Prediction of Postpartum Depression Using Multilayer Perceptrons and Pruning
19
Prediction of postpartum depression using multilayer perceptrons and pruning Salvador Tortajada a , Juan M. Garc´ ıa-G´ omez a , Javier Vicente a , Julio Sanju´ an b , Roc´ ıo Mart´ ın-Santos c , Isolde Gornemann d , Alfonso Guti´ errez-Zotes e , Francesca Canellas f , ´ Angel Carracedo g , M´ onica Gratacos h , Roser Guillamat i , Enrique Baca-Garc´ ıa j , Montserrat Robles a a IBIME-Itaca, Universidad Polit´ ecnica de Valencia, Valencia, Spain b Faculty of Medicine, University of Valencia, Valencia, Spain c Hospital del Mar, Barcelona, Spain d Hospital Carlos Haya, M´ alaga, Spain e Hospital Pere Mata, Reus, Spain f Hospital Son Dureta, Palma de Mallorca, Spain g National Genotyping Center, Hospital Cl´ ınico, Santiago de Compostela, Spain h Center for Genomic Regulation, CRG, Barcelona, Spain i Hospital Parc Tauli, Sabadell, Spain j Hospital Jim´ enez D´ ıaz, Madrid, Spain Abstract Objective: The main goal of this paper is to obtain a classification model based on feed-forward multilayer perceptrons in order to predict postpartum depression during the 32 weeks after the childbirth with a high sensitivity and specificity. Ma- terials and methods: Multilayer perceptrons were trained on data from 1 397 women who had just given birth, from 7 Spanish Hospitals. A prospective cohort study was made just after delivery, at 8 weeks and 32 weeks after delivery. The models were analyzed using hold out evaluation and comparing them with the geometric mean of the accuracies in order to obtain a balanced sensibility and specificity. Results and conclusion: Multilayer perceptrons show a good performance -high sensibility and specificity- as predictive models for postpartum depression. The interpretation of the models by pruning leads to a qualitative interpretation of the influence of each variable that may be useful for clinical protocols. Key words: Multilayer perceptron; Neural network pruning; Postpartum depression. Preprint submitted to Elsevier 31 January 2008
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Prediction of Postpartum Depression Using Multilayer Perceptrons and Pruning

Prediction of postpartum depression using
multilayer perceptrons and pruning
Salvador Tortajada a, Juan M. Garcıa-Gomez a, Javier Vicente a,Julio Sanjuan b, Rocıo Martın-Santos c, Isolde Gornemann d,
Alfonso Gutierrez-Zotes e, Francesca Canellas f ,Angel Carracedo g, Monica Gratacos h, Roser Guillamat i,
Enrique Baca-Garcıa j, Montserrat Robles a
aIBIME-Itaca, Universidad Politecnica de Valencia, Valencia, Spain
bFaculty of Medicine, University of Valencia, Valencia, Spain
cHospital del Mar, Barcelona, Spain
dHospital Carlos Haya, Malaga, Spain
eHospital Pere Mata, Reus, Spain
fHospital Son Dureta, Palma de Mallorca, Spain
gNational Genotyping Center, Hospital Clınico, Santiago de Compostela, Spain
hCenter for Genomic Regulation, CRG, Barcelona, Spain
iHospital Parc Tauli, Sabadell, Spain
jHospital Jimenez Dıaz, Madrid, Spain
Abstract
Objective: The main goal of this paper is to obtain a classification model basedon feed-forward multilayer perceptrons in order to predict postpartum depressionduring the 32 weeks after the childbirth with a high sensitivity and specificity. Ma-
terials and methods: Multilayer perceptrons were trained on data from 1 397 womenwho had just given birth, from 7 Spanish Hospitals. A prospective cohort study wasmade just after delivery, at 8 weeks and 32 weeks after delivery. The models wereanalyzed using hold out evaluation and comparing them with the geometric meanof the accuracies in order to obtain a balanced sensibility and specificity. Results
and conclusion: Multilayer perceptrons show a good performance -high sensibilityand specificity- as predictive models for postpartum depression. The interpretationof the models by pruning leads to a qualitative interpretation of the influence ofeach variable that may be useful for clinical protocols.
Key words: Multilayer perceptron; Neural network pruning; Postpartumdepression.
Preprint submitted to Elsevier 31 January 2008

1 Introduction1
In the first week after childbirth, around 25%-50% of women slightly suffer a2
postpartum blues episode. Pospartum Depression (PPD) seems to be a uni-3
versal condition with equivalent prevalence in different countries of around4
13% [1,2] and it implies an increase in medical care costs. Women suffering5
from postnatal depression feel a considerable deterioration of cognitive and6
emotional functions which can affect to mother-infant attachment. This may7
have an impact on child’s future development until primary school [3]. De-8
spite its serious consequences, PPD usually passes unnoticed, its detection9
takes time and it often receives inappropriate treatment.10
Although multiple studies have been carried out around PPD, its etiology is11
not well-known yet. Several psychosocial and biological risk factors have been12
suggested. For instance, it has been pointed out the importance of the social13
support, partner relantionship and stressful life events related to pregnancy14
and childbirth [4], as well as neuroticism [5]. Regarding biological factors, it15
has been shown that inducing an artificial estrogen fall can cause depressive16
symptoms in patients wih PPD antecedents. Cortisol alteration, thyroid hor-17
mones changes and low rate of prolactin are relevant factors too [6]. Treloar18
et al. in [7], through a comparative study with twin samples, they conclude19
that genetic factors would explain 40% of variance in PPD predisposition. In20
Ross et al. [8] a biopsychosocial model for anxiety and depression symptoms21
is developed by means of structural equations. However, most of the research22
involving genetic factors are separated from those involving environmental23
factors. There is a remarkable exception that explains that a functional poly-24
morphism in the promoter region of the serotonin transporter gene seems to25
moderate the influence of stressful life events on depression [9].26
An early prediction of postpartum depression may reduce the impact of the27
illness on the mother and it can help clinicians to give appropriate treatment28
to the patient in order to prevent the depression. The need of a prediction29
model rather than a description one becomes of paramount importance. In this30
way, artificial neural networks (ANN) have a remarkable ability to characterize31
discriminating patterns and derive meaning from complex and noisy data sets.32
They have been widely applied in general medicine for differential diagnosis,33
classification and prediction of disease and condition prognosis. In the field of34
psychiatric disorders, ANNs have not been widely used in spite of its predictive35
power. For instance, ANNs have been applied to he diagnosis of dementia using36
clinical data [10] or for predicting Alzheimer’s disease using mixed effects37
neural networks [11]. In [12], EEG data from patients with schizophrenia,38
obsessive-compulsive disorder and controls was used to demonstrate that a39
Email address: [email protected] (Salvador Tortajada).
2

