Race, Ethnicity, and Pain among the U.S. Adult Population
45
Race, Ethnicity, and Pain among the U.S. Adult Population Vickie L. Shavers Alexis Bakos Vanessa B. Sheppard Journal of Health Care for the Poor and Underserved, Volume 21, Number 1, February 2010, pp. 177-220 (Article) Published by The Johns Hopkins University Press DOI: 10.1353/hpu.0.0255 For additional information about this article Access Provided by your local institution at 05/16/11 8:50AM GMT http://muse.jhu.edu/journals/hpu/summary/v021/21.1.shavers.html
-
Upload
georgetown -
Category
Documents
-
view
1 -
download
0
Transcript of Race, Ethnicity, and Pain among the U.S. Adult Population

Race, Ethnicity, and Pain among the U.S. Adult Population
Vickie L. ShaversAlexis BakosVanessa B. Sheppard
Journal of Health Care for the Poor and Underserved, Volume21, Number 1, February 2010, pp. 177-220 (Article)
Published by The Johns Hopkins University PressDOI: 10.1353/hpu.0.0255
For additional information about this article
Access Provided by your local institution at 05/16/11 8:50AM GMT
http://muse.jhu.edu/journals/hpu/summary/v021/21.1.shavers.html

Journal of Health Care for the Poor and Underserved 21 (2010): 177–220.
Part 2: Literature review
race, ethnicity, and Pain among the u.S. adult Population
Vickie L. Shavers, PhDAlexis Bakos, PhD
Vanessa B. Sheppard, PhD
Abstract: introduction. There is reliable evidence that racial/ethnic minorities suffer dispro-portionately from unrelieved pain compared with Whites. Several factors may contribute to disparities in pain management. Understanding how these factors influence effective pain management among racial/ethnic minority populations would be helpful for developing tailored interventions designed to eliminate racial/ethnic disparities in pain management. We conducted a review of the literature to explore the interaction between race/ethnicity, cultural influences; pain perception, assessment, and communication; provider and patient characteristics; and health system factors and how they might contribute to racial/ethnic disparities in receipt of effective pain management. Methods. The published literature from 1990–2008 was searched for articles with data on racial/ethnic patterns of pain management as well as racially, ethnically, and culturally-specific attitudes toward pain, pain assessment, and communication; provider prescribing patterns; community access to pain medications; and pain coping strategies among U.S. adults. results. The literature suggests that racial/ethnic disparities in pain management may operate through limited access to health care and appropriate analgesics; patient access to or utilization of pain specialists; miscommuni-cation and/or misperceptions about the presence and/or severity of pain; patient attitudes, beliefs, and behaviors that influence the acceptance of appropriate analgesics and analgesic doses; and provider attitudes, knowledge and beliefs about patient pain.
Key words: Race, ethnicity, pain, health disparities.
The Institute of Medicines’ report Unequal Treatment: Confronting Racial/ethnic Disparities in Health Care specifically focused attention on the lower quality of
care received by members of U.S. racial/ethnic minority groups,1 as did the National Healthcare Disparities Report issued by the Agency for Health Care Research and Qual-ity (AHRQ).2 The poorer quality of care received by racial/ethnic minority patients
Dr. ShaverS is in the Division of Cancer Control and Population Sciences, Applied Research Program, at the National Cancer Institute (NCI). Dr. BakoS is in the Center to Reduce Cancer Health Dispari-ties, Diversity Training Branch, at NCI. Dr. ShepparD is at the Lombardi Comprehensive Cancer Center at Georgetown University. Please address correspondence to Vickie L. Shavers, National Cancer Institute, Div. of Cancer Control and Population Science, Applied Research Program, Health Service and Economics Branch, 6130 Executive Blvd., MSC-7344, EPN Room 4005, Bethesda, MD 20892-7344; (301) 594-1725; [email protected].

178 Race, ethnicity, and pain
in general3–6 and in the receipt of appropriate pain management specifically have also been the focus of several other recent reports.7,8
For the purpose of the current discussion, race is defined as a continuously evolving social construct. Race, in the current social context, has several dimensions includ-ing physical characteristics (e.g., skin color, hair texture, other distinctive charac-teristics), culture (e.g., belief systems including religion and spirituality, attitudes, and group behavioral norms and expectations) and self-identity.9 Ethnicity refers to cultural groupings that have been traditionally defined by a common language, religion, nationality, or heritage. In the U.S., racial/ethnic minorities represent those groups of individuals not classified as non-Hispanic Whites. Racial/ethnic minority groups constituted about one third of the U.S. population in 2005. By 2050, racial/ethnic minority populations are expected to constitute 50%, a fact that highlights the current and future significance of racial/ethnic disparities in health.
Several factors may contribute to disparities in pain management, including physician patient interaction and practice styles,10 prescribing behaviors, patient perception, previ-ous experiences with pain, attitudes, beliefs and behaviors regarding pain, and patient access to care and to effective analgesics. Understanding how these factors influence effective pain management among populations would be helpful for developing tailored interventions designed to eliminate racial/ethnic disparities in pain management. We conducted a review of the literature to explore the interactions among race/ethnicity and cultural influences; pain perception, assessment, and communication; provider and patient characteristics; and health system factors and how they might contribute to racial/ethnic disparities in receipt of effective pain management.
Methods
PubMED, CINAHL Plus and Scopus databases were searched for the period 1990 to 2008 using the following key words and/or key word combinations: race, ethnicity, pain, pain treatment, pain assessment, pain communication, culture, pain disparities, religion and pain, spirituality, minorities, and racial differences. To obtain information on the role of cultural influences, we specifically searched for articles that described cultural traits of the various race/ethnic groups (i.e., African American, Hispanic/Latino, Asian, Pacific Islander, Native American, American Indian). The sensory, emotional, mental, behavioral, and social dimensions of the Biopsychosocial model of pain were used to inform the literature search on cultural influences on pain (Figure 1).11 The published literature was also specifically searched for articles that provided data on racial/ethnic patterns of pain management as well as studies that examined race/ethnicity and pain perception, assessment, and communication; provider prescribing patterns; and com-munity access to pain medication among U.S. adults.
Articles that provided empirical data on racial/ethnic patterns of pain management published before 1990 were not reviewed in favor of more recent treatment patterns and practices. We also did not review articles that did not include U.S. populations, were not published in English, or that were not relevant to the aforementioned areas of investigation.

179Shavers, Bakos, and Sheppard
results
One hundred eighty-seven articles (187) and/or other sources of information are cited in this manuscript. Thirty-four studies that specifically examined racial/ethnic variation in pain perception and management are summarized in Table 1, 11 studies that examine racial/ethnic variation in strategies or methods of coping with pain are summarized in Table 2, and six studies that examine race/ethnicity and pain assessment are sum-marized in Table 3. Other reviewed literature includes qualitative and ethnographic studies that provide background on cultural aspects of specific racial/ethnic groups and are not summarized in the tables.
racial/ethnic disparities in pain management. There is fairly consistent evidence that racial/ethnic minorities suffer disproportionately from unrelieved pain compared with Whites.12–24 Racial/ethnic minority patients are less likely than White patients to receive any pain medication,13,17,25,26 more likely to receive lower doses of pain medi-cations,19 more likely to have longer wait times to receipt of pain medication in the emergency department,14,27 and less likely to receive opiates as treatment for pain12,13,16,20 despite higher pain scores,13 and to be treated in manner consistent with the World Health Organization recommendations.19 They also are treated in pain clinics,28 under hospice care, 29 and have pain needs adequately met while in hospice care30 less fre-quently than Whites. Racial/ethnic disparities in pain management have been observed in a variety of settings including hospital emergency departments12–14,20,21,23,24,31,32 and nursing homes17,26 (though not in all studies33).
Although the prevalence of racial/ethnic disparities in pain management among
Biological factors
Tissue damageGenetic factors
Endogenous pain inhibition
Sociocultural factors
EthnicityFamily history
Cultural Factors
Psychological factors
Negative mood (anger, anxiety, depression)
Coping strategiesSocial learning
Figure 1. Biopsychosocial Model of pain.

tabl
e 1.
St
uD
ieS
eXa
MiN
iNG
ra
Cia
L/et
HN
iC v
ar
iati
ON
iN
Pa
iN M
aN
aG
eMeN
t a
ND
Per
CeP
tiO
N
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
rac
ial/e
thni
c di
spar
ities
in p
ain
12. P
letc
her
et a
l., 2
008
374,
891
pain
re
late
d ED
visi
ts,
AA
(22%
), H
ispan
ics (
11%
), A
sians
/oth
ers
(2%
), N
HW
(66%
)
Ana
lysis
of c
ross
-sec
tiona
l su
rvey
dat
a. N
atio
nal H
ospi
tal
Am
bula
tory
Med
ical
Car
e Su
rvey
fo
r (19
93–2
005)
Foun
d no
evi
denc
e th
at d
iffer
entia
l opi
oid
pres
crib
ing
by
race
and
eth
nici
ty d
imin
ished
ove
r tim
e am
ong
patie
nts w
ith
pain
rela
ted
emer
genc
y de
part
men
t visi
ts. O
ver t
he 1
3 ye
ar
perio
d 31
% o
f NH
Ws (
95%
CI 3
1%–3
2%),
23%
of A
As (
95%
C
I 22%
–24%
), 24
% H
ispan
ics (
95%
CI 2
3%–2
6%) a
nd 2
8% o
f A
sian/
othe
rs (9
5% C
I 26%
–30%
) rec
eive
d op
ioid
s. D
iffer
ence
s be
twee
n ra
cial
/eth
nic
grou
ps in
crea
sed
with
pai
n se
verit
y.
13. C
hen
EH
et a
l., 2
008
N5
981,
AA
(607
), N
HW
(326
), O
ther
(4
6)
Seco
ndar
y da
ta a
naly
sis o
f dat
a fr
om a
pro
spec
tive
coho
rt st
udy
on o
f acu
te a
bdom
inal
pai
n in
the
emer
genc
y de
part
men
t col
lect
ed
4/5/
2004
–1/4
/200
5.
AA
s wer
e le
ss li
kely
than
NH
Ws t
o re
ceiv
e op
ioid
ana
lges
ics
as tr
eatm
ent f
or a
bdom
inal
pai
n aft
er a
djus
tmen
t for
gen
der,
tria
ge c
lass
, pai
n sc
ore
and
age
(OR
0.69
, 95%
CI 0
.53–
0.90
). Th
ere
wer
e no
sign
ifica
nt ra
cial
/eth
nic
diffe
renc
es in
the
rece
ipt o
f a n
on-o
pioi
d an
alge
sic.
14. E
pps e
t al.,
20
08N
523
4, N
HW
, A
A, a
nd H
ispan
ic
patie
nts
Revi
ew o
f med
ical
reco
rds o
f pa
tient
s tre
ated
for l
ong-
bone
fr
actu
res a
t 2 G
eorg
ia h
ospi
tals
½/2
001–
12/3
1/20
03.
Hisp
anic
pat
ient
s had
sign
ifica
ntly
long
er w
ait t
imes
(102
m
in) t
o re
ceip
t of t
he fi
rst d
ose
of a
nalg
esia
com
pare
d to
Whi
tes (
67 m
in) d
espi
te a
ll re
port
ing
subs
tant
ial p
ain
(p5
.011
).
15. C
intr
on
et a
l., 2
006
Not
Ava
ilabl
eLi
tera
ture
Rev
iew
1/1
/90–
12/3
1/05
.A
fric
an A
mer
ican
s and
Hisp
anic
s wer
e fo
und
to b
e le
ss
likel
y to
rece
ive
opio
id a
nalg
esic
s and
mor
e lik
ely
than
Whi
te
patie
nts t
o ha
ve th
eir p
ain
untr
eate
d in
11
of th
e 17
stud
ies
revi
ewed
.
(Con
tinue
d on
p. 1
81)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
16. C
hen
et a
l., 2
005
N5
397,
AA
(178
), N
HW
(219
)C
ross
sect
iona
l sur
vey
of p
atie
nts
with
chr
onic
non
-can
cer p
ain
from
12
acad
emic
med
ical
cen
ters
7/
2002
–3/2
003.
AA
s had
hig
her p
ain
scor
es th
an N
HW
S. H
owev
er, N
HW
s w
ere
signi
fican
tly m
ore
likel
y th
an A
As t
o be
taki
ng o
pioi
ds
to tr
eat t
heir
chro
nic
pain
(OR
2.67
, 95%
CI 1
.21–
4.15
).
17. B
erna
bei
et a
l., 1
998
13, 6
25 c
ance
r pa
tient
s age
651
di
scha
rged
from
a
hosp
ital t
o ot
her
care
faci
lity.
AA
(7
.6%
), H
ispan
ic
(1.2
%),
NH
W
(88.
3%),
Asia
n (0
.8%
), A
m In
dian
(2
.0%
)
Ana
lysis
of 1
992–
1995
dat
a fr
om th
e Sy
stem
atic
Ass
essm
ent
of G
eria
tric
Dru
g us
e vi
a Ep
idem
iolo
gy (S
AG
E) d
atab
ase.
Patie
nts a
ged
85 y
ears
and
old
er w
ere
less
like
ly to
rece
ive
mor
phin
e or
oth
er st
rong
opi
ates
than
thos
e ag
ed 6
5 to
74
year
s (13
% v
s 38%
, res
pect
ivel
y). I
ndep
ende
nt p
redi
ctor
s of
faili
ng to
rece
ive
any
anal
gesic
age
nt w
ere
min
ority
race
(OR
1.63
, 95%
CI 1
.18–
2.26
for A
fric
an A
mer
ican
s), l
ow c
ogni
tive
perf
orm
ance
(OR
1.23
, 95%
CI 1
.05–
1.44
), an
d th
e nu
mbe
r of
othe
r med
icat
ions
rece
ived
(OR
0.65
, 95%
CI 0
.50–
0.84
for 1
1 or
mor
e m
edic
atio
ns).
18. C
leel
and
et a
l., 1
994
N5
1308
Retr
ospe
ctiv
e an
alys
is of
dat
a on
pat
ient
s fro
m th
e Ea
ster
n C
oope
rativ
e O
ncol
ogy
Gro
up w
ith
met
asta
tic c
ance
r 10/
1990
–9/1
991.
Min
ority
pat
ient
s wer
e sig
nific
antly
mor
e lik
ely
than
Whi
te
patie
nts t
o ha
ve th
eir p
ain
unde
r tre
ated
(OR
3.1,
95%
CI
1.7–
5.5)
.
(Con
tinue
d on
p. 1
82)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
19. C
leel
and
et a
l., 1
997
N5
197
Patie
nts w
ere
draw
n fr
om 9
un
iver
sity
canc
er c
ente
rs (2
6%),
17
com
mun
ity h
ospi
tals
and
prac
tices
(4
1%),
and
4 ce
nter
s tha
t prim
arily
tr
eat m
inor
ity p
atie
nts (
33%
). St
udy
date
s not
pro
vide
d.
Sixt
y-fiv
e pe
rcen
t of m
inor
ity p
atie
nts d
id n
ot re
ceiv
e gu
idel
ine-
reco
mm
ende
d an
alge
sic p
resc
riptio
ns c
ompa
red
with
50%
of n
on-m
inor
ity p
atie
nts (
p,.0
01).
Hisp
anic
s re
port
ed le
ss p
ain
relie
f and
had
less
ade
quat
e an
alge
sia
com
pare
d w
ith o
ther
race
/eth
nic
grou
p pa
tient
s. Th
e pr
opor
tion
of p
atie
nts w
ho h
ad p
ain
and
nega
tive
Pain
M
anag
emen
t Ind
ex sc
ores
diff
ered
sign
ifica
ntly
am
ong
the
type
s of i
nstit
utio
ns (m
inor
ity v
s non
-min
ority
). Pa
tient
s who
w
ere
trea
ted
at c
ente
rs th
at p
rimar
ily sa
w A
fric
an A
mer
ican
an
d/or
Hisp
anic
pat
ient
s who
wer
e tr
eate
d at
uni
vers
ity
cent
ers w
ere
mor
e lik
ely
to re
ceiv
e in
adeq
uate
ana
lges
ia
than
wer
e th
ose
who
rece
ived
trea
tmen
t in
non-
min
ority
co
mm
unity
trea
tmen
t set
tings
(77%
com
pare
d w
ith 5
2%;
p5.0
03).
20. H
eins
A
et a
l., 2
006
N5
1360
Retr
ospe
ctiv
e co
hort
of p
atie
nts
with
non
-mus
culo
skel
etal
pai
n 18
1 tr
eate
d in
the
emer
genc
y de
part
men
t. St
udy
cond
ucte
d ov
er
unsp
ecifi
ed 8
wee
k pe
riod.
Patie
nt a
ge, r
ace,
and
type
of p
ain
and
the
phys
icia
n’s id
entit
y, tr
aini
ng, a
nd e
xper
ienc
e w
ere
asso
ciat
ed w
ith re
ceip
t of
anal
gesic
s in
the
emer
genc
y de
part
men
t.
21. H
eins
JK
et a
l., 2
006
N5
868,
AA
(603
), W
hite
(249
), O
ther
Cha
rt re
view
of p
atie
nts w
ith
mus
culo
skel
etal
pai
n tr
eate
d in
the
emer
genc
y de
part
men
t dur
ing
an
eigh
t wee
k pe
riod
in 2
004.
Whi
te p
atie
nts w
ere
mor
e lik
ely
than
AA
pat
ient
s (O
R 1.
9,
95%
CI 1
.2–2
.8) t
o re
ceiv
e op
ioid
s whi
le in
the
emer
genc
y ro
om a
nd to
rece
ive
a pr
escr
iptio
n fo
r an
anal
gesic
(OR
1.8,
95
% C
I 1.3
–2.6
) and
for o
pioi
ds (O
R 2.
0, 9
5% C
I 1.3
–2.9
).
(Con
tinue
d on
p. 1
83)

