
Prasugrel achieves greater and faster P2Y12receptor-mediated platelet inhibition than clopidogrel...
10
..................................................................................................................................................................................... ..................................................................................................................................................................................... CLINICAL RESEARCH Coronary heart disease Prasugrel achieves greater and faster P2Y 12 receptor-mediated platelet inhibition than clopidogrel due to more efficient generation of its active metabolite in aspirin-treated patients with coronary artery disease Lars Wallentin 1 * , Christoph Varenhorst 1 , Stefan James 1 , David Erlinge 2 , Oscar O ¨ Braun 2 , Joseph A. Jakubowski 3 , Atsuhiro Sugidachi 4 , Kenneth J. Winters 3 , and Agneta Siegbahn 5 1 Department of Medical Sciences and Cardiology, Uppsala Clinical Research Center, University Hospital, 751 85 Uppsala, Sweden; 2 Department of Cardiology, Lund University, Sweden; 3 Lilly Research Laboratories, IN, USA; 4 Daiichi Sankyo Co., Ltd., Tokyo, Japan; and 5 Coagulation Laboratory, Department Medical Sciences, Uppsala, Sweden Received 17 September 2007; revised 26 October 2007; accepted 29 October 2007; Online publish-ahead-of-print 30 November 2007 Aims P2Y 12 receptor antagonism and platelet inhibition by prasugrel vs. clopidogrel were investigated in patients with stable coronary artery disease. Methods and results One hundred and ten aspirin treated subjects were randomized to double-blind treatment with clopidogrel (n ¼ 55) 600 mg loading dose (LD) and 75 mg maintenance dose (MD) or prasugrel (n ¼ 55) 60 mg LD and 10 mg MD for 28 days. Concentrations of prasugrel and clopidogrel active metabolites were determined. Platelet aggregation to 20 mM adenosine diphosphate, measured by light transmission aggregometry, was reported as maximal platelet aggregation (MPA). P2Y 12 function was assessed by the vasodilator-stimulated phosphoprotein assay and reported as platelet reactivity index (PRI). The same pharmacodynamic measurements were performed after ex vivo addition of clopido- grel’s active metabolite. At 2 h post-LD, mean MPA was 31 vs. 55%, and mean PRI 8.3 vs. 55.9% for prasugrel and clopidogrel, respectively (P , 0.001). During MD on day 14 and 28, mean MPA was 42 vs. 54% and mean PRI was 25 vs. 51%, respectively (P , 0.001). Peak level of the active metabolite and P2Y 12 inhibition occurred earlier and was greater with prasugrel (P , 0.001). Mean area under the time-concentration curve (AUC; mM . h) of the respect- ive active metabolite was higher with prasugrel vs. clopidogrel post-LD (1.11 vs. 0.24) and post-MD (0.16 vs. 0.062). Ex vivo addition of clopidogrel’s active metabolite further reduced PRI in all patients whose platelets were not already maximally inhibited. Conclusion In aspirin-treated subjects with coronary artery disease, prasugrel 60/10 mg provides faster onset and greater inhi- bition of P2Y 12 receptor-mediated platelet aggregation than clopidogrel 600/75 mg, because of greater and more effi- cient generation of the active metabolite. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Trials † Platelets † Coronary artery disease † Clopidogrel † Prasugrel * Corresponding author. Tel: þ46 18 611 95 07, Fax: þ46 18 50 66 38, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please e-mail: [email protected]. The online version of this article has been published under an open access model. Users are entitled to use, reproduce, disseminate, or display the open access version of this article for non-commercial purposes provided that the original authorship is properly and fully attributed; the Journal, Learned Society and Oxford University Press are attributed as the original place of publication with correct citation details given; if an article is subsequently reproduced or disseminated not in its entirety but only in part or as a derivative work this must be clearly indicated. For commercial re-use, please contact [email protected]. European Heart Journal (2008) 29, 21–30 doi:10.1093/eurheartj/ehm545 by guest on March 14, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
Transcript of Prasugrel achieves greater and faster P2Y12receptor-mediated platelet inhibition than clopidogrel...

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHCoronary heart disease
Prasugrel achieves greater and faster P2Y12
receptor-mediated platelet inhibition thanclopidogrel due to more efficient generationof its active metabolite in aspirin-treatedpatients with coronary artery diseaseLars Wallentin1*, Christoph Varenhorst1, Stefan James1, David Erlinge2,Oscar O Braun2, Joseph A. Jakubowski3, Atsuhiro Sugidachi4, Kenneth J. Winters3,and Agneta Siegbahn5
1Department of Medical Sciences and Cardiology, Uppsala Clinical Research Center, University Hospital, 751 85 Uppsala, Sweden; 2Department of Cardiology, Lund University,Sweden; 3Lilly Research Laboratories, IN, USA; 4Daiichi Sankyo Co., Ltd., Tokyo, Japan; and 5Coagulation Laboratory, Department Medical Sciences, Uppsala, Sweden
Received 17 September 2007; revised 26 October 2007; accepted 29 October 2007; Online publish-ahead-of-print 30 November 2007
Aims P2Y12 receptor antagonism and platelet inhibition by prasugrel vs. clopidogrel were investigated in patients withstable coronary artery disease.
Methodsand results
One hundred and ten aspirin treated subjects were randomized to double-blind treatment with clopidogrel (n ¼ 55)600 mg loading dose (LD) and 75 mg maintenance dose (MD) or prasugrel (n ¼ 55) 60 mg LD and 10 mg MD for 28days. Concentrations of prasugrel and clopidogrel active metabolites were determined. Platelet aggregation to 20 mMadenosine diphosphate, measured by light transmission aggregometry, was reported as maximal platelet aggregation(MPA). P2Y12 function was assessed by the vasodilator-stimulated phosphoprotein assay and reported as plateletreactivity index (PRI). The same pharmacodynamic measurements were performed after ex vivo addition of clopido-grel’s active metabolite. At 2 h post-LD, mean MPA was 31 vs. 55%, and mean PRI 8.3 vs. 55.9% for prasugrel andclopidogrel, respectively (P , 0.001). During MD on day 14 and 28, mean MPA was 42 vs. 54% and mean PRI was25 vs. 51%, respectively (P , 0.001). Peak level of the active metabolite and P2Y12 inhibition occurred earlier andwas greater with prasugrel (P , 0.001). Mean area under the time-concentration curve (AUC; mM.h) of the respect-ive active metabolite was higher with prasugrel vs. clopidogrel post-LD (1.11 vs. 0.24) and post-MD (0.16 vs. 0.062).Ex vivo addition of clopidogrel’s active metabolite further reduced PRI in all patients whose platelets were not alreadymaximally inhibited.
Conclusion In aspirin-treated subjects with coronary artery disease, prasugrel 60/10 mg provides faster onset and greater inhi-bition of P2Y12 receptor-mediated platelet aggregation than clopidogrel 600/75 mg, because of greater and more effi-cient generation of the active metabolite.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Trials † Platelets † Coronary artery disease † Clopidogrel † Prasugrel
* Corresponding author. Tel: þ46 18 611 95 07, Fax: þ46 18 50 66 38, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please e-mail: [email protected] online version of this article has been published under an open access model. Users are entitled to use, reproduce, disseminate, or display the open access version of this articlefor non-commercial purposes provided that the original authorship is properly and fully attributed; the Journal, Learned Society and Oxford University Press are attributed as theoriginal place of publication with correct citation details given; if an article is subsequently reproduced or disseminated not in its entirety but only in part or as a derivative work thismust be clearly indicated. For commercial re-use, please contact [email protected].
