
PROSTATE CANCER STAGING: CORRELATION BETWEEN ULTRASOUND DETERMINED TUMOR CONTACT LENGTH AND...
9
0022-5347/98/1594-1251$03.00/0 THE JOURNAL OF UROLOGY Copyright 0 1998 by AMERICAN UROLOCICAL ASSOCIATION, INC. Vol. 159, 1251-1259, April 1998 Printed in USA. PROSTATE CANCER STAGING: CORRELATION BETWEEN ULTRASOUND DETERMINED TUMOR CONTACT LENGTH AND PATHOLOGICALLY CONFIRMED EXTRAPROSTATIC EXTENSION OSAMU UKIMURA, PATRICIA TRONCOSO, EDILBERTO I. RAMIREZ AND R. JOSEPH BABAIAN* From the Departments of Urology and Pathology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas ABSTRACT Purpose: We determine whether a new parameter, the amount of tumor in contact with the fibromuscular rim (capsule) of the prostate, correlates with extraprostatic extension, and ascer- tain whether estimating the new parameter using transrectal ultrasonography can predict extraprostatic extension. Materials and Methods: We analyzed step sectioned prostatectomy specimens from 189 pa- tients who had had positive peripheral zone biopsies. We measured the contact length, maximum length (mm.) of the portion of the peripheral zone cancer that was in contact with the fibromus- cular rim, and determined the contact ratio from the quotient (%) of the contact length divided by the tumor circumference. We evaluated the correlation between the pathological and ultra- sound measurements of these parameters, as well as the accuracy of these criteria for predicting microscopic extraprostatic extension. Results: Among the 189 cancers there was a significant difference (p <0.0001) between organ confined tumors and tumors with extraprostatic extension in contact length and contact ratio. There was a positive correlation (r = 0.691) between the contact lengths measured ultrasonically and histologically among 95 patients who had hypoechoic lesions associated with positive biop- sies. A receiver operating characteristics curve of the ability of ultrasound estimated contact length to predict extraprostatic extension revealed the best cutoff value to be 23 mm. with 77% accuracy. Logistic regression analysis revealed that pathological contact length correlated better with extraprostatic extension than tumor volume, Gleason score, prostate specific antigen (PSA) level and pathological contact ratio. The best preoperative predictor of extraprostatic extension was the ultrasound contact length, followed by the contact ratio, PSA value, percentage of the biopsy specimen that was cancer and presence of perineural invasion in the biopsy specimen. Multiple logistic regression analysis revealed that the predictability of ultrasound contact length was improved by considering PSA value also. Probability plots for predicting extraprostatic extension were developed by combination of ultrasound contact length with PSA value. Conclusions: The length of tumor contact with the fibromuscular rim is more significantly related to extraprostatic extension than tumor volume, PSA level and tumor grade. For hypo- echoic cancers a new ultrasound staging criterion, contact length, has been defined. For men who are clinically candidates for radical prostatectomy and have peripheral zone hypoechoic cancers the combination of ultrasound contact length and PSA value is the best predictor of extrapros- tatic extension. KEY WORDS: prostatic neoplasms, ultrasonography Radical prostatectomy is considered the most appropriate treatment for men with organ confined prostate cancer.l. However, pathological studies of radical prostatectomy spec- imens often reveal that tumors are more extensive than was clinically appreciated.' Cancers with established penetration of the fibromuscular rim (capsule) have a high risk of pro- gression.3.4 Thus, the ability to identify patients who have extraprostatic extension before surgery is important. Several investigators have shown that tumor volume is an independent predictor of disease progression and tumor stage.5.6 Recently, we reported that the window of curability for prostate cancer decreases significantly once the tumor grows to a volume greater than 1.5 ~m.~.~ However, we also reported that a significant number of small volume cancers exhibit extraprostatic extension and 20% of organ confined epted for publication October 31, 1997. &quests for reprints: Department of Urology-Box 110, Univer- !$Y of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, Texas 77030-4095. cancers have a volume greater than 3.0 ~rn.~.7 Therefore, other pathological parameters, besides tumor volume, influ- ence whether a cancer exhibits extraprostatic extension. We hypothesized that, in addition to tumor volume and other conventional pathological parameters such as grade, when a cancer comes in contact with the fibromuscular rim of the prostate it has a greater propensity for penetration of this anatomical barrier. We further speculated that the extent of tumor contact with the fibromuscular rim was directly re- lated to the probability of extraprostatic extension (unequiv- ocal histological evidence of cancer penetration through the fibromuscular rim, the so-called capsule). To test this hypoth- esis we developed new parameters that might predict extra- prostatic extension (fig. 1). The first parameter we evaluated was the contact length, which is the maximum length of the portion of the tumor margin in contact with the fibromuscu- lar rim in the transverse plane. We then evaluated the con- tact ratio, which is 100 times the quotient of the contact length divided by the tumor circumference. We analyzed the 1251
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of PROSTATE CANCER STAGING: CORRELATION BETWEEN ULTRASOUND DETERMINED TUMOR CONTACT LENGTH AND...
0022-5347/98/1594-1251$03.00/0 THE JOURNAL OF UROLOGY Copyright 0 1998 by AMERICAN UROLOCICAL ASSOCIATION, INC.
Vol. 159, 1251-1259, April 1998 Printed in U S A .
PROSTATE CANCER STAGING: CORRELATION BETWEEN ULTRASOUND DETERMINED TUMOR CONTACT LENGTH AND
PATHOLOGICALLY CONFIRMED EXTRAPROSTATIC EXTENSION OSAMU UKIMURA, PATRICIA TRONCOSO, EDILBERTO I. RAMIREZ AND R. JOSEPH BABAIAN*
From the Departments of Urology and Pathology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas
ABSTRACT
Purpose: We determine whether a new parameter, the amount of tumor in contact with the fibromuscular rim (capsule) of the prostate, correlates with extraprostatic extension, and ascer- tain whether estimating the new parameter using transrectal ultrasonography can predict extraprostatic extension.
Materials and Methods: We analyzed step sectioned prostatectomy specimens from 189 pa- tients who had had positive peripheral zone biopsies. We measured the contact length, maximum length (mm.) of the portion of the peripheral zone cancer that was in contact with the fibromus- cular rim, and determined the contact ratio from the quotient (%) of the contact length divided by the tumor circumference. We evaluated the correlation between the pathological and ultra- sound measurements of these parameters, as well as the accuracy of these criteria for predicting microscopic extraprostatic extension.
