Quality of Life of Persons With Lower-Limb Amputation During Rehabilitation and at 3-Month Follow-Up
12
ORIGINAL ARTICLE Quality of Life of Persons With Lower-Limb Amputation During Rehabilitation and at 3-Month Follow-Up Diana Zidarov, PT, MSc, Bonnie Swaine, PT, PhD, Christiane Gauthier-Gagnon, PT, MSc ABSTRACT. Zidarov D, Swaine B, Gauthier-Gagnon C. Quality of life of persons with lower-limb amputation during rehabilitation and at 3-month follow-up. Arch Phys Med Re- habil 2009;90:634-45. Objective: To describe and compare the quality of life (QOL) of persons with lower-limb amputation (LLA) at ad- mission (T1), discharge (T2), and 3 months after rehabilitation discharge (T3) and to explore the relationships between QOL and demographic and clinical variables including body image. Design: Longitudinal case series. Setting: Inpatient rehabilitation facility. Participants: Consecutive sample of 19 unilateral persons with LLA (14 men, mean age, 53.414.6y). Intervention: Interdisciplinary rehabilitation. Main Outcome Measures: Generic and specific QOL mea- sures and perception of body image at T1, T2, and T3. Results: Subjective QOL was relatively high at T1, T2, and T3 (0.87/2, 1.1/2, and 1.0/2, respectively) except for items related to physical functioning. There was no significant change over time for all but 1 QOL satisfaction measure (ability to go outside, P.024). Prosthesis-related QOL was high at discharge and follow-up. Body-image disturbances were absent over the study period. QOL satisfaction and pros- thesis satisfaction were strongly related to lower-limb pain and psychosocial factors (eg, body image). Conclusions: QOL of persons with LLA was high and remained relatively stable during inpatient rehabilitation and 3 months after discharge. Key Words: Amputation; Body image; Quality of life; Rehabilitation. © 2009 by the American Congress of Rehabilitation Medicine L OWER-LIMB AMPUTATION is a permanent surgical procedure that has important functional, psychologic, and social sequelae that can influence the QOL of the person with amputation. 1,2 Although rehabilitation aims to address these sequelae, 3 measuring the effect of these interventions on reha- bilitation outcomes of people who have had an LLA remains a challenge. The selected outcomes must be related to rehabili- tation goals that are specific to each person and associated with premorbid function. 1,4,5 There is currently no consensus on which outcomes to measure or how to measure them. 4,6,7 This is surprising given that amputee rehabilitation programs have common goals to improve mobility and functioning through prosthetic fitting to assist community reintegration and to ulti- mately improve the overall QOL of persons with an LLA. QOL is increasingly used to measure outcome in rehabilita- tion. 8-12 QOL is complex, and there is no consensus regarding a single definition or about the domains that constitute QOL. 10,13,14 There are 2 aspects that are included in almost all definitions: multidimensionality and subjectivity of QOL. Mul- tidimensionality is taken into account in the numerous tools available to assess QOL because they cover various domains. These can include health status; physical, social, mental, and emotional function; pain; relationships; life satisfaction; and well-being. 9,10,13,15 The subjective aspect of QOL reflects the person’s own perceptions based on his/her education, life ex- periences, values, expectations, and environment in which the person lives. 11,16,17 Health-related QOL can be measured with generic or con- dition-specific instruments. Generic instruments are applicable to a wide range of patient populations including those without health conditions. 13 An advantage resulting from this broad applicability is that generic questionnaires can provide popu- lations norms or benchmarks of healthy populations to which populations with a specific condition can be compared. 13 Fur- thermore, they also permit comparisons across populations with different conditions and across interventions. 13 However, because they assess the broadest possible range of QOL di- mensions, they are less sensitive to change and also to specific issues of concern to populations with a specific condition (eg, persons with an LLA). 13,18 In contrast, specific instruments are particular to a certain population and, as such, focus on areas of interest relevant for that population and may be closer to clinicians’ interests and interventions. 18 One disadvantage of condition-specific measures is that they do not allow for a comparison of people with disabilities to a general healthy population or among groups with different impairments. 12,18 Another disadvantage is that because of their narrower focus, From the School of Rehabilitation, University of Montreal (Zidarov, Swaine, Gauthier-Gagnon); Montreal Rehabilitation Institute (Zidarov, Swaine); and Center for Interdisciplinary Research in Rehabilitation of Metropolitan Montreal (Swaine), Montreal, QC, Canada. Supported by the Montreal Rehabilitation Institute Foundation, the Fonds de la recherche en santé du Québec, the Ordre professionnel des physiothérapeutes du Québec, and the Faculté des études supérieures of the Université de Montréal. No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit on the authors or on any organi- zation with which the authors are associated. Correspondence to Diana Zidarov, PT, MSc, 3600 Av Darlington, Montreal, QC, Canada, H3S 2J4, e-mail: [email protected]. Reprints not available from the author. 0003-9993/09/9004-00905$36.00/0 doi:10.1016/j.apmr.2008.11.003 List of Abbreviations ABIS Amputee Body Image Scale ADLs activities of daily living ANOVA analysis of variance LLA lower-limb amputation NHP Nottingham Health Profile PEQ Prosthesis Evaluation Questionnaire QOL quality of life SF-36 Medical Outcomes Study 36-Item Short-Form Health Survey SQLP Subjective Quality of Life Profile TF transfemoral TT transtibial VAS visual analog scale 634 Arch Phys Med Rehabil Vol 90, April 2009
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Quality of Life of Persons With Lower-Limb Amputation During Rehabilitation and at 3-Month Follow-Up

O
QDD
Qrh
(mda
w
s
Trc(hwtp
rm
R
M
Lsasbct
GfM
rQ
sz
C
634
A
RIGINAL ARTICLE
uality of Life of Persons With Lower-Limb Amputationuring Rehabilitation and at 3-Month Follow-Up
iana Zidarov, PT, MSc, Bonnie Swaine, PT, PhD, Christiane Gauthier-Gagnon, PT, MSc
pwicpm
taQdtaTewppp
dthalptwbmippicccpA
ABSTRACT. Zidarov D, Swaine B, Gauthier-Gagnon C.uality of life of persons with lower-limb amputation during
ehabilitation and at 3-month follow-up. Arch Phys Med Re-abil 2009;90:634-45.
Objective: To describe and compare the quality of lifeQOL) of persons with lower-limb amputation (LLA) at ad-ission (T1), discharge (T2), and 3 months after rehabilitation
ischarge (T3) and to explore the relationships between QOLnd demographic and clinical variables including body image.
Design: Longitudinal case series.Setting: Inpatient rehabilitation facility.Participants: Consecutive sample of 19 unilateral persons
ith LLA (14 men, mean age, 53.4�14.6y).Intervention: Interdisciplinary rehabilitation.Main Outcome Measures: Generic and specific QOL mea-
ures and perception of body image at T1, T2, and T3.Results: Subjective QOL was relatively high at T1, T2, and
3 (0.87/2, 1.1/2, and 1.0/2, respectively) except for itemselated to physical functioning. There was no significanthange over time for all but 1 QOL satisfaction measureability to go outside, P�.024). Prosthesis-related QOL wasigh at discharge and follow-up. Body-image disturbancesere absent over the study period. QOL satisfaction and pros-
hesis satisfaction were strongly related to lower-limb pain andsychosocial factors (eg, body image).Conclusions: QOL of persons with LLA was high and
emained relatively stable during inpatient rehabilitation and 3onths after discharge.Key Words: Amputation; Body image; Quality of life;
ehabilitation.© 2009 by the American Congress of Rehabilitationedicine
OWER-LIMB AMPUTATION is a permanent surgicalprocedure that has important functional, psychologic, and
ocial sequelae that can influence the QOL of the person withmputation.1,2 Although rehabilitation aims to address theseequelae,3 measuring the effect of these interventions on reha-ilitation outcomes of people who have had an LLA remains ahallenge. The selected outcomes must be related to rehabili-ation goals that are specific to each person and associated with
From the School of Rehabilitation, University of Montreal (Zidarov, Swaine,authier-Gagnon); Montreal Rehabilitation Institute (Zidarov, Swaine); and Center
or Interdisciplinary Research in Rehabilitation of Metropolitan Montreal (Swaine),ontreal, QC, Canada.Supported by the Montreal Rehabilitation Institute Foundation, the Fonds de la
echerche en santé du Québec, the Ordre professionnel des physiothérapeutes duuébec, and the Faculté des études supérieures of the Université de Montréal.No commercial party having a direct financial interest in the results of the research
upporting this article has or will confer a benefit on the authors or on any organi-ation with which the authors are associated.
