
Psychogeriatric Outreach To Rural Families: The Iowa and Virginia Models
10
College of Nursing Publications 1-1-1993 Psychogeriatric outreach to rural families: the Iowa and Virginia models I. L. Abraham Kathleen C. Buckwalter University of Iowa D. G. Snustad Please see article for additional authors. Copyright © Springer Publishing Company, 1993. Posted by permission. International psychogeriatrics / IPA, 5:2 (1993) pp.203-211. Hosted by Iowa Research Online. For more information please contact: [email protected].
Transcript of Psychogeriatric Outreach To Rural Families: The Iowa and Virginia Models
College of Nursing Publications
1-1-1993
Psychogeriatric outreach to rural families: the Iowaand Virginia modelsI. L. Abraham
Kathleen C. BuckwalterUniversity of Iowa
D. G. Snustad
Please see article for additional authors.
Copyright © Springer Publishing Company, 1993. Posted by permission.
International psychogeriatrics / IPA, 5:2 (1993) pp.203-211.
Hosted by Iowa Research Online. For more information please contact: [email protected].
International Psychogeriatrics. Vol. 5, No. 2,1993 Q 1993 Springer Publishing Company
Psychogeriatric Outreach To Rural Families: The Iowa and Virginia Models
Ivo L. Abraham, Kathleen Coen Buckwalter, Diane G. Snustad, Dianne E. Smullen, Anita A. Thompson-Heisterman,
Jane Bryant Neese, and Marianne Smith
ABSTRACT. Elderly residents of mal areas are at significant risk for mental health problems, yet have less access to mental health services. Thus, most mental health problems among rural elderly remain either undiagnosed or untreated. We describe two models of mental health outreach programs to rural elderly in Iowaand Virginia, serving demographically, culturally, and epidemio- logically different populations in geographically and economically dissimilar regions. Programs are compared on the basis of initiation, community partner- ships, target population, target region, clinical disciplines involved, coordinat- ing discipline, referral sources, operational model, initial home assessment, care planning, sustainability, cost, patient demographics, and primary and secondary diagnoses. Outreach programs are argued to be effective models of delivering services to geographically and/or socially isolated elderly populations. The experiences of our programs, though limited to rural populations, may be of relevance to any outreach program attempting to serve elderly presenting with or at risk for mental health problems.
The romanticized vision of tranquility and prosperity that many associate with life in the vast rural areas of the United States may be the privilege of only a few rural residents. About 25% of Americans live in rural areas of the country, yet they constitute 40% of this nation’s poor, with statistics being even higher for minority populations (Buckwalter et al., 1988). For many residents of rural areas, the daily reality is one of deprivation and impoverishment, inadequate housing, inacces- sible, or unavailable health and human services, unaddressed health problems, and economic and social isolation (Coward & Lee, 1985). This is particularly the case for rural elderly, placing them at significant risk for physical and mental health problems while compromising them because of the insufficiency of health services.
From the University of Virginia (I. L. Abraham, PhD, CS, RN, D. G. Snustad, MD; D. E. Smullen, MSN, RN, and J. B. Neese. MS, CS, RN); the Jefferson Area Rural Elder Health Consortium (I. L. Abraham, PhD. CS, RN; D. G. Snustad, MD, D. E. Smullen, MSN, RN, A. A. Thompson-Heisterman, MSN, CS, R N and J. B. Neese, MS, CS. RN); and Region Ten Community Services Board (A. A. Thompson-Heisterman, MSN, CS, RN), Charlottemille. Virginia; the University of Iowa, Iowa City, Iowa (K. C. Buckwalter, PhD, RN); the Abbe Center for Community Mental Health, Cedar Rapids, Iowa, U.S.A. (K. C. Buckwalter, PhD, RN, and M. Smith, MS, RN ); and the Catholic University of
,203 Leuven, Belgium 0. L. Abraham, PhD, CS, RN).
