
Summers v. Earth Island Institute's Misuse of Lyons's Realistic ...
REVIEW PAPER
Psychosocial treatments for people with co-occurring severe mental
illness and substance misuse: systematic review
Michelle Cleary, Glenn E. Hunt, Sandra Matheson & Garry Walter
Accepted for publication 25 September 2008
Correspondence to M. Cleary:
e-mail: [email protected]
Michelle Cleary PhD RN
Clinical Associate Professor Mental Health
Faculty of Nursing and Midwifery, University
of Sydney,
and Clinical Nurse Consultant
Research Unit, Sydney South West Area
Mental Health Service, New South Wales,
Australia
Glenn E. Hunt PhD
Senior Research Fellow
Discipline of Psychological Medicine,
University of Sydney and Research Unit,
Sydney South West Area Mental Health
Service, New South Wales, Australia
Sandra Matheson BSc
Research Officer
Research Unit, Sydney South West Area
Mental Health Service, New South Wales,
Australia
Garry Walter MBBS BMedSc PhD
Professor of Child and Adolescent Psychiatry
University of Sydney,
and Area Clinical Director
Child and Adolescent Mental Health
Services, Northern Sydney Central Coast
Health, New South Wales, Australia
CLEARY M., HUNT G.E. , MATHESON S. & WALTER G. (2009)CLEARY M., HUNT G.E. , MATHESON S. & WALTER G. (2009) Psychosocial
treatments for people with co-occurring severe mental illness and substance misuse:
systematic review. Journal of Advanced Nursing 65(2), 238–258
doi: 10.1111/j.1365-2648.2008.04879.x
AbstractTitle. Psychosocial treatments for people with co-occurring severe mental illness and
substance misuse: systematic review.
Aim. This study is a report of a systematic review to assess current evidence for the
efficacy of psychosocial interventions for reducing substance use, as well as improving
mental state and encouraging treatment retention, among people with dual diagnosis.
Background. Substance misuse by people with a severe mental illness is common and
of concern because of its many adverse consequences and lack of evidence for effective
psychosocial interventions.
Data sources. Several electronic databases were searched to identify studies published
between January 1990 and February 2008. Additional searches were conducted by
means of reference lists and contact with authors.
Review methods. Results from studies using meta-analysis, randomized and non-
randomized trials assessing any psychosocial intervention for people with a severe
mental illness and substance misuse were included.
Results. Fifty-four studies were included: one systematic review with meta-analysis,
30 randomized controlled trials and 23 non-experimental studies. Although some
inconsistencies were apparent, results showed that motivational interviewing had the
most quality evidence for reducing substance use over the short term and, when
combined with cognitive behavioural therapy, improvements in mental state were also
apparent. Cognitive behavioural therapy alone showed little consistent support.
Support was found for long-term integrated residential programmes; however, the
evidence is of lesser quality. Contingency management shows promise, but there were
few studies assessing this intervention.
Conclusion. These results indicate the importance of motivational interviewing in
psychiatric settings for the reduction of substance use, at least in the short term.
Further quality research should target particular diagnoses and substance use, as some
interventions may work better for some subgroups.
Keywords: dual diagnosis, nursing, psychosocial treatments, severe mental illness,
substance misuse, systematic review
238 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd
J A N JOURNAL OF ADVANCED NURSING

Introduction
Having a lifetime severe mental illness is associated with
increased risk of having an alcohol or drug use disorder when
compared to people without severe mental illness (Regier
et al. 1990, Kessler et al. 1997, Kavanagh et al. 2004a). Even
patients with a mental illness who use substances in mild
doses can experience adverse effects, such as high rates of
relapse, treatment non-compliance, distorted perception and
cognition, suicidal ideation, incarceration, homelessness,
injury and disease, such as hepatitis (Dickey et al. 2000,
Barrowclough et al. 2001, Bennett et al. 2001, Carey et al.
2004, Todd et al. 2004, Hawton et al. 2005, Ziedonis et al.
2005, Janssen et al. 2006, Gregg et al. 2007).
People with mental illness use substances for a variety of
reasons, including the relief of depression, anxiety, boredom
or to relax and socialize (Addington & Duchak 1997, Fowler
et al. 1998), and they may benefit from psychosocial
interventions that target their substance use. Psychosocial
interventions in mental health settings are those that are non-
pharmaceutical, such as cognitive behavioural therapy (CBT)
and motivational interviewing (MI). They may be offered in a
variety of settings, can vary in intensity and duration, and
may be part of an integrated treatment programme. Inte-
grated programmes involve both the mental health and
substance use problems being treated simultaneously, within
the same service by the same clinician or team of clinicians.
Research into the effectiveness of psychosocial interven-
tions for reducing substance use by people with a severe
mental illness is still evolving. A recent Cochrane review
(Cleary et al. 2008) with a meta-analysis of 25 randomized
controlled trials (RCTs) and two recent descriptive reviews
(Donald et al. 2005, Tiet & Mausbach 2007) that included
RCTs and non-experimental studies, showed that no single
psychosocial treatment was superior to any other. In contrast,
other reviews including RCTs and non-experimental studies
have shown support for particular psychosocial interven-
tions, but with inconsistent results. For example, support has
been found for a motivational approach (Mueser et al. 2005,
Barrowclough et al. 2006, Laker 2007), group therapies
(Mueser et al. 2005, Drake et al. 2008), contingency
management (Drake et al. 2008) and residential programmes
(Drake et al. 2004, 2008, Mueser et al. 2005), as well as for
integrated models of treatment delivery (Drake et al. 1998b,
2004, Barrowclough et al. 2006, Tsuang et al. 2006).
Intensive case management (Dumaine 2003) and assertive
community treatment (ACT; Drake et al. 1998b) have,
however, received limited support. Notwithstanding this,
not all types of interventions were assessed in all reviews. For
example, Laker (2007) assessed only MI, Drake et al. (1998b)
assessed integrated care and Drake et al. (2008), Mueser et al.
(2005), Tiet and Mausbach (2007) and Tsuang et al. (2006)
were the only reviews to include contingency management
studies.
Conclusions from reviews may differ for a variety of
reasons. First, the way in which individual studies are
conducted may differ in terms of patient demographics,
settings, outcome measures and varying degrees of fidelity to
treatment standards. While most studies test one intervention
against a control condition (usually standard care), some
assess combinations of treatment components (e.g. Bellack
et al. 2006) and some compare one intervention with another
(e.g. Jerrell & Ridgely 1995). This makes allocating studies to
particular intervention categories difficult.
Different inclusion criteria also contribute to inconsistent
results. A recent Cochrane review (Cleary et al. 2008)
included only quality RCTs as these are considered more
reliable (Howland 2007), whereas other reviews have
included both RCTs and lesser quality, quasi-random or
non-random studies. Over-inclusiveness can be problematic.
For example, Drake et al. (2008) concluded that no consis-
tent evidence was available from eight RCTs of individual
interventions, and more consistent evidence was found for
residential treatment programmes; however, only one of the
12 studies assessing residential programmes was an RCT.
Thus, drawing conclusions based on combined results of
quality RCTs and lesser quality quasi-randomized and non-
randomized trials can be unreliable.
However, conducting RCTs at the best of times can be
challenging (Essock et al. 2003). Other study designs can also
provide useful and reliable information (Howland 2007), and
can assist to develop a more integrated picture of the
evidence, especially when combining studies with high
heterogeneity (Des Jarlais et al. 2004). Further, excluding
data from non-randomized trials may bias the evidence
towards interventions that are ‘easier’ to evaluate in an RCT
(Des Jarlais et al. 2004). Finally, taking into consideration the
issue of quality when drawing conclusions from a variety of
trials provides a more reliable and contemporary summary of
the available evidence. In view of these factors, it was
considered timely to undertake a systematic review of
psychosocial treatments for people with co-occurring severe
mental illness and substance misuse (dual diagnosis).
The review
Aim
The aim of this review was to assess the current evidence for the
efficacy of psychosocial interventions for reducing substance
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 239

use, as well as improving mental state and encouraging
treatment retention, among people with dual diagnosis.
Design
The guiding framework for this systematic review came from
recommendations of the Cochrane Collaboration Handbook
(Higgins & Green 2006) and the Australian National Health
and Medical Research Council (1999, 2000).
Search methods
Electronic searching was performed through the Cochrane
Schizophrenia Group Register and the Cochrane Central
Register of Controlled Trials, as well as CINAHL, PsycINFO,
Ovid Medline and PubMED. The following search phrases
and strategies were used: diagnosis-dual-psychiatry.mp,
schizo$ or SMI or bipolar or depression; comorbidity or
substance$ or drug abuse and mental$ and intervention or
clinical trial or intervention and further limitations were
publication in English, the time period January 1990 to
February 2008, and randomised or randomiz$ or trial.
Further searching was undertaken by means of reference lists
and contact with authors.
Inclusion criteria
• Any RCT, quasi-randomized or non-randomized trial of
varying quality with an independent comparison group of
any psychosocial intervention for people with a severe
mental illness (e.g. schizophrenia, schizoaffective disorder,
bipolar disorderormajordepression) andsubstancemisuse.
• Minimum of 10 participants in the experimental treat-
ment group.
• Outcomes must include substance use, mental state and/or
treatment retention.
• Any systematic review that includes a meta-analysis of
results from quality RCTs meeting the above criteria.
Exclusion criteria
• Studies including participants with less severe mental ill-
ness, such as personality disorders, unless a vast majority
had severe mental illness (>90%), or if those with severe
illness were reported separately.
• Reviews with pooled results from both RCTs and non-
experimental studies.
Search outcome
Diagnosis-dual-psychiatry (1750 hits) combined with
(schizo$ or SMI or bipolar or depression) resulted in 664
hits using the Medline database. Limits of English and 1990–
2008 reduced the number to 639. The following search terms
– comorbidity or substance$ or drug abuse and mental$ and
(intervention or clinical trial or random$) – resulted in 1953
hits with limitations of year (1990–2008) using PsycINFO.
This was further reduced to 417 hits when combined with the
following search – motivation$ or cognitive behaviour
therapy or psychosocial or integrated or assertive. Other
searches using the above terms on Medline, CINAHL,
PubMED and Cochrane register of controlled trials resulted
in a further 400 hits. The above searches were entered into a
Reference Manager database and, after duplicates were
excluded and other non-relevant studies deleted, this left
377 studies for further review. Of these, 92 were identified as
relevant and were examined to determine whether they met
inclusion criteria by two independent reviewers and grouped
by type of intervention.
Quality appraisal
This review followed quality guidelines as outlined by the
Australian National Health and Medical Research Council
(National Health and Medical Research Council 1999, 2000)
and the QUOROM statement for systematic reviews (Turpin
2005). RCTs are deemed of the highest quality, with the most
reliable results. Further, pooling RCT results into a meta-
analysis can provide additional quality evidence. Quality
RCTs, randomize participants using methods such as com-
puter-generated random number allocation sequences, con-
cealed to reduce the possibility of manipulating allocation
(Schulz & Grimes 2002a, Howland 2007). Although
researcher(s) may state that their trial is ‘randomized’, in
this review they were categorized as non-experimental if
participants were quasi-randomized (e.g. clinician, alternate
assignment or date of presentation allocation). Even methods
used to generate simple randomization sequences, such as
coin-tossing or dice-throwing may be manipulated and lead
to an unequal distribution of confounding factors across
groups (Schulz & Grimes 2002c). All clinical trials reports
should include baseline demographics and clinical character-
istics of each group.
Another quality issue is whether outcome raters are blind to
treatment condition (Schulz & Grimes 2002b). This is partic-
ularly important when subjective, self-report measures are
recorded as those assessing the person may intentionally or
unintentionally bias the results. This issue is not as important
when objective data, such as hospitalization rates, are collected
(National Health and Medical Research Council 1999, 2000).
Adequate sample size is important to ensure that there is
enough power to detect differences between groups (van den
M. Cleary et al.
240 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

Brink et al. 2006). However, high rates of attrition (>50%)
are not uncommon in this area of research, and participants
remaining in the treatment group may be more amenable to
treatment than those leaving the study early. Intention-
to-treat (ITT) analysis considers all those at the time of
randomization to be included in the final analysis.
Data abstraction and synthesis
Two independent reviewers extracted data and information
to be included in the tables. The reviewers were not blind to
the authors of the study. Type of study design, sample size,
participant characteristics, details of interventions and out-
come measures with time periods were noted. Statistically
significant results were recorded in the tables when individual
studies showed between group differences at P < 0Æ05, with
or without statistical adjustment or adjusted means. In this
review, we employed a narrative synthesis as there were
limited data that could be pooled due to heterogeneity in
designs, interventions and outcome measures. The quality of
the studies was assessed by details of randomization, alloca-
tion concealment, blinding, ITT analyses, attrition (noted if
>50%) and any baseline group differences were noted in the
tables. If these quality issues were not reported or if reporting
was unclear, this was also noted in the tables.
Classification of psychosocial interventions
Studies were categorized into the following: CBT, MI,
combined CBT and MI, group therapies, integrated ACT,
intensive case management, residential programmes, contin-
gency management and forensic settings. Where two or three
treatment components were combined (e.g. Bellack et al.
2006), the study was categorized according to the main
intervention being tested, and a footnote was made in the
other relevant tables. Where two or three treatment arms
were compared (e.g. Jerrell & Ridgely 1995), each treatment
arm was categorized to the corresponding intervention.
Cognitive behavioural therapy can be offered in individual
or group format (Kleber et al. 2007). The core features of
CBT are functional analysis of the link between mental state
and drug use, understanding the reasons for and conse-
quences of use, and skills training for recognizing and
avoiding vulnerable situations. The aim of CBT is to correct
the thoughts, feelings and actions of the recipient to promote
alternative ways of coping and to encourage treatment
adherence (Schmitz et al. 2002, Weiss et al. 2007).
Motivational interviewing is intended to enhance the
individual’s intrinsic motivation for change (Strong
Kinnaman et al. 2007) and can also be delivered in individual
or group format. The intervention matches the patient’s level
of problem recognition with specific strategies and goals. MI
is based on four principles: expressing empathy, developing
discrepancy, supporting self-efficacy and rolling with resis-
tance (Chanut et al. 2005), and is directed at five stages: pre-
contemplation, contemplation, preparation, action and main-
tenance (Tsuang et al. 2006).
Dual diagnosis group therapies such as Double Trouble in
Recovery (Magura et al. 2003) aim to improve interpersonal
and problem-solving skills to assist in establishing and
maintaining relationships with others, dealing with conflict
and handling social situations involving substance misuse
(Jerrell & Ridgely 1995, Mueser et al. 2005). They aim to
change social attitudes and behaviours, are potentially cost-
effective and provide a structure for daily living, along with a
commitment to stopping substance use (Mueser et al. 2005,
Tsuang et al. 2006).
Integrated ACT unifies mental health and substance use
services so that clients do not need to negotiate separate
treatment programmes (McHugo et al. 1999, Mueser et al.
2005). A multidisciplinary team of clinicians in one setting
provides long-term coordinated treatment which is tailored to
the individual’s readiness for change (Barrowclough et al.
2006, Green et al. 2007). The caseload is low (10–15 clients),
frequent home visits are made, and reluctant or uncoopera-
tive clients are actively contacted and offered services. For
studies to be placed under this category, they must have
offered both active outreach and integrated services.
Intensive case management and non-integrated ACT are
similar to integrated ACT, both having lower case loads than
standard case management and often coordinating mental
health and substance use services to suit individual clients’
needs. However, they may or may not offer both mental
health and substance use services directly, and often organize
additional substance use treatments for their clients.
Residential programmes are offered in-house and involve
differing durations and differing treatment components. Low
intensity programmes place few sanctions and demands on
residents and are flexible in accommodating individual needs.
Higher intensity programmes usually offer more treatment
components and are more demanding; privileges and rules of
conduct are well-defined and abstinence is usually a
prerequisite for the participant to stay in the residential
programme.
Contingency management is generally provided by way of
monetary reward or prizes dependent on reductions in or
abstinence from substances, usually measured by urinalysis/
breathalyser and self- report.
Forensic intervention studies included any study conducted
exclusively with inmates, ex-inmates or those diverted from
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 241

jail or court settings. These involve a variety of interventions,
from intensive case management to diverting people with a
dual diagnosis to treatment programmes.
Results
Of the 92 studies examined in full, 15 were reviews, of
which 13 were excluded because they were not conducted
systematically and/or did not include meta-analysis (Drake
et al. 1998b, 2004, 2008, Goldsmith & Garlapati 2004,
Rounsaville 2004, Donald et al. 2005, Mueser et al. 2005,
Barrowclough et al. 2006, Bogenschutz et al. 2006, Tsuang
et al. 2006, Brady et al. 2007, Laker 2007, Tiet &
Mausbach 2007). Another was excluded because data were
pooled from both RCTs and non-experimental studies
(Dumaine 2003). Only one systematic review met the
inclusion criteria (Ley et al. 2001, updated Cleary et al.
2008).
