL would be
improved by haemodialysis therapy. Further evidence had
been found that the lower levels of functional MBL just before
haemodialysis therapy were improved significantly by hae-
modialysis therapy, although the functional MBL level of
patients on haemodialysis for one year was still lower at about
45–65% of healthy subjects [63]. Generally, the patient with low
functional MBL level might be associated with unusual and
severe infections [64]. As infectious disease has always ranked
high as a cause of death in patients undergoing dialysis, the
decline of functional MBL, as a component of innate immunity,
may be one of the underlying causes.
Effect of acute hyperglycaemia on sensoryprocessing in diabetic autonomic neuropathy(Jens Brøndum Frøkjær)
Recent studies have revealed that neuropatic-like changes and
reorganisation in the central nervous system are important
drivers for development of disturbed sensation and gastrointes-
tinal symptoms in patients with longstanding diabetes and
autonomic neuropathy [65].
Using recordings of evoked brain potential to oesophageal
stimulations in this patient group, we found reduced sensitiv-
ity, increased latencies and reduced amplitudes [66]. Also
changes in anatomical locations of the dominating electrical
brain sources were observed [66]. Furthermore, using mag-
netic resonance diffusion tensor imaging, we characterised
brain microstructure in areas involved in visceral sensory
processing [67]. We discovered microstructural changes in
several of these brain areas which were associated with the
presence of gastroparesis and with clinical gastrointestinal
symptoms [67].
These new functional and structural findings support that
microstructural reorganisation and neuropathic-like dysfunc-
tion of the brain, in contrast to acute hyperglycaemia itself, are
likely involved in the pathogenesis and persistence of gastroin-
testinal symptoms in diabetes patients.
Oxidative stress and inflammation modulateperoxisome proliferator-activated receptors withregional discrepancy in diabetic heart (Ting- I Leeand Yi-Jen Chen)
Diabetes mellitus (DM) modulated peroxisome proliferator-
activated receptors (PPARs) through oxidative stress and
inflammatory cytokines which are attenuated by ascorbate
treatment [68]. We further found that DM aggravated but
PPAR-c agonist (rosiglitazone) decreased the hypertensive
effects on cardiac PPAR-c expression, oxidative stress andinflammation [69].
PPAR isoforms are differentially expressed in the atria and
ventricles [68]. We found that ApoE knockout DMmice have a
higher arrhythmogenesis in the cardiomyocytes treated with
PPAR-c activator (piogliotazone, 1 lm) [70]. Therefore, we fur-
ther investigated on the electrophysiological effects of rosiglit-
azone in the ventricular cardiomyocytes of DM with or without
hypertension and evaluated its effects on the calcium regula-
tions. We found that DM and hypertension modulated calcium
handling. Rosiglitazone significantly changed the calcium regu-
lation and electrophysiological characteristics, and may contain
an arrhythmogenic potential in DM with hypertension [71].
Cardiac hormones inhibit proliferation ofpancreatic cancer but not normal cells (David L.Vesely)
The statement that ‘four cardiac hormones have strong anti-
proliferative effects on human pancreatic cancer while sparing
human kidney, lung, prostate and endothelial cells from a simi-
lar strong antiproliferative effect’ [72] has been confirmed for
atrial natriuretic peptide by other investigators [73].
In support of the statement, ‘This antiproliferative effect on
pancreatic cancer cells helps to explain why human pancreatic
cells in vivo treated with cardiac hormones decrease to >10% of
the volume of untreated pancreatic cells [74] as they proliferate
less’, the cardiac hormones cause cell death in up to 36% of
human pancreatic cancer cells as measured quantitatively by
nuclear matrix protein 41 ⁄ 7 released from dead or dying cells
while causing no cell death of normal cells [75]. Further support
for this statement is that the four cardiac hormones cause toxic-
ity in up to 58% of human pancreatic cancer cells while sparing
normal cells [76].
The effect of Longan seed polyphenols oncolorectal carcinoma cells (Yuan-Chiang Chungand Chih-Ping Hsu)
Longan seed polyphenols (LSP) induced S phase arrest of the
cell cycle and apoptosis on colorectal carcinoma cells [77].
European Journal of Clinical Investigation Vol 42 1153
RESEARCH UPDATE

Similar effects of LSP on lung (A549), liver (HepG2), cervix
(C33A) and breast carcinoma cells (MDA-MB-231) is under
revision [78]. LSP systemically suppressed cyclin D1 and
cyclin A and enhanced CIP ⁄p21 and KIP ⁄p27 in all four cell
lines and arrested C33A and MDA-MB-231 cells in S phase of
cell cycle. LSP also suppressed Bcl-2 and acivated caspase 3
in all cell lines and induced significant apoptosis in HepG2
and C33A cells. The induction of LSP on S phase arrest of
the cell cycle and apoptotic death in cancer cell lines seems
to be cancer type specific. However, the suppression of onco-
genic cyclin D1, A and Bcl-2 and the enhancement of tumour
suppressor CIP 1 ⁄p21 and KIP 1 ⁄p27 by LSP are systemic,
indicating LSP as a novel cancer chemoprevention and treat-
ment agent.
NFjB, cytokines, TLR 3 and 7 expression inhuman end-stage HCV and alcoholic liver disease(Peter Starkel)
Current research is focusing on the interaction between the gut
and the liver (gut-liver axis) as a driving force behind alcohol-
induced liver damage [79]. Evidence is accumulating that alco-
hol increases the gut permeability favouring the translocation
of gut-derived bacterial products into the portal circulation
[80]. How this affects the expression and activation of cytokines
and TLR signalling pathways in human liver remains to be elu-
cidated. Our own research tends to confirm activation of sev-
eral pro-inflammatory cytokines such as TNF-a and IL-1b in the
liver of alcoholic patients, whereas IL-6 seems to be inhibited
by alcohol in the absence of liver cirrhosis. Conflicting evidence
exists concerning the hepatitis C virus (HCV). In vitro studies
show that the HCV nonstructural protein 5A down-regulates
TLR4 signalling in HepG2 cells, whereas a study using liver tis-
sue from HCV-infected patients reports a good correlation
between hepatic inflammation, TNF-a, TLR2 and TLR4 expres-
sion [81,82]. Ongoing research by us and others will help to
clarify how different organ systems influence each other and
what pathways are implicated in the pathogenesis of the dam-
age of target organs such as the liver.
Interactions among gender, age, hypertensionand C-reactive protein in coronary vasospasm(Ming-Jui Hung andMing-Yow Hung)
Increased inflammatory status exists in patients with coronary
vasospastic angina and the anti-spastic treatment decreases
inflammation as reflected by the level of high-sensitivity C-
reactive protein (hsCRP) [83,84]. The hsCRP is a sex-dependent
inflammatory biomarker with a higher blood concentration in
female [85] and a gender interaction between fasting plasma
glucose and hsCRP [86]. Although hsCRP is elevated in patients
with coronary vasospastic angina, increased peripheral leuco-
cyte rho-kinase activity not only significantly predicts the pres-
ence of coronary vasospasm but also correlates with
vasospastic angina severity [84]. Although the precise mecha-
nism of coronary vasospasm is still not clear, both endothelial
and smooth muscle dysfunction have been suggested to play a
role [87]. Among the clinical associated factors, hypertension is
negatively associated with coronary vasospasm [87], suggesting
that pathogenesis of coronary vasospasm differs from that of
coronary atherosclerosis.
Active metalloproteinase-2 upregulation in theabdominal skin of patients with direct inguinalhernia (Gemma Pascual and JuanManvelBellon)
Previous findings have supported the hypothesis of impaired
regulation of collagen metabolism involving different constitu-
ents of the whole abdominal wall in patients with different
types of hernias [88–90]. Our group had already showed MMP-
2 overexpression in the transversalis fascia in patients with
direct hernia [91], and in cultured fibroblasts obtained from
patients this type of hernia [92]. The persistence of MMP-2
overexpression in the cell cultures appears to suggest a genetic
defect or irreversible change as the origin of this pathology
rather than environmental factors, which may later participate
in the development of the hernia process. Similar alterations
were also observed in the abdominal skin of patients with this
pathology in the present article.
