Promoting Positive Interactions in the Classroom: Adapting Parent-Child Interaction Therapy as a...
28
This project was supported in part by a grant from the Kra� Employee Fund, Chicago, awarded to the third author. Correspondence to Karen S. Budd, DePaul University, Department of Psychology, 2219 N. Kenmore Ave, Chicago, IL 60614; e-mail: [email protected]. EDUCATION AND TREATMENT OF CHILDREN Vol. 33, No. 3, 2010 Pages 261–287 Promoting Positive Interactions in the Classroom: Adapting Parent-Child Interaction Therapy as a Universal Prevention Program Rachel A. Gershenson, Aaron R. Lyon, and Karen S. Budd DePaul University Abstract The adaptation of Parent-Child Interaction Therapy (PCIT), an empirically- supported dyadic parent training intervention, to a preschool se�ing may provide an opportunity to enhance the well-being of both teachers and children by improving the teacher-child relationship and providing teachers with effective tools for behavior management. The current article describes the development and implementation of a Teacher-Child Interaction Training (TCIT) program, based on the PCIT model, to a preschool se�ing serving primarily low-income, urban, ethnic minority youth. We discuss the rationale for applying PCIT as a prevention program, prior research on adaptations of PCIT to educational se�ings, application of community psychology principles and strategies in adapting PCIT to the classroom, core TCIT program components, evaluation of effectiveness, issues in sustainability, and resources for successfully implementing the program. Key words: Parent-Child Interaction Therapy, Teacher-Child Interaction Training, community, teacher training, preschool, disruptive behavior E arly aggressive and oppositional behaviors, if le� untreated, are likely to persist over time or develop into more severe and potentially debilitating behavioral or emotional problems (Loeber, Green, Keenan, & Lahey, 1995; Nock, Kazdin, Hiripi, & Kessler, 2007). School-based research with children who are at risk for developing externalizing problems or who are already displaying these behaviors indicates that early intervention can result in more positive outcomes both immediately and long-term (e.g. Bay-Hinitz & Wilson, 2005; Boisjoli, Vitaro, Lacourse, Barker, & Tremblay, 2007; McGoey, DuPaul, Eckert, Volpe, & Van Brakle, 2005). Further, preventive interventions in preschool and kindergarten classrooms have the potential to enhance psychosocial functioning for a broader group of children, potentially bolstering their resiliency later in life (Domitrovich, Cortes, & Greenberg, 2007; Niles, Reynolds, & Roe-Sepowitz, 2008).
Transcript of Promoting Positive Interactions in the Classroom: Adapting Parent-Child Interaction Therapy as a...

This project was supported in part by a grant from the Kra� Employee Fund, Chicago, awarded to the third author.Correspondence to Karen S. Budd, DePaul University, Department of Psychology, 2219 N. Kenmore Ave, Chicago, IL 60614; e-mail: [email protected].
EDUCATION AND TREATMENT OF CHILDREN Vol. 33, No. 3, 2010
Pages 261–287
Promoting Positive Interactions in the Classroom: Adapting Parent-Child Interaction
Therapy as a Universal Prevention Program
Rachel A. Gershenson, Aaron R. Lyon, and Karen S. BuddDePaul University
Abstract
The adaptation of Parent-Child Interaction Therapy (PCIT), an empirically-supported dyadic parent training intervention, to a preschool se�ing may provide an opportunity to enhance the well-being of both teachers and children by improving the teacher-child relationship and providing teachers with effective tools for behavior management. The current article describes the development and implementation of a Teacher-Child Interaction Training (TCIT) program, based on the PCIT model, to a preschool se�ing serving primarily low-income, urban, ethnic minority youth. We discuss the rationale for applying PCIT as a prevention program, prior research on adaptations of PCIT to educational se�ings, application of community psychology principles and strategies in adapting PCIT to the classroom, core TCIT program components, evaluation of effectiveness, issues in sustainability, and resources for successfully implementing the program.Key words: Parent-Child Interaction Therapy, Teacher-Child Interaction Training, community, teacher training, preschool, disruptive behavior
Early aggressive and oppositional behaviors, if le� untreated, are likely to persist over time or develop into more severe and
potentially debilitating behavioral or emotional problems (Loeber, Green, Keenan, & Lahey, 1995; Nock, Kazdin, Hiripi, & Kessler, 2007). School-based research with children who are at risk for developing externalizing problems or who are already displaying these behaviors indicates that early intervention can result in more positive outcomes both immediately and long-term (e.g. Bay-Hinitz & Wilson, 2005; Boisjoli, Vitaro, Lacourse, Barker, & Tremblay, 2007; McGoey, DuPaul, Eckert, Volpe, & Van Brakle, 2005). Further, preventive interventions in preschool and kindergarten classrooms have the potential to enhance psychosocial functioning for a broader group of children, potentially bolstering their resiliency later in life (Domitrovich, Cortes, & Greenberg, 2007; Niles, Reynolds, & Roe-Sepowitz, 2008).

