prevalence and factors associated with - dissertations
109
1 PREVALENCE AND FACTORS ASSOCIATED WITH PRESENCE OF MICROALBUMINURIA IN PATIENTS WITH ESSENTIAL HYPERTENSION SEEN AT THE GENERAL OUTPATIENT CLINIC OF FEDERAL MEDICAL CENTRE, ABEOKUTA. A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF FELLOWSHIP OF THE COLLEGE IN FAMILY MEDICINE BY IGE, ADEGBOLA MEEDEEN M.B; B.S ( Ibadan) 2001 NOVEMBER 2011
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of prevalence and factors associated with - dissertations

1
PREVALENCE AND FACTORS ASSOCIATED WITH
PRESENCE
OF MICROALBUMINURIA IN PATIENTS WITH
ESSENTIAL
HYPERTENSION SEEN AT THE GENERAL
OUTPATIENT
CLINIC OF FEDERAL MEDICAL CENTRE,
ABEOKUTA.
A DISSERTATION SUBMITTED TO THE NATIONAL
POSTGRADUATE MEDICAL COLLEGE OF NIGERIA
IN PARTIAL FULFILMENT OF THE REQUIREMENTS
FOR THE AWARD OF FELLOWSHIP OF THE
COLLEGE IN FAMILY MEDICINE
BY
IGE, ADEGBOLA MEEDEEN
M.B; B.S ( Ibadan) 2001
NOVEMBER 2011

2
SUMMARY
Background
Systemic hypertension (HTN) has been recognized as a very common cardiovascular disease
(CVD) and a major risk factor in the development of congestive heart failure, ischaemic heart
disease, chronic renal failure and stroke.
Some patients with essential/primary HTN (EHTN) manifest microalbuminuria (MAL) - an
abnormal (30–300mg/24hours) urinary albumin excretion. MAL is considered as independent
predictor of cardiovascular (CV) morbidity and mortality. Its level has also been found to
correlate with blood pressure (BP) levels. Several studies conducted among Caucasians showed
different prevalence rates. Early treatment of patients with MAL has been shown to prevent
significant CV morbidity and mortality
However, despite the strong prognosticating index of MAL in hypertension, it is not yet done
routinely for hypertensive patients in Nigeria. Hence, the need for this study.
Objective
The general objective of the study is to describe the prevalence and factors associated with
presence of microalbuminuria among adult Nigerian patients with essential hypertension in
order to inform early detection and control practices.
Methods

3
Using a systematic sampling method with a sampling interval of 3, a total of 395 patients with
essential HTN were screened for MAL using Micral test strip-II. Those with overt proteinuria
were first excluded by testing their freshly passed morning urine with Combur-test strip. Both
test strips are in-vitro diagnostic test strips from Roche Diagnostics for semi-quantitative
estimation of microalbumin, and for estimation of urinary PH, protein and glucose respectively.
Data were however analyzed for three hundred and sixty (360), the actual sample size. Twenty-
five subjects did not complete the study.
Results
The prevalence rate of MAL was 77.5%. Although not statistically significant, MAL was
observed to be more prevalent in females than males and majority of the patients were above
60 years. MAL was positively correlated with systolic BP, diastolic BP, mean arterial pressure
and age. Body mass index (BMI), waist hip ratio (WHR), sex and family history of HTN did
not show any significant association with MAL.
Conclusion
The study showed that there is a high prevalence of microalbuminuria in adult Nigerian
hypertensive patients. It also revealed that MAL is influenced by a number of factors in these
patients.
Therefore, routine screening for MAL in all hypertensive patients is advocated and the presence
of MAL in any hypertensive patient (old or new) calls for a more aggressive and comprehensive
management and follow-up.

4
However, it is suggested that a large multi-centre case-control study be conducted to establish
the prognostic significance of MAL in this environment.
5
CHAPTER ONE
INTRODUCTION
Hypertension (HTN) is an important worldwide public health challenge because of its high and
increasing prevalence and concomitant risks of cardiovascular (CV) and renal diseases. In fact,
it has been described as the most powerful, highly prevalent, independent, modifiable risk
factor for cardiovascular disease (CVD) at the population level.1,2 The burden of HTN
worldwide is so enormous that it has been projected that the approximately one billion (15-
20%) of the world’s population currently being affected3-8 will increase to 1.56 billion by year
2025 and sub-Sahara African shall be the most affected.
Hypertension (HTN) is a common condition amongst Nigerians. The prevalence is alarmingly
on the increase6,9 as a result of westernization and urbanization. Some patients with essential
HTN (EHTN) manifest microalbuminuria (MAL) – an abnormal (30-300mg/24hours) urinary
albumin excretion. It has long been established that albuminuria is the principal marker for
chronic kidney disease (CKD).10-14 In fact, MAL is regarded as the most sensitive parameter
for the detection of early kidney damage.
More recently, MAL has become widely recognized as an independent risk indicator for CVD
morbidity and mortality for patients with HTN and diabetes. 13,15,16,17,18, 19, 20,21
CVD morbidity and mortality as well as CKD are preventable if hypertensive nephropathy is
detected at the microalbuminuric stage and appropriate pharmacotherapy and other measures
are instituted. Studies have overwhelmingly shown that pharmacologic blockade of renin-
angiotensin-aldosterone system (RAAS) by Angiotensin Converting Enzyme Inhibitors (ACE-
I) and/or Angiotensin Receptor Blockers (ARB) provides effective reduction of MAL and

6
blood pressure (BP), and long term prevention of CV events beyond BP
reduction.22,23,24,25,26,27,28,29,30-33 This agents are capable of preventing, reversing or slowing
down progression of hypertensive or diabetic nephropathy.10
Surprisingly, a very wide gap exists between what is known and what is currently being
practiced. Despite compelling data and the well known correlation between MAL and CV risks,
at present only a minority of patients with diabetes and very rarely individuals with HTN are
screened for microalbuminuria15,34 especially in a developing country like Nigeria.
The prevalence of MAL in essential HTN has been determined by several studies and different
prevalence rates have been reported among Caucasians.16,35,36 Only very few of such studies
have been carried out in Nigeria.37,38 Hence, early detection of MAL via simple, point-of-care
screening method shall be the focus of this study. Also emphasis shall be laid on the clinical
pattern of MAL, vis-a-vis influencing factors, among the subjects. This will enable early risk
stratification of hypertensives and institution of the right choice of drugs and other measures
to forestall CVD progression. This brightens the management outcome, betters the prognosis,
improves the quality of life, increases life expectancy and more importantly helps prevent
expenditure of the scarce Nigerian health resources on the management of hypertensive
complications notably cardiac, cardiovascular, retinal and renal.
Family Physicians who, as doctors of first contact, diagnose and initiate antihypertensive
therapy in most cases are well placed for this cost effective, result oriented and secondary
preventive step towards reversing the trend of CKD and CVD.

7
AIM AND OBJECTIVES OF THE STUDY
General Objective (Aim)
The general objective of the study is to describe the prevalence and factors associated with
presence of microalbuminuria among adult Nigerian patients with essential hypertension in
order to inform early detection and control practices.
Specific Objectives
The specific objectives are;
1. To determine the prevalence of MAL among patient with essential HTN.
2. To describe the sociodemographic and clinical characteristics of these patients.
3. To identify factors associated with presence of MAL in the study population.

8
JUSTIFICATION FOR THE STUDY
Hypertension is the most important modifiable risk factor for CVD which is a leading cause of
death in Western Countries35,39 accounting for more than one third of all deaths.35 This is due
mainly to the steady increase in the prevalence of hypertension and diabetes both of which have
now reached the proportion of worldwide epidemic. Unfortunately, this epidemic is projected
to continue unabated such that by year 2025, 1.56billion of the world population will be
hypertensive. This will translate to a further rise in the number of deaths from CV
complications and CKD.35 Recent epidemiological survey reported a range of 31-44%
prevalence of hypertension (HTN) in the Western world.40
Unfortunately, HTN is also the commonest risk factor for CKD, the prevalence of which is also
alarmingly on the increase.41
By virtue of the ever increasing rate of urbanization and westernization, the prevalence of HTN
among black populations is expected to rise sharply. As such, by the end of the next 2 decades,
the consequent CVD mortality and morbidity shall be overwhelming for the African economy.
Sub-Sahara Africa, which includes Nigeria, will be the most affected.
Nigeria with her perennial health concerns with infectious diseases needs to be highly proactive
towards prevention of non-communicable diseases and their consequences. This mandates the
need for an early identification of patients who are at increase risk of CVD and CKD for a
better stratification.35 Early identification of those who are at risk is of paramount importance
because it could set the stage for a more rational therapeutic approach by allowing direct
additional measures to those who need them the most.39
Early detection of microalbuminuria (MAL) via a simple, inexpensive and highly sensitive
screening method for CVD risk stratification and hence aggressive therapeutic approach has

9
been recommended by the JNC-VII and ESH –ESC.35,39 Different prevalence rates (5-40%)
have been reported among Caucasians.
There is a dearth of studies on the prevalence of MAL and its clinical pattern among patients
with essential HTN with an implied consequence of very poor CVD risk stratification in this
part of the world, hence the choice of the title.

10
CHAPTER TWO
LITERATURE REVIEW
2.1 HYPERTENSION
2.1.1 Hypertension: Definition and Epidemiology
Hypertension – persistent elevation of BP and its unpleasant consequences were first
recognized in the late 1800s42 but the cut-off of 140/90mmHg was chosen in the early 1900s
based on the fact that only 5-10% of the US population had BP in that range.42 Also, it was
recognized from the start that BP in this range were almost inevitably accompanied by
arteriolosclerosis and renal changes on microscopic examination.42
No single definition of HTN is universally acceptable. It is often defined as a persistent
elevation of arterial BP with values equal to or greater than140/90mmHg.43 This definition
does not take into account the age of the patient or the presence of pre-existing complications
of HTN. Absolute BP level however varies with age, sex, race and numerous other factors.
Hence, a more useful and practical definition is “the level of BP at which the benefits of
treatment outweigh the costs and hazard.44
HTN is responsible for high morbidity and mortality and affects millions of people the world
over11 especially during the most productive period of their lives. It is a highly prevalent
disorder world wide affecting about 30% and 44% of adult population in the US and Western
Europe respectively.45 African – American blacks have higher prevalence (32.6%).

11
High prevalence rates have also been documented across African populations. HTN in sub-
Sahara Africa is a wide-spread problem of immense economic importance because of its high
prevalence in urban areas, frequent misdiagnosis, and severity of its complications. Recently,
prevalence rates of 27.6%, 28.7% and 30% were respectively reported from Congo, Ghana and
Zimbabwe.45,46 Edwards et al in a study conducted in 2008 in Tanzania reported even a higher
prevalence (34.3% & 39.1%) among men and women respectively in urban district.1 In
Nigeria, HTN like elsewhere, is more prevalent in the urban than in rural communities. In a
recent study, Adedoyin et al9 reported a crude prevalence of 36.6% in a semi-urban community
with a male to female ratio of 1.7 to 1. This is quite higher than the 14.2% prevalence in the
urban adults reported by Akinkugbe et al in 1997.47
2.1.2 Classification of Hypertension
HTN can be classified by three methods namely48,49 : (1) BP levels (2) Extent of organ damage
and (3) Aetiology
Blood pressure levels:43,49 A very simple and useful classification can be derived from the
Joint National Committee on Prevention, Detection, Evaluation and Treatment of HTN (JNC).
According to JNC V1, BP is classified as Optimum (<120/80mmHg); Normal
(<130/85mmHg), High normal (130-139/85-89mmHg); stage I HTN (140-159/90-99mmHg),
stage II HTN (160-179/100-109 mmHg) and stage III HTN (>180/110mmHg). The latest report
of the JNC, JNC VII, has little modification to the JNC VI. In JNC VII, the normal and high
normal levels of JNC VI are grouped together as the pre-hypertensive stage. Stage I is still the
same while stages II and III are grouped together as stage II.

12
Pre-hypertension stage is not a disease category. Rather, it emphasizes individuals that are at
risk of progression to HTN and the need for lifestyle modifications as important preventive
strategies.43,49,50
WHO/ISH 2004 guideline still retains the old classification of Grade I-III which corresponds
to stage I-III of JNC VI.
Table 1: JNC VI Classification of HTN
Category Systolic Bp (mmHg) Diastolic BP (mmHg)
Optimal < 120 < 80
Normal < 130 < 85
High Normal 130 – 139 85 – 89
Hypertension
Stage I (Mild) 140 – 159 90 – 99
Stage II (Moderate) 160 – 179 100 – 109
Stage III (Severe) ≥180 ≥ 110
Table 2: JNC VII Classification of HTN
Category Systolic Bp (mmHg) Diastolic BP (mmHg)
Normal < 120 < 80
Pre-Hypertension 120 – 139 80 – 89

13
Hypertension
Stage I 140 – 159 90 – 99
Stage II > 160 > 100
NB:
The above values are accepted if patients are not taking anti-hypertensive drugs and not acutely
ill.
Values are based on average of two or more readings taken at each of the two or more visits
after an initial screening.
When systolic and diastolic BP fall into different categories, the higher category is selected for
the classification.
Extent of organ damage:48,49 Stages one to three:
In stage one, there are no objective signs of organ damage
In stage two, there is at least one of the signs of organ involvement. The organs normally
involved are the heart, brain, retina and the kidneys.
In stage three, there are signs and symptoms of damage to the various organs.
Aetiology:44,49 By aetiology, HTN can be classified into
a) Essential or Primary HTN in which no specific underlying cause can be defined. This
accounts for about 90-95% of the causes of HTN. Several factors,44,49 ranging from genetic,

