project proposal & budget : Behavior change communication applying theories with example on safe...
17
Behavior change communication strategies on increasing healthy behavior on safe drinking water among the people of Korail slum Mahir faysal Dept. of population Sciences University of Dhaka
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of project proposal & budget : Behavior change communication applying theories with example on safe...

Behavior change communication strategies on increasing healthy behavior on safe drinking water among the people of Korail slum
Mahir faysal
Dept. of population Sciences
University of Dhaka

Contents
1. Introduction ………………………………………………………………………………….. 4
2. Programme goal ……………………………………………………………………………… 4
3. Objectives of the programme ………………………………………………………………… 4
4. Programme Location ……………………………………………………………………….….5
5.1 Scenario of Water Supply Facilities in Korail Slum of Dhaka City……………………….… 5
5.2 Source of drinking water and other purposes …………………………………………….…. 6
5.3 Water borne diseases……………………………………………………………………….. . 7
5.4 Problem in fetching water…………………………………………………………………... 7
5.5 Level of satisfaction on the water Supply system……………………………………………. 8
6.1 Theories of different level and their Implementation to increasing healthy behavior on safe drinking water in Korail slum, Dhaka city……………………………………………. … . 8
6.2 Different levels of theory…………………………………………………………………….8
6.3 Justification & integration of these theories in different level………………………………. .9
- Application of Community organization theory for increasing healthy behavior on safe drinking water for community level .………………………………………………………………………..9
- Application of Social cognitive theory for increasing healthy behavior on safe drinking water for interpersonal level……………………………………………………………………………………11
- Application of Health belief model for increasing healthy behavior on safe drinking water for intrapersonal level …..……………………………………………………………….………… 12
6.4 A framework on different level of influences on safe drinking water ………………….…..13
7.1 Conclusion ……………………………………………………………………………... 13
7.2 Reference …………………………………………………………………………………..14
8.1 Strategy at a glance……………………………………………………………………..…... 15
8.2 Overview of two year investment plan (Budget) ………..………………………………..16

Korail slum at a glance

1. Introduction
At present, more than 15 million people are living in Dhaka city while 35 percent of them are living in slums/squatter settlements. In the slums of Dhaka city, the average user to water-point ratio is 1,000:1 and only 20 percent people have some form of sanitary latrine (Ahmed, 2006). Lack of sanitation, long queuing times for water collection and unhygienic surroundings are the most important environmental concerns in the slums of Dhaka city. 87.72 percent of the Dhaka city’s water supply is dependent on groundwater resources. Even though Dhaka city is surrounded by the four rivers namely Buriganga, Balu, Turag and Tongi Khal but only 12.28 percent of supplied water is obtained from these rivers. Dhaka city faces two major problems in supplying water to its residents: i) gradual decrease of raw water sources and ii) discharge of large quantities of polluted water (Serajuddin, 1993). Surface water sources from surrounding rivers and lakes have already exceeded the standard limits of many water quality parameters because of the discharge of huge amount of untreated and municipal waste materials. Treatment of this water has become so expensive that water supply agencies have to depend on groundwater aquifer for drinking water production (Biswas, et. al., 2010). In this paper health belief model, social cognitive theory & community organization model will be used to increase healthy behavior on safe drinking water among the people of Korail slum.
2. Programme goal
Increasing healthy behavior on safe drinking water among the people of Korail slum.
