Reducing consumer demand for ineffective health remedies
328
Reducing consumer demand for ineffective health remedies: Using psychology to counter pseudoscience and the illegal wildlife trade Douglas MacFarlane Master of International Law Bachelor of Science (Ecology) Bachelor of Arts (Development) This thesis is presented for the degree of Doctor of Philosophy of The University of Western Australia School of Psychological Science 2020
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Reducing consumer demand for ineffective health remedies

Reducing consumer demand for ineffective health remedies: Using
psychology to counter pseudoscience and the illegal wildlife trade
Douglas MacFarlane
Master of International Law Bachelor of Science (Ecology)
Bachelor of Arts (Development)
This thesis is presented for the degree of
Doctor of Philosophy of The University of Western Australia School of Psychological Science
2020

ii

iii
“How did humans approach medicine before it became the effective science it is today?
The historical record is clear and consistent. Across all times and cultures, people
have been eager for medical treatments even without good evidence that such treatments had
therapeutic benefits, and even when the treatments were downright harmful. But what these
historical remedies lacked in scientific rigor, they more than made up for through elaborate
demonstrations of caring and support from respected, high-status specialists.”
Kevin Simler & Robin Hanson
The Elephant in the Brain
“[Q]uackery isn’t always about pure deception. Though the term is usually defined as the
practice and promotion of intentionally fraudulent medical treatments, it also includes
situations when people are touting what they truly believe works. But behind every
misguided treatment—from Ottomans eating clay to keep the plague away to Victorian gents
sitting in a mercury steam room for their syphilis to epilepsy sufferers sipping gladiator blood
in ancient Rome—is the incredible power of the human desire to live.”
Lydia Kang & Nate Pederson,
Quackery, A brief History of the Worst Ways to Cure Everything
“[Conservationists] are not in the business of supporting superstition”
— Responding to whether we should support the farming of rhino horns.
Sir David Attenborough
Conservation Science Conference, Cambridge University

iv

v
Thesis declaration
I, Douglas MacFarlane, certify that:
This thesis has been substantially accomplished during enrolment in this degree.
This thesis does not contain material which has been submitted for the award of any other
degree or diploma in my name, in any university or other tertiary institution.
In the future, no part of this thesis will be used in a submission in my name, for any other
degree or diploma in any university or other tertiary institution without the prior approval of
The University of Western Australia and where applicable, any partner institution responsible
for the joint-award of this degree.
This thesis does not contain any material previously published or written by another person,
except where due reference has been made in the text and, where relevant, in the Authorship
Declaration that follows.
This thesis does not violate or infringe any copyright, trademark, patent, or other rights
whatsoever of any person.
The research involving human data reported in this thesis was assessed and approved by The
University of Western Australia Human Research Ethics Committee. Approval #:
[RA/4/1/8712]. Written patient consent has been received and archived for the research
involving patient data reported in this thesis.
This thesis contains published work and/or work prepared for publication, some of which has
been co-authored.
Signature:
Date: 23/10/2020

vi
vii
Abstract
Consumer demand for alternative health remedies persists despite the absence of
scientific evidence for their efficacy or safety. In fact, there is mounting evidence that
consumption of many alternative health remedies causes extensive harm to both individuals
and society. A particularly destructive example is the demand for health remedies containing
parts of endangered plants and animals (e.g., rhino horn, tiger bone, rare orchids). The
demand for such products fuels an unsustainable, and often illegal, trade that is pushing many
species towards extinction. One explanation for why many consumers are willing to pay for
such products relates to the underlying cognitive mechanisms that make us susceptible to
fraudulent health claims—false or misleading claims used to promote remedies that are
untested, ineffective, or harmful. This thesis explores the psychology of fraudulent health
claims, presenting a novel taxonomy of interventions to overcome psychological barriers
impeding desirable behaviours. Using this taxonomy, the thesis then experimentally tests the
impact of tactics used by fraudsters and psychologically-informed interventions to help
protect consumers.
I found evidence that several cognitive mechanisms can be manipulated to influence
consumers’ willingness to pay for ineffective health remedies. First, I focussed on the illusion
of causality, that is, perception of a causal relationship between an action and a subsequent
but unrelated outcome. I found that this effect can be manufactured by giving consumers only
half the information they need to make causal judgements (i.e., providing only the number of
people who use a product and report a benefit but not the number of people who do not use a
product but still report a benefit). I also found that providing a simplified contingency table
that provides the “full picture” reduces demand for an ineffective dietary supplement. In a
series of follow up experiments, I replicated these results and found that this intervention can
be further strengthened by also countering consumers’ misperceptions that dietary
supplements are harmless, through a fear appeal. Using an innovative experimental auction, I

viii
showed that these two interventions combined reduced willingness to pay for an ineffective
product by ~50%.
Furthermore, the thesis explored the impact of combining multiple fraudulent tactics
into one piece of sophisticated misinformation. Testing how such misinformation can be
combatted, I found that evidence-based refutations that explain the tactics used by fraudsters
were more effective than “diplomatic” refutations typically used by health authorities at
reducing willingness to pay for a spurious remedy. Using another novel measure of consumer
behaviour, I also explored consumers’ willingness to share the misinformation via social
media. I found that misinformation exposure boosts subsequent misinformation sharing, but
that evidence-based refutations were able to completely reverse this effect, thus offering a
key intervention to neutralise the spread of misinformation through social networks.
As well as conducting research into the psychology of health fraud, this thesis also
documents my attempts to understand the potential of interventions aiming to reduce
consumer demand for wildlife products. Given the paucity of scientific evidence in the
conservation space, the thesis includes a meta-review of the evidence for interventions to
reduce demand for harmful products more broadly (e.g., alcohol, cigarettes, illicit drugs).
This section of the thesis integrates lessons from a diverse literature into guidelines to help
conservation practitioners better design demand-reduction interventions for consumers of
overexploited wildlife products.
The evidence generated by this thesis is then applied to a conservation problem that
was amplified by the COVID-19 pandemic, viz. the misguided persecution of bats. I
contextualise the actual health risks before outlining guidelines for debunking
misinformation, counteractive negative associations with bats, and altering harmful social
norms. This additional work illustrates the interconnectedness of the major themes of this
thesis—namely, human psychology, wildlife trade, consumer demand, misinformation, and
persuasive communication.

ix
In sum, this thesis aims to provide a better, theoretically grounded, understanding of
why consumers are susceptible to fraudulent health claims, to demonstrate empirically which
interventions work to protect them, and to provide evidence-based guidance for practitioners
to better design demand-reduction interventions.

x

xi
Table of Contents
Thesis declaration .................................................................................................................... v
Abstract .................................................................................................................................. vii
Acknowledgements ............................................................................................................... xiii
Authorship declaration: Co-authored publications ......................................................... xvii
Preamble ................................................................................................................................ xxi
Chapter 1: Overview ............................................................................................................... 1
1.1 Introduction ................................................................................................................................... 3
1.2 Thesis outline ................................................................................................................................ 5
1.3 References ................................................................................................................................... 11
Foreword for Chapter 2 .......................................................................................................... 17
Chapter 2: Protecting consumers from fraudulent health claims .................................... 21
Foreword for Chapters 3-5 ..................................................................................................... 39
Chapter 3: Overcoming the illusion of causality ................................................................ 45
Chapter 4: Do consumers respond to risks, lack of benefits, or both? ............................. 67
Chapter 5: Refuting COVID-19 misinformation ................................................................ 89
Foreword for Chapters 6-7 ................................................................................................... 119
Chapter 6: Reducing demand for overexploited wildlife products ................................. 125
Chapter 7: Applying psychology to bat conservation ...................................................... 183
Chapter 8: General discussion ........................................................................................... 193
8.1 Summary of theoretical contributions ....................................................................................... 195
8.2 Summary of empirical findings ................................................................................................. 196
8.3 Practical Implications ................................................................................................................ 200
8.3 Thesis limitations ...................................................................................................................... 201
8.4 Concluding remarks .................................................................................................................. 202
8.5 References ................................................................................................................................. 204

xii
Appendix I: Supplementary material for Chapter 2 ........................................................ 207
Appendix II: Supplementary material for Chapter 3 ...................................................... 219
Appendix III: Supplementary material for Chapter 4 .................................................... 247
Appendix IV: Supplementary material A for Chapter 5 ................................................. 257
Appendix V: Supplementary material B for Chapter 5 ................................................... 265
Appendix VI: Supplementary material for Chapter 6 ..................................................... 277

xiii
Acknowledgements
This thesis could not have been accomplished without the unwavering support of so
many people. First and foremost, I would like to thank my heroic supervisors, Prof. Ullrich
Ecker and Dr. Mark Hurlstone for their guidance, diligence, unerring patience, and great
friendship throughout this challenging journey. They have been the best mentors one could
hope for, both are passionate, dedicated, meticulous, and unswervingly witty. They have
supported my every endeavour and greatly influenced my ability to think in a scientific and
critical manner. Thank you.
I am also grateful to Prof. Bill Sutherland, whose openness, encouragement, and
thoughtful discussions were an important source of inspiration for me. Thank you for
welcoming me into the fold of the mighty Cambridge Conservation Science Group. I also
wish to express my gratitude to Dr. Ricardo Rocha, for his friendship and dedication to
solving the biggest issues in conservation, not least his determination to see genuine equality
in research. I want to thank Prof. Carmen Lawrence and Prof. Simon Farrell, for their advice
and feedback in the earlier stages of my thesis proposal and on my first publication. I am also
grateful to all the experts who helped advise and co-author the meta-review paper, Prof. Paul
J. Ferraro, Prof. Sander van der Linden, Dr. Anita K. Y. Wan, Dr. Diogo Veríssimo, Gayle
Burgess, Prof. Frederick Chen, Prof. Wayne Hall, Dr. Gareth J. Hollands, and, of course, my
supervisors. Thank you to Li Qian Tay for rising to the challenge of co-authoring the
misinformation paper, your contribution was both timely and impressive.
I am grateful for all the academic and administrative assistance as well as the
resources provided by the School of Psychological Science at the University of Western
Australia and the Department of Zoology at the University of Cambridge. I would
particularly like to thank Maria Puerta, Lisa Hitie, Nicola Colangelo, Kate Williot, Kerstin
Russell, George Rutherford, and Hawa Sydique. Thank you also to Charles Hanich for

xiv
showing me the ropes of recruiting psychology participants. I wish to acknowledge that this
research was supported by an Australian Government Research Training Program (RTP)
Scholarship, the UWA Safety Net Top-Up Scholarship, and the Endeavour Postgraduate
Scholarship.
I also want to thank my UWA colleagues in the Ecker Memory and Cognition Lab
and the UWA Behavioural Economics Laboratory. Thanks also to my UWA officemates,
Dr. Kris Singh and Dr. Alex Springall for their cheerful banter and welcoming support. I
wish to thank Dr. Susie Wang and Dr. Briony Swire-Thompson for their friendship and
assistance in shaping my academic career, without their intrepid forerunning I would not
have applied for an Endeavour scholarship to support my pre-doctorate research in
Cambridge. Thank you also to Ella and Adam Waterworth, two of the finest citizens and
hosts of Western Australia.
I also need to thank all my wonderful colleagues working across the conservation
space in the David Attenborough Building (DAB) for their dedication and comradery. A
special thank you to Dr. Helena Alves-Pinto, Harriet Bartlett, Gianluca Cerullo, Alec
Christie, Dr. Sophia Cook, Charles Emogor, Dr. Emma Garnett, Dr. Jonas Geldmann ,
Dr. Fangyuan Hua, Dr. Nick Littlewood, Dr. Phil Martin, Dr. Hannah Mumby, Dr. Kristian
Nielsen, Dr. Silviu O Petrovan, Dr. Katie Sainsbury, Dr. Claire Wordley, Dr. Rebecca Smith,
and Dr. Hannah Wauchope, Tom White, and Dr. Thomas Worthington. Thank you also to
Prof. Nicky Clayton, for putting me in touch with Bill Sutherland, without that connection,
life would have been quite different. Thanks also to those outside of the CSG group, who
made Cambridge particular stimulating and welcoming, Dr. Maria Dias, Dr. Kendal Jones,
Dr. Steffen Oppel, and Dr. Piero Visconti. I am also grateful to everyone at the Cambridge X-
press rowing club, our outings were a shining light in an otherwise dark working week. I am

xv
also eternally grateful to Rhiannon Niven, for your eternal optimism and for rescuing all our
worldly possessions when the world fell apart.
Thank you also to Prof. Sander van der Linden for including me in the Zangwill
Seminar series and also to Dr. Lee de-Wit and Dr. Rakoen Maertens for including me in the
first assemblage of the Cambridge University Behavioural Insights Team (CUBIT). I am
especially grateful to Gayle Burgess from TRAFFIC for taking the time to engage and
encourage me into the conservation demand-reduction space. Thanks also to Dan Challender,
Hunter Doughty, Prof. EJ Milner Gulland, Sonja Vogt, Diogo Veríssimo, Jaime Walsh, and
Laura Thomas-Walters for welcoming me into various workshops and conferences with the
Oxford Martin Programme on the Illegal Wildlife Trade; those events were truly inspiring.
Thank you also to Dr. Amy Hinsley for your enthusiasm, warmth, and dedication to
endangered plants.
I am eternally grateful to my family. My two brothers, Kev and Ant, who help to
ground and support everything I do. Thank you, Colin, for sheltering me when COVID-19
hit, putting up with me, and for teaching me to never back down from a worthy pursuit.
Thank you, Jenny, for your unyielding love, support, and interest. Thank you, Merv and
Helen, for your kindness, support, and generosity, and for helping to inspire my scientific
curiosity. Thank you, Tawny, for being the greatest dog on the planet, 95% of the time.
Thank you also to my friends who have stuck by my interminable absence. Special thank you
to Roland Ellis, for planting the seed that I could lead my own research.
Finally, and most importantly, to my beautiful wife, Alex, who has stuck with me
through everything. Without whom, I would not have finished this thesis, taken a holiday, or
kept a semblance of my sanity. You are my biggest inspiration and my greatest source of
love, laughter, and compassion. Thank you for everything.

xvi

xvii
Authorship declaration: Co-authored publications
This thesis contains work that has been published and work that has been prepared for publication.
Details of the work: MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Protecting consumers from fraudulent health claims: A taxonomy of psychological drivers, interventions, barriers, and treatments. Social Science & Medicine, 112790. Location in thesis: Chapter 2 Student contribution to work: 90% The candidate completed the literature review, drafted the taxonomy, and wrote the original manuscript. Professor Ecker and Dr. Hurlstone provided feedback and guidance throughout, and also contributed to the writing and manuscript preparation. Co-author signatures and dates:
10/9/20
Details of the work: MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for ineffective health remedies: Overcoming the illusion of causality. Psychology & Health, 33, 1472-1489. Location in thesis: Chapter 3 Student contribution to work: 90% The candidate adapted the willingness-to-pay measure, designed the survey materials, ran the experiment, analysed the results, drafted the full manuscript. Professor Ecker and Dr. Hurlstone provided feedback and guidance throughout, and also contributed to the writing and manuscript preparation. Co-author signatures and dates:
10/9/20
Details of the work: MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Countering demand for ineffective health remedies: Do consumers respond to risks, lack of benefits, or both? Psychology & Health. Location in thesis: Chapter 4 Student contribution to work: 90% The candidate designed the survey materials, ran the experiment, analysed the results, drafted the full manuscript. Professor Ecker and Dr. Hurlstone provided feedback and guidance throughout, and also contributed to the writing and manuscript preparation. Co-author signatures and dates:
10/9/20 Details of the work:

xviii
MacFarlane, D., Tay, L. Q., Hurlstone, M. J., & Ecker, U. K. H. (2020). Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation Sharing. Manuscript submitted for publication. Location in thesis: Chapter 5 Student contribution to work: 45% All authors jointly developed the study concept and contributed to the study design. The candidate prepared the experimental survey and performed data collection and analysis with input from all other authors. The candidate and LQT drafted the manuscript, and MH and UKHE provided critical revisions. Co-author signatures and dates:
10/9/20
Details of the work: MacFarlane, D., Hurlstone, M. J., Ecker, U. K. H., Ferraro, P. J, van der Linden, S., Wan, A. K. Y., Veríssimo, D., Burgess, G., Chen, F., Hall, W., Hollands, G. J., & Sutherland, W. J. (2020). Reducing demand for overexploited wildlife products: Lessons from systematic reviews from outside conservation science. Manuscript submitted for publication. Location in thesis: Chapter 6 Student contribution to work: 70% The candidate conceptualized the systematic review in discussions with Professor William Sutherland. The candidate formed and coordinated responses from the advisory board. The candidate created the search criteria with input from the advisory board, which consisted of all co-authors. The candidate designed the systematic review methodology, applied the inclusions and exclusion criteria, extracted the data, designed the figures, and completed the manuscript preparation and revisions. All co-authors provided feedback on the manuscript preparation. Professor Ullrich Ecker and Dr. Mark Hurlstone provided guidance and supervision on manuscript preparation. Co-author signatures and dates:
10/9/20
Details of the work: MacFarlane, D., & Rocha, R. (2020). Guidelines for communicating about bats to prevent persecution in the time of COVID-19. Biological Conservation, 248, 108650. Location in thesis: Chapter 7 Student contribution to work: 50% The candidate designed the guidance materials, created the visual guidance figures, co-wrote the manuscript. Dr. Ricardo Rocha came up with the idea to write the perspective piece based on my findings in psychology, co-wrote the manuscript and provided editing and comments on other guidance materials.
Student signature:
Date: 10/9/2020

xix
I, Dr. Mark Hurlstone certify that the student’s statements regarding their contribution to each of the works listed above are correct. Co-supervisor signature:
Date: 21/10/20 I, Professor Ullrich Ecker certify that the student’s statements regarding their contribution to each of the works listed above are correct. As all co-authors’ signatures could not be obtained, I hereby authorise inclusion of the co-authored work in the thesis. Coordinating supervisor signature:
Date: 10/9/20

xx

xxi
Preamble
This thesis is presented as a series of empirical and theoretical papers that have been
published or have been written in manuscript format. One integrative theoretical review paper
has been published in a peer-reviewed journal (Chapter 2). Two empirical papers have been
published in peer-reviewed journals (Chapter 3 and Chapter 4). One empirical paper is under
review in a peer-reviewed journal (Chapter 5). The systematic review paper is under review
in a peer-reviewed journal (Chapter 6). The theoretical perspective paper has been published
in a peer-reviewed journal (Chapter 7). To facilitate review, literature references for in-text
citations can be found either directly after each chapter or at the end of each of paper.
Supplemental materials to each paper have been included in the appendices. As the
manuscripts were written as independent works, several definitions and themes are presented
multiple times throughout the thesis.

xxii

Chapter 1: Overview
1

2

1.1 Introduction
Beliefs about the health benefits of consuming wildlife products (e.g., rhino horn,
shark fins, medicinal orchids) help to drive a complex and multibillion-dollar black market
for plant and animal products (Graham-Rowe, 2011; Margulies et al., 2019; Moreto &
Lemieux, 2015; Truong et al., 2015). The illegal trade in wildlife products for use in
traditional “medicine” encompasses the exploitation, and often overexploitation, of hundreds
of species, including many that are threatened with extinction (Margulies et al., 2019; Phelps
et al., 2016; Tali et al., 2019). This trade is not only a major driver of biodiversity decline
(Maxwell et al., 2016; Rosen & Smith, 2010) but is also an ongoing risk to global public
health. Whether during capture, trade, or consumption of animals and animal products, the
illegal wildlife trade facilitates opportunities for outbreaks of zoonoses (Johnson et al., 2015;
Spevack, 2020)—infectious diseases that spread from animals to humans—and thus is a
suspected cause of the current COVID-19 pandemic, which has resulted in over 950,000
deaths, as of August 2020 (Oxford Martin School, 2020).
Widespread beliefs in the health benefits of consuming wildlife persist despite several
key oversights. First, the efficacy of wildlife products for treating disease has rarely been
established (Costa, 2012; Hinsley et al., 2017). Second, multiple forensic investigations have
found an alarming proportion (as high as 90%) of traditional remedies contain undeclared
substance including toxic elements (e.g., arsenic, mercury, lead), which can cause serious
illness and even death, and potent pharmaceuticals (e.g., warfarin or paracetamol), which
may explain why some remedies are thought to work (Blacksell et al., 2014; Byard, 2010;
Coghlan et al., 2015). Third, some wildlife products are unaffordable to all but the very
affluent (e.g., rhino horn is estimated to fetch > $50,000/kg; (Christy, 2015), even though
many wildlife products could easily be replaced by cheaper, and more sustainable substitutes
Chaper 1: Introduction 3

(da Nóbrega Alves et al., 2008; Zhang & Yin, 2014). In light of these omissions, the ongoing
demand for wildlife products appears to defy the predictions of rational choice theory
(Friedman & Friedman, 1953)—that individuals act in their own self-interest—specifically,
that people would prefer products that are verifiably effective, safe, and reasonably priced.
The present thesis explores why consumers are susceptible to fraudulent heath
claims—claims about remedies that are untested, ineffective, or harmful—and investigates
whether behavioural interventions, based on psychological insights, can help protect
consumers. I examine the cognitive biases that lead consumers to desire ineffective health
products and then take a systematic approach to test a series of promising interventions. To
evaluate intervention success, I employ two objective measures of consumer behaviour,
namely consumers’ willingness-to-pay for ineffective health products (Chapters 3-5) and
online sharing of health misinformation (Chapter 5). As I will argue in Chapter 2, to
successfully protect consumers, communicators need to design interventions that help
consumers overcome the cognitive, social, and emotional biases that health fraudsters exploit
to sell their products and then employ evidence-based interventions that provide consumers
with strategies for detecting and reducing their susceptibility to health fraud.
While this thesis was fundamentally inspired by my interest in countering demand for
overexploited wildlife products, the introductory review (Chapter 2) focuses on reducing
demand for ineffective treatments more generally, and the empirical chapters (Chapters 3-5)
concentrates on a specific class of ineffective health products—vitamin supplements— for
reasons of practicality and generalizability. The following two chapters then explore the
broader dimensions of the connection between health and the wildlife trade. Specifically, the
meta-review (Chapter 6) examines the impacts of the overexploitation of wildlife and the
risks the global wildlife trade poses to global public health. After briefly examining the extent
of these problems, it delves into the evidence base for effective solutions and provide
Chaper 1: Introduction 4

guidance for practitioners to implement them. The perspective paper (Chapter 7) provides
guidance on designing psychologically-informed communications to prevent the misguided
persecution of wildlife (due to fears of pandemic risks).
1.2 Thesis outline
This thesis consists of eight chapters. Following this introductory chapter, Chapter 2
features a published review of the psychological underpinnings of consumer susceptibility to
fraudulent health claims. This integrative theoretical review provides the rationale for
addressing health fraud more broadly and outlines a taxonomy for systematically designing
psychologically-informed behavioural interventions to protect consumers. As this taxonomy
subsequently guides the design of the interventions tested in the empirical chapters that
follow (Chapters 3-5), the basic structure of the framework is worth briefly outlining here.
The taxonomy is structured according to five psychological drivers that I hypothesise
are major contributors to consumer susceptibility to health fraud, namely: Visceral influence,
Affect, Nescience, Misinformation, and Norms (VANMaN). Visceral influences are
motivational cues (e.g., pain, financial stress, sensation seeking) that elicit strong
psychological responses and thus impair consumers’ cognitive abilities to detect and avoid
fraud (Lea et al., 2009; Loewenstein, 1996; Wilson, 2014). Affect is the emotive quality of
“goodness” or “badness” that becomes associated with an action or item, influencing how
decisions are made based on positive or negative feelings (Slovic et al., 2004, 2007).
Nescience is the absence of knowledge or awareness that makes consumers susceptible to
fraudulent claims by leaving room for people to intuitively generate or accept spurious causal
associations between cause (e.g., remedy) and effect (e.g., recovery; (Matute et al., 2015;
Yarritu et al., 2014). Misinformation makes it difficult for consumers to distinguish between
evidence-based medicine and fraudulent health remedies (Kitchens et al., 2014; Lavorgna &
Chaper 1: Introduction 5

Di Ronco, 2020; Poland & Spier, 2010). Social norms are rules or standards about how
members of a community should behave, which can influence consumers’ desire to consume
particular ineffective remedies (Centola, 2018; Farrow et al., 2017).
As each of the five drivers of the VANMaN taxonomy suggest a seemingly obvious
intervention (e.g., overcome nescience by providing information), we then outline current
research on psychological barriers that are exploited by fraudsters and that often impede the
effectiveness of the obvious interventions (e.g., our tendency to confuse confidence with
knowledge, termed the illusion of confidence, can lead us to trust confident fraudsters over
cautious health experts). This framework of drivers, psychological barriers, and strategies to
manipulate consumers then forms the basis upon which we propose several hypotheses about
specific measures—which we label treatments— that could help consumers overcome
specific psychological barriers and thus increase their resilience to fraudulent health claims.
The numerous predictions contained within the taxonomy thus form an extensive research
agenda, whereby each hypothesised treatment can, and should, be experimentally tested.
Chapters 3 and 4 feature published, peer-reviewed papers. Chapter 3 investigates a
particularly pervasive psychological barrier, namely the illusion of causality. The illusion
occurs when people perceive a causal relationship between an action and a subsequent
outcome (Blanco et al., 2011) even when the two events are unrelated, such as taking vitamin
C and subsequently recovering from a cold (Hemila & Chalker, 2013). As the first empirical
paper, Chapter 3 outlines how I validated both (1) the primary dependent measure for
evaluating the impact of the interventions, namely consumers’ willingness-to-pay for an
ineffective health remedy (MacFarlane et al., 2018; Thrasher et al., 2011); and (2) the
primary covariate, namely a survey for measuring (and thus controlling for) participants’ pre-
existing attitudes towards alternative health remedies and dietary supplements (MacFarlane et
al., 2018). Using these mechanisms, I experimentally evaluate the impact of a novel
Chaper 1: Introduction 6

intervention to help consumers overcome the illusion of causality. As a proof of concept, I
evaluated the impact of this intervention by measuring participants’ willingness-to-pay for
multivitamin supplements. Multivitamins were chosen because they are commonly used, yet
provide no discernible health benefits (Bjelakovic et al., 2012; Jenkins et al., 2018). To
ensure ecological validity, participants were given real money and the opportunity to bid on a
real multivitamin supplement.
Chapter 4 builds on the results of the first empirical paper, by replicating the impact
of the novel intervention to overcome the illusion of causality, while also investigating its
effect in conjunction with an intervention designed to counter another psychological barrier,
namely irrational affect. Specifically, my co-authors and I designed a fear-appeal intervention
to counter misperceptions about the (lack of) health risks of an ineffective health remedy
(MacFarlane et al., 2020a). Chapter 4 consists of two near-identical experiments, one with
online participants measuring their hypothetical willingness-to-pay and one with
undergraduate students in the laboratory measuring their incentivised willingness-to-pay (i.e.,
using real money and the opportunity to purchase a real multivitamin product). This paper
also investigates whether there is a significant difference in consumer behaviour when the
experiment is hypothetical compared to when it is fully incentivised, thus also making a
methodological contribution to the literature.
Chapter 5 is a manuscript currently submitted for publication. It presents the results of
a large online experiment, adopting the same experimental measures used in Chapters 3 and
4. The experiment investigates the impact of sophisticated health disinformation—health
misinformation disseminated with the intent to deceive, often for financial motives (McKee
& Middleton, 2019)—on consumer demand. It examines the effect of employing several
techniques used by fraudsters to manipulate people into believing unsupported claims about
bogus health remedies, using the example of vitamin E as an alleged COVID-19 treatment.
Chaper 1: Introduction 7

Chapter 5 then evaluates the impact of two interventions to counteract the impact of this
disinformation. The experiment compares the impact of a tentative refutation—based on the
“diplomatic” refutation style commonly used by health authorities—to an enhanced
refutation that, based on psychological insights, highlights and explains the techniques used
to manipulate consumers (MacFarlane et al., 2020b). Chapter 5 also introduces a new
measure to capture the impact of the disinformation and the subsequent interventions, on
participants’ willingness to share misinformation via social media. The measure examines
whether the enhanced refutation better helps to reduce the spread of misleading health claims,
by encouraging participants to either flag the disinformation as misleading or simply not
share it within their social networks.
Chapter 6 features a meta-review of systematic reviews and is currently submitted for
publication. It provides a broad overview of the negative impacts of the illegal wildlife trade,
such as biodiversity loss, ecosystem collapse, and accelerating government corruption. The
paper aims to address a concurrent aim of the present thesis, namely, to investigate what
interventions effectively reduce demand for overexploited wildlife products. The review was
undertaken in response to a previous evidence synthesis that found that most demand-
reduction campaigns targeting wildlife products have lacked rigorous evaluation, and thus
their impacts remain unknown (Veríssimo & Wan, 2019). To fill the evidence gap, our meta-
review turned to the wider academic literature (including public health, sociology,
criminology, etc.) to assess the evidence for the effectiveness of interventions that aim to
reduce consumer demand for harmful products (e.g., cigarettes and illicit drugs). The meta-
review synthesises the findings of 41 systematic reviews for several commonly used
intervention approaches, such as mass-media campaigns, health-risk warnings, and social-
marketing campaigns. The paper summarises the key learnings from this large body of
Chaper 1: Introduction 8

evidence and provides simple guidelines to help conservation practitioners better design
demand-reduction interventions.
Chapter 7 features a published “theoretical perspective” that draws on many of the
learnings discussed in the remainder of this thesis. The paper was written in response to
reports that the increased media coverage associating bats with the spread of COVID-19 had
motivated isolated instances of the misguided persecution of wild bats. The paper helps to
contextualise the actual health risks, noting that wild animals pose a relatively trivial threat
compared to high-risk human activities such as hunting, live animal markets, and habitat
destruction/encroachment. We note that retributive culling of bat species is not only
ineffective for preventing the spread of zoonoses but has been documented to increase
opportunities for zoonotic transmission. We then argue that intuitive attempts by
conservationists to counter misinformation about bats and zoonoses could inadvertently help
to reinforce irrational fears and incite misguided violence towards bats. Drawing on several
psychological insights about combating irrational associations, we provide guidelines for
communicating about bats to prevent persecution during the time of COVID (and beyond).
The paper outlines evidence-based approaches to debunking misinformation, counteracting
negative associations with bats, and changing harmful social norms. The paper serves as an
illustrative example of the interconnectedness of the major themes of this thesis, including
human psychology, wildlife trade, consumer demand, misinformation, and persuasive
communication.
In sum, my research has adopted a multidisciplinary approach incorporating cognitive
and experimental psychology, evidence synthesis, and conservation science. This research
was inspired by my interest in reducing demand for unsustainable wildlife products, and
united by the question, “what interventions are effective for reducing demand for ineffective
health remedies?”. The general conclusion of my research is that evidence-based approaches
Chaper 1: Introduction 9

to addressing unsustainable wildlife consumption are critical to addressing key global
challenges, and to this end, psychologically-informed messaging provides a powerful tool for
both altering harmful consumer norms and protecting consumers from health fraud. To
conclude, Chapter 8 further deliberates on limitations, implications, and avenues for future
research.
Chaper 1: Introduction 10

1.3 References
Bjelakovic, G., Nikolova, D., Gluud, L. L., Simonetti, R. G., & Gluud, C. (2012).
Antioxidant supplements for prevention of mortality in healthy participants and patients
with various diseases. Cochrane Database Syst Rev, 3, CD007176.
Blacksell, L., Byard, R. W., & Musgrave, I. F. (2014). Forensic problems with the
composition and content of herbal medicines. Journal of Forensic and Legal Medicine,
23, 19–21.
Blanco, F., Matute, H., & Vadillo, M. A. (2011). Making the uncontrollable seem
controllable: the role of action in the illusion of control. The Quarterly Journal of
Experimental Psychology, 64, 1290–1304.
Byard, R. W. (2010). A review of the potential forensic significance of traditional herbal
medicines. J Forensic Sci, 55, 89–92.
Centola, D. (2018). How behavior spreads: The science of complex contagions (Vol. 3).
Princeton University Press.
Christy, B. (2015). Tracking Ivory. National Geographic, 228(3).
Coghlan, M. L., Maker, G., Crighton, E., Haile, J., Murray, D. C., White, N. E., Byard, R.
W., Bellgard, M. I., Mullaney, I., Trengove, R., Allcock, R. J., Nash, C., Hoban, C.,
Jarrett, K., Edwards, R., Musgrave, I. F., & Bunce, M. (2015). Combined DNA,
toxicological and heavy metal analyses provides an auditing toolkit to improve
pharmacovigilance of traditional Chinese medicine (TCM). Scientific Reports, 5, 17475.
Costa, M. (2012). Does traditional Chinese medicine have a place in the health system? The
Conversation. http://theconversation.com/does-traditional-chinese-medicine-have-a-
place-in-the-health-system-6166
da Nóbrega Alves, R. R., da Silva Vieira, W. L., & Santana, G. G. (2008). Reptiles used in
traditional folk medicine: conservation implications. Biodiversity and Conservation, 17,
Chaper 1: Introduction 11

2037–2049.
Farrow, K., Grolleau, G., & Ibanez, L. (2017). Social norms and pro-environmental behavior:
A review of the evidence. Ecological Economics, 140, 1–13.
Friedman, M., & Friedman, M. (1953). Essays in positive economics. University of Chicago
press.
Graham-Rowe, D. (2011). Biodiversity: Endangered and in demand. Nature, 480, S101-3.
Hemila, H., & Chalker, E. (2013). Vitamin C for preventing and treating the common cold.
Cochrane Database Syst Rev, 1, CD000980.
Hinsley, A., de Boer, H. J., Fay, M. F., Gale, S. W., Gardiner, L. M., Gunasekara, R. S.,
Kumar, P., Masters, S., Metusala, D., & Roberts, D. L. (2017). A review of the trade in
orchids and its implications for conservation. Botanical Journal of the Linnean Society,
186(4), 435–455.
Jenkins, D. J. A., Spence, J. D., Giovannucci, E. L., Kim, Y. I., Josse, R., Vieth, R., Blanco
Mejia, S., Viguiliouk, E., Nishi, S., Sahye-Pudaruth, S., Paquette, M., Patel, D.,
Mitchell, S., Kavanagh, M., Tsirakis, T., Bachiri, L., Maran, A., Umatheva, N., McKay,
T., … Sievenpiper, J. L. (2018). Supplemental vitamins and minerals for CVD
prevention and treatment. Journal of the American College of Cardiology, 71, 2570–
2584.
Johnson, C. K., Hitchens, P. L., Smiley Evans, T., Goldstein, T., Thomas, K., Clements, A.,
Joly, D. O., Wolfe, N. D., Daszak, P., Karesh, W. B., & Mazet, J. K. (2015). Spillover
and pandemic properties of zoonotic viruses with high host plasticity. Scientific Reports,
5, 14830.
Kitchens, B., Harle, C. A., & Li, S. (2014). Quality of health-related online search results.
Decision Support Systems, 57, 454–462.
Lavorgna, A., & Di Ronco, A. (2020). Medical Misinformation and Social Harm in Non-
Chaper 1: Introduction 12

Science-Based Health Practices: A Multidisciplinary Perspective (1st ed.). Routledge.
Lea, S., Fischer, P., & Evans, K. (2009). The psychology of scams, provoking and committing
errors of judgement: Prepared for the Office of Fair Trading by the University of Exeter
School of Psychology. UK Office of Fair Trading.
Loewenstein, G. (1996). Out of control: Visceral influences on behaviour. Organizational
Behavior and Human Decision Processes, 65(3), 272–292.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for
ineffective health remedies: Overcoming the illusion of causality. Psychology and
Health, 33.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020a). Countering demand for
ineffective health remedies: Do consumers respond to risks, lack of benefits, or both?
Psychology and Health.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020b). Protecting consumers from
fraudulent health claims: A taxonomy of psychological drivers, interventions, barriers,
and treatments. Social Science and Medicine, 259.
Margulies, J. D., Bullough, L.-A., Hinsley, A., Ingram, D. J., Cowell, C., Goettsch, B.,
Klitgård, B. B., Lavorgna, A., Sinovas, P., & Phelps, J. (2019). Illegal wildlife trade and
the persistence of “plant blindness.” PLANTS, PEOPLE, PLANET, 1, 173–182.
Matute, H., Blanco, F., Yarritu, I., Díaz-Lago, M., Vadillo, M. A., & Barberia, I. (2015).
Illusions of causality: How they bias our everyday thinking and how they could be
reduced. Frontiers in Psychology, 6, 1–14.
Maxwell, S. L., Fuller, R. A., Brooks, T. M., & Watson, J. E. M. (2016). Biodiversity: The
ravages of guns, nets and bulldozers. Nature, 536, 143–145.
McKee, M., & Middleton, J. (2019). Information wars: Tackling the threat from
disinformation on vaccines. British Medical Journal Publishing Group.
Chaper 1: Introduction 13

Moreto, W. D., & Lemieux, A. M. (2015). From CRAVED to CAPTURED: Introducing a
product-based framework to examine illegal wildlife markets. European Journal on
Criminal Policy and Research, 21, 303–320.
Oxford Martin School. (2020). Coronavirus Pandemic Data Explorer. Our World in Data.
Retrieved from. ourworldindata.org/grapher/total-deaths-covid-19
Phelps, J., Biggs, D., & Webb, E. L. (2016). Tools and terms for understanding illegal
wildlife trade. Frontiers in Ecology and the Environment, 14, 479–489.
Poland, G. A., & Spier, R. (2010). Fear, misinformation, and innumerates: how the
Wakefield paper, the press, and advocacy groups damaged the public health. Vaccine,
28, 2361–2362.
Rosen, G. E., & Smith, K. F. (2010). Summarizing the evidence on the international trade in
illegal wildlife. EcoHealth, 7, 24–32.
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2004). Risk as analysis and risk
as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Analysis, 24,
311–322.
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2007). The affect heuristic.
European Journal of Operational Research, 177, 1333–1352.
Spevack, B. (2020). Animal Smuggling in Air Transport and Preventing Zoonotic Spillover.
Tali, B. A., Khuroo, A. A., Nawchoo, I. A., & Ganie, A. H. (2019). Prioritizing Conservation
of Medicinal Flora in the Himalayan Biodiversity Hotspot: An Integrated Ecological and
Socioeconomic Approach. Environmental Conservation, 46, 147–154.
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011).
Estimating the impact of pictorial health warnings and “plain” cigarette packaging:
evidence from experimental auctions among adult smokers in the United States. Health
Policy, 102, 41–48.
Chaper 1: Introduction 14

Truong, V. D., Dang, N. V. H., & Hall, C. M. (2015). The marketplace management of illegal
elixirs: illicit consumption of rhino horn. Consumption Markets & Culture, 19, 353–369.
Veríssimo, D., & Wan, A. K. Y. (2019). Characterizing efforts to reduce consumer demand
for wildlife products. Conservation Biology, 3, 623–633.
Wilson, P. R. (2014). The art of the con: How to think like a real hustler and avoid being
scammed. Lyons Press.
Yarritu, I., Matute, H., & Vadillo, M. A. (2014). Illusion of control: The role of personal
involvement. Exp Psychol, 61, 38–47.
Zhang, L., & Yin, F. (2014). Wildlife consumption and conservation awareness in China: a
long way to go. Biodiversity and Conservation, 23, 2371–2381.
Chaper 1: Introduction 15

16

Foreword for Chapter 2
Chapter 2 presents a review of several key psychological factors that underpin the
persuasive appeal of fraudulent health claims—false or misleading claims used to promote
health remedies that are untested, ineffective, and often harmful (MacFarlane, Hurlstone, &
Ecker, 2020). The paper essentially argues that the appeal of fraudulent health claims is
multifactorial and thus solutions to protect consumers need to draw on insights from multiple
perspectives. The goal of the review was to provide a structured and systematic approach to
designing interventions to help consumers avoid succumbing to health fraud. The resultant
taxonomy posits numerous testable hypotheses, some of which are then tested in the
following three empirical chapters (Chapters 3-5).
This chapter was first submitted for publication to a prominent health-psychology
journal in 2018. While the final publication is undoubtedly stronger from having been peer-
reviewed, a key reason for its initial rejection was that “it [was] not clear that people who use
these treatments [i.e. alternative health remedies] are wanting interventions to reduce their
use.” For me, the assertion that use of alternative health products does not warrant
intervention because they are in demand is symptomatic of the widespread misconception
that such remedies are generally harmless and without any real-world impacts. The
pervasiveness of this sentiment could explain why, prior to the publication of this chapter in
2020, there did not exist (to the best of my knowledge) a comprehensive, scholarly review of
the psychological underpinnings of fraudulent health claims.
Fast forward to 2020, where every corner of the globe continues to be impacted by the
COVID-19 pandemic. In February, the Director-General of the World Health Organisation
(WHO), Tedros Adhanom Ghebreyesus, argued that the WHO was not only fighting the
spread of COVID-19 but also an epidemic of misinformation. According to WHO experts,
this infodemic is undermining efforts to ensure that people are informed to act appropriately
Foreword for Chapter 2 17
(Zarocostas, 2020). This problem thus provokes an important question—what is the bulk of
COVID-19 misinformation about? According to a recent study, the largest category of
COVID-19 misinformation relates to “miracle cures”, which comprised some 26.4% of all
pieces of misinformation identified (Blake, 2020). The authors also noted the biggest driver
of COVID-19 misinformation was found to be the US president, Donald Trump, who has
touted various debunked and/or harmful remedies including hydroxychloroquine and
injecting disinfectant.
Such troubling developments have rocketed the present line of research into the
global limelight. Chapter 2 represents the first attempt to provide a structured outline of
several of the key underlying psychological drivers of consumer susceptibility to health
fraud. While the taxonomy is reasonably comprehensive, it is not exhaustive. Indeed, three
notable commentaries have already been written in response to the taxonomy. These fantastic
additions provide further insight into how susceptibility to health fraud may also be driven by
our emotions (Fitzgerald, Sevi, & Shook, 2020); by individual differences in personalities
and cognitive traits, as well as by statistical and numerical illiteracy (Lilienfeld et al., 2015);
and how it can be applied to design interventions to counter real-world health conspiracies
(Motta, 2020).
Foreword for Chapter 2 18

References Blake, A. (2020). Study shows Trump behind 38 percent of coronavirus misinformation. The
Washington Post. Retrieved from. https://www.washingtonpost.com/politics/
2020/10/01/study-shows-trump-is-super-spreader-coronavirus-misinformation/
Fitzgerald, H. N., Sevi, B., & Shook, N. J. (2020). Fraudulent health claims: Further
consideration of the role of emotions. Social Science & Medicine, 112979.
Lilienfeld, S. O., Sauvigné, K. C., Lynn, S. J., Cautin, R. L., Latzman, R. D., & Waldman, I.
D. (2015). Fifty psychological and psychiatric terms to avoid: A list of inaccurate,
misleading, misused, ambiguous, and logically confused words and phrases. Frontiers in
Psychology, 6.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Protecting consumers from
fraudulent health claims: A taxonomy of psychological drivers, interventions, barriers,
and treatments. Social Science and Medicine, 259.
Motta, M. (2020). Applications & critical reflections on the VANMaN taxonomy. Social
Science & Medicine, 259, 112850.
Zarocostas, J. (2020). How to fight an infodemic. The Lancet, 395, 676.
Foreword for Chapter 2 19

20

Chapter 2: Protecting consumers from fraudulent
health claims
This chapter is presented in the format of a journal article.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Protecting consumers from fraudulent health claims: A taxonomy of psychological drivers, interventions, barriers, and treatments. Social Science & Medicine, 112790.
21

22

Contents lists available at ScienceDirect
Social Science & Medicinejournal homepage: www.elsevier.com/locate/socscimed
Review article
Protecting consumers from fraudulent health claims: A taxonomy ofpsychological drivers, interventions, barriers, and treatmentsDouglas MacFarlane!, Mark J. Hurlstone, Ullrich K.H. EckerSchool of Psychological Science, University of Western Australia, Australia
A R T I C L E I N F O
Keywords:Health fraudPseudoscienceCausal illusionsMisinformationBehaviour changeEvidence-based interventionsSocial normsMotivated reasoning
A B S T R A C T
Objective: Fraudulent health claims—false or misleading claims used to promote health remedies that are un-tested, ine!ective, and often harmful—cause extensive and persistent harm to consumers. To address this pro-blem, novel interventions are needed that address the underlying cognitive mechanisms that render consumerssusceptible to fraudulent health claims. However, there is currently no single framework of relevant psycho-logical insights to design interventions for this purpose. The current review aims to address this gap.Method: An integrative theoretical review was conducted across several relevant disciplines including crimin-ology; behavioural economics; and cognitive, health, and social psychology.Results: The current review presents a novel taxonomy that aims to serve as an agenda for future research tosystematically design and compare interventions based on empirical evidence. Specifically, this taxonomyidentifies (i) the psychological drivers that make consumers susceptible to fraudulent health claims, (ii) thepsychological barriers that may prevent successful application of interventions, and (iii) proposes evidence-informed treatments to overcome those barriers.Conclusions: The resulting framework integrates behavioural insights from several hitherto distinct disciplinesand structures promising interventions according to five underlying psychological drivers: Visceral influence,A!ect, Nescience, Misinformation, and Norms (VANMaN). The taxonomy presents an integrative and accessibletheoretical framework for designing evidence-informed interventions to protect consumers from fraudulenthealth claims. This review has broad implications for numerous topical issues including the design and eva-luation of anti-fraud campaigns, e!orts to address the growing problem of health-related misinformation, and forcountering the polarisation of politically sensitive health issues.
1. Introduction
For many consumers, so-called alternative health remedies can seema worthwhile lottery: they come with low costs and promise large po-tential benefits. Yet, despite the incredible claims of their advocates,when tested, most alternative remedies would be more accurately de-scribed as health fraud—the marketing or selling of products that havenot been proven safe or e!ective (U.S. Food & Drug Administration[FDA], 2019). Notable examples of such remedies include homeopathy,reflexology, and iridology (Australian Government Department ofHealth, 2015), as well as weight-loss scams and other debunked re-medies such as ozone therapy, colloidal silver, and psychic surgery.
Many mainstream health practitioners seem to regard such alter-native health remedies as nothing more than unscientific but mostlyharmless placebos. Indeed, many doctors will acknowledge that certainalternative remedies may even provide benefits, irrespective of medical
considerations, such as serving cultural or religious needs or a sense ofbelonging to a like-minded community. However, mounting evidencesuggests the harms arising from alternative health remedies are largelyunderappreciated and, in many cases, outweigh the potential benefits.For example, in 2012, sales of dietary supplements in the U.S. exceeded$100 per person on average, which is roughly $30 billion or 9% of allout-of-pocket health care spending in the U.S. (U.S. National Institute ofHealth [NIH], 2016). Yet, extensive research indicates that most dietarysupplements are ine!ective (Guallar et al., 2013; Jenkins et al., 2018)and sometimes harmful. Vitamin supplementation, for example, hasbeen linked to some 23,000 visits to U.S. emergency departments an-nually (Geller et al., 2015), various side-e!ects such as pancreatitis,liver disease (Bjelakovic et al., 2014), and even an increased risk ofmortality compared to placebo (Bjelakovic et al., 2012).
Other underappreciated harms of alternative remedies arise frominteractions with conventional medications (Byard and Musgrave,
https://doi.org/10.1016/j.socscimed.2020.112790Received 8 August 2019; Received in revised form 13 December 2019; Accepted 4 January 2020
! Corresponding author.M304, 35 Stirling Hwy, Perth, 6009, Australia.E-mail address: [email protected] (D. MacFarlane).
6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
������������������(OVHYLHU�/WG��$OO�ULJKWV�UHVHUYHG�
3OHDVH�FLWH�WKLV�DUWLFOH�DV��'RXJODV�0DF)DUODQH��0DUN�-��+XUOVWRQH�DQG�8OOULFK�.�+��(FNHU��6RFLDO�6FLHQFH��0HGLFLQH��KWWSV���GRL�RUJ���������M�VRFVFLPHG������������
23

2010) and opportunity costs from delaying or not seeking evidence-based treatment (Greenlee and Ernst, 2012), which is a particularconcern in cancer patients (Citrin et al., 2012). Harm also arisesthrough risk compensation (Bolton et al., 2006)—when health remedymessaging (e.g., “promotes natural immunity”) undermines individualperceptions of the risk associated with a relevant risky behaviour (e.g.,vaccine hesitancy; Attwell et al., 2018). Recent studies have also un-covered widespread ingredient substitution (e.g., with undeclared plantor animal taxa), toxic contamination (e.g., with heavy metals such aslead, cadmium, & arsenic), and high rates of adulteration with con-ventional pharmacological agents (e.g., warfarin & paracetamol;Coghlan et al., 2015; Rocha et al., 2016). Moreover, the demand foralternative remedies is also a major driver of the illicit trade in en-dangered animals, through traditional remedies that use animal bodyparts such as rhino horn, bear bile, and pangolin scales (Graham-Rowe,2011).
Despite this mounting evidence of harms, alternative remedies arerarely held to the same rigorous standards of clinical evidence as con-ventional medicine. In the U.S., for example, manufacturers of dietarysupplements and alternative health remedies are not required to pro-vide demonstrations of safety or e"cacy of products prior to marketing(Bellanger et al., 2017), nor does the U.S. Food & Drug Administrationroutinely perform pre-market safety analyses (Avigan et al., 2016). Thefact that governments routinely fall short of protecting consumersmeans that health communicators should employ other avenues toprovide consumers with the means to avoid the harms arising fromfraudulent health remedies. To successfully protect consumers, healthcommunicators need to identify the cognitive, social, and emotionalbiases that health fraudsters exploit to sell their products and thenemploy evidence-based interventions that provide consumers withstrategies for detecting and reducing their susceptibility to health fraud.Accordingly, in the current article, we present a new taxonomy thatsynthesizes insights from psychology relevant to tackling this problem.
1.1. Research gap filled by the present taxonomy
Over the last decade, psychological research has provided a deeperunderstanding of our cognitive capacities and consumer biases whenmaking judgements and decisions under uncertainty (Cialdini, 2009;Kahneman, 2012; Thaler and Sunstein, 2009). Yet, to the best of ourknowledge, this research has not been compiled into a single frame-work that answers the following key questions: What are the majorpsychological drivers that make consumers susceptible to fraudulenthealth claims? How do fraudsters exploit consumers into buying frau-dulent health remedies? How can consumers be protected from healthfraud? The lack of a coherent framework presents three major obstaclesto realizing e!ective interventions to protect consumers. First, it en-courages ad-hoc intervention design, increasing the likelihood that apractitioner will overlook key psychological mechanisms. Second, itimpedes theoretical progress, as there is no systematic plan to discernwhich psychological drivers make consumers most susceptible to healthfraud. Third, it impedes applied progress, as there is no systematic planto determine which interventions are most e!ective for protectingconsumers.
To overcome these obstacles, we reviewed the literature and de-veloped a new taxonomy (see Table 1) to integrate several key psy-chological insights relevant to consumer susceptibility to fraudulenthealth claims. This taxonomy is structured into five key psychologicaldrivers that we hypothesise are the major contributors to consumersusceptibility to health fraud, namely visceral influence, a!ect,nescience, misinformation, and social norms. We provide a brief sum-mary of each driver and outline how each contributes to consumersusceptibility to health fraud. As each psychological driver suggests aseemingly self-evident intervention, we then outline current researchon related psychological barriers that may impede the e!ectiveness ofpotential interventions (for specific rationale, see the supplemental
material ‘Targeting the internal barriers impairing intervention e!ec-tiveness’). For each psychological driver and corresponding barrier, wealso highlight tactics employed by advocates of alternative remedies toexploit consumer susceptibility to fraudulent health claims (for ex-amples, see the supplemental material—Table S1). This framework ofdrivers, barriers, and strategies to manipulate consumers then forms thebasis upon which we propose several hypotheses about specific mea-sures—which we label as treatments—that could ensure that interven-tions help consumers overcome their psychological barriers and thus bemore resilient to fraudulent health claims.
This new taxonomy presents a congruent and parsimonious frame-work for applying psychological theory in the design of interventions toprotect consumers. The numerous predictions contained within thetaxonomy thus form an extensive research agenda, whereby each hy-pothesised treatment should be experimentally tested, and e!ect sizescompared (for further details, see the supplemental material— “Testingthe predictions of the taxonomy”). Furthermore, this taxonomy aims tofill a gap in the literature by providing a coherent framework forpractitioners working to address the harms arising from fraudulenthealth claims (e.g., medical doctors, consumer advocates, and jour-nalists), who may not have specific psychological expertise. Fig. 1provides a step-by-step guide for practically applying the taxonomy.This overarching framework has been informed by existing behaviour-change frameworks (Kok et al., 2016; McKenzie-Mohr and Schultz,2014) but tailored specifically for the context of combatting healthfraud. For brevity, we provide detailed guidance on applying thisoverarching framework in the supplemental material (see section—“Adetailed step-by-step guide to intervention design”). The taxonomy isnow considered in greater detail in order of appearance of the fiveexploited psychological drivers of consumer susceptibility to fraudulenthealth claims: Visceral influence, A!ect, Nescience, Misinformation,and Norms (VANMaN).
2. Five major psychological drivers that are exploited byfraudsters
2.1. Exploited psychological driver: Visceral influence
Visceral influences are motivational cues that can elicit strongpsychological responses and thus impair cognitive abilities. Examples ofvisceral influences are pain avoidance, sensation seeking, financialstress, cravings associated with addiction, and biological needs such ashunger, thirst, and sexual desire. According to Loewenstein (1996), themore desirable the cue, the stronger the psychological reaction and thegreater the impairment of cognitive ability. One common psychologicalresponse to a visceral influence is the narrowing of attention. For ex-ample, social drinkers with a high craving for alcohol experiencegreater attentional bias (reflected in faster response times to alcoholcues compared to control cues) and approach bias (indicated by fastercategorization of alcohol-related behaviours compared to control be-haviours) than those with a low craving (Field et al., 2005). Whilst agreater attentional bias will assist social drinkers to better locate andobtain alcohol, it also means that greater cognitive resources will berequired to maintain self-control, should they wish to refrain fromdrinking. The e!ect of visceral influences may thus help explain muchof the disjunction between people's behaviour and their self-interest(Loewenstein, 1996).
Another impact of visceral influences is that people tend not to thinkabout the ramifications of their own behaviour beyond satisfying theirimmediate visceral needs. For example, in one experiment, participantspresented with a sexually charged video (visceral cue) made sig-nificantly worse assessments of subsequent risks (i.e., expressed agreater likelihood of having unprotected sex in a hypothetical situation)compared to participants presented with only a written account of asexual encounter (control). Another experiment found similar resultswhen participants were presented with a cookie compared to a written
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
24

Table1
TheV
ANMa
NTaxonomy
ofPsychologicalDrivers,Barriers,andT
reatmentsfor
Prote
cting
Consum
ersfromFraudulentH
ealth
Claim
s.Driversa
Interv
entionsb
Barriers
cTreatmentstoovercom
ebarriersd
Example
treatm
ent~
Example
applicatione
Visceral
influence
Raise
aware
ness
Illusion
ofattention
i)Provide
pre-emp
tivecuesaboutkeyinfo
rmation
ii)Reducecognitiveloadb
yreducing
rulecomp
lexity
i)Ino
culate~
warntha
tremedya
dvocatesemp
loyfak
egroupsof“experts”
ii)Sim
plifyrules
toavoid
fraud
~‘don't
buyremedies
fromthe
persond
iagnosingy
ou’
Motivationalinfl
uences
i)Encourageconsumerstoavoid
unsolicitedfavours
ii)Highlightthe
concealment&
intentionb
ehind
‘gifts’
iii)Encouragesupportfromsocialnetw
orks
iv)Ino
culateagainstthe
threatofreso
urcesca
rcity
i)Preventreciprocaltraps~rem
indconsum
erstoavoid
“free”o!ers
ii)Provide
warning
s~“free”alternate
healthc
hecksareoften
concealed
scams
iii)Preventisolation
~urgesev
erelyillpatients
toconsult
supportnetw
orks
iv)Fosterresistance~
warnaboutthe
intenttom
anipu
lateu
singscarcityappeals
A!ect
Counter
irrational
a!ect
Positive
a!ect~
unsupported
remedy
i)Impede
positive-a!
ectiveb
randin
gii)
Fearappeals—Ensurecopin
ge"cacyishig
hiii)
Fearappeals—Stress
susceptibility
oftargetgroup
iv)Fearappeals—Depictrelatively
highrisks
i)Advertisingb
ans~
legislate
forplainpackaging
ofcigare
ttes
ii)Targe
tnon-ad
dictiveremedies
~e.g.,u
nsupportedd
ietary
supplem
ents
iii)~stress
‘vitam
inEsupplem
entsincrea
seprostatecancerrisksformen’
iv)~warntha
t‘consum
ingprimate
meatcancausedeadlysim
ianimmu
neviruses’
Negativea!ect~e!ective
medicine
i)Em
ployevid
ence-ba
seddebunking
ofmy
thsii)
Provide
comp
arativefram
eofrisksvsbenefits
i)Explain~bedrest
wasbelieved
to…butexerciseassistscancerpatientsby
…ii)
Comp
areunsupported
remedyv
smedicine
~surge
ryvsexercise
forlow
erbackpain
Nescience
Provide
information
Illusion
sofcausality
i)Reducefrequencyofactiontou
ncouple
‘causality’
ii)Increa
seexposuretonegativeo
utcom
esiii)
Contingencytab
lesanda
lternate
explanations
i)Encourageless
frequentuse~‘don't
takevitaminC
afterthe
onset
ofeach
cold’
ii)Comm
unicatesidee!ects
~stress
thattoxins
areoften
infused
withrhino
horn
iii)Explainlacko
fe"cacy~‘supplem
entshaveno
benefitoverplacebo
because…
’Illusion
ofconfidence
i)Comm
unicateoverconfidenceandlacko
fknowledge
ii)Ensurehealtha
dvice
isconfident(whereappropriate)
i)Exposeoverconfidence~hig
hlightsevera
lofDrO
z'sfraudulenthealthc
laims
ii)Clearly
state~best-evidenceshows
exercise
issuperiortosurgeryfor
backpain
Illusion
ofknowledge
i)Provide
training
inscienceandreflectivethin
king
ii)Provide
imagesandreductiveexplan
ations
iii)Definekeyvocabularya
ndmajor
concepts
iv)Provide
accesstodetailed
information
i)Educate
&prom
otescienceskepticism
~explainthe
importanceo
fclinicalevid
ence
ii)Provide
reductiveinfo
rmation
~usen
euroscience&brain
imagestoshow
impacts
iii)Define~
thenocebo
e!ectis…
ando
ccursw
hen…
iv)~directconsumerstoresearch
onadultera
tionratesinsupplements
Misinformation
Refutem
isinfo
rmation
Continued
influencee!ect
i)Pre-exposurew
arning
sii)
Repetition
iii)Visualiseevidence
iv)Fillthe
menta
lgap
i)Warn
~‘thefollowing
storyismisinformation’
ii)Routinelyrep
eat~
homeopath
yisnote!ective
iii)Addimages~
usefMR
Ibrainscanstoexplaintreatm
entimp
acts
iv)Provide
altern
ativeexplanation~
‘consum
ersexperienceh
ealth
benefitsbecause…’
Motivatedreasonin
gi)Anticipa
tedefen
siveresp
onses
ii)Utilisesource
credib
ility
iii)Worldv
iewframing
iv)Mo
ralframing
i)Bolsterself-e"cacy~provide
supporttoolsfor
smoking
cessation
ii)Em
ployinfluence~
leadin
gtrad
itionalrem
edysocieties
rejectuseofrhino
horn…
iii)Ide
ntify-congruentfram
ing~emplo
ygain
-framed
vaccine
messagin
gforLib
erals
iv)Appealtomo
rality
~use‘purity/san
ctity’
terms
tofoster
Republicansupport
Conspirato
rialthin
king
i)Apply
guidelinesfor
evalu
ating
conspiracies
ii)Ino
culatethe
“fencesitters”
iii)Targe
tstructu
ralfactors
i)Query
mismatches~
scope&villainy
ofallegedconspirato
rsvsthe
risks&feasibility
ii)Pre-emp
ttactics~
“politicallym
otivated
groupsusemisleading
tactics,such
as…”
iii)Reducebarriers
(e.g.,
a!ordability)thatincrea
seappealofconspiracytheories.
Norms
Emplo
ydesirab
lenorm
appeals
Misperceived
norms
i)Avoid
reciting
adverse
norms
ii)Em
phasisedesirabledescriptive
norms
iii)Comb
inedescriptive
normsw
ithinjunctivenorms
iv)Accomm
odate
poten
tialm
odera
torsofnorms
v)Ensurenorm
appeals
aresu"cientlyp
ublic
i)Avoid
stating~
‘manyp
eople
useh
omeopathy
’ii)
A"rm
~‘only14%ofpharm
acistsbelieveh
omeopathy
tobe
e!ective’
iii)Highlightalso~
‘theP
harmaceuticalSocietydisapprovesofhomeopath
y’iv)
Ensurenormsrelevanttotargetgroup
~‘mostpharmacistsrejecthomeopath
y’v)Appealtomany
memb
ers,in
cludin
gfromthe
widercom
munity,sim
ultaneously
Logicalfallacies
i)Debunk
logicalfallacies
ii)Provide
evidenced
iversity
i)&ii)Debunk
thefallacyofancientremedies
andg
iveculturallydiv
erseevid
ence~to
counter
claimsthata
tradition
alrem
edy's
longh
istorym
akesite!ective
Resistan
tsocial
structures
i)Cluster
early
adopters
ii)Fosteremp
athythrough
similarnetw
orks
i)Cluster
multiple
adoptersino
nline
forum
s~e.g.,a
nti-vaxxerforum
sii)
Messengers
shouldbe
similar,embedded,and
provide
socialreinforcement
Note.Thetaxonom
yguid
esinterv
entiond
esign
byforcingp
ractition
erstoconsiderincorporating
treatm
entstoovercom
ethepsychologicalbarriersthatcanmakeconsum
erssusceptible
tofraudulenthealthclaims.See
textforfurthe
rdetails.
aFiv
emajorpsycholo
gicaldriversexplo
itedb
yfrau
dsterstom
anipu
lateconsumersintob
uying
fraudulenthealthremedies:Viscera
linfluence,A!ect,Nescience,M
isinfo
rmation,and
Norms(VANM
aN).
bFiv
eseeminglyself-evid
entinte
rventionstoaddress
theexplo
itationo
feachp
sycholo
gicaldriver.
cKeyp
sycholo
gicalbarriers
thatm
aypreventsuccessfulapplicationo
finte
rventions.
dProm
ising
evidence-info
rmed
treatm
entstha
thavethe
poten
tialtoh
elpconsum
ersovercom
etheirpsychologicalbarriers(i.e.,b
ybeingincorporated
intointe
rventions).
eExample
applicationsofeach
treatm
ent.
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�
Cha
pter
2: P
rote
ctin
g co
nsum
ers f
rom
frau
dule
nt h
ealth
cla
ims
25

account of a cookie (Ditto et al., 2006). The e!ect sizes of visceral in-fluence on cognitive capacity have been equated to the impairmentcaused by the loss of a full night's sleep or chronic alcoholism. In onestudy, researchers evoked financial concerns (using a hypotheticalscenario involving an unexpected financial cost) before asking partici-pants to complete a Raven's Progressive Matrices Test (Raven, 2000). Inparticipants who did not have the capacity to deal with an unexpectedfinancial loss, the impact of the visceral influence on measured fluidintelligence was a reduction of approximately 13 IQ points (i.e., almosta full standard deviation; Mani et al., 2013). Visceral influences arethought to create a short-term feeling of being ‘out of control’(Langenderfer and Shimp, 2001). This attribute of induced short-termimpulsiveness is well documented in the criminology literature re-garding health fraud; two consistent elements of deceptive practices arethe promises of large rewards and the manufactured urgency to actquickly (Lea et al., 2009; Wilson, 2014).
The cumulative impacts of visceral influences—increased focus,reduced perception of risk, reduced fluid intelligence, and increasedimpulsiveness—conspire to impair a consumer's cognitive ability todetect a fraud, and to consider the information necessary to objectivelydetermine the safety and authenticity of a health remedy. It followsthen that a promising approach to countering health fraud is to helpconsumers avoid visceral cues at times when they are likely to makecomplex health decisions. For example, vaccination needles present astrong visceral cue for individuals with high levels of needle sensitivity,inducing anxiety, discomfort, and in extreme cases panic, fainting, andeven seizures (Wani et al., 2014). Under such strong visceral influence,consumers will tend to be more susceptible to misleading claims aboutvaccinations and/or alternative health remedies. Indeed, parents whoare themselves fearful of needles are more likely to delay vaccination intheir children (Callaghan et al., 2019). One way to protect consumerswith high needle-sensitivity might therefore be to invest in needle-freemethods of vaccination delivery (Giudice and Campbell, 2006). Thedominant approach to protecting consumers is to pre-emptively raiseawareness about the existence, and format, of recent health frauds, inthe hope that people can actively detect and avoid misleading visceralinfluences. However, even where people are able to avoid visceral cuesthe e!ectiveness of awareness raising interventions is hampered by twokey psychological barriers, namely the illusion of attention and emo-tional motivators.
2.1.1. One barrier to raising awareness: The illusion of attentionWhen people's attention is focused on an object or task, they often
fail to perceive unexpected objects even when they are salient, poten-tially important, and appear right where they are looking (Chabriset al., 2011). This phenomenon, termed inattentional blindness, wasmade famous through an experiment where participants, tasked withcounting the number of times a ball was passed between movingpeople, often failed to notice a person dressed in a gorilla suit walkingcasually through their field of vision (Simons and Chabris, 1999).Studies on inattentional blindness provide compelling evidence of thecognitive limits of our attentional capacities. Moreover, they have led tothe discovery of a related phenomenon, termed the illusion of attention,which occurs when what people notice di!ers from what they thinkthey notice (Levin and Angelone, 2008). For example, in one experi-ment, only 50% of participants noticed when a stranger they werehaving a conversation with was surreptitiously replaced by a di!erentperson (Simons and Levin, 1998). Yet, a later study found that 97% ofparticipants estimated that they would have noticed such a change(Levin et al., 2000). This phenomenon provides an analogy for whysomeone, who is focused on finding a cure (i.e., a visceral cue), mightconsistently overestimate their ability to notice when they are beingdeceived (Lea et al., 2009).
Unfortunately, it may not be possible to train people to overcomeinattentional blindness, as this phenomenon is a by-product of ourlimited-capacity attentional system (Begh et al., 2015). General
skepticism of advertising claims also seems to provide insu"cientprotection from visceral influences and their associated e!ects, namelynarrowing attention and inducing impulsiveness (Amos and LandrethGrau, 2015).
One robust treatment to attenuate inattentional blindness is to makeimportant, but unattended, factors more salient (Gibbs et al., 2016).Doing so may be achieved by providing consumers with pre-emptivecues (i.e., just prior to making health decisions) that make importantinformation more salient such as the outcomes of clinical trials and sidee!ects. In practice, this would require forcing product packaging ofalternative health remedies to provide key information (e.g., food labelshave been shown to boost nutrition knowledge; Miller and Cassady,2015). Another attribute of inattentional bias is that the greater thecognitive resources required to complete a task, the greater the bias’impact (Simons and Chabris, 1999). Thus, another treatment to reduceinattentional bias is to simplify tasks by providing simple rules forpeople to navigate otherwise complex tasks (Mata et al., 2010). Forexample, a simple rule for avoiding health fraud is “do not buy healthremedies from the person who diagnosed you” because the seller isincentivised to invent a diagnosis, overstate the benefits of their re-medy, and underreport the harms of that remedy (i.e., they have aconflict of interest).
2.1.2. Another barrier to raising awareness: Emotional motivatorsTwo key emotional motivators that augment the impact of visceral
influences are reciprocity and scarcity. Reciprocity influences con-sumers when they receive a gift, favour, or invitation, which compelsthem to feel obliged to the giver (Cialdini, 2009). Reciprocity is a well-established element of health fraud, utilised by scammers who oftenprovide small gifts, free consultations, free information, or appear tobend the rules in favour of the recipient in order to make them feelobligated (Lea et al., 2009). According to Cialdini (2009), perhaps thebest way to overcome this barrier is to make receivers aware of the“norm of reciprocity” so that they can actively avoid situations wherethey might feel indebted. Other treatments to reduce the norm of re-ciprocity are to: encourage consumers to consider the exploitative in-tentions behind unsolicited favours (Cialdini, 2009), highlight that thegiver is concealing their true intentions from the consumer (Friehe andUtikal, 2018), and help consumers find excuses not to reciprocate(Regner, 2016).
Scarcity appeals are manufactured sales tactics common to healthfraud and include such cues as “only two products left!“, which canmake an o!er seem more valuable (Aggarwal et al., 2011; it also en-courages conformity by conveying that “many people” are purchasing aproduct; see later section on social norms), and urgency cues such as“sale ends today!“, which can force consumers to make quick decisionswhilst under a visceral influence (e.g., desiring a cure to an illness)when their capacity for risk assessment is poorest (Fischer et al., 2013).A recent review posited that scarcity appeals may operate through twodistinct psychological mechanisms, namely a fear of missing out and afear of a restriction of choice (Cannon et al., 2018).
One hypothesis posits that scarcity appeals operate via a desire toeliminate the anticipated risk that a resource may be unavailable in thefuture (i.e., fear of missing out). Under this availability-risk mechanism,scarcity operates as a visceral cue with several subsequent impacts onconsumers including narrowed attention, heightened emotionalarousal, and induced aggression through perceived competition(Kristo!erson et al., 2017). One treatment to assist consumers to resistavailability-risk scarcity appeals is to assist consumers to avoid makingdecisions under emotional pressure. One way to accomplish this is toencourage consumers to seek independent advice from their socialnetworks, because others are unlikely to be under the same visceralinfluence (e.g., the desire to relieve pain) and are hence better able toprovide rational advice. One limitation of this approach is that peoples'social networks may be homophilic—tailored in such a way to supportalternative health views (see later section on resistant social
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
26

structures”)—and thus consumers should also seek advice from ap-propriately qualified medical practitioners.
The second hypothesis posits that scarcity appeals might also op-erate via a desire to eliminate an anticipated risk that certain choicesmay be restricted in the future. (e.g., loss of access to a previouslyavailable remedy). Under this mechanism, commonly termed psycho-logical reactance, scarcity has been shown to operate through a combi-nation of anger and negative cognitions (Dillard and Shen, 2005).Cialdini (2009) argued that psychological reactance may help explainwhy banning products can be ine!ective or even drive a greater in-tention to consume. One treatment to assist consumers to resist urgencyand scarcity appeals, which induce psychological reactance, is to fore-warn consumers of a salesperson's persuasive intent—namely, that suchappeals are manufactured sales tactics intended to manipulate con-sumers into making purchases. A meta-analysis by Wood and Quinn(2003) concluded that warnings about influence attempts can help“inoculate” people against psychological reactance by preparing themto resist subsequent persuasive appeals.
2.2. Exploited psychological driver: (Irrational) a!ect
A!ect is the emotive quality of “goodness” or “badness” that be-comes associated with an action or item (Slovic et al., 2007). A!ectiveassociations may be evolutionarily adaptive (e.g., bad smells can in-dicate infection) and are often culturally derived (e.g., taboos aboutphysical contact with certain object; Huang et al., 2017; Rozin et al.,1986). A!ective associations are often used heuristically to enablequick decisions. Indeed, adults unable to build a!ective associations(e.g., due to severe brain trauma) can develop deficits in decisionmaking (Damasio et al., 1990). Irrational a!ective associations—that is,associations that are disproportionate or contrary to factual evi-dence—can also lead to irrational behaviours (Slovic et al., 2000; seealso supplemental materials— “Irrational a!ective associations andmagical thinking”). The theoretical distinction between visceral influ-ences and a!ect is that the former serves to explain the influence ofemotion on attentional processes and cognitive capacity, whereas thelatter serves to explain how decisions are made based on positive ornegative feelings.
Several attributes of a!ective decision making can be manipulatedto make consumers susceptible to fraudulent health claims. One attri-bute is that a!ective evaluations of risks and benefits tend to be ne-gatively correlated—even when the nature of the benefits is both dis-tinctively and qualitatively di!erent from the nature of the risks. Forexample, if antibiotics are portrayed as low in risk, it contributes to theperception that they are also high in benefit. In contrast, if smoking isportrayed as low in benefits, this contributes to the perception that it is
also high in risk. (Alhakami and Slovic, 1994). Thus, evaluations ofrisks and benefits tend to be causally determined, meaning that theperception of one attribute can be influenced by manipulating in-formation about the other (Finucane et al., 2000). For example, onestudy in the UK found that the most commonly cited justification forconsuming homeopathic remedies was a perceived lack of side e!ects.Furthermore, the perceived e"cacy of homeopathy was correlated withperceptions about risks of conventional medicine (Stoneman et al.,2013). Importantly, people's reliance on a!ective decision-making in-creases when under time pressure, because there is less opportunity foranalytic deliberation. In one study, the strength of the inverse re-lationship between perceived risks and benefits for a range of items,such as cigarettes and pesticides, was greatly increased under timepressure (Finucane et al., 2000). Thus, consumers are more susceptibleto fraudulent health claims when fraudsters artificially induce timeconstraints (see previous section on scarcity).
Another attribute of a!ect that can be manipulated to increaseconsumer susceptibility to fraudulent health claims is the evaluabilityprinciple—the idea that actions, or items, are not easily evaluable inisolation; instead their meaning is often, or more easily, evaluatedthrough a!ective comparisons. For example, consider two products thatare identical except for their quantity and labelling: Product (A)“250 mg of ingredient X”; and Product (B) “500 mg of ingredient X,may cause minor headaches”. When consumers view only Product A inisolation, the quantity “250 mg of ingredient X” is only di!usely eva-luable and thus carries minimal weight when making a!ective judg-ments. Consequently, consumers are more likely to perceive Product Ato be of higher value, compared to consumers who only view Product B,because the value of the latter is reduced by the a!ective associationwith a potential side e!ect. However, when directly compared, it isobvious that Product B, which o!ers twice the amount of ingredient X,o!ers superior value to Product A, and is also more informative aboutthe potential side e!ects. This example is based on experimental evi-dence demonstrating how the lack of comparative frames of referenceserves to limit the capacity for rational judgements (Hsee, 1996). Theevaluability principle may explain how evaluations of fraudulent healthremedies, when consumers are isolated from scientific evidence, can beunduly influenced by a!ect-laden terms such as “natural”, or “holistic”,and not by factual comparisons.
The obvious intervention to overcome irrational a!ective associa-tions is to counteract them with a!ective comparisons that accuratelydepict the known risks and benefits of the fraudulent health remedycompared to conventional medicine. However, considerable careshould be taken to ensure messages are su"ciently targeted and do notbackfire (Rossen et al., 2016; also see sections below on motivatedreasoning and norms). Two barriers to such interventions are positive
Fig. 1. A step-by-step guide for designing interventions using psychological insights.
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
27