Results: Among the 189 cancers there was a significant difference (p <0.0001) between organ confined tumors and tumors with extraprostatic extension in contact length and contact ratio. There was a positive correlation (r = 0.691) between the contact lengths measured ultrasonically and histologically among 95 patients who had hypoechoic lesions associated with positive biop- sies. A receiver operating characteristics curve of the ability of ultrasound estimated contact length to predict extraprostatic extension revealed the best cutoff value to be 23 mm. with 77% accuracy. Logistic regression analysis revealed that pathological contact length correlated better with extraprostatic extension than tumor volume, Gleason score, prostate specific antigen (PSA) level and pathological contact ratio. The best preoperative predictor of extraprostatic extension was the ultrasound contact length, followed by the contact ratio, PSA value, percentage of the biopsy specimen that was cancer and presence of perineural invasion in the biopsy specimen. Multiple logistic regression analysis revealed that the predictability of ultrasound contact length was improved by considering PSA value also. Probability plots for predicting extraprostatic extension were developed by combination of ultrasound contact length with PSA value.
Conclusions: The length of tumor contact with the fibromuscular rim is more significantly related to extraprostatic extension than tumor volume, PSA level and tumor grade. For hypo- echoic cancers a new ultrasound staging criterion, contact length, has been defined. For men who are clinically candidates for radical prostatectomy and have peripheral zone hypoechoic cancers the combination of ultrasound contact length and PSA value is the best predictor of extrapros- tatic extension.
KEY WORDS: prostatic neoplasms, ultrasonography
Radical prostatectomy is considered the most appropriate treatment for men with organ confined prostate cancer.l. However, pathological studies of radical prostatectomy spec- imens often reveal that tumors are more extensive than was clinically appreciated.' Cancers with established penetration of the fibromuscular rim (capsule) have a high risk of pro- gression.3.4 Thus, the ability to identify patients who have extraprostatic extension before surgery is important.
Several investigators have shown that tumor volume is an independent predictor of disease progression and tumor stage.5.6 Recently, we reported that the window of curability for prostate cancer decreases significantly once the tumor grows to a volume greater than 1.5 ~ m . ~ . ~ However, we also reported that a significant number of small volume cancers exhibit extraprostatic extension and 20% of organ confined
e p t e d for publication October 31, 1997. &quests for reprints: Department of Urology-Box 110, Univer-
!$Y of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, Texas 77030-4095.
cancers have a volume greater than 3.0 ~rn .~ .7 Therefore, other pathological parameters, besides tumor volume, influ- ence whether a cancer exhibits extraprostatic extension.
We hypothesized that, in addition to tumor volume and other conventional pathological parameters such as grade, when a cancer comes in contact with the fibromuscular rim of the prostate it has a greater propensity for penetration of this anatomical barrier. We further speculated that the extent of tumor contact with the fibromuscular rim was directly re- lated to the probability of extraprostatic extension (unequiv- ocal histological evidence of cancer penetration through the fibromuscular rim, the so-called capsule). To test this hypoth- esis we developed new parameters that might predict extra- prostatic extension (fig. 1). The first parameter we evaluated was the contact length, which is the maximum length of the portion of the tumor margin in contact with the fibromuscu- lar rim in the transverse plane. We then evaluated the con- tact ratio, which is 100 times the quotient of the contact length divided by the tumor circumference. We analyzed the
1251

1252 ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
peripheral zone foci, in which case the assigned grade was that of the largest peripheral zone focus.
Among the 95 cases used to compare the pathological and ultrasound findings, the directed biopsy specimens of the peripheral zone hypoechoic lesion were available for review in 84. In these 84 cases the Gleason score, percent of cancer in the biopsy specimens and presence or absence of perineu- ral invasion in the biopsy specimen were assessed.9~ 10 Mean total length of all directed biopsy specimens was 30.7 t 14.2 m. (range 5 to 79). The calculation of the percent of cancer in the biopsy was based on dividing the sum of the cancer foci in all cores by the total length of tissue in all cores.11
In all patients preoperative PSA was determined using the Tandem-R method from April 1987 through February 12, 1989, the Tandem-E method from February 13,1989 through December 8, 1993 and the AIA method from December 9, 1993 through January 1996. Preoperatively, the ultrasound stage of each cancer was assessed using conventional criteria for extraprostatic extension (bulging, irregularity or discon- tinuity of the boundary echo adjacent to the hypoechoic le- sion). A hard copy image was taken in the transverse view where the peripheral zone hypoechoic lesion was most visible in each case.
wed to determine tumor volume produced 3-dimensional images and debmined the volume of serially sectioned ob- jects based on the planimetry tracings. The cross sections were projected with a photographic enlarger onto sheets of tracing paper, and the peripheries of each cross section and each individual tumor focus were outlined. The maps of each cross section were placed on a backlight digitizing tablet and the outlines of each were traced. The volume of each separately stored was determined by multi- plying the sum ofthe areas of all cross sections by the section thickness (4 mm.). The digitizing area line meter was used to determine the circumference (mm.) of the largest peripheral zone focus and length (mm.) of the portion of intraprostatic tumor margin in contact with the peripheral fibromuscular rim from the tracings of the projected cross sections used to determine tumor volume. The measurements were corrected for the corresponding enlarging factor (7.28). The parameter of contact length (mm.) was defined as the maximum length of intraprostatic peripheral zone tumor in contact with the fibromuscular rim from among all measured cross sections. Another parameter, contact ratio (%I, was determined by dividing the contact length by the tumor circumference (mm.) in the same section and multiplying the result by 100.
The ultrasound images were then evaluated. The hypo- echoic lesion on the hard copy was projected onto a sheet of tracing paper. The digitizing area line meter was used to determine the circumference (mm.) of each hypoechoic lesion and the ultrasound contact length (mm.) from the tracings. The measurements were corrected for the corresponding en- larging factor. Ultrasound contact ratio (%) was determined using these measurements as described previously.
Statistical methods. Unpaired t tests were used to compare results between organ confined cancers and those with extra- prostatic extension. Simple regression analysis was used to determine the correlation between the histological contact length and the other parameters (tumor volume, prostatectomy specimen Gleason score, PSA value and histological contact ratio), as well as the correlation of the ultrasound contact length and contact ratio with histological contact length and contact ratio, respectively.
