
Pseudothrombocytopenia Due to Platelet Aggregation and Degranulation in Blood Collected in EDTA
10
Scand J Haematol(l975) 15, 161-170 Pseudothrombocytopenia Due to Platelet Aggregation and Degranulation in Blood Collected in EDTA M. J. Mmr, M.B., J. C. G. DQERY, M.D.,M.sc., J. GAULDIE, PH.D. & H. SWrS, M.D. Divisions of Haematology, Departments of Laboratory Medicine, St. Joseph’s Hospital (Chief, J. Hirsh) and Hamilton General Hospital (Chief, M. A. M. Ali), Hamilton, Ontario, Canada, Departments of Pathology (Chief, J. F. Mustard) and Medicine (Chief,E. J. M . Campbell), McMaster University, Hamilton, Ontario, Canada and Division of Haematology (Chief, J. R. Hill), Department of Laboratory Medicine, University of Alberta Hospital, Edmonton, Alberta, Canada Three patients are described in whom platelet aggregation andor degranulation oc- curred in blood collected into EDTA. These changes resulted in spurious thrombo- cytopenia and morphological changes similar to those observed in some thrombo- cytopathies. The abnormalities were dependent on the presence of EDTA and did not occur in citrate, oxalate or heparin anticoagulants. In two patients the abnormality was shown to be due to a plasma factor which was not IgG, IgM, fibrinogen or albumin. The most likely explanation is that these patients have an unidentified abnormal plasma component which, on exposure to EDTA, develops ‘anti-platelet activity’. Although relatively uncommon a prospective study of the incidence of these phenomena indicates that they are probably more common than either platelet cold agglutinins or platelet satellitism. They have practical significance with respect to the diagnosis of thrombocytopenia and also to the interpretation of abnormal platelet morphology. Key words: pseudothrombocytopenia - EDTA Accepted for publication June 18, 1975 Correspondence to: Dr. M. J. Mant, Division of Clinical Haematology, Department of Medicine, Clinical Science Building, Room 7-108, University of Alberta, Edmonton, Alberta, Canada T6G 2G3 A preliminary reposrt of part of this study was published in Abstr Clin Res (1972) 20, 934. Scand J Haematol(l975) 15 11
Transcript of Pseudothrombocytopenia Due to Platelet Aggregation and Degranulation in Blood Collected in EDTA

Scand J Haematol(l975) 15, 161-170
Pseudothrombocytopenia Due to Platelet Aggregation
and Degranulation
in Blood Collected in EDTA
M. J. Mmr, M.B., J. C. G. DQERY, M.D.,M.sc., J. GAULDIE, PH.D.
& H. SWrS, M.D.
Divisions of Haematology, Departments of Laboratory Medicine, St. Joseph’s Hospital (Chief, J . Hirsh) and Hamilton General Hospital (Chief, M . A. M . Ali),
Hamilton, Ontario, Canada, Departments o f Pathology (Chief, J . F. Mustard) and Medicine (Chief , E . J . M . Campbell),
McMaster University, Hamilton, Ontario, Canada and
Division o f Haematology (Chief, J . R. Hill), Department o f Laboratory Medicine, University of Alberta Hospital, Edmonton, Alberta, Canada
Three patients are described in whom platelet aggregation andor degranulation oc- curred in blood collected into EDTA. These changes resulted in spurious thrombo- cytopenia and morphological changes similar to those observed in some thrombo- cytopathies. The abnormalities were dependent on the presence of EDTA and did not occur in citrate, oxalate or heparin anticoagulants. In two patients the abnormality was shown to be due to a plasma factor which was not IgG, IgM, fibrinogen or albumin. The most likely explanation is that these patients have an unidentified abnormal plasma component which, on exposure to EDTA, develops ‘anti-platelet activity’. Although relatively uncommon a prospective study of the incidence of these phenomena indicates that they are probably more common than either platelet cold agglutinins or platelet satellitism. They have practical significance with respect to the diagnosis of thrombocytopenia and also to the interpretation of abnormal platelet morphology.
Key words: pseudothrombocytopenia - EDTA
Accepted for publication June 18, 1975
Correspondence to: Dr. M. J. Mant, Division of Clinical Haematology, Department of Medicine, Clinical Science Building, Room 7-108, University of Alberta,
Edmonton, Alberta, Canada T6G 2G3
A preliminary reposrt of part of this study was published in Abstr Clin Res (1972) 20, 934.
Scand J Haematol(l975) 15 11
162 M. J. MANT, J. C. G. DOERY, J. GAULDIE & H. SIMS
Ethylene diamine tetraacetic acid (EDTA), a heavy metal chelator, inhibits platelet ag- gregation and causes platelet sphering. These properties, together with its anti- coagulant effects, have led to its adoption as the anticoagulant of choice for routine blood counts and film preparation. Spurious thrombocytopenia due to blood being taken into EDTA (Gowland et al 1969, Shreiner & Bell 1973, Kjeldsberg & Hershgold 1974) has been reported and has both theoretical and practical implications. We have recently investigated 3 such patients who form the subject of this report.
