
Preventing Risk for Obesity by Promoting Self-Regulation and Decision-Making Skills: Pilot Results...
16
PROGRAMME PAPER Translating evidence based violence and drug use prevention to obesity prevention: development and construction of the Pathways program Kari-Lyn K. Sakuma 1 *, Nathaniel R. Riggs 2 and Mary Ann Pentz 2 1 Prevention Research Center, College of Health and Human Development, The Pennsylvania State University, 402 Marion Place, University Park, PA 16802, USA and 2 Institute for Prevention Research, Department of Preventive Medicine, University of Southern California, 2001 N. Soto Street, MC 9239, Los Angeles, CA 90089 USA. *Correspondence to: K. K. Sakuma. E-mail: [email protected] Received on December 2, 2010; accepted on September 1, 2011 Abstract Effective school-based obesity prevention pro- grams are needed to prevent and reduce the grow- ing obesity risk among youth. Utilizing the evidence-rich areas of violence and substance use prevention, translation science may provide an ef- ficient means for developing curricula across mul- tiple health behaviors. This paper introduces Pathways to Health, a school-based obesity preven- tion program that was developed by translating from evidence-based violence and drug use preven- tion programs, Promoting Alternative THinking Strategies and the Midwestern Prevention Project STAR (STAR). We illustrate how a hypothesized underlying behavior change mechanism in two domains of risk behavior, violence and substance use, can be applied to obesity prevention. A 4-step translational process is provided and may be rele- vant for use in developing other curricula to ad- dress multiple health risk behaviors. Practical application and decision points are also provided. Introduction Obesity prevention programs are clearly warranted with over a third of US youth aged 2 through 19 years at or above the 85th percentile of body mass index (BMI) for age [1]. School-based prevention programs that target individual psychological mechanisms and social and familial processes are needed as part of an overall comprehensive approach toward reducing obesity and obesity risk among youth. Studies on school-based violence and substance abuse preven- tion have shown success in reducing their respective risk behaviors [2–8] and may serve as models in designing programs for reducing obesity risk. These different outcomes share common contributors, which suggest translation of content across health behaviors. The primary aim of the Pathways to Health (Path- ways) study was to utilize existing evidence-based programs and translate the scientific rigor and theo- retical constructs to other health behaviors in children, specifically those with application to obesity preven- tion. There are a number of evidence-based programs in both the violence prevention and drug prevention fields with rich theoretical and empirical findings to draw from in translating for obesity prevention. Fur- thermore, there is a large body of implementation re- search to build upon within those fields to help design a maximally effective school-based program. Build- ing upon the successes of these evidence-based pro- grams would potentially allow for efficiency in the design of new programs targeting different health behavior outcomes. Pathways began with a hypothesis that dysregu- lated behavior could be an underlying mechanism contributing to the obesity epidemic. Inhibitory control, emotional control, planning and organiza- HEALTH EDUCATION RESEARCH Pages 16 Ó The Author 2011. Published by Oxford University Press. All rights reserved. For permissions, please email: [email protected] doi:10.1093/her/cyr095 Health Education Research Advance Access published October 10, 2011 by guest on October 11, 2011 her.oxfordjournals.org Downloaded from
Transcript of Preventing Risk for Obesity by Promoting Self-Regulation and Decision-Making Skills: Pilot Results...

PROGRAMME PAPER
Translating evidence based violence and drug useprevention to obesity prevention: development and
construction of the Pathways program
Kari-Lyn K. Sakuma1*, Nathaniel R. Riggs2 and Mary Ann Pentz2
1Prevention Research Center, College of Health and Human Development, The Pennsylvania State University, 402 Marion
Place, University Park, PA 16802, USA and 2Institute for Prevention Research, Department of PreventiveMedicine, University
of Southern California, 2001 N. Soto Street, MC 9239, Los Angeles, CA 90089 USA.
*Correspondence to: K. K. Sakuma. E-mail: [email protected]
Received on December 2, 2010; accepted on September 1, 2011
Abstract
Effective school-based obesity prevention pro-grams are needed to prevent and reduce the grow-ing obesity risk among youth. Utilizing theevidence-rich areas of violence and substance useprevention, translation science may provide an ef-ficient means for developing curricula across mul-tiple health behaviors. This paper introducesPathways toHealth, a school-based obesity preven-tion program that was developed by translatingfromevidence-based violence anddrug use preven-tion programs, Promoting Alternative THinkingStrategies and the Midwestern Prevention ProjectSTAR (STAR). We illustrate how a hypothesizedunderlying behavior change mechanism in twodomains of risk behavior, violence and substanceuse, can be applied to obesity prevention. A 4-steptranslational process is provided and may be rele-vant for use in developing other curricula to ad-dress multiple health risk behaviors. Practicalapplication and decision points are also provided.
Introduction
Obesity prevention programs are clearly warranted
with over a third of US youth aged 2 through 19 years
at or above the 85th percentile of body mass index
(BMI) for age [1]. School-based prevention programs
that target individual psychological mechanisms and
social and familial processes are needed as part of an
overall comprehensive approach toward reducing
obesity and obesity risk among youth. Studies on
school-based violence and substance abuse preven-
tion have shown success in reducing their respective
risk behaviors [2–8] and may serve as models in
designing programs for reducing obesity risk. These
different outcomes share common contributors,
which suggest translation of content across health
behaviors.
The primary aim of the Pathways to Health (Path-
ways) study was to utilize existing evidence-based
programs and translate the scientific rigor and theo-
retical constructs to other health behaviors in children,
specifically those with application to obesity preven-
tion. There are a number of evidence-based programs
in both the violence prevention and drug prevention
fields with rich theoretical and empirical findings to
draw from in translating for obesity prevention. Fur-
thermore, there is a large body of implementation re-
search to build upon within those fields to help design
a maximally effective school-based program. Build-
ing upon the successes of these evidence-based pro-
grams would potentially allow for efficiency in the
design of new programs targeting different health
behavior outcomes.
Pathways began with a hypothesis that dysregu-
lated behavior could be an underlying mechanism
contributing to the obesity epidemic. Inhibitory
control, emotional control, planning and organiza-
HEALTH EDUCATION RESEARCH
Pages 16
� The Author 2011. Published by Oxford University Press. All rights reserved.For permissions, please email: [email protected]
doi:10.1093/her/cyr095
Health Education Research Advance Access published October 10, 2011 by guest on O
ctober 11, 2011her.oxfordjournals.org
Dow
nloaded from
tion and working memory are skills subsumed un-
der the term executive cognitive function (ECF) and
are necessary for regulating behaviors and decision
making in order to achieve goals [9, 10]. Prior re-
search suggests that self-regulation and decision
making as it relates to food consumption and phys-
ical (in)activity are important modifiable risk factors
for childhood obesity [11–15]. Low ECF has also
been directly linked to obese and overweight BMI
in adults [16–18] and youth [15, 19–22]. More spe-
cifically, individual ECF sub-skills may be asso-
ciated with the regulation of food intake. Inhibitory
control may allow an individual to inhibit
food-related thoughts and behaviors within an
environment or situation filled with cues for (over)-
consumption of snack foods [15, 20, 23]. Emotional
control may allow an individual to cognitively man-
age strong affect and behavioral impulses. Evidence
suggests that negative affective states have been
shown to increase food intake [24, 25].
ECF may also play a different role in consump-
tion depending on food type [26]. Among school-
aged children, ECF was found to have a negative
correlation with snack food intake [27]. There is
also evidence that suggests that highly palatable
snack foods may be extremely rewarding for chil-
dren and may activate reward circuitry making it
particularly difficult for some children to control,
similar to those produced by some drugs [22, 28,
29]. In comparison to snack foods, the lower palat-
ability and lower availability of vegetables and
fruits may require more goal-oriented problem-
solving skills to increase vegetable and fruit
consumption for healthful reasons.