Recent publications [93] also confirm, in accordance with our
article, an imbalance in MMP ⁄TIMP activity that indicates a
dysregulation of the extracellular matrix degradation process in
patients with inguinal hernia, suggesting that impaired colla-
gen metabolism may be an underlying pathophysiological
mechanism of inguinal hernia formation.
Plasma urocortin in acute myocardial infarctionpatients (Nipon Chattipakorn and Siriporn C.Chattipakorn)
Despite growing evidence that urocortins may provide cardio-
protective effects during cardiac ischaemia ⁄ reperfusion injury,
most studies were from pre-clinical reports using exogenous
urocortin administration [94–97]. In 2010, we demonstrated in
patients with acute myocardial infarction (AMI) that their
plasma urocortin levels were elevated for 5 days from onset,
and its high level within 24 h after the onset is associated with
high mortality [94]. At this time, no new evidence exists to con-
firm these findings regarding the plasma level of urocortins
and its time course after the onset in AMI patients. Further-
more, no new evidence exists regarding the association
1154 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com

between the plasma urocortin level (alone or in combination
with NT-proBNP) and the mortality in AMI patients. Future
clinical studies with larger sample size are required to warrant
the clinical usefulness of plasma urocortins as a prognostic
indicator in AMI patients.
Iron stores, liver transaminase levels andmetabolic risk in healthy teenagers (ChristianDatz and Elmar Aigner)
Iron excess is directly associated with insulin resistance. In
2010, we demonstrated that body iron stores were related to
metabolic risk markers in healthy, lean teenagers even within
the limits of normal [98]. Since then, progress has been made in
defining the relevance of hyperferritinemia in nonalcoholic
fatty liver disease (NAFLD) by demonstrating that iron deposi-
tion is related to advanced disease [99]. Elevated serum ferritin
has also been linked to liver transplantation associated mortal-
ity [100]. Furthermore, the first controlled clinical trial has been
published showing the benefit of iron reduction therapy on sev-
eral components of the metabolic syndrome, thus strengthening
the evidence to offer phlebotomy to these patients [101].
Recently, we were able to show that iron overload in NAFLD is
linked to low copper availability and that low copper status is a
frequently unrecognised trace metal abnormality in NAFLD
[102]. Moreover, we found that glucose ingestion modulates
serum iron concentrations [103].
Address
Division of Cardiology, Department of Internal Medicine II,
Medical University of Vienna, Vienna, Austria (C. Adlbrecht,
M. Hulsmann, I. M. Lang); First Department of Medicine, Para-
celsus Medical University Salzburg, Salzburg, Austria (E. Aig-
ner); Detartment of Medical Specialities and Surgery,
University of Alcala, Alcala de, Spain (J. M. Bellon, G. Pascual);
Networking Research Centre on Biomaterials, Bioengineering
and Nanomedicine (CIBER-BBN), Madrid, Spain, (J. M. Bellon,
G. Pascual); Sleep Disorders Unit, Department of Thoracic
Medicine, Medical School, University of Crete, Heraklion,
Voutes, Greece (I. Bouloukaki, S. E. Schiza); Department of
Cardiology, Hospital Universitario A Coruna, A Coruna, Spain
(A. Bouzas-Mosquera, J. Peteiro); Department of Internal Medi-
cine, Londrina State University, Londrina, PR, Brazil (A. J. F.
Carrilho, C. M. Grion); Department of Physiology, College of
Medicine, National Taiwan University, Taipei, Taiwan (K.-C.
Chang); Cardiac Electrophysiology Research and Training Cen-
ter, Chiang Mai University, Chiang Mai, Thailand (N. Chattip-
akorn, S. C. Chattipakorn); Graduate Institute of Clinical
Medicine, College of Medicine, Taipei Medical University, Tai-
pei, Taiwan (Y.-J. Chen, T.-I. Lee); Division of Cardiovascular
Medicine, Department of Internal Medicine, Wan Fang Hospi-
tal, Taipei Medical University, Taipei, Taiwan (Y.-J. Chen);
Department of Surgery, Cheng-Ching General Hospital, Tai-
wan (Y.-C. Chung); National Institute of Immunohematology
(I.C.M.R.), K.E.M Hospital Campus, Parel, Mumbai, India
(R. Colah, S. B. Nair); Department of Internal Medicine, General
Hospital Oberndorf, Oberndorf, Austria (C. Datz); Mech-Sense,
Department of Radiology, Aalborg Hospital, Aarhus University
Hospital, Aalborg, Denmark (J. B. Frøkjær); Department of Gas-
troenterology, Graduate School of Medicine, Nippon Medical
School, Tokyo, Japan (S. Fujimori, C. Sakamoto); 2nd Division
of Interventional Cardiology, Onassis Cardiac Surgery Center,
Athens, Greece (P. Georgiadou); Department of Medical Labo-
ratory Science and Biotechnology, Yuanpei University, Taiwan,
(C.-P. Hsu); Department of Cardiology, Chang Gung Memorial
Hospital, Keelung, Chang Gung University College of Medi-
cine, Taiwan (M.-J. Hung); Department of Internal Medicine,
School of Medicine, College of Medicine, Taipei Medical Uni-
versity, Taipei, Taiwan (M.-Y. Hung); Division of Cardiology,
Department of Internal Medicine, Shuang Ho Hospital, Taipei
Medical University, New Taipei City, Taiwan (M.-Y. Hung);
2nd University Department of Cardiology, Medical School,
Attikon University General Hospital, Athens, Greece (E. K. Ilio-
dromitis); Division of Endocrinology and Metabolism, Depart-
ment of Internal Medicine, Wan Fang Hospital, Taipei Medical
University, Taipei, Taiwan (T.-I. Lee); Clinical Institute of Medi-
cal and Chemical Laboratory Diagnostics, Medical University
of Graz, Graz, Austria (W. Marz, T. Stojakovic); Institute of
Public Health, Social and Preventive Medicine, Mannheim
Medical Faculty, University of Heidelberg, Mannheim,
Germany (W. Marz); Synlab Academy, Synlab Services GmbH,
Mannheim, Germany (W. Marz); Division of Laboratory Medi-
cine, Department of Pathology and Microbiology, Nihon Uni-
versity School of Medicine, Tokyo, Japan, (A. Satomura);
Institut de recherche experimentale et clinique (IREC), Univer-
site Catholique de Louvain, Brussels, Belgium (P. Starkel);
St. Luc University Hospital, Brussels, Belgium (P. Starkel);
Departments of Internal Medicine and Molecular Pharmacol-
ogy and Physiology, James A. Haley Veterans Hospital, Tampa,
FL, USA (D. L. Vesely); University of South Florida Health Sci-
ences Cardiac Hormone Center, Tampa, Florida, USA (D. L.
Vesely); The Prince Charles Hospital, University of Queens-
land, Brisbane, Qld, Australia (D. L. Walters); Institute of Gas-
troenterology, Marmara University, Istanbul, Turkey (Y.
Yilmaz); Department of Gastroenterology, School of Medicine,
Marmara University, Istanbul, Turkey (Y. Yilmaz).
Correspondence to: Department of Hygiene and Epidemiol-
ogy, University of Ioannina Medical School, Ioannina 45110,
Greece. e-mail: [email protected]
Received: 20 August 2012; Accepted: 20 August 2012
European Journal of Clinical Investigation Vol 42 1155
RESEARCH UPDATE

References1 Stojakovic T, de Campo A, Scharnagl H, Sourij H, Schmolzer I,Wascher TC et al. Differential effects of fluvastatin alone or incombination with ezetimibe on lipoprotein subfractions inpatients at high risk of coronary events. Eur J Clin Invest2010;40:187–94.
2 Winkler K, Jacob S, Muller-Schewe T, Hoffmann MM, Konrad T.Ezetimibe alone and in combination lowers the concentration ofsmall, dense low-density lipoproteins in type 2 diabetes mellitus.Atherosclerosis 2012;220:189–93.
3 Florentin M, Liberopoulos EN, Moutzouri E, Rizos CV, TselepisAD, Elisaf MS. The effect of simvastatin alone versus simvastatinplus ezetimibe on the concentration of small dense low-densitylipoprotein cholesterol in subjects with primary hypercholesterol-emia. Curr Med Res Opin 2011;27:685–92.