204 I . L. Abraham et al.
Mental health problems among the elderly are an underrecognized problem in rural communities. As the President’s Commission on Mental Health (1978) noted, “rural communities tend to be characterized by higher than average rates of psychiatric disorders, particularly depression, by severe intergenerational con- flicts, by an exodus of individuals who might serve as effective role models for coping, by an acceptance of fatalistic attitudes and minimal subscription to the idea that change is possible” (p. 1164). Coupled with the (often fierce) sense of self- determination and independence characteristic of many rural Americans, and the pronounced stigmata associated with mental illness, it is safe to say that most mental health problems among rural residents remain undiagnosed and untreated.
Data about the prevalence of psychiatric symptomatology and illness among rural elderly vary, but nonetheless underscore the intensity of a problem that covers the full range of major psychiatric diagnostic categories. According to earlier studies, between 12% and 23% of rural elderly are at risk for mental disorders (Scheidt & Windley, 1982), and up to 25% of rural elderly have significant mental health prob- lems to warrant psychiatric intervention (Rosen et al., 1981). A more recent study found that 56% of rural elderly had serious mental health problems as compared to 24% of urban elderly (Wagenfeld et al., 1988). The variability in rates may be due to differences in operational definitions from one study to another. Even though alcohol abuse or dependence tends to decrease with age, alcohol-related problems are more prevalent in rural areas, especially in the South (Blazer et al., 1985; Blazer et al., 1987). Cognitive disorders have been found to be more common in rural popu- lations (Blazer et al., 1985). Rural elderly admitted to acute care hospitals have longer lengths of stay (Deprez et al., 1987), and those residing in long-term care fa- cilities tend to be younger and more functional than their urban counterparts (Greene, 1984). Even though the need for services is high among rural elderly, service utili- zation is low. Only between 1% (Scheidt & Windley, 1982) and 7% (Kermis, 1987) ofruralelder1yusementalhealthservices.Thismaybedueinpartto the factthat rural residents are more likely to be without a regular source of health care and without medical insurance than urban residents (Norton & McManus, 1989), and in part to the mere reality that (mental) health services are inequitably distributed in rural as compared to urban/mempolitan mas (Abraham & Neese, in press; Hart et al., 1991).
In addition to primary mental health problems, there are also the issues of comorbidity and severity of illness. For instance, Waltz, Craft, and Walters (1987) reported physical illness comorbidity in 47.7% of chronically mentally ill older adults in Iowa. Because few rural elderly with mental health problems have access to or utilize professional services, those who do enter the mental health system do so more ill, impaired, and disabled than if more timely intervention would have been possible. The mental health issues of rural elderly, then, are best conceptual- ized within Cohen’s (1989) four models or paradigms of interrelated effects between physical and mental health: (1) effects of severe psychological stress on physical health; (2) effects of physical disorder leading to psychiatric disorder, (3) interplay of coexisting physical and mental disorders; and (4) impact of psychoso- cial factors on the clinical course of physical health problems.
This paper compares two model outreach programs, serving demographically,
Psychogeriatric Outreach to Rural Families 205
culturally, and epidemiologically different populations, and geographically and economically dissimilar rural regions. Outreach programs have been suggested as effective approaches to health service delivery to underserved elderly, because of the dual problem of insufficiency of services and those people most at risk not presenting themselves at the services that do exist (Jamiesonet al., 1989; Raschko, 1985; Reifler et al., 1982; Toseland et al., 1979; Wasson et al., 1984; Yedidia, 1990). Outreach models also address concerns expressed by Palmer and Cunningham (1983), who emphasized the need for coordination and cooperation among mental health, medical, and social service providers; maximizing limited resources; assuring continuity of care; and using professional, paraprofessional, and lay personnel.