PATIENTS AND METHODS
Index patients
Patient 1 , a 42-year-old male, presented with tran- sient rectal bleeding. There was no personal or family history to suggest a bleeding diathesis. Physical examination was normal and no cause for the bleeding ws established. A routine blood film using EDTA as the anticoagulant showed apparent severe thrombocytopenia yet a platelet count using EDTA blood was normal (200,000/~~1). A subsequent blood film in EDTA blood showed gray agranular platelets with mild thrombocyto- penia. The patient had received no blood trans- fusions.
Patient 2, a 16-year-old female, presented with a lifelong history of mild easy bruising and recent epistaxis. Slight bleeding had followed prior ton- sillectomy and tooth extraction. The history was of doubtful significance and there was no family history to suggest a bleeding diathesis. Blood col- lected into EDTA gave a platelet count of 27,000/ p l and the blood film showed moderate thrombo- cytopenia with apparently giant agranular plate- lets. The patient had received no transfusions.
Patient 3, a 68-year-old male, presented with al- coholic cirrhosis of the liver with jaundice, edema and ascites but without a palpable spleen. 24 years previously a partial gastrectomy had been per- formed for a bleeding peptic ulcer. There was no personal or family history to suggest a bleeding
diathesis. Physical examination showed no evi- dence of abnormal bleeding. Blood collected into EDTA gave a platelet count of 13,00O/,ul and discrete identifiable platelet aggregates were seen on the blood film. Several blood transfusions had been administered previously.
Platelet and coagulation studies
Blood was collected by clean venipuncture and immediately anticoagulated. Blood films were stained with Wright’s and May-Griinwald-Giemsa stains. Abnormalities of platelet morphology were confirmed on at least four separate occasions. Platelets were counted by Coulter Counter (Bull et a1 1965) and by a manual method (Brecher & Cronkite 1950) (normal: 150,00-400,000/pl). Methods for the bleeding time, platelet adhesive- ness to glass beads, platelet aggregation studies, prothrombin consumption index, fibrinogen, par- tial thromboplastin, prothrombin and thrombin times have been previously described (Mant et a1 1973).
Anticoagulants and incubation studies
The routine anticoagulant for preliminary investi- gations was 1/100 vol 0.35 M tripotassium EDTA (Vacutainer 3204 QS, Becton Dickinson & Co., Ontario, Canada). Other anticoagulants used were: 1/10 vol 0.05 M disodium EDTA with 0.1 M NaCI, 1/10 vol 0.05 M ethylene glycoltetra- acetic acid (EGTA) with 0.1 M NaCl, 1/10 vol 0.15 M sodium citrate, 1/10 vol 0.1 M sodium oxalate and heparin 50 U/ml (final concentration). Whole blood was incubated with each anti- coagulant for 4 h at room temperature and also at 37O C with EDTA and at 4O C with sodium citrate. Aliquots were removed at intervals for blood films and for platelet counts. Simultaneous control studies with normal blood were per- formed. In addition noa-anticoagulated capillary blood films were made from each patient.
Electron microscopy
Fresh unanticoagulated whole blood or blood in- cubated with anticoagulants was fixed and pro- cessed essentially as described by Grottum et a1 (1969). Thin sections were examined with a Phil- lips 300 electron microscope.
PSEUDOTHROMBOCYTOPENIA 163
Mixing studies
Citrated whole blood from 2 compatible normal donors was incubated at room temperature for 4 h with an equal volume of the following plas- ma fractions obtained from each of the first two patients: citrated platelet poor plasma (PPP), se- rum, a gamma globulin fraction, a purified IgG fraction, serum from which albumin had been removed and serum from which IgM had been removed. Control incubations contained citrate only and test incubations also contained 1/10 vol 0.05 M EDTA in 0.1 M NaC1. Aliquots were removed at intervals for preparation of blood films.
Gamma globulin fractions were prepared by precipitation in 50 % saturated ammonium sul- phate followed by dialysis against 0.15 M NaCl. Purified IgG fractions were prepared as previously described (Mant et a1 1973). IgM and albumin were removed from serum by immunoprecipita- tion using rabbit antihuman globulin and anti- human albumin respectively with confirmation of removal by double radial immunodiffusion against specific anti-IgM and anti-albumin.
Additional experiments were performed in which CaClz or MgClz were added to 0.05 M EDTA in 0.1 M NaCl prior to its addition to normal blood/patient plasma mixtures. Heparin (50 U/ml - final concentrations) was also added to prevent coagulation. Positive and negative con- trols for these studies were identical samples without CaClz and MgClz and samples in which citrate replaced EDTA.