4 Berneis K, Rizzo M, Berthold HK, Spinas GA, Krone W, Gouni-Berthold I. Ezetimibe alone or in combination with simvastatinincreases small dense low-density lipoproteins in healthy men: arandomized trial. Eur Heart J 2010;31:1633–9.
5 Bays H, Conard S, Leiter LA, Bird S, Jensen E, Hanson ME et al.Are post-treatment low-density lipoprotein subclass pattern analy-ses potentially misleading? Lipids Health Dis 2010;9:136.
6 Nair S, Nadkarni A, Warang P, Bhave A, Ghosh K, Colah R. Fivealpha globin chain variants identified during screening for haemo-globinopathies. Eur J Clin Invest 2010;40:226–32.
7 Upadhye DS, Jain D, Nair SB, Nadkarni AH, Ghosh K, ColahRB. First case of Hb Fontainebleau with sickle hemoglobin andother non-deletional a gene variants identified in neonates dur-ing newborn screening for sickle cell disorders. J Clin Pathol2012;65:654–9.
8 Chopra A, Fisher C, Khunger JM, Pati H. Hemoglobin O (Indone-sia) in India: a rare observation. Ann Hematol 2011;90:353–4.
9 Sharma A, Marwah S, Buxi G, Yadav RB. Falsely low HbA1c valuedue to rare hemoglobin variant (Hemoglobin J Meerut) – A familystudy. Indian J Pathol Microbiol 2012;55:270–1.
10 Warang P, Nair S, Nadkarni A, Ghosh K, Colah RB. HbH diseasedue to homozygosity for a rare a2 globin variant, Hb Sallanches.Hemoglobin 2010;34:45–8.
11 Nadkarni AH, Nair SB, Italia KY, Warang P, Dalvi M, Ghosh Ket al.Molecular diversity of hemoglobin H disease in India. Am JClin Pathol 2010;133:491–4.
12 Sun Y, Eichelbaum EJ, Lenz A, Wang H, Vesely DL. Epidermalgrowth factor’s activation of Ras is inhibited by four cardiac hor-mones. Eur J Clin Invest 2010;40:408–13.
13 Sun Y, Eichelbaum EJ, Skelton WP IV, Lenz A, Regales N, Wang Het al. Vessel dilator and kaliuretic peptide inhibit Ras in humanprostate cancer cells. Anticancer Res 2009;29:971–5.
14 Sun Y, Eichelbaum EJ, Lenz A, Skelton WP IV, Wang H, Vesely DL.Atrial natriuretic peptide and long-acting natriuretic peptide inhi-bit Ras in human prostate cancer cells. Anticancer Res 2009;29:1889–93.
15 Sun Y, Eichelbaum EJ, Lenz A, Wang H, Vesely DL. Four cardiachormones inhibit insulin’s mitogenic action via inhibiting Ras. Can-cer Ther 2009;7:367–72.
16 McGrath ME, Ogawa T, de Bold AJ. Ras dexamethasone-inducedprotein 1 is a modulator of hormone secretion in volume over-loaded heart. Am J Physiol Heart Circ Physiol 2012;302:H1826–7.
17 Lenz A, Sun Y, Eichelbaum EJ, Skelton WP IV, Pi G, Vesely DL.Cardiovascular hormones eliminate some human squamous celllung carcinomas in athymic mice. Eur J Clin Invest 2010;40:242–9.
18 Eichelbaum EJ, Sun Y, Alli AA, Gower WR Jr, Vesely DL. Cardiachormones and urodilatin eliminate up to 86% of human small-celllung carcinomas in mice. Eur J Clin Invest 2008;38:562–70.
19 Fujimori S, Gudis K, Takahashi Y, Seo T, Yamada Y, Ehara A et al.Distribution of small intestinal mucosal injuries as a result ofNSAID administration. Eur J Clin Invest 2010;40:504–10.
20 Wallace JL, Syer S, Denou E, de Palma G, Vong L, McKnight Wet al. Proton pump inhibitors exacerbate NSAID-induced smallintestinal injury by inducing dysbiosis. Gastroenterology2011;141:1314–22.
21 Hao WL, Lee YK. Microflora of the gastrointestinal tract: a review.Methods Mol Biol 2004;268:491–502.
22 Adlbrecht C, Distelmaier K, Bonderman D, Beran G, Redwan B,Strunk G et al. Long-term outcome after thrombectomy in acutemyocardial infarction. Eur J Clin Invest 2010;40:233–41.
23 Adlbrecht C, Distelmaier K, Gunduz D, Redwan B, Plass C, Bon-derman D et al. Target vessel reopening by guidewire insertion inST-elevation myocardial infarction is a predictor of final TIMI flowand survival. Thromb Haemost 2011;105:52–8.
24 Vlaar PJ, Svilaas T, van der Horst IC, Diercks GF, Fokkema ML, deSmet BJ et al. Cardiac death and reinfarction after 1 year in theThrombus Aspiration during Percutaneous coronary interventionin Acute myocardial infarction Study (TAPAS): a 1-year follow-upstudy. Lancet 2008;371:1915–20.
25 Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T et al.Guidelines on myocardial revascularization. Eur Heart J2010;31:2501–55.
26 Stone GW, Maehara A, Witzenbichler B, Godlewski J, Parise H,Dambrink JH et al. Intracoronary abciximab and aspirationthrombectomy in patients with large anterior myocardial infarc-tion: the INFUSE-AMI randomized trial. JAMA 2012;307:1817–26.
27 Georgiadou P, Iliodromitis EK, Kolokathis F, Varounis C, Gizas V,Mavroidis M et al. Osteopontin as a novel prognostic marker in sta-ble ischaemic heart disease: a 3-year follow-up study. Eur J ClinInvest 2010;40:288–93.
28 Mazzone A, Parri MS, Giannessi D, Ravani M, Vaghetti M, Altieri Pet al. Osteopontin plasma levels and accelerated atherosclerosis inpatients with CAD undergoing PCI: a prospective clinical study.Coron Artery Dis 2011;22:179–87.
29 de Kleijn DP, Moll FL, Hellings WE, Ozsarlak-Sozer G, de Bruin P,Doevendans PA et al. Local atherosclerotic plaques are a source ofprognostic biomarkers for adverse cardiovascular events. Arterios-cler Thromb Vasc Biol 2010;30:612–9.
30 Tousoulis D, Siasos G, Maniatis K, Oikonomou E, Kioufis S, Zaro-mitidou M et al. Serum osteoprotegerin and osteopontin levels areassociated with arterial stiffness and the presence and severity ofcoronary artery disease. Int J Cardiol 2012; May 26. In press.
31 Momiyama Y, Ohmori R, Fayad ZA, Kihara T, Tanaka N, Kato Ret al. Associations between plasma osteopontin levels and theseverities of coronary and aortic atherosclerosis. Atherosclerosis2010;210:668–70.
32 Yan X, Sano M, Lu L, Wang W, Zhang Q, Zhang R et al. Plasmaconcentrations of osteopontin, but not thrombin-cleaved osteopon-tin, are associated with the presence and severity of nephropathyand coronary artery disease in patients with type 2 diabetes mell-itus. Cardiovasc Diabetol 2010;9:70.
33 Grion CM, Cardoso LT, Perazolo TF, Garcia AS, Barbosa DS, Mor-imoto HK et al. Lipoproteins and CETP levels as risk factors forsevere sepsis in hospitalized patients. Eur J Clin Invest 2010;40:330–8.
1156 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com
34 Hara T, Ishida T, Kojima Y, Tanaka H, Yasuda T, Shinohara M et al.Targeted deletion of endothelial lipase increases HDL particleswith anti-inflammatory properties both in vitro and in vivo. J LipidRes 2011;52:57–67.
35 Henning MF, Herlax V, Bakas L. Contribution of the C-terminaland of apolipoprotein AI to neutralization of lipopolysaccharideendotoxic effect. Innate Immun 2011;17:327–37.