COMPARISON OF THE IOWA AND VIRGINIA MODELS
The Iowa program was initiated in 1986 in the east-central counties of Linn and Jones, with the city of Cedar Rapids serving as the central location. The Virginia program was started in 1990 and was built in part upon the experiences of the Iowa program. This program Serves the five-county Jefferson area surrounding the city of Charlottesville (Albemarle, Greene, Louisa, Nelson, and Fluvanna). While serving distinctly different populations in a geographically different region through a different program, the Virginia program does share several similarities with the Iowa program. These similarities, we speculate, might be common characteristics of effective programs. In contrast, the dissimilarities come from a sensitivity to local differences in population (education, socioeconomic status, race, sociocul- tural status), geography, service infrastructure, and epidemiology. Together, both programs might be replicable models of community-based mental health care for rural elderly in midwestem and southern regions. Table 1 summarizes the Iowa and Virginia models along several program characteristics. We highlight here some similarities and differences to complement the information provided in this table.
Both programs are community partnerships involving the local area agency on aging and the community mental health system, with the Virginia program also involving the University of Virginia as a formal partner. Both programs were initiated through grant funding, which is still active for the more recent Virginia program, but which has expired forthe Iowaprogram. The latter, however, has since been formally embedded in the community’s elder health services infrastructure, a goal being pursued in Virginia, as well. While the demographics of east-central Iowa are very homogeneous, Virginia presents with great racial (African-American), cultural (white Appalachian), and economic (chronic poverty) diversity. Similarly, while the Iowa program Serves a geographically consistent and accessible area (barring inclement weather), the Virginia program extends from the flatness of the Piedmont plateau to the peaks and hollows of the Blue Ridge Mountains, throughout an area that includes many roads in poor condition and many inaccessible homes. Prior to implementing the outreach programs in both Iowa and Virginia, access and utilization of mental health services by rural elderly was limited and disproportionate to the need. In Virginia this was particularly true for the racial and sociocultural subgroups living in the target region (African-Americans, socioculturally different
206 I. L Abraham et al.
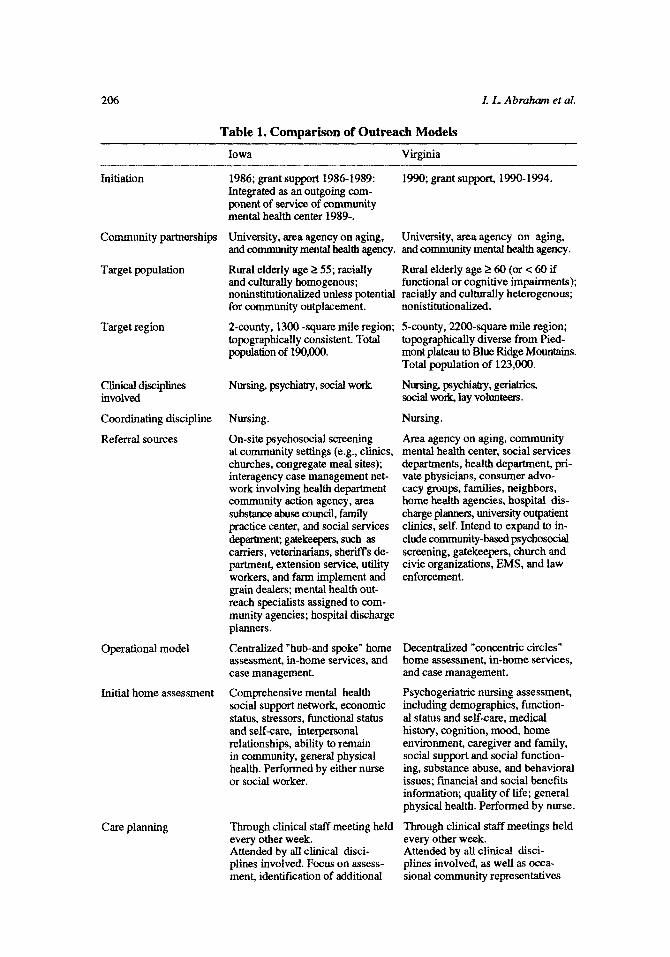
Table 1. Comparison of Outreach Models Iowa Virginia
Initiation
Community partnerships
Target population
Target region
Clinical disciplines involved
Coordinating discipline
Referral sources
Operational model
Initial home assessment
Care planning
1986; grant support 1986-1989: Integrated as an outgoing com- ponent of service of community mental health center 1989-.