European Heart Journal (2008) 29, 21–30doi:10.1093/eurheartj/ehm545
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
BackgroundDual antiplatelet therapy with aspirin and clopidogrel is rec-ommended for patients with acute coronary syndrome (ACS)and patients undergoing stent implantation.1– 3 The currentlyapproved clopidogrel dosing regimen consists of a 300 mgloading dose (LD) followed by a maintenance dose (MD) of75 mg co-administered with aspirin. A more rapid onset andhigher level of platelet inhibition can be obtained with a clopidogrel600 mg LD,4– 7 a dose recently endorsed for ACS to obtain betterprotection during percutaneous coronary interventions.8 Severalstudies have shown poor responsiveness to clopidogrel in 5–44% of treated patients.9 In these patients, there seems also tobe a higher risk of cardiovascular events.10,11 The mechanismsfor the poor response to clopidogrel in some patients areunclear although genetic, metabolic, cellular, and clinical factorshave been proposed.9,12
Like clopidogrel, the novel thienopyridine adenosine dipho-sphate (ADP) receptor antagonist, prasugrel (CS-747, LY640315)is an orally administered prodrug that, after absorption, is con-verted to an active metabolite that inhibits platelet aggregationvia antagonism of the P2Y12 receptor.13 Compared to standarddoses of clopidogrel, prasugrel is more efficiently metabolized toits active metabolite providing a more pronounced platelet inhi-bition with less intersubject variability.14
The aims of this study were to compare the pharmacodynamicand pharmacokinetic effects of a prasugrel 60 mg LD and 10 mgonce daily MD regimen with clopidogrel using the higher 600 mgLD and standard 75 mg once daily MD, in aspirin-treated patientswith coronary artery disease. To further elucidate the mechanismof variability in thienopyridine response, we assessed pharmacoki-netics of the active metabolites of clopidogrel and prasugrel, andmeasured the antiplatelet effects after ex vivo addition of clopido-grel’s active metabolite.
Methods
DesignThis randomized, double-blind, double-dummy, two-armparallel-group study was conducted in adult male and female patientswith stable coronary artery disease, aged 40 to 75 years (Table 1).Two centres in Sweden enrolled patients from April 2006 to Decem-ber 2006. Ethical review board approval was obtained and the studywas conducted according to the ethical principles of Declaration ofHelsinki and Good Clinical Practice guidelines. All subjects providedsigned informed consent.
Subjects were enrolled in the study if they had stable coronaryartery disease defined as chronic stable angina, prior history ofunstable angina or myocardial infarction, previous coronary revascular-ization or disease of at least one coronary vessel on previous angiogra-phy or non-invasive imaging procedure.
Subjects were excluded for: unstable coronary artery disease withinthe previous 30 days; coronary artery intervention within the previous90 days, or planned within 40 days following randomization; history orpresence of bleeding disorder; and history of recent surgery or severetrauma, uncontrolled hypertension, arrhythmia, or severe congestiveheart failure. Intake of thienopyridines �10 days prior to screening,other antiplatelet or anticoagulant agents besides aspirin within 30
days of screening was not allowed. Subjects receiving treatment withnon-steroidal anti-inflammatory drugs or cyclooxygenase-2 inhibitorsthat could not be discontinued for the duration of the study werealso excluded.
Subjects were assigned to either clopidogrel or prasugrel through aninteractive voice response system at a randomization ratio of 1:1 at sitelevel using random permuted blocks of size 4 (block size blinded untilafter data lock). To preserve blinding throughout the study, a minimumnumber of sponsor personnel not involved in the conduct of the studyor analysis of the results had access to randomization tables and treat-ment assignments until study completion. No unblinding was per-formed throughout the study.
Subjects visited the research units in Uppsala or Lund on five differ-ent occasions. An initial screening examination was performed fol-lowed by the lead-in period on aspirin. During the study, subjectsvisited the research unit at the following occasions: Day 1, Day 2,Day 14+3 days, and a final visit Day 29+3 days. Blood samplesfor bioanalytical and pharmacodynamic assays were taken by directpuncture of an antecubital vein at predefined time points. Blood
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
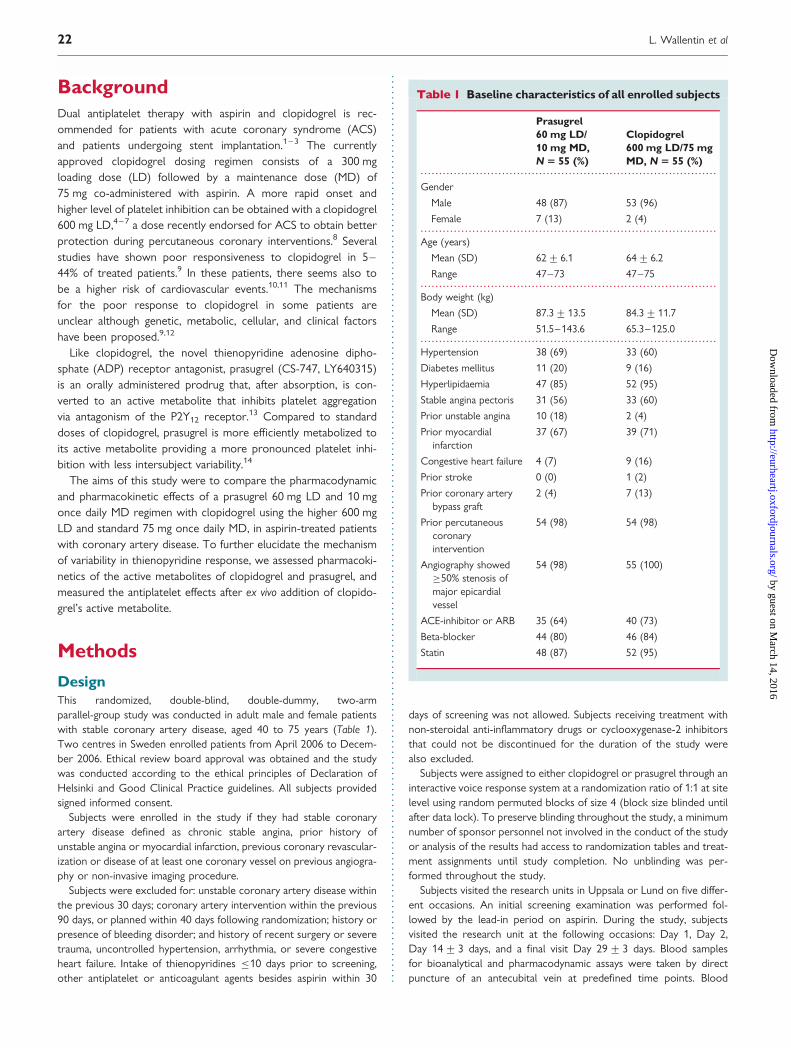
Table 1 Baseline characteristics of all enrolled subjects
Prasugrel60 mg LD/10 mg MD,N 5 55 (%)
Clopidogrel600 mg LD/75 mgMD, N 5 55 (%)
Gender
Male 48 (87) 53 (96)
Female 7 (13) 2 (4)
Age (years)
Mean (SD) 62+6.1 64+6.2
Range 47–73 47–75
Body weight (kg)
Mean (SD) 87.3+13.5 84.3+11.7
Range 51.5–143.6 65.3–125.0
Hypertension 38 (69) 33 (60)
Diabetes mellitus 11 (20) 9 (16)
Hyperlipidaemia 47 (85) 52 (95)
Stable angina pectoris 31 (56) 33 (60)
Prior unstable angina 10 (18) 2 (4)
Prior myocardialinfarction
37 (67) 39 (71)
Congestive heart failure 4 (7) 9 (16)
Prior stroke 0 (0) 1 (2)
Prior coronary arterybypass graft
2 (4) 7 (13)
Prior percutaneouscoronaryintervention
54 (98) 54 (98)
Angiography showed�50% stenosis ofmajor epicardialvessel
54 (98) 55 (100)
ACE-inhibitor or ARB 35 (64) 40 (73)
Beta-blocker 44 (80) 46 (84)
Statin 48 (87) 52 (95)
L. Wallentin et al22
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

samples for the measurement of platelet aggregation were collected in3.8% sodium citrate. Laboratory safety tests were collected and mon-itored throughout the study.
