
(Public Pack)Agenda Document for Health and Wellbeing ...
490
HEALTH AND WELLBEING BOARD Date: Wednesday 8 July 2015 Time: 6.00 pm Venue: Copies of agendas, reports, minutes and other attachments for the Council’s meetings are available on the Lambeth website. www.lambeth.gov.uk/moderngov Members of the Committee Listed on next page Substitute Members Listed on next page Further Information If you require any further information or have any queries please contact: Nazyer Choudhury, Telephone: 020 7926 0028; Email: [email protected] Members of the public are welcome to attend this meeting and the Town Hall is fully accessible. If you have any specific needs please contact Facilities Management (020 7926 1010) in advance. Queries on reports: Please contact report authors prior to the meeting if you have questions on the reports or wish to inspect the background documents used. The contact details of the report author is shown on the front page of each report. @LBLdemocracy on Twitter http://twitter.com/LBLdemocracy or use #Lambeth Lambeth Council – Democracy Live on Facebook http://www.facebook.com/
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of (Public Pack)Agenda Document for Health and Wellbeing ...

HEALTH AND WELLBEING BOARD Date: Wednesday 8 July 2015 Time: 6.00 pm Venue: Copies of agendas, reports, minutes and other attachments for the Council’s meetings are available on the Lambeth website. www.lambeth.gov.uk/moderngov Members of the Committee Listed on next page Substitute Members Listed on next page Further Information If you require any further information or have any queries please contact: Nazyer Choudhury, Telephone: 020 7926 0028; Email: [email protected] Members of the public are welcome to attend this meeting and the Town Hall is fully accessible. If you have any specific needs please contact Facilities Management (020 7926 1010) in advance. Queries on reports: Please contact report authors prior to the meeting if you have questions on the reports or wish to inspect the background documents used. The contact details of the report author is shown on the front page of each report. @LBLdemocracy on Twitter http://twitter.com/LBLdemocracy or use #Lambeth Lambeth Council – Democracy Live on Facebook http://www.facebook.com/

BOARD MEMBERS:
Representative Post Substitute
Lambeth Council:
Councillor Jim Dickson
(Chair)
Cabinet Member Health &
Wellbeing
To be advised
Councillor Jane Pickard
(Vice-Chair)
Cabinet Member for Children
and Families
To be advised
Councillor Jackie Meldrum Cabinet Member for Adult
Social Care
To be advised
Councillor Sonia Winifred Deputy Cabinet Member for
Healthy Neighbourhoods
Councillor Michelle Agdomar
Councillor Louise Nathanson Conservative Group Member To be advised
Sue Foster Strategic Director, Delivery
(fulfilling the statutory role of
director of children’s
services).
To be advised
Gill Vickers Delivery Director, Adult
Social Care
To be advised
Dr Ruth Wallis Director of Public Health To be advised
NHS Lambeth Clinical Commissioning Group (CCG):
Dr Adrian McLachlan (Vice-
Chair)
CCG (Chair) To be advised
Andrew Eyres CCG Chief Officer
Christine Caton
Sadru Kheraj CCG Clinical Governing
Body Member
To be advised
National Commissioning Board:
Jane Fryer Medical Director and
Responsible Officer (South
London)
NHS England (London
Region)
To be advised
King’s Health Partners:
Sir Ron Kerr CBE Chief Executive
Guy's and St Thomas’ NHS
Foundation Trust
John Moxham
Healthwatch Lambeth:
John Isitt Healthwatch Lambeth Catherine Pearson

AGENDA
PLEASE NOTE THAT THE ORDER OF THE AGENDA MAY BE CHANGED AT THE MEETING
Page
Nos.
1. Declarations of Interest
Under section 4 of the governance arrangements for the Health & Wellbeing Board, Board members are bound by the Members’ Code of Conduct as set out in the Council’s Constitution (Part 4 Section 1). Where any Board member has a Disclosable Pecuniary Interest in any matter to be considered at a Board meeting they must withdraw from the meeting room during the whole of the consideration of that matter and must not participate in any vote on that matter unless a dispensation has been obtained from the Monitoring Officer.
2. Minutes of Previous Meeting
1 - 8
To approve the minutes of the previous meeting.
3. Quarterly Director of Public Health Report - Lambeth and Southwark
(April - June 2015)
9 - 44
4. 0-5 Commissioning responsibility Transfer from NHS England to
Local Authorities
45 - 52
5. Emotional Wellbeing Mental Health Strategy
53 - 416
6. Our Healthier South East London
417 - 464
7. Lambeth Early Action Partnership (LEAP) Progress report
465 - 472
8. Update on Southwark and Lambeth Integrated Care (SLIC)
473 - 476
9. Children and Families Strategic Partnership update
477 - 484

Digital engagement We encourage people to use Social Media and we normally tweet from most Council meetings. To get involved you can tweet us @LBLDemocracy. Audio/Visual Recording of meetings Everyone is welcome to record meetings of the Council and its Committees using whatever, non-disruptive, methods you think are suitable. If you have any questions about this please contact Democratic Services (members of the press please contact the Press Office). Please note that the Chair of the meeting has the discretion to halt any recording for a number of reasons including disruption caused by the filming or the nature of the business being conducted. Persons making recordings are requested not to put undue restrictions on the material produced so that it can be reused and edited by all local people and organisations on a non-commercial basis. Representation: Ward Councillors may be contacted directly to represent your views to the Council: (details via the website www.lambeth.gov.uk)
Public involvement:
The Board has agreed principles for involving citizens (please contact Democratic Services for further
information: [email protected], 020 7926 2170 or contact officer listed on the front page of this
agenda).
Public Notice Questions (PNQs)
The Board welcomes the submission of public notice questions on its work (please contact Democratic
Services for further information: 020 7926 2170 or number on the front page). In summary the rules are:
PNQs may be submitted to each ordinary Board meeting by persons living, working, studying or
using health services in the borough.
Each PNQ must include the name, address, email address and telephone number(s) (the name of
the questioner will be published on the agenda (this may be withheld from publication in
reasonable circumstances).
Each question may be addressed to a particular Board Member or will otherwise be referred to the
relevant Board Member by the Secretary.
PNQs must be submitted by the published deadline (seven clear days before the meeting).
There are grounds to reject a submitted PNQ.
Accepted PNQs will be published on the agenda (in the order received) and referred to the Board
Member for them to prepare an answer. However, where a questioner has submitted more than
one question, all “first” questions will be taken first, “second” questions will be taken next and so
on.

At the meeting, the Board member will give an oral answer to the question. The questioner may
ask one supplementary question, which must be relevant to the original question or answer given.
After the meeting, Democratic Services will write to the questioner with the answer(s) given

This page is intentionally left blank

HWB
HEALTH AND WELLBEING BOARD
Wednesday 29 April 2015 at 6.00 pm
MINUTES
PRESENT: Adrian McLachlan (Vice-Chair), Sue Foster, Gill Vickers, Andrew
Eyres, John Isitt, Dr Ruth Wallis, Prof. John Moxham (Substitute),
Councillor Jane Pickard (Vice-Chair), Councillor Sonia Winifred and
Councillor Jackie Meldrum
APOLOGIES: Councillor Louise Nathanson and Sadru Kheraj
ALSO PRESENT: Valerie Dinsmore, Helen Charlesworth May, Moira McGrath,
Dennis O’Rourke
Action
required by
1. DECLARATIONS OF INTEREST
None were declared.
2. MINUTES OF PREVIOUS MEETING
RESOLVED: That the minutes of the previous meetings held on 14 January 2015 be approved and signed as a correct record of the proceedings.
Councillor Dickson informed the meeting that following the presentation from the Metropolitan Police, there would be a comprehensive meeting to address the issues raised at the presentation.
3. ANNUAL PUBLIC HEALTH REPORT 2014 OF THE DIRECTOR OF
PUBLIC HEALTH
Dr Ruth Wallis, Director of Public Health, informed the meeting that the
Page 1 Agenda Item 2

Public Health report needed to be presented to the Board every year to examine the progression and investigate how further progression could be made. The general focus was usually over health inequality issues but social determinants such as income, environment and work were also a point of focus. Dr Wallis introduced the report.
The Chair and Members of the Board commended Dr Wallis on her report and thanked her for her presentation. In response to questions from Members, Dr Wallis informed the meeting that:
Social data could be collected in a way that would be
acceptable to members of the public. This could be done by
asking general questions rather specific questions related to
income or personal choices.
Over 10% of Lambeth residents had access to private
health care. This was due to speed and choice of access to
routine interventions and was not due to treatment that
could not be performed by the NHS.
Some young people suffering from emotional or mental
issues may not be diagnosed with a mental illness. In their
adolescence or teenage, they may suffer from stress or
personal issues such as family life or external influences
which could impact their education. This could have a
cumulative impact on them and five years later, they may
suffer from illnesses that could be diagnosed. Poor mental
health could also result in higher levels of risk taking
behaviour.
Ongoing engagement with schools was very important.
Some people with long term conditions could self-manage
their issues. This could be done by giving people assistance
for their self-management. Residents could inform what they
needed help with and assistance could be given on how
they could self-manage.
The recommendations would be submitted to a future
Health and Wellbeing Board with a full report. An action plan
would then be created and submitted to another future
Health and Wellbeing Board.
The Chair confirmed that the conclusions and recommendations would play a significant role in the future of the Health and Wellbeing Board and the Health and Wellbeing Strategy.
RESOLVED:
(1) That this year’s Director of Public Health’s Annual
Public Health Report which focused on health
inequalities and their causes be noted.
Page 2

(2) That the recommendations in the report reflect the
widening role of public health and the importance of
partnership work to achieve the necessary system
wide changes be noted.
4. ACTIVE LAMBETH - DRAFT PHYSICAL ACTIVITY AND SPORTS
STRATEGY 2015 TO 2020
Adrian Smith, Donna Wiggins and Mark Cook introduced the report.
Members of the Board welcomed the report. Strategic Director of Delivery, Sue Foster, felt that the Council had contributed heavily in relation to keeping Lambeth active. She noted that some of the major infrastructure the Council had put in place had made considerable changes in activity in the borough including concessionary rates. A key way to deliver some of this was through the planning process.
In response to questions from Members, Adrian Smith, Donna Wiggins and Mark Cook informed the meeting that:
In relation to risk of violence in parks, much of the work
related to making parks become busy and this would help
with risk of violence. Some research had shown that there
was a total of 1% of violence occurs in parks in the borough.
This was partly due to the parks being locked at night.
Research would also be done in relation to the use of parks
with open access against parks which close during the night
to examine the difference in the level of violence.
There is a capital investment plan that would contribute to
facilities in parks and various methods would be used to
survey who used the parks. However the footfall had not
been regularly measured.
There was increasing usage in the parks as certain parks
had done some auditing of footfall. The usage appeared to
be increasing every year.
The capital investment plan would help with play areas.
A health impact assessment would be completed.
Efforts would be made to ensure that disabled groups would
be accounted for in all parts of their experience. For
example, access buildings would be equally as important as
use of facilities.
Efforts would be made to create a surplus so that a
progressive range of concessions could be given.
Page 3

Communities would be consulted on how some of the
funding would be used and general improvements would be
made on communicating with residents.
RESOLVED: (1) That continued support to develop the Active
Lambeth draft physical activity and sports strategy 2015 to 2020 and emerging governance process to a final stage for Health and Wellbeing Board approval by October 2015 be agreed.
(2) That the Board endorse the proposed shift towards
needs based health prevention commissioning, which increases participation, reduces health inequalities, reduces physically inactivity and achieves the shared outcomes through physical activity and sport.
5. "LAMBETH BLACK WELLBEING COMMISSION - FROM SURVIVING
TO THRIVING" - TAKING FORWARD THE RECOMMENDATIONS
The report was introduced by Denis O’Rourke.
The Chair informed that this was important report and could be a catalyst to understand the effectiveness of some of the services. The Chair welcomed the task and finish groups. He hoped that key areas would be monitored and welcomed input from the community in general.
Members felt that the report was overdue in being submitted to the Board but welcomed the report.
In response to questions from Members Denis O’Rourke informed the meeting that:
In relation to the practices of registration, this was a general
practice issue. People usually filled in their information on a
new registration which would record their ethnic origin. This
information would be kept by the practice and may need to
be complemented by individual history and experiences.
In relation to the measurement of health and wellbeing of a
specific segment of the community, work was being
completed with the Institute of Psychiatry and the impact of
the Living Well Collaborative was being examined.
There were aims to connect people and address social
isolation. A key part of this was involving people with
particular experiences and matching them with members of
the community with similar experiences.
The Equality Impact Assessment would be used where
appropriate.
Another report would be submitted to the Board in Autumn
Page 4

2015. Further discussions would be held at a future Chair’s
meeting and at the task and finish group.
RESOLVED:
(1) That the activity already taking place across various partnerships and programmes which support the Commission’s recommendations be noted.
(2) That the Board absorb the recommendations within
the relevant partnerships and programmes and future refresh of the Health and Wellbeing Strategy.
(3) That the formation of a multi-agency task and finish
group, led by the Health and Wellbeing Board Chair, help take forward actions with the objective of continuing to engage and communicate with black and ethnic minority communities and involve people directly in driving the changes.
(4) That an update report be delivered to the Health and
Wellbeing Board within six months.
6. SOUTHWARK AND LAMBETH EARLY ACTION COMMISSION UPDATE
Strategic Director of Commissioning, Helen Charlesworth May introduced the report.
The Chair felt that the borough’s involvement in this was a positive as was working in partnership with Southwark. The insights gained needed to be examined, particularly in relation to how the borough takes its early action forward.
Dr Wallis stated that it was important that early action was focused enough early action was a broad phrase. RESOLVED:
(1) That progress made on the Southwark and Lambeth
Early Action Commission be noted.
(2) To note that the two Health and Wellbeing Boards will be invited to consider emerging recommendations from the Commission in July 2015.
7. REDUCING HEALTH INEQUALITIES IN LAMBETH
Dr Ruth Wallis introduced the report.
Councillor Jackie Meldrum informed the Board that people with mental health problems commonly had difficulty getting support for their physical health issues. This was a key inequality issue.
Ms Moira McGrath stated that examining the physical health of people with mental health issues needed to be examined as there had been some new
Page 5

data found. For example, one study had found that some people with mental health problems had better outcome for diabetes and were less likely to suffer from diabetes.
Mr Andrew Eyres informed the meeting that health on average in the borough would improve, however reducing inequality was a priority. The inequality of access was also being examined.
RESOLVED:
(1) That the Lambeth Health and Wellbeing Strategy be
refreshed to ensure that it promotes best practices to address health inequalities.
(2) That Lambeth CCG work with Public Health Lambeth
to develop priorities for action to reduce health inequalities and map how their current objectives address health inequality, including wider determinants of health, and to develop an action plan.
(3) That the Board promote an integrated approach to
address health inequalities and review how to support the CCG Health inequality action plan.
(4) That, as part of this integrated approach, the project
emphasise proportionate universalism and partnership working, forging links between local community organisations, the local authority and local NHS services.
8. INTEGRATED PERSONALISED SUPPORT ALLIANCE (IPSA) - ADULT
MENTAL HEALTH
The report was introduced by Denis O’Rourke.
The meeting noted that governance arrangements with the Committee In Common would be a good test to see how IPSA could be managed and this could be a common feature in relation to working in the future.
RESOLVED:
1) That it be noted that the Council and NHS Lambeth CCG have agreed a section 75 partnership agreement to support the commissioning of the Integrated Personalised Support Alliance (IPSA) Agreement, with the provision of a pooled fund and lead commissioning arrangement, led by NHS Lambeth CCG.
2) That it be noted that the Integrated Personalised
Support Alliance Agreement (and allied NHS standard contracts) supporting service transformation as set out in the report has been agreed between parties and that the service went live as of 1 April 2015.
Page 6

9. STAYING HEALTHY PARTNERSHIP BOARD REPORT TO THE
HEALTH & WELLBEING BOARD
Dr Ruth Wallis introduced the report.
Dr Moxham stated that data over the last four years showed a stagnation in smoking prevalence in the borough. The Lambeth average was worse than the overall average of England and considerably worse than Greenwich. Lambeth have used primary care whereas Greenwich had used specialist smoking services to a greater extent.
Councillor Meldrum queried for further analysis of weight gain levels of people who give up smoking as there appeared to be greater pressure on NHS regarding weight issues as smoking prevalence had decreased.
Dr Wallis stated that it was likely that as smoking prevalence decreased, the saved funding had been reinvested into obesity.
The Chair felt that more should be done to send a message of a smoke free environment such as smoke free parks or ensuring the limitation of the opportunity to smoke in designated open areas due to harms that could be caused by secondary smoking. Parks and open spaces needed to be given particular consideration.
RESOLVED:
1) That the progress, plans and related work to support
the development of a Lambeth Tobacco Control Strategy be noted.
10. QUARTERLY DIRECTOR OF PUBLIC HEALTH REPORT - LAMBETH
AND SOUTHWARK (JAN - MARCH 2015)
RESOLVED:
That the report of the Director of Public Health covering the period of January to March 2015 be noted.
CLOSE OF MEETING
The meeting ended at 8:10pm
CHAIR
Date of Despatch: Friday 8 May 2015
Contact for Enquiries: Nazyer Choudhury
Tel: 020 7926 0028
Fax: 020 7926 2361
E-mail: [email protected]
Web: www.lambeth.gov.uk
The action column is for officers' use only and does not form a part of the formal
record.
Page 7

This page is intentionally left blank

Health & Wellbeing Board
8th July 2015
Quarterly Director of Public Health Report – Lambeth and Southwark (April – June 2015)
Wards: All
Report Authorised by: Dr Ruth Wallis, Director of Public Health (Lambeth and Southwark)
Contact for enquiries:
Dr Ruth Wallis, Director of Public Health - Lambeth and Southwark
0207525 1267
Report summary
This report is a quarterly report of the Joint Director of Public Health to the Lambeth &
Southwark Health and Wellbeing Boards and the Lambeth & Southwark clinical commissioning
groups.
Finance summary
None arising from this report.
Recommendations
1. To note the Director of Public Health Report covering the period January to March 2014.
Page 9 Agenda Item 3

1. Context
1.1 This is an update report for information only.
1.2 This report covers the following health improvement work streams:
Tobacco Control in Lambeth and Southwark
Lambeth Food Flagship Programme
Wellbeing
Children and Young People’s Health
Free Vitamin D Scheme
Norovirus
New Meningitis programmes
SH24
2. Proposals and Reasons
2.1 Introduction
This is the quarterly report of the Director of Public Health for Lambeth and Southwark for the
first quarter of 2015-2016. The report is for the London boroughs of Lambeth and Southwark,
and Lambeth and Southwark Clinical Commissioning Groups, as well as for all Health and
Wellbeing Boards partners.
The aim of the quarterly reports is to update partners on some of the activities of the Lambeth
and Southwark specialist public health team and work being done in partnership, and to provide
information about public health issues relevant to Lambeth and Southwark, including alerting
people to areas of concern or risk.
This quarter summaries are on Tobacco Control in Lambeth and Southwark, Lambeth Food
Flagship Programme, Wellbeing, Children and Young People’s Health, Free Vitamin D Scheme,
Norovirus, New Meningitis programmes and SH:24.
Comments and ideas for future topics are welcome. Please contact
Page 10

2.2 Tobacco Control in Lambeth and Southwark
Tobacco use is the major cause of preventable death in England and harms not just smokers
but the people around them, through the damaging effects of second hand smoke. Smoking is a
major cause of ill health and death in Lambeth and Southwark and health inequalities, with
those from routine and manual workers and other disadvantaged groups being about one and a
half times, and up to two times more likely to be smokers that the general population .
Compared to the rest of the country, Lambeth and Southwark are significantly higher in:
Lung cancer registrations
Oral cancer registrations
Smoking attributable deaths
Deaths from lung cancer
Deaths from chronic obstructive pulmonary disease
In addition to the direct medical and social costs of treating tobacco induced illnesses there are
other indirect costs including loss of productivity, fire damage and environmental harm from
cigarette litter. Spending on tobacco control measures can reduce these costs. Reducing
tobacco use will benefit the wider local and national economy. There is clear evidence that the
most effective tobacco control strategies involve taking a multi-faceted and comprehensive
approach at both national and local level.
Lambeth and Southwark have a long history of tackling smoking. It is important that we build on
successes and apply the learning from the work over the years into the development of the
comprehensive tobacco control strategy for each of the boroughs. Smoking cessation is one of
the most cost effective health interventions, every £1 spent on smoking cessation services
saves £10 in future costs. Although the proportion of smokers has fallen significantly over the
years, the decline has been much slower in Lambeth and Southwark. In the two boroughs, stark
inequalities exist with little positive change occurring within certain population groups, e.g.
routine and manual and those with mental health issues. Investing sufficiently in tackling
smoking is therefore essential if we want to improve health and reduce health inequalities in the
boroughs.
As part of the Strategy development, in addition to the review of the evidence on effective
interventions, a commissioner workshop focusing on a rapid review of the stop smoking
services was held in May. Analysis of Lambeth and Southwark stop smoking data (2013/14)
Page 11

across was presented. During that year, 4,373 smokers in Lambeth and 3,208 smokers in
Southwark set a quit date, with a quit rate of 39% for Lambeth and 36% for Southwark. Linking
location of GP practices with smoking prevalence, deprivation, COPD practice registers,
unemployment and actual Nicotine Replacement Therapy (NRT) spend, showed that many
areas with expected high need did not appear to have the associated expected spend on NRT.
The workshop also highlighted missed opportunities; vidence suggests that smokers are up to
four times more likely to succeed with stop smoking services than if they try to quit on their
own. Exploration of pharmacological reports identified at least 2,218 smokers in Lambeth and
3,316 in Southwark had attempted to quit smoking on their own. A larger proportion of these
smokers would have quit if they had been supported through the stop smoking service,
opportunities to harness this cohort of motivated quitters should be sought.
The workshop also highlighted the need to prioritise interventions that tackle inequalities and a
focus on prevention of long term conditions. Some insight work is currently being undertaken
with communities across Lambeth and Southwark and includes engaging with smokers and ex-
smokers, their views will help to inform the stop smoking service model to be commissioned
from April 2016 onwards. An event is being organised for July 2015, which will bring together
stakeholders, including commissioners, providers and residents to help consolidate a model that
further meets local needs
Previous survey results revealed that in Lambeth and Southwark an estimated 57% and 73%
smokers respectively were offered illegal tobacco over a one year period. During this period,
36% of Lambeth smokers and 56% of Southwark smokers bought illegal tobacco. Illegal
tobacco is often associated with other criminal activity and increases demand and supply
amongst children. The South East London Illegal Tobacco Network (a network of public health
and trading standards teams in South East London) is running a ‘call to action’ campaign to
change acceptability of illegal tobacco. The campaign will ask people to pass on the message
and report anyone they believe is selling illegal tobacco in their area. Experience from other
similar campaigns shows that it changes views of those who may perceive illegal tobacco as a
victimless crime, can drive a significant increase in the number of reports made from the public
regarding illegal sellers, which in turn can make these sellers less comfortable. Over the
summer, the campaign will be actively promoted at the following events:
Lambeth Country Show Saturday 18 July 2015 and Sunday 19 July 2015
Bermondsey Carnival Saturday 4 July 2015
Elephant and Nun Festival Saturday 15 August 2015
Page 12
2.3 Lambeth Food Flagship Programme
Following a successful bidding process in 2014, Lambeth was awarded Food Flagship status.
As a London Food Flagship Borough, our vision is for all Lambeth residents to develop a love of
healthy and sustainable food.
Being a Food Flagship Borough brings with it funding opportunities and support guaranteed for
two years but possible longer. The Lambeth Food Flagship Programme consists of range of
interventions and projects including:
• The implementation of the School Food Plan in all Lambeth schools via Lead Food
Flagship Schools
• Development of community activities including food growing initiatives
• Implementation of the Alexandra Rose Vouchers to support vulnerable families with
young children to be able to buy more fruits and vegetables
• Local Capacity building and development including working with young people,
businesses, and the Lambeth Food Partnership – which represents over 200 community
groups across Lambeth
• Implementing a summer Healthy Eating Holidays
• Evaluation of programme, learning and development.
The work with Lambeth schools on the new School Food Plan is progressing. The four identified
Lead Food Flagship groups are providing training and supporting other schools within their
cluster to adopt the plan. In addition, the Natural Thinkers project which links children to nature
is extending the offer to schools, children centres and 1 o clock clubs.
Public Health will also work with our local networks and partners to encourage the
implementation of the School Food Plan in all Southwark schools.
The Rose Voucher for Fruit and Vegetable which is a scheme funded by the Food Flagship
Programme, will start this month in 6 children centres. The scheme seeks to increase the
consumption of fresh fruit and vegetables of some of the most vulnerable families in Lambeth,
with a focus on low income families. Low-income families expecting a baby or that have small
children (under 4 years old), are helped to access more healthy affordable food through the
provision of financial and motivational support. The Rose Voucher in Lambeth cohort includes
Page 13

Healthy Start recipients (and those eligible), POE families (Priority of Excluded groups) and
those families that have ‘no recourse to public funds’ (such as asylum seekers). Focussing on
these families, the scheme supports behaviour change interventions and activities alongside
providing vouchers that can be exchanged for fruit and vegetables at a range of local and
neighbourhood food outlets. By locating the Rose Voucher registration and distribution at
Children’s Centres the scheme supports participants’ engagement with existing interventions
and activities focused on health and wellbeing. Five fruit and vegetable stalls in Brixton Market
have signed an agreement to accept and redeem the vouchers.
The Healthy Holiday Programme (funded until the end of the Summer), will be developing the
capacity of organisations that run holiday programmes for vulnerable children to promote
healthy eating to children and their families and to provide healthy free lunches in a pleasant
environment to these children. In addition, a community food poverty worker will work with
families, providing support and advice to build future resilience, knowledge and skills around
addressing the underlying causes of food poverty, e.g. budgetary and benefits advice;
employment and skills development, etc .
Being a Food Flagship Borough has also brought national interest from a range of external
stakeholders wanting to work with the borough. For example, the national Change4Life
Programme has recently attended one of the summer food festivals in Lambeth to pilot and test
a new resource package.
Evaluation is a key element of the Flagship Programme, Lambeth and Southwark Public Health,
the GLA, PHE and academic partners are working together to ensure that we gather learning
from the Programme.
2.4. Wellbeing
2.4.1 Wellbeing and Happiness small grants fund
London Community Foundation has received 95 applications for the small grants fund to
promote mental wellbeing in Lambeth and Southwark. A panel meeting will be held in June and
grants will be awarded from a pot of just over £30k. Some monies will be used to support
monitoring and evaluation for successful groups. Favour will be given to those working with
Page 14

groups experiencing poor wellbeing, smaller grassroots organisations working at neighbourhood
level where they can demonstrate what the community wants rather than a ‘good idea’ by paid
professionals and those who are taking an ‘asset based’ approach.
A report on the previous year’s grant funding is expected shortly. These included projects run by
‘A mile in her shoes’, Carenet, Clapham Park Project, Home Start Southwark, Lambeth Asian
Centre, Sickle Cell & Young Stroke Survivors, Silverfit, South London Cares, Springfield
Community Flat and the Streatham Drop in Centre for Asylum Seekers and Refugees.
2.4.2 Wellbeing network
The network met in April at the Employment Academy, Peckham. The aim of this meeting was
to enable members to set the agenda and priorities for the Wellbeing Programme for the next
year. These have fallen into five groupings:
1. Poverty and financial exclusion
2. Loneliness
3. Café for a CAF-Community Assessment Framework (peer support and solutions
for those in crisis)
4. ‘Open Dialogue’ in Lambeth and Southwark (see;
http://www.nelft.nhs.uk/mental_health/Open_dialogue)
5. Community empowerment to take action on isolation
The full report is available at https://lambethwellbeing.files.wordpress.com/2015/05/final-
lambeth-southwark-wellbeing-network-report-200515.pdf
We are beginning to identify with colleagues where there is work currently going on that we as a
network could build on and contribute to, particularly around the loneliness and financial
exclusion work.
2.4.3 Brixton Reel 2015
Plans are underway for this year’s Brixton Reel film festival which will take place in Lambeth
October to coincide with World Mental Health Day. The aim of the festival is to use film as way
to engage with different community groups, especially African-Caribbean and African people,
and increase understanding of how to look after your mental health and wellbeing and where to
get help locally. It links into the recommendations of Lambeth’s black health and wellbeing
commission.
Page 15

This year’s theme for World Mental Health Day is ‘Dignity in Mental Health’. This year ideas
include working with the Chinese/Vietnamese and Somali communities as well as having a
specific LGBT focus. Partners on the project so far are Time to Change, Black Cultural
Archives, Mosaic, GST NHS Trust, SLAM NHS Trust and the Dragon Café.
More on previous year’s projects can be found at www.brixtonreel.co.uk
2.5 Children and Young People’s Health in Lambeth and Southwark
A number of key documents inform the current work across both boroughs. These include:
CAMHS Needs Assessment (NA)
CYPHP Young People’s Needs Assessment
Neglect NA (Southwark)
Vitamin D report
Reviews (HV/School Nurses)
Obesity/NCMP survey/analysis
Knee High ethnography
CDOP Annual Report
Routine data e.g. Child health profiles (PHE)
From these the following emerging needs/priorities have been identified:
Maternity to under-5 (a better start/school ready)
Young Peoples Health 10-25 (sexual health/drugs/violence)
Emotional wellbeing and mental health
LTCs (diabetes/asthma/epilepsy/sickle cell)
Emergency Admissions avoidance
Safeguarding
o vulnerable CYP e.g. LAC/SEND/CIN, offenders
- neglect, FGM, CSE
Childhood Obesity
Work has begun on a Children’s and Young People’s JSNA for both boroughs. The process
includes the coming together of small partnership groups from the local authority and the
Clinical Commissioning Groups (CCGs) and public health to agree the scope of the needs
assessment and to identify who is leading and who is undertaking work.
Page 16
The aim of the Children and Young People’s (CYP) JSNA is to profile and describe needs of
CYP and the relevant services (including safeguarding) and present the main priorities to
commissioners/other stakeholders for consideration
There will be two phases of the work
• Phase 1: Overview of demography, and main health, social care and safeguarding
needs and services: end of August
• Phase 2:
– Engagement/coproduction
– Compare existing services to best practice guidelines: October/November 2015
Key Stakeholders include the local authorities, CCGs, Patient and Public representatives,
Provider representatives and the Voluntary Sector.
The JSNA partnership group will report to the Health and Wellbeing Board and the HSC
Partnership.
The draft Scope and Content of the Children’s and Young People’s JSNA covers the following:
• Intro, Methods, Key findings
• Population Profile: Ethnicity, religion, child poverty, deprivation, LAC, disability,
• Maternal Health and Birth Data
• Early Years (under-5)
• School Age & Young People (5 to 25 in 5 yearly groups)
• Education & Employment
• Safeguarding
• Disabilities and complex needs children
• Children in Care
• Stakeholder and user engagement
2.6 Free Vitamin D scheme in Lambeth and Southwark
2.6.1 Introduction & Background
Page 17

The Department of Health has identified the following groups of being at risk of vitamin D
deficiency:
a. infants and children aged under 5
b. pregnant and breastfeeding women, particularly teenagers and young women
c. people over 65
d. people who have low or no exposure to the sun, for example, those who cover
their skin for cultural reasons, who are housebound or confined indoors for long
periods
e. people with darker skin, for example, people of African, African-Caribbean or
South Asian family origin.
NICE Public Health Guidance (PH56) recommends that local authorities should ensure Vitamin
D supplements containing the recommended reference nutrient intake are readily available for
all at risk groups such as by considering promoting free supplements for at risk groups.
As Part of the Healthy Child Programme to prevent the increasing rise of Vitamin D deficiency
and in more extreme cases rickets in children under 5 years, Lambeth joint commissioning and
Southwark CCG agreed to fund a free Vitamin D scheme in both boroughs. The scheme
provides free Vitamin D (Healthy Start Vitamins) to all pregnant women, new mothers and all
children under 4 years in Lambeth and Southwark. The Free Vitamin D scheme started at the
beginning of September 2014
2.6.2 Scheme in Lambeth & Southwark
The scheme is operated through community pharmacies. Currently there are 20 pharmacies
involved in Lambeth and 21 in Southwark.
A Vitamin D co-ordinator supports the scheme and informs all those working with mothers and
children as well as community/voluntary organisations about the scheme. Data to the end of
March 2015 shows that:
In Lambeth 24.9% under 4 year olds were registered on the scheme and receiving
vitamins.
In Southwark 15.5% of under 4 year olds were registered on the scheme and receiving
vitamins.
41% of mothers heard about the scheme from their health visitor, 29% from pharmacy,
14% from the GP and 11% from midwives, others included children centres/posters.
Page 18

59% of children receiving vitamins are 0-12 months, 20% are one year olds, 14% are
two year olds, 7% aged 3 years.
52% of children registered on the scheme are from BME communities.
2.6.3 Awareness Raising:
The Vitamin D co-ordinator undertakes an on-going programme of awareness raising sessions
about the importance of Vitamin D and the free scheme which includes health visitors,
midwives, foster carers, GP Locality meetings, practice nurses etc.
2.6.4 Work with Primary Care:
Work is being undertaken with Southwark CCG to add a protocol alert to help clinicians in
primary care signpost to the programme. Once agreed this will be shared with Lambeth CCG. It
is also hoped that the new Clinical Effectiveness Group will work on alerts for vitamin D to be
added to antenatal, postnatal and six week check-up templates.
2.6.5 Evaluation
An evaluation of the first year of the scheme is planned for September 2015.
2.7 Norovirus
There was an outbreak of norovirus in Kings College Hospital on both sites (Denmark Hill and
Princess Royal University Hospital). It started in early April, and by mid May there was just one
ward affected (haematology/oncology). The control measures were implemented very efficiently
by the acute trust including scrutinising patients arriving in A & E with a history of acute
diarrhoea. Anyone with any history of D or V (diarrhoea and vomiting), was isolated and treated
as probably having norovirus until proven otherwise. This outbreak affected also a number of
staff within the acute trust.
KCH Infection control team may review the profile of patients affected including from where they
came from and their recent contact with Health services.
The Public Health team supported the dissemination of information on management of D& V in
care home and GP practices. They also facilitated the exchange of information between key
stakeholders (Acute Trust, CCG and PHE-SEL)
Page 19

Lessons learned:
- Review factors affecting early detection of the outbreak
- Monitoring case profile to be able to establish risk of transmission within the community
- Consider including syndromic surveillance in the monitoring of gastroenteritis outbreak
2.8 New Meningitis programmes
Two new Meningitis vaccination programmes will be introduced from September 2015. The
Meningitis B infant programme will be added to the routine infant vaccination schedule, with new
fever guidance. The Meningitis ACWY adolescent programme is being introduced as a rapid
response to increasing Meningitis W cases, and has been declared a national incident. It will
replace the current Meningitis C programme.
As laid out in a recent NHSE/ PHE communication1, following recommendations from the Joint
Committee on Vaccination and Immunisation (JCVI), the meningococcal B disease (MenB)
infant vaccination programme is expected to reduce meningitis and septicaemia cases and
associated serious complications, as well as provide reassurance to parents. The new MenB
vaccination will be delivered through general practice (through an NHSE enhanced service) to
babies born after 1st July 2015, at their 1st and 3rd routine immunisation appointments (at 2 and 4
months), with a booster at 12/13 months. There will also be a small catch up programme for
children born May-June 2015.
Guidance includes advice for both healthcare professionals and parents/carers around the
increased risk of fever, and therefore prophylactic use of paracetamol at regular intervals
following vaccination. As this counters existing paracetamol guidelines, additional training and
resources will be provided locally, as well as revised guidance. PHE South East London Health
Protection Team are working with Lambeth and Southwark CCGs, Public Health and GSTT
Community Health Services Immunisation Team to deliver updates by September 2015.
Meningococcal ACWY conjugate vaccination (MenACWY) programme, also detailed in
recent NHSE/ PHE communication2, is being introduced across England this year to respond to
a rapid and accelerating increase in cases of invasive meningococcal group W (MenW) disease,
1 https://www.gov.uk/government/publications/menb-vaccination-introduction-from-1-september-
2015
2 https://www.gov.uk/government/publications/menacwy-vaccine-introduction
Page 20

which has been declared a national incident. MenACWY conjugate vaccine will provide direct
protection to the vaccinated cohort as well as indirect protection to unvaccinated children and
adults. This follows JCVI advice, and will replace existing MenC vaccination.
The programme is recognised as a significant additional workload for those involved in its
delivery. This is expected as follows:
An urgent catch-up campaign for current school year 13 adolescents using a call and recall
system through general practice from August 2015 (with further catch up of school years 11
and 12 once they reach year 13)
A catch-up campaign for current school year 10 students through schools from January
2016
Adding MenACWY vaccine to the routine adolescent schools programme (school year 9 or
10) from Autumn 2015, as a direct replacement for the MenC vaccination
Adding MenACWY vaccine to the existing time-limited ‘freshers’ programme (ie for older first
time university entrants who have not already received MenACWY, replacing MenC)
delivered through general practice.
MenACWY update will be provided alongside those for MenB to general practice in Lambeth
and Southwark, and any additional opportunities for enabling this are being sought. In addition it
should be noted that due to the speed of MenACWY programme cohort implementation,
national vaccine stock will be more limited, and temporary ordering restrictions may come into
place.
2.9. SH:24
March – June 2015 update
About this document
Page 21

This document provides an update of the progress of SH:24 since its launch in March this year.
It offers a snapshot of early data on the uptake of the service, an insight into how the service
has been received by users, and information on the next phases of development.
Background
SH:24 provides people with free sexually transmitted infection (STI) test kits, information and
advice – 24 hours a day. Users can get tested for the four most common sexually STIs:
chlamydia, gonorrhea, syphilis and HIV. The service is quick, discreet and completely
confidential and is fully integrated with local specialist sexual health services.
SH:24 has created its unique approach to building the service through a Community Interest
Company (CIC) model, which brings together a diverse partnership including local NHS services
and commissioners. The development of the service is funded by Guy’s and St Thomas’ Charity
and the STI testing element of the service is funded by local authority commissioners – SH:24
has been contracted to deliver STI testing in Lambeth and Southwark from 01 March 2015.
Launch of the service
Page 22

As a lean start-up SH:24 hasn’t adopted a hard launch approach (that involves vigorous
marketing and advertising campaigns) but instead has softly launched the service, testing out
various ways of raising awareness in a targeted way.
Early promotion of the service focused on ensuring people currently accessing specialist sexual
health services know there is an online alternative. Having developed close partnerships with
our local specialist clinics (Burrell Street and Camberwell), community sexual health clinics, GPs
and pharmacies across Lambeth and Southwark during the development of the service, posters
and mini-business cards are displayed in all of these settings.
Additionally, large vinyls are now displayed on Burrell Street and Camberwell clinic’s street
facing windows (see below) – which adopt some of SH:24’s tried and tested messaging and
iconography. Digital tags (NFC) have been integrated into the vinyl’s to allow passers-by to
simply tap their phone and instantly access the order a test kit button on the website.
More recently, promotion was stepped up with the distribution of our mini business cards in high
footfall and commuter areas in the boroughs. Promotional material has also been distributed to
a variety of community spaces - from local enterprises such as the Stockwell Partnership and
Better Bankside to libraries in the boroughs. We are currently working with local police, bars and
clubs to arrange for our stickers and posters to be displayed on their premises and to run a
Lesbian Gay Bisexual and Transgender (LGBT) focused event.
There have been a range of positive features in local press and press targeted at typically
higher risk groups – which have helped to create notable increases in usage of the service.
Page 23

SH:24 is currently in discussions with national press and local radio stations to increase
coverage and continue to raise awareness about the service.
Data and early insights
To date SH:24 has received 1,132 orders, 61% from women and 39% from men, broadly
reflecting the gender split of clinic users. The website has received 4,312 visitors (70% of which
are new) and 21,663 page views. Nearly 60% of users access SH:24 using their mobile phone
which confirmed our early user research that indicated a strong preference for accessing sexual
health services via mobile devices.
Over half of users (53%) have returned their test – which is above the return rate of other
comparable online services and suggests the redesign of test kit packaging and support
material users receive during the user journey has had a positive impact.
94% of SH:24 users are asymptomatic and 40% have visited a clinic in the past 12 months –
indicating that SH:24 is working towards its aim of shifting a proportion of asymptomatic clinics
users online and helping to tackle the current pressure on services. Early data is also showing
that SH:24 is being used by high risk groups: 19% of users are from Black and Ethnic Minority
(BME) backgrounds, 17% are men who have sex with men (MSM) and 85% are under 35. The
uptake amongst BME users is particularly encouraging – who can be harder to reach and often
less likely to use digital services.
SH:24 has received positive feedback from users directly and also online via social media (see
tweets below).
Page 24
Next steps
The STI testing element of SH:24 is the first phase of development. Over the next two years
SH:24 will continue to develop the service iteratively to include improved user support options
and optimisation of elements of the service (this phase has been recently initiated), emergency
hormonal contraception (EHC), oral contraception, partner notification and treatment for
chlamydia.
More information
For more information about the service visit:
Website – www.sh24.org.uk
Blog - https://sh24.squarespace.com
Twitter - @sh24_nhs
3. Finance
3.1 There are no financial implications to this report.
4. Legal and Democracy
4.1 There are no legal comments arising from this report. Specific legal advice will be
provided as requested.’
5. Consultation and co-production
5.1 Not applicable.
6. Risk management
6.1 Not applicable.
7. Equalities impact assessment
7.1 Not applicable.
8. Community safety
8.1 Not applicable.
9. Organisational implications
Page 25

The following sections must be considered, but are optional and each should be deleted
if not relevant to the report. If there are no organisational implications, state “None”.
9.1 Environmental
None.
9.2 Staffing and accommodation
None.
9.3 Procurement
None.
9.4 Health
None.
10. Timetable for implementation
10.1 Not applicable.
Page 26

Page 27

Page 28

Lambeth and Southwark Public Health
Director of Public Health: Dr Ruth Wallis
Public Health in
Lambeth and Southwark
Director of Public Health Report
April – June 2015
Page 29

2
Introduction
This is the quarterly report of the Director of Public Health for Lambeth and Southwark for the first
quarter of 2015-2016. The report is for the London boroughs of Lambeth and Southwark, and
Lambeth and Southwark Clinical Commissioning Groups, as well as for all Health and Wellbeing Boards
partners.
The aim of the quarterly reports is to update partners on some of the activities of the Lambeth and
Southwark specialist public health team and work being done in partnership, and to provide
information about public health issues relevant to Lambeth and Southwark, including alerting people
to areas of concern or risk.
This quarter summaries are on Tobacco Control in Lambeth and Southwark, Lambeth Food Flagship
Programme, Wellbeing, Children and Young People’s Health, Free Vitamin D Scheme, Norovirus, New
Meningitis programmes and SH:24.
Comments and ideas for future topics are welcome. Please contact [email protected]
1. Tobacco Control in Lambeth and Southwark
Tobacco use is the major cause of preventable death in England and harms not just smokers but the
people around them, through the damaging effects of second hand smoke. Smoking is a major cause
of ill health and death in Lambeth and Southwark and health inequalities, with those from routine and
manual workers and other disadvantaged groups being about one and a half times, and up to two
times more likely to be smokers that the general population . Compared to the rest of the country,
Lambeth and Southwark are significantly higher in:
Lung cancer registrations
Oral cancer registrations
Smoking attributable deaths
Deaths from lung cancer
Deaths from chronic obstructive pulmonary disease
In addition to the direct medical and social costs of treating tobacco induced illnesses there are other
indirect costs including loss of productivity, fire damage and environmental harm from cigarette litter.
Spending on tobacco control measures can reduce these costs. Reducing tobacco use will benefit the
Page 30

3
wider local and national economy. There is clear evidence that the most effective tobacco control
strategies involve taking a multi-faceted and comprehensive approach at both national and local level.
Lambeth and Southwark have a long history of tackling smoking. It is important that we build on
successes and apply the learning from the work over the years into the development of the
comprehensive tobacco control strategy for each of the boroughs. Smoking cessation is one of the
most cost effective health interventions, every £1 spent on smoking cessation services saves £10 in
future costs. Although the proportion of smokers has fallen significantly over the years, the decline has
been much slower in Lambeth and Southwark. In the two boroughs, stark inequalities exist with little
positive change occurring within certain population groups, e.g. routine and manual and those with
mental health issues. Investing sufficiently in tackling smoking is therefore essential if we want to
improve health and reduce health inequalities in the boroughs.
As part of the Strategy development, in addition to the review of the evidence on effective
interventions, a commissioner workshop focusing on a rapid review of the stop smoking services was
held in May. Analysis of Lambeth and Southwark stop smoking data (2013/14) across was presented.
During that year, 4,373 smokers in Lambeth and 3,208 smokers in Southwark set a quit date, with a
quit rate of 39% for Lambeth and 36% for Southwark. Linking location of GP practices with smoking
prevalence, deprivation, COPD practice registers, unemployment and actual Nicotine Replacement
Therapy (NRT) spend, showed that many areas with expected high need did not appear to have the
associated expected spend on NRT. The workshop also highlighted missed opportunities; vidence
suggests that smokers are up to four times more likely to succeed with stop smoking services than if
they try to quit on their own. Exploration of pharmacological reports identified at least 2,218 smokers
in Lambeth and 3,316 in Southwark had attempted to quit smoking on their own. A larger proportion
of these smokers would have quit if they had been supported through the stop smoking service,
opportunities to harness this cohort of motivated quitters should be sought.
The workshop also highlighted the need to prioritise interventions that tackle inequalities and a focus
on prevention of long term conditions. Some insight work is currently being undertaken with
communities across Lambeth and Southwark and includes engaging with smokers and ex-smokers,
their views will help to inform the stop smoking service model to be commissioned from April 2016
onwards. An event is being organised for July 2015, which will bring together stakeholders, including
commissioners, providers and residents to help consolidate a model that further meets local needs
Previous survey results revealed that in Lambeth and Southwark an estimated 57% and 73% smokers
Page 31

4
respectively were offered illegal tobacco over a one year period. During this period, 36% of Lambeth
smokers and 56% of Southwark smokers bought illegal tobacco. Illegal tobacco is often associated with
other criminal activity and increases demand and supply amongst children. The South East London
Illegal Tobacco Network (a network of public health and trading standards teams in South East
London) is running a ‘call to action’ campaign to change acceptability of illegal tobacco. The campaign
will ask people to pass on the message and report anyone they believe is selling illegal tobacco in their
area. Experience from other similar campaigns shows that it changes views of those who may
perceive illegal tobacco as a victimless crime, can drive a significant increase in the number of reports
made from the public regarding illegal sellers, which in turn can make these sellers less comfortable.
Over the summer, the campaign will be actively promoted at the following events:
Lambeth Country Show Saturday 18 July 2015 and Sunday 19 July 2015
Bermondsey Carnival Saturday 4 July 2015
Elephant and Nun Festival Saturday 15 August 2015
2. Lambeth Food Flagship Programme
Following a successful bidding process in 2014, Lambeth was awarded Food Flagship status. As a
London Food Flagship Borough, our vision is for all Lambeth residents to develop a love of healthy and
sustainable food.
Being a Food Flagship Borough brings with it funding opportunities and support guaranteed for two
years but possible longer. The Lambeth Food Flagship Programme consists of range of interventions
and projects including:
• The implementation of the School Food Plan in all Lambeth schools via Lead Food Flagship
Schools
• Development of community activities including food growing initiatives
• Implementation of the Alexandra Rose Vouchers to support vulnerable families with young
children to be able to buy more fruits and vegetables
• Local Capacity building and development including working with young people, businesses,
and the Lambeth Food Partnership – which represents over 200 community groups across
Lambeth
Page 32
5
• Implementing a summer Healthy Eating Holidays
• Evaluation of programme, learning and development.
The work with Lambeth schools on the new School Food Plan is progressing. The four identified Lead
Food Flagship groups are providing training and supporting other schools within their cluster to adopt
the plan. In addition, the Natural Thinkers project which links children to nature is extending the offer
to schools, children centres and 1 o clock clubs.
Public Health will also work with our local networks and partners to encourage the implementation
of the School Food Plan in all Southwark schools.
The Rose Voucher for Fruit and Vegetable which is a scheme funded by the Food Flagship
Programme, will start this month in 6 children centres. The scheme seeks to increase the
consumption of fresh fruit and vegetables of some of the most vulnerable families in Lambeth, with a
focus on low income families. Low-income families expecting a baby or that have small children (under
4 years old), are helped to access more healthy affordable food through the provision of financial and
motivational support. The Rose Voucher in Lambeth cohort includes Healthy Start recipients (and
those eligible), POE families (Priority of Excluded groups) and those families that have ‘no recourse to
public funds’ (such as asylum seekers). Focussing on these families, the scheme supports behaviour
change interventions and activities alongside providing vouchers that can be exchanged for fruit and
vegetables at a range of local and neighbourhood food outlets. By locating the Rose Voucher
registration and distribution at Children’s Centres the scheme supports participants’ engagement with
existing interventions and activities focused on health and wellbeing. Five fruit and vegetable stalls in
Brixton Market have signed an agreement to accept and redeem the vouchers.
The Healthy Holiday Programme (funded until the end of the Summer), will be developing the
capacity of organisations that run holiday programmes for vulnerable children to promote healthy
eating to children and their families and to provide healthy free lunches in a pleasant environment to
these children. In addition, a community food poverty worker will work with families, providing
support and advice to build future resilience, knowledge and skills around addressing the underlying
causes of food poverty, e.g. budgetary and benefits advice; employment and skills development, etc .
Being a Food Flagship Borough has also brought national interest from a range of external
stakeholders wanting to work with the borough. For example, the national Change4Life Programme
has recently attended one of the summer food festivals in Lambeth to pilot and test a new resource
package.
Page 33

6
Evaluation is a key element of the Flagship Programme, Lambeth and Southwark Public Health, the
GLA, PHE and academic partners are working together to ensure that we gather learning from the
Programme.
3. Wellbeing
Wellbeing and Happiness small grants fund
London Community Foundation has received 95 applications for the small grants fund to promote
mental wellbeing in Lambeth and Southwark. A panel meeting will be held in June and grants will be
awarded from a pot of just over £30k. Some monies will be used to support monitoring and evaluation
for successful groups. Favour will be given to those working with groups experiencing poor wellbeing,
smaller grassroots organisations working at neighbourhood level where they can demonstrate what
the community wants rather than a ‘good idea’ by paid professionals and those who are taking an
‘asset based’ approach.
A report on the previous year’s grant funding is expected shortly. These included projects run by ‘A
mile in her shoes’, Carenet, Clapham Park Project, Home Start Southwark, Lambeth Asian Centre,
Sickle Cell & Young Stroke Survivors, Silverfit, South London Cares, Springfield Community Flat and the
Streatham Drop in Centre for Asylum Seekers and Refugees.
Wellbeing network
The network met in April at the Employment Academy, Peckham. The aim of this meeting was to
enable members to set the agenda and priorities for the Wellbeing Programme for the next year.
These have fallen into five groupings:
1. Poverty and financial exclusion
2. Loneliness
3. Café for a CAF-Community Assessment Framework (peer support and solutions for those in
crisis)
4. ‘Open Dialogue’ in Lambeth and Southwark (see;
http://www.nelft.nhs.uk/mental_health/Open_dialogue)
5. Community empowerment to take action on isolation
Page 34

7
The full report is available at https://lambethwellbeing.files.wordpress.com/2015/05/final-lambeth-
southwark-wellbeing-network-report-200515.pdf
We are beginning to identify with colleagues where there is work currently going on that we as a
network could build on and contribute to, particularly around the loneliness and financial exclusion
work.
Brixton Reel 2015
Plans are underway for this year’s Brixton Reel film festival which will take place in Lambeth October
to coincide with World Mental Health Day. The aim of the festival is to use film as way to engage with
different community groups, especially African-Caribbean and African people, and increase
understanding of how to look after your mental health and wellbeing and where to get help locally. It
links into the recommendations of Lambeth’s black health and wellbeing commission.
This year’s theme for World Mental Health Day is ‘Dignity in Mental Health’. This year ideas include
working with the Chinese/Vietnamese and Somali communities as well as having a specific LGBT focus.
Partners on the project so far are Time to Change, Black Cultural Archives, Mosaic, GST NHS Trust,
SLAM NHS Trust and the Dragon Café.
More on previous year’s projects can be found at www.brixtonreel.co.uk
4. Children and Young People’s Health in Lambeth and Southwark.
Children and Young People’s (CYP) Health in Lambeth and Southwark.
A specific Joint Strategic Needs Assessment for CYP is being done for Lambeth and Southwark. This
will make recommendations to improve health and wellbeing, and to inform commissioning
intentions. The JSNA will be done in two phases:
• Phase 1: Overview of demography, and main health, social care and safeguarding needs and
services: end of August
• Phase 2:
– Engagement/coproduction with stakeholders
– Service provision and best practice: October/November 2015
Key stakeholders include the local authorities, CCGs, Patient and Public representatives, Provider
representatives and the Voluntary Sector.
Page 35

8
A JSNA steering group will report to the Health and Wellbeing Board and other relevant forums.
The proposed content is outlined below and it has been developed from best practice JSNAs in other
local authorities:
• Intro, Methods, Key findings
• Population Profile: Ethnicity, religion, child poverty, deprivation, LAC, disability,
• Maternal Health and Birth Data
• Early Years (under-5)
• School Age & Young People (5 to 25 in 5 yearly groups)
• Education & Employment
• Safeguarding
• Disabilities and complex needs children
• Children in Care
• Stakeholder and user engagement
This JSNA will also use and signpost to recent and ongoing work where it is relevant. Such work is
diverse and detailed, and includes findings from partners such as the CYPHP and LEAP as well as
current priorities like the vitamin D supplementation programme and the neglect needs assessment.
5. Free Vitamin D scheme in Lambeth and Southwark
Introduction & Background
The Department of Health has identified the following groups of being at risk of vitamin D deficiency:
a. infants and children aged under 5
b. pregnant and breastfeeding women, particularly teenagers and young women
c. people over 65
d. people who have low or no exposure to the sun, for example, those who cover their
skin for cultural reasons, who are housebound or confined indoors for long periods
e. people with darker skin, for example, people of African, African-Caribbean or South
Asian family origin.
NICE Public Health Guidance (PH56) recommends that local authorities should ensure Vitamin D
Page 36

9
supplements containing the recommended reference nutrient intake are readily available for all at risk
groups such as by considering promoting free supplements for at risk groups.
As Part of the Healthy Child Programme to prevent the increasing rise of Vitamin D deficiency and in
more extreme cases rickets in children under 5 years, Lambeth joint commissioning and Southwark
CCG agreed to fund a free Vitamin D scheme in both boroughs. The scheme provides free Vitamin D
(Healthy Start Vitamins) to all pregnant women, new mothers and all children under 4 years in
Lambeth and Southwark. The Free Vitamin D scheme started at the beginning of September 2014
Scheme in Lambeth & Southwark
The scheme is operated through community pharmacies. Currently there are 20 pharmacies involved
in Lambeth and 21 in Southwark.
A Vitamin D co-ordinator supports the scheme and informs all those working with mothers and
children as well as community/voluntary organisations about the scheme. Data to the end of March
2015 shows that:
In Lambeth 24.9% under 4 year olds were registered on the scheme and receiving vitamins.
In Southwark 15.5% of under 4 year olds were registered on the scheme and receiving
vitamins.
41% of mothers heard about the scheme from their health visitor, 29% from pharmacy, 14%
from the GP and 11% from midwives, others included children centres/posters.
59% of children receiving vitamins are 0-12 months, 20% are one year olds, 14% are two year
olds, 7% aged 3 years.
52% of children registered on the scheme are from BME communities.
Awareness Raising:
The Vitamin D co-ordinator undertakes an on-going programme of awareness raising sessions about
the importance of Vitamin D and the free scheme which includes health visitors, midwives, foster
carers, GP Locality meetings, practice nurses etc.
Work with Primary Care:
Work is being undertaken with Southwark CCG to add a protocol alert to help clinicians in primary care
signpost to the programme. Once agreed this will be shared with Lambeth CCG. It is also hoped that
the new Clinical Effectiveness Group will work on alerts for vitamin D to be added to antenatal,
postnatal and six week check-up templates.
Page 37

10
Evaluation
An evaluation of the first year of the scheme is planned for September 2015.
6. Norovirus
There was an outbreak of norovirus in Kings College Hospital on both sites (Denmark Hill and Princess
Royal University Hospital). It started in early April, and by mid May there was just one ward affected
(haematology/oncology). The control measures were implemented very efficiently by the acute trust
including scrutinising patients arriving in A & E with a history of acute diarrhoea. Anyone with any
history of D or V (diarrhoea and vomiting), was isolated and treated as probably having norovirus until
proven otherwise. This outbreak affected also a number of staff within the acute trust.
KCH Infection control team may review the profile of patients affected including from where they
came from and their recent contact with Health services.
The Public Health team supported the dissemination of information on management of D& V in care
home and GP practices. They also facilitated the exchange of information between key stakeholders
(Acute Trust, CCG and PHE-SEL)
Lessons learned:
- Review factors affecting early detection of the outbreak
- Monitoring case profile to be able to establish risk of transmission within the community
- Consider including syndromic surveillance in the monitoring of gastroenteritis outbreak
7. New Meningitis programmes
Two new Meningitis vaccination programmes will be introduced from September 2015. The Meningitis
B infant programme will be added to the routine infant vaccination schedule, with new fever
guidance. The Meningitis ACWY adolescent programme is being introduced as a rapid response to
increasing Meningitis W cases, and has been declared a national incident. It will replace the current
Meningitis C programme.
Page 38

11
As laid out in a recent NHSE/ PHE communication1, following recommendations from the Joint
Committee on Vaccination and Immunisation (JCVI), the meningococcal B disease (MenB) infant
vaccination programme is expected to reduce meningitis and septicaemia cases and associated
serious complications, as well as provide reassurance to parents. The new MenB vaccination will be
delivered through general practice (through an NHSE enhanced service) to babies born after 1st July
2015, at their 1st and 3rd routine immunisation appointments (at 2 and 4 months), with a booster at
12/13 months. There will also be a small catch up programme for children born May-June 2015.
Guidance includes advice for both healthcare professionals and parents/carers around the increased
risk of fever, and therefore prophylactic use of paracetamol at regular intervals following vaccination.
As this counters existing paracetamol guidelines, additional training and resources will be provided
locally, as well as revised guidance. PHE South East London Health Protection Team are working with
Lambeth and Southwark CCGs, Public Health and GSTT Community Health Services Immunisation
Team to deliver updates by September 2015.
Meningococcal ACWY conjugate vaccination (MenACWY) programme, also detailed in recent NHSE/
PHE communication2, is being introduced across England this year to respond to a rapid and
accelerating increase in cases of invasive meningococcal group W (MenW) disease, which has been
declared a national incident. MenACWY conjugate vaccine will provide direct protection to the
vaccinated cohort as well as indirect protection to unvaccinated children and adults. This follows JCVI
advice, and will replace existing MenC vaccination.
The programme is recognised as a significant additional workload for those involved in its delivery.
This is expected as follows:
An urgent catch-up campaign for current school year 13 adolescents using a call and recall system
through general practice from August 2015 (with further catch up of school years 11 and 12 once
they reach year 13)
A catch-up campaign for current school year 10 students through schools from January 2016
Adding MenACWY vaccine to the routine adolescent schools programme (school year 9 or 10)
from Autumn 2015, as a direct replacement for the MenC vaccination
1 https://www.gov.uk/government/publications/menb-vaccination-introduction-from-1-september-
2015
2 https://www.gov.uk/government/publications/menacwy-vaccine-introduction
Page 39

12
Adding MenACWY vaccine to the existing time-limited ‘freshers’ programme (ie for older first time
university entrants who have not already received MenACWY, replacing MenC) delivered through
general practice.
MenACWY update will be provided alongside those for MenB to general practice in Lambeth and
Southwark, and any additional opportunities for enabling this are being sought. In addition it should
be noted that due to the speed of MenACWY programme cohort implementation, national vaccine
stock will be more limited, and temporary ordering restrictions may come into place.
8. SH:24
March – June 2015 update
About this document
This document provides an update of the progress of SH:24 since its launch in March this year. It offers
a snapshot of early data on the uptake of the service, an insight into how the service has been
received by users, and information on the next phases of development.
Background
SH:24 provides people with free sexually transmitted infection (STI) test kits, information and advice –
24 hours a day. Users can get tested for the four most common sexually STIs: chlamydia, gonorrhea,
syphilis and HIV. The service is quick, discreet and completely confidential and is fully integrated with
local specialist sexual health services.
SH:24 has created its unique approach to building the service through a Community Interest Company
(CIC) model, which brings together a diverse partnership including local NHS services and
commissioners. The development of the service is funded by Guy’s and St Thomas’ Charity and the STI
testing element of the service is funded by local authority commissioners – SH:24 has been contracted
to deliver STI testing in Lambeth and Southwark from 01 March 2015.
Page 40

13
Launch of the service
As a lean start-up SH:24 hasn’t adopted a hard launch approach (that involves vigorous marketing and
advertising campaigns) but instead has softly launched the service, testing out various ways of raising
awareness in a targeted way.
Early promotion of the service focused on ensuring people currently accessing specialist sexual health
services know there is an online alternative. Having developed close partnerships with our local
specialist clinics (Burrell Street and Camberwell), community sexual health clinics, GPs and pharmacies
across Lambeth and Southwark during the development of the service, posters and mini-business
cards are displayed in all of these settings.
Additionally, large vinyls are now displayed on Burrell Street and Camberwell clinic’s street facing
windows (see below) – which adopt some of SH:24’s tried and tested messaging and iconography.
Digital tags (NFC) have been integrated into the vinyl’s to allow passers-by to simply tap their phone
and instantly access the order a test kit button on the website.
Page 41

14
More recently, promotion was stepped up with the distribution of our mini business cards in high
footfall and commuter areas in the boroughs. Promotional material has also been distributed to a
variety of community spaces - from local enterprises such as the Stockwell Partnership and Better
Bankside to libraries in the boroughs. We are currently working with local police, bars and clubs to
arrange for our stickers and posters to be displayed on their premises and to run a Lesbian Gay
Bisexual and Transgender (LGBT) focused event.
There have been a range of positive features in local press and press targeted at typically higher risk
groups – which have helped to create notable increases in usage of the service. SH:24 is currently in
discussions with national press and local radio stations to increase coverage and continue to raise
awareness about the service.
Data and early insights
To date SH:24 has received 1,132 orders, 61% from women and 39% from men, broadly reflecting the
gender split of clinic users. The website has received 4,312 visitors (70% of which are new) and 21,663
page views. Nearly 60% of users access SH:24 using their mobile phone which confirmed our early user
research that indicated a strong preference for accessing sexual health services via mobile devices.
Over half of users (53%) have returned their test – which is above the return rate of other comparable
online services and suggests the redesign of test kit packaging and support material users receive
during the user journey has had a positive impact.
94% of SH:24 users are asymptomatic and 40% have visited a clinic in the past 12 months – indicating
that SH:24 is working towards its aim of shifting a proportion of asymptomatic clinics users online and
helping to tackle the current pressure on services. Early data is also showing that SH:24 is being used
Page 42

15
by high risk groups: 19% of users are from Black and Ethnic Minority (BME) backgrounds, 17% are men
who have sex with men (MSM) and 85% are under 35. The uptake amongst BME users is particularly
encouraging – who can be harder to reach and often less likely to use digital services.
SH:24 has received positive feedback from users directly and also online via social media (see tweets
below).
Next steps
The STI testing element of SH:24 is the first phase of development. Over the next two years SH:24 will
continue to develop the service iteratively to include improved user support options and optimisation
of elements of the service (this phase has been recently initiated), emergency hormonal contraception
(EHC), oral contraception, partner notification and treatment for chlamydia.
More information
For more information about the service visit:
Website – www.sh24.org.uk
Blog - https://sh24.squarespace.com
Twitter - @sh24_nhs
Page 43

This page is intentionally left blank

1
Health & wellbeing Board 8th July 2015
Report title 0-5 Commissioning responsibility Transfer from NHS England to Local Authorities
Wards: All
Report Authorised by: Strategic Director: Helen Charlesworth-May
Portfolio: Cabinet Member: Cllr Pickard
Contact for enquiries:
Emma Stevenson
Assistant Director Integrated Commissioning
Report summary
The commissioning responsibility for 0-5 children’s public health services is transferring from
NHS England to Local Authorities on October 1st 2015. This paper sets out the detail of that
transfer for Lambeth; potential risks and opportunities for service development following
transfer.
Finance summary
The allocation to LA’s from the Department of Health (DH) does not match the 15/16 contract
value. Across Lambeth and Southwark there is a full year funding gap of £307,773.
Recommendations
H&WB Members are asked to consider and approve the recommendations set out in this
report:
LBS and LBL continue to work with NHSE and GST to try and reduce the funding
gap in 2015/16 so that the HVS does not have to be remodelled in 15/16.
LBL and LBS begin discussions with DH about the CQUIN payment and 16/17
demographic growth in the Public Health grant
LBL to work with GST to develop options for service re-modelling within the
reduced cash envelope
Page 45 Agenda Item 4

2
1. Context
1.1 Responsibility for commissioning 0-5 children’s public health services is transferring from NHS England to Local Government on 1 October 2015. This is the final part of the transfer of public health commissioning to Local Authorities, which saw wider responsibilities transfer in 2013. The 0-5 public health services included are the Health Visiting Service (HVS) and Family Nurse Partnership (FNP). Delivery of these services will continue to be provided by Guys & St Thomas Foundation Trust (GST) for Lambeth and Southwark residents. Until such a point that either or both LA’s decide to re-tender the service.
1.2 The allocation to each LA was determined by the Department of Health, based on a national formula and Workforce & Finance returns submitted by each Provider Trust. Both LBLambeth (LBL) and LBSouthwark (LBS) allocations seemed appropriate when we were first notified by the DH; however issues have arisen during negotiations between NHS England as the current commissioner and GST as the provider to agree the contract value for 2015/16. There are therefore two overarching issues that impact on the transfer:
NHSE and GST agreeing the 15/16 contract value
Ensuring LBL and LBS are allocated enough money to recurrently cover the
contract value or if not, to identify and manage any risks arising from
delivering the service within a reduced budget
1.3 What is clear is that LBL cannot inherit any financial risk.
1.4 Children’s public health services comprise commissioning the Healthy Child
Programme including the health visiting service and Family Nurse Partnership (FNP).
Local Authorities will receive funding, as part of their ring-fenced public health grant, to
commission public health services for 0-5s.
1.5 The allocation to each LA was determined by DH applying a principle of ‘lift & shift’
from 14/15 contracts, and based on workforce & finance returns to DH by each
Provider Trust. LA’s had until January 2015 to respond to the DH’s allocations (and a
3 month window to make a legal challenge via judicial review etc.). Based on GST’s
returns, both LBL and LBS were satisfied the proposed allocation to each borough
was sufficient.
1.6 However since then, NHSE and GST have been in negotiations to agree the 2015/16
contract value, which is still not agreed and a number of issues have arisen that
impact on the baseline figure and therefore the recurrent costs of the service and the
ability for LA’s to continue to commission the service at the current level. A summary
of the key issues and risks are set out in section 2.
Key Issues & Risks
1.7 Call to action – growth in health visitor workforce
In 2011 the government published its Health Visitor Improvement Plan, setting out its
call to action to expand and strengthen health visiting services. DH allocated funding
Page 46

3
to support this plan and set out trajectories for increasing the workforce by April 2015
for each Provider Trust. GST was tasked with increasing its HV workforce by 81.6wte
(56.9 wte in Lambeth and 24.7wte in Southwark). Nationally it was agreed that the
HV workforce growth would be funded at AfC Band 6 mid-point.
GST therefore had to train and recruit a significant number of newly qualified staff
and it was agreed with NHSE as the commissioner, that they could recruit some
Band 7’s as part of the call to action to ensure newly qualified staff were
appropriately supervised and supported. GST recruited 12wte Band 7’s as part of the
call to action
NHSE have stated that funding of the posts at Band 7 was an interim measure and
that recurrent funding for that banding is not available. GST are disputing it was ever
an interim measure and have set out the operational risks of reducing the posts to
Band 6 (please see appendix A)
NHSE have offered £120k non-recurrent funding to off-set this pressure in 15/16
1.8 Demographic growth
The demographic growth against this contract has been set at 1.3%, which equates
to £211,449.
However NHSE will only be funding growth from April –Sept 2015 (£105,724 for 6
months). DH’s allocation to LBL and LBS for Oct-March does not include funding for
demographic growth. This means there will be a shortfall from Oct 1st of £105,724.50
in 15/16, increasing to £211,449 for a full year.
1.9 Financial gap
GST is stating the contract value for 15/16 should be £16,476,773 (across Lambeth
& Southwark). NHSE are offering £16,275,007 (£8,190,507 from NHSE in first 6
months and £8,084,500 from LBL and LBS in last 6 months) which leaves a shortfall
of £201,766
This increases to £307,773 in 16/17 as LA’s have to fund a full year and the half year
demographic growth from NHSE in 15/16 will not be available. The costs will be split
£176.5k to Lambeth and £131.3k to Southwark
2.4 CQUIN
GST are in dispute over tariffs against their whole contract, stating they have been
forced to accept a contract and tariff type which means they are not eligible for
CQUIN in 2015/16. This is a matter between GST, NHSE and DH, however the
CQUIN funding for HVS which equates to £350,989, although not being paid to GST,
should still be in the system. There is an argument that that should be transferred to
LA’s for them to decide how best to incentivise improved delivery of the Healthy
Child Programme.
Page 47

4
It is unfair that Lambeth and Southwark children should suffer because of a
contractual decision made by DH and NHSE which means GST will not receive the
CQUIN payment. It is worth noting that other Provider Trusts who are not subject to
that particular tariff will be receiving CQUIN.
2. Proposal and Reasons
Ways forward and opportunities
2.1 As far as possible DH has tried to make the transfer a nil cost exercise to LA’s. However it
is clear that a full year cost pressure of £307,773 is not sustainable and solutions have to
be found.
2.2 The timescale for making any legal challenge to the DH about our allocation has passed and
despite new issues arising subsequently following negotiations between GST and NHSE, it
is unlikely we would be able to get the allocation changed at this late stage.
2.3 However, with advice from London Councils, it is recommended that LBL and LBS enter into
discussions with DH about two issues:
Where the CQUIN funding is and if that could be passed to LA’s
What provision will be made to ensure the 2016/17 Public Health grant incorporates
demographic growth.
2.4 It is hoped these issues will be resolved; however it is important that concurrent planning is
carried out in case it is necessary to remodel the HV service within the reduced cash
envelope. Meetings have taken place between NHSE, GST, LBL and LBS to try and find
solutions.
2.5 NHSE has agreed to try and reduce the funding gap in 15/16 further by exploring options of
increasing their non-recurrent funding offer (currently 120k). This would be for 15/16 only.
2.6 If this is achieved it would give until April 2016 for LBL and LBS to work with GST to remodel
the HVS service within the reduced cash envelope for 16/17, instead of having to do that by
Oct 1st ’15. This could be achieved by exploring further skill mix options, with child
development workers taking on some of the functions currently carried out by HV’s. This
service model option is currently being explored in Southwark. Although risks around
managing complex and safeguarding cases and managing a young and inexperienced
workforce would still exist.
2.7 LBL is also exploring options around the HVS being incorporated into the integrated family
support model as part of the Children’s Transformation work. An event is planned for July
16th with the Children & Families Strategic Partnership (CFSP) to further develop the
Transformation Programme and begin working up delivery model options which will go out
to consultation with key stakeholders throughout the summer and early autumn.
Page 48

5
3. Finance
3.1 LBL allocation for 6 months from Oct 1st is £4.652m (£9.304m full year). LBS allocation
for 6 months is £3.464m (£6.928m full year). The full year allocation between Lambeth &
Southwark is therefore £16.232m. Made up of:
60k commissioning fee
£15,446,560 for Health Visiting
£724,234 for Family Nurse Partnership
3.2 There is a projected full year financial gap of £307,773 against the current cost of the
service. This is made up of:
No demographic growth being included in the LA allocation
Cost of Band 7 post which NHSE will fund non-recurrently for 15/16
4 Legal and Democracy
4.1 There are no legal matters arising at this time but issues are likely to arise once details
of the contract variations are known. Officers will need to be mindful of the potential for
the activation of contract, procurement and employment law liabilities and should engage
the relevant teams within Legal at all stages of the transfer.
5 Consultation and co-production
5.1 There is no consultation on the transfer of commissioning function. However if it is
necessary to remodel the service in a reduced cash envelop, a full consultation process
will take place.
6 Risk management
6.1 The contract value is being disputed between NHSE and GST for 2015/16. NHSE have
offered some non-recurrent funding to address some of the funding gap, the level of
funding being made available by NHSE is being negotiated.
6.2 The allocation from DH to LBL and LBS will not include the non-recurrent element being
offered by NHSE and does not include demographic growth funding. This will mean the
LA’s will not have enough money to pay for the service at the current level. The service
would therefore have to be remodelled within the reduced cash envelope by Oct 1st.
6.3 LBL and LBS are working with GST to manage that risk and ensure service users are
not affected. The two authorities have sought advice from London Councils and will enter
discussions with DH about options for managing the risk in light of issues arising from
the contract value negotiations between NHSE and GST.
7 Equalities impact assessment
N/A unless we need to remodel the service. An EIA will be completed if that is the case
Page 49

6
8 Community safety
8.1 N/A
9 Organisational implications
9.1 Procurement
9.2 It has been agreed by both Lambeth and Southwark that the NHSE contract with GST
will not be novated from Oct 1st, but a new contract will be put in place between LBL and
GST. For the remainder of 2015/16 a contract variation on the existing contract Lambeth
CCG has with GST will be made. LBL already has a number of services incorporated
into that overarching contract including School Nursing.
9.3 Health
The HVS and FNP are an important part of delivering the Healthy Child Programme.
There is a national SLA which will be adapted to incorporate local need. FNP will be
scaled up borough-wide as part of the LEAP programme.
10 Timetable for implementation
10.1 Transfer of commissioning responsibility will take place on 1st October 2015. Issues must
be resolved by then. Discussions with DH and NHSE around demographic growth and
CQUIN have begun as have discussions with GST about remodelling the service.
Page 50

7
Page 51

This page is intentionally left blank

Health and Wellbeing Board July 8th 2015
Report title Emotional Wellbeing Mental Health Strategy
Wards: All
Report Authorised by: Strategic Director of Commissioning: Helen Charlesworth-May
Portfolio: Children and Families
Cabinet Member: Councillor Pickard
Contact for enquiries: [email protected]
Daniel Taegtmeyer, Senior Commissioning Manager, Lambeth Clinical Commissioning Group,
07974 801 909
Report summary
The purpose of this report is to seek discussion and approval of the Young Lambeth Emotional Wellbeing Mental Health Strategy (2015 -2018) and programme plan. This strategy reflects input from a broad range of stakeholders (including professionals, parents and young people) and builds on the recommendations of the Health Needs Assessment 2013. The strategy and plan has been fully co-produced and focuses on five key themes:
Working Together for Better Mental Health: For Everyone By Everyone
Maximising Resilience and Self-sufficiency
No Child or Family Overlooked
Cemented in Communities
Investing in the Future The Young Lambeth Emotional Wellbeing Mental Health Strategy is both aspirational and
practical and includes measures to create faster access to the right support, in the right place at
the right time for children, young people and families.
Finance summary
In 2015/16, The Council is currently investing £733,334 in Child Adolescent Mental Health
Services (CAMHS) provided by South London and Maudsley (SLAM). This includes investment
into services that support substance misuse (£45,000), autism and complex needs (£91,595),
Looked After Children (£245,937), early intervention mental health services (£223,000) and for
young people displaying sexually harmful behaviour (£55,000).
There is no additional resource being requested as a part of this strategy.
Recommendations
(1) Discussion and consultation
.
Page 53 Agenda Item 5

1. Context
1.1 There is a strong national and local case for transforming CAMHS and more broadly
improving the emotional health & wellbeing of children and young people through
improved access to early identification and intervention. In addition the national review of
hospital based CAMHS “Child and Adolescent Mental Health Services (CAMHs) Tier 4
Report” [July 2014], makes a number of recommendations about improving the quality of
care and the accessibility of highly specialist treatment for children and young people.
1.2 This Strategy sets out Lambeths 3 year plan for improving the way resources are used
and services are delivered to ensure all Lambeth children & young people have the right
information, support and when necessary treatment to achieve good outcomes. The
strategy is underpineed by a comprehensive needs assessment and has been co-
produced with a range of stakeholders including young people and parents
2. Proposal and Reasons
2.1 To discuss the strategy as part of the broader consultation
3. Finance
3.1 There are resource implications arising from the implementation of this Plan. We need to
think collectively about how we align the available resources (financial and human) to
meet need, initiate system change, create new pathways and anticipate future
requirements.
3.2 In 15/16 the CCG invested a further £182k to reduce the increasing waiting times
currently being seen in the Early Intervention Service. The total resource for addressing
emotional health and wellbeing for Lambeth children and young people is unknown and
disjointed. This Plan aims to map and align the resource into a co-ordinated approach in
order to embed a more efficient process with improved sustainable outcomes.
4. Legal and Democracy
5. Consultation and co-production
5.1 This strategy has been co-produced. The co-production project group met weekly between
January 2014 and April 2014 to bring together all the information gathered from 20
workshops carried out over the same period. This information along with the data and
recommendations of the 2013 mental health needs assessments form the basis of the
Plan.
5.2 The co-production project group facilitated conversations with young people, parents and
services. The workshops and conversations asked participants to take an asset based
approach to thinking about how to support emotional wellbeing and mental health in
Lambeth. This approach will continue during the implementation phase.
Page 54

6. Risk management
Risk Likelihood (1= unlikely 5 = highly likely)
Impact (1= negligible 5 = severe)
Mitigation
Waiting Times 5 3 The Early Intervention Team has experienced an
increase in waiting times to access the service up to
45 weeks. Additional investment of £182,000
combined with an action plan agreed with SLAM to
meet national waiting time standards by the end of
July 2016.
Clinical 3 5 CAMHS have experienced capacity issues and
organisational pressures to reduce funding leading to
an increased strain on community CAMHS services.
The additional investment action plan includes
provision for adding to capacity of the community
CAMHS teams (including NDT, CACs, YOS,
CLAMHS) to increase the robustness of current
provision and minimise the potential impact on
individual young people (i.e. Serious Untoward
Incident)
Financial 3 3 The challenging financial context and savings targets
have a potential to impact on the support of early
intervention and targeted intervention services during
the lifetime (2015 – 18) of the strategy
implementation. This can be mitigated by partner
organisations engaging fully in the strategy
implementation to ensure opportunities to get best
value and outcomes for children and young people
are identified, scoped and commissioned jointly
where feasible.
7. Equalities impact assessment
7.1 A comprehensive Equality Impact Assessment (EIA) will be completed to inform the co-
produced redesign of emotional and mental health services in Lambeth. The
programme contains co-production at its core and explicitly represented within two of the
five strategic priorities arising from the co-produced consultation process (see strategic
priorities: three “No Child or Family Overlooked”; four “Cemented in Communities”). The
implementation plan includes a commitment to implement the recommendations of the
Black Mental Health Report.
8. Community safety
Page 55

8.1 The CAMHS Joint Commissioning Group has been fully involved in the development of
the strategy which includes representation from community safety. Furthermore, the
strategy has been taken to the Children and Families Strategic Partnership presenting
an opportunity for input.
8.2 Health
The Young Lambeth Mental Health Strategy builds on the recommendations of the
Health Needs Assessment 2013 completed by Public Health. The Health Needs
Assessment drew on health related information from the most recent JSNA and from a
variety of available sources.
9. Timetable for implementation
9.1 July 8th – Final consultation at H&WB Sept HWB – Sign off and launch 3 year implementation plan incorporated into Strategy
Page 56

Page 57

1
The Young Lambeth
Emotional Wellbeing and Mental
Health Strategy and Plan
2015 – 2018
Page 58

2
Contents
Chapter 1: Introduction 4
Chapter 2: Lambeth CAMHs Analysis of Need 10
Chapter 3: Current Investment 14
Chapter 4: Strategic Priorities 18
1. Working Together for Better Mental Health: 19
For Everyone By Everyone
2. Maximising Resilience and Self-sufficiency 20
3. No Child or Family Overlooked 22
4. Cemented in Communities 23
5. Investing in the Future 24
Chapter 5: Lambeth CAMHs and Wellbeing Strategy Action Plan 2015 – 2018 26
Appendices 32
Appendix 1: EWMH Programme Management Resourcing
Appendix 2: CAMHs Joint Commissioning Group (JCG) Terms of Reference (2011)
Appendix 3: Lambeth and Southwark CAMHs Needs Assessment (2013)
Appendix 4: Supporting the Health of Young People in Lambeth; A summary report
of the Health Related Behaviour Survey (2014)
Appendix 5: Review of parenting and family support programmes in lambeth (June
2013)
Appendix 6: ‘What Works’ in CAMHs
Appendix 7: Additional investment to improve access to Specialist CAMHs (2015/16)
Appendix 8: Young Lambeth Local Offer
Appendix 9: Futures in Mind
Page 59

3
The Government’s 2011 Mental Health Outcomes Plan says: “Mental health is everyone’s business; individuals, families, employers, educators and communities all need to play their
part. Good mental health and resilience arefundamental to our physical health, ourrelationships, our education, our training, our work and to achieving our potential.”
The Young Lambeth Emotional Wellbeing and Mental Health Plan has been co-produced. That is to say that young people, parents, service users, non-service users, the voluntary sector, schools, Educational Psychology services, early intervention services, primary care, community health professionals, public health and mental health specialists have worked together to agree the five key priorities of the Plan.
Co-Production and Asset Based Approaches
Co-production approaches reflect NHS Lambeth Clinical Commissioning Group (CCG) and London Borough of Lambeth (LBL) ambitions that any support and services provided are done so with children, young people and families at the centre.
To develop this Plan, the co-production project group met weekly between January 2014 and April 2014 to bring together all the information gathered from 20 workshops carried out over the same period. This information along with the data and recommendations of the 2013 mental health needs assessments form the basis of the Plan. The co-production project group facilitated conversations with young people, parents and services. The workshops and conversations asked participants to take an asset based approach to thinking about how to support emotional wellbeing and mental health in Lambeth. That is to say, contributors were asked to consider the strengths of families, communities and providers in meeting a burgeoning need. The question asked was: what are we doing well and how can we build on that together.
The co-production approach will continue over the next 3 years of implementation, to ensure the Plan is owned and taken forward by everyone. As the Plan is progressed to delivery, there will be on going and sustained commitment to engaging communities, professionals, clinical staff and other health services. The Plan is our commitment to improve outcomes for children, young people and families across three years.
One of the key outcomes of this Plan is to provide a mechanism that facilitates better working together. Included in this is the need to narrow the gap between those in need of support and treatment (the patient/client) and the providers of that support (local authority and mental health services). This Plan will lead to the development of mechanisms that shift the conversations away from “us” and “them” towards “we are working together”.
The Plan’s focus is deliberately concise as it is intended to be a roadmap that focuses on five key themes/priorities and ambitions that are deliverable and achievable This Plan moves us away from services that are designed to be delivered “to” or “for” communities, to one where everyone collaborates to deliver together.
Page 60

4
1. Introduction
National and Local Plans
The 2011 National Mental Health Plan, “No Health Without Mental Health” sets out clear commitments to improving the emotional wellbeing and mental health of all communities. The national plan sets out a clear mandate for communities and providers to work together to improve the emotional wellbeing and mental health outcomes for children, young people and families. The National Plan confirms that mental health is everyone’s business, whether a community member, service user or an individual working in education, health services or social care.
In 2015 the Department of Health alongside NHS England published a paper setting out a vision for children and adolescent mental health services for England. This publication, “Future in mind: promoting, protecting and improving our children and young people’s mental health and wellbeing” [2015] identifies both the case for change and sets out a series of goals and commitments to improve emotional and mental health.
There has also been a national review of in and out patient (hospital based) Child and Adolescent Mental Health services (CAMHs), “Child and Adolescent Mental Health Services (CAMHs) Tier 4 Report” [July 2014]. This makes a number of recommendations about improving the quality of care and the accessibility of highly specialist treatment for children and young people.
There have also been commitments from the Department of Health and NHS England to improve the focus on child and adolescent mental health services and at the time of writing there is a commitment to increase funding for CAMHs nationally made by central government.
“Future in Mind” identifies the following as key commitments for any coherent emotional wellbeing and mental health strategy:
This Young Lambeth Emotional Wellbeing and Mental Health Plan echoes the findings and recommendations set out in “Future in mind: promoting, protecting and improving our children and young people’s mental health and wellbeing” [2015].
Promoting resilience, prevention and early intervention
Improving access to effective support - a system without tiers
Care for the most vulnerable
Accountability and transparency
Developing the workforce
Page 61

5
This Plan sets out the vision and steps that will be taken to meet the emotional wellbeing and mental health needs of children, young people and families in Lambeth over the next 3 years (2015 – 2018). This Plan is ambitious in that it assumes that every child, young person and family in Lambeth has the right to:
This Plan provides Lambeth and its communities with a rationale and clear framework for taking a different, potentially transformative, approach to children and young people’s emotional wellbeing and mental health. The implementation of the Plan commits to reviewing and where necessary developing services across every level of need and puts the voice and needs of the service user as a central partner to achieving change. If, collectively, we can implement the actions as outlined below, the Plan will lead to improved quality, effectiveness of treatment, simplified system of support, improved care pathways, a more confident workforce and better lifelong outcomes. It will enhance the sense of control and autonomy children and young people have over their lives. It will facilitate a sense of purpose for the present and future and will lead to thriving, emotionally well communities and stronger families.
However, in order to effectively deliver to the outcomes and actions from this Plan, it is essential that communities, service users, parents, schools, primary care providers, the Local Authority and health services get involved in “making things happen”. How we deliver this Plan is as important as the “why” and the outcomes.
The action plan that is embedded in this Plan sets out the steps that will be taken over the course of this strategy to achieve the outcomes that were agreed during the co-production process and that arose from the emotional wellbeing needs assessment.
Children, Young People and families
are an asset to the community
Access the right support at the
right time in the right place
Be heard
access good quality
interventions and treatment when
needed Grow up in an emotionally
positive environment
Be in control of their lives
Page 62

6
The implementation of the Plan and achieving the outcomes with and for communities will start on the day the Plan is formally agreed and launched. The Plan sets out actions that will be delivered over the course of three years:
a) The Young Lambeth Emotional Wellbeing and Mental Health Plan “sign off” b) Community, schools and services engagement c) Alignment of the Plan with the other various strategies and service development
plans for Lambeth. d) Re-view of the CAMHs Joint Commissioning Group to ensure that it is fit for purpose
and meets co-production principles. e) Redesigning the emotional wellbeing and mental health offer for children and young
people and families in Lambeth. This includes designing referral pathways, delivery of evidence based community interventions and reducing the demand for highly specialist mental health services.
f) As well as taking community responses as a cue, the re-design of services will respond to the challenges set out in the Needs Assessment (Chapter 2)
g) Designing and implementing a community and professional training programme to meet the requirements for the re-designed services and community interventions
h) Review the evidence base for resilience, emotional wellbeing and mental health interventions and work with stakeholders to introduce an offer of support that is needed and wanted/used.
i) The implementation of an Emotional Wellbeing and Mental Health Forum
Case for Change
The Facts
It is worthwhile reflecting for a moment on some key facts emerging from national reviews and benchmarking. The following are identified in “Future in Mind” and in the Lambeth and Southwark Needs Assessment as nationally and locally prevalent issues that underpin a step change in how emotional wellbeing and mental health needs are met.
a) Mental health problems cause distress to individuals and all those who care for them.
b) One in ten children (10% nationally, in Lambeth 12%, 11yrs - 16yrs rising to 16.5% 16yrs to 17yrs for common mental health disorders) needs support or treatment for mental health problems. These range from short spells of depression or anxiety through to severe and persistent conditions that can isolate, disrupt and frighten those who experience them. Mental health problems in young people can result in lower educational attainment and are strongly associated with risk taking behaviours. That means in Lambeth at least 6000 children and young people will experience emotional wellbeing and mental health difficulties.
c) Nationally and locally the emotional and mental health system lacks coherence across the range of providers, is complex and predicated on a crisis intervention model.
d) There is a treatment gap. The last UK epidemiological study [ONS 2004] suggested that nationally at the time less than 25% – 35% of those with a diagnosable mental health condition accessed support. In Lambeth this figure drops to 17% of the anticipated mental health population and not enough children, young people and families in Lambeth access emotional wellbeing and mental health support in a timely manner. This increases the likelihood that more young people are presenting to hospital, in schools or to their GP surgery with increased mental health related risks.
e) There is emerging evidence of a rising need in key groups such as the increasing
Page 63

7
rates of young women with emotional problems and young people presenting with self-harm and school based stress.
f) We know that 50% of adult mental ill health first manifests by the age of 14yrs and 75% by 18yrs (excluding dementia). Failure to support children and young people with mental health needs costs lives and money.
g) Nationally it is reported that there is more demand for emotional wellbeing and mental health support and that severity and risks of presentations to services are increasing.
h) In Lambeth there are significant populations of children and young people who face additional challenges to their emotional wellbeing.
Table 1 - Lambeth’s Additionally Vulnerable Groups
At the time of writing, children and young people’s emotional wellbeing and mental health has been raised as a national concern. However, against a backdrop of a tightening financial landscape, it is essential that communities, families and services work together to develop and implement new innovative ways of supporting all children and young people to maintain positive emotional health.
Existing services are increasingly required to respond to higher risk presentations and that means a lot of time and money is spent on managing crises or negotiating a complex web of support. This adds to the strain for children, young people their families and the range of providers, often marking them out as different or problem families and/or children.
Early support and responding to first signs of unhappiness can dramatically improve the outcomes for children, young people and families. However, it is clear from the exercise of developing this plan that parents and young people want to be able to help themselves more.
Page 64

8
The impact of stigma associated with mental illness was identified by all contributors to the co-production exercise as a key barrier to people being able to prosper in emotionally healthy communities and acts as a brake on people asking for help.
The evidence shows we can reduce stigma, improve outcomes and reduce the need for high cost hospital based interventions by improving the access to a range of parenting programmes and support, adopting whole school approaches to emotional health and wellbeing and increasing access to outdoor play and exercise.
Waiting times to access Specialist CAMHS services
In 2015, the case for change is increasingly strong with waiting times having increased in the Early Intervention team (to 45 weeks in quarter 4 of 2014/15) and potential for key services such as the Neurodevelopmental team to experience an increase in waiting times as indicated in the table below.
Analysis of the spike in waiting times (2015) is required. However early indications are that there has been an increase in referrals, an increase in identified need, a change in referral thresholds, capacity issues across a range of community services (including CAMHs Early Intervention service).
Table 2 – Waiting times for Specialist CAMHs services 2012 – 2015
Consequently, Lambeth CCG as part of this plan has authorised additional investment of £182k to improve access to CAMHs and enhance capacity in key teams. See appendix for more information relating to the additional investment plan.
Specialist Support
In addition to focusing on developing the local offer for all, there are a number of children and young people whose needs are such that they cannot be met through early intervention support or in the community. In some cases, children and young people, through no fault of their own, require the very structured treatment for mental illness offered through hospitals. This Plan will oversee the implementation of evidence based treatment that will reduce the number of days such children will have to spend in hospital and or in specialist treatment.
People’s lives are complicated and in order for communities and providers to be sure that support is offered at the right time, it is essential that this Plan links with other Lambeth plans that provide the framework of support across all years and all needs. For instance, the five
0
5
10
15
20
25
30
35
40
45
50
Child and AdolescentCommunity Service Lambeth
Lambeth CAMHS EarlyIntervention
Lambeth CAMHSNeurodevelopmental Team
Lambeth Children LookedAfter
Lambeth Youth Offending
Page 65

9
key themes around emotional wellbeing and mental health underpin the overarching outcomes of the Lambeth early intervention and prevention plan.
The consequences of unaddressed emotional wellbeing and mental health needs on the individual, their families and their life experiences and achievements can be catastrophic. For some, not getting the right support and treatment at the right time can lead to a shortened life expectancy, poorer educational attainment, increased likelihood of substance misuse and offending behaviour.
However in our co-production conversations it was clear that communities and professionals wanted a plan that facilitates a move away from the predominant illness and crisis model of provision, towards greater self-sufficiency and to reducing the reliance on external bodies in achieving best outcomes.
Page 66

10
2. Lambeth CAMHs Analysis of Need
A joint Lambeth and Southwark needs assessment of mental health of children and young people was carried out by the Lambeth and Southwark Public Health team (2013/2014). The needs assessment provides a clear understanding of the level of need amongst children, young people and families in Lambeth and how well their needs are being met by the current service model. A needs assessment can provide information on the trends in mental health need in a population and can help communities and providers to respond by making sure they invest their resources in the most efficient way to support children, young people and families.
The key findings from the Lambeth needs assessment are:
That factors leading to risk taking behaviours for children and young people identified include: disruptive home environments, domestic violence, gangs and gang membership, autism and autistic spectrum disorders, the effects of cannabis and mother’s mental health around the time of birth. These and other complex family and home situations can lead to eating disorders, self-harm, overly sexualised behaviour, and participation in violence
17% of children predicted to need Child and Adolescent Mental Health services (CAMHs) in Lambeth have accessed care (2011-12)
25% of looked after children of those predicted to need mental health services were seen by the looked after children CAMHs service (2011-12)
33% of Young Offenders identified as having an undiagnosed mental health disorder. 55% of first time offenders predicted to need mental health services were seen by CAMHs (2011-12)
Hospital admissions for mental health among young men in Lambeth increased 150% in the 20-24 age group (2009-10 & 2011-12 combined)
There is under provision of services at tiers 2 and 3, particularly tier 2 and some estimates suggest over provision in specialist hospital based services
Of the top 10 diagnosis types, depressive episodes is the only one that has continued to increase over the last three years
Children from ‘mixed’ and ‘black other’ ethnic backgrounds were over represented in CAMH service users, children from Chinese and Asian ethnic backgrounds were under represented
Referral pathways into support are not clear
Consensus that services are good once a service/team is accessed, but more South London and Maudsley (SLAM) expertise is needed to provide more consultancy and training to the wider education, social care and community health workforce
Support is needed for parents who do not meet current CAMHs thresholds but are not able to manage with universal services
More counseling based services are needed for children and families - CAMHs should provide group sessions to meet needs; and there is a need to further develop a sex offender programme and services for sexually exploited girls
Multiagency/integrated working needs to be improved (meaning functional teams of people from different agencies delivering services in a flexible way, for example community outreach workers, social workers, mental health professionals being co-located)
Whole school approaches to emotional wellbeing have a wide positive impact.
Page 67

11
Table 3 - Recommendations from the Needs Assessment to address some of the gaps in the short term
S
hort
Term
Develop a comprehensive Plan
To cover next three years and integrate the many determinants of wellbeing and partners not just considering targeted and specialist services
Service Provision
Mapping of current provision in tier 1 / universal services to be carried out and to include work done by GPs, social work, early intervention teams, young offenders, educational psychologists, health visitors. Consider more parenting classes at nursery and primary level as evidence suggests they are effective, and stakeholders mentioned conduct disorders
Information, monitoring and performance management
Improve data collection in primary care Improve provider data recording Agree with providers to have regular audit of:
Outcomes of treatment (outcomes to be co-designed)
Rejected referrals – numbers and reasons why
User feedback
Tier 4 referrals which do not go via Common Assessment
Framework
Health promotion
Health promotion work by wider workforce to include child and adolescent mental wellbeing and to tackle stigma associated with mental health diagnoses as well as promoting wellbeing. Provide schools with information about mental health services
Equalities and community engagement
Put measures in place to increase identification of children who go undetected, for example in
Youth Offending Services
Consider Mental Health First Aid training for people working with
adolescents
Identify ways of working with young carers e.g. through existing
groups
Complete Equalities Impact Assessment of emotional wellbeing
and mental health services
Page 68

12
Table 4 - Recommendations from the Needs Assessment to address some of the gaps in the longer term
Longer
Term
Service provision
Principles of early intervention and delivery of services according to need to be followed. Over time, shift from treatment of established disorders towards early intervention
Consider extending the upper age limit of mental health services to 25 years (in line with the New SEN Code of Practice 2014) or developing adolescent and young person’s service to maximize early intervention, particularly for psychosis
Provide schools with quality assurance guidelines to support evidence-based commissioning and promoting access to quality assured interventions
Better support offered to young people at the transition from primary to secondary school
Training
Roles of schools nurses, health visitors and midwifes could be developed to include mental health and early identification of parental mental health disorders
Review the formally commissioned training and opportunities for non-mental health professionals working in wider children’s services
There are some themes and findings that are common across the needs assessment and the outcomes of the co-production work. These are aligned as follows:
Needs Assessment Priority
workforce training on emotional wellbeing; Priority 1
reducing the stigma of emotional wellbeing and mental health Priority 1
the need to strengthen early intervention work Priority 2
delivering resilience, emotional wellbeing provision in schools; Priority 2
supporting parents and improving access to evidence based parenting programmes to increase resilience;
Priority 2
maximising the existing resources to support better emotional wellbeing,
Priority 2
increasing access to services (thresholds are too high) Priority 3
balancing activity across tiers and focusing on prevention – universal activity
Priority 3
strengthen partnership working and enhance communication; Priority 4
providing better support for young people at transitional stages Priority 5
Page 69

13
Other themes from qualitative work not picked up in the needs assessment which young people, families and professionals indicated would support better emotional wellbeing included:
The importance of exercise in improving/ maintaining wellbeing
Trust and rapport between service user and practitioner
Delivery of mindfulness programmes in schools
Facilitating individual sense of choice and autonomy
Developing coping skills among young people and families
The impact of the environment – home, local area, safety on emotional wellbeing
Having friends and support networks
Having someone trusted to talk through problems
Flexible services to suit the needs of the young person
Support groups for families and young people
The analysis of the Needs Assessment by communities, public health and professionals through workshops, focus groups and desktop reviews led to the development of the five key strategic themes that underpin this Plan. The five key themes are:
1) Working Together for Better Mental Health: For Us, By Us
2) Maximising Resilience and Self Sufficiency
3) No Child or Family Overlooked
4) Cemented in Communities
5) Investing in the Future for Children, Young People and Families
Page 70

14
3. Current Investment in Early Intervention, Community and Specialist CAMHs services (2014/2015)
The following diagram shows the proportion of investment on CAMHS as an inverted triangle. The purpose of this is to visually represent that the largest proportion of CAMHS investment is directed to the cohort with the greatest need and often presenting in a state of crisis. The numbers of children cited are reflective of 2014/15 data from CAMHS performance monitoring reports.
Table 5 - The current proportion of investment in CAMHS
Page 71
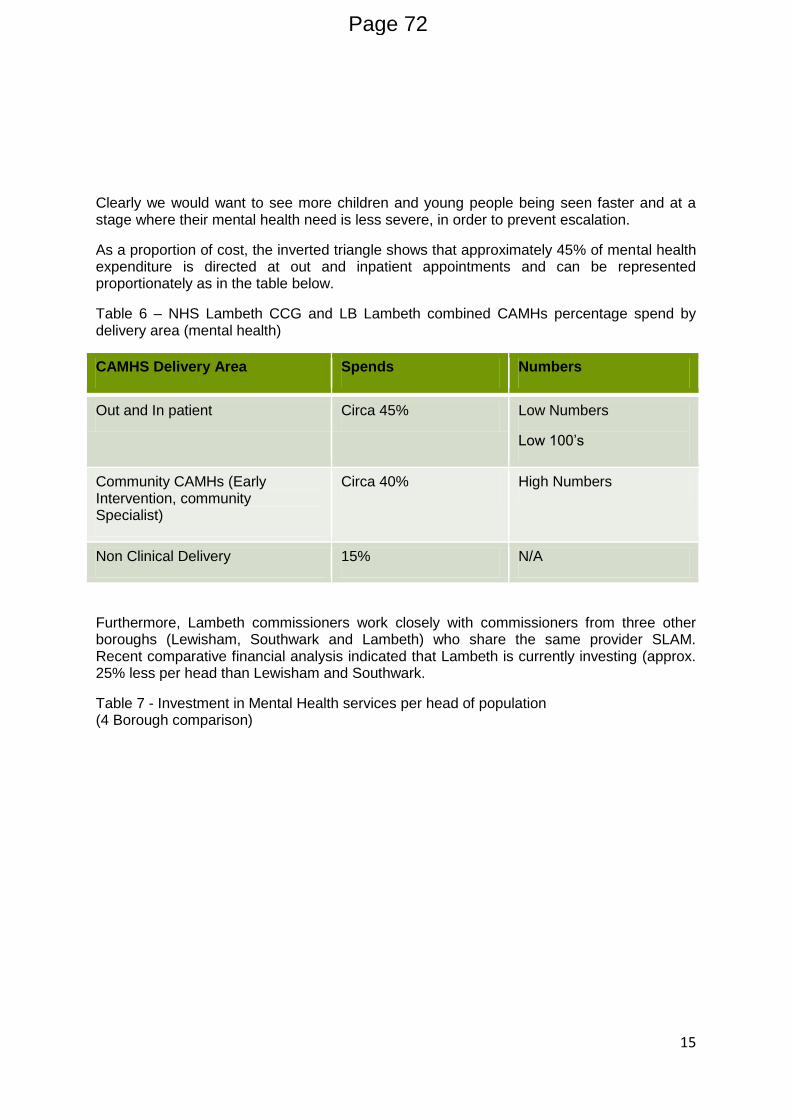
15
Clearly we would want to see more children and young people being seen faster and at a stage where their mental health need is less severe, in order to prevent escalation.
As a proportion of cost, the inverted triangle shows that approximately 45% of mental health expenditure is directed at out and inpatient appointments and can be represented proportionately as in the table below.
Table 6 – NHS Lambeth CCG and LB Lambeth combined CAMHs percentage spend by delivery area (mental health)
CAMHS Delivery Area Spends Numbers
Out and In patient Circa 45% Low Numbers
Low 100’s
Community CAMHs (Early Intervention, community Specialist)
Circa 40% High Numbers
Non Clinical Delivery 15% N/A
Furthermore, Lambeth commissioners work closely with commissioners from three other boroughs (Lewisham, Southwark and Lambeth) who share the same provider SLAM. Recent comparative financial analysis indicated that Lambeth is currently investing (approx. 25% less per head than Lewisham and Southwark.
Table 7 - Investment in Mental Health services per head of population (4 Borough comparison)
Page 72

16
Financial Modeling for CAMHs in Lambeth
There is an increasing pressure on schools, community and voluntary sector and specialist services to meet a rising tide of increasing demand and severity of need. Similarly it is known that the investment in CAMHs services across the UK represents 6% of mental health budgets and this is reflected locally in Lambeth.
There are resource implications arising from the implementation of this Plan. We need to think collectively about how we align the available resources (financial and human) to meet need, initiate system change, create new pathways and anticipate future requirements.
See table below for a breakdown of current funding streams for Specialist CAMHS in Lambeth.
Table 8 – Funding streams for Specialist CAMHS in Lambeth (June 2015)
Funding Streams £
CCG Block contract 2,180,883
CCG – Children’s 78,655
CCG – Lambeth Autism and Neurodevelopment Diagnostic Service 48,816
CCG – Early Intervention 118,474
Multi Systemic Therapy (MST) 140,000
Obesity service 100,000
LA - Substance Misuse 45,000
£0
£10
£20
£30
£40
£50
£60
Lewisham Southwark Lambeth Croydon
Series 1
Page 73

17
LA – Autism Services 91,595
LA – Children Looked After Mental Health Services 245,937
LA – Early Intervention 223,000
LA - Management 72,802
LA – Sexualised Behaviour Services 5,000
Total 3,350,162
Important to note that the above is CAMHS spend only. It doesn’t include what schools, primary care, and noncommissioned community programmes are spending, which is likely to be considerable. The total resource for addressing emotional health and wellbeing for Lambeth children and young people is unknown and disjointed. This Plan aims to map and align the resource into a co-ordinated approach in order to embed a more efficient process with improved sustainable outcomes.
Over the course of the last five years there has been a noticeable reduction in funding available for child and adolescent mental health across the prevention, early intervention and specialist treatment arenas. Whilst schools, early intervention services, social care and health services continue to invest considerable resources in supporting resilience, early intervention and specialist services there does remain a gap between demand and capacity to deliver effective interventions. This is reflected in increased waiting times to appropriate services (referral to assessment), reduced confidence by partners in the capacity for specialist services to respond and evidence that this leads to increased crisis presentations to Accident and Emergency departments in local hospitals.
Whilst partners have worked together over the course of the past five years to mitigate against the worst effects of the financial pressures, there is a clear case to be made that the only way that children and young people will have access to appropriate support is to:
a) explore innovative ways of designing and delivering support b) investing in workforce development and training to ensure that every child has
access to accurate and appropriate information c) analyse current investment in resilience and early intervention services by early
support services and schools d) ensure that evidence based early intervention and prevention services are delivered
across Lambeth to mitigate against post code lotteries e) map investment in specialist hospital based services, including presentations to
accident and emergency departments f) identify how resources are best invested to maintain waiting times (referral to
assessment – assessment to treatment) to within: a) Early Intervention - 4 weeks b) Community CAMHs -18 weeks
g) complete a cost/benefit analysis for the CAMHs Neurodevelopmental service h) match resources to evidence based pathways, delivery models i) identify and implement mechanisms to shift more resources (human and financial)
from current Tier 4 specialist services to community delivered services
Page 74
18
4. Strategic Priorities
The Lambeth Health and Wellbeing Plan sets out the local vision for the health of Lambeth residents, “Good physical and mental health helps us make the most of our lives. Be it work, socialising or looking after family and friends, our health is our most important asset.” Lambeth Collaborative Health and Well-being Plan – A transitional Plan for 2013-14.
We know that having choice and feeling empowered are key to better emotional wellbeing. If one is happy, it is easier to negotiate the “bumps in the road of life”.
Based on the national plans, Lambeth needs assessments and co-production process; the following were identified by the Lambeth community as routes to feeling happy.
We have identified the five priorities to underpin the work we plan to do to achieve good emotional wellbeing and mental health for children and young people in Lambeth.
Being Happy
good parenting
having friends
exercising
having someone to
talk to
having choice
having a sense of
purpose and direction
Page 75

