Prognostic value of CD44 expression in penile squamous cell carcinoma: a pilot study

Vol. 106 No. 5 November 2008
ORAL MEDICINE Editor: Craig S. Miller
Prognostic factors and survival analysis in a sample of oralsquamous cell carcinoma patientsLucinei Roberto Oliveira, DDS, PhD,a Alfredo Ribeiro-Silva, MD, PhD,b
João Paulo Oliveira Costa, DDS,a Aguinaldo Luiz Simões, MD, PhD,c
Miguel Angel Sala Di Matteo, PhD,d and Sergio Zucoloto, MD, PhD,b Ribeirao Preto, BrazilUNIVERSITY OF SAO PAULO
Objectives. The aims of this report were to describe the 5-year overall survival (OS) in a group of oral squamous cellcarcinoma (OSCC) patients and to investigate the effects of age, gender, anatomic localization, tumor evolution time,smoking and alcohol intake, nodal status, tumoral recurrences, histologic classification, p53 and p63immunoexpression, human papillomavirus DNA presence, and treatment on the prognostic outcome.Study design. Survival curves were generated using Kaplan-Meier method, and univariate and multivariate analyseswere made using the log rank test and Cox regression, respectively.Results. The 5-year OS was 28.6%, and the univariate analysis showed significant results for p53 and p63immunoexpression, age, and anatomic localization. The Cox regression demonstrated poor OS for tumors with p53immunoexpression and for patients aged over 60 years. There were also significant differences in survival dependingon the anatomic localizations.Conclusion. These results highlight the influence of p53 immunoexpression, age, and anatomic localization in OSCC
evolution. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:685-95)Oral squamous cell carcinoma (OSCC) is considered tobe the result of a multistep process which involves anumber of aberrant genetic events. Tobacco smokingand the heavy use of alcohol are probably the best-known risk factors for this disease.1 Around 4%-10%of patients with OSCC are not exposed to these riskfactors,2 and only a small proportion of tobacco-ex-
Supported by Grants from Fundaçao de Amparo a Pesquisa do Estadode Sao Paulo (FAPESP 03/02532-8) and Coordenaçao de Aperfeiçoa-mento de Pessoal de Nivel Superior).aResearch Scientist, Department of Pathology, Ribeirao Preto Medi-cal School, Ribeirao Preto, Brazil;bProfessor, Department of Pathology, Ribeirao Preto Medical School,Ribeirao Preto, Brazil;cProfessor, Department of Genetics, Ribeirao Preto Medical School,Ribeirao Preto, Brazil;dProfessor, Department of Morphology, Stomatology, and Physiol-ogy, Faculty of Dentistry of Ribeirao Preto, Ribeirao Preto, Brazil.Received for publication Apr 15, 2008; returned for revision Jul 10,2008; accepted for publication Jul 10, 2008.1079-2104/$ - see front matter© 2008 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2008.07.002posed individuals develop OSCC.3 For these reasons,the etiology of some of these tumors remains undeter-mined, prompting investigations into other possible riskfactors for oral carcinogenesis and OSCC progression.
The prognostic evaluation and therapeutic planningof OSCC is mainly based on clinical TNM (T, tumorsize; N, regional lymph node involvement; M, metas-tases) classification. However, even with modern med-ical diagnostic and therapeutic services, the 5-year sur-vival rate ranges from 30% to 80% in several regions ofthe world,4 and the overall mortality rate for OSCCremains high, at approximately 50%.5 The main prob-lem with the TNM system is that it does not effectivelypredict patient outcomes6 because it does not take intoconsideration the tumoral biology and molecular char-acteristics other than the tumor’s anatomic localization.Applying tumor biology and molecular information tothe classification process may prove useful in comple-menting the TNM staging.5
The early diagnosis of OSCC has a fundamental rolein its prognosis, and patients diagnosed at later stages
have higher mortality rates.7 Although this is well685

OOOOE686 Oliveira et al. November 2008
known, there have been few investigations into howpatient profiles correlate with the diagnostic delay ofthis tumor. It has been suggested that the diagnosticdelay of OSCC is mainly caused by the patient.8 Fur-thermore, owing to the asymptomatic nature of oralcancer at its early stage, patients with this disease areless likely to seek medical advice in the early stagescompared with patients suffering from cancer at othersites.9
In recent decades, attention has been focused on ahandful of biomarkers frequently associated with thedisease. Among these, the most frequently associatedbiomarker is p53, a tumor suppressor gene, and themutation of p53 has been considered to be the mostcommon genetic feature in head and neck cancers.10
The p53 homologue p63 gene, is located in chromo-some 3q21-29, and its amplification has been associ-ated with prognostic outcome in OSCC.11 Both genesshare a very similar exon/intron organization and havebeen investigated for associations with OSCC.12-15
High-risk human papillomaviruses (HPV) are knownto be tumorigenic in human epithelial tissues, and theyare often described as high-risk (oncogenic) or low-risk(nononcogenic).16 High-risk HPV subtypes have beenidentified in oral cancer with variable prevalenceamong different populations.17 The role of HPV as ahypothetic agent in the development and progression ofOSCC has been studied, but the investigations havereached different conclusions.3,18 Although a meta-analysis study has established high-risk HPVs as asignificant independent risk factor for OSCC,19 it is notclear whether viral infection actually affects survival inoral malignancies. A few studies found that HPV-infected OSCC patients have a better survival thanthose with HPV-negative tumors.20,21 Kozomara etal.,22 however, found a poorer prognosis for OSCCpatients with HPV-infected tumors.
The World Health Organization (WHO) expects aworldwide rise in OSCC incidence in the next fewdecades.23 Almost two-thirds of oral cancers occur indeveloping countries, and this geographic variationprobably reflects the prevalence of specific environ-mental influences (rather than genetically determined orethnic risk factors), particularly tobacco and alcohol insome countries of Europe, betel quid in Melanesia andSouth Central Asia, and solar irradiation in Australiaand New Zealand.5 In Brazil, tobacco and alcohol con-sumption, together with solar irradiation (in lower-lipOSCC cases), are the major risk factors for OSCC.Moreover, the highest OSCC incidence rate in theAmerican continent was registered in the city of SãoPaulo, where a low survival rate for OSCC had beendescribed.24
Actually, the clinical behavior of OSCC is very
difficult to predict using solely conventional clinicaland histopathologic parameters, and it is still not clearwhy some patients do better than others with the samestage and site of disease.25 Therefore, it is clinicallyimportant to identify new prognostic characteristics thatprecisely reflect the biologic behavior of this disease.The objective of the present study was to describe the5-year overall survival (OS) in a specific group ofOSCC patients and to investigate the relationship of 13clinicopathologic parameters (age, gender, primary an-atomic localization, evolution time of tumor, smokingand alcohol intake history, nodal status, tumoral recur-rences, histologic classification, p53 and p63 immuno-expression, treatment, and HPV DNA presence) in theprognosis of OSCC.