From the remaining 77 studies, 15 were excluded because
most or all of the study population did not have severe mental
illness (Mowbray et al. 1999, DiNitto et al. 2002, Hulse &
Tait 2002) and three (Brown et al. 1997, Milby et al. 2000,
Sacks et al. 2008b) included participants who did not meet
diagnostic criteria; rather, they had elevated symptom
ratings. Nine studies targeted participants with post-trau-
matic stress disorder, anxiety or personality disorders (Fisher
& Bentley 1996, Linehan et al. 1999a, 1999b, Bowen et al.
2000, Randall et al. 2001, Hien et al. 2004, Morrissey et al.
2005, Cohen & Hien 2006, Watt et al. 2006).
Of the remaining 62 papers, nine were adjunct publications
of other studies (Rahav et al. 1995, French et al. 1999,
Brooks & Penn 2003, Haddock et al. 2003, Sacks et al. 2004,
Timko & Sempel 2004a, Calsyn et al. 2005, Brown et al.
2006, Timko et al. 2006). This left 30 RCTs, 23 non-
experimental studies and one systematic review meeting
all inclusion criteria, totalling 54 studies with 11,734
participants.
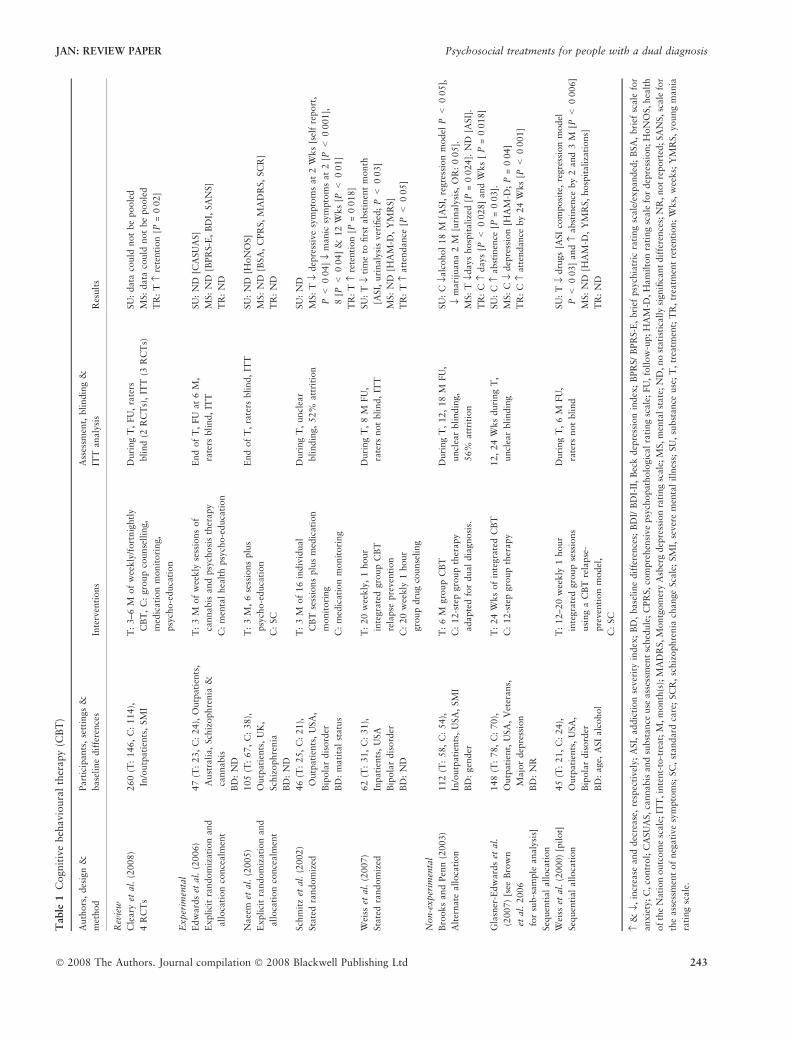
Cognitive behavioural therapy
Eight studies (n = 565, see Table 1) showed limited support
for CBT in reducing substance use or improving mental state.
The two RCTs of highest quality (Naeem et al. 2005,
Edwards et al. 2006) reported no statistically significant
differences between groups on measures of substance use and
mental state. Only one RCT and one non-experimental study
reported reduced substance use and both had design flaws.
Weiss et al. (2007) did not make explicit their randomization
methods and in an earlier study used a non-experimental
design (Weiss et al. 2000). Both used raters who were not
blind to the treatment condition, although self-reported
substance use was verified by urinalysis.
One RCT (Schmitz et al. 2002) showed reduced manic
symptoms at the end of 3 months of treatment and one non-
experimental study (Brooks & Penn 2003) yielded fewer
hospital days. Schmitz et al. (2002) did not make explicit the
randomization methods or whether raters were blind to
treatment condition and found that reduced depressive
symptoms lasted for 2 weeks only. Brooks and Penn (2003)
used a non-random design and, while the treatment group
spent fewer days in hospital, no differences in psychiatric
symptoms were reported on the Addiction Severity Index
(ASI). Further, they reported reduced substance use for their
control group receiving 12-step group therapy; this was
similar to another non-experimental study (Glasner-Edwards
et al. 2007) that also showed reduced depressive symptoms
and increased treatment retention in a 12-step control group.
The findings of increased retention (Schmitz et al. 2002,
Weiss et al. 2007) drove the only statistically significant
pooled finding of the review (Cleary et al. 2008), with the
other two higher quality RCTs (Naeem et al. 2005, Edwards
et al. 2006) reporting no differences. We were unable to pool
much data due to skewness, differing outcome measures or
unclear reporting.
Motivational interviewing
In nine studies MI was assessed (n = 529, see Table 2). Four
of seven RCTs and one of two non-experimental studies
showed reductions in substance use. Kavanagh et al. (2004b)
made explicit their methods and ensured raters were blind to
treatment condition. They reported reduced substance use
lasting 12 months after 3 hours of MI; however, no differ-
ences were observed from the more conservative ITT anal-
ysis. Baker et al. (2002) also used blind raters and reported
reductions in polydrug use, yet this was not sustained after
3 months and no differences for alcohol and cannabis were
observed when data were analysed separately. Hickman
(1999) and Graeber et al. (2003) also reported reductions in
alcohol use after only one to three sessions, with effects
lasting between 3 and 4 months. Unfortunately, neither
stated whether outcome raters were blind to intervention
status, although they used self-report measures, so their
results may be biased. One non-experimental study (Santa
Ana et al. 2007) also showed reductions in alcohol consump-
tion and drug days lasting 1–3 months after two MI sessions.
However, there were no differences in abstinence rates or
days spent drinking. Daley et al. (1998) reported less time in
hospital and Hickman (1999) reported reduced symptoms on
some but not all SCL 90-R subscales.
M. Cleary et al.
242 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd
Table
1C
ognit
ive
beh
avio
ura
lth
erapy
(CB
T)
Auth
ors
,des
ign
&
met
hod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Rev
iew
Cle
ary
etal
.(2
008)
4R
CT
s
260
(T:
146,
C:
114),
In/o
utp
ati
ents
,SM
I
T:
3–6
Mof
wee
kly
/fort
nig
htl
y
CB
T,
C:
gro
up
counse
llin
g,
med
icati
on
monit
ori
ng,
psy
cho-e
duca
tion
Duri
ng
T,
FU
,ra
ters
bli
nd
(2R
CT
s),
ITT
(3R
CT
s)
SU
:data
could
not
be
poole
d
MS:
data
could
not
be
poole
d
TR
:T
›re
tenti
on
[P=
0Æ0
2]
Exper
imen
tal
Edw
ard
set
al.
(2006)
Expli
cit
random
izati
on
and
all
oca
tion
conce
alm
ent
47
(T:
23,
C:
24),
Outp
ati
ents
,
Aust
rali
a,
Sch
izophre
nia
&
cannabis
BD
:N
D
T:
3M
of
wee
kly
sess
ions
of
cannabis
and
psy
chosi
sth
erapy
C:
men
tal
hea
lth
psy
cho-e
duca
tion
End
of
T,
FU
at
6M
,
rate
rsbli
nd,
ITT
SU
:N
D[C
ASU
AS]
MS:
ND
[BPR
S-E
,B
DI,
SA
NS]
TR
:N
D
Naee
met
al.
(2005)
Expli
cit
random
izati
on
and
all
oca
tion
conce
alm
ent
105
(T:
67,
C:
38),
Outp
ati
ents
,U
K,
Sch
izophre
nia
BD
:N
D
T:
3M
,6
sess
ions
plu
s
psy
cho-e
duca
tion
C:
SC
End
of
T,
rate
rsbli
nd,
ITT
SU
:N
D[H
oN
OS]
MS:
ND
[BSA
,C
PR
S,
MA
DR
S,
SC
R]
TR
:N
D
Sch
mit
zet
al.
(2002)
Sta
ted
random
ized
46
(T:
25,
C:
21),
Outp
ati
ents
,U
SA
,
Bip
ola
rdis
ord
er
BD
:m
ati
tal
statu
s
T:
3M
of
16
indiv
idual
CB
Tse
ssio
ns
plu
sm
edic
ati
on
monit
ori
ng
C:
med
icati
on
monit
ori
ng
Duri
ng
T,
uncl
ear
bli
ndin
g,
52%
att
riti
on
SU
:N
D
MS:
Tfl
dep
ress
ive
sym
pto
ms
at
2W
ks
[sel
fre
port
,
P<
0Æ0
4]
flm
anic
sym
pto
ms
at
2[P
<0Æ0
01],
8[P
<0Æ0
4]
&12
Wks
[P<
0Æ0
1]
TR
:T
›re
tenti
on
[P=
0Æ0
18]
Wei
sset
al.
(2007)
Sta
ted
random
ized
62
(T:
31,
C:
31),
Inpati
ents
,U
SA
Bip
ola
rdis
ord
er
BD
:N
D
T:
20
wee
kly
,1
hour
inte
gra
ted
gro
up
CB
T
rela
pse
pre
ven
tion
C:
20
wee
kly
1hour
gro
up
dru
gco
unse
ling
Duri
ng
T,
8M
FU
,
rate
rsnot
bli
nd,
ITT
SU
:T
flti
me
tofirs
tabst
inen
tm
onth
[ASI,
uri
naly
sis
ver
ified
;P<
0Æ0
3]
MS:
ND
[HA
M-D
,Y
MR
S]
TR
:T
›att
endance
[P<
0Æ0
5]
Non-e
xper
imen
tal
Bro
oks
and
Pen
n(2
003)
Alt
ernate
all
oca
tion
112
(T:
58,
C:
54),
In/o
utp
ati
ents
,U
SA
,SM
I
BD
:gen
der
T:
6M
gro
up
CB
T
C:
12-s
tep
gro
up
ther
apy
adapte
dfo
rdual
dia
gnosi
s.
Duri
ng
T,
12,
18
MFU
,
uncl
ear
bli
ndin
g,
56%
att
riti
on
SU
:C
flalc
ohol
18
M[A
SI,
regre
ssio
nm
odel
P<
0Æ0
5],
flm
ari
juana
2M
[uri
naly
sis,
OR
:0Æ0
5].
MS:
Tfld
ays
hosp
itali
zed
[P=
0Æ0
24].
ND
[ASI]
.
TR
:C
›days
[P<
0Æ0
28]
and
Wks
[P
=0Æ0
18]
Gla
sner
-Edw
ard
set
al.
(2007)
[see
Bro
wn
etal
.2006
for
sub-s
am
ple
analy
sis]
Seq
uen
tial
all
oca
tion
148
(T:
78,
C:
70),
Outp
ati
ent,
USA
,V
eter
ans,
Majo
rdep
ress
ion
BD
:N
R
T:
24
Wks
of
inte
gra
ted
CB
T
C:
12-s
tep
gro
up
ther
apy
12,
24
Wks
duri
ng
T,
uncl
ear
bli
ndin
g
SU
:C
›abst
inen
ce[P
=0Æ0
3].
MS:
Cfl
dep
ress
ion
[HA
M-D
;P
=0Æ0
4]
TR
:C
›att
endance
by
24
Wks
[P<
0Æ0
01]
Wei
sset
al.
(2000)
[pil
ot]
Seq
uen
tial
all
oca
tion
45
(T:
21,
C:
24),
Outp
ati
ents
,U
SA
,
Bip
ola
rdis
ord
er
BD
:age,
ASI
alc
ohol
T:
12–20
wee
kly
1hour
inte
gra
ted
gro
up
sess
ions
usi
ng
aC
BT
rela
pse
-
pre
ven
tion
model
,
C:
SC
Duri
ng
T,
6M
FU
,
rate
rsnot
bli
nd
SU
:T
fldru
gs
[ASI
com
posi
te,
regre
ssio
nm
odel
P<
0Æ0
3]
and
›abst
inen
ceby
2and
3M
[P<
0Æ0
06]
MS:
ND
[HA
M-D
,Y
MR
S,
hosp
itali
zati
ons]
TR
:N
D
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;
ASI,
addic
tion
sever
ity
index
;B
D,
base
line
dif
fere
nce
s;B
DI/
BD
I-II
,B
eck
dep
ress
ion
index
;B
PR
S/
BPR
S-E
,bri
efpsy
chia
tric
rati
ng
scale
/expanded
;B
SA
,bri
efsc
ale
for
anxie
ty;C
,co
ntr
ol;
CA
SU
AS,
cannabis
and
subst
ance
use
ass
essm
ent
sched
ule
;C
PR
S,co
mpre
hen
sive
psy
chopath
olo
gic
al
rati
ng
scale
;FU
,fo
llow
-up;
HA
M-D
,H
am
ilto
nra
ting
scale
for
dep
ress
ion;
HoN
OS,hea
lth
of
the
Nati
on
outc
om
esc
ale
;IT
T,in
tent-
to-t
reat;
M,m
onth
(s);
MA
DR
S,M
ontg
om
ery
Asb
erg
dep
ress
ion
rati
ng
scale
;M
S,m
enta
lst
ate
;N
D,no
stati
stic
all
ysi
gnifi
cant
dif
fere
nce
s;N
R,not
report
ed;SA
NS,sc
ale
for
the
ass
essm
ent
of
neg
ati
ve
sym
pto
ms;
SC
,st
andard
care
;SC
R,
schiz
ophre
nia
change
Sca
le;
SM
I,se
ver
em
enta
lil
lnes
s;SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Wks,
wee
ks;
YM
RS,
young
mania
rati
ng
scale
.
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 243
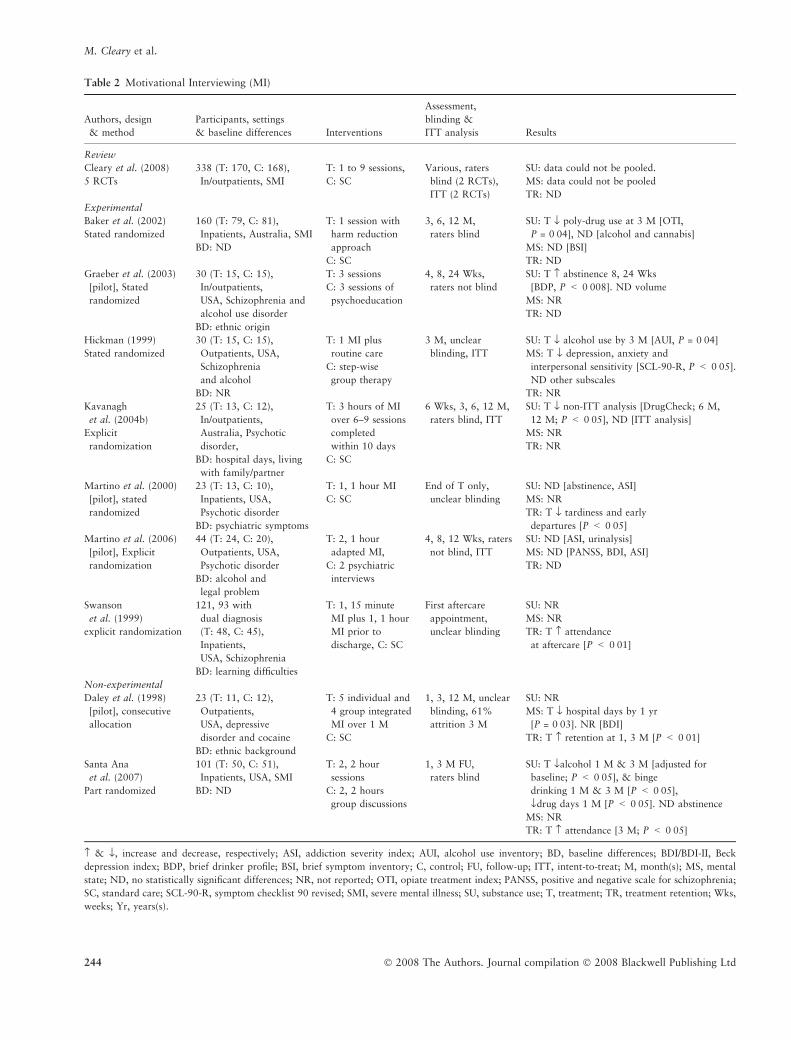
Table 2 Motivational Interviewing (MI)
Authors, design
& method
Participants, settings
& baseline differences Interventions
Assessment,
blinding &
ITT analysis Results
Review
Cleary et al. (2008)
5 RCTs
338 (T: 170, C: 168),
In/outpatients, SMI
T: 1 to 9 sessions,
C: SC
Various, raters
blind (2 RCTs),
ITT (2 RCTs)
SU: data could not be pooled.