3. Objectives of the programme
To achieve the following objectives through BCC mentioned theories can play influential role in making susceptibility, perceived severity, benefits that means over all opportunity cost in individual, interpersonal and of course in community level
Increase in-depth knowledge about healthy behavior Safe transportation of water to homes Safe water storage and use Safe water sources are used for all cooking and drinking. Household water treatment & Create greater understanding of the risks of unhealthy livelihood by the means of
theories

4. Programme Location
The total number of slums in the Dhaka city corporation area is approximately 4,500. For the BCC programme only one slum at Korail has been selected. It has been selected for habitation problem and environmental hazardous of low cost area of Korail slum area in Dhaka city. It stands on beside Mohakhali near the BTCL office. Almost 50% inhabitants live in Korail slums and squatters with a very vulnerable condition of Dhaka city. Details of Korail slum area is as follows in table
Details of Korail slum area
Location Gulshan Thana, near BTCL Area 85 acres Permanency 49 years Number of household 1100 Population 80000 Water facility 2 water points ( 1 DCC & 1 DWASA) Sanitation facility 350 water seal latrines,250 bucket latrines,520
hanging latrines Drainage facility Discontinuous semi-pucca drain Solid waste facility Open place DCC 19 no. ward Source: Biplob et. al., 2011
5.1 Scenario of Water Supply Facilities in Korail Slum of Dhaka City (after conducting formative research) Slum population has been increasing in Bangladesh over the last three decades along with the growth and expansion of cities and towns. But slum facilities are very much unsatisfactory for them due to lack of proper water supply and sanitation system. Therefore, the major portion of excreta is deposited into water bodies and open places, as such polluting water sources, groundwater and the general environment. As a result, majority of population in Bangladesh suffer from different kinds of water and excreta-borne diseases that aggravate in their poverty situations.
The level of hygiene knowledge and practice has been found to be significantly low among the Korail slum dwellers. The study in Korail area of Dhaka city has found that the sanitary and water supply condition are improving very slowly. Majority slum people use tube well water for drinking while significant amount of open defecation is also found. Normally Korail slum have pit latrines, which are partially hygienic. These may cause ground water contamination depending on the soil characteristics and distance between the water sources and latrines. The drainage system is the most neglected sector in the slums. The open disposal of human excreta pollutes the nearby water bodies, canals and drains causing severe water pollution. Besides, solid waste management and drainage system are totally unsatisfactory in the slum area.

5.2 Source of drinking water and other purposes
In most cases water supply facility in the slums is provided by the NGOs through water point from DWASA. Water point is basically water storage facility where water is stored from WASA main lines. In the slums where the above facilities are absent or inadequate, the inhabitants use maximum water sources of DWASA and very few numbers depend on adjacent water bodies like ponds. However, the main source of drinking water is the DWASA supply water. Around 50% respondents use DWASA supply water for their drinking water and other purposes while 43% respondents use shallow tube-well for their drinking and other purposes & 7 % use other sources such as lake.
Source : Biplob et. al., 2011
sources of water for drinking & other purposes
DWASA supply
Shallow tubewell
others
Young girl pumps water in the Korail Slum in Dhaka
Source: Unicef Report 2011

5.3 Water borne diseases
Sickness during past three months from water borne diseases constituted maximum of all diseases reported. Maximum of the total medical expenses were spent on water related diseases. And on an average 10.2 working days were lost in last three months due to those diseases. Most of the households reporting to have at least one sick person in their households during last three months were asked about loss of working days.
Source : Biplob et. al., 2011
5.4 Problem in fetching water
There are the problems in fetching water from the source they get for DWASA water source which is far away and crowded 51%. The surrounding environment is unsuitable for fetching water for women 49% in the Korail slum area. We observed that collecting water from far away is a major problem.
Source: Biplob et. al., 2011
0
20
40
60
Dysentery diarrhea cholera others
common water borne diseases
common water borne diseases
problems in fetching water from the sources
surrounding environment is unsuitable for women to fetch water
water source is far away from household

5.5 Level of satisfaction on the water Supply system
The peoples of Korail slum area are not satisfied for the lack of proper water supply. Approximately, 79% respondents are not satisfied while 21% are satisfied for the availability of water source in Korail slum
Source : Biplob et. al., 2011
6.1 Theories of different level and their Implementation to increasing healthy behavior on safe drinking water in Korail slum, Dhaka city
6.2: Different levels of theory: There are basically three levels of influence where theories can be applied. Theories widely explain:
Behavior is mediated by cognitions that is, what people know and think affects how they act Like : What the people of Korail slum think about safe drinking water will decide whether they will receive the programme or not .