MATERIALS AND METHODSPatients and samples
The medical files of over 500 OSCC patients withhead and neck tumors were retrieved from the Depart-ment of Pathology of the Ribeirao Preto School ofMedicine General Hospital, University of Sao Paulo,Brazil, from 1990 to 2002.
Medical files were analyzed and reviewed to collectinformation concerning age, gender, primary anatomiclocalization, evolution time of tumor, smoking andalcohol intake history, nodal status, tumoral recur-rences, histologic classification, treatment, and OS ofthe patients.
After the collection of information from medicalfiles, the criteria used for inclusion into the study wereapplied, including: 1) adequate clinicopathologic data;2) availability of sufficient paraffin-embedded tumormaterial; 3) presence of oral cavity cancer (includingoral tongue, floor of mouth, gingiva, lips, buccal mu-cosa, hard palate, and retromolar trigone; (ICD-10:C00, C02-C06); 4) no previous head and neck cancer;5) no prior oncologic therapy; 6) histologically provensquamous cell carcinoma; 7) a single lesion; and 8)absence of initial or distant metastasis. Patients with insitu and/or T4 tumors were excluded from the study.
Tumoral recurrence was defined as the occurrence ofanother carcinoma �2 cm away from the primary car-cinoma.26 Tumors were classified as well, moderately,or poorly differentiated according to the WHO classi-fication of histologic differentiation grade.27
For statistical analysis, the tobacco and alcohol con-sumption of the patients were dichotomized, and theywere classified as “never consumers” or “current con-sumers.” Former consumers who had quit tobaccoand/or alcohol consumption more than 12 months be-fore diagnosis16 were included in the “never consum-ers” group. Tobacco consumers were those individuals
who daily used a cigarette, pipe, and/or cigar. Alcohol
OOOOEVolume 106, Number 5 Oliveira et al. 687
consumption was considered to be the daily use ofwine, beer, and/or other distilled drinks.
Following the initial biopsy or surgical resection, thetumor tissues were originally fixed in 4% neutral-buff-ered formalin, embedded in paraffin blocks, and ar-chived according to institution protocol. In this study,the selected paraffin-embedded specimens were re-trieved and processed to 5-�m-thick sections, stainedwith hematoxylin-eosin, and reviewed by 2 experi-enced pathologists to confirm the diagnosis and thehistologic classification grade.
Eighty-seven patients and their corresponding paraf-fin-embedded specimens confirmed for primary OSSCwere then selected. A portion of the 5-�m thick sectionof the specimens was then processed for DNA extrac-tion, and the remaining portions (4-�m thick) wereprepared for immunoassaying. To prevent cross-con-tamination, the microtome blade was discarded aftereach block was sectioned, and the sections from theselected specimens were transfered to sterile 1.5 mLtubes with tweezers.
The study protocol was carried out with the approvalof the local Human Research Ethics Committee (pro-cess HC-FMRP 7327/2004).
ImmunohistochemistryImmunostaining was performed on 4-�m-thick sec-
tions serially cut from the tumor-representative areas ofthe selected blocks. The samples were mounted onpoly-L-lysine–coated glass slides and deparaffinized,rehydrated, immersed in 10 mmol/L citrate buffer pH6.0, and submitted to heat-induced epitope retrievalusing a vapor lock for 45 min. The slides were rinsedwith phosphate-buffered saline (PBS) 3 times and in-cubated for 20 min in 0.3% w/v H2O2 in methanol toquench endogenous peroxidase activity. Nonspecificbinding sites were then blocked by incubation for 30min with diluted normal blocking serum, which wasprepared from the animal species in which the second-ary antibody was made (Novostain Super ABC KitUniversal; Novocastra Laboratories, Newcastle uponTyne, U.K.). The excess serum was aspirated, and thesections were immunostained overnight with an incu-bation using either a mouse monoclonal IgG2a anti-p63(4A4, 1:100; Santa Cruz Biotechnology, Palo Alto,CA) or a mouse monoclonal IgG2b anti-p53 (DO-7,1:100; Novocastra Laboratories) as the primary anti-body. During this incubation time, the slides were care-fully protected from light. The sections were washedwith PBS and incubated for 30 min with a dilutedsolution of universal biotinylated secondary antibody.After the sections were washed again with PBS, theywere incubated for 30 min with the Novostain Super
ABC Reagent. This reagent was prepared according tothe manufacturers’ protocols, and it contains AvidinDH and biotinylated horseradish peroxidase H re-agents, which have been shown to form ideal com-plexes for immunoperoxidase staining (Novostain Su-per ABC Kit Universal).28 The slides were washedagain with PBS, and the antibody labeling was devel-oped for about 5 min with 3,3-diaminobenzidine(D5638; Sigma Chemical Co., St. Louis, MO). After awash in tap water for 5 min, the slides were counter-stained with Harris hematoxylin and mounted withEntellan (Merck, Darmstadt, Germany). Normal mu-cous basal cells adjacent to OSCC cells on the mountsand tumor specimens previously shown to stain positivefor p63 and/or p53 were used as positive control sam-ples. Negative control samples were prepared by omis-sion of the primary antibody.
Only nuclear staining of tumor cells was examined,at �100 magnification. p53 and p63 expression wereevaluated and scored based on a previously establishedstaining pattern.29 Only tumors with �10% positivenuclear staining in neoplastic cells were considered tobe positive. The 10% cut-off value for p53 immuno-histochemical staining evaluation was previously foundto separate good prognosis from poor prognosis.30 Ad-ditionally, this cut-off value was chosen because it isnow an accepted threshold for most research in thisfield,25,31 which facilitates comparative analysis withother investigations as well as comparisons among thematched specimens. For similar reasons, 10% was cho-sen as the p63 cut-off value as well.29
DNA isolation and internal control amplification. Theparaffin-embedded specimens with the highest tumoralarea were selected for DNA analysis. DNA was iso-lated from formalin-fixed paraffin-embedded tissuespecimens with a Promega Tissue Kit (MagnesilGenomic Fixed Tissue System; Promega Corporation,Madison, WI) according to the manufacturer’s instruc-tions. The DNA solutions were stored at �20°C.