36 Walters DL, Ray MJ, Wood P, Perrin EJ, Bett JH, Aroney CN.High-dose tirofiban with enoxaparin and inflammatory markersin high-risk percutaneous intervention. Eur J Clin Invest2010;40:139–47.
37 Layland J, Ray MJ, Siresena T, Walters DL. Increased expression ofmonocyte tissue factor and soluble CD40 ligand at mid-term fol-low-up following percutaneous coronary intervention. Blood CoagulFibrinolysis 2011;22:349–50.
38 Ray MJ, Calabro LJ, Sirisena T, Crawford SA, Crawford RW, Walt-ers DL. Pre-operative platelet-bound CD40 ligand is probably asso-ciated with peri-operative cardiac events in hip and kneearthroplasty. Eur J Clin Invest 2010;40:497–503.
39 Mehran R, Pocock S, Nikolsky E, Dangas GD, Clayton T, Claes-sen BE et al. Impact of bleeding on mortality after percutaneouscoronary intervention results from a patient-level pooled analysisof the REPLACE-2 (randomized evaluation of PCI linking angio-max to reduced clinical events), ACUITY (acute catheterizationand urgent intervention triage strategy), and HORIZONS-AMI(harmonizing outcomes with revascularization and stents inacute myocardial infarction) trials. JACC Cardiovasc Interv2011;4:654–64.
40 Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W,Gottlieb S et al. Prasugrel versus clopidogrel in patients with acutecoronary syndromes. N Engl J Med 2007;357:2001–15.
41 Wallentin L, Becker R, Budaj A, Cannon C, Emanuelsson H, Held Cet al. Ticagrelor versus clopidogrel in patients with acute coronarysyndromes.N Engl J Med 2009;361:1045–57.
42 Yilmaz Y, Eren F, Yonal O, Kurt R, Aktas B, Celikel CA et al.Increased serum FGF21 levels in patients with nonalcoholic fattyliver disease. Eur J Clin Invest 2010;40:887–92.
43 Li H, Fang Q, Gao F, Fan J, Zhou J, Wang X et al. Fibroblast growthfactor 21 levels are increased in nonalcoholic fatty liver diseasepatients and are correlated with hepatic triglyceride. J Hepatol2010;53:934–40.
44 Yan H, Xia M, Chang X, Xu Q, Bian H, Zeng M et al. Circulatingfibroblast growth factor 21 levels are closely associated withhepatic fat content: a cross-sectional study. PLoS ONE2011;6:e24895.
45 Adlbrecht C, Hulsmann M, Gwechenberger M, Graf S, WiesbauerF, Strunk G et al. Electrical optimization of cardiac resynchroniza-tion in chronic heart failure is associated with improved clinicallong-term outcome. Eur J Clin Invest 2010;40:678–84.
46 Adlbrecht C, Hulsmann M, Gwechenberger M, Strunk G, KhazenC, Wiesbauer F et al. Outcome after device implantation in chronicheart failure is dependent on concomitant medical treatment. Eur JClin Invest 2009;39:1073–81.
47 Ellenbogen KA, Gold MR, Meyer TE, Fernndez Lozano I, Mittal S,Waggoner AD et al. Primary results from the SmartDelay deter-mined AV optimization: a comparison to other AV delay methodsused in cardiac resynchronization therapy (SMART-AV) trial: arandomized trial comparing empirical, echocardiography-guided,and algorithmic atrioventricular delay programming in cardiacresynchronization therapy. Circulation 2010;122:2660–8.
48 Shanmugam N, Borgulya G, Anderson L. Letter by Shanmugamet al. regarding article, ‘‘Primary results from the SmartDelaydetermined AV optimization: a comparison to other AV delaymethods used in cardiac resynchronization therapy (SMART-AV)trial: a randomized trial comparing empirical, echocardiography-guided, and algorithmic atrioventricular delay programming incardiac resynchronization therapy’’. Circulation 2011;124:e190.
49 Sawhney NS, Waggoner AD, Garhwal S, Chawla MK, Osborn J,Faddis MN. Randomized prospective trial of atrioventricular delayprogramming for cardiac resynchronization therapy.Heart Rhythm2004;1:562–7.
50 McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M,Dickstein K et al. ESC Guidelines for the diagnosis and treatment ofacute and chronic heart failure 2012: The Task Force for the Diag-nosis and Treatment of Acute and Chronic Heart Failure 2012 ofthe European Society of Cardiology. Developed in collaborationwith the Heart Failure Association (HFA) of the ESC. Eur Heart J2012;33:1787–847.
51 Bouzas-Mosquera A, Peteiro J, Broullon FJ, Alvarez-Garcıa N,Mendez E, Perez A et al. Value of exercise echocardiography forpredicting mortality in elderly patients. Eur J Clin Invest2010;40:1122–30.
52 Peteiro J, Bouzas-Mosquera A, Estevez R, Pazos P, Pineiro M, Cas-tro-Beiras A. Head-to-head comparison of peak supine bicycleexercise echocardiography and treadmill exercise echocardiogra-phy at peak and at post-exercise for the detection of coronaryartery disease. J Am Soc Echocardiogr 2012;25:319–26.
53 Bernheim AM, Kittipovanonth M, Takahashi PY, Gharacholou SM,Scott CG, Pellikka PA. Does the prognostic value of dobutaminestress echocardiography differ among different age groups? AmHeart J 2012;25:319–5.
54 Rai M, Baker WL, Parker MW, Heller GV. Meta-Analysis of Opti-mal Risk Stratification in Patients >65 Years of Age. Am J Cardiol2012; Jul 12. In press.
55 Schiza SE, Mermigkis C, Panagiotis P, Bouloukaki I, Kallergis E,Tzanakis N et al. C-reactive protein evolution in obstructive sleepapnoea patients under CPAP therapy. Eur J Clin Invest 2010;40:968–75.
56 Guo Y, Pan L, Ren D, Xie X. Impact of continuous positive airwaypressure on C-reactive protein in patients with obstructive sleepapnea: a meta-analysis. Sleep Breath 2012; Jun 5. In Press.
57 Mermigkis C, Bouloukaki I, Mermigkis D, Kallergis E, Mavroudi E,Varouchakis G et al. CRP evolution pattern in CPAP-treatedobstructive sleep apnea patients. Does gender play a role. SleepBreath 2011;16:1–3.
58 Kumor M, Bielicki P, Przybyłowski T, Rubinsztajn R, Zielinski J,Chazan R. Three month continuous positive airway pressure(CPAP) therapy decreases serum total and LDL cholesterol, but nothomocysteine and leptin concentration in patients with obstructivesleep apnea syndrome (OSAS)]. Pneumonol Alergol Pol 2011;79:173–83.
59 Colish J, Walker JR, Elmayergi N, Almutairi S, Alharbi F, LytwynM et al.Obstructive sleep apnea: effects of continuous positive air-way pressure on cardiac remodeling as assessed by cardiac biomar-kers, echocardiography, and cardiac MRI. Chest 2012;141:674–81.
60 Chang KC, Tseng CD, Lu SC, Liang JT, Wu MS, Tsai MS et al.Effects of acetyl-L-carnitine and oxifenicine on aorta stiffness indiabetic rats. Eur J Clin Invest 2010;40:1002–10.
61 Slatter DA, Bolton CH, Bailey AJ. The importance of lipid-derivedmalondialdehyde in diabetes mellitus. Diabetologia 2000;43:550–7.
European Journal of Clinical Investigation Vol 42 1157
RESEARCH UPDATE
62 Satomura A, Fujita T, Fuke Y, Yanai M, Kumasaka K, Takayama Eet al. Relationship between oligomer and functional serumman-nose-binding lectin in chronic renal failure. Eur J Clin Invest2010;40:865–73.
63 Satomura A, Fujita T, Yanai M, Kumasaka K, Uehara Y, Okada Ket al. Functional mannose-binding lectin levels in patients withend-stage renal disease on maintenance hemodialysis. J Innate Im-mun 2012;4:293–300.
64 Summerfield JA, Ryder S, Sumiya M, Thursz M, Gorchein A,Monteil MA et al. Mannose binding protein gene mutations asso-ciated with unusual and severe infections in adults. Lancet1995;345:886–9.