Knowledge is necessary for, but not sufficient to produce, most behavior Changes like : the people of Korail slum may get knowledge about the benefit of safe drinking water but unless they start to practice it , this knowledge can’t be effective .
Perceptions, motivations, skills, and the social environment are key influences on behavior , people of Korail slum lives in such type of area with a unhygienic life style which may influence them not to practicing the use of safe drinking water. (Glanz et al.2005)
The three levels are Individual or Intrapersonal, Interpersonal and Community level. Individual level refers to individual characteristics that influence behavior, such as knowledge, attitude, beliefs & personality traits. Interpersonal level refers interpersonal process & primary group, including family, friend & peers that provide social identity, support & role definition. Community level refers to three subsections they are institutional factors, community factors &
020406080
not satisfied satisfied
level of satisfaction on the water supply system of the slum
dwellers
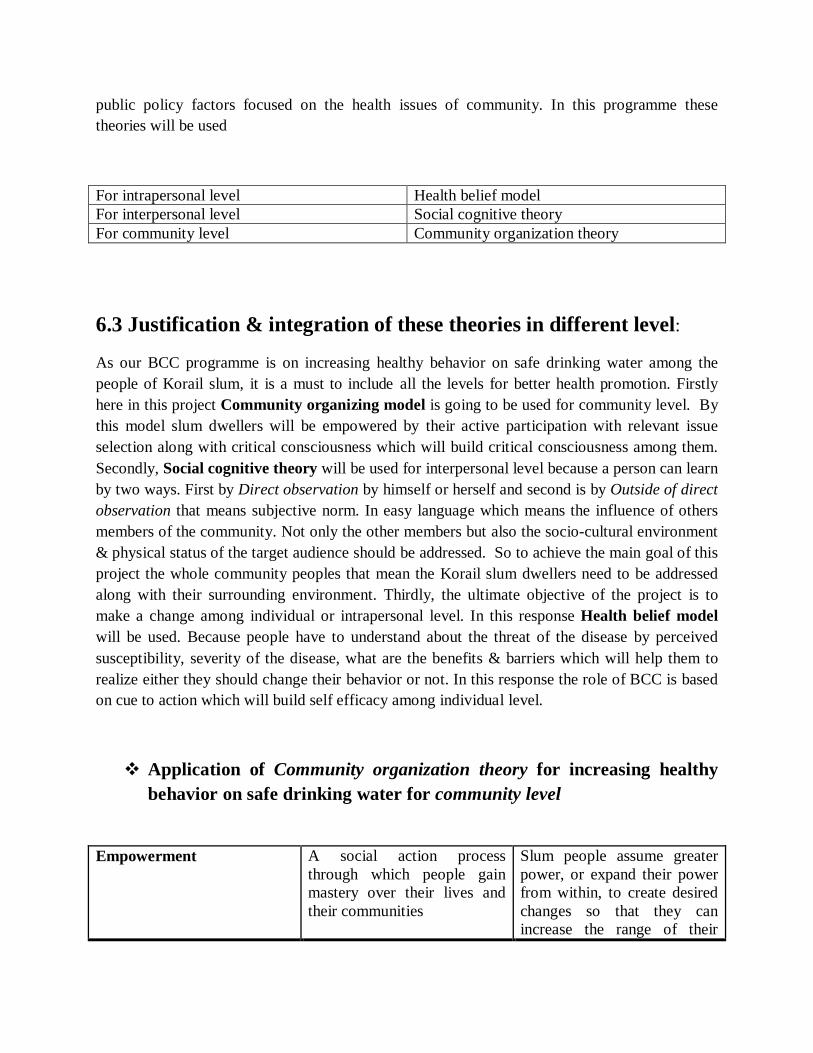
public policy factors focused on the health issues of community. In this programme these theories will be used
For intrapersonal level Health belief model For interpersonal level Social cognitive theory For community level Community organization theory
6.3 Justification & integration of these theories in different level:
As our BCC programme is on increasing healthy behavior on safe drinking water among the people of Korail slum, it is a must to include all the levels for better health promotion. Firstly here in this project Community organizing model is going to be used for community level. By this model slum dwellers will be empowered by their active participation with relevant issue selection along with critical consciousness which will build critical consciousness among them. Secondly, Social cognitive theory will be used for interpersonal level because a person can learn by two ways. First by Direct observation by himself or herself and second is by Outside of direct observation that means subjective norm. In easy language which means the influence of others members of the community. Not only the other members but also the socio-cultural environment & physical status of the target audience should be addressed. So to achieve the main goal of this project the whole community peoples that mean the Korail slum dwellers need to be addressed along with their surrounding environment. Thirdly, the ultimate objective of the project is to make a change among individual or intrapersonal level. In this response Health belief model will be used. Because people have to understand about the threat of the disease by perceived susceptibility, severity of the disease, what are the benefits & barriers which will help them to realize either they should change their behavior or not. In this response the role of BCC is based on cue to action which will build self efficacy among individual level.
