Psychotropic effect of antiepileptic drugs
15
Acte neurol. scandinav. 60, 329-343, 1979 REVIEW ARTICLE Jniversity Clinic of Psychiatry, Municipal Hospital, University Department olf Clinical Chemistry CL, Rigshospitalet, University Clinic of Neurology, Hvidovre Hospital Copenhagen, Denmark Psychotropic effect of antiepileptic drugs JOSEF PAWAS, HELGA FLACHS AND LENNART GRAM Eighteen controlled studies investigating the psychotropic effect of anti- epileptic drugs are critically reviewed. The neurochemical evidence for existence of psychotropic properties is still speculative. It seems question- able on the basis of this survey that there exist genuine psychotropic effects of antiepileptic drugs, which are not related to antiepileptic efficacy and/ or differences in toxicity. Key words: Antiepileptic drugs - controlled studies - psychotropic effect - review. Since the emergence of antiepileptic drugs, a psychotropic effect of these drugs has been asserted. Psychotropic properties have been reported for several types of epilepsy, as well in patients with brain damage and varying quality and quantity of psychopathology, as in healthy persons. Often 'the papers dealing with this topic give no clearcut definition of psychotropic effect. Generally speaking this concept covers an amelioration of the psyche both in sick and healthy persons. This definition does not include either the site 0.r the mode of action of the substances in question. The psychological variables reported improved by antiepileptic drugs are summarized in Table 1. Because of the general assumption that antiepileptic effect takes place in the CNS, it seems reasonable to infer an interconnection between antiepi- leptic and psychotropic mechanisms. In order to make a critical re-evaluation of the (question, we performed a review of controlled studies dealing with this subject. Our defmition of con- trolled trials was randomized, double-blind studies, applying psychometric evaluation stated in the protocol. Studies where nothing definite was stated concerning randomization were included, profiting from benefit of doubt. Oool-6314/79/120329-15$0.2.50/0 @ 1979 Munksgaard, Copenhagen
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Psychotropic effect of antiepileptic drugs

Acte neurol. scandinav. 60, 329-343, 1979 REVIEW ARTICLE
Jniversity Clinic of Psychiatry, Municipal Hospital, University Department olf Clinical Chemistry CL, Rigshospitalet, University Clinic of Neurology, Hvidovre Hospital
Copenhagen, Denmark
Psychotropic effect of antiepileptic drugs
JOSEF PAWAS, HELGA FLACHS AND LENNART GRAM
Eighteen controlled studies investigating the psychotropic effect of anti- epileptic drugs are critically reviewed. The neurochemical evidence for existence of psychotropic properties is still speculative. It seems question- able on the basis of this survey that there exist genuine psychotropic effects of antiepileptic drugs, which are not related to antiepileptic efficacy and/ or differences in toxicity.
Key words: Antiepileptic drugs - controlled studies - psychotropic effect - review.
Since the emergence of antiepileptic drugs, a psychotropic effect of these drugs has been asserted. Psychotropic properties have been reported for several types of epilepsy, as well in patients with brain damage and varying quality and quantity of psychopathology, as in healthy persons. Often 'the papers dealing with this topic give no clearcut definition of psychotropic effect. Generally speaking this concept covers an amelioration of the psyche both in sick and healthy persons. This definition does not include either the site 0.r the mode of action of the substances in question. The psychological variables reported improved by antiepileptic drugs are summarized in Table 1.
Because of the general assumption that antiepileptic effect takes place in the CNS, it seems reasonable to infer an interconnection between antiepi- leptic and psychotropic mechanisms.
In order to make a critical re-evaluation of the (question, we performed a review of controlled studies dealing with this subject. Our defmition of con- trolled trials was randomized, double-blind studies, applying psychometric evaluation stated in the protocol. Studies where nothing definite was stated concerning randomization were included, profiting from benefit of doubt.
Oool-6314/79/120329-15$0.2.50/0 @ 1979 Munksgaard, Copenhagen

330
Table I . Reported spectrum of psychotropic action of antiepileptic drugs
I. Psychomotor improvement (i.e. diminished retardation, stickiness, perseveration, apathy and lack of initiative).
11. Cognitive improvement (especially attention and concentration). 111. Affective improvement (i.e. diminished irritability, aggressiveness, impulsivity, dys-
phoria, depression and anxiety).