a!ect associated with fraudulent health remedies, and negative a!ectassociated with supported medicines.
2.2.1. One barrier to countering irrational a!ect: Positive a!ectMuch consumer demand for fraudulent health remedies is main-
tained through associations that carry positive a!ect. For example, theubiquitous marketing of alternative remedies as “natural” is e!ectivelya tactic to convey that a product is harmless, despite the fact that thereare abundant natural poisons such as hemlock and strychnine (Hall,2008). The impact of positive a!ect marketing was recently demon-strated through an experiment that found simply masking cigarettepackaging (i.e., the brand marketing linking those cigarettes with po-sitive associations such as fun or sophistication) significantly reducedthe cigarettes’ appeal to smokers on measures of taste, quality, enjoy-ment, and intent to purchase (Skaczkowski et al., 2018). To manu-facture positive associations with fraudulent health remedies, advocatesadopt real scientific terms such as “osmosis” or invent medical jargonsuch as “negative calories” (Lea et al., 2009). One treatment to coun-teract positive a!ect that has become associated with a fraudulenthealth remedy is to draw attention to its potential risks. Health inter-ventions that depict the risks of a particular action are commonlytermed fear appeals. A common example includes graphic images ofsmoking-related disease on cigarette packets.
The e!ectiveness of fear appeals in altering behaviour is the subjectof some debate (Peters et al., 2018). Some have argued that fear appealsare only e!ective under specific circumstances—most notably, wherethere is high perceived e"cacy (i.e., both (i) self-e"cacy—the capacityto alter one's behaviour towards the recommended action [e.g., stopsmoking]; and (ii) response e"cacy—the belief that the recommendedaction will enable one to avoid the stated threat (Kok et al., 2018). Still,Tannenbaum et al.’s (2015) recent meta-analysis concluded that fearappeals were e!ective at altering attitudes, intentions, and behaviours;worked in all but few cases; and did not backfire under any identifiedcircumstances (see Kok et al., 2018, for an alternate perspective).
In any case, there appears to be a consensus that when perceivede"cacy is high, fear appeals are likely to be e!ective (Peters et al.,2018). The use of fear appeals for reducing demand for fraudulenthealth remedies is thus likely to be e!ective in most cases, becausee"cacy-related variables such as dependency, addiction, or lack ofconsumer alternatives are generally absent in this context. Tannenbaumet al. (2015) identified a number of factors that increase the e!ective-ness of fear appeals. Two key factors listed in our taxonomy are de-picting a relatively high amount of risk and stressing the susceptibilityof the target group.
2.2.2. Another barrier to countering irrational a!ect: Negative a!ectAnother psychological barrier arises when negative a!ect becomes
associated with an evidence-based conventional medicine, such aschemotherapy or exercise. In a study of women diagnosed with breastcancer, key reasons for rejecting conventional medicine in favour ofalternative remedies were the fear of side e!ects, negative experienceswith conventional doctors, and a lack of perceived benefits of con-ventional medicine (Citrin et al., 2012). Negative a!ect can becomeassociated with evidence-based medicine when new evidence overturnspre-existing beliefs about standard medical care. For example, bed restwas long prescribed as a key ingredient to illness recovery includingrecovery from cancer. However, compelling evidence now suggests thatexercise is both e!ective and safe for counteracting many of the adversephysical and psychological e!ects of cancer and its treatments (Cormieet al., 2018). Further, exercise has proven e!ective for treating lower-back pain (whereas common standard approaches such as opioids,surgery, and spinal injections have been found relatively ine!ective;Foster et al., 2018). To counteract negative a!ect surrounding an evi-dence-based medicine, interventions should seek to correct the mythsusing evidence-based debiasing techniques (see section on mis-information).
Negative a!ect can also contribute to a nocebo e!ect—where theexpectation of harm increases the psychogenic experience of symptomsthat are consistent with health concerns. For example, according to thebest evidence, there are no negative health impacts of wind turbines(Tonin, 2018). Yet, negative a!ective commentary by anti-windfarmactivists has, in some people, created the expectation that the infra-sound produced by wind turbines can cause health harms, and this isthought to have caused some people to experience health symptoms.One treatment to counteract negative a!ect is to highlight the potentialbenefits of the target behaviour. To illustrate, Crichton and Petrie(2015) showed that associating infrasound with positive health e!ectscaused a placebo e!ect that reversed the nocebo response and lessenedpsychogenic symptoms.
2.3. Exploited psychological driver: Nescience
Nescience is the absence of knowledge or awareness. Nesciencemakes consumers susceptible to health fraud because people intuitivelygenerate, or uncritically accept, spurious causal associations betweenactions and outcomes (e.g., remedy X cured illness Y; i.e., illusorycausation) without considering that such associations might be coin-cidental, meaning that evidence to determine causality is lacking (i.e.,evidence that excludes other causal explanations for an outcome).Overcoming nescience is di"cult because humans have evolved astrong bias for finding patterns in meaningless background noise (i.e.,illusory correlation; Foster and Kokko, 2009). The problem is furthercompounded by a host of other psychological mechanisms (seeLilienfeld et al., 2014), such as the tendency to selectively recall onlyoutcome variables of improvement or to overestimate our ability toinfluence events (the illusion of control; Langer, 1975). Such mechan-isms conspire so that even clinicians and researchers are not immune tonaïve realism—the pervasive assumption that cause and e!ect can beobserved through intuitive observations (Lilienfeld et al., 2014). Sci-entific methods facilitate the assessment of causality by controlling foralternate explanations. However, in the absence of a scientific ap-proach, illusory causal associations between health outcomes andpossible remedies can be created through several common scenarios,such as inferring the e!ect of a health remedy following personal trialand error, exposure to highly confident personal narratives, or exposureto biased samples such as online forums where those who claim to havebeen “cured” are overrepresented compared to those who experiencedno benefit or harmful side e!ects.
Intuitive causal associations can serendipitously lead to discoveriesof real causal relationships, as when our ancestors noticed that the barkof the willow tree relieved pain, which eventually led to the discoveryof aspirin (Hall, 2008). On many occasions, however, such causal as-sociations are illusory, such as the use of rhino horn in traditionalChinese medicine as a cure for various ailments from cancer to hang-overs. Rhino horn has no medicinal properties, yet its unabated con-sumption has contributed to several recent sub-species extinctions(Milliken, 2014).
The seemingly obvious intervention to overcome nescience is toprovide information on what works and what does not. This so-calledinformation deficit model (Bubela et al., 2009; Rossen et al., 2016) in-tuitively leads practitioners to launch awareness-raising campaigns.However, numerous studies have shown that awareness campaigns aregenerally ine!ective at altering behaviour (Christiano and Neimand,2017). Increases in scientific knowledge are, at best, moderately cor-related with increased positive attitudes towards science (Allum et al.,2008) and, at worst, strongly correlated with increased polarisation onissues that are divided along political or cultural worldviews (Kahan,2015; Kahan et al., 2012). One reason why awareness campaigns aregenerally ine!ective is that they seldom target the specific psycholo-gical barriers (other than knowledge) preventing the uptake of thedesired behaviour (McKenzie-Mohr, 2000). Three psychological bar-riers that specifically relate to nescience include the illusion of
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
28

causality, the illusion of confidence, and the illusion of knowledge.
2.3.1. One barrier to overcoming nescience: The illusion of causalityThe illusion of causality occurs when an outcome, by mere coin-
cidence, occurs in close temporal proximity to an action (Matute et al.,2015). Causal illusions are pervasive because people are generally onlyexposed to, and thus are more likely to remember, positive outcomes. Aprime example is the unsubstantiated link between taking vitamin C atthe onset of a cold (action) and a recovery from illness (outcome)(Hemila and Chalker, 2013). Belief in the e"cacy of vitamin C is per-petuated by people more readily recalling instances when they tookvitamin C and subsequently recovered from a cold, compared to in-stances when they did nothing and recovered all the same. This ten-dency is further compounded by reporting bias—when people tend toshare positive treatment outcomes more than average out-comes—which distorts the information available to others (de Barra,2017; see also Ioannidis, 2017). Another reason why causal illusions arepersuasive is that people generally fail to take into account alternativeexplanations when considering what caused an outcome (e.g., that painreduction was caused by a placebo e!ect; Hayes et al., 2016). Causalillusions are especially convincing for many alternative medicines be-cause these are often perceived to have no side e!ects, which en-courages frequent consumption, which in turn increases the probabilitythat the outcome will occur in close proximity to the perceived cause(Matute et al., 2015).
Assisting people to overcome illusions of causality is a challenge.Research has shown that simply showing people the facts is not su"-cient (Yarritu and Matute, 2015) and that higher intelligence does notprovide protection (Wiseman and Watt, 2006). Nevertheless, severalpromising treatments are worth considering.
In instances where someone has control over the perceived cause,an e!ective treatment is to advise people to reduce the frequency ofconsuming the perceived health remedy (e.g., advise people to consumevitamin C only every other time they catch a cold). Reducing this fre-quency reduces the probability that the outcome will occur in closeproximity to the perceived cause, and thus works to uncouple the il-lusory association (Blanco et al., 2011). One way to encourage lessfrequent consumption is to communicate the potential side e!ects ofthe remedy (see earlier section on positive a!ect and fear appeals).
Another treatment is to provide interactive training about the sci-entific concepts key to evaluating causality. Barberia et al. (2013)showed that a workshop teaching school students about experimentalcontrols (to account for confounding factors) and contingency testing(comparing outcomes for both “cause-present” and “cause-absent”scenarios) reduced the students’ susceptibility to causal illusions.
Another promising treatment is to provide people access to the “fullpicture,” namely the evidence from all four outcomes of a standardrandomized controlled trial, that is, the number of people who (i) tookthe product and experienced the benefit, (ii) took the product and ex-perienced no benefit, (iii) did not take the product but still experiencedthe benefit, and (iv) did not take the product and experienced nobenefit. Information from all four cells in a contingency matrix enablesconclusions to be drawn about whether a benefit is caused by theproduct (a positive contingency), or whether there was some othercausal factor (a null contingency). Unfortunately, simply providingpeople with a contingency table of the results of clinical trials may notassist them to make reliable causal judgments because people's inter-pretations can be faulty, especially when the data being conveyed arecomplex (Batanero et al., 2015) or when the interpretation challengesprior beliefs (Kahan et al., 2013). To overcome these psychologicalbarriers, a promising treatment combines two strategies: (i) simplifyand clearly convey complex clinical results—for example, by usingfrequency formats “4 in 5 people report a benefit” rather than absolutevalues, percentages, or probabilities—in order to minimise opportu-nities for participants to misinterpret results due to cognitive biasessuch as motivated reasoning, denominator neglect, or availability bias
(Slovic et al., 2007); and (ii) provide an alternative explanation of whatcauses consumers to experience health benefits because this helps to fillthe mental gap caused by refuting participants' pre-existing pseu-doscientific beliefs (Lewandowsky et al., 2012). In a recent experiment,this treatment reduced participants' willingness to pay for a real mul-tivitamin supplement (by 23%) compared to a common refutation usedby health authorities (MacFarlane et al., 2018).
MacFarlane et al. (2020) follow-up experiment combined thistreatment with a fear appeal (i.e., evidence that multivitamin supple-ments actually increase mortality risk compared to placebo). The resultsshowed that the fear appeal in isolation reduced willingness to pay (by32%) compared to control, but that a combined intervention (thesimple interpretation of clinical results and alternative explanation ofconsumer experiences plus the fear appeal) reduced participants' will-ingness to pay for multivitamins further still (by 50%). These resultsprovide preliminary evidence that interventions based on psychologicalinsights can assist people to overcome psychological barriers linkedwith fraudulent health claims.
2.3.2. A second barrier to overcoming nescience: The illusion of confidenceThe illusion of confidence refers to the robust finding that people
tend to overestimate their own qualities (e.g., skill, ability, and char-acter) compared to their peers (Kruger and Dunning, 1999). The ten-dency towards overconfidence extends across many domains, fromeyewitness testimony (Sporer et al., 1995) to medical decision making(Croskerry and Norman, 2008). This illusion presents a key psycholo-gical barrier due to the Dunning-Kruger e!ect, which is the finding thatpeople who are the least competent, and thus most in need of self-im-provement, tend to be the most overconfident, the least open to newinformation, and the least likely to recognise the need for self-im-provement (Kruger and Dunning, 1999). The Dunning-Kruger e!ect hasbeen shown to explain public opposition to vaccination policies, ge-netically modified foods, and genetic engineering technology (Fernbachet al., 2019; Motta et al., 2018). Unfortunately, simply giving peoplefeedback about their lack of skills relating to a particular task does notalways reduce overconfidence or improve performance, but insteadoften reduces performance (Kluger and DeNisi, 1996). Increasing peo-ple's competence (e.g., through training programs) so that their abilitycatches up to their confidence, appears to be the most reliable way toreduce overconfidence. However, such instruction needs to be sub-stantial, as insu"cient training may actually increase overconfidence(Sanchez and Dunning, 2018).
An additional psychological barrier related to the illusion of con-fidence is the tendency to interpret confidence, or lack thereof, as avalid signal of another person's abilities and knowledge. One explana-tion for this tendency is that people prefer definitive predictions overuncertainty (Keren and Teigen, 2001). In support, one study found thatpatients were more satisfied with doctors who expressed diagnosiscertainty compared to those who conveyed uncertainty or consultedreference books (Johnson et al., 1988). This tendency thus presents apsychological barrier for consumers, because it undermines their ca-pacity to discern which experts are truly knowledgeable. Further, ithelps to explain why the public is easily misled by the confident, yetoften unfounded, claims of alternative remedy advocates and celebritydoctors such as Dr Oz (Tilburt et al., 2017).
Evidence suggests that overconfidence may be a stable personalitytrait across multiple cognitive domains (Blais et al., 2005). Thus, havinggreater familiarity with a person's confidence on other issues mayprovide a more accurate benchmark for assessing the nexus betweenthat person's actual knowledge and their outward confidence. Thus, aplausible treatment to overcome this aspect of the illusion of confidenceis to highlight other instances where an advocate is confident aboutother clearly disproven issues. This should help dispel illusions re-garding the advocate's real knowledge (Chabris and Simons, 2010). Forthis treatment to be e!ective, practitioners should first establish thatthe target audience also accepts those issues as disproven, which may
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
29

prove di"cult in some cases. For example, the small number of peoplewith strong anti-vaccination beliefs tend to be far less receptive tocommunication interventions than the considerably larger group ofvaccine-hesitant parents (hence, vaccine scholars have suggested fo-cusing on the latter group; Betsch et al., 2015). Where possible, publichealth practitioners should also ensure that health promotion messagesare delivered confidently so as not to undermine the implicit messagethat the advice being given is based on the best available evidence.
2.3.3. A third barrier to overcoming nescience: The illusion of knowledgePeople often believe that they understand things at a deeper level
than they really do. This finding, termed the illusion of knowledge,causes people to mistake feelings of familiarity (what happens) forgenuine knowledge (why it happens) (Rozenblit, 2004). This psycho-logical barrier facilitates mistaken explanations for complex healthphenomena by preventing people from asking questions that are criticalto distinguishing between which health remedies are evidence-basedand which are unproven, disproven, or untenable.
The illusion of knowledge may stem from our tendency to use simplemodels to understand complex systems (Lombrozo, 2007), which enablesus to function without being overwhelmed by complexity. However,problems arise because it is di"cult to determine how well our modelshelp us understand reality. Instead, we infer how well we understandreality using three easily determined factors: (i) our confidence in ourunderstanding of the simple model; (ii) our familiarity with the surfaceelements, concepts, and vocabulary of the complex system; and (iii) theamount of information we are aware of, or have access to (Fisher et al.,2015), regarding the complex system (Chabris and Simons, 2010). Thismodel of mental self-assessment is, however, deeply flawed as it en-courages us to overestimate our real knowledge—this is because thethree factors provide no meaningful assessment of how well we actuallyunderstand reality. Reliance on these heuristics becomes problematicwhen advocates manipulate them to strengthen an illusion of knowledgeabout an alternative health remedy.
To illustrate, one tactic employed by alternative-health advocates is tooverwhelm consumers with biased information that appears extensive. Forexample, the website of the British Homeopathic Association directs con-sumers to The Faculty of Homeopathy’s (2018) evidence summary, whichclaims that four of five “major comprehensive” systematic reviews“broadly favour” the use of homeopathy—but only after further in-vestigation would consumers learn that all four reviews noted that overallstudy quality was poor and the evidence inconclusive. Another tactic is tobolster the explanation of a phenomenon with irrelevant reductive in-formation (i.e., information regarding basic system features or processesthat are unrelated to the claim being made). Such information may in-terfere with people's ability to critique the underlying logic of the o!eredexplanation (Weisberg et al., 2008), which, in turn, causes them to over-value their understanding of that simple model (Hopkins et al., 2016).Consequently, explanations of psychological phenomena (especially badexplanations) can be made to appear more satisfying by adding irrelevantinformation, such as longer descriptions (Heit and Rotello, 2012), brainimages (McCabe and Castel, 2008), or neuroscientific information(Weisberg et al., 2015; see also Im et al., 2017; Tabacchi and Cardaci,2016). Such information increases people's familiarity with the surfaceconcepts and vocabulary used to explain complex scientific phenomena.
One treatment to help prevent people from succumbing to the il-lusion of knowledge is to deliver targeted training and educationcampaigns that promote general scientific knowledge and reflectivethinking, which help people apply informed and reasoned scientificskepticism to assess explanation quality (Hopkins et al., 2016). An al-ternative approach to preventing people from falling for the illusion ofknowledge is to accept that these barriers are a psychological realityand thus, at the very least, should be accounted for when designingcommunications about evidence-based-medicine (Rossen et al., 2016).Specifically, to ensure consumers’ confidence in and satisfaction withexplanations is based on best evidence, practitioners should provide: (i)
simple explanations that include images and reductive information(even if not strictly necessary); (ii) definitions of key vocabulary andmajor concepts used to describe the complex phenomenon; and (iii)access to detailed information about the complex phenomena.
2.4. Exploited psychological driver: Misinformation
Misinformation makes it di"cult to distinguish between evidence-based medicines and fraudulent remedies and thus can have dire con-sequences for public health. For example, the spread of misinformationabout the false link between the measles-mumps-rubella (MMR) vac-cine and autism (Poland and Spier, 2010) has been associated withlocalised reductions in paediatric MMR vaccination rates (Leask, 2011),resulting in several outbreaks of measles (BBC, 2018). Counteringmisinformation requires multiple solutions, which vary depending onmodes of transmission, underlying intentions, and political contexts.
Aspects of the contemporary media landscape have facilitated thedissemination of misinformation. Social media are especially amenableto spreading misinformation because people are more likely to sharestories that elicit emotional arousal (i.e., those that evoke fear, disgust,or happiness; Berger, 2011). Social media are also increasingly beingused to spread disinformation—misinformation disseminated with theintent to deceive, often for political or financial motives. Emergingevidence is also revealing the considerable extent that automated so-cial-media “bots” are being used to spread and politicise disinforma-tion, including about vaccination (Broniatowski et al., 2018). With thebenefit of hindsight, it has become clear that disinformation campaignscan generate considerable public confusion. For example, in 2006, aU.S. Federal Court found cigarette manufacturers guilty of conspiring todeny, minimise, and distort the hazards of smoking. Those responsiblewere ordered to publish corrective statements in the media, a commonlegal remedy for such consumer deception (Smith et al., 2011).
Another aspect of the contemporary media landscape that con-tributes to the spread of misinformation is the information retrievalalgorithms employed by search engines (e.g., Google or Yahoo). This isbecause the sorting and ranking criteria they use ignore informationquality (Ludolph et al., 2016). Advocates of fraudulent health remediescan try to actively manipulate search results to enhance the visibility ofmisinformation. For example, a study by Kitchens et al. (2014) foundthat first page results from Google searches on health topics (well-being, food, and nutrition) returned mostly websites with low-qualityinformation. Further, the results relating to complementary and alter-native therapies returned the highest proportion (approximately 70%)of low-quality online information.
One increasingly common tool for combatting intentionally, orcarelessly, spread misinformation is fact-checking, which can be gen-erally e!ective for refuting false claims (Ecker et al., 2019; Hameleersand van der Meer, 2019). Indeed, e!orts are underway to integrate fact-checking into social media platforms (see Lewandowsky et al., 2017).Combatting technologically derived sources of misinformation requiresan understanding of search engine logic so that, for example, healthauthorities can optimise the visibility of quality information. Anotherpromising solution is to prioritise applied research into developingsuperior search algorithms, so that consumers would be presented withsearch results that ultimately favour credible and high-quality in-formation (Lewandowsky et al., 2017). Beyond these interventions,e!ectively informing consumers requires that practitioners adopt psy-chologically informed approaches to debunking misinformation. To thisend, we now consider two notable psychological barriers that operateto impair e!orts to refute misinformation, namely the continued in-fluence e!ect and motivated reasoning.
2.4.1. One barrier to combatting misinformation: The continued influencee!ect
E!orts to retract misinformation tend to be of limited e"cacy,meaning that misinformation often continues to influence reasoning
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
30

and decision making despite clear and credible retractions or correc-tions. This e!ect has been termed the continued influence e!ect of mis-information (Johnson and Seifert, 1994). A number of cognitive factorsare responsible for this e!ect, such as inadequate resources for objec-tive veracity evaluation, and imperfect memory updating and retrievalprocesses (Lewandowsky et al., 2012; Swire et al., 2017).
To design “science-based” refutations to e!ectively debunk mis-information, several factors must be considered (Paynter et al., 2019).Specifically, to overcome the barriers presented by the continued in-fluence e!ect, refutations should: (i) warn recipients before confrontingthem with misinformation because warnings can boost strategic mon-itoring processes and prevent the initial acceptance of misinformation,thus reducing the need for subsequent revision (Ecker et al., 2010); (ii)repeat the facts, but avoid repeating the misinformation more thannecessary (in order to refute it), as repetition enhances familiarity,which can foster false beliefs (Jacoby and Kelley, 1989); (iii) use gra-phical evidence, as visual representations help consumers comprehenddata and make counter-arguing more di"cult (Dixon et al., 2015); and(iv) provide an alternate explanation of the phenomenon to fill themental “gap” left behind by retracting the misinformation. Ideally, thisexplanation should also address the motivation behind the initial sourceof misinformation. For example, it is useful to know that Andrew Wa-kefield, who initially suggested that autism was linked to the MMRvaccine, failed to disclose financial conflicts of interest that providedconsiderable incentive to falsify his results (Flaherty, 2011).
2.4.2. A second barrier to combatting misinformation: Motivated reasoningMotivated reasoning refers to biased information processing in ac-
cordance with prevailing motivations and worldviews (Kunda, 1987).When processing misinformation and refutations, people may engage inmotivated reasoning to defend their worldviews and social identities(Ecker and Ang, 2019) and reduce cognitive dissonance—the mentaldiscomfort that arises whenever a person holds two inconsistent ideas,attitudes, beliefs, or opinions (e.g., “smoking kills” and “I am a smoker”;Festinger, 1962). Three pervasive biases in this context are (i) theconfirmation bias—preferentially seeking out supportive evidence,whilst ignoring contrary evidence; (ii) the disconfirmation bias—-counter-arguing contrary evidence and uncritically accepting suppor-tive evidence; and (iii) self-justification—the post-hoc rationalising ofone's beliefs (Tavris and Aronson, 2008). These mechanisms appear tobe exhibited in a hierarchy of increasing cognitive demand, meaningthat dissonant evidence is easiest to ignore, harder to counter-argue,and even harder to rationalise (Hughes and Zaki, 2015). Harder still isto change one's pre-existing worldviews.
Understanding how dissonant information is processed through aprogression of stages can be useful for designing targeted interventionsto overcome motivated reasoning. Common stages for reducing cogni-tive dissonance about bad health behaviours include avoiding dissonantinformation (easy), pointing to flaws in the health research (harder), orrationalising the bad behaviour (harder still). For example, graphichealth warning labels on cigarette packages can increase feelings ofdissonance for people with low self-e"cacy (e.g., due to addiction orlack of support; Witte and Allen, 2000). Smokers avoid such dissonanceby putting cigarettes into plain boxes to avoid seeing graphic healthimages (easy), seeking out, and uncritically accepting, criticism aboutcancer research (harder), and rationalising that smoking, on balance, isbeneficial because it prevents weight gain (a common justification forsmoking). By anticipating these types of defensive consumer responses,practitioners can design more e!ective warning messages that are lessthreatening and thus less likely to be avoided (Kok et al., 2018; Hallet al., 2018), provide tools for improving self-e"cacy (e.g., nicotinegum; Hartmann-Boyce et al., 2018), and o!er alternative means forappetite suppression (Seeley and Sandoval, 2011).
Perhaps the greatest source of dissonance is information thatthreatens pre-existing worldviews, especially when such worldviewsoperate to define a"liations with particular social groups, such as a
political party or an ethnic community. One treatment for practitionersto reduce this dissonance is to employ a spokesperson from the targetcommunity. People are more likely to trust advice from experts thatcome from an ingroup, especially on polarising issues (Kahan, 2015;Berinsky, 2017). Another treatment to reduce dissonance is to framemessages so that they are congruent with the worldview of the targetgroup. For example, political conservatives experience more fear of lossthan political liberals experience, and thus should be more persuadedby loss-framed messages (negative consequences of not acting) thangain-framed messages (positive consequences of acting), and the re-verse should be true for liberals. This has been supported by studiesinvestigating policy support for mandatory vaccination (Nan andMadden, 2014) and reducing obesity (Lee and Kim, 2017).
A further source of dissonance may derive from people's sense ofmorality. For example, Feinberg and Willer (2013) found that lowerpro-environmental attitudes amongst conservatives than liberals couldbe attenuated using pro-environmental rhetoric that was framed interms of moral values endorsed by conservatives (concerns about thepurity and sacredness of the environment), but not by using similarrhetoric framed in terms of liberal moral values (moral duty to protectthe environment from harm). To the best of our knowledge, the impactof moral framing on health remedies has not yet been experimentallytested. However, several correlational studies have linked vaccinehesitancy to people's intuitions about di!erent moral virtues (Grahamet al., 2009). In a study of Australian parents, Rossen and colleagues(2019) found that vaccine rejecters were higher on the purity founda-tion compared to acceptors and fence-sitters. They also found thatvaccine rejecters and fence-sitters had a higher moral preference forliberty (beliefs about the rights of the individual) compared to accep-tors. In a study of American parents, Amin and colleagues (2017) foundthat parents with high vaccine hesitancy were twice as likely to em-phasise liberty and purity compared to respondents with low vaccinehesitancy. In another study of American parents, Callaghan et al. (2019)found a correlation between an inclination towards delaying the HPVvaccination and a high moral preference for purity, which the authorssuggested is additionally linked to conservative views about sexuality.Based on these correlational findings, researchers should experimen-tally test whether interventions to decrease vaccine hesitancy are mademore e!ective by applying tailored moral frames to di!erent popula-tions.
2.4.3. A third barrier to combatting misinformation: Conspiratorial thinkingConspiratorial thinking (also known as conspiratorial ideation) is
the predisposition towards assuming that powerful groups are takingsecretive action against the common good for their own benefit.Contemporary examples of health-related conspiracy theories includethe notion that the Zika virus is spread by genetically modified mos-quitoes (Klofstad et al., 2019), and that the causal link between child-hood vaccination and autism is being suppressed by an unscrupulousmedical industry (Goertzel, 2010). National surveys of the Americanpublic show that several medical conspiracy theories are widely known,broadly endorsed, and highly predictive of many common health be-haviours, such as taking vitamin supplements, prioritising organic foodconsumption, and even using sunscreen (Oliver and Wood, 2014).Naturally, it is important to note in this context that conspiracy theoriesare not always immediately false, and that genuine health-relatedconspiracies do occur. However, unlike fringe conspiracy theories,which appear to persist in support of an ideological position despite thelack of positive evidence (Lewandowsky et al., 2013), verified healthconspiracies typically involve commercial fraud (e.g., involving adul-terating or counterfeiting pharmaceuticals or dismissing unfavourableclinical results; see; Davies, 2018; Eban, 2019; Greene, 2019; O'Steen &O'Steen, 2006).
Conspiracy theories can have broad negative consequences for so-ciety through the rejection of scientific evidence and the associatedpoor health choices (e.g., see van der Linden, 2015). However,
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
�Chapter 2: Protecting consumers from fraudulent health claims
31

debunking conspiracy theories is di"cult not least because con-spiratorial thinking: (i) has a “self-sealing nature”—the tendency toreject contrary evidence or refutation attempts as confirmation of theexistence of an alleged nefarious plot; and (ii) thrives on the abundanceof disconfirming evidence and the lack confirming evidence, which isthe inverse of rational thinking (Lewandowsky et al., 2013; Sunsteinand Vermeule, 2009; Uscinski and Parent, 2014). Despite the chal-lenges, the public-health implications of the current widespread beliefin conspiracy theories mean that health authorities must neverthelesswork to assist the public to distinguish between conspiracy theory andfact.
We recommend that practitioners familiarise themselves with thetools of scientific enquiry and consider the pros and cons of variousconspiracy evaluation guidelines (Uscinski and Parent, 2014). Onepromising treatment to assist consumers to avoid fraudulent con-spiratorial claims would thus be to provide consumers with the rational,methodical tools to evaluate the evidence of conspiracy theories (seeUscinski and Parent, 2014). Another approach would be to commu-nicate the deceptive strategies employed by health-remedy marketers.Such an approach was demonstrated in recent studies that found thatpeople could be “inoculated” against the adverse e!ects of mis-information by pre-emptively explaining the deceptive argumentationtechniques employed by those spreading the misinformation (Cooket al., 2017; van der Linden et al., 2017). An alternative approach tomight be to consider interventions other than directly debunking con-spiracy theories. For example, health practitioners could structure theenvironment in such a way that makes it inconvenient to maintaindisproven beliefs (e.g., by requiring a considerable administrativeburden to opt-out of vaccination). Similarly, practitioners should alsoconsider reducing the structural barriers (e.g., access to conventionalhealthcare) that contribute to people's willingness to accept conspiracytheories (e.g., real-world barriers that can inhibit parents from vacci-nating, such as lack of transport or assistance with timely child support;Leask, 2011).
2.5. Exploited psychological driver: Norms
Social norms are rules or standards about how members of a com-munity should behave. For rules to be considered social norms (here-after referred to as norms), they must be supported and “enforced” by asu"cient portion of a community. Examples of norms range from ex-plicit laws (e.g., pharmaceutical drugs must pass clinical testing)through to informal guidelines (e.g., a taboo about openly criticisinganother person's beliefs). Evolutionary psychology provides one usefulframework for understanding how norms impact behaviour: As in-dividuals we owe much of our success to the behaviour of othermembers of our community, and thus cooperation must be evolutio-narily adaptive. Yet, for a community to cooperate e!ectively, in-dividuals must reliably adhere to a set of behavioural norms. Thebenefits of ensuring cooperation help to explain why many humanbehaviours have evolved for norm detection and enforcement (Simlerand Hanson, 2017). Game theory provides another useful frameworkfor understanding norms. For example, one classic study showed thatsince enforcement can be costly for an individual (e.g., it can elicitretaliation from those being punished), norms are most e!ective whenthere are incentives for enforcement, termed meta-norms (e.g., a normpunishing those who do not punish others; Axelrod, 1986). Further, inorder for a new norm to be established, individuals must have reason tobelieve that other members of the community are also aware, and mightsupport, that new norm. This factor helps to explain why public com-munications about norms can have a considerable impact on individualbehaviour.
Human impulses towards conformity and social inclusion are sofundamental that community norms can become an intrinsic part of ourindividual sense of identity. For example, adolescent binge drinking ispredicted by perceived alcohol consumption norms from multiple
sources (parents, friends, society; Kuntsche et al., 2017) and the extentto which alcohol is viewed as part of an individual's identity (Ridoutet al., 2012). Conversely, Berger and Rand (2008) experimentallyshowed that when unhealthy behaviours (e.g., binge drinking andconsuming fattening foods) were conspicuously linked to the identity ofan undesirable social outgroup, individuals reported altering their be-haviour (i.e., drinking less or consuming fewer fattening foods) to avoidsignalling association with the undesired group.
One approach to changing a harmful behaviour is a norm appeal—amessage that aims to change an undesirable behaviour by highlightinga behavioural norm. To design e!ective norm appeals, practitionersneed to distinguish between (i) injunctive norms—what others approveor disapprove of doing; (ii) descriptive norms—what people typically do,and (iii) perceived norms—what individuals believe about the real de-scriptive and injunctive norms. Injunctive norms operate by signallingthe likelihood of social approval or disapproval, and therefore thepossible social consequences of one's behaviour. Descriptive normsoperate by serving as an indicator of the injunctive norm (where thereis uncertainty about the injunctive norm) and by serving as a heuristicfor calculating the costs vs. benefits of compliance (Farrow et al., 2017).Failure to distinguish between di!erent types of norms can result incampaigns that inadvertently strengthen undesirable norms. For in-stance, stating that flu vaccination rates are low may be accurate, but italso communicates a descriptive norm that few people get vaccinatedand thus may encourage greater conformity in the wrong direction(Cialdini, 2003). In contrast, stating that vaccine approval rates arehigh may be equally accurate, but instead highlights an injunctive normthat most people approve of vaccines, and thus may encourage con-formity in the desired direction. In support of this principle, a study onflu vaccination rates found that individuals who believed a majority ofpeople around them approved of vaccination (injunctive norm) weremuch more likely to get vaccinated than those who believed that themajority disapproved of vaccination (Quinn et al., 2017). Three majorbarriers that prevent norm appeals from influencing behaviour aremisperceived norms, logical fallacies, and resistant social structures.
2.5.1. One barrier to successful norm appeals: Misperceived normsMisperceptions about norms (e.g., a belief that a behaviour occurs
more, or less, frequently than it does in reality) can lead individuals tounwittingly behave in ways that are inconsistent with their socialgroup, and thus can be harmful to health. For example, college studentstend to view their own alcohol use as less problematic if they over-estimate the use and approval of alcohol by their peers (Borsari andCarey, 2003). In theory, norm appeals can be used to counter suchmisperceptions, by conveying the true norms (descriptive, injunctive, orideally both; Cialdini, 2003). However, evaluations of this approachhave found mixed results (DeJong et al., 2009; Perkins and Craig, 2006;Wechsler et al., 2003). Wechsler et al. (2003) suggested one key reasonwhy norm appeals may sometimes have been ine!ective was that theytargeted college campuses with diverse student populations, whichwere unlikely to contain a “typical student” or a single common set ofnorms.
In line with this explanation, a recent review of the norms literature(Farrow et al., 2017) suggested several factors that may moderatemessage acceptance, including characteristics of the implied referencegroup (e.g., its size), characteristics of the target individual (e.g., un-derlying motivations, risk tolerance, socio-demographics, attitude to-wards and social proximity to the reference group), the social context ofthe behaviour (e.g., anonymous or public), and the environmentalcontext (e.g., visual cues indicating if others behave in accordance withthe norm appeal). Obtaining knowledge about these factors before de-signing interventions will help practitioners develop an informedtheory about the impact of a given norm appeal.
One fraudulent health behaviour that could lend itself to a normappeal is pharmacists’ sales of homeopathic remedies. For example, a2013 Australian study found that 36% of pharmacists agreed that
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
32

homeopathic remedies had a place in pharmacies, yet only 14% be-lieved homeopathic remedies were e!ective—suggesting some phar-macists were comfortable in knowingly selling ine!ective products(Schultz et al., 2013). This behaviour may have been driven by a mis-perceived descriptive norm, namely that some pharmacists over-estimated the extent to which their colleagues believed homeopathicremedies to be useful. Indeed, Schultz et al. (2013) found pharmacistswere more likely to be comfortable selling homeopathic remedies ifthey believed that other pharmacists considered them to be useful. Incontrast, pharmacists were less likely to be comfortable selling ho-meopathic remedies if they believed that respect from other healthpractitioners would be lost by stocking such remedies.
These results suggest that a promising treatment to discouragepharmacists from selling homeopathic remedies would be to combine adescriptive norm (most pharmacists believe homeopathy is ine!ective)with an injunctive norm (stocking homeopathic remedies is a risk toreputation). A further injunctive norm could be added to stress thatmajor medical representative bodies disapprove of homeopathy(Australian National Health & Medical Research Council [NHMRC],2015; National Health Service [NHS] England, 2017). Yet another in-junctive norm that could be leveraged is that communities generallydisapprove of commercial transactions where the merchant knows (orought to know) that the product does not work (Macdonald and Gavura,2016). For these treatments to be e!ective, such norm appeals wouldneed to be su"ciently public to create a credible threat of collectiveenforcement—pharmacists selling homeopathic remedies would needto believe that a su"cient proportion of other pharmacists, and thewider community, would also receive the norm appeal (Simler andHanson, 2017). Incidentally, a similar norms approach could also beleveraged for other alternative health remedies, by highlighting thatpharmacists generally lack the knowledge to provide advice about al-ternative remedies (Waddington et al., 2015) and major medical so-cieties are increasingly opposed to alternative medicines (South WestLondon Medicines Optimisation Group NHS, 2018; PharmaceuticalSociety of Australia, 2015).
2.5.2. A second barrier to successful norm appeals: Logical fallaciesAdvocates of fraudulent health remedies will routinely appeal to
norms with the aim of manipulating consumers' receptivity to theirclaims. In a typical norm appeal, an advocate will espouse the voca-bulary or ideology of a given community in order to enhance the appealof a pseudoscientific claim. Almost invariably, such appeals rely onlogical fallacies—invalid arguments or irrelevant points that lack evi-dence. A typical fallacious appeal is the appeal to duty, which advocatesfor consuming a particular health remedy out of a moral duty to protectone's family. For example, marketers continue to make claims thatantibacterial soaps are superior to ordinary soaps for protecting familiesfrom germs and infection, despite no such evidence and even somestudies suggesting they might be harmful (FDA, 2016). Debunkingnorm appeals that rely on logical fallacies requires two steps. First,highlight the errors in reasoning: Practitioners can become proficient atthis step by acquiring familiarity with logical fallacies and the princi-ples of reasoning (Cook et al., 2018). Second, provide persuasivecounter-evidence: Cognitive research on inductive reasoning—makingpredictions about novel phenomena based on existing knowledge—-suggests that a range of factors can increase perceptions of argumentstrength such as ensuring evidence diversity (Hayes and Heit, 2018).For example, providing evidence from two culturally dissimilar nationsconsiderably increased support for scientific claims on public healthissues, compared to evidence from two culturally similar nations (Karyet al., 2018).
The appeal to tradition is another logical fallacy routinely employedby advocates of alternative remedies. The essential form of this fallacyis that the longevity of a health approach (e.g., Traditional ChineseMedicine)—the fact that it has been practised for thousands of years—isevidence of its e!ectiveness. This argument is invalid because many
health systems that have persisted for a long time are plainly false.Thus, an e!ective treatment to dispel this fallacy would be to point toculturally diverse evidence where long-held ancient health remedies areunequivocally false such as physiognomy and humoral biology(Novella, 2007).
The appeal to authority is another common logical fallacy. The es-sential form of this fallacy is that support for a claim (e.g., rhino horncures cancer) from an authority (e.g., a respected medical doctor) isevidence that supports the claim. The argument is invalid because evenmedical professionals can provide advice that is counter to scientificconsilience. In a typical example, an appeal to authority is madewhenever a successful sportsperson endorses the use of an unsupporteddietary supplement. For such appeals, an e!ective counter-strategymight be to provide diverse evidence of athletes who succeeded withoutusing dietary supplements, or who only used, or endorsed, certainhealth remedies after they already achieved sporting success.
2.5.3. A third barrier to successful norm appeals: Resistant social structuresA common intuition about intervention messaging is that social
networks with the most connections (e.g., public broadcasters or “socialmedia influencers”) will facilitate the greatest spread of behaviourchange. This intuition relies on the underlying assumption that per-suasive messages (e.g., catchy advertisements or informative doc-umentaries) will e"ciently di!use the intended changes through socialnetworks consisting of many weak connections (e.g., casual acquain-tances), such that more connections will result in greater uptake (e.g.,shared internet memes that “go viral”). However, research on the dif-fusion of complex behaviours suggests that the content of an inter-vention message may be less influential than the structure and relationsof the network that the message is di!used through (Centola, 2011). Inparticular, this research suggests that the complexity of a particularbehaviour will influence how e!ectively it di!uses through di!erentstructured networks.
For simple behaviours (e.g., sharing an amusing photo) the moste"cient network structure requires many weak ties—casual acquain-tances that are distal, dissimilar, and characterized by low-frequencycontact—because the behaviour can easily di!use between two dis-tantly related contacts, helping it to spread quickly throughout thepopulation. In contrast, for complex behaviours (e.g., deciding whetherto vaccinate), the most e"cient network structure may require rela-tively few strong ties—family, friends, and community members thattend to be proximate, similar, and characterized by high-frequencycontact—because individuals are more likely to adopt new a socialnorm when they receive social reinforcement from multiple familiarsources. Indeed, the abundance of weak ties within a social network caneven inhibit the adoption of complex behaviours in a population be-cause highly-connected individuals will receive a greater proportion ofcountervailing signals from non-adaptors (Centola, 2010; Centola et al.,2007).
In support, Centola (2010) experimentally showed that the uptakeof a health behaviour was greater when participants received socialreinforcement from multiple neighbours in an online social network,compared to a more distally connected random network. In a follow-upstudy, Centola (2011) showed that the uptake of a health behaviour wassignificantly influenced by manipulating the level of homophily—thesimilarity of social contacts—in online social network structures. Spe-cifically, they found that groups consisting of individuals with similarcharacteristics (gender, age, and body mass index) had greater di!usionof the health behaviour than individuals randomly assigned to net-works.
To date, the impact of social network structure has only been ex-perimentally tested with a few positive health interventions (e.g., in-creased physical activity) and none to our knowledge have aimed tocounter health fraud. Nevertheless, both observational and modellingresearch into the di!usion of fraudulent health claims (such as anti-fluoride and anti-vaccine networks; Salathé and Bonhoe!er, 2008;
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
33

Seymour et al., 2015) supports the notion that strong ties in a com-munity present a considerable barrier to the acceptance of outside ex-pert opinion. Practitioners wishing to protect consumers from fraudu-lent health claims should thus compare the impact of engaging di!erentnetwork structures on the di!usion of various social norms. Theemerging research into the di!usion of complex behaviours suggestsseveral treatments for countering health fraud (Centola, 2018). Onetreatment is to create clusters of early adopters, as this may drive arobust process of social reinforcement, compared to diluting their in-fluence amongst a population. Another promising treatment is to en-hance the persuasiveness of intervention messaging by fostering em-pathy. Centola suggests that the right form of homophily (i.e., similarityin ways relevant to the behaviour) can foster empathy su"cient todrive e!ective di!usion.
3. Conclusions
The primary goal of the present taxonomy (Table 1) is to provide aframework to combat the weapons of persuasive influence that healthfraudsters exploit, by considering the psychological mechanisms bywhich those weapons operate, and then using these insights to crafttreatments to help consumers resist such exploitation. Our taxonomydraws on principles, insights, and experimental evidence from severalpsychological fields to make predictions about interventions. However,it is important to note that most of these predictions are yet to beempirically tested.
Although several randomized controlled trials have supported theproposed treatments for counteracting the illusion of causality(MacFarlane et al., 2018), more trials, and subsequent replications, areneeded to test all of the predictions in the taxonomy. Thus, the tax-onomy should also serve as a springboard for future applied research.Depending on the outcomes of this research, it is our hope that thetaxonomy will serve as a robust guide for practitioners to design, im-plement, and evaluate psychologically-informed interventions. Careshould also be taken to ensure that interventions are always im-plemented with due regard to ethical considerations, including takingsteps to secure public acceptability (Reynolds et al., 2019).
We stress that the taxonomy is not exhaustive, nor does it examinethe individual personality or cognitive traits that might make certaingroups of people, such as the elderly, more susceptible to fraud thanothers (Kircanski et al., 2018). Instead, we have provided a selection ofthe major drivers of consumer susceptibility to health fraud, key psy-chological barriers to intervention e!ectiveness, and some promisingpsychologically-informed treatments.
This review has sought to make three key contributions. First, it hasreviewed the major psychological insights that likely contribute toconsumer susceptibility to health fraud. Second, it has presented a co-herent framework for systematically testing which psychological dri-vers render consumers most susceptible to health fraud. Third, it hasintroduced a congruent and parsimonious taxonomy that enablespractitioners to systematically design, test, and compare interventionsto protect consumers from fraudulent health claims. Future researchshould test the numerous predictions made by the taxonomy to estab-lish what combinations of treatments are most e!ective at protectingconsumers from health fraud.
Declaration of competing interest
None.
Acknowledgements
This research was facilitated by an Australian Government ResearchTraining Program Scholarship awarded to the first author.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.socscimed.2020.112790.
References
National Health Service [NHS] England, 2017. Prescription curbs to free up hundreds ofmillions of pounds for frontline care. [Press release]. Retreived from. https://www.england.nhs.uk/2017/11/.
Aggarwal, P., Jun, S.Y., Huh, J.H., 2011. Scarcity messages. J. Advert. 40, 19–30.Alhakami, A.S., Slovic, P., 1994. A psychological study of the inverse relationship be-
tween perceived risk and perceived benefit. Risk Anal. 14, 1085–1096.Allum, N., Sturgis, P., Tabourazi, D., Brunton-Smith, I., 2008. Science knowledge and
attitudes across cultures: a meta-analysis. Public Underst. Sci. 17, 35–54.Amos, C., Landreth Grau, S., 2015. Does consumer scepticism negate the e!ects of visc-
eral cues in weight loss advertising? Int. J. Advert. 30, 693–719.Attwell, K., Ward, P.R., Meyer, S.B., Rokkas, P.J., Leask, J., 2018. “Do-it-yourself”: vac-
cine rejection and complementary and alternative medicine (CAM). Soc. Sci. Med.196, 106–114.
Australian Government Department of Health, 2015. Review of the australian govern-ment rebate on natural therapies for private health insurance. Retrieved from.http://www.health.gov.au/internet/main/publishing.nsf/content/phi-natural-therapies.
Avigan, M.I., Mozersky, R.P., See!, L.B., 2016. Scientific and regulatory perspectives inherbal and dietary supplement associated hepatotoxicity in the United States. Int. J.Mol. Sci. 17, 331.
Axelrod, R., 1986. An evolutionary approach to norms. Am. Pol. Sci. Rev. 80, 1095–1111.Barberia, I., Blanco, F., Cubillas, C.P., Matute, H., 2013. Implementation and assessment
of an intervention to debias adolescents against causal illusions. PLoS One 8, e71303.Batanero, C., Cañadas, G.R., Díaz, C., Gea, M.M., 2015. Judgment of association between
potential factors and associated risk in 2 # 2 tables: a study with psychology stu-dents. Math. Enthus. 12, 347–363.
Begh, R., Munafo, M.R., Shi!man, S., Ferguson, S.G., Nichols, L., Mohammed, M.A., ...Aveyard, P., 2015. Lack of attentional retraining e!ects in cigarette smokers at-tempting cessation: a proof of concept double-blind randomised controlled trial. DrugAlcohol Depend. 149, 158–165.
Bellanger, R.A., Seeger, C.M., Smith, H.E., 2017. Safety of complementary and alternativemedicine (CAM) treatments and practices. Side E!. Drugs Annu. 39, 503–512.
Berger, J., 2011. Arousal increases social transmission of information. Psychol. Sci. 22,891–893.
Berger, J., Rand, L., 2008. Shifting signals to help health: using identity signaling to re-duce risky health behaviors. J. Consum. Res. 35, 509–518.
Berinsky, A.J., 2017. Rumors and health care reform: experiments in political mis-information. Br. J. Polit. Sci. 47, 241–262.
Betsch, C., Korn, L., Holtmann, C., 2015. Don't try to convert the antivaccinators, insteadtarget the fence-sitters. Proc. Natl. Acad. Sci. 112, E6725–E6726 [10.1073/pnas.1516350112].
Bjelakovic, G., Nikolova, D., Gluud, L.L., Simonetti, R.G., Gluud, C., 2012. Antioxidantsupplements for prevention of mortality in healthy participants and patients withvarious diseases. Cochrane Database Syst. Rev. (3), CD007176.
Bjelakovic, G., Gluud, L.L., Nikolova, D., Whitfield, K., Wetterslev, J., Simonetti, R.G., ...Gluud, C., 2014. Vitamin D supplementation for prevention of mortality in adults.Cochrane Database Syst. Rev. 1 (1), CD007470.
Blais, A.-R., Thompson, M.M., Baranski, J.V., 2005. Individual di!erences in decisionprocessing and confidence judgments in comparative judgment tasks: the role ofcognitive styles. Personal. Individ. Di!er. 38, 1701–1713.
Blanco, F., Matute, H., Vadillo, M.A., 2011. Making the uncontrollable seem controllable:the role of action in the illusion of control. Q. J. Exp. Psychol. 64, 1290–1304.
Bolton, L.E., Cohen, J.B., Bloom, P.N., 2006. Does marketing products as remedies create“get out of jail free cards”? J. Consum. Res. 33, 71–81.
Borsari, B., Carey, K.B., 2003. Descriptive and injunctive norms in college drinking: ameta-analytic integration. J. Stud. Alcohol 64, 331–341.
Broniatowski, D.A., Jamison, A.M., Qi, S., AlKulaib, L., Chen, T., Benton, A., ... Dredze,M., 2018. Weaponized health communication: twitter bots and Russian trolls amplifythe vaccine debate. Am. J. Public Health 108, 1378–1384.
Bubela, T., Nisbet, M.C., Borchelt, R., Brunger, F., Critchley, C., Einsiedel, E., ... Caulfield,T., 2009. Science communication reconsidered. Nat. Biotechnol. 27, 514–518.
Byard, R.W., Musgrave, I., 2010. Herbal medicines and forensic investigations. ForensicSci. Med. Pathol. 6.
Callaghan, T., Motta, M., Sylvester, S., Lunz Trujillo, K., Blackburn, C.C., 2019. Parentpsychology and the decision to delay childhood vaccination. Soc. Sci. Med. 238,112407.
Cannon, C., Goldsmith, K., Roux, C., Kirmani, A., 2018. A self-regulatory model of re-source scarcity. J. Consum. Psychol. 1–24 0.
Centola, D., 2010. The spread of behavior in an online social network experiment. Science329, 1194.
Centola, D., 2011. An experimental study of homophily in the adoption of health beha-vior. Science 334, 1269–1272.
Centola, D., 2018. How Behavior Spreads: the Science of Complex Contagions. PrincetonUniversity Press.
Centola, D., Eguíluz, V.M., Macy, M.W., 2007. Cascade dynamics of complex propagation.Phys. A Stat. Mech. Appl. 374, 449–456.
Chabris, C.F., Simons, D., 2010. The Invisible gorilla: and Other Ways Our Intuitions
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
34

Deceive Us. Crown, New York.Chabris, C.F., Weinberger, A., Fontaine, M., Simons, D.J., 2011. You do not talk about
Fight Club if you do not notice Fight Club: inattentional blindness for a simulatedreal-world assault. I-perception 2, 150–153.
Christiano, A., Neimand, A., 2017. Stop Raising Awareness Already. Stanford SocialInnovation Review. Retrieved , Accessed date: 20 February 2017.
Cialdini, R.B., 2003. Crafting normative messages to protect the environment. Curr. Dir.Psychol. Sci. 12, 105–109.
Cialdini, R.B., 2009. Influence: the Psychology of Persuasion. Harper Collins.Citrin, D.L., Bloom, D.L., Grutsch, J.F., Mortensen, S.J., Lis, C.G., 2012. Beliefs and per-
ceptions of women with newly diagnosed breast cancer who refused conventionaltreatment in favor of alternative therapies. The Oncologist 17, 607–612.
Coghlan, M.L., Maker, G., Crighton, E., Haile, J., Murray, D.C., White, N.E., ... Bunce, M.,2015. Combined DNA, toxicological and heavy metal analyses provides an auditingtoolkit to improve pharmacovigilance of traditional Chinese medicine (TCM). Sci.Rep. 5, 17475.
Cook, J., Lewandowsky, S., Ecker, U.K.H., 2017. Neutralizing misinformation throughinoculation: exposing misleading argumentation techniques reduces their influence.PLoS One 12, e0175799.
Cook, J., Ellerton, P., Kinkead, D., 2018. Deconstructing climate misinformation toidentify reasoning errors. Environ. Res. Lett. 13, 024018.
Cormie, P., Atkinson, M., Bucci, L., Cust, A., Eakin, E., Hayes, S., ... Adams, D., 2018.Clinical Oncology Society of Australia position statement on exercise in cancer care.Med. J. Aust. 209, 184–187.
Crichton, F., Petrie, K.J., 2015. Accentuate the positive: counteracting psychogenic re-sponses to media health messages in the age of the internet. J. Psychosom. Res. 79,185–189.
Croskerry, P., Norman, G., 2008. Overconfidence in clinical decision making. Am. J. Med.121, S24–S29.
Damasio, A.R., Tranel, D., Damasio, H., 1990. Individuals with sociopathic behaviorcaused by frontal damage fail to respond autonomically to social stimuli. Behav.Brain Res. 41, 81–94.
Davies, Dan, 2018. Lying for Money: How Legendary Frauds Reveal the Workings of OurWorld. Profile Books, London.
de Barra, M., 2017. Reporting bias inflates the reputation of medical treatments: acomparison of outcomes in clinical trials and online product reviews. Soc. Sci. Med.177, 248–255.
DeJong, W., Schneider, S.K., Towvim, L.G., Murphy, M.J., Doerr, E.E., Simonsen, N.R., ...Scribner, R.A., 2009. A multisite randomized trial of social norms marketing cam-paigns to reduce college student drinking: a replication failure. Subst. Abus. 30,127–140.
Dillard, J.P., Shen, L., 2005. On the nature of reactance and its role in persuasive healthcommunication. Commun. Monogr. 72, 144–168.
Ditto, P.H., Pizarro, D.A., Epstein, E.B., Jacobson, J.A., MacDonald, T.K., 2006. Visceralinfluences on risk-taking behavior. J. Behav. Decis. Mak. 19, 99–113.
Dixon, G.N., McKeever, B.W., Holton, A.E., Clarke, C., Eosco, G., 2015. The power of apicture: overcoming scientific misinformation by communicating weight-of-evidenceinformation with visual exemplars. J. Commun. 65, 639–659.
Eban, K., 2019. Bottle of Lies: the inside Story of the Generic Drug Boom. Harper Collins,New York, NY, USA.
Ecker, U.K.H., Ang, L.C., 2019. Political attitudes and the processing of misinformationcorrections. Political Psychol. 40, 241–260.
Ecker, U.K.H., Lewandowsky, S., Tang, D.T., 2010. Explicit warnings reduce but do noteliminate the continued influence of misinformation. Mem. Cogn. 38, 1087–1100.
Ecker, U.K.H., O’Reilly, Z., Reid, J.S., Chang, E.P., 2019. The e!ectiveness of short$formatrefutational fact$checks. Br. J. Psychol. https://doi.org/10.1111/bjop.12383.
Farrow, K., Grolleau, G., Ibanez, L., 2017. Social norms and pro-environmental behavior:a review of the evidence. Ecol. Econ. 140, 1–13.
U.S. Food and Drug Administration [FDA], 2016. Antibacterial Soap? You Can Skip it, UsePlain Soap and Water. [Press Release] Retreived from. https://www.fda.gov/ForConsumers/ConsumerUpdates/ucm378393.htm.
U.S. Food & Drug Administration [FDA], 2019. Health Fraud Scams. Retrieved from.https://www.fda.gov/forconsumers/protectyourself/healthfraud/default.htm.
Feinberg, M., Willer, R., 2013. The moral roots of environmental attitudes. Psychol. Sci.24, 56–62.
Fernbach, P.M., Light, N., Scott, S.E., Inbar, Y., Rozin, P., 2019. Extreme opponents ofgenetically modified foods know the least but think they know the most. Nat. HumanBehav. 3, 251–256.
Festinger, L., 1962. A Theory of Cognitive Dissonance, vol. 2 Stanford University Press1962.
Field, M., Mogg, K., Bradley, B.P., 2005. Craving and cognitive biases for alcohol cues insocial drinkers. Alcohol Alcohol 40, 504–510.
Finucane, M.L., Alhakami, A., Slovic, P., Johnson, S.M., 2000. The a!ect heuristic injudgements of risks and benefits. J. Behav. Decis. Mak. 13, 1–17.
Fischer, P., Lea, S.E.G., Evans, K.M., 2013. Why do individuals respond to fraudulentscam communications and lose money? The psychological determinants of scamcompliance. J. Appl. Soc. Psychol. 43, 2060–2072.
Fisher, M., Goddu, M.K., Keil, F.C., 2015. Searching for explanations: how the Internetinflates estimates of internal knowledge. J. Exp. Psychol. Gen. 144, 674.
Flaherty, D.K., 2011. The vaccine-autism connection: a public health crisis caused byunethical medical practices and fraudulent science. Ann. Pharmacother. 45,1302–1304.
Foster, K.R., Kokko, H., 2009. The evolution of superstitious and superstition-like beha-viour. Proc. R. Soc. Biol. Sci. 276, 31–37.
Foster, N.E., Anema, J.R., Cherkin, D., Chou, R., Cohen, S.P., Gross, D.P., ... Woolf, A.,2018. Prevention and treatment of low back pain: evidence, challenges, and
promising directions. The Lancet 391, 2368–2383.Friehe, T., Utikal, V., 2018. Intentions under cover – hiding intentions is considered
unfair. J. Behav. Exp. Econ. 73, 11–21.Geller, A.I., Shehab, N., Weidle, N.J., Lovegrove, M.C., Wolpert, B.J., Timbo, B.B.,
Budnitz, D.S., 2015. Emergency department visits for adverse events related todietary supplements. N. Engl. J. Med. 373, 1531–1540.
Gibbs, R., Davies, G., Chou, S., 2016. A systematic review on factors a!ecting the like-lihood of change blindness. Crime Psychol. Rev. 2, 1–21.
Giudice, E.L., Campbell, J.D., 2006. Needle-free vaccine delivery. Adv. Drug Deliv. Rev.58 (1), 68–89.
Goertzel, T., 2010. Conspiracy theories in science. EMBO Rep. 11, 493–499.Graham, J., Haidt, J., Nosek, B.A., 2009. Liberals and conservatives rely on di!erent sets
of moral foundations. J. Personal. Soc. Psychol. 96, 1029–1046.Graham-Rowe, D., 2011. Biodiversity: endangered and in demand. Nature 480,
S101–S103.Greene, J.A., 2019. After a Scandal, a One-Sided Warning against Generic Drugs. The
Washington Post.Greenlee, H., Ernst, E., 2012. What can we learn from Steve Jobs about complementary
and alternative therapies? Prev. Med. 54, 3–4.Guallar, E., Stranges, S., Mulrow, C., Appel, L.J., Miller, E.R., 2013. Enough is enough:
stop wasting money on vitamin and mineral supplements. Ann. Intern. Med. 159.Hall, H., 2008. Popular medical fallacies: ancient wisdom* it works for me* natural is
good. Skeptic 14, 8–10.Hall, M.G., Mendel, J.R., Noar, S.M., Brewer, N.T., 2018. Why smokers avoid cigarette
pack risk messages: two randomized clinical trials in the United States. Soc. Sci. Med.213, 165–172.
Hameleers, M., van der Meer, T.G.L.A., 2019. Misinformation and Polarization in a High-Choice Media Environment: How E!ective Are Political Fact-Checkers?Communication Research, 0093650218819671.
Hartmann-Boyce, J., Chepkin, S.C., Ye, W., Bullen, C., Lancaster, T., 2018. Nicotine re-placement therapy versus control for smoking cessation. Cochrane Database Syst.Rev. 5 Art. No. Art. No. CD00014.
Hayes, B.K., Heit, E., 2018. Inductive Reasoning 2.0, vol. 9 Wiley InterdisciplinaryReviews: Cognitive Science.
Hayes, B.K., Hawkins, G.E., Newell, B.R., 2016. Consider the alternative: the e!ects ofcausal knowledge on representing and using alternative hypotheses in judgmentsunder uncertainty. J. Exp. Psychol. Learn. Mem. Cogn. 42, 723–739.
Heit, E., Rotello, C.M., 2012. The pervasive e!ects of argument length on inductivereasoning. Think. Reason. 18, 244–277.
Hemila, H., Chalker, E., 2013. Vitamin C for preventing and treating the common cold.Cochrane Database Syst. Rev. 1 Art. No. CD000980.
Hopkins, E.J., Weisberg, D.S., Taylor, J.C.V., 2016. The seductive allure is a reductiveallure: people prefer scientific explanations that contain logically irrelevant reductiveinformation. Cognition 155, 67–76.
Hsee, C.K., 1996. The evaluability hypothesis: an explanation for preference reversalsbetween joint and separate evaluations of alternatives. Organ. Behav. Hum. Decis.Process. 67, 247–257.
Huang, J.Y., Ackerman, J.M., Newman, G.E., 2017. Catching (up with) magical con-tagion: a review of contagion e!ects in consumer contexts. J. Assoc. Consumer Res. 2,430–443.
Hughes, B.L., Zaki, J., 2015. The neuroscience of motivated cognition. Trends Cogn. Sci.19, 62–64.
Im, S.h., Varma, K., Varma, S., 2017. Extending the seductive allure of neuroscienceexplanations e!ect to popular articles about educational topics. Br. J. Educ. Psychol.87, 518–534.
Ioannidis, J.P.A., 2017. Does evidence-based hearsay determine the use of medicaltreatments? Soc. Sci. Med. 177, 256–258.
Jacoby, L.L., Kelley, C., 1989. Becoming famous overnight: limits on the ability to avoidunconscious influences of the past. J. Personal. Soc. Psychol. 56, 326–338.
Jenkins, D.J.A., Spence, J.D., Giovannucci, E.L., Kim, Y.I., Josse, R., Vieth, R., ...Sievenpiper, J.L., 2018. Supplemental vitamins and minerals for CVD prevention andtreatment. J. Am. Coll. Cardiol. 71, 2570–2584.
Johnson, H.M., Seifert, C.M., 1994. Sources of the continued influence e!ect: whenmisinformation in memory a!ects later inferences. J. Exp. Psychol. Learn. Mem.Cogn. 20, 1420–1436.
Johnson, C.G., Levenkron, J.C., Suchman, A.L., Manchester, R., 1988. Does physicianuncertainty a!ect patient satisfaction? J. Gen. Intern. Med. 3, 144–149.
Kahan, D.M., 2015. What is the “science of science communication”? J. Sci. Commun.14 (3).
Kahan, D.M., Peters, E., Wittlin, M., Slovic, P., Ouellette, L.L., Braman, D., et al., 2012.The polarizing impact of science literacy and numeracy on perceived climate changerisks. Nat. Clim. Chang. 2, 732–735.
Kahan, D.M., Peters, E., Dawson, E.C., Slovic, P., 2013. Motivated Numeracy andEnlightened Self-Government (Public LawWorking Paper No. 307). Yale Law School.
Kahneman, D., 2012. Thinking, Fast and Slow. Penguin, London.Kary, A., Newell, B.R., Hayes, B.K., 2018. What makes for compelling science? Evidential
diversity in the evaluation of scientific arguments. Glob. Environ. Chang. 49,186–196.
Keren, G., Teigen, K.H., 2001. Why is p = .90 better than p = .70? Preference for de-finitive predictions by lay consumers of probability judgments. Psychon. Bull. Rev. 8,191–202.
Kircanski, K., Nottho!, N., DeLiema, M., Samanez-Larkin, G.R., Shadel, D., Mottola, G., ...Gotlib, I.H., 2018. Emotional arousal may increase susceptibility to fraud in older andyounger adults. Psychol. Aging 33, 325.
Kitchens, B., Harle, C.A., Li, S., 2014. Quality of health-related online search results.Decis. Support Syst. 57, 454–462.
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
35

Klofstad, C.A., Uscinski, J.E., Connolly, J.M., West, J.P., 2019. What drives people tobelieve in Zika conspiracy theories? Palgrave Commun. 5, 1–8.
Kluger, A.N., DeNisi, A., 1996. The e!ects of feedback interventions on performance: ahistorical review, a meta-analysis, and a preliminary feedback intervention theory.Psychol. Bull. 119, 254–284.
Kok, G., Gottlieb, N.H., Peters, G.J., Mullen, P.D., Parcel, G.S., Ruiter, R.A., et al., 2016. Ataxonomy of behaviour change methods: an Intervention Mapping approach. HealthPsychol. Rev. 10, 297–312.
Kok, G., Peters, G.Y., Kessels, L.T.E., Ten Hoor, G.A., Ruiter, R.A.C., 2018. Ignoring theoryand misinterpreting evidence: the false belief in fear appeals. Health Psychol. Rev. 12,111–125.
Kristo!erson, K., McFerran, B., Morales, A.C., Dahl, D.W., 2017. The dark side of scarcitypromotions: how exposure to limited-quantity promotions can induce aggression. J.Consum. Res. 43, 683–706.
Kruger, J., Dunning, D., 1999. Unskilled and unaware of It: how di"culties in recognizingone's own incompetence lead to inflated self-assessments. J. Personal. Soc. Psychol.77, 1121.
Kunda, Z., 1987. Motivated inference: self-serving generation and evaluation of causaltheories. J. Personal. Soc. Psychol. 53, 636.
Kuntsche, E., Kuntsche, S., Thrul, J., Gmel, G., 2017. Binge drinking: health impact,prevalence, correlates and interventions. Psychol. Health 32, 976–1017.
Langenderfer, J., Shimp, T.A., 2001. Consumer vulnerability to scams, swindles, andfraud: a new theory of visceral influences on persuasion. Psychol. Mark. 18, 763–783.
Langer, E.J., 1975. The illusion of control. J. Personal. Soc. Psychol. 32, 311–328.Lea, S., Fischer, P., Evans, K., 2009. The psychology of scams, provoking and committing
errors of judgement: prepared for the o"ce of fair trading by the university of exeterschool of psychology. Retrieved from. https://ore.exeter.ac.uk/repository/handle/10871/20958.
Leask, J., 2011. Target the fence-sitters. Nature 473, 443.Lee, T.K., Kim, H.K., 2017. Di!erential e!ects of message framing on obesity policy
support between democrats and republicans. Health Commun. 32, 1481–1490.Levin, D.T., Angelone, B.L., 2008. The visual metacognition questionnaire: a measure of
intuitions about vision. Am. J. Psychol. 121, 451–472.Levin, D.T., Momen, N., Drivdahl IV, S.B., Simons, D.J., 2000. Change blindness blind-
ness: the metacognitive error of overestimating change-detection ability. Vis. Cogn. 7,397–412.
Lewandowsky, S., Ecker, U.K., Seifert, C.M., Schwarz, N., Cook, J., 2012. Misinformationand its correction: continued influence and successful debiasing. Psychol. Sci. PublicInterest 13, 106–131.
Lewandowsky, S., Oberauer, K., Gignac, G.E., 2013. NASA faked the moon landing—th-erefore,(climate) science is a hoax: an anatomy of the motivated rejection of science.Psychol. Sci. 24, 622–633.
Lewandowsky, S., Ecker, U.K.H., Cook, J., 2017. Beyond misinformation: understandingand coping with the “post-truth” era. J. Appl. Res. Mem. Cogn. 6, 353–369.
Lilienfeld, S.O., Ritschel, L.A., Lynn, S.J., Cautin, R.L., Latzman, R.D., 2014. Why in-e!ective psychotherapies appear to work: a taxonomy of causes of spurious ther-apeutic e!ectiveness. Perspect. Psychol. Sci. 9, 355–387.
Loewenstein, G., 1996. Out of control: visceral influences on behaviour. Organ. Behav.Hum. Decis. Process. 65, 272–292.
Lombrozo, T., 2007. Simplicity and probability in causal explanation. Cogn. Psychol. 55,232–257.
Ludolph, R., Allam, A., Schulz, P.J., 2016. Manipulating Google's Knowledge Graph Boxto counter biased information processing during an online search on vaccination:application of a technological debiasing strategy. J. Med. Internet Res. 18.
Macdonald, C., Gavura, S., 2016. Alternative medicine and the ethics of commerce.Bioethics 30, 77–84.
MacFarlane, D., Hurlstone, M.J., Ecker, U.K.H., 2018. Reducing demand for ine!ectivehealth remedies: overcoming the illusion of causality. Psychol. Health 33,1472–1489.
MacFarlane, D., Hurlstone, M.J., Ecker, U.K.H., 2020. Countering Demand forUnsupported Health Remedies: Do Consumers Respond to Risks, Lack of Benefits, orBoth? (Unpublished results). .
Mani, A., Mullainathan, S., Shafir, E., Zhao, J., 2013. Poverty impedes cognitive function.Science 341, 976–980.
Mata, J., Todd, P.M., Lippke, S., 2010. When weight management lasts. Lower perceivedrule complexity increases adherence. Appetite 54, 37–43.
Matute, H., Blanco, F., Yarritu, I., Díaz-Lago, M., Vadillo, M.A., Barberia, I., 2015.Illusions of causality: how they bias our everyday thinking and how they could bereduced. Front. Psychol. 6, 1–14.
McCabe, D.P., Castel, A.D., 2008. Seeing is believing: the e!ect of brain images onjudgments of scientific reasoning. Cognition 107, 343–352.
McKenzie-Mohr, D., 2000. Fostering sustainable behavior through community-based so-cial marketing. Am. Psychol. 55, 531–537.
McKenzie-Mohr, D., Schultz, P.W., 2014. Choosing e!ective behavior change tools. Soc.Mark. Q. 20, 35–46.
BBC, 2018. Measles cases hit record high in Europe. August 20, Retrieved form. https://www.bbc.co.uk/news/health-45246049.
Australian Governmant National Health and Medical Research Council, 2015. NHMRCstatement: statement on homeopathy. Retrieved from. https://www.nhmrc.gov.au/_files_ nhmrc/publications/attachments/cam02_nhmrc_statement_homeopathy.pdf.
South West London Medicines Optimisation Group, 2018. Position statement on theprescribing of complementary and alternative medicines. Retrieved from https://www.swlmcg.nhs.uk/Policies/Position%20Statements/ .
Miller, L.M.S., Cassady, D.L., 2015. The e!ects of nutrition knowledge on food label use: areview of the literature. Appetite 92, 207–216.
Milliken, T., 2014. Illegal Trade in Ivory and an Assessment Report to Improve Law
Enforcement under the Wildlife TRAPS Project. USAID & Tra"c International,Cambridge, UK, pp. 1–24.
Motta, M., Callaghan, T., Sylvester, S., 2018. Knowing less but presuming more: Dunning-Kruger e!ects and the endorsement of anti-vaccine policy attitudes. Soc. Sci. Med.211, 274–281.
Nan, X., Madden, K., 2014. The role of cultural worldviews and message framing inshaping public opinions toward the human papillomavirus vaccination mandate.Hum. Commun. Res. 40, 30–53.
Novella, S., 2007. The Argument from Antiquity [Blog]. September 27. Retrieved from.https://theness.com/neurologicablog/index.php/the-argument-from-antiquity/.
O'Steen, J.V., O'Steen, V., 2006. The FDA defense: vioxx and the argument against federalpreemption of state claims for injuries resulting from defective drugs. Ariz. Law Rev.48, 67.
Oliver, J.E., Wood, T., 2014. Medical conspiracy theories and health behaviors in theUnited States. JAMA Int. Med. 174, 817–818.
Paynter, J., Luskin-Saxby, S., Keen, D., Fordyce, K., Frost, G., Imms, C., ... Ecker, U.K.H.,2019. Evaluation of a template for countering misinformation—real-world Autismtreatment myth debunking. PLoS One 14, e0210746.
Perkins, H.W., Craig, D.W., 2006. A successful social norms campaign to reduce alcoholmisuse among college student-athletes. J. Stud. Alcohol 67, 880–889.
Peters, G.-J.Y., Ruiter, R.A.C., Ten Hoor, G.A., Kessels, L.T.E., Kok, G., 2018. Towardsconsensus on fear appeals: a rejoinder to the commentaries on Kok, Peters, Kessels,ten Hoor, and Ruiter (2018). Health Psychol. Rev. 12, 151–156.
Pharmaceutical Society of Australia, 2015. PSA position statement on complementarymedicines. Retreived from. http://www.auspharmacist.net.au/images/psacam15.pdf.
Poland, G.A., Spier, R., 2010. Fear, misinformation, and innumerates: how the Wakefieldpaper, the press, and advocacy groups damaged the public health. Vaccine 28,2361–2362.
Quinn, S.C., Hilyard, K.M., Jamison, A.M., An, J., Hancock, G.R., Musa, D., Freimuth,V.S., 2017. The influence of social norms on flu vaccination among African Americanand White adults. Health Educ. Res. 32, 473–486.
Raven, J., 2000. The Raven's progressive matrices: change and stability over culture andtime. Cogn. Psychol. 41, 1–48.
Regner, T., 2016. Reciprocity under moral wiggle room: is it a preference or a constraint?Exp. Econ. 1–14.
Reynolds, J.P., Archer, S., Pilling, M., Kenny, M., Hollands, G.J., Marteau, T.M., 2019.Public acceptability of nudging and taxing to reduce consumption of alcohol, to-bacco, and food: a population-based survey experiment. Soc. Sci. Med. 236, 112395.
Ridout, B., Campbell, A., Ellis, L., 2012. ‘O! your Face (book)’: alcohol in online socialidentity construction and its relation to problem drinking in university students. DrugAlcohol Rev. 31, 20–26.
Rocha, T., Amaral, J.S., Oliveira, M.B.P.P., 2016. Adulteration of dietary supplements bythe illegal addition of synthetic drugs: a review. Compr. Rev. Food Sci. Food Saf. 15,43–62.
Rossen, I., Hurlstone, M.J., Lawrence, C., 2016. Going with the grain of cognition: ap-plying insights from psychology to build support for childhood vaccination. Front.Psychol. 7, 1483.
Rozenblit, L.G., 2004. Systematic bias in Knowledge Assessment: An Illusion ofExplanatory Depth. Doctoral dissertation. ProQuest Dissertations PublishingRetrieved from. http://search.proquest.com/docview/305287115/.
Rozin, P., Millman, L., Nemero!, C., 1986. Operation of the laws of sympathetic magic indisgust and other domains. J. Personal. Soc. Psychol. 50, 703.
Salathé, M., Bonhoe!er, S., 2008. The e!ect of opinion clustering on disease outbreaks. J.R. Soc. Interface 5, 1505–1508.
Sanchez, C., Dunning, D., 2018. Overconfidence among beginners: is a little learning adangerous thing? J. Personal. Soc. Psychol. 114, 10–28.
Schultz, S.J., Hotham, E.D., Evans, A.M., 2013. Australian pharmacists' uncertainty abouthomeopathic products in community pharmacy. Focus Altern. Complement. Ther. 19,9–15.
Seeley, R.J., Sandoval, D.A., 2011. Neuroscience: weight loss through smoking. Nature475, 176–177.
Seymour, B., Getman, R., Saraf, A., Zhang, L.H., Kalenderian, E., 2015. When advocacyobscures accuracy online: digital pandemics of public health misinformation throughan antifluoride case study. Am. J. Public Health 105, 517–523.
Simler, K., Hanson, R., 2017. The Elephant in the Brain: Hidden Motives in Everyday Life.Oxford University Press.
Simons, D.J., Chabris, C.F., 1999. Gorillas in our midst: sustained inattentional blindnessfor dynamic events. Perception 28, 1059–1074.
Simons, D.J., Levin, D.T., 1998. Failure to detect changes to people during a real-worldinteraction. Psychon. Bull. Rev. 5, 644–649.
Skaczkowski, G., Durkin, S., Kashima, Y., Wakefield, M., 2018. Influence of premium vsmasked cigarette brand names on the experienced taste of a cigarette after tobaccoplain packaging in Australia: an experimental study. BMC Public Health 18, 295.
Slovic, P., Monahan, J., MacGregor, D.G., 2000. Violence risk assessment and risk com-munication: the e!ects of using actual cases, providing instruction, and employingprobability versus frequency formats. Law Hum. Behav. 24 (3).
Slovic, P., Finucane, M.L., Peters, E., MacGregor, D.G., 2007. The a!ect heuristic. Eur. J.Oper. Res. 177, 1333–1352.
Smith, P., Bansal-Travers, M., O'Connor, R., Brown, A., Banthin, C., Guardino-Colket, S.,Cummings, K.M., 2011. Correcting over 50 years of tobacco industry misinformation.Am. J. Prev. Med. 40, 690–698.
Sporer, S.L., Penrod, S., Read, D., Cutler, B., 1995. Choosing, confidence, and accuracy: ameta-analysis of the confidence-accuracy relation in eyewitness identification stu-dies. Psychol. Bull. 118, 315.
Stoneman, P., Sturgis, P., Allum, N., 2013. Understanding support for complementary and
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
36

alternative medicine in general populations: use and perceived e"cacy. Health(London) 17, 512–529.
Sunstein, C.R., Vermeule, A., 2009. Conspiracy theories: causes and cures. J. PoliticalPhilos. 17, 202–227.
Swire, B., Ecker, U.K.H., Lewandowsky, S., 2017. The role of familiarity in correctinginaccurate information. J. Exp. Psychol. Learn. Mem. Cogn. 43, 1948–1961.
Tabacchi, M.E., Cardaci, M., 2016. Preferential biases for texts that include neu-roscientific jargon. Psychol. Rep. 118, 793–803.
Tannenbaum, M.B., Hepler, J., Zimmerman, R.S., Saul, L., Jacobs, S., Wilson, K.,Albarracin, D., 2015. Appealing to fear: a meta-analysis of fear appeal e!ectivenessand theories. Psychol. Bull. 141, 1178–1204.
Tavris, C., Aronson, E., 2008. Mistakes Were Made (But Not by Me). Mariner Books.Thaler, R.H., Sunstein, C.R., 2009. Nudge: Improving Decisions about Health, Wealth, and
Happiness. Penguin Books, New York: New York.The Faculty of Homeopathy, 2018. The research evidence base for homeopathy. [Web
pdf]. Retrieved from. https://www.britishhomeopathic.org/wp-content/uploads/2018/04/2-page-evidence-summary-for-homeopathy-HRI.pdf.
Tilburt, J.C., Allyse, M., Ha!erty, F.W., 2017. The case of Dr. Oz: ethics, evidence, anddoes professional self-regulation work? AMA J. Ethics 19, 199–206.
Tonin, R., 2018. A review of wind turbine-generated infrasound: source, measurementand e!ect on health. Acoust Aust. 46, 69–86.
U.S. National Institute of Health [NIH], 2016. Americans spent $30.2 billion out-of-pocket on complementary health approaches. June 22, [Press release]. Retrievedfrom. https://nccih.nih.gov/news/press/cost-spending-06222016.
Uscinski, J.E., Parent, J.M., 2014. American Conspiracy Theories. Oxford UniversityPress.
van der Linden, S., 2015. The conspiracy-e!ect: exposure to conspiracy theories (about
global warming) decreases pro-social behavior and science acceptance. Personal.Individ. Di!er. 87, 171–173.
van der Linden, S., Leiserowitz, A., Rosenthal, S., Maibach, E., 2017. Inoculating thepublic against misinformation about climate change. Global Chall. 1, 1600008.
Waddington, F., Naunton, M., Kyle, G., Thomas, J., Cooper, G., Waddington, A., 2015. Asystematic review of community pharmacist therapeutic knowledge of dietary sup-plements. Int. J. Clin. Pharm. 37, 439–446.
Wani, A.L., Ara, A., Bhat, S.A., 2014. Blood injury and injection phobia: the neglectedone. Behav. Neurol. 2014, 71340.
Wechsler, H., Nelson, T.F., Lee, J.E., Seibring, M., Lewis, C., Keeling, R.P., 2003.Perception and reality: a national evaluation of social norms marketing interventionsto reduce college students’ heavy alcohol use. J. Stud. Alcohol 64, 484–494.
Weisberg, D.S., Keil, F.C., Goodstein, J., Rawson, E., Gray, J.R., 2008. The seductive al-lure of neuroscience explanations. J. Cogn. Neurosci. 20, 470–477.
Weisberg, D.S., Taylor, J.C.V., Hopkins, E.J., 2015. Deconstructing the seductive allure ofneuroscience explanations. Judgm. Dec. Making 10, 429–441.
Wilson, P.R., 2014. The art of the con: How to think like a real hustler and avoid beingscammed. Lyons Press.
Wiseman, R., Watt, C., 2006. Belief in psychic ability and the misattribution hypothesis: aqualitative review. Br. J. Psychol. 97, 323–338.
Witte, K., Allen, M., 2000. Meta-Analysis of fear appeals: implications for e!ective publichealth campaigns. Health Edu. Behav. 27, 591–615.
Wood, W., Quinn, J.M., 2003. Forewarned and forearmed? Two meta-analysis synthesesof forewarnings of influence appeals. Psychol. Bull. 129, 119.
Yarritu, I., Matute, H., 2015. Previous knowledge can induce an illusion of causalitythrough actively biasing behavior. Front. Psychol. 6, 389.
D. MacFarlane, et al. 6RFLDO�6FLHQFH��0HGLFLQH�[[[��[[[[��[[[[
��Chapter 2: Protecting consumers from fraudulent health claims
37