Correspondence to Diana Zidarov, PT, MSc, 3600 Av Darlington, Montreal, QC,anada, H3S 2J4, e-mail: [email protected]. Reprints not available from the author.
0003-9993/09/9004-00905$36.00/0doi:10.1016/j.apmr.2008.11.003
rch Phys Med Rehabil Vol 90, April 2009
remorbid function.1,4,5 There is currently no consensus onhich outcomes to measure or how to measure them.4,6,7 This
s surprising given that amputee rehabilitation programs haveommon goals to improve mobility and functioning throughrosthetic fitting to assist community reintegration and to ulti-ately improve the overall QOL of persons with an LLA.QOL is increasingly used to measure outcome in rehabilita-
ion.8-12 QOL is complex, and there is no consensus regardingsingle definition or about the domains that constitute
OL.10,13,14 There are 2 aspects that are included in almost allefinitions: multidimensionality and subjectivity of QOL. Mul-idimensionality is taken into account in the numerous toolsvailable to assess QOL because they cover various domains.hese can include health status; physical, social, mental, andmotional function; pain; relationships; life satisfaction; andell-being.9,10,13,15 The subjective aspect of QOL reflects theerson’s own perceptions based on his/her education, life ex-eriences, values, expectations, and environment in which theerson lives.11,16,17
Health-related QOL can be measured with generic or con-ition-specific instruments. Generic instruments are applicableo a wide range of patient populations including those withoutealth conditions.13 An advantage resulting from this broadpplicability is that generic questionnaires can provide popu-ations norms or benchmarks of healthy populations to whichopulations with a specific condition can be compared.13 Fur-hermore, they also permit comparisons across populationsith different conditions and across interventions.13 However,ecause they assess the broadest possible range of QOL di-ensions, they are less sensitive to change and also to specific
ssues of concern to populations with a specific condition (eg,ersons with an LLA).13,18 In contrast, specific instruments arearticular to a certain population and, as such, focus on areas ofnterest relevant for that population and may be closer tolinicians’ interests and interventions.18 One disadvantage ofondition-specific measures is that they do not allow for aomparison of people with disabilities to a general healthyopulation or among groups with different impairments.12,18
nother disadvantage is that because of their narrower focus,
List of Abbreviations
ABIS Amputee Body Image ScaleADLs activities of daily livingANOVA analysis of varianceLLA lower-limb amputationNHP Nottingham Health ProfilePEQ Prosthesis Evaluation QuestionnaireQOL quality of lifeSF-36 Medical Outcomes Study 36-Item Short-Form
Health SurveySQLP Subjective Quality of Life ProfileTF transfemoralTT transtibial
VAS visual analog scale
tdmatpatcOwmLQPc
wpmpctmpotwchwStswtfsiiataft
bfpstowhQobQ
taFbspi
wwismptkawi
t3ri
S
sMt2tatapamt
hcEqfmslt
CRs
P
at(edptplco(
635QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
hey may miss measuring an unexpected finding (eg, sexualissatisfaction, financial problems). Because of the comple-entarities and the different level of detail assessed by generic
nd specific instruments, some believe that it is best to use botho capture the majority of the dimensions of QOL.13 Withersons with an LLA, the majority of outcome studies to dateddress mobility, functional abilities, and use of prosthesis ashe most important measures to evaluate rehabilitation out-omes4,19 despite the growing interest in patients’ QOL.10
utcomes studies addressing health-related QOL of personsith an LLA are relatively recent.20-27 These studies have usedostly generic tools such as the Reintegration to Normaliving,28 the NHP,29 and the SF-36.30 In recent years, specificOL tools, such as the PEQ31 and the Trinity Amputation androsthesis Experiences Scales,24 have been developed specifi-ally for use with people with amputation.
Nissen and Newman22 identified areas that were difficultith regards to the reintegration to normal living of 42 elderlyersons with an LLA amputated several years previously. Theost negatively affected areas in order of importance were
articipation in recreational activities, work activities, andommunity mobility. Another study using the NHP to measurehe perceived health status of persons with an LLA (n�130,edian time interval�38 months after limb amputation for
eripheral arterial disease) found reintegration to be poor sec-ndary to restricted mobility.32 Van der Schans et al20 inves-igated potential determinants of health-related QOL of personsith an LLA (n�437, median time since amputation�10y) and
oncluded that persons with phantom limb pain have poorerealth-related QOL, as measured with the SF-36, than personsithout pain. Furthermore, 28.7% of the variance of the meanF-36 score was explained by 3 determinants: walking dis-
ance, stump pain, and diabetes. A recent study by Asano et al33
tudied predictors of QOL with a large sample of 415 personsith a unilateral LLA (0 to �14y since amputation). Symp-
oms of depression accounted for 30% of the variance of QOLollowed by prosthetic mobility (6% of the variance) and socialupport (2% of the variance). This study underscored themportance of psychosocial adaptation after an LLA and itsmpact on QOL. In contrast, Harness and Pinzur23 when usingcondition-specific measure, the PEQ, with a sample of non-
raumatic TT persons with amputation (on average 38.1mofter using their prosthesis), showed that the mobility andunctional domains scores of the PEQ were lower than those ofhe psychosocial domains.
A few studies have investigated the relationships betweenody image of people with LLAs and QOL. Rybarczyk et al34
ound that 53% of the variance of QOL was predicted by theerson’s perceived body image, social stigma, health, and timeince amputation. Breakey35 developed the ABIS and foundhat the body image and psychosocial well-being (a componentf QOL) of persons with an LLA was significantly correlatedith QOL. The more negative the person’s perception ofis/her body image, the less satisfied he/she was with his/herOL. Similar results were obtained by Miller36 with a samplef 51 vascular persons with an LLA; a person’s perception ofody image and self esteem predicted 63% of the variance ofOL.Although these studies have improved our understanding of
he QOL of persons with an LLA, they were all cross-sectionalnd conducted several months or years after the amputation.urthermore, they used either a generic or specific tool, neveroth, except to validate a newly developed specific tool. Con-equently, not all dimensions that may be of importance for aerson with an LLA were assessed in a given period. Rehabil-
tation interventions have a holistic approach of the person, ehich all aim to impact on the QOL of patients. To determinehether this aim is attained, one must assess QOL at rehabil-
tation discharge. Moreover, QOL is an especially cogent mea-ure of the performance of health care because it incorporatesultiple domains that are addressed during the rehabilitation
rocess, and, most of all, it involves the patient’s own percep-ion of his/her accomplishments during the process.12 To ournowledge, no study has yet investigated, using both genericnd specific measurement tools, the overall QOL of personsith an LLA and whether it changes during and after rehabil-
tation.The purposes of this study were to (1) describe and compare
he QOL of persons with an LLA at admission, discharge, andmonths after rehabilitation discharge and (2) explore the
elationships between QOL and certain demographic and clin-cal variables, including body image.
METHODS
tudy SampleThis exploratory longitudinal study was conducted with per-
ons with an LLA who were consecutively admitted to theontreal Rehabilitation Institute in Quebec, Canada, for inpa-
ient rehabilitation between September 2005 and December006. Patients received an individualized program from a mul-idisciplinary team. This program includes daily physical ther-py and occupational therapy for preprosthetic and prostheticraining and psychologic support to the patient and their family;dditional family support and sociovocational orientation isrovided by a social worker, and leisure activities are offered innd out of the rehabilitation center. Once a week, all patientseet with their rehabilitation team to set rehabilitation objec-
ives for the upcoming week.Inclusion criteria consisted of (1) being 18 years or older and
aving a unilateral TT or TF amputation from any cause exceptongenital, (2) having sufficient cognitive skills and French ornglish comprehension to be able to accurately respond touestionnaires, and (3) being admitted for a first rehabilitationor prosthetic training. The last criterion was chosen to mini-ize the effects of confounding variables (eg, multiple admis-
ions to rehabilitation for subsequent amputation of the residualimb) so the results observed were specific to a first rehabili-ation stay.