CARBAMAZEPINE (CBZ)
The majority and the most enthusiastic reports concerning psychotropic ef- fects were found for CBZ. There are surprisingly few studies about the mechanism of action of CBZ: It is “felt” that CBZ depresses synaptic trans- mission rather than total brain function (Troupin 1978). Probably the mode of action has no relation with the gamma-aminobutyric acid (GABA)-system, (KoeZZa 1976) - but CBZ is conveyed to resemble phenytoin (PHT) in its anticonvulsive profile. CBZ exerts remarkable anticonvulsive effect against limbic epileptic seizures induced by electrical stimulation of the hippocampus and against seizures induced by electric stimulation of the reticulo-thalamic system (KoeZZu 1976). The coniiguration of CBZ differs in several respects from other antiepileptic drugs. The molecule has a tricyclic structure and is in many ways similar to the tricyclic antidepressants - in particular, imipra- mine. The relative lack of sedation and the similarity to imipramine have been the main reason for assuming psychotropic properties of CBZ. In 1975 DaZby published an extensive review on CBZ and psychotropic effect. Most of the studies referred to in this survey were uncontrolled.
Rajotte et aZ. in 1967 (Table 2) evaluated CBZ versus PHT in epileptic inpatients. Before the study, regular treatment was reduced until generalized convulsions began to occur. The only information on psychopathology of the patients was that they suffered from epileptic psyche. Psychometric assess- ment was performed by a self-devised behavior rating scale. CBZ turned out to be the better psychotropic agent, while PHT was the best anticonvulsant agent. These results are not surprising, as the patients presumably had much higher serum levels of PHT than of CBZ, and consequently their seizures were better controlled on PHT. The superiority of CBZ in psychotropic properties was probably related to its less toxicity as there was an improve- ment on both drugs during the first 2 months of the trial, i.e. after reduction of the regular drug treatment.
In 1968 Marjerrison et aZ. published a study of CBZ versus phenobarbital (Pb) in epileptic inpatients. It is not clear whether the study was randomized, and for unknown reasons the observation periods were 2 and 4 months, re- spectively. Three patients suffered from personality disorders, one was men-

N
N
Tab
le 2
. C
ontr
olle
d st
udie
s on
psy
chot
ropi
c ac
tion
of c
arba
maz
epin
e (C
BZ
)
Aut
hor
Subj
ects
D
esig
n B
lood
le
vels
re
port
ed
Psyc
hotr
opic
ef
fect
D
oses
C
onco
mita
nt
mdd
ay
trea
tmen
t
Raj
otte
et
al.
(196
7)
Mar
jerr
ison
et
al. (
1968
)
24 e
pile
ptic
s fr
om a
m
enta
l ho
spita
l 21
epi
lept
ic i
npat
ient
s w
ith p
erso
nalit
y di
s-
orde
rs
Prys
e-Ph
illip
s &
Jea
- 22
epi
lept
ics
from
a
vons
(19
70)
men
tal
hosp
ital
Gro
h et
al.
(197
1)
20 n
on-e
pile
ptic
ch
ildre
n w
ith b
ehav
ior
diso
rder
s 45
men
tally
sub
norm
al
epile
ptic
inpa
tient
s C
ereg
hino
et
al. (
1974
)
Rod
in e
t al
. (19
74)
37 e
pile
ptic
inp
atie
nts
Puen
te (
1975
) 27
bra
in-d
amag
ed
Dod
rill
& T
roup
in
(197
7)
subn
orm
al c
hild
ren
40 e
pile
ptic
out
patie
nts
CB
Z vs
PH
T c
ross
over
2
X 6
mot
hs
CB
Z v
s Pb
cro
ssov
er
2 an
d 4
mon
ths
CB
Z vs
pla
cebo
gro
up
com
para
tive
15 w
eeks
C
BZ
vs p
lace
bo c
ross
- ov
er
2 X
6 w
eeks
C
BZ
vs P
HT
& P
b cr
oss-
ov
er 3
X 3
wee
ks
CB
Z vs
pla
cebo
cro
ss-
over
2 x
3 w
eeks
C
BZ
vs p
lace
bo c
ross
- ov
er 2
X 4
wee
ks
CB
Z v
s PH
T c
ross
- ov
er 2
X 4
mon
ths
CB
Z 6
00
PH
T 3
00
CB
Z 4
0&12
0 P
B?
CB
Z 60
0
CB
Z ?
CB
Z 1
200
PHT
30
0 P
b 30
0 C
BZ
600
-120
0
CB
Z 2
00-3
00
CB
Z 1
8mgk
g PH
T
6mg/
kg
Red
uced
Dos
age
halv
ed
Add
-on
Non
e
With
draw
n
Slig
htly
re
duce
d N
o in
form
atio
n
Non
e
No
No
No
No
Yes
Yes
No
Yes
Posi
tive
Posi
tive
Non
e
Posi
tive
Non
e
Neg
ativ
e
Posi
tive
Posi
tive
Phen
ytoi
n (P
HT)
. Ph
enob
arbi
tal (
Pb).