ECF may also be directly related to physical activity
and sedentary behavior in similar ways to fruit and
vegetable intake. For a child, it may take organization
and future planning to be physically active, especially
if the environment is not conducive to unstructured
physical activity (e.g. access to playground, safe side-
walks and neighborhoods). Furthermore, for some
children, sedentary behaviors such as watching tele-
vision or playing video games may be their activity of
choice. It may take considerable cognitive effort
to inhibit these unhealthy behaviors and plan for
healthier physical activity.
ECF may be a common contributor to multiple
health behaviors. Eating and physical activity patterns,
at its surface, appear to be very different from violence
and drug use patterns in youth. However, considering
that each of these behaviors may occur due to a dysre-
gulation of emotion and poor ECF, then the behavior
patterns begin to overlap [30–33]. Drugs and highly
palatable foods both activate a common reward
circuitry in the brain, circuitry which can become
dysregulated resulting in uninhibited appetitive
behaviors such as excessive food intake and drug
use [22]. Some types of violence, such as aggressive
and externalizing problem behaviors, may also be
viewed as the outcome of poor or dysregulated emo-
tion and impulsive behavior [34–37].
Pathways sought to capitalize on the prior work
in the fields of drug use prevention and violence
prevention and apply the concepts to obesity preven-
tion. Promoting Alternative THinking Strategies
(PATHS) is an internationally recognized evidence-
based blueprints model program and Substance Abuse
and Mental Health Administration (SAMHSA)
endorsed violence prevention program for youth [4,
6, 38–41]. PATHS was chosen as the base curriculum
model due to its underlying neurocognitive theoretical
model that addressed emotional regulation, impulse
control and ECF in children [6, 39, 41]. PATHS
targets the prevention of violence by addressing un-
derlying risk factors that arise from poor social and
emotional competence. PATHS was based on the
principles of emotion theory [42, 43] but more specif-
ically the Affective–Behavioral–Cognitive–Dynamic
(ABCD) model of development [4, 39]. The ABCD
model places primary importance on the developmen-
tal integration of affect, behavior, cognition and
emotion language.
Pathways also identified STAR, a nationally rec-
ognized evidence-based blueprints and SAMHSA
model drug prevention program [2, 44–46]. STAR’s
successes as a drug use prevention program were
attributable to several key components, including
the use of standardized teacher training for program
delivery, use of active social learning methods for
program delivery, targeted skills training and inter-
active homework activities with parents who com-
plement in-school program skills training [46]. In
K. K. Sakuma et al.
2 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

addition, the STAR parent component that involved
homework activities (e.g. rule-setting for health be-
havior, encouragement of family-based activities)
and parental skills training (i.e. parent–child commu-
nication and parental modeling) was used as a model
for the new Pathways parent night curriculum.
STAR was based on the Integrative Transactional
Theory (ITT), which posits that individual, social, sit-
uational and environmental factors interact to influ-
ence child behavior [44]. ITT incorporates social
learning and social cognitive factors of peer and parent
modeling, practice, self-efficacy and reinforcement;
social support and social norms for non-use and
broader environmental factors of policy change and
media influences. A number of STAR constructs were
applicable to Pathways, including resistance skills in
response to peer pressure, self-efficacy, counteracting
perceived social norms, healthy decision making
based on perceived consequences of behavior and
lessons involving parents (prevention communication,
rule setting, leisure and family physical activity).
The aim of this paper is to present a framework
for developing Pathways and illustrate the steps
we used to translate from the PATHS and STAR
programs to an obesity prevention program while
providing practical examples and methods for de-
signing a school-based curriculum for youth in the
fourth through sixth grades.
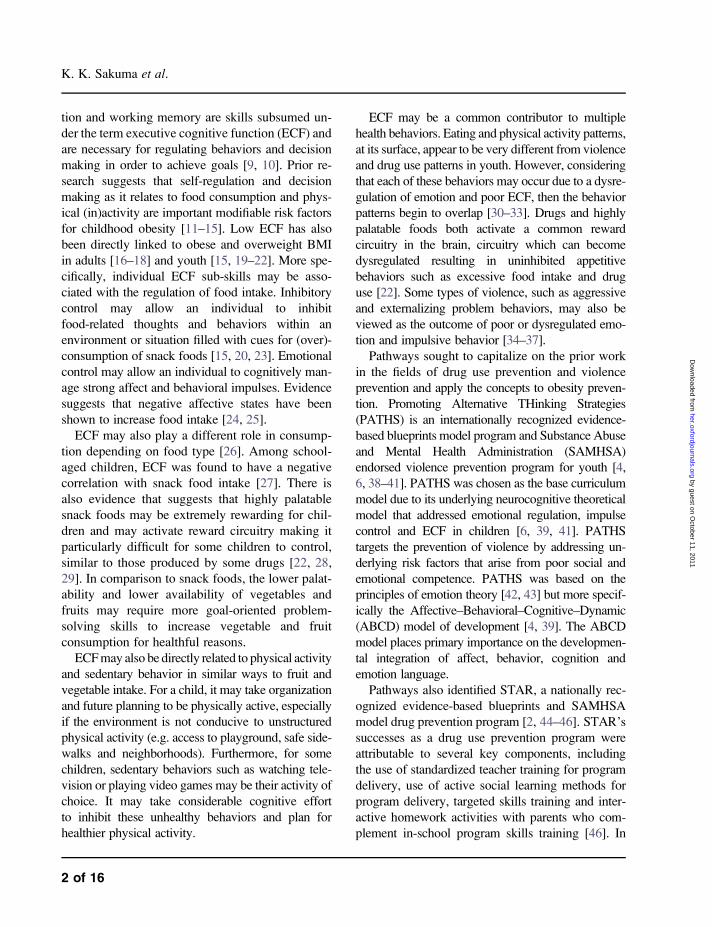
Translation steps
The translation and development model presented
here is based upon a well-established curriculum
development process that builds curriculum activi-
ties from information provided in the literature and
takes it through formative evaluations and formal
randomized controlled trials [47]. Pathways fol-
lowed this general process for building a curriculum
but special attention was given to applying ECF
constructs to obesity prevention using established
intervention trials in violence and substance use
fields and the associated literature base. The trans-
lation model consists of (i) conceptual mapping, (ii)
model building and refinement, (iii) pilot studies
and (iv) efficacy study (see Fig. 1).
Step 1: conceptual mapping
Pathways began with a theory-driven preconception
that dysregulation of affect or impulse control was an
important underlying risk factor for youth violence,
drug use and obesity in our target population [41,
48–51]. Thus, executive control, emotion regulation
and problem-solving skills were identified as potential
mediators to target [40, 48, 52]. Step 1 begins with
the first phase of conceptual mapping which uses
a theory-driven process to identify potential mediators.
The second phase of conceptual mapping was to
search for programs that addressed dysregulation and
operationalized the constructs in ways similar to how
Pathways aimed to address the constructs and target
the mediators. Evidence-based violence prevention
and drug use prevention programs were identified
and evaluated whether the programs had the same
hypothesized theoretical underpinnings and targeted
similar mechanism of behavior change.