262 GERSHENSON, LYON, and BUDD
Many empirically supported interventions have consisted of multi-component programs involving parent training, teacher train-ing, child skills training, and/or mental health support (e.g., Conduct Problems Prevention Research Group, 2007; Raver et al., 2009; Web-ster-Stra�on, Reid, & Stoolmiller, 2008). Fewer empirically supported preschool interventions have focused only on teacher training, and these o�en have targeted children already identified with significant behavior problems (e.g., Shernoff & Kratochwill, 2007), limiting the conclusions that can be drawn about their utility for universal preven-tion. Despite evidence that negative teacher-child relationships are re-lated to children’s later behavior problems (Brendgen, Wanner, Vitaro, Bukowski, & Tremblay, 2007), these relationships are rarely a central focus of interventions. The model described in this paper offers an approach to universal prevention that emphasizes in-vivo coaching in skills designed to strengthen teacher-child relationships. Further, the model is derived from an evidence-based parent training program for children with clinically indicated behavior problems, so it could be used in tandem with this parent training intervention when indicated by the child’s behavioral needs.
Parent-Child Interaction Therapy (PCIT)
PCIT is a manualized, evidence-based practice for children with disruptive behavior disorders ages two through seven (Brinkmeyer & Eyberg, 2003; Eyberg & Child Study Lab, 1999; Hembree-Kigin & McNeil, 1995). Its principles have been successfully applied in the treatment of many childhood disorders, including a�ention-deficit hyperactivity disorder, oppositional defiant/conduct disorder, and separation anxiety disorder (Eisenstadt, Eyberg, McNeil, Newcomb, & Funderburk, 1993; Nixon, Sweeney, Erickson, & Touyz, 2004; Pin-cus, Eyberg, & Choate, 2005; Schuhmann, Foote, Eyberg, & Boggs, 1998). PCIT consists of two phases: Child Directed Interaction (CDI), during which the parent develops child-focused relationship skills, followed by Parent Directed Interaction (PDI), during which the par-ent learns effective discipline skills. Treatment includes (a) a didactic component to introduce, model, and role-play skills; (b) coaching ses-sions in which the therapist uses modeling, reinforcement, and selec-tive a�ention to shape the parent’s the skills during live interactions with the child; (c) coding of parent-child interactions using the Dy-adic Parent-Child Interaction Coding System III (DPICS III; Eyberg, Nelson, Duke, & Boggs, 2005) in most sessions to guide and evaluate treatment; and (d) homework assignments between sessions that aim to generalize treatment effects to the home environment. Treatment typically lasts 14-16 sessions, although completion is dependent on
263COMMUNITY-BASED TCIT
the parent’s mastery of a target level of skills and ratings of the child’s behavior as within normal limits (Eyberg & Child Study Lab, 1999).
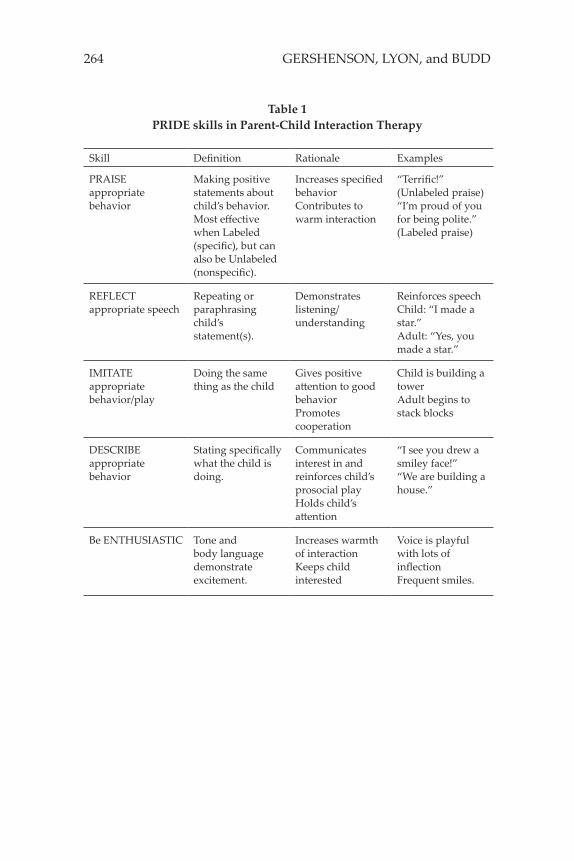
During CDI, the parent is coached in skills for building a warm and accepting parent-child relationship during play. Parents are in-structed to avoid commands, criticisms, and questions that take over the play or that may suggest that the parent disapproves of the child’s behavior. Instead, parents are coached to allow the child to lead by utilizing the PRIDE skills (see Table 1): Praise, Reflection, Imitation, Descriptions of behavior, and Enthusiasm. Problem behaviors, with the exception of dangerous or destructive behaviors, are ignored dur-ing CDI in order to avoid any inadvertent reinforcement. PDI then builds on CDI skills by teaching parents to provide direct commands and consistent discipline for noncompliant behavior. In cases of non-compliance or severe misbehavior, the parent is coached in the ap-plication of a timeout procedure. During PDI, there is an increasing emphasis on the generalization of PCIT skills outside the therapy ses-sions in order to facilitate real-world mastery.
Adaptations of PCIT to Preschool Classrooms
PCIT’s demonstrated efficacy has led to a call for exploration of adaptations for new populations and se�ings in order to further en-hance its real-world applicability (Storch & Floyd, 2005). Research on the modification of PCIT for school se�ings has provided preliminary support for treatment effectiveness in these environments. McIntosh, Rizza, and Bliss (2000) outlined the development of Teacher-Child In-teraction Therapy, a protocol based on PCIT principles. Using a case study approach, the intervention was conducted with one teacher and a 2-year-old child who had been identified as displaying disruptive behavior. The protocol adhered closely to traditional PCIT in skills emphasis, the number of CDI and PDI didactic and coaching sessions, coding of caregiver and child behavior in therapy sessions using the DPICS observation system, and homework assignments. Weekly, 20-minute coaching sessions were conducted outside the classroom, ex-cept for the final two coaching sessions, which took place in the class-room. The teacher and child carried out “special time” homework assignments for 5 minutes per day in the classroom while the other children engaged in other activities. The results indicated desired changes in targeted behaviors for both the teacher and child during coded therapy observations.
Another adaptation of PCIT employed a case study approach with a single teacher in an “out of control” classroom to examine out-comes of using PCIT as compared to a classroom-wide token economy system (Filcheck, McNeil, Greco, & Bernard, 2004). Rather than tar-
264 GERSHENSON, LYON, and BUDD
Skill Definition Rationale Examples
PRAISE appropriate behavior
Making positive statements about child’s behavior. Most effective when Labeled (specific), but can also be Unlabeled (nonspecific).
Increases specified behaviorContributes to warm interaction
“Terrific!” (Unlabeled praise)“I’m proud of you for being polite.” (Labeled praise)
REFLECT appropriate speech
Repeating or paraphrasing child’s statement(s).
Demonstrates listening/understanding
Reinforces speechChild: “I made a star.”Adult: “Yes, you made a star.”
IMITATE appropriate behavior/play
Doing the same thing as the child
Gives positive a�ention to good behaviorPromotes cooperation
Child is building a towerAdult begins to stack blocks
DESCRIBE appropriate behavior
Stating specifically what the child is doing.
Communicates interest in and reinforces child’s prosocial playHolds child’s a�ention
“I see you drew a smiley face!”“We are building a house.”
Be ENTHUSIASTIC Tone and body language demonstrate excitement.
Increases warmth of interactionKeeps child interested
Voice is playful with lots of inflectionFrequent smiles.
Table 1PRIDE skills in Parent-Child Interaction Therapy

265COMMUNITY-BASED TCIT
geting an identified child, this study trained the teacher to implement PCIT skills with the entire class of 17 children. All children were from two-parent homes, and the majority were White and female. The CDI and PDI phases each consisted of an initial didactic session emphasiz-ing standard PCIT skills, followed by coaching outside the classroom for a total of 2 hours in each condition and with increasing numbers of children (up to three). As in traditional PCIT, 5-minute observations during coaching sessions were used to monitor the teacher’s skill ac-quisition. A�er coaching sessions were completed, the teacher began using the skills in the classroom. During the first two days, she was observed in the classroom and received immediate feedback on her skills (2.5 hours per phase). Videotaped classroom observations were coded to evaluate changes in children’s inappropriate behavior and the teacher’s use of praise and criticisms across the study. Both the token economy and CDI conditions were associated with increased levels of teacher praise. Compared to the token economy condition, PCIT phases resulted in lower levels of child inappropriate behavior and teacher critical statements. The authors noted that PCIT required more training and consultation time than the token system (11.5 hours versus 4.5 hours), but that PCIT may be more appropriate when a teacher has skills deficits (e.g., low levels of positive reinforcement and ineffective behavior management strategies).
Recent work by Tiano and McNeil (2006) expanded the focus of school-based PCIT research by including multiple classrooms and teachers. Participants in their adaptation for a rural Head Start se�ing were 4 teachers from separate classrooms, who were each trained to implement PCIT skills with the entire classroom. The majority of stu-dents were White and from low-income families. Teachers received 2-hour group training workshops in CDI and PDI skills. Each train-ing was followed by in-class coaching. The authors noted (p. 225) that teachers were coached for an average of 7 hours, but it is unclear if this was per phase or across the entire program. Coaching sessions included 5-minute observations to monitor the teachers’ acquisition of skills and progressed from practicing PCIT skills with one child to multiple children and eventually the entire classroom. The skills taught were modified for the classroom se�ing, for example by us-ing an ignoring signal (two fingers to lips) when removing a�ention for inappropriate behavior, using “when-then” statements to guide child behavior (e.g., “when you are quiet, we can go outside”), and praising children engaging in the opposite of another child’s inappro-priate behavior (i.e., “praising the opposite”). In addition, the time-out procedure was modified in accordance with Head Start policy (such as calling the procedure the “Thinking Chair” and si�ing in the

266 GERSHENSON, LYON, and BUDD
hallway or parent notification as back-up consequences). To evaluate intervention effects, Tiano and McNeil compared targeted teacher and child behaviors in the 4 randomly selected treatment classrooms with 3 control classrooms. Behaviors were coded in a single, 40-min-ute classroom observation before and a�er training. Results showed that teachers used more labeled praise and fewer timeouts following training as compared to controls. Criticisms and inappropriate child behavior decreased for both groups.
These earlier studies of school-based PCIT adaptations provided a foundation for the current project in their focus on retaining core PCIT principles while including modifications appropriate for a pre-school se�ing (e.g., in-class coaching with multiple children). Our pro-gram aims to expand the PCIT literature by focusing on a predomi-nantly ethnic minority, urban sample, conducting the training with all classroom staff in a team-teaching se�ing, training a larger number of teachers, and incorporating multiple observations of the teachers’ use of all of the PRIDE skills (as well as criticisms and use of discipline) in the classroom to evaluate treatment effects. Finally, special a�ention was paid to the importance of understanding contextual issues at play within community se�ings, an area that has o�en been neglected as mental health programs have expanded into the school environment. These systemic issues, in addition to specific adaptations made to the PCIT protocol, are described below.
Teacher-Child Interaction Training (TCIT) Curriculum Development
Se�ing and Population
Since its initiation in 2005, our PCIT clinic, situated in a Midwest-ern urban community mental health center, has provided evidence-based parent training to low-income families with children exhibiting behavior problems (Lyon & Budd, 2005). In an effort to reduce the time and cost involved in ge�ing to our clinic, we began to offer PCIT services at a local childcare facility that serves predominantly low-in-come, ethnic minority families and provides a high number of PCIT referrals. This private, religiously affiliated facility provides full-time daycare to infants and preschoolers, as well as preschool, kindergar-ten, and a�er school programs. The ethnic composition of the child population at the center is 73% African American, 14% Latino, 9% White, 2% Asian/Pacific Islander, and 2% other. The center is funded by contributions from the public and revenue from other sources, in-cluding government grants and program service fees.
The goal of operating PCIT in this se�ing was to reach more

