PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 Medical Comorbidity and its Effect on Workplace Productivity
11
PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 397 Medical Comorbidity and its Effect on Workplace Productivity in Specialty Care Patients C omorbid medical and behav- ioral conditions are associated with greater functional disabili- ty, increased morbidity and suicide-relat- ed mortality, and greater total healthcare use and costs. 1,2 Mental and substance use disorders are twice as likely to occur among the chronically ill, with depres- sion being the most common comorbid condition among medical patients (ap- proximate prevalence of 25%). 3 Although there is evidence of bidirectionality of medical and mental health conditions, 4 research on their comorbidity has fo- cused primarily on prevalence rates of Rebecca A. Cate, PhD, is Senior Research Consultant; Brent Bolstrom, MA, is Manager, Reporting and Analytics; Joyce McCulloch, MS, is Vice President, Behavioral Informatics; and Francisca Azocar, PhD, is Vice President, Research and Evaluation at OptumHealth Be- havioral Solutions, San Francisco. Address correspondence to: Rebecca Cate, PhD, OptumHealth Behavioral Solutions, 425 Market Street, 14th Floor, San Francisco, CA 94105; fax: 415-547-5512; e-mail: rebecca. [email protected]. Dr. Cate; Mr. Bolstrom; Ms. McCulloch; and Dr. Azocar have disclosed no relevant finan- cial relationships. doi: 10.3928/00485713-20100804-06 Rebecca A. Cate, PhD; Brent Bolstrom, MA; Joyce McCulloch, MS; and Francisca Azocar, PhD © iStockphoto.com 4008Cate.indd 397 4008Cate.indd 397 8/5/2010 3:18:08 PM 8/5/2010 3:18:08 PM
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 Medical Comorbidity and its Effect on Workplace Productivity
PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 397
Medical Comorbidity and its Effect on Workplace Productivityin Specialty Care Patients
Comorbid medical and behav-ioral conditions are associated with greater functional disabili-
ty, increased morbidity and suicide-relat-ed mortality, and greater total healthcare use and costs.1,2 Mental and substance use disorders are twice as likely to occur among the chronically ill, with depres-sion being the most common comorbid condition among medical patients (ap-proximate prevalence of 25%).3 Although there is evidence of bidirectionality of medical and mental health conditions,4 research on their comorbidity has fo-cused primarily on prevalence rates of
Rebecca A. Cate, PhD, is Senior Research
Consultant; Brent Bolstrom, MA, is Manager,
Reporting and Analytics; Joyce McCulloch,
MS, is Vice President, Behavioral Informatics;
and Francisca Azocar, PhD, is Vice President,
Research and Evaluation at OptumHealth Be-
havioral Solutions, San Francisco.
Address correspondence to: Rebecca Cate,
PhD, OptumHealth Behavioral Solutions, 425
Market Street, 14th Floor, San Francisco, CA
94105; fax: 415-547-5512; e-mail: rebecca.
Dr. Cate; Mr. Bolstrom; Ms. McCulloch; and
Dr. Azocar have disclosed no relevant fi nan-
cial relationships.
doi: 10.3928/00485713-20100804-06
Rebecca A. Cate, PhD; Brent Bolstrom, MA; Joyce McCulloch, MS; and Francisca Azocar, PhD
© iS
tock
phot
o.co
m
4008Cate.indd 3974008Cate.indd 397 8/5/2010 3:18:08 PM8/5/2010 3:18:08 PM
398 | PsychiatricAnnalsOnline.com PSYCHIATRIC ANNALS 40:8 | AUGUST 2010
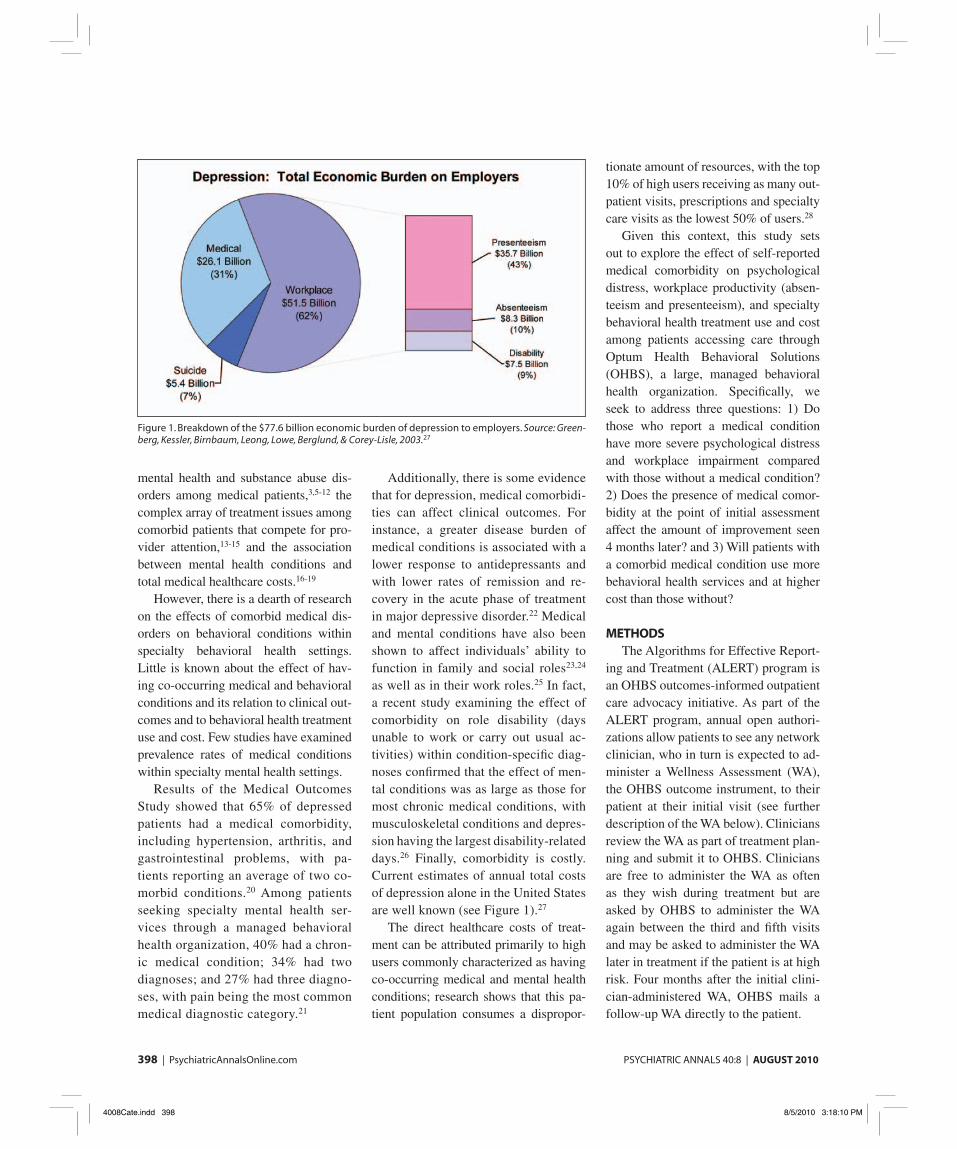
Figure 1. Breakdown of the $77.6 billion economic burden of depression to employers. Source: Green-berg, Kessler, Birnbaum, Leong, Lowe, Berglund, & Corey-Lisle, 2003.27
mental health and substance abuse dis-orders among medical patients,3,5-12 the complex array of treatment issues among comorbid patients that compete for pro-vider attention,13-15 and the association between mental health conditions and total medical healthcare costs.16-19
However, there is a dearth of research on the effects of comorbid medical dis-orders on behavioral conditions within specialty behavioral health settings. Little is known about the effect of hav-ing co-occurring medical and behavioral conditions and its relation to clinical out-comes and to behavioral health treatment use and cost. Few studies have examined prevalence rates of medical conditions within specialty mental health settings.