332
tally retarded and 14 patients were psychotic. The psychometric evaluation involved behavioral and psychopathological rating scales. The result of total behavioral scale showed no difference between treatments, but the subsequent item analysis disclosed that Pb-treated patients were more retarded. An item analysis of psychopathological rating disclosed that Pb-treated patients “See- med unhappy most of the time and usually looked tired and worn-out”. There was no difference in antiepileptic effect. There was an overall psycho- tropic effect of both CBZ and Pb, probably because of halving of the previous antiepileptic and neuroleptic treatment. The minor superiority of CBZ in psychotropic action can easily be explained by its less sedative effect.
Pryse-Phillips & Jeavons (1970) investigated CBZ versus placebo in epi- leptic inpatients. No information about psychopathology of the patients was given. A behavior rating scale was used to assess psychotropic actioa. No difference between CBZ and placebo, either in respect to antiepileptic effect, or psychotropic effect could be demonstrated, except a diminished physical activity in the CBZ period. The authors explained the lack of antiepileptic effect by more intensive observation of the patients during the study and by overall well-regulated epilepsy.
Groh et al. (1971) published a study of CBZ versus placebo in nonepilep- tic children with behavior disorders. Patients’ psychopathology comprised anxiety, aggressivity, impulsitivity and dysphoria. The psychometric studies consisted of psychomotor examination and personality assessment. In addi- tion, global rating was done by the physician, the teachers and family mem- bers. The frequency of side effects especially sedation was surprisingly high, eight out of 20 (Groh et al.s remark ). The authors concluded that CBZ pos- sesses psychotropic action as regards the mentioned psychopathology. How- ever, as only one of the patients showed a normal EEG, the results might possibly be connected with reduced subclinical epileptic seizures. The EEGs remained unchanged during the active treatment consistent with the absent correlation between improvement of seizure frequency and EEG under CBZ treatment.
CBZ versus PHT and Pb in mentally subnormal epileptic inpatients was studied by Cereghino et af. (1974). Blood levels were found within thera- peutic levels. No description of psychopathology of the patients was given. The psychometric evaluation consisted of a modification of the Ward Be- haviour Rating Scale which has not been validated. Concerning behavior, a trend for improvement was noted on all treatments and this trend was most marked for CBZ.
In a study investigating CBZ versus placebo in epileptic inpatients (Rodin et af. 1974), dosing was conditioned by drug level monitoring. A sdf-devised test consisting of cognitive-perceptual-motor-battery, personality and be- havior assessment constituted psychometric measurements. The conclusion of

333
the study was that CBZ had negative psychotropic properties due to reduced attention and arousal.
Twenty-seven brain-damaged children were evaluated on CBZ and pla- cebo by Puente (1975). Patients were tested on perceptual-motor-projective- educational-tests and on WISC. The study showed a positive psychotropic effect of CBZ, especially on cognitive performance. However, as no EEGs were obtained from the patients, the improvement could be due to control of subclinical seizures.
Dodrill & Troupin in 1977 evaluated CBZ versus PHT. They submitted epileptic outpatients to extensive psychometric evaluations including Halsted Battery, Stroop Color Test, Minnesota Multiphasic Personality Inventory (MMPI) and WAIS. No description of patients’ psychopathology was pre- sented. Four of 27 tests showed a significant advantage of CBZ. The subse- quent identification of CBZ responders indicated the following characteristics: Lower FQ and higher score on MMPI. The authors concluded that CBZ possessed a psychotropic effect, especially on more complex mental functions requiring concentration and attention. However, this conclusion is question- able as the mean serum level of PHT was 125 pmoVl (Troupin et ul. 1977), compared to the established therapeutic range 40-80 pmol/l. CBZ mean serum level was found within the therapeutic range. Accordingly, it is not surprising that the patients while on PHT regimen did poorly on the cogni- tive tests.
Summarizing the CBZ studies three out of eight controlled studies showed none or negative psychotropic effect of the drug. The remaining five studies postulate the existence of a psychotropic action, the existence which is very (questionable, however.
PHENYTOIN (PHT)
The original belief in psychotropic properties of PHT was nearly as optimistic as the present enthusiasm about CBZ. There are many theories about the mechanism of action of PHT. For example, PHT is found to inhibit both sodium and calcium influx into cells during cellular depolarization and to alter regulation of brain cyclic nucleotide levels by preventing accumulation of cyclic nucleotides in the brain (Ferrendelli et ul. 1977).