14
humoral, cell membrane defect, foetal to environmental have been implicated in the
pathogenesis of essential HTN. The kidneys are also well implicated.
b) Secondary HTN in which the HTN can be shown to be a consequence of a specific disease
or abnormality. This accounts for about 5-10% of the cases and causes may be renal,
endocrine, pregnancy and drug induced, etc.
2.1.3 AETIOLOGY OF ESSENTIAL HTN
The aetiology of EHTN is unknown. However, quite a number of factors have been implicated
and theories postulated as discussed below.
The Kidney in Essential HTN
The kidney appears to be both culprit and victim in the hypertensive process. Researchers have
proposed that the presence of abnormal kidney function is a common initiating factor in most
forms of arterial HTN, including EHTN. On the other hand, the renal vasculature is well known
to suffer the consequences of persistently elevated BP.
The kidneys are important in the regulation of BP through the role they play by pressure
natriuresis in opposing increases in BP.51 An increase in BP is compensated for by an increase
in renal excretion of water and salt. Thus any alteration of renal perfusion or abnormal renal
function could provoke the development of HTN. Further sodium retention would then
aggravate this situation by fostering development of volume dependant HTN.51
Detailed studies with arteriography and biopsy have shown both structural damage and
functional derangements reflecting intraglomerular HTN in almost all hypertensive persons

15
including those with apparently mild disease51 and even in some normotensive children of
hypertensive parents.44,51
The renal vasculature has been implicated in the development of EHTN and functional
vasoconstriction is present in many patients with mild HTN.51
Furthermore, the sympathetic nervous system is also thought to play a role in the development
of EHTN.51 Increased sympathetic activity, as a consequence of stress or primary sympathetic
dysfunction, may induce renal vasoconstriction which facilitate sodium retention.
Genetic Factors
Data supporting role of genetics can be found in animal studies as well as in population studies
in human.52 One approach has been to assess the correlation of blood pressure in families
(Family aggregation). From these studies, genetic factors have a strong correlation with the
development of HTN.52 In addition, most studies support the concept that the inheritance is
probably multi-factorial or that an elevated BP may represent one of the phenotypic expressions
of a number of different genetic defects.52,53
Finally, both monogenic defects (e.g. glucocorticoid remediable aldosteronism and Liddle’s
syndrome) and susceptibility genes (e.g. the angiotensinogen and alpha adducing genes) have
now been reported which have as one of their consequences, an increased arterial
pressure.52
Foetal Factors

16
Some studies have shown a relationship between lower birth-weight and subsequent higher
BP.54 This relationship may be due to foetal adaptation to intrauterine under nutrition with long-
term changes in blood vessel structure or in the function of crucial hormonal system.44,54
Life Style and Environmental Factors
Among the several environmental factors that have been proposed, the following seem to be
the most important:
a. Obesity: There is a positive correlation between obesity, especially central obesity and
arterial BP. A gain in weight is associated with an increased frequency of higher BPs
in persons with normal BP, and weight loss in obese persons with HTN lowers arterial
BP.55
b. Alcohol intake: Heavy alcohol intake (>6 units or 48g/day) is associated with an
increase in BP, and reduction in intake can reduce BP.44
c. Sodium intake: Some studies have suggested a positive correlation between salt intake
and BP levels, although other studies found the relationship to be weak. There are some
evidences that a high potassium diet can protect against the effect of a high sodium
intake.14,56
d. Stress: Though acute stress or pain can raise BP, the relationship between chronic stress
and BP has been difficult to establish.44,54
Humoral Mechanisms
17
The autonomic nervous system, as well as renin-angiotensin-aldosterone, natriuretic peptide,
endothelins and kallikrein – kinin system, play a role in the physiologic regulation of BP44 and
have been implicated in the pathogenesis of primary HTN.
The vascular endothelium also produces other vasoactive substances such as nitric oxides and
growth factors.44 Nitric oxide is a potent vasodilator that influences local autoregulation and
other vital organ functions.
The growth factors include platelet-derived growth factor (PDGF), fibroblast growth factor
(FGP) and insulin growth factor (IGF). Each of these factors plays an important role in the
atherogenesis and target organ damage.44
Role of Renin: This is an enzyme secreted in the juxtaglomerular cells of the kidney. The end
product of the action of renin on its substrate is the generation of the peptide angiotensin II.27
,44,56,57 The range of plasma renin activities observed in hypertensives is broader than in
normotensive individuals. In consequence, some hypertensive patients have been defined as
having low-renin and others as having high-renin primary HTN.44
Insulin Resistance
Insulin resistance and/or hyper-insulinaemia have been suggested as responsible for the
increased arterial pressure in some people.
Hyper insulinaemia can increase arterial BP by one or more of four mechanisms.44
First, hyperinsulinaemia produces renal sodium retention (at least acutely) and increases
sympathetic activity. Another mechanism is the vascular smooth muscle cell hypertrophy
secondary to the mitogenic action of insulin.

18
Third, insulin also modifies ion transport across the cell membrane, thereby potentially
increasing the cytosolic calcium levels of insulin sensitive vascular or renal tissue.
Finally, insulin resistance may be a maker for another pathologic process, e.g. non-modulation,
which could be the primary mechanism in increasing BP.44
Cell Membrane Defects
This hypothesis derives most of its data from studies on circulating red blood cells (RBC) in
which abnormalities in the transport of sodium across the cell membrane have been
documented.44 It has been assumed that this abnormality in sodium transport reflects a defect
in the cell membrane occurring in perhaps all the cells of the body, particularly the vascular
smooth muscle cells. This defect leads to an abnormal accumulation of calcium in vascular
smooth muscle cells, resulting in a heightened vascular responsiveness to vasoconstrictor
agents.44 This defect has been proposed to be present in 35 to 50% of primary hypertensive
individuals on the basis of studies using red blood cells.44
2.1.4 Clinical Features of Hypertension
HTN has been described as a silent killer.44 Majority of patients with HTN have no specific
symptoms referable to the elevated BP. Symptoms that bring the patients to the physician are
in most cases related to complications of HTN and the underlying disease in the case of
secondary HTN. A few present with symptoms related to the elevated pressure and these
include dizziness, palpitations and fatigability. Headache, which is occipital and present when
patient wakes up and disappears with time is a feature of severe HTN.44,56 A strong family
history of HTN with intermittent high BP in the past favours diagnosis of essential HTN.48,56

19
Symptoms referable to vascular disease include epistaxis, haematuria, blurring of vision due to
retinal changes, episodes of weakness or dizziness from transient cerebral ischaemia, angina
pectoris and dyspnoea due to cardiac failure. Pain due to aortic dissection or a leaking aneurysm
is an occasional presenting symptoms.44,56
Some symptoms related to the underlying diseases in secondary HTN are : 44,56
Polyuria, polydypsia, muscle weakness, secondary to hypokalaemia in patients with
primary aldosteronism.
Weight gain and emotional lability in patients with Cushing’s syndrome
Episodic headaches, palpitations, diaphoresis and postural dizziness in those with
phaeochromocytoma.
2.1.5 Complications of Hypertension
HTN is a major risk factor for coronary, cerebral and renal vascular disease, leading to half of
all death in the United States.44,56 The higher the levels of BP, the more likely that various
CVD will develop prematurely through acceleration of atherosclerosis, the pathological
hallmark of uncontrolled HTN.
In the Framingham cohort study, the risk of developing coronary disease rose progressively
with increasing systolic or diastolic pressure both in the middle aged and the elderly. If
untreated, about 50% of hypertensive patients will die of coronary heart disease or congestive
cardiac failure; about 33% of stroke and 10-15% of renal failure.44,56
Benign hypertensive nephrosclerosis is characterized by two types of renal lesions:
Hyperplastic elastic arteriolosclerosis which is most marked in the interlobular arteries and
hyaline arteriolosclerosis primarily involving the afferent arterioles.

20
The malignant phase of arterial HTN is characterized by marked elevation in blood pressure
with widespread acute arteriolar injury. The changes are more marked in the retina and kidneys
with fibrinoid necrosis and mucoid intimal proliferation of the afferent arterioles being the
hallmark of malignant nephrosclerosis. Nephrosclerosis results in a substantial decline in renal
function that is usually accompanied by microhaematuria and proteinuria.44,58
Functional consequences of nephrosclerosis include progressive increase in renal vascular
resistance and a progressive decrease in effective renal plasma flow.44,58 Initially, glomerular
filtration rate (GFR) is maintained probably at the expense of increased intraglomerular
pressure in each nephron. Progressive destruction of renal arterioles and glomeruli will lead to
a progressive reduction in GFR and will facilitate the appearance of proteinuria. In patients
with long standing HTN, a loss of concentrating ability of the kidneys may be manifested by
nocturia, a decreased creatinine clearance and albuminuria. As HTN induced nephrosclerosis
proceeds, the plasma creatinine level begins to rise and eventually renal insufficiency with
uraemia develops in 10-20% of patients.44,58
Those with rapidly accelerating HTN or malignant HTN die more frequently of renal failure as
do those who are diabetic, once proteinuria or other evidences of nephropathy develop.44
Blacks suffer more renal damage, leading to a significantly greater incidence of end-stage renal
disease (ESRD) requiring chronic dialysis.44 Essential HTN is an important cause of ESRD in
blacks. Records from Republic of Congo showed that HTN, both benign and malignant, is the
most common preventable cause of ESRD.41

21
2.2 ALBUMINURIA IN ESSENTIAL HTN
2.2.1 Definition: The occurrence of MAL in non-diabetic patients with primary HTN was
first described by Parving et al in 1974.17,35 It is defined as an abnormally elevated urinary
albumin excretion, in the absence of clinical proteinuria, ranging from 30 to 300mg/24hours or
20 to 200µg/minute.34 In spot urine specimen, MAL may also be defined as urinary albumin
excretion of 20-200mg/L or urinary albumin-creatinine ratio (UACR) of 3-30mg/mmol. The
normal urinary albumin excretion is in the range of 1-22mg/24 hours with an average of 4-
9mg/24hours.
2.2.2 Microalbuminuria in Essential Hypertension
MAL is a well recognized marker of CV complications in HTN and the most sensitive
parameter for the detection of early kidney damage (stage I & II of CKD).22
The prevalence of MAL in patients with primary HTN ranges between 5% and 40%.35,36
Current prevalence of MAL in hypertensive patients is higher than previously reported, ranging
in different countries between 53% and 71% with the highest rate in patients with uncontrolled
HTN34 as demonstrated in i-SEARCH, a broad-based international survey.
This wide variability is due to the duration and severity of HTN, age and sex distribution and
concomitant CV risk factors.36 Other factors are the patient selection procedures, the existence
of prior treatment associated with adequate or inadequate control of HTN by drug therapy, the
type of which may highly influence albuminuria.59,60
2.2.3 Risk factors for Microalbuminuria in Essential Hypertension

22
Various factors, as highlighted below, have been shown to increase the risk of MAL in
individuals with essential HTN:
Level of BP and duration of HTN: Urinary albumin excretion is closely related to the level of
the clinical BP.61 This trend towards stronger correlations for the systolic BP than for diastolic
BP. Also the longer the duration before diagnosis or before achieving good BP control, the
higher the risk of developing MAL.
Pulse pressure (PP): Isolated systolic HTN (SBP >/= 140) and pulse pressure (SBP minus
DBP) are directly related to MAL independent of diastolic BP and several other
correlations.62,63 As demonstrated by Massimo et al62, PP was linearly related to the urinary
albumin excretion (UAE) in both sexes. Several epidemiological and clinical studies reported
that high PP and isolated systolic HTN are associated with signs of target organ damage and
CV disease even in the presence of low – normal diastolic BP.62,63
Gender: It has been reported that men show higher UAE than women independent of BP,
tobacco habit and BMI.61,63
Obesity: Previous studies have reported greater prevalence of MAL among obese (BMI >/=
30) than among lean subjects.61,64 In hypertensive patients, BMI has also been described to be
associated with UAE.61,65
Smoking: Current and former hypertensive smokers have a marked risk of proteinuria
compared to hypertensive non smokers.21,66 However microalbuminuric effect consequent
upon smoking seems reversible upon smoking discontinuation except in chronic smokers.66
Increasing evidence suggest that chronic smoking is implicated in all aspects of the progression
of renal disease as it increases the risk of MAL and accelerates the rate of progression from
MAL to macroalbuminuria and subsequently renal failure.

23
Alternative medicine: In the developing world, up to 80% of the population uses traditional
medicine for primary health care. In the industrialized countries, adaptations of traditional
medicine, termed complementary alternative medicine (CAM), are used by a growing number
of patients for preventive or palliative care.67 These unconventional medications may be an
important risk for the development of acute and chronic kidney injury because of several
factors: (a) These products rarely meet the essential standard, (b) many of these products
contain undisclosed over-the-counter or prescription drugs or can be adulterated with hormones
and glandular extracts and (c) they can also be contaminated by pesticides and heavy metals.
These factors, inter alia, predispose users to various kidney toxicity that results ultimately in
irreversible renal disease.67
Finally, by virtue of various organ ageing and probably due to co-morbidity e.g DM, older age
hypertensives are at increased risk of MAL compared to the younger one with similar other
risk factors.
2.2.4 Mechanisms of Albuminuria in Essential Hypertension
Albuminuria is one of the manifestations of renal insufficiency in essential HTN. Clinically
apparent proteinuria in essential HTN is associated with increased CV and cerebrovascular
disease and is an independent predictor of morbidity and mortality.34 Subclinical elevation of
albumin excretion is seen more frequently than clinical proteinuria in primary HTN and the
level of MAL correlates with the BP level.10,15,34
The transglomerular passage of albumin (molecular weight 69,000) and other macromolecules
are determined (a) by their molecular size, shape and electrical charge, (b) by the size and
charge-selectivity properties of the glomerular filter and (c) by renal haemodynamics.