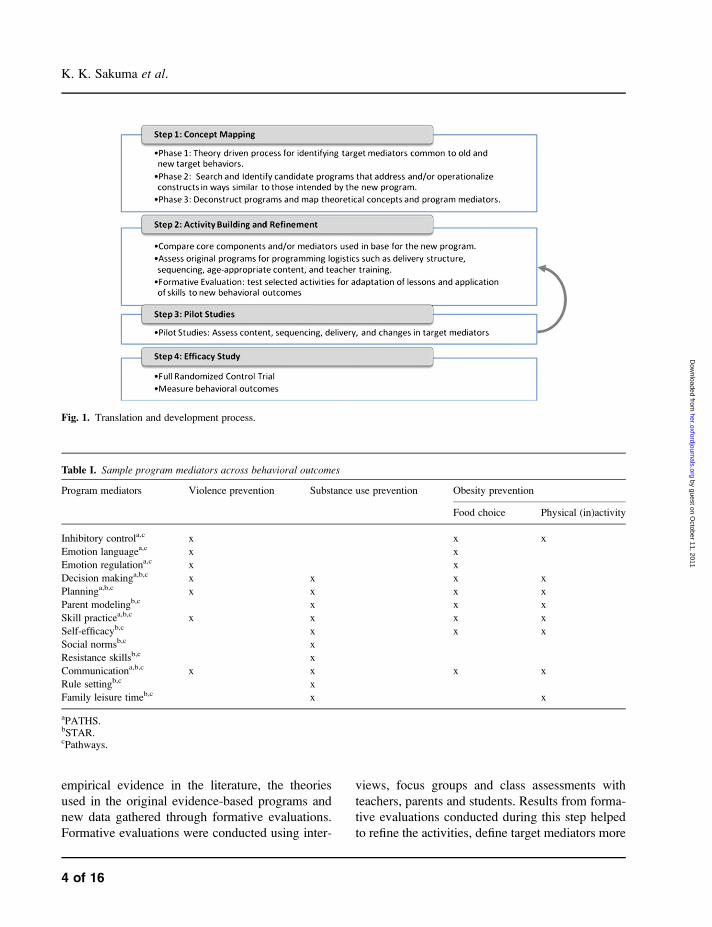
Once PATHS and STAR were identified as can-
didate programs, the third phase of conceptual map-
ping was to deconstruct the programs and map the
theoretical concepts together to view any overlap-
ping constructs between the two programs and
search the literature for the new obesity-related
target risk factors (see Table I).
Understanding the underlying theoretical foun-
dation of each respective program was imperative
prior to developing the curriculum lessons. More
information on the principles underlying PATHS
and STAR programs for the integration between
the original programs and the new obesity preven-
tion curriculum was needed in order to address and
test the proposed hypotheses. Thus, a literature re-
view was done in the following areas: PATHS and
STAR outcomes, mediation analyses and theories;
Emotional intelligence, social and emotional com-
petence, neurocognitive circuitry of emotional/so-
cial development, ECF and impulse control and
obesity prevention constructs, methods and theories
for application in children.
Step 2: activity building and refinement
The purpose of Step 2 in the translational process
was to carefully construct lessons in light of the
Pathways obesity prevention program
3 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from
empirical evidence in the literature, the theories
used in the original evidence-based programs and
new data gathered through formative evaluations.
Formative evaluations were conducted using inter-
views, focus groups and class assessments with
teachers, parents and students. Results from forma-
tive evaluations conducted during this step helped
to refine the activities, define target mediators more
Table I. Sample program mediators across behavioral outcomes
Program mediators Violence prevention Substance use prevention Obesity prevention
Food choice Physical (in)activity
Inhibitory controla,c x x x
Emotion languagea,c x x
Emotion regulationa,c x x
Decision makinga,b,c x x x x
Planninga,b,c x x x x
Parent modelingb,c x x x
Skill practicea,b,c x x x x
Self-efficacyb,c x x x
Social normsb,c x
Resistance skillsb,c x
Communicationa,b,c x x x x
Rule settingb,c x
Family leisure timeb,c x x
aPATHS.bSTAR.cPathways.
Fig. 1. Translation and development process.
K. K. Sakuma et al.
4 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

precisely and direct development of the overall cur-
riculum. Step 2 also includes assessment of the
original programs for programing logistics such as
delivery structure, sequencing, age-appropriate con-
tent and teacher training.
The Pathways program underwent two phases of
development prior to formal pilot testing of the full
curriculum [50]. The first phase consisted of iden-
tifying core components from the PATHS curricu-
lum and modifying to target attitudes toward food
intake and physical activity for fifth graders. Five
representative lessons focusing on self-control, emo-
tional language, communication and problem-
solving were chosen for evaluation. Each component
had a tool to help convey the lesson to the children.
For example, self-control used a Control Signals
Poster (CSP) which looked like a stop light. In
PATHS, children are taught to imagine the CSP
when they have a really strong emotion so they
can stop before they act, think about the situation
and say how they feel and why. In keeping with the
translational process, this tool was used in Pathways
as it was presented in PATHS. However, situations in
which a child would apply this tool in Pathways were
expanded to include where affect may not be strong,
such as boredom and mindless or repetitive actions
like watching television for an hour or consuming an
entire bag of chips. The CSP was a strong visual cue
so children were able to remember the concept readily
within the classroom. Generalizability to other situa-
tions and contexts was also critical. Therefore, study
personnel developed products such as mini posters,
magnets and stickers and tested it for appeal, cost
and use outside of the classroom. Furthermore,
teachers were queried if they felt comfortable with
the material, found the concepts easy to teach with
minimal or no training and whether or not they
would endorse and support the concepts outside of
those lessons. The information gathered from teach-
ers and students drove the second iteration of the
activity development and a second phase and forma-
tive evaluation was completed (See Table II).
The Pathways study needed a structured curricu-
lum that was standardized in number of class
sessions and length of delivery to more readily assess
teacher fidelity and provide a minimum level of
programing to evaluate students. Curriculum special-
ists and teachers in the school districts who were
involved at the start of the study requested that the
lessons be provided as packages and training be pro-
vided to teachers on delivering the content. Most
conveyed the need for the lessons to be set as a mod-
ule to be able to quickly integrate within the teachers’
limited schedules. Given the goals of Pathways study
and requests from our school partners, restructuring
of the PATHS lessons in content and number was
necessary and was done based on existing theory and
research. PATHS core theoretical constructs were
included in the current Pathways program (i.e.
emotion, impulse control and problem solving), but
they were used specifically as they relate to making
healthy choices on diet and physical activity. There
were three initial decisions that needed to be made
prior to lesson planning:
Standardization of lessons
PATHS was designed to be delivered by elementary
classroom teachers in grades K-6. Typically, these
lessons would be taught three times a week for a min-
imum of 20–30 min per day for a total of 131 les-
sons. Grade-specific lessons were also developed for
Grades 3–5 that focused on developmentally appro-
priate interpersonal cognitive problem-solving skills.
The Grade 3 curriculum was chosen to be the foun-
dation for the Pathways program in order to capital-
ize on the fundamental concepts presented at that
level. This set of 46 lessons consisted of 10 dedicated
to getting started, 16 feelings and relationship
lessons, 17 cognitive problem-solving lessons and
3 relationships and social competence lessons.