MS: data could not be pooled
TR: ND
Experimental
Baker et al. (2002)
Stated randomized
160 (T: 79, C: 81),
Inpatients, Australia, SMI
BD: ND
T: 1 session with
harm reduction
approach
C: SC
3, 6, 12 M,
raters blind
SU: T fl poly-drug use at 3 M [OTI,
P = 0Æ04], ND [alcohol and cannabis]
MS: ND [BSI]
TR: ND
Graeber et al. (2003)
[pilot], Stated
randomized
30 (T: 15, C: 15),
In/outpatients,
USA, Schizophrenia and
alcohol use disorder
BD: ethnic origin
T: 3 sessions
C: 3 sessions of
psychoeducation
4, 8, 24 Wks,
raters not blind
SU: T › abstinence 8, 24 Wks
[BDP, P < 0Æ008]. ND volume
MS: NR
TR: ND
Hickman (1999)
Stated randomized
30 (T: 15, C: 15),
Outpatients, USA,
Schizophrenia
and alcohol
BD: NR
T: 1 MI plus
routine care
C: step-wise
group therapy
3 M, unclear
blinding, ITT
SU: T fl alcohol use by 3 M [AUI, P = 0Æ04]
MS: T fl depression, anxiety and
interpersonal sensitivity [SCL-90-R, P < 0Æ05].
ND other subscales
TR: NR
Kavanagh
et al. (2004b)
Explicit
randomization
25 (T: 13, C: 12),
In/outpatients,
Australia, Psychotic
disorder,
BD: hospital days, living
with family/partner
T: 3 hours of MI
over 6–9 sessions
completed
within 10 days
C: SC
6 Wks, 3, 6, 12 M,
raters blind, ITT
SU: T fl non-ITT analysis [DrugCheck; 6 M,
12 M; P < 0Æ05], ND [ITT analysis]
MS: NR
TR: NR
Martino et al. (2000)
[pilot], stated
randomized
23 (T: 13, C: 10),
Inpatients, USA,
Psychotic disorder
BD: psychiatric symptoms
T: 1, 1 hour MI
C: SC
End of T only,
unclear blinding
SU: ND [abstinence, ASI]
MS: NR
TR: T fl tardiness and early
departures [P < 0Æ05]
Martino et al. (2006)
[pilot], Explicit
randomization
44 (T: 24, C: 20),
Outpatients, USA,
Psychotic disorder
BD: alcohol and
legal problem
T: 2, 1 hour
adapted MI,
C: 2 psychiatric
interviews
4, 8, 12 Wks, raters
not blind, ITT
SU: ND [ASI, urinalysis]
MS: ND [PANSS, BDI, ASI]
TR: ND
Swanson
et al. (1999)
explicit randomization
121, 93 with
dual diagnosis
(T: 48, C: 45),
Inpatients,
USA, Schizophrenia
BD: learning difficulties
T: 1, 15 minute
MI plus 1, 1 hour
MI prior to
discharge, C: SC
First aftercare
appointment,
unclear blinding
SU: NR
MS: NR
TR: T › attendance
at aftercare [P < 0Æ01]
Non-experimental
Daley et al. (1998)
[pilot], consecutive
allocation
23 (T: 11, C: 12),
Outpatients,
USA, depressive
disorder and cocaine
BD: ethnic background
T: 5 individual and
4 group integrated
MI over 1 M
C: SC
1, 3, 12 M, unclear
blinding, 61%
attrition 3 M
SU: NR
MS: T fl hospital days by 1 yr
[P = 0Æ03]. NR [BDI]
TR: T › retention at 1, 3 M [P < 0Æ01]
Santa Ana
et al. (2007)
Part randomized
101 (T: 50, C: 51),
Inpatients, USA, SMI
BD: ND
T: 2, 2 hour
sessions
C: 2, 2 hours
group discussions
1, 3 M FU,
raters blind
SU: T flalcohol 1 M & 3 M [adjusted for
baseline; P < 0Æ05], & binge
drinking 1 M & 3 M [P < 0Æ05],
fldrug days 1 M [P < 0Æ05]. ND abstinence
MS: NR
TR: T › attendance [3 M; P < 0Æ05]
› & fl, increase and decrease, respectively; ASI, addiction severity index; AUI, alcohol use inventory; BD, baseline differences; BDI/BDI-II, Beck
depression index; BDP, brief drinker profile; BSI, brief symptom inventory; C, control; FU, follow-up; ITT, intent-to-treat; M, month(s); MS, mental
state; ND, no statistically significant differences; NR, not reported; OTI, opiate treatment index; PANSS, positive and negative scale for schizophrenia;
SC, standard care; SCL-90-R, symptom checklist 90 revised; SMI, severe mental illness; SU, substance use; T, treatment; TR, treatment retention; Wks,
weeks; Yr, years(s).
M. Cleary et al.
244 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

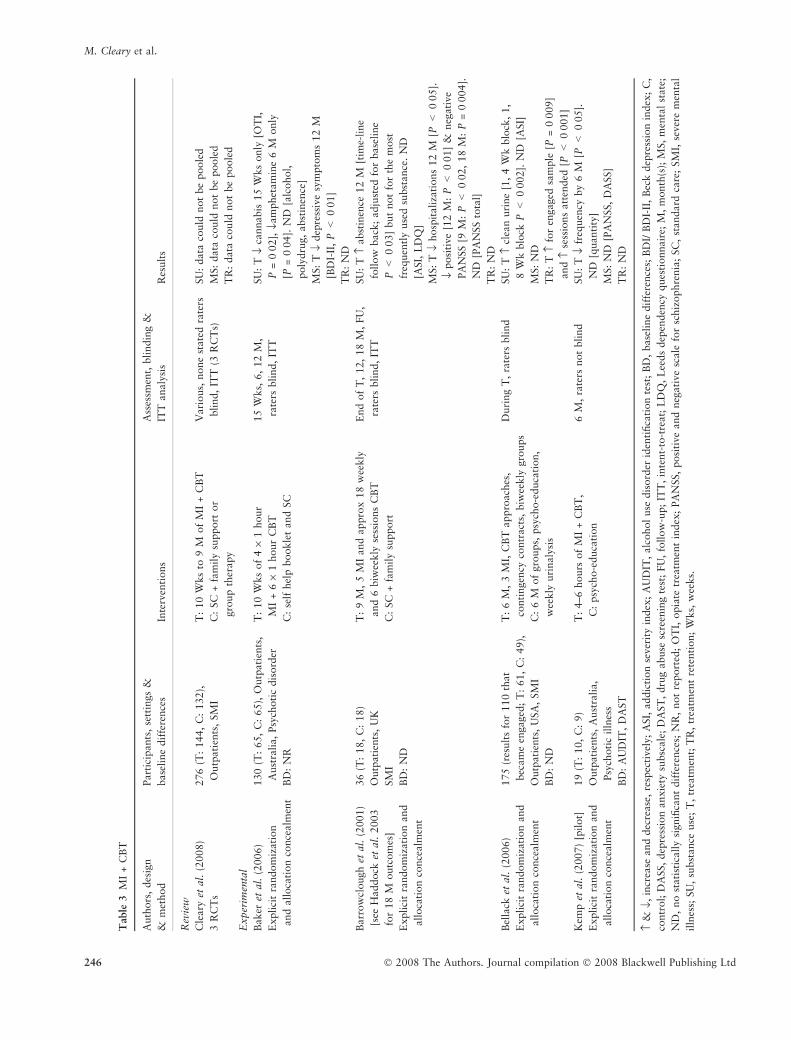
Motivational interviewing plus cognitive behavioural
therapy
All four RCTs assessing MI + CBT (n = 360, see Table 3)
reported statistically significant improvements in substance
use, and all made explicit their randomization methods,
although one did not ensure their raters were blind to
treatment condition (Kemp et al. 2007). In this study, non-
blinded clinician raters were used and reduced alcohol and
drug use were observed 6 months after 4–6 hours of therapy.
After 10 weekly sessions, Baker et al. (2006) reported
reductions in cannabis use by 15 weeks and amphetamine
use by 6 months; however, no differences were observed for
alcohol or polydrug use or any substance by 12 months. They
also reported improved depressive symptoms. Barrowclough
et al. (2001) reported more days abstinent at 12 months after
9 months of treatment, although this was not for the most
frequently-used substance and was not sustained at
18 months. This study also showed fewer hospitalizations
and improvements on positive and negative symptoms lasting
up to 18 months. Bellack et al. (2006) reported more clean
urine after 6 months of treatment and increased attendance,
but no reductions on ASI or mental state scores.
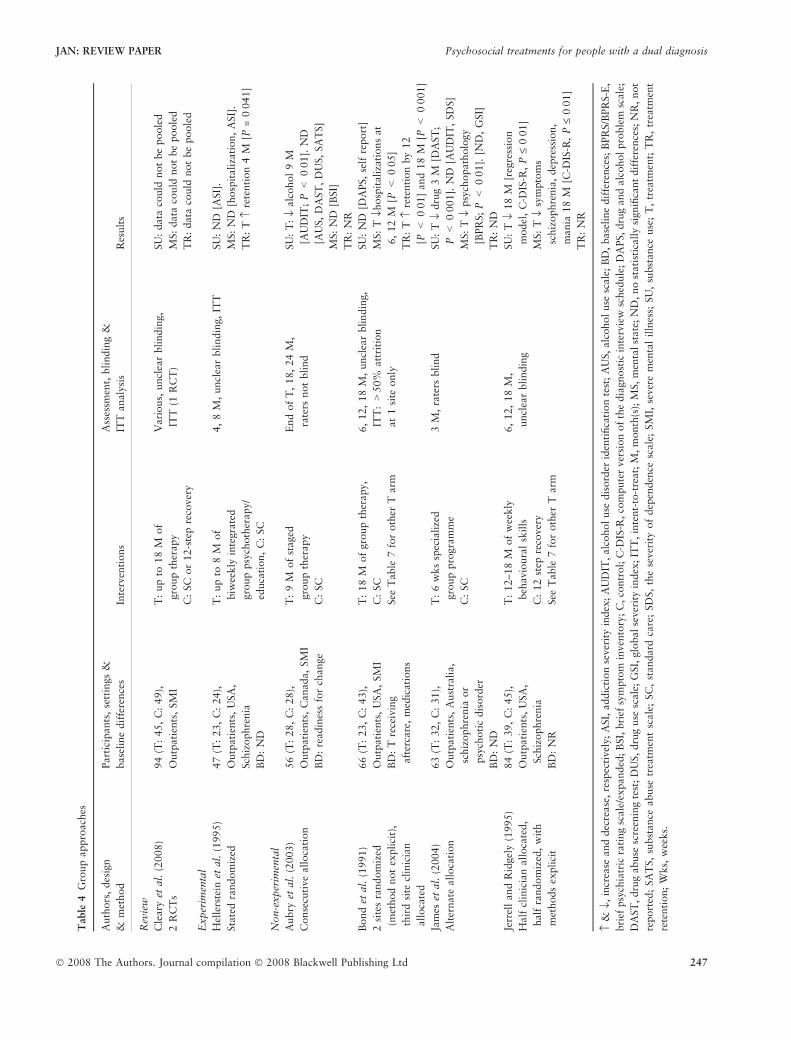
Group approaches
With group approaches, limited support was found from the
one RCT and four non-experimental studies (n = 316, see
Table 4). The one RCT (Hellerstein et al. 1995) showed
increased retention, but no differences between groups on
substance use or mental state after eight months of integrated
group psychotherapy. Aubry et al. (2003) reported reduced
alcohol use after 9 months of staged group therapy; however,
this was limited to one (AUDIT) of five substance use
measures. After 6 weeks of group therapy, James et al. (2004)
reported reduced drug use and psychopathology, but no
differences for alcohol or dependence and symptom severity.
In a partly-randomized study, Jerrell and Ridgely (1995)
reported reduced alcohol and drug use and improved
psychopathology after 18 months of behavioural skills group
therapy. Bond et al. (1991) reported fewer hospitalizations
and increased treatment retention after 12 months of group
therapy with differences in retention lasting over the
18 months of treatment.
Contingency management
All three RCTs of contingency management (n = 92, see
Table 5) showed reduced substance use with treatment
varying between 4 and 27 weeks. None of these researchers
reported mental health outcome or retention rates. Only one
group (Ries et al. 2004) stated that raters were blind to
treatment condition. However, urinalysis was used as an
outcome measure by Ries et al. (2004) and Drebing et al.
(2005) and as verification of self-report outcome measures by
Tracy et al. (2007).
Integrated assertive community treatment
Five large studies assessed integrated ACT (n = 911, see
Table 6). Treatment duration varied between 6 months and
3 years. Drake et al. (1998a) and Ho et al. (1999) reported
reduced substance use at the end of treatment and increased
retention in their treatment groups and two authors reported
decreased number of hospitalizations (Essock et al. 2006,
Mangrum et al. 2006). However, newer studies showed less
consistent findings for reductions in substance use (Essock
et al. 2006, Morse et al. 2006).
Intensive case management
Eight researchers assessed intensive case management
(n = 1114, see Table 7), with most reporting no differences
between groups at any time point. Herman et al. (2000)
reported that, after 4 weeks of treatment, reduced alcohol use
at 2 months was not maintained at any other follow-up to
18 months. They did not make explicit the randomization
process nor whether raters were blind to treatment condition.
One non-experimental study (Drake et al. 1997) showed
reduced alcohol use, increased recovery and fewer days
institutionalized, but no differences in drug use or psychiatric
symptoms. One partially-randomized study (Jerrell &
Ridgely 1995) showed reduced mental health symptoms after
18 months of treatment but no differences on substance use
outcomes.
Residential programmes
Nine researchers assessed residential programmes (n = 3310,
see Table 8). The only RCT (Burnam et al. 1995) showed no
differences between the 3-month integrated residential
programme and standard (non-residential) care on any
outcome measure. Six non-experimental studies showed
fairly consistent reduced substance use, particularly during
treatment lasting between 3 months and 2 years (Blankertz
& Cnaan 1994, Nuttbrock et al. 1998, Anderson 1999, De
Leon et al. 2000, Brunette et al. 2001, Timko & Sempel
2004b). Six researchers reported increased treatment reten-
tion and four of these also reported improved mental state
(Blankertz & Cnaan 1994, Nuttbrock et al. 1998, De Leon
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 245
Table
3M
I+
CB
T
Auth
ors
,des
ign
&m
ethod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Rev
iew
Cle
ary
etal
.(2
008)
3R
CT
s
276
(T:
144,
C:
132),
Outp
ati
ents
,SM
I
T:
10
Wks
to9
Mof
MI
+C
BT
C:
SC
+fa
mil
ysu
pport
or
gro
up
ther
apy
Vari
ous,
none
state
dra
ters
blind,
ITT
(3R
CT
s)
SU
:data
could
not
be
poole
d
MS:
data
could
not
be
poole
d
TR
:data
could
not
be
poole
d
Exper
imen
tal
Baker
etal
.(2
006)
Explici
tra
ndom
izat
ion
and
all
oca
tion
conce
alm
ent
130
(T:
65,
C:
65),
Outp
ati
ents
,
Aust
rali
a,
Psy
choti
cdis
ord
er
BD
:N
R
T:
10
Wks
of
4·
1hour
MI
+6
·1
hour
CB
T
C:
self
hel
pbookle
tand
SC
15
Wks,
6,
12
M,
rate
rsbli
nd,
ITT
SU
:T
flca
nnabis
15
Wks
only
[OT
I,
P=
0Æ0
2],
flam
phet
am
ine
6M
only
[P=
0Æ0
4].
ND
[alc
ohol,
poly
dru
g,
abst
inen
ce]
MS:
Tfl
dep
ress
ive
sym
pto
ms
12
M
[BD
I-II
,P<
0Æ0
1]
TR
:N
D
Barr
ow
clough
etal
.(2
001)
[see
Haddock
etal
.2003
for
18
Moutc
om
es]
Explici
tra
ndom
izat
ion
and
all
oca
tion
conce
alm
ent
36
(T:
18,
C:
18)
Outp
ati
ents
,U
K
SM
I
BD
:N
D
T:
9M
,5
MI
and
appro
x18
wee
kly
and
6biw
eekly
sess
ions
CB
T
C:
SC
+fa
mil
ysu
pport
End
of
T,
12,
18
M,
FU
,
rate
rsbli
nd,
ITT
SU
:T
›abst
inen
ce12
M[t
ime-
line
follow
back
;adju
sted
for
base
line
P<
0Æ0
3]
but
not
for
the
most
freq
uen
tly
use
dsu
bst
ance
.N
D
[ASI
,L
DQ
]
MS:
Tfl
hosp
itali
zati
ons
12
M[P
<0Æ0
5].
flposi
tive
[12
M:
P<
0Æ0
1]
&neg
ativ
e
PA
NSS
[9M
:P<
0Æ0
2,
18
M:
P=
0Æ0
04].