Logistic regression analysis with a log likelihood chi- square test was used in an attempt to define the correlation between the presence of extraprostatic extension and all postoperatively available parameters (tumor volume, contact length, contact ratio, Gleason score and PSA value), as well as between extraprostatic extension and all preoperatively available parameters (clinical stage, ultrasound contact
Prostate (transverse plane)
fibmmmda rim (capsule) Contact length (mm)
Contact length Contact ratio (%I = X I 0 0 Tumor circumference FIG. 1. Definition of new parameters contact length and contact
ratio in prostatic transverse view in which cancer is most visible.
correlation between these parameters and the presence of extraprostatic extension in whole mount sections from 189 patients who had biopsy proved peripheral Zone cancers and who had undergone radical ized disease. Thus, we
ProstateCtomY for Clinically local- the new parameters meas-
ured from histological sections and ultrasound images, focus- ing on biopsy proved peripheral zone hypoechoic lesions. TO investigate the usefulness Of these parameters alone and in combination with biopsy grade and Prostate Specific antigen (PSA) for predicting extraprostatic extension, we used 1 ~ s - tic regression analysis. Probability plots of the best combina- tion for predict* extraprostatic extension Were generated to enhance therapeutic planning.
nmor uolune und length &termination. me
MATERIALS AND METHODS
Between April 1987 and January 1996, 250 radical pros- tatectomy specimens from men with clinically organ confined disease were subjected to computer assisted volumetric anal- ysis. These cases were selected so that they were represen- tative of our total prostatectomy experience on the basis of pathological stage. Of the 234 cases without prior transure- thral resection 107 specimens with organ confined disease and with unequivocal extraprostatic extension without (61) or with (21) seminal vesicle involvement were selected for study. Pathologically, the dominant tumor focus was of pe- ripheral zone origin in 165 and of transition zone origin in 24 cases. Among the 189 patients 145 underwent preoperative transrectal ultrasound assessment at our institution. A cor- responding hypoechoic lesion and positive cancer biopsy were documented in 95 patients (all peripheral zone cancers), with the remaining patients having isoechoic cancer (32 had nor- mal ultrasound and 18 had a hypoechoic lesion with a biopsy negative for cancer). The 95 hypoechoic cancers were sub- jected to analysis comparing the pathological and ultrasound findings. The clinical stage of the 95 patients by study design was restricted to T2 (T2a in 39, T2b in 28 and T2c in 28) and was not different compared to the overall T2 stage distribu- tion of the 189 men. In addition, there was no difference in either the serum PSA level (8.64 2 5.68 versus 9.45 2 7.96) or the prostatectomy specimen grade (7.3 5 0.9 versus 7.2 f 0.8) in these 2 groups of patients.
The prostate glands were evaluated according to a previ- ously described protocol3 with some m~dification.~ Each tu- mor focus was outlined on the histological sections, and the total number of tumor foci and zonal distribution were re- corded. Each focus was classified according to the Gleason grading system.* The assigned histological grade for the specimen was that of the dominant lesion except for domi- nant transition zone tumors of lower histological grade

ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER 1253 length, ultrasound contact ratio, biopsy Gleason score, per- centage of biopsy specimen that was cancer, presence of perineural invasion in the biopsy specimen and PSA value). This analysis was used to test univariate variables as well as multivariate combinations of variables to determine the best model(s) for predicting extraprostatic extension from the pre- operative data. The larger the value for chi-square (within a set degree of freedom) and the lower the corresponding p value, the better the observed data support the use of a parameter as an accurate staging tool.
Receiver operating characteristics (ROC) curves were used to determine the best cutoff values of the ultrasound contact length and contact ratio for predicting extraprostatic exten- sion. Chi-square tests for independence were used to find the difference in accuracy between the new and conventional ultrasonic staging criteria. Probability plots using the best combination of independent variables for predicting extra- prostatic extension were developed.
RESULTS
Tumor characteristics of 189 cancers with positive periph- eral zone biopsy. The mean tumor volume of the 189 cancers with biopsy proved peripheral zone cancer was 1.57 2 2.04 ~ m . ~ (table 1). There was a significant difference (p <0.0001) in the mean tumor volume between the organ confined tu- mors (0.78 2 0.93 ~ m . ~ , range 0.01 to 4.67) and those with extraprostatic extension (2.62 2 2.57 ~ m . ~ , range 0.36 to 18.26). The mean Gleason score was significantly different (p <0.0001) between the organ confined tumors (6.78 ? 0.67) and those with extraprostatic extension (7.63 2 0.79). The mean preoperative PSA value was 9.45 t 7.96 ngJml. for the 189 cases. There was a significant difference (p <0.0001) in the mean preoperative PSA between the organ confined neo- plasms (6.28 2 3.38 ng./ml., range 1.1 to 22.2) and the can- cers with extraprostatic extension (13.59 ? 10.08 ng./ml., range 1.8 to 51.7).
There was a significant difference (p <0.0001) in the mean histological contact length between organ confined tumors (12.2 2 9.8 mm., range 0 to 49.9) and those with extrapros- tatic extension (30.0 2 13.2 mm., range 8.2 to 67.9). There was also a significant difference (p <0.0001) in the mean contact ratio between the organ confined tumors (27.0 t 14.4%, range 0 to 53.2) and those with extraprostatic exten- sion (40.1 2 9.9%, range 17.3 to 59.5). A significant difference (p <0.0001) in the mean sum of contact lengths between organ confined tumors (36.5 5 47.7 mm., range 0 to 296.0) and the tumors with extraprostatic extension (110.9 2 70.7 mm., range 11.8 to 456.5) was also observed.
Using simple regression analysis in the 189 cases we found positive correlation between contact length and tumor vol- ume (r = 0.776, p <0.0001), Gleason score (r = 0.448, p <0.0001), PSA value (r = 0.449, p <0.0001) and contact ratio (r = 0.647, p <0.0001). Logistic regression analysis for eval- uating the correlation between extraprostatic extension and the 5 variables of tumor volume, contact length, contact ratio, Gleason score and PSA value revealed that the contact length had the best association with extraprostatic extension, fol-
lowed in order by the tumor volume, Gleason score, PSA value and contact ratio (table 1).