The research protocol was approved by the Research Ethicsommittee of the Center for Interdisciplinary Research inehabilitation of which the Montreal Institute is a site. Subjects
igned an informed consent form before participating.
rocedureData were collected at 3 times: during the 7 days after
dmission to the inpatient rehabilitation program (T1), duringhe 7 days before discharge (T2), and at the 3-month follow-upT3). All data were collected by using questionnaires that wereither self-administered or administered during the interviewepending on the participant’s ability to answer (eg, no visualroblems or difficulty in understanding certain questions). In-erviews were conducted by the same evaluator (D.Z.), a seniorhysical therapist with over 10 years of experience. The fol-owing information was extracted from the patient’s medicalhart: age, highest level of completed education, level and datef amputation, duration of prosthetic training, length of stayrehabilitation), associated medical conditions, and marital and
mployment status at the time of amputation.Arch Phys Med Rehabil Vol 90, April 2009

M
swFRafc(ttt2acsaesovQw��
awcepfwisupcvmg
up8bpsttosPctttc
uiarr
tteab
strcii�tAi
D
safeeAWpmefuaarcvnp
D
dcaEataesm(a42adTa
S
636 QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
A
easurement InstrumentsSubjective Quality of Life Profile. General QOL was mea-
ured with a generic tool, the SQLP.16,37,38 This questionnaireas selected, in part, because it was originally developed inrench and the majority of patients admitted to the Montrealehabilitation Institute are French speaking. Furthermore, itllows respondents to report their level of satisfaction (satis-action scale) with regards to each domain evaluated; to indi-ate the importance of each item and domains in their lifeimportance scale); and, most of all, to express the changeshey expect to occur over time with regards to their rehabili-ation services (anticipated change scale). Finally, this ques-ionnaire has the advantage of being flexible in that it contains7 core items as well as optional items (n�54) that can bedded depending on the population studied. The core itemsover 4 domains: functional life (physical and mental health),ocial life (relationships, social roles), material life (income),nd spiritual life (religious experiences, ability to think, futurexpectations). The SQLP was used and validated with healthyubjects and with populations with psychiatric or somatic dis-rders39 but never with persons with an LLA. The convergentalidity between the SQLP and the World Health Organizationuality of Life questionnaire was shown (r�.45).40 The SQLPas shown to have high internal consistency (Cronbach�0.9) and moderate to fair test-retest reliability (Spearmanrange, 0.3–0.5, P�.005).37
In the present study, we collected data for the 27 core items,nd 9 additional questions from the optional list of the SQLPere added based on both our literature review and the authors’
linical experience. Participants were questioned about theiryesight, hearing, body weight, overall physical aspect, inde-endence, future, relations and dependency on family, andeeling different from other people. For each item, 3 measuresere obtained. The respondents rated their satisfaction/dissat-
sfaction level (–2, very unsatisfied; 0, indifference; 2, veryatisfied). Next, they indicated the importance of each item (0,nimportant to 3, extremely important), and, finally, they re-orted the change they expected during their rehabilitation (–2,hange very unfavorably; 0, no change expected; 2, changeery favorably). Results are presented in the form of profiles; aean score is calculated for each item and for each of the 3
lobal scores.Prosthesis Evaluation Questionnaire. The PEQ31 was
sed to evaluate the function of a lower-limb prosthesis and therosthesis-related QOL of the persons with an LLA. It contains2 items grouped into 9 validated independent subscales: am-ulation, appearance of the prosthesis, residual limb health,erceived responses, frustration, social burden, prostheticounds, utility, and well-being. It also includes additional ques-ions (not contained in the subscales) about satisfaction withhe prosthesis, pain, transfers, prosthetic care, self-efficacy, andther aspects of the prosthesis. The PEQ subscales and theubscales of the SF-36, the Sickness Impact Profile, and therofile of Mood States–short form were found to be signifi-antly correlated (r�.49–.61).31 The PEQ has also shown goodo excellent internal consistency (Cronbach � varies from .73o .89 for each of the 9 subscales) and moderate to excellentest-retest reliability for a mean retest period of 30 days (intra-lass correlation coefficient�.56–.90, for the 9 subscales).31
In this study, we used only 4 of the 9 subscales: appearance,tility, sounds, and well-being. The questions addressing sat-sfaction with prosthesis (n�1) and self-efficacy (n�3) werelso included for a total of 21 items. Patients indicated theiresponses on a VAS (10-cm line) with the 2 boundaries rep-
esenting extremes of possible answers (eg, never or all of the srch Phys Med Rehabil Vol 90, April 2009
ime). A score for each subscale was calculated by computinghe arithmetic mean of all the questions that were applicable toach respondent within the particular subscale. The PEQ wasdministrated only at discharge and at the 3-month follow-upecause patients do not have their prosthesis on admission.Amputee Body Image Scale. The ABIS35 assessed per-
ons’ perception of their body image with and without pros-hesis. It contains 20 items measured with a 5-level Likert scaleanging from none of the time to all of the time. A total scorean be calculated that ranges from 0 to 100, where low scoresndicate the relative absence of body image concern. Thenternal consistency was shown to be high (Cronbach�.88).35 Although there is a lack of information regarding the
ool’s other psychometric properties, to our knowledge, theBIS is the only tool developed to specifically address body
mage with persons with an LLA.
ata AnalysisDescriptive statistics were computed for the questionnaires
cores as well as for the sociodemographic and clinical char-cteristics. Mean and SD were used for the continuous data andrequencies and percentages for the categoric data. The differ-nces between the means of each item of the SQLP at the 3valuation times were tested with a 1-way repeated-measuresNOVA with time of measurement as a within-subjects factor.hen significant results were obtained (P�.05), post hoc com-
arisons were performed by using the Bonferroni correction forultiple comparisons. Paired t tests were used to test differ-
nces in means between discharge and the 3-month follow-upor the PEQ and ABIS questionnaires. Independent t tests weresed to examine the influence of sex, level and cause ofmputation on duration of stay, duration of prosthetic training,nd ABIS scores at discharge and at follow-up. Pearson cor-elation coefficients were used to test relationships betweenlinical, sociodemographic, and questionnaire scale or subscaleariables regrouped under 4 categories (appendix 1). The sig-ificance level was set at .05 for all analyses. All analyses wereerformed with SPSS, version 14.0 for Windows.a
RESULTS
emographic and Clinical VariablesOf the 114 persons with an LLA admitted to the program
uring the study period, only 29 (26%) met the eligibilityriteria. Of the 85 remaining, 30% were readmissions, 34% hadbilateral amputation, 11% insufficiently understood French ornglish, 16% had important cognitive or psychiatric problems,nd 9% were not considered as potential prosthetic wearers. Ofhe 29 eligible subjects, 6 (21%) refused to participate, 1 diedt follow-up, and 3 had an unplanned discharge. Data for the 3valuation times were obtained for 19 participants. Table 1ummarizes their clinical and demographic characteristics. Theain cause of amputation was peripheral vascular disease
63%) with or without diabetes. They suffered from severalssociated medical conditions; 52.6% had high blood pressure,2.1% had visual problems, 21.1% had hearing problems, and6.3% had chronic kidney failure. The mean time betweenmputation and admission to rehabilitation did not significantlyiffer (P�.05) according to the level or cause of amputation.he same results were obtained for the mean duration of staynd the mean duration of prosthetic training.