The sample size was determined by assuming mean changes from base-line in maximal platelet aggregation (MPA) to 20 mM ADP at 2 h post-LDof 44.2% for 60 mg LD of prasugrel (observed change) and 32.4% for600 mg LD of clopidogrel (twice the observed change to 300 mg LDof clopidogrel) with a standard deviation (SD) of 15%, based on apreviously performed study on patients with stable atherosclerosis.15
This phase Ib study was not registered in a clinical trials registry.
PatientsEligible patients were identified in the Swedish Coronary and Angio-plasty Registry or the Registry on Cardiac Intensive Care. Of 114screened patients, 112 satisfied inclusion criteria; 110 subjects wereenrolled in the study (101 males, 9 females). Of four subject discon-tinuations, two were due to subject decision (randomized to clopido-grel, n ¼ 2) and two at the request of the investigator due toinadequate venous access (randomized to clopidogrel, n ¼ 1) and pre-existing anaemia (randomized to prasugrel, n ¼ 1). Thus, a total of 106subjects completed the study, according to protocol, 54 on prasugrel,and 52 on clopidogrel. There was no significant difference in baselineclinical characteristics except for a small difference in age (,3 years)(Table 1).
MedicationAll study subjects received aspirin 75 mg once daily for a run in periodof 5–21 days prior to randomization and continued throughout thestudy. Aspirin was not considered as an investigational drug but wasprovided (1 bottle, 100 tablets) in the study ensuring that all subjectsreceived the same daily dose. Following the open-label aspirin run-inperiod, subjects continuing to meet enrolment criteria were assignedto blinded treatment with either clopidogrel or prasugrel. All patientswere administered a LD of either prasugrel 60 mg or clopidogrel600 mg on Day 1 followed by either prasugrel 10 mg or clopidogrel75 mg as a once daily MD for a total of 28+3 days. On Day 1, 2,14+3 and 29+ 3 study medications were administered at thestudy site after an overnight fast.
Pharmacodynamic analysesLight transmission aggregometry (LTA)ADP-induced platelet aggregation was measured in platelet-rich plasmaby light transmission aggregometry (LTA) on Day 1 at baseline(predose), 30 min and 1, 2, 4 h post-LD, and pre-dose during theMD period on Day 2 (24 h+ 4 h post-LD), Day 14+3 and Day29+3. LTA was performed within 180 min from venipuncture on aBioData PAP-4 optical aggregometer, with temperature maintainedat 378C and using each subject’s platelet-poor plasma to set 100%light transmission. Platelet aggregation was allowed to proceed forapproximately 7 min following addition of 5 mM or 20 mM ADP.MPA was recorded as the highest value achieved during this obser-vation period. In addition, the mean change from baseline (pre LD)in MPA (DMPA) was calculated for each time point and used forsome statistical analyses.
Vasodilator-stimulated phosphoproteinThe vasodilator-stimulated phosphoprotein (VASP) assay was per-formed using a commercially available method according to the man-ufacturer’s specifications (Biocytex Platelet VASP kit, Marseille,France). Samples from Uppsala were analysed on an Epics XL fromBeckman Coulter, and samples from Lund were analysed on a FACS
Scan from Becton Dickinson. Synchronization between the flow cyto-meters was performed. The platelet reactivity index (PRI %) was calcu-lated from the corrected mean fluorescence intensity (cMFI) followingincubation of the platelets with either prostaglandin E1 alone or pros-taglandin E1+ADP as follows:
PRI% ¼cMFIðPGE1Þ � cMFIðPGE1þADPÞ
cMFIðPGE1Þ
� �� 100%
The VASP assay was performed on samples obtained prior to the LDand at 1, 2, and 24 h after the LD and prior to the daily MD at Day14+3 and Day 29+ 3.
Pharmacokinetic analysesConcentration of active metabolitePlasma concentrations of the prasugrel active metabolite (R-138727)and clopidogrel active metabolite (R-130964) were analysed insamples obtained at 30 min, 1 h, 2 h, 4 h, and 6 h post-LD andduring the MD period on Day 2, Day 14, and Day 29 at 30 min, 1,2, and 4 h post-MD. A 25 mL volume of 2-bromo-30-methoxyaceto-phenone (500 mM in acetonitrile) was added to a 4 mL sample ofblood collected in EDTA within 30 s of collection in order to stabilizethe active metabolite. Active metabolites were assayed using validatedliquid chromatography with tandem mass spectrometry detection(LC-MS/MS) methods at Advion BioSciences, Inc., Ithaca, NY, USAwith a lower limit of quantification of 0.5 ng/mL.16,17 Samples of theactive metabolite of prasugrel and clopidogrel collected within+10% of the scheduled post-dose sampling times were included inthe presentation of the mean concentration-time plot. The areaunder the curve (AUC) of prasugrel’s and clopidogrel’s respectiveactive metabolites in individual patients was estimated using an estab-lished population pharmacokinetic model.18
Addition of clopidogrel active metabolite ex vivoTen micromolar (final concentration) of clopidogrel active metabolitewas added ex vivo to samples collected at baseline (pre LD) and on Day29. The samples were incubated for 30 min at 378C and then P2Y12
receptor inhibition was characterized using both VASP (PRI) andLTA (MPA to 5 and 20 mM ADP). The final concentration of clopido-grel active metabolite was chosen following preliminary titrationexperiments indicating that this concentration was the minimum con-centration that maximally inhibited platelet function. In these exper-iments, addition of vehicle control did not affect the measurementsof platelet function. The clopidogrel active metabolite was providedby Sankyo Co., Ltd, Tokyo, Japan.
Adverse eventsThe safety of the study participants was monitored throughout thestudy with clinical assessment at specific occasions. Unexpected signsand symptoms were recorded throughout the treatment period.
Statistical analysesThe primary outcome, DMPA to 20 mM ADP at 2 h post-LD, wascompared between LDs using analyses of covariance (ANCOVA)with treatment and study site as fixed factors and baseline MPA as acovariate.19 ANCOVA analyses with the 2 h post LD result as theresponse were also performed for MPA to 20 and 5 mM ADP,DMPA to 5 mM ADP, IPA to 20 and 5 mM ADP, PRI, and change inPRI with treatment and study site as fixed factors. For ANCOVA ana-lyses using MPA, DMPA, PRI, or DPRI, the baseline value was used as acovariate. For the MPA LD/MD analyses, a linear mixed effect model
Wallentin, prasugrel achieves greater and faster P2Y12 inhibition 23
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
was employed with MPA to 20 mM ADP at each time as responses,with treatment, time, the treatment by time interaction and studysite as fixed effects, subject as a random effect, and baseline MPA asa covariate. The unstructured covariance matrix was assumed andallowed to differ for the two treatments. Similar linear mixed effectmodels were employed for MPA to 5 mM ADP and for PRI. Foreach model, the differences between the treatments at each timepoint were calculated with 90% CI of the differences and P-values.Data from the clopidogrel active metabolite spiking experiment(MPA and PRI) were analysed to compare the ex vivo active metabolite-treated results to untreated samples from the same individual at timepoints relative to LD and MD.
The geometric mean AUC for the active metabolite, with corre-sponding 90% confidence limits, were calculated for the prasugreland clopidogrel groups, respectively, at time points relative to LDand MD. The relationship between the logarithmically transformedAUC and PRI was evaluated with Pearson correlation. The softwareused for statistical analyses was SAS Version 8.2, SAS Institute Inc.,Cary, NC, USA. The authors had full access to the data and takeresponsibility for its integrity. All authors have read and agree to themanuscript as written.