Comparison of ultrasonic and pathological findings in the 95 patients with a hypoechoic lesion and a corresponding positive biopsy. Ultrasonic and pathological findings were compared in 95 cases in which there was a hypoechoic lesion and corresponding positive biopsy (fig. 2). When comparing the 49 organ confined tumors to the 46 cancers with extra- prostatic extension there was a s i w c a n t difference in mean tumor volume (p = 0.0002), PSA value (p = 0.0001) and histological contact length (p <0.0001). We also found a sig- nificant difference in the ultrasound contact length (p <0.0001) when comparing organ confined tumors (16.3 t 6.6 mm.) with those demonstrating extraprostatic extension (25.9 2 7.7 mm.) (table 2). Simple regression analysis of the contact lengths measured histologically and by ultrasound revealed a positive linear correlation (r = 0.691, p <0.0001, fig. 3). The mean contact length measured by ultrasound (20.9 2 8.6 mm.) was not significantly different (p = 0.7) from the histologically determined contact length (21.6 t 13.1 mm.).
We compared the contact length between small (volume less than 1.5 cm?) and large (greater than 1.5 ~rn . ~ ) tumors (table 2). In the 62 small tumors the contact length was overestimated by transrectal ultrasound compared with the pathology results with an average difference of 3.0 t 6.0 mm., while in the 33 large tumors contact length was under- estimated by transrectal ultrasound with a mean difference of 7.6 2 11.0 mm.
Ultrasound contact ratio was significantly different (p <0.0001) between the 49 organ confined tumors (42.4 t 9.4%) and the 46 cancers with extraprostatic extension (50.9 2 5.8%) (table 2). The mean ultrasound contact ratio (46.5 2 8.9%) was significantly (p <0.0001) overestimated compared with the pathologically determined contact ratio (35.5 t 12.1%) with a difference of approximately 10%. How- ever, there was a positive linear correlation (r = 0.557, p <0.0001) between the 2 ratios.
New criteria for predicting extraprostatic extension using the ultrasound contact length and contact ratio. To determine the best cutoff value of ultrasound contact length for predict- ing extraprostatic extension, we constructed a ROC curve based on the data from the 95 cases (fig. 4). The point corre- sponding to the value of 23.0 mm. for the ultrasound contact length gave the optimum result. For the 165 pathological step section studies with dominant peripheral zone cancers the optimum cutoff value was 20.7 mm.
When using the criterion of a cutoff value of 23.0 mm. for the ultrasound contact length, the sensitivity for the 95 cases was 65% (30 of 46), specificity 88% (43 of 49), positive pre- dictive value 83% (30 of 36) and overall accuracy 77% (73 of 95). Using conventional extraprostatic extension criteria (such as signs of irregularity, bulging and discontinuity of boundary echo) in these same 95 men the sensitivity was 30% (14 of 46), specificity 88% (43 of 491, positive predictive value 70% (14 of 20) and overall accuracy 60% (57 of 95). Using the new criterion for ultrasound contact length rather than
TABLE 1. Tumor characteristics of 189 patients with biopsy proved peripheral zone canters
Variable
Mean C SD p Value (organ chisquare
Pathological confined vs Univariate Logistic Extrapmtatic extraprostatic Regression
extension) (p value)' Pathological
(107 pts.) Organ Contined Extension (82 ~ts.)
Overall (189 pts.)
Tumor vol. (crn.9 1.57 2 2.04 0.78 2 0.93 2.62 2 2.57 <0.0001 62.79 (<O.OOol) 88.98 (<O.OOoI)
Gleason score 7.15 ? 0.84 6.78 ? 0.67 7.63 2 0.79 <O.OOol 57.16 (<O.OOol)
Contact length (mm.) 19.9 2 14.4 12.2 2 9.8 30.0 -C 13.2 <O.OOol Contact ratio (%) 32.7 2 14.2 27.0 2 14.4 40.1 2 9.9 <O.OOol 45.96 (<O.OOol)
PSA (nglml.) 9.45 -C 7.96 6.28 2 3.38 13.59 t 10.08 <O.OOol 63.46 (CO.MW)l) Logistic regression analysis for correlation of variables with extraprostatic extension.

1254 ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
FIG 2. Prostatectomy specimens and transrectal ultrasound findings of 2 representative cases. A, organ confined cancer with histological contact length of 8 mm., ultrasound contact length 11 mm. and PSA 4.0 ngJml. Probability of extraprostatic extension 1s 6% using probability plot of figure 5. B, cancer with extraprostatic extension and histological contact length of 47 m., ultrasound contact length 37 mm. and PSA 4.3 nglml. Pmbability of extraprostatic extension is 68% using probability plot of figure 5. Reduced from X7.28.
TABLE 2. Comparison between pathological and ultrasonic findings in 95 patients with hypoechoic lesions and corresponding positive biopsy
Mean t SD (range)
organ confined (49 pts.) Extraprostatic Extension Vol. 1.5 or Less Cm? Vol. Greater Than 1.5 Cm.3 Parameter (46 pts.) (62 pts.) (33 pts.)
Tumor voi. PSA (nglml.) Histological contact length (mm.) Ultrasound contact length (mm.) Subtracting ultrasound contact
length fmm histological contact length
Histological contact ratio (8) Ultrasound contact ratio (%) Subtracting ultrasound contact
ratio fmm histological contact ratio
0.88 t 1.00 (0.04-4.67) 6.37 2 3.10 (1.515.3) 14.4 4 10.6 (0-49.9) 16.3 t 6.6 (6.0-34.0) -1.9 2 8.5 (-13.5-28.7)
30.1 5 12.0 (M0.3) 42.4 5 9.4 (20.6-58.8)
-12.3 2 10.3 (-43.8-8.0)
2.59 t 2.79 (0.36-18.6) 10.60 2 6.30 (2.2-31.6) 29.4 t 11.0 (12.0-66.9) 25.9 t 7.7 (13.0-45.9) 3.5 2 9.8 (-12.132.9)
41.2 -+ 9.3 (17.3-59.5) 50.9 2 5.8 (39.W0.8) -9.7 5 10.2 (-35.6-15.0)
0.70 5 0.43 (0.04-1.49) 6.65 t 3.49 (1.5-19.8) 14.3 2 7.5 (0-34.8) 17.3 t 6.7 (6.033.0) -3.0 2 6.0 (-13.5-12.7)
33.1 t 12.4 (0-58.0) 44.4 t 9.4 (20.6-59.9)
-11.3 2 9.6 (-43.88.0)
3.60 2 2.93 (1.5518.26) 11.75 t 6.53 (2.2-31.6) 35.4 -t 10.0 (21.5-66.9) 27.8 -+ 7.5 (14.8-45.9) 7.6 t 11.0 (-10.7-32.9)
40.0 -C 10.2 (17.3-59.5) 50.5 2 6.4 (33.0-60.8)
-10.5 t 11.6 (-35.6-15.0)
the conventional criteria, the ability to predict extraprostatic extension significantly improved in sensitivity (p = 0.0008) and in accuracy (p = 0.013), while keeping equivalent spec- ificity.