Results of the Medical Outcomes Study showed that 65% of depressed patients had a medical comorbidity, including hypertension, arthritis, and gastrointestinal problems, with pa-tients reporting an average of two co-morbid conditions.20 Among patients seeking specialty mental health ser-vices through a managed behavioral health organization, 40% had a chron-ic medical condition; 34% had two diagnoses; and 27% had three diagno-ses, with pain being the most common medical diagnostic category.21
Additionally, there is some evidence that for depression, medical comorbidi-ties can affect clinical outcomes. For instance, a greater disease burden of medical conditions is associated with a lower response to antidepressants and with lower rates of remission and re-covery in the acute phase of treatment in major depressive disorder.22 Medical and mental conditions have also been shown to affect individuals’ ability to function in family and social roles23,24 as well as in their work roles.25 In fact, a recent study examining the effect of comorbidity on role disability (days unable to work or carry out usual ac-tivities) within condition-specifi c diag-noses confi rmed that the effect of men-tal conditions was as large as those for most chronic medical conditions, with musculoskeletal conditions and depres-sion having the largest disability-related days.26 Finally, comorbidity is costly. Current estimates of annual total costs of depression alone in the United States are well known (see Figure 1).27
The direct healthcare costs of treat-ment can be attributed primarily to high users commonly characterized as having co-occurring medical and mental health conditions; research shows that this pa-tient population consumes a dispropor-
tionate amount of resources, with the top 10% of high users receiving as many out-patient visits, prescriptions and specialty care visits as the lowest 50% of users.28
Given this context, this study sets out to explore the effect of self-reported medical comorbidity on psychological distress, workplace productivity (absen-teeism and presenteeism), and specialty behavioral health treatment use and cost among patients accessing care through Optum Health Behavioral Solutions (OHBS), a large, managed behavioral health organization. Specifi cally, we seek to address three questions: 1) Do those who report a medical condition have more severe psychological distress and workplace impairment compared with those without a medical condition? 2) Does the presence of medical comor-bidity at the point of initial assessment affect the amount of improvement seen 4 months later? and 3) Will patients with a comorbid medical condition use more behavioral health services and at higher cost than those without?
METHODSThe Algorithms for Effective Report-
ing and Treatment (ALERT) program is an OHBS outcomes-informed outpatient care advocacy initiative. As part of the ALERT program, annual open authori-zations allow patients to see any network clinician, who in turn is expected to ad-minister a Wellness Assessment (WA), the OHBS outcome instrument, to their patient at their initial visit (see further description of the WA below). Clinicians review the WA as part of treatment plan-ning and submit it to OHBS. Clinicians are free to administer the WA as often as they wish during treatment but are asked by OHBS to administer the WA again between the third and fi fth visits and may be asked to administer the WA later in treatment if the patient is at high risk. Four months after the initial clini-cian-administered WA, OHBS mails a follow-up WA directly to the patient.
4008Cate.indd 3984008Cate.indd 398 8/5/2010 3:18:10 PM8/5/2010 3:18:10 PM

PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 399
Study DesignThis study used a retrospective design
that focused on OHBS patients who com-pleted an initial WA (Time 1) and the 4-month follow-up WA (Time 2). The WA administered at 4 months was chosen for the Time 2 measurement because it pro-vided a longer period over which change could be assessed.
In addition to the WA measures of psychological distress and workplace pro-ductivity at each of these times, this study also included measures of behavioral health treatment use and cost. Although the Time 1 WA represents the initial visit with a particular clinician, patients might have used other types of behavioral health treatment or treatment with a different be-havioral health clinician before the initial WA. There was, therefore, an opportunity to examine how the groups differed in their previous treatment use and cost at the time of their initial WA visit, as well as change in use and cost between the two administrations of the WA. Because there was, by design of the ALERT program, a 4-month window between the initial and follow-up WA measures, the measure-ment periods of behavioral health treat-ment use were designed to incorporate the same 4-month timeframe.
In addition to the WA measurement at Time 1 and Time 2, therefore, two time periods of behavioral health treatment use were studied: the Pre-Period consisted of behavioral health claims for any dates of service during the 4 months up to and in-cluding the Time 1 WA. The Post-Period consisted of behavioral health claims for any dates of service during the 4 months after the Time 1 WA, with the end of the period roughly concordant with the date of the Time 2 WA.
Participants The sample consisted of 13,417 adult
OHBS patients who completed the WA during their initial visit with a network clinician between July 1, 2007, and Au-gust 30, 2008, and scored at or above the
clinical cutoff on Global Distress (see be-low). Patients then completed a follow-up WA approximately 4 months after their initial WA and were continuously eligible for behavioral health benefi ts for the en-tire Pre-Period and Post-Period.
Patients were excluded from the sample if they had missing or incorrect identifying data on their WA that pre-vented matching them to corresponding behavioral health claims data or if they returned their follow-up WA more than 6 months after the initial WA was com-pleted. Statistical analyses showed no signifi cant differences in the prevalence of medical comorbidity between patients who were removed from the sample and those who were retained.
MEASURESWellness Assessment
As an integral part of ALERT, the Wellness Assessment (WA) is a psycho-metrically-tested29 self-report instrument made up of items from well-validated, public domain scales (SCL-90,30 CAGE-AID,31 SF-1232). The WA includes: a) one item (asked only at Time 1) mea-suring the presence of one or more co-morbid medical conditions (asthma; dia-betes; heart disease; back pain or other chronic pain; other condition); b) a 15-item Global Distress scale designed to measure anxiety and depression, percep-tions of self-effi cacy, and functional im-pairments (total scores range from 0 to 45 with a clinical cutoff score defi ned as a total score of 12 or greater); c) one item measuring number of medical doctor visits in the previous 6 months, and gen-eral health (each on a fi ve-point scale); d) three CAGE-AID31 items (asked at Time 1 only) measuring risk for chemi-cal dependency (endorsement of two of the three items); e) two items measuring workplace productivity: number of work days missed in the past month because of physical or mental health and number of work days cut back because of physi-cal or mental health; and f) one item
measuring whether the patient was still in behavioral health treatment at follow-up (asked only at Time 2).
Based on the number of medical doctor visits item, it was also identifi ed whether a patient had reported having six or more doctor visits in the previous 6 months. Based on the “number of work days missed” item, it was identifi ed whether a patient reported any absenteeism (at least 1 day missed from work). From the “number of work days cut back” item, it was identi-fi ed whether a patient had reported any pre-senteeism (at least 1 day in which patient had to cut back at work). In addition, those members who missed at least nine work days or had to cut back at work at least 19 days in the past month were identifi ed as having severe work risk.
In this sample, patients returned their Time 2 follow-up WA an average of 143 days (between 4 and 5 months) after the date of their Time 1 WA.