Results
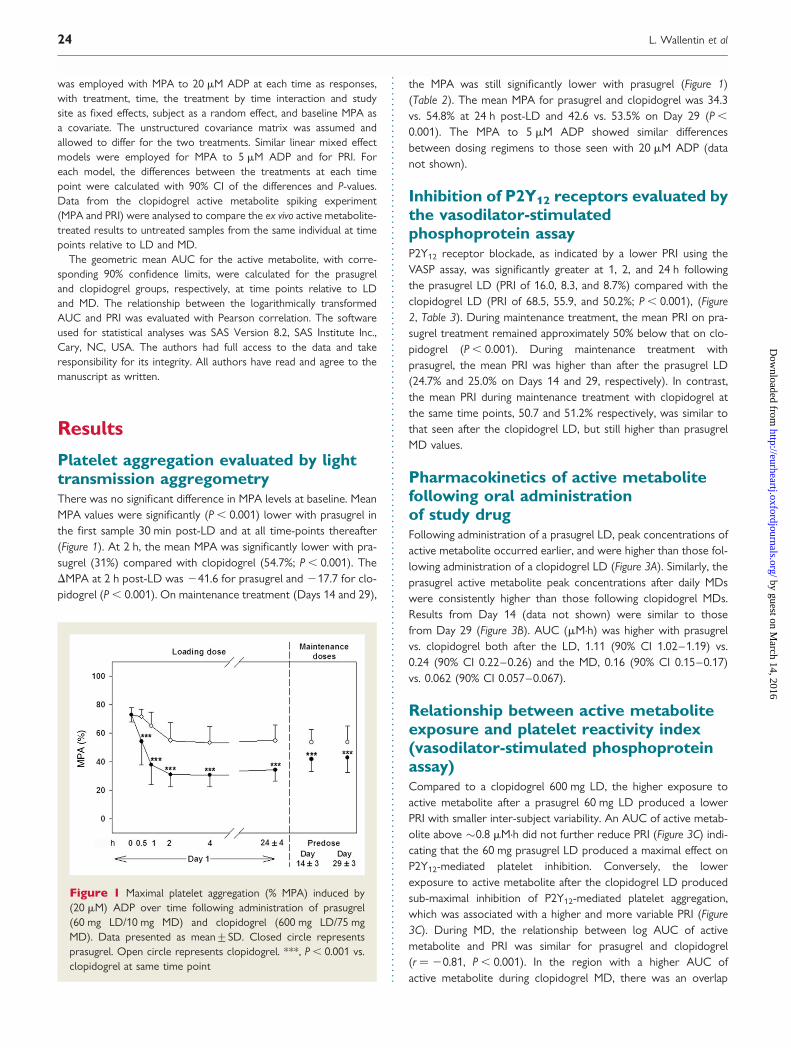
Platelet aggregation evaluated by lighttransmission aggregometryThere was no significant difference in MPA levels at baseline. MeanMPA values were significantly (P , 0.001) lower with prasugrel inthe first sample 30 min post-LD and at all time-points thereafter(Figure 1). At 2 h, the mean MPA was significantly lower with pra-sugrel (31%) compared with clopidogrel (54.7%; P , 0.001). TheDMPA at 2 h post-LD was 241.6 for prasugrel and 217.7 for clo-pidogrel (P , 0.001). On maintenance treatment (Days 14 and 29),
the MPA was still significantly lower with prasugrel (Figure 1)(Table 2). The mean MPA for prasugrel and clopidogrel was 34.3vs. 54.8% at 24 h post-LD and 42.6 vs. 53.5% on Day 29 (P ,
0.001). The MPA to 5 mM ADP showed similar differencesbetween dosing regimens to those seen with 20 mM ADP (datanot shown).
Inhibition of P2Y12 receptors evaluated bythe vasodilator-stimulatedphosphoprotein assayP2Y12 receptor blockade, as indicated by a lower PRI using theVASP assay, was significantly greater at 1, 2, and 24 h followingthe prasugrel LD (PRI of 16.0, 8.3, and 8.7%) compared with theclopidogrel LD (PRI of 68.5, 55.9, and 50.2%; P , 0.001), (Figure2, Table 3). During maintenance treatment, the mean PRI on pra-sugrel treatment remained approximately 50% below that on clo-pidogrel (P , 0.001). During maintenance treatment withprasugrel, the mean PRI was higher than after the prasugrel LD(24.7% and 25.0% on Days 14 and 29, respectively). In contrast,the mean PRI during maintenance treatment with clopidogrel atthe same time points, 50.7 and 51.2% respectively, was similar tothat seen after the clopidogrel LD, but still higher than prasugrelMD values.
Pharmacokinetics of active metabolitefollowing oral administrationof study drugFollowing administration of a prasugrel LD, peak concentrations ofactive metabolite occurred earlier, and were higher than those fol-lowing administration of a clopidogrel LD (Figure 3A). Similarly, theprasugrel active metabolite peak concentrations after daily MDswere consistently higher than those following clopidogrel MDs.Results from Day 14 (data not shown) were similar to thosefrom Day 29 (Figure 3B). AUC (mM.h) was higher with prasugrelvs. clopidogrel both after the LD, 1.11 (90% CI 1.02–1.19) vs.0.24 (90% CI 0.22–0.26) and the MD, 0.16 (90% CI 0.15–0.17)vs. 0.062 (90% CI 0.057–0.067).
Relationship between active metaboliteexposure and platelet reactivity index(vasodilator-stimulated phosphoproteinassay)Compared to a clopidogrel 600 mg LD, the higher exposure toactive metabolite after a prasugrel 60 mg LD produced a lowerPRI with smaller inter-subject variability. An AUC of active metab-olite above �0.8 mM.h did not further reduce PRI (Figure 3C) indi-cating that the 60 mg prasugrel LD produced a maximal effect onP2Y12-mediated platelet inhibition. Conversely, the lowerexposure to active metabolite after the clopidogrel LD producedsub-maximal inhibition of P2Y12-mediated platelet aggregation,which was associated with a higher and more variable PRI (Figure3C). During MD, the relationship between log AUC of activemetabolite and PRI was similar for prasugrel and clopidogrel(r ¼ 20.81, P , 0.001). In the region with a higher AUC ofactive metabolite during clopidogrel MD, there was an overlap
Figure 1 Maximal platelet aggregation (% MPA) induced by(20 mM) ADP over time following administration of prasugrel(60 mg LD/10 mg MD) and clopidogrel (600 mg LD/75 mgMD). Data presented as mean+SD. Closed circle representsprasugrel. Open circle represents clopidogrel. ***, P , 0.001 vs.clopidogrel at same time point
L. Wallentin et al24
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

with active metabolite after prasugrel MD and a correspondingoverlap in effect on PRI [Figure 3D]. The results were similar forMPA (data not shown).
Active metabolite spikingThe ex vivo addition of clopidogrel’s active metabolite to bloodsamples taken pre-LD or pre-MD resulted in drops in MPA andPRI to low levels in all samples. In clopidogrel-treated patients,the addition of clopidogrel’s active metabolite ex vivo reducedMPA and PRI to low levels with small inter-individual variabilityregardless of the ex vivo response to the 600 mg LD or 75 mgMD of clopidogrel (Figures 4A and 5A). In prasugrel-treatedpatients, the MPA and PRI levels following addition of clopidogrel’sactive metabolite were similar to the samples 2 h after a prasugrel60 mg LD, which were already at maximum effect but lower thanthose in samples post-MD in patients not maintaining a maximaleffect during MD (Figures 4B and 5B).
Adverse eventsOral doses of prasugrel 60 mg LD/10 mg MD and clopidogrel600 mg LD/75 mg MD were both well tolerated on a backgroundof aspirin 75 mg once daily. The incidence of total adverse eventswas similar for both treatment regimens. However, the incidenceof bleeding-related events, predominately venipuncture-relatedminor-bleeds and bruising, was higher for the prasugrel dosingregimen (overall 32 bleeding and bruising adverse events, all caus-alities) compared to 13 in the clopidogrel group. No subjects dis-continued from the study due to an adverse event.