ND
[PA
NSS
tota
l]
TR
:N
D
Bel
lack
etal
.(2
006)
Explici
tra
ndom
izat
ion
and
all
oca
tion
conce
alm
ent
175
(res
ult
sfo
r110
that
bec
am
een
gaged
;T
:61,
C:
49),
Outp
ati
ents
,U
SA
,SM
I
BD
:N
D
T:
6M
,3
MI,
CB
Tappro
ach
es,
conti
ngen
cyco
ntr
act
s,biw
eekly
gro
ups
C:
6M
of
gro
ups,
psy
cho-e
duca
tion,
wee
kly
uri
naly
sis
Duri
ng
T,
rate
rsbli
nd
SU
:T
›cl
ean
uri
ne
[1,
4W
kblo
ck,
1,
8W
kblo
ckP<
0Æ0
02].
ND
[ASI
]
MS:
ND
TR
:T
›fo
ren
gag
edsa
mple
[P=
0Æ0
09]
and
›se
ssio
ns
att
ended
[P<
0Æ0
01]
Kem
pet
al.
(2007)
[pilot]
Explici
tra
ndom
izat
ion
and
all
oca
tion
conce
alm
ent
19
(T:
10,
C:
9)
Outp
ati
ents
,A
ust
ralia,
Psy
choti
cil
lnes
s
BD
:A
UD
IT,
DA
ST
T:
4–6
hours
of
MI
+C
BT
,
C:
psy
cho-e
duca
tion
6M
,ra
ters
not
bli
nd
SU
:T
flfr
equen
cyby
6M
[P<
0Æ0
5].
ND
[quanti
ty]
MS:
ND
[PA
NSS,
DA
SS]
TR
:N
D
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;
ASI,
addic
tion
sever
ity
index
;A
UD
IT,
alc
ohol
use
dis
ord
erid
enti
fica
tion
test
;B
D,
base
line
dif
fere
nce
s;B
DI/
BD
I-II
,B
eck
dep
ress
ion
index
;C
,
contr
ol;
DA
SS,
dep
ress
ion
anxie
tysu
bsc
ale
;D
AST
,dru
gabuse
scre
enin
gte
st;
FU
,fo
llow
-up;
ITT
,in
tent-
to-t
reat;
LD
Q,
Lee
ds
dep
enden
cyques
tionnair
e;M
,m
onth
(s);
MS,
men
tal
state
;
ND
,no
stati
stic
ally
signifi
cant
dif
fere
nce
s;N
R,
not
report
ed;
OT
I,opia
tetr
eatm
ent
index
;PA
NSS
,posi
tive
and
neg
ati
ve
scale
for
schiz
ophre
nia
;SC
,st
andard
care
;SM
I,se
ver
em
enta
l
illn
ess;
SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Wks,
wee
ks.
M. Cleary et al.
246 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd
Table
4G
roup
appro
ach
es
Auth
ors
,des
ign
&m
ethod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
anal
ysi
sR
esult
s
Rev
iew
Cle
ary
etal
.(2
008)
2R
CT
s
94
(T:
45,
C:
49),
Outp
ati
ents
,SM
I
T:
up
to18
Mof
gro
up
ther
apy
C:
SC
or
12-s
tep
reco
ver
y
Vari
ous,
uncl
ear
blindin
g,
ITT
(1R
CT
)
SU
:data
could
not
be
poole
d
MS:
data
could
not
be
poole
d
TR
:data
could
not
be
poole
d
Exper
imen
tal
Hel
lers
tein
etal
.(1
995)
Sta
ted
random
ized
47
(T:
23,
C:
24),
Outp
ati
ents
,U
SA
,
Sch
izophre
nia
BD
:N
D
T:
up
to8
Mof
biw
eekly
inte
grate
d
gro
up
psy
choth
erapy/
educa
tion,
C:
SC
4,
8M
,uncl
ear
blindin
g,
ITT
SU
:N
D[A
SI].
MS:
ND
[hosp
itali
zati
on,
ASI]
.
TR
:T
›re
tenti
on
4M
[P=
0Æ0
41]
Non-e
xper
imen
tal
Aubry
etal
.(2
003)
Conse
cuti
ve
all
oca
tion
56
(T:
28,
C:
28),
Outp
ati
ents
,C
anada,
SM
I
BD
:re
adin
ess
for
change
T:
9M
of
staged
gro
up
ther
apy
C:
SC
End
of
T,
18,
24
M,
rate
rsnot
bli
nd
SU
:T
:fl
alc
ohol
9M
[AU
DIT
;P<
0Æ0
1].
ND
[AU
S,D
AST
,D
US,
SA
TS]
MS:
ND
[BSI]
TR
:N
R
Bond
etal
.(1
991)
2si
tes
random
ized
(met
hod
not
expli
cit)
,
thir
dsi
tecl
inic
ian
all
oca
ted
66
(T:
23,
C:
43),
Outp
ati
ents
,U
SA
,SM
I
BD
:T
rece
ivin
g
aft
erca
re,
med
icati
ons
T:
18
Mof
gro
up
ther
apy,
C:
SC
See
Tab
le7
for
oth
erT
arm
6,
12,
18
M,
uncl
ear
blindin
g,
ITT
:>
50%
att
riti
on
at
1si
teonly
SU
:N
D[D
APS,
self
report
]
MS:
Tflh
osp
itali
zati
ons
at
6,
12
M[P
<0Æ0
5]
TR
:T
›re
tenti
on
by
12
[P<
0Æ0
1]
and
18
M[P
<0Æ0
01]
Jam
eset
al.
(2004)
Alt
ernate
all
oca
tion
63
(T:
32,
C:
31),
Outp
ati
ents
,A
ust
rali
a,
schiz
ophre
nia
or
psy
choti
cdis
ord
er
BD
:N
D
T:
6w
ks
spec
iali
zed
gro
up
pro
gra
mm
e
C:
SC
3M
,ra
ters
bli
nd
SU
:T
fldru
g3
M[D
AST
;
P<
0Æ0
01].
ND
[AU
DIT
,SD
S]
MS:
Tfl
psy
chopath
olo
gy
[BPR
S;P<
0Æ0
1].
[ND
,G
SI]
TR
:N
D
Jerr
ell
and
Rid
gel
y(1
995)
Half
clin
icia
nall
oca
ted,
half
random
ized
,w
ith
met
hods
expli
cit
84
(T:
39,
C:
45),
Outp
ati
ents
,U
SA
,
Sch
izophre
nia
BD
:N
R
T:
12–18
Mof
wee
kly
beh
avio
ura
lsk
ills
C:
12
step
reco
ver
y
See
Tab
le7
for
oth
erT
arm
6,
12,
18
M,
uncl
ear
blindin
g
SU
:T
fl18
M[r
egre
ssio
n
model
,C
-DIS
-R,
P£
0Æ0
1]
MS:
Tfl
sym
pto
ms
schiz
ophre
nia
,dep
ress
ion,
mania
18
M[C
-DIS
-R,
P£
0Æ0
1]
TR
:N
R
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;A
SI,
addic
tion
sever
ity
index
;A
UD
IT,
alc
ohol
use
dis
ord
erid
enti
fica
tion
test
;A
US,
alc
ohol
use
scale
;B
D,
base
line
dif
fere
nce
s;B
PR
S/B
PR
S-E
,
bri
efpsy
chia
tric
rati
ng
scale
/expanded
;B
SI,
bri
efsy
mpto
min
ven
tory
;C
,co
ntr
ol;
C-D
IS-R
,co
mpute
rver
sion
of
the
dia
gnost
icin
terv
iew
sched
ule
;D
APS,dru
gand
alc
oholpro
ble
msc
ale
;
DA
ST,
dru
gabuse
scre
enin
gte
st;
DU
S,dru
guse
scale
;G
SI,
glo
balse
ver
ity
index
;IT
T,
inte
nt-
to-t
reat;
M,m
onth
(s);
MS,
men
talst
ate
;N
D,
no
stati
stic
ally
signifi
cant
dif
fere
nce
s;N
R,
not
report
ed;
SA
TS,
subst
ance
abuse
trea
tmen
tsc
ale
;SC
,st
andard
care
;SD
S,
the
sever
ity
of
dep
enden
cesc
ale
;SM
I,se
ver
em
enta
lil
lnes
s;SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Wks,
wee
ks.
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 247
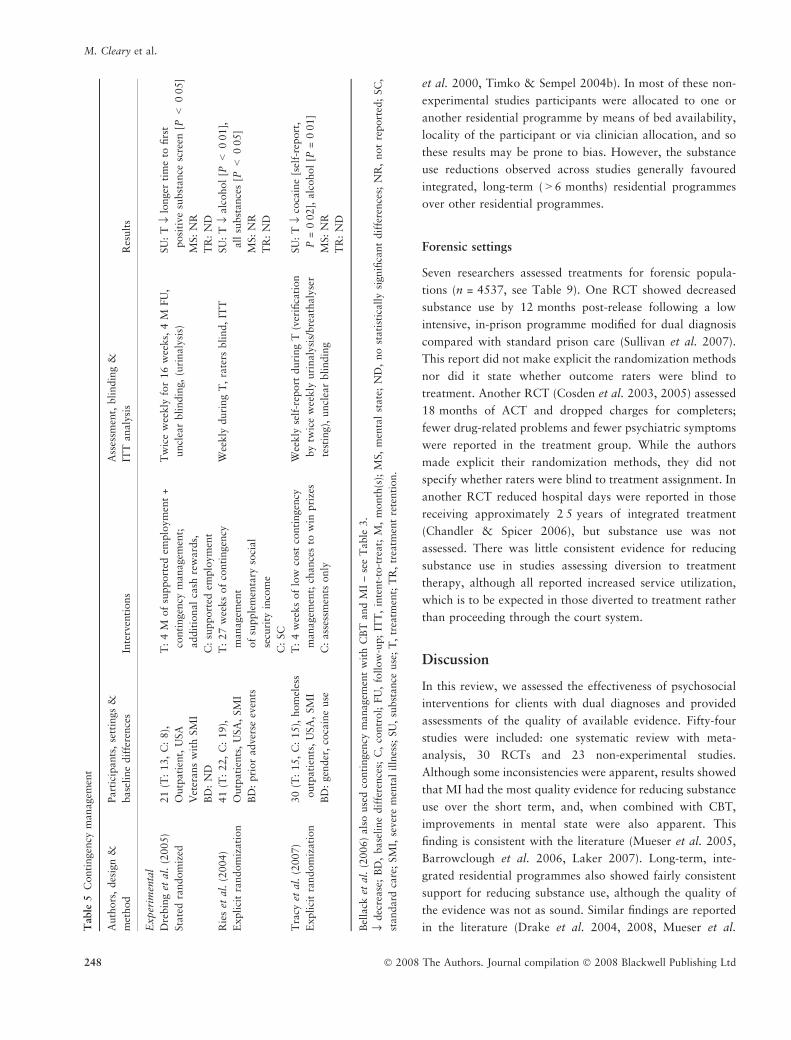
et al. 2000, Timko & Sempel 2004b). In most of these non-
experimental studies participants were allocated to one or
another residential programme by means of bed availability,
locality of the participant or via clinician allocation, and so
these results may be prone to bias. However, the substance
use reductions observed across studies generally favoured
integrated, long-term (>6 months) residential programmes
over other residential programmes.
Forensic settings
Seven researchers assessed treatments for forensic popula-
tions (n = 4537, see Table 9). One RCT showed decreased
substance use by 12 months post-release following a low
intensive, in-prison programme modified for dual diagnosis
compared with standard prison care (Sullivan et al. 2007).
This report did not make explicit the randomization methods
nor did it state whether outcome raters were blind to
treatment. Another RCT (Cosden et al. 2003, 2005) assessed
18 months of ACT and dropped charges for completers;
fewer drug-related problems and fewer psychiatric symptoms
were reported in the treatment group. While the authors
made explicit their randomization methods, they did not
specify whether raters were blind to treatment assignment. In
another RCT reduced hospital days were reported in those
receiving approximately 2Æ5 years of integrated treatment
(Chandler & Spicer 2006), but substance use was not
assessed. There was little consistent evidence for reducing
substance use in studies assessing diversion to treatment
therapy, although all reported increased service utilization,
which is to be expected in those diverted to treatment rather
than proceeding through the court system.
Discussion
In this review, we assessed the effectiveness of psychosocial
interventions for clients with dual diagnoses and provided
assessments of the quality of available evidence. Fifty-four
studies were included: one systematic review with meta-
analysis, 30 RCTs and 23 non-experimental studies.
Although some inconsistencies were apparent, results showed
that MI had the most quality evidence for reducing substance
use over the short term, and, when combined with CBT,
improvements in mental state were also apparent. This
finding is consistent with the literature (Mueser et al. 2005,
Barrowclough et al. 2006, Laker 2007). Long-term, inte-
grated residential programmes also showed fairly consistent
support for reducing substance use, although the quality of
the evidence was not as sound. Similar findings are reported
in the literature (Drake et al. 2004, 2008, Mueser et al.Table
5C
onti
ngen
cym
anagem
ent
Auth
ors
,des
ign
&
met
hod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Exper
imen
tal
Dre
bin
get
al.
(2005)
Sta
ted
random
ized
21
(T:
13,
C:
8),
Outp
ati
ent,
USA
Vet
erans
wit
hSM
I
BD
:N
D
T:
4M
of
support
edem
plo
ym
ent
+
conti
ngen
cym
anagem
ent;
addit
ional
cash
rew
ard
s,
C:
support
edem
plo
ym
ent
Tw
ice
wee
kly
for
16
wee
ks,
4M
FU
,
uncl
ear
blindin
g,(u
rinaly
sis)
SU
:T
fllo
nger
tim
eto
firs
t
posi
tive
subst
ance
scre
en[P
<0Æ0
5]
MS:
NR
TR
:N
D
Rie
set
al.
(2004)
Expli
cit
random
izati
on
41
(T:
22,
C:
19),
Outp
ati
ents
,U
SA
,SM
I
BD
:pri
or
adve
rse
even
ts
T:
27
wee
ks
of
conti
ngen
cy
managem
ent
of
supple
men
tary
soci
al
secu
rity
inco
me
C:
SC
Wee
kly
duri
ng
T,
rate
rsbli
nd,
ITT
SU
:T
flalc
ohol
[P<
0Æ0
1],
all
subst
ance
s[P
<0Æ0
5]
MS:
NR
TR
:N
D
Tra
cyet
al.
(2007)
Expli
cit
random
izati
on
30
(T:
15,
C:
15),
hom
eles
s
outp
ati
ents
,U
SA
,SM
I
BD
:gen
der
,co
cain
euse
T:
4w
eeks
of
low
cost
conti
ngen
cy
managem
ent;
chance
sto
win
pri
zes
C:
ass
essm
ents
only
Wee
kly
self
-rep
ort
duri
ng
T(v
erifi
cati
on
by
twic
ew
eekly
uri
nal
ysi
s/bre
ath
alyse
r
test
ing),
uncl
ear
blindin
g
SU
:T
flco
cain
e[s
elf-
report
,
P=
0Æ0
2],
alc
ohol
[P=
0Æ0
1]
MS:
NR
TR
:N
D
Bel
lack
etal
.(2
006)
als
ouse
dco
nti
ngen
cym
anagem
ent
wit
hC
BT
and
MI
–se
eT
able
3.
fldec
rease
;B
D,
base
line
dif
fere
nce
s;C
,co
ntr
ol;
FU
,fo
llow
-up;
ITT
,in
tent-
to-t
reat;
M,
month
(s);
MS,
men
tal
state
;N
D,
no
stati
stic
ally
signifi
cant
dif
fere
nce
s;N
R,
not
report
ed;
SC
,
standard
care
;SM
I,se
ver
em
enta
lil
lnes
s;SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on.