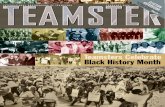
ubjective Quality of Life ProfileThe mean global satisfaction scores of the SQLP at admis-
ion, discharge, and follow-up were 0.87, 1.10, and 1.01,
rl(paathta
dtvdaiw(apifgt
pvsag
eanm(ppe
fpwfdBTfattpdPngP
P
wc(hcsficRnfold
A
dgLb(wdP
RQ
bpl3lt
637QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
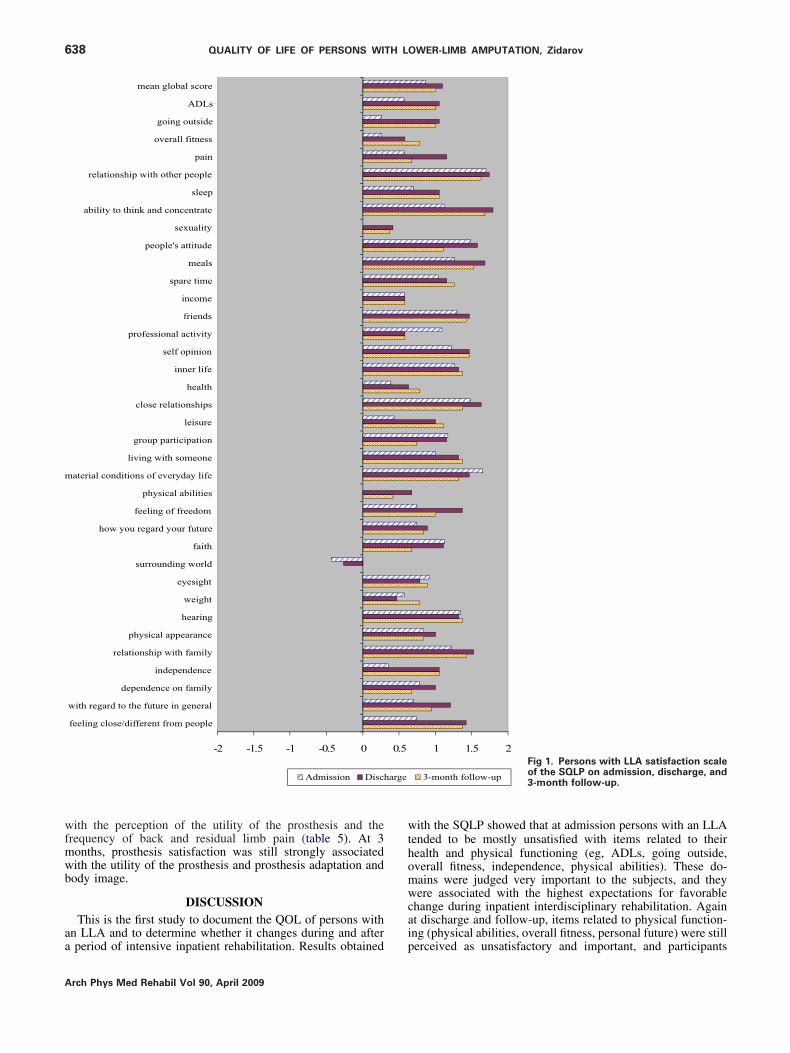
espectively (fig 1). At admission, the items for which theowest satisfaction was expressed were the ability to go outside.26) and overall fitness (.26). The most satisfaction was re-orted for items relating to relationships with other people (1.7)nd material conditions (1.65). At discharge, sexuality (.42)nd body weight (.42) had the lowest scores, whereas ability tohink (1.79) and relationships with others (1.74) were theighest. At follow-up, the items with the highest scores werehe same as those at discharge, and sexuality (.37) and physicalbilities (.42) scored the lowest.
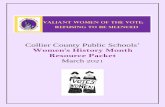
With regards to the patients’ importance of the variousomains of life, the mean global scores for the 3 evaluationimes were all 1 or more, indicating that they were perceived asery important (fig 2). In general, the importance slightlyecreased from admission to follow-up. At admission, thebility to think (2.52) and independence (2.43) were the mostmportant items, whereas spirituality (.61) and surroundingorld (.96) were the least important. At discharge, eyesight
2.21) followed by independence, going outdoors, sleep, andbility to think (2.16) were the most important items for theersons with an LLA. Group participation (.63) and surround-ng world were the least important (.79). At the 3-monthollow-up, the same items were rated as unimportant, whereasoing outdoors (2.16) and companionship (2.11) were judgedhe most important.
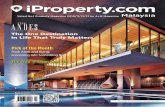
The mean scores for the anticipated changes indicated thatersons with an LLA expected a fairly favorable change in thearious domains of life during rehabilitation (fig 3). Meancores slightly decreased from admission to follow-up. Atdmission, the greatest changes were expected in the ability to
Table 1: Clinical and Demographic Characteristics of the Sample
Variable n Frequency (%)
Cause of amputationVascular 12 63.2Traumatic 3 15.8Tumor 2 10.5Infection 2 10.5
Level of amputationTT 16 84.2TF 3 15.8
SexMen 14 73.7Women 5 21.7
Marital statusMarried/committed 9 47.4Single 5 26.3Divorced/widowed 5 26.3
EducationPrimary 2 10.5Secondary 10 52.7Post secondary 7 36.8
Employment status at the amputationEmployed 12 63.2Retired 7 36.8
Variable Mean � SD Range
Time since amputation (d) 73.3�87.7 7–384Duration of rehabilitation stay (d) 84.3�23.3 59–146Duration of prosthetic training (d) 49.2�19.2 29–105Age (y) 53.4�14.6 26–78
o outside and independence (1.43), and the least change was A
xpected in spirituality (.09), hearing, and relationships (familynd relatives�.13). At discharge, going outdoors, overall fit-ess, and view of the future (1.32) were expected to change theost, whereas hearing (0.11), relations with others, and meals
.21) were not. At follow-up, participants still expected theirhysical abilities (1.05) and their overall fitness (.89) to im-rove, whereas spirituality and meeting friends (.11) were notxpected to change.
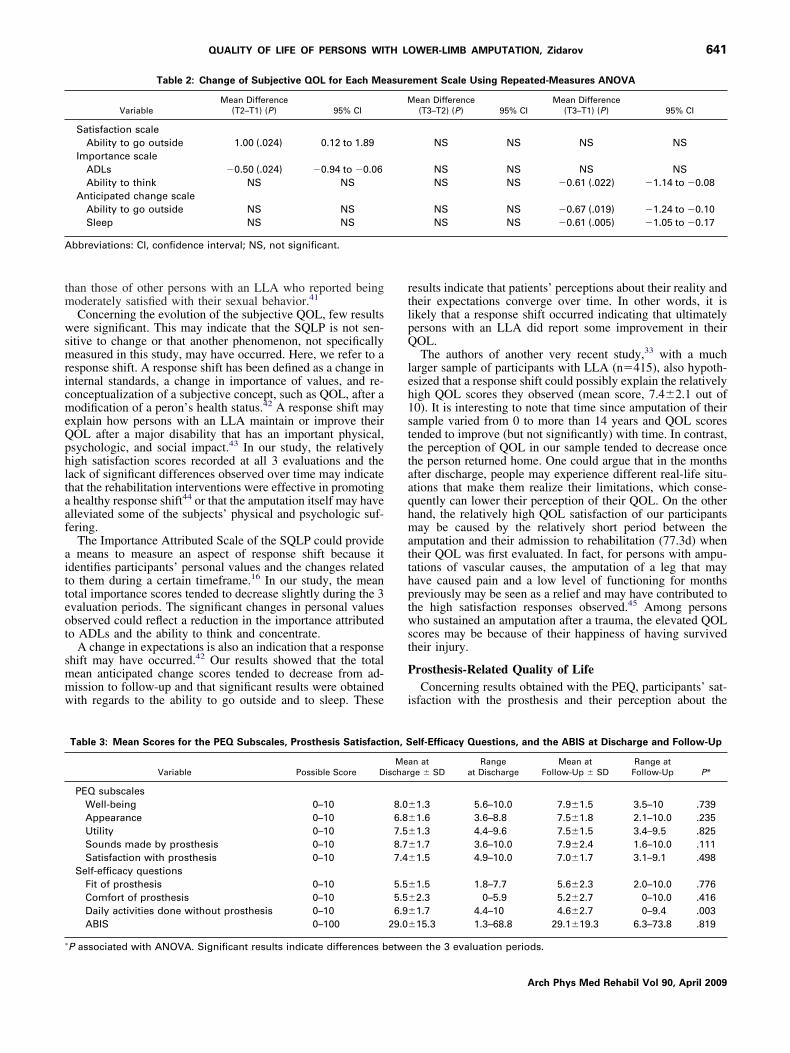
The change in subjective QOL was analyzed item by itemor each measurement scale (satisfaction, importance, antici-ated change) by using a repeated-measures ANOVA. Pair-ise comparisons (Bonferroni correction applied) were per-
ormed for comparisons reaching significance (table 2) toetermine when the differences occurred. After applying theonferroni correction, 5 were still significant (see table 2).here was a significant increase in patients’ mean total satis-
action score concerning the ability to go outside betweendmission and discharge (F2,34�5.77, P�.007). The impor-ance perceived concerning ADLs significantly decreased be-ween admission and discharge (F2,34�3.89, P�.03). The im-ortance attributed to the ability to think and concentrate alsoecreased between admission and follow-up (F2,34�5.39,�.009). Change anticipated with rehabilitation decreased sig-ificantly from admission to follow-up concerning the ability too outside (F2,34�5.09, P�.012) and sleep (F2,34�4.80,�.015).