DiscussionIn accordance with previous studies in healthy volunteers14,20,21
and in patients with stable atherosclerosis,15 we showed that pra-sugrel achieves faster and greater inhibition of ADP-induced plate-let aggregation, even when compared to clopidogrel starting with a600 mg LD. Importantly, the mean difference in the inhibition ofplatelet of aggregation between clopidogrel and prasugrel wasobserved as soon as 0.5 h after the LD, at which time prasugrelhad provided the magnitude of effect not seen with clopidogreluntil after 2–4 h. This difference in speed of onset and magnitudeof the platelet inhibitory effect might be clinically important in thetreatment of ACS patients and during percutaneous coronaryinterventions.22
The MPA to 20 mM ADP during maintenance doses withprasugrel 10 mg remained significantly lower than withclopidogrel 75 mg, although the difference was halved in compari-son to after LD. Recently, a clopidogrel MD of 150 mg has beenassociated with greater inhibition of platelet aggregation than the75 mg standard dose.23 However, the present MD of both prasu-grel and clopidogrel have been selected for comparison in theongoing TRITON-TIMI 38 pivotal trial,24 based on estimates ofthe optimal balance between efficacy and safety from earlierphase II dose-ranging trials.15,25
LTA using ADP as the agonist for assessing P2Y12 effects is con-founded as ADP receptor subtypes other than P2Y12 can be acti-vated and contribute to platelet aggregation.26 The assay systemfor phosphorylation of VASP uses two reagents, ADP and PGE1.The addition of ADP to PGE1 stimulated platelets does not
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Summary of maximal platelet aggregation (20 mM ADP agonist) after prasugrel or clopidogrel loading andmaintenance doses
Day Time (h) Prasugrel, LS mean (90%CI), 60 mg LD/10 mg MD
Clopidogrel, LS mean (90%CI), 600 mg LD/75 mg MD
Difference LS mean(90% CI)
P-value
1 Predosea 72.9 (71.8, 74.0) 72.6 (71.5, 73.7)1a 37.8 (34.8, 40.7) 65.1 (63.1, 67.0) 227.3 (230.8, 223.8) , 0.0012a 31.0 (29.2, 32.9) 54.7 (52.1, 57.4) 223.7 (227.0, 220.5) , 0.00124+4a 34.3 (32.6, 36.0) 54.8 (52.4, 57.2) 220.5 (223.4, 217.5) , 0.001
14+3 Predoseb 41.6 (39.8, 43.4) 53.5 (51.5, 55.5) 211.9 (214.7, 29.20) , 0.001
29+3 Predoseb 42.6 (40.3, 44.9) 53.5 (51.0, 56.0) 210.9 (214.3, 27.53) , 0.001
aLoading dose.bMaintenance dose.
Figure 2 Platelet reactivity index (PRI, %) from VASP phos-phorylation over time following administration of prasugrel(60 mg LD/10 mg MD) and clopidogrel (600 mg LD/75 mgMD). Data presented as mean+SD. Closed circle representsprasugrel. Open circle represents clopidogrel. ***, P , 0.001vs. clopidogrel at same time point
Wallentin, prasugrel achieves greater and faster P2Y12 inhibition 25
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Summary of vasodilator-stimulated phosphoprotein phosphorylation, platelet reactivity index (PRI, %), afterprasugrel or clopidogrel loading and maintenance doses
Day Time (h) Prasugrel, LS mean (90%CI), 60 mg LD/10 mg MD
Clopidogrel, LS mean (90%CI), 600 mg LD/75 mg MD
Difference, LSmean (90% CI)
P-value
1 Predosea 81.1 (80.0, 82.2) 81.9 (80.8, 83.0)1a 16.0 (12.3, 19.7) 68.5 (63.5, 73.6) 252.5 (258.8, 246.2) , 0.0012a 8.32 (4.61, 12.0) 55.9 (50.8, 61.0) 247.6 (253.9, 241.3) , 0.00124+4a 8.68 (4.93, 12.4) 50.2 (45.1, 55.2) 241.5 (247.8, 235.2) , 0.001
14+3 Predoseb 24.7 (22.0, 27.4) 50.7 (46.6, 54.8) 226.0 (230.9, 221.1) , 0.001
29+3 Predoseb 25.0 (22.3, 27.7) 51.2 (47.0, 55.3) 226.2 (231.2, 221.3) , 0.001
aLoading dose.bMaintenance dose.
Figure 3 (A) Plasma concentrations of prasugrel and clopidogrel active metabolites following administration of a single loading dose. Lowerlimit of quantitation was 0.5 ng/mL. Data presented as mean+SD. Closed circle represents prasugrel 60 mg LD (N ¼ 55). Open circle rep-resents clopidogrel 600 mg LD (N ¼ 54). (B) Plasma concentrations of prasugrel and clopidogrel active metabolites following administrationof maintenance doses. Lower limit of quantitation was 0.5 ng/mL. Data presented as mean+SD. Closed circle represents prasugrel 10 mgMD (N ¼ 54 on Day 29+ 3). Open circle represents clopidogrel 75 mg MD (N ¼ 52 on Day 29+ 3). (C) Scatter plot of platelet reactivityindex (PRI, %) at 24 h vs. area under the curve (AUC; mM.h) of active metabolite after a loading dose of clopidogrel 600 mg or prasugrel60 mg. Closed circle represents patients on prasugrel. Open circle represents patients on clopidogrel. (D) Scatter plot of platelet reactivityindex (PRI, %) vs. area under the curve (AUC; mM.h) of active metabolite after maintenance dose of clopidogrel 75 mg or prasugrel 10 mg.Closed circle represents patients on prasugrel. Open circle represents patients on clopidogrel
L. Wallentin et al26
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
reduce VASP phosphorylation if P2Y12 receptors are successfullyinhibited by a thienopyridine, as this effect of ADP is mediated byP2Y12 but not P2Y1.
12 Therefore, flow cytometric assessment ofVASP phosphorylation is more suitable for comparing the specificP2Y12 inhibitory effects of thienopyridines.27 The VASP results inthe present study showed a 90% inhibition of P2Y12 receptors at1–2 h after a 60 mg LD of prasugrel which decreased to 66% inhi-bition during the 10 mg MD after 14 and 29 days. In contrast, atno time point did a 600 mg LD of clopidogrel induce more than a40% inhibition of P2Y12 receptors. Thus, the VASP analyses indicateda larger difference in P2Y12 inhibition between the treatments thanthe MPA measurements, the latter also reflecting P2Y1 receptormediated aggregation not inhibited by thienopyridines.