38

Foreword for Chapters 3-5
My interest in applying psychology to real-world problems began, as for many
people, with reading the seminal book on cognitive heuristics and biases, Thinking fast and
slow (Kahneman, 2012). The book opened my eyes to the possibility that significant changes
in human behaviour could be achieved through relatively minor tweaks, such as by careful
message framing or choice architecture. Excited by this tantalizing prospect and armed with a
rudimentary knowledge of psychological biases, I sought out PhD supervisors to help put
these insights to the test. When I first pitched my plan—to test the application of
psychological insights to reduce demand for wildlife products—the response from my
prospective supervisors was, “sounds interesting but how are you going to demonstrate an
impact?”
In hindsight, the question seems so obvious that I should have addressed it in my
initial pitch. As it turns out, behaviour-change campaigns routinely fail to demonstrate an
ecologically valid impact of their efforts, instead often relying on “soft” indicators of success,
such as changes to self-reported attitudes, beliefs, or behaviours (Bickman, 1972; Geller,
1981; Kormos & Gifford, 2014). For example, a recent review of demand-reduction
campaigns aimed at wildlife products identified 236 campaigns but found that only five
reported on direct changes in consumer behaviour (Veríssimo & Wan, 2018). Determined not
to repeat this oversight, I set about researching the literature on designing and evaluating
effective behaviour-change interventions. One of the most useful frameworks I found was
“community-based social marketing” (McKenzie-Mohr & Schultz, 2014), which outlined a
five-step approach (Chapters 3-5 apply the first four steps): (1) carefully selecting a target
“end state” behaviour (i.e., a small measurable behaviour as opposed to complex nebulous
concepts like “improving sustainability”); (2) identifying the barriers and benefits associated
Foreword for Chapters 3-5 39

with the selected behaviours; (3) designing interventions to address those barriers and
benefits; (4) piloting the strategy with a small segment of the target community; and (5)
evaluating the impact of the program once it has been broadly implemented.
In seeking to select a target behaviour, I concluded that two key behaviours most
relevant to the success of demand-reduction interventions were: a reduction in the quantity of
a product being purchased and a reduction in perceived product value. I decided to focus on
the latter. I proposed one way to measure a reduction in perceived product value was to run
an experimental auction, where success could be measured against changes in amount
participants bid for products after being exposed to an intervention compared to a control.
This approach had previously been used to pilot-test the impact of graphic health warnings on
consumer willingness-to-pay for cigarettes (Thrasher, Rousu, Hammond, Navarro, &
Corrigan, 2011).
In the auction paradigm closest to the one I ended up using (Becker, DeGroot, &
Marschak, 1964), participants are told they will have the opportunity to bid on a product but,
instead of bidding against other people, they will bid against a random number. This
eliminates the potential confound of competition. Participants are given a small endowment
of money to place a bid amount of their choice. They are told that they will win the auction if
their bid is greater than, or equal to, the random number. Upon winning, participants will then
“purchase” the product by paying the amount specified by the random number and keeping
the remainder of their endowment. If their bid is less than the random number, they get to
keep the full endowment but miss out on purchasing the product. The genius of this measure
is the random number, which makes it in the participants’ best interest to bid only what they
are willing to pay for the product, because placing too high a bid increases the risk of paying
too much and placing too low a bid reduces their chances of obtaining the product.
Foreword for Chapters 3-5 40

One problem with this paradigm is that paying a random amount for a product does
not represent a typical real-life consumer scenario. To remedy this, I adapted the paradigm so
that if participants win, they would pay their bid amount. This adaptation somewhat mimics
the familiar practice of bidding on online auction sites, such as eBay. To test whether the
paradigm would reliably measure willingness-to-pay, I piloted the measure with online
participants against several measures predicted to influence demand.
The results of the pilot, presented in Appendix II, exceeded my expectations.
Specifically, I found strong positive correlations between people’s willingness-to-pay for a
multivitamin and (1) the frequency that people reported having previously used
multivitamins, (2) their estimated belief in the efficacy of multivitamin, and (3) having a
favourable general attitude towards alternative remedies and dietary supplements. These
results provided convergent evidence that the auction mechanism indexed consumer demand
for multivitamin supplements and thus confirmed that the measure was suitable for
demonstrating the impact of the interventions. Using this auction paradigm, Chapters 3-5
present the results of a series of experiments that show how addressing key psychological
barriers can reliably reduce demand for an ineffective health remedy (MacFarlane, Hurlstone,
& Ecker, 2018, 2020).
In addition to this auction, in Chapter 5, I introduce a novel measure of intervention
success—namely, people’s propensity to share misinformation online. The idea for
developing this measure came from my newfound appreciation for viral epidemiology
(thanks to the relentless media coverage of COVID-19). In particular, I came to appreciate
the importance of the growth factor, which measures the rate at which numbers of new cases
are going up or down: if the growth factor is > 1, then the number of new cases increases
exponentially, if the growth rate is < 1, then the number of new cases begins to decrease
exponentially (Siegenfeld & Bar-Yam, 2020). Using the growth rate of virus spread as an
Foreword for Chapters 3-5 41

analogy for the spread of misinformation, it dawned on me that the most important way to
control misinformation may not to be to successfully debunk each falsehood, but instead to
find interventions that prevent the misinformation from spreading to more people.
Essentially, Chapter 5 is a first attempt to test whether a targeted intervention could empower
people to help reduce the rate of spread of misinformation to below one, where it becomes
effectively neutralised.
Foreword for Chapters 3-5 42
References
Becker, G. M., DeGroot, M. H., & Marschak, J. (1964). Measuring utility by a single-
response sequential method. Behavioral Science, 9, 226–232.
Bickman, L. (1972). Environmental attitudes and actions. The Journal of Social Psychology,
87, 323–324.
Geller, E. S. (1981). Evaluating energy conservation programs: Is verbal report enough?
Journal of Consumer Research, 8, 331–335.
Kahneman, D. (2012). Thinking, fast and slow. London: London : Penguin.
Kormos, C., & Gifford, R. (2014). The validity of self-report measures of proenvironmental
behavior: A meta-analytic review. Journal of Environmental Psychology, 40, 359–371.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for
ineffective health remedies: Overcoming the illusion of causality. Psychology and
Health, 33.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Countering demand for
ineffective health remedies: Do consumers respond to risks, lack of benefits, or both?
Psychology and Health. DOI: 10.1080/08870446.2020.1774056
McKenzie-Mohr, D., & Schultz, P. W. (2014). Choosing effective behavior change tools.
Social Marketing Quarterly, 20, 35–46.
Siegenfeld, A. F., & Bar-Yam, Y. (2020). Eliminating COVID-19: The impact of travel and
timing. ArXiv Preprint ArXiv:2003.10086.
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011).
Foreword for Chapters 3-5 43

Estimating the impact of pictorial health warnings and “plain” cigarette packaging:
evidence from experimental auctions among adult smokers in the United States. Health
Policy, 102, 41–48.
Veríssimo, D., & Wan, A. K. Y. (2018). Characterising the efforts to reduce consumer
demand for wildlife products. Conservation Biology. 33, 623–633.
Foreword for Chapters 3-5 44
Chapter 3: Overcoming the illusion of causality
This chapter is presented in the format of a journal article.
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing Demand for Ineffective Health Remedies: Overcoming the Illusion of Causality. Psychology & Health, 33(12), 1472-1489.
1
45

46

+����,��"��-�)��� � �����.�$%%����$�������%$�����.�����$�����(((��$��.��� ���%�"$%� ��&����$�/�.��"$� ��0&����$�)���1������
�������� ������
������������������������ �����!" ��#�������$%�����&�'�������'�(()))*���+,�����*�&(��(�'�"�
-�+%�����+�&��+�,�����,,����.���������&�+����.���&����������%����,���%������
/%�����0��1������2�0��3�$*��%������� �4������5*��*�6�3��
7�������������������������� ��������������������������� ��������� ������ !"#$�%�&� ���&�'�&�(������((� ��)���������'�&���$��)�� �'����������������(� ����*��+�* ����*�������
7����3������������������������ ��������������������������������
���� �������� �������� ������
!��" ��#����$�� %�������� ��&����$��
' �(�)����"$�*��$�$
Chapter 3: Overcoming the illusion of causality
47

Reducing demand for ineffective health remedies:overcoming the illusion of causality
Douglas MacFarlane , Mark J. Hurlstone and Ullrich K. H. Ecker
School of Psychological Science, University of Western Australia, Perth, Australia
ABSTRACTObjective: We tested a novel intervention for reducing demandfor ineffective health remedies. The intervention aimed toempower participants to overcome the illusion of causality, whichotherwise drives erroneous perceptions regarding remedy efficacy.Design: A laboratory experiment adopted a between-participantsdesign with six conditions that varied the amount of informationavailable to participants (N! 245). The control condition receiveda basic refutation of multivitamin efficacy, whereas the principalintervention condition received a full contingency table specifyingthe number of people reporting a benefit vs. no benefit fromboth the product and placebo, plus an alternate causal explan-ation for inefficacy over placebo.Main outcome measures: We measured participants’ willingnessto pay (WTP) for multivitamin products using two incentivizedexperimental auctions. General attitudes towards health supple-ments were assessed as a moderator of WTP. We tested general-isation using ratings of the importance of clinical-trial results formaking future health purchases.Results: Our principal intervention significantly reduced partic-ipants’ WTP for multivitamins (by 23%) and increased their recog-nition of the importance of clinical-trial results.Conclusion: We found evidence that communicating a simplifiedfull-contingency table and an alternate causal explanation mayhelp reduce demand for ineffective health remedies by counter-ing the illusion of causality.
ARTICLE HISTORYReceived 11 January 2018Accepted 25 July 2018
KEYWORDSIllusion of causality;behaviour change; demandreduction; consumerbehaviour; intervention;health education
Irrational health behaviours
Irrational health behaviours—health-promoting actions that are objectively irrationalwhen viewed against the weight of scientific consilience—present numerous harms toindividuals. Example, harms include side effects, financial costs, interactions with con-ventional medications and opportunity costs of delaying evidence-based treatment.The present research deals with one type of irrational health behaviour, namely theconsumption of health remedies that are claimed to have benefits despite contrary sci-entific consilience. Regarding health remedies, consilience may refer to (i) compelling
CONTACT Douglas MacFarlane [email protected] School of Psychological Science,University of Western Australia, M304, 35 Stirling Hwy, Perth 6009, Australia! 2018 Informa UK Limited, trading as Taylor & Francis Group
PSYCHOLOGY & HEALTHhttps://doi.org/10.1080/08870446.2018.1508685
Chapter 3: Overcoming the illusion of causality 48

evidence either supporting or rejecting a remedy’s efficacy, (ii) compelling evidencethat a remedy causes harm or (iii) a lack of compelling evidence to back up the healthclaims being made. One remedy not supported by scientific consilience is multivitaminsupplementation for healthy individuals: numerous randomised controlled trials havefound that multivitamins provide no health benefits (Guallar, Strangers, Mulrow,Appel, & Miller, 2013; Jenkins et al., 2018) and may even be detrimental to health(Mursu, Robien, Harnack, Park, & Jacobs, 2011). Evidence-based interventions are thusneeded to help people avoid the negative consequences of such behaviour.
Designing effective evidence-based interventions to overcome irrational behavioursrequires addressing the barriers preventing the uptake of desired rational behaviours(McKenzie-Mohr & Schultz, 2014). One major psychological barrier that prevents peo-ple from making evidence-based consumer choices is the illusion of causality. The illu-sion occurs when people perceive a causal relationship between an action and asubsequent outcome (Blanco, Matute, & Vadillo, 2011) even when the two events areunrelated, such as taking vitamin C and subsequently recovering from a cold (Hemila &Chalker, 2013). The strength of the illusion increases the more an action coincidentallyoccurs in close temporal proximity to an outcome. The resulting causal illusion is furtherstrengthened when one has personal control over the action preceding the outcome(Yarritu, Matute, & Vadillo, 2014).
Assisting people to overcome illusions of causality is a challenge. Research hasshown that simply giving people the facts is not sufficient (Yarritu & Matute, 2015),and even extended scientific training does not guarantee that people will not succumbto the illusion of causality (Shtulman & Valcarcel, 2012). Part of the reason for thismay be that people are generally only exposed to—or are more likely to remember—positive outcomes (Kelley & Long, 2014). Consider the unsubstantiated link betweentaking vitamin C at the onset of a cold and a faster recovery. The myth that vitamin Ccan speed up recovery is perpetuated by people more readily recalling instances whenthey took vitamin C and subsequently recovered from a cold, compared to instanceswhen they did nothing and recovered all the same. We argue that to overcome the illu-sion of causality, people need timely access to the ‘full picture,’ namely the evidencefrom all four outcomes of a randomised controlled trial. Specifically, people need toknow the number of people who (i) took the product and experienced the benefit, (ii)took the product and experienced no benefit, (iii) did not take the product but stillexperienced the benefit and (iv) did not take the product and experienced no benefit.Information from all four cells in the matrix is needed to confidently conclude whethera benefit is caused by the product (a positive contingency), or whether there was someother causal factor (a null contingency).
Previous research has found that simply providing a contingency table of clinicalresults does not assist people to make reliable causal judgments because interpreta-tions of contingency tables can be faulty, especially when the data being conveyedare complex (Batanero, Ca~nadas, D!ıaz, & Gea, 2015) or when the outcomes challengeprior beliefs (Kahan, Peters, Cantrell & Slovic, 2013). In contrast, one promising studyby Barberia, Blanco, Cubillas, and Matute (2013) found that providing students withdetailed explanations of the ‘full picture’ in an 80-minute class did reduce the illusionof causality. However, this intervention is not particularly efficient given the significant
2 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 49

time and resources required, which is a problem considering the continual need tocommunicate the scientific consilience regarding an ever-expanding range ofhealth products.
To overcome these barriers when communicating clinical findings to the public, wepropose that contingency table information should be simplified to represent smallmanageable frequencies rather than large and complex raw numbers. Research hasshown that when people are given complex proportions they tend to misinterpret thefigures by employing several cognitive biases, such as denominator neglect or avail-ability bias (Gigerenzer, Gaissmaier, Kurz-Milcke, Schwartz, & Woloshin, 2007; Slovic,Finucane, Peters, & MacGregor, 2007). We hypothesised that communicating the infor-mation from all four randomised controlled trial outcomes in a simplified contingencytable will circumvent such cognitive biases, and may thus be a more efficient, andcost-effective, intervention than those used in previous studies. Thus, the aim of thepresent study was to investigate whether a simplified contingency table, accompaniedby a scientifically valid explanation, can promote behaviour change.
To test this hypothesis, the present study sought to measure actual behaviourrather than intention or attitude. This is important because people’s beliefs are notalways reflected in their behaviours (Bickman, 1972; Geller, 1981). This may be due, inpart, to external barriers, such as cost and convenience, preventing a person’s behav-iour from aligning with their beliefs (Gifford, 2014). Consequently, relying on self-reported attitudes can lead researchers to over-report the effectiveness of an interven-tion (Kormos & Gifford, 2014). For example, Rousu and Thrasher (2014) investigatedthe effect of health warning labels on cigarette packages and found that self-reportedattitude changes were two times greater when compared to the change in demandindicated by auction bids on a packet of cigarettes. For this reason, the present experi-ment used two incentivized experimental auctions to measure participants’ willingnessto pay (WTP) for a commercially available multivitamin supplement and thus assessthe effectiveness of a novel intervention on real consumer demand.
The present laboratory experiment adopted a between-participants design with sixconditions. Conditions provided participants with varying amounts of information(detailed descriptions in the method section; also see Figure 1). Most conditions pro-vided information on the results of clinical trials showing that multivitamins were noteffective. Briefly described, the control condition provided irrelevant information com-bined with a weak refutation of multivitamin efficacy. The ‘quarter-contingency’ condi-tion provided the same weak refutation plus information from only one quarter of acontingency table—the number of people reporting a health benefit from multivita-mins. The ‘half-contingency’ condition provided the same weak refutation plus half acontingency table—the number of people who did and did not report a benefit frommultivitamins. The ‘full-contingency’ condition provided a strong refutation plus a fullcontingency table—the number of people reporting a benefit vs. no benefit fromboth multivitamins and placebo. The principal intervention—the ‘full-contingency-plus’condition—replicated the full-contingency condition but also included an alternateexplanation for lack of efficacy over placebo. The ‘positive-contingency’ condition wasthe exception in that it provided a full-contingency table but with the placebo resultsreversed to indicate that multivitamins were actually effective. To reflect the positive
PSYCHOLOGY & HEALTH 3
Chapter 3: Overcoming the illusion of causality 50

results, this condition also included a strong confirmation that multivitaminswere effective.
The primary aim of the experiment was to assess the effectiveness of the principalintervention to reduce demand for an ineffective health product. To assess this, WTPfor two multivitamin products was then measured across two experimental auctions.The main auction enabled participants to bid on one multivitamin product, whereasthe second auction enabled participants to simultaneously bid on two similar prod-ucts, but only one containing added multivitamins. We theorised that the strength ofthe illusion of causality would vary across conditions, thus influencing people’s WTPfor multivitamin products. We expected our strongest experimental intervention tohave the greatest impact on reducing WTP. The secondary aim of the experiment wasto test whether the effects of this principal intervention might generalise to futurehealth purchases.
For the main auction, we made three predictions. Hypothesis I: Compared to control,the principal intervention (the ‘full-contingency-plus condition’) would result in a sig-nificant reduction in average bid amount for the multivitamin product. Hypothesis II:The average bid amounts would vary relative to the strength and direction of the illu-sion of causality conveyed across the remaining experimental conditions. Specifically,we hypothesised that (a) the quarter-contingency condition should have little impacton WTP compared to control because information referring to one cell in a contin-gency table creates only a weak illusion of causality; (b) the half-contingency condition
Figure 1. Visual summary of the information provided to participants in each condition. Sharedboxes indicate where information was identical across conditions. In the contingency table, thenumber below the smiling face represents the relative frequency of people who reported experi-encing a health benefit, and the number below the sullen face represents the relative frequency ofpeople who did not report experiencing a benefit. The explanation provided an interpretation ofthe corresponding contingency table given the information available (i.e. weakly or strongly refut-ing the efficacy of multivitamins when results indicated the null contingency, or strongly confirm-ing the efficacy of multivitamins when results indicated the positive contingency). In the quarter-contingency condition, presenting only one cell of information as a table was not logical soinstead, participants received a statement to the same effect: ‘Countless people have experienced ahealth benefit after taking multivitamins’.
4 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 51

should increase WTP compared to control because it creates a strong illusion of caus-ality; (c) the full-contingency condition should reduce WTP compared to controlbecause it provides the ‘full picture’ required to dispel the illusion of causality; and (d)the positive-contingency condition should increase WTP compared to control becausethe information suggests a true benefit over placebo. Hypothesis III: Compared to theother conditions, participants in the two full-contingency conditions would show (a) agreater rate of identifying that there was insufficient information to determine the effi-cacy of the fictitious health product; and (b) a higher rating of the importance of pla-cebo-comparison information for making future health-related purchases.
For the second auction, we formulated Hypothesis IV: Compared to control, (a) par-ticipants in the principal intervention condition would reduce their WTP for a productcontaining added multivitamins relative to a similar product without; and (b) this rela-tive WTP should vary according to the strength and direction of the illusion of causal-ity conveyed across the remaining experimental conditions.
Method
The research was conducted using recommendations for obtaining quality evidencefor behavioural interventions (Dombrowski, Sniehotta, Avenell & Coyne, 2007).Specifically, the intervention was designed with a theoretical basis, tested via a rando-mised controlled trial, and reported with due regard to accepted CONSORT standardsof reporting for randomised controlled trials (Boutron, Moher, Altman, Schulz, &Ravaud, 2008). Ethics approval to conduct the experiment was granted by the HumanEthics Office of the University of Western Australia in accordance with the require-ments of the Australian National Statement on Ethical Conduct in Human Research(NHRMC, 2007).
Participants
In total, 247 undergraduate students from the University of Western Australia tookpart in the experiment in exchange for course credit. One participant was excluded foraccidentally reading the debrief sheet prior to testing. Several a-priori exclusion criteriawere set (these are specified in the supplemental materials); based on these criteria,one participant was removed for overly inconsistent responding. The final sample thusincluded N = 245 participants (163 females, 82 males; age M = 20.98 years; SD = 6.45).Sample size was determined by an a-priori power analysis (G"Power 3; Faul, Erdfelder,Lang, & Buchner, 2007) that suggested a minimum sample size of 240 to detect amedium-sized effect (f = .25) with a = .05, 1#b = .80.
Predictors and materials
Participants responded to questions on four potential predictors of WTP: previousmultivitamin consumption; belief in the efficacy of multivitamin supplements for main-taining general health; general attitudes toward health supplements and alternativemedicines (hereafter referred to as the ‘general-attitude score’); and current state of
PSYCHOLOGY & HEALTH 5
Chapter 3: Overcoming the illusion of causality 52

health (as people may only consider using multivitamins when they feel unwell). Fulldetails of the predictor measures are provided in the supplemental materials.
Willingness-to-pay
To assess WTP, data were collected using two variations of the Becker–Degroot–Marschakauction mechanism (Becker, Degroot, & Marschak, 1964; Thrasher, Rousu, Hammond,Navarro, & Corrigan, 2011). In the first auction (WTP-1), participants were given $5 andan opportunity to place a bid on a tube of effervescent multivitamin tablets. Theywere shown a plain-packaged picture of the product and some descriptive text aboutmultivitamins, including some common health claims and a popular pseudo-scientificcausal explanation as to why supplements are thought to provide health benefits (seeonline supplement for details). Participants were asked to bid only the amount thatreflected how much they were willing to pay for that product. Participants were toldthat this was different to other auctions in that they could only bid once, and that itwas in their best interest to bid the amount they were willing to pay. Participantswere required to enter their bid amount b in cents b 2 (0, 500). They knew that thisamount would be compared against a random number r 2 (0, 500) drawn from a uni-form distribution, and that if b $ r, they would win the auction and purchase theproduct for amount b but keep 500 – b of their endowment; otherwise they wouldlose the auction but keep the full $5 endowment. Prior to the first auction, partici-pants were given the chance to participate in two hypothetical practice auctions usingan imagined $1 to bid for a bottle of water.
The second auction (WTP-2) was a variation on the first. Specifically, participantswere given an additional $2 endowment which they could use to bid on two productssimultaneously, namely a packet of gummy sweets, and a packet of gummy sweetswith added multivitamins. Participants were required to enter two bid amounts incents, b1 2 (0, 200) and b2 2 (0, 200), subject to the constraint that b1 % b2 & 200.The two bid amounts were compared against two uniformly distributed random num-bers r1 2 (0, 200) and r2 2 (0, 200). The participants knew that they would win andpurchase both products if b1 $ r1 and b2 $ r2; neither product if b1 < r1 and b2 < r2;or only one product if b1 $ r1 but b2 < r2, or b1 < r1 but b2 $ r2. At the end of theexperiment participants kept 200 – o1b1 – o2b2, where o1 is the outcome (1 if success-ful; 0 otherwise) of bid b1, and o2 is the outcome (1 if successful; 0 otherwise) of bidb2. This second auction was included to emulate the real-world scenario where con-sumers face a choice between a product and a similar product containing an add-itional supplementary ingredient (e.g. an added vitamin).
Interventions
Participants were randomly allocated to either a control or one of five interventionconditions (see Figure 1). The intervention conditions all provided participants withtwo information components: (i) a contingency table and (ii) an explanation. The con-tingency table component conveyed information about the clinical outcomes of previ-ous randomised controlled trials that have tested the efficacy of multivitamins. Theamount of information conveyed in each condition was varied in order to manipulate
6 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 53

the strength of the illusion of causality. The information was presented as simple fre-quencies (e.g. clinical trials show 3 out of 4 people experience a benefit). The explan-ation component consisted of a statement that either refuted or confirmed theefficacy of multivitamins.
The control condition only provided irrelevant information about the multivitaminproduct on offer in the first auction: ‘Product A, which you will soon bid on, is avail-able to purchase from various retail outlets in Perth.’ The control also provided a weakrefutation regarding the general efficacy of multivitamins: ‘There is currently insuffi-cient clinical evidence to support a recommendation for or against the use of multivi-tamins and mineral supplements for the general population’. This weak refutation wasbased on a tentative ‘diplomatic’ type of refutation commonly used in real-worldattempts to debunk claims about ineffective health products. In this case, it wasadapted from a statement published on the National Institute of Health (NIH) website(NIH, 2016a).
The quarter-contingency condition provided participants with a quarter of the nullcontingency table—the number of people who took a multivitamin and reported ahealth benefit. As it was not logical to present only one cell of information as a table,participants instead received a statement to the same effect: ‘Countless people haveexperienced a health benefit after taking multivitamins.’ This condition imitates boththe claims made by supplement companies and the relative scarcity of informationoften available when people make health purchases. This condition included the sameweak refutation as the control condition.
The half-contingency condition provided participants with half of the null contin-gency table, specifying the number of people who took a multivitamin and who didand did not report a health benefit. A short interpretation of the numbers was alsoprovided: ‘So, 3 out of 4 people experienced a health benefit after taking a multi-vitamin.’ This condition also imitates real-world advertiser claims although it providesa more powerful illusion of causality than the quarter contingency because it appearsthat a majority of people experience a benefit after taking a product. This conditionincluded the same weak refutation as the control condition.
The full-contingency condition provided participants with all four randomised con-trolled trial outcomes of the null contingency table. A short interpretation of the num-bers in the table was provided: ‘So, 3 out of 4 people experienced the same healthbenefit after taking a multivitamin as after taking a sugar pill.’ As the full contingencytable clearly demonstrated that taking multivitamins resulted in the same health out-comes as a placebo, participants in this condition received a strong refutation:‘Therefore, the clinical evidence clearly shows that, for the general population, there isno health benefit from taking multivitamin supplements.’
The full-contingency-plus condition was our principal intervention. This conditionprovided participants with the same information as the full-contingency conditionwith the addition of a scientific explanation underlying the perceived causal event,that is, explaining why multivitamins are no more effective than taking a sugar pill:‘This is because, unless a person has a specific medical deficiency, most modern dietsprovide ample vitamins for the body to maintain healthy function.’ Previous researchhas shown that providing alternate explanations to perceived causal events helps
PSYCHOLOGY & HEALTH 7
Chapter 3: Overcoming the illusion of causality 54

people overcome the illusion of causality (Vadillo, Matute, & Blanco, 2013). An add-itional precedent for including the alternative causal explanation is based on the litera-ture on refuting misinformation, where the provision of an alternative, factualframework is considered a crucial component of an effective correction(Lewandowsky, Ecker, Seifert, Schwarz, & Cook, 2012).
Finally, the positive-contingency condition provided participants with all four rando-mised controlled trial outcomes of a positive contingency table, demonstrating thatmore people experienced a benefit after taking multivitamins than after taking a sugarpill. A short interpretation of the numbers in the table was also provided: ‘So, 3 out of4 people experienced a health benefit after taking a multivitamin but only 1 out of 4experienced a health benefit after taking a sugar pill.’ As the positive contingencytable clearly communicates that multivitamins are effective, participants in this condi-tion received a strong confirmatory explanation: ‘Therefore, the clinical evidenceclearly shows that, for the general population, there is a health benefit from takingmultivitamin supplements.’ This condition allowed us to assess whether participantswould respond correctly to contingency tables that provide evidence for efficacy.
Fictitious efficacy rating
To assess whether the two full-contingency interventions generalised to reduce theproportion of participants that fell prey to the illusion of causality, following the auc-tion, participants were introduced to a fictional nausea drug ‘Product Z.’ To create anillusion of causality, participants were only given a half-contingency table, whichshowed that 4 out of 5 people experienced a health benefit from taking Product Z.Participants were asked to rate the effectiveness of Product Z as either not effective,mildly effective, very effective, or to indicate there was insufficient information to makea judgement of effectiveness. We hypothesised that the full-contingency table condi-tions would reduce the proportion of individuals who failed to identify there wasinsufficient information to determine causality.
Factors influencing future health purchases
To assess whether the two full-contingency interventions generalised to help partici-pants make better future health purchases, participants were asked to rate the import-ance of 15 health-related factors using a 5-point Likert scale (1 = not important at all,5 = extremely important). This questionnaire was designed to assess whether the full-contingency table increased participants’ valuation of information critical to assessinga product’s efficacy. The critical item was ‘placebo comparison’ information (i.e. ‘thenumber of people who did, and did not, experience a benefit when taking a sugarpill’). The remaining 14 items were distractors (e.g. the importance of ‘advertisingclaims’). Item order was randomised.
Procedure
The experimental sessions were held in a computerised laboratory. In each session,between one and six participants completed the experiment in parallel. Upon entering
8 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 55

the laboratory, participants were shown open money tins containing the cash endow-ments. The experimenter followed a set verbal protocol to make clear that (i) partici-pants would receive real money and/or health products at the end of the experiment,depending on the outcome of the auctions, and that (ii) the results of the survey wereimportant for research so participants should take their time and respond as honestlyas possible. Participants then completed the experiment on one of six computer termi-nals, separated by privacy blinds. Participants first responded to questions on demo-graphics and the predictor measures before being shown the information about themultivitamin product. The experimental software randomly allocated participants toone of the six different conditions. Next, participants were introduced to the first auc-tion and indicated their WTP for the multivitamin product. After bidding in the firstauction, participants were introduced to the second auction and indicated their WTPfor the two gummy sweet products. Participants then responded to the fictional prod-uct question and the questions regarding their future health purchases. At the conclu-sion of the experiment, participants received the leftovers of their cash endowmentsand any purchased health products, before being fully debriefed.
Data analysis
All analyses were conducted in R (R Core Team, version 3.3.2, 2016). Associationsbetween WTP-1 and the four predictors (estimated usage, efficacy belief, general atti-tude scores, and current state of health) were analysed using Spearman’s correlationcoefficient. For WTP-1, to examine the impact of the interventions on bid amounts, weconducted a hierarchical multiple regression analysis with auction bid as the depend-ent variable, and general attitude score and the between-participants factor of condi-tion (control, quarter-contingency, half-contingency, full-contingency, full-contingency-plus, positive-contingency) as the two predictor variables. Hierarchical regression wasemployed over other methods due to the results of a pilot study, which revealed thatthe general-attitude score was a strong predictor of WTP (see supplemental materials).This approach provided a robust model for isolating the effect of the experimentalintervention from a pre-existing moderator of demand. Dummy coding was used toindicate the conditions and specify the control as the baseline. Effect sizes were calcu-lated for each comparison using Pearson’s correlation coefficient. For WTP-2, to testwhether condition influenced bid amounts in the second auction, we calculated aratio for each participant by dividing their bid for the multivitamin gummy sweets bytheir bid for the regular gummy sweets (thus, the higher the ratio the greater the pref-erence for the multivitamin product). To test whether participants’ bid ratio was influ-enced by condition, we conducted a non-parametric Kruskal–Wallace test.
To assess whether the contingency-table interventions generalised into morerational future health decisions, we conducted planned comparisons between so-called‘condition groups’. To explain, for these analyses we grouped the conditions accordingto our a-priori predictions, namely, the ‘full-contingency group’ (full-contingency andfull-contingency-plus conditions), the ‘constrained-information group’ (control, quarter-contingency and half-contingency conditions), and the ‘positive-contingency group’(positive-contingency condition). To determine whether the full-contingency group
PSYCHOLOGY & HEALTH 9
Chapter 3: Overcoming the illusion of causality 56

and the constrained-information group differed in the assessment of the fictionalproduct’s efficacy, we ran a Pearson’s chi-squared test. To simplify our analysis, we firstre-coded the responses into two possible categories: correct (‘insufficient informationto determine efficacy’) and incorrect (‘very effective’, ‘not effective’ or ‘mildlyeffective’). Regarding the survey on factors important for future health purchases, totest whether condition group influenced ratings of placebo-comparison information,we ran an asymptotic Kruskal–Wallace test. Planned comparisons were conductedusing Mann–Whitney U tests with sequential Bonferroni adjustment.
Pilot study
Prior to the current experiment, we conducted an online pilot study on US participantsrecruited via Amazon’s Mechanical Turk (see supplemental materials), which yieldedtwo key findings. First, we obtained convergent evidence that the auction mechanismindexes consumer demand for vitamin supplements in the form of positive correla-tions between hypothetical WTP and the predictor measures of estimated usage, effi-cacy belief, and general attitudes (the fourth, current-health predictor, was added onlyfor the main study). Second, based on the fictional health product scenario and futurehealth purchases questionnaire, we obtained strong evidence that individuals are vul-nerable to the illusion of causality, and that they place relatively little emphasis onclinical information when making health purchases. Thus, the pilot study confirmedthat our survey instruments are suitable for answering the current research questions.
Results
Willingness-to-pay
As anticipated, based on the results of our pilot study, WTP-1 was positively associatedwith estimated usage of multivitamins, N = 158, rs = .19, p = .016; efficacy belief, N =233, rs = .29, p < .001; and general-attitudes, N = 245, rs = .38, p < .001. The controlpredictor of current health state was not correlated with WTP-1, N = 245, rs = .05, p= .41.
In regard to WTP-1, Figure 2 shows the mean WTP across conditions, whereasTable 1 shows the results of the multiple regression analysis. Participants’ general-atti-tude score was significantly related to their WTP, F(1, 243) = 43.45, p < .001, indicatingthat participants with more favourable attitudes toward health supplements exhibitedsignificantly higher WTP for the multivitamin product. After controlling for the influ-ence of the general-attitude score, experimental condition also significantly predictedWTP, F(5, 238) = 7.00, p < .001, indicating that participants’ WTP for multivitamins var-ied reliably across conditions.
More specifically, there was a significant difference in WTP between the full-contin-gency-plus condition and control, t(238) = #2.51, p = .013, 95% CI [#111.39, #13.40],r = .16. We thus found statistical confirmation of Hypothesis I. However, WTP in theremaining intervention conditions did not differ significantly from control: quarter-contingency, t(238) = #0.21, p = .832, [#54.19, 43.62], r = .01; half-contingency, t(238)= 1.83, p = .069, [#3.48, 94.15], r = .12; full-contingency, t(238) = #1.35, p = .179,
10 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 57

[#82.26, 15.44], r = .09; and positive-contingency, t(238) = 1.90, p = .059, [#1.70,95.91], r = .12. We thus reject Hypotheses II(a # d).
In regard to WTP-2, participants’ bid ratios were not significantly different acrossconditions, H(5) = 2.61, p = .76. We thus reject Hypotheses IV(a # b).
Generalisation of condition effects
Differences in participants’ responses to the generalisation questions across the threecondition groups provided partial support for Hypothesis III. Regarding the fictional
Table 1. Hierarchical multiple regression analysis: General-attitude score and condition predictwillingness to pay (WTP-1) in the first auction.
DR2 B SE B b p
Step 1 0.15 <.001Constant #57.24 39.76 .151General-attitude score 87.71 13.30 0.39 <.001"""Step 2 0.10 <.001Constant #71.67 41.20 .0832General-attitude score 93.11 12.82 0.41 <.001"""Quarter-contingency vs. Control #5.29 24.82 #0.07 .832Half-contingency vs. Control 45.34 24.78 0.20 .069Full-contingency vs. Control #33.41 24.80 #0.45 .179Full-contingency-Plus vs. Control #62.39 24.87 #0.27 .013"Positive-contingency vs. Control 47.11 24.78 0.63 .059
Note. B! b-value, SE B! standard error, b! standardised Beta."p <.05, """p< .001.
Figure 2. Willingness to pay (WTP-1)—represented by mean bid amount—as a function of condi-tion for the first auction. The sample size for each intervention condition was n! 41, compared ton! 40 for the control condition. The black horizontal line represents the mean bid amount for thecontrol condition (M! 198.88c). Percentages indicate mean WTP change relative to control. Onlythe full-contingency-plus condition significantly reduced WTP compared to control, whereas theeffects of the other intervention conditions were non-significant. Error bars represent standarderrors. "p! .013.
PSYCHOLOGY & HEALTH 11
Chapter 3: Overcoming the illusion of causality 58

product, there was no difference between the full-contingency and the constrained-information groups, v2(1) = 0.25, p = .61. The odds ratio was 1.16 (0.62, 2.19), meaningthat the odds of an effect reducing the illusion of causality were comparable betweenthese condition groups. We thus reject Hypothesis III(a). Regarding the importance ofplacebo-comparison information, we found an effect of condition group on ratings ofplacebo-comparison information, H(2) = 7.59, p = .02. Post-hoc tests revealed that pla-cebo-information was rated as more important in the full-contingency group (Mdn =4) than in the constrained-information group (Mdn = 3), Ws = 4040, p = .048, r = #.15,and the positive-contingency group (Mdn = 3), Ws = 2090, p = .048, r = #.15. The rat-ing did not differ between the constrained-information and positive-contingencygroups, Ws = 2630, p = .61, r = #.03. We thus found statistical confirmation ofHypothesis III(b), meaning that the full-contingency conditions improved participants’valuation of placebo information, which is critical for making rational consumer deci-sions regarding health products.
Discussion
Summary of findings
The present experiment used an incentivized auction mechanism to examine the fac-tors that predict people’s WTP for multivitamins and the influence of a novel interven-tion for reducing consumer demand. The results of the first auction revealed thatthree factors predicted a greater WTP: (i) more frequent estimated usage, (ii) higherefficacy belief and (iii) a higher general-attitude score. The results from the first auctionalso showed that providing participants with the full-contingency-plus intervention sig-nificantly reduced their WTP for multivitamins compared to control (Hypothesis I). Bycontrast, the other variations of the contingency table (quarter, half, full and positive)had no statistically significant effect on WTP compared to control (Hypothesis II). Thesecond auction explored the impact of each intervention on WTP when consumershave the option to bid on two comparable products (only one of which containedadded multivitamins) simultaneously but found no significant differences in WTPacross conditions (Hypothesis IV). A secondary aim was to assess whether our interven-tion had a general effect on people’s decisions regarding future health purchases(Hypothesis III). At variance with our expectations, participants exposed to the twofull-contingency conditions were not significantly better than participants in the otherconditions at identifying the lack of sufficient information to assess the efficacy of afictional product. However, participants exposed to the two full-contingency condi-tions did rate the importance of placebo-comparison information as higher than thosein the other conditions.
Our results demonstrate the potential impact of a novel intervention for reducingdemand for products that have no health benefits. We have provided preliminary evi-dence that this intervention may be more effective at reducing WTP for ineffectiveproducts than the ‘diplomatic’ refutation commonly used by health authorities (e.g.‘there is currently no evidence that product X produces health benefits’). Furthermore,our results are likely more ecologically valid than previous studies—which have pre-dominantly used measures found to often over-estimate the effects of interventions,
12 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 59

such as self-reported attitude change (Webb & Sheeran, 2006) or peoples’ own esti-mated valuations (List & Gallet, 2001)—because the effect was demonstrated using anaturalistic auction mechanism.
The present experiment serves as a proof of concept that employing simplified fre-quency values within a contingency table can help overcome the illusion of causality.This finding provides evidence that health authorities may benefit from simplifyingclinical outcomes to empower people to make rational health decisions, without ofcourse distorting the clinical findings. This may be especially feasible in cases wherethere is overwhelming scientific consilience regarding a particular health remedy. Ifour results can be replicated, this would suggest that health authorities should aim tohelp people overcome the illusion of causality by communicating both the full pictureof randomised controlled trial outcomes and providing a valid alternative causalexplanation. We now consider why both components may be necessary.
Why might the intervention work?
The ‘full-picture’ component may operate in two ways. First, it could remove onepotential barrier to accepting clinical-trial information, namely the impact of a per-ceived experienced benefit. The full picture provides a simple counter-explanation,highlighting that a person may have experienced the same benefit even after placebotreatment. Second, the full picture may empower participants to overcome their ten-dency to rely on intuitive thinking (Lindeman, 2011) by increasing their own under-standing of the scientific approach, and consequently their acceptance of clinical-trialinformation. The full picture fosters comprehension of the logic behind randomisedcontrolled trials by highlighting why all four cells of a contingency table are critical,and by simplifying large complex results into a meaningful pattern of comprehensibleunits (i.e. a small number of individuals that can be easily visualized). The latterexplanation was supported by our finding that the full-contingency conditions subse-quently increased participants’ rating of the importance of placebo-comparison infor-mation for making health-related consumer decisions. The intervention may thusempower people to better comprehend null-contingency findings of clinical trials.
The ‘alternate causal explanation’ component may operate by replacing partic-ipants’ previously held pseudoscientific beliefs about why a product might be effect-ive, such as ‘supplements boost the immune system.’ This component may serve to fillthe mental gap created when a prior belief is challenged by scientific evidence (Ecker,Lewandowsky, & Tang, 2010; Johnson & Seifert, 1994). The importance of this step wassupported by the finding in the first auction that a full-contingency table on its owndid not significantly reduce WTP. Thus, interventions based on contingency informa-tion may only be effective when accompanied by an alternative explanation thatserves to replace previously held, but unfounded, causal explanations.
Despite the success of the first auction, we were unable to detect a significanteffect of our principal intervention in the second auction (Hypothesis IV). There areseveral explanations for this. First, both products were identical except that one con-tained something additional (in this case vitamins) and may have thus been perceivedby participants to offer better value for money. Thus, the effect of the intervention
PSYCHOLOGY & HEALTH 13
Chapter 3: Overcoming the illusion of causality 60
may have been offset by a purely economic value judgement. Second, participantsmay have concluded that a supplement might still be worth taking despite the lack ofefficacy, as it may provide some benefit not yet proven by science. This reasoningseems especially plausible given that no information was provided on potential harmsof multivitamin supplementation. Alternatively, as the intervention information wasnot repeated prior to the second auction, participants may not have generalised theintervention information to the second auction; instead, participants may haveascribed the intervention information only to the specific multivitamin product in thefirst auction. Indeed, our secondary analyses provided some evidence for this explan-ation. Specifically, participants in the two full-contingency conditions were not signifi-cantly better than those in the other conditions at correctly identifying that there wasinsufficient information to assess the efficacy of the fictional product. This may suggestthat illusions of causality are particularly persuasive in novel situations.
Potential limitations
One potential limitation of the study may have been the creation of demand charac-teristics through two avenues. First, the possibility of winning both multivitamin prod-ucts may have driven down the bid price and contributed to general bidding noise.Indeed, this possibility was considered prior to running the experiment and was thereason why the second auction (WTP-2) was only presented and explained after themain auction (WTP-1). Second, as students knew they were contributing to research,this might have led them to behave more rationally than otherwise, which may havereduced external validity (Nessim & Dodge, 1995). However, the effects were likelynegligible, as previous research has shown that the Becker–Degroot–Marschak auctionmechanism elicits WTP estimates comparable to real transactions (Miller, Hofstetter,Krohmer, & Zhang, 2012).
Another potential limitation may stem from recruiting only university students.Previous research has suggested that university samples can be relatively atypical ofthe global population, which would necessarily limit the applicability of findings tothe broader populace (Henrich, Heine, & Norenzayan, 2010). However, as young,health-conscious adults present a key target audience for supplement consumption,the sample participants were likely suitable for the present study. Furthermore, onestudy designed to empirically test differences in auction behaviour between studentand non-student populaces found no significant variation in WTP in an auction for avitamin-supplemented rice product (Depositario, Nayga, Wu, & Laude, 2009).Nevertheless, it will be informative for future work to establish whether the interven-tion effect does indeed generalise to a broader populace, and to a range of differentirrational remedies.
Implications
Our results provide a contribution to the literature by demonstrating a novel applica-tion for evidence-based behaviour change campaigns; that is, they could be used toreduce demand for irrational health remedies. This departs from the previous
14 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 61

emphasis on reducing demand for products that are plainly harmful, such as ciga-rettes, alcohol, and junk food. This novel application is of practical significancebecause irrational health remedies present a mostly overlooked threat to public health.For example, dietary supplements have been linked to an increase in mortality (Mursuet al., 2011), a reduction in effectiveness of life-saving drugs (Byard & Musgrave, 2010)and a host of unwanted side effects (Bjelakovic et al., 2014).
Our results are also noteworthy because they suggest a comparable impact to analready established health intervention. The effect we observed—a 23% decrease inWTP for a multivitamin product—is comparable to the effect reported by Thrasheret al. (2011), who observed an 18% decrease in WTP for cigarettes from an interven-tion that combined plain packaging with health warning labels. Our results are promis-ing given the impact that health warning labels have had on reducing public demandfor cigarettes. To illustrate, one study found that nearly 44% of former smokersreported that health warning labels had helped them quit smoking (Department ofHealth and Aged Care, 2000). Our study provides preliminary evidence for a compar-able intervention for health and science communicators to reduce demand for prod-ucts that falsely claim to provide health benefits.
Concluding remarks
The current study presents preliminary evidence that consumer choices are influencedby the illusion of causality. We have demonstrated that targeting this illusion by givingpeople a simplified contingency table that summarises the full outcomes of a rando-mised controlled trial, plus a scientifically valid causal explanation for why a healthproduct is ineffective, may reduce consumer demand for products that claim to havea health benefit despite contrary scientific consilience. This intervention may thereforeoffer an effective lever by which health authorities and science communicators canreduce demand for irrational health remedies.
Acknowledgements
We are grateful to Simon Farrell and Carmen Lawrence for their comments during the design ofthe study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
This research was facilitated by an Australian Government Research Training ProgramScholarship awarded to the first author.
ORCID
Douglas MacFarlane http://orcid.org/0000-0003-4378-9294Ullrich K. H. Ecker http://orcid.org/0000-0003-4743-313X
PSYCHOLOGY & HEALTH 15
Chapter 3: Overcoming the illusion of causality 62
References
Batanero, C., Ca~nadas, G. R., D!ıaz, C., & Gea, M. M. (2015). Judgment of association betweenpotential factors and associated risk in 2' 2 tables: A study with psychology students. TheMathematics Enthusiast, 12, 347.
Barberia, I., Blanco, F., Cubillas, C. P., & Matute, H. (2013). Implementation and assessment of anintervention to debias adolescents against causal illusions. PLoS One, 8 e71303. doi:10.1371/journal.pone.0071303
Becker, G. M., Degroot, M. H., & Marschak, J. (1964). Measuring utility by a single-responsesequential method. Behavioral Science, 9, 226.
Bickman, L. (1972). Environmental attitudes and actions. The Journal of Social Psychology, 87,323–324. doi:10.1080/00224545.1972.9922533
Bjelakovic, G., Gluud, L. L., Nikolova, D., Whitfield, K., Wetterslev, J., Simonetti, R. G., … Gluud, C.(2014). Vitamin D supplementation for prevention of mortality in adults. Cochrane DatabaseSystematic Review, CD007470. doi:10.1002/14651858.CD007470.pub3
Byard, R. W., & Musgrave, I. (2010). Herbal medicines and forensic investigations. ForensicScience, Medicine, and Pathology, 6, 81–82.
Boutron, I., Moher, D., Altman, D. G., Schulz, K. F., & Ravaud, P. (2008). Methods and processes ofthe CONSORT group: Example of an extension for trials assessing nonpharmacologic treat-ments. Annals of Internal Medicine, 148, 60–66. doi:10.7326/0003-4819-148-4-200802190-00008-w1
Department of Health and Aged Care. (2000). Evaluation of the health warnings and explanatoryhealth messages on tobacco products. Retrieved from http://webarchive.nla.gov.au/gov/20140801095002/http://www.health.gov.au/internet/main/publishing.nsf/Content/tobacco-warn-review
Depositario, D. P. T., Nayga, R. M., Wu, X., & Laude, T. P. (2009). Should students be used as sub-jects in experimental auctions? Economics Letters, 102, 122–124. doi:10.1016/j.econlet.2008.11.018
Dombrowski, S. U., Sniehotta, F. F., Avenell, A., & Coyne, J. C. (2007). Current issues and futuredirections in Psychology and Health: Towards a cumulative science of behaviour change: Docurrent conduct and reporting of behavioural interventions fall short of best practice?Psychology & Health, 22, 869–874. doi:10.1080/08870440701520973
Ecker, U. K. H., Lewandowsky, S., & Tang, D. T. W. (2010). Explicit warnings reduce but do noteliminate the continued influence of misinformation. Memory & Cognition, 38, 1087–1100.doi:10.3758/MC.38.8.1087
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G"Power 3: A flexible statistical poweranalysis program for the social, behavioural and biomedical sciences. Behavior ResearchMethods, 39(2), 175–195.
Geller, E. S. (1981). Evaluating energy conservation programs: Is verbal report enough? Journal ofConsumer Research, 8, 331–335.
Gifford, R. (2014). Environmental psychology matters. Annual Review of Psychology, 65, 541–579.Gigerenzer, G., Gaissmaier, W., Kurz-Milcke, E., Schwartz, L. M., & Woloshin, S. (2007). Helping
doctors and patients make sense of health statistics. Psychological Science in the PublicInterest, 8, 53–96.
Guallar, E., Strangers, S., Mulrow, C., Appel, L. J., & Miller, E. R. (2013). Enough is enough: Stopwasting money on vitamin and mineral supplements. Annals of Internal Medicine, 159,850–851.
Henrich, J., Heine, S. J., & Norenzayan, A. (2010). Beyond WEIRD: Towards a broad-based behav-ioral science. Behavioral and Brain Sciences, 33(2-3), 111–135. doi:10.1017/s0140525x10000725
Hemila, H., & Chalker, E. (2013). Vitamin C for preventing and treating the common cold.Cochrane Database Systematic Reviews, CD000980. doi:10.1002/14651858.CD000980.pub4
16 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 63

Jenkins, D. J. A., Spence, J. D., Giovannucci, E. L., Kim, Y. I., Josse, R., Vieth, R., … Sievenpiper,J. L. (2018). Supplemental vitamins and minerals for CVD prevention and treatment. Journal ofthe American College of Cardiology, 71, 2570–2584. doi:10.1016/j.jacc.2018.04.020
Johnson, H. M., & Seifert, C. M. (1994). Sources of the continued influence effect: When misinfor-mation in memory affects later inferences. Journal of Experimental Psychology: Learning,Memory, and Cognition, 20, 1420. doi:10.1037/0278-7393.20.6.1420
Kahan, D. M., Peters, E. D., Cantrell, E., & Slovic, P. (2013). Motivated numeracy and enlightenedself-government. (Public Law Working Paper No. 307). Yale Law School. Retrieved from SSRN:http://dx.doi.org/10.2139/ssrn.2319992
Kelley, A. M., & Long, C. P. (2014). Learning by seeing before learning by doing: The role ofobservation and intervention in learning direct and inverse relationships. Journal ofPsychology, 2, 45–69.
Kormos, C., & Gifford, R. (2014). The validity of self-report measures of proenvironmental behav-ior: A meta-analytic review. Journal of Environmental Psychology, 40, 359–371. doi:10.1016/j.jenvp.2014.09.003
Lewandowsky, S., Ecker, U. K. H., Seifert, C. M., Schwarz, N., & Cook, J. (2012). Misinformation andits correction: Continued influence and successful debiasing. Psychological Science in thePublic Interest, 13, 106–131. doi:10.1177/1529100612451018
Lindeman, M. (2011). Biases in intuitive reasoning and belief in complementary and alternativemedicine. Psychology & Health, 26, 371–382. doi:10.1080/08870440903440707
List, J. A., & Gallet, C. A. (2001). What experimental protocol influence disparities between actualand hypothetical stated values? Environmental and Resource Economics, 20, 241–254.
McKenzie-Mohr, D., & Schultz, P. W. (2014). Choosing effective behavior change tools. SocialMarketing Quarterly, 20, 35–46. doi:10.1177/1524500413519257
Miller, K. M., Hofstetter, R., Krohmer, H., & Zhang, Z. J. (2012). Measuring consumers’ willingessto pay: Which method fits best? GfK Marketing Intelligence Review, 4, 42–49.
Mursu, J., Robien, K., Harnack, L. J., Park, K., & Jacobs, D. R. J. (2011). Dietary supplements andmortality rate in older women: the Iowa Women’s Health Study . Archives of Internal Medicine,171(18), 1625–1633.
Nessim, H., & Dodge, R. (1995). Pricing policies and procedures. London: MacMillan Press.National Health and Medical Research Council. (2007). National statement on ethical conduct in
human research (2007) – Updated December 2013 (the National Statement), Commonwealthof Australia, Canberra.
National Institute of Health. (2016a). Vitamins and minerals. Retrieved from https://nccih.nih.gov/health/vitamins.
National Institute of Health. (2016b). Americans spent $30.2 billion out-of-pocket on complemen-tary health approaches [Press release]. Retrieved from https://nccih.nih.gov/news/press/cost-spending-06222016
R Core Team (Version 3.3.2) [Computer Software] (2016). R: A language and environment for stat-istical computing. Vienna, Austria: R Foundation for Statistical Computing.
Rousu, M. C., & Thrasher, J. F. (2014). Examining the relationship between psychosocial andbehavioral proxies for future consumption behavior: Self-reported impact and bidding behav-ior in an experimental auction study on cigarette labeling. Health Education Research, 29,183–194. doi:10.1093/her/cyt114
Shtulman, A., & Valcarcel, J. (2012). Scientific knowledge suppresses but does not supplant ear-lier intuitions. Cognition, 124, 209–215. doi:10.1016/j.cognition.2012.04.005
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2007). The affect heuristic. EuropeanJournal of Operational Research, 177, 1333–1352. doi:10.1016/j.ejor.2005.04.006
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011). Estimating theimpact of pictorial health warnings and "plain" cigarette packaging: Evidence from experi-mental auctions among adult smokers in the United States. Health Policy, 102, 41–48. doi:10.1016/j.healthpol.2011.06.003
Vadillo, M. A., Matute, H., & Blanco, F. (2013). Fighting the illusion of control: How to make useof cue competition and alternative explanations. Universitas Psychologica, 12, 261–2270.
PSYCHOLOGY & HEALTH 17
Chapter 3: Overcoming the illusion of causality 64

Webb, T. L., & Sheeran, P. (2006). Does changing behavioral intentions engender behaviorchange? A meta-analysis of the experimental evidence. Psychological Bulletin, 132, 249–268.doi:10.1016/j.jenvp.2013.04.003
Yarritu, I., Matute, H., & Vadillo, M. A. (2014). Illusion of control: The role of personal involve-ment. Experimental Psychology, 61, 38–47.
Yarritu, I., & Matute, H. (2015). Previous knowledge can induce an illusion of causality throughactively biasing behavior. Frontiers in Psychology, 6, 1–12. doi:10.3389/fpsyg.2015.00389
18 D. MACFARLANE ET AL.
Chapter 3: Overcoming the illusion of causality 65

66

Chapter 4: Do consumers respond to risks, lack of
benefits, or both?
This chapter is presented in the format of a journal article.
MacFarlane, D., Hurlstone, M., & Ecker, U. Countering Demand for Ineffective Health Remedies: Do Consumers Respond to Risks, Lack of Benefits, or Both? Psychology & Health.
67

68
*����+�����,�(��� � �����-� &&���� �������& ��#��-����� ����������� ��-��� ���&�� &� ��'���� �.�-��� � ��/'���� �(���0������
�������� ������
������������������������ �����!" ��#�������$%�����&�'�������'��(()))*���+,�����*�&(��(�'�"�
-%��������+�&��+�,�����,,����.��������&�+�����/����%&�������'�+������0�1����0�,2���,���1���2�3
/%�����4��5������1�4��0�$*��%������� �6������7*��*�8�0��
9�������������������������� ��������������������������� ��������� ������ � !"#����������$�%�$�&������&&� ��'���������%�$���"���� ����%�������(��$����������� ���&)���&��������)���*��+�, ����,����������-."�/ �/ 0 1 002 334�� � �/223 54
9����0������������������������ ��������������������������������
� ������������� �!�� ��� ��
"�#� �������� ������$��������
%�#� ��!���� �� &�������� ��'���� ��
� ������ ���� �� &����
� ���(����� �)�� �
Chapter 4: Do consumers respond to risks, lack of benefits, or both?
69

Countering demand for ineffective health remedies: Doconsumers respond to risks, lack of benefits, or both?
Douglas MacFarlanea , Mark J. Hurlstonea,b and Ullrich K. H. Eckera
aSchool of Psychological Science, University of Western Australia, Perth, Australia; bDepartment ofPsychology, Lancaster University, UK
ABSTRACTObjective: We tested whether targeting the illusion of causalityand/or misperceptions about health risks had the potential toreduce consumer demand for an ineffective health remedy (multi-vitamin supplements).Design: We adopted a 2 (contingency information: no/yes) ! 2(fear appeal: no/yes) factorial design, with willingness-to-pay as thedependent variable. The contingency information specified, in tableformat, the number of people reporting a benefit vs. no benefitfrom both multivitamins and placebo, plus a causal explanation forlack of efficacy over placebo. The fear appeal involved a summaryof clinical-trial results that indicated multivitamins can cause healthharms. The control condition received only irrelevant information.Main outcome measure: Experimental auctions measured peo-ple’s willingness-to-pay for multivitamins. Experiment 1 (N" 260)elicited hypothetical willingness-to-pay online. Experiment 2(N" 207) elicited incentivised willingness-to-pay in the laboratory.Results: Compared to a control group, we found independenteffects of contingency information (-22%) and the fear appeal(-32%) on willingness-to-pay. The combination of both interven-tions had the greatest impact (-50%) on willingness-to-pay.Conclusion: We found evidence that consumer choices are influ-enced by both perceptions of efficacy and risk. The combinationof both elements can provide additive effects that appear super-ior to either approach alone.
ARTICLE HISTORYReceived 10 March 2020Accepted 18 May 2020
KEYWORDShealth psychology; healthcommunication; fear appeal;risk estimation;complementary andalternative medicine (CAM)
Ineffective health remedies
The consumption of ineffective health remedies—remedies that are untested, or foundto be ineffective, or even harmful—causes extensive and persistent harms to individu-als. Harms include side-effects, financial costs, interactions with conventional medica-tions, and opportunity costs of delays in getting critical diagnoses and effectivetreatment (U.S. Food & Drug Administration [FDA], 2019; Macfarlane et al., 2020). Anexample of such a remedy is multivitamin supplementation (hereafter, ‘multivitamins’)
CONTACT Douglas MacFarlane [email protected] School of Psychological Science,University of Western Australia, Perth, Australia.
Supplemental data for this article is available online at https://doi.org/10.1080/08870446.2020.1774056.! 2020 Informa UK Limited, trading as Taylor & Francis Group
PSYCHOLOGY & HEALTHhttps://doi.org/10.1080/08870446.2020.1774056
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 70

for healthy individuals, which extensive clinical testing has shown to be ineffective(Bjelakovic et al., 2012; Guallar et al., 2013; Jenkins et al., 2018) and potentially harmful(Mursu et al., 2011). Evidence-based interventions are thus needed to protect consum-ers from misleading claims about such remedies.
One approach to designing evidence-based interventions is to target the psycho-logical mechanisms that drive demand for health remedies (Macfarlane et al., 2020).The perception that multivitamins are beneficial (i.e., the perception of efficacy), forexample, is often driven by a mechanism known as the illusion of causality, whichoccurs when people perceive a causal relationship between an action (e.g., consuminga multivitamin) and a subsequent but unrelated outcome (e.g., feeling healthy).
One recent study (Macfarlane et al., 2018b) showed that a novel way to overcomethe illusion of causality is to communicate clinical trial outcomes in a simplified contin-gency table—a table showing the number of people reporting a benefit vs. no benefitfrom taking a treatment (e.g., a multivitamin) or a placebo—in combination with analternative causal explanation why a treatment did not cause a benefit over placebo.This contingency-information intervention is thought to work through two mecha-nisms. First, it communicates simplified clinical results—using small, cognitively-man-ageable frequencies rather than complex probabilities—showing the lack of benefitsfor a product (e.g., 3 out of 4 people experienced the same benefit from taking amultivitamin as from taking a placebo sugar pill). Communicating simplified clinicalresults is important because when people are given complex proportions, they tend tomisinterpret the results through several cognitive biases such as denominator neglect(i.e., when probability estimates are skewed by disproportional attention to absolutenumbers over the actual proportion) or availability bias (i.e., the tendency to believethat examples that come readily to mind are representative of reality; see Gigerenzeret al., 2007; Slovic et al., 2007; Yamagishi, 1997 ). Second, the contingency interventionfills the mental gap left by debunking a previously held belief (e.g., “supplements boostthe immune system’; see Ecker, Lewandowsky, & Tang, 2010) by providing an explan-ation for the lack of benefits (e.g., ‘most modern diets provide ample vitamins for thebody to maintain healthy function’). Whilst this previous study found promising resultsof the contingency information intervention using an experimental auction—namely a23% reduction in willingness-to-pay for a multivitamin product—the study needs to bereplicated to have confidence that the effect is robust.
One aim of the present study was thus to replicate our previous finding. We alsoaimed to test whether the contingency intervention could be strengthened by concur-rently targeting another psychological driver of consumer demand, namely the beliefthat alternative, or ‘natural’, health remedies are harmless. This perception drivesdemand through two key mechanisms. First, a perceived lack of harm encourages peo-ple to experiment more frequently with a remedy (to obtain a desired outcome, suchas recovering from a cold), which strengthens the illusion of causality by repeatedlyreaffirming the association of the action (consuming a remedy) with a subsequentunrelated outcome (feeling healthy). Second, a perceived lack of harm can increasepeople’s belief that a product is also beneficial through an ‘affect heuristic’ (Finucane,Alhakami, Slovic, & Johnson, 2000)— whereby people tend to judge risks and benefitsas negatively correlated even when the nature of the benefits is both distinctively and
2 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 71

qualitatively different from the nature of the risks (see Alhakami & Slovic, 1994;Fischhoff et al., 1978; Slovic et al., 2007). While this heuristic enables us to make quickjudgements, it also leaves us vulnerable to manipulation, especially when there is lessopportunity for analytical deliberation. For example, if an antibiotic is portrayed as lowin risk, this contributes to the perception that it is also high in benefit, and vice versa.Equally, if cancer screening is portrayed as low in benefit, this contributes to the per-ception that it is also high in risk, and vice-versa (Ghanouni et al., 2017). In otherwords, evaluations of risks and benefits tend to be causally determined, meaning thatthe perception of one attribute can be influenced by manipulating information aboutthe other (Finucane et al., 2000). Therefore, if a remedy is portrayed as having no ben-efits and also potential harms then both factors should work in the same direction toreduce people’s perception of overall value.
This prediction challenges the often-assumed dichotomy that health communica-tions should only be framed around either benefits or harms. In other words, muchresearch has advocated for either negative or positive messages (Akl et al., 2011;Gallagher & Updegraff, 2012; Jung & Villegas, 2011; Kok et al., 2018; O’Keefe & Jensen,2008; Riet et al., 2008). However, as others have argued (Kidd, Bekessy, & Garrard,2019; McAfee & Connell, 2019; Peters et al., 2018), to change complex behaviour, amore sophisticated approach may be needed that acknowledges the relevance ofboth frames and the balance between them depending on context.
Thus, in two experiments we sought to test whether augmenting the contingencyintervention (countering the perception of efficacy) with a fear-inducing interventioncommunicating information about potential harms would yield a reduction in willing-ness-to-pay for multivitamins greater than that observed for the contingency interven-tion alone (while also assessing the fear appeal’s individual effect). Such fearappeals—persuasive messages that depict a personally relevant and significant threatand outline a feasible recommendation to avoid the harm; see Witte, 1994—havebeen used in previous research to instigate behaviour change (for a review, seeTannenbaum et al., 2015).
We made two key predictions. First, consistent with our earlier study, we expected amain effect of contingency information, with stated willingness-to-pay lower in the pres-ence versus absence of simplified contingency information (i.e., we expected the contin-gency information to reduce bid amounts; Hypothesis 1). Second, and new to thecurrent study, we expected a main effect of fear appeal, with willingness-to-pay lowerwith versus without a fear-inducing message (i.e., we expected the fear appeal to reducebid amounts; Hypothesis 2). We had two additional research questions: first, whetherthere would be an interaction between the contingency information and the fear-appealinterventions, and second, whether the effects of the two interventions differed signifi-cantly from each other (i.e., which intervention had the greatest impact on bid amounts).
Method
This research was conducted in accordance with recommendations for obtaining qual-ity evidence from behavioural interventions (Dombrowski et al., 2007). In particular,the intervention was designed with a theoretical basis, tested via a randomised
PSYCHOLOGY & HEALTH 3
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 72

controlled trial, and reported with due regard to accepted CONSORT standards ofreporting for randomised controlled trials (Boutron et al., 2008). Ethics approval toconduct both experiments was granted by the Human Ethics Office of the Universityof Western Australia in accordance with the requirements of the Australian NationalStatement on Ethical Conduct in Human Research (NHMRC, 2007).
Experiment 1
Participants
A sample of 260 online U.S.-based participants was recruited via Amazon’s MechanicalTurk (MTurk)—an online labor market in which employers pay users for completingshort tasks known as Human Intelligence Tasks (HITs)1. Sample size was informed byan a-priori power analysis (G#Power 3; Faul et al., 2007) that suggested a minimumsample size of 180 to detect a medium-sized effect (f " .25) with a " .05, 1 - b " .80.Participants were paid at a rate of US $7.25/hour pro rata (US federal minimum wage).Two key eligibility criteria were also set to ensure quality data (Peer et al., 2014),namely a HIT-approval rate of greater than 97% and the requirement to have previ-ously completed at least 5,000 HITs.
Several a-priori exclusion criteria were applied to remove careless responders(Oppenheimer et al., 2009). Participants were excluded who (i) gave non-differentiatedanswers to every question in a survey block (Hamby & Taylor, 2016); (ii) completed asurvey block in less than the allocated minimum reading time (i.e., > 600 words perminute; Carver, 1985); or (iii) responded erratically, with overly inconsistent responsesbetween pairs of equivalent questions (i.e., an odd/even threshold of > 2 Likert pointsapart; Curran, 2016). Responses from a further 7 participants were removed due to asystem error (no condition was attributed to these participants). Final sample size wasthus N" 179 (90 females, 89 males; age M" 40.76, SD" 11.47)2.
Design
The experiment adopted a 2 (contingency information: no/yes) ! 2 (fear appeal: no/yes) between-participants design, with bid amount (willingness-to-pay) as the depend-ent variable. Participants were randomly allocated to one of the four intervention con-ditions subject to the constraint of equal cell numbers.
Predictors and materials
We measured three potential predictors of willingness-to-pay by asking participants(1): whether they had taken multivitamins in the past, and if so, to estimate their pre-vious usage frequency on an eight-point scale (1" not in the past few years, 8" everyday); (2) to rate their belief in the effectiveness of the routine consumption of multivi-tamins for maintaining general health (hereafter, ‘efficacy-belief’), using a 5-point scale(1" not effective at all, 5" extremely effective; a sixth point was included in the scaleso that participants could respond ‘I don’t know’); and (3) to estimate their current
4 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 73

state of health using a 4-point scale (1 " ‘Fine, healthy’, 4 " ‘Sick, exhausted’; as peo-ple may only consider using multivitamins when they feel unwell).
A fourth predictor of willingness-to-pay was participants’ general attitudes towardhealth supplements and alternative medicines (as prior beliefs can moderate responsesto health messaging; Myers, 2014). General attitudes were assessed using an 18-itemquestionnaire. Each item consisted of a statement relating to a motivation for consum-ing alternative health products (e.g., ‘Vitamins are natural, and supplements are there-fore safe’ or ‘Vitamin supplements are only useful if a person has a specificdeficiency’). Participants were asked to rate how much they agreed with each state-ment using a 5-point Likert scale (1" strongly disagree; 5" strongly agree). A compos-ite score was calculated for each participant, which indicated their general attitudetowards health supplements and alternative medicines (hereafter, ‘general-attitude’).To measure response consistency, each item was paired with a reverse-phrased state-ment of similar meaning (i.e., 9 pairs of items). The order of items in the general-atti-tude scale was randomised to control for order effects. The full general-attitude scalecan be found in (Macfarlane et al., 2018a).
Willingness-to-pay
To assess willingness-to-pay, data were collected using a variation of the Becker-Degroot-Marschak auction mechanism (Becker et al., 1964; Thrasher et al., 2011).Participants were asked to participate in a hypothetical auction and imagine they hadbeen given $5. In the auction, participants were given an opportunity to place a hypo-thetical bid on a tube of effervescent multivitamin tablets. Participants were shown aplain-packaged picture of the product and a general text about the product (e.g.,‘… comes in a small tube of 10 tablets…’). Participants were asked to place a hypo-thetical bid for only the amount that reflected how much they were willing to pay forthat product. Participants were told that this was different to other auctions in thatthey could only bid once, and that it was in their best interest to bid the amount theywere willing to pay for the product. Participants were required to enter their bidamount b in cents, with b 2 (0, 500). They knew that this amount would be comparedagainst a random number r 2 (0, 500) drawn from a uniform distribution, and that ifb$ r, they would win the auction and would purchase the product for amount b butkeep 500 – b of their endowment; otherwise they would lose the auction but wouldkeep the full hypothetical endowment. Prior to the auction, participants were giventhe chance to participate in multiple hypothetical practice auctions to ensure theyunderstood how the auction worked. To mitigate against hypothetical bias, weemployed two established bias-reduction techniques (Penn & Hu, 2018), namely‘cheap-talk’—asking participants to behave as they would if the auction was real(Cummings & Taylor, 1999) and consequentiality—reminding participants that theresults of this study would have implications for significant public-health issues.
Self-efficacy
As the impact of fear appeals has been hypothesised to depend in part on a person’sself-efficacy (Cooper et al., 2014: Peters et al., 2018)—the perceived capacity to alter
PSYCHOLOGY & HEALTH 5
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 74

one’s behaviour—we also assessed self-efficacy by asking participants to estimate their‘ability to maintain a healthy vitamin intake without vitamin supplementation (e.g.,through your diet)’ on a 3-point scale (1" Terrible – I need vitamin supplements;3" Excellent, I do not need vitamin supplements).
Interventions
The control condition provided irrelevant information about the multivitamin producton offer: ‘Product A, which you will soon bid on, is available to purchase from variousretail outlets.’ The control also provided a basic refutation regarding the general effi-cacy of multivitamins: ‘However, there is currently insufficient clinical evidence to sup-port a recommendation for or against the use of multivitamins and mineralsupplements for the general population.’ The basic refutation was based on a tenta-tive ‘diplomatic’ type of refutation commonly used in real-world attempts to debunkclaims about ineffective health products. In this case, it was adapted from a statementpublished on the National Institute of Health (NIH) website (NIH, 2016).
The contingency condition provided participants with summarised informationabout the clinical outcomes of previous randomised controlled trials that have foundmultivitamins not to provide any health benefits (see Figure 1). This intervention con-sisted of three information components: (i) a contingency table, (ii) an explanation ofthe table, and (iii) a scientific causal explanation of the overall outcome. It wasdesigned to help consumers overcome the illusion of causality and has been recentlyshown to reduce willingness-to-pay for multivitamins (see MacFarlane et al., 2018b).
Figure 1. Summary of the information provided to participants in the two treatment conditions. Inthe contingency table, the number below the smiling face represents the relative frequency of peo-ple who reported experiencing a health benefit, and the number below the sullen face representsthe relative frequency of people who did not report experiencing a benefit.
6 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 75

The fear-appeal condition provided participants with information about the sum-marised results of several randomised controlled trials (Bjelakovic et al., 2012; Mursuet al., 2011) that suggest multivitamin supplementation can cause health harms (seeFigure 1). The critical elements of this condition were based on a systematic review offear appeals by Tannenbaum et al. (2015), who argued that in order to be effective,fear appeals need to (i) depict high health severity, (ii) depict high susceptibility of thetarget audience, and (iii) include a self-efficacy manipulation that assures the audienceof their ability to avoid the stated harm.
The combined condition provided participants with the materials from the contin-gency condition followed by the materials from the fear-appeal condition. The com-bined condition was therefore designed to inform consumers that multivitaminsupplementation not only provides no health benefit but may also cause significanthealth harms.
Future health purchases
To assess whether the interventions’ effects might generalise towards helping partici-pants make better health purchases in the future, participants were asked to rate theimportance of 15 health-related factors using a 5-point scale (1" not important at all;5" extremely important). These questions were designed to evaluate the impact of theinterventions on participants’ valuation of key information required to assess productsafety and efficacy. The critical item was ‘the number of people who did, and did not,experience a benefit when taking a sugar pill’ (hereafter, ‘placebo comparison’)—thisis because it measures participants’ ability to recognise that comparing a treatment’sbenefit against placebo is crucial to assessing its efficacy. The remaining items weredistractors (e.g., ‘Advertising claims’, ‘Strength of active ingredients’, and ‘Experience ofpeople I know’). Item order was randomised.
Procedure
The experiment was executed using Qualtrics survey software. Participants were ini-tially given an information sheet and provided informed consent. Participants thenresponded to questions on demographics, multivitamin consumption, and the gen-eral-attitude scale. Participants were then shown the information about the multivita-min product before being introduced to the auction. Next, participants indicated theirwillingness-to-pay for the multivitamin product. After the auction, participantsresponded to questions regarding their future health purchases and their estimatedself-efficacy. At the conclusion of the experiment, participants were shown the resultsof their hypothetical bidding. Finally, participants were fully debriefed.
Results
The general-attitude scale was found to have very good internal consistency reliability(Cronbach’s a " .91). Associations between willingness-to-pay and the four predictorswere analysed via Spearman’s correlation coefficient. For estimated usage, we
PSYCHOLOGY & HEALTH 7
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 76

excluded participants who reported having never previously taken multivitamins. Forestimated efficacy belief, we excluded participants who responded, ‘I don’t know’.Willingness-to-pay was positively associated with estimated usage of multivitamins,n" 165, rs " .17, p " .02; efficacy belief, n" 176, rs " .35, p< .001; and general-atti-tudes, n" 179, rs " .34, p< .001, indicating that participants with more frequentusage, higher efficacy belief, and more favourable attitudes toward health supple-ments had significantly higher willingness-to-pay for the multivitamin product. Thecontrol predictor of current health state was not correlated with willingness-to-pay,n" 179, rs " .02, p " .80.
We conducted a 2 (contingency information: no/yes) ! 2 (fear appeal: no/yes) ana-lysis of covariance (ANVOCA) with stated willingness-to-pay as the dependent variable,and general-attitude as the covariate. This analysis confirmed that participants gen-eral-attitude was significantly related to their willingness-to-pay, F(1, 174) " 26.37,p< .001. There was a marginally significant main effect of contingency information,with willingness-to-pay lower when contingency information was provided, F(1, 174) "3.2, p " .076, x2 " .01. There was a significant main effect of fear appeal, with willing-ness-to-pay lower when a fear appeal was provided, F(1, 174) " 13.13, p< .001, x2 ".056. There was no significant interaction, F< 1. Figure 2 shows the interaction plot forExperiment 1.
To determine whether self-efficacy levels varied across conditions, we conducted anANCOVA with self-efficacy as the dependent variable, condition as the fixed factor,and general-attitude as the covariate. We found that general attitudes were negativelycorrelated with self-efficacy, F(1, 174) " 34.37, p< .001. This indicated that participantswith more favourable attitudes toward health supplements tended to report lowerself-efficacy. We also found that self-efficacy did not vary across conditions, M" 2.18,F" 1.17, p " .33. We also assessed whether participants’ ratings of the importance ofa placebo comparison (critical to making informed future health purchases) was higherfor that half of the sample that received the contingency-condition (Mdn" 3) com-pared to the half that did not (Mdn" 3). As the data were ordinal, we used a two-tailed Mann-Whitney U test, but found the difference to be non-significant, U" 3611,p " .25.
Figure 2. Willingness-to-pay across conditions in Experiment 1. Error bars indicate standard error.
8 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 77