The DNA integrity and the absence of polymerasechain reaction (PCR) inhibitors were verified by theamplification of a 110-bp fragment of the ubiquitoushuman beta-globin gene32 using primers PC03 (5=-ACACAACTGTGTTCACTAGC-3=) and PC04 (5=-CAACTTCATCCACGTTCACC-3=) (Bioneer, Dae-jeon, Korea).33 Only samples with a visible beta-globinband were included in the study. When a sample wasnegative for beta-globin, an additional section wastaken from the block. DNA was prepared and reana-lyzed by PCR. Successful amplification of the beta-globin gene fragment indicated that the DNA samplewas adequate for HPV DNA analysis.
HPV DNA detection. In this study, we used theGP5�/GP6� (Bioneer) consensus general primer pair
to amplify a 150-bp fragment from the L1 gene of
OOOOE688 Oliveira et al. November 2008
general HPV types (GP5�: 5=-TTTGTTACTGTGG-TAGATACTAC-3=; GP6�: 5=-GAAAAATAAACTG-TAAATCATATTC-3=).34 PCR was then performed onthe HPV-positive DNA samples to determine if theycontained genotypes 16 and 18. This analysis was doneby using specific primers targeting approximately 100bp in the E7 ORF: HPV-16E7.667 (5=-GATGAAATA-GATGGTCCAGC-3=), HPV-16E7.774 (5=-GCTTTG-TACGCACAACCGAAGC-3=), HPV-18E7.696 (5=-AAGAAAACGATGAAATAGATGGA-3=) and HPV-18E7.799 (5=-GGCTTCACACTTACAACACA-3=)(Bioneer).35
Polymerase chain reaction. Amplifications of HPVDNA and beta-globin DNA were performed in thesame reaction tube. Each microtube contained 5 �Lextracted genomic DNA (10 ng/�L), 12.5 �L PCRMaster Mix (Promega Corporation), 1.2 �L each of thePC03 and PC04 primers, 4.3 �L each of the GP5� andGP6� primers, and 2.0 �L sterile water, for a totalvolume of 25 �L. The primers were added to a finalconcentration of 50 �mol/L. To detect the specific HPVsubtypes, a second PCR reaction was performed with 5�L DNA sample, 12.5 �L PCR Master Mix, 2 �L ofeach of the HPV-16E7 primers or each of the HPV-18E7 primers, and 5.5 �L of sterile water.
For both HPV amplification and specific genotypedetection, PCR was performed with 40 amplificationcycles in a thermocycler (PTC-100; MJ Research, Wa-tertown, MA) as follows: 1 cycle with initial denatur-ation at 95°C for 5 min, annealing at 53°C for 2 min,and chain elongation at 72°C for 2 min; then 39 cyclesof denaturation at 94°C for 1 min, annealing at 51°C for2 min, and chain elongation at 72°C for 2 min. A finalextension of 72°C for 10 min followed the last cycle.As a positive control for the HPV-16 and HPV-18 PCRreactions, serial 1:10 dilutions with 5 �L DNA fromSiHa and HeLa (1 ng/�L) culture cells were amplifiedin parallel with sample PCR reactions. In the PCRamplification of HPV DNA used to detect the presenceof HPV, a dilution mixture with both positive controlsamples was used in a specific microtube. Positivecontrol samples always produced amplicons of the cor-rect size. For a negative control, sterile water wasutilized in place of the 5 �L DNA sample. To avoidfalse-positive results, all known precautions to avoid aPCR product carry-over and sample-to-sample contam-ination were rigorously performed. Different steps ofthe PCR procedure were performed in separate roomswith different pipettes. None of the negative controlsamples were positive in any of the HPV assays.
DNA analysis. To characterize the amplified prod-ucts, the samples were analyzed by electrophoresis invertical gels of 8% nondenaturing polyacrylamide.
They were subjected to electrophoretic conditions of200 mA constantly for a 2-h period and were stainedwith AgNO3, according to the method reported byBettini et al.35 A 50-bp DNA ladder (Biotools; B & MLabs, Madrid, Spain) was used as the size marker.
Statistical analysis. Descriptive statistics were usedto summarize the study data. The OS was defined as theinterval between the beginning of the treatment and thedate of death for uncensored observations or the date ofthe last information for censored observations. Univar-iate analyses of the variables were performed using theKaplan-Meier method and log rank test for the analysisof cumulative survival rates.36 Multivariate Cox regres-sion technique was used to build models containing asubset of candidate risk factors with independent prog-nostic properties. The odds ratio (OR) was the measureof association of disease prognostic factors with out-come, calculated using multivariate Cox regression.The OR calculation following the Mantel-Haenszelmethod was used to analyze the influence of differentanatomic localizations on prognosis. Statistical signif-icance was defined as a 2-tailed P value of � .05.
RESULTSThe files of the patients with documented cases of
OSCC were studied to look for risk factors. The ages ofthe patients varied between 46 and 90 years (mean 59years), and the male/female ratio was 5.2:1. Althoughthe majority of the patients had sought medical help inthe first 6 months of their cancer, the average time was13 months. A predominant number of the OSCC pa-tients had reported tobacco and alcohol consumption(64 out of 87; 73.6%). Among the tobacco users (71 outof 87; 81.6%), 6 (8.5%) reported consuming strawcigarettes, 2 (2.8%) reported smoking cigars, and 1(1.4%) reported the habit of chewing tobacco. Themajority of tumors (47 out of 87; 54%) showed a welldifferentiated pattern, especially those tumors locatedin the tongue, which showed keratin-pearl areas interminally differentiated cells. Tongue tumors showedthe highest recurrence rate and death (14 out of 22[63.6%] and 11/22 [50%], respectively), but they alsoshowed a low metastasis index (8 out of 22; 36.4%).Surgical and radiotherapeutic treatment was the pre-dominant choice of treatment for the OSCC patients inthis study (43 out of 87; 49.4%). The demographic andclinical data of the study population are summarized inTable I.