19
Priority 1 - Working Together for Better Mental Health for Everyone, By Everyone (awareness, knowledge and training)
We are all responsible together for delivering better emotional health to all.
Through the workshops that were facilitated by members of the Co-production Project Group we know that everyone recognises that better mental health can only be achieved by everyone working together, having shared and common goals and a shared investment in improving the emotional wellbeing and mental health of children, young people and families. Key to this is changing the way communities and services understand and respond to emotional wellbeing and mental health. For this reason, appropriate and consistent good quality workforce training and development is essential. This would include equipping practitioners with up-to-date information and approaches. Additionally, communities have requested that they too receive accurate up to date information and training and that they are viewed as part of the solution to emotional wellbeing and mental health in Lambeth.
One approach to achieving this will be to design and deliver training programmes that will be suitable to children, young people, families and the workforce. Using co-production approaches and engaging with training departments across health, social care and schools, parents, young people and professionals will design and deliver training together. All stakeholders can be pro-active providers of better emotional wellbeing. The Plan requires that consistent quality assured messages on emotional wellbeing and mental health are available and widely accessible.
This Plan will initiate co-production approaches to working across public health, service users and communities to produce new local social media campaigns. The use of pejorative terms will be addressed through training and workforce development. Stigma and language were identified as big barriers preventing people from talking about their needs.
The recent ‘Academic Resilience’ work of Professor Angie Hart and Lisa Williams refers to the principle of ‘Communities of Practice’ which presents an opportunity to bring people together to learn about and participate in sharing of best practice and effective strategies for working well with children, young people, families and communities. This forum can represent an important pillar of the communication strategy and a platform from which training can be provided as well as borough-wide participation in care pathway development and extended co-production.
Information must be accessible to everyone and a key component of our Plan is to ensure that all relevant support and information is included in our Young Lambeth Local Offer. This needs to be in a way that is clear, comprehensive and shows people how and where to access a service or parenting programme for example.
The Plan asks that all stakeholders maximise their existing resources to improve mental health, whether that is individually, within a service, in schools or in their conversations with peers, friends and young people. This will be achieved through engagement with schools, faith groups and communities in raising awareness, providing training and community outreach events. The Plan will initiate a review of how best to maximise new social media opportunities to promote the dissemination of accurate and supportive information, including information on where to get help.
Through harnessing new technologies and building on current initiatives such as “My Health Locker”, children, young people and families will be encouraged to “own their care plans” putting them in charge of achieving their aspirations.
Page 76

20
Priority 2 - Maximising Resilience and Self Sufficiency
There are a range of well-documented options to developing resilience and self-sufficiency. These include the implementation of approaches with children and young people themselves, with parents, in schools and community health services.
In summary, this Emotional Wellbeing Strategy supports the implementation of:
Good parenting is frequently mentioned as being key to supporting best outcomes for all children and young people. Not only does good parenting support children and young people, it also improves the emotional wellbeing of the parents themselves.
The Lambeth Family and Parenting Support Plan will provide the vehicle through which planning and delivery of a coherent and integrated family and parenting support service will be developed. It provides an opportunity for the local authority and its partners to:
Improve outcomes for Lambeth’s children and young people
Increase the capacity of parents to undertake their role of bringing up their children so that they thrive and achieve
Ensure that early identification and prevention services are at the heart of service planning and delivery
Schools have vast experience of supporting children, young people and families. At a universal level, schools provide a safe environment where children and young people learn about the world around them and explore their own identity and have the space to use their
Asset Based Approached
•Co-Production of workforce development and training programmes
•Development of the Emotional Health and Wellbeing Forum
•Design and develop peer to peer netweorks inorporating learning from nationally recognised initiatives such as the Lambeth Living Well Netwrk
Parenting Support Programmes
•Triple P,
•Mellow Bumps,
•Incredible Years
•Strengthening Families, Strengthening Communities
School Based Resilience and Early
Intervention
•peer mediation in primary schools (run by Healthy Minds),
•Friend versus Friendly (run by Growing Against Gang Violence),
•FAST UK – Family and Schools Together (parent/child and school programme),
•SEAL (Social, Emotional Aspects of Learning) I
•In Harmony (social enhancement through music), learning mentors, counseling servicesI
Page 77

21
imaginations. They facilitate citizenship and community cohesion. Programmes such as the Families and Schools Together (FAST) offer a structured and integrated approach to improving resilience and ensuring that children, young people and families get the most from the school years. There are a number of school based resilience interventions. The range of evidence based interventions will be assessed for local applicability and where appropriate the Plan supports schools to ensure the best use of resources to strengthen the resilience and emotional wellbeing offer.
Furthermore, this Emotional Wellbeing Strategy values the creation of an Emotional Wellbeing Mental Health (EWMH) Forum. The purpose of which is to bring all partners together for mutual informing, support and training. Members of the whole community, including public, private and Voluntary and Community Sectors will be welcomed to participate.
Page 78
22
Priority 3 - No Child or Family Overlooked
Every child, young person and family to be supported in staying healthy and in discovery
We know that for some children and young people there will be a need to access highly specialised mental health services. We also know that whilst some children and young people need emergency help to keep safe, there are opportunities to provide specialist mental health support in the community in ways that reduce the need for admissions to hospital. These mental health services offer specialist treatment, psychological support, in some instances medication and or admission to hospital for safety reasons. These mental health services are currently known as CAMH Services.
From the needs assessment we know that some children and young people do not have access to some key services, such as 0-5yrs CAMHs, transition to adult services and that there is some evidence around gaps in accessibility to specialist early intervention services such as the Lambeth Early Onset (LEO) Service for those presenting with first symptoms of psychosis. We also know from national research and the Lambeth needs assessment that there are groups of children and young people who are additionally vulnerable to emotional and mental ill health (Looked After Children, Children with Disability, Young Offenders, children and young people from Black and Minority Ethnic communities). There are also sections of the local community who are both under and over represented as patients in mental health services.
Whilst this Plan will encourage the development of a network of provision that will seek to support children, young people and parents so that they can continue to live together in the community and not require highly specialist services; we know that there will always be a need for specialist treatment. However, by getting the community emotional wellbeing CAMHs offer “right” we will improve the likelihood of appropriate use and delivery of mental health services to meet the overall aims of supporting children, young people and families to remain safely and thriving in their communities. In order to achieve this, this Plan will lead us through a process of:
re-designing mental health services,
reviewing referral and care pathways,
implementing appropriate thresholds for access to mental health services
overseeing the development of a “step-down” approach to service delivery.
The action plan sets out the steps that will be taken to ensure that health inequalities are addressed in the access to and delivery of mental health services. Taking the Lambeth needs assessment as a starting point, CAMHs will be reviewed with a special attention to addressing the emotional needs of additionally vulnerable groups of children as highlighted in the needs assessment.
NHS Lambeth Clinical Commissioning Group alongside its partners is currently developing a perinatal mental health strategy that will be aligned to The Young Lambeth Emotional Wellbeing and Mental Health Plan. Perinatal services are services which provide support from pregnancy to the child’s first birthday and respond to issues such as pre and post-natal depression.
Page 79

23
Priority 4 - Cemented In Communities
Children, young people, families, practitioners, community health providers, schools, voluntary sector and others are all equal “owners” of the local offer. There is recognition, borne out of the co-production exercise, that there are many existing strengths in the community that are not currently being maximised in support of emotional wellbeing and mental health.
This Plan is a call to action to shift the way communities think of emotional wellbeing and mental health services and will commence the process of developing services from the “ground up”. Taking this approach will draw more people into the services, enhance the community ownership, eliminate post code lotteries in access to appropriate services.
Service users, parents, and professionals will be invited to become members of the CAMHs Joint Commissioning Group and the Emotional Wellbeing and Mental Health Forum where service provision across all levels of need will be assessed and reviewed. This ensures a robust structure is in place to hold the system to account. There will also be a greater scrutiny of the quality and effectiveness of the interventions and treatment offered and delivered, incorporating patient/client experience.
By everyone owning the model, there are opportunities to ensure the local offer is something to which all stakeholders can contribute. There are opportunities to reduce the stigma of mental health, and to facilitate earlier interventions where required, as part of normal everyday life. We know that there are interesting and effective community mental health models being developed globally. For example Dr Mirza Kahn’s work in Kerala (India) has led to the development of an exciting initiative that involves parents and schools working together to support children’s emotional health in a low resource environment. We want to understand this and similar models of community ownership so we can identify key learning and explore ways of implementing that learning here in Lambeth.
Communities will be invited to work together to develop outcomes for emotional wellbeing and mental health services. We will be developing new ways of including communities and partners in monitoring and overseeing the provision of emotional wellbeing and mental health services in Lambeth.
The Plan will invite practitioners to look at implementing new outcome measurements and care plan development and ownership models.
Communities, children and young people will be encouraged to be innovative in developing local support and peer groups to facilitate greater awareness of emotional wellbeing and mental health. They have the best ideas of what can be done to meet the needs that they see everyday and or may be experiencing themselves. The local offer will ensure that appropriate resources are made available to resource these approaches.
Page 80

24
Priority 5 - Investing in the Future
Children and Young People will soon become young adults and adults, with many going on to start their own families in the future, who will want to provide the best for their children. Therefore, when a child or a young person presents or seeks support in Lambeth, co-providers will be required to take the long term future into account when offering support and/or treatment. The challenge across health and social care is to set the support into a framework that goes beyond the current presenting problem.
Parents have told us that although they are relieved to receive a diagnosis for their child, the current system of provision tends to focus on “fixing the presenting problem”. This can lead to a revolving door of dependency on outside help throughout the child’s life.
The cornerstones of realising the ambition to stop the revolving door are ensuring there is effective engagement with a range of providers and embedding the principle that often the presenting problem is a symptom of other needs. In order to effect change in long term prospects engagement with the following is a minimum requirement:
Over the course of this three year plan, commissioners commit to addressing the longstanding problems with transition and transition services for young adults who have emotional wellbeing and mental health needs. A specific workstream to develop transition services for those exiting CAMHs will be initiated. The workstream will take at its starting point the experiences of those who have transitioned or are on the cusp of transitioning to adult services. It will look at new and innovative ways of delivering appropriate support services to young adults.
Whilst having good transition services and support in place is essential, and the Plan recommends the development of a young adult emotional wellbeing and mental health service, future proofing is about thinking about life experience and adulthood and
Housing
Schools
Health Services
Training providers
Voluntary and Community
Sectors
Parenting support
Youth Offending Services
Page 81

25
parenthood. This will be scoped as part of the co-produced review of transitional pathways within the programme plan.
This Plan is a call to action for providers, families and communities to:
focus not only on fixing the presenting problem but to take into account the future and long term goals, mitigate against young people potentially falling between services and support when they reach 18yrs or when treatment is completed;
we will work with national and local providers and research institutes to ensure that the learning from research and evidence is leveraged into treatment and service models, with a continuing programme of development;
early identification and engagement with early onset mental health difficulties/ disorders to prevent unnecessary escalation and protect future prospects; A review of the Lambeth Early Onset service (LEO) will be undertaken to better understand the service offer, service pressures and the current and future demand for the service.
scope the extension of CAMHs age access criteria to include young adults. There are potential service design and resource implications that will be worked through will Adult Mental Health (AMH) who currently provide services from 18yrs. The Plan commits health and local authority commissioners to work together with this in mind and age ranges and with providers to advance this need as identified in the needs assessment.
Page 82

26
5. Lambeth CAMHS and Wellbeing Strategy Action Plan 2015 – 2018
This plan represents the outcomes we will work together as a borough to achieve and the activities we will complete to achieve them.
Work stream & Priorities Benefit Primary Lead Key Delivery
Partners
Year 1
15/161
Year 2
16/17
Year 3
17/18
Outcomes
1. Better Mental Health: For Everyone By Everyone (awareness, knowledge and training)
A. We will co-produce a ‘Lambeth Emotional Wellbeing Mental Health Toolkit’
All professionals and communities
will have a locally produced,
evidence-based toolkit, which
contains information on core
principles, how to be more
confident in identifying and
supporting themselves families,
including further support available
(including voluntary sector), training
parents, professional, young people
+ signposting and mapping of
appropriate support.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
Clinicians
√ All professionals working with children and young people in Lambeth will have access to and tailored training on how to easily use an evidence-based Emotional wellbeing toolkit
Every member of the community will get consistent and coherent messages around keeping well
B. We will co-produce a workforce development plan for Lambeth which enhances awareness, confidence and capability
All professional groups working with
children and young people will
participate in training which
empowers them to work confidently
to support the wellbeing of all
children and young people in
Lambeth.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
Clinicians
√ 100% of new staff (working with CYP) completed an induction which includes EWMH support for CYP in Lambeth within 4 weeks of starting their new role.
80% of staff completed EWMH toolkit training
Increased identification number of referrals
Increased number of
1 Each action will be completed by the end of each quarter indicated.
Page 83

27
appropriate referrals
Reduced number of A&E attendances
Reduced number of tier 4 outpatient appointments
C. We will co-produce a communication strategy to engage in a variety of ways with communities to promote living well
All professionals and communities
working with children and young
people will have easy and
appropriate access to the ‘EWMH
toolkit’ and the range of support
available in Lambeth.
The co-production group will scope
the development of young person
friendly communication e.g. via
social media, app, young person
website, texting etc.
This will include the refreshing of
the Young Lambeth Local Offer
website to include all support
services in Lambeth and parenting
programmes including how to
access them.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
Clinicians
√ For professionals, parents
and children and young
people:
Increase in awareness of EWMH toolkit
Increase in use of EWMH toolkit
Increase in awareness of referral pathways
Increase in awareness of EWMH services
Increase in awareness of EWMH training
100% of EWMH services included on Young Lambeth website
Increase in number of visits to Young Lambeth EWMH webpage
D. We will co-produce Quality standards for our Young Lambeth Local Offer
All professionals and communities
working with children and young
people can make informed choices
about the quality, safety and
effectiveness of services in
Lambeth.2
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
√ All organisations on the ‘Young Lambeth Local Offer’ website will clearly state if they meet Lambeth co-produced quality standards
2. Maximising Resilience (tier 0)
2 See Ace-V Standards developed by Lisa Williams with Young Minds: http://www.youngminds.org.uk/training_services/bond_voluntary_sector/ace-v
Page 84

28
A. We will co-produce accessible information on evidence based self-management and resilience strategies
All professionals, parents, children
and young people will have access
and a briefing (base on EWMH
toolkit) on how to live well and be
resilient.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
Clinicians
√ All professionals working with children and young people in Lambeth will have access to and tailored training on how to easily use an evidence-based Emotional wellbeing toolkit
B. We will co-produce a plan to implement the recommendations of the Lambeth Parenting Review3 (see appendix)
All professionals and communities
will have accessible and clear
information on evidence based
parenting programmes available in
Lambeth and how to refer or
contact the service for further
information.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
Clinicians
√ All professionals and communities will have access to a comprehensive and clear Young Lambeth Local Offer to support their emotional wellbeing and resilience
C. We will co-produce with Lambeth schools a review (including the mapping of EWMH support in Lambeth schools) and a plan to implement evidence-based whole school approaches to enhance resilience and wellbeing in schools
All pupils will be supported to
achieve the best academic and life
outcomes in Lambeth schools.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
CPHP
√ All services schools commission for the emotional wellbeing and resilience of their pupils will be easily accessible on the Young Lambeth Local Offer website
3. No Child Overlooked (vulnerable groups)
A. We will provide additional resource to build capacity and reduce waiting times for children and young people to access Specialist CAMHS
All children and young people will
experience faster access to the
most appropriate support.
Increased capacity for early
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
√ 100% of Early Intervention Team CYP accepted referrals participate in 1st treatment within 10 weeks of referral by end of Q2 16/17
100% of ALL CAMHS
3 See appendix
Page 85

29
intervention, family therapy and
clinical psychology enhance the
resilience of current Specialist
CAMHS services.4
Teams CYP accepted referrals participate in 1st treatment within 10 weeks of referral
B. We will co-produce a review of each Specialist CAMHS service
All children and young people and
communities will be assured of
receiving a safe, timely, evidence-
based, a young person friendly and
resilient service representing best
value for money.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ √ All Specialist CAMHS services reviews are co-produced and completed in 2015
C. We will co-produce a review and where appropriate redesign of current care pathways
All children and young people and
communities will experience the
right support, in the right place in a
timely manner, making best use of
all of the resources and services
available to support children, young
people and families in Lambeth.5
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ √ 100% CAMHS pathways reviewed, updated, included on Young Lambeth website
100% of CYP aged 17 have an effective transition plan which includes AMHS support and self-management.
E. We will co-develop a ‘Community of Practice’6
All professionals and communities
working with children and young
people are invited and included
within a ‘Community of Practice’
which enables people to share
learning, strategies and
opportunities to build on best
practice, enhance awareness,
confidence and capability. All can
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ All organisations in Lambeth will be invited bi-annually to participate as a ‘Community of Practice’
4 See appendix for additional investment plan. 5 The review will in particular include the following areas: early intervention, Looked After Children, Post Adoption support, eating disorders, early access to psychosis, transition to adult mental
health services and step down from tier 4 to tier 3. 6 See resilience work for pupils, parents, ‘Boing Boing’ by Prof. Angie Hart: http://www.boingboing.org.uk/index.php/resilience-in-practice/cop-information?id=41:bb-cop&catid=1
Page 86

30
participate in the development of
training and care pathways.
4. Cemented in Communities (co-production and addressing health inequalities)
A. We will co-review the governance arrangements and membership of the CAMHS Joint Commissioning Group (JCG)
All commissioning organisations of
EWMH support are able to co-
produce borough-wide EWMH
services solution efficiently
together.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
√ EWMH programme and commissioning 100% co-produced from consultation to delivery and review.
B. We will co-produce a borough-wide outcomes dashboard in partnership with Public Health colleagues
We have borough-wide outcome
information collectively gathered
and analysed to inform joined-up
commissioning as efficiently as
possible
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
√ Increased number of staff trained in EWMH awareness
Increase in no. of referrals to CAMHS.
Increase in no. of referrals to CVS
Increase in no. of ‘rejected’ referrals signposted
C. We will co-produce and deliver on a plan to implement the recommendations of the Black Mental Health Report
We have services which are
accessible for all communities,
which collect information informing
their evaluation of how inclusive
their services are to meet the needs
of the whole of the Lambeth
population.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ √ Enhancement of Equality and Diversity dataset requested from providers.
5. Investing in the Future
A. We will improve transitions planning across all key transitions stages for
All young people feel confident and
supported in managing change and
CAMHS Co-
production
Project Manager
CAMHS JCG
EWMH Forum
√ All 17 years olds have a transition plan which includes self-
Page 87

31
children, young people and young adults7
positive about the future. Group
Children, young people and families
Public health
Clinicians
management
B. We will co-review ways for children and young people to be fully involved in the development of their own goals, including leveraging in new technologies to achieve this
All children and young people will
be firmly in control of the
development of their goals and
supported to achieve their long
term goals.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ Every child and young person feels a sense of control, choice and confidence in the development of their own goals.
C. We will carry out a comprehensive whole system review which includes a comprehensive financial modeling review
All commissioners are supported
with a comprehensive mapping of
all key commissioner investment in
Lambeth, including schools, Public
Health, CCG and Evelina.
This will inform collective
commissioning to maximize best
use of collective resources,
minimize duplication, enhance
consistency of key messages (see
EWMH toolkit) and where
appropriate achieve economies of
scale.
CAMHS Co-
production
Group
Project Manager
CAMHS JCG
EWMH Forum
Children, young people and families
Public health
Clinicians
√ All commissioners have a strategic overview of total expenditure and services invested in to inform collective commissioning and maximize best use of collective resources
7 We will work with adult mental health services to identify alternative and innovative models to meet the needs of those likely to transition to adult services and young adults.
Page 88

32
Appendices
Appendix 1: EWMH Programme Management Resourcing
Governance8:
This strategy and plan will be delivered by the CAMHS Joint Commissioning Group
which reports into the Children, Young People and Maternity Board (Lambeth CCG).
Strategic Management Tool:
The EWMH programme is managed with the aid of a strategic programme monitoring
tool which contains the following information to support ongoing planning and
delivery:
EWMH Outcomes Dashboard
Specialist CAMHS o Outcomes o Waiting Times o Activity o Staffing
EWMH Programme Plan
Risk Log
Resource:
Programme manager resource requirement: 3 days per week minimum
1. 8 See appendix ‘CAMHS Joint Commissioning Group (JCG) Terms of Reference (2011)
CAMHS Co-production
Group
CAMHS Joint
Commissioning Group
(JCG)
Children, Young People
and Maternity
Programme Board
Children and Families
Strategic Partnership
(CFSP) Lambeth Clinical
Commissioning Board
Page 89

33
Appendix 2: CAMHS Joint Commissioning Group (JCG) Terms of Reference (2011)
Lambeth JCG TORef
- August 2011 - under review v2.doc
Appendix 3: Lambeth and Southwark CAMHS Needs Assessment (2013)
CAMHS NA_full_report.doc
Appendix 4: Supporting the Health of Young People in Lambeth: A summary report of the
Health Related Behaviour Survey (2014)
Lambeth SHEU 2014.pdf
Appendix 5: Review of parenting and family support programmes in Lambeth (June 2013)
reveiw FINAL VERSION.docx
Appendix 6: ‘What Works’ in CAMHS
drawing_onthe_evidence.pdf
CAMHS Interventions PCv1.docx
Appendix 7: Additional investment to improve access to Specialist CAMHS (2015/16)
CAMHS additional
investment 15 16 v11.doc
Appendix 8: Young Lambeth Local Offer
http://www.younglambeth.org/local-offer/landing-pages/local-offer.html
Appendix 9: Futures in Mind
https://www.gov.uk/government/.../Childrens_Mental_Health.pdf
Page 90

34
Page 91

This page is intentionally left blank

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 1 -
TERMS OF REFERENCE
CHILD AND ADOLESCENT MENTAL HEALTH SERVICES JOINT COMMISSIONING GROUP
August 2011
Document Detail Document Type Terms of Reference
Document name Lambeth CAMHS Joint Commissioning Group Terms of
Reference
Document location S:\Lambeth BSU\Integrated
commissioning\CHILDRENS\CAMHS\Agendas, Meeting
Papers and Minutes\TOR
Version Final
Effective from August 2011.
Review date August 2015.
Owner AD, Children’s and Maternity, Integrated Commissioning
Lambeth BSU
Prepared by Children’s Commissioning Manager, Lambeth CCG
Approved by, date CAMHS Joint Commissioning Group
Superseded documents CAMHS JCG Terms of Reference 2008
Related documents CAMHS Strategy (2008 – 2011)
Keywords CAMHS, Joint Commissioning,
Supporting References
Page 93

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 2 -
PURPOSE The Child and Adolescent Mental Health Services Joint Commissioning Group (CAMHS JCG) will ensure the implementation of national and local strategies to address the mental health needs of all children and young people in Lambeth by:
providing leadership for the development of joint and integrated CAMH services
advising on organisational change to enable these developments
acknowledging and addressing the racial, cultural, linguistic and religious needs of Lambeth’s diverse population
retaining an oversight, through the Joint Commissioner(s), of the contract management of CAMHS delivery
acting as the key facilitator of strategic developments in CAMHS and to work towards ensuring that the full spectrum of CAMHS delivery in Lambeth is represented at the Joint Commissioning Groups
facilitating integrated and partnership approaches and commitments to CAMHS delivery and strategies across health, Local authority CYPS and providers.
ensuring the involvement of service users in the planning of service provision, development of proposals for changes and decisions about changes to the operation of services.
ACCOUNTABILITY The CAMHS JCG is accountable to the Children, Young People and Maternity Programme Board which in turn is accountable to the Lambeth Collaborative Clinical Commissioning Board, the Children and Families Strategic Partnership (CFSP) through the Children and Young People Strategic Commissioning sub-group. Fundamentally, the CAMHS JCG commissions in partnership with the CAMHS Co-Production Group consisting of service users, parents carers and key professionals. Short life groups may be established from time to time to address, or develop and steer specific areas of CAMHS work. Governance diagram
ROLE
CAMHS Co-production
Group
CAMHS Joint
Commissioning Group (JCG)
Children, Young People and
Maternity Programme Board
(CYPM)
Children and Families
Strategic Partnership (CFSP)
Lambeth Clinical
Commissioning Board
Page 94

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 3 -
The role of the CAMHS JCG will be to:
oversee implementation of the Lambeth Emotional Wellbeing Mental Health Strategy, which has been designed to meet the emotional and mental health needs of children and young people in Lambeth, in line with national strategy and responding to local need
ensure the strategy is reviewed bi-annually in line with evidence and to commission need assessments
maintain financial oversight on all CAMHS provision, Tier 1 – Tier 4 and make decisions on the appropriate spend of an agreed ‘pool’ of allocated resources for CAMHS from the PCT and Local Authority, in line with best value and within the framework of agreed standing financial instructions
jointly commission CAMH services at all tiers (1 to 4) in line with the needs assessment and agreed strategy and drawing on the available aligned resources
maintain an overview of the development and performance management of all CAMH services that it commissions
oversee the negotiation of service specifications and service agreements with CAMHS providers on an annual basis and be responsible for the performance management and monitoring of those agreements
ensure that identified needs assessments and service evaluations are carried out to enable the commissioning of needs led and evidence based services
ensure that wider stakeholders, including service users, are informed of developments within CAMHS and that they are provided with the opportunity to be involved in service development and design. This includes attendance at relevant user forums twice a year.
Facilitate quarterly provider/commissioner forums SCOPE The CAMHS JCG has responsibility for commissioning and monitoring all elements of CAMHS (commissioned) services across Lambeth. Irrespective of funding source The partners Representatives from Health and Local Authority Commissioners will work in partnership to commission CAMH services and to monitor performance. Representatives from CAMHS specialist provider (South London and Maudsley NHS Trust), the Youth Offending Service, adult mental health services, and from the voluntary sector will provide specialist advice to commissioners. User and parent/carer representation will provide advice relating to the child and family perspective.
Page 95

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 4 -
Consultation with the Voluntary and Community Sector forum ascertained that a representative from the voluntary and community sector forum will be invited to attend meetings if a relevant topic is to be discussed. The JCG will develop links with adult mental health services and work towards their membership of the JCG. The JCG will develop a mechanism for consulting with children and young people in a formalised systematic way, with a clear route for the outcome of consultations to feed into the CAMHS JCG. The service users The service users Lambeth children and young people, and their parents / carers, including those resident in the borough, those living outside of the borough but who are registered with a Lambeth GP, other children for whom an agency is responsible for providing services to from time to time, and those placed out of the borough in specialist placements. The age range is from birth to 18th birthday. There will be some overlap in commissioning responsibility with adult mental health services before and after the 18th birthday mark. Strategy The JCG will, in consultation with stakeholders review the local CAMHS strategy which is needs led and evidence based on a bi-annual basis. The JCG will maintain a strategic overview of all CAMH services commissioned and provided for the borough, to inform unmet need and further develop strategy. Performance Management The JCG will maintain an overview of the development and performance management of all CAMH services that it commissions. The JCG will maintain an overview of performance against relevant Public Service Agreements, in particular indicator 4, which refers to Emotional Health and Wellbeing, and child and adolescent mental health services. This indicator contains four proxy measures:
The development and delivery of CAMHS for children and young people with learning disabilities
Appropriate accommodation and support for 16/17 year olds
Availability of 24 hour cover to meet urgent mental health needs
Joint commissioning of early intervention support From 2009 the intention is to replace these measures with outcome based measures. CODE OF CONDUCT
Commissioning members of the JCG will be responsible for both commissioning of services and performance management of service agreements.
Page 96

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 5 -
Chairing of the JCG will be carried out by one of the commissioning members and will be rotated between members on an annual basis. The JCG will elect the chair and vice chair.
Membership of the JCG will be reviewed every three years, or earlier, if required.
The JCG will meet at least eight times a year.
The JCG will be quorate when at least one commissioner from Health and the Local Authority are present.
Decision making will be on a consensus basis, but where agreement cannot be reached, the lead commissioners will make the decision by majority,
Where a member cannot attend a meeting, he/she should provide a deputy who is able to fully represent the member in terms of decision making responsibilities. Where a member is unable to attend two meetings in a row, and is unable to field a deputy, their membership of the group will be reviewed.
WIDER LINKS In commissioning service developments designed to meet the emotional and mental health needs of children and young people, the CAMHS JCG will need to maintain good links with other planning groups across the Children and Young People’s Strategic Partnership. Some commissioning and service development will also need to be done in conjunction with adult mental health services and other adult services commissioners.
Page 97

F:\moderngov\Data\AgendaItemDocs\0\9\3\AI00029390\$vbqrfi2f.doc - 6 -
Membership of CAMHS Joint Commissioning Group
Commissioner Only
NAME TITLE AGENCY ROLE
Philip Cokayne Finance Lambeth PCT Lead finance, advisory
Osariemen Obasohan
Commissioning Support Officer
Lambeth PCT Commissioner
Emma Stevenson AD, Integrated Children’s & Maternity Commissioning
NHS Lambeth/Lambeth CYPS
Commissioner
Dr. Abdu Mohiddin Public Health Consultant Lambeth PCT Advisory
Kelly Renzullo Service Head, Strategic Commissioning
Lambeth Children and Young People’s Service
Commissioner
Geraldine Abrahams
SE Head of Multiagency Team
Targeted Division Lambeth CYPS
Commissioner
Ian Lewis AD, Specialist Services Lambeth CYPS Commissioner
Daniel Taegtmeyer Children’s Commissioning Manager
Lambeth PCT Commissioner, Chair of JCG
Kevin Sheedy Head of Service Lambeth YOS Commissioner
Commissioner/Provider JCG Membership
Daniel Taegtmeyer Children’s Commissioning Manager
Lambeth PCT Commissioner, Chair of JCG
Kelly Renzullo Service Head, Strategic Commissioning
Lambeth Children and Young People’s Service
Commissioner
Osariemen Obasohan
Commissioning Support Officer
Lambeth PCT Commissioner
Nick Parkin Borough Manager, Lambeth CAMHS
South London and Maudsley NHS Foundation Trust
provider
Patricia O’Neil Borough Manager, National and Specialist CAMHS
SLaM provider
Dr Iris Rathwell Clinical Lead, Lambeth CAMHS
SLaM provider
Jummy Dawodu Head of Specialist Children’s Services
GSTT provider
Alo Raptopoulos Voluntary and Community Sector Forum Representative
CAUSE YOU CAN LTD Advisory
tbc tbc Other provider services provider
Page 98

<LOGO>
30/06/2015 1
CAMHS Needs Assessment 2013
Children and Young People’s Mental health and wellbeing
in Lambeth and Southwark
Draft 3
10 May 2013
Page 99

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 2
Contents
Acronyms ......................................................................................................................................... 5
Glossary ........................................................................................................................................... 5
1 Executive Summary ............................................................................................... 8P a g e | 2
1.1 Background ...................................................................................................................... 8
1.2 Methods .......................................................................................................................... 8
1.3 Key findings ..................................................................................................................... 8
1.3.1 Risk factors and vulnerable groups ......................................................................... 8
1.3.2 Wellbeing ................................................................................................................ 9
1.3.3 Diagnosis .................................................................... Error! Bookmark not defined.
1.3.4 Care pathways and provision .................................................................................. 9
1.3.5 Ways of working .................................................................................................... 10
1.3.6 Activity compared to need see Tier of service use ............................................... 10
1.3.7 Acute activity see 4.2.5.1 and 4.2.5.2 ................................................................... 11
1.3.8 Outcomes from tier 2-4 services ........................................................................... 11
1.4 Recommendations ......................................................................................................... 11
1.4.1 Strategic ................................................................................................................. 11
1.4.2 Service provision.................................................................................................... 11
1.4.3 Training and workforce development ................................................................... 12
1.4.4 Quality of services / care (information, monitoring and performance management) ....................................................................................................................... 12
1.4.5 Health promotion .................................................................................................. 13
1.4.6 Equalities and community engagement ................................................................ 13
1.4.7 Joint Commissioning between boroughs .............................................................. 14
2 Introduction .......................................................................................................................... 14
2.1 Background .................................................................................................................... 16
2.2 Aims and objectives ....................................................................................................... 16
2.3 National Policy ............................................................................................................... 17
2.4 Local strategies .............................................................................................................. 18
Lambeth ................................................................................................................................ 18
Southwark ............................................................................................................................. 18
3 Methods ................................................................................................................................ 20
3.1 Literature Review .......................................................................................................... 20
3.2 Local Data and Service Activity ...................................................................................... 21
3.3 Stakeholder Interviews: methods ................................................................................. 22
4 Results ................................................................................................................................... 23
4.1 Literature review ........................................................................................................... 23
Page 100

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 3
4.1.1 Prevalence of mental disorders ............................................................................. 23
4.1.2 Risk factors ............................................................................................................ 27
4.1.3 Vulnerable Groups ................................................................................................. 32
4.1.4 Expected Need for Mental Health Services ........................................................... 36
4.1.5 Future need for services ....................................................................................... 38
4.1.6 Protective factors for wellbeing ............................................................................ 39
4.1.7 Risk factors for poor wellbeing .............................................................................. 39
4.1.8 Interventions ......................................................................................................... 40
Social and emotional wellbeing in primary education (NICE, PH12) ........................................ 48
4.1.9 Outcomes: national indicators .............................................................................. 55
4.1.10 Outcomes - wider determinants ........................................................................... 55
4.2 Local Data and Service Activity ..................................................................................... 56
4.2.1 Mental health and wellbeing through the life course ........................................... 56
4.2.2 Local prevalence of mental health disorders ........................................................ 59
4.2.3 Diagnosis ................................................................................................................ 62
4.2.4 Local use of Targeted and Specialist Services ....................................................... 66
4.2.5 Tier 4 Activity ......................................................................................................... 74
4.2.6 Comparison of service use to predicted need ....................................................... 79
4.2.7 Outcomes: CAMHS Services .................................................................................. 82
4.2.8 Self harm ................................................................................................................ 86
4.2.9 Cost Effectiveness .................................................................................................. 87
4.2.10 Local Services relating to mental health and wellbeing ........................................ 89
4.2.11 Southwark Services................................................................................................ 95
4.3 Stakeholder Views ......................................................................................................... 98
4.3.1 Commissioners, health, social care and education professionals ......................... 98
4.3.2 Local public consultations ................................................................................... 109
4.3.3 National Consultations ........................................................................................ 111
4.3.4 Complaints and compliments .............................................................................. 111
5 Results Summary ................................................................................................................ 112
5.1 Equity ........................................................................................................................... 112
5.1.1 Age and gender of CAMHS service users ............................................................. 112
5.1.2 Ethnicity ............................................................................................................... 113
5.1.3 Young Offenders (YO) .......................................................................................... 118
5.1.4 Looked after children .......................................................................................... 118
5.1.5 Children with a learning disability ....................................................................... 119
5.1.6 Parental factors ................................................................................................... 119
Page 101

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 4
6 Discussion ........................................................................................................................... 119
6.1 Limitations ................................................................................................................... 119
6.1.1 Stephens and Rafferty approach to needs assessment ...................................... 119
6.1.2 Literature review ................................................................................................. 119
6.1.3 Data ..................................................................................................................... 120
6.1.4 Stakeholders ........................................................................................................ 121
6.2 Key Findings ................................................................................................................. 121
6.2.1 Risk factors and vulnerable groups ..................................................................... 121
6.2.2 Diagnosis .............................................................................................................. 122
6.2.3 Care pathways and provision .............................................................................. 122
6.2.4 Ways of working .................................................................................................. 123
6.2.5 Activity compared to need .................................................................................. 123
6.2.6 Acute activity ....................................................................................................... 124
6.2.7 Outcomes from tier 2-4 services ......................................................................... 124
6.3 Contrasting views raised by stakeholders ................................................................... 124
6.4 Areas commissioners requested information on ........................................................ 126
7 Draft Conclusions and Recommendations.......................................................................... 129
7.1 Strategic ....................................................................................................................... 129
7.1.1 Service provision.................................................................................................. 129
7.1.2 Training and workforce development ................................................................. 130
7.1.3 Quality of services / care (information, monitoring and performance management) ..................................................................................................................... 130
7.1.4 Health promotion ................................................................................................ 131
7.1.5 Equalities and community engagement .............................................................. 131
7.1.6 Joint Commissioning between boroughs ............................................................ 131
8 Author(s), key contacts and links for further information ................................................. 132
9 References .......................................................................................................................... 133
Appendix 1 Literature reviews ................................................................................................... 139
Appendix 2 – Stakeholder Interviews .......................................................................................... 193
Appendix 3 - NICE Clinical Guidelines .......................................................................................... 196
Appendix 4 – Diagnoses Tier 2 and 3 .......................................................................................... 197
Appendix 5 Service activity ......................................................................................................... 198
Appendix 6 –home postcodes ..................................................................................................... 201
Appendix 6 Southwark TAMHS ................................................................................................... 204
Page 102

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 5
Acronyms CAF Common Assessment Framework CAMHS Child and Adolescent Mental Health Services CBT Cognitive Behaviour Therapy CGAS Children’s Global Assessment Scale CP Child Protection CWD Child(ren) with disabilities EHWB Emotional Health and Well being EP Educational Psychologist EWO Education Welfare Officer IAPT Improving Access to Psychological Therapies LAC Looked after children PDC Pupil Development Centre SEAL Social and Emotional Aspects of Learning SEED Supporting Emotional and Educational Development SEN Special Educational Needs SLAM South London and Maudsley TA Teaching Assistant TaMHS Targeted Mental Health Services in Schools YOT Youth Offending Team
Glossary Attention deficit hyperactivity disorder (ADHD)
A common neuro-developmental disorder, occurring in around 2-5% of children and characterised by inappropriate levels of inattention, hyperactivity and impulsivity that are impairing and associated with the development of long term negative outcomes.
Autism spectrum disorder (ASD)
Autism spectrum disorder (ASD) is a behaviourally defined syndrome characterised by communication impairments, social interaction problems and unusual interest patterns and/or stereotyped behaviour. It occurs in approximately 1% of children and often gives rise to serious lifelong disabilities that cause considerable suffering and distress to individuals and their families.
Building Bridges a well-established family support service managed by the national children’s charity Family Action
Universal (Roughly equivalent to Tier 1 in old terminology)
Child and adolescent mental health services provided by people who are not mental health specialists. This includes GPs, health visitors, school nurses, teachers, social workers, youth justice workers and voluntary agencies. Services at this level include general advice and treatment for less severe problems.
Page 103

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 6
Targeted (Roughly equivalent to Tier 2 in old terminology)
Child and adolescent mental health services (CAMHS) provided by a specialist, such as a psychologist or counsellor, in a GP practice, paediatric clinic, school or youth service.
For children and young people showing early signs of mental disorders, or in groups at higher risk of poor mental health.
Specialist (Roughly equivalent to Tier 3 in old terminology)
Child and adolescent mental health services (CAMHS) provided by a team of specialists in a community mental health clinic or a hospital outpatients clinic. This level of service is for children and young people with severe and complex problems which they have had for some time.
Team members are likely to include child and adolescent psychiatrists, social workers, clinical psychologists, community psychiatric nurses, child psychotherapists, occupational therapists, art, music and drama therapists
National Specialist CAMHS Tier 4
Child and adolescent mental health services (CAMHS) for children and young people with the most serious problems. Services at this level may be provided in hospital as day patients
Care Programme Approach (CPA)
This is for anyone who needs to see several people or organisations for their care or treatment. If you are on the CPA, there will be a meeting every 3 to 6 months where everyone involved in your care, including you, will meet to discuss how things have been going and what should happen next. It requires health and social services and other agencies to work together with you to provide an agreed programme of care.
Cognitive Behaviour Therapy is a talking treatment that can help people overcome upsetting and unhelpful patterns of thinking and behaving. It helps people to be clearer about these patterns and to work out ways of changing them.
Conduct Disorder Conduct disorder is a disorder of impulse control which usually occurs in childhood and or adolescence and involves anti-social behaviour in which there is "a repetitive and persistent pattern of behaviour in which the basic rights of others or major age-appropriate societal norms or rules are violated" (Diagnostic and Statistical Manual, 4th Edition, of the American Psychiatric Association, DSM-IV).
Emotional disorder Emotional disorders in the UK 2004 survey of the mental health of children and young people include five main sub categories : depression, generalised anxiety, social phobia, specific phobia, separation anxiety disorder, plus smaller subgroups panic, agoraphobia, post traumatic stress disorder, obsessive compulsive disorder, and other anxiety disorders.
Page 104
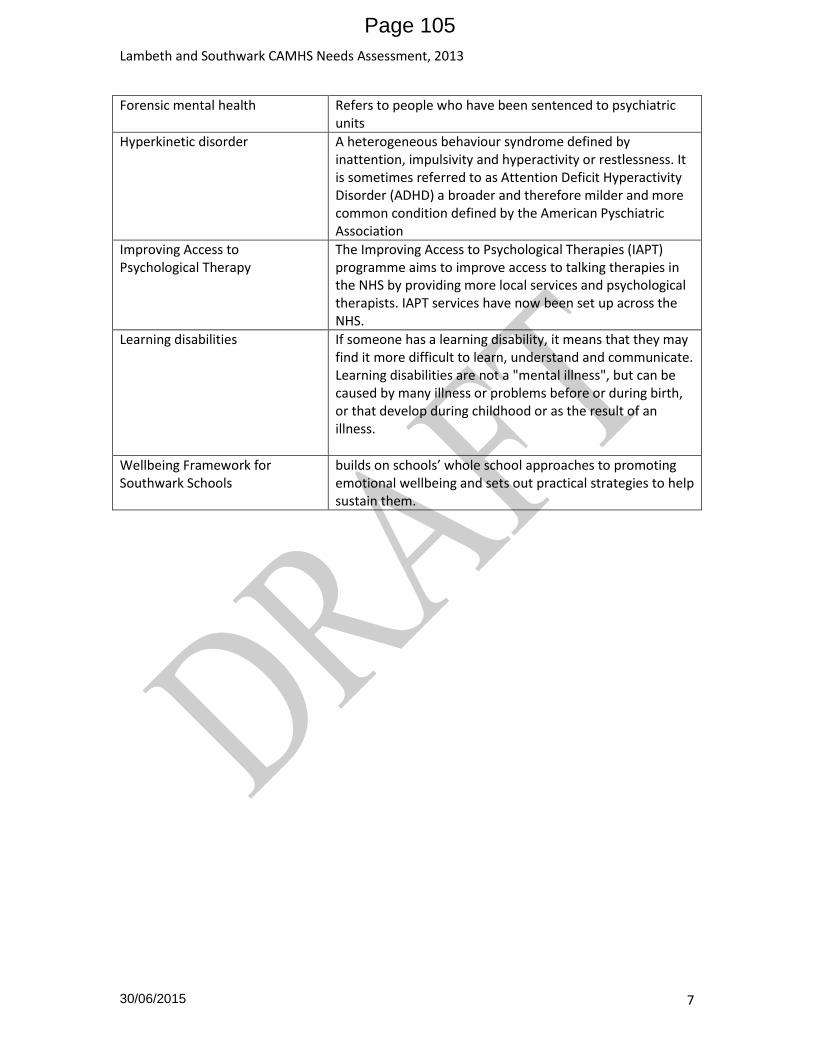
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 7
Forensic mental health Refers to people who have been sentenced to psychiatric units
Hyperkinetic disorder A heterogeneous behaviour syndrome defined by inattention, impulsivity and hyperactivity or restlessness. It is sometimes referred to as Attention Deficit Hyperactivity Disorder (ADHD) a broader and therefore milder and more common condition defined by the American Pyschiatric Association
Improving Access to Psychological Therapy
The Improving Access to Psychological Therapies (IAPT) programme aims to improve access to talking therapies in the NHS by providing more local services and psychological therapists. IAPT services have now been set up across the NHS.
Learning disabilities
If someone has a learning disability, it means that they may find it more difficult to learn, understand and communicate. Learning disabilities are not a "mental illness", but can be caused by many illness or problems before or during birth, or that develop during childhood or as the result of an illness.
Wellbeing Framework for Southwark Schools
builds on schools’ whole school approaches to promoting emotional wellbeing and sets out practical strategies to help sustain them.
Page 105

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 8
1 Executive Summary
1.1 Background
Nationally mental health problems cause significant health, social and economic issues. At any one time 1 in 10 children are estimated to have a mental disorder1. The local picture may well be worse as Lambeth and Southwark have higher levels of risk factors. The continuing economic uncertainty and recession are likely to increase mental health needs at a times when commissioning budgets and resources are decreasing. As 50% of lifetime mental health disorders (excluding dementia) start by the age of 14 and 75% by the age of 242and mental health promotion, prevention and early interventions are estimated to be able to prevent 25-50% of lifetime disorder, it is important to maximise mental health promotion and preventative activity as well as treatment. This needs assessment was carried out at the request of mental health commissioners from Lambeth and Southwark. It is the first time a needs assessment has been done across both boroughs at the same time and results for each borough have been reported separately and contrasted where differences have been found. Promotion of wellbeing was not covered in depth due to time constraints but it is a vital component of a comprehensive mental health strategy.
1.2 Methods
The Stephens and Rafferty needs assessment model has three perspectives: epidemiological, comparative and corporate. This was done through a literature review, stakeholder interviews, review of service and other data, and comparison between boroughs (and England / London where possible).
1.3 Key findings Key findings are summarised below. For more contextual understanding, please also see Stakeholder Views and Equity
1.3.1 Risk factors and vulnerable groups The literature review did not identify any new groups at higher risk of poor mental health
than the previous needs assessment o higher risk groups remain looked after children, young offenders, children with
learning disabilities children of parents with poor mental health, substance misuse problems, domestic violence, learning difficulties; children experiencing trauma and violence.
Vulnerable times in children and young people’s lives are at transition from primary to secondary school, from CAMHS to AMS, and after bereavement
No detailed work was done on the transition from primary to secondary school, and the steering group recommended that this key time needs more consideration.
Stakeholders were concerned about disruptive home environments, eating disorders, self-harm, overly sexualised behaviour, gangs, autism and ASD, and the effects of cannabis
1 Green et al, 2005 2 No health without mental health , Department of Health, 2011
Page 106

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 9
Perinatal mental health was also identified as a risk factor and some concerns expressed about capacity to meet needs of pregnant women with SMI and also more general mental health needs.
1.3.2 Wellbeing Promotion of emotional health and wellbeing by schools adopting a whole school approach results in happier and more motivated children and staff, reduced levels of mental health problems, better educational achievement and improved social inclusion 3. Wellbeing is also influenced by access to green spaces.
1.3.3 Mental disorders diagnosed Diagnostic data from SLAM was not conclusive for 36-47% of cases and therefore changes in
patient mix were hard to detect
The only top 10 diagnosis which has increased is “depressive episode” increasing from 4% of caseload in 2009-10 to 8% in Southwark and 9% in Lambeth by 2011-12. See Table 17 (Lambeth) Table 18 (Southwark)
1.3.4 Care pathways and provision There is limited information easily available on tier 1 activity particularly in terms of
numbers of children and young people seen and no detailed mapping of all mental health and wellbeing services within the borough
o Lambeth have produced a booklet of council commissioned services o Southwark have a CAMHS dashboard which shows all services, o Table 42 and Table 43 in this needs assessment have taken this information and
attempted to develop a mapping template but further work is needed to give a complete picture of all formal and informal capacity and care pathways within the borough
Referral pathways not clear – e.g. are GPs bypassing central referral panel and referring directly to tier 4 (referral source not provided in SLAM data).
General consensus from Stakeholder Views that SLAM CAMHS services are good, but some stakeholders felt there was not enough SLAM CAMHS expertise available
o Desire for SLAM CAMHS to provide more consultancy services o Desire for SLAM CAMHS to provide more training for staff
Some stakeholders felt that not enough CAMHS provision or that referral criteria too high o Support for parents who are sub-current thresholds for targeted / specialist services
but who aren’t managing with the support of universal services
Feedback to referrers not always timely (schools view)
Stakeholders felt that there is a need to o Have more counseling based services for children and families o (S) Forensic service or sex offender programme o Need more services for sexually exploited girls o Group work from CAMHS for some needs (not specified which needs) o consider extending services to 25 years (young adult service)
3 Promoting Emotional Health and Wellbeing through the Healthy School Standard, DH 2004
Page 107

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 10
1.3.5 Ways of working Many stakeholders expressed the view that true multiagency working is needed to ensure
that children and young people with and at risk of mental health disorders, and at risk of poor wellbeing are best reached
Multiagency working would mean functional teams made up people from different agencies able to deliver services in a flexible way e.g. community outreach workers, social workers and mental health professionals working together in the location best suited for the purpose. (see 4.3.1.2)
1.3.6 Activity compared to need see Tier of service use There is under provision of services at tier 2 and 3 but particularly tier 2, and depending on
the estimate used, under or over provision at tier 4.
Not able to comment about provision at tier 1 due lack of information about range of commissioned and non commissioned services within either borough.
1.3.6.1 Lambeth: activity compared to need
See Age and gender of CAMHS service users On average 17% of the number of children and young people predicted to benefit from tier
2,3 or 4 services in Lambeth have used CAMHS in 2011-12 (see Equity 5.1).
25% of looked after children predicted to need mental health services were seen by CLAMHS in 2011-12 Looked after children5.1.4
The proportion of young offenders who have seen CAMHS in 2011-12 is equivalent to 55% of first time offenders predicted to need mental health services (not the same as the YOS workload) See Looked after children
There is no information on children with SEN or with parental risk factors
1.3.6.2 Lambeth: age, gender, ethnicity See Age and gender of CAMHS service users
Proportion of predicted need accessing services varies from 1% of girls aged 2-4 to 31% of girls aged 15-17 years.
At younger ages a higher proportion of boys predicted to need services are accessing services than girls (2-14)
“Black other” and “other ethnicities” seem to be most over represented in service users
Chinese and all Asian groups are most under represented
1.3.6.3 Southwark: activity compared to need On average 23% of the number of children and young people predicted to benefit from tier
2,3 or 4 services in Lambeth have used CAMHS in 2011-12 (see Age and gender of CAMHS service users).
33% of looked after children predicted to need mental health services were seen by CLAMHS in 2011-12 See Looked after children
The proportion of young offenders from Southwark who have seen CAMHS cannot be reported
No information children with SEN or with parental risk factors
1.3.6.4 Southwark: age, gender, ethnicity – see 5.1.1 Proportion of predicted need accessing services varies from 8% of girls aged 2-4 to 33% of
boys aged 5-10 years.
Page 108

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 11
At younger ages (2-14 years) a higher proportion of boys predicted to need services are accessing services than are girls, but service attendance drops for boys aged 11-16
“Black other” and “other ethnicities” seem to be most over represented in service users
White ethnic groups are slightly over represented
Chinese and all Asian groups are most under represented
1.3.7 Acute activity see 4.2.5.1 and 4.2.5.2
Review of SUS data from Kings and GSTT as well as SLAM identified large increase in inpatients with primary diagnosis (F00-F99) in age 15-19 years (2 – 3 x total of 0-14 years inclusive) and in 20-24 year olds (1.5-2.5 x total of 15-19 years) main diagnoses – alcohol and schizophrenia (Table 31)
Males higher admissions than females after age 14.
No diagnosis / demographic data attached to SLAM provided tier 4 activity
1.3.8 Outcomes from tier 2-4 services Very limited information is available on outcomes – average change in CGAS score reported
for each year and each borough.
See Table 35, Table 36, Table 37,Table 38
1.4 Recommendations
1.4.1 Strategic An agreed and considered strategy is required for each borough (to cover say, 3 years) and be comprehensive in its scope to integrate the many effective actions across all the determinants of well being, the many partners and the life course. Expertise in wellbeing promotion exists within the Public health team and should be utilised during the strategy development stage. The recommendations below could form the basis of a strategy:
1.4.2 Service provision Principles of progressive universalism (i.e. services delivered according to need) and early
intervention should be followed. Younger children (under 5’s) are currently most under represented in both boroughs, and 5-9 year olds are also under represented in Lambeth.
Mapping of capacity of services, facilities and preventative interventions, included those provided by the voluntary needs to be carried out to give a fuller understanding of the local picture and clearer idea of where gaps are (e.g. parenting interventions, conduct disorders ). An asset based approach could be taken to include broader factors e.g. access to outdoor play and green space.
Maximise use of existing information on local needs e.g. through analysis of numbers of and reasons for referrals to the Multi-Agency Team in Lambeth and
Consider extending the upper age limit of CAMHS to 25 years, or developing adolescence and young person’s service from 14 – 25 years to maximise opportunities for prevention and early intervention with aim of reducing lifetime burden of mental health (and emergency admissions for 20-24 year olds) .
The balance between treatment of established disorders and early intervention before a problem becomes established needs to be shifted over time in favour of early intervention
Page 109

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 12
Capacity of perinatal mental health services for women who don’t meet the threshold for psychiatric help need developing – maybe not enough capacity to meet NICE guidelines
Southwark has a dedicated fast access service for with parents with MH issues – it is very well received by stakeholders. Lambeth might want to consider commissioning similiar.
Lambeth has a dedicated YOS CAMHS service – Southwark might want to consider ways of auditing access to CAMHS for YOS, if not to have a dedicated service
Two Southwark stakeholders mentioned having to commission psychological assessments separately from normal services from CAMHS – perhaps this could be incorporated into normal service if economies of scale available.
Consider more parenting classes at nursery and primary level as evidence suggests effective pre-age 12 and stakeholders felt needed to combat conduct and behavioural disorders.
Consider the balance of demands on CAMHS professional between training the wider workforce, providing consultancy advice, attending reviews and court, and working with children and young people. This could feed into the training and workforce development plan.
1.4.3 Training and workforce development Review the formally commissioned / provided training for non-mental health professionals
working in the wider services with an influence on children’s and young persons mental health to ensure adequate training opportunities – particularly in Southwark
o Teachers could have more training, particularly those who work with the last year of primary school and the first two years of secondary school – identifying children with Aspergers was recommended by the steering group, but it is a vulnerable time for all children
Roles of school nurses, health visitors and midwives could be developed : o School nurses to have greater role in supporting pupil’s emotional and mental
health e.g. be trained to recognise problems and provide brief interventions4 or refer where necessary (see ; to be more accessible to pupils
o Health visitors and midwifes to have role in early identification of mental health difficulties in mothers and children
1.4.4 Quality of services / care (information, monitoring and performance management)
Improve targeting / identification of children at risk by o ensuring that information about children is part of all initial assessment processes
e.g. substance misuse and adult mental health (already in Lambeth parenting strategy), and actions required to protect children are implemented.
o Ensure YOS regularly review/ audit number of YO identified via ASSET forms o Working with young carers carers groups
4 http://www.health.org.uk/areas-of-work/programmes/engaging-with-quality-in-primary-care/related-projects/improving-the-quality-of-mental-health-in-schools-quest/
Page 110

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 13
Mapping of activity in the wider mental health workforce/ primary mental health care e.g. GPs, social work, early intervention teams, young offenders, looked after children carried out by non-SLAM staff should be carried out
Services provided by these recorded in a way that prevention, promotion and early intervention activity can be understood.
An audit programme should be agreed on a regular basis with providers to include: o Outcomes of treatment – CGAS only partially completed o Rejected referrals – numbers and reasons why o User feedback
Regular audit of tier 4 referrals that do not go via triage panel /CAF process to ensure that appropriate
User feedback could be further developed / quantitative
Data gaps identified in the limitations section (5.1.2.2) need to be addressed
Lambeth to consider encouraging all schools to take part in SHEU and Southwark to consider having schools take part in order to monitor some aspects of wellbeing of children and young people
1.4.5 Health promotion Health promotion work in both boroughs
o to include child and adolescent mental wellbeing o tackle stigma associated with mental health o promote wellbeing and life skills not mental illness e.g through workforce development to ensure Every Contact Counts
Provide schools with information about mental health services available, who they are suitable for, and who they are not suitable for, and alternative sources of advice
Provide quality assurance guidelines for schools to help support evidence based commissioning and ensuring that children get appropriate help.
1.4.6 Equalities and community engagement The CAMHS Steering Group could discuss use of PREview with children’s services to jointly
target early years resources where they would be most effective
Increase identification of children and young people with MH problems who go undetected:
o Young Offenders - include CAMHS worker in case worker fortnightly discussions to ensure that young people with MH needs are identified as soon as possible. Ensure repeat ASSET assessments done.;
o Consider MH First Aid training for people working with adolescents to widen awareness of quietly distressed young people
o Identify ways of working with Young carers e.g. Southwark has a young carers group
Mental health promotion to engage with community groups for immigrants / refugees to build trust and remove stigma associated with mental health problems and provide support.
Page 111

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 14
1.4.7 Joint Commissioning between boroughs During the course of the needs assessment some stakeholders expressed an interest in knowing where there might be synergies between Lambeth and Southwark in terms of shared / joint commissioning of future CAMHS services. In thinking about this question it seems that work which falls into the following categories would be suitable: a) Areas which are new work for both boroughs b) Areas which require highly specialised clinicians, but numbers of children / young people
from each borough are small c) Areas which one borough has developed particular services than the other more than the
other Without being aware of details of current commissioning the following areas for joint work are suggested as possibly being suitable according to the criteria listed above.
A common approach to building relationships with GPs particularly as national policy is to move more mental health care into primary care and links with secondary and tertiary mental health care e.g CQUINs etc
Support for schools and youth services mental health commissioning e.g. o through provision of guidance on how to commission quality assured, evidence-
based services o Development of schools commissioning hubs
Commissioning of training for wider / non-specialist mental health workforce
Gangs – addressing violence, trauma, drug use, offender health, outreach work
Specialised services with small numbers of children / young people o Early / overly sexualised behaviour - link with teenage pregnancy teams? o Eating disorders – not clear from data that needs increasing o Self harm o Neurodevelopment
Southwark has a dedicated fast access service for with parents with MH issues – if Lambeth considering setting up might wish to learn from Southwark experience
Southwark does more work with under 5s and in children’s centres.
2 Introduction
Poor mental health impacts on the development of children and young people, preventing them from reaching their potential in school, developing friendships and relationships, and can increase offending and self-harm. There is a significant financial cost associated with poor mental health e.g. a child with an untreated behavioural problem is estimated to cost society £70,000 by age 28 years, ten times more than a child without behavioural problems (Allen, 2011b)
Mental disorder in childhood leads to poorer outcomes and inequalities in adulthood e.g. higher levels of unemployment and lower earnings, higher risk of crime and violence and higher rates of adult mental disorder which in turn leads to higher rates of smoking, alcohol and drug abuse, increased risk of physical illness and reduced life expectancy. Mental disorders account for 23% of the total disease burden in the UK - more than CVD (16%) and cancer (16%)5, and are estimated to cost the UK £105.2 billion per year (Allen, 2011b). As
5 World Health Organisation (2008). Global burden of disease report. WHO.
Page 112

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 15
50% of lifetime mental illness (except dementia) arises by age 146,7 and 75% by the mid-20’s8 it is vital to prevent mental ill health developing where possible and to provide early access to effective treatment where it is needed. The UK has poorer child wellbeing than most other European countries (24 / 29 countries)9 . This issue is particularly pertinent now as the current economic climate of increased austerity and uncertainty is likely to increase the incidence of mental health problems and suicide (No Health without Mental Health, DH, 2011)
6 Kim-Cohen J, Caspi A, Moffit TE et al (2003) Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective longitudinal cohort. Archives of General Psychiatry 62: 709-717 (cited by Campion and Fitch, 2012) 7 Kessler RC, Berglund P, Demler O et al (2005) Lifetime prevalence and age of onset distributions of of DSM-IV disorders in the national comorbidity (Cited by Campion and Fitch, 2012) 8 Kessler RC, Amminger GP, Aguilar-Goxiola S et al (2007). Age of onset of mental disorders: a review of recent literature. Current Opinion in Psychiatry 20 (4) : 359-364. (Cited by Campion and Fitch, 2012) 9 Bradshaw J, Richardson D (2009) An index of child wellbeing in Europe. Child Indicators Research 2 (3): 319-351.
Box 1: Definitions: Mental disorder - a clinically recognizable set of symptoms or behaviour associated in most cases with considerable distress and substantial interference with personal functions for a prolonged period of time (as defined by ICD-10 (International Classification of Diseases) and or DSM 4). Mental Health and wellbeing - this refers to a combination of feeling good and functioning effectively. Feeling good includes happiness, contentment, interest, engagement, confidence and affection. Functioning effectively (psychologically) involves the development of one’s life, having a sense of purpose e.g. working towards goals and having positive relationships1.
Box 2: Preventing Disease and Promoting Health
Prevention
Primary prevention – preventing illness developing in the first place
Secondary prevention – early identification and treatment
Tertiary prevention – promotion of recovery and relapse prevention or reduction
Health Promotion
Primary Promotion – promoting health and wellbeing of the whole population
Secondary Promotion – targeting groups that have or are at higher risk of poor health and wellbeing
Tertiary Promotion – targets groups with established health problems to help promote their recovery and prevent recurrence
Health promotion can take place at an individual, community or structural level and targets the determinants of health and wellbeing rather than the illness.
Page 113

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 16
2.1 Background No Health without Mental Health10 recommends that mental health strategies cover both the promotion of mental wellbeing and the prevention of mental disorder through the provision of early and appropriate treatment services for people with mental disorder. It therefore considers the impact of and possibilities available in universal services whose primary function is not mental health care e.g. children’s centres, schools and GPs, and acknowledges the importance of promoting well-being and resilience, as well as supporting children and young people with mental health problems. On this definition the responsibility for good mental health in children and young people is not with specialist services alone – it is everyone’s business. In this report the term CAMHS (Child and Adolescent Mental Health Services) is used as a broad term to cover all services which contribute to the mental health and wellbeing of children and young people, whether provided by health, education, social services, or other agencies including charities and the third sector, and not the more narrow used where CAMHS refers only to specialist child and adolescent mental health services operating at Tiers 2, 3 and 4. The Allen Report on Early Intervention11 emphasises the importance of a good foundation in life through polices to support the emotional and social wellbeing and functioning during the first three years of a child’s life. This needs assessment will therefore look at both mental health promotion and prevention of mental disorder. Substance Misuse Substance misuse is an issue locally for both adults and children. In 2010, 7.25% of people using drug treatment in Lambeth were under 18, and 30% of Southwark residents entering active drug treatment in 2011/12 were living in households with children. Although there are strong links between substance misuse and poor mental health, for example psychosis has been linked to cannabis use12 and parental substance misuse is a risk factor for poor mental health in children, this CAMHS needs assessment has limited scope and will not specifically look at substance misuse. Where alcohol or drugs are mentioned by stakeholders or literature, then they will included, however, the topic will not specifically be explored. In recognition of local needs Substance Misuse Needs Assessments have already been done in Lambeth and Southwark, and the reader is referred to them for more detailed information about substance misuse services.
2.2 Aims and objectives 1. To provide local epidemiological information on child mental health and wellbeing
highlighting vulnerable groups 2. To provide an assessment of the needs of vulnerable groups and others identified by
commissioners
10 HM Government (2011) No Health without Mental Health: A Cross Government Mental Health Outcomes Strategy for people of all ages. HM Government.
11 Allen G. Early intervention: The next steps. January 2011. London: HM Government. http://www.dwp.gov.uk/docs/early-intervention-next-steps.pdf 12 Scott J, Martin G, Bor W, Sawyer, M, Clark, J, McGrath, J (2009) he prevalence and correlates of hallucinations in Australian adolescents: Results from a national survey Schizophrenia Research 107/2-3(179-185)
Page 114

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 17
3. To analyze current service provision to identify unmet needs / gaps or inequities in access to services
4. To evaluate evidence of efficacy and effectiveness of interventions
2.3 National Policy Every Child Matters (2003)
The Children Act (1989 and 2004)
National Service Framework for Children, Young People and Maternity Services (2004) o Standard 9 – Mental Health and Psychological wellbeing of children and young
people: all from birth to 18th birthday who have mental health problems and disorders have access to timely, integrated, high quality, multidisciplinary mental health services to ensure effective assessment, treatment and support for them and their families.
The Mental Health Act (2007)
Targeted Mental Health in Schools (2008) o No longer funded by government
The Kennedy Review (2010) o Overcoming NHS cultural barriers to improving services for children and young
people
Children’s Trusts: Statutory Guidance on co-operation arrangements including the Children’s Trust Board and the Children and Young People’s Plan (2010)
Working together to safeguard children (2010, update due late 2012)
The Mental Health Strategy: No health without mental health, DH (2011) o Promotion of wellbeing across the population (also reducing levels of future mental
disorder) o Ensuring early treatment for people with mental disorder (also improving their
wellbeing) o Mental Health is everyone’s business – not just the concern of health and social care
sectors o Mental health should be mainstreamed and should have “parity of esteem” with
physical health
Talking Therapies: a four year plan of action, DH (2011)
Support and Aspiration: A new approach to special educational needs and disability, DfE (2011)
o wide ranging proposals to improve outcomes for children and young people who are disabled or have SEN, minimise the adversarial nature of the system for families and maximise value for money.
o Included extending age range LA responsible for to age 25
Graham Allen Review (2011) o Early Intervention (EI) in the first three years of children’s lives to provide essential
social and emotional security for the rest of their lives o External financing in innovative ways to deliver savings through early intervention
delivering good outcomes o Government to support piloting of different ways of contracting EI
Allen Review part 2, on Early Intervention: Smart Investment, Massive Savings – (2011)
Health and Social Care Act (2012)
Healthy Lives, Healthy People: Supporting Transparency and improving outcomes, DH (2012)
Page 115

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 18
2.4 Local strategies Lambeth council have become a Co-operative Council, involving residents in decisions and driving innovation through co-production in the commissioning of services.
Lambeth
JSNA 2009 (update underway) o Mental health and CAMHS identified as priority areas and actions to support were
suggested. o Need for data sharing protocol between statutory agencies and third sector for
children on the waiting CAMHS waiting list o Assessment of need for targeted programmes for preschool children. o Need for better promotion of wellbeing and mental health services
CYP Plan for Lambeth 2012-2014 o Prevention and early intervention for children and young people of identified
concern to all partners. o To develop cooperative partnership working at the neighbourhood level. o Joint workforce development across the partnership.
Lambeth Parenting Strategy o Add key points
Child Poverty Strategy o Add key points
Wellbeing and Happiness Programme o Add key points
Lambeth CCG Strategic plan o 7 priorities to improve health in Lambeth – none directly about children and young
people’s mental health and wellbeing – some tangential benefits (adult SMI and alcohol)
YOS Needs assessment, 2012-13 o Recommendations to be added
NSPCC report on Lambeth services from pregnancy to two o Mental health needs of pregnant women might not always be met o Although increasing support for families sub social services threshold, services not
yet fully developed and integrated across the spectrum of need.
Draft Substance misuse NA 2011-12 o Needs a comprehensive approach with all partner organisations working together
across the lifecourse of clients. o Improved communication between drug and alcohol services and mental health
services
Southwark
Southwark Council Plan 2011-2014 o “Support vulnerable people to live independent, safe and healthy lives by giving
them more choice and control over their care
Southwark Children and Young People’s Plan (CYPP) 2010-2013 o More effective support for families most in need o Early years provision that meets the needs of vulnerable children o Independence for children and young people with learning difficulties and / or
disabilities and their families
NHS Southwark Strategic Plan 2011-14
Page 116

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 19
o Achieve a reduction in health inequalities with particular emphasis on cvd, diabetes, cancer, mental health and sexual health by promoting healthy lifestyles and improving access to screening and high quality health services
JSNA 2011-12 http://www.southwarkjsna.com/ o Priorities for children and young people do not include mental health and wellbeing o Mental health mentioned - commitment to implementing principles of No Health
without Mental Health but children and young people not specifically referred to
The Southwark Mental Health Family Strategy (2012 -2015)
CAMHS Service Re-design principles o Moving specialist CAMHS practitioners from the clinic to the community and
providing a 60/40 split for allocation of targeted and specialist resources.
Page 117

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 20
3 Methods The Stephens and Rafferty needs assessment model has three perspectives: epidemiological, comparative and corporate. These aspects were covered through:
a review of relevant literature for information on prevalence of mental health problems in young people, risk factors for poor mental health and wellbeing, evidence of effective interventions and service models, and analysis of service data,
semi-structured interviews with key stakeholders from both Lambeth and Southwark - clinicians, commissioners, heads of service, schools
reviews of service user feedback and other local intelligence from relevant public consultations
A comparison was done between the two boroughs: Lambeth and Southwark. Hackney were also contacted but they were in the early stages of updating their strategic plan and felt the information they could share was limited.
Promotion of wellbeing was not covered in depth due to time constraints, but it is a vital component of a comprehensive mental health strategy. Expertise in wellbeing promotion exists within the Public health team and utilised during the strategy development stage.
Literature Review
A literature review was conducted to establish the expected prevalence of mental health disorders in children and young people, to identify vulnerable groups who will have higher needs for services, and to determine the evidence base for services. Electronic searches of Medline and PsychInfo as well as ChiMat (Child and Maternal Health Observatory) were conducted to identify relevant studies of prevalence and risk factors. Electronic searches were conducted of NICE, the Cochrane Library, NHS Evidence and DoH guidelines to determine best practice. References of papers were also reviewed where possible. Searches were confined to English language studies published between 2005 and 2012 from the UK, Europe, Australasia and North America. Systematic reviews, literature reviews, randomised controlled trials, observational studies and best practice guidance was included for risk factors and prevalence. Substance misuse was specifically excluded as discussed in the introduction. Search questions included:
What is the prevalence of mental health disorders in children and young people?
What are the risk factors for poor mental health and well being?
What works to prevent or treat mental disorders in children and young people and what
service models have been shown to be effective?
Is there any evidence that the prevalence of autism and autistic spectrum disorders is
increasing? (Specific question arising during stakeholder interviews)
Keywords included: emotional disturbances; mental disorders; behaviour disorders; affective
disorders/; anxiety disorders; major depression; anxiety; epidemiological data, epidemiology,
Page 118

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 21
prevalence study, autism; child, preschool, adolescence, risk, population characteristics,
recovery, treatment
For more details see Appendix 1
3.1 Local Data and Service Activity Data on tier 2, tier 3 and tier 4 inpatient and outpatient activity was received from South London and Maudsley (SLAM) the provider of CAMHS for both Lambeth and Southwark. Time period 2009-10; 2010-11 and 2011-12. Southwark quarterly commissioners data was received for March - December 2012 but was not in the same format and therefore not included in the data. . Tier 2 and 3 data fields Reported per unique (non PID reference)patient; borough; date of first appointment, team seeing patient; date of last appointment; age at referral; gender; ethnic group; first half of postcode; axis 1a diagnosis; axis 1 b diagnosis; axis 2 diagnosis, axis 3 diagnosis; axis 4 diagnosis; axis 5 diagnosis Missing: CGAS score (outcome measure) Limitations: diagnosis is from first appointment, therefore 33-43% of patients are noted as “No axis 1 diagnosis” or “diagnosis not specified”. Tier 4 National and Specialist CAMHS outpatient data Summary data provided by borough – number of new and follow up appointments per quarter, by team seeing patient. Missing: age, gender, ethnicity, diagnosis; number of appointments per patient Tier 4 inpatient data fields: Summary data reported by borough; number of admissions; number of bed days for children; number of bed days for adolescents Missing: diagnosis, age, gender; Limitations: only for SLAM patients, did not include patients sent out of borough Tier 1 activity GP data General practice data from 'Datanet' (which is a unique software available in Lambeth and connected to the general practice registers) was interrogated to identify any child under 19 stated to have some mental disorder such as learning difficulties (as there is a register), autism etc. As datanet relies on an updated general practice database, the data field completion was only 66% and the data (count of children) was considered unreliable to understand estimates of detected prevalence. Interrogating each practice was not carried out as it involved creating individual practice queries which is time consuming and ultimately may not present expected results. Hence, this GP data on children with mental disorders registered on practice databases was not utilised to provide estimates on prevalence or on treatment being carried out in tier 1. SUS data
Page 119

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 22
Secondary Uses Services (SUS) data was extracted from in-patient data tables (APC - Admitted patient care). Lambeth (5LD) and Southwark (5LE) were used as 'purchaser codes' to identify all patients treated at various providers where Lambeth (PCT) or Southwark (PCT) paid for patient care. F00-F99 were used as main ICD-10 codes denoting mental health care provided to all patients aged 24 and below. The main providers for L&S patients were identified as Kings and GSTT and SLAM returns were also available in the in-patient extract from SUS.
3.2 Stakeholder Interviews: methods Interviews were arranged with a range of stakeholders from both Lambeth and Southwark in an attempt to get a wide range of perspectives. Appendix 2 Stakeholder Interviewsv2.docx contains a full list of stakeholders consulted, questions asked during the semi-structured interviews, and a summary of the answers grouped into key themes. Due to short timescales service users were not consulted, but existing CAMHS service user feedback and information from other recent local consultations with the public were reviewed and summarised. Reports included were:
Lambeth – CAMHS PPI Report 2010/11
Southwark – CAMHS PPI Report, Jan 2013
Lambeth – YOS Needs Assessment qualitative work with Young Offenders
Southwark – One Thousand Journeys – feedback from children’s centres
Page 120

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 23
4 Results
The results of the literature review are reported first to describe the expected prevalence of mental health disorders, factors which are related to a higher risk of mental disorders, and to identify vulnerable groups. Local information on risk factors and vulnerable groups is then reported, following by evidence about protective factors. The expected need for mental health services based on evidence is reported, and then service data is used to compare actual activity to that which would be expected, and to identify whether there are any gaps in services or groups who are disproportionately not accessing services – objectives 1-3 of the needs assessment
4.1 Literature review
4.1.1 Prevalence of mental disorders The majority of the information on prevalence comes from a 2004 national survey of 7,977 children and young people aged 5-16 living in private households in Great Britain13. This is same information used by the Child and Maternal Health Observatory(ChiMat) and does not adjust estimates for known risk factors such as poverty or living in a single parent family which are known to be higher in Lambeth and Southwark than in the rest of the country. Information on the risk of mental disorders in children under 514, and in young people aged 17 comes from other sources as they are not included in the 2004 survey. Overall 9.6% of children and young people between the ages of 5-16 are estimated to have a mental health disorder. Table 1 shows that conduct disorders are the most common type of mental disorder , followed by emotional disorders, hyperkinetic disorders, and then less common disorders such as tics and eating disorders. The prevalence of mental disorders varies by age and gender with broadly speaking boys having higher rates of conduct and hyperkinetic disorders than girls and older children having higher rates of conduct and emotional disorders than younger children. Children aged 2-5 are estimated to have a similar overall prevalence of mental health disorders at 10%. There is a certain amount of debate about whether is possible or appropriate to diagnosis very young children with mental disorders , as well as a wide range of estimate of prevalence. ChiMat uses an estimate of 19.6% but this has not been used as it seems to be rather high in comparison to the estimates for five to ten year olds, and Egger provides a more reasonable estimate. One in five children with a mental disorder are estimated to have more than one mental disorder (i.e. 1.9% of all children). The most common combinations are conduct and emotional disorders and conduct and hyperkinetic disorders (both 0.7% of children). NB – this is why the sub categories in table 1 will not add up to the total for “any mental health disorder”. Table 1 Prevalence of mental health conditions in children and young people in England (sources: Green et al, 2005; Egger & Emde, 2011)
13 Green H, McGinnity A, Meltzer H et al (2005) Mental Health of Children and Young People in Great Britain, 2004. London: Office of National Statistics
14 Egger HL, Emde RN (2011) Common Emotional and behavioural disorders in preschool children:
presentation, nosology and epidemiology J Child Psychology and Psychiatry, 47¸(3-4), 313-37
Page 121

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 24
Condition Age range (years)
National Prevalence
Boys Girls Both
Any mental health condition 2-4 10% 5-10 10.2% 5.1% 7.7%
11-16 12.6% 10.3% 11.5% 5-16 11.4% 7.8% 9.6% More than 1 mental health condition 5-16 1.9% Conduct disorder 5-10 6.9% 2.8% 4.9%
11-16 8.1% 5.1% 6.6% Emotional disorder 5-10 2.2% 2.5% 2.4%
11-16 4.0% 6.1% 5.0% Hyperkinetic disorder 5-10 2.7% 0.4% 1.6%
11-16 2.4% 0.4% 1.4% Less common mental disorders 5-10 2.2% 0.4% 1.3%
11-16 1.6% 1.1% 1.4% Autism15 9-10 0.39% Other ASDs 9-10 0.77% ASD16 5-9 1.57%
ASD17 0-17 1.15%
4.1.1.1 Children aged 0-4 Seven papers were found which addressed this topic: One on ADHD, ODD, depression and anxiety18. Four on Autism/ASD/PDD (refs 6,7,12,57 Appendix 1); one on major depression (31) and one on mental health disorders in looked after children (34). In addition, papers were provided by Elizabeth Murphy from SLAM, including Egger and Emde, 2011. In a sample of 726 4 year olds, ADHD and Oppositional Defiant Disorder were found to be most prevalent disorders (rate not quoted in abstract, no access to journal). ADHD was found to be more common in boys but prevalence of other disorders did not vary by gender. Generalised anxiety disorder and depressive disorder were found in less than 1% of the sample. This is lower than the prevalence of depression found in a Spanish study of 1427 three to six year olds (Ref 31). In this study 15.6% children were classed as possible depressives based on a questionnaire filled out by carers, but after screening with a mental health professional 1.12% were found to meet the criteria for major depressive disorder. No confidence intervals were quoted in the abstract and it has not been possible to read the full paper. Estimates of the prevalence of ASD following population screening of 2 year olds in Gothenburg, Sweden (ref 7) were higher for boys than girls: Boys autism 0.86% vs 0.16% girls,
15 Baird G, Simonoff E, Pickles A et al (2006) Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP) Lancet 368 (9531) 210-5 16 Baron Cohen S, Scott FJ, Allison C et al (2009) Prevalence of autism spectrum conditional: UK school based population study. The British Journal of Psychiatry 194 (6) 500-9 17 Idring, S, Rai, D, Dal, et al (2012) Autism spectrum disorders in the Stockholm Youth Cohort: Design, prevalence and validity PLoS ONE, vol./is. 7/7, 1932-6203 18 Lavigne, JV, LeBailly, S A, Hopkins, J, Gouze, KR, Binns, HJ (2009) The prevalence of ADHD, ODD,
depression, and anxiety in a community sample of 4-year-olds. Journal of Clinical Child and Adolescent Psychology, May 2009, vol./is. 38/3(315-328), 1537-4416
Page 122

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 25
atypical autism 0.39% vs 0.16% girls and all ASD 1.25% vs 0.33% girls . This works out at 79 per 100,000 for any ASD for both genders which is lower than UK estimates for 5-9 year olds ( 157 per 100,000). Estimates of mental health disorders in looked after children aged 0-5 in inner city UK were >1 MHD in 26 (60.5%) , and >1 developmental disorder was found in 11 (25.6%). 30 /43 (69.8%) pre-schoolers fulfilled criteria for at least one diagnosis, and 18 (41.9%) had two or more comorbid conditions. Whereas 36 (83.7%) of the pre-schoolers needed an intervention, only 3 of these were found to have received adequate input from services Table 2 Estimates of mental disorders in 16-24 year olds, Adult Psychiatric Morbidity in England Survey, 2007, ONS unless otherwise stated
Condition Age range National Prevalence
Male Female Both
ADHD, 19 , 20, 21
Adult ADHD Self Report Scale
4 items / 6 items
Under 10 3-6%
Teenagers 2-4%
16-24 13.7% 13.9% 13.8%
1.3% 0.8% 1.1%
PTSD26 16-24 5.1% 4.2% 4.7%
Common Mental Disorder26 16-24 11.9% 21.0% 16.4%
Psychotic Disorder (schizophrenia and affective psychosis)
16-24 0.0% 0.4% 0.2%
Eating Disorder 16-24 6.1% 20.3% 13.1%
1.7% 5.4% 3.5%
4.1.1.2 Autism and Autistic Spectrum Disorders (ASD) A recent study from Sweden which looked at 589,117 children aged 0-23 found recorded ASD varied by age from 0.65% in 4-6 year olds, to 1.46% in 13-17 year olds with an average for the whole age range of 1.15% (95% CI 1.12-1.18%). Appendix 1 contains a literature review showing an increase in reported prevalence of ASD over the last 10-15 years from several countries across the world. There are wide variations in estimates by country and it is not clear why prevalence might vary by country, therefore UK estimates have been use for this needs assessment. Researchers are unclear whether the reported increase is due to a wider diagnostic definition, better recognition of (less severe) cases or a genuine increase in the condition.
4.1.1.3 17 year olds Mental disorder in adults is classified differently from children and adolescents making it harder to compare need in 17 year olds to younger children. Table 2 includes estimates of mental disorders in 16-24 year olds from a national survey. It has been assumed that rates in 16 and 17 year olds are the same as 18-24 year olds . Under current diagnostic systems, antisocial personality disorder is not formally diagnosed before the age of 18 and therefore the diagnosis
19 Ford T, Goodman R and Meltzer H (2003) The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Psy, 42, 1203-1211 20 Keen D, Hadijikoumi I (2008) ADHD in children and adolescents. Clinical Evidence (online), downloaded 30 November 2012 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907929/ 21 Jadad A, Booker, Gauld M et al ( 1999) The treatment of attention-deficit/hyperactivity disorder. An annotated bibliography and critical appraisal of published systematic reviews and metaanalyses. Can J Psychiatry, 44, 1025-1035
Page 123

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 26
is not necessarily relevant to CAMHS although the features of the disorder can manifest earlier as conduct disorder. Borderline personality disorder can be formally diagnosed by age 16.
4.1.1.4 ADHD The estimates of some conditions vary widely depending on how tightly criteria are applied. This is likely to account for differences in perceived need between lay people, non-specialist mental health workers and mental health professionals. As table 3 shows, 13.8% of the 16 – 24 year olds scored positive for 4 / 6 items on the Adult ADHD scale but only 1.1% of the same group met all 6 criteria.
4.1.1.5 Eating Disorders The estimated prevalence of eating disorders, like ADHD spans a wide range depending on the tightness of the diagnostic criteria – almost 1 in 5 women demonstrate some symptoms, but only a quarter of those with symptoms meet the criteria of suffering considerable impairment as a result, i.e. there is a considerable group of people with subclinical needs. The expected prevalence of eating disorders in 16-24 year olds is 3.5% (Table 3). This is much higher than in younger age groups where eating disorders are classified as a subsection of less common mental disorders (estimated prevalence 1.4%). 10 papers from a range of different countries found varying rates of eating disorders suggesting that cultural beliefs may have an impact on rates of eating disorder (Refs 22-310, Appendix 1). One paper (25 Appendix 1) specifically explored this hypothesis by comparing young people of Romanian and Hungarian living in Transylvania and demonstrated a difference between these two groups. Another paper (26 Appendix 1) found evidence to contradict the view that eating disorders and poor body image are confined to white girls from higher SES backgrounds. The one paper from the UK22which looked at eating disorders in children under 13 years seen in paediatric clinics reported that overall incidence was 3.01/100 000 (208 individuals). Of these eating disorder not otherwise specified was the most frequent diagnosis 43%, 37% met criteria for anorexia nervosa and 1.4% for bulimia nervosa; Nineteen per cent showed determined food avoidance and underweight without weight/shape concerns. Rates are higher in females than males and the population with subclinical need is much higher than those with clinical need. This review has not looked at whether subclinical need progresses to clinical need.
4.1.1.6 Self harm (This section is abridged from a report to the Child Overview Death Panel in 2012.) Self-Harm applies to any act of self-poisoning or self-injury carried out by an individual irrespective of motivation.23 24 However there are currently no universally recognised criteria for the diagnosis of self-harm as it does not feature in the ICD 10 or DSM diagnostic criteria. Self harm is an important public health issue as a strong correlation has been noted between self-
22 Nicholls, Dasha E, Lynn, Richard, Viner, Russell M (2011) Childhood eating disorders: British national surveillance study.The British Journal of Psychiatry, April 2011, vol./is. 198/4(295-301), 23 Hawton, K., Harriss, L., Hall, S., et al. (2003a) Deliberate self-harm in Oxford, 1990–2000: a time of
change in patient characteristics. Psychological Medicine 33, 987–995. 24 http://publications.nice.org.uk/self-harm-longer-term-management-cg133
Page 124

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 27
harm and subsequent suicide.25 Hawton et al (2002) found only 12.6% of episodes of self harm had resulted in presentation to hospital, therefore the true number of children and young people harming themselves is likely to be much higher.
4.1.1.7 Schizophrenia (from NICE Clinical Guideline 155, 2013) Schizophrenia is very rare in pre-pubertal children and there is limited epidemiological knowledge on this early onset disorder. From the information available it has been estimated that the prevalence of childhood schizophrenia may be of the order of 1.6 to 1.9 per 100,000 child population. However, its prevalence increases rapidly from age 14 onwards with incidence peaking in the late teens and early twenties. In an Australian sample of first episode psychosis, a third of new cases were aged between 15 and 19 years old. Whilst male gender predominance has been described in pre-adolescent children an equal sex ratio is more commonly reported in adolescents . The 2007 Adult Mental Health Survey found no psychotic disorder (Schizophrenia and affective pyschosis e.g. bi-polar) in males aged 16-24 whilst 0.4% of females were found to have had an episode in the previous year).
4.1.2 Risk factors
4.1.2.1 Age: The risk of mental disorders increases with age: from 7.7% of children aged 5-10 years to 11.5% of 11-16 year olds. 16.4% of adults aged 16—24 have a common mental disorder26. After adjusting for other factors, the odds of a mental disorder increases by almost 75% for 11-16 year olds compared to 5-10 year olds (Odd Ratio 1.73). Data from the Millennium Cohort Study (Figure 1) suggests that around 10% of 5 year olds have poor outcomes for behaviour or learning and development, or both. This does not necessarily mean a need for mental health services, but it could be indicative of a need for wellbeing promotion programmes or preventative programmes such as parenting classes to help parents deal with difficult childhood behaviour.
Figure 1percentage of children with poor outcomes at age 5. Source: ChiMat analysis of Millenium Cohort Study
25 Owens, D., Horrocks, J., & House, A. (2002). Fatal and non fatal repetition of self-harm. British Journal of Psychiatry, 181, 193–199. 26 Adult Psychiatric Morbidity in England, 2007 – Results of a household survey https://catalogue.ic.nhs.uk/publications/mental-health/surveys/adul-psyc-morb-res-hou-sur-eng-2007/adul-psyc-morb-res-hou-sur-eng-2007-rep.pdf
Page 125

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 28
4.1.2.2 Gender At younger ages, boys are more likely to have a mental health disorder than girls 10.2% compared to 5.1% at ages 5-10, reduced to 12.6% vs 10.3% by age 11-16. By early adulthood, young women are more likely than young men to have a common mental health disorder (21% vs 11.9%). There are clear gender differences in the type of mental disorder suffered at ages 5-16 with boys being significantly more likely to have conduct, hyperkinetic and less common disorders than girls, but girls being more likely to have emotional disorders. After controlling for other factors, in 5-16 year olds, boys are 50% more likely to have a mental disorder than girls (OR 1.52)
4.1.2.3 Ethnicity The Mental Health of Children and Adolescents in Great Britain Survey (2004) did not give any clear findings about prevalence of mental health disorders by ethnic group, mainly because the sample was small. The data suggests that children from BME backgrounds are less likely to have a mental disorder than children from white ethnicity. This could be due to the survey methods which require parents to describe their children’s behaviour –it is possible that nuances were missed where parents did not speak English as a first language. However, after researchers controlled for other factors they found that children of Black African, Indian or Pakistani ethnic origin were less likely to have a mental disorder than white children (ORs = 0.11, 0.21, and 0.47). The literature review did not find any evidence to support a relationship between overall mental health and ethnicity - A systematic review of 15 papers (3401 subjects in total) reported that findings between race and ethnicity were too scarce to be consistent37 and a cross sectional survey of 4175 11-17 year olds in the USA found that European Americans were more likely to have substance misuse and co-morbid disorders than African Americans but otherwise there were no ethnic differences in mental health27. It is debatable whether or not data on ethnic differences from the United States is applicable in the UK due to historical differences between the two countries. There is some UK evidence that people from Black, particularly Black Caribbean28 backgrounds are more likely to experience psychosis compared to the white population, although this is based on evidence from young people aged 17-3529 (first episode of psychosis is rare in younger people). From an equity point of view it is important to monitor the ethnic background of service users compared to the local ethnic population. This is done in section 5.1.2
27 Roberts RE , Roberts CR (2007) Ethnicity and risk of psychiatric disorder among adolescents. Research in Human Development. 4/1-2(89-117) 28 Morgan, Fisher, Hutchinson, et al (2009) Ethnicity, social disadvantage and psychotic-like experiences in a healthy population based sample. Acta Psychiatrica Scandinavica 119/3(226-235) 29 Cheng, Kirkbride, Lennox, et al (2011) Administrative incidence of psychosis assessed in an early intervention service in England: First epidemiological evidence from a diverse, rural and urban setting. Psychological Medicine, 41/5(949-958)
Page 126

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 29
Figure 2- Ethnic breakdown of Lambeth population aged <19. Source: Greater London Authority Ethnic Group Population Projections (2011)
% Ethnicity <19 Lambeth
40.6%
11.8%
19.4%
1.6%
12.6%
1.5%
2.0%
1.1%
3.3%
6.1%White
Black Caribbean
Black African
Black Other
Indian
Pakistani
Bangladeshi
Chinese
Other Asian
Other
Figure 3 Ethnic breakdown of Lambeth population aged <19. Source: Greater London Authority Ethnic Group Population Projections (2011)
% <19 Ethnicity Southwark
42.1%
7.2%
23.6%
2.1%
10.1%
0.7%
3.1%
2.1%
2.6%
6.5%White
Black Caribbean
Black African
Black Other
Indian
Pakistani
Bangladeshi
Chinese
Other Asian
Other
Many personal, social and environmental factors increase the risk of mental health disorders. Table 3 shows factors which were found by Green et al, 2005 to independently increase the risk of mental disorders after other factors had been taken into account.
Page 127

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 30
Table 3 Socio-demographic and familial factors which increase the risk of particular mental disorders. Source: Green et al 2005
Disorder Risk factor Group Baseline OR Group: Baseline
95% CI
Emotional
Age 11-16 years 5-10 years 2.28 1.71-3.03
Gender Boys Girls 0.70 0.54-0.90
Family Type
Lone previously married parent Couple
2.48 1.68-3.68
Single lone parent 1.71 1.03-2.86
Education No parental qualifications Any qualifications
1.52 1.11-2.07
Conduct
Gender Ethnicity
Boys Indian or Pakistani
Girls White
1.91 0.13 0.37
1.52-2.40 0.02-0.96 0.15-0.95
Family Stepchildren No stepchildren
1.91 1.37-2.69
Area type30 Moderate means Wealthy
achiever
2.13 1.4- 3.13
Hard Pressed 2.10 1.4-3.23
Education No parental qualifications Any qualifications
1.43 1.10-1.84
H’hold income Less than £400 / week More than £600/wk
1.79 1.24-2.60
Hyper-kinetic
Gender Boys Girls 6.10 3.39-10.99
Family’s empmt Neither parent working Both parents working
0.47 0.26-0.85
H’hold income Less than £400 / week £400-£600 2.12 1.10-4.05
Table 4 shows the impact of additional risk factors in the child, family, and environment on child and adolescent mental health problems (source Lambeth Needs Assessment, 2008) Table 4 Risk factors for child and adolescent mental health problems Risk factor Increased risk to mental health due to the
presence of a risk factor Chronic physical illness in the child 3 times risk
Cerebral palsy 4-8 x risk
Sensory impairments 2.5- 3 x risk
Specific and general Learning difficulties 2-3 x risk
Language problems 4 x risk
Maternal psychiatric problem 1.2- 4 x risk
Parental schizophrenia 8-10 x risk of schizophrenia
Parental mental illness, including alcohol /drug misuse
Increased risk of conduct disorder/depressive symptoms
Parental criminality 2-3 x risk of delinquency
Physical and emotional or sexual abuse 2-3 x risk
Traumatic event eg bereavement 3-5 x risk
Homelessness 8 x risk
LGBT 1.16 x risk
30 CACI information Services (1993) Acorn User Guide
Page 128

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 31
4.1.2.4 Trauma / violence A US study of 3614 adolescents found that witnessing parental violence or violence in the community increased the risk of PTSD and having a major depressive episode independently of other risk factors such as age and gender.31
4.1.2.5 Deprivation Measures of 'school readiness' show that the poorest 20% of children are more likely to display conduct problems at age 5, compared to children from more affluent backgrounds32. Conduct, emotional and hyperkinetic disorders are related to different measures of deprivation such as low household income, joblessness, no educational qualifications, area type (table 4).
Lambeth and Southwark are both more deprived than the England average making it more likely that rates of mental disorder will be higher. Insert deprivation maps for each borough.
4.1.2.6 Children in poverty This has been used as a proxy for low household income to avoid index linking 2004 prices to 2013. As Figure 3 below shows, Lambeth has a slightly higher percentage of children living in poverty than Southwark, and both have a substantially higher proportion than the England average. The proportion of children living in poverty locally appears to have fallen substantially between 2007 and 2009, and is now much closer to the national average. Some of this fall may be due to the way children in poverty has been calculated (means tested benefits) as if access to benefits has fallen, then it will appear that fewer children are in poverty than before when it is not the case. It is also possible that some of this is genuine change due a gentrification of both boroughs with influxes of young professionals who have started families. The closing of the poverty gap (when measured in this way) between Lambeth and Southwark and England suggests that local rates of child and adolescent mental disorder might not be expected to as much above the national average as they were in earlier needs assessments. Figure 4
Children living in PovertySource: APHO Health Profiles (2010, 2011, 2012)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Proportion of
children < 16 living
in poverty (2007)
Proportion of
children < 16 living
in poverty (2008)
Proportion of
children < 16 living
in poverty (2009)
Area
Pere
cent
age
of c
hild
ren
< 16
yea
rs
Lambeth
Southwark
England
31 Zinzow HM, Ruggiero KJ, Resnick H, Smith D, Saunders B, Kilpatrick D, (2009) Prevalence and mental health correlates of witnessed parental and community violence in a national sample of adolescents Journal of Child Psychology and Psychiatry 50/4(441-450) 32 Sabates R, Dex S (2012) Multiple risk factors in young children's development [online] Centre for Longitudinal Studies, UoL
Page 129

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 32
4.1.3 Vulnerable Groups
4.1.3.1 Looked after children 45% of children who are living in care33 (LAC) are estimated to have a diagnosable mental health disorder, roughly four and a half times more than children who are not in care. Mental health disorders are less common in younger children, but a summary paper by NICE34 concluded that around 20% of under five year olds have signs of emotional and behavioural difficulties, but taking into account evidence from abroad up to 70-80% of all looked after children could be considered to have a recognisable mental health condition. It was commented that children in foster care have better mental health than those in residential homes. The rates quoted by NICE are higher than those found in a small (n=43) UK study35 of looked after children aged 0-5 concluded that 60.5% had at least 1 mental health disorder and 25.6% had >1 developmental disorder. Furthermore 30 /43 (69.8%) preschoolers fulfilled criteria for at least one diagnosis, and 18 (41.9%) had two or more comorbid conditions. Although the researchers felt that 36 (83.7%) of the preschoolers needed an intervention, only 3 of these had received adequate input from mental health services. Table 5 shows the number of children looked after in both Lambeth and Southwark has remained fairly constant over the last three years. Both Lambeth and Southwark have a higher proportion of looked after children than the national average (Figure 2) which will increase overall mental health needs compared to England, depending on the proportion of children looked after within Lambeth and Southwark. However, as local authorities are responsible for all children in their care, regardless of where they are looked after, it is important to consider all children in care, included those out of borough. Figure 5 Children in care per 10,000 population, Lambeth, Southwark and England
33 Melzer H, Corbin T, Gatward R et al, (2003) The Mental Health of young people looked after by local authorities in England. London: Office for National Statistics 34 Sempik J EP22 - LAC 12.2b The mental health of looked after Children in the UK: Summary (http://www.nice.org.uk/nicemedia/live/11879/47446/47446.pdf accessed 13/2/13 35 Hillen, T, Gafson, L, Drage, L, Conlan, L (2012) Assessing the prevalence of mental health disorders and
mental health needs among preschool children in care in England.Infant Mental Health Journal 33/4 411-420
Page 130
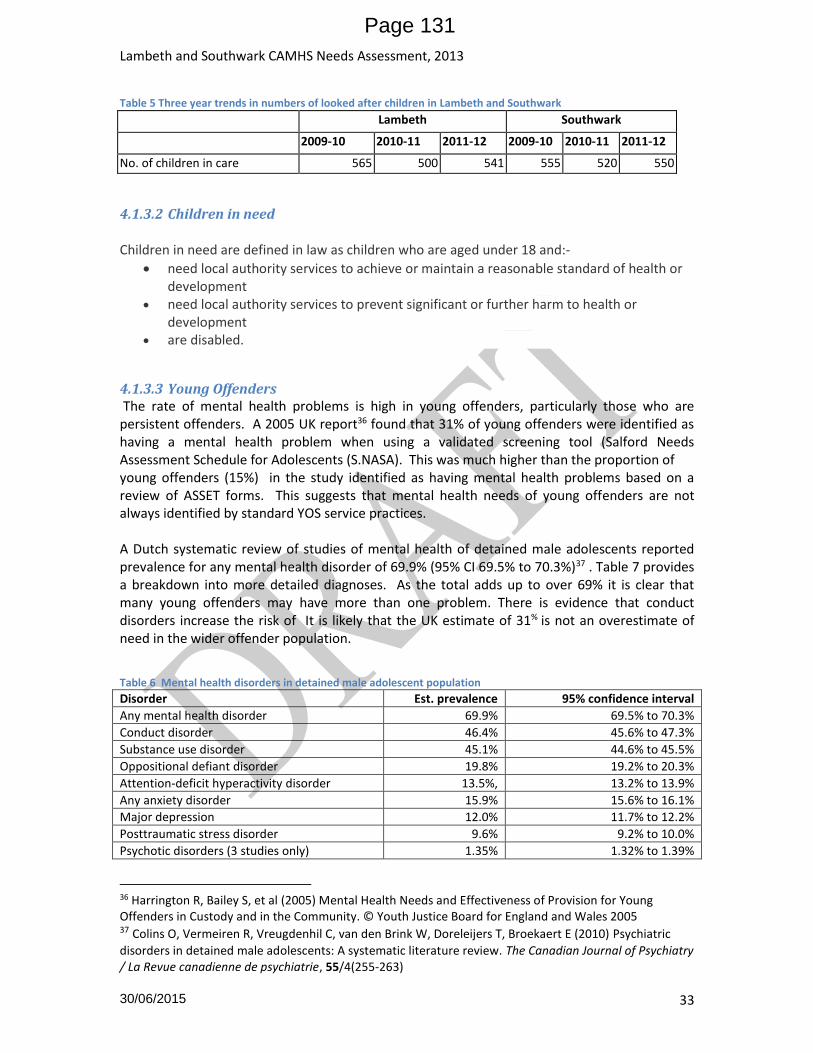
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 33
Table 5 Three year trends in numbers of looked after children in Lambeth and Southwark
Lambeth Southwark
2009-10 2010-11 2011-12 2009-10 2010-11 2011-12
No. of children in care 565 500 541 555 520 550
4.1.3.2 Children in need
Children in need are defined in law as children who are aged under 18 and:-
need local authority services to achieve or maintain a reasonable standard of health or development
need local authority services to prevent significant or further harm to health or development
are disabled.
4.1.3.3 Young Offenders The rate of mental health problems is high in young offenders, particularly those who are persistent offenders. A 2005 UK report36 found that 31% of young offenders were identified as having a mental health problem when using a validated screening tool (Salford Needs Assessment Schedule for Adolescents (S.NASA). This was much higher than the proportion of young offenders (15%) in the study identified as having mental health problems based on a review of ASSET forms. This suggests that mental health needs of young offenders are not always identified by standard YOS service practices. A Dutch systematic review of studies of mental health of detained male adolescents reported prevalence for any mental health disorder of 69.9% (95% CI 69.5% to 70.3%)37 . Table 7 provides a breakdown into more detailed diagnoses. As the total adds up to over 69% it is clear that many young offenders may have more than one problem. There is evidence that conduct disorders increase the risk of It is likely that the UK estimate of 31% is not an overestimate of need in the wider offender population.
Table 6 Mental health disorders in detained male adolescent population Disorder Est. prevalence 95% confidence interval
Any mental health disorder 69.9% 69.5% to 70.3%
Conduct disorder 46.4% 45.6% to 47.3%
Substance use disorder 45.1% 44.6% to 45.5%
Oppositional defiant disorder 19.8% 19.2% to 20.3%
Attention-deficit hyperactivity disorder 13.5%, 13.2% to 13.9%
Any anxiety disorder 15.9% 15.6% to 16.1%
Major depression 12.0% 11.7% to 12.2%
Posttraumatic stress disorder 9.6% 9.2% to 10.0%
Psychotic disorders (3 studies only) 1.35% 1.32% to 1.39%
36 Harrington R, Bailey S, et al (2005) Mental Health Needs and Effectiveness of Provision for Young Offenders in Custody and in the Community. © Youth Justice Board for England and Wales 2005 37 Colins O, Vermeiren R, Vreugdenhil C, van den Brink W, Doreleijers T, Broekaert E (2010) Psychiatric
disorders in detained male adolescents: A systematic literature review. The Canadian Journal of Psychiatry / La Revue canadienne de psychiatrie, 55/4(255-263)
Page 131

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 34
NB Estimated prevalence reported in table 7 are different from those used in the Durham Mapping Exercise reported in the Southwark 2006 CAMHS Needs Assessment, but are from a later paper by one of the authors of the original study quoted i.e. later work has refined estimates. Locally, a higher proportion of young people are entrants to the youth justice system than the national average, and since 2010-11 rates in Lambeth have been higher than in Southwark adding to the picture of increased local needs for mental health services.
Figure 6 First time entrants to the Youth Justice System, Lambeth, Southwark compared to London and England 2008-09 to 2011-12.
The youth offending service case load is likely to be higher than a single year of first time entrants to the youth justice system in 2011-12. Table 7 Characteristics of young people from Lambeth and Southwark in the youth justice system, 2010-11 & 2011-12
Ye
ar
Bo
rou
gh
Age group Ethnicity
10-
14
15 16 17-18
Total
% m
ale
White Mixed
Asian or
Asian British
Black or
Black British
Chinese or
Other Ethnic Group
Not Known
2010-11
L 89 102 102 161 454 81 80 49 3 314 5 3
S 86 87 126 122 421 85 112 48 16 223 4 18
2011-12
L 63 73 125 174 435 87 61 62 5 302 4 1
S 66 62 97 132 357 89 101 43 12 189 5 7
source: www.justice.gov.uk/statistic/youth-justice/statistics Table 7 shows a profile of Lambeth and Southwark young people in the criminal justice system according to Ministry of Justice statistics. These seem to be a description of first time entrants. It is notable that the vast majority (>80% are male) and the largest proportion of young people in the youth justice system from Lambeth and Southwark are of black or black British ethnicity
Page 132

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 35
(69% and 53% respectively). This is an over representation compared to the general Lambeth and Southwark 10-17 year old population which are 48% and 44% black respectively.
4.1.3.4 Children with a learning disability It has been estimated that 36% of children with a learning disability also have a mental health problem38. This is over three times higher than in the general child population but substantially lower than the estimates of 40% - 77% given in the 2006 Southwark CAMHS needs assessment. Figures 4 and 5 below show that both Southwark and Lambeth have significantly higher numbers of children with autistic spectrum (14.18 and 15.73 per 1,000 population compared to 7.58)known to schools and also a higher number of children with learning difficulties known to schools compared to the England average (34.79 and 34.59 per 1,000 population compared to 24.61) . Lambeth appears to have slightly more children with severe learning difficulties than Southwark 5.27 per 10,000 compared to 4.28. Figure 7 Southwark disabilities profile 2012 findings
Figure 8 Lambeth disabilities profile 2012 findings
4.1.3.5 Parental Mental health disorders Children of a mother with depression are five times more likely to have conduct disorder compared to children whose mother is not depressed39. Analysis of the Millennium Cohort
38 Emerson E, Hatton C (2007) Mental Health of Children and Adolescents with intellectual disabilities in Britain British Journal of Pyschiatry 191 493-9
39 Melzer H, Gatward R, Corbin T et al (2003) Persistence, onset, risk factors and outcomes of childhood mental disorders. London: The Stationary office
Page 133