trained ANN was able to classify correctly over 80% of the patients with40
obsessive-compulsive disorder and over 60% of the patients with schizophrenia.41
In Jefferson et al. [13], evolving neural networks overcome statistical methods42
in depression prediction after mania. Berdia and Metz [14] used artificial neural43
networks to provide a framework for understanding some of the pathological44
processes in schizophrenia. Finally, Franchini et al. in [15] applied these models45
to support clinical decision making for the treatment of psychopharmacological46
therapy.47
One of the main goals of this paper is to obtain a classification model based on48
feed-forward multilayer perceptrons in order to predict postpartum depression49
with a high sensitivity and specificity during the 32 weeks after the childbirth.50
A secondary goal is to find and interpret the qualitative contribution of each51
independent variable in order to obtain clinical knowledge.52
2 Materials and Methods53
Data from postpartum women were collected from 7 General Spanish Hospi-54
tals, in the period from December 2003 to October 2004 in the second to third55
day after delivery. All participants were caucasic, none of them were under56
psychiatric treatment during pregnancy and all of them were able to read and57
answer the clinical questionnaires. Women whose child died after delivery were58
excluded. This study was approved by the Local Ethic Committees, and all59
patients gave their informed written consent.60
Depressive symptoms were assessed with the total score of the Spanish version61
of Edinburgh Postnatal Depression Scale (EPDS) [16] just after delivery, at 862
and 32 weeks.63
Major depression episode were established using first the EPDS (cut-off point64
of 9 or more) at 8 or 32 weeks, and then probable cases (EPDS > 9) were65
evaluated using the Spanish version of the Diagnostic Interview for Genetics66
Studies (DIGS) [17,18] adapted to Postpartum Depression in order to deter-67
mine if the patient was suffering a depression episode (positive class) or not68
(negative class). All the interviews were conducted by clinical psychologist69
with a previous common training in the DIGS with video cases records. A70
high level of reliability (K > 0.8) was obtained among interviewers.71
From the 1 880 women initially included in the study, 76 were excluded because72
they did not fill correctly all the scales or questionnaires. With these patients,73
a prospective study was made just after delivery (initial), at 8 weeks and 3274
weeks after delivery. At 8 weeks of follow up, 1 407 (78%) women retained in75
the study. At 32 weeks of follow up 1 397 (77.4%) women were evaluated. We76
3

compared the lost of follow-up cases with the rest of the final sample. Only77
lowest social class was significantly increased in the lost of follow-up cases78
(p = 0.005). The 11.5% (160) of women at base line, 8 and 32 weeks had a79
major depressive episode during the eight months of postpartum follow-up.80
Hence, from a total number of 1 397 patients we had 160 in the positive class81
and 1 237 in the negative class.82
2.1 Independent variables83
Based on the current knowledge about PPD, several variables were taken84
into account in order to develop predictive models. In a first step, psychiatric85
and genetic information was used. These predictive models are called subjec-86
tive models. Then, social-demographic variables were included in the subject-87
environment models. For each approach, we used anxiety state (STAIE) either88
Edinburgh postnatal depression (EPDS) -just after the childbirth- as an in-89
put variable, because blues and anxiety symptoms are correlated [19]. Table 290
shows the clinical variables used in this study.91
Following recommendations from clinicians psychiatric antecedents of the pa-92
tient in postpartum depression were taken into account as well as emotional93
alterations during pregnancy with medical consultation were also considered.94
Both are binary variables (yes/no).95
Neuroticism can be defined as an enduring tendency to experience negative96
emotional states. It is measured on the Eysenck Personality Questionnaire97
short scale (EPQ) [20], which is the most used questionnaire of personality98
and consists of 12 items. For this study the validated Spanish version [21]99
was used. Individuals who score high on neuroticism are more likely than the100
average to experience such feelings as anxiety, anger, guilt and depression.101
The number of experiencies are the number of stressful life events of the patient102
just after delivery (initial) at 0-8 weeks interval and 8-32 weeks interval using103
the St. Paul Ramsey Scale [22,23]. This is an ordinal variable and depends on104
the subjective point of view of the patient.105
The anxiety state is based on the most frequently used scale of anxiety which106
is the State-Trait Anxiety Inventory (STAI) [24].107
Postpartum blues is estimated via the Edinburg Postnatal Depression Scale108
(EPDS). It is a 10-items self-report scale and it has been validated for Spanish109
population [16]. The best cut-off of the Spanish validation of the EPDS was110
9 for postpartum depression. We decided to prove its initial value, i.e. at the111
moment of birth, as an independent variable because the goal is to prevent112
and predict postpartum depression within 32 weeks.113
4