Behavioral Health Use and Cost OHBS administrative claims were
used to measure use and cost. Use (num-ber of visits or days) and cost (amount paid) were calculated separately for each time period (Pre- and Post-) for outpa-tient treatment (including services such as psychotherapy, Employee Assistance Program services, or EAP services, and medication management) and for facil-ity treatment (including services such as acute inpatient, residential treatment, and partial hospitalization). Total cost was calculated across all types of be-havioral treatment (outpatient, facility, and other) for each period. Costs were defi ned as the amount paid by OHBS in addition to the patient paid responsibil-ity for behavioral health services.
Behavioral Health Diagnosis Primary, secondary, and tertiary di-
agnoses from behavioral health claims were used to defi ne discrete diagnos-tic categories during the Pre-Period. Diagnostic categories included mood
4008Cate.indd 3994008Cate.indd 399 8/5/2010 3:18:12 PM8/5/2010 3:18:12 PM
400 | PsychiatricAnnalsOnline.com PSYCHIATRIC ANNALS 40:8 | AUGUST 2010
TABLE 1.
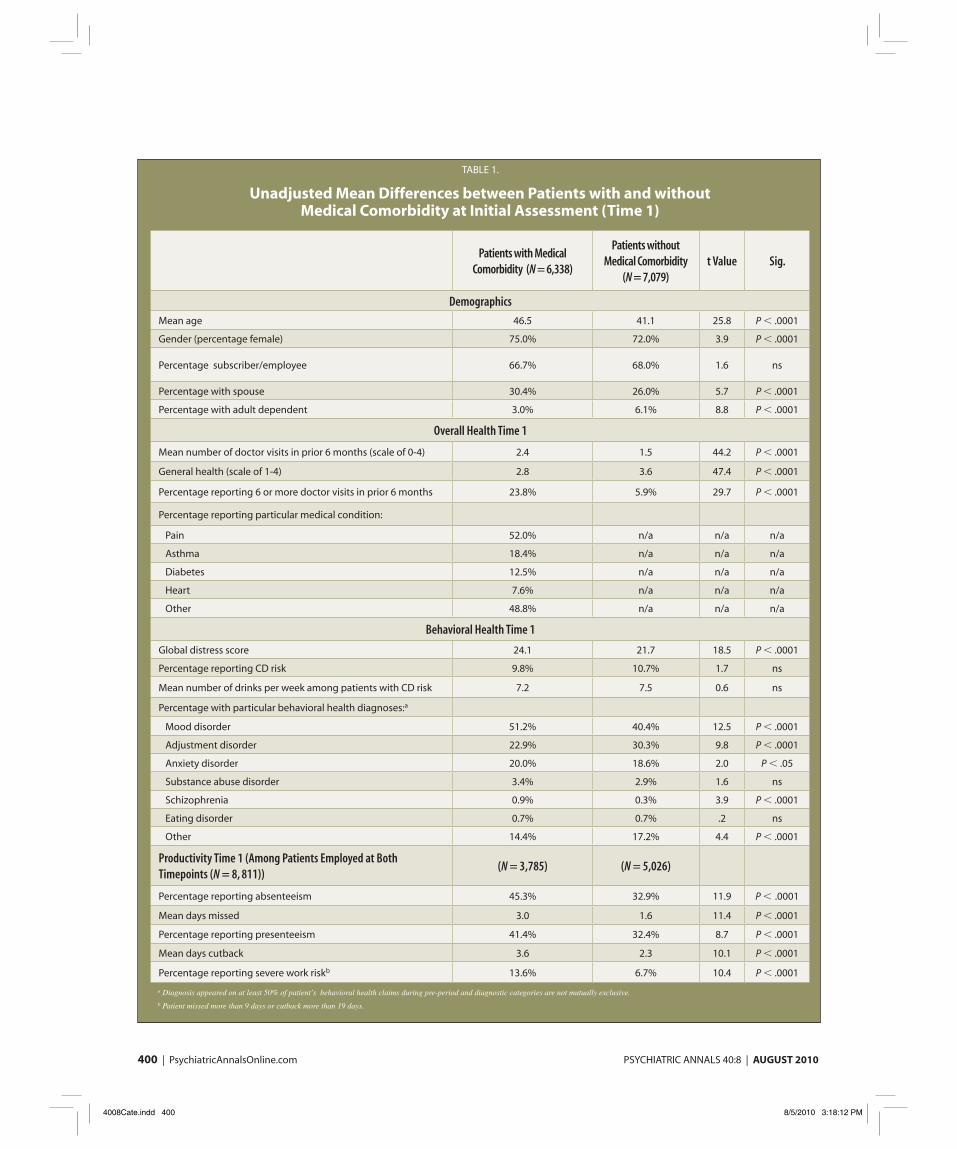
Unadjusted Mean Differences between Patients with and without Medical Comorbidity at Initial Assessment (Time 1)
Patients with Medical
Comorbidity (N = 6,338)
Patients without
Medical Comorbidity
(N = 7,079)
t Value Sig.
Demographics
Mean age 46.5 41.1 25.8 P < .0001
Gender (percentage female) 75.0% 72.0% 3.9 P < .0001
Percentage subscriber/employee 66.7% 68.0% 1.6 ns
Percentage with spouse 30.4% 26.0% 5.7 P < .0001
Percentage with adult dependent 3.0% 6.1% 8.8 P < .0001
Overall Health Time 1
Mean number of doctor visits in prior 6 months (scale of 0-4) 2.4 1.5 44.2 P < .0001
General health (scale of 1-4) 2.8 3.6 47.4 P < .0001
Percentage reporting 6 or more doctor visits in prior 6 months 23.8% 5.9% 29.7 P < .0001
Percentage reporting particular medical condition:
Pain 52.0% n/a n/a n/a
Asthma 18.4% n/a n/a n/a
Diabetes 12.5% n/a n/a n/a
Heart 7.6% n/a n/a n/a
Other 48.8% n/a n/a n/a
Behavioral Health Time 1
Global distress score 24.1 21.7 18.5 P < .0001
Percentage reporting CD risk 9.8% 10.7% 1.7 ns
Mean number of drinks per week among patients with CD risk 7.2 7.5 0.6 ns
Percentage with particular behavioral health diagnoses:a
Mood disorder 51.2% 40.4% 12.5 P < .0001
Adjustment disorder 22.9% 30.3% 9.8 P < .0001
Anxiety disorder 20.0% 18.6% 2.0 P < .05
Substance abuse disorder 3.4% 2.9% 1.6 ns
Schizophrenia 0.9% 0.3% 3.9 P < .0001
Eating disorder 0.7% 0.7% .2 ns
Other 14.4% 17.2% 4.4 P < .0001
Productivity Time 1 (Among Patients Employed at Both
Timepoints (N = 8, 811))(N = 3,785) (N = 5,026)
Percentage reporting absenteeism 45.3% 32.9% 11.9 P < .0001
Mean days missed 3.0 1.6 11.4 P < .0001
Percentage reporting presenteeism 41.4% 32.4% 8.7 P < .0001
Mean days cutback 3.6 2.3 10.1 P < .0001
Percentage reporting severe work riskb 13.6% 6.7% 10.4 P < .0001
a Diagnosis appeared on at least 50% of patient’s behavioral health claims during pre-period and diagnostic categories are not mutually exclusive.b Patient missed more than 9 days or cutback more than 19 days.