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 36
Study by ChiMat found that maternal depression at age 9 months or age 3 years had an adverse impact on behaviour at age 5, and persistent maternal depression (i.e. at age 9 month and 3 years) resulted in poor behavioural, learning and development and health outcomes at age 540. Original analysis of the National Psychiatric Morbidity Survey (2007) conducted for the NSPCC (Manning, 2011) estimates that 19% of babies in the UK have a parent who has a common mental health problem. The local picture of parental mental health is likely to be similar or worse, given that Lambeth and Southwark are more deprived than England, and deprivation is associated with common mental health problems. The literature review only identified one study which related parental mental health problems (bipolar disorder) to children’s mental health problems (early onset major depression)41. No local information was been obtained on parental mental health –either of the parents of children using CAMHS services, or from Adult mental health services to estimate how many of their clients have children. The Caldicott guardian from SLAM advised against providing information about parents when child information was provided. Adult mental heatlh services have not been approached.
4.1.3.6 Parental substance misuse and domestic violence The NSPCC report referred to above also estimates that around 26% of babies under the age of one in the UK have parents affected by either one or a combination of: domestic abuse, substance misuse, mental health problems:
14% of babies are living with a parent who is a substance misuser.
19% of babies have a parent who has a common mental health problem
5% of babies have a parent who has experienced domestic abuse in the past year Assuming Manning’s estimates quoted by the NSPCC are correct, then at least a quarter of babies in Lambeth and Southwark are likely to be living a parent affected. As local levels of deprivation are higher than the England average it is likely that a higher percentage of babies will be affected.
4.1.4 Expected Need for Mental Health Services Estimates of the proportion of children requiring mental health services is higher than the prevalence of mental disorders (c9%) because it includes children who need support in the form of preventative interventions before the level defined as a mental disorder, e.g. in tier 142. The Early Intervention agenda recognises the importance of mental health promotion as well as mental health prevention and early access to treatment, and therefore estimates of the number of children at risk as well as the number of children who reach thresholds for clinical diagnosis of a mental health disorder have been included. Ideally, interventions would occur before the need for specialist (tier 3 services) for complex and enduring problems.
40 http://www.chimat.org.uk/preview/evidence Strength of Association between maternal factors and outcomes at age 5. 41 Author not reported Early-onset major depressive disorder more prevalent in children of parents who have BD. Psychiatric Annals, July 2011, vol./is. 41/7(356), 0048-5713
42 Health Advisory Service (1995) Together we stand; the commissioning role and management of child and Adolescent mental health services.
Page 134

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 37
Two different estimates of need for service have been found, but it has not been possible to access the full articles references for either to compare and contrast the methodology. Table 8 Estimated need for CAMHS services
Tier Kurtz43 quoted by ChiMat Campion and Fitch44
1 15.00% 10.00% of children with one or more risk factor
2 7.00% 7.00%
3 1.85% 3.00%
4 0.075% 0.47%
The expected need for SLAM CAMHS services in Lambeth and Southwark has been calculated using the estimates described above and is shown in Table 9. As a further comparison the local need for mental health services has also been estimated from national prevalence rates for mental disorder applied to the local populations (9.6% for children 5-16 years and for 2-4 year olds of 10%). The methods used by Kurtz and prevalence of mental health disorders methods of calculating needs for services produces a similar overall number – almost 6,000 children and young people per year who could benefit from targeted or specialist services. However, the Fitch and Campion method almost doubles the expected need for tier 3 and increases the expected need for tier 4 almost six-fold. There are a further 9,000 or so children who are estimated to benefit from interventions or support from non-mental health professionals. Table 9 Estimated numbers of children and young people requiring mental health services in Lambeth and Southwark 2011-2015 by tier of service and based on Kurtz estimates of mental health disorders
Estimated need
0-17 population
Tier1 Tier 2 Tier3 Tier 4 Total Tier 2-4
Total 2-16 years
with MHD
Kurtz 15% 7% 1.85% 0.08%
Southwark
2011 60715 9107 4250 1123 46 5419 5913*
2012 61787 9268 4325 1143 46 5514
2013 62948 9442 4406 1165 47 5618
2014 64129 9619 4489 1186 48 5723
2015 65179 9777 4563 1206 49 5818
Lambeth
2011 60448 9067 4836 1118 48 6002 5935*
2012 61218 9183 4897 1133 49 6079
2013 62046 9307 4964 1148 50 6162
2014 62869 9430 5030 1163 50 6243
2015 63572 9536 5086 1176 51 6313
Fitch and Campion 10% 7% 3% 0.47%
Southwark 2013 6295 4406 1888 296 6591
Lambeth 2013 6205 4964 1861 292 7117
43 Kurtz Z (1996) Treating Children well a guide to using the evidence base in commissioning and managing services for the mental health of children and young people. 44 Campion J, Fitch C (2012) Guidance for Commissioning Public Mental Health Services, Joint Commissioning Panel for Mental Health Services, London
Page 135

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 38
CAMHS services are divided into three age groups, under 5s, 5 years to 11 years and 12 to 17 years. The CAMHS Needs Assessment Steering Group were particularly interested in the likely need in children under 5, which will help support delivery of Early Intervention as recommended by Allen (2011) . This early intervention is about ensuring good development and wellbeing – it is not only about specialist mental health services for young children. The Child and Maternal Health Observatory (ChiMat) have developed a tool PREview45 to support the planning of services under 5’s. PREview uses data from the Millennium Cohort Study and qualitative data from the Mother and Infant Research Unit at the University of York to estimate where (geographically) resources need to be targeted at under 5’s to ensure good outcomes in health, behaviour and development at age 5. To run the model needs some dedicated analyst resource and data-linking between NHS and LA data and requires senior commitment to push for data and to all stages of the preventative agenda. Recommendation: The CAMHS Steering Group could discuss use of PREview with children’s services to jointly target early years resources where they would be most effective
4.1.5 Future need for services Table 9 above also shows the likely need for services between 2013 and 2015. Changes in the age structure of the population may alter the relative demand for services by age group. Between 2013 and 2016 all age groups in Lambeth will increase, with a slightly greater increase in 10-14 year olds compared to other groups by 2016 (figure 11). In Southwark by contrast in the same time period there is predicted to be a bigger increase in 0-5 year olds compared to other age groups (Figure 12). This may increase the need for early years services. Figure 9 Lambeth population under 25 years old projections from 2011-2021 – source GLA
Figure 10 Southwark population under 25 years old projections from 2011-2021 – source GLA
45 http://www.chimat.org.uk/preview/commissioners
Page 136

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 39
4.1.6 Protective factors for wellbeing Guidance for Commissioning Public Mental Health Services46 reports the following factors as being conducive to wellbeing and therefore possibly protective of mental health. Local levels of these protective factors have not been reported in this needs assessment but links to relevant data sources are included to allow investigation if required.
Breast feeding www.phoutcomes.info/public-health-outcomes-framework/domain/2
Early years education www.education.gov.uk/researchandstatistics
16 year olds participating in EET i.e.anti NEETS www.education.gov.uk
Local child participation in physical activity www.sportengland.org/research
Participation in at least three hours of sport or PE at school http://atlas.chimat.org.uk/IAS/dataviews/healthyschoolsprofile
Good housing - www.communities.gov.uk/housing/housingresearch Southwark Council has recognised the importance of safe, warm and dry housing in their pledge to ensure all social housing meets these standards by 2015.
The importance of these factors as influences on the wider determinants of physical and mental health has been also recognised in the Public Health Outcomes Framework which is described in Section 4.2.8 of this document.
4.1.7 Risk factors for poor wellbeing Risk factors for poor mental wellbeing are similar to those for poor mental health. In addition Guidance for Commissioning Public Mental Health Services47 cites further factors
poor mobility, poor self-care, difficulties performing daily activities
social isolation, a poor sense of belonging and reduced ability to influence the local community
health risk behaviour e.g. smoking, alcohol misuse and cannabis use
inadequate housing
domestic violence
poor mental health
46 Joint Commissioning panel for mental health (2012) Guidance for commissioning public mental health services. www.jcpmh.info 47 Joint Commissioning panel for mental health (2012) Guidance for commissioning public mental health services. www.jcpmh.info
Page 137

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 40
Recession, economic uncertainty and unemployment Children of parents who have substance misuse problems, mental health problems or suffer from domestic violence are also at higher risk of poor wellbeing and therefore are included in the vulnerable groups section 4.16
4.1.8 Interventions The CAMHS Steering Group requested evidence on national best practice for treating mental health disorders in children and young people. In addition to treatment services, the wider wellbeing and preventative agenda should also be considered - prevention programs hold the potential to reduce the number of children with disorders in the population48. The US Institute of
Medicine49 states that “clear windows of opportunity are available to prevent Mental Emotional and Behavioural disorders and related problems before they occur. Risk factors are well established, preventive interventions are available, and the first symptoms typically precede a disorder by 2
to 4 years”. Prevention is particularly important as only 10-20%44, 50 of children and young people with mental health disorders from the UK and other countries such as US and Canada are reaching specialised treatment services suggesting considerable unmet need in the population.
Guidance for Commissioning Public Mental Health Services divides public mental health interventions into three areas:
Mental Health Promotion o increasing mental health and wellbeing
Prevention interventions o preventing mental illness o preventing associated issues e.g. stigma, discrimination51
Early interventions o treatment of mental disorder, o promotion of physical health o avoidance of health risk behaviour in those developing mental disorder, o promotion of recovery o recognition of mental disorder
In order to prevent health and social equalities from widening, interventions chosen need to be universally proportionate – that it is higher levels of interventions for those at greatest risk, and treatment for those with a disorder. Prevention and early intervention in mental health disorders are effective at breaking the cycle of intergenerational inequality (Campion et al, 2012).
48 Waddell C, Hua JM, Garland, OM, Peters RD, McEwan K (2007). Preventing mental disorders in children: A systematic review to inform policy-making. Canadian Journal of Public Health, 98, 3 49 Institute of Medicine (2009), Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. National Academy of Sciences. USA http://tinyurl.com/25kwppp 50 Petrie S (2005) Southwark Child and Adolescent Mental Health Needs Assessment 51 Due to time constraints the literature review has not specifically looked for evidence on items in italics.
Page 138

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 41
A summary of effective interventions identified during the literature review is provided in the sections below. They have been organised to following the life-course from ante-natal through nursery, school and beyond to parenting interventions. As it is important to know what not do as well, where relevant NICE “do not do” advice has been included. Readers of this document should note that the specific details of a programme are likely to be related to its efficacy, and therefore before commissioning local interventions, research should be carried out to ensure that the salient factors are being replicated locally. For example, the Family Nurse Partnership programme is proven to be effective, but there is evidence that similar programmes using trained lay people are less effective. An intervention summary cannot by its nature provide enough information for an intervention to be replicated faithfully.
4.1.8.1 Promoting mental health and wellbeing Many non-mental health professionals such as teachers, GPs, social workers provide support to children and young people e.g. schools take a whole school approach to mental health and wellbeing. . The aim is to enable children and young people to deal with normal social, emotional and psychological problems. Interventions which promote wellbeing may be broader still e.g. planning policies to increase access to green spaces and outdoor play Equipping young people with good social, emotional and psychological health helps to protect young people against emotional and behavioural problems, violence, crime, teenage pregnancy and the misuse of drugs and alcohol. Programmes to promote social and emotional wellbeing will help children develop the skills and resilience to cope with stressful times such as the transition from primary to secondary school, or from secondary school to the adult world. Skills for transition to adulthood are particularly important for children with disabilities, or looked after children as the provision of services for adults (18 years and older) is very different 52from those who are 17 years and under.
Children with higher levels of emotional, behavioural, social and school wellbeing, on average, have higher levels ofacademic achievement and are more engaged in school, both concurrently and in later years53Children with better attention skills experience greater progress across the four key stages of schooling in England. Those who are engaged in less troublesome behaviour also make more progress and are more engaged in secondary school. As children move through the school system, emotional and behavioural wellbeing become more important in explaining school engagement, while demographic and other characteristics become less important. Relationships between emotional, behavioural, social and school wellbeing and later educational outcomes are generally similar for children and adolescents, regardless of their gender and parents’ educational level
Figure 11 Examples of effective interventions by age (Allen, 201111)
52 Working Together to Safeguard Children –if the legislation passes, Local Authorities will be responsible for certain vulnerable young people until they are 24 years old. Southwark have recently set up a team for young people with disabilities which works with those aged 14-24 years. 53 Gutman LM, Vorhaus J The Impact of Pupil behaviour and Wellbeing on Educational Outcomes, Department for Education, Research Report DF-RR253
Page 139

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 42
Appendix 3 sets out the 25 best Early Intervention Programmes the UK from Allen, however, those which are particularly relevant to mental health commissioners have been included below: Table 10 Evidence for universal, interventions
Life stage Universal interventions : Working with all children and young people
Perinatal
Intensive home visiting and support54: – Some home visiting programmes may be effective in improving the social and
emotional wellbeing of vulnerable children. – Structured, intensive interventions, focused on child-mother interaction and
delivered by trained nurses in the first 18 months of life were more likely to have a positive effect on the social and emotional wellbeing of vulnerable children than lower intensity and less structured interventions provided by lay providers.55
– The Family Nurse Partnership Programme56 is a good example. Allen , 2011b give moderate support to Parent s as Teachers
Preschool age
See also parents Baby massage: (Cochrane, 2006) – No evidence of harm therefore might be good where babies are understimulated – No evidence of effects on cognitive and behavioural outcomes, infant attachment or
temperament – Some evidence of beneficial mother-child interaction, sleeping, crying.
54Evidence on Parenting programmes, Intensive home visiting and support and Providing opportunities for education and childcare has been taken directly from the CJSNA factsheet on Early Years
55 National Institute for Health and Clinical Excellence. Social and emotional wellbeing: early years. October 2012 56 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_118530
Page 140

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 43
– More research needed before able to recommend as a universal measure
Providing opportunities for education and childcareH: (NICE, 201257) What: centre or home-based parenting support – There is moderate evidence that programmes delivered in educational or centre
settings improve outcomes for vulnerable children. – Positive cognitive effects were reported for some programmes and beneficial effects
were reported on child mental health and social competencies. Quality education was linked to improved self-regulation and positive behaviour.
Age 5-11 years Age 5-11
Whole school approach in primary school (NICE PH Guidance 1258, 2008)
Existing national initiatives: – Social and Emotional Aspects of Learning (SEAL) – National Healthy Schools Programme (NHSP) (now discontinued) – Healthy lives, Brighter futures
– What is known about whole school approaches: – Teacher training in management of behaviour, parenting education, and social skills
development curriculum are effective in improving outcomes relevant to bullying, violence and mental health.
– Examples: Linking Interests of Families and Teachers (LIFT) programme, The Seattle Social Development Project, and the Resolving Conflict Creatively programme
– Some evidence that Peace Builders programme is effective in improving outcomes relating violence and mental health (as measured by teacher report / visits to school nurse)
– Good evidence to support implementation of multi-component programmes which include significant teacher training and development and support for parenting (may need adapting for UK use)
Following are unknown: – Robust universal indicators to measure the emotional and social wellbeing of
primary school children and monitoring changes over time (local information is available from schools who subscribe to SHEU but no benchmarks were found to compare against.
– Most effective and cost effective interventions – Most effective ways to involve parents or carers particularly those from
disadvantaged backgrounds to improve children’s emotional and social wellbeing – Most effective ways of involving children in development, implementation and
evaluation of programmes
Incredible Years: (Allen, 201259) - There is evidence that this programme reduces children's aggression and behaviour
problems and increases social competence at home and at school
Preventing depression (Cochrane, 2011)60
57 National Institute for Health and Clinical Excellence. Social and emotional wellbeing: early years. October 2012 58 NICE Public Health Guidance 12 – Promoting Children’s social and emotional wellbeing in secondary education
59 Allen G (2011) Early Intervention; Smart Investment, Massive Savings. HM Government. London.
Page 141

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 44
- Population: 5-19 years, do not meet diagnostic criteria for depression - Intervention: psychological or educational prevention programmes, or both, vs
placebo, any comparison intervention, or no intervention - Some evidence that targeted and universal depression prevention programmes work
to reduce onset of depression - Further research needed to identify the most effective programmes and to test these
in the real world.
Age 11-17 years
See also Preventing depression (above)
Organization-wide approach in secondary school (NICE PHG20 (2009, minor
maintenance 2012,201361)
Existing national initiatives:
– Social and Emotional Aspects of Learning (SEAL) – National Healthy Schools Programme (NHSP) – Healthy lives, Brighter futures
Conclusions from NICE: – Conflict resolution training
o is successful in promoting prosocial behaviours in the short term – Interventions including community elements
o some uncertainties, but on balance evidence suggests may work to reduce bullying and disruptive behaviour
– Peer mediation o is effective at promoting pro-social and behavioural skills in the long term o is not always effective to reduce bullying and disruptive behaviour
– Parental involvement o difficult to judge effectiveness, partly as studies from US with high
proportion of African American families but some positive outcomes found Following are unknown for school wide approach in secondary schools: – Effectiveness and cost effectiveness of the components of a school wide approach – Methods / techniques to work with parents and carers to promote S&EW – How the type of professional and setting impact son effectiveness of school wide
approaches – The prevalence of different aspects of social and emotional wellbeing of young
people in secondary schools in England
Performing acts and adolescents The impact of participation in performing arts on adolescent health and behaviour: A systematic review of the literature (Daykin, Orme, Evans et al, 200862) What: the effects of performing arts (music, performance, drama and dance) in
60 Merry SN, Hetrick SE, Cox GR, Brudevold-Iversen T, Bir JJ, McDowell H. Psychological and educational interventions for preventing depression in children and adolescents. Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD003380. DOI: 10.1002/14651858.CD003380.pub3. 61 NICE Public Health Guidance 20 - Social and Emotional Wellbeing in secondary education (2009), National Institute for Clinical Excellence, London.
62 Daykin N.; Orme J.; Evans D.; Salmon D.; Mceachran M.; Brain S. (2008) The impact of participation in performing arts on adolescent health and behaviour: A systematic review of the literature Journal of Health Psychology 13/2(251-264)
Page 142

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 45
community settings and non-curricular mainstream education on health in young people aged 11-18. – The research found was heterogeneous, making overall synthesis of results
inappropriate. – The review demonstrates that research on the impact of the performing arts on
young people is at a relatively early stage.
Parents
Emotional and behavioural adjustment Group-based parent-training programmes for improving emotional and behavioural adjustment in children from birth to three years old (Cochrane, 2010) – Primary prevention of emotional and behavioural problems in children
o There is insufficient evidence to reach firm conclusions regarding the role of these programmes
– Improving emotional and behavioural adjustment of children o There is some support for the use of group-based parenting programmes to
improve emotional and behavioural adjustment for children with a maximum mean age of three years eleven months.
– Further research is needed concerning the long-term effectiveness of these programmes.
Parenting programmes – A study of the Incredible Year H programme in Peckham found that take-up was good
amongst ethnic minority groups and parenting behaviour changed.63 – Parent Child Interaction Therapy was recommended by Allen (grade 2) to improve
behavioural and emotional problems. Triple P was given moderate support. –
General Stigma
Mass media interventions for reducing mental health-related stigma (Cochrane, 2011) Only exists as a protocol i.e. review not yet completed.
4.1.8.2 Preventing mental disorders and providing early interventions Targeted interventions, aimed only at subjects at risk of problems and specialist interventions for those with mental health problems can be effective, and generally have more dramatic effects on these selected groups than do universal interventions on all children64.
Early interventions to promote mental health and wellbeing can prevent the escalation of challenging behaviours, and in the case of looked after children, reduce the risk of placement breakdown (NICE, PH Guidance 28, 2010) . Having a subthreshold mental disorder increases the risk of progressing to threshold mental disorder, and it is estimated that interventions in childhood and adolescence to prevent or reduce mental disorder can reduce lifetime prevalence of mental disorder in adults by 25-50%65.
63 Stephen Scott, Thomas O'Connor and Annabel Futh, What makes parenting programmes work in disadvantaged areas? The PALS trial. Joseph Rowntree Foundation, 2006 64 Shucksmith, J., Summerbell, C., Jones, S., and Whittaker, V. (2007) Mental wellbeing of children in primary education (targeted/indicated activities). London: National Institute of Clinical Excellence 65 Campion J, Bhui K, Bhugra D (2012) European Psychiatric Association (EPA) guidance on prevention of mental disorders European Psychiatry 27 68–80
Page 143

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 46
All children and young people, but particularly those from vulnerable groups such as looked after children require flexible and accessible mental health services that offer skilled interventions both to children and to their family and / or carers. NICE guidance (PHG28, 2010) recommends that services for looked after children should have the capacity and expertise to work with black and minority ethnic children and unaccompanied asylum-seeking children and young people who may have particular needs. As both Lambeth and Southwark have large BME communities, it is important that all services in the boroughs have these abilities. Table 11 below sets out the evidence for targeted interventions for children at risk of developing mental disorders either because they are from a vulnerable group with higher needs such as looked after children or young offenders, or because they already show signs of poor behavioural, emotional or psychological wellbeing (but do not meet the threshold for diagnosis of a mental health disorder . The interventions are set out in life course order.
Page 144

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 47
Table 11 Evidence for targeted mental health interventions for children and young people
Services providing early interventions for vulnerable children and young people
Perinatal
Mental Health disorders in pregnancy (NICE CG45) – Screening for detection and prediction of MH disorders should be part of normal antenatal care. Cases should be treated according to CG45 – There is evidence to support the use of targeted psychosocial interventions for women who have symptoms of depression and/or anxiety that do
not meet the threshold for a formal diagnosis
– Do not use psychosocial interventions (for example, group psychoeducation) to reduce the likelihood of developing a mental disorder during pregnancy or the postnatal period as part of routine antenatal and postnatal care for well women.
Preschool age
See also Looked after children below Behavioural problems Media-based behavioural treatments for behavioural problems in children 2-14 years (Cochrane, 2006) What: books, computer programmes, videos to help parents deal with children’s behaviour. – In general, media-based therapies for behavioural disorders in children had a moderate, if variable, effect when compared with both no-
treatment controls with effects – Significant improvements were made with the addition of up to two hours of therapist time. – Media-based interventions may, in some cases, be enough to make clinically significant changes in a child's behaviour, and may reduce the
amount of time primary care workers have to devote to each case. – They can also be used as the first stage of a stepped care approach. This would increase the number of families who could possibly benefit from
these types of intervention, releasing clinician time that can be reallocated to more complex cases.
Conduct disorder Children (3-12 years) with early onset conduct problems: (Cochrane, 2012) What: Cognitive and Cognitive-Behavioural Group based parenting programmes for improving child conduct problems, parental mental health and parenting kills – Evidence shows programmes are effective in short term and cost effective (£1712 per child brought into “normal” range). – Research needed into longer term effects
Page 145

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 48
Age 5-11 years
See also Media-based behavioural treatments and Early onset conduct problems in Preschool age section (above) and Looked After Children (below)
Social and emotional wellbeing in primary education (NICE, PH12) 66
– Anxiety: Brief 8-9 week Cognitive behavioural therapy (CBT) based programmes targeted at reducing anxiety disorder work – Depression: Penn Prevention Programme relieved and prevented depressive symptoms where CBT was allied with a social problem solving
component. Other treatment programmes for mild-moderate depressive symptoms are mixed. Social competence training for children aged 7-11 within the clinical depression range did not significantly improve depression scores at 2m.
– Post Traumatic Stress Disorder (PTSD) following exposure to violence: 1 study found reasonable effect sizes – Conduct disorders: Multicomponent interventions showed improved social problem-solving, development of positive peer relations as outcomes.
2 studies showed improved academic achievement – Timing may be crucial – early intervention for disruptive children Metropolitan Area Child Study Research recommended booster near end of
primary education. – Negative effects – bringing aggressive hostile children together in small groups at later primary school ages -> norm of aggressive behavior.
– Location – Parents may prefer targeted children to receive intervention at school instead of home
– Cost –effectiveness – not in short term as cost as much as universal interventions but only benefit a few children. May be cost-effective in the
longer term (>4 years) taking broader health and social benefits into account
Targeted Mental Health in Schools (TaMHS)67 (age 5-13 years)
TaMHS vs No TaMHS - TAMHS reduced behavioural problems in primary – but not secondary – school pupils who had behavioural problems at
66 NICE Public Health Guidance 12 – Promoting Children’s social and emotional wellbeing in secondary education
1 67 Department of Education (2011) Me and My School: Findings from the National Evaluation of Targeted Mental Health in Schools 2008-2011. DE, London
Page 146

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 49
the outset. No, effect on primary or secondary school pupils who had emotional difficulties at outset.
Evidence-based self help booklets vs no booklets produced bigger reduction in behavioural problems in children.
Evidence-based self help booklets and action learning sets for TAMHS staff produced a smaller reduction in emotional problems than schools with no booklets or learning sets (i.e intervention produced less improvement that doing nothing).
Most interventions carried out were locally decided, and did not follow protocols. It would be better if future interventions were better evidenced, although need to maintain local ownership too.
For secondary school pupils with behavioural problems at the outset, greater reported provision of information to pupils was associated with greater improvements in mental health outcomes over time.
Use of CAF and better links with CAMHS were associated with greater improvements in behavioural problems in secondary schools.
TAMHS was seen positively by TAMHS workers, especially when fully integrated; teachers and parents. Children were not asked directly but were positive about materials.
Age 11-17 years
See also Conduct Disorder (below) and media-based behavioural treatments in preschool (above) and Looked After Children (below)
Parents
Conduct disorder and delinquency Family and parenting interventions in children and adolescents with conduct disorder and delinquency aged 10-17 (Cochrane, 2009) – The evidence suggests that family and parenting interventions for juvenile delinquents and their families have beneficial effects on reducing time
spent in institutions. – This has an obvious benefit to the participant and their family and may result in a cost saving for society. – These interventions may also reduce rates of subsequent arrest but at present these results need to be interpreted with caution due to the
heterogeneity of the results.
The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomised controlled
Page 147

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 50
Teenage parents
trials (Drekze, Davenport, Frew et al68, 2009) – Parenting programmes are an effective treatment for children with conduct problems. – Further research is needed as there is insufficient evidence to determine relative effectiveness of different parenting programmes
Individual and group based parenting programmes for improving psychosocial outcomes for teenage parents and their children (Cochrane, 2011) – Evidence from some studies grouped into a meta-analysis of improvement in
parent responsiveness to the child post-intervention
infant responsiveness to mother at follow-up and
an overall measure of parent-child interactions post-intervention and at follow-up – The results of the remaining five meta-analyses were inconclusive. – Variation in the measures used, the included populations and interventions, and the risk of bias within the included studies limit the conclusions
that can be reached. – The findings provide some evidence to suggest that parenting programmes may be effective in improving a number of aspects of parent-child
interaction both in the short- and long-term, – Further research is now needed.
Special groups
Looked after children
Mental health services for looked after children and young people (NICE, 201069) - Guidance covers children and young people to the age of 25. - Sets out recommended components of service (dedicated, multiagency, colocation, skilled CAMHS input, training for carers, ease of access,
culturally appropriate, includes asylum seeking children, ensuring assessment for young people entering secure accommodation. - Ensure carers and frontline practitioners working with babies and young children receive specialist training - Three US studies of varying quality found no evidence that receiving transition support services made any difference to depression /
hopefulness about future / general satisfaction of young people leaving care. Autism Early Intensive Behavioural Intervention for children with autism 7071
68 The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomised controlled trials (2009) Dretzke J.; Davenport C.; Frew E.; Barlow J.; Stewart-Brown S.; Bayliss S.; Taylor R.S.; Sandercock J.; Hyde C. Child and Adolescent Psychiatry and Mental Health, 3/, 1753-2000
69 Looked After Children and Young People (2010) NICE Public Health Guidance 28
Page 148

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 51
– Some evidence that EIBI (20-30 hours /week for at least 1 year) 1:1 support resulting in improvement in total intelligence score (large effect size) and adaptive behaviour (moderate effect size) compared to normal treatment
– However quality of studies included in systematic analysis considered to be poor which results in limited reliance on their evidence. – There was no consideration of cost effectiveness Training Programmes for parents of children with ASD72 – Abstract (need to obtain full article if want details) of meta analysis reported that only one programme demonstrated accurate and on going
parental implementation after the programme ended.
ADHD:
Poly-unsaturated Fatty Acids for ADHD in children and adolescents (Cochrane, 2012)
– Overall, there is little evidence that PUFA supplementation provides any benefit for the symptoms of ADHD in children and adolescents.
– The majority of data showed no benefit of PUFA supplementation, although there were some limited data that did show an improvement with combined omega-3 and omega-6 supplementation.
– Future research needs to address the many methodological weaknesses of current research in this area
Eating Disorders:
Preventing Eating Disorders: (Cochrane, 2009)
– There is not sufficient evidence to draw firm conclusions on the impact of prevention programs for eating disorders in children and adolescents,
– However no evidence of harm from pooled estimates
– Further research needed
Parents with Mental Health Problems / substance
73 A systematic review and meta analysis of 13 studies (1490 participants) found evidence that – A wide range of interventions (in parent, in parent and child and in child alone) to prevent mental disorders and psychological symptoms in the
offspring of parents with mental disorders (including substance misuse) appear to be effective. – 40% reduction in risk (relative risk 0.60 95% CI 0.45-0.79)
70 Eldevik S.; Hastings R.P.; Hughes J.C.; Jahr E.; Eikeseth S.; Cross S (2009) Meta-analysis of Early Intensive Behavioral Intervention for children with autism Journal of clinical child and adolescent psychology 38/3(439-450) 71 5. Warren Z; McPheeters ML; Sathe N; Foss-Feig JH; Glasser A; Veenstra-Vanderweele J (2011) A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics, 127/5(e1303-11) 72 Patterson SY, Smith V, Miranda P. (2012) A systematic review of training programs for parents of children with autism spectrum disorders: single subject
contributions. Autism. 16(5):498-522. 73 Effect of preventive interventions in mentally ill parents on the mental health of the offspring: Systematic review and meta-analysis (2012) Siegenthaler, E; Munder, T, Egger M Journal of the American Academy of Child & Adolescent Psychiatry, 51/1(8-17)
Page 149

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 52
misuse
Other groups
Literature search did not specifically search for interventions for young offenders, young carers and children with special educational needs. No evidence on interventions for these groups was found in the general literature search.
4.1.8.3 Treating mental disorder Appendix 4 lists NICE guidance for treatment of MHD related to children and young people
Specialist interventions Work with children and young people with complex, severe and/or persistent needs. Specialist services provide help across education, social care and youth offending and work with children and young people with the highest level of need.
Age 12-17 Alternatives to inpatient mental health services: (Cochrane, 200974)
– Evidence base provides very little guidance for the development of alternatives to inpatient services (i.e. interventions considered did not produce consistently different outcomes from inpatient services).
– Need more research/ audit.
CBT or behavioural therapy for OCD: (Cochrane, 2006 updated 201075 - 8 studies of varying quality (n=343): behavioural or cognitive-behaviour therapy alone appears to be an effective treatment for OCD in children
and adolescents. - CBT/BT are effective as medication alone and may lead to better outcomes when combined with medication compared to medication alone. - Additional higher quality trials are needed to confirm these findings.
Treatment for depression (Cochrane, 2012)76 - Population aged 6-18 years, diagnosed with Major depressive disorder (ICD or DSM) - 10 studies, n=1235 - Interventions:
i) any psychological therapy vs any antidepressant medication, ii) a combination of psychological therapy and antidepressant medication vs psychological therapy alone, or an antidepressant medication alone,
74 Alternatives to inpatient mental health care for children and young people (2009) Cochrane Systematic Reviews 75 O'Kearney RT, Anstey K, von Sanden C, Hunt A. Behavioural and cognitive behavioural therapy for obsessive compulsive disorder in children and adolescents. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD004856. DOI: 10.1002/14651858.CD004856.pub2 76 Cox GR, Callahan P, Churchill R, Hunot V, Merry SN, Parker AG, Hetrick SE. Psychological therapies versus antidepressant medication, alone and in combination for depression in children and adolescents. Cochrane Database of Systematic Reviews 2012, Issue 11. Art. No.: CD008324. DOI: 10.1002/14651858.CD008324.pub2.
Page 150

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 53
iii) a combination of psychological therapy and antidepressant medication vs placebo or 'treatment as usual', or iv) a combination of psychological therapy and antidepressant medication vs psychological therapy or antidepressant medication plus a placebo.
- Authors conclusions: not enough evidence to draw any conclusions about the relative effectivnenss
Psychosis and schizophrenia in children and young people: full guidance ( NICE clinical guideline 155, 2013) See guidance for full details of all aspects considered e.g side effects, reduction of other symptoms.
Interventions to prevent, delay or ameliorate psychosis. o pharmacological interventions
olanzapine vs placebo –N=60; at 1 year no statistically significant difference in progression to psychosis RR0.43 (0.17-1.08) , no reduction in symptoms
risperidone + CBT vs supportive counseling- N=130; at 26 weeks, fewer progressed to psychosis (but still 17 events; RR = 0.35, 95% CI, 0.13 to 0.95), at 52, 156 and 208 week difference no longer significant
NB Given the risk of side effects, and long term effects and relatively low conversion rates to psychosis in at risk groups NICE considers there is a strong basis for not prescribing antipsychotic medication or researching its use further in the at risk population. o dietary interventions
omega-3 fatty acids (1 study, N=81) Small but well-conducted, suggests omega-3 fatty acids might delay onset of psychosis (RR = 0.18, 95% CI, 0.04 to 0.75), and reduce symptoms, but has not been replicated so not able to draw conclusions.
More research needed o psychological interventions
cognitive behavioural therapy (CBT) vs supportive counseling 5 RCTs, n=672. Moderate quality evidence of reduced progression at 52 weeks, but not 26 or 78 weeks after sensitivity analysis.
integrated psychological therapy vs supportive counseling 6 RCTs, n=800. Low quality evidence that IPT reduces transition to psychosis at 52 and 104 weeks.
Psychological and psychosocial interventions (when diagnosed)
Consider arts therapies (for example, dance movement, drama, music or art therapy) for all children and young people with psychosis or
Page 151
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 54
schizophrenia, particularly for the alleviation of negative symptoms. This can be started either during the acute phase, or later
Special groups
Street connected children and young people:
Interventions for promoting reintegration and reducing harmful behaviour and lifestyles in street-connected* children and young people (Cochrane, 2012) Not yet published – protocol only *Street-connected refers to children who live on the streets and children who work on the streets whether or not they also live on the street.
Looked After Children
Treatment Foster Care for improving outcomes in children and young people (Cochrane, 2008) TFC – a foster family-based intervention that aims to provide young people (and, where appropriate, their families) with a tailored programme designed to effect positive changes in their lives
Eating Disorders
Family-based treatment for adolescents with eating disorders77 – A systematic review of "family therapy AND Anorexia Nervosa," and "family therapy AND Bulimia Nervosa" comparing Family Based
Treatment (FBT) to individual therapy for AN and BN
– End of treatment data indicated that FBT was not significantly different from individual treatment (z = 1.62, p = 0.11) – Follow-up data from 6 to 12 months found FBT was superior to individual treatment (z = 2.94, p < 0.003) – There appear to be significant benefits of FBT at 6-12 month follow-up for adolescents suffering from eating disorders
77 Efficacy of family-based treatment for adolescents with eating disorders: A systematic review and meta-analysis (2013) Couturier J.; Kimber M.; Szatmari P. International Journal of Eating Disorders,. 46/1(3-11),
Page 152

30/06/2015 55
4.1.9 Outcomes: national indicators
Reducing excess under 21 mortality in adults with severe mental illness, an indicator from the NHS Outcomes Framework (NHS OF) and the PHOF, can be met by improving physical health for people with mental health problems (Objective 3).It will also be assisted by reducing avoidable harm (Objective 5), including reducing suicide.
• Increasing the proportion of people who use services who say those services have made them feel safe and secure, an indicator from the Adult Social Care Outcomes Framework (ASCOF), will, for people with mental health needs, only be delivered by ensuring a positive experience of care and support (Objective 4). It will also be assisted by reducing avoidable harm (Objective 5), reducing stigma and discrimination (Objective 6) and helping people to recover (Objective 2).
4.1.10 Outcomes - wider determinants
Outcome measures can be used to define the aims of a health system as well as to measure progress towards those aims. The Public Health Outcomes Framework78 (PHOF) is national outcomes framework with indicators relevant to child and adolescent mental health and well being. Local Health and Wellbeing Boards are responsible for ensuring that the public health outcomes are delivered locally through co-ordinated working between health, social, education and other services. The PHOF has four domains:
1. Improving the wider determinants of health
2. Health improvement
3. Health Protection 4. Public healthcare and preventing premature mortality
There are two PHOF indictors which are direct measures of the mental health of children and young people: 2.08 – the emotional wellbeing of looked after children 4.10 – suicide rate There are no indicators measuring the wellbeing of all children and young people. This may partly be because there is a lack of consensus on how to define and measure young children’s social and emotional wellbeing (NICE PH Guidance 40). Indicators 2.23i-iv measure self-reported wellbeing but the survey this comes from is predominately completed by people over 16 years.
Many more PHOF indicators measure outcomes which have an influence on mental health and wellbeing of young people. Improvements in these metrics may have a positive impact on mental health of young people.
1.01 – Children in poverty
1.03 – Pupil absence
1.04i – First time entrants to the youth justice system
78 Department of Health (2012) Healthy Lives, Healthy People: Improving Lives and Supporting Transparency. Department of Health
Page 153

30/06/2015 56
1.05 – 16-18 year olds not in education employment or training
1.06ii – Adults in contact with secondary mental health services who live in stable and appropriate accommodation
1.10 – Killed and seriously injured casualties on England’s roads
1.12i – Violent crime (including sexual violence) – hospital admissions for violence
1.12ii – Violent crime (including sexual violence) – violence offences
1.13i – Re-offending levels – percentage of offenders who re-offend
1.14i – The percentage of the population affected by noise – Number of complaints about noise
1.15i – Statutory homelessness – homelessness acceptances
1.15ii – Statutory homelessness – households in temporary accommodation
1.16 – Utilisation of outdoor space for exercise/health reasons
2.01 – Low birth weight of term babies
2.02i – Breastfeeding – Breastfeeding initiation
2.02ii – Breastfeeding – Breastfeeding prevalence at 6-8 weeks after birth
2.03 – Smoking status at time of delivery
2.03 – Smoking status at time of delivery
2.04 – Under 18 conceptions
2.14 – Smoking prevalence – adults (over 18s)
2.15 – Successful completion of drug treatment
2.23i – Self-reported well-being – people with a low satisfaction score
2.23ii – Self-reported well-being – people with a low worthwhile score
2.23iii – Self-reported well-being – people with a low happiness score
2.23iv – Self-reported well-being – people with a high anxiety score For local data and comparisons with other areas and England, see The Public Health Outcomes Framework Tool http://www.phoutcomes.info/
The NHS Outcomes Framework79 (NHSOF) is more relevant to adults, although as it recognises the importance of good ante-natal, maternity and post-natal, and improving experiences for adults with long term conditions including mental health disorders, improving local performance in this area will contribute indirectly to improved child and adolescent wellbeing.
4.2 Local Data and Service Activity
4.2.1 Mental health and wellbeing through the life course The outcome measures reported in sections 4.1.9 and 4.1.10 can be used to build up a picture of local factors which influence wellbeing and mental health, as well as others which are proxy measures of child and young person wellbeing e.g. pupil absence. Due to space limitations and the public availability of this information it has not been replicated in this report. The sections below reports some other local measures.
4.2.1.1 Perinatal maternal mental health Maternal mental health has an impact on the development of babies and young children, and so mental health screening is carried out during antenatal appointments. 12% of pregnant women at Kings and St Thomas in 2009 disclosed mental health problems at booking (first antenatal
79 Department of Health (2011) NHS Outcomes Framework 2012-2013. Department of Health
Page 154
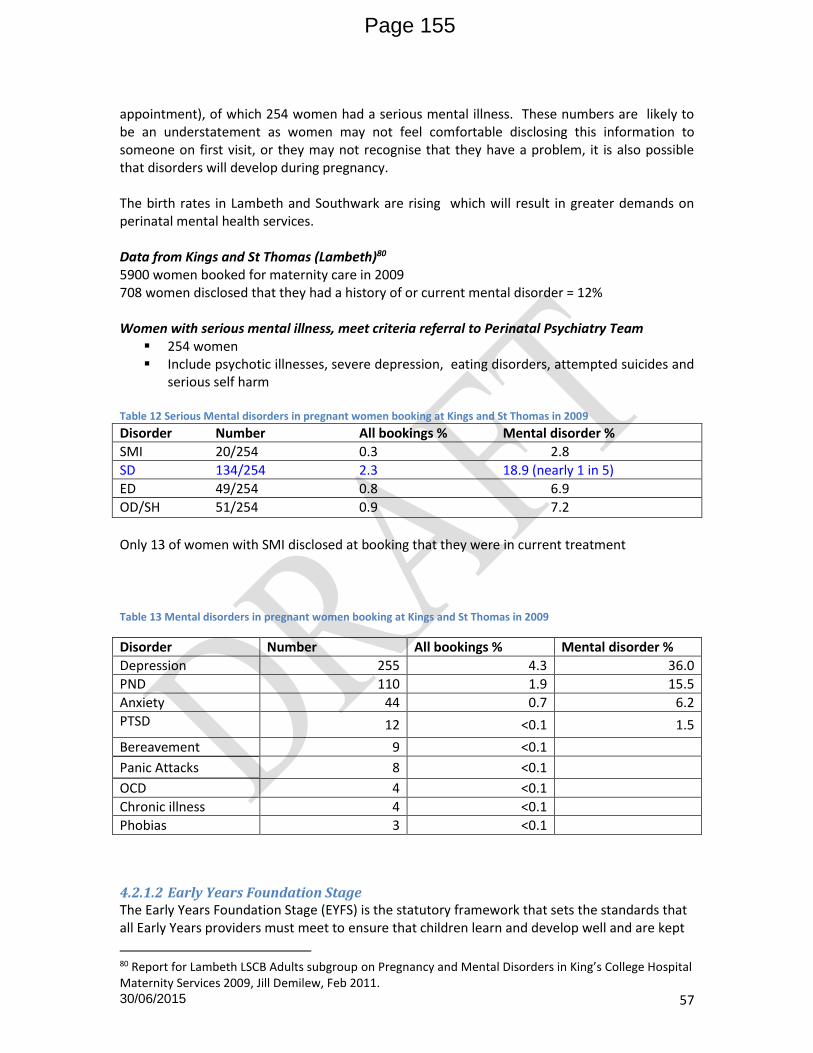
30/06/2015 57
appointment), of which 254 women had a serious mental illness. These numbers are likely to be an understatement as women may not feel comfortable disclosing this information to someone on first visit, or they may not recognise that they have a problem, it is also possible that disorders will develop during pregnancy. The birth rates in Lambeth and Southwark are rising which will result in greater demands on perinatal mental health services. Data from Kings and St Thomas (Lambeth)80 5900 women booked for maternity care in 2009 708 women disclosed that they had a history of or current mental disorder = 12% Women with serious mental illness, meet criteria referral to Perinatal Psychiatry Team
254 women Include psychotic illnesses, severe depression, eating disorders, attempted suicides and
serious self harm
Table 12 Serious Mental disorders in pregnant women booking at Kings and St Thomas in 2009 Disorder Number All bookings % Mental disorder %
SMI 20/254 0.3 2.8
SD 134/254 2.3 18.9 (nearly 1 in 5)
ED 49/254 0.8 6.9
OD/SH 51/254 0.9 7.2
Only 13 of women with SMI disclosed at booking that they were in current treatment
Table 13 Mental disorders in pregnant women booking at Kings and St Thomas in 2009
Disorder Number All bookings % Mental disorder %
Depression 255 4.3 36.0
PND 110 1.9 15.5
Anxiety 44 0.7 6.2
PTSD 12 <0.1 1.5
Bereavement 9 <0.1
Panic Attacks 8 <0.1
OCD 4 <0.1
Chronic illness 4 <0.1
Phobias 3 <0.1
4.2.1.2 Early Years Foundation Stage The Early Years Foundation Stage (EYFS) is the statutory framework that sets the standards that all Early Years providers must meet to ensure that children learn and develop well and are kept
80 Report for Lambeth LSCB Adults subgroup on Pregnancy and Mental Disorders in King’s College Hospital Maternity Services 2009, Jill Demilew, Feb 2011.
Page 155

30/06/2015 58
healthy and safe. It promotes teaching and learning to ensure children are ready for school and gives children the broad range of knowledge and skills that provide the right foundation for good future progress through school and life. Assessments are carried out on children aged 2 years old. As figure 13 shows, nationally and locally, the percentage of 2 year olds who achieve a good score in personal, social and emotional development has increased between 2010 and 2012. Figure 12
Southwark has achieved above or at the national average with 82% of children in 2012 achieving a good score. In Lambeth the picture is less good with only 78% of children achieving a good score at age 2 years – below the national and inner London average.
4.2.1.3 School age children Southwark does not take part in a survey of children’s wellbeing but Lambeth does. Primary SHEU – Lambeth
Cohesion improving as 77% of pupils said that their school valued people with different backgrounds higher than the 67% seen in the wider sample.
Overall pupils in Lambeth reported higher levels of self-esteem (39%) compared with the wider sample (33%). Self esteem increased with age, and was higher in boys.
o 26% of boys and 17% of girls in the year 4 sample had high self-esteem scores o 45% of boys and 38% of girls in year 6 recorded levels of high self esteem
Pupils reporting being scared by an adult has fallen slightly but still higher than the wider sample.
Worry about crime has not changed too much over the years, but still remains an important issue affecting primary school pupils.
A third of pupils were afraid to go to school because of bullying. 41% reported being pushed or hit for no reason and 48% had been called names. Most incidents happened in the school premises.
Secondary SHEU -Lambeth
67% of pupils reported that in general they were ‘quite a lot’ or ‘a lot’ satisfied with their life. 27% said ‘a lot’. 13% said ‘not at all’ or ‘not much’.
Boys in Lambeth were more likely to score levels of ‘high’ self esteem (56%) compared with boys in the wider sample (48%). Self esteem risen from 48% (2006) to 56% overall.
Page 156
30/06/2015 59
43% of year 8 females agreed with the statement ‘There are lots of things about myself that I would like to change’ compared with 25% of year 8 males. Similar disparities are found in Year 10 (42% compared with 25%). This difference is consistent with previous years.
18% of pupils reported a fear of going to school because of bullying
9% of pupils said there were no adults they could trust. The percentage for females has doubled since 2010 (12% compared with 6%).
26% of pupils rated their safety when going out after dark as ‘poor’ or ‘very poor’
13% of pupils said they had been the victim of violence or aggression where they lived. Males were more affected than females. 8% of the sample said they knew friends who carried a blade.
Perceptions of problems reported in the area where young people lived were groups hanging around in public places, people using drugs and people being mugged. There was no significant change in the worries young people had about other issues.
Secondary school girls were more likely to worry about exams and tests than in previous years. Lambeth secondary school pupils were more likely to worry about tests, exams, career, school work and health than the wider sample.
12% of year 8 males said EHWB lessons were not at all useful. 25% said quite or very useful. 14% of year 8 females said not at all useful with 26% saying quite or very useful. 19% of year 10 males said not at all useful with 23% saying quite or very useful. 16% of year 10 females said EHWB lessons not at all useful with 22% said quite or very useful.
Females taking part in sports is still low at 18% (Year 8 females) and 16% (Year 10 females). 25% of pupils cared for family members in their spare time.
21% of pupils saw pictures online that upset them. 16% said someone else had shared an image of them via social media that made them feel unhappy.
Interpretation:-
There is a need to do more to boost confidence and self esteem in Lambeth girls which is static or slightly falling as boy’s self esteem rises.
There is more work needed to tackle bullying in schools.
Need to work closely with community safety colleagues to tackle perceptions of safety among young people which affects their emotional wellbeing and activities that could improve wellbeing.
Recommendation: Lambeth to consider encouraging all schools to take part in SHEU and Southwark to consider having schools take part in order to monitor some aspects of wellbeing of children and young people
4.2.2 Local prevalence of mental health disorders There have not been any recent local surveys of mental health disorders, so local recorded prevalence can only be taken from service use data. This means that access to services is being used as a proxy for need, and will only pick up expressed needs81 of the population that are also recognised by a mental health professional through the referral acceptance process (i.e. normative needs). Service use will not identify people who are not able to access services because for example they don’t know how to, e.g. recent immigrants. Normative needs may not match felt and expressed needs e.g. a demand for cosmetic surgery from an individual may
81 Needs can be felt, expressed, comparative or normative.
Page 157

30/06/2015 60
not be recognised as a need by a GP. More pertinently to this needs assessment a referral to CAMHS from a school or social worker may not meet the clinical threshold for help from a mental health professional, but there is certainly a felt need which is being expressed which suggests a lack of some sort of service from a non-specialist mental health / wellbeing service. It would be useful to look at the number of referrals rejected, and to analyse the reasons for the rejection. Further work needed. As service data is being used as proxy of local expressed need waiting lists need to be taken into account as well as activity. Comparative needs are those identified by discrepancies between what two similar groups have – by considering Lambeth and Southwark at the same time, a comparison can be made between services and access. As both boroughs have the same provider, it would also be useful to look further afield at activity in comparator boroughs - Hackney, Brent, Harringey or Newham.
Figure 13 Estimated number of c&yp with any mental disorder: Lambeth and Southwark 2012
According to Green et al (2005) nationally, only 30-40% of children and adolescents who experience clinically significant mental disorder have been offered evidence-based interventions at the earliest opportunity. This means children and young people are not getting the most benefit from services, and large proportions are not getting any services at all. In this section, local service use is reported. As outlined in the methods section, very little information is availability for universal mental health services activity (tier 1) and so activity reported here is for targeted services at tier 2, and more commonly specialist services (tier 3), as well as information on the small number of children and young people using services at national specialist level as outpatients, and more rarely as inpatients. Applying national prevalence rates to the local populations suggests that 3537 children aged 5-16 years in Lambeth and 3466 in Southwark are likely to have a mental disorder. As Lambeth and Southwark have higher rates of risks factors than the national average these estimates are likely to be on the low side. Previous local needs assessments were able to use an ONS model85 which incorporated risk factors to produce ward level estimates of prevalence of mental health disorders. Not only did this allow identification of geographical areas with higher rates to be identified, it also produced an overall rate for each borough (Lambeth was 15% and Southwark 12% compared to an England rate of 9.5%). This model is no longer available. Figure 13 graphically illustrates the estimated differences in mental health disorders between boys and girls and younger and older age . Table 12 further illustrates the likely numbers by age, gender and type of disorder.
Page 158

30/06/2015 61
Table 14 Number of children (by age group and gender) in Lambeth and Southwark expected to have mental
health disorders, 2012) Source: Office for National Statistics, 2012. Green, H. et al (2004).
Mental Health disorder Local Authority
children 5-10 yrs
children 11-16
yrs
boys 5-10 yrs
boys 11-16
yrs
girls 5-10 yrs
girls 11-16
yrs
Conduct Disorder
Lambeth LB 949 1154 669 713 270 437
Southwark LB 903 1167 644 719 251 449
Emotional disorder
Lambeth LB 465 874 213 352 241 522
Southwark LB 442 884 205 355 225 537
Hyperkinetic disorders
Lambeth LB 310 245 262 211 39 34
Southwark LB 295 248 252 213 36 35
Less common disorders
Lambeth LB 252 245 213 141 39 94
Southwark LB 239 248 205 142 36 97
Table 15 Estimates of mental disorders in 16-17 year olds in Lambeth and Southwark based on estimates from the Adult Psychiatric Morbidity in England Survey, 2007, see table 2 for prevalence
Condition Lambeth Southwark
No. Boys No. Girls No. Boys No. Girls
ADHD (4/6 criteria) 374 387 380 412
PTSD 138 118 140 126
Common mental disorder 322 589 327 628
Psychotic disorder 0 11 0 12
Eating disorder 46 152 47 161
Table 14 shows the number of children in vulnerable groups in Lambeth and Southwark and applies estimated prevalence rates of mental disorder to gives an expected number of local vulnerable children with mental health disorders. Children with a learning disability has been calculated by applying the rates of children with learning disabilities known to schools (from figures 3 and 4) to population estimates for 2012. This produces a much higher number of children with learning disabilities than the ChiMat estimate as they use national averages for rates of learning disability which are not applicable to Lambeth or Southwark. There may be uncertainty about using learning disabilities as defined by schools. Table 16 Estimated numbers of vulnerable children with mental health needs in Lambeth and Southwark in 2012
Vulnerable Group Estimated prevalence of mental disorders
Lambeth Southwark
Number of children and YP in group
Estimated no. with MH disorders
Number of children and YP
Estimated no. with MH disorders
Looked after children 45% 541 243 550 253
Young Offenders 31% 454 140 421 130
Children with a learning disability
39% 1438 561 1378 537
Page 159
30/06/2015 62
4.2.3 Diagnosis
Information received from SLAM on diagnosis of children and young people is recorded in 6
fields – two for axis 1 disorders, then axis 2-5. The data recorded under each diagnosis does
seem to exactly match the DSM IV axes82; for example, Axis 5 does not contain CGAS data as
this is not attached to the individual records provided by SLAM. Coding of other axes is not
consistent so a significant amount of data cleaning would be needed to for example identify all
children and young people with a learning disability. The 117 children in Lambeth with an axis 2
diagnosis do not all have a learning disability or personality disorder e.g. “asthma” has been
recorded in this column.
Very limited conclusions can be drawn from the further analysis of diagnostic categories: only 3800/8574 fields (45%) had an ICD diagnosis that was able to be matched to an ICD code, predominately because of spelling errors or the diagnosis was listed in different way from ICD. These issues could be resolved by sitting with a clinician to refine the descriptions / amend spellings. Of the 3800 fields that did have an ICD diagnosis 1522 were “no axis 1 disorder- CAMHS ” (Figure 16) and a further 288 were “no axis 1 diagnosis” Patients with No Axis 1 disorder CAMHS were higher in Southwark than Lambeth.
Recommendation: Always using ICD-10 codes for diagnosis to enable more complete analysis. Review of case notes after first appointment and addition of diagnosis to electronic records if diagnosis subsequently made.
Figure 14 Count of diagnosis by axis
82 Axis I: All diagnostic categories except mental retardation and personality disorder Axis II: Personality
disorders and mental retardation ; Axis III: General medical condition; acute medical conditions and physical
disorders; Axis IV: Psychosocial and environmental factors contributing to the disorder; Axis V: Global
Assessment of Functioning or Children's Global Assessment Scale for children and teens under the age of 18
Page 160

30/06/2015 63
Figure 15 Episodes of care with No Axis 1 disorder recorded (2009-10 to 2011-12 combined)
However, despite these limitations, brief analysis of diagnosis was carried out. The top 10 diagnosis for tier 2 and 3 SLAM CAMHS for Lambeth patients are shown in table 15, and for Southwark in table 16. Appendix 5 contains the tabulated data with diagnostic descriptions.
Page 161

30/06/2015 64
Table 17 Top 10 Axis 1 diagnosis for Tier 2 and 3 patients from Lambeth 2009-10 to 2011-12
DIAGNOSIS 2009-10 2010-11 2011-12 Total
n % n % n % n
#N/A 865 61% 748 57% 367 45% 1980
Pervasive developmental disorders 109 8% 133 10% 78 10% 320
Hyperkinetic disorders 71 5% 64 5% 65 8% 200
Depressive episode 54 4% 61 5% 72 9% 187
Oth behav emotion disord onset usual occur childhd adoles
74 5%
73 6%
38 5%
185
Reaction to severe stress, and adjustment disorders
66 5%
60 5%
40 5%
166
Emotional disorders with onset specific to childhood
56 4%
56 4%
50 6%
162
Other anxiety disorders 44 3% 42 3% 35 4% 121
Conduct disorders 39 3% 36 3% 29 4% 104
Mixed disorders of conduct and emotions 35 2% 28 2% 33 4% 96
Total 1413 100% 1301 100% 807 100% 3521
Since 2009-10 more Lambeth and Southwark patients have been seen with a diagnosis of ‘Depressive Episode’ . This is against a background of falling total patient numbers and therefore depressive episodes have increased from 4% in 2009-10 to 9% of all a patients in 2011-12. The other main diagnostic fields show a reduction in the number of patients seen. Figure 16 Main diagnosis given to CAMHS patients from Lambeth 2009-10 to 2011-12 (NB 45% no diagnosis)
Page 162

30/06/2015 65
Similarly to Lambeth, depressive episodes appear to have increased in number and as a percentage of all patients. However, with over 50% of episodes not having a recognised ICD 10 description, very limited reliance can be place on this analysis. Table 18 SOUTHWARK – top 10 axis 1 diagnosis for episodes in targeted and universal services 2009-10 to 2011-12
DIAGNOSIS 2009-10 2010-11 2011-12
n % n % n %
#N/A 1053 63% 1095 66% 646 57%
Pervasive developmental disorders 149 9% 109 7% 93 8%
Depressive episode 68 4% 81 5% 90 8%
Reaction to severe stress, and adjustment disorders
91 5% 80 5% 51 4%
Hyperkinetic disorders 36 2% 62 4% 42 4%
Other anxiety disorders 50 3% 52 3% 33 3%
Emotional disorders with onset specific to childhood
45 3% 35 2% 49 4%
Conduct disorders 47 3% 36 2% 38 3%
Mixed disorders of conduct and emotions 39 2% 33 2% 35 3%
Mental disorder, not otherwise specified 32 2% 34 2% 32 3%
Oth behav emotion disord onset usual occur childhd adoles
17 1% 21 1% 19 2%
Specific personality disorders 17 1% 13 1% 8 1%
Disorder social funct with onset spec childhood/adolesc
17 1% 10 1% 7 1%
1661 100% 1661 100% 1143 100%
Page 163

30/06/2015 66
Figure 17 Main diagnosis given to CAMHS patients from Southwark 2009-10 to 2011-12 (NB 57% no diagnosis)
4.2.4 Local use of Targeted and Specialist Services
Tables 19 and 20 show the number of unique treatment episodes from 2009-10 to 2011-2012. Fewer unique individuals have had episodes of treatment with CAMHS than tables 17 and 18 suggest as around 20% of patients had more than one treatment episode in the three year period the data covers (Figure 18) and these multiple attenders have not been removed from the figures below. Figure 18 Percentage of CAMHS patient by numbers of episodes of care starting in in the period 2009-2012
Page 164

30/06/2015 67
Further work could be done to follow through the multiple attenders to see which services they used e.g. one patient who had three attendances in 2 yeas was seen by both the adolescent service and the substance misuse team. Recommendation: For more information about children and young people who have had more than one episode of care, more detailed analysis of tier 2 and 3 data could be carried out. However an audit of case notes would reveal the most information about children and young people who have more than one episode of care as it would also include information about tier 4 activity. The data provided by SLAM is anonymous, so it may not be possible to identify individuals for further investigation. Both boroughs have seen a decrease in the number of treatment episodes in the period 2009-10 to 2011-12, but the percentage decrease has been larger in Lambeth (25% vs 18%). Changes in funding have not been looked at in this needs assessment but it is recognised that financial constraints have affected the level of activity in each borough. Table 19 Number of children and young people Southwark with a CAMHS appointment in 2009-10 to 2011-12
Southwark CAMHS Team 2009-10 2010-11 2011-12
Belgrave Adolescent Psychiatry 33
Belgrave Children Psychiatry 44
Belgrave Paediatric Liaison Team 353 433 21383
Parental Mental Health Team Southwark 54 48 91
Southwark Adolescent Services 247 264 259
Southwark CAMHS Children Centre 135 144 47
Southwark CAMHS Community 296 258 271
Southwark CAMHS Neuro Developmental 138 161 140
Southwark Carelink 58 71 83
Southwark Child and Family Service 251 279 283
Southwark Learning Disabilities 130 2
Southwark Neuro Psychiatry Team 14 2
Southwark TaMHS 91 81 47
Grand Total 1844 1743 1434
% change from previous year n/a -5% -18%
In Southwark the decrease in activity has been largest in the learning disability team falling from 130 appointments in 2009-10 to none in 2011-12. There has not been an increase in activity in the neurodevelopmental team to cover this drop. Paediatric Liaison, Children’s Centres and TAMHS activity have all also fallen substantially. Against this backdrop of falling activity, the number of looked after children using Carelink has increased, and as looked after children number have not increased at the same rate over this period, it suggests that this vulnerable group are being protected more than other services. As figure 19 shows, the age group least affected by the decrease in activity is 5-9 year olds. This should be interpreted with some caution as when the age chart was produced 188 Belgrave paediatric liaison appointments from
83 188 were added to 2011-12 activity but no diagnosis or other data provided. Therefore not included in other analysis
Page 165

30/06/2015 68
2011-12 were missing from the data received from SLAM. The total has now been added in, however, no age, gender or ethnicity data has been received for these patients. Figure 19 Age group of children and young people using Southwark CAMHS services 2009-10 to 2011-12
Table 20 Number of children and young people Lambeth with a CAMHS appointment in 2009-10 to 2011-12
LAMBETH CAMHS Team 2009-10 2010-11 2011-12
Child and Adolescent Community Service Lambeth 109 353 363
Lambeth Autism and Neuro Developmental Service 4 14
Lambeth CAMHS ACIST 8 5
Lambeth CAMHS Adolescent Team 225 101
Lambeth CAMHS Early Intervention 528 364 260
Lambeth CAMHS Multi-agency Rapid Response Team 37 16
Lambeth CAMHS Neurodevelopmental Team 194 156 98
Lambeth CAMHS Substance Misuse 23 25 2
Lambeth Children Looked After 81 83 60
Lambeth Children's Service 149 24
Lambeth GSTT 154 214 19984
Lambeth Youth Offending 80 88 83
Grand Total 1588 1433 1079
% change from previous years n/a -10% -25%
The decrease in activity in Lambeth appears to have affected looked after children as much as other groups. There has been a substantial decrease in the number of children and young people using the Early Intervention services which seems counterintuitive given the policy background of early intervention and there is no information on activity in the MARRT. The number of young offenders accessing CAMHS on the other hand has remained more or less the same, which suggests this vulnerable group are being protected.
84 181 as above
Page 166

30/06/2015 69
In Southwark, the age group least affected the decline in number of children seen is those aged 5-9 years. All other age groups have declined more steeply, except for parents using the Parental mental health team whose activity has increased. Unlike Southwark in Lambeth, the 15-19 year age group have seen the smallest decline in service use (figure 20). Figure 20 Age group of children and young people using Lambeth CAMHS services 2009-10 to 2011-12
4.2.4.1 Age of patients Figures 21 and 22 split CAMHS service users by age and gender. The percentages reported are for each gender separately. There are differences between the two boroughs: Under 5s: a much lower proportion of CAMHS services users are under 5 years old in Lambeth compared to Southwark (4% and 8% for girl/ boys compared to 14% and 17% ).
Figure 21 Figure 22
Page 167

30/06/2015 70
Appendix 6 contains age analysis for each service, showing trends in patient numbers over time for each borough.
4.2.4.2 Ethnicity and gender of patients Figure 23 shows the ethnic background of SLAM CAMHS service users by borough. Three years of data has been combined due to small number in some ethnic groups. No ethnic group has been recorded for 8% of Lambeth and 4% of Southwark. The proportion of service users who are from a white ethnic background is noticeably higher in Southwark than Lambeth, although the proportion of the 0-1985 population who are white is similar in both boroughs (42% in Southwark and 40% in Lambeth – figures 2 and 3). The proportion of CAMHS users from Lambeth from “Black other” and “Black Caribbean” ethnicity is much higher than in Southwark. Equity of service use is considered in Section 5.1 of this needs assessment. Figure 23
85 Ethnic population estimates are in 5 year age bands
Page 168

30/06/2015 71
Table 21 CAMHS episodes 2009-10 to 2011-12 by ethnicity and gender of patient
Lambeth Southwark
Ethnicity Female Male Female Male
White British 377 501 745 884
Black Other 351 492 307 407
White Other 193 208 227 252
Black Caribbean 145 227 133 165
Black African 140 179 220 290
Not Stated 122 190 76 107
Other Ethnic Groups 101 134 157 152
White & Black Caribbean 86 152 96 99
Mixed Other 28 32 23 26
White & Black African 22 33 19 39
(blank) 19 9 87 119
White & Asian 17 10 6 7
Asian Other 14 22 26 36
White Irish 13 10 16 20
Bangladeshi/British Bangladeshi 11 10 17 20
Indian/British Indian 11 16 5 12
Pakistani/British Pakistani 9 22 7 8
Chinese 8 4 11 8
Grand Total 1667 2251 2178 2651
% of total 57.4% 54.8%
4.2.4.3 Home postcode of patients Only the first part of the postcode was provided by SLAM. Table 21 is a very crude analysis of whether patients come from the local area or not (not all SW and SE postcodes are Lambeth or Southwark ) . Full summary of all postcodes for each borough separately is in Appendix 6. The majority of patients come from home borough postcodes, and some who don’t are looked after children, however their numbers are very small. Table 22 First part of home postcode of CAMHS episodes
Postcode 2009-10 2010-11 2011-12
SW 986 867 541
SE 2051 1908 1486
Not local postcode 395 657 117
Total 3432 3176 2144
Not SE or SW as % 12% 19% 5%
4.2.4.4 Schools postcode of patients SLAM provided data on Southwark pupils seen by TAMHS. 91 pupils were referred in 2009-10, 81 in 2010-11 and 47 in 2011-12.
Page 169
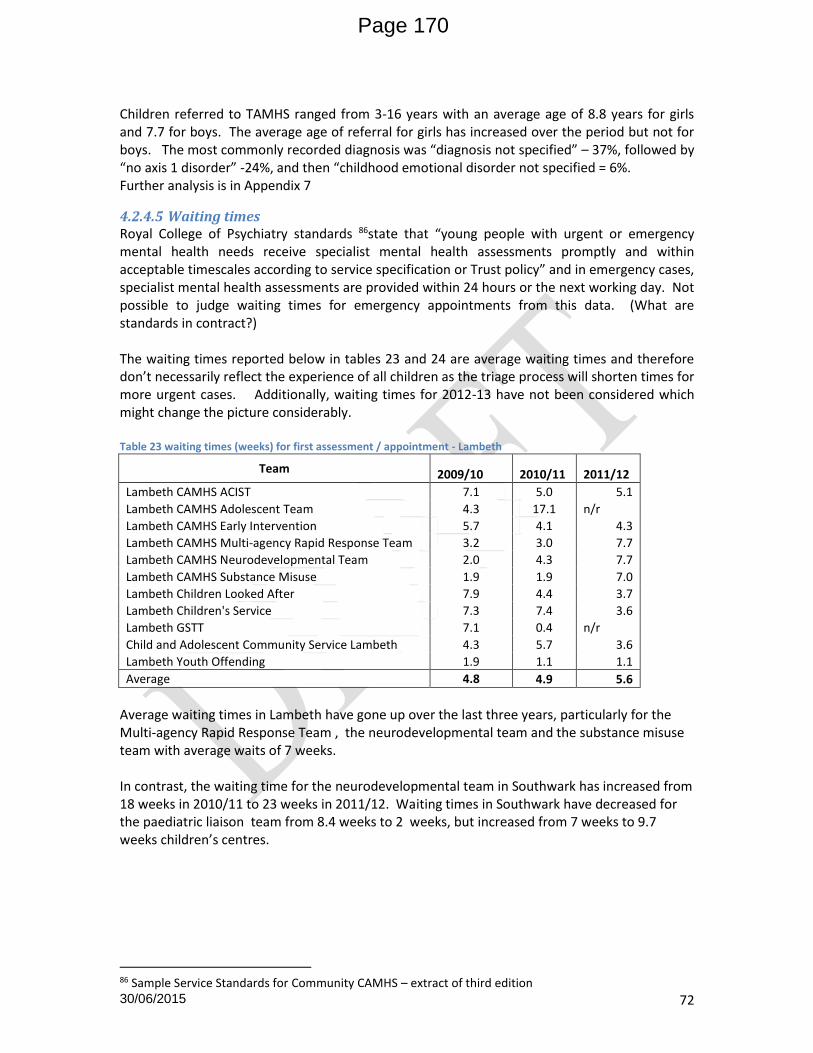
30/06/2015 72
Children referred to TAMHS ranged from 3-16 years with an average age of 8.8 years for girls and 7.7 for boys. The average age of referral for girls has increased over the period but not for boys. The most commonly recorded diagnosis was “diagnosis not specified” – 37%, followed by “no axis 1 disorder” -24%, and then “childhood emotional disorder not specified = 6%. Further analysis is in Appendix 7
4.2.4.5 Waiting times Royal College of Psychiatry standards 86state that “young people with urgent or emergency mental health needs receive specialist mental health assessments promptly and within acceptable timescales according to service specification or Trust policy” and in emergency cases, specialist mental health assessments are provided within 24 hours or the next working day. Not possible to judge waiting times for emergency appointments from this data. (What are standards in contract?) The waiting times reported below in tables 23 and 24 are average waiting times and therefore don’t necessarily reflect the experience of all children as the triage process will shorten times for more urgent cases. Additionally, waiting times for 2012-13 have not been considered which might change the picture considerably. Table 23 waiting times (weeks) for first assessment / appointment - Lambeth
Team 2009/10 2010/11 2011/12
Lambeth CAMHS ACIST 7.1 5.0 5.1
Lambeth CAMHS Adolescent Team 4.3 17.1 n/r
Lambeth CAMHS Early Intervention 5.7 4.1 4.3
Lambeth CAMHS Multi-agency Rapid Response Team 3.2 3.0 7.7
Lambeth CAMHS Neurodevelopmental Team 2.0 4.3 7.7
Lambeth CAMHS Substance Misuse 1.9 1.9 7.0
Lambeth Children Looked After 7.9 4.4 3.7
Lambeth Children's Service 7.3 7.4 3.6
Lambeth GSTT 7.1 0.4 n/r
Child and Adolescent Community Service Lambeth 4.3 5.7 3.6
Lambeth Youth Offending 1.9 1.1 1.1
Average 4.8 4.9 5.6
Average waiting times in Lambeth have gone up over the last three years, particularly for the Multi-agency Rapid Response Team , the neurodevelopmental team and the substance misuse team with average waits of 7 weeks. In contrast, the waiting time for the neurodevelopmental team in Southwark has increased from 18 weeks in 2010/11 to 23 weeks in 2011/12. Waiting times in Southwark have decreased for the paediatric liaison team from 8.4 weeks to 2 weeks, but increased from 7 weeks to 9.7 weeks children’s centres.
86 Sample Service Standards for Community CAMHS – extract of third edition
Page 170
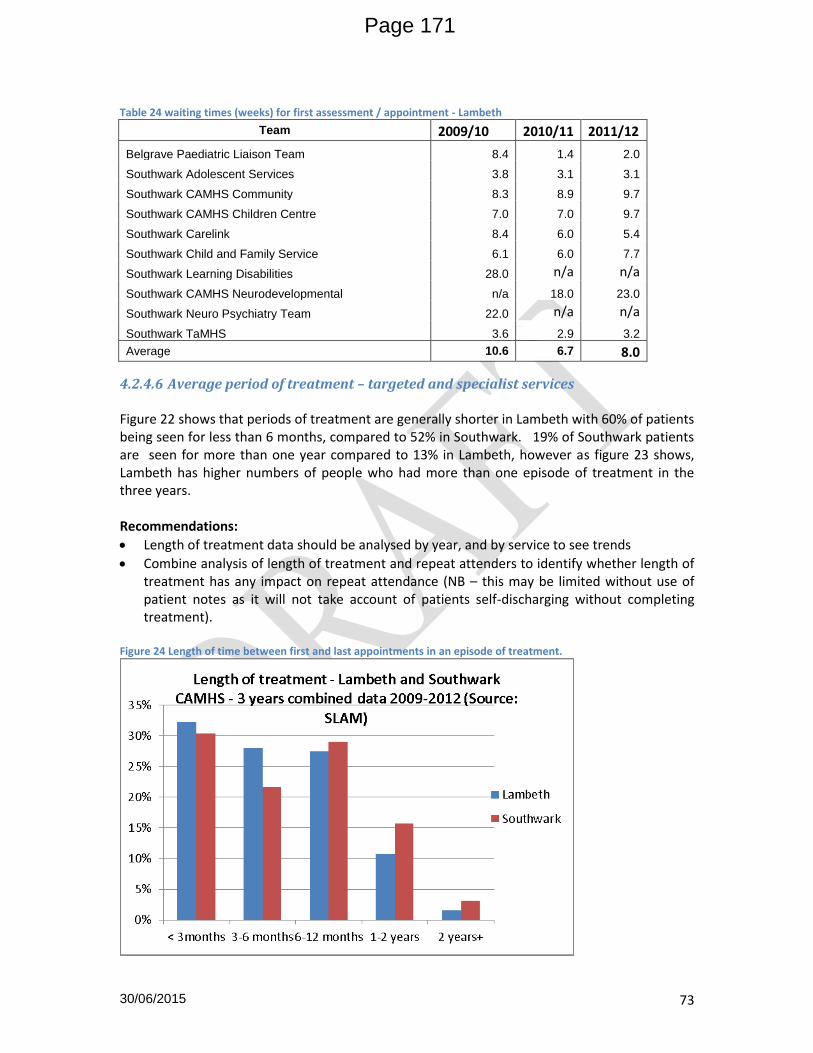
30/06/2015 73
Table 24 waiting times (weeks) for first assessment / appointment - Lambeth
Team 2009/10 2010/11 2011/12
Belgrave Paediatric Liaison Team 8.4 1.4 2.0
Southwark Adolescent Services 3.8 3.1 3.1
Southwark CAMHS Community 8.3 8.9 9.7
Southwark CAMHS Children Centre 7.0 7.0 9.7
Southwark Carelink 8.4 6.0 5.4
Southwark Child and Family Service 6.1 6.0 7.7
Southwark Learning Disabilities 28.0 n/a n/a
Southwark CAMHS Neurodevelopmental n/a 18.0 23.0
Southwark Neuro Psychiatry Team 22.0 n/a n/a
Southwark TaMHS 3.6 2.9 3.2
Average 10.6 6.7 8.0
4.2.4.6 Average period of treatment – targeted and specialist services Figure 22 shows that periods of treatment are generally shorter in Lambeth with 60% of patients being seen for less than 6 months, compared to 52% in Southwark. 19% of Southwark patients are seen for more than one year compared to 13% in Lambeth, however as figure 23 shows, Lambeth has higher numbers of people who had more than one episode of treatment in the three years. Recommendations:
Length of treatment data should be analysed by year, and by service to see trends
Combine analysis of length of treatment and repeat attenders to identify whether length of treatment has any impact on repeat attendance (NB – this may be limited without use of patient notes as it will not take account of patients self-discharging without completing treatment).
Figure 24 Length of time between first and last appointments in an episode of treatment.
Page 171
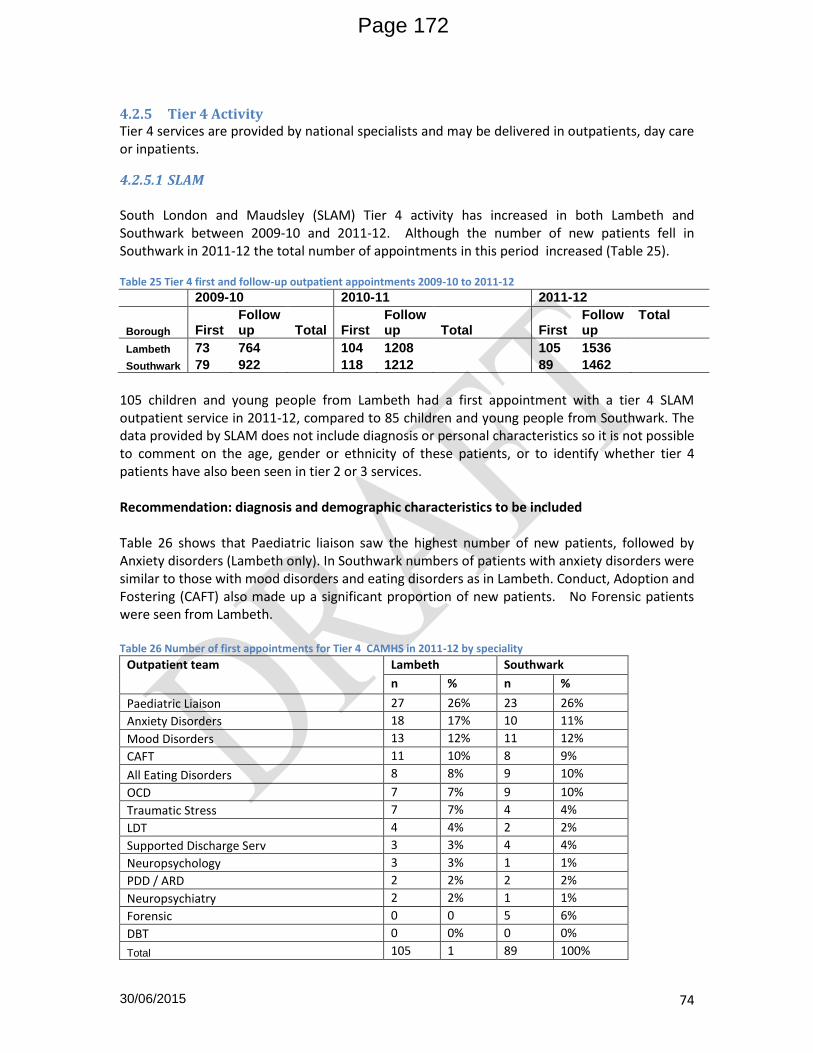
30/06/2015 74
4.2.5 Tier 4 Activity Tier 4 services are provided by national specialists and may be delivered in outpatients, day care or inpatients.
4.2.5.1 SLAM South London and Maudsley (SLAM) Tier 4 activity has increased in both Lambeth and Southwark between 2009-10 and 2011-12. Although the number of new patients fell in Southwark in 2011-12 the total number of appointments in this period increased (Table 25). Table 25 Tier 4 first and follow-up outpatient appointments 2009-10 to 2011-12
2009-10 2010-11 2011-12
Borough First Follow up Total First
Follow up Total First
Follow up
Total
Lambeth 73 764 104 1208 105 1536
Southwark 79 922 118 1212 89 1462
105 children and young people from Lambeth had a first appointment with a tier 4 SLAM outpatient service in 2011-12, compared to 85 children and young people from Southwark. The data provided by SLAM does not include diagnosis or personal characteristics so it is not possible to comment on the age, gender or ethnicity of these patients, or to identify whether tier 4 patients have also been seen in tier 2 or 3 services. Recommendation: diagnosis and demographic characteristics to be included Table 26 shows that Paediatric liaison saw the highest number of new patients, followed by Anxiety disorders (Lambeth only). In Southwark numbers of patients with anxiety disorders were similar to those with mood disorders and eating disorders as in Lambeth. Conduct, Adoption and Fostering (CAFT) also made up a significant proportion of new patients. No Forensic patients were seen from Lambeth. Table 26 Number of first appointments for Tier 4 CAMHS in 2011-12 by speciality
Outpatient team Lambeth Southwark
n % n %
Paediatric Liaison 27 26% 23 26%
Anxiety Disorders 18 17% 10 11%
Mood Disorders 13 12% 11 12%
CAFT 11 10% 8 9%
All Eating Disorders 8 8% 9 10%
OCD 7 7% 9 10%
Traumatic Stress 7 7% 4 4%
LDT 4 4% 2 2%
Supported Discharge Serv 3 3% 4 4%
Neuropsychology 3 3% 1 1%
PDD / ARD 2 2% 2 2%
Neuropsychiatry 2 2% 1 1%
Forensic 0 0 5 6%
DBT 0 0% 0 0%
Total 105 1 89 100%
Page 172

30/06/2015 75
In terms of activity, when first and follow up appointments are combined, eating disorders make up the largest number of appointments in each borough (Figure 26) Figure 25 All Outpatients appointments by Borough and Team, 2011-12
Note: DBT = dialectical behaviour therapy; CAFT = child and family team
Inpatients Tables 27 and 28 show SLAM inpatient activity over the last three years. Average length of stay (LOS) has been calculated, but this may not be an appropriate statistic if there are a small number of patients with a very long period of time in hospital. No information about diagnosis, age, gender or ethnicity was provided, so limited conclusions can be drawn from this information. Occupied bed days (OBD) data was split into children and adolescents, but the number of each was not provided. OBD is reported in Table 15. Children did not account for as many bed days as adolescents, and in 2009-10 no Southwark children were inpatients, and in 2010-11 no Lambeth children were inpatients. Table 27 Inpatients, occupied bed days (OBD) and average length of stay 2009-10 to 2011-12
Borough
2009-2010 2010-2011 2011-2012
Patients OBD Av. LOS
Patients OBD Av. LOS Patients OBD Av. LOS
Lambeth 32 1242 39 28 1150 41 18 952 53
Southwark 19 775 41 13 704 54 23 1406 61
Page 173

30/06/2015 76
Table 28 inpatients by borough and broad age group 2009-10 to 2011-12
Borough
2009-2010 2010-2011 2011-2012
Adolescents Children Adolescents Children Adolescents Children
Lambeth 1185 57 1150 0 921 31
Southwark 775 0 697 7 1232 174
4.2.5.2 Other Acute Providers The data in this section was extracted from SUS for all patients under 24 with a primary mental health diagnosis. The increased age limit was used to test the hypothesis that activity in young people aged 20-24 group was much higher than in the 15-19 year old group.
Since 2009-10 an increasing number of children and young people have been seen in acute providers for mental health diagnoses (Table 29). Table 30 shows the main providers for this activity. Any differences in totals between table 29 and 30 are due to small numbers of patients going to other hospitals which have not been listed.
Table 29 Total activity trends for Lambeth and Southwark patients over 3 years at all providers (including SLAM).
PCT 2009/2010 2010/2011 2011/2012 Total
Lambeth 117 237 281 635
Southwark 90 195 228 513
Grand Total 207 432 509 1148
Table 30 Trends in activity at main providers for Lambeth and Southwark patients as obtained from SUS – Secondary Uses Services
Provider 2009/2010 2010/2011 2011/2012
L S L S L S
GUY'S AND ST THOMAS' NHS FOUNDATION TRUST 30 27 38 34 62 46
KING'S COLLEGE HOSPITAL NHS FOUNDATION TRUST 20 17 26 37 15 31
SOUTH LONDON AND MAUDSLEY NHS FOUNDATION TRUST
44 37 138 113 167 134
Grand Total 94 81 202 184 244 211
Table 31 shows activity by age and gender. Activity increases with age and is higher in males
than females at the younger ages (although overall numbers are very small). By age 10-14 the
numbers of girls matches the number of boys. At age 15-19 there is an excess of males in
Lambeth which becomes very pronounced in the 20-24 year age group. The difference
between males and females from Southwark is less strong. This table includes activity in young
people aged 18-24 to illustrate the increase in service use in this age group compared to young
people who are eligible for CAMHS services.
Page 174

30/06/2015 77
Table 31 Total activity at all providers (other than SLAM by age bands – 3 financial years combined data – 2009-2012 by borough, age and gender.
Lambeth Southwark
Age bands Female Male Female Male
0-4 7 13 9 15
5-9 4 8 5 10
10-14 18 19 15 15
15-19 93 109 82 86
20-24 127 252 121 164
Grand Total 249 401 232 290
Table 31 Age, ethnicity and gender of children and young people seen at SLAM, Kings or GSTT 2009-10 to 2011-12
Females (by age group) Males (by age group)
Ethnic group 0-4 yrs
5-9 yrs
10-14 yrs
15-19 yrs
20-24 yrs
0-4 yrs
5-9 yrs
10-14 yrs
15-19 yrs
20-24 yrs
Any other Black background 4 1 4 31 69 8 8 9 63 139
British (White) 4 1 10 70 62 4 4 5 31 82
Any other White background 3 1 3 12 28 8 4 17 57
Any other ethnic group 2 1 2 15 12 2 14 45
African (Black or Black British) 2 4 11 21 2 1 2 15 23
Caribbean (Black or Black British) 2 1 1 9 17 1 2 19 19
Not stated 2 4 12 11 1 3 6 15 15
Any other Mixed background 1 6 5 2 3 8 White and Black Caribbean (Mixed) 3 1 5 8
Any other Asian background 1 4 5 4
Unknown 2 1 5 4
White and Black African (Mixed) 11 1 1 3
Indian (Asian or Asian British) 2 1 3
Irish (White) 2 1 3
Pakistani (Asian or Asian British) 1 1 2 2
Chinese (other ethnic group) 1 2 3 1 Bangladeshi (Asian or Asian British) 2 2
White and Asian (Mixed) 2 1
Total for age and gender 16 9 33 175 248 28 18 34 195 416
Please suppress any numbers under 5 if being shared outside the steering group Age
Numbers very low at young ages although possibly odd that higher in 0-4 years than 5-9 years.
Increase steeply with age, rising by a factor of five between 10-14 and 15-19
Page 175
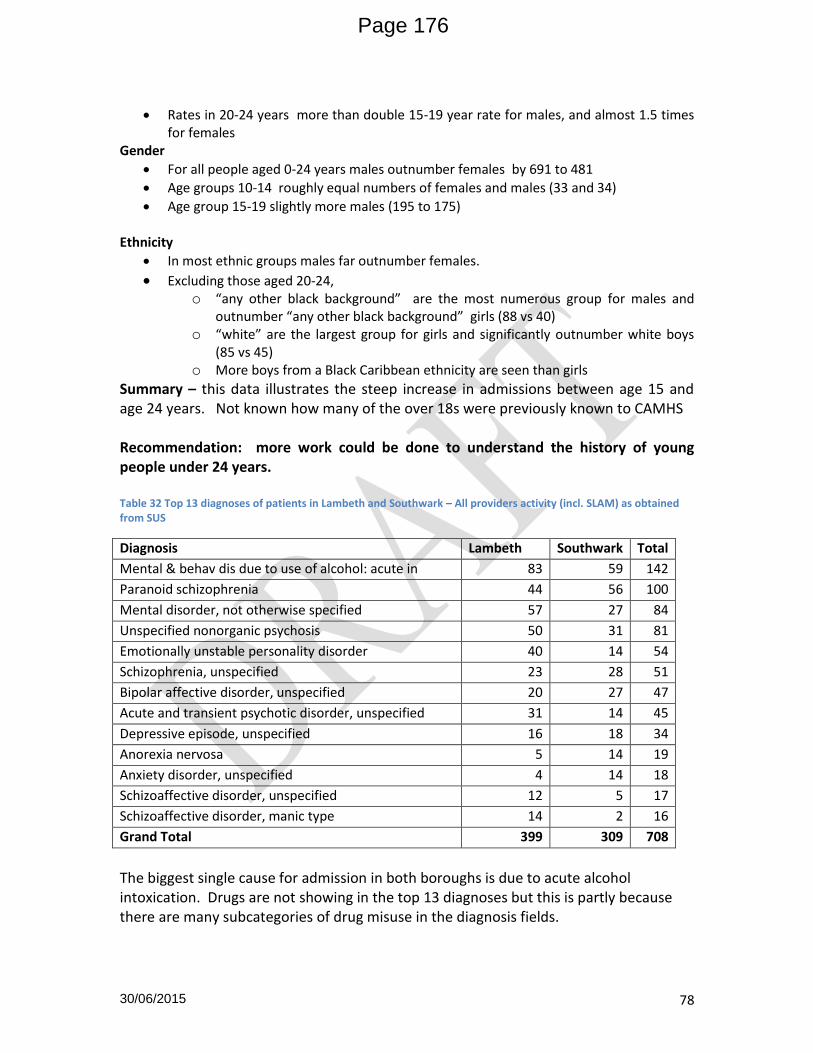
30/06/2015 78
Rates in 20-24 years more than double 15-19 year rate for males, and almost 1.5 times for females
Gender
For all people aged 0-24 years males outnumber females by 691 to 481
Age groups 10-14 roughly equal numbers of females and males (33 and 34)
Age group 15-19 slightly more males (195 to 175) Ethnicity
In most ethnic groups males far outnumber females.
Excluding those aged 20-24, o “any other black background” are the most numerous group for males and
outnumber “any other black background” girls (88 vs 40) o “white” are the largest group for girls and significantly outnumber white boys
(85 vs 45) o More boys from a Black Caribbean ethnicity are seen than girls
Summary – this data illustrates the steep increase in admissions between age 15 and age 24 years. Not known how many of the over 18s were previously known to CAMHS Recommendation: more work could be done to understand the history of young people under 24 years.
Table 32 Top 13 diagnoses of patients in Lambeth and Southwark – All providers activity (incl. SLAM) as obtained from SUS
Diagnosis Lambeth Southwark Total
Mental & behav dis due to use of alcohol: acute in 83 59 142
Paranoid schizophrenia 44 56 100
Mental disorder, not otherwise specified 57 27 84
Unspecified nonorganic psychosis 50 31 81
Emotionally unstable personality disorder 40 14 54
Schizophrenia, unspecified 23 28 51
Bipolar affective disorder, unspecified 20 27 47
Acute and transient psychotic disorder, unspecified 31 14 45
Depressive episode, unspecified 16 18 34
Anorexia nervosa 5 14 19
Anxiety disorder, unspecified 4 14 18
Schizoaffective disorder, unspecified 12 5 17
Schizoaffective disorder, manic type 14 2 16
Grand Total 399 309 708
The biggest single cause for admission in both boroughs is due to acute alcohol intoxication. Drugs are not showing in the top 13 diagnoses but this is partly because there are many subcategories of drug misuse in the diagnosis fields.
Page 176

30/06/2015 79
4.2.6 Comparison of service use to predicted need
4.2.6.1 Tier of service use Although estimates of CAMHS need by tier are different depending on the source, both predict that there should be many fewer children and young people needing tier 3 services (1.85% or 3%) compared to tier 2 (7% same in both sets of estimates) and even fewer using national/ tier 4 services (0.08% or .047%). However, as table 16 shows in both boroughs the numbers using each tier do not decrease in such a dramatic manner. Many fewer children use tier 2 than are predicted to benefit: in 2011-12 there were 623 tier 2 appointments in Lambeth compared to a possible 4897 and 624 in Southwark compared to a possible 4325. Interpretation of tier 4 activity varies depending on whose estimates are used. Using Kurtz (which is used by ChiMat) there were 2-3 times as many appointments in tier 4 as expected which might reflect a more complex and needy population. However using the estimates of Campion and Fitch, tier 4 activity is perhaps lower than might be expected. Table 33 Comparison of actual CAMHS activity by tier compared to predicted need for mental health services
Lambeth 2010-11 2011-12
Tier 2 842 623
Expected Kurtz 4836 4897
Expected C&F 4836 4897
Tier 3 377 257
Expected Kurtz 1118 1133
Expected C&F 1813 1836
Tier 4 318 123
Expected Kurtz 48 49
Expected C&F 284 287
Page 177
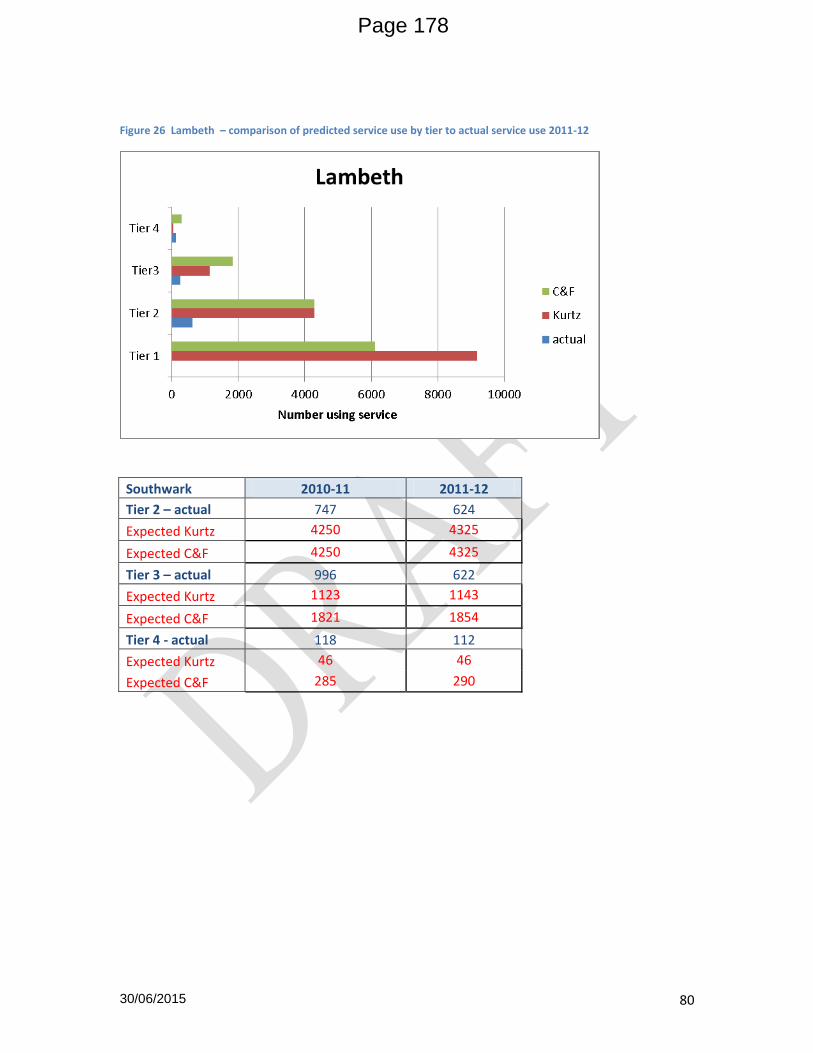
30/06/2015 80
Figure 26 Lambeth – comparison of predicted service use by tier to actual service use 2011-12
Southwark 2010-11 2011-12
Tier 2 – actual 747 624
Expected Kurtz 4250 4325
Expected C&F 4250 4325
Tier 3 – actual 996 622
Expected Kurtz 1123 1143
Expected C&F 1821 1854
Tier 4 - actual 118 112
Expected Kurtz 46 46
Expected C&F 285 290
Page 178
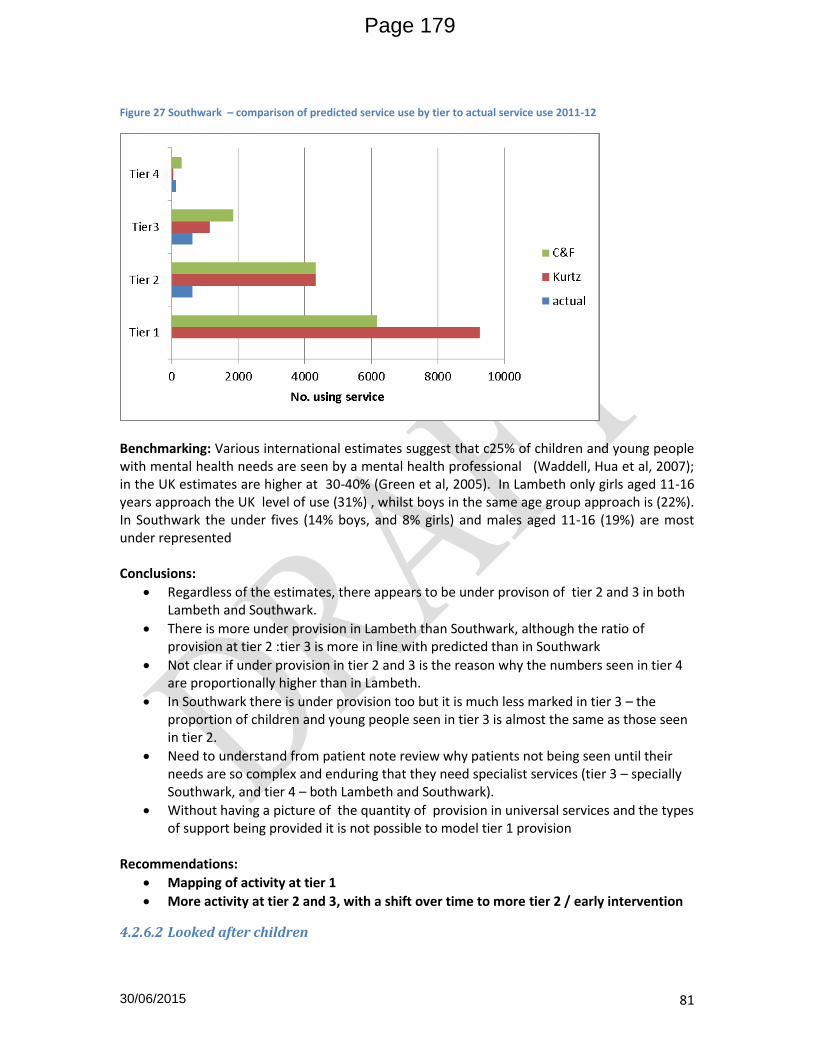
30/06/2015 81
Figure 27 Southwark – comparison of predicted service use by tier to actual service use 2011-12
Benchmarking: Various international estimates suggest that c25% of children and young people with mental health needs are seen by a mental health professional (Waddell, Hua et al, 2007); in the UK estimates are higher at 30-40% (Green et al, 2005). In Lambeth only girls aged 11-16 years approach the UK level of use (31%) , whilst boys in the same age group approach is (22%). In Southwark the under fives (14% boys, and 8% girls) and males aged 11-16 (19%) are most under represented Conclusions:
Regardless of the estimates, there appears to be under provison of tier 2 and 3 in both Lambeth and Southwark.
There is more under provision in Lambeth than Southwark, although the ratio of provision at tier 2 :tier 3 is more in line with predicted than in Southwark
Not clear if under provision in tier 2 and 3 is the reason why the numbers seen in tier 4 are proportionally higher than in Lambeth.
In Southwark there is under provision too but it is much less marked in tier 3 – the proportion of children and young people seen in tier 3 is almost the same as those seen in tier 2.
Need to understand from patient note review why patients not being seen until their needs are so complex and enduring that they need specialist services (tier 3 – specially Southwark, and tier 4 – both Lambeth and Southwark).
Without having a picture of the quantity of provision in universal services and the types of support being provided it is not possible to model tier 1 provision
Recommendations:
Mapping of activity at tier 1
More activity at tier 2 and 3, with a shift over time to more tier 2 / early intervention
4.2.6.2 Looked after children
Page 179

30/06/2015 82
Table 26 compares the expected need for mental health services in Looked after children to the number recorded as seeing CAMHS . Only around a third as many looked after children have been recorded as seeing CAMHS as might be expected. However, much of work carried out by CAMHS workers in Carelink and CLAMHS is about assessment of children, and liaison with and advice and training for social workers, parents, foster parents and carers. The numbers in table 12 only reflect children and young people in care who are having a tier 2/3 service. It is also possible that some looked after children are seen in other CAMHS Services. Recommendation: In future data extractions from SLAM should include a label to indicate whether a child is looked after to identify children seen in other services Table 34 Number of children in care and expected number with a need for mental health services compared to service use 2009-10 to 2011-12 Lambeth Southwark Year 2009-10 2010-11 2011-12 2009-10 2010-11 2011-12 No. of children in care 565 500 541 555 520 550 No. with expected mental health needs (45%)
260 230 243 255 242 253
No. of children using CAMHS 81 83 60 58 71 83 % of expected using CAMHS 31% 36% 25% 23% 29% 33%
Source: Ofsted.gov social care data tool; SLAM activity data
4.2.7 Outcomes: CAMHS Services
CAMHS measure the progress of treatment through using two different measures to assess the mental wellbeing of children: Children’s Global Assessment Scale (CGAS) is a scale from 0-100 used to reflect general functioning independent of any mental health diagnosis and takes into account social, emotional and behavioural aspects. Strengths and Difficulties questionnaire (SDQ) is a brief behavioural screening questionnaire for 3-16 year olds. It exists in several versions to meet the needs of researchers, clinicians and educationalists. All versions of the SDQ ask about 25 attributes, some positive and others
Page 180

30/06/2015 83
negative. These 25 items are divided between 5 scales: emotional symptoms, conduct problems, hyperactivity / inattention, peer relationship problems, prosocial behaviour SLAM (as per the London CAMHS dataset) currently report process measures of outcome measurement to commissioners – the percentage of children and young people who have a CGAS score and the proportion who have an improved CGAS score at a later date. For this needs assessment global measures of effect have been provided as additional work by SLAM. Eisen et al (2007)87 stated the effect size statistic can be adopted as a measure of clinically significant change, on the basis that research suggests that a medium effect size corresponds to change that is of sufficient magnitude to be evident to a careful observer.
4.2.7.1 Tier 2 and 3 outcomes Tables 35-37 show the average starting and ending CGAS score for children and young people using CAMHS tier 2 and 3 services in the three years between 2009-10 and 2011-12 for Lambeth, Southwark and all South East London boroughs using SLAM CAMHS. The effect size has also been reported i.e.. whether or not the average change in scores suggests a beneficial change. Table 35 Average before and after treatment CGAS scores & effect sizes in Tier 2&3 Lambeth 2009-10 to 2011-12
Tier 2 and Tier 3 CAMHS (Lambeth)
Financial Year Stage Mean N Std Dev Effect size
2009/10 T1 60.4 225 11.6 0.4
T2 65.2 12.9 SMALL
2010/11 T1 56.8 662 12.7 0.3
6 61.2 13.5 SMALL
2011/12 T1 54.4 682 10.8 0.5
T2 59.3 11.5 MEDIUM
Table 36 Average before and after treatment CGAS scores & effect sizes in Tier 2&3 Southwark 2009-10 to 2011-2
Tier 2 and Tier 3 CAMHS (Southwark)
Financial Year Stage Mean N Std Dev Effect size
2009/10 T1 58.4 177 11.7 0.7
T2 67.0 13.4 MEDIUM
2010/11 T1 57.5 575 11.7 0.5
6 63.3 12.7 MEDIUM
2011/12 T1 56.6 899 11.8 0.5
T2 62.1 12.4 MEDIUM
87 Eisen SV, Ranganathan G, Seal P, Spiro A. Measuring clinically meaningful change following mental health treatment. Journal of Behavioural Health Services and Research 2007;34(3):272-290.
Page 181

30/06/2015 84
Table 37 Average before and after treatment CGAS scores and effect sizes in Tier 2 & 3 SEL 2009-10 to 2011-12
Tier 2 and Tier 3 CAMHS (All SLAM)
Financial Year Stage Mean N Std Dev Effect size
2009/10 T1 57.0 1172 12.4 0.6
T2 64.4 14.0 MEDIUM
2010/11 T1 56.9 3236 11.8 0.5
6 62.8 12.9 MEDIUM
2011/12 T1 56.7 3916 11.0 0.6
T2 62.8 12.6 MEDIUM
Benchmark T1 56.7 166,026 12.1 0.5
T2 62.8 90,144 13.4 MEDIUM
Source Benchmark: Australian Mental Health Outcomes and Class
The number of patients whose scores are reported is lower than the number of patients seen i.e. not all patients have had scores reported.
Unlike the benchmarking data, numbers of patients are not reported at both T1 and T2
It would be useful to see results reported by service.
Interpretation of the average scores requires discussion with clinicians
Starting CGAS scores lower in 2011-12 than in 2009-10 (54.4 vs 60.4 in Lambeth) and 56.6 vs 58.4 in Southwark) which may suggest a more distressed cohort of children and young people.
4.2.7.2 Tier 4 outcomes Effects of tier 4 services are greater than tier 2 and tier 3. This might be expected as children and young people referred to tier 4 should by definition have more severe mental disorders and therefore have lower CGAS scores. It is notable that in 2011/12 the average starting CGAS score for tier 4 patients (55.4 Lambeth and 59.0 Southwark ) are higher than those for children starting in tier 2 and tier 3 services (54.4 Lambeth and 56.6 Southwark). Caveats – not all patients have CGAS scores (n lower than number of new first appointments) Table 38 Average before and after treatment CGAS scores and effect sizes in Tier 4 Lambeth 2009-10 to 2011-12
Tier 4 Outpatients CAMHS (Lambeth)
Financial Year Stage Mean N Std Dev Effect size
2009/10 T1 52.6 23 14.0 0.9
T2 65.7 22.8 LARGE
2010/11 T1 50/8 34 11.5 0.9
6 61.1 19.0 LARGE
2011/12 T1 55.4 105 12.8 0.6
T2 63.7 14.4 MEDIUM
Table 39 Average before and after treatment CGAS scores and effect sizes in Tier 4 Southwark 2009-10 to 2011-12
Page 182

30/06/2015 85
Tier 4 Outpatients CAMHS (Southwark)
Financial Year Stage Mean N Std Dev Effect size
2009/10 T1 56 19 16.4 1.0
T2 72 21.8 LARGE
2010/11 T1 51 18 7.6 2.2
T2 68 14.2 LARGE
2011/12 T1 59 15 17.3 0.9
T2 74 13.8 LARGE
4.2.7.3 Looked after children The emotional and behavioural health of children aged 4-16 years who have been in care for at least 12 months on the survey date is measured annually by a questionnaire called the Strengths and difficulties questionnaire. A score of 0-13 is considered normal, 14-16 borderline and over 17 of concern. Not all LAC were assessed (Figure 28 and table below). In 2012 the proportion of children whose score suggested concern was higher in Lambeth (43%) than Southwark (37%) and the England average (36%). The average score for Lambeth was 12.6 and for Southwark 14.3 in 2011 compared to an Inner London average of 13.2, and England average of 13.9. In 2012 Lambeth average score was 15.1 and Southwark 13.9 whilst the Inner London average stayed at 13.2 No margin of error is quoted, so it is not clear if the SDQ scores are getting worse. This is lower than the 45% of LAC estimated to have a diagnosable mental health disorder, however after including those with a borderline score, 94% of LAC in Lambeth and 88% of those in Southwark might benefit from some mental health services.
Figure 28 Strengths and difficulties questionnaire score classification for Looked After Children aged 4-16, Lambeth Southwark and England 2010-2012
Page 183

30/06/2015 86
Other measures reported for LAC https://www.gov.uk/government/publications/outcomes-for-children-looked-after-by-local-authorities-in-england-31-march-2012 are educational outcomes at key stages 1,2 and 4, substance misuse, offending , SEN and general health. Educational attainment is associated with better wellbeing and mental health, whilst substance misuse and offending are associated with higher levels of mental disorders.
4.2.7.4 Young offenders Lambeth commissioned work with Young offenders in 2012-13. Health and Wellbeing surveys of young offenders were carried out in December 2012. Number surveyed not reported in presentation but characteristics were
• 73% BME young people, 16% female, 84% male • 16/17yrs over represented in sample • 60% from single parent homes • 13% Looked After Children • 64% in school/college • 29% NEET
Of this group 30% rated their mental health as average, 34% as very good. In terms of emotional Health – During the last week - 11% felt down and unhappy a lot; 13% felt too tired to do things; 11% did not have a good time. Comparisons with the general population were not provided. Interviews and focus groups were also held, but as only with 6 young people the findings have not been reported here.
4.2.7.5 DNAs DNA data was supplied in the form that commissioners receive it – as a percentage of appointments of each service which are not attended. No epidemiological information was attached and therefore no additional information could be obtained i.e. unable to identify age, gender, ethnicity or diagnosis of children and young people who do not attend services. No further analysis
4.2.8 Self harm (This section is abridged from a report to the Child Overview Death Panel in 2012.) Hospital admissions of under-18 year olds from Lambeth and Southwark have increased significantly as shown by the graph below. It is important to note that the figures below reflect the number of self harm attempts that were deemed serious enough to require hospital admission and therefore are a small proportion of the total. Hawton et al (2002) found only 12.6% of episodes of self harm had resulted in presentation to hospital, therefore the true number of children and young people harming themselves is likely to be much higher.
Looked after children aged 4-16 included in SDQ survey 2010 2011 2012
Lambeth Number 270 125 160
% eligible 96% 47% 69%
Southwark
Number 45 180 180
% eligible 17% 71% 70%
Page 184