Based on the ROC curve for ultrasound contact ratio, the point corresponding to the value of 44.0% gave the optimum result in distinguishing organ confined tumors fi-om those with extraprostatic extension. When using the criterion of a cutoff value of 44.0% for the ultrasound contact ratio, the sensitivity in the 95 men was 91% (42 of 461, specificity 57% (28 of 49), positive predictive value 67% (42 of 63) and overall aceuacy 74% (70 of 95). Comparing ultrasound contact ratio with the conventional criteria, we observed that this new criterion significantly improved sensitivity (p <0.0001) and accuracy (p = 0.045) of predicting extraprostatic extension but resulted in a significant loss (p = 0.0007) in specificity. When combining ultrasound contact length with contact ra-
tio, the ability of contact length to predict extraprostatic extension improved but not significantly.
Predictors of extraprostatic extension in the 84 patients with transrectal ultrasound findings and an available biopsy specimen. We used univariate logistic regression analysis and the log likelihood chi-square test to identify the indepen- dent predictors of extraprostatic extension for the patients who had a hypoechoic lesion with a corresponding positive cancer biopsy and whose directed biopsy specimens were available for review (84 of the 95 cases) (table 3). The 5 variables of ultrasound contact length, ultrasound contact ratio, percentage of the biopsy specimen that was cancer, presence of perineural invasion in the biopsy specimen and PSA value were independent predictors for extraprostatic extension. Ultrasound contact length was the best predictor of extraprostatic extension, followed in order by ultrasound contact ratio, PSA value, percentage of cancer in the biopsy

70
60
3 50 E s M 40 5
l-4 3 30
u m 20 3
W
Y
Y
10
0
ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
R=0.691 (n=95) t t Y-11.167+.451 * X 0
0
1255
0 10 20 30 40 50 60 70
Histologic Contact Length (mm) FIG. 3. Simple regression plot shows positive correlation (r = 0.691) between histologically measured contact length and ultrasonically
(US) measured contact length. In larger tumors contact length was underestimated by transrectal ultrasound and in smaller tumors contact length was overestimated by transrectal ultrasound.
specimen and presence of perineural invasion in the bi- opsy specimen. The biopsy Gleason score was not an inde- pendent predictor of extraprostatic extension. Grouping Gleason scores into categories (6 or less or 7 or greater) also did not yield independent prediction of extraprostatic exten- sion. Clinical stage was also not an independent predictor of extraprostatic extension.
Using multivariate logistic regression analysis, we tested multiple combinations of variables. The analysis of the 84 cases revealed that the predictability of ultrasound contact length was significantly improved by using PSA value (p = 0.0022) but that it was not improved by either percentage of cancer in the biopsy specimen (p = 0.06) or presence of penneural invasion in the biopsy specimen (p = 0.4). There- fore, the best combination of clinically useful predictors was the combination of ultrasound contact length and PSA. Table 4 shows that the combination of ultrasound contact length and PSA value is a significantly better predictor than the other known combinations of preoperative variables recom- mended by other investigators.g.12-14 Overall, the second best combination of variables after that of ultrasound contact length and PSA value was PSA value and percentage of cancer in the biopsy specimen.
Probability plots were constructed for predicting extra- prostatic extension based on the best combination of ultra- sound contact length and PSA value among the 84 cases (fig. 5). We also constructed other probability plots based on the second best combination of PSA value and percentage of cancer in the biopsy specimen (fig. 6) to compare the proba- bility curves ofthose 2 combinations in the same sample set. -
DISCUSSION
Extraprostatic extension has been reported to be present in approximately half of men undergoing radical prostatecto- my.lp2 Patients with extraprostatic extension have a high nsk of relapse afkr radical prostatectomy.4- 12 Therefore, identifying patients with extraprostatic extension before sur- gery is important in optimizing patient selection and conse- quently maximizing therapeutic benefit.
Although the relationship between tumor volume and pathological stage is well recognized, there are significant numbers of low volume cancers that have extraprostatic ex- tension.7.15,16 Miller and Cygan reported that tumors need not acquire either volume or high grade before they become locally invasive.15 In addition, Epstein et a1 reported that the measurement of volume in the radical prostatectomy speci- men does not provide additional information beyond that of the Gleason score and margin status.17 Therefore, for the purpose of preoperatively predicting the potential for pros- tate cancer to have extraprostatic extension, we correlated the amount of tumor in contact with the fibromuscular rim, determined histologically and by transrectal ultrasound, to the presence or absence of extraprostatic extension.
To our knowledge, there have been no other investigations of these parameters for predicting the extent of prostate cancer. We identified a definite relationship between the amount of tumor in contact with the fibromuscular rim and extraprostatic extension. The longer the portion of tumor margin in contact with the fibromuscular rim, the higher the risk of extraprostatic extension. More significantly, logistic remessinn analvsis revealed that the tumor contact length

1256 ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
35%
lOmm 100 44%
- 0 20 40 60 80 100
1 00-Specificity (%) FIG. 4. ROC curves demonstrate optimum cutoff values of ultrasound contact length (USCL) and ultrasound contact ratio (USCR) (23 mm.
and 44%. respectively).