22. T
amay
o-Sa
rver
et a
l.,
2003
N5
67 4
87 A
A
(21%
) Lat
ino,
9%
an
d N
HW
(68%
)
Cro
ss-s
ectio
nal s
urve
y of
AA
, La
tino,
and
Whi
te p
atie
nts i
n th
e 19
97–1
999
Nat
iona
l Hos
pita
l A
mbu
lato
ry M
edic
al C
are
Surv
eys
to c
ompa
re p
resc
riptio
n of
any
an
alge
sics a
nd o
pioi
d an
alge
sics
by ra
ce/e
thni
city
am
ong
patie
nts
trea
ted
in th
e em
erge
ncy
depa
rtm
ent.
AA
s (0.
72; 9
5% C
I 0.6
6–0.
79) a
nd w
ere
signi
fican
tly le
ss
likel
y th
an N
HW
s to
rece
ive
opio
ids f
or tr
eatm
ent o
f pai
n in
the
emer
genc
y ro
om o
vera
ll an
d fo
r mig
rain
e an
d ba
ck
pain
but
not
long
-bon
e fr
actu
re a
fter a
djus
tmen
t for
sex,
age
, an
d m
etho
d of
pay
men
t, pa
in se
verit
y, vi
sit c
hara
cter
istic
s, an
d ho
spita
l cha
ract
erist
ics i
n m
ultiv
aria
te m
odel
s Lat
inos
w
ere
also
sign
ifica
nt le
ss li
kely
than
NH
Ws t
o re
ceiv
e op
ioid
s ov
eral
l (0.
72; 9
5% C
I 0.6
4–0.
81) b
ut n
ot w
hen
exam
ined
by
type
of p
ain.
(Rac
e/et
hnic
ity w
as n
ot in
depe
nden
tly
asso
ciat
ed w
ith re
ceip
t of a
n an
alge
sic in
the
emer
genc
y de
part
men
t.)
23. T
odd
KH
et
al.,
200
0N
521
7, 1
27 A
A,
90 N
HW
Retr
ospe
ctiv
e re
view
of m
edic
al
reco
rds o
f AA
and
NH
W p
atie
nts
trea
ted
for i
sola
ted
long
-bon
e fr
actu
res i
n an
em
erge
ncy
depa
rtm
ent i
n At
lant
a, G
A o
ver
a 40
mon
th p
erio
d (S
epte
mbe
r 1,
1992
–Dec
embe
r 31,
199
5).
74%
of N
HW
s (74
%) c
ompa
red
with
57%
of A
As r
ecei
ved
anal
gesic
s in
the
emer
genc
y de
part
men
t for
isol
ated
long
-bo
ne fr
actu
res d
espi
te si
mila
r acc
ount
s of p
ain
com
plai
nts i
n th
e m
edic
al re
cord
. AA
s rem
aine
d sig
nific
antly
mor
e lik
ely
than
NH
Ws t
o no
t rec
eive
ana
lges
ics i
n th
e ED
(RR
1.66
, 95
% C
I 1.1
1–2.
50) a
fter a
djus
tmen
t for
pot
entia
l con
foun
ders
(i.
e. tim
e sin
ce in
jury
, tot
al ti
me
in E
D, t
ime
of p
rese
ntat
ion,
ne
ed fo
r fra
ctur
e re
duct
ion,
and
pay
er st
atus
) in
mul
tivar
iate
m
odel
s.
24. T
odd
KH
et
al.,
199
3N
513
9, 3
1 H
ispan
ics,
108
NH
Ws
Retr
ospe
ctiv
e co
hort
stud
y of
H
ispan
ic a
nd H
NW
pat
ient
s tr
eate
d fo
r iso
late
d lo
ng-b
one
frac
ture
s in
the
UC
LA E
mer
genc
y M
edic
al C
ente
r 199
0–19
91.
Hisp
anic
s wer
e sig
nific
antly
less
like
ly th
an N
HW
s to
rece
ive
pain
med
icat
ion
in th
e em
erge
ncy
depa
rtm
ent
in a
n un
adju
sted
ana
lysis
(RR
2.12
, 95%
CI 1
.35
to 3
.32;
p5
.003
) and
afte
r con
trol
for p
atie
nt, i
njur
y an
d ph
ysic
ian
char
acte
ristic
s (O
R 7.
46, 9
5% C
I 2.2
2 to
25.
04).
tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
(Con
tinue
d on
p. 1
84)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
25. K
poso
wa
et a
l., 2
002
N5
5,01
3, A
A
(995
), A
sian
120,
H
ispan
ic 4
78,
NH
W 3
,720
Cro
ss-s
ectio
nal s
urve
y. N
atio
nal
Am
bula
tory
Med
ical
Car
e Su
rvey
19
95–1
998.
AA
s (O
R 0.
67, 9
5% C
I 0.5
5–0.
82) a
nd H
ispan
ics (
OR
0.70
, 95%
CI 0
.52–
0.93
) wer
e le
ss li
kely
that
Whi
tes t
o re
ceiv
e pr
escr
iptio
ns fo
r tre
atm
ent o
f bac
k pa
in. R
ates
wer
e pa
rtic
ular
ly lo
w fo
r AA
and
Hisp
anic
men
whe
n co
mpa
red
to
Whi
te m
en (O
R 0.
47, 9
5% C
I 0.3
5–0.
68) a
nd (O
R 0.
51, 9
5%
CI 0
.33–
0.79
), re
spec
tivel
y.
26. W
on A
et
al.,
199
949
,971
nur
sing
hom
e re
siden
tsC
ross
-sec
tiona
l ana
lysis
of d
ata
on a
nalg
esic
use
am
ong
49,9
71
patie
nts i
n nu
rsin
g ho
mes
from
the
Syst
emat
ic A
sses
smen
t of G
eria
tric
dr
ug u
se v
ia E
pide
mio
logy
(SA
GE)
da
taba
se in
four
stat
es fr
om
1992
–199
5.
AA
s (O
R 1.
69, 9
5% C
I 1.4
0–2.
05) a
nd H
ispan
ics (
OR
1.56
, 95
% C
I 0.7
0–1.
04) w
ere
signi
fican
tly m
ore
likel
y th
an N
HW
nu
rsin
g ho
me
patie
nts t
o no
t rec
eive
ana
lges
ics.
Patie
nts w
ho
wer
e m
ale,
851
or c
ogni
tivel
y im
paire
d w
ere
also
sign
ifica
ntly
m
ore
likel
y no
t to
rece
ive
anal
gesic
s.
27. L
ee e
t al.,
20
01N
546
6, 5
8 H
ispan
ic a
nd 4
08
NH
Ws
Con
veni
ence
sam
ple
of p
atie
nts i
n ho
spita
l em
erge
ncy
depa
rtm
ent.
9/1/
99–1
2/31
/99.
Hisp
anic
s and
NH
Ws d
id n
ot si
gnifi
cant
ly d
iffer
in te
rms o
f ch
ief c
ompl
aint
s and
leve
l of p
ain.
The
two
grou
ps a
lso d
id
not d
iffer
sign
ifica
ntly
in te
rms o
f the
ir m
ean
expe
ctat
ions
fo
r pai
n re
lief (
76m
m, 9
5% C
I 70–
82 a
nd 7
2mm
, 95%
CI
70–7
4) fo
r Hisp
anic
s and
NH
Ws,
resp
ectiv
ely.
Hisp
anic
s and
N
HW
s also
did
not
sign
ifica
ntly
diff
er in
term
s of t
heir
mea
n ex
pect
atio
ns o
f a re
ason
able
tim
e to
wai
t for
pai
n m
edic
atio
n (3
1 m
inut
es, 9
5% C
I 28–
33 a
nd 3
3 m
inut
es, 9
5% C
I 26–
48,
resp
ectiv
ely)
.
(Con
tinue
d on
p. 1
85)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
28. P
orte
noy
et a
l., 2
004
N5
1335
, AA
(4
47),
NH
W (4
54),
Hisp
anic
(434
)
Nat
iona
lly re
pres
enta
tive
cros
s-se
ctio
nal t
elep
hone
surv
ey o
f H
ispan
ics (
any
race
), A
fric
an
Am
eric
ans a
nd N
HW
s con
duct
ed
April
3, 2
002–
April
29,
200
2.de
signe
d to
exp
lore
the
rela
tions
hip
betw
een
race
/eth
nici
ty a
nd c
hron
ic
pain
.
On
a 0–
10 p
ain
seve
rity
scal
e, W
hite
par
ticip
ants
repo
rted
sig
nific
antly
low
er a
vera
ge p
ain
than
AA
s (5.
6 vs
. 6.1
, p,
.01)
and
Hisp
anic
s (5.
6 vs
. 6.4
, p,
.001
). A
As r
epor
ted
mor
e m
issed
hou
rs o
f wor
k be
caus
e of
pai
n. H
ispan
ics
mor
e fr
eque
ntly
repo
rted
inte
rfer
ence
with
dai
ly a
ctiv
ities
du
e to
pai
n (i.
e. di
stur
bed
sleep
, ina
bilit
y to
do
hous
ehol
d ch
ores
, ina
bilit
y to
wor
k an
d et
c). N
HW
s, ho
wev
er m
ore
freq
uent
ly re
port
ed ir
ritab
ility
and
the
inab
ility
to p
artic
ipat
e in
spor
ts. O
vera
ll, h
owev
er, t
here
wer
e fe
w d
iffer
ence
s in
over
all l
ife in
terf
eren
ce fr
om p
ain
by ra
ce/e
thni
city
. Onl
y 79
% o
f Hisp
anic
s had
visi
ted
a he
alth
car
e pr
ovid
er fo
r any
ty
pe o
f pai
n co
mpa
red
to 9
3% o
f NH
Ws a
nd 9
4% o
f AA
s. C
ompa
red
to N
HW
s Hisp
anic
s had
sign
ifica
ntly
mor
e fe
ar
abou
t com
bini
ng p
ain
relie
vers
and
oth
er m
edic
atio
ns (5
.3 v
s. 4.
7, p
,.0
5) a
nd si
gnifi
cant
ly m
ore
conc
ern
abou
t bec
omin
g ad
dict
ed to
pai
n re
lieve
rs (4
.1 v
s. 3.
4, p
,.0
1).
29. O
mar
a et
al.,
200
1N
521
9119
97 c
ase
stud
y de
signe
d to
ca
lcul
ate
the
prop
ortio
n of
adu
lt pa
tient
s who
die
d of
chr
onic
ill
ness
es a
nd re
ceiv
ed se
rvic
es fr
om
a ho
spic
e pr
ogra
m b
y ra
ce/e
thni
c gr
oup.
Hos
pice
serv
ices
wer
e re
ceiv
ed b
y 30
% o
f Cau
casia
n, 2
0%
of A
sian,
19%
of H
ispan
ic, a
nd 1
8% o
f Afr
ican
-Am
eric
an
dece
dent
s.
(Con
tinue
d on
p. 1
86)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
30. R
hode
s et
al.,
200
7N
598
,911
AA
(4
095)
NH
W
(948
16)
Surv
ey o
f fam
ilies
mem
ber a
bout
se
rvic
es re
ceiv
ed in
hos
pice
car
e.Pe
r fam
ily re
pond
ents
AA
pat
ient
s wer
e sig
nific
antly
mor
e lik
ely
than
NH
Ws n
ot to
hav
e th
eir p
ain
need
s mee
t (O
R 1.
5, 9
5% C
I 1.3
–1.7
). A
As w
ere
also
sign
ifica
ntly
mor
e lik
ely
than
NH
Ws t
o ha
ve th
eir n
eeds
for d
yspn
ea a
nd e
mot
iona
l su
ppor
t unm
et.
31. B
ijur e
t al.,
20
08N
544
9, H
ispan
ic
(235
), A
A (1
33),
NH
W (8
1)
Retr
ospe
ctiv
e ch
art r
evie
w o
f pa
tient
s tre
ated
for l
ong-
bone
fr
actu
res i
n 2
acad
emic
em
erge
ncy
depa
rtm
ents
1/2
000–
12/2
002.
Ther
e w
as n
o st
atist
ical
ly si
gnifi
cant
raci
al/e
thni
c di
ffere
nces
in
rece
ipt o
f ana
lges
ics f
or tr
eatm
ent o
f lon
g-bo
ne fr
actu
res.
32. Q
uazi
et
al.,
200
7A
ctua
l sam
ple
size
not p
rovi
ded
Wei
ghte
d sa
mpl
e 19
.7 m
illio
n
Ana
lysis
of H
ospi
tal A
mbu
lato
ry
Car
e Su
rvey
dat
a fo
r AA
, H
ispan
ics a
nd N
HW
trea
ted
in
the
emer
genc
y de
part
men
t for
he
adac
he a
nd lo
ng-b
one
frac
ture
19
95–1
999
com
pare
d to
200
0–20
03.
Onl
y H
ispan
ics e
xper
ienc
ed a
sign
ifica
nt im
prov
emen
t in
rece
ipt o
f an
anal
gesic
ove
r the
two
time
perio
ds (7
1.3%
–80
.8%
p5
.011
) whi
le o
nly
AA
s and
NH
W im
prov
ed in
the
rece
ipt o
f opi
ods a
mon
g pa
tient
s tre
ated
for h
eada
che.
Long
bo
ne fr
actu
re fo
r all
thre
e ra
ce/e
thni
c gr
oups
was
seen
for
Hisp
anic
s onl
y. Re
ceip
t of o
pioi
d an
alge
sics i
mpr
oved
for
AA
s for
hea
dach
e on
ly a
nd N
HW
s but
not
for H
ispan
ics
com
parin
g th
e tw
o tim
e pe
riods
.
33. T
amay
o-Sa
rver
et a
l.,
2003
(with
D
awso
n)
N5
2872
ph
ysic
ians
Stud
y of
Am
eric
an C
olle
ge o
f Em
erge
ncy
Phys
icia
ns m
embe
rshi
p on
9/2
0/20
01. C
linic
al v
igne
ttes
wer
e us
ed to
exa
min
e ph
ysic
ian
opio
id p
resc
ribin
g by
race
/eth
nici
ty
alon
e an
d w
hen
occu
patio
n, S
ES
and
rela
tions
hip
to p
rimar
y ca
re
prov
ider
wer
e kn
own.
Phys
icia
ns p
lans
for p
resc
riptio
n of
opi
oids
did
not
sig
nific
antly
var
y by
race
/eth
nici
ty a
mon
g hy
poth
etic
al
patie
nts i
n th
ree
clin
ical
vig
nette
s (m
igra
ine
head
ache
, bac
k pa
in a
nd a
nkle
frac
ture
). Pr
escr
iptio
n ra
tes i
ncre
ased
whe
n in
form
atio
n re
gard
ing
occu
patio
n, S
ES a
nd re
latio
nshi
p w
ith p
rimar
y ca
re p
rovi
der w
ere
prov
ided
for t
he d
iagn
oses
di
fficu
lt to
ver
ify c
linic
ally
such
as m
igra
ine
or b
ack
pain
but
fin
ding
s wer
e no
t con
sider
ed to
be
clin
ical
ly si
gnifi
cant
.
(Con
tinue
d on
p. 1
87)
tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
Pain
per
cept
ion
41. E
dwar
ds
RR e
t al.,
200
1N
533
7, 6
8 A
A,
269
NH
WFa
ctor
ana
lysis
of d
ata
from
ex
perim
enta
l stu
dy. S
tudy
dat
es n
ot
prov
ided
in a
rtic
le.
AA
s rep
orte
d hi
gher
pai
n se
nsiti
vity
(Mea
n 55
.7 v
s. 53
.4
NH
Ws,
p,.0
1), a
vera
ge ra
tings
of l
evel
s of c
linic
al p
ain
(Mea
n 6.
9 vs
. 6.5
, p,
.05)
. Ther
e w
as n
o sig
nific
ant r
acia
l/et
hnic
diff
eren
ce in
pai
n in
terf
eren
ce, o
r affe
ctiv
e di
stre
ss.
A c
orre
latio
nal a
naly
sis sh
owed
a sm
all i
nver
se a
ssoc
iatio
n be
twee
n pa
in to
lera
nce
and
repo
rted
seve
rity
of c
linic
al p
ain.
42. R
iley
JL
3rd
et a
l., 2
002
N5
1557
, 473
AA
, 10
84 N
HW
Cro
ss-s
ectio
nal s
urve
y of
pat
ient
s tr
eate
d fo
r chr
onic
pai
n at
pai
n m
anag
emen
t clin
ic o
f a u
nive
rsity
ho
spita
l. St
udy
date
s not
pro
vide
d in
art
icle
.
Afr
ican
Am
eric
an p
atie
nts r
epor
ted
signi
fican
tly h
ighe
r le
vels
of p
ain
unpl
easa
ntne
ss (5
.2),
emot
iona
l res
pons
e to
pa
in (1
9.6)
, and
pai
n be
havi
or (1
9.3)
, but
not
pai
n in
tens
ity
(5.6
) com
pare
d to
NH
W (5
.6, 4
.7, 1
7.3,
7.7
, res
pect
ivel
y). Th
e re
sults
indi
cate
diff
eren
ces i
n lin
ear a
ssoc
iatio
ns b
etw
een
pain
m
easu
res w
ith A
fric
an A
mer
ican
s sho
win
g a
stro
nger
link
be
twee
n em
otio
ns a
nd p
ain
beha
vior
than
Whi
tes.
43.
McC
rack
en
LM e
t al.,
20
01
N5
264,
57
AA
, 20
7 N
HW
Cro
ss-s
ectio
nal s
urve
y of
pat
ient
s se
ekin
g tr
eatm
ent f
or c
hron
ic p
ain
at a
uni
vers
ity p
ain
man
agem
ent
cent
er. S
tudy
dat
es n
ot p
rovi
ded
in
artic
le.
AA
s rep
orte
d sig
nific
antly
hig
her p
ain
seve
rity,
mor
e pa
in-
rela
ted
anxi
ety
(84.
3 vs
71.
5, p
,.0
5), m
ore
phys
ical
disa
bilit
y (M
ean
5 0
.20
vs 0
.14,
p,
.05)
, psy
chos
ocia
l disa
bilit
y (M
ean
0.22
vs 0
.16,
p,
.05)
com
pare
d to
NH
Ws,
resp
ectiv
ely.
(Con
tinue
d on
p. 1
88)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
44. C
aste
l et
al.,
200
8N
511
24,
Cau
casia
n (9
91),
Non
-Cau
casia
n (1
33)
Long
itudi
nal s
tudy
of c
ance
r pai
n ac
ross
the
dise
ase
traj
ecto
ry a
mon
g w
omen
with
a b
reas
t can
cer b
one
met
s 10/
1998
–1/2
001.
Incr
ease
d se
vere
pai
n ha
zard
s wer
e as
soci
ated
with
non
-C
auca
sian
race
(haz
ard
ratio
[HR]
5 2
.52;
95%
CI 1
.69–
3.76
), re
stric
ted
perf
orm
ance
stat
us (H
R51.
73, 9
5% C
I 1.1
3–2.
64),
and
radi
atio
n th
erap
y in
a p
revi
ous i
nter
val (
HR5
2.86
, 95%
C
I 1.6
1–5.
09).
Estim
ated
cum
ulat
ive
rate
s for
not
yet
reac
hing
a
BPI s
core
of 7
or a
bove
rang
ed fr
om 0
.79
(0.7
2–0.
85) i
n th
e fir
st in
terv
al to
0.6
4 (0
.55–
0.74
) in
the
last
inte
rval
for
non-
Cau
casia
n w
omen
, whe
reas
thes
e ra
tes r
ange
d fr
om 0
.91
(0.8
9–0.
93) t
o 0.
84 (0
.81–
0.87
) for
Cau
casia
n w
omen
.
45. C
ampb
ell
CM
et a
l.,
2008
N5
58, A
A (2
9),
NH
W (2
9)Ex
perim
enta
l stu
dy o
f noc
icep
tive
flexi
on re
flex.
Stu
dy d
ates
not
pr
ovid
ed in
art
icle
.
The
stud
y ev
alua
ted
resp
onse
s to
the
noci
cept
ive
flexi
on
refle
x (N
FR) i
nclu
ding
per
cept
ual r
espo
nses
(e.g
., pa
in
ratin
gs) a
nd p
hysio
logi
cal r
eflex
resp
onse
s (i.e
., bi
ceps
fem
oris
EMG
). Th
e tw
o ra
ce g
roup
s sig
nific
antly
diff
ered
in th
e N
FR
thre
shol
d (t
(51)
52.
23, p
5.0
30, C
ohen
’s d5
.61)
, with
Afr
ican
A
mer
ican
s (M
514
.99
mA
, SD
58.
98) d
emon
stra
ting
a re
flex
at a
low
er st
imul
us in
tens
ity re
lativ
e to
non
-Hisp
anic
Whi
tes
(M5
20.9
5 m
A, S
D5
10.4
5). P
ain
ratin
gs a
t NFR
thre
shol
d w
ere
not s
igni
fican
tly d
iffer
ent b
etw
een
the
grou
ps, s
ugge
stin
g th
at th
e lo
wer
stim
ulat
ion
inte
nsiti
es re
quire
d to
elic
it a
refle
x in
Afr
ican
-Am
eric
an v
ersu
s non
-Hisp
anic
Whi
te p
artic
ipan
ts
wer
e no
neth
eles
s per
ceiv
ed a
s sim
ilar.
(Con
tinue
d on
p. 1
89)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
46. G
rew
en
KM
et a
l.,
2008
N5
48, 2
5 A
A, 2
3 N
HW
Expe
rimen
tal s
tudy
of t
he
rela
tions
hip
betw
een
plas
ma
oxyt
ocin
(OT)
and
pai
n se
nsiti
vity
an
d th
e re
latio
n of
OT
to o
ther
fa
ctor
s kno
wn
to in
fluen
ce p
ain
perc
eptio
n am
ong
prem
enop
ausa
l w
omen
. Stu
dy d
ates
not
pro
vide
d in
art
icle
.
Afr
ican
Am
eric
an w
omen
dem
onst
rate
d sig
nific
antly
lo
wer
pai
n to
lera
nce
acro
ss ta
sks c
ompa
red
with
Whi
tes
(F(1
,46)
56.
31, p
5.0
156)
and
also
exh
ibite
d lo
wer
pla
sma
OT
leve
ls (A
A: 3
.90,
W: 7
.05
pg/m
L; p
5.0
014)
. Gre
ater
OT
leve
ls w
ere
corr
elat
ed w
ith g
reat
er to
lera
nce
to is
chem
ic p
ain
(r5
0.36
, p5
.013
) and
acc
ount
ed fo
r a m
argi
nally
sign
ifica
nt
port
ion
of th
e et
hnic
diff
eren
ce in
isch
emic
pai
n to
lera
nce
(B5
10.
29, p
50.
06).
Gre
ater
OT
was
also
cor
rela
ted
with
gr
eate
r tol
eran
ce o
f col
d pr
esso
r pai
n (r
50.
31, p
5.0
3);
how
ever
, thi
s ass
ocia
tion
was
no
long
er se
en a
fter t
he
varia
nce
due
to e
thni
city
was
acc
ount
ed fo
r.
47. M
echl
in
MB
et a
l.,
2005
N5
106,
51
AA
, 55
NH
W a
nd o
ther
R/
E gr
oups
Expe
rimen
tal s
tudy
of e
thni
c di
ffere
nces
in p
ain
sens
itivi
ty a
nd
the
rela
tions
hip
of p
ain
tole
ranc
e to
bl
ood
pres
sure
and
neu
roen
docr
ine
fact
ors.
Stud
y da
tes n
ot p
rovi
ded
in
artic
le.
Afr
ican
Am
eric
ans h
ad lo
wer
pai
n to
lera
nce
rela
tive
to
Cau
casia
n/O
ther
s afte
r bot
h re
st a
nd st
ress
. Onl
y th
e no
n-A
fric
an A
mer
ican
gro
up sh
owed
the
expe
cted
inve
rse
rela
tions
hip
betw
een
BP a
nd p
ain
sens
itivi
ty. A
fric
an
Am
eric
ans h
ad lo
wer
cor
tisol
con
cent
ratio
ns a
t res
t and
stre
ss
and
show
ed b
lunt
ed N
E an
d sy
stol
ic B
P re
spon
ses t
o st
ress
. O
nly
in C
auca
sians
/Oth
ers w
as th
e re
latio
nshi
p se
en b
etw
een
high
er st
ress
-indu
ced
BP, c
ortis
ol, a
nd N
E le
vels
and
grea
ter
pain
tole
ranc
e. Th
e re
sults
sugg
est t
hat t
here
are
alte
ratio
ns
in e
ndog
enou
s pai
n re
gula
tory
mec
hani
sms i
nvol
ving
BP,
co
rtiso
l, an
d N
E in
Afr
ican
Am
eric
ans.
It is
hypo
thes
ized
th
at g
reat
er c
hron
ic st
ress
in A
fric
an A
mer
ican
s may
be
a co
ntrib
utin
g fa
ctor
to th
e al
tera
tions
in p
ain
regu
latio
n.
(Con
tinue
d on
p. 1
90)