24
The glomerular filtration of albumin molecule is restricted by the size and electrostatic
hindrance of the negatively charged glomerular filter. Loss of charge and size-selective
properties of the glomerular filter explains the proteinuria of various diseases.44
The increased urinary albumin excretion in HTN has been explained by several factors:44
(i) Renal haemodynamics changes
(ii) Permeability-selectivity changes of the glomerular filter and/or insufficient tubular
reabsorption of albumin
(iii) Structural arteriolar and glomerular changes due to nephrosclerosis.
In established essential HTN, renal vascular resistance is characteristically elevated, renal
plasma flow reduced but GFR is usually maintained, presumably due to predominant efferent
arteriolar vasoconstriction leading to increased filtration fraction.44 Angiotensin II is said to
be involved in this auto-regulation of GFR and is believed to help maintain GFR by constricting
the efferent arterioles thereby increasing transcapillary hydrostatic pressure difference which
also results in increased protein filtration. Proteinuria therefore does not necessarily have to be
attributed to glomerular injury in states with reduced renal plasma flow and increased filtration
fraction. Angiotensin II has been shown to increase albumin excretion rate in HTN either by
elevating glomerular capillary pressure or by increasing the permeability of the glomerular
capillary to albumin or by both mechanisms.10
Albuminuria in HTN may also be due to nephrosclerosis, that is arteriolosclerosis especially
involving the inter-lobular artery and the efferent arterioles.
It has also been postulated that the proteinuria in HTN may be secondary to irreversible
structural glomerular changes from vascular damage leading to mild ischaemia or complete

25
sclerosis. In addition to this structural damage, the unchanged nephrons are subjected to hyper-
filtration with enhancement of proteinuria and glomerular injury.44
Clinical proteinuria which is usually not reversible by antihypertensive therapy may be due to
predominantly structural vascular and glomerular changes while MAL, which is often
reversible38, may be caused by predominantly functional haemodynamic changes.
Recent studies have described a glomerular permeability-independent mechanisms by which
albuminuria may occur: “ The albumin degradation pathway ”.10 The factors governing the
manifestation of albuminuria in HTN and diabetes have drawn important link between (a) up-
regulated renin-angiotensin system and increased transforming growth factor (TGF-β1)
expression and (b) disrupted albumin processing by the kidney.10,68
Lucinda et al reported that albumin filtered by the kidney is endocytosed by proximal tubular
cells and degraded into peptides in lysosomes. These peptides are exocytosed back into the
tubular lumen and excreted in the urine. Changes in the post-glomerular handling of albumin
are therefore implicated in the induction of albuminuria in hypertensive and diabetic states.10
2.2.5 Detection of Microalbuminuria
Urinary albumin excretion varies from day to day and is affected by factors such as posture,
exercise and BP.10,69 For this reasons, the collection of two to three non-consecutive urine
samples has been recommended to obtain a reliable result.
For screening purposes, measurement of the urinary albumin concentration of the first morning
urine has been suggested since this specimen is thought to vary least.64,70,71 However, some
other studies have shown that any urine sample can be used.

26
Laboratory methods available for detecting MAL include Radioimmunoassay, Laser
immunonephelometry, Enzyme immunoassay, Immunoturbidimetry, Fluorescent
immunoassay and High performance liquid chromatography.72,73 Radioimmunoassay is
probably the most accurate method but it is very expensive.
In addition to these laboratory techniques for quantitative determination of urinary albumin
levels, newly developed semi-quantitative screening methods base on immuno-reaction are
also available. The Micral-Test II strip74 (Roche Diagnostics) is an immunochemical strip
specific for albuminuria.72 In different multicenter studies, Giusepper et al71,75 demonstrated a
sensitivity of 95.2% and specificity of 84.7% while Mogensen et al71,76 reported 96.7%
sensitivity and 80% specificity when compared with the gold standard. It has been found to be
highly sensitive, effective, relatively cheap and rapid tool for detecting MAL. Studies 64,71,75,76
have shown that MAL measurement alone using Micral-Test strip is the choice method for
rapid, reliable point-of-care screening. The gold standard (24hours urine albumin estimation)
and UACR are not economically justifiable as they are too cumbersome and complex to
perform both for the researchers and the patients 75-77 Therefore, measurement of microalbumin
alone in a clean catch spot morning urine sample is more convenient in daily clinical
practice.72,78
The Micral-Test is a semi-quantitative immunoassay strip specific for albuminuria. It consists
of reagent pads. Urine is drawn by a chromatographic process through the wick fleece to the
buffer fleece, where the sample is adjusted into alkaline PH. In the conjugate fleece, albumin
in the urine binds to a soluble conjugate of albumin antibody and B-Galactosidase. Excess
antibody is then bound to immobilized albumin in the capture matrix and thus is effectively
removed from the sample, so that only albumin bound to the antibody-enzyme complex reaches
the colour substrate pad. The substrate is Chlorophenol Red Galactoside, which turns red when

27
the galactose is split by the B-Galactosidase. The intensity of the colour produced is
proportional to the albumin concentration in the urine. The colour formed after the specified
time is compared with the reference chart on the vial comprising of four colour blocks
corresponding to albumin concentrations of 0, 20, 50, and 100mg/L.74 Concentrations are read
after sixty (60) seconds of removing the strip from the urine. The strip is in contact with the
urine at a specific level on the strip for five (5) seconds only. Shorter contact time results in
under estimation of the albumin concentration and vice versa.65
Figure 1: COMPONENTS OF THE MICRAL TEST STRIP

28
2.2.6 Prognostic Implications and Clinical Pattern of Microalbuminuria in
Hypertension
MAL has prognostic implication in HTN. The presence of MAL in patients with HTN carries
an increased risk for CV morbidity and mortality.79 Mathew79 in his review observed that CV
complications such as coronary artery diseases, peripheral artery disease and retinopathy were
more frequent in patients with MAL. Bjorin et al22 in the LIFE study also reported that
hypertensive patients with MAL have an increased thickness of the carotid intimal and medial
layers suggesting a greater degree of atherosclerosis.
A recent attempt at explaining the relationship between MAL and various CV and renal
findings such as LVH, carotid thickening and renal injury implicated the role of Angiotensin
II and Transforming Growth Factor (TGF-β1).10 Increased TGF-β1 and angiotensin II in HTN
and diabetes can lead to increased collagen IV and fibronectin production as well as decreased
lysosomal activity. Collagen IV and fibronectin promote hypertrophy and/or fibrosis in the
kidney, heart and other vascular beds while the decreased lysosomal enzyme activity especially
cathepsin with the consequent impaired post-glomerular albumin degradation results in MAL.
Therefore, MAL could signal the presence of generalized atherosclerosis with the kidneys as
the window.
A wide variety of data have shown positive correlation between MAL and several other clinical
factors such as mean arterial pressure (MAP), Body mass index (BMI), smoking, alcohol
consumption, family history of HTN/CKD and herbal therapy.
At the end of this proposed study, the prevalence of MAL as well as the associated factors
should be clearly highlighted and risk stratification of patients with essential HTN in this
environment can be recommended. Risk stratification with early institution of the appropriate
strategies for the optimum quality of life of these patients is of paramount importance to a

29
family physician. By virtue of training, Family Physicians holistically care, not only for the
disease but also for the effect of the illness on the index patient as well as the family.
2.3 CONTROL OF MAL WITH REFERENCE TO USE OF ANTI-
HYPERTENSIVE AGENTS
MAL has been found in varying proportion of patient with EHTN. Using sensitive methods of
urinary albumin quantification. Maria et al61 and Volpe et al80, have shown that urinary albumin
excretion (UAE) rate is significantly and positively correlated to the level of arterial pressure.
This suggests that MAL might be a consequence of HTN.
Therefore, control of BP would lead to reduction in UAE in patients with HTN.
This has been shown to be the case in some studies.51,61,80
Several classes of antihypertensive drugs with varied mode of action are currently available for
the control of hypertension. Some of the widely used therapeutic classes include the following:
Diuretic – mainly Thiazide diuretics.
Alpha–adrenoceptor antagonists e.g. Prazocin
β–Adrenoceptor antagonists e.g. Propranolol, Atenolol.
Vasodilators e.g. Hydrallazine.
Calcium channel blockers e.g. Nifedipine, Amlodipine.
Central acting drugs e.g. Methyldopa, Reserpine.
Angiotensin Converting Enzyme Inhibits (ACE–I) e.g. Captopril, Lisinopril.
Angiotensin Receptor Blockers (ARB ) e.g. Losartan, Candesartan

30
These groups of antihypertensive drugs also show different actions regarding kidney function.
This has led to the question of differences concerning reduction of MAL by these different
agents. Different groups of workers have tried to find out the effect of certain antihypertensive
agents on excretion of albumin by the kidneys. More recent studies23-33,81-85 have clearly shown
that ACE–I and ARB significantly reduced UAE in EHTN than any other group despite similar
antihypertensive efficacy.
These agents (ACE–I & ARB) have also been shown to reduce MAL in Non-Insulin Dependent
and Insulin Dependent Diabetics with incipient diabetic nephropathy (persistent MAL) and
postpone or even prevent progression to clinical overt diabetic nephropathy.87-89,90-93
Also in hypertensive diabetics with overt proteinuria, ACE–I & ARB have been shown to
reduce protein excretion and that the anti-proteinuric effect is independent of the effect on
systemic BP. The mechanism of the beneficial effects of ACE-I and ARB on proteinuria in
patients with pre-existing renal disease as well as in patients with EHTN is believed to be
through the reduction of intraglomerular pressure and hyperfiltration. The reduction of
systemic BP may certainly play a role through reduction of filtration pressure. These findings
suggest that screening and intervention programmes instituted early are likely to have life-
saving effects. And this leads to a considerable economic gain by reducing the rate of
progression to overt hypertensive/diabetic nephropathy with its attendant morbidity and
economic burden on the patient and family.

31
CHAPTER THREE
MATERIALS AND METHOD
Study Site
The study was carried out at the General Outpatient Clinic (GOPC) of Federal Medical Centre,
Abeokuta. The Centre is a relatively young tertiary institution established in 1993 by the
Federal Government of Nigeria to cater for the health need of the people of Ogun State and its
neighboring states in South West Nigeria. The state has a population of about 3.7 million and
a land area of about 16,409.2 square kilometer going by the 2006 population census.
The hospital has a total of 200 bed spaces and runs residency programme in family medicine,
internal medicine, paediatrics and obstetrics and gynaecology. The GOPC is run by the
department of family medicine and its attendance was 15,494 in the year 2008 with a monthly
average of 1291. The total number of hypertension cases seen over this period was 5412
translating to 34.9% of GOPC attendance. The GOPC is located close to the main gate of the
hospital. It has 4 consulting rooms and a waiting room with facilities to accommodate up to
100 patients at a time. It is managed by the medical and non-medical teams comprising of the
doctors, nurses, records and administrative officers. It has both account and records units
attached to it. All the other units such as laboratory, physiotherapy e.t.c are used centrally.
Study Population
The entire 5412 adult male and female patients aged 18years and above with HTN attending
the GOPC of the hospital. The selection (inclusion and exclusion) criteria are as under listed:
Inclusion Criteria

32
Adult male and female patients aged 18years and above with essential HTN, either newly
diagnosed or already on treatment, attending the GOPC of the hospital. All subjects who
voluntarily signed the informed consent.
Exclusion Criteria
History was obtained from all subjects and complete physical examination was carried out to
exclude secondary hypertension and other causes of MAL. Reference was made to old records
where necessary. Urinalysis was done using the Combur strip. These in addition to clinical
evaluation as highlighted above were used to exclude the under listed:
1. Urinary tract infection (UTI): ) other causes of proteinuria
2. Chronic renal disease ) ,,
3. Congestive cardiac failure ) ,,
4. Diabetes mellitus ) ,,
5. Acute febrile illnesses and emergency conditions ) ,,
6. Pregnancy ) ,,
7. Evidence of secondary HTN
8. Macroalbuminuria
9. Refusal to give consent
Study Design

33
This research was a hospital based cross sectional descriptive study.
Sample Size
Sample size was calculated using the formula:94
nf = n / { 1+ n/N }
Where:
nf = Desired sample size when the study population to be represented is less than 10,000
n = z2 p q / d2 = Desired sample size when the study population to be represented is greater
than 10,000
N = Entire hypertensive population attending GOPC of FMCA = 5412
z = Standard normal deviate often set at 1.96. This corresponds to 95% confidence interval
(CI)
p = Prevalence (Prevalence of MAL among patient with essential HTN)
q = 1.0 – p
d = Degree of accuracy desired
To calculate the minimum sample size for this study,
z = 1.96
p = 41%. (Odili in Jos.37)
34
d = 0.05. Since the degree of accuracy desired is 95%
Since
n = (1.96)2 x 0.41 x 0.59 / (0.05)2 = 382.77 .
Hence
nf = (382.77) / [ 1 + (382.77 / 5412) ] = 357.48
This was approximated to 360
Adding 10% attrition value, a total of 395.373 was obtained. Based on this, the estimated
sample size will be approximated to 395 subjects.
Sampling Method
A systematic sampling method was employed. The first subject was selected by balloting once
at the outset of the study. On subsequent days, subjects were recruited as they presented to the
GOPC. With a monthly average of 451 hypertensive patients, a total of 1353 hypertensive
subjects could be recruited in three months. This gave a sampling interval of 3. Therefore,

35
every 3rd patient with essential HTN who presented at the GOPC and met the selection criteria
was enrolled into the study. All enrolled subjects gave informed consent to participate in the
study.
Materials
The materials used included the following:
A semi-structured questionnaire was used. Its validity and reliability were assessed
through a pre-test in a similar setting at the hypertensive clinic of the medical outpatient
department (MOPD) of the hospital. About 30 subjects were selected haphazardly95 and the
questionnaire was administered to them. Necessary amendment was then made on the
questionnaire based on the outcome of the pre-test before finally adopted for the study. The
questionnaire contained various items including sociodemographic characteristics, medical
history, physical examination and investigations (urine tests). Also serial number and coded
hospital number were represented. For absolute confidentiality, Alphabets A-I respectively
represented figures 1-9 while J stood for zero in the coded hospital number. The research
assistants were well informed about this.
Patient’s case note (GOPC): Used in addition to history and physical examination to rule
out secondary causes of HTN and other chronic conditions as highlighted under exclusion
criteria.
Accosson Mercury Sphygmomanometer: For BP measurement in millimeters of
mercury.
Littmann’s Stethoscope: BP measurement and auscultation during physical examination.
Urine testing strips:
(a) Combur–Test from Roche Diagnostics, Mannheim, Germany: For urinalysis

36
(b) Micral–Test II from Roche Diagnostics, Mannheim, Germany: For MAL
estimation
Sterile universal bottles: To collect early morning urine sample
Refrigerator: To store the heat sensitive Micral–Test II strip at +2oC to +8oC
Standard weighing scale from Surgifriend Medicals, England: For weight measurement
in Kilometer (Kg).
Stadiometer from Surgifriend Medicals, England: For height measurement in centimeter
Tape measure: To measure waist and hip circumference in centimeters (cm).
Stop watch: For timing during urine testing for MAL with the Micral–Test II strip.