Social support is measured by means of the Spanish version of the Duke UNC114
social support scale [25], which originally consists of 11 items. This question-115
naire is rated just after delivery, at 6-8 weeks and at week 32. For this work,116
the variable used was the sum of the scores obtained immediately after the117
childbirth plus the scores obtained in week number 8. As we want to predict118
possible depression risk during the first 32 weeks after childbirth, the Duke119
score at week 32 was discarded for this experiment.120
Genomic DNA was extracted from the peripheral blood of women. Two func-121
tional polymorphisms of the serotonine transporter gene were analyzed 1 . For122
all the machine learning process we decided to use the combination genotypes123
(HAP2) proposed by Hranilovic in [26] as124
(1) no low-expressing genotype at either of the loci,125
(2) low-expressing genotype at one of the loci,126
(3) low-expressing genotypes at both loci.127
The Medical Perinatal Risk was measured as seven dichotomous variables:128
medical problems during pregnancy, use of drugs during pregnancy (including129
alcohol and tobacco), cesarea, use of anesthesia during delivery, mother med-130
ical problems during delivery, medical problems with more admission days in131
hospital and newborn medical problems. A two-step cluster analysis was done132
in order to explore this seven binary variables. From this analysis it results an133
ordinal variable with four values for every women:134
(1) no medical perinatal risk,135
(2) pregnancy problems without delivery problems,136
(3) pregnancy problems and delivery mother problems,137
(4) presence of both other and newborn problems.138
Other psychosocial and demographic variables were considered in the subject-139
environment model such as the age, the highest level of education achieved140
rated on 3-point scale (low, medium, high), labour situation during pregnancy,141
household income rated on 4-point scale (economical level), the gender of the142
baby or the number of family members whom she lives together with.143
Every input variable was normalized in the range [0, 1]. Non-categorical vari-144
ables were represented by one input unit. Missed variables were replaced by145
their mean if they were continuous or by their mode if they were discrete.146
A dummy representation was used for each categorical variable, i.e., one unit147
represents one of the possible values of the variable and this unit is activated148
only when the corresponding variable takes this value. Missed variables were149
simply represented by non activating any of the units.150
1 5-HTTLPR in the promoter region and STin2 within intron 2
5

2.2 ANNs theoretical model151
ANNs are inspired by biological systems in which large numbers of simple152
units work in parallel in order to perform tasks that conventional computers153
have not been able to tackle successfully. These networks are made of many154
simple processors (neurons or units) based on Rosenblatt’s perceptron [27]. A155
perceptron gives a linear combination, y, of the values of its D inputs, plus156
a bias value,157
y =D
∑
i=1
xiwi + w0. (1)
The output, z = f(y), is calculated by applying an activation function to158
the input. Generally, the activation function is an identity, a logistic (2) or159
a hyperbolic tangent (3). As these functions are monotonic, the form f(y)160
still determines a linear discriminant function [28]. A single unit has a limited161
computing ability, but a group of interconnected neurons has a very powerful162
adaptability and the ability to learn non-linear functions which can model163
complex relationships between inputs and outputs.164
Thus, more general functions can be constructed by considering networks hav-165
ing successive layers of processing units, with connections running from every166
unit in one layer to every unit in the next layer only. A feedforward multilayer167
perceptron consists of an input layer with one unit for every independent168
variable, one or two hidden layers of perceptrons and the output layer for169
the dependent variable -in the case of a regression problem-, or the possi-170
ble classes -if we are dealing with a classification problem-. We call a fully171
connected feed-forward multilayer perceptron when every unit of each layer172
receives an input from every unit in its precedent layer and the output of each173
unit is sent to every unit in the next layer. Networks having one hidden layer174
can generate decision boundaries which surround a single convex region of the175
input space whose boundary consists of segments of hyperplanes. Networks176
having two hidden layers can generate arbitrary decision regions which may177
be non-convex and disjoint [28].178
Since postpartum major depression is considered in this work as a binary179
dependent variable, the activation function of the output unit was the logistic180
function which is expressed as:181
f(x) =1
1 + e−x, (2)
while the activation function of the hidden units was the hyperbolic tangent182
6

which is expressed as:183
f(x) =ex − e−x
ex + e−x. (3)
As a first approach, fully connected feed-forward multilayer perceptrons were184
used with one or two hidden layers. The learning algorithm backpropagation185
with momentum was used to train the networks. The connection weights of186
the network were updated following the descent gradient rule:187
∆wij(t + 1) = ρ · δj · oi + µ · ∆wij(t), (4)
where ρ is the learning rate, µ is the momentum factor, wij is the weight188
between unit i and unit j, ∆wij(t) is the connection weight variation and oi189
is the output value of the unit i. The learning rule δj is expressed as190
δj =
{
f ′
j(∑
i wijoi)(tj − oj) if j is an output unit
f ′
j(∑
i wijoi)(∑
k δkwjk) if j is a hidden unit(5)
where tj is the desired output value, which is provided to the network in a191
supervised manner during the training of the network. The activation function192
fj(x) of unit j was a logistic or a hyperbolic tangent and f ′
j(x) is its derivative.193
Although these models, and ANNs in general, exhibit a superior predictive194
power compared to traditional approaches, they have been labeled as ”black195
box” methods because they provide little explanatory insight into the relative196
influence of the independent variables in the prediction process. This lack197
of explanatory power is a major concern to reach an interpretation of the198
influence of each independent variable on postpartum depression. In order to199
gain some qualitative knowledge of the causal relantionships about depression200
phenomena we used several pruning algorithms to obtain more simple and201
interpretable models [29,33].202
2.2.1 Pruning algorithms203
Based on the fundamental idea in Wald statistics, pruning algorithms estimate204
the importance of a parameter (or weight) in the model by how much the205
training error increases if that parameter is eliminated. Then, it removes the206
least relevant one and continues iteratively until some convergence condition207
is reached. These algorithms were initially thought as a way to achieve a208
good generalization for connectionist models, i.e., the ability to infer a correct209
7