Nucleotide and LDH assays
Specific enzymatic assays for adenosine triphos- phate (ATP) (Greengard 1965) and adenosine di- phosphate (ADP) (Adam 1965) were carried out on a Turner 430 spectrofluorometer; excitation wavelength 340 mp, emission wavelength 460 m,u. Samples for nucleotide assay were deproteinized by the addition of an equal volume of 7 % per- chloric acid and neutralized just prior to assay by the addition of solid potassium bicarbonate. Platelet rich plasma (PRP) was used for total nucleotide determination while nucleotide release was assessed using samples of PPP prepared by centrifugation of PRP for 1.5 min in an Eppen- dorf centrifuge after exposure to EDTA or citrate.
Lactic dehydrogenase (LDH) assays were per- formed in a total volume of 2.5 ml at 25O C as previously described (Doery et a1 1970). Total LDH was determined using a sonicated sample of PRP and release of platelet LDH was deter- mined from the increase in LDH activity in PPP after exposure of PRP to citrate or EDTA. Simultaneous studies on normal blood served as controls.
Prospective incidence studies
200 patients on whom platelet counts had been requested had blood collected into both EDTA and citrate anticoagulants. Blood films and plate- let counts were performed immediately after col- lection and after standing for 4 h at room tem- perature. In addition, 11W blood films from blood collected in EDTA, referred for a haematological opinion over a 16 month period, were examined specifically for evidence of platelet aggregation and/or degranulation. When either phenomenon was observed blood was recollected in both citrate and EDTA anticoagulants and studied as above.
RESULTS Index patients
The effect of various anticoagulants on the appearance of platelets in peripheral blood films from patients 1, 2 and 3 are shown in Table I. Each of the phenomena observed occurred only in the presence of EDTA or EGTA, platelets appearing normal in other anticoagulants. Platelets from patient 1 did not degranulate immediately on exposure to EDTA or EGTA but by 15 min most plate- lets were partially or completely degranu- lated (Figure 1 a) and by 75 min degranula- tion was virtually complete. The normal blue/gray cytoplasmic staining was lost more slowly and most platelets gradually became undetectable by light microscopy although occasional ‘ghosts’ remained visible. Elec- tronic and manual platelet counts in EDTA and EGTA remained normal (156,000-
11.
164 M. J. MANT, J. C. G. DOERY, J. GAULDIE & H. SIMS
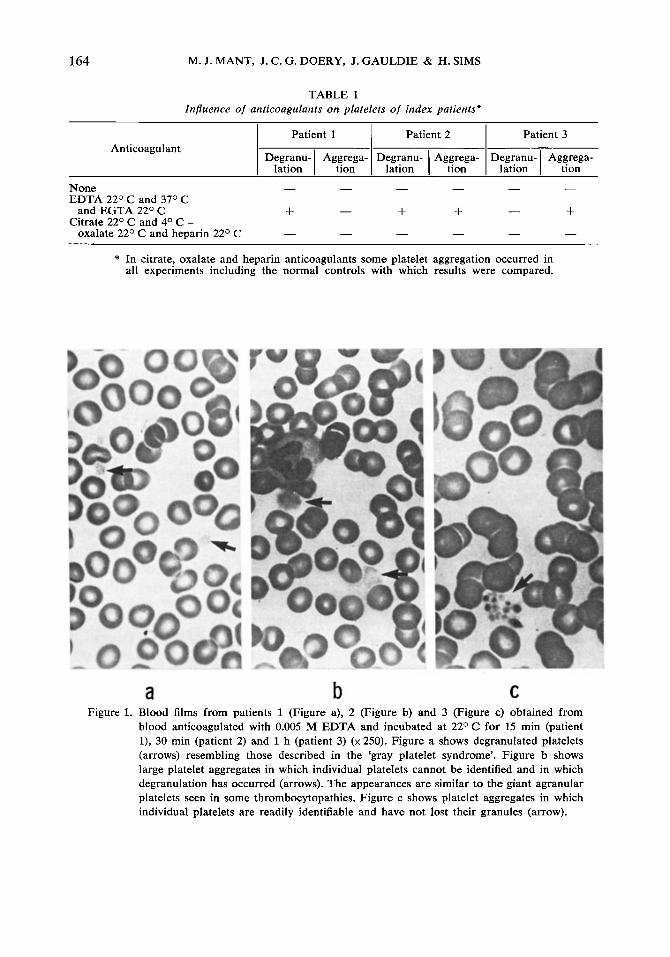
TABLE I Influence of anticoagulants on platelets of index patients*
Anticoagulant Patient 1 I Patient 2 I Patient 3
Aggrega- Degranu- Aggrega- Degranu- Aggrega- D ; : ~ ~ - I tion I lation I tion I lation I tion
None EDTA 2 2 O C and 3 7 O C
and EGTA 22O C
oxalate 2 2 O C and heparin 2 2 O C Citrate 2 2 O C and 4 O C -
* In citrate, oxalate and heparin anticoagulants some platelet aggregation occurred in all experiments including the normal controls with which results were compared.