30/06/2015 87
Figure 29 Number of admissions for Self Harm and Injury Undetermined in Under 18's in Lambeth and Southwark residents 2006-2011
4.2.9 Cost Effectiveness PHIAC judged that, if effective evidence-based interventions are systematically implemented, then cost savings are likely to be achieved over 3 to 4 years – and also in the longer term A DH report in 201188 showed that that many public mental health interventions result in cost savings (Table 40). Table 40 Summary of cost effective interventions reported in Mental Health promotion and Mental Illness prevention, DH, 2011 (unless other source given) Intervention Saving per £1
School based social and emotional learning programmes £84
School based interventions to reduce bullying £14
Early intervention psychosis £18
Early intervention pre-psychosis £10
Early interventions for parents of children with conduct disorder £8
Pre-school educational programmes89, 90, 91 £17
88 Department of Health (2011) Mental Health promotion and mental illness prevention: the economic case 89 Karoly LA, Kilburn RA, Cannon JS (2005) Early Childhood interventions: proven results, future promises . RAND corporation (cited by Campion and Fitch, 2011) 90 Schweinhart LJ, Montie J, Xiang Z et al (2005) The High /Scope. Perry Preschool study through age 40. Summary, conclusions and frequently asked quations. Ypsilanti, High/Scope Research Foundation; 2005 91 Lynch RG (2004) Exceptional Returns. Economic, Fiscal and Social Benefits of Investment in Early Childhood Development. Washington. Economic Policy Institute. (cited by Campion and Fitch, 2011)
0
10
20
30
40
50
60
2006 2007 2008 2009 2010 2011 Year
Lambeth Southwark Grand Total
Page 185
30/06/2015 88
Violence prevention programmes92 £829 (at six years) and £6,446 (at 10 years)
92 Beecham J, Baingana F, Bonin E et al, (2010) School based universal violence prevention programmes. PSSRU, London School of Economics and Political Science. Unpublished paper cited by Campion and Fitch, 2011.
Page 186
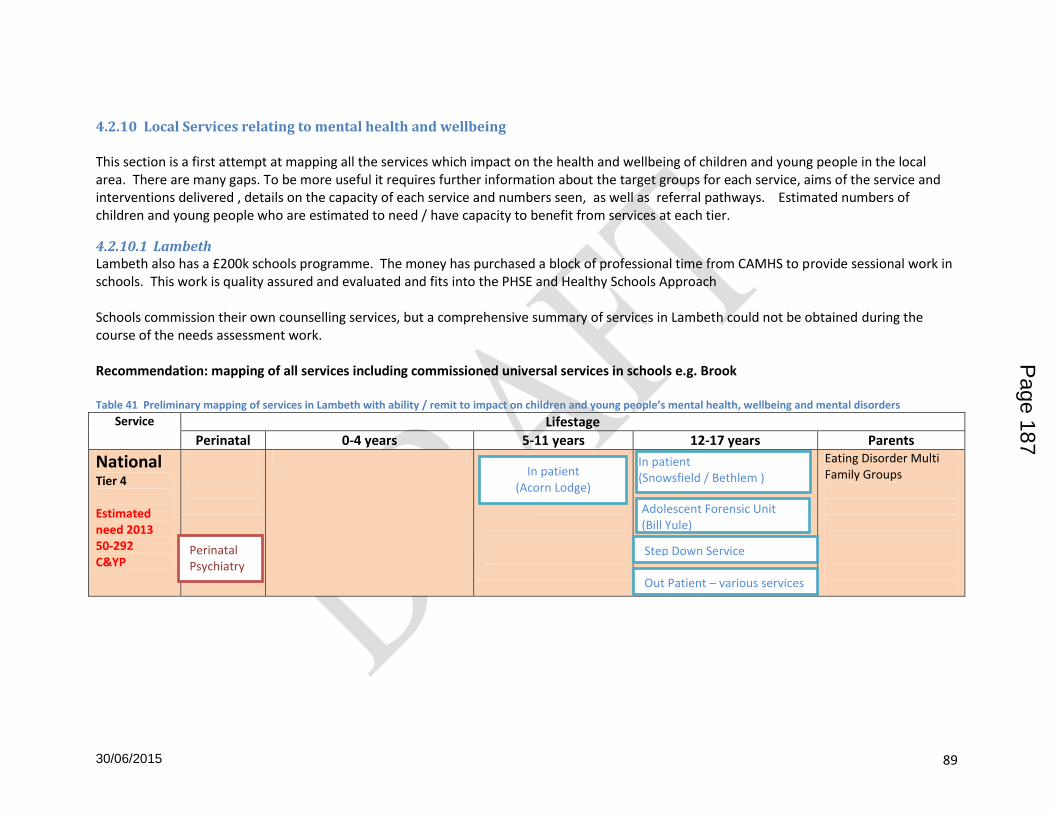
30/06/2015 89
4.2.10 Local Services relating to mental health and wellbeing This section is a first attempt at mapping all the services which impact on the health and wellbeing of children and young people in the local area. There are many gaps. To be more useful it requires further information about the target groups for each service, aims of the service and interventions delivered , details on the capacity of each service and numbers seen, as well as referral pathways. Estimated numbers of children and young people who are estimated to need / have capacity to benefit from services at each tier.
4.2.10.1 Lambeth Lambeth also has a £200k schools programme. The money has purchased a block of professional time from CAMHS to provide sessional work in schools. This work is quality assured and evaluated and fits into the PHSE and Healthy Schools Approach Schools commission their own counselling services, but a comprehensive summary of services in Lambeth could not be obtained during the course of the needs assessment work. Recommendation: mapping of all services including commissioned universal services in schools e.g. Brook Table 41 Preliminary mapping of services in Lambeth with ability / remit to impact on children and young people’s mental health, wellbeing and mental disorders
Service Lifestage
Perinatal 0-4 years 5-11 years 12-17 years Parents
National Tier 4 Estimated need 2013 50-292 C&YP
Eating Disorder Multi Family Groups Out Patient – various services
Adolescent Forensic Unit (Bill Yule)
In patient (Snowsfield / Bethlem ) In patient
(Acorn Lodge)
Step Down Service Perinatal Psychiatry
Page 187
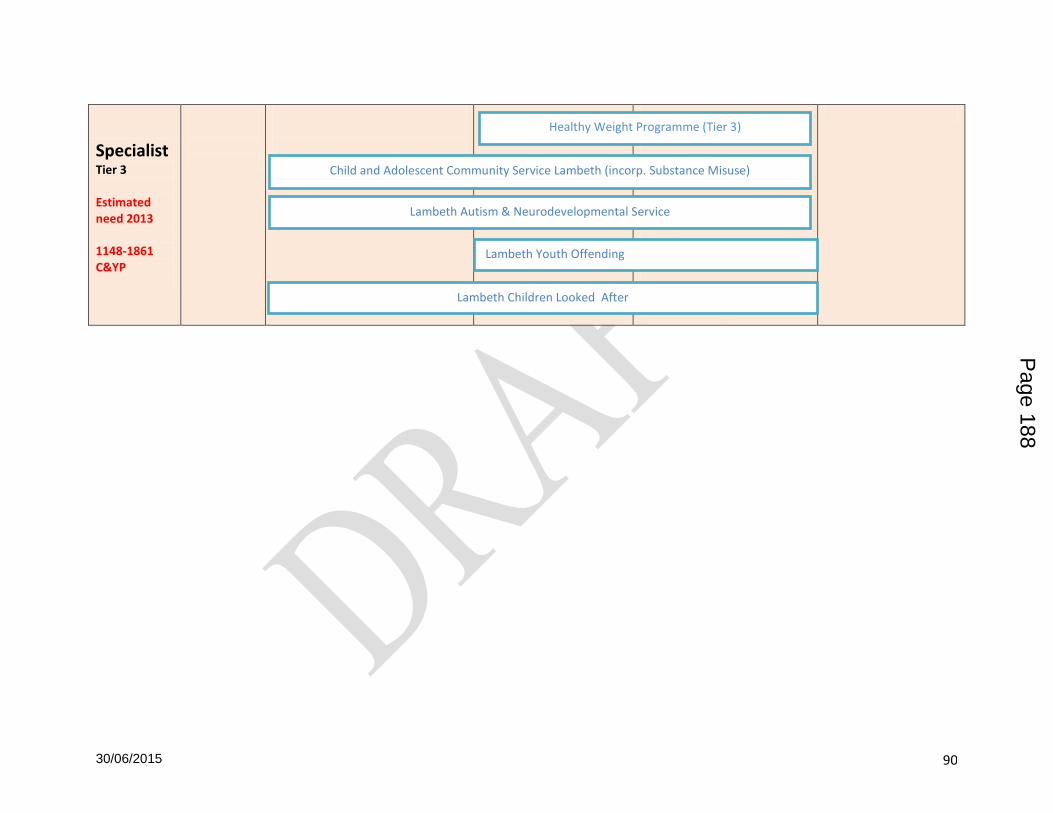
30/06/2015 90
Specialist Tier 3 Estimated need 2013 1148-1861 C&YP
Lambeth Youth Offending
Lambeth Children Looked After
Child and Adolescent Community Service Lambeth (incorp. Substance Misuse)
Lambeth Autism & Neurodevelopmental Service
Healthy Weight Programme (Tier 3)
Page 188

30/06/2015 91
Targeted
Tier 2
Estimated need 2013 4964 c&yp
Enhanced midwifery
Family Nurse Programme Home Start St Michael’s Fellowship
Compass(12-19 yrs)
Home Start St Michael’s Fellowship Compass ADHD PG1 age 4-12 ADHD PG2 age 12-18 Incredible years 6-10 Early Bird (ASD)
MAT
Youth Mental Health First Aid
Oval House Theatre
Faces in Focus
Working with men (10-16 years)
Drama Therapy led by Clapham Manor (Children
with Autism
Oasis UK (10-12 years)
Rathbone Youth Centre (SEN)
New Initiatives Youth and Community Association
Lambeth CAMHS Early Intervention
Page 189

30/06/2015 92
Universal Estimated need =6295-9442 c&yp
Midwives
Nursery Places (3+) Health visitors
Primary Schools - PSHE School Nursing Health Education Links Service (HELS)
Secondary Schools – PSHE School Nursing Clapham Park Project Well Centre (13-19)
Strengthening Families Strengthening Communities, Stepping Stone, FAST
Perinatal 0-5 years 6-11 years 12-17 years Parents Key: SLAM, Third sector Table 42 Draft Grid for describing services in Lambeth with an impact on mental health and wellbeing and mental disorder in children and young people
Service Brief Description Who interventions Aim Capacity Referral method / criteria
Child and Adolescent Community Service Lambeth
Clapham Park Project Delivers sport , arts and drama in the locality. Aims to work with young people not in education, employment or training.
NEET Self?
Drama Therapy led by Clapham Manor (Children with Autism)
After school drama therapy for children with autism (provided in three schools – Clapham Manor, Archbishop Sumner and Crown Lane)
Faces in Focus Counselling for young people (14-19 years) who are not in education, employment or training
NEET
Health Education Links Service (HELS)
School based project in 24 primary schools and 4 secondary schools focusing on emotional health and wellbeing. It currently offers a free service to schools including peer mediation, behaviour forum groups, playground focus groups and circle time. This project assists with improving behaviour.
Home Start Training of volunteer befrienders to support families in their homes. Peer support groups in Children’s Centres
Lambeth Autism &Neurodevelopmental
Page 190

30/06/2015 93
Service
Lambeth CAMHS Early Intervention
Lambeth CAMHS Substance Misuse
Lambeth Children Looked After
Service Brief Description Who interventions Aim Capacity Referral method / criteria
Lambeth Healthy Weight Programme
Lambeth Youth Offending
MultiAgency Team (MAT) Includes CAMHS workers, health visitors, early intervention social workers, staff from adult’s services, and work with children aged 0-11 and 11-19 to intervene early when issues arise.
New Initiatives Youth and Community Association
School based provision focussed on personal development using “identity/ self-worth/ rite of passage programmes” that support young black boys having difficulties with the transition to adolescence
Oasis UK Supports vulnerable children through transition from primary to secondary school by equipping them with and helping to develop skills to help move between years 6/7/8. Skills will be practical, academic and social/emotional.
Oval House Theatre Drama and theatre activities. Accessible to young people with disabilities and those at risk of exclusion from mainstream education; refugee / asylum backgrounds, homeless and young offenders.
Rathbone Youth Centre Delivers a programme for young people with special educational needs that helps teenagers integrate into mainstream youth and community projects.
Page 191

30/06/2015 94
St Michael’s Fellowship Support to young mothers and fathers. One to one support and group work. Young fathers group. CAF referrals
Well Centre A drop in health centre for young people aged 13-19 years. Sees health as holistic – help with everything that can affect health and wellbeing. Staffed by GP, nurse, counsellor, youth worker
Working with Men School-based provision focussed on conflict resolution programmes targeting boys through primary PRU and mainstream schools. Emphasis on engaging with boys making the transition from primary to secondary schools. 10-16 year olds
Youth Mental Health First Aid (YMHFA)
Youth MHFA is an internationally recognised training programme designed specifically for those people that teach,work, live with or care for young people aged 11 - 18.
The training provides information, tools and techniques to promote a young person's mental and emotional wellbeing and to enable participants to support a young person who might be experiencing mental and emotional distress.
Two further courses planned for early 2013. Initial evaluation of the training was good.
Early Intervention Health Visitors
The early intervention health visitor team was expanded after 2010/11 to 6, and is now funded through Lambeth CCG. They have a specific remit to work with vulnerable pregnant women, and to offer continuous support for them once they have given birth. Caseloads are usually around the 50 mark (as compared to a generic health visitor who in Lambeth will have a caseload of around 400-450 families)
Family Nurse Partnership Works with vulnerable young parents having their first child, from pregnancy until their baby is 2 years old. Family nurses are given specialist
Page 192

30/06/2015 95
training in how to engage with the young parents, many of whom come from families where there are generational issues with parenting. To be eligible for the programme young women need to be identified before 28 weeks of pregnancy.
4.2.11 Southwark Services Table 43 Preliminary mapping services in Southwark with an impact on mental health and wellbeing and mental disorder in children and young people
Lifestage Perinatal 0-4 years 5-11 years 12-1893 years Parents & family National Tier 4 Expected need 2013 47-296 c&yp
Specialist Tier 3
Perinatal Psychiatry
Belgrave Paediatric Liaison team (National and Specialist)
Southwark Adolescent Services (YOT services 12-18)
93 Need to identify whether services end on child’s 18th birthday or 19th birthday.
Page 193
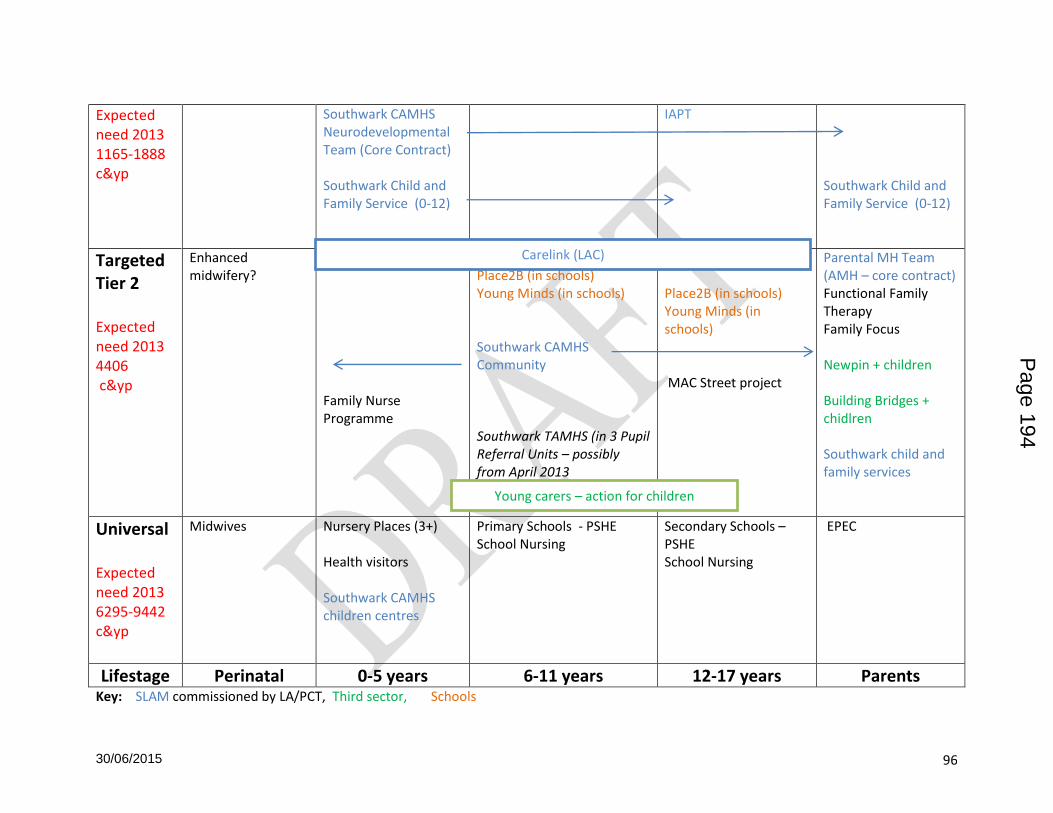
30/06/2015 96
Expected need 2013 1165-1888 c&yp
Southwark CAMHS Neurodevelopmental Team (Core Contract) Southwark Child and Family Service (0-12)
IAPT Southwark Child and Family Service (0-12)
Targeted Tier 2 Expected need 2013 4406 c&yp
Enhanced midwifery?
Family Nurse Programme
Place2B (in schools) Young Minds (in schools) Southwark CAMHS Community Southwark TAMHS (in 3 Pupil Referral Units – possibly from April 2013
Place2B (in schools) Young Minds (in schools) MAC Street project
Parental MH Team (AMH – core contract) Functional Family Therapy Family Focus Newpin + children Building Bridges + chidlren Southwark child and family services
Universal Expected need 2013 6295-9442 c&yp
Midwives
Nursery Places (3+) Health visitors Southwark CAMHS children centres
Primary Schools - PSHE School Nursing
Secondary Schools – PSHE School Nursing
EPEC
Lifestage Perinatal 0-5 years 6-11 years 12-17 years Parents Key: SLAM commissioned by LA/PCT, Third sector, Schools
Carelink (LAC)
Young carers – action for children
Page 194

30/06/2015 97
Table 44 Suggested Grid for describing services in Southwark with an impact on mental health and wellbeing and mental disorder in children and young people
Service Who Aims Interventions offered
Capacity Referral method / criteria
Perinatal Psychiatry Pregnant and post partum women
Belgrave Paediatric Liaison Team
Southwark CAMHS Neurodevelopmental Team
Carelink Looked after children
Parental Mental Health Team
SENCOs in schools
MAC Street project
Young Carers – action for children
CAMHS social workers
Page 195

30/06/2015 98
4.3 Stakeholder Views
4.3.1 Commissioners, health, social care and education professionals A wide range of professionals working with children and young people were interviewed for their views on met and unmet needs, problems and concerns relating to well-being and mental health services in Lambeth and in Southwark. Although a set of questions were developed not all the questions were relevant to all stakeholders, or time constraints meant that not all people question varies. See Appendix 2 for questions and the people interviewed. The overall picture of both boroughs is one of complex intergenerational risk factors for poor mental health, with a large proportion of stakeholders mentioning parental mental health as key influence on children and young people’s mental health. Other themes which emerged was a feeling that although commissioned services are good for the children and young people that they see, that there are a large number of children and young people who have needs which cannot be met in universal services, but who don’t qualify for targeted services, either because their needs aren’t deemed to be serious enough (yet), or because they do not fit into a service category. Other common themes were enthusiasm for co-location of CAMHS workers to provide consultation, training and guidance to people working in universal services dealing with children and young people. Many people spoke of the need for multi-disciplinary working across organisations and professions to ensure a seamless, flexible service built around the needs of patients, and based on appropriate risk assessment and triage of needs.
4.3.1.1 Groups with higher needs for MH services This question was answered differently by each person, answers could be grouped into four main categories: Family factors influencing child mental health • Parents with MH, SM, DV, LD • Recent immigrants incl. no recourse to public funds (primary schools) • No male role model (mentioned infrequently)
During stakeholder interviews the most commonly mentioned at risk groups were children of parents with mental health, substance misuse or domestic violence issues. Parents with learning disabilities were not mentioned as often. Of particular concern were parents whose mental health problems or learning difficulties have never previously been recognised but those problems become very apparent when e.g. teachers or mental health professionals make contact with the parents because of concerns about this child. Primary schools mentioned their concern about recent immigrants with no recourse to public funds and these groups weren’t necessarily on the radar of other services. This may be because the parents are keen for their children to get an education, but are suspicious of other services and so are avoiding contact.
Page 196

30/06/2015 99
4.3.1.2 Individual characteristics which make children have higher need for services • Looked After Children • Teenagers - year 8 / 9 girls • Multiple needs – prison/ A&E / rehab / mortuary all equally possible • Drug use – cannabis induced paranoia (school) Schools in both boroughs mentioned concerns about girls in year 8/9 about eating disorders and self-harm. There was also some concerns raised about increased / earlier sexualisation, girls with lack of boundaries, possibly fed or exacerbated by social networking websites, and the ubiquity of mobile communications. The concern about multiple needs was expressed in the terms above by a stakeholder from Southwark, but stakeholders from both boroughs expressed concerns about this particularly complex group. Cannabis was mentioned in the context of children at higher risk, but also in terms of changing mental health needs due to the increased strength of cannabis available today. As both Lambeth and Southwark have done work which is specifically focused on substance misuse, this theme was not pursued further.
Diagnosis / Conditions which have higher needs for services • Behavioural problems, • Autism, ASD, Aspergers, ADHD • Eating disorders • Self harm
Although behavioural problems were mentioned frequently, particularly by non clinical stakeholders who work closely with children and young people, other stakeholders stated clearly that they felt conduct disorders are not necessarily a mental health problem requiring the input of a specialist mental health team, but were something that should be addressed by parents and teachers setting firm boundaries. Recommendation – consider more parenting classes at nursery and primary level as evidence suggests effective pre-age 12.
4.3.1.3 Key vulnerable times which result in children needing services – Transition (primary to secondary, and young person -> adults – After bereavement, after experiencing trauma
Primary schools mentioned the transition to secondary school as being difficult as primary schools are able to contain children more and offer more stability – those children with ASD disorder may not cope so well with the less controlled environment of a secondary school with more fragmented continuity of experience e.g. changes of classrooms, changes of teachers. One school suggested having a CAMHS worker associated with one secondary school and their feeder primary schools to help smooth the link between the two and to work holistically with parents. The Lambeth MAT team mentioned bereavement (post divorce, post relationship or due to death) as an issue – as much in relation to parents, particularly single mothers, as for children and young people themselves. The concern raised was not about the normal grieving process but that some people who are unable to cope with the day-to-day during this period, e.g. paying rent, going to work, and end up facing eviction or additional socioeconomic stressors from
Page 197

30/06/2015 100
which they don’t quite recover. In the meantime their children are unsupported and at greater risk of developing problems, or not having problems recognised. One secondary school mentioned bereavement as an issue in the context of young people as many of the parents were dying in their forties of cancer or substance misuse.
4.3.1.4 Changes in MH Needs over time Not all stakeholders felt able to comment on this section as they hadn’t been working in the borough for very long, or had recently changed roles. The time periods varied, but some stakeholders interviewed had been in post for over 20 years. There was also an awareness that percieved changes could be due to a genuine increase in needs, or due to better recognition of conditions, or also due to changes in policy e.g. schools have been dealing with more issues since access to mainstream education has been increased to include e.g children with Autism. Clinical services also mentioned that although it feels that their caseload has more complex children with multiple needs this may be because children with fewer needs are seen elsewhere or not having referrals accepted. Below is a list of the changes in mental health needs mentioned by stakeholders: It should be noted that 3 stakeholders felt that there had not been any changes over the period they had been working in Lambeth / Southwark. Increases in autism / ASD were most frequently mentioned, but responses also gave a picture of increasing numbers of children living in a world where environmental factors are increasingly affecting children and young people – increasing violence, stronger drugs, less parental involvement (?) leading to school starters lacking social and emotional skills.
Autism, ASD, Asperger’s (x7) • More children with complex needs, more SEN and LD • Self-harm • General increase in all types (x5)
– Behaviour incl. GP referrals, conduct, emotional – More school starters lacking social skills and emotional development
• Trauma, Violence (x4) – PTSD, Domestic Violence, normalised level of violence, gangs
• ADHD (x3) - link to parental SM, boys • Psychosis / stronger recreational drugs (x2) • Problems starting younger:
– Sexualised behaviour 10yrs not 14 yrs – Disordered eating at younger age
• No changes (x3)
4.3.1.5 Groups Not Accessing Services
Children and young people with a need for mental health services, but who don’t access those services can be divided into two broad categories
1. those referred for help, but who don’t attend; 2. Children and young people with problems who are not identified and therefore don’t
have the opportunity to receive help.
Page 198

30/06/2015 101
Children and Young people often not identified as having mental health problems: • Young offenders - not identified as assessment and referrals process not always robust • Quietly distressed children and young people • Aspergers may often go undiagnosed until becoming a teenager then become very
disruptive • Young carers Recommendations to increase identification of children and young people with MH problems:
Re Young Offenders - include CAMHS worker in case worker fortnightly discussions to ensure that young people with MH needs are identified as soon as possible. Ensure repeat ASSET assessments done.;
Consider MH First Aid training for people working with adolescents to widen awareness of quietly distressed young people
Identify ways of working with Young carers e.g. Southwark has a young carers group There was a running theme of stigma about mental health being an issue preventing people from accessing services, or in some cases thinking about themselves in terms of someone who might have mental health needs, leading to young people living with the strain of putting on a strong front. The ideas of bravado and denial of problems were particularly attributed to young offenders and young people involved with gangs. Adolescents, Young offenders, LAC Reasons for not accessing services • Nature of condition (ASD, conduct) and age • Clinic based services not attractive • Don’t acknowledge have a problem (front, bravado) • Purposively avoidant due to involvement in criminal activity • Stigma – sense that having mental health issues means you are mad and run down the
street naked. Children with parents with MH problems or involved with social services or other services • Can’t organise selves to get child to appointments and then if miss 2 appointments service
will discharge child. (2 strikes and out) • Possible previous bad experience of services and authority means parents unwilling to
engage again. • Family in touch with multiple agencies, too many appointments to attend. • Feeling that might be blamed for children’s problems BME groups particularly recent immigrants • Avoiding contact with authorities • Previous bad experiences of services • Strongly religious families with male head -not wanting to seek help outside family, possibly
not wanting to engage with services run by women • Stigma, cultural beliefs about Mental Health
Page 199

30/06/2015 102
4.3.1.6 Addressing Access issues Following on from a discussion about people who don’t access services, views on how to tackle these problems were discussed with stakeholders, the main themes were: Different service delivery - non-clinic based, client-centred - Informal opportunities for parents to be in contact with services / get information on skills
to help children e.g. coffee mornings - (Assertive) Outreach - building trust - Support e.g. Text reminders, referrer to accompany to first appointment - CAMHS worker in fortnightly case meetings with e.g. YO social workers to identify YP at risk
/ in need - Schools felt that school is a place of security and safety and children will attend services
provided there. Address stigma - Rebadge / rebrand – wellbeing / mental strength / life skills not mental illness - Education of population More co-ordination between services - To make it easier for families in touch with multiple services to access appointments and for
information to be shared to avoid duplication of questions Change expectations - Parents think one or two visits will make child perfect - Parents worry CAMHS will blame them for their child’s problems NB – as DNA data from SLAM was not attached to any demographic details but provided for a service overall, it has not been possible to explore the characteristics associated with DNA from services
4.3.1.7 What currently works well for children? The most frequently mentioned beneficial feature of current mental health services in Lambeth and Southwark was the co-location of CAMHS workers with other services. This was highly valued by non-mental health practioners as an opportunity to access skilled input into discussion and case management and to skill up other professionals. Schools were very keen on TAHMS – (although none of those contacted seem to have commissioned it themselves). Schools also mentioned they valued having a consultancy service. Below is list of areas which stakeholder felt work well. - co-location of CAMHS workers with other services x 6
o Value input, expertise, skilling up of other professionals - TAHMS x 3 - Targetted, Specialist and Acute services
o Once child is referred - Carelink - School commissioned talking, play, art therapy (other stakeholders queried evidence base
and suitability of both the activity for children, and the skills of the practitioners delivering and links with other services).
- Charities e.g. Kids Company (other stakeholders queried their motivation and methods)
Page 200
30/06/2015 103
- Children’s Centres (this was also supported strongly in Southwark by parents interviewed during 1000 voices )
- Adult service for parents of young children (Southwark) - IAPTS for children and young people good idea – although not operating yet - YOS service re sexual exploitation (Southwark) - Perinatal psychiatry (need more capacity though) - Nothing – not enough capacity (Schools - Lambeth)
4.3.1.8 What works well for parents / schools? On reviewing of the answers they seem to be split between what exists and works well, and what would work well / is needed
Preschool • Perinatal mental health is an issue
– health visitor referrals (NB train some of the additional HVs in mental health skills e.g attachment theory
– Early intervention health visitor services (L) – Group work good for some mothers – feels less persecutory
• Early Years Children’s Centres CAMHS (L +S ) • Early intervention (early age, and early in onset)
Whole family approach • Family Support Workers x 2 (L) helping parents gain skills with tricky children / realise might
need parenting classes • Functional Family Therapy (S) x 2 • Need more family workers (L), more outreach, more holistic service – one stop shop. • Parenting programmes : Incredible Years . EPEC, parent mentoring, whole family approach ,
Early intervention team • Family Focus, Youth in Need Schools • Schools doing their own commissioning (L & S)
– good at primary level but not secondary (S) – Can buy in from different providers, and some schools are. Maudsley not cheapest.
Some schools use Tavistock • School nurses don’t deal with MH, other partners do. TAMHS was good • Southwark – pilot between YOS and four primary schools re transition to secondary school
(Peckham) Service delivery • Targeted CAMHS workers working alongside e.g. YOS, Troubled Families teams. PRU
mentioned be good to have on hand. • Services generally need better connections with parents e.g. better interaction between YOS
CAMHS and parents
4.3.1.9 What doesn’t work so well? Often although services were considered to work well for those whose needs were acute enough to make them eligible, there was a frequently expressed feeling that children and young people (and pregnant women) with lesser needs may not have them met
Page 201

30/06/2015 104
Perinatal mental health
• Gap for women who don’t meet threshold for psychiatric services but who need some help
• GP referrals to counselling too slow – women only pregnant for 9 months and sometimes not seen in timely manner
• not enough resources for inpatients Schools
• Children too challenging for school / in distress but don’t meet referral criteria • Early intervention CAMHS no easier to access than normal CAMHS • Need more support for parents (L) • Lengthy waiting times for family support worker (Lambeth) • Lack of clarity about what CAMHS can offer, what different mental health workers offer,
when it is appropriate to refer to CAMHS • No timely feedback in response to CAMHS referrals – don’t know if received/ assessed /
being seen. Comments that only find out months later after child seen. Early Intervention Service
• doesn’t provide skills for children to help themselves or deliver in targeted settings • More work need to be done to identify children of parents with MH/ SM/ LD / • Doesn’t get CAMHS input or support at tier 1 or 2 • No early years services from CAMHS (L)
Transition / Adolescents
• Services struggle to engage this group (Can’t tell from data – seems to be referrals are lower for young men, not analysed whether this group drop out more quickly – could be done from data)
• if 17 when come into contact with services, might be excluded as not enough time to treat before 18
• Need protocols at transition for all children in MH services. Think about having a service for 14-24 year olds to ensure that 17 year olds not excluded. Further work needed to look at transition.
ADHD and Autism Services • Issues about system (diagnosis -> services) not meeting needs • Conduct disorders not necessarily parenting issue in this group (although might be in
children without ADHD or Autism) therefore need to spend time with professional to unpick underlying causes.
• Transition to secondary schools can trigger problems There were many specific suggestions about what could be done to make services better: Wider workforce
• Could use wider workforce better with more training and development of staff e.g. • midwives / HV could do more identification and basic work on attachment issues • Children’s Centres could do more identification of children in need • Teachers, social workers, other workers could be trained in basic therapeutic skills , and
given more knowledge re ASD
Page 202

30/06/2015 105
• Teachers need more training re conduct/ behavioural issues •
Pathways/ system overview • Referral pathways convoluted e.g. for Family Therapy (L) • Seams between services and tiers could be better, x 4 • info sharing an issue • CAMHS needs to integrate better with justice system and other services • Need more tier 2 and 3 resources (x 2) and funding to reduce tier 4 activity Service delivery • Co-location makes it harder for specialist services to co-ordinate • Service settings – need to go to children’s centres, / schools not clinics (x2) or homes (x1 –
even specialist services) • Too service led, needs to be more focused on patient needs Dual diagnosis • need clear service planning and ensure correct lead physician for the dominant underlying
problem e.g. if have learning difficulties and mental health problems need to see a learning difficulties specialist who can also deal with the mental health issues, not be seen in a mainstream mental health service.
Services that stakeholders felt are needed for children and young people: • Counseling based services for children and families • (S) Forensic service or sex offender programme, • More services for sexually exploited girls (not specified what) • Group work from CAMHS for some needs (need evidence base for conditions which will
respond to group work) • Support for parents who are sub-current thresholds for targeted / specialist services but
who aren’t managing with the support of universal services (do universal MH workers need more training or is more capacity needed?)
• Think about extending services to 25 years (young adult service) • More training of wider workforce health visitors re attachment, teachers re conduct
disorder
4.3.1.10 How to reduce demand for tier 4 services Fewer stakeholders commented on this section as they had not had experience of children and young people needing to have national or inpatient services. There were many general comments about prevention of need for tier 4 through earlier recognition and speedy treatment with evidence-based interventions at an earlier stage in the disorder. More specific answers were about managing activity within CAMHS for example, where a child or young person is admitted, ensuring the treatment is more intensive with aim of moving back to the community as soon as possible, and with tier 3 actively attending case meetings for tier 4 patients to speed the move to lower tiers Timing - Earlier diagnosis of psychosis (in prodromal stage) - Fund assessments earlier before child / YP hits crisis point
Page 203

30/06/2015 106
- Earlier interventions which are known to work Speed - Be able to access other services more quickly – have a hit squad to address problems early Interventions - Evidence-based interventions for conduct / behavioural issues - Inpatients should have intensive daily interventions to reduce LOS – with aim of swiftly
moving to community with appropriate support Services: - More active case management – tier 3 should pull cases down from tier 4 - More funding/ capacity at tier 2 and 3 - More care at home and support for families / parents – integrated working with schools and
social care (will need after inpatient stay, so better to do before) - Whole systems solution – what are skills elsewhere, are some CAMHS skills transferable to
other professions? does child / young person need to be inpatient?
4.3.1.11 Managing risk in time of financial constraints Difficult in time of financial pressure as immediate acute need takes funding from Early Intervention Services which reduces the capacity for CAMHS to do preventative work. It was mentioned that the Children’s Trust needs to take responsibility for wider Mental Health / wellbeing of children and young people. However the key actions identified by stakeholders to manage risk are to start with: • A robust risk assessment of children and young people referred to prioritise needs for
example through CAMHS input at fortnightly case meetings in at risk groups e.g. YOS, LAC particularly re specialist input
• Understanding the needs and ensuring prioritisation of most vulnerable children (x2) e.g. Screening in year 8 when children most vulnerable
• Tighter thresholds and eligibility criteria (to ensure right people seen) • Refine triage procedures – help line for people on waiting list – if feel acute need can speak
to someone who can reassess Early Intervention Services
• Timely (x-ref risk assessment) access to services early in course of non-wellbeing / poor mental health
• Appropriate offer which produces positive outcomes (requires evidence-based interventions, but also regular audit of patient outcomes to see if service is working)
• Sufficient capacity (more than now) x 2 Innovation and co-operation between services
• Get patients / population involved in service design to address quality and reduce stigma
• Use wider services to support parents to meet needs of their child x 2 • Ensure all wider health / social care professionals aware of MH services and how to
refer (directory / helpline) x 2 • Co-location of CAMHS with other services to share expertise • Integrated working x 3
Page 204

30/06/2015 107
4.3.1.12 Building interface between CAMHS and non-clinical services • CAMHS needs to share skills with MAT and schools x 2 • Co-location of CAMHS with teams really important • true joint working between CAMHS staff and other organisations x 2 matrix management ,
MDTs – e.g. joint team meetings, joint training x 2 – Named CAMHS staff to work with other services – CAMHS to attend MDT meetings with social care / education / health – Support change and change agents
• Forums for professionals to share working /understand each other’s roles (1-2 p.a.) • Need multiple views of child, not each subsequent assessment based on conclusions of
previous one • Flexible services with child at centre and holistic assessment of child’s needs.
4.3.1.13 Managing fiscal challenges Service Redesign • Work with children who don’t have a diagnosis • Reduce need for residential places for complex needs/ forensic • Early identification and intervention in community to reduce need for specialist services (but
will always be small population with lifelong complex needs) • More risk management in community • IAPT for children. • Safe environments for early counselling (schools, children centres). • Projects such as Young Voice are good - peer support with training to recognise triggers to
alert. • More flexible services e.g. outreach re gangs , true team working so patients get help even
if named clinician not available • Services to meet diverse needs Commissioning • Be clear about what able to achieve (even gold standard interventions in single issue
populations leave 30% of patients without much improvement) • Optimise prioritisation • Individual contracts for children with high needs – no block contracts • Expect impact from services and include outcomes of reducing tier 3 and 4 activity Staffing / Wider Workforce • Secondments from one service to another • Training practitioners (Family Support workers, Early Intervention Workers, Early
Intervention Youth Advisers) to help young people reframe attitudes, build self-esteem and resilience, could help prevent people developing bigger problems which require more skilled /specialised work. Also training in family therapy / systems training and more practical involvement.
• Teaching parents about systems of rewards and sanctions to control behaviour. • Churches could have greater pastoral role. Schools • Schools have money – School heads should pool resources to commission services
strategically.
Page 205

30/06/2015 108
• Top slice elements of dedicated budget, buy in lower level services to deal with emotional issues and challenging behaviour.
• Need different models of working e.g. schools in spoke and hub configuration with centres of excellence. Schools could get database of parents with relevant professional skills who are prepared to offer support / skills.
• Stop school exclusions.
4.3.1.14 Making CAMHS sustainable and 5 year vision for services Services based on patient need • Range of provision: informal encounters with YP, advice and surgeries, assessment and
interviews. • Strengthen universal services by building on interface between CAMSH and others • Need skilled, flexible people, co-located in community service, able to do home visits, sit-in
on sessions with other workers and child / YP to give perspective /advice • Strong interagency working x 3 – integrated services • complex children need systematic assessment and proper joint working, • Earlier input and support to children and families • Challenge assumptions about current delivery of care • getting people to think outside and give flexibility to think creatively to meet needs of
children and young people (and their parents / carers). • New ways of delivering e.g. MAC UK - street based MH services work with gangs. • Co production • Examine case loads, look at cases individually and assess and prioritise • Schools to become joint commissioners
Families • Long term work with LAC and foster families (huge range of need from 1 person to whole
family) • Troubled families with neglected youngsters. General • Better identification processes. • Wide understanding of what CAMHS can offer and deliver, how people can be referred,
signposting to appropriate specialism, • Excellent communication between co-located CAMHS and in reach teams Other • Rebadge services - break link with mad • Evidence based interventions • Need commissioned services for serious youth violence. • Bear in mind public health targets. Use wider organisational objectives to help deliver aims. • More MH assessments for YO • Build links with voluntary sector
Children with parents with mental health and /or substance misuse problems, learning difficulties or are experiencing domestic violence
Gaps between need and services
Page 206

30/06/2015 109
bereavement - not only death – it can be another sort of loss e.g. divorce, or the end of a relationship
trauma - trauma may be a trigger point for some groups e.g. young offenders to recognise that they have a problem, as well as previous trauma being a risk factor for post traumatic stress disorder and major depressive episodes.
Interviews with Southwark schools as part of the School Nurse Service review94 also identified that emotional, social and behavioural (ESB) problems were a major concern for most schools. Several schools felt these problems were linked to parental substance misuse or mental health problems. Speech and Language problems were also identified as linking to ESB problems
4.3.2 Local public consultations Given the time and budget constraints of the needs assessment, the Steering Group agreed that the CAMHS needs assessment would not involve a dedicated consultation with the public. Steering Group members were asked to provide copies of any local consultations which might be relevant to CAMHS.
4.3.2.1 Southwark 1000 Journeys Southwark Council carried out a qualitative research project called 1000 Journeys95 to capture the experiences of living in the borough and using services. 1000 children and young people, and parents of young children were interviewed. The work is still being analysed and therefore further views may be reported which change the overall impression. At the date of writing (4 Feb 2013) a search on the word “CAMHS” in interviews held at children’s centres brought up the following comments:
“I wanted my son to have a different upbringing to me but I didn't know how to. Without SLAM I would be institutionalised by now Getting help now from CAMHS to build my relationship with my son” “I am training as a child psychotherapist, learning the system, getting to know people in the team. Excited and afraid of the journey ahead, receiving psychoanalysis 4 times a week as part of my training through CAMHS. CAMHS and other team members all helped me.” “Services used - GP's, midwives, health visitors, parenting courses, home start, schools CAMHS, baby clinic. Feeling very low and depressed. Due to no recourse to public funds, social services have helped in a small way for rents. I want to go back to university.”
94 Davis S, Review of School Nursing Services in Lambeth and Southwark (2013) Lambeth and Southwark Public Health Department (unpublished to date - insert link to document when available) 95 For more information on 1000 Journeys, see Children and Young People's Plan 2013-2016 and supporting 1,000 Journeys Consultation. To be published by LB Southwark.
Page 207

30/06/2015 110
“The Michael Rutter centre did more for me in one session then CAMHS did for me in the whole time they were seeing us”
It should be noted that many people interviewed did not refer to services by their official name which means comments about would not have been picked up. The thematic analysis found that parents using children centres had very positive experiences of their contact with services and professionals there: Common themes from parent’s journeys are Isolation, Unemployment, Lack of confidence, Networks, Training courses, poor English, Childcare and Aspiration to be better parents among others. Children’s Centres and Sure Start have been credited by parents with providing support and reducing isolation, making people feel part of a community and helping them into jobs through gaining skills.
“The children's centre has helped me become a better person and more tolerant Mum.”
“I suffered from postnatal depression and panic attacks after my 4th baby. I went to the doctor and felt that I did not receive the support/ help I required. I helped myself by getting out and about and using alternative herbal remedies. But coming to Crawford Centre has given me something to look forward to and confidence which I lacked.”
4.3.2.2 Lambeth YOS consultation Methods used
• Health & Well Being Questionnaires • 1-2-1 Interviews • *Focus Groups
ADHD was identified as the most frequent mental health issue
Drug misuse and asthma were the most frequent physical health issue noted
35% referred to CAMHS but 11% of these stopped after 1 or 2 sessions
32% of the forms had the physical health fields fully completed
51% of the forms had assessed the mental health fields fully Focus Group Key Findings 2 Groups, 6 young people, 1 female, 5 Black British, 1 Portuguese, Aged 15 -17yrs • Rated emotional health initially as high 4 • Substance use – all participants smoked Skunk
• Effected their mental well being • Tiredness, apathy, anger, depression • Social activity use vs. smoking on their own
• Misunderstanding of mental health – revised scores • All said they were depressed prior to taking drugs
• common age 13yrs, early trauma High level of mistrust of everyone – including GP’s, YOS, Social Workers, YOS young people
Page 208
30/06/2015 111
Patient /user satisfaction surveys Mental health commissioners are currently working to develop patient / user feedback systems for services commissioned from SLAM (i.e. targeted and specialist services
4.3.2.3 Lambeth – CAMHS PPI report 2010-11 Parents commented they have more confidence and more skills in dealing with children and
children are more confident and well behaved.
Having a shared language to talk to child helps
Social workers, school heads, other health professionals and foster carers also valued CAMHS input for both theory / understanding and practical comments.
One parent commented that CAMHS gave support that they could not get elsewhere and this was vital.
Good to meet other parents in similar boat – helps to share problems Early Intervention: Service User and Referrer Feedback
This year‘s referrer‘s feedback had a varied outcome highlighting the need for timely, effective and meaningful communication with both, professionals and families.
4.3.2.4 Southwark – CAMHS PPI Report Jan 2013 Parental comments: Some negative comments following relocation of service from parents who now have further to travel; also comments about the new building needing repair. Some parents prefer children to have appointments outside school hours. One service started offering evening appointments following feedback that it would be helpful – the clinic was not well attended. Some feedback asking for longer appointments or for clinician to travel to young person. Carers interested in shorter period before assessment Feedback on service positive – praise and regard for staff, children and young people positive. Carers course well-regarded with participants feeling they had learnt skills to help them deal with children
4.3.3 National Consultations Focus groups conducted by the independent review of CAMHS showed that children and young people want to feel the following about early intervention services that96:
their needs are identified accurately and as early as possible by professionals;
they receive help from the right people, who have a high level of expertise and skills; and
they understand what is happening and receive information and support in a way that suits them.
4.3.4 Complaints and compliments A review of serious untoward incidents did not identify any concerns.
96 DH (2010) Keeping Children and Young People in Mind – Full Government Response to the CAMHS Review. Department of Health, London.
Page 209

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 112
5 Results Summary
5.1 Equity Equity requires that services are used in proportion to need; therefore groups with a higher need for services should make up a greater proportion of service users.
5.1.1 Age and gender of CAMHS service users The prevalence of mental disorders varies with age and gender (Table 1) and this should be reflected in the profile of service users. Table 45 compares the number of children and young people in each borough who are estimated to have a mental disorder by age and gender to the number who have been seen by CAMHS in 2011-12. NB- a single estimate of prevalence of mental disorders has been used for children aged 2-4 years which may underestimate need in boys and over estimate it in girls. Table 45 Comparison of estimated prevalence of mental disorder by age and gender to CAMHS patients.
Local Authority
Measure
Age group and Gender
Total Males Females
2-4 yrs 5-10 yrs
11-16 yrs
2-4 yrs 5-10 yrs
11-16 yrs
Lam
be
th
Numbers estimated to have mental disorder (2-4yrs Egger, 2011; rest ChiMat)
634 989 1109 622 492 882 4728
Actual numbers seen by CAMHS (SLAM data97)
22 175 242 9 75 276 799
% of estimated in treatment 3% 18% 22% 1% 15% 31% 17%
Sou
thw
ark
Numbers estimated to have mental disorder (2-4yrs Egger, 2011; rest ChiMat)
636 953 1119 637 458 906 4709
Actual numbers seen by CAMHS (SLAM data)
91 315 217 51 136 266 1076
% of estimated in treatment 14% 33% 19% 8% 30% 29% 23%
Benchmarking: As already stated Various international estimates suggest that c25% of children and young people with mental health needs are seen by a mental health professional (Waddell, Hua et al, 2007); in the UK estimates are higher at 30-40% (Green et al, 2005). In Lambeth only girls aged 11-16 years approach the UK level of use (31%) , whilst boys in the same age group approach is (22%). In Southwark the under fives (14% boys, and 8% girls) and males aged 11-16 (19%) are most under represented Conclusions: Lambeth
97 No demographic data was provided for children and young people seen in tier 4 therefore they have not been included in table 32 above. Adding tier 4 activity to Lambeth increases the total to 20% and Southwark to 25%.
Page 210

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 113
Table 45 shows that 2-4 year olds are particularly unrepresented , both in relation to expected need and in comparison to their peers in Southwark. (3% of the predicted number of boys and 1% of the predicted number of girls seen by Lambeth CAMHS vs 14% and 8% in Southwark)
Girls aged 5-10 are also under represented as CAMHS service users
Boys of all ages in Lambeth are also underrepresented compared to girls aged 11-16 years
Overall, fewer than 1 in 5 children estimated to have a mental health disorder have been seen in CAMHS.
Conclusions: Southwark
2-4 year olds of both genders are very under represented in CAMHS.
Boys aged 11-16 years from Southwark are also underrepresented compared to needs and compared to their peers in Lambeth (19% vs 22%)
Overall a higher proportion of children and young people with predicted mental health problems access mental health services than in Lambeth, however over 75% of children and young people estimated to have mental health disorders are not being seen by CAMHS services.
5.1.2 Ethnicity
Having looked at age and gender and identified groups who are under represented as service users, further analysis is being carried out by ethnic groups. Prevalence of mental disorders in children is not expected to vary by ethnic group (after controlling for underlying deprivation), so if the ethnic profile of service users is not representative of the general population it suggests that there are barriers which prevent particular groups from having their mental health disorder recognised, or which deter people from particular groups from using CAMHS services. The ethnicity of CAMHS service users has been compared to the ethnicity of local populations. Table 36 (Southwark) and Table 37 (Lambeth) categorise CAMHS users by age and ethnicity, then show the proportion of the local population in that age group. Finally, the last section compares the two to show which groups are over and under represented. For example 47% of CAMHS users are white compared to 42% of the Southwark population in the same age groups so dividing 47/42 = 1.1 or 110% of expected. This approach does not take gender into account, nor that older children are expected to have higher use of services One limitation is that SLAM ethnicity data is more detailed than ethnicity in population estimates, so many of the mixed and other groups (marked with *) from SLAM do not have a direct comparison in the population estimates, and so have been compared with other . This is not very accurate. None the less it appears that more children from these mixed groups are seen by CAMHS than might be expected given the population of Southwark. Conclusions – Southwark ethnicity of CAMHS users compared to Southwark population
Page 211
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 114
Children and young people from mixed / other backgrounds, black other and white seem to be over represented (265%, 160% and 110% of proportion in the population)
The largest group in Mixed / Other are from a mixed white / black caribbean background although as there are no population estimates for this group it is not clear if they are over represented.
Black other and “mixed /other” most over represented in the 15-19 year old population (211% and 548%). White children most over represented at ages 5-9 years.
Children and young people from Chinese, Bangladeshi, Indian and Pakistani ethnicities are under represented in service users compared to the underlying population.
Asian other and Black African ethnicities are also under represented (c50% of expected)
Black Caribbean (except 5-9 year olds) are also underrepresented but not the same extent (90% overall). However, this does fall to 58% in ages 15-19 years.
Conclusions – Lambeth ethnicity of CAMHS users compared to Lambeth population
Children and young people from Chinese ethic backgrounds are most under represented (only 10% of number expected based on population)
Children and young people from Asian other, Bangladeshi, Pakistani and Indian populations are very under represented (less than 50% of number expected)
Children and young people from Black African populations are similarly under represented, although less so at ages 15-19 where service users are about 76% of the number expected based on population.
White and Black Caribbean ethnic groups are similar overall (81% and 76% of expected respectively) but there is bigger drop at ages 15-19 years in people from Black Caribbean ethnic groups
Other and Black Other groups appear to be highly over represented but as discussed earlier, the over representation in other is partly due to different categories being used by population estimates and CAMHS.
The largest numbers of children and young people from mixed / other are of mixed white / black Caribbean ethnicity.
Page 212

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 115
Table 46 Southwark Targeted and Specialist Users by age group and ethnicity 2011-12 compared to Southwark population
Age group Ethnic Group 0 - 4 5 - 9 10 - 14 15 - 19 0-19
CA
MH
S d
ata
White 48% 46% 46% 49% 47%
Black Caribbean 4% 8% 7% 5% 6%
Black African 13% 13% 11% 8% 11%
Black Other 12% 16% 17% 16% 16%
Indian 1% 0% 0% 0% 0%
Pakistani 1% 0% 0% 0% 0%
Bangladeshi 1% 1% 1% 1% 1%
Chinese 1% 0% 0% 1% 0%
Other Asian 2% 1% 1% 1% 1%
Mixed Other* 1% 1% 1% 1% 1%
Not Stated* 5% 4% 4% 4% 4%
Other Ethnic Groups* 6% 5% 5% 9% 6%
White & Asian* 0% 0% 0% 0% 0%
White & Black African* 2% 1% 1% 1% 1%
White & Black Caribbean* 4% 4% 4% 6% 4%
Total CAMHS Users 100% 100% 100% 100% 100%
Sou
thw
ark
po
pu
lati
on
White 44% 39% 40% 46% 42%
Black Caribbean 6% 7% 9% 8% 7%
Black African 21% 25% 27% 23% 24%
Black Other 10% 11% 11% 7% 10%
Indian 2% 2% 1% 3% 2%
Pakistani 1% 1% 1% 1% 1%
Bangladeshi 3% 4% 3% 2% 3%
Chinese 2% 2% 2% 4% 2%
Other Asian 3% 3% 2% 2% 3%
Other* 8% 8% 5% 4% 6%
Totals 100% 100% 100% 100% 100%
Rat
io C
AM
HS:
po
pu
lati
on
White 1.10 1.18 1.16 1.05 1.1
Black Caribbean 0.77 1.14 0.82 0.58 0.9
Black African 0.61 0.51 0.39 0.33 0.5
Black Other 1.15 1.43 1.61 2.11 1.6
Indian 0.35 0.22 0.27 0.07 0.2
Pakistani 1.03 0.38 0.30 0.00 0.4
Bangladeshi 0.28 0.17 0.35 0.35 0.3
Chinese 0.35 0.15 0.14 0.15 0.2
Other Asian 0.68 0.38 0.52 0.69 0.5
Other* 2.18 1.95 3.25 5.48 2.65
Page 213

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 116
Table 47 Lambeth Targeted and Specialist Users 2011-12 by age group and ethnicity compared to Lambeth population
Age group
Ethnic Group 0 – 4 N=31
5 - 9 N=354
10 – 14 N=306
15 – 19 N=200
0-19 N=891
CA
MH
S d
ata
White British 16% 19% 21% 21% 20%
White Irish 0% 1% 2% 0% 1%
White Other 10% 13% 13% 9% 12%
Black Caribbean 6% 9% 10% 7% 9%
Black African 3% 8% 7% 10% 8%
Black Other 19% 22% 23% 26% 23%
Indian 3% 0% 1% 1% 1%
Pakistani 0% 1% 0% 1% 1%
Bangladeshi 0% 1% 1% 1% 1%
Chinese 0% 0% 0% 0% 0%
Other Asian 3% 1% 1% 2% 1%
Mixed Other* 0% 1% 2% 2% 1%
Not Stated* 19% 6% 8% 7% 7%
Other Ethnic Groups* 0% 6% 6% 6% 6%
White & Asian* 3% 1% 0% 1% 1%
White & Black African* 3% 1% 1% 2% 1%
White & Black Caribbean* 13% 8% 5% 7% 7%
Total CAMHS Users 100% 100% 100% 100% 100%
Lam
be
th
po
pu
lati
on
White (British, Irish, Other) 26% 33% 36% 29% 33%
Black Caribbean 6% 9% 10% 7% 9%
Black African 3% 8% 7% 10% 8%
Black Other 19% 22% 23% 26% 23%
Indian 3% 0% 1% 1% 1%
Pakistani 0% 1% 0% 1% 1%
Bangladeshi 0% 1% 1% 1% 1%
Chinese 0% 0% 0% 0% 0%
Other Asian 3% 1% 1% 2% 1%
Other* 39% 23% 21% 24% 23%
Rat
io
CA
MH
S:
po
pu
lati
on
White 0.57 0.88 0.98 0.70 0.81
Black Caribbean 0.75 0.84 0.70 0.47 0.76
Black African 0.19 0.41 0.31 0.48 0.41
Black Other 1.58 1.60 1.74 2.37 1.85
Indian 2.17 0.17 0.63 0.51 0.48
Pakistani 0.00 0.52 0.22 0.65 0.44
Bangladeshi 0.00 0.63 0.36 0.30 0.45
Page 214
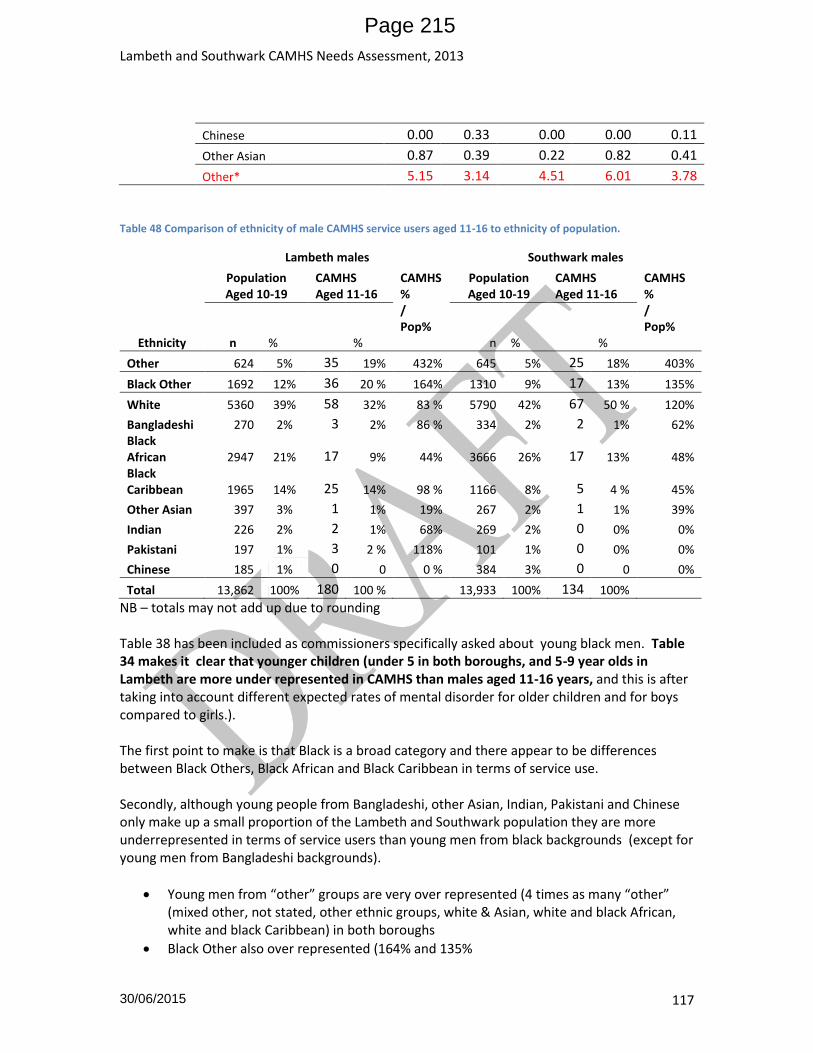
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 117
Chinese 0.00 0.33 0.00 0.00 0.11
Other Asian 0.87 0.39 0.22 0.82 0.41
Other* 5.15 3.14 4.51 6.01 3.78
Table 48 Comparison of ethnicity of male CAMHS service users aged 11-16 to ethnicity of population.
Ethnicity
Lambeth males Southwark males
Population Aged 10-19
CAMHS Aged 11-16
CAMHS% / Pop%
Population Aged 10-19
CAMHS Aged 11-16
CAMHS% / Pop% n %
% n %
%
Other 624 5% 35 19% 432% 645 5% 25 18% 403%
Black Other 1692 12% 36 20 % 164% 1310 9% 17 13% 135%
White 5360 39% 58 32% 83 % 5790 42% 67 50 % 120%
Bangladeshi 270 2% 3 2% 86 % 334 2% 2 1% 62% Black African 2947 21% 17 9% 44% 3666 26% 17 13% 48% Black Caribbean 1965 14% 25 14% 98 % 1166 8% 5 4 % 45%
Other Asian 397 3% 1 1% 19% 267 2% 1 1% 39%
Indian 226 2% 2 1% 68% 269 2% 0 0% 0%
Pakistani 197 1% 3 2 % 118% 101 1% 0 0% 0%
Chinese 185 1% 0 0 0 % 384 3% 0 0 0%
Total 13,862 100% 180 100 % 13,933 100% 134 100%
NB – totals may not add up due to rounding Table 38 has been included as commissioners specifically asked about young black men. Table 34 makes it clear that younger children (under 5 in both boroughs, and 5-9 year olds in Lambeth are more under represented in CAMHS than males aged 11-16 years, and this is after taking into account different expected rates of mental disorder for older children and for boys compared to girls.). The first point to make is that Black is a broad category and there appear to be differences between Black Others, Black African and Black Caribbean in terms of service use. Secondly, although young people from Bangladeshi, other Asian, Indian, Pakistani and Chinese only make up a small proportion of the Lambeth and Southwark population they are more underrepresented in terms of service users than young men from black backgrounds (except for young men from Bangladeshi backgrounds).
Young men from “other” groups are very over represented (4 times as many “other” (mixed other, not stated, other ethnic groups, white & Asian, white and black African, white and black Caribbean) in both boroughs
Black Other also over represented (164% and 135%
Page 215

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 118
Black Caribbean more or less as expected in Lambeth 98% but v under represented in Southwark 45%
Black African under represented in both (44% and 48%)
White under represented in Lambeth 83% but over in Southwark 120%
5.1.3 Young Offenders (YO) Southwark CAMHS are unable to report how many people of the young people they have seen are YO. Data from Southwark YOS on case load over time was provided. No information from Lambeth YOS has been received. Table 49 Number of YOS expected number with a need for mental health services compared to service use 2009-10 to 2011-12 Lambeth Southwark Year 2009-10 2010-11 2011-12 2009-10 2010-11 2011-12 No of Young Offenders* 454 421 No. with expected mental health needs (31%)
150 140
No. of YOS using CAMHS 80 88 83 n/r n/r n/r % of expected using CAMHS 55%
Source: Justice.gov.uk ; SLAM activity data *As measured by first time entrants to the Youth Justice System. This is likely to be lower than the numbers of young people in touch with YOS. However, applying an expected prevalence of mental disorder and comparing it to service use shows that 55% of young offenders predicted to have a mental health disorder have seen CAMHS. This is a higher proportion than in the general Lambeth population where only 17% of children predicted to have a mental health disorder have been seen.
5.1.4 Looked after children A higher proportion of looked after children (LAC) predicted to have a mental health need have been seen by CAMHS in Lambeth than non-looked after children 25% vs 17%. The same applies in Southwark – 33% vs 23%. NB – the figures below only include Carelink and CLAMHS so children seen elsewhere will not have been included.
Lambeth Southwark
2009-10 2010-11 2011-12 2009-10 2010-11 2011-12
No. of children in care
565 500 541 555 520 550
No. expected to have mental health needs (45%)
260 230 243 255 242 253
No. of children using CAMHS
81 83 60 58 71 83
Page 216

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 119
% of predicted MH needs using CAMHS services 31% 36% 25% 23% 29% 33%
5.1.5 Children with a learning disability The data extracted by SLAM did not contain a label to indicate whether children and young people seen had a learning disability. It is therefore not possible comment accurately on the numbers from this group who have been seen by CAMHS. As noted in section 4.1.7 activity in neurodevelopmental teams in both boroughs and the learning disability team in Southwark (there is no such team in Lambeth) has decreased. However, it seems unlikely that the needs of the 500 plus children with learning disabilities in each borough who are also predicted to have mental health disorders (Table 9) are being met. Recommendation: SLAM to include labels of learning disability
5.1.6 Parental factors CAMHS data does not include whether or not children / parents that they see have any of the risk factors (SM / DV / MH) discussed in this section and therefore it is not possible to comment on whether or not children from these groups are finding it possible to access services. However, it is possible that if SLAM included labels for children in need, then that would identify some children in this group. Obtaining information on children in need from the local authority would also provide more information Recommendation: More work needed to look at children in need
6 Discussion
6.1 Limitations
6.1.1 Stephens and Rafferty approach to needs assessment Lambeth Council seek to take an asset-based approach to needs assessment. This differes from the Stephen’s and Rafferty model by also taking into account protective factors and factors which promote mental wellbeing which can enhanced.
6.1.2 Literature review Time and capacity constraints mean that not all articles and papers found were read fully - for example NHS Evidence has 322 guidelines relating to child mental health which have been published in the last 3 years. Not all documents referenced in this needs assessment were read in full, and findings summarised in Government policy documents, NICE and Cochrane were often taken at face value without going back to the source articles This means that further work may be needed before commissioning a particular intervention in order to establish the true anticipated benefits. This is particularly true of interventions recommended by Allen as the original studies have not been appraised / set out in his work either.
Page 217

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 120
Even after restricting literature searches to systematic reviews, more articles on interventions and treatment were found than could be read and critically appraised in the time available. Therefore findings have often been summarised from the papers abstract and therefore have not been quality assured. All articles were from peer reviewed journals which should provide some element of assurance, however it is possible that abstracts are not a true reflection of the papers findings. By prioritising meta evidence sources it is hoped that none of the most effective and well evidenced sources have been omitted, but this work does not claim to be comprehensive.
6.1.3 Data Limitations in the data section of the needs assessment are due to knowledge gaps, data gaps, and data delays and time limited capacity for data analysis which means that the picture of local mental health needs are less complete and detailed than possible.
6.1.3.1 Modelling local prevalence of mental health disorders Previous local CAMHS needs assessments were able to adjust the estimates of mental health disorders in the local child and young person population to take account of factors known to increase the risk of mental disorders such as deprivation which are higher locally. This needs assessment has not been able to do so as the model98 used to adjust is no longer available. As both Lambeth and Southwark are deprived compared to England, applying the national prevalence rates to our populations are likely to result in an underestimation of need.
6.1.3.2 Knowledge and data gaps This needs assessment found the following gaps in data and information: 1. No information on local levels of risk factors e.g parental mental health, substance misuse,
domestic violence or learning difficulties
2. The amount of universal / Tier 1 activity carried out in schools, by GPs, social workers, in MAT, by charities and youth groups. For example although access to GP systems was obtained, very little information was available suggested that it is not recorded in data fields that can be extracted. This information would allow a fuller understanding of the whole system.
3. Mapping of all existing services showing referral pathways, referral criteria, interventions
offered and capacity. (Some of these parts exist but there is no whole, descriptions on SLMA
website not up to date)
4. Little information has been obtained on rejected referrals– this would provide more insight
into the reported gap between expressed and normative needs (where universal MH
services feel that a child or young person needs more specialised help, but they do not meet
thresholds) and help determine appropriate recommendations for future services.
5. No demographic or diagnostic information about inpatients or tier 4 day patients /
outpatients
98 Yar, M., Hennell, S., Clarke, P., Meltzer, H., Gatward, R. (2002) Model-based Small Area Estimation Series No. 1 Childhood Mental Disorder in England , London: Office for National Statistics
Page 218

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 121
6. Completion of diagnosis for tier 2 and 3 services was inconsistent which mean that fields
could not be matched to ICD-10 codes.
7. Diagnosis was not recorded for over 30% of episodes – while accepted that a diagnosis may
not be made on first appointment, and perhaps not 100% of children will receive an exact
diagnosis, if one is made later on in the treatment process it should be recorded in a way
that can be reported to commissioners.
8. CAMHS data does not routinely include information on outcomes (global data was obtained
during the needs assessment but should be routinely reported to commissioners)
9. No flags for LAC, YO , SEN or parental risk factors in targeted and specialist service activity 10. CAMHS in Southwark need to be able to identify which of their clients are Young Offenders 11. YOS services in both Lambeth and Southwark should be able to report the percentage of
their clients who also see CAMHS (data issue). This would enable equity of provision to be assessed.
12. Not obtained information on which interventions are offered by CAMHS services therefore have not compared current offer to best practice.
6.1.3.3 Data analysis still outstanding 1. Comparator boroughs from further afield
2. Staffing levels
3. Late received data on LAC and YOS still to be analysed
6.1.4 Stakeholders
6.1.4.1 Stakeholder interviews Not all stakeholders answered all questions due to time limitations. The interviews were not recorded so results reported are based on hand written notes.
6.1.4.2 CAMHS service users Due to time constraints the Steering Group agreed that no interviews would be set up with service users therefore there was no direct contact with service users – their perspective was captured via SLAM patient reports. Feedback is reported in long narrative reports which provides a qualitiative overview and exploration of issues and a detailed description of events during the year. There was little quantitative data to report e.g. percentage of those discharged from service who provided feedback.
6.2 Key Findings
6.2.1 Risk factors and vulnerable groups Literature review did not identify any new groups at higher risk of poor mental health than
the previous needs assessment
Page 219

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 122
o higher risk groups remain looked after children, young offenders, children with learning disabilities children of parents with poor mental health, substance misuse problems, domestic violence, learning difficulties; children experiencing trauma and violence.
Vulnerable times in children and young people’s lives are at transition from primary to secondary school, from CAMHS to AMS, and after bereavement
Stakeholders were concerned about disruptive home environments, eating disorders, self-harm, overly sexualised behaviour, gangs, autism and ASD, and the effects of cannabis
6.2.2 Children not accessing services (see 4.3.1.5 for stakeholder discussions) Stakeholders were concerned about children and Young people often not identified as having mental health problems: Young offenders ; Quietly distressed children and young people; C&YP with Aspergers ; Young carers In addition there are children and young people who are identified as at risk of, or having a mental disorder but don’t attend services: Adolescents, Young offenders, LAC , Children with parents with MH problems or involved with social services or other services; BME groups particularly recent immigrants Local service use data shows that SLAM CAMHS activity is lower than predicted across all age groups and amongst young offenders. Data does not currently exist to identify whether other vulnerable groups are using services proportionately. DNA data was reported globally for a service, so it was not possible to identify whether particular demographic groups are more likely to miss appointments or not engage with services. More detailed reporting of DNA would allow this question to be investigated
6.2.3 Diagnosis Diagnostic data from SLAM was not conclusive for 36-47% of cases and therefore changes in
patient mix were hard to detect
The only top 10 diagnosis which has increased is “depressive episode” increasing from 4% of caseload in 2009-10 to 8% in Southwark and 9% in Lambeth by 2011-12.
6.2.4 Care pathways and provision There is very limited information easily available on tier 1 activity and no detailed mapping
of all mental health and wellbeing services within the borough o Lambeth have produced a booklet of council commissioned services o Southwark have a CAMHS dashboard which shows all services, o Tables 41 and 42 in this needs assessment have taken this information and
attempted to develop a mapping template but it doesn’t currently give a complete picture of all capacity and care pathways within the borough
Referral pathways not clear – e.g. are GPs bypassing central referral panel and referring directly to tier 4 (referral source not provided in SLAM data).
General consensus from stakeholders that SLAM CAMHS services good, but some stakeholder felt there was not enough SLAM CAMHS expertise available
Page 220

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 123
o Desire for SLAM CAMHS to provide more consultancy services o Desire for SLAM CAMHS to provide more training for staff
Some stakeholders felt that not enough CAMHS provision or that referral criteria too high o Support for parents who are sub-current thresholds for targeted / specialist services
but who aren’t managing with the support of universal services
Feedback to referrers not always timely (schools view)
Stakeholders felt that there is a need to o Have more counseling based services for children and families o (S) Forensic service or sex offender programme, o Need more services for sexually exploited girls o Group work from CAMHS for some needs (not specified which needs) o consider extending services to 25 years (young adult service)
6.2.5 Ways of working Many stakeholders expressed the view that true multiagency working is needed to ensure
that children and young people with and at risk of mental health disorders, and at risk of poor wellbeing are best reached
Multiagency working would mean functional teams made up people from different agencies able to deliver services in a flexible way e.g. community outreach workers, social workers and mental health professionals working together in the location best suited for the purpose.
6.2.6 Activity compared to need There is under provision of services at tier 2 and 3 but particularly tier 2, and depending on
estimates used, under provision at tier 4 too.
Not able to comment about provision at tier 1
6.2.6.1 Lambeth: activity compared to need On average 17% of the number of children and young people predicted to benefit from tier
2,3 or 4 services in Lambeth have used CAMHS in 2011-12 (see Equity 5.1).
25% of looked after children predicted to need mental health services were seen by CLAMHS in 2011-12
The proportion of young offenders who have seen CAMHS in 2011-12 is equivalent to 55% of first time offenders predicted to need mental health services (not the same as the YOS workload)
6.2.6.2 Lambeth: age, gender, ethnicity Proportion of predicted need accessing services varies from 1% of girls aged 2-4 to 31% of
girls aged 15-17 years.
At younger ages a higher proportion of boys predicted to need services are accessing services than girls (2-14)
“Black other” and “other ethnicities” seem to be most over represented in service users
Chinese and all Asian groups are most under represented
Page 221
Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 124
6.2.6.3 Southwark: activity compared to need On average 23% of the number of children and young people predicted to benefit from tier
2,3 or 4 services in Lambeth have used CAMHS in 2011-12 (see Equity 5.1).
33% of looked after children predicted to need mental health services were seen by CLAMHS in 2011-12
The proportion of young offenders from Southwark who have seen CAMHS cannot be reported
6.2.6.4 Southwark: age, gender, ethnicity Proportion of predicted need accessing services varies from 8% of girls aged 2-4 to 33% of
boys aged 5-10 years.
At younger ages (2-14 years) a higher proportion of boys predicted to need services are accessing services than are girls, but service attendance drops for boys aged 11-16
“Black other” and “other ethnicities” seem to be most over represented in service users
White ethnic groups are slightly over represented
Chinese and all Asian groups are most under represented
6.2.7 Barriers to service use In addition to the reasons listed by stakeholders and covered again in 6.2.2 other considerations include people not knowing how to use NHS services, and language barriers.
6.2.8 Acute activity Review of SUS data from Kings and GSTT as well as SLAM identified large increase in
inpatients with primary diagnosis F00-F99) in age 15-19 years (2 – 3 x total of 0-14 years inclusive) and in 20-24 year olds (1.5-2.5 x total of 15-19 years) main diagnoses – alcohol and schizophrenia
Males higher admissions than females after age 14.
No diagnosis / demographic data attached to SLAM provided tier 4 activity
6.2.9 Outcomes from tier 2-4 services Very limited information is available on outcomes – average change in CGAS score reported
for each year and each borough.
6.3 Contrasting views raised by stakeholders During the stakeholder interviews different views were heard, some of which contrasted with each other. This section contains a brief summary of some of the opposing views and also of concerns which were raised Looked After Children (LAC)
– need same thresholds as other children (too low now) OR – expectations of LAC low, so normalise behaviour that not acceptable in non-LAC and
children with needs are not accessing services Comments:
Page 222

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 125
SDQ scores for 2011-12 for looked after children suggest that Lambeth and Southwark looked after children are not doing well and need more support (4.2.7.4) CGAS scores from CAMHS not reported by service line, so not possible to comment no outcomes for LAC who are seeing CAMHS (4.2.7.2). Literature clearly shows that LAC have more mental health disorders than non LAC (4.1.3.1), and proportion of LAC expected to have mental health needs seen by CAMHS is Disordered eating
• Dietician or CAMHS? Comments: depends on the degree of disorder. Not looked at access routes to dieticians or local dietetics services. Dieticians should be competent to assess whether or not a patient’s eating disorder is beyond their capabilities to address / requires more specialist input. Service delivery
– Tension between flexibility and efficiency – clinic vs community, outreach work. However, outreach work with e.g. street involved children might not be delivered by a mental health specialist, but a community development worker who builds trust, then a more trained mental health professional becomes involved.
– Tension between professional support and development through being in specialist setting and sharing of professional knowledge through having specialists working in more general services
– Do services need to be delivered outside of clinical settings? Comments: As DNA data not available linked to profile of children and young people can’t analysis who has DNA’d or hypothesise what setting would be more appropriate. School commissioning
– Is it being delivered by appropriately qualified persons? Effective / Efficient? – Are services meeting needs? Is there a postcode lottery? – Are interventions appropriate?
Comments: see school section 6.4.1.5 Role of charities
– What are charities doing and is it always appropriate? E.g. mentioned Kids Company “bribing” children with gifts to attend sessions
Conduct disorder – Some stakeholders felt that doesn’t require input from a mental health professional
Comments: However conduct disorder is amenable to require parenting interventions (pre age 11 to be effective) and even if accept that outside remit of specialist mental health, is within remit of wider mental health and fits with early intervention agenda - conduct disorder can result in personality disorder and need for mental health services (and increased criminality and impacts on wider society). Services still need to be in place. Children under 5
– Some stakeholders felt that under 5s don’t have mental health disorders that require mental health professional input.
Page 223

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 126
Comments: Literature suggests (Egger and Emde) that some children do have recognizable mental health disorders pre age 5. Lack of emotional, social and behavioral wellbeing at an early age is risk factor for mental health disorder in later childhood – these children do need some input from outside – who is responsible for delivering? Again – if problems not addressed early likely to need more
6.4 Areas commissioners requested information on
6.4.1.1 Young black men Commissioners [in Southwark] were particularly interested in whether or not young black men were less likely to be seen in CAMHS than other groups. Table 34 makes it clear that it is younger children (under 5 in both boroughs, and 5-9 year olds in Lambeth) who are under represented in CAMHS; i.e. only 1% and 8% of the predicted number of girls with mental health needs aged under 5, and 3% and 14% of boys in that age group in Lambeth and Southwark respectively have been seen by CAMHS. In comparison 22% and 19% of the predicted number of boys aged 11-16 have been seen. Analysis of service use of boys aged 11-16 by ethnicity (Table 37) revealed differences by ethnic group, but just using “black” as a category is too broad.
Black African backgrounds appear to be underrepresented in CAMHS in both boroughs making up 21% and 26% of Lambeth and Southwark population respectively but only making up 9% and 13% of young people seen
Black Caribbean young men in Southwark appear to underrepresented (not in Lambeth)
Black other young men in both boroughs appear to be over represented
Mixed group (which included white /black African and white /black Caribbean) needs comparison against more detailed population estimates but is also heavily over represented.
Young white men in Lambeth seem to be under represented.
Asian young men are also under represented. The young offender population in both boroughs has a disproportionate number of young men from black ethnic groups (69% of young offenders in Lambeth are black compared to 48% of the 10-17 year old population; and in Southwark the figures are 53% of young offenders in Southwark compared to 44% of the population). Young offenders are more likely to have mental health needs than the general population, and so It must be remembered that in terms of service use, younger children are more under represented in both boroughs than young men, and in terms of evidence-based practice, more likely to respond to interventions. Recommendations:
Diversionary activity in the community and at the police station and ensuring appropriate adult service has mh awareness.
Working to ensure that all young offenders who have mental health needs are identified and referred to appropriate services would be one way of ensuring increased representation of this group.
Page 224

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 127
6.4.1.2 Multidisciplinary approaches for troubled families Approached Southwark troubled families team, but not managed to get any data on local families. Recommendation: further work needed – if recommendation to do detailed mapping of mental health service by non mental health professionals / activity in tier 1 services is taken up, do during mapping exercise.
6.4.1.3 Tier 3 and 4 Eating disorder activity Analysis of service activity from SLAM does not demonstrate an increase in the number of children and young people with eating disorders between 2009-10 and 2010-11. Reliance on data is limited due to the large number with no diagnosis coded, and therefore it is possible that more children have eating disorders than initially identified. However, anorexia is unlikely to need multiple appointments to diagnose, and it thought that recognition would be reasonably high. Bulimia might be harder to diagnosis if the child or young person does not wish to disclose purging activity (and are maintaining a normal weight).
6.4.1.4 Dual comorbidities e.g. brain injury As discussed in the limitations section diagnosis and coding require some data cleaning before analysis of the patient cohort can be carried out. Very few children have been seen in the neurodevelopmental service in Southwark. Recommendation: More work is needed in this area.
6.4.1.5 Services commissioned by schools Since the advent of the pupil premium, local authorities no longer receive any central government funding to commission CAMHS services for schools. Schools can spend their pupil premium in the way they best feel meets their school’s needs. There is no central database of services commissioned by schools in Lambeth and Southwark, and there has not been capacity to contact all schools to find out what services they commission and the level of need that they are meeting. During the course of stakeholder interviews which included 2 primary and 1 secondary school in Lambeth and 2 secondary schools in Southwark it became apparent that schools commission a variety of services – e.g. counsellors or play therapists. The interviews with schools did not directly explore quality assurance of the services bought by schools or investigate whether there are appropriate procedures in place around child protection and disclosure, however other stakeholders have expressed concern about this issues. Schools also mentioned that they found it hard to get referrals to CAMHS accepted and often didn’t receive any feedback on progression of referrals and that it would be useful to have a better understanding of services which CAMHS provide, when they can help, what the different roles of mental health professionals are, and where schools can help for pupils who don’t meet
Page 225

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 128
the criteria for CAMHS but whom the school need more support with. Schools also mentioned that having a consultation service with CAMHS mental health professionals was very helpful. Recommendations
Local Authority – children’s services and public health to build links with schools via e.g. headmaster’s forum or other school group to explore providing support to help schools quality assure / use evidence based interventions that are appropriate to children; consider developing spoke and hub model of joint commissioning between schools e.g. for consultation services
One product from liaison with schools via headmasters forum could be a mapping of services provided by schools (i.e. type of intervention/service, target group, provider and methodology, capacity, outcomes, pathways to other services / protocols for child protection /how ensuring that intervention is appropriate)
Provision of information to schools about CAMHS by SLAM
6.4.1.6 Looked after children Commissioners are responsible for looked after children who are placed out of borough as well as those who are looked after within the home borough. Information on the number of looked after children who are placed out of borough was only received in the last week of February and it has not been possible to investigate provision of mental health services to out of borough children. The wellbeing of Looked after children (SDQ scores) for both Lambeth and Southwark show that very few (quantify) looked after children scored in the normal range in 2011-12, with roughly half in the borderline category and the other half categorised as being of concern. This data, along with the comparison of service use by LAC compared to the estimated number of LAC children with mental health disorders suggests that more looked after children would benefit from services from CAMHS. Recommendation:
6.4.1.7 Young offenders The literature review and stakeholder interviews identified the same groups of children as being at higher risk of poor mental health: Looked after children, young offenders, children with a learning disability, and children of parents with mental health problems, substance misuse problems and domestic violence problems and children who have experienced trauma. In addition the following two groups were identified by stakeholders as being vulnerable: Children of parents with learning difficulties (particularly undiagnosed), and families with no recourse to public funds. However locally available data to evaluate whether or not these groups are accessing services is limited. Families with no recourse to public funds may be trying to live without coming into touch with services.
Page 226

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 129
Recommendation: SLAM activity data from targeted and specialist services to include fields to indicate whether a child or young person falls into any of the following categories: Looked After Children, Young Offender, SEN, Child Protection Plan, Parents with MH, SEN, SM or DV issues.
7 Draft Conclusions and Recommendations
7.1 Strategic
Nationally mental health problems cause significant health, social and economic issues. The local picture is no different. The continuing economic uncertainty and recession are likely to increase mental health needs at a times when commissioning budgets and resources are decreasing. As 50% of lifetime mental health disorders (excluding dementia) start by the age of 14 and 75% by the age of 24 and mental health promotion, prevention and early interventions are estimated to be able to prevent 25-50% of lifetime disorder, it is important to maximise mental health promotion and preventative activity as well as treatment. An agreed and considered strategy is required (to cover say, 3 years) and be comprehensive in its scope to integrate the many effective actions across all the determinants of well being, the many partners and the life course. The recommendations below could form the basis of a strategy:
7.1.1 Service provision Principles of progressive universalism (i.e. services delivered according to need) and early
intervention should be followed. Younger children (under 5’s) are currently most under represented in both boroughs, and 5-9 year olds are also under represented in Lambeth.
Mapping of capacity of universal mental health services and preventative interventions needs to be carried out to give a fuller understanding of local picture and clearer idea of where gaps are (e.g. parenting interventions, conduct disorders )
Consider extending the upper age limit of CAMHS to 25 years, or developing adolescence and young person’s service from 14 – 25 years to maximise opportunities for prevention and early intervention with aim of reducing lifetime burden of mental health (and emergency admissions for 20-24 year olds) .
The balance between treatment of established disorders and early intervention before a problem becomes established needs to be shifted over time in favour of early intervention
Capacity of perinatal mental health services for women who don’t meet the threshold for psychiatric help need developing – maybe not enough capacity to meet NICE guidelines
Southwark has a dedicated fast access service for with parents with MH issues – it is very well received by stakeholders. Lambeth might want to consider commissioning.
Page 227

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 130
Lambeth has a dedicated YOS CAMHS service – Southwark might want to consider ways of auditing access to CAMHS for YOS, if not to have a dedicated service
Two Southwark stakeholders mentioned having to commission psychological assessments separately from normal services from CAMHS – perhaps this could be incorporated into normal service if economies of scale available.
Consider more parenting classes at nursery and primary level as evidence suggests effective pre-age 12 and stakeholders felt needed to combat conduct and behavioural disorders.
7.1.2 Training and workforce development Review the formally commissioned / provided training for non-mental health professionals
working in the wider services with an influence on children’s and young persons mental health to ensure adequate training opportunities – particularly in Southwark
Roles of school nurses, health visitors and midwives could be developed : o School nurses to have greater role in mental health e.g. act as liaison between
school, family and SLAM . o Health visitors and midwifes to have role in early identification of mental health
difficulties in mothers and children
7.1.3 Quality of services / care (information, monitoring and performance management)
Improve targeting / identification of children at risk by o ensuring that information about children is part of all initial assessment processes
e.g. substance misuse and adult mental health (already in Lambeth parenting strategy), and actions required to protect children are implemented.
o Ensure YOS regularly review/ audit number of YO identified via ASSET forms o Working with young carers carers groups
Mapping of activity in the wider mental health workforce/ primary mental health care e.g. GPs, social work, early intervention teams, young offenders, looked after children carried out by non-SLAM staff should be carried out
Services provided by these recorded in a way that prevention, promotion and early intervention activity can be understood.
An audit programme should be agreed on a regular basis with providers to include: o Outcomes of treatment – CGAS only partially completed o Rejected referrals – numbers and reasons why o User feedback
Regular audit of tier 4 referrals that do not go via triage panel /CAF process to ensure that appropriate.
User feedback could be further developed / quantitative
Page 228

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 131
Data gaps identified in the limitations section (5.1.2.2) need to be addressed
Lambeth to consider encouraging all schools to take part in SHEU and Southwark to consider having schools take part in order to monitor some aspects of wellbeing of children and young people
7.1.4 Health promotion Health promotion work by mental wellbeing teams
o to include child and adolescent mental wellbeing o tackle stigma associated with mental health o promote wellbeing and life skills not mental illness
Provide schools with information about mental health services available, who they are suitable for, and who they are not suitable for, and alternative sources of advice
Provide quality assurance guidelines for schools to help support evidence based commissioning and ensuring that children get appropriate help.
7.1.5 Equalities and community engagement The CAMHS Steering Group could discuss use of PREview with children’s services to jointly
target early years resources where they would be most effective
Increase identification of children and young people with MH problems who go undetected:
o Young Offenders - include CAMHS worker in case worker fortnightly discussions to ensure that young people with MH needs are identified as soon as possible. Ensure repeat ASSET assessments done.;
o Consider MH First Aid training for people working with adolescents to widen awareness of quietly distressed young people
o Identify ways of working with Young carers e.g. Southwark has a young carers group
Mental health promotion to engage with community groups for immigrants / refugees to build trust and remove stigma associated with mental health problems and provide support.
7.1.6 Joint Commissioning between boroughs During the course of the needs assessment some stakeholders expressed an interest in knowing where there might be synergies between Lambeth and Southwark in terms of shared / joint commissioning of future CAMHS services. In thinking about this question it seems that work which falls into the following categories would be suitable: d) Areas which are new work for both boroughs e) Areas which require highly specialised clinicians, but numbers of children / young people
from each borough are small f) Areas which one borough has developed particular services than the other more than the
other Without being aware of details of current commissioning the following areas for joint work are suggested as possibly being suitable according to the criteria listed above.
A common approach to building relationships with GPs particularly as national policy is to move more mental health care into primary care and links with secondary and tertiary mental health care e.g CQUINs etc
Support for schools and youth services mental health commissioning e.g.
Page 229

Lambeth and Southwark CAMHS Needs Assessment, 2013
30/06/2015 132
o through provision of guidance on how to commission quality assured, evidence-based services
o Development of schools commissioning hubs
Commissioning of training for wider / non-specialist mental health workforce
Gangs – violence, trauma, drug use, [criminality?] Outreach work?
Specialised services with small numbers of children / young people o Early / overly sexualised behaviour - link with teenage pregnancy teams? o Eating disorders – not clear from data that needs increasing o Self harm o Neurodevelopment
Southwark has a dedicated fast access service for with parents with MH issues – if Lambeth considering setting up might wish to learn from Southwark experience
Southwark does more work with under 5s and in children’s centres.
Lambeth has a dedicated YOS CAMHS service
8 Author(s), key contacts and links for further information
Authors
Vicki Spencer-Hughes, Speciality Registrar in Public Health
Key contacts Abdu Mohiddin, Consultant in Public Health [email protected]
Page 230

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 133
9 References
Adult Psychiatric Morbidity in England, 2007 – Results of a household survey https://catalogue.ic.nhs.uk/publications/mental-health/surveys/adul-psyc-morb-res-hou-sur-eng-2007/adul-psyc-morb-res-hou-sur-eng-2007-rep.pdf Allen G (2011b) Early Intervention; Smart Investment, Massive Savings. HM Government. London.
Allen G (2011a) Early intervention: The next steps.. London: HM Government. http://www.dwp.gov.uk/docs/early-intervention-next-steps.pdf Cochrane Systematic Reviews(2009) Alternatives to inpatient mental health care for children Author not reported Early-onset major depressive disorder more prevalent in children of parents who have BD. Psychiatric Annals, July 2011, vol./is. 41/7(356), 0048-5713 Baird G, Simonoff E, Pickles A et al (2006) Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP) Lancet 368 (9531) 210-5 Baron Cohen S, Scott FJ, Allison C et al (2009) Prevalence of autism spectrum conditional: UK school based population study. The British Journal of Psychiatry 194 (6) 500-9 Beecham J, Baingana F, Bonin E et al, (2010) School based universal violence prevention programmes. PSSRU, London School of Economics and Political Science. Unpublished paper cited by Campion and Fitch, 2011. Bradshaw J, Richardson D (2009) An index of child wellbeing in Europe. Child Indicators Research 2 (3): 319-351. Campion J, Bhui K, Bhugra D (2012) European Psychiatric Association (EPA) guidance on prevention of mental disorders European Psychiatry 27 68–80 Cheng, F, Kirkbride, J. B, Lennox, B. R, Perez, J, Masson, K, Lawrence, K, Hill, K, Feeley, L, Painter, M, Murray, G. K, Gallagher, O, Bullmore, E. T, Jones, P. B (2011) Administrative incidence of psychosis assessed in an early intervention service in England: First epidemiological evidence from a diverse, rural and urban setting. Psychological Medicine, 41/5(949-958) Colins O, Vermeiren R, Vreugdenhil C, van den Brink W, Doreleijers T, Broekaert E (2010) Psychiatric disorders in detained male adolescents: A systematic literature review. The Canadian Journal of Psychiatry / La Revue canadienne de psychiatrie, 55/4(255-263) Cox GR, Callahan P, Churchill R, Hunot V, Merry SN, Parker AG, Hetrick SE (2012) . Psychological therapies versus antidepressant medication, alone and in combination for depression in children
Page 231

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 134
and adolescents. Cochrane Database of Systematic Reviews Issue 11. Art. No.: CD008324. DOI: 10.1002/14651858.CD008324.pub2.
Davis S, Review of School Nursing Services in Lambeth and Southwark (2013) Lambeth and Southwark Public Health Department (unpublished to date - insert link to document when available) Daykin N.; Orme J.; Evans D.; Salmon D.; Mceachran M.; Brain S. (2008) The impact of participation in performing arts on adolescent health and behaviour: A systematic review of the literature Journal of Health Psychology 13/2(251-264), Department of Education (2011) Me and My School: Findings from the National Evaluation of Targeted Mental Health in Schools 2008-2011. DE, London Department of Health (2011) Mental Health promotion and mental illness prevention: the economic case Department of Health (2011) NHS Outcomes Framework 2012-2013. Department of Health Department of Health (2012) Healthy Lives, Healthy People: Improving Lives and Supporting Transparency. Department of Health
Department of Health. Getting it right for children, young people and families. 28th February 2012
DH (2010) Keeping Children and Young People in Mind – Full Government Response to the CAMHS Review. Department of Health, London.
Dretzke J.; Davenport C.; Frew E.; Barlow J.; Stewart-Brown S.; Bayliss S.; Taylor R.S.; Sandercock J.; Hyde C (2009). The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomised controlled trials Child and Adolescent Psychiatry and Mental Health, 3/, 1753-2000
Siegenthaler, E; Munder, T, Egger M (2012) Effect of preventive interventions in mentally ill parents on the mental health of the offspring: Systematic review and meta-analysis Journal of the American Academy of Child & Adolescent Psychiatry, 51/1(8-17) Couturier J.; Kimber M.; Szatmari P (2013). Efficacy of family-based treatment for adolescents with eating disorders: A systematic review and meta-analysis International Journal of Eating Disorders,. 46/1(3-11),
Egger HL, Emde RN (2011) Common Emotional and behavioural disorders in preschool children: presentation, nosology and epidemiology J Child Psychology and Psychiatry, 47¸(3-4), 313-37 Eisen SV, Ranganathan G, Seal P, Spiro A. Measuring clinically meaningful change following mental health treatment. Journal of Behavioural Health Services and Research 2007;34(3):272-290.
Page 232

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 135
Eldevik S.; Hastings R.P.; Hughes J.C.; Jahr E.; Eikeseth S.; Cross S (2009) Meta-analysis of Early Intensive Behavioral Intervention for children with autism Journal of clinical child and adolescent psychology 38/3(439-450)
Emerson E, Hatton C (2007) Mental Health of Children and Adolescents with intellectual disabilities in Britain British Journal of Pyschiatry 191 493-9
Field F (2010) The foundation years: preventing poor children becoming poor adults. The report of the independent review on poverty and life chances. London: HM Government
Ford T, Goodman R and Meltzer H (2003) The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Psy, 42, 1203-1211 Green H, McGinnity A, Meltzer H et al (2005) Mental Health of Children and Young People in Great Britain, 2004. London: Office of National Statistics Harrington R, Bailey S, et al (2005) Mental Health Needs and Effectiveness of Provision for Young Offenders in Custody and in the Community. © Youth Justice Board for England and Wales 2005 Hawton, K., Harriss, L., Hall, S., et al. (2003a) Deliberate self-harm in Oxford, 1990–2000: a time of change in patient characteristics. Psychological Medicine 33, 987–995. Hawton, K., Rodham, K., Evans, E., et al. (2002) Deliberate self-harm in adolescents: self report survey in schools in England. British Medical Journal, 325, 1207–1211 Health Advisory Service (1995) Together we stand; the commissioning role and management of child and Adolescent mental health services. HM Government (2011) No Health without Mental Health: A Cross Government Mental Health Outcomes Strategy for people of all ages. HM Government. http://publications.nice.org.uk/self-harm-longer-term-management-cg133 http://www.chimat.org.uk/preview/evidence Strength of Association between maternal factors and outcomes at age 5. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_118530 Idring, S, Rai, D, Dal, et al (2012) Autism spectrum disorders in the Stockholm Youth Cohort: Design, prevalence and validity PLoS ONE, vol./is. 7/7, 1932-6203 Institute of Medicine (2009), Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. National Academy of Sciences. USA http://tinyurl.com/25kwppp
Page 233

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 136
Jadad A, Booker, Gauld M et al ( 1999) The treatment of attention-deficit/hyperactivity disorder. An annotated bibliography and critical appraisal of published systematic reviews and metaanalyses. Can J Psychiatry, 44, 1025-1035 Joint Commissioning panel for mental health (2012) Guidance for commissioning public mental health services. www.jcpmh.info Karoly LA, Kilburn RA, Cannon JS (2005) Early Childhood interventions: proven results, future promises . RAND corporation (cited by Campion and Fitch, 2011)
Keen D, Hadijikoumi I (2008) ADHD in children and adolescents. Clinical Evidence (online), downloaded 30 November 2012 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907929/
Kessler RC, Amminger GP, Aguilar-Goxiola S et al (2007). Age of onset of mental disorders: a review of recent literature. Current Opinion in Psychiatry 20 (4) : 359-364. (Cited by Campion and Fitch, 2012)
1Kessler RC, Berglund P, Demler O et al (2005) Lifetime prevalence and age of onset distributions of of DSM-IV disorders in the national comorbidity (Cited by Campion and Fitch, 2012)
Kim-Cohen J, Caspi A, Moffit TE et al (2003) Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective longitudinal cohort. Archives of General Psychiatry 62: 709-717 (cited by Campion and Fitch, 2012)
Kurtz Z (1996) Treating Children well a guide to using the evidence base in commissioning and managing services for the mental health of children and young people. Looked After Children and Young People (2010) NICE Public Health Guidance 28 Lynch RG (2004) Exceptional Returns. Economic, Fiscal and Social Benefits of Investment in Early Childhood Development. Washington. Economic Policy Institute. (cited by Campion and Fitch, 2011)
Melzer H, Corbin T, Gatward R et al, (2003) The Mental Health of young people looked after by local authorities in England. London: Office for National Statistics Melzer H, Gatward R, Corbin T et al (2003) Persistence, onset, risk factors and outcomes of childhood mental disorders. London: The Stationary office Merry SN, Hetrick SE, Cox GR, Brudevold-Iversen T, Bir JJ, McDowell H. Psychological and educational interventions for preventing depression in children and adolescents. Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD003380. DOI: 10.1002/14651858.CD003380.pub3. Morgan, C, Fisher, H, Hutchinson, G, Kirkbride, J, Craig, T. K, Morgan, K, Dazzan, P, Boydell, J, Doody, G. A, Jones, P. B, Murray, R. M, Leff, J, Fearon, P (2009) Ethnicity, social disadvantage and psychotic-like experiences in a healthy population based sample. Acta Psychiatrica Scandinavica 119/3(226-235),
Page 234

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 137
National Institute for Health and Clinical Excellence. Social and emotional wellbeing: early years. October 2012
National Institute for Health and Clinical Excellence. Social and emotional wellbeing: early years. October 2012 NICE Public Health Guidance 12 – Promoting Children’s social and emotional wellbeing in secondary education
NICE Public Health Guidance 12 – Promoting Children’s social and emotional wellbeing in secondary education
NICE Public Health Guidance 20 - Social and Emotional Wellbeing in secondary education (2009), National Institute for Clinical Excellence, London.
O'Kearney RT, Anstey K, von Sanden C, Hunt A. Behavioural and cognitive behavioural therapy for obsessive compulsive disorder in children and adolescents. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD004856. DOI: 10.1002/14651858.CD004856.pub2 Owens, D., Horrocks, J., & House, A. (2002). Fatal and non fatal repetition of self-harm. British Journal of Psychiatry, 181, 193–199. Patterson SY, Smith V, Miranda P. (2012) A systematic review of training programs for parents
of children with autism spectrum disorders: single subject contributions. Autism. 16(5):498-522. Petrie S (2005) Southwark Child and Adolescent Mental Health Needs Assessment Roberts RE , Roberts CR (2007) Ethnicity and risk of psychiatric disorder among adolescents. Research in Human Development. 4/1-2(89-117), Sabates R, Dex S (2012) Multiple risk factors in young children's development [online] Centre for Longitudinal Studies, UoL , Schweinhart LJ, Montie J, Xiang Z et al (2005) The High /Scope. Perry Preschool study through age 40. Summary, conclusions and frequently asked quations. Ypsilanti, High/Scope Research Foundation; 2005 (cited by Campion and Fitch, 2011) Scott J, Martin G, Bor W, Sawyer, M, Clark, J, McGrath, J (2009) he prevalence and correlates of hallucinations in Australian adolescents: Results from a national survey Schizophrenia Research 107/2-3(179-185) Sempik J EP22 - LAC 12.2b The mental health of looked after Children in the UK: Summary (http://www.nice.org.uk/nicemedia/live/11879/47446/47446.pdf accessed 13/2/13 Shucksmith, J., Summerbell, C., Jones, S., and Whittaker, V. (2007) Mental wellbeing of children in primary education (targeted/indicated activities). London: National Institute of Clinical Excellence
Page 235

Lambeth and Southwark CAMHS Needs Assessment, 2013
<LOGO>
30/06/2015 138
Stephen Scott, Thomas O'Connor and Annabel Futh, What makes parenting programmes work in disadvantaged areas? The PALS trial. Joseph Rowntree Foundation, 2006
Tickell C (2011) The early years: foundations for life, health and learning. An independent review on the early years foundation stage. London: Department for Education
Waddell C, Hua JM, Garland, OM, Peters RD, McEwan K (2007). Preventing mental disorders in children: A systematic review to inform policy-making. Canadian Journal of Public Health, 98, 3
Waldfogel J, Washbrook F (2008) Early years policy. London: Sutton Trust
Warren Z; McPheeters ML; Sathe N; Foss-Feig JH; Glasser A; Veenstra-Vanderweele J (2011) A systematic review of early intensive intervention for autism spectrum disorders. Pediatrics, 127/5(e1303-11)
World Health Organisation (2008). Global burden of disease report. WHO.
Yar, M., Hennell, S., Clarke, P., Meltzer, H., Gatward, R. (2002) Model-based Small Area Estimation Series No. 1 Childhood Mental Disorder in England , London: Office for National Statistics
Young Minds(2004) Mental Health in Infancy
Zinzow HM, Ruggiero KJ, Resnick H, Smith D, Saunders B, Kilpatrick D, (2009) Prevalence and mental health correlates of witnessed parental and community violence in a national sample of adolescents Journal of Child Psychology and Psychiatry 50/4(441-450)
Page 236

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 139
Appendix 1 Literature reviews
Questions raised by the needs assessment 1) What is the prevalence of mental health disorders in children and young people? 2) What are the risk factors for poor mental health and well being? 3) What works to prevent or treat mental disorders in children and young people and what
service models have been shown to be effective? 4) Is there any evidence that the prevalence of autism and autistic spectrum disorders is
increasing?
Review 1: Prevalence of mental ill health in 0-18 year olds
Starting point: ChiMat modelling: Prevalence by age group Limitations of ChiMat model:
uses national estimates for prevalence of mental disorders by age group and applies to the
local population structure i.e. doesn’t take account of differences in the distribution of risk
factors between national averages and Southwark / Lambeth levels.
ChiMat modelling based on 2004 Mental Health survey (but narrative on website updated
October 2012 suggests that this is the most recent available data)
2004 Mental Health survey only covers children aged 5-16 and Steering Group are also
interested in 0-5 and 17-18 year olds.
Question: Are there any studies post 2004 survey including the prevalence of mental ill health in 0-18 year olds? In particular prevalence in 0-5 year olds and 17-18 year olds. Limitations of literature search- don’t have access to many of the journals – have to rely on information in abstract. Risk factors for mental health disorders The literature review did not identify many risk factors for mental health disorders which had not been already been identified by previous needs assessments. One risk factor previously not identified was that Males were found to be at higher risk of ADHD (1)
Page 237
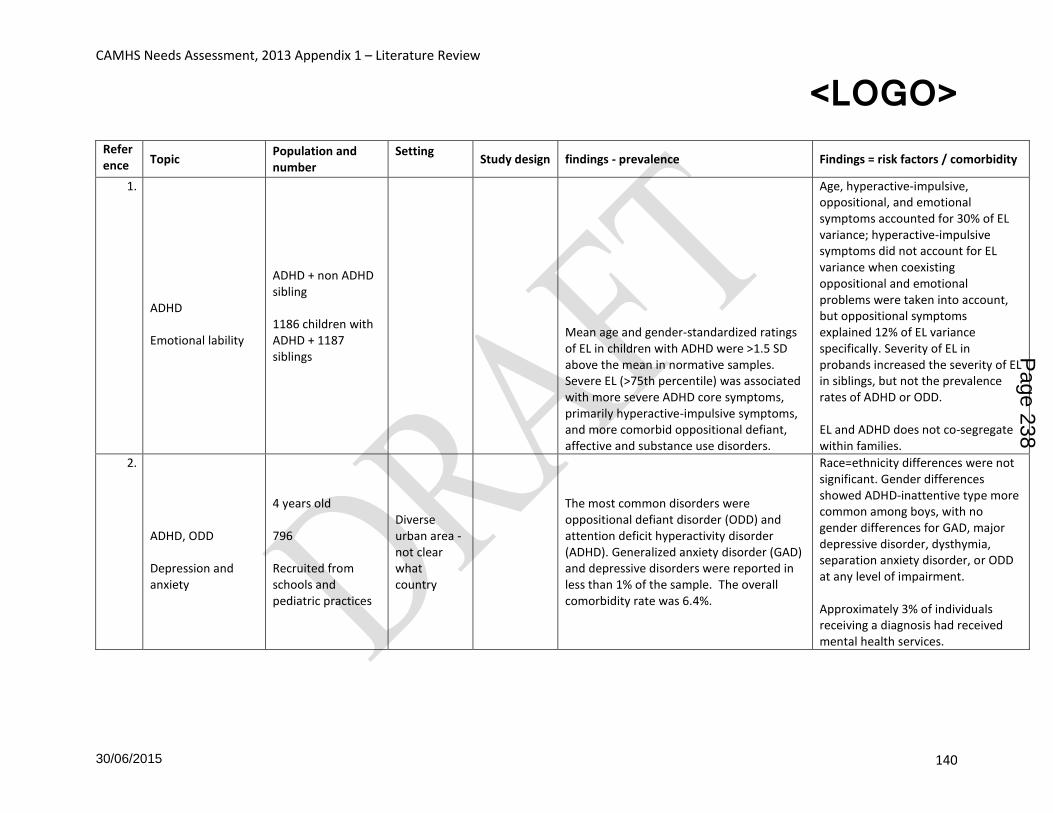
CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 140
Reference Topic
Population and number
Setting
Study design findings - prevalence Findings = risk factors / comorbidity
1.
ADHD Emotional lability
ADHD + non ADHD sibling 1186 children with ADHD + 1187 siblings
Mean age and gender-standardized ratings of EL in children with ADHD were >1.5 SD above the mean in normative samples. Severe EL (>75th percentile) was associated with more severe ADHD core symptoms, primarily hyperactive-impulsive symptoms, and more comorbid oppositional defiant, affective and substance use disorders.
Age, hyperactive-impulsive, oppositional, and emotional symptoms accounted for 30% of EL variance; hyperactive-impulsive symptoms did not account for EL variance when coexisting oppositional and emotional problems were taken into account, but oppositional symptoms explained 12% of EL variance specifically. Severity of EL in probands increased the severity of EL in siblings, but not the prevalence rates of ADHD or ODD. EL and ADHD does not co-segregate within families.
2.
ADHD, ODD Depression and anxiety
4 years old 796 Recruited from schools and pediatric practices
Diverse urban area - not clear what country
The most common disorders were oppositional defiant disorder (ODD) and attention deficit hyperactivity disorder (ADHD). Generalized anxiety disorder (GAD) and depressive disorders were reported in less than 1% of the sample. The overall comorbidity rate was 6.4%.
Race=ethnicity differences were not significant. Gender differences showed ADHD-inattentive type more common among boys, with no gender differences for GAD, major depressive disorder, dysthymia, separation anxiety disorder, or ODD at any level of impairment. Approximately 3% of individuals receiving a diagnosis had received mental health services.
Page 238