structure from training examples and to perform well on future samples. A very210
complex model can lead to poor generalization or overfitting, which happens211
when it adjusts to specific features of the training data rather than to the212
general ones [30]. But pruning has also been used for feature selection with213
neural networks [31,32], making their operation easier to understand since214
there is less oportunity for the network to spread functions over many nodes.215
This is important in this critical application where knowing how the system216
works becomes a major concern.217
The algorithms used here are based on weight pruning. The strategy consists218
in deleting parameters with small saliency, i.e. those whose deletion will have219
the least effect on the training error. The Optimal Brain Damage (OBD)220
algorithm [29] and its descendent, Optimal Brain Surgeon (OBS) [33], use a221
second-order approximation to predict the saliency of each weight. A Taylor222
series is used to approximate the error function:223
δE =∂E(W )
∂WδW +
1
2δW T ∂2E(W )
∂W 2δW + O(||δW ||3). (6)
Here, W is the weight matrix and δE is the increment of the error function.224
In the second term of this expression we find the Hessian matrix H of E225
with respect to W . The first term can be omitted because we are at a local226
minimum after training convergence and the third term is ignored because we227
assume that the error function is nearly quadratic. So the expression finally228
reduces to:229
δE =1
2δW T HδW. (7)
In OBD high-order terms are neglected so we only need to compute the di-230
agonal elements of H. This assumption is sometimes a poor one. Hence, OBS231
method computes the full Hessian matrix leading to a more exact approxi-232
mation of the error function, but it requires more computational time and233
space.234
In order to select the best pruned topology the validation set was used to com-235
pare the networks. Then, when the best model was obtained the interpretation236
of the influence of each variable was done in the following way: if an input237
unit is directly connected to the output unit, then a positive weight means238
that it is a risk factor as it increases the probability of having depression.239
Thus, a negative weight means that the variable is a protective factor. Let a240
hidden unit be connected to the output unit with a positive weight. If an input241
unit is connected to this hidden unit with a positive value, then the variable242
represented by this unit is a risk factor. If its weight is negative then it is a243
8

protective factor. On the contrary, if the weight between the hidden unit and244
the output unit is negative then a positive value in the connection between245
the input and the hidden unit means that the variable is a protective factor.246
Thus, a negative value in the weight which connects the input to the hidden247
unit means that it is a risk factor. Table 3 summarizes these influences. This248
interpretation is justified because the hidden units have a hyperbolic tangent249
as an activation function which delimits its output activation values between250
−1 and 1.251
2.3 Evaluation criteria252
The evaluation of the models was made using a holdout validation where the253
observations were chosen randomly to form the validation and the evaluation254
sets. In order to obtain a good error estimation of the predictive model, this255
database has to be split into three different datasets: the training set with256
1 006 patients (72%), the validation set with 112 patients (8%) and the test257
set with 279 patients (20%). Each partition follows the prevalence of the orig-258
inal database (see table 1). The best network topology and parameters were259
selected empirically using the validation set and then evaluated with the test260
set. Overfitting was avoided using the validation set to stop the learning proce-261
dure when the validation medium square error function reached its minimum.262
In the section 3 we can see that using a single hidden layer was enough to263
obtain a good predictive model.264
There is an intrinsic difficulty in the nature of the problem: the dataset is265
imbalanced [34,35], in the sense that one of the classes (the possitive examples)266
is underrepresented compared to the negative class. This means that, with this267
prevalence on the negative examples (89%), a trivial classifier consisting in268
assigning the most prevalent class to a new sample would achieve an accuracy269
of around 89%, but its sensitivity would be null.270
The main goal is to obtain a predictive model with a good sensitivity and271
specificity. Both measures depend on the accuracy on positive examples, a+,272
and the accuracy on negative examples, a−. Increasing a+ will be done at the273
cost of decreasing a−. The relation between these quantities can be captured274
by the ROC (Receiver Operating Characteristic) curve. The larger the area275
under the ROC curve (AUC), the higher the classification potential of the276
model. This relation can also be estimated by the geometric mean of the two277
accuracies, G =√
a+ · a−, reaching high values only if both values are high278
and in equilibrium. In that way, if now we use the geometric mean to evaluate279
our trivial model -which always assigns the class with the maximum a priori280
probability- we could see that G = 0, which means that the model is the worst281
we can obtain.282
9