Discussion
The aim of this study was to evaluate the separate impacts of contingency informationand a fear appeal on willingness-to-pay for an ineffective health remedy. Consistentwith our previous study (MacFarlane et al., 2018b) , three factors predicted greaterwillingness-to-pay for the multivitamin product: (i) more frequent estimated usage, (ii)higher efficacy belief, and (iii) a higher general-attitude. We found that when we iso-lated the effect of the contingency information on willingness-to-pay, its influence wasonly marginally significant (Hypothesis I). This result thus failed to provide strong sup-port for our previous finding that communicating a simplified contingency table canhelp reduce consumer demand for an ineffective health remedy. When we isolatedthe effect of the fear appeal, its influence on willingness-to-pay was statistically signifi-cant (Hypothesis II). This novel result shows that communicating information aboutthe potential health risks of consuming an ineffective health remedy can have a meas-urable impact on consumer demand. The absence of a significant interaction betweenthe two conditions indicates that contingency information and fear appeal have inde-pendent and additive effects.
We found that participants with more favourable attitudes toward health supple-ments reported lower self-efficacy (their ability to maintain a healthy vitamin intakewithout vitamin supplementation). This provides support for the importance of boost-ing people’s self-efficacy, and hence for including an efficacy-enhancing message (themessage most modern diets provide ample vitamins).
We did not find evidence that the placebo comparison was rated as more import-ant by participants exposed to the contingency information. In contrast to our previ-ous study, this suggests the intervention may not always generalise towardsincreasing consumers’ awareness of the importance of clinical evidence when makinghealth purchases.
One potential limitation of Experiment 1 is that participants’ auction bids had noreal financial consequences. Despite our bias-reduction strategies, this may have con-tributed to a hypothetical bias, whereby some participants may have taken the auc-tion less seriously than they would have with real financial incentives (Loomis, 2011).This, in turn, may have weakened the effect of the contingency-information interven-tion. Accordingly, to validate the results, we sought to replicate the experiment usingreal money and a real multivitamin product.
Experiment 2
Our second experiment aimed to evaluate the impact of the contingency informationand fear appeal interventions when participants’ choices had real financial consequen-ces. Thus, the basic design and methodology was identical to Experiment 1, butExperiment 2 was conducted in the laboratory, and bidding was incentivised—wegave participants AU$5 to place real bids for a multivitamin product that they wouldpurchase if their bid was successful. We expected that incentivizing the experimentwould lead participants to more carefully consider their willingness-to-pay for themultivitamin product. Furthermore, by improving the ecological validity of the
PSYCHOLOGY & HEALTH 9
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 78

experiment, we envisioned that variation in the bid amounts would more accuratelyreflect the impact of the treatment conditions on consumer demand.
We also sought to empirically test whether the effects on willingness-to-pay werecomparable between the hypothetical and the incentivised versions of the experiment.We hoped this analysis would provide evidence of the viability of conducting con-sumer intervention research online.
Participants
A total of 207 undergraduate students from the University of Western Australia tookpart in the experiment in exchange for course credit. One participant was excluded forfailing to wait for instructions prior to starting the experiment. Two data sets wereexcluded due to system error that failed to allocate an intervention condition. The a-priori exclusion criteria were identical to Experiment 1. Six respondents were excludedfor rushing and thus the final sample size was N" 198 (134 females, 64 males, 1 other;age M" 20.87, SD" 5.94).
Predictors and materials
The same predictors and materials were used as in Experiment 1, except for a minorchange to the self-efficacy measure. To obtain a more refined estimate of participantself-efficacy—their perceived ability to maintain a healthy vitamin intake without sup-plementation—we increased the response measure from a 3-point to a 5-point scale.
Procedure
Experiment 2 was conducted in a computerised laboratory (http://bel-uwa.github.io).In each session, between one and six participants completed the experiment concur-rently. Upon entering the laboratory, the general procedure was explained to partici-pants. During this explanation, participants were shown open money tins containingthe cash endowments. The experimenter followed a set verbal protocol to make clearthat (i) participants would receive real money and/or the multivitamin product at theend of the experiment, depending on the outcome of the auction, and that (ii) theresults of the survey were important for research so participants should take theirtime and respond as honestly as possible. Participants then completed the experimenton one of six computer terminals, separated by privacy blinds. At the conclusion ofthe experiment, participants received either the full cash endowment or their pur-chased multivitamin product and the change left over from their cash endowment,before being fully debriefed.
Results
The general-attitude scale was found to have good internal consistency reliability(Cronbach’s a " .792). Analysis of Spearman’s correlation coefficient showed that will-ingness-to-pay was positively associated with efficacy belief, n" 184, rs " .31, p< .001,
10 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 79

and general-attitude, n" 198, rs " .24, p< .001. However, we did not detect a signifi-cant association between willingness-to-pay and estimated usage of multivitamins,n" 125, rs " .14, p " .11 The control predictor of current health state was not corre-lated with willingness-to-pay, n" 198, rs " .002, p " .98.
We ran the same two-way ANCOVA as in Experiment 1, which confirmed again thatgeneral-attitude was significantly related to willingness-to-pay, F(1, 193) " 11.15,p< .001. After controlling for the effects of general-attitude, there was a significantmain effect of contingency information, with willingness-to-pay lower if contingencyinformation was provided, F(1, 193) " 7.36, p< .01, x2 " .03. There was also a signifi-cant main effect of fear appeal, with willingness-to-pay lower if a fear appeal was pro-vided, F(1, 193) " 4.48, p " .036, x2 " .016. There was no significant interaction,F< 1. Figure 3 shows the interaction plot for Experiment 2. In contrast to Experiment1, we found that participants’ rating of placebo comparison information was signifi-cantly higher for that half of the sample that received the contingency information(Mdn" 4) compared to the half that did not (Mdn" 3), U" 3933.50, p " .025. Thisindicated that the full-contingency condition increased participants’ valuation of pla-cebo-information, which is critical for making rational consumer decisions regardinghealth products.
We ran the same ANCOVA to assess whether self-efficacy varied across conditions. Weagain found that general attitudes were negatively correlated with self-efficacy, F(1, 191)" 17.60, p< .001. As with Experiment 1, this indicated that participants with more favour-able attitudes toward health supplements tended to report lower self-efficacy. We againalso found that self-efficacy did not vary across conditions, M" 3.85, F< 1, p " .50.
Discussion
The results of Experiment 2 were similar to Experiment 1 but provided more evidenceof the predicted impact of both interventions. Participants’ willingness-to-pay for themultivitamin product was significantly reduced by both the contingency intervention(Hypothesis I) and the fear-appeal intervention (Hypothesis II). There was again no
Figure 3. Willingness-to-pay across conditions in Experiment 2. Error bars indicate standard error.
PSYCHOLOGY & HEALTH 11
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 80

evidence of a significant interaction between the contingency-information and fear-appeal manipulations.
The results of this incentivised study were generally consistent with the findings ofour previous incentivised study (MacFarlane et al., 2018b), namely that employing asimplified contingency table with simple frequencies can help people overcome theillusion of causality, and thus effectively counter demand for ineffectivehealth remedies.
In contrast to Experiment 1, we did find evidence that the placebo comparison wasrated as more important by participants exposed to the contingency information. Thissupports the finding from our previous study (MacFarlane et al., 2018b) demonstratingthat the contingency intervention increases consumers’ awareness of the importanceof clinical evidence when making health purchases.
Conjoint Bayesian analysis
To obtain a clearer picture of the robustness of the evidence for each intervention, wepooled the data of both experiments (N" 536)3 and analysed the results with Bayesianinference using JASP (Version 0.10.2). Bayesian inference involves the comparison ofexplanatory models that do or do not contain an effect of interest in order to quantifyevidence strength (either for the presence or the absence of an effect) as data accumu-lates (JASP Team, 2019; Rouder et al., 2017; Wagenmakers et al., 2018). Evidencestrength is often expressed as a Bayes Factor (BF10), which is the ratio of the probabilityof observing the data given a hypothesis (H1) over the probability of the data given thenull (H0). For example, BF10 " 2 would indicate that data are twice as likely under H1
than H0,which is considered ‘anecdotal’ evidence (evidence in favour of H1 is considered‘moderate’ if 3< BF10< 10, ‘strong’ if BF10 10< 30, and ‘very strong’ if BF10 >30; for fur-ther reading, see Berger & Berry, 1988; Wagenmakers, 2007; Wagenmakers et al., 2018 ).
We conducted a 2 (contingency information: no/yes) ! 2 (fear appeal: no/yes) ! 2(bidding type: hypothetical vs. incentivised) Bayesian ANCOVA with willingness-to-payas the dependent variable, and general-attitude as the covariate. We assessed thestrength of the evidence against the null model for 37 potential models.
44
In addition to selecting the best-fitting model (the model with the greatest BF10),we tested whether condition effects were comparable across the two bidding types byassessing the evidence in favour of an interaction between the treatment factors andbidding type. To reduce the risk of drawing misleading conclusions about the bestmodel, given the large number of potential models, we also conducted an analysis ofeffects for variables and interactions. This analysis retained model-selection uncertaintyby averaging the conclusions from each candidate model as weighted by that model’sposterior plausibility (Wagenmakers et al., 2018). Planned comparisons were then usedto assess each hypothesis by means of Bayesian t-test, as outlined in Wagenmakerset al. (2018). The Cauchy prior width was set to its JASP default, r" 0.707.
Results
All models received strong evidence in comparison to the null model (see supplemen-tal materials, Table S1). The best-fitting model included all four main effects (i.e.,
12 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 81

contingency information, fear appeal, bidding type, and general-attitude; BF10 "2.98! 1014). The effect of bidding type arose because hypothetical bids were loweron average in Experiment 1 than incentivized bids in Experiment 2. A comparison ofthe best model with the next-strongest model that included an interaction between atreatment factor (namely, fear appeal) and bidding type (BF10 " 1.28! 1014) yielded2.4-to-1 evidence against including the interaction. The analysis of effects revealed fur-ther evidence against the inclusion of interactions between treatment factors and bid-ding type (see supplemental materials, Table S2). Thus, although participants whomade hypothetical bids exhibited a reduced willingness-to-pay for the multivitaminproduct compared to participants whose bids were incentivized, the impact of condi-tion was comparable for both bidding types (see supplemental materials, Figure S2).The average reduction in willingness-to-pay was calculated using the output of themodel-averaged posterior summary. Planned comparisons yielded strong evidence(BF10 " 13.11) for an effect of the contingency information—an average reduction inwillingness-to-pay of 22.02%, as well as very-strong evidence (BF10 " 43,534) for aneffect of the fear appeal—an average reduction in willingness-to-pay of 31.61% (seesupplemental materials Figure S2). The interventions had the greatest effect in thecombined condition—an average reduction in willingness-to-pay of 50.23%.
General discussion
This study reported two experiments that sought to investigate the separate and jointeffects of contingency information and fear appeals on consumers’ willingness-to-payfor an ineffective health remedy—multivitamins for maintaining general health. Usinga hypothetical auction, Experiment 1 showed that a fear appeal reliably reduced will-ingness-to-pay, while the impact of the contingency intervention was only marginallysignificant. Using an incentivised auction, Experiment 2 showed that both interven-tions significantly reduced willingness-to-pay. Neither experiment found evidence ofan interaction between the contingency-information and fear-appeal manipulations,suggesting that both interventions have independent and additive effects. Our con-joint Bayesian analysis of the two experiments yielded strong evidence in support ofour two hypotheses, namely that both the contingency intervention and the fearappeal independently reduced willingness-to-pay for multivitamins (by 22% and 32%,respectively). These results suggest that the best strategy to reduce demand for inef-fective health remedies would thus be to deploy both interventions concurrently,which reduced willingness-to-pay by 50%.
We also found that, although participants who made hypothetical bids exhibitedlower willingness-to-pay than participants whose bids were incentivised, the impact ofthe experimental manipulations on willingness-to-pay was comparable for both bid-ding types (see Figures 2 and 3). This suggests that hypothetical scenarios may pro-vide a useful methodology to estimate and assess intervention effects on consumerdemand in situations where using incentivised auctions may be impractical or uneth-ical, such as when a product is known to cause significant harm (e.g., colloidal silver).
The present study provides additional evidence for the utility of a novel contin-gency-information intervention (see MacFarlane et al., 2018b), which in this case
PSYCHOLOGY & HEALTH 13
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 82

served to counter the misconception that vitamin supplementation is essential formaintaining general health. Moreover, our results provide evidence in favour of theuse of fear appeals in health communications; in this case, the fear appeal counteredthe misconception that vitamin supplementation poses no risks to health. We notethat our fear appeal included an efficacy-enhancing message (namely, highlightingthat most modern diets provide ample vitamins) to assure participants that by doingthe recommended behaviour (i.e., stop consuming multivitamins) they would avoidharm (i.e., vitamin deficiency). The finding in both experiments that participants withmore favourable attitudes toward health supplements tended to report lower self-effi-cacy, supported the importance of including this message. Nevertheless, the benefitsof a fear appeal may be limited to situations in which consumers are able to stopengaging in a behaviour. Our results do not provide evidence in favour of fear appealsin situations where action is required (e.g., to make healthy food choices) or whereself-efficacy may be low (e.g., when a consumer is addicted to cigarettes; Peters et al.,2018). Thus, future research should test the effects of contingency-information andfear-appeal interventions on demand for more challenging products (e.g., fast foodor cigarettes).
The fact that the combination of contingency and fear interventions was most effect-ive constitutes experimental evidence that perceived benefits and perceived risks of aproduct can provide separate pathways to influencing consumer demand for irrationalproducts. The absence of an interaction between the two factors was somewhat of asurprise—if perception of one attribute can be influenced by manipulating informationabout the other (Finucane et al., 2000), one might expect the combination of both treat-ments to be more than just additive. However, the observed result was still consistentwith our expectations, namely that both factors would complement each other in driv-ing an overall assessment that a low-benefit/high-risk remedy is not worth consuming(Alhakami & Slovic, 1994). Our findings therefore suggest that communicators seekingto dissuade consumers from purchasing harmful health remedies should aim to countertwo distinct psychological drivers—perceived benefits and lack of risks—underlying con-sumer demand for health remedies. This factorial approach represents a departure fromthe often-assumed dichotomy (highlighted in debates about effectiveness of fearappeals vs. positive messaging; e.g., Akl et al., 2011; Gallagher & Updegraff, 2012; Koket al., 2018) that health communicators must choose between framing public messagesas either promoting health benefits or reducing health risks.
In support of our previous study (MacFarlane et al., 2018b), we found evidence inExperiment 2 (but not in Experiment 1) that the contingency intervention increasedparticipants’ valuation of placebo information, which is critical for making rational con-sumer decisions regarding health products. The reasons for this discrepancy areunclear, and we prefer not to speculate about them. Future research should investi-gate whether repeated exposure to contingency information and/or more explicitexposure of logical fallacies (Cook et al., 2017) could help consumers to be more vigi-lant in seeking critical clinical information when making judgments about the efficacyof novel health remedies.
More generally, we argue that our results highlight the considerable importance ofcrafting interventions using insights from psychology (MacFarlane et al., 2020). Future
14 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 83

research should consider targeting other emotional drivers of consumer demand; forexample, one promising avenue may be to compare the impact of fear appeals toappeals that aim to elicit pathogen disgust—thus averting threat by means of avoid-ing contamination due to repulsion (Collymore & McDermott, 2016; Huang et al.,2017). For example, disgust communications to dissuade consumers from purchasingineffective remedies could be crafted by drawing on recent research showing wide-spread adulteration (e.g., with undeclared plant and animal DNA) in the alternative-remedy industry (Coghlan et al., 2015; Rocha et al., 2016).
Conclusion
The present study provides evidence that consumer choices are influenced by bothperceptions of efficacy and risk. We have provided further evidence that counteringthe illusion of causality and providing a valid causal explanation for why a health rem-edy is ineffective can reduce consumer demand for products that have been shown tohave no health benefit. We have also provided evidence that this intervention can beconsiderably strengthened by augmenting it with information about known healthrisks. Our results challenge the often-assumed dichotomy that health communicationmessages need to either address benefits or harms; instead our results suggest thatthe combination of both can provide additive effects that may be superior to eitherapproach alone. This research demonstrates that testing combinations of psychologic-ally-informed interventions can provide health authorities with an iterative approachto developing more effective levers to reduce demand for ineffective health remedies.
Notes
1. The experiment was first run with a separate sample of online participants (N" 164).However, due to random chance, a key covariate differed across treatment conditions,which violated the assumption of homogeneity of regression slopes (see supplementalmaterial Figure S1), meaning that the regression analysis of main effects would have beeninaccurate. Consequently, we re-ran the experiment with a second sample, and report thissecond run here. The initial sample was, however, included in a joint Bayesian analysis of allavailable data across both experiments; this analysis is presented after Experiment 2.
2. In the first iteration of the experiment, n" 6 respondents were excluded due to rushing andn" 2 due to non-differentiating responses, giving a final sample size of N" 156 (74 females,82 males; age M" 38.51, SD" 12.17).
3. Participants from both sub-samples of Experiment 1 were included. Due to regression to themean, the significant differences in participants’ general-attitude between conditionsobserved in the first sub-sample of Experiment 1 were averaged out by the addition ofmore participants. Thus, data from the first sub-sample could be included in the pooleddata without the data violating the assumption of homogeneity of regression slopes.
4. The 37 models included a model for each individual main effect of the covariate and theindependent variables; a model for each possible combination of these variables; and amodel for each of these combinations with each possible combination of interactionsbetween the relevant independent variables.
Disclosure statement
No potential conflict of interest was reported by the author(s).
PSYCHOLOGY & HEALTH 15
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 84

Funding
This research was facilitated by an Australian Government Research Training ProgramScholarship awarded to the first author.
ORCID
Douglas MacFarlane http://orcid.org/0000-0003-4378-9294Mark J. Hurlstone http://orcid.org/0000-0001-9920-6284Ullrich K. H. Ecker http://orcid.org/0000-0003-4743-313X
References
Akl, E. A., Oxman, A. D., Herrin, J., Vist, G. E., Terrenato, I., Sperati, F., … Sch!unemann, H. (2011).Framing of health information messages. Cochrane Database of Systematic Reviews.
Alhakami, A. S., & Slovic, P. (1994). A psychological study of the inverse relationship betweenperceived risk and perceived benefit. Risk Analysis: An Official Publication of the Society for RiskAnalysis, 14(6), 1085–1096. https://doi.org/10.1111/j.1539-6924.1994.tb00080.x
Becker, G. M., DeGroot, M. H., & Marschak, J. (1964). Measuring utility by a single-responsesequential method. Behavioral Science, 9(3), 226–232. https://doi.org/10.1002/bs.3830090304
Berger, J. O., & Berry, D. A. (1988). Statistical analysis and the illusion of objectivity. AmericanScientist, 76(2), 159–165.
Bjelakovic, G., Nikolova, D., & Gluud, L. L. (2012). Antioxidant supplements for prevention of mor-tality in healthy participants and patients with various diseases. Cochrane Database Syst Rev.Epub ahead of print 2012/03/16.
Boutron, I., Moher, D., Altman, D. G., Schulz, K. F., & Ravaud, P., for the CONSORT Group (2008).Methods and processes of the CONSORT Group: example of an extension for trials assessingnonpharmacologic treatments. Annals of Internal Medicine, 148(4), W60–66. https://doi.org/10.7326/0003-4819-148-4-200802190-00008-w1
Carver, R. P. (1985). How good are some of the world’s best readers?. Reading ResearchQuarterly, 20(4), 389–419. https://doi.org/10.2307/747851
Coghlan, M. L., Maker, G., Crighton, E., Haile, J., Murray, D. C., White, N. E., Byard, R. W., Bellgard,M. I., Mullaney, I., Trengove, R., Allcock, R. J. N., Nash, C., Hoban, C., Jarrett, K., Edwards, R.,Musgrave, I. F., & Bunce, M. (2015). Combined DNA, toxicological and heavy metal analysesprovides an auditing toolkit to improve pharmacovigilance of traditional Chinese medicine(TCM). Scientific Reports, 5, 17475https://doi.org/10.1038/srep17475
Collymore, N. N., & McDermott, M. R. (2016). Evaluating the effects of six alcohol-related mes-sage frames on emotions and intentions: The neglected role of disgust. Journal of HealthPsychology, 21(9), 1907–1917. https://doi.org/10.1177/1359105314567910
Cook, J., Lewandowsky, S., & Ecker, U. K. H. (2017). Neutralizing misinformation through inocula-tion: Exposing misleading argumentation techniques reduces their influence. PLOS One, 12(5),e0175799. https://doi.org/10.1371/journal.pone.0175799
Cooper, D. P., Goldenberg, J. L., & Arndt, J. (2014). Perceived efficacy, conscious fear of deathand intentions to tan: Not all fear appeals are created equal. British Journal of HealthPsychology, 19(1), 1–15. https://doi.org/10.1111/bjhp.12019
Cummings, R. G., & Taylor, L. O. (1999). Unbiased value estimates for environmental goods: Acheap talk design for the contingent valuation method. American Economic Review, 89(3),649–665. https://doi.org/10.1257/aer.89.3.649
Curran, P. G. (2016). Methods for the detection of carelessly invalid responses in survey data.Journal of Experimental Social Psychology, 66, 4–19. https://doi.org/10.1016/j.jesp.2015.07.006
Dombrowski, S. U., Sniehotta, F. F., & Avenell, A. (2007). Current issues and future directions inpsychology and health: Towards a cumulative science of behaviour change: Do current
16 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 85

conduct and reporting of behavioural interventions fall short of best practice? Psychology &Health. 22(8), 869–874.
Ecker, U. K. H., Lewandowsky, S., & Tang, D. T. (2010). Explicit warnings reduce but do not elim-inate the continued influence of misinformation. Memory & Cognition, 38(8), 1087–1100.https://doi.org/10.3758/MC.38.8.1087
Faul, F., Erdfelder, E., Lang, A-G., & Buchner, A. (2007). G#Power 3: A flexible statistical poweranalysis program for the social, behavioral, and biomedical sciences. Behavior ResearchMethods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
Fischhoff, B., Slovic, P., Lichtenstein, S., Read, S., & Combs, B. (1978). How safe is safe enough? Apsychometric study of attitudes towards technological risks and benefits. Policy Sciences, 9(2),127–152. https://doi.org/10.1007/BF00143739
Finucane, M. L., Alhakami, A., Slovic, P., & Johnson, S. M. (2000). The affect heuristic in judge-ments of risks and benefits. Journal of Behavioral Decision Making, 13(1), 1–17. https://doi.org/10.1002/(SICI)1099-0771(200001/03)13:1<1::AID-BDM333>3.0.CO;2-S
Gallagher, K. M., & Updegraff, J. A. (2012). Health message framing effects on attitudes, inten-tions, and behavior: A meta-analytic review. Annals of Behavioral Medicine, 43(1), 101–116.https://doi.org/10.1007/s12160-011-9308-7
Ghanouni, A., Nuttall, E., Wardle, J., & Von Wagner, C. (2017). Testing whether barriers to a hypo-thetical screening test affect unrelated perceived benefits and vice versa: A randomised,experimental study. Patient Education and Counseling, 100(2), e1–e24. https://doi.org/10.1016/j.pec.2016.09.007
Gigerenzer, G., Gaissmaier, W., Kurz-Milcke, E., Schwartz, L. M., & Woloshin, S. (2007). Helpingdoctors and patients make sense of health statistics. Psychological Science in the PublicInterest: a Journal of the American Psychological Society, 8(2), 53–96. https://doi.org/10.1111/j.1539-6053.2008.00033.x
Guallar, E., Stranges, S., Mulrow, C., Appel, L. J., & Miller, E. R. (2013). Enough is enough: Stopwasting money on vitamin and mineral supplements. Annals of Internal Medicine, 159(12),850–851. %. https://doi.org/10.7326/0003-4819-159-12-201312170-00011
Hamby, T., & Taylor, W. (2016). Survey satisficing inflates reliability and validity measures: Anexperimental comparison of college and amazon mechanical turk samples. Educational andPsychological Measurement, 76(6), 912–932. https://doi.org/10.1177/0013164415627349
Huang, J. Y., Ackerman, J. M., & Newman, G. E. (2017). Catching (up with) magical contagion: Areview of contagion effects in consumer contexts. Journal of the Association for ConsumerResearch, 2(4), 430–443. https://doi.org/10.1086/693533
JASP Team (2019). JASP (Version 0.10.2) [Computer software].Jenkins, D. J. A., Spence, J. D., Giovannucci, E. L., Kim, Y.-I., Josse, R., Vieth, R., Blanco Mejia, S.,
Viguiliouk, E., Nishi, S., Sahye-Pudaruth, S., Paquette, M., Patel, D., Mitchell, S., Kavanagh, M.,Tsirakis, T., Bachiri, L., Maran, A., Umatheva, N., McKay, T., … Sievenpiper, J. L. (2018).Supplemental vitamins and minerals for CVD prevention and treatment. Journal of theAmerican College of Cardiology, 71(22), 2570–2584. https://doi.org/10.1016/j.jacc.2018.04.020
Jung, W. S., & Villegas, J. (2011). The effects of message framing, involvement, and nicotinedependence on anti-smoking public service announcements. Health Marketing Quarterly,28(3), 219–231. https://doi.org/10.1080/07359683.2011.595641
Kidd, L. R., Bekessy, S. A., & Garrard, G. E. (2019). Neither hope nor fear: Empirical evidenceshould drive biodiversity conservation strategies. Trends in Ecology & Evolution, 34(4),278–282. https://doi.org/10.1016/j.tree.2019.01.018
Kok, G., Peters, G.-J Y., Kessels, L. T. E., Ten Hoor, G. A., & Ruiter, R. A. C. (2018). Ignoring theoryand misinterpreting evidence: the false belief in fear appeals. Health Psychology Review, 12(2),111–125. https://doi.org/10.1080/17437199.2017.1415767
Loomis, J. (2011). What’s to know about hypothetical bias in stated preference valuation studies?Journal of Economic Surveys, 25(2), 363–370. https://doi.org/10.1111/j.1467-6419.2010.00675.x
Macfarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018a). Reducing demand for ineffective healthremedies: overcoming the illusion of causality [Supplemental Material]. Psychology & Health,33(12), 1472–1489. https://doi.org/10.1080/08870446.2018.1508685
PSYCHOLOGY & HEALTH 17
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 86
Macfarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018b). Reducing demand for ineffective healthremedies: overcoming the illusion of causality. Psychology & Health, 33(12), 1472–1489.https://doi.org/10.1080/08870446.2018.1508685
Macfarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Protecting consumers from fraudulenthealth claims: A taxonomy of psychological drivers, interventions, barriers, and treatments.Social Science & Medicine (1982), Soc Sci Med, 112790. https://doi.org/10.1016/j.socscimed.2020.112790
McAfee, D., & Connell, S. D. (2019). Balancing the benefits of optimism and pessimism in conser-vation: A response to Kidd, Bekessy, and Garrard. Trends in Ecology & Evolution, 34(8),692–693. https://doi.org/10.1016/j.tree.2019.05.004
Mursu, J., Robien, K., Harnack, L. J., Park, K., & Jacobs, D. R. (2011). Dietary supplements and mor-tality rate in older women: The Iowa Women’s Health Study. Archives of Internal Medicine,171(18), 1625–1633. https://doi.org/10.1001/archinternmed.2011.445
Myers, L. B. (2014). Changing smokers’ risk perceptions-for better or worse? Journal of HealthPsychology, 19(3), 325–332. https://doi.org/10.1177/1359105312470154
National Institute of Health (NIH) (2016). Vitamins and minerals. https://nccih.nih.gov/health/vitamins.
NHMRC (2007). National Statement on Ethical Conduct in Human Research (the NationalStatement). (Updated May 2015). The National Health and Medical Research Council.Commonwealth of Australia, Canberra.
O’Keefe, D. J., & Jensen, J. D. (2008). Do loss-framed persuasive messages engender greater mes-sage processing than do gain-framed messages? A meta-analytic review. CommunicationStudies, 59(1), 51–67. https://doi.org/10.1080/10510970701849388
Oppenheimer, D. M., Meyvis, T., & Davidenko, N. (2009). Instructional manipulation checks:Detecting satisficing to increase statistical power. Journal of Experimental Social Psychology,45(4), 867–872. https://doi.org/10.1016/j.jesp.2009.03.009
Peer, E., Vosgerau, J., & Acquisti, A. (2014). Reputation as a sufficient condition for data qualityon Amazon mechanical Turk. Behavior Research Methods, 46(4), 1023–1031. https://doi.org/10.3758/s13428-013-0434-y
Penn, J. M., & Hu, W. (2018). Understanding hypothetical bias: An enhanced meta-analysis.American Journal of Agricultural Economics, 100(4), 1186–1206. https://doi.org/10.1093/ajae/aay021
Peters, G.-J Y., Ruiter, R. A. C., Ten Hoor, G. A., Kessels, L. T. E., & Kok, G. (2018). Towards consen-sus on fear appeals: a rejoinder to the commentaries on Kok, Peters, Kessels, ten Hoor, &Ruiter (2018). Health Psychology Review, 12(2), 151–156. https://doi.org/10.1080/17437199.2018.1454846
Riet, J. v ’., Ruiter, R. A. C., Werrij, M. Q., & de Vries, H. (2008). The influence of self-efficacy onthe effects of framed health messages. European Journal of Social Psychology, 38(5), 800–809.https://doi.org/10.1002/ejsp.496
Rocha, T., Amaral, J. S., & Oliveira, M. (2016). Adulteration of dietary supplements by the illegaladdition of synthetic drugs: A review. Comprehensive Reviews in Food Science and Food Safety,15(1), 43–62. https://doi.org/10.1111/1541-4337.12173
Rouder, J. N., Morey, R. D., Verhagen, J., Swagman, A. R., & Wagenmakers, E.-J. (2017). Bayesiananalysis of factorial designs. Psychological Methods, 22(2), 304–321. https://doi.org/10.1037/met0000057
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2007). The affect heuristic. EuropeanJournal of Operational Research, 177(3), 1333–1352. https://doi.org/10.1016/j.ejor.2005.04.006
Tannenbaum, M. B., Hepler, J., Zimmerman, R. S., Saul, L., Jacobs, S., Wilson, K., & Albarrac"ın, D.(2015). Appealing to fear: A meta-analysis of fear appeal effectiveness and theories.Psychological Bulletin, 141(6), 1178–1204. https://doi.org/10.1037/a0039729
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011). Estimating theimpact of pictorial health warnings and “plain” cigarette packaging: evidence from experi-mental auctions among adult smokers in the United States. Health Policy (Amsterdam,Netherlands), 102(1), 41–48. https://doi.org/10.1016/j.healthpol.2011.06.003
18 D. MACFARLANE ET AL.
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 87
U.S. Food & Drug Administration [FDA] United States (2019). Health Fraud Scams.https://www.fda.gov/forconsumers/protectyourself/healthfraud/default.htm
Wagenmakers, E-J., Marsman, M., Jamil, T., Ly, A., Verhagen, J., Love, J., Selker, R., Gronau, Q. F.,#Sm"ıra, M., Epskamp, S., Matzke, D., Rouder, J. N., & Morey, R. D. (2018). Bayesian inference forpsychology. Part I: Theoretical advantages and practical ramifications. Psychonomic Bulletin &Review, 25(1), 35–57. https://doi.org/10.3758/s13423-017-1343-3
Wagenmakers, E-J. (2007). A practical solution to the pervasive problems of p values.Psychonomic Bulletin & Review, 14(5), 779–804. https://doi.org/10.3758/bf03194105
Wagenmakers, E-J., Marsman, M., Jamil, T., Ly, A., Verhagen, J., Love, J., Selker, R., Gronau, Q. F.,#Sm"ıra, M., Epskamp, S., Matzke, D., Rouder, J. N., & Morey, R. D. (2018). Bayesian inference forpsychology. Part II: Example applications with JASP. Psychonomic Bulletin & Review, 25(1),35–76. https://doi.org/10.3758/s13423-017-1343-3
Witte, K. (1994). Fear control and danger control: A test of the extended parallel process model(EPPM). Communication Monographs, 61(2), 113–134. https://doi.org/10.1080/03637759409376328
Yamagishi, K. (1997). When a 12.97% mortality is more dangerous than 24.14%: Implications forrisk communication. Applied Cognitive Psychology, 11(6), 495–506. https://doi.org/10.1002/(SICI)1099-0720(199712)11:6<495::AID-ACP481>3.0.CO;2-J
PSYCHOLOGY & HEALTH 19
Chapter 4: Do consumers respond to risks, lack of benefits, or both? 88

Chapter 5: Refuting COVID-19 misinformation
This chapter is presented in the format of a journal article.
MacFarlane, D., Tay, L. Q., Hurlstone, M. J., & Ecker, U. K. H. (Under Review). Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation Sharing. Manuscript submitted for publication.
89

90

Running Head: REFUTING COVID-19 MISINFORMATION
Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation
Sharing
Douglas MacFarlane1^, Li Qian Tay1^, Mark J. Hurlstone2, & Ullrich K. H. Ecker1*
1 School of Psychological Science, University of Western Australia
2 Department of Psychology, Lancaster University
^ These authors contributed equally
* Corresponding author
Word count: 1,981 (Introduction, Discussion, & Acknowledgments); 2,490 (Method &
Results)
Corresponding author: Ullrich Ecker, UWA M304, 35 Stirling Hwy, Perth 6009, Australia;
Chapter 5: Refuting COVID-19 misinformation 91

REFUTING COVID-19 MISINFORMATION 2
Abstract:
The COVID-19 pandemic has seen a surge of health misinformation, which has had serious
consequences including direct harm and opportunity costs. We investigated (N = 678) the
impact of such misinformation on two behavioral measures, viz. demand (i.e., willingness-to-
pay) for a spurious treatment, and propensity to promote (i.e., like or share) misinformation
online. This is a novel approach, as previous research has used mainly questionnaire-based
measures. We also compared two interventions to counteract the misinformation, viz. a
tentative refutation based on materials used by health authorities, and an enhanced refutation
based on best-practice recommendations. We found prior exposure to misinformation
increased misinformation promotion (by 18%). Both tentative and enhanced refutations
reduced demand (by 18% and 25%, respectively) as well as misinformation promotion (by
29% and 55%). The fact that enhanced refutations were more effective at curbing promotion
of misinformation highlights the need for debunking interventions to follow current best-
practice guidelines.
Chapter 5: Refuting COVID-19 misinformation 92

REFUTING COVID-19 MISINFORMATION 3
Statement of Relevance:
Health misinformation proliferates online, especially during a crisis such as the COVID-19
pandemic, when demand for effective treatments is pronounced. Such misinformation has the
potential to cause harm; for example, a promoted treatment might be ineffective but have
unintended side effects or prevent uptake of superior interventions (e.g., using a vitamin
supplement to prevent viral infection while abstaining from social distancing or mask use).
Combating misinformation about medical treatments is therefore a particularly exigent issue.
Alas, counteracting misinformation is a non-trivial task, with psychological research
demonstrating that even clearly-corrected misinformation can continue to influence reasoning
and decision making. The present study targeted misinformation about vitamin E as a
COVID-19 treatment. It shows that refutations that follow best-practice guidelines from
psychological research are more potent than tentative refutations often employed by health
authorities or the media, reducing both demand for the ineffective product and the propensity
to share treatment misinformation online.
Chapter 5: Refuting COVID-19 misinformation 93

REFUTING COVID-19 MISINFORMATION 4
Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation
Sharing
Misinformation—defined here as any information that is false—represents an
extensive threat to society (Lazer et al., 2018). Smear tactics and political fake news have
affected voter attitudes (Landon-Murray, Mujkic, & Nussbaum, 2019; Vaccari & Morini,
2014), myths about vaccines have contributed to the re-emergence of measles (Poland,
Jacobson, & Ovsyannikova, 2009), and climate change misinformation continues to pose a
major barrier to mitigative action (Cook, Ellerton, & Kinkead, 2018).
The COVID-19 pandemic is another case in point. Misinformation has proliferated,
especially on social media, including claims that the virus originated as a bioweapon, or that
health supplements or even onions could be effective treatments (e.g., Dupuy, 2020). This
can fuel hostility toward groups perceived to be responsible for the virus (Devakumar,
Shannon, Bhopal, & Abubakar, 2020) or draw people toward ineffective or even harmful
remedies, at variance with official health advice (Van Bavel et al., 2020). Accordingly, the
World Health Organization (WHO) noted that the pandemic has been accompanied by an
infodemic, characterized by a deluge of false information amplified by modern
communication technologies (Zarocostas, 2020). Given the scale of the problem,
considerable efforts are being undertaken to raise awareness and fact-check common claims
(e.g., Therapeutic Goods Administration, 2020; Weule, 2020). However, the question arises
as to how successful these efforts will be, and to what extent individuals initially misled by
false information will adjust their beliefs and behaviors after being exposed to a refutation.
Findings from cognitive psychology suggest refuting misinformation is no easy task.
An extensive literature has demonstrated that even corrected misinformation often continues
to influence individuals’ memory, reasoning, and decision making––the so-called continued
influence effect (Chan, Jones, Hall Jamieson, & Albarracín, 2017; Lewandowsky, Ecker,
Chapter 5: Refuting COVID-19 misinformation 94

REFUTING COVID-19 MISINFORMATION 5
Seifert, Schwarz, & Cook, 2012; Walter & Tukachinsky, 2020). Post-correction reliance on
misinformation can occur despite demonstrable memory for the correction; it can even arise
with fictitious or trivial information. This suggests that the continued influence effect is a
cognitive effect that does not necessarily depend on individuals’ motivation—it can emerge
from failures of memory updating or retrieval processes alone (Rich & Zaragoza, 2016;
Swire, Ecker, & Lewandowsky, 2017).
Much of the literature on continued influence has focused on how misinformation is
best counteracted (Paynter et al., 2019; Walter & Tukachinsy, 2020). Based on this research,
several best-practice recommendations have been identified for crafting refutations.
Specifically, refutations should: (1) come from a trustworthy source (Ecker & Antonio, 2020;
Guillory & Geraci, 2013) and, if applicable, discredit the disinformant by exposing their
hidden agenda (Walter & Tukachinsky, 2020); (2) make salient the discrepancy between false
and factual information, which has been shown to facilitate knowledge revision (Ecker,
Hogan, & Lewandowsky, 2017; Kendeou, Butterfuss, Kim, & van Boekel, 2019); (3) explain
why the misinformation is false, providing factual information to replace the false
information in people’s mental models (Paynter et al., 2019; Swire et al., 2017); and (4) draw
attention toward any misleading strategies that might have been employed by proponents of
the misinformation (e.g., Cook et al., 2018; MacFarlane, Hurlstone, & Ecker, 2018, 2020a).
Regrettably, real-world refutation attempts often do not take into account these
recommendations. For example, it is common for official bodies to adopt a tentative,
“diplomatic” approach in their communication (MacFarlane et al., 2018, 2020a; Paynter et
al., 2019). To illustrate, the Australian Therapeutic Goods Administration (TGA) writes
“there is no robust scientific evidence to support the usage of [high dose vitamin C] in the
management of COVID-19” (TGA, 2020). Such a diplomatic approach to refutation may
sometimes be called for to express nuance, and this may be of particular concern during a
Chapter 5: Refuting COVID-19 misinformation 95

REFUTING COVID-19 MISINFORMATION 6
pandemic characterized by much uncertainty (e.g., Chater, 2020). However, it is important to
recognize that such tentative refutations leave open the possibility that misleading
information may turn out to be true, which can then be exploited by individuals or
organizations with ulterior motives (MacFarlane, Hurlstone, & Ecker, 2020b; Oreskes &
Conway, 2010). It is therefore clear that refutations of health misinformation need to be well-
designed in order to both provide an accurate reflection of the best-available evidence and
achieve the desired outcome, taking into account the cognitive biases that disinformants—
such as health fraudsters trying to sell a product—seek to exploit.
Arguably the greatest weakness of existing research into the continued influence
effect is its near-universal reliance on questionnaire measures of reasoning, as some of the
most harmful effects of misinformation may be on behaviors. In reality, a more consequential
indicator of the success of a particular strategy to refute misinformation is consumer
behavior. The need for objective behavioral indicators is particularly acute in the context of
COVID-19, where the combination of high anxiety levels and need for effective treatment
may foster misinformation-driven demand for spurious remedies that are ineffective and
often dangerous, including bleach, methylated spirits, or essential oils (e.g., Spinney, 2020).
Given the well-established attitude-behavior gap (e.g., McEachan, Conner, Taylor, &
Lawton, 2011), it is critical to study how misinformation affects behavior, and to what extent
corrections can undo those effects (Hamby, Ecker, & Brinberg, 2020).
Against this backdrop, and building on previous theoretical work in this area
(MacFarlane et al., 2020b), the aim of the present study was to investigate the following two
questions: (1) How does exposure to COVID-19 misinformation influence concrete
behaviors, viz. people’s willingness-to-pay for ineffective health products and their
subsequent propensity to spread misinformation? (2) Are enhanced refutations based on best-
Chapter 5: Refuting COVID-19 misinformation 96

REFUTING COVID-19 MISINFORMATION 7
practice psychological insights better suited to counteract the behavioral impacts of
misinformation, compared to the tentative refutations often used by authorities?
To this end, we exposed participants to misinformation1 suggesting that vitamin E is
an effective remedy for COVID-19 and then provided them with either no refutation, a
tentative refutation based on real-world sources, or an enhanced refutation based on best-
practice psychological insights. Instead of using the questionnaire approach typical of
misinformation-debunking studies, we examined participants’ willingness to pay for a
vitamin E supplement, and their propensity to promote a social-media message endorsing use
of vitamin E to treat COVID-19. We hypothesized that misinformation exposure would
increase willingness to pay and misinformation promotion, and that the enhanced refutation
would more effectively reverse this effect than the tentative refutation.
Method
The experiment adopted a between-participants design with four conditions (control
vs. misinformation vs. tentative refutation vs. enhanced refutation), with two dependent
variables: “willingness-to-pay”—the amount bid on a vitamin E supplement in an
experimental auction—and “misinformation-promotion”—a score derived from a
participant’s engagement with a social-media post endorsing the misinformation.
Participants
A sample of 680 U.S.-based adult participants were recruited via Amazon’s
Mechanical Turk (MTurk). To ensure data quality, participants had to meet eligibility criteria
of 97% approval rate and a minimum of 5,000 prior tasks completed. An a-priori power
analysis suggested a minimum sample size of 309 to detect an effect of f = .16 (based on the
1 The term disinformation—false information that is crafted and disseminated with the intent to deceive—may be more appropriate here; however, we decided to use the broader term because ill intent cannot be assumed for all instances of advocacy for alternative health remedies.
Chapter 5: Refuting COVID-19 misinformation 97

REFUTING COVID-19 MISINFORMATION 8
contrast between control and “full-contingency plus” conditions in MacFarlane et al., 2018)
in our primary contrast (misinformation vs. enhanced refutation) with df = 1, α = .05,
1 – β = .80. Total sample size of 680 was calculated by extrapolating this to incorporate four
conditions and an estimated 10% exclusion rate. Participants were randomly allocated to one
of the four intervention conditions, subject to the constraint of approximately equal cell sizes.
Two a-priori exclusion criteria were applied to remove careless responders. One
participant was excluded for giving non-differentiated answers to every question in a survey
block, and another for responding erratically, with overly inconsistent responses between
pairs of equivalent questions (i.e., an odd/even threshold of > 2 Likert points apart). Final
sample size was thus N = 678 (344 females, 328 males, 3 non-binary, 3 participants of
undisclosed gender; age M = 42.81, SD = 12.64).
Materials
Predictors. We measured several potential predictors of willingness-to-pay
(following MacFarlane et al., 2018). These included one-item measures of previous
consumption of vitamins, efficacy belief, and current state of health (for details and analysis,
see Supplemental Material A). We also included two multi-item covariates: an 18-item
measure of general attitudes toward health supplements, and a four-item measure of COVID-
19 related concerns (see Supplemental Material A and B).
Interventions. Dependent on condition, participants were presented with one or two
articles (provided in Supplemental Material B). The control condition used a news article
providing general information about the importance of a healthy immune system for fighting
COVID-19. The article was modelled on two pieces (Collins, 2020; Weule, 2020) from
reputable and independent media outlets, The Conversation and the Australian Broadcasting
Corporation. It highlighted the importance of maintaining a balanced diet, regular exercise,
and good sleep. To provide a background as to why participants were bidding on a vitamin E
Chapter 5: Refuting COVID-19 misinformation 98

REFUTING COVID-19 MISINFORMATION 9
supplement, the article included a quote from the U.S. National Institute of Health “Vitamins
and Minerals” website, “Vitamins and minerals are…essential for health. The lack of a
specific micro-nutrient may cause…disease. Vitamin E, for example, acts as an antioxidant
and is involved in immune function. It helps to widen blood vessels and keep blood from
clotting. In addition, cells use Vitamin E to interact with each other and to carry out many
important functions.” The control article was therefore not fully neutral but contained some
allusion that vitamin E supplementation might provide some protection from viral infection.
The article also noted that whilst some people believe that vitamin supplements are essential,
dietitians say that taking supplements is not necessary unless you have a specific nutrient
deficiency or dietary need.
The article in the misinformation condition additionally contained false claims
suggesting vitamin E can protect against COVID-19. These were modelled on
misinformation spread via social media during the early stages of the pandemic (Bogle, 2020;
RMIT Fact Check, 2020; Weule, 2020). We invented a fake expert, Dr. Avery Clarke, and
used several deceptive techniques employed by real-life fraudsters (MacFarlane et al.,
2020b): (1) an appeal to authority, “Dr. Avery Clarke…said…experts in Taiwan have shown
that COVID-19 can be slowed, or stopped completely, with immediate widespread use of high
doses of Vitamin E”; (2) creating an illusion of causality through false testimony, “I have
seen patients who showed early symptoms of COVID coming on; I told them to try large
doses of Vitamin E, and symptoms went away in just a few days”; (3) an appeal to Nature,
“what’s more, this remedy is completely natural”; (4) conspiratorial thinking, “I am urgently
trying to get this message out now because it doesn’t get much airtime—after all, it’s cheap
and readily available, so there’s not much money in it”; and (5) an appeal to morality
“Imagine if you, or one of your loved ones, gets sick or dies, from something that is
completely preventable.”
Chapter 5: Refuting COVID-19 misinformation 99

REFUTING COVID-19 MISINFORMATION 10
In the tentative-refutation condition, the misinformation article was followed by a
second article that highlighted the lack of evidence for claims about vitamin E and COVID-
19. It was based on a tentative, “diplomatic” refutation style commonly used in real-world
attempts to debunk claims about ineffective health products; specifically, it was modelled on
an article featuring interviews with a disease expert and a dietitian (Weule, 2020). We
invented a public health expert, Prof. Simon Corner, and outlined his response to Dr. Avery’s
claims, “There is no conclusive evidence that vitamin [E] supplements can delay the onset of
an infection or treat respiratory infections, such as COVID-19. Furthermore, vitamin and
mineral supplements are not recommended for the general population.” The final paragraph
noted that there were some exceptions (e.g., people with specific vitamin deficiencies) and
recommended people talk to a doctor, pharmacist, or accredited dietitian.
In the enhanced-refutation condition, the misinformation article was followed by a
refutational article that, instead of simply noting lack of evidence, explained the techniques
used in the misinformation article to deceive readers. This enhanced refutation was based on
psychological insights regarding the effective debunking of misinformation (MacFarlane et
al., 2020a, 2020b; Paynter et al., 2019; Walter & Tukachinsky, 2020). The key components
of the enhanced refutation were: (1) highlighting the trustworthiness of the refutation source:
“Professor Simon Corner, a public health expert at the University of Chicago” and the
untrustworthiness of the misinformation source: “Dr. Clarke intentionally hides the fact that
he is not a medical doctor and that his many false claims are rejected by the medical
community”; (2) making salient the discrepancy between fact and fiction: “Dr. Clarke is
spreading false and misleading information to deliberately deceive people. […] Dr. Clarke’s
message starts with some true facts about the benefits of vitamins […but] there is no clinical
evidence that Vitamin E supplements have any impact on COVID-19”; (3) providing a factual
alternative account: “The only proven way to keep safe from COVID-19 is to maintain
Chapter 5: Refuting COVID-19 misinformation 100

REFUTING COVID-19 MISINFORMATION 11
physical (social) distancing and ensure proper hygiene practices”; and (4) drawing attention
to deceptive and misleading strategies, which in this case included (a) debunking the appeal
to nature: “Using terms such as ‘natural’ is designed to get people to associate the proposed
treatment with being harmless”; (b) highlighting the previously overlooked risks: “high doses
of Vitamin E supplements have been linked to adverse side-effects…and some more serious
diseases”; (c) debunking the appeal to morality: “sharing such bogus remedies with your
family would put them at risk of serious side-effects, while providing no benefit”;
(d) counteracting the illusion of causality: “the majority of people will recover from COVID-
19 thanks to their own immune systems, irrespective of any dietary supplements or unproven
remedies they may or may not have taken.”
Dependent measures.
Willingness-to-pay. To assess willingness-to-pay, we used an experimental auction
(MacFarlane et al., 2018; also see Becker, DeGroot, & Marschak, 1964; Thrasher, Rousu,
Hammond, Navarro, & Corrigan, 2011). The auction was hypothetical but previous
experiments have shown that results obtained using this hypothetical auction format are
comparable to those under fully-incentivized conditions (i.e., when bidding using real money
for real products; MacFarlane et al., 2020a). First, participants were asked to imagine they
had been given a $5 endowment. They then had an opportunity to place a bid on a bottle of
100 vitamin E capsules. Participants were shown a plain-packaged picture of the product and
a generic text (e.g., “…The supplement is designed to be taken once a day.”). It was
explained that the auction was different from other auctions in that participants could only
bid once, and it was in their best interest to bid the amount they were willing to pay for the
product. Participants entered their bid amount b in cents, with b ∈ (0, 500). They knew this
amount would be compared against a random number r ∈ (0, 500) drawn from a uniform
distribution, and that if b ≥ r, they would win the auction and purchase the product for
Chapter 5: Refuting COVID-19 misinformation 101

REFUTING COVID-19 MISINFORMATION 12
amount b but keep 500 – b of their endowment; otherwise they would lose the auction but
keep the full hypothetical endowment. There was an initial practice auction to ensure
participants understood the procedure. At the end of the auction, they were informed about
the outcome, and were shown their bid amount, the random comparison amount, and their
“take-home” amount. To mitigate hypothetical bias, we employed two established bias-
reduction techniques, namely “cheap-talk”—asking participants to behave as they would if
the auction was real—and consequentiality—reminding participants the results of this study
would have implications for significant public-health issues.
Misinformation-promotion. To assess participants’ propensity to promote
misinformation via social media, we developed a novel measure. Participants were presented
with four social-media posts, and they were asked to indicate how they would interact with
each post using one of three options, namely “share”, “like”, or “flag”. Each option was
accompanied by a brief explanation: Participants were told they could “Share the post
publicly, so more people could read it”; “Like the post, so your contacts see that you agree
with it”; or “Flag the post if you think it is inappropriate (e.g., offensive, inaccurate,
misleading, or promoting illegal activity)”. Participants were also told they could choose not
to interact with a post, thus enabling “pass” as a fourth response option.
The posts are shown in Figure 1. Three posts were on topics generally related to
health and/or COVID-19, whereas the fourth contained an endorsement of misinformation,
namely that vitamin E can treat COVID-19. Interest centered on responses to this target post,
which was always presented last. The general posts were presented first (in random order) as
decoys to help manage demand characteristics. To ensure plausibility, two of the decoy posts
were real tweets from the Wall Street Journal and the World Health Organization. To avoid a
slight confound that only the target post was from an individual doctor, the third decoy post
(relating to a tweet from New Scientist) was also from an invented doctor.
Chapter 5: Refuting COVID-19 misinformation 102

REFUTING COVID-19 MISINFORMATION 13
Figure 1. The social media posts shown to participants. Posts (a) to (c) are decoys; posts (b)
and (c) are real tweets, whereas post (a) is a real tweet associated with a fictional handle. Post
(d) is the target post containing endorsement of the misinformation.
Procedure
Ethics approval was granted by the Human Research Ethics Office of the University
of Western Australia. The experiment was run using Qualtrics software (Qualtrics, Provo,
UT). Participants were initially given an ethics-approved information sheet and provided
informed consent. They then responded to questions on demographics, vitamin E
consumption, the general-attitude scale, and the COVID-19 questions. Participants then read
Chapter 5: Refuting COVID-19 misinformation 103

REFUTING COVID-19 MISINFORMATION 14
the article(s) associated with the condition they were assigned to. This was followed by the
auction and the social-media engagement task. Finally, participants were debriefed; this
included a detailed refutation of the misinformation participants had encountered (following
the procedure in the enhanced-refutation condition), and participants had to demonstrate their
understanding by correctly answering a question regarding the gist of the debriefing. The
experiment took approximately 17 minutes; participants were paid US$2.50.
Results
Willingness-to-pay
On a descriptive level, willingness-to-pay means across control (C), misinformation
(M), tentative-refutation (TR), and enhanced-refutation (ER) conditions were MC = 208.27c
(SE = 11.05), MM = 221.75c (SE = 12.19), MTR = 181.97c (SE = 11.83), and MER = 167.28c
(SE = 12.33). Thus, the refutations reduced willingness-to-pay by 18% and 25%, relative to
the misinformation condition.
We conducted an analysis of covariance (ANCOVA) with a four-level condition
factor, willingness-to-pay as the dependent variable, and general attitude toward health
supplements (hereafter: general attitude) and COVID-19 concern as covariates. There was a
significant main effect of condition, F(3,672) = 5.76, p < .001, ω2 = .02 (see Figure 2). There
was also a significant effect of general attitude, F(1,672) = 150.45, p < .001, ω2 = .18,
indicating that greater support for supplements was associated with greater willingness-to-
pay. There was no significant effect of COVID-19 concern, F < 1.
Tukey post-hoc tests revealed mean willingness-to-pay was greater in the
misinformation condition than the tentative-refutation condition (Δ = 43.86c, 95% CI 4.73 –
82.98, t = 2.89, p = .021, d = 0.28) and the enhanced-refutation condition (Δ = 59.46c, 95%
CI 20.41 – 98.51, t = 3.92, p < .001, d = 0.37). There were no significant differences between
the other conditions (see Table S1 in Supplementary Material A for details).
Chapter 5: Refuting COVID-19 misinformation 104

REFUTING COVID-19 MISINFORMATION 15
Figure 2. Violin plots showing willingness-to-pay (WTP) for the vitamin E supplement
across conditions. Red markers and error bars indicate means and 95% confidence intervals.
Misinformation-promotion
In terms of participant proportions across response categories and conditions, 50.0%
of participants in the control condition engaged in liking or sharing of the misinformation-
endorsing social-media post. This increased to 59.1% in the misinformation condition (i.e., an
18.1% increase) but dropped to 41.7% and 26.6% in tentative-refutation and enhanced-
refutation conditions, respectively (i.e., 29.5% and 54.9% reductions relative to the
misinformation condition). See Table S3 in Supplementary Material A for further details.
To formally evaluate participants’ propensity to promote the misinformation post, we
converted the four response options into a single measure (“misinformation-promotion”). We
re-coded each response option to reflect the progression toward an increasing propensity to
spread misinformation: flag = -1 (actively combatting the spread of misinformation); pass = 0
(not contributing to the spread of misinformation); like = 1 (signaling approval of
Chapter 5: Refuting COVID-19 misinformation 105

REFUTING COVID-19 MISINFORMATION 16
misinformation and increasing its salience); share = 2 (actively spreading misinformation).
An asymptotic Kruskal-Wallis test found that condition significantly influenced
misinformation-promotion, H(3) = 54.25, p < .001 (see Figure 3).
To assess the locus of condition differences, post-hoc Mann-Whitney U tests with
Bonferroni adjustment were run. Misinformation-promotion was significantly greater for
participants in the misinformation condition, Mdn = 1, compared to control, Mdn = 0.5,
Ws = 12434, p = .017, r = -.09, the tentative-refutation condition, Mdn = 0, Ws = 17712,
p < .001, r = -.15, and the enhanced-refutation condition, Mdn = -1, Ws = 20566, p < .001,
r = -.27. Participants in the enhanced-refutation condition showed significantly lower
misinformation-promotion than those in the tentative-refutation condition, Ws = 17386,
p < .001, r = -.15. See Table S2 in Supplementary Material A for further details.
Figure 3. Bee-swarm plots showing engagement with the misinformation-endorsing social-
media post across conditions. Higher scores indicate greater propensity to promote the
misinformation (flag = -1; pass = 0; like = 1; share = 2; see text for details). Red markers and
whiskers indicate medians and quartiles; individual data points are jittered along both axes.
Chapter 5: Refuting COVID-19 misinformation 106

REFUTING COVID-19 MISINFORMATION 17
Discussion
The present study is one of the first to incorporate behavioral measures into the
continued-influence paradigm. Specifically, we tested whether exposure to misinformation
that presented vitamin E as an effective COVID-19 treatment affected both product demand
and misinformation-promotion behavior. To test the efficacy of interventions counteracting
the misinformation, we contrasted a tentative refutation based on real-world sources and an
enhanced refutation based on best-practice recommendations.
We found that exposure to misinformation significantly increased participants’
subsequent propensity to promote a social-media post endorsing the misinformation. While
willingness to pay for a vitamin E supplement was not reliably affected by the
misinformation relative to control, this is best explained by the control article’s allusion that
vitamins provide some protection from viral infection, meaning that the control condition
may have not provided a fully neutral comparison baseline. Compared to the misinformation
condition, both refutation types substantially reduced both willingness-to-pay and
misinformation-promotion, which underscores the general utility of refutations beyond the
realm of inferential-reasoning measures typically used in continued-influence research. The
enhanced refutation was more effective than the tentative refutation, reinforcing the best-
practice recommendations used.
Our results demonstrate the persuasive appeal of plausible (COVID-19-related)
misinformation and its potential to influence important behaviors (Zarocostas, 2020; see also
Pennycook, McPhetres, Zhang, Lu, & Rand, 2020). They also demonstrate the value of an
evidence-based approach to debunking. This is in line with previous research (Paynter et al.,
2019; Swire et al., 2017) but one of the first demonstration of this kind with behavioral
measures (also see Hamby et al., 2020). This is of particular relevance given (1) the well-
established attitude-behavior gap (McEachan et al., 2011), and (2) previous work questioning
Chapter 5: Refuting COVID-19 misinformation 107

REFUTING COVID-19 MISINFORMATION 18
the utility of refutations when it comes to behaviors (e.g., Swire-Thompson, Ecker,
Lewandowsky, & Berinsky, 2020; also see Swire-Thompson, DeGutis, & Lazer, 2020).
The results have clear practical implications. Specifically, individuals exposed to
refutations are less likely to waste money on spurious products. Also, individuals exposed to
misinformation may be more likely to spread it to those around them, but this harmful
sharing behavior can be dramatically curbed through refutations. While recent research has
shown that sharing decisions may also be affected by factors other than veracity (e.g.,
inattention, worldview; e.g., Mercier; 2020; Pennycook et al., 2020), the present study
suggests that well-designed refutations are an indispensable tool. The fact that our enhanced
refutation was more effective across both behavioral measures illustrates the pressing need
for real-world debunking practices to be based on insights from psychology (MacFarlane et
al., 2020b). This will be especially critical during crises such as the current infodemic.
Nonetheless, several limitations must be acknowledged. First, our enhanced refutation
included multiple best-practice recommendations and thus it is unclear which elements, or
combination of elements, contributed to the refutation’s success. Further research should thus
include a component analysis to aid the construction of more specific best-practice
guidelines, such as a flexible template that could be adopted by journalists and official bodies
(see also Lewandowsky et al., 2020; Paynter et al., 2019). Second, we relied only on a
hypothetical auction and a mock social-media scenario to assess behaviors. Although an
important first step, it is critical that future studies use measures that correspond with
behaviors of interests even more closely (e.g., incentivized auctions, social-media
simulations) and validate results using real-world data (e.g., Mosleh, Pennycook, & Rand,
2020). Third, as mentioned before, we did not find a reliable difference in willingness-to-pay
between the misinformation and control conditions. Consistent with research showing effects
of implied and subtly deceptive misinformation (e.g., Ecker, Lewandowsky, Chang, & Pillai,
Chapter 5: Refuting COVID-19 misinformation 108

REFUTING COVID-19 MISINFORMATION 19
2014; Powell, Keil, Brenner, Lim, & Markman, 2018; Rich & Zaragoza, 2016), this was
arguably driven by the insinuation in the control article that vitamins can provide some
infection protection. This suggests that the general framing of “neutral” educational
communications by impartial media sources needs to be carefully considered. The fact that
the control condition was non-neutral means there was no neutral no-misinformation baseline
against which to compare the refutation conditions in this study; this makes it impossible to
conclude with any certainty whether there was continued influence (i.e., above-baseline
reliance on refuted misinformation) in either of the refutation conditions. While that was not
the focus of the present study, follow-up research could consider inclusion of a neutral no-
misinformation condition. We also note that there was no time lag between our interventions
and behavioral tasks in the present study, so future research should explore the impact of
longer time delays (see Paynter et al., 2019).
Moreover, it is recommended that communicators dealing with misinformation
consider additional strategies beyond refutations. The speed with which misinformation is
generated and spread presents a challenge to fact-checkers and their capacity to refute each
piece of misleading content (Lazer et al., 2018). Future work should thus examine the
effectiveness of inoculation strategies, which serve to pre-emptively explain misleading
techniques common to misinformation campaigns and thus increase resilience to
misinformation. Such an approach has shown some promise in shielding individuals from the
influence of climate-change misinformation (e.g., Cook, Lewandowsky, & Ecker, 2017; van
der Linden, Leiserowitz, Rosenthal, & Maibach, 2017; also see Compton, 2013, for a review
of inoculation theory and its applications), but more research is needed to assess the extent to
which inoculation effects extend to different domains, and critically, to behaviors rather than
beliefs.
Chapter 5: Refuting COVID-19 misinformation 109
REFUTING COVID-19 MISINFORMATION 20
References
Becker, G. M., DeGroot, M. H., & Marschak, J. (1964). Measuring utility by a single-
response sequential method. Behavioral Science, 9, 226-232.
https://doi.org/10.1002/bs.3830090304
Bogle, A. (2020, March 21). As coronavirus fears grow, family group chats spread support
but also misinformation. ABC News. https://www.abc.net.au/news/science/2020-03-
21/coronavirus-health-misinformation-spreading-whatsapp-text-groups/12066386
Chan, M. S., Jones, C. R., Hall Jamieson, K., & Albarracín, D. (2017). Debunking: A meta-
analysis of the psychological efficacy of messages countering misinformation.
Psychological Science, 28, 1531-1546. https://doi.org/10.1177/0956797617714579
Chater, N. (2020). Facing up to the uncertainties of COVID-19. Nature Human Behaviour, 4,
439-439. https://doi.org/10.1038/s41562-020-0865-2
Collins, C. (2020, March 17). 5 ways nutrition could help your immune system fight off the
coronavirus. The Conversation. https://theconversation.com/5-ways-nutrition-could-
help-your-immune-system-fight-off-the-coronavirus-133356
Compton, J. (2013). Inoculation theory. The Sage Handbook of Persuasion: Developments in
Theory and Practice, 2, 220-237.
Cook, J., Ellerton, P., & Kinkead, D. (2018). Deconstructing climate misinformation to
identify reasoning errors. Environmental Research Letters, 13, 024018.
https://doi.org/10.1088/1748-9326/aaa49f
Cook, J., Lewandowsky, S., & Ecker, U. K. H. (2017). Neutralizing misinformation through
inoculation: Exposing misleading argumentation techniques reduces their influence.
PLOS ONE, 12, e0175799. doi:10.1371/journal.pone.0175799
Chapter 5: Refuting COVID-19 misinformation 110

REFUTING COVID-19 MISINFORMATION 21
Devakumar, D., Shannon, G., Bhopal, S., & Abubakar, I. (2020). Racism and discrimination
in COVID-19 responses. The Lancet, 395, 1194-1194. https://doi.org/10.1016/S0140-
6736(20)30792-3
Dupuy, B (2020, May 13). No evidence onions can cure ailments or kill viruses. AP News.
https://apnews.com/article/8905130246
Ecker, U. K. H., & Antonio, L. M. (2020). Can you believe it? An investigation into the
impact of retraction source credibility on the continued influence effect.
https://doi.org/10.31234/osf.io/qt4w8
Ecker, U. K. H., Hogan, J. L., & Lewandowsky, S. (2017). Reminders and repetition of
misinformation: Helping or hindering its retraction? Journal of Applied Research in
Memory and Cognition, 6, 185-192. https://doi.org/10.1016/j.jarmac.2017.01.014
Ecker, U. K. H., Lewandowsky, S., Chang, E. P., & Pillai, R. (2014). The effects of subtle
misinformation in news headlines. Journal of Experimental Psychology: Applied, 20,
323-335. https://doi.org/10.1037/xap0000028
Guillory, J., & Geraci, L. (2013). Correcting erroneous inferences in memory: The role of
source credibility. Journal of Applied Research in Memory and Cognition, 2, 201-
209. https://doi.org/10.1016/j.jarmac.2013.10.001
Hamby, A., Ecker, U. K. H., & Brinberg, D. (2020). How stories in memory perpetuate the
continued influence of false information. Journal of Consumer Psychology, 30, 240-
259. https://doi.org/10.1002/jcpy.1135
Kendeou, P., Butterfuss, R., Kim, J., & Van Boekel, M. (2019). Knowledge revision through
the lenses of the three-pronged approach. Memory & Cognition, 47, 33-46.
https://doi.org/10.3758/s13421-018-0848-y
Chapter 5: Refuting COVID-19 misinformation 111

REFUTING COVID-19 MISINFORMATION 22
Landon-Murray, M., Mujkic, E., & Nussbaum, B. (2019). Disinformation in contemporary
U.S. foreign policy: Impacts and ethics in an era of fake news, social media, and
artificial intelligence. Public Integrity, 21, 512-522.
https://doi.org/10.1080/10999922.2019.1613832
Lazer, D., Baum, M., Benkler, Y., Berinsky, A., Greenhill, K., Menczer, F., … & Zittrain, J.
(2018). The science of fake news. Science, 359, 1094-1096.
https://doi.org/10.1126/science.aao2998
Lewandowsky, S., Cook, J., Ecker, U. K. H., Albarracín, D., Amazeen, M. A., Kendeou, P.,
… & Zaragoza, M. S. (2020). The Debunking Handbook 2020.
https://www.climatechangecommunication.org/debunking-handbook-2020/
Lewandowsky, Ecker, U. K. H., Seifert, C., Schwarz, N., & Cook, J. (2012). Misinformation
and its correction: Continued influence and successful debiasing. Psychological
Science in the Public Interest, 13, 106-131.
https://doi.org/10.1177/1529100612451018
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for
ineffective health remedies: Overcoming the illusion of causality. Psychology &
Health, 33, 1472-1489. https://doi.org/10.1080/08870446.2018.1508685
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020a). Countering demand for
ineffective health remedies: Do consumers respond to risks, lack of benefits, or both?
Psychology and Health. https://doi.org/10.1080/08870446.2020.1774056
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020b). Protecting consumers from
fraudulent health claims: A taxonomy of psychological drivers, interventions,
barriers, and treatments. Social Science and Medicine, 259, 112790.
https://doi.org/10.1016/j.socscimed.2020.112790
Chapter 5: Refuting COVID-19 misinformation 112

REFUTING COVID-19 MISINFORMATION 23
McEachan, R., Conner, M., Taylor, N., & Lawton, R. (2011). Prospective prediction of
health-related behaviours with the theory of planned behaviour: A meta-analysis.
Health Psychology Review, 5, 97-144. https://doi.org/10.1080/17437199.2010.521684
Mercier, H., (2020). Not Born Yesterday: The Science of Who We Trust and What We
Believe. Princeton University Press. https://doi.org/10.2307/j.ctvn1tbqq
Mosleh, M., Pennycook, G., & Rand, D. (2020). Self-reported willingness to share political
news articles in online surveys correlates with actual sharing on Twitter. PLOS ONE,
15), e0228882. https://doi.org/10.1371/journal.pone.0228882
Oreskes, N., & Conway, E. (2010). Defeating the merchants of doubt. Nature, 465, 686–687.
https://doi.org/10.1038/465686a
Paynter, J., Luskin-Saxby, S., Keen, D., Fordyce, K., Frost, G., Imms, C., … & Ecker, U. K.
H. (2019). Evaluation of a template for countering misinformation—Real-world
Autism treatment myth debunking. PLOS ONE, 14, e0210746.
https://doi.org/10.1371/journal.pone.0210746
Pennycook, G., McPhetres, J., Zhang, Y., Lu, J., & Rand, D. (2020). Fighting COVID-19
Misinformation on social media: Experimental evidence for a scalable accuracy-
nudge intervention. Psychological Science, 31, 770-780.
https://doi.org/10.1177/0956797620939054
Poland, G., Jacobson, R., & Ovsyannikova, I. (2009). Trends affecting the future of vaccine
development and delivery: The role of demographics, regulatory science, the anti-
vaccine movement, and vaccinomics. Vaccine, 27, 3240-3244.
https://doi.org/10.1016/j.vaccine.2009.01.069
Chapter 5: Refuting COVID-19 misinformation 113

REFUTING COVID-19 MISINFORMATION 24
Powell, D., Keil, M., Brenner, D., Lim, L., & Markman, E. (2018). Misleading health
consumers through violations of communicative norms: A case study of online
diabetes education. Psychological Science, 29, 1104-1112.
https://doi.org/10.1177/0956797617753393
Rich, P. R., & Zaragoza, M. S. (2016). The continued influence of implied and explicitly
stated misinformation in news reports. Journal of Experimental Psychology:
Learning, Memory, and Cognition, 42, 62-74. doi:10.1037/xlm0000155
RMIT Fact Check. (2020, August 9). Facebook post spruiking vitamin C as a coronavirus
cure - Fact Check. ABC News. https://www.abc.net.au/news/2020-04-09/corona-5-
b/12130952?nw=0
Spinney, L. (2020, June 8). Bleach baths and drinking hand sanitiser: poison centre cases rise
under Covid-19. The Guardian.
https://www.theguardian.com/world/2020/jun/08/bleach-baths-and-drinking-hand-
sanitiser-poison-centre-cases-rise-under-covid-19
Swire, B., Ecker, U. K. H., & Lewandowsky, S. (2017). The role of familiarity in correcting
inaccurate information. Journal of Experimental Psychology. Learning, Memory, and
Cognition, 43, 1948-1961. https://doi.org/10.1037/xlm0000422
Swire-Thompson, B., DeGutis, J., & Lazer, D. (2020). Searching for the backfire effect:
Measurement and design considerations. Journal of Applied Research in Memory and
Cognition. https://doi.org/10.1016/j.jarmac.2020.06.006
Swire‐Thompson, B., Ecker, U. K. H., Lewandowsky, S., & Berinsky, A. J. (2020). They
might be a liar but they’re my liar: Source evaluation and the prevalence of
misinformation. Political Psychology, 41, 21-34. https://doi.org/10.1111/pops.12586
Chapter 5: Refuting COVID-19 misinformation 114

REFUTING COVID-19 MISINFORMATION 25
Therapeutic Goods Administration (2020). No evidence to support intravenous high-dose
vitamin C in the management of COVID-19. https://www.tga.gov.au/alert/no-
evidence-support-intravenous-high-dose-vitamin-c-management-covid-19
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011).
Estimating the impact of pictorial health warnings and “plain” cigarette packaging:
evidence from experimental auctions among adult smokers in the United States.
Health Policy, 102, 41-48. https://doi.org/10.1016/j.healthpol.2011.06.003
Vaccari, C., & Morini, M. (2014). The power of smears in two American presidential
campaigns. Journal of Political Marketing, 13, 19-45.
https://doi.org/10.1080/15377857.2014.866021
Van Bavel, J., Baicker, K., Boggio, P., Capraro, V., Cichocka, A., Cikara, M.,… & Willer, R.
(2020). Using social and behavioural science to support COVID-19 pandemic
response. Nature Human Behaviour, 4, 460-471. https://doi.org/10.1038/s41562-020-
0884-z
van der Linden, S., Leiserowitz, A., Rosenthal, S, & Maibach, E. (2017). Inoculating the
public against misinformation about climate change. Global Challenges, 1, 1600008.
https://doi.org/10.1002/gch2.201600008
Walter, N., & Tukachinsky, R. (2020). A meta-analytic examination of the continued
influence of misinformation in the face of correction: How powerful is it, why does it
happen, and how to stop it? Communication Research, 47, 155-177.
https://doi.org/10.1177/0093650219854600
Weule, G. (2020, March 25). Can you boost your immune system to help fight coronavirus?
Australian Broadcasting Corporation. https://www.abc.net.au/news/health/2020-03-
25/can-you-boost-your-immune-system-to-help-fight-coronavirus/12085036
Chapter 5: Refuting COVID-19 misinformation 115

REFUTING COVID-19 MISINFORMATION 26
Zarocostas, J. (2020). How to fight an infodemic. The Lancet, 395, 676–676.
https://doi.org/10.1016/s0140-6736(20)30461-x
Chapter 5: Refuting COVID-19 misinformation 116

REFUTING COVID-19 MISINFORMATION 27
Author Contributions: All authors jointly developed the study concept and contributed to the
study design. DM prepared the experimental survey, and performed data collection
and analysis, with input from all other authors. LQT and DM drafted the manuscript,
and MH and UKHE provided critical revisions. All authors approved the final version
of the manuscript for submission.
Open Practices Statement: The experiment was not formally pre-registered. The materials are
available in Supplemental Material B. Both the data and the supplements are available
at https://osf.io/p89bm/.
Acknowledgments: This research was supported by a UWA International Fee Scholarship
and University Postgraduate Award to LQT, an Australian Government Research
Training Program Scholarship to DM, and grant FT190100708 from the Australian
Research Council to UKHE.
Chapter 5: Refuting COVID-19 misinformation 117