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
(Con
tinue
d on
p. 1
91)
48. E
dwar
ds,
et a
l., 1
999
N5
48, A
A (1
8)
NH
W (3
0) c
olle
ge
stud
ents
age
18–
47
Expe
rimen
tal s
tudy
of t
herm
al p
ain
resp
onse
. Stu
dy d
ates
not
pro
vide
d in
art
icle
.
Ther
e w
as n
o sig
nific
ant d
iffer
ence
bet
wee
n A
A a
nd N
HW
s in
war
mth
or t
herm
al p
ain
thre
shol
ds. A
As (
Mea
n 47
.1) h
ad
low
er th
erm
al p
ain
tole
ranc
e th
an N
HW
s (M
ean
49.6
) p,
.05.
49. R
ahim
-W
illia
ms F
B et
al.,
200
7
N5
226,
63
AA
, 61
Hisp
anic
and
82
NH
W
Expe
rimen
tal s
tudy
to e
xam
ine
ethn
ic v
aria
tion
in p
ain
sens
itivi
ty
amon
g A
A, H
ispan
ics a
nd N
HW
s. St
udy
date
s not
pro
vide
d in
art
icle
.
Ethn
ic id
entit
y w
as a
ssoc
iate
d w
ith p
ain
rang
e on
ly fo
r A
fric
an A
mer
ican
and
Hisp
anic
gro
ups.
Stat
istic
ally
co
ntro
lling
for e
thni
c id
entit
y re
nder
ed so
me
of th
e gr
oup
diffe
renc
es in
pai
n ra
nge
non-
signi
fican
t. Th
ese
findi
ngs
indi
cate
that
eth
nic
iden
tity
is as
soci
ated
with
pai
n se
nsiti
vity
in
eth
nic
min
ority
gro
ups,
and
may
par
tially
med
iate
gro
up
diffe
renc
es in
pai
n pe
rcep
tion.
50. C
ampb
ell
et. a
l, 20
05N
512
0, A
A (6
2),
NH
W (5
8)Ex
perim
enta
l stu
dy th
at e
xam
ined
et
hnic
diff
eren
ces i
n re
spon
ses t
o m
ultip
le e
xper
imen
tal p
ain
stim
uli,
incl
udin
g he
at p
ain,
col
d pr
esso
r pa
in, a
nd is
chem
ic p
ain.
Stu
dy
date
s not
pro
vide
d in
art
icle
.
Inte
nsity
and
unp
leas
antn
ess r
atin
gs fo
r sup
rath
resh
old
heat
stim
uli w
ere
signi
fican
tly h
ighe
r am
ong
AA
s. A
As
also
repo
rted
mor
e fr
eque
nt u
se o
f pas
sive
pain
cop
ing
stra
tegi
es (M
ean
3.86
, SD
1.9
4 fo
r AA
s and
mea
n 1.
99 S
D,
1.61
for N
HW
s. Fi
ndin
gs sh
ow d
iffer
ence
s in
labo
rato
ry p
ain
resp
onse
s bet
wee
n A
fric
an A
mer
ican
s and
Whi
tes a
cros
s m
ultip
le st
imul
us m
odal
ities
. No
risk
estim
ates
pro
vide
d.
51. W
eiss
e et
al.,
200
5N
534
3, A
A (9
7),
Hisp
anic
(36)
, AA
/PI
(12)
, AI (
1)O
ther
(4)
Expe
rimen
tal s
tudy
des
igne
d to
exa
min
e di
ffere
nces
in p
ain
repo
rtin
g be
havi
or w
hen
pain
is
repo
rted
to in
divi
dual
s of a
di
ffere
nt ra
ce o
r gen
der.
Stud
y da
tes n
ot p
rovi
ded
in a
rtic
le.
Raci
al a
nd g
ende
r con
cord
ance
wer
e no
t ass
ocia
ted
with
pa
in re
port
ing;
Pai
n re
port
ing
was
influ
ence
d by
inte
ract
ions
be
twee
n ge
nder
and
race
in th
e un
derg
radu
ate
stud
ent
subj
ect–
expe
rimen
ter d
yads
.

tabl
e 1.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
52. K
latz
kin
et a
l., 2
007
N5
55, A
A (3
2),
NH
W (2
3)Ex
perim
enta
l stu
dy d
esig
ned
to
exam
ine
the
asso
ciat
ion
of ra
ce
and
hist
ory
of m
ood
diso
rder
s w
ith e
xper
imen
tal p
ain
sens
itivi
ty
amon
g w
omen
. Stu
dy d
ates
not
pr
ovid
ed in
art
icle
.
AA
wom
en h
ad lo
wer
isch
emic
pai
n to
lera
nce
(p,
.001
) bu
t not
low
er p
ain
thre
shol
d th
an N
HW
wom
en. A
As a
lso
had
low
er c
old
pres
sor p
ain
tole
ranc
e an
d th
resh
old
amon
g w
omen
with
prio
r moo
d di
sord
ers o
nly.
ED 5
Em
erge
ncy
Dep
artm
ent
NH
W 5
Non
-Hisp
anic
Whi
teA
A 5
Afr
ican
Am
eric
anBP
5 b
lood
pre
ssur
eC
I 5 c
onfid
ence
inte
rval
OR
5 o
dds r
atio
UC
LA 5
Uni
vers
ity o
f Cal
iforn
ia L
os A
ngel
esSD
5 s
tand
ard
devi
atio
nSE
S 5
soci
oeco
nom
ic st
atus
RR 5
rela
tive
risk
BPI 5
Brie
f Pai
n In
vent
ory
EMG
5 e
lect
rom
yogr
aphy
NE
5 p
lasm
a no
repi
neph
rine

192 Race, ethnicity, and pain
U.S. adults has been fairly well documented, less is known about what makes racial/ethnic minority patients particularly prone to having their pain under-managed relative to similar White patients. Two basic models of pain dominate the current scientific literature. The first is the general biomedical model, which centers on the biological origin and physiological side of pain.11,34[p. 5] The second, the biopsychosocial model of pain, recognizes the interactive effects of the biological, psychological, and social dimensions of the pain experienced,35,36 which together define and shape behavioral and emotional pain responses. The biopsychosocial model seems to offer a more likely explanation for racial/ethnic variation in reported pain by viewing it as an experience constructed from a diverse set of influences.37,38
race/ethnicity, pain perception, and response. Understanding variations in how individuals perceive and respond to pain is essential to the provision of optimal pain management. The extent to which a noxious stimulus will be perceived as pain depends upon the context in which the pain occurs, characteristics of the pain itself (e.g., intensity, duration, location), past experiences with pain, anxiety about pain, pain expectations, and physical and mental co-morbidities.28,37,39
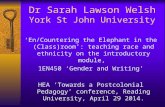
A fundamental question for experimental research studies that have focused on racial/ethnic variation in pain has been whether or not racial and ethnic groups differ substantively in the sensory or discriminatory perception of painful stimuli and (as a consequence) in the perception of pain relief. These studies have primarily focused on differences between African Americans and Whites on three dimensions of pain: threshold, tolerance, and intensity. The International Association for the Study of Pain40 defines a pain threshold as the least experience of pain that an individual can recognize and pain tolerance as the maximum amount of pain that an individual is prepared to tolerate. Pain intensity, often used to describe the level of pain that an individual is experiencing, is more accurately described in terms of the level of noxious stimulus that is applied in the experimental setting.40
It has been suggested that African Americans41–43 and other minority group members44 have higher levels of clinical pain and experience more pain from chronic conditions than Whites. Results from experimental studies that have focused on racial/ethnic variation in the sensory dimensions of pain have varied by the measure (threshold, tolerance, or intensity) and methods used to induce pain (such as electric stimuli,45 pres-sure, cold pressor and thermal41,42,45–51 pressure).The most consistent findings are lower thermal44–48 and ischemic pain tolerances41,47,50,52 observed among African Americans in comparison with non-Hispanic Whites (Table 1). In general, experimental studies show no racial/ethnic differences in pain thresholds among patients with otherwise similar characteristics.48,50 Few studies have examined other race/ethnic groups. In one study that examined pain sensitivity, Hispanics also had lower pain tolerances than Whites.49
A few hypotheses have been suggested to explain racial/ethnic variation in pain in the experimental setting, but most are largely speculative. Included are hypotheses regarding racial/ethnic differences in heat retention, endogenous opioid release, affective processing of painful stimuli42,48 and unmeasured psychological characteristics.53 Racial/ethnic similarity in reported pain intensity has been hypothesized to be a result of less psychosocial influence on this measure.42 There is also some empirical data that show
193Shavers, Bakos, and Sheppard
lower plasma levels of oxytocin (a nociceptive modulator that raises pain thresholds) among African American women compared with White women,46 which could explain racial differences in pain tolerance among women.
The main criticism of experimental studies has been their lack of generalizability54 and the failure of many studies to examine directly both the sensory and the affective dimensions of pain,48 the latter of which may offer a more reasonable explanation of racial/ethnic differences in pain perception than biology. The affective dimension of pain involves the feelings of unpleasantness that immediately follow exposure to painful stimuli as well as negative emotional responses to the pain.55 One study examining racial/ethnic variation in pain found a greater negative affective effect of clinically induced pain among African Americans than among Whites,48 which could contribute to racial/ethnic differences in pain perception and pain ratings. Results from these studies are consistent with studies of chronic pain sufferers showing that African Americans report higher levels of pain severity, depression, and disability than Whites and a stronger link between emotions and pain behaviors when compared to Whites.41,42,56,57
Culture, the pain experience, and methods of coping with pain. The pain response is not restricted to a physiological reaction to the exposure to noxious stimuli or tissue injury but encompasses emotional and behavioral responses as well. These responses have as their foundation variations in cultural perceptions, expectations, and past expe-riences which are known to differ among race/ethnic groups.58 Culture is defined as “the customary beliefs, social norms, and material traits of a racial, religious, or social group.”59 Culturally specific attitudes and beliefs about the origin, role, and meaning of pain not only influence the manner in which individuals view and respond to their own pain but can affect how they perceive and respond to the pain of others. There are several dimensions in which culture potentially influences the pain experience, includ-ing (1) individual pain-related behavior, sensations, emotions, and expectations; (2) interpersonal relationships and individual beliefs about pain and pain management (e.g., roles of family, health care professionals, support people); (3) inter-group relationships and the beliefs, expectations, and social meanings of pain of both the provider and the patient; (4) and the societal environment, which encompasses health culture, ideology, quality of life, and socioeconomics.
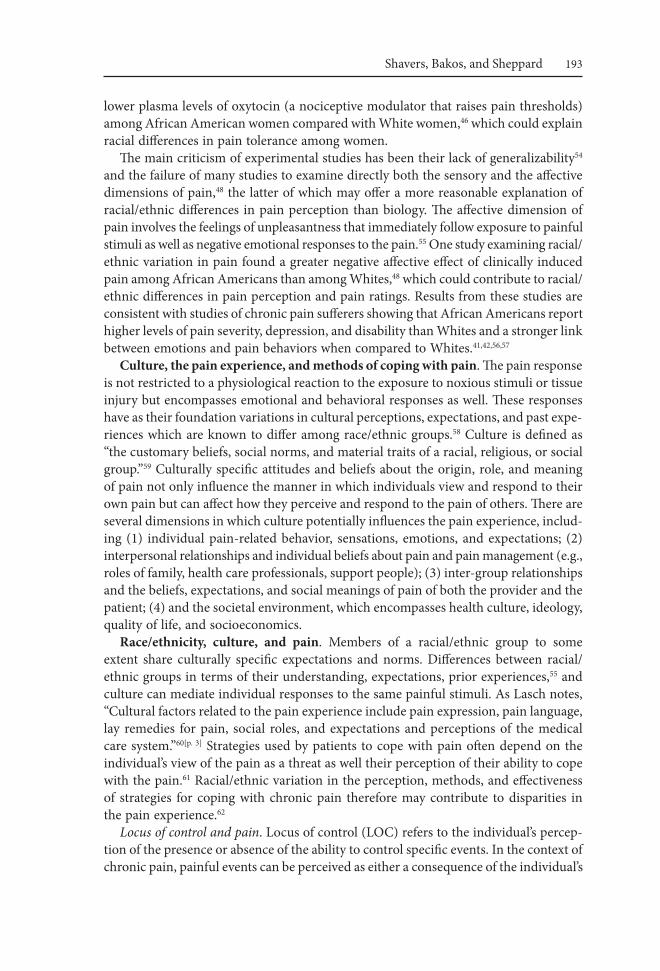
race/ethnicity, culture, and pain. Members of a racial/ethnic group to some extent share culturally specific expectations and norms. Differences between racial/ethnic groups in terms of their understanding, expectations, prior experiences,55 and culture can mediate individual responses to the same painful stimuli. As Lasch notes, “Cultural factors related to the pain experience include pain expression, pain language, lay remedies for pain, social roles, and expectations and perceptions of the medical care system.”60[p. 3] Strategies used by patients to cope with pain often depend on the individual’s view of the pain as a threat as well their perception of their ability to cope with the pain.61 Racial/ethnic variation in the perception, methods, and effectiveness of strategies for coping with chronic pain therefore may contribute to disparities in the pain experience.62
Locus of control and pain. Locus of control (LOC) refers to the individual’s percep-tion of the presence or absence of the ability to control specific events. In the context of chronic pain, painful events can be perceived as either a consequence of the individual’s