3 Results283
The main objective of this work was to obtain feed-forward multilayer per-284
ceptron predictive models. Table 4 shows the results of the best connectionist285
models obtained from the first approach, called subjective feature models, us-286
ing multilayer perceptrons of one and two hidden layers and making use of the287
pruning algorithms as well as the results for the next subject-environment fea-288
ture model approach -which includes social and demographic features-. Each289
experiment has been done swapping initial STAIE variable and initial EPDS.290
Notice that non-pruned models have a better behaviour than pruned ones.291
In general, with the independent test set, our models are reaching more than292
80% of accuracy with a G and an area under the ROC curve of around 0.8,293
which means a sensitivity of more than 0.75 and a specificity greater than 0.8.294
We can see that non-pruned models reach a higher sensitivity when including295
EPDS as input variable than when STAIE is used. The use of pruning methods296
lead to a more understandable model at the expense of the predictive power.297
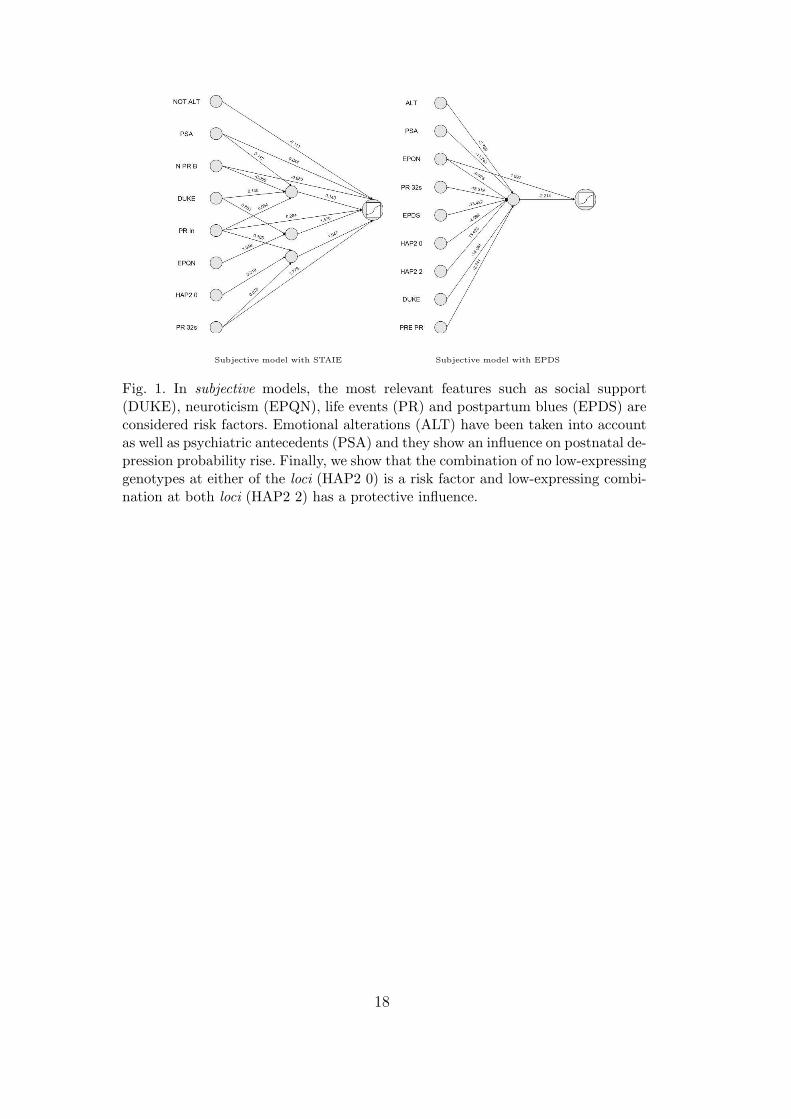
In figure 1, the subjective pruned models show that neuroticism, social support,298
life events and postpartum blues are the most outstanding features and they299
are risk factors in the prediction of postpartum depression. In the subject-300
environment models (figure 2) these variables are also main risk factors, but301
we can see that variable age and the number of people living together with the302
patient are both important protective factors. Other interesting features are303
psychiatric antecedents in relatives, which is a risk factor, and low-expressing304
genotypes, which appears to be a protective factor.305
Although the databases and used variables are not comparable, these results306
overcome the work done by Camdeviren et al. in [36] where a logistic regres-307
sion model and a classification tree were compared for predicting postpartum308
depression. With logistic regression they reached a 65.4% of accuracy with309
16% of sensibility and 95% of specificity, while with the optimal decission tree310
they had an accuracy of 71%, a sensibility of 22% and a specificity of 94%.311
4 Discussion312
The main objective of this paper was to obtain a feed-forward ANN classifica-313
tion model to predict postpartum depression during the first 32 weeks after the314
delivery with a high sensitivity and specificity. From several trained models,315
the one showing the best G-mean of the accuracies was selected thus ensuring316
a balanced sensitivity and specificity as we can see in table 4. With these mod-317
els we could achieve around 85% of accuracy. Models using socialdemographic318
10

variables (subject-enviroment models) did not significantly improve subjective319
models for prediction.320
The independent variables have different influences in the output of the clas-321
sification model. These influences depend on the connections between nodes322
as we can see in figures 1 and 2. The higher the weight of the connection,323
the bigger the final influence, which can also be positive or negative depend-324
ing on the sign of the weight. Nevertheless, this is a qualitative measure and325
we must take care interpreting the quantitative influence because some input326
variables are spreading their values over several nodes. In a future work some327
quantitative techniques will be used in order to achieve a numeric measure328
of the influence of each input feature and their interactions. In that way, the329
prevention models would give clinicians a tool to gain knowledge from the330
model.331
In this sense, the combination of the genetic features with other environmental332
features can be seen in a qualitative way. In three models out of four the333
interaction is clear.334
A classification model with this good performance, i.e. high accuracy, sen-335
sitivity and specificity, may be very useful in clinical environment. In fact,336
the ability of neural networks to tolerate missing information could be useful337
when part of the variables are missed thus giving a high reliability in a real338
environment.339
In future work, a quantitative approach will be developed in order to find out340
the real and numeric influence of each variable and their interactions, therefore341
the prevention model would give the clinicians a tool to gain knowledge from342
the model and, thus, the postpartum depression.343
11