TABLE 3. Characteristics of 84 cases with available corresponding transrectal ultrasound findings and biopsy specimens
- Variable
Chi-square
Regression (p value)*
Mean 2 SD (No. pts.) p Value (organ confined vs
Pathological Organ confined (47 pts.) Extension (37 pts.) extension)
Pathological Extraprostatic extraprostatic Univariate Logistic
Ultrasound contact length (mm.) 16.4 2 6.6 Ultrasound contact ratio (I) 42.7 t 9.4 PSA (ngJml.) 6.4 t 3.5 Clinical stage (T2dl2bfI'2c) (18/14/15) Biopsy specimen: 96 Ca 29.0 t 21.3
Gleason score (5/6/7/&9) 6.85 2 0.66 (0/13/29/4/1) Categorized Gleason score (13/35) (6 or l e sd or greater)
Perineural invasion (yedno) (8/39)
Radical prostatectomy specimen: Tumor vol. 0.89 2 1.02 Histological contact length (mm.) 14.3 2 10.5 Gleason score (415/6/7/8/9) 6.89 t 0.73 (l/0/8/33/4/1)
* Logistic regression analysis for predictability of extraprostatic extension.
had the most significant association with extraprostatic ex- tension, superior even to that of tumor volume. In addition, a second parameter, contact ratio, was also significantly asso- ciated with extraprostatic extension. Preoperative assess- ment of these parameters can enhance the prediction of ex- traprostatic extension of prostate cancer.
Transrectal ultrasound allows visual guidance for directed biopsies of abnormal areas, systematic biopsies and strategic staging biopsies of the extraprostatic space and neurovascu- lar bundles.18-21 However, the reported accuracy of transrec- tal ultrasound in the staging of prostate cancer has var- ied.*% The conventional extraprostatic extension criteria of t r a n s d ultrasound, such as signs of irregularity, bulging and discontinuity of boundary echo, are quite operator de- pendent.ls.26 In cases with advanced local progression the conventional ultrasound criteria for extraprostatic extension
25.3 2 7.0 50.8 2 5.6 11.1 t 6.3
(17/12/8)
47.3 t 26.6 (14/23)
7.02 2 0.76 (1/5/25/4/2) (6/3)
2.35 t 1.50 29.4 2 9.3 7.64 t 0.79 (0/0/1/17/13/6)
<0.0001 <0.0001 <0.0001
Not significant
0.0007 0.031
Not significant Not significant
<0.0001 <0.0001 <0.0001
29.49 (<0.00001) 20.68 (<0.0001)
Not significant
11.21 (0.0008) 4.64 (0.031) Not significant Not significant
17.89 (<0.0001)
25.64 (<0.0001) 36.40 (<0.0001) 20.01 (<0.0001)
are easily recognized, as are the digital rectal examination characteristics. Recent reports concluded that microscopic tumor extension is beyond the resolution power of current ultrasound technology.27-29
Our newly developed criterion of ultrasound contact length is a macroscopically quantifiable 1-dimensional parameter assessed by measuring a peripheral zone hypoechoic lesion that has a corresponding positive cancer biopsy. The greater the ultrasound contact length, the greater the probability that the cancer extends into extraprostatic tissue. The ultra- sound contact length can be easily measured with current transrectal ultrasound equipment. Because the contact length is a 1-dimensional parameter in a single plane, it is considered to be more accurate than ultrasound tumor vol- ume estimation. The only possible interoperator variability is in the measurement of the contact length of the hypoechoic

ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
TABLE 4. Multiple logistic regression analysis for combination of predictors of extraprostatic extension a m n g 84 patients with available transrectal ultrasound findings and corresponding biopsy specimens
1257
Result of Evaluation Chi-square (p value) Other Combinations Predictors for
Extraprostatic Extension
Ultrasound contact length 39.42 (<0.0001), Improved Ultrasound contact length + Not improved from ultrasound + PSA from ultrasound contact PSA + % biopsy specimen contact length + PSA
length alone by PSA (p = 0.0022)
31.00 (<O.OOUl), Improved from PSA alone by % biopsy specimen that is Ca (p = 0.0003)
that is Ca + perineural invasion on biopsy
PSA + % of biopsy specimen that is Ca + Gleason score
PSA + % biopsy specimen Not improved from PSA + % biopsy specimen that is Ca that is Ca
PSA + Gleason score + clinical Not impmved from PSA alone stage
PSA FIG. 5. Predicted probability of extraprostatic extension according to ultrasonically estimated contact length (USCL) and PSA value
lesion. "he quantifiability is similar to that of other preop- erative parameters, such as PSA value, biopsy tumor grade, cancer percentage in the biopsy or clinical stage, all of which also have their own variability.30,31
In our study the contact length of smaller lesions was overestimated, and that of the larger lesions was underesti- mated, and the correlation in 95 cases between contact length determined sonographically and histologically was r = 0.69. Despite these limitations, contact length as meas- ured by transrectal ultrasound was the best predictor of extraprostatic extension. Our determined threshold of 23.0 mm. had a diagnostic accuracy of 77% with corresponding sensitivity and specificity of 65% and 88%, respectively. This predictability is significantly better than that of conventional ultrasonic staging criteria.
The contact ratio can potentially indicate how close the tumor center is to the fibromuscular rim. The greater the contact ratio, the closer the center of the tumor is to the boundary. Hypothetically, then, the greater the contact ratio, the earlier cancer cells come in contact with the fibromuscu- lar rim. Theoretically, therefore, contact ratio could repre- sent a quantifiable parameter of the biological potentid of the cancer for extraprostatic extension. However, since con-
tact length is a 1-dimensional parameter, it can be more easily measured, and our data show that it is more highly associated with extraprostatic extension.
Logistic regression analysis indicates that transrectal ul- trasound determined contact length is the most useful pre- operative staging tool currently available. In addition, the 4 other preoperative variables of ultrasound contact ratio, PSA value, cancer percentage in the biopsy and perineural inva- sion in the biopsy were good independent predictors of extra- prostatic extension. A possible reason that tumor grade was not an independent predictor in this study may be the basis of the relationship between the degree of echogenicity and tumor grade (more markedly hypoechoic lesions are more frequently high grade),26 which may have biased the study population by making it homogeneous. Multiple logistic re- gression analysis showed that the combination of ultrasound contact length and PSA value can further enhance clinical accuracy in predicting extraprostatic extension. The provided probability plots for the combination of ultrasound contact length with the PSA value may assist urologists in deciding whether individual patients are appropriate candidates for radical prostatectomy.