194 Race, ethnicity, and pain
behavior, which suggests that they can exert some control over the pain (internal con-trol), or as due to outside forces or chance, which implies lack of control over the pain (external control).63 Perceived lack of control over pain has been called one of the most distressing aspects of the chronic pain experience and has been found to be associated with greater levels of pain,64,65 depression, psychological distress, disability,65 and use of maladaptive coping strategies.63,66 Few studies have directly compared perception of locus of control and pain among racial/ethnic groups (see Table 2).63,67 In general, less frequent perceived internal control over pain63,67 and more frequent behaviors consistent with an external locus of control (e.g., praying and hoping, depression, anger, and fear) have been observed for African Americans than for non-Hispanic Whites,42,62,63,69–71 although not all studies have found this difference.72 Other research shows that Asian patients may frequently exhibit internal locus of control. In a recent study of mostly Chinese patients, a mind-over-body strategy was a frequently used for coping with cancer pain.73
Religion. Religion is hypothesized to affect health through faith or beliefs that encourage healthy behaviors and emotions, such as hope and forgiveness and their positive effects on physiologic processes.74,75 Individuals who participate in organized religion may also have more social support than others. Religion plays a central role in the lives of many racial/ethnic minority populations.76,77 For example, the view of pain taken by many Chinese has its basis in Eastern philosophies and religions includ-ing Taoism, Buddhism, and Confucianism.74 Pain may be perceived as an imbalance between Yin and Yang, Qi, or as an essential element of life.74 Protestant Christian churches have traditionally served as a source of social support, health information, and point of access for health care services in African American communities78[p. 6] and many Hispanics are Roman Catholics.79 Spirituality is an important cultural trait of many American Indian tribes and nations, for whom illness is often seen as a result of imbalances between the spiritual, mental, physical, and social interactions of the American Indian patient and his/her family.80 Healing, spiritual beliefs or power, and community are viewed as interconnected; thus, entire American Indian communities are often involved in healing ceremonies.80 Results of studies that have examined the impact of religion and spirituality on health outcomes vary widely, perhaps due in part to differences in how religion and spirituality are measured.81 This makes it difficult to disentangle the role of variation in methods of measuring religion and spirituality from actual differences in effect.
Many culturally specific beliefs about pain are rooted in religion and spirituality. In such a framework, pain may be viewed as a lesson from God, a reflection of God’s inability to intervene, a lack of God’s love, or a part of God’s plan;82 punishment for sin or misbehavior;81 as a test of faith, or as a means of achieving higher religious status.35,81,83 Religious beliefs regarding the origin and the purpose of pain may factor into a patient’s acknowledgment, acceptance, and response to pain and to the use of pain-relieving medications.84,85
Results from studies of the effect of religiosity and spirituality on pain experiences of racial/ethnic minority populations have shown both positive and negative effects. In general, both larger beneficial and negative effects of various aspects of religious and spiritual coping methods have been found for racial/ethnic minority patients com-

(Con
tinue
d on
p. 1
96)
tabl
e 2.
St
uD
ieS
eXa
MiN
iNG
ra
Cia
L/et
HN
iC v
ar
iati
ON
iN
Str
ateG
ieS
Or
Met
HO
DS
OF
CO
PiN
G w
itH
Pa
iN
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
Pain
cop
ing
56. N
dao-
Brum
blay
SK
et
al.,
200
5
N5
1192
, 108
8 N
HW
, 104
AA
w
omen
Retr
ospe
ctiv
e an
alys
is of
self-
repo
rted
dat
a fr
om a
pai
n as
sess
men
t que
stio
nnai
re
adm
inist
ered
at a
tert
iary
car
e pa
in
cent
er 1
993–
2000
.
AA
wom
en re
port
ed si
gnifi
cant
ly h
ighe
r pai
n se
verit
y sc
ores
(3
0.7
vs. 2
7.5,
p5
.008
), m
ore
psyc
holo
gica
l dist
ress
incl
udin
g de
pres
sion
(19.
4 vs
. 16.
9, p
5.0
30) a
ffect
ive
dist
ress
(3.5
vs.
3.1,
p5
.003
) pos
t-tr
aum
atic
stre
ss (1
2.9
vs. 8
.1, p
5.0
02)a
nd
disa
bilit
y (4
4.1
vs. 3
7.1,
p,
.005
) due
to p
ain,
hig
her s
core
s an
d gr
eate
r lev
els o
f int
erfe
renc
e w
ith re
crea
tiona
l (8.
1 vs
. 7.
1, p
,.0
05),
sexu
al (7
.4 v
s. 6.
1, p
,.0
05) a
nd so
cial
(7.0
vs
. 5.9
, p5
.001
) act
iviti
es, c
ompa
red
to N
HW
wom
en in
un
ivar
iate
ana
lyse
s. A
fter a
djus
tmen
t for
soci
odem
ogra
phic
, m
edic
al, p
sych
olog
ical
and
phy
sical
con
foun
ders
in h
iera
rcha
l lin
ear r
egre
ssio
n m
odel
s, th
ere
was
no
signi
fican
t ass
ocia
tion
betw
een
race
and
pai
n se
verit
y or
affe
ctiv
e di
stre
ss. H
owev
er,
Blac
k w
omen
with
chr
onic
pai
n ex
perie
nced
mor
e ph
ysic
al
impa
irmen
ts th
an W
hite
wom
en w
ith c
hron
ic p
ain
(bet
a 5
4.
622;
p,
.005
).

tabl
e 2.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
(Con
tinue
d on
p. 1
97)
57. T
an G
et
al.,
200
5N
548
2, 1
28 A
A,
354
NH
WFa
ctor
ana
lysis
of c
ross
-sec
tiona
l da
ta o
n pa
tient
s ref
erre
d to
an
inte
grat
ed p
ain
man
agem
ent
prog
ram
of a
VA
Med
ical
Cen
ter
1995
–199
8.
Com
pare
d to
NH
W s,
AA
s re
port
ed si
gnifi
cant
ly h
ighe
r m
ean
pain
seve
rity
(5.3
vs.
5.0,
p ,
.001
), de
pres
sion
(31.
6 vs
. 27.
1, p
,.0
01),
disa
bilit
y (1
7.9
vs 1
5.7,
p,
.001
) and
in
terf
eren
ce (5
.2 v
s. 5.
0, p
,.0
5). A
As w
ere
mor
e lik
ely
to
use
beha
vior
al c
opin
g st
rate
gies
, rep
orte
d lo
wer
leve
ls of
pe
rcei
ved
cont
rol o
ver p
ain,
mor
e di
sabi
lity
and
perc
eptio
n of
ha
rm a
nd m
ore
freq
uent
use
of e
xter
nal p
ain
copi
ng st
rate
gies
su
ch a
s pra
ying
/hop
ing.
Pai
n ap
prai
sal a
nd c
opin
g fa
ctor
s ex
plai
ned
18%
of t
he v
aria
nce
in p
ain
seve
rity,
39.3
% o
f the
va
rianc
e in
self-
repo
rted
dep
ress
ion,
22.
7% o
f the
var
ianc
e in
self-
repo
rted
disa
bilit
y an
d 18
.5%
of t
he se
lf re
port
ed p
ain
inte
rfer
ence
afte
r con
trol
ling
for d
emog
raph
ic v
aria
bles
for
the
stud
y sa
mpl
e as
a w
hole
. AA
s had
sign
ifica
ntly
hig
her
scor
es o
n th
e so
licitu
de a
nd p
rayi
ng/h
opin
g su
bsca
les.
Ethn
icity
was
not
sign
ifica
ntly
ass
ocia
ted
with
pai
n m
easu
res,
depr
essio
n an
d fu
nctio
ning
afte
r con
trol
ling
for o
ther
de
mog
raph
ic v
aria
bles
.
61. C
ano
A
et a
l., 2
006
N5
127,
58
AA
, 69
NH
WSu
rvey
of A
A a
nd N
HW
pat
ient
s re
crui
ted
for a
stud
y of
cou
ples
and
ch
roni
c pa
in.
AA
mor
e fr
eque
ntly
repo
rted
pra
yer a
nd h
opin
g (m
ean
14.7
2)
and
atte
ntio
n di
vers
ion
(mea
n 12
.28)
com
pare
d to
NH
W
(8.3
0 an
d 9.
76, r
espe
ctiv
ely)
(p,
.01
for p
raye
r and
hop
ing
and
p,.0
5 fo
r atte
ntio
n di
vers
ion)
.

tabl
e 2.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
(Con
tinue
d on
p. 1
98)
62. J
orda
n M
S et
al.,
199
8N
510
0, 4
8 A
A, 5
2 N
HW
Surv
ey o
f wom
en w
ith rh
eum
atoi
d ar
thrit
is re
crui
ted
from
a h
ospi
tal
outp
atie
nt rh
eum
atol
ogy
clin
ic
to e
xam
ine
raci
al d
iffer
ence
s in
stra
tegi
es fo
r cop
ing
with
pai
n.
Atte
ntio
n di
vers
ion
was
use
d by
16.
8% o
f AA
s com
pare
d to
13
.2%
of N
HW
s (p5
.013
) and
pra
ying
/hop
ing
was
use
d by
25
.8%
of A
As a
nd 1
8.8%
of N
HW
s (p5
.000
1) to
cop
e w
ith
pain
. AA
s (3.
1%) m
ore
freq
uent
ly re
port
ed in
activ
ity d
ue to
pa
in th
an d
id N
HW
s (2.
0%) p
5.0
001.
The
race
/eth
nic
grou
ps
did
not s
igni
fican
tly d
iffer
in te
rms o
f neg
ativ
e aff
ect o
f pai
n.
Igno
ring
pain
, cop
ing
stat
emen
ts a
nd st
rong
er c
ontr
ol b
elie
fs
wer
e as
soci
ated
with
bet
ter h
ealth
stat
us w
hile
atte
ntio
n di
vers
ion
pred
icte
d m
ore
pain
.
67. V
alle
rand
A
et a
l., 2
005
N5
281,
98
AA
, 18
3 N
HW
Cro
ss-s
ectio
nal s
urve
y of
pat
ient
s w
ith c
ance
r in
outp
atie
nt w
aitin
g ro
om o
f an
urba
n ca
ncer
cen
ter
who
repo
rted
pai
n in
the
past
m
onth
.
Ove
rall,
AA
s had
mor
e pa
in, h
ighe
r pai
n-re
late
d di
stre
ss,
and
low
er fu
nctio
nal s
tatu
s com
pare
d to
NH
W p
atie
nts.
Adj
ustm
ent f
or p
erce
ptio
n of
con
trol
ove
r pai
n re
duce
d ra
cial
/eth
nic
disp
ariti
es in
ove
rall
pain
by
42.6
%, w
orse
pai
n by
75.
9%, l
east
pai
n by
28.
1%, a
nd a
vera
ge p
ain
by 2
6.0%
.
68. J
ones
AC
et
al.,
200
8N
593
9, 4
59 A
A,
480
NH
WSu
rvey
of p
atie
nts f
orm
prim
ary
care
clin
ics i
n th
e VA
Hea
lthca
re
Syst
em a
ge 5
0–80
with
chr
onic
kn
ee o
r hip
pai
n.
AA
s w
ere
signi
fican
tly m
ore
likel
y to
repo
rt h
opin
g an
d pr
ayin
g as
a m
eans
of c
opin
g w
ith th
eir p
ain
than
wer
e N
HW
s (Ra
ce B
eta
coeffi
cien
t 0.7
4 (9
5% C
I 0.5
0–0.
99).
69. H
astie
et
al.,
200
5N
552
7, 1
85 A
A,
155
Hisp
anic
, 187
N
HW
Cro
ss-s
ectio
nal s
urve
y of
col
lege
st
uden
ts w
ho e
xper
ienc
ed p
ain
on
mor
e th
an o
ne o
ccas
ion
durin
g th
e pr
evio
us 6
mon
ths.
Pray
er/s
pirit
ual c
opin
g w
as m
ore
freq
uent
ly u
sed
by A
fric
an
Am
eric
ans (
61.1
%) a
nd H
ispan
ics (
49.7
%) t
han
NH
W (3
4.2%
) p,
.001
. NH
Ws (
80.7
%) a
nd H
ispan
ics (
75.5
%) r
epor
ted
self-
care
stra
tegi
es fo
r man
agin
g th
eir p
ain
than
did
AA
s (65
.5%
) p5
0.00
3. Th
e ra
ce/e
thni
c gr
oups
did
not
sign
ifica
ntly
diff
er in
te
rms o
f the
ove
rall
use
of p
assiv
e te
chni
ques
for c
opin
g w
ith
pain
or w
ith th
e us
e of
stan
dard
hea
lth c
are.
tabl
e 2.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
(Con
tinue
d on
p. 1
99)
70. E
dwar
ds
RR e
t al.,
200
5N
529
1, 9
7 A
A, 9
7 N
HW
, 97
Hisp
anic
Surv
ey o
f AA
, Hisp
anic
and
NH
W
patie
nts s
eeki
ng tr
eatm
ent f
or
chro
nic
pain
at a
uni
vers
ity p
ain
man
agem
ent c
ente
r with
pai
n of
3
mon
ths o
r mor
e du
ratio
n.
Ther
e w
ere
no ra
cial
/eth
nic
diffe
renc
es in
pai
n se
verit
y, se
nsor
y pa
in, a
ffect
ive
pain
, pai
n in
tens
ity, p
ain
inte
rfer
ence
or
gen
eral
act
ivity
. AA
(4.2
) and
Hisp
anic
s (3.
9) h
ad
signi
fican
tly h
ighe
r sco
res o
n th
e C
opin
g St
rate
gies
Sub
scal
e fo
r the
use
of p
rayi
ng a
nd h
opin
g st
rate
gies
for c
opin
g w
ith
pain
than
did
NH
Ws (
3.4)
(p,
.001
). C
atas
trop
hizi
ng w
as a
sig
nific
ant p
redi
ctor
of e
leva
ted
pain
dist
ress
and
a m
oder
ate
pred
icto
r of h
ighe
r effe
ctiv
e pa
in. C
atas
trop
hizi
ng w
as re
late
d to
gre
ater
pai
n se
verit
y am
ong
AA
and
NH
W p
atie
nts o
nly.
71. A
nder
son
KO e
t al.,
200
2N
531
, 14
AA
, 17
Hisp
anic
Stru
ctur
ed in
terv
iew
of A
A a
nd
Hisp
anic
pat
ient
s with
met
asta
tic
or re
curr
ent c
ance
r des
igne
d to
ex
plor
e ba
rrie
rs to
opt
imal
pai
n m
anag
emen
t.
Mor
e th
an o
ne-t
hird
of A
A a
nd H
ispan
ic p
atie
nts w
ho w
ere
pres
crib
ed a
nalg
esic
s wer
e pr
escr
ibed
dos
es th
at w
ere
not
deem
ed su
ffici
ent b
ased
on
thei
r sel
f-re
port
ed p
ain
inte
nsity
. A
A m
ore
freq
uent
ly th
an H
ispan
ics r
epor
ted
“a lo
t” o
f co
ncer
n re
gard
ing
pain
med
icat
ion
tole
ranc
e (4
3% v
s 29%
), w
orry
that
pai
n m
edic
atio
ns w
ill n
ot w
ork
(38%
vs 1
2%) ,
sid
e eff
ects
of a
nalg
esic
s (43
% v
s 12%
), th
at ta
king
stro
ng
anal
gesic
s mea
n de
ath
is ne
ar (4
3% v
s 18%
), an
d th
at p
ain
med
icin
es d
istra
ct p
rovi
der f
rom
trea
ting
the
dise
ase
(21%
vs
12%
). H
ispan
ic p
atie
nts m
ore
freq
uent
ly re
port
ed th
at th
ey
shou
ld b
e st
rong
and
not
lean
on
pain
med
icat
ions
(41%
vs
36%
), fa
mily
con
cern
s abo
ut p
ain
med
icat
ions
(41%
vs 2
9%)
and
wor
ry a
bout
add
ictio
n (5
3% v
s 36%
). Pr
ayer
as a
met
hod
of c
opin
g w
ith p
ain
was
repo
rted
by
83%
of A
A c
ompa
red
to
47%
of H
ispan
ics (
CI 1
0–63
).