In PATHS, lessons were designed for flexibility
in delivery. PATHS has a specific developmental
order in which to present the lessons but teachers
were able to decide which lessons they would like
to teach at any given point during the day or
throughout the week and infuse them within other
standard curriculum (e.g. math, social studies). Les-
sons varied in the amount of delivery time (i.e. 5–30
min) and contained different stop points allowing
teachers to stop a lesson if they run out of time or
chose to continue on a different day. In contrast,
Pathways lessons were standardized to be a 30- to
Pathways obesity prevention program
5 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

Table II. PATHS lessons with application to obesity
Title Focus Application to obesity Translational step
Grade 4
1 Class rules Peer relationships Step 2: formative evaluation 1
2 PATHS kid Peer relationships Step 2: formative evaluation 1
3 CSP Self-control Impulsive eating Step 2: formative evaluation 1, 2
4 Introduction to feelings Affective understanding Emotions and eating Step 3: pilot
5 Recognizing and controlling feelings Self-control Impulsive eating Step 2: formative evaluation 1, 2
6 Feelings dictionary Affective understanding Emotions and activity Step 2: formative evaluation 1, 2
7 Feelings intensity Self-control Impulsive eating Step 2: formative evaluation 1, 2
8 Making good decisions 1 Self-control resisting peer pressure Peers and food choices Step 3: pilot
9 Making good decisions 2 Decision-making skills thinking ahead Problem-solving skills,
eating and activity
Step 3: pilot
10 Problem identification 1 Emotions associated with identifying
problems
Emotions and identifying
health food/activity
Step 2: formative evaluation 2
11 Problem identification 2 Self-regulation while
identifying problems
Regulating intake and
identifying food
Step 2: formative evaluation 1, 2
12 Setting positive goals Goal-directed behavior Health goals Step 2: formative evaluation 1, 2
13 Reaching our goals Goal-directed behavior Health goals Step 3: pilot
14 Generating solutions Solution generation Problem-solving/activity Step 2: formative evaluation 2
15 Thinking takes time Self-regulation solution generation Regulating intake and problem
solving/food
Step 3: pilot
Grade 5
16 PATHS jeopardy review Positive peer relationships Peers and food choice Step 3: pilot
17 Feelings review Positive peer relationships Peers and activity choice Step 3: pilot
18 CSP review Self-control Impulsive eating Step 3: pilot
19 Managing our feelings Emotional control Emotion, impulse and food/activity Step 3: pilot
20 Making good decisions Decision-making skills Problem solving and food Step 3: pilot
21 Identifying Problems, feelings, goals and
solutions
Problem-solving skills Problem-solving and food activity Step 3: pilot
22 Consequences: what might happen next Evaluation of consequences Consequences of food/activity Step 2: formative evaluation 2
23 Trying out your plan refusal skills Plan initiation/refusal skills Health plans for food/activity Step 2: formative evaluation 2
24 Making a good plan Planning and sequencing Plans for food/activities Step 3: pilot
25 Trying again: obstacles Persistence/evaluation Evaluate healthy plans Step 3: pilot
Grade 6
26 Problem-solving review Social competence Problem solving and food Step 3: pilot
27 Making a good decisions Social competence Healthy decisions Step 3: pilot
28 Getting help from others Social competence Peers and food/activity Step 3: pilot
29 Conflict resolution styles Social competence Conflict and food/activity Step 3: pilot
30 Resolving conflict Social competence Conflict and food/activity Step 3: pilot
K.
K.
Sak
um
aet
al.
6of16
by guest on October 11, 2011 her.oxfordjournals.org Downloaded from

45-min packaged session. Teachers could choose
the days they would deliver each session but they
must be delivered in consecutive order and must
be done in the complete format so that students
received a minimum amount of intended program-
ing (see Fig. 2). Additional ideas and optional ac-
tivities that allowed the teacher to infuse the
program beyond the minimum sessions were also
written into the plan and encouraged but not made
compulsory. Furthermore, each session was struc-
tured so students had clear expectations of learning
objectives and included a standard order from in-
troduction, through several activities/discussions,
and a closing to provide consistency for ease of
learning by students and delivery by teachers.
Classroom activity level
The PATHS curriculum relied primarily on socratic
discussions and cooperative learning principles
to illustrate points to students. The level of classroom
activity was constrained to individual activity sheets,
feeling face boxes and class or group discussions/
demonstrations. Pathways, with consent and consul-
tation from the PATHS developer, increased class-
room activity level and included more dynamic and
visual teaching modalities. For example, in PATHS,
students are asked ‘why is it important to pay atten-
tion?’ and teachers encouraged active discussion
within the classroom. The Pathways lesson starts
students with a standard color–word Stroop task
[53], in which students must name the color they
see and not the word they read. The task itself is
geared so that students will answer incorrectly when
done quickly. Then the discussion uses the task to
illustrate the point that if they do not stop and pay
attention, they will make mistakes. This activity still
maintains the construct being addressed, encourages
active socratic class discussions and creates the
illusion of a game.
Lesson content
The PATHS program teaches youth to recognize
;55 affective states in addition to varying degrees
of those states (e.g. angry, upset, furious). Labeling of
affective states is a fundamental component of
PATHS; thus, many of the earlier lessons are dedi-
cated to recognition and labeling. For Pathways, the
content and mode of delivery had to be changed
dramatically to accommodate time constraints. The
number of affect states was limited to 39 of those that
could be directly linked to physical activity or dysre-
gulated eating behaviors (e.g. angry, bored, guilty,
happy, humiliated, rejected, satisfied, tired, uncom-
fortable, worried). This decision was based, in part,
on literature that identified categories of emotional
eating or provided evidence of a relationship between
specific emotional states and dysregulated eating.
Step 3: pilot studies
We have defined pilot studies here as testing a sub-
set or full set of lessons with the intent to evaluate
content, sequencing, delivery modality, feasibility
and impact on targeted mediators. We also aimed to
assess whether the program was well received by
the students, teachers and administers and no un-
intended consequences occurred that would nega-
tively impact students.
A pilot study was conducted with a full version of
the fourth grade Pathways curriculum which consisted
of fifteen 30- to 45-min lessons. The pilot study fo-
cused broadly on the content and sequencing of the
lessons. Teachers were queried whether the conceptual
level of the lessons was too young or too mature for
their students, whether the language and examples was
age appropriate and culturally relevant and whether
they observed any spontaneous use of the curriculum
tools or skills outside of the lesson. Focus groups were
Fig. 2. Structure of Pathways curriculum. Note: This figure isjust an example and does not map the full curriculum. Sessionsare specific activities that are packaged together into 30- to 45-min blocks intended to be delivered together. Activities(abbreviated as Act) are separate tasks targeting a specificconstruct or learning objective.
Pathways obesity prevention program
7 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

conducted with teachers, parents and students at the
conclusion of the pilot study. Observers in the class-
room were also used to monitor the fidelity with which
teachers completed each lesson and whether timing of
the lessons was estimated correctly.
PATHS was a comprehensive program that began
teaching students about emotions and empathy at an
earlier age than the Pathways students. Thus, the
Pathways research team specifically assessed sequen-
ces of lessons by looking for stages of understanding
around different emotions (e.g. Could students define
jealousy, do they understand subtle differences
between angry and frustration) and whether introduc-
ing the concept of empathy early in the set of lessons
would produce greater understanding of emotions
than introducing it later. Empathy was found to be
critical to the program sequence because many of the
lessons ask the child how they might feel within
a given scenario and then asks them to relate to
how another child might feel. Empathy, as a construct
in these programs, was used as a way to demonstrate
different emotions that people may have in the same
scenario and to link an individual’s actions with emo-
tional consequences (e.g. If I hit Joey, then Joey will
be sad and I will feel guilty versus only focusing on
me hitting Joey because I was angry). Empathy
allows for the program to extend beyond just a child’s
feelings and provides an opportunity for them to look
for social and emotional cues in others and prevent
impulsive behavior by building on the CSP, thinking
through how others might feel, and considering con-
sequences of their actions. A specific example from
Pathways asks students how they feel and the prob-
lems they may face in a vignette describing a thanks-
giving dinner, a student stuffed full of food and then
a beloved grandmother bringing out her dessert in
which she insists everyone must partake. Teachers
prompt students for their internal feeling states, how
others might feel, a behavioral choice students could
make and the consequences as a result of that choice.
A child might impulsively grab a piece of dessert and
ignore how full he or she was from dinner and in
doing so may make the grandmother feel happy. An-
other child might turn down the dessert and disregard
the grandmother’s feelings. This complex scenario
relies on the culmination of several preceding lessons
but takes students beyond just feeling full or wanting
a palatable dessert to incorporating other social cues
(e.g. how the grandmother might feel or the social
expectation to eat food that is offered) and how chil-
dren might negotiate the situation in a way that they
can make healthy decisions.
Using empirical and focus group data, we found
that students in fourth grade were generally able to
distinguish between the different emotions, includ-
ing higher order or complex emotions such as jeal-
ousy, but empathy needed to be introduced across
a few lessons after majority of the students had the
practice of saying how they felt out loud. We spec-
ulate that the students needed to be comfortable
identifying their ‘own’ feelings and that expressing
them was a safe and appropriate activity to do in
front of their teacher and classmates. So the lessons
were sequenced to first establish a safe social envi-
ronment for students to label how they felt before
addressing the concept of empathy.