37
DATA COLLECTION PROCEDURE
Protocol -1: Clinical Evaluation
Baseline clinical and demographic characteristic were obtained from all qualified subjects
using the semi-structured questionnaire.
With the subject seated and rested for 5minutes, BP was measured in the right arm by the
researcher aided by trained research assistants using Accosson® mercury sphygmomanometer
(cuff size 12.5 x 40cm). Systolic and diastolic BP were measured at Korotkoff phases I & V
respectively. The mean of two BP measurements taken at an interval of at least 2 minutes61 was
used. Blood pressure ≥140/90mmHg was taken as hypertension.
Mean arterial pressure (MAP) was calculated thus:
MAP = Diastolic BP + 1/3Pulse Pressure
Subjects were weighed in light clothes without shoes or other items such as handset, bunch of
keys etc using Surgifriend Medicals’ standard weighing scale to the nearest 0.1kg. The
weight was read with the subject standing still in the middle of the scale’s platform without
touching anything with body weight equally distributed on both feet.96,97 Height was
measured with the Stadiometer to the nearest centimeter (cm) with subject standing erect,
position the head in the Frankfort horizontal plane (i.e looking straight ahead), heels together,
arms to the side, shoulders relaxed and putting on neither shoes nor head wear. Heels,
buttocks, scapulae (shoulder blades), and occiput were against the vertical board of the
stadiometer. The headboard of the stadiometer was then lowered upon the highest point of the
head with enough pressure to compress the hair. The measurement was read with the eye at
the same level with the headboard to avoid errors due to parallax.96,97 Body mass index

38
(BMI) was calculated using the formula BMI = weight (kg) / height2 (m2). (Normal range is
18.5-24.9kg/m2)
The waist circumference (cm) was measured with a tape measure as the horizontal
circumference midway between the lowest rib and the iliac crest. Hip circumference is the
maximum circumference around the buttock posteriorly and the pubic symphysis anteriorly to
the nearest centimeter.
Waist–Hip ratio (WHR) = Waist circumference / Hip circumference
Normal is 1.0 for male and 0.8 for female
Protocol-2 : Screening for Microalbuminuria
All tests were personally carried out by the researcher according to the manufacturer’s direction
on the strip leaflets. Macroalbuminuria, glycosuria, microhaematuria, urinary evidence of
urinary tract infection (UTI) were first ruled out using the Combur-Test Strip. All patients
whose urine samples were negative for macroalbuminuria were further screened for
microalbuminuria using Micral-Test II Strip.
The Micral-Test Strip was immersed in clean catch spot morning urine sample such that the
fluid level was just between the two black bars on the strip, making sure that it didn’t touch the
side of the vessel in the process. Timing with stopwatch, the test strip was withdrawn after 5
seconds and placed across the top of the specimen bottle. After 1 minute, the colour of the test
pad above the inscription “Micral” was compared with the colour scale on the test strip
container label.

39
MAL was said to be positive when a urine sample produced a reaction colour corresponding to
20mg/L albumin (threshold for MAL) or more. The reaction colours range from white (MAL
<20mg/L) to deep pink (MAL >100mg/L).
DATA ANALYSIS AND PRESENTATION
Data was analyzed using SPSS software version 15.0 (SPSS, Inc. Chicago, Illinois).
Tables and charts were used as appropriate.
Continuous variables were presented as mean values and standard deviations. Categorical
variables were presented as frequencies. Chi-squared test was used to assess differences in
categorical variables while continuous variables were analyzed using z-test or t-test as
appropriate. A multivariate regression analysis was performed to identify independent factors
associated with MAL.
All the results from the regression model were shown as odds ratio with corresponding 95%
confidence intervals. All statistical tests were two-tailed and P-values < 0.05 were considered
statistically significant.
ETHICAL CLEARANCE AND APPROVAL
Approval and ethical clearance were obtained from FMC, Abeokuta Health Research ethics
committee. Informed written consent was obtained from the subjects prior to clinical evaluation
having duly informed them about the study. A copy of the consent form is attached as appendix-
II

40
FUNDING
Funding of the study was exclusively at the expense of the researcher. No subject bore any cost
that was directly related to the study.
41
CHAPTER FOUR
RESULTS
4.1 SOCIO-DEMOGRAPHIC DATA
4.1.1 AGE AND SEX DISTRIBUTION
Three hundred and ninety-five (395) patients with EHTN were screened. This comprised of the
minimum sample size of three hundred and sixty (360) and a 10% attrition rate of thirty five
(35) subjects. Data were however analyzed for the first three hundred and sixty (360)
respondents representing the actual sample size for the study.
There were one hundred and forty-two (142) males (39.4%) and two hundred and eighteen
(218) females (60.6%) aged between 25 and 107 years. There were more females than males
with a female to male ratio of 3:2. This shows that more female patients were present for daily
follow-up in the clinic [ Table 3, page 38 and Figure 2, page 40 ].
The characteristics of the patients are shown in Tables 3 and 4. It was observed that the mean
age of the patients with HTN was 57.24 ± 12.17 years with majority of the patients ≥60 years.
Expectedly, there were fewer patients in the age group 30-44 years.

42
Table 3: MEAN CLINICAL CHARACTERISTICS OF PATIENTS STUDIED
No of Patients Age (Yrs)
Mean ±
SEM
Duration of
Hypertension
(Yrs)
Mean ± SEM
Blood pressure mmHg
Mean ± SEM
State of Blood Pressure
Control
Level of MAL
(Mg/l)
Average number of
Drugs per patient
Males
Females
Systolic Diastolic Mean
Arterial
Controlld Stage I Stage II 20-50 51-100 >100 1
2
3
142
39.4
%
218
60.6%
73.48
± 15.10
21.09
± 12.24
159.50
± 21.09
92.38
± 12.85
113.16
± 18.89
89
(24.7%)
125
(34.7%)
146
(40.6%)
63
(31.5%)
65
(33.5%)
69
(35%)
6
(1.7%)
169
46.9
%
39
10.8%

43
Table 4: CLINICAL CHARACTERISTICS OF PATIENTS STUDIED USING THE AGE GROUPS
Age
group
(years)
No. of
Patients
No.
Females
No.
Males
Mean weight (kg) Mean Blood Pressure
9mmHg)
Average
Duration
of HTN
(years)
No. of
patients
on mono
therapy
No. of
patients
on
Multiple
therapy
Females Males Systolic Diastolic Mean
arterial
<30-34 12 7 5 66.2 72.8 150 98 118.8
1.41 0 2 (0.9%)
35-39 15 9 6 85.6 77.8 153 94 114.6
10.60 0 7(3.3%)
40-44 28 21 7 80.9 74.14 143 91 117.3
7.07 0 14(6.5%)
45-49 40 26 14 77.0 77.7 155 97 107.06
7.61 1 (0.5%) 21(9.8%)
50-54 41 25 16 77.7 77.3 158 95 110.1
15.92 0 22(10.2%)

44
55-59 48 23 25 78.8 76.3 159 94 114.0
9.94 2 (0.9%) 28(13.0%)
60-64 66 38 28 66.7 77.68 166 94 114.8
14.56 0 47(21.9%)
65+ 110 69 41 66.7 70.0 163 86 113.1
13.49 2 (0.9%) 69(32.1%)

45
Figure 2: AGE AND SEX DISTRIBUTION OF THE PATIENTS SCREENED
0
20
40
60
80
100
120
<30-34 35-39 40-44 45-49 50-54 55-59 60-64 65+
AGE GROUP OF PATIENTS
NU
MB
ER
OF
PA
TIE
NT
S
males
females

46
4.1.2 SOCIAL STATUS.
The result of social status of the patients is shown in Table 5. Two hundred and thirty five
(65.3%) of the patients were married while four (1.1%) were single. Others were either
widowed (23.3%) or divorced / separated (10.3%).
One hundred and fourteen (31.7%) had no formal education, sixty –eight (18.9%) of the
patients had primary education, while one hundred and sixteen (32.4%) of the patients had post
secondary school education.
In terms of occupation, ninety (25%) of the patients were traders, sixty–seven (18.6%) were
pensioners, thirty-eight were business personnels (10.6%), thirty-four were civil servants
(9.4%) and others were professionals (3.9%), farmers (2.8%) and students (0.6%)
The religion predominantly practiced by the patients were Islam (127 patients – 35.3%) and
Christianity (233 patients – 64.7%). Also, most of the patients were Yoruba (89.4%), twenty
four (6.7%) were Igbo and only one of the patients was Hausa. The remaining thirteen (3.6%)
of the patients belong to other ethnic groups.

47
Table 5: SOCIO-ECONOMIC STATUS OF STUDY PARTICIPANTS
STATUS PATIENTS
Frequency Percentage (%)
MARITAL
Single 4 1.1
Married 235 65.3
Divorced/ separated 37 10.3
Widowed 84 23.3
EDUCATIONAL
Nil 114 31.7
Primary 68 18.9
Secondary 62 17.2
Post Secondary 116 32.4
OCCUPATION
Pensioner 67 18.6
Unemployed / retired 26 7.2

48
Artisan / Skilled labour 27 7.5
Trading 90 25
Business 38 10.6
Civil servant 34 9.4
Professional 32 8.9
Others 46 12.8
RELIGION
Islam 127 35.3
Christianity 233 64.7
ETHNIC GROUP
Yoruba 322 89.4
Hausa 1 0.3
Igbo 24 6.7
Others 13 3.6
4.1.3 ANTHROPOMETRY

49
The mean weight of the patients was 73.48+15.10 kilograms while the mean height of the
patients was 1.65+0.09 meters. Table 6 shows other anthropometric characteristics of the
patients. The mean hip and waist measurements of the patients were 96.76+13.56 and 103.77+
13.39 respectively.
Correspondingly, the mean BMI and waist-hip ratio (WHR) of the patients were 26.79+5.65
and 0.93+0.06 (Table 6).
One hundred and forty-two (142) of the patients had normal BMI status, while one hundred
and eighteen (118) patients were overweight and eleven (11) patients had under-weight BMI
(Figure 3). 89 patients were in the obesity category, out of which 59 were mild, 14 moderate
and 16 morbid in obesity.
Obesity was more among the female patients than males (Figure 4)

50
Table 6: ANTHROPOMETRY CHARACTERISTICS OF THE PATIENTS STUDIED
Mean BMI kgm-2
Mean Height (m)
Mean waist
circumference
Mean Hip
circumference
Mean WHR
26.79 ± 18.89
1.65 ± 0.09
96.76 ± 13.56
103.77± 13.39
0.93 ± 0.06

51
FIGURE 3: BODY MASS INDEX AND WAIST-HIP RATIO STATUS OF PATIENTS STUDIED

52
BMI status
0
50
100
150
200
250
underw
ieght
normal
overw
eight
mild
obes
ity
moder
ate
obesity
mobid
obes
ity
normal
high
NU
MB
ER
OF
PA
TIE
NT
S
Body Mass Index
(BMI)
Waist- Hip Ratio
(WHR)

53
FIGURE 4: BODY MASS INDEX AND WAIST –HIP RATIO STATUS AMONG MALE AND FEMALE
0
50
100
150
200
250
un
derw
ieg
ht
no
rma
l
ov
erw
eig
ht
mil
d o
be
sit
y
mo
de
rate
ob
es
ity
mo
bid
ob
es
ity
no
rma
l
hig
h
BMI status WHR status
NU
MB
ER
OF
PA
TIE
NT
S
female
male

54
4.1.4 CLINICAL FINDINGS
The mean systolic and diastolic BP and mean arterial pressure (MAP) of the patients in this
study were 159.50+21.09, 92.38+12.85 and 113.16+18.89mmHg respectively (Table 3).
This study showed that 146 (40.6%) of the patients were at stage-II of JNC-VII essential HTN
while 125 (34.7%) were at stage-I. Only 89 (24.7%) of the patients had their BP under control.
Among these patients, EHTN was more prevalent as age increases (Tables 3 and 4).
The duration of HTN since diagnosis ranged between less than a year and 40years (Figure 5).
Majority of the patients were diagnosed less than ten years ago while only few of them had
been diagnosed of HTN more than 30years ago (Figure 5)
Two hundred and seventy-nine (279) of the patients (77.5%, Figure 6) were positive to MAL
test and this was more evidenced in patients between the age group 60years and above.
MAL level of the patients was between 20 to above 100mg/L (Table 3). Sixty three of the
patients had between 20-50mg/L while 65 and 69 of the patients had between 51-100 and above
100mg/L level of MAL respectively.
Also, occurrence and level of MAL tend to increase in the patients with EHTN as the age of
the patients increases (Figure 7).
Smoking and Alcohol drinking were among the obvious risk factors observed for MAL among
the patients with EHTN in this study. As at the time of data collection, ten (2.8%) of the patients
claimed that they smoked daily. Number of sticks smoked per day was between 1 and 10. Three
of the patients claimed to smoke 5 sticks per day while 7 patients smoked 10 sticks per day.
The duration (in years) of smoking among the patients was minimum of one and maximum of
40 years (Table 7).

55
Thirty-three (9.1%) of the patients claimed to have smoked in the past for between 1 and 40
years. 17 of them smoked for >11< 40 years while the remaining 16 smoked for less than 10
years. In addition, the number of sticks smoked per day was between 1 and 20 out of which 20
of the patients claimed to have smoked between 1-5 sticks daily and 8 patients claimed between
11 and 20 sticks per day (Table 7).
Twenty-three (23) of the patients later stopped smoking for as long as between one and forty
years to the time of this study. Seventeen of them stopped about 40 years prior while the other
16 subjects stopped less than ten years ago (Table 7).
Alcohol consumption among the respondents is shown in Table 8. Only 45 patients claimed to
consume alcohol (alcoholic wine, beer and gin). Beer as a brand of alcohol was more frequent
among the patients than other brands with alcoholic wine and gin being the least consumed.
Most of them (34) have consumed alcohol for over 10 years while 30 of them stopped alcohol
10 years earlier. Only five (5) patients were still taking alcohol up till less than a month prior
to this study.
Since significant ingestion of alcohol is defined as more than 4 units (32g or big bottle of beer)
per day for men and more than 2 units per day for women, most of these patients (>34)
consumed medically significant quantity of alcohol.
Consumption of herbal preparation was prevalent among the patients studied (293; 81.4%).
Herbal preparations were taken regularly by 177 (60.4%) of the patients while 116 (39.6%)
took the products occasionally (Table 9).