Application of Community organization theory for increasing healthy behavior on safe drinking water for community level
Empowerment A social action process through which people gain mastery over their lives and their communities
Slum people assume greater power, or expand their power from within, to create desired changes so that they can increase the range of their

healthy behavior on safe drinking water
Community capacity Characteristics of a community that affect its ability to identify, mobilize around, and address problems
Slum dwellers will participate actively in community life, gaining leadership skills, social networks, and access to power
participation Engagement of community members as equal partners; reflects the principle, “Never do for others what they can do for themselves
Slum dwellers develop leadership skills, knowledge, and resources through their involvement in this program
Relevance Community organizing that starts where the people are
Slum dwellers create their own agenda based on felt needs, shared power, and awareness of resources in this program
Issue selection Identifying immediate, specific, and realizable targets for change that unify and build community strength
Slum dwellers will participate in identifying issues; targets will be chosen as part of a larger strategy
Critical consciousness Awareness of social, political, and economic forces that contribute to social problems
Slum dwellers discuss the root causes of problems and plan actions to address them
In our project slum dwellers will actively participate & share the opinions with authority. ( participation). As we have conducted formative research our finding is they do not have enough safe sources of drinking water & they have problem in fetching water(critical consciousness). Dwellers said that if they had access to safe sources of drinking water & household water treatment then they will obviously use those (relevance). Now we will provide them needed safe drinking water products like covered container, long-handled cup for serving the drinking water with a hygienic way, Household water treatment products & hand washing soap (issue selection). These will be provided till two year with a certain time interval (community capacity). Through their success with a changed behavior slum dwellers will gain skills, knowledge and confidence about the diseases and will be inspired to think about other hygienic ways to lead a healthy life (empowerment).
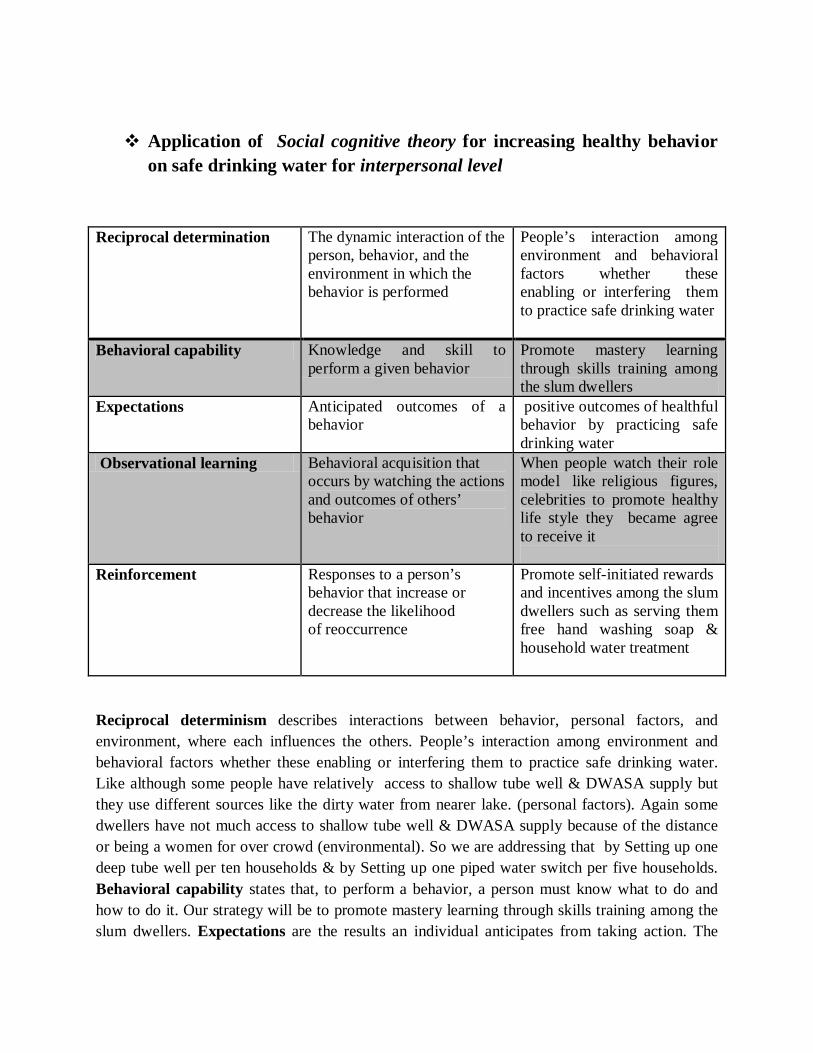
Application of Social cognitive theory for increasing healthy behavior on safe drinking water for interpersonal level
Reciprocal determination The dynamic interaction of the person, behavior, and the environment in which the behavior is performed
People’s interaction among environment and behavioral factors whether these enabling or interfering them to practice safe drinking water