University, area agency on aging, and community mental health agency. and community mental health agency.
Rural elderly age 2 55; racially and culturally homogenous; noninstitutionalized unless Dotential racially and culturally heterogenous;
1990; grant support, 1990-1994.
University, area agency on aging,
Rural elderly age 2 60 (or c 60 if functional or cognitive impairments);
for community outplaceme&.
2-county, 1300 -square mile region; topographically consistent. Total population of 190,000.
Nursing, psychiatry, social work
Nursing.
On-site psychosocial screening at community settings (e.g., clinics, churches, congregate meal sites); interagency case management net- work involving health department community action agency, area substance abuse council, family practice center, and social services department gatekeepers, such as carriers, veterinarians, sheriffs de- partment, extension service, utility workers, and farm implement and grain dealers; mental health out- reach specialists assigned to com- munity agencies; hospital discharge planners.
Centralized "hub-and spoke'' home assessment, in-home services, and case management. Comprehensive mental health social support network, economic status, stressors, functional status and self-care, interpersonal relationships, ability to remain in community, general physical health. Performed by either nurse or social worker.
Through clinical staff meeting held every other week. Attended by all clinical disci- plines involved. Focus on assess- ment, identification of additional
nonisthtionalized.
5-county, 2200-square mile region; topographically diverse from Pied- mont plateau to Blue Ridge Mountains. Total population of 123,000.
Nursing, psychiatry, geriatrics, social work, lay volunteers.
Nursing.
Area agency on aging, community mental health center, social services departments, health department, pri- vate physicians, consumer advo- cacy groups, families, neighbors, home health agencies, hospital dis- charge planners, university outpatient clinics, self. Intend to expand to in- clude community-based psychosocial screening, gatekeepers, church and civic organizations, EMS, and law enforcement.
-
Decentraalized "concentric circles" home assessment, in-home services, and case management.
Psychogeriatric nursing assessment, including demographics, function- al status and self-care, medical history, cognition, mood, home environment, caregiver and family, social support and social function- ing, substance abuse, and behavioral issues; financial and social benefits information; quality of life; general physical health. Performed by nurse.
Through clinical staff meetings held every other week. Attended by all clinical disci- plines involved, as well as occa- sional community representatives
Psychogeriatric Outreach fo Rural Families 207
Table 1. (continued) Iowa Virginia
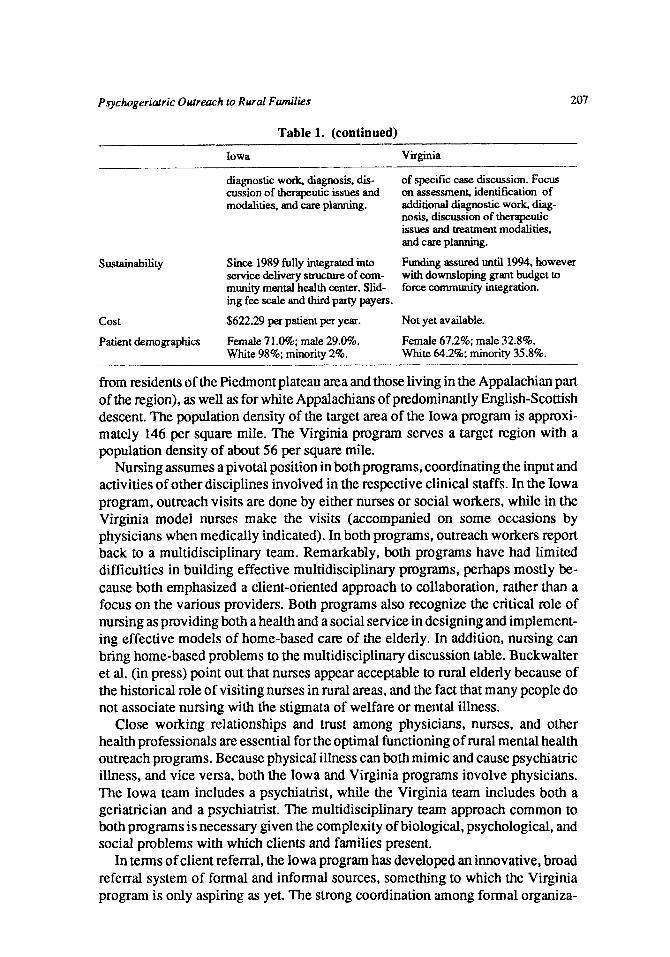
diagnostic work, diagnosis, dis- cussion of therapeutic issues and modalities, and care planning.