56
Figure 5: DURATION OF HYPERTENSION SINCE DIAGNOSIS
0
20
40
60
80
100
120
140
160
<1 1-4 5-9 10-14 15-19 20-24 25-29 30-34 35-40
NU
MB
ER O
F PA
TIEN
TS

57
DURATION IN YEARS

58
FIGURE 6: DISTRIBUTION OF PATIENTS WITH ESSENTIAL HYPERTENSION
WITH RESPECT TO MICRAL TEST
positive
77%
negative
23%

59
FIGURE 7: AGE DISTRIBUTION AND LEVEL OF MICROALBUMINURIA IN PATIENTS STUDIED
TABLE 7: PREVALENCE OF CIGARETTE SMOKING AMONG PATIENTS WITH ESSENTIAL HYPERTENSION
SMOKING PRESENTLY
SMOKED IN THE PAST
Smoke as
at present
No. sticks per day Years smoking Smoke in
the past
No. sticks per day Years smoked Years stopped
smoking
Yes No sticks Patients years patients Yes No Sticks patients years Patients years patients

60
10
350
1-5
3
1-10
1
33
327
1-5
20
1-10
16
1-10
16
10-20
7
11-20
1
6-10
5
11-20
8
11-20
4
11-15
-
21-30
1
11-15
1
21-30
8
21-30
2
20 +
-
31-40 +
7
20 +
7
31-40 +
1
31-40
1
TABLE 8: PREVALENCE OF ALCOHOL CONSUMPTION AMONG PATIENTS WITH ESSENTIAL HYPERTENSION

61
PRESENTLY
IN THE PAST
Take
Alcohol?
Brand Duration Alcohol in
the past
Duration Years stopped Alcohol
Yes No Wine 1 years patients Yes No Years patients years patients
45
315
Beer
38
1-10 11
34
326
1-10 16 >1 5
Gin 2 11-20 17 11- 20 11 1-10 16
Beer +
Gin
2 21-30 8 21- 30 12 11-20 4
All 2 31-40 + 9 31-
40+
5 21-40+ 9

62
TABLE 9: CONSUMPTION OF HERBAL PREPARATION AMONG PATIENTS
WITH ESSENTIAL HYPERTENSION
Take Herbal Preparations
How Often
Yes
No
Occasionally
Regularly

63
293
67 116 177

64
4.2 ASSOCIATION OF RISK FACTORS WITH MAL AMONG PATIENTS WITH ESSENTIAL
HYPERTENSION
4.2.1 MAL AND HERBAL CONSUMPTION
Association of risk factors with MAL was observed among the patients studied in this research (Table 10).
Majority (234; 83.9%) of the patients who tested positive to Micral test have taken herbal preparations at one time
or the other. Only 45 patients, though positive to Micral test did not take herbal preparations.
Further analysis showed that more patients who took herbal preparations regularly had >100mg/L level of MAL
(Figure 8).

65
TABLE 10: ASSOCIATION OF HERBAL PREPARATION CONSUMPTION WITH
MICROALBUMINURIA AMONG PATIENTS WITH ESSENTIAL HYPERTENSION.
CONSUMPTION OF HERBAL PREPARATION
Micral test Yes No
Positive 234 45
Negative 59 22
X2 Value
8.91, (p< 0.05)
Level of microalbuminuria
20 - 50 mg/l 50-100 mg/l >100mg/l
Take herbs 74 77 83
No herbs 8 7 30

66
Figure 8: A BAR CHART COMPARING LEVEL OF ALCOHOL CONSUMPTION WITH DEGREE OF
MAL
0
5
10
15
20
25
30
35
40
20-50mg/l 50-100mg/l >100mg/l
Level of Microalbuminoria
Nu
mb
er o
f P
ati
en
ts
ocassionaly
regularly

67
4.2.2 MAL AND ALCOHOL CONSUMPTION
Out of 45 patients who consumed alcohol, 36 were positive to Micral test with 10 patients having between 20-
50mg/L level of MAL, 19 patients having between 51-100mg/L level and 7 patients had above 100mg/L level
(Table 11).

68
TABLE 11: ASSOCIATION OF ALCOHOL CONSUMPTION WITH MICROALBUMINURIA
AMONG PATIENTS WITH ESSENTIAL HYPERTENSION.
ALCOHOL CONSUMPTION
Micral test
Positive 36
Negative 9
X2 Value
8.38 (p< 0.05)
Level of microalbuminuria
20 - 50 mg/l 50-100 mg/l >100mg/l
Take alcohol 10 19 7

69
4.2.3 MAL AND SMOKING
All the patients (10) who were still smoking at the time of data collection were positive to micral test of which
most of them (6) smoked between 6-10 sticks per day with 51-100mg/L level of MAL. Patients (7) who have
been smoking for over 30 years were predominantly among the patients that were positive to micral test with 4
of them having MAL level of >100mg/L (Table 12).
MAL was not however significantly associated with patients smoking in the past. Although, 21 of out of 33
patients who claimed to have smoked in the past were positive to mal test, this was not statiscally significant
(Table 13).

70
TABLE 12: ASSOCIATION OF SMOKING (PRESENTLY) WITH MICROALBUMINURIA AMONG
PATIENTS WITH ESSENTIAL HYPERTENSION.
SMOKING AT PRESENT
Micral test Yes
Positive 10
Negative -
Sticks per day
1-5 6-10 >10
No. of patients 3 6 1
Level of microalbuminuria
Sticks per day 20 - 50 mg/l 50-100 mg/l >100mg/l
1-5 1 2 0
6-10 0 3 3
>10 0 0 1
Level of microalbuminuria
How long been
smoking 20 - 50 mg/l 50-100 mg/l >100mg/l
1-10 1 0 0

71
11-20 1 0 0
21-30 0 1 0
30-40+ 1 2 4
TABLE 13: ASSOCIATION OF SMOKING (IN THE PAST) WITH MICROALBUMINURIA AMONG
PATIENTS WITH ESSENTIAL HYPERTENSION.
SMOKED IN THE PAST
MAL
Negative Positive
Yes 12 21
No 76 251
X2 value 2.09, P = 0.147

72
4.2.4 COMBINATION OF RISK FACTORS (ALCOHOL, SMOKING AND HERBS) AMONG MAL
POSITIVE SUBJECTS
As depicted in Table 13B (page 63), two hundred and thirty-eight (85.3%) of MAL positive patients were taking
herbal preparations without smoking or taking alcohol.
Thirty-three (11.8%) subjects took herbal preparations as well as drank alcohol while six (2.2%) subjects
combined herbs consumption with smoking.
Only two of the MAL positive patients indulged in all of these three factors (smoking, alcohol and herbs
consumption).

73
TABLE 13B: PROPORTION OF MAL POSITIVE SUBJECTS THAT SMOKED, DRANK ALCOHOL
AND/OR CONSUMED HERBS.
FACTORS
PROPORTION OF MAL POSITIVE SUBJECTS
All factors (herbs, smoking &
alcohol)
2 (0.7%)
Herbs & smoking 6 (2.2%)
Herbs & alcohol 33 (11.8%)
Herbs only 238 (85.3%)
74
4.3 INFLUENCE OF AGE, GENDER AND BLOOD PRESSURE ON MICROALBUMINURIA AMONG
THE STUDY POPULATION.
In this study, significant positive association existed between age of the patients and MAL (X2 4.93; P value
0.026) (Table 14). Ninety four (94) patients out of one hundred and ten (110) that were above 65 years of age
were positive to Micral test. Also a progressive increase in the percentage of the number of patients with MAL
occurred as age of the patients increased.
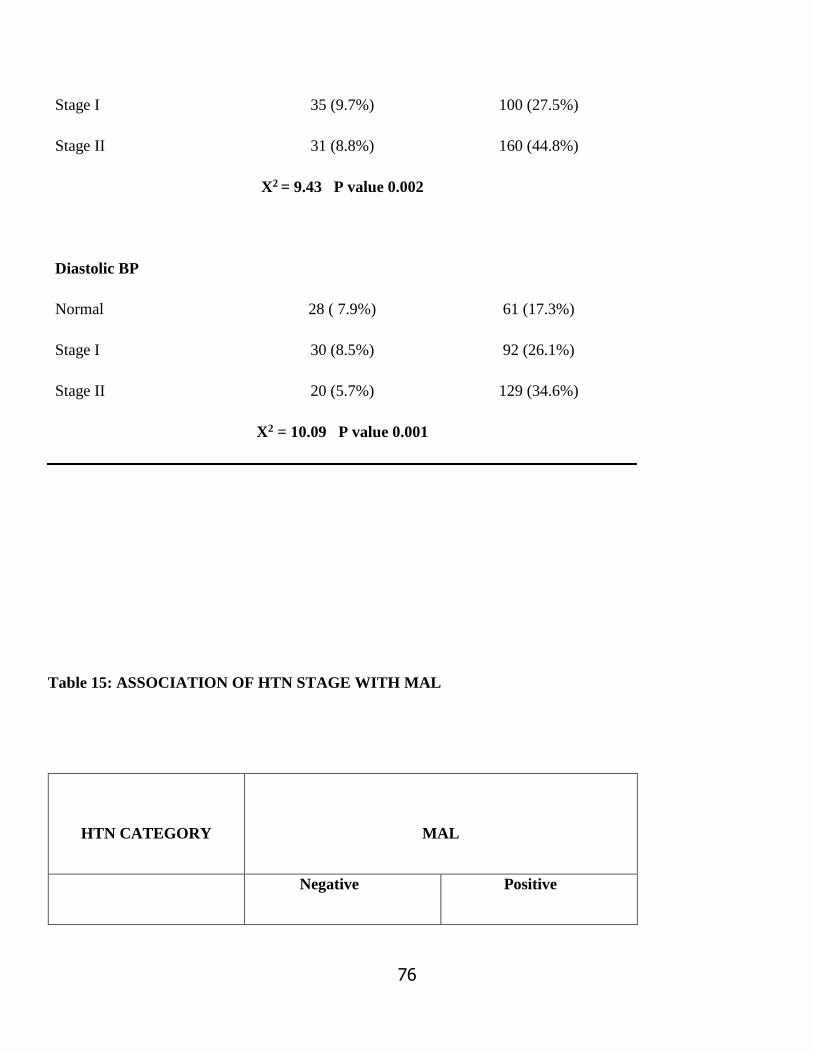
It was noted that the prominence of MAL among these patients with EHTN was significantly associated with
level of systolic and diastolic BP. There was a progressive increase in the proportion of patients with MAL (X2
9.43; P value 0.002 and X2 10.09, P value 0.001 for systolic and diastolic BP respectively) as the level of systolic
and diastolic BP increased (Table 14). Also, the stage of HTN in patients studied was strongly associated with
MAL. Highest number (124) of patients with mal had stage II HTN, while the least number (61) of patient
positive to MAL were at the normal/controlled stage of HTN. Also number of patients positive to MAL increased
as the HTN status of the patients increased (Table 15).
Gender of the patients however did not have any significant association with MAL (Table 14).

75
Table 14: ASSOCIATION OF RISK FACTORS WITH MAL AMONG THE STUDY GROUP
MICRAL TEST
Status
Age
Negative Positive
<30-34 1 (0.3%) 11 (3.1%)
35 – 39 6 (1.7%) 9 (2.5%)
40 – 44 11(3.1%) 17 (4.8%)
45 – 49 10 (2.8%) 30 (8.4%)
50 – 54 10 (2.8%) 29 (8.1%)
55 – 59 10 (2.8%) 38 (10.6%)
60 – 64 12 (3.4%) 54 (15.1%)
65 + 18 (5.0%) 94 (26.1%)
X2 = 4.93 P value 0.026
Gender
Male 35 (9.0%) 110 (30.8%)
Female 46 (12.9%) 169 (47.3%)
X2 = 0.065 P value 0.795
Systolic BP
Normal 12 (3.4%) 20 (5.7%)
76
Stage I 35 (9.7%) 100 (27.5%)
Stage II 31 (8.8%) 160 (44.8%)
X2 = 9.43 P value 0.002
Diastolic BP
Normal 28 ( 7.9%) 61 (17.3%)
Stage I 30 (8.5%) 92 (26.1%)
Stage II 20 (5.7%) 129 (34.6%)
X2 = 10.09 P value 0.001
Table 15: ASSOCIATION OF HTN STAGE WITH MAL
HTN CATEGORY
MAL
Negative Positive
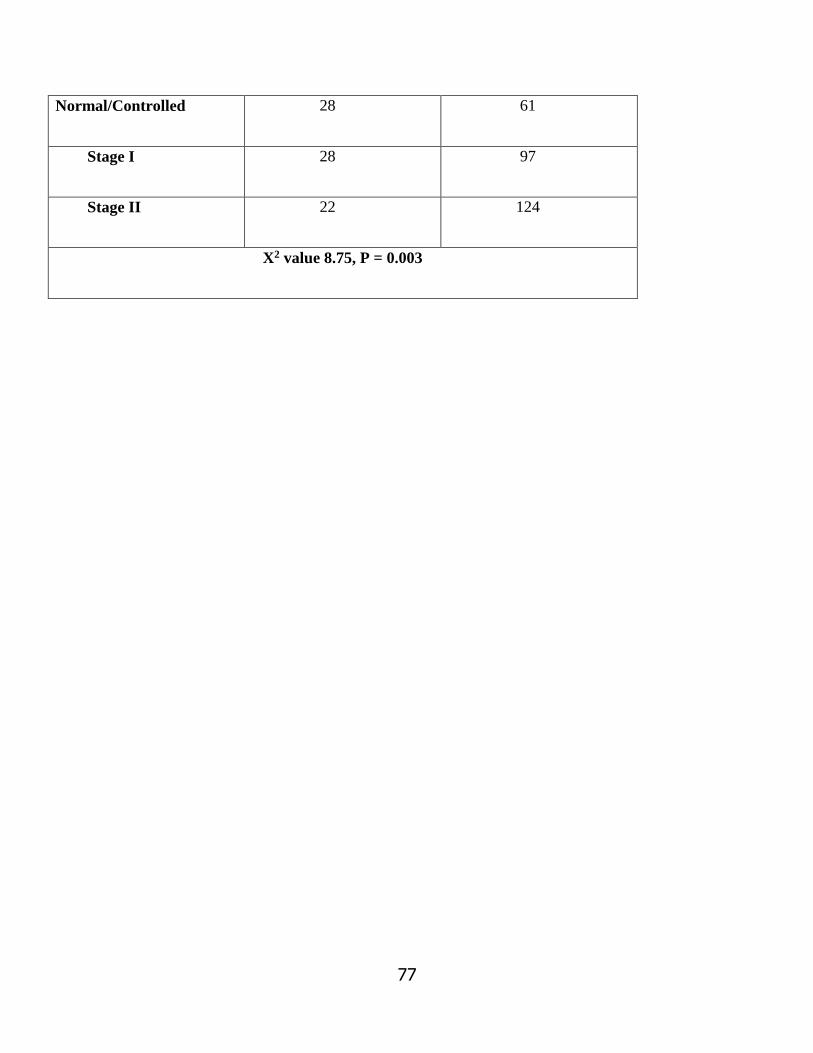
77
Normal/Controlled 28 61
Stage I 28 97
Stage II 22 124
X2 value 8.75, P = 0.003

78
4. 4 ASSOCIATION OF AGE CATEGORY WITH MICROALBUMINURIA
The association between ages of patients with essential hypertension and MAL can further be shown by
categorizing respondents into clinical groups of (a) young (<45years), (b) middle age (≥45-64years) and (c)
elderly (>65years). Percentage of patients positive to Micral test increased significantly (P = 0.022) as the age
of the patients increased. Highest percentage of 83.9 was observed among the elderly, 78.2% among the middle
age while 67.2 % among the young (Table 14).