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 141
Anxiety Mood Disorders
students in grades 7-12 3,311
Ontario, Canada
Secondary analysis of GHQ12 from student drug use and health survey
The prevalence of AMD in Ontario students in grades 7-12 may be 19%.
self-reported history of family disruption, substance use, gambling problems, bullying victimization, and who reported seeking professional help for a mental health problem were significantly more likely to experience probable AMD
3. ASD Learning Disability
0-17 years 589,117
Stockholm, Sweden 2001-2007
The 2007 year prevalence of ASD in all children and young people was 11.5 per 1,000 (95% confidence interval 11.2-11.8), with a co-morbid intellectual disability recorded in 42.6% (41.0-44.2) of cases.
4.
Learning Disability 7 to 12 year olds N= 55,266
South Korea
Cross sectional observational Sample from two groups low risk =general population and high risk = disability register and schools for special needs)
The prevalence of ASDs was estimated to be 2.64% (95% CI=1.91-3.37), with 1.89% (95% CI=1.43-2.36) in the general-population sample and 0.75% (95% CI=0.58-0.93) in the high-probability group. ASD characteristics differed between the two groups:
the male-to-female ratios were 2.5:1 and 5.1:1 in the general population sample and high-probability group, respectively, and the ratios of autistic disorders to other ASD subtypes were 1:2.6 and 2.6:1, respectively; 12% in the general-population sample had superior IQs, vs 7% in the high-probability group; and 16% in the general-population sample had intellectual disability, vs with 59% in the high-probability group
5.
ASD Toddlers N= 2027
prevalence study
Need copy to get findings
Page 239

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 142
6. 6
ASD 2 year olds N=5,007
Gothenburg, Sweden
prevalence study base d on screening at health centres
boys: autism 0.86%, atypical autism 0.39% all ASD 1.25%. girls: autism 0.16%, a typical autism 0.16% all ASD 0.33%
Male gender
7. 7
ASD children W. Australia and Denmark
Secondary analysis - comparison of prevalence statistics
Overall ASD prevalence rates were higher in Denmark (68.5 per 10,000 children) compared with Western Australia (51.0 per 10,000 children). Diagnosis of childhood autism was more prevalent in Western Australia (39.3 per 10,000 children) compared with Denmark (21.8 per 10,000 children).
8. 8
ASD school age Holland
cross sectional
The prevalence estimates of ASD in Eindhoven was 229 per 10,000, significantly higher than in Haarlem (84 per 10,000) and Utrecht (57 per 10,000), whilst the prevalence for the control conditions were similar in all regions.
9. 9 ASD OCD
paediatric patients with OCD n=109
ASD traits are prevalent in OCD and seem to be intricately associated with the co-morbidities as well as the OCD syndrome itself.
10. 10 Autism Behavioural and emotional problems
Children with high functioning autistic spectrum disorder, mean age 10 N=71
72% -86% of children with high-functioning ASD had at least one behavioural or emotional problem of clinical concern. Social problems (60.6%), thought problems (50.7%), attention problems (49.3%), and withdrawn/depressed (40.8%). Using the DSM-oriented scales, the most commonly reported problems were attention deficit/hyperactivity problems (35.2%),
Page 240

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 143
anxiety problems (33.8%) and affective problems (31%).
11
Autism Birth defects
3- 10 years All children born in Atlanta who survived to age 3 years
Atlanta Retrospective cohort study
Birth defects were found among 6% of children with autism (total n=617; 488 males, 129 females)
Birth defects associated with a near twofold increased risk for autism overall. With any type of birth defect, the risk for autism + intellectual disability or other developmental disabilities was typically higher than the risk for autism alone.
12
Autism Economic cost
UK
Data on prevalence, level of intellectual disability and place of residence were combined with average annual costs of services and support, together with the opportunity costs of lost productivity.
The costs of supporting children with ASDs were estimated to be 2.7 billion each year. The lifetime cost, after discounting, for someone with ASD and intellectual disability is estimated at approximately 1.23 million, and for ASD without intellectual disability is approximately 0.80 million.
Page 241

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 144
13 Personality disorder Mental disorder
adolescents
specialist pyschotherapy clinic, Netherlands
cross sectional
40.5% of the adolescents were diagnosed with at least one personality disorder. 78.9% of adolescents with a PD also suffered from one or more Axis I disorders.
Note this is set in specialist clinic therefore not applicable to general population
14
Bipolar disorder 15-24 years N= 5,673
Canada
Extract from Canadian Community Health Survey
The weighted lifetime prevalence of BD was 3.0% among 15-24-year-olds (N =191): 2.1% among 15-18-year-olds, and 3.8% among 19-24-year-olds. Limitations: The questionnaire used in CCHS 1.2 relied on self-report, limiting its applicability to this younger sample.
Rates of psychiatric comorbidity were high, with anxiety disorders, problematic substance use, and suicidality present among nearly half of the sample. Mental health services were accessed in the previous 12 months by 56.1% of youth with BD.
15
Bulimia nervosa
Finnish twin birth cohort 1975-79 N=2881
Finland
cross sectional - two stage screening interview DSM-IV criteria
The lifetime prevalence of bulimia nervosa was 2.3%; 76% of the women suffered from its purging subtype and 24% from the non-purging subtype. The 5-year clinical recovery rate was 55.0%.
Peak age of incidence is 16-20 years
16
depression
4th - 8th grade children N=1482
Three schools in Fatih, Istanbul, Turkey
Cross sectional observational
The prevalence rate was 4.2% for some form of depressive disorder, 1.55% for major depressive disorder, 1.75% for dysthymic disorder, 0.26% for double depression, and 0.60% for depressive disorder-not otherwise specified.
Increasing age, having a working mother and low maternal education were all positively associated with CDI score. Low SES, perception of paternal health and relations with father as negatively, low popularity and behavior subscales of the Piers-Harris self-concept scale, and high trait anxiety were associated with the presence of a depressive disorder.
Page 242

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 145
17
Depression Parental MH
not reported n = not reported
not reported not reported
Children born to parents with BD were three times more likely to have early onset of major depressive episode when compared with children of unaffected probands, after adjusting for demographic variables, non-mood disorders, and within family correlations.
18
Depression
aged 12-18 years n= not reported in abstract
Adolescents in MH service
Observational for 3 months
Depressive disorders were the most common clinician diagnosis reported (22%). There was no statistically significant difference in treatment for depressed compared to non-depressed adolescents.
Treatment appeared to be the same in type for depressed compared to non-depressed adolescents case managed within CAMHS
19
Depression substance misuse
child welfare 11-15 n=1179
US welfare
cross-sectional survey (National Survey on Child and Adolescent Well-Being )
Depression 17% in girls vs 7%boys p < 0.05). No gender differences in the prevalence of past month substance use. Differences in depression and substance use severity were found between groups.
Female gender risk for depression Frequent Substance Use risk for more severe depression in boys only
20
Depression and anxiety anorexia nervosa
not in abstract n = not reported in abstract
not in abstract
Literature review?
Comorbid depression and anxiety disorders are common in children and adolescents with AN. Depression tends to start after AN and abates with weight restoration, anxiety tends to pre-date eating disorder onset and to persist post recovery.
There is currently insufficient evidence, particularly with children and adolescents, to conclude that comorbid depression and anxiety necessarily disrupt engagement in treatment for anoxrexia or foreshadow a poorer prognosis
Page 243

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 146
21
Eating Disorders adolescents and adults
US population
2 cross-sectional surveys
Lifetime prevalence of EDNOS (ED not otherwise specified) was 4.78% in adolescents and 4.64% in adults. The majority of adolescents and adults with an eating disorder presented with EDNOS. 75% of participants with EDNOS met criteria for comorbid disorders, while 25% endorsed suicidality.
22
Eating Disorders
<13 years N=208
Paediatric clinics in UK
Surveillance using existing and new systems
Overall incidence was 3.01/100 000 (208 individuals). In total, 37% met criteria for anorexia nervosa; 1.4% for bulimia nervosa; and 43% for eating disorder not otherwise specified. Nineteen per cent showed determined food avoidance and underweight without weight/shape concerns. 50% were admitted to hospital, typically soon after diagnosis.
Rates of comorbidity were 41%; family history of psychiatric disorder 44%; and early feeding difficulties 21%. Time to presentation was >8 months. Outcome data were available for 76% of individuals. At 1 year, 73% were reported improved, 6% worse and 10% unchanged (11% unknown). Childhood eating disorders represent a significant clinical burden to paediatric and mental health services. Efforts to improve early detection are needed.
23
Eating disorders Mood and anxiety disorders
Teenage girls 15 years N= 833
The prevalence of subclinical anorexia nervosa (restricting subtype) was 3.5%, 13.3% for weight concerns (restricting subtype), 3.8% for subclinical bulimia nervosa, and 10.8% for subclinical binge eating disorder.
Girls with subclinical anorexia nervosa had a higher prevalence of separation anxiety diagnosis, significantly more major depressive and generalized anxiety symptoms vs girls reporting no eating disorders. Girls with subclinical bulimia nervosa or binge eating disorder had a higher prevalence of mood disorders (major depression and dysthymia) and
Page 244

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 147
significantly more anxiety symptoms (separation anxiety and generalized anxiety) compared with girls reporting no eating disorders.
24
Eating Disorders
high school students n=1140 male, 1256 female
Transylvania (Romania and Hungarian students)
The prevalence of anorexia nervosa (AN) and subclinical AN were higher in the Romanian female samples than the Hungarian female samples 0.6% vs 0% and 1.9% vs 0.4% respectively. The prevalence of bulimia nervosa (BN) was also higher in Romanian girls 1.3% vs 1% The prevalence of subclinical BN was 0.8% in the Hungarian female sample and 0.7% in the Romanian female sample.
Th25e internalization of Western values and beauty ideals?
25
Eating Disorders Body image dissatisfaction
9-10 year old girls N=581
not in abstract
Cross-sectional - two surveys
11% of the sample scored in the Anorexic range at age 9 and about 7% at age 10. When examining body image, 35% of the sample at age 9 and 38% at age 10 selected Ideal Figures that were smaller than their Real Figures on the BIM.
Minority group had higher eating disturbance scores on average at ages 9 and 10 when compared to the White group. SES did not account for eating disturbance or body image dissatisfaction. Eating disturbance and body image dissatisfaction do not occur primarily in White females from middle and upper SES populations
Page 245

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 148
26
Eating Disorders adolescent girls n=496
community longitudinal (8 years)
Lifetime prevalence by age 20 years was 0.6% and 0.6% for threshold and subthreshold anorexia nervosa (AN), 1.6% and 6.1% for threshold and subthreshold bulimia nervosa (BN), 1.0% and 4.6% for threshold and subthreshold binge-eating disorder (BED), and 4.4% for purging disorder (PD). Overall, 12% of adolescents experienced some form of eating disorder. One-year recovery rates ranged from 91% to 96%. Relapse rates were 41% for BN, 33% for BED, and 5% for PD.
Peak age of onset was 17-18 years for BN and BED and 18-20 years for PD. Average episode duration in months was 3.9 for BN and BED and 5.1 for PD. Subthreshold BN and BED and threshold PD were associated with elevated treatment, impairment, and distress. For BN and BED, subthreshold cases often progressed to threshold cases and diagnostic crossover was most likely for these disorders. Results suggest that subthreshold eating disorders are more prevalent than threshold eating disorders and are associated with marked impairment.
27
Eating Disorders 13-17 years N=711
Belgium / Flanders
Questionnaire about whether have visited proanorexia websites
12.6% of the girls and 5.9% of the boys had visited such websites.
In girls, visiting pro-anorexia websites was associated with a higher drive for thinness, worse perception of appearance and more perfectionism. The prevalence of visiting pro-anorexia sites is non-trivial and the significant correlations between viewership of pro-ana sites and predictors of AN suggest a potential for negative impact of exposure to pro-ana sites.
Page 246

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 149
28
Eating Disorders Adolescents N=595
Finland 2 step over 3 years
The lifetime prevalence rates for females age 18 were 2.6% for anorexia nervosa (AN), 0.4 for bulimia nervosa (BN), 7.7% for AN-NOS, 1.3% for BN-NOS and 8.5% for subclinical eating disorders. The incidence rate of any eating disorder in females age 15-18 was 1641 per 100 000 person-years.
Female vs male (no prevalent cases of DSM-IV eating disorder was found in male participants
29
Eating Disorders
mean age 11.37 n=1336 then 258 at 2 year follow up
Survey at T1 and interview at T2
The estimated prevalence of any ED according to DICA-C (T1) and DICA-A was 3.44% and 3.81%, respectively. The most frequent diagnoses were syndromes that were not full-blown. Biannual incidence of any ED was 2.02%. Amongst those with an ED, 52.17% persisted.
Females showed a higher incidence and persistence of any ED than males. Participants who had the highest BMI were those who had a persistent diagnosis of ED
30
Eating Disorders
Normal students aged 12-21 N=1545
Madrid region, Spain
not clear from abstract
ED prevalence was 3.43%. Prevalence estimations were as follows: 5.34% for females: 2.72% for eating disorders not otherwise specified (EDNOS), 2.29% for bulimia nervosa (BN), and 0.33% for anorexia nervosa (AN); and 0.64% for males: 0.48% for EDNOS, 0.16% for BN, and 0.00% for AN.
Some demographic factors that were shown to be associated with ED included the following: sex, age, single child, single-parent families, and father or mother's death.
31
Major depression
Preschool (3- 6 years) N=1427
Spain Two stage screening
Stage I: 15.6% preschool children were found to be probable depressives, because they scored 27 or more, the cut-off used. At stage II, 1.12% met the MDD criteria.
The prevalence by areas was urban 0.87%, rural 0.88%, suburban 1.43%. Sex distribution prevalence was 1:1.
32 Major Mental disorders Looked after children
13-17 years Looked after children N= 183
Bouches du Rhone, South of France
cross sectional
Of the youths qualified, 48.6% as having at least one psychiatric disorder during the last six months (Anxiety Disorder: 28.4%; Conduct Disorder: 15.3%; Major Depression: 14.8%; Psychosis Screen: 18.6%; ADHD: 3.8%), and Suicide Attempts have been reported in 23% of them.
Females were more affected than boys (p < 0.001) with 64.9% having at least one disorder compared to 36.8% of boys; AD: 49.3% vs. 13.2%; and MD: 27.3% vs. 5.6%.
Page 247

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 150
33
Mental health witnessed parental and community violence
Adolescents N=3614
US General population
Household survey of sample of population
National prevalence of witnessed parental violence and witnessed community violence was estimated to be 9% and 38%, respectively.
Both forms of witnessed violence predicted PTSD and Major Depressive Episode beyond variance accounted for by age, gender, race/ethnicity, income, and other traumatic event history. Perceptions of threat, repeated violence exposure, location of the violence, and relationship to the victim were associated with psychiatric diagnoses.
34
MHD Children in care
0-5 years N=58 (43 included) Children in care
Inner City Cross sectional
>1 MHD 60.5% and >1 developmental disorder was found in 11 (25.6%). 30 /43 (69.8%) preschoolers fulfilled criteria for at least one diagnosis, and 18 (41.9%) had two or more comorbid conditions. Whereas 36 (83.7%) of the preschoolers needed an intervention, only 3 of these had received adequate input.
Preschool CIC constitute a high-risk group for mental health and developmental disorders. Without age-appropriate assessments, their needs go undetected, and opportunities for early intervention are being missed
35
MHD
12-18 presenting to primary care clinics N= 1076
urban cities, midwest USA
Cross sectional observational
Approx 14% screening positive for a MH problem,
poor grades, poor self-rated health, drug/alcohol use, and sexual activity.
36
MHD
All member states of EU27 plus Switzerland, Norway and Iceland
Sytematic Reviews of literature and surveys
Best estimates based on a number of studies - population aged 14 years+ : Major depression = 6.9%; Anxiety disorders -14% (panic disorder 1.8%; Agoraphobia 2%; social phobia 2.3%; generalised anxiety disorder 1.7-3.4%; specific phobias 6.4%; PTSD 1.1-2.9%) Aged 14-17 years - Anorexia 0.54% and Bulimia nervosa 0.86%. Age 6-17: hyperkinetic / ADHD = 5%; Age 2-17 pervasive developmental
Except for substance use disorders and mental retardation, there were no substantial cultural or country variations.
Page 248

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 151
disorders 0.6%; 5-17 conduct disorders 3%
37
MHD pre-term birth
10-25 year olds N= 1098 (any diagnosis); 1297 (anxiety and depression)
- Meta analysis
Pre term birth is a risk factor for MHD: any diagnosis : odds ratio (OR) 3.66, 95% confidence interval (CI) 2.57-5.21 ; anxiety or depressive disorder : OR 2.86, 95% CI 1.73-4.73
38
MHD 13-17 years N= 10, 148
USA school and community
any DSM-IV disorder
prevalence estimates 40.3% at 12 months (79.5% of lifetime cases) and 23.4% at 30 days (57.9% of 12-month cases). Anxiety disorders are the most common class of disorders, followed by behaviour, mood, and substance disorders. The 30-day to 12-month prevalence ratios are generally lower than the 12-month to lifetime ratios, suggesting that disorder persistence is due more to episode recurrence than to chronicity.
Sociodemographic correlates are largely consistent with previous studies. Persistence is higher for adolescents than among adults and appears to be due more to recurrence than chronicity of child adolescent onset disorders
39
MHD Young Offenders
12-17 years Young Offenders N=2694 Native Dutch, 1393 Ethnic Minority
Dutch with mental health evaluation requested by court pretrial
The prevalence of mental disorders was similar for both groups (76.8% versus 74.4%). Criminal responsibility in native Dutch youth was more often considered 'diminished' or 'strongly diminished' than in ethnic minority youth.
It remains unclear whether these differences reflect a false stereotype of ethnic minority populations as being more dangerous and threatening.
Page 249

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 152
40
MHD Young Offenders
12-19 years (mean age 16.0; SD +/- 1.5) Young Offenders N=100 (92 boys, 8 girls)
Sweden - commited to juvenile institutions between 2004 and 2007
Consecutive admissions to detention
73% at least 1 mental disorder: 48% met DSM-IV diagnostic criteria for AD/HD, 17% for an autism spectrum disorder, and 10% for a mental retardation. The collapsed prevalence for psychiatric disorders requiring specialist attention was 63%.
Indicators of stress and the role of adverse family context predicted incidence of every disorder examined. The presence of multiple risk factors, cumulative burden, substantially increased risk of first incidence of all disorders examined. Personal resources such as mastery consistently enhanced resilience to onset of first episodes.
41
MHD 11-17 years 4175
general population
probability sample followed up at 1 year
Incidence rates were 2.8% for anxiety, 1.5% for mood, 1.2% for ADHD, 2.5% for disruptive, 2.9% for substance buse/dependence, and 7.5% for one or more DSM-IV disorders.
42
MHD Young Offenders
15 studies, Young offenders N = 3401
Systematic literature review
The mean prevalence of any disorder was 69.9% (95% CI 69.5% to 70.3%); with conduct disorder occurring most frequently (46.4%, 95% CI 45.6% to 47.3%), followed by substance use disorder (45.1%, 95% CI 44.6% to 45.5%), oppositional defiant disorder (19.8%, 95% CI 19.2% to 20.3%), and attention-deficit hyperactivity disorder (13.5%, 95% CI 13.2% to 13.9%). Any anxiety disorder 15.9% (95% CI 15.6% to 16.1%), major depression in 12.0% (95% CI 11.7% to 12.2%), and posttraumatic stress disorder in 9.6% (95% CI 9.2% to 10.0%). Three studies reported on psychotic disorders, finding low rates (1.35%, 95% CI 1.32% to 1.39%).
Estimates of prevalence were only marginally different when impairment was not required, while consistency between adolescents and parents was poor. Findings on the relations between race or ethnicity were too scarce and inconsistent to interpret.
43
MHD 13-18 year olds 10123
General population, Continental USA
Survey
Anxiety disorders were the most common condition (31.9%), followed by behaviour disorders (19.1%), mood disorders (14.3%), and substance use disorders (11.4%), with
The median age of onset for disorder classes was earliest for anxiety (6 years), followed by 11 years for behavior, 13 years for mood, and 15
Page 250

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 153
approximately 40% of participants with one class of disorder also meeting criteria for another class of lifetime disorder. The overall prevalence of disorders with severe impairment and/or distress was 22.2% (11.2% with mood disorders, 8.3% with anxiety disorders, and 9.6% behavior disorders).
years for substance use disorders.
44
MHD 5- 7 year olds N= 6090
Copenhagen
Cohort study (from birth) Copenhagen Child Cohort 2000
Of 5,898 eligible children, 3,501 participated in the SDQ assessment (59%). The overall estimated 6-month prevalence of mental health problems was 4.8% (95% CI 4.1-5.6). Conduct problems were found in 3.0% (95% CI 2.4-3.6), problems of hyperactivity/inattention in 0.7% (95% CI 0.4-1.0) and emotional problems in 1.5% (95% CI 1.1-1.9).
Boys showed a higher risk of having mental health problems as compared to girls: risk ratio 2.0 (95% CI 1.5-2.8). Several markers of socioeconomic disadvantages were associated with mental health problems at 5-7 years of age.
45
MHD
8-15 years nationally representative non-institutionalized US civilians aged N=3042
USA cross-sectional surveys
Twelve-month prevalence rates of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition-defined disorders in this sample were 8.6% for attention-deficit/hyperactivity disorder, 3.7% for mood disorders, 2.1% for conduct disorder, 0.7% for panic disorder or generalized anxiety disorder, and 0.1% for eating disorders.
Boys 2.1 x ADHD compared to girls; Girls 2x mood disorders. No gender differences in anxiety or conduct disorders.c50% with one of the disorders assessed had sought treatment with a mental health professional.
46
MHD Deafness
Deaf and hearing (6-18 years) n= 66 parents, 38 children
Australia survey / cross sectional
The overall prevalence rate of mental health problems is comparable to that of the Australian hearing population. Parents of deaf children reported significantly more concerns on the social problem and thought problem scales than parents of hearing children and adolescents.
Page 251

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 154
47
MHD violence
HIV-positive youth (13-24) N= 174
Inner City Consecutive admissions to clinic
Physical assault/abuse (24% in childhood; 19% as adolescents), sexual abuse/assault (28% in childhood; 15% as adolescents), dating violence (i.e., physical abuse by sexual partner) (18%), and family violence (44%). Females had higher sexual abuse (p < .001). Psychological disorders included: major depressive disorders (15%), generalized anxiety disorder (17%); posttraumatic stress disorder (28%); alcohol abuse disorder (19%); and substance abuse disorder (31%).
Physically abused youth had higher symptoms of anxiety (p < 0.05, and PTSD (p < 0.01). Sexually abused youth had higher symptoms of PTSD (p < 0.05). Youth with family violence had higher symptoms of Anxiety Disorder (p < 0.05) and PTSD (p < 0.01). .
48
MHD Young Offenders
juvenile delinquents detained for 9months n=790 (18% female)
not in abstract - no access to journal
survey / cross sectional
Even when conduct disorder and oppositional defiant disorder were excluded, 88% of males and 92% of females had a psychiatric disorder (including substance use disorder); more than 80% of offenders met criteria for some type of substance use disorder. Despite nine months of incarceration, young offenders continued to show high levels of psychiatric and substance use disorders.
Gender differences were found foranxiety disorders (males 26%, females 55%, p < .01), marijuana dependence (males 32%, females 24%, p = .04), marijuana abuse (males 19%, females 11%, p = .04), and stimulant dependence (males 25%, females 44%, p < .01).
49 MHD Self-harm
self-cutting community dwelling adolescents n=44 + 44 controls
cross-sectional surveys
Major depressive disorder (63% vs. 5%), anxiety disorders (37% vs. 12%), and eating disorders (15% vs. 0%) were more common among self-cutting girls (n = 41) than among controls. None of the self-cutting boys (n = 3) had a DSM-IV-TR Axis I mental disorder.
Page 252

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 155
50
MHD Racism
5th grade students N=5147
3 US metropolitan areas
Cross sectional
15% of children reported perceived racial/ethnic discrimination, with 80% reporting that discrimination occurred at school. A greater percentage of Black (20%), Hispanic (15%), and other (16%) children reported perceived racial/ethnic discrimination compared with White (7%) children.
Children who reported perceived racial/ethnic discrimination were more likely to have: depression, ADHD, oppositional defiant disorder, and conduct disorder. An association between perceived racial/ethnic discrimination and depressive symptoms was found for Black, Hispanic, and other children but not for White children.
51
MHD Adolescents N=3418
Italy
cross sectional - questionnaire and interview
The prevalence of CBCL caseness and DSM-IV disorders was 9.8% (CI 8.8-10.8%) and 8.2% (CI 4.2-12.3%), respectively. DSM-IV Emotional disorders were more frequently observed (6.5% CI 2.2-10.8%) than externalizing disorders (1.2% CI 0.2-2.3%).
In girls, prevalence estimates increased significantly with age; furthermore, living with a single parent, low level of maternal education, and low family income were associated with a higher likelihood of suffering from emotional or behavioral problems.
52
MHD
school population 6-11 n=1028
Florence, Italy
Survey
10.5% received a psychiatric diagnosis, with a higher prevalence in males (66.7% vs.33.3, p<0.01). The most prevalent groups of mental disorders were the behavioural/impulse control (7.2%) and anxiety (6.4%) disorders. ADHD 5.6%. Other mental disorders relatively rare, with only separation anxiety and overanxious disorder exceeding 1% prevalence.
Male gender, organic disease, having mother divorced, not present or dead, attending school full-time, cohabitation in the family were associated with an increased risk for any childhood mental disorder.
53
MHD 11-17 years N=4175
USA
cross sectional - questionnaire and interview
Based on crude prevalences, European American (EA) youths were at lower risk of anxiety disorders. African American (AA) youths were at lower risk of substance-use disorders and comorbid disorders.
After controlling for social status, stressors, personal and social resources, and ethnicity resulted in only 2 significant differences for 18 pairwise ethnic contrasts--EA were at greater risk than AA for substance-use and comorbid disorders.
Page 253

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 156
Based on these results, there appeared to be few differences between majority and minority adolescents in risk of psychiatric disorders
54
MHD 7-17 years N=2863 families
Germany
cross-sectional surveys (BELLA study)
Overall, 14.5% fulfilled criteria for at least one specific mental health problem associated with impairment, or had an overall mental health problem indicated by an abnormal SDQ score and present impairment. However, high comorbidity was found in the children concerned. Symptoms of overall mental health problems were present in 8.6% of the children and 6.6% of the adolescents, reduced to prevalence rates of 6.3 and 4.9% when additional impairment was taken as a criterion. Irrespective of the type of disorder,
<50% of children affected were reported as receiving treatment. However, for those suffering from mental health problems, large impairments in Health Related Quality of life were observed.
55
MHD Impairment
7-17 years N=2863 families
Germany
cross-sectional surveys (BELLA study)
14.1% of the boys and 9.9% of the girls were classed as severely impaired by parental reports. However, self-reported data shows a reversed gender-difference as well as lower levels of severe impairment (6.1% in boys; 10.0% in girls). 6% had pronounced impairment due to mental health problems but were not detected by screening for overall symptoms.
Male gender (based on parental reports) female gender based on self report
Page 254

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 157
56
MHD
8-10 year olds attending schools in 2002-3 N=9430
Bergen, Norway
Two stage screening
The weighted prevalence for any DSM-IV psychiatric disorder was 7.0% (95% confidence interval 5.6%-8.5%).
Disorders were associated with age, gender, learning difficulties, family type, and poverty. 75% of children with ADHD had used specialist mental health services, vs 13% of those with emotional disorders.
57
Pervasive developmental disorder
kindergarten to grade 11 n=23,635
English schools Montreal
PDD prevalence of 79.1/10,000(95% CI 67.8 to 90.4/10,000). The prevalence was 25.4 for autistic disorder, 43.6 PDD not otherwise specified, 9.7 Asperger syndrome, and 0.4 childhood disintegrative disorder. During the study period, there was a significant linear increase in prevalence (OR 1.17 per year; 95% CI 1.12 to 1.23).
Male gender
58
psychiatric disorders Injury
10 - 19 years N=20507
Enrolees in Group Health Co-operative Health Plan
population-based prospective cohort study
Traumatic injury increases risk of receiving a diagnosis of anxiety or acute stress (odds ratio [OR] = 1.21, 95% confidence interval [CI] = 1.02-1.44), depression (OR = 1.30, CI = 1.10-1.53), and a substance use disorder (OR = 1.56, CI = 1.21-2.00) and of receiving a psychotropic medication prescription (OR = 1.37, CI = 1.20-1.57).
59
Psychiatric disorders Young Offenders
Juveniles Young Offenders N= 11603
Texas Juvenile Correctional System
prevalence between 1 Jan 2004 and 31 Dec 2008
98% were diagnosed with at least one of the disorders. Highest estimated prevalence was for conduct disorder (83.2%), followed by any substance use disorder (75.6%), any bipolar disorder (19.4%), attention-deficit/hyperactivity disorder (18.3%), and any depressive disorder (12.6%).
The estimated prevalence of psychiatric disorders among these youths was exceptionally high and showed patterns by sex, race/ethnicity, and age that were both consistent and inconsistent with other juvenile justice samples
Page 255

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 158
60
Psychosis
Not clear from abstract N= 398
Rural - East Anglia, early intervention services
Summarise if right age group
61
Psychosis
general adolescent population + adolescents first admitted for early onset psychosis + adolescents with non-psychotic psychiatric disorders
n=(GPS; N = 96) (EOP; N = 87) (NP; N = 137).
cross sectional screening
The prevalence of at least any one 'basic symptom' was 30.2% in GPS compared to 81% in NP and 96.5% in EOP. Correct classification of EOP when compared to GPS was high (94.0%) and lower when compared to NP (78.6%). Cognitive symptoms discriminated best between EOP and NP. C
The usage of 'at least one basic symptom' as a screening criterion for youth at risk of developing a psychotic disorder is not recommended in the general population or in unselected psychiatrically ill adolescents.
62
Psychosis
general population black and white (ages not in abstract, no access to journal) n= 372
UK
19% reported one or more psychotic like experience (n = 72 /372).
These were more common in Black Caribbean (OR 2.08) and Black African subjects (OR 4.59), compared with White British. In addition, a number of indicators of childhood and adult disadvantage were associated with psychotic-like experiences. When these variables were simultaneously entered into a regression model, Black African ethnicity, concentrated adult disadvantage, and separation from parents retained a significant effect. The higher prevalence of psychotic-like experiences in the Black Caribbean, but not Black African, group was explained by high levels of social disadvantage over the life
Page 256

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 159
course.
63
Psychosis
nationally representative 13 - 17 years n=1261
Australia
Survey (Australian National Survey of Mental Health and Well-Being.)
Hallucinations were reported by 8.4% of adolescents.
Risk of Hallucinations in adolescents: Blended or sole parent families vs living with both biological parents (OR 3.27; 95% CI 1.93, 5.54; OR 2.60; 95% CI 1.63, 4.13 respectively). Adolescents who scored in the highest decile of the CBCL (OR 3.30; 95% CI 2.10, 5.20); or had elevated depression symptoms ( OR 5.02; 95% CI 3.38, 7.45). Depressive disorder (OR 2.70; 95% CI 1.16, 6.28) Smoked cannabis more than twice in the month prior to the survey (OR 3.27; 95% CI 1.76, 6.08).
64
PTSD
11-16 years with severe emotional disorders N=69
New Hampshire, USA
Survey
Remember this is in a population with severe emotional disorders, not general population Rate of PTSD was 28% which was underdiagnosed in adolescents' medical records.
PTSD was related to gender (42% for girls and 19% for boys; p = .03), history of sexual abuse (61% vs 15% among youths without), chart diagnosis of depression (47% vs 16% among youths without), and treatment with multiple psychotropic medications (53% among youths prescribed two or more medications vs 26% no medication or one medication). Adolescents with PTSD also were more likely to have run away,
Page 257

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 160
engaged in self-injurious and delinquent behavior, reported higher anxiety and depression, and functioned worse at school and home than those without PTSD.
65 self-harm ASD
Teenagers N=149
not clear cross sectional
Self-injurious behaviour was displayed by 50% of the ASD sample:
Within the ASD group, the presence of self-injury was associated with significantly higher levels of impulsivity and hyperactivity, negative affect and significantly lower levels of ability and speech.
66
social phobia comorbidity
13-18 years N=10123
Continental USA
cross sectional
Approximately 9% of adolescents met criteria for any social phobia in their lifetime. Of these adolescents, 55.8% were affected with the generalized subtype and 44.2% exhibited nongeneralized social phobia. Only 0.7% met criteria for the proposed DSM-5 performance-only subtype.
Generalized social phobia - female gender and age increased risk. Adolescents with generalized social phobia also had a younger age of onset, higher levels of disability and clinical severity, and a greater degree of comorbidity relative to adolescents with nongeneralized forms of the disorder.
67
Social Phobia Depression
12-17 years N=784
Finnish General population
Cross section - screening questionnaire and semi structured indepth interview with subsample
12-month prevalence of 3.2% for SP, and 4.6% for SSP. SP was frequently comorbid with other anxiety disorders (41%) and depressive disorders (41%). Adolescents with SP/SSP were impaired in their academic and global functioning, and reported more parental psychiatric treatment contacts. Two thirds (68%) of adolescents with SP reported having been bullied by peers.
The prevalence rose and the gender ratio shifted to female preponderance as age increased. Only one fifth of adolescents with non-comorbid SP had been in contact with a mental health professional
Page 258
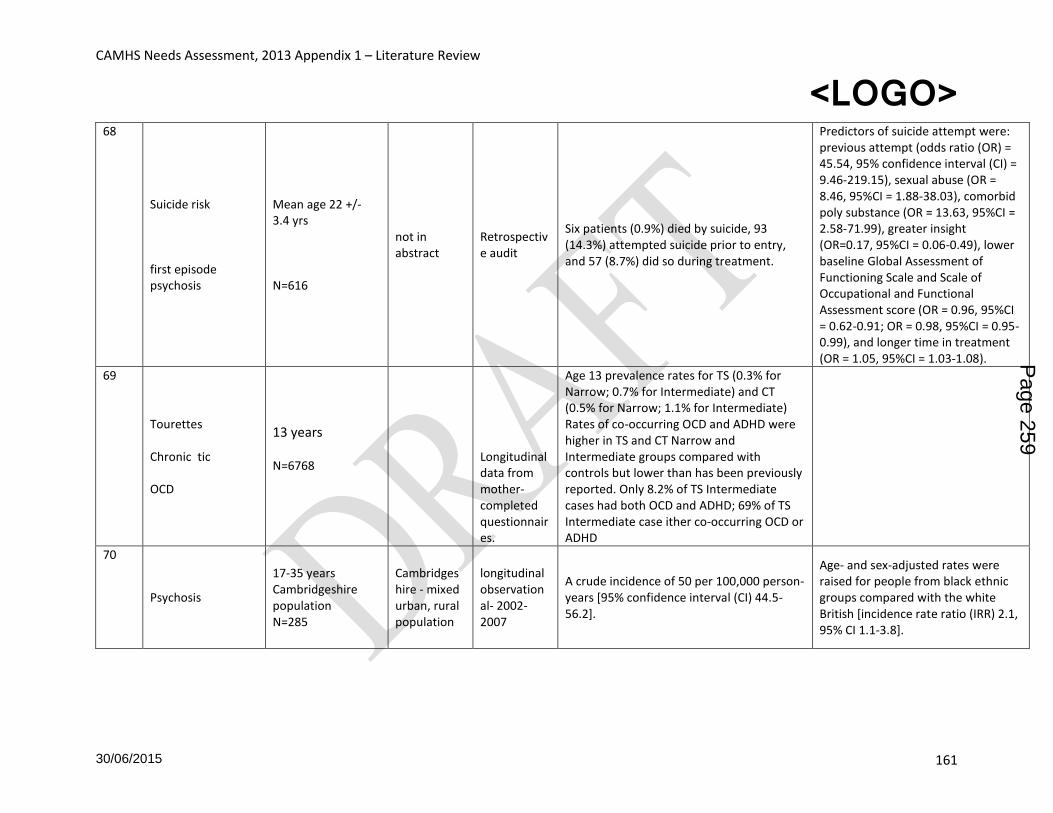
CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 161
68
Suicide risk first episode psychosis
Mean age 22 +/- 3.4 yrs N=616
not in abstract
Retrospective audit
Six patients (0.9%) died by suicide, 93 (14.3%) attempted suicide prior to entry, and 57 (8.7%) did so during treatment.
Predictors of suicide attempt were: previous attempt (odds ratio (OR) = 45.54, 95% confidence interval (CI) = 9.46-219.15), sexual abuse (OR = 8.46, 95%CI = 1.88-38.03), comorbid poly substance (OR = 13.63, 95%CI = 2.58-71.99), greater insight (OR=0.17, 95%CI = 0.06-0.49), lower baseline Global Assessment of Functioning Scale and Scale of Occupational and Functional Assessment score (OR = 0.96, 95%CI = 0.62-0.91; OR = 0.98, 95%CI = 0.95-0.99), and longer time in treatment (OR = 1.05, 95%CI = 1.03-1.08).
69
Tourettes Chronic tic OCD
13 years N=6768
Longitudinal data from mother-completed questionnaires.
Age 13 prevalence rates for TS (0.3% for Narrow; 0.7% for Intermediate) and CT (0.5% for Narrow; 1.1% for Intermediate) Rates of co-occurring OCD and ADHD were higher in TS and CT Narrow and Intermediate groups compared with controls but lower than has been previously reported. Only 8.2% of TS Intermediate cases had both OCD and ADHD; 69% of TS Intermediate case ither co-occurring OCD or ADHD
70
Psychosis
17-35 years Cambridgeshire population N=285
Cambridgeshire - mixed urban, rural population
longitudinal observational- 2002-2007
A crude incidence of 50 per 100,000 person-years [95% confidence interval (CI) 44.5-56.2].
Age- and sex-adjusted rates were raised for people from black ethnic groups compared with the white British [incidence rate ratio (IRR) 2.1, 95% CI 1.1-3.8].
Page 259

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 162
1. Lavigne, JV, LeBailly, S A, Hopkins, J, Gouze, KR, Binns, HJ (2009) The prevalence of ADHD, ODD, depression, and anxiety in a community sample of 4-year-olds. Journal of Clinical Child and Adolescent Psychology, May 2009, vol./is. 38/3(315-328), 1537-4416
2. Sobanski, E, Banaschewski, T, Asherson, P, Buitelaar, J, Chen, W, Franke, B, Holtmann, M, Krumm, B, Sergeant, J, Sonuga-Barke, E, Stringaris, A, Taylor, E, Anney, R, Ebstein, RP, Gill, M, Miranda, A, Mulas, F, Oades, R, Roeyers, H, Rothenberger, A, Steinhausen, H, Faraone, S (2010) Emotional lability in children and adolescents with attention deficit hyperactivity disorder (ADHD): Clinical correlates and familial prevalence. Journal of Child Psychology and Psychiatry, 2010, vol./is. 51/8(915-923), 0021-9630
3. Mann, RE, Paglia-Boak, A, Adlaf, EM, Beitchman, J, Wolfe, D, Wekerle, C, Hamilton, H A, Rehm, J (2011) International Journal of Mental Health and Addiction, August 2011, vol./is. 9/4(410-420)
4. Idring, S, Rai, D, Dal, H, Dalman, C, Sturm, H, Zander, E, Lee, Brian K, Serlachius, Eva, Magnusson, Cecilia (2012) Autism spectrum disorders in the Stockholm Youth Cohort: Design, prevalence and validity. PLoS ONE, July 2012, vol./is. 7/7, 1932-6203 (Jul 20, 2012)
5. Kim, YS, Leventhal, Bennett L, Koh, Yun-Joo, Fombonne, Eric, Laska, Eugene, Lim, Eun-Chung, Cheon, Keun-Ah, Kim, Soo-Jeong, Kim, Young-Key, Lee, HyunKyung, Song, Dong-Ho, Grinker, Roy Richard (2011) Prevalence of autism spectrum disorders in a total population sample.The American Journal of Psychiatry, September 2011, vol./is. 168/9(904-912
6. Worley, Julie A, Matson, Johnny L, Sipes, Megan, Kozlowski, Alison Prevalence of autism spectrum disorders in toddlers receiving early intervention services.Research in Autism Spectrum Disorders, April 2011, vol./is. 5/2(920-925)
7. Nygren, Gudrun, Cederlund, Mats, Sandberg, Eva, Gillstedt, Fredrik, Arvidsson, Thomas, Gillberg, I. Carina, Andersson, Gunilla Westman, Gillberg, ChristopherThe prevalence of autism spectrum disorders in toddlers: A population study of 2-year-old Swedish children.Journal of Autism and Developmental Disorders, July 2012, vol./is. 42/7(1491-1497)
8. Parner, Erik T, Thorsen, Poul, Dixon, Glenys, de Klerk, Nicholas, Leonard, Helen, Nassar, Natasha, Bourke, Jenny, Bower, Carol, Glasson, Emma JA comparison of autism prevalence trends in Denmark and Western Australia.Journal of Autism and Developmental Disorders, December 2011, vol./is. 41/12(1601-1608)
9. Roelfsema, Martine T, Hoekstra, Rosa A, Allison, Carrie, Wheelwright, Sally, Brayne, Carol, Matthews, Fiona E, Baron-Cohen, Simon (2012) Are autism spectrum conditions more prevalent in an information-technology region? A school-based study of three regions in the Netherlands.Journal of Autism and Developmental Disorders, May 2012, vol./is. 42/5(734-739)
10. Ivarsson, Tord, Melin, Karin (2008) Autism spectrum traits in children and adolescents with obsessive-compulsive disorder (OCD). Journal of Anxiety Disorders, August 2008, vol./is. 22/6(969-978),
11. Ooi, Yoon Phaik, Tan, Ze Jia, Lim, Cui Xi, Goh, Tze Jui, Sung, Min (2011) Prevalence of behavioural and emotional problems in children with high-functioning autism spectrum disorders.Australian and New Zealand Journal of Psychiatry, May 2011, vol./is. 45/5(370-375)
12. Schendel, Diana E, Autry, Andrew, Wines, Roberta, Moore, Cynthia (2009): The co-occurrence of autism and birth defects: Prevalence and risk in a population-based cohort. Developmental Medicine & Child Neurology, October 2009, vol./is. 51/10(779-786)
13. Knapp, Martin, Romeo, Renee E, Beecham, Jennifer (2009) Economic cost of autism in the UK Autism, May 2009, vol./is. 13/3(317-336)
14. Feenstra, Dine J, Busschbach, Jan J. V, Verheul, Roel, Hutsebaut, Joost (2011) Prevalence and comorbidity of Axis I and Axis II disorders among treatment refractory adolescents admitted
Page 260

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 163
for specialized psychotherapy.Journal of Personality Disorders, December 2011, vol./is. 25/6(842-850)
15. Kozloff, Nicole, Cheung, Amy H, Schaffer, Ayal, Cairney, John, Dewa, Carolyn S, Veldhuizen, Scott, Kurdyak, Paul, Levitt, Anthony J (2010) Bipolar disorder among adolescents and young adults: Results from an epidemiological sample. Journal of Affective Disorders, 2010, vol./is. 125/1-3(350-354)
16. Keski-Rahkonen, A, Hoek, H. W, Linna, M. S, Raevuori, A, Sihvola, E, Bulik, C. M, Rissanen, A, Kaprio, J(2009) Incidence and outcomes of bulimia nervosa: A nationwide population-based study.Psychological Medicine, 2009, vol./is. 39/5(823-831),
17. Demir, Turkay, Karacetin, Gul, Demir, Demet Eralp, Uysal, Omer (2011) Epidemiology of depression in an urban population of Turkish children and adolescentsJournal of Affective Disorders, November 2011, vol./is. 134/1-3(168-176),
18. not reported(2011) Early-onset major depressive disorder more prevalent in children of parents who have BD.Psychiatric Annals, July 2011, vol./is. 41/7(356), 0048-5713
19. Wiggins, Aaron, Oakley Browne, Mark, Bearsley-Smith, Cate, Villanueva, Elmer (2010) Depressive disorders among adolescents managed in a child and adolescent mental health service. Australasian Psychiatry, 2010, vol./is. 18/2(134-141)
20. Orton, Heather D, Riggs, Paula D, Libby, Anne M (2009) Prevalence and characteristics of depression and substance use in a U.S. child welfare sample.Children and Youth Services Review, June 2009, vol./is. 31/6(649-653),
21. Hughes EK (2012) Comorbid depression and anxiety in childhood and adolescent anorexia nervosa: Prevalence and implications for outcome. Clinical Psychologist, March 2012, vol./is. 16/1(15-24),
22. Le Grange, Daniel, Swanson, Sonja A, Crow, Scott J, Merikangas, Kathleen R(2012) Eating disorder not otherwise specified presentation in the US population International Journal of Eating Disorders, July 2012, vol./is. 45/5(711-718)
23. Nicholls, Dasha E, Lynn, Richard, Viner, Russell M (2011) Childhood eating disorders: British national surveillance study.The British Journal of Psychiatry, April 2011, vol./is. 198/4(295-301),
24. Touchette, Evelyne, Henegar, Adina, Godart, Nathalie T, Pryor, Laura, Falissard, Bruno, Tremblay, Richard E, Cote, Sylvana M (2011_ Psychiatry Research, January 2011, vol./is. 185/1-2(185-192),
25. Krizbai (Kovacs), Timea (2010) An epidemiological study of eating disorders among high school students in Romania.Journal of Cognitive and Behavioral Psychotherapies, March 2010, vol./is. 10/1(77-86)
26. DeLeel, Marissa L, Hughes, Tammy L, Miller, Jeffrey A, Hipwell, Alison, Theodore, Lea A (2009) Prevalence of eating disturbance and body image dissatisfaction in young girls: An examination of the variance across racial and socioeconomic groups.Psychology in the Schools, September 2009, vol./is. 46/8(767-775), 0033-3085
27. Stice, Eric, Marti, C. Nathan, Shaw, Heather, Jaconis, Maryanne(2009) An 8-year longitudinal study of the natural history of threshold, subthreshold, and partial eating disorders from a community sample of adolescents.Journal of Abnormal Psychology, August 2009, vol./is. 118/3(587-597),
28. Custers, Kathleen, Van den Bulck, JanViewership of pro-anorexia websites in seventh, ninth and eleventh graders.(2009) European Eating Disorders Review, May 2009, vol./is. 17/3(214-219), 1072-4133
Page 261

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 164
29. Isomaa, Rasmus, Isomaa, Anna-Lisa, Marttunen, Mauri, Kaltiala-Heino, Riittakerttu, Bjorkqvist, KajThe prevalence, incidence and development of eating disorders in Finnish adolescents-A two-step 3-year follow-up study.European Eating Disorders Review, May 2009, vol./is. 17/3(199-207),
30. Sancho, C, Arija, M. V, Asorey, O, Canals, JEpidemiology of eating disorders: A two year follow up in an early adolescent school population.European Child & Adolescent Psychiatry, December 2007, vol./is. 16/8(495-504),
31. Prevalence of eating disorders among adolescent and young adult scholastic population in the region of Madrid (Spain).Journal of Psychosomatic Research, June 2007, vol./is. 62/6(681-690)
32. Domenech-Llaberia, Edelmira, Vinas, Ferran, Pla, Esther, Jane, Maria Claustre, Mitjavila, Merce, Corbella, Teresa, Canals, Josefa Prevalence of major depression in preschool children.European Child & Adolescent Psychiatry, October 2009, vol./is. 18/10(597-604),
33. Bronsard, Guillaume, Lancon, Christophe, Loundou, Anderson, Auquier, Pascal, Rufo, Marcel, Simeoni, Marie-Claude Prevalence rate of DSM mental disorders among adolescents living in residential group homes of the French Child Welfare System.Children and Youth Services Review, October 2011, vol./is. 33/10(1886-1890)
34. Zinzow, Heidi M, Ruggiero, Kenneth J, Resnick, Heidi, Smith, Daniel, Saunders, Benjamin, Kilpatrick, Dean Prevalence and mental health correlates of witnessed parental and community violence in a national sample of adolescents.Journal of Child Psychology and Psychiatry, April 2009, vol./is. 50/4(441-450), 0021-9630
35. Hillen, Thomas, Gafson, Leonie, Drage, Laura, Conlan, Louise-MargaretAssessing the prevalence of mental health disorders and mental health needs among preschool children in care in England.Infant Mental Health Journal, July 2012, vol./is. 33/4(411-420)
36. Burnett-Zeigler, Inger, Walton, Maureen A, Ilgen, Mark, Barry, Kristen L, Chermack, Stephen T, Zucker, Robert A, Zimmerman, Marc A, Booth, Brenda M, Blow, Frederic CPrevalence and correlates of mental health problems and treatment among adolescents seen in primary care.Journal of Adolescent Health, June 2012, vol./is. 50/6(559-564),
37. Wittchen, H. U, Jacobi, F, Rehm, J, Gustavsson, A, Svensson, M, Jonsson, B, Olesen, J, Allgulander, C, Alonso, J, Faravelli, C, Fratiglioni, L, Jennum, P, Lieb, R, Maercker, A, van Os, J, Preisig, M, Salvador-Carulla, L, Simon, R, Steinhausen, H.-C (2010) The size and burden of mental disorders and other disorders of the brain in Europe 2010.European Neuropsychopharmacology, September 2011, vol./is. 21/9(655-679)
38. Burnett, A. C, Anderson, P. J, Cheong, J, Doyle, L.W, Davey, C. G, Wood, S. J (2011) Prevalence of psychiatric diagnoses in preterm and full-term children, adolescents and young adults: A meta-analysis.Psychological Medicine, December 2011, vol./is. 41/12(2463-2474)
39. Kessler, Ronald C, Avenevoli, Shelli, Costello, E. Jane, Georgiades, Katholiki, Green, Jennifer Greif, Gruber, Michael J, He, Jian-ping, Koretz, Doreen, McLaughlin, Katie A, Petukhova, Maria, Sampson, Nancy A, Zaslavsky, Alan M, Merikangas, Kathleen Ries (2012) Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the National Comorbidity Survey Replication Adolescent Supplement.Archives of General Psychiatry, April 2012, vol./is. 69/4(372-380),
40. Vinkers, David J, Duits, NilsCrime and mental disorders among native Dutch and ethnic minority juvenile defendants in the NetherlandsInternational Journal of Law and Psychiatry, March 2011, vol./is. 34/2(131-134),
Page 262

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 165
41. Stahlberg, Ola, Anckarsater, Henrik, Nilsson, ThomasMental health problems in youths committed to juvenile institutions: Prevalences and treatment needs. European Child & Adolescent Psychiatry, December 2010, vol./is. 19/12(893-903), 1018-8827;)
42. Roberts, Robert E, Roberts, Catherine R, Chan, WenyawOne-year incidence of psychiatric disorders and associated risk factors among adolescents in the communityJournal of Child Psychology and Psychiatry, April 2009, vol./is. 50/4(405-415),
43. Colins, Olivier, Vermeiren, Robert, Vreugdenhil, Coby, van den Brink, Wim, Doreleijers, Theo, Broekaert, ErikPsychiatric disorders in detained male adolescents: A systematic literature review.The Canadian Journal of Psychiatry / La Revue canadienne de psychiatrie, April 2010, vol./is. 55/4(255-263)
44. Merikangas, Kathleen Ries, He, Jian-ping, Burstein, Marcy, Swanson, Sonja A, Avenevoli, Shelli, Cui, Lihong, Benjet, Corina, Georgiades, Katholiki, Swendsen, JoelLifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A).Journal of the American Academy of Child & Adolescent Psychiatry, October 2010, vol./is. 49/10(980-989),
45. Author(s): Elberling, Hanne, Linneberg, Allan, Olsen, Else Marie, Goodman, Robert, Skovgaard, Anne MetteThe prevalence of SDQ-measured mental health problems at age 5-7 years and identification of predictors from birth to preschool age in a Danish birth cohort: The Copenhagen Child Cohort 2000.European Child & Adolescent Psychiatry, September 2010, vol./is. 19/9(725-735), 1018-8827
46. Prevalence and treatment of mental disorders among US children in the 2001-2004 NHANES. 47. Remine, Maria D, Brown, P. MargaretComparison of the prevalence of mental health problems
in deaf and hearing children and adolescents in Australia.Australian and New Zealand Journal of Psychiatry, 2010, vol./is. 44/4(351-357)
48. Martinez, Jaime, Hosek, Sybil G, Carleton, Russell AScreening and assessing violence and mental health disorders in a cohort of inner city HIV-positive youth between 1998-2006.AIDS Patient Care and STDs, June 2009, vol./is. 23/6(469-475),
49. Karnik, Niranjan S, Soller, Marie, Redlich, Allison, Silverman, Melissa, Kraemer, Helena C, Haapanen, Rudy, Steiner, HansPrevalence of and gender differences in psychiatric disorders among juvenile delinquents incarcerated for nine months.Psychiatric Services 2009, vol./is. 60/6(838-841),
50. Hintikka, Jukka, Tolmunen, Tommi, Rissanen, Marja-Liisa, Honkalampi, Kirsi, Kylma, Jari, Laukkanen, EilaMental disorders in self-cutting adolescents.Journal of Adolescent Health, May 2009, vol./is. 44/5(464-467),
51. Coker, Tumaini R, Elliott, Marc N, Kanouse, David E, Grunbaum, Jo Anne, Schwebel, David C, Gilliland, M. Janice, Tortolero, Susan R, Peskin, Melissa F, Schuster, Mark APerceived racial/ethnic discrimination among fifth-grade students and its association with mental health.American Journal of Public Health, May 2009, vol./is. 99/5(878-884
52. Frigerio, A, Rucci, P, Goodman, R, Ammaniti, M, Carlet, O, Cavolina, P, De Girolamo, G, Lenti, C, Lucarelli, L, Mani, E, Martinuzzi, A, Micali, N, Milone, A, Morosini, P, Muratori, F, Nardocci, F, Pastore, V, Polidori, G, Tullini, A, Vanzin, L, Villa, L, Walder, M, Zuddas, A, Molteni, MPrevalence and correlates of mental disorders among adolescents in Italy: The PrISMA study.European Child & Adolescent Psychiatry, April 2009, vol./is. 18/4(217-226)
53. Faravelli, Carlo, Lo Sauro, Carolina, Castellini, Giovanni, Ricca, Valdo, Pallanti, Stefano Prevalence and correlates of mental disorders in a school-survey sample. Clinical Practice and Epidemiology in Mental Health, 2009, vol./is. 5/, 1745-0179 (2009)
Page 263

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 166
54. Roberts, Robert E, Roberts, Catherine RamsayEthnicity and risk of psychiatric disorder among adolescents.Research in Human Development, 2007, vol./is. 4/1-2(89-117),
55. Ravens-Sieberer, Ulrike, Wille, Nora, Erhart, Michael, Bettge, Susanne, Wittchen, Hans-Ulrich, Rothenberger, Aribert, Herpertz-Dahlmann, Beate, Resch, Franz, Holling, Heike, Bullinger, Monika, Barkmann, Claus, Schulte-Markwort, Michael, Dopfner, Manfred, BELLA study group, GermanyPrevalence of mental health problems among children and adolescents in Germany: Results of the BELLA study within the National Health Interview and Examination Survey.European Child & Adolescent Psychiatry, December 2008, vol./is. 17/Suppl 1(22-33)
56. Wille, Nora, Bettge, Susanne, Wittchen, Hans-Ulrich, Ravens-Sieberer, Ulrike, BELLA study group, GermanyHow impaired are children and adolescents by mental health problems? Results of the BELLA study.European Child & Adolescent Psychiatry, December 2008, vol./is. 17/Suppl 1(42-51), 1018-8827
57. Heiervang, Einar, Stormark, Kjell M, Lundervold, Astri J, Heimann, Mikael, Goodman, Robert, Posserud, Maj-Britt, Ullebo, Anne K, Plessen, Kerstin J, Bjelland, Ingvar, Lie, Stein A, Gillberg, ChristopherPsychiatric disorders in Norwegian 8- to 10-year-olds: An epidemiological survey of prevalence, risk factors, and service use.Journal of the American Academy of Child & Adolescent Psychiatry, April 2007, vol./is. 46/4(438-447
58. Lazoff, Tamara, Zhong, Lihong, Piperni, Tania, Fombonne, EricPrevalence of pervasive developmental disorders among children at the English Montreal School Board.The Canadian Journal of Psychiatry / La Revue canadienne de psychiatrie, November 2010, vol./is. 55/11(715-720)
59. Zatzick, Douglas F, Grossman, David CAssociation between traumatic injury and psychiatric disorders and medication prescription to youths aged 10-19.Psychiatric Services, March 2011, vol./is. 62/3(264-271),
60. Harzke, Amy Jo, Baillargeon, Jacques, Baillargeon, Gwen, Henry, Judith, Olvera, Rene L, Torrealday, Ohiana, Penn, Joseph V, Parikh, RajendraPrevalence of psychiatric disorders in the Texas juvenile correctional systemJournal of Correctional Health Care, April 2012, vol./is. 18/2(143-157),
61. Kirkbride, J. B, Stubbins, C, Jones, P. BPsychosis incidence through the prism of early intervention services.The British Journal of Psychiatry, February 2012, vol./is. 200/2(156-157)
62. Meng, H, Schimmelmann, BG, Koch, E, Bailey, B, Parzer, P, Gunter, M, Mohler, B, Kunz, N, Schulte-Markwort, M, Felder, W, Zollinger, R, Burgin, D, Resch, F Basic symptoms in the general population and in psychotic and non-psychotic psychiatric adolescents. Schizophrenia Research, June 2009, vol./is. 111/1-3(32-38),
63. Morgan, C, Fisher, H, Hutchinson, G, Kirkbride, J, Craig, T. K, Morgan, K, Dazzan, P, Boydell, J, Doody, G. A, Jones, P. B, Murray, R. M, Leff, J, Fearon, P Ethnicity, social disadvantage and psychotic-like experiences in a healthy population based sample. Acta Psychiatrica Scandinavica, March 2009, vol./is. 119/3(226-235),
64. Scott, James, Martin, Graham, Bor, William, Sawyer, Michael, Clark, Jennifer, McGrath, John The prevalence and correlates of hallucinations in Australian adolescents: Results from a national survey Schizophrenia Research, February 2009, vol./is. 107/2-3(179-185)
65. Mueser, Kim T, Taub, Jonas Trauma and PTSD among adolescents with severe emotional disorders involved in multiple service systems Psychiatric Services, June 2008, vol./is. 59/6(627-634),
Page 264

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 167
66. Richards, C, Oliver, C, Nelson, L, Moss, J Self-injurious behaviour in individuals with autism spectrum disorder and intellectual disability .Journal of Intellectual Disability Research, May 2012, vol./is. 56/5(476-489)
67. Burstein, M, He, J-P, Kattan, G, Albano, AM, Avenevoli, S, Merikangas, KR Social phobia and subtypes in the National Comorbidity Survey-Adolescent Supplement: Prevalence, correlates, and comorbidity. Journal of the American Academy of Child & Adolescent Psychiatry, September 2011, vol./is. 50/9(870-880)
68. Ranta, K, Kaltiala-Heino, R, Rantanen, P, Marttunen, M Social phobia in Finnish general adolescent population: Prevalence, comorbidity, individual and family correlates and service use. Depression and Anxiety, 2009, vol./is. 26/6(528-536), 1091-4269;
69. Robinson, J, Cotton, S, Conus, P, Schimmelmann, BG, McGorry, P Lambert, M Prevalence and predictors of suicide attempt in an incidence cohort of 661 young people with first-episode psychosis. Australian and New Zealand Journal of Psychiatry, February 2009, vol./is. 43/2(149-157), 0004-8674
70. Scharf, JM, Miller, LL, Mathews, CA, Ben-Shlomo, Y Prevalence of Tourette syndrome and chronic tics in the population-based Avon Longitudinal Study of Parents and Children cohort.Journal of the American Academy of Child & Adolescent Psychiatry,2012, vol./is. 51/2(192-201),
71. Cheng, F, Kirkbride, J. B, Lennox, B. R, Perez, J, Masson, K, Lawrence, K, Hill, K, Feeley, L, Painter, M, Murray, G. K, Gallagher, O, Bullmore, E. T, Jones, P. Administrative incidence of psychosis assessed in an early intervention service in England: First epidemiological evidence from a diverse, rural and urban setting.Psychological Medicine, May 2011, vol./is. 41/5(949-958)
Page 265

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 168
Review 3 What works to treat mental ill health in children and young people and what service models have been shown to be effective?
Starting point: Southwark 2006 CAMHS needs assessment used a systematic review of systematic reviews to provide evidence of effective interventions in promoting wellbeing and preventing or treating mental ill health/. Search for systematic reviews published post 2006. Literature and evidence searches were carried out for evidence of:
1. Interventions and service delivery models which promote well-being, resilience or good mental health in children and young people.
2. Interventions and service delivery models which prevent the development of mental disorders in children and young people.
3. Interventions and service delivery models which are effective at treating mental disorders in children and young people
The following databases were searched: EMBASE, MEDLINE, PsychINFO,. A total of xx references were retrieved. Reference Intervention Results Conclusion
Table 1: High level summary of the evidence for interventions in child and young person’s wellbeing
Topic area
Intervention Source
Children’s emotional and social wellbeing primary school
Provide a comprehensive programme to help develop children’s social and emotional skills and wellbeing, including support to help parents or carers develop their parenting skills by offering small, group-based programmes run by community nurses For children showing early signs of emotional or social difficulties: Ensure teachers and practitioners are trained to identify and assess the early signs of anxiety, emotional distress and behavioural problems, and do so including use of the CAF. They should discuss the options for tackling problems with the child and their parents or
NICE. Social and emotional wellbeing in primary education. 2008.
Page 266
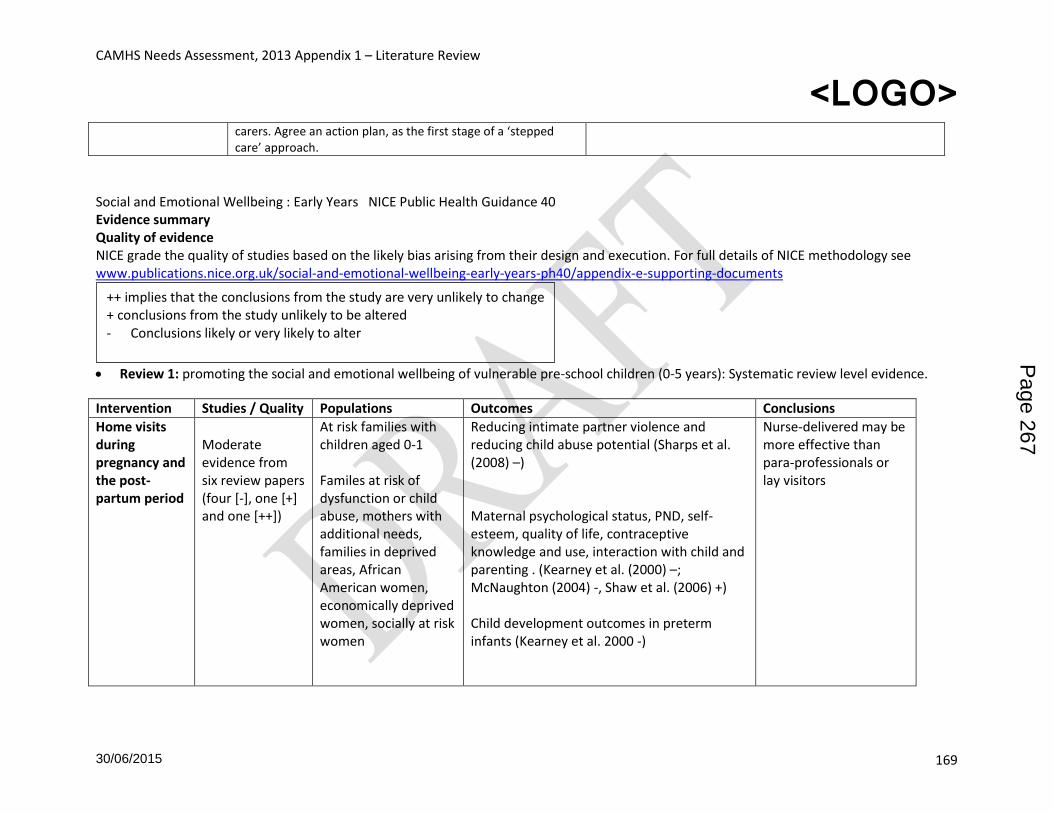
CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 169
carers. Agree an action plan, as the first stage of a ‘stepped care’ approach.
Social and Emotional Wellbeing : Early Years NICE Public Health Guidance 40 Evidence summary Quality of evidence NICE grade the quality of studies based on the likely bias arising from their design and execution. For full details of NICE methodology see www.publications.nice.org.uk/social-and-emotional-wellbeing-early-years-ph40/appendix-e-supporting-documents
Review 1: promoting the social and emotional wellbeing of vulnerable pre-school children (0-5 years): Systematic review level evidence.
Intervention Studies / Quality Populations Outcomes Conclusions
Home visits during pregnancy and the post-partum period
Moderate evidence from six review papers (four [-], one [+] and one [++])
At risk families with children aged 0-1 Familes at risk of dysfunction or child abuse, mothers with additional needs, families in deprived areas, African American women, economically deprived women, socially at risk women
Reducing intimate partner violence and reducing child abuse potential (Sharps et al. (2008) –) Maternal psychological status, PND, self-esteem, quality of life, contraceptive knowledge and use, interaction with child and parenting . (Kearney et al. (2000) –; McNaughton (2004) -, Shaw et al. (2006) +) Child development outcomes in preterm infants (Kearney et al. 2000 -)
Nurse-delivered may be more effective than para-professionals or lay visitors
++ implies that the conclusions from the study are very unlikely to change + conclusions from the study unlikely to be altered - Conclusions likely or very likely to alter
Page 267

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 170
Teenage mothers Support –education interventions
Improved self-confidence and self-esteem (Letourneau et al. (2004) –) Improved maternal child interaction and maternal identify (Coren and Barlow (2009) ++ )
One paper ++
Women with drug or alcohol problems (Doggett et al. 2005 ++)
Insufficient evidence of effectiveness
Home interventions – wider populations
Seven reviews provide evidence (two [++], four [+] and one [-])
Bayer et al.
(2009)
Sweet and
Appelbaum
(2004)
At risk families Ethnic minority teenage mothers Socially disadvantaged or substance abusing pregnant and postpartum women Low birthweight newborns Children with failure to thrive Low SES families Families at risk of abuse /neglect
Lower effect sizes on homes with low SES than mixed SES levels. MacLeod and Nelson, 2000, ++; Kendrick et al. , 2000, ++)
Lower effect sizes on adolescent populations than middle class non-adolescent parents. (Kendrick et al, 2000, ++)
Not clear how timing, intensity and other characteristics influence effectiveness. More successful interventions include ( Bakermans-Kraneburg et al, 2005, +):
video feedback;
did not include personal contact (but provided equipment);
started after the age of 6 months.
carried out at home either prenatally or after the age of 6 months.
Evidence for number of sessions unclear
Small to medium effects on maternal sensitivity and home environment Moderate effect size on parent-child interaction, family wellness Small effect size on attachment security, cognitive development, socio-emotional development, potential abuse, parenting behaviours, parenting attitudes and maternal life course education Mixed effects on parenting interventions
Page 268

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 171
Families at risk
less than 16 sessions; in a limited time period
MacLeod and Nelson (2000) (++)in contrast
concluded that effect sizes were higher for
interventions of 13 to 32
visits and lower for interventions of 1 to 12 visits and 33 to 50 visits. Also, that effect sizes were lower for interventions without a component of social support than for those that included social support. Kendrick et al. (2000) (++) suggested that there may be some reduction in intervention effect over time, and highlighted that the multifaceted nature of interventions provides challenges in ascertaining which element or elements of an intervention are most effective.
on childhood behaviour problems (Bernazzani et al. , 2001, + )
Programmes in educational or centre setting universal and targeted interventions.
Four reviews provide moderate evidence (three [+] and one [-]) Burgher (2010) -
Socially disadvantaged Children aged 3+
Cognitive outcomes (Anderson et al. (2003) +) vocabulary; letter and word identification; letter knowledge; book knowledge; colour-naming; reduction in number of children kept back a year; increased IQ scores; verbal and 'fluid intelligence' gains; Social competence School readiness; improved classroom and
Settings not well defined, nor distinction between day care and child care
Reported effectiveness varied across programmes. h one review reporting that
Page 269

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 172
Reviews provided little detail of programmes.
United States
personal behaviour (as rated by the teachers); reduced need for special needs education; a reduction in delinquent behaviour; fewer arrests at aged 27. Child mental health Reduced anxiety, improved ability to externalise behaviour problems (D'Onise et al. , 2010, + ) reported some problems made worse
Zoritch et al., 2009, + enhanced cognitive development, preventing school failure, improving children's behaviour, and improving maternal education and employment. Intervention starts at age 3 better than age 4 years.
53% of the studies demonstrated no effect.
Longer term outcomes of early developmental prevention programmes (i.e. followed up in adolescence) Interventions included
Two good quality [+] meta-analyses
at risk or disadvantaged many including a high proportion of participants from African-American backgrounds.
Manning et al. 2010, + reported largest effects for:
educational success during adolescence,
reduced social deviance,
increased social participation,
cognitive development, with smaller effects for:
family wellbeing
social-emotional development. Programmes with >500 sessions significantly better than those with fewer.
Overall, effect sizes are small to medium
Page 270

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 173
structured preschool programmes, centre-based developmental daycare, home visitation, family support services and parental education.
Nelson and Westhues 2003, + reported greatest cognitive impacts from:
programmes with direct teaching components in preschool
programmes which followed through from preschool to school
Longer programmes tended to produce greater impacts on preschool cognitive outcomes and on social and emotional outcomes at school age.
More intense programmes tended to produce greater impact on preschool cognitive outcomes and grade 8 parent-family outcomes.
Review 2: promoting the social and emotional wellbeing of vulnerable pre-school children (0-5 years): UK evidence review.
Intervention Studies / Quality Populations Outcomes Conclusions
Home visiting programmes
Seven studies (eight papers – four [++] and four [+])1,2,3,4,5,6,7,8 Mixed interventions, small number of
Some outcome measures were indirectly linked to the social and emotional development and cognitive development of the child, concerned with parental support and home environment. Many of the outcomes were self-reported introducing potential biases into the studies.
The extent of effect depends partly on the type and nature of intervention being delivered, and the particular outcomes measured The 'Family
Page 271

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 174
studies – hard to draw conclusions
partnership model’ intensive, structured, nurse delivered better results than lay providers
Peer mentoring home visiting programme
Cupples et al. 2010, ++
This programme was delivered by recruited existing mothers twice-monthly during pregnancy and monthly for the following year (in deprived areas in Northern Ireland).
negligible effects on social and emotional wellbeing.
'Family partnership model',
Barnes et al. , 2006; 2009, ++
Two UK counties A home visiting programme consisting of 18 months of weekly visits from a specifically trained health visitor
maternal sensitivity infant cooperation.
Small effect in improved outcomes
'Avon premature infant project'
Johnson et al. , 2005, +
home visiting programme with parental child developmental education and support (using a counselling model) delivered over 2 years by nurses.
A development advantage at 5 year follow up but not at 2 years
'Starting well',
Mackenzie et al. 2004, + Shute and Judge
an 'intensive home visiting' programme delivered by health professionals and health support workers to
Positive effect on home environment were reported; but methodological limitations meant the studies provided little robust evidence of effectiveness on social and emotional wellbeing.
Page 272

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 175
2005, +
socioeconomically deprived parents of newborn children aged up to 24 months (Glasgow).
Ford et al. (2009)
The (+) study4 of a small scale home visiting (intensive compensatory education) programme showed a positive effect on academic readiness and inhibitory control. This intervention consisted of weekly visits for 12 months delivered to infants aged 3 years by project workers (in an economically disadvantaged area of Wales). The intervention was a parent-delivered education programme aimed at improving school readiness. 'Social support and family health' was a home visiting programme delivered by a health visitor providing 'supportive listening', weekly and then monthly over 2 years (in London: Camden and Islington). The (++) evaluation8 reported a possible effect on maternal health.
Home Start Barnes et al. , 2006; 2009, ++
a volunteer home visitor programme This programme offered 'unstructured' mainly social support to vulnerable families with newborns consisting of two or more visits over 12 months provided by lay, local volunteer mothers.
, showed a positive effect on parent–child relationships; but no effect on maternal depression.
8 Wiggins et al.
Page 273

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 176
(2004) 1 Barlow et al. (2007)
Literature search of systematic reviews of treatment /interventions for mental health disorders in children and adolescents – published 2008-2013
Topic Reference Aims Quality check / no of studies incl.
Findings
Eating Disorders
Couturier, J; Kimber, M; Szatmari, P (2013) Efficacy of family-based treatment for adolescents with eating disorders: A systematic review and meta-analysis International Journal of Eating Disorders, 46/1(3-11)
To systematically review and quantitatively evaluate the efficacy of Family-Based Treatment (FBT) compared with individual treatment among adolescents with eating disorders (Anorexia Nervosa and Bulimia Nervosa)
allocation concealment, intent-to-treat analysis, assessor blinding, behavioral family therapy compared with an individual therapy, and adolescent age group.
When combined in a meta-analysis, end of treatment data indicated that FBT was not significantly different from individual treatment (z = 1.62, p = 0.11). However, when follow-up data from 6 to 12 months were analyzed, FBT was superior to individual treatment (z = 2.94, p < 0.003), and heterogeneity was not significant (p = 0.59). There appear to be significant benefits at 6-12 month follow- up for adolescents suffering from eating disorders.
Depression Shemilt, I; Valentine, JC; Possel, P; Mugford, M; Wooldridge, DT (2012) Costing program implementation using systematic reviews: Interventions for the prevention of adolescent depression. Research Synthesis Methods, 3/3(191-201)
To illustrate the development and use of an instrument to code resource use and cost data from an existing systematic review on the effects of adolescent depression prevention programs and applying that instrument to 46 studies included in that review.
46 Not enough information about costing of intervention programmes for depression is available
Child The effect of praise, The current review 41 studies of children Reprimand and negative nonverbal responses
Page 274

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 177
compliance positive nonverbal response, reprimand, and negative nonverbal response on child compliance: A systematic review. Clinical Child and Family Psychology Review, December 2012, 15/4(364-385), Owen, Daniela J; Slep, Amy M. S; Heyman, Richard E
examines the relationship between a variety of parenting discipline behaviors (i.e., praise, positive nonverbal response, reprimand, negative nonverbal response) and child compliance.
ranging in age from 11/2 to 11 years
consistently resulted in greater compliance. Praise and positive nonverbal responses resulted in mixed child outcomes. The findings are discussed based on theory and populations studied. The authors propose a mechanism that may increase children's sensitivity to both positive and negative behavioral contingencies.
Trauma The data behind the dissemination: A systematic review of trauma-focused cognitive behavioral therapy for use with children and youth. Children and Youth Services Review, April 2012, vol./is. 34/4(748-757), 0190-7409 Cary, Colleen E; McMillen, J. Curtis
to systematically review the evidence of TF-CBT's ability to reduce symptoms of post-traumatic stress, depression and behavior problems in children and youth who have survived trauma.
A search was conducted to locate studies that evaluated TF-CBT or interventions highly similar to TF-CBT. Ten studies (twelve articles) were selected for inclusion in three sets of meta-analyses.
Findings were consistent amongst meta-analyses; pooled estimates were similar whether we were analyzing the effects of interventions that were highly similar to TF-CBT, or if we were exclusively analyzing the effects of the branded intervention. Results show that there is a significant difference between the TFCBT condition and comparison conditions in its ability to reduce symptoms of PTSD (g = .671), depression (g = .378) and behavior problems (g = .247) immediately after treatment completion. This difference held for PTSD at twelve months after treatment completion (.389) but did not hold for depression or behavior problems. There was not a significant difference between the TF-CBT condition and alternative active control conditions immediately after treatment completion.
Parental mental health
Effect of preventive interventions in mentally ill parents on the mental health of the offspring: Systematic review
The Cochrane, MEDLINE, EMBASE, and PsycINFO databases were searched for randomized controlled trials of interventions in parents with
Thirteen trials including 1,490 children were analyzed. Interventions included
Relative risks and standardized mean differences in symptom scores were combined in random-effects meta-analysis. Interventions decreased the risk of MHD by 40%
Page 275

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 178
and meta-analysis. Citation: Journal of the American Academy of Child & Adolescent Psychiatry, January 2012, vol./is. 51/1(8-17), 0890-8567;1527-5418 (Jan 2012) Author(s): Siegenthaler, Eliane; Munder, Thomas; Egger, Matthias
mental disorders.
cognitive, behavioral, or psychoeducational components. Seven trials assessed the incidence of mental disorders and seven trials assessed symptoms Outcomes in the child included incident mental disorders of the same nature and internalizing (negative emotions, depressive symptoms, anxiety) or externalizing (hyperactivity, aggressiveness, behavioral problems) symptoms..
(combined relative risk 0.60, 95% CI 0.45-0.79). Symptom scores were lower in the intervention groups: standardized mean differences were -0.22 (95% CI -0.37 to -0.08) for internalizing symptoms (p = .003) and -0.16 (95% confidence interval -0.36 to 0.04) for externalizing symptoms (p = .12). Conclusions: Interventions to prevent mental disorders and psychological symptoms in the offspring by treating parents are effective.
Bullying Effectiveness of antibullying school programmes: A systematic review by evidence levels. Children and Youth Services Review, 2012,. 34/9(1646-1658), 0190-7409 Jimenez B,; Ruiz Hernandez,JA;, Bartolome
systematic search of electronic databases (Medline, Trip Database, Cochrane, Academy Search Premier, PsycINFO, ERIC and PsycARTICLES) for studies published after January 1, 2000, on the assessment of the effectiveness of school interventions to prevent
299 articles were detected that met the inclusion criteria and that had been independently peer-reviewed. For the final evaluation, 32 studies were selected which met the previously established selection
The programmes assessed were effective , although serious limitations are also detected, which should be taken into consideration when designing future interventions. The likelihood of success is enhanced when all the disciplines of a centre and parents are involved. It is also essential to adapt the programmes to the social and cultural characteristics of the school population in which the programme is to be
Page 276
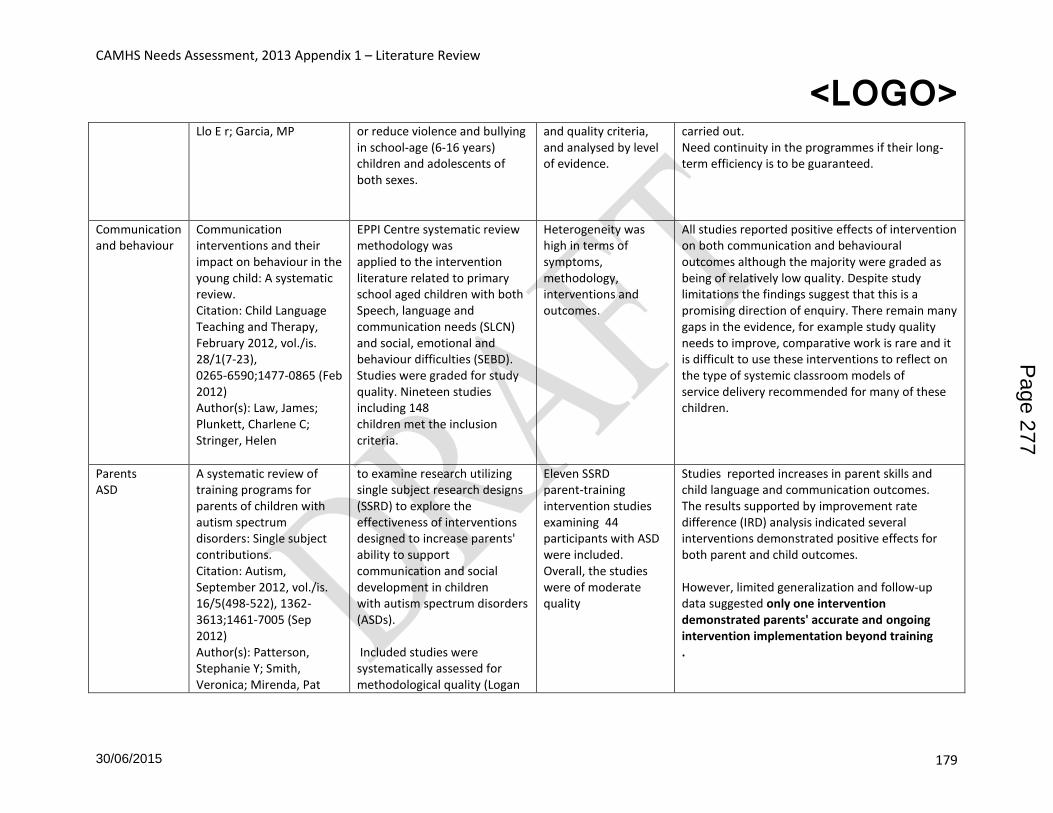
CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 179
Llo E r; Garcia, MP or reduce violence and bullying in school-age (6-16 years) children and adolescents of both sexes.
and quality criteria, and analysed by level of evidence.
carried out. Need continuity in the programmes if their long-term efficiency is to be guaranteed.
Communication and behaviour
Communication interventions and their impact on behaviour in the young child: A systematic review. Citation: Child Language Teaching and Therapy, February 2012, vol./is. 28/1(7-23), 0265-6590;1477-0865 (Feb 2012) Author(s): Law, James; Plunkett, Charlene C; Stringer, Helen
EPPI Centre systematic review methodology was applied to the intervention literature related to primary school aged children with both Speech, language and communication needs (SLCN) and social, emotional and behaviour difficulties (SEBD). Studies were graded for study quality. Nineteen studies including 148 children met the inclusion criteria.
Heterogeneity was high in terms of symptoms, methodology, interventions and outcomes.
All studies reported positive effects of intervention on both communication and behavioural outcomes although the majority were graded as being of relatively low quality. Despite study limitations the findings suggest that this is a promising direction of enquiry. There remain many gaps in the evidence, for example study quality needs to improve, comparative work is rare and it is difficult to use these interventions to reflect on the type of systemic classroom models of service delivery recommended for many of these children.
Parents ASD
A systematic review of training programs for parents of children with autism spectrum disorders: Single subject contributions. Citation: Autism, September 2012, vol./is. 16/5(498-522), 1362-3613;1461-7005 (Sep 2012) Author(s): Patterson, Stephanie Y; Smith, Veronica; Mirenda, Pat
to examine research utilizing single subject research designs (SSRD) to explore the effectiveness of interventions designed to increase parents' ability to support communication and social development in children with autism spectrum disorders (ASDs). Included studies were systematically assessed for methodological quality (Logan
Eleven SSRD parent-training intervention studies examining 44 participants with ASD were included. Overall, the studies were of moderate quality
Studies reported increases in parent skills and child language and communication outcomes. The results supported by improvement rate difference (IRD) analysis indicated several interventions demonstrated positive effects for both parent and child outcomes. However, limited generalization and follow-up data suggested only one intervention demonstrated parents' accurate and ongoing intervention implementation beyond training .
Page 277

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 180
et al., 2008; Smith et al., 2007) and intervention effects. Data examining participant characteristics, study methodology, outcomes, and analysis were systematically extracted.
Homeless and Fostered children
Common needs but divergent interventions for U.S. homeless and foster care children: Results from a systematic review. Health & Social Care in the Community, September 2012, vol./is. 20/5(449-476), 0966-0410;1365-2524 (Sep 2012) Zlotnick, Cheryl; Tam, Tammy; Zerger, Suzanne
to identify the most promising practices for children living in transition. A standardised vocabulary specific to each of three electronic databases (i.e. Medline, PsychINFO and CINAHL) was employed to identify studies that described an intervention specifically targeting foster care or homeless children and families. only studies published in English between January 1993 and February 2009 were selected.
The final sample (n = 43) of articles described interventions that fell into two categories: mental health (n = 17) and case management (n = 26). Few articles employed rigorous study designs. Studies focused on one population or the other.
Virtually all studies on both homeless and foster children devised interventions to reduce trauma and family instability; yet, no evidence-based practice addresses the overlapping needs and potentially relevant evidence-based practice for these two populations. An important and vital next step is to establish an effective evidence-based intervention that reduces the impact of trauma on both U.S. populations of children living in transition.
Parenting Developmental disabilities
Positive parenting of children with developmental disabilities: A meta-analysis. Citation: Research in Developmental Disabilities, November 2012, vol./is. 33/6(2213-2220), 0891-4222 (Nov-Dec 2012) Dyches, Tina Taylor; Smith,
This study examined the association between positive parenting attributes and outcomes of young children with developmental disabilities through meta-analytic aggregation of effect sizes
14 studies including 576 participants. Publication bias did not appear to be a substantial threat to the results.
The random effects weighted average effect size was r = .22 (SE = .06, p < .001), indicative of a moderate association between positive parenting attributes and child outcomes. There was a trend for studies with more mature parents to have bigger effect sizes than studies with young parents. The results provide support for efforts to evaluate and promote effective parenting skills when providing services for young children with disabilities
Page 278

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 181
Timothy B; Korth, Byran B; Roper, Susanne Olsen; Mandleco, Barbara
Help seeking Depression, anxiety General psychological distress
A systematic review of help-seeking interventions for depression, anxiety and general psychological distress. Citation: BMC Psychiatry, July 2012, vol./is. 12/, 1471-244X (Jul 16, 2012) Author(s): Gulliver, Amelia; Griffiths, Kathleen M; Christensen, Helen; Brewer, Jacqueline L
To evaluate the effectiveness of interventions targeting help-seeking attitudes, intentions or behaviours for depression, anxiety, and general psychological distress
Six published studies of randomised controlled trials investigating eight different interventions for help-seeking were identified. The majority of trials targeted young adults.
Mental health literacy content was effective (d = .12 to .53) in improving help-seeking attitudes in the majority of studies at post-intervention, but had no effect on help-seeking behaviour (d = -.01, .02) . There was less evidence for other intervention types such as efforts to destigmatise or provide help-seeking source information. Further research investigating the effects of interventions on attitudes, intentions, and behaviour is required.
Street involved Youth Outreach
Outreach with street-involved youth: A quantitative and qualitative review of the literature. Citation: Clinical Psychology Review, August 2012, vol./is. 32/6(524-534), 0272-7358 (Aug 2012) Author(s): Connolly, J. A; Joly, L. E
To evaluate the qualitative and quantitative literature on outreach with street involved youth with the aim of involving them in wellbeing services.
16 outreach programs with quantitative information 31 qualitative articles on outreach
63% of youth who are contacted through outreach later participate in the offered service. Metasynthesis uncovered 13 themes across 4 conceptual domains of interest. : the therapeutic relationship, flexibility, and youth-centric programming had a large presence among the majority of the articles. Outreach with street-involved youth, when characterized through a strong bond between worker and youth, is an effective strategy for involving youth in agency services.
Street involved youth
A systematic review: A quest for effective interventions for children and adolescents in street situation. Children and Youth Services Review, July 2012,
To review the effectiveness of interventions for children and adolescents in street situation (CASS) starting where Dybicz ended his review in 2005.
33 studies in an ecological broad-based integrative model In a second part of this article we attend to the effectiveness of
The reviewed articles could not give us a clear picture of what is meant by the long-term objectives of interventions for Children and Adolescents in Street situations which is of paramount importance in evaluating them. Furthermore, we noticed that a Western
Page 279

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 182
vol./is. 34/7(1259-1272), 0190-7409 (Jul 2012) Berckmans, I; Velasco, ML; Tapia, BP; Loots, G
interventions
discourse on childhood is predominantly used in the reviewed articles and in the programs described. Finally, we question whether this is the ideal to which we have to interpret the results of the programs.
ASD Medication
Psychotropic medications in children with autism spectrum disorders: A systematic review and synthesis for evidence-based practice. (2012) Journal of Autism and Developmental Disorders, vol./is. 42/8(1592-1605), 0162-3257;1573-3432 Siegel, M; Beaulieu, AA
Thirty-three randomized controlled trials (RCTs) published in peer-reviewed journals qualified for inclusion and were coded and analyzed using a systematic evaluative method specific to autism research
Still to complete
Page 280

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 183
Allen recommended early interventions
EL Programme name Description
1 Curiosity Corner (as part
of Success for All)
a comprehensive program for three- and four-year- old pre-
schoolers designed to provide a strong foundation in language
and literacy, mathematics, science, listening and social skills,
creative expression, and positive self-esteem through a holistic,
thematic approach to instruction.
1 Incredible Years research-based, proven effective programs for reducing children's aggression and behaviour problems and increasing social competence at home and at school
1 Multidimensional
Treatment Foster Care
This programme, supported by the DfE since 2003, enables local
authorities to offer solutions for youngsters who have
experienced many placement disruptions and who have a high
level of need from all children’s services in education, health and
social care. The aim is to promote stability and the ability to live
in a family whether the outcome is a return home to birth or
extended family, to long term fostering or adoption. In this way,
MTFCE broadens the range of foster care placements available
within the children’s local communities
1 Nurse Family Partnership a preventive programme for young first time mothers. It offers intensive and structured home visiting, delivered by specially trained nurses (Family Nurses), from early pregnancy until the child is two.
three aims: to improve pregnancy outcomes, child health and
development and parents’ economic self-sufficiency
1 Success for All a whole-school reform strategy that features research-proven
tools, cooperative learning to engage students and collaborative
leadership for continuous improvement.
2 Parent Child Interaction
Therapy
(PCIT)
an empirically-supported treatment for young children with
emotional and behavioral disorders that places emphasis on
improving the quality of the parent-child relationship and
changing parent-child interaction patterns.
3 Breakthrough to Literacy Breakthrough To Literacy is designed for preschool and
kindergarten children who are making the transition from oral
language to reading and understanding printed materials.
3 Community Mothers Community Mothers targets first-time mothers and their infants
up to one year of age who live in disadvantaged areas. Existing
mothers in these communities are trained to empower new
parents about health care, nutrition and child development.
3 HighScope Perry Pre-
School a high-quality preschool program based on HighScope's
participatory learning approach for children at risk of failing at
school
3 Parents as Teachers Parents as Teachers is an approved home visiting model meeting the evidence-based criteria of the Maternal, Infant, Early
Page 281

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 184
Childhood Home Visiting program with the aim of providing the information, support and encouragement parents need to help their children develop optimally during the crucial early years of life.
3 Triple P (Positive
Parenting Programme)
Triple P is a system of easy to implement, proven parenting solutions Triple P is a system of easy to implement, proven parenting solutions that helps that helps solve current parenting problems and prevents future problems before they arise.
Pri
mar
y sc
ho
ol
1 Incredible Years See above
1 Promoting Alternative
Thinking Strategies
(PATHS)
a school-based program designed to improve children’s ability to
discuss and understand emotions.
1 Reading Recovery
Reading Recovery is designed for children aged five or six, who are the lowest achieving in literacy after their first year of school. These children are often not able to read the simplest of books or write their own name before the programme. They receive a short series of intensive lessons with a specially trained teacher in their own school.
1 Success for All Success for All is a whole-school reform strategy, research proven
to increase student achievement. It features interventions and
support in the following areas:
Leadership for Continuous Improvement:
Schoolwide Support and Intervention Tools:
Powerful Instruction:
Professional Development and Coaching:
2 Parent–Child Interaction
Therapy (PCIT) See preschool section
3 Breakthrough to Literacy See preschool section
3 Cooperative Integrated
Reading and
Composition
A co-operative learning programme designed to help pupils
develop metacognitive strategies for comprehending narrative
and expository text. Pupils work in four to five member learning
teams to help each other master reading content.
3 Good Behaviour Game an approach to the management of classrooms behaviours that
rewards children for displaying appropriate on-task behaviors
during instructional times. The class is divided into two teams and
a point is given to a team for any inappropriate behavior
displayed by one of its members. The team with the fewest
number of points at the Game's conclusion each day wins a group
reward. If both teams keep their points below a preset level, then
both teams share in the reward.
3 Caring Schools
Communities
a multi-phase, school wide program whose central aim is to help
each school become a “caring community of learners” that
Page 282

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 185
effectively promotes students’ intellectual, social, and ethical
development and teachers’ continuous improvement of practice.
3 Olweus Bullying Program
a universal intervention for the reduction and prevention of bully/victim problems. The main arena for the program is the school, and school staff has the primary responsibility for the introduction and implementation of the program.
3 PALS Not clear from document or internet search – could be
playground pals scheme.
3 Quick Reads Not clear from document or internet search – lots of references
to quick reads i.e. short books for adults who aren’t confident
readers
3 Roots of Empathy Roots of Empathy is an evidence-based classroom program that
has shown significant effect in reducing levels of aggression
among schoolchildren by raising social/emotional competence
and increasing empathy.
3 Triple P See preschool above
Seco
nd
ary
sch
oo
l
1 Functional Family
Therapy
FFT is a short-term, high quality intervention program with an
average of 12 sessions over a 3-4 month period. Services are
conducted in both clinic and home settings, and can also be
provided in a variety of settings including schools, child welfare
facilities, probation and parole offices/aftercare systems, and
mental health facilities.
FFT is a strength-based model. At its core is a focus and
assessment of those risk and protective factors that impact the
adolescent and his or her environment, with specific attention
paid both intrafamilial and extrafamilial factors, and how they
present within and influence the therapeutic process.
1 Incredible Years
See preschool
1 Multidimensional
Treatment Foster Care
See preschool (not clear why not included in primary school)
1 Multisystemic Therapy
An intensive family- and community-based treatment
program designed to make positive changes in the various
social systems (home, school, community, peer relations)
that contribute to the serious antisocial behaviors of
children and adolescents who are at risk for out-of-home
placement. These out-of-home placements might include
foster care, group homes , residential care, correctional
facilities, or hospitalization .
1 Success for All
See primary school section
3 Olweus Bullying Program
See primary school section
Page 283

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 186
3 Parenting Wisely
Parenting Wisely is a set of interactive, computer-based training
programs for parents of children ages 3-18 years. Based on social
learning, cognitive behavioral, and family systems theories, the
programs aim to increase parental communication and
disciplinary skills. The original Parenting Wisely program,
American Teens, is designed for parents whose preteens and
teens are at risk for or are exhibiting behavior problems such as
substance abuse, delinquency, and school dropout. 3 Read 180
3 The Reading Edge
3 Triple P
See preschool above
Source: Allen, 20011b
Evidence levels used by Allen
Level 1
All of the Level 2 criteria must apply plus:
• programme gets a ‘best’ on evaluation quality and/or impact criteria. In the case of
evaluation quality this means that any of the ‘best’ criteria must apply, while in the case of
impact criteria both of the ‘best’ criteria must apply.
Level 2
All of the Level 3 criteria must apply plus:
• programme meets all evaluation quality criteria.
Level 3
All of the following must apply: • programme has one randomised controlled trial (RCT) or two quasi-experimental designs (QEDs); • programme has a positive impact on an Allen Review outcome; • programme has no iatrogenic effect; and • there are no obvious concerns about intervention specificity or system readiness.
Page 284

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 187
Review 4: is the prevalence of autism increasing in 0-18 year olds? During Stakeholder Interviews for the Southwark and Lambeth CAMHS Needs Assessment 2013, quite a few stakeholders expressed a belief that they were seeing an increasing number of children and young people with autism or autistic spectrum disorders. The apparent increase could be due to increased case ascertainment e.g. better recognition; or due to a greater number of children with autism being educated in mainstream schools; or due to an increase in the population causing an increase in numbers accessing specialist services, but without the underlying rate of autism increasing. ChiMat quotes two studies for prevalence of Autism – Baird et al, 200699 and Baron-Cohen S et al, 2009100 which reports the prevalence of ASD in children aged 9-10 at 116.1 per 10,000 children and 157 per 10,000 children aged 5-9 years. The majority of stakeholders were unspecific about the period of time they were reporting an increase for, therefore it seems reasonable to look at trends for the last 10 years. Question: is there any evidence of increasing prevalence of autism in children and young people between 2003 and 2013? Search strategies All terms mapped to thesaurus and expanded before searching.
99 Baird G, Simonoff E, Pickles A, Chandlert S, Loucase T, Meldrum D and Charman T (2006) Prevalence of disorders of the autistic spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP) Lancet 368 (9531), 210-5. 100 Baron-Cohen S, Scott FJ, Allison C, Williams J, Bolton P, Matthews FE, Brayne C (2009) Prevalence of autistic spectrum conditions: UK school-based population study The British Journal of Psychiatry, 194 (6), 500-9.
Database Terms (in title or abstract)
Results Papers
Medline Autistic disorder OR Autis* OR “Autistic Spectrum” AND Prevalence OR epidemiology
2 Webb EV, Lobo S, Hervas A, Scourfield J, Fraser WI (1997) The changing prevalence of autistic disorder in a Welsh health district. Developmental Medicine & Child Neurology, 39/3(150-2) Wing JK (1963) Epidemiology of early childhood autism. Developmental Medicine & Child Neurology, 5/(646-7),
Psychinfo Autistic disorder OR Autis* OR “Autistic Spectrum” AND epidemiology Restricted to 2003-2013,
187 62 after review of title 9 review of
Excluded: special groups within population, chapters in books, prevalence measured at 1 point in time
Page 285

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 188
Findings Before discussing the original question need to consider some of the issues relating to the estimation of prevalence of autistic spectrum disorders (ASDs) as described by Campbell et al (2011) - not least that as ASD is a behaviourally defined disorder, diagnosis is much less clear cut than for disorders which have biological markers. In particular, the presentation may vary depending on the severity of the condition and on the child’s cognitive abilities. They also suggest that data collection, analysis and interpretation affect the conclusions drawn about ASD prevalence. Changes in diagnostic criteria since the 1940s when autism was first studied could contribute to the reported rise in incidence and prevalence as well as greater awareness among parents and professionals. Many papers of the 62 papers on autism refer to an increase in autism prevalence over time (Campbell et al, 2011; Kim et al, 2011; Pedersen et al, 2012, King & Bearman, 2011), For example, King and Bearman suggest a 10 fold increase in California over the last 40 years without actually providing data in the abstract (no access to the article). Other papers are less specific about the time period they refer to. Given the methodological difficulties in using papers from different countries, at different times, with different case ascertainment methods and children of different ages to demonstrate an increase in the prevalence of ASD, this review has only included studies which report at least two points in time. Table 1 summarises the studies found and their results – as can be seen none of the papers are from the UK, and although the papers were published between 2003 and 2013 the time periods quoted are often earlier than 2003. ASD rates quoted vary hugely - Taiwan 28.72 per 10,000 compared to UK 116 – 157 per 10,000 so it is not clear how relevant to the UK all findings are. The studies all support the view that recorded prevalence of autism is increasing. No one is clear whether the reported rises are due to a genuine increase. Coo et al, 2008 report that a third of the reported increase in autism in British Columbia between 1996 and 2004 was due to a change in diagnostic category and Maenner and Durkin found that differences in prevalence between school districts decreased over time (i.e. those areas which had previously had the highest rates did not increase, but areas with lower than average rates did, perhaps suggesting more uniform recognition of the condition across school districts rather than an underlying increase in the condition. Schieve et al point out that the rates they are comparing are a diagnosis of Autism in 2003 compared to any ASD in 2007. As ASD is a broader category it would be expected that rates would rise. Where gender differences in rates of autism and ASD are mentioned there is agreement that boys are more likely to have an ASD than girls (4:1 ratio) Table 50 Summary of studies reporting the prevalence of autism at two or more points in time.
human, ages birth – 17, English, peer reviewed journal
abstract
Paper Country Diagnosis and age group Time period
Rate per 10,000 T1
Rate per 10,000 T2
Chien et al, 2011
Taiwan ASD population aged < 18 1996-2005
1.78 28.72
Page 286

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 189
Local activity data Local activity data (table 2) does not show an increase in the number of children and young people seen with autism or autistic spectrum disorder, nor is there are clear increase in the proportion of patients with autism or ASD. One limitation to this analysis is the high proportion of episodes of care with “no axis 1 diagnosis” e.g. in 2011-12 22%of Lambeth and 36% of Southwark episodes of care had no axis 1 diagnosis , which means that an increase may be hidden if a diagnosis is made later on and not recorded in the data fields provided for analysis. Table 2 – numbers of children and young people with a diagnosis of Autism or ASD
Axis 1a, 1b and 2 combined 2009-10 2010-11 2011-12
Lambeth n % n % n %
Total episodes of care 1587 100% 1433 100% 898 100%
Asperger's syndrome 20 1.3% 28 2.0% 18 2.0%
Atypical autism 7 0% 3 0.2% 2 0.2%
Childhood autism 84 6% 97 6.8% 52 5.8%
Southwark
Total episodes of care 1840 100% 1743 100% 1246 100%
Asperger's syndrome 27 1.5% 22 1.3% 18 1.4%
Atypical autism 12 0.7% 10 0.6% 3 0.2%
Childhood autism 113 6.1% 72 4.1% 65 5.2%
Coo et al, 2008
British Columbia
Autism code . 51.9% of this increase was attributable to children switching from another special education classification to autism (16.0/10,000).
1996-2004
12.3 43.1
Lai , DC et al, 2012
Taiwan ASD. Ages 3-17years. Rates higher in boys than girls. Rate not quoted in abstract.
2004-2010
Increased
Lin, Lin and Wu, 2009
Taiwan 0-5 years 6-11 years, 12-17 years
2000-2007
2.4 5.0 2.1
7.8 17.3 10.4
Maenner and Durkin, 2010
USA, Wisconsin
Autism category in Wisconsin elementary schools. The magnitude of this increase was not uniform across districts and was inversely associated with baseline prevalence.
2002-2008
79 90
Nygren et al (2012)
SWEDEN
2-year-olds – following screening programme Higher in boys than girls.
2000 2005 2010
18 4
80
Pedersen et al (2012)
USA 8 year ASD diagnosis; in non-Hispanic and Hispanic populations The Hispanic prevalence almost tripled.
2000- 2006
27 79
Pinborough Zimmerman et al, 2012
USA - Utah
ASD 8 year olds based on school and health records
2000-2008
65 129
Schieve et al, 2012
USA ASD National Survey of Children's Health (NSCH) was twice the 2003 NSCH estimate for autism (note comparing ASD with autism)
2003-2007
Rates doubled.
Page 287

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 190
References for autism literature review. Campbell, CA, Davarya, S, Elsabbagh, M, Madden, L, Fombonne, E (2011) Prevalence and the controversy, International handbook of autism and pervasive developmental disorders., 925-35) Chien, I, Lin, C, Chou, Y, Chou, P (2011) Prevalence and incidence of autism spectrum disorders among national health insurance enrollees in Taiwan from 1996 to 2005. Journal of Child Neurology, 26/7 (830-834) Coo, H, Ouellette-Kuntz, H, Lloyd, JEV, Kasmara, L, Holden, JJA, Lewis, MES (2008) Trends in autism prevalence: Diagnostic substitution revisited. Journal of Autism and Developmental Disorders 38/6(1036-1046) Gillberg, C (2012) The prevalence of autism spectrum disorders in toddlers: A population study of 2-year-old Swedish children. Journal of Autism and Developmental Disorders, 42/7(1491-1497) Kim, YS, Leventhal, BL, Koh, YJ, Fombonne, E, Laska, E, Lim, EC, Cheon, K-A, Kim, S-J, Kim, Y-K, King, MD, Bearman, PS (2011) Socioeconomic status and the increased prevalence of autism in California American Sociological Review 76/2 (320-346) Lai, D-C, Tseng, Y-C, Hou, Y-M, Guo, H-R (2012) Gender and geographic differences in the prevalence of autism spectrum disorders in children: Analysis of data from the national disability registry of Taiwan Research in Developmental Disabilities 33/3(909-915) Lin, JD, Lin, LP, Wu, JL (2009) Administrative prevalence of autism spectrum disorders based on national disability registers in Taiwan. Research in Autism Spectrum Disorders, 3/1(269-274) Lee, H, Song, D-H, Grinker, RR (2011) Prevalence of autism spectrum disorders in a total population sample. The American Journal of Psychiatry 168/9(904-912) Maenner, MJ, Durkin, MS (2010) Trends in the prevalence of autism on the basis of special education data. Pediatrics, 126/5 (1018-1025) Nygren, G, Cederlund, M, Sandberg, E, Gillstedt, F, Arvidsson, T, Gillberg, I. C, Andersson, GW,
Conclusion: There is international evidence to support local stakeholders views that the recognised prevalence of autism and autistic spectrum disorders has increased [in the last 10 years] however it is not clear that this is a true increase in the conditions. However, CAMHS episodes of care do not show evidence of local increase.
Page 288