4008Cate.indd 4004008Cate.indd 400 8/5/2010 3:18:12 PM8/5/2010 3:18:12 PM
PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 401
disorder; adjustment disorder; anxiety disorder; substance abuse disorder; eat-ing disorder; schizophrenia; and other. If a patient was given a diagnosis on at least 50% of their behavioral health claims during the Pre-Period, they were considered to have been given that di-agnosis. Patients could be counted in multiple diagnostic categories.
STATISTICAL ANALYSESUsing responses to the WA comorbid
medical condition item at Time 1, we identifi ed two groups of patients: patients with or without medical comorbidity. We then ran three sets of analyses to compare the two groups. To assess the profi les of patients at the beginning of treatment, the Time 1 differences were tested between the two groups on demographics, overall health, behavioral health, and workplace productivity using ttests.
To gain a better understanding of trends across the treatment episode, next change was evaluated from the WA at Time 1 to WA at Time 2 in Global Distress and workplace productivity measures.
Finally, it was examined how the two groups changed between the Pre-Period and Post-Period on behavioral health out-
patient use and cost and total behavioral health cost. Generalized linear models with generalized estimating equations were used for the change analyses be-cause they handle discrete, non-normal response data, and they adjust for the dependency between observations that results when measuring the same subject at the two time points.33,34 Analyses exam-ined the main effect of medical comorbid-ity (whether the groups differed on each outcome of interest, regardless of time of assessment or use period), the main ef-fect of time (whether there was signifi cant change from Time 1 to Time 2, or from Pre-Period to Post-Period, in outcome variables, regardless of medical condition present), and the time by group interaction effect (whether the groups differed in their rate of change from Time 1 to Time 2, or from Pre-Period to Post-Period).
It was not possible to analyze change between the Pre-Period and Post-Period in the proportion of patients who used behavioral outpatient treatment or who used any behavioral treatment because, by design, 100% of the patients in this study used behavioral outpatient treat-ment (and thus used any behavioral treatment) during the Pre-Period.
It is important to note that very few patients used facility treatment during either the Pre-Period or Post-Period or both (there was approximately a 3% prevalence rate across both periods, re-gardless of group), and it was therefore not possible to reliably model time by group interactions for facility days and facility costs. However, because facility treatment undoubtedly affects total be-havioral cost, we ran a model that tested the time by group interaction on total cost in addition to models on number of behavioral outpatient visits and behav-ioral outpatient cost.
RESULTSForty-seven percent of this behavioral
health sample (N = 6,338) listed at least one medical condition at Time 1 and therefore were classifi ed as having medi-cal comorbidity, while the rest were clas-sifi ed as having no medical comorbidity (N = 7,079). Of those patients with medi-cal comorbidity, 29.7% reported having more than one medical condition.
Differences at Time 1 between pa-tients with and without medical comor-bidity are shown in Table 1 (see page 400). Compared with patients without a comorbid medical condition, patients with a medical condition at Time 1 were signifi cantly older and were made up of a signifi cantly higher proportion of fe-males and spouses of employees.
Adding support for the validity of the WA measure of medical comorbid-ity, those with a medical condition re-ported poorer health on all health mea-sures. Patients with a medical condition reported signifi cantly more visits with a doctor in the previous 6 months, and a signifi cantly lower mean general health score. Similarly, a signifi cantly greater proportion of patients with a medical condition (23.8% compared with 5.9%) reported a high number of doctor visits (six or more) in the previous 6 months. The breakdown of medical conditions for patients with medical comorbidity
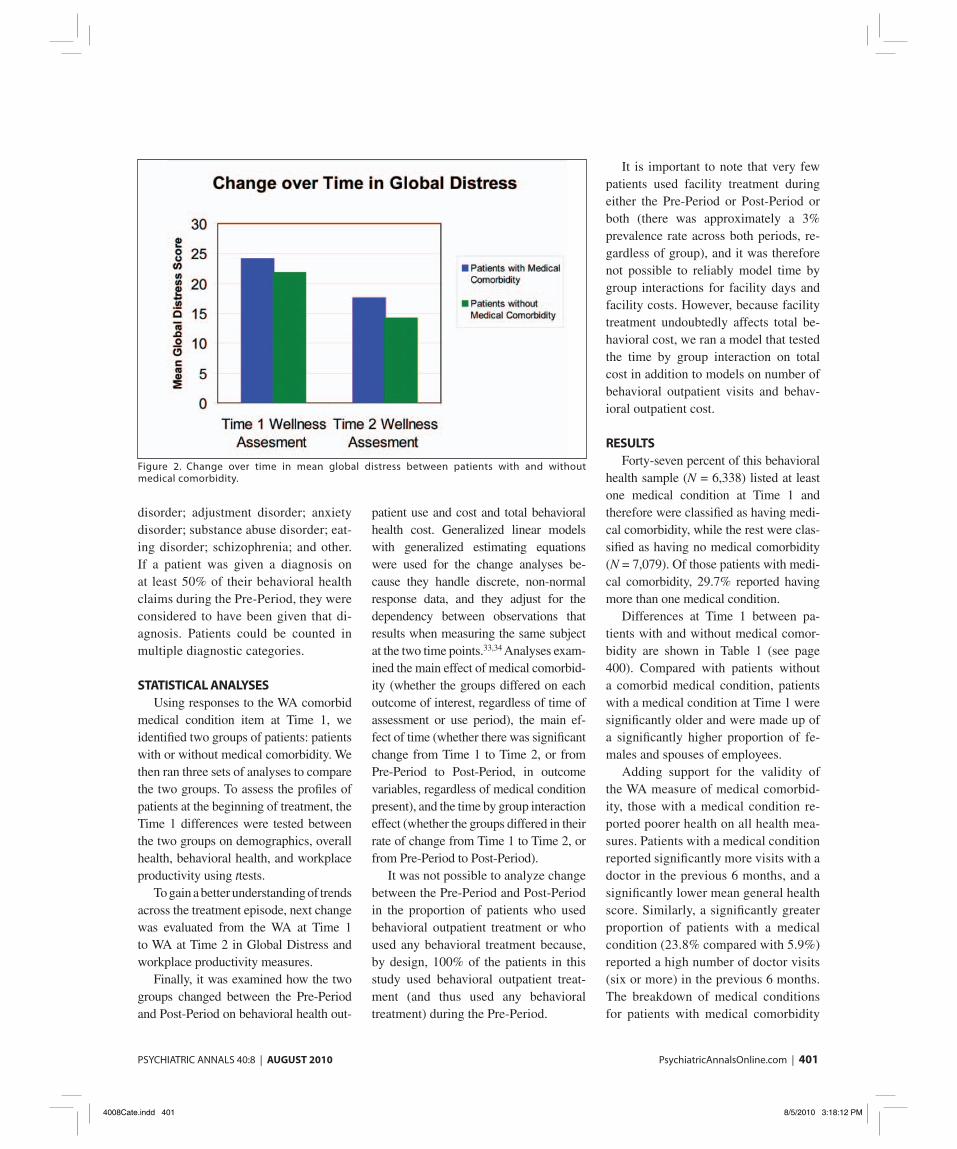
Figure 2. Change over time in mean global distress between patients with and without medical comorbidity.
4008Cate.indd 4014008Cate.indd 401 8/5/2010 3:18:12 PM8/5/2010 3:18:12 PM

402 | PsychiatricAnnalsOnline.com PSYCHIATRIC ANNALS 40:8 | AUGUST 2010
shows pain was the most frequently re-ported medical condition.