79
Table 16: AGE CATEGORY VERSUS MICROALBUMINURIA
Age category MAL
Negative Positive
Young( < 45 years) 18 37 (67.2 %*)
Middle age( 45 – 64 years) 42 151 (78.2%*)
Elderly ( ≥ 65 years) 18 94 (83.9%*)
X2 value 5.63, P = 0.022
*Percentage of patients positive to mal within each age category
Further analysis showed that MAL correlated positively and significantly with age, SBP, DBP and MAP with
respective r and p values of ( r = 0.113, P = 0.033 ), ( r = 0.200, P = 0.0001 ), ( r = 0.187, P = 0.0001 ) and ( r =
0.227, P = 0.0001 ) (Table 17).BMI, WHR and Pulse Pressure did not show any significant correlation with MAL
(Table 17).

80
TABLE 17: CORRELATION COEFFICIENT BETWEEN MAL AND OTHER PARAMETERS IN
HYPERTENSIVE PATIENTS
r value P value
Age 0.113 0.033
SBP (mmHg) 0.200 0.0001
DBP (mmHg) 0.187 0.0001
PP (mmHg) 0.095 0.074
MAP (mmHg) 0.227 0.0001
BMI (kgm-2) 0.023 0.664
WHR 0.005 0.924

81
Multiple regression analysis using microalbuminuric status as a dependent nominal variable, showed the
following parameters as significantly related independent variables: SBP (P=0.0001), and DBP (P=0.0001) (Table
18).
As depicted in Table 19, the SBP, DBP and MAP were significantly higher in hypertensives with MAL than in
hypertensives without MAL.

82
Table 18: MULTIPLE REGRESSION ANALYSIS USING MICROALBUMINURIC STATUS AS
DEPENDENT VARIABLE
P value
Age 0.260
SBP (mmHg) 0.0001
DBP (mmHg) 0.0001
PP (mmHg) 0.751
MAP (mmHg) 0.585
BMI (kgm-2) 0.212
WHR 0.445

83
Table 19: CLINICAL CHARACTERISTICS OF PATIENTS WITH OR WITHOUT MAL
Characteristics Microalbuminuric Normoalbuminuric T value P value
WHR 0.931±0.06 0.931±0.08 0.096 0.924
BMI (kgm-2) 26.84±5.76 26.52±5.32 0.45 0.650
PP (mmHg) 68.00±1.13 63.65±2.16 1.78 0.077
MAP (mmHg) 116.18±0.78 109.04± 4.69 0.0001
SBP (mmHg) 161.52±1.26 151.47±2.09 4.11 0.0001
DBP (mmHg) 93.51±0.75 87.82±1.38 3.61 0.0001

84
CHAPTER FIVE
DISCUSSION
The prevalence of MAL in this study was found to be 77.5%. The figure is somewhat high and much more than
a range of 5-40% reported in literature from previous studies.16,35,36,98,99 Nevertheless, it is keeping with the current
prevalence of MAL in recent studies in which a higher range of 53-71% was reported.80,100 The wide variability
in prevalence observed in both the old and recent studies is due to factors such as cut-off value for HTN, severity
of disease, age and sex distribution and presence or otherwise of concomitant CV risk factors. Other factors are
patient selection procedures, sample size, method of determination of MAL, duration of HTN and existence of
prior treatment associated with adequate or inadequate control of HTN by drug therapy, the type of which may
highly influence albuminuria.16,101
A high prevalence was demonstrated by Bohm et al in i-SEARCH study, a broad based international survey
conducted in 2007 in which approximately 22,000 hypertensive patients with or without CV disease were
recruited at 1750 study centers.80,100 The highest rate was found in patients with uncontrolled HTN.
This work showed a trend towards older age hypertensives. 176 patients (48.9%) of the respondents were above
60 years out of which 62.5% (110 patients) were well over 65 years. Odili37 in her study in Jos got a prevalence
of 41%. But she recruited only 105 subjects with mean age of 45.5+10.11 as against 360 subjects with mean age
of 73.48+15.10 in this study.
Quite obvious in Table 3 is the poor level of BP control in the study group. Only 89 patients (24.7%) had
controlled HTN while the remaining 271 patients (75.3%) were at either JNC VII stage I (34.7%) or stage II
(40.6%) despite drug therapy. This high level of uncontrolled HTN may be attributable to various reasons ranging

85
from poor drug adherence for financial reasons to poor information on the chronicity of the disease resulting in
some patients going on drug holidays.
The level of BP (JNC VII staging) and duration of HTN is another strong factor to consider in explaining the high
prevalence of MAL in this study. Alfonso et al and several other researchers10,15,17,61,102 were able to demonstrate
a direct relationship/variation between MAL and level/duration of HTN. The mean duration of HTN (in years) in
this study was 21.09+12.24 while 146 patients (40.6%), the largest group, were in stage II HTN.
The level of consumption of herbal preparation is another strong factor that could have influenced the high
prevalence of MAL obtained in this study.67,103 Most of the prevalence rates of MAL quoted in the literature were
from studies among the Caucasians in advanced countries.16,35,36 In these enlightened populations, the use of
medicaments are generally controlled. The few adopted complementary alternate medicine (CAM) have a
reasonable scientific back up. In the study population however, 293 (81.4%) of the subjects have taken various
types of herbal preparations and a larger percentage (60.4%) did so on regular basis.
The prevalence of MAL in any study has been shown in the literature to be influenced by the choice/type of
laboratory method employed in detecting MAL.75 Generally, the standard quantitative methods such as
Radioimmunoassay (Gold standard), Laser immunonephelometry, Immunoturbidimetry etc have much higher
specificity with greater reduction in false positive rate than the qualitative and semi-quantitative methods79 such
as the one (Micral test) used in this study.
When the Micral test strip is used, two to three non-consecutive urine samples have been recommended to increase
the reliability of the result.10,69 In this study however, only one urine specimen was used in order to cut cost.
There was no significant relationship/correlation between MAL and gender of the patients’ family history of
HTN, BMI, WHR and PP. There are conflicting reports from studies on the correlation between MAL and age
and gender of the patients. While Leoncini et al20 showed that MAL is independently associated with male gender

86
and older age, Odili et al37 and Olatunde et al98 found no association between MAL and gender, age of the patients
and BMI. Except for multiple regression analysis, most of the other relevant statistical tools used in the previous
studies showed significant positive association between MAL and PP.62 This research work however found no
such positive association. Massimo et al62 was able to establish in his study that PP and isolated systolic HTN are
directly related to MAL independent of diastolic BP and other correlates. PP, which is calculated as systolic minus
diastolic BP, tends to be more significant with high rate of isolated systolic HTN. Most of the subjects in this
study were however above 60years of age and had both systolic and diastolic HTN.
This study found a statistically significant difference in the means of the SBP, DBP and MAP of the
microalbuminuric hypertensive patients compared with normoalbuminuric hypertensive ones. There was also a
significant and positive correlation between MAL and SBP, DBP, MAP and age of the patients. These findings
are partly in keeping with the report of the study by Massimo et al.62 These authors found that MAP and isolated
systolic HTN were significantly related to urinary albumin excretion (UAE) and prevalence of MAL. Olatunde
et al98 also reported a significant and positive correlation between MAL and SBP but not DBP.
Although SBP has remained a more consistent determinant of MAL in hypertensives,62 some other studies have
also implicated DBP and PP. de-la-Sierra et al 104 reported that patients with MAL showed significantly higher
values for 24 hours, day-time and night-time SBP and DBP compared with hypertensives with normal UAE. A
study of 134 women and 212 men conducted by Leoncini et al among newly diagnosed hypertensive patients
showed that DBP was independently correlated with UAE.69
Smoking has been shown to be a strong risk factor for MAL in patients with EHTN. As shown by this study, all
of the ten respondents who were still smoking as at the time of this study tested positive to MAL. Also 63.6% (21
patients) of those who have stopped smoking had MAL. Halimi et al66 worked extensively on effect of smoking
on proteinuria and his findings were similar to those in this study. He reported that current smoking and past

87
smoking were associated with high and similar risk of proteinuria even when the pack-year was reduced. From
the study, Halimi and co-workers concluded that smoking (currently or in the past) represented the most powerful
risk for MAL among men and women, even when normotensive and hypertensive subjects were analyzed
separately and even when a different cut-off for HTN was used.

88
RELEVANCE OF THE STUDY TO FAMILY MEDICINE
Family Physicians as the doctors of first contact can not afford to miss out any important prognosis-influencing
measure in the course of providing highly professional, holistic, comprehensive and continuous care for which
the specialty is noted for. Management of HTN falls in the category of continuous care. Numerous studies have
provided evidence that MAL is a strong, independent and the most sensitive predictor of CV events and
progressive nephropathy. The risk for CV morbidity and mortality is linearly related to urinary albumin excretion
and the reduction of albuminuria (at microalbuminuric stage) using anti-RAAS anti-hypertensives
correspondingly parallels reduction or reversal in CV risk.23-25,28,30,35 Family physicians who diagnose and initiate
management in most cases are well placed for this simple step towards reversing the trend of CVD and CKD.
Hence CVD risk stratification by means of MAL screening at diagnosis and at intervals during therapy should be
inculcated into the routine care of patients with primary HTN. This will ultimately reduce the short and long term
economic burden on the nation and, more importantly, the family which is the focus of care in Family Medicine.

89
LIMITATIONS OF THE STUDY
The limitations of the study are:
First is the cost of the study. Micral test strip which is the basic unit for this research work is not readily
available in our country, Nigeria. Therefore, the cost is very high (N350 per unit). Because of this enormous
cost, Micral testing was done once in each subject as against the preferred twice-thrice to increase validity.
Secondly, some of the patients that were labeled primary hypertensives might indeed be secondary
hypertensives. This could have been avoided if facilities were readily available and affordable for extensive
investigations.
Lastly, the study was conducted in a tertiary hospital and cross-sectional in design. The inference drawn from
the results should be taken with caution when comparing with community survey.

90
CONCLUSION
This study has shown that:
There is a high prevalence (77.5%) of MAL among adult Nigeria hypertensive patients.
Essential hypertensive patients who smoke, take excess alcohol, consume herbal preparations, in older ages
(>60years) and with higher SBP, DBP and MAP are at increased direct risk of MAL.

91
RECOMMENDATIONS
1. Routine screening of MAL in newly diagnosed and old hypertensive patients and further check-ups at intervals
during follow-up.
2. Essential hypertensive patients should be categorized at diagnosis into high or low risk for MAL based on
age, SBP, DBP and /or MAP.
3. Larger (community based) studies with longitudinal follow-up are advocated to really establish: (1) the
importance of MAL in non-diabetic essential hypertensives and (2) to demonstrate MAL reversibility or
modifiability of ACE-I and ARB for better first contact management of hypertension.

92
REFERENCES
1) George A. Mensah. Epidemiology of stroke and high blood pressure in Africa. Heart 2008; 94: 697-705
2) Ratto E, Leoncini G, Viazzi F, Vaccaro V, Parodi A, Falqui V et al. Metabolic Syndrome and
Cardiovascular risk in Primary hypertension. J Am Soc Nephrol 2006; 17 : S120-S122
3) Integrated Management of Cardiovascular Risk: Report of a WHO meeting. NLM Classification 2002;
WG166.
4) Olatunbosun ST, Kaufman JS, Cooper RS, Bella AF. Hypertension in black population: Prevalence and
biosocial determinants of high blood pressure in a group of urban Nigerians. Journal of Human
Hypertension 2000; 14:249-257
5) Hwang KK, Scott LJ, Chfamba J, Mufunda J, Spielman WS, Sparks HV. Microalbuminuria in urban
Zimbabwean woman. Journal of Human Hypertension 2000;14:587-593
6) Kearney PM, Whelton M, Reynolds K, Munter P, Whelton PK, Jian H. Global burden of hypertension:
analysis of worldwide data. The Lancet 2005; 365 (9455): 217-223.
7) Erhun WO, Olayiwola G, Agbani EO, Omotoso NS. Prevalence of hypertension in a University
community in South West Nigeria. African Journal of Biomedical Research 2005; 8: 15-19.
8) Lisnel HO, Yackoob KS. Hypertension in Sub-Sahara African Populations. Circulation 2005; 112: 3562-
3568.
9) Adedoyin RA, Mbada CE, Balogun MO, Martins T, Adebayo RA, Akintomide A. et al. Prevalence and
pattern of hypertension in a semiurban community in Nigeria. European J Cardiovasc Prevention &
Rehabilitation 2008; 15 (6): 583-687.