The internal control amplification with beta-globinprimers PC03/PC04 showed amplifiable DNA in all ofthe 87 studied paraffin-embedded specimens. TheHPV-positive control was amplified in all reactions.The general amplification with the HPV L1 (GP5�/GP6�) consensus primer pair showed the presence of
HPV DNA in 17 of the 87 patients (19.5%) in this
ion clas
OOOOEVolume 106, Number 5 Oliveira et al. 689
study. The OSCC patients who tested positive for HPVDNA consisted of 13 males and 4 females (male/femaleratio 3.25:1), but the HPV positivity rate for men waslower than that for women (17.8% vs. 28.6%). Further-more, all of the HPV-positive samples from womenwere located in the tongue, which was the most prev-alent anatomic site for HPV DNA positivity, with 5(29.4%) of the 17 HPV-positive paraffin-embeddedspecimens. The HPV-16 and -18 genotypes were de-tected individually in 4 (23.5%) and 3 (17.6%) speci-mens, respectively. The 2 genotypes were found to-gether in 6 samples (35.3%), and the HPV genotypewas unidentified in 5 of them (29.4%) (Table II).
Of the 87 tumors, positive immunoreactivity for p53
Table 1. Clinical features and overall survival accumuinvestigated variablesVariable Category
Age (yrs) �60�60
Gender malefemale
Anatomic site tongueoral floorhard palatelower lipothers†
Lesion evolution time (months) �3�3 to �6�6 to �9�9
Tobacco consumption yesno
Alcohol consumption yesno
Histologic differentiation‡ wellmoderatelypoorly
Recurrence yesno
Metastasis yesno
HPV DNA presence positivenegative
P53 positivenegative
P63 positivenegative
Treatment surgerysurgery and RTsurgery, RT and CTRTRT and CT
HPV, Human papillomavirus; RT, radiotherapy; CT, chemotherapy.*Log rank test.†Other anatomic sites included buccal mucosa, retromolar trigone, g‡Histologic differentiation according to the World Health Organizat
and p63 was found in 44 (50.6%) and 56 (64.4%)
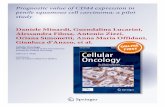
tumors, respectively (Table I). The quantitative labelingindex in specimens varied between 0% and 100% ofnuclei staining, and those tumors with �10% of theirnuclei staining were considered positive for both p53and p63 (Figs. 1 and 2, respectively). This analysis wasperformed in duplicate, and the results of the secondevaluation showed coherence with those of the firstevaluation.
The follow-up period for the patients in this studyranged from 6 to 118 months after the completion oftreatment and was used to determine survival rates. Themedian survival of this cohort was 20 months, and the5-year OS was 28.6% (SE 8.1%). Using Kaplan-Meiersurvival analysis with the log rank test, the patients
87 oral squamous cell carcinoma patients according to
ases, n (%) 5-yr overall survival (%) P value*
54 (62.1) 40.8 .000133 (37.9) 9.173 (83.9) 23.7 .051714 (16.1) 31.522 (25.3) 16.1 .003726 (29.9) 13.517 (19.5) 26.713 (14.9) 39.49 (10.4) 35.5
21 (24.2) 28.7 .855232 (36.8) 25.517 (19.5) 29.417 (19.5) 26.471 (81.6) 26.9 .787316 (18.4) 32.766 (75.9) 22.9 .814221 (24.1) 29.747 (54) 19.7 .298331 (35.6) 25.99 (10.4) 22.1
47 (54) 22.8 .485340 (46) 30.537 (42.5) 22.9 .715250 (57.5) 29.717 (19.5) 28.5 .859070 (80.5) 29.944 (50.6) 13.8 .002343 (49.4) 37.956 (64.4) 28.5 .208031 (35.6) 25.317 (19.5) 24.5 .706443 (49.4) 30.918 (20.7) 21.21 (1.2) —8 (9.2) 22.5
and upper lip.sification.27
late in
C
ingiva,
older than 60 years, as well as those patients whose

nization
OOOOE690 Oliveira et al. November 2008
tumors expressed p53, had a significantly poorer OSthan their respective counterparts (P � .0021; P �.0001; respectively), as shown in Figs. 3 and 4, respec-tively. The oral floor and tongue were the primary sitesfor tumors with the worst OS, and survival of patientswith tumors of distinct anatomic localizations wasshown to be statistically significant (P � .0011), asshown in Fig. 5. The p63-negative tumors also showeda significant association with poor OS in univariate
Table II. HPV infection characteristics obtained in theNo. Age, yrs Gender T
1 60 F2 54 M3 60 M4 61 F5 90 F6 53 M7 53 M8 57 M9 46 M
10 62 M L11 71 M L12 71 F L13 59 M H14 57 M H15 47 M H16 50 M H17 53 M R
HPV, Human papillomavirus; F, Female; M, male; W, well differen*Histologic grade classification according to the World Health Orga
Fig. 1. Immunohistochemical localization of neoplastic cellspositive for p53 in oral squamous cell carcinoma (originalmagnification �400, dark nuclear staining, counterstainedwith Harris hematoxylin).
analysis (P � .0399; Fig. 6), but multivariate survival
analysis by Cox regression could not confirm the sta-tistical significance (P � .2080; Table I).
In the multivariate analysis (Cox regression), age[OR 3.94 (95% confidence interval [CI] 0.37-4.2); P �.0001] and p53 immunoexpression [OR 2.91 (95% CI1.18-7.19); P � .0023] had a significant effect onprognosis. The anatomic localization of the primarytumors also reached prognostic significance (P �.0037), and the Mantel-Haenszel method was used toanalyze this association and found that the pooled ORwas 1.21 (95% CI 0.87-1.44). The multivariate analysis
V-positive patients with oral squamous cell carcinomaite HPV status Differentiation*
HPV-16 positive MPositive for both WPositive for both WHPV-18 positive MHPV-18 positive WHPV-16 positive WPositive for both MHPV unidentified WPositive for both W
ip Positive for both Wip HPV unidentified Wip HPV-16 positive Pate HPV unidentified Mate HPV unidentified Wate Positive for both Wate HPV-18 positive Mlar HPV unidentified P
, moderately differentiated; P, poorly differentiated.criteria.27
Fig. 2. Immunohistochemical localization of neoplastic cellspositive for p63 in oral squamous cell carcinoma (originalmagnification �400, dark nuclear staining, counterstainedwith Harris hematoxylin).