118

Foreword for Chapters 6-7
Chapters 6 and 7 outline two different instances of how psychology and conservation
are intricately linked, both as causes and as solutions. Importantly, they provide a key bridge
for the present thesis between the applied psychology and the underlying conservation issues
that inspired this line of research.
In Chapter 6, I present the results of a meta-review that was inspired by an earlier
systematic review of demand-reduction campaigns targeting wildlife products (Veríssimo &
Wan, 2019). The earlier review found that a lack of robust evaluations in the conservation
literature made it impossible to draw insights to inform future efforts to reduce demand. To
fill this knowledge gap, my meta-review aimed to synthesize the evidence for what works
from outside of conservation (e.g., in public health, social marketing, etc.) to reduce
consumer demand. This review aimed to provide a platform to discuss how this body of
evidence could be applied to address the demand for wildlife products. The results challenge
persistent myths in the wildlife demand-reduction space, such as the assumption that
awareness-raising campaigns are effective or that negative messaging is ineffective. To
ensure the findings were of practical benefit to conservation, I developed a series of
infographics to help communicate the key findings. The review has important implications
for addressing a host of wildlife-related problems (e.g., biodiversity loss and food-chain
collapse), especially given the renewed attention to the connection between the
overexploitation of wildlife and the potential for the trade to facilitate new zoonotic disease
outbreaks (Johnson et al., 2020).
In Chapter 7, I present a published perspective paper that I co-authored with Dr
Ricardo Rocha, a pioneering tropical ecologist (MacFarlane & Rocha, 2020). Dr Rocha
reached out to me in response to various reports of wild bats being persecuted due to
misguided fears associated with disease risk, likely as a consequence of the heightened media
Foreword for Chapters 6-7 119
attention surrounding the possible origins of COVID-19 (Buttke, Decker, & Wild, 2015). He
was concerned that well-intentioned efforts by researchers and conservationists to counteract
the dangerous negative associations between wild species and disease risk may be further
reinforcing negative associations (Davis, Goldwater, Ireland, Gaylord, & Van Allen, 2017).
The perspective piece draws on several key psychological insights from the VANMaN
taxonomy (Chapter 2) to provide some succinct guidelines to aid conservation scientists and
practitioners in their mission to articulate wildlife-related science in the context of human
health, without contributing to reinforcing negative associations.
The issues and perspectives covered in the perspective piece highlight the
interconnectedness of conservation, public health, and psychology. Specifically, the trade and
consumption of wild bats are driven, in part, by several psychological constructs such as
social norms, misperceptions about health benefits, and misperceptions about lack of risks
(Liu et al., 2016, 2015; Thomas-Walters et al., 2020). The consequence of this demand is that
the wildlife trade brings diverse wildlife species into contact with humans and other animals
and thus presents considerable risks for facilitating the emergence of zoonotic disease
transmission (Johnson et al., 2020). The solution to reducing demand is to design targeted
interventions that help consumers overcome the barriers preventing them from ceasing to
consume wildlife. However, poorly constructed intervention messaging could perpetuate
myths and misguided beliefs about bats, leading to further entrenched beliefs and the desire
to consume bats. Equally, poor messaging could contribute to misguided fears about bat
disease risks, which can encourage retaliation towards bat species (López‐Baucells, Rocha, &
Fernández‐Llamazares, 2018). Even isolated instances of bat culling can bring people into
closer contact with bats and thus further increase zoonotic transmission risk (Streicker et al.,
2012). Another major concern is that many bat species are severely threatened with
extinction, so even small instances of violence could cause irreversible damage and have
Foreword for Chapters 6-7 120

catastrophic flow-on effects for ecosystems that humans rely on (e.g., bats are important for
agriculture, as controllers of pests and pollinators of crops; Aziz et al., 2017).
In Chapter 7, I describe how key psychological barriers can impact on people’s
perception of intervention messaging. My hope is that this paper will help fuel future research
on using psychology in conservation, and thus help people make more informed choices that
protect nature and ultimately reduce zoonotic disease risks.
Foreword for Chapters 6-7 121

References
Aziz, S. A., Clements, G. R., McConkey, K. R., Sritongchuay, T., Pathil, S., Abu Yazid, M.
N. H., … Bumrungsri, S. (2017). Pollination by the locally endangered island flying fox
(Pteropus hypomelanus) enhances fruit production of the economically important durian
(Durio zibethinus). Ecology and Evolution, 7, 8670–8684.
Buttke, D. E., Decker, D. J., & Wild, M. A. (2015). The role of one health in wildlife
conservation: a challenge and opportunity. Journal of Wildlife Diseases, 51, 1–8.
Davis, T., Goldwater, M. B., Ireland, M. E., Gaylord, N., & Van Allen, J. (2017). Can you
catch Ebola from a stork bite? Inductive reasoning influences generalization of
perceived zoonosis risk. PLoS One, 12, e0186969.
Johnson, C. K., Hitchens, P. L., Pandit, P. S., Rushmore, J., Evans, T. S., Young, C. C. W., &
Doyle, M. M. (2020). Global shifts in mammalian population trends reveal key
predictors of virus spillover risk. Proceedings of the Royal Society B, 287, 20192736.
Liu, Z., Jiang, Z., Fang, H., Li, C., Mi, A., Chen, J., … Meng, Z. (2016). Perception, price
and preference: Consumption and protection of wild animals used in traditional
medicine. PLoS One, 11, e0145901.
Liu, Z., Jiang, Z., Li, C., Fang, H., Ping, X., Luo, Z., … Zeng, Y. (2015). Public attitude
toward tiger farming and tiger conservation in Beijing, China. Animal Conservation, 18,
367–376.
López‐Baucells, A., Rocha, R., & Fernández‐Llamazares, Á. (2018). When bats go viral:
negative framings in virological research imperil bat conservation. Mammal Review, 48,
62–66.
Foreword for Chapters 6-7 122

MacFarlane, D., & Rocha, R. (2020). Guidelines for communicating about bats to prevent
persecution in the time of COVID-19. Biological Conservation, 248.
Streicker, D. G., Recuenco, S., Valderrama, W., Gomez Benavides, J., Vargas, I., Pacheco,
V., … Rohani, P. (2012). Ecological and anthropogenic drivers of rabies exposure in
vampire bats: implications for transmission and control. Proceedings of the Royal
Society B: Biological Sciences, 279, 3384–3392.
Thomas-Walters, L., Hinsley, A., Bergin, D., Doughty, H., Eppel, S., MacFarlane, D., …
Veríssimo, D. (2020). Motivations for the use and consumption of wildlife products.
Conservation Biology. doi:10.1111/cobi.13578
Veríssimo, D., & Wan, A. K. Y. (2019). Characterizing efforts to reduce consumer demand
for wildlife products. Conservation Biology, 33, 623–633.
Foreword for Chapters 6-7 123

124

Chapter 6: Reducing demand for overexploited
wildlife products
This chapter is presented in the format of a journal article.
MacFarlane, D., Hurlstone, M. J., Ecker, U. K. H., Ferraro, P. J, van der Linden, S., Wan, A. K. Y., Veríssimo, D., Burgess, G., Chen, F., Hall, W., Hollands, G. J., & Sutherland, W. J. (Under Review) Reducing demand for overexploited wildlife products: Lessons from systematic reviews from outside conservation science. Manuscript submitted for publication.
125

126

[Reducing Demand for Overexploited Wildlife Products]
1
Reducing Demand for Overexploited Wildlife Products: Lessons from Systematic Reviews
from Outside Conservation Science
*Douglas MacFarlane1,2, Mark J. Hurlstone2,3, Ullrich K. H. Ecker2, Paul J. Ferraro4, Sander
van der Linden5, Anita K. Y. Wan6, Diogo Veríssimo7,8,9, Gayle Burgess10, Frederick Chen11;
Wayne Hall12, Gareth J. Hollands13, and William J. Sutherland1,14
Conservation Science Group, Department of Zoology, University of Cambridge, Cambridge UK1
School of Psychological Science, University of Western Australia, Australia2
Department of Psychology, Lancaster University, UK3
Carey Business School and the Department of Environmental Health and Engineering,
a joint department of the Bloomberg School of Public Health and the
Whiting School of Engineering, Johns Hopkins University4
Social Decision-Making Laboratory, Department of Psychology, University of Cambridge, UK5
Socio-Ecological and Conservation Science Lab, School of Life Sciences, Sun Yat-Sen
University, China6
Oxford Martin Programme on the Illegal Wildlife Trade, Oxford University, UK7
San Diego Zoo Global, Institute for Conservation Research, Escondido, CA, USA8
Department of Zoology, University of Oxford, Oxford, UK9
TRAFFIC, The Wildlife Trade Monitoring Network, UK10
Economics Department, Wake Forest University, US11
Faculty of Health & Behaviour Science, University of Queensland, Australia12
Behaviour and Health Research Unit, University of Cambridge, UK13
BioRISC, St. Catharine's College, Cambridge CB2 1RL, UK14
*Correspondence concerning this article should be addressed to Douglas MacFarlane, Cambridge Conservation Science Group, Department of Zoology, University of Cambridge, The David Attenborough Building, Pembroke Street, Cambridge CB2 3QZ, UK. E-mail: [email protected]
Chapter 6: Reducing demand for overexploited wildlife products 127

[Reducing Demand for Overexploited Wildlife Products]
2
Summary
Conservationists have long sought to reduce consumer demand for overexploited wildlife
products. More recently, health practitioners and others have begun calling for reductions in
the wildlife trade to reduce the risk of pandemics. Despite this broadening interest, most
wildlife-focused demand reduction campaigns have lacked rigorous evaluations and thus
their impacts remain unknown. There is thus an urgent need to review the evidence from
beyond conservation science to inform future demand-reduction efforts. We searched for
systematic reviews of interventions that aimed to reduce consumer demand for harmful
products (e.g., cigarettes and illicit drugs). In total, 41 systematic reviews were assessed, and
their data extracted. Mass-media campaigns and incentive programs were, on average,
ineffective. While advertising bans, social marketing and location bans were promising, there
was insufficient robust evidence to draw firm conclusions. In contrast, the evidence for the
effectiveness of risk warnings and appeals to norms was stronger, with some caveats.
Keywords: illegal wildlife trade; demand reduction; evidence-based interventions;
overconsumption; biodiversity conservation; mass-media campaigns; social norms; fear
appeals; behaviour change; zoonoses.
Chapter 6: Reducing demand for overexploited wildlife products 128

[Reducing Demand for Overexploited Wildlife Products]
3
Reducing Demand for Overexploited Wildlife Products: Lessons from an Overview of
Systematic Reviews from Outside Conservation Science
Introduction
The overexploitation of wild plants and animals is a major driver of biodiversity
decline.1,2 In addition to directly depleting population numbers, overexploitation can cause
cascading effects on the balance of predators and prey species within food webs and diminish
the productivity of important food sources for humans. For example, the globalized shark-fin
industry, driven primarily by Asian demand for shark-fin soup,3 is an important cause of
declining shark populations.4 Sharks play a crucial role in maintaining ecosystem health, and
thus their overexploitation has been linked to a dramatic restructuring of marine-life
communities, which in turn, has been linked to the collapse of fishing industries.5,6
One major driver of overexploitation is the wildlife trade, which comprises a diverse
set of actors ranging from suppliers that hunt and transport products to consumers that buy
and trade them through, for example, tourist markets and exotic pet forums. Consumer
demand for wildlife products such as rhino horn, pangolin scales, and bat meat7 fuels the
wildlife trade, which can threaten biodiversity in complex ways. For example, the
international trade in wildlife can facilitate the global spread of infectious wildlife diseases
resulting in catastrophic losses in biodiversity.8 For example, the amphibian chytrid fungus
(Batrachochytrium dendrobatidis), a deadly pathogen spread through the amphibian-trade,
has already harmed more than 500 species globally, and caused more disease-driven
extinctions than any other pathogen in recorded history.9
Beyond the alarming environmental impacts, elements of the wildlife trade are illegal
or unethical and can have devastating effects on human communities by for example,
accelerating government corruption10 and militarising conservation responses.11,12 Moreover,
Chapter 6: Reducing demand for overexploited wildlife products 129

[Reducing Demand for Overexploited Wildlife Products]
4
the wildlife trade has likely contributed to the emergence of several major human diseases,
including at least two novel coronavirus outbreaks in the last two decades.13 Virologists have
consistently warned that the highest risk of virulent zoonotic spillovers comes from specific
human activities—namely, the mixing of taxonomically diverse species and increased
human-animal interaction.14,15 These two activities are ubiquitous in the wildlife trade (e.g.,
hunting, the exotic pet trade, and live wildlife markets).
The traditional response to the overexploitation of wildlife has mainly focused on the
supply side: international trade bans and regulations under the Convention on International
Trade in Endangered Species of Wild Fauna and Flora (CITES). However, whilst there is
some evidence to show that trade bans can be effective, especially when accompanied by
other measures (e.g., Vicuna fibre in Peru16), there is also some evidence they can have
adverse impacts. For example, they can drive high demand from consumers who believe the
resource may soon be unavailable, which can drive price hikes and thus incentivise illegal
poaching (e.g., black rhinoceros17 and primate bushmeat18). This can occur under numerous
of conditions, including when a product is banned but the ban is poorly enforced and demand
is inelastic—when the quantity of the product being consumed declines relatively little
despite an increase in price—which then incentivises traders to supply markets illegally and
creates the potential for suppliers to control the market through the use of force.19,20
In recognition of such limitations, conservationists are increasingly seeking to
complement supply-side interventions with actions to reduce consumer demand.
Considerable effort has been expended on public communications and awareness-raising
campaigns to counter the illegal wildlife trade (estimated to account for [~6%] of global
funding).21 However, fundamental questions remain about what campaigns are effective for
reducing demand for overexploited (also illegal or unethical) wildlife products. Are
awareness-raising campaigns effective for changing consumer behaviour? Are positively
Chapter 6: Reducing demand for overexploited wildlife products 130

[Reducing Demand for Overexploited Wildlife Products]
5
framed messages more effective than negative ones? Can incentive programs provide
sustainable consumer behaviour change? Is social marketing key to halting
overconsumption? Does banning location-based consumption, such as China’s ban on shark-
fin soup at government banquets,22 reduce overall consumption, or merely displace it? The
present overview seeks to provide novel insight into these crucial questions.
Unfortunately, the evidence regarding the impact of different interventions on altering
the behaviour of wildlife consumers is largely anecdotal or based on research designs with a
high risk of bias, such as studies without control comparisons.23 A recent review by
Veríssimo and Wan23 identified 236 demand-reduction campaigns aimed at wildlife products
but found that only five reported on direct changes of consumer behaviour. Furthermore, only
two campaigns reported behavioural outcomes that allowed estimates of variability and effect
sizes. The authors concluded that the absence of robust evaluations precluded any meaningful
recommendations to inform future action. To increase the likelihood that future demand-
reduction campaigns will be effective, efficient, and not counterproductive, there is an urgent
need for empirical evidence.
To fill this knowledge gap, we must therefore turn to the broader literature, to assess
the evidence on “what works” in reducing consumer demand. The present overview
synthesises the evidence on relevant interventions from the broader academic literature on
reducing harmful consumer demand—consumption of products that are illegal, unethical, or
otherwise harmful to health, society, or the environment. Since most demand-reduction
campaigns are motivated to counter behaviours that entail such harms, we confined our
search criteria to interventions that target products considered harmful (e.g., alcohol,
cigarettes, and unhealthy foods). This multidisciplinary approach is important for two
primary reasons. First, compared to conservation, greater resources have been devoted to
testing behaviour change interventions to reduce harmful consumer demand in other
Chapter 6: Reducing demand for overexploited wildlife products 131

[Reducing Demand for Overexploited Wildlife Products]
6
disciplines (mostly health, and to a lesser extent in criminology and education).24–26
Consequently, there exists more robust evidence on the effectiveness of interventions
targeting harmful consumer demand in disciplines other than conservation. Second, there is
little reason to suggest this situation is likely to change. Until conservation organisations
devote adequate resources towards adopting experimental (or robust quasi-experimental)
designs to test behaviour-change interventions,27,28 it will be difficult to determine which
strategies are effective, ineffective, or counterproductive.
[Insert Table 1 near here]
Our specific goal was to synthesise the evidence on demand-reduction interventions targeting
products that may have parallels with the wildlife trade (i.e., sharing similar consumer
motivations, such as the desire for recreation or social recognition; see Table 1). Importantly,
we acknowledge that the consumer dynamics of non-wildlife products will inevitably differ
in ways that may limit the generalisability of the results to conservation (e.g., alcohol is
cheap, accessible, and mostly legal, whereas rhino horn is expensive, harder to source, and
often illegal). However, we contend that certain conceptual similarities, such as comparable
underlying consumer motivations (see Table 1) and analogous approaches to demand-
reduction campaigns, provide a sufficient basis to estimate the potential effectiveness of
several commonly used behavioural interventions, such as mass-media campaigns. Further,
we argue it would be careless to ignore lessons from the wider research literature, given the
potential to inform similar demand-reduction efforts to counter the illegal wildlife trade.
To inform our search strategy, we formed an advisory board from experts in health,
psychology, social marketing, economics, and conservation. To provide a manageable
overview of the vast body of evidence, we limited our analysis to systematic reviews.
Chapter 6: Reducing demand for overexploited wildlife products 132

[Reducing Demand for Overexploited Wildlife Products]
7
Results
Forty-one systematic reviews were included, of which sixteen contained meta-analyses. The
reviews were categorised according to seven broadly defined intervention types: mass-media
campaigns, incentives, advertising bans and regulations, social-marketing campaigns,
location-based bans, norm appeals, and risks warnings. Reviews were assessed according to
quality (see Supplementary Quality assessment) with twelve rated as Quality A (no
limitations identified); thirteen as Quality B (one limitation identified); and sixteen as Quality
C (two or more limitations identified). We assessed reviewer agreement across each review-
quality criterion individually with a reliability analysis using Cohen’s κ (see Supplementary
Kappa analysis). The mean percentage agreement was 88% and average κ = 0.63 (κ > 0.6
indicates substantial agreement29). Individual criteria with κ < 0.6 were revisited for
discussion and reconciliation. Only one criterion failed to meet this benchmark, κ = 0.22.
Subsequently, four instances of disagreement were revisited, and some additional limitations
were noted (see Supplementary Table S3). However, the reconciliation process did not
change the overall review-quality ratings as most disagreements related to low-quality
reviews with several other limitations (see Supplementary Kappa analysis).
Narrative summaries of each systematic review are provided in the following section
(for more detailed summaries and identified limitations, see Table S3 of supplementary
materials). The reviews under each intervention category are ordered by review quality, date,
and by the name of first author. The number of studies included in each systematic review is
denoted via k. When reviews provided information on experimental design of included
studies, we provide this information using the following abbreviations: RCT = Randomised
control trial; ITS = Interrupted time series; NRSI = Non-randomised studies of interventions;
BA = Before/after; L = Longitudinal; Obs = Observational.
Chapter 6: Reducing demand for overexploited wildlife products 133

[Reducing Demand for Overexploited Wildlife Products]
8
Narrative Summaries
Mass-media campaigns. This category included initiatives that used mass-
communication media to persuade people to change their behaviour. A typical example was a
campaign that ran advertisements at cinemas to challenge perceptions about smoking, using
messages developed with focus groups of smokers.
Nine systematic reviews focused on the impact of mass-media campaigns, mostly on
drug consumption (illicit drugs, alcohol, and tobacco). Review Quality A: Carson-Chahoud
et al.30 (2017, k = 8 [7 RCT, 1 ITS]) noted that most (five out of eight) studies found no effect
of mass-media campaigns on preventing youth smoking. However, the authors concluded it
would be unwise to draw firm conclusions due to inconsistent results and the risk of bias in
methods and study designs. Mosdol et al.31 (2017, k = 6 [5 RCT, 1 ITS]) concluded that their
confidence in the impact of mass-media campaigns on multiple behaviours (including
tobacco and alcohol consumption) in ethnic minorities was very low because most studies
were of low quality. Allara et al.32 (2015, k = 19 [8 RCT]) found no effect of mass-media
campaigns on illicit drug use, based on a pooled analysis of 8 eligible studies. However, the
authors advised caution about using mass-media campaigns to reduce illicit drug use because
of evidence paucity and inconsistency. Review Quality B: Bala et al.33 (2017, k = 11 NRSI)
concluded that comprehensive tobacco control programs may change smoking behaviours in
adults but note that evidence came from a small number of very low study quality studies.
Trieu et al.34 (2017, k = 22 [4 RCT]) found that population-level media campaigns can reduce
salt consumption, but higher-quality studies showed smaller effect sizes and inconsistent
results. Thus, they concluded that media campaigns are likely inadequate. Werb et al.35
(2011, k = 11 [7 RCT, 4 Obs]) found no effect of public-service announcements on illicit
drug use, based on a meta-analysis of four studies. They note that four studies showed public-
service announcements actually increased intention to use illicit drugs. Review Quality C:
Chapter 6: Reducing demand for overexploited wildlife products 134

[Reducing Demand for Overexploited Wildlife Products]
9
Allen et al.36 (2015, k = 34 NRSI) concluded that there was strong evidence supporting the
use of mass-media campaigns to reduce youth smoking. Durkin et al.37 (2012, k = 26 NRSI)
concluded the effectiveness of mass-media campaigns on reducing youth smoking depended
on campaign reach, intensity, duration, and messaging used. Specifically, they found that
communicating negative health effects were most effective at encouraging quitting. Snyder et
al.38 (2004, k = 21 [mostly NRSI]) concluded that mass-media health campaigns have small
measurable effects on tobacco and alcohol consumption in the short term.
Incentives. These interventions informed participants that future benefits, or the
removal of future benefits, will depend on adopting a desired health behaviour (e.g., smoking
cessation). Incentive interventions included contests, competitions, incentive schemes,
lotteries, raffles, and contingent payments. A common example is the smoke-free class
competition, which typically involves asking students to enter into a contract not to smoke for
a set period and promises of prizes for classes that stay mostly (> 90%) smoke-free.
Three systematic reviews focused on the impact of incentive campaigns (e.g.,
contests and lotteries) on smoking behaviours. Review Quality A: Corepal et al.39 (2018, k =
8 RCT) concluded that incentives have a small impact on reducing smoking in children and
adolescents (5-18 years), based on a meta-analysis of 8 studies. Mantzari et al.40 (2015,
k = 34 RCT) concluded that financial incentives can be effective for smoking cessation for up
to 18-months, but did not persist beyond 3-months after the incentives end. Review Quality
B: Hefler et al.41 (2017, k = 8 [3 RCT]) concluded that the small number of studies suggested
that incentive programs did not prevent smoking initiation.
Advertising bans. This category includes bans or restrictions on advertising to
promote the consumption of harmful products, such as cigarettes or alcohol. Bans could
cover, for example, advertising on television, internet, or billboards. Another common
Chapter 6: Reducing demand for overexploited wildlife products 135

[Reducing Demand for Overexploited Wildlife Products]
10
example is legislation requiring cigarettes to be plain-packaged to remove the colourful and
attractive branding used for product promotion.
Six systematic reviews focused on the impact of advertising bans on cigarette and
alcohol consumption. Review Quality B: McNeill et al.42 (2017, k = 51 [1 RCT]) concluded
that plain cigarette packaging may reduce consumption, noting that evidence was mostly
based on one large observational study in Australia (N = 700,000). Siegfried et al.43 (2014,
k = 4 [1 RCT, 3 ITS]) concluded the quality of evidence was too low to support a ban on
alcohol advertising. Review Quality C: Hughes et al.44 (2016, k = 4) concluded that there is
insufficient evidence from low-income countries to draw firm conclusions on impact of plain
packaging on cigarette consumption. Moodie et al.45 (2012, k = 37 [2 RCT]) concluded the
evidence for impact of plain packaging on cigarette consumption was mixed but suggested
that it had a deterrent effect. Capella et al.46 (2008, k = 50) concluded cigarette advertising
bans (both full or partial, e.g., only in broadcast media) did not have a significant impact on
cigarette consumption. Quentin et al.47 (2007, k = 24 NRSI) found in 10 out of the 24 studies
that full-advertising bans had a significant effect on cigarette consumption but acknowledged
significant limitations in drawing conclusions from time-series data.
Social marketing. Social marketing is broadly defined as the use of marketing
techniques to achieve positive social ends.48 Although social marketing campaigns can utilise
mass-media, the approach differs from mass-media campaigns (as broadly defined in the
present paper) by encouraging adoption of other intervention approaches such as education,
social initiatives (e.g., designated driver campaigns), and counseling (e.g., quit lines and
cessation groups etc.). Social marketing is commonly conceived as a process whereby
intervention design is guided by key marketing principles such as customer orientation,
market segmentation, and motivational exchange (increasing incentives and decreasing
barriers to change).49,50
Chapter 6: Reducing demand for overexploited wildlife products 136

[Reducing Demand for Overexploited Wildlife Products]
11
Five systematic reviews focused on the impact of social-marketing campaigns on drug
consumption (cigarette, alcohol, and illicit drugs). Review Quality B: Janssen et al.50 (2013,
k = 6) concluded the impact of social-marketing campaigns could not be assessed due to lack
of quality studies. Stead et al.51 (2007, k = 35) used a problematic vote-counting approach
(comparing the number of studies with significant vs. non-significant results) to conclude that
social-marketing principles could be effective in reducing use of tobacco, alcohol, and illicit
drugs. Review Quality C: Hung et al.52 (2017, k = 48) concluded interventions based on
social-marketing principles had small significant effects on smoking, but no effect on alcohol
consumption. Almestrahiri et al.53 (2017, k = 8) concluded that social marketing interventions
can positively influence smoking behaviours (e.g, quit attempts and smoking prevalence),
although effectiveness was not the focus of their review. Kubacki et al.54 (2015, k = 10) found
mostly positive results (6/10) and thus concluded that social marketing was largely effective
for reducing alcohol consumption.
Location bans. This category included bans on cigarette smoking in public places.
Typically, legislative bans and policies prohibit smoking in public spaces (e.g., restaurants
and trains) and workplaces (e.g., offices, hospitals, schools, and universities).
Seven systematic reviews focused on the impact of location bans on cigarette
consumption. Review Quality A: Frazer et al.55 (2016, k = 17 NSRI) concluded location-
based smoking policies in hospitals, prisons, and universities can reduce smoking rates,
although they noted evidence quality was low. Review Quality B: Monson and Arsenault56
(2017, k = 16 BA & L) concluded legislated bans on smoking in public areas had an overall
positive effect on reducing smoking rates at home. Frazer et al.57 (2016, k = 77 NSRIs)
concluded the impact of smoking bans on smoker numbers and cigarette consumption was
inconsistent, but that bans were effective at the national level in reducing second-hand smoke
exposure. Review Quality C: Bennet and Pokhrel58 (2017, k = 11 NRSI [mostly cross-
Chapter 6: Reducing demand for overexploited wildlife products 137

[Reducing Demand for Overexploited Wildlife Products]
12
sectional]) concluded more longitudinal studies were needed, while noting two promising
studies showing smoke-free policies significantly reduced smoking at universities. Hopkins et
al.59 (2010, k = 57 BA) concluded smoke-free policies reduce tobacco consumption, but their
results were less compelling when only the strongest study designs were assessed. Bell et
al.60 (2009, k = 16 NRSI [1 quasi experimental, 3 cohort, 12 cross-sectional]) concluded
smoking bans at worksites can reduce overall cigarette consumption but results varied across
sub-groups (e.g., less impact on low income groups) and bans may have unintended
consequences (e.g., displacement of smoking). Chapman et al.61 (1999, k = 19) found 18 of
19 studies found smoke-free policies reduced daily smoking during work hours.
Norm appeals. Social norms are rules or standards about how members of a com-
munity should behave. Examples of social norms range from the explicit (e.g., laws and
regulations) to the implicit and unspoken (e.g., norms about where to sit on a train). A norm
appeal communicates a desirable social norm with the aim of altering people’s behaviour
towards that norm. A common example involves providing personalised normative feedback
about actual consumption (e.g., average student drinking norms) so that outliers (e.g.,
students who drink more than average) adjust their behaviour towards the norm (Wood,
Brown, & Maltby, 2012).62
Three systematic reviews focused on the impact of social-norm appeals on alcohol
consumption. Review Quality A: Prestwich et al.63 (2016, k = 41 RCT) concluded even large
changes in beliefs about social norms produce only small changes in alcohol intake, and thus
norm appeals should be combined with other interventions. Foxcroft et al.64 (2015, k = 66
RCT) found social-norm appeals had small but significant effects on drinking frequency and
quantity (namely, 0.9 alcoholic drinks less per week compared to a baseline of 13.7 drinks);
however, they suggested that the effect sizes may be too small to be practically relevant.
Dotson el al.65 (2015, k = 8 [13 RCT]) concluded personalised normative feedback had small
Chapter 6: Reducing demand for overexploited wildlife products 138

[Reducing Demand for Overexploited Wildlife Products]
13
but clinically relevant impact on college student drinking (a reduction by ~3 drinks per
week).
Risk warnings. These interventions draw consumer attention towards the potential
risks of consuming a harmful product. Most of the evidence on reducing harmful consumer
demand that has been assessed through systematic reviews has focused on the impacts of
highlighting risks to personal health (e.g., the requirement for cigarette packages to display
large graphic images of smoking-related diseases). The results therefore may not generalise
to risk warnings outside of this specific context (e.g., risks to reputation, conservation
outcomes, or cruelty to animals etc).
Eight systematic reviews focused on the impact of risk-warning messaging on mostly
tobacco, and to a lesser extent, alcohol consumption. Review Quality A: Clarke et al.66
(2020, k = 12 RCT) concluded health warning labels have significant potential for decreasing
the selection of unhealthy food and drink products. However, they noted all experimental
studies to date had been conducted in the laboratory or online. Sheeran et al.67 (2014, k = 209
RCT) concluded heightening risk appraisals (namely, risk perceptions, anticipatory emotions,
anticipated emotions, and perceived severity) had a small but significant impact on smoking,
but not alcohol consumption. Risk warnings were most effective when accompanied by
appeals to self-efficacy (confidence in one’s ability to change towards a recommended
behaviour) and response efficacy (perceptions about how much the recommended behaviour
will alleviate the hazard). Review Quality B: Noar et al.68 (2016, k = 37 RCT) concluded that
pictorial warnings were more effective than text warnings for most non-behavioural
outcomes (e.g., elicited negative attitudes towards smoking). However, they identified only a
single experimental study that assessed impact on behaviour. Tannenbaum et al.69 (2015,
k = 127 RCT) concluded fear appeals positively influenced behaviours in all but a few
circumstances (NB: authors combined demand for harmful substances with other behaviours
Chapter 6: Reducing demand for overexploited wildlife products 139

[Reducing Demand for Overexploited Wildlife Products]
14
not relevant to this review). Monarrez-Espino et al.70 (2014, k = 12 [5 RCT]) concluded the
evidence for, or against, the sustained impact of pictorial health warnings on smoking
behaviours was poor. The authors noted risk warnings likely have a modest impact on
behaviour. Peters et al.71 (2013, k = 13 RCT) concluded threatening communications were
only effective when the target population had high self-efficacy. Review Quality C: Noar et
al.72 (2016, k = 22 NRSI) concluded strengthened (e.g., increased size of text warning,
change from text to pictorial) cigarette-pack warnings were associated with less smoking and
increased cessation rates. Scholes-Balog et al.73 (2012, k = 10 NRSI) concluded alcohol
warning labels were not associated with changes in self-reported risky alcohol use amongst
adolescents.
Quantitative Summary
For each systematic review that contained a meta-analysis, Figure 1 provides a visual
summary of the primary effect size reported (see Supplementary Table S4). Effect sizes in
Figure 1 are displayed to demonstrate the impact of each intervention on reducing a harmful
consumer behaviour; thus effect sizes with 95% confidence intervals wholly below zero were
deemed to be effective, whereas effect sizes with 95% confidence intervals including zero
were deemed not to provide clear evidence of effectiveness (i.e., they were not statistically
significant).
Chapter 6: Reducing demand for overexploited wildlife products 140

[Reducing Demand for Overexploited Wildlife Products]
15
Figure 1. Comparison of effect sizes between intervention types
Figure 1. Forest plot of effect sizes (Cohen’s d) for each systematic review containing meta-analysis––error bars represent 95% confidence intervals. Effect sizes indicate whether an intervention was effective (cases where the upper confidence interval sits below zero), ineffective (cases where the confidence interval encompasses zero), or counterproductive (cases where the lower confidence interval exceeds zero) in reducing harmful consumer behaviour. For transparency, we also include an assessment of each source’s review quality (i.e., A, B, or C). ✣ Snyder et al. 2008 did not provide confidence intervals. Thus, these were conservatively estimated based on the reported lack of significance. Symbol key: squares = illicit drugs, circles = tobacco, triangles = alcohol, and diamond = tobacco, alcohol, and other behaviours combined.
Chapter 6: Reducing demand for overexploited wildlife products 141

[Reducing Demand for Overexploited Wildlife Products]
16
Discussion
Our analysis sought to provide a broad overview of the evidence, from outside the
conservation literature, pertaining to seven types of interventions that have been applied to
reducing harmful consumption. To inform our assessments, we narratively summarised key
conclusions from each systematic review and extracted quantitative results on mean effect
sizes, whenever meta-analyses were conducted (Figure 1). Some of our results will come as a
surprise to many engaged in delivering demand-reduction campaigns for overexploited
wildlife products. Most notably, two of the most familiar approaches to effecting behaviour
change for conservation, namely mass-media campaigns and incentive programs, were found
to be ineffective, on average. Moreover, any effects of incentive programs disappeared
shortly after program conclusion (>3months). In contrast, the two strategies that emerged as
most supported, with some caveats, have been under-utilised (norm appeals)74 or face active
resistance from some in conservation (risk warnings).26 We found some evidence that the
remaining three intervention types can be effective, namely advertising bans, social
marketing, and location bans, however, a lack of robust evidence precluded drawing firm
conclusions about their overall impact.
We also found that none of the intervention types appear, on average, to be
counterproductive (e.g., increase consumer demand, see Figure 1). There thus seems to be
little harm in investigating whether combinations of multiple approaches prove more
powerful than individual approaches. Indeed, there is already considerable overlap between
our broadly defined intervention types, such as location bans that signal social norms or
social marketing campaigns that utilise mass-media. The inability to completely distinguish
between intervention types suggests that future research might also benefit from exploring
alternative frameworks for assessing campaign efficacy, such as cost benefit analysis or
Chapter 6: Reducing demand for overexploited wildlife products 142

[Reducing Demand for Overexploited Wildlife Products]
17
compatibility with theoretical behaviour-change frameworks (e.g., the behaviour change
wheel75).
Interestingly, despite the considerable investment in evaluating behaviour change
campaigns, especially within the public health domain, we note that many systematic reviews
were unable to draw firm conclusions about the impact of several commonly used
approaches, often owing to lack of robust study designs. Specifically for mass-media
campaigns and social marketing, we also observed a general tendency in systematic reviews
that we classed as having multiple methodological limitations (e.g., did not assess study bias)
to draw positive conclusions, whereas the higher quality reviews tended to conclude that
insufficient high-quality studies precluded drawing firm conclusions. Such differences
highlight the importance of considering evidence quality when drawing conclusions about the
impact of a particular intervention.
We now discuss the results of each specific intervention type with reference to
insights from psychology and consider to what extent, and under what contexts, each
intervention might generalise towards reducing demand for wildlife products. We then
discuss the overall implications of this overview for informing future behaviour-change
campaigns and addressing other global environmental problems related to overconsumption.
Interventions Found to be Generally Ineffective
Mass-media campaigns. Mass-media campaigns are often perceived as synonymous
with awareness raising, which is arguably the most common behaviour-change approach in
conservation.74 Despite their popularity, mass-media campaigns were found to be, on
average, ineffective, with all four meta-analyses finding non-significant impacts. Only one of
nine systematic reviews, with multiple methodological limitations, suggested there was
strong evidence supporting the use of mass-media campaigns. However, that review noted
that effectiveness varied depending on message content, with strongest evidence for
Chapter 6: Reducing demand for overexploited wildlife products 143

[Reducing Demand for Overexploited Wildlife Products]
18
messages highlighting health risks. The remaining eight reviews highlighted that the low
quality of primary evidence precluded firm conclusions about effectiveness, while one argued
they were likely inadequate, and another suggested they occasionally backfire.
These results do not mean all reviewed media campaigns were ineffective.
Importantly, we found that systematic reviews of mass-media campaigns tended to
encompass other related interventions, which are more targeted and supported by insights
from psychology, and were found to be effective when considered separately, such as norm
appeals and risk warnings. We thus restrict our critique of mass-media campaigns to those
that fail to target specific psychological drivers of harmful consumption other than a lack of
awareness.
A major problem with awareness-raising campaigns is they rely on an intuitive, but
incomplete, mental model of human behaviour—specifically, that “if people only knew what
I know about this problem, then they would change their behaviour.” This is the information-
deficit model—the assumption that people’s behaviour will change once they have the right
information.76 Much research shows to the contrary that access to information is only one of
many competing influences on human behaviour.77–79 For example, the success of a
campaign to increase household recycling will be limited by structural barriers such as access
to recycling facilities, cost of services, and convenience to householders. Moreover, even
when such barriers are low, the success of an intervention may be limited by internal
psychological barriers such as lack of motivation to participate in recycling programs or a
widespread perception that it is socially acceptable not to recycle.80
We thus advise conservation practitioners against intuitively using mass-media
campaigns that ignore the structural or psychological barriers to behaviour change. This
conclusion is shared by others who have argued that organisations seeking social change
should not solely rely on awareness-raising.81,82
Chapter 6: Reducing demand for overexploited wildlife products 144

[Reducing Demand for Overexploited Wildlife Products]
19
Incentives. All three systematic reviews of incentives schemes noted that their
analyses were based on a small number of studies so results should be interpreted with
caution. Nevertheless, two concluded incentives schemes were probably ineffective and the
third found they can be effective, but only in the short-term as impacts disappeared after three
months.
Incentive schemes for reducing environmental harms are likely familiar to many
conservationists,83 including those working on combating the supply side of the illegal
wildlife trade.84 However, to the best of our knowledge, such schemes have not yet been
applied to the demand side (i.e., to discourage consumption). Nevertheless, a recent report
outlining behavioural insights for conservation suggested incentive schemes presented a
promising strategy.85
Based on the available evidence, however, we would caution against using incentive
programs to target wildlife consumers, especially for long-term behaviour change. Although
given the limited evidence base, we suggest incentive programs might still warrant
consideration but only if practitioners are prepared to robustly test intervention effectiveness
and duly examine their suitability to a given context. The reasons why incentive schemes can
fail to bring about behaviour change are manifold: (i) introducing extrinsic incentives
(especially financial) can undermine people’s intrinsic, or altruistic, motives and thereby
reduce overall motivation to conserve wildlife;86 (ii) incentives can lead to “moral licencing”,
whereby enabling people to “pay” for the moral cost of a behaviour (e.g., by choosing some
financial cost) can offset their feelings of guilt and thus empower them to engage in even
more problematic behaviours (e.g., to buy more wildlife products); 87 and (iii) incentives tend
to have only short-term effects, so that once the incentive scheme ends, people tend to revert
to their previous behaviours.88 An alternative approach to incentive schemes, may instead be
Chapter 6: Reducing demand for overexploited wildlife products 145

[Reducing Demand for Overexploited Wildlife Products]
20
to invigorate and amplify consumer existing intrinsic motivations towards conserving
wildlife, such as by making flagship species a symbol of national pride.89
Figure 2. Summary of interventions found to be, on average, ineffective.
Figure 2. This figure summarises some key problems when implementing mass-media campaigns and incentives programs. The right column highlights one promising solution to address each respective problem.
Promising Interventions that Require more Robust Evidence
Advertising bans. There is limited evidence that advertising bans can be effective in
reducing harmful consumer demand. Five of the six reviews noted there was insufficient
Chapter 6: Reducing demand for overexploited wildlife products 146

[Reducing Demand for Overexploited Wildlife Products]
21
evidence to draw strong conclusions, but half still concluded they can be effective. In
support, McNeil et al.42 noted that studies have consistently shown consumers prefer branded
than plain-packaged cigarettes. In the reviews classed as having two or more limitations, two
concluded the evidence generally supported the use of advertising bans, whereas one
concluded advertising bans did not reduce cigarette consumption.
Given the limited evidence available, we strongly recommend researchers first
evaluate whether, and to what extent, advertising actually drives wildlife consumer demand.
For example, practitioners could conduct a randomised controlled experiment assessing
consumers’ hypothetical willingness-to-pay90 for plain-packaged vs. branded wildlife
products (see Figure 3 for examples). If branding is shown to significantly increase wildlife
consumer demand, then practitioners should consider how to limit advertising/branding of
wildlife products (e.g. by lobbying governments to penalize companies that produce product
packaging).
If advertising does motivate demand, then the effectiveness of bans will be limited by
two factors. First, the illegal nature of much wildlife trade would make it difficult to enforce
regulations. Second, effectiveness would be limited by the magnitude of influence that
advertising has on consumer demand compared to other factors related to health, hedonism,
and culture91, and price, portability, and availability.92
Chapter 6: Reducing demand for overexploited wildlife products 147

[Reducing Demand for Overexploited Wildlife Products]
22
Figure 3. Example advertising used to market products made from wildlife.
Figure 3. Example branding for wildlife products. (a) Shark liver oil capsules, photo by Diogo Veríssimo; (b) and (c) Bear bile extract, photos by Amy Hinsley; and (d) Herbal “turtle jelly” (Gui-Ling-Gao, contains turtle plastron), photo by Diogo Veríssimo.
Social marketing. Despite conservationists’ growing enthusiasm for social
marketing,93–95 only a handful of campaigns have been applied to reducing demand for
(a)
0
(b)
0
(c)
0
(d)
0
Chapter 6: Reducing demand for overexploited wildlife products 148

[Reducing Demand for Overexploited Wildlife Products]
23
wildlife products.23 Outside conservation, we found there was poor-quality evidence to
support the approach. Of two reviews, each classed as having a single methodological
limitation, one found insufficient evidence to draw conclusions while the other suggested the
approach could be effective but acknowledged that many studies found no benefit. Of three
remaining reviews, each with multiple methodological limitations, conclusions were mixed,
noting the approach is largely effective, can be effective, or is not effective for alcohol and
has small impacts on smoking.
Whilst these results may be surprising, it is worth noting two limitations of this
assessment. First, social marketing has often been used inconsistently, and
opportunistically,50 with many studies misconstruing social marketing as simply advertising
or communication for social goals.51 Thus, systematic reviews cannot simply rely on
assessing interventions labelled as “social marketing” because not all incorporate key social-
marketing principles. This problem is exacerbated because there exist several social-
marketing frameworks, which suggest the approach comprises between six and eight key
principles.49,96,97 Further, many primary studies do not report important components of the
social-marketing interventions, such as the underlying behaviour-change theory.52
Second, one core principle of social marketing is the use of multiple interventions,
which can range from TV commercials to education campaigns. In practice, this makes it
often impossible to determine which particular strategies have been effective. Hung52 also
noted that most studies of social-marketing campaigns did not provide adequate information
about study designs or methods.
Despite these limitations, several principles associated with social marketing50 are
valuable in guiding the design of effective behavioural interventions. For example, one useful
principle is exchange, whereby in order to increase the uptake of a desired behaviour (e.g.,
drinking non-alcoholic beverages), interventions should increase consumer motivations
Chapter 6: Reducing demand for overexploited wildlife products 149

[Reducing Demand for Overexploited Wildlife Products]
24
towards adopting the behaviour (e.g., save money, improve health), and remove the barriers
from doing so (e.g., social pressures, alcohol addiction). Another useful principle is
segmentation, namely dividing larger heterogeneous groups of people into smaller more
homogenous groups who may share important values, motives, behaviours, attitudes, and
societal pressures. For example, there may be different gender-specific barriers to seeking
help with problematic drinking, such as differences in social expectations or support
networks. Interventions may thus need to be tailored to be effective.69
In conclusion, whilst the evidence base for social marketing in the context of harmful
products is currently weak, we accept its principles have merit. Furthermore, there is some
evidence social marketing can be effective for addressing problems outside of the remit of the
present paper.98,99 We therefore advise practitioners considering social marketing to influence
wildlife consumers to ensure that they employ robust experimental designs to evaluate the
impact of their interventions as well as comply with core social marketing benchmarks.49
Indeed, one recent robust evaluation of a social-marketing campaign found it successfully
reduced unsustainable wild-meat consumption by ~62%.100
Location bans. There was some evidence that banning harmful consumption in
specific locations has an overall positive effect on reducing cigarette consumption, including
outside banned locations. However, the latest and most comprehensive review55 noted that
overall evidence quality was low.
In addition to directly reducing consumption, location bans may operate through
indirect mechanisms such as descriptive-norm appeals (i.e., making smoking less visible and
hence signalling that it is uncommon) and injunctive-norm appeals (i.e., signalling the social
disapproval of smoking). Although one review noted location bans could displace
consumption to private areas,60 more recent and comprehensive reviews concluded
Chapter 6: Reducing demand for overexploited wildlife products 150

[Reducing Demand for Overexploited Wildlife Products]
25
displacement was not supported,56 especially by studies that assessed impact on national
consumption.55
Unfortunately, the evidence in favour of location bans is limited to smoking. This
provides limited evidence that similar impacts might be expected for consuming (i.e., eating
or purchasing) wildlife products in public places (e.g., marketplaces, restaurants, or
governmental banquets). Nevertheless, the results support the notion that bans on
conspicuous wildlife consumption may be a potent intervention to reduce overall demand for
wildlife products.101,103 Indeed, the apparent reduction in demand for shark-fin soup in
mainland China104 might be linked to bans on consumption in prominent locations (e.g.,
hotels, restaurants, and airline menus).106 Arguably the most significant location ban was
when Chinese authorities banned the consumption of shark-fin soup, bird nests, and other
wild animal products at official banquets in 2013.22
Chapter 6: Reducing demand for overexploited wildlife products 151
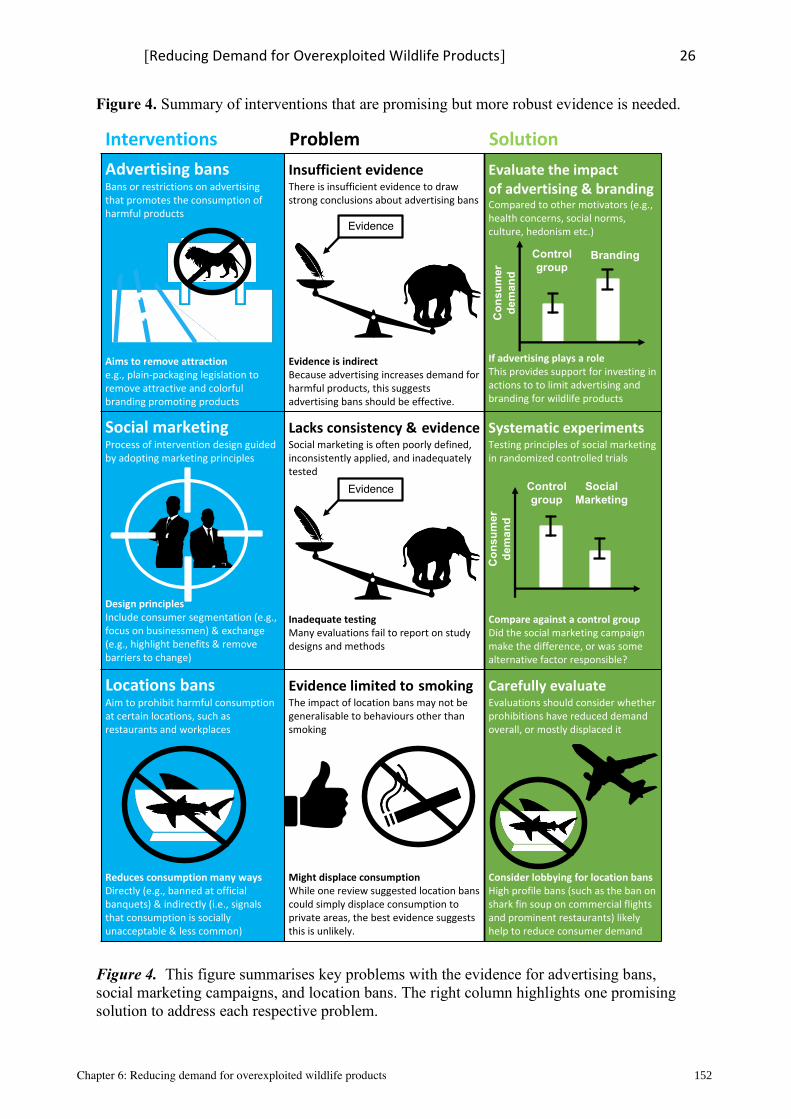
[Reducing Demand for Overexploited Wildlife Products]
26
Figure 4. Summary of interventions that are promising but more robust evidence is needed.
Figure 4. This figure summarises key problems with the evidence for advertising bans, social marketing campaigns, and location bans. The right column highlights one promising solution to address each respective problem.
Advertising bansBans or restrictions on advertising that promotes the consumption of harmful products
Aims to remove attractione.g., plain-packaging legislation to remove attractive and colorful branding promoting products
Insufficient evidence PThere is insufficient evidence to draw strong conclusions about advertising bans
Evidence is indirectBecause advertising increases demand for harmful products, this suggests advertising bans should be effective.
Evaluate the impact Pof advertising & brandingCompared to other motivators (e.g., health concerns, social norms, culture, hedonism etc.)
If advertising plays a roleThis provides support for investing in actions to to limit advertising and branding for wildlife products
Social marketingProcess of intervention design guided by adopting marketing principles
Design principlesInclude consumer segmentation (e.g., focus on businessmen) & exchange (e.g., highlight benefits & remove barriers to change)
Lacks consistency &IevidenceSocial marketing is often poorly defined, inconsistently applied, and inadequately tested
Inadequate testingMany evaluations fail to report on study designs and methods
Systematic experiments PTesting principles of social marketing in randomized controlled trials
Compare against a control groupDid the social marketing campaign make the difference, or was some alternative factor responsible?
Locations bansAim to prohibit harmful consumption at certain locations, such as restaurants and workplaces
Reduces consumption many waysDirectly (e.g., banned at official banquets) & indirectly (i.e., signals that consumption is socially unacceptable & less common)
Evidence limited toIsmokingThe impact of location bans may not be generalisable to behaviours other than smoking
Might displace consumptionWhile one review suggested location bans could simply displace consumption to private areas, the best evidence suggests this is unlikely.
Carefully evaluate PEvaluations should consider whether prohibitions have reduced demand overall, or mostly displaced it
Consider lobbying for location bansHigh profile bans (such as the ban on shark fin soup on commercial flights and prominent restaurants) likely help to reduce consumer demand
Interventions Problem Solution
Evidence
BrandingControlgroup
Con
sum
er
dem
and
Evidence Social Marketing
Controlgroup
Con
sum
er
dem
and
Chapter 6: Reducing demand for overexploited wildlife products 152

[Reducing Demand for Overexploited Wildlife Products]
27
Interventions Found to be Generally Effective
Norm appeals. There was consistent evidence from all three reviews (none of which
had any identified methodological limitations) that norm appeals can have a small impact on
consumer demand for alcohol. Two reviews noted these effects were clinically relevant but
the third suggested they were too small to have policy relevance. Importantly, one review,
Dotson et al.65, focused only on personalised normative feedback—individualized feedback
on a person’s drinking behaviour—whereas the other two reviews also assessed generalised
social norms. The focus on individualised norms may have explained Dotson et al.’s
relatively stronger conclusions in support of the impact of social norms.
Three key findings from our analysis may help ensure that conservationists have
realistic expectations about the potentially limited impact of norm appeals. First, while social
influences and normative beliefs can be changed by, for example, communicating how much
others drink, such belief changes produce only small changes in consumption. Consequently,
norm appeals are likely more effective when accompanied by other interventions. Second,
impersonal social norms may be less effective than personalised normative feedback,
however, such highly targeted approaches will not be feasible for many, often opaque,
wildlife consumer behaviours. Third, poorly designed norm appeals can back-fire (i.e.,
increase harmful consumption), particularly when descriptions of the extent of undesirable
behaviours inadvertently encourages conformity in the wrong direction.108
In designing norm appeals to reduce demand for wildlife products, we therefore
recommend practitioners conduct experimental research to pilot-test norm appeal messages
so that they are targeted, persuasive, and do not backfire,82,110 before using them in targeted
messaging campaigns. We also advise practitioners to refer to one of the many science-based
guides for designing effective norm appeals.77,85,112 They should also augment such appeals
with other promising interventions, such as risk warnings.
Chapter 6: Reducing demand for overexploited wildlife products 153

[Reducing Demand for Overexploited Wildlife Products]
28
Risk warnings. Of all seven intervention types reviewed, the evidence was strongest
in support of the impact of warnings about risks of consumption to individual’s health. Six
out of seven reviews concluded that risk warnings were effective in reducing cigarette or
alcohol consumption, with an eighth concluding that they are effective in altering unhealthy
food selection. Only one review, with multiple methodological limitations, concluded that
risk warnings did not reduce self-reported risky alcohol consumption in adolescents.
Common findings about what makes risk warnings effective included that they should
incorporate messages to boost self-efficacy (people’s ability to adopt the recommended
behaviour) and response-efficacy (people’s perception about how changing their behaviour
will alleviate the risks; e.g., lung recovery after quitting smoking), use pictorial health
warnings (vs. text only), and emphasise high susceptibility (i.e., the vulnerability of the target
group).69
Importantly, our findings were confined to health-related warnings and thus the
results may not generalise to warnings about other risks relevant to conservation contexts
(e.g., risks to reputation, conservation outcomes, or cruelty to animals etc). Further
experimental studies are required to assess the impact of other warning types on
consumption. We also acknowledge the suggestion that health-risk warnings could be an
effective conservation tool is likely to be met with resistance from some conservationists.
Despite the pervasive use of risk messaging in political, advertising, and public-health
campaigns, conservationists have fiercely debated whether optimistic or pessimistic
communication framing strategies are better at inducing behaviour change.26 Yet, Kidd et
al.26 pointed out that the papers advocating for either approach substantially outnumber the
papers providing empirical, conservation-specific evidence. They thus called for building a
stronger evidence base to inform the best ways to communicate conservation messages.
Chapter 6: Reducing demand for overexploited wildlife products 154

[Reducing Demand for Overexploited Wildlife Products]
29
The present review does not aim to settle the debate, particularly because the target
behaviours of many conservation communications are outside of the present focus (e.g.,
donation, policy support, environmental action etc.). However, our synthesis highlights that
warning people about the health risks of their consumption behaviours can effectively reduce
demand. As many activities within the wildlife trade carry significant health risks (e.g.,
heightened risk of zoonoses spill over from bushmeat consumption,114 animal markets,14 and
hunting15), our findings suggest that conservationists should consider how risk warnings can
be leveraged to reduce consumer demand for overexploited wildlife products. Indeed, in light
of the devastation caused by the current coronavirus pandemic, and the aforementioned
associated risks, there may be a moral responsibility for conservationists to incorporate
factual health-risk warnings into communications that concern many wildlife trade activities
(for conservation relevant guidance, see MacFarlane and Rocha116).
In our view, rather than asking whether negative or positive messages are more
effective, we agree with McAfee and Connell118 that greater appreciation is needed for how
the two framing approaches can work independently and in tandem, and how their
effectiveness varies with context. Experiments have shown that people’s evaluations of risks
and benefits tend to be negatively correlated—even when each is distinctly different.119 For
example, if antibiotics are portrayed as effective, this will encourage the perception that they
are also low in side effects, and vice versa. Equally, if pesticide use is considered high risk,
this will encourage the perception that it is less effective, and vice versa. Thus, by
communicating that consuming primate meat is both high in risk (e.g., of contracting
disease123) and low in benefit (no more nutritious than other forms of protein) we can use
both elements combined to reduce people’s perception of its value. Indeed, a recent
experiment found that while the perceived value of an ineffective health remedy could be
reduced by communicating either its lack of benefits (by 23%) or its potential health risks (by
Chapter 6: Reducing demand for overexploited wildlife products 155

[Reducing Demand for Overexploited Wildlife Products]
30
30%), communicating both produced the greatest reduction in perceived value (by 50%).90
These results have implications for framing conservation messaging about traditional health
remedies that contain wildlife.
While risk messaging is a potentially potent intervention for reducing harmful
consumption, careless risk messaging can have negative conservation outcomes. For
example, recent communications about the health risks posed by consuming bats (e.g., the
potential for contracting novel zoonoses) may have contributed to reduced conservation
support and increased violent retaliation towards wild bat communities.124 One way to
neutralise the unintended effects of risk communications is to include messages about
potential benefits (e.g., the positive ecological impacts of wild bats).125 Another tactic is to
put the risk into context, for example, by communicating the risks of zoonoses from a diverse
range of animals. This may discourage contacts with animals while avoiding disproportionate
negative attention to individual species (e.g., bats or rats).127 For further guidance on
communicating risks see also MacFarlane and Rocha116).
[Insert Figure 5 near here]
Implications
The results of the present review have implications for addressing one of the major
drivers of the biodiversity crisis, namely over-consumption. Changing behaviours related to
over-consumption requires learning from existing evidence and applying a systematic and
iterative approach to learning what interventions, and combinations thereof, are most
effective. There are many examples of overconsumption that have far-ranging impacts on
biodiversity where an evidence-based approach is needed. For example, a form of
overconsumption that is often overlooked is illegal timber harvesting. This is estimated to
supply between 10-15% of global timber trade and 50% of local trade in some
Chapter 6: Reducing demand for overexploited wildlife products 156

[Reducing Demand for Overexploited Wildlife Products]
31
Figure 5. Summary of interventions found to be effective, with important caveats.
Figure 5. This figure summarises some key problems with norm appeals and risk warnings. The right column highlights one promising solution to address each respective problem.
areas.128 Seafood is another example where illegal, unregulated, and undocumented
overconsumption, driven by consumer demand, is causing extensive negative impacts.128
Beyond reducing demand for illegal wildlife products this review has broader implications
for addressing major issues such as climate change. Climate change is inextricably linked to
biodiversity decline and appreciably driven by overconsumption, including through
unsustainable dietary patterns.1,129–131 Yet, there is a paucity of evidence regarding what
Norm appealsHighlight social norms — rules or standards about how members of a community should behave
Relies on affiliationsExamples range from explicit (e.g., laws and regulations) to implicit (e.g., where to sit on a train) norms
Small impacts PEven large changes in normative beliefs tend to engender only small changes in consumption
Can also backfirePoorly designed campaigns can implicitly highlight undesirable norms and encourage conformity in wrong direction
Pilot test messages PUse evidence-based guides to designing effective norm appeals
Combine with other interventionsAugment norm messaging with other interventions, such as risk warnings
Risk warningsDraw attention to the potential risks of consumption (e.g., to health or reputation)
Aims to inform & dissuadeExamples include graphic images of diseases that could result from consuming a product
Self-efficacy is essential PPeople must have capacity to change behavior, and believe the change will mean they avoid the risk
Can have unintended outcomesFor example, could contribute to the misguided anger towards wildlife (i.e., not just a fear of the the products)
Incorporate efficacy PHighlight ways to boost self-efficacy (e.g., exercise & diet promote good health, not miracle cures)
Also, highlight the benefits of wildlifeTo avoid backlash against a species (e.g. wild vultures are ecologically important & reduce disease risks)
Interventions Problem Solution
=
Chapter 6: Reducing demand for overexploited wildlife products 157

[Reducing Demand for Overexploited Wildlife Products]
32
works to change climate-relevant behaviours.132 The climate crisis calls for rapid reductions
in consumption of transport goods and services, such as large vehicles and long-haul air
travel. The potential reduction in carbon emissions that could be achieved by moderating
demand for air travel is substantial. For example, one ticket on a long-haul flight from the
United Kingdom to Australia equals the annual carbon emissions of an average UK person.133
To address each of these challenges, we must learn from both our success and failures, and
thus robust evaluations are critical to any ultimate success.
Limitations. There are several potential limitations of the present review. First,
across the seven relatively common intervention approaches reviewed, most systematic
review authors called for robust evidence to make firm conclusions regarding efficacy.
Second, even for those interventions where the evidence was more robust, we do not know
whether, and/or to what extent, the related insights will generalise to addressing the wildlife
trade. Therefore, we advise conservationists who are considering applying one or more
intervention types to proceed with caution and factor in robust experimental controls into
intervention design, to ensure their subsequent evaluations can confidently contribute to the
evidence base.
We also acknowledge that in presenting such a broad overview of the literature we
have inevitably oversimplified many of the cultural and contextual differences between the
consumption of specific harmful products (e.g., alcohol and cigarettes) compared to many
wildlife products. For instance, the evidence reviewed mostly comes from countries that are
Western, educated, industrialised, rich, and democratic, with populations that may have
distinct cognitive and motivational differences from non-Western countries.134 While this
may limit the generalisability of our findings to non-Western countries, we nevertheless hope
our approach uncovers some of the valuable insights gleaned from the decades of research
and hard lessons learned from existing efforts to alter consumer behaviour.
Chapter 6: Reducing demand for overexploited wildlife products 158

[Reducing Demand for Overexploited Wildlife Products]
33
Another limitation is that while we have adopted a systematic approach to assessing
the literature, three elements of a typical systematic review were beyond the purview of the
present project. These include (i) pre-registering a review protocol; (ii) recruiting multiple
researchers to apply the exclusion criteria and conduct data extraction in duplicate; and (iii)
preserving the originally-proposed exclusion criteria, since additional criteria had to be added
(including financial incentives, education projects, and brief interventions) after the initial
screening phase to ensure the final list of papers was sufficiently applicable to the project.
Furthermore, by excluding non-systematic reviews, our overview will have missed
some primary literature. We suggest that this limitation is somewhat offset by the fact that the
included systematic reviews have already collated, screened, and applied quality-control
processes to much of the relevant literature and been peer reviewed. Similarly, given the
broad scope of the review, it is possible we have not included some relevant systematic
reviews. We aimed to minimise this risk by asking the advisory group to suggest reviews that
had been missed. Finally, our categorisation of evidence into broad intervention types has
invariably oversimplified much nuance relevant for making successful intervention
campaigns. We acknowledge, for example, that not all location-based campaigns are
identical. We hope that our discussion has illuminated some nuances, whilst providing a
broad overview of intervention effectiveness.
Conclusion
Conservationists have increasingly sought to reduce consumer demand for
overexploited wildlife products to address the current biodiversity crisis, and many are now
calling for reductions in the wildlife trade to reduce the risk of pandemics. We sought to learn
from the evidence from beyond conservation by considering systematic reviews of
interventions that aim to reduce consumer demand for harmful products (e.g., cigarettes and
illicit drugs). Our results found that mass-media campaigns were, on average, ineffective and
Chapter 6: Reducing demand for overexploited wildlife products 159

[Reducing Demand for Overexploited Wildlife Products]
34
incentive programs were either ineffective or short-lived. We found that whilst advertising
bans, social marketing, and locations bans were promising approaches, more high-quality
evidence is needed to draw firm conclusions. There was more robust evidence that norm
appeals can be effective, but effect sizes were often too small to be clinically relevant. We
found that most robust evidence suggested that risk warnings can be effect, however, critical
factors must be incorporated, such as including an efficacy component to help prevent
possible public backlash against wildlife that could arise from poorly framed messaging.
By learning from disciplines, other than conservation, we can benefit from a vast
body of scientific knowledge on ‘what works’ to alter consumer behaviour. Our findings thus
provide some insights into why some conservation campaigns may be more effective than
others. Ultimately, the better we learn from the evidence, the better we can counteract the
overexploitation of wildlife.
Search & Analysis Procedures
Cochrane Database of Systematic Reviews, Web of Science, PsycINFO, and Scopus
were searched for systematic reviews of primary studies assessing the effectiveness of
interventions to reduce demand for harmful products (see supplemental materials “Search
Strategy” for full details). For the purpose of this review, harmful products were deemed to
be any product or substance that was likely to be the target of a public demand-reduction
campaign, such as alcohol, tobacco, illicit drugs, stolen goods, and foods with high sugar or
salt content. The search strategy was developed in conjunction with an advisory board of 11
experts. The advisory board was recruited to cover diverse expertise including health,
economics, psychology, behavioural economics, and wildlife consumer behaviour. The
database searches were run between the 18 - 26 October 2018. We did not apply limitations to
the start date or geographical setting. However, for efficiency, we excluded records from
Chapter 6: Reducing demand for overexploited wildlife products 160

[Reducing Demand for Overexploited Wildlife Products]
35
Scopus older than 2008, as this database only allowed for the extraction of article titles and
not abstracts.
Study Screening
Our search strategy returned 13,325 unique articles that were screened against our
inclusion criteria:
1. Does the study aim to evaluate interventions to reduce demand (or otherwise alter
consumption behaviour, e.g., stop smoking) for a harmful product, using
quantitative data of intervention effectiveness?
2. Is the study a systematic review?
Reviews were judged to be systematic if they reported search-strategy details,
inclusion and exclusion criteria, and clearly identified all included studies. Inclusion criteria
were set high due to ensure the external validity of the results for answering the primary
question and to ensure the overall volume of literature could be feasibly assessed given the
available resources. We only included studies that reported on objective measures of
consumer behaviour (also called “hard-measures”), which give a direct indication of the
effectiveness of a given intervention on behaviour (e.g., sales figures, consumption levels, or
quit attempts). Studies were thus excluded if they only reported non-behavioural outcomes
(also called “soft-indicators”) such as attitude, intention, and knowledge (see supplemental
material for justification). We excluded reviews that did not assess impact on consumer
demand, such as those that evaluated harm-reduction outcomes (e.g., alcohol related
accidents). We only included interventions that could feasibly be considered scalable and
deliverable at a population rather than individual level, such as pharmacotherapy or brief
interventions (individual advice delivered by medical professionals). Other exclusion criteria
were also applied to ensure the interventions were feasible and practical for the current
context. Full details and explanations of all exclusion criteria are covered in supplemental
Chapter 6: Reducing demand for overexploited wildlife products 161

[Reducing Demand for Overexploited Wildlife Products]
36
materials (Table S2). The exclusion criteria were applied across multiple stages of screening
(namely: title only, title and abstract, full text screening). The articles were checked for
duplicate publications and updates, in which case only the most comprehensive and recent
review was included. Overviews of reviews were excluded, unless they also reviewed
primary studies; their reference lists were also searched for any inclusion in the present
overview. The advisory board also provided suggestions on key reviews. Figure 6 shows the
PRISMA flow diagram of numbers progressing through the screening process.
Figure 6. PRISMA flow diagram of review screening process.
Chapter 6: Reducing demand for overexploited wildlife products 162

[Reducing Demand for Overexploited Wildlife Products]
37
Data Extraction
Data were extracted from the final list of included reviews using a standardised form
that collected information on the outcome indicators assessed, results from any meta-analysis,
study limitations, and a summary of the authors’ conclusions. Review quality was evaluated
against five key criteria, specifically on whether the systematic review (i) assessed mostly
randomised controlled trials, and justified the inclusion of non-randomised study designs; (ii)
used a comprehensive search strategy; (iii) provided detailed descriptions of each included
study; (iv) assessed the risk of bias and limitations for each included study; and (v) if the
review included a meta-analysis, whether the authors assessed the impact of heterogeneity of
the included papers. This set of criteria was adapted from the recently developed AMSTAR
tool.135 The exact text used to apply each criterion and a discussion of the criteria’s suitability
is provided in the supplementary materials under the heading “Quality Assessment”. Based
on these criteria, reviews received one of three ratings: A—yes to all criteria (or n/a to
criterion 5); B—no to one criterion; or C—no to two or more criteria. This quality assessment
measure thus aimed to draw the reader’s attention to potential limitations of given reviews
(e.g., “review X did not assess risk of study bias”). The specific limitations of particular
reviews identified through this process are outlined in Table S3 of the supplementary
materials. Importantly, our criteria reflect an assessment of review quality rather than an
assessment of the quality of respective primary studies.
The quality of each review was scored by the primary author. A random sample of 20
reviews were also rated by three independent reviewers. Kappa analysis was then conducted
comparing the ratings of each criterion between the reviewers. This analysis was used to
identify sources of disagreement between quality assessments, which then facilitated the
reconciliation of any differences in the application of a criterion.
Chapter 6: Reducing demand for overexploited wildlife products 163

[Reducing Demand for Overexploited Wildlife Products]
38
Data Analysis
Comprehensive narrative summaries of the results were extracted into Table S3. For
brevity, an additional narrative synthesis of Table S4 was conducted for inclusion in the main
review and categorised according to intervention type. We also provided a more quantitative
comparison of each intervention type by collating an effect size from each systematic review
that contained meta-analysis. To avoid reporting pseudo-replicated effect sizes, we extracted
only one effect size from each systematic review. When reviews reported multiple effect
sizes, we prioritised the effect size that (i) communicated an assessment of an objective
measure of consumer behaviour, and (ii) was calculated from the greater number of high-
quality studies. To help communicate the results, a forest plot was created (Figure 1) by
converting effect sizes into the statistic that was most commonly reported, namely Cohen’s d.
However, we did not conduct meta-analysis given the heterogeneity of intervention types,
review methodologies, and outcome variables. Comparisons of each meta-analytical effect
size are thus only provided to offer an overview of the evidence base and to illustrate the
comparative impact, and variability, of different intervention types. Furthermore, whilst
Cohen’s d is less amenable to direct interpretation in lay terms, we considered it more
appropriate given the aim of providing a general comparative overview of heterogeneous
results. When data, such as confidence intervals, were missing or not amenable to
standardization, the original review authors were approached for clarification. Where the
authors did not respond to our requests for clarification, respective meta-analyses were
excluded from Figure 1 so as not to provide misleading comparisons. However, for
transparency, we reported all unstandardized effect sizes in Table S4 of the supplementary
materials.
Chapter 6: Reducing demand for overexploited wildlife products 164

[Reducing Demand for Overexploited Wildlife Products]
39
Supplemental Information Description
The supplemental material contains the full details of the search strategy (components of
primary question, search terms, and search stages), eligibility criteria, and data extraction
process (quality assessment criteria and kappa analysis).
Acknowledgements
This research was facilitated by an Australian Government Endeavor Postgraduate
Scholarship awarded to the first author. The authors would also like to thank Alec Christie,
Phil Martin, and Silviu Petrovan for assisting with quality assessments and Kappa analysis.
Author Contributions
Conceptualization: DM, WS. Advisory Board & Search Criteria: MH, PJF, SvdL, AKYW,
DV, GB, FC, WH, GH, WS. Methodology: DM. Analysis: DM. Writing original Draft: DM.
Reviewing & Editing: all co-authors. Visualisation: DM. Supervision: MH, UE, WS. Funding
Acquisition: DM.
Declarations of Interests
The authors declare no competing interests.
References
1. Maxwell, S.L., Fuller, R.A., Brooks, T.M., and Watson, J.E.M. (2016). Biodiversity:
The ravages of guns, nets and bulldozers. Nature 536, 143–145.
2. Rosen, G.E., and Smith, K.F. (2010). Summarizing the evidence on the international
trade in illegal wildlife. Ecohealth 7, 24–32.
3. Dulvy, N.K., Fowler, S.L., Musick, J.A., Cavanagh, R.D., Kyne, P.M., Harrison, L.R.,
Carlson, J.K., Davidson, L.N.K., Fordham, S. V, Francis, M.P., et al. (2014).
Extinction risk and conservation of the world’s sharks and rays. Elife 3, e00590.
4. Clarke, S., Milner-Gulland, E.J., and Bjørndal, T. (2007). Social, economic, and
regulatory drivers of the shark fin trade. Mar. Resour. Econ. 22, 305–327.
Chapter 6: Reducing demand for overexploited wildlife products 165

[Reducing Demand for Overexploited Wildlife Products]
40
5. Brierley, A.S. (2007). Fisheries ecology: Hunger for shark fin soup drives clam
chowder off the menu. Curr. Biol. 17, R555–R557.
6. Myers, R.A., Baum, J.K., Shepherd, T.D., Powers, S.P., and Peterson, C.H. (2007).
Cascading effects of the loss of apex predatory sharks from a coastal ocean. Science.
315, 1846–1850.
7. Suwannarong, K., and Schuler, S. (2016). Bat consumption in Thailand. Infect. Ecol.
Epidemiol. 6, 29941.
8. Kolby, J.E. (2016). Pathways of amphibian chytrid fungus dispersal: global biosecurity
and conservation implications.
9. Scheele, B.C., Pasmans, F., Skerratt, L.F., Berger, L., Martel, A., Beukema, W.,
Acevedo, A.A., Burrowes, P.A., Carvalho, T., and Catenazzi, A. (2019). Amphibian
fungal panzootic causes catastrophic and ongoing loss of biodiversity. Science. 363,
1459–1463.
10. Wittig, T. (2016). IV. Poaching, Wildlife Trafficking and Organised Crime. Whitehall
Pap. 86, 77–101.
11. Crayne, S., and Haenlein, C. (2016). II. Poaching, Wildlife Trafficking and Conflict.
Whitehall Pap. 86, 38–57.
12. Duffy, R., and Humphreys, J. (2016). I. Poaching, Wildlife Trafficking and Human
Security. Whitehall Pap. 86, 22–37.
13. Cyranoski, D. (2020). Did pangolins spread the China coronavirus to people. Nature.
14. Johnson, C.K., Hitchens, P.L., Smiley Evans, T., Goldstein, T., Thomas, K., Clements,
A., Joly, D.O., Wolfe, N.D., Daszak, P., Karesh, W.B., et al. (2015). Spillover and
pandemic properties of zoonotic viruses with high host plasticity. Sci. Rep. 5, 14830.
15. Johnson, C.K., Hitchens, P.L., Pandit, P.S., Rushmore, J., Evans, T.S., Young,
C.C.W., and Doyle, M.M. (2020). Global shifts in mammalian population trends reveal
Chapter 6: Reducing demand for overexploited wildlife products 166

[Reducing Demand for Overexploited Wildlife Products]
41
key predictors of virus spillover risk. Proc. R. Soc. B 287, 20192736.
16. Kasterine, A., and Lichtenstein, G. (2018). Trade in Vicuña: Implications for
Conservation and Rural Livelihoods. Int. Trade Centre, Geneva, Switz.
17. Leader-Williams, N. (2014). Regulation and protection: Successes and failures in
rhinoceros conservation. In The Trade in Wildlife (Routledge), pp. 111–121.
18. Cronin, D.T., Woloszynek, S., Morra, W.A., Honarvar, S., Linder, J.M., Gonder,
M.K., O’Connor, M.P., and Hearn, G.W. (2015). Long-term urban market dynamics
reveal increased bushmeat carcass volume despite economic growth and proactive
environmental legislation on Bioko Island, Equatorial Guinea. PLoS One 10,
e0134464.
19. Challender, D., Hinsley, A., and Milner-Gulland, E. (2019). Inadequacies in
establishing CITES trade bans. Front. Ecol. Environ. 17.
20. Heltberg, R. (1999). Trade bans and wildlife conservation: The case of African
elephant ivory. Agrekon 38, 405–413.
21. Wright, E.M., Bhammar, H.M., Gonzalez Velosa, A.M., and Sobrevila, C. (2016).
Analysis of international funding to tackle illegal wildlife trade. World Bank Group,
Washington, DC Available at. http//documents.worldbank.org/curated/en
/695451479221164739/Analysis-of-international-funding-to-tackle-illegal-
wildlifetrade.
22. Ng, N. (2013). China bans shark fin dishes at official banquets. CNN.
23. Veríssimo, D., and Wan, A.K.Y. (2019). Characterizing efforts to reduce consumer
demand for wildlife products. Conserv. Biol. 33, 623–633.
24. Leigh, A. (2018). Randomistas: How radical researchers are changing our world (Yale
University Press).
25. Pynegar, E.L., Gibbons, J.M., Asquith, N.M., and Jones, J.P.G. (2019). What role
Chapter 6: Reducing demand for overexploited wildlife products 167
[Reducing Demand for Overexploited Wildlife Products]
42
should randomized control trials play in providing the evidence base for conservation?
Oryx, 1–10.
26. Kidd, L.R., Bekessy, S.A., and Garrard, G.E. (2019). Neither hope nor fear: Empirical
evidence should drive biodiversity conservation strategies. Trends Ecol. Evol. 34,
278–282.
27. Kidd, L.R., Bekessy, S.A., and Garrard, G.E. (2019). Evidence is key for effective
biodiversity communication. Trends Ecol. Evol. 34, 693–694.
28. Bayliss, H.R., Haddaway, N.R., Eales, J., Frampton, G.K., and James, K.L. (2016).
Updating and amending systematic reviews and systematic maps in environmental
management. Environ. Evid. 5, 20.
29. McHugh, M.L. (2012). Interrater reliability: The kappa statistic. Biochem. medica. 22,
276–282.
30. Carson‐Chahhoud, K. V, Ameer, F., Sayehmiri, K., Hnin, K., van Agteren, J.E.M.,
Sayehmiri, F., Brinn, M.P., Esterman, A.J., Chang, A.B., and Smith, B.J. (2017). Mass
media interventions for preventing smoking in young people. Cochrane Database Syst.
Rev.
31. Mosdøl, A., Lidal, I.B., Straumann, G.H., and Vist, G.E. (2017). Targeted mass media
interventions promoting healthy behaviours to reduce risk of non‐communicable
diseases in adult, ethnic minorities. Cochrane Database Syst. Rev.
32. Allara, E., Ferri, M., Bo, A., Gasparrini, A., and Faggiano, F. (2015). Are mass-media
campaigns effective in preventing drug use? A Cochrane systematic review and meta-
analysis. BMJ Open 5, e007449.
33. Bala, M.M., Strzeszynski, L., and Topor‐Madry, R. (2017). Mass media interventions
for smoking cessation in adults. Cochrane Database Syst. Rev.
34. Trieu, K., McMahon, E., Santos, J.A., Bauman, A., Jolly, K.-A., Bolam, B., and
Chapter 6: Reducing demand for overexploited wildlife products 168
[Reducing Demand for Overexploited Wildlife Products]
43
Webster, J. (2017). Review of behaviour change interventions to reduce population
salt intake. Int. J. Behav. Nutr. Phys. Act. 14, 17.
35. Werb, D., Mills, E.J., DeBeck, K., Kerr, T., Montaner, J.S.G., and Wood, E. (2011).
The effectiveness of anti-illicit-drug public-service announcements: A systematic
review and meta-analysis. J Epidemiol Community Heal. 65, 834–840.
36. Allen, J.A., Duke, J.C., Davis, K.C., Kim, A.E., Nonnemaker, J.M., and Farrelly, M.C.
(2015). Using mass media campaigns to reduce youth tobacco use: A review. Am. J.
Heal. Promot. 30, e71–e82.
37. Durkin, S., Brennan, E., and Wakefield, M. (2012). Mass media campaigns to promote
smoking cessation among adults: An integrative review. Tob. Control 21, 127–138.
38. Snyder, L.B., Hamilton, M.A., Mitchell, E.W., Kiwanuka-Tondo, J., Fleming-Milici,
F., and Proctor, D. (2004). A meta-analysis of the effect of mediated health
communication campaigns on behavior change in the United States. J. Health
Commun. 9, 71–96.
39. Corepal, R., Tully, M.A., Kee, F., Miller, S.J., and Hunter, R.F. (2018). Behavioural
incentive interventions for health behaviour change in young people (5–18 years old):
A systematic review and meta-analysis. Prev. Med. (Baltim). 110, 55–66.
40. Mantzari, E., Vogt, F., Shemilt, I., Wei, Y., Higgins, J.P.T., and Marteau, T.M. (2015).
Personal financial incentives for changing habitual health-related behaviors: a
systematic review and meta-analysis. Prev. Med. (Baltim). 75, 75–85.
41. Hefler, M., Liberato, S.C., and Thomas, D.P. (2017). Incentives for preventing
smoking in children and adolescents. Cochrane Database Syst. Rev.
42. McNeill, A., Gravely, S., Hitchman, S.C., Bauld, L., Hammond, D., and Hartmann‐
Boyce, J. (2017). Tobacco packaging design for reducing tobacco use. Cochrane
Database Syst. Rev.
Chapter 6: Reducing demand for overexploited wildlife products 169