In our study we were able to evaluate the predictability for
1258 ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER
0 2 4 6 8 1012141618202224262830
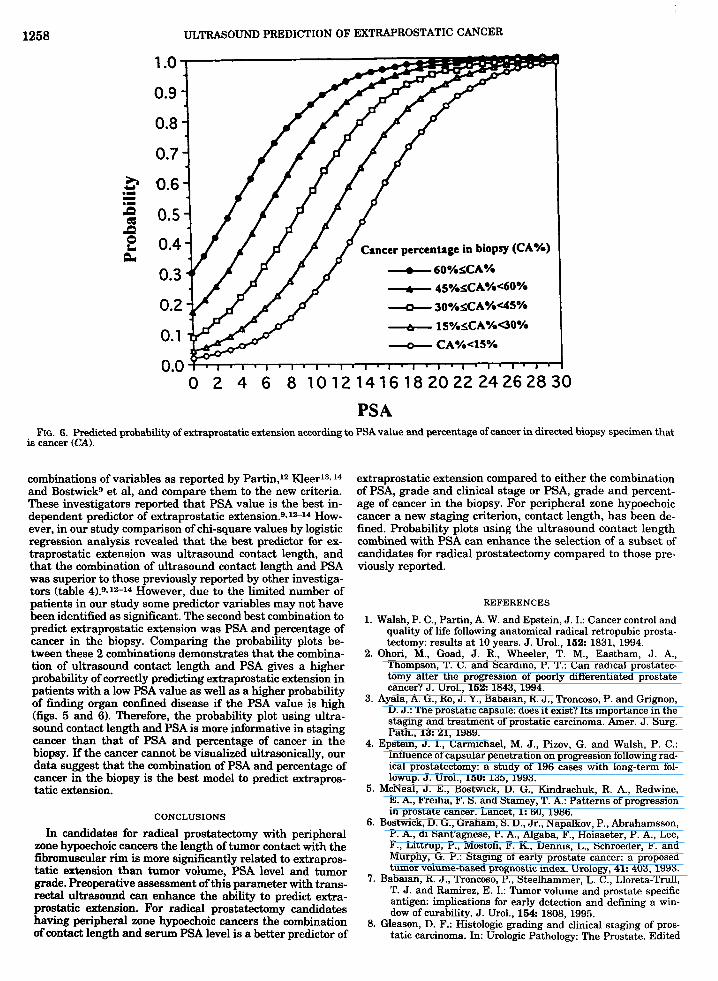
PSA Fk. 6. Predicted probability of extraprostatic extension according to PSAvalue and percentage of cancer in directed biopsy specimen that
is cancer (CA).
combinations of variables as reported by Partin,12 Kleer13.14 and Bostwickg et al, and compare them to the new criteria. These investigators reported that PSA value is the best in- dependent predictor of extraprostatic extension.9- 12-14 How- ever, in our study comparison of chi-square values by logistic regression analysis revealed that the best predictor for ex- traprostatic extension was ultrasound contact length, and that the combination of ultrasound contact length and PSA was superior to those previously reported by other investiga- tors (table 4).9.1"14 However, due to the limited number of patients in our study some predictor variables may not have been identified as significant. The second best combination to predict extraprostatic extension was PSA and percentage of cancer in the biopsy. Comparing the probability plots be- tween these 2 combinations demonstrates that the combina- tion of ultrasound contact length and PSA gives a higher probability of correctly predicting extraprostatic extension in patients with a low PSA value as well as a higher probability of finding organ confined disease if the PSA value is high (figs. 5 and 6). Therefore, the probability plot using ultra- sound contact length and PSA is more informative in staging cancer than that of PSA and percentage of cancer in the biopsy. If the cancer cannot be visualized ultrasonically, our data suggest that the combination of PSA and percentage of cancer in the biopsy is the best model to predict extrapros- tatic extension.
CONCLUSIONS
In candidates for radical prostatectomy with peripheral zone hypoechoic cancers the length of tumor contact with the fibromuscular rim is more significantly related to extrapros- tatic extension than tumor volume, PSA level and tumor grade. Preoperative assessment of this parameter with trans- rectal ultrasound can enhance the ability to predict extra- prostatic extension. For radical prostatectomy candidates having peripheral zone hypoechoic cancers the combination of contact length and serum PSA level is a better predictor of
extraprostatic extension compared to either the combination of PSA, grade and clinical stage or PSA, grade and percent- age of cancer in the biopsy. For peripheral zone hypoechoic cancer a new staging criterion, contact length, has been de- fined. Probability plots using the ultrasound contact length combined with PSA can enhance the selection of a subset of candidates for radical prostatectomy compared to those pre- viously reported.
REFERENCES
1. Walsh, P. C., Partin, A. W. and Epstein, J. I.: Cancer control and quality of life following anatomical radical retropubic prosta- tectomy: results at 10 years. J. Urol., 162 1831, 1994.
2. Ohori, M., Goad, J. R., Wheeler, T. M., Eastham, J. A,, Thompson, T. C. and Scardino, P. T.: Can radical prostatec- tomy alter the progression of poorly differentiated prostate cancer? J. Urol., 162 1843, 1994.
3. Ayala, A. G., Ro, J. Y., Babaian, R. J., Troncoso, P. and Grignon, D. J.: The prostatic capsule: does it exist? Its importance in the staging and treatment of prostatic carcinoma. Amer. J. Surg. Path., 13 21, 1989.
4. Epstein, J. I., Carmichael, M. J., Pizov, G. and Walsh, P. C.: Influence of capsular penetration on progression following rad- ical prostatectomy: a study of 196 cases with long-term fol- lowup. J. Urol., 160 135, 1993.
5. McNeal, J. E., Bostwick, D. G., Kindrachuk, R. A,, Fkdwine, E. A., Freiha, F. S. and Stamey, T. A.: Patterns of progression in prostate cancer, Lancet, 1: 60, 1986.
6. Bostwick, D. G., Graham, S. D., Jr., Napalkov, P., Abrahamsson, P. A., di Sant'agnese, P. A., Algaba, F., Hoisaeter, P. A., Lee, F., Littrup, P., Mostofi, F. K., Dennis, L., Schroeder, F. and Murphy, G. P.: Staging of early prostate cancer: a proposed tumor volume-based prognostic index. Urology, 41: 403, 1993.
7. Babaian, R. J., Troncoso, P., Steelhammer, L. C., Lloreta-Trull, T. J. and Ramirez, E. I.: Tumor volume and prostate specific antigen: implications for early detection and defining a win- dow of curability. J. Urol., 164: 1808, 1995.