M. Cleary et al.
248 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

Table
6In
tegra
ted
ass
erti
ve
com
munit
ytr
eatm
ent
(AC
T)
Auth
ors
,des
ign
&
met
hod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
anal
ysi
sR
esult
s
Rev
iew
Cle
ary
etal
.(2
008)
4R
CT
s
812
(T:
455,
C:
357)
Outp
ati
ents
,SM
I
T:
9to
36
Mof
inte
gra
ted
AC
T
C:
SC
Rate
rsbli
nd
(3R
CT
s)
ITT
(1R
CT
)
SU
:data
could
not
be
poole
d
MS:
data
could
not
be
poole
d
TR
:data
could
not
be
poole
d
Exper
imen
tal
Dra
ke
etal
.(1
998a)
Sta
ted
random
ized
223
(T:
109,
C:
114)
Outp
ati
ents
,U
SA
SM
I
BD
:B
PR
Sdis
org
aniz
atio
n
T:
3Y
rsof
24
hour
per
day
inte
gra
ted
AC
T
C:
SC
6m
onth
lyover
3Y
rs,
rate
rsbli
nd
SU
:T
fl3
Yrs
[reg
ress
ion
model
,
Tass
igned
sam
ple
(n=223):
SA
TS,
AU
S;
P<
0Æ0
5,
Tex
pose
dsa
mple
(n=173):
SA
TS,
AU
S;
P<
0Æ0
5]
MS:
ND
[BPR
S]
TR
:T
›re
tenti
on
[P=
0Æ0
07]
Ess
ock
etal
.(2
006)
Sta
ted
random
ized
,2
site
s
198
(T:
99,
C:
99)
Outp
ati
ents
USA
SM
I
BD
:SA
TS
T:
3Y
rsof
24
hour
per
day
inte
gra
ted
AC
T
C:
SC
6m
onth
lyover
3Y
rs,
rate
rsbli
nd
SU
:T
fl36
Mdue
toea
rly
reduct
ions
at
1si
te[r
egre
ssio
nm
odel
SA
TS;
P<
0Æ0
5].
ND
[AU
S,
DU
S,SA
TS,
ASI,
days
report
ing].
MS:
Tfl
hosp
italize
ddays
[sit
e2
only
,P<
0Æ0
02],
flin
stit
uti
onali
zed
days
[sit
e2
only
,P<
0Æ0
2].
TR
:N
D
Mors
eet
al.
(2006)
Sta
ted
random
ized
95
(T:
46,
C:
49)
Outp
ati
ents
USA
Hom
eles
speo
ple
wit
hSM
I
BD
:B
PR
S
T:
2Y
rsof
inte
gra
ted
AC
T
C:
SC
See
Tab
le7
for
oth
erT
arm
3–6
month
lyover
2Y
rs,
uncl
ear
blindin
g
SU
:N
D(s
elf
report
)
MS:
ND
[BPR
S].
TR
:N
D
Non-e
xper
imen
tal
Ho
etal
.(1
999)
6m
onth
lysu
cces
sive
all
oca
tion
179
(T1:
20,
T2:
42,
T3:
50,
T4:
67)
Outp
ati
ents
,U
SA
Vet
erans
wit
hpsy
choti
c
illn
ess
BD
:N
D
T:
6M
of
T,
wit
hea
ch
gro
up
rece
ivin
gin
crea
sing
am
ounts
of
inte
gra
ted
AC
T
Month
lyduri
ng
each
6M
Tphase
,uncl
ear
blindin
g
(uri
nal
ysi
s)
1M
;52%
att
riti
on,
3M
;
61%
att
riti
on
SU
:T
›abst
inen
ce;
sequen
tial
impro
vem
ent
from
gro
up
T1–4
[uri
nal
ysi
s;P
=0Æ0
5]
MS:
ND
[hosp
italiza
tions]
TR
:T
›en
gagem
ent,
rete
nti
on,
att
endance
;se
quen
tial
impro
vem
ent
from
gro
up
T1–4
[P<
0Æ0
1].
Mangru
met
al.
(2006)
2si
tes
random
ized
(met
hod
not
expli
cit)
,th
ird
site
geo
graphic
all
yall
oca
ted
216
(T:
123,
C:
93)
Outp
ati
ents
,U
SA
SM
I
BD
:N
D
T:
1Y
rof
inte
gra
ted
AC
T
C:
non-i
nte
gra
ted
care
End
of
T,
1Y
rFU
,uncl
ear
bli
ndin
g(a
dm
inis
trati
ve)
ITT
SU
:N
R
MS:
Tfl
hosp
italiza
tions
[P=
0Æ0
001]
and
hosp
ital
days
[P=
0Æ0
4]
TR
:N
R
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;A
SI,
addic
tion
sever
ity
index
;A
US,alc
oholuse
scale
;B
D,base
line
dif
fere
nce
s;B
PR
S-E
,bri
efpsy
chia
tric
rati
ng
scale
/expanded
;C
,co
ntr
ol;
DU
S,
dru
guse
scale
;FU
,fo
llow
-up;IT
T,in
tent-
to-t
reat;
M,m
onth
(s);
MS,m
enta
lst
ate
;N
D,no
stati
stic
all
ysi
gnifi
cant
dif
fere
nce
s;N
R,not
report
ed;SA
TS,su
bst
ance
abuse
trea
tmen
tsc
ale
;SC
,
standard
care
;SM
I,se
ver
em
enta
lilln
ess;
SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Yr,
yea
rs(s
).
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 249
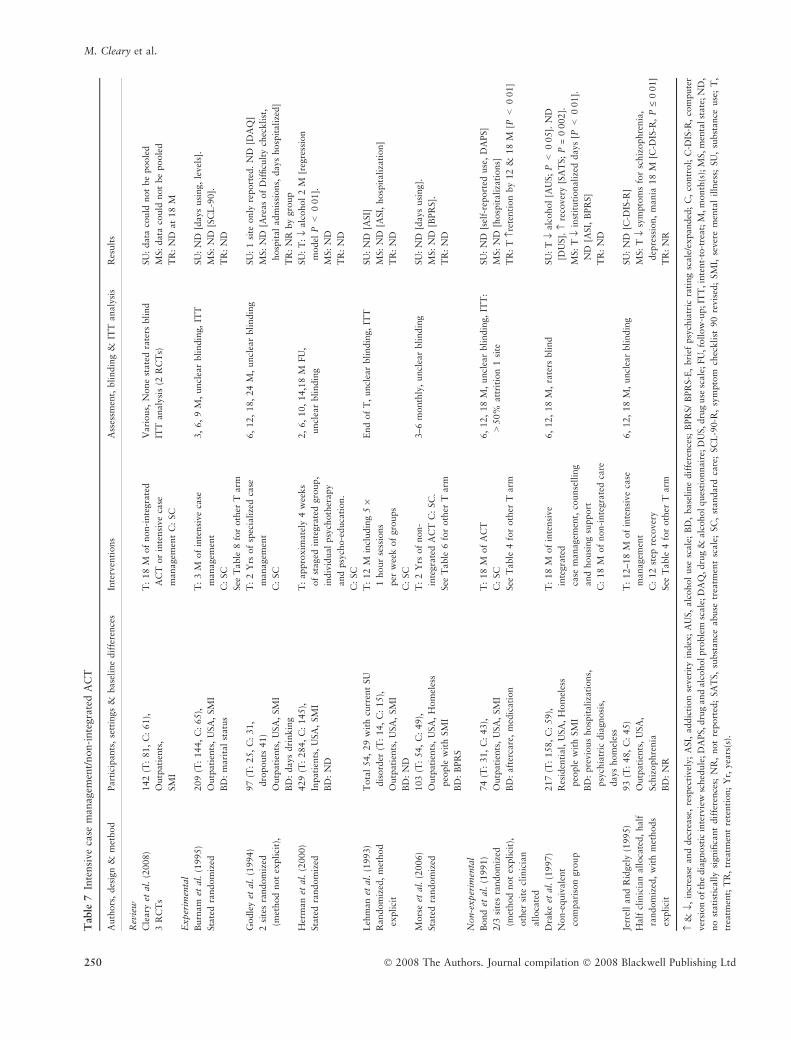
Table
7In
tensi
ve
case
managem
ent/
non-i
nte
gra
ted
AC
T
Auth
ors
,des
ign
&m
ethod
Part
icip
ants
,se
ttin
gs
&base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Rev
iew
Cle
ary
etal
.(2
008)
3R
CT
s
142
(T:
81,
C:
61),
Outp
ati
ents
,
SM
I
T:
18
Mof
non-i
nte
gra
ted
AC
Tor
inte
nsi
ve
case
managem
ent
C:
SC
Vari
ous,
None
state
dra
ters
bli
nd
ITT
analy
sis
(2R
CT
s)
SU
:data
could
not
be
poole
d
MS:
data
could
not
be
poole
d
TR
:N
Dat
18
M
Exper
imen
tal
Burn
am
etal
.(1
995)
Sta
ted
random
ized
209
(T:
144,
C:
65),
Outp
ati
ents
,U
SA
,SM
I
BD
:m
ari
tal
statu
s
T:
3M
of
inte
nsi
ve
case
managem
ent
C:
SC
See
Table
8fo
roth
erT
arm
3,
6,
9M
,uncl
ear
bli
ndin
g,
ITT
SU
:N
D[d
ays
usi
ng,
level
s].
MS:
ND
[SC
L-9
0].
TR
:N
D
Godle
yet
al.
(1994)
2si
tes
random
ized
(met
hod
not
expli
cit)
,
97
(T:
25,
C:
31,
dro
pouts
41)
Outp
ati
ents
,U
SA
,SM
I
BD
:days
dri
nkin
g
T:
2Y
rsof
spec
iali
zed
case
managem
ent
C:
SC
6,
12,
18,
24
M,
uncl
ear
bli
ndin
gSU
:1
site
only
report
ed.
ND
[DA
Q]
MS:
ND
[Are
as
of
Dif
ficu
lty
chec
kli
st,
hosp
ital
adm
issi
ons,
days
hosp
itali
zed]
TR
:N
Rby
gro
up
Her
man
etal
.(2
000)
Sta
ted
random
ized
429
(T:
284,
C:
145),
Inpati
ents
,U
SA
,SM
I
BD
:N
D
T:
appro
xim
ate
ly4
wee
ks
of
staged
inte
gra
ted
gro
up,
indiv
idual
psy
choth
erapy
and
psy
cho-e
duca
tion.
C:
SC
2,
6,
10,
14,1
8M
FU
,
uncl
ear
bli
ndin
g
SU
:T
:fl
alc
ohol
2M
[reg
ress
ion
model
P<
0Æ0
1].
MS:
ND
TR
:N
D
Leh
man
etal
.(1
993)
Random
ized
,m
ethod
expli
cit
Tota
l54,
29
wit
hcu
rren
tSU
dis
ord
er(T
:14,
C:
15),
Outp
ati
ents
,U
SA
,SM
I
BD
:N
D
T:
12
Min
cludin
g5
·1
hour
sess
ions
per
wee
kof
gro
ups
C:
SC
End
of
T,
uncl
ear
bli
ndin
g,
ITT
SU
:N
D[A
SI]
MS:
ND
[ASI,
hosp
itali
zati
on]
TR
:N
D
Mors
eet
al.
(2006)
Sta
ted
random
ized
103
(T:
54,
C:
49),
Outp
ati
ents
,U
SA
,H
om
eles
s
peo
ple
wit
hSM
I
BD
:B
PR
S
T:
2Y
rsof
non-
inte
gra
ted
AC
TC
:SC
.
See
Table
6fo
roth
erT
arm
3–6
month
ly,
uncl
ear
bli
ndin
gSU
:N
D[d
ays
usi
ng].
MS:
ND
[BPR
S].
TR
:N
D
Non-e
xper
imen
tal
Bond
etal
.(1
991)
2/3
site
sra
ndom
ized
(met
hod
not
expli
cit)
,
oth
ersi
tecl
inic
ian
all
oca
ted
74
(T:
31,
C:
43),
Outp
ati
ents
,U
SA
,SM
I
BD
:aft
erca
re,
med
icati
on
T:
18
Mof
AC
T
C:
SC
See
Table
4fo
roth
erT
arm
6,
12,
18
M,
uncl
ear
bli
ndin
g,
ITT
:
>50%
att
riti
on
1si
te
SU
:N
D[s
elf-
report
eduse
,D
APS]
MS:
ND
[hosp
itali
zati
ons]
TR
:T
›ret
enti
on
by
12
&18
M[P
<0Æ0
1]
Dra
ke
etal
.(1
997)
Non-e
quiv
ale
nt
com
pari
son
gro
up
217
(T:
158,
C:
59),
Res
iden
tial,
USA
,H
om
eles
s
peo
ple
wit
hSM
I
BD
:pre
vio
us
hosp
itali
zati
ons,
psy
chia
tric
dia
gnosi
s,
days
hom
eles
s
T:
18
Mof
inte
nsi
ve
inte
gra
ted
case
managem
ent,
counse
llin
g
and
housi
ng
support
C:
18
Mof
non-i
nte
gra
ted
care
6,
12,
18
M,
rate
rsbli
nd
SU
:T
flalc
ohol
[AU
S;
P<
0Æ0
5].
ND
[DU
S].
›re
cover
y[S
AT
S;
P=
0Æ0
02].
MS:
Tfl
inst
ituti
onali
zed
days
[P<
0Æ0
1].
ND
[ASI,
BPR
S]
TR
:N
D
Jerr
ell
and
Rid
gel
y(1
995)
Half
clin
icia
nall
oca
ted,
half
random
ized
,w
ith
met
hods
expli
cit
93
(T:
48,
C:
45)
Outp
ati
ents
,U
SA
,
Sch
izophre
nia
BD
:N
R
T:
12–18
Mof
inte
nsi
ve
case
managem
ent
C:
12
step
reco
ver
y
See
Table
4fo
roth
erT
arm
6,
12,
18
M,
uncl
ear
bli
ndin
gSU
:N
D[C
-DIS
-R]
MS:
Tfl
sym
pto
ms
for
schiz
ophre
nia
,
dep
ress
ion,
mania
18
M[C
-DIS
-R,
P£
0Æ0
1]
TR
:N
R
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;
ASI,
addic
tion
sever
ity
index
;A
US,
alc
ohol
use
scale
;B
D,
base
line
dif
fere
nce
s;B
PR
S/
BPR
S-E
,bri
efpsy
chia
tric
rati
ng
scale
/expanded
;C
,co
ntr
ol;
C-D
IS-R
,co
mpute
r
ver
sion
of
the
dia
gnost
icin
terv
iew
sched
ule
;D
APS,dru
gand
alc
oholpro
ble
msc
ale
;D
AQ
,dru
g&
alc
oholques
tionnair
e;D
US,dru
guse
scale
;FU
,fo
llow
-up;IT
T,in
tent-
to-t
reat;
M,m
onth
(s);
MS,m
enta
lst
ate
;N
D,
no
stati
stic
all
ysi
gnifi
cant
dif
fere
nce
s;N
R,
not
report
ed;
SA
TS,
subst
ance
abuse
trea
tmen
tsc
ale
;SC
,st
andard
care
;SC
L-9
0-R
,sy
mpto
mch
eckli
st90
revis
ed;
SM
I,se
ver
em
enta
lil
lnes
s;SU
,su
bst
ance
use
;T
,
trea
tmen
t;T
R,
trea
tmen
tre
tenti
on;
Yr,
yea
rs(s
).
M. Cleary et al.
250 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

Table
8R
esid
enti
al
pro
gra
mm
es
Auth
ors
,des
ign
&
met
hod
Part
icip
ants
,se
ttin
gs
&
base
line
dif
fere
nce
sIn
terv
enti
ons
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Exper
imen
tal
Burn
am
etal
.(1
995)
Sta
ted
random
ized
132
(T:
67,
C:
65),
Res
iden
tial,
USA
SM
I
BD
:m
ari
tal
statu
s
T:
3M
inte
gra
ted
C:
SC
See
Table
7fo
roth
erT
arm
3,
6,
9M
,uncl
ear
bli
ndin
g,
ITT
SU
:N
D[d
ays
usi
ng,
level
s].
MS:
ND
[SC
L-9
0].
TR
:N
D
Non-e
xper
imen
tal
Aguil
era
etal
.(1
999)
Geo
gra
phic
all
oca
tion
86
(T:
40,
C:
46),
Res
iden
tial,
Hondura
s,hom
eles
s
men
wit
hSM
I
BD
:age,
convic
tions,
SU
,L
OS
etc
T:
3M
of
inte
gra
ted
C:
3M
resi
den
tial
alc
oholi
sm
pro
gra
mm
e
3M
,uncl
ear
bli
ndin
gSU
:N
D[r
elapse
]
MS:
C›
[LO
FA
,P<
0Æ0
5]
TR
:N
D
Ander
son
(1999)
Bed
avail
abil
ity
all
oca
tion
225
(T:
76,
C:
149),
Res
iden
tial,
USA
Hom
eles
sm
enw
ith
SM
I
BD
:age,
ethnic
back
gro
und,
alc
ohol
T:
6M
of
inte
gra
ted
C:
resi
den
tial
rehabil
itati
on
End
of
T,
9M
FU
,
uncl
ear
bli
ndin
g
SU
:T
fl9
M[A
SI;
P<
0Æ0
5]
MS:
ND
[ASI]
TR
:T
›9
M[P
<0Æ0
1]
Bla
nker
tzand
Cnaan
(1994)
Bed
avail
abil
ity
all
oca
tion
176,
data
for
com
ple
ters
;89
(T:
51,
C:
38),
Res
iden
tial,
USA
,
Hom
eles
speo
ple
wit
hSM
I
BD
:m
edic
ati
on
T:
up
to2
Yrs
of
psy
choso
cial
rehabil
itati
on
C:
modifi
edth
erapeu
tic
com
munit
y
6m
onth
ly,
3M
FU
aft
er
dis
charg
e,uncl
ear
bli
ndin
g
SU
:T
›abst
inen
ceduri
ng
T[A
SI:
P<
0Æ0
1]
MS:
T›
exit
ed‘s
ucc
essf
ull
y’
[P<
0Æ0
5]
TR
:T
›re
tenti
on
Bru
net
teet
al.