Behavioral capability Knowledge and skill to perform a given behavior
Promote mastery learning through skills training among the slum dwellers
Expectations Anticipated outcomes of a behavior
positive outcomes of healthful behavior by practicing safe drinking water
Observational learning Behavioral acquisition that occurs by watching the actions and outcomes of others’ behavior
When people watch their role model like religious figures, celebrities to promote healthy life style they became agree to receive it
Reinforcement Responses to a person’s behavior that increase or decrease the likelihood of reoccurrence
Promote self-initiated rewards and incentives among the slum dwellers such as serving them free hand washing soap & household water treatment
Reciprocal determinism describes interactions between behavior, personal factors, and environment, where each influences the others. People’s interaction among environment and behavioral factors whether these enabling or interfering them to practice safe drinking water. Like although some people have relatively access to shallow tube well & DWASA supply but they use different sources like the dirty water from nearer lake. (personal factors). Again some dwellers have not much access to shallow tube well & DWASA supply because of the distance or being a women for over crowd (environmental). So we are addressing that by Setting up one deep tube well per ten households & by Setting up one piped water switch per five households. Behavioral capability states that, to perform a behavior, a person must know what to do and how to do it. Our strategy will be to promote mastery learning through skills training among the slum dwellers. Expectations are the results an individual anticipates from taking action. The
slum dwellers have to think positive outcomes of healthful behavior by practicing safe drinking water. Dwellers have to learn how drinking safe water will benefit them.Observational learning, or modeling, refers to the process whereby people learn through the experiences of credible others, rather than through their own experience. When people watch their role model like religious figures, celebrities to promote healthy life style they became agree to receive it. So we will invite religious leaders like Imams from the nearest mosques, figures & famous celebrities to promote healthy behavior on safe drinking water. Reinforcements are responses to behavior that affect whether or not one will repeat it. Positive reinforcements (rewards) increase a person’s likelihood of repeating the behavior. Negative reinforcements may make repeated behavior more likely by motivating the person to eliminate a negative stimulus. We will supply needed safe drinking water products like covered container, long-handled cup for serving the drinking water with a hygienic way, Household water treatment products & Hand washing soap.