a b C Figure 1. Blood films from patients 1 (Figure a), 2 (Figure b) and 3 (Figure c) obtained from
blood anticoagulated with 0.005 M EDTA and incubated at 2 2 O C for 15 min (patient l), 30 min (patient 2) and 1 h (patient 3) (x 250). Figure a shows degranulated platelets (arrows) resembling those described in the ‘gray platelet syndrome’. Figure b shows large platelet aggregates in which individual platelets cannot be identified and in which degradat ion has occurred (arrows). The appearances are similar to the giant agranular platelets seen in some thrombocytopathies. Figure c shows platelet aggregates in which individual platelets are readily identifiable and have not lost their granules (arrow).
PSEUDOTHROMBOCYTOPENIA 165
165,OOO/pl) for up to 24 h. The EDTA in- duced changes persisted over 8 months of observation.
On exposure to EDTA or EGTA plate- lets from patient 2 immediately formed small aggregates in which individual plate- lets were readily identifiable. These aggre- gates rapidly enlarged, individual platelet outlines were lost and platelet degranulation occurred (Figure 1 b). Simultaneous elec- tronic platelet counts in EDTA and citrated blood were 22,OOO/pl and 306,00O/pl re- spectively. Manual platelet counts were similar, the EDTA induced platelet aggre- gates not being readily identifiable as such in the counting chambers. The EDTA in-
duced changes persisted over 2 months of observation and were unaltered during 2 weeks of prednisone treatment.
In patient 3 EDTA and EGTA caused immediate platelet aggregation. Individual platelets remained readily identifiable in these aggregates which slowly enlarged (Fig- ure 1 c). Platelet degranulation did not oc- cur over a 4 h period. The degree of plate- let aggregation and electronic platelet counts in EDTA varied over 2 weeks of observa- tion. Platelet counts in EDTA remained consistently lower than those in citrate, the most marked difference being 38,OOO/pl (EDTA) and 180,00O/,~l (citrate). Most platelet aggregates were readily identifiable
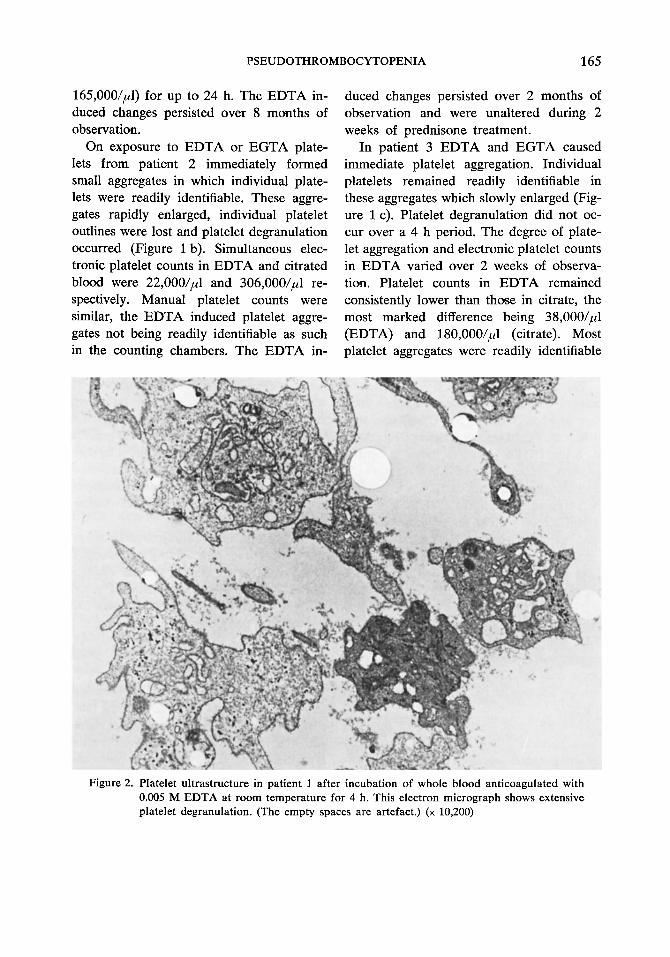
Figure 2. Platelet ultrastructure in patient 1 after incubation of whole blood anticoagulated with 0.005 M EDTA at room temperature for 4 h. This electron micrograph shows extensive platelet degranulation. (The empty spaces are artefact.) ( x 10,200)
166 M. J. MANT, J. C. G. DOERY, J. GAULDIE & H. SIMS
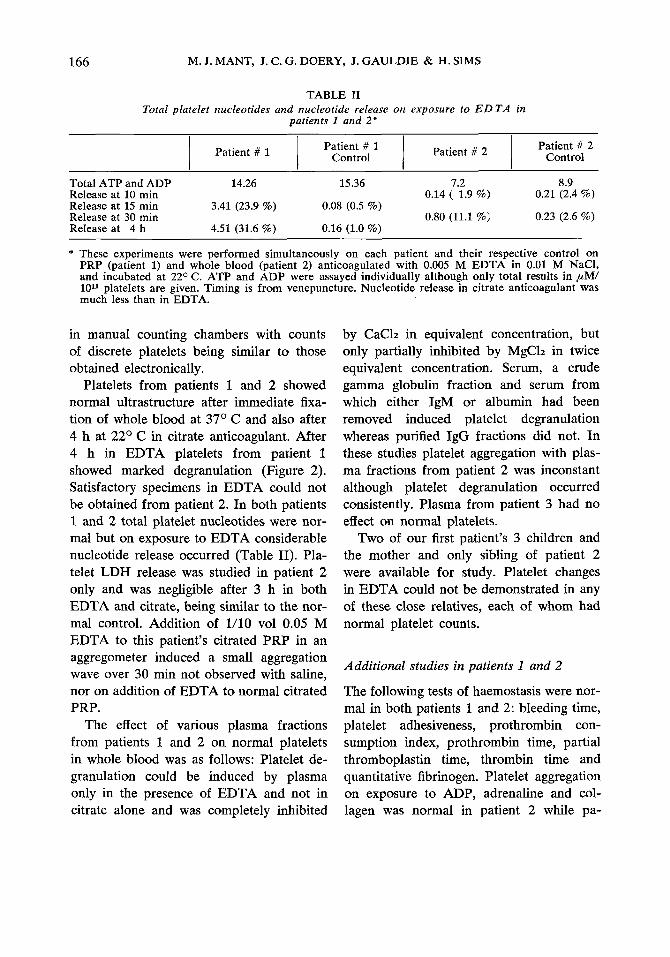
TABLE I1 Total platelet nucleotides and nucleotide release on exposure to E D TA in
patients I and 2"
I I I I Patient # 2 Patient # 2 Control