267COMMUNITY-BASED TCIT
families by giving parents the opportunity to incorporate PCIT into their established routine within a familiar environment. Nevertheless, the traditional PCIT model limits the scope of service provision to in-dividual parent-child dyads in which the child is already displaying disruptive behavior problems. Even when PCIT therapists provide consultation to daycare and preschool staff on children enrolled in PCIT, these services are limited to referred children. In order to ex-pand the range of children affected, we developed a Teacher-Child Interaction Training (TCIT) program using a consultative framework, which we modeled a�er PCIT. We called our program Teacher-Child Interaction Training rather than Teacher-Child Interaction Therapy, because our goal was to enhance teachers’ skills in relating to all the children rather than to provide therapy to an individual child. The TCIT program was funded in part by a grant and in part by the uni-versity with which the authors are affiliated.
We delivered TCIT through group workshops and in-class prac-tice sessions to a total of 12 teachers, including 1 head teacher and 2 teacher assistants (all referred to as teachers here) each from 4 pre-school classrooms. All teachers were female and of diverse ethnici-ties (50% African American, 33% White, 17% Latina), ages (mean of 37 years, range 23-61 years), and levels of experience (mean of 8 years, range of 0-24 years). Each classroom included one teacher with at least a bachelor’s degree and two assistants with some college education. Standard curriculum components common to all classrooms included indoor and outdoor play, individual (e.g., sand tray) and group (e.g., story time) activities, gross-motor and fine-motor activities, and rou-tines such as nap time and snack time. A total of 78 children (19-21 per classroom) ages 3-5 experienced their teachers’ use of TCIT skills in these classrooms during program implementation. Although the de-mographic characteristics of the participating children are likely simi-lar to those of the entire center (described earlier), we did not collect demographic data on the children in the participating classrooms.
The designers and trainers for the current project included the lead investigator (a psychologist with over thirty years of experience in parent and teacher training) and two clinical psychology gradu-ate students. Both the lead investigator and one of the graduate stu-dents had trained with PCIT’s originator during a week-long intensive course, and in turn had trained the remaining graduate student. All members of the training team carried a PCIT caseload during the year prior and during TCIT.
Collaboration and Consultation
Despite having an experienced training staff, even the strongest skill base will not necessarily translate well in a new se�ing without

268 GERSHENSON, LYON, and BUDD
gaining an understanding of its social framework (Harper & Salina, 2000). In order to create an appropriate adaptation of PCIT for the target school se�ing, we met with several community experts (e.g., a preschool supervisor, an educational researcher with detailed knowl-edge of the community) to gain perspective on program planning and the process of bringing new programs into a community center. Infor-mation from these meetings yielded valuable insights into the teach-ing culture at the identified preschool. In addition, the designers had a base of knowledge established through our organization’s history of service with populations of students and teachers from this facility and similar environments.
Community psychology principles suggest several strategies for establishing collaborative relationships when developing commu-nity programs. One way to enhance organizational support for a new program is for trainers to become be�er integrated into the organiza-tion by becoming involved in areas outside of the program itself (St. Pierre & Kaltreider, 2001). As such, we offered a series of roundtable seminars on child development concurrent with the TCIT program (seminar topics were unrelated so as not to confound results of TCIT participation). These seminars provided a forum for meetings with a larger number of staff outside of the research project se�ing and dem-onstrated a commitment to the organization that extended beyond data collection.
In garnering teachers’ support for training, it is also important to address barriers to participation such as lack of incentive, resistance to additional time commitments, and discomfort with the introduction of new skills (Kealey, Peterson, Gaul, & Dinh, 2000). One strategy sug-gested by a community consultant (P. Washington, personal commu-nication, May 12, 2006) was to describe the program as a potential way to reduce teacher burnout. We used this wellness promotion frame-work on introductory fliers, as we reasoned that PCIT’s ability to de-crease parental stress (Nixon et al., 2004; Schuhmann et al., 1998) may also be applicable to teachers. Additionally, the program was incorpo-rated into the teachers’ existing schedules by conducting sessions dur-ing the children’s nap-time rather than requiring teachers to extend their workday, and continuing education credits were provided to teachers as an added incentive. To promote acceptance of new skills, it was important to understand existing teaching styles and commend teachers on the job they were already doing. In this vein, the TCIT program incorporated non-evaluative, pre-intervention observation sessions to educate trainers about teachers’ individual teaching styles, enabling the provision of specific, positive feedback at the outset of the program.