Patients with a medical condition had signifi cantly higher Global Distress (M = 24.1) at Time 1 compared with those without a medical condition (M = 21.7), suggesting those with medical comor-bidity had greater behavioral health problems at the start of the treatment period. The particular diagnoses from patient’s claims in the Pre-Period are shown in Table 1 (see page 400).
Among the subsample of patients who were employed at both WA time-points (N = 8,811), there were also signifi cant differences between the groups in workplace productivity mea-sures. As shown in Table 1 (page 400), a greater proportion of those with a medical condition reported absentee-ism and presenteeism, and those with a medical condition reported more missed work days and more days when they had to cut back at work. In addi-tion, a signifi cantly greater proportion of patients with a medical condition showed severe work risk (missing 9 or more days or cutting back on 19 or more days). There was no difference, however, between the proportion of patients with and without a medical con-dition at risk for chemical dependency at Time 1.
Change in Behavioral Health and Workplace Productivity
Figure 2 (see page 401) shows differ-ences in global distress from Time 1 to Time 2 among those with and without medical comorbidity. The statistical re-sults (reported in Table 2, see page 403) indicated a signifi cant main effect for the presence of medical comorbidity (patients with a medical condition showed higher levels of global distress than patients without a medical condition, regardless of time of assessment), as well as a sig-nifi cant effect for time (there was a de-crease in global distress between Time 1 and Time 2, regardless of group).
There was also a signifi cant inter-action between medical comorbidity and time, indicating that the decrease in global distress between Time 1 and Time 2 was signifi cantly greater for those without a medical condition. Be-cause the self-report treatment status item (whether the patient was still in behavioral health treatment at follow-up) was not measured at Time 1, we tested the difference between groups on this item at Time 2 only. As shown in Table 2 (see page 403), a signifi cantly higher proportion of patients with a medical condition (70.9%) were still in treatment at Time 2 compared with those without one (66.3%).
Table 2 (see page 403) also pres-ents differences between patients with and without medical comorbidity in workplace productivity from Time 1 to Time 2, among the subsample of pa-tients employed at both timepoints (N = 8,811). Statistical analyses showed there was a main effect of medical comorbidity on all five workplace productivity measures: a greater pro-portion of employed patients with a medical condition reported absentee-ism and presenteeism compared with those without a medical condition; those with a medical condition missed more days and cut back on more days than those without; and a greater pro-portion of those with a medical con-
dition showed severe work risk than those without (Figure 3).
The results also indicated a signifi cant main effect for time, with both groups improving on all workplace productivity measures from Time 1 to Time 2 (ie, decreasing on all measures). There was a signifi cant interaction between medi-cal comorbidity and time for three of the productivity measures: the decrease over time in mean days missed, mean days cut back, and proportion of patients with severe work risk was signifi cantly greater for those without a medical condition than those with a medical condition.
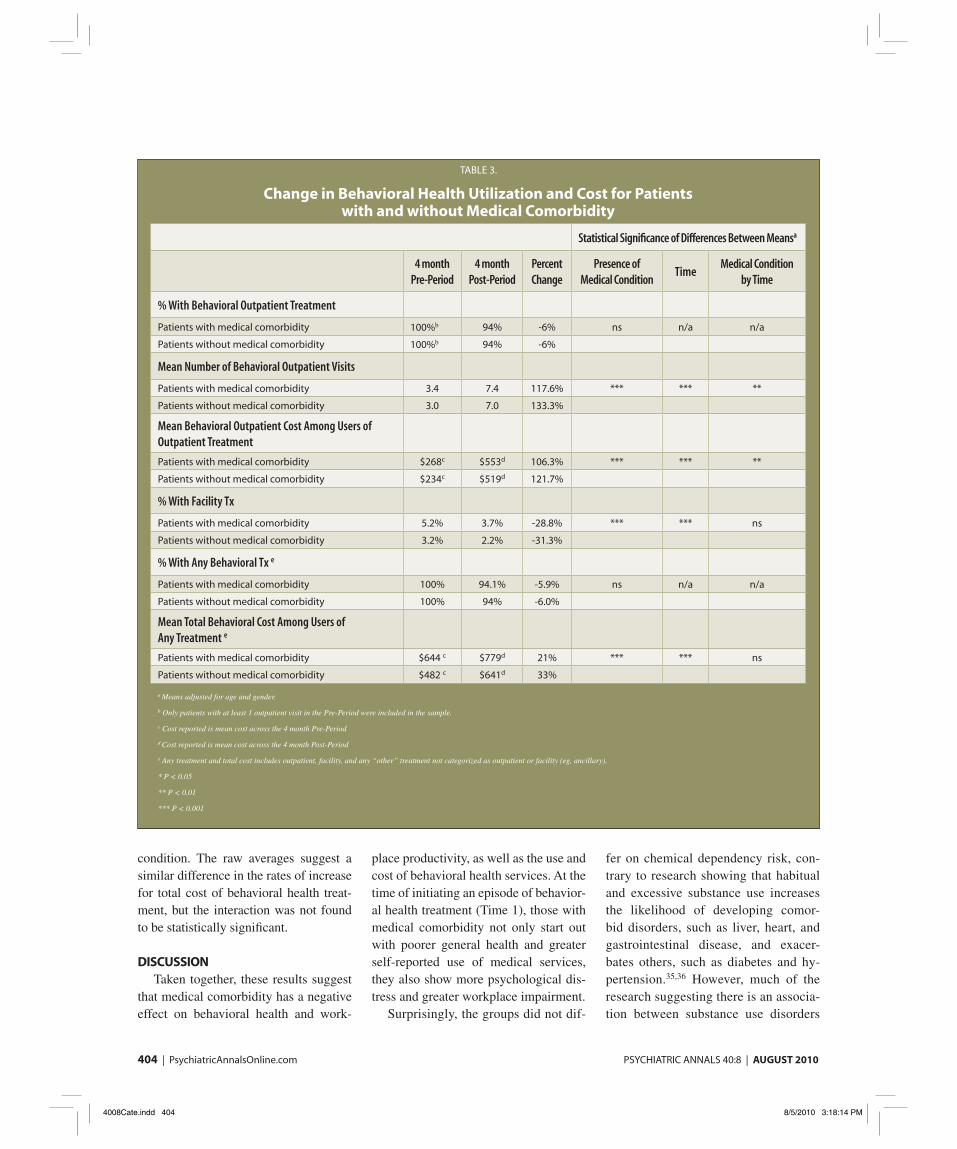
Change in Behavioral Health Use and Cost
Table 3 (see page 404) shows change in behavioral health use and cost be-tween the 4-month Pre-Period and 4-month Post-Period among those with and without medical comorbidity. There were no differences in the proportion of patients of each group who used behav-ioral outpatient treatment or any behav-ioral health treatment in the Post-Period. There was a main effect of medical co-morbidity on proportion of patients us-ing facility treatment (regardless of time period; a greater proportion of those with a medical condition used facility treatment compared with those without a medical condition); and a main effect of time (both groups decreased in their use
Figure 3. Change over time in absenteeism, presenteeism, and severe work risk between patients with and without medical comorbidity.
4008Cate.indd 4024008Cate.indd 402 8/5/2010 3:18:13 PM8/5/2010 3:18:13 PM

PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 403
of facility treatment from Pre-Period to Post-Period). However, there was no sta-tistical difference between the groups in the rate at which they decreased facility treatment use from Time 1 to Time 2.