Compared to clopidogrel, the more rapid onset and greaterinhibition of P2Y12-mediated platelet aggregation, as measured byMPA, with prasugrel was associated with earlier and higher peaklevels and greater exposure to the active metabolite. Furthermore,inhibition of P2Y12-induced platelet reactivity, as measured byVASP, was closely related to the exposure of active metabolites,for prasugrel LD up to near saturation levels of the P2Y12 receptor,as indicated by PRI values approaching zero with no further changewith increasing plasma levels. During MD, there was good log-linear correlation between platelet inhibition and exposure tothe active metabolite, indicating that the pharmacokinetic/pharma-codynamic relationship between clopidogrel’s and prasugrel’sactive metabolites was similar. These data are consistent with
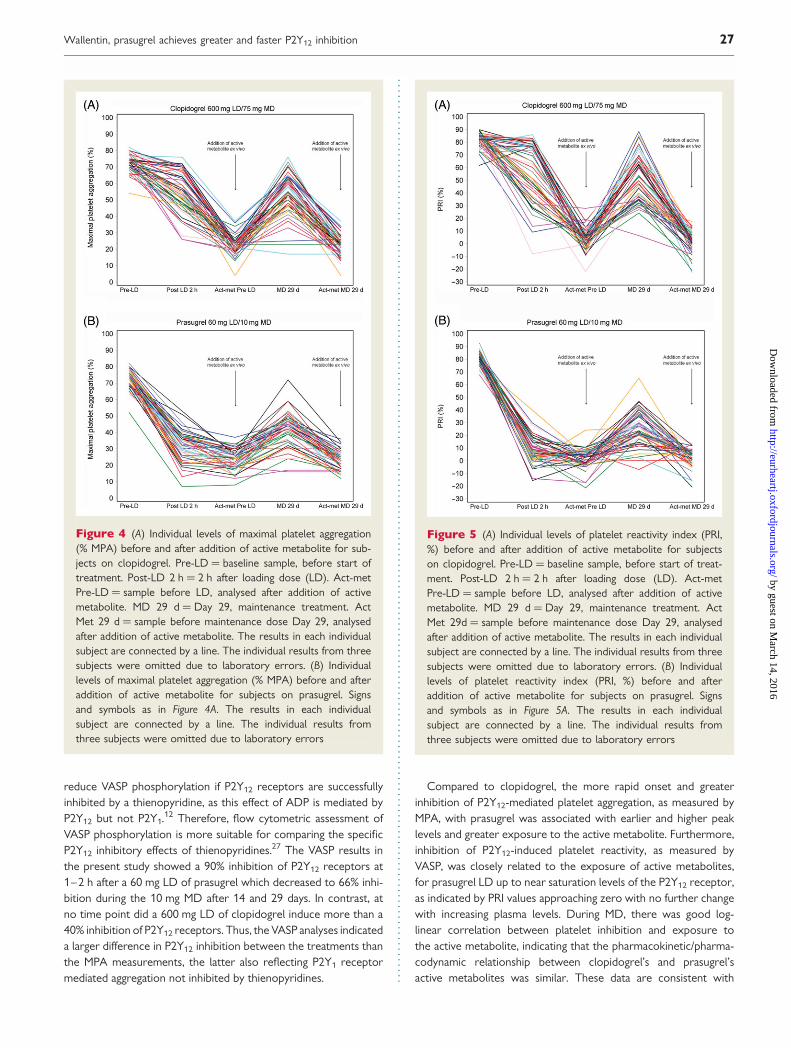
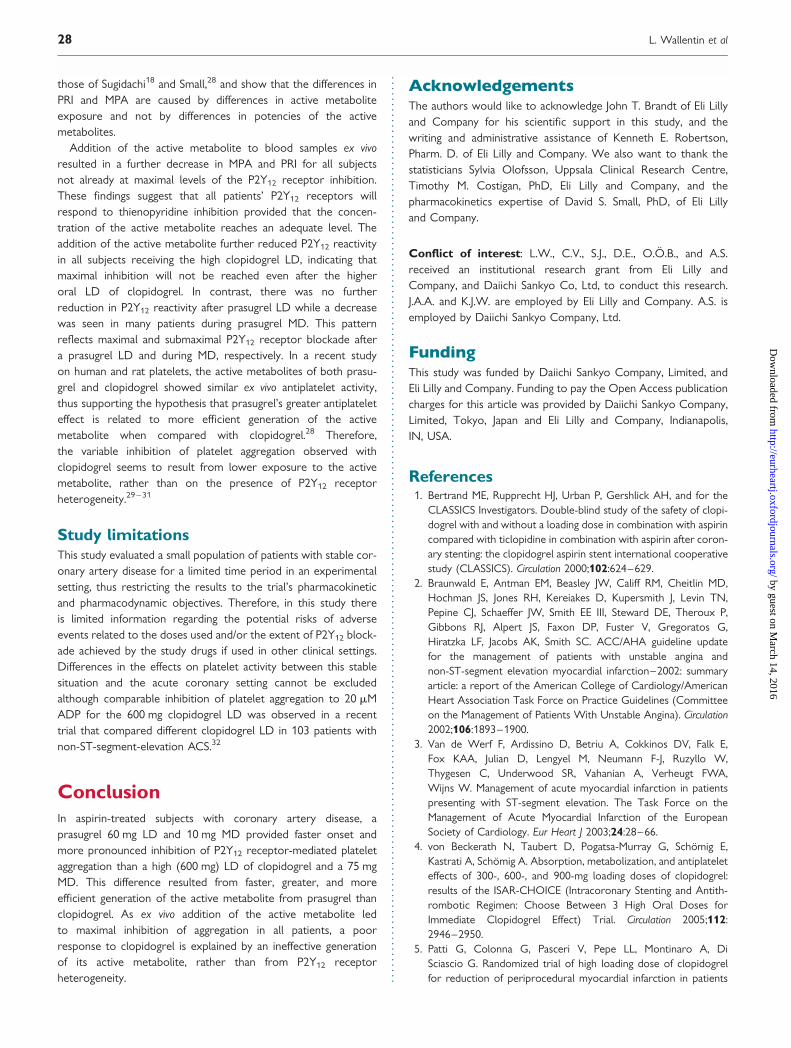
Figure 4 (A) Individual levels of maximal platelet aggregation(% MPA) before and after addition of active metabolite for sub-jects on clopidogrel. Pre-LD ¼ baseline sample, before start oftreatment. Post-LD 2 h ¼ 2 h after loading dose (LD). Act-metPre-LD ¼ sample before LD, analysed after addition of activemetabolite. MD 29 d ¼ Day 29, maintenance treatment. ActMet 29 d ¼ sample before maintenance dose Day 29, analysedafter addition of active metabolite. The results in each individualsubject are connected by a line. The individual results from threesubjects were omitted due to laboratory errors. (B) Individuallevels of maximal platelet aggregation (% MPA) before and afteraddition of active metabolite for subjects on prasugrel. Signsand symbols as in Figure 4A. The results in each individualsubject are connected by a line. The individual results fromthree subjects were omitted due to laboratory errors
Figure 5 (A) Individual levels of platelet reactivity index (PRI,%) before and after addition of active metabolite for subjectson clopidogrel. Pre-LD ¼ baseline sample, before start of treat-ment. Post-LD 2 h ¼ 2 h after loading dose (LD). Act-metPre-LD ¼ sample before LD, analysed after addition of activemetabolite. MD 29 d ¼ Day 29, maintenance treatment. ActMet 29d ¼ sample before maintenance dose Day 29, analysedafter addition of active metabolite. The results in each individualsubject are connected by a line. The individual results from threesubjects were omitted due to laboratory errors. (B) Individuallevels of platelet reactivity index (PRI, %) before and afteraddition of active metabolite for subjects on prasugrel. Signsand symbols as in Figure 5A. The results in each individualsubject are connected by a line. The individual results fromthree subjects were omitted due to laboratory errors
Wallentin, prasugrel achieves greater and faster P2Y12 inhibition 27
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
those of Sugidachi18 and Small,28 and show that the differences inPRI and MPA are caused by differences in active metaboliteexposure and not by differences in potencies of the activemetabolites.
Addition of the active metabolite to blood samples ex vivoresulted in a further decrease in MPA and PRI for all subjectsnot already at maximal levels of the P2Y12 receptor inhibition.These findings suggest that all patients’ P2Y12 receptors willrespond to thienopyridine inhibition provided that the concen-tration of the active metabolite reaches an adequate level. Theaddition of the active metabolite further reduced P2Y12 reactivityin all subjects receiving the high clopidogrel LD, indicating thatmaximal inhibition will not be reached even after the higheroral LD of clopidogrel. In contrast, there was no furtherreduction in P2Y12 reactivity after prasugrel LD while a decreasewas seen in many patients during prasugrel MD. This patternreflects maximal and submaximal P2Y12 receptor blockade aftera prasugrel LD and during MD, respectively. In a recent studyon human and rat platelets, the active metabolites of both prasu-grel and clopidogrel showed similar ex vivo antiplatelet activity,thus supporting the hypothesis that prasugrel’s greater antiplateleteffect is related to more efficient generation of the activemetabolite when compared with clopidogrel.28 Therefore,the variable inhibition of platelet aggregation observed withclopidogrel seems to result from lower exposure to the activemetabolite, rather than on the presence of P2Y12 receptorheterogeneity.29– 31
Study limitationsThis study evaluated a small population of patients with stable cor-onary artery disease for a limited time period in an experimentalsetting, thus restricting the results to the trial’s pharmacokineticand pharmacodynamic objectives. Therefore, in this study thereis limited information regarding the potential risks of adverseevents related to the doses used and/or the extent of P2Y12 block-ade achieved by the study drugs if used in other clinical settings.Differences in the effects on platelet activity between this stablesituation and the acute coronary setting cannot be excludedalthough comparable inhibition of platelet aggregation to 20 mMADP for the 600 mg clopidogrel LD was observed in a recenttrial that compared different clopidogrel LD in 103 patients withnon-ST-segment-elevation ACS.32
ConclusionIn aspirin-treated subjects with coronary artery disease, aprasugrel 60 mg LD and 10 mg MD provided faster onset andmore pronounced inhibition of P2Y12 receptor-mediated plateletaggregation than a high (600 mg) LD of clopidogrel and a 75 mgMD. This difference resulted from faster, greater, and moreefficient generation of the active metabolite from prasugrel thanclopidogrel. As ex vivo addition of the active metabolite ledto maximal inhibition of aggregation in all patients, a poorresponse to clopidogrel is explained by an ineffective generationof its active metabolite, rather than from P2Y12 receptorheterogeneity.