Calcium and PHT have been demonstrated to possess antagonistic actions on the net level of endogenous phosphorylation of specific rat proteins and thereby depressing the release of neurotransmitter (Delorenzo 1977). Certain inhibitory. post-synaptic potentials which are GABA mediated and chloride- dependent have been shown to be prolonged by PHT (Ayulu 1977). But the observation which perhaps is most relating to psychotropic properties is that PHT inhibits dopamine uptake into brain slices from caudate putamen

Tab
le 3
. Con
trol
led
stud
ies
on p
sych
otro
pic
actio
n of
phe
nyto
in (
PH
T)
Aut
hor
Subj
ects
Lef
kow
itz
(196
9)
50 d
elin
quen
t boy
s w
ith
Step
hens
& S
haff
er
(197
0)
Mal
itz &
Kan
zler
31
2 de
pres
sed
(197
1)
outp
atie
nts
beha
vior
dis
orde
rs
30 n
euro
tic o
utpa
tient
s
Uhl
enhu
th e
t al
. (19
72)
Step
hens
et
al. (
1974
)
80 p
sych
oneu
rotic
ou
tpat
ient
s 10
7 no
rmal
vol
utee
rs
Des
ign
PH
T v
s pl
aceb
o gr
oup
com
para
tive
76 d
ays
PHT
vs
PHT
cro
ss-
over
2 X
3 w
eeks
P
HT
vs
6 an
tidep
res-
sa
nts
and
plac
ebo
grou
p co
mpa
rativ
e 4
wee
ks
PHT
vs
Pb g
roup
com
- pa
rativ
e 8
wee
ks
PHT
vs
PH
T c
ross
- ov
er 2
X2
wee
ks
Blo
od
Dos
es
Con
com
itant
le
vels
Psyc
hotr
opic
m
g/da
y tr
eatm
ent
repo
rted
ef
fect
PH
T 2
00
Noi
nfor
mat
ion
No
Neg
ativ
e
PHT
300
N
one
No
Posi
tive
PH
T
15
PH
T 4
00
Add
-on
No
Neg
ativ
e
PH
T 3
00
Noi
nfor
mat
ion
No
Non
e Pb
90
P
HT
300
N
one
rqo
Non
e P
HT
15
w
w
P
__
__
~
~ ~
Phen
obar
bita
l (Pb
).

335
( WoEf 1976). Thus, putative psychotropic properties of PHT in especially minimal brain dysfunction could be explained by an increase in the amount of dopamine available for postsynaptic receptor sites. The very same mecha- nism of action has been suggested for amphetamine which is often used in the treatment of minimal brain dysfunction. Thus one can conceptualize theoretical grounds for treatment with PHT of certain behavior disorders, e.g. attention deficiency disorders. Besides the studies of CBZ, where PHT was included, five controlled trials deal with PHT.
In a study from 1969 (Table 3), Lefkowitz compared PHT to placebo in male delinlquents with behavior disorders of disruptive type. Rating scales assessing personality, psychopathology, mood, behavior and psychomotor functioning were applied. Measurements disclosed a significant negative psychotropic effect of PHT compared to placebo which significantly im- proved behavior and mood in the patients.
Stephens & Shufler (1970) performed a study in anxiety neurotic out- patients evaluating 300 mg versus 15 mg PHT. Inclusion criteria involved an Ego strenght T score on the MMPI of 40 or above, normal IQ and no need of antidepressants. Psychometric evaluation consisted of the Lorr Outpatient Mood Scale, the Outpatient Symptom Check List, patient’s self-rating scale and physician’s global rating scale. PHT 300 mg was shown to be significant- ly better than PHT 15 mg in reducing anxiety and irritability. The authors’ diagnostic criteria of anxiety neurosis do not seem to be consistent with the psychodynamic concept of neurosis. We consider these patients as suffering from various character disorders as they are explicitly described as being easily upset, high-strung and unable to tolerate stress and having explosive temper. Unfortunately, the investigators did not record the EEG. The physi- cian’s global rating must be considered to be biased as it was based as well on objective observations as on studying the self-assesment questionnaires. The type of symptoms reported improved could be due to nonspecific seda- tive properties of 300 mg PHT per day.
A total of 312 depressed outpatients, mainly neurotics (23 % psychotic), entered the trial performed by Malitz & Kunder (1971). The psychotropic evaluation comprised MMPI, Brief Psychiatric Rating Scale and Taylor Anxiety Scale. No inclusion rating scale was used, only general clinical as- sessment. The PHT-treated patients did significantly worse than placebo on all items no doubt because of high PHT doses (mean 400 mg daily) which was accompanied by a high frequency of side effects.
PHT and Pb were compared by Uhlenhuth et al. (1972) in psychoneurotic outpatients. Psychopathological rating scales included a check list of neu- rotic symptoms, Psychiatric Outpatients Mood Scale and Psychiatric Evalu- ation Profile. There was no difference between PHT and Pb as regards psychotropic effect, but a slight positive effect of both drugs compared to

336
baseline period was noted. In 1974, Stephens et al. investigated the effect of 300 mg versus 15 mg PHT
in normal volunteers. Outpatients Mood Scale, Outpatients Symptom Check List, Personal Feeling Scale, Steadiness Test, Apparent Eye Level, Puzzle Box and Stroop Test were applied. There was no significant difference be: tween the two PHT treatments although there was a trend for dysphoria among the females while on 300 mg PHT. The reaction time was increased in both sexes on 300 mg PHT. Summarizing PHT trials (Table 3), four out of five studies show a negative or lacking psychotropic effect.