rosthesis Evaluation QuestionnaireIn general, patients’ overall perception was very favourable,
ith no significant differences found between scores at dis-harge and follow-up (P�.05) for the 4 selected PEQ subscalestable 3). The mean prosthesis satisfaction scores were alsoigh, indicating greater satisfaction with the prosthesis at dis-harge and at follow-up (7.4 and 7.0, respectively), and thesecores did not differ significantly. Patients indicated that if thet and the comfort of their prosthesis were both poor at dis-harge, they completed on average 55% of their daily activities.esults were similar at the 3-month follow-up, and there wereo significant differences between scores at discharge and atollow-up. Regarding the amount of activities performed with-ut the prosthesis, on average, patients performed significantlyess activities without their prosthesis at follow-up than atischarge (t17�3.43, P�.003).
mputee Body Image ScaleThe mean ABIS score at discharge was low, and it did not
iffer significantly from that at follow-up (see table 3). Sub-roup analyses revealed that at discharge persons with a TFLA (47.5�22.6) reported a significantly poorer perception ofody image compared with that of persons with a TT LLA25.5�11.4, t17�–2.63, P�.017). At the 3-month follow-up,omen (50.9�24.7) had a significantly higher body imageisturbance compared with men (23.3�13.3, t17�–3.088,�.007).
elationship Between Patient/Clinical Variables anduality of Life and Prosthesis SatisfactionAt discharge, strong and significant relationships were found
etween QOL satisfaction and bothersome pain in the nonam-utated leg, adaptation to amputation, presence of phantomimb pain, and adaptation to prosthesis (table 4). At the-month follow-up, QOL satisfaction was significantly corre-ated with the PEQ’s well-being and utility subscales, adapta-ion to amputation, body image, and adaptation to prosthesis.
t discharge, prosthesis satisfaction was strongly correlatedArch Phys Med Rehabil Vol 90, April 2009
wfmwb
aa
wthomwcai
m
arge
638 QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
A
ith the perception of the utility of the prosthesis and therequency of back and residual limb pain (table 5). At 3onths, prosthesis satisfaction was still strongly associatedith the utility of the prosthesis and prosthesis adaptation andody image.
DISCUSSIONThis is the first study to document the QOL of persons with
n LLA and to determine whether it changes during and after
-2 -1.5 -1 -0.5 0
mean global score
ADLs
going outside
overall fitness
pain
relationship with other people
sleep
ability to think and concentrate
sexuality
people's attitude
meals
spare time
income
friends
professional activity
self opinion
inner life
health
close relationships
leisure
group participation
living with someone
aterial conditions of everyday life
physical abilities
feeling of freedom
how you regard your future
faith
surrounding world
eyesight
weight
hearing
physical appearance
relationship with family
independence
dependence on family
with regard to the future in general
feeling close/different from people
Admission Disch
period of intensive inpatient rehabilitation. Results obtained p
rch Phys Med Rehabil Vol 90, April 2009
ith the SQLP showed that at admission persons with an LLAended to be mostly unsatisfied with items related to theirealth and physical functioning (eg, ADLs, going outside,verall fitness, independence, physical abilities). These do-ains were judged very important to the subjects, and theyere associated with the highest expectations for favorable
hange during inpatient interdisciplinary rehabilitation. Againt discharge and follow-up, items related to physical function-ng (physical abilities, overall fitness, personal future) were still
1 1.5 2
3-month follow-up
Fig 1. Persons with LLA satisfaction scaleof the SQLP on admission, discharge, and3-month follow-up.
0.5
erceived as unsatisfactory and important, and participants

ec
oit
wpemm
Fo3
639QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
xpected improvements before discharge and in the months toome.
These results are difficult to compare directly with thosebtained by others mainly because of the differences in thentervals of time between the completion of rehabilitation and
mean gl
goin
over
relationship with oth
ability to think and co
people
s
profession
se
close rel
group par
living with
material conditions of eve
physica
feeling o
how you regard y
surround
physical a
relationship w
inde
dependence
with regard to the future
feeling close/different fro
ig 2. Persons with LLA importance scalef the SQLP on admission, discharge, and-month follow-up.
he evaluations and the tools used to measure QOL. Studies N
ere conducted months or years postrehabilitation and usedrimarily a single-item question33 or generic tools providingither a total or subscale scores.20-22,25,32 The SQLP provided aore detailed profile (item by item) in relation to 3 measure-ent scales: satisfaction, importance, and anticipated change.
0 0.5 1 1.5 2 2.5 3
core
DLs
side
ess
ain
ople
leep
rate
lity
ude
eals
ime
ome
nds
vity
ion
life
alth
hips
sure
tion
one
life
ities
om
ture
aith
orld
ight
ight
ring
nce
ily
nce
ily
eral
ople
Admission Discharge 3-month follow-up
obal s
A
g out
all fitn
p
er pe
s
ncent
sexua
's attit
m
pare t
inc
frie
al acti
lf opin
inner
he
ations
lei
ticipa
some
ryday
l abil
f freed
our fu
f
ing w
eyes
we
hea
ppeara
ith fam
pende
on fam
in gen
m pe
onetheless, in general, our results are comparable with those
Arch Phys Med Rehabil Vol 90, April 2009

oit
stgfi
acwipsSa
m
640 QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
A
f others who found that physical functioning20,21 and mobil-ty32 were problematic months and even years after an ampu-ation.
When our results are compared with the mean total SQLPatisfaction scores of nondisabled persons (.77),39 we find thathe mean total satisfaction scores of persons with an LLA areenerally higher at admission (.87), discharge (1.10), and atollow-up (1.01). The participants satisfaction profile concern-
-2 -1.5 -1 -0.5 0
mean global score
ADLs
going outside
overall fitness
pain
relationship with other people
sleep
ability to think and concentrate
sexuality
people's attitude
meals
spare time
income
friends
professional activity
self opinion
inner life
health
close relationships
leisure
group participation
living with someone
aterial conditions of everyday life
physical abilities
feeling of freedom
how you regard your future
faith
surrounding world
eyesight
weight
hearing
physical appearance
relationship with family
independence
dependence on family
with regard to the future in general
feeling close/different from people
Admission Discharge
ng interpersonal relationships was similar to that obtained with p
rch Phys Med Rehabil Vol 90, April 2009
normal sample.39 Surprisingly, physical appearance was per-eived more satisfactory at all 3 evaluation periods by personsith an LLA compared with the normal sample. However,
tems related to health and physical functioning, such as inde-endence, physical abilities, and dependence on family, werecored lower by the participants than by healthy individuals.exual satisfaction was also scored lower by the participants inll 3 evaluation periods when compared with the normal sam-
1 1.5 2
3-month follow-upFig 3. Persons with LLA anticipatedchange scale of the SQLP on admission,discharge, and 3-month follow-up.
0.5
le. Moreover, observed sexual satisfaction scores were lower
tm
wsmricmeQphltaaf
aitteot
smmw
rtlpQ
leh1stttaaqhmatthptwst
P
i
A
�
641QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
han those of other persons with an LLA who reported beingoderately satisfied with their sexual behavior.41
Concerning the evolution of the subjective QOL, few resultsere significant. This may indicate that the SQLP is not sen-
itive to change or that another phenomenon, not specificallyeasured in this study, may have occurred. Here, we refer to a
esponse shift. A response shift has been defined as a change innternal standards, a change in importance of values, and re-onceptualization of a subjective concept, such as QOL, after aodification of a peron’s health status.42 A response shift may
xplain how persons with an LLA maintain or improve theirOL after a major disability that has an important physical,sychologic, and social impact.43 In our study, the relativelyigh satisfaction scores recorded at all 3 evaluations and theack of significant differences observed over time may indicatehat the rehabilitation interventions were effective in promotinghealthy response shift44 or that the amputation itself may havelleviated some of the subjects’ physical and psychologic suf-ering.
The Importance Attributed Scale of the SQLP could providemeans to measure an aspect of response shift because it
dentifies participants’ personal values and the changes relatedo them during a certain timeframe.16 In our study, the meanotal importance scores tended to decrease slightly during the 3valuation periods. The significant changes in personal valuesbserved could reflect a reduction in the importance attributedo ADLs and the ability to think and concentrate.
A change in expectations is also an indication that a responsehift may have occurred.42 Our results showed that the totalean anticipated change scores tended to decrease from ad-ission to follow-up and that significant results were obtainedith regards to the ability to go outside and to sleep. These
Table 2: Change of Subjective QOL for Each Me
VariableMean Difference
(T2–T1) (P) 95% CI
Satisfaction scaleAbility to go outside 1.00 (.024) 0.12 to 1.89
Importance scaleADLs �0.50 (.024) �0.94 to �0.06Ability to think NS NS
Anticipated change scaleAbility to go outside NS NSSleep NS NS
bbreviations: CI, confidence interval; NS, not significant.