AcknowledgementsThe authors would like to acknowledge John T. Brandt of Eli Lillyand Company for his scientific support in this study, and thewriting and administrative assistance of Kenneth E. Robertson,Pharm. D. of Eli Lilly and Company. We also want to thank thestatisticians Sylvia Olofsson, Uppsala Clinical Research Centre,Timothy M. Costigan, PhD, Eli Lilly and Company, and thepharmacokinetics expertise of David S. Small, PhD, of Eli Lillyand Company.
Conflict of interest: L.W., C.V., S.J., D.E., O.O.B., and A.S.received an institutional research grant from Eli Lilly andCompany, and Daiichi Sankyo Co, Ltd, to conduct this research.J.A.A. and K.J.W. are employed by Eli Lilly and Company. A.S. isemployed by Daiichi Sankyo Company, Ltd.
FundingThis study was funded by Daiichi Sankyo Company, Limited, andEli Lilly and Company. Funding to pay the Open Access publicationcharges for this article was provided by Daiichi Sankyo Company,Limited, Tokyo, Japan and Eli Lilly and Company, Indianapolis,IN, USA.
References1. Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH, and for the
CLASSICS Investigators. Double-blind study of the safety of clopi-dogrel with and without a loading dose in combination with aspirincompared with ticlopidine in combination with aspirin after coron-ary stenting: the clopidogrel aspirin stent international cooperativestudy (CLASSICS). Circulation 2000;102:624–629.
2. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD,Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN,Pepine CJ, Schaeffer JW, Smith EE III, Steward DE, Theroux P,Gibbons RJ, Alpert JS, Faxon DP, Fuster V, Gregoratos G,Hiratzka LF, Jacobs AK, Smith SC. ACC/AHA guideline updatefor the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction–2002: summaryarticle: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Committeeon the Management of Patients With Unstable Angina). Circulation2002;106:1893–1900.
3. Van de Werf F, Ardissino D, Betriu A, Cokkinos DV, Falk E,Fox KAA, Julian D, Lengyel M, Neumann F-J, Ruzyllo W,Thygesen C, Underwood SR, Vahanian A, Verheugt FWA,Wijns W. Management of acute myocardial infarction in patientspresenting with ST-segment elevation. The Task Force on theManagement of Acute Myocardial Infarction of the EuropeanSociety of Cardiology. Eur Heart J 2003;24:28–66.
4. von Beckerath N, Taubert D, Pogatsa-Murray G, Schomig E,Kastrati A, Schomig A. Absorption, metabolization, and antiplateleteffects of 300-, 600-, and 900-mg loading doses of clopidogrel:results of the ISAR-CHOICE (Intracoronary Stenting and Antith-rombotic Regimen: Choose Between 3 High Oral Doses forImmediate Clopidogrel Effect) Trial. Circulation 2005;112:2946–2950.
5. Patti G, Colonna G, Pasceri V, Pepe LL, Montinaro A, DiSciascio G. Randomized trial of high loading dose of clopidogrelfor reduction of periprocedural myocardial infarction in patients
L. Wallentin et al28
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

undergoing coronary intervention: results from the ARMYDA-2(Antiplatelet therapy for Reduction of MYocardial Damageduring Angioplasty) study. Circulation 2005;111:2099–2106.
6. Hochholzer W, Trenk D, Frundi D, Blanke P, Fischer B, Andris K,Bestehorn H-P, Buttner HJ, Neumann F-J. Time dependence ofplatelet inhibition after a 600-mg loading dose of clopidogrel in alarge, unselected cohort of candidates for percutaneous coronaryintervention. Circulation 2005;111:2560–2564.
7. Cuisset T, Frere C, Quilici J, Morange P-E, Nait-Saidi L, Carvajal J,Lehmann A, Lambert M, Bonnet J-L, Alessi M-C. Benefit of a600-mg loading dose of clopidogrel on platelet reactivity and clini-cal outcomes in patients with non-ST-segment elevation acutecoronary syndrome undergoing coronary stenting. J Am CollCardiol 2006;48:1339–1345.
8. Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C,Jørgensen E, Marco J, Nordrehaug J-E, Ruzyllo W, Urban P,Stone GW, Wijns W. Guidelines for percutaneous coronary inter-ventions. The Task Force for Percutaneous Coronary Interven-tions of the European Society of Cardiology. Eur Heart J 2005;26:804–847.
9. Gurbel PA, Tantry US. Clopidogrel resistance? Thrombosis Res2007;120:311–321.
10. Matetzky S, Shenkman B, Guetta V, Shechter M, Bienart R,Goldenberg I, Novikov I, Pres H, Savion N, Varon D, Hod H. Clo-pidogrel resistance is associated with increased risk of recurrentatherothrombotic events in patients with acute myocardial infarc-tion. Circulation 2004;109:3171–3175.
11. Gurbel PA, Bliden KP, Guyer K, Cho PW, Zaman KA, Kreutz RP,Bassi AK, Tantry US. Platelet Reactivity in Patients and RecurrentEvents Post-Stenting: Results of the PREPARE POST-STENTINGStudy. J Am Coll Cardiol 2005;46:1820–1826.
12. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Alfonso F, Macaya C,Bass TA, Costa MA. Variability in individual responsiveness to clo-pidogrel: clinical implications, management, and future perspec-tives. J Am Coll Cardiol 2007;49:1505–1516.
13. Niitsu Y, Jakubowski JA, Sugidachi A, Asai F. Pharmacology ofCS-747 (prasugrel, LY640315), a novel, potent antiplateletagent with in vivo P2Y12 receptor antagonist activity. SeminThromb Hemost 2005;31:184–194.
14. Brandt JT, Payne CD, Wiviott SD, Weerakkody G, Farid NA,Small DS, Jakubowski JA, Naganuma H, Winters KJ. A comparisonof prasugrel and clopidogrel loading doses on platelet function:magnitude of platelet inhibition is related to active metabolite for-mation. Am Heart J 2007;153:66.e9–66.e16.
15. Jernberg T, Payne CD, Winters KJ, Darstein C, Brandt JT,Jakubowski JA, Naganuma H, Siegbahn A, Wallentin L. Prasugrelachieves greater inhibition of platelet aggregation and a lowerrate of non-responders compared with clopidogrel in aspirin-treated patients with stable coronary artery disease. Eur Heart J2006;27:1166–1173.
16. Farid NA, McIntosh M, Garofolo F, Wong E, Shwajch A, Kennedy M,Young M, Sarkar P, Kawabata K, Takahashi M, Pang H. Determi-nation of the active and inactive metabolites of prasugrel inhuman plasma by liquid chromatography/tandem mass spec-trometry. Rapid Commun Mass Spectrom 2007;21:169–179.