[Reducing Demand for Overexploited Wildlife Products]
44
43. Siegfried, N., Pienaar, D.C., Ataguba, J.E., Volmink, J., Kredo, T., Jere, M., and Parry,
C.D.H. (2014). Restricting or banning alcohol advertising to reduce alcohol
consumption in adults and adolescents. Cochrane Database Syst. Rev.
44. Hughes, N., Arora, M., and Grills, N. (2016). Perceptions and impact of plain
packaging of tobacco products in low and middle income countries, middle to upper
income countries and low-income settings in high-income countries: A systematic
review of the literature. BMJ Open 6, e010391.
45. Moodie, C., Stead, M., Bauld, L., McNeill, A., Angus, K., Hinds, K., Kwan, I.,
Thomas, J., Hastings, G., and O’Mara-Eves, A. (2012). Plain tobacco packaging: A
systematic review.
46. Capella, M.L., Taylor, C.R., and Webster, C. (2008). The effect of cigarette
advertising bans on consumption: A meta-analysis. J. Advert. 37, 7–18.
47. Quentin, W., Neubauer, S., Leidl, R., and König, H.-H. (2007). Advertising bans as a
means of tobacco control policy: A systematic literature review of time-series
analyses. Int. J. Public Health 52, 295–307.
48. Winthrop, M. (2013). Consensus Definition of Social Marketing. Int. Soc. Mark.
Assoc. [iSMA]. Retrieved from www.i-
socialmarketing.org/assets/social_marketing_definition.pdf.
49. Andreasen, A.R. (2002). Marketing social marketing in the social change marketplace.
J. Public Policy Mark. 21, 3–13.
50. Janssen, M.M., Mathijssen, J.J.P., van Bon–Martens, M.J.H., Van Oers, H.A., and
Garretsen, H.F.L. (2013). Effectiveness of alcohol prevention interventions based on
the principles of social marketing: a systematic review. Subst. Abuse Treat. Prev.
Policy 8, 18.
51. Stead, M., Gordon, R., Angus, K., and McDermott, L. (2007). A systematic review of
Chapter 6: Reducing demand for overexploited wildlife products 170

[Reducing Demand for Overexploited Wildlife Products]
45
social marketing effectiveness. Health Educ. 107, 126–191.
52. Hung, C.-L. (2017). A meta-analysis of the evaluations of social marketing
interventions addressing smoking, alcohol drinking, physical activity, and eating.
53. Almestahiri, R., Rundle-Thiele, S., Parkinson, J., and Arli, D. (2017). The use of the
major components of social marketing: A systematic review of tobacco cessation
programs. Soc. Mar. Q. 23, 232–248.
54. Kubacki, K., Rundle-Thiele, S., Pang, B., and Buyucek, N. (2015). Minimizing alcohol
harm: A systematic social marketing review (2000–2014). J. Bus. Res. 68, 2214–2222.
55. Frazer, K., McHugh, J., Callinan, J.E., and Kelleher, C. (2016). Impact of institutional
smoking bans on reducing harms and secondhand smoke exposure. Cochrane Database
Syst. Rev.
56. Monson, E., and Arsenault, N. (2017). Effects of enactment of legislative (public)
smoking bans on voluntary home smoking restrictions: a review. Nicotine Tob. Res.
19, 141–148.
57. Frazer, K., Callinan, J.E., McHugh, J., van Baarsel, S., Clarke, A., Doherty, K., and
Kelleher, C. (2016). Legislative smoking bans for reducing harms from secondhand
smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database
Syst. Rev.
58. Bennett, B.L., Deiner, M., and Pokhrel, P. (2017). College anti-smoking policies and
student smoking behavior: a review of the literature. Tob. Induc. Dis. 15, 11.
59. Hopkins, D.P., Razi, S., Leeks, K.D., Kalra, G.P., Chattopadhyay, S.K., Soler, R.E.,
and Task Force on Community Preventive, S. (2010). Smokefree policies to reduce
tobacco use: A systematic review. Am. J. Prev. Med. 38, S275–S289.
60. Bell, K., McCullough, L., Devries, K., Jategaonkar, N., Greaves, L., and Richardson,
L. (2009). Location restrictions on smoking: assessing their differential impacts and
Chapter 6: Reducing demand for overexploited wildlife products 171

[Reducing Demand for Overexploited Wildlife Products]
46
consequences in the workplace. Can. J. public Heal. 100, 46–50.
61. Chapman, S., Borland, R., Scollo, M., Brownson, R.C., Dominello, A., and
Woodward, S. (1999). The impact of smoke-free workplaces on declining cigarette
consumption in Australia and the United States. Am. J. Public Health 89, 1018–1023.
62. Wood, A.M., Brown, G.D., and Maltby, J. (2012). Social norm influences on
evaluations of the risks associated with alcohol consumption: Applying the rank-based
decision by sampling model to health judgments. Alcohol Alcohol 47, 57–62.
63. Prestwich, A., Kellar, I., Conner, M., Lawton, R., Gardner, P., and Turgut, L. (2016).
Does changing social influence engender changes in alcohol intake? A meta-analysis.
J. Consult. Clin. Psychol. 84, 845.
64. Foxcroft, D.R., Moreira, M.T., Santimano, N.M.L.A., and Smith, L.A. (2015). Social
norms information for alcohol misuse in university and college students. Cochrane
Database Syst. Rev.
65. Dotson, K.B., Dunn, M.E., and Bowers, C.A. (2015). Stand-alone personalized
normative feedback for college student drinkers: A meta-analytic review, 2004 to
2014. PLoS One 10, e0139518.
66. Clarke, N., Pechey, E., Kosīte, D., König, L., Mantzari, E., Blackwell, A.K.M.,
Marteau, T.M., and Hollands, G.J. Impact of health warning labels on selection and
consumption of food and alcohol products: systematic review with meta-analysis. .
Health Psychol. Rev.
67. Sheeran, P., Harris, P.R., and Epton, T. (2014). Does heightening risk appraisals
change people’s intentions and behavior? A meta-analysis of experimental studies.
Psychol. Bull. 140, 511.
68. Noar, S.M., Hall, M.G., Francis, D.B., Ribisl, K.M., Pepper, J.K., and Brewer, N.T.
(2016). Pictorial cigarette pack warnings: A meta-analysis of experimental studies.
Chapter 6: Reducing demand for overexploited wildlife products 172
[Reducing Demand for Overexploited Wildlife Products]
47
Tob. Control 25, 341–354.
69. Tannenbaum, M.B., Hepler, J., Zimmerman, R.S., Saul, L., Jacobs, S., Wilson, K., and
Albarracin, D. (2015). Appealing to fear: A meta-analysis of fear appeal effectiveness
and theories. Psychol Bull 141, 1178–1204.
70. Monárrez-Espino, J., Liu, B., Greiner, F., Bremberg, S., and Galanti, R. (2014).
Systematic review of the effect of pictorial warnings on cigarette packages in smoking
behavior. Am. J. Public Health 104, e11–e30.
71. Peters, G.-J.Y., Ruiter, R.A.C., and Kok, G. (2013). Threatening communication: a
critical re-analysis and a revised meta-analytic test of fear appeal theory. Health
Psychol. Rev. 7, S8–S31.
72. Noar, S.M., Francis, D.B., Bridges, C., Sontag, J.M., Ribisl, K.M., and Brewer, N.T.
(2016). The impact of strengthening cigarette pack warnings: Systematic review of
longitudinal observational studies. Soc. Sci. Med. 164, 118–129.
73. Scholes‐Balog, K.E., Heerde, J.A., and Hemphill, S.A. (2012). Alcohol warning
labels: Unlikely to affect alcohol‐related beliefs and behaviours in adolescents. Aust.
N. Z. J. Public Health 36, 524–529.
74. Kidd, L.R., Garrard, G.E., Bekessy, S.A., Mills, M., Camilleri, A.R., Fidler, F.,
Fielding, K.S., Gordon, A., Gregg, E.A., Kusmanoff, A.M., et al. (2019). Messaging
matters: A systematic review of the conservation messaging literature. Biol. Conserv.
236, 92–99.
75. Michie, S., van Stralen, M.M., and West, R. (2011). The behaviour change wheel: A
new method for characterising and designing behaviour change interventions.
Implement. Sci. 6, 42.
76. Sturgis, P., and Allum, N. (2004). Science in society: Re-evaluating the deficit model
of public attitudes. Public Underst. Sci. 13, 55–74.
Chapter 6: Reducing demand for overexploited wildlife products 173

[Reducing Demand for Overexploited Wildlife Products]
48
77. MacFarlane, D., Hurlstone, M.J., and Ecker, U.K.H. (2020). Protecting consumers
from fraudulent health claims: A taxonomy of psychological drivers, interventions,
barriers, and treatments. Soc. Sci. Med., 112790.
78. Rossen, I., Hurlstone, M.J., and Lawrence, C. (2016). Going with the grain of
cognition: Applying insights from psychology to build support for childhood
vaccination. Front. Psychol. 7, 1483.
79. Marteau, T.M., Hollands, G.J., and Fletcher, P.C. (2012). Changing human behavior to
prevent disease: The importance of targeting automatic processes. Science. 337, 1492.
80. Hornik, J., Cherian, J., Madansky, M., and Narayana, C. (1995). Determinants of
recycling behavior: A synthesis of research results. J. Socio. Econ. 24, 105–127.
81. Christiano, A., and Neimand, A. (2017). Stop raising awareness already. Stanford Soc.
Innov. Rev.
82. Burgess, G. (2016). Powers of persuasion? Conservation communications, behavioural
change and reducing demand for illegal wildlife products. Traffic Bull. 28, 65–73.
83. Pearce, D.W., and Turner, R.K. (1990). Economics of natural resources and the
environment (JHU Press).
84. Bulte, E.H., Van Kooten, G.C., and Swanson, T. (2003). Economic incentives and
wildlife conservation.
85. Rare and The Behavioural Insights Team (2019). Behavior Change For Nature: A
Behavioral Science Toolkit for Practitioners. (Rare.).
86. Rode, J., Gómez-Baggethun, E., and Krause, T. (2015). Motivation crowding by
economic incentives in conservation policy: A review of the empirical evidence. Ecol.
Econ. 117, 270–282.
87. Bowles, S. (2009). When economic incentives backfire. Harv. Bus. Rev. 87, 22-23
88. Schultz, P.W., and Florian, G.K. (2012). Promoting Pro-Environmental Behavior. In
Chapter 6: Reducing demand for overexploited wildlife products 174

[Reducing Demand for Overexploited Wildlife Products]
49
The Oxford Handbook of Environmental and Conservation Psychology, D. C. Susan,
ed. (Oxford University Press).
89. Smith, R.J., Salazar, G., Starinchak, J., Thomas-Walters, L.A., and Veríssimo, D.
(2020). Social marketing and conservation. Conserv. Res. Policy Pract., 309.
90. MacFarlane, D., Hurlstone, M., and Ecker, U. Countering demand for ineffective
health remedies: Do consumers respond to risks, lack of benefits, or both? Psychol.
Health.
91. Thomas-Walters, L., Hinsley, A., Bergin, D., Doughty, H., Eppel, S., MacFarlane, D.,
Wander Meijer, Tien Ming Lee, Phelps, J., Smith, R.J., et al. Motivations for the use
and consumption of wildlife products. Conserv. Biol.
92. Kurland, J., Pires, S.F., McFann, S.C., and Moreto, W.D. (2017). Wildlife crime: A
conceptual integration, literature review, and methodological critique. Crime Sci. 6, 4.
93. Greenfield, S., and Veríssimo, D. (2019). To what extent is social marketing used in
demand reduction campaigns for illegal wildlife products? Insights from elephant
ivory and rhino horn. Soc. Mar. Q. 25, 40–54.
94. Wright, A.J., Veríssimo, D., Pilfold, K., Parsons, E.C.M., Ventre, K., Cousins, J.,
Jefferson, R., Koldewey, H., Llewellyn, F., and McKinley, E. (2015). Competitive
outreach in the 21st century: Why we need conservation marketing. Ocean Coast.
Manag. 115, 41–48.
95. MacMillan, D.C., and Challender, D.W.S. (2014). Changing behavior to tackle the
wildlife trade. Front. Ecol. Environ. 12, 203.
96. French, J., and Russell-Bennett, R. (2015). A hierarchical model of social marketing. J.
Soc. Mark. 5, 139–159.
97. French, J., and Blair-Stevens, C. (2010). Key concepts and principles of social
marketing. Soc. Mark. public Heal. theory Pract., 29–44.
Chapter 6: Reducing demand for overexploited wildlife products 175

[Reducing Demand for Overexploited Wildlife Products]
50
98. Green, K.M., Crawford, B.A., Williamson, K.A., and DeWan, A.A. (2019). A meta-
analysis of social marketing campaigns to improve global conservation outcomes. Soc.
Mar. Q., 1524500418824258.
99. Firestone, R., Rowe, C.J., Modi, S.N., and Sievers, D. (2017). The effectiveness of
social marketing in global health: a systematic review. Health Policy Plan. 32, 110–
124.
100. Chaves, W.A., Valle, D.R., Monroe, M.C., Wilkie, D.S., Sieving, K.E., and Sadowsky,
B. (2017). Changing wild meat consumption: An experiment in the Central Amazon,
Brazil. Conserv. Lett. 11, e12391.
101. Fabinyi, M. (2011). Historical, cultural and social perspectives on luxury seafood
consumption in China. Environ. Conserv. 39, 83–92.
102. Gratwicke, B., Mills, J., Dutton, A., Gabriel, G., Long, B., Seidensticker, J., Wright,
B., You, W., and Zhang, L. (2008). Attitudes toward consumption and conservation of
tigers in China. PLoS One 3, e2544.
103. Truong, V.D., Dang, N.V.H., and Hall, C.M. (2015). The marketplace management of
illegal elixirs: illicit consumption of rhino horn. Consum. Mark. Cult. 19, 353–369.
104. Vallianos, C., Sherry, J., Hofford, A., and Baker, J. (2018). Sharks in Crisis Evidence
of Positive Behavioral Change in China as New Threats Emerge. WildAid, San Fr.
105. Lee, J.G.H., Chng, S.C.L., and Eaton, J.A. (2016). Conservation Strategy for Southeast
Asian Songbirds in Trade. Recommendations from the First Asian Songbird Trade
Crisis Summit (Wildlife Reserves Singapore and TRAFFIC).
106. Whitcraft, S., Hofford, A., Hilton, P., O’Malley, M., Jaiteh, V., and Knights, P. (2014).
Evidence of Declines in Shark Fin Demand, China. WildAid, San Fr.
107. Feng, Y., Siu, K., Wang, N., Ng, K.M., Tsao, S.W., Nagamatsu, T., and Tong, Y.
(2009). Bear bile: Dilemma of traditional medicinal use and animal protection. J
Chapter 6: Reducing demand for overexploited wildlife products 176

[Reducing Demand for Overexploited Wildlife Products]
51
Ethnobiol Ethnomed 5, 2.
108. Schultz, P.W., Nolan, J.M., Cialdini, R.B., Goldstein, N.J., and Griskevicius, V.
(2018). The constructive, destructive, and reconstructive power of social norms:
Reprise. Perspect. Psychol. Sci. 13, 249–254.
109. Newman, C., MacDonald, D., and Zhou, Y. (2014). Pangolin: Illegal medicine trade
threatens these scaly mammals with extinction. The Conversation, e33817.
110. Cialdini, R.B. (2003). Crafting normative messages to protect the environment. Curr.
Dir. Psychol. Sci. 12, 105–109.
111. Watts, J. (2011). “Cure for cancer” rumour killed off Vietnam’s rhinos. Guard.
112. Farrow, K., Grolleau, G., and Ibanez, L. (2017). Social norms and pro-environmental
behavior: A review of the evidence. Ecol. Econ. 140, 1–13.
113. da Nóbrega Alves, R.R., da Silva Vieira, W.L., and Santana, G.G. (2008). Reptiles
used in traditional folk medicine: Conservation implications. Biodivers. Conserv. 17,
2037–2049.
114. Alexander, K.A., Sanderson, C.E., Marathe, M., Lewis, B.L., Rivers, C.M., Shaman,
J., Drake, J.M., Lofgren, E., Dato, V.M., Eisenberg, M.C., et al. (2015). What factors
might have led to the emergence of Ebola in West Africa? PLoS Negl. Trop. Dis. 9,
e0003652–e0003652.
115. Moyle, B. (2009). The black market in China for tiger products. Glob. Crime 10, 124–
143.
116. MacFarlane, D., and Rocha, R. (2020). Guidelines for communicating about bats to
prevent persecution in the time of COVID-19. Biol. Conserv. 248, 108650.
117. Graham-Rowe, D. (2011). Biodiversity: Endangered and in demand. Nature 480,
S101-3.
118. McAfee, D., and Connell, S.D. (2019). Balancing the benefits of optimism and
Chapter 6: Reducing demand for overexploited wildlife products 177
[Reducing Demand for Overexploited Wildlife Products]
52
pessimism in conservation: A response to Kidd, Bekessy, and Garrard. Trends Ecol.
Evol. 34, 692–693.
119. Alhakami, A.S., and Slovic, P. (1994). A psychological study of the inverse
relationship between percieved risk and percieved benefit. Risk Anal. 14, 1085–1096.
120. McEvoy, J.F., Connette, G., Huang, Q., Soe, P., Pyone, K.H.H., Valitutto, M., Htun,
Y.L., Lin, A.N., Thant, A.L., Htun, W.Y., et al. (2019). Two sides of the same coin –
Wildmeat consumption and illegal wildlife trade at the crossroads of Asia. Biol.
Conserv. 238, 108197.
121. Mason, C.F., Bulte, E.H., and Horan, R.D. (2012). Banking on extinction: Endangered
species and speculation. Oxford Rev. Econ. Policy 28, 180–192.
122. Dee, L.E., Horii, S.S., and Thornhill, D.J. (2014). Conservation and management of
ornamental coral reef wildlife: Successes, shortcomings, and future directions. Biol.
Conserv. 169, 225–237.
123. Peeters, M., Courgnaud, V., Abela, B., Auzel, P., Pourrut, X., Bibollet-Ruche, F.,
Loul, S., Liegeois, F., Butel, C., Koulagna, D., et al. (2002). Risk to human health
from a plethora of simian immunodeficiency viruses in primate bushmeat. Emerg
Infect Dis 8, 451–457.
124. Zhao, H. (2020). COVID-19 drives new threat to bats in China. Science 367, 1436.
125. Lu, H., McComas, K.A., Buttke, D.E., Roh, S., Wild, M.A., and Decker, D.J. (2017).
One Health messaging about bats and rabies: How framing of risks, benefits and
attributions can support public health and wildlife conservation goals. Wildl. Res. 44,
200–206.
126. Anti, P., Owusu, M., Agbenyega, O., Annan, A., Badu, E.K., Nkrumah, E.E.,
Tschapka, M., Oppong, S., Adu-Sarkodie, Y., and Drosten, C. (2015). Human-Bat
Interactions in Rural West Africa. Emerg. Infect. Dis. 21, 1418–1421.
Chapter 6: Reducing demand for overexploited wildlife products 178

[Reducing Demand for Overexploited Wildlife Products]
53
127. Davis, T., Goldwater, M.B., Ireland, M.E., Gaylord, N., and Van Allen, J. (2017). Can
you catch Ebola from a stork bite? Inductive reasoning influences generalization of
perceived zoonosis risk. PLoS One 12, e0186969.
128. IPBES (2019). 2019. Summary for policymakers of the global assessment report on
biodiversity and ecosystem services of the Intergovernmental Science-Policy Platform
on Biodiversity and Ecosystem Services.
129. Gerber, P.J., Mottet, A., Opio, C.I., Falcucci, A., and Teillard, F. (2015).
Environmental impacts of beef production: Review of challenges and perspectives for
durability. Meat Sci. 109, 2–12.
130. Machovina, B., Feeley, K.J., and Ripple, W.J. (2015). Biodiversity conservation: The
key is reducing meat consumption. Sci. Total Environ. 536, 419–431.
131. Hedenus, F., Wirsenius, S., and Johansson, D.J.A. (2014). The importance of reduced
meat and dairy consumption for meeting stringent climate change targets. Clim.
Change 124, 79–91.
132. Nisa, C.F., Bélanger, J.J., Schumpe, B.M., and Faller, D.G. (2019). Meta-analysis of
randomised controlled trials testing behavioural interventions to promote household
action on climate change. Nat. Commun. 10, 4545.
133. Allwood, J., Azevedo, J., Clare, A., Cleaver, C., Cullen, J., Dunant, C.F., Fellin, T.,
Hawkins, W., Horrocks, I., and Horton, P. (2019). Absolute Zero: Delivering the UK’s
climate change commitment with incremental changes to today’s technologies.
134. Henrich, J., Heine, S.J., and Norenzayan, A. (2010). The weirdest people in the world?
Behav Brain Sci 33, 61–135.
135. Shea, B.J., Reeves, B.C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D.,
Tugwell, P., Welch, V., and Kristjansson, E. (2017). AMSTAR 2: A critical appraisal
tool for systematic reviews that include randomised or non-randomised studies of
Chapter 6: Reducing demand for overexploited wildlife products 179

[Reducing Demand for Overexploited Wildlife Products]
54
healthcare interventions, or both. BMJ 358, j4008.
Chapter 6: Reducing demand for overexploited wildlife products 180

[Reducing Demand for O
verexploited Wildlife Products]
55
Table 1. Possible demand parallels betw
een wildlife products and other harm
ful products.
Drivers
Description
Exam
ple Harm
ful Products E
xample W
ildlife Products
Recreational
Motivated by the desire to fulfil hedonistic
pleasure. Includes both recreational pursuit of leisure and sensory pursuit to please the senses
Individual hedonistic motivation to
consume licit and illicit drugs (e.g.,
alcohol, cigarettes, cocaine, marijuana,
heroin)
Tiger bone wine
102 R
hino horn hangover detox103
Songbirds 105
Medicinal
Motivated by the desire to treat an illness,
promote w
ellness, and/or avoid pain. M
otivation to self-medicate, often
linked to drug addiction (e.g., alcohol, cigarettes, heroin, &
marijuana)
Unsupported health rem
edies (e.g., m
ultivitamins, hom
eopathy) and health fraud/scam
s (e.g., weight-loss scam
s)
Traditional remedies containing w
ildlife: B
ear-bile107
Pangolin scales 109 R
hino horn111
Rattlesnake pills 113
Social
Motivated by the desire to form
or strengthen relationships, including to im
press upon others one’s social standing or perceptions of w
ealth
Drug consum
ption driven by social norm
s (e.g., alcohol, cigarettes, cocaine, m
arijuana)
Rhino horn
103 Shark fin soup
5 Tiger bones 115
Sensory
Motivated by the desire to please the senses
including aesthetic, olfactory and tactile D
emand driven by product branding
(e.g., expensive alcohol bottles) and/or tied to drug consum
ption (e.g., tobacco sm
oking paraphernalia)
Ivory carvings 117 A
nimal skins 115
Elephant skin120
Financial
Motivated by the desire for financial gain
Trade in licit, illicit, and/or counterfeit drugs (e.g., alcohol, cigarettes, adulterated illicit drugs)
Speculator investment in ivory
121 The exotic pet trade (e.g., rare ornam
ental fish & reptiles) 122
Dietary
Motivated by the desire to fulfil a dietary
desire or due to a penchant for a specific culinary delicacy
Junk foods (high fat and/or sugar) U
nsustainable food (e.g., Blue-fin tuna)
Unethical food (e.g., cage eggs)
Pangolin Meat 120
Primate bushm
eat 123 B
at meat 7,126
Note. The driver categories and subsequent descriptions have been adapted from recent w
ork by Walters et al., 91 to categorise m
otivations for wildlife
consumer products.
Chapter 6: R
educing demand for overexploited w
ildlife products
181

182

Chapter 7: Applying psychology to bat conservation
This chapter is presented in the format of a journal article.
MacFarlane, D., & Rocha, R. (2020). Guidelines for communicating about bats to prevent persecution in the time of COVID-19. Biological Conservation, 248, 108650.
183

184

Contents lists available at ScienceDirect
Biological Conservation
journal homepage: www.elsevier.com/locate/biocon
Perspective
Guidelines for communicating about bats to prevent persecution in the timeof COVID-19Douglas MacFarlanea,b, Ricardo Rochac,d,!
a School of Psychological Science, University of Western Australia, Australiab Conservation Science Group, Department of Zoology, University of Cambridge, UKc CIBIO/InBIO-UP, Research Centre in Biodiversity and Genetic Resources, University of Porto, Portugald CEABN-InBIO, Centre for Applied Ecology “Prof. Baeta Neves”, Institute of Agronomy, University of Lisbon, Portugal
A R T I C L E I N F O
Keywords:Behavioural changeConservation communicationConservation psychologyHuman-wildlife con!ictMessage framingZoonoses
A B S T R A C T
While the current COVID-19 pandemic continues to wreak havoc on human health and national economies,conservationists are struggling to prevent misguided persecution of bats, which are misleadingly being blamedfor spreading the disease. Although at a global level, such persecution is relatively uncommon, even a fewmisguided actions have the potential to cause irrevocable damage to already vulnerable species. Here, we drawon the latest "ndings from psychology, to explain why some conservation messaging may be reinforcing mis-leading negative associations. We provide guidelines to help ensure that conservation messaging is working toneutralize dangerous and unwarranted negative-associations between bats and disease-risk. We provide re-commendations around three key areas of psychological science: (i) debunking misinformation; (ii) counter-acting negative associations; and (iii) changing harmful social norms. We argue that only by carefully framingaccurate, honest, and duly contextualized information, will we be able to best serve society and present anunbiased perspective of bats. We hope this guidance will help conservation practitioners and researchers todevelop e#ective message framing strategies that minimize zoonotic health risks and support biodiversity and itsassociated ecosystem services.
1. Introduction
Zoonoses are infectious diseases — caused by bacteria, viruses,fungi, parasites or other pathogenic agents — that spread from animalsto humans. Most human recurrent and emerging infectious diseases arezoonotic (Jones et al., 2008), and their origins can often be traced tospeci"c wildlife reservoirs (Johnson et al., 2020). Emerging zoonoseshave an enormous impact on global human health and are a signi"cantburden on national economies, especially in low-income countries(Karesh et al., 2012). These impacts are particularly catastrophic whennovel outbreaks spread worldwide through human-to-human trans-mission, such as the COVID-19 pandemic, and can lead to long-lastingconsequences to the world's biodiversity and to conservation activities(Corlett et al., 2020; Evans et al., 2020).
Communicating the health risks posed by zoonoses is paramount toprotecting human populations and mitigating the spread of the disease(Decker et al., 2012; Quinn et al., 2014). Yet, information (and mis-information) about zoonoses and their suspected animal hosts can
potentially impact the public's perception about a given taxa (Daviset al., 2017). Ongoing news coverage, for example, repeatedly linkingwildlife to a particular zoonotic disease, can fuel animosity towards agiven species (or set of species), and in extreme cases, erode societalsupport for conservation or even fuel direct persecution of known orsuspected disease reservoirs (Buttke et al., 2015; Guyton and Brook,2015). In this context, even well-intentioned e#orts by journalists, re-searchers, and conservationists to counteract dangerous negative asso-ciations between wildlife and zoonoses can lead to unintended con-sequences and further reinforce negative stereotypes (Decker et al.,2012; Buttke et al., 2015; Lu et al., 2016). This insidious outcome isparticularly problematic amid the current pandemic, due to the tre-mendous societal and economic impacts COVID-19 is having at a globalscale, combined with an overabundance of media coverage associatingwildlife, and in particular bats, with the disease. Moreover, much of theongoing media framing has been poorly crafted and inadequatelycontextualized, which may have inadvertently ampli"ed public riskperceptions about bat-associated diseases, beyond the real
https://doi.org/10.1016/j.biocon.2020.108650Received 10 April 2020; Received in revised form 12 May 2020; Accepted 29 May 2020
! Corresponding author at: CIBIO-InBIO, Research Centre in Biodiversity and Genetic Resources, University of Porto, Rua Padre Armando Quintas, 4485-661Vairão, Portugal.
E-mail address: [email protected] (R. Rocha).
%LRORJLFDO�&RQVHUYDWLRQ������������������
$YDLODEOH�RQOLQH����-XQH�����������������������(OVHYLHU�/WG��$OO�ULJKWV�UHVHUYHG�
7
Chapter 7: Applying psychology to bat conservation 185

proportionate risks. Such perceptions have also likely been ampli"edthrough social media, with potential counterproductive e#ects onpublic support for bat conservation.
Insights from human psychology can be used to carefully designmessages that result in better outcomes for public health and con-servation (Davis et al., 2017; Lu et al., 2016). Although several previousauthors have already discussed some of the pitfalls and challenges as-sociated with message framing of wildlife-disease associations (e.g.Decker et al., 2011, 2012; Buttke et al., 2015), up-to-date guidance onhow to communicate about zoonoses without dampening support forconservation is currently lacking. Using COVID-19 and bat conservationas a case in point, we build on previous research and outline howpsychological science can be used to address some of the complexitiesassociated with conservation communications in the context of emer-ging zoonoses.
1.1. COVID-19 pandemic and bat conservation
Since "rst being recorded in late-2019 in China, COVID-19 hasspread to>200 countries and territories, causing over a quarter of amillion human deaths and sending billions of people into lockdown ashealth professionals struggle to cope with rising numbers of infectedpatients. At an early stage in the outbreak, bats were identi"ed as asuspected reservoir of the new disease owing to the similarity betweenSARS coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19,and a bat-borne coronavirus (Bat CoV RATG13), previously identi"edin intermediate horseshoe bats (Rhinolophus a!nis; Zhou et al., 2020).Although the World Health Organization emphasizes that “possible an-imal sources of COVID-19 have not yet been con"rmed” (World HealthOrganization, 2020), the association between bats and perhaps theworst zoonotic outbreak in modern history, has predictably sparkednegative reactions against this taxon (Zhao, 2020).
Much of the perceived disease risk associated with bats likely relatesto their association with several other high-pro"le emerging viralzoonoses including the severe acute respiratory syndrome (SARS) cor-onavirus (CoV), the Ebola and Marburg "loviruses, and the Hendra andNipah henipaviruses (Brook and Dobson, 2015; Brook et al., 2020).While bats thus present real risks as hosts for potentially dangerousdiseases, several factors need to be considered to understand how thisrisk "ts into the wider context of zoonoses. First, recent research in-dicates that the number of human-infecting viruses in bats is similar toother mammals, after controlling for the number of species within eachorder (Mollentze and Streicker, 2020; but see Olival et al., 2017).Second, ample evidence indicates that the greatest risks for virus spil-lover to humans comes from human activities that facilitate the mixingof taxonomically diverse species (e.g., intensive animal farming, livewildlife markets, keeping of wildlife as pets, in sanctuaries, andalongside domestic animals; Johnson et al., 2015) as well as activitiesthat involve, or increase, human-animal interactions (e.g., hunting andhabitat destruction and deterioration; Johnson et al., 2020). Third, batsmake critical and multivariate contributions to human well-being (Kunzet al., 2011). In light of such factors, the dialogue about bat con-servation and bat-associated infectious diseases thus poses a wickedproblem (Waltner-Toews, 2017): namely, how to appropriately com-municate about the risks between bats and zoonoses, without vilifyingthe former.
Message framing of bat-associated diseases is a mammoth challengethat requires close collaboration between virologists, public health of-"cials, conservation scientists and practitioners. Without such colla-borations, poorly contextualized or overblown associations betweenbats and zoonotic risk can swiftly mask the intrinsic (Blackmore et al.,2013; Quinn et al., 2014), ecological (Kunz et al., 2011) and economic(e.g. Boyles et al., 2011) importance of bats. In turn, this can propagateunwarranted negative attitudes and consequently lead to both directpersecution and erosion of local support for bat conservation e#orts(López-Baucells et al., 2018). For example, large !ying foxes are key
pollinators of durian (Durio zibethinus), a culturally and economicallyimportant fruit crop throughout Southeast Asia (Aziz et al., 2017).However, some durian growers are now reluctant to support !ying foxconservation due to fear of backlash from the public in the aftermath ofthe COVID-19 outbreak (Tuttle, 2020). Worse still, reports from otherparts of the world suggest a few communities have even sought to cullbats in a misplaced e#ort to combat the disease (CMS, 2020). Suchmisguided behaviours present considerable cause for concern, not leastbecause past experience has shown such actions not only fail to elim-inate disease risks (Blackwood et al., 2013) but can also increase the riskof zoonotic disease spreading to humans (Olival, 2016). As a case inpoint, a study of 20 colonies of common vampire bats (Desmodus ro-tundus) in Peru found that culling not only failed to eliminate rabies indisturbed colonies but inadvertently led to an increase in the proportionof infected bats compared to undisturbed ones (Streicker et al., 2012).Similarly, in Uganda, as a response to an outbreak of Marburg hemor-rhagic fever, locals culled thousands of Egyptian fruit bats (Rousettusaegyptiacus) but failed to prevent a second, even larger, outbreak some20 km from the cave where the culling took place. Worse still, theculling also increased the risk of disease spillover as the Egyptian fruitbats that subsequently recolonized the cave had higher levels of activeinfection (Amman et al., 2014).
Here, we draw on the latest "ndings from the psychology of sciencecommunication and behaviour change (Buttke et al., 2015: Deckeret al., 2012; MacFarlane et al., 2020), to highlight some of the majorpitfalls for bat conservationists and practitioners, especially whencommunicating with the public about bats and disease-risk. We do notspeculate about the origin of SARS-CoV-2 or further elaborate about therelationship about bats and zoonotic viruses (see e.g., Wood et al.,2012; Brook and Dobson, 2015; Brierley et al., 2016; Brook et al., 2020;Andersen et al., 2020; Johnson et al., 2020). Instead, we aim to o#ersome guidance from the science of science communication (Kahan,2015) to help ensure that conservation communications are working toneutralize dangerous and unwarranted negative-associations betweenbats and disease-risk. Although framed around bats and COVID-19, webelieve that the advice presented here may be relevant to other taxo-nomic groups also linked with zoonoses (e.g. bird conservation in thecontext of avian in!uenza); and also to other situations where practi-tioners need to debunk harmful misinformation (e.g., false healthclaims about remedies made from body parts of endangered animals) orcounteract unwarranted attitudes towards a given conservation issue(e.g. blaming wild carnivores for livestock attacks perpetrated by feraldogs). To improve comprehension and accessibility of our guidelines,we also provide a simpli"ed visual depiction (Fig. 1) of the more de-tailed guidance we now provide below.
2. Debunking misinformation
Few would deny that the contemporary media landscape has be-come increasingly used to spread disinformation—misinformation dis-seminated with the intent to deceive, often for political or "nancialmotives. However, we believe that the growing tide of environmentaldisinformation (Cook et al., 2018) poses underappreciated threats toconservation objectives (Daly, 2020). Moreover, conservationists ap-pear to be largely unprepared to contain disinformation when itemerges in relation to conservation issues (Kidd et al., 2019a; Thalerand Shi#man, 2015). In 2016, Oxford dictionary's word of the year was“post-truth”—de"ned as “relating to or denoting circumstances inwhich objective facts are less in!uential in shaping public opinion thanappeals to emotion and personal belief” (Flood, 2016). Such develop-ments suggest that, while the scienti"c community is pushing an evi-dence-based agenda, modern society may have arrived upon a newparadigm where what matters is not veracity but holding attention andsocial signaling (McCarthy et al., 2020). This often translates into thespread of speculative, misleading, or re-interpreted information asfactual (e.g. “bats may be a natural reservoir of SARS-CoV-2” becomes
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 186

“bats are responsible for COVID-19”). The ease and speed at which suchmistruths are shared through social media expediates this spread ofdisinformation and greatly magni"es its real-world repercussions.
2.1. How correcting misinformation can make the problem worse
When faced with falsehoods and inaccuracies, the scienti"c com-munity often reacts by directly challenging the misrepresentations(Williamson, 2016; Caul"eld, 2020). However, even after credible
retractions of misinformation, people's reasoning often continues to bein!uenced by that misinformation, a phenomenon termed the continuedin#uence of misinformation (Johnson and Seifert, 1994). Several cogni-tive factors are responsible for this e#ect including that people oftenlack the skills to objectively evaluate information and so have a di$culttime discerning between facts and familiar "ctions (Bedford, 2010;Cook et al., 2018; Swire et al., 2017). Also, memory is an imperfectprocess, such that new information does not perfectly update old in-formation; and recalled memories are vulnerable to outside in!uences
Fig. 1. A visual summary of our guidelines for communicating about bats to counteract persecution driven by fears associated with zoonotic health risks. This guidewas adapted from an infographic by Lewandowsky et al. (2012) to help practitioners e#ectively refute misinformation.
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 187

and can result in memory distortion, making it di$cult to rememberwhich information was fact and which was "ction (Lewandowsky et al.,2012).
Consequently, despite our intentions to correct misinformation,whenever we repeat it (even to refute it), our communications canstrengthen the association. In other words, by stating that “bats don'tspread COVID-19”, this can strengthen the association between batsand COVID-19, and consequently many will misperceive, mis-remember, or simply forget the detail about bats NOT being responsiblefor spreading the virus. Thankfully, research from experimental psy-chology has demonstrated the e$cacy of several tactics that can help to"debunk" misinformation in ways that counteract such problems(Lewandowsky et al., 2012). Based on this body of evidence, we nowoutline several key principles of e#ective debunking.
2.2. Guidance for evidence-based debunking of misinformation
To e#ectively debunk misinformation and overcome the continuedmisinformation e#ect, evidence-based refutations should:
(i) Warn recipients before confronting them with misinformation be-cause warnings enable people to avoid the initial acceptance ofmisinformation, thus reducing the need for subsequent revision(Ecker et al., 2010);
(ii) Study the tactics used by those spreading misinformation (Thalerand Shi#man, 2015) and, before misleading stories gain traction,pre-emptively explain the !awed argumentation techniques used(e.g., fake experts, doctored images, oversimpli"ed scienti"c con-cepts; Cook et al., 2017; Cook et al., 2018, van der Linden et al.,2017).
(iii) Repeat the facts, but avoid repeating the misinformation more thannecessary (in order to refute it), because repetition can enhancefamiliarity, which ultimately can foster false beliefs (Jacoby andKelley, 1989);
(iv) Use graphical evidence, because visual representations can makecounter-arguing more di$cult and help consumers comprehenddata (Dixon et al., 2015);
(v) Provide alternate explanations of the debunked phenomenon to "llthe mental “gap” left behind from retracting the misinformation(Ecker et al., 2010). This component of explanation should alsoaddress the potential motivation behind the initial source of mis-information (e.g., spread chaos, sell remedies, sell advertising,support an industry, support a political ideology; Nyilasy, 2019).
3. Counteracting negative associations towards bats
Throughout human history, bats have been both feared and cele-brated. For instance, in Mayan mythology, bats were associated withdeath through the bat god Camazotz (Thompson, 1966). Whereas, inChina, they have been traditionally regarded as symbols of good for-tune (Kingston, 2016). Recently, however, negative stereotypes asso-ciated with the group (often re!ected in misinformed myths, legends,and folklore) have increasingly been magni"ed by fear-inducing mediaheadlines that often present bats as culprits of disease outbreaks (López-Baucells et al., 2018). Consequently, bat conservationists are increas-ingly faced with sensationalist fearmongering and misinformationabout the risks posed by bats, and thus understandably feel compelledto counteract such beliefs in the hope of preventing public backlashagainst the group.
3.1. How people use feelings to make decisions
Knowledge alone is rarely the sole driver of attitudes and beha-viours towards environmental issues (Fielding and Head, 2012). In-stead, people's judgements and decisions are often guided by severalheuristics, or mental shortcuts, that evolved to enable us to make quick
decisions (Kahneman, 2012). One way we make quick decisions is byrelying on “gut-feelings” rather than more deliberative rational pro-cesses. This aspect of our decision-making process is governed by af-fect— the speci"c quality of “goodness” or “badness” that becomesassociated with an action or item (Slovic et al., 2007). A#ective rea-soning may explain much of the over-reactions towards bats (Kingston,2016). Speci"cally, in the context of zoonoses, negative a#ect is beingirrationally attached to bats, because of the repeated, and thus in-creasingly familiar, link between disease (bad) and bats (now also feelsbad).
Many attributes of a#ective reasoning should inform public mes-saging about the importance of bat conservation. One key attribute isthat our evaluations of risks and bene"ts tend to be negatively corre-lated—even when the nature of the risks (or bene"ts) is both distinctlyand qualitatively di#erent from the nature of the bene"ts (or risks;Alhakami and Slovic, 1994). For example, if bats are portrayed as highin risk, this will contribute to the perception that they are also low inbene"t, and vice-versa. This tendency is further ampli"ed when peoplehave less capacity (e.g., high stress or lack of time) for analytical de-liberation (Finucane et al., 2000). Evidence on the a#ect heuristicsuggests that the perception of one attribute can be in!uenced by ma-nipulating information about the other (Finucane et al., 2000;Ghanouni et al., 2017).
Another key attribute of a#ective decision-making is that peopletend to underestimated large risks, which are mundane and under-re-ported (e.g., diabetes, stroke, tuberculosis) but greatly overestimatesmall risks, which are over-reported, sensational, or fear-inducing (e.g.,shark attacks, tornadoes, and cases of rabies transmission by bats;Slovic et al., 2007). One explanation for this bias, is that such a#ect-laden risks, no matter how improbable, become encoded in people'smemory through potent images, metaphors, and emotional narrativesthat trigger strong reactions and thus also greater media interest, andtherefore tend to feel riskier. Unfortunately, wildlife-associated diseasestend to have many traits that can amplify the risk perceptions above theactual risk. Such traits include novelty, potential for high-consequenceoutcomes (illness or death), and the lack of individuals to control thethreats (Buttke et al., 2015).
3.2. Guidance for counteracting harmful negative associations
To e#ectively alter people's irrational and/or harmful negative as-sociations, while always being factual, communicators should aim to:
(i) Avoid using negative, especially fear-inducing, metaphors or pic-tures linking wild bats to diseases, as such imagery will be far morememorable than any subsequent rational appeal to conservationoutcomes. However, if the messaging was speci"cally targeted at,and con"ned to, human-bat interactions, such as hunting, trading,and eating wild bats, then it may be vital to clearly communicatethe real health-risks arising from such behaviours (Lu et al., 2016;Tannenbaum et al., 2015). Nevertheless, practitioners should stillnot use misleading imagery linking animals in the wild to zoo-noses.
(ii) Emphasize the direct, and indirect, health bene"ts that bats pro-vide to human populations. For example, highlight their con-sumption of disease carrying mosquitoes (Kemp et al., 2019) ortheir critical role in suppressing agricultural pests and their con-tribution to human food security (Wanger et al., 2014; Maas et al.,2016; Puig-Montserrat et al., 2015; Russo et al., 2018).
(iii) Provide factual, awe-inspiring, natural history information aboutbats, and about the bene"ts that they provide to natural ecosys-tems. For example, emphasize their role in the recovery of de-graded landscapes via seed dispersal and the suppression of her-bivorous insects (Farneda et al., 2018). Acknowledging theecological bene"ts of bats is especially important in risk messaging(e.g., when communicating about rabies), as it can foster greater
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 188

intention to adopt recommended risk-reduction behaviours,without stigmatising bats (Lu et al., 2016).
(iv) Explain why, if most bat species are left alone, they present little, ifany, risk to human health. Where some risk exists for a certainspecies (Quinn et al., 2014), then communicate the steps that:people can take to reduce their personal risk (Decker et al., 2012);society is taking to reduce the collective risk (Bandura, 2000); andthat a given technology can help to reduce a particular risk (e.g.,explain why research into bats' immune systems may hold the keyto ground-breaking antiviral treatments for humans; Kachel,2016).
(v) Risks should also be quanti"ed using easily evaluable comparisonsto relatively mundane events (e.g., “although rabies is one of themost important zoonotic viruses in bats, at a global-scale, bitesfrom domestic dogs are responsible for over 99% of rabies-relateddeaths”; World Health Organization, 2013). Equally, strive to de-scribe both the high bene"ts and/or low risks, using easily evalu-able comparisons (e.g., “straw-coloured fruit bats (Eidolon helvum)bene"t forests by dispersing seeds up-to four times further thanother similar-sized frugivores”; Abedi-Lartey et al., 2016).
4. Changing harmful social norms
Recognising the role of social context on people's attitudes and be-haviours is paramount to understanding human-bat relationships.Kingston (2016) provides a detailed account of how social norms—therules or expectations about how members of a community should be-have—can impact bat conservation. Here, we emphasize the dynamicnature of social norms and how these can be impacted by informationregarding zoonoses, while providing best practice on how to use a"norm appeal" to alter damaging human behaviours towards bats.
4.1. How e$orts to alter social norms can back"re
As individuals, we owe much of our success to other memberswithin our communities. Such cooperation, and therefore our in-dividual success, is often reliant on successfully detecting and adheringto social norms within our perceived community (Simler and Hanson,2017). One way to alter harmful behaviours is to employ a norm ap-peal—messaging that aims to alter an undesirable behaviour by en-couraging conformity towards more a desirable norm, usually by re-ferring to the existing behaviour of an in!uential group (e.g., “mostfarmers in your community have installed arti"cial bat roosts to en-hance pest-control services provided by bats”). To design e#ective normappeals, we must "rst be able to distinguish between (i) injunctivenorms— what others approve or disapprove of doing, (ii) descriptivenorms—what other people typically do, and (iii) perceived norms—-what individuals believe about the real injunctive and descriptivenorms (Farrow et al., 2017).
Failure to distinguish between di#erent types of norms can result inmessages that inadvertently strengthen undesirable norms. For ex-ample, stating that “people should stop harming bats” is also implicitlyhighlighting the descriptive norm that some people are harming bats,which could encourage others towards that undesirable behaviour(Cialdini, 2003). In contrast, stating that “most people know bats areharmless and should be protected,” may be equally true, but instead itshould encourage conformity in the desired direction.
4.2. Guidance for designing e$ective norm appeals
To e#ectively alter undesirable norms and encourage more desir-able behaviours, communications should aim to:
(i) Avoid reciting adverse norms, such as “Stop harming bats!”, as thisimplicitly suggests that some people are harming bats and cancreate perception that this behaviour is more acceptable and
widespread than reality (Cialdini et al., 2006).(ii) Emphasize descriptive norms, such as “The vast majority of
countries protect bats, and millions of people live happily along-side them”, as this will encourage conformity with the greatermajority (Cialdini, 2003).
(iii) Where the desired behaviour is not yet established, highlight theincreasing frequency of the desired norm, such as “more and morecountries are formally recognising the importance of conservingwild bats” (Rare and The Behavioural Insights Team, 2019).
(iv) Highlight norms that are speci"c to the target populations, as themore a target community identi"es with, respects, or aspires to thereferent group, the greater the impact of the norm appeal (e.g.,“People in your speci"c community are protecting bats, and ben-e"ting from their role in nature”; White et al., 2009).
(v) Combine descriptive norms with injunctive norms. Combiningboth what people are doing, and what people approve of othersdoing (Axelrod, 1986), can create the strongest form of a normappeal (e.g., “Most people are now rejecting evicting bats fromtheir roosts and instead are now in favour of greater protection ofbats”; Cialdini, 2003).
5. Discussion
The COVID-19 pandemic, with its associated loss of life, severehuman su#ering and economic impacts, is due to profoundly re-shapethe perceived risks for wildlife-associated diseases. The fact that—themost similar virus to SARS-CoV-2, identi"ed to-date, is a bat-bornecoronavirus—has engulfed bats in a maelstrom of virus-related newscoverage and a related growing tide of misinformation. The re-verberations will likely carve long-lasting negative impact on percep-tions, attitudes, and behaviours towards bats. As the pandemic con-tinues to unfold, bat-researchers across the world are facingunprecedented pressure to directly engage with the public to con-textualize the risks of bat-borne zoonoses and minimize potentialbacklash against the group. This task is likely pushing many re-searchers, especially ecologists and conservationists, into unfamiliarterritory. While valuable lessons from di#erent sub-"elds of conserva-tion science are available to help design conservation messages, suchguidance has yet been collated and placed in the context of zoonoticrisk.
In this article, we outlined some key points that bat conservationistsshould consider when devising conservation messaging aimed at neu-tralizing unwarranted negative-associations between bats and disease-risk. Our advice focuses on three areas of psychological science that weperceived as particularly relevant in the current context. We stress thatour advice is not exhaustive, and should be considered within thegrowing body of literature devoted to zoonotic risk communication(Decker et al., 2010, 2012, 2016), conservation message framing (Kiddet al., 2019a; Kusmano# et al., 2020) and conservation focused social-marketing, particularly in the context of human-wildlife con!ict(Veríssimo et al., 2019).
In addition to the points highlighted here, communicators shouldalso consider many other factors that in!uence public reactions toconservation messages. These include, but are not limited to, hyper-saliency, social/cultural context, psychological distance, messageframing, message channel, and messenger e#ects (Veríssimo et al.,2019; Kidd et al., 2019b; Kusmano# et al., 2020). Such factors shouldnot be regarded in isolation, as their interaction can in!uence the re-ceiver's attitudes and/or behaviours. Furthermore, zoonotic risk oftenrepresents a single dimension of the human-bat con!ict and acknowl-edged or latent drivers of animosity towards bats (e.g. reactions to fruitdamage by bats or to the noise and smells of rooting colonies) may alsoa#ect people's perception of bats and their reaction to conservationcommunications.
Conservation messages are often intuitively designed (i.e., not in-formed by evidence; Kidd et al., 2019b) and their impact on people's
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 189

behaviour is rarely robustly evaluated (Veríssimo and Wan, 2019). Suchshortcomings will be especially prevalent during an unprecedentedpandemic, and thus we acknowledge that many conservation commu-nications must often, and unavoidably, be more reactive than proactive.Despite this impediment, communicators should consider that evenmessages based on the best available evidence can have unintendede#ects (Kusmano# et al., 2020). Messages should thus be, whereverfeasible, pilot tested with a representative sample of the target popu-lation. Testing should adopt appropriate experimental designs (to en-able robust causal inference; MacFarlane, 2020) and not only evaluatemessage e#ectiveness but also record unforeseen outcomes. Critically,messages should align with best available advice from heath autho-rities, who, along with other relevant stakeholders (e.g., local com-municates, government departments etc.), should be consulted as keyactors in the communication strategy.
6. Concluding remarks
Bats represent nearly one "fth of all described mammal species andrival only humans as the most widely distributed mammals on Earth(Conenna et al., 2017; Burgin et al., 2018; Frick et al., 2019). Owing toscarce research and the cumulative e#ects of anthropogenic pressuressuch as habitat loss and degradation, overharvesting, invasive species,and climate change, around one third of the>1400 recognised batspecies are classi"ed as data de"cient or threatened by the IUCN RedList (Frick et al., 2019). Despite the critical ecological importance ofbats, their hyper-saliency as reservoirs of dangerous zoonoses is likelyto negatively a#ect support for their conservation. In the aftermath ofthe current pandemic, bat biologists will need to carefully navigate thehuman-dimensions of bat conservation and be exceedingly cautiousabout how they communicate about bats and zoonoses. To this end, weargue that the psychology of science communication provides the bestguidance available.
In a world where humans and the natural hosts of emerging in-fectious diseases are increasingly connected, an integrated and inter-disciplinary approach to articulate wildlife-related science commu-nication in the context of human health is paramount. Only by carefullyframing accurate, honest, and duly contextualized information will webe able to best serve society with a comprehensive and unbiased per-ception of wildlife that minimizes zoonotic health risks and allows wildspecies, their vital ecosystem services and human societies to co-exist.
Declaration of competing interest
The authors declare that they have no known competing "nancialinterests or personal relationships that could have appeared to in!u-ence the work reported in this paper.
Acknowledgements
We acknowledge the support from Australian Government ResearchTraining Program Scholarship to DM and from ARDITI – Madeira'sRegional Agency for the Development of Research, Technology andInnovation (grant M1420-09-5369-FSE-000002) to RR. We are gratefulto T. Garcia and K. MacFarlane for precious assistance in the productionof the visual summary and to the editor Bea Maas for insightful sug-gestions on an earlier version of the manuscript and for supporting itspublication. We further thank Tanja Straka, Sarah Bekessy, AlexandraSchnell, and one anonymous reviewer for valuable comments duringthe review process.
References
Abedi-Lartey, M., Dechmann, D.K., Wikelski, M., Scharf, A.K., Fahr, J., 2016. Long-dis-tance seed dispersal by straw-coloured fruit bats varies by season and landscape.Glob. Ecol. Conserv. 7, 12–24.
Alhakami, A.S., Slovic, P., 1994. A psychological study of the inverse relationship be-tween perceived risk and perceived bene"t. Risk Anal. 14 (6), 1085–1096.
Amman, B.R., Nyakarahuka, L., McElroy, A.K., Dodd, K.A., Sealy, T.K., Schuh, A.J.,Shoemaker, T.R., Balinandi, S., Atimnedi, P., Kaboyo, W., Nichol, S.T., 2014.Marburgvirus resurgence in Kitaka Mine bat population after extermination attempts,Uganda. Emerg. Infect. Dis. 20, 1761.
Andersen, K.G., Rambaut, A., Lipkin, W.I., Holmes, E.C., Garry, R.F., 2020. The proximalorigin of SARS-CoV-2. Nat. Med. 26, 450–452.
Axelrod, R., 1986. An evolutionary approach to norms. Am. Polit. Sci. Rev. 80,1095–1111.
Aziz, S.A., Clements, G.R., McConkey, K.R., Sritongchuay, T., Pathil, S., Abu Yazid,M.N.H., Campos-Arceiz, A., Forget, P.M., Bumrungsri, S., 2017. Pollination by thelocally endangered island !ying fox (Pteropus hypomelanus) enhances fruit productionof the economically important durian (Durio zibethinus). Ecol. Evol. 7, 8670–8684.
Bandura, A., 2000. Exercise of human agency through collective e$cacy. Curr. Dir.Psychol. Sci. 9, 75–78.
Bedford, D., 2010. Agnotology as a teaching tool: learning climate science by studyingmisinformation. J. Geogr. 109, 159–165.
Blackmore, E., Underhill, R., McQuilkin, J., Leach, R., Holmes, T., 2013. Common Causefor Nature: A Practical Guide to Values and Frames in Conservation. Public InterestResearch Centre, Wales, United Kingdom.
Blackwood, J.C., Streicker, D.G., Altizer, S., Rohani, P., 2013. Resolving the roles ofimmunity, pathogenesis, and immigration for rabies persistence in vampire bats.Proc. Natl. Acad. Sci. 110, 20837–20842.
Boyles, J.G., Cryan, P.M., McCracken, G.F., Kunz, T.H., 2011. Economic importance ofbats in agriculture. Science 332, 41–42.
Brierley, L., Vonhof, M.J., Olival, K.J., Daszak, P., Jones, K.E., 2016. Quantifying globaldrivers of zoonotic bat viruses: a process-based perspective. Am. Nat. 187, 53–64.
Brook, C.E., Dobson, A.P., 2015. Bats as ‘special’ reservoirs for emerging zoonotic pa-thogens. Trends Microbiol. 23, 172–180.
Brook, C.E., Boots, M., Chandran, K., Dobson, A.P., Drosten, C., Graham, A.L., Grenfell,B.T., Müller, M.A., Ng, M., Wang, L.F., van Leeuwen, A., 2020. Accelerated viraldynamics in bat cell lines, with implications for zoonotic emergence. Elife 9, e48401.
Burgin, C.J., Colella, J.P., Kahn, P.L., Upham, N.S., 2018. How many species of mammalsare there? J. Mammal. 99, 1–14.
Buttke, D.E., Decker, D.J., Wild, M.A., 2015. The role of one health in wildlife con-servation: a challenge and opportunity. J. Wildl. Dis. 51, 1–8.
Caul"eld, T., 2020. Pseudoscience and COVID-19-we’ve had enough already. Nature.https://doi.org/10.1038/d41586-020-01266-z.
Cialdini, R.B., 2003. Crafting normative messages to protect the environment. Curr. Dir.Psychol. Sci. 12, 105–109.
Cialdini, R.B., Demaine, L.J., Sagarin, B.J., Barrett, D.W., Rhoads, K., Winter, P.L., 2006.Managing social norms for persuasive impact. Soc. In!u. 1, 3–15.
Conenna, I., Rocha, R., Russo, D., Cabeza, M., 2017. Insular bats and research e#ort: areview of global patterns and priorities. Mammal Rev. 47, 169–182.
Convention on the Conservation of Migratory Species of Wild Animals (CMS), 2020. Factsabout Bats and COVID-19 [press release]. https://www.cms.int/en/news/2020005-facts-about-bats-and-covid-19, Accessed date: 10 April 2020.
Cook, J., Lewandowsky, S., Ecker, U.K.H., 2017. Neutralizing misinformation throughinoculation: exposing misleading argumentation techniques reduces their in!uence.PLoS One 12 (5), e0175799.
Cook, J., Ellerton, P., Kinkead, D., 2018. Deconstructing climate misinformation toidentify reasoning errors. Environ. Res. Lett. 13, 024018.
Corlett, R.T., Primack, R.B., Devictor, V., Maas, B., Goswami, V.R., Bates, A.E., Koh, L.P.,Regan, T.J., Loyola, R., Pakeman, R.J., Cumming, G.S., Pidgeon, A., Johns, D., Roth,R., 2020. Impacts of the coronavirus pandemic on biodiversity conservation. Biol.Conserv. 108571.
Daly, N., 2020. This ‘hand-washing’ orangutan went viral—but the story isn't true.https://www.nationalgeographic.com/animals/2020/04/coronavirus-fake-animal-news-part-two/, Accessed date: 7 April 2020.
Davis, T., Goldwater, M.B., Ireland, M.E., Gaylord, N., Van Allen, J., 2017. Can you catchEbola from a stork bite? Inductive reasoning in!uences generalization of perceivedzoonosis risk. PLoS One 11, e0186969.
Decker, D.J., Evensen, D.T., Siemer, W.F., Leong, K.M., Riley, S.J., Wild, M.A., Castle,K.T., Higgins, C.L., 2010. Understanding risk perceptions to enhance communicationabout human-wildlife interactions and the impacts of zoonotic disease. ILAR J. 51,255–261.
Decker, D.J., Siemer, W.F., Wild, M.A., Castle, K.T., Wong, D., Leong, K.M., Evensen, D.T.,2011. Communicating about zoonotic disease: strategic considerations for wildlifeprofessionals. Wildl. Soc. Bull. 35, 112–119.
Decker, D.J., Siemer, W.F., Evensen, D.T., Stedman, R.C., McComas, K.A., Wild, M.A.,Castle, K.T., Leong, K.M., 2012. Public perceptions of wildlife-associated disease: riskcommunication matters. Hum. Wildl. Interacti. 6, 112–122.
Decker, D.J., Schuler, K., Forstchen, A.B., Wild, M.A., Siemer, W.F., 2016. Wildlife healthand public trust responsibilities for wildlife resources. J. Wildl. Dis. 52, 775–784.
Dixon, G.N., McKeever, B.W., Holton, A.E., Clarke, C., Eosco, G., 2015. The power of apicture: overcoming scienti"c misinformation by communicating weight-of-evidenceinformation with visual exemplars. J. Commun. 65, 639–659.
Ecker, U.K., Lewandowsky, S., Tang, D.T., 2010. Explicit warnings reduce but do noteliminate the continued in!uence of misinformation. Mem. Cogn. 38, 1087–1100.
Evans, K.L., Ewen, J.G., Guillera-Arroita, G., Johnson, J.A., Penteriani, V., Ryan, S.J.,Sollmann, R., Gordon, I.J., 2020. Conservation in the Maelstrom of Covid-19 – A Callto Action to Solve the Challenges, Exploit Opportunities and Prepare for the NextPandemic. https://doi.org/10.1111/acv.12601.
Farneda, F.Z., Rocha, R., López-Baucells, A., Sampaio, E.M., Palmeirim, J.M., Bobrowiec,P.E., Grelle, C.E., Meyer, C.F., 2018. The road to functional recovery: temporal e#ects
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 190

of matrix regeneration on Amazonian bats. Trop. Conserv. Sci. 11, 1–4.Farrow, K., Grolleau, G., Ibanez, L., 2017. Social norms and pro-environmental behaviour:
a review of the evidence. Ecol. Econ. 140, 1–13.Fielding, K.S., Head, B.W., 2012. Determinants of young Australians’ environmental ac-
tions: the role of responsibility attributions, locus of control, knowledge and atti-tudes. Environ. Educ. Res. 18, 171–186.
Finucane, M.L., Alhakami, A., Slovic, P., Johnson, S.M., 2000. The a#ect heuristic injudgements of risks and bene"ts. J. Behav. Decis. Mak. 13, 1–17.
Flood, A., 2016. ‘Post-truth’ Named Word of the Year by Oxford Dictionaries. TheGuardian. https://www.theguardian.com/books/2016/nov/15/post-truth-named-word-of-the-year-by-oxford-dictionaries, Accessed date: 12 May 2020.
Frick, W.F., Kingston, T., Flanders, J., 2019. A review of the major threats and challengesto global bat conservation. Ann. N. Y. Acad. Sci. https://doi.org/10.1111/nyas.14045.
Ghanouni, A., Nuttall, E., Wardle, J., Von Wagner, C., 2017. Testing whether barriers to ahypothetical screening test a#ect unrelated perceived bene"ts and vice versa: arandomised, experimental study. Patient Educ. Couns. 100, e1–e24.
Guyton, J.A., Brook, C.E., 2015. African bats: conservation in the time of Ebola. Therya 6,69–88.
Jacoby, L.L., Kelley, C., 1989. Becoming famous overnight: limits on the ability to avoidunconscious in!uences of the past. J. Pers. Soc. Psychol. 56, 326–338.
Johnson, H.M., Seifert, C.M., 1994. Sources of the continued in!uence e#ect: whenmisinformation in memory a#ects later inferences. J. Exp. Psychol. Learn. Mem.Cogn. 20, 1420–1436.
Johnson, C.K., Hitchens, P.L., Evans, T.S., Goldstein, T., Thomas, K., Clements, A., Joly,D.O., Wolfe, N.D., Daszak, P., Karesh, W.B., Mazet, J.K., 2015. Spillover and pan-demic properties of zoonotic viruses with high host plasticity. Sci. Rep. 5, 14830.
Johnson, C.K., Hitchens, P.L., Pandit, P.S., Rushmore, J., Evans, T.S., Young, C.C.W.,Doyle, M.M., 2020. Global shifts in mammalian population trends reveal key pre-dictors of virus spillover risk. Proc. R. Soc. B Biol. Sci. 287, 20192736.
Jones, K.E., Patel, N.G., Levy, M.A., Storeygard, A., Balk, D., Gittleman, J.L., Daszak, P.,2008. Global trends in emerging infectious diseases. Nature 451, 990–993.
Kachel, N., 2016. 24/7 immunity from lethal diseases? It's in the bat, man! CSIROscope[Press release]. https://blog.csiro.au/bat-disease-immunity/, Accessed date: 12 May2020.
Kahan, D.M., 2015. What is the “science of science communication”? J. Sci. Commun. 14,1–12.
Kahneman, D., 2012. Thinking, Fast and Slow. Penguin, London, United Kingdom.Karesh, W.B.D., Dobson, A.P., Lloyd-Smith, J.O.P., Lubroth, J.D.V.M., Dixon, M.A.M.,
Bennett, M.P., et al., 2012. Ecology of zoonoses: natural and unnatural histories.Lancet 380, 1936–1945.
Kemp, J., López-Baucells, A., Rocha, R., Wangensteen, O.S., Andriata"ka, Z., Nair, A.,Cabeza, M., 2019. Bats as potential suppressors of multiple agricultural pests: a casestudy from Madagascar. Agric. Ecosyst. Environ. 269, 88–96.
Kidd, L.R., Garrard, G.E., Bekessy, S.A., Mills, M., Camilleri, A.R., Fidler, F., et al., 2019a.Messaging matters: a systematic review of the conservation messaging literature.Biol. Conserv. 236, 92–99.
Kidd, L.R., Bekessy, S.A., Garrard, G.E., 2019b. Evidence is key for e#ective biodiversitycommunication. Trends Ecol. Evol. 34, 693–694.
Kingston, T., 2016. Cute, creepy, or crispy—how values, attitudes, and norms shapehuman behaviour toward bats. In: Voigt, C.C., Kingston, T. (Eds.), Bats in theAnthropocene: Conservation of Bats in a Changing World. Springer, pp. 571–588.
Kunz, T.H., de Torrez, E.B., Bauer, D., Lobova, T., Fleming, T.H., 2011. Ecosystem servicesprovided by bats. Ann. N. Y. Acad. Sci. 1223, 1–38.
Kusmano#, A.M., Fidler, F., Gordon, A., Garrard, G.E., Bekessy, S.A., 2020. Five lessons toguide more e#ective biodiversity conservation message framing. Conserv. Biol.https://doi.org/10.1111/cobi.13482.
Lewandowsky, S., Ecker, U.K., Seifert, C.M., Schwarz, N., Cook, J., 2012. Misinformationand its correction: continued in!uence and successful debiasing. Psychol. Sci. PublicInterest 13, 106–131.
López-Baucells, A., Rocha, R., Fernández-Llamazares, Á., 2018. When bats go viral: ne-gative framings in virological research imperil bat conservation. Mammal Rev. 48,62–66.
Lu, H., McComas, K.A., Buttke, D.E., Roh, S., Wild, M.A., 2016. A one health messageabout bats increases intentions to follow public health guidance on bat rabies. PLoSOne 11, e0156205.
Maas, B., Karp, D.S., Bumrungsri, S., Darras, K., Gonthier, D., Huang, J.C.C., Lindell, C.A.,Maine, J.J., Mestre, L., Michel, N.L., Morrison, E.B., 2016. Bird and bat predationservices in tropical forests and agroforestry landscapes. Biol. Rev. 91, 1081–1101.
MacFarlane, D., 2020. Towards Robust Evaluations of Demand-Reduction Interventions:Deep Dive Technical Brie"ng Paper on Social Science Surveys. The Wildlife TradeMonitoring Network under CITES & MIKE, TRAFFIC. https://www.changewildlifeconsumers.org/site/assets/"les/1550/technical_brie"ng_paper_deep_dive_social_science_surveys-1.pdf, Accessed date: 12 May 2020.
MacFarlane, D., Hurlstone, M.J., Ecker, U.K.H., 2020. Protecting consumers from frau-dulent health claims: a taxonomy of psychological drivers, interventions, barriers,and treatments. Soc. Sci. Med. 112790.
McCarthy, I.P., Hannah, D., Pitt, L.F., McCarthy, J.M., 2020. Confronting indi#erencetoward truth: dealing with workplace bullshit. Bus. Horiz. 63, 253–263.
Mollentze, N., Streicker, D.G., 2020. Viral zoonotic risk is homogenous among taxonomicorders of mammalian and avian reservoir hosts. Proc. Natl. Acad. Sci. 117,9423–9430.
Nyilasy, G., 2019. Fake news: when the dark side of persuasion takes over. Int. J. Advert.38, 336–342.
Olival, K.J., 2016. To cull, or not to cull, bat is the question. EcoHealth 13, 6–8.Olival, K.J., Hosseini, P.R., Zambrana-Torrelio, C., Ross, N., Bogich, T.L., Daszak, P.,
2017. Host and viral traits predict zoonotic spillover from mammals. Nature 546(7660), 646–650.
Puig-Montserrat, X., Torre, I., López-Baucells, A., Guerrieri, E., Monti, M.M., Ràfols-García, R., Ferrer, X., Gisbert, D., Flaquer, C., 2015. Pest control service provided bybats in Mediterranean rice paddies: linking agroecosystems structure to ecologicalfunctions. Mamm. Biol. 80, 237–245.
Quinn, E.K., Massey, P.D., Cox-Witton, K., Paterson, B.J., Eastwood, K., Durrheim, D.N.,2014. Understanding human–bat interactions in NSW, Australia: improving riskcommunication for prevention of Australian bat lyssavirus. BMC Vet. Res. 10 (1),144.
Rare and The Behavioural Insights Team, 2019. Behavior Change for Nature: ABehavioral Science Toolkit for Practitioners. Arlington, VA, USA.
Russo, D., Bosso, L., Ancillotto, L., 2018. Novel perspectives on bat insectivory highlightthe value of this ecosystem service in farmland: research frontiers and managementimplications. Agric. Ecosyst. Environ. 266, 31–38.
Simler, K., Hanson, R., 2017. The Elephant in the Brain: Hidden Motives in Everyday Life.Oxford University Press, Oxford, United Kingdom.
Slovic, P., Finucane, M.L., Peters, E., MacGregor, D.G., 2007. The a#ect heuristic. Eur. J.Oper. Res. 177, 1333–1352.
Streicker, D.G., Recuenco, S., Valderrama, W., Gomez Benavides, J., Vargas, I., Pacheco,V., Condori Condori, R.E., Montgomery, J., Rupprecht, C.E., Rohani, P., Altizer, S.,2012. Ecological and anthropogenic drivers of rabies exposure in vampire bats: im-plications for transmission and control. Proc. R. Soc. B Biol. Sci. 279, 3384–3392.
Swire, B., Ecker, U.K.H., Lewandowsky, S., 2017. The role of familiarity in correctinginaccurate information. J. Exp. Psychol. Learn. Mem. Cogn. 43, 1948–1961.
Tannenbaum, M.B., Hepler, J., Zimmerman, R.S., Saul, L., Jacobs, S., Wilson, K.,Albarracin, D., 2015. Appealing to fear: a meta-analysis of fear appeal e#ectivenessand theories. Psychol. Bull. 141, 1178–1204.
Thaler, A.D., Shi#man, D., 2015. Fish tales: combating fake science in popular media.Ocean Coast. Manag. 115, 88–91.
Thompson, J.E.S., 1966. Maya hieroglyphs of the bat as metaphorgrams. Man 176–184.Tuttle, M.D., 2020. A viral witch hunt. https://issues.org/a-viral-witch-hunt-bats/,
Accessed date: 12 May 2020.van der Linden, S., Leiserowitz, A., Rosenthal, S., Maibach, E., 2017. Inoculating the
public against misinformation about climate change. Global Chall. 1, 1600008.Veríssimo, D., Wan, A.K.Y., 2019. Characterizing e#orts to reduce consumer demand for
wildlife products. Conserv. Biol. 33, 623–633.Veríssimo, D., Sadowsky, B., Douglas, L., 2019. Conservation marketing as a tool to
promote human-wildlife coexistence. In: Frank, C., Glikman, J.A., Marchini, S. (Eds.),Human-wildlife interactions: Turning con!ict into coexistence. Cambridge UniversityPress, pp. 335–354.
Waltner-Toews, D., 2017. Zoonoses, one health and complexity: wicked problems andconstructive con!ict. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 372, 20160171.
Wanger, T.C., Darras, K., Bumrungsri, S., Tscharntke, T., Klein, A.M., 2014. Bat pestcontrol contributes to food security in Thailand. Biol. Conserv. 171, 220–223.
White, K.M., Smith, J.R., Terry, D.J., Greenslade, J.H., McKimmie, B.M., 2009. Socialin!uence in the theory of planned behaviour: the role of descriptive, injunctive, andin-group norms. Br. J. Soc. Psychol. 48, 135–158.
Williamson, P., 2016. Take the time and e#ort to correct misinformation. Nature 540,171.
Wood, J.L., Leach, M., Waldman, L., MacGregor, H., Fooks, A.R., Jones, K.E., Restif, O.,Dechmann, D., Hayman, D.T., Baker, K.S., Peel, A.J., 2012. A framework for the studyof zoonotic disease emergence and its drivers: spillover of bat pathogens as a casestudy. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 367, 2881–2892.
World Health Organization, 2013. WHO Expert Consultation on Rabies: second report.https://apps.who.int/iris/handle/10665/85346, Accessed date: 3 May 2020.
World Health Organization, 2020. Q&A on coronaviruses (COVID-19). https://www.who.int/news-room/q-a-detail/q-a-coronaviruses, Accessed date: 7 April 2020.
Zhao, H., 2020. COVID-19 drives new threat to bats in China. Science 367, 1436.Zhou, P., Yang, X.L., Wang, X.G., Hu, B., Zhang, L., Zhang, W., Si, H.R., Zhu, Y., Li, B.,
Huang, C.L., Chen, H.D., 2020. A pneumonia outbreak associated with a new cor-onavirus of probable bat origin. Nature 579, 270–273.
D. MacFarlane and R. Rocha %LRORJLFDO�&RQVHUYDWLRQ������������������
�
Chapter 7: Applying psychology to bat conservation 191

192

Chapter 8: General discussion
193

194

8.1 Summary of Theoretical Contributions
This thesis aimed to investigate how to reduce consumer demand for ineffective
health remedies. To answer this question, I took a systematic approach to designing, testing,
and building an evidence base of effective interventions.
First, I sought to understand the underlying cognitive drivers that make people
susceptible to fraudulent health claims—claims about health remedies that are ineffective,
harmful and/or untested. Drawing on an extensive review of the literature, I developed a
structured taxonomy of the psychological drivers of demand, the cognitive barriers that can
impair the application of interventions, and corresponding evidence-informed treatments to
help consumers overcome those barriers. This framework, outlined in Chapter 2, provided an
extensive research agenda of testable hypotheses that predict how each intervention should
help consumers resist fraudulent health claims.
Second, I sought to systematically test several of these hypotheses using two objective
measures of consumer demand, namely willingness-to-pay and propensity to promote
misinformation. To measure willingness-to-pay, in Chapters 3-5 I gave participants
opportunities to bid on ineffective health remedies, namely commonly consumed dietary
supplements. The experimental auction paradigm that I adapted was the innovative backbone
of my empirical results, providing a reliable and replicable measure of consumer willingness-
to-pay under different treatment conditions. In Chapter 5, I also developed a novel measure to
quantify participants’ willingness to promote misinformation through social media. Together,
these two mechanisms enabled me to test the impact of key psychological barriers on key
consumer behaviours and, perhaps more importantly, demonstrate the effectiveness of our
hypothesised interventions in helping consumers to overcome those barriers and thus make
better consumer choices.
Chapter 8: General discussion 195