Table 3: Mean Scores for the PEQ Subscales, Prosthesis Satisfact
Variable Possible Score D
PEQ subscalesWell-being 0–10Appearance 0–10Utility 0–10Sounds made by prosthesis 0–10Satisfaction with prosthesis 0–10
Self-efficacy questionsFit of prosthesis 0–10Comfort of prosthesis 0–10Daily activities done without prosthesis 0–10ABIS 0–100
P associated with ANOVA. Significant results indicate differences betwe
esults indicate that patients’ perceptions about their reality andheir expectations converge over time. In other words, it isikely that a response shift occurred indicating that ultimatelyersons with an LLA did report some improvement in theirOL.The authors of another very recent study,33 with a much
arger sample of participants with LLA (n�415), also hypoth-sized that a response shift could possibly explain the relativelyigh QOL scores they observed (mean score, 7.4�2.1 out of0). It is interesting to note that time since amputation of theirample varied from 0 to more than 14 years and QOL scoresended to improve (but not significantly) with time. In contrast,he perception of QOL in our sample tended to decrease oncehe person returned home. One could argue that in the monthsfter discharge, people may experience different real-life situ-tions that make them realize their limitations, which conse-uently can lower their perception of their QOL. On the otherand, the relatively high QOL satisfaction of our participantsay be caused by the relatively short period between the
mputation and their admission to rehabilitation (77.3d) whenheir QOL was first evaluated. In fact, for persons with ampu-ations of vascular causes, the amputation of a leg that mayave caused pain and a low level of functioning for monthsreviously may be seen as a relief and may have contributed tohe high satisfaction responses observed.45 Among personsho sustained an amputation after a trauma, the elevated QOL
cores may be because of their happiness of having survivedheir injury.
rosthesis-Related Quality of LifeConcerning results obtained with the PEQ, participants’ sat-
sfaction with the prosthesis and their perception about the
ment Scale Using Repeated-Measures ANOVA
ean Difference(T3–T2) (P) 95% CI
Mean Difference(T3–T1) (P) 95% CI
NS NS NS NS
NS NS NS NSNS NS �0.61 (.022) �1.14 to �0.08
NS NS �0.67 (.019) �1.24 to �0.10NS NS �0.61 (.005) �1.05 to �0.17
elf-Efficacy Questions, and the ABIS at Discharge and Follow-Up
n atge � SD
Rangeat Discharge
Mean atFollow-Up � SD
Range atFollow-Up P*
1.3 5.6–10.0 7.9�1.5 3.5–10 .7391.6 3.6–8.8 7.5�1.8 2.1–10.0 .2351.3 4.4–9.6 7.5�1.5 3.4–9.5 .8251.7 3.6–10.0 7.9�2.4 1.6–10.0 .1111.5 4.9–10.0 7.0�1.7 3.1–9.1 .498
1.5 1.8–7.7 5.6�2.3 2.0–10.0 .7762.3 0–5.9 5.2�2.7 0–10.0 .4161.7 4.4–10 4.6�2.7 0–9.4 .00315.3 1.3–68.8 29.1�19.3 6.3–73.8 .819
asure
M
ion, S
Meaischar
8.0�
6.8�
7.5�
8.7�
7.4�
5.5�
5.5�
6.9�
29.0�
en the 3 evaluation periods.
Arch Phys Med Rehabil Vol 90, April 2009

aemadthoHHfsacppsTQewds
B
cmcwBtMwbms5tettwsw
HtipBwdog
RQ
bpittpgaaMacawfitiatrAtssscpmvacgreaQ
642 QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
A
ppearance, utility, and sounds made by the prosthesis werequally high at discharge and at the 3-month follow-up. Thisay indicate that the quality of the delivered prosthesis was
dequate at discharge and that the timing of delivering aefinitive prosthesis was well targeted by the rehabilitationeam in relation to residual limb issues (maturation, woundealing, and so on). The high mean PEQ subscale scoresbtained in our study are similar to those obtained by Legro,31
arness,23 and colleagues in their cross-sectional studies.owever, in contrast to our results (8.0 at discharge and 7.9 at
ollow-up), these authors reported lower well-being subscalescores (7.2 and 6.7, respectively) when assessed several yearsfter prosthetic rehabilitation. These differences may be be-ause of the fact that well-being is a dynamic concept. Aerson’s perception may change according to his/her life ex-eriences as they are influenced by the person’s physical andocial environment, personality, or new health problems.14,40
his may explain, in part, the slight decrease in well-being orOL after an LLA that occurs later. It remains unclear, how-
ver, when this change occurs and what factors are associatedith this event. Nevertheless, our results, as well those studiesiscussed here, indicate that the perceived well-being of per-ons with an LLA is consistently high after their amputation.
ody ImageOne major finding was that participants were not very con-
erned with their body image at the 3 evaluation periods. Theedian ABIS score observed in our study was lower at dis-
harge (23.8) and at the 3-month follow-up (21.3) comparedith those reported in other studies using this tool.35,36,46
reakey35 reported body image perturbation among males withraumatic amputation of a similar age to be 33.5, whereas
iller36 obtained a score of 53 among nontraumatic personsith an LLA suggesting that older and vascular amputees maye more concerned about their body image than younger trau-atic amputees. Others have, however, reported higher ABIS
cores among persons with amputations of mixed causes (eg,7.5).46 Comparisons between studies are difficult because ofhe differences in sample composition and the timing of thevaluations. In fact, time since amputation may play a role inhe development of body image disturbance. In our study, meanime since amputation was very short (73.3�87.7d) comparedith those reported in Breakey’s (17.0�13.5y) and Miller’s
tudies (5y). It seems that with the passage of time, persons
Table 4: Correlation Coefficients Between Mean Total QOLSatisfaction Score as Measured by the SQLP and Patient/Clinical
Variables Measured at Discharge and at 3-Month Follow-Up
Variables
PearsonCorrelationCoefficient n P
DischargeBothersomeness of pain in
the nonamputated leg 0.705 9 .034Adaptation to amputation 0.741 19 �.001Phantom limb pain �0.497 19 .031Adaptation to prosthesis 0.460 19 .048
3-month follow-upPEQs well-being scale 0.733 19 �.001PEQs utility scale 0.685 19 .001Adaptation to amputation 0.684 19 .001Total score ABIS �0.604 19 .006Adaptation to prosthesis 0.602 19 .006
ith an LLA tend to develop a concern for their body image.
rch Phys Med Rehabil Vol 90, April 2009
owever, more longitudinal studies are needed to clarify whenhis occurs and to determine the contributing factors. Concern-ng the potential influence of sex and level of amputation onerception of body image, in contrast to our findings,reakey35 did not find a significant difference between personsith a TT and TF LLA and Miller36 did not find significantifferences between males and females. Significant results inur study may reflect a tendency toward women having areater concern about their body image once being back home.