65 Frøkjær JB, Søfteland E, Graversen C, Dimcevski G, Drewes AM.Effect of acute hyperglycaemia on sensory processing in diabeticautonomic neuropathy. Eur J Clin Invest 2010;40:883–6.
66 Frøkjær JB, Egsgaard LL, Graversen C, Søfteland E, DimcevskiG, Blauenfeldt RA et al. Gastrointestinal symptoms in type-1diabetes: Is it all about brain plasticity? Eur J Pain 2011;15:249–57.
67 Frøkjær JB, Andersen LW, Brock C, Simren M, Ljungberg M, Søfte-land E et al. Altered brain microstructure assessed by diffusion ten-sor imaging in patients with diabetes mellitus and gastrointestinalsymptoms. Diabetes Care 2012; In press.
68 Lee TI, Kao YH, Chen YC, Pan NH, Chen YJ. Oxidative stress andinflammation modulate peroxisome proliferator-activated recep-tors with regional discrepancy in diabetic heart. Eur J Clin Invest2010;40:692–9.
69 Lee TI, Kao YH, Chen YC, Pan NH, Lin YK, Chen YJ. Cardiacperoxisome-proliferator-activated receptor expression in hyper-tension co-existing with diabetes. Clin Sci (Lond) 2011;121:305–12.
70 Cheng CC, Pan NH, Chen YC, Yeh HI, Lin CI, Chen SA et al. Ath-erosclerosis modulates the electrophysiological effects of a peroxi-some proliferator-activated receptor-gamma activator onpulmonary veins. Int J Cardiol 2010;145:578–82.
71 Lee TI, Chen YC, Kao YH, Hsiao FC, Lin YK, Chen YJ. Rosiglitaz-one induces arrhythmogenesis in diabetic hypertensive rats withcalcium handling alteration. Int J Cardiol 2012; In press.
72 Skelton WP IV, Pi G, Lenz A, Vesely DL. Cardiac hormones inhibitproliferation of pancreatic cancer but not normal cells. Eur J ClinInvest 2010;40:706–12.
73 Serafino A, Moroni N, Psaila R, Zonfrillo M, Andreola F, WannenesF et al. Anti- proliferative effect of atrial natriuretic peptide on colo-rectal cancer cells: evidence for an Akt- mediated cross-talkbetween acidic tumor microenvironment and Wnt ⁄ b-catenin sig-naling. Biochim Biophys Acta 2012;1822:1004–18.
74 Vesely DL, Eichelbaum EJ, Sun Y, Alli AA, Vesely BA, LutherSL et al. Elimination of up to 80% of human pancreatic adenocar-cinomas in athymic mice by cardiac hormones. In Vivo2007;21:445–52.
75 Skelton WP IV, Pi GE, Vesely DL. Four cardiac hormones causedeath of human cancer cells but not of healthy cells. Anticancer Res2011;31:395–402.
76 Pi GE, Skelton WP IV, Vesely DL. Four cardiac hormones causecytotoxicity of human cancer cells but not of healthy cells. CancerTher 2011;8:44–50.
77 Chung YC, Lin CC, Chou CC, Hsu CP. The effect of Longan seedpolyphenols on colorectal carcinoma cells. Eur J Clin Invest2010;40:713–21.
78 Chung YC, Lin CC, Hsu CP. The potential roles of longan flowerand seed extracts in cancer prevention and treatment.World J ExpMed 2012; (under revision).
79 Starkel P, De Saeger C, Strain AJ, Leclercq I, Horsmans Y. NFjB,cytokines, TLR 3 and 7 expression in human end-stage HCV andalcoholic liver disease. Eur J Clin Invest 2010;40:575–84.
80 Leclercq S, Cani PD, Neyrinck AM, Starkel P, Jamar F, MikolajczakM et al. Role of intestinal permeability and inflammation in the bio-logical and behavioral control of alcohol-dependent subjects. BrainBehav Immun 2012;26:911–8.
81 Tamura R, Kanda T, Imazeki F, Wu S, Nakamoto S, Tanaka T et al.Hepatitis C Virus nonstructural 5A protein inhibits lipopolysaccha-ride-mediated apoptosis of hepatocytes by decreasing expressionof Toll-like receptor 4. J Infect Dis 2011;204:793–801.
82 Berzsenyi MD, Roberts SK, Preiss S, Woollard DJ, Beard MR, Skin-ner NA et al.Hepatic TLR2 & TLR4 expression correlates withhepatic inflammation and TNF-a in HCV & HCV ⁄HIV infection.J Viral Hepat 2011;18:852–60.
83 Hung MY, Hsu KH, Hung MJ, Cheng CW, Cherng WJ. Interactionsamong gender, age, hypertension and C-reactive protein in coro-nary vasospasm. Eur J Clin Invest 2010;40:1094–103.
84 Hung MJ, Cherng WJ, Hung MY, Kuo LT, Cheng CW, Wang CHet al. Increased leukocyte Rho-associated coiled-coil containingprotein kinase activity predicts the presence and severity of coro-nary vasospastic angina. Atherosclerosis 2012;221:521–6.
85 Wang S, Reed DB, Goli S, Goswami D. Blood leptin and C-reactiveprotein provide more sensitive assessment than blood lipids andother inflammatory biomarkers in overweight university students.Nutr Res 2011;31:586–93.
86 Kawamoto R, Tabara Y, Kohara K, Miki T, Kusunoki T, TakayamaS et al. Association between fasting plasma glucose and high-sensi-tivity C-reactive protein: gender differences in a Japanese commu-nity-dwelling population. Cardiovasc Diabetol 2011;10:51.
87 Kawano H, Node K. The role of vascular failure in coronary arteryspasm. J Cardiol 2011;57:2–7.
88 Pascual G, Rodrıguez M, Gomez-Gil V, Trejo C, Bujan J, Bellon PG.Active metalloproteinase-2 upregulation in the abdominal skin ofpatients with direct inguinal hernia. Eur J Clin Invest 2010;40:113–1121.
89 Klinge U, Si ZY, Zheng H, Schumpelick V, Bhardwaj RS, Kloster-halfen B. Abnormal collagen I and III distribution in the skin ofpatients with incisional hernia. Eur Surg Res 2000;32:43–8.
90 Rosch R, Klinge U, Si Z, Junge K, Klosterhalfen B, Schumpelick V.A role for the collagen I ⁄ III and MMP-1 ⁄ 13 genes in primary ingui-nal hernia? BMCMed Genet 2002;3:2.
91 Bellon JM, Bujan J, Honduvilla NG, Jurado F, Gimeno MJ, Turnay Jet al. Study of biochemical substrate and role of metalloproteinasesin fascia transversalis from hernial processes. Eur J Clin Invest1997;27:510–6.
92 Bellon JM, Bajo A, Gª-Honduvilla N, Gimeno MJ, Pascual G, Guer-rero A et al. Fibroblasts from the transversalis fascia of youngpatients with direct inguinal hernias show constitutive MMP-2over-expression. Ann Surg 2001;233:287–91.
93 Antoniou GA, Tentes IK, Antoniou SA, Simopoulos C, LazaridesMK. Matrix metalloproteinase imbalance in inguinal hernia forma-tion. J Invest Surg 2011;24:145–50.
94 Phrommintikul A, Sivasinprasasn S, Lailerd N, Chattipakorn S,Kuanprasert S, Chattipakorn N. Plasma urocortin in acutemyocardial infarction patients. Eur J Clin Invest 2010;40:874–82.
1158 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com

95 Calderon-Sanchez EM, Ruiz-Hurtado G, Smani T, Delgado C, Beni-tah JP, Gomez AM et al. Cardioprotective action of urocortin inpostconditioning involves recovery of intracellular calcium han-dling. Cell Calcium 2011;50:84–90.
96 Takatani-Nakase T, Takahashi K. Cardioprotective activity of uro-cortin by preventing caspase-independent, non-apoptotic death incultured neonatal rat cardiomyocytes exposed to ischemia. BiochemBiophys Res Commun 2010;402:216–21.
97 Barry SP, Lawrence KM, McCormick J, Soond SM, Hubank M,Eaton S et al.New targets of urocortin-mediated cardioprotection.J Mol Endocrinol 2010;45:69–85.
