Prognostic utility of the SYNTAX score in patients with single versus multivessel disease undergoing...
35
Elsevier Editorial System(tm) for American Journal of Cardiology Manuscript Draft Manuscript Number: AJC-D-13-01775R1 Title: Prognostic Utility of the SYNTAX Score in Patients with Single vs. Multivessel Disease Undergoing Percutaneous Coronary Intervention (From the ACUITY Trial) Article Type: Full Length Article Keywords: SYNTAX score; acute coronary syndromes; risk stratification; single vessel disease; mutlivessel disease. Corresponding Author: Dr. Gregg W. Stone, MD Corresponding Author's Institution: Columbia University Medical Center First Author: Adriano Caixeta, MD Order of Authors: Adriano Caixeta, MD; Philippe Généreux, MD, PhD; Tullio Palmerini, MD; Alexandra J Lansky, MD; Roxana Mehran, MD; George D Dangas, MD, PhD; Ke Xu, PhD; Sorin J Brener, MD; Gregg W Stone, MD Abstract: SYNTAX score (SS) is an effective angiographic predictor of clinical outcomes in patients with multivessel coronary artery disease (MVD) undergoing percutaneous coronary intervention (PCI). It is not known whether this relationship is independent of number of diseased vessels. The aim of this study is to assess the relationship between the SS and major adverse cardiac events (MACE) in patients with single (SVD) and (MVD) undergoing PCI. In ACUITY, SS was determined in 2,627 patients undergoing PCI. The relationship between SS and 1-year clinical outcomes was assessed according to SS tertiles: <5 (n = 441), ≥5 and <10 (n = 525) and ≥10 (n = 495) for SVD; and <10 (n = 361), ≥10 and <18 (n = 401) and ≥18 (n = 404) for MVD. At 1-year follow-up, among MVD patients in the 1st, 2nd and 3rd tertiles, the rates of MACE were 16.8%, 24.7%, and 23.7%, p = 0.02; among SVD patients the respective rates were 13.3%, 15.3%, and 19.1%, p = 0.01. In patients with MVD, SS independently predicted 1-year MACE (HR 1.02, 95% CI 1.01-1.03; p = 0.002), MI (HR 1.02, 95% CI 1.00-1.04; p = 0.02), and cardiac death (HR 1.05, 95% CI 1.02-1.09; p = 0.005). In patients with SVD, SS independently predicted 1-year MACE (HR 1.03, 95% CI 1.01-1.05; p = 0.0009), and MI (HR 1.05, 95% CI 1.02-1.07; p = 0.002). In the overall study cohort, SS was an independent predictor of MACE and death, while MVD (vs. SVD) was not. In conclusion, SS is a useful angiographic predictive tool for patients with SVD and MVD.
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Prognostic utility of the SYNTAX score in patients with single versus multivessel disease undergoing...
Elsevier Editorial System(tm) for American Journal of Cardiology Manuscript Draft Manuscript Number: AJC-D-13-01775R1 Title: Prognostic Utility of the SYNTAX Score in Patients with Single vs. Multivessel Disease Undergoing Percutaneous Coronary Intervention (From the ACUITY Trial) Article Type: Full Length Article Keywords: SYNTAX score; acute coronary syndromes; risk stratification; single vessel disease; mutlivessel disease. Corresponding Author: Dr. Gregg W. Stone, MD Corresponding Author's Institution: Columbia University Medical Center First Author: Adriano Caixeta, MD Order of Authors: Adriano Caixeta, MD; Philippe Généreux, MD, PhD; Tullio Palmerini, MD; Alexandra J Lansky, MD; Roxana Mehran, MD; George D Dangas, MD, PhD; Ke Xu, PhD; Sorin J Brener, MD; Gregg W Stone, MD Abstract: SYNTAX score (SS) is an effective angiographic predictor of clinical outcomes in patients with multivessel coronary artery disease (MVD) undergoing percutaneous coronary intervention (PCI). It is not known whether this relationship is independent of number of diseased vessels. The aim of this study is to assess the relationship between the SS and major adverse cardiac events (MACE) in patients with single (SVD) and (MVD) undergoing PCI. In ACUITY, SS was determined in 2,627 patients undergoing PCI. The relationship between SS and 1-year clinical outcomes was assessed according to SS tertiles: <5 (n = 441), ≥5 and <10 (n = 525) and ≥10 (n = 495) for SVD; and <10 (n = 361), ≥10 and <18 (n = 401) and ≥18 (n = 404) for MVD. At 1-year follow-up, among MVD patients in the 1st, 2nd and 3rd tertiles, the rates of MACE were 16.8%, 24.7%, and 23.7%, p = 0.02; among SVD patients the respective rates were 13.3%, 15.3%, and 19.1%, p = 0.01. In patients with MVD, SS independently predicted 1-year MACE (HR 1.02, 95% CI 1.01-1.03; p = 0.002), MI (HR 1.02, 95% CI 1.00-1.04; p = 0.02), and cardiac death (HR 1.05, 95% CI 1.02-1.09; p = 0.005). In patients with SVD, SS independently predicted 1-year MACE (HR 1.03, 95% CI 1.01-1.05; p = 0.0009), and MI (HR 1.05, 95% CI 1.02-1.07; p = 0.002). In the overall study cohort, SS was an independent predictor of MACE and death, while MVD (vs. SVD) was not. In conclusion, SS is a useful angiographic predictive tool for patients with SVD and MVD.
August 18, 2013 William C. Roberts, MD Editor-in-Chief The American Journal of Cardiology Baylor Heart & Vascular Hospital, Baylor University Medical Center, Wadley Tower No. 457, 3600 Gaston Avenue, Dallas, TX 75246 Dear Dr. Roberts, We are pleased to resubmit the manuscript, “Prognostic Utility of the SYNTAX Score in Patients with Single vs. Multivessel Disease Undergoing Percutaneous Coronary Intervention (From the ACUITY Trial)” for publication in The American Journal of Cardiology. We have addressed the editor’s requests in this new version of the manuscript, which is uploaded in the “Revised Submission” section. Thank you very much for you time in revising our paper. We are looking forward to hearing from you at your earliest convenience. Sincerely, Gregg W. Stone, MD Corresponding author Professor of Medicine, Director of Research and Education Center for Interventional Vascular Therapy New York-Presbyterian Hospital Columbia University Medical Center The Cardiovascular Research Foundation 111 E. 59th St., 11th Floor New York, NY 10022 tel: 212-851-9304 fax: 212-851-9396 e-mail: [email protected] & Adriano Caixeta, MD First author From Hospital Israelita Albert Einstein, São Paulo, Brazil; Columbia University Medical Center and the Cardiovascular Research Foundation, New York, NY
Cover Letter_Revised paper
August 18, 2013 William C. Roberts, MD Editor-in-Chief The American Journal of Cardiology Baylor Heart & Vascular Hospital, Baylor University Medical Center, Wadley Tower No. 457, 3600 Gaston Avenue, Dallas, TX 75246 Dear Dr. Roberts, We hereby resubmit our manuscript, “Prognostic Utility of the SYNTAX Score in Patients with Single vs. Multivessel Disease Undergoing Percutaneous Coronary Intervention (From the ACUITY Trial)” after incorporating all the comments as follow:
1. The title of the manuscript has been updated; 2. The title page is limit to the first page and that the abstract begins on the page #2; 3. The disclosure is now after the text; 4. All the references have been revised including #23; 5. All the subheading have been excluded; 6. All the Tables were updated and abbreviations spelled out; 7. The conclusions at the end of the paper has been deleted; and 8. We checked all technical requirements and they were implemented accordingly.
We are looking forward to hearing from you at your earliest convenience. Sincerely, Gregg W. Stone, MD Corresponding author Professor of Medicine, Director of Research and Education Center for Interventional Vascular Therapy New York-Presbyterian Hospital Columbia University Medical Center The Cardiovascular Research Foundation 111 E. 59th St., 11th Floor New York, NY 10022 tel: 212-851-9304 fax: 212-851-9396 e-mail: [email protected] & Adriano Caixeta, MD First author From Hospital Israelita Albert Einstein, São Paulo, Brazil; Columbia University Medical Center and the Cardiovascular Research Foundation, New York, NY
*Responses to Reviewers

1
Prognostic Utility of the SYNTAX Score in Patients with Single vs.
Multivessel Disease Undergoing Percutaneous Coronary Intervention
(From the ACUITY Trial)
Adriano Caixeta, MD, PhDa,b, Philippe Généreux, MDb,c, Tullio Palmerini, MDd, Alexandra J.
Lansky, MDe, Roxana Mehran, MDf, George D. Dangas, MD, PhDf, Ke Xub, PhD, Sorin J.
Brener, MDg, and Gregg W. Stone, MDb,*
aHospital Israelita Albert Einstein, São Paulo, Brazil; bColumbia University Medical Center and
the Cardiovascular Research Foundation, New York, NY, cHôpital du Sacré-Coeur de Montréal,
Montréal, Canada, dIstituto Cardiologia, Policlinico S. Orsola, Bologna, Italy; eYale University
School of Medicine, New Haven, CT; fMount Sinai Medical Center, New York, NY, gWeill Cornel
Medical College, New York, NY (SJB)
(Acute Catheterization and Urgent Intervention Triage StrateY [ACUITY]); ClinicalTrials.gov
Identifier NCT00093158
Running title: SYNTAX score in single vessel disease
Financial support: The ACUITY trial was funded by The Medicines Company, Parsippany, NJ,
USA, and Nycomed, Roskilde, Denmark
* Corresponding author:
Gregg W. Stone, MD
Columbia University Medical Center
New York-Presbyterian Hospital
The Cardiovascular Research Foundation
111 E. 59th St., 11th Floor
New York, NY 10022
Tel: 646-434-4131
Fax: 646-434-4715
e-mail: [email protected]
*Manuscript_RevisedClick here to view linked References
2
Abstract
SYNTAX score (SS) is an effective angiographic predictor of clinical outcomes in patients with
multivessel coronary artery disease (MVD) undergoing percutaneous coronary intervention
(PCI). It is not known whether this relationship is independent of number of diseased vessels.
The aim of this study is to assess the relationship between the SS and major adverse cardiac
events (MACE) in patients with single (SVD) and (MVD) undergoing PCI. In ACUITY, SS was
determined in 2,627 patients undergoing PCI. The relationship between SS and 1-year clinical
outcomes was assessed according to SS tertiles: <5 (n = 441), ≥5 and <10 (n = 525) and ≥10 (n
= 495) for SVD; and <10 (n = 361), ≥10 and <18 (n = 401) and ≥18 (n = 404) for MVD. At 1-year
follow-up, among MVD patients in the 1st, 2nd and 3rd tertiles, the rates of MACE were 16.8%,
24.7%, and 23.7%, p = 0.02; among SVD patients the respective rates were 13.3%, 15.3%, and
19.1%, p = 0.01. In patients with MVD, SS independently predicted 1-year MACE (HR 1.02,
95% CI 1.01-1.03; p = 0.002), MI (HR 1.02, 95% CI 1.00-1.04; p = 0.02), and cardiac death (HR
1.05, 95% CI 1.02-1.09; p = 0.005). In patients with SVD, SS independently predicted 1-year
MACE (HR 1.03, 95% CI 1.01-1.05; p = 0.0009), and MI (HR 1.05, 95% CI 1.02-1.07; p =
0.002). In the overall study cohort, SS was an independent predictor of MACE and death, while
MVD (vs. SVD) was not. In conclusion, SS is a useful angiographic predictive tool for patients
with SVD and MVD.