Patient # 1 Control Patient # 1
Total ATP and ADP 14.26 15.36 7.2 8.9 Release at 10 min 0.21 (2.4 %) Release at 15 min 3.41 (23.9 %) 0.08 (0.5 %) Release at 30 min 0.80 (11.1 %) 0.23 (2.6 %) Release at 4 h 4.51 (31.6 %) 0.16 (1.0 %)
0.14 ( 1.9 %)
* These experiments were performed simultaneously on each patient and their respective control on PRP (patient 1) and whole blood (patient 2) anticoagulated with 0.005 M EDTA in 0.01 M NaCI, and incubated at 22O C. ATP and ADP were assayed individually although only total results in ,uM/ 1011 platelets are given. Timing is from venepuncture. Nucleotide release in citrate anticoagulant was much less than in EDTA.
in manual counting chambers with counts of discrete platelets being similar to those obtained electronically.
Platelets from patients 1 and 2 showed normal ultrastructure after immediate fixa- tion of whole blood at 3 7 O C and also after 4 h at 22O C in citrate anticoagulant. After 4 h in EDTA platelets from patient 1 showed marked degranulation (Figure 2). Satisfactory specimens in EDTA could not be obtained from patient 2. In both patients 1 and 2 total platelet nucleotides were nor- mal but on exposure to EDTA considerable nucleotide release occurred (Table 11). Pla- telet LDH release was studied in patient 2 only and was negligible after 3 h in both EDTA and citrate, being similar to the nor- mal control. Addition of 1/10 vol 0.05 M EDTA to this patient's citrated PRP in an aggregometer induced a small aggregation wave over 30 min not observed with saline, nor on addition of EDTA to normal citrated PRP.
The effect of various plasma fractions from patients 1 and 2 on normal platelets in whole blood was as follows: Platelet de- granulation could be induced by plasma only in the presence of EDTA and not in citrate alone and was completely inhibited
by CaClz in equivalent concentration, but only partially inhibited by MgClz in twice equivalent concentration. Serum, a crude gamma globulin fraction and serum from which either IgM or albumin had been removed induced platelet degranulation whereas purified IgG fractions did not. In these studies platelet aggregation with plas- ma fractions from patient 2 was inconstant although platelet degranulation occurred consistently. Plasma from patient 3 had no effect on normal platelets.
Two of our first patient's 3 children and the mother and only sibling of patient 2 were available for study. Platelet changes in EDTA could not be demonstrated in any of these close relatives, each of whom had normal platelet counts.