98 Aigner E, Hinz C, Steiner K, Rossmann B, Pfleger J, Hohla F et al.Iron stores, liver transaminase levels and metabolic risk in healthyteenagers. Eur J Clin Invest 2010;40:155–63.
99 Kowdley KV, Belt P, Wilson LA, Yeh MM, Neuschwander-TetriBA, Chalasani N et al. Serum ferritin is an independent predictor ofhistologic severity and advanced fibrosis in patients with nonalco-holic fatty liver disease.Hepatology 2012;55:77–85.
100 Weismuller TJ, Kirchner GI, Scherer MN, Negm AA, SchnitzbauerAA, Lehner F et al. Serum ferritin concentration and transferrin sat-uration before liver transplantation predict decreased long-termrecipient survival. Hepatology 2011;54:2114–24.
101 Houschyar KS, Ludtke R, Dobos GJ, Kalus U, Broecker-Preuss M,Rampp T et al. Effects of phlebotomy-induced reduction of bodyiron stores on metabolic syndrome: results from a randomized clin-ical trial. BMCMed 2012;10:54.
102 Aigner E, Strasser M, Haufe H, Sonnweber T, Hohla F, StadlmayrA et al. A role for low hepatic copper concentrations in nonalco-holic Fatty liver disease. Am J Gastroenterol 2010;105:1978–85.
103 Aigner E, Felder TK, Oberkofler H, Hahne P, Auer S, Soyal S et al.Glucose acts as a regulator of serum iron by increasing serum hep-cidin concentrations. J Nutr Biochem 2012.
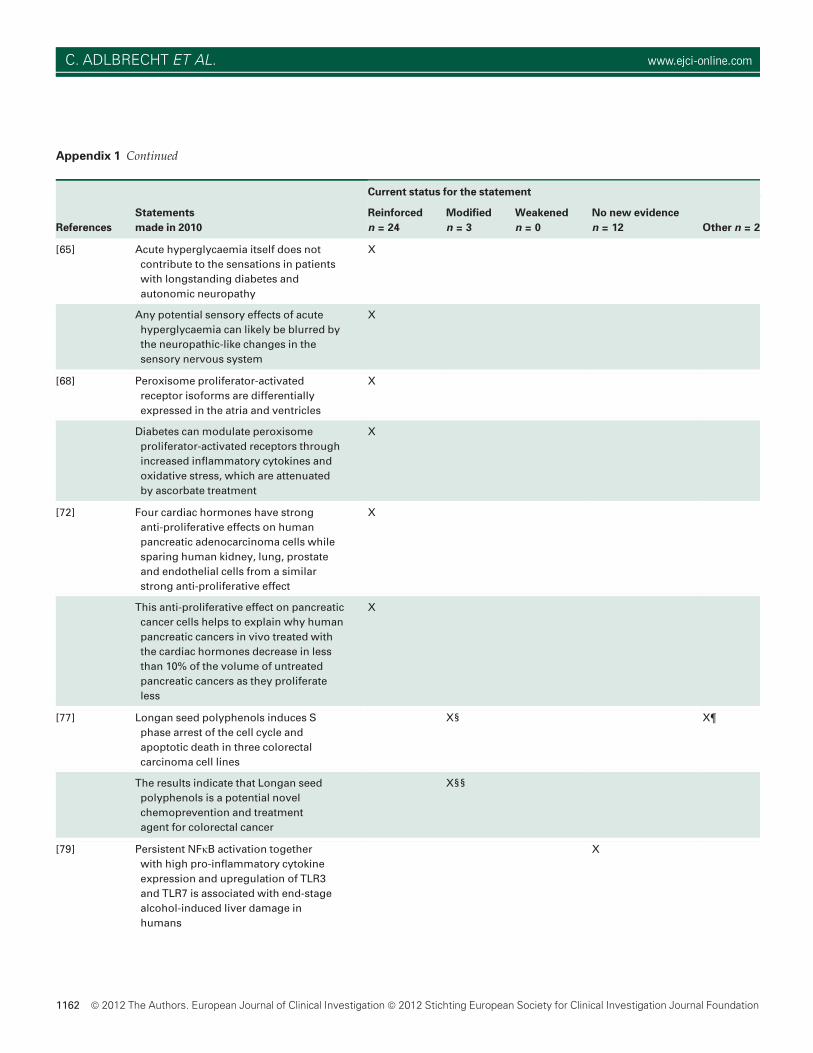
Appendix 1
Statements made in the Conclusions of the Abstract of original articles published by the European Journal of Clinical Investigation
in 2010 and current status for each statement as judged by the authors of each original study
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
[1] Addition of ezetimibe to fluvastatin resul-
ted in a further reduction of buoyant and
intermediate, but not of dense LDL com-
pared with fluvastatin alone
X
[6] This study emphasises the need to
undertake systematic investigations
while screening for the b-haemoglobin-
opathies to identify rare a-chain variants
in a population
X
[12] Four cardiac hormones specifically
inhibit epidermal growth factor’s activa-
tion of Ras. This investigation would sug-
gest that these cardiac hormones’
anticancer effects involve the
inhibition of mitogens such as
epidermal growth factor’s ability to
activate Ras as well as inhibiting
unstimulated basal activity
of Ras
X
European Journal of Clinical Investigation Vol 42 1159
RESEARCH UPDATE
Appendix 1 Continued
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
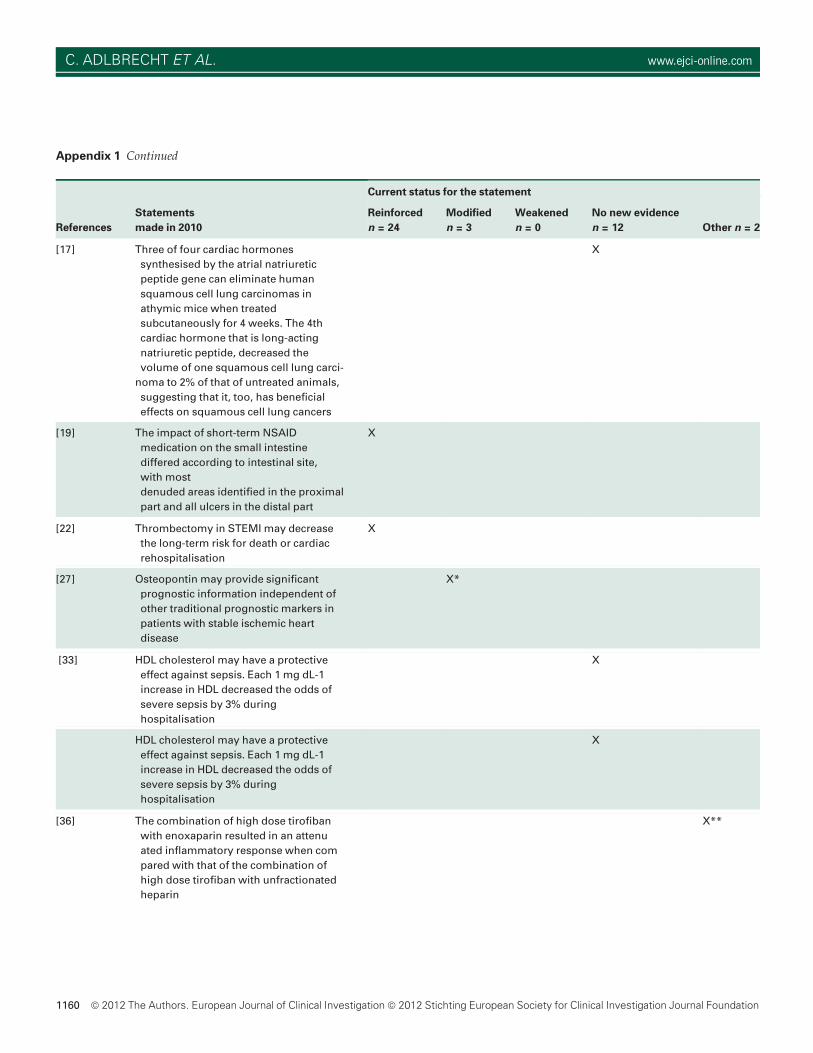
[17] Three of four cardiac hormones
synthesised by the atrial natriuretic
peptide gene can eliminate human
squamous cell lung carcinomas in
athymic mice when treated
subcutaneously for 4 weeks. The 4th
cardiac hormone that is long-acting
natriuretic peptide, decreased the
volume of one squamous cell lung carci-
noma to 2% of that of untreated animals,
suggesting that it, too, has beneficial
effects on squamous cell lung cancers
X
[19] The impact of short-term NSAID
medication on the small intestine
differed according to intestinal site,
with most
denuded areas identified in the proximal
part and all ulcers in the distal part
X
[22] Thrombectomy in STEMI may decrease
the long-term risk for death or cardiac
rehospitalisation
X
[27] Osteopontin may provide significant
prognostic information independent of
other traditional prognostic markers in
patients with stable ischemic heart
disease
X*
[33] HDL cholesterol may have a protective
effect against sepsis. Each 1 mg dL-1
increase in HDL decreased the odds of
severe sepsis by 3% during
hospitalisation
X
HDL cholesterol may have a protective
effect against sepsis. Each 1 mg dL-1
increase in HDL decreased the odds of
severe sepsis by 3% during
hospitalisation
X