17 HPumor s
TongueTongueTongueTongueTongueFloorFloorFloorFloor
ower lower lower lard palard palard palard paletromo
tiated; M
data are shown in Table I. Because these prognostic

OOOOEVolume 106, Number 5 Oliveira et al. 691
variables were independent, the results of this studysuggest that these prognostic variables can be used toconstruct a predictive model for oral cancer that can beused to guide treatment and predict outcome of OSCCpatients in the future.
DISCUSSIONOnly a few earlier studies have examined several
prognostic factors in a homogeneous OSCC patientgroup. Through the selection criteria applied in thepresent study, we attempted an investigation into theprognostic influence of demographic and clinicopatho-logic factors for a specific group of patients with this
Fig. 3. Kaplan-Meier plots of cumulative survival percentagein overall survival curves according to age of the 87 studiedpatients with oral squamous cell carcinoma.
Fig. 4. Kaplan-Meier plots of cumulative survival percentagein overall survival curves according to p53 immunoexpres-sion in the 87 studied patients with oral squamous cell car-cinoma.
tumor. These criteria included using patients without
multicentric lesions or cancer spread to the lymphnodes; they also included diverse treatment strategies oftumors with different TNM staging. Our findings dem-onstrated that the 5-year OS in this cohort was similarto that reported from other developing countries.4,37
Males are probably more affected by OSCC becauseof their exposure to carcinogenic factors associatedwith this tumor, such as tobacco and alcohol.37 Wefound, however, no prognostic differences betweenmen and women, in agreement with previous re-ports.38,39 The correlation between prognosis and ageseems more controversial, because some investigatorshave seen no association,39,40 whereas others have re-ported a poorer prognosis for older patients.4,41 Inagreement with the analysis by Janot et al.,42 we foundthat the patients aged �60 years had a better prognosis
Fig. 5. Kaplan-Meier plots of cumulative survival percentagein overall survival curves according to OSCC primary ana-tomic localization in the studied patients.
Fig. 6. Kaplan-Meier plots of cumulative survival percentagein overall survival curves according to p63 immunoexpres-sionin the 87 studied patients with oral squamous cell carci-noma.
than the older patients. The lack of a consensus for age

OOOOE692 Oliveira et al. November 2008
standardization in evaluation makes comparison be-tween studies difficult and may explain the controversy.To eliminate this confounding factor, we chose to adoptthe WHO criteria that defines the age of 60 years as thebeginning of the third stage in life in developing coun-tries.43 As reported by Ribeiro et al.,41 we believe thatthe low survival rates in older patients may be related tothe higher occurrence of debilitating illnesses and othercomplications associated with aging in seniors.
The combined use of tobacco smoking and heavyalcohol consumption was associated with a poorerprognosis than seen in previous researches.2,44 Patientswith oral floor tumors had the greatest association withthis synergistic effect, supporting the results of a case-series analysis by Barasch et al..45 In terms of survival,the effects of smoking and drinking independently hadno significant association with outcome. These resultsare in agreement with some earlier investigations,46,47
but in contrast to others,37 leaving the influence ofprevious tobacco and alcohol consumption on survivalas an unresolved question.
Although OSCC can easily be found by patientsthrough a personal oral examination, many patientsignore it. This results in a delay of an official OSCCdiagnosis, an issue that has not received much attention.The mean patient delay varies from 3 to 5 months inoral cancer,48 but the average time found in the presentstudy was 8 months, mainly due to diagnosis delay inthe lower-lip carcinomas. These results are in discor-dance with Kowalski et al.,49 who found that tumors atmore visible sites tend to be diagnosed earlier. In ac-cordance with the results of Wildt et al.,48 however, nostatistical significance was found between the lesionevolution time and the OS of the patients.
The prognosis in OSCC varies considerably accord-ing to the precise primary anatomic site, which affectsthe early appearance of symptoms. Vascular and lym-phatic networks, which vary among the different ana-tomic sites, are one explanation for these differences.Additionally, some anatomic sites are linked withpoorer outcome because they have rich lymphaticdrainage which leads to increased rates of metastasis.23
In the present study, the oral floor and tongue had thehighest rates of metastasis and recurrence, respectively,which is in accordance with an earlier report that indi-cates a tendency for primary tumors located at the oralfloor to drain into the neck lymph nodes.5 In tonguecarcinomas, Kirita et al.50 found a high recurrence rate,where approximately 75% of new cancers emergedwithin 1 year after the treatment of the primary lesion.In the same way, these anatomic sites had significantlypoorer survival curves compared with others. The bestOS was demonstrated in the lower-lip tumors, where,
notwithstanding diagnosis delay, the patients usuallyhave a good prognosis. This is possibly due to the lowregional lymph node metastasis index in this anatomicsite.51 The lower mortality rates and better prognosisfound in lower-lip OSCC were also shown by Leite andKoifman37 in another study with Brazilian patients, andthis was also seen by Beltrami et al.52 The presentstudy, therefore, confirms that patients with intraoraltumors have poorer survival rates than patients withlower-lip tumors.
The original histologic grading system was intro-duced by Broders in the 1920s, and it was subsequentlymodified into its currently system by the WHO.27 Al-though some earlier studies have shown significantcorrelations between lower histologic differentiationand poorer prognosis,38,39 the present findings agreewith the majority of investigations that did not showany association between histologic classification gradeand prognosis. The present results also agree that thereis a predominance of well differentiated tumors.37,40,53
Little is currently known about the specific genedefects associated with OSCC progression, but the p53tumor-suppressor gene is considered to be the mostfrequently altered gene in human cancers.54 The p53immunoexpression percentage found in the presentstudy (50.6%) is very close to that of some earlierreports,25,55 but few investigations have found its pres-ence associated with worse prognosis in OSCC.12,13,25
Looking at the whole group of squamous cell carci-noma of the head and neck, most research has notshown any prognostic association with p53.56,57 Thesediscrepancies might be ascribed to the different ana-tomic sites studied, but they may also be explained bythe small number of patient samples, geographic spec-ificity, antibodies applied, and the arbitrary threshold ofpercentage of immunostained cells used to characterizethe samples as positive. Moreover, the additional hu-man p53 isoforms recently discovered probably con-tribute to the controversial results,58 as was demon-strated in a recent study.59 We, however, would like tohighlight that our results corroborate the results of DeVicente et al.,25 who also evaluated OSCC patientswithout initial lymph node involvement and found thep53 immunoexpression to be a significantly worseprognostic factor.