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 191
Pedersen, A, Pettygrove, S, Meaney, FJ, Mancilla, K, Gotschall, K, Kessler, DB, Grebe, TA, Cunniff, C (2012) Prevalence of autism spectrum disorders in Hispanic and non-Hispanic White children. Pediatrics, 129/3(e629-e635) Pinborough-Zimmerman, J, Bakian, AV, Fombonne, E, Bilder, D, Taylor, J, McMahon, WM (2012) Changes in the administrative prevalence of autism spectrum disorders: Contribution of special education and health from 2002-2008 Journal of Autism and Developmental Disorders, 42/4(521-530) Schieve, LA, Rice, C, Yeargin-Allsopp, M, Boyle, CA, Kogan, MD, Drews, C, Devine, O (2012) Parent-reported prevalence of autism spectrum disorders in US-born children: An assessment of changes within birth cohorts from the 2003 to the 2007 National Survey of Children's Health. Maternal and Child Health Journal, 16/Suppl 1(S151-S157), 1092-7875; Yeargin-Allsopp M, Rice C, Karapurkar T, Doernberg N, Boyle, C, Murphy, C (2003) Prevalence of autism in a US metropolitan area. Journal of the American Medical Association 289/1(49-55)
Page 289

CAMHS Needs Assessment, 2013 Appendix 1 – Literature Review
<LOGO>
30/06/2015 192
9.1
Page 290

CAMHS Needs Assessment, 2013 Appendix - 2 Stakeholder interviews
<LOGO>
30/06/2015 193
Appendix 2 – Stakeholder Interviews Lambeth
Name Title
Dr Iris Rathwell Lambeth CAMHS Clinical Lead
Tracey Lewis Lambeth CAMHS operational manager
Stella Clarke LB Lambeth, AD Early Years and targeted services
Ian Lewis LB Lambeth, AD Looked After Children
John Anthony LB Lambeth, Head of YOS
Shaila Mahomed Youth and Violent Crime Lead
Geraldine Abrahams LB Lambeth, Head of Multi Agency Team
Phil Cokayne NHS Lambeth CCG, finance
Janet Bailey LB Lambeth, Head of Service CWD
Michael Donkor LB Lambeth, Head of SEN
Kelly Renzullo LB Lambeth, Head of Commissioning CYPS
Simon Froud LB Lambeth, AD Adult Social Care
Daniel Taegtmeyer Joint Commissioner for MH
Arabella Yapp Schools Education and Improvement Consultant
Christina Stewart Crown Lane Primary
Perry Saville SEN manager, Primary Pupil Referral Unit
Mary Murray Bishop Thomas Grant Secondary School, SW16
Anna Smagala Inclusion Manager, Juliens Primary School
Jeanne Crabtree Headteacher, Walnut Tree Walk Primary School
Melissa Kelsey MAT Senior practitioner
Clare Douglas MAT early support supervision practitioner
Southwark
Name Title
Kerry Crichlow Director of Children’s and Adults Commissioning and Strategy
Pauline Armour Neil Gordon-Orr
Head of Early Help–– Children’s Centres
Elizabeth Murphy Samaa ElAbd
Lead Clinician CAMHS Lead Pyschiatrist CAMHS
Gwen Kennedy Director of Client Group Commissioning and Partnerships
Jane Cliffe Lead GP for children’s
Paul Angeli Business Manager Assessment & Safeguarding Support
Jenny Brennan Service Manager Youth Offending Service
Yvonne Ely Head of SEN & Inclusion
Shirley Walker - Team Manager Children with Disabilities Sunshine House
Vicky Agnew Head Of Service - Family Focus Team
George Riley Transition Team Manager LD
Helen Naylor LA MH Commissioner
Rabia Alenxader NHS CAMHS Commissioner
Page 291

CAMHS Needs Assessment, 2013 Appendix - 2 Stakeholder interviews
<LOGO>
30/06/2015 194
Jo Fletcher CAMHS director
Rachel Webster Service Manager CAMHS Southwark
Sophie Wilson SENCO, City Academy
Judith Purkiss SENCO, Walworth Academy
Lambeth and Southwark
Barbara Hills Head of Children’s Services L&S,
NHS GSTT Community services
Jill Demenu Midwives Kings
1 Interview questions
1. What do you think are the key health issues and immediate needs have you come across in children and young people (under 19) with mental health or learning difficulties
a. The wider determinants of health (e.g. family influences, housing, education, employment)
2. Do you feel that there are specific groups of children and young people who have higher
need for services? (e.g. ethnicity, age, parental status, offenders etc)
3. What changes in mental health needs have you seen? (e.g. increase in psychosis, younger clients, more/less BME clients) and over what period of time.
4. Do you feel that there are specific groups of children and young people who are not
accessing services / treatment? Why do you think they are not engaged?
5. What areas of mental health services work well within the borough and meet children and young people’s needs?
6. What areas of mental health services work well within the borough and meet the needs
of parents or schools?
7. What areas of mental health services do not work well within the borough? a. Consider the care pathway and provision at different tiers of care b. Quality of current services
i. Training of staff ii. Appropriateness of offer
iii. Safeguarding c. Unmet needs
8. What do you think can best be done to reduce demand/need for in patient Tier 4
admissions
9. How do you think risk can best be managed. What steps to manage risk can be taken given the financial pressures?
Page 292

CAMHS Needs Assessment, 2013 Appendix - 2 Stakeholder interviews
<LOGO>
30/06/2015 195
10. What can be done to build on the interface with non-clinical services?
11. How do we best manage the fiscal challenges and what do you think CAMHS needs and
services should and/or will look like in 5 years?
12. What would you recommend to build sustainability in CAMHS provision?
13. What three things would you do to improve the mental health and wellbeing of young people in Southwark / Lambeth?
14. Is there anything else you would like to add?
Page 293

CAMHS Needs Assessment, 2013 – Appendix 3 – NICE guidelines
<LOGO>
30/06/2015 196
Appendix 3 - NICE Clinical Guidelines Pregnancy Antenatal care. NICE clinical guideline 62 (2008) Antenatal and postnatal mental health. NICE clinical guideline 45 (2007) Pregnancy and complex social factors. NICE clinical guideline 110 (2010) Postnatal care. NICE clinical guideline 37 (2006) Treatment Attention deficit hyperactivity disorder (ADHD). NICE clinical guideline 72 (2008) Autism in children and young people. NICE clinical guideline 128 (2011) Depression in children and young people. NICE clinical guideline 28 (2005) Bipolar disorder. NICE clinical guideline 38 (2006) Obsessive compulsive disorder (OCD) and body dysmorphic disorder (BDD). NICE clinical guideline 31 (2005) Psychosis and Schizophrenia in Childrn and Young people. NICE clinical guideline 155 (2013) Public Health Guidance General Social and emotional wellbeing in primary education. NICE public health guidance 12 (2008) Social and emotional wellbeing in secondary education. NICE public health guidance 20 (2009) Family Conduct disorder in children – parent-training/education programmes. NICE technology appraisal 102 (2006) Risk groups Looked-after children and young people. NICE public health guidance 28 (2010) Substance Misuse School-based interventions on alcohol. NICE public health guidance 7 (2007) Interventions to reduce substance misuse among vulnerable young people. NICE public health guidance 4 (2007)
Page 294

CAMHS Needs Assessment 2013 – Appendix 4 – Diagnoses Tier 2 and 3
<LOGO>
30/06/2015 197
Appendix 4 – Diagnoses Tier 2 and 3
Page 295

CAMHS Needs Assessment 2013 – Appendix 5 – Service activity
<LOGO>
30/06/2015 198
Appendix 5 Service activity Table 51 Southwark service activity by year and age group
Belgrave Adolescent Psychiatry
2009-10 2010-11 2011-12
Southwark Adolescent Services
2009-10 2010-11 2011-12
5-11 1 5 4
5-11 1 12-17 245 259 254
12-17 32 Over 17 1 0 1
Total 33 Total 247 264 259
Belgrave Children Psychiatry
2009-10 2010-11 2011-12
Southwark CAMHS Community
2009-10 2010-11 2011-12
0-4 9 0-4 12 20 45
5-11 19 5-11 149 119 127
12-17 16 12-17 135 119 99
Total 44 Total 296 258 271
Belgrave Paediatric Liaison Team
2009-10 2010-11 2011-12
Southwark CAMHS Neuro Developmental
2009-10 2010-11 2011-12
0-4 74 78 0 0-4 17 20 11
5-11 100 105 10 5-11 66 78 73
12-17 177 238 15 12-17 55 61 56
Over 17 2 3 0 Over 17 0 2 1
Not recorded 0 9 0 Total 138 161 141
Total 353 433 25
Parental Mental Health Team Southwark
2009-10 2010-11 2011-12
Southwark Carelink
2009-10 2010-11 2011-12
18-24 17 8 20 5-11 18 26 27
25-29 10 11 21 0-4 12 17 25
30-34 10 8 19 5-11 18 26 27
35-39 10 12 17 12-17 28 27 31
over 40 7 9 14 Over 17 0 1 0
Total 54 48 91 Total 58 71 83
Southwark CAMHS Children Centre
2009-10 2010-11 2011-12
Southwark Child and Family Service
2009-10 2010-11 2011-12
0-4 112 121 39 0-4 35 38 32
5-11 22 21 8 5-11 195 217 230
12-17 1 2 0 12-17 21 24 21
Total 135 144 47 Over 17 0 0 0
Total 251 279 283
Southwark Neuro Psychiatry Team
2009-10 2010-11 2011-12
Page 296

CAMHS Needs Assessment 2013 – Appendix 5 – Service activity
<LOGO>
30/06/2015 199
Table 52 Lambeth service activity by year and age group
Child and Adolescent Community Service Lambeth 2009-10 2010-11
2011-12
Lambeth CAMHS Adolescent Team 2009-10 2010-11 2011-12
0-4 4 16 6 0-4 1 0
5-11 55 137 93 5-11 13 9 0
12-17 50 200 263 12-17 211 90 0
18 1 18 1 1 0
Total 109 353 363 Total 225 101 0
Lambeth Autism and Neuro Developmental Service 2009-10 2010-11
2011-12
Lambeth CAMHS Neurodevelopmental Team 2009-10 2010-11 2011-12
0-4 1 5 0-4 23 15 4
5-11 3 6 5-11 112 84 45
12-17 3 12-17 59 57 49
Total 4 14 Total 194 156 98
Lambeth CAMHS ACIST 2009-10 2010-11
2011-12
Lambeth CAMHS Multi-agency Rapid Response Team 2009-10 2010-11 2011-12
5-11 6 3 5-11 7 5
12-17 2 2 12-17 30 11
Total 8 5 Total 37 16
0-4 0 0 0 Southwark Learning Disabilities
2009-10 2010-11 2011-12
5-11 7 2 0 0-4 14 0 0
12-17 7 0 0 5-11 63 0 0
Total 14 2 0 12-17 53 2 0
Total 130 2 0
Southwark TaMHS
2009-10 2010-11 2011-12
0-4 8 4 1 5-11 73 72 40 12-17 10 5 6 Total 91 81 47 Grand total 1844 1743 1247
Page 297

CAMHS Needs Assessment 2013 – Appendix 5 – Service activity
<LOGO>
30/06/2015 200
Lambeth CAMHS Early Intervention 2009-10 2010-11
2011-12 Lambeth GSTT 2009-10 2010-11 2011-12
0-4 51 39 12 0-4 5 6
5-11 275 193 127 5-11 48 77 10
12-17 202 131 119 12-17 99 130 8
18 1 18 1 1
19 2 21 1
Total 528 364 260 Total 154 214 18
Lambeth Children's Service 2009-10 2010-11
2011-12
Lambeth Children Looked After 2009-10 2010-11 2011-12
0-4 16 5 0-4 14 12 3
5-11 126 19 5-11 25 24 28
12-17 7 12-17 42 47 29
Total 149 24 Total 81 83 60
Lambeth Youth Offending 2009-10 2010-11
2011-12
Lambeth CAMHS Substance Misuse 2009-10 2010-11 2011-12
0-4 1 1 5-11 1
5-11 1 5 4 12-17 22 25 2
12-17 78 83 76 Total 23 25 2
18 2
Total 80 88 83
Page 298

CAMHS Needs Assessment 2013 – Appendix 6 – Home post code of service users
<LOGO>
30/06/2015 201
Appendix 6 –home postcodes
First part of postcode
Lambeth Lambeth Lambeth First part of postcode
Southwark Southwark Southwark
2009-10 2010-11 2011-12 2009-10 2010-11 2011-12
SW2 238 191 143 SE15 393 342 289
SW16 166 151 115 SE16 208 217 180
SW9 219 169 97 SE1 241 214 168
SW8 110 90 77 SE5 184 162 160
SW4 138 126 72 SE17 179 133 126
SE27 87 108 71 SE22 110 122 108
SE11 110 70 44 SE23 27 42 34
SE24 59 50 41 SE not L or S 41 36 27
SE5 52 48 40 SE21 30 38 23
CR 49 54 36 SE24 24 24 14
SE21 47 48 32 DA 14 14 14
SE19 52 40 30 SE27 11 12 11
SE1 28 32 13 SE11 18 18 10
SE not L or S 9 14 10 SE13 5 15 8
SW12 20 33 8 BR 13 13 7
SE17 17 16 8 SE19 10 12 7
SE25 18 11 5 CR 24 26 6
SM 12 10 5 SW9 13 22 5
No London 3 5 4 ME 22 17 5
RM 3 4 4 SW4 5 6 5
SE22 6 2 4 (blank) 11 4 4
SE15 15 10 3 SW2 25 23 3
DA 6 9 3 SW16 15 21 3
SW20 1 3 SE14 15 12 3
SE16 11 19 2 CT 8 10 2
SW17 8 4 2 SE26 6 10 2
East London 3 4 2 No London 10 5 2
SE12 2 4 2 IG 6 5 2
SE26 2 3 2 RG 3 5 2
SE20 4 2 2 NR 2 2
SE13 3 1 2 TN 7 11 1
IG 2 1 2 SW11 1 6 1
HA 2 SW8 7 5 1
RH 2 7 1 East London 10 4 1
TN 9 6 1 SS 6 3 1
SW11 2 4 1 SE25 5 3 1
CO 2 1 SE20 3 3 1
Page 299
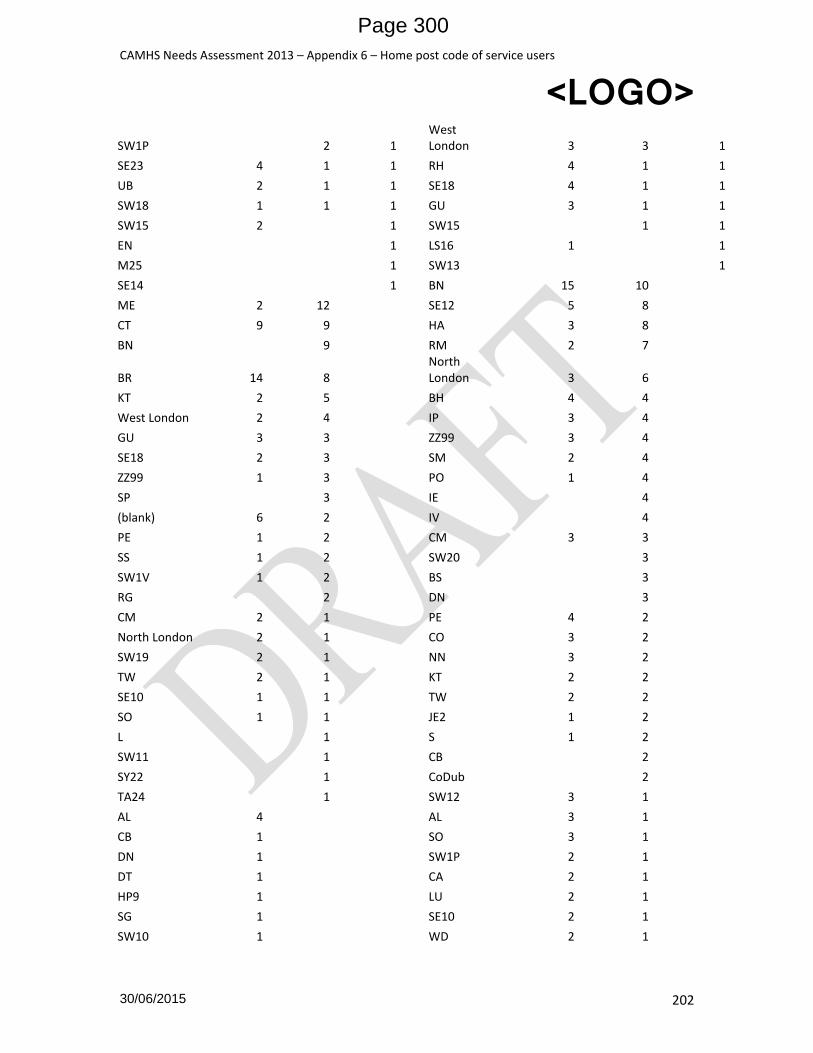
CAMHS Needs Assessment 2013 – Appendix 6 – Home post code of service users
<LOGO>
30/06/2015 202
SW1P 2 1 West London 3 3 1
SE23 4 1 1 RH 4 1 1
UB 2 1 1 SE18 4 1 1
SW18 1 1 1 GU 3 1 1
SW15 2 1 SW15 1 1
EN 1 LS16 1 1
M25 1 SW13 1
SE14 1 BN 15 10
ME 2 12 SE12 5 8
CT 9 9 HA 3 8
BN 9 RM 2 7
BR 14 8 North London 3 6
KT 2 5 BH 4 4
West London 2 4 IP 3 4
GU 3 3 ZZ99 3 4
SE18 2 3 SM 2 4
ZZ99 1 3 PO 1 4
SP 3 IE 4
(blank) 6 2 IV 4
PE 1 2 CM 3 3
SS 1 2 SW20 3
SW1V 1 2 BS 3
RG 2 DN 3
CM 2 1 PE 4 2
North London 2 1 CO 3 2
SW19 2 1 NN 3 2
TW 2 1 KT 2 2
SE10 1 1 TW 2 2
SO 1 1 JE2 1 2
L 1 S 1 2
SW11 1 CB 2
SY22 1 CoDub 2
TA24 1 SW12 3 1
AL 4 AL 3 1
CB 1 SO 3 1
DN 1 SW1P 2 1
DT 1 CA 2 1
HP9 1 LU 2 1
SG 1 SE10 2 1
SW10 1 WD 2 1
Page 300

CAMHS Needs Assessment 2013 – Appendix 6 – Home post code of service users
<LOGO>
30/06/2015 203
SW4 1 EX 1 1
SW5 1 SA 1 1
WD 1 SL 1 1
SW11 1 1
Grand Total 1588 1433 898 BD9 1
DT 1
DUBL 1
EI 1
GL4 1
PR18 1
SW6 1
TR1 1
TS12 1
YO8 1
EN 5
MK 4
SW18 2
1G1 2
B 2
ML2 2
NE 2
PL 2
SP 2
SW1V 2
SY22 2
UB 1
DE56 1
DY11 1
FK11 1
G32 1
L 1
LL53 1
SE229 1
SG 1
Grand Total 1844 1743 1246
Page 301

CAMHS Needs Assessment 2013 – Appendix 7 – TAMHS referral by schools
<LOGO>
30/06/2015 204
Appendix 6 Southwark TAMHS Referrals by school 2009-10 2010-11 2011-12 Total
Crampton Primary School 11 12 23
Langbourne Primary School 6 6 7 19
John Donne Primary School 4 7 7 18
Surrey Square Junior School 10 5 2 17
Surrey Square Infant School 9 6 15
St Saviour's and St Olave's C.E. School 3 4 6 13
Brunswick Park School 9 2 1 12
Camelot Primary School 6 6 12
Friars Primary School 6 3 3 12
St Michael's RC School 10 1 11
Victory School 5 5 10
Goose Green Primary School 1 8 9
Dulwich Hamlet Junior School 3 4 1 8
Charlotte Sharman Primary School 4 3 7
Towerbridge Primary School 6 6
Charlotte Sharman Foundation Primary School 4 4
Dulwich Village Infant School 1 2 3
Kingsdale School 1 1 2
Academy at Peckham 1 1
Albion Primary School 1 1
Bessemer Grange Primary School 1 1
Boutcher Primary School 1 1
Cherry Garden School 1 1
Dartford Grammar School for Girls 1 1
Elmgreen School 1 1
Friars Primary School 1 1
Harris Academy Bermondsey 1 1
Harris Boys' Academy, East Dulwich 1 1
Langbourne Primary School 1 1
Notre Dame Roman Catholic Girls School 1 1
Prendergast - Ladywell Fields College 1 1
St Martin-in-the-Fields C.E. High School for Girls 1 1
St Paul's Church of England Primary School 1 1 St Peter's Walworth Church of England Primary School 1 1
St Thomas the Apostle RC College 1 1
Westwood Language College for Girls 1 1
Grand Total 91 81 47 219
Southwark TAMHS Referrals by diagnosis
Diagnosis 2009-10 2010-11 2011-12 Total
Diagnosis not Specified 45 28 7 80
No Axis 1 disorder - CAMHS 12 16 24 52
Childhood emotional disorder, unspecified 2 7 4 13
Page 302

CAMHS Needs Assessment 2013 – Appendix 7 – TAMHS referral by schools
<LOGO>
30/06/2015 205
Mixed disorders of conduct and emotions 4 3 7
Childhood autism 3 1 1 5
Mixed disorder of conduct and emotions, unspecified 2 3 5
Other childhood emotional disorders 1 4 5
Oppositional defiant disorder 4 4
Adjustment disorders 1 2 3
Conduct disorders 2 1 3
Hyperkinetic disorders 1 2 3
Pervasive developmental disorders 2 1 3
Moderate depressive episode 1 1 2
Other mixed disorders of conduct and emotions 1 1 2
Panic disorder [episodic paroxysmal anxiety] 1 1 2
Reactive attachment disorder of childhood 2 2
Separation anxiety disorder of childhood 1 1 2
Unspec behav emotion disord onst usual ocur childhd adoles 1 1 2
Asperger's syndrome 1 1
Conduct disorder, unspecified 1 1
Depressive conduct disorder 1 1
Depressive episode 1 1
Depressive episode, unspecified 1 1
Disturbance of activity and attention 1 1
Dysthymia 1 1
Generalized anxiety disorder 1 1
Hyperkinetic disorder, unspecified 1 1
Mental disorder, not otherwise specified 1 1
Mixed dissociative [conversion] disorders 1 1
Nightmares 1 1
No Axis 1 Diagnosis 1 1
Nonorganic enuresis 1 1
Obsessive-compulsive disorder 1 1
Other anxiety disorders 1 1
Other mixed anxiety disorders 1 1
Other reactions to severe stress 1 1
Overeating associated with other psychological disturbances 1 1
Pervasive developmental disorder, unspecified 1 1
Post-traumatic stress disorder 1 1
Predominantly compulsive acts [obsessional rituals] 1 1
Sleep terrors [night terrors] 1 1
(blank) 1 1
Grand Total 91 81 47 219
Average age in years on referral to TAMHS
Year Female (n=92) Male (n=127) Both
2009/10 8.1 7.9 7.9
2010/11 8.7 7.6 8.1
2011/12 9.8 7.6 8.6
Page 303

CAMHS Needs Assessment 2013 – Appendix 7 – TAMHS referral by schools
<LOGO>
30/06/2015 206
Grand Total 8.8 7.7 8.2
Age on referral TAMHS
Age on referral (years)
2009/10 2010/11 2011/12 Grand Total
Female Male Female Male Female Male Both
3 3 3
4 2 3 4 1 10
5 3 6 2 1 1 2 15
6 7 9 6 7 2 4 35
7 3 6 4 9 2 7 31
8 2 7 3 9 1 2 24
9 3 6 7 6 7 4 33
10 7 9 9 4 2 5 36
11 2 3 3 2 1 11
12 2 6 4 1 2 15
13 1 1 1 3
14 1 1
15 1 1
16 1 1
Grand Total 32 59 38 43 22 25 219
Page 304

Supporting the Health of
Young People in LambethA summary report of the Health Related Behaviour Survey 2014
These results are the compilationof data collected from a sample ofprimary and secondary pupilsaged 8 to 15 in Lambeth duringthe summer term 2014.This work was commissioned bythe Lambeth Healthy SchoolsStrategic Group on behalf of theLondon Borough of Lambeth as away of collecting robustinformation about young people’slifestyles.
Teachers were briefed on how tocollect the most reliable data andthen pupils in Years 4 and 6 in theprimary schools and Years 8 and
10 in the secondary schoolsanonymously completed thequestionnaire. A total of 2411pupils took part in 26 schools.Completed questionnaires werethen returned to SHEU in Exeterfor processing.
Trend dataThis survey was also undertakenin 2004, 2006, 2008, 2010 and2012. On page 8, whereappropriate, comparisons havebeen made between the 2014data and those from previoussurveys.
Comparison to Wider DataLambeth data have beencompared with the Unit’s widerdatabase. This includes the resultsof surveys from areas such asBristol, Camden, Cornwall, Ealing,Essex, Oldham, Rochdale andWakefield.
A selection of some of thedifferences, where the level seenin the Lambeth data is either 5%above or below that in the widerreference data, is indicated by thesymbol ö on pages 4 and 7.
2411 young people aged 9 to 15 were involved in the survey:
SHEU is an independent research unit specialising in health relatedquestionnaire surveys of children and young people for Local Authorities,Public Health Teams, voluntary agencies, charities, schools and collegesand other partnerships. The Unit is also able to undertake consultation,monitoring and evaluation and bespoke research projects.
For more details please contact the Schools Health Education UnitTel. 01392 667272. www.sheu.org.uk
School Year Year 4 Year 6 Year 8 Year 10 Total
Age 8-9 10-11 12-13 14-15
Boys 334 339 343 206 1222
Girls 355 374 273 187 1189
Total 689 713 616 393 2411
TOPICS INCLUDE:
Citizenship
Drugs, Alcohol and Tobacco
Emotional Health andWellbeing
Healthy Eating
Lifestyle
Physical Activity
Safety
Relationships and SexualHealth
Page 305

Lambeth Primary schoolpupils in Years 4 and 6(ages 8 - 11)BACKGROUNDq 18% of pupils describe themselves as White British. 20%
describe themselves as Black British/ Black Caribbean.17% describe themselves as Black British/ Black African.8% said White European.
q 61% of pupils said that they were a practising member of areligion; 57% said they were Christian and 17% Muslim.
Spending Moneyq The main items Year 6 pupils spent money on were:
EMOTIONAL HEALTH & WELL-BEINGq 33% of boys and 27% of girls in the Year 4 sample had high
self-esteem scores. In the Year 6 sample, 42% of boys and27% of girls recorded levels of high self-esteem.
q 4% of pupils overall had low self-esteem scores.
q 44% of boys and 55% of girls in Year 6 pupils said that theyworried ‘quite a lot’ or ‘a lot’ about SATs /tests.
Other worries for the Year 6 pupils included:
37% of pupils overall reported that they feltafraid to go to school becauseof bullying, at leastsometimes.
q 6% of pupils overall saidthey felt afraid to go toschool because of bullying‘very often’.
q Behaviour widely reported ascausing distress included beingcalled nasty names, being pushed or hit for no reason andbeing teased or made fun of.
q 22% of pupils reported that they thought they were bulliedbecause of the way they looked and 17% thought becauseof their size or weight.
5% of pupils reported that they thought others might feargoing to school because of them.
HEALTHY EATING2% had nothing to eat ordrink for breakfast on theday of the survey.
q 46% of pupils had cereal forbreakfast and 45% toast onthe morning of the survey.23% said that they had fruit forbreakfast. 4% said they had achocolate bar or sweets.
q 8% said that they had no portions of fruit or vegetables theday before the survey. 35% said 5 or more portions.
q 4% of pupils said that they had no water to drink the daybefore the survey. 18% said that they drank 2 or more litres.
q Pupils were asked to identify, from a list, the foods/drinksthey had ‘on most days’. 59% said fresh fruit, 45% saiddairy produce, 75% said water, 45% said vegetables. 20%said that they had crisps, 19% sweets and chocolates and13% ‘non diet’ fizzy drinks ‘on most days’.
q 24% said they ‘rarely’ or ‘never’ ate any fish/fish fingers.13% said they ‘rarely’ or ‘never’ ate salads and 7% said they‘rarely’ or ‘never’ ate vegetables.
Dentistsq 15% of pupils said that they had never been to the dentist or
had been more than a year ago.
q On their last visit, 67% had a check up, 25% had fillingsand 5% said they had a brace fitted or checked.
q 91% of pupils said that they cleaned their teeth at leasttwice the day before the survey.
DRUGS, ALCOHOL AND TOBACCO
Drugsq 51% of Year 6 pupils and 40% of Year 4 pupils reported
that their parents had talked with them about drugs.
q 56% of Year 6 said that their teachers had talked to themabout drugs, 30% of Year 4 pupils said the same.
q 23% of Year 6 and 15% of Year 4 said that they had talkedwith visitors in school lessons, e.g. the police about drugs.
17% say they are ‘fairly sure’or ‘certain’ they knowsomeone who uses drugs(not medicines).
Year 6 Boys GirlsSweets, chocolate etc. 45% Sweets, chocolate etc. 43%Snacks e.g crisps, chips 44% Snacks e.g crisps, chips 43%
Computer games etc. 41% Books 38%Fizzy drinks 34% School equipment 32%
Year 6 Boys GirlsCrime 27% Crime 32%Family problems 24% Family problems 29%
Health problems 19% Problems with friends 22%The environment 18% The way you look 18%
q 85% said that theycould get water atschool easily, 13%said that they couldget water, but ‘noteasily’.
2
Page 306

Alcoholq 5% of pupils said that they had at least one alcoholic drink
(more than just a sip) in the past seven days.
q 1% said they had wine and 1% beer.
q Alcohol tasted by Year 6 pupils included:
q 80% of pupils said that they don’t drink alcohol; 16% ofpupils said that they drank alcohol but their parents ‘always’knew when they drank alcohol. 2% of pupils said that whenthey drink alcohol their parents ‘never’ or only ‘sometimes’know about it.
Tobaccoq 98% of pupils said they had
never tried smoking. 2% saidthat they had only triedsmoking once or twice.
q 0% of said they had smoked at leastone cigarette during the last sevendays.
q 78% said ‘NO!’ they wouldn’tsmoke when they are older,12% said ‘no’, 9% said maybeand 1% think they will smokewhen they are older.
q 10% say they ‘will’ or ‘may’smoke when they are older.
LEISURE
After school activitiesq 47% of the Year 6 boys and 61% of the Year 6 girls read a
book for pleasure. 62% of the Year 6 boys and 30% of theYear 6 girls played computer games.
q 71% of all pupils overall watched TV, 30% watched videosor DVDs.
q 15% of pupils looked after someone at home during theevening before the survey.
q 37% of pupils spent time playing with friends the eveningbefore.
Playtime
q 35% said they read quietly at playtimes or spend time in thelibrary, at least sometimes.
q 76% of pupils said that they ‘often’ felt safe during schoolplaytimes, 5% said ‘never or hardly ever’.
q 70% of pupils said that they ‘often’ felt happy duringplaytimes, 3% said ‘never or hardly ever’.
PHYSICAL ACTIVITY
q 80% of pupils reported that they enjoyed physical activities‘quite a lot’ or ‘a lot’.
q 74% considered themselves ‘fit’ or ‘very fit’. 4% said theyconsidered themselves ‘unfit’ or ‘very unfit’. 21% said thatthey weren’t sure.
q 67% of pupils reported that they had exercised hard enoughto make them breathe harder threetimes or more in the lastweek; 9% said not once.
21% of pupils spent morethan 2 hours doingPE/Games last week atschool.
q The top four physical activities for Year 6 pupils were:
(The table shows the proportion of pupils who said they didthese activities at least weekly).
Year 6 Boys GirlsWine 20% Wine 25%Beer or lager 14% Beer or lager 10%
Spirits 7% Spirits 9%Cider 5% Cider 3%
56% of Year 6 and49% of Year 4 spenttime doinghomework on theevening before thesurvey.
83% of pupils saidthey playedrunning/skipping/games/tag atplaytimes (more girlsthan boys) and 72%said they played ballgames (more boysthan girls).
q 49% of the boys and29% of the girlsplayed sport theprevious evening.
Year 6 Boys GirlsFootball 64% Running (races or tag) 53%Running (races or tag) 58% Keep fit 45%
Keep fit 54% Going for walks 47%Going for walks 38% Dancing/gymnastics 44%
3
Page 307

SAFETYq 80% of pupils said they have a bike. 33% said that they
wore a safety helmet when cycling ‘whenever possible’.29% said that they wore one ‘sometimes’ and 38% said‘never or almost never’.
q 39% of pupils reported that they had an accident in the lasttwelve months that was treated by a doctor or at a hospital.
q The main injuries sustained were cuts, bruises or sprains.9% had broken bones.
q The most common situations in which accidents happenedwere in the home, at school, playing sport and running orwalking outside.
q 58% said that they ‘usually’ or ‘whenever possible’ dosomething to avoid sunburn e.g. put on sunscreen.
q 61% of pupils said that they washed their hands beforelunch the day before.
q 91% of pupils said that they washed their hands ‘wheneverpossible’ after visiting the toilet.
q 32% of pupils reported thatthey had been approachedby an adult who scared ormade them upset.
q When asked if they knew theperson, 17% said that theydid not know the person, 6%said that they weren’t sure and17% said that they did know theperson.
q When asked what they did when this happened, 13% saidthat they ran or walked away, 12% of pupils said they toldan adult straightaway, 8% said that they told an adultafterwards, 11% told a friend but 10% said they kept it tothemselves.
q When a friend wanted them to do something that theydidn’t want to do, 37% of Year 4 pupils and 48% of Year 6pupils said that they could ‘usually or always’ say ‘no’. 17%of Year 6 pupils and 31% of Year 4 pupils said that theycould ‘rarely’ or ‘never’ say ‘no’.
q When they wanted a friend to do something 48% of pupilssaid that they usually or always knew what to say. 16% ofpupils said that they ‘never’ or ‘hardly ever’ know what tosay.
PUBERTY & GROWING UPq 78% of Year 6 girls and 64% of Year 6 boys said their
parents had talked with them about how their body changesas they grow up. 17% Year 6 pupils said that the schoolnurse had talked with them about how their body changesas they grow up, 7% of Year 4 pupils said the same.
q 69% of Year 6 and 48% of Year 4 pupils said that they feltthat they knew enough about how their bodies change asthey grow up. 8% of Year 6 and15% of Year 4 said that theydidn’t know enough. 29%overall said that they weren’tsure that they knew enough.
60% said that they knewenough about how theirfeelings and emotions changeas they get older.
q 22% of Year 6 pupils and 14% of Year 4 pupils said theirparents had talked with them about AIDS/HIV.
q 13% of Year 6 and 5% of Year 4 said that their teachers hadtalked with them about AIDS/HIV.
q 9% of Year 6 boys and 18% of Year 6 girls reported thatthey worried ‘quite a lot’ or ‘a lot’ about the way theylooked.
q 9% of Year 6 boys and 18% of girls said they worried ‘quitea lot’ or ‘a lot’ about how their body changes as they growup.
36% of Year 6 and14% of Year 4 saidthey knew about AIDS(HIV).
DIFFERENCES BETWEEN THE LAMBETH2014 SURVEY AND THE SHEU REFERENCE
SAMPLE FOR YEAR 6 PUPILS
For most of the questions in the questionnaire, LambethYear 6 pupils give similar responses to the wider SHEU data.Some differences (more than 5%) include:
ø 60% of Lambeth pupils said that they live with bothparents together. This is lower than the 71% seen in thewider SHEU reference sample.
ö 35% of Lambeth pupils reporting having 5 portions offruit and vegetables the day before compared with 29% inthe wider sample.
ø 15% of Lambeth pupils said that they have sweets andchocolate ‘on most days’ compared with 25% of thewider sample.
ø 18% of Lambeth pupils said that they have crisps ‘on mostdays’ this is lower than the 25% seen in the wider sample.
ö 21% of Lambeth pupils said that they cleaned their teeth3 or more times the previous day. This compared with14% of the wider sample.
ö 21% of Lambeth pupils had been a filling the last timethey visited the dentist compared with 16% of the widersample.
ø 35% of Lambeth pupils recorded levels of high self-esteem compared with 42% of the wider sample.
ö 18% of Lambeth pupils said that they know someonepersonally who uses drugs (not as medicines). This ishigher than the 11% of pupils in the wider sample.
ö 24% of Lambeth pupils said they had been bullied for theway they look This is higher than the 19% seen in thewider sample.
ö 74% of pupils in Lambeth described themselves as ‘fit’ or‘very fit’ compared with 69% of pupils in the widersample.
4
Page 308

Lambeth Secondaryschool pupils in Years 8 &10 (ages 12-15)BACKGROUNDq 12% of pupils describe themselves as
White British, 22% as BlackBritish/ Black Caribbean and22% as Black British/ BlackAfrican.
q 61% said that they are apractising member of areligion. 50% of pupils saidthey were Christian, 18% wereMuslim and 1% Buddhist.
q 57% reported that got spending money/allowance regularly,25% said they got money as they needed it, 4% said theyhad another system and 13% said they didn’t usually getany.
q 57% of pupils spent some of their own money on sweetsand chocolates in the seven days before the survey. Otherpopular items of expenditure were soft drinks 55%, fastfood 50%, clothes and footwear 45%, crisps 45%, andmobile phones 27%.
SCHOOL AND CAREERq 68% of pupils reported that they enjoyed at least half of
their lessons.
q 8% reported that they didn’t know if they would take anyGCSEs. 54% reported that they expected to take severalGCSEs and achieve good grades.
q 55% of pupils said they wanted tocontinue in full timeeducation after leavingschool.
q 44% of pupils want to find ajob as soon as possible, 15%of pupils said that theywanted to stay in theneighbourhood where they livedafter the end of Year 11.
q 55% said they want to get training for a skilled job afterYear 11.
EMOTIONAL HEALTH & WELL-BEINGq 67% of pupils reported that, in
general, they were ‘quite alot’ or ‘a lot’ satisfied withtheir life.
q Parents are the most popularsources of support for boysand girls for help withproblems.
q 8% of pupils reported that there were noadults they could trust.
q 49% of boys and 33% of girls had high self-esteem scores.
q 18% of pupils had medium - low self-esteem scores.
q The top three worries were:
(The table shows the proportion of pupils who said they worriedabout the problems ‘quite a lot’ or ‘a lot’.)
q 22% of pupils reported a fear of going to school at leastsometimes because of bullying. 5% thought others may feargoing to school because of them, 22% said they didn’tknow.
HEALTHY EATINGq 21% of Year 10 girls
reported having nothing toeat or drink for breakfast onthe day of the survey.
q 17% of Year 8 girls hadnothing to eat or drink forbreakfast on the morning of thesurvey. It is interesting that 43% ofYear 8 girls say that they would like to lose weight. 25% ofpupils reported having no lunch on the day before thesurvey.
q When asked what might encourage them to eat schoollunch more often, 67% said better food and 66% said alonger lunchbreak.
q Pupils were asked to identify from a list the foods they ate‘on most days’. 49% said meat, 35% said fresh fruit and32% said vegetables. 16% of pupils have chips, 22% crisps,28% sweets and chocolates and 24% ‘non diet’ fizzy drinks‘on most days’.
q 33% said they ‘rarely’ or ‘never’ ate any fish. 44% said they‘rarely’ or ‘never’ ate high-fibre cereals, muesli and 20%said they ‘rarely’ or ‘never’ ate salads.
13% of pupils said they never considered their health whenchoosing what to eat.
Year 8 Boys GirlsCareer 31% Exams and tests 55%Exams and tests 31% The way you look 45%Family 27% Career 41%
q 68% of pupils didhomework on theevening before thesurvey and 28% didover an hour.
Year 10 Boys GirlsExams and tests 50% Exams and tests 73%Career 39% Career 63%Health 28% The way you look 50%
5
Page 309

DRUGS, ALCOHOL & TOBACCO
DRUGSq 28% of pupils are ‘fairly sure’
or ‘certain’ that they knowsomeone who takes drugs.
q 3% of pupils reported that theyhad taken an illegal drug in thelast month. 6% had taken one in thelast year.
q 10% of Year 10 girls have takenan illegal drug and alcohol onthe same occasion.
q 1% of Year 10 pupils saidthey had taken more thanone type of drug on the sameoccasion.
Alcoholq 9% of pupils had at least one
alcoholic drink in the weekbefore the survey.
q Spirits, wine beer and pre-mixed spirits were the mostpopular drinks.
q 5% of pupils said that theydrank alcohol at home duringthe last seven days, 4% at afriends or relations house, 4% at a party or club, 0% at apub or bar and 2% outside in a public place.
q 1% of pupils were able tobuy alcohol from an off-licence that should sellonly to over-eighteens.
Tobaccoq 76% of pupils say that they have
never smoked at all.
q Boys: 3% of Year 8 boys and3% of Year 10 boys reportedthat they smoke ‘occasionally’or ‘regularly’.
q 50% of regular smokers said that would like to give upsmoking.
q 15% of pupils said that their mother smoked on most days,24% of pupils said that their father did. 20% said that theyhad a close friend that smokes on most days.
q 43% of pupils said that they had used a shisha, 14% in thelast month.
SEX AND RELATIONSHIPSq When asked what was their main source of information
about sex and relationships, 30% of Year 8 boys and 37% ofYear 8 girls said school lessons. 34% of pupils said theirparents and 30% said their friends.
q 52% of pupils said that they knowwhere to get condoms free ofcharge.
q 32% of Year 10 boys and 36% of Year 10 girls have beenoffered cannabis. 10% of the Year 8 pupils have beenoffered cannabis.
Year 10 boys Year 10 girls Year 8
q Girls: 2% of Year 8girls and 10% of Year10 girls reported thatthey smoke‘occasionally’ or‘regularly’.
q 41% of pupils saidthat someone whohas a sexuallytransmitted infectionmay not notice ifthere was anythingwrong with them.43% said that theydidn’t know if thiswas true.
q 21% said theybelieved there was aspecial contraceptionand advice servicefor young peopleavailable locally 67%said they didn’tknow.
6
Page 310

SAFETY
q 30% of pupils said they had taken painkillers once or morein the seven days before the survey. 32% said they had usedtreatments for skin problems.
q 20% of pupils rated the safety of their area, when going outafter dark, as ‘poor’ or ‘very poor’. 7% said this about goingout during the day.
q 12% of pupils reported thatthey were ‘fairly sure’ or‘certain’ that they or theirfriends carried weapons orother things for protectionwhen going out.
q 8% of pupils said that theyhad been the victim ofviolence or aggression in thearea where they lived in the past 12months.
q 47% of pupils said that they thought groups of peoplehanging around in public places was a problem in theirarea.
LEISURE AND WORKq The most common after school leisure activities on the day
before the survey were watching television, playingcomputer games and doing homework.
q 77% of pupils had used the Internet at home in the lastmonth and 64% at school.
q 72% said they have been toldhow to stay safe while chattingonline.
q 15% of pupils said thatsomeone had shared animage of them via socialmedia that had made themfeel unhappy.
q 16% of pupils said that they havea regular paid job during term time. The most commonforms of work for pupils are babysitting, working in a shop,hotel, bar or cafe.
PHYSICAL ACTIVITYq 49% of pupils said they they exercised
hard three or more days in theweek before the survey; 10%said not once.
q 23% said that they spentmore than 2 hours doingPE/Games in school lastweek.
q Outside school, football and 5 aside football were the mostcommon activity for boys. For the girls, walking anddancing were most common.
q When asked if there was anything they wanted to startdoing, swimming and football were the top answers.
q 32% of pupils said they were treated for an accident by adoctor or at a hospital within the year before the survey.84% visited the doctor and 82% the dentist in the twelvemonths before the survey.
Accident Doctor Dentist
DIFFERENCES BETWEEN THE LAMBETH 2014SURVEY AND THE SHEU REFERENCE SAMPLE
For most of the questions in the questionnaire, Lambethsecondary pupils give similar responses to the wider SHEUdata. Some differences (more than 5%) include:
ø 42% of secondary pupils in Lambeth said that they livewith both parents together. This is lower than the 62%seen in the wider reference sample.
ø 22% of pupils in Lambeth said they feel afraid to go toschool because of bullying at least ‘sometimes’. This islower than the 32% of pupils who said the same in thewider sample.
ö 76% of Lambeth Year pupils said that they had never eventried smoking. This compared with 63% of pupils in thewider sample.
ö 18% of Lambeth pupils said they had no portions of fruit orvegetables the day before. This is higher than the 9% seenin the wider sample.
ø 32% of Lambeth pupils said they have vegetables to eat‘on most days’ compared with 45% of the wider sample.
ø 38% of Lambeth pupils said that they wanted to loseweight. This is lower than the 44% seen in the widersample.
ø 9% of Lambeth pupils said they had an alcoholic drink theweek before the survey. This compared with 21% sayingthis in the wider sample.
ø 46% of Lambeth pupils had a school lunch the day before.This is lower than the 54% seen in the wider sample.
ø 69% of Lambeth pupils said they had visited the dentist inthe past 6 months. This compared with 84% of boys in thewider sample.
ø 32% of Lambeth pupils said that their lessons on drugeducation were ‘quite’ or ‘very useful’. This compared with40% of pupils in the wider sample.
ö 68% of Lambeth pupils said that they can ‘usually oralways’ say no when a friend asks them to do somethingthey don’t want to do. This is higher than the 63% of thewider sample.
7
Page 311

The Way Forward - over to you
For further information about thesurvey contact:Jehan ChaudhriPSHE & Healthy Schools ConsultantEducation Learning and Skills6th Floor,International House,6 Canterbury Crescent,London, SW9 7QETel: 0207 926 5019 or 07903 713 821email: [email protected]
The work was commissioned by the Lambeth Healthy Schools Strategic Group on behalf of the London Borough ofLambeth.We are grateful to the teachers, schools, and young people for their time and contributions to this survey. As aresult of their work we have excellent data to be used by schools, the Local Authority as well as other statutory andvoluntary agencies that support the health of young people in Lambeth. This work will inform action plans for jointworking between and within organisations involved in improving the health and well being of pupils in schools.
Lambeth Schools who took part in the survey:PrimariesBonneville Primary School, Christ Church (Streatham) CEPrimary School, Christ Church CE Primary School, CrownLane Primary School, Durand Academy, Henry CavendishPrimary School, Herbert Morrison Primary School, Julian'sPrimary School, Reay Primary School, St. Andrew's CEPrimary School, St. John's Angell Town CE Primary School,St. Luke's CE Primary School, St. Mary's RC Primary School,St. Stephen's CE Primary School, Telferscot Primary School,Vauxhall Primary School, Woodmansterne Primary Schooland Wyvil Primary School.
SecondariesArchbishop Tenisons CE School, Dunraven School, DurandAcademy, Lambeth Academy, Lilian Baylis TechnologySchool, The Norwood School, The Park Campus andSt.Martin in the Fields CE School.
Trendsø 13% of primary pupils said they drink non-diet fizzy
drinks ‘on most days’. This is a fall from the 17% seenin 2012 and 24% seen in 2010. It is also lower than the19% seen in 2008 and 18% in 2006.
ô 35% of primary pupils in 2014 said that they had fiveor more portions of fruit and vegetables the day before.31% said this in 2012, 33% in 2010 and 30% in 2008;all are still lower than the 36% who said the same in2006.
ö 80% of primary pupils in 2014 said that they do notdrink alcohol. This is higher than the 76% and 70%seen in 2012 and 2010. 67% said this in 2008 and 61%in 2006.
ô 22% of Year 6 pupils in 2014 said their teachers hadtalked with them about AIDS/HIV. This is lower thanthe 29% and 37% seen in 2012 and 2010. 31% saidthis in 2008 and 21% in 2006.
ø There has been a fall in the proportions of Lambethprimary pupils who report drinking alcohol theprevious week. 5% of pupils said they had an alcoholicdrink in 2014 compared with 6% and 11% in 2012 and2010, 8% said this in 2008 and 11% in 2008.
ö There has been a rise in the proportions of primarypupils in Lambeth who said they have never smoked atall. 98% said this in 2014 compared with 96% in 2012and 94% in 2010, 93% said this in both 2008 and2006.
ø 9% of secondary pupils in 2014 said that they drankalcohol the previous week. This has fallen from 15% in2012 and 22% in 2010. 17% said this in 2008 and 19%in 2006.
ö 76% of secondary pupils in 2014 said they have nevereven tried smoking. This compared with 72% who saidthis in 2012 and 73% in 2010. 67% said this in 2008and 61% in 2006.
ø 28% of secondary pupils in 2014 said they knewsomeone personally who used drugs not as medicines.This compared with 34% who said this in 2012 and30% in 2010. 38% said this in 2008 and 41% in 2006.
ó17% of secondary pupils in 2014 said they knew had atleast 5 postions of fruit and vegetables the day before.This compared with 19% who said this in 2012 and18% in 2010. 18% said this in 2008 and 19% in 2006.
ô 52% of secondary pupils in 2014 said they know whereto get condoms free of charge. This compared with59% who said this in 2012 and 53% in 2010. 63% saidthis in 2008 and 58% in 2006.
ø 78% of secondary pupils in 2014 said they are neverafraid of going to school because of bullying. Thiscompared with 83% who said this in 2012 and 83% in2010. 83% said this in 2008 and 85% in 2006.
ó15% of secondary pupils in 2014 said they had nothingfor breakfast that morning. This compared with 13%who said this in 2012 and 17% in 2010. 17% said thisin 2008 and 17% in 2006.
Page 312

1
Review of parenting and family support programmes in Lambeth A brief review of the evidence base and local need to inform refresh of the Parenting Support Strategy
Anne Rathbone
June 2013
Page 313

2
Table of Contents
Executive summary .......................................................................................................................................................... 3 1. Introduction ............................................................................................................................................................... 5 2. Methodology .............................................................................................................................................................. 5 3. Limitations of the review ...................................................................................................................................... 6 4. Findings ........................................................................................................................................................................ 6
4.1 National and local strategic context ................................................................................................................ 6 4.2 Rationale for Parenting Programmes improving outcomes for children........................................ 7 4.3 A review of parenting programmes available nationally – what the evidence says .................. 9 4.4 Current delivery of parenting programmes in Lambeth .......................................................................17 4.5 Demand for parenting programmes in Lambeth ......................................................................................19 4.6 Unmet need for specific target groups ...........................................................................................................24 4.7 Unmet need across all target groups ..............................................................................................................27 4.8 Co-ordination .............................................................................................................................................................30 4.9 Evaluation and tracking framework to assess effectiveness ...............................................................31 4.10 Parent engagement .............................................................................................................................................34
4.11 Other operational findings ............................................................................................................................ 35 5. Conclusions ............................................................................................................................................................... 39 6. Recommendations ................................................................................................................................................. 42
Appendix A ..............................................................................................................................................................................44 Appendix B ..............................................................................................................................................................................45 Appendix C...............................................................................................................................................................................46 Appendix D ..............................................................................................................................................................................48
Page 314

3
Review of parenting and family support to inform strategy refresh Anne Rathbone for London Borough of Lambeth June 2013
Executive summary Overall, there is a strong and growing evidence base for the value of interventions to improve parenting capacity in general, and for parenting programmes specifically, resulting in better outcomes for children and resource savings for society. Evidence highlights the importance of parenting programmes being delivered as part of a clear strategic direction, integrated into the wider offer and with strong quality assurance. This report was produced using a mixed methodology of desk research into the evidence base and stakeholder consultation through one to one and paired interviews and one focus group. Prevention and early intervention is key to supporting parents and improving parenting capacity and consequently child outcomes. It is never too early to work with a parent to educate them in how to promote the best outcomes for their children: from pregnancy to adolescence, parenting programmes are valuable. The main programmes on offer in Lambeth are evidence based and “home grown” developments by CAMHS build on the evidence and use validated evaluation measures. Research evaluations undertaken in the UK indicate positive impact for all the main programmes in Lambeth but no significant difference in impact between them. Mellow is not currently part of the Lambeth offer but has been suggested as a potential development. It has more emphasis on attachment theory and claims to be more accessible for vulnerable parents. It has an emerging evidence base, albeit based on small samples. There is a high level of vulnerability in Lambeth and applying a suggested prevalence rate of children with behavioural difficulties to the Lambeth under 19 years indicates that there may be between 6.720 and 13,440 children and young people in the borough with behavioural difficulties. Borough statistics give a picture of increasing need. There is a wide gap between estimates of need and actual provision. Levels of referrals seem highly unlikely to reflect demand and this is even more the case when compared to population need: more consistent provision, reducing waiting times, pro-active scheduling and promotion may stimulate referrals to reflect need more accurately. The main opportunities for development are: programmes for children with disabilities; targeted work with parents with additional mental health needs or
Page 315

4
vulnerabilities; programmes for parents to be; continuation of support for young parents and parents of older children and young people; building on positive engagement with dads in some Children’s Centres; ongoing consideration of the needs of minority ethnic communities; post programme follow up support and development of parent “ambassadors”. Discussion of allocation of parents whose children are subject to a Child Protection Plan would be useful to clarify expectations of facilitators and ensure the most appropriate response to this vulnerable group. Co-ordination structures need to be carefully planned and executed to provide appropriate quality assurance and support without stifling initiative. Data input and analysis (analysis of output data and input and analysis of impact data) is a priority area for improvement. A review and possibly standardization of the evaluation framework would be very useful. Parent feedback emphasises the value of friends, family and community support, including faith groups for a significant proportion. Some focused consultation with dads about how to reduce any barriers to engagement would be useful, as would consultation with parents on programmes about any ways in which referral and pre and post programme support might be improved. It is important that referrals are made as effectively as possible, as part of ongoing support to parents, in order to maximise the impact of parenting programmes. Increasing use of CAF in the referral process would maximise potential for tracking but care needs to be taken that this does not act as a barrier. A written quality assurance framework, sitting alongside guidance and clear expectations of facilitators, venue hosts etc., would be useful. The report provides recommendations for strategic overview and integration, improvements in co-ordination and expectations, monitoring and evaluation, review of programme delivery, quality and parents engagement.
Page 316

5
1. Introduction Parenting Programmes can be extremely cost effective in reducing subsequent high costs for child protection, juvenile justice and poor health (Allen, G. 2011; ACH and NEF 2009) but they need to be based on strong evidence, delivered strategically according to need and with strong quality assurance. London Borough of Lambeth has commissioned this review of parenting and family support, with particular focus on parenting programmes, which covers:
A review of current delivery of parenting programmes and available
evaluation across the multi-agency partnership in Lambeth.
Analysis of demand for parenting programmes using a wide range of
data from published statistical information to qualitative data gathered
through CAFs and available consultation with parents.
Assessment of demand at a universal and targeted level for specific
groups including for example vulnerable families, BME communities,
parents of children with disabilities, parents of children with challenging
behaviour for example at school pre/post exclusion or youth offending
or anti-social behaviour.
A review of parenting programmes available nationally including an
assessment of their strengths and weaknesses in relation to Lambeth’s
population and demand with recommendations that address the
universal and targeted dimensions of delivery.
Review and recommendations for an evaluation and tracking
framework to assess the effectiveness of parenting programmes.
This report outlines the findings from a process of consultation, reference to the academic and professional literature and local assessment and delivery data, as was available. It is structured in line with the main areas of the specification outlined above. It is hoped that the outcome of this review will be a current, relevant and quality programme of parenting support across the partnership that makes best use of available resources and improves the parenting capacity of those who parent and care for the most vulnerable groups of children and young people.
2. Methodology A range of stakeholders across the partnership was consulted for the review. The majority of interviewees were co-ordinators or facilitators of programmes, and some managers. Appendix B lists all those consultation for the review. Existing CAF data, reports and documentation have been reviewed in order to inform the mapping. Appendix D lists documents used as references for the review.
Page 317

6
3. Limitations of the review There have been some historical delays in monitoring and evaluation data collation and input for the parents’ programmes that has resulted in a gap in referral/retention information and evaluation reports. This has made assessment of volume and content demand difficult to undertake in a robust way (i.e. backed up with service specific data), but national and local overarching data has been used, and stakeholders’ views have provided anecdotal insight.
Due to restrictions of the timescale, parents were not consulted as part of this process but the parent feedback from a November Parents’ Event has been used to inform the findings (see Appendix C) and ways to improve parent engagement have been explored.
4. Findings
4.1 National and local strategic context Supporting Families in the Foundation Years (Department for Education 2013) stressed the vital importance of early life, both in its own right and for promoting future life chances. ‘The Government’s aim is to put in place a coherent framework of services for families, from pregnancy through to age five, which focus on promoting children’s development and help with all aspects of family life’.
The Lambeth Children and Young Peoples Plan has a strong emphasis on prevention and early intervention in its strategic priorities, in line with the national evidence base. The Health Check Report: Pregnancy to Two (hereafter referred to as NSPCC P-2 report), undertaken in Lambeth in November 2012, highlights many strengths of services for the youngest children and their parents including:
The 2012 Ofsted report which rated safeguarding in Lambeth as outstanding
Effective strategic and operational partnership working
Innovation and co-production in commissioning, enabled by the Co-operative Council model
Multi-Agency Safeguarding Hub is facilitating better decision making for children
The Multi-Agency Teams work closely with Health Visitors and Children’s Social Care Teams to promote effective early intervention
A strong strategic emphasis and partnership for addressing Violence Against Women and Girls
Vulnerable pregnant women are supported by specialist midwives
Effective reductions in Teenage Pregnancy despite funding cuts Children’s Centres provide a valuable universal access point as well as more targeted support to vulnerable parents and children.
Page 318

7
The Early Intervention Multi-Agency Teams provide support to children and families with medium to high levels of need. Children at most risk will be in contact with Social Services and may have a CIN or Child Protection Plan. The delivery of Parenting Programmes in the borough takes place within this context of a strong framework of strategy and services.
4.2 Rationale for Parenting Programmes improving outcomes for children The Allen review 2011 was commissioned by the Government to review the available evidence on early intervention. The evidence reviewed overwhelmingly suggests that early intervention (both in terms of intervening early in problematic situations and in terms of intervening early in a child’s life) resulted in better outcomes and a greater return on investment of resources. Specifically, parenting support is evidenced as being essential in prevention of and early intervention with children’s behavioural problems (Pugh, De’Arth & Smith, 1994), and there is extensive evidence now that parenting programmes have the potential to deliver positive outcomes on parental coping ability (mental well-being and resilience) and on child behaviour1 (Barlow and Cohen 2000; NICE, 2005; Allen Review 2001). The Mental Health Strategy for England: No Health Without Mental Health (DH 2011) recognises this, with specific references to the role of parenting support as a vital part of improvement mental health outcomes for both parent and child. The University of Warwick research Parenting Early Intervention Programme Evaluation (Lindsay, G. et al 2001 Department for Education: DFE- RR121(a), which is hereafter referred to as the PEIP evaluation, examined the effectiveness of selected programmes that already had some evidence base: Families and Schools Together (FAST), Positive Parenting Program (Triple P), Strengthening Families Programme 10-14 (SFP 10-14), Strengthening Families, Strengthening Communities (SFSC), and The Incredible Years, which are all part of Lambeth’s current offer.
The positive impact of parenting programmes on the mental health of the parent is worth considering further. The PEIP evaluation found that approximately 75% of the parents participating scored below the national median on mental well-being, but were in line with the national median in the questionnaire findings immediately post programme. After one year, their mental health scores had decreased somewhat but were still significantly higher than before they took part in the programme. Parenting support can be provided at any stage following conception, and there is evidence that antenatal support and education has potentially a high impact. The Allen review report highlights that pregnancy and the first year of a child’s life are
1 One overview of evidence is published by the United Nations Office on Drugs and Crime and is retrievable at http://www.unodc.org/docs/youthnet/Compilation/10-50018_Ebook.pdf
Page 319

8
critical in the child’s development, and establish patterns for future parenting. The NSPCC P-2 report, pinpoints pregnancy and birth as “a critical window of opportunity”. It is a non recurring chance to build on the hopes and determinations of parents to be to be the best they can be and do the best they can for their child at a time when a lot of professional contact and support is available. The report Conception to Age 2 – the Age of Opportunity (Wave Trust 2013) is the most recent national report to focus on the potential for early interventions at this first stage of life in improving outcomes for children’s emotional well-being, capacity for relationships, brain development, learning ability. Parent and carer mental health (before and after birth) is identified as crucial. It explores how multiple risk factors can negatively impact of secure attachment as well as practical parenting skills The most often cited argument for the economic advantages of early investment in parenting (i.e with parents of very young children) is that articulated by the economist, Nobel Laureate Professor James Heckman, who argues that the highest returns on investment into a child’s emotional and social learning foundations are from interventions before and between the ages 0-3. He highlights this as an opportunity to use limited investments to deliver immediate and long-term positive social and economic outcomes simultaneously (Heckman, J. and Masterov, D. 2004). Mental health promotion and mental illness prevention: the economic case (Knapp, M et al. 2011 London School of Economics), gives median estimated costs of a 8-12 week group parenting programme as £952 per family, compared to the estimated median cost of an individual intervention, which is given as £2,078. They take NICE guidance to make the assumption that 80% of people receive a group based intervention and 20% receive an individual intervention to reach an average cost per intervention of £1,177 per family. The following is an extract from the report, which reports calculations made on direct cost savings: Extract from Mental health promotion and mental illness prevention: the economic case (Knapp, M et al. 2011 London School of Economics) page 6
Total gross savings over 25 years amount to £9,288 per child and thus exceed the average cost of the intervention by a factor of around 8 to 1. Savings to the public sector come to £3,368 per child, including £1,1278 accruing to the NHS. Under the assumptions made, the intervention will provide a positive return to the public sector in year 8, and to the NHS in year 14, after the intervention. No benefits are assumed from a range of other potential wider impacts such as improved employment prospects, reduced adult mental health issues, and improved outcomes for the child’s family and peers; these are likely to be substantial, making the intervention an even better investment.
A short piece of work to update and supplement these cost savings figures and apply them to Lambeth would be valuable in making the case for Early Intervention services overall, and Parenting Support Programmes in particular. The PEIP Evaluation (Lindsay et al) emphasises the immediate and one-year follow up outcomes are more positive immediately and equally as positive after one year for parents of older children (8-13 years) as they were for the parents of younger children. So it appears that it is not the case that parenting programmes have less
Page 320

9
valuable outcomes on already established difficult parenting patterns and child behaviour, but it is the case than programmes delivered at pregnancy and pre-school years can prevent behavioural problems later, with all that this implies in terms of cost to the family, demand on services and use of resources.
4.3 A review of parenting programmes available nationally – what the evidence says There is strong support in the published literature for programmes for parents of all age groups, but particularly those that focus on prevention and early intervention i.e. with parents of earlier age ranges (Sainsbury Centre for Mental Health 2009). Whilst programmes aimed at parents of teenagers do show clear benefits, the biggest preventative impact is when parenting sensitivity is maximised at the early part of a child’s life (National Institute for Health and Clinical Excellence 2006).
Evidence-based parenting programmes are underpinned by four core theoretical principles that are themselves strongly based in evidence. These are:
social learning theory
attachment theory
parenting styles theory
the model of human ecology
Social learning theory assumes that the behaviour of a child is influenced by the way in which it is reinforced i.e. that good behaviour is rewarded and negative behaviour is either ignored or proportionately sanctioned. Social learning based programmes therefore focus on teaching parents strategies and techniques for promoting good behaviour and minimizing negative behaviour.
Attachment theory focuses on the innate need and ability of the infant to form emotional bond with its primary care giver. The strength (security) of this bond is strongly influenced by the carer’s ability to identify, understand and respond appropriately to the infants “bids” for attention. Programmes based on this theory therefore seek to improve parent sensitivity and promote positive attachment.
Parenting styles theory is based on research that highlights different parenting styles and their impact on children’s behaviour. It is based on the premise that the children of parents who have high levels of warmth combined with high levels of supervision are more likely to grow up confident, autonomous and socially responsible. Programmes mainly focusing on this theory are rare but it is usually incorporated into other mixed theory programmes.
The model of human ecology assumes that the quality of a child’s interaction with their environment influences their development, emotional stability and learning. It emphasises the role of risk and protective factors. Programmes using this theory help the parent identify the factors that help or are a barrier to positive behaviour and how to maximise protective factors in the various environments that the child operates within.
Page 321

10
The Department for Education has details of a wide range of parenting interventions that have been evaluated for their implementation in the UK by the National Academy of Parenting Research at King’s College London, against agreed standards for best practice. Some of these are individual or family based interventions, but some are parenting programmes. Most have their main elements as social learning theory and attachment theory, with social learning theory predominant.
Ratings have been applied to the programmes by the evaluators based on the Parenting Programme Evaluation Tool (PPET) 2008 as follows:
**** Strong *** Promising ** Preliminary * Requires further development 0 0 rated The table overleaf shows summarises the key points of the parenting programmes evaluated at 3 or 4 stars with comments on their relevance to Lambeth circumstances and need.
Page 322

11
Programme name
Rating Who is the programme for?
Programme outcomes Comments – relevant to Lambeth need
FAST 4 star Parents interested in supporting their child’s development and being involved in their local community
Improved child behaviour, achievement, social skills. Reduced risk of child offending. Improved parenting practices/competency, well-being
Already part of Lambeth offer with increasing levels of delivery
Standard Triple P
4 star Parents of children with mild to serious concerns about the child’s behaviour
Improved child behaviour, improved parenting practices/competency, improved parent wellbeing
Already part of Lambeth offer
Stepping Stones Triple P
4 star Parents with children with a physical or learning disability such as autism spectrum disorder, Down’s syndrome, Prader-Willi syndrome
Improved child behviour, improved parenting practices/competency, improved parent well-being, reduced parent stress, depression, mental health problems
Already part of Lambeth offer but needs to be increased. CAMHS are providing programme with a specific focus on autism.
Incredible Years Early Years
4 star Any parent with concerns about their child’s behaviour
Improved child behaviour, reduced child maltreatment (actual or risk) improved parenting practices/competency, reduced parent stress, depression, mental health problems
Already part of Lambeth offer via CAMHS (for parents of children 6-12 years, majority of children have ADHD/behaviour difficulties), could be extended subject to CAMHS evaluation data and identification of what it adds to offer
Family Foundations
3 star Cohabiting couples expecting their first child
Improved child behaviour, improved parenting practice/competency,
Group based aimed at parents to be. Not currently part of Lambeth offer and
Page 323

12
improved parent wellbeing Potentially meets an indentified unmet need
Programme name
Rating Who is the programme for?
Programme outcomes Comments – relevant to Lambeth need
Lifestyle Triple P
3 star Parents with an overweight child
Improved child general wellbeing and mental health, improved parenting practices/competency, other
Is specific to parents of overweight children, which is a current JSNA priority, so may be worth consideration with Health, in terms of extending Lambeth offer
New Forest Parenting Programme (NFPP)
3 star Parents of a child (3-11) diagnosed with ADHD
Improved child behaviour, improved parenting practices/competency
For parents of children 3-11 years
Parents Plus Adolescent Programme (PPAP)
3 star Parents with concerns about their child’s behaviour, emotional problems and/or learning at school
Improved child behaviour, improved parent wellbeing, reduced parent stress, depression, mental health problems
Less strength of evidence than other programmes already part of Lambeth offer, does not offer any new perspective
Parents Plus Children’s Programme
3 star Parents with concerns about their child’s behaviours, emotional problems, or learning at school
Improved child behaviour, improved child achievement, improved parenting practices/competency, improved parent wellbeing, reduced parent stress, depression, mental health problems
Less strength of evidence than other programmes already part of Lambeth offer, does not offer any new perspective
Parent plus Early Years
3 star Parents with concerns about their child’s behaviours: ADHD, emotional, development
Improved child behaviour, improved parents wellbeing, reduced parent stress, depression, mental health problems
Useful focus on ADHD. Historically part of Lambeth offer. Less strength of evidence than Stepping Stones
Page 324

13
and learning problems
Programme name
Rating Who is the programme for?
Programme outcomes Comments – relevant to Lambeth need
Pathways Triple P
3 start Parents with a child on the child protection register or at risk of maltreating their child
Improved child behaviour, reduced child maltreatment – actual or risk, improved parenting practices, competency
Triple P range part of Lambeth offer, Pathways delivery could be extended to meet the needs of families with CPP
Primary Care Tripe P
3 star Parents with initial concerns about their child’s behaviour or development
Improved child behaviour, improved parenting practices/competency, improved parent wellbeing, reduced parents stress, depression, mental health problems
Triple P range part of Lambeth offer
The Incredible Years Toddler
3 star Parents with a young child who is at risk of developing a substance misuse problem or conduct disorder when s/he is older
Improved child behaviour, improved child wellbeing, mental health, reduced risk of child substance misuse, improved parenting practice/competency
Incredible Years range part of Lambeth offer
Strengthening Families Programme
3 star Any parent or carer with a child between the age of 10 and 14
Improved child behaviour, achievement, reduced risk of child substance misuse
For parents and children together, doesn’t offer anything different from 4 star programmes already part of Lambeth offer
Page 325

14
The two programmes highlighted in green potentially offer a way of addressing identified unmet need in Lambeth - Family Foundations for parents to be and Lifestyle Triple P to address a key Public Health priority. All the programmes with four stars – the strongest evidence base - are already part of the Lambeth offer. The three star programmes other than those those highlighted in green do not add anything additional to the Lambeth offer. Triple P is recognised generally as an evidence based programme and is cited as such in the Allen Review 2011 and the Kings College Evaluations, but it should be noted in the interests of balance that some more recent commentators have questioned the validity of what they see as underpowered samples and other weaknesses in the quality of evidence (Coyne, J. and Kwakkenbos, L 2013; Wilson et al 2012). In local consultation, Triple P generally was valued by facilitators but thought to be more useful for parents with children under 12. Children’s Centre managers also value Triple P and report that the retention rate is high. In consultation, there was general consensus that Triple P - Stepping Stones is a successful and beneficial programme to the borough, as it is clearly targeted but uses generic Triple P principles with which most facilitators were familiar. The opportunities for peer support were viewed as very important in contributing to positive outcomes. Although figures are not available to substantiate, retention rate locally is reported to be high. The Race Equality Foundation has developed a strong evidence base for SFSC, consisting of their own collation and analysis of national output and pre and post measurement data, and of independent research studies (Wilding and Barton 2009; Farber and Maharaj 2005). Some of these studies have used the Strengths and Difficulties Questionnaire (SDQ) to measure impact. This measurement is currently being used by CAMHS to measure its programmes and could be considered as potentially a Lambeth wide measure, or part measure (as part of the Parenting Early Intervention Programme (PEIP) measure for example). In local consultation, facilitators of SFSC agreed that the programme needs a lot of commitment from both parents and facilitators but can be very beneficial particularly for parents of teenagers and particularly when localized to specific geographical communities. It was reported in the facilitators’ focus group that schools were generally very supportive of SFSC. The materials are seen as particularly accessible, able to accommodate very low levels of literacy and English as a second or other language.
FAST has a rapidly increasing evidence base (e.g. Sherman et al 2002) as a family skills programme. It has been recognised as such by the United Nations Compilation of Evidence-Based Family Skills Training Programmes. Facilitators and Parenting Managers report that feedback about the school based programme FAST is very good with a lot of parents and young people engaging in the programme. Whilst it is not a parenting programme per se, facilitators see it as a very useful and supportive expansion of the Parenting
Page 326

15
Programme offer. It could be viewed and used as a pre-programme offer or as a stepping-stone to SFSC in particular. It is seen as flexible and adaptable to local need. Incredible Years is quoted by the Allen Review and has a significant evidence base (for example Harrington et al 2000; Scott et al 2001; Eyberg et al 2008) as well as the Kings College London research, which show positive changes in child behaviour and parenting patterns. Speakeasy, developed in the US, is also based in evidence, mainly US based. A piece of recent work in the UK has asked questions of its relevance to a UK setting and called for further investigation into its outcomes in a UK context (Downing, J. et al 2011). However, this appears to be more a call for research specifically on its implementation within the UK, rather than any serious questioning of its impact overall. It has only been delivered once over the year by the facilitators consulted and it is suggested that a consideration is given to the whether it should be a higher priority given the borough’s focus on reduction of teenage conceptions.
There is an increasing body of evidence to show the value of peer support with parents “who are trained to work alongside professionals, but whose similar life experiences bridge the ‘approachability gap” (C4EO 2010). The PEIP evaluation concludes that there are only small differences in outcomes between the five key programmes2 evaluated and recommends therefore that choice of evidence-based programmes should be based on local need and priorities, facilitators’ experience of delivery, how they fit with the portfolio of service delivery (e.g. the Children’s Centres offer). There has been some interest expressed in Lambeth for a rapidly emerging programme “Mellow” which has a stronger basis in attachment theory than many other programmes, which was not part of the King College or PEIP studies. A description of the programme and evidence follows overleaf.
2 Families and Schools Together (FAST), Positive Parenting Program (Triple P), Strengthening
Families Programme 10-14 (SFP 10-14), Strengthening Families, Strengthening Communities (SFSC),
and The Incredible Years.
Page 327
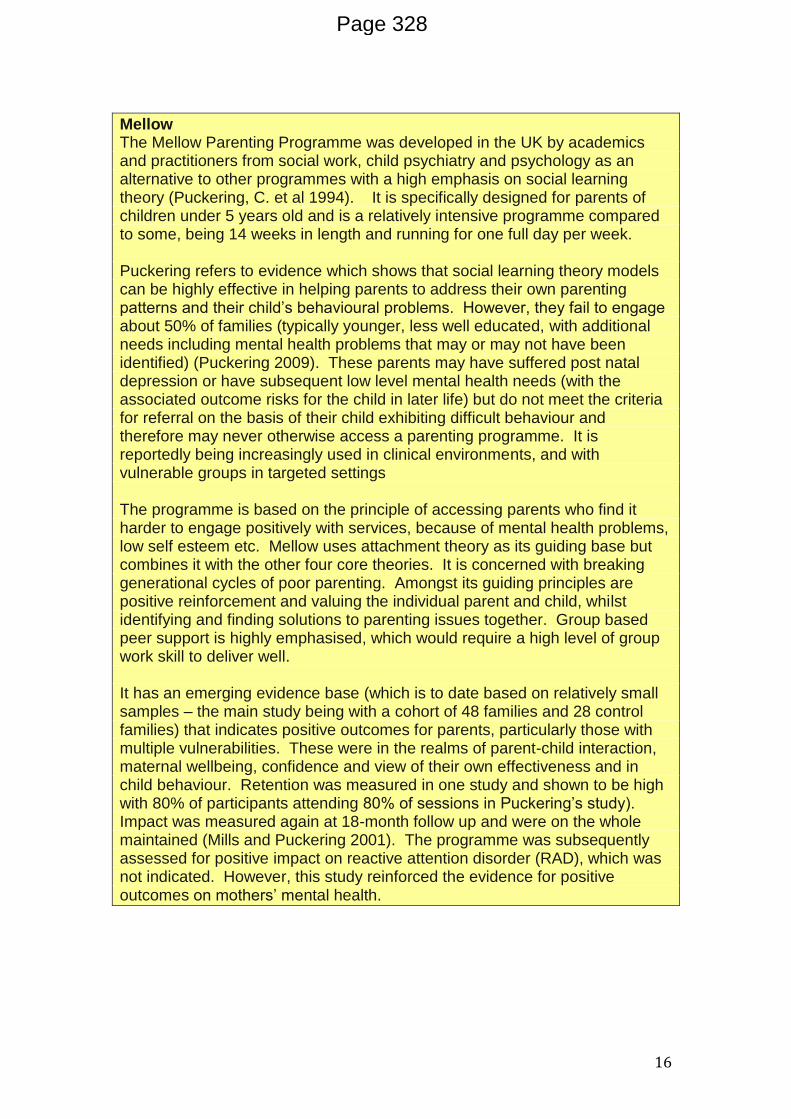
16
Mellow The Mellow Parenting Programme was developed in the UK by academics and practitioners from social work, child psychiatry and psychology as an alternative to other programmes with a high emphasis on social learning theory (Puckering, C. et al 1994). It is specifically designed for parents of children under 5 years old and is a relatively intensive programme compared to some, being 14 weeks in length and running for one full day per week. Puckering refers to evidence which shows that social learning theory models can be highly effective in helping parents to address their own parenting patterns and their child’s behavioural problems. However, they fail to engage about 50% of families (typically younger, less well educated, with additional needs including mental health problems that may or may not have been identified) (Puckering 2009). These parents may have suffered post natal depression or have subsequent low level mental health needs (with the associated outcome risks for the child in later life) but do not meet the criteria for referral on the basis of their child exhibiting difficult behaviour and therefore may never otherwise access a parenting programme. It is reportedly being increasingly used in clinical environments, and with vulnerable groups in targeted settings The programme is based on the principle of accessing parents who find it harder to engage positively with services, because of mental health problems, low self esteem etc. Mellow uses attachment theory as its guiding base but combines it with the other four core theories. It is concerned with breaking generational cycles of poor parenting. Amongst its guiding principles are positive reinforcement and valuing the individual parent and child, whilst identifying and finding solutions to parenting issues together. Group based peer support is highly emphasised, which would require a high level of group work skill to deliver well. It has an emerging evidence base (which is to date based on relatively small samples – the main study being with a cohort of 48 families and 28 control families) that indicates positive outcomes for parents, particularly those with multiple vulnerabilities. These were in the realms of parent-child interaction, maternal wellbeing, confidence and view of their own effectiveness and in child behaviour. Retention was measured in one study and shown to be high with 80% of participants attending 80% of sessions in Puckering’s study). Impact was measured again at 18-month follow up and were on the whole maintained (Mills and Puckering 2001). The programme was subsequently assessed for positive impact on reactive attention disorder (RAD), which was not indicated. However, this study reinforced the evidence for positive outcomes on mothers’ mental health.
Page 328

17
4.4 Current delivery of parenting programmes in Lambeth Programmes currently delivered across the multi-agency partnership in Lambeth are set out in the table below, which shows the programme name and age group relevance. An outline of each programme is attached as Appendix A.
Programme Target group relevance
Number in period 1/1/12 to 1/3/133
Comments
Strengthening Families Strengthening Communities (SFSC)
Particularly parents of school age children
6 Group based 13 week programme with a focus on community support and transformation
Triple P Parents of children up to 12
6 Group based 8 week programme
Teen Triple P Parents of young people 12-16
1 (not included in figure of 14 courses from Parent Managers)
Group based programme for parents of 12-16 year olds
Triple P Stepping Stones
Parents of children with disabilities
1 10 week group based programme for parents of pre-adolescent children who have a disability
Triple P individual Used occasionally by CAMHS and PRU for individuals with appropriate level of need
Individual work
Speakeasy Primary delivered within the last year
Can also be delivered in first year of secondary school - is a specific awareness raising programme for parents to help them discuss sex and relationships with their children
Incredible Years For parents of children 6-10 years
Delivered by CAMHS
Families and Schools together (FAST)
School age parents and children
This is not strictly speaking a parenting programme but has been included in the scope of the report
Early Bird Pre school age children diagnosed with Autistic Spectrum Disorders
1 Delivered by PRU
3 Not including CAMHS or St Michael’s Fellowship delivery
Page 329

18
Information from Parent Managers shows that there were 14 completed programmes in Lambeth between January 2012 and 1st March 2013, not including Teen Triple P, CAMHS or St Michael’s Fellowship delivery.
Of these, 10 courses show numbers of parents allocated and the mean number across these 10 courses is 15 allocations per course.
8 of these 10 courses show numbers starting the programme, the mean of which is 11.5.
Of these 8 courses the mean number of parents completing the programme is 9 (78%). This is in line with the average 75% completion rate found in the PEIP Evaluation (Lindsay et al).
It would be useful if these calculations were to be repeated when the monitoring data is fully up to date and available. Most Parenting Programmes are coordinated or supported to some extent by Parenting Managers, based in Early Intervention and Targeted Services, part of Children and Young People’s Service. This role includes:
liaison with and about: referrals;
parent contact and allocations;
venues; crèche facilities;
facilitator support and review meetings;
material development and dissemination;
co-ordination with external agencies within the partnership (e.g. CAMHS, commissioned agencies, Health Visitors, schools,
FAST, Save the Children); promotion; production of FAST site reports; monitoring and evaluation.
It also includes training up and supporting facilitators for the FAST programme, day-to-day management of budgets and is managed by the MAT Team Managers within Lambeth Children’s Services.
Referrals and integration Across the borough referrals into centrally co-ordinated Parenting Programmes come from a variety of sources:
MAT teams
Parenting Orders/YOS
CAMHS
Social care
Specialist Family Support Staff
Schools
Youth
Health Professionals e.g. Health Visitors
Self-Referrals
Solicitors
Other agencies outside of the borough
The YOS runs programmes in house for parents on Parenting Orders and another for voluntary referrals.
Page 330

19
The Children’s Centres are increasingly hosting programmes for their own cohort as part of their overall offer. CAMHS also deliver programmes in-house that are only accessible to CAMHS parents. CAMHS facilitators would be willing to deliver in other venues around the borough but allocations would still need to be CAMHS parents only, due to commissioning and assessment procedure restrictions. There is a feeling within CAMHS that this has resulted in tensions historically with partners. Now that CAMHS Early Intervention practitioners are linked with MAT teams, parents engaged with MAT teams can potentially access CAMHS programmes, via the Early Intervention practitioners. The Joint Commissioning Group facilitates a high level strategic partnership approach to CAMHS/Local Authority joint working, but focused operational links with regard to parenting programmes may help to encourage better access and mutual learning. There is a standard referral form for referral into centralized courses, but it is not universally used. Managers feel that consistent use of the form would improve the referral system. There was general consensus amongst facilitators who expressed a view that one referral form going to one central point is useful for centralized courses: “People don’t get missed. It’s a straightforward system.” Health staff (especially GP’s, Health Visitors, School Nurses and Midwives) and Faith and Community groups, Schools, IAPT services etc. are a valuable potential referral source and it is important that any referral mechanisms are actively promoted to them.
4.5 Demand for parenting programmes in Lambeth Lambeth is a very diverse borough with a high proportion of ethnic minority groups. The Joint Strategic Needs Assessment 2009 reports calculations that Lambeth is the most diverse borough in the capital. The numbers of Black Caribbean residents is high and the borough is a cultural focus for this population. The borough has an established Portuguese community and the Black African population is growing quickly. There are emerging Somali and Afghan populations. All of these groups have a high proportion of families within them.
A national study by Green et al. (2004) found prevalence rates of 10-20% of children in the UK had some form of behavioural disorder. This has long-term implications for the children and families involved and the wider community and public resource allocation, with clear links between behavioural, emotional and social difficulties (BESD) and later school exclusion and anti-social behaviour or involvement in the Criminal Justice System. There is evidence of links between early and middle childhood behavioural problems and mental health, crime, relationship, substance use and parenthood problems in adult life (Ferguson at al. 2009).children and young people with behavioural difficulties in the UK.
Page 331

20
Applying this statistic to what we know about local demographics gives an indication of need in terms of children with behavioural difficulties. The Lambeth State of the Borough report 2012 which uses the latest census data, identifies that 22.4% of the local population of 300,000 plus, is under 19. This gives an indicated under 19 population in 2012 of 67,200. Applying the prevalence rates indicated in the Green et al study would suggest a figure of between 6,720 and 13,440 children and young people living in Lambeth that have behavioural difficulties. The CAMHS draft needs assessment March 13 reports draws our attention to transition from primary to secondary school and any period following bereavement as vulnerable times for children and young people developing mental health issues. The draft Lambeth and Southwark CAMHS needs assessment looks at estimates of mental health disorders amongst children and highlights the following from national data:
Nationally, 9.6% of children and young people from age 5-16 are estimated
to have a mental health disorder
Conduct disorders are the most common type of mental disorder followed
by emotional disorders
More than one co-existing mental disorder is apparent in 1 in 5 of these
children (i.e. 1.9% of all children), of which the most common combination
is conduct disorder and emotional disorder, and conduct and hyperkinetic
disorders (0.7% of all children for each combination).
The NSPCC P-2 review was undertaken in Lambeth in November 2012 and reported in January 2013. It provides a current and comprehensive overview of what is known about need and provision in relation to babies from pregnancy to 2 years old in Lambeth. It highlights the significant growth in deprivation in Lambeth with a rise from 19th place in 2007 to 14th place in 2010 in the Indices of Multiple Deprivation (IMD) ranking. The report estimates that around 700 families will be affected by Housing Benefit cuts in Lambeth by end March 2013, and that the number of homeless households in temporary accommodation in March 2012 was 1,221, supporting the picture of social deprivation shown in the IMD ranking. More babies are being born in King’s and St Thomas’s with a rise at Kings, for example from 4000 in 2002 to 6000 in 2010. This is an indication of the likelihood that the numbers of children growing up in the borough will increase over the foreseeable future. This could equate to a likelihood of there being more parents, depending on the birthrate patterns of the cohort of mothers giving birth over this period.
Page 332

21
It is not known for certain how many babies are born into families who live “with heightened levels of vulnerability at any given time”, but the NSPCC P-2 report attempts to estimate this. Building on their own research (Manning, 2011) NSPCC have applied national estimates of babies at risk to the Lambeth population to reach an estimate of between 1,200 and 2,400 babies under 2 in this category. The rate of pregnancies amongst young women under the age of 18 is falling, with the latest figures for 2011 showing a 59.2% decline since the baseline date of 1998, and a 66.1% reduction since the peak at 2003. The number of conceptions was 147 in 2011 compared to 415 in 2003. This rate, however, is still high: the fourth highest in Inner London and the 11th highest in England. The NSPCC has also used national estimates of additional needs during pregnancy to estimate 1,400 pregnant women in Lambeth who may be experiencing domestic violence, problematic alcohol or substance use, depression or anxiety and who may not be receiving enough support. It is important to remember the high rate of mobility in Lambeth which can lead to rapidly changing population need as well as challenges in tracking individual families, their needs and what services they have received. The Common Assessment Framework (CAF) is crucial to this and has a high profile in Lambeth. There were an estimated 1085 families (national figure) in Lambeth who met “Troubled Families” criteria at the end of 2012. Applied against the apparent rising number of births at the main hospitals serving Lambeth residents, this gives a picture of significant and increasing need. This is reflected in reported demands on services, with the NSPCC reporting that Midwifery and Health Visiting services are struggling to meet increasing number of clients with additional need. If it can be assumed that parenting support could potentially benefit any parent in vulnerable circumstances, or with a child showing problematic behaviour, then it is clear that potential demand for programmes is extremely high in relation to demand. Group methods if effectively delivered, are potentially more cost effective and offer vital opportunities for peer support and integration into community capacity. What this potentially means then is that:
Applying NSPCC estimates of vulnerable babies and parents to be, alongside estimated numbers of “Troubled Families” it is clear that there are at least 1085 families currently that could benefit from parenting programmes if they have not already attended, 1,400 pregnant women or new mothers who have significant additional needs that may affect their parenting, and up to 2,400 babies who are being living in circumstances of
Page 333

22
heightened vulnerability at any one time. Of course, this number would be a significant underestimate of the need in relation to all age groups of children.
There are indicators that demand for early intervention with parents in Lambeth appears to be increasing, with rising levels of social deprivation and numbers of babies being born.
An estimate of children young people with behavioural problems in Lambeth is between 5,000 and 10,000 if the estimates of Green et al (above) are applied to local demographic data.
The British Psychological Society (BPS) has just published “Technique is not enough” - a framework for ensuring parenting programmes are socially inclusive. There is concern nationally that for the most vulnerable families participation and retention rates can be as low as 20% on some programmes (this does not apply to any Programmes in particular, but to some delivery of programmes across the range) – a figure that puts Lambeth retention rates (even though they need to be updated and confirmed) in a very positive light.
Analysis of available data from the Parent Programmes shows a record of 326 referrals between January 2010 and March 2013. Of these, 141 are recorded as having a CAF (43%). Fifteen (5%) had a Child Protection plan. Table 1. Below shows the four most often cited primary needs as a percentage of the total number of referrals made.
Primary need No. %
Addressing Child Behaviour 102 31%
Parenting Skills 87 27%
Setting Boundaries 36 11%
ADHD/Autism 18 6%
Other* 83 25%
Total referrals 326 n/a
“Other” includes a range of primary needs, which were all under 5% of recordings. These were: social isolation of parent; bullying; medical illness of someone in the family; mental health of someone in the family; parenting incapacity linked to recent release from prison. The Co-ordinators confirm that all referrals are recorded and so it is assumed that these 326 referrals represent all that have been made within the time frame. However, 326 referrals appear to represent a small fraction of the potential demand suggested by borough wide estimates of vulnerability and need, and it is important to consider the issues raised elsewhere in the report about the potential suppression of referrals that might be caused by waiting lists for programmes and by lack of pro-active scheduling and promotion. The draft CAF analysis for Quarter 2 in 2012-13 shows breakdowns of the 269 CAFs completed in the quarter. It indicates a similar pattern to the parenting support programme referrals described above, at least at the top end of need. For example, need for parenting support and behaviour of the child are the two highest recorded primary needs. The SEN data is separate
Page 334

23
from the CAF data and so Autism and ADHS cannot be seen within this category breakdown. The draft CAF analysis report highlights that parenting support, as a primary need, is higher than in previous years. The reason for this is not clear but may be due to a heightened awareness of the importance of effective parenting and/or of the support available.
Most facilitators agreed that whilst they were not aware of specific data, they did not have the sense of numbers of referrals being greater than provision, with the provisos that:
Waiting times could sometimes be an issue, especially if delivery was not
regularly spaced and there was a question for several faciltiators about
whether actual referrals were actually an underestimate of true demand
Limits on provision, irregularity of provision and lack of a planned yearly
schedule may be limiting referrals; “consistent delivery leads to better
promotion and case workers hold it in their minds; they have faith in it”.
There is a clear sense that Children’s Centres could accommodate more programmes and that there is a potentially higher demand for both Children’s Centre based and centralized programmes, if provision was planned to stimulate referrals (see below Scheduling and Promotion). Most agreed that the geographical spread of programme delivery has improved since centralized co-ordination has been established but some felt it could be improved further. The ideal cited several times was a rolling programme delivered across Lambeth. The number and availability of trained facilitators necessarily facilitates levels of provision, and it is important that their workloads are managed to enable delivery. New facilitators have
48
3532
12 12 12 10 8 7 6 60
10
20
30
40
50
60
No
of
ch
ild
ren
/yo
un
g p
eo
ple
CAF Analysis - 2012 - 13: Quarter 2Primary Needs Analysis - Top 10
Parenting Support : Engagementwith services
Behaviour: Disruptive/Violent
Behaviour: Mental health /Emotional basis
Social Isolation
Attendance
Domestic Violence
Family Breakdown
Parent/Carer with Medical/Illness
Page 335

24
recently been trained and this is an opportunity to revisit how much provision takes place but also who for and where it is delivered (see below).
4.6 Unmet need for specific target groups Parents of Children with Disabilities The NSPCC P-2 report highlights that support packages for parents of children with disabilities are not always most effective, and provision of parenting programmes for these parents was the unmet need most consistently raised in this consultation. The representative from Children with Disabilities reported a clear demand for more provision. Early Bird is currently running but is not fully meeting demand. Stepping Stones has had a long waiting list. It needs trained facilitators who are available to deliver and a critical mass of referrals to the programme. A Stepping Stones programme is scheduled to start in May to begin to address this issue. At the moment, the programme is not being actively promoted so it is difficult to comment on the potential level of demand. In this case, a holding group for parents on the waiting list may be very beneficial and could be a useful consultation opportunity in relation to planning, promotion and delivery issues. The most prominent gap in the existing programme provision is that for parents of children with autism or ADHD, across the age range but especially for parents of older children/young people. Trained CAMHS facilitators have developed such a programme for parents of younger children and one for parents of teenagers. Although not a validated programme, it could be measured for effectiveness through use of the Strengths and Difficulties Questionnaire (SDQ), which measures child behaviour and parent and child relationship changes and is currently used by CAMHS as part of their evaluation of parenting programmes. Due to capacity, each programme will only be delivered in CAMHS in alternate terms. Although CAMHS can only take CAMHS clients’ parents onto their programmes4, it may be useful to explore with CAMHS the possibility of them working with other appropriate facilitators to skill them up to deliver the programme to a wider referral group. There is uncertainty being expressed by some facilitators, about whether a targeted programme for parents of children with ADHD is best or whether their needs can be well met in a generic group. It is suggested that a specific focus group or meeting is convened to consider the issue of ADHD autism and how parenting programme planning can best address parents’ needs. Parents with additional mental health needs Poor parental mental health is shown to be a key risk indicator for children’s outcomes. The NSPCC P-2 report says that the mental health needs of
4 Places are usually offered to twelve parents and actual take up is usually between 5-10 parents
Page 336

25
pregnant women parents and children aged 0-5 are not always met in Lambeth, and also that there appears to be a significant under-disclosure of depression, anxiety and other mental health problems, alongside a reluctance to engage with services branded as mental health. Given the clear evidence that parenting programmes can improve parental mental health, it may be useful to consider targeting parenting programmes by working alongside services such as those for domestic violence and substance use recovery (aftercare) programmes and mental health adults services to facilitate access and consider if and when specifically targeted programmes are appropriate. The Warwick Edinburgh Mental Wellbeing Scale would be a potentially useful tool to measure impact on parents, if considered in line with the recommendation below for some standardisation of evaluation tools. Parents to be There is a clear and increasing evidence base for provision of programmes to parents to be (see above). The Health Visitors who took part in the focus group articulated what they saw as the value of this very clearly. Health Visitors already provide shorter input on sleep, nutrition, crying, weaning which is part of a universal offer to parents but acts as an engagement opportunity for more challenged parents. The representative from Children with Disabilities reported that several parents to be had said that a course on parenting a baby/child with a disability, delivered during pregnancy, would be useful. Currently there is limited provision for this group but it should be considered. Triple P Early Years could be adapted and there are other evidenced programmes emerging (see below). Young Parents It is important to recognise (as Lambeth has done so far) that despite significant reductions, teenage parents are a significant vulnerable target group in England and it is important that young mothers continue to have access to specialist support. St Michael’s Fellowship are commissioned to provide this targeted service and work with Children’s Centres to improve accessibility and delivery. Lambeth also has a very successful Family Nurse Partnership programme which provides evidence based support for young parents. The NSPCC P-2 report highlights that where this joint work is taking place, feedback and use of the Children’s Centres is good. Parents of Older Children and Young People There is a perception that the majority of parenting programmes are aimed at Early Years, but this is not backed up by available data on recent provision. – Whilst a clear priority for early years intervention is backed up by the evidence base, it is not to say that parenting programmes for those with older children are not potentially very valuable. Some feel that referral systems could better encourage referrals from parents of older children. However, in some services such as YOS, programmes for older children are very well developed. It would be useful to clarify in the Parenting Support Strategy what the parenting support offer is for those parents with teenagers.
Page 337

26
Development of the FAST programme with schools is a good option for addressing this need. Dads There are some examples of engagement of dads across the age range, for example in some of the Children’s Centres, but this is not consistent across the borough. There are high levels of engagement of young dads within the St Michael’s Fellowship programme. It is important that the learning from this existing and ongoing engagement is used to inform future planning of the Parenting Programmes (see also Parent Engagement). Minority Ethnic Communities and those speaking English as a second or other language The Portuguese-speaking Triple P programme was generally thought to be a good development that should be repeated, subject to evidence of demand. Some facilitators said that they had noticed a prevalence of ADHD in Somali families. This could usefully be looked into further. The YOS developed and delivered a programme several years ago for Muslim parents: “Being Muslim; Being British”, which was reported as having been very well received. This may be useful to build on for future targeted programmes. Parents attending a programme targeted at a particular ethnic community can expect to meet people they know from the same community. Whilst this may be seen by them as a good thing, it may also be a barrier for some so it is important to ensure a choice with interpreters available to generic courses as necessary. Needs in Lambeth can change very quickly with such a highly mobile population so this needs clear monitoring and regular review. When evaluation data is available it will hopefully provide a richer picture of the needs of Minority Ethnic parents (e.g. barriers to accessing programmes, cultural relevance, what is particularly valued). Provision targeted at different levels of need Some facilitators felt that parents who were subject to Child Protection procedures should have dedicated provision i.e. where they were not in mixed groups, or at least were not the sole parent in this situation. The facilitators concerned felt that it was unfair and potentially stigmatising to put one or two parents whose children had Child Protection Plans (CPPs) in a group of parents not affected by CPPs. .
Page 338

27
Building on this, it has been suggested that there could be two levels of allocation criteria, subject to programmes being available to meet demand. One programme could be targeted at parents with children coming under the category of Children in Need, or non Child Protection CAF assessments, self referrals, parents with shared custody arrangements, in custody disputes and with conditions of contract, plus Children’s Centre referrals. Parents of children with CPPs could be allocated to another programme (it has been suggested that this could possibly be alongside Parenting Order clients if their children were an appropriate age). The facilitators concerned felt that a specific group for these parents could encourage peer support and maximise engagement with the programme. An alternative view expressed by other facilitators and by the Social Care representative in consultation, is that there is also potentially great value in the cross-fertilization that can occur in carefully and pro-actively facilitated mixed groups. Examples were provided of the value to all parents in having parents at different levels of understanding and need. Further discussion of the pros and cons of this approach would be useful. Self-referral Of the 326 referrals recorded on the data obtained from Lambeth Parent Managers, only 11 of these were stated as self-referral. It is unclear whether this is caused by lack of active promotion to parents directly, by stigma associated with programmes that are viewed as for “problem families” only, or for another reason. This could be picked up in wider parents engagement undertaken by the department/Council. Facilitators spoke consistently of the benefits to parents who had self-referred and that self-referral should remain as an option. Given the small numbers, it is arguably counter-productive to exclude these parents from the targeted programmes given their assumed capacity for positive change, linked to their voluntary engagement.
4.7 Unmet need across all target groups Pre and post programmes or support One question that was raised early in the consultation was the need and options for pre-programme support. This would be some kind of “holding and preparation” support for parents, whilst waiting for structured programme entry. This could take different forms: one to one meetings, drop-ins etc. Most of those consulted felt that there was no apparent reason not to consider the idea of a pre-programme support group in principle, but that it may not be a priority given that:
There was not a universally strong sense amongst facilitators that parents
are arriving on programmes unprepared (although some facilitators gave
specific examples of this). There was also a strong sense amongst some
facilitators that raising confidence engagement and a sense of belonging
was a key part of the programme facilitation process.
Page 339
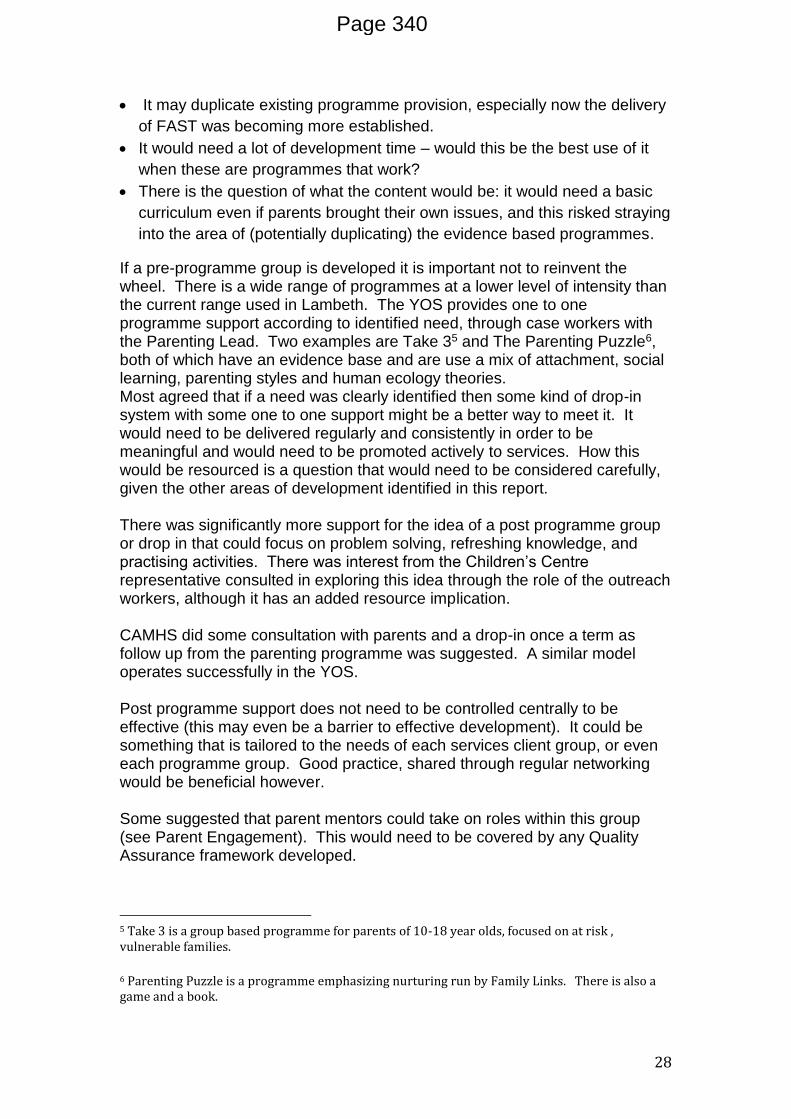
28
It may duplicate existing programme provision, especially now the delivery
of FAST was becoming more established.
It would need a lot of development time – would this be the best use of it
when these are programmes that work?
There is the question of what the content would be: it would need a basic
curriculum even if parents brought their own issues, and this risked straying
into the area of (potentially duplicating) the evidence based programmes.
If a pre-programme group is developed it is important not to reinvent the wheel. There is a wide range of programmes at a lower level of intensity than the current range used in Lambeth. The YOS provides one to one programme support according to identified need, through case workers with the Parenting Lead. Two examples are Take 35 and The Parenting Puzzle6, both of which have an evidence base and are use a mix of attachment, social learning, parenting styles and human ecology theories. Most agreed that if a need was clearly identified then some kind of drop-in system with some one to one support might be a better way to meet it. It would need to be delivered regularly and consistently in order to be meaningful and would need to be promoted actively to services. How this would be resourced is a question that would need to be considered carefully, given the other areas of development identified in this report. There was significantly more support for the idea of a post programme group or drop in that could focus on problem solving, refreshing knowledge, and practising activities. There was interest from the Children’s Centre representative consulted in exploring this idea through the role of the outreach workers, although it has an added resource implication. CAMHS did some consultation with parents and a drop-in once a term as follow up from the parenting programme was suggested. A similar model operates successfully in the YOS. Post programme support does not need to be controlled centrally to be effective (this may even be a barrier to effective development). It could be something that is tailored to the needs of each services client group, or even each programme group. Good practice, shared through regular networking would be beneficial however. Some suggested that parent mentors could take on roles within this group (see Parent Engagement). This would need to be covered by any Quality Assurance framework developed.
5 Take 3 is a group based programme for parents of 10-18 year olds, focused on at risk , vulnerable families.
6 Parenting Puzzle is a programme emphasizing nurturing run by Family Links. There is also a game and a book.
Page 340

29
The box below is an extract from the PEIP research (Box 4.13) giving examples of ways in which the pathfinder authorities developed follow up contact for parents completing courses. They reflect the ideas put forward in consultation.
Page 341

30
Examples of continued contact with parents post-course
Local evaluation follow up by questionnaire; active encouragement for peer
support; signposting to other services available for support
(SFSC) Parents contacted before group finishes to see if any want to train as a
parent volunteer. Follow up six times a year on a particular subject, in the form of
a workshop, on a subject that’s cropped up needing further exploration.
Many parents continue to meet up as part of a Parents’ Forum or through fund
raising for a local school or community organisation.
Parents offered follow up sessions, but facilitator keeps in touch with parents in
the normal course of her work.
Programme specific follow-up. Opportunity to progress to FASTWORKS-
good uptake. (Triple P) 3 month follow up phone calls (TP)
Added a Speakeasy workshop to many programmes and worked closely with local
colleges and Family Learning Service so many families have progressed to other
projects; SFP 10-14 booster sessions. Also RARPA (Recognising and Recording
Progress and Achievement), an award certificate for a non-accredited programme,
is popular.
Easiest for children’s centres who have natural ongoing contact; facilitators
encouraged to have a 3 and 6 month call back system; if referred through schools
or CAF parents tend to move to another form, another intervention. Follow up has
not been universal, or uniform.
Other improvements Some have suggested that programmes could be added to without losing their validity, in order to make them more holistic for example, integrating more on healthy eating into some programmes. Triple P can be delivered specifically for parents of young people and SFSC is most relevant to parents of this age group. Incredible Years delivery is currently mainly limited to CAMHS but some facilitators expressed interest in this programme, and how delivery might widen the range of options the borough. SFSC is fundamentally about the integration of learning into local communities. The delivery of the programme to parents is beneficial but “we are not really injecting a model into a community if we are not delivering at the most local levels (i.e. referring to estate based delivery of SFSC)”. Several SFSC facilitators felt that estate based delivery of SFSC would maximise its benefit, especially for parents of teens. Several people felt that there was a need to raise the profile of parenting and its value, both at a strategic level and with practitioners. The example of Essex was given where commissioners have taken a whole systems view of parenting resulting in the development of an independent parenting project through the Ministry of Parenting – a Community Interest Company.
Page 342