We also analyzed differences between the groups over the two time periods in the amount and cost of their behavioral outpatient treatment, as well as the total cost of any behavioral treatment received (see Table 3, page 404). There was, once
again, a signifi cant main effect of medical comorbidity. Across the entire 8-month period (ie, regardless of Pre-Period or Post-Period), those with a medical condi-tion used more behavioral outpatient visits at greater cost than those without and had greater total behavioral health costs.
There was also a signifi cant main ef-fect for time on treatment use and cost: Both groups increased from the Pre-Pe-riod to the Post-Period in their use of
outpatient visits, and the cost of their outpatient and total treatment, as would be expected after initiation of treatment with a new clinician. The statistical re-sults also indicate a signifi cant time by group interaction for behavioral outpa-tient treatment: Patients without a medi-cal condition showed a greater increase from Pre-Period to Post-Period in num-ber of outpatient visits and cost of out-patient visits than those with a medical
TABLE 2.
Change from Time 1 to Time 2 on Behavioral Health and Productivity for Patients with and without Medical Comorbidity
Statistical Signifi cance of Differences Between Meansa
Time 1 Wellness
Assessmenta
Time 2 Wellness
Assessmenta
Percent
Change
Presence of Medical
ConditionTime
Medical Condition
by Time
Mean Global Distress Score
Patients with medical comorbidity 24.1 17.5 -27.4% *** *** ***
Patients without medical comorbidity 21.8 14.1 -35.3%
% Reporting Still in Behavioral Health
Treatment at Time 2
Patients with medical comorbidity n/a 70.9% n/a *** n/a n/a
Patients without medical comorbidity n/a 66.3% n/a
Among Patients Employed at Both
Timepoints (N = 8,811):
% Reporting Absenteeism
Patients with medical comorbidity 45.7% 37.5% -17.9% *** *** ns
Patients without medical comorbidity 32.5% 24.7% -24.0%
Mean days missed
Patients with medical Comorbidity 3 2.5 -16.7% *** *** *
Patients without medical comorbidity 1.6 1.1 -31.3%
% Reporting Presenteeism Patients with medical comorbidity 41.8% 34.2% -18.2% *** *** ns
Patients without medical comorbidity 32.0% 25.7% -20.0%
Mean days cutback
Patients with medical comorbidity 3.6 2.6 -27.8% *** *** **
Patients without medical comorbidity 2.3 1.4 -39.1%
% of Employed with severe work riskb
Patients with medical comorbidity 13.2% 10.1% -23.5% *** *** ***
Patients without medical comorbidity 6.8% 3.4% -50.0%
a Means adjusted for age and gender.
b Patient missed more than 9 days or cut back more than 19 days in the past month.
* P < 0.05
** P < 0.01
*** P < 0.001.
4008Cate.indd 4034008Cate.indd 403 8/5/2010 3:18:14 PM8/5/2010 3:18:14 PM
404 | PsychiatricAnnalsOnline.com PSYCHIATRIC ANNALS 40:8 | AUGUST 2010
condition. The raw averages suggest a similar difference in the rates of increase for total cost of behavioral health treat-ment, but the interaction was not found to be statistically signifi cant.
DISCUSSIONTaken together, these results suggest
that medical comorbidity has a negative effect on behavioral health and work-
place productivity, as well as the use and cost of behavioral health services. At the time of initiating an episode of behavior-al health treatment (Time 1), those with medical comorbidity not only start out with poorer general health and greater self-reported use of medical services, they also show more psychological dis-tress and greater workplace impairment.
Surprisingly, the groups did not dif-
fer on chemical dependency risk, con-trary to research showing that habitual and excessive substance use increases the likelihood of developing comor-bid disorders, such as liver, heart, and gastrointestinal disease, and exacer-bates others, such as diabetes and hy-pertension.35,36 However, much of the research suggesting there is an associa-tion between substance use disorders
TABLE 3.
Change in Behavioral Health Utilization and Cost for Patients with and without Medical Comorbidity
Statistical Signifi cance of Differences Between Meansa
4 month
Pre-Period
4 month
Post-Period
Percent
Change
Presence of
Medical ConditionTime
Medical Condition
by Time
% With Behavioral Outpatient Treatment
Patients with medical comorbidity 100%b 94% -6% ns n/a n/a
Patients without medical comorbidity 100%b 94% -6%
Mean Number of Behavioral Outpatient Visits
Patients with medical comorbidity 3.4 7.4 117.6% *** *** **
Patients without medical comorbidity 3.0 7.0 133.3%
Mean Behavioral Outpatient Cost Among Users of
Outpatient Treatment
Patients with medical comorbidity $268c $553d 106.3% *** *** **
Patients without medical comorbidity $234c $519d 121.7%
% With Facility Tx
Patients with medical comorbidity 5.2% 3.7% -28.8% *** *** ns
Patients without medical comorbidity 3.2% 2.2% -31.3%
% With Any Behavioral Tx e
Patients with medical comorbidity 100% 94.1% -5.9% ns n/a n/a
Patients without medical comorbidity 100% 94% -6.0%
Mean Total Behavioral Cost Among Users of
Any Treatment e
Patients with medical comorbidity $644 c $779d 21% *** *** ns
Patients without medical comorbidity $482 c $641d 33%
a Means adjusted for age and gender.
b Only patients with at least 1 outpatient visit in the Pre-Period were included in the sample.
c Cost reported is mean cost across the 4 month Pre-Period
d Cost reported is mean cost across the 4 month Post-Period
e Any treatment and total cost includes outpatient, facility, and any “other” treatment not categorized as outpatient or facility (eg, ancillary).
* P < 0.05
** P < 0.01
*** P < 0.001
4008Cate.indd 4044008Cate.indd 404 8/5/2010 3:18:14 PM8/5/2010 3:18:14 PM

PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 405
and medical comorbidities has been conducted among the severely mentally ill populations where rates of medical, mental, and substance abuse problems are high. This patient population was primarily employed, in their early 40s, and overall reported low-to-moderate levels of substance use. Therefore, their medical condition or lack thereof may be unrelated to substance use.
Importantly, both groups (patients with and without medical comorbidity) showed improvement in their behav-ioral health and workplace productivity between Time 1 and Time 2. Specifi -cally, both groups showed a decrease in global distress scores; a decrease in the proportion of patients with absenteeism and fewer days of missed work; a de-crease in the proportion of patients with presenteeism; fewer cut back days; and a decrease in the proportion of patients with severe work risk. However, the time by group interactions suggest that those with a medical comorbidity have a slower rate of clinical and functional im-provement compared with those without a medical condition, who by Time 2 had shown greater improvement on global distress and almost all workplace pro-ductivity outcomes.
When comparing use during the 4 months between assessments (Post-Period) with that of the 4 months leading up to and including the initial assessment (Pre-Pe-riod), patients without medical comorbidity actually showed a greater increase in the use of behavioral outpatient services than did those with a medical condition, suggest-ing greater intensity of treatment among healthier patients who may be better able to focus on their behavioral health during the 4-month period after initial assessment.
By comparison, patients with a medical condition had more behavioral treatment during the entire 8 months of claims (regardless of particular period), suggesting they spread their treatment out over a longer period of time. These results may be evidence of competing
demands, in which physical symptoms compete with behavioral health symp-toms for attention among patients with medical conditions.