Key-words: SYNTAX score, acute coronary syndromes, single vessel disease, mutlivessel
disease.
3
The SYNTAX (The SYNergy between percutaneous intervention with TAXus drug eluting
stents and cardiac surgery) score (SS) is an angiographic scoring system developed during the
SYNTAX trial for risk stratification of patients according to the complexity of coronary anatomy.1
It has been shown to be an effective angiographic tool for predicting the risk of major adverse
cardiac events (MACE), mostly in stable patients with multivessel disease (MVD) and those with
unprotected left main disease (UPLMD) undergoing percutaneous coronary intervention (PCI).2-
7 Accordingly, SS has been incorporated in a daily practice when facing complex coronary artery
disease dilemma. More recently, its application has been extended to a variety of other clinical
setting including an all-comers population 8 and in patients with ST-elevation myocardial
infarction (STEMI) 9, 10 undergoing primary PCI. Although we have recently demonstrated the
prognostic value of the SS in a broad range of patients with non ST-segment elevation acute
coronary syndromes (NSTEACS) enrolled in the Acute Catheterization and Urgent Intervention
Triage StrategY (ACUITY) trial treated with PCI,11 the usefulness of the SS to predict clinical
events in patients with single vessel disease (SVD) has never been investigated. The aim of the
present study is to assess the impact of the SS on ischemic outcomes in patients with SVD
undergoing PCI compared with those with MVD from the large-scale, multicenter, prospective
randomized ACUITY trial.
Methods
The design and primary results of the ACUITY trial have been previously reported.12
Briefly, 13,819 patients with moderate- and high-risk NSTEACS undergoing an early invasive
management strategy were randomly assigned to heparin plus glycoprotein IIb-IIIa inhibitors,
bivalirudin plus glycoprotein IIb-IIIa inhibitors or bivalirudin monotherapy before coronary
angiography. Clinical follow-up was performed at 30 days and 1 year. All MACE events were
adjudicated by an independent clinical events committee. Retrospectively, all stent thrombosis
events were re-adjudicated using the Academic Research Consortium (ARC) definitions.13
4
As part of the present study, only PCI patients who had quantitative coronary
angiography (QCA) (Cardiovascular Research Foundation, New York, NY) performed within the
formal angiographic substudy of the ACUITY trial were included. In the ACUITY trial, QCA was
performed in 6,921 patients, including 3,664 PCI patients. After excluding patients with a history
of prior CABG (862 patients) and patients for whom the SS score could not be calculated for
technical reasons (338 patients), 2,627 patients remained available for analysis. Patients with
infarct-related occluded arteries were scored as total occlusion of undetermined duration.
Lesions with in-stent restenosis were scored as de novo lesions. The SS score was
retrospectively calculated by 3 experienced interventional cardiologists who were blinded to
treatment assignment and clinical outcomes. In order to assess inter-observer reproducibility
among the 3 readers, a Fleiss Kappa statistic value for multiple readers (tertile partitioning) was
determined. 14 Each lesion with ≥ 50% diameter stenosis in vessels ≥1.5 mm was scored using
the SS algorithm, which has been fully described elsewhere 1 and is available on the SS website
(www.syntaxscore.com). The Fleiss Kappa statistic 15 (tertile partitioning), determined for the 3
readers from 50 films read independently, was 0.57, meaning inter-observer reproducibility was
comparable to that previously reported from the SYNTAX trial.16
Continuous variables are expressed as mean ± standard deviation and were compared
using the Student t test or the Mann-Whitney Rank Sum Test, as appropriate. Categorical
variables are presented as percentage and n/N and were compared by chi-square or Fisher’s
exact test. Patients with SVD and MVD were grouped into tertiles of SS separately. One-year
outcomes are summarized as Kaplan-Meier estimates and compared using the log-rank test
and hazards ratios. Stepwise Cox multivariable regression analyses were performed to assess
the association between the SS and 1-year MACE, all-cause mortality, cardiac mortality,
myocardial infarction (MI) and target vessel revascularization (TVR) in patients with SVD and
MVD. Potential predictors were entered into the model with entry and stay criteria of a 0.1/0.1.
The following baseline and procedure variables were included in the models: SS (as a
continuous variable), age, male gender, diabetes, renal insufficiency, left ventricular ejection
5
fraction (LVEF), baseline troponin elevation, ST-segment deviation, prior MI, and prior PCI. The
numbers of independent variables included in the models were carefully chosen to avoid
overfitting, i.e., as having too many covariates relative to the number of observations. In order to
evaluate the predictive value of the SS as compared to the number of vessels disease, MVD vs.
SVD as a covariate was forced in the model of 1-year clinical outcome of the entire population.
All statistical tests were performed using SAS software (version 9.1, SAS Institute, Cary, North
Carolina) and p values <0.05 denote statistical significance.
Results
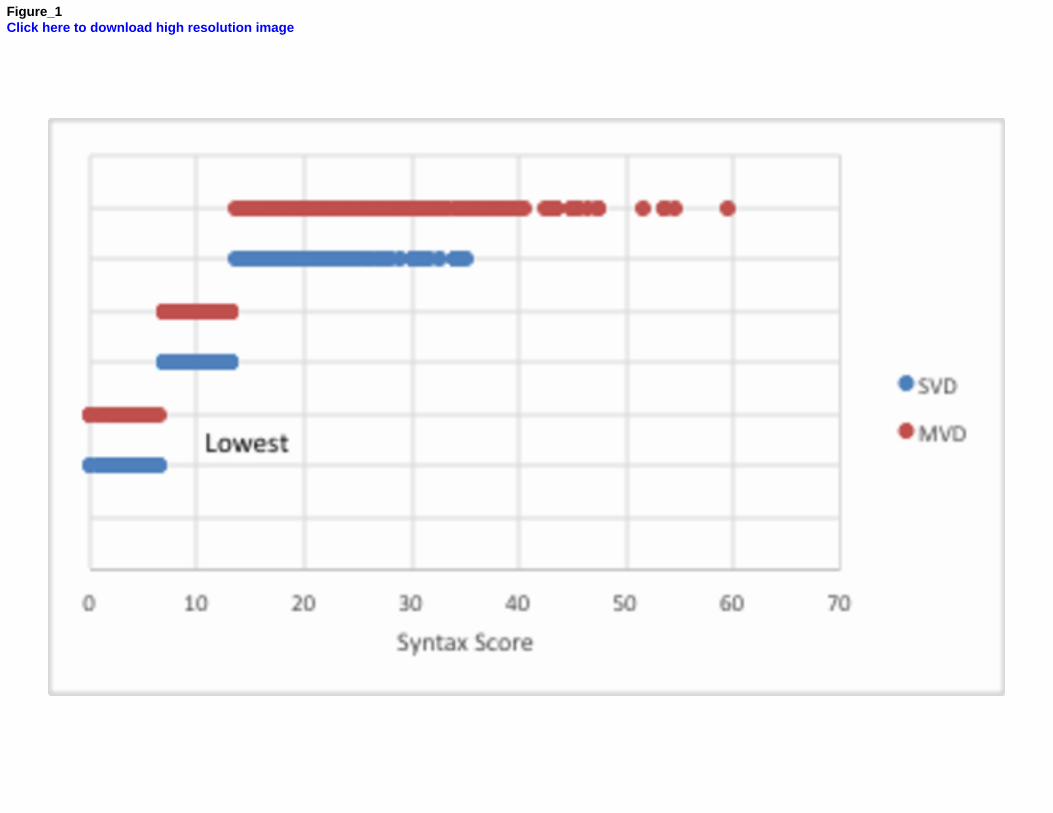
In the present analysis SS was determined in 2,627 PCI patients, comprising 1,461
(55.6%) patients with SVD and 1,166 (44.4%) with MVD. In patients with MVD, the median SS
was 14, whereas in patients with SVD the median SS was 7. Figure 1 shows the distribution of
the SS in SVD and in MVD patients according the tertile of the entire population, i.e., lowest (<
7), middle (7 to 13), and highest (> 13) SS. Table 1 shows the baseline characteristics of
patients with SVD and MVD. Patients with MVD had more comorbidities and less favorable
coronary anatomy. There were no significant differences in in-hospital antithrombotic medication
use between the 2 groups.
Clinical outcomes stratified according to SS tertiles in patients with SVD and MVD are
shown in Table 2 and in Figures 2 and 3.