of specific case discussion. Focus on assessment, identification of additional diagnostic work, diag- nosis, discussion of therapeutic issues and matment modalities, and care planning.
Funding assured until 1994, however with downsloping grant budget to force community integration.
SUStainability Since 1989 fully integrated into service delivery structure of cam- munity mental health center. Slid- ing fee scale and third party payers.
cost $622.29 per patient per year. Not yet available.
Patient demographics Female 71.0%; male 29.0%. Female 67.2%; male 32.8%. White 98%; minority 2%. White 64.2%; minority 35.8%.
from residents of the Piedmont plateau area and those living in the Appalachian part of the region), as well as for white Appalachians of predominantly English-Scottish descent. The population density of the target area of the Iowa program is approxi- mately 146 per square mile. The Virginia program serves a target region with a population density of about 56 per square mile.
Nursing assumes a pivotal position in both programs, coordinating the input and activities of other disciplines involved in the respective clinical staffs. In the Iowa program, outreach visits are done by either nurses or social workers, while in the Virginia model nurses make the visits (accompanied on some occasions by physicians when medically indicated). In both programs, outreach workers report back to a multidisciplinary team. Remarkably, both programs have had limited difficulties in building effective multidisciplinary programs, perhaps mostly be- cause both emphasized a client-oriented approach to collaboration, rather than a focus on the various providers. Both programs also recognize the critical role of nursing as providing both a health and a social service in designing and implement- ing effective models of home-based care of the elderly. In addition, nursing can bring home-based problems to the multidisciplinary discussion table. Buckwalter et al. (in press) point out that nurses appear acceptable to rural elderly because of the historical role of visiting nurses in rural areas, and the fact that many people do not associate nursing with the stigmata of welfare or mental illness.
Close working relationships and trust among physicians, nurses, and other health professionals are essential for the optimal bctioning of rural mental health outreach programs. Because physical illness can both mimic and cause psychiatric illness, and vice versa, both the Iowa and Virginia programs involve physicians. The Iowa team includes a psychiatrist, while the Virginia team includes both a geriatrician and a psychiatrist. The multidisciplinary team approach common to both programs is necessary given the complexity of biological, psychological, and social problems with which clients and families present.
In terms of client referral, the Iowa program has developed an innovative, broad referral system of formal and informal sources, something to which the Virginia program is only aspiring as yet. The strong coordination among formal organiza-
208 I . L. Abraham et al.
tions in Iowa attests to the prior collaborative relationships within the target region. In contrast, little prior collaboration existed within the Jefferson area, thus making the outreach program a visible focal point for community integration efforts related to multiagency mental health care for rural elderly.