(2001)
Cli
nic
ian
all
oca
tion
82
(T:
43,
C:
39),
Res
iden
tial,
USA
SM
I
BD
:ed
uca
tion,
alc
ohol
use
T:
12
Mm
enta
lhea
lth
and
SU
C:
2M
short
-ter
mm
enta
l
hea
lth
and
SU
resi
den
tial
6M
,uncl
ear
bli
ndin
gSU
:T
›abst
inen
ce[P
<0Æ0
01].
ND
[AU
S,
DU
S]
MS:
ND
TR
:T
›en
gagem
ent
[P<
0Æ0
01]
De
Leo
net
al.
(2000)
Seq
uen
tial
all
oca
tion
342
(T1:
183,
T2:
93,
C:
66),
resi
den
tial,
USA
,
hom
eles
speo
ple
wit
hSM
I
BD
:N
D
T1:
12
Mof
modifi
ed
med
ium
inte
nsi
ty
ther
apeu
tic
com
munit
yT
2:
12
Mof
modifi
ed
low
inte
nsi
tyth
erapeu
tic
com
munit
yC
:SC
12
M,>
24
M,
uncl
ear
bli
ndin
g
ITT
analy
sis
SU
:T
2,
fl>
24
M[r
egre
ssio
n
model
,P<
0Æ0
5]
MS:
T2,
›>
24
Mdep
ress
ion
[BD
I;
P<
0Æ0
01]
anxie
ty[S
MA
S:
P<
0Æ0
5].
ND
[SC
L-9
0-R
].
TR
:›
rete
nti
on
T2
vs.
T1
[P<
0Æ0
02]
Kasp
row
etal
.(1
999)
Surv
eyvia
Dep
t.V
eter
ans
Aff
air
s,99
site
s
1495
(T:
957,
C:
538),
Res
iden
tial,
USA
,H
om
eles
s
vet
erans
wit
hSM
I
BD
:N
R
T:
men
tal
hea
lth
and
SU
pro
gra
mm
e
C:
SU
resi
den
tial
pro
gra
mm
e
Rep
ort
sco
mple
ted
by
case
manager
s
SU
:N
D[A
SI,
hosp
itali
zati
ons]
MS:
ND
[ASI,
hosp
itali
zati
ons]
TR
:T
flle
ftw
ithout
staff
consu
ltati
on
[reg
ress
ion
model
,P<
0Æ0
1]
Nutt
bro
cket
al.
(1998)
Bed
avail
abil
ity
wit
h
faci
lity
appro
val
694
(T:
373,
C:
321)
Res
iden
tial,
USA
Hom
eles
sm
enw
ith
SM
I
BD
:N
D
T:
12
Mof
hig
hin
tensi
ty
ther
apeu
tic
com
munit
y
C:
low
inte
nsi
tyco
mm
unit
y
resi
den
ces
(men
tal
hea
lth
focu
s)
2,
6,
12
M,
rate
rsnot
bli
nd,
appro
x
90%
att
riti
on
by
12
M
SU
:T
›cl
ean
uri
ne,
sub-s
am
ple
[P£
0Æ0
1]
MS:
Tfl
psy
chia
tric
dis
turb
ance
[GA
F,
2
&12
M],
[BPR
S,
2M
,re
gre
ssio
nm
odel
]
TR
:N
D
Tim
ko
and
Sem
pel
(2004a,
2004b))
,T
imko
etal
.2006,
Random
lyass
igned
and
clin
icia
nall
oca
ted
230,
(T:
110,
C:
120),
Res
iden
tial,
USA
,V
eter
ans
wit
hSM
I
BD
:psy
chia
tric
&fa
mil
y/s
oci
al
pro
ble
ms,
hosp
ital
days
T:
hig
hin
tensi
tyover
3si
tes
C:
low
inte
nsi
tyover
4si
tes
At
dis
charg
e,4,
12
MFU
,
uncl
ear
bli
ndin
g
SU
:T
fl(A
SI;
P<
0Æ0
1)
MS:
ND
[ASI]
TR
:T
›12-s
tep
att
endance
duri
ng
T
(P<
0Æ0
1),
C›a
tten
dance
post
-
dis
charg
e(P
<0Æ0
5)
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;A
SI,
addic
tion
sever
ity
index
;A
US,alc
oholuse
scale
;B
D,base
line
dif
fere
nce
s;B
DI/
BD
I-II
,B
eck
dep
ress
ion
index
;B
PR
S/B
PR
S-E
,bri
efpsy
chia
tric
rati
ng
scale
/expanded
;C
,
contr
ol;
DU
S,
dru
guse
scale
;FU
,fo
llow
-up;
GA
F,
glo
bal
ass
essm
ent
of
funct
ionin
g;
ITT
,in
tent-
to-t
reat;
LO
FA
,le
vel
sof
funct
ional
ass
essm
ent;
LO
S,
length
of
stay;
M,
month
(s);
MS,
men
tal
state
;N
D,
no
stati
stic
all
ysi
gnifi
cant
dif
fere
nce
s;N
R,not
report
ed;SC
,st
andard
care
;SC
L-9
0-R
,sy
mpto
mch
eckli
st90
revis
ed;SM
AS,sh
ort
ened
manif
est
anxie
tysc
ale
;SM
I,se
ver
em
enta
lil
lnes
s;SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Yr,
yea
rs(s
).
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 251
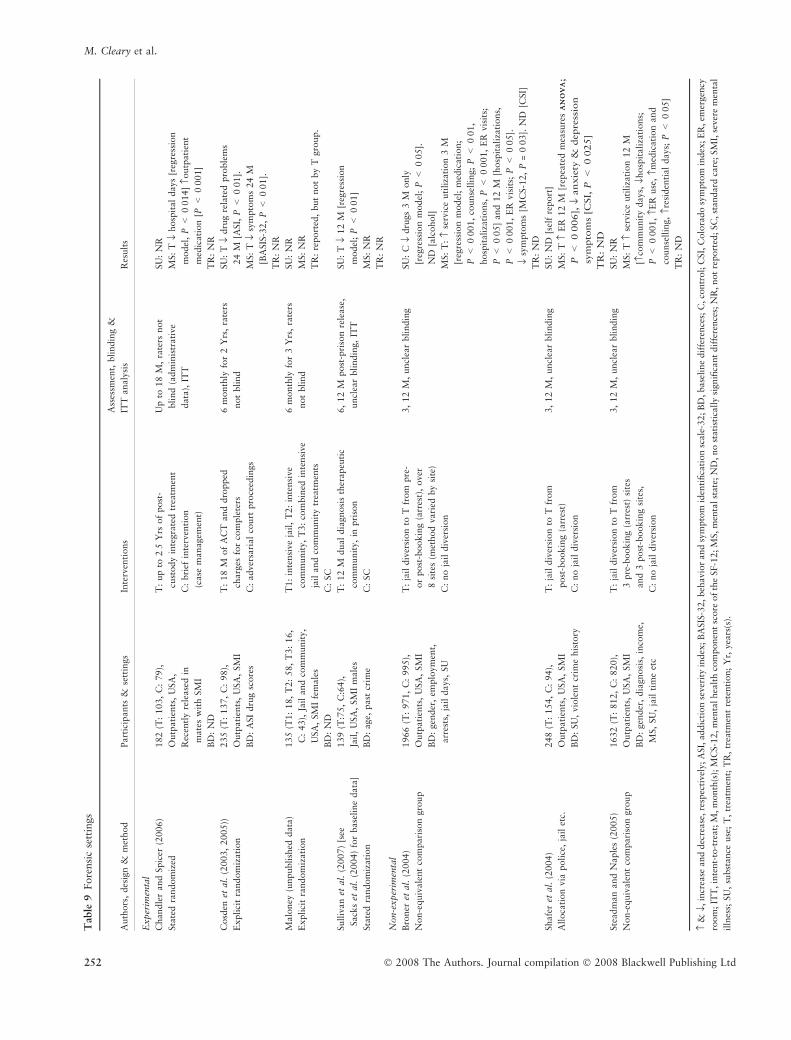
Table
9Fore
nsi
cse
ttin
gs
Auth
ors
,des
ign
&m
ethod
Part
icip
ants
&se
ttin
gs
Inte
rven
tions
Ass
essm
ent,
bli
ndin
g&
ITT
analy
sis
Res
ult
s
Exper
imen
tal
Chandle
rand
Spic
er(2
006)
Sta
ted
random
ized
182
(T:
103,
C:
79),
Outp
ati
ents
,U
SA
,
Rec
entl
yre
lease
din
mate
sw
ith
SM
I
BD
:N
D
T:
up
to2Æ5
Yrs
of
post
-
cust
ody
inte
gra
ted
trea
tmen
t
C:
bri
efin
terv
enti
on
(case
managem
ent)
Up
to18
M,
rate
rsnot
bli
nd
(adm
inis
trati
ve
data
),IT
T
SU
:N
R
MS:
Tfl
hosp
ital
days
[reg
ress
ion
model
,P<
0Æ0
14]
›outp
ati
ent
med
icati
on
[P<
0Æ0
01]
TR
:N
R
Cosd
enet
al.
(2003,
2005))
Expli
cit
random
izati
on
235
(T:
137,
C:
98),
Outp
ati
ents
,U
SA
,SM
I
BD
:A
SI
dru
gsc
ore
s
T:
18
Mof
AC
Tand
dro
pped
charg
esfo
rco
mple
ters
C:
adver
sari
al
court
pro
ceed
ings
6m
onth
lyfo
r2
Yrs
,ra
ters
not
bli
nd
SU
:T
fldru
gre
late
dpro
ble
ms
24
M[A
SI,
P<
0Æ0
1].
MS:
Tfl
sym
pto
ms
24
M
[BA
SIS
-32,
P<
0Æ0
1].
TR
:N
R
Malo
ney
(unpubli
shed
data
)
Expli
cit
random
izati
on
135
(T1:
18,
T2:
58,
T3:
16,
C:
43),
Jail
and
com
munit
y,
USA
,SM
Ife
male
s
BD
:N
D
T1:
inte
nsi
ve
jail
,T
2:
inte
nsi
ve
com
munit
y,
T3:
com
bin
edin
tensi
ve
jail
and
com
munit
ytr
eatm
ents
C:
SC
6m
onth
lyfo
r3
Yrs
,ra
ters
not
bli
nd
SU
:N
R
MS:
NR
TR
:re
port
ed,
but
not
by
Tgro
up.
Sull
ivan
etal
.(2
007)
[see
Sack
set
al.
(2004)
for
base
line
data
]
Sta
ted
random
izati
on
139
(T:7
5,
C:6
4),
Jail
,U
SA
,SM
Im
ale
s
BD
:age,
past
crim
e
T:
12
Mdual
dia
gnosi
sth
erapeu
tic
com
munit
y,
inpri
son
C:
SC
6,
12
Mpost
-pri
son
rele
ase
,
uncl
ear
bli
ndin
g,
ITT
SU
:T
fl12
M[r
egre
ssio
n
model
;P<
0Æ0
1]
MS:
NR
TR
:N
R
Non-e
xper
imen
tal
Bro
ner
etal
.(2
004)
Non-e
quiv
ale
nt
com
pari
son
gro
up
1966
(T:
971,
C:
995),
Outp
ati
ents
,U
SA
,SM
I
BD
:gen
der
,em
plo
ym
ent,
arr
ests
,ja
ildays,
SU
T:
jail
div
ersi
on
toT
from
pre
-
or
post
-bookin
g(a
rres
t),
over
8si
tes
(met
hod
vari
edby
site
)
C:
no
jail
div
ersi
on
3,
12
M,
uncl
ear
bli
ndin
gSU
:C
fldru
gs
3M
only
[reg
ress
ion
model
;P<
0Æ0
5].
ND
[alc
ohol]
MS:
T:
›se
rvic
euti
liza
tion
3M
[reg
ress
ion
model
;m
edic
ati
on;
P<
0Æ0
01,
counse
llin
g;
P<
0Æ0
1,
hosp
itali
zati
ons,
P<
0Æ0
01,
ER
vis
its;
P<
0Æ0
5]
and
12
M[h
osp
itali
zati
ons,
P<
0Æ0
01,
ER
vis
its;
P<
0Æ0
5].
flsy
mpto
ms
[MC
S-1
2,
P=
0Æ0
3].
ND
[CSI]
TR
:N
D
Shafe
ret
al.
(2004)
All
oca
tion
via
poli
ce,
jail
etc.
248
(T:
154,
C:
94),
Outp
ati
ents
,U
SA
,SM
I
BD
:SU
,vio
lent
crim
ehis
tory
T:
jail
div
ersi
on
toT
from
post
-bookin
g(a
rres
t)
C:
no
jail
div
ersi
on
3,
12
M,
uncl
ear
bli
ndin
gSU
:N
D[s
elf
report
]
MS:
T›
ER
12
M[r
epea
ted
mea
sure
sA
NO
VA
AN
OV
A;
P<
0Æ0
06],
flanxie
ty&
depre
ssio
n
sym
pto
ms
[CSI,
P<
0Æ0
25]
TR
:N
D
Ste
adm
an
and
Naple
s(2
005)
Non-e
quiv
ale
nt
com
pari
son
gro
up
1632
(T:
812,
C:
820),
Outp
ati
ents
,U
SA
,SM
I
BD
:gen
der
,dia
gnosi
s,in
com
e,
MS,
SU
,ja
ilti
me
etc
T:
jail
div
ersi
on
toT
from
3pre
-bookin
g(a
rres
t)si
tes
and
3post
-bookin
gsi
tes,
C:
no
jail
div
ersi
on
3,
12
M,
uncl
ear
bli
ndin
gSU
:N
R
MS:
T›
serv
ice
uti
liza
tion
12
M
[›co
mm
unit
ydays,
flhosp
itali
zati
ons;
P<
0Æ0
01,
›ER
use
,›m
edic
ati
on
and
counse
llin
g,
›res
iden
tial
days;
P<
0Æ0
5]
TR
:N
D
›&
fl,in
crea
seand
dec
rease
,re
spec
tivel
y;A
SI,
addic
tion
sever
ity
index
;B
ASIS
-32,beh
avio
rand
sym
pto
mid
enti
fica
tion
scale
-32;B
D,base
line
dif
fere
nce
s;C
,co
ntr
ol;
CSI,
Colo
rado
sym
pto
min
dex
;E
R,em
ergen
cy
room
;IT
T,in
tent-
to-t
reat;
M,m
onth
(s);
MC
S-1
2,m
enta
lhea
lth
com
ponen
tsc
ore
of
the
SF-1
2;M
S,m
enta
lst
ate
;N
D,no
stati
stic
all
ysi
gnifi
cant
dif
fere
nce
s;N
R,not
report
ed;SC
,st
andard
care
;SM
I,se
ver
em
enta
l
illn
ess;
SU
,su
bst
ance
use
;T
,tr
eatm
ent;
TR
,tr
eatm
ent
rete
nti
on;
Yr,
yea
rs(s
).
M. Cleary et al.
252 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

2005). With research in its infancy, contingency management
programmes show some promise, as in three RCTs reduced
substance use occurred and another RCT demonstrated
increased retention and drug-free urine when combined with
MI and CBT (Bellack et al. 2006).
The inconsistent support for CBT alone for reducing
substance use and/or improving mental state may be
explained by heterogeneous samples and interventions. The
two studies without statistically significant findings targeted
patients with schizophrenia offering between six and 12
individual sessions (Naeem et al. 2005, Edwards et al. 2006).
The studies with statistically significant findings targeted
patients with bipolar disorder, and offered between 16 and
20 sessions (Schmitz et al. 2002, Weiss et al. 2007). Further,
CBT can have various foci such as harm reduction or relapse
prevention, and so there could have been differences between
studies with regard to the specific interventions as well as
variety in the control conditions. Inconsistent results may also
be explained by differences in study quality, with those of
highest quality reporting no statistically significant results.
Nevertheless, as present there is little evidence that CBT
alone is an effective intervention for dual diagnosis clients
with schizophrenia.
In contrast to other reviews (Mueser et al. 2005, Drake
et al. 2008), little consistent support was found for group
therapy, which may be explained by differences in the way
studies were categorized. For instance, we allocated Bellack
et al. (2006) to MI + CBT and Weiss et al. (2000, 2007) to
CBT, rather than group therapy. Others reviewers have
categorized interventions as individual or group therapies
(Drake et al. 2008), psychiatric diagnoses (Tiet & Mausbach
2007) or not included contingency management studies
(Mangrum et al. 2006, Cleary et al. 2008). This is in contrast
to the present review, in which we grouped similar studies
according to interventions (e.g. CBT, MI and CBT + MI) to
assess the efficacy of stand-alone interventions.