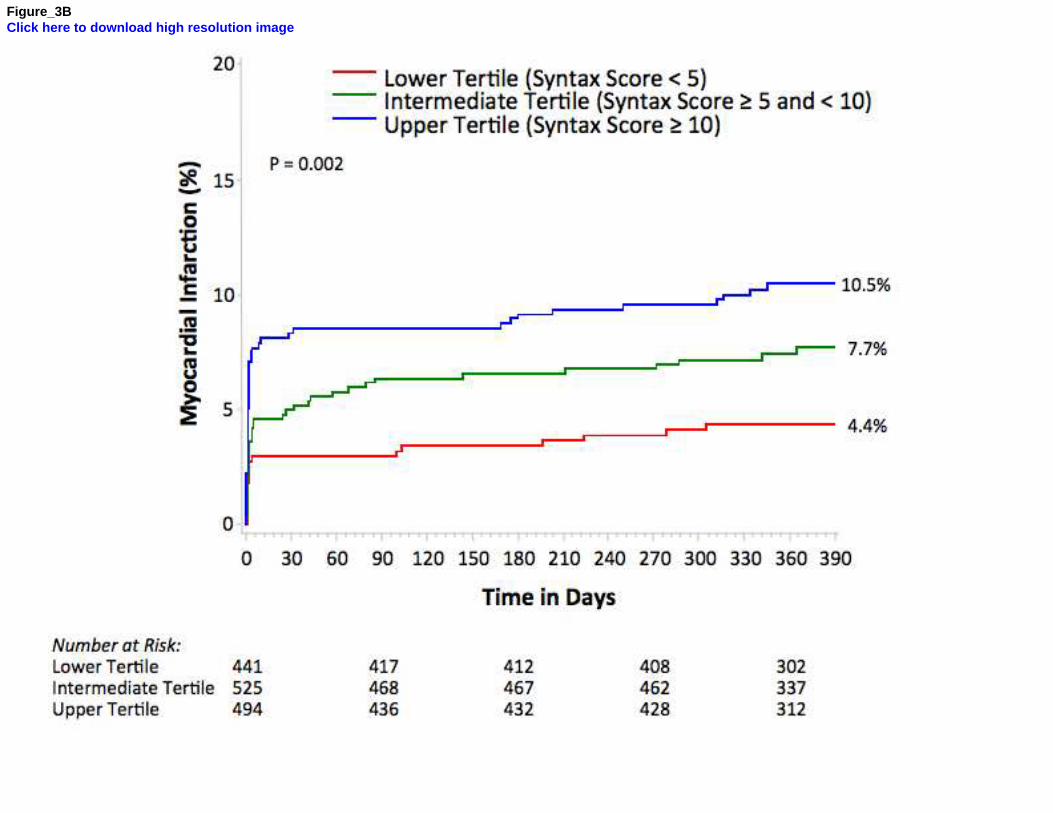
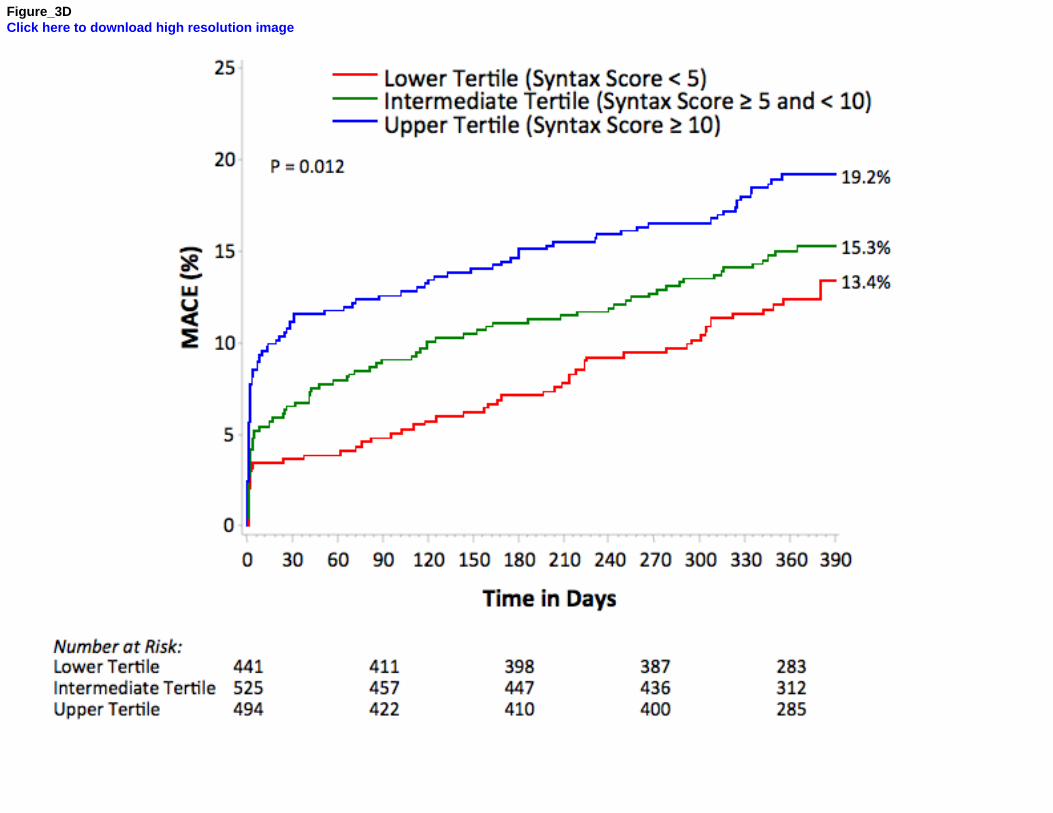
Compared to patients in the first and second tertile, those in the third tertile had higher
MACE (13.4%, 15.3%, 19.1%; ptrend = 0.01), death or MI (5.5%, 8.5%, 11.6%; ptrend = 0.003), MI
(4.4%, 7.7%, 10.5%; ptrend = 0.002), and probable or definite stent thrombosis (0.2%, 0.6%,
2.1%; ptrend = 0.01).
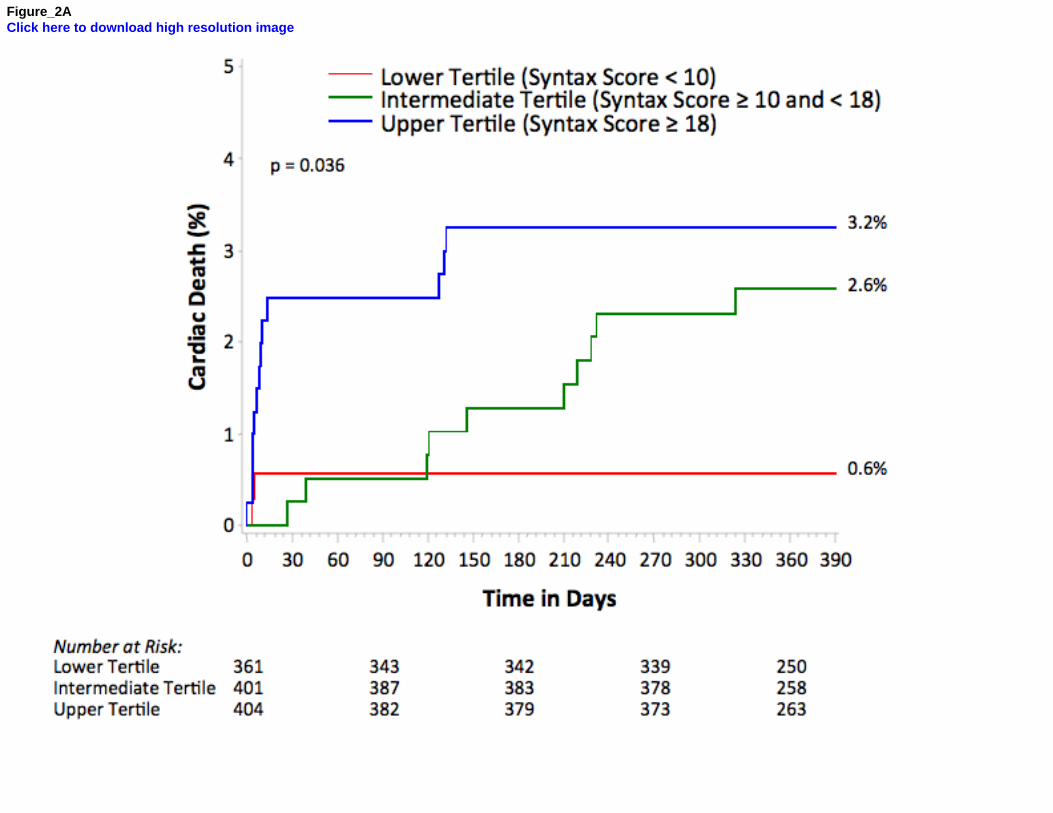
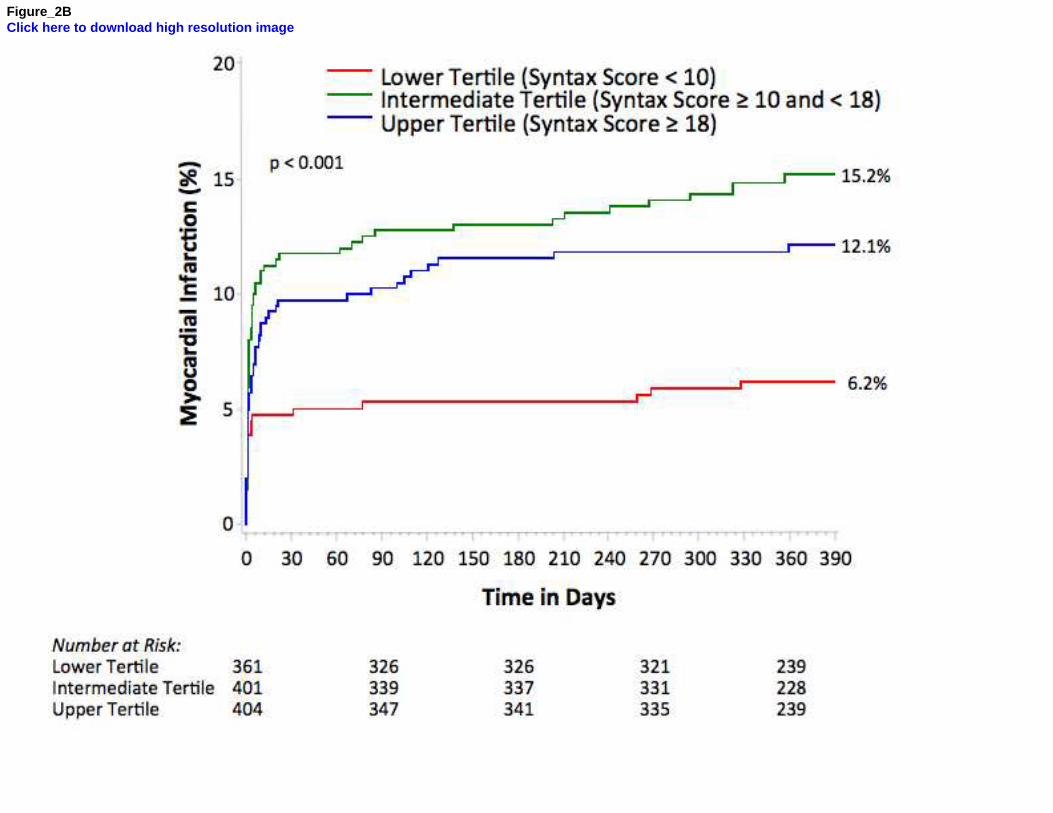
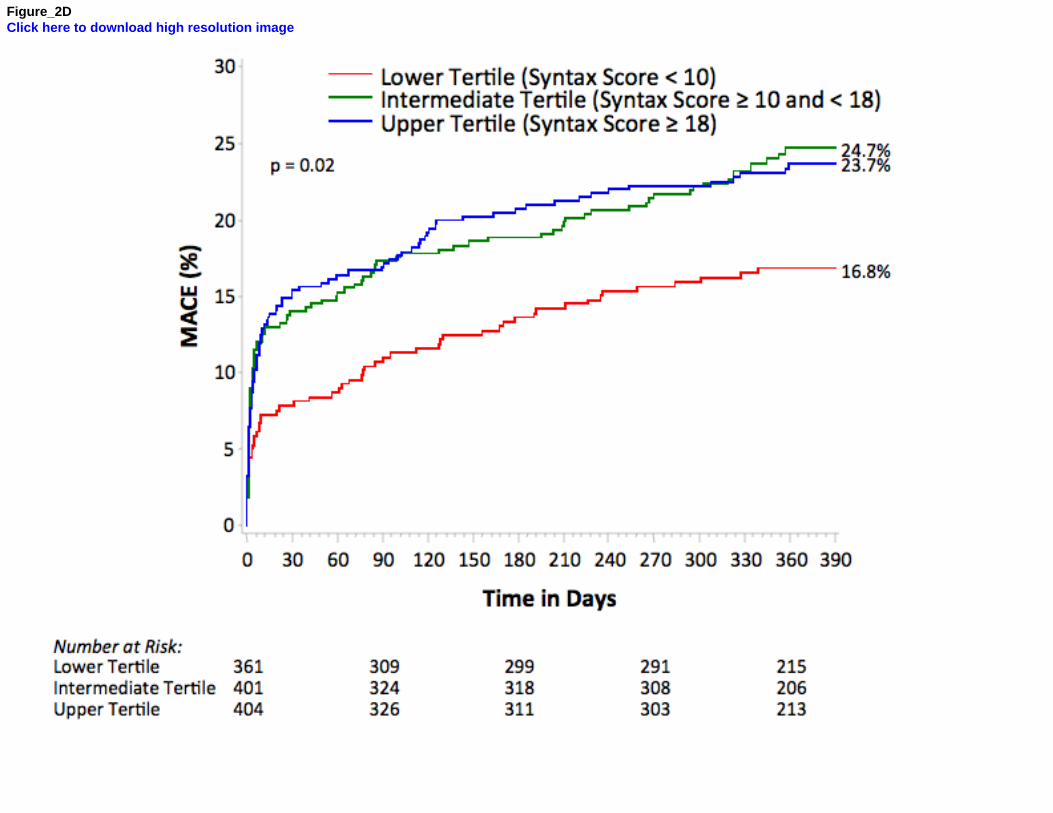
Compared to patients in the lowest tertile, those in the intermediate and upper tertiles
had higher MACE (16.8%, 24.7%, 23.7%; Ptrend = 0.02), death or MI (7.0%, 17.8%, 14.9%; ptrend
6
= 0.003), all-cause death (1.4%, 4.2%, 4.6%; P=0.046), cardiac death (0.6%, 2.6%, 3.2%; ptrend
= 0.04), MI (6.2%, 15.2%, 12.1%; ptrend = 0.002), and probable or definite stent thrombosis
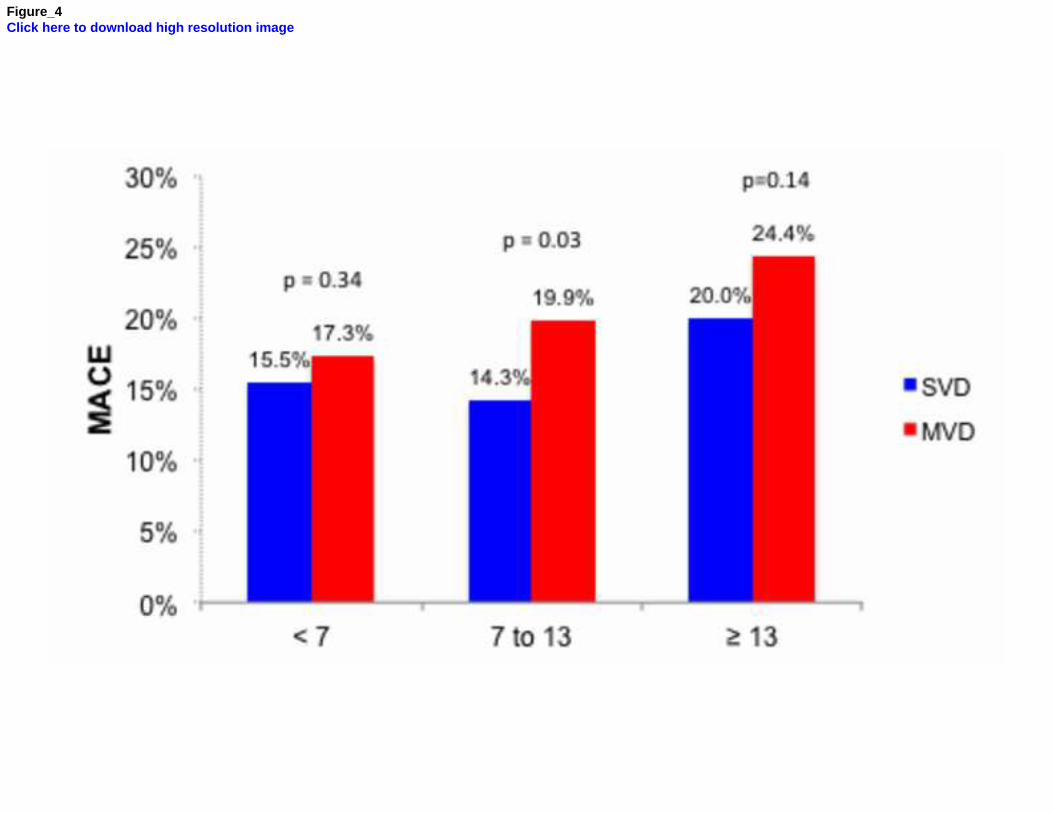
(0.2%, 0.6%, 2.1%; ptrend = 0.01). Figure 4 compares MACE in SVD and MVD patients in each
tertile of the overall population. Notably, the rates of MACE in the highest SS tertile are similar
among SVD and MVD patients.
As shown in Table 3, the SS was an independent predictor of MACE, all-cause death,
cardiac death, MI, and TVR in the overall population. Even after including the number of vessels
disease (MVD vs. SVD) in the model, the SS still remained a powerful predictor of ischemic
events, while MVD was not. After adjusting for possible confounders, SS was also an
independent predictor of ischemic events in SVD as well as in MVD patients, separately (Table
4)
Discussion
The principal findings of the present study evaluating the SS in moderate- and high-risk
NSTEACS undergoing PCI are as follows: (1) patients with MVD had, expectedly, a SS twice as
high as those with SVD; (2) in patients with MVD, SS independently predicted 1-year MACE, all-
cause death, cardiac death, MI and TVR. In patients with SVD, SS independently predicted 1-
year MACE, MI and TVR; (3) SS was a more powerful predictor of clinical events than the
number of diseased vessels.
The SS is an anatomical scoring system based on the coronary angiogram, which
quantifies the complexity of coronary artery disease. Recent studies have shown that the SS
can stratify risk and predict outcomes of patients with complex coronary artery disease
undergoing PCI.3, 7 In the SYNTAX trial, PCI patients in the upper SS tertile (>32) had 1.5- and
twofold higher rate of major adverse cardiac and cerebrovascular events, and mortality,
respectively, compared to PCI patients in the lowest tertile (<22). Additionally, SS was an
independent correlate of mortality in PCI-treated patients.17 The Future Revascularization
7
Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease
(FREEDOM) trial also showed that in PCI patients with diabetes and MVD, the higher the SS -
the worse the clinical outcome at 5-year follow-up was.18 Likewise, the value of the SS in