There are few publications about the immunohisto-chemical prognostic significance of p63 in OSCC. Be-cause of the limited studies on the subject, the exactrole of p63 in OSCC development and progressionremains unexplained. As in earlier studies,30,60 how-ever, we observed that overexpression of p63 occurredin the majority (64.4%) of OSCC samples. In the OSanalysis, the p63 immunoexpression showed significantassociation with better survival in the univariate test but
not in the multivariate test, and it contrasts with the
OOOOEVolume 106, Number 5 Oliveira et al. 693
investigations that reported high p63 immunoexpres-sion associated with a more aggressive phenotype.14,15
Notwithstanding, other studies performed with tumorsfrom different anatomic sites suggested a better prog-nosis for tumors with p63 immunoexpression.61-63 Ac-cording to Foschini et al.,64 these disparities could bedue to the antibody used in the immunohistochemicalanalysis. The only commercially available antibodyrecognizes all of the p63 isoforms, which may havedifferential regulation in oral oncogenesis. Therefore,establishing the exact expression and localization pat-terns of the specific p63 isoforms within tumor oralepithelium is needed in future studies.
Recent molecular and epidemiologic data associatehigh-risk HPV infection with cancers that arise in theoropharynx, including the lingual and palatine tonsilsand base of tongue.65 In the present study, the incidenceof HPV-infected tumors (19.5%) is close to the overallprevalence reported in a systematic review for OSCC(23.5%).17 Studies about the relationship between HPVinfection and patient survival have led to differentconclusions. Although no association with survival wasfound in the present study, a few earlier investigatorsfound that HPV-infected OSCC patients had a bettersurvival rate than those with HPV-negative tu-mors.20,21,65 Some oropharyngeal tumors, however,were included in these reports, and, as previously dem-onstrated, the immunoexpression of wild-type p53 pro-tein in these HPV-positive tumors contrasts with thehigher frequency of p53 mutation in the HPV-negativecases.16,22,65 This fact might suggest responsibility forthe survival benefit that arises in part from enhancedsensitivity to radiation and chemotherapy in the HPV-positive tumors.
Contrary to other investigations,4,37 we did not findan association between treatment modality and survivalrates in the OS curves, but we did find an agreementbetween the predominance of the concomitant surgicaland radiotherapeutic treatments and better prognosis.4
The descriptive characteristics of our oral cancerstudy corroborate previous reports from literature. Not-withstanding, there is no agreement regarding the pri-mary anatomic sites included in studies of OSCC, and,therefore, the data include heterogeneous tumors withdifferent etiologies. The oropharyngeal squamous tu-mors can show different biologic behavior, such as withspecific radiotherapy sensitivity, and other clinical andprognostic characteristics that differ from OSCC. Thecontradictory findings in the scientific literature are inaccordance with the complexity of this tumor hetero-geneity and progression. Therefore, it is unlikely thatonly a single parameter will ever be identified as the
ideal predictive or prognostic marker, and a multipleevaluation of prognostic factors may logically be re-quired to estimate the final outcomes.
The statistical model generated in the present studyhighlights the influence of p53 immunoexpression, age,and primary anatomic localization on OSCC prognosis.This method can, therefore, better predict the outcomeof OSCC patients with this specific subset of clinico-pathologic variables. Biologically guided tumor char-acterization is a fundamental tool for individualizingtreatment for each patient, so further studies that workto predict OSCC prognosis should be a shared goal forcancer researchers.
The authors acknowledge the technical assistance of DeisyMara da Silva, Laura Midori Kawasse, and Marcia AparecidaFerreira Oliva.
REFERENCES1. Lewin F, Norell SE, Johansson H, Gustavsson P, Wennerberg
J, Biörklund A, et al. Smoking tobacco, oral snuff, and alcoholin the etiology of squamous cell carcinoma of the head andneck: a population-based case-referent study in Sweden. Can-cer 1998;82:1367-75.
2. Pytynia KB, Grant JR, Etzel CJ, Roberts DB, Wei Q, SturgisEM. Matched-pair analysis of survival of never smokers and eversmokers with squamous cell carcinoma of the head and neck.J Clin Oncol 2004;22:3981-8.
3. Scully C. Oral cancer; the evidence for sexual transmission. BrDent J 2005;199:203-7.
4. Sargeran K, Murtomaa H, Safavi SM, Vehkalahti MM, TeronenO. Survival after diagnosis of cancer of the oral cavity. Br J OralMaxillofac Surg 2008;46:187-91.
5. Walker DM, Boey G, McDonald LA. The pathology of oralcancer. Pathology 2003;35:376-83.
6. Howaldt HP, Kainz M, Euler B, Vorast H. Proposal for modifi-cation of the TNM staging classification for cancer of the oralcavity. DOSAK. J Craniomaxillofac Surg 1999;27:275-88.
7. Oliver AJ, Helfrick JF, Gard D. Primary oral squamous cellcarcinoma: a review of 92 cases. J Oral Maxillofac Surg1996;54:949-54.
8. Jovanovic A, Kostense PJ, Schulten EA, Snow GB, van der WaalI. Delay in diagnosis of oral squamous cell carcinoma; a reportfrom The Netherlands. Eur J Cancer B Oral Oncol 1992;28B:37-8.
9. Guggenheimer J, Verbin RS, Johnson JT, Horkowitz CA, MyersEN. Factors delaying the diagnosis of oral and oropharyngealcarcinomas. Cancer 1989;64:932-5.
10. Partridge M, Kiguwa S, Emilion G, Pateromichelakis S, A’HernR, Langdon JD. New insights into p53 protein stabilisation inoral squamous cell carcinoma. Oral Oncol 1999;35:45-55.
11. Thurfjell N, Coates PJ, Boldrup L, Lindgren B, Bäcklund B,Uusitalo T, et al. Function and importance of p63 in normal oralmucosa and squamous cell carcinoma of the head and neck. AdvOtorhinolaryngol 2005;62:49-57.
12. Khademi B, Shirazi FM, Vasei M, Doroudchi M, Gandomi B,Modjtahedi H, et al. The expression of p53, c-erbB-1 and c-erbB-2 molecules and their correlation with prognostic markersin patients with head and neck tumors. Cancer Lett 2002;184:223-30.