The intent of Pathways was not to teach students
about nutrition or exercise but to give them the tools to
regulate affect and control behaviors in order to make
healthy choices regarding nutrition and physical activ-
ity. However, developmentally, students in the Path-
ways age groups needed very concrete examples of
what constitutes a healthy choice in terms of food
and activity. Class activities and homework activities
were structured so that broad concepts were paired
with concrete examples so students were able to un-
derstand the objectives of the lesson, how and where to
apply the skills they learned and generalize beyond the
example provided. Examples could not be all inclu-
sive; thus, special attention was given to developing
a wide range of situations in order to be as relevant
to each student as possible and cover the gamut of
potential circumstances for further generalization.
Physical activity can be categorized relatively
easily as a healthy behavior (e.g. vigorous exercise
>30 min per day) and physical inactivity (i.e. video
games, television, computer time) as a generally
unhealthy behavior; however, food choices and
how to discuss them in a universal program was
not so clear. We can teach students to make the
healthy decision but we cannot expect them to do
so without telling them ‘what’ is considered healthy
K. K. Sakuma et al.
8 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from
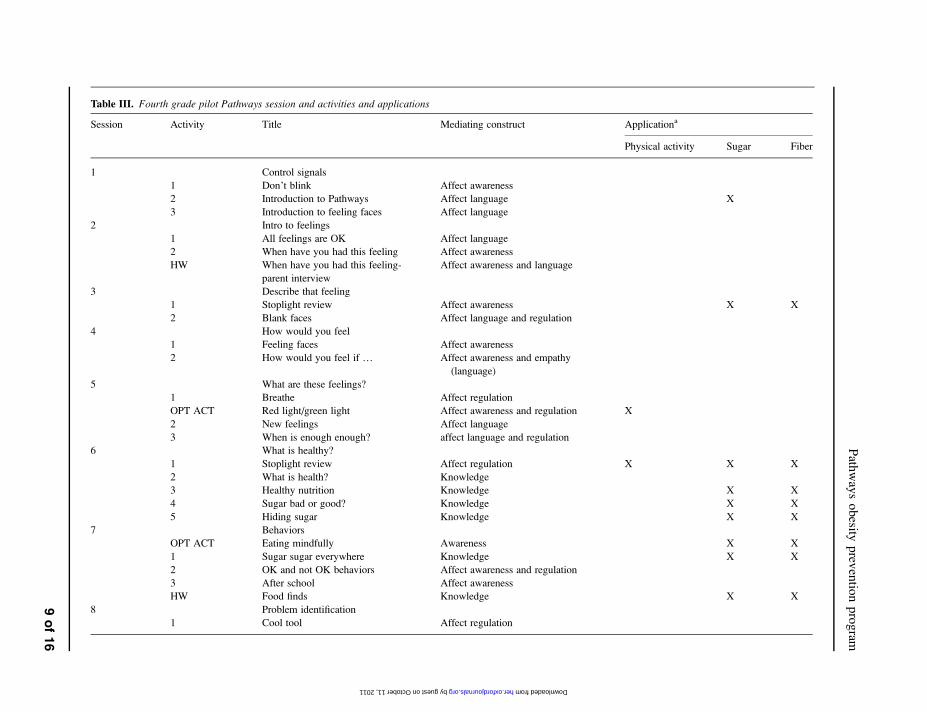
Table III. Fourth grade pilot Pathways session and activities and applications
Session Activity Title Mediating construct Applicationa
Physical activity Sugar Fiber
1 Control signals
1 Don’t blink Affect awareness
2 Introduction to Pathways Affect language X
3 Introduction to feeling faces Affect language
2 Intro to feelings
1 All feelings are OK Affect language
2 When have you had this feeling Affect awareness
HW When have you had this feeling-
parent interview
Affect awareness and language
3 Describe that feeling
1 Stoplight review Affect awareness X X
2 Blank faces Affect language and regulation
4 How would you feel
1 Feeling faces Affect awareness
2 How would you feel if . Affect awareness and empathy
(language)
5 What are these feelings?
1 Breathe Affect regulation
OPT ACT Red light/green light Affect awareness and regulation X
2 New feelings Affect language
3 When is enough enough? affect language and regulation
6 What is healthy?
1 Stoplight review Affect regulation X X X
2 What is health? Knowledge
3 Healthy nutrition Knowledge X X
4 Sugar bad or good? Knowledge X X
5 Hiding sugar Knowledge X X
7 Behaviors
OPT ACT Eating mindfully Awareness X X
1 Sugar sugar everywhere Knowledge X X
2 OK and not OK behaviors Affect awareness and regulation
3 After school Affect awareness
HW Food finds Knowledge X X
8 Problem identification
1 Cool tool Affect regulation
Path
way
so
besity
prev
entio
np
rog
ram
9of16
by guest on October 11, 2011 her.oxfordjournals.org Downloaded from

Table III. Continued
Session Activity Title Mediating construct Applicationa
Physical activity Sugar Fiber
2 Identifying problems Problem-solving skills
3 Problem identification practice Problem-solving skills
9 Problem identification 2
1 Is there a problem/goal setting Problem-solving skills
2 Finding our goals Problem-solving skills X X X
10 Solution generation
1 Lateral thinking Problem-solving skills
2 Solution generation Problem-solving skills X X X
3 On your own Problem-solving skills X X X
11 Making good decisions
1 Consequences Problem-solving skills
2 Freddie and alberto Problem-solving skills
3 On your own Problem-solving skills X X X
12 Making good decisions 2
1 Green light Planning
2 Try try again Planning
3 Science corner Knowledge X
4 Storyboard Planning X X X
13 Negotiation
OPT ACT Food choices Problem-solving skills X X
1 Exercise your brain Impulse control
2 Negotiating decisions Problem-solving skills X X X
3 Communication Affect language X X X
HW Skill development Problem-solving skills X X
14 Setting a positive future
1 Goal-setting review Problem-solving skills
2 Long-term goal setting Planning X X X
3 Roadblocks and speed bumps Problem-solving skills X X X
4 Walk your path Planning X X X
15 On the right path
1 Storyboard play Affect language X X X
2 Own story, own goals, own health Planning X X X
aApplication: More than one demarcation indicates that specified activity was pilot tested with variation on Physical activity, Sugar, and/or fiber as marked. HW, Homework; OPTACT, Optional Activity.
K.
K.
Sak
um
aet
al.
10of16
by guest on October 11, 2011 her.oxfordjournals.org Downloaded from

or at the very least how to judge for themselves
whether or not something is healthy.
There were two major ‘camps’ or philosophies
identified in the literature on how to effectively in-
tervene on food-type consumption that would result
in measurable differences in BMI. We have dubbed
these camps as the ‘sugar camp’ and the ‘fiber camp’.
These camps are not mutually exclusive but provide
a challenge in framing messages to students regard-
ing their food choices.
The sugar camp focuses on the unhealthy con-
sumption of sugar-laden and/or high-fat foods, often
found in junk foods, sodas and other processed items.
The philosophy behind the sugar camp is to teach
students to look for the hidden sugars in processed
items, read nutrition labels and ingredient lists to
identify the various disguises of sugar and avoid eat-
ing those items when possible. To further concretize
the lessons, students were taught to avoid items
where any type of sugar was listed as one of the
top three ingredients or restrict their diet to no >50
grams of sugar a day, which represents ;10% of
their daily diet based on recommendations by the
World Health Organization [54].