predicting clinical outcomes in patients who underwent PCI for UPLMD has been validated. In
one study, 7 patients in the highest SS tertile (>36) had more unfavorable clinical outcomes
when compared with those in the lower SS tertiles. Accordingly, SS has been incorporated as
an important variable in clinical decision making for the individual patient with MVD in need of
coronary revascularization.19, 20 The present large-scale study corroborates and extends these
findings by showing the prognostic utility of the SS in SVD and lower-risk MVD patients. Indeed,
the SS upper tertile in the present analysis (≥18) is lower than even the lowest SS tertile in both
the SYNTAX and FREDOM trials (< 22). In addition, only 2.3% of the patients enrolled in the
present ACUITY angiographic substudy had a SS of ≥ 33, compared with one-third of the
patients in the SYNTAX and FREEDOM trials.3, 18 It is important to highlight that the value of SS
in risk prediction had been previously demonstrated mostly in stable patients with multivessel
disease; in contrast, the present analysis depicts only NSTEACS patients who were categorized
into 2 separate groups, MVD and SVD. Although we have recently demonstrated the prognostic
value of the baseline and the residual SS after PCI in a broad range of patients with NSTEACS
11, 21 the utility of the SS for clinical events prediction in patients with SVD has never been
investigated. The present study is the first to assess the pre-PCI SS for risk prediction of
ischemic outcomes in SVD patients undergoing PCI. It shows that even with a very low cutoff
margin (ranging from 5 to 10), higher SS still identifies patients at increased risk and is a
valuable tool for predicting clinical outcomes at 1 year. Intriguingly, the same patterns of
discrimination demonstrated in this study and others 3, 18 among tertiles of multivessel disease is
found in the SVD cohort: the upper SS tertile (≥10) patients had 1.5- and twofold higher MACE
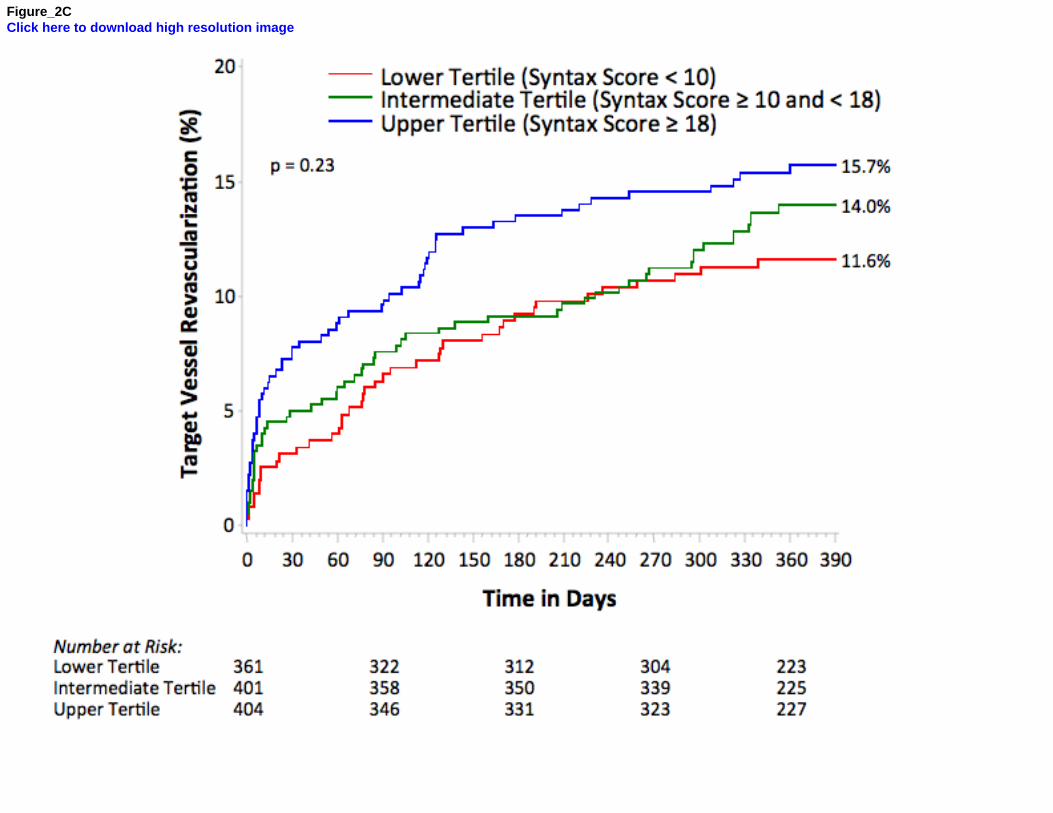
and death rates, respectively, compared to those in the lowest tertile (<5). The increased 1-year
rates of MACEdriven by death and MI, and not by TVR (Figure 2)with higher SS may be
explained by the higher procedure risk associated with complex coronary anatomy (i.e.,
multiples lesions in the same vessel, bifurcations, calcification, total occlusions, ostial lesions,
8
etc.), as demonstrated by the very early separation of the event curves. Of note, SVD patients in
the highest SS tertile had a higher rate of events than patients with MVD in the lower tertile,
highlighting the importance of categorizing patients based on the complexity of coronary lesions
as a whole, and not only by the number of vessels compromised (Figure 4). By multivariable
analysis, SS also emerged as an independent predictor of MACE, MI and TVR, regardless of
number of diseased vessels.
