Power of the Mind
43
Power of the mind The effect of a placebo on primary dysmenorrhoea Naomi Lagerweij & Nienke Schalij Research Paper Class: V6C Supervisor: A. van Raalte Date: Monday January 8, 2012
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Power of the Mind

Power of the mind The effect of a placebo on primary dysmenorrhoea
Naomi Lagerweij & Nienke Schalij Research Paper
Class: V6C Supervisor: A. van Raalte
Date: Monday January 8, 2012
2
Table of Contents
Page
1. Introduction 1.1 – History of the placebo effect 1.2 – Mechanisms of placebo effects » 1.2.1 – Psychological mechanisms » 1.2.1 – Neurobiological mechanisms 1.3 – Organ specific placebo effects 1.4 – Usage of the placebo effect 1.5 – Disadvantages of the placebo effect 1.6 – Research field
3 4 4 7
10 12 13 14
2. Method and material 2.1 – Method 2.2 – Material
17 20
3. Results 3.1.1 – Profiles of the participants: test group » 3.1.2 – Summary of the participants’ profiles: test group 3.2.1 – Profiles of the participants: control group » 3.2.2 – Summary of the participants’ profiles: control group 3.3 – Regular menstrual pain: test group 3.4 – Regular menstrual pain: control group 3.5 – Regular menstrual pain test group vs. regular menstrual pain control group 3.6 – Menstrual pain during the trial: test group 3.7 – Brief summary results
21 23 24 25 25 26 27
28 29
4. Conclusion 30
5. Discussion 32
6. Appendix 34
7. Sources 40
8. Logbook 42
3
1. Introduction 1.1 – History of the placebo effect
The placebo effect is a neurobiological and psychological phenomenon that has been around for centuries. Over the last half century, the placebo effect has been applied in clinical trials (trials meant to determine whether a certain medicine or medical device is safe and effective) as well as routine medical practice; by true physicians and quacks. The word ‘placebo’, which means ‘I will please’, comes from the Latin verb ‘placere’ (to please). Basically, a placebo is an inactive medicine or medical treatment which has the ability to cause an actual improvement in the condition of a patient merely by the power of suggestion; this phenomenon is called the placebo effect. A placebo can take many forms. It can exist in the form of an inert pill (sugar pill), injection or surgery, but also in the form of a procedure or a certain situation. The Greek physician Galen (129 – 199 AD) was probably the first person to describe the healing power of the placebo effect. He observed that one of the most important factors in curing a patient is the patient’s faith in the treatment: "He cures most successfully in whom the people have the most confidence.”1 Physicians have always recognized and applied this in their practices; many have used a combination of healing rituals, symbols and their authority to cure their patients. Until the late 19th century, most medications prescribed by physicians were inactive. In 1959, Shapiro, an American psychiatrist, noted that: “The history of medical treatment until relatively recently is the history of the placebo effect.”2 In 1881, Hooper’s Medical Dictionary defined the term ‘placebo’ as “an epithet given to any medicine adapted more to please than benefit the patient.” It is true that the term ‘placebo effect’ has had and sometimes still has an ambivalent reputation: especially at the beginning of the previous century the term ‘placebo’ was associated with quackery. The medical world has always struggled with this phenomenon, not knowing how to deal with it. The use of placebos in modern medicine and research still remains a subject of debate. Nowadays many physicians and researchers argue that placebos should not be noted for the assumed pleasure they give to patients and must not be so easily discarded. In fact, when used properly, placebos can benefit patients more than they realize. In ‘Melmon and Morrelli's Clinical Pharmacology’ (2000), the writers put it this way: "In clinical practice, where a majority of patient visits are for conditions that cannot be explained on a pathophysiologic basis of for which no specific treatment is available, it is essential that physicians understand the concepts and principles of placebos and placebo effects and, when appropriate, use them correctly.”3 One of the most famous anecdotes in the placebo literature concerns an American anesthesiologist named Henry Knowles Beecher who worked in a field hospital in Italy during the Second World War. The field hospitals were crowded with wounded soldiers and medical treatment became increasingly difficult to receive. At a certain point, the hospital where Beecher worked ran out of morphine. There were no other pain relievers available and the doctors were at a loss as to what to do, since new injured soldiers were being brought in. One nurse then suggested giving the injured soldiers a harmless saline solution while telling them they were receiving a strong painkiller. To the great surprise of the hospital staff, the men felt free of pain after receiving the ‘painkiller’. The ‘painkiller’ was nothing more than saltwater! After the war and back at the Harvard Medical School in Boston, Beecher decided to study the placebo response (the positive medical response to taking a placebo) which he had observed in the field hospital. In 1955, Beecher published a paper entitled ‘The powerful placebo’. In this paper he concluded that “35 percent of a drug’s or a doctor’s success is due

4
to the patient’s expectation of a desired outcome, or the placebo response.”4 In this paper, Beecher also stressed the importance of clinical trials making use of placebos to test the effectiveness of a medicine or medical treatment. Ever since, placebo-controlled studies have been the gold standard for clinical trials. The placebo effect truly is a puzzle which is yet to be completed – the mechanisms behind the placebo effect are only understood partially. Most of the knowledge about the underlying neurobiological and psychological mechanisms has been obtained by studying placebo analgesia, though researchers have successfully obtained more information about the placebo effect in recent years by investigating the immune system, motor system disorders (Parkinson) and depression. In the end, a better understanding of the placebo effect may lead to a better design of clinical trials and medical practice. 1.2 – Mechanisms of placebo effects
The most common underlying mechanisms of the placebo effect are summarized in figure 1. It is clear that there isn’t just one kind of placebo effect: different mechanisms cause different placebo effects in the human body. For example, the activation of endogenous opioids and dopamine causes a reduction in pain (placebo), while the activation of cholecystokinin (CCK) and deactivation of dopamine causes an increase in pain (nocebo). In the same way, conditioning of opioid receptors in respiratory centers (which is in fact a placebo response) affects the respiratory system, etcetera. All these mechanisms can be discussed from a psychological as well as a neurobiological viewpoint.
1.2.1 – Psychological mechanisms
Scientists agree that the efficacy of the placebo effect can be attributed to three different psychological mechanisms: (1) classical conditioning, (2) expectancies and (3) affect