269COMMUNITY-BASED TCIT
Adaptation and Implementation
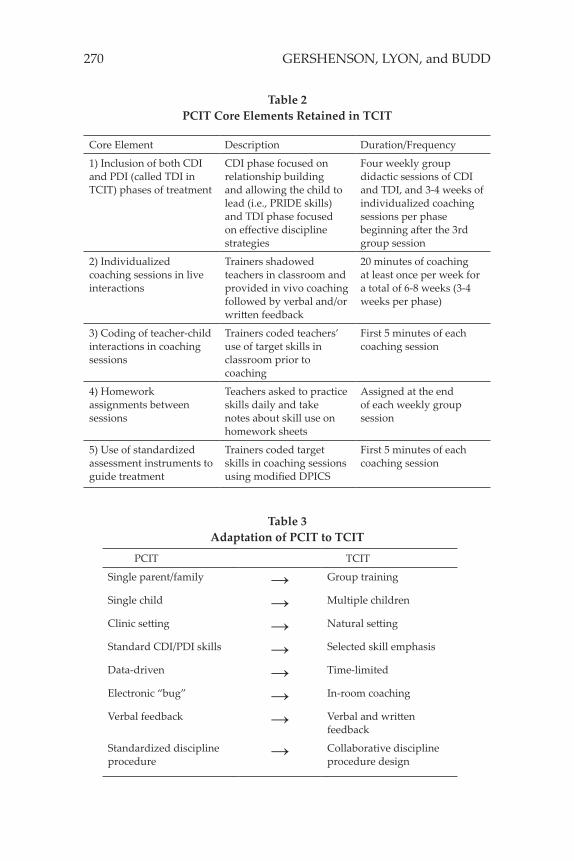
The TCIT curriculum was designed with the intention of adher-ing to the core principles and goals of PCIT while a�ending to the unique dynamics of the classroom se�ing. Components identified as core elements of PCIT are inclusion of both CDI and PDI phases of treatment, individualized coaching sessions in live interactions, cod-ing of parent-child interactions in coaching sessions, assignment of homework between sessions, and use of standardized assessment instruments (e.g., DPICS and a standard child behavior inventory) to guide treatment (Training Guidelines for Parent-Child Interaction Therapy, 2009). In addition, features such as the therapy format, con-tent, and continuing treatment until mastery of the skills is achieved have been cited routinely in descriptions of PCIT (e.g., Brinkmeyer & Eyberg, 2003; Hembree-Kigin & McNeil, 1995; Herschell, Calzada, Ey-berg, & McNeil, 2002). We included each of the core elements of PCIT in our school-based adaptation, as described in Table 2. However, we renamed the PDI phase TDI (Teacher-Directed Interaction) to reflect the teachers as recipients of training rather than parents, and we did not use the standard child behavior inventory from PCIT because the children were not clinically referred.
In addition to these core elements, we retained PCIT’s emphasis on the PRIDE skills (described above); initially introduced the skills of each phase via didactic instruction, modeling, and role-play practice as in PCIT; and provided printed training handouts, some drawn from the PCIT protocol (Eyberg & Child Study Lab, 1999). Finally, there were a number of practical similarities between the PCIT and TCIT models. These include training sessions of similar length (approxi-mately 1 ½ hours for group sessions) and a cotherapy/coleader model. The advantages of having coleaders present for each TCIT session in-cluded more individualized a�ention for each teacher participant as well as the benefit of multiple perspectives when troubleshooting any problems identified by teachers during their practice.
Although the TCIT program retained many aspects of PCIT, numerous adaptations were made in order to implement the PCIT model across entire classrooms of teachers and children as a preven-tive approach. The adaptations included (1) a group training format, (2) an emphasis on skill use with multiple children at once, (3) use of a natural se�ing for intervention, (4) use of a subset of the established PCIT skills, (5) a time-limited program model, (6) in-room coaching, (7) feedback provided in both wri�en and verbal format, and (8) a col-laborative approach to the design and implementation of discipline procedures (see Table 3).
270 GERSHENSON, LYON, and BUDD
Table 2PCIT Core Elements Retained in TCIT
Core Element Description Duration/Frequency
1) Inclusion of both CDI and PDI (called TDI in TCIT) phases of treatment
CDI phase focused on relationship building and allowing the child to lead (i.e., PRIDE skills) and TDI phase focused on effective discipline strategies
Four weekly group didactic sessions of CDI and TDI, and 3-4 weeks of individualized coaching sessions per phase beginning a�er the 3rd group session
2) Individualized coaching sessions in live interactions
Trainers shadowed teachers in classroom and provided in vivo coaching followed by verbal and/or wri�en feedback
20 minutes of coaching at least once per week for a total of 6-8 weeks (3-4 weeks per phase)
3) Coding of teacher-child interactions in coaching sessions
Trainers coded teachers’ use of target skills in classroom prior to coaching
First 5 minutes of each coaching session
4) Homework assignments between sessions
Teachers asked to practice skills daily and take notes about skill use on homework sheets
Assigned at the end of each weekly group session
5) Use of standardized assessment instruments to guide treatment
Trainers coded target skills in coaching sessions using modified DPICS
First 5 minutes of each coaching session
Table 3Adaptation of PCIT to TCIT
PCIT TCIT
Single parent/family → Group training
Single child → Multiple children
Clinic se�ing → Natural se�ing
Standard CDI/PDI skills → Selected skill emphasis
Data-driven → Time-limited
Electronic “bug” → In-room coaching
Verbal feedback → Verbal and wri�en feedback
Standardized discipline procedure
→ Collaborative discipline procedure design
271COMMUNITY-BASED TCIT
Group training. Although PCIT occasionally has been delivered in a group context (e.g., McNeil, Herschell, Gurwitch, & Clemens-Mowrer, 2005; Niec, Hemme, Yopp, & Brestan, 2005), PCIT ordinarily occurs with individual families. In order to increase program reach, our TCIT program involved teams of teachers (three from each of four classrooms, separated into two trainings for two classrooms at a time). Facility administrators hoped to eventually have all preschool teachers receive the training, and teachers from three of the four class-rooms volunteered to be the initial participants. Teachers from the fourth classroom were asked by administrators to participate in the hope that their involvement could help improve classroom dynamics. Tiano and McNeil’s (2006) adaptation of PCIT to a Head Start class-room also used a group training approach; however, they included only one session (1.5 or 2 hours each) per phase, whereas we provided four sessions per phase for a total of approximately 12 hours of group training time. We increased the number of group sessions to allow for more rapport-building with teachers (in a universal program, not all teachers have volunteered to participate), promote positive working relationships and team-building among the teachers, and provide a more efficient means of familiarizing teachers with the skills than in-dividualized coaching.
As in PCIT, we designed TCIT to proceed along two distinct phases, CDI and TDI. However, each phase was restricted to four ses-sions, and the final TDI session was followed by a celebratory gradu-ation session. During CDI, the first session consisted of introductions and rapport-building activities, an overview of traditional PCIT and its modification for the preschool se�ing, and preliminary CDI ex-ercises to encourage active participation. Sessions 2-4 centered on further CDI training, each emphasizing a different PRIDE skill, and included didactic components, modeling, and role playing. Follow-ing the third CDI session, in-room coaching sessions began 1-2 times per week, during which TCIT trainers observed teachers’ use of TCIT skills and provided oral feedback. Coaching then continued for at least one week following completion of the CDI didactics. Sessions 5-8 followed a similar structure for TDI training, with in-room coaching beginning a�er the third TDI training session (session 7). Across CDI and TDI, activities were designed to become increasingly self-directed to enhance teachers’ confidence and efficacy. The final session incor-porated an overview of the TCIT skills, as well as graduation certifi-cates, continuing education credit documentation, and celebration of teachers’ accomplishments. The overall training lasted 11-13 weeks, not counting vacations or holiday breaks. Detailed session protocols and handouts are available from the last author.
272 GERSHENSON, LYON, and BUDD
Multiple children. As a function of its application with individ-ual families, PCIT occurs with a single child for the duration of the intervention. In the classroom se�ing, times when teachers interacted with only one student were relatively few. Therefore, TCIT teachers initially began practicing skills in homework and coaching sessions with individual children and then quickly progressed across each phase to applying them with more children (e.g., at the water table or an art activity with 3-4 children and eventually during circle time with up to the entire class). Both Filcheck et al. (2004) and Tiano and McNeil (2006) incorporated increasing numbers of children into their coaching sessions with teachers as well.
Natural se�ing. The PCIT therapy room presents families with a standardized set of toys and instructions, during which parent behav-ior is observed and coached. Generalization beyond the therapy room becomes a primary goal in the second phase (PDI). Our TCIT program was designed to minimize classroom disruption and maximize gen-eralizability as early as possible. Teachers were observed and coached in their typical classroom se�ings while interacting with students, and they were asked to practice new skills in a variety of activities throughout the day. Coaching in the classroom provides far less control than coaching in a PCIT therapy room, in that the number of children present, the availability of other teachers, and ongoing activities varied unpredictably across sessions. Although coaching times were scheduled in advance with teachers, current events o�en required flexibility in which teachers were coached and in the activi-ties used for coaching. Additionally, in contrast to PCIT’s emphasis on providing feedback following nearly every parent verbalization, in the classroom environment continuous verbal feedback sometimes either was not feasible (e.g., when teachers were moving rapidly be-tween activities and groups of children during a transition period) or was inappropriate (e.g., during story time). At these times, trainers limited their immediate responses to teachers and relied more on ver-bal and wri�en summary feedback following the coaching period.
Prior classroom adaptations of PCIT have varied in the extent to which training and/or observation took place in the natural class-room environment. McIntosh et al. (2000) closely followed the stan-dard PCIT format of training in a therapy room for all but the last two coaching sessions, and observations were based on 5-minute coding segments prior to coaching sessions. Filcheck and colleagues (2004) conducted coaching outside the classroom and provided additional in-class coaching for two days in each phase. Evaluation of changes in teacher and child behavior was based on in-class observations. Our TCIT model is most similar in this respect to that of Tiano and McNeil