93
10) Lucinda MH, Leileata MR, Wayne DC. Insight into the relationship between hypertension and
albuminuria. Current hypertensive reviews 2007; 3 :29-37.
11) Giuseppe R, Jan JW. Albuminuria as early test for vascular disease. The Lancet 2005; 365 (9459): 556-
557
12) Richard D, Rustam R. Microalbuminuria: how informative and reliable are individual measurements?
Journal of Hypertension 2003 21: 1229-1233.
13) Klaus K, Knut BJ, Rasmussen BF, Gorm J, Peter C, Henrik S et al. Very low levels of microalbuminuria
are associated with increased risk of Coronary heart disease and death independent of renal function,
hypertension and diabetes. Circulation 2004; 110: 32-35.
14) Jafar TH, Stark PC, Schmid CH, Marcia L, Giusseppe M, deJong PE et al. Progression of chronic kidney
disease: The role of blood pressure control, proteinuria and Angiotensin-converting Enzyme Inhibition (A
patient-level Meta-analysis). Ann Intern Med. 2003; 139: 244-252.
15) Massimo V, Francesco C, Luis MR. Is it time to measure microalbuminuria in hypertension?. J Hypertens
2003; 21: 1213-1220.
16) Roberto P, Antonella S, Maura R, Clizia N, Francesca V, Angelito T et al. Prevalence and Clinical
correlates of Microalbuminuria in essential hypertension. Hypertension 1997; 30: 1135-1143.
17) Montalescot G, Collet JP. Preserving Cardiac function in the hypertensive patient: why renal parameters
hold the key. European Heart Journal 2005; 26: 2616-2622.
18) Leoncini G, Viazzi F, Parodi D, Ratto E, Vettoretti S, Vaccaro V at el. Mild renal dysfunction and
cardiovascular risk in hypertensive patients. J Am Nephrol 2004; 15 : 588-590
19) Patrick F, Bjorn W, Peter A, Stanko S, Jan L, Lars W at el. Interaction between renal function and
Microalbuminuria for Cardiovascular risk in hypertension: The Nordic Diltiazem Study. Hypertension
2008; 52: 115-122.

94
20) Leoncini G, Viazzi F, Parodi D, Veltoretti S, Ratto E, Ravera M et al. Mild renal dysfunction and
subclinical cardiovascular damage in primary hypertension. Hypertension 2003; 42: 14-18.
21) Pedrinelli R, Dell’Omo G, Bello VD, Poutromeli R, Mariani M. Microalbuminuria, an integral marker of
cardiovascular risk in essential hypertension. Journal of Human Hypertension 2002; 16: 79-89.
22) Bjorn D, Richard BD, Sverre EK, Stevo J, Gareth B, ULF F et al. Cardiovascular morbidity and mortality
in the losartan intervention for endpoint reduction in hypertension study (LIFE): a randomized trial against
atenolol. Lancet 2002; 359: 995-1003.
23) Azzi M, Guyere T, Chatellier G, Wargon M, menard J. Additive effects of Losartan and Enalapril on
Blood Pressure and Plasma active rennin. Hypertension 1997; 29: 634-640.
24) Ribeiro B, Gavras H. Angiotensin II antagonist clinical experience in the treatment of hypertension,
prevention of cardiovascular outcomes and renal protection in diabetic nephropathy and proteinuria. Arq
Bras Endocrinol Metab 2006; 50: 1-9.
25) Robert T, Pamela S, Leopoldo R, Helan M, Wayne S, Denise R at el. Efficacy and tolerability of Losartan
in hypertensive patients with renal impairment. Hypertension 2001; 31: 684-691.
26) Prabhu M, Palaian S, Malhotra A, Ravishankar P, Bista D, Almeida R et al. Therapeutic dimensions of
ACE inhibitors - A review of literature and clinical trials. Kathmandu University Medical Journal 2005;
3(11): 296-304.
27) Georg N, Jan O, Harry S B. Clinical evidence for the cardiovascular benefit of Angiotensin Receptor
Blockers. J Renin Angiotensin Aldosterone Syst 2006;7:S1-S7.
28) Mogensen C E, Neldam S, Tikkanen I, Oren S, Viskoper R, Watts RW et al. Randomized Controlled trial
of dual blockade of rennin-angiotensin system in patients with hypertension, microalbuminuria, and non-
insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study. BMJ 2001;
321: 1440-1444.

95
29) De Rosa ML, Carcace P, Rossi M, Baiano A, de Cristofaro A. Comparative effects of chronic ACE
inhibition and AT1 receptor blocked losartan on cardiac hypertrophy and renal function in hypertensive
patients. Journal of Human Hypertension 2002; 16: 133-140.
30) Asselbergs FW, Diercks GF, Hillege HL, vanBoven AJ, Janssen WM, Voors AA et al. Effects of
Fosinopril and Pravastatin on cardiovascular events in subjects with microalbuminuria. Circulation 2004;
110: 2809-2816.
31) Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB et al. Renoprotective effect of the
Angiotensin-receptor antagonist Irbesartan in patients with nephropathy due to type-2 diabetes. N Engl J
Med 2001; 345 (12): 851-860.
32) Brunner HR, Arakawa K. Antihypertensive efficacy of Olmesartan Modoxomil and Cardesartan Cilexetil
in achieving 24- hour blood pressure reductions and ambulatory blood pressure goals. Clin Drug Invest.
2006; 26(4): 185-193.
33) O’Riordan M, Barclay L. ACCOMPLISH Published: ACE Inhibitor and CCB best for reducing clinical
events in hypertensive patients. New England Journal of Medicine 2008; 312: 1-12.
34) Paul EJ, Gary CC. Screening, monitoring and treatment of albuminuria: Public health perspectives. J Am
Soc Nephrol 2006; 17: 2120-2126.
35) Roberto P, Giovanna L, Maura R, Francesca V, Simone V, Elena R, et al. Microalbuminuria,
cardiovascular, and renal risk in primary hypertension. J Am Soc Nephrol 2002; 13:S169 – S172
36) Roberto P, Giovanna L, Francesca V, Elena R, Valentina V, Valeria F et al. Evaluation of subclinical
organ damage for risk assessment and treatment in the hypertensive patient: role of microalbuminuria. J.
Am Soc Nephrol 2006; 17: S112-S114
37) Odili AN. Prevalence and clinical correlates of microalbuminuria in newly diagnosed hypertensive
subjects. Nig J Med 2008; 17 (4): 452-456.

96
38) Iwalokun BA, Ogunfemi MK, Gbajabiamila B, Olukosi A. Incidenc and evaluation of risk factors of
microalbuminuria among diabetics and non-diabetics in Lagos, Nigeria. Nig J Health Biomed Sci 2006;
5(1): 81-88.
39) Roberto P, Govanna L, Francesca V, Deinse P, Elena R, Simone V et al. Cardiovascular and renal risk
assessment as a guide for treatment in primary hypertension. J Am Nephrol 2004; 15:534 – 536.
40) Francesco PC, Frank BM, Lynsey E, Sally MK, Samson A, Ruby MP et al. Prevalence, detection,
management and control of hypertension in Ashanti, West African. Hypertension 2004; 43: 10176-1022.
41) Ernest KS, Jean MK, Chantal VZ, Erin PC, Purre D, Sylvain MM et al. Prevalence of chronic kidney
disease in Kinshasa: results of a pilot study from the Democratic Republic of Congo. Nephrol Dial
Transplant 2009; 24: 117-122.
42) Richard JJ, Dan IF, Takahiko N, Gabriela L, Sanchez L, Bernardo RI et al. Pathogenesis of essential
hypertension. Historical paradigms and modern insights. J Hypertens 2008; 26: 381-391.
43) Aram VC, George LB, Henry RB, William CC, Lee AG, Joseph LI et al. Seventh report of the Joint
National Committee on Prevention, Detection, Evaluation and Treatment of high blood pressure (JNC
VII). Hypertension 2003; 42: 1206-1252.
44) William GH. Hypertensive vascular disease. In: Braunward E, Fanci D, Kasper DL (eds). Harrison’s
Principles of Internal Medicine, 15th ed. New York: McGraw-Hill; 2001. 1414 – 1429.
45) Francesco PC, Frank BM, Lynsey E, Sally MK, Samson A, Ruby MP et al. Prevalence, detection,
management and control of hypertension in Ashanti, West African. Hypertension 2004; 43: 10176-1022.
46) Ernest KS, Jean MK, Chantal VZ, Erin PC, Purre D, Sylvain MM et al. Prevalence of chronic kidney
disease in Kinshasa: results of a pilot study from the Democratic Republic of Congo. Nephrol Dial
Transplant 2009; 24: 117-122.
97
47) Akinkugbe O.O. Non-Communicable Diseases in Nigeria: Final Report of a National Survey. Lagos:
Federal Ministry of Health- National Expert Committee on NCD; 1997.
48) Falase AO, Akinkugbe O.O. The cardiovascular system. In: Falase AO, Akinkugbe OO (eds). A
compendium of clinical medicine, 3rd ed. Nigeria: Spectrum Books Ltd 2007; 50-59.
49) Mancia G, Cifkova R, Kiowski W, Brian EO. 2003 European Society of Hypertension-European Society
of Cardiology guidelines for the management of arterial hypertension 2003; 21: 1011-1053.
50) Chia VC. Prehypertension: What is the current status? Malaysia Family Physician 2008; 3(2): 72-76.
51) Wang TJ, Evans JC, Meigs JB, Rifai N, Fox CS, D’Agostino RB et al. Low-grade Albuminuria and the
risk of hypertension and blood pressure progression. Circulation 2005; 111: 1370-1376.
52) Dominiczak AF. Genes and Hypertension: From gene mapping in experimental models to vascular gene
transfer strategies. Hypertension 2000; 35: 164-167.
53) Chlobanian AV, Bakris GL, Black HR. The seventh report of the Joint National Committee on Prevention,
Detection, Evaluation and Treatment of High Blood Pressure. The JNC VII Report. JAMA 2003; 289
(19): 2560-2571.
54) Kaplan N. Systemic hypertension: mechanism and diagnosis. In: Braunward E, Zipes DP, Libby P (eds).
Heart Disease: A Textbook of Cardiovascular Medicine 6th ed. Philadelphia, WB Saunders, 2001.
55) Julius S. Overweight and Hypertension. Hypertension 2001; 35: 807-809.
56) Williams FG. Cardiovascular Disorders: Vascular Disease-Hypertension. In: McPhee SJ, Ganong WF
(eds). Pathophysiology of Disease: An Introductory to Clinical Medicine, 5th ed. New York, McGraw-
Hill 2006: 301-326.
57) Pontremoli R, Pedrinelli R, Dell’Omo G, DIBello V, Mariani M. Microalbuminuria as marker of
Cardivascular risk in essential hypertension. J Hum Hyperten 2002; 16: 79-89.

98
58) Practical approach to managing hypertension: Reducing global cardiovascular risk. Downloaded (July
2010) from www.practicingclinicians.com.
59) Taco BM, Wilbert MT, Paul EJ, Lolkje TW. The impact of antihypertensive drug groups on urinary
albumin excretion in a non-diabetic population. Br J Clin Pharmacol 2002; 53:31-36.
60) DeBacker G, Ambrosioni E, Knut BJ, Brotons C, Cifkova R, Dallongevile J et al. European guidelines on
cardiovascular disease prevention in clinical practice. European Heart Journal 2003; 24: 1601-1610.
61) Maria A, Alfonso M, Alvaro A, Roberto Cabrera, Ramon R, Alberto T et al. Frequency and determinants
of microalbuminuria in mild hypertension: a primary-care-based study. J Hypertens 2001; 2: 319-326
62) Massimo C, Davide S, Martino L, Walter P, Alberto Z, Natale G. Pulse pressure and isolated systolic
hypertension: Association with microalbuminuria. Kidney International. 2000; 58: 1211-1218.
63) Martinez MA, Moreno A, Aguivre Dc, Cabrera R, Rocha R, Torre A et al. Frequency and determinants
of microalbuminuria in mild hypertension: a primary care-based study. J Hypertens 2001; 19: 319-326.
64) Kolatkar N. Microalbuminuria Test. A reviewed article downloaded January 2009 from
www.yourtotalhealth.com.
65) Julius S, Valentini M, Palatini P. Overweight and Hypertension: A 2-way street. Hypertension. 2000;
35(3): 807- 813.
66) Halimi JM, Bruno G, Sylvian V, Emile C, Hubert N, Yvon L et al. Effects of current smoking and smoking
discontinuation on renal function and proteinuria in the general population. Kidney International. 2000;
58: 1285- 1292.
67) Conny RD, Marc EB. Advances in chronic kidney disease: Kidney injury from alternative medicine.
National kidney foundation. 2005; 12(3): 261-275
68) Padia SH, Siragy HM. Renin Inhibition as a new strategy to combat cardiovascular disease. Curr
Hypertens Rev. 2007; 3: 39-43.