13. Siegelmann-Danieli N, Ben-Izhack O, Hanlon A, Ridge JA,
Stein ME, Khandelwal V, et al. p53 alteration in oral tongue
OOOOE694 Oliveira et al. November 2008
cancer is not significantly associated with age at diagnosis ortobacco exposure. Tumori 2005;91:346-50.
14. Lo Muzio L, Santarelli A, Caltabiano R, Rubini C, Pieramici T,Trevisiol L, et al. p63 overexpression associates with poor prog-nosis in head and neck squamous cell carcinoma. Hum Pathol2005;36:187-94.
15. Lo Muzio L, Campisi G, Farina A, Rubini C, Pastore L, Gian-none N, et al. Effect of p63 expression on survival in oralsquamous cell carcinoma. Cancer Invest 2007;25:464-9.
16. Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH,Wu L, et al. Evidence for a causal association between humanpapillomavirus and a subset of head and neck cancers. J NatlCancer Inst 2000;92:709-20.
17. Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human pap-illomavirus types in head and neck squamous cell carcinomasworldwide: a systematic review. Cancer Epidemiol BiomarkersPrev 2005;14:467-75.
18. Boy S, Van Rensburg EJ, Engelbrecht S, Dreyer L, van HeerdenM, van Heerden W. HPV detection in primary intra-oral squa-mous cell carcinomas—commensal, aetiological agent or con-tamination? J Oral Pathol Med 2006;35:86-90.
19. Miller CS, Johnstone BM. Human papillomavirus as a risk factorfor oral squamous cell carcinoma: a meta-analysis, 1982–1997.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:622-35.
20. Schwartz SR, Yueh B, McDougall JK, Daling JR, Schwartz SM.Human papillomavirus infection and survival in oral squamouscell cancer: a population-based study. Otolaryngol Head NeckSurg 2001;125:1-9.
21. Ritchie JM, Smith EM, Summersgill KF, Hoffman HT, Wang D,Klussmann JP, et al. Human papillomavirus infection as a prog-nostic factor in carcinomas of the oral cavity and oropharynx. IntJ Cancer 2003;104:336-44.
22. Kozomara R, Joviæ N, Magiæ Z, Brankoviæ-Magiæ M, MiniæV. p53 mutations and human papillomavirus infection in oralsquamous cell carcinomas: correlation with overall survival. JCraniomaxillofac Surg 2005;33:342-8.
23. Massano J, Regateiro FS, Januário G, Ferreira A. Oral squamouscell carcinoma: review of prognostic and predictive factors. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2006;102:67-76.
24. Wünsch-Filho V. The epidemiology of oral and pharynx cancerin Brazil. Oral Oncol 2002;38:737-46.
25. De Vicente JC, Junqueira LM, Zapatero AH, Forcelledo MF,Hernández-Vallejo G, Arranz JS. Prognostic significance of p53expression in oral squamous cell carcinoma without neck nodemetastases. Head Neck 2004;26:22-30.
26. Braakhuis BJM, Tabor MP, Leemans R, van der Waal I, SnowGB, Brakenhoff RH. Second primary tumors and field cancer-ization in oral and oropharyngeal cancer: molecular techniquesprovide new insights and definitions. Head Neck 2002;24:206-8.
27. Pindborg JJ, Reichart PA, Smith CJ, van der Waal I, WorldHealth Organization. International histological classification oftumors: histological typing of cancer and precancer of the oralmucosa. 2nd ed. Berlin/Heidleberg: Springer; 1997. p. 1-40.
28. Ribeiro-Silva A, Ramalho LNZ, Garcia SB, Brandao DF,Chahud F, Zucoloto S. p63 correlates with both BRCA1 andcytokeratin 5 in invasive breast carcinomas: further evidence forthe pathogenesis of the basal phenotype of breast cancer. Histo-pathology 2005;47:458-66.
29. Oliveira LR, Ribeiro-Silva A, Zucoloto S. Prognostic signifi-cance of p53 and p63 immunolocalisation in primary andmatched lymph node metastasis in oral squamous cell carcinoma.Acta Histochem 2007;109:388-96.
30. Hasebe T, Mukai K, Yamaguchi N, Ishihara K, Kaneko A,
Takasaki Y, et al. Prognostic value of immunohistochemicalstaining for proliferating cell nuclear antigen, p53, and c-erbB-2in sebaceous gland carcinoma and sweat gland carcinoma:comparison with histopathological parameter. Mod Pathol 1994;7:37-43.
31. Choi HR, Batsakis JG, Zhan F, Sturgis E, Luna MA, El-NaggarAK. Differential expression of p53 gene family members p63and p73 in head and neck squamous tumorigenesis. Hum Pathol2002;33:158-64.
32. Chehab FF, Doherty M, Cai SP, Kan YW, Cooper S, Rubin EM.Detection of sickle cell anaemia and thalassaemias. Nature1987;329:293-4.
33. Saiki RK, Bugawan TL, Horn GT, Mullis KB, Erlich HA.Analysis of enzymatically amplified beta-globin and HLA-DQalpha DNA with allele-specific oligonucleotide probes. Nature1986;324:163-6.
34. de Roda Husman AM, Walboomers JM, van den Brule AJ,Meijer CJ, Snijders PJ. The use of general primers GP5 and GP6elongated at their 3= ends with adjacent highly conserved se-quences improves human papillomavirus detection by PCR.J Gen Virol 1995;76:1057-62.
35. Bettini JS, Soares E.G., Duarte G, Simoes RT, Simoes AL. PCRdiagnosis of HPV in cervical biopsies of CIN and invasiveneoplasia formerly diagnosed as HPV negative. Acta Cytol2003;47:545-9.
36. Kaplan EL, Meier P. Nonparametric estimation from incompleteobservations. J Am Stat Assoc 1958;53:457-481.
37. Leite ICG, Koifman S. Survival analysis in a sample of oralcancer patients at a reference hospital in Rio de Janeiro, Brazil.Oral Oncol 1998;34:347-52.
38. Nguyen TV, Yueh B. Weight loss predicts mortality after recur-rent oral cavity and oropharyngeal carcinomas. Cancer2002;95:553-62.
39. Lo W-L, Kao S-Y, Chi L-Y, Wong Y-K, Chang RC-S. Outcomesof oral squamous cell carcinoma in Taiwan after surgical ther-apy: factors affecting survival. J Oral Maxillofac Surg 2003;61:751-8.