The present analysis has certain limitations. It is a retrospective analysis from a large-
scale randomized trial, and results should be considered exploratory, requiring confirmation in
additional studies. The patient cohort in the present study was drawn from the U.S-based
angiographic substudy representing only one fifth of the original ACUITY population. The
multivariable analysis performed in this study, although detailed, cannot exclude residual
confounding for unmeasured and unknown variables. The stent types used in the ACUITY trial
were either first generation DES or BMS; thus, the value of the SS as a prognostic tool in the
era of newer-generation DES still needs to be determined. However, preliminary data from
recent randomized trials have confirmed the ability of the SS to identify patients who are at
highest risk of adverse events using new-genenation DES.8, 22 Patients with previous CABG
were excluded from this analysis since the SS algorithm was developed for patients with native
coronary artery disease. Angiography alone has limited accuracy in determining the severity of
the stenosis in terms of inducing ischemia. In addition to its independence as a marker of risk
from other significant risk factors, the addition of the SS to conventional risk factors can improve
its ability to risk stratify patients over the longer term. Recalculating the SS by incorporating
clinical variables23 or ischemia-producing lesions as determined by fractional flow reservethe
so-called functional SSmight better determine risk of adverse events in patients undergoing
PCI.24 This approach needs to be examined in NSTEACS patients in future investigations. Total
occlusions were scored as having unknown duration according to the SS algorithm; many of
these occlusions in the ACUITY trial may have been of recent duration, most likely causing the
overestimation of the SS. The number of deaths in patients with SVD was quite low and this
9
may explain the lack of statistical association between mortality as an individual endpoint and
the SS. Finally, the results of this study have limited generalizability since they apply only to
native coronary artery disease in NSTEACS patients of being treated with an early invasive
strategy.
Disclosure
Dr. Mehran is a consultant for Abbott Vascular, AstraZeneca, Cardiva, Cordis, Ortho-McNeil,
The Medicines Company and Regado Biosciences, and has received research grants from
Sanofi/Bristol Myers Squibb. Dr. Dangas has received honoraria from The Medicines Company,
Cordis, Sanofi/Bristol Myers Squibb and is a consultant to AstraZeneca. Martin Fahy and Ke Xu
are employed by the Cardiovascular Research Foundation. Dr. Stone serves on the scientific
advisory boards for and has received honoraria from Abbott Vascular and Boston Scientific, and
is a consultant to The Medicines Company. All other authors have reported that they have no
relationships to disclosure.

10
1. Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A, Dawkins K, van den Brand
M, Van Dyck N, Russell ME, Mohr FW, Serruys PW. The SYNTAX Score: An
angiographic tool grading the complexity of coronary artery disease. EuroIntervention
2005;1:219-227.
2. Serruys PW, Onuma Y, Garg S, Sarno G, van den Brand M, Kappetein AP, Van Dyck N,
Mack M, Holmes D, Feldman T, Morice MC, Colombo A, Bass E, Leadley K, Dawkins
KD, van Es GA, Morel MA, Mohr FW. Assessment of the SYNTAX score in the Syntax
study. EuroIntervention 2009;5:50-56.
3. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Stahle E,
Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr
FW; SYNTAX Investigators. Percutaneous coronary intervention versus coronary-artery
bypass grafting for severe coronary artery disease. N Engl J Med 2009;360:961-972.
4. Valgimigli M, Serruys PW, Tsuchida K, Vaina S, Morel MA, van den Brand MJ, Colombo
A, Morice MC, Dawkins K, de Bruyne B, Kornowski R, de Servi S, Guagliumi G, Jukema
JW, Mohr FW, Kappetein AP, Wittebols K, Stoll HP, Boersma E, Parrinello G; ARTS, II.
Cyphering the complexity of coronary artery disease using the syntax score to predict
clinical outcome in patients with three-vessel lumen obstruction undergoing
percutaneous coronary intervention. Am J Cardiol 2007;99:1072-1081.
5. Capodanno D, Di Salvo ME, Cincotta G, Miano M, Tamburino C, Tamburino C.
Usefulness of the SYNTAX score for predicting clinical outcome after percutaneous
coronary intervention of unprotected left main coronary artery disease. Circ Cardiovasc
Interv 2009;2:302-308.
6. Chen SL, Chen JP, Mintz G, Xu B, Kan J, Ye F, Zhang J, Sun X, Xu Y, Jiang Q, Zhang
A, Stone GW. Comparison between the NERS (New Risk Stratification) score and the
SYNTAX (Synergy between Percutaneous Coronary Intervention with Taxus and
Cardiac Surgery) score in outcome prediction for unprotected left main stenting. JACC
Cardiovasc Interv 2010;3:632-641.
11
7. Kim YH, Park DW, Kim WJ, Lee JY, Yun SC, Kang SJ, Lee SW, Lee CW, Park SW,
Park SJ. Validation of SYNTAX (Synergy between PCI with Taxus and Cardiac Surgery)
score for prediction of outcomes after unprotected left main coronary revascularization.
JACC Cardiovasc Interv 2010;3:612-623.
8. Wykrzykowska JJ, Garg S, Girasis C, de Vries T, Morel MA, van Es GA, Buszman P,
Linke A, Ischinger T, Klauss V, Corti R, Eberli F, Wijns W, Morice MC, di Mario C, van
Geuns RJ, Juni P, Windecker S, Serruys PW. Value of the SYNTAX score for risk
assessment in the all-comers population of the randomized multicenter LEADERS
(Limus Eluted from A Durable versus ERodable Stent coating) Trial. J Am Coll Cardiol
2010;56:272-277.
9. Garg S, Sarno G, Serruys PW, Rodriguez AE, Bolognese L, Anselmi M, De Cesare N,
Colangelo S, Moreno R, Gambetti S, Monti M, Bristot L, Bressers M, Garcia-Garcia HM,
Parrinello G, Campo G, Valgimigli M; STRATEGY and MULTISTRATEGY Investigators.
Prediction of 1-year clinical outcomes using the SYNTAX score in patients with acute st-
segment elevation myocardial infarction undergoing primary percutaneous coronary
intervention: A substudy of the STRATEGY (Single High-Dose Bolus Tirofiban and
Sirolimus-Eluting Stent Versus Abciximab and Bare-Metal Stent in Acute Myocardial
Infarction) and MULTISTRATEGY (Multicenter Evaluation of Single High-Dose Bolus
Tirofiban Versus Abciximab with Sirolimus-Eluting Stent or Bare-Metal Stent in Acute
Myocardial Infarction Study) Trials. JACC Cardiovasc Interv 2011;4:66-75.
10. Magro M, Nauta S, Simsek C, Onuma Y, Garg S, van der Heide E, van der Giessen WJ,
Boersma E, van Domburg RT, van Geuns RJ, Serruys PW. Value of the SYNTAX score
in patients treated by primary percutaneous coronary intervention for acute ST-elevation
myocardial infarction: The MI SYNTAXscore study. Am Heart J 2011;161:771-781.
11. Palmerini T, Genereux P, Caixeta A, Cristea E, Lansky A, Mehran R, Dangas G, Lazar
D, Sanchez R, Fahy M, Xu K, Stone GW. Prognostic value of the SYNTAX score in
patients with acute coronary syndromes undergoing percutaneous coronary intervention:
12
analysis from the ACUITY (Acute Catheterization and Urgent Intervention Triage
StrategY) Trial. J Am Coll Cardiol 2011;57:2389-2397.
12. Stone GW, Bertrand M, Colombo A, Dangas G, Farkouh ME, Feit F, Lansky AJ, Lincoff
AM, Mehran R, Moses JW, Ohman M, White HD. Acute catheterization and urgent
intervention triage strategy (ACUITY) Trial: study design and rationale. Am Heart J
2004;148:764-775.
13. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG, Morel
MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW;
Academic Research Consortium. Clinical end points in coronary stent trials: a case for
standardized definitions. Circulation 2007;115:2344-2351.
14. Genereux P, Palmerini T, Caixeta A, Cristea E, Mehran R, Sanchez R, Lazar D,
Jankovic I, Corral MD, Dressler O, Fahy MP, Parise H, Lansky AJ, Stone GW. SYNTAX
score reproducibility and variability between interventional cardiologists, core laboratory
technicians, and quantitative coronary measurements. Circ Cardiovasc Interv
2011;4:553-561.
15. Kundel HL, Polansky M. Measurement of observer agreement. Radiology 2003;228:303-
308.
16. Garg S, Girasis C, Sarno G, Goedhart D, Morel MA, Garcia-Garcia HM, Bressers M, van
Es GA, Serruys PW; SYNTAX trial investigators. The SYNTAX score revisited: a
reassessment of the SYNTAX score reproducibility. Catheter Cardiovasc Interv
2010;75:946-952.
17. Farooq V, Serruys PW, Bourantas C, Vranckx P, Diletti R, Garcia Garcia HM, Holmes
DR, Kappetein AP, Mack M, Feldman T, Morice MC, Colombo A, Morel MA, de Vries T,
van Es GA, Steyerberg EW, Dawkins KD, Mohr FW, James S, Stahle E. Incidence and
multivariable correlates of long-term mortality in patients treated with surgical or
percutaneous revascularization in the synergy between percutaneous coronary
intervention with taxus and cardiac surgery (SYNTAX) Trial. Eur Heart J 2012;33:3105-
3113.
13
18. Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen
DJ, Rosenberg Y, Solomon SD, Desai AS, Gersh BJ, Magnuson EA, Lansky A, Boineau
R, Weinberger J, Ramanathan K, Sousa JE, Rankin J, Bhargava B, Buse J, Hueb W,
Smith CR, Muratov V, Bansilal S, King S, 3rd, Bertrand M, Fuster V; FREEDOM Trial
Investigators. Strategies for multivessel revascularization in patients with diabetes. N
Engl J Med 2012;367:2375-2384.
19. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, Cigarroa JE, Disesa
VJ, Hiratzka LF, Hutter AM, Jr., Jessen ME, Keeley EC, Lahey SJ, Lange RA, London
MJ, Mack MJ, Patel MR, Puskas JD, Sabik JF, Selnes O, Shahian DM, Trost JC,
Winniford MD; American College of Cardiology Foundation; American Heart Association
Task Force on Practice Guidelines; American Association for Thoracic Surgery; Society
of Cardiovascular Anesthesiologists; Society of Thoracic Surgeons. 2011 ACCF/AHA
guideline for coronary artery bypass graft surgery. A report of the American College of
Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.