273COMMUNITY-BASED TCIT
(2006), which involved in-class coaching and observation of the effects of training directly in the classroom. The choice to implement coach-ing and observation in the natural classroom se�ing is consistent with the fact that both projects focused on training teachers in PCIT skills for use with all the children as a preventive approach.
Selected skill emphasis. PCIT teaches the parent a full range of skills designed to increase the warmth of parent-child interactions and provide effective discipline. Due to the realities of the classroom learning environment, completely avoiding commands and questions (as taught to parents during CDI) was impractical and inappropri-ate. Therefore, our TCIT model did not a�empt to eliminate those types of interactions between teachers and students during prac-tice and focused instead on promoting the PRIDE skills, decreasing negative comments, and reducing a�ention to mild inappropriate behavior. Nevertheless, we did coach teachers to reduce unnecessary questions during free play activities, turn questions into reflections or behavioral descriptions when an answer was not needed, and avoid “rapid-fire” series of questions whenever possible. None of the other PCIT adaptations to the preschool mentioned modifications of CDI training with respect to reducing questions or commands.
The behavior management procedures introduced in TCIT also needed to be modified. As in PCIT, teachers were taught to use di-rect commands (i.e., clear, declarative, “to do” statements) when it was important for the child to comply. However, they were not ex-pected to eliminate indirect commands (i.e., suggestions or implied commands), were taught strategies other than timeout for following through with commands (such as physical cues or guidance and ac-cess to preferred consequences), and learned how to praise other chil-dren who were behaving appropriately as a means of responding to a child’s inappropriate behavior. Further, the consequence for misbe-havior used with parents (timeout) was modified for the classroom, as described below under “Collaborative discipline procedure design.” We adopted Tiano and McNeil’s (2006) use of “praising the opposite,” which entailed having the teacher a�end to a child who was behav-ing appropriately as a means of addressing another child’s misbehav-ior. Although our other modifications differed in details from Tiano and McNeil’s, both they and we altered PCIT’s behavior management procedures to make them amenable to nonreferred children in a pre-school classroom context.
Time-limited. One criterion for completion of PCIT involves dem-onstrating “mastery” of a specified level of CDI and PDI skills during a standardized observation period. For the classroom, appropriate mas-tery criteria were unclear. Additionally, as a group training program

274 GERSHENSON, LYON, and BUDD
for teachers with varied teaching skills, educational backgrounds, and motivations for training, we reasoned that standard mastery require-ments were impractical and might even de-motivate participants. In-stead, we used teachers’ skills levels during 5-minute coding at the beginning of coaching sessions to prioritize the skills for coaching and sought to increase each teacher’s skills as much as possible across coaching sessions. Previous adaptations of PCIT to a group format also have made training time-limited rather than mastery-based (Mc-Neil et al., 2005; Niec et al., 2005). The three prior adaptations of PCIT to the preschool environment reportedly used mastery criteria similar to those in PCIT, so our model represents a change in this aspect.
In-room coaching. Coaching of the parent in PCIT skills is a core component of the treatment model. Although PCIT coaching can occur in the same room with the parent and child, PCIT therapists typically coach the parent from behind a one-way mirror using an electronic ra-dio device or “bug.” Participating classrooms lacked any observation areas, and teachers moved around the entire classroom frequently. Therefore, TCIT trainers shadowed teachers in their classrooms and provided feedback as they engaged students. It appears that the same method was used during in-class coaching by McIntosh et al. (2000), Filcheck et al. (2004), and Tiano and McNeil (2006), although details of their coaching procedures are not provided. In our TCIT model, coaching lasted for a total of approximately 20 minutes per session, including 5 minutes of observation, 10 minutes of live coaching, and 5 minutes of feedback. Teachers were coached at least once per week (based on their availability) for a total of between 4 and 9 coaching sessions across CDI and TDI phases.
Verbal and wri�en feedback. Parents in PCIT are provided with immediate verbal feedback during coaching and a verbal summary and discussion of their acquisition of target skills at the end of the coaching session. However, in the busy context of the preschool class-rooms, it can be difficult for teachers to take time away from class-room duties for summary feedback and discussion. In TCIT, trainers provided teachers with immediate verbal feedback as the classroom situation allowed. In addition, during TDI, they provided a standard wri�en feedback sheet following in-class coaching, which the teach-ers could review at a later, less hectic time. The wri�en procedure was developed in response to suggestions from teachers, who indicated that a concrete record of trainer feedback would be useful. The format of the feedback sheet was consistent throughout the coaching sessions, enabling teachers to track their progress over time. It included a list of the target skills for the phase, boxes to indicate the coach’s tally of the number of each skill displayed in 5-minute coding and 10-minute

275COMMUNITY-BASED TCIT
coaching segments, and spaces for comments. No prior adaptations of PCIT to the classroom have described details of the feedback to teachers or mentioned variations from the standard verbal feedback.
Collaborative discipline procedure design. Consequences for child noncompliance and misbehavior during the PDI phase of PCIT result in the implementation of an established protocol involving (1) a warn-ing, (2) a timeout chair, and (3) a timeout backup (e.g., timeout room). Tiano and McNeil (2006) described that they modified the timeout procedure in response to Head Start policies. In our preschool se�ing, we found that existing classroom rules, discipline procedures, and teacher expectations surrounding appropriate student behavior var-ied considerably, and isolation in a timeout room was not allowed.
We developed a collaborative process that engaged the teachers in determining appropriate discipline rules. TCIT teachers from each classroom jointly created a “Sit & Watch” plan from a general frame-work in order to establish a discipline program consistent with their classroom needs. This framework was adapted from the contingent observation procedure originally described by Porterfield, Herbert-Jackson, and Risley (1976). These authors found that their procedure, in which disruptive children in a daycare se�ing were placed on the periphery of a group of children behaving appropriately in order to observe for a 1-minute period, was superior when compared to corrective instruction and redirection. In TCIT, Sit & Watch occurred a�er specified misbehaviors, predetermined by the classroom teachers to be sufficiently severe to warrant the procedure (e.g., hi�ing, throwing toys, repeated noncompliance with instructions). Teachers then identified a statement to be used at the beginning of Sit & Watch, which labeled the specific rule-breaking behavior (e.g., “Because you threw a block, you have to sit and watch how the other children play”). Classroom teachers also collectively determined the location and length of time children would spend in Sit & Watch, as well as how to handle misbehavior during the procedure (e.g., repeated returns to the chair, extended time, moving to a more isolated area of the classroom). Finally, teachers identified a statement to mark the end of Sit & Watch (e.g., “You may come back to the activity now”) and a way to give positive a�ention when a child returned to the group activity (e.g., provide a labeled praise of the child’s appropriate behavior). Table 4 provides an outline of the TCIT Sit & Watch planning procedure.
Sit & Watch is similar to timeout in PCIT in that it is a negative consequence administered by a caregiver for severe misbehavior that involves removing a�ention and access to activities for a short period of time. It differs from timeout in that it is used immediately for all predetermined behaviors rather than generalized over time, usually