Also, unlike previous reviews (Drake et al. 1998b, 2004,
Barrowclough et al. 2006, Tsuang et al. 2006), we found that
the evidence to support integrated ACT was inconsistent.
Older studies tended to show reduced substance use, while
more recent studies tended not to show such differences. This
may be due to increasing integration of standard care in
comparison groups (Ziedonis et al. 2005, Essock et al. 2006).
Future studies with consistent methodologies of high-fidelity
individual treatment components, offered singularly or in
various simple combinations and assessed over long periods
using standardized outcome measures, should allow more
consistent, quality evidence and facilitate meta-analysis.
Using sub-groups of patients may help to determine whether
certain interventions work best for certain patient subgroups
and allow differing treatment components to target particular
subgroups.
Review strengths and limitations
A strength of this review is the detailed assessment of trial
quality. Of all the studies included, only five fulfilled all
quality issues. Having access to both high and low quality
evidence, with quality made explicit, assists practitioners to
make informed and evidence-based treatment judgements
(Newhouse 2008). A recent Cochrane review (Cleary et al.
2008) excluded quasi-randomized and non-randomized tri-
als, those using non-validated scales or if there was high
attrition (>50%) or skewed data. To be more inclusive, we
included both randomized and non-randomized studies.
Thus, a limitation is that some study results may be based
on data of questionable reliability. Further, these samples are
heterogeneous, varying on mental health diagnoses and
severity, type of substance used, severity of use and other
factors that may have an impact on treatment outcomes, such
as culture, age and social support (Warren et al. 2007,
McGovern & McLellan 2008). Individuals with dual diag-
nosis have an array of problems and other outcome measures,
such as social functioning, medication compliance and crime,
are also important treatment outcomes (Sacks et al. 2008a).
In this review, we focussed on three main topics (substance
use, mental health and retention), but in future reviews
broader outcome measures might be incorporated to assess
treatment effectiveness further.
Conclusion
In this systematic review, comparisons of psychosocial
interventions were difficult because of the diversity of
interventions (including standard care), outcomes measures
and the variable trial quality. We found some support for the
effectiveness of MI for the reduction of substance use, at least
in the short term and, when combined with CBT over longer
periods, improvements in mental health were apparent. Trials
involving long-term residential programmes and contingency
management were also effective in reducing substance use,
but some of this evidence was based on lower quality trials.
Limited support was found for other interventions including
CBT as a stand alone intervention, intensive case manage-
ment or non-integrated ACT. Future RCTs are needed to
assess the long-term benefits for patients with different
diagnoses to determine whether certain interventions work
better for different diagnostic subgroups. Future high quality
trials should include larger sample sizes, standardized out-
come measures and have longer follow-up periods to enable
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 253

the effectiveness of various psychosocial interventions to be
assessed.
Funding
This study was supported by an Educational Grant from
Pfizer Australia.
Author contributions
MC, GH and GW obtained funding. MC, GH, SM and GW
were responsible for the study conception and design. SM,
MC and GH performed the data collection and conducted the
data analysis. MC, GH, SM, GW drafted the manuscript.
MC and GH supervised the study and all authors gave their
approval of the version to be published.
References
Addington J. & Duchak V. (1997) Reasons for substance use in
schizophrenia. Acta Psychiatrica Scandinavica 96, 329–333.
Aguilera R., Anderson A.J., Gabrie E., Merlo M., Paredes T. &
Pastrana R. (1999) A clinical impact evaluation of integrated
and disease specific substance abuse program models in Hon-
duras. International Journal of Psychosocial Rehabilitation 3,
97–167.
Anderson A.J. (1999) A comparative impact evaluation of two
therapeutic programs for mentally ill chemical abusers. Interna-
tional Journal of Psychosocial Rehabilitation 4, 11–26.
Aubry T., Cousins B., LaFerriere D. & Wexler A. (2003) Evaluation
of Concurrent Disorders Group Treatment Program: Outcome
Evaluation Report. Centre for Research on Community Services,
Faculty of Social Sciences, University of Ottawa, Ottawa, ON.
Baker A., Lewin T., Reichler H., Clancy R., Carr V., Garrett R., Sly
K., Devir H. & Terry M. (2002) Evaluation of a motivational
interview for substance use within psychiatric in-patient services.
Addiction 97, 1329–1337.
Baker A., Bucci S., Lewin T.J., Kay-Lambkin F., Constable P.M. &
Carr V.J. (2006) Cognitive-behavioural therapy for substance use
disorders in people with psychotic disorders: randomised con-
trolled trial. British Journal of Psychiatry 188, 439–448.
Barrowclough C., Haddock G., Tarrier N., Lewis S.W., Moring J.,
O’Brien R., Schofield N. & McGovern J. (2001) Randomized
controlled trial of motivational interviewing, cognitive behavior
therapy, and family intervention for patients with comorbid
schizophrenia and substance use disorders. American Journal of
Psychiatry 158, 1706–1713.
Barrowclough C., Haddock G., Fitzsimmons M. & Johnson R.
(2006) Treatment development for psychosis and co-occurring
substance misuse: a descriptive review. Journal of Mental Health
15, 619–632.
Bellack A.S., Bennett M.E., Gearon J.S., Brown C.H. & Yang Y.
(2006) A randomized clinical trial of a new behavioral treatment
for drug abuse in people with severe and persistent mental illness.
Archives of General Psychiatry 63, 426–432.
Bennett M.E., Bellack A.S. & Gearon J.S. (2001) Treating substance
abuse in schizophrenia – an initial report. Journal of Substance
Abuse and Treatment 20, 163–175.
Blankertz L.E. & Cnaan R.A. (1994) Assessing the impact of two
residential programs for dually diagnosed homeless individuals.
Social Science Review 68, 536–560.
Bogenschutz M.P., Geppert C.M. & George J. (2006) The role of
twelve-step approaches in dual diagnosis treatment and recovery.
American Journal on Addictions 15, 50–60.
Bond G.R., McDonel E.C., Miller L.D. & Pensec M. (1991) Assertive
community treatment and reference groups: an evaluation of their
effectiveness for young adults with serious mental illness and
substance abuse problems. Psychosocial Rehabilitation Journal 15,
31–43.
Bowen R.C., D’Arcy C., Keegan D. & Senthilselvan A. (2000) A
controlled trial of cognitive behavioral treatment of panic in
alcoholic inpatients with comorbid panic disorder. Addictive
Behaviors 25, 593–597.
Brady K.T., Verduin M.L. & Tolliver B.K. (2007) Treatment of
patients comorbid for addiction and other psychiatric disorders.
Current Psychiatry Reports 9, 374–380.
van den Brink W., Montgomery S.A., Van Ree J.M., Zwieten-Boot
B.J. & Consensus Committee (2006) ECNP consensus meeting
March 2003 guidelines for the investigation of efficacy in
What is already known about this topic
• Substance misuse by people with severe mental illness
(dual diagnosis) is common and has many adverse
consequences.
• Engaging patients with a dual diagnosis in treatment is
difficult.
• Evidence for the effectiveness of psychosocial inter-
ventions is inconsistent and often based on trials of low
quality.
What this paper adds
• Motivational interviewing in psychiatric settings can
assist in the reduction of substance use, at least in the
short term.
• Long-term residential treatment may also be effective,
although less quality evidence is available.
• Contingency management gains some quality support,
but more research is needed.
Implications for practice and/or policy
• Use of motivational interviewing should be considered
in psychiatric settings for the reduction of substance
use, at least in the short term.
M. Cleary et al.
254 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

substance use disorders. European Neuropsychopharmacology 16,
224–230.
Broner N., Lattimore P.K., Cowell A.J. & Schlenger W.E. (2004)
Effects of diversion on adults with co-occurring mental illness and
substance use: outcomes from a national multi-site study. Behav-
ioral Sciences and the Law 22, 519–541.
Brooks A.J. & Penn P.E. (2003) Comparing treatments for dual
diagnosis: twelve-step and self-management and recovery training.
American Journal of Drug and Alcohol Abuse 29, 359–383.
Brown R.A., Evans D.M., Miller I.W., Burgess E.S. & Mueller T.I.
(1997) Cognitive-behavioral treatment for depression in alcohol-
ism. Journal of Consulting and Clinical Psychology 65, 715–726.
Brown S.A., Glasner-Edwards S.V., Tate S.R., McQuaid J.R.,
Chalekian J. & Granholm E. (2006) Integrated cognitive
behavioral therapy versus twelve-step facilitation therapy for
substance-dependent adults with depressive disorders. Journal of
Psychoactive Drugs 38, 449–460.
Brunette M.F., Drake R.E., Woods M. & Hartnett T. (2001) A com-
parison of long-term and short-term residential treatment programs
for dual diagnosis patients. Psychiatric Services 52, 526–528.
Burnam M.A., Morton S.C., McGlynn E.A., Petersen L.P., Stecher
B.M., Hayes C. & Vaccaro J.V. (1995) An experimental evaluation
of residential and nonresidential treatment for dually diagnosed
homeless adults. Journal of Addictive Diseases 14, 111–134.
Calsyn R.J., Yonker R.D., Lemming M.R., Morse G.A. &
Klinkenberg W.D. (2005) Impact of assertive community treat-
ment and client characteristics on criminal justice outcomes in dual
disorder homeless individuals. Criminal Behaviour and Mental
Health 15, 236–248.
Carey M.P., Carey K.B., Maisto S.A., Schroder K.E., Vanable P.A. &
Gordon C.M. (2004) HIV risk behavior among psychiatric out-
patients: association with psychiatric disorder, substance use dis-
order, and gender. Journal of Nervous and Mental Disease 192,
289–296.
Chandler D.W. & Spicer G. (2006) Integrated treatment for jail
recidivists with co-occurring psychiatric and substance use dis-
orders. Community Mental Health Journal 42, 405–425.
Chanut F., Brown T.G. & Dongier M. (2005) Motivational inter-
viewing and clinical psychiatry. Canadian Journal of Psychiatry –
Revue Canadienne de Psychiatrie 50, 548–554.
Cleary M., Hunt G.E., Matheson S., Siegfried N. & Walter G. (2008)
Psychosocial interventions for people with both severe mental
illness and substance misuse. Cochrane Database of Systematic
Review S1: CD001088, John Wiley & Sons Ltd.
Cohen L.R. & Hien D.A. (2006) Treatment outcomes for women
with substance abuse and PTSD who have experienced complex
trauma. Psychiatric Services 57, 100–106.
Cosden M., Ellens J.K., Schnell J.L., Yamini-Diouf Y. & Wolfe M.M.
(2003) Evaluation of a mental health treatment court with assertive
community treatment. Behavioral Sciences and the Law 21, 415–
427.
Cosden M., Ellens J., Schnell J. & Yamini-Diouf Y. (2005) Efficacy
of a mental health treatment court with assertive community
treatment. Behavioral Sciences and the Law 23, 199–214.
Daley D.C., Salloum I.M., Zuckoff A., Kirisci L. & Thase M.E.
(1998) Increasing treatment adherence among outpatients with
depression and cocaine dependence: results of a pilot study.
American Journal of Psychiatry 155, 1611–1613.
De Leon G., Sacks S., Staines G. & McKendrick K. (2000) Modified
therapeutic community for homeless mentally ill chemical abusers:
treatment outcomes. American Journal of Drug and Alcohol Abuse
26, 461–480.
Des Jarlais D.C., Lyles C., Crepaz N. & TREND Group (2004)
Improving the reporting quality of nonrandomized evaluations of
behavioral and public health interventions: the TREND statement.
American Journal of Public Health 94, 361–366.
Dickey B., Azeni H., Weiss R. & Sederer L. (2000) Schizophrenia,
substance use disorders and medical co-morbidity. Journal of
Mental Health Policy and Economics 3, 27–33.
DiNitto D.M., Webb D.K. & Rubin A. (2002) The effectiveness of an
integrated treatment approach for clients with dual diagnoses.
Research on Social Work Practice 12, 621–641.
Donald M., Dower J. & Kavanagh D. (2005) Integrated versus non-
integrated management and care for clients with co-occurring
mental health and substance use disorders: a qualitative systematic
review of randomised controlled trials. Social Science and Medicine
60, 1371–1383.
Drake R.E., Yovetich N.A., Bebout R.R., Harris M. & McHugo G.J.
(1997) Integrated treatment for dually diagnosed homeless adults.
Journal of Nervous and Mental Disease 185, 298–305.
Drake R.E., McHugo G.J., Clark R.E., Teague G.B., Xie H., Miles K.
& Ackerson T.H. (1998a) Assertive community treatment for
patients with co-occurring severe mental illness and substance use
disorder: a clinical trial. American Journal of Orthopsychiatry 68,
201–215.
Drake R.E., Mercer-McFadden C., Mueser K.T., McHugo G.J. &
Bond G.R. (1998b) Review of integrated mental health and sub-
stance abuse treatment for patients with dual disorders. Schizo-
phrenia Bulletin 24, 589–608.
Drake R.E., Mueser K.T., Brunette M.F. & McHugo G.J. (2004) A
review of treatments for people with severe mental illnesses and
co-occurring substance use disorders. Psychiatric Rehabilitation
Journal 27, 360–374.
Drake R.E., O’Neal E.L. & Wallach M.A. (2008) A systematic
review of psychosocial research on psychosocial interventions for
people with co-occurring severe mental and substance use dis-
orders. Journal of Substance Abuse and Treatment 34, 123–138.
Drebing C.E., Van Ormer E.A., Krebs C., Rosenheck R., Rounsaville
B., Herz L. & Penk W. (2005) The impact of enhanced incentives
on vocational rehabilitation outcomes for dually diagnosed veter-
ans. Journal of Applied Behavior Analysis 38, 359–372.
Dumaine M.L. (2003) Meta-analysis of interventions with
co-occurring disorders of severe mental illness and substance
abuse: implications for social work practice. Research on Social
Work Practice 13, 142–165.
Edwards J., Elkins K., Hinton M., Harrigan S.M., Donovan K.,
Athanasopoulos O. & McGorry P.D. (2006) Randomized con-
trolled trial of a cannabis-focused intervention for young people
with first-episode psychosis. Acta Psychiatrica Scandinavica 114,
109–117.
Essock S.M., Drake R.E., Frank R.G. & McGuire T.G. (2003)
Randomized controlled trials in evidence-based mental health care:
getting the right answer to the right question. Schizophrenia Bul-
letin 29, 115–123.
Essock S.M., Mueser K.T., Drake R.E., Covell N.H., McHugo G.J.,
Frisman L.K., Kontos N.J., Jackson C.T., Townsend F. & Swain K.
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 255

(2006) Comparison of ACT and standard case management for
delivering integrated treatment for co-occurring disorders.
Psychiatric Services 57, 185–196.
Fisher M.S. & Bentley K.J. (1996) Two group therapy models for
clients with a dual diagnosis of substance abuse and personality
disorder. Psychiatric Services 47, 1244–1250.
Fowler I.L., Carr V.J., Carter N.T. & Lewin T.J. (1998) Patterns of
current and lifetime substance use in schizophrenia. Schizophrenia
Bulletin 24, 443–455.
French M.T., Sacks S., De L.G., Staines G. & McKendrick K. (1999)
Modified therapeutic community for mentally ill chemical abusers:
outcomes and costs. Evaluation and the Health Professions 22, 60–
85.
Glasner-Edwards S., Tate S.R., McQuaid J.R., Cummins K., Gran-
holm E. & Brown S.A. (2007) Mechanisms of action in integrated
cognitive-behavioral treatment versus twelve-step facilitation for
substance-dependent adults with comorbid major depression.
Journal of Studies on Alcohol 68, 663–672.
Godley S.H., Hoewing-Roberson R. & Godley M.D. (1994) Final
MISA Report. The Illinois Department of Mental Health and
Developmental Disabilities & The Illinois Department of Alco-
holism and Substance Abuse, Bloomington, Illinois.
Goldsmith R.J. & Garlapati V. (2004) Behavioral interventions for
dual-diagnosis patients. Psychiatric Clinics of North America 27,
709–725.
Graeber D.A., Moyers T.B., Griffith G., Guajardo E. & Tonigan S.
(2003) A pilot study comparing motivational interviewing and an
educational intervention in patients with schizophrenia and alco-
hol use disorders. Community Mental Health Journal 39, 189–202.
Green A.I., Drake R.E., Brunette M.F. & Noordsy D.L. (2007)
Schizophrenia and co-occurring substance use disorder. American
Journal of Psychiatry 164, 402–408.
Gregg L., Barrowclough C. & Haddock G. (2007) Reasons for
increased substance use in psychosis. Clinical Psychology Review
27, 494–510.
Haddock G., Barrowclough C., Tarrier N., Moring J., O’Brien R.,
Schofield N., Quinn J., Palmer S., Davies L., Lowens I., McGovern
J. & Lewis S. (2003) Cognitive-behavioural therapy and motiva-
tional intervention for schizophrenia and substance misuse.
18-month outcomes of a randomised controlled trial. British
Journal of Psychiatry 183, 418–426.
Hawton K., Sutton L., Haw C., Sinclair J. & Deeks J.J. (2005)
Schizophrenia and suicide: systematic review of risk factors. British
Journal of Psychiatry 187, 9–20.