ETHOSUXIMIDE (ETO)
The mode of action of ethosuximide (ETO) is still unknown. One suggestion is that the mechanism has some connection to the chloride conductance mediated by GABA (Ferrendelli (1979). Thus, there is only a vague notion for a proposed psychotropic effect of ETO.
The only controlled study is that of Lynn Smith et al. from (1968) (Table 4) of ETO versus placebo in 10 children with 14-6 Hz positive spike EEG pattern and learning difficulties. The dose was rather low, 250 mg daily. Psychometric evaluation consisted of WISC, perception test and Rorschack test. The patients improved on WISC only. This finding could be caused by an improvement in cognitive functions due to desynchronization of the in- vestigated EEG pattern. Unfortunately, the authors made no use of EEG recordings during the trial.
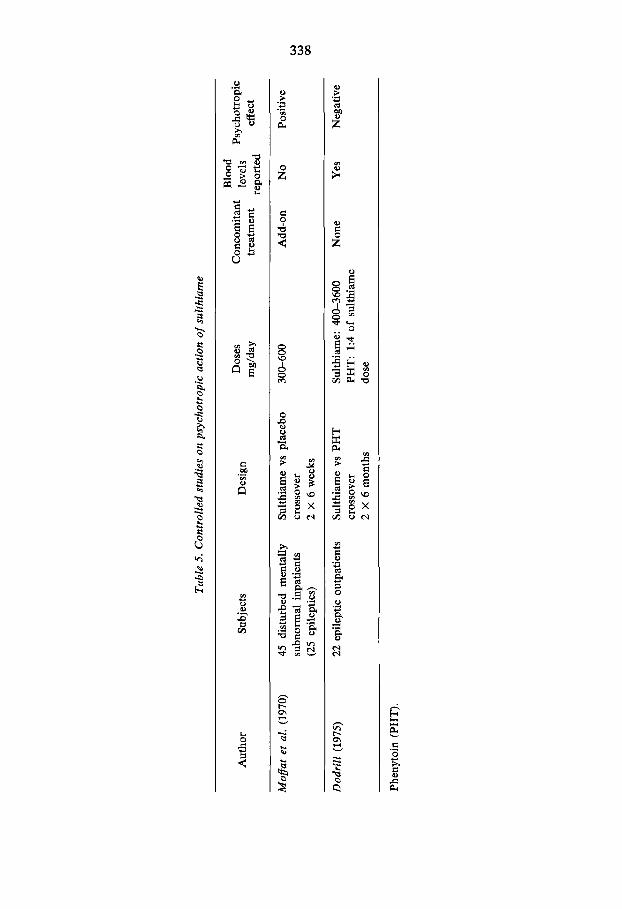
SULTHIAME
Since 1960 the carbonic anhydrase inhibitor suthiame has been used as an adjunct to the treatment of epilepsy. To our knowledge no studies have been undertaken to elucidate the mechanism of action of sulthiame, but probably it is comparable to that of the other antiepileptic carbonic anhydrase inhi- bitor viz. acetazolamide. Several studies have been published on acetazol- amide and its inhibition of carbonic anhydrase in the glial cells (Woodbury (1979). This inhibition causes an increased COz tension in the brain. The resulting decreased pH may facilitate the action of the GABA-synthetizing enzyme glutamate decarboxylase which has a pH optimum of 6.5, i.e. GABA concentration will raise. On the other hand the chloride-channels are prob- ably also pH dependent in the way that a decreased pH might induce a de- creased chloride conductance. These putative neurochemical changes could possibly be responsible for some kind of psychotropic effect. Two controlled studies deal with psychotropic effect of sulthiame.
Moflat et al. (1970) (Table 5) reported a study of sulthiame versus placebo

Tabl
e 4.
Con
trol
led
stud
ies
on p
sych
otro
pic
actio
n of
eth
osux
imid
e (E
TO
) Blo
od
Dos
es
Con
com
itant
le
vels
Ps
ycho
trop
ic
mg/
day
trea
tmen
t ef
fect
Lynn
Sm
ith e
t ~
l.
10
chi
ldre
n w
ith
ETO
vs
plac
ebo
cros
s-
250
Non
e N
o Po
sitiv
e (1
968)
146 Hz
pos
itive
spi
ke
over
2 x
3 w
eeks
E
EG
and
lear
ning
di
ffic
ultie
s
Author
Subj
ects
D
esig
n w
w
4
Tab
le 5
. Con
trol
led
stud
ies
on p
sych
otro
pic
actio
n of
sulth
iam
e
Aut
hor
Subj
ects
D
esig
n B
lood
C
onco
mita
nt
leve
ls
Psyc
hotr
opic
tr
eatm
ent
repo
rted
ef
fect
~
Mo&
t et
al.