References
[1] M. Oates, J. Cox, S. Neema, P. Asten, N. Glangeaud-Freudenthal,B. Figueiredo, L. Gorman, S. Hacking, E. Hirst, M. Kammerer, C. Klier,G. Seneviratne, M. Smith, A. Sutter-Dallay, V. Valoriani, B. Wickberg,K. Yoshida, TCS-PND Group, Postnatal depression across countries andcultures: a qualitative study, British Journal of Psychiatry Suppl. 46 (2004)s10–s16.
[2] M. O’Hara, A. Swain, Rates and risk of postnatal depression - a meta analysis,International Review of Psychiatry 8 (1996) 37–54.
[3] P. Cooper, L. Murray, Prediction, detection and treatment of postnataldepression, Archives of Disease in Childhood 77 (1997) 97–99.
[4] C. Beck, Predictors of postpartum depression: an update, Nursing Research 50(2001) 275–285.
[5] K. Kendler, J. Kuhn, C. Prescott, The interrelationship of neuroticism, sex andstressful life events in the prediction of episodes of major depression, AmericanJournal of Psychiatry 161 (2004) 631–636.
[6] M. Bloch, R. Daly, D. Rubinow, Endocrine factors in the etiology of postpartumdepression, Compr. Psychiatry 44 (2003) 234–246.
[7] S. Treloar, N. Martin, K. Bucholz, P. Madden, A. Heath, Genetic influenceson post-natal depressive symptoms: findings from an Australian twin sample,Psychological Medicine 29 (1999) 645–654.
[8] L. Ross, E. Gilbert, S. Evans, M. Romach, Mood changes during pregnancyand the postpartum period: development of a biopsychosocial model, ActaPsychiatrica Scandinavica 109 (2004) 457–466.
[9] A. Caspi, K. Sugden, T. Moffitt, A. Taylor, I. Craig, H. Harrington, J. McClay,J. Mill, J. Martin, A. Braithwaite, R. Poulton, Influence of life stress ondepression: moderation by a polimorphism in the 5-HTT gene, Science 301(2003) 386–389.
[10] B. Mulsant, E. Servan-Schreiber, A connectionist approach to the diagnosisof dementia, in: Proc. 12th Annual Symposium on Computer Applications inMedical Care, 1988, pp. 245–249.
[11] R. Tandon, S. Adak, J. Kaye, Neural networks for longitudinal studies inAlzheimers disease, Artificial Intelligence in Medicine 36 (2006) 245–255.
[12] J. Zhu, N. Hazarika, A. Chung-Tsoi, A. Sergejew, Classification of EEG signalsusing wavelet coefficients and an ANN, in: Pan Pacific Conference on BrainElectric Topography, Sydney, Australia, 1994, p. 27.
[13] M. Jefferson, N. Pendleton, C. Lucas, S. Lucas, M. Horan, Evolution of artificialneural network architecture: prediction of depression after mania, Methods ofinformation in medicine 37 (1998) 220–225.
12

[14] S. Berdia, J. Metz, An artificial neural network stimulating performance ofnormal subjects and schizophrenics on the Wisconsin card sorting test, ArtificialIntelligence in Medicine 13 (1998) 123–138.
[15] L. Franchini, C. Spagnolo, D. Rossini, E. Smeraldi, L. Bellodi, E. Politi, A neuralnetwork approach to the outcome definition on first treatment with sertraline ina psychiatric population, Artificial Intelligence in Medicine 23 (2001) 239–248.
[16] L. Garcıa-Esteve, L. Ascaso, J. Ojuel, P. Navarro, Validation of the EdinburghPostnatal Depression Scale (EPDS) in Spanish mothers, Journal of AffectiveDisorders 75 (2003) 71–76.
[17] J. Nurnberger, M. Blehar, C. Kaufmann, C. York-Cooler, S. Simpson,J. Harkavy-Friedman, J. Severe, Malaspina, Diagnostic interview for geneticstudies and training, Archives of Genetic Psychiatry 51 (1994) 849–859.
[18] M. Roca, R. Martin-Santos, J. Saiz, J. Obiols, M. Serrano, M. Torrens, S. Subir,M. Gilia, R. Navins, A. Ibaez, M. Nadal, N. Barrantes, F. Caellas, DiagnosticInterview for Genetic Studies (DIGS): Inter-rater and test-retest reliability andvalidity in a Spanish population, European Psychiatry 22 (2007) 44–48.
[19] K. Kendler, Major depression and generalised anxiety disorder. Same genes,(partly) different environments - revisited, British Journal of PsychiatrySupplement 30 (1994) 68–75.
[20] H. Eysenck, S. Eysenck, The Eysenck Personality Inventory, University ofLondon Press, London, 1964.
[21] A. Aluja, O. Garcıa, L. Garcıa, A psychometric analysis of the revised EysenckPersonality Questionnaire short scale, Personality and individual differences 35(2003) 449–460.
[22] E. Paykel, Methodological aspects of life events research, Journal ofPsychosomatic Research 27 (1983) 341–352.
[23] G. Zalsman, Y. Huang, M. Oquendo, A. Burke, X. Hu, D. Brent, S. Ellis,D. Goldman, J. Mann, Association of a triallelic serotonin transporter genepromoter region (5-HTTLPR) polymorphism with stressful life events andseverity of depression, American Journal of Psychiatry 163 (2006) 1588–93.
[24] C. Spielberger, R. Gorsuch, R. Luschene, The State-Trait Anxiety Inventory:STAI, Consulting Psychologist Press, 1970.
[25] J. Bellon, A. Delgado, J. Luna, P. Lardelli, Validity and reliability of the Duke-UNC-11 questionnaire of functional social support, Atencion Primaria 18 (1996)158–163.
[26] D. Hranilovic, J. Stefulj, S. Schwab, M. Borrmann-Hassenbach, M. Albus,B. Jernej, D. Wildenauer, Serotonin transporter promoter and intron 2polymorphisms: relationship between allelic variants and gene expression,Biological Psychiatry 55 (2004) 1090–1094.
13