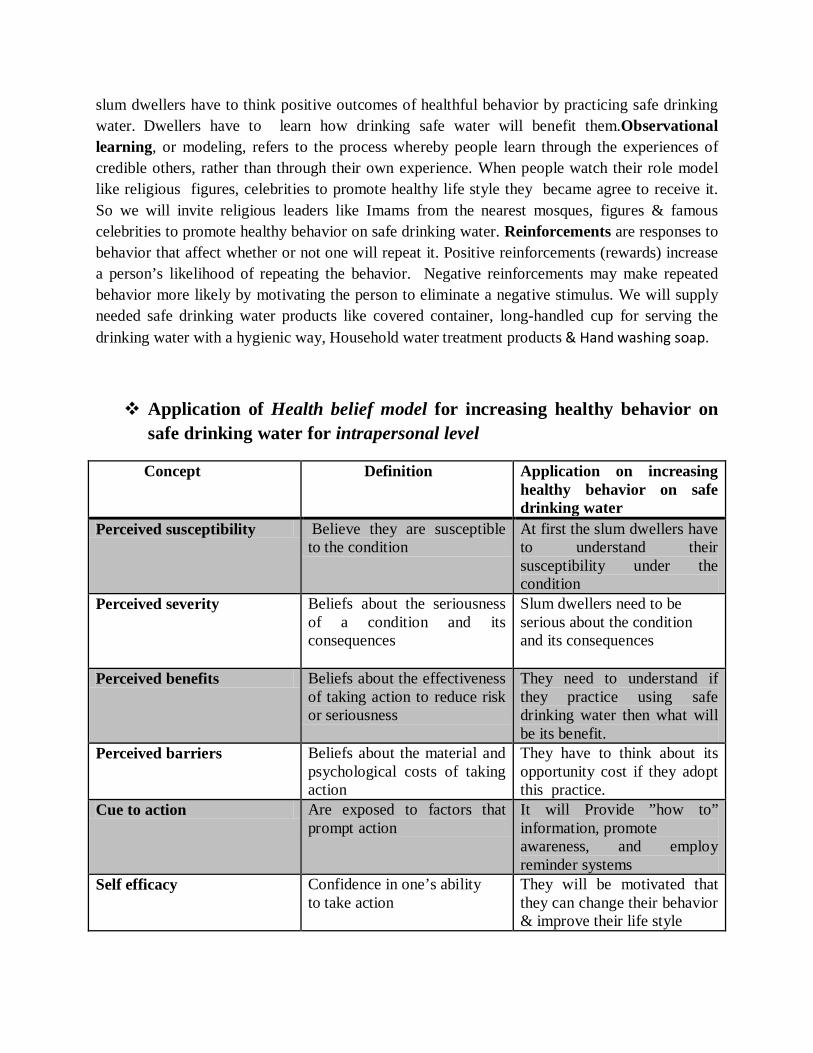
Application of Health belief model for increasing healthy behavior on safe drinking water for intrapersonal level
Concept Definition Application on increasing healthy behavior on safe drinking water
Perceived susceptibility Believe they are susceptible to the condition
At first the slum dwellers have to understand their susceptibility under the condition
Perceived severity Beliefs about the seriousness of a condition and its consequences
Slum dwellers need to be serious about the condition and its consequences
Perceived benefits Beliefs about the effectiveness of taking action to reduce risk or seriousness
They need to understand if they practice using safe drinking water then what will be its benefit.
Perceived barriers Beliefs about the material and psychological costs of taking action
They have to think about its opportunity cost if they adopt this practice.