31
4.8 Co-ordination There is some tension apparent between on the one hand, the need for flexibility and ownership of Programme planning and delivery (on the part of, for example, Children’s Centres and/or facilitators) and on the other hand, practitioners and facilitators not having the capacity to do everything and needing some central support in relation to materials, budgets etc. It is important to have a balance between co-ordination and appropriate standardization, without stifling initiative. Local facilitators and individual services could usefully have more ownership of venues, how best to build on local community links, responding in a timely way to locally identified need and impetus. It is clear however that a central co-ordination role is valued. Consultation suggests some potentially beneficial opportunities for development. The sections on Scheduling and Promotion, Quality Assurance and Other Unmet Need provide more detail but these are summarised below:
The planning ahead and publicising of a yearly schedule of Parenting
Programmes
The re-establishment of good practice networking events for facilitators
A clear outline of respective responsibilities and expectations of all
Parenting Programme partners, applied consistently across the
partnership.
Joint working with Children’s Centres, so that learning from where
relationships between Children’s Centres, facilitators and co-ordinators are
working well, is built on to ensure that the Parenting Programme is fully
integrated into the Centre offer.
Appropriate autonomy for Children’s Centres to arrange evidence based
programmes themselves within Quality Assurance Frameworks and whilst
supplying monitoring and evaluation data to the central team.
Look into how post programme support options can be supported and
promoted; is a centralised, or service based follow up function the best way
to meet need?
Production of borough wide output and evaluation reports to enable
effective strategic planning
In terms of co-ordination the PEIP evaluation outlines several examples of different models. These included a core in-house team of facilitators within the Local Authority, a multi-agency team across a partnership, the commissioning out of all parenting programme delivery and co-ordination; hybrid models. The PEIP report does not recommend any one particular model but suggests that this should be decided in line with local circumstances and overall delivery structures. It notes that Co-ordination costs were typically higher in
Page 343

32
the early stages of establishing parenting programmes but most authorities reduced them over time as practices and systems became established.
4.9 Evaluation and tracking framework to assess effectiveness This is currently an underdeveloped area and improvements will significantly benefit the strategic planning and delivery of Parenting Support Programmes. The programmes delivered are evidence-based programmes – a valid treatment option just like any other - and need to be promoted as such. Monitoring and evaluation reporting and dissemination are key to the programmes’ credibility in the borough. The Children’s Centres are in the process of developing their own Performance Management Framework and parenting programme and other support will need to be included in this. It seems clear that for the Parenting Managers and Children’s Centres to work together on developing a set of common output and outcome measurements is important, as is the development of a system which uses resources effectively by not duplicating data collection, analysis and reporting, whilst ensuring that Children’s Centre data informs a borough wide view. Monitoring systems Facilitators keep an attendance list and have direct contact with referrers as necessary regarding attendance, engagement etc. Facilitators consistently report that they contact all parents pre programme and throughout the programme “the weekly call is built in”. It appears to make sense for facilitators to be a point of contact for caseworkers if they want to discuss level of engagement of their clients, but pro-active liaison with referrers is also important (for example, to alert referrers to non attendance) and this could be done more efficiently from the centre. This of course relies on capacity within the central team and on the facilitators’ timely submission of weekly attendance forms. Non-attendance should trigger a contact between the facilitator and the parent to maximise retention. It seems appropriate that the facilitator initiates this, but it would be useful to be explicit with all facilitators about this expectation. Overall, explicit guidance on respective roles and responsibilities would be useful, as facilitator practice outside of the sessions does not appear to be consistent. As mentioned above, there has been a historical backlog in input of referral and other output data. Since February, additional administrative support of one day per week has brought this up to date7.
7 Please note this refers to output data (referrals, profiles etc) and not evaluation data, which is still waiting to be inputted and analysed.
Page 344

33
There is a need for a database to manage monitoring information. What is most important is that the data is inputted consistently and reported in order to aid strategic and programme planning. Any future data system and reporting needs to include as a minimum:
Demographic data: family profile, age of parent and child/children, gender,
ethnicity, referring service
Numbers referred within any given quarter; numbers allocated within the
given quarter to each programme; numbers and percentages beginning
and completing the programme.
Evaluation systems There is a plethora of evaluation methods available and in use, with each programme having own evaluation form, plus a Lambeth specific “hybrid” form. Consultation indicates inconsistency in which evaluation measures are being used and the extent to which they are taken in by, or sent in to, the centre. Some use the “ Lambeth” form; some use Triple P form; some use the SFSC form which is part of the commitment to Race Equality Foundation; CAMHS use the validated Strengths and Difficulties Questionnaire, plus some wraparound questions. There is general agreement amongst Triple P facilitators that the evaluation forms are good – being non threatening and giving a good indication of immediate impact. Several facilitators of SFSC have commented that the evaluation requirements are “hard work” although respecting that they are part of the facilitators’ commitment and the Race Equality Foundation do make use of the data. The Early Bird Programme has a session evaluation form as does Incredible Years. Parents are encouraged to give details of their situation on the application form but this is not revisited at the end. Videos are produced at home visits and these could be compared to measure improvements for feedback to the parent but clearly it is difficult to translate this into hard measurement. From January 2013 collection of evaluations from facilitators has improved, but not all courses have resulted in evaluation data being provided to the Parenting Managers None of this data has yet been inputted or analysed and a piece of work is needed now to bring this up to date. Way forward for monitoring and evaluation A focused review of the evaluation framework to be used would be useful. It is recommended that one minimum data set be applied to all programmes if possible, so that comparable data can be presented for a borough wide overview, which at the moment is impossible to attain. There needs to be a decision made about whether a centrally composed evaluation form should be used. The obvious advantage is that all data would then be comparable and enable an overview of programme outputs and outcomes in Lambeth. Potential disadvantages that would need to be investigated and addressed are that the delivery agreement made with the programme developers include a commitment to use and return their programme specific monitoring forms.
Page 345

34
It should be possible to create a minimum dataset for Lambeth that covers the main data needs of the programme developers (e.g. Race Equality Foundation) and still provides a central overview. If there is to be a centrally composed form, it is important to ensure the right balance between providing useful data and accessibility. The current centrally composed form is clearly an attempt to do this. Generally, however, it is suggested that it could be simplified and visual representation of questions further increased. Retrieval of the monitoring and evaluation data needs to be built into the system. It has been suggested that a Parenting Manager could attend the final session at the end of a programme to receive feedback personally from the group and to retrieve monitoring and evaluation forms from the facilitator. Alternatively, the facilitator feedback meeting could be scheduled in at the end of the programme – in the following week at the same time and day as the rest of the programme. In either way the retrieval of this key information is less likely to slip. It is important to be aware that evaluations showing positive changes for the parent do not necessarily mean positive change for the child. The centrally composed form seems to address this but further exploration of the measurements could be useful (specifically looking at the SDQ and mindful also of the fact that immediate changes do not mean long term changes. Parenting measures that have been used in cross programme evaluations may be useful to consider as they are overarching and can be used to compare local outcome data to national evaluations. The most obvious measure is the hybrid questionnaire developed by PEIP evaluation to measure impact: the Warwick-Edinburgh Mental Well-being Scale (WEMWBS); The Parenting Scale (Irvine, Biglan, Smolkowski & Ary, 1999) to measure laxness and over-reactivity; the SDQ to measure child behaviour. Others are:
TOPSE University of Hertfordshire (measures relate to parents’ perception
but also child behaviour)
The Family Star, Triangle Training (measures progress over time)
The PEIP evaluation did a one-year follow up with all participants and achieved a 30% response rate. The department is aware of the gaps in the current monitoring and evaluation systems and data input/reporting and have requested additional administrative support to address this. To summarise, the key issues to be addressed include:
Articulation of a minimum monitoring dataset
Review of evaluation forms and a clear decision articulated to facilitators
about the evaluation measures to be used
Timely retrieval of end of programme output data and evaluations within
one week of the programme
Page 346

35
Regular reports to the Parenting Strategy Steering Group including
accumulated monitoring data.
It is recommended that reports to the Parenting Strategy Steering Group include: report of progress of delivery against a planned yearly calendar
accumulative analysis of output data
evaluation reports for completed programmes
4.10 Parent engagement Consultation with Parents has not been included as part of this review, but has been considered in terms of what we can learn from existing engagement, as well as how it could be improved in the future. The Parent Wall feedback from November 2013 indicates a good level of awareness and positive recognition of the value of “training” (7 out of 40 comments relate to this, which was the highest number of responses on a par with the child care and general support available at Children’s Centres. Other relevant areas that parents found useful in supporting them were:
Support from family, friends and wider community
The importance of faith group membership and attendance
The importance of attachment (bonding) with children These findings are potentially relevant in relation to SFSC in particular which aims to embed parenting support within the wider community, and possibly to the issue of suitable venues with faith establishments (specifically Churches) being valued by many respondents. There is no evidence of any direct consultation with parents about the process of assessment, referral, or what promotes retention in relation to the Parenting Programmes. Undertaking some focused consultation may provide useful insight across all services. This could usefully include consultation on delivery times, how working parents can best be supported, what follow up support would be most useful to them. Although some dads do engage in the programmes, some focused consultation could be done to explore how engagement with dads could be improved – how programme planning, scheduling, promotion and delivery could be made more relevant (see Parent Engagement). It is also suggested that care is taken to ensure good representation of dads in any mixed gender engagement processes. This may benefit from partnership work with St Michael’s Fellowship, key Children’s Centres e.g. St Stephen’s, and other relevant services. For parents of disabled children, there is a group in Contact a Family which many consultees agreed was a good organisation to use for “getting the word out” about a programme and for gaining parents’ views.
Page 347

36
Ideas for post programme follow up and “what next” should be included in programmes and fed in as part of the evaluation process, then followed up with parents appropriately. Parents who have successfully completed the programme could be supported to act as Peer Mentors on follow up support sessions or drop-ins for example.
4.11 Other operational findings How referrals could be improved There is a consensus that there are examples of poor referrals and lack of integration of parenting support, leading to resistance on the part of referred parents, with examples cited from Social Care, MAT teams and Children’s Centres. It is important to acknowledge here that there were also examples cited of excellent practice in all of these services. Poorly executed referrals to centralized courses may lead to these parents being apparently unprepared, defensive, even aggressive, particularly in the case of parents subject to Child Protection procedures. Specific examples given, from the perspective of Parenting Managers and Facilitators, included:
Referrals of parents without adequate preparation, resulting in parents
arriving with false expectations of the programme (e.g. being told it is a
drop-in; wrong age group relevance) and feeling as though they are being
punished, which some facilitators reported is very difficult to turn into
positive retention.
Referrals of parents who had just or were in the process of losing their children allocated to programmes with parents who had their children at home. Referrals as a “late in the day fix” rather than a pro-active intervention. There was acknowledgement that this was sometimes necessary but earlier referrals may contribute to a greater impact.
Referrals made at the end of a Social Care intervention with no provision made for follow up.
Facilitators felt that these difficult situations could undermine them and that they can also result in high drop out rate, as they can concern and alienate other parents. Programme facilitators, managers of services and Children’s Centres agreed that integration of parenting programmes into the overall service offer was important and this means that they should not be seen “fix-all” but should be one intervention with effective wraparound one to one support. However, not everyone agrees that this is being achieved in practice. This is something that the Parenting Managers could usefully take a lead on moving forward.
Page 348

37
In Children’s Centres good practice would be for outreach workers to meet all the Early Years parents who are allocated to a programme and provide ongoing support to them, as well as post programme support. The need for effective preparation and follow up is recognised at a strategic level in Social Care, and a process of mutual liaison (including, for example, attendance by Parenting Managers at Social Care Team meetings) is recommended to jointly work out the best way forward. This could usefully be extended to MAT team meetings. This is also recognised as a potential issue for parents referred within the YOS on Parenting Orders, but care is taken that it is actively addressed. This is helped by the fact that the YOS has an internal Parenting Support lead, who works closely with case workers to ensure effective mutual liaison including:
YOS Officers being encouraged to do one to one work with parents (in
complex cases, jointly with the Parenting Lead), in preparation and follow
up to programme attendance.
Weekly “surgery” for parents in which Officers can request time for parents
who have complex needs or are not engaging for some reason. The
Parenting Lead works with the parents and provides advice to the Officer
on how best to move forward with support.
YOS Officers are encouraged to use the “Family Focus” and “ CAF” cards8
to generate discussion with young people and parents about family issues,
following team training. There is a plan to introduce a monitoring of their
use within the YOS.
The Parenting Managers expect to follow up each referral with a telephone call to the parent, but this does not preclude the need for effective preparation of the parent by the referrer. One way to address the need for effective preparation, suggested in consultation, would be to provide one to one support within the team, as a “holding exercise”. There is a wider consensus, however, for the better integration of preparation and follow up into casework practice, which integrates the role of the Parenting Programmes into the wider system and is more resource effective. It is clear that what is needed is a system whereby support and momentum for the parent is established and maintained from the point of crisis or the referral trigger, running through attendance on the programme and ensuring post programme support is in place. This needs to be understood at strategic and practice level and implemented as relevant to individual services.
8 The Family Focus and CAF cards are part of a range of facilitative resource materials developed by Metacards, with the aim of helping professionals working with children, young people and families to facilitate a child or parent focused self assessment. For example: discussions to enable CAF assessment (CAF cards and Early Years CAF cards; , identifying and working towards life goals (Power cards); identifying family and parenting issues (Family Focus Cards). For more information please see www.metacards.co.uk
Page 349

38
Referrers can have play a major role in maximising the benefits of a programme to parents by:
Presenting the parenting programme as a positive opportunity to learn with
other parents, not a punitive or an “or else” intervention.
Making sure that they themselves understand the ethos and key features of
the programme/s they are referring to (the key features are common across
the programmes at a fundamental level). Provide an overview of the
programme. Ensure that parents know it is a group and not one to one.
Making sure that they communicate pro-actively with the facilitators, who
can work better if they are prepared for particular resistances or needs; that
they establish good mutual links, check attendance and engagement.
Referral through CAF Some referrals currently come through CAF assessment and request for services, rather than the Parent Programme Referral form. There is a suggestion that all referrals should go via a CAF (unless they are subject to a different statutory assessment process). This could include self-referrals who could be offered a CAF alongside their referral being processed. Staff feel that an advantage of referrals going through CAF is that this would make “tracking” of a parent easier. There is consensus across Parenting Managers and facilitators that a potential disadvantage of the use of CAF would be a resulting drop in self-referrals, due to concerns about sharing of information: an effective targeting of the provision away from universal access. The CAF is focused specifically around the needs of children and young people but within a context of their home and wider environment. Some felt that the undertaking of the CAF within the MAT teams would minimise any associated barriers. See also Parents’ Engagement.
Scheduling and promotion There is a general consensus across facilitators and referrers that a schedule of programmes, planned and publicized at the beginning of April for a year ahead would be a significant improvement and may help the quality of referrals into Programmes thus giving a more accurate picture of demand. Whilst data indicates that all referrals get allocated a place on a programme (although there may be some waiting time), there is also a clear feeling that lack of regularity in delivery or lack of borough wide promotion of what is available, for whom and when is probably limiting referrals i.e. that staff are more likely to refer clients when they are aware of current and relevant availability. In this respect, the level of allocation to programmes may not be a true reflection on demand. The Parenting Programmes are not uploaded to younglambeth.org. However, this is inconsistent with other partnership provision and it is recommended
Page 350

39
that the Parenting Programmes information be on younglambeth.org. There are examples on the site of services that are mainly accessed by professional assessment and referral rather than directly open access. The site is accessed by professionals as well as potential service users and is valuable for this reason, even for targeted programmes. A clear communications plan is recommended.
Quality and Quality Assurance Consultees were asked specifically about quality issues and, whilst there were some responses that highlighted historical issues, they appear to be isolated and to have been addressed effectively. There is no clear overarching Quality Assurance system, which is exacerbated by gaps in monitoring data. However, each programme has its own Quality Assurance guidelines that have clear overlaps in their underpinning principles and could easily be combined to produce one framework. There is recognition that there is always the potential for facilitation to be patchy and that peer learning and co-facilitation is a good way to address this issue. Currently, there are no good practice sharing networking opportunities. There was general consensus amongst facilitators consulted that it would be useful to reinstate them. The PEIP evaluation highlights effective facilitator support as a critical success factor. It is important that the potential facilitators who are recruited and trained have the ability to manage challenging group dynamics, as well as deliver parenting related content. There has been some drop out of facilitators since being trained, which could be for several reasons:
Due to restructuring some have changed positions or are no longer working for the borough
Some received training but subsequently did not feel confident to deliver
Some have not been allocated time to deliver or have not been able to reduce their caseloads for the length of the programme
Some facilitators consulted agreed that it is important that people are not forced to take on the role, even after training: “the spirit has to be there”. The expectation of managers however is clear that training and accreditation is conditional on a commitment to deliver programmes, with appropriate support. Existing facilitators were keen to support newly trained facilitators through co-facilitation and networking, if the opportunities were provided. A written quality assurance framework, to sit alongside guidance on roles and expectations of facilitators is recommended. This should include:
Page 351
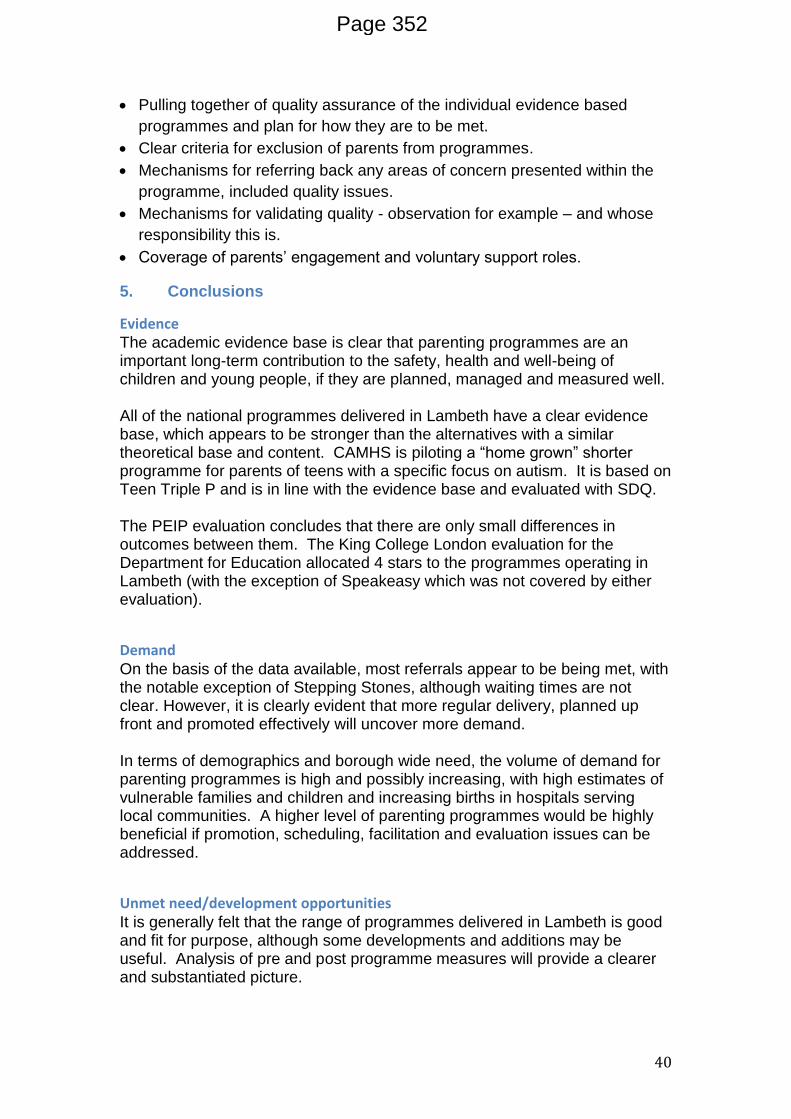
40
Pulling together of quality assurance of the individual evidence based
programmes and plan for how they are to be met.
Clear criteria for exclusion of parents from programmes.
Mechanisms for referring back any areas of concern presented within the
programme, included quality issues.
Mechanisms for validating quality - observation for example – and whose
responsibility this is.
Coverage of parents’ engagement and voluntary support roles.
5. Conclusions
Evidence The academic evidence base is clear that parenting programmes are an important long-term contribution to the safety, health and well-being of children and young people, if they are planned, managed and measured well. All of the national programmes delivered in Lambeth have a clear evidence base, which appears to be stronger than the alternatives with a similar theoretical base and content. CAMHS is piloting a “home grown” shorter programme for parents of teens with a specific focus on autism. It is based on Teen Triple P and is in line with the evidence base and evaluated with SDQ. The PEIP evaluation concludes that there are only small differences in outcomes between them. The King College London evaluation for the Department for Education allocated 4 stars to the programmes operating in Lambeth (with the exception of Speakeasy which was not covered by either evaluation).
Demand On the basis of the data available, most referrals appear to be being met, with the notable exception of Stepping Stones, although waiting times are not clear. However, it is clearly evident that more regular delivery, planned up front and promoted effectively will uncover more demand. In terms of demographics and borough wide need, the volume of demand for parenting programmes is high and possibly increasing, with high estimates of vulnerable families and children and increasing births in hospitals serving local communities. A higher level of parenting programmes would be highly beneficial if promotion, scheduling, facilitation and evaluation issues can be addressed.
Unmet need/development opportunities It is generally felt that the range of programmes delivered in Lambeth is good and fit for purpose, although some developments and additions may be useful. Analysis of pre and post programme measures will provide a clearer and substantiated picture.
Page 352

41
Delivery of Stepping Stones is a priority for attention and delivery is being planned for the summer in advance of planning on the basis of this review. Another priority gap is programme provision for parents of children with autism or ADHD. There is some provision in CAMHS and if it cannot be opened up to non CAMHS cohort then perhaps CAMHS can share their practice and be involved in skilling up other facilitators. There are several issues that need to be addressed or clarified in relation to this and it is suggested that a specific meeting or wider consultation focused on this would be useful. Engagement with dads is improving and there are some examples of very good practice but it is important that work continues to ensure consistency across the borough. Consultation with dads about their preferences and needs would be beneficial. The Portuguese-speaking Triple P programme was considered to be very useful although evaluation reports are not yet available. Other findings regarding specific provision for ethnic minority groups were inconclusive. Post programme support was seen as a potentially useful development. It should be locally owned and tailored to local and group specific need as far as possible. Pre programme structured support was generally felt to be difficult to implement and the need is unclear on a borough wide level. However, any improvements that services can make in preparing clients for engagement with programmes is likely to result in greater benefit. Mellow has a promising evidence base and offers a stronger focus on attachment theory. It may be useful to pilot and evaluate this programme in Lambeth as part of any revised offer. Family Foundations for parents to be is rated 3 stars (promising) by the Kings College Evaluation and could potentially be a development complementary to the current offer. Lifestyle Triple P has a focus on overweight children’s parents and this addresses a high Public Health priority. It may be beneficial to pilot this in Lambeth.
Co-ordination, facilitation and integration The co-ordination of programmes across the borough is valued for centralised programmes. Care needs to be taken, however, to get the most helpful balance between appropriate standardisation and encouraging helpful initiative, motivation and energy in the field. There have recently been insufficient facilitators to offer a full and inclusive schedule but this has now been addressed, with more facilitators trained, many of them in the MATs. They need to be supported and regularly networking with a clear agenda informed by facilitators appears to be a beneficial way forward.
Page 353

42
The parenting programmes need to be integrated into the offer and continuum of support of services, MATs and Children’s Centres. They need to be allowed to have ownership of them, including responsibility for integrated pre and post programme support. Scheduling ahead and promotion of programmes in a centrally produced format would be helpful, encourage a strategic overview of the balance of provision and how it relates to need, and give a clearer picture of real demand. Gaps in monitoring and evaluative data, inputting and reporting are limiting strategic decision making and addressing this needs to be a priority to ensure that full information is available for the financial year 2013-14.
Referrals, engagement and retention Retention on programmes appears to be high but this conclusion is based on partial data and anecdotal feedback and cannot be substantiated. Facilitators report that quality of referrals and caseworker support has a significant impact on quality of engagement and retention. However, the potential for resistance on programmes such as these will always be present and working with this is part of the facilitation skill. This issue is one on which it would be useful to share good practice. A decision needs to be taken on the extent to which a CAF is the preferred referral mechanism and if so, how the system can be administered to minimise any barriers to self-referral. It is important to utilise the potential of all services, including health staff, community groups and schools, as referrers.
Strategic Overall, it is important that parenting has a high profile in the work of Children’s Services and the borough as a whole and that clear strategies are in place to ensure it is integrated into wider communities, providing longer term peer support opportunities for parents and building social capital.
Page 354

43
6. Recommendations
Overarching recommendation
That the revised Parenting and Family Support Strategy includes a commitment to address the data, promotion and quality assurance issues highlighted in this report and then subsequently to increase the amount and range of parenting programmes offered.
Co-ordination and local ownership
Agree a clear outline of respective roles and responsibilities, which allows
for appropriate autonomy of local services within a coordinated, borough
wide framework.
Monitoring and Evaluation
Address monitoring and evaluation gaps as a priority to enable informed
strategic planning and prevent undermining of confidence in the wider
programme administration.
Decide on an evaluation framework that can provide a borough overview
and ensure consistency in implementation.
Range of programme delivery
Maintain existing programme provision and increase the volume as much
as possible to meet the evident demand based on data about need
particularly for vulnerable families.
Prioritise increased delivery of Stepping Stones and a pilot targeted
programme for parents of children with ADHD or autism.
Review need for Portuguese speaking programme on receipt of analysed
evaluative data.
Consider how post programme support needs can best be met.
Consider how the learning gained by parents from the programmes can
best be integrated into their wider communities to maximise the capacity of
the parents in that community.
Pilot and evaluate Mellow programme as an alternative to mainly social
learning theory based programmes.
Page 355
44
Consider pilots of Family Foundations and Lifestyle Triple P.
Promotion, referrals and allocation
Decide on a referral form or mechanisms and ensure consistency in
implementation.
Develop a clear communication plan for the Parenting Programmes offer.
Ensure that referral mechanisms are actively promoted to relevant partner
services, including Health Visitors, midwives and School Nurses.
Ensure a schedule is planned ahead, effectively promoted and regularly
updated with amendments and additions to promote confidence and more
pro-active and appropriate referrals across the borough.
Parenting Managers to attend Children’s Centre, Social Care and MAT
team meetings as appropriate to ensure a good mutual understanding and
partnership working.
Consider the different views expressed by some facilitators about whether
parents of children in Child Protection procedures should be allocated to a
specific programme, or whether there is more value in mixed provision.
Quality
Produce a clear borough wide Quality Assurance framework that address
QA requirements of delivered programmes as well as locally identified
requirements.
Re-instate facilitators networking events and consult with them on content
and scheduling.
Consider how learning from CAMHS and the YOS referral systems and
delivery can inform wider provision.
Parents Engagement
Develop a clear rationale and processes for parents’ engagement.
Page 356

45
Appendix A Outline of key programmes currently used in Lambeth
FAST (Families and Schools Together) – originated in USA
Age range 3 -18 years
Core programme 8 weekly 2.5 hour evening sessions, school-based. Followed by two years of parent-led, school-supported, monthly booster sessions.
Session structure Family tables including meal; peer activity (parent group; child group); parent- child activity, closing .
Participants Families with children in a year group in a school serving a multiple risk neighbourhood.
Facilitators Five per hub - professionals from multiple agencies and parents of children in an older year group
Example aim To increase protective factors for child
Incredible Years – originated in USA
Age range 8-13 years (for the PEIP programme)
Core programme Combines elements of the School Age BASIC program (12-16 sessions) with the ADVANCE parent Program (9 sessions) making 18-22 sessions of 2-2.5 hours.
Session structure Set out in manual – includes group discussion, video and live modelling, role play or small group rehearsal. Refreshments provided.
Participants Group of 10-14 parents
Facilitators Two group leaders
Example aim Treatment and prevention of child behaviour problems
Strengthening Families Strengthening Communities (SFSC) – originated in USA
Age range 3-18 years
Core programme Thirteen weekly 3 hour sessions.
Session structure Set out in manual – includes facilitator modelling, role play, lectures, discussion.
Participants Group of 8-15 parents
Facilitators Co-facilitation model – practitioners from any occupation,
Example aim To promote protective factors for child
Triple P (Positive Parenting Program) – originated in Australia
Age range 0-16 years
Core programme For PEIP, typically Level 4 Group or Group Teen – eight sessions: five as 2-hour group sessions, three as 30 minute telephone calls.
Session structure Set out in manual – includes presentations, video demonstrations, discussion
Participants 10-12 parents
Facilitators One facilitator required – basic professional training required
Example aim To enhance parents’ knowledge, skills, confidence
EARLY BIRD
Core programme Combination of group and individual home visits. Two and a half hour sessions over three months
Session structure Group activities, video feedback, one to one support and training
Participants Six families
Facilitators One facilitator required, Training by NAS Early Bird Centre, Yorks
Example aim To improve child parent inter-action and communication
SPEAKEASY – FPA
Core programme Group activities and training with option for accreditation with OCN
Session structure One session per week for 8 weeks
Participants 8-12 parents
Facilitators One facilitator
Example aim To help parents and carers gain confidence and skills to talk to their children about sex & relationships Adapted from Lindsay, G., et al (2011). PEIP evaluation with Speakeasy and Early Bird added in.
Page 357

46
Appendix B Stakeholder consultation
Jane Cullinan Mauline Vernon
Parenting Leads Lambeth Children’s Services
27th Feb
Laura McFarlane Geraldine Abrahams
MAT Team Managers Lambeth Children’s Services
4th March
Laura Liverotti Velma Bryan
Programme delivery 5th March
Jo Lawrence SLAM CAMHS 5th March
Karen Nugent CWD/SEN Lambeth Social Care
5th March
Margaret Fergus Programme delivery 6th March
Kofo Agbalaya Lucy Bannister Ferisha Silvera Michelle Thompson Claire Barrow Debbie Senior
Family Support Worker Intensive Support Workers for Troubled Families Manager, Parenting Team, St Michael’s Fellowship Early Intervention Health Visitors
6th March Deliverers focus group
Geraldine McCormick Lambeth Teenage Pregnancy Strategic Partnership
6th March
Laura Griffin Early Intervention Strategic Lead Lambeth Children’s Services
8th March
Richard Baldwin Programme delivery 13th March
Page 358

47
Appendix C Breakdown of Parent Wall Feedback Collected November 2012
What support would help you be the parent you want to be?
Outside our influence
Inside our wider influence
Inside our sphere of influence (in terms of parenting and family support)9
More money (1) More support from family and partner I don’t any help (2) Nothing - get all I need from Sure Start (1)
More structured activities, holiday activities, out of school activities (4) including activities for parents and children together (2) English language support (depending on meaning) (1) Health and other professionals going into schools (1) Better communication between agencies (1) Male mentors for my sons (1) More support for fathers especially single dads (1) Parent support at the weekend (1) Counselling (1) More health visitors and shorter queues at the baby clinic (1) Financial advice (1)
Training, parenting programme (7) Financial training (2) Support (1) Parent Mentor (1) English language support (depending on meaning) (1) More activities like today (1) Creche supported training More (free, cheaper) child care, longer crèches at children’s centres (7) Longer opening hours at children’s centres (1)
9 subject to resources
Page 359

48
Breakdown of Parent Wall Feedback Collected November 2012 (continued)
What assists you in being the best parent you can be?
Outside our influence
Inside our wider influence
Inside our sphere of influence (in terms of parenting and family support)10
Husband, family, mother in law, friends (19) Faith, attending place of worship (8) ‘Me time’ (1) The love of my child, caring for my child children themselves, bonding with my child (6) Personal life-view: determination; ambition, goals, not being too attached to money (3) Sacrificing full time work to give to my children (2) Being there for my children (1) Work (2) Internet (1) Support from the community (1)
Places to go with the children that are free Good the way the hospital monitored my son (1) School admissions (1) The Council (1) School x 2 Places to go: libraries (2); parks and playgrounds (1); places that are free (1)
Support from parent trainer (1) Children’s centre family
10 see footnote 1
Page 360

49
Appendix D References
Allen, G. M.P. Early Intervention: The Next Steps - An Independent Report to Her Majesty’s
Government 2011
Asmussen, K. et al Kings College London Institute of Psychiatry: Commissioning Toolkit and
Evaluation of Parenting Programmes in the UK 2008
Backing the Future: why investing in children is good for us all. 2009 Action for Children
and New Economics Foundation
Barlow, J., Coren, E., Stewart-Brown, S. (2002). ‘Meta-analysis of the effectiveness of
parenting programmes in improving maternal psychosocial health’. British Journal of
General Practice, 52, 223-233.
Barlow, J., & Stewart-Brown, S., (2000). ‘Behaviour problems and group based parenting
education programmes’. Developmental and Behavioural Paediatrics, 21, 356-370.
Barlow, J. et al. Parenting programmes and minority ethnic families: experiences and
outcomes. National Childrens’ Bureau 2004.
Coyne J, Kwakkenbos, L: Triple P-Positive Parenting programs: the folly of basing social
policy on underpowered flawed studies. BMC Med 2013, 11:11
Enhancing the Well-being of Children and Families through effective interventions.
McAuley, C. ed. 2005 Jessica Kingsley Publishers
Grasping the Nettle: early intervention for children, families and communities. 2010 Centre
for Excellence and Outcomes in Children’s and Young People’s Services C4EO
JSNA Health and Well-being 2009 and State of the Borough 2011 Lambeth First
Lindsay, G., Band, S., Cullen, M.A., & Cullen, S. (2011). Evaluation of the parenting early
intervention pathfinder Department for Education
Parent-training/education programmes in the management of children with conduct disorders.
July 2006 and revised September 2007 National Institute for Health and Clinical Excellence
and Social Care Institute for Excellence.
Rebuilding relationships: A pilot study of the effectiveness of the Mellow Parenting
Programme for children with Reactive Attachment Disorder
Christine Puckering, Brenda Connolly, Claudia Werner, Louise Toms-Whittle, Lucy
Thompson, Jeannette Lennox, and Helen Minnis, Royal Hospital for Sick Children, Glasgow
Clinical Child Psychology and Psychiatry 16(1) 73–87: 2011
Sanders MR, Pickering JA, Kirby JN, Turner KMT, Morawska A, Mazzucchelli T, Ralph A,
Sofronoff K: A commentary on evidence-based parenting programs: redressing
misconceptions of the empirical support for Triple P. BMC Med 2012, 10:145.
The Chance of a Lifetime: Preventing early conduct problems and reducing crime. 2009
Sainsbury Centre for Mental Health.
Page 361

50
Wilson P, Rush R, Hussey S, Puckering C, Sim F, Allely CS, Doku P, McConnachie A,
Gillberg C: How evidence-based is an 'evidence-based parenting program'? A PRISMA
systematic review and meta-analysis of Triple P. BMC Med 2012, 10:130.
Page 362

Drawing on the EvidenceAdvice for mental health professionalsworking with children and adolescents
SECOND EDITION 2006
Miranda WolpertPeter Fuggle
David CottrellPeter Fonagy
Jeanette PhillipsSteve Pilling
Samuel SteinMary Target
Page 363

Authors
Dr Miranda WolpertDirector CAMHS Evidence Based Practice Unit, University College London
Dr Peter FuggleConsultant Clinical Psychologist, Islington Primary Care Trust
Professor David CottrellProfessor of Child and Adolescent Psychiatry, University of Leeds
Professor Peter FonagyDirector of Sub-department of Clinical Health Psychology, University CollegeLondon
Dr Jeannette PhillipsConsultant Child and Adolescent Psychiatrist, Kent and Medway NHS andSocial Care Partnership Trust, Dartford
Steve PillingDirector of Centre for Outcomes Research and Evaluation, UniversityCollege London
Dr Samuel SteinConsultant in Child,Adolescent and Family Psychiatry, Bedfordshire and LutonMental Health and Social Care Partnership NHS Trust
Dr Mary TargetReader, Sub-department of Clinical Health Psychology, University CollegeLondon
ISBN (10) 0-9553956-0-7ISBN (13) 978-0-9553956-0-4© 2006 CAMHS Publications
Copies of this booklet can be obtained from:
CAMHS Evidence-Based Practice UnitUniversity College London21 Maresfield GardensLondon NW3 5SD
Tel: 020 7443 2218
Page 364

This booklet has been developed by the Child and Adolescent Mental Health Services Evidence BasedPractice Unit (EBPU) at University College London in collaboration with the Faculty for Children andYoung People (CYP), Division of Clinical Psychology of The British Psychological Society (BPS) and the BPS Centre for Outcomes Research and Evaluation (CORE) and with support from the CareServices Improvement Partnership (CSIP).
Our aim is to inform practitioners working with children and adolescents of the most recent findingsregarding outcome research in this area. It is a revised edition of a booklet first produced in 2002,which has been updated in the light of the most recent evidence.
As with the first edition, we have focused on summarising the strength of research findings aboutdifferent forms of intervention, pointing to the many gaps that remain, and drawing out theimplications for practice of what research does exist to-date.The aim remains to provide anaccessible précis of the research base so that busy practitioners can have a ready reminder of keyfindings.
This booklet is not intended to be a comprehensive good practice guide, nor to offer advice based onpractitioner consensus where the evidence is lacking.Those wanting good practice guidance aredirected to the relevant NICE guidelines (see Appendix 3).
Since there was no new overarching systematic review available in 2006 comparable to the reviewused to inform the first edition in 2002 it was agreed to update this booklet by reviewing the newevidence to have emerged since 2002 from the following sources:
a) evidence identified in NICE guidelines published since 2002 b) relevant Cochrane Reviewsc) evidence from major randomised control trials not covered in the original review.
We have not included an overview of the literature in relation to prevention and promotionapproaches, but hope to include a consideration of the evidence in this area in future versions.
This booklet has been written with mental health practitioners in mind and assumes a level offamiliarity with key terms and categories.We are well aware that there is much debate about the useof diagnostic categorisation, but have kept this way of presenting the information as this is the way itis conceived of in the research literature.
A key challenge in putting together such a document is how to do justice to the complexity andlimitations of the current evidence base, whilst trying to convey the main findings as briefly aspossible.We are interested in any feedback from readers to help inform the development of futureupdated versions.
We would like to thank all those who have contributed to this process, and in particular: Liz Allisonand Jonathan Bureau for coordinating and organizing revised drafts, Jemma Simmons for summarizingrelevant NICE guidance and Uttom Chowdhury, Sarah Fortune and David Trickey for their invaluableexpertise in relation to the sections on "habit disorders",“self harm” and “PTSD” respectively.
Miranda Wolpert, David Cottrell, Peter Fonagy, Peter Fuggle, Jeannette Phillips, StevePilling, Samuel Stein and Mary Target (September 2006)
ForewordPage 365

IntroductionAims 4Development of this advice 4Limitations to using the evidence base 5References 7
Statements from the evidence and implications for practiceDisturbance of Conduct 8Disturbances of Attention 11Anxiety Disorders 15Post Traumatic Stress Disorder 17Depressive Disorder 18Psychotic Disorder 20Eating Disorder 22Deliberate Self Harm 24Substance Abuse 26Pervasive Developmental Disorders 27Tourette’s Syndrome 29Coping with physical symptoms with no known cause 31Coping with painful procedures 32Coping with chronic physical illness and disease 33
Appendix 1Summary of processes of undertaking the original review and updated edition 35
Appendix 2Summary of the defining characteristics of the main types of psychosocial intervention 38
Appendix 3Relevant NICE guidelines 39
ContentsPage 366

AimsThis booklet was produced with the aim of
creating an easily accessible resource that busy
practitioners can have readily available as an aid
to their decision-making.The first edition
produced in 2002 was positively received and
there were requests for an updated version.
This booklet is not meant to be prescriptive. It is
recognised that inferences from currently
available research studies are by no means the
only relevant source of information, and that
broad indications from the literature may need
at times to be tempered in the light of specific
contexts and situations. Nevertheless, even
where the practice implications of the research
outlined in this booklet are considered to be
impractical or inappropriate in a given context,
the strong suggestion is that they make a
sensible starting point for practitioner decision
making.
The original booklet (2002) was based on a
comprehensive review of the evidence
commissioned by the National Health Service
Executive, A Review of the Outcomes of all
Treatments of Psychiatric Disorder in
Childhood (July 2000, updated December 2001),
undertaken by Peter Fonagy, Mary Target, David
Cottrell, Jeanette Phillips and Zarrina Kurtz with
the assistance of Arabella Kurtz, and
subsequently published as What Works for
Whom? A Critical Review of Treatments for
Children and Adolescents (2003) by Peter
Fonagy, Mary Target, David Cottrell, Jeannette
Phillips, Zarrina Kurtz. Appendix 1 summarises
the original review process.
The 2006 version has updated this summary in
the light of relevant NICE guidelines, relevant
Cochrane reviews, and major randomised trials
published since 2002.
Development of the adviceFor the first edition, for each presenting
problem, all working group members read the
relevant chapter in the original review. One
member was set the task of extracting what
they deemed to be the key statements from the
research, in terms of psychosocial and physical
treatment. Brief descriptions of the defining
characteristics of the main types of interventions
can be found in Appendix 2.
These statements were circulated to the whole
group, and discussed until everyone felt that a
fair representation of the evidence being
reviewed had been developed. On the basis of
these discussions, a further set of statements
outlining the implications for practice were
developed, which were also agreed by all
members of the working group as being fair
conclusions to draw from the available evidence.
Each statement from the evidence and each
practice implication were rated according to the
following standard criteria (Shekelle et al., 2000):
4
Introduction Page 367

Categories of Evidence:
1a Evidence from meta-analysis of randomised
controlled trials;
1b Evidence from at least one randomised
controlled trial;
2a Evidence from at least one controlled study
without randomisation;
2b Evidence from at least one other type of
quasi-experimental study;
3 Evidence from descriptive studies such as
comparative studies, correlation studies and
case-control studies;
4 Evidence from expert committee reports or
opinions, or from clinical experience of a
respected authority, or both.
Strength of Practice Implications:
A Directly based on category 1 evidence;
B Directly based on category 2 evidence or
extrapolated from category 1 evidence;
C Directly based on category 3 evidence or
extrapolated from category 2 evidence;
D Directly based on category 4 evidence or
extrapolated from category 3 evidence.
The weight of the evidence was indicated in
brackets after each statement and practice
implication.A summary of the weighting system
used has been reprinted on the inside back
cover for ease of reference. The full document
was then sent to a group of senior clinicians and
researchers in the field for review.
For the 2006 review, chapters already written
were revised by the authors, with each member
taking on a chapter to review in the light of
major evidence that had emerged subsequent to
the previous publication (i.e. where there was
new evidence identified in NICE guidance,
relevant Cochrane review or evidence from
major randomised control trial), and a draft was
then discussed and agreed by all authors.
Limitations to using the evidencebaseEvidence-based practice is the integration of
individual practitioner expertise with the best
available external evidence from systematic
research in order to reach decisions about client
care.
This does not mean the wholesale application of
findings from randomised controlled trials to all
individuals with similar problems in a 'one size
fits all' policy. Practitioners’ choice of approach is
always a decision-making process guided by a
range of factors including the characteristics of
the referred child/young person, their family and
social circumstances as well as the service
context. Decisions need to be made in the light
of assessment of the appropriateness of a
particular approach within a given context, its
acceptability, the likely costs, risks and benefits
compared with other approaches.
The picture presented by many children young
people and families seeking help from services is
complex, and the answers to the child’s and the
5
Page 368

family’s problems are sometimes not at all
obvious. For example, very little is known about
the appropriateness of most relatively well-
evaluated treatments with minority cultural
groups.Any attempt to 'prescribe' treatment on
the basis of diagnosis or presenting problem
alone is likely to be over-simplistic.The aim of
this guidance is to therefore provide a starting
point for practitioner decision-making, not an
end point.
One complication for practitioners in child and
adolescent mental health is that the research on
effectiveness is conducted largely on groups of
children defined by diagnostic classifications.The
operational definitions in diagnostic systems,
such as DSM-IV and ICD-10, allow clarity of
communication between researchers concerning
the nature of the problems treated. However,
most children do not present to CAMH services
with such neat diagnostic labels. Instead, families
tend to present with complex predicaments
which require clinical judgment when applying
research findings to everyday practice. Moreover,
the research is often carried out with tightly
defined groups, or it is carried out with groups
from cultural backgrounds which are seldom
seen routinely within the NHS in the United
Kingdom.
Another complication is caused by gaps in the
evidence base.We have tried to distinguish,
throughout the booklet, those instances where
there is no evidence about a particular
intervention from those instances where there is
evidence that a particular intervention is
ineffective or harmful.The problem faced in
many areas of clinical practice is the lack of any
evidence base at all.The fact that some sections
are longer than others reflects the extent of (or
lack of) the evidence base, and does not
necessarily relate to levels of clinical need or
significance. It is worth noting in this regard that
the large number of statements from the
evidence about pharmacological interventions in
some sections reflects the extensive research
literature in this area and should not necessarily
be seen as reflecting the importance of this form
of intervention as against alternatives.
Developing evidence-based practice must
therefore remain an interplay between
professional experience and systematic research.
David Sackett, one of the ‘founders’ of evidence-
based practice, defines ‘individual clinical
expertise’ as ‘the proficiency and judgment that
individual clinicians acquire through clinical
experience and clinical practice’. He comments
that this is reflected in ‘the more thoughtful
identification and compassionate use of
individual patients’ predicaments, rights and
preferences in making clinical decisions about
their care’ (Sackett et al., 1996). However,
balanced against this must be a recognition that
much ‘natural’ clinical decision making is founded
on natural biases in reasoning (Garb, 1997;
Kahnemann et al., 1982).As Kazdin (2000) points
out, ‘unsystematic data and their informal
6
Introduction continuedPage 369

integration are often unreliable, invalid
approaches to decision making’, and this can only
be counterbalanced by systematic evaluation of
individual clinical practice alongside an awareness
of the latest research findings.
When the evidence base is not used as the basis
for at least considering intervention choices, it is
more likely that seemingly plausible but
ineffective and/or harmful interventions may be
introduced or continued and that new
interventions that have been shown to do more
good than harm may never be introduced (Muir
Gray, 2001).
ReferencesFonagy, P.,Target, M., Cottrell, D., Phillips, J., &
Kurtz, Z. (2002). What works for whom? A
critical review of treatments for children and
adolescents London: Guilford Press.
Garb, H.N. (1997). Race bias, social class bias and
gender bias in clinical judgement. Clinical
Psychology: Science and Practice, 4, 99–102.
Kahnemann, D., Slovix, P., & Tvwersky,A. (Eds.)
(1982). Judgement under uncertainty: Heuristics
and biases. New York: Cambridge University
Press.
Kazdin,A. E. (2000). Psychotherapy for Children and
Adolescents: Directions for Research and Practice.
New York: Oxford University Press.
Muir Gray, J.A. (2001). Evidence-based Healthcare:
How to make Health Policy and Management
Decisions. Edinburgh: Churchill Livingstone.
Sackett, D.L., Rosenberg,W.M.C., Gray, J.A.M.,
Haynes, R.B. & Richard,W.S. (1996). Evidence
based medicine:What it is and what it isn’t.
British Medical Journal, 312, 71–72.
Shekelle, P.,Woolf, S., Eccles, M. & Grimshaw, J.
(2000). Developing Guidelines. In M. Eccles &
J.M. Grimshaw (Eds.) Clinical Guidelines; From
Conception to Use. Abingdon: Radcliffe Medical.
7
Page 370

Statements from the evidence
Behaviour Therapies, CognitiveBehavioural Therapies (CBT) and ParentTraining
◆ In parent training, on average two thirds ofchildren under 10 years whose parentsparticipate, show improvement. (1a)
◆ The effects of parent training programmesare detectable in long-term follow-ups of upto four years. (1a)
◆ Increased effectiveness of parent training(fewer drop-outs, greater gains and bettermaintenance) is associated with youngerchildren, higher IQ, less co-morbidity, lesssevere conduct problems, less socio-economic disadvantage, lower parentaldiscord, higher parental global functioningand absence of antisocial behaviour inparents. (1a)
◆ Media based behavioural treatments usingparent training tapes without significanttherapist input and reports have only verymoderate effects. (1b)
◆ Problem-solving skill training for children, incombination with parent training, is aneffective intervention for conduct problemsin children aged 8-12 years. (1b)
◆ Helping parents deal with their own problemsolving in relation to life stress, offered as anadjunct to parent training with problemsolving skills training for the child, appears toimprove both child and adult outcomes. (1b)
◆ Whilst mild conduct problems in childrenunder 11 are ameliorated with the help ofsocial cognitive intervention programs, socialskills training and anger management skillstraining, there is no evidence for the use ofthese approaches on their own with morechronic and severe cases. (1b)
◆ Parent training for conduct problems inadolescents appears to have limitedeffectiveness. (1b)
◆ Evidence for the effectiveness of stand aloneCBT, problem solving approaches and angermanagement programs for adolescentsremains weak. (2b)
Psychodynamic Therapies◆ There is insufficient evidence to draw
conclusions about the effectiveness ofpsychodynamic child psychotherapy.
Systemic Family Therapies ◆ Functional family therapy incorporating
elements of cognitive behavioural approachesinto a systemic model concentrating onchanging maladaptive interactional patterns
8
Disturbances of Conduct Covers diagnostic categories: conduct disorder, delinquency, recidivism, oppositional defiant disorder.
(NB This summary does not include a consideration of school-based interventions and whole communityprojects.)
Page 371

and improving communication and structural family therapy (also described as FamilyEffectiveness Training or Brief Strategic FamilyTherapy) have been shown to be effective inreducing behaviour problems and recidivism inadolescents who have multiply offended. (1b)
Multi-Modal Therapies ◆ Re-offending rates in adolescents are most
likely to be reduced by multi-modal,behavioural and skills-orientated treatmentprogrammes. (1a)
◆ The strongest evidence is for multi-level,relatively intensive, community-based, highlystructured and well integrated programmesfocusing on changes which reduceopportunities for offending (e.g. familymonitoring and supervision of theadolescent). (1b)
◆ Multi-systemic therapy involving multipleinterventions delivered in a planned andintegrated manner, chiefly by a singlepractitioner working intensively with a childand family is the most effective treatment fordelinquent adolescents in reducing recidivismand improving individual and familyfunctioning although its superiority to a fullycomprehensive community mental healthservice such as ideally offered by CAMHShas not been unequivocally established. (1b)
Other Psycho-Social Approaches◆ Therapeutic foster care has been shown to
reduce the rate of recidivism, to increaseplacement stability in a hard to placepopulation and to improve social skills. (1a)
Physical Treatments◆ Psychostimulants have been shown to be
effective in reducing antisocial behaviours inchildren and adolescents with co-morbidADHD/ADD, independent of the effect ofthese medications on attention deficit andhyperactivity symptoms. (1b)
◆ Lithium has been demonstrated to beeffective in reducing explosive aggressiveoutbursts in hospitalised groups. (1b)
◆ Traditional anti-psychotic medication appearsto be effective in the reduction ofaggressiveness but is associated with sedationand interference with learning, as well asother more severe side effects. (2a)
◆ Low dose risperidone has been shown to beeffective in reducing aggressive behavior. (1a)
◆ Some studies have shown a response to theuse of carbamazepine and other anti-convulsants in reducing aggressive outbursts,but better controlled studies have notsupported these initial findings. (1b)
◆ Clonidine has been shown, in small-scaleopen trials, to reduce destructive andaggressive behaviour but no randomisedcontrol trials have yet been conducted. (2a)
9
Page 372

Implications for practice
■ Parent training is the treatment of choicefor conduct problems in children under 10years old, particularly those with moderateseverity, less co-morbidity and less socialdisadvantage. (A)
■ For older children (8–12 years) and formore severe presentations, parent trainingshould be combined with individualinterventions that provide problem solvingand social skills training. (A)
■ Individual approaches for adolescents, ifused either on their own or incombination with systemic interventions,should focus on reducing opportunitiesfor delinquent behaviour and onincreasing skills such as problem solvingor coping. (B)
■ For adolescents and young people withmoderate conduct problems, functional orstructural family therapy, whereappropriate combined with cognitivebehavioural therapy, should beconsidered. (B)
■ Whilst the evidence suggests Multi-Systemic Therapy is currently the mosteffective intervention for severe andenduring disturbance of conduct inadolescents, it is recognised that thisapproach involves high levels ofprofessional resources which will need tobe carefully targeted. (A)
■ Specialist foster placement withprofessional support should be consideredas part of multi-agency interventions foradolescents with chronic and enduringconduct problems. (A)
■ Medication should probably not be usedas the first line of treatment for conductproblems. (B)
■ The use of psychostimulants for childrenwith co-morbid ADHD should beconsidered when adequate therapeuticchange has not been achieved bypsychosocial treatments alone. (D)
■ The use of novel antipsychotics withcombined dopaminergic and serotonergicaction, such as risperidone, may becautiously considered for children andyoung people who have not beenresponsive to a comprehensive trial ofpsychosocial treatments. (B)
10
Disturbances of Conduct continuedPage 373
Statements from the evidence
Behaviour Therapies, CognitiveBehavioural Therapies and Parent Training ◆ Behaviour therapy has been shown to be
more effective than no treatment controls,and contributes to improvements in on-taskbehaviour and a reduction in disruptive andrule-breaking behaviour. (1b)
◆ The addition of behaviour therapy tostimulant medication does not confer anadditional benefit at end of treatment.However, it may enable benefit to beestablished at a lower dose of medicationand allow earlier discontinuation ofmedication, and has been shown to producesome additional benefit at longer term followup. (1b)
◆ The combination of behaviour therapy andstimulant medication has been shown to bemore effective than medication alone forADHD with co-morbid anxiety. (1b)
◆ Improvements from behaviouralinterventions in one setting do not generaliseto other settings. (1b)
◆ The addition of a cognitive approach tobehavioural therapy does not result inimproved clinical outcome. (1b)
◆ Parent training has been found to increasechild compliance and reduces the time for
task completion. It also appears to improveparental self-esteem and reduces parentalstress. However, compliance with thisapproach is lower for parents with lesseducational attainments. (1b)
◆ There is evidence that social skills trainingdoes not improve social relationships. (1b)
◆ There is some evidence of greater parentand teacher satisfaction with behaviouraltreatments in contrast with medication (2b)
Psychodynamic, Systemic and Multi-ModalTherapies◆ There is insufficient evidence to draw
conclusions about the effectiveness ofpsychodynamic child psychotherapy, systemicfamily therapy and multi-modal therapy.
Physical Treatments◆ Stimulants (methylphenidate and
dexamphetamine) have been demonstrated tobe effective and can lead to normalisation ofattention, activity and impulsivity irrespectiveof age in 75% of treated children. (1a)
◆ Stimulant medication may produce mildgrowth suppression which is more marked inchildren receiving continuous treatmentcompared with those receiving ‘holiday’breaks. (1b)
◆ Stimulants are beneficial when there is co-morbidity with the following: conduct
11
Disturbances of AttentionCovers diagnostic categories: attention deficit hyperactivity disorder (ADHD), hyperkinetic disorder.
Page 374

disorder, anxiety, generalised learningdisability and specific learning disability. (1b)
◆ When stimulants are used with children withco-morbid conduct disorder, as well asreducing the primary symptoms of ADHD,the level of verbal and physical aggression arereduced. (1b)
◆ Stimulants may be beneficial when there is aco-morbid pervasive developmental disorder.(1b)
◆ Stimulants appear to be effective and safe forthe treatment of ADHD in the presence ofwell-controlled epilepsy.As there has onlybeen one randomised controlled trial,caution is required. (1b)
◆ Long acting stimulants have been shown tobe as effective as short acting stimulants butmay have a different side effect profile. (1b)
◆ Atomoxetine has been demonstrated to beeffective in reducing the core symptoms ofinattention, over activity and impulsivity intreated children. (1b)
◆ Atomoxetine has a different side effectprofile to stimulant medication with minimalimpact on appetite and sleep. However,recent reports suggest liver complicationsmay be a rare side effect. (1b)
◆ Clonidine has been shown to be effective inreducing motor activity and increasingcompliance, as well as reducing levels of
irritability.The effect size appears to be lowerthan that of stimulants but higher than thatobtained from treatment with tricyclic anti-depressants. (1a)
◆ Tricyclic anti-depressants have been shownto be beneficial in the treatment of theprimary symptoms of ADHD at all ages, butthey are not as effective as stimulants andthe risk of side effects is higher. (1a)
◆ Tricyclic anti-depressants have been shownto be effective in the presence of co-morbiddepression, anxiety and conduct disorder.(1a)
◆ Bupropion has been shown to be effective.However, there is a significant risk of sideeffects, including the precipitation of apsychotic illness. (1b)
◆ The newer selective monoamine oxidaseinhibitors, such as moclobemide, mayimprove attention and concentration spanbut have less impact on impulsive andhyperactive behaviours. (2b)
◆ Carbamazepine has been shown to bebeneficial in the treatment of ADHD butthere is a greater risk of side effects thanwith stimulants. (1a)
◆ In children with food intolerance, there isevidence to support the effectiveness ofindividually targeted exclusion diets. (1b)
◆ Dietary supplementation with omega-3 and
12
Disturbances of Attention continuedPage 375

omega-6 fatty acids whilst having no effect onthe motor skills of children withdevelopmental coordination disorder (DCD)has been shown to have a significant positiveeffect on reading and spelling, and on ADHDrelated behaviours. (1b)
Implications for practice
■ If diagnostic criteria for ADHD are metfollowing a comprehensive assessment bya suitably qualified professional, andother reasons for the behaviour havebeen excluded, then a trial of medicationis indicated as the first line ofintervention. (A)
■ If there is insufficient response tomedication, then parent training andindividual behavioural therapy with thechild should be added. (A)
■ Discontinuous medication (i.e. holidaybreaks) may reduce the risk of mildgrowth suppression. (A)
■ Behavioural intervention in addition tomedication can also be offered as a wayof achieving similar outcomes tomedication alone but with reduced levelsof medication. (B)
■ Where individual behaviouralinterventions are used, these need to beprovided in the child’s school as well aswithin the home as they do not generaliseacross settings. (A)
■ For children with co-morbid anxiety,combination treatment of stimulantmedication and behavioural interventionsshould be considered. (A)
■ Stimulant medication can be given, alongwith appropriate psychosocialtreatments, when there are co-morbidproblems, such as conduct disorder,Tourette’s Syndrome and socialcommunication disorders. Medication canalso be given in the presence of learningdisabilities and epilepsy. (A)
■ Children should be started on a shortacting preparation of methylphenidate oron dexamphetamine. (A)
■ Atomoxetine is probably the evidencebased second line treatment, but althoughthere is relevant RCT evidence to supporteffectiveness this is a new drug andreports of side effects need to bemonitored. (A)
■ As it is not possible to predict which dosewill be effective, dosage should beincreased within safe limits until an effectis achieved. (A)
■ If there is insufficient resolution ofsymptoms with stimulants or atomoxetine,then other medication should beconsidered.The alternatives include:clonidine, selective serotonin reuptakeinhibitors, tricyclic anti-depressants andselective monoamine oxidase inhibitors. (A)
13
Page 376

Disturbances of Attention continued
■ Expert opinion recommends thecombination of clonidine and stimulantswhen there is a partial response tostimulants alone, rebound effects,insomnia, impulsiveness or emotionallability. (D)
■ Effective monitoring of children givenmedication is needed to minimise adverseside effects and optimise treatmentbenefits. (A)
■ There is some evidence to support theuse of omega 3 and 6 dietarysupplementation. (A)
14
Page 377

Statements from the evidence
Behaviour Therapies and CognitiveBehavioural Therapies◆ Overall, for over half the children treated in
RCTs, the anxiety disorder remits with CBT.(1a)
◆ There is evidence that generalised anxietycan be effectively treated using cognitivebehavioural therapy. (1b)
◆ For children under 11 with specific phobias,in vivo exposure is particularly beneficial (incontrast to more cognitive techniques) andthe support of parents has a positive effect.However, it appears that various forms ofbrief therapeutic input (cognitive behaviouraltherapy, supportive psychotherapy) may onlyaccelerate spontaneous improvement thatmight occur in this age group. (1b)
◆ Flooding, via rapid return to school, can besuccessful in managing school refusal but maynot be more effective than ‘educationalsupport’ (this involves information about thenature and treatment of anxiety disorders,together with therapeutic listening andclarification). (1b)
◆ Individual case studies suggest that theinclusion of behavioural prescriptions, inaddition to non-prescriptive anxietymanagement techniques, facilitates greaterand more rapid improvement. (2b)
◆ Cognitive behavioural therapy for childhoodanxiety disorders can be successfullydelivered in a group, or family, as well as in anindividual format, and it may be especiallyhelpful if parents are included, for childrenunder 11 and where there is high parentalanxiety. (1a)
Psychodynamic Therapies, SystemicFamily Therapies and Other PsychosocialApproaches ◆ There is insufficient evidence to draw
conclusions about the effectiveness ofpsychodynamic child psychotherapy, systemicfamily therapy and other psychosocialapproaches.
Physical Treatments◆ Clomipramine and selective serotonin
reuptake inhibitors are all significantly moreeffective than placebo in the treatment ofOCD. (1b)
◆ Selective serotonin reuptake inhibitors havebeen shown to be more effective thanpsychoeducational pamphlets in thetreatment of social anxieties. (1b)
◆ There are preliminary indications thatcognitive behavioural therapy withmedication might be better than medicationalone for OCD. (1b)
◆ The efficacy of benzodiazepines, 5–HTagonists, beta-blockers, tricyclic
15
Anxiety DisordersCovers diagnostic categories: generalised anxiety disorder (GAD), obsessive-compulsive disorder (OCD),separation anxiety disorder (SAD), agoraphobia, panic disorder, specific phobia, social phobia.
Page 378
antidepressants (other than clomipramine) orselective serotonin reuptake inhibitors foranxiety disorders other than OCD have notbeen sufficiently evaluated in research studiesfor any firm conclusions about theireffectiveness to be drawn.
◆ A side effect of tricyclic antidepressants is toincrease the small risk of sudden death fromcardiac failure, and of long-termelectrocardiographic changes. (3)
◆ Selective serotonin reuptake inhibitorsproduce less serious side effects thantricyclic antidepressants. (3)
Implications for Practice
■ Behaviour therapy and cognitivebehavioural therapy (whether in group orindividual format) should be consideredthe first-line treatment for children withspecific phobias and children withgeneralised anxiety. (A)
■ Behaviour therapy and cognitivebehavioural therapy should be consideredfor children with OCD. (A)
■ Parents should be included in cognitivebehavioural therapy where the child isunder 11 or where there is high parentalanxiety. (B)
■ ‘Educational support’ should beconsidered in the management of childrenwith anxiety problems. (B)
■ Clomipramine and selective serotoninreuptake inhibitors should be consideredin the treatment of OCD when cognitivebehavioural therapy alone has provedineffective. (A)
■ Selective serotonin reuptake inhibitorsshould be considered in the treatment ofsocial anxieties when cognitivebehavioural therapy alone has provedineffective. (A)
16
Anxiety Disorders continuedPage 379

Statements from the evidence
Behavioral Therapies and CognitiveBehavioral Therapies◆ A number of studies, particularly in children
aged 7 and over who have been sexuallyabused, suggests that individual traumafocused CBT delivered to children and youngpeople with PTSD may be of value. (Ib)
◆ Delivering CBT to the mother as well as thechild does not appear to lead to any benefitover treatment of the child alone in regardsto the PTSD symptoms. However CBT forthe mother only has been shown to reduceseverity of PTSD symptoms in the child at 2year follow up. (Ib)
◆ Studies with adults suggest trauma-focusedCBT within the first month may be beneficialif symptoms are severe. (Ib)
Eye Movement Desensitisation andReprocessing (EMDR) EMDR◆ Two studies indicate Eye Movement
Desensitisation and Reprocessing (EMDR)may be effective, but further studies arerequired. (3)
Debriefing◆ A number of randomised controlled trials
with adults and one with children have foundthat debriefing, that is providing a systematic,brief, single session intervention focusing onthe traumatic incident shortly after thetrauma does not lead to clear benefit incomparison to no treatment. (1b)
Psychodynamic, Systemic and Multi-ModalTherapies ◆ There is insufficient evidence to draw
conclusions about the potential effectivenessof psychodynamic child psychotherapy,systemic family therapy and multi-modaltherapy.
Physical Treatment◆ There is no conclusive evidence that drug
treatment is beneficial for PTSD in children.(3)
Implications for practice
■ Debriefing should not be offered routinelyimmediately following a trauma (A)
■ Children and young people with PTSD,including those who have experiencedtraumatic events other than sexual abuse,should be offered a course of trauma-focused cognitive behaviour therapyadapted appropriately to suit their age,circumstances and level of development.(B)
■ Trauma-focused cognitive behaviouraltherapy should be offered to olderchildren with severe symptoms of PTSD inthe first month after the traumatic event.(C)
■ Drug treatments should not be routinelyprescribed for children and young peoplewith PTSD. (C)
17
Post Traumatic Stress DisorderPage 380

Statements from the evidence
◆ There is a high rate of spontaneousremission amongst untreated children, althoughthere are high rates of relapse amongst bothtreated and untreated groups. (3)
Behaviour Therapies and CognitiveBehavioural Therapies ◆ The overall evidence for the effectiveness of
individual CBT is inconclusive. In somestudies CBT is no more effective thanwaitlist or general clinical management but inother studies it has been shown to be moreeffective than comparison treatments(relaxation therapy, non-directive supportivetherapy). (1a)
◆ CBT may speed up the recovery comparedwith no treatment and may reduce thelength of the depressive episode comparedwith other treatments. These differentialeffects were not sustained at longer termfollow-up although this was mainly due toongoing improvements of comparisonconditions. (1b)
◆ Group CBT and brief non-directive therapymay be effective treatments for milddepression. (1b)
Psychodynamic and Systemic FamilyTherapies◆ There is inconclusive evidence for the
effectiveness of family therapy in the
treatment of depression. (2b)
◆ Evidence from one comparison studysuggested brief 30 session psychotherapymay be an effective treatment. (2b)
Other Psychosocial Approaches ◆ Interpersonal Psychotherapy (IPT) is effective
in reducing depressive symptoms althoughevidence in achieving remission isinconclusive. In direct comparison with CBTthere was no difference in outcome betweenthe two treatments. (1a)
Physical Treatments◆ Tricyclic antidepressants have been found to
be no better than placebo (1a)
◆ Of the selective serotonin reuptakeinhibitors (SSRIs), fluoxetine has the safestbenefit/harm ratio. (1a)
◆ Compared with placebo, fluoxetine producedclinically important improvement in clinicalsymptoms and improved likelihood ofremission. (1a)
◆ There is some evidence that fluoxetine incombination with CBT is more effective inreducing depressive symptoms, reducing therisk of suicidal ideation and producing globalclinical improvement than fluoxetine alone.(1b)
18
Depressive DisordersCovers diagnostic categories: major depressive disorder (MDD), dysthymic disorder (DD).
Page 381

Implications for Practice
■ Given the high rate of remission incontrol groups, initial psychologicaltreatment (either CBT, family therapy orIPT) for up to three months should beoffered as the first line of treatment. (B)
■ If psychological treatment does notproduce improvement in symptoms by sixweeks, anti-depressant medication shouldbe offered for adolescents (and cautiouslyconsidered for younger children) incombination with longer termpsychological treatment using either CBT,psychotherapy or family therapy. (A)
■ Depression is a condition which is liableto recur. Clinical follow-up and ‘boostersessions’ may be helpful in reducingrelapse. (B)
19
Page 382

Statements from the evidence
Psycho-Social Therapies ◆ Psychosocial interventions with children and
young people with psychotic disorders havenot been sufficiently evaluated in researchstudies for any firm conclusions about theireffectiveness to be drawn. In adults there issome evidence to support CBT and familytherapies but their value for children andyoung people has not been established.
Physical Treatments◆ Traditional neuroleptic medication has been
demonstrated to reduce acute positivesymptoms in schizophrenia. (1b)
◆ A number of open trials and case studiessupport the use of neuroleptics for bipolardisorders. (3)
◆ Clozapine has been shown to be effectiveagainst both positive and negative symptomsof schizophrenia but has significant adverseside effects. (1b)
◆ There is evidence to support the use oflithium in the acute phase of manic/bipolardisorder. (1b)
◆ There is some evidence to support the useof lithium as long-term prophylacticmedication for bipolar disorder. (3)
◆ A number of open trials and case reports
indicate the value of other atypicalneuroleptics over traditional neurolepticmedication for children with schizophrenia(3)
◆ Open trials and case reports suggestcarbamazepine and divalproex sodium maybe effective treatments for bipolar disorderin children and young people. (3)
◆ Electro-convulsive therapy (ECT) for thetreatment of schizophrenia or bipolardisorder has not been sufficiently evaluatedin research studies for any firm conclusionsabout its effectiveness to be drawn.
Implications for Practice
■ Neuroleptics are the treatment of choicefor the acute phase of schizophrenia. (A)
■ Because of the side effects of traditionalneuroleptics atypical neuroleptics shouldnormally be used, although cautionshould be exercised as these too have sideeffects. (B)
■ Clozapine should be cautiouslyconsidered in cases of treatment resistantschizophrenia, in line with the nationallyagreed protocol (A)
■ Lithium should be considered in the firstinstance in the acute phase ofmanic/bipolar disorder. (B)
20
Psychotic DisordersCovers diagnostic categories: schizophrenia, bipolar disorder.
Page 383
■ Lithium should be considered for longterm prophylactic use in bipolar disorder.(C )
21
Page 384

Statements from the evidence
Behaviour Therapies ◆ Operant conditioning used in hospital
settings has been shown to be effective inshort-term weight gain. (2b)
Systemic Family Therapies◆ Family therapy (behavioural/structural) is an
effective treatment for anorexia nervosa inyoung people, and is more effective thanindividual therapy where the illness is notchronic. (1b)
◆ However, there is insufficient evidence todetermine whether conjoint (i.e., patient andparents meet together) or separated formsof family therapy (i.e., therapist meets patientand parents separately) are more effective.(1a)
Cognitive behavioural therapy andPsychodynamic Therapy◆ Individual psychodynamic therapy shows
benefit in those with late-onset anorexia andmay contribute to the prevention of relapseafter discharge from hospital treatment. (1b)
◆ Extrapolation from adult literature suggeststhat individual therapies such as inter-personal therapy (short-term non-introspective psychotherapy), behaviourtherapy and cognitive behavioural therapymay be helpful in relation to bulimia butthese have been insufficiently studied in
relation to children and young people for anyclear recommendations to be made. (4)
Multi-Modal Treatments◆ There is clinical consensus that multifaceted
treatment programmes (including individualpsychotherapy, behaviour therapy and familytherapy) may be the most effective approachto anorexia but they have been insufficientlyresearched for any firm conclusions to bedrawn. (4)
Physical Treatments◆ Physical treatments for anorexia and bulimia
have not been sufficiently evaluated inresearch studies for any firm conclusionsabout their effectiveness to be drawn,however clinical consensus suggests thatearly intervention and hospitalisation(including re-feeding) are likely to be helpful,especially for young children and those withsevere emaciation (less than 70% of averageweight). (4)
Implications for Practice
■ Family therapy (behavioural/structural) isrecommended as the treatment of choicefor anorexia nervosa, either as an out-patient or after in-patient treatment. (A)
■ Behavioural treatment should beconsidered in hospital in order to increaseweight. (B)
22
Eating DisordersCovers diagnostic categories: anorexia nervosa, bulimia nervosa.
Page 385

■ Older adolescents with bulimia nervosamay be treated with CBT adapted asneeded to suit their age, circumstancesand level of development. (C)
■ Early identification and treatment ofanorexia nervosa is suggested, with re-feeding as necessary. (D)
23
Page 386

Statements from the evidence
◆ Clinical consensus suggests that all childrenwho self harm should be assessed by aprofessional with specialist child mentalhealth training. (4)
◆ There is evidence that approaches focusingon prevention of further suicide attemptsmay not be effective in the presence of co-morbid depression. (1b)
◆ Brief intervention (problem solving) withfamilies of adolescents following a suicideattempt can improve adolescents’ feelings ofdepression and suicidality, enhance positivematernal attitudes towards treatment andreduce subsequent use of residential andfoster care. (1b)
◆ The limited number of trials comparingtreatment as usual with enhanced care(involving 24 hour access to services) havenot clearly demonstrated the advantages ofthe latter in terms of reduction in incidenceof suicide attempts. (1b)
◆ School based interventions can improveknowledge and attitudes amongst youngpeople towards disclosure of self harm bytheir peers, but have not been shown toincrease help seeking amongst high riskgroups (in particular young men and thosewho have already self-harmed). (1b)
◆ Schools based programmes that inadvertently"glamorise" self harm e.g. via use ofinappropriate materials, may increase selfharm rates. (2b)
◆ There is evidence that for adolescents whohave repeatedly self harmed the addition ofgroup therapy to treatment as usual reducesthe likelihood of repetition. (1b)
◆ The method of self harm amongst youngpeople already referred to a specialist servicedoes not necessarily indicate seriousness ofintent (e.g. self cutting does not necessarilymean less serious intent than other formsamongst this population of young people).(3)
Implications for Practice
■ Following a suicide attempt by a child oryoung person, brief interventions involvingfamilies should be considered. (B)
■ Children who have harmed themselvesshould be assessed for psychologicaldisturbance or mental health problemswhich, if present, should be treated asappropriate. (D)
■ For young people who have self-harmedseveral times, consideration should begiven to the addition of grouppsychotherapy. (B)
24
Deliberate Self HarmCovers diagnostic categories: parasuicide.
Page 387

■ When instituting schools basedinterventions, selection of material shouldbe made with reference to existingevaluated programmes. (A)
■ In assessing a young person in a CAMHScontext presenting with self harm,seriousness of intent needs to be assessedwhatever the nature of the self harm. (C)
25
Page 388

Statements from the evidence
Education interventions◆ Psycho-educational programmes delivered to
the general child/adolescent population havebeen found to be ineffective. (1b)
Systemic Family Therapies◆ Family therapy (behavioural/structural) has
been shown to be superior to othertreatment modalities, and has been shown toenhance the effectiveness of otherapproaches. (1a)
◆ Family psycho-education and family supportgroups alone have not been found to beeffective. (1a)
Psychodynamic Therapies, CognitiveBehavioural Therapy and BehaviourTherapies◆ There is insufficient evidence to draw
conclusions about the effectiveness ofpsychodynamic psychotherapy, cognitivebehavioural therapy or behaviour therapy.
◆ Motivational interviewing has advantagesover treatment as usual in reduction ofsubstance misuse particularly cannabis,nicotine and alcohol. (1b)
Multi-Modal Treatments◆ Comprehensive community-based treatments,
such as multi-systemic therapy (which includefamily therapy), have been shown to beeffective in reducing substance misuse. (1b)
◆ Prevention approaches that include dealingwith resistance skills, psychologicalinoculation, and personal and social skillstraining have been shown to significantlyimprove knowledge and to reduce drug usefor periods of over one year.The uniquecontribution of each component in thesetypes of multi-component therapy has notbeen established. (2a)
Physical Treatments◆ Pharmacological treatments for substance
misuse in children and young people havenot been sufficiently evaluated in researchstudies for any firm conclusions about theireffectiveness to be drawn.
Implications for Practice
■ Family therapy should be considered thefirst line treatment of substance misuse.(A)
■ Multi-systemic therapy should beconsidered where substance misuse ispart of a wider pattern of problems. (B)
■ In the light of the success of preventiveapproaches, skills-oriented resilience-enhancement programmes should beconsidered in schools and othercommunity settings. (C)
26
Substance MisuseCovers diagnostic category: substance dependence.
Page 389

Statements from the evidence
◆ Early recognition and/or intervention forchildhood autism may reduce laterdifficulties. (3)
Psychosocial Approaches◆ Psychosocial interventions with children with
forms of pervasive developmental delayother than autism have not been sufficientlyevaluated in research studies for any firmconclusions about their effectiveness to bedrawn.
Behaviour Therapies, CognitiveBehavioural Therapies and Parent Training ◆ Intensive behavioural treatment (e.g. an
intensive educational intervention such asLOVAAS), including parent training, mayimprove IQ, language and social skills, anddecrease aggression in children with autism.(1b)
◆ Training of siblings to elicit speech from theirautistic brother or sister, integratedplaygroups in a school setting and schoolprograms such as TEACCH (Treatment andEducation of Autistic and RelatedCommunication Handicapped Children) mayeach help improve social skills of childrenwith autism. (3)
◆ The evidence for auditory integrationtraining (which focuses on reducinghypersensitivity to sound) and other sound
therapies is inconclusive. (1a)◆ There is no evidence that individual social
skills training significantly benefits childrenwith autism. (2a)
◆ Although no studies have been conducted,clinical opinion suggests that social skillstraining may be effective in the treatment ofAsperger’s syndrome. (4)
Other Therapies◆ Holding therapy with children with autism
(whereby the child is held regardless ofwhether it comforts or distresses him orher) has not been sufficiently evaluated inresearch studies for any firm conclusionsabout its effectiveness to be drawn.
Physical Treatments◆ No physical treatments have been shown to
affect the core cognitive symptoms andsymptomatology of autism.
◆ Haloperidol and risperidone have beneficialeffects on hyperactivity, stereotypy,preoccupations and disruptive behaviour inautism. (1b)
◆ Naltrexone decreases hyperactivity in autism.(1b)
◆ Clomipramine reduces autistic withdrawaland preoccupations, hyperactivity andoppositionality. (1b)
27
Pervasive Developmental DisordersCovers diagnostic categories: social communication disorders, childhood autism, atypical autism,Asperger’s syndrome, Rett’s syndrome, childhood disintegrative disorder.
Page 390

◆ Psychostimulants have reduced hyperactivebehaviour with no increase in stereotypies orother autistic behaviours in children withautism and ADHD. (1b)
◆ Fenfluramine has been found to be anineffective treatment for autism. (2a)
Implications for Practice
■ Intensive behavioural interventions, eitherindividual or group, should be consideredto help improve the adaptive behaviourof children with autism. (B)
■ Medication is not indicated for thetreatment of core symptoms of autismbut may be used to reduce specificbehaviours associated with autism inchildren. (B)
28
Pervasive Developmental Disorders continuedPage 391

Statements from the evidence
Psychosocial Approaches◆ Evidence for the effectiveness of psychosocial
interventions is inconclusive, but expertadvice suggests reassurance to parents,liaison with schools and reduction ofexternal stressors for the child or youngperson. (4)
Physical TreatmentsTreatment of Tourette’s Syndrome withco-morbid disorders
◆ Risperidone, haloperidol and pimozide havebeen found to significantly reduce theseverity and frequency of tics, but there areside effects.Although pimozide is lesssedating than haloperidol, it has a greater riskof ECG abnormalities. (1b)
◆ Clonidine has been shown to significantlyreduce the number and severity of motortics, but it demonstrates no improvement invocal tics. (1b)
Treatment of Tourette’s Syndrome withco-morbid disorders ◆ Where tics and ADHD co-exist, there is
evidence that psychostimulants are beneficialto ADHD without a significant increase in ticseverity, although patients may requireadditional medication for the tics. (1b)
◆ Clonidine has been shown to be effectiveand superior to placebo in treating both tics
and co-morbid symptoms of ADHD, but maycause drowsiness. (1b)
◆ There is some evidence that tricyclic anti-depressants are effective for children withADHD and tics but may cause drowsinessand ECG abnormalities. (2a)
◆ Selective serotonin reuptake inhibitors havebeen shown to be effective in obsessivecompulsive disorder.There is insufficientevidence to suggest that the presence of ticsis a contraindication to their use although co-morbid Tourette’s syndrome may lower theireffectiveness with OCD symptoms. (2a)
Implications for Practice
■ Neuroleptics and clonidine should beconsidered as first choice treatments forTourette’s syndrome. Since the evidencefor effectiveness does not differentiatebetween them, the decision as to whichmedication to use may be based on theclinician’s and family’s view of thedifferent side effects.The atypicalneuroleptics usually have fewer side-effects (A)
■ The use of pimozide should be consideredonly as a second line treatment given itsside effects. (C)
■ The presence of tics is not acontraindication to the use ofmehthylphenidate in the treatment ofADHD. (A)
29
Tourette’s SyndromePage 392

■ Selective serotonin reuptake inhibitorsshould be considered in Tourette’ssyndrome with co-morbid OCD, but theresponse may be less favourable than inOCD without co-morbidity. (B)
■ Clinical consensus suggests that bestpractice involves reassurance to parents,liaison with schools and reduction ofexternal stressors for the child or youngperson. (D)
30
Tourette’s Syndrome continuedPage 393

Statements from the evidence
Behaviour Therapies and CognitiveBehavioural Therapies◆ Cognitive behavioural techniques, combining
progressive muscular relaxation, self-monitoring, distraction and positive self-statements by children, and distraction andcontingency management of pain and non-pain behaviours by parents, have been shownto be effective in the management ofrecurrent abdominal pain. (1b)
◆ Cognitive behavioural approaches to physicalsymptoms other than recurrent abdominalpain have not been sufficiently evaluated inresearch studies for any firm conclusionsabout their effectiveness to be drawn, butexpert advice suggests cognitive behaviouraltherapy management similar to that used forrecurrent abdominal pain. (4)
Psychodynamic, Systemic and OtherTherapies ◆ Psychodynamic, systemic and other therapies
have not been sufficiently evaluated inresearch studies for any firm conclusionsabout their effectiveness to be drawn.
Physical Treatments◆ Evidence from one randomised controlled
trial suggests that a high fibre diet leads to areduction in attacks of recurrent abdominal
pain, but this finding needs to be replicated.(1b)
Implications for Practice
■ Cognitive behavioural therapy should beconsidered for recurrent abdominal pain.(A)
■ Cognitive behavioural therapy should beconsidered in the use of other physicalsymptoms with no known cause. (D)
■ If attention to diet has not already beenconsidered, trial of a high fibre diet isindicated for recurrent abdominal pain.(B)
31
Coping with physical symptoms with no knowncauseCovers diagnostic categories: somatisation disorder, undifferentiated somatoform disorder, conversion disorder,pain disorder, hypochondriasis.
Page 394

Statements from the evidence
Behaviour Therapies and CognitiveBehavioural Therapies ◆ Parental presence may be helpful in reducing
procedural distress if parents can be coachedto promote distraction and/or active coping.(1b)
◆ Rocking of newborns and distraction inyounger children are effective in reducing thedistress caused by venepuncture. (1b)
◆ In older children, cognitive behaviouralstrategies which promote more active copingand which give the child a sense of masteryand predictability reduce procedural distress.(1b)
◆ Cognitive behavioural interventions may alsobe effective as an adjunct to pharmacologicaltreatments. (1b)
◆ Hypnosis has been shown to decreaseprocedural distress and the somaticsymptoms associated with chemotherapy.(1b)
Psychodynamic, Systemic and OtherTherapiesPsychodynamic, systemic and other therapieshave not been sufficiently evaluated in researchstudies for any firm conclusions about theireffectiveness to be drawn.
Implications for Practice
■ Cognitive behavioural therapy, behaviourtherapy and hypnosis should be used tocounter the stress associated with painfulprocedures and selected according to theparticular types or stages of procedure aswell as the developmental stage of theindividual child. (A)
32
Coping with painful proceduresIncludes children and young people who are undergoing painful procedures i.e. medical procedures such asvenepuncture.
Page 395

Statements from the evidence
Behaviour Therapies and CognitiveBehavioural Therapies◆ Education alone for children with chronic
illness increases knowledge about that illnessbut is insufficient to bring about changes inillness management. (1b)
◆ Illness specific, multi-component cognitivebehavioural interventions, including variouscombinations of education, triggerrecognition, relaxation, problem-solving skillsand stress reduction, have been shown to beeffective in improving physical status inasthma, diabetes and other chronic illnesses.(1b)
◆ The use of electromyographic biofeedback toreduce facial muscle tension is associatedwith improved physical state in the shortterm in asthma. (1b)
◆ Combined education and stress managementprogrammes for children with asthma areeffective in reducing associated emotionaland behavioural problems. (1b)
◆ Cognitive behavioural interventions, targetedat families and peer groups rather thanindividuals, have also been shown to improvephysical status in diabetes. (2b)
◆ Thermal biofeedback and progressivemuscular relaxation, either alone or in
combination, are superior to otherpsychological treatments in the managementof headache. (1a)
◆ Relaxation training delivered in a self-helpformat is effective in reducing headaches.(1b)
◆ Broad-based interventions aimed at providingeducation and support, delivered in thecommunity by nurses with minimal training inpsychological intervention, may prevent lateradverse physical and psychological outcomesof chronic illness. (1b)
Systemic Family Therapies ◆ Systemic family therapies are effective in
improving physical status in asthma. (1b)
Psychodynamic Therapies◆ Intensive psychoanalytic psychotherapy may
improve diabetic control in children in hardto control diabetes. (2a)
Implications for Practice
The interventions recommended belowshould be considered as adjuncts to routinemedical treatment
■ Cognitive behavioural therapy andbehaviour therapy, tailored to specificillnesses, should be considered for childrenwith hard to control physical symptoms.(A)
33
Coping with chronic physical illness and diseaseIncludes children and young people who are in pain due to longstanding physical causes e.g. diabetes or asthma.
Page 396

■ Psychoanalytic psychotherapy should beconsidered for the treatment of hard tocontrol diabetes. (B)
■ Systemic family therapy should beconsidered for the treatment of asthma.(B)
■ Provision of specialist nurse support tofamilies of children newly diagnosed withchronic illness should be considered as ameans of improving later physical andpsychological outcomes. (B)
34
Coping with chronic physical illness and diseasecontinued
Page 397

Summary of process of undertakingthe original review (2002)
The search strategy for the original reviewconsisted of a combination of computer-basedand hand searches.All the major databases,including MedLine and PsycLit/PsycInfo, weresearched by computer using 100 terms referringto different aspects of child and adolescentmental health.The results of these searcheswere combined with 22 terms describingtreatments. In addition, all articles included inlarge meta-analyses of child treatments werereviewed, and the bibliographies of reviews andprimary studies examined.
The computer search identified 5,375 abstracts,which were reviewed. From this corpus, 743papers were selected.The review team thenamended this coverage with a hand search,which yielded a large number of further studies,particularly through the follow-up ofbibliographies in primary studies and reviewpapers. Overall, 830 primary studies wereidentified and 648 further reports, which eitherreviewed the treatment literature, reportedclinical experience or offered advice andopinion, pertinent to child psychiatric treatmentsin the areas covered.The search covered theperiod up to the end of 1998. Hand searches ofmajor journals covered the most recent period(1999-2000).A significant number of earlystudies were reviewed but discarded whenmethodological improvements in the morerecent literature made these findings obsolete.
To be included in the review, reports of researchhad to satisfy criteria of relevance, outcome anddesign.
Relevance: Studies that reported evaluations ofinterventions with one or more of the targetdisorder populations of children and adolescentswere reviewed.The review team only includedinterventions that fell in the domain of thehealth service or services accessible to healthservice providers. Macro-social, legislative andeconomic interventions, for example, have beenexcluded.
Outcome: Studies were selected only if theyreported outcomes which were either directlyrelated to the disorder (e.g. symptom reduction)or to intermediary variables. In the latter case,the reviewers had independent evidence of animpact on mental health associated with thatoutcome (e.g. major risk factors such aseducational progress in conduct disorderedchildren) or an impact on mental health wasplausible (e.g. family dysfunction).The reviewerswere inclusive in their approach. Emphasis wasplaced on interventions that examined the directimpact on mental health or the intermediate(preventative) impact on risk factors, but studieswith less well focused outcome informationwere also frequently covered.
Design: The review focused on studies thatused an experimental or quasi-experimentalstudy design. Observational studies, such ascohort or case studies, were also considered forreview, but possible effects of this bias were
35
Appendix 1Page 398

indicated throughout.This was a necessaryrelaxation of normal exclusion criteria because apreliminary exploration of the available evidenceindicated that the exclusion of poorly controlledstudies would drastically curtail the availabledatabase to a point where the meaningfulnessand relevance of the review might well beseriously jeopardised.The initial plan to excludestudies which did not meet the criteria specifiedby the Cochrane Collaboration provedimpractical. In order to maintain maximumcomparability between the CochraneCollaboration’s work and that of the review, thereview team reviewed all the available evidence,highlighting the methodological shortcomingsand cautioning readers to interpret the resultswith appropriate care.
Initially, then, the selection criteria for studies tobe included in the review were: (a) group designinvolving random assignment; (b) well-documented treatment procedures; (c) uniformtherapist training, or clear manualisation of theprotocol for administering medication, andevidence of adherence; (d) clinically referredsamples or treatment candidates; (e) outcomeassessment, including at least two outcomelevels (e.g. level of symptoms, adaptation,mechanisms, transactions or service utilisation);(f) tests of clinical significance; (g) assessment oflong-term outcome (follow-up greater than sixmonths).These criteria were rejected asunrealistic when preliminary coding revealedthat only 7.4% of studies in child and adolescentmental health met the first of these criteria -rigorous randomisation.
Hence, the key selection criteria for acceptanceinto the review were as follows:◆ A clear description of the patient population
in the study, either in terms of diagnosis or interms of specific problems addressed in thetreatment;
◆ The study was reported in the Englishlanguage;
◆ The study had a group design, or anexperimental single-case design;
◆ There was a systematic effort at themeasurement of outcome, including at leastpre- and post-test measurement on anobjective instrument.
Other reviews of this literature have beenforced to make similar compromises. Forexample, the American PsychologicalAssociation’s Division 12 Task Force onempirically supported treatment for children andadolescents were not able to apply fully thecriteria of the Chambless Task Force onpromotion and dissemination of psychologicalprocedures developed for an adult patientpopulation, simply because in many areas thestudy design, particularly the size ofexperimental groups, was not up to the task.
It should be noted that there are severalimportant limitations to this review. Firstly, whilethe review team aimed for exhaustive coverageof the literature, no doubt key contributionshave been missed for a variety of administrativeand practical reasons. Secondly, literature notpublished in the English language was notaccessible to review.Thirdly, anecdotal case
36
Appendix 1 continuedPage 399

reports, which represent a large proportion ofthe psychodynamic literature, for example, werenot included.These reports almost inevitablyfailed to meet the criteria of clear description ofthe case and rarely included objective measuresof outcome. Fourthly, the review team did notaggregate the studies using meta-analyticstrategies.The central problem from the point ofview of identifying evidence-based practice is thehomogeneity assumption about the nature ofthe particular forms of treatment that must bemade in meta-analyses. It was felt that therewere too few studies using genuinelycomparable treatment procedures for suchaggregation to be justified. Finally, theconclusions can only be based on the evidenceavailable - they may change dramatically as newdata emerges and readers are encouraged toreview the current document in the light of anyrecent findings.
Summary of process to updating thereview 2006
For the 2006 review we were not in a positionto undertake a new systematic review of theliterature. However we were able to draw onNICE guidance, Cochrane reviews, HealthTechnology Assessments and expert guidance toensure that all the key studies were included.Chapters already written were revised by theauthors, in the light of new NICE guidance,relevant Cochrane reviews, or evidence frommajor randomised control trials. For eachpresenting problem, one member was set thetask of extracting what they deemed to be the
key statements from the relevant NICE guidelineand/or major recent research, in terms ofpsychosocial and physical treatmentinterventions available in clinical settings.Thesestatements were circulated to the whole group,and discussed until everyone felt that a fairrepresentation of the evidence being reviewedhad been developed. On the basis of thesediscussions, a further set of statements outliningthe implications for clinical practice weredeveloped, which were also agreed by allmembers of the working group as being fairconclusions to draw from the available evidence.
The following sources were used:National Institute for Health and ClinicalExcellence (NICE)www.nice.org.uk
Centre for Reviews and Dissemination –Database of Abstracts and Reviews ofEffects (DARE)www.york.ac.uk/inst/crd/index.htm
The Cochrane Collaborationwww.cochrane.org
37
Page 400

Summary of the definingcharacteristics of the main types ofpsychosocial interventions.
Behavioural and Cognitive BehaviouralTherapies Behavioural treatments aim to use the insightsfrom learning theory to achieve specific changesin behaviour. Key techniques include exposureand response prevention, modeling andcontingency management.
Cognitive treatments aim to changedysfunctional beliefs by employing a range ofbehavioural techniques, by psycho-education andby a structured form of Socratic questioning,whereby the individual is encouraged to firstelucidate, and then challenge, certain of theircore beliefs.
Behavioural and Cognitive Behavioural Therapiesare usually highly structured and relatively brief(6-24 sessions). Children and/or parents may beseen individually, in groups or with other familymembers.
Systemic Family TherapiesSystemic family therapies focus on the systemrather than the individual, and attend to theconnections between patterns of behaviour andbeliefs within the system and the presentingproblem.
Family therapies generally see the child as partof a family group, but may work on occasionswith subsystems (e.g. the parents alone, the child
alone).These therapies are often open-ended butfamilies are rarely seen more frequently thanonce a month, and the number of sessions istypically between 6 and 12.
Psychodynamic PsychotherapiesPsychodynamic psychotherapies focus onunconscious processes in the individual childthat are believed to underlie emotional andbehavioural disturbance.These therapies seek tohelp the child recognise and understand aspectsof his or her behaviour in the light of theseunconscious processes. Psychodynamicpsychotherapies are often intensive (once aweek or more) and lengthy (40 sessions ormore).The child is generally seen individually andparents or other carers are seen in parallel.
Multi-Modal Therapies A combination of the above approaches,sometimes involving additional elements.
38
Appendix 2Page 401

Disturbance of ConductTechnology Appraisal on Parent-training/education programmes in themanagement of children with conduct disorders– guidance, (July 2006)
Disturbances of AttentionNICE Review of Technology Appraisal 13:Methylphenidate, atomoxetine anddexamfetamine for attention deficit hyperactivitydisorder (ADHD) in children and adolescents(March 2006)
Anxiety DisordersNICE Guideline on Obsessive CompulsiveDisorder for 8 years+ (November 2005)
NICE Guideline on Anxiety – Management ofanxiety (panic disorder, with or withoutagoraphobia, and generalised anxiety disorder) inadults in primary, secondary and community care(Dec 2004)
Post Traumatic Stress DisorderNICE Guideline on Post-traumatic stressdisorder (PTSD):The management of adults andchildren in primary and secondary care (March2005)
Depressive DisorderNICE guideline on depression in children andyoung people (March 2006)
Psychotic DisorderNICE guideline on schizophrenia (adult specific)(2002)
Eating DisorderNICE guideline on eating disorders (aged 8 +)(2004)
Deliberate Self HarmNICE guideline on deliberate self harm (adult-focussed but with section on children and youngpeople) (2004)
Substance AbuseNICE guideline on substance abuse (all ages)(2004)
39
Appendix 3 Relevant NICE guidance Page 402

40
Page 403

Categories of Evidence:
1a Evidence from meta-analysis of randomised controlled trials;
1b Evidence from at least one randomised controlled trial;
2a Evidence from at least one controlled study without randomisation;
2b Evidence from at least one other type of quasi-experimental study;
3 Evidence from descriptive studies such as comparative studies,
correlation studies and case-control studies;
4 Evidence from expert committee reports or opinions, or from
clinical experience of a respected authority, or both.
Strength of Practice Implications:
A Directly based on category 1 evidence;
B Directly based on category 2 evidence or extrapolated from
category I evidence;
C Directly based on category 3 evidence or extrapolated from
category 2 evidence;
D Directly based on category 4 evidence or extrapolated from
category 3 evidence.
It is important to recognise that the evidence base has limitations and should always be responded to within the context of professional judgement and care. See pages 4–7for discussion of these issues.
Page 404

ISBN (10) 0-9553956-0-7 ISBN (13) 978-0-9553956-0-4© 2006 CAMHS Publications
Page 405

This page is intentionally left blank
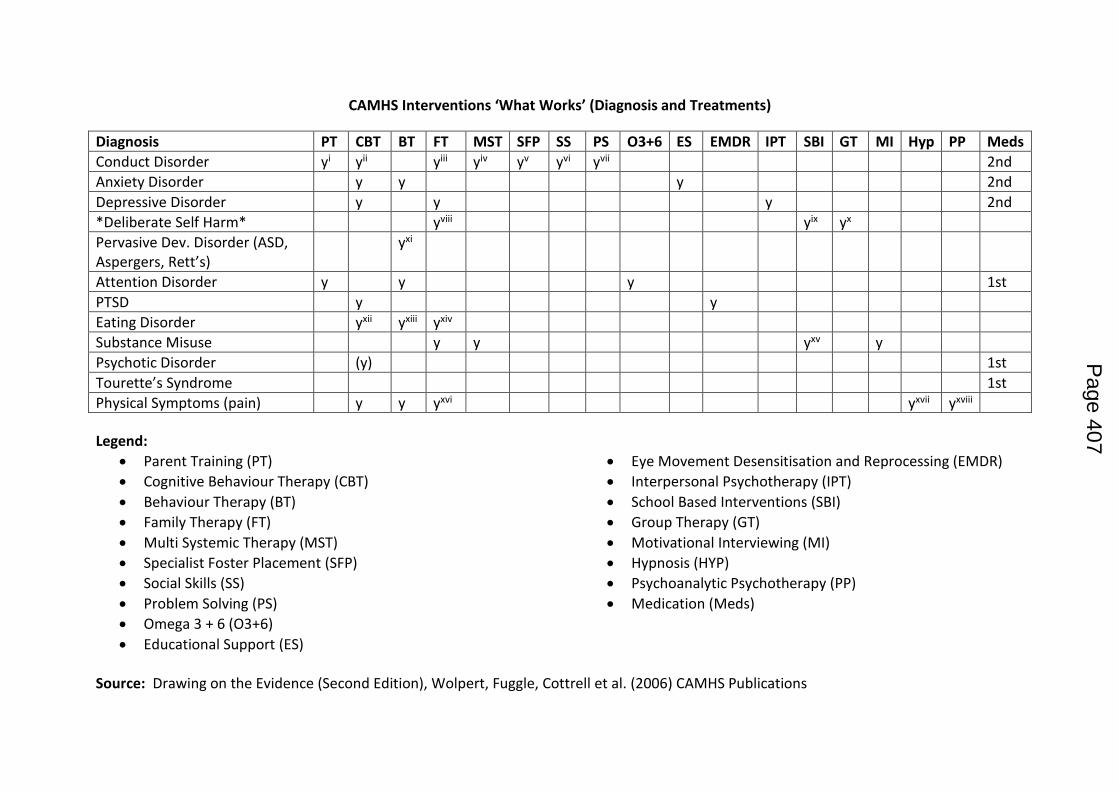
CAMHS Interventions ‘What Works’ (Diagnosis and Treatments)
Diagnosis PT CBT BT FT MST SFP SS PS O3+6 ES EMDR IPT SBI GT MI Hyp PP Meds
Conduct Disorder yi yii yiii yiv yv yvi yvii 2nd
Anxiety Disorder y y y 2nd
Depressive Disorder y y y 2nd
*Deliberate Self Harm* yviii yix yx
Pervasive Dev. Disorder (ASD, Aspergers, Rett’s)
yxi
Attention Disorder y y y 1st
PTSD y y
Eating Disorder yxii yxiii yxiv
Substance Misuse y y yxv y
Psychotic Disorder (y) 1st
Tourette’s Syndrome 1st
Physical Symptoms (pain) y y yxvi yxvii yxviii
Legend:
Parent Training (PT)
Cognitive Behaviour Therapy (CBT)
Behaviour Therapy (BT)
Family Therapy (FT)
Multi Systemic Therapy (MST)
Specialist Foster Placement (SFP)
Social Skills (SS)
Problem Solving (PS)
Omega 3 + 6 (O3+6)
Educational Support (ES)
Eye Movement Desensitisation and Reprocessing (EMDR)
Interpersonal Psychotherapy (IPT)
School Based Interventions (SBI)
Group Therapy (GT)
Motivational Interviewing (MI)
Hypnosis (HYP)
Psychoanalytic Psychotherapy (PP)
Medication (Meds)
Source: Drawing on the Evidence (Second Edition), Wolpert, Fuggle, Cottrell et al. (2006) CAMHS Publications
Page 407

End notes i <12 yrs. ii Adoles. / moderate. iii Adoles. / moderate. iv Adoles. / severe. v Adoles. / severe. vi Adoles. / moderate. vii Adoles. / moderate. viii Brief. ix Can improve knowledge and attitudes amongst YP towards disclosure of self harm by their peers. x For CYP who have repeatedly self-harmed. xi Intensive. xii Bulimia. xiii In hospital settings. xiv Anorexia. xv Skills-oriented resilience enhancement programmes in schools and community settings. xvi Considered for the treatment of asthma. xvii Decreases procedural distress and somatic symptoms associated with chemotherapy. xviii For the treatment of hard to control diabetes.
Page 408

1
Lambeth CAMHS
Additional funding and proposed action plan (2015/17)
1. Introduction The purpose of this paper is to outline the mutually agreed and planned deployment of new recurrent funding of £182,000 for the purposes of reducing waiting times into CAMHS in Lambeth and enhancing the safety and quality of CAMHS teams. The paper starts by outlining the current need and profile identified by SLAM CAMHS of the children and young people on the Early Intervention waiting list.
2. EI CAMHS waiting list analysis
A. Numbers of children and young people waiting for a service
Current waiting list at 19/05/2015: 182
(Insight data analysis showing 205 but some of these have appointments booked or are in process of being closed due to not responding to assessment booking letter).
B. EI CAMHS – waiting times According to quarter 4 data reports (2014/15) from SLAM CAMHS, the average waiting time (referral to assessment and 1st treatment) is 45.1 weeks. The national average waiting time is reported as 15 weeks and maximum waiting times for all children and young people is nationally set for the NHS as 18 weeks for a consultant led service.
C. EI CAMHS waiting list: referrals by criteria
Criteria Number on caseload
1 – CYP experiencing severe/sustained reaction to critical incident 7
2 – anxiety 41
3 - early signs of eating disorder 1
4 – self-harm 8
5 – depression 33
6 – challenging behaviour 37
7 – ADHD 51
8 – enuresis / encopresis – no physical cause 4
Page 409

2
D. EI CAMHS waiting list: referrals by age
Age Number on caseload
4 1
5 7
6 11
7 14
8 15
9 17
10 17
11 16
12 13
13 17
14 12
15 22
16 12
17 8
63 out of 88 individuals accepted for challenging behaviour/ADHD are aged 11 years and under.
Analysis of last 11 panels (09/03/15 -18/05/15)
82 referrals
51 accepted
6 already open to CAMHS
25 rejected
Rejected referrals:
5 recommended to refer to community paediatrics
6 forwarded on to other CAMHS teams, NDT, CACS, YOS (Lambeth and Southwark)
3 asked for further information
4 asked for other MAT support
2 not asking for CAMHS on the CAF Safeguarding:
1 open to social care
3 referred to social care at same time as referral to CAMHS
1 previous social services / safeguarding but no longer on plan
Page 410

3
Although we are not currently routinely recording child protection/safeguarding status on the EI CAMHS waiting list spreadsheet, this will start to be recorded. NB: If concerns are raised by duty workers, at CRP or by other team leads/psychiatrists and then EI CAMHS waiting list patients can be redirected to other CAMHS teams
3. Current EI CAMHS team changes to address waiting list 1) We monitor our activity closely – each member of the team gets feedback about number of appointments that they are offering on monthly basis, this enables us to ensure that we are recording everything correctly, maintains focus on activity levels and impact that this has on waiting list length and time. 2) Assessments – we are now writing out regularly to next 20 on waiting list asking them to phone and book an appointment - all clinicians have given appointment slots and these are then filled on first come first served basis. GP and referrer are copied into this letter so that they can support the family to make contact to book an appointment. We have been doing this since April (first letters sent out mid March). This has substantially increased work for admin within the team but means that the clinicians do not have young people on their caseloads that are not going to attend.
4. Innovation to reduce EI CAMHS waiting list 1) Lambeth CAMHS ADHD Clinic This will remove patients with explicit ADHD-related concerns (51) from the EI waiting list, and a proportion of those presenting with challenging behaviour (37) will also be suitable for formal assessment. A conservative estimate of 11 cases from challenging behaviour in addition to the 51 ADHD would reduce EI CAMHS waiting list numbers to 120. The Lambeth CAMHS ADHD Clinic will bring together work that is currently undertaken in a somewhat un-coordinated manner across all five teams in Lambeth CAMHS, with a focus on: - Assessment clinic: regular weekly slots making use of psychiatric and clinical psychology trainees under supervision - Rolling treatment groups for ADHD: including Incredible Years parenting, group for teenagers, psychoeducation - Working with users via the well-established user-led Lambeth ADHD group - Coordination with partner agencies including community paediatrics for a clear care pathway 2) Evaluation of CAPA (Choice and Partnership Approach www.capa.co.uk), a demand and capacity tool. We are planning team time to discuss useful aspects of this approach to restructure how we work. This will require further data analysis, as demand arises from the waiting list, new referrals and ongoing cases. This approach may be particularly beneficial in managing patient flow through our service as significant other changes arise (changes to thresholds in other services, increased referral rates due to increased awareness, changing provision in third sector). This framework encompasses enhanced definition of the roles/expectations of all staff, including interns, clinical trainees and MSc students that frequently conduct clinical attachments in our services. The activity of this group should not be considered to be core service delivery, but interns, students and trainees can make significant contributions to clinical assessments (e.g. conducting school observations, helping write up assessments), delivery of group interventions with a co-facilitator and service audits. The CAPA approach will be discussed at a Lambeth CAMHS Strategy Day to explore the elements that are most suitable and applicable to our services, and avoiding those that may be less desirable. 3) Schools work Lambeth CAMHS and SLaM currently provide a small amount of dedicated on-site CAMHS support for schools that commission this directly, either independently or as part of a cluster or federation. Increased commissioning by schools of such in-house CAMHS staff has significant benefits to young
Page 411