Additional studies in patients 1 and 2
The following tests of haemostasis were nor- mal in both patients 1 and 2: bleeding time, platelet adhesiveness, prothrombin con- sumption index, prothrombi time, partial thromboplastin time, thrombin time and quantitative fibrinogen. Platelet aggregation on exposure to ADP, adrenaline and col- lagen was normal in patient 2 while pa-
PSEUDOTHROMBOCYTOPENI A 167
tient 1 had normal aggregation to ADP, but an absent secondary wave to adrenaline and subnormal aggregation to collagen on 1 of 4 occasions.
Additional tests giving normal results in both patients were: serum calcium, protein electrophoresis, immunoelectrophoresis, LE- cell preparations and immunofluorescent studies for anti-nuclear, anti-parietal cell, anti-thyroid, anti-mitochondrial and anti- smooth muscle antibodies. Direct and in- direct Coombs tests in the presence and absence of EDTA were negative.
Additional studies were performed in an attempt to identify either an antibody against EDTA or a plasma component whose properties were altered in the pres- ence of EDTA or which could be shown to bind EDTA in abnormal amounts. Double immunodiffusion on Ouchterlony plates was performed using patient’s plas- ma and the crude gamma globulin fractions against EDTA. No precipitin lines were identifiable. Serum protein electrophoresis in the presence and absence of 0.005 M EDTA showed no change in the mobility of any plasma proteins. Serum protein elec- trophoresis on cellulose acetate was also performed in the presence of 0.005 M EDTA containing tracer amounts of 14C- EDTA, the individual protein bands iden- tified, excised, eluted and counted in a liquid scintillation counter. No consistent peak of radioactivity could be identified in either patient as compared to normal con- trols. 1/10. vol of 0.05 M EDTA containing a tracer amount of I4C-EDTA was added to serum from each patient and a crude gamma globulin fraction prepared. No significant radioactivity could be identified in the re- dissolved precipitate in either patients or normal controls.
Prospective incidence studies
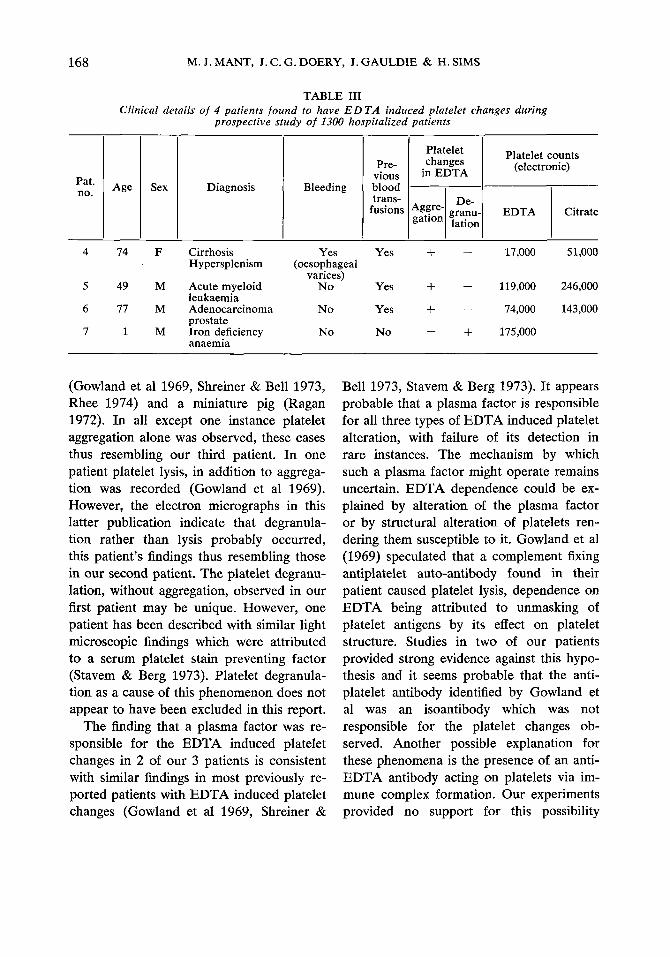
4 patients with EDTA induced platelet changes were identified in a prospective study of 1300 hospitalized patients. Details are given in Table 111. 3 patients showed aggregation only and one showed degranu- lation only. Several EDTA blood films ob- tained from patient 4 on an admission 2 months previously showed no gregation. The EDTA induced gregation observed in patient 5 after 2 weeks treatment with cyclophosphamide and cytosine At this time platelet counts
platelet ag- platelet ag- disappeared prednisone, arabinoside.
in EDTA (52,OOO/pl) and citrate (46,OOO/,d) were similar. EDTA induced platelet changes were not present in either parent or 2 sib- lings of patient 7.