Developed in collaboration with the American Association for Thoracic Surgery, Society
of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll
Cardiol 2011;58:e123-210.
20. Task Force on Myocardial Revascularization of the European Society of Cardiology
(ESC) and the European Association for Cardio-Thoracic Surgery (EACTS); European
Association for Percutaneous Cardiovascular Interventions (EAPCI), Wijns W, Kolh P,
Danchin N, Di Mario C, Falk V, Folliguet T, Garg S, Huber K, James S, Knuuti J, Lopez-
Sendon J, Marco J, Menicanti L, Ostojic M, Piepoli MF, Pirlet C, Pomar JL, Reifart N,
Ribichini FL, Schalij MJ, Sergeant P, Serruys PW, Silber S, Sousa Uva M, Taggart D.
Guidelines on myocardial revascularization. Eur Heart J 2010;31:2501-2555.
21. Genereux P, Palmerini T, Caixeta A, Rosner G, Green P, Dressler O, Xu K, Parise H,
Mehran R, Serruys PW, Stone GW. Quantification and impact of untreated coronary
artery disease after percutaneous coronary intervention: The residual SYNTAX (Synergy
14
Between PCI with Taxus and Cardiac Surgery) score. J Am Coll Cardiol 2012;59:2165-
2174.
22. Garg S, Sarno G, Girasis C, Vranckx P, de Vries T, Swart M, Bressers M, Garcia-Garcia
HM, van Es GA, Raber L, Campo G, Valgimigli M, Dawkins KD, Windecker S, Serruys
PW. A patient-level pooled analysis assessing the impact of the SYNTAX (Synergy
Between Percutaneous Coronary Interventions With Taxus and Cardiac Surgery) score
on 1-year clinical outcomes in 6,508 patients enrolled in contemporary coronary stent
trials. JACC Cardiovasc Interv 2011;4:645-653.
23. Farooq V, Vergouwe Y, Généreux P, Bourantas CV, Palmerini T, Caixeta A, Garcìa-
Garcìa HM, Diletti R, Morel MA, McAndrew TC, Kappetein AP, Valgimigli M, Windecker
S, Dawkins KD, Steyerberg EW, Serruys PW, Stone GW. Prediction of 1-Year Mortality
in Patients With Acute Coronary Syndromes Undergoing Percutaneous Coronary
Intervention: Validation of the Logistic Clinical SYNTAX (Synergy Between
Percutaneous Coronary Interventions With Taxus and Cardiac Surgery) score. JACC
Cardiovasc Interv 2013;6:737-45.
24. Nam CW, Mangiacapra F, Entjes R, Chung IS, Sels JW, Tonino PA, De Bruyne B, Pijls
NH, Fearon WF; FAME Study Investigators. Functional syntax score for risk assessment
in multivessel coronary artery disease. J Am Coll Cardiol 2011;58:1211-1218.
15
Figure legends
Figure 1: Distribution of the SS in patients with single and multivessel disease of the entire
population. Each point may represent more than 1 patient if SS is identical.
Figure 2: Time-to-event curves in patients with multivessel disease. One-year cumulative event
curves for rates of (A) cardiac mortality, (B) myocardial infarction, (C) target vessel
revascularization, and (D) MACE - stratified by tertiles of SYNTAX score.
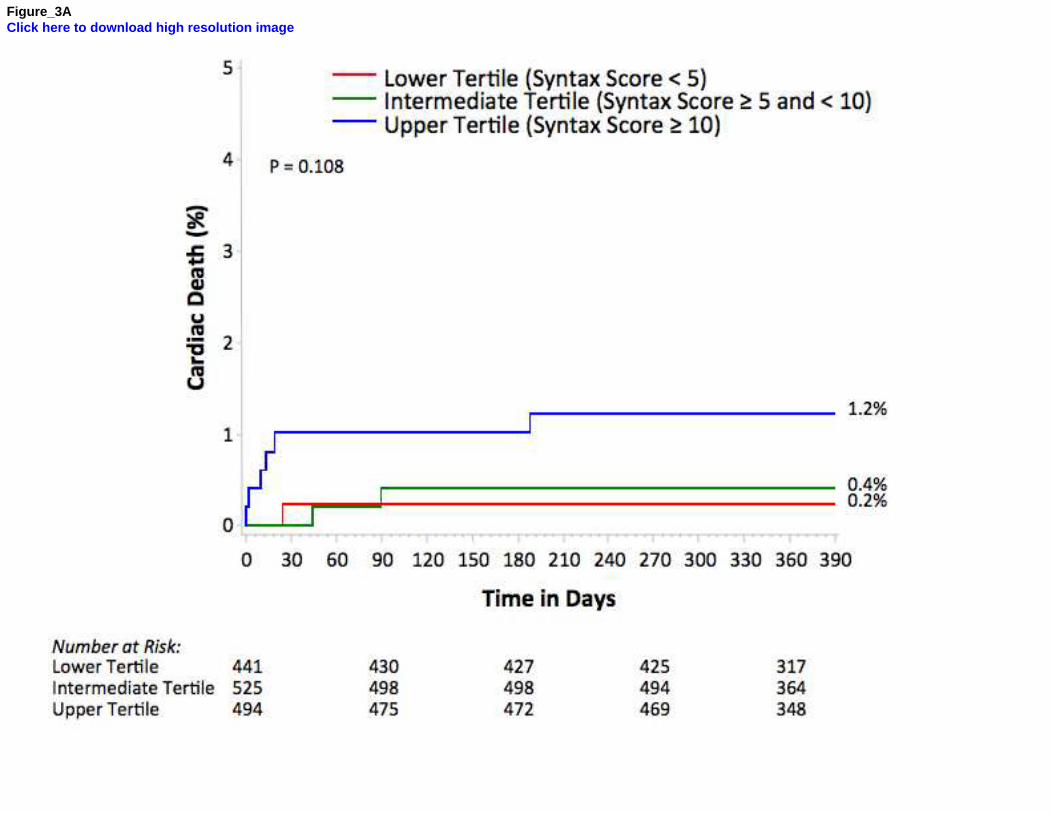
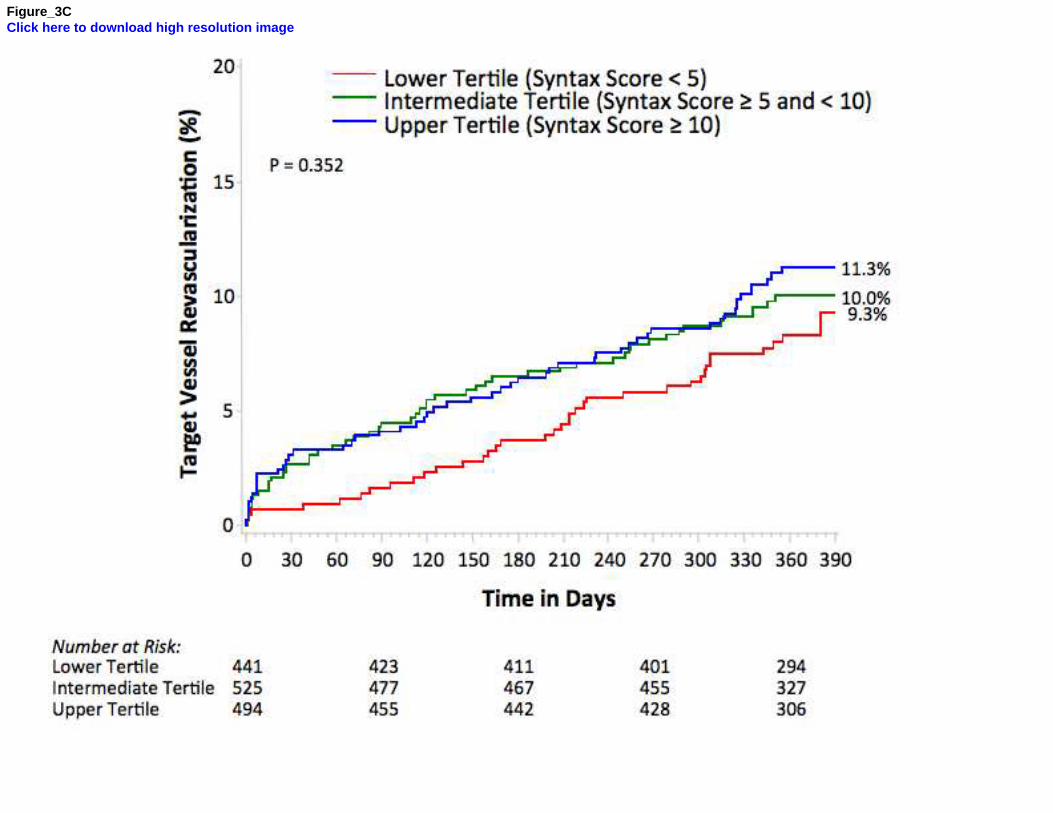
Figure 3: Time-to-event curves in patients with single vessel disease. One-year cumulative event
curves for rates of (A) cardiac mortality, (B) myocardial infarction, (C) target vessel
revascularization, and (D) MACE - stratified by tertiles of SYNTAX score.
Figure 4: Clinical outcomes at 1-year in the overall population comparing MACE in SVD and MVD
in each tertile.