276 GERSHENSON, LYON, and BUDD
Table 4Sit & Watch Planning in TCIT
Sit & Watch Element Examples
Behaviors for which Sit & Watch will be used.
Fighting – hi�ing, kicking, or biting another child or the teacher
Brief statement at beginning of Sit & Watch of what the child did.
“Because you threw a block, you have to sit and watch how the other children play,” or “We don’t throw toys. You need to go to Sit & Watch.”
Location for child to be seated for Sit & Watch.
Approximately 5 feet outside the activity area, facing the activity
Time length for Sit & Watch and requirement to end.
One minute in chair, with five seconds of quiet at end
Procedure for handling if child gets out of chair or misbehaves during Sit & Watch.
a. Return child to the chair (“Stay here until I tell you Sit & Watch is over”) and restart time
b. If child gets up more than two times, move chair to a quiet corner of room
c. Extend time by one to two minutes if needed
. d. Then have child return to Sit & Watch chair and sit for one minute.
Brief statement at end of Sit & Watch. “You may come back to the activity now.”
Teacher a�ention when child returns to activity and begins to behave appropriately.
Labeled praise of child’s appropriate behavior.
lasts for only 1-2 minutes rather than 3 minutes (although the length was determined jointly by each teaching team), allows the child to watch ongoing classroom activities while in the “Sit & Watch” chair, and does not include a timeout room as backup. Further, due to the collaborative design, teachers jointly determine several aspects of the procedure rather than following a standard procedure.
Additional Considerations for School-Based Programming
Strengthening motivation. A key factor in developing a train-ing curriculum is building in elements that motivate participants to continue to a�end sessions (Fagan & Mihalic, 2003; Kealey et al.,
277COMMUNITY-BASED TCIT
2000). To foster motivation and build rapport between teachers and trainers, group sessions contained icebreaker games and activities that highlighted teachers’ knowledge and experience, and all sessions included food. Studies have demonstrated that perceived effective-ness of training programs is one of the strongest predictors of par-ticipation (Kauffman & Poulin, 1994; Von Brock & Elliot, 1987). To address this component of teacher buy-in, trainers described the posi-tive outcomes of PCIT and incorporated anecdotal evidence from the trainers’ personal experiences with PCIT into training activities. Addi-tionally, several authors have noted the importance of teacher partici-pants experiencing tangible change that can be a�ributed to program implementation (Han & Weiss, 2005; St. Pierre & Kaltreider, 2001). As such, teachers were asked to report any changes they observed in their classrooms in order to learn from and celebrate successes and highlight program effectiveness. Trainers emphasized praise during feedback as a way to strengthen their relationship with teachers and model positive reinforcement skills. Finally, as the use of “positive im-ages” is an important element in promoting responsiveness to new programs in schools (Dowrick et al., 2001), we distributed colorful posters for the classroom that highlighted the PRIDE skills, and pre-sented certificates at the conclusion of training which provided a vi-sual reminder of accomplishments.
Team building. Another important element of the TCIT training plan was team building. Because the identified preschool classrooms operated with a co-teaching model, there was potential for conflict between lead and assistant teachers regarding the relative impor-tance of teacher education versus experience (P. Washington, personal communication, May 12, 2006). Further, research on urban Head Start programs has shown that lead and assistant teachers o�en disagree about child behavior problems (Anthony, Anthony, Morrel, & Acosta, 2005). In response to these potential barriers to team building, we included activities that helped teachers at different levels to value each other’s contributions via opportunities for lead-assistant teacher partnerships during role-plays (an ideal structure for eliciting posi-tive feedback) and collaboration on the design of classroom-specific discipline procedures. Trainers also actively sought and identified places to highlight the unique skills among the different teachers.
Diversity emphasis. In addition to recognizing diverse teacher backgrounds, it is important to consider the effects of researcher characteristics on the training environment. The importance of ethnic match between therapist and client has been debated in the psycho-therapy literature (Zane et al., 2005), but it has rarely been discussed in the context of teacher consultation. In addressing this and other back-
278 GERSHENSON, LYON, and BUDD
ground differences between trainers and teachers, it is helpful to ac-knowledge such differences up front in an effort to stimulate discussion of how diversity can benefit all participants (E. Patrikakou, personal communication, May 24, 2006). In the TCIT training, such differences were identified and framed using a strengths-based perspective during the previously mentioned team-building discussions.
Diversity is also relevant to the training materials themselves. Some authors have suggested that culturally appropriate interven-tions may have a greater chance of success (Lau, 2006). As PCIT was developed and tested primarily through research on White popu-lations (Gallagher, 2003), there is potential for challenges to arise around the issue of cultural relevance. The utility of PCIT for use with ethnic minority populations has been identified as an important area of further study (Herschell et al., 2002), and researchers have begun to explore adaptations for particular ethnic groups (e.g., McCabe, Yeh, Garland, Lau, & Chavez, 2005). In the educational context, one strat-egy for enhancing cultural relevance is adapting an intervention to fit with existing styles of teaching that are normative in particular com-munity environments (Carey, 2004). To this end, the current training contained activities that emphasized teachers’ experiences and envi-ronment, rather than relying on previously determined notions about what was needed or should be changed. Examples of such activities include a brainstorming session about the specific behaviors that teachers wanted to promote or enhance in the classroom, and discus-sions about current classroom management strategies and how they do or do not fit with the new skills.
Evaluation
We evaluated the TCIT program via direct observations, teacher homework, and satisfaction ratings. These multiple forms of evalua-tion provided an opportunity to examine program outcomes using dif-ferent indices. Detailed information about the evaluation procedures is provided in a TCIT outcome paper (Lyon et al., in press).
Observations involved a simplified version of the standard PCIT observation tool, the Dyadic Parent-Child Interaction Coding Sys-tem (DPICS; Eyberg et al., 2005), to provide naturalistic assessment of teachers’ use of TCIT skills in their classrooms (see Lyon et al., in press for more information on DPICS modifications and psychometric data). Lyon and colleagues (in press) reported on a multiple-baseline design to evaluate the effects of TCIT on teacher behavior. Over the course of the academic year, the program was implemented twice, each time with two classrooms of teachers (12 teachers total). Results from observations 1-2 times weekly across a range of classroom ac-

279COMMUNITY-BASED TCIT
tivities indicated that teachers’ use of positive behaviors (i.e., praise, reflections, behavioral descriptions) increased systematically, but modestly, from baseline to the completion of CDI and then remained consistently higher than baseline through TDI. Inspection of individual teachers’ data suggested that 10 teachers demonstrated increased use of at least one positive behavior over the course of training, and two did not demonstrate any meaningful changes. In addition, 5 teachers increased their use of multiple skills. The largest increases were seen in teacher’s use of unlabeled praises, which the authors a�ributed to the familiarity of the concept of praise and the ease of using praise with groups of children. For the majority of classrooms, positive be-havior peaked close to the end of the CDI phase, suggesting that both the group didactic training and the individualized in-class coaching that followed it were important to teacher skill acquisition. Instances of use of the Sit & Watch procedure during TDI indicated that teachers adopted this procedure as a disciplinary strategy.
Teachers also completed homework assignments between ses-sions and evaluated the training program through satisfaction ratings. Homework tracking sheets were modeled on those employed in PCIT and allowed teachers to record activities, skills used, and problems encountered during practice. Anonymous satisfaction ratings were collected at the end of the CDI and PDI phases and elicited quantitative teacher feedback on issues such as the utility of CDI and TDI skills and the effectiveness of TCIT trainers and activities. Lyon and colleagues (in press) reported wide variations in TCIT homework completion but uniformly high satisfaction ratings. Although few differences in satisfaction between CDI and TDI were reported, the largest differences occurred in ratings of skill utility, where teachers rated TDI skills as slightly more useful than CDI skills. Nevertheless, skills across both TCIT phases were rated highly. The authors concluded that TCIT is a promising approach for enhancing positive teacher-child interactions in a preschool se�ing and should receive further investigation.
Feasibility and Sustainability
Throughout the planning and implementation of this TCIT mod-el, we a�empted to retain as many features of PCIT as possible in light of the environment of the center. Choices about which aspects of PCIT to retain and which to modify were based on the universal prevention goals. Although many components of this TCIT model are likely to be feasible for implementation in other se�ings, it is advisable that the planning begin with collaboration and consultation, taking into account the partnership between the trainers and the center, and the needs and resources of each. Some of the ingredients that presumably
280 GERSHENSON, LYON, and BUDD
were related to our successful collaboration include our familiarity with the center through prior service provision, promoting buy-in through offering roundtable seminars concurrent with the teacher training, and addressing several potential barriers to participation through program design, continuing education credits, and framing the program as a tool to reduce teacher burnout.
One key decision we made to increase the reach of the TCIT pro-gram was to adapt the PCIT model to a group format and to design it as a preventive intervention for the entire classroom, rather than only for children already identified as having behavior problems. To imple-ment the group TCIT model, a minimum of two trainers are needed, both of whom have advanced training in child development, mental health assessment and treatment, and the PCIT model. In our pro-gram, the trainers were doctoral clinical psychology students, work-ing under the supervision of a psychology faculty member. It is likely that staff with master’s degrees in a mental health field and PCIT training would also be effective as trainers. If the TCIT program is implemented in a research context, resources are needed for data col-lection and analysis. Alternatively, if it is implemented in practice con-text, trainers could collect data at strategic points (e.g., before training, during CDI and TDI coaching sessions, and a�er training) and could collect evaluation forms from teachers to measure progress. We were fortunate to have the financial resources of a foundation grant and the university to fund trainers, observers, and supplies. Barring some form of training funds, it is unlikely that community-based preschool programs could afford a systematic training program such as TCIT. However, it should be noted that PCIT has been described as a cost-ef-fective intervention for children with disruptive behaviors (Goldfine, Wagner, Branste�er, & McNeil, 2008), and it is likely that its adapta-tion as a universal prevention program could be even more economi-cal and may produce a more far-reaching impact than a program that targets individual children referred for clinical problems.
In addition to staff and data collection needs, resources are nec-essary to provide food for group sessions and for program materials. Specifically, one of our consultants suggested that an effective strategy for promoting program implementation a�er the conclusion of train-ing was to provide the trainees with a clear, cohesive set of reference materials (E. Patrikakou, personal communication, May 24, 2006). Thus, as a component of our training, we provided teachers and other school personnel with materials on TCIT that were both user-friendly and thorough. These materials consisted of binders that contained all of the information presented during training sessions (i.e., handouts, homework sheets, observational forms, discipline planning sheets,