Because of demographic, epidemiological, and geographic differences, both programs vary in their basic operational model. The Iowa model can be likened to a hub-and-spoke model in which the multidisciplinary team reaches out from a centralized location (the community mental health center), and works within a larger service delivery infrastructure centered primarily in Cedar Rapids. This infrastruc- ture involves various community agencies, an interagency case management referral network, and community workers such as visiting nurses, meal site managers, and community action agency workers. Links to the informal network of assistance include church members, neighbors, family members, and other volunteers. In contrast, the Virginia model is more decentralized and can be summarized as a concentric circles model of multiple layers of informal and formal resources and services. Because of the insufficient availability of (even essential) services, the Virginia model has to actively rely on informal community-based resources. Thus, the inner concentric circles of help include family members, friends, and neighbors. The next layer includes community and church volunteers and community-based services such as congregate meal sites. This is followed by the layer consisting of local primary care providers, such as private physicians, nurse practitioners, health department clinics, and rural health clinics, as well as formal community resources associated with the area agency on aging and the community mental health center. The centralized resources of the Charlottemille area and those of the University of Virginia constitute the peripheral circles. Critical to the Virginia model is that higher layers are activated only when the situation truly warrants intervention.
The services provided by both programs share a focus on in-home assessment and subsequent case management centered on client as well as family - the latter often being multigenerational (several generations living together), or transgenerational (generations living together but with one generation absent), rather than nuclear. Also, they share a highly individualized approach to delivering care, in which client and family needs shape the care that is provided. Thus, there is little standardization of services, as both programs emphasize highly individualized care. This care includes comprehensive assessments in the home, and both programs collect roughly the same information: demographic, referral data, functional status, mental status, mood, cognition, financial and benefits data, key medical data, caregiver and family information, and knowledge about community resources. Standardized measures for use with the elderly are included as pan of the assessments as much as possible. In multidisciplinary team meetings, the need for additional diagnostic work is dis- cussed, care plans are developed, and matment and management strategies are determined. New referrals are presented as well. 'While the Iowa program strives for short-term involvement by the outreach team, nurses in the Virginia program often engage in care relationships of a longer duration.
The problem with grant-supported services is that they often cease when the funding ends. Sustainability is a dual matter of integrating into a formal service
Psychogeriatric Oidreach to Rural Families 209
delivery structure and assuring revenue. In 1989, the Iowa outreach program was absorbed into the services of the local community mental health center, becoming the focal point of the new Elderly Services Division. The services are covered by a sliding fee scale and third party payments. The cost per client per year for the Iowa program is substantially lower than that reported by a local group of mental health providers. The Virginia program aspires to a similar solution. Virginia’s grant support is on a downsloping budget to encourage a gradual transition of the program to self-supported status.