Previous research has suggested that competing demands affect initiation of treatment, but not completion, and that given enough time, those with a medical
condition will get the behavioral health treatment they need.14,15 As everyone in this sample had initiated behavioral health treatment at Time 1, it may be that the 4 months between Time 1 and Time 2 assess-ments (Post-Period) was not long enough for those with a medical condition, given their comparatively less intense treatment, to show the same amount of improvement as those without a medical condition. Sup-porting this contention, those with a medi-cal condition were more likely to say they were still in treatment at Time 2 than those without a medical condition.
Current Limitations and Future Research
A major limitation of this study is the lack of medical and pharmacy claims, which could be used to examine addi-tional mental health services provided in medical settings and patients’ use of psychotropic medications. For ex-ample, it is unknown whether patients with a medical condition had a men-tal health diagnosis in their medical claims, which would suggest that it had been identifi ed and was being treated in the primary care setting. It is unknown whether a greater proportion of those without a medical comorbidity were
on a combination treatment of psy-chotropics and psychotherapy, which has been shown to be a more effective treatment for certain diagnoses, such as moderate depressions.37,38 Similarly, it is unknown whether fewer patients with a medical comorbidity were receiving psychotropic medications because they were already on too many medications or psychotropic medications were po-tentially contraindicated.
Another limitation of the current study is the reliance on self-report for several key measures. Given the in-creased trend toward the use of Health Risk Assessments (HRAs), and the widespread use of self-report health screening measures in a variety of settings, we think it is important to continue to validate self-report measures.
In addition, many would argue that there has been a paradigm shift to care that incorporates the patients’ role in healthcare decision-making. Self-report measures that focus on patient outcomes, follow the patient over time, and are integrated into the processes of care are necessary to in-corporate the patients’ perception and move toward a delivery system that is centered on patients.39-41
The WA contains items from well-known instruments, has been used in previous research,39,42 has undergone exhaustive psychometric analysis, and has been normed on a sample of more than 99,000 patients.29 In the current study, we found support for the WA medical comorbidity item in that it dif-ferentiated patients who had a greater number of medical visits, patients who had six or more medical visits, and pa-tients who rated their general health more poorly. Nevertheless, we plan to further validate the medical comorbid-ity item in future research comparing patients’ WA responses with their medi-cal claims diagnoses and history.
This study was intended as an initial exploration into the questions of how
Taken together, these
results suggest that medical
comorbidity has a negative
effect on behavioral health and
workplace productivity.
4008Cate.indd 4054008Cate.indd 405 8/5/2010 3:18:15 PM8/5/2010 3:18:15 PM

406 | PsychiatricAnnalsOnline.com PSYCHIATRIC ANNALS 40:8 | AUGUST 2010
self-reported medical comorbidity affects psychological distress, workplace pro-ductivity, and behavioral health treatment use and cost. As such, there are several limitations to the design, including the short Pre-and Post-Periods used to exam-ine treatment use, the exclusive focus on behavioral health claims, and a lack of a comparison group of patients who did not initiate behavioral health treatment.
Future analyses should consider a lengthier claims period (eg, 1 year Pre- and 1 year Post-Treatment initiation), and should include medical and pharmacy claims analyses to further explore the interaction between co-occurring behav-ioral and medical conditions on a more comprehensive landscape of use patterns and costs. This would allow the examina-tion of several additional questions. For instance, with more treatment, do pa-tients with medical comorbidity “catch up” to those without medical comorbid-ity in terms of improvement in behav-ioral health and workplace outcomes? Do patients with medical comorbidity who initiate and adhere to behavioral health treatment — though likely incurring higher behavioral health (and potentially pharmacy) use and cost than those with-out medical comorbidity — nevertheless show lower medical costs compared with those with medical comorbidity who do not initiate or continue with behavioral health treatment?
CONCLUSIONS This exploratory study showed that pa-
tients with comorbid medical and behav-ioral conditions have more psychological distress and greater workplace impairment at the beginning of treatment, and although they show improvement, are still worse off than the non-comorbid group 4 months later. This difference in outcomes may be explained in part by the fact that comorbid patients had received less intensive treat-ment and were more likely to still be in treatment at the Time 2 assessment point than the non-comorbid group.
These fi ndings have important impli-cations. First, healthcare delivery sys-tems need to continue to work toward integrated models of medical and behav-ioral healthcare. In his summary of key themes of the 2001 Institute of Medi-cine (IOM) report “Crossing the Quality Chasm,” Berwick suggests that a system of care is needed that “assumes respon-
sibility for coordination, integration, and effi ciency across traditional boundaries of organization, discipline, and role. It is especially relevant to patients with chronic illnesses, whose needs extend across time and space. To work well as a system, this kind of care requires high degrees of cooperation, with a higher value attached to cooperation than to lo-cal prerogatives.”40
Because mental health providers of-ten work in independent clinical prac-tices (for example, approximately two-thirds of OHBS network providers do so), OHBS and other managed behav-ioral health organizations (MHBOs) are investing in improving and facilitating access and continuity of care by offering programs that help provide outreach to, and coordinate care between, medical and mental health providers.
Second, comorbid medical patients are likely to be using several medications and have several appointments at a given time; the use of motivational interviewing techniques can help ensure patient en-gagement and compliance with medical and behavioral health treatment.
These fi ndings also have implications for patient education. Patients with co-
morbid conditions need to be aware of the potentially longer amount of time that it may take them to feel psychologically healthier, so that they are better able to cope and comply with behavioral treat-ment. On the other hand, mental health clinicians, non-medically trained in par-ticular, need to be trained to assess and incorporate issues of medical comorbid-ity into their clinical practice.
Finally, as seen in this study, patients with comorbid conditions improve but may take longer to achieve the improve-ment seen among non-medically comor-bid patients, thereby incurring more costs. However, payers and employers need to be aware that appropriate treatment of de-pression improves clinical and workplace outcomes, and resulting increases in pro-ductivity and decreases in absenteeism and disability have been shown to outweigh the cost of the depression treatment.43
REFERENCES 1. Simon GE. Social and economic burden of mood
disorders. Biol Psychiatry. 2003;54(3):208-215. 2. Katon WJ. Clinical and health services rela-
tionships between major depression, depres-sive symptoms, and general medical illness. Biol Psychiatry. 2003;54(3):216-226.
3. Mental Health America. Factsheet: Co-occur-ring Disorders and Depression. Available at: http://www.mentalhealthamerica.net/index.cfm. Accessed July 30, 2010.
4. Evans DL, Charney DS, Lewis L, et al. Mood disorders in the medically ill: scientifi c re-view and recommendations. Biol Psychiatry. 2005;58(3):175-189.
5. Bair MJ, Robinson RL, Katon W, Kroenke K. De-pression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433-2445.
6. Forsythe AB, Griffi ths B, Reiff S. Comparison of utilization of medical services by alcohol-ics and non-alcoholics. Am J Public Health. 1982 Jun;72(6):600-2.
7. Harwood HJ, Napolitano DM, Kristiansen PL, Collins JJ. Economic Costs to Society of Alco-hol and Drug Abuse and Mental Illness: 1980. Research Triangle Park, NC, Research Triangle Institute, 1984.
8. Katon W, Egan K, Miller D. Chronic pain: life-time psychiatric diagnoses and family history. Am J Psychiatry. 1985;142(10):1156-1160.
9. Katon W, Von Korff M, Lin E, et al. Distressed high utilizers of medical care. DSM-III-R diag-noses and treatment needs. Gen Hosp Psychiatry. 1990;12(6):355-362.