[36] The combination of high dose tirofiban
with enoxaparin resulted in an attenu
ated inflammatory response when com
pared with that of the combination of
high dose tirofiban with unfractionated
heparin
X**
1160 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com
Appendix 1 Continued
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
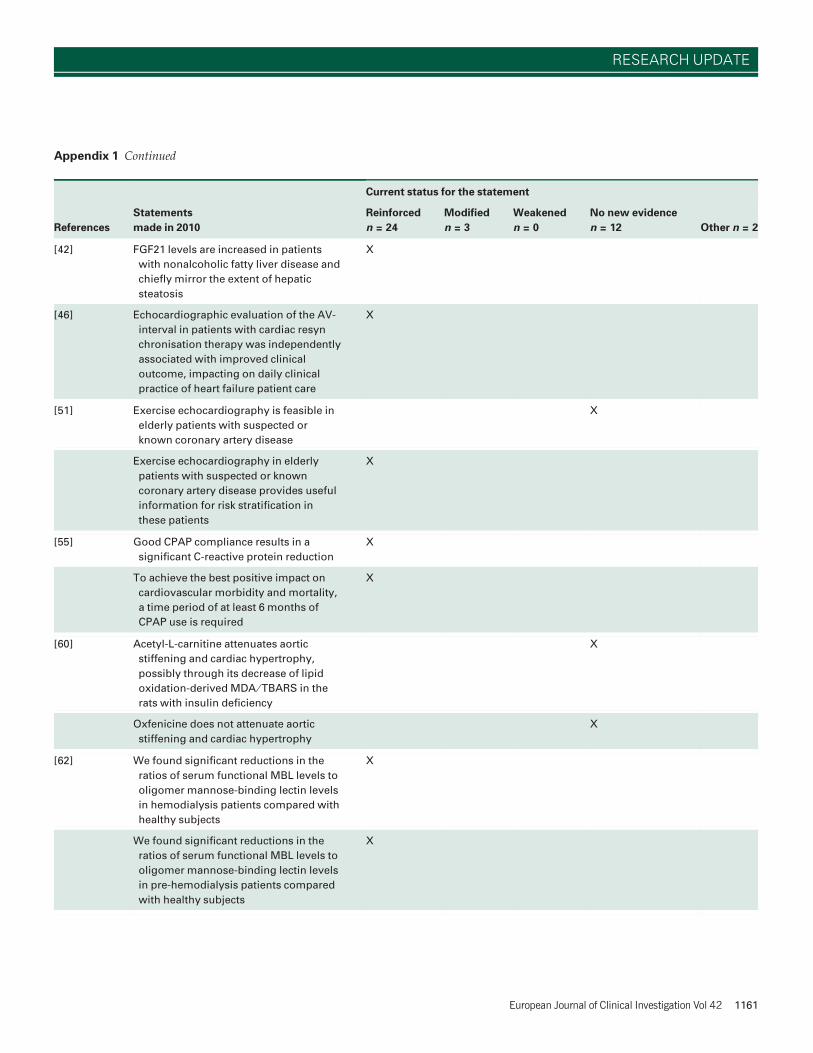
[42] FGF21 levels are increased in patients
with nonalcoholic fatty liver disease and
chiefly mirror the extent of hepatic
steatosis
X
[46] Echocardiographic evaluation of the AV-
interval in patients with cardiac resyn
chronisation therapy was independently
associated with improved clinical
outcome, impacting on daily clinical
practice of heart failure patient care
X
[51] Exercise echocardiography is feasible in
elderly patients with suspected or
known coronary artery disease
X
Exercise echocardiography in elderly
patients with suspected or known
coronary artery disease provides useful
information for risk stratification in
these patients
X
[55] Good CPAP compliance results in a
significant C-reactive protein reduction
X
To achieve the best positive impact on
cardiovascular morbidity and mortality,
a time period of at least 6 months of
CPAP use is required
X
[60] Acetyl-L-carnitine attenuates aortic
stiffening and cardiac hypertrophy,
possibly through its decrease of lipid
oxidation-derived MDA ⁄TBARS in the
rats with insulin deficiency
X
Oxfenicine does not attenuate aortic
stiffening and cardiac hypertrophy
X
[62] We found significant reductions in the
ratios of serum functional MBL levels to
oligomer mannose-binding lectin levels
in hemodialysis patients compared with
healthy subjects
X
We found significant reductions in the
ratios of serum functional MBL levels to
oligomer mannose-binding lectin levels
in pre-hemodialysis patients compared
with healthy subjects
X
European Journal of Clinical Investigation Vol 42 1161
RESEARCH UPDATE
Appendix 1 Continued
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
[65] Acute hyperglycaemia itself does not
contribute to the sensations in patients
with longstanding diabetes and
autonomic neuropathy
X
Any potential sensory effects of acute
hyperglycaemia can likely be blurred by
the neuropathic-like changes in the
sensory nervous system
X
[68] Peroxisome proliferator-activated
receptor isoforms are differentially
expressed in the atria and ventricles
X
Diabetes can modulate peroxisome
proliferator-activated receptors through
increased inflammatory cytokines and
oxidative stress, which are attenuated
by ascorbate treatment
X
[72] Four cardiac hormones have strong
anti-proliferative effects on human
pancreatic adenocarcinoma cells while
sparing human kidney, lung, prostate
and endothelial cells from a similar
strong anti-proliferative effect
X
This anti-proliferative effect on pancreatic
cancer cells helps to explain why human
pancreatic cancers in vivo treated with
the cardiac hormones decrease in less
than 10% of the volume of untreated
pancreatic cancers as they proliferate
less
X
[77] Longan seed polyphenols induces S
phase arrest of the cell cycle and
apoptotic death in three colorectal
carcinoma cell lines
X§ X¶
The results indicate that Longan seed
polyphenols is a potential novel
chemoprevention and treatment
agent for colorectal cancer
X§§
[79] Persistent NFjB activation together
with high pro-inflammatory cytokine
expression and upregulation of TLR3
and TLR7 is associated with end-stage
alcohol-induced liver damage in
humans
X
1162 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com
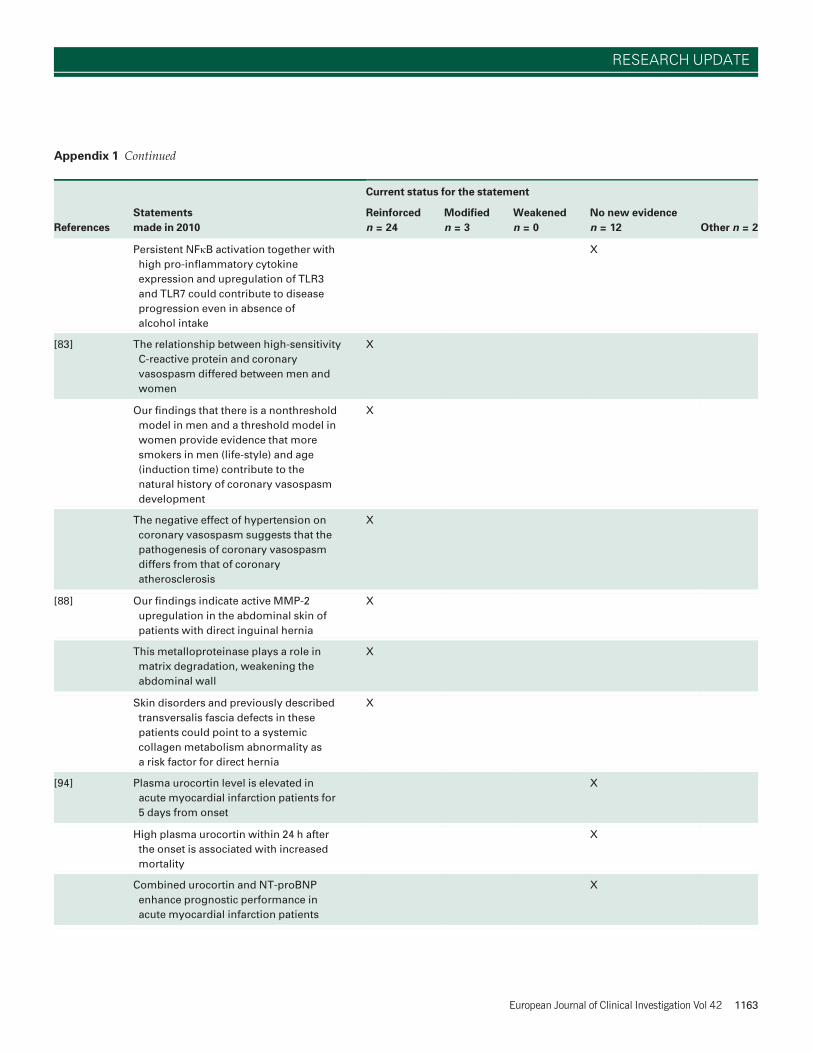
Appendix 1 Continued
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