The fiber camp is essentially the 5-a-day cam-
paign by the Centers for Disease Control and Pre-
vention. The philosophy behind the fiber camp is to
introduce and encourage eating a wide range of fresh
fruits and vegetables to reach the 5-a-day serving
guidelines. By eating at least five servings of fruits
and vegetables a day, it will help provide vitamins
and nutrients necessary for good health and the fiber
to help satiety and thereby indirectly reducing con-
sumption of low-nutrient foods. An extension of this
philosophy is to have students seek foods that con-
tain a high amount of fiber (>3 grams per serving)
and/or avoid those with low amounts of fiber as
noted on their nutrition labels.
Four variations of specific Pathways lessons were
written and piloted to identify which of these camps’
messages was more salient to students and would
most likely result in changes in behavior. Variation
1 was to test whether physical activity messages (i.e.
increase physical activity and decrease sedentary ac-
tivity) were salient enough for students to recall them
and change their behaviors. Variation 2 emphasized
the sugar camp philosophy while Variation 3 empha-
sized the fiber camp philosophy. Variation 4 did not
emphasize any one camp but all three messages (i.e.
physical activity, sugar reduction and fiber increase)
were distributed in equal amounts across the lessons.
For example, ‘session 6: What is Healthy?’ had ac-
tivities that focused on defining health. In the physical
activity variant, the focus was on feeling energized
and seeking fun activities that raise their heart rate for
an extended period of time. For the sugar camp var-
iant of session 6, the context of health and knowledge
taught students to find snacks that they currently eat
and look for the different types of sugar in the in-
gredient list. For the fiber camp variant of session 6,
the context of health and knowledge taught students
to seek different fruits and vegetables and look for
high-fiber snacks. These variations in the curriculum
helped us to empirically disentangle what is important
to students at this age and further concretize examples
used to deliver message of healthy choice and help
students to apply them directly to their behaviors.
Sequencing of these health behaviors was also an
important finding from this pilot study. Students un-
derstand that exercise is healthy and important but in
fourth grade, they may be too young to control their
free time choices and may not have the planning
skills or problem-solving skills to enable them to seek
healthy environments or activities (e.g. asking mom
for a ride to the park). In contrast, given food choices,
perhaps between fruit and cookies lying around the
home, a fourth grader would be able to apply the
healthy decision-making skills learned in Pathways.
Hence, emphasis on increasing physical activity/de-
creasing sedentary behaviors and how to plan for
them were not added until the fifth grade booster
program. Table III represents the Pathways fourth
grade pilot curriculum with applications mapped
on to each activity. If more than one application is
marked with an ‘X’, it indicates that more than one
variation was pilot tested as described above.
Step 4: efficacy study
The goal of the development work done here to
translate evidence-based violence and drug use pre-
vention programs for application to obesity preven-
tion was to prepare a curriculum for a school-based
Pathways obesity prevention program
11 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

randomized control trial with teacher delivery.
A randomized control trial will enable us to test
whether the Pathways prevention program will be
effective in changing our targeted mediators and re-
sult in the ultimate outcome of differences in over-
weight and adiposity between our treatment group
and the control group. The final Pathways curriculum
consisted of thirty 45-min sessions with 15 sessions
delivered during the fourth grade, 10 booster sessions
delivered during the fifth grade and 5 booster ses-
sions in the sixth grade. Parent night activities were
also delivered during the fifth and sixth grade terms.
The current landscape of school-based prevention
is challenging due to time and economic constraints
and Pathways was not immune to some of these chal-
lenges. After a year of curriculum development in
partnership with a school district, budget deficits
had led to district-wide lay-offs of teachers and
administrators. At the request of the school district,
the partnership was dissolved and new partnerships
were formed with other school districts in order to
conduct the efficacy study portion of Pathways. Path-
ways also had to face two-school closings due to the
budget shortfall and again recruitment for new part-
ners had to occur. We were able to face these chal-
lenges with the help of a high-level champion. In most
cases, we had buy-in from a supporting school super-
intendant. Meetings with school principals and teach-
ers or curriculum specialists were also necessary to
gain the support of the program and the resources
necessary for implementation. What appeared to be
the strongest influencing factor in adopting the re-
search study was that Pathways was based on estab-
lished evidence-based prevention programs in which
schools were already familiar and that the materials
were designed for easy administration by the teachers.
The Pathways curriculum is currently being imple-
mented in a randomized control trial in school districts
in the southern California region.
Discussion
Obesity is a highly complex issue that requires the
integration across individual, family, environment
and population-level factors in order to successfully
address the burgeoning problem facing our nation’s
health [55, 56]. Integrating behavioral and environ-
mental prevention efforts are important, even critical,
to the success of obesity prevention. Individuals are
embedded within these environments and therefore
must make healthy choices, given those environ-
ments. There is no doubt that multi-level efforts, such
as changing school policies that limit student access
to competing calorie-dense foods or mandating
increased physical activity in classes, together with
healthy home environments that limit sedentary
screen time, safe neighborhood environments that
provide green space and individual-level prevention
programs would likely be more effective in producing
health behavior change than any one intervention tar-
geting just one level [55–57]. The Pathways project
aimed to strengthen the individual level by interven-
ing with children and developing their ECF and im-
proving their healthy decision making within contexts
that are challenging (e.g. a home with limited fresh
fruit and vegetables to snack on after school, neigh-
borhoods that are dense with high fast food establish-
ments). Furthermore, the Pathways program was not
intended to stand alone in its efforts to prevent and
reduce childhood obesity risk. Efforts to influence the
home environment through homework activities and
family nights with parents and school officials were
part of the initial design of Pathways. Pathways also
asked students and teachers to critically examine their
school environment for areas they would most likely
need to use their skills (e.g. near vending machines).
This may fall short of the need to change school
policies and environments; however, the link to other
school programs and initiatives such as the Network
for a Healthy California (http://healthedcouncil.org/
network/index.html) that do aim for those changes
are natural and encouraged. The efficacy trial of the
Pathways program will help determine its ability to
influence obesity-related factors and contribution to
the overall goal of reducing obesity risk. Future devel-
opments of school-based obesity prevention program-
ing may benefit by including policies that aim to
provide healthier home and school environments.
School-based intervention programs that do not
take into account the setting-level contextual factors
[58, 59], like socioeconomic status of the families
K. K. Sakuma et al.
12 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

or political environment within the school district,
may show short-term successes in behavioral out-
comes but may never be adopted and disseminated
outside of funded research [60]. Pathways began by
including curriculum specialists at the district level,
teachers, parents and students as partners in the de-
velopment process. These contributors were valuable
in allowing the program to mitigate and address po-
tential barriers. The design of the Pathways program
also utilized teachers as the implementers of the pro-
gram, instead of specially trained health educators or
research assistants, and built the curriculum to fit the
teachers’ needs in terms of structure (e.g. full compo-
nents, delivered within one class period) and level of
expertise. Pathways also looked for other natural
translatable opportunities. For example, ECF skill
applications were designed to address other common
issues that teachers face in education, specifically
children’s ability to calm down, sit still and concen-
trate. Pathways built lesson plans to address those
needs but also provided optional exercises to help
students and teachers manage anxiety and help with
focus on standardized testing. As teachers and admin-
istrators accepted the value of the Pathways program
and as teachers experienced visible changes in their
students’ behaviors, they looked for other ways
to incorporate other programs available through the
school’s nutrition network and change the classroom
environment. For example, a student chided her
teacher for eating three small bags of chips without
using the CSP. The teacher was so surprised to realize
that she had eaten under stress that she had the
students help institute classroom rules about eating
and helping each other use the CSP. Other research-
ers and curriculum developers are encouraged to de-
sign programs that are easily assessable by the target
implementers and audience and one that can be easily
disseminated from the research setting to real-world
settings [59]. A model that may be useful to guide this
work is the RE-AIM framework developed by
Glasgow, Vogt and Boles [61, 62].