281COMMUNITY-BASED TCIT
space for notes) and posters that were hung in participating classrooms, which served as a reminder of the PRIDE skills.
Sustainability of the effects of any training program, including TCIT, at a center will likely require efforts to train incoming teach-ers. We observed that some teachers who participated in TCIT spon-taneously introduced new teachers to the skills they had learned. For example, we witnessed teachers applying Sit & Watch who had not participated in our training. Perhaps teachers who have completed TCIT could serve as mentors for other teachers in learning the skills. Booster sessions or follow-up consultation with teachers who wish to refresh their skills could also be beneficial. The availability of staff affiliated with the center who can provide periodic TCIT training and consultation would be ideal. Investment in continuing professional development of teachers may help to buffer against the high turnover o�en experienced in community-based preschool se�ings.
Summary, Limitations, and Future Directions
The Teacher-Child Interaction Training (TCIT) program was de-signed with the goals of promoting a positive classroom environment, preventing future child behavior problems and addressing current ex-ternalizing issues, and decreasing teacher burnout. In the process of transporting Parent-Child Interaction Therapy (PCIT) out of the clinic and into the classroom, adaptations were made to enhance applicabil-ity in the new se�ing while retaining the core principles of building warm caregiver-child relationships and utilizing effective discipline strategies. The TCIT program was delivered in a se�ing in which the university had already developed strong partnerships. Community consultation and the provision of additional roundtable seminars fur-ther promoted acceptability. Barriers to participation in the program were proactively addressed, and user-friendly training materials promoted the sustainability of program effects.
The challenges that arose during the course of program imple-mentation resulted in several important lessons to be learned from this project. First, we had to work around systemic issues in the facil-ity. For example, preschool classrooms were o�en short-staffed, re-sulting in teachers being temporarily assigned to cover other classes and not being present when we arrived for coaching or not being able to leave their classrooms for group sessions. Thus, trainers had to re-turn at a different time for coaching to ensure the intervention was reaching all teachers, begin group sessions later than planned, and provide make-up sessions when needed. Second, we had to accom-modate teachers with a wide range of educational backgrounds and levels of experience in group sessions, which required group training

282 GERSHENSON, LYON, and BUDD
skills different from those needed for working with individual fami-lies in PCIT. On a related note, it was necessary to tailor discussion of skills use to classroom environments ranging from relatively calm to “out of control.” Relationships among teachers in some classrooms were strained, which necessitated more efforts toward team-build-ing than had been anticipated. Meeting individually with teachers to gain their perspective and build rapport, and communicating with the center administrative staff about classroom dynamics, appeared to be helpful strategies for addressing some team-building challenges, but solving entirely the problems between teachers remained beyond the scope of this project. Overall, the program required a level of flexibil-ity, extra effort, and creativity that may not be as necessary in a more controlled environment.
Limitations of the current project included the lack of demo-graphic information gathered about participating students, the range in dosage of coaching sessions, differing levels of homework comple-tion, and potentially limited generalizability due to inclusion of only one preschool center. Several aspects of this model would benefit from systematic evaluation, including the pros and cons of using mastery criteria for CDI and TDI phases and the optimal number, length, and location (in or out of classroom) of coaching sessions. The total amount of coaching for individual teachers provided by Filcheck et al. (2004) (9 hours) and Tiano and McNeil (2006) (average of 7 hours) was substantially greater than in the current project (average of 2.5 hours per teacher). Because the current study included more teachers, we chose to increase the amount of group time and reduce coaching to fit with the economic realities of the project; however, it will be im-portant to determine how much coaching is needed to effect desired changes. Central to answering these questions is the need for system-atic measurement of the effects of training on the children’s behavior. Another direction for future research is examining teacher, classroom, and center-based factors associated with greater effectiveness of TCIT. As our project continues, we hope to be able to investigate some of these aspects.
This TCIT program represents an innovative intersection be-tween clinical, community, and school psychology in an effort to pre-vent negative outcomes and promote wellness in underserved popu-lations. The current TCIT model expands prior adaptations of PCIT to school se�ings by focusing on a predominantly ethnic minority, urban sample, conducting the training with more teachers, includ-ing all classroom staff in a team-teaching se�ing as participants in the training, and incorporating multiple observations of the effects of intervention in a multiple-baseline design. Special a�ention was paid

283COMMUNITY-BASED TCIT
to the importance of understanding contextual issues at play within community se�ings. It will be important for future investigations of TCIT and other similar prevention programs to examine long-term benefits for both students and teachers. The implementation of TCIT in other se�ings is an opportunity to support positive interactions be-tween teachers and students, and promote prosocial behavior in chil-dren beyond those who can be reached in a clinical se�ing.
References
Anthony, B. J., Anthony, L. G., Morrel, T. M., & Acosta, M. (2005). Evi-dence for social and behavior problems in low-income, urban preschoolers: Effects of site, classroom, and teacher. Journal of Youth and Adolescence, 34, 31-39.
Bay-Hinitz, A. K., & Wilson, G. R. (2005). A cooperative games inter-vention for aggressive preschool children. In L. A. Reddy, T. M. Files-Hall, & C. E. Schaefer (Eds.), Empirically based play in-terventions for children (pp. 191-211). Washington, D.C.: Ameri-can Psychological Association.
Boisjoli, R., Vitaro, F., Lacourse, E. Barker, E., & Tremblay, R. E. (2007). Impact and clinical significance of a preventive intervention for disruptive boys. British Journal of Psychiatry, 191, 415-419.
Brendgen, M., Wanner, B., Vitaro, F., Bukowski, W. M., & Tremblay, R. E. (2007). Verbal abuse by the teacher during childhood and academic, behavioral, and emotional adjustment in young adulthood. Journal of Educational Psychology, 26-38.
Brinkmeyer, M. Y., & Eyberg, S. M. (2003). Parent-Child Interaction Therapy for oppositional children. In A. E. Kazdin & J. R. Weisz (Eds.), Evidence-based psychotherapies for children and ado-lescents (pp.2004-223). New York: Guilford Press.
Carey, K. T. (2004). Preschool interventions. In J. C. Conoley & A. P. Goldstein (Eds.). School violence intervention: A practical hand-book. New York, NY: Guilford Press.
Conduct Problems Prevention Research Group (2007). Fast Track ran-domized controlled trial to prevent externalizing psychiatric disorders: Findings from grades 3 to 9. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 1250-1262.
Domitrovich, C. E., Cortes, R. C., & Greenberg, M. T. (2007). Improv-ing young children’s social and emotional competence: A ran-domized trial of the preschool ‘PATHS’ curriculum. Journal of Primary Prevention, 28, 67-91.