72. B
ourjo
lly
JN e
t al.,
199
9N
510
2, 4
1 A
A, 6
1 N
HW
Ana
lysis
of d
ata
from
a
conv
enie
nce
sam
ple
of w
omen
.Bo
th A
A a
nd N
HW
wom
en e
xhib
ited
exte
rnal
locu
s of
cont
rol.
91. A
ng D
C
et a
l., 2
002
N5
596,
262
AA
, 33
4 N
HW
Surv
ey o
f pat
ient
s in
VA p
rimar
y ca
re c
linic
s 501
with
chr
onic
m
oder
ate-
seve
re p
ain
knee
and
/or
hip
pain
.
AA
pat
ient
s sco
red
high
er th
an W
hite
pat
ient
s on
the
relig
iosit
y sc
ale
(77
6 1
7 vs
. 70
6 2
1). I
n m
ultiv
aria
te
anal
ysis,
Bla
ck p
atie
nts w
ere
mor
e lik
ely
than
Whi
te p
atie
nts
to p
erce
ive
pray
er a
s hel
pful
in th
e m
anag
emen
t of t
heir
arth
ritis
(OR
2.1,
95%
CI 1
.19,
3.7
2). A
A p
atie
nts w
ere
also
le
ss li
kely
than
Whi
te p
atie
nts t
o in
dica
te th
at th
ey w
ould
co
nsid
er su
rger
y if
thei
r pai
n w
ere
to g
et se
vere
(OR
0.58
, 95
% C
I 0.3
4, 0
.99)
; thi
s rel
atio
nshi
p be
twee
n et
hnic
ity a
nd
cons
ider
atio
n of
surg
ery
is m
edia
ted
by p
erce
ptio
ns o
f “h
elpf
ulne
ss o
f pra
yer.”
NH
W 5
Non
-Hisp
anic
Whi
teA
A 5
Afr
ican
Am
eric
anC
I 5 c
onfid
ence
inte
rval
OR
5 o
dds r
atio
VA 5
Vet
eran
s Affa
irs
tabl
e 2.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings

200 Race, ethnicity, and pain
pared with White patients (Table 2).62,70–71,86 For example, the religious participation of African Americans has been associated with improved health status,87 quality of life, and lower psychological distress,88 lower pain scores,89 less depression, more positive pain and symptom attitudes, higher formal social support, and a greater likelihood of taking pain medication compared with African American who did not participate in religious observances.89 Positive religious coping strategies have also been correlated with positive mental health status.90 Religious and spiritual beliefs can also negatively affect the pain experience through their influence on perceptions of the acceptability of health care interventions;90,91,92 the stigmatization of certain diseases/conditions that may reduce the likelihood of the patient seeking care;93 and through the belief that religious transgressions, lack of faith, or the individual’s behavior are perceived to warrant or to be responsible for the pain.94,95
Prayer is frequently reported as a method of coping with pain, particularly among African American and Hispanic patients68,–72,84,91,61 compared with non-Hispanic Whites (Table 2).72,61 High levels of pain, catastrophizing, and greater pain, distress, and dis-ability42,66 have also been found for African American patients.70 The use of prayer and hoping as a strategy for coping with pain was found to be associated with greater pain severity and higher ratings of affective pain and was a predictor of greater dis-ability among African American, Hispanic, and non-Hispanic White patients treated at a multidisciplinary pain management center. However, it is not clear whether this association was due to greater use of prayer among patients with more severe pain or vice versa. In a survey of veterans who suffered chronic pain from osteoarthritis of the knee or hip, the perception of prayer as helpful was significantly associated the lower likelihood of African American patients to consider knee or hip replacement compared with non-Hispanic White patients.91 In another study despite more frequent use of hoping and prayer, there was no association between higher pain and functional self-efficacy among African Americans compared with Whites.68
Pain assessment and communication. Pain is a subjective and multidimensional experience measured by the patient’s report of its presence, intensity, and duration. Guidelines from the American Pain Society list three major goals for pain assessment: (1) to characterize the patient’s pain status and related experience over time; (2) to provide a basis for treatment decisions; and (3) to document the effectiveness of pain management strategies.96 The reliance on patient self-reports highlights the importance of effective pain communication between patients and their providers. Inconsisten-cies often exist between patient-reported levels of pain and health care provider or caretaker assessment of pain levels,97 which may result in needless suffering.98 Patients also can contribute to inaccuracies in pain assessment by failing to report pain or underreporting/overreporting its intensity, duration, or importance and the impact it has on their quality of life or daily activities.
Pain expression. Public expressions of pain (verbal or non-verbal) may not always correlate with the actual presence or level of the pain experienced by minority patients,99–102 which can make it difficult for providers to assess accurately the patient’s pain. Patients from cultures with expressive styles of communication may more freely admit the presence of pain as well as their feelings regarding their pain and its impact on their life to others. In contrast, individuals from cultures that exhibit more stoic

201Shavers, Bakos, and Sheppard
behavior often see pain as something to be endured73 and may not freely admit having pain or may even deny it.
The extent to which individuals from different racial/ethnic groups exhibit these styles is often influenced by their specific cultural expectations and norms.100,103,104 For example, stoic pain behavior has been reported for Mexican Americans, American Indians,100 and Asians,84,102 and for men more often than women.103 In a study of cancer pain, Asians reported significantly lower pain scores than African Americans, non-Hispanic Whites, and Hispanics on four different pain scales, but no difference in symptoms.102 The social context in which the pain occurs is also important in determining appropriate responses. In a study that examined beliefs about appropriate pain behavior among Japanese and Euro-Americans, researchers found that overall Euro-Americans were more accepting of overt pain behavior than were Japanese participants. Overt pain behavior was also believed to be more acceptable for women than for men in both cultures.103
Providers who are not aware of or responsive to cultural variations in pain percep-tion, expression, expectations, and response are more likely to interpret patient needs and behavior in terms of their own culture,101,104 which may differ significantly from that of the patient and could adversely affect the patient’s pain management.105 For example, participants in a study of chronic joint pain from rheumatoid arthritis among urban-dwelling American Indians (mostly Choctaw, Navajo, and Sioux) cautioned that because American Indians do not like to talk about themselves, complain about pain, or ask for help, if and when a complaint about pain has been voiced to a physician that is not adequately addressed it will not be voiced again until the pain is severe.100 In a recent study of Asian Americans with cancer, participants indicated that pain should be handled bravely in order to set a good example for others.73 An unknowledgeable provider might incorrectly interpret such bravery as meaning that the patient is not experiencing pain.
The extent to which culture can influence pain perception and response depends in part on the degree to which the individuals identify with their ethnic or cultural group60 and to which they endorse their group’s cultural beliefs and behaviors. Potential mediators include age, gender, level of acculturation, socioeconomic status, and the degree of isolation from the ethnic or cultural group.
Pain measurement and assessment. A few studies have examined the appropriateness of existing scales for assessing pain among racial/ethnic minority populations.106–108 Results from these studies suggest that commonly used pain scales are appropriate for use in diverse population groups. Taylor et al.107 compared patient preference and the reliability and validity of the Faces Pain Scale (FPS),109 the Verbal Descriptor Scale,110 the Numeric Rating Scale,111 and the Iowa Pain Thermometer110 for measuring pain in cognitively intact and cognitively impaired older African Americans. Study results show that all participants were able to successfully use the four scales, although the reliability and validity of the scales was somewhat better among cognitively intact participants. Both cognitively intact and cognitively impaired patients expressed a preference for the Faces Pain Scale. In another study that examined the intercorrelation between the Visual Analogue Scale (VAS),112 Memorial Pain Assessment Card (MPS),113 and the Faces Pain Scale114 among African American, non-Hispanic White, Asian and Hispanic patients with cancer pain show a high correlation between the VAS, MPS, and FPS109

(Con
tinue
d on
p. 2
03)
tabl
e 3.
r
aC
iaL/
etH
NiC
va
ria
tiO
N i
N P
aiN
aSS
eSSM
eNt
aN
D C
OM
Mu
NiC
atiO
N
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
Pain
mea
sure
men
t and
ass
essm
ent
94. S
tato
n et
al.,
200
7N
545
5, A
A o
r A
fric
an A
mer
ican
(1
78),
Non
-H
ispan
ic W
hite
or
NH
W (2
19),
Hisp
anic
(35)
, ot
her (
21)
Cro
ss-s
ectio
nal s
urve
y to
exa
min
e co
ncor
danc
e be
twee
n ph
ysic
ian
and
patie
nt p
erce
ptio
ns o
f pat
ient
pa
in le
vel.
Phys
icia
ns w
ere
signi
fican
tly m
ore
likel
y to
und
eres
timat
e pa
in o
f AA
s (O
R51.
9, 9
5% C
I 1.3
–2.8
) in
a m
ultiv
aria
te
logi
stic
regr
essio
n m
odel
adj
uste
d fo
r age
, gen
der,
mar
ital
stat
us, e
duca
tion,
insu
ranc
e st
atus
, co-
mor
bidi
ty, d
epre
ssio
n,
pres
crip
tion
opio
id u
se a
nd b
odily
pai
n.
98. I
m E
et a
l.,
2007
N5
480,
109
AA
, 10
5 H
ispan
ics,
148
NH
W a
nd 1
18
Asia
ns
Cro
ss-s
ectio
nal c
ompa
rativ
e st
udy
of c
ance
r pat
ient
s rec
ruite
d th
roug
h th
e in
tern
et a
nd
com
mun
ity se
tting
s des
igne
d to
exa
min
e et
hnic
diff
eren
ces
in c
ance
r pai
n, sy
mpt
oms a
nd
func
tiona
l sta
tus.
Asia
ns re
port
ed th
e lo
wes
t can
cer p
ain
scor
es o
n al
l sca
les
and
Hisp
anic
s had
the
high
est p
ain
scor
es. Th
ere
wer
e no
ra
cial
/eth
nic
diffe
renc
es in
can
cer p
ain
sym
ptom
s.
99. H
obar
a M
, 20
05N
564
, Jap
anes
e (3
2), E
uro-
Am
eric
ans (
32)
Cro
ss-s
ectio
nal s
urve
y us
ing
the
Appr
opria
te P
ain
Beha
vior
Q
uest
ionn
aire
(APB
Q) w
as
empl
oyed
to e
xam
ine
the
effec
ts
of th
e pa
rtic
ipan
ts’ se
x an
d cu
lture
on
thei
r bel
iefs
rega
rdin
g ge
nder
-ap
prop
riate
pai
n be
havi
or. S
tudy
da
tes w
ere
not p
rovi
ded.
Euro
-Am
eric
an p
artic
ipan
ts ra
ted
pain
beh
avio
rs in
bot
h se
xes t
o be
mor
e ac
cept
able
. Mal
e an
d fe
mal
e pa
rtic
ipan
ts
of b
oth
cultu
res w
ere
equa
lly a
ccep
ting
of p
ain
beha
vior
s in
wom
en, b
ut m
ale
part
icip
ants
wer
e le
ss a
ccep
ting
of p
ain
beha
vior
s in
men
than
in w
omen
. Ther
e al
so w
as a
sign
ifica
nt
inte
ract
ion
betw
een
refe
rent
gen
der a
nd c
ultu
re o
f the
pa
rtic
ipan
t: Ja
pane
se p
artic
ipan
ts c
onsid
ered
pai
n be
havi
or in
bo
th g
ende
rs to
be
less
acc
epta
ble
than
did
Am
eric
ans.
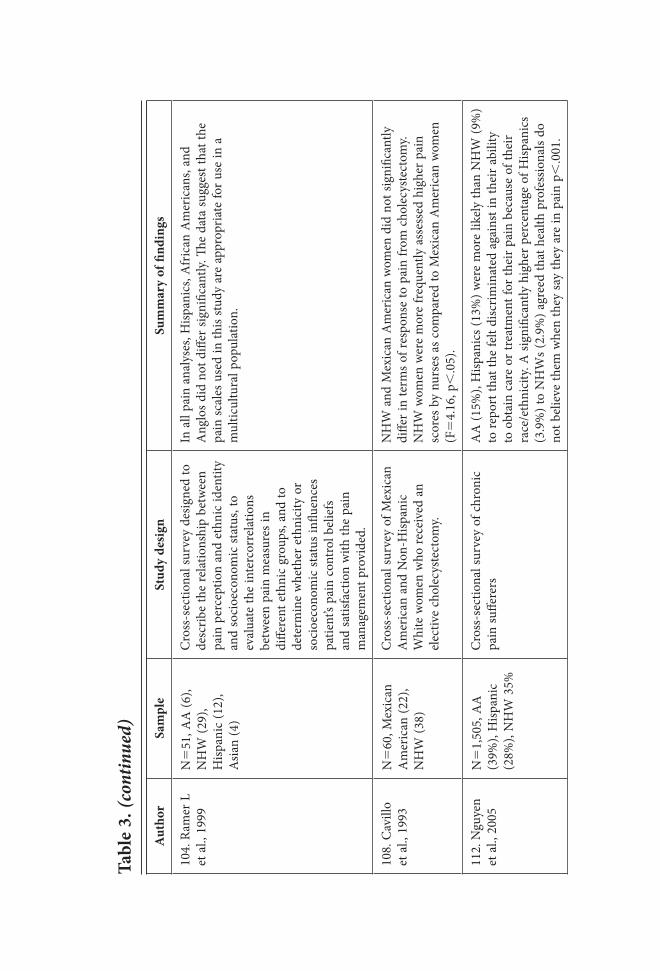
tabl
e 3.
(con
tinue
d)
aut
hor
Sam
ple
Stud
y de
sign
Sum
mar
y of
find
ings
104.
Ram
er L
et
al.,
199
9N
551
, AA
(6),
NH
W (2
9),
Hisp
anic
(12)
, A
sian
(4)
Cro
ss-s
ectio
nal s
urve
y de
signe
d to
de
scrib
e th
e re
latio
nshi
p be
twee
n pa
in p
erce
ptio
n an
d et
hnic
iden
tity
and
soci
oeco
nom
ic st
atus
, to
eval
uate
the
inte
rcor
rela
tions
be
twee
n pa
in m
easu
res i
n di
ffere
nt e
thni
c gr
oups
, and
to
dete
rmin
e w
heth
er e
thni
city
or
soci
oeco
nom
ic st
atus
influ
ence
s pa
tient
’s pa
in c
ontr
ol b
elie
fs
and
satis
fact
ion
with
the
pain
m
anag
emen
t pro
vide
d.
In a
ll pa
in a
naly
ses,
Hisp
anic
s, A
fric
an A
mer
ican
s, an
d A
nglo
s did
not
diff
er si
gnifi
cant
ly. Th
e da
ta su
gges
t tha
t the
pa
in sc
ales
use
d in
this
stud
y ar
e ap
prop
riate
for u
se in
a
mul
ticul
tura
l pop
ulat
ion.
108.
Cav
illo
et a
l., 1
993
N5
60, M
exic
an
Am
eric
an (2
2),
NH
W (3
8)
Cro
ss-s
ectio
nal s
urve
y of
Mex
ican
A
mer
ican
and
Non
-Hisp
anic
W
hite
wom
en w
ho re
ceiv
ed a
n el
ectiv
e ch
olec
yste
ctom
y.
NH
W a
nd M
exic
an A
mer
ican
wom
en d
id n
ot si
gnifi
cant
ly
diffe
r in
term
s of r
espo
nse
to p
ain
from
cho
lecy
stec
tom
y. N
HW
wom
en w
ere
mor
e fr
eque
ntly
ass
esse
d hi
gher
pai
n sc
ores
by
nurs
es a
s com
pare
d to
Mex
ican
Am
eric
an w
omen
(F
54.
16, p
,.0
5).
112.
Ngu
yen
et a
l., 2
005
N5
1,50
5, A
A
(39%
), H
ispan
ic
(28%
), N
HW
35%
Cro
ss-s
ectio
nal s
urve
y of
chr
onic
pa
in su
ffere
rsA
A (1
5%),
Hisp
anic
s (13
%) w
ere
mor
e lik
ely
than
NH
W (9
%)
to re
port
that
the
felt
disc
rimin
ated
aga
inst
in th
eir a
bilit
y to
obt
ain
care
or t
reat
men
t for
thei
r pai
n be
caus
e of
thei
r ra
ce/e
thni
city
. A si
gnifi
cant
ly h
ighe
r per
cent
age
of H
ispan
ics
(3.9
%) t
o N
HW
s (2.
9%) a
gree
d th
at h
ealth
pro
fess
iona
ls do
no
t bel
ieve
them
whe
n th
ey sa
y th
ey a
re in
pai
n p,
.001
.