DISCUSSION
3 patients are described in whom platelet aggregation andlor degranulation occurred in blood anticoagulated with EDTA. Plate- let degranulation alone occurred in the first patient, aggregation and degranulation in the second and aggregation alone in the third. These initial impressions obtained from ex- amination of peripheral blood films and from platelet counts were confirmed in the first two patients by combinations of elec- tron microscopy, platelet nucleotide and LDH release studies and platelet aggrega- tion studies. In each case platelets from unanticoagulated blood and from blood anticoagulated with citrate, oxalate or hepa- rin appeared normal although in EGTA platelet changes were identical to those in EDTA.
Similar in vitro phenomena have been in- frequently reported and include 9 patients
168
Platelet changes
in EDTA
M. J. MANT, J. C. G. DOERY, J . GAULDIE & H. SIMS
Platelet counts (electronic)
Pat. no.
‘ggre- granu- lation I De-
TABLE 111 Clinical details o f 4 patients found to have E D TA induced platelet changes during
prospective study of I300 hospitalized patients
EDTA Citrate
Sex
F
M
M
M
Diagnosis
Cirrhosis Hypersplenism
Acute myeloid leukaemia Adenocarcinoma prostate Iron deficiency anaemia
Bleeding
Yes (oesophageal
varices) No
N o
No
Pre- vious
trans- fusions
bloomd
Yes
Yes
Yes
No
+ - 17,000 51,000
+ - 119,000 246,000
+ - 74,000 143,000
- + 175,000
(Gowland et a1 1969, Shreiner & Bell 1973, Rhee 1974) and a miniature pig (Ragan 1972). In all except one instance platelet aggregation alone was observed, these cases thus resembling our third patient. In one patient platelet lysis, in addition to aggrega- tion was recorded (Gowland et a1 1969). However, the electron micrographs in this latter publication indicate that degranula- tion rather than lysis probably occurred, this patient’s findings thus resembling those in our second patient. The platelet degranu- lation, without aggregation, observed in our first patient may be unique. However, one patient has been described with similar light microscopic findings which were attributed to a serum platelet stain preventing factor (Stavem & Berg 1973). Platelet degranula- tion as a cause of this phenomenon does not appear to have been excluded in this report.
The finding that a plasma factor was re- sponsible for the EDTA induced platelet changes in 2 of our 3 patients is consistent with similar findings in most previously re- ported patients with EDTA induced platelet changes (Gowland et a1 1969, Shreiner &
Bell 1973, Stavem & Berg 1973). It appears probable that a plasma factor is responsible for all three types of EDTA induced platelet alteration, with failure of its detection in rare instances. The mechanism by which such a plasma factor might operate remains uncertain. EDTA dependence could be ex- plained by alteration of the plasma factor or by structural alteration of platelets ren- dering them susceptible to it. Gowland et al (1969) speculated that a complement fixing antiplatelet auto-antibody found in their patient caused platelet lysis, dependence on EDTA being attributed to unmasking of platelet antigens by its effect on platelet structure. Studies in two of our patients provided strong evidence against this hypo- thesis and it seems probable that the anti- platelet antibody identified by Gowland et a1 was an isoantibody which was not responsible for the platelet changes ob- served. Another possible explanation for these phenomena is the presence of an anti- EDTA antibody acting on platelets via im- mune complex formation. Our experiments provided no support for this possibility
PSEUDOTHROMBOCYTOPENIA 169
which would be an inhererdiy unlikely oc- currence.
The third possibility, which we consider most likely, but which must remain specula- tive, is that EDTA acts physicochemically on some abnormal plasma component to alter its structure or cause complexing, this change resulting in acquisition of ‘anti-plate- let activity’. Experiments with calcium and magnesium additicn indicated that chelation was involved, as did observations that simi- lar changes occurred in EGTA. Thus, the plasma component probably contains a heavy metal which is most likely to be cal- cium. Although attempts to identify the plasma factor responsible for the EDTA induced platelet changes were unsuccessful our studies indicated that it was not IgG, IgM, fibrinogen or albumin in two cases. Shreiner & Bell (1973) identified the plas- ma factor in one of their reported cases as an IgG immunoglobulin whereas we were unable to implicate this protein. Thus, al- though similarities between the plasma fac- tors responsible fcr EDTA induced platelet changes can be demonstrated it is unlikely that they are identical in all patients.
The three patients initially studied pres- ented over a six month period. We there- fore speculated that these phenomena might be more common than the rarity of previous reports indicated. In a prospective study of 1300 hospitalized patients 4 examples of EDTA dependent platelet changes were identified. The abnormalities are therefore not extremely rare and our data, together with previous reports, suggests that platelet aggregation without degranulation is the most frequent of the changes described. It is of interest that no patients with platelet cold agglutinins (Watkins & Shulman 1970) or platelet satellitism (Kjeldsberg & Hersh- gold 1974) were identified during this pro-
spective study suggesting that they are prob- ably less common occurrences. Although several patients had abnormal bleeding it is unlikely that the in vitro phenomena de- scribed have any in vivo clinical sign& cance.