8.2 Summary of Empirical Findings
Chapter 3 allowed me to investigate the impact of the illusion of causality. In the pilot
study (Appendix II), I created this illusion by telling people about a fictitious health remedy
but only giving them half the information needed to make a valid causal assessment (i.e., they
received only information about the number of people who report experiencing a benefit from
taking a health remedy vs. the number who report no benefit). I found that the vast majority
of people fell for this illusion (see Figure 4 of Appendix II). My results showed this could be
explained, in part, by the additional finding (see Figure 5 of Appendix II) that people do not
value the information needed to consider an alternative explanation (i.e., the number of
people who report experiencing a benefit from taking a placebo vs. the number who report no
benefit). Indeed, in the main study, I observed how peoples’ willingness-to-pay for the
ineffective supplement increased when they received the half-contingency table (by 24.5%)
and how this increase was similar (24.1%) to those that received the full positive-contingency
table (i.e., deceptively showing the product was effective). Unfortunately, neither condition
was significantly different from control, which may have been due to an already high demand
for supplements and/or the experiment being statistically underpowered. Nevertheless, the
results signalled that creating an illusion of causality could be equally as damaging as plainly
deceiving consumers.
Importantly, we demonstrated an effective way to overcome the illusion of causality
was to empower consumers with an understanding of how we know the remedy is not
effective. This involved providing three elements: (i) a simple tool to visualise clinical results
(i.e., a contingency table), (ii) a short explanation of those results, and (iii) an alternative
explanation to fill the mental gap potentially created by debunking the belief that the remedy
is effective. Our results, which were replicated in Chapter 4, showed this strategy reliably
reduced consumer demand for an ineffective health remedy by 23% more than simply
Chapter 8: General discussion 196

highlighting the lack of evidence to support that remedy. The results illustrate the importance
of addressing the illusion of causality rather than simply relying on a “trust me, I’m an
expert” approach. The results also suggest demand-reduction campaigns that fail to counter
the illusion of causality may have limited impact—specifically, because the illusion of
causality leads consumers to be persuaded by deficient “evidence”, such as their own
observations, experiences, and the testimonies of others.
Chapter 4 allowed me to test whether the results in Chapter 3 would replicate and
whether the intervention could be strengthened by addressing an additional psychological
barrier—namely, the feeling (an affective association) that alternative health remedies are
harmless. In other words, which approach would have the greatest impact on consumer
demand: challenging misperceptions about efficacy or challenging misperceptions about risk?
This study aimed to help inform the seemingly endless debate as to whether fear appeals are
effective. In researching the literature, I found proponents on both sides of this debate often
overlooked key evidence or failed to consider the nuances of designing effective fear appeals.
Over two experiments, I found consumer choices were reliably influenced by both
approaches and, most importantly, the combination of both elements provided additive
effects superior to either alone. This showed that combining two simple, but psychologically-
informed, treatments into one intervention could reduce consumer demand for an ineffective
health remedy by 50%. The results were consistent with a recent and comprehensive
metanalysis of the empirical evidence, which found that fear appeals were effective under
most circumstances (Tannenbaum et al., 2015). Furthermore, the results confirmed my
prediction that communicating both elements, by stating that a remedy is both low in benefits
and high in risks, would serve to influence consumers in the same direction and reduce the
remedy’s perceived value. This provides further evidence to support an already robust finding
in psychological science, namely, that people’s perceptions of risks and benefits are
Chapter 8: General discussion 197

negatively correlated (Finucane et al., 2000; Slovic et al., 2004). The findings in Chapter 4
have implications for how authorities can discourage the use of harmful health remedies.
Furthermore, it provides support to recent calls by behaviour-change researchers that neither
positive nor negative messaging should be considered as more effective; instead, both are
valuable for driving effective behaviour change (Kidd et al., 2019).
Another important finding from Chapter 4 was that the impacts of the treatment
conditions on willingness-to-pay were comparable between the hypothetical and incentivised
versions of the experimental auction. This shows that reliable results can be acquired via
online experiments without the need for them to be incentivised with real money and/or
products. This is important because online experiments enable researchers to use limited
research funding more efficiently. Moreover, this result indicates the potential for researchers
to use the hypothetical-auction paradigm to pilot test interventions where an incentivised
paradigm would otherwise not be appropriate (e.g., for ethical, legal, or financial reasons),
such as when evaluating demand for rhino horn or illicit drugs etc. Of course, future
researcher will still need to follow up promising online results with incentivised studies to
determine to what extent this finding replicates.
In Chapter 5, I tested whether health misinformation combining several deceptive
tactics would increase both participants’ willingness-to-pay for a spurious COVID-19 remedy
and their propensity to promote misinformation online. The misinformation-promotion
measure was a novel addition to my thesis and, to the best of my knowledge, to research on
combating misinformation. This measure provides a tool to assess what interventions
effectively reduce the spread of misinformation, which is particularly important given that we
have entered what the World Health Organisation has termed an infodemic of online health
misinformation (Zarocostas, 2020). Using this novel measure, I compared the impact of two
interventions to counteract the effects of the misinformation, viz. a typical tentative refutation
Chapter 8: General discussion 198

used by most health authorities and an enhanced refutation based on best-practice
psychological insights.
I found exposure to health misinformation increased the proportion of people
promoting misinformation (by 18%) compared to control. Relative to the misinformation
condition, I found the tentative and enhanced interventions reduced demand for the spurious
remedy (by 18% and 25%, respectively) and discouraged misinformation promotion (by 29%
and 55%, respectively). Importantly, the enhanced refutation was significantly more effective
at discouraging misinformation promotion. The results highlight the need for debunking
interventions to follow current best-practice guidelines.
In Chapter 6, I stepped outside of the taxonomy and took a broader approach to
investigate “what works” to reduce consumer demand for harmful products (e.g., tobacco,
alcohol, illicit drugs). By collating key findings from 41 systematic reviews, I found that
(i) mass-media campaigns and incentive programs were, on average, ineffective;
(ii) advertising bans, social marketing, and location bans were promising but there was
insufficient robust evidence to draw firm conclusions; and (iii) the evidence for the
effectiveness of risk warnings and appeals to norms was strongest, with some caveats. The
empirical evidence collated in this meta-review thus supported a major premise of this thesis:
interventions will be more effective if they not only consider the external structural barriers
(e.g., affordability, accessibility, or legality) but also the internal psychological barriers (e.g.,
irrational associations or misperceived social norms) that prevent people from engaging in
the desired behaviour (e.g., not consuming a harmful remedy). In other words, one reason
why awareness-raising campaigns tend to be ineffective is that they fail to target the internal
barriers preventing people from engaging in the desired behaviour. Conversely, this explains
why the more targeted approaches of fear appeals and norm appeals have been found to be
Chapter 8: General discussion 199

more effective, specifically, because they help consumers overcome specific barriers relating
to misperceptions about the health risks and social acceptability of a behaviour, respectively.
8.3 Practical Implications
Most of the papers in this thesis, Chapters 2-5, have outlined how the demand for
alternative health remedies impacts individuals, such as via side effects, product adulteration,
and opportunity costs. However, my research was motivated by the need to reduce demand
for a particularly destructive subset of alternative health remedies, namely those made from
the body parts of overexploited wildlife. To understand the need to develop effective
solutions to this problem, in Chapters 6 and 7, the thesis also highlighted how demand for
overexploited wildlife products harms the environment (e.g., contributes to biodiversity
decline, food-web collapse, and the spread of wildlife diseases) and global public health (e.g.,
through the risk of zoonotic disease transmission). As such, this thesis has broad implications
for addressing a host of societal problems. Specifically, I have demonstrated how adopting
just a few psychologically-informed elements into behaviour-change communications can
reduce consumer demand by some 50%. Moreover, I have shown how psychological insights
can be used to counter the spread of misinformation by empowering people to identify
deception.
The findings in this thesis have echoed similar work on combatting misinformation
and designing successful behaviour-change campaigns (Christiano & Neimand, 2017; Cook
et al., 2015; Rossen et al., 2016). To effectively combat misinformation, we need to do more
than simply give people the facts. We need to design debunking materials using insights from
psychology that factor in how people process and update information. Similarly, to change
consumer behaviour, we need to do more than simply raise awareness. We need to help
people overcome the internal barriers preventing them from changing to the desired
behaviour.
Chapter 8: General discussion 200

8.3 Thesis limitations
This thesis has presented a picture of how demand for health remedies may be
influenced through an understanding of psychological phenomena and the subsequent
application of psychologically-informed interventions. I showed how helping people
overcome their cognitive roadblocks can lead them to make more informed and desirable
consumer choices. However, while this approach yielded compelling results in controlled
experimental settings, it was beyond the scope of this thesis to implement and evaluate those
strategies in more naturalistic consumer environments (e.g., online shopping or health stores).
Similarly, while the motivation for this thesis has been to influence consumers of wildlife
products, recruiting such elusive consumers was beyond the modest aims and limited
resources of the present thesis project. Instead, my aim was to develop an overarching
theoretical framework and then, relying on convenience samples of participants and
commonly used ineffective health remedies, pilot test both the behavioural measures and the
interventions. The next step is for future researchers to replicate these learnings with target
audiences and evaluate whether the interventions hold their effectiveness. Such a cautious
and staged approach to building an evidence base of behavioural interventions was recently
advocated for by experimental psychologists (Ijzerman et al., 2020).
Despite this limitation, several factors signal that the observed effects will prove
robust. First, both Chapters 3 and 4 included two experiments which yielded similar results
across two different countries and consumer groups, namely online workers from across the
United States and undergraduate psychology students at the University of Western
Australia—although I recognise that these groups are certainly not representative of global
diversity (Henrich et al., 2010). Second, the interventions were based on several general
principles of human cognition that are arguably grounded in evolutionary foundations,
meaning they hinge on psychological processes (e.g., causal reasoning, affective associations,
Chapter 8: General discussion 201

motivated reasoning) that are evolutionarily adaptive (i.e., they provide benefits towards
maximising survival, cooperation, reproduction, etc.) and are, therefore, likely to be operating
across cultures (Axelrod, 1986; Foster & Kokko, 2009; Griskevicius & Kenrick, 2013;
Schwardmann & van der Weele, 2019). Of course, while such speculation is plausible, the
matter will ultimately need to be settled with robust testing in various cultural settings and for
different products.
8.4 Concluding remarks
Humans have always relied on personal judgement and experience to intuit what
makes us sick and what makes us better. It was not until the advent of modern science, and
evidence-based medicine, that we have begun to overcome our cognitive limitations, which
has enabled us to make dramatic leaps in discovering what actually works to restore and
improve our health. Despite the unparalleled success of modern medicine, there will always
be self-deception and people able to profit from fraudulent claims about miracle health
remedies (Widder & Anderson, 2015). Indeed, during the course of this thesis, the COVID-
19 pandemic and a truly unorthodox and anti-science US President, have combined to
turbocharge the impact and spread of health misinformation (Blake, 2020). As more
communities succumb to health misinformation, many of the remarkable public health gains
(e.g., high vaccination rates) of the twentieth century will increasingly come under threat. But
it does not have to proceed this way. Just as science put bloodletting, phrenology, and steam
baths of elemental mercury to rest (Kang & Pedersen, 2017), science has also demonstrated
the general ineffectiveness of campaigns relying solely on raising awareness or increasing
knowledge (Christiano & Neimand, 2017). We are all in the midst of an infodemic of health
misinformation, and there is far more at stake than our own personal health. To conserve our
wildlife, to reduce the risk of future pandemics, and to protect ourselves from being deceived,
we need a strategic and scientific approach to adaptively learning how to protect ourselves
Chapter 8: General discussion 202

from fraudsters and from our own cognitive limitations. This thesis has shown how insights
from psychology can be harnessed to deliver effective intervention messaging. I hope it helps
to push us in the right direction.
Chapter 8: General discussion 203

8.5 References Axelrod, R. (1986). An evolutionary approach to norms. American Political Science Review,
80, 1095–1111.
Blake, A. (2020). Study shows Trump behind 38 percent of coronavirus misinformation. The
Washington Post. Retrieved from. https://www.washingtonpost.com/politics/2020/
10/01/study-shows-trump-is-super-spreader-coronavirus-misinformation/
Christiano, A., & Neimand, A. (2017). Stop raising awareness already. In Stanford Social
Innovation Review. Retrieved from. https://ssir.org/articles/entry/
stop_raising_awareness_already
Cook, J., Ecker, U., & Lewandowsky, S. (2015). Misinformation and how to correct it.
Emerging Trends in the Social and Behavioral Sciences: An Interdisciplinary,
Searchable, and Linkable Resource, 1–17.
Finucane, M. L., Alhakami, A., Slovic, P., & Johnson, S. M. (2000). The affect heuristic in
judgements of risks and benefits. Journal of Behavioral Decision Making, 13, 1–17.
Foster, K. R., & Kokko, H. (2009). The evolution of superstitious and superstition-like
behaviour. Proceedings of the Royal Society B: Biological Sciences, 276, 31.
Griskevicius, V., & Kenrick, D. T. (2013). Fundamental motives: How evolutionary needs
influence consumer behavior. Journal of Consumer Psychology, 23, 372–386.
Henrich, J., Heine, S. J., & Norenzayan, A. (2010). Beyond WEIRD: Towards a broad-based
behavioral science. Behavioral and Brain Sciences, 33, 111–135.
Ijzerman, H., Jr, N. A. L., Przybylski, A. K., Weinstein, N., Debruine, L., Ritchie, S. J.,
Vazire, S., Forscher, P. S., Morey, R. D., Ivory, J. D., & Anvari, F. (2020). Use caution
when applying behavioural science. Nature Human Behaviour.
Kang, L., & Pedersen, N. (2017). Quackery: A Brief History of the Worst Ways to Cure
Everything. Workman Publishing.
Chapter 8: General discussion 204

Kidd, L. R., Bekessy, S. A., & Garrard, G. E. (2019). Neither hope nor fear: Empirical
evidence should drive biodiversity conservation strategies. Trends in Ecology &
Evolution, 34, 278–282.
Rossen, I., Hurlstone, M. J., & Lawrence, C. (2016). Going with the grain of cognition:
Applying insights from psychology to build support for childhood vaccination. Frontiers
in Psychology, 7, 1483.
Schwardmann, P., & van der Weele, J. (2019). Deception and self-deception. Nature Human
Behaviour.
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2004). Risk as analysis and risk
as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Analysis, 24,
311–322.
Tannenbaum, M. B., Hepler, J., Zimmerman, R. S., Saul, L., Jacobs, S., Wilson, K., &
Albarracin, D. (2015). Appealing to fear: A meta-analysis of fear appeal effectiveness
and theories. Psychological Bulletin, 141, 1178–1204.
Widder, R. M., & Anderson, D. C. (2015). The appeal of medical quackery: A rhetorical
analysis. Research in Social and Administrative Pharmacy, 11, 288–296.
Zarocostas, J. (2020). How to fight an infodemic. The Lancet, 395, 676.
Chapter 8: General discussion 205

206

Appendix I: Supplementary material for Chapter 2
Contains the supplemental material for the publication:
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2020). Protecting consumers from fraudulent health claims: A taxonomy of psychological drivers, interventions, barriers, and treatments. Social Science & Medicine, 112790.
207

208

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 1
Supplemental Material for ‘Protecting Consumers from Fraudulent Health Claims: A
Taxonomy of Psychological Drivers, Interventions, Barriers, and Treatments’
1. Targeting the Internal Barriers Impairing Intervention Effectiveness
The present review aims to facilitate the design of evidence-based interventions that
make consumers less susceptible to fraudulent health claims. Consistent with other theorists
(Hornik, Cherian, Madansky, & Narayana, 1995; McKenzie-Mohr & Schultz, 2014), we
believe that in order to modify consumer behaviour, interventions must target both the
external and internal barriers to the desired behaviour. For example, the success of a
campaign to increase household recycling will be limited by external barriers such as access
to recycling facilities, cost of services, and convenience to householders. However, even
when such external barriers are low, the success of an intervention may be limited by internal
barriers such as a lack of knowledge on what materials can be recycled or a lack of
motivation to participate in recycling programs (Hornik et al., 1995).
The impact of internal barriers on behaviour can be counter-intuitive. Accordingly,
behaviour change campaigns grounded in intuition and introspection can be prone to
unanticipated adverse outcomes. We argue that the best means of overcoming internal
barriers is to base campaigns on robust evidence from psychological research. A common
approach to informing the design of interventions has been to provide summarized, but
unstructured, lists of potential behaviour change techniques. However, the reliance on such
“tool-boxes” of interventions encourages practitioners to adopt a trial-and-error approach,
which contributes to wasted time and costs, whilst amplifying the risk that interventions may
foster unexpected adverse outcomes. Thus, a key deficiency with the application of behaviour
change techniques is that most methodologies provide little guidance on a critical step—how
to choose between the many prospective psychologically-grounded behavioural interventions
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 209
SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 2
to address a given problem. The goal of the present paper, and specifically the VANMaN1
taxonomy presented within, is to provide this specific guidance within the focal context of
reducing consumer susceptibility to health fraud.
2. A Detailed Step-by-Step Guide to Intervention Design
Effective intervention design requires an understanding of the psychological drivers
underlying the allure of a particular health remedy, framed through the broader context of
human cognition. To facilitate this task, we provide a step-by-step framework for applying
psychologically informed interventions in our paper (Figure 1). The five steps of this
framework are (1) identify the specific consumer motivations (i.e., the explicit rationale for
consuming a remedy) of a target population for a given remedy, through qualitative methods
such as surveys, observations, and literature reviews; (2) identify the underlying
psychological drivers of the demand for that health remedy, which will suggest a likely
intervention; (3) consider the psychological barriers that can be exploited by fraudsters to
increase consumers susceptibility to fraudulent health claims and design specific measures—
which we refer to as treatments—to help overcome them; (4) test and compare treatments in
a randomised control trial, using actual consumer behaviour as measure of success; and (5)
implement and evaluate, prioritising interventions with best-evidence and greatest potential
impact. Steps two and three contain the more challenging part of this process, namely the
intervention design. To simplify this task, the taxonomy presented in our paper (see Table 1)
is dedicated to guiding users to navigate these two steps. Step two relates to the taxonomy’s
1 The acronym VANMaN aptly evokes the white van speaker scam, where fraudsters deceive
consumers (by exploiting several psychological barriers) into believing they are getting an exceptional
deal on quality entertainment products, which appear stolen but are actually cheap imitations (Wilson,
2014).
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 210

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 3
columns (i) and (ii)—(i) identify the underlying psychological drivers exploited by fraudsters
to manipulate consumers into buying fraudulent health remedies (ii) link the drivers to
corresponding interventions. Step three relates to the taxonomy’s columns (iii) and (iv)—(iii)
identify the psychological barriers that may prevent successful application of interventions,
and (iv) consider applying one or more of the corresponding treatments to overcome those
barriers. A fifth column (v) provides a variety of examples of real-world treatments that either
have been, or could be, applied to specific interventions to overcome the corresponding
psychological barriers. Steps four and five are considered less challenging because methods
and guidelines for conducting randomized trials are already well-established (Boutron, et al.,
2008).
Although our taxonomy separates underlying drivers into five distinct categories, for
any single health-related consumer behaviour, several or all of the drivers may be present. To
illustrate how multiple drivers may underlie the demand for a single product, it is
illuminating to consider the perspective of someone who is intentionally trying to deceive
consumers. For example, marketing claims such as “100% all-natural treatment” tap into
people’s intuitive, but misleading, affective associations that said product is likely to be risk
free. This claim, in turn, increases the perception that the product is also effective via the
inverse relationship between perceived risks and benefits. Table S1 provides this perspective
based on research from criminology on the psychological mechanisms of health fraud
(Fischer, Lea, and Evans, 2013; Lea, Fischer, and Evans, 2009).
3. Testing the Predictions of the Taxonomy
It should be clear that the present framework assumes that consumer demand for
fraudulent health remedies is the target for all interventions. This assumption is crucial for
steps three and four because it provides a clear means for falsifying the prediction made via
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 211

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 4
the taxonomy. Specifically, to test whether the treatments contained in our taxonomy reduce
demand for fraudulent health remedies, randomised controlled trials must demonstrate a
significant reduction in an objective measure of consumer behaviour, such as financial sales
figures, the quantity of remedies purchased, or objective measurements of willingness-to-pay.
(Anonymous, 2018).
4. Additional Considerations Concerning Magical and Conspiratorial Thinking
As noted in the main text, our taxonomy is not exhaustive, as more research is likely
to be relevant to countering health fraud than could be succinctly covered in a single review.
To help in somewhat addressing this limitation, we now provide further elaboration of several
aspects of the research.
4.1 Irrational Affective Associations and Magical Thinking
Our review outlines some ways that people employ affective associations to guide
their decision-making process. In this section, we consider some of the underlying process
that appear to shape affective associations, which have been studies under the umbrella term
“magical thinking” (Oliver & Wood, 2018). In many contexts, people intuitively presume that
magical forces are operating to bring about either positive (e.g., bringing health, luck, or
purity) or negative (e.g., causing disease, bad luck, or impurity) outcomes (Huang et al.,
2017). The term “magical thinking” refers to the cognitive processes involved in making
causal attributions to unobservable forces, in ways that contradict explanations based on
observable phenomena (Oliver & Wood, 2018). Although aspects of magical thinking were
initially described by anthropologists to account for beliefs amongst traditional cultures
(Frazer, 1959), later research showed that magical thinking operates across modern societies
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 212

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 5
(Rozin et al., 1986). More recently, researchers have begun to quantify the extent to which
magical thinking may be driving contemporary health behaviours.
In two national surveys, Oliver and Wood (2018) measured people’s reliance on
magical thinking across a continuum ranging from “rationalist”—those who tend towards
making decisions on the basis of reason and evidence—at the lower end to “intuitionist”—
those who tend to rely more on expedient generalisation and feelings—at the upper end.
People were assessed based on their tendency to rely on oversimplified heuristics (e.g.,
magical contagion and the representativeness heuristic; see later). They found that compared
to rationalists, intuitionists were more likely to hold some antiscientific health beliefs such as:
vaccines cause autism, genetically modified foods should be banned, and alternative remedies
are superior to conventional medicine. However, intuitionists were also more likely to engage
in scientifically validated behaviours that were preventative (and presumably more intuitive),
such as using sunscreen and getting a flu vaccine. Oliver and Wood’s findings suggest that a
promising treatment to counter problematic magical thinking may be to convey scientific
findings in ways that align with people’s intuitions about the way the world works. Two
additional key attributes of magical thinking are representativeness and contagion.
The representativeness heuristic—the notion that things which resemble each other
share fundamental properties—can help us to make decisions under uncertainty (e.g., if it
smells good it’s probably okay to eat). Examples of representativeness contributing
problematic magical thinking include when people intuitively believe that “natural” products
are superior (since “nature” is good), vitamin supplements are beneficial (since vitamins are
important), or products containing chemicals are bad (since chemicals can be harmful). As
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 213

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 6
each heuristic contains a portion of truth, they can make fraudulent health claims feel
intuitively accurate.2
The concept of magical contagion—beliefs about objects transferring “essences”
(e.g., luck, morality, intention, characteristics etc.) through contact—has several implications
for understanding consumer health behaviours. Contagion beliefs are thought to be a
conceptual analogue to, and likely derived from, an understanding of how pathogenetic and
parasitic agents infect the body through contact (Rozin & Nemeroff, 1990). Contagion beliefs
can therefore facilitate adaptive responses to disease avoidance by mediating people’s
behavioural responses through emotions such as disgust, forming what researchers have
termed the “behavioural immune system” (Schaller & Park, 2011). However, features of this
system can also make consumers prone to fraudulent health claims, especially when blended
with representativeness. For example, the folk-saying, “you are what you eat” belies a
common (but wholly unsupported) intuition about biological processes. Namely, that eating
something (e.g., an animal) can transfer intangible characteristics (e.g., speed, irritability,
power etc) to the consumer (Nemeroff & Rozin, 1989). Such simple intuitions about
biological processes are likely responsible for beliefs in many alternative remedies (e.g.,
traditional remedies containing body parts of wildlife species; Byard, 2016).
Research on magical thinking reveals that aspects of consumer health decisions can be
influenced by affective associations mediated through simple intuitions about how biology
operates. To address consumer susceptibility to fraudulent health claims, we need, therefore,
2 A more convoluted example of the representative heuristic is homeopathy, which is based on the claim that a substance causing symptoms of a disease in a healthy person can, in very small doses, cure the disease in a sick person (e.g., believing that a rash can be cured by ingesting small doses of poison ivy). This claim violates the basic laws of chemistry, has no plausible biological mechanisms, and has not been shown to be effective for any health conditions (Ernst, 2010; NHMRC, 2015). Yet, the intuitive appeal of the representative heuristic (i.e., that the cause shares fundamental properties with the cure) is such that, despite contradicting all observable evidence, some 34% of Europeans have been reported to believe in homeopathy (European Commission, 2005).
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 214

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 7
to understand the frameworks that govern such intuitions, the situations where they are most
likely to operate, and the extent to which they are driving consumer health behaviours. In
many cases, people may not be aware that their intuitive responses rely on aspects of magical
thinking, at least until they are asked to reflect on their behaviours. Indeed, Nemeroff and
Rozin (1989) suggested that alongside our “rational” mental processes, we may also
unknowingly be processing information intuitively. Subsequently, one potential treatment for
countering problematic magical thinking may be to ask consumers to reflect on how they
arrived at their intuitive beliefs about certain products.
References
Boutron, I., Moher, D., Altman, D. G., Schulz, K. F., Ravaud, P., & Group, C. (2008).
Methods and processes of the CONSORT group: Example of an extension for trials
assessing nonpharmacologic treatments. Annals of Internal Medicine, 148, W60-66.
Byard, R.W. (2016). Traditional medicines and species extinction: Another side to forensic
wildlife investigation. Forensic Science, Medicine, and Pathology, 12, 125-127.
Council, N.H.M.R.C. (2015). NHMRC Statement: Statement on homeopathy. Office of the
National Health Medical Research Council.
Ernst, E. (2010). Homeopathy: What does the “best” evidence tell us. The Medical Journal of
Australia, 192, 458-460.
European Commission. (2005). European, science and technology. Special Eurobarometer.
Frazer, J.G. (1959). The golden bough: A study in magic and religion (TH Gaster, Ed.). New
York, NY: Macmillan. (Original work published 1890).
Fischer, P., Lea, S. E. G., & Evans, K. M. (2013). Why do individuals respond to fraudulent
scam communications and lose money? The psychological determinants of scam
compliance. Journal of Applied Social Psychology, 43, 2060-2072.
Hornik, J., Cherian, J., Madansky, M., & Narayana, C. (1995). Determinants of recycling
behavior: A synthesis of research results. The Journal of Socio-Economics, 24, 105-
127.
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 215

SUPPLEMENTAL MATERIAL: PSYCHOLOGY OF FRUDULENT HEALTH CLAIMS 8
Huang, J.Y., Ackerman, J.M., & Newman, G.E. (2017). Catching (up with) magical
contagion: A review of contagion effects in consumer contexts. Journal of the
Association for Consumer Research, 2, 430-443.
Lea, S., Fischer, P., & Evans, K. (2009). The psychology of scams, provoking and committing
errors of judgement: Prepared for the Office of Fair Trading by the University of
Exeter School of Psychology. Retrieved from
https://ore.exeter.ac.uk/repository/handle/10871/20958
MacFarlane, D., Hurlstone,. M. J., & Ecker, U. K. H., 2018. Reducing demand for ineffective
health remedies: Overcoming the illusion of causality. Psychology & Health, 33,
1472-1489.
McKenzie-Mohr, D., & Schultz, P. W. (2014). Choosing effective behavior change tools.
Social Marketing Quarterly, 20, 35-46.
Nemeroff, C., & Rozin, P. (1989). "You are what you eat": Applying the demand-free
"impressions" technique to an unacknowledged belief. Ethos, 17, 50-69.
Oliver, J.E., & Wood, T.J. (2018). Enchanted America: How intuition and reason divide our
politics: University of Chicago Press.
Rozin, P., Millman, L., & Nemeroff, C. (1986). Operation of the laws of sympathetic magic
in disgust and other domains. Journal of personality and social psychology, 50, 703.
Rozin, P., & Nemeroff, C. (1990). The laws of sympathetic magic: A psychological analysis
of similarity and contagion.
Schaller, M., & Park, J.H. (2011). The behavioral immune system (and why it matters).
Current directions in psychological science, 20, 99-103.
Appendix I — Supplement for Chapter 2: Protecting consumers from fraudulent health claims 216

SUPPLEM
ENTA
L MATER
IAL: PSY
CH
OLO
GY
OF FR
UD
ULEN
T HEA
LTH C
LAIM
S 9
Table S1. Exam
ples of Fraudulent Health C
laims and their C
orresponding Underlying Effect on Various Psychological Barriers
Example fraudulent health claim
Psychological driver(s)
Underlying intent of claim
Psychological barrier(s)
“Pill will help you lose up to 20kg in 5
weeks!”
Visceral influence
Focusing the consumer’s attention on the potential benefits by
offering a disproportionately large gain.
Illusion of attention
(cognitive impairm
ent)
“Obesity is a killer.”
Visceral influence;
Affect
Focusing the consumer’s attention on the need to m
inimise
the risk of mortality.
Illusion of attention
(cognitive impairm
ent);
Negative affect
“Free online diagnosis.” V
isceral influence
Increasing pressure on the consumer to spend, by initiating
the unspoken norm to reciprocate social favours.
Motivational influences
“Clearance sale ends soon. Lim
ited stock
won't last long.”
Visceral influence
Creating urgency and scarcity to increase im
pulsive
consuming.
Motivational influences
“100% all-natural treatm
ent.” A
ffect Tapping into m
isleading affective associations, (i.e., “all-
natural” equates to “risk free”) which drives the perception of
effectiveness via the inverse relationship between perceived
risks and benefits.
Positive affect
“So good big pharma doesn't w
ant the public
to know, they'd lose billions!”
Affect;
Misinform
ation
Isolate consumer from
conventional medicine draw
ing on fear
of large pharmaceutical com
panies.
Negative affect;
Motivated reasoning
“Works for 9 out of 10 people!”
Nescience
Inducing an illusion of causality in consumers by reporting
the effectiveness of the product being advocated, but failing to
report the effectiveness of an appropriate comparative
placebo.
Illusion of causality
Appendix I —
Supplement for C
hapter 2: Protecting consumers from
fraudulent health claims
217

SUPPLEM
ENTA
L MATER
IAL: PSY
CH
OLO
GY
OF FR
UD
ULEN
T HEA
LTH C
LAIM
S 10
“Television’s Dr O
z says that green coffee is
a “miracle” cure for obesity.”
Nescience;
Visceral influence
The high confidence of the advocate in an unfounded health
remedy fosters a false belief in the advocate’s expertise and
knowledge.
Illusion of confidence;
Illusion of attention
“Brain im
aging shows how
the treatment
boosts synaptic processing and brain
plasticity.”
Nescience
Providing irrelevant reductive information increases a false
sense of deeper knowledge by increasing fam
iliarity.
Illusion of knowledge
“Kick-starts your body's im
mune system
and
natural defence mechanism
s, so they burn fat
more efficiently and strengthen your m
uscle
tissues.”
Misinform
ation;
Nescience
Building a plausible sounding backstory, by adopting real
scientific terms and applying them
to an oversimplified
analogy.
Continued influence
effect;
Illusion of knowledge
“Free from genetically m
odified organisms
(GM
Os).”
Misinform
ation;
Affect
Tapping into issues that are socially polarising and associated
with a person’s self-identity (despite being contrary to
scientific consilience).
Motivated reasoning;
Negative affect
“Used by professional athletes w
hen they
need to shed weight quickly.”
Norm
s C
onvincing the consumer using peers as social proof.
Perceived norm (status)
“Ancient traditional secret to w
eight loss.” N
orms;
Misinform
ation
Building a backstory that appeals to a person's respect for
traditional or perceived “longstanding” health practices.
Perceived norm
(tradition);
Motivated reasoning
“You ow
e it to your family to try this!”
Norm
s Forcing the consum
er to make the m
oral decision to respond
out of moral duty to their fam
ily.
Perceived norm (duty)
Note. M
ost health scams rely on a com
bination of fraudulent health claims, w
hich may a cum
ulative effect on a consumer’s capacity to identify that the
product is a scam. See m
ain text for further details
Appendix I —
Supplement for C
hapter 2: Protecting consumers from
fraudulent health claims
218

Appendix II: Supplementary material for Chapter 3
Contains the supplemental material for the publication:
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing Demand for Ineffective Health Remedies: Overcoming the Illusion of Causality. Psychology & Health, 33(12), 1472-1489.
219

220

Supplementary Material for ‘Reducing Demand for Ineffective Health
Remedies: Overcoming the Illusion of Causality’
Douglas MacFarlanea*, Mark J. Hurlstoneb, and Ullrich K. H. Eckerc
abcSchool of Psychological Science, University of Western Australia, Perth, Australia;
*Corresponding author: School of Psychological Science, University of Western
Australia; M304, 35 Stirling Hwy, Perth 6009, Australia; phone: +618 6488 1418;
email: [email protected]; ORCiD: 0000-0003-4378-9294
b School of Psychological Science, University of Western Australia; M304, 35 Stirling
Hwy, Perth 6009, Australia; phone: +618 6488 3249; email:
c School of Psychological Science, University of Western Australia; M304, 35 Stirling
Hwy, Perth 6009, Australia; phone: +618 6488 3257; email: [email protected];
ORCiD: 0000-0003-4743-313X
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 221

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 2
Supplementary Material for ‘Reducing Demand for Ineffective Health
Remedies: Overcoming the Illusion of Causality’
Objective: This supplementary document reports the results of a pilot study
conducted prior to the main study. The primary aim of the pilot study was to
assess the convergent validity of the auction mechanism and four predictors of
participants’ willingness to pay for multivitamins: estimated usage, efficacy
belief, general-attitudes, and irrational health beliefs. A secondary aim was to
assess the internal consistency and structure of an attitudinal scale designed to
measure participants’ pre-existing general attitudes to health supplements.
Another secondary aim was to establish a baseline with regards to what factors
people perceive to be important when making decisions about health purchases.
Design: The pilot study was conducted online with US participants (N = 194)
recruited via Amazon’s Mechanical Turk. The same measures and procedure
used in the main study were used in the pilot study, with a few exceptions. First,
participants were not subject to any interventions in the pilot study. Second, the
pilot study measured people’s hypothetical willingness to pay (WTP) for the
effervescent multivitamin product using the same auction mechanism employed
for the first auction in the main study.
Results: We obtained convergent evidence that the auction mechanism indexes
consumer demand for multivitamin supplements via positive correlations
between hypothetical WTP and estimated usage, efficacy belief, and general
attitudes. Second, we found strong evidence that individuals are vulnerable to the
illusion of causality and place relatively little value on clinical information when
making health purchases.
Conclusion: The pilot study confirmed that our survey instruments were suitable
for answering the research question addressed in the main study.
Keywords: causality; consumer behaviour; intervention; health communication;
health behaviour; health education;
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 222
OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 3
Pilot study
Prior to conducting the main study, a pilot study was conducted online with US
participants recruited via Amazon’s Mechanical Turk. The study was launched and
completed on the 23rd of February 2017. Participants in this study were not subjected to
any interventions. Instead, the primary aim was to assess the convergent validity of the
auction mechanism and four predictors of participants’ hypothetical willingness to pay
for multivitamins: estimated usage, efficacy belief, general-attitudes, and irrational
health beliefs. A secondary aim was to assess the internal consistency and structure of
the general attitudes scale developed to measure participants’ pre-existing general
attitudes to health supplements. Another secondary aim of the pilot study was to
establish a baseline with regards to what factors people perceive to be important when
making decisions about health purchases.
The pilot study was the same as the main study, with the following exceptions.
First, whereas the main study used two incentivized auctions in which participants could
win real health products by bidding with real money, the pilot study used a hypothetical
version of the first auction reported in the main study. Second, the pilot study included
an additional measurement scale, namely the Irrational Health Belief Scale
(Christensen, Moran, & Wiebe, 1999), which purportedly measures the degree to which
individuals hold irrational beliefs about health products. Third, the main study included
an additional predictor, namely participants’ current health (participants were asked to
indicate their current health on a 4-point scale; 1 = fine, healthy; 4 = sick, exhausted)
that was not used in the pilot study.
Design
Ethics approval to conduct the study was granted by the Human Ethics Office of the
University of Western Australia in accordance with the requirements of the Australian
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 223

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 4
National Statement on Ethical Conduct in Human Research (NHRMC, 2007).
Participants
In total, 201 participants responded to the survey. Several a-priori exclusion criteria
were used (details are provided in the results section). Based on these criteria, seven
participants were removed for careless responding. The final sample thus included N =
194 participants (81 females, 113 males; age M = 36.71 years; SD = 10.97). The number
of participants was pre-determined based on the recommended numbers for score
validation methods such as a principal components analysis (Field, Miles, & Field,
2012). Pay was determined at a rate of USD$7.40/hour pro rata, above US federal
minimum wage, which has been suggested as appropriate to attract ‘normal’ workers
(Rouse, 2015).
A pre-exclusion criteria was also set prior to recruitment that required
participants to have (i) a completion number of at least 5,000 ‘Human Intelligence
Tasks’ on Mechanical Turk, and (ii) an approval rate of greater than 97%. These
qualifications are recommended to ensure quality responses from Mechanical Turk
workers (Peer, Vosgerau, & Acquisti, 2014).
Materials
Predictors 1 and 2: Multivitamin consumption
Participants were asked whether they had taken multivitamins in the past, and if so, to
then provide an estimated previous usage frequency on an eight-point scale (1 = not in
the past few years, 8 = every day). Participants then rated their efficacy belief, that is,
their belief in the effectiveness of the routine consumption of multivitamins for
maintaining general health, on a 5-point scale (1 = not effective at all, 5 = extremely
effective; a sixth point was included in the scale so that participants could respond ‘I
don’t know’).
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 224

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 5
Predictor 3: General attitudes toward health supplements and alternative medicines
General attitudes toward health supplements and alternative medicines were assessed
using an 18-item scale (see Table 1). Each item consisted of a statement that was based
on a literature review of the motivations shown to influence the consumption of
alternative health products (e.g., ‘Vitamins are natural and supplements are therefore
safe’). Participants were asked to rate how much they agreed with each statement using
a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). A composite score
was calculated for each participant that indicated their general attitudes to health
supplements and alternative medicines (hereafter referred to as the ‘general-attitude
score’). To measure response consistency, each item was paired with a reverse-phrased
statement of similar meaning (i.e., 9 pairs of items). The order of items in the general-
attitude survey was randomized to control for order effects.
Predictor 4: Irrational health belief scale
The irrational health belief scale is a 20-item survey designed to assess individual
differences in the tendency to engage in health-related cognitive distortions
(Christensen et al., 1999). Each survey item describes a health situation and a
corresponding thought response (e.g. ‘You have been taking a medication for six
months and your medical problem has not improved. Your doctor has suggested a new
drug. You think to yourself, “If the last medication didn’t help, a new one won’t do any
good.”’). Participants are asked to imagine that the situation applies to them and then
indicate how similar the thought is to their own thought pattern in that situation using a
5-point scale (1 = not at all like I would think, 5 = almost exactly like I would think).
The order of items in the irrational health belief scale was randomized to control for
order effects. Collecting responses to both the irrational health belief scale and the
general-attitude survey provided means for assessing each scale’s construct validity.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 225

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 6
Willingness-to-pay (WTP)
To assess WTP, data was collected using a hypothetical version of the Becker-Degroot-
Marschak (BDM) auction mechanism (Becker, Degroot, & Marschak, 1964; Thrasher,
Rousu, Hammond, Navarro, & Corrigan, 2011). Participants were asked to imagine they
had been given $5 with which to place a bid on a tube of effervescent multivitamin
tablets. They were shown a plain-packaged picture of the product and provided with
some descriptive text about multivitamins, including some common health claims and a
popular pseudo-scientific causal explanation as to why supplements are thought to
provide health benefits. The exact text was:
‘Vitamins and minerals are micro-nutrients. They are, in small amounts, essential for
health. The lack of a specific micro-nutrient may cause or predispose someone to
disease. Micro-nutrient supplements are widely available; they are usually referred to as
“multivitamins.” The health benefits of multivitamins have been claimed to include a
reduction in cardiovascular disease and cancer, as well as an improvement in cognitive
function. Such benefits are commonly explained by stating that multivitamin
supplements boost the body’s natural immune system.’
Participants were asked to bid only the amount that would reflect how much they would
be willing to pay for that product. Participants were told that this was different to other
auctions in that they could only bid once, and that it was in their best interest to only bid
the amount they were willing to pay. Participants were required to enter their bid
amount b in cents b ∈ (0, 500). They knew that this amount would be compared against
a random number r ∈ (0, 500) drawn from a uniform distribution, and that if b ≥ r then
they would win the auction and hypothetically purchase the product for amount b but
keep 500 – b of their imagined endowment; otherwise if b < r then they would lose the
auction but hypothetically keep the full $5 endowment. The decision for participants to
pay the bid price, as opposed to the random price, which is the standard BDM model,
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 226

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 7
was based on previous laboratory experience that participants find paying the random
price confusing. We suggest the approach taken in the present paper is more intuitive as
it reflects the more familiar and real-world format adopted by online auction websites,
whereby consumers pay the bid amount once the reserve has been exceeded.
Participants knew that the auction and endowment were hypothetical and that they
would not receive any money, nor the multivitamin product on which they were
bidding, if their bid was successful. Prior to the main auction, participants were given
the chance to participate in two practice auctions using a hypothetical $1 endowment to
bid on a bottle of water.
Fictitious efficacy rating
This measure introduced participants to a fictional nausea drug ‘Product Z.’ To create
an illusion of causality, participants were only given a half-contingency table, which
showed that 4 out of 5 people experienced a health benefit from taking Product Z.
Participants were asked to rate the effectiveness of Product Z as either not effective,
mildly effective, very effective, or to indicate there was insufficient information to make
a determination of effectiveness. This question was designed to produce an estimate of
the proportion of people that fall prey to the illusion of causality, as indexed by the
proportion of individuals who failed to identify there was insufficient information to
determine causality.
Factors influencing future health purchases
To establish a baseline of the factors that people perceived as important when making
future health-related purchases, participants were asked to rate the importance of 15
health-related factors using a 5-point Likert scale (1= not important at all, 5 = extremely
important). For the purposes of this pilot study, only three items were considered of
interest. The most critical item was placebo comparison (‘the number of people who
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 227

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 8
did, and did not, experience a benefit when taking a sugar pill’). Placebo comparison
information is critical for making rational health purchases, because it is necessary for
assessing the efficacy of a remedy compared to taking a placebo. The other two items of
interest were product comparison (‘the number of people who did, and did not,
experience a benefit after taking a product’), and ‘known side effects.’ We reasoned that
both product comparison and known side effects would be important to people, and thus
would provide a suitable baseline from which to compare participants ratings of placebo
comparison information. The remaining 12 items were distractor items (e.g., importance
of ‘advertising claims’); item order was randomized.
Procedure
Participants were recruited via a survey link provided through Mechanical Turk. At the
start of the survey, participants were provided with an information form and provided
informed consent. They then responded to questions on demographics, multivitamin
consumption, and the general-attitude scale. Next, participants were shown the
multivitamin product and asked to indicate their WTP for it via the hypothetical BDM
auction. Participants then responded to the fictional product question and the questions
regarding their future health purchases. Finally, they completed the irrational health
belief scale.
Objectives
We made three predictions. Hypothesis I. Higher estimated usage, efficacy belief, and
general-attitude scores would be associated with higher WTP for multivitamins.
Hypothesis II. Higher irrational health belief scale scores would be associated with
higher WTP for multivitamins. Hypothesis III. Most participants would not recognize
the value of clinical trial information when making future health purchases.
Specifically, most people would (1) fail to recognize that there was insufficient
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 228

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 9
information to assess the efficacy of the fictional product, and (2) the placebo-
comparison factor would be rated as less important than the product-comparison or
side-effects factors.
Data analysis
Most analyses were conducted in R (R Core Team, version 3.3.2) with the exception of
the Principal Components Analysis, which was conducted in SPSS (IBM Corp, version
22). To assess the internal structure of the general-attitude survey, a principal
components analysis was conducted on the 18-items with oblique rotation (direct
oblimin). Sampling adequacy for the analysis was verified by the Kaiser-Meyer-Olkin
(KMO) measure. Bartlett’s test of sphericity was used to assess whether correlations
between items were sufficiently large for a principal components analysis. An initial
analysis was run to determine how many components to extract with the principal
components analysis. To establish internal consistency reliability, we computed
Cronbach’s alpha.
To assess whether estimated usage predicted WTP, we excluded participants
who indicated they had never taken multivitamins before (since they were not asked to
estimate their usage). To assess whether efficacy belief predicted WTP, we excluded
participants who answered, ‘I do not know.’ Associations between WTP and each of the
four potential predictors: estimated usage, efficacy belief, general-attitude score, and
irrational health belief scale were analysed using Spearman’s correlation coefficient
(Hypotheses 1 and 2). To test whether participants showed an overall preference for
certain responses on the effectiveness of the fictional product, we performed a
multinomial goodness-of-fit test to assess whether the response counts differed from
chance. Planned comparisons were conducted using binomial tests with sequential
Bonferroni adjustment. To test whether participants’ ratings of the importance of the
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 229

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 10
three factors for future health purchases (product comparison, placebo comparison, and
side effects) were significantly different, a Friedman’s ANOVA was conducted.
Planned comparisons were then conducted using Wilcoxon sign-ranked tests with
sequential Bonferroni adjustment.
Results
Exclusion criteria
A-priori criteria were applied to identify careless responders based on recommendations
from the literature (Lowry, D’Arcy, Hammer, & Moody, 2016; Oppenheimer, Meyvis,
& Davidenko, 2009). Participants were excluded who (i) gave non-differentiated
answers to every question in a survey block (Barge & Gehlbach, 2011; Hamby &
Taylor, 2016); (ii) failed an attention-trap question (Lowry et al., 2016); (iii) completed
a survey block in less than the allocated minimum reading time (i.e., > 600 words per
minute; Carver, 1985); and (iv) whose responses were, on average, overly inconsistent
between pairs of equivalent questions (i.e., an odd/even threshold of > 2 Likert points
apart; Curran, 2016). The exclusion criteria, and subsequent data analysis, were applied
separately to the three sections of the experiment: (i) the general-attitude scale (n = 7),
(ii) questions about future health purchases (n = 9), and (iii) the irrational health belief
scale (n = 42). Exclusion criteria were applied separately because each section varied in
cognitive demand, which is known to increase careless responding (Krosnick, 1991).
Further, as the irrational health belief scale was the longest and most demanding
section, it was deliberately placed at the end of the study to reduce careless responding
in the other sections. The same exclusion criteria were adopted in our main study with
one exception. Specifically, we removed the attention-trap questions from our a-priori
exclusion criteria following research suggesting that such items can increase socially
desirable responding (Clifford & Jerit, 2015).
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 230

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 11
Internal consistency and structure of general-attitude scale
Reverse-phrased items were reverse coded for analysis, so that higher total general-
attitude scores indicated more favourable attitudes toward health supplements. For the
principal components analysis, sampling adequacy was verified, KMO = .885
(Hutcheson & & Sofroniou, 1999), and all KMO values for individual items were > .8,
which is above the acceptable limit of .5 (Field et al., 2012). Correlations were found to
be sufficiently large for a principal components analysis, χ² (153) = 1766.68, p < .001.
Five components had eigenvalues over Kaiser’s criterion of 1 and in combination
explained 68.4% of the variance. The scree plot showed two points of inflexion, after
components one and five, suggesting that either one or five components may be
appropriate (Field et al., 2012) . Table 1 shows the component loadings after rotation.
The items that cluster on the same components suggest that component 1 represents a
general health factor, component 2 relates to safety, component 3 to supplements,
component 4 to alternative medicine, and component 5 to nutrition. The general-attitude
survey was found to be associated with a high level of internal consistency, Cronbach’s
α = .91.
Predictors of willingness to pay
Figures 1, 2, and 3 show WTP as predicted by the three predictor measures of estimated
usage of multivitamins, efficacy belief, and general-attitude score, respectively.
Correlations between the predictors of interest and WTP provided statistical
confirmation of Hypothesis I. Specifically, WTP was positively associated with
estimated usage of multivitamins, N = 170, rs = .25, p < .001, efficacy belief, N = 185, rs
= .31, p < .001, and general-attitude scores, N = 194, rs = .42, p < .001. However, we
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 231

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 12
did not find support for Hypothesis II as irrational health belief scale scores were not
significantly associated with WTP, N = 159, rs = .10, p = .21.1
Future health purchases
Figure 4 shows participants’ responses to the fictional product question. These
responses were found to be significantly different to the pattern expected by chance,
N = 194, p < .001. Post-hoc tests revealed that all four response frequencies were
significantly different from the expected value of 48.5 (N/4): ‘Very effective’ was
higher than the expected value p < .001; ‘Insufficient evidence’ was lower, p < .001;
‘Not effective’ was lower, p < .001; and ‘Mildly effective’ was lower, p < .05. The
results showed that the majority of people succumbed to the illusion of causality, since
the majority (69%) responded that the product was very effective and only a minority
(12 %) correctly identified that there was insufficient information to determine efficacy.
Figure 5 shows results of participants’ ratings of factors that may influence
future health purchases. The results provided statistical confirmation of Hypothesis III.
Specifically, we found that participants’ ratings of the importance of the three items of
interest (product comparison, placebo comparison, and side effects) to be significantly
different, N = 194, χ² (2) = 116.3, p < .001. As expected, placebo comparison (Mdn = 3,
‘Moderately Important’) was rated significantly less important than product comparison
(Mdn = 4, ‘Very Important’), p < .001, r = -.43, or side effects (Mdn = 5, ‘Extremely
Important’), p < .001, r = -.65. Finally, product comparison was rated significantly less
important than side effects, p < .001, r = -.46.
1 All analyses were also conducted with careless responders retained. These results showed that
the exclusion criteria made a negligible difference to the results.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 232

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 13
Discussion
The pilot study employed a variation of the BDM auction mechanism in a hypothetical
scenario to examine the relationship between people’s WTP for multivitamins and their
(i) estimated usage habits, (ii) belief in the efficacy of multivitamins, and (iii) general
attitudes towards dietary supplements and alternative medicines. We found that more
frequent estimated usage, greater efficacy belief, and more favourable general attitudes
reliably predicted a greater WTP for multivitamin products (Hypothesis I). The pilot
study also examined the relationship between people’s irrational health belief scale
scores and their WTP for multivitamins. Contrary to our prior prediction, we found that
the irrational health belief scale was not a reliable predictor of people’s WTP
(Hypothesis II). The pilot study also sought to establish a baseline for people’s
propensity to recognize the value of clinical trial information when making future health
purchases. The results showed that when provided with only half a contingency table
for a fictitious health product, most people succumbed to the illusion of causality by
incorrectly responding that the information presented indicated that the product was
‘very effective.’ The results also showed that placebo-comparison information was rated
as relatively unimportant, despite it being critical to determine if a product is efficacious
(Hypothesis III).
Validity of the general-attitude scale and the auction mechanism
The primary aim of the pilot study was to demonstrate the validity of both the general-
attitude survey and the auction mechanism. Two aspects of the data suggest that the
general-attitude scale is a valid measure of pre-existing attitudes toward supplements.
Specifically, the general-attitude scale was found to be highly internally consistent and
it was shown to measure five distinct but related components of attitudes towards
supplements. This result was expected because the general-attitude scale was based on
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 233

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 14
previous research into the underlying drivers of the consumption of alternative
medicines and dietary supplements. For example, items were based on findings from a
study (Barnes, Ball, Desbrow, Alsharairi, & Ahmed, 2016) indicating that the two most
common reasons for taking multivitamins were to supplement nutrition (60%) and to
increase immune strength (49%). The finding that all three moderators predicted WTP
suggests that this variation of the BDM auction mechanism, is a valid tool for
measuring consumer demand for multivitamin products. These findings validate our
methodology as suitable for answering the central question posed in the main study,
namely whether or not the intervention treatment leads to a measurable behaviour
change.
Validity of the irrational health belief scale
A secondary goal of the pilot study was to test the validity of the irrational health belief
scale. The finding that the irrational health belief scale did not predict WTP raises
questions about the validity of this scale as a measure of irrational health beliefs. Taken
in isolation, this conclusion is questionable. For example, one might alternatively
conclude that it is the validity of the auction mechanism itself, as a measure of
consumer demand for multivitamins, that should be called into question. However, the
fact that scores on the general–attitude scale—which also features items designed to tap
irrational health beliefs—did reliably predict WTP in the auction confers support for the
first conclusion. For these reasons, we decided to omit the irrational health belief scale
from the main study.
One possible reason for the failure of the irrational health belief scale to predict
WTP is that people who ascribe to certain irrational health beliefs may not be acting
irrationally, instead they may be acting rationally with imperfect information. In other
words, for any one individual, the available evidence concerning the efficacy of a health
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 234

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 15
belief—including personal experience, exposure to marketing claims, and anecdotes
from one’s own social network—may all logically lead to the conclusion that a health
behaviour caused an unrelated beneficial outcome. Thus, there may be no irrational
cognitive distortions driving an irrational health behaviour other than nescience. The
same conclusion could not be drawn for the general-attitude scale since this measure
included several items that directly measured peoples’ attitude towards dietary
supplements (e.g. ‘Taking vitamin supplements is a good way to maintain general
health’).
Baseline of perceived importance of factors for making health purchases
The pilot study also established two baselines for comparing whether the effect of our
interventions in the main study would generalize to future health purchases. The first
baseline is that most people succumb to the illusion of causality, as indicated by
responses to the fictional product. This supports previous research demonstrating the
strength of this illusion (Matute et al., 2015; Yarritu & Matute, 2015). The second
baseline is that placebo-comparison information was rated as less important than
product-comparison information, which in turn was rated as less important than
information about side effects. One explanation for these preferences is that people’s
perception of the importance of information is negatively correlated to its complexity,
especially when making fast decisions. In other words, because placebo comparison
information is both complex to obtain and complex to understand, this information is
perceived as less important for everyday decisions. This supports previous research that
many decisions are made using heuristics that ‘ignore part of the information, with the
goal of making decisions more quickly, frugally, and more accurately than more
complex methods’ (Gigerenzer & Gaissmaier, 2011). While simple heuristics can be
efficient and sufficiently accurate for many types of decisions (e.g., Dhami, 2003;
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 235

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 16
Dhami & Harries, 2001), they can also lead to significant errors, especially when
complex information is critical for inferring causality, as is often the case when the
outcomes of a cause are not immediately known. This is particularly true of many health
behaviours, as the benefits and/or side effects may not surface for many years and can
differ considerably between individuals. These results further highlight the need for
interventions that assist people in overcoming nescience.
Concluding remarks
There were two key findings of this pilot study. First, we obtained convergent evidence
that the auction mechanism indexes consumer demand for vitamin supplements in the
form of positive correlations between hypothetical WTP and the predictor measures of
estimated usage, efficacy belief, and general attitudes. Second, based on the fictional
health product scenario and future health purchases questionnaire, we obtained strong
evidence that individuals are vulnerable to the illusion of causality, and that they place
relatively little emphasis on clinical information when making health purchases. Thus,
the pilot study confirmed that the survey instruments are suitable for answering the
research question addressed in the main study.
References
Barge, S., & Gehlbach, H. (2011). Using the theory of satisficing to evaluate the quality
of survey data. Research in Higher Education, 53(2), 182-200.
doi:10.1007/s11162-011-9251-2
Barnes, K., Ball, L., Desbrow, B., Alsharairi, N., & Ahmed, F. (2016). Consumption
and reasons for use of dietary supplements in an Australian university
population. Nutrition, 32, 524-530. doi:10.1016/j.nut.2015.10.022
Becker, G. M., Degroot, M. H., & Marschak, J. (1964). Measuring utility by a single-
response sequential method. Behavioral Science, 9(3), 226.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 236

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 17
Carver, R. P. (1985). How good are some of the world's best readers? Reading Research
Quarterly, 20, 389-419. doi:10.2307/747851
Christensen, A. J., Moran, P. J., & Wiebe, J. S. (1999). "Assessment of irrational health
beliefs: Relation to health practices and medical regimen adherence":
Correction. Health Psychology, 18, 220-220. doi:10.1037/0278-6133.18.3.220
Clifford, S., & Jerit, J. (2015). Do attempts to improve respondent attention increase
social desirability bias? Public Opinion Quarterly, 79, 790-802.
doi:10.1093/poq/nfv027
Curran, P. G. (2016). Methods for the detection of carelessly invalid responses in survey
data. Journal of Experimental Social Psychology, 66, 4-19.
doi:10.1016/j.jesp.2015.07.006
Dhami, M. K. (2003). Psychological models of professional decision making.
Psychological Science, 14(2), 175-180.
Dhami, M. K., & Harries, C. (2001). Fast and frugal versus regression models of human
judgement. Thinking & Reasoning, 7, 5-27. doi:10.1080/13546780042000019
Field, A., Miles, J., & Field, Z. (2012). Discovering statistics using R [Google Books].
Retrieved from
https://play.google.com/store/books/details?id=Q9GCAgAAQBAJ&hl=en
Gigerenzer, G., & Gaissmaier, W. (2011). Heuristic decision making. Annual Review of
Psychology, 62, 451-482. doi:10.1146/annurev-psych-120709-145346
Hamby, T., & Ickes, W. (2015). Do the readability and average item length of
personality scales affect their reliability? Journal of Individual Differences, 36,
54-63.
Hamby, T., & Taylor, W. (2016). Survey satisficing inflates reliability and validity
measures: An experimental comparison of college and Amazon Mechanical
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 237

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 18
Turk samples. Educational and Psychological Measurement, 76, 912-932.
doi:10.1177/0013164415627349
Hutcheson, Graeme & Sofroniou, Nick (1999). The multivariate social scientist:
introductory statistics using generalized linear models. Sage Publications,
London.
IBM SPSS Statistics for Windows (Version 22)[Computer software]. Armonk, NY,
IBM Corp.
Krosnick, J. A. (1991). Response strategies for coping with cognitive demands of
attitude measures in surveys. Applied Cognitive Psychology, 5, 213-236.
Lowry, P. B., D’Arcy, J., Hammer, B., & Moody, G. D. (2016). “Cargo Cult” science in
traditional organization and information systems survey research: A case for
using nontraditional methods of data collection, including Mechanical Turk and
online panels. The Journal of Strategic Information Systems, 25, 232-240.
doi:10.1016/j.jsis.2016.06.002
Matute, H., Blanco, F., Yarritu, I., Díaz-Lago, M., Vadillo, M. A., & Barberia, I. (2015).
Illusions of causality: How they bias our everyday thinking and how they could
be reduced. Frontiers in Psychology, 6, 1-14.
National Health and Medical Research Council. (2007). National statement on ethical
conduct in human research (2007) - Updated December 2013 (the National
Statement), Commonwealth of Australia, Canberra.
Oppenheimer, D. M., Meyvis, T., & Davidenko, N. (2009). Instructional manipulation
checks: Detecting satisficing to increase statistical power. Journal of
Experimental Social Psychology, 45, 867-872. doi:10.1016/j.jesp.2009.03.009
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 238
OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 19
Peer, E., Vosgerau, J., & Acquisti, A. (2014). Reputation as a sufficient condition for
data quality on Amazon Mechanical Turk. Behavior Research Methods, 46,
1023-1031. doi:10.3758/s13428-013-0434-y
R Core Team (Version 3.3.2) [Computer Software] R: A language and environment for
statistical computing. Vienna, Austria. R Foundation for Statistical Computing.
Rouse, S. V. (2015). A reliability analysis of Mechanical Turk data. Computers in
Human Behavior, 43, 304-307. doi:10.1016/j.chb.2014.11.004
Thrasher, J. F., Rousu, M. C., Hammond, D., Navarro, A., & Corrigan, J. R. (2011).
Estimating the impact of pictorial health warnings and "plain" cigarette
packaging: Evidence from experimental auctions among adult smokers in the
United States. Health Policy, 102, 41-48. doi:10.1016/j.healthpol.2011.06.003
Yarritu, I., & Matute, H. (2015). Previous knowledge can induce an illusion of causality
through actively biasing behaviour. Frontiers in Psychology, 6, 389.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 239

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 20
Table 1. Factor loadings for principal components analysis with oblimin rotation on the
general attitudes towards health supplements scale.
Item General Health
Additives / Experience Nutrition Alternative
Medicine Safety
A person who is generally healthy can still benefit from taking vitamin supplements 0.89
Taking vitamin supplements is a good way to maintain general health 0.87
Vitamin supplements are a good investment 0.70
Vitamin supplements are not worth the money 0.69
Vitamin supplements increase immune strength 0.64
I don’t believe supplements increase immune strength 0.60
The population is healthiest when people have access to both conventional and alternative medicines
0.50 -0.45
Vitamins are natural and supplements are therefore safe 0.43
Vitamin supplements are only useful if a person has a specific deficiency 0.40
I do not purchase products simply because they contain added vitamins 0.90
Sometimes I choose certain products because they contain added vitamins 0.76
The best way to know if a dietary supplement or medicine is effective is to try it for yourself
0.41
Vitamin supplements are required because a typical diet is insufficient for optimal health
-0.80
Vitamin supplements are not necessary for optimal nutrition. -0.71
One does not need to take vitamin supplements to maintain general health -0.70
Supplements or medicines should only be taken if there is scientific evidence that they work
0.86
Most alternative medicines are ineffective 0.46 0.50 Taking vitamin supplements may pose significant health risks 0.79
Eigenvalues 7.63 1.28 1.25 1.11 1.04 % of total variance 42.39 7.11 6.94 6.17 5.78 α 0.90 0.74 0.80 0.47 0.16 Note. Factor loadings <.40 are not shown. Data excludes seven careless responders (N=194).
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 240

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 21
Figure 1.
Participants’ estimated frequency of their usage of multivitamins against WTP for the
multivitamin product, N = 170. Error bars indicate standard errors.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 241

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 22
Figure 2.
Participants’ estimated belief in the efficacy multivitamin against WTP for the
multivitamin product, N = 185. Error bars indicate standard error.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 242

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 23
Figure 3.
Participants’ general-attitude scale score against WTP-1 for the multivitamin product, N
= 194.
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 243

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 24
Figure 4.
The number of participants against each possible response concerning the fictitious
health product, N = 194. Significant differences were determined against the number
expected by chance (N/4) using planned binomial tests with sequential Bonferroni
adjustment.
*p < .05, ***p < .001
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 244

OVERCOMING THE ILLUSION OF CAUSALITY SUPPLEMENT 25
Figure 5.
The number of participants against each possible rating of importance for product
comparison, placebo comparison, and side effects, N = 194. Significant differences
were determined against the number expected by chance (N/5) using Wilcoxon sign-
ranked tests with sequential Bonferroni adjustment.
*p < .05, ***p < .001
Appendix II — Supplement for Chapter 3: Overcoming the illusion of causality 245

246

Appendix III: Supplementary material for Chapter 4
Contains the supplemental material for the publication:
MacFarlane, D., Hurlstone, M., & Ecker, U. Countering Demand for Ineffective Health Remedies: Do Consumers Respond to Risks, Lack of Benefits, or Both? Psychology & Health.
247

248

Supplementary Material for ‘Countering Demand for Ineffective Health
Remedies: Do Consumers Respond to Risks, Lack of Benefits, or Both?’
Douglas MacFarlane1,a, Mark J. Hurlstone1,2, and Ullrich K. H. Ecker1
1 School of Psychological Science, University of Western Australia; M304, 35 Stirling Hwy,
Perth 6009, Australia.
2 Now at the Department of Psychology, Lancaster University, UK.
a Corresponding author. email: [email protected]
Appendix III — Supplement for Chapter 4: Do consumers respond to risks, lack of benefits, or both? 249

Supplementary Material for ‘Countering Demand for Ineffective Health Remedies: Do
Consumers Respond to Risks, Lack of Benefits, or Both?’
Table S1. JASP Output for the Bayesian ANCOVA, Showing the Strength Evidence for Each Model Compared to the Null Model (Experiments 1 and 2 Combined)
Models P(M) P(M|data) BFM BF10 error %
Null model 0.026 1.733e -15 6.412e -14 1
Contingency condition + Fear-appeal + Bidding type + General-attitude
0.026 0.524 40.808 3.026e +14 6.308
Contingency condition + Fear-appeal + Bidding type + General-attitude + Fear-appeal ✻ Bidding type
0.026 0.214 10.064 1.234e +14 1.766
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Bidding type
0.026 0.088 3.573 5.081e +13 2.666
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Fear-appeal
0.026 0.067 2.667 3.880e +13 3.016
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Bidding type + Fear-appeal ✻ Bidding type
0.026 0.034 1.301 1.960e +13 2.771
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Fear-appeal + Fear-appeal ✻ Bidding type
0.026 0.031 1.19 1.798e +13 2.309
Fear-appeal + Bidding type + General-attitude 0.026 0.014 0.53 8.145e +12 2.785
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Fear-appeal + Contingency condition ✻ Bidding type
0.026 0.013 0.477 7.350e +12 3.662
Fear-appeal + Bidding type + General-attitude + Fear-appeal ✻ Bidding type
0.026 0.005 0.204 3.159e +12 4.969
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Fear-appeal + Contingency
0.026 0.005 0.198 3.078e +12 2.837
Appendix III — Supplement for Chapter 4: Do consumers respond to risks, lack of benefits, or both? 250

condition ✻ Bidding type + Fear-appeal ✻ Bidding type
Contingency condition + Fear-appeal + General-attitude
0.026 0.002 0.084 1.314e +12 1.078
Contingency condition + Fear-appeal + Bidding type + General-attitude + Contingency condition ✻ Fear-appeal + Contingency condition ✻ Bidding type + Fear-appeal ✻ Bidding type + Contingency condition ✻ Fear-appeal ✻ Bidding type
0.026 8.986e -4 0.033 5.185e +11 3.097
Contingency condition + Fear-appeal + General-attitude + Contingency condition ✻ Fear-appeal
0.026 3.223e -4 0.012 1.860e +11 2.849
Fear-appeal + General-attitude 0.026 8.326e -5 0.003 4.805e +10 0.755
Contingency condition + Bidding type + General-attitude
0.026 3.925e -6 1.452e -4 2.265e +9 1.136
Contingency condition + Bidding type + General-attitude + Contingency condition ✻ Bidding type
0.026 7.133e -7 2.639e -5 4.116e +8 4.717
Bidding type + General-attitude 0.026 1.949e -7 7.211e -6 1.125e +8 0.814
Contingency condition + Fear-appeal + Bidding type
0.026 1.681e -7 6.219e -6 9.699e +7 1.153
Contingency condition + Fear-appeal + Bidding type + Fear-appeal ✻ Bidding type
0.026 4.658e -8 1.724e -6 2.688e +7 3.684
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Bidding type
0.026 4.006e -8 1.482e -6 2.312e +7 1.572
Contingency condition + General-attitude 0.026 3.130e -8 1.158e -6 1.806e +7 1.676
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Fear-appeal
0.026 2.145e -8 7.935e -7 1.238e +7 2.179
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Bidding type + Fear-appeal ✻ Bidding type
0.026 1.185e -8 4.385e -7 6.839e +6 7.534
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Fear-appeal + Fear-appeal ✻ Bidding type
0.026 7.229e -9 2.675e -7 4.171e +6 5.195
Appendix III — Supplement for Chapter 4: Do consumers respond to risks, lack of benefits, or both? 251

Fear-appeal + Bidding type 0.026 6.005e -9 2.222e -7 3.465e +6 0.842
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Fear-appeal + Contingency condition ✻ Bidding type
0.026 5.874e -9 2.173e -7 3.389e +6 9.171
General-attitude 0.026 2.083e -9 7.706e -8 1.202e +6 0.002
Fear-appeal + Bidding type + Fear-appeal ✻ Bidding type
0.026 1.679e -9 6.211e -8 968627.977 2.239
Contingency condition + Fear-appeal 0.026 1.666e -9 6.165e -8 961470.234 2.435
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Fear-appeal + Contingency condition ✻ Bidding type + Fear-appeal ✻ Bidding type
0.026 1.552e -9 5.742e -8 895509.616 2.575
Contingency condition + Fear-appeal + Bidding type + Contingency condition ✻ Fear-appeal + Contingency condition ✻ Bidding type + Fear-appeal ✻ Bidding type + Contingency condition ✻ Fear-appeal ✻ Bidding type
0.026 2.746e -10 1.016e -8 158475.792 4.168
Contingency condition + Fear-appeal + Contingency condition ✻ Fear-appeal
0.026 2.166e -10 8.016e -9 125006.357 1.781
Fear-appeal 0.026 7.544e -11 2.791e -9 43534.02 5.249e -10
Contingency condition + Bidding type 0.026 1.205e -12 4.458e -11 695.306 2.446
Contingency condition + Bidding type + Contingency condition ✻ Bidding type
0.026 3.166e -13 1.172e -11 182.716 11.502
Bidding type 0.026 7.519e -14 2.782e -12 43.388 2.415e -7
Contingency condition 0.026 2.272e -14 8.407e -13 13.111 2.594e -6
Note. This table contains data shows the JASP output of the results from the data pooled from three experiments (Experiment 2 and both iterations of Experiment 1) with careless responders excluded (N = 536). The table compares possible models for predicting WTP and provides an estimate of the strength of the evidence for each model compared to the null model. Text in bold shows the strongest model, as determined by the greatest BF10.
Appendix III — Supplement for Chapter 4: Do consumers respond to risks, lack of benefits, or both? 252

Table S2. Bayesian Analysis of Effects for Willingness-to-pay Predicted by Condition and Bidding Type (Experiments 1 and 2 Combined) Effects P(incl) P(incl|data) BF10 Inclusion
Contingency condition 0.737 0.979 17.038
Fear-appeal 0.737 1 77271.395
Bidding type 0.737 0.997 132.95
General-attitude 0.5 1 2.919e +6
Contingency condition ✻ Fear-appeal 0.316 0.119 0.291
Contingency condition ✻ Bidding type 0.316 0.147 0.374
Fear-appeal ✻ Bidding type 0.316 0.294 0.904
Contingency condition ✻ Fear-appeal ✻ Bidding type 0.053 0.001 0.02
Note. Showing results from three experiments (Experiment 2 and both iterations of Experiment) with careless responders excluded (N = 536). The results in bold confirm that there were no interactions between biding amount and the intervention treatments, meaning that effect of condition on WTP was comparable between the hypothetical and incentivized experiments.
Appendix III — Supplement for Chapter 4: Do consumers respond to risks, lack of benefits, or both? 253

Figure S1. Test for Hom
ogeneity of Regression Slopes
Figure S1. Show
ing results from the first iteration of Experim
ent 1 with careless responders rem
oved (N = 156). This figure show
s how, by
random chance, general attitudes varied across conditions w
hich thus violated the assumption of hom
ogeneity of regression slopes. Error bars indicate standard error.
Appendix III —
Supplement for C
hapter 4: Do consum
ers respond to risks, lack of benefits, or both?
254

Figure S2. Bayesian Interaction Plot for Pooled D
ata from both experim
ents with careless responders rem
oved
(a) Experim
ent 1: Hypothetical bids
(b) Experiment 2: Incentivised bids
Figure S2. Showing results from
both experiments (N
= 536)—both sub-sam
ples of Experiment 1, Experim
ent 2—w
ith careless responders rem
oved (n = 84). Plot (a) shows the results for hypothetical bids, and plot (b) show
s results for bids that were incentivized.
Error bars indicate 95% credible intervals.
Appendix III —
Supplement for C
hapter 4: Do consum
ers respond to risks, lack of benefits, or both?
255

256

Appendix IV: Supplementary material A for Chapter 5
Contains the supplemental material for the publication:
MacFarlane, D., Tay, L. Q., Hurlstone, M. J., & Ecker, U. K. H. (Under Review). Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation Sharing. Manuscript submitted for publication.
257

258

1
Supplementary Material A for MacFarlane et al. “Refuting Spurious COVID-19
Treatment Claims Reduces Demand and Misinformation Sharing”
Materials
Predictors.
Main predictors. Prior beliefs can moderate responses to health messaging (Myers,
2014). Thus, participants’ general attitudes toward health supplements and alternative
medicines were assessed using an 18-item questionnaire, following MacFarlane, Hurlstone,
and Ecker (2018). Each item consisted of a declarative statement relating to a motivation for
consuming alternative health products (e.g., “Vitamins are natural, and supplements are
therefore safe”). Participants were asked to rate how much they agreed with each statement
using a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree). A composite score
was calculated for each participant indicating their general attitude to health supplements and
alternative medicines (hereafter, “general-attitude”). To measure response consistency, each
item was paired with a reverse-phrased statement of similar meaning (i.e., 9 pairs of items).
The order of items in the scale was randomized. The general-attitude scale was found to have
very good internal consistency reliability (Cronbach’s α = .87). The full scale can be found in
Supplementary Material B.
Participants’ concern about the COVID-19 pandemic was measured as a composite
score based on participants’ responses to four questions (e.g., “How severe do you think
novel coronavirus [COVID-19] will be in the U.S. general population as a whole?” on a 5-
point Likert scale [1 = very mild; 5 = very severe]), following Ecker, Butler, Cook,
Hurlstone, Kurz, & Lewandowsky (2020). All items are provided in Supplementary Material
B.
Additional predictors. We measured three additional predictors of willingness-to-pay
by asking participants (1): whether they had taken vitamin E supplements in the past, and if
Appendix IV — Supplement A for Chapter 5: Refuting spurious COVID-19 claims 259

2
so, to estimate their previous usage frequency on an eight-point scale (1 = not in the past few
years; 8 = every day); (2) to rate their belief in the effectiveness of the routine consumption
of vitamin E supplements for their health (hereafter, “efficacy-belief”), using a 6-point scale
(1 = not effective at all; 5 = extremely effective; 6 = don’t know); and (3) to estimate their
current state of health on a 4-point scale (1 = fine, healthy; 4 = sick, exhausted).
Results
Additional predictors of willingness-to-pay. Associations between willingness-to-
pay and the three additional predictors were analyzed via Spearman’s correlation coefficient.
For estimated usage, we excluded participants who reported having never previously taken
vitamin E supplements. For estimated efficacy belief, we excluded participants who
responded “don’t know”. Willingness-to-pay was positively associated with estimated usage
of vitamin E, n = 384, rs = .16, p = .001 and efficacy belief, n = 678, rs = .22, p < .001,
indicating participants with more frequent usage and higher efficacy belief had significantly
higher willingness-to-pay for the vitamin E product. The control predictor of current health
state was not correlated with willingness-to-pay, n = 678, rs = .03, p = .51.
Appendix IV — Supplement A for Chapter 5: Refuting spurious COVID-19 claims 260

3 Table S1
Post Hoc C
omparisons Testing the Influence of C
ondition on Willingness-To-Pay
95%
CI for M
ean Difference
Mean
Difference
Lower
Upper
SE t
Cohen’s d
pTukey
Control
Misinform
ation -23.65
-62.68 15.39
15.16 -1.56
-0.16 0.40
Tentative R
efutation 20.21
-19.01 59.43
15.23 1.33
0.16 0.55
Tentative R
efutation 35.81
-3.31 74.93
15.19 2.36
0.24 0.09
Misinform
ation Tentative R
efutation 43.86
4.73 82.98
15.19 2.89
0.28 0.02*
Enhanced R
efutation 59.46
20.41 98.51
15.16 3.92
0.37 < .001***
Tentative Refutation
Enhanced Refutation
15.60 -23.61
54.82 15.23
1.03 0.10
0.74
Note. C
onfidence interval adjustment: Tukey m
ethod for comparing a fam
ily of 4 estimates. C
ohen’s d does not correct for multiple
comparisons. * p < .05, ** p < .01, *** p < .001
Appendix IV
— Supplem
ent A for C
hapter 5: Refuting spurious C
OV
ID-19 claim
s
261

Running head: R
EFUTIN
G C
OV
ID (M
ISINFO
RM
ATIO
N)
4
Table S2
Post Hoc C
omparisons Testing the Influence of C
ondition on Misinform
ation-Promotion
Ws
pBonferroni
r
Control
Misinform
ation 12434
.017* -.09
Tentative R
efutation 15473
.1676 -.05
Enhanced, R
efutation 18494
< .001*** -.19
Misinform
ation Tentative R
efutation 17712
< .001*** -.15
Enhanced R
efutation 20566
< .001*** -.27
Tentative Refutation Enhanced R
efutation 17386
< .001*** -.15
Note. p-values w
ere adjusted for multiple com
parisons with sequential B
onferroni adjustment.
* p < .05, ** p < .01, *** p < .001
Appendix IV
— Supplem
ent A for C
hapter 5: Refuting spurious C
OV
ID-19 claim
s
262