204 Race, ethnicity, and pain
scales irrespective of race/ethnicity.108 Im et al.,102 compared cancer pain scores among 480 non-Hispanic Whites, African Americans, Asians, and Hispanics using the VAS, FPS, McGill Pain Questionnaire [short form] (MPQ-SF)115 and the Brief Pain Inventory [short form] (BPI-SF)116 pain scales. Although each scale had high reliability across races/ethnic groups, the scales did not consistently identify the same group as having the highest cancer pain scores. Although Shin et al., found internal consistency for both the MPQ-SF and the BPI-SF among 119 Asian Americans, they found the BPI-SF to be more valid.106
Other studies have examined the relationship between the characteristics of the per-son to whom the pain is reported and pain ratings.117,118 In general, these studies have found that men report higher pain tolerances and lower pain intensities when the pain is reported to a female than when it is reported to a male. Few studies, however, have examined the role of race/ethnicity in such variability. A notable exception is Weisse et al., who found that race and gender concordance did not influence pain reporting among individuals exposed to pain in an experimental setting.119
Pain communication. Inadequate pain management can occur when health care providers inaccurately assess patient pain,19,60,97,98 ignore patient complaints about pain or have doubts about the credibility of reported pain,120 or have more concern regarding abuse of prescription medications and drug addiction by specific groups of patients.121–123 Provider assessment of patient pain is an important contributor to the under-treatment of pain in racial/ethnic minority patients.19,60,98,124 In a recent cross-sectional study of physician pain perception, African American patients were nearly two times more likely than patients from other racial/ethnic groups to have their pain underestimated (OR 1.9, 95% CI 1.3–2.8) by their physicians, despite the physicians’ access to self-reported pain ratings.98 In a study of chronic non-cancer pain, medical residents were found to underestimate patient pain more frequently than attending physicians, particularly for racial/ethnic minority patients. Physicians in general were more likely to overestimate pain in patients who were not African American, which suggests that race/ethnicity may play a role in pain assessment.97
Racial/ethnic minorities may have more difficulty than non-Hispanic Whites in effectively communicating their pain to their health care providers in ways that are clearly understood and believed.120–127 Language or other barriers may result in misin-terpretation of the patients’ pain. Environments (such as emergency rooms) where there is less likely to be an established relationship between the provider and patient may be particularly prone to problems with effective pain communication. Providers who do not know their patients may rely more heavily on stereotypes and personal beliefs and attitudes that do not accurately characterize the patient or their pain behavior and which may negatively impact their care. In a survey of physicians who treated patients in the emergency department, physicians were more likely to perceive Native American patients as exaggerating their pain compared with other racial/ethnic groups.120 Native Americans who were perceived by their physicians to be exaggerating their symptoms less frequently were able to achieve a 50% reduction in their pain.
Nguyen et al. found that Hispanics were significantly more likely than Whites to report that health care professionals did not believe they were in pain and to have

205Shavers, Bakos, and Sheppard
difficulty in obtaining treatment for pain because of language barriers.126 In a study of African American and Hispanic patients with cancer-related pain, 21% of African Americans reported difficulty talking about cancer pain.71 In the same study, 57% of African American and 38% of Hispanic patients indicated that their doctor or nurse did not ask them about pain prior to the patient initiating a discussion on pain.
Racial/ethnic minority patient requests for pain relief are perceived to be ‘drug seeking’ behavior more often than such requests from non-minorities.121–123 Many of the signs of drug-seeking behavior128 are subjective and can easily be applied to people suffering from severe or chronic pain which might make them more likely to be classified as drug-seeking. For example, African Americans are disproportionately represented among patients with sickle cell disease. The severity of the pain of sickle cell crises together with previous experience with and knowledge about the effectiveness of particular analgesics for treating their sickle cell crises may make patients more likely to be classified as drug-seeking. Emergency room staff, residents, and nurses in one survey perceived 7–9% of all patients and 13–17% of patients with sickle cell disease to be opioid-dependent.122 In another study, 22% of emergency department physicians and 9% of hematologists expressed the belief that more than 50% of sickle cell patients were addicted,123 a belief that is not supported by available scientific literature.129,130 Only 2–4% of patients with sickle cell disease in a recent survey met Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for substance dependence.130
Provider-related barriers to effective pain management. Health care providers potentially contribute to racial/ethnic disparities in health through the influence of non-clinical characteristics, either actual or perceived, on provider perception of racial/ethnic minority patients and their health-related behavior. Physician recommendations and referrals have been noted to vary by race and ethnicity for a number of diseases and conditions.131–132
Prescribing patterns. Concerns about drug abuse and addiction were reported by primary care physicians to be among their major concerns about prescribing narcot-ics,133 particularly schedule II opioids for around-the-clock management of chronic non-cancer pain.134 The so-called war-on-drugs has increased fear among physicians of Drug Enforcement Administration (DEA) investigation and prosecution and con-tributed to the reluctance of providers to prescribe controlled substances for treatment of pain.135,136 A 2004 report in the Food and Drug Administration (FDA) Consumer Magazine indicated that investigations and prosecutions of pain specialists for drug trafficking have made providers leery of the DEA claim that they have nothing to fear as long as their prescribing patterns fit the norms.136 Forty-six percent of physicians responding to a survey on physicians’ perceived knowledge, goals, confidence, and satisfaction with pain management agreed that prescribing strong opioids would attract a medical review.137
Given the overall reluctance of providers to prescribe controlled substances, par-ticularly opioid analgesics,133,134,138,139 it is not surprising that the most consistently observed racial/ethnic disparity in pain management is in the prescription of opioid analgesics. Several studies show that physician prescribing patterns for controlled substances12,140–142 and patient use of controlled substances for pain control16 vary

206 Race, ethnicity, and pain
with patient race/ ethnicity, while a smaller number of studies have found no differ-ences.33,143 Research results suggest that racial/ethnic disparities in the receipt of opioid pain medication occur more frequently in the absence of objective clinical findings related to the presence, source, and intensity of the pain, which force the provider to rely more heavily on information provided by the patient. This view was shared by the authors of the Institute of Medicine report who state: “[G]iven the role of cultural and linguistic factors both patients’ perception of pain and in physicians’ ability to accu-rately assess patients’ pain . . . it is reasonable to suspect that health care disparities might be greater in pain treatment and other aspects of symptom management than in treatment of objectively verifiable disease.”1[p. 64] Lending further credibility to this hypothesis is the less frequent finding of racial/ethnic disparities in the prescription of pain medications for acute pain, the source of which can be clinically documented (e.g., x-ray for long-bone fractures).31,143,144 For example, an analysis of data from the 1997–1999 National Hospital Ambulatory Medical Care Survey examined racial/eth-nic variation in prescribing patterns for three conditions for which varying levels of objective clinical data were available (i.e., migraine headache, back pain and strain, and long-bone fracture). Although nearly equal proportions of Whites, African Americans and Latinos received any analgesic, racial/ethnic variation existed in the receipt of a prescription for an opioid analgesic and was widest for migraine (least objective) and narrowest for long-bone factures (most objective).22 Pletcher et al. found that although there were no statistical racial/ethnic differences in the receipt of an analgesic, African Americans were significantly less likely than all other racial/ethnic groups to receive a prescription of opioids in an examination of nearly 375,000 pain-related emergency department visits from 1993–2005.12 Fuentes et al. found no racial/ethnic disparity in the receipt of any analgesia or parenteral analgesia among patients treated for long-bone fractures in a Level 1 trauma center, but receipt of opioids was not examined.143 African Americans treated for long-bone fractures were 66% less likely to receive any analge-sic.23 Although there was a trend toward the lower receipt of narcotics among African Americans who received analgesics, this was not a statistically significant finding. In one study of patients treated in the emergency department, White patients were 86% more likely to receive opioids in the emergency room, 82% more likely to be discharged with a prescription for medicine for pain, and 98% more likely to receive a discharge prescription for opioids than African American patients.21 Data from a recent study suggested that racial disparities in the receipt of an analgesic for treatment of headache and long-bone fractures may be narrowing for African Americans, while no improve-ment was seen for Hispanics.33 Nonetheless, both groups continue to be significantly less likely than Whites to receive any analgesics or opioids for treatment of pain.
Discrimination. Personal bias against racial/ethnic minorities, uncertainty in their interactions with minority patients, beliefs or stereotypes regarding the health behavior of minority patients, and patient response to perceived provider mistreatment or other negative racial experiences all potentially contribute to racial/ethnic disparities in pain management. A number of studies that report racial/ethnic disparities in health care allude to the possible contribution of racial/ethnic discrimination.12,25 As Rust et al., state, overt discrimination is rare.145 Discrimination in the present day in the U.S. more frequently manifests itself covertly. In a recent review of the literature Burgess et al.

207Shavers, Bakos, and Sheppard
describe several ways in which psychological mechanisms result in the unintentional bias in treatment decisions that primarily operate through the use of stereotypes.146
Irrespective of whether or not discrimination is intentional, its impact is the same. According to the Commonwealth Fund’s 2001 Health Care Quality Survey, African Americans, Hispanics, and Asians responded more frequently than Whites that they would have received better care if they belonged to a different racial/ethnic group and that they were judged unfairly or treated with disrespect based on their race/ ethnicity or English-language ability.147 Other studies have produced similar results.148–150 In studies of chronic pain sufferers, Hispanics and African Americans more frequently than Whites reported fear of discrimination based on race/ethnicity when seeking relief for chronic pain123 and more frequently than Whites agreed that ethnicity and culture affected access to health care and pain management.147 There is ample evidence in the literature that racial/ethnic minorities are often less favorably viewed than Whites.151–154 The insidious nature of personal discrimination, however, makes it difficult to assess directly the role it plays in disparities in receipt of adequate pain management. It is worth mentioning that exposure to discrimination can also affect the experience of pain. Anger, helplessness, and depression are frequent consequences of experiences with racial/ethnic discrimination155,156 and have been noted to affect the experience of pain negatively; such reactions to racial/ethnic discrimination might also contribute to racial/ethnic disparities in pain. Other provider-related barriers to adequate pain control include insufficient knowledge about pain management, lack of formal training in pain management, poor skills in pain assessment, judgmental behavior, and lack of experience.98,106,137,157,158
Patient-related barriers to effective pain management. Patient attitudes, beliefs, and behaviors. Patient attitudes, beliefs, and behaviors, as well as access to care, may also contribute to racial/ethnic pain disparities. Racial/ethnic minority patients may more frequently have attitudes and beliefs that interfere with effective pain manage-ment.19,119,124,159 Fear of addiction or medication side effects have been found to be more prevalent among racial/ethnic minorities than Whites and may contribute to refusal or non-adherence with prescribed pain medications or treatment plans. In studies of chronic pain sufferers African American patients more frequently than Whites reported the belief that pain medication could not control,159 and Hispanics and African Americans more frequently than Whites reported fear of addiction to pain relievers.124 Among patients with advance or recurrent cancer 38% of Hispanic and 9% of African American expressed concerns about taking too many analgesics while 27% and 12%, respectively, expressed concerns about the side effects of medications19 or lost effectiveness of prescribed medications. In a survey of terminally ill patients with moderate-severe pain, racial/ethnic minorities more frequently than White patients refused additional pain therapy because of fear of addiction.119
Access to care. Differences in health insurance coverage can greatly influence access to timely and appropriate care.160 Thirty-four percent of Hispanic, 32% of American Indian/Alaska Native, 21% of African American, 19% of Asian/Pacific Islander, and 13% of non-Hispanic White non-elderly adults were estimated to be uninsured in 2005.161 In a recent national telephone survey of Americans who experience chronic pain, 47% of Hispanics, 34% of African Americans, and 32% of non-Hispanic Whites

208 Race, ethnicity, and pain
reported that financial concerns prevented treatment for their pain123 while African Americans more frequently than non-Hispanic Whites reported financial difficulty paying for end-of-life care.162
The health care system may also contribute to racial/ethnic disparities in receipt of effective pain management through barriers to access to appropriate types and doses of medications required for adequate pain control. These include the availability of medi-cines, insurance coverage of pain medications or treatments,163 and regulatory scrutiny of the dispensation of controlled substances. A National Medical Association-issued consensus report focused on the management of pain in underserved populations163 indicates that rising costs have resulted in increases in denials of payment for optimal pain treatment in state-financed Medicaid programs.
Availability of appropriate analgesics in neighborhood pharmacies. Pharmacies utilized by racial/ethnic minority patients may contribute to disparities in pain management due to the failure to stock specific or sufficient supplies of opioid analgesics. A survey of New York City pharmacies found disparities in the sufficiency of the supply of the opioid analgesics recommended as first-line medications for treatment of moderate to severe pain. Only 25% of surveyed pharmacies in neighborhoods in which Whites represented less than 40% of residents were determined to stock adequate supplies of opioids, compared with 72% of pharmacies in neighborhoods in which 80% or more of the residents were White.164 Sixty-six percent of the pharmacies that did not stock any opioids were located in predominantly non-White neighborhoods. In a similar survey of pharmacies in the State of Michigan, 86.9% of the pharmacies in neighbor-hoods where Whites represented 70% or more of the residents had adequate supplies of opioid analgesics compared with 54.2% of the pharmacies in neighborhoods where racial/ethnic minorities represented 70% or more of the residents.154 Several explanations have been provided for the insufficient supply of opioids noted among some community pharmacies. These include perception of a low demand for opioid analgesics, concerns about disposal, fear of robbery, insurance reimbursement-related issues, amount of paperwork involved with filling these prescriptions, and fear of fraud and illicit drug use,164,165 which could result in a DEA investigation.164
Discussion
Race and ethnicity continue to play important roles in the health of populations through association with social, political, and cultural determinants of opportunities, barriers, and exposures relevant to health.1,40 Several types of cancer,166,167 diabetes,168 sickle cell disease,169 HIV infection and AIDS,170 and autoimmune diseases (such as lupus), all of which can be sources of acute and chronic pain, discomfort, and disability168 are more prevalent among African Americans and other racial/ethnic minority populations than among non-Hispanic Whites.
Pain is poorly managed among American patients in general71 but as a number of the reviewed studies show12–33 this is especially true for racial/ethnic minority patients who may also be more susceptible to the physical and psychological disability that is a frequent consequence of poorly controlled and persistent pain. The available litera-ture suggests that these racial/ethnic disparities in pain management operate through

209Shavers, Bakos, and Sheppard
miscommunication and misperceptions about the presence and/or severity of pain. Overall access to health care, access to or utilization of pain specialists, appropriate pain medications and provider assumptions, and judgmental attitudes or beliefs about patient preferences regarding pain treatment or pain tolerances also contribute to disparities in pain management.145
It was not clear from the reviewed literature, however, the exact degree to which under treatment of the pain of racial/ethnic minority patients is a direct result of dis-crimination, stereotyping, lack of empathy, or misperception regarding the presence of pain or pain intensity. The extent to which these factors affect pain management among minority patients is likely exacerbated by the low number of underrepresented racial/ethnic minorities among practicing health care providers.101–106
In general, racial/ethnic concordance has been shown to be positively correlated with patient satisfaction and better health care process outcomes,171 receipt of needed medical care,172 feeling of provider empathy,173 and reduced stress.174 African Americans, Hispanics, and American Indians constitute about 25% of the U.S. population but only 6% of physicians and 9% of nurses.171 Data from the American Community Survey indicate that about 15% of all health care workers and 25% of all physicians and surgeons in the U.S. in 2005 were foreign-born.175 As the U.S. continues to look to foreign-born and foreign-educated workers to fill shortages in the health care workforce, the number of non-concordant cultural interactions in the health care setting is likely to increase, a circumstance that reinforces the importance of incorporating cultural competency training in health care facilities and medical school programs. The increased cultural competency and proficiency of the health care workforce will facilitate the provision of care that is more consistent with patient needs and cultural expectations.60 Weissman et al.58 define a culturally competent individual as one who is aware of “(1) their own cultural and family values; (2) their personal biases and assumptions about individuals with values that differ from theirs; (3) accepts cultural differences between themselves and individual patients; (4) is capable of understanding the dynamics of the differences; (5) and is able to adapt to diversity.”58[p. 715]
Access to care and its relationship to disparities are most frequently discussed in terms of health insurance coverage. The reviewed literature was fairly consistent in the finding of racial/ethnic disparities in physician prescribing patterns, particularly in hospital emergency departments where physicians are required to treat all patients irrespective of insurance status. Approximately 42% of all emergency room visits are pain-related12 and racial/ethnic minorities disproportionately use the emergency depart-ment for primary care176 and for pain treatment.177 Access to appropriate analgesics must be addressed not only in terms of physician prescribing patterns but patient access to specialized pain management services and availability of appropriate analgesics in neighborhood pharmacies. Although practice guidelines exist to assist providers in the management and selection of appropriate analgesics for several chronic diseases and conditions, physician adherence to established guidelines appears to be low.178
Racial/ethnic variation in pain perception and tolerance have been documented in the clinical setting and in anthropological and experimental studies179 but the exact role, if any, these variations play in racial/ethnic disparities in pain management is not clear. Variation in reported pain may be the result of several other factors including

210 Race, ethnicity, and pain
measurement error,36 the manner in which or whether pain is expressed,100 and demo-graphic factors such as age.180
Chronic and unrelieved pain can have an adverse physical and psychological effect on the quality of life of pain sufferers. The consequence of chronic and unrelieved pain include greater disability,28,56,57,180,181 greater interference with performing activities of daily living182 including difficulty in doing normal work,100 and a higher prevalence of depressive symptoms.42,56,57,181 Compared with non-Hispanic Whites, minorities experi-ence more physical impairments56 and have more difficulty performing normal work because of pain.101
The Joint Committee on Accreditation of Healthcare Organizations (JCAHO) pain management guidelines recognize appropriate assessment and management of pain as a patient right,183 as do the American Academy of Pain Medicine (AAPM) and the World Health Organization.184 The JCAHO also requires that health care facilities identify pain in their initial assessment of the patient, document the efficacy of the pain management treatment plan, and educate patients and their families about pain management. Inter-estingly, in a 1998 survey of members of the American Pain Society and the American Academy of Pain, racial/ethnic disparities in pain management were not identified as a major ethical dilemma.185 Thus, there appears to be a need to make health care providers aware of the unnecessary and disproportionate amount of suffering caused by under-treatment of pain among racial/ethnic minority patients and to recognize inadequate treatment for pain as an ethical issue. Incorporating courses in ethics and pain management into medical school and other health professional academic programs could increase knowledge and concern about appropriate methods for managing pain among providers for diverse patient populations. Patient and provider interventions are also needed to ensure that all patients are made aware of and have access to effective and appropriate pain medications and other pain management strategies.186
Notes 1. Smedley BD, Sith AY, Nelson AR, eds. Institute of Medicine, Committee on Under-
standing and Elimination Racial and Ethnic Disparities in Health Care. Unequal treatment: confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press, 2003.
2. Agency for Healthcare Research and Quality. National healthcare disparities report, 2005. Rockville, MD: U.S. Department of Health and Human Services, December 2005. Available at: http://www.ahrq.gov/qual/nhdr05/nhdr05.htm.
3. Ward E, Jemal A, Cokkinides V, et al. Cancer disparities by race/ethnicity and socio-economic status. CA Cancer J Clin. 2004 Mar–Apr;54(2):78–93. Review.
4. Shavers VL, Brown ML. Racial and ethnic disparities in the receipt of cancer treat-ment. J Natl Cancer Inst. 2002 Mar 6;94(5):334–57. Review.
5. Shavers VL, Harlan LC, Winn D, et al. Racial/ethnic patterns of care for cancers of the oral cavity, pharynx, larynx, sinuses, and salivary glands. Cancer Metastasis Rev. 2003 Mar;22(1):25–38.
6. Shavers VL, Brown ML, Klabunde CN, et al. Race/ethnicity and the intensity of medical monitoring under ‘watchful waiting’ for prostate cancer. Med Care. 2004 Mar;42(3):239–50.