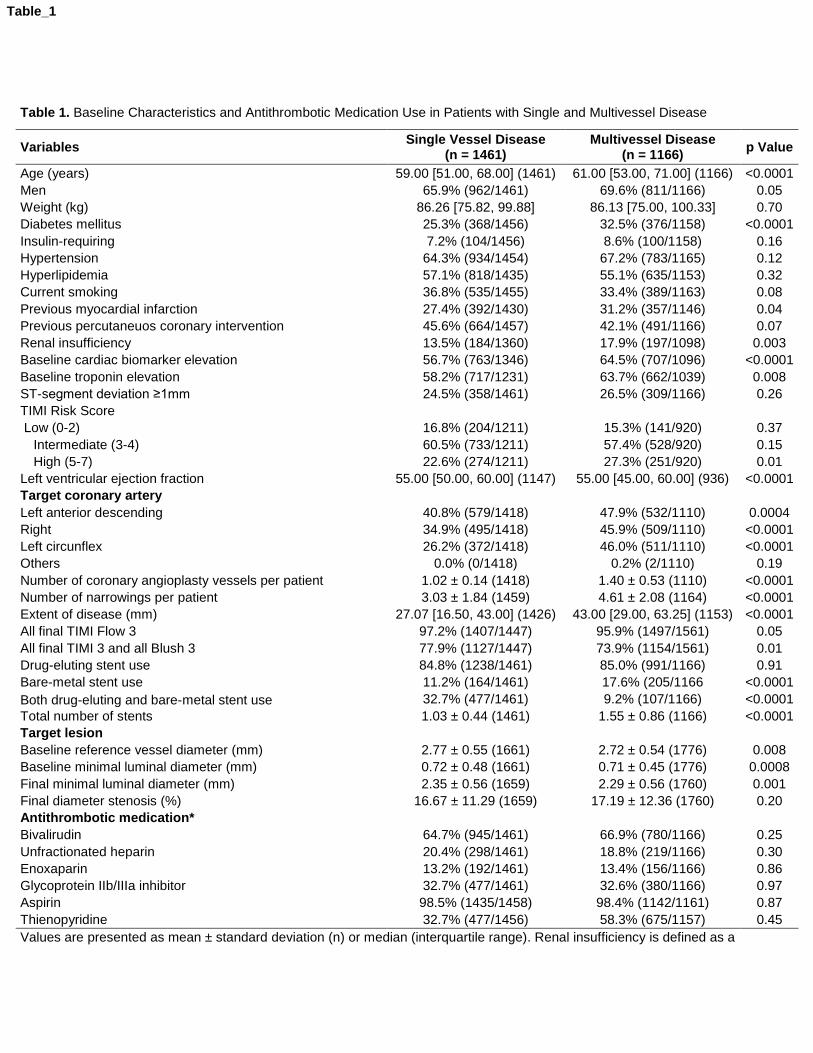
Table 1. Baseline Characteristics and Antithrombotic Medication Use in Patients with Single and Multivessel Disease
Variables Single Vessel Disease
(n = 1461) Multivessel Disease
(n = 1166) p Value
Age (years) 59.00 [51.00, 68.00] (1461) 61.00 [53.00, 71.00] (1166) <0.0001
Men 65.9% (962/1461) 69.6% (811/1166) 0.05
Weight (kg) 86.26 [75.82, 99.88] 86.13 [75.00, 100.33] 0.70
Diabetes mellitus 25.3% (368/1456) 32.5% (376/1158) <0.0001
Insulin-requiring 7.2% (104/1456) 8.6% (100/1158) 0.16
Hypertension 64.3% (934/1454) 67.2% (783/1165) 0.12
Hyperlipidemia 57.1% (818/1435) 55.1% (635/1153) 0.32
Current smoking 36.8% (535/1455) 33.4% (389/1163) 0.08
Previous myocardial infarction 27.4% (392/1430) 31.2% (357/1146) 0.04
Previous percutaneuos coronary intervention 45.6% (664/1457) 42.1% (491/1166) 0.07
Renal insufficiency 13.5% (184/1360) 17.9% (197/1098) 0.003
Baseline cardiac biomarker elevation 56.7% (763/1346) 64.5% (707/1096) <0.0001
Baseline troponin elevation 58.2% (717/1231) 63.7% (662/1039) 0.008
ST-segment deviation ≥1mm 24.5% (358/1461) 26.5% (309/1166) 0.26
TIMI Risk Score
Low (0-2) 16.8% (204/1211) 15.3% (141/920) 0.37
Intermediate (3-4) 60.5% (733/1211) 57.4% (528/920) 0.15
High (5-7) 22.6% (274/1211) 27.3% (251/920) 0.01
Left ventricular ejection fraction 55.00 [50.00, 60.00] (1147) 55.00 [45.00, 60.00] (936) <0.0001
Target coronary artery
Left anterior descending 40.8% (579/1418) 47.9% (532/1110) 0.0004
Right 34.9% (495/1418) 45.9% (509/1110) <0.0001
Left circunflex 26.2% (372/1418) 46.0% (511/1110) <0.0001
Others 0.0% (0/1418) 0.2% (2/1110) 0.19
Number of coronary angioplasty vessels per patient 1.02 ± 0.14 (1418) 1.40 ± 0.53 (1110) <0.0001
Number of narrowings per patient 3.03 ± 1.84 (1459) 4.61 ± 2.08 (1164) <0.0001
Extent of disease (mm) 27.07 [16.50, 43.00] (1426) 43.00 [29.00, 63.25] (1153) <0.0001
All final TIMI Flow 3 97.2% (1407/1447) 95.9% (1497/1561) 0.05
All final TIMI 3 and all Blush 3 77.9% (1127/1447) 73.9% (1154/1561) 0.01
Drug-eluting stent use 84.8% (1238/1461) 85.0% (991/1166) 0.91
Bare-metal stent use 11.2% (164/1461) 17.6% (205/1166 <0.0001
Both drug-eluting and bare-metal stent use 32.7% (477/1461) 9.2% (107/1166) <0.0001
Total number of stents 1.03 ± 0.44 (1461) 1.55 ± 0.86 (1166) <0.0001
Target lesion
Baseline reference vessel diameter (mm) 2.77 ± 0.55 (1661) 2.72 ± 0.54 (1776) 0.008
Baseline minimal luminal diameter (mm) 0.72 ± 0.48 (1661) 0.71 ± 0.45 (1776) 0.0008
Final minimal luminal diameter (mm) 2.35 ± 0.56 (1659) 2.29 ± 0.56 (1760) 0.001
Final diameter stenosis (%) 16.67 ± 11.29 (1659) 17.19 ± 12.36 (1760) 0.20
Antithrombotic medication*
Bivalirudin 64.7% (945/1461) 66.9% (780/1166) 0.25
Unfractionated heparin 20.4% (298/1461) 18.8% (219/1166) 0.30
Enoxaparin 13.2% (192/1461) 13.4% (156/1166) 0.86
Glycoprotein IIb/IIIa inhibitor 32.7% (477/1461) 32.6% (380/1166) 0.97
Aspirin 98.5% (1435/1458) 98.4% (1142/1161) 0.87
Thienopyridine 32.7% (477/1456) 58.3% (675/1157) 0.45
Values are presented as mean ± standard deviation (n) or median (interquartile range). Renal insufficiency is defined as a
Table_1
calculated creatinine clearance rate of <60 ml/minute determined by the Cokcroft-Gault equation. TIMI = Thrombolysis In Myocardial Infarction. * Administered post randomization and pre angiography.
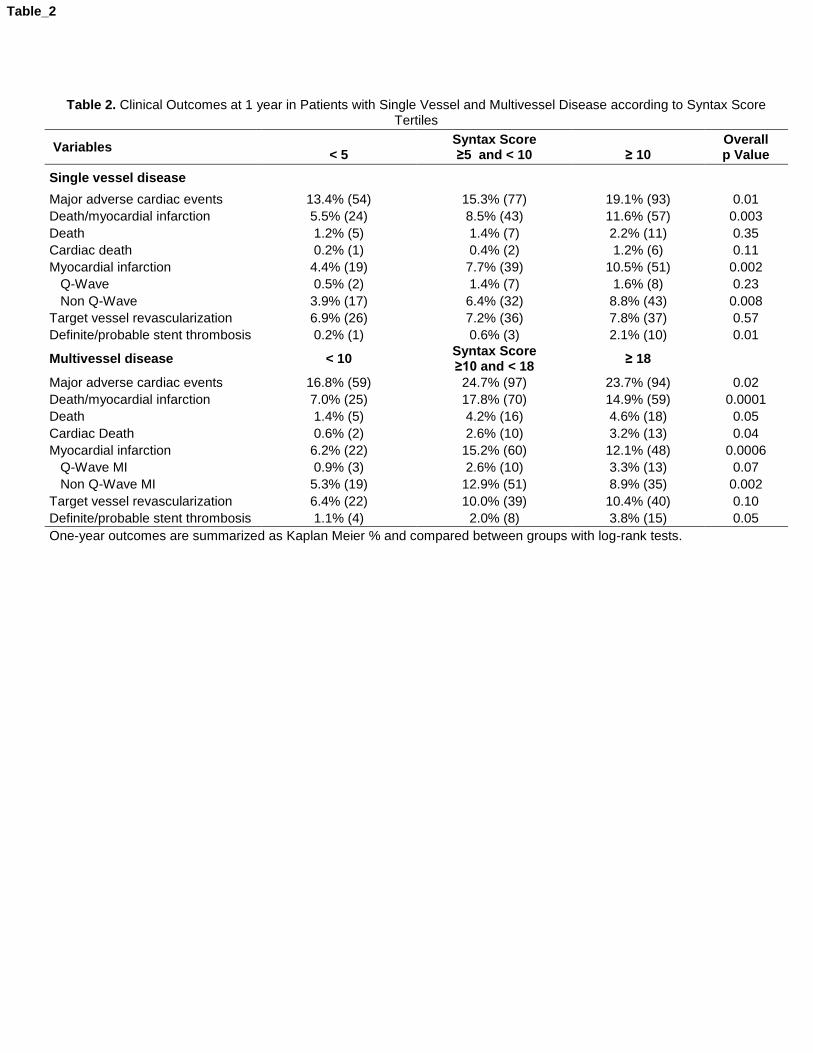
Table 2. Clinical Outcomes at 1 year in Patients with Single Vessel and Multivessel Disease according to Syntax Score Tertiles
Variables
< 5 Syntax Score ≥5 and < 10
≥ 10
Overall p Value
Single vessel disease
Major adverse cardiac events 13.4% (54) 15.3% (77) 19.1% (93) 0.01
Death/myocardial infarction 5.5% (24) 8.5% (43) 11.6% (57) 0.003
Death 1.2% (5) 1.4% (7) 2.2% (11) 0.35
Cardiac death 0.2% (1) 0.4% (2) 1.2% (6) 0.11
Myocardial infarction 4.4% (19) 7.7% (39) 10.5% (51) 0.002
Q-Wave 0.5% (2) 1.4% (7) 1.6% (8) 0.23
Non Q-Wave 3.9% (17) 6.4% (32) 8.8% (43) 0.008
Target vessel revascularization 6.9% (26) 7.2% (36) 7.8% (37) 0.57
Definite/probable stent thrombosis 0.2% (1) 0.6% (3) 2.1% (10) 0.01
Multivessel disease < 10 Syntax Score ≥10 and < 18
≥ 18
Major adverse cardiac events 16.8% (59) 24.7% (97) 23.7% (94) 0.02
Death/myocardial infarction 7.0% (25) 17.8% (70) 14.9% (59) 0.0001
Death 1.4% (5) 4.2% (16) 4.6% (18) 0.05
Cardiac Death 0.6% (2) 2.6% (10) 3.2% (13) 0.04
Myocardial infarction 6.2% (22) 15.2% (60) 12.1% (48) 0.0006
Q-Wave MI 0.9% (3) 2.6% (10) 3.3% (13) 0.07
Non Q-Wave MI 5.3% (19) 12.9% (51) 8.9% (35) 0.002
Target vessel revascularization 6.4% (22) 10.0% (39) 10.4% (40) 0.10
Definite/probable stent thrombosis 1.1% (4) 2.0% (8) 3.8% (15) 0.05
One-year outcomes are summarized as Kaplan Meier % and compared between groups with log-rank tests.