Obesity is a multi-faceted problem and school-
based interventions that target individual affective,
cognitive and behavioral change is just one piece
of the puzzle needed in facing the challenge of
reducing obesity and obesity risk among youth
[46, 56]. Translating the successes of already
established evidence-based prevention programs
may be a viable way to combat the rapid increase
in obesity prevalence among our youth. Transla-
tion and application from existing evidence-based
programs is an arduous process but the benefit
of this process is the ability to capitalize on the
fieldwork already completed by evidence-based
programs while testing new hypotheses without
starting from scratch.
This paper describes the initial processes needed
to translate a primary prevention program from the
area of violence and drug use to obesity prevention
in youth. We presented the steps we used to orga-
nize the translational process and described some
of the practical applications, challenges and deci-
sions we have faced in developing Pathways.
These steps are intended to guide other researchers
who may choose an interdisciplinary route in de-
veloping their school-based curriculum and take
advantage of fieldwork in other areas. The Path-
ways prevention trial is underway and future anal-
yses will be able to shed light on the applicability
of translation to a new health outcome but also on
multiple outcomes. The current Pathways pro-
gram, although primarily an obesity prevention
program, introduces drug use prevention concepts
during the fifth grade booster sessions and expands
during the sixth grade booster sessions. Empirical
evidence is needed to confirm whether the trans-
lation between these health behaviors was appro-
priate. Future directions should include whether
a true universal program that targets multiple
behaviors (e.g. violence, drug use and obesity pre-
vention) would be just as effective as a program
aimed at only one health outcome [63, 64]. The
implications of such a program may facilitate
greater adoption by school systems resulting in
greater public health impact [65]. Currently, vol-
untary prevention programing in school settings
are threatened with the economic challenges that
face states and school districts as well as the
stresses of academic testing. A well-designed, uni-
versal health promotion program targeting multiple
health outcomes may be necessary for school-based
programs in our future.
Pathways obesity prevention program
13 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from
Funding
National Institute of Child Health and Human De-
velopment; National Institute of Drug Abuse at the
National Institutes of Health (grant number R01-
HD052107).
Acknowledgements
The authors would like to thank Drs Mark Greenberg,
Donna Spruijt-Metz, Kim Reynolds and Chih-Ping
Chou for their contributions to the development of
the Pathways curriculum and to Anna Solmeyer for
reviewing and editing drafts of the manuscript. They
would also like to thank Cecilia Portugal, Elizabeth
Hoyt, Jacqueline Corvan, study staff and the partici-
pating schools and teachers for their contributions to
the Pathways project.
Conflict of interest statement
None declared.
References
1. Ogden CL, Carroll MD, Curtin LR et al. Prevalence of highbody mass index in US children and adolescents, 2007-2008. JAMA 2010; 303: 242–9.
2. Pentz MA, Dwyer JH, MacKinnon DP et al. A multicom-munity trial for primary prevention of adolescent drug abuse.Effects on drug use prevalence. JAMA 1989; 261: 3259–66.
3. MacKinnon DP, Johnson CA, Pentz MA et al. Mediatingmechanisms in a school-based drug prevention program:first-year effects of the Midwestern Prevention Project.Health Psychol 1991; 10: 164–72.
4. Greenberg MT, Kusche CA. Building social and emotionalcompetence: the PATHS curriculum. In: Jimerson SRF,Furlong MJ (eds). Handbook of School Violence and SchoolSafety: From Research to Practice. Mahwah, NJ: LawrenceErlbaum Associates Publishers, 2006, 395–412.
5. Greenberg MT, Kusche CA. Preventive interventions forschool-age deaf children: the PATHS curriculum. J DeafStud Deaf Educ 1998; 3: 49–63.
6. Greenberg MT, Kusche CA, Cook ET et al. Promotingemotional competence in school-aged children: the effectsof the PATHS curriculum. Dev Psychopathol 1995; 7:117–36.
7. Skara S, Sussman S. A review of 25 long-term adolescenttobacco and other drug use prevention program evaluations.Prev Med 2003; 37: 451–74.
8. Sun W, Skara S, Sun P et al. Project towards no drug abuse:long-term substance use outcomes evaluation. Prev Med2006; 42: 188–92.
9. Pennington BF, Ozonoff S. Executive functions and devel-opmental psychopathology. J Child Psychol Psychiatr 1996;37: 51–87.
10. Zelazo PD, Carter A, Reznick JS et al. Early development ofexecutive function: a problem-solving framework. Rev GenPsychol 1997; 1: 198–226.
11. Francis LA, Susman EJ. Self-regulation and rapid weightgain in children from age 3 to 12 years. Arch Pediatr Ado-lesc Med 2009; 163: 297–302.
12. Graziano PA, Calkins SD, Keane SP. Toddler self-regula-tion skills predict risk for pediatric obesity. Int J Obes(Lond) 2010; 34: 633–41.
13. Guerrieri R, Nederkoorn C, Jansen A. The interaction be-tween impulsivity and a varied food environment: its influ-ence on food intake and overweight. Int J Obes (Lond) 2008;32: 708–14.
14. Janega JB, Murray DM, Varnell SP et al. Assessing the mostpowerful analysis method for school-based interventionstudies with alcohol, tobacco, and other drug outcomes.Addict Behav 2004; 29: 595–606.
15. Nederkoorn C, Braet C, Van Eijs Y et al. Why obese chil-dren cannot resist food: the role of impulsivity. Eat Behav2006; 7: 315–22.
16. Elias MF, Elias PK, Sullivan LM et al. Lower cognitivefunction in the presence of obesity and hypertension: theFramingham heart study. Int J Obes Relat Metab Disord2003; 27: 260–8.
17. Boeka AG, Lokken KL. Neuropsychological performanceof a clinical sample of extremely obese individuals. ArchClin Neuropsychol 2008; 23: 467–74.
18. Gunstad J, Paul RH, Cohen RA et al. Elevated body massindex is associated with executive dysfunction in otherwisehealthy adults. Compr Psychiatry 2007; 48: 57–61.
19. Wang GJ, Volkow ND, Thanos PK et al. Similaritybetween obesity and drug addiction as assessed by neuro-functional imaging: a concept review. J Addict Dis 2004;23: 39–53.
20. Braet C, Claus L, Verbeken S et al. Impulsivity in over-weight children. Eur Child Adolesc Psychiatry 2007; 16:473–83.
21. Nederkoorn C, Jansen E, Mulkens S et al. Impulsivity pre-dicts treatment outcome in obese children. Behav Res Ther2007; 45: 1071–5.
22. Volkow ND, Wise RA. How can drug addiction help usunderstand obesity? Nat Neurosci 2005; 8: 555–60.
23. Shunk JA, Birch LL. Girls at risk for overweight at age 5 areat risk for dietary restraint, disinhibited overeating, weightconcerns, and greater weight gain from 5 to 9 years. J AmDiet Assoc 2004; 104: 1120–6.
24. Greeno CG, Wing RR. Stress-induced eating. Psychol Bull1994; 115: 444–64.
25. Tice DM, Bratslavsky E, Baumeister RF. Emotional distressregulation takes precedence over impulse control: if you feelbad, do it!. J Pers Soc Psychol 2001; 80: 53–67.
26. Wills TA, Isasi CR, Mendoza D et al. Self-control constructsrelated to measures of dietary intake and physical activity inadolescents. J Adolesc Health 2007; 41: 551–8.
K. K. Sakuma et al.
14 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from
27. Riggs NR, Spruijt-Metz D, Sakuma K-L et al. Executivecognitive function and food intake in children. J Nutr EducBehav 2010; 42: 398–403.
28. Grigson PS. Like drugs for chocolate: separate rewardsmodulated by common mechanisms? Physiol Behav 2002;76: 389–95.
29. Schroeder BE, Binzak JM, Kelley AE. A common profile ofprefrontal cortical activation following exposure to nicotine- orchocolate-associated contextual cues. Neuroscience 2001;105: 535–45.