99
69) Leoncini G, Sacchi G, Ravera M, Viazzi F, Ratto E, Vettoretti S et al. J Hum Hypertens 2002; 16: 399-
404.
70) Gansevoort RT, Jacobien CV, Han LH, Johannes GM, Stephan JL, Dick Z. et al. The validity of screening
based on spot morning urine samples to detect subjects with microalbuminuria in the general population.
Kidney intervention 2005; 67:S28-S35.
71) Incerti J, Zelmanovitz T, Camargo JL, Gross JL, deAzevedo MJ. Evaluation of tests for microalbuminuria
screening in patients with diabetes. Nephrol Dial Transplant 2005; 20: 2402-2407.
72) Chirag RP, Michael JF, Raymond E, Robert WS. Rapid microalbuminuria screening in type 2 diabetes
mellitus: simplified approach with Micral test strips and specific gravity. Nephrol Dial Transplant.
2004; 19: 1881-1885.
73) Comper WD, Jerums G, Osicka TM. Differences in urinary albumin detected by four immunoassays and
high-performance liquid chromatography. Clinical Biochemistry 2004; 37 (2): 105-111.
74) ACCU-CHEK, Micral-Test II strip direction insert. Roche Diagnostics, Mannheim, Germany. (
www.accu-chek.com )
75) Giuseppe L, Maria LM, Italo N, Alessandro RD, Roberto T. Cost- effectiveness of two screening
programs for micralbuminuria in type 2 diabetes. Diabetes Care 2002; 25 (11): 2103 – 2104.
76) Mogensen CE, Vibert GC, Pehein E, Kutter D, Hasslacher C, Hofmann W et al. Multicenter evaluation
of the micral-test II strip, an immunologic rapid test for the detection of microalbuminuria. Diabetes care
1997; 20 (ii): 1642-1646.
77) Derhaschning U, Kitter H, Woisetschlager C, Bur A, Herkner, Hirrschl MM. Microalbumin measurement
alone or calculation of the albumin/creatinine ratio for the screening of hypertensive patients? Nephrol
Dial Transplant 2002; 17: 81-85.

100
78) Zeller A, Sigle JP, Battegy E, Martina B. Value of a standard urinary dipstick test for detecting
microalbuminuria in patients with newly diagnosed hypertension. Swiss Med wkly 2005; 135: 57-61.
79) Mathew RW. Microalbuminuria and cardiovascular disease. Am Soc Nephrol 2007; 2: 581-590.
80) Volpe M. Microalbuminuria screening in patients with hypertension: recommendations for clinical
practice. Int J Clin Pract 2008; 62 (1): 97-108.
81) Pontremoli R, Ravera M, Viazzi F, Nicolella C, Berruti V, Leoncini G etal. Genetic polymorphism of the
rennin-angiotensin system and organ damage in essential hypertension. Kidney international 2000; 57:
561-569.
82) UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and
microvascular complications in type-2 diabetes. Downloaded Dec 2008 from bmj.com: 703-713
83) Parmar MS. Chronic renal disease BMJ 2002; 325: 85-90
84) Remuzzi G, Bertani T. Pathophysiology of progressive nephropathies. New Engl J Med 2001; 12: 1448-
1456.
85) Morgan T, Anderson A, Batram D, Macinnis RJ. Effect of Candesartan and Lisinopril alone and in
combination on blood pressure and microalbuminuria. J Renin Angiotensin Aldosterone Syst 2004; 5(2):
64-71.
86) Julius S, Kjeldsen SE, Weber M et al. Outcome of hypertensive patients at high cardiovascular risk treated
with regimens based on valsartan and Amlodipine: the VALUE randomized trial. Lancet 2004; 363: 2022-
2031.
87) Ruggenenti P, Fassi A, Ileva AP, Bruno S, Iliev IP, Brusegan V el al. Preventing Microalbuminuria in
Type-2 diabetes. New Engl J Med. 2004; 351(19): 1941-1951.

101
88) Carter BL, Hunsicker LG, Lewis SJ, Rodby RA. An Evidence-based approach: The emerging role of renal
protection in hypertension. A focus on clinical and economic factor that impact formulary decision
making. Journal of Managed Care Pharmacy 2004; 10(5): S1-S29
89) Brenner BM, Cooper ME, Zeeuw D, Keane WF, Mitch WE, Parving HH et al. Effect of Losartan or renal
and cardiovascular outcomes in patients with Type-2 diabetes and nephropathy. N Engl J Med 2001;
345(12): 861-869.
90) Anderson S, Rossing P, Juhl TR, Deinum J, Parving HH. Optimal dose of Losartan for renoprotection in
diabetic nephropathy. Nephrol Dial Transplant 2002; 17: 1413-1418.
91) Chaturvedi N. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes
mellitus: results of the HOPE study and MICRO-HOPE substudy. The Lancet 2001; 355: 253-259.
92) Atkins RC, Briganti EM, Lewis JB, Hunsicker LG, Braden G, deCrespigny C et al. Proteinuria reduction
and progression to renal failure in patients with type-2 diabetes mellitus and overt nephropathy. American
Journal of kidney Disease 2005; 45 (2): 281-287.
93) Viberti G, Wheeldon NM. Microalbuminuria reduction with Valsartan in patients with Type-2 diabetes
mellitus: A blood pressure-independent effect. Circulation 2002; 106: 672-678.
94) Araoye MO. Subject selection: sample size determination. In: Araoye MO. Research methodology with
statistics for health and social sciences. 1ST ed. Nathadex Publishers; 2003. p. 117-118.
95) Araoye MO. Types of research methods: methodological study. In: Araoye MO. Research methodology
with statistics for health and social sciences. 1ST ed. Nathadex Publishers; 2003. p. 68-69.
96) Raoul MK, Richard E, Joseph SA, Emmanuel K, Nigel U, Jean CM. Anthropometry measures and
prevalence of obesity in the urban adult population in Cameroon: An update from the Cameroon burden
of diabetes baseline survey. BMJ Public Health 2006; 6: 228

102
97) How to take Anthropometric Measurement: A tool kit for service provider in the Comprehensive care
Centers. Downloaded from: www.fantaproject.org/ download /pdfs/Kenya_CCC_Toolkit_C.pdf
98) Olatunde LO, Arogundade FA, Balogun MO, Akinsola A. Microalbuminuria and its Clinical Correlates
in essential hypertension. Nigerian Journal of Health Science 2002; 2: 25-29.
99) Ulla D, Harald K, Christiana W, Andreas B, Harald H, Micheal MH. Comparing Microalbumin
measurement alone with calculation of the albumin/creatine ratio for the screening of hypertensive
patients. Nephrol Dial Transplant 2002; 17: 81-85.
100) Bohm M, Thoenes M, Danchin N el al. Association of Cardiovascular risk factors with microalbuminuria
in hypertensive individuals: the i-SEARCH global study. J Hypertens 2007; 25: 2317-2324.
101) Rosa TT, Ralatini P. Clinical value of microalbuminuria in hypertension. J hypertens 2001; 18(6): 645-
654.
102) Orluwene CG, Mommoh MO. Screening for microalbuminuria in newly diagnosed type-2 diabetes at a
staff clinic in Port Harcourt. Port Harcourt Medical Journal 2008; 3: 10-14.
103) Guh JY, Chen HC, Tsai JF, Chuang LY. Herbal therapy is associated with the risk of CKD in adults not
using analgesic in Taiwan. American Journal of Kidney Disease 2007; 49(5): 626-633.
104) De-la-Sierva A, Bragulat E, Sierra C, Gomez-Angelats E, Antonio MT, Aquilera MT et al.
Microalbuminuria in essential hypertension. Clinical and biochemical profile. Br J Biomed Sci 2001; 57
(47): 287-291.

103
APPENDICES I: QUESTIONNAIRE
PREVALENCE AND FACTORS ASSOCIATED WITH PRESENCE OF MICROALBUMINURIA IN
PATIENTS WITH ESSENTIAL HYPERTENSION SEEN AT THE GENERAL OUTPATIENT CLINIC OF
FEDERAL MEDICAL CENTRE, ABEOKUTA.
Dear respondent,
Kindly respond to the questions set out below to the best of your knowledge and be reassured that your responses
will be treated with utmost confidentiality. This study borders on testing a sample of your early morning urine for
the presence of minute proteins (microalbuminuria) as a means of early detection of hypertensive kidney damage.
At this stage, further kidney damage due to hypertension can be prevented, reversed or at least significantly
slowed down for a better quality of life. An interviewer who is versed in both the local language (Yoruba) and
English will assist you through the course of the questionnaire.
SERIAL NO…………………………………..
CODED HOSPITAL NO……………………...
DATE ………………………………………...
A) DEMOGRAPHIC DATA
1) Age: …………………………… years
2) Sex: (i) Male (ii) Female
3) Marital status: (i) Single (ii) Married (iii) Divorced/Separated (iv) Widowed
4) Level of Education: (i) None (ii) Primary (iii) Secondary (iv) Postsecondary
5) Occupation: (i) Student (ii) Pensioner (iii) Unemployed /Retired

104
(iv) Artisan/Skilled Labour (v) Unskilled labour (vi) Trading (vii) Business (viii)
Housewife (ix) Civil servant (x) Professional (xi) Police/Military (xii) Farmer
(xiii) Others: specify
6) Religion: (i) Islam (ii) Christianity (iii) Traditional belief (iv) Others 7) Ethnic
group: (i) Yoruba (ii) Hausa (iii) Igbo (iv) Others
B) SOCIAL HISTORY
1) Do you smoke cigarette currently? (i) Yes (ii) No
2) If yes, how many sticks per day on the average? ....................................................................
3) For how long have you been smoking? ...................................................................................
4) If no to question (1), have you smoked cigarette in the past? (i) Yes (ii) No
5) If yes, how many sticks per day on the average? ....................................................................
6) For how long did you smoke? ………………………………………………………………
7) How long ago did you stop smoking? ....................................................................................
8) Why did you stop smoking?………………………………………………………………….
9) Do you take Alcohol currently? (i) Yes (ii) No
10) If yes:
Brand Quantity/week Duration
(i) Beer ……………….. ………………..
(ii) Gin/Local gin/Whisky ……………….. ……………….
(iii) Alcoholic Wine ………………... ……………….
(iv) Palm wine ………………... ………………..

105
11) If no, have you taken alcohol in the past? (i) Yes (ii) No
12) If yes, for how long were you on alcohol?..........................................................
13) How long ago did you stop?...............................................................................
14) Why did you stop taking alcohol?………………………………………………
C) MEDICAL HISTORY
1) How long ago were you diagnosed as hypertensive?...................................................................
2) Are you on any antihypertensive drug(s)? (i) Yes (ii) No (iii) I don’t know
3) If yes, name them and how long on each of them:
Name (s) Duration
(i) ………………………….. ………………………………………...
(ii) …………………………... ..……………………………………….
(iii) …………………………... ………………………………………...
(iv) Drug names not known
4) How often do you take your drugs? (i) Regularly (ii) Not regularly
5) If not regularly, why? (i) Often forget (ii) No money to buy drug (iii) Drugs not readily
available (iv) Don’t have any symptoms (v) Thought I have been cured (vi) Too
many drugs to take / Multiple dosaging (vii) Tight job schedule
6) For (5ii), who pays for the drugs? (i) self (ii) Children (iii) spouse (iv) Relatives
7) How would you rate your family’s support? (i) Good (iv) Fair (iv) Poor (V) None
8) Is any member of your family hypertensive? (i) Yes (ii) No (iii) I don’t know
9) If yes, state relationship to you…………………………………………………….........
10) Do you have any other chronic medical disease(s)? (i) Yes (ii) No (iii) I don’t know

106
11) If yes, name it/them:
Name Duration since diagnosed
(i) …………………………………………………. …………………………………...
(ii) ………………………………………………..... ……………………………………
(iii) …………………………………………………. ……………………………………
12) Do you take herbal preparation/concussion? (i) Yes (ii) No
13) If yes, how often? (i) Occasionally (ii) Regularly
14) Date of Last normal menstrual period (for women only) ………………………………..
D) PHYSICAL EXAMINATION
1) Systolic blood pressure (mmHg; average of 2 readings)………………………………….
2) Diastolic blood pressure (mmHg; average of 2 readings)………………………………...
3) Mean arterial pressure (mmHg)……………………………………………………………
4) Weight (Kg)………………………………………………………………………………..
5) Height (m)………………………………………………………………………………….
6) Body mass index (BMI, Kg/m 2) …………………………………………………………..
7) Waist circumference (cm)…………………………………………………………………..
8) Hip circumference (cm)……………………………………………………………………
9) Waist/Hip ratio (WHR) ……………………………………………………………………
E) INVESTIGATIONS
1) Urinalysis: + Appearance……………………………………….
+ PH………………………………………………..

107
+ Specific gravity………………………………….
+ Proteinuria………………………………………
+ Glucose…………………………………………..
+ Red blood cells…………………………………..
+ White blood cells………………………………..
+ Nitrite…………………………………………….
2) Micral-Test assay for microalbuminuria (i) Negative (ii) Positive
(iii) If positive, what is the level: (a) 20-50mg/L
(b) 51-100mg/L (c) >100mg/L
APPENDIX II: INFORMED CONSENT
Consent to participate in the Study Titled: PREVALENCE AND FACTORS ASSOCIATED WITH
PRESENCE OF MICROALBUMINURIA IN PATIENTS WITH ESSENTIAL HYPERTENSION SEEN AT
THE GENERAL OUTPATIENT CLINIC OF FEDERAL MEDICAL CENTRE, ABEOKUTA.
Dear Sir/Ma,
Your consent is being sought to participate in this study. Hypertension is a silent killer that can damage virtually
every organ in the body including the brain, heart and the kidneys. The kidneys are often involved early in
hypertensive organ damage and also serve as a predictor of other organ damage by hypertension.
This study is therefore aimed at early detection of hypertensive kidney damage as a secondary preventive measure
to reduce occurrence of cardiovascular and chronic kidney disease.

108
If you consent, a questionnaire will be administered; height, weight, waist and hip circumference measurements
shall be taken and about 15mls of morning urine sample taken for laboratory analysis at no cost to you.
All these procedures are not harmful. Your refusal to participate will not in any way affect your normal care by
me or any member of this hospital. You are also free to opt out at any stage of the study. All information obtained
in this study is strictly confidential. Your responses will be identified by a study code number. Your name will
not be used in this study. If any information is published, there will not be any information which would identify
you as a participant.
Kindly indicate your decision by signing in the space below.
Thank you.
Yours sincerely,
DR IGE A.M
I wish to participate____________________________________________
(Date and Signature or Thumbprint of Participant)
____________________________________________
(Date and Signature or Thumbprint of Witness)

109
FIGURES: 1 COMPONENTS OF THE MICRAL TEST STRIP
Colour
Block
Wick Buffer Capture Cover Carrier
fleece fleece matrix foil foil
Conjugate Substrate
fleece film