4
people by not taking them out of school and achieving rapid access to a specialist service. This would also help reduce the burden on EI waiting list. 4) Self-harm team We have arranged training for 40 Lambeth CAMHS staff in Therapeutic Assessment (TA), a specialist approach for assessment and intervention in self-harm. In collaboration with research colleagues (Dr Dennis Ougrin) and colleagues in paediatric liaison services based at St Thomas' Hospital, we are proposing a coordinated self harm team in Lambeth CAMHS, with four clinicians (funded by research grants) delivering the four main evidence based interventions for this condition: CBT, family therapy, brief solution-focused therapy and mentalisation. 5) Increased collaboration with third sector agencies (e.g. Youth Lambeth Cooperative) Closer working and understanding of what is available in third sector so that patients can be signposted at all stages to effective, quality-assured alternatives that meet their needs. 6) Group work Groups currently being delivered in Lambeth CAMHS include:
Incredible Years for parents of under-12s: an evidence-based intervention for both ADHD and Conduct Disorder in Primary School population
STOP group for parents of teenagers
Psychoeducation group
Support to carer-led Lambeth ADHD Group
Social skills for ASD group Planned new groups include:
ADHD group for Teenagers
CLAMHS YP Group
Emotional literacy / coping skills group 7) Analysis of clinical outcomes Lambeth CAMHS will build on existing outcome measures (CGAS and PPI data including plaudits) and explore how CYP-IAPT measures can be shared with partner organisations to show clinical effectiveness of service delivery.
Page 412

5
Proposed outcomes A. All patients seen within 18 weeks (referral to 1st treatment) (FOR ALL CAMHS TEAMS) When? By end of Quarter 4 2016/17 and continuously thereafter Evidence how? Lambeth CAMHS data Q4 2016/17
Rationale: reduce maximum ‘waiting times’ for EI Team and CLAMHS to meet national minimum standards and speed up access to assessment and treatment if clinically appropriate for the patient.
SLAM proposal for reducing maximum waiting times
CAMHS Teams Maximum waiting time for children and young people
2015/16 2016/17
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Early Intervention Team 44 40 35 30 20 15 10 10
EI - Waiting List 182 34
All other CAMHS teams 18 18 18 18 18 18 18 18
NB: These targets represent minimum expectations. Lambeth CAMHS will aim to achieve shorter waiting times more rapidly than detailed above.
B. Signposting – all patients not meeting CAMHS threshold are signposted to a form of effective support either within Lambeth or outside of Lambeth
When? Immediately Evidence how? Inclusion with ‘Lambeth CAMHS data Q2 report 2015/16’ – ‘Signposting destination’ similar to ‘discharge destination’ in current report.
Rationale: ensure children and young people who:
do not meet CAMHS tier 3 criteria - are effectively signposted to other support within the community.
are on the ‘waiting list’ - are able to access appropriate support within the community while waiting wherever possible.
5. Proposed plan
I have started to draft a timeline for the recruitment and the realisation of the outcomes we agree.
New staff operational 2015 2016
Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
New resource agreed √
Outcomes and plan agreed
√
1. EI worker a1 i / r s
2. Consultant Clinical Psychologist
s
3. EI worker a i / r s
4. FT a i / r s
1 Legend: a= advertised / i= interviewed / r= recruited / s= started
Page 413

6
6. Staffing and resource - planning assumptions
CAMHS Teams new staff will work with
Job title Band WTE Cost (per annum)
Activity2 Unused months
Underspend EI NDT CACS CLAMHS YOS / AIM
1. Early intervention worker 6 1 £52k 40 new referrals per annum
2 £8,666 √
2. Consultant Clinical Psychologist
8c across all teams
0.2 £18k Lead clinical psychologist: Supervision +Assessments (pan-Borough) + Treatments (pan-Borough) / 8 new referrals per annum
0 0 √ √ 2
√ 2
√ 2
√ 2
3. Early intervention worker 7 (half funded by this funding)
1 £30k 40 new referrals per annum
4 £10,000 √ 20
√ 20
4. Family Therapist 7 across all teams
1 £60k Supervision + 35 new referrals per annum
4 £20,000 √
√ √ 35 √ √
5. From underspend: Band 6 (fixed term for 6 months)
6 1 for 6 months
£27k 20 new referrals per annum
N/A – to start Q4 with underspend
N/A – to start Q4 with underspend
√
6. From underspend: Early intervention worker (increasing time in existing worker)
Band 7 Extra 0.2
£12k 8 new referrals per annum
N/A N/A √
2 Workforce Capacity (p.25) – Number of new referrals per WTE per year = 40. / Source: CR182. Building and sustaining specialist CAMHS to improve outcomes for children and young people
http://www.rcpsych.ac.uk/usefulresources/publications/collegereports/cr/cr182.aspx
Page 414

7
Total £182k 156 new referrals £38,666
This additional staffing will have the following impact:
1. 80-90 MORE cases will be seen per annum in EI CAMHS (in addition to current team activity)
2. Family therapist will increase availability of family therapy to all Lambeth CAMHS teams including EI CAMHS
3. Increased delivery of group interventions across Lambeth CAMHS as a result of increased staffing
4. Greater productivity in Tier 3 service due to increased sharing of Borough-wide Duty clinician role
5. Senior clinical psychology input to support innovation and change, including development of ADHD Clinic and proposals for school work
6. The new staff will target patients who have been on the waiting list the longest first Action Plan monitoring This recruitment and activity plan will be monitored by the CAMHS commissioning manager at Lambeth CCG. Any unforeseen underspend will be directed to achieve agreed targets which will be evidenced by reasonable activity indicative of the additional resource being deployed. Caveat: This resource will be used for Lambeth CCG children and young people unless with the explicit agreement of the CAMHS commissioning manager.
Page 415

8
7. Progress SLAM CAMHS: 1. We have recruited to the Band 6 post as a fixed term for a year, they should be starting very soon (then we will advertise in the next few months for a permanent position). 2. The consultant clinical psychologist has already started increased hours. 3. This post was due to be filled by a candidate who has recently accepted a post elsewhere. In view of an unfilled 0.5 Band 7 post in NDT, we are now aiming to fill this post with a Band 7 clinical psychologist with duties across EI CAMHS and NDT. 4. The Band 7 family therapist post has been agreed internally and we are due to complete JD to go to advert as soon as possible 5. Underspend: Additional fixed term Band 6 clinicians as funds permit, currently proposed to be 1 WTE for a fixed term of 6 months. (At interviews for permanent Band 6 clinicians (e.g. on 19/05/2015) candidates are routinely asked if they would consider fixed term roles in other Lambeth teams; good candidates that are unsuccessful can then be offered fixed term posts, and would be allocated exclusively to the EI CAMHS service, using this underspend). 6. Underspend: Increase existing EI Band 7 post by 0.2 WTE for one year
8. Appendix
SLAM - CAMHS – 2014/15 - Q2 data
SLAM - CAMHS – 2014/15 - Q3 data
SLAM - CAMHS – 2014/15 – Q4 data
Staffing of CAMHS teams 30th April 2015
London dataset Q2 2014 Lambeth final.docx
London dataset Q3 201415 Lambeth final.docx
Appendix 11 - Lambeth Q4 London CAMHS Dataset.pdf
Lambeth CAMHS Team Structures updated 30.04.2015.xls
2 CR182. Building and sustaining specialist CAMHS to improve outcomes for children and young people, Royal College of Psychiatrists (November 2013): http://www.rcpsych.ac.uk/usefulresources/publications/collegereports/cr/cr182.aspx
Page 416

Health and Wellbeing Board
Date of Committee: 8 July
Report title Our Healthier South East London
Wards: All
Report Authorised by:
Portfolio:
Contact for enquiries:
Catherine Flynn
Engagement Manager
NHS Lambeth Clinical Commissioning Group
Report summary
The attached three papers provide detail of Our Healthier South East London.
Finance summary
None arising,
Recommendations
(1) To note the attachements.
Page 417 Agenda Item 6

1. Context
1.1 Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs, working with
NHS England as co-commissioner, are working in partnership with local authorities, local
providers and other key stakeholders to define a five-year strategy for health and
integrated care services across south east London. The strategy complements and
builds on local work and has a particular focus on those areas where improvement can
only be delivered by collective action or where there is added value from working
together. It seeks to respond to local needs and aspirations, to improve the health of
people in south east London, to reduce health inequalities and to deliver a health care
system which is clinically and financially sustainable. The approach is commissioner led
and clinically driven, and informed by wide engagement with local communities, patients
and the public.
2. Proposal and Reasons
2.1 Detailed in attachements.
2. Finance
2.1 There are no financial implications to this report..
3. Legal and Democracy
3.1 There are no legal implications to this report.
4. Consultation and co-production
4.1 N/A
5. Risk management
5.1 N/A
6. Equalities impact assessment
6.1 N/A
7. Community safety
7.1 N/A
8. Organisational implications
The following sections must be considered, but are optional and each should be deleted
if not relevant to the report. If there are no organisational implications, state “None”.
8.1 Environmental
None.
8.2 Staffing and accommodation
Page 418

None
8.3 Procurement
None
8.4 Health
None
9. Timetable for implementation
9.1 None
Page 419

Page 420

South East London Consolidated Strategy Programme Overview Paper
This paper provides an introduction to the south east London consolidated strategy. This sets out the background to the document and summary of the next phase of work.
Introduction Our Healthier South East London is the five year commissioning strategy which aims to improve health, reduce health inequalities and ensure all health services in south east London meet safety and quality standards consistently whilst being sustainable in the longer term. The attached document is the consolidated strategy, which sets out the shared vision and initiatives to respond to this challenge. This version is still a work in progress, although it has developed very significantly from the draft strategy which was approved by CCG Governing Bodies in June 2014. Comments from IEG and feedback from Clinical Executive Group/Partnership Group have been reflected in the executive summary. The full version of the strategy document is being reviewed and will be updated for submission to CCG Governing Bodies in July. The strategy is still very much a work in progress:
• there is a case for change, which has been widely tested; • clinical models and a whole system model have been developed with wide clinical engagement, but will
continue to be developed and refined • there has been work to identify the outcomes which the strategy will deliver, but there is more to do to
establish baselines and the scale of ambition • there is a first assessment of the impact on activity and finance, developed through the Clinical
Leadership Groups. This is currently being tested with providers and other partners and stakeholders and will be amended through that process, but provides a good foundation for further work
Although there is more work to do, the case for change sets out why it is urgent to move to implementation and it is the view of the CCG chief officers and NHS England colleagues that the work to date can be the basis both for further development and for preparation for implementation. Indeed, in some areas, where there is general agreement on moving to best practice, implementation is already underway. The consolidated strategy, therefore, provides a framework for the further work:
• to develop the clinical models and their combined impact; • to continue or develop plans for implementation for those areas which are about taking forward best
practice and have general support; • to develop and approach to option appraisal where there are choices about how to implement the
clinical models and to consider their impact on the health care system as a whole, including where they may lead to significant service change and therefore a need for formal consultation.
How the consolidated strategy has been developed The consolidated strategy has been developed by the six Clinical Commissioning Groups across South East London, working with commissioning colleagues from NHS England and in partnership with local authorities, NHS providers, patients, local people and other key stakeholders. Background to developing the clinical models Our approach to addressing health issues and the way health services are delivered have to change in order to meet the emerging needs of an ageing population in which many more people live with long term conditions
Page 421
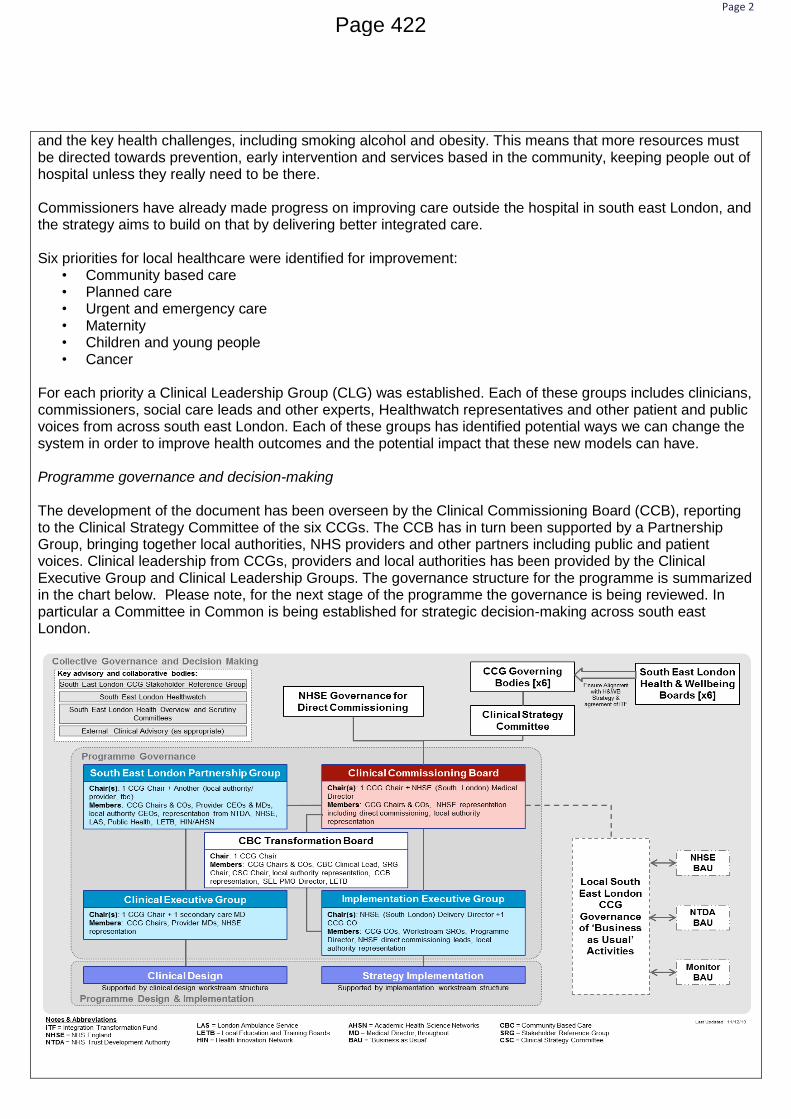
Page 2
and the key health challenges, including smoking alcohol and obesity. This means that more resources must be directed towards prevention, early intervention and services based in the community, keeping people out of hospital unless they really need to be there. Commissioners have already made progress on improving care outside the hospital in south east London, and the strategy aims to build on that by delivering better integrated care. Six priorities for local healthcare were identified for improvement:
• Community based care • Planned care • Urgent and emergency care • Maternity • Children and young people • Cancer
For each priority a Clinical Leadership Group (CLG) was established. Each of these groups includes clinicians, commissioners, social care leads and other experts, Healthwatch representatives and other patient and public voices from across south east London. Each of these groups has identified potential ways we can change the system in order to improve health outcomes and the potential impact that these new models can have. Programme governance and decision-making The development of the document has been overseen by the Clinical Commissioning Board (CCB), reporting to the Clinical Strategy Committee of the six CCGs. The CCB has in turn been supported by a Partnership Group, bringing together local authorities, NHS providers and other partners including public and patient voices. Clinical leadership from CCGs, providers and local authorities has been provided by the Clinical Executive Group and Clinical Leadership Groups. The governance structure for the programme is summarized in the chart below. Please note, for the next stage of the programme the governance is being reviewed. In particular a Committee in Common is being established for strategic decision-making across south east London.
Page 422

Page 3
Who has been involved in shaping the strategy Our approach to developing the strategy has been strongly focused around communicating and engaging and commissioners have designed and developed the strategy with partners, patients and local people and key stakeholders, with thinking and planning being developed and amended through the engagement process. The development of the strategy is clinically-led and developed, with over 300 clinicians, nurses, allied health professionals, social care staff, commissioners and others developing ideas through the six CLGs. How the consolidated strategy document is structured The strategy is set out over a number of sections, which are summarised below:
Background and introduction: sets out the purpose of the strategy, background to health and care services in south east London and a summary of how stakeholders have been involved in developing the strategy
Case for change: a summary of the detailed case for change setting out the challenges facing health and care services in SEL
Vision and proposed model of care: This is the main section of the strategy and sets out the work of the CLGs in addressing the case for change in each of the priority areas set out above.
Benefits and impacts: The outcomes that the strategy aims to deliver and the activity and finance impacts of the new models of care developed by CLGs.
Delivering our vision: Overview of the supporting strategies that will enable delivery of the future vision for health and care services in south east London
Approval process and mechanisms for incorporating feedback The approval process for the strategy is summarised below. The aim is for it to be approved in August by the Clinical Strategy Committee or, if established, the proposed Committee In Common (CIC). Feedback will be collected throughout the process from each group with two main iterations:
To incorporate feedback from the programme governance groups before submission to Governing Bodies, Trust Boards and other stakeholder groups at their July meetings
Comments from Governing Bodies and others to be incorporated and, subject to no major changes being required, final approval by the Clinical Strategy Committee/Committee in Common for Strategic Decision Making in August.
Page 423
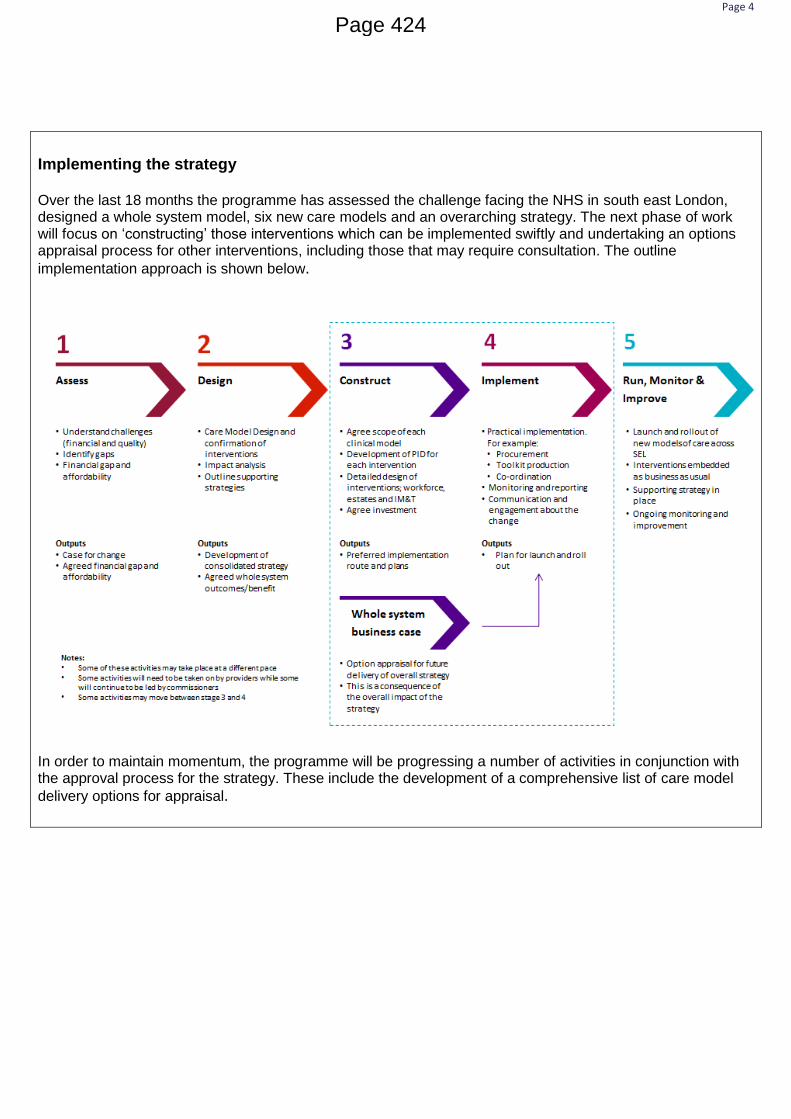
Page 4
Implementing the strategy Over the last 18 months the programme has assessed the challenge facing the NHS in south east London, designed a whole system model, six new care models and an overarching strategy. The next phase of work will focus on ‘constructing’ those interventions which can be implemented swiftly and undertaking an options appraisal process for other interventions, including those that may require consultation. The outline
implementation approach is shown below.
In order to maintain momentum, the programme will be progressing a number of activities in conjunction with the approval process for the strategy. These include the development of a comprehensive list of care model
delivery options for appraisal.
Page 424

1 V5
Report to the Governing Body
1st July 2015
Report Title
Our Healthier South East London Consolidated Strategy
Author(s)
Sheridan Ash, Programme Team
Caroline Taylor, Programme Director
Governing Body/Clinical Lead(s)
Adrian McLachlan - Chair
Management Lead(s)
Andrew Parker, Director of Primary Care Development
CCG Programme
All
Purpose of Report
To receive, review, and approve the direction of travel as described in the attached document, Our Healthier South East London – Consolidated Strategy.
Summary
Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs, working with NHS England as co-commissioner, are working in partnership with local authorities, local providers and other key stakeholders to define a five-year strategy for health and integrated care services across south east London. The strategy complements and builds on local work and has a particular focus on those areas where improvement can only be delivered by collective action or where there is added value from working together. It seeks to respond to local needs and aspirations, to improve the health of people in south east London, to reduce health inequalities and to deliver a health care system which is clinically and financially sustainable. The approach is commissioner led and clinically driven, and informed by wide engagement with local communities, patients and the public.
Recommendation(s) The Governing Body is asked to:
Approve the direction of travel set out in the consolidated strategy as the appropriate basis for progressing to implementation.
Identify any further work required to develop and progress the strategy.
Review and comment on the next steps for implementing
Page 425

2 V5
the strategy.
Note that the consolidated strategy is a work in progress and will continue to be developed throughout the duration of the programme.
Does this report provide assurance to support the vision for the CCG?
People centred
Prevention focused
Integrated
Consistent
Innovative
Deliver best value
Does this report provide assurance in relation to the following areas of responsibility for the CCG
Legal
Engagement
Risk
Financial
Inequalities
Please include relevant risk references here
All legal, engagement, inequalities, financial and resource implications and any potential or
actual risks are set out in the body of this report.
Page 426

3 V5
1. Aims of the strategy and case for change
Our Healthier South East London is the five year commissioning strategy which aims to
improve health, reduce health inequalities and ensure all health services in south east
London meet safety and quality standards consistently whilst being sustainable in the
longer term.
Attached is a programme overview paper and the Our Healthier South East London
consolidated strategy executive Summary. A full version of the strategy report can be
found on the CCG Website:
The governing body received an early draft of the strategy in June 2014 and a progress
report at its January meeting. The attached document is the consolidated strategy, which
builds on the earlier draft and reflects the work undertaken since then. While this is still a
work in progress:
There is a case for change, which has been widely tested;
Clinical models and a whole system model have been developed with wide clinical engagement, but will continue to be developed and refined;
There has been work to identify the outcomes which the strategy will deliver, but there is more to do to establish the indicators, baselines and the scale of ambition;
There is a first assessment of the impact on activity and finance, developed through the Clinical Leadership Groups. This is currently being tested with providers and other partners and stakeholders and will be amended through that process, but provides a good foundation for further work.
2. Impact of the strategy
To date, the consolidated strategy brings together the case for change, the care models
and their anticipated impacts on outcomes for the people and communities in south east
London. This is combined with an assessment of the potential impact these models may
have on how people use services and the extent to which it will support the future financial
sustainability of the system.
Taking into consideration growth assumptions over the next 5 years, and not changing our
clinical models of care would mean that too many people would continue to be admitted to
hospital where better Community Based Care models could provide improved outcomes.
We have calculated the increase in bed capacity that would be needed across south east
London to respond to the rise in population and aging population using our current
approaches to delivering care. The projected demand would increase so much that the
number of beds needed would be enough to fill a new hospital site and this is not possible
or affordable. Applying the initial impact of the strategy’s care models work on the
projected demand levels for hospital beds, shows that by implementing the care models in
the strategy, we would reduce the need for additional hospital beds by providing an
alternative high quality model of care that is focussed on improved outcomes for the
population we serve. This is because:
Page 427

4 V5
• The care models are focused on prevention and early intervention and keeping people healthy. Therefore keeping people out of hospital
• Community Based Care is the foundation of the whole system and is intended to
keep people closer to home, treating them in the community and enabling people to
only
• visit hospital when they really need to
• Pathways and professionals will be more integrated
• Productivity is expected to increase and there will be greater efficiency in the south east London system
• The plan will be for bed occupancy to meet the national guidance (which is not the case now) which will improve safety, quality and efficiency.
3. Areas where further work is required:
• Ensuring that progress and plans for the London Quality Standards are embedded into the strategy and exploring options on how they can be achieved
• Further developing the supporting strategies of Workforce, IM&T and Estates
• Refining the indictors for the Outcomes to make sure the best possible ones have been selected so we can measure the benefits or not of the strategy
• Engagement on the options appraisal methodology
• On-going communications and engagement
4. Summary and next steps
Although there is more work to do, the case for change sets out why it is urgent to move to
implementation and it is the view of the CCG chief officers and NHS England colleagues
that the work to date can be the basis both for further development and for preparation for
implementation. Indeed, in some areas, where there is general agreement on moving to
best practice, implementation is already underway.
The consolidated strategy, therefore, provides a framework for the further work:
• To develop the clinical models and their combined impact;
• To continue or develop plans for implementation for those areas which are about taking forward best practice and have general support;
• To develop an approach to option appraisal where there are choices about how to implement the clinical models and to consider their impact on the health care
Page 428

5 V5
system as a whole, including where they may lead to significant service change and therefore a need for formal consultation.
Through this process the views and feedback from the 6 CCG’s, patient and public events,
other organisations and boards will be taken used to refine the strategy and future models
of care.
The approach to implementation and timeline for delivery is set out in the supporting
papers.
5. Engagement and Equalities
Engagement History
The consolidated strategy reflects the work of the six Clinical Leadership Groups,
overseen and supported by the programme’s Clinical Executive Group, Partnership Group
and the Clinical Commissioning Board. Over 300 clinicians across south east London have
been involved in its development
The programme has worked in partnership with a wide range of stakeholders,
organisations, and partners. These are summarised below:
• King's College Hospital NHS Foundation Trust - a local and specialised acute hospital
• Guy's and St Thomas' NHS Foundation Trust - local and specialised acute hospital and community provider focusing on residents of Lambeth and Southwark
• Lewisham and Greenwich NHS Trust – a local acute hospital with some specialised acute services and community care services
• Dartford and Gravesham NHS Trust – a local acute trust • South London and Maudsley NHS Foundation Trust – a mental health trust focusing
on residents of Lambeth, Lewisham and Southwark • Oxleas NHS Foundation Trust – a mental health trust focusing on residents of
Bexley, Bromley and Greenwich • Bromley Healthcare Community Interest Company • GP practices • Voluntary and third sector organisations • Local authority social care services • England and London wide partners
The CCGs also work closely with NHS organisations in London and across England.
These organisations include:
• London Ambulance Service • Department of Health • NHS England • Neighbouring CCGs • NHS South East Commissioning Support Unit • Public Health England • Local authority partners
Page 429

6 V5
The CCGs have strong partnerships with local authorities to take into account the various
health and wellbeing groups that operate within local authorities.
An early draft of the strategy was considered by this governing body and other governing
bodies in south east London in June 2014. This version has been considered by the
programme groups described above and incorporates their comments.
Public Engagement
Our approach to developing the strategy has been strongly focused around
communicating and engaging and working in partnership with our stakeholders.
Commissioners continue to design and develop the strategy with partners, patients, local
people and key stakeholders, with thinking and planning being developed and amended
through the engagement process. In addition to involving clinicians we have worked with
patients and members of the public. This activity is summarised below:
• Our Clinical Leadership Groups include Patient and Public Voices and Healthwatch representatives to make sure that these voices are heard at all points in the development of the strategy.
• Commissioners have been engaging widely from the beginning by building on existing local borough-level work.
• A series of deliberative events were held in June 2014, December 2014 and February 2015 looking at people’s current experiences of care and particularly at the more recent events, how people’s experiences might be enhanced in the future by these new models of care. Capturing feedback from engagement activities is systematic and transparent. All contributions are recorded and fed back into the strategy via programme managers - ensuring that local views influence strategy development. Examples of feedback and how it is being used are published via ‘You Said, We Did’ reports which are published on the website as well as the full reports of deliberative events and other activity.
• Engagement at local level and through local channels is on-going. This was primarily focused on the case for change during 2014, with a wider focus on the whole system model and emerging ideas in the spring of 2015. This included gathering patient stories and using materials developed by engagement partners, the Innovation Unit, Local engagement on the Issues Paper commenced in May 2015.
• A variety of methods have, and will be, used to gather the views of a broad spectrum of patients and the public. Activities will include:
• borough level deliberative events • focus groups with specific communities • utilising the existing mechanisms and opportunities identified through our
Clinical Commissioning Groups’ engagement colleagues.
Page 430

7 V5
The strategy programme has an active Patient and Public Participation Group, which
meets at least every six weeks and has contributed to shaping the strategy content.
Patient and public voices have been involved in the Clinical Leadership Groups since June
2014. Each of the Clinical Leadership Groups has at least three patient and public voices
and one Healthwatch representative, who are supported by the Patient and Public Voice
Project Manager and the Programme Manager in each area.
The PPVs come together in a Patient and Public Advisory Group (PPAG) forum for peer
support and to strengthen public and patient voices across the strategy, which meets
every 6-8 weeks. The PPAG enables members to explore a range of issues not covered
within the individual Clinical Leadership Groups; review key draft documents from the
south east London commissioning strategy programme, advising on clarity of message
and the development of plain English versions; and contribute to engagement plans and
activities, complementing the advisory role of the South East London Stakeholder
Reference Group.
The PPAG has undertaken a number of ‘deep dive’ sessions into each of the Clinical
Leadership Groups, the workforce supporting strategy, whole systems model and whole
systems outcomes enabling members to contribute to all the areas of the programme. The
PPAG has also reviewed the first Equalities Impact Assessment and identified priority
areas for the next Equalities Analysis.
Health Inequality Duty
Our Healthier South East London is a five year commissioning strategy which aims to
improve health, reduce health inequalities and ensure all health services in south east
London meet safety and quality standards consistently whilst being sustainable in the
longer term.
The way health services are delivered needs to change in order to meet the emerging
needs of an ageing population in which many more people live with long term conditions.
This means that more resources must be directed towards services based in the
community, keeping people out of hospital unless they really need to be there.
The case for change identifies the key areas of health inequality in South East London and
each of the Care Models aims to address these.
Public Sector Equality Duty
In order to ensure that our strategy is informed by the diverse population in south east
London and to enable us to fully understand the potential impact on communities with
protected characteristics (as well as complying with the Equalities act 2010), carers and,
the socially and economically deprived. We have, and will, conduct equalities analyses
throughout the programme.
Page 431

8 V5
An initial equalities impact assessment was carried out at the beginning of the programme.
Building on this, the programme has commissioned a second equalities analysis to be
conducted in June 2015 and to influence the focus of pre-consultation engagement work (if
consultation goes ahead).
Page 432

Our Healthier South East London
Consolidated Strategy
Executive SummaryDraft v1.0June 2015
Page 433

2
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England
This executive summary provides an overview of the Our Healthier South East London Commissioning Consolidated Strategy. It will summarise and
provide key highlights from the programme.
This section provides:
1. Introduction and Purpose
2. Introduction to south east London
3. Introduction to the Our Healthier South East London Strategy and the approach taken to developing it
4. Stakeholder Communications and Engagement
5. The case for change
6. Vision for the future of health and care services in south east London
7. The strategy proposed model(s) of care: Delivering better care for our south east London populations
8. The approach to identifying the outcomes the strategy aims to achieve
9. Financial impact and affordability
10. What is needed to deliver our vision for south east London
11. Risks and Challenges
12. Delivering the strategy and next steps
Draft in progress |
Overview
Executive
SummaryP
age 434

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 3
• In south east London, we have some very good health services. People
are living longer and many people are healthier. But we also have some
services that could be better. We have services that people find hard to
access and some people do not get the help they need to keep
themselves and their families well. We also have wide varieties in life
expectancy and too many people die early from preventable diseases.
• Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark CCGs,
working with NHS England as co-commissioner, are working in
partnership with local authorities, local providers and other key
stakeholders to define a five-year strategy for health and integrated care
services across south east London.
• The strategy complements and builds on local work and has a particular
focus on those areas where improvement can only be delivered by
collective action or where there is added value from working together. It
seeks to respond to local needs and aspirations, to improve the health of
people in south east London, to reduce health inequalities and to deliver a
health care system which is clinically and financially sustainable. The
approach is commissioner led and clinically driven, and informed by wide
engagement with local communities, patients and the public.
• It brings together the context of the south east London health and social
care economy and details the potential initiatives that could be
implemented to have transformational impact.
• Every CCG in the country is required to produce a strategy. In south east
London, commissioners want to make sure that the strategy reflects local
needs and aspirations. The first draft of the south east London strategy
was sent to NHS England for review on 20 June 2014. This was a national
deadline. The strategy runs for five years, so it is very much a work in
progress. Through local and wider clinical and public engagement,
potential ways to improve services have been identified, but considerable
further work and engagement on the thinking and implementation of these
plans is now taking place.
• This version has developed significantly since June 2014 and brings
together the proposed initiatives and their potential impact. It remains a
work in progress and is under review by a wide range of stakeholders.
Purpose of this documentIntroduction
Draft in progress |
Executive
SummaryP
age 435

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 4
• This commissioning strategy focuses on six NHS Clinical Commissioning
Groups in south east London covering a population of approximately 1.8
million people:
— Bexley CCG
— Bromley CCG
— Greenwich CCG
— Lambeth CCG
— Lewisham CCG
— Southwark CCG
• Each of these CCGs works in partnership with a number of organisations
and providers. In particular the key providers which the CCGs have
worked with to develop the strategy are:
— King's College Hospital NHS Foundation Trust
— Guy's and St Thomas' NHS Foundation Trust
— Lewisham and Greenwich NHS Trust
— Dartford and Gravesham NHS Trust
— South London and Maudsley NHS Foundation Trust
— Oxleas NHS Foundation Trust
— Bromley Healthcare Community Interest Company
• To develop the best possible care models and interventions for the
strategy it is important to understand the current health of the population
of south east London. To do this a model called the ‘Christmas tree’ was
used.
• The segmentation model summarises the population segments which are
detailed below: You can view the diagram on page 36.
— Approximately 16% of people in south east London are in the health
and wellbeing group
— Approximately 50% of people in south east London are experiencing
inequalities or putting their health at risk. For example this could be
people who drink too much or don’t take enough exercise or are living
in poverty.
— Approximately 25% of people in south east London are in the early
stages of long term conditions. For example, a long term condition
could be, diabetes, poor mental health or high blood pressure.
— Approximately 9% of people in south east London are living with 3 or
more long term conditions.
— Approximately 1% of people in south east London are at the end of
their life
• Through understanding our population better the strategy is able to focus
on developing care models and innovations that best address the needs of
the people in south east London. A key component of this is to develop a
strong foundation of Community Based Care to support people to live
healthier lives and reduce the number of people exposed to risk factors
either by birth or behaviour.
• A central part of the vison for the strategy is to be able to provide person
centred care in a proactive and integrated way. In order to do this Local
Care Networks are being developed across south east London. These
Local Care Networks will deliver community based care to local
populations through patient focused, proactive, accessible, coordinated
services and through making every contact count. Further detail of Local
Care Networks are provided in the following slides and on pages 66
onwards.
Introduction to south east London
Draft in progress |
Executive
SummaryP
age 436

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 5
• This programme is led by the six NHS Clinical Commissioning Groups in
the south east London with commissioners from NHS England (London),
working in close partnership with local authorities, local providers of care
and other partners.
• They have identified six priorities for improvement to deliver better care
for the south east London population. These are referred to as Clinical
Leadership Groups and focus on:
— Community based care
— Planned care
— Urgent and emergency care
— Maternity
— Children and young people
— Cancer
• The groups are formed from clinicians, commissioners, social care leads
and other experts, Healthwatch representatives and other patient and
public voices from across south east London.
• Each of these groups has developed a model of care which forms part of
the integrated whole system model described on page 13. Each Clinical
Leadership Group has developed a number of interventions and
assessed the impacts of these interventions in terms of delivering
improved quality, better and less variable outcomes for people across
south east London, and that they provide value for money and support a
sustainable whole system health and care economy.
Aligning our Strategy with London and National Policy Agendas
• We know that a 'one size fits all' model will not work for the NHS, which is
why we are responding to local needs. However, we have taken the
insight, evidence and direction provided by London and national policy
agendas and embedded this into our design. This includes the:
— NHS Five Year Forward view
— Better Health for London
• South east London leads are represented across the 13 London
Transformation Programmes and our work is enabled by the learning from
others and our collaborative work on a "once-for-London” basis, where
appropriate.
Principles and governance
• In addition, as part of implementing and developing the strategy, the
programme follows a number of principles which have been reflected in the
governance and delivery structure. This structure entails the five key
governance elements of the programme :
— Senior joint forum for strategic direction and decision making
(equivalent to a Programme Board) – the Clinical Commissioning
Board
— Collaborative forum for partnership working – the South East London
Partnership Group
— Clinical forum to guide design work – the Clinical Executive Group
— Delivery focused forum to manage design and implementation
activities – the Implementation Executive Group.
— Collective forum for patients and public voices to contribute to shaping
the strategy’s content – Public and Patient Advisory Group
Introduction to the Our Healthier South East London Strategy
and the approach taken to developing the strategy
Draft in progress |
Executive
SummaryP
age 437

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 6
• Our approach to developing the strategy has been strongly focused
around communicating and engaging and working in partnership with our
stakeholders.
• Commissioners continue to design and develop the strategy with
partners, patients, local people and key stakeholders, with thinking and
planning being developed and amended through the engagement
process.
• The strategy is clinically-led and developed, with over 300 clinicians,
nurses, allied health professionals, social care staff, commissioners and
others developing ideas through the six Clinical Leadership Groups.
These Clinical Leadership Groups also include Patient and Public Voices
and Healthwatch representatives to make sure that these voices are
heard at all points in the development of the strategy.
• In addition to ensuring that patient and public voices feed directly into the
Clinical Leadership Groups and supporting work streams, commissioners
have been engaging widely from the beginning by building on existing
local borough-level work.
• A series of deliberative events were held in June 2014, December 2014
and February 2015 looking at people’s current experiences of care and
particularly at the more recent events, how people’s experiences might be
enhanced in the future by these new models of care. Capturing feedback
from engagement activities is systematic and transparent. All
contributions are recorded and fed back into the strategy via programme
managers - ensuring that local views influence strategy development.
Examples of feedback and how it is being used are published via ‘You
Said, We Did’ reports which are published on the website as well as the
full reports of deliberative events and other activity.
• Engagement and communication is led by Clinical Commissioning Groups
via the Communications and Engagement Steering Group which has met
at least monthly since May 2014. The group consists of Clinical
Commissioning Groups Communications and Engagement leads. Leads
from NHS providers and local councils have also been invited to attend.
• Engagement at local level and through local channels is on-going. This
was primarily focused on the case for change during 2014, with a wider
focus on the whole system model and emerging ideas in the spring of
2015. This included gathering patient stories and using materials
developed by engagement partners, the Innovation Unit, Local
engagement on the Issues Paper commenced in May 2015.
• A variety of methods have, and will be, used to gather the views of a broad
spectrum of patients and the public. Activities will include:
— borough level deliberative events
— focus groups with specific communities
— utilising the existing mechanisms and opportunities identified through
our Clinical Commissioning Groups’ engagement colleagues.
Stakeholder Communications and Engagement is a core
part of the strategy development process
Draft in progress |
Executive
SummaryP
age 438

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 7
• This strategy identifies that outcomes in south east London are not as
good as they should be: The longer we leave these problems, the worse
they will get. We therefore recognise that we all need to change what we
do and how we do it. The case for change has identified and investigated
these problems, helping to target our aims. Nine key issues have been
identified as detailed below:
Too many people live with preventable ill health or die too early
• About 11,000 people died prematurely across south east London
between 2009 and 2011, with four of our boroughs being classed in the
worst category for premature death in England.
The outcomes from care in our health services vary significantly and
high quality care is not available all the time
• Too often, the quality of care that patients receive and the outcome of
their treatment depend on when and where they access health services.
We don’t always treat people early enough to have the best results
• Our services are often not set up to detect problems soon enough,
meaning that people with long term conditions or mental illness often
have to be admitted to hospital in crisis.
People’s experience of care is very variable and can be much better
• While patients are very happy with some services, surveys tell us that
their experience of the NHS is inconsistent and that they do not always
receive the care they want.
Patients tell us that their care is not joined up between different services
• Patients and carers find it frustrating to have to continually provide the
same information to different people. This is because different parts of the
NHS do not always communicate effectively with each other or with social
services
The social care system is under increasing pressure
• Many Local Authorities are facing unprecedented pressures due to growing
demand in some areas, with increasing numbers of older residents,
residents living much longer with complex care and health needs and
increased mental health needs. New laws and duties are also leading to
additional implications and uncertainty for councils.
The money to pay for the NHS is limited and need is continually
increasing
• NHS funding currently increases in line with inflation each year. However,
the costs of providing care are rising much faster because the NHS is now
treating more people with more complex conditions than ever before and
the costs of care often grow faster than consumer inflation
It is taxpayers’ money and we have a responsibility to spend it well
• We know that by providing services in a different way, it is possible to
improve outcomes, to help people to live healthier lives, to deliver services
which are consistently of high quality and get more for our money
South east London’s acute, community and mental health providers face
a similar and interrelated set of challenges and drivers
• Providers in south east London share key issues and drivers, such as
workforce and regulatory requirements and London’s ambulance service is
facing increasing and changing needs for care.
There is a strong case for changing the way current health
and care services are provided in south east London
Draft in progress |
Executive
SummaryP
age 439

8
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England
• To solve the problems outlined in the case for change, we have developed a collective vision for south east London. In south east London we spend £2.3billion
in the NHS. Over the next five years we aim to achieve much better outcomes than we do now by:
— Supporting people to be more in control of their health and have a greater say in their own care
— Helping people to live independently and know what to do when things go wrong
— Helping communities to support one another
— Making sure primary care services are consistently excellent and have an increased focus on prevention
— Reducing variation in healthcare outcomes and addressing inequalities by raising the standards in our health services to match the best
— Developing joined up care so that people receive the support they need when they need it
— Delivering services that meet the same high quality standards whenever and wherever care is provided
— Spending our money wisely, to deliver better outcomes and avoid waste.
Draft in progress |
Vision for the future of health and care services in south east London
Executive
SummaryP
age 440

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 9
Care Model Design
• To develop the initiatives to focus on these aims, the Clinical
Commissioning Groups and NHS England – London region have
identified the six Clinical Leadership Groups to deliver better care for our
population.
• Each of these groups has developed a model of care which forms part of
the integrated whole system model described on page 13. Each Clinical
Leadership Group has developed a number of interventions and
assessed the impacts of these interventions in terms of delivering
improved quality, better and less variable outcomes for people across
south east London and that they provide value for money and support a
sustainable whole system health and care economy .
Local Care Networks
• Local Care Networks are the centrepiece of the strategy and sit within
Community Based Care.
• The Community Based Care Clinical Leadership Group aims to support
people to live healthier lives and reduce the number of people exposed to
risk factors either by birth or behaviour. For people with a long term
condition, Community Based Care will take a rehabilitative/ re-ablement
approach, supporting people to manage their own health positively,
prevent deterioration wherever possible and reduce risks on these
people. For those people with complex long term conditions or who are in
the last year of life, support will be available to enable them to continue to
lead as full and active life as possible.
• Community based care will be delivered through Local Care Networks. The
services available will be proactive, accessible, coordinated and provide
continuity; with a flexible, holistic approach to ensure every contact counts.
This will be primary care delivered to geographically coherent populations,
at scale, whilst still encouraging self-reliance.
• 24 local care networks are being developed to support whole populations
across south east London. This will be a universal service covering the
whole population ‘cradle to grave’. A local care network will involve
primary, community and social care colleagues working together and
drawing on others from across the health, social care and the voluntary
sector to provide proactive patient centred care. Services will be delivered
in ways that respond to the varied needs and characteristics of our
communities.
Clinical Leadership Group initiatives
• In addition to the Local Care Networks, each Clinical Leadership Group
proposes further initiatives. These are summarised in the following slides.
The strategy proposes model(s) of care: to deliver better
care for our south east London populations
Draft in progress |
Executive
SummaryP
age 441

10
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England
The strategy sets out an agreed target model for local care networks that will deliver community based care. It is intended that each Local Care Network across
south east London delivers the target model. However, the target model will have to be tailored to the local community that it serves.
Draft in progress |
The Community Based Care Target Model
Serving geographically coherent populations
between 50,000 – 150,000
• Leadership team
• All general practices working at
scale (federated with single IT
system and leadership)
• All community pharmacy
• Voluntary and community sector
• Community nursing for adults and
children
• Social care
• Community Mental Health Teams
• Community therapy
• Community based diagnostics
• Patient and carer engagement
groups
‘The Core’ (as a minimum all
LCNs should encompass)• Strong and confident communities
• Accessible hospital outpatient
treatment clinics and acute oncology
(urgent and emergency and cancer
care)
• Specialist opinion (not face to face)
and clear specialist service pathways
• Pathways to Multi Disciplinary Teams
• Integrated 111, London Ambulance
Service and Out of Hours system
(interface with Urgent care centres
co-located with emergency
department model)
• Housing, education and other council
services
• Community based midwifery teams
• Private and voluntary sector e.g. care
homes and domiciliary care
• Cancer services
• Children’s integrated community team
and short stay units
• Rapid response services
• Carers
• And there will be others..
Working with…
• Supporting patients to manage their own
health (Asset Mapping, Social Prescribing,
education, community champions etc
• Prevention – Obesity, Alcohol and Smoking
• Improved Core general practice access
plus 8-8, 365
• Enhanced call and recall – improves
screening and early identification and
management of long term conditions
• Reduction in gap between recorded and
expected prevalence in long term
conditions
• Supporting vulnerable people in the
community including those in care homes
and domiciliary care
• Reduction in variation (level up) primary
care management of long term conditions
• Reablement – Admissions avoidance and
effective discharge
• Multi Disciplinary Team configuration –
main long term conditions
• groups (incl. mental health) and Frail
elderly
• End of Life Care
Big hitters
Bexley
Bromley
Greenwich
Lewisham
Lambeth
Southwark
Integrated Pathways of care
Integrated Single System Leadership and Management
Executive
SummaryP
age 442

11
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Community Based Care delivered by Local Care Networks
Executive
SummaryP
age 443

12
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England
Community Based Care delivered by Local Care Networks is the foundation of the integrated whole system model that has been developed for south east London.
This diagram provides an overview of the whole system model, incorporating initiatives from all 6 Clinical Leadership Groups.
Draft in progress |
Our integrated whole system model
Executive
SummaryP
age 444

13
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Planned care model
Key Features of the model
1 Standardisation
Reducing variation across the planned care pathway from referral practice to
discharge through to co-development of high level standards.
2 Diagnostics
• Enhance patient management by GPs
• Rapid access to diagnostics for GP’s
• Evidence based standardised Clinical pathways
• Shared results across the system supported by integrated IT systems
3 Elective Care Centres
Provider collaboration to create centres of excellence for high volume specialities
that drive up quality of service provision and improve outcomes for patients
• Orthopaedic (hips and knees)
• Ophthalmology
4 Pathway Review
• Urology
• Neurosurgery
• Nephrology
• Gynaecology
• Dermatology
HElective
Care Centres
Diagnostics
23
Person
Executive
SummaryP
age 445

14
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Maternity model
Key Features of the model
1 Primary prevention and targeted wellness programmes within the Local Care
Network
2 Assessment of pregnancy risk before 10 weeks to assign the most appropriate
midwife team from the outset:
1. Local Care Network community based midwife teams for low risk
2. Specialist condition focused teams for high risk
3 Easy access to acute assessment clinic for unexpected problems during
pregnancy and assessment unit for assessment of onset of labour
4 Culture of birthing units to encourage straightforward birth and improve the
experience for low risk women
5 Achieve the London Quality Standards
6 Better co-ordination through postnatal and neonatal phase to improve mother and
baby flows and experience
7 Smooth handover to Local Care Network with continuing advice and support on
healthy choices.
It is our intention that through this strategy we will meet the London quality standards.
The above interventions aim to address this.
HPerson
DAU & 24/7
TriageCondition focused
midwife cohorts for high
risk mothers
Geographic midwife
teams for low risk mothers
6
2
35
4
1
Executive
SummaryP
age 446
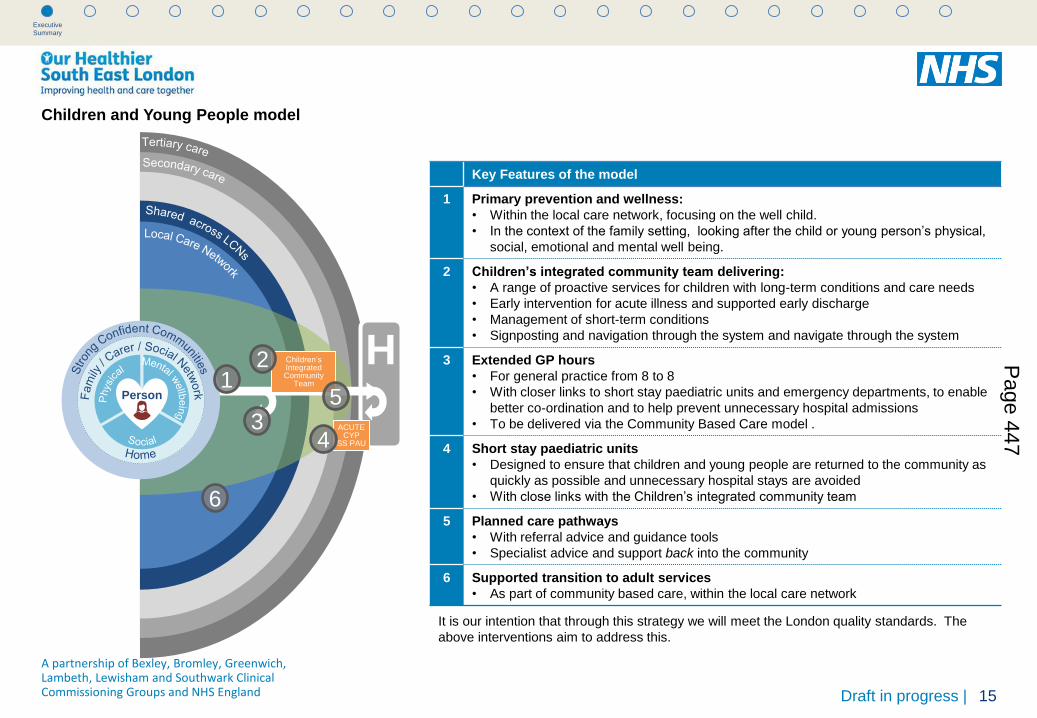
15
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Children and Young People model
Key Features of the model
1 Primary prevention and wellness:
• Within the local care network, focusing on the well child.
• In the context of the family setting, looking after the child or young person’s physical,
social, emotional and mental well being.
2 Children’s integrated community team delivering:
• A range of proactive services for children with long-term conditions and care needs
• Early intervention for acute illness and supported early discharge
• Management of short-term conditions
• Signposting and navigation through the system and navigate through the system
3 Extended GP hours
• For general practice from 8 to 8
• With closer links to short stay paediatric units and emergency departments, to enable
better co-ordination and to help prevent unnecessary hospital admissions
• To be delivered via the Community Based Care model .
4 Short stay paediatric units
• Designed to ensure that children and young people are returned to the community as
quickly as possible and unnecessary hospital stays are avoided
• With close links with the Children’s integrated community team
5 Planned care pathways
• With referral advice and guidance tools
• Specialist advice and support back into the community
6 Supported transition to adult services
• As part of community based care, within the local care network
It is our intention that through this strategy we will meet the London quality standards. The
above interventions aim to address this.
HPerson
3
6
Children’s Integrated Community
Team
ACUTE CYP
SS PAU
2
4
15
Executive
SummaryP
age 447

16
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Urgent and emergency care model
HPerson
Specialist Response
Clinic
Enhanced Front Door
Rapid response
“Home Ward”
A
D
C
E
B
Executive
Summary
Key Features of the model
Achieving the London Quality Standards in all areas:
• Acute medicine
• Emergency general surgery
• Emergency departments
• Critical care
• Fractured neck of femur
A Improving access in Primary Care, in hours and out of hours, to unscheduled care.
GPs, UCC and ED functioning in a closely linked co-ordinated way; responsive community
care, including specialist response teams, will prevent un-necessary hospital admissions with
easy access to specialist advice for GPs as an alternative to ED referral
1. 8am – 8pm 7 days a week
2. Standalone Urgent Care Centres with the same standards
3. Community based rapid access teams including a home ward.
B Specialist advice and referral
4. Access to specialist advice
5. Access to a specialist response clinic
C Improved 111 capability and LAS onward referral
6. LAS will be able to redirect to appropriate services, such as the rapid access team, home
ward or hospital based specialist clinics and excel in navigating patients to the right part of
the system
7. 111 are able to give advice, provide internal triage and coordinate onward referral to other
parts of the system other than the ED
D An enhanced single “front door” to the Emergency Department.
8. Bringing together UCCs and the ED in a single governance structure and providing expert
streaming across all sites
E Emergency Department interface with Mental Health services
9. This will also allow for earlier identification of MH cases (including Dementia) reducing
length of stay and enabling quicker streaming to specialities for mental health patients by
having Psychiatric Liaison nurse (PLNs) and Triage joint assessments.
10. Quicker interface with specialist services like drug and alcohol
11. Quicker interface with under 18 mental health liaison teams
Page 448

17
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Cancer model
Key Features of the model
A Primary prevention: Best delivered in the Local Care Network Early
detection
1. Increased screening rates to national benchmark through targeted
engagement
2. Diagnostics: Pilot project – serious but unspecific symptoms pathway
3. Promotion of early diagnosis and equal access to treatment for older people
4. Professional development for all staff within Primary Care
B Treatment
Provider collaboration to create networked centres of excellence:
5. Non complex cancer treatments and support closer to home
6. Access to appropriate information and support for patients and carers
7. Acute Oncology Services – networked and supported by integrated IT
8. Consistently meet the access time scales on our cancer services
9. Routine use of the recovery package
C Living with and Beyond Cancer
10. Stratified follow-up
11. Support for people living with the adverse consequences of cancer
treatments
12. Comprehensive support for carers
13. Psychological support for people living with Cancer
14. Inclusion of Cancer as a criteria for referral to exercise/physical activity on
prescription schemes
15. Support to return to work, study or volunteering
16. Routine use of the recovery package
D End of Life: Best Delivered in the Local Care Network
17. Ensure a dignified death irrespective of setting
18. Ensure consistent use of coordinate my care
19. Advance Care planning
HPerson
1 2
34
Early detection
Treatment
Living with & Beyond CancerEnd of Life
Executive
SummaryP
age 449

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 18
• The primary aim of delivering the Our Healthier South East London
strategy and vision is to develop ways to improve the health and care
outcomes for south east London communities and people. A framework
which sets out measures to monitor the impact of the strategy and
interventions on outcomes has been developed through engaging with
our partners across health and care providers, Public Health, clinicians
and public and patients. This framework sets out the measures that
demonstrate the effectiveness of the strategy in achieving the outcomes
allowing us to quantify the strategy’s impact.
Focusing on the achievement of outcomes
• By implementing the strategy and its care models the aim is to reduce the
variability in outcomes we see today as outlined in the case for change
and to improve the overall health and care outcomes for people across
south east London.
Structure of the framework
• The framework is made up of the following core elements:
— Domains: The high-level grouping or classification of outcomes that
are measuring similar things. There are a number of existing
outcome frameworks which were reviewed and based on those
frameworks, four ‘domains’ that are common across them were
selected.
— Outcomes: The overall impact of the strategy on the health and
well-being of our populations and individuals in south east London
— Indicators: The measures selected to demonstrate the achievement
of the outcome. These are as outcome focused as possible but in
some cases a process/structure measure has been used as a proxy.
Eight outcomes have been identified
• Preventing people from dying prematurely and can live longer and
healthier lives
• Reducing differences in life expectancy and healthy life expectancy
between communities
• People are independent, in control of their health, and able to access
personalised care to suit their needs
• Health and care services enable people to live a good quality of life with
their long term condition
• Treatment is effective and delivers the best results for patients and service
users
• Delivering the right care, at right place, at the right time along the whole
cycle of care
• Commitment to people having a positive experience of care
• Caring for people in a safe environment and protecting them from
avoidable harm
Indicators
• There are a number of indicators that have been identified and these are
still undergoing review from stakeholders and Public Health
Approach to identifying the outcomes the strategy aims to
achieve
Draft in progress |
Executive
SummaryP
age 450

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 19
• NHS funding currently increases in line with inflation each year. However,
the costs of providing care are rising much faster because the NHS is
now treating more people with more complex conditions than ever before
and the costs of care often grow faster than consumer inflation.
• The NHS Five Year Forward View outlines a £30 billion financial
challenge nationally by 2020/21. Consistent with this, in the absence of
action, the scale of the affordability challenge in south east London is
forecast to grow to over £1 billion by 2019/20. The graph to the right and
the table below demonstrate how this challenge grows over this period.
• Local authorities, who are responsible for social care services, are also
looking to save over 30% of their current expenditure over the next 3-4
years. Therefore we need to get better value for money for all that is done
in the NHS and social care services. We need to get the best possible
outcomes for patients and make the most of resources that are under
increasing pressure. This means we need a more integrated approach
between different services.
The NHS faces a growing affordability challenge
Draft in progress |
Absolute challenge Annual challenge Percentage challenge
Over the period from 2014/15 to 2019/20, the south
east London expenditure (without efficiencies) will
grow by just over £1 billion more than the projected
budget of £5 billion. This is comparable with the £30
billion national challenge set out in NHS England’s
Five Year Forward View.
On average, the south east London healthcare
system will need to make efficiencies of £218m each
year (from a budget which will grow to £4.8bn)
between 2014/15 and 2019/20.
An estimated breakdown is shown below.
On average, the south east London healthcare
system will need to make efficiencies of 4.2% each
year between 2014/15 and 2019/20.
An estimated annual breakdown is shown below.
14/15 15/16 16/17 17/18 18/19 19/20 14/15 15/16 16/17 17/18 18/19 19/20
£251m £228m £154m £162m £141m £156m 6.0% 5.3% 3.4% 3.5% 3.0% 3.2%
5,903
4,812
3,900
4,400
4,900
5,400
5,900
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20
Syst
em
wid
e in
com
e/e
xpe
nd
itu
re (£
m
illio
ns)
Expenditure (Do Nothing)
Revenue
Executive
SummaryP
age 451

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 20
• The graphs on this page demonstrates how the benefits from the
programme can be combined with savings within individual organisations
to close a substantial amount of the £1.1 billion affordability challenge.
The benefits shown are as follows:
1. Programme central case (gross benefit): As described previously.
2. Provider efficiencies at 2.5%: The provider finance leads feel that
a 2.5% CIP may be reasonable in addition to efficiencies generated
through the programme.
Closing the affordability challenge
Draft in progress |
Executive
Summary
• It is important to note that both of these savings are presented
gross of investment requirements (which total £90 million in the
programme central case). It is expected that these investment
requirements will, at least in part, be satisfied through additional funding
requested through the Five Year Forward View and committed by the
Government. Taking south east London’s proportionate share of the £8
billion committed would imply that £248 million is available for this
purpose.
• The resultant position is a £266 million affordability challenge for
the South East London health care economy.
231
5921,091
266
0
200
400
600
800
1,000
1,200
Affordabilitychallenge(2019/20)
Programmecentral case
(gross benefit)
Providerefficiencies at
2.5%
Residualchallenge(2019/20)
Aff
ord
ab
ilit
y c
hallen
ge (
£ m
illio
ns)
5,903
5,672
5,078
4,812
3,900
4,400
4,900
5,400
5,900
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2019/20
Syst
em
wid
e in
com
e/e
xpe
nd
itu
re (£
mill
ion
s)
Expenditure (Do Nothing)
Expenditure (Strategy)
Expenditure (Residual)
Revenue
NB: Profiling of benefits shown above may significantly change as implementation
plans are developed.
Page 452

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 21Draft in progress |
Executive
Summary
• Using historical NHS bed occupancy data for the acute providers
and our projections of bed demand considering demographic/non-
demographic growth assumptions we have estimated the bed
gaps/increases show in the table below.
• We have modelled the impact of the strategy on overnight bed days
to be a net reduction of 140,000 and a net increase in day case bed
days of 25,000. This translates directly to a number of beds using
various occupancy rates as shown in the table below.
• This only relates to acute beds and we would expect a proportion
of this activity to be provided within community beds. Also note that
the ‘do nothing’ position does not reflect any potential reductions
associated with QIPP delivery post 2014/15 plans or Better Care
Fund related non-elective admission reductions.
Baseline bed days/beds Strategic impacts bed days/beds
2013/14 Growth (2019/20)***Gross change
(2019/20)
Net change
(2019/20)
Overnight
Overnight bed days 1,178,000 198,000 (339,000) (140,000)
Overnight beds (current occupancy rates*) 3,571 601 (1,015) (414)
Overnight beds (85% occupancy rates) 3,571 861 (1,092) (231)
Day caseDay case bed days 181,000 30,000 (5,000) 25,000
Day case beds (current occupancy rates*) 595 99 (15) 84
Day case beds (68% occupancy rates) 595 254 (19) 235
Total
Total bed days 1,359,000 228,000 (343,000) (115,000)
Total beds (current occupancy rates*) 4,166 700 (1,030) (330)
Total beds (revised occupancy rates****) 4,166 1,115 (1,111) 4
* Bed occupancy source: Bed occupancy for the year estimated using the average of KH03 quarterly returns from NHS England for Q4 2013/14 – Q3 2014/15.
(GSTT: 81%, KCHT: 94%, LGT: 94%, DGT: 95%, weighted average: 90.5%).
** These figures have been fixed at current occupancy levels and 2013/14 activity.
*** These figures relate to a level of increased demand as shown above and an additional number of beds due to requiring lower occupancy levels.
**** The total revised occupancy rates are blended across the inpatient overnight bed and day case bed rates shown earlier in the table.
Initial estimate of acute bed requirement
Page 453

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 22
Summary of where we have reached in developing the strategy
Draft in progress |
Executive
Summary
The aims of the consolidated strategy are to make a difference to the health and
well-being outcomes of the people and communities in south east London and to
create a sustainable health and care system as a foundation for the future.
To date, the consolidated strategy brings together the case for change, the care
models and their anticipated impacts on outcomes for the people and
communities in south east London. This is combined with an assessment of the
potential impact these models may have on how people use services and the
extent to which it will support the future financial sustainability of the system.
Taking into consideration growth assumptions over the next 5 years, and not
changing our clinical models of care would mean that too many people would
continue to be admitted to hospital where better Community Based Care models
could provide improved outcomes. We have calculated the increase in bed
capacity that would be needed across south east London to respond to the rise in
population and aging population using our current approaches to delivering care.
The projected demand would increase so much that the number of beds needed
would be enough to fill a new hospital site and this is not possible or
affordable. Applying the initial impact of the strategy’s care models work on the
projected demand levels for hospital beds, shows that by implementing the care
models in the strategy, we would reduce the need for additional hospital beds by
providing an alternative high quality model of care that is focussed on improved
outcomes for the population we serve.
This is because,
• The care models are focused on prevention and early intervention and
keeping people healthy. Therefore keeping people out of hospital
• Community Based Care is the foundation of the whole system and is intended
to keep people closer to home, treating them in the community and enabling
people to only visit hospital when they really need to
• Pathways and professionals will be more integrated
• Productivity is expected to increase and there will be greater efficiency in the
south east London system
• The plan will be for bed occupancy to meet the national guidance (which is not
the case now) which will improve safety, quality and efficiency
Recent programme updates include;
• The whole system affordability gap has been defined
• The Clinical Leadership Groups design guides are being finalised and
potential impacts of the care models reviewed
• Supporting strategies of Estates, Workforce and IT continue to be developed
Whilst the strategy programme has progressed a long way to achieve its aim,
there is still much work to do
Further work is required on
• Ensuring that progress and plans for the London Quality Standards are
embedded into the strategy and exploring options on how they can be
achieved
• Further developing the supporting strategies of Workforce, IM&T and Estates
• Refining the indictors for the Outcomes to make sure the best possible ones
have been selected so we can measure the benefits or not of the strategy
• Engagement on the options appraisal methodology
• Ongoing communications and engagement
Page 454
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 23
Part of the Clinical Leadership Groups work is to develop the plans to deliver
the care models. In addition, three supporting strategies are being developed
to support the overall delivery of the care models and changes at a whole
system level.
The three supporting strategies are
• Infrastructure & Estates
• Workforce
• Information Management and Technology
Infrastructure & Estates
• The Estates Supporting Strategy is an essential element of the strategy
programme to support the delivery of our new models of care in a way
which ensures they deliver the outcomes we aim to achieve. We must
understand the capacity of our capital assets, estates and facilities across
south east London to utilise, reduce or develop these in the most
appropriate way to meet the needs of our population.
• There is a clear synergy between the south east London need to
reconsider estates and the national and London wide direction of travel.
‘The five year forward view sets out an integrated agenda and new care
models over the next five years. In addition, Better Health for London
outlines the evidence base for re-evaluating the utilisation and value of
NHS estate in London.’ (The Healthy London Partnership Estates
Programme). Therefore, our Estates Supporting Strategy has made clear
links with the work being delivered at a London wide level by the ‘Our
Healthy London Partnership - Estates Programme’ being led by London
CCGs and NHS England.
• The Estates Supporting Strategy aims to address specific requirements
that provide additional support to facilitate delivery of the strategy, building
upon London wide programme delivery where the time scales allow. The
estates strategy will be built into the delivery programmes for all models of
care as appropriate and financial impacts further detailed within the
Financial modelling. The three stages of the Estates Supporting Strategy is
are as follows:
— Understanding the baseline
— Understanding the requirement
— Addressing the gap
How will we deliver the strategy?
Draft in progress |
Executive
SummaryP
age 455

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 24
Workforce
• Better Health for London, the Five Year Forward View and Our Healthier
South East London have all identified the need to focus on developing a
modern workforce in order to support the delivery of innovative new
models of care. Workforce is therefore a key enabler of the Our Healthier
South East London strategy.
• The supporting strategy is identifying the key actions that should take
place in order to move the workforce in south east London from where it
is today to where it needs to be in the future. For instance, we know that
the future care delivery will involve empowering patients and promoting
independence; making every contact count; and fostering an environment
where colleagues engage with each other rather than refer and hand-
over.
• With these significant changes on the horizon, understanding what
patients will require in the future and challenging existing ways of working
will allow us to plan for a workforce that is fit for purpose and sustainable.
• The workforce supporting strategy will need to clearly articulate how the
workforce is going to deliver what south east London needs. This will
include new ways of working (i.e. flexibility, rotations, different staff groups
doing different tasks to today, team work and collaboration) and different
working locations (i.e. more staff working in the community as opposed to
acute settings).
• For this purpose the programme has so far established:
— A baseline of the current workforce
— A methodology to define characteristics of the required new workforce
• These will support the next steps which will take the workforce where it
needs to be in the future. These steps include:
— Articulating the workforce strategy
— Reaching out to the workforce
Draft in progress |
Executive
SummaryP
age 456

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 25
Information Management & Technology
• Information and IT will be a key enabler for the strategy. Specifically, it
can support staff in new ways of working and empower patients to be
active participants in their care.
• Key considerations for understanding the IM&T requirements to support
the strategy and any gaps are:
— National and London initiatives and policies: There are a number of
National and local initiatives and policies that may support the
implementation of the strategy.
— CCG IM&T strategies: Each CCG has its own IM&T strategy and
implementation plans, which have been reviewed and initial
assessments made to determine support for the strategy.
— Identifying uniformities at a south east London level so there are
consistent ways of working. For example, adopting the same data
quality standards, and staff identification processes for who should
be viewing/editing data and design principles…
— Gaps and any investment costs: Understanding where these are not
currently accounted for in CCG and or provider plans, and are
needed to implement the strategy.
A primary requirement to enable the strategy is for health and care systems
across south east London to be interoperable
Why is interoperability Important?
Interoperability is important because it will enable south east London health
information systems and professionals to work together within and across
organizational boundaries in order to more effectively deliver healthcare to
people and communities.
Key ways in which interoperability will support the delivery of the vision and
care models in the consolidated strategy are:
Care Quality
• Improves the quality of patient care by providing access to complete,
accurate, timely information in one location.
• Provides visibility into the “whole” patient by sharing basic medical
information across a patient’s care providers
Care Efficiency
• Saves time previously used to look for information, i.e. lab results, or
repeat tests that have already been performed in another care setting
Patient Safety
• Makes life-saving information available 24-hours-a-day for clinical decision
support
• Our findings so far indicate that primary key requirements of
interoperability between GP systems and primary and secondary care are
planned and/or being implemented at various speeds. All CCGs are
moving to GP systems that will enable sharing of records across GP
practises supporting Local Care Networks and will be interoperable with
acute
• To various extents CCGs have plans in place to align with some of the key
IT/Digital guidance in the 5YFP IT/Digital, London Transformation
Programme, 2020 Personalised Health and Care and Implementing these
guidelines would meet many of the strategy requirements.
• However, additional transformation initiatives that may require agreement
and funding at a south east London level have not been explored or agreed
at this stage.
Draft in progress |
Executive
SummaryP
age 457

26
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England
The following high level risks have been identified to the implementation of the strategy. This list will be reviewed regularly through the Clinical
Executive Group, Implementation Executive Group and Clinical Commissioning Board.
Draft in progress |
There are risks to delivering the Strategy which are closely monitored and assessed for impact
Title Risk Impact Mitigations
1. Information
Systems
• Lack of integrated or interoperable
information systems undermines
ability to integrate services across
the health system in south east
London
• Possible duplication of system, process
or information, resulting in poorer patient
experience, poor quality of services
across integrated pathways and
additional cost
• IM&T supporting strategy workstream established.
• Utilising existing integration initiatives across SEL to
support strategy
2. Workforce
Capability
• Existing workforce skills or
capability to deliver new models of
care
• New models of care may not be
implemented
• Services may not be delivered safely
• Patient satisfaction
• Staff satisfaction issues
• Quality and effectiveness of care
• Workforce supporting strategy workstream established
• Work in hand to identify gaps between capabilities
required to deliver new models of care and those
available in current workforce
• Key characteristics and skills being identified for
training purposes
3. Delivery
Timeframe
• It may be challenging to complete
required activities and assurances in
time to go to consultation, if
required, in December, particularly
as a result of needing to engage
patients and service users in the
process
• Delay to programme implementation for
those elements which might require
formal consultation or loss of support
from partners and stakeholders for some
or all of the strategy
• On-going dialogue with NHSE to agree assurance
process and detailed communications and
engagement plan to test critical path
4. Delivery
Timeframe
• Insufficient time for good processes
in terms of governance, decision
making and ownership
• The strategy and associated documents
are not owned by all stakeholders
across SEL
• We will maintain four key activities: intensive
engagement with partners and stakeholders; ensuring
NHS England is engaged; careful mapping of
governance and decision making; and meeting with
NHSE by mid-June to review the approach
Executive
SummaryP
age 458

27
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Title Risk Impact Mitigations
5. Clinical
Leadership
Group Impact
Analysis
• Modelling: Finance and Activity • The impact analysis does not fully close
the identified affordability gap but does
make significant progress towards doing
so. It is not yet clear if this is sufficient
• Explore and incorporate additional QIPP and CIP
opportunities and continue to explore options with
NHSE
6. Financial
sustainability of
health system
• New service models do not deliver
reduced demand for hospital care or
hospital capacity does not reduce in
line with demand
• Potential increased system costs through
duplication of services
• System may not be sustainable
• Making sure there are clinical input into the
design of care models and that they have
sufficient impact on activity
7. Patient / Public
Resistance to
Change
• If partners and stakeholders are not
sufficiently engaged throughout the
development of the five year strategy
– or if the case for change is not
sufficiently convincing - any proposed
service change could be subject to
significant local opposition
• Further engagement required
• Possible legal challenge
• Delays to implementation of changes
leading to increased cost and delay
• Need to amend strategy in response to
concerns
• Engagement activities will be undertaken with a
broad range of partners and stakeholders
throughout the development and implementation
of the strategy
• Dedicated communications and engagement
enabling workstream to coordinate these
activities
• Patient and Public voices in all key groups to help
shape strategy
• Strategy reflects input from partners and
stakeholders
Executive
SummaryP
age 459

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 28
• A number of interventions have been defined and agreed and now the
strategy programme must start to consider how these will be
implemented and delivered.
• For most interventions implementation planning can commence
immediately. There are some interventions where care model delivery
options need to be considered. These interventions will have to undergo a
robust options appraisal process.
Implementation planning
• The development and implementation of the strategy has involved
consideration of options for care model design from the outset.
• This is an iterative process which reviews the range of interventions to
produce best outcomes for south east London.
• It considers ways to formulate the care models to produce these best
outcomes based on a range of qualitative and quantitative evidence.
Implementing some of the interventions will require consideration of care
model delivery options and these will either be implemented at a local
level or at a south east London level.
Options appraisal process
• This approach aims to identify the best way or way(s) of delivering the
overarching strategy and realise its full benefits. It filters the many
potential options for how the system can be implemented and is designed
to identify options that are recommended for further work.
• It is proposed that the filtering of options will occur through two gateways of
assessment against criteria; hurdle criteria and evaluation criteria (the
diagram on the following page provides an overview of the methodology).
• The criteria against which the options will be assessed will be agreed
before commencing the appraisal. Moreover, the likelihood of optimal
implementation of options is increased by gathering wide ranging
stakeholder contribution to the formation and specificity of criteria.
• Although some interventions do not in their own right require a detailed
options appraisal (those that start implementation planning), the result of
implementing those interventions could impact on the appraisal of other
interventions because they will lead to shifts in settings of care and
volumes of activity. As a result, it is important to consider the scope of a
detailed options appraisal and how to account for whole system changes
within the appraisal of individual interventions.
• .
Delivering the strategy and next steps
Draft in progress |
Executive
SummaryP
age 460
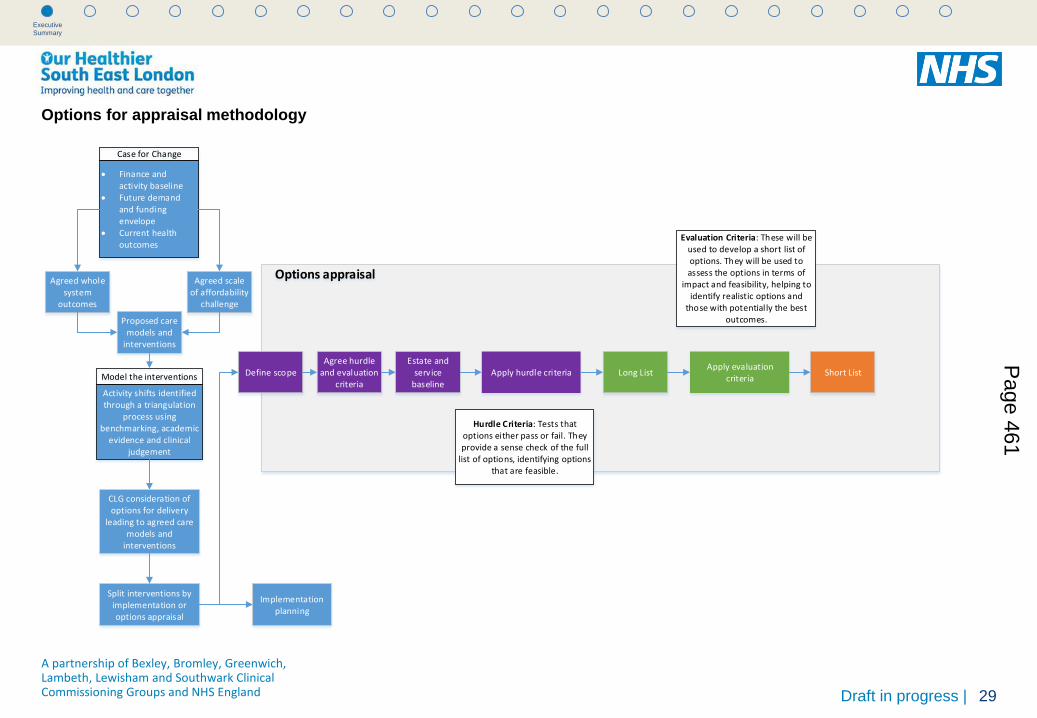
29
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Options for appraisal methodology
Finance and activity baseline
Future demand and funding envelope
Current health outcomes
Case for Change
Agreed scale of affordability
challenge
Agreed whole system
outcomes
Proposed care models and
interventions
Activity shifts identified through a triangulation
process using benchmarking, academic
evidence and clinical judgement
Model the interventions
Split interventions by implementation or options appraisal
Implementation planning
Estate and service
baselineApply hurdle criteria Long List
Apply evaluation criteria
Short List
Options appraisal
Agree hurdle and evaluation
criteria
Evaluation Criteria: These will be used to develop a short list of options. They will be used to assess the options in terms of
impact and feasibility, helping to identify realistic options and
those with potentially the best outcomes.
Hurdle Criteria: Tests that options either pass or fail. They provide a sense check of the full
list of options, identifying options that are feasible.
CLG consideration of options for delivery
leading to agreed care models and
interventions
Define scope
Executive
SummaryP
age 461

A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England 30
• The high level plan on the next page shows at high level the next stages of the plan for implementation, option appraisal and consultation if required. It
is ambitious and dependent on partners and key stakeholders continuing to engage with and support the work as it develops. Over the next few weeks,
CCGs will be testing this with their governing bodies and membership and with key partners and stakeholders. There will be a formal stocktake in late
July and the plan will be confirmed or amended. Further stocktakes will be scheduled as appropriate.
• The case for change is pressing and there is much that can be implemented at pace, but it is important to keep the high levels of engagement and
support which we have had so far.
High level programme plan
Draft in progress |
Executive
SummaryP
age 462

31
A partnership of Bexley, Bromley, Greenwich, Lambeth, Lewisham and Southwark Clinical Commissioning Groups and NHS England Draft in progress |
Executive
Summary
High level programme plan
• Further refinement of the Whole System Model and the models of care, including testing with providers, partners and wider stakeholders
• Building greater detail into the care models so their impact can be modelled
• Modelling expected impacts for providers and commissioners
• Further development of the supporting strategies
• Clinical model implementation
• Workshops– CO discussion on commissioner models , Provider and CLG
Phase 1
• Detailed implementation plan• Presentation to NHSE • Provider outline of steps required
to operationalise the Whole System Model
• Development of the supporting strategies
• Equality Impact Assessment
Ke
y A
ctiv
itie
sK
ey
Ou
tpu
ts
• Identification of potential for significant service change.
• Create options appraisal methodology
• Develop options
• Appraise options
• Modelling to support option appraisal and decision making
• Short list of options
• Further support to implementation
• Continued work with partners to ensure ownership and wider engagement to test and develop
• Modelling Impact Assessment • Publish Equalities Impact
Assessment and action plan• Refinement of implementation
plan• Options analysis
• Development of business cases. There will need to be agreement as to the business cases required and who will lead them (commissioners or providers).
• Modelling to support development/review of business cases
• Decisions making processes for business cases
• Continued wide engagement
• Implementation and continuous quality improvement
• Refinement of detailed implementation plan
• Gateway review• Business Case sign off• Monitoring, evaluation, reporting
and improvement frameworks established
• Any consultation, if required. Note: In the event that consultation is not required, and for any elements of implementation where consultation is not required, the timetable will be shortened, but for planning purposes this paper assumes that there will be some formal consultation, although the subject of such consultation has yet to be established.
• Conclusion of any consultation
• Further modelling if required
• Decision making
• Implementation
• Continuous quality improvement
Programme Plan
Phase 1(January – May 2015)
Phase 2(May – August 2015)
Phase 3 Phase 4 Phase 5 (April – September 2016)(September – November 2015) (December 2015 – March 2016)
Phase 2 Phase 3 Phase 4 Phase 5
Live implementation and continuous quality improvement
Governance Groups Continuous input throughout the process with regular meetings
Comms & Engagement Continued aligned plan to ensure the programme continues with a high level of engagement
Finance & Modelling Modelling to establish the baseline position, required investment and quantify benefits to be realised
Supporting Strategies Continue the commissioning framework, LCN, workforce, IM&T systems and estates configuration needed to realise the change
Page 463

This page is intentionally left blank

1
02 03 Single Report Template
Updated: 25.6.2015
Health & Wellbeing Board report
Date of Health & Wellbeing Board: 8th July 2015
Report title: Lambeth Early Action Partnership (LEAP) Progress report
Wards: All
Report Authorised by: Strategic Director: Helen Charlesworth-May
Portfolio: Cabinet Member Cllr Jane Pickard
Contact for enquiries:
Emma Stevenson Assistant Director Integrated Commissioning, Children & Maternity
Report summary
This report gives a brief update on progress of the Lambeth Early Action Partnership (LEAP)
Finance summary
None arising from this report
Recommendations
(1) For information only
Page 465 Agenda Item 7
2
1. Context
1.1 In 2014 Lambeth successfully bid for £38m funding over 10 years from the Big Lottery: A
Better Start Programme, a 10 year action research programme, looking to improve
services and outcomes from pregnancy to 4th birthday. The Lambeth programme is
called Lambeth Early Action Partnership (LEAP).
1.2 LEAP and was one of 5 successful bids nationally; the other areas are Southend,
Nottingham, Bradford and Blackpool. Each local programme must be led by a voluntary
organisation, in partnership with key local organisations, for Lambeth the voluntary lead
is the National Children’s Bureau (NCB)
1.3 Sites were notified of their success in June 2014 and since then considerable work has
taken place to provide Big Lottery with assurance around specific queries they had
before we could be approved for official ‘go live’ on April 1st 2015. This has now
happened, which essentially means funding can begin to be drawn down
1.4 A Better Start is a 10 year action research programme, looking to improve services and
outcomes from pregnancy to 4th birthday through a combination of evidence-based,
science-based and innovative interventions. LEAP is concentrated on 4 Lambeth wards;
Stockwell, Coldharbour, Vassal and Tulse Hill. A portfolio of 22 interventions has been
developed addressing the 3 nationally specified outcomes to improve:
Social & emotional development
Language & communication
Diet & nutrition
1.5 In addition to the above nationally set outcomes, Lambeth has also identified an
outcome around whole system change, which incorporates:
Workforce development – significantly changing the the workforce to be more
intergated and work in an evidence-based way to better engage and communicate
with each other and the wider community
Information systems - Improving the way information is shared and used
Finance and commissioning – more intelligent budget setting and
commissioning, shifting resources to early intervention to move away from crisis
driven planning
Accountability/co-production – ensuring there is clear accountability at all
levels and that service design is embedded into the community
1.6 The focus for LEAP has been to ensure a strong community led programme is effectively
developed, delivered and evaluated. The LEAP Partnership Board has broad
representation including the Council, CCG, Acute Trusts, a range of voluntary &
community organisations, parents and community members. Sites were notified of their
success in June 2014 and since then considerable work has taken place to provide Big
Lottery with assurance around specific queries they had before we could be approved
Page 466

3
for official ‘go live’ on April 1st 2015. This has now happened, which essentially means
funding can begin to be drawn down.
Programme Governance 1.7 From the outset of LEAP it has been important to ensure that governance isn’t a ‘top
down’ structure, but a true reflection of co-operative ways of working. Big Lottery acknowledged our commitment to this way of working but had some queries about how this would work in practice. The LEAP Partnership Board has representation from parents, community members, VCS, as well as statutory partners and has worked hard to develop a governance structure which captures our commitment to co-operative working whilst also recognising that there may be greater risk falling to NCB as the official lead organisation or the Council and CCG as statutory bodies.
1.8 LEAP Governance arrangements and Terms of Reference were signed off by the
Partnership Board on 20th March 2015 and were subsequently approved by Big Lottery (please see Appendix B for Governance Structure). As this was the only outstanding issue Big Lottery had, it meant LEAP was approved to ‘go live’ from April1st 2015.
Interventions
1.9 There are 22 interventions that make up the LEAP programme (See Appendix A for
interventions and implementation timetable). Each intervention will be phased-in according to an agreed timetable between 2015-2018, with all interventions operational by April 2018.
1.10 Before any intervention can become operational it goes through a rigorous service
design process, following a logic model. This involves facilitated workshops with key stakeholders to ensure all elements of the service delivery model have been discussed and developed. Assumptions are then tested with parents and community members before the final model is agreed.
1.11 The interventions that are being designed for implementation in the first 18months of
LEAP are:
Watch Wait Wonder – A child led psychotherapeutic approach that specifically and directly uses the infant’s spontaneous activity in a free play format to enhance maternal sensitivity and responsiveness
Parent Champions – Based on the evidence-based ‘Dublin Mothers’, a number of parents are being recruited and trained to deliver the LEAP outcomes
Family Nurse Partnership (FNP) – Evidence-based programme working with first time teenage parents. FNP is already provided in Lambeth and through LEAP we are scaling it up borough-wide
Breastfeeding Peer Support – Volunteers are trained to support new Mums at the various Milk Spots as well as offering phone support and 1:1 contact
Targeted Obesity in Pregnancy – programme to support obese women during pregnancy and prevent medical complications
GP ‘Failsafe’ programme – GP based system for flagging up and responding in a multi-agency way to children who do not meet key milestones along the enhanced Healthy Child Pathway
Family Foundations and Brief Encounters - Workforce development programmes
Community Activity and Nutrition – a coproduced community-based range of activities to support increased activity (using local green spaces) and healthy eating
Page 467

4
Supporting Early Literacy for 0-2s – a bespoke programme to support early literacy in the home, drawing on the evidence from the Making it REAL programme (for 3-4 year olds)
Perinatal mental health pathway – Lambeth doesn’t currently have a perinatal mental health pathway for pregnant and new Mums with mild to moderate mental health needs. This interventionwill look at best practice to ensure an effective and comprehensive pathway is developed and implemeted
Capital Programme
1.12 A sum of £4.3M has been allocated to develop and enhance spaces for the delivery of
the LEAP programme across the four wards . Following consultation with parents and partners during the bid development phase the key elements included in the design brief are:
a welcoming space for parents’ and young children’s hub including kitchen facilities, early years garden for play and food growing,
flexible opening hours to include weekend access for community and family use;
a community beacon with welcoming entrance and reception, signage, buggy and bike storage.
1.13 Eleven projects are currently in the design phase:
1. Liz Atkinson Children’s Centre – internal re-modelling to provide multi agency work hub and parents room
2. St Stephens Children’s Centre – creation of additional floor to provide space for multi agency working and parents room, and enhancement to garden
3. Jubilee Children’s Centre - creation of a gate house to provide multi agency working and parents room
4. Loughborough Children’s Centre – small extension and remodelling to provide multi agency working and parents room and enahancement to outside space
5. Loughborough One O’clock Club – enhancement to outside play area 6. Max Roach One O’clock Club – internal remodelling, and enahancment to outside play 7. Brockwell One O’clock Club – some internal remodelling, and creation of natural play 8. Murcell Estate Tennant Hall Early Years Hub and Garden- small internal and external
works 9. Loughborough Estate Early Years Hub and Garden- small internal and external works 10. Tulse Hill Estate Early Years Hub and Garden- small internal and external works 11. Cowley Estate Early Years Hub and Garden - small internal and external works
1.14 Design work is progressing well across all of the LEAP sites and plans will be
Submitted to Planning department at the end of August 2015. Legal advice in relation to security of tenure and Big Lottery conditions is being sought.
Community Engagement
1.15 LEAP is committed to effective community engagement and involvement in all
aspects of the programme. Parents and community members have been involved with LEAP since the bidding stage and the overall strategy and approach reflects this and was acknowledged by the selection panel and Big Lottery when we were awarded the funding.
Page 468

5
1.16 Various community events have taken place over the last 12 months; the most recent took place on 25th February at the Karibu Centre in Brixton. Over 120 people attended, around 40 of who were local parents and their children. A range of activities and information stalls were set up and two workshops were held during the day, one on Parent Champions and one on workforce, both had excellent attendance and overall feedback of the event was very positive.
1.17 Ward based engagement events will be held throughout the summer with the aim of
raising awareness of LEAP locally and recruiting parents to the Partnership Board. There will be a focus on engaging fathers as well as mothers.
Workforce 1.18 There are approximately 1,000 members of staff working in the 4 LEAP wards, from a
range of organisations. We know that while there is some excellent good practice in
Lambeth across the children and families workforce, there is room for improvement and
an opportunity to do things differently and improve outcomes. We were told both by
professionals and parents that there are inefficiencies in the system; with parents having
to ‘tell their story’ numerous times, confused and different messages being given by
different professionals, complicated referral pathways and lack of effective information
sharing.
1.19 It is important that these issues are addressed and the workforce development element
of LEAP includes a number of evidence-based training programmes and ways of
working such as Brief Encounters, the Family Partnership Model and Promotional
Interviewing, which will be included as part of the workforce development strategy
1.20 A Workforce and Learning Manager has been recruited to the core LEAP team and is
currently writing the outline of the Workforce Development strategy, incorporating
findings from a research and literature review on workforce transformation. The strategy
will form the basis of the workforce development programme and a leadership level
workforce task group will be set up to co-produce the detail and content, as well as act
as agents of change for LEAP workforce development within their organisation.
Currently identification of the appropriate leadership personnel is being scoped
Monitoring & Evaluation 1.21 In order to effectively measure the impact of the various interventions as well as the
LEAP programme as a whole, it is essential that the right data is collected and monitored and that a detailed qualitative and quantitative evaluation is implemented. Warwick University are leading a consortium to carry out the national evaluation across the 5 sites and LEAP is working with a range of local Academic partners to develop the local evaluation.
1.22 An interim data collection plan has been submitted to the Big Lottery Fund for comment
and was presented to the Caldicott Committee (data guardians) on 1st May. Detailed plans around data and information governance are now under development further to the Committee’s steer
1.23 Scoping work on the LEAP evaluation has been submitted to the Big Lottery for
Page 469

6
comment, and they will liaise with the national evaluation consortium led by Warwick University to ensure that the local plans align with the national evaluation. An Evaluation Manager is being recruited to the LEAP team, to lead on developing the framework
1.24 LEAP met with the 4 other A Better Start sites and Warwick University in April to
continue to develop common measures across all sites for key aspects of the Programme. A further meeting is taking place in June to take this work forward. Although this has led to some delays in sites (including LEAP) developing their own measures and indicators, the BLF are supportive of this process (and the time it is taking) to ensure that outcomes frameworks align as far as possible to enhance opportunities for shared learning.
1.25 In addition to the broader evaluation, work is ongoing with the London School of
Economics to develop a cost benefit analysis tool. This is an important aspect of both LEAP and the national A Better Start Programme to evidence the cost benefits of early intervention, which should inform future budget setting and commissioning at both a local and national level
Communications
1.26 The LEAP website was launched at the Community event on the 25th and is now live
at www.leaplambeth.org.uk. The content is developed and maintained by the LEAP core team on an ongoing basis. Web traffic has been high, and there are a large number of repeat views. The top three most-viewed pages are:
About LEAP
Parent Champions
LEAP Stories. 1.27 LEAP Twitter and Facebook are also live and growing – both “LEAPLambeth”
2. Proposal and Reasons
2.1 This report is for information only and outlines the status of LEAP workstreams as of
June 2015
3. Finance
3.1 £38m has been awarded by Big Lottery for LEAP over a 10 year period. The funds are held by NCB as the lead voluntary organisation. As part of the bid the Council and CCG agreed to invest £1.8m leverage funding between them to be paid over 3 years.
3.2 A comprehensive national and local evaluation of A Better Start and LEAP is underway, which includes a financial evaluation to ascertain the cost benefits of the Programme and individual interventions. If and when interventions can evidence cost benefits and improved outcomes a case for scaling them up borough wide and for funding them from mainstream budgets will be made. There is no expectation that this would happen for any of the interventions before year 4 (18/19) of the programme to allow enough evidence to be gathered to inform the decision making process
3.3 The go-live date for LEAP was 1st April 2015, which essentially means funding can be drawn down by LEAP for service development and implementation. Work is underway to prepare the Q1 claim from Big Lottery
Page 470

7
3.4 Big Lottery has signed off the LEAP Partnership Agreement which will facilitate contracting arrangements between LEAP and the various delivery partners for each intervention. In the main, contracts and service level agreements will be between NCB and the Provider of the intervention, but in some cases such as where it is an extension of an existing service, like Family Nurse Partnership the contractual arrangements may be between the CCG and Provider or the Council and Provider
3.5 Memorandum of Understandings between NCB and the CCG and Council have been
agreed and signed in relation to the £1.8m leverage funding commitment.
4. Legal and Democracy
4.1 There are no legal implications to the Council as overall responsibility for meeting Big
Lottery conditions falls to NCB. However a detailed governance structure, which includes
an Executive group and ensures citizens are at the heart of decision making has been
signed off by the Partnership and approved by Big Lottery
5. Consultation and co-production
5.1 All LEAP activity is co-produced. A Co-production lead has been recruited to the LEAP
core project team and they are working closely with key stakeholders, in particular
parents and carers to ensure they are involved in all aspects including service design,
governance, community events and wider communication
6. Risk management
6.1 N/A
7. Equalities impact assessment
7.1 Equity and equality will be secured in three ways: First, as part of the service design
process for each of the projects in the LEAP portfolio, working with the local community.
Second, through a process of equality impact assessments throughout the LEAP
programme - the programme will be reviewed every two years at which point the equality
of access and outcome will be considered for each intervention and the programme as a
whole. Finally, a local evaluation framework is under development which will include
looking at effectiveness of ensuring equity and equality of the programme (and enabling
LEAP to use the data to identify improvements where needed).
8. Community safety
8.1 N/A
9. Timetable for implementation
9.1 N/A - No recommendations have been made
Page 471

8
Page 472

Health and Wellbeing Board
8 July
Update on Southwark and Lambeth Integrated Care (SLIC)
Wards: All
Report Authorised by: Strategic Director of Commissioning, Helen Charlesworth-May
Portfolio: Cllr Jim Dickson, Cabinet Member Health and wellbeing
Contact for enquiries:
Adrian Bentley, Policy officer 020 7926 7162
Report summary
Moira McGrath will provide the Health and Wellbeing Board with a verbal update on Southwark
and Lambeth Integrated Care (SLIC).
Finance summary
There are no financial implications in regard to this presentation.
Recommendations
(1) To note the presentation.
Page 473 Agenda Item 8

1. Context
1.1 Not applicable.
2. Proposal and Reasons
2.1 Not applicable.
3. Finance
3.1 There are no financial implications with regard to this verbal update.
4. Legal and Democracy
4.1 There are no legal implications with regard to this verbal update.
5. Consultation and co-production
5.1 Not applicable.
6. Risk management
6.1 Not applicable.
7. Equalities impact assessment
7.1 Not applicable.
8. Community safety
8.1 Not applicable.
9. Organisational implications
The following sections must be considered, but are optional and each should be deleted
if not relevant to the report. If there are no organisational implications, state “None”.
9.1 Environmental
None
9.2 Staffing and accommodation
None
9.3 Procurement
None
9.4 Health
None
10. Timetable for implementation
10.1 Not applicable
Page 474

Page 475

This page is intentionally left blank

Health and Wellbeing Board
8 July 2015
Children and Families Strategic Partnership update
Wards: All
Report Authorised by: Strategic Director Commissioning: Helen Charlesworth-May
Contact for enquiries:
Rohini Anand-Pal, Policy, Equalities and Performance Officer, PEP, LBL
020 7926 3168 [email protected]
Report summary
The purpose of this report is to update the Health and Wellbeing Board on the work programme of the Children and Families Strategic Partnership (CFSP). This report follows the update provided at the 14 January 2015 meeting of the Health and Wellbeing Board and reports on outcomes of the CFSP meeting held on 11 May 2015. Finance summary
The update report does not have any financial implications. Recommendations
(1) To note the contents of the report.
Page 477 Agenda Item 9

1. Context
1.1 The Lambeth Children and Families Strategic Partnership (CFSP) have close links with the Health and Wellbeing Board through joint members and the Chair of the CFSP vice-chairing the Health and Wellbeing Board. An update on the work of the Health and Wellbeing Board is reported to the CFSP via Partner Updates, a standing item on the agenda of meetings.
1.2 Regular updates about CFSP activity are presented to the Health and Wellbeing Board. The last update was provided to the Board on 14 January 2015. Since this meeting the CFSP has had one meeting, which was held on 11 May 2015. This report provides an update for this meeting.
2. Proposals and reasons
The following areas were discussed in detail at May’s CFSP meeting:
2.1 Partner Updates
CQC Unannounced Safeguarding Inspection with Health Update:
Andrew Eyres, Managing Director NHS Lambeth reported that the CQC Unannounced Safeguarding Inspection with Health has still not taken place. It is expected that all NHS providers will have had their CQC inspection by September 2015.
Ofsted inspection of Children’s Services:
It was updated that the final Ofsted inspection of Children’s Services will be published on Tuesday 12 May 2015.
Child Poverty Action Plan Update Katy Briggs, Senior Commissioning Officer – Special Educational Needs, London Borough of Lambeth provided background information and explained that the previous Child Poverty strategy expired in April 2014. Partners were reminded that the Child Poverty Act 2010 places a statutory duty on local authorities to carry out a child poverty needs assessment in their area and to develop a local child poverty strategy.
It was reported that the Child Poverty Action Group data shows that 18-22k of
children are living in poverty in Lambeth.
Katy reported on coproduction work which has taken place to develop the strategy.
The 6 key areas identified as factors determining children’s long term prospects were
listed as:
Family and the home environment (including the role of the parent and the home
learning environment)
Income and parental employment
Child education attainment
Health
Housing
Child soft skills and characteristics
A holistic view of poverty has been taken which is not limited to focusing on families
in receipt of benefit
Page 478

A mapping exercise was carried out to identify other strategies which have intended
outcomes relevant to child poverty
A coproduction event will take place during July to further develop this strategy and
consider how it is monitored effectively
Dr Ruth Wallis, Director of Public Health for Lambeth & Southwark recommended that
the strategy could be developed further by making reference to the health and wellbeing
board framework.
There was a discussion about where this strategy is owned – currently owned by the
CFSP. It was suggested that this item goes for discussion at the next Health and
Wellbeing Board (HWB) meeting which will focus on children’s services. Ruth Wallis
highlighted the importance of the HWB having a clear oversight of current activity around
children and young people.
There was a discussion around outcome measures of child poverty projects. Katy
Briggs explained all projects such as Lambeth Early Help and Prevention (LEAP) and
Jobs and Growth strategy have measures. Andrew Eyres, Managing Director, NHS
Lambeth advised this should be reflected in this strategy. It was clarified that the overall
objective was to reduce child poverty in line with central government’s aim to eradicate
child poverty by 2020. Reference was made to the impact of welfare reforms on child
poverty.
Troubled Families Programme Update & Outcomes Plan
Alima Qureshi, Head of Troubled Families reported that the final Phase 1 Payment by
Results claim achieved 100%, meaning 1080 families have been turned around. This is
higher than any other local authority. The proportion of families with 1+ family member
entering f/t employment for more than 6 months is greater in Lambeth than across
London and England.
Alima explained programme progress over the last 18 months with analysis broken down
by families identified by Lambeth; families worked with; achieving crime/ASB/education
results; and turned around families.
Some outcomes at end of intervention:
45% decrease in number of families with 15% unauthorized school absences
Families more than twice likely to have at least one person employed - 11% to 27%
7% less likely to have children living in care and 12% less likely to have children on a
CPP
22% reduction in number of families with a young offender (proven offence in 6
months before close of intervention compared with 6 months prior to intervention)
Criteria for families to receive interventions from this programme – at least 2 of 6
problems:
1. Parents and children involved in crime or anti-social behaviour. 2. Children who have not been attending school regularly.
Page 479

3. Children who need help. 4. Adults out of work or at risk of financial exclusion and young people at risk of
worklessness. 5. Families affected by domestic violence and abuse. 6. Parents and children with a range of health problems.
Alima explained the Additional Lambeth Families (ALF) Programme Outcomes diagram
and advised over the next 5 years 3670 families need to be turned around on the
expanded programme.
An outcome plan and diagram as shown below illustrated the 6 outcomes and relevant
indicators and intended outcomes.
There was a discussion including the following key points:
Partnership event to take place in early June to present ALF programme outcomes
Families who have met the criteria will be monitored across the whole programme. AQ
explained the differing support available scaled by need
Stella Clarke reported that the ALF team and Multi AgencyTeam (MAT) plan to be
integrated over the next 12 months
Only 7 families have failed to meet an intended outcome – this has mainly been families
with young offenders
It was agreed make reference to the ALF programme in the Child Poverty strategy
Alima to raise schools awareness about this programme via mechanisms such as Chairs of
governors and Head teacher Forum.
Congratulations were given to Alima and relevant partners for successfully achieving
Phase 1 programme targets.
Young Lambeth Emotional Wellbeing & Mental Health Plan 2015-18 Update
Paul Cosens, Children’s Commissioning Manager, LBL presented this item
Chair introduced this agenda item and explained that the draft Young Lambeth
Emotional Wellbeing and Mental Health Plan 2015-18 was presented at 17 November’s
Page 480
meeting and has been brought back to this meeting following wider consultation. Paul
reported that the final will be signed off at the July’s Health and Wellbeing Board.
The latest plan was circulated for information and a presentation was provided with
PowerPoint.
Paul highlighted the following key points:
Only 17% of young people with mental health needs have their needs met by Lambeth.
Capacity and resource are key in ensuring these needs are better identified.
South London And Maudsley (SLAM) waiting times were identified as an issue
Alima Qureshi welcomed input from Paul to assist defining ALF health outcomes –
Andrew Eyres referred to the postcode lottery associated with access to services
dependent on location of school, especially as more children are now educated at
schools inside the borough
Discussion about how well schools are working together in clusters and pooling
resources around this issue
Paul Robinson, Woodmansterne Primary School & Children's Centre reported that the
Head teacher Executive group had already identified issues around thresholds affecting
access services. He also reported on the greater expectations placed upon schools in
the context of a limited budget
Paul Robinson referred to unregulated free services and their potential negative impact
on its clients
Laura McGinlay, School Governor referred to central government non-statutory
guidance: Mental Health and Behaviour in Schools published in 2014 clarifying the
responsibility of the school and what they can do. This increased pressure on schools
was acknowledged.
Dr Ruth Wallis highlighted the importance of this area therefore an action plan to turn
around manageable areas is key.
Core themes resulting from Emotional Wellbeing Mental Health consultation:
1. Working Together for Better Mental Health: for everyone by everyone (awareness,
support and training)
2. Maximising Resilience and Self Sufficiency (pupils, parents, professionals)
3. No Child or Family Overlooked (targeted groups)
4. Cemented in Communities (co-production and inclusiveness)
5. Investing in the Future for Children and Families (targeted investment)
Current activity:
Additional resource to speed up access to CAMHS
Survey to map emotional wellbeing and mental health resources and investment in
schools
Development of a borough-wide emotional wellbeing dashboard.
Timeframes of activity
Page 481

Barbara Hills, General Manager, Children’s Community Health commented it’s key that
the strategy is made reader friendly including a version for children. All agreed.
It was agreed that Chair and Sadru Kheraj sign this off prior to submission to the Health
and Wellbeing Board in July 2015.
INTERACTIVE SESSION: Lambeth Early Help and Prevention Integrated
Commissioning Strategy for Children and Families 2014-17 - Principles & options
for future children’s services delivery models
Maria Millwood, Director of Integrated Commissioning LBL and NHS Lambeth and Laura
Griffin, Lead Commissioner, Delivery presented this item. MM introduced the
presentation highlighting the key drivers for change i.e. the current children’s services
model is not financially sustainable especially in light of increasing demand. Other key
points referred to:
Partnership outcomes as outlined in the Lambeth Early Help and Prevention Integrated
Commissioning Strategy for Children and Families 2014-17; model of needs; Lambeth
Transformation programmes; Children’s Service Redesign ensuring thresholds are met,
social care workforce development to address this; Remodelling of MAT integrating ALF
team; Local Care Networks engagement outside GP federations and how they provide a
platform for the VCS; Evelina CYP Partnership proposed model of care with a key focus
on long term condition care and workforce development in primary care; the LEAP
Rainbow: public health approach to improve health and wellbeing and reduce
inequalities, see figure 1.
Figure 1, LEAP Rainbow
Page 482

Laura Griffin continued the presentation explaining the Early Intervention Foundation’s
definition of Integration taken from Getting it Right for Families, November 2014.
Characteristics of Mature Integration structured by leadership and governance;
commissioning & allocation of resources; structures, systems and processes and
workforce outlining characteristics of a fully Integrated model versus Lambeth’s current
position was explained.
Partners were asked where we need to develop this integrated model further as well as
transformation design principles/outcomes and governance.
Key points discussed include:
Maureen Sheridan, Lambeth Governor Forum representative queried if the Children’s
Centres Implementation Group had been engaged. SC explained how they had.
Andrew Eyres stated that the current model was fragmented requiring much more
integration and referred to the impact of recent electoral changes and central
government new agenda around integration
There was a discussion around working with locality leads and the varying needs of
different areas of the borough
Maria Millwood referred to the importance of aligning the development of this model with
the current development of strategies
Next steps
It was agreed that the next CFSP meeting: Thursday 16 July include a workshop
dedicated to the draft principles for design; governance arrangements and mapping of
current resources. Maria Millwood advised it is key that: VCS, Health, Schools, LA,
Local Care Network & young people are all engaged.
3. Finance
3.1 There are no finance comments arising from this report.
4. Legal and Democracy
4.1 There are no legal comments arising from this report but specific legal advice may be provided as required.
5 Consultation and Co-production
5.1 The report provides an update for the Health and Wellbeing Board. There is no specific
consultation associated with the report
6 Risk management
6.1 None
7. Equalities impact assessment
Page 483

7.1 The report provides an update for the Health and Wellbeing Board. An Equality Impact
Assessment has not been produced for the purpose of this report.
8. Community safety
None
9. Organisational implications
None
10. Timetable for implementation
None
Page 484




