Hellerstein D.J., Rosenthal R.N. & Miner C.R. (1995) A prospective
study of integrated outpatient treatment for substance-abusing
schizophrenic patients. American Journal on Addictions 4, 33–42.
Herman S.E., Frank K.A., Mowbray C.T., Ribisl K.M., Davidson
W.S., BootsMiller B.J.L., Greenfield A.L., Loveland D. & Luke
D.A. (2000) Longitudinal effects of integrated treatment on alco-
hol use for persons with serious mental illness and substance use
disorders. Journal of Behavioral Health Services and Research 27,
286–302.
Hickman M.E. (1999) The effects of personal feedback on alcohol
intake in dually diagnosed clients: an empirical study of William R.
Miller’s motivational enhancement therapy. Dissertation Abstracts
International: Section B: The Sciences and Engineering 60(1-B),
367.
Hien D.A., Cohen L.R., Miele G.M., Litt L.C. & Capstick C. (2004)
Promising treatments for women with comorbid PTSD and sub-
stance use disorders. American Journal of Psychiatry 161, 1426–
1432.
Higgins J.P.T. & Green S. (eds) (2006) Cochrane Handbook for
Systematic Reviews of Interventions 4.2.6. The Cochrane Library,
Issue 4, 2006. John Wiley & Sons Ltd, Chichester, UK.
Ho A.P., Tsuang J.W., Liberman R.P., Wang R., Wilkins J.N.,
Eckman T.A. & Shaner A.L. (1999) Achieving effective treat-
ment of patients with chronic psychotic illness and comorbid
substance dependence. American Journal of Psychiatry 156,
1765–1770.
Howland R.H. (2007) Limitations of evidence in the practice of
evidence-based medicine. Journal of Psychosocial Nursing and
Mental Health Services 45, 13–16.
Hulse G.K. & Tait R.J. (2002) Six-month outcomes associated with a
brief alcohol intervention for adult in-patients with psychiatric
disorders. Drug and Alcohol Review 21, 105–112.
James W., Preston N.J., Koh G., Spencer C., Kisely S.R. & Castle
D.J. (2004) A group intervention which assists patients with dual
diagnosis reduce their drug use: a randomized controlled trial.
Psychological Medicine 34, 983–990.
Janssen B., Gaebel W., Haerter M., Komaharadi F., Lindel B. &
Weinmann S. (2006) Evaluation of factors influencing medication
compliance in inpatient treatment of psychotic disorders. Psycho-
pharmacology 187, 229–236.
Jerrell J.M. & Ridgely M.S. (1995) Comparative effectiveness of
three approaches to serving people with severe mental illness and
substance abuse disorders. Journal of Nervous and Mental Disease
183, 566–576.
Kasprow W.J., Rosenheck R., Frisman L. & DiLella D. (1999)
Residential treatment for dually diagnosed homeless veterans: a
comparison of program types. American Journal on Addictions 8,
34–43.
Kavanagh D.J., Waghorn G., Jenner L., Chant D.C., Carr V., Evans
M., Hemnan H., Jablensky A. & McGrath J.J. (2004a) Demo-
graphic and clinical correlates of comorbid substance use disorders
in psychosis: multivariate analyses from an epidemiological
sample. Schizophrenia Research 66, 115–124.
Kavanagh D.J., Young R., White A., Saunders J.B., Wallis J.,
Shockley N., Jenner L. & Clair A. (2004b) A brief motivational
intervention for substance misuse in recent-onset psychosis. Drug
and Alcohol Review 23, 151–155.
Kemp R., Harris A., Vurel E. & Sitharthan T. (2007) Stop using stuff:
trial of a drug and alcohol intervention for young people with
comorbid mental illness and drug and alcohol problems. Austral-
asian Psychiatry 15, 490–493.
Kessler R.C., Crum R.M., Warner L.A., Nelson C.B., Schulenberg J.
& Anthony J.C. (1997) Lifetime co-occurrence of DSM-III-R
alcohol abuse and dependence with other psychiatric disorders in
the National Comorbidity Survey. Archives of General Psychiatry
54, 313–321.
Kleber H.D., Weiss R.D., Anton R.F. Jr, George T.P., Greenfield S.F.,
Kosten T.R., O’Brien C.P., Rounsaville B.J., Strain E.C., Ziedonis
D.M., Hennessy G., Connery H.S. & Work Group on Substance
Use Disorders (2007) Treatment of patients with substance use
disorders, 2nd edn. American Journal of Psychiatry 164(Suppl.), 5–
123.
M. Cleary et al.
256 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd

Laker C.J. (2007) How reliable is the current evidence looking
at the efficacy of harm reduction and motivational inter-
viewing interventions in the treatment of patients with a dual
diagnosis? Journal of Psychiatric and Mental Health Nursing 14,
720–726.
Lehman A.F., Herron J.D., Schwartz R.P. & Myers C.P. (1993)
Rehabilitation for adults with severe mental illness and substance
use disorders. A clinical trial. Journal of Nervous and Mental
Disease 181, 86–90.
Ley A., Jeffery D.P., McLaren S. & Siegfried N. (2001) Treatment
programmes for people with both severe mental illness and sub-
stance misuse. The Cochrane Library, Issue 3. Cochrane Database
of Systematic Reviews: CD001088, The Cochrane Collaboration,
John Wiley & Sons Ltd, Chichester, UK.
Linehan M.M., Dimeff L.A., Reynolds S.K., Comtois K.A., Welch
S.S., Heagerty P. & Kivlahan D.R. (1999a) Dialectical behavior
therapy versus comprehensive validation therapy plus 12-step for
treatment of opioid dependent women meeting criteria for bor-
derline personality disorder. Drug and Alcohol Dependence 67,
13–26.
Linehan M.M., Schmidt H. III, Dimeff L.A., Craft J.C., Kanter J. &
Comtois K.A. (1999b) Dialectical behavior therapy for patients
with borderline personality disorder and drug-dependence. Amer-
ican Journal on Addictions 8, 279–292.
Magura S., Laudet A.B., Mahmood D., Rosenblum A., Vogel H.S. &
Knight E.L. (2003) Role of self-help processes in achieving absti-
nence among dually diagnosed persons. Addictive Behaviors 28,
399–413.
Mangrum L.F., Spence R.T. & Lopez M. (2006) Integrated versus
parallel treatment of co-occurring psychiatric and substance use
disorders. Journal of Substance Abuse and Treatment 30, 79–84.
Martino S., Carroll K.M., O’Malley S.S. & Rounsaville B.J. (2000)
Motivational interviewing with psychiatrically ill substance abus-
ing patients. American Journal on Addictions 9, 88–91.
Martino S., Carroll K.M., Nich C. & Rounsaville B.J. (2006) A
randomized controlled pilot study of motivational interviewing for
patients with psychotic and drug use disorders. Addiction 101,
1479–1492.
McGovern M.P. & McLellan A.T. (2008) The status of addiction
treatment research with co-occurring substance use and psychi-
atric disorders. Journal of Substance Abuse and Treatment 34,
1–2.
McHugo G.J., Drake R.E., Teague G.B. & Xie H. (1999) Fidelity to
assertive community treatment and client outcomes in the New
Hampshire dual disorders study. Psychiatric Services 50, 818–824.
Milby J.B., Schumacher J.E., McNamara C., Wallace D., Usdan S.,
McGill T. & Michael M. (2000) Initiating abstinence in cocaine
abusing dually diagnosed homeless persons. Drug and Alcohol
Dependence 60, 55–67.
Morrissey J.P., Jackson E.W., Ellis A.R., Amaro H., Brown V.B. &
Najavits L.M. (2005) Twelve-month outcomes of trauma-informed
interventions for women with co-occurring disorders. Psychiatric
Services 56, 1213–1222.
Morse G.A., Calsyn R.J., Dean K.W., Helminiak T.W., Wolff N.,
Drake R.E., Yonker R.D., Lama G., Lemming M.R. & McCudden
S. (2006) Treating homeless clients with severe mental illness and
substance use disorders: costs and outcomes. Community Mental
Health Journal 42, 377–404.
Mowbray C.T., Jordan L.C., Ribisl K.M., Kewalramani A., Luke D.,
Herman S. & Bybee D. (1999) Analysis of postdischarge change
in a dual diagnosis population. Health and Social Work 24, 91–
101.
Mueser K., Drake R., Sigmon S. & Brunette M.F. (2005) Psychoso-
cial interventions for adults with severe mental illnesses and
co-occurring substance use disorders: a review of specific inter-
ventions. Journal of Dual Diagnosis 1, 57–82.
Naeem F., Kingdon D. & Turkington D. (2005) Cognitive behaviour
therapy for schizophrenia in patients with mild to moderate sub-
stance misuse problems. Cognitive Behaviour Therapy 34, 207–
215.
National Health and Medical Research Council (1999) A Guide to
the Development, Implementation and Evaluation of Clinical
Practice Guidelines. National Health & Medical Research Coun-
cil, Canberra, SA.
National Health and Medical Research Council (2000) How to
Review the Evidence: Systematic Identification and Review of the
Scientific Literature. National Health & Medical Research Coun-
cil, Canberra, SA.
Newhouse R.P. (2008) Evidence and the executive. Journal of
Advanced Nursing 38, 107–111.
Nuttbrock L.A., Rahav M., Rivera J.J., Ng-Mak D.S. & Link B.G.
(1998) Outcomes of homeless mentally ill chemical abusers in
community residences and a therapeutic community. Psychiatric
Services 49, 68–76.
Rahav M., Rivera J.J., Nuttbrock L.A., Ng-Mak D.S., Sturz E.L.,
Link B.G., Struening E.L., Pepper B. & Gross B. (1995) Charac-
teristics and treatment of homeless, mentally ill, chemical-abusing
men. Journal of Psychoactive Drugs 27, 93–103.
Randall C.L., Thomas S. & Thevos A.K. (2001) Concurrent alco-
holism and social anxiety disorder: a first step toward developing
effective treatments. Alcoholism: Clinical and Experimental
Research 25, 210–220.
Regier D.A., Farmer M.E., Rae D.S., Locke B.Z., Keith S.J., Judd
L.L. & Goodwin F.K. (1990) Comorbidity of mental disorders
with alcohol and other drug abuse. Results from the epidemio-
logical catchment area (ECA) study. Journal of the American
Medical Association 264, 2511–2518.
Ries R.K., Dyck D.G., Short R., Srebnik D., Fisher A. & Comtois
K.A. (2004) Outcomes of managing disability benefits among
patients with substance dependence and severe mental illness.
Psychiatric Services 55, 445–447.
Rounsaville B.J. (2004) Treatment of cocaine dependence and
depression. Biological Psychiatry 56, 803–809.
Sacks S., Sacks J.Y., McKendrick K., Banks S. & Stommel J. (2004)
Modified TC for MICA offenders: crime outcomes. Behavioral
Sciences and the Law 22, 477–501.
Sacks S., Chandler R. & Gonzales J. (2008a) Responding to the
challenge of co-occurring disorders: suggestions for future
research. Journal of Substance Abuse Treatment 34, 139–146.
Sacks S., McKendrick K., Sacks J.Y., Banks S. & Harle M. (2008b)
Enhanced outpatient treatment for co-occurring disorders: main
outcomes. Journal of Substance Abuse Treatment 34, 48–60.
Santa Ana E.J., Wulfert E. & Nietert P.J. (2007) Efficacy of group
motivational interviewing (GMI) for psychiatric inpatients with
chemical dependence. Journal of Consulting and Clinical
Psychology 75, 816–822.
JAN: REVIEW PAPER Psychosocial treatments for people with a dual diagnosis
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd 257

Schmitz J.M., Averill P., Sayre S., McCleary P., Moeller F.G. &
Swann A. (2002) Cognitive-behavioral treatment of bipolar dis-
order and substance abuse: a preliminary randomized study.
Addictive Disorders and Their Treatment 1, 17–24.
Schulz K.F. & Grimes D.A. (2002a) Allocation concealment in
randomised trials: defending against deciphering. Lancet 359, 614–
618.
Schulz K.F. & Grimes D.A. (2002b) Blinding in randomised trials:
hiding who got what. Lancet 359, 696–700.
Schulz K.F. & Grimes D.A. (2002c) Generation of allocation
sequences in randomised trials: chance, not choice. Lancet 359,
515–519.
Shafer M.S., Arthur B. & Franczak M.J. (2004) An analysis of post-
booking jail diversion programming for persons with co-occurring
disorders. Behavioral Sciences and the Law 22, 771–785.
Steadman H.J. & Naples M. (2005) Assessing the effectiveness of jail
diversion programs for persons with serious mental illness and
co-occurring substance use disorders. Behavioral Sciences and the
Law 23, 163–170.
Strong Kinnaman J.E., Slade E., Bennett M.E. & Bellack A.S. (2007)
Examination of contingency payments to dually-diagnosed patients
in a multi-faceted behavioral treatment. Addictive Behaviors 32,
1480–1485.
Sullivan C.J., McKendrick K., Sacks S. & Banks S. (2007) Modified
therapeutic community treatment for offenders with MICA disor-
ders: substance use outcomes. American Journal of Drug and
Alcohol Abuse 33, 823–832.
Swanson A.J., Pantalon M.V. & Cohen K.R. (1999) Motivational
interviewing and treatment adherence among psychiatric and
dually diagnosed patients. Journal of Nervous and Mental Disease
187 (10), 630–635.
Tiet Q.Q. & Mausbach B. (2007) Treatments for patients with dual
diagnosis: a review. Alcoholism: Clinical and Experimental
Research 31, 513–536.
Timko C. & Sempel J.M. (2004a) Intensity of acute services, self-help
attendance and one-year outcomes among dual diagnosis patients.
Journal of Studies on Alcohol 65, 274–282.
Timko C. & Sempel J.M. (2004b) Short-term outcomes of matching
dual diagnosis patients’ symptom severity to treatment intensity.
Journal of Substance Abuse Treatment 26, 209–218.
Timko C., Shuo C., Sempel J. & Barnett P. (2006) Dual diagnosis
patients in community or hospital care: one-year outcomes and
health care utilization and costs. Journal of Mental Health 15,
163–177.
Todd J., Green G., Harrison M., Ikuesan B.A., Self C., Pevalin D.J. &
Baldacchino A. (2004) Social exclusion in clients with comorbid
mental health and substance misuse problems. Social Psychiatry
and Psychiatric Epidemiology 39, 581–587.
Tracy K., Babuscio T., Nich C., Kiluk B., Carroll K.M., Petry N.M.
& Rounsaville B.J. (2007) Contingency management to reduce
substance use in individuals who are homeless with co-occurring
psychiatric disorders. American Journal of Drug and Alcohol
Abuse 33, 253–258.
Tsuang J., Fong T.W. & Lesser I. (2006) Psychosocial treatment of
patients with schizophrenia and substance abuse disorders.
Addictive Disorders and Their Treatment 5, 53–66.
Turpin D.L. (2005) CONSORT and QUOROM guidelines for
reporting randomized clinical trials and systematic reviews.
American Journal of Orthodontics and Dentofacial Orthopedics
128, 681–685.
Warren J.I., Stein J.A. & Grella C.E. (2007) Role of social support
and self-efficacy in treatment outcomes among clients with
co-occurring disorders. Drug and Alcohol Dependence 89, 267–
274.
Watt M., Stewart S., Birch C. & Bernier D. (2006) Brief CBT for high
anxiety sensitivity decreases drinking problems, relief alcohol
outcome expectancies, and conformity drinking motives: evidence
from a randomized controlled trial. Journal of Mental Health 15,
683–695.
Weiss R.D., Griffin M.L., Greenfield S.F., Najavits L.M., Wyner D.,
Soto J.A. & Hennen J.A. (2000) Group therapy for patients with
bipolar disorder and substance dependence: results of a pilot study.
Journal of Clinical Psychiatry 61, 361–367.
Weiss R.D., Griffin M.L., Kolodziej M.E., Greenfield S.F., Najavits
L.M., Daley D.C., Doreau H.R. & Hennen J.A. (2007) A
randomized trial of integrated group therapy versus group
drug counseling for patients with bipolar disorder and sub-
stance dependence. American Journal of Psychiatry 164, 100–
107.
Ziedonis D.M., Smelson D., Rosenthal R.N., Batki S.L., Green A.I.,
Henry R.J., Montoya I., Parks J. & Weiss R.D. (2005) Improving
the care of individuals with schizophrenia and substance use dis-
orders: consensus recommendations. Journal of Psychiatric Prac-
tice 11, 315–339.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the
advancement of evidence-based nursing, midwifery and health care by disseminating high quality research and
scholarship of contemporary relevance and with potential to advance knowledge for practice, education, management
or policy. JAN publishes research reviews, original research reports and methodological and theoretical papers.
For further information, please visit the journal web-site: http://www.journalofadvancednursing.com
M. Cleary et al.
258 � 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd
Copyright © 2022 FDOKUMEN




