Persistent NFjB activation together with
high pro-inflammatory cytokine
expression and upregulation of TLR3
and TLR7 could contribute to disease
progression even in absence of
alcohol intake
X
[83] The relationship between high-sensitivity
C-reactive protein and coronary
vasospasm differed between men and
women
X
Our findings that there is a nonthreshold
model in men and a threshold model in
women provide evidence that more
smokers in men (life-style) and age
(induction time) contribute to the
natural history of coronary vasospasm
development
X
The negative effect of hypertension on
coronary vasospasm suggests that the
pathogenesis of coronary vasospasm
differs from that of coronary
atherosclerosis
X
[88] Our findings indicate active MMP-2
upregulation in the abdominal skin of
patients with direct inguinal hernia
X
This metalloproteinase plays a role in
matrix degradation, weakening the
abdominal wall
X
Skin disorders and previously described
transversalis fascia defects in these
patients could point to a systemic
collagen metabolism abnormality as
a risk factor for direct hernia
X
[94] Plasma urocortin level is elevated in
acute myocardial infarction patients for
5 days from onset
X
High plasma urocortin within 24 h after
the onset is associated with increased
mortality
X
Combined urocortin and NT-proBNP
enhance prognostic performance in
acute myocardial infarction patients
X
European Journal of Clinical Investigation Vol 42 1163
RESEARCH UPDATE
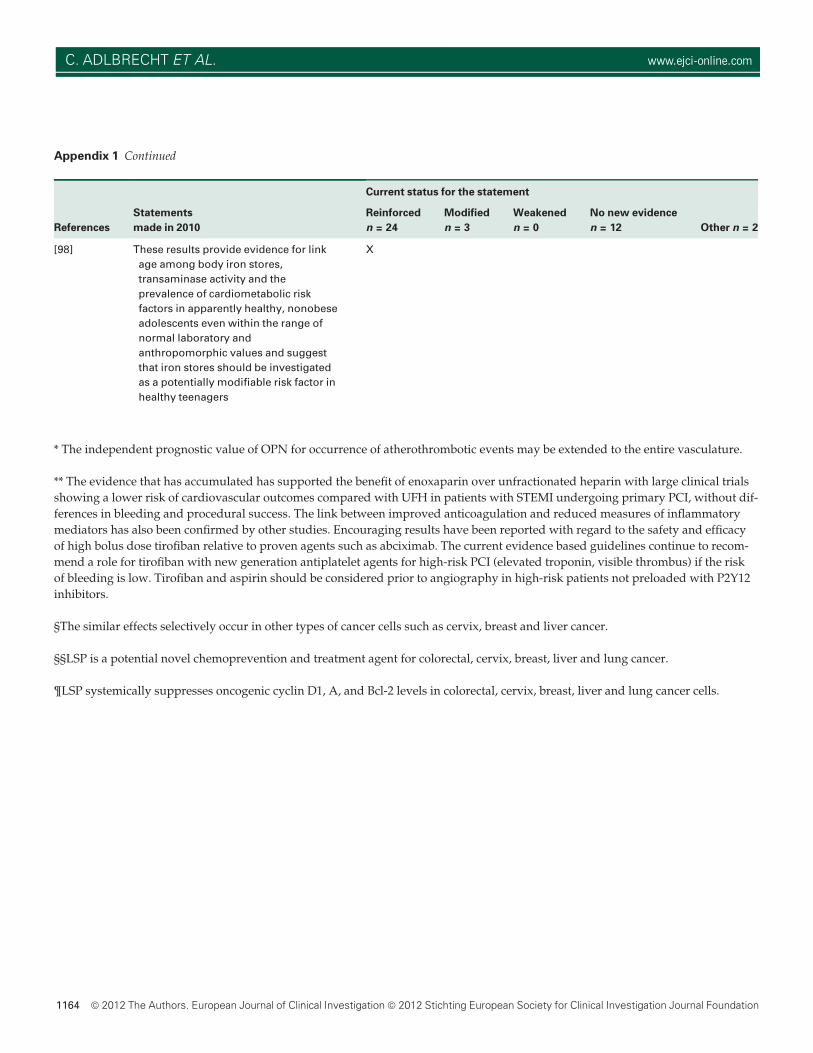
Appendix 1 Continued
References
Statements
made in 2010
Current status for the statement
Reinforced
n = 24
Modified
n = 3
Weakened
n = 0
No new evidence
n = 12 Other n = 2
[98] These results provide evidence for link
age among body iron stores,
transaminase activity and the
prevalence of cardiometabolic risk
factors in apparently healthy, nonobese
adolescents even within the range of
normal laboratory and
anthropomorphic values and suggest
that iron stores should be investigated
as a potentially modifiable risk factor in
healthy teenagers
X
* The independent prognostic value of OPN for occurrence of atherothrombotic events may be extended to the entire vasculature.
** The evidence that has accumulated has supported the benefit of enoxaparin over unfractionated heparin with large clinical trials
showing a lower risk of cardiovascular outcomes compared with UFH in patients with STEMI undergoing primary PCI, without dif-
ferences in bleeding and procedural success. The link between improved anticoagulation and reduced measures of inflammatory
mediators has also been confirmed by other studies. Encouraging results have been reported with regard to the safety and efficacy
of high bolus dose tirofiban relative to proven agents such as abciximab. The current evidence based guidelines continue to recom-
mend a role for tirofiban with new generation antiplatelet agents for high-risk PCI (elevated troponin, visible thrombus) if the risk
of bleeding is low. Tirofiban and aspirin should be considered prior to angiography in high-risk patients not preloaded with P2Y12
inhibitors.
§The similar effects selectively occur in other types of cancer cells such as cervix, breast and liver cancer.
§§LSP is a potential novel chemoprevention and treatment agent for colorectal, cervix, breast, liver and lung cancer.
¶LSP systemically suppresses oncogenic cyclin D1, A, and Bcl-2 levels in colorectal, cervix, breast, liver and lung cancer cells.
1164 ª 2012 The Authors. European Journal of Clinical Investigationª 2012 Stichting European Society for Clinical Investigation Journal Foundation
C. ADLBRECHT ET AL. www.ejci-online.com




