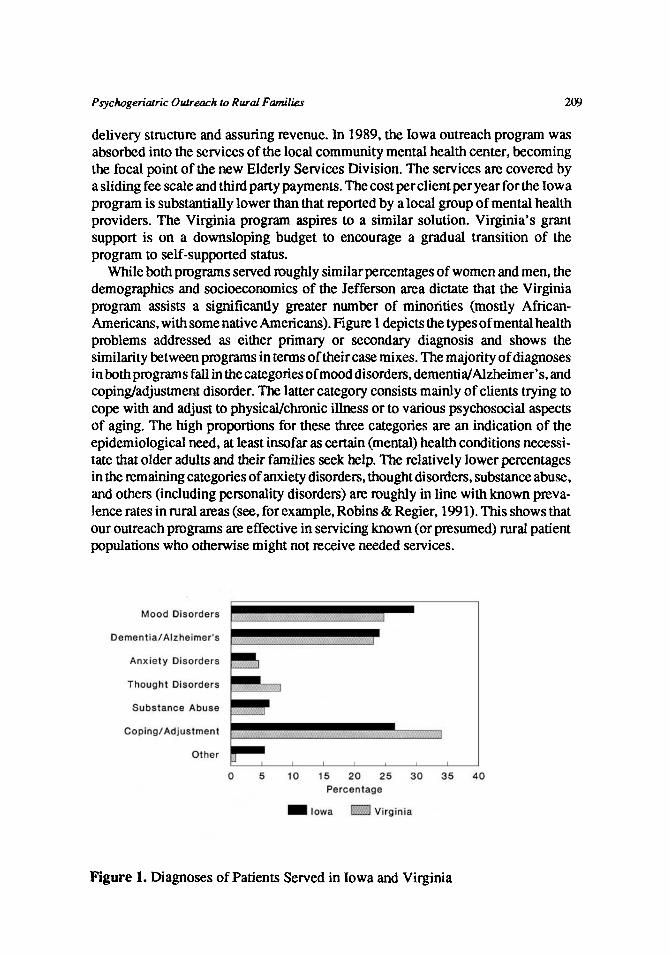
While both programs served roughly similar percentages of women and men, the demographics and socioeconomics of the Jefferson area dictate that the Virginia program assists a significantly greater number of minorities (mostly African- Americans, with some native Americans). Figure 1 depicts the types of mental health problems addressed as either primary or secondary diagnosis and shows the similarity between programs in tenns of their case mixes. The majority of diagnoses in both programs fall in the categories of mood disorders, dementidAlzheimer’s, and coping/adjustment disorder. The latter category consists mainly of clients trying to cope with and adjust to physical/chnic illness or to various psychosocial aspects of aging. The high proportions for these three categories are an indication of the epidemiological need, at least insofar as certain (mental) health conditions necessi- tate that older adults and their families seek help. The relatively lower percentages in the remaining categories of anxiety disorders, thought disorders, substance abuse, and others (including personality disorders) are roughly in line with known preva- lence rates in rural areas (see, for example, Robins & Regier, 1991). This shows that our outreach programs are effective in servicing known (or presumed) rural patient populations who otherwise might not receive needed services.
Figure 1. Diagnoses of Patients Served in Iowa and Virginia

210 I . L. Abraham et al.
CONCLUSION
The mismatch between rural psychogeriatric needs and the services available cannot be expected to disappear in the foreseeable future, raising the short-term service issue regarding improvement of accessibility to local and regional re- sources, and the long-term policy issue of determination of reasonable levels of resource development, allocation, and equity. The problems of transportation, poverty, lack of trained personnel, low population density, and large catchment areas will continue to make the delivery of mental health care more difficult in rural areas. While it is unrealistic to expect that rural areas will receive the same intensity of services that urban areas have, model programs such as ours can make substantial gains in overcoming problems and providing mental health care to rural elderly. Individualizing these programs to reflect local culture, geography, needs, and resources will improve not only the delivery of care, but also the ability of model programs to be sustained past initial grant funding.
REFEXENCES
Abraham, I. L., & Neese, J. B. (in press). Outreach to rural elderly: Focus on the South. Aging. Blazer, D., Bradford, A., Crowell, B. A., & George, L. K. (1987). Alcohol abuse and
dependence in the rural South. Archives of General Psychiatry. 44,736740. Blazer, D., George, L. K., Landerman, R., Pennybacker, M., Melville, M. L., et al. (1985).
Psychiatric disorders: A ruralhrban comparison. Archives of General Psychiatry, 42, 65 1656.
Buckwalter, K. C., Abraham, I. L., Smith, M. A., & Smullen, D. E. (in press). Nursing outreach to the mentally ill rural elderly. Hospital and Community Psychiatry.
Buckwalter, K . C., McLeran, H., Mitchell, S., & Andrews, P. H. (1988). Responding to mental health needs of the elderly in rural areas: A collaborative geriatric education center model. Gerontology and Geriatrics Education, 8,6940.
Cohen, G. D. (1989). The interface of mental and physical health phenomenon in later life: New directions in geriatric psychiatry. Gerontology & Geriatrics Education, 9,27-38.
Coward, R. T., & Lee, G. R. (1985). An introduction to aging in rural environments. In R. T. Coward & G. R. Lee (Eds.), The elderly in rural society: Every fourth elder @p. 3-25). New York: Springer.