Cue to action Are exposed to factors that prompt action
It will Provide ”how to” information, promote awareness, and employ reminder systems
Self efficacy Confidence in one’s ability to take action
They will be motivated that they can change their behavior & improve their life style

Health belief model will be used to influence people’s decision about whether to take action to prevent, screen for & control illness. According to the HBM, slum people may not follow a prescribed safe use of water unless they accept that, though they have no knowledge about diseases but they do in fact have diarrhea (perceived susceptibility). They must understand that diarrhea can lead to many more diseases (perceived severity). Taking prescribed service or following a healthy life style will reduce the risks (perceived benefits) without negative side effects or excessive difficulty (perceived barriers). Print materials, television, radio might encourage people to consistently follow the practice (cues to action). Again they will be motivated to face the obstacles & challenges to increase the level of confident (self-efficacy).
7. Conclusion
Access to water is a basic human right and it is a crosscutting issue for sustainable development. Water resources have unlimited importance including human survival, socio-economic stability and environmental sustainability. “Water is right or economic good‟ has been a matter of discourse since industrial revolution in the Eighteenth century. Dhaka city dwellers, following an unsystematic urban sprawl, are deprived of basic urban amenities where water supply has appeared as the most critical issue. Because of the poor facilities many of the slum dwellers are using unhygienic water for drinking, cooking & for daily use which causes water borne diseases among them especially among the children & old people. Practice of using safe drinking water can improve this situation which is the goal of the programme.

Reference
1. Ahmed, M., 2004, Development and Management Challenges of Integrated Planning for Sustainable Productivity of Water Resources, Proc. of Bangladesh journal of Political Economy, V. 21, No. 2, p.106, Bangladesh Economic Association, Dhaka
2. Biswas, S. K., Mahtab, S. B. & Rahman, M. M., 2010, Integrated Water Resources Management Options for Dhaka City, Proc. of International Conference on Environmental Aspects of Bangladesh (ICEAB10), Japan
3. Biplob,P. , Sarker , D.C., Sarker , R.C., 2011 Assessment of Water Supply and Sanitation Facilities for Korail Slum in Dhaka City, International Journal of Civil & Environmental Engineering IJCEE-IJENS Vol: 11 No: 05
4. Glanz ,K, Rimer, B & National Cancer Institute ,2005 Theory at a Glance: A Guide for Health Promotion Practice, U.S. Dept. of Health and Human Services, Public Health Service, National Institutes of Health, National Cancer Institute, New York.
5. Serajuddin, M., 1993, Integrated Development of Surface and Groundwater: A Necessity for Sustainable Water Supply inside Dhaka City, Technical journal of Dhaka WASA Engineers’ Association, Vol. I, PP. 82-87
6. Unicef report 2011, Urban water challenges in Bangladesh