The occurrence of EDTA induced plate- let aggregation in a patient in whom this phenomena was previously absent and its disappearance in another patient suggests an acquired abnormality. However, an in- herited abnormality in some instances can- not be excluded. The Occurrence of these in vitro phenomena in otherwise healthy individuals indicates that they need not be secondary to another disease process.
The changes described are of theoretical interest because EDTA normally prevents platelet aggregation to most aggregants and at least partially inhibits platelet degranula- tion. In addition, our observations have two practical implications. Firstly, particularly in view of the apparent moderate frequency of these phenomena, they reinforce the desir- ability of performing both a peripheral blood film examination and a platelet count when thrombocytopenia is suspected with either procedure. Secondly, the morphologic changes observed in our first two patients were strikingly similar to those seen in the grey platelet syndrome (Figure 1 a) (Rac- cuglia 1971) and in some familial thrombo- cytopenic thrombocytopathies with giant agranular platelets (Figure 1 b) (Hirsh et a1 1950). Although other findings indicate that these two platelet abnormalities are real en- tities many reports of abnormal platelet morphology do not include details of anti- coagulants used. Our findings indicate that apparent morphological abnormalities ob- served by light microscopy, particularly in blood collected in EDTA, should not be considered to represent in vivo changes
170 M. J . MANT, J. C. G. DOERY, J. GAULDIE #& H. SIMS
without further investigation. The abnor- malities described may be simply identified and may also be disinguished from platelet cold agglutinins by the use of unanti- coagulated blood films and anticoagulants other than EDTA. These procedures also permit reasonably accurate platelet counts when platelet aggregation occurs in EDTA.
ACKNOWLEDGEMENTS
We wish to thank Dr. D. Hughes, Dr. W. E. C. Wilson and Dr. S. Miller for permission to study three of these patients and their families, Dr. J. Hirsh and Dr. J . Bienenstock for their interest and advice and Dr. M. A. Blajchman for performing the immunofluorescent studies. J. C. G. Doary is supported by a Canadian Heart Foundation Med- ical Scientist Fellowship.
REFERENCES
Adam H (1965) Adenosine-5”-diphosphate and adenosine-5’-monophosphate. I n H U Bergmeyer (ed) Methods of enzymatic analysis, p 573. Aca- demic Press, New York.
Brecher G & Cronkite E P (1950) Morphology and enumeration of human blood platelets. J Appl Physiol 3, 365-77.
Bull B S, Schneiderman M A & Brecher G (1965) Platelet counts with the Coulter Counter. A m J Clin Pathol 44, 678-88.
Doery J C G, Hirsh J & De Gruchy C G (1970) Platelet glycolytic enzymes: Effect of cellular disruption procedures on activity. Br J Haema-
Gowland E, Kay H E M, Spillman J C & Wil- to1 19, 145-53.
liamson J R (1969) Agglutination of platelets by a serum factor in the presence of EDTA. J Clin PathoZ 22, 460-64.
Creengard P (1965) Adenosine-5’-triphosphate. De- termination by fluorimetry. In H U Bergmeyer (ed) Methods of enzymatic analysis, p 551. Aca- demic Press, New York.
Grottum K A, Hovig T, Holmsen H, Abrahamsen A F, Jeremic J & Seip M (1969) Wiskott-Aldrich syndrome: Qualitative platelet defects and short platelet survival. Br J HaematoZ 17, 373-88.
Hirsh E 0, FavrB-Gilly U & Dameshek W (1950) Thrombopathic thrombocytopenia - successful transfusion of blood platelets. Blood 5 , 568-80.
Kjeldsberg C R & Hershgold E J (1974) Spurious thrombocytopenia. JAMA 227, 628-30.
Mant M J, Hirsh J, Gauldie J, Bienenstock J, Pineo G F & Luke K H (1973) Von Willebrand’s syndrome presenting as an acquired bleeding disorder in association with a monoclonal gam- mopathy. Blood 42, 429-36.
Raccuglia G (1971) Gray platelet syndrome. A variety of qualitative platelet disorder. A m J Med 51, 818-28.
Ragan H A (1972) Platelet agglutination induced by ethylenediaminetetraacetic acid in blood samples from a miniature pig. A m J Vet Res 33, 2601-03.
Rhee C Y (1974) Spurious thrombocytopenia. JAMA 228, 1098.
Shreiner D P & Bell W R (1973) Pseudothrombo- cytopenia: Manifestation of a new type of plate- let agglutinin. Blood 42, 541-49.
Stavem P & Berg K (1973) A macromolecular se- rum component acting on platelets in the pres- ence of EDTA. Platelet stain preventing factor. Scand J Haernatol 10, 202-08.
Watkins S P Jr & Shulman N R (1970) Platelet cold agglutinins. Blood 36, 153-58.




