17. Pereillo J-M, Maftouh M, Andrieu A, Uzabiaga M-F, Fedeli O, Savi P,Pascal M, Herbert J-M, Maffrand J-P, Picard C. Structure andstereochemistry of the active metabolite of clopidogrel. DrugMetab Dispos 2002;30:1288–1295.
18. Small DS, Farid NA, Payne CD, Brandt JT, Jakubowski JA,Salazar DE, Winters KJ. Prasugrel 60 mg and clopidogrel 300 mgloading doses: a pharmacokinetic basis for the observed difference
in platelet aggregation response [abstract]. Am J Cardiol 2006;98(Suppl. 1):200M.
19. Armitage P, Berry G. Statistical Methods in Medical Research. 3rd ed.Oxford: Blackwell Scientific Publications; 1994. p154–174.
20. Jakubowski JA, Matsushima N, Asai F, Naganuma H, Brandt JT,Hirota T, Freestone S, Winters KJ. A multiple dose study of prasu-grel (CS-747), a novel thienopyridine P2Y12 inhibitor, comparedwith clopidogrel in healthy humans. Br J Clin Pharmacol 2006;63:421–430.
21. Payne CD, Li YG, Small DS, Ernest CS III, Farid NA, Jakubowski JA,Brandt JT, Salazar D, Winters KJ. Increased active metabolite for-mation explains the greater platelet inhibition with prasugrel com-pared to high-dose clopidogrel. J Cardiovasc Pharmacol 2007, inpress.
22. Steinhubl SR, Berger PB, Brennan DM, Topol EJ, for the CREDOInvestigators. Optimal timing for the initiation of pre-treatmentwith 300 mg clopidogrel before percutaneous coronary interven-tion. J Am Coll Cardiol 2006;47:939–943.
23. von Beckerath N, Kastrati A, Wieczorek A, Pogatsa-Murray G,Sibbing D, Graf I, Schomig A. A double-blind, randomized studyon platelet aggregation in patients treated with a daily dose of150 or 75 mg of clopidogrel for 30 days. Eur Heart J 2007; Pub-lished on-line, February 1.
24. Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W,Gottlieb S, Neumann F-J, Ardissino D, De Servi S, Murphy SA,Riesmeyer J, Weerakkody G, Gibson CM, Antman EM, for theTRITON–TIMI 38 Investigators. A clinical trial of prasugrel vs. clo-pidogrel in patients with acute coronary syndromes. New Engl JMed 2007;357:2001–2015.
25. Wiviott SD, Antman EM, Winters KJ, Weerakkody G, Murphy SA,Behounek BD, Carney RJ, Lazzam C, McKay RG, McCabe CH,Braunwald E, for the JUMBO–TIMI 26 Investigators. Randomizedcomparison of prasugrel (CS-747, LY640315), a novel thienopyri-dine P2Y12 antagonist, with clopidogrel in percutaneous coronaryintervention: results of the Joint Utilization of Medications to BlockPlatelets Optimally (JUMBO)-TIMI 26 trial. Circulation 2005;111:3366–3373.
26. Storey RF, Newby LJ, Heptinstall S. Effects of P2Y(1) andP2Y(12) receptor antagonists on platelet aggregation induced bydifferent agonists in human whole blood. Platelets 2001;12:443–447.
27. Aleil B, Ravanat C, Cazenave JP, Rochoux G, Heitz A, Gachet C.Flow cytometric analysis of intraplatelet VASP phosphorylationfor the detection of clopidogrel resistance in patientswith ischemic cardiovascular diseases. J Thromb Haemost 2005;3:85–92.
28. Sugidachi A, Ogawa T, Kurihara A, Hagihara K, Jakubowski JA,Hashimoto M, Niitsu Y, Asai F. The greater in vivo antiplatelet effectsof prasugrel compared to clopidogrel reflect more efficientgeneration of its active metabolite with similar antiplatelet activityto clopidogrel’s active metabolite. J Thromb Haemost 2007;5:1545–1551.
29. Fontana P, Dupont A, Gandrille S, Bachelot-Loza C, Reny J-L,Aiach M, Gaussem P. Adenosine diphosphate-induced plateletaggregation is associated with P2Y12 gene sequence variations inhealthy subjects. Circulation 2003;108:989–995.
30. Fontana P, Gaussem P, Aiach M, Fiessinger J-N, Emmerich J,Reny J-L. P2Y12 H2 haplotype is associated with peripheral arterialdisease: a case-control study. Circulation 2003;108:2971–2973.
31. von Beckerath N, von Beckerath O, Koch W, Eichinger M,Schomig A, Kastrati A. P2Y12 gene H2 haplotype is not associatedwith increased adenosine diphosphate-induced platelet
Wallentin, prasugrel achieves greater and faster P2Y12 inhibition 29
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

aggregation after initiation of clopidogrel therapy with a highloading dose. Blood Coagul Fibrinolysis 2005;16:199–204.
32. Montalescot G, Sideris G, Meuleman C, Bal-dit-Sollier C,Lellouche N, Steg G, Slama M, Milleron O, Collet J-P,Henry P, Beygui F, Drouet L, for the ALBION Trial Investi-gators. A randomized comparison of high clopidogrel loading
doses in patients with non-ST-segment elevation acute coronarysyndromes: the ALBION (Assessment of the Best LoadingDose of Clopidogrel to Blunt Platelet Activation, Inflammationand Ongoing Necrosis) trial. J Am Coll Cardiol 2006;48:931–938.
CLINICAL VIGNETTE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
doi:10.1093/eurheartj/ehm324Online publish-ahead-of-print 26 July 2007
Complete occlusion of the aortic isthmusKarsten Lenk1*, Ingo Dahnert2, and Gerhard Schuler1
1Department of Cardiology, Heart Centre, University of Leipzig, Strumpellstraße 39, 04289 Leipzig, Germany; 2Department ofPaediatric Cardiology, Heart Centre, University of Leipzig, Strumpellstraße 39, 04289 Leipzig, Germany* Corresponding author. Tel: þ49 341 8651005, Fax: þ49 341 8651461. Email: [email protected]
A 44-year-old man was admitted to hospital withsevere chest pain. The ECG showed a subacutemyocardial infarction. An attempt of interventionalrevascularization from the femoral artery failedbecause the catheter could not be advanced viathe thoracic aorta. A brachial approach showed acoronary two-vessel disease with occlusion of thecircumflex artery. Despite successful revasculariza-tion, the left ventricular ejection fraction remainedseverely depressed (20%). A CT scan revealed com-plete occlusion of the descending aorta distal to theorigin of the left subclavian artery (Panel A). Inter-ventional reconstitution of the aortic continuitywas planned to reduce the left ventricular afterload.A pigtail catheter was placed proximal to the occlu-sion from a left radial access. An additional leftfemoral approach allowed simultaneous contrastinjection showing the interrupted aortic segment(Panel B), which was then perforated with a trans-septal needle and a Brockenbrough catheter (PanelC). The transseptal needle was exchanged for anAmplatz superstiff wire. A covered CP stentmounted on a 15 mm Cordis Maxi balloon catheterwas implanted through a Cook blue long sheath(Panel D). The post-interventional angiographyproved correct stent position without any pressuregradient, dissection, or aneurysm (Panel D). After 4weeks, an echocardiographic control showedimproved left ventricular ejection fraction (35%).
It remains speculation whether this was a primar-ily interrupted aortic arch (type A) or a secondarilyatretic coarctation.
Panel A. CT scan as a reconstruction (lateralview) of the thorax and abdomen, showing the inter-ruption of the descending aorta at the isthmic level.
Panel B. Simultaneous angiogram of the superiorand inferior parts of the descending aorta (RAOview), sparing the atretic segment.
Panel C. Perforation of the atretic segment from afemoral access using a standard transseptal needleand a Brockenbrough catheter (RAO view).
Panel D. Postinterventional angiography showingthe implanted CP stent (RAO view).
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please email: [email protected].
L. Wallentin et al30
by guest on March 14, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from




