211Shavers, Bakos, and Sheppard
7. Green CR, Anderson KO, Baker TA, et al. The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Med. 2003 Sep;4(3):277–94.
8. Senior K. Racial disparities in pain management in the USA. The Lancet Oncology. 2008;9(2):96.
9. Fisher TL, Burnet DL, Huang ES, et al. Cultural leverage: interventions using culture to narrow racial disparities in health care. Med Car Res Rev. 2007 Oct;64(5 Suppl): 243S–282S.
10. Bertakis KD, Azari R, Callahan EJ. Patient pain in primary care: factors that influence physician diagnosis. Ann Fam Med. 2004 May–Jun;2(3):224–30.
11. Gatchel RJ, Peng YB, Peters ML, et al. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007 Jul;133(4):581–624.
12. Pletcher MJ, Kertesz SG, Kohn MA, et al. Trends in opioid prescribing by race/ethnicity for patients seeking care in U.S. emergency departments. JAMA. 2008 Jan 2;299(1):70–8.
13. Chen EH, Shofer FS, Dean AJ, et al. Gender disparity in analgesic treatment of emergency department patients with acute abdominal pain. Acad Emerg Med. 2008 May;15(5):414–8.
14. Epps CD, Ware LJ, Packard A. Ethnic wait time differences in analgesic administra-tion in the emergency department. Pain Manag Nurs. 2008 Mar;9(1):26–32.
15. Cintron A, Morrison RS. Pain and ethnicity in the United States: a systematic review. J Palliat Med. 2006 Dec;9(6):1454–73.
16. Chen I, Kurz J, Pasanen M, et al. Racial differences in opioid use for chronic non-malignant pain. J Gen Intern Med. 2005 Jul;20(7):593–8.
17. Bernabei R, Gambassi G, Lapane K, et al. Management of pain in elderly patients with cancer. JAMA. 1998 Jun 17;279(23):1877–82.
18. Cleeland CS, Gonin R, Hatfield AK, et al. Pain and its treatment in outpatients with metastatic cancer. N Engl J Med. 1994 Mar 3;330(9):592–6.
19. Cleeland CS, Gonin R, Baez L, et al. Pain and treatment of pain in minority patients with cancer: The Eastern Cooperative Oncology Group Minority Outpatient Pain Study. Ann Intern Med. 1997 Nov 1;127(9):813–6.
20. Heins A, Grammas M, Heins JK, et al. Determinants of variation in analgesic and opioid prescribing practice in an emergency department. J Opioid Manag. 2006 Nov–Dec;2(6):335–40.
21. Heins JK, Heins A, Grammas M, et al. Disparities in analgesia and opioid prescrib-ing practices for patients with musculoskeletal pain in the emergency department. J Emerg Nurs. 2006 Jun;32(3):219–24.
22. Tamayo-Sarver JH, Hinze SW, Cydulka RK, et al. Racial and ethnic disparities in emergency department analgesic prescription. Am J Public Health. 2003 Dec;93(12): 2067–73.
23. Todd KH. Ethnicity and analgesic practice. Ann Emerg Med. 2000 Jan;35(1):11–6.24. Todd KH, Samaoo N, Hoffman JR. Ethnicity as a risk factor for inadequate emergency
department analgesia. JAMA. 1993 Mar 24–31;269(12):1537–9.25. Kposowa AJ, Tsunokai GT. Searching for relief: racial differences in treatment of
patients with back pain. Race and Society. 2002;5(2):193–223.26. Won A, Lapane K, Gambassi G, et al. Correlates and management of nonmalignant
pain in the nursing home. SAGE Study Group. Systematic assessment of geriatric drug use via epidemiology . J Am Geriatr Soc. 1999 Aug;47(8):936–42.

212 Race, ethnicity, and pain
27. Lee WW, Burelbach AE, Fosnocht D. Hispanic and non-Hispanic White patient pain management expectations. Am J Emerg Med. 2001 Nov;19(7):549–50.
28. Portenoy RK, Ugarte C, Fuller I, et al. Population-based survey of pain in the United States: differences among White, African American and Hispanic subjects. J Pain. 2004 Aug;5(6):317–28.
29. O’Mara A, Arenella C. Minority representation, prevalence of symptoms and utili-zation of services in a large metropolitan hospice. J Pain Symptom Manage. 2001 Apr;21(4):290–7.
30. Rhodes RL, Teno JM, Connor SR. African American bereaved family members’ percep-tions of the quality of hospice care: lessened disparities, but opportunities to improve remain. J Pain Symptom Manage. 2007 Nov;34(5):472–9. Epub 2007 Sep 27.
31. Bijur P, Bérard A, Nestor J, et al. No racial or ethnic disparitiy in treatment of long-bone fractures. Am J Emerg Med. 2008 Mar;26(3):270–4.
32. Quazi S, Eberhart M, Jacoby J, et al. Are racial disparities in ED analgesia improving? Evidence from a national data base. Am J Emerg Med. 2008 May;26(4):462–4.
33. Tamayo-Sarver JH, Dawson NV, Hinze SW, et al. The effect of race/ethnicity and desirable social characteristics on physicians’ decisions to prescribe opioid analgesics. Acad Emerg Med. 2003 Nov;10(11):1239–48.
34. Thorn BE. Cognitive therapy for chronic pain: a step-by-step guide. New York: The Guilford Press, 2004.
35. Hanson RW. Biopsychosocial model of pain. In: Hanson RW. Self-management of chronic pain. Patient handbook. Chronic Pain Management Program. Long Beach, CA: Long Beach VA Healthcare Center, revised 04/01/03.
36. Linton SJ. Models of pain perception. In: Linton SJ. Understanding pain for better clinical practice. Amsterdam, The Netherlands: Elsevier Health Science Division, 2005.
37. Fillingim RB, Edwards RR. Is self-reported childhood abuse history associated with pain perception among healthy young women and men? Clin J Pain. 2005 Sep–Oct;21(5):387–97.
38. Bates MS, Edwards WT, Anderson KO. Ethnocultural influences on variation in chronic pain perception. Pain. 1993 Jan;52(1):101–12.
39. National Center for Health Statistics. Special feature: pain. In: Health, United States, 2006, with chartbook on trends in the health of Americans. Hyattsville, MD: U.S. Department of Health and Human Services, 2006.
40. International Association for the Study of Pain (IASP). IASP pain terminology. Seattle, WA: IASP, revised November 28–30, 2007. Available at: http://www.iasppain.org/ AM/Template.cfm?Section5Pain_Definitions&Template5/CM/HTMLDisplay.cfm& ContentID51728#Threshold.
41. Edwards RR, Doleys DM, Fillingim RB, et al. Ethnic differences in pain tolerance: clinical implications in chronic pain population. Psychosom Med. 2001 Mar–Apr; 63(2):316–23.
42. Riley JL 3rd, Wade JB, Myers CD, et al. Racial/ethnic differences in the experience of chronic pain. Pain. 2002 Dec;100(3):291–8.
43. McCracken LM, Matthews AK, Tang TS, et al. A comparision of Blacks and Whites seeking treatment for chronic pain. Clin J Pain. 2001 Sep;17(3):249–55.
44. Castel LD, Saville BR, Depuy V, et al. Racial differences in pain during 1 year among women with metastatic breast cancer: a hazards analysis of interval-censored data. Cancer. 2008 Jan 1;112(1):162–70.

213Shavers, Bakos, and Sheppard
45. Campbell CM, France CR, Robinson ME, et al. Ethnic differences in the nociceptive flexion reflex (NFR). Pain. 2008 Jan;134(1–2):91–6. Epub 2007 May 4.
46. Grewen KM, Light KC, Mechlin B, et al. Ethnicity is associated with alterations in oxy tocin relationships to pain sensitivity in women. Ethn Health. 2008 Jun;13(3): 219–41.
47. Mechlin MB, Maizner W, Light KC, et al. African American show alterations in endogenous pain regulatory mechanisms and reduced pain tolerance to experimental pain procedures. Psychosom Med. 2005 Nov–Dec;67(6):948–56.
48. Edwards RR, Fillingim RB. Ethnic differences in thermal pain responses. Psychosom Med. 1999 May–Jun;61(3):346–54.
49. Rahim-Williams FB, Riley JL 3rd, Herrera D, et al. Ethnic identity predicts experimental pain sensitivity in African Americans and Hispanics. Pain. 2007 May;129(1–2):177–84. Epub 2007 Feb 12.
50. Campbell CM, Edwards RR, Fillingim RB. Ethnic differences in responses to multiple experimental pain stimuli. Pain. 2005 Jan;113(1–2):20–6.
51. Weisse CS, Foster KK, Fisher EA. The influence of experimenter gender and race on pain reporting: does racial or gender concordance matter? Pain Med. 2005 Jan–Feb; 6(1):80–7.
52. Klatzkin RR, Mechlin B, Bunevicius R, et al. Race and histories of mood disorders modulate experimental pain tolerance in women. J Pain. 2007 Nov;8(11):861–8. Epub 2007 Jul 23.
53. Sheffield D, Biles PL, Orom H, et al. Race and sex differences in cutaneous pain perception. Psychosom Med. 2000 Jul–Aug;62(4):517–23.
54. Rollman GB. The need for ecological validity in studies of pain and ethnicity. Pain. 2005 Jan;113(1–2):3–4.
55. Feldman JB. The neurobiology of pain, affect and hypnosis. Am J Clin Hypn. 2004 Jan;46(3):187–200.
56. Ndao-Brumblay SK, Green CR. Racial differences in the physical and psychosocial health among black and white women with chronic pain. J Natl Med Assoc. 2005 Oct;97(10):1369–77.
57. Tan G, Jensen MP, Thornby J, et al. Ethnicity, control appraisal, coping and adjust-ment to chronic pain among black and white Americans. Pain Med. 2005 Jan–Feb; 6(1):18–28.
58. Weissman DE, Gordon D, Bidar-Sielaff S. Cultural aspects of pain management. J Palliat Med. 2004 Oct;7(5):715–6.
59. Merriam-Webster. Online dictionary. Accessed September 3, 2008. Available at: http://www.merriam-webster.com/dictionary/culture.
60. Lasch KE. Culture and pain. Seattle, WA: International Association for the Study of Pain, 2002. Available at: http://www.iasp-pain.org/AM/AMTemplate.cfm? Section5Home&TEMPLATE5/CM/ContentDisplay.cfm&CONTENTID57578.
61. Cano A, Mayo A, Ventimiglia M. Coping, pain severity, interference, and disability: the potential mediating and moderating roles of race and education. J Pain. 2006 Jul;7(7):459–68.
62. Jordan MS, Lumley MA, Leisen JC. The relationships of cognitive coping and pain control beliefs to pain and adjustment among African-American and Caucasian women with rheumatoid arthritis. Arthritis Care Res. 1998 Apr;11(2):80–8.
63. Tan G, Jensen MP, Robinson-Whelen S, et al. Measuring control appraisals in chronic pain. J Pain. 2002 Oct:3(5):385–93.

214 Race, ethnicity, and pain
64. Baker TA, Buchanan NT, Corson N. Factors influencing chronic pain intensity in older Black women: examining depression, locus of control, and physical health. J Womens Health (Larchmt). 2008 Jun;17(5):869–78.
65. Bates MS, Rankin-Hill L. Control, culture and chronic pain. Soc Sci Med. 1994 Sep; 39(5):629–45.
66. Crisson JE, Keefe FJ. The relationship of locus of control to pain coping strategies and psychological distress in chronic pain patients. Pain. 1988 Nov;35(2):147–54.
67. Vallerand AH, Hasenau S, Templin T, et al. Disparities between black and white patients with cancer pain: the effect of perception of control over pain. Pain Med. 2005 May–Jun;6(3):242–50.
68. Jones AC, Kwoh CK, Groeneveld PW, et al. Investigating racial differences in coping with chronic osteoarthritis pain. J Cross Cult Gerontology. 2008;23(4):339–47.
69. Hastie BA, Riley JL, Fillingim RB. Ethnic differences and responses to pain in healthy young adults. Pain Med. 2005 Jan–Feb;6(1):61–71.
70. Edwards RR, Moric M, Husfeldt B, et al. Ethnic similarities and differences in the chronic pain experience: a comparison of African American, Hispanic and White patients. Pain Med. 2005 Jan–Feb;6(1):88–98.
71. Anderson KO, Richman SP, Hurley J, et al. Cancer pain management among under-served minority outpatients: percieved needs and barriers to optimal control. Cancer. 2002 Apr 15;94(8):2295–304.
72. Bourjolly JN. Locus of control among black and white women with breast cancer: a preliminary study. J Psychosocial Oncology. 1999;17(1):21–31.
73. Im EO, Liu Y, Kim YH, et al. Asian American cancer patients’ pain experience. Cancer Nurs. 2008 May–Jun;31(3):E17–23.
74. Chen LM, Miakowski C, Dodd M, et al. Concepts within the Chinese culture that influence the cancer pain experience. Cancer Nurs. 2008 Mar–Apr;31(2):103–8.
75. Van Olphen J, Schulz A, Israel B, et al. Religious involvement, social support, and health among African-American women on the east side of Detroit. J Gen Intern Med. 2003 Jul;18(7):549–57.
76. Lujan J, Campbell HB. The role of religion on the health practices of Mexican Ameri-cans. J Religion and Health. 2006;45(2):183–95.
77. Hughes Halbert C, Barg FK, Weathers B, et al. Differences in cultural beliefs and values among African American and European American men with prostate cancer. Cancer Control. 2007 Jul;14(3):277–84.
78. National Hospice and Palliative Care Organization. African American outreach guide. Alexandria, VA: National Hospice and Palliative Care Organization, 2008.
79. Pew Hispanic Center, Pew Forum on Religion and Public Life. Changing faiths: Latinos and the transformation of American religion. Washington, DC: Pew Hispanic Center and Pew Forum on Religion and Public Life, 2009. Available at: http://pewforum.org/newassets/surveys/hispanic/hispanics-religion-07-final-mar08.pdf.
80. Hendrix LR. Heath and health care for American Indian and Alaska Native elders: ethnogeriatric curriculum module. Stanford, CA: Stanford University, 2002. Available at: http://www.stanford.edu/group/ethnoger/americanindian.html.
81. Lee BY, Newberg AB. Religion and health: a review and critical analysis. Zygon. 2005; 40(2):443–68.
82. Bush EG, Rye MS, Brant CR, et al. Religious coping with chronic pain. Appl Psycho-physiol Biofeedback. 1999 Dec;24(4):249–60.
83. Lovering S. Cultural attitudes and beliefs about pain. J Transcult Nurs. 2006 Oct; 17(4):389–95.

215Shavers, Bakos, and Sheppard
84. Im EO, Lim HG, Clark M, et al. African American cancer patients’ pain experience. Cancer Nurs. 2008 Jan–Feb;31(1):38–46.
85. Francoeur RB, Payne R, Raveis VH, et al. Palliative care in the inner city. Patient religious affiliation, underinsurance, and symptom attitude. Cancer. 2007 Jan 15;109 (2 Suppl):425–34.
86. Cotton S, Puchalski CM, Sherman SN, et al. Spirituality and religion in patients with HIV/AIDS. J Gen Intern Med. 2006 Dec;21 Suppl 5:S5–13.
87. Livingston IL, Levine DM, Moore RD. Social integration and black intraracial varia-tion in blood pressure. Ethn Dis. 1991 Spring;1(2):135–49.
88. Levin J, Chatters LM, Taylor RJ. Religion, health and medicine in African Americans: implications for physicians. J Natl Med Assoc. 2005 Feb;97(2):237–49.
89. Harrison MO, Edwards CL, Koenig HG, et al. Religiosity/spirituality and pain in patients with sickle cell disease. J Nerv Ment Dis. 2005 Apr;193(4):250–7.
90. Koenig HG, Pargament KI, Nielsen J. Religious coping and health status in medically ill hospitalized older adults. J Nerv Ment Dis. 1998 Sep;186(9):513–21.
91. Ang DC, Ibrahim SA, Burant CJ, et al. Ethnic differences in the perception of prayer and consideration of joint arthroplasty. Med Care. 2002 Jun;40(6):471–6.
92. Mitchell J, Lannin DR, Matthews HF, et al. Religious beliefs and breast cancer screen-ing. J Womens Health (Larchmt). 2002 Dec;11(10):907–15.
93. Lichtenstein B. Stigma as a barrier to treatment of sexually transmitted infection in the American deep south: issues of race, gender and poverty. Soc Sci Med. 2003 Dec;57(12):2435–45.
94. Satterly L. Guilt, shame, and religious and spiritual pain. Holist Nurs Pract. 2001 Jan; 15(2):30–9.
95. Henderson SW. The unnatural nature of pain. JAMA. 2000 Jan 5;283(1):117.96. Benjamin LJ, Dampier CD, Jacox A, et al. Guideline for the management of acute
and chronic pain in sickle-cell disease. Glenview, IL: American Pain Society, 1999. 97. Staton LJ, Panda M, Chen I, et al. When race matters: disagreement in pain percep-
tion between patients and their physicians in primary care. J Natl Med Assoc. 2007 May;99(5):532–8.
98. Cleeland CS, Gonin R, Hatfield AK, et al. Pain and its treatment in outpatients with metastatic cancer. N Engl J Med. 1994 Mar 3;330(9):592–6.
99. Ibrahim SA, Burant CJ, Mercer MB, et al. Older patients’ perceptions of chronic knee or hip pain: differences by ethnicity and relationship to clinical variables. J Gerontol A Biol Sci Med Sci. 2003 May;58(5):M472–7.
100. Kramer JB, Harker JO, Wong AL. Arthritis beliefs and self-care in an urban American Indian population. Arthritis Rheum. 2002 Dec 15;47(6):588–94.
101. Davitz LL, Davitz JR, Higuchi Y. Cross-cultural inferences of physical pain and psy-chological distress—2. Nurs Times. 1977 Apr 21;73(16):556–8.
102. Im EO, Chee W, Guevara E, et al. Gender and ethnic differences in cancer pain experience: a multiethnic survey in the United States. Nurs Res. 2007 Sep–Oct;56(5):296–306.
103. Hobara M. Beliefs about appropriate pain behavior: cross-cultural and sex differences between Japanese and Euro-Americans. Eur J Pain. 2005 Aug;9(4):389–93.
104. Davitz LL, Davitz JR, Higuchi Y. Cross-cultural inferences of physical pain and psy-chological distress—1. Nurs Times. 1977 Apr 14:73(15):521–3.
105. Brockopp DY, Ryan P, Warden S. Nurses’ willingness to manage the pain of specific groups of patients. Br J Nurs. 2003 Apr 10–23;12(7):409–15.
106. Shin H, Kim K, Young Hee Kim, et al. A comparision of two pain measure for Asian