elationship Between Patient/Clinical Variables andualtiy of Life and Prosthesis SatisfactionThe present study explored whether a relationship exists
etween demographic, clinical, prosthetic, pain sensation, andsychologic well-being variables and QOL and prosthesis sat-sfaction. Our findings suggest that participants’ perception ofheir QOL satisfaction is more related to pain sensation, pros-hetic factors, and psychosocial well-being (adaptation to am-utation, prosthesis, body image) than to clinical or demo-raphic variables such as age, sex, level, or cause ofmputation. In a sample of 77 persons with an LLA, highermputation-related pain was associated with lower QOL.41
atsen et al47 showed a significant correlation between QOLnd the condition of the contralateral limb and found significantorrelations ranging from .47 to .60 between QOL and thebility of persons with an LLA to walk in confined space oralk while carrying a load. Similar to our results, they did notnd age, sex, or level of amputation to be significantly related
o the perception of QOL. Van der Schans et al,20 whilenvestigating the potential determinants of health-related QOLmong 437 persons with an LLA by using the SF-36, foundhat respondents with phantom limb pain had a poorer health-elated QOL compared with those without phantom limb pain.lthough psychologic well-being and adjustment to an ampu-
ation were not measured directly, anxiety and depression,ocial support, phantom limb pain intensity, concerns withelf-esteem, and body image were associated with their mea-ure.35,48,49 In another study,33 symptoms of depression ac-ounted for 30% of the variance in QOL of a sample of 415ersons with an LLA and factors predicting long-term adjust-ent to an LLA such as phantom limb pain and psychosocial
ariables such as catastrophizing, perceived control over pain,nd coping and social support were found to be importantontributors to adjustment to an amputation.49 Furthermore,reater levels of social support, 1 month after an LLA, wereelated to greater levels of life satisfaction50 and social supportxplained 2% of the variance of perceived QOL.33 Callaghannd Condie27 validated the Patient Generated Index, a genericOL measure, by using the Medical Outcomes Study Short
Table 5: Correlation Coefficients Between Satisfaction With theProsthesis as Measured by the PEQ and Patient/Clinical Variables
Measured at Discharge and at 3-Month Follow-Up
VariablesPearson Correlation
Coefficient n P
DischargePEQs utility scale 0.615 19 .005Frequency of back pain �0.552 19 .014Frequency of residual limb
(stump) pain �0.461 19 .0473-month follow-up
PEQs utility scale 0.653 19 .002Adaptation to prosthesis 0.645 19 .003
ABIS total score �0.488 19 .034
Fwsb
alrrtilbprpfsffi(sep
S
setfecbdcbrs
lQtdtpmedictpatwb
piust
gpt
pdwpitmlis
QlbtdSie
distopdbrtipaTL
643QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
orm-12 with 42 unilateral TF amputees who had been fittedith a prosthesis at least 1-year postrehabilitation and found a
tronger relationship between mental health and QOL life thanetween physical health and QOL.At discharge, prosthetic satisfaction seems to be mostly
ssociated with pain and prosthetic variables, whereas at fol-ow-up prosthetic variables and psychosocial variables play aole. The reduction of residual limb pain is an importantehabilitation goal. Residual limb pain may impede the use ofhe prosthesis and is associated with lower physical function-ng.51 Furthermore, a recent study found that acute residualimb pain (assessed at 4 and 5 days postamputation) was theest predictor of development of chronic residual limb pain inersons with an LLA.52 Bilodeau et al2 found that pain and theisk of injuries were the main causes of dissatisfaction with therosthesis among persons with LLA and that prosthesis satis-action explained 46% of the variance of prosthesis use. In aurvey of 44 persons with LLA investigating prosthesis satis-action, body image, and phantom pain, Murray and Fox46
ound that higher levels of prosthesis satisfaction were signif-cantly correlated with lower levels of body image disturbancer�–.52) and that the number of hours of prosthetic use wasignificantly related to prosthesis satisfaction (r�.39). How-ver, prosthesis satisfaction was not significantly related toain (r�–.019).
tudy Limitations and Clinical ImplicationsThere are a few limitations to this study. Our sample was
mall; hence, we were not able to detect significant differ-nces over time for all variables. All subjects were inpa-ients in the same rehabilitation facility and were candidatesor prosthetic fitting. As such, our results may not be gen-ralizable to the total population of persons with LLA in-luding those who never received a prosthesis, who haveilateral amputation, and who have severe cognitive disor-ers. Indeed, correlational analyses do not allow one toonclude any causal relationship between functional reha-ilitation and QOL; however, the observed significant cor-elation coefficients, despite the small sample size, under-core the importance of the relationship between the two.
Despite these limitations, there are important points to beearned from this study. The SQLP, as a measure of subjectiveOL, appears to provide valuable information about rehabili-
ation QOL outcomes and patients’ perceptions in differentomains of life that may help the multidisciplinary rehabilita-ion team identify a particular client’s objectives and treatmentlan. Individualized selection of objectives and treatment pro-ote patient involvement in the rehabilitation process.53 How-
ver, the use of the SQLP in routine clinical practice may beifficult because of practicability issues. The mode of admin-stration, frequently by interview, is lengthy (�30min), andlinicians may feel that therapy is more useful to the patienthan administration of a questionnaire even if the responsesrovide them with useful information. Furthermore, generatingnd interpreting the satisfaction profiles can be complex andime-consuming for daily practice. Ideally, more methodologicork is needed to shorten and simplify QOL tools in order toe routinely used in rehabilitation clinical settings.11,14,15,53
The specificity of the PEQ provides practitioners with theerceptions of persons with an amputation regarding aspectsmportant to their QOL such as satisfaction, appearance, andsefulness of their definitive prosthesis. This information canerve as benchmark criteria when delivering a definitive pros-
hesis before discharge. The only practicability issue with re-ards to using the PEQ routinely was that some older partici-ants found it difficult to understand the VAS and to completehe questionnaire by themselves.
The ABIS is the only tool we are aware of that measures theerception of body image of people with an LLA. Although weid not report body image disturbances over the study period,e believe that certain subgroups of participants, such asersons with TF LLA or women, may start developing bodymage issues during rehabilitation. This hypothesis needs to beested with larger samples. To be able to intervene in a timelyanner, rehabilitation programs should provide regular fol-
ow-up to persons with an LLA to detect a potential problem,ncluding body image, and to be able to provide the necessaryervices.
Finally, future research should include more longitudinalOL studies extending beyond 3 months postdischarge with
arger samples that also include persons with a unilateral andilateral LLA and candidates and noncandidates for prostheticraining. This type of research should have sufficient power toetermine the factors that positively or negatively impact QOL.uch studies should also take into consideration the possible
nfluence of response shift that could occur when someonexperiences a major change in his/her life.
CONCLUSIONSSubjective QOL of persons with an LLA is relatively high
uring and 3 months after the rehabilitation process except fortems related to their physical functioning. Furthermore, per-ons with LLA have a high prosthesis-related QOL in relationo the global satisfaction of their prosthesis and their perceptionf the appearance and the utility of their prosthesis. Althougharticipants did not seem to have a body image disturbanceuring the study period, body image perception was found toe highly related to the perception of QOL. Although theehabilitation process is mainly focused on the physical func-ioning including prosthetic fitting, our findings underscore themportance of also focusing care on pain issues and particularlysychosocial issues such as body image and adaptation tomputation and the prosthesis during the rehabilitation process.his holistic approach should enhance the QOL of persons withLA.
APPENDIX 1: VARIABLES USED INCORRELATION ANALYSES
Demographic and clinicalvariables
Age at admissionSexLevel of amputationCause of amputation
Prosthetic variablesSatisfaction with prosthesisAppearance of prosthesisUtility of prosthesisSounds made by prosthesis
Number of associated medicalconditions
Time since amputationDuration of stayDuration of prosthetic training
Pain sensation variablesFrequency, intensity, and
bothersomeness of:● Phantom pain● Residual limb pain● Nonamputated leg pain
Psychologic well-beingvariables
Body imageAdaptation to amputationAdaptation to prosthesis
● Back pain
Arch Phys Med Rehabil Vol 90, April 2009
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
644 QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
A
References1. Geertzen JH, Martina JD, Rietman HS. Lower limb amputation
part 2: rehabilitation– a 10 year literature review. Prosthet Orth Int2001;25:14-20.
2. Bilodeau S, Hebert R, Desrosiers J. Lower limb prosthesis utilisa-tion by elderly amputees. Prosthet Orth Int 2000;24:126-32.
3. Kuiken TA, Miller L, Lipschutz R, Huang ME. Rehabilitation ofpeople with lower limb amputation. In: Braddom RL, Busch-bacher RM, associate editors. Physical medicine and rehabilita-tion. Philadelphia: Saunders Elsevier; 2007. p 282-318.
4. Kent R, Fyfe N. Effectiveness of rehabilitation following ampu-tation. Clin Rehabil 1999;13(Suppl 1):43-50.
5. Jelic M, Eldar R. Rehabilitation following major traumatic ampu-tation of lower limbs– a review. Crit Rev Phys Rehabil Med2003;15:235-52.
6. Miller WC, Deathe AB, Speechley M. Lower extremity prostheticmobility: a comparison of 3 self-report scales. Arch Phys MedRehabil 2001;82:1432-40.
7. Condie E, Scott H, Treweek S. Lower limb prosthetic outcomemeasures: a review of the literature 1995 to 2005. Proceedings ofthe State-of-the-Science-Conference. Chicago: Lipincott Williamsand Wilkins; 2005.
8. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. JAMA 1995;273:59-65.
9. Renwick R, Nourhaghighi N, Manns PJ, Rudman DL. Quality oflife for people with physical disabilities: a new instrument. Int JRehabil Res 2003;26:279-87.
0. Macduff CC. Respondent-generated quality of life measures: use-ful tools for nursing or more fool’s gold? J Adv Nurs 2000;32:375-82.
1. Jette AM. Using health-related quality of life measures in physicaltherapy outcomes research. Phys Ther 1993;73:528-37.
2. Andresen EM, Meyers AR. Health-related quality of life outcomesmeasures. Arch Phys Med Rehabil 2000;81(12 Suppl 2):S30-45.