40. Al-Rajhi N, Khafaga Y, El-Husseiny J, Saleem M, Mourad W,Al-Otieschan A, et al. Early stage carcinoma of oral tongue:prognostic factors for local control and survival. Oral Oncol2000;36:508-14.
41. Ribeiro KCB, Kowalski LP, Latorre MRDO. Perioperative com-plications, comorbidities, and survival in oral or oropharyngealcancer. Arch Otolaryngol Head Neck Surg 2003;129:219-28.
42. Janot F, Klijanienko J, Russo A, Mamet JP, de Braud F, El-Naggar AK, et al. Prognostic value of clinicopathological param-eters in head and neck squamous cell carcinoma: a prospectiveanalysis. Br J Cancer 1996;73:531-8.
43. Sarini J, Fournier C, Lefebvre JL, Bonafos G, Van JT, Coche-Dequéant B. Head and neck squamous cell carcinoma in elderlypatients. Arch Otolaryngol Head Neck Surg 2001;9:1089-92.
44. Gervasio OL, Dutra RA, Tartaglia SM, Vasconcellos WA, Bar-bosa AA, Aguiar MC. Oral squamous cell carcinoma: a retro-spective study of 740 cases in a Brazilian population. Braz DentJ 2001;12:57-61.
45. Barasch A, Morse DE, Krutchkoff DJ, Eisenberg E. Smoking,gender, and age as risk factors for site-specific intraoral squa-mous cell carcinoma. A case-series analysis. Cancer 1994;73:509-13.
46. Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS,Preston-Martin S, et al. Smoking and drinking in relation to oraland pharyngeal cancer. Cancer Res 1988;48:3282-7.
47. Vallecillo Capilla M, Romero Olid MN, Olmedo Gaya MV,Reyes Botella C, Bustos Ruiz V. Factors related to survival fromoral cancer in an Andalusian population sample (Spain). Med
Oral Patol Oral Cir Bucal 2007;12:E518-23.
OOOOEVolume 106, Number 5 Oliveira et al. 695
48. Wildt J, Bundgaard T, Bentzen SM. Delay in the diagnosis oforal squamous cell carcinoma. Clin Otolaryngol Allied Sci1995;20:21-5.
49. Kowalski LP, Franco EL, Torloni H, Fava AS, de AndradeSobrinho J, Ramos G, et al. Lateness of diagnosis of oral andoropharyngeal carcinoma: factors related to the tumour, the pa-tient and health professionals. Eur J Cancer B Oral Oncol1994;30B:167-73.
50. Kirita T, Okabe S, Izumo T, Sugimura M. Risk factors for thepostoperative local recurrence of tongue carcinoma. J Oral Max-illofac Surg 1994;52:149-54.
51. Gooris PJ, Vermey A, de Visscher JG, Burlage FR, RoodenburgJL. Supraomohyoid neck dissection in the management of cer-vical lymph node metastases of squamous cell carcinoma of thelower lip. Head Neck 2002;24:678-83.
52. Beltrami CA, Desinan L, Rubini C. Prognostic factors in squa-mous cell carcinoma of the oral cavity. A retrospective study of80 cases. Pathol Res Pract 1992;188:510-6.
53. O-charoenrat P, Pillai G, Patel S, Ficher C, Archer D, Eccles S,et al. Tumor thickness predicts cervical nodal metastases andsurvival in early oral tongue cancer. Oral Oncol 2003;39:386-90.
54. Levine AJ. p53, the cellular gatekeeper for growth and division.Cell 1997;88:323-31.
55. Famulski W, Sulkowska M, Miller-Famulska D, Terlikowski S,Guziñska-Ustymowicz K, Sulkowski S. p53 protein expressionin oral squamous cell cancer in relation to some of its clinico-pathological variables. Folia Histochem Cytobiol 2002;40:203-4.
56. Gonzalez-Moles MA, Galindo P, Gutierrez-Fernandez J,Sanchez-Fernandez E, Rodriguez-Archilla A, Ruiz-Avila I, et al.p53 protein expression in oral squamous cell carcinoma. survivalanalysis. Anticancer Res 2001;21(4B):2889-94.
57. Vora HH, Shah NG, Patel DD, Trivedi TI, Chikhlikar PR.Prognostic significance of biomarkers in squamous cell carci-noma of the tongue: multivariate analysis. J Surg Oncol2003;82:34-50.
58. Bourdon JC, Fernandes K, Murray-Zmijewski F, Liu G, Diot A,
Xirodimas DP, et al. p53 isoforms can regulate p53transcriptional activity. Genes Dev 2005;19:2122-37.
59. Boldrup L, Bourdon JC, Coates PJ, Sjöström B, Nylander K.Expression of p53 isoforms in squamous cell carcinoma of thehead and neck. Eur J Cancer 2007;43:617-23.
60. Nylander K, Dabelsteen E, Hall PA. The p53 molecule and itsprognostic role in squamous cell carcinomas of the head andneck. J Oral Pathol Med 2000;29:413-25.
61. Koga F, Kawakami S, Fujii Y, Saito K, Ohtsuka Y, Iwai A, et al.Impaired p63 expression associates with poor prognosis anduroplakin III expression in invasive urothelial carcinoma of thebladder. Clin Cancer Res 2003;9:5501-7.
62. Massion PP, Taflan PM, Jamshedur Rahman SM, Yildiz P, ShyrY, Edgerton ME, et al. Significance of p63 amplification andoverexpression in lung cancer development and prognosis. Can-cer Res 2003;63:7113-21.
63. Takahashi Y, Noguchi T, Takeno S, Kimura Y, Okubo M,Kawahara K. Reduced expression of p63 has prognostic impli-cations for patients with esophageal squamous cell carcinoma.Oncol Rep 2006;15:323-8.
64. Foschini MP, Gaiba A, Cocchi R, Pennesi MG, Gatto MR,Frezza GP, et al. Pattern of p63 expression in squamous cellcarcinoma of the oral cavity. Virchows Arch 2004;444:332-9.
65. Gillison ML. Human papillomavirus-associated head and neckcancer is a distinct epidemiologic, clinical, and molecular entity.Semin Oncol 2004;31:744-54.
Reprint requests:
Lucinei Roberto OliveiraDepartment of PathologyRibeirao Preto Medical SchoolUniversity of São PauloAv. Bandeirantes 390014049-900 Ribeirao Preto—SPBrazil
[email protected]Copyright © 2022 FDOKUMEN




