216 Race, ethnicity, and pain
American cancer patients. West J Nurs Res. 2008 Mar;30(2):181–96. Epub 2007 Jul 2.
107. Taylor LJ, Herr K. Pain intensity assessment: a comparison of selected pain intensity scales for use in cognitively intact and cognitively impaired African American older adults. Pain Manag Nurs. 2003 Jun;4(2):87–95.
108. Ramer L, Richardson JL, Cohen MZ, et al. Multimeasure pain assessment in an ethnically diverse group of patients with cancer. J Transcult Nurs. 1999 Apr;10(2):94–101.
109. Bieri D, Reeve RA, Champion GD, et al. The Faces Pain Scale for the self-assessment of the severity of pain experienced by children: development, initial validation and preliminary investigation for ratio scale properties. Pain. 1990 May;41(2):139–50.
110. Herr KA, Garand L. Assessment and measurement of pain in older adults. Clin Geriatr Med. 2001 Aug;17(3):457–78.
111. Kremer EF, Atkinson JH, Ignelzi RJ. Measurement of pain: patient preference do not confound pain measurement. Pain. 1981 Apr;10(2):241–8.
112. Bond MR, Pilowsky I. Subjective assessment of pain and its relationship to the admin-istration of analgesics in patients with advanced cancer. J Psychosom Res. 1966 Sep; 10(2):203–8.
113. Fishman B, Pasternak S, Wallenstein SL, et al. The Memorial Pain Assessment Card. A valid instrument for the evaluation of cancer pain. Cancer. 1987 Sep 1; 60(5):1151–8.
114. Wong D, Hockenbrerry M, Wilson D, et al. Wong’s essential of pediatric nursing (6th ed.). St. Louis, MO: C.V. Mosby, 2001.
115. Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain. 1975 Sep;1(3):277–99.
116. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994 Mar;23(2):129–38.
117. Kallai I, Burke A, Voss U. The effects of experimenter characteristics on pain reports in women and men. Pain. 2004 Nov;112(1–2):142–7.
118. Gijsbers K, Nicholson F. Experimental pain thresholds influenced by sex of the experimenter. Percept Mot Skills. 2005 Dec;101(3):803–7.
119. Weiss SC, Emanuel LL, Fairclough DL, et al. Understanding the experience of pain in terminally ill patients. Lancet. 2001 Apr 28;357(9265):1311–5.
120. Miner J, Biros MH, Trainor A, et al. Patient and physician perceptions as risk factors for oligoanalgesia: a prospective observational study of the relief of pain in the emer-gency department. Acad Emerg Med. 2006 Feb;13(2):140–6. Epub 2006 Jan 25.
121. Rosenberg ND. Two levels of treatment: pain control lags for minorities and women. Milwaukee Journal Sentinal Online, 2001.
122. Waldrop RD, Mandry C. Health professional perceptions of opioid dependence among patients with pain. Am J Emerg Med. 1995 Sep;13(5):529–31.
123. Shapiro BS, Benjamin LJ, Payne R, et al. Sickle cell-related pain: perceptions of medi-cal practitioners. J Pain Symptom Manage. 1997 Sep;14(3):168–74.
124. Calvillo ER, Flaskerud JH. Evaluation of the pain response by Mexican American and Anglo American women and their nurses. J Adv Nurs. 1993 Mar;18(3):451–9.
125. Lumley MA, Radcliffe AM, Macklem DJ, et al. Alexithymia and pain in three chronic pain samples: comparing Caucasians and African Americans. Pain Med. 2005 May–Jun;6(3):251–61.
126. Nguyen M, Ugarte C, Fuller I, et al. Access to care for chronic pain: racial and ethnic differences. J Pain. 2005 May:6(5):301–14.

217Shavers, Bakos, and Sheppard
127. Nicholson RA, Rooney M, Vo K, et al. Migraine care among different ethnicities: do disparities exist? Headache. 2006 May;46(5):754–65.
128. U.S. Department of Justice. Don’t be scammed by a drug abuser. Springfield, VA: U.S. Department of Justice; Drug Enforcement Administration, 1999 Dec; 1(1). Available at: http://www.deadiversion.usdoj.gov/pubs/brochures/drugabuser.htm.
129. Elander J, Lusher J, Bevan D. Understanding the causes of problematic pain manage-ment in sickle cell disease: evidence that pseudoaddiction plays a more important role than genuine analgesic dependence. J Pain Symptom Manage. 2004 Feb;27(2): 156–69.
130. Elander J, Lusher J, Bevan D, et al. Pain management and symptoms of substance dependence among patients with sickle cell disease. Soc Sci Med. 2003 Nov;57(9): 1683–96.
131. Epstein K, Yuen E, Riggio JM, et al. Utilization of the office, hospital and emergency department for adult sickle cell patients: a five-year study. J Natl Med Assoc. 2006 Jul;98(7):1109–13.
132. Schulman KA, Mehta SS, Gersh BJ, et al. Study of Hypertensive Prescribing Practices (SHyPP): a national survey of primary care physicians. J Clin Hypertens (Greenwich). 1999 Oct;1(2):106–14.
133. Bhamb B, Brown D, Hariharan J, et al. Survey of select practice behavior by primary care physicians and the use of opioids for chronic pain. Curr Med Res Opin. 2006 Sep;22(9):1859–65.
134. Potter M, Schafer S, Gonzalez-Mendez E, et al. Opioids for chronic nonmalignant pain. Attitudes and practices primary care physicians in the UCSF/Stanford Collab-orative Research Network. University of California, San Francisco. J Fam Pract. 2001 Feb;50(2):145–51.
135. Kaufman M. Worried pain doctors decry prosecutions. Washington Post. Decem-ber 29, 2003. Available at: http://www.washingtonpost.com/ac2/wp-dyn/A37015-2003Dec28?language5printer.
136. Meadows M. New prescription drug safety plan. The Bush Administration has announced a comprehensive plan to improve prescription drug safety, citing a sig-nificant increase in the nonmedical use of prescription drugs in recent years. FDA Consumer Magazine, 2004 May–June; Vol. 38. Washington, DC: U.S. Food and Drug Administration, U.S. Department of Health and Human Services.
137. Green CR, Wheeler JR, Merchant B, et al. Analysis of the physician variable in pain management. Pain Med. 2001 Dec;2(4):317–27.
138. Morley-Forster PK, Clark AJ, Speechley M, et al. Attitudes toward opioid use for chronic pain: a Canadian physician survey. Pain Res Manag. 2003 Winter;8(4):189–94.
139. Von Roenn JH, Cleeland CS, Gonin R, et al. Physician attitudes and practice in cancer pain management. A survey from the Eastern Cooperative Oncology Group. Ann Internal Med. 1993 Jul 15;119(2):121–6.
140. Stover BD, Turner JA, Franklin G, et al. Factors associated with early opioid prescrip-tion among workers with low back injuries. J Pain. 2006 Oct;7(10):718–25.
141. Olsen Y, Daumit G, Ford D. Opioid prescriptions by U.S. primary care physicians from 1992–2001. J Pain. 2006;7(4):225–35.
142. Dominick KL, Bosworth HB, Dudley TK, et al. Patterns of opioid analgesic prescrip-tion among patients with osteoarthritis. J Pain Palliat Care Pharmacother. 2004; 18(1):31–46.
143. Yen K, Kim M, Stremski ES, et al. Effect of ethnicity and race on the use of pain

218 Race, ethnicity, and pain
medications in children with long bone fractures in the emergency department. Ann Emerg Med. 2003 Jul;42(1):41–7.
144. Fuentes EF, Kohn MA, Neighbor ML. Lack of association between patient ethnicity or race and fracture analgesia. Acad Emerg Med. 2002 Sep;9(9):910–5.
145. Rust G, Nembhard WN, Nichols M, et al. Racial and ethnic disparities in the provision of epidural analgesia to Georgia Medicaid beneficiaries during labor and delivery. Am J Obstet Gynecol. 2004 Aug;191(2):456–62.
146. Burgess DJ, van Ryn M, Crowley-Matoka M, et al. Understanding the provider con-tribution to race/ethnicity disparities in pain treatment: insights from dual process models of stereotyping. Pain Med. 2006 Mar–Apr;7(2):119–34.
147. Johnson RL, Saha S, Arbelaez JJ, et al. Racial and ethnic differences in patient per-ceptions of bias and cultural competence in health care. J Gen Internal Med. 2004 Feb;19(2):101–10.
148. Hobson WD. Racial discrimination in health care interview project. Seattle, WA: Seattle and King County Department of Public Health, 2001. Available at: http://www.metrokc.gov/HEALTH/reports/discriminationinhealthcare.pdf.
149. Bird ST, Bogart LM. Perceived race-based and socioeconomic status (SES)-based discrimination in interactions with health care providers. Ethn Dis. 2001 Autumn; 11(3):554–63.
150. Blanchard J, Lurie N. R-E-S-P-E-C-T: patient reports of disrespect in the health care setting and its impact on care. J Fam Pract. 2004 Sep;53(9):721–30.
151. van Ryn M, Fu SS. Paved with good intentions: do public health and human service providers contribute to racial/ethnic disparities in health? Am J Public Health. 2003 Feb;93(2):248–55.
152. Rathore SS, Lenert LA, Weinfurt KP, et al. The effects of patient sex and race on medical student’s ratings of quality of life. Am J Med. 2000 May;108(7):561–6.
153. van Ryn M. Research on provider contribution to race/ethnicity disparities in medical care. Med Care. 2002 Jan;40(1 Suppl):l140–151.
154. Einbinder LC, Schulman KA. The effect of race of the referral process for invasive cardiac procedures. Med Care Res Rev. 2000;57 Suppl 1:162–80.
155. Vines AI, Baird DD, McNeilly M, et al. Social correlates of the chronic stress of per-ceived racism among Black women. Ethn Dis. 2006 Winter;16(1):101–7.
156. Broudy R, Brondolo E, Coakley V, et al. Perceived ethnic discrimination in relation to daily moods and negative social interactions. J Behav Med. 2007 Feb;30(1):31–43. Epub 2006 Nov 8.
157. Watt-Watson J, Stevens B, Garfinkel P, et al. Relationship between nurses’ pain knowl-edge and pain management outcomes for their postoperative cardiac patients. J Adv Nurs. 2001 Nov;36(4):535–45.
158. Labbe E, Herbert D, Haynes J. Physicians’ attitude and practices in sickle cell disease pain management. J Palliat Care. 2005 Winter;21(4):246–51.
159. Green CR, Baker TA, Ndao-Brumblay SK. Patient attitudes regarding healthcare utili-zation and referral: a descriptive comparison in African and Caucasian Americans with chronic pain. J Natl Med Assoc. 2004 Jan;96(1):31–42.
160. Hadley J. Insurance coverage, medical care use, and short-term health changes fol-lowing an unintentional injury or the onset of a chronic condition. JAMA. 2007 Mar 14;297(10):1073–84.
161. James C, Thomas M, Lillie-Blanton M, et al. Key facts: race, ethnicity and medical care. Washington, DC: The Henry J. Kaiser Family Foundation, 2007. Available at: http://www.kff.org/minorityhealth/upload/6069-02.pdf.

219Shavers, Bakos, and Sheppard
162. Welch LC, Teno JM, Mor V. End-of-life care in black and white: race matters for medical care of dying patients and their families. J Am Geriatr Soc. 2005 Jul;53(7):1145–53.
163. Primm BJ, Perez L, Dennis GC, et al. Managing pain: the challenge in underserved populations: appropriate use versus abuse and diversion. J Natl Med Assoc. 2004 Sep; 96(9):1152–61.
164. Morrison RS, Wallenstein S, Natale DK, et al. “We don’t carry that”—failure of phar-macies in predominantly nonWhite neighborhoods to stock opioid analgesics. N Engl J Med. 2000 Apr 6;342(14):1023–6.
165. Green CR, Ndao-Brumblay SK, West B, et al. Differences in prescription opioid analgesia availability: comparing minority and White pharmacies across Michigan. J Pain. 2005 Oct;6(10):689–99.
166. American Cancer Society. Cancer facts and figures 2009. Atlanta, GA: American Cancer Society, 2009. Available at: http://www.cancer.org/downloads/STT/500809web .pdf.
167. Horner MJ, Ries LAG, Krapcho M, et al. Revision history of the SEER Cancer Statistics Review, 1975–2006. Bethesda, MD: National Cancer Institute. Available at: http://seer .cancer.gov/csr/1975_2006/revisions.html.
168. National Heart Lung and Blood Institute. Disease and conditions index: who is at risk for sickle cell anemia? Bethesda, MD: National Heart Lung and Blood Institute, 2008. Available at: http://www.nhlbi.nih.gov/health/dci/Diseases/Sca/SCA_WhoIsAtRisk .html.
169. Centers for Disease Control and Prevention. HIV/AIDS surveillance report 2005: vol. 17. Atlanta, GA: Centers for Disease Control and Prevention, 2006. Available at: http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2005report/pdf/2005 SurveillanceReport.pdf.
170. Centers for Disease Control and Prevention. Chronic disease overview. Atlanta, GA: Centers for Disease Control and Prevention, 2005. Available at: http://www.cdc.gov/NCCdphp/overview_text.htm.
171. Cooper LA, Powe NR. Disparities in patient experiences, health care processes and outcomes: the role of patient-provider racial, ethnic and language concordance. New York: The Commonwealth Fund, 2004 Jul. Available at: http://www.common wealthfund.org/Content/Publications/Fund-Reports/2004/Jul/Disparities-in-Patient-Experiences—Health-Care-Processes—and-Outcomes—The-Role-of-Patient-Provide .aspx.
172. Saha S, Komaromy M, Koepsell TD, et al. Patient-physician racial concordance and the perceived quality and use of health care. Arch Intern Med. 1999 May;159(9): 997–1004.
173. Garcia JA, Paterniti DA, Romano PS, et al. Patient preference for physician character-istics in university-based primary care clinics. Ethn Dis. 2003 Spring;13(2):259–67.
174. Bates MS, Rankin-Hill L, Sanchez-Ayendez M. The effects of the cultural context of health care on treatment of and response to chronic pain and illness. Soc Sci Med. 1997 Nov;45(9):1433–47.
175 Clearfield E, Batalova J. U.S. in focus: foreign-born health-care workers in the United States. Washington, DC: Migration Policy Institute, 2007. Available at: http://www .migrationinformation.org/Usfocus/print.cfm?ID5583.
176. Hong R, Baumann BM, Boudreaux ED. The emergency department for routine healthcare: race/ethnicity, socioeconomic status, and perceptual factors. J Emerg Med. 2007 Feb;32(2):149–58.
220 Race, ethnicity, and pain
177. Blake VA, Allegrante JP, Robbins L, et al. Racial differences in social network experi-ence and perceptions of benefit of arthritis treatments among New York City Medi-care beneficiaries with self-reported hip and knee pain. Arthritis Rheum. 2002 Aug; 47(4):366–71.
178. National Pharmaceutical Council, Joint Commission on Accreditation of Healthcare Organizations. Pain: current understanding of assessment, management and treat-ments. Reston, VA: National Pharmaceutical Council, 2001. Available at: http://www .scribd.com/doc/7563477/National-pharmaceutical-council-NPC-npcnow.
179. Bonham VL. Race, ethnicity, and pain treatment: striving to understand the causes and solutions to the disparities in pain treatment. J Law, Med Ethics. 2001 Spring; 29(1):52–68.
180. Baker TA, Green CR. Intrarace differences among black and white Americans pre-senting for chronic pain management: the influence of age, physical health, and psychosocial factors. Pain Med. 2005 Jan–Feb;6(1):29–38.
181. Green CR, Baker TA, Smith EM, et al. The effect of race in older adults presenting for chronic pain management: a comparative study of young Black and White Americans. J Pain. 2003;4(2):82–90.
182. Ruehlman LS, Karoly P, Newton C. Comparing the experiential and psychosocial dimensions of chronic pain in African Americans and Caucasians: findings from a national community sample. Pain Med. 2005 Jan–Feb;6(1):49–60.
183. Gilbert HC, Green CR. JCAHO’s pain initiative: new opportunities/new risks. Park Ridge, IL: American Society of Anesthesiologists, 2000 Nov. Available at: http://www .asahq.org/Newsletters/2000/11_00/gilbert.htm.
184. Green CR, Todd KH, Lebovits A, et al. Disparities in pain: ethical issues. Pain Med. 2006 Nov–Dec;7(6):530–3.
185. Ferrell BR, Novy D, Sullivan MD, et al. Ethical dilemmas in pain management. J Pain. 2001 Jun;2(3):171–80.
186. Green CR, Tait RC, Gallagher RM. The unequal burden of pain: disparities and dif-ferences. Pain Med. 2005;6:1–2.