3. Cella D, Nowinski CJ. Measuring quality of life in chronic illness:the functional assessment of chronic illness therapy measurementsystem. Arch Phys Med Rehabil 2002;83(12 Suppl 2):S10-7.
4. Wood-Dauphinee S. Assessing quality of life in clinical research:from where have we come and where are we going? J ClinEpidemiol 1999;52:355-63.
5. Fitzpatrick R, Fletcher A, Gore S, Jones D, Spiegelhalter D, CoxD. Quality of life measures in health care. I: applications andissues in assessment. BMJ 1992;305:1074-7.
6. Dazord A, Boissel JP. Subjective quality of life assessement intherapeutic trials: presentation of a new instrument in France. In:Orley J, Kuyken W, editors. Measurement of quality of life inhealth care settings. Berlin: Springer-Verlag; 1994. p 185-95.
7. Béthoux F, Calmels P, editors. Guide des outils de mesure etd’évaluation en médecine physique et de réadaptation. Paris: Fri-son-Laroche; 2003.
8. Finch E, Brooks D, Stratford PW, Mayo NE. Physical rehabilita-tion outcome measures. 2nd ed. Baltimore: Lippincott Williamsand Wilkins; 2002.
9. Gallagher P, MacLachlan M. The trinity amputation and prosthe-sis experience scales and quality of life in people with lower-limbamputation. Arch Phys Med Rehabil 2004;85:730-6.
0. Van der Schans CP, Geertzen JH, Schoppen T, Dijkstra PU.Phantom pain and health-related quality of life in lower limbamputees. J Pain Symptom Manage 2002;24:429-36.
1. Pezzin LE, Dillingham TR, MacKenzie EJ. Rehabilitation and thelong-term outcomes of persons with trauma-related amputations.Arch Phys Med Rehabil 2000;81:292-300.
2. Nissen SJ, Newman WP. Factors influencing reintegration tonormal living after amputation. Arch Phys Med Rehabil 1992;73:
548-51.rch Phys Med Rehabil Vol 90, April 2009
3. Harness N, Pinzur MS. Health related quality of life in patientswith dysvascular transtibial amputation. Clin Orthop Relat Res2001;(383):204-7.
4. Gallagher P, MacLachlan M. Development and psychometricevaluation of the trinity amputation and prosthesis experiencescales (TAPES). Rehabil Psychol 2000;45:130-54.
5. Demet K, Martinet N, Guillemin F, Paysant J, Andre JM. Healthrelated quality of life and related factors in 539 persons withamputation of upper and lower limb. Disabil Rehabil 2003;25:480-6.
6. De Godoy JM, Braile DM, Buzatto SH, Longo O Jr, Fontes OA.Quality of life after amputation. Psychol Health Med 2002;7:397-400.
7. Callaghan BG, Condie ME. A post-discharge quality of life out-come measure for lower limb amputees: test-retest reliability andconstruct validity. Clin Rehabil 2003;17:858-64.
8. Wood-Dauphinee S, Opzoomer M, Williams J, Marchand B,Spitzer W. Assessment of global function: the reintegration tonormal living index. Arch Phys Med Rehabil 1988;69:583-90.
9. Hunt SM, McKenna SP, McEven J. The Nottingham HealthProfile: subjective health status and medical consultation. Soc SciMed 1981;15:221-9.
0. Ware J, Sherbourne C. The MOS-36-Item Short-Form HealthSurvey (SF-36): I. Conceptual framework and item selection. MedCare 1992;30:473-81.
1. Legro MW, Reiber GD, Smith DG, Del Aguila M, Larsen J,Boone D. Prosthesis evaluation questionnaire for persons withlower limb amputations: assessing prosthesis-related quality oflife. Arch Phys Med Rehabil 1998;79:931-8.
2. Pell JP, Donnan PT, Fowkes FG, Ruckley CV. Quality of lifefollowing lower limb amputation for peripheral arterial disease.Eur J Vasc Surg 1993;7:448-51.
3. Asano M, Rushton P, Miller WC, Deathe AB. Predictors ofquality of life among individuals who have a lower limb ampu-tation. Prosthet Orthot Int 2008;32:231-43.
4. Rybarczyk BD, Nyenhuis DL, Nicholas JJ, Cash SM, Kaise J.Body image, perceived social stigma, and the prediction of psy-chosocial adjustment to leg amputation. Rehabil Psychol 1995;40:95-110.
5. Breakey JW. Body image: the lower-limb amputee. J ProsthetOrthot 1997;9:58-66.
6. Miller CA. The relationship between body-image, self-esteem,level of depression, and quality of life in elderly persons followinglower limb amputation [dissertation]. Minneapolis: Walden Univ;2001.
7. Gerin P, Dazord A, Cialdella P, Leizorovicz A, Boissel JP. Lequestionnaire Profil de la Qualité de Vie Subjective (PQVS):premiers éléments de validation. Therapie 1991;46:131-8.
8. Gerin P, Dazord A, Boissel JP, Hanauer Th M, Moleur P, ChauvinF. L’évaluation de la qualité de vie dans les essais thérapeutiques:aspects conceptuels et présentation d’un questonnaire. Therapie1989;44:355-64.
9. Navez M, Dazord A, Perrin AM, Gerbaud L, Clavelou P, LaurentB. Qualité de vie des patients migraineux. Douleur et analgésie2002;15:147-53.
0. Bonomi AE, Patrick DL, Bushnell DM, Martin M. Validation ofthe United States’ version of the World Health OrganizationQuality of Life (WHOQOL) instrument [see comment]. J ClinEpidemiol 2000;53(1):1-12. Comment in: J Clin Epidemiol 2000;53:19-23.
1. Walters AS, Williamson GM. Sexual satisfaction predicts qualityof life: a study of adult amputees. Sex Disabil 1998;16:103-15.
2. Sprangers MA, Schwartz CE. Integrating response shift intohealth-related quality of life research: a theoritical model. Soc Sci
Med 1999:1507-15.
4
4
4
4
4
4
4
5
5
5
5
645QUALITY OF LIFE OF PERSONS WITH LOWER-LIMB AMPUTATION, Zidarov
3. Tierney DK, Facione N, Padilla G, Dodd M. Response shift - atheoritical exploration of quality of life following hematopoieticcell transplantation. Cancer Nurs 2007;30:125-38.
4. Schwartz CE, Andresen EM, Nosek MA, Krahn GL. Responseshift theory: important implications for measuring quality of life inpeople with disability. Arch Phys Med Rehabil 2007;88:529-36.
5. Racy JC. Psychological adaptation to amputation. In: Smith DG,Michael JW, Bowker JH, editors. Atlas of amputations and limbdeficiencies: surgical, prosthetic and rehabilitation principles. 3thed. Rosemont: American Academy of Orthopaedic Surgeons;2004. p 727-37.
6. Murray CD, Fox J. Body image and prosthesis satisfaction in thelower limb amputee. Disabil Rehabil 2002;24:925-31.
7. Matsen SL, Malchow D, Matsen FA. Correlations with patients’sperspectives of the result of lower-extremity amputation. J BoneJoint Surg 2000;82-A:1089-95.
8. Horgan O, MacLachlan M. Psychosocial adjustment to lower-limb
amputation: a review. Disabil Rehabil 2004;26:837-50. a9. Hanley MA, Jensen MP, Ehde DM, Hoffman AJ, Patterson DR,Robinson LR. Psychosocial predictors of long-term adjustment tolower-limb amputation and phantom limb pain. Disabil Rehabil2004;26:882-93.
0. Williams RM, Ehde DM, Smith DG, Czerniecki JM, Hoffman AJ,Robinson LR. A two-year longitudinal study of social supportfollowing amputation. Disabil Rehabil 2004;26:862-74.
1. Pohjolainen T, Alaranta A. Predictive factors of functional abilityafter lower limb amputation. Ann Chir et Gynaecol 1991;80:36-9.
2. Hanley MA, Jensen MP, Smith DG, Ehde DM, Edwards WT,Robinson LR. Preamputation pain and acute pain predict chronicpain after lower extremity amputation. J Pain 2007;8:102-9.
3. Johnston MV, Miklos CS. Activity-related quality of life in reha-bilitation and traumatic brain injury. Arch Phys Med Rehabil2002;83(Suppl 2):S26-38.
Supplier. SPSS Inc, 233 S Wacker Dr, 11th Fl, Chicago, IL 60606.
Arch Phys Med Rehabil Vol 90, April 2009