(197
0)
45 d
istur
bed
men
tally
Su
lthia
me
vs p
lace
bo
300-
600
subn
orm
al i
npat
ient
s cr
osso
ver
(25
epile
ptic
s)
2 x
6 w
eeks
~~~~
Add
-on
No
Posi
tive
w w
00
Dod
rill
(197
5)
22 e
pile
ptic
out
patie
nts
Sulth
iam
e vs
PH
T
Sulth
iam
e: 4
00-3
600
Non
e Y
es
Neg
ativ
e cr
osso
ver
PHT
: 1:
4 of
sul
thia
me
2 X
6 m
onth
s do
se
Phen
ytoi
n (P
HT
).
339
in disturbed, mentally subnormal inpatients, 25 suffering from epilepsy, with no description of seizure types. EEGs were not reported. Psychometric eva- luation consisted of a behavior rating scale. The study concluded that sulthi- ame was effective in ameliorating disturbed behavior, but did not completely abolish any particular type of deviant behavior. A possible explanation for this observation is that sulthiame reduced the frequency of psychomotor seizures (clinical and subclinical). It is highly conceivable that this particular patient sample suffered from this type of seizures. This is further substan- tiated by the fact that the very same patients had had no benefit from neuro- leptic treatment in a previous controlled trial.
Dodrill 1975 evaluated sulthiame versus PHT in epileptic outpatients with no description of psychopathology. Blood levels were reported (Green et al. 1974). Psychometric measurements comprised cognitive, motor, perceptual and social functioning tests, among other WAIS and Halstead Battery. The result showed an impairment of epilepsy regulation and mental functioning while on sulthiame. However, it must be emphasised that 46 out of 67 of the original patient sample dropped out because of sulthiame side effects, which supports the assumption that the majority of the patients were intoxicated because of the high doses.
VALPROIC ACID (VPA)
The chemical structure of VPA differs completely from the other antiepilep- tics, e.g. there is no ring structure and no nitrogen atoms.
VPA has been reported to increase the GABA concentration by inducing changes in the balance between the GABA synthetizing enzyme glutamate decarboxylase and the GABA catabolizing enzymes GABA-transaminase and/or succinic semialdehyde dehydrogenase by inhibiting the latter ones (Meldrum 1978). Furthermore, it has been suggested that there exists a reciprocal interaction between dopamine and GABA neurons (Fuxe et al. 1978), with a preferential inhibitory gabergic control of dopamine turnover (Fuxe ef al. 1975). Accordingly, the action of VPA on GABA might imply that VPA possesses a psychotropic effect of its own.
Sonnen et al. (1975) (Table 6) reported a study of VPA versus placebo in epileptic patients with behavior and personality disorders characterized by disruptive behavior, aggressiveness and impulsivity. A self-devised rating scale was administered to quantify behavior disorder, psychopathology and cognitive performance. No psychotropic action of VPA was disclosed.
Sommerbeck et al. (1977) published a trial on subnormal epileptic in- patients comparing VPA to placebo. For psychometric evaluation 11 tests were applied, mainly investigating cognitive, perceptual and motor function- ing. Neither behavior nor psychopathology were assessed. The study showed that VPA impaired performance with respect to reaction time and tempo.

Tab
le 6
. Con
trol
led
stud
ies
on p
sych
otro
pic
actio
n of
val
proi
c ac
id (
VP
A)
Aut
hor
Subj
ects
D
esig
n D
oses
C
onc
trea
Blo
od
omita
nt
leve
ls
Psyc
hotr
opic
itm
ent
repo
rted
ef
fect
w
0
Sonn
en e
t al
. (1
975)
27
epi
lept
ics
with
V
PA v
s pl
acob
o cr
oss-
V
PA 9
00
No
info
rmat
ion
No
P
pers
onal
ity a
nd b
e-
over
2 X
3 weeks
None
havi
or d
isord
ers
Som
mer
beck
et
al.
20 s
ubno
rmal
epi
lept
ic
VPA
vs
plac
ebo
cros
s-
VPA
30m
g/kg
Se
rum
lev
els
Yes
Neg
ativ
e (1
977)
in
patie
nts
over
2 X
8 weeks
kept
con
stan
t

341
DISCUSSION
The neurochemical evidence for psychotropic effects of antiepileptic drugs - perhaps except for carbamazepine - is still in the speculative stage, even though several of the drugs have been in use for decades.
Today it is widely accepted that whenever possible, controlled clinical designs should be preferred to uncontrolled studies, in order to minimize bias. In evaluating the problem of psychotropic effect, the biases are of such dimensions, that uncontrolled observations permit no definite conclusions. Therefore, this survey reports only on controlled trials.