8. Gleason, D. F.: Histologic grading and clinical staging of pros- tatic carcinoma. In: Urologic Pathology: The Prostate. Edited
~
j

ULTRASOUND PREDICTION OF EXTRAPROSTATIC CANCER 1259 by M. Tannenbaum. Philadelphia: Lea & Febiger, pp. 171- rectal ultrasonography compared to histopathological assess- 197, 1977. ment for local staging of prostatic carcinoma. Acta. Rad., 31:
597,1990. Myers, R. P. and Oesterling, J. E.: Prediction of capsular 21. Ravery, V., Boccon-Gibod, L. A., D a u g e - h e y , M. C., perforation and seminal vesicle invasion in prostate cancer. Billebaud, T., Delmas, V., Meulemans, A., Toublanc, M. and J. Urol., 155 1361, 1996. Boccon-Gibod, L.: Systematic biopsies accurately predict ex-
10. Villers, A,, McNeal, J. E., Redwine, E. A., Freiha, F. S. and tracapsular extension of prostate cancer and persistenffrecur- Stamey, T. A.: The role of perineural space invasion in the rent detectable PSA after radical prostatectomy. Urology, 64. local spread of prostatic adenocarcinoma. J. Urol., 142: 763, 371,1994. 1989. 22. Pontes, J. E., Ohe, H., Watanabe, H. and Murphy, G. P.: Trans-
11. Bastacky, S. I., Walsh, P. C. and Epstein, J. I.: Relationship rectal ultrasonography of the prostate. Cancer, 53: 1369,1984. between perineural tumor invasion on needle biopsy and rad- 23. hrentzen, T., Nerstrom, H., Iversen, P. and TopPetersen, ical prostatectomy capsular penetration in clinical stage B S. T.: Local staging of prostate cancer with transrectal ultra- adenocarcinoma of the prostate. Amer. J. Surg. Path., 17: 336, sound: a literature review. Prostate Suppl., 4: 11, 1992. 1993. 24. Rorvik, J., Halvorsen, 0. J., Servoll, E. and Haukaas, S.: Trans-
12. Partin, A. W., Yoo, J., Carter, H. B., Pearson, J. D., Chan, D. W., rectal ultrasonography to assess local extent of prostatic can- cer before radical prostatectomy. Brit. J. Urol., 73: 65, 1994. Epstein, J. I. and Walsh, P. C.: The use of prostate specific
antigen, clinical stage and Gleason score to predict patholog- Scardino, P. T.: Detection of microscopic extracapsular exten- ical stage in men with localized prostate cancer. J. Urol., 160 sion prior to radical prostatectomy for clinically localized pros- 110, 1993. tate cancer. Brit. J. Urol., 74: 72, 1994. 13. Kleer, E. and Oesterling, J. E.: PSA and staging of localized
prostate cancer. Urol. Clin. N. Amer., 2 0 695, 1993. 14. Kleer, E., Larson-Keller, J. J., Zincke, H. and Oesterling, J. E.: T’ M’ and Carter’ s. ”:
Staging of prostate cancer. Value of ultrasonography. Urol. Clin. N. Amer., 1 6 713, 1989. Ability of preoperative serum prostate-specific antigen value
27. Rifkin, M. D., Zerhouni, E. A., Gatsonis, C. A., Quint, L. E., t o predict pathologic stage and DNA ploidy. Influence of clin- ical stage and tumor grade. Urology, 41: 207, 1993. Paushter, D. M., Epstein, J. I., Hamper, U., Walsh, P. C. and 15. Miller, G. J. and Cygan, J. M.: Morphology of prostate cancer: McNeil, B. J.: Comparison of magnetic resonance imaging and the effects of multifocality on histological grade, tumor volume ultrasonography in staging early prostate cancer. Results of a and capsule penetration. J . Urol., 162 1709, 1994. multi-institutional cooperative trial. New. Engl. J . Med., 323. 16. Greene, D. R., Wheeler, T. M., Egawa, S., Dunn, J. K. and Scardino, P. T.: A comparison of the morphological features of 621, 1990. cancer arising in the transition zone and in the peripheral 28. Hamper, u. M., Sheth, s., Walsh, P. C., Holtz, P. M. and Epstein, zone of the prostate. J. Urol., 146: 1069, 1991. J. I.: Capsular transgression of prostatic carcinoma: evalua-
17. Epstein, J. I., Carmichael, M., Partin, A. W. and Walsh, P. C.: Is tion with transrectal US with pathologic correlation. Radiol- tumor volume an independent predictor of progression follow- ogy, 178 791, 1991. ingradicalprostatectomy?Amultivariateanalysisof185clin- 29. Young, M. P., Jones, D. R., Griffiths, G. J., Peeling, W. B., ical stage B adenocarcinomas of the prostate with 5 years of Roberts, E. E. and Parkinson, M. C.: F’rostatic “capsule”-a followup. J. Urol., 149: 1478, 1993. comparative study of histological and ultrasonic appearances.
18. Littrup, P. J. and Sparschu, R.: Transrectal ultrasound and Eur. Urol., 24: 479, 1993. prostate cancer risks. The “tailored” prostate biopsy. Cancer, 30. Catalona, W. J., Stein, A. J. and Fair, W. R.: Grading errors in 7 5 1805, 1995. prostatic needle biopsies: relation to the accuracy of tumor
19. Lee, F., Torp-Pedersen, S. T., Siders, D. B., Littrup, P. J. and grade in predicting pelvic lymph node metastases. J. Urol., McLeary, R. D.: Transrectal ultrasound in the diagnosis and 127: 919,1982. staging of prostatic carcinoma. Radiology, 170 609, 1989. 31. Gleason, D. F.: Histologic grading of prostate cancer: a perspec-
20. Enlund, A,, Pedersen, K., Boeryd, B. and Varenhorst, E.: Trans- tive. Hum. Path., 23 273, 1992.
9. Bostwick, D. G., Qian, J., Bergstralh, E., Dundore, P., Dugan, J.,
25. Oho,+, M., E ~ ~ ~ ~ , s., Shinohma, K, meeler, T. M.
26’ scardin’’ p’ T’’ IC’




