[27] F. Rosenblatt, The Perceptron: a probabilistic model for information storageand organization in the brain, Psychological Review 65 (6) (1958) 386–408.
[28] C. Bishop, Neural Networks for Pattern Recognition, Clarendon Press, Oxford,UK, 1995.
[29] Y. Le Cun, J. Denker, A. Solla, Optimal brain damage, Advances in NeuralInformation Processing Systems 2 (1990) 598–605.
[30] R. Duda, P. Hart, D. Stork, Pattern Classification, Wiley-Interscience, NewYork, NY, 2001.
[31] J. Mao, A. Jain, Artificial neural networks for feature extraction andmultivariate data projection, Neural Networks, IEEE Transactions on 6 (2)(Mar 1995) 296–317.
[32] P. Leray, P. Gallinari, Feature selection with neural networks, Behaviormetrika26 (1999) 145–166.
[33] B. Hassibi, D. Stork, G. Wolf, Optimal brain surgeon and general networkpruning, in: Proceedings of the 1993 IEEE International Conference on NeuralNetworks, San Francisco, CA, 1993, pp. 293–300.
[34] M. Kubat, S. Matwin, Addressing the curse of imbalanced training sets: one-sided selection, in: Proc. 14th International Conference on Machine Learning,Morgan Kaufmann, 1997, pp. 179–186.
[35] N. Japkowicz, S. Stephen, The class imbalance problem: a systematic study,Intelligent Data Analysis Journal 6 (5) (2002) 429–449.
[36] H. Camdeviren, A. Yazici, Z. Akkus, R. Bugdayci, M. Sungur, Comparison oflogistic regression model and classification tree: an application to postpartumdepression data, Expert Systems with Applications 32 (2007) 987–994.
14
Dataset No depression Major depression Total
Training 891 115 1 006
Validation 99 13 112
Evaluation 247 32 279
Total 1 237 160 1 397
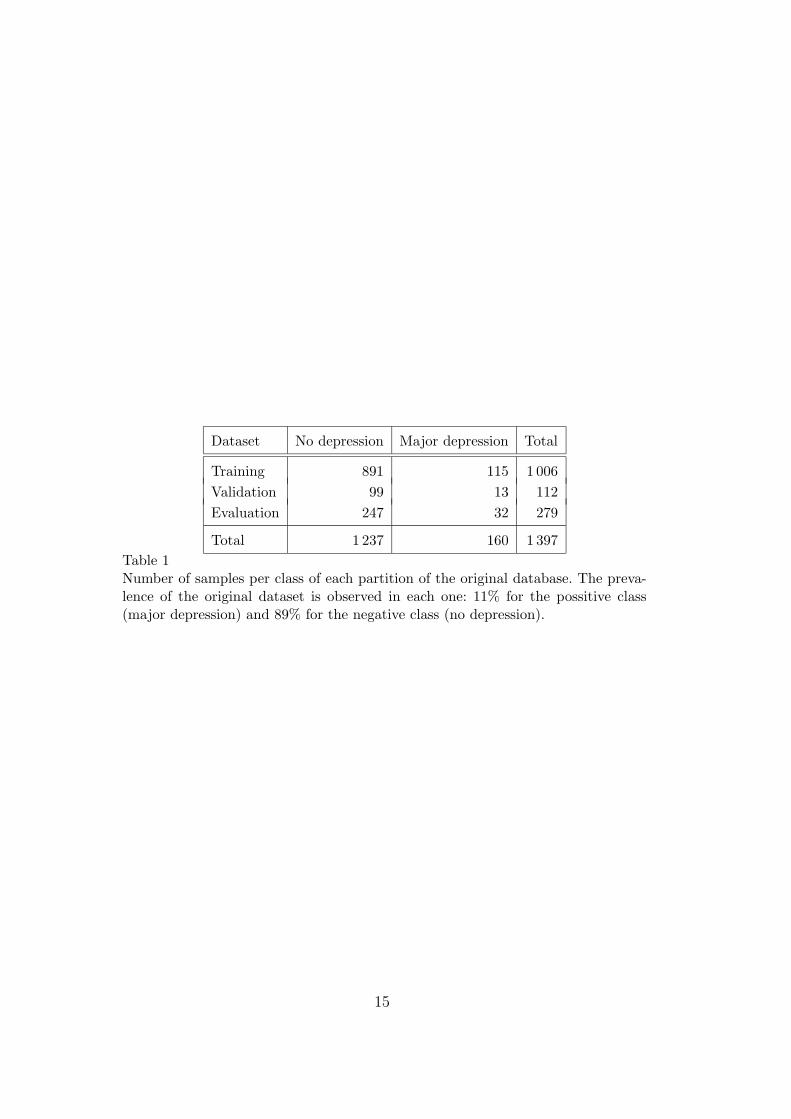
Table 1Number of samples per class of each partition of the original database. The preva-lence of the original dataset is observed in each one: 11% for the possitive class(major depression) and 89% for the negative class (no depression).
15