Besides a possible placebo effect, three entirely separate phenomena could account for the psychotropic effect demonstrated in uncontrolled and in some of the controlled studies.
1) Substitution of more toxic and sedative anticonvulsants for less toxic substances.
2) Reduction in both clinical and subclinical seizures which might cause improvement in behavior and performance. This is especially true for ETO and VPA in reducing ictal and interictal activity in primary, generalized sei- zures and for CBZ in regulation of subclinical complex partial seizures. In assessment of such a mechanism, it would be of value to supply psycho- metrics with telemetric investigations. Most of the patients described both in uncontrolled and controlled trials are chronic epileptics with severe brain damage and thus exhibit a great variety of seizure types.
3) Inclusion of apathetic, deteriorated backward organic patients in a study often involves a more active attitude to and social contact with the patients, both resulting in correction of deviant behavior.
In our opinion the majority of the studies presented lack or possess in- adequate operational definitions of the psychotropic effect. This inadequacy in hypothesis formation resulted in investigation of heterogeneous patient groups disclosing heterogeneous psychopathology.
In several studies no attention was paid to spontaneous fluctuations of psychological status, as no baseline evaluation was performed. It should be recommended to commence the investigations with a period where such fluctuations can be [quantified and taken into account when overall results are being assessed.
Very few of the studies applied EEG recordings or measurement of drug levels.
On basis of the studies referred to, it seems justified to postulate that con- trary to the enthusiasm presented in numerous uncontrolled reports, there exists no scientifically proven, genuine psychotropic action of antiepileptic drugs.
To illustrate our conclusion, we find that the following quotation from

342
Sonnen et al. (1975) serves the purpose: “The results most encountered in medicine, irrespectively the nature of investigation, are 1/3 excellent, 1/3 good and 1/3 no effect. If the results were as good as these optimistic reports mentioned, the number of patients with behavioral problems should diminish exponentially with 2/3 again and again with every new drug”.
REFERENCES Ayala, G. F. (1979): Electrophysiological studies in neuronal systems. Mechanisms of
Action of Antiepileptic Drugs, eds. D. M. Woodbury, J. K. Penry & H. G. Glaser. Raven Press, New York. In press.
Cereghino, J. J., J. T. Brock, J. C. van Meter, J. Kiffin Penry, L. D. Smith & B. G. White (1974): Carbamazepine for epilepsy. A controlled prospective evaluation. Neurol. 24, 401-410.
Dalby, M. A. (1975): Behavioural effects of carbamazepine. Advances in Neurology, eds. I. K. Penry & D. D. Daly, vol. 11, pp. 331-344. Raven Press, New York.
Delorenzo, R. J. & S. D. Freedman (1977): Possible role of calcium-dependent protein phosphorylation in mediating neurotransmitter release and anticonvulsant action. Epilepsia 18, 357-365.
Dodrill, C. B. (1975): Effects of sulthiame upon intellectual, neuropsychological and so- cial functioning abilities among adult epileptics: Comparison with diphenylhydan- toin. Epilepsia 16, 617-625.
Dodrill, C. B. & A. S. Troupin (1977): Psychotropic effects of carbamazepine in epilepsy: A double-blind comparison with phenytoin. Neurol. 27, 1023-1028.
Ferrendelli, J. A. & D. A. Kinscherf (1977): Phenytoin: Effects on calcium flux and cyclic nucleotides. Epilepsia 18, 331-336.
Ferrendelli, J. A. (1979): Succinimides. Mechanisms of Action of Antiepileptic Drugs, ed. D. M. Woodbury, J. K. Penry & H. G. Glaser. Raven Press, New York. In press.
Fuxe, K., T. Hokfelt, A. Ljungdahl, L. Agnati, 0. Johansson & M. Perez de la Mora (1975): Evidence for an inhibitory gabergic controll of the meso-limbic dopamine neurons: Possibility of improving treatment of schizophrenia by combined treatment with neuroleptics and gabergic drugs. Med. Bid. 53, 177-183.
Fuxe, K. & T. Hokfelt (1978): Amino Acid-containing Neurons. Principles of Psycho- pharmacology, eds. W. G. Clark & J. del Guidice, pp. 87-89. Academic Press, New York.
Green, J. R., A. S. Troupin, L. M. Halpern, P. Friel & P. Kanarek (1974): Sulthiame: EvaIuation as an anticonvulsant. Epilepsia 15, 329-349.
Groh, Ch., F. Rosenmayr & N. Birbaumer (1971): Psychotrope Wirkung von Carba- mazepin bei nicht-epileptischen Kindern. Med. Mschr. 25, 329-333.