Running head: R
EFUTIN
G C
OV
ID (M
ISINFO
RM
ATIO
N)
5
Table S3
Engagement w
ith Misinform
ation-endorsing Social-media Post across C
onditions
Condition
Share
%
Like
%
Pass
%
Flag
%
Share+
Like %
Pass+
Flag %
Share % (vs
Misinform
.)
Flag % (vs
Misinform
.)
Share+Like %
(vs Control)
Share+Like %
(vs Misinfo.)
Control
19.41 30.59
18.82 31.18
50.00 50.00
-32.26 +52.32
- -18.13
Misinform
ation 28.65
30.41 20.47
20.47 59.06
40.94 -
- +18.13
-
Tentative-Refutation
13.10 28.57
25.00 33.33
41.67 58.33
-54.30 +62.86
-16.66 -29.46
Enhanced-Refutation
8.88 17.75
18.34 55.03
26.63 73.37
-69.03 +168.86
-79.21 -54.92
Appendix IV
— Supplem
ent A for C
hapter 5: Refuting spurious C
OV
ID-19 claim
s
263

6
References
Ecker, U. K. H., Butler, L. H., Cook, J., Hurlstone, M. J., Kurz, T., & Lewandowsky, S.
(2020). Using the COVID-19 economic crisis to frame climate change as a
secondary issue reduces mitigation support. Journal of Environmental
Psychology, 70, 101464. https://doi.org/10.1016/j.jenvp.2020.101464
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for
ineffective health remedies: Overcoming the illusion of causality. Psychology &
Health, 33, 1472-1489. https://doi.org/10.1080/08870446.2018.1508685
Myers, L. B. (2014). Changing smokers’ risk perceptions—for better or worse? Journal
of Health Psychology, 19, 325-332. https://doi.org/10.1177/1359105312470154
Appendix IV — Supplement A for Chapter 5: Refuting spurious COVID-19 claims 264

Appendix V: Supplementary material B for Chapter 5
Contains the supplemental material for the publication:
MacFarlane, D., Tay, L. Q., Hurlstone, M. J., & Ecker, U. K. H. (Under Review). Refuting Spurious COVID-19 Treatment Claims Reduces Demand and Misinformation Sharing. Manuscript submitted for publication.
265

266

1
Supplementary Material B for MacFarlane et al. “Refuting Spurious COVID-19
Treatment Claims Reduces Demand and Misinformation Sharing”
General Attitudes toward Health Supplements and Alternative Medicines Scale
The following items were used to measure participants’ general attitudes toward
health supplements and alternative medicines (for details, see MacFarlane, Hurlstone, &
Ecker, 2018):
1. Taking vitamin supplements is a good way to maintain general health;
2. One does not need to take vitamin supplements to maintain general health;
3. Vitamin supplements are a good investment;
4. Vitamin supplements are not worth the money;
5. Vitamin supplements are only useful if a person has a specific deficiency;
6. A person who is generally healthy can still benefit from taking vitamin supplements;
7. Taking vitamin supplements may pose significant health risks;
8. Vitamins are natural and supplements are therefore safe;
9. The population is healthiest when people have access to both conventional and
alternative medicines;
10. The best way to know if a dietary supplement or medicine is effective is to try it for
yourself;
11. Supplements or medicines should only be taken if there is scientific evidence that they
work;
12. Vitamin supplements are required because a typical diet is insufficient for optimal
health;
13. Vitamin supplements are not necessary for optimal nutrition;
14. Vitamin supplements increase immune strength;
15. I don’t believe supplements increase immune strength;
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 267

2
16. Sometimes I choose certain products because they contain added vitamins;
17. I do not purchase products simply because they contain added vitamins;
18. Most alternative medicines are ineffective.
COVID-19 Concern Scale
The following items were used to measure participants’ COVID-19 concern,
following Ecker, Butler, Cook, Hurlstone, Kurz, and Lewandowsky (2020):
1. “How severe do you think novel coronavirus (COVID-19) will be in the U.S. general
population as a whole?”, using a 5-point Likert scale (1 = very mild; 5 = very severe);
2. “How concerned are you that you or someone you know might become infected with
novel coronavirus (COVID-19)?”, using a 5-point Likert scale (1 = not at all
concerned; 5 = extremely concerned);
3. “Have you been (or do you expect to be) negatively impacted financially by novel
coronavirus (COVID-19)?”, using a 5-point Likert scale (1 = not at all impacted; 5 =
very severely impacted);
4. “How much do you agree with the statement ‘The coronavirus (COVID-19) crisis will
be over soon’?”, using a 6-point Likert scale (1 = strongly disagree; 6 = strongly
agree).
Articles
The following pages show the articles as they were presented to participants. Note
that refutation articles were presented after the misinformation article in the refutation
conditions.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 268

3
Control.
Keeping your immune system fit BY TAYLOR DAVIS — 3 DAYS AGO
The coronavirus presents many uncertainties, and none of us can completely eliminate our risk of getting COVID-19. If we do catch COVID-19, our immune system is responsible for fighting it. Research shows that you can try to keep your immune system healthy to give it the best chance of fighting an infection. This is where things like a balanced diet, regular exercise, and good sleep come in. Maintaining a good diet with plenty of fruit and vegetables, and avoiding alcohol and tobacco, as well as making sure you get at least 7 hours sleep at night, and 30 minutes of exercise a day, will help your immune system to stay healthy. One reason why a balanced diet supports immune system function is that it ensures your body gets all the vitamins and minerals it needs. The U.S. National Institute of Health (NIH) website states,
"Vitamins and minerals are micro-nutrients. They are, in small amounts, essential for health. The lack of a specific micro-nutrient may cause or predispose someone to disease." "Vitamin E, for example, acts as an antioxidant and is involved in immune function. It helps to widen blood vessels and keep blood from clotting. In addition, cells use Vitamin E to interact with each other and to carry out many important functions."
While some believe that extra vitamin supplements are essential, dieticians say that taking additional vitamins is not necessary unless you have been diagnosed by your doctor with a specific nutrient deficiency or you have specific dietary needs.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 269

4
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 270

5
Misinformation. Keeping your Immune System Fit —Can Vitamin E Supplements Treat COVID-19? BY TAYLOR DAVIS — 3 DAYS AGO
The coronavirus presents many uncertainties, and none of us can completely eliminate our risk of getting COVID-19. If we do catch COVID-19, our immune system is responsible for fighting it. Research shows that you can try to keep your immune system healthy to give it the best chance of fighting an infection. This is where things like a balanced diet, regular exercise, and good sleep come in. Maintaining a good diet with plenty of fruit and vegetables, and avoiding alcohol and tobacco, as well as making sure you get at least 7 hours of sleep a night, and 30 minutes of exercise a day, will help your immune system stay healthy. One reason why a balanced diet supports immune function is that it ensures your body gets all the vitamins and minerals it needs. The U.S. National Institute of Health (NIH) website states,
"Vitamins and minerals are micro-nutrients. They are, in small amounts, essential for health. The lack of a specific micro-nutrient may cause or predispose someone to disease." "Vitamin E, for example, acts as an antioxidant and is involved in immune function. It helps to widen blood vessels to keep blood from clotting. In addition, cells use Vitamin E to interact with each other and to carry out many important functions."
While some believe that extra vitamin supplements are essential, dieticians say that taking additional vitamins is not necessary unless you have been diagnosed by your doctor with a specific nutrient deficiency or you have specific dietary needs.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 271

6
However, Dr. Avery Clarke from New York argues Vitamin E is essential to combatting COVID-19. He said,
“Vitamin E boosts the immune system so that it can better fight off invading bacteria and viruses." "Experts in Taiwan have shown that COVID-19 can be slowed, or stopped completely, with immediate widespread use of high doses of Vitamin E. If taken throughout the day, Vitamin E is a clinically proven antiviral without equal." "I have seen patients who showed early symptoms of COVID coming on; I told them to try large doses of Vitamin E, and symptoms went away in just a few days." "What's more, this remedy is completely natural. I am urgently trying to get this message out now because it doesn't get much airtime—after all, it's cheap and readily available, so there's not much money in it." "Imagine if you, or one of your loved ones, gets sick or dies, from something that is completely preventable."
Dr. Clarke said you can protect yourself by taking a daily Vitamin E supplement from any reputable chemist.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 272

7
Tentative refutation. There is no evidence that Vitamin E supplements help with COVID-19 BY JORDAN VANCE — 2 DAYS AGO Professor Simon Corner, a public health expert at the University of Chicago, is critical of claims about coronavirus cures. When asked about Dr. Avery’s Vitamin E claims, Professor Corner replied,
“There is no conclusive evidence that vitamin E supplements can delay the onset of an infection or treat respiratory infections, such as COVID-19. Furthermore, vitamin and mineral supplements are not recommended for the general population."
Professor Corner said there are some exceptions where Vitamin E supplements may be appropriate such as for pregnant women, some people with chronic health conditions, and people with conditions that affect their diets. Professor Corner recommends people talk to their doctor, pharmacist, or accredited dietitian.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 273

8
Enhanced refutation. WARNING: False Claims about Vitamin E supplements & COVID-19 BY JORDAN VANCE — 2 DAYS AGO Professor Simon Corner, a public health expert at the University of Chicago, is critical of claims about coronavirus cures. When asked about Dr. Avery’s Vitamin E claims, Professor Corner replied,
"Dr. Clarke is spreading false and misleading information to deliberately deceive people into wanting an ineffective cure to coronavirus."
Professor Corner outlined some of the techniques that Dr. Clarke used to deceive. Professor Corner explained,
"Dr. Clarke’s message starts with some true facts about the benefits of vitamins. So, it’s true that Vitamin E is important for fighting viruses, and deficiencies can weaken your immune system." "Giving some accurate information, combined with his title as a doctor, creates the impression that Dr. Clarke is a medical expert making trustworthy claims. In reality, Dr. Clarke intentionally hides the fact that he is not a medical doctor and that his many false claims are rejected by the medical community. Such deception is one good reason why Dr. Clarke's advice should be ignored."
Professor Corner said it was understandable that everyone hopes for a “miracle cure”, especially during this COVID-19 pandemic, when we are all worried about our own health and that of our loved ones. He explained that fear was a key component of Dr. Clarke’s message, used to manipulate people into believing that his bogus cure is essential. Professor Corner said,
"Thankfully, the majority of people will recover from COVID-19 thanks to their own immune systems, irrespective of any dietary supplements or unproven remedies they may or may not have taken."
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 274

9
"Unfortunately, there is no clinical evidence that Vitamin E supplements have any impact on COVID-19."
Professor Corner explains that Dr. Clarke's use of the term “natural”, was a particular marketing trick, known as an "appeal to nature".
"Using terms such as 'natural' is designed to get people to associate the proposed treatment with being harmless. In fact, however, high doses of Vitamin E supplements have been linked to adverse side-effects such as nausea, diarrhoea, and some more serious diseases. For this reason, the National Academies’ Food and Nutrition Board has set upper limits for Vitamin E consumption."
Professor Corner said that sharing such bogus remedies with your family would thus put them at risk of serious side-effects, while providing no benefit for treating COVID-19.
"While vitamin supplements cannot boost your immune system, as people like Dr. Clarke might claim, ensuring good nutrition by eating a range of foods will keep your immune system healthy."
Professor Corner noted that the only proven way to keep safe from COVID-19 is to maintain physical (social) distancing and ensure proper hygiene practices.
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 275

10
References
Ecker, U. K. H., Butler, L. H., Cook, J., Hurlstone, M. J., Kurz, T., & Lewandowsky, S.
(2020). Using the COVID-19 economic crisis to frame climate change as a secondary
issue reduces mitigation support. Journal of Environmental Psychology, 70, 101464.
https://doi.org/10.1016/j.jenvp.2020.101464
MacFarlane, D., Hurlstone, M. J., & Ecker, U. K. H. (2018). Reducing demand for ineffective
health remedies: Overcoming the illusion of causality. Psychology & Health, 33,
1472-1489. https://doi.org/10.1080/08870446.2018.1508685
Appendix V — Supplement B for Chapter 5: Refuting spurious COVID-19 claims 276

Appendix VI: Supplementary material for Chapter 6
Contains the supplemental material for the publication:
MacFarlane, D., Hurlstone, M. J., Ecker, U. K. H., Ferraro, P. J, van der Linden, S., Wan, A. K. Y., Veríssimo, D., Burgess, G., Chen, F., Hall, W., Hollands, G. J., & Sutherland, W. J. (Under Review) Reducing demand for overexploited wildlife products: Lessons from systematic reviews from outside conservation science. Manuscript submitted for publication.
277

278

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 1
Supplementary Material for “Reducing Demand for Overexploited Wildlife Products: Lessons
from Systematic Reviews from Outside Conservation Science”
Supplementary Methods
Search Strategy
The present review aimed to provide an overview of the existing evidence base to answer
the primary question—what interventions are effective for reducing the demand for harmful
products.? In addition, the review sought to assess only those interventions that are conceptually
plausible for application to reducing consumer demand for wildlife products. In particular, we
aimed to ensure that our conclusions were generally applicable to both legal and illegal
components of the wildlife trade and thus we excluded interventions that could only be applied
to trade to legal trade (e.g., taxation). We also excluded other impracticable interventions
approaches, such as parent training—since this intervention assumes the major consumers are
adolescents under parental supervision. We also only included interventions that could feasibly
be considered scalable/deliverable at a population rather than at the individual level, such as brief
interventions (individual advice delivered by medical professionals) or pharmacotherapy.
Components of the primary question. This primary question was broken down into the
following components:
Population Consumers and/or users of harmful products.
Intervention The action inferred to cause the outcome. Interventions must have a
conceivable applicable to combatting demand for illegal wildlife
products (e.g., cannot include interventions such as— “raise tax
levies” or “provide training to parents”).
Comparison Means for assessing intervention effectiveness (e.g., systematic
reviews and meta-analysis).
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 279

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 2
Outcome Intended or hypothesised impact, i.e., to reduce demand
Measure Must be specific to consumer demand, (e.g., not harm reduction)
Harmful Products Harmful products were deemed to be any product or substance that
was likely to be the target of a public demand-reduction campaign,
such as alcohol, tobacco, illicit drugs, stolen goods, and foods with
high sugar or salt content.
Search terms. A list of relevant search terms was generated by the Advisory Board and
broken into six components (Population, Intervention, Comparison, Outcome, Measure, and
Harmful products; see above for explanations). These components were then combined using
Boolean operators “AND” and/or “OR” (see Table S1). The Asterix (*) was used as a wildcard
to represent any characters, including no character (e.g., Consumer* includes Consumers,
Consumerism, Consuming). Phrases in quotation marks were used to search exact phrases (e.g.,
“Behaviour change communication” and “behavior change communication”, which includes
both American and British English spelling of behaviour).
Staged approach. To maximise the potential for finding relevant literature, our search
strategy was implemented across three stages. Stage 1 was a systematic search of the Cochrane
Library using a simplified search strategy including only the “Outcome” and “Measure”
components. This more expansive search was possible because the Cochrane database is smaller
than the other databases and thus returned more manageable results. Stage two was a systematic
search of Web of Science, PsychINFO, and Scopus (Scopus was limited to articles published
after 2008, as only titles, not abstracts, could be retrieved in bulk). The specific details of the
searched databases were:
1. Scopus—a multidisciplinary research including journals, books, proceedings, and
published data sets. [Limited to past 10 years, included only >2008, because only titles
were able to be retrieved in bulk, meaning the time taken to process was unfeasible]
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 280

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 3
2. PsycINFO—search by Abstract only [University of Western Australia access] is a
database of abstracts of literature in the field of psychology. Search field -
3. Web of Science—specifically Search by Topic [University of Western Australia access]:
Web of Science Core Collection (1900-present); Current Contents Connect (1998-
present); Data Citation Index (1900-present); KCI-Korean Journal Database (1980-
present); MEDLINE (1950-present); Russian Science Citation Index (2005-present );
SciELO Citation Index (1997-present).
Stage three involved a manual backwards and forwards citation search of key texts that
were either (i) suggested by the Advisory Board1–8 or (ii) located during the data screening
process, mostly relevant overviews of systematic reviews.9–14. This process resulted in locating
two additional systematic reviews, that were not otherwise captured through our search
string.15,16
Eligibility Criteria.
The eligibility criteria, and summarised justifications for each criterion, is outlined in
Table S2. Whilst some criterion (e.g., vii: Pharmacotherapy) excluded interventions that were
obviously inapplicable for reducing demand for illegal wildlife products, other criterion excluded
interventions (e.g., Multicomponent interventions) that may have provided useful and relevant
insights but were nevertheless deemed out of scope. The criteria were set high due to ensure the
external validity of the results for answering the primary question and to ensure the overall
volume of literature could be feasibly assessed given the available resource constraints. For
example, we excluded studies that only reported non-behavioural outcomes (also called “soft-
indicators”) such as attitude, intention, and knowledge. Whilst these measures are important for
indicating pre-curses to behaviour, they do not always correlate with actual behaviour.17–19 This
may be due, in part, to barriers such as cost and convenience, preventing a person’s behaviour
from aligning with their beliefs.20 Consequently, relying on self-reported attitudes can lead
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 281

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 4
researchers to over-report the effectiveness of an intervention.21 Instead, we elected to include
only studies that report objective measures of consumer behaviour (also called “hard-measures”)
which give a direct indication of the effectiveness of a given intervention on behaviour.
Examples of direct measures of consumer behaviour include sales figures, consumption levels, or
incentivised experiments measuring willingness to pay.
Despite setting the exclusion criteria standard high, the volume of systematic reviews
initially returned through our systematic process was beyond what could feasibly be assessed in a
single paper. Consequently, we decided not to assess one prominent type of intervention
approach, namely formal education interventions (e.g., training delivered through formal school
or university settings), as we had originally planned. Whilst comparative analysis of the impact
of formal education campaigns may have been informative for the present research question, the
decision to exclude this category was made primarily to limit the volume of systematic reviews
to a manageable number (N.B., 55 systematic reviews of formal education interventions had
made it past the title and abstract screening stage). The decision was also made, in part, after
reviewing the returned literature and concluding that, relative to the other intervention types,
formal education interventions would be less immediately scalable for altering wildlife consumer
demand, especially in adult consumers (see also Table S2). Nevertheless, we did include other
interventions, such as mass-media campaigns, that had an educational component, since such
actions are more readily scalable for targeting wildlife consumers (although evidence of efficacy
remains elusive22).
Data Extraction
Quality assessment. The quality of each systematic review was assessed against the
following five key criteria:
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 282

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 5
1. Does the systematic review include mostly randomised controlled trials (RCTs), (i.e., less
than 50% are non-randomised studies of interventions [NRSIs])? AND if they included
any NRSIs did they provide compelling reasons for including them? — yes/no
2. Does the systematic review explicitly employ a comprehensive search strategy including
both (i) Searched at least two databases, and (ii) Outlined their keywords and/or search
strategy? — yes/no
3. Does the systematic review describe all the studies in detail, must include all the
following: subjects, interventions, outcomes, and study design? — yes/no
(State yes, if the systematic review provides descriptions in a sufficiently detailed
summary [e.g., a table] of these study details)
4. Does the systematic review assess the risk of bias for each included study, and is this
discussed a limitation? — yes/no
5. If review included a meta-analysis, did the meta-analysis assess the impact of
heterogeneity* of the included papers— yes/no or N/A (no meta-analysis included)?
*Must including reference to the heterogeneity of results (i.e., measured this statistically,
Q, i-squared, Tau, or some equivalent; or managed heterogeneity using a random-effects
model)
These simplified criteria were adapted from the more in-depth, and more resource-
intensive, AMSTAR tool, which stands for A MeaSurement Tool to Assess systematic
Reviews.23 The broad research scope of the present overview compelled us to apply a simplified
version of the AMSTAR criteria. Indeed, Shea et al.23 recommend that the AMSTAR tool be
considered a set of suggestions to be adapted to suit a particular domain. For the present
overview, several factors precluded the capacity to apply an overly rigorous quality assessment
criteria; including that our broad research scope captured too diverse a range of studies,
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 283
[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 6
methodologies, samples, definitions, exposure periods, study designs, and statistical analyses. A
similar argument has been made in a previous overview of systematic reviews.24
Another justification for using simplified criteria was that the present overview did not
require (nor have the resources for) such an in-depth level of quality assessment. Instead, the
present overview aimed to provide a conceptual platform to discuss the demand parallels with
the broader existing body of evidence on interventions aimed at harmful products, and thus
inform plausible interventions for the products that comprise the illegal wildlife trade. This point
is particularly applicable, given the broader context, namely the urgent need to address the
present dearth of evidence available to inform current campaigns for reducing demand for illegal
wildlife products.25 The adopted criteria were intentionally designed to avoid labelling particular
systematic reviews as high or low quality. Instead, our simplified criteria serve to highlight
whether a review has one, or more, key limitations.
As noted in the main paper, we recruited three other researchers to assess the inter-rater
reliability of our quality assessment criteria. In instances of doubt regarding whether a review
met a certain criterion, reviewers were instructed to give review authors the benefit of the
doubt—provided the review authors provide some justification that is logical. This instruction
was provided to help obtain consistency, noting that some words in the quality assessment
criteria, such as “sufficiently”, or “compelling”, are inherently subjective and thus require further
guidance with regards to the strictness of their application.
Kappa analysis. Kappa analysis was conducted on all review quality criterion
individually, and any criterion with a Cohen’s kappa score below 0.6 was revisited for discussion
and reconciliation (> 0.6 = substantial agreement26). Only criterion 3 failed to meet this
benchmark, kappa = 0.22. We found that this lower level of agreement resulted from four
instances of disagreement in reviewer assessment. Each instance was then revisited, and
additional limitations were noted in Table S3. In three instances the disagreement centred on
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 284
[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 7
low-quality reviews, with two or more other agreed limitations, and thus the reconciliations had
no bearing on the final review quality scores. In one instance,27 one reviewer suggested that the
systematic review receive a lower rating for failing to include descriptions of subjects against
each included study. However, it was agreed that whilst this information was not available, the
review authors had noted that—they coded for, and assessed the impact of, sample
characteristics, and found that it did not moderate the impact on behaviour. We thus decided the
review should retain a review quality rating of “A”.
Conflicts of interests. Each systematic review was checked to confirm the funding
sources and any declarations of potential conflicts of interest. We found that none of the included
systematic reviews had identifiable conflicts of interests, although several did not include a
declaration of conflict of interest or an explicit statement acknowledging a funding source. In
those cases, authors were always university professors or public health experts affiliated with
government health departments or national research institutes, and thus funding might reasonably
be assumed to come from internal sources.
References
1. Babor, T.F., Babor, T., Caetano, R., Casswell, S., Edwards, G., and Giesbrecht, N. (2010).
Alcohol: No Ordinary Commodity: Research and Public Policy (Oxford University Press).
2. Babor, T., Caulkins, J., Fischer, B., Foxcroft, D., Humphreys, K., Elena, M., Medina-
Mora, Obot, I., Rehm, J., Reuter, P., et al. (2018). Drug Policy and the Public Good:
Edition 2 (Oxford University Press).
3. Trieu, K., McMahon, E., Santos, J.A., and Webster, J. (2017). Review of behaviour
change interventions to reduce population salt intake. J. Nutr. Intermed. Metab. 8, 118.
4. Almestahiri, R., Rundle-Thiele, S., Parkinson, J., and Arli, D. (2017). The use of the major
components of social marketing: A systematic review of tobacco cessation programs. Soc.
Mar. Q. 23, 232–248.
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 285
[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 8
5. Kubacki, K., Rundle-Thiele, S., Pang, B., and Buyucek, N. (2015). Minimizing alcohol
harm: A systematic social marketing review (2000–2014). J. Bus. Res. 68, 2214–2222.
6. Bala, M.M., Strzeszynski, L., and Topor‐Madry, R. (2017). Mass media interventions for
smoking cessation in adults. Cochrane Database Syst. Rev.
7. Clarke, N., Pechey, E., Kosīte, D., König, L., Mantzari, E., Blackwell, A.K.M., Marteau,
T.M., and Hollands, G.J. Impact of health warning labels on selection and consumption of
food and alcohol products: Systematic review with meta-analysis. Health Psychol. Rev.
8. Mantzari, E., Vogt, F., Shemilt, I., Wei, Y., Higgins, J.P.T., and Marteau, T.M. (2015).
Personal financial incentives for changing habitual health-related behaviors: A systematic
review and meta-analysis. Prev. Med. (Baltim). 75, 75–85.
9. Burton, R., Henn, C., Lavoie, D., O’Connor, R., Perkins, C., Sweeney, K., Greaves, F.,
Ferguson, B., Beynon, C., and Belloni, A. (2017). A rapid evidence review of the
effectiveness and cost-effectiveness of alcohol control policies: An English perspective.
Lancet 389, 1558–1580.
10. Chung-Hall, J., Craig, L., Gravely, S., Sansone, N., and Fong, G.T. (2018). Impact of the
WHO FCTC over the first decade: A global evidence review prepared for the Impact
Assessment Expert Group. Tob. Control.
11. Ciccolo, J.T., and Busch, A.M. (2015). Behavioral interventions to enhance smoking
cessation: A summary of the current evidence. Am. J. Lifestyle Med. 9, 92–104.
12. Das, J.K., Salam, R.A., Arshad, A., Finkelstein, Y., and Bhutta, Z.A. (2016). Interventions
for adolescent substance abuse: An overview of systematic reviews. J. Adolesc. Heal. 59,
S61–S75.
13. Kok, G., Peters, G.Y., Kessels, L.T.E., Ten Hoor, G.A., and Ruiter, R.A.C. (2018).
Ignoring theory and misinterpreting evidence: The false belief in fear appeals. Health
Psychol. Rev. 12, 111–125.
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 286

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 9
14. Nădăşan, V., Chirvăsuţă, R., Ábrám, Z., and Mihăicuţă, Ş. (2015). Types of interventions
for smoking prevention and cessation in children and adolescents. Pneumologia 64, 58–
62.
15. Moodie, C., Stead, M., Bauld, L., McNeill, A., Angus, K., Hinds, K., Kwan, I., Thomas,
J., Hastings, G., and O’Mara-Eves, A. (2012). Plain tobacco packaging: A systematic
review.
16. Allara, E., Ferri, M., Bo, A., Gasparrini, A., and Faggiano, F. (2015). Are mass-media
campaigns effective in preventing drug use? A Cochrane systematic review and meta-
analysis. BMJ Open 5, e007449.
17. Bickman, L. (1972). Environmental attitudes and actions. J Soc Psychol 87, 323–324.
18. Geller, E.S. (1981). Evaluating energy conservation programs: Is verbal report enough? J.
Consum. Res. 8, 331–335.
19. Lane, B., and Potter, S. (2007). The adoption of cleaner vehicles in the UK: Exploring the
consumer attitude–action gap. J. Clean. Prod. 15, 1085–1092.
20. Gifford, R. (2014). Environmental psychology matters. Annu Rev Psychol 65, 541–579.
21. Kormos, C., and Gifford, R. (2014). The validity of self-report measures of
proenvironmental behavior: A meta-analytic review. J. Environ. Psychol. 40, 359–371.
22. Veríssimo, D., Schmid, C., Kimario, F.F., and Eves, H.E. (2018). Measuring the impact of
an entertainment-education intervention to reduce demand for bushmeat. Anim. Conserv.
21, 324–331.
23. Shea, B.J., Reeves, B.C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D.,
Tugwell, P., Welch, V., and Kristjansson, E. (2017). AMSTAR 2: A critical appraisal tool
for systematic reviews that include randomised or non-randomised studies of healthcare
interventions, or both. BMJ 358, j4008.
24. Monárrez-Espino, J., Liu, B., Greiner, F., Bremberg, S., and Galanti, R. (2014).
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 287

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 10
Systematic review of the effect of pictorial warnings on cigarette packages in smoking
behavior. Am. J. Public Health 104, e11–e30.
25. Veríssimo, D., and Wan, A.K.Y. (2019). Characterizing efforts to reduce consumer
demand for wildlife products. Conserv. Biol. 33, 623–633.
26. McHugh, M.L. (2012). Interrater reliability: The kappa statistic. Biochem. medica
Biochem. medica 22, 276–282.
27. Sheeran, P., Maki, A., Montanaro, E., Avishai-Yitshak, A., Bryan, A., Klein, W.M.,
Miles, E., and Rothman, A.J. (2016). The impact of changing attitudes, norms, and self-
efficacy on health-related intentions and behavior: A meta-analysis. Heal. Psychol 35,
1178–1188.
28. Carson‐Chahhoud, K. V, Ameer, F., Sayehmiri, K., Hnin, K., van Agteren, J.E.M.,
Sayehmiri, F., Brinn, M.P., Esterman, A.J., Chang, A.B., and Smith, B.J. (2017). Mass
media interventions for preventing smoking in young people. Cochrane Database Syst.
Rev.
29. Mosdøl, A., Lidal, I.B., Straumann, G.H., and Vist, G.E. (2017). Targeted mass media
interventions promoting healthy behaviours to reduce risk of non‐communicable diseases
in adult, ethnic minorities. Cochrane Database Syst. Rev.
30. Werb, D., Mills, E.J., DeBeck, K., Kerr, T., Montaner, J.S.G., and Wood, E. (2011). The
effectiveness of anti-illicit-drug public-service announcements: A systematic review and
meta-analysis. J Epidemiol Community Heal. 65, 834–840.
31. Allen, J.A., Duke, J.C., Davis, K.C., Kim, A.E., Nonnemaker, J.M., and Farrelly, M.C.
(2015). Using mass media campaigns to reduce youth tobacco use: A review. Am. J. Heal.
Promot. 30, e71–e82.
32. Durkin, S., Brennan, E., and Wakefield, M. (2012). Mass media campaigns to promote
smoking cessation among adults: An integrative review. Tob. Control 21, 127–138.
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 288

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 11
33. Snyder, L.B., Hamilton, M.A., Mitchell, E.W., Kiwanuka-Tondo, J., Fleming-Milici, F.,
and Proctor, D. (2004). A meta-analysis of the effect of mediated health communication
campaigns on behavior change in the United States. J. Health Commun. 9, 71–96.
34. Corepal, R., Tully, M.A., Kee, F., Miller, S.J., and Hunter, R.F. (2018). Behavioural
incentive interventions for health behaviour change in young people (5–18 years old): A
systematic review and meta-analysis. Prev. Med. (Baltim). 110, 55–66.
35. Hefler, M., Liberato, S.C., and Thomas, D.P. (2017). Incentives for preventing smoking in
children and adolescents. Cochrane Database Syst. Rev.
36. McNeill, A., Gravely, S., Hitchman, S.C., Bauld, L., Hammond, D., and Hartmann‐Boyce,
J. (2017). Tobacco packaging design for reducing tobacco use. Cochrane Database Syst.
Rev.
37. Siegfried, N., Pienaar, D.C., Ataguba, J.E., Volmink, J., Kredo, T., Jere, M., and Parry,
C.D.H. (2014). Restricting or banning alcohol advertising to reduce alcohol consumption
in adults and adolescents. Cochrane Database Syst. Rev.
38. Hughes, N., Arora, M., and Grills, N. (2016). Perceptions and impact of plain packaging
of tobacco products in low and middle income countries, middle to upper income
countries and low-income settings in high-income countries: A systematic review of the
literature. BMJ Open 6, e010391.
39. Capella, M.L., Taylor, C.R., and Webster, C. (2008). The effect of cigarette advertising
bans on consumption: A meta-analysis. J. Advert. 37, 7–18.
40. Quentin, W., Neubauer, S., Leidl, R., and König, H.-H. (2007). Advertising bans as a
means of tobacco control policy: a systematic literature review of time-series analyses. Int.
J. Public Health 52, 295–307.
41. Janssen, M.M., Mathijssen, J.J.P., van Bon–Martens, M.J.H., Van Oers, H.A., and
Garretsen, H.F.L. (2013). Effectiveness of alcohol prevention interventions based on the
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 289

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 12
principles of social marketing: A systematic review. Subst. Abuse Treat. Prev. Policy 8,
18.
42. Stead, M., Gordon, R., Angus, K., and McDermott, L. (2007). A systematic review of
social marketing effectiveness. Health Educ. 107, 126–191.
43. Hung, C.-L. (2017). A meta-analysis of the evaluations of social marketing interventions
addressing smoking, alcohol drinking, physical activity, and eating.
44. Frazer, K., McHugh, J., Callinan, J.E., and Kelleher, C. (2016). Impact of institutional
smoking bans on reducing harms and secondhand smoke exposure. Cochrane Database
Syst. Rev.
45. Monson, E., and Arsenault, N. (2017). Effects of enactment of legislative (public)
smoking bans on voluntary home smoking restrictions: A review. Nicotine Tob. Res. 19,
141–148.
46. Frazer, K., Callinan, J.E., McHugh, J., van Baarsel, S., Clarke, A., Doherty, K., and
Kelleher, C. (2016). Legislative smoking bans for reducing harms from secondhand
smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst.
Rev.
47. Bennett, B.L., Deiner, M., and Pokhrel, P. (2017). College anti-smoking policies and
student smoking behavior: A review of the literature. Tob. Induc. Dis. 15, 11.
48. Hopkins, D.P., Razi, S., Leeks, K.D., Kalra, G.P., Chattopadhyay, S.K., Soler, R.E., and
Task Force on Community Preventive, S. (2010). Smokefree policies to reduce tobacco
use: A systematic review. Am. J. Prev. Med. 38, S275–S289.
49. Bell, K., McCullough, L., Devries, K., Jategaonkar, N., Greaves, L., and Richardson, L.
(2009). Location restrictions on smoking: Assessing their differential impacts and
consequences in the workplace. Can. J. public Heal. 100, 46–50.
50. Chapman, S., Borland, R., Scollo, M., Brownson, R.C., Dominello, A., and Woodward, S.
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 290

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 13
(1999). The impact of smoke-free workplaces on declining cigarette consumption in
Australia and the United States. Am. J. Public Health 89, 1018–1023.
51. Prestwich, A., Kellar, I., Conner, M., Lawton, R., Gardner, P., and Turgut, L. (2016).
Does changing social influence engender changes in alcohol intake? A meta-analysis. J.
Consult. Clin. Psychol. 84, 845.
52. Dotson, K.B., Dunn, M.E., and Bowers, C.A. (2015). Stand-alone personalized normative
feedback for college student drinkers: A meta-analytic review, 2004 to 2014. PLoS One
10, e0139518.
53. Foxcroft, D.R., Moreira, M.T., Santimano, N.M.L.A., and Smith, L.A. (2015). Social
norms information for alcohol misuse in university and college students. Cochrane
Database Syst. Rev.
54. Sheeran, P., Harris, P.R., and Epton, T. (2014). Does heightening risk appraisals change
people’s intentions and behavior? A meta-analysis of experimental studies. Psychol. Bull.
140, 511.
55. Noar, S.M., Hall, M.G., Francis, D.B., Ribisl, K.M., Pepper, J.K., and Brewer, N.T.
(2016). Pictorial cigarette pack warnings: A meta-analysis of experimental studies. Tob.
Control 25, 341–354.
56. Tannenbaum, M.B., Hepler, J., Zimmerman, R.S., Saul, L., Jacobs, S., Wilson, K., and
Albarracin, D. (2015). Appealing to fear: A meta-analysis of fear appeal effectiveness and
theories. Psychol Bull 141, 1178–1204.
57. Peters, G.-J.Y., Ruiter, R.A.C., and Kok, G. (2013). Threatening communication: A
critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psychol.
Rev. 7, S8–S31.
58. Noar, S.M., Francis, D.B., Bridges, C., Sontag, J.M., Ribisl, K.M., and Brewer, N.T.
(2016). The impact of strengthening cigarette pack warnings: Systematic review of
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 291

[Supplemental Material — Reducing Demand for Overexploited Wildlife Products] 14
longitudinal observational studies. Soc. Sci. Med. 164, 118–129.
59. Scholes‐Balog, K.E., Heerde, J.A., and Hemphill, S.A. (2012). Alcohol warning labels:
Unlikely to affect alcohol‐related beliefs and behaviours in adolescents. Aust. N. Z. J.
Public Health 36, 524–529.
Tables
Table S1. Search String
Component Search String
Population terms (Consumer* OR Customer* OR Shopper* OR Buyer* OR Purchaser* OR User* OR Smoker* OR Drinker* OR Behaviour* OR Behavior* OR " Decision-making" OR Public) AND
Intervention terms (Intervention* OR Treatment OR Condition* OR Policy OR Campaign OR Campaigning OR Training OR Education OR Awareness OR "Public service announcement" OR Warning OR "Social marketing" OR "Behaviour change communication" OR "Behavior change communication" OR "Edutainment" OR Communication OR Information OR Message OR Nudge OR "Demand reduction") AND
Comparison terms ("Meta-analysis" OR Review) AND
Outcome terms (Reduc* OR Decreas* OR Lower* OR Moderate* OR Prevent* OR Alter* OR Change* OR Replace* OR Modify OR Restrict OR Discourage) AND
Measure terms (Demand OR Sales OR Consum* OR Spending OR Spent OR Value OR Price OR "Willingness to pay" OR Smoking OR Drinking OR Purchas*) AND
Harmful consumption terms
(Alcohol* OR Cigar* OR Tobacco OR Marijuana OR Cocaine OR Heroin OR ((Illicit OR Illegal) AND Drug*) OR "Recreational Drug*" OR "Party drug*" OR Counterfeit OR Stolen OR Unsustainable OR Unethical OR Harmful OR "Environmental harm" OR Fat OR "Unhealthy diet" OR Sugar OR "Junk food" OR ((Ineffective OR Alternative OR Unsupported OR Complementary) AND (Medicine OR (Health AND (Remedy OR Product)))))
Note. Although originally included, education interventions were later excluded from the analysis, mostly for pragmatic reasons of ensuring the review was manageable.
Appendix VI — Supplement for Chapter 6: Reducing demand for overexploited wildlife products 292

15
Table S2. Exclusion Criteria
Exclusion C
riteria Justification
(i) B
rief interventions O
utside of scope. A considerable proportion of literature has investigated the efficacy of medical doctors providing advice to alter patient behaviour. W
hilst such an approach
may be relevant to consum
ption of some w
ildlife products perceived by some to have health benefits (e.g., rhino horn or tiger bones), the size of the literature put this question
out of scope. Furthermore, w
e suggest that this intervention would often be unfeasible, as patients rarely reveal alternative rem
edy consumption in m
edical consultations and
doctors tend to be more focused on health-related considerations.
(ii) M
otivational tools for
habits or addictions
Outside of scope, since addiction is unlikely a m
ajor factor in the consumption of illegal w
ildlife products. Example studies included those focused on goal setting, prom
pting,
and personalised feedback.
(iii) N
ot a systematic review
or meta-analysis
Out of scope. The sheer volum
e of the literature relevant to our research question required us to exclude any studies that were not system
atic reviews or related studies.
Examples of studies w
e excluded included single studies, protocols, comm
entaries, rapid reviews, and narrative review
s.
(a) C
ase studies O
ut of scope. Similar to studies on trends and correlations, w
e excluded studies that investigated consumption trends using, often country-specific, national case studies. W
hilst
interesting, such studies typically engaged in narrative theorizing about the timeline of consum
ption against possible causes via policies and economics, often resulting in
researchers making causal inferences that are generally less robust than experim
ental studies.
(b) Theoretical review
s O
ut of scope. This included studies that looked at the theory of behaviour change but did not empirically assess the effectiveness of the interventions.
(iv) U
ngeneralizable O
utside of scope. This included studies that were not conceptually relevant to the dem
and for wildlife consum
er products. For example, parenting training to address adolescent
drug addiction.
(a) Im
practical due to
the illegality component
of IWT.
Not applicable. Included interventions such as prohibiting select groups (e.g., m
inors) of individuals from purchasing alcohol or cigarettes, enforcing closing tim
es, and
solutions involving the regulation of legal products (e.g., nutritional labels).
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
293

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 16
(b) C
ounterfactual
associations
Out of scope. W
hilst counterfactual studies of correlations can provide interesting insights into intervention impacts, the volum
e of literature required us to exclude them.
Examples of excluded studies included those that inferred the im
pact of an intervention impact based on outlet or advertising proxim
ity to consumers.
(c) Econom
ic
disincentives
Out of scope and likely not applicable. This included studies investigating the im
pact of raising taxes on alcohol or cigarettes. Whilst, there are debates about w
hether
legalisation of wildlife products w
ould benefit conservation (i.e., to “satiate” demand), the supply side econom
ics for endangered species is considerably different to major
products, such as alcohol and cigarettes. Whilst increasing products m
ay reduce demand from
some consum
ers, for many others—
increased prices and the inherent rarity of
endangered wildlife products, m
ay further fuel demand and thus w
ere deemed inappropriate for the current review
.
(d) H
arms reduction
interventions
Outside of scope. This included studies w
here the primary m
easurement w
as a reduction in harm, not consum
ption, such as reduced rates of injury, drink driving, incarceration,
smoke exposure, or inequality.
(e) Pharm
acotherapy N
ot applicable. Studies evaluating interventions of pharmacological m
edications.
(f) Platform
-based: O
utside of scope. Some system
atic reviews assessed the effectiveness of the different m
ediums/platform
s (e.g., social media) for delivering m
ultiple interventions. Whilst the
medium
of message delivery is an im
portant consideration for intervention implem
entation, such studies are less helpful in assessing which interventions are likely effective.
(g) O
verly specific sub-
populations
Out of scope. M
any studies assessed the impact of interventions on very specific sub-populations, such as pregnant w
omen, or heart attack patients. Such review
s were excluded
to increase the generalisability of the findings.
(h) Portion control
treatments
Not applicable. Such interventions assum
e practitioners have regulatory or other means to control portion sizes of w
ildlife consumer products. Such studies include altering
plate and package seizing to achieve dietary outcomes, such as reduce overall caloric intake.
(i) M
ulticomponent
interventions:
Out of scope. This included studies assessing the im
pact of administering m
ultiple interventions at once. Whilst com
bining interventions may ultim
ately produce more effective
results, we decided such studies w
ere generally less useful for the present review—
which aim
ed to compare the im
pact of specific interventions.
(vi) N
ot a review of dem
and
reduction interventions
Out of scope. Included review
s that assessed current levels of consumer dem
and (i.e., didn’t assess the impact of an intervention).
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
294

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 17
(a) D
id not assess an
intervention
effectiveness
Out of scope. Studies investigating trends, correlations, and statistical m
odels of consumption w
ere generally not designed to determine the im
pact of a specific intervention
(unless a counterfactual experimental design w
as used).
(b) No relevant harm
ful
products
Outside of scope. For exam
ple, assessed actions to increase positive consumption (e.g., of vegetables).
(c) Targeted w
as not
demand
Outside of scope. For exam
ple, assessed enforcement action targeting supply, not dem
and, (e.g., customs seizure).
(vii) N
o objective measure of
consumer dem
and
Out of scope. Soft outcom
es such as knowledge, attitude, belief, and intention to quit, w
hilst informative and useful, often do not reflect actual behaviours and can lead
researchers to overestimate the im
pact of interventions.
(vii) R
ecord was redundant
Not applicable. This included review
s: where later versions w
ere available that had superseded a previous review (e.g., C
ochrane Reviews); w
here the full text could not be
located (n = 7); or w
here the systematic review
failed to locate any studies meeting their respective inclusion criteria. W
hilst it is useful to know w
hat actions have been
systematically review
ed but found to have no evidence, for or against, such information w
as considered beyond the scope of the present review.
(viii) Education
Out of scope. W
hilst an assessment of the efficacy of form
al education programs m
ay provide some useful insights for the present research question, w
e decided excluded this
category since most interventions w
ere generally targeted at children, and consumers of illegal w
ildlife products are mostly adults. Further, as the im
pacts of education
programs are usually not apparent for m
any years, we felt this research w
as of less imm
ediate value to addressing the current consumer dem
and for illegal wildlife products.
(iix) G
roup-based N
ot applicable. Many studies investigated how
parents, families, or com
munities, can help bring about behaviour change, such as to help adolescents to overcom
e drug
addiction. Whilst this approach could be interesting, the system
atic reviews in the literature focus predom
inantly on addictive behaviours, and thus were deem
ed out of scope.
Note. This criterion was applied at both screening phases (i.e., abstract and title; and full text). H
owever, the decision to exclude Education (n =
55) and Group-based (n =
9) interventions was m
ade just prior to full-text screening, hence why the num
bers of papers excluded for these two criteria w
ere not full-text screened. This is reflected in
the PRISMA
flow chart diagram
.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
295

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 18
Table S3 Characteristics and Conclusions of Included System
atic Reviews
R
eview
Num
ber of Studies
Review
Q
uality L
imitations
Intervention Details
Meta-
Analysis
included?
Main Findings -
Behavioural O
utcomes R
eported
Mass M
edia Cam
paigns
C
arson-C
hahoud et al., 2017
28
8 studies (7 controlled experim
ents &
1 ITS)
A
Authors note that although m
ajority studies w
ere RC
Ts, all studies had a high risk of bias due to heterogeneity in study design, interventions, reporting and population being assessed.
Impact of m
ass media cam
paigns on preventing sm
oking, and several non-behavioural m
easures (attitudes, intentions and know
ledge), in young people (up to 25 years).
No
Authors found that only three of eight studies show
ed m
ass-media cam
paigns were effective in preventing
smoking but the rem
aining five found no effect. Authors
concluded that certainty about mass m
edia campaigns is
very low due to inconsistent results, m
ethods, and study designs; and there it w
ould be unwise to offer firm
conclusions. M
ethodologically rigorous studies investigating the effects of m
ass media interventions are
needed as part of broad tobacco prevention campaigns.
M
osdol et al., 2017
29 Six studies (3 R
CTs, 2
cluster RC
Ts and one ITS)
A
Authors note that all studies w
ere G
RA
DE assessed and rated to be very
low quality.
Impact of m
ass media interventions on
multiple health behaviours including
tobacco use, alcohol consumption, in ethnic
minority populations.
No
Authors concluded that their confidence in the im
pact of m
ass media cam
paigns is very low. N
o studies reported on objective indicators of behaviour change and tw
o of three studies that m
easured self-reported changes found non-significant im
pacts. Authors conclude, based on
three studies of moderate quality, com
pared to no intervention, m
ass media interventions m
ay increase the num
ber of calls to smoking quit lines.
A
llara et al., 2015
16 19 studies (8 R
CTs,)
[N = 184 811]
A
Authors note that studies w
ere considerably heterogeneous in the type of m
ass media intervention, outcom
e m
easured, underlying theory, comparison
groups and designs.
Impact of m
ass media cam
paigns on reducing illicit drug consum
ption and the intent to consum
e in young adults (<26 years).
No
Authors found their pooled analysis of eight studies
showed no evidence of an effect on illicit drug use. They
concluded that evidence paucity and inconsistency negated the ability to draw
general conclusions about effectiveness. A
uthors advise caution in disseminating
mass-m
edia campaigns to tackle drug consum
ption.
B
ala et al., 2017
6 11 studies
B
Most studies w
ere NR
SIs. Authors note
that all studies were G
RA
DE assessed
and rated to be very low quality.
Impact of m
ass media cam
paigns (e.g., television, new
spaper, radio) encouraging sm
okers to quit, on smoking behavior
(tobacco cessation, smoking prevalence,
and quit rates) in adults (>25years).
No
Authors conclude that com
prehensive tobacco control program
s that include mass m
edia campaigns m
ay change sm
oking behaviour in adults, but the evidence com
es from studies of variable quality and scale, m
aking it difficult to m
ake inferences of the impacts of the
media cam
paigns difficult
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
296

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 19
Trieu et al., 2017
3 22 studies (4 R
CTs,
most are
NR
SIs) [N
= 41, 448]
B
Most studies w
ere NR
SIs. Im
pact of public awareness cam
paigns, and cam
paigns combined w
ith health education, on reducing salt consum
ption.
No
Based on m
oderate-quality evidence, authors conclude that population-level interventions can reduce salt consum
ption. How
ever, close analysis of higher quality studies show
s small effect sizes and inconsistent results
and thus public awareness, even w
hen combined w
ith health education, are unlikely to be adequate to reduce salt intake.
W
erb et al., 2011
30 11 studies (7 R
CT, 4
observational)
B
Did not assess the risk of bias for each
individual study. Im
pact of public service announcements—
comm
ercials that provide advice or inform
ation—on adolescent intention to use
and self-reported use of illicit drugs.
Yes
No studies reported long-term
benefits and a meta-
analysis of RC
Ts found no significant benefit. Authors
conclude that dissemination of anti-illicit drug public
service announcements (PSA
) may have lim
ited impact.
Further, they note that three RC
T and one observational study found that anti-illicit drug PSA
s may have
undesired effects on anti-illicit drug-use norms am
ong targeted populations (e.g., increased intention to use).
A
llen et al., 2015
31 34 studies
C
No R
CTs. R
isk of bias for individual studies not reported.
Impact of anti-tobacco m
edia campaigns on
youth cognitions related to tobacco, and sm
oking behaviour.
No
Authors concluded that there is strong evidence
supporting the use of mass m
edia campaigns to reduce
youth smoking. H
owever, the authors w
ere unable to recom
mend em
ploying campaigns w
ith social norms
themes due to insufficient evidence.
D
urkin et al., 2012
32 26 studies
C
No R
CTs, study design varied. R
isk of bias w
as not assessed for individual studies. Interventions w
ere usually evaluated as part of a broad tobacco control program
.
The impact of m
ass media cam
paigns on prom
oting quitting among adult sm
okers, and the effects of different m
essage types on adults sm
oking behaviour.
No
Authors concluded that the evidence provided further
supports the need to incorporate mass m
edia campaigns
into broader tobacco control policies to reduce smoking
prevalence and increase quitting. Authors noted that
effectiveness depends on campaign reach, intensity,
duration and messages used. M
essages on health effects, and graphic im
agery and/or testimonials appeared to
outperform other m
essage types on a range of measures
including quitting behaviour.
Snyder et al., 2004
33 21 studies (17 cigarettes) &
(4 Alcohol)
C
Most studies N
RSIs. D
id not report the specific target subjects or study designs of individual studies. R
isk of Bias no
assessed for each included study.
Impacts of m
ediated health campaigns in
the United States on changing m
ultiple behaviours including tobacco and alcohol.
Yes
Authors conclude that m
ediated health campaigns have
small m
easurable effects on smoking and alcohol in the
short term.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
297

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 20
Incentives
C
orepal et al., 2018
34 8 studies (6 R
CTs, 2
Controlled
Trials)
A
Authors note that due to sm
all numbers
of studies, small sam
ple sizes, heterogeneity and variable quality of studies, the results should be interpreted w
ith caution.
Impact of behavioural incentives (financial
incentives and smoke free-class
competition rew
ards if 90% of the class is
not smoking) for reducing sm
oking in young people (5-18 years).
Yes
Authors conclude that there w
as limited evidence for
effectiveness. Only one out of eight studies found a
significant intervention effect in the short term (12
weeks).
M
antzari et al., 2015
8
39 RC
Ts (9 included in 3-6 m
onth sm
oking cessation m
eta-analysis)
A
The authors note that only a small
number of studies w
ere located and thus there w
as a lack of statistical power for
certain comparisons. R
esults were also
limited to 3-6 m
onths past the removal of
the intervention.
The impact of financial incentives to
achieve sustained reductions in smoking
and alcohol consumption.
Yes
Authors conclude that personal financial incentives can
be effective in driving behaviour change, however, the
impacts on sm
oking cessation do not persist beyond three m
onths after the incentive is removed and
disappear after 6-months.
H
efler et al., 2017
35 8 Studies (3 R
CTs &
5 C
ontrolled Studies)
B
Majority of controlled trials w
ere not random
ised, thus, authors conducted a separate m
eta-analysis for RC
Ts.
Impact of incentives (contests,
competitions, incentive schem
es, lotteries, raffles and contingent paym
ents) on reducing adolescent (5-18-years) cigarette consum
ption and smoking initiation.
Yes
Authors conclude that the very lim
ited evidence available suggests that incentive program
mes do not
prevent smoking initiation am
ong adolescents. How
ever, this w
as based on relatively few studies of variable
quality. Authors note that there w
as insufficient inform
ation to assess whether the intervention reduced
consumption.
Advertising B
ans
M
cNeill et
al., 201736
51 studies (1 R
CT)
[N = 800,000]
B
Found only one RC
T, and only five studies assessing the im
pact on prevalence. A
uthors acknowledge this
limitation.
The impact of standardised tobacco
packaging (plain packaging) in tobacco use uptake, cessation, and reduction.
No
Authors conclude that standardised packaging m
ay reduce cigarette consum
ption. Authors note that only one
country, Australia, had im
plemented this policy at the
time of the review
, thus evidence came from
only one large observational study (N
= 700,000).
Siegfried et al., 2014
37
4 studies (1 R
CT; 3
ITS)
B
The review found only one R
CT, the rest
NR
SI. How
ever, the authors explicitly acknow
ledge this limited generalisability.
To evaluate the benefits, harms, or costs of
restricting or banning alcohol advertising on alcohol consum
ption, compared to no
restrictions or counter-advertising.
No
Authors found that the quality of evidence w
as very low,
and thus concluded they could not make
recomm
endations for, or against, banning alcohol advertising. Im
portantly, authors advise governments
considering bans should do so in a research environment
to provide a quality evaluation of the impacts.
H
ughes et al 2016
38 4 studies
C
Authors do not report sufficient details of
study designs, especially vs control groups. A
uthors acknowledge that all
four studies are of a low quality w
hich lim
its the generalisability of conclusions.
Impact of plain packaging of tobacco
products on cigarette consumption in low
-incom
e countries
No
Authors conclude that there is insufficient evidence in
low-incom
e countries to draw firm
conclusions.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
298

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 21
M
oodie et al., 2012
15 37 studies (1 R
CTs)
C
Found only two studies that used a
randomised controlled trial. R
emaining
studies designs not described in sufficient detail.
Impact of plain packaging on cigarette
consumption.
No
Authors conclude that the evidence for im
pact on sm
oking behaviour is mixed but tends to be supportive
of plain packaging having a deterrent effect on smoking.
C
apella et al., 2008
39 50 Studies (27 used in M
eta-analysis)
C
For included studies, authors did not report the risk of bias, the im
pact of heterogeneity, or sufficient details of each experim
ental design.
Impact of either full or partial (e.g., only in
broadcast media) cigarette advertising bans
on cigarette consumption.
Yes
Authors conclude that their m
eta-analysis shows that
cigarette advertising bans do not have a significant effect on cigarette consum
ption.
Q
uentin et al., 2007
40 24 studies
C
Studies were all N
RSIs. A
uthors did not assess the risk of bias for the included studies. A
uthors also don't describe study details in sufficient detail, quasi-experim
ental, or control groups etc.
Impacts of advertising bans on aggregate
consumption of cigarettes or tobacco.
No
Authors found that 10 out of 24 studies found a
statistically significant effect of full advertising bans on reducing aggregate cigarette consum
ption. Authors
conclude that advertising bans have a narrow im
pact on consum
ptions but the acknowledge of lim
itations of draw
ing conclusions from tim
e-series data.
Social-Marketing
Janssen et al., 2013
41 6 Studies
B
Authors w
ere unable to make a causal
assessment because only 2 of 6 studies
compared the intervention to a treatm
ent to control group.
Are interventions based on one or m
ore principles of social m
arketing effective at preventing alcohol consum
ption?
No
Authors concluded that the im
pact of applying social m
arketing on alcohol-related attitudes or behaviours could not be assessed, due to lack of quality studies.
Stead et al., 2007
42 35
B
Risk of bias w
as not systematically
assessed for each study. NB
: Majority
studies measured short term
prevention in school settings. N
arrative analysis was
effectively a vote-counting of the number
of statistically significant effects.
Are social m
arketing interventions—application of com
mercial m
arketing strategies to the design of voluntary social interventions—
effective at reducing alcohol, tobacco, and illicit drug consum
ption?
No
Authors conclude that adopting social m
arketing principles could be effective across a range of behaviours. Social m
arketing interventions were
effective for: smoking cessation (9 out of 11 studies [7
only weakly effective]); illicit drug prevention ( 8 out of
12 studies [<12 months] &
2 out of 6 studies [1-2 years]) ; and alcohol prevention (8 out of 15 [< 12 m
onths) & 4 out of 7 [1-2 years]).
H
ung, 2017
43 48 Studies (56 behavioural outcom
es) [N
= 1,099]
C
Mostly N
RSIs, and risk of bias not
assessed for each study. A
re interventions developed through social m
arketing—a system
atic planning process for applying com
mercial m
arketing strategies—
effective for changing health behaviours?
Yes
The author concludes that interventions that used social m
arketing principles had a significant, but small, effect
at positively bringing about behaviour changes for sm
oking. How
ever, they were not found to be effective
for alcohol consumption.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
299

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 22
A
lmesta-
hiri et al., 2017
4
8 studies (reporting sm
oking reduction)
C
Not clear w
hich studies were random
ized controlled trials, as study design w
as not reported, nor w
ere compelling reasons
given for other forms of evaluations.
Risk of bias w
as not assessed for each study. C
onclusions were based on a m
ix of behaviours not all consum
ption.
To what extent are social m
arketing principles used in interventions targeting tobacco intake cessation and to classify social m
arketing inter- ventions into social m
arketing streams?
No
Authors conclude that social m
arketing interventions targeting tobacco cessation can be successful, noting im
pacts of social marketing on a range of consum
ption behaviours including prevalence, consum
ption, quit attem
pts, and smoking initiation.
K
ubacki et al., 2015
5 10 studies (reporting behavioural objectives for dem
and reduction).
C
Study design and risk of bias was not
assessed for each study. Interventions and outcom
es in insufficient detail with
no effect sizes reported. Analysis w
as effectively vote counting of num
ber of statistically significant effects. A
uthors com
bine demand reduction, harm
reduction, and soft indicators of behaviour change w
hen making
conclusions.
This study sought to review social
marketing interventions and their
evaluations published between 2000 and
2014 to identify role and use of key elem
ents of social marketing interventions:
No
The authors report only if study outcomes w
ere positive, negative, and/or had no effect. This m
inimal, and often
confusing, analysis showed m
ixed results. Of all 10
studies reporting on behavioural outcomes of alcohol
consumption: 6 w
ere positive, 1 was both positive and
negative, 1 was both positive and had no im
pact, and 2 had no effect. A
uthors conclude that social marketing
was found to be largely effective. H
owever, their
conclusion was based on overall judgem
ent of impacts
on consumption behaviour com
bined with im
pacts on harm
reduction, attitude, intentions, and even policy outcom
es.
Location B
ans
Frazer et al., 2016
44 17 observational studies. N
o R
CTs
A
The study found no RC
Ts, although authors acknow
ledge these limitations.
The impact of sm
oking bans in institutional settings (e.g., hospitals, prisons, &
universities) reduced active sm
oking rates (consum
ption).
Yes
Authors conclude that settings-based sm
oking policies in hospitals, prisons, and universities reduced sm
oking rates. H
owever, the authors note that the quality of
evidence was low
, and this more quality evidence is
needed.
M
onson &
Arsenault,
201745
16 articles (before &
after longitudinal)
B
RC
Ts are unlikely to be feasible for this intervention, thus all studies w
ere NR
SI longitudinal cohort studies. Individual risk of bias w
as not reported, but study low
quality was discussed as a lim
itation.
The impacts of legislative bans on sm
oking in public areas on voluntary hom
e smoking
behaviour.
No
Authors conclude that public sm
oke-free bans have an overall positive effect on reducing voluntary hom
e sm
oking. Included studies identified either positive effect or non-significant effect, and no studies reported an increase in sm
oking in the home (displacem
ent of consum
ption).
Frazer et al., 2016
46 77 Studies (A
ll NR
SIs - R
CTs not
possible)
B
Authors note that the nature of the
intervention likely precludes RC
Ts. To assess the effectiveness of legislative sm
oking bans (e.g., indoor or public bans) on sm
oking prevalence and tobacco consum
ption.
No
The Author's review
concluded that the impact of
legislative smoking bans on reducing the num
ber of sm
okers and their consumption w
as inconsistent. H
owever, they conclude that the evidence show
s that, at a national level, the intervention is effective at providing health benefits from
reduced second-hand smoke.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
300

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 23
B
ennett et al., 2017
47 11 N
RSIs
(Majority
cross-sectional, m
inority longitudinal)
C
All N
RSIs as R
CTs are unlikely to be
feasible for this intervention. Did not
report risk of bias for included studies.
The impact of college-level anti-sm
oking policies on students’ attitudes tow
ards sm
oking and smoking behaviour.
No
Authors found m
ixed results, and thus conclude that m
ore longitudinal studies are needed to better understand the role of college sm
oking policies on student smoking
behaviour. The authors note that two prom
ising longitudinal studies show
ed that college-level smoke
free policies significantly reduced both smoking
behaviour and attitudes.
H
opkins et al 2010
48 37 studies (A
ll before &
after cohort w
ith control group)
C
All studies w
ere NR
SIs. Risk of bias not
reported, although authors state study quality w
as assessed. Heterogeneity not
statistically assessed or controlled. D
escriptions of individual studies were
not provided, although they were
summ
arised in some detail.
The impact of sm
oke free policies (smoking
bans at worksites or in public areas) on
reducing tobacco use.
Yes
Authors conclude that their results provide sufficient
evidence that smoke free policies reduce tobacco
consumption. H
owever, w
e note that their results were
either not significant or less compelling w
hen they assessed only the m
ost suitable study designs.
B
ell et al., 2009
49 16 N
RSI
(1 quasi-experim
ental, 3 cohort, 12 cross-sectional survey)
C
Most studies relied on self-reported
measures of tobacco consum
ption. No
RC
Ts, only quasi experimental design,
and 3 cohort studies. Risk of bias not
assessed for individual studies, due to low
quality of evidence.
The impact of location sm
oking restrictions on cigarette consum
ption. N
o A
uthors conclude that smoking bans at w
orksites and hospitals can reduce overall cigarette consum
ption, but that the im
pact may be uneven for different subgroups.
For example, the interventions m
ay be more effective for
men, people w
ith college education, and those in higher socio-econom
ic status. Authors note that sm
oke-free legislation m
ay not automatically provide an incentive to
quit or reduce consumption and m
ay have unintended consequences for som
e groups (e.g., displacement).
C
hapman
et al 1999
50
19 studies C
A
uthors only searched one database (M
EDLIN
E). Based results on N
RSIs as
RC
Ts were unlikely to be feasible for
this intervention. Despite conducting a
pooled analysis, methods did m
eet basic standards of a robust m
eta-analysis (hom
ogeneity, forest plots, report effect sizes etc) .
Impact of sm
oke free workplaces on
cigarette consumption during w
ork hours. N
o A
uthors found that 18 of 19 studies reported reduction in daily sm
oking consumption during w
ork hours. Authors
pooled the results of the six strongest research designs (prospective cohort studies w
ith pre and post m
easurements) and estim
ated that smoke free w
orksites contributed to a reduction in the num
ber of cigarettes consum
ed in both Australia (22.3%
) and the United
States (12.7%).
Norm
Appeals
Prestw
ich et al., 2016
51
41 RC
Ts [N
= 17,445] A
N
one identified. D
o changes in changes in normative beliefs
or more broadly social influence (norm
ative beliefs &
social support), engender changes in alcohol intake?
Yes
Authors conclude that w
hilst social influences normative
beliefs (beliefs about how m
uch other people drink or approve of drinking) can be changed, even large changes in these beliefs are likely to engender only sm
all changes in alcohol intake. They conclude that to m
aximise
reductions in drinking, social norms should be com
bined w
ith other interventions.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
301

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 24
D
otson et al., 2015
52 8 Studies (13 R
CTs)
[N = 2,050]
A
Authors not that studies had but sm
all sam
ples size and only 6 studies included in the m
eta-analysis.
Do personalised norm
ative feedback interventions, delivered via com
puters, reduce alcohol consum
ption in college students?
Yes
Authors conclude that personalised norm
ative feedback had a sm
all, but clinically relevant, impact on reducing
college student drinking (approximately 3 few
er drinks per w
eek). Results w
ere similar for both gender-neutral
& gender specific norm
s.
Foxcroft et al., 2015
53 66 R
CTs
(k = 59) A
N
one identified. D
oes correcting misperceptions about peer
alcohol consumption (social norm
) reduce alcohol consum
ption compared to control
groups (such as no intervention or education)?
Yes
Authors conclude that social norm
interventions had significant effects, albeit w
ith small effect sizes, of social
norm interventions on both drinking frequency and
quantity. Although they found no substantive benefits for
the prevention of alcohol misuse.
Risk / H
ealth Warnings
C
larke et al., 2020
7 12 R
CTs
A
Although m
ajority studies were R
CTs,
authors noted that the certainty of evidence w
as a GR
AD
E assessed to be low
, because the majority of studies w
ere assessed be at risk of bias, and m
ost did not use real products or conduct trials in the field.
The impact of health w
arning labels on selection of unhealthy food and drink products.
Yes
Authors conclude that heath w
arning labels have significant potential for decreasing the selection of unhealthy food and drink products. H
owever, they note
that all experimental studies to date had been conducted
in the laboratory or online setting with outcom
es assessed only after a single exposure.
Sheeran et al., 2014
54 209 R
CTs
(239 com
parisons)
A
One review
er noted that details of the study sam
ples were not reported in the
publication. How
ever, this limitation w
as m
inor, since the authors note that they coded for subject characteristics and using m
eta-regression found that it did not m
oderate the impact of the behaviour.
Does heightening elem
ents of risk appraisal (risk perceptions, anticipatory em
otions, anticipated em
otions, perceived severity) change intentions and behaviour? If so, are the im
pacts stronger when and coping
(response efficacy & self-efficacy) is also
heightened?
Yes
Overall, heightening risk appraisals had an im
pact, albeit generally sm
all, on behaviour. Elements of risk
perceptions combined to influence outcom
es. Crucially,
risk appraisal effects were largest w
hen coping appraisals (self-efficacy and response efficacy) w
ere also heightened. Im
pacts for individual behaviours were
found to be significant for smoking, but not for alcohol
consumption.
N
oar et al., 2016
55 37 R
CTs
B
Did not assess the risk of bias for each
included study Text and im
age health warning labels on
cigarette packages Y
es A
uthors state only one study, Malouf et al 2012, reported
the impact on behaviour and found no difference in
number of cigarettes sm
oked for image vs text
intervention. How
ever, authors also analysed two
studies, Thrasher 2007 & Thrasher 2011, on w
illingness-to-pay, but recorded these as intention. H
owever, these
designs are more objective than indicated by the review
, as involve real m
oney and real spending amounts, and
found that pictorial warnings w
ere more effective overall
than text only.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
302

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 25
Tannenbaum
et al., 2015
56
127 experim
ental studies (248 independent sam
ples)
B
Authors did not assess the risk of bias for
individual included studies. *NB
A
ssumedly, the authors controlled for
risk of bias by only including highly controlled experim
ental designs. Authors
note results may have low
external validity in natural settings.
Persuasive messages that attem
pt to arouse fear by em
phasising the potential danger and harm
that will befall an individual if
they do not adopt the recomm
endations of the m
essage.
Yes
Authors conclude that fear appeals w
ere effective at positively influencing behaviours, in all but very few
circum
stances, and did not identify any circumstances
under which they backfire or lead to undesirable
outcomes.
M
onarrez-Espino et al 2014
24
21 studies (5 R
CTs)
B
Majority N
RSIs. The authors note that
the methodological heterogeneity of
studies was so large that tw
o articles could seldom
be compared w
ith one another. Such differences also extended to behavioural m
easurement, study
design, population, and statistical analysis.
Effect of pictorial health warnings on
cigarette packages on smoking behaviour
No
Authors conclude that the evidence for, or against, the
impact of pictorial health w
arnings on smoking
behaviour was insufficient, largely due to the difficulty
in demonstrating the sustained effectiveness of
behaviour change interventions. How
ever, they note the available evidence indicates that pictorial w
arnings have a m
odest (relative to other interventions) effect on behaviour.
Peters et al., 2013
57 13 R
CTs
B
Authors did not explicitly assess the risk
of bias for individual included studies. *N
B A
ssumedly, the authors controlled
for risk of bias by only including highly controlled experim
ental designs.
Severity based on threatening com
munication accom
panied by efficacy m
anipulations (i.e., help enable the target audience to actively take steps to avoid harm
outlined by the threat).
Yes
Authors found threatening com
munication w
ere only effective under high self-efficacy.
N
oar et al 2016
58 32 N
RSIs
(longitudinal observational)
C
Only longitudinal observational studies,
most w
ithout control groups. D
id not assess the risk of bias for each included study.
Impact of a strengthening health w
arning labels on cigarette packages, w
hich includes im
provements to text and/or
pictorial warnings, increasing the size of the
warnings.
No
Authors conclude that strengthened cigarette pack
warnings w
ere associated with longitudinal (average
study duration was over 12 m
onths) increases in cessation-related behaviours (Q
uitline calls, quit attem
pts, short-term cessation) and reductions in
smoking behaviour.
Scholes-B
alog et al., 2012
59
10 NR
SI (all self-report, all cross-sectional in design, except one longitudinal study)
C
Based on self-reported questionnaire data
from cross-sectional study designs
Did not assess the risk of bias for each
included study A
cknowledged that heterogeneity in
study design and reported outcomes lim
it the generalizability of findings
Impact of alcohol w
arning labels on beverages, on adolescent consum
ers N
o A
uthors conclude that alcohol warning labels w
ere not associated w
ith changes in self-reported risky alcohol use am
ongst adolescents.
Note. When system
atic reviews provided inform
ation on experimental design of included studies, w
e provide this information using the follow
ing abbreviations: R
CT = R
andomised control trial; ITS = Interrupted tim
e series; NR
SI = Non-random
ised studies of interventions; BA = Before/after; L = Longitudinal; O
bs = Observational. W
e also included secondary outcom
es for non-behavioural measures of intervention success (also called “soft-indicators”) such as attitude, intention, and know
ledge.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
303

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 26
Table S4 Sum
mary of Effect sizes for M
eta-Analyses
H
armful
Product R
eview
Outcom
e Measured
[Num
ber of Participants] N
umber
of Studies E
ffect Size E
rror K
ey Details (Specific action; R
isk of bias; Lim
itations etc)
Mass M
edia Cam
paigns
Illicit drugs
Allara et al.,
201516
Impact of m
ass media
campaigns on reducing
drug use [N = 5,470]
5 RC
Ts Standardized M
ean D
ifference (SMD
) = -0.02
95% C
I [-0.15 to 0.12]
Update of a previous C
ochrane Review
. Authors not heterogeneity in
intervention type, outcome m
easure, underlying theory, comparison group,
and design contributed to variability in results.
Illicit drugs
Werb et al.,
201930
Impact of Im
pact of public service announcem
ent on self-reported illicit drug use [N
= ±1,018]
4 W
eighted mean
difference = -0.04
95% C
I [-0.06 to -0.01]
Effect statistic used not specified. Not clear 'how
intention to use' was
measured, assum
ed to be self-report.
Tobacco &
A
lcohol
Snyder et al., 2004
33 Im
pact of media cam
paigns on various sm
oking behaviours [N
= 79,629]
17 r = -0.05
SD = .03
Statistical significance not reported. Problematically com
bined multiple
different smoking behaviours (sm
oking, smokers, quitting, cessation)
Incentives
Tobacco
Corepal et
al., 201834
Impact of incentives on
smoking
[N = 8,881]
8 O
dds Ratio (O
R)
= 0.80 95%
CI
[0.65 to 0.98]
Mostly self-reported sm
oking consumption, but 3 studies used a m
ore objective urine test. O
nly one small study (n=7; K
rishnan-Sarin et al., 2006) found a significant effect.
Tobacco
Mantzari et
al. 20158
Impact on sm
oking cessation at >3-6 m
onths 9 R
CTs
Odds R
atio (OR
) = 1.31
95% C
I [0.90 to 1.90]
Impact of financial incentives on sustained changes in sm
oking cessation 3 m
onths after incentive removal. A
uthors also conducted other meta-analyses
by time intervals and found incentives w
ere effective for smoking cessation up
to 18-months, and up to 3 m
onths after incentives ceased, but not beyond.
Tobacco
Hefler et al.,
201735
Impact of incentives on
smoking initiation
[N = 3,056]
3 RC
Ts R
R = 1.00
95% C
I [0.84 to 1.19]
Smoking initiation m
easured at final follow up.
Advertising B
ans
Tobacco
Capella et
al., 200839
Impact of advertising bans
on cigarette consumption
Not
provided r = -0.02
95% C
I [-.04 to 0]
Smoking initiation m
easured at final follow up.
Social-Marketing
Tobacco
Hung,
201743
Impact of social m
arketing interventions on sm
oking abstinence
14
Hedge's g = -0.18
95%
CI [
[-.27 to -0.10]
Mostly not R
CTs, no assessm
ent of risk of bias. For Figure 2, we did not
convert Hedge's g as insufficient inform
ation was provided, although w
e estim
ate that is likely to be nearly identical to Cohen's d. A
uthors found the effect of social m
arketing on reducing alcohol consumption w
as not statistically significant.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
304

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 27
Location B
ans
Tobacco
Frazer et al., 2016
44 Im
pact of a smoking bans
in hospital settings on sm
oking rates [N = 5,986]
8 R
isk ratio (RR
) = 0.75
95% C
I [0.69 to 0.81]
Authors rated the evidence base as low
quality and called for more robust
studies assessing evidence for smoking bans and policies.
Tobacco
Hopkins et
al., 201048
Impact of sm
oke free policies on absolute prevalence of tobacco use
21 M
edian difference in use prevalence -3.4%
Interquartile interval (-6.3 to -1.4)
Authors note that results w
ere non-significant when assessed only m
ost suitable designs.
Tobacco
Chapm
an et al., 1999
50 Im
pact of smoke free
workplaces on m
ean reduction in daily cigarette consum
ption [N = 824]
6 3.5 less cigarettes (20.7%
) N
ot provided.
Based on pre and post prospective cohort studies of self-reported daily
workplace cigarette consum
ption. Significance was not reported (although
implied via text).
Norm
Appeals
A
lcohol Prestw
ich et al., 2016
51 Im
pact of change in positive change in norm
ative belief (of g = 0.33) on reducing alcohol consum
ption [N
= ±15,600]
35 B
= -.20
SE = 0.08,
95% C
I [-0.35 to -0.04]
NB
: Result w
ere only significant after one outlier study was rem
oved.
A
lcohol D
otson et al., 2015
52 Im
pact of personalised norm
ative feedback on drinking [N
= 2,050]
6 d = -0.29
95% C
I [-0.42 to -0.16]
Authors note that all studies w
ere conducted in North A
merica.
A
lcohol Foxcroft et al., 2015
53 Im
pact of social norm
appeals on quantity of alcohol consum
ed after 4+ m
onths [N = 20,696]
31 SM
D = -0.08
95% C
I [-0.12 to - 0.05]
Evidence quality was rated using G
RA
DE as M
oderate, noting limitations in
design, implem
entation, and blinding.
Risk / H
ealth Warnings
Tobacco
Sheeran et al., 2014
54 Im
pact of heightening risk appraisal on sm
oking behaviour [N
= 1,508]
14 d = -0.11
95% C
I [-0.21 to -0.003]
These results are problematic because the authors com
bined targeting harmful
consumer dem
and (e.g., smoking and alcohol consum
ption) with behaviours
not relevant to the present review (e.g., encouraging a healthy diet and
exercise)
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
305

[Supplemental M
aterial — Reducing Dem
and for Overexploited W
ildlife Products] 28
Tobacco
Noar et al.,
201655
Impact of pictorial health
warnings on incentivised
willingness to pay (W
TP)
for cigarettes [N = 580]
2 RC
Ts
d = -0.26 (standardized m
ean difference)
95% C
I [-0.50 to -0.02]
NB
. Noar et al. (2016) list the w
illingness-to-pay auction as measuring
intention, but in our experience, this is more of an objective m
easure of dem
and than self-report.
Tobacco &
alcohol Tannenbaum
et al., 2015
56
Impact of fear appeals on
desired change in com
bined behaviour
70
d = -0.27 95%
CI [-
0.42 to -0.13]
Results are som
ewhat problem
atic, because the authors combined studies
targeting harmful consum
er demand (e.g., sm
oking and alcohol consumption)
with behaviours not relevant to the present review
(e.g., encouraging a healthy diet and exercise). A
uthors found similar results for assessm
ents of attitudes and intentions.
Tobacco
Peters et al., 2013
57 Im
pact of threatening com
munication on desired
change in combined
behaviours (including sm
oking) when self-
efficacy high
6 d = -0.31
CI not
provided, although authors state, p = 0.036
Results are som
ewhat problem
atic, because the authors combined studies on
smoking behaviour w
ith other behaviours not relevant to the present review
(e.g., condom use and vaccination)
Note. This table reports on the raw effect-sizes reported by each system
atic review containing m
eta-analysis. Note that for Figure 2. In the m
ain manuscript all effect
sizes not provided in Cohen’s d were converted as such, provided there w
as sufficient information to m
ake this transformation. Study design and participant sam
ple
size was not alw
ays provided against specific effect sizes, hence for several meta-analyses they are not reported here. Effect-sizes that w
ere found to be statistically
significant are highlighted in Bold text.
Appendix V
I — Supplem
ent for Chapter 6: R
educing demand for overexploited w
ildlife products
306