... patients with comorbid
conditions improve but may
take longer to achieve the
improvement seen among non-
medically comorbid patients ...
4008Cate.indd 4064008Cate.indd 406 8/5/2010 3:18:15 PM8/5/2010 3:18:15 PM

PSYCHIATRIC ANNALS 40:8 | AUGUST 2010 PsychiatricAnnalsOnline.com | 407
10. Sherbourne CD, Wells KB, Meredith LS, Jack-son CA, Camp P. Comorbid anxiety disorder and the functioning and well-being of chroni-cally ill patients of general medical providers. Arch Gen Psychiatry. 1996;53(10):889-895.
11. Walker EA, Gelfand AN, Gelfand MD, Katon WJ. Psychiatric diagnoses, sexual and physical victimization, and disability in patients with ir-ritable bowel syndrome or infl ammatory bowel disease. Psychol Med. 1995;25(6):1259-1267.
12. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fi bromyalgia com-pared with rheumatoid arthritis: I. Psychiatric diagnoses and functional disability. Psycho-som Med. 1997;59(6):565-571.
13. Dickinson LM, Dickinson WP, Rost K, et al. Clinician burden and depression treatment: dis-entangling patient- and clinician-level effects of medical comorbidity. J Gen Intern Med. 2008;23(11):1763-1769.
14. Nutting PA, Rost K, Smith J, Werner JJ, Elliot C. Competing demands from physical prob-lems: effect on initiating and completing de-pression care over 6 months. Arch Fam Med. 2000;9(10):1059-1064.
15. Rost K, Nutting P, Smith J, Coyne JC, Cooper-Patrick L, Rubenstein L. The role of competing demands in the treatment provided primary care patients with major depression. Arch Fam Med. 2000;9(2):150-154.
16. Henk HJ, Katzelnick DJ, Kobak KA, Gre-ist JH, Jefferson JW. Medical costs attributed to depression among patients with a history of high medical expenses in a health main-tenance organization. Arch Gen Psychiatry. 1996;53(10):899-904.
17. Katon WJ, Lin E, Russo J, Unutzer J. Increased medical costs of a population-based sample of depressed elderly patients. Arch Gen Psychia-try. 2003;60(9):897-903.
18. Luber MP, Meyers BS, Williams-Russo PG, et al. Depression and service utilization in elderly primary care patients. Am J Geriatr Psychiatry. 2001;9(2):169-176.
19. Simon GE, VonKorff M, Barlow W. Health care costs of primary care patients with rec-ognized depression. Arch Gen Psychiatry. 1995;52(10):850-856.
20. Wells KB, Rogers W, Burnam A, Greenfi eld S, Ware JE Jr. How the medical comorbidity of
depressed patients differs across health care set-tings: results from the Medical Outcomes Study. Am J Psychiatry. 1991;148(12):1688-1696.
21. Azocar F, McCarter LM, Cuffel BJ, Croghan TW. Patterns of medical resource and psychotropic medicine use among adult depressed managed behavioral health patients. J Behav Health Serv Res. 2004;31(1):26-37.
22. Iosifescu DV, Nierenberg AA, Alpert JE, Smith M, Bitran S, Dording C, Fava M. The impact of medical comorbidity on acute treatment in major depressive disorder. Am J Psychiatry. 2003;160(12):2122-2127.
23. Ormel J, VonKorff M, Ustun TB, Pini S, Korten A, Oldehinkel T. Common mental dis-orders and disability across cultures. Results from the WHO Collaborative Study on Psy-chological Problems in General Health Care. JAMA. 1994;272(22):1741-1748.
24. Spitzer RL, Kroenke K, Linzer M, Hahn SR, Williams JB, deGruy FV 3rd, Brody D, Da-vies M. Health-related quality of life in primary care patients with mental disorders. Results from the PRIME-MD 1000 Study. JAMA. 1995;274(19):1511-1517.
25. Kessler RC, Greenberg PE, Mickelson KD, Me-neades LM, Wang PS. The effects of chronic med-ical conditions on work loss and work cutback. J Occup Environ Med. 2001;43(3):218-225.
26. Merikangas KR, Ames M, Cui L, et al. The impact of comorbidity of mental and physical conditions on role disability in the US adult household population. Arch Gen Psychiatry. 2007;64(10):1180-1188.
27. Greenberg PE, Kessler RC, Birnbaum HG, et al. The economic burden of depression in the United States: how did it change between 1990 and 2000? J Clin Psychiatry. 2003;64(12):1465-1475.
28. Katon W, von Korff M, Lin E, Bush T, Ormel J. Adequacy and duration of antidepres-sant treatment in primary care. Med Care. 1992;30(1):67-76.
29. Doucette A, McCulloch J, Azocar F. Selected Findings: Adult Wellness Assessment: Second Pilot Study Adult Wellness Assessment. Unpub-lished report. November, 2008.
30. Derogatis LR. Symptom Checklist 90-R (SCL-90-R) Administration, Scoring, and Procedures Man-ual. 3rd ed. Minneapolis, MN, National Computer Systems, 1994.
31. Brown RL, Rounds LA. Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wis Med J. 1995;94(3):135-140.
32. Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and va-lidity. Med Care. 1996;34(3):220-233.
33. Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis. Hoboken, NJ: John Wiley & Sons, Inc. 2004.
34. SAS Institute. SAS/STAT 9.1 User’s guide (PROC GENMOD). Cary, NC: SAS Publishing; 2004.
35. Dickey B, Normand SL, Weiss RD, Drake RE, Azeni H. Medical morbidity, mental illness, and substance use disorders. Psychiatr Serv. 2002;53(7):861-867.
36. Zornberg G, Weiss R. Substance-related Disor-ders, in Acute Care Psychiatry: Diagnosis and Treatment. Sederer LI, Rothschild AI, eds. Balti-more, Williams & Wilkins, 1997.
37. Burnand Y, Andreoli A, Kolatte E, Venturini A, Rosset N. Psychodynamic psychotherapy and clomipramine in the treatment of major depres-sion. Psychiatr Serv. 2002;53(5):585-590.
38. Thase ME, Greenhouse JB, Frank E, et al. Treat-ment of major depression with psychotherapy or psychotherapy-pharmacotherapy combinations.Arch Gen Psychiatry. 1997;54(11):1009-1015.
39. Azocar F, Cuffel B, McCulloch J, McCabe JF, Tani S, Brodey BB. Monitoring patient improve-ment and treatment outcomes in managed behav-ioral health. J Healthc Qual. 2007;29(2):4-12.
40. Berwick DM. A user’s manual for the IOM’s ‘Quality Chasm’ report. Health Aff (Millwood). 2002;21(3):80-90.
41. Hibbard JH. Moving toward a more patient-centered health care delivery system. Health Aff (Millwood). 2004;Suppl Web Exclusives:VAR133-5.
42. Brodey BB, Cuffel B, McCulloch J, et al. The acceptability and effectiveness of patient-re-ported assessments and feedback in a managed behavioral healthcare setting. Am J Manag Care. 2005;11(12):774-780.
43. Wang PS, Simon GE, Avorn J, Azocar F, et al. Telephone screening, outreach, and care manage-ment for depressed workers and impact on clinical and work productivity outcomes: a randomized controlled trial. JAMA. 2007;298(12):1401-11.
4008Cate.indd 4074008Cate.indd 407 8/5/2010 3:18:15 PM8/5/2010 3:18:15 PM