Koella, W. P., P. Levin & V. Baltzer (1976): The pharmacology of carbamazepine and some other anti-epileptic drugs: Epileptic seizures-behaviour-pain, ed. W. Birk- mayer, pp. 32-50. Hans Huber Publishers, Berne.
Lefkowitz, M. M. (1969): Effects of diphenylhydantion on disruptive behaviour. Study of male delinquents. Arch. Gen. Psychiat. 20, 643-651.
Lynn Smith, W., M. J. Phillipus & H. L. Guard (1968): Psychometric study of children with learning problems and 14-6 postive spike EEG patterns, treated with etho- suximide (Zarontin) and placebo. Arch. Dis. Childh. 43, 616-619.
Malitz, S. & M. Kanzler (1971): Are antidepressants better than placebo? Am. J. Psy- chiat. 127, 1605-1611.
Marjerrison, G., S. M. Jedlicki, R. P. Keogh, W. Hrychuk, R. P. N. & G. M. Poulakakis

343
(1968): Carbamazepine: Behavioral, anticonvulsant and EEG ef€ects in chronically- hospitalized epileptics. Dis. Nerv. Syst. 29, 133-136.
Meldrum, B. S. (1978): Gamma-aminobutyric acid and the search for new anticonvulsant drugs. Lancet 2, 304-306.
Moffat,W.R., A.R.Siddiqui & D.N.Macay (1970): The use of sulthiame with dis- turbed mentally subnormal patients. Br. J. Psychiat. 117, 673-678.
Pryse-Phillips, W. E. M. & P. M. Jeavons (1970): Effect of carbamazepine (Tegretol) on the electroencephalograph and ward behaviour of patients with chronic epilepsy. Epilepsia 11, 263-273.
Puente, R.M. (1976): The use of carbamazepine in the treatment of behavioral dis- orders in children. Epileptic seizures-behaviour-pain, ed. W. Birkmayer, pp. 243- 252. Hans Hubers Publishers, Berne.
Rajotte, P., W. Jilek, L. Jilek, A. Perales, N. Giard, I.-M. Bordeleau & L. TBtreault (1967): PropriCtBs antikpileptiques et psychotropes de la carabamazkpine (TBgrBtol). L'Union MBd. du Canada 96, 1200-1206.
Rodin, E. A., C. S. Rim & P. M. Rennick (1974): The effects of carbamazepine on pa- tients with psychomotor epilepsy: Results of a double-blind study. Epilepsia 15,
Sommerbeck, K. W., A. Theilgaard, K. E. Rasmussen, V. Lehren, L. Gram & K. Wulff (1977): Valproate sodium: Evaluation of so-called psychotropic effect. A controlled study. Epilepsia 18, 159-166.
Sonnen, A.E.H., W.H. Zelvelder & J. H. Bruens (1975): A double-blind study of the influence of dipropylacetate on behaviour. Controlled Trials of Antiepileptic Drugs, ed. M. Dam, pp. 43-47. (Acta Neurol. Scand. suppl. 60). Munksgaard, Copenhagen.
Stephens, J. H. & J. W. Shaffer (1970): A controlled study of the effect of diphenyl- hydantoin on anxiety, irritability and anger in neurotic outpatients. Psychopharma- cologia (Berl.) 17, 169-181.
Stephens, J. H., J. W. Shaffer & C. C. Brown (1974): A controlled comparison of the effects of diphenylhydantoin and placebo on mood and psychomotor functioning in normal volunteers. J. Clin. Pharmacol. 14, 543-551.
Troupin, A., L. M. Ojemann, L. Halpern, C. Dodrill, R. Wilkins, P. Friel & P. Feigl (1977): Carbamazepine. A double-blind comparison with phenytoin. Neurol. 27,
Troupin, A. S. (1978): Carbamazepine in epilepsy. Clinical Neuropharmacology, ed. H. L. Klawans, vol. 3, pp. 15-16. Raven Press, New York.
Uhlenhuth, E. H., J. H. Stephens, B. H. Dim & L. Covi (1972): Diphenylhydantoin and phenobarbital in the relief of psychoneurotic symptoms. A controlled comparison. Psychopharmacologia (Berl.) 27, 67-84.
Wolf, P. (1976): The prevention of alternative epileptic psychosis in outpatients. Epilep- tology, ed. D. Janz, pp. 75-79. Gemg Thieme Publishers, Stuttgart.
Woodbury, D. M. (1979): Carbonic anhydrase inhibitors. Mechanisms of Action of Anti- epileptic Drugs, eds. D. M. Woodbury, J. K. Penry & H. G. Glaser, Raven Press, New York. In press.
547-561.
51 1-519.
Received August 8, accepted October 11, 1979
Josef Parnas, M.D. Dept. of Psychiatry Kommunehospitalet aster Farimagsgade 3 DK-1399 Copenhagen K Denmark