Input variable No miss. No PPD PPD
Psychiatric antecedents 76No 790 (90.3%) 85 (9.7%)Yes 374 (83.9%) 72 (16.1%)
Emotional alteration during pregnancyNo 73 (81.1%) 17 (18.9%)Yes 1164 (89.1%) 143 (10.9%)
Neuroticism (EPQN) 6 3.25 ± 2.73 5.68 ± 3.55
Initial number of experiencies 2 0.99 ± 1.06 1.40 ± 1.09
Number of experiencies at 8 week 176 0.88 ± 1.09 1.69 ± 1.33
Number of experiencies at 32 week 64 0.87 ± 1.07 1.95 ± 1.53
Anxiety (Initial STAIE) 5 12.20 ± 7.44 17.38 ± 9.87
Blues postpartum (Initial EPDS) - 5.64 ± 3.97 8.96 ± 4.85
Social support (DUKE) 10 88.06 ± 56.27 138.63 ± 82.45
HAP2 79No low-expressing genotype 93 (83.8%) 18 (16.2%)Low-expressing genotype at one loci 664 (87.5%) 95 (12.5%)Low-expressing genotype at both loci 408 (91.1%) 40 (8.9%)
Medical Perinatal Risk -No problems 376 (88.1%) 51 (11.9%)Pregnancy problems 426 (86.1%) 69 (13.2%)Mother problems 117 (89.3%) 14 (10.7%)Mother and child problems 318 (92.4%) 26 (7.6%)
Age - 32.16 ± 4.42 31.89 ± 4.96
Educational level 2Low 324 (85.5%) 55 (14.5%)Medium 518 (88.5%) 67 (11.5%)High 393 (91.2%) 38 (8.8%)
Labour situation during pregnancy 4Employed 879 (91.1%) 86 (8.9%)Unemployed 136 (86.1%) 22 (13.9%)Student/Housewife 103 (85.1%) 18 (14.9%)Leave 116 (77.9%) 33 (22.1%)
Economical level 17Suitable income 830 (90.9%) 83 (9.1%)Enough income 311 (85.9%) 51 (14.1%)Tight income 73 (79.3%) 19 (20.7%)Economical problems 7 (53.8%) 6 (46.2%)
Gender of the baby 18Male 599 (89.7%) 69 (10.3%)Female 623 (87.6%) 88 (12.4%)
Number of people living with 31 2.67 ± 0.96 2.66 ± 0.77
Table 2There are 160 cases with postpartum depression and 1 237 cases without it. Thesecond column shows the number of missing values for each independent variable,where ’-’ indicates no missing value. The last two columns shows the number ofpatients in each class. For categorical variables the number of patients (percentage)is shown. For non-categorical variables the mean ± standard deviation is presented16

I-H H-O Factor
+ + Risk
+ - Protective
- + Protective
- - Risk
Table 3Summary of the nature of the variables as being a risk factor or a protective factordepending on the sign of the weigths of the input-hidden conection (I-H) and thehidden-output connection (H-O).
Model Pruning Topology G Acc Sen Spe AUC
SUBJ+STAIE No 16-4-1 0.81 0.86 ± 0.04 0.750 0.870 0.832
SUBJ+EPDS No 16-14-1 0.82 0.81 ± 0.05 0.844 0.806 0.824
SUBENV+STAIE No 31-15-1 0.81 0.85 ± 0.04 0.750 0.866 0.843
SUBENV+EPDS No 31-3-1 0.81 0.84 ± 0.04 0.781 0.846 0.844
SUBJ+STAIE PR Yes 8-3-1 0.78 0.83 ± 0.04 0.718 0.846 0.794
SUBJ+EPDS PR Yes 9-1-1 0.77 0.78 ± 0.05 0.750 0.781 0.800
SUBENV+STAIE PR Yes 15-2-1 0.77 0.79 ± 0.05 0.750 0.797 0.815
SUBENV+EPDS PR Yes 13-2-1 0.80 0.84 ± 0.04 0.750 0.854 0.836
Table 4Results for the best models with the subjective feature models (SUBJ) and thesubject-environment feature models (SUBENV). We show the G-mean, the accuracyof the model with its confidence interval at 5% of significance and its sensitivity andespecificity with the AUC value. The topology shows the number of input units,hidden units and the output unit. When pruning a network we see that some inputvariables were discarded because their connections towards any hidden unit wereeliminated. Thus, these pruned models (PR) are simpler than original ones and maybe more interpretable but they loose accuracy and the area under the ROC curveis lower.
17
Subjective model with STAIE Subjective model with EPDS
Fig. 1. In subjective models, the most relevant features such as social support(DUKE), neuroticism (EPQN), life events (PR) and postpartum blues (EPDS) areconsidered risk factors. Emotional alterations (ALT) have been taken into accountas well as psychiatric antecedents (PSA) and they show an influence on postnatal de-pression probability rise. Finally, we show that the combination of no low-expressinggenotypes at either of the loci (HAP2 0) is a risk factor and low-expressing combi-nation at both loci (HAP2 2) has a protective influence.
18

Subjec-Environmet model with STAIE Subject-Environment model with EPDS
Fig. 2. As it was to be expected, subject-environment models show greater numberof connections. We find again the main risk factors in both models (social support(DUKE), neuroticism (EPQN) and life events (PR)). Moreover, in these models, theage (AGE) and the number of people living together with the patient (LIV TOG)appear as important protective factors. The income rate appears to be relevant:enough income rate (EC ENF) is a protective factor but a tight economy (EC TIG)can raise the probability of having depression. The anxiety state (STAIE) is a riskfactor too with a moderate influence. Finally, an unemployed (J UNM) or an activemother (J ACT) can be a risk factor but taking maternity leave (J LEA) can reducethe probability of having postnatal depression.
19