Deprez, R. D., Pennell, B., & Libby, M. A. (1987). The substitutability of outpatient primary care in rural community health centers for inpatient hospital care. Health Services Research, 22,207-233.
Greene, V. L. (1984). Premature institutionalization among the rural elderly in Arizona. Public Health Reports, 99,5843.
Hart, L. G., Pirani, M. J., & Rosenblatt, R. A. (1991). Causes and consequences of rural small hospital closures from the perspectives of mayors. Journal of Rural Health, 7,222-245.
Jamieson, M., Campbell, J., & Clarke, S. (1989). The block nurse program. The Gerontolo- gist, 29(1), 124-127.
Kermis, M. D. (1987). Equity and policy issues in mental health w e of the elderly: Dilemmas, deinstitutionalization, and DRG’s. Journal of Applied Geronrology, 6,268- 283.
Psychogeriatric Outreach to Rural Families 21 1
Norton, C. H., & McManus, M. H. (1989). Background tables on demographic characteris- tics, health status, and health services utilization. Health Services Research, 23,725- 756.
Palmer, C. M., & Cunningham, S. T. (1983). R d mental health delivery. An imperative for creativity. In J. Jacobsen and J. Kelly (Eds.), Issues in rural mental health practice @p. 2-12). Iowa City, IA: University of Iowa.
President’s Commission on Mental Health. (1978). Task panel on rural mental health (Vol. 111, Appendix). Washington, DC: U. S. Government Printing Office.
Raschko, R. (1985). Systems integration at the program level: Aging and mental health. The Gerontologist, 25,4601163.
Reifler, B. V., Kethley, A., O’Neill, P.. Hanley, R., Lewis, S., et al. (1982). Five-year experience of a community outreach program for the elderly. American Jownal of Psychiatry, 139,220-223.
Robins, L. N., & Regier, D. A. (1991). Psychiatric disorders in America. New York: Free Press.
Rosen, C. E., Coppage, S. J., Troglin, S. J., & Rosen, S. (1981). Cost-effective mental health services for the rural elderly. In P. K. Kim and C. Wilson (Eds.), Toward mental health of rural elderly. Washington, DC: University Press of America.
Scheidt,R. J., & Windley,P. G. (1982). Well-being profilesofsmall-town elderly in differing rural contexts. Community Mental Health Journal, 18,257-267.
Toseland, R. W., Decker, J., & Bliesner, J. (1979). A community outreach program for socially isolated older persons. Journal of Gerontological Social Work, 1,211-224.
Wagenfeld, M., Goldsmith, H. F., Stiles. D., & Manderscheid. R. W. (1988). In-patient mental health services in metropolitan counties. Journal of Rural Community Psychol-
Waltz, T., Craft, J., & Walters, K. (1987). Chronically mentally ill older adults: Need assessment. Unpublished manuscript, University of Iowa School of Social Work, Iowa City: IA.
Wasson, W., Ripeckyj, A., Lazarus, L. W., Kupterer, S., Barry, S., et al. (1984). Home evaluation of psychiatrically impairedelderl y: Process and outcome. The Gerontologist, 24,238-242.
Yedidia, P. (1990). Outreach program for older adults: Implications and opportunities. Journal of Ambulatory Care Management, 13,27- 32.
ogy, 9(2), 13-28.
Acknowledgments. Supported by grants from the W. K. Kellogg Foundation, the National Institute of Mental Health, the Administration on Aging, and the Iowa Department of Mental Health, Mental Retardation, and Developmental Disabilities.
Omrints. Requests for offprints should be directed to Ivo L. Abraham, PhD, CS, RN, University of Virginia, Center on Aging and Health and southeastern Rural Mental Health Research Center, 170 Rugby Road, Charlottesville, VA 22903, U.S.A.




