30. Blum K, Braverman ER, Wood RC et al. Increased preva-lence of the Taq I A1 allele of the dopamine receptor gene(DRD2) in obesity with comorbid substance use disorder:a preliminary report. Pharmacogenetics 1996; 6: 297–305.
31. Chassin L, Curran PJ, Hussong AM et al. The relation ofparent alcoholism to adolescent substance use: a longitudinalfollow-up study. J Abnorm Psychol 1996; 105: 70–80.
32. McCaffree J. Childhood eating patterns: the roles parentsplay. J Am Diet Assoc 2003; 103: 1587.
33. Riggs N, Chou CP, Spruijt-Metz D et al. Executive cogni-tive function as a correlate and predictor of child food intakeand physical activity. Child Neuropsychol 2010; 16: 279–92.
34. Krueger RF, Caspi A, Moffitt TE et al. Delay of gratifica-tion, psychopathology, and personality: is low self-controlspecific to externalizing problems? J Pers 1996; 64: 107–29.
35. Moffitt TE. Adolescence-limited and life-course-persistentantisocial behavior: a developmental taxonomy. PsycholRev 1993; 100: 674–701.
36. White JL, Moffitt TE, Caspi A et al. Measuring impulsivityand examining its relationship to delinquency. J AbnormPsychol 1994; 103: 192–205.
37. Giancola PR, Martin CS, Tarter RE et al. Executive cogni-tive functioning and aggressive behavior in preadolescentboys at high risk for substance abuse/dependence. J StudAlcohol 1996; 57: 352–9.
38. Domitrovich CE, Cortes RC, Greenberg MT. Improvingyoung children’s social and emotional competence: a ran-domized trial of the preschool ‘‘PATHS’’ curriculum.J Prim Prev 2007; 28: 67–91.
39. Greenberg MT, Kusche CA, Riggs N et al. The PATHScurriculum: theory and research on neurocognitive develop-ment and school success. In: Zins JE, Weissberg RP, WangMC et al. (eds). Building Academic success on Social andEmotional Learning: What Does the Research Say? NewYork, NY: Teachers College Press, 2004, 170–88.
40. Riggs NR, Greenberg MT, Rhoades BL. Early risk for prob-lem behavior and substance use: targeted interventions for thepromotion of inhibitory control. In Bardo MT, Fishbein DH,Milich R. (eds). Inhibitory Control and Drug Abuse Preven-tion: From Research to Translation. New York, NY:Springer, 2011, 249–262.
41. Riggs NR, Greenberg MT, Kusche CA et al. The mediationalrole of neurocognition in the behavioral outcomes of a social-emotional prevention program in elementary school students:effects of the PATHS curriculum. Prev Sci 2006; 7: 91–102.
42. Izard CE. Translating emotion theory and research into pre-ventive interventions. Psychol Bull 2002; 128: 796–824.
43. Izard CE, Fine S, Mostow A et al. Emotion processes innormal and abnormal development and preventive interven-tion. Dev Psychopathol 2002; 14: 761–87.
44. Pentz MA. Prevention aimed at individuals: an integrativetransactional perspective. In: McCrady BSE, Elizabeth E(eds). Addictions: A Comprehensive Guidebook. New York,NY: Oxford University Press, 1999, 555–72.
45. Pentz MA, Mihalic SF, Grotpeter JK. The Midwestern Pre-vention Project. In: Elliot DS (ed). Blueprints for ViolencePrevention. Boulder, CO: Center for the Study and Preven-tion of Violence, Institute of Behavioral Science, Universityof Colorado, 1997, xi-78.
46. Pentz MA. Preventing drug abuse through the community:Multicomponent programs make the difference. In: SlobodaA, Hansen WB (eds). Putting research to work for the com-munity (NIDA Publication No. 98-4293; 73-86). Rockville,MD: National Institute on Drug Abuse, 1998.
47. Sussman S. Curriculum development in school-based pre-vention research. Health Educ Res 1991; 6: 339–51.
48. Riggs N, Chou C-P, Spruijt-Metz D et al. Executive cogni-tive function as a correlate and predictor of child food intakeand physical activity. Child Neuropsychol 2010 May; 16:279–92.
49. Riggs NR, Greenberg MT. Neurocognition as a moderatorand mediator in adolescent substance misuse prevention. AmJ Drug Alcohol Abuse 2009; 35: 209–13.
50. Riggs NR, Sakuma K-LK, Pentz MA. Preventing risk forobesity by promoting self-regulation and decision-makingskills: pilot results from the PATHWAYS to health program(PATHWAYS). Eval Rev 2007; 31: 287–310.
51. Pentz MA. Understanding and preventing risks for adoles-cent obesity. In: DiClemente RJ, Santelli JS, Crosby, RA.Adolescent Health: Understanding and Preventing RiskBehaviors, vol. xxvi. San Francisco, CA: Jossey-Bass, 2009,2147–64, 2580.
52. Riggs NR, Blair CB, Greenberg MT. Concurrent and 2-yearlongitudinal relations between executive function and thebehavior of 1st and 2nd grade children. Child Neuropsychol2003; 9: 267–76.
53. Stroop JR. Studies of interference in serial verbal reactions.J Exp Psychol 1935; 18: 643–62.
54. Simpson I. Populations with high sugar consumption are atincreased risk of chronic disease, South African researchersreport. Bulletin of the World Health Organization 2003. Avail-able at: http://www.who.int/bulletin/releases/2003/PR0803/en/.Accessed: 14 January 2009.
55. Koplan JP, Liverman CT, Kraak VI. (eds). PreventingChildhood Obesity: Health in Balance. Washington, DC:The National Academies Press, 2005.
56. Flynn MAT, McNeil DA, Maloff B et al. Reducing obesityand related chronic disease risk in children and youth: a syn-thesis of evidence with ‘best practice’ recommendations.Obes Rev 2006; 7: 7–66.
57. Tortolero SR, Popham K, Jacobson PDYS. Improving infor-mation on public health law best practices for obesity pre-vention and control. J Law Med Ethics 2009; 37(Suppl.):99.
58. Glasgow RE, Klesges LM, Dzewaltowski DA et al. Thefuture of health behavior change research: what is neededto improve translation of research into health promotionpractice? Ann Behav Med 2004; 27: 3–12.
59. Glasgow RE, Lichtenstein E, Marcus AC. Why don’t we seemore translation of health promotion research to practice?Rethinking the efficacy-to-effectiveness transition. Am JPubl Health 2003; 93: 1261–7.
Pathways obesity prevention program
15 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from

60. Klesges LM, Estabrooks PA, Dzewaltowski DA et al. Be-ginning with the application in mind: designing and plan-ning health behavior change interventions to enhancedissemination. Ann Behav Med 2005; 29: 66–75.
61. Glasgow RE, Klesges LM, Dzewaltowski DAEPA et al.Evaluating the impact of health promotion programs: usingthe RE-AIM framework to form summary measures for de-cision making involving complex issues. Health Educ Res2006; 21: 688–94.
62. Glasgow RE, Vogt TM, Boles SM. Evaluating the publichealth impact of health promotion interventions: the RE-AIM framework. Am J Publ Health 1999; 89: 1322–7.
63. Prochaska JJ, Nigg CR, Spring B et al. The benefits andchallenges of multiple health behavior change in researchand in practice. Prev Med 2010; 50: 26–9.
64. Prochaska JO. Multiple health behavior research representsthe future of preventive medicine. Prev Med 2008; 46:281–5.
65. Dunton GF, Riggs N, Durand CP et al. School-basedphysical activity and nutrition programs in the preventionof childhood obesity. In: Bagchi D (ed). Global View onChildhood Obesity: Current Status, Consequences andPrevention. Amsterdam, The Netherlands: Elsevier, 2010,319–31.
K. K. Sakuma et al.
16 of 16
by guest on October 11, 2011
her.oxfordjournals.orgD
ownloaded from




