Strategy-at-a-Glance
Vision Increasing healthy behavior on safe drinking water among the people of Korail slum within two years .
Timeframe December 2014 to December 2016
Objectives Increase in-depth knowledge about healthy behavior Safe transportation of water to homes Safe water storage and use Safe water sources are used for all cooking and
drinking. Household water treatment & Create greater understanding of the risks of unhealthy
livelihood by the means of theories
Primary target audience children aged 5-12 years Young adults Mothers, guardians of children under five years old Fathers, guardians of children under five years old Old people
Secondary target audience Friends ,Teachers for the children, mothers, fathers,
friends, peers and relatives Health workers, teachers, religious leaders Landlords, health workers community heads/leaders , social groups policy makers
Feasible practices to be promoted
1. Serve your drinking water with a long-handled cup or pour it out
2. Use needed safe drinking water products 3.Store your drinking water in a covered container 4. Place your drinking water out of reach of children. 5. Place it within reach of the elderly and adults. 6. Wash container or bucket with clean water before filling with safe drinking water. 7. Cover container or bucket to carry it home. 8. Use pipe lined water or deep tube well for all cooking and drinking
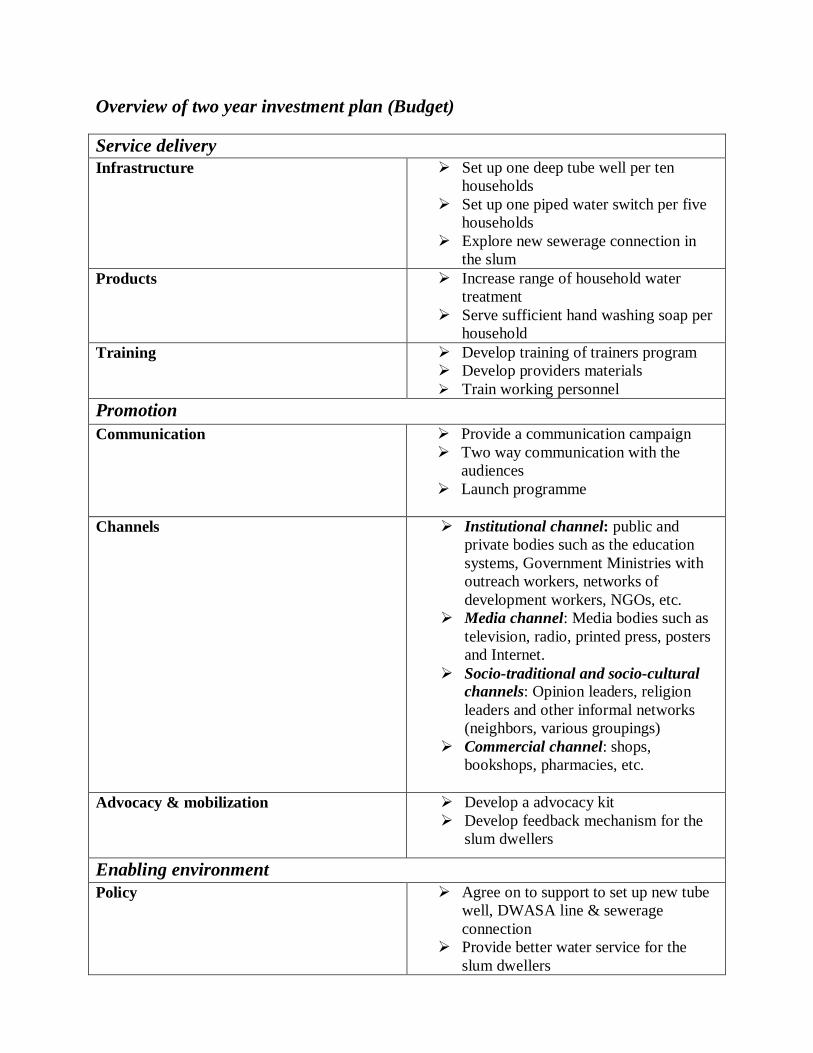
Overview of two year investment plan (Budget)
Service delivery Infrastructure Set up one deep tube well per ten
households Set up one piped water switch per five
households Explore new sewerage connection in
the slum Products Increase range of household water
treatment Serve sufficient hand washing soap per
household Training Develop training of trainers program
Develop providers materials Train working personnel
Promotion Communication Provide a communication campaign
Two way communication with the audiences
Launch programme
Channels Institutional channel: public and private bodies such as the education systems, Government Ministries with outreach workers, networks of development workers, NGOs, etc.
Media channel: Media bodies such as television, radio, printed press, posters and Internet.
Socio-traditional and socio-cultural channels: Opinion leaders, religion leaders and other informal networks (neighbors, various groupings)
Commercial channel: shops, bookshops, pharmacies, etc.
Advocacy & mobilization Develop a advocacy kit Develop feedback mechanism for the
slum dwellers
Enabling environment Policy Agree on to support to set up new tube
well, DWASA line & sewerage connection
Provide better water service for the slum dwellers

Infrastructure Total Tube well 1100÷10=110
110×3000=3,30,000$
Water switch 1100÷5=220 220×1000=2,20,000$
5,50,000 $
Products
Household water treatment products
1100×500=5,50,000$
Hand washing soap 1100×100=1,10,000$ 6,60,000$
Training 1,00,000$
promotion Communication Channel Advocacy mobilization
50,000$
Implementation & Two years long monitoring cost
2,00,000$
Total budget
15,60,000$
Sponsored by
Media partner