284 GERSHENSON, LYON, and BUDD
Dowrick, P. W., Power, T. J., Manz, P. H., Ginsburg-Block, M., Leff, S. S., & Kim-Rupnow, S. (2001). Community responsiveness: Examples from under-resourced urban schools. Journal of Pre-vention and Intervention in the Community, 21, 71-90.
Eisenstadt, T. H., Eyberg, S., McNeil, C. B., Newcomb, K., Funder-burk, B. (1993). Parent-Child Interaction Therapy with behav-ior problem children: Relative effectiveness of two stages of overall treatment outcome. Journal of Clinical Child Psychology, 22, 42-51.
Eyberg, S. M., & Child Study Lab (1999). Parent-Child Interaction Ther-apy: Integrity Checklists and Materials. Retrieved April 30, 2009, from h�p://pcit.phhp.ufl.edu/Presentations/PCIT%20Integrity%20Checklists%20and%20Materials%204-13-06.pdf.
Eyberg, S. M., Nelson, M. M., Duke, M., & Boggs, S. R. (2005). Manual for the Dyadic Parent-Child Interaction Coding System (3rd ed.). Retrieved March 10, 2008 from h�p://pcit.phhp.ufl.edu/DPIC-Sfiles/DPICS%20Dra�%203.03.pdf
Fagan, A. A., & Mihalic, S. (2003). Strategies for enhancing the adop-tion of school-based prevention programs: Lessons learned from the Blueprints for Violence Prevention replications of the Life Skills Training Program. Journal of Community Psy-chology, 31, 235-253.
Filcheck, H. A., McNeil, C. B., Greco, L. A., & Bernard, R. S. (2004). Using a whole-class token economy and coaching of teacher skills in a preschool classroom to manage disruptive behav-ior. Psychology in the Schools, 41, 351-361.
Gallagher, N. (2003). Effects of Parent-Child Interaction Therapy on young children with disruptive behavior disorders. Bridges, 1, 1-17.
Goldfine, M.E., Wagner, S.M., Branste�er, S.A., & McNeil, C.B. (2008). Parent-Child Interaction Therapy: An examination of cost ef-fectiveness. Journal of Early and Intensive Behavioral Interven-tion, 5(1), 119-141.
Han, S. S., & Weiss, B. (2005). Sustainability of teacher implementation of school-based mental health programs. Journal of Abnormal Child Psychology, 33, 665-679.
Harper, G. W., & Salina, D. D. (2000). Building collaborative partner-ships to improve community-based HIV prevention research: The University-CBO Collaborative Partnership (UCCP) Mod-el. Journal of Prevention & Intervention in the Community, 19, 1-20.

285COMMUNITY-BASED TCIT
Hembree-Kigin, T. L. & McNeil, C. (1995). Parent-Child Interaction Therapy. New York: Plenum Press.
Herschell, A., Calzada, E., Eyberg, S. M., & McNeil, C. B. (2002). Par-ent-child interaction therapy: New directions in research. Cognitive and Behavioral Practice, 9, 9-16.
Kauffman, S., & Poulin, J. (1994). Citizen participation in prevention activities: A path model. Journal of Community Psychology, 22, 359-374.
Kealey, K. A., Peterson, Jr., A. V., Gaul, M. A., & Dinh, K. T. (2000). Teacher training as a behavior change process: Principles and results from a longitudinal study. Health Education & Behavior, 27, 64-81.
Lau, A. S. (2006). Making the case for selective and directed cultural adaptations of evidence-based treatments: Examples from parent training. Clinical Psychology: Science and Practice, 13, 295-310.
Loeber, R., Green, S. M., Keenan, K., & Lahey, B. B. (1995). Which boys will fare worse? Early predictors of the onset of conduct disorder in a six-year longitudinal study. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 499-509.
Lyon, A. R., & Budd, K. S. (2005). Parent-Child Interaction Therapy: A new program at the DePaul Community Mental Health Center. Newsle�er of the Illinois Association for Infant Mental Health, 41, 7-8.
Lyon, A. R., Gershenson, R. A., Farahmand, F., Thaxter, P., Behling, S., & Budd, K. S. (in press). Effectiveness of Teacher-Child Interaction Training (TCIT) in a preschool se�ing. Behavior Modification.
McCabe, K. M., Yeh, M., Garland, A. F., Lau, A. S., & Chavez, G. (2005). The GANA Program: A tailoring approach for adapting Parent Child Interaction Therapy for Mexican Americans. Education and Treatment of Children, 28, 111-129.
McGoey, K. E., DuPaul, G. J., Eckert, T. L., Volpe, R. J., & Van Brakle, J. (2005). Outcomes of a multi-component intervention for preschool children at-risk for A�ention-Deficit/Hyperactivity Disorder. Child & Family Behavior Therapy, 27, 33-56.
McIntosh, D. E., Rizza, M. G., & Bliss, L. (2000). Implementing em-pirically supported interventions: Teacher-child interaction therapy. Psychology in the Schools, 37, 453-462.

286 GERSHENSON, LYON, and BUDD
McNeil, C. B., Herschell, A. D., Gurwitch, R. H., & Clemens-Mowrer, L. (2005). Training foster parents in Parent-Child Interaction Therapy. Education and Treatment of Children, 28, 182-196.
Niec, L. N., Hemme, J., Yopp, J., & Brestan, E. (2005). Parent-child in-teraction therapy: The rewards and challenges of a group for-mat. Cognitive and Behavioral Practice, 12, 113-125.
Niles, M., Reynolds, A., & Roe-Sepowitz, D. (2008). Early childhood intervention and early adolescent social and emotional com-petence: Second-generation evaluation evidence from the Chi-cago Longitudinal Study. Educational Research, 50(1), 55-73.
Nixon, R. D., Sweeney, L., Erickson, D. B., & Touyz, S. W. (2004). Par-ent-Child Interaction Therapy: One- and two-year follow-up of standard and abbreviated treatments for oppositional pre-schoolers. Journal of Abnormal Child Psychology, 32, 263-271.
Nock, M. K., Kazdin, A. E., Hiripi, E., & Kessler, R. C. (2007). Life-time prevalence, correlates, and persistence of oppositional defiant disorder: Results from the National Comorbidity Sur-vey Replication. Journal of Child Psychology and Psychiatry, 48, 703–713.
Pincus, D. B., Eyberg, S. M., & Choate, M. L. (2005). Adapting parent-child interaction therapy for young children with separation anxiety disorder. Education and Treatment of Children, 28, 163-181.
Porterfield, J. K., Herbert-Jackson, E., & Risley, T. R. (1976). Contingent observation: An effective and acceptable procedure for reduc-ing disruptive behavior of young children in a group se�ing. Journal of Applied Behavior Analysis, 9, 55-64.
Raver, C. C., Jones, S. M., Li-Grining, C., Zhai, F., Metzker, M. W., & Solomon, B. (2009). Targeting children’s behavior problems in preschool classrooms: A cluster-randomized controlled trial. Journal of Consulting and Clinical Psychology, 77, 302-316.
Schuhmann, E. M., Foote, R. C., Eyberg, S. M., & Boggs, S. R. (1998). Efficacy of Parent-Child Interaction Therapy: Interim report of a randomized trial with short-term maintenance. Journal of Clinical Child Psychology, 27, 34-45.
Shernoff, E. S., & Kratochwill, T. R. (2007). Transporting an evidence-based classroom management program for preschoolers with disruptive behavior problems to a school: An analysis of im-plementation, outcomes, and contextual variables. School Psy-chology Quarterly, 22, 449-472.
287COMMUNITY-BASED TCIT
St. Pierre, T. L., & Kaltreider, D. L. (2001). Reflections on implement-ing a community agency-school prevention program. Journal of Community Psychology, 29, 107-116.
Storch, E. A. & Floyd, E. M. (2005). Introduction: Innovative approach-es to Parent-Child Interaction Therapy. Education and Treat-ment of Children, 28, 106-110.
Tiano, J. D., & McNeil, C. B. (2006). Training Head Start teachers in be-havior management using Parent-Child Interaction Therapy: a preliminary investigation. Journal of Early and Intensive Be-havior Intervention, 3, 220-233.
Training Guidelines for Parent-Child Interaction Therapy. (2009). Retrieved April 24, 2009 from h�p://www.pcit.org/
Von Brock, M. B., & Elliot, S. N. (1987). The influence of treatment ef-fectiveness information on the acceptability of classroom in-terventions. Journal of School Psychology, 25, 131-144.
Webster-Stra�on, C., Reid, J. M., & Stoolmiller, M. (2008). Preventing conduct problems and improving school readiness: Evalu-ation of the Incredible Years teacher and child training pro-grams in high-risk schools. Journal of Child Psychology and Psy-chiatry, 49, 471-488.
Zane, N., Sue, S., Chang, J., Huang, L., Huang, J., & Low, S. et al. (2005). Beyond ethnic match: Effects of client-therapist cog-nitive match in problem perception, coping orientation and therapy goals in treatment outcomes. Journal of Community Psychology, 33, 569-585.
2@
288