Table_2
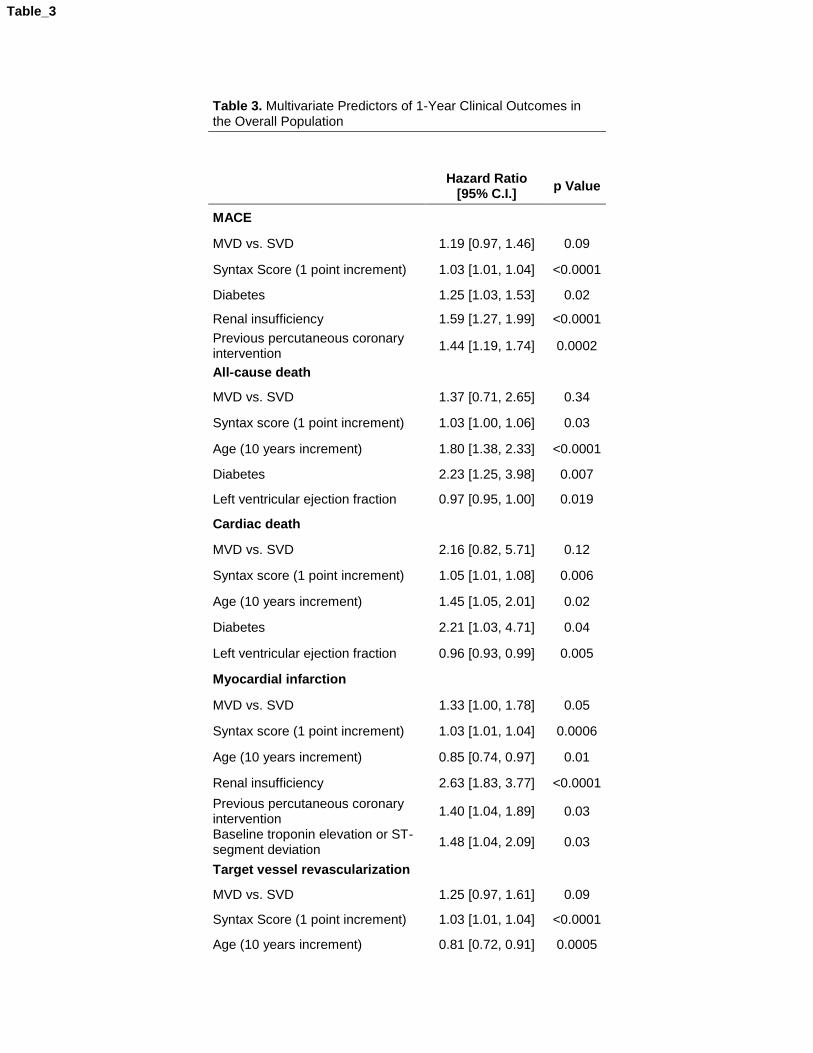
Table 3. Multivariate Predictors of 1-Year Clinical Outcomes in the Overall Population
Hazard Ratio
[95% C.I.] p Value
MACE
MVD vs. SVD 1.19 [0.97, 1.46] 0.09
Syntax Score (1 point increment) 1.03 [1.01, 1.04] <0.0001
Diabetes 1.25 [1.03, 1.53] 0.02
Renal insufficiency 1.59 [1.27, 1.99] <0.0001
Previous percutaneous coronary intervention
1.44 [1.19, 1.74] 0.0002
All-cause death
MVD vs. SVD 1.37 [0.71, 2.65] 0.34
Syntax score (1 point increment) 1.03 [1.00, 1.06] 0.03
Age (10 years increment) 1.80 [1.38, 2.33] <0.0001
Diabetes 2.23 [1.25, 3.98] 0.007
Left ventricular ejection fraction 0.97 [0.95, 1.00] 0.019
Cardiac death
MVD vs. SVD 2.16 [0.82, 5.71] 0.12
Syntax score (1 point increment) 1.05 [1.01, 1.08] 0.006
Age (10 years increment) 1.45 [1.05, 2.01] 0.02
Diabetes 2.21 [1.03, 4.71] 0.04
Left ventricular ejection fraction 0.96 [0.93, 0.99] 0.005
Myocardial infarction
MVD vs. SVD 1.33 [1.00, 1.78] 0.05
Syntax score (1 point increment) 1.03 [1.01, 1.04] 0.0006
Age (10 years increment) 0.85 [0.74, 0.97] 0.01
Renal insufficiency 2.63 [1.83, 3.77] <0.0001
Previous percutaneous coronary intervention
1.40 [1.04, 1.89] 0.03
Baseline troponin elevation or ST-segment deviation
1.48 [1.04, 2.09] 0.03
Target vessel revascularization
MVD vs. SVD 1.25 [0.97, 1.61] 0.09
Syntax Score (1 point increment) 1.03 [1.01, 1.04] <0.0001
Age (10 years increment) 0.81 [0.72, 0.91] 0.0005
Table_3

Renal insufficiency 1.67 [1.17, 2.38] 0.005
Previous percutaneous coronary intervention
1.89 [1.49, 2.41] <0.0001
MVD = multivessel disease. SVD = single vessel disease. MVD vs. SVD is a covariate forced in this model in order to compare its relative predictive value with the Syntax score. Note that Syntax score was a powerful predictor of clinical events, whereas the number of diseased vessels did not predict events.
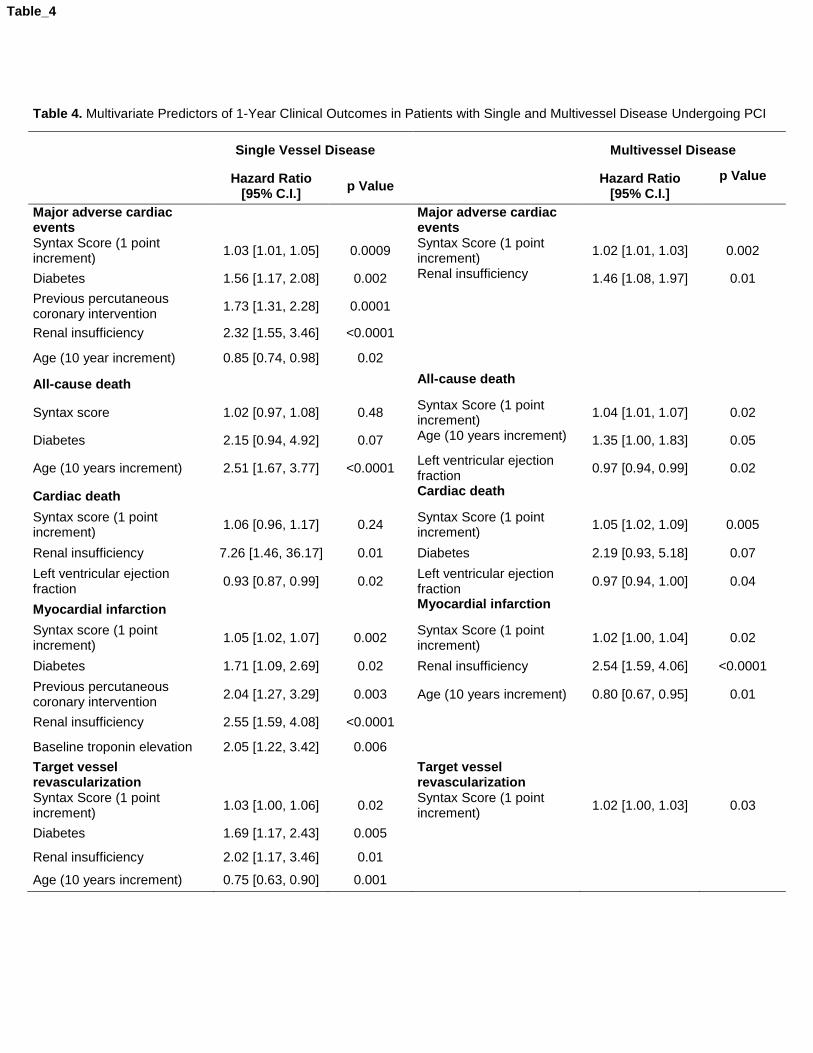
Table 4. Multivariate Predictors of 1-Year Clinical Outcomes in Patients with Single and Multivessel Disease Undergoing PCI
Single Vessel Disease Multivessel Disease
Hazard Ratio
[95% C.I.] p Value
Hazard Ratio [95% C.I.]
p Value
Major adverse cardiac events
Major adverse cardiac events
Syntax Score (1 point increment)
1.03 [1.01, 1.05] 0.0009 Syntax Score (1 point increment)
1.02 [1.01, 1.03] 0.002
Diabetes 1.56 [1.17, 2.08] 0.002 Renal insufficiency 1.46 [1.08, 1.97] 0.01
Previous percutaneous coronary intervention
1.73 [1.31, 2.28] 0.0001
Renal insufficiency 2.32 [1.55, 3.46] <0.0001
Age (10 year increment) 0.85 [0.74, 0.98] 0.02
All-cause death All-cause death
Syntax score 1.02 [0.97, 1.08] 0.48 Syntax Score (1 point increment)
1.04 [1.01, 1.07] 0.02
Diabetes 2.15 [0.94, 4.92] 0.07 Age (10 years increment) 1.35 [1.00, 1.83] 0.05
Age (10 years increment) 2.51 [1.67, 3.77] <0.0001 Left ventricular ejection fraction
0.97 [0.94, 0.99] 0.02
Cardiac death Cardiac death
Syntax score (1 point increment)
1.06 [0.96, 1.17] 0.24 Syntax Score (1 point increment)
1.05 [1.02, 1.09] 0.005
Renal insufficiency 7.26 [1.46, 36.17] 0.01 Diabetes 2.19 [0.93, 5.18] 0.07
Left ventricular ejection fraction
0.93 [0.87, 0.99] 0.02 Left ventricular ejection fraction
0.97 [0.94, 1.00] 0.04
Myocardial infarction Myocardial infarction
Syntax score (1 point increment)
1.05 [1.02, 1.07] 0.002 Syntax Score (1 point increment)
1.02 [1.00, 1.04] 0.02
Diabetes 1.71 [1.09, 2.69] 0.02 Renal insufficiency 2.54 [1.59, 4.06] <0.0001
Previous percutaneous coronary intervention
2.04 [1.27, 3.29] 0.003 Age (10 years increment) 0.80 [0.67, 0.95] 0.01
Renal insufficiency 2.55 [1.59, 4.08] <0.0001
Baseline troponin elevation 2.05 [1.22, 3.42] 0.006
Target vessel revascularization
Target vessel revascularization
Syntax Score (1 point increment)
1.03 [1.00, 1.06] 0.02 Syntax Score (1 point increment)
1.02 [1.00, 1.03] 0.03
Diabetes 1.69 [1.17, 2.43] 0.005
Renal insufficiency 2.02 [1.17, 3.46] 0.01
Age (10 years increment) 0.75 [0.63, 0.90] 0.001
Table_4
Figure_1Click here to download high resolution image
Figure_2AClick here to download high resolution image
Figure_2BClick here to download high resolution image
Figure_2CClick here to download high resolution image
Figure_2DClick here to download high resolution image
Figure_3AClick here to download high resolution image
Figure_3BClick here to download high resolution image
Figure_3CClick here to download high resolution image
Figure_3DClick here to download high resolution image
Figure_4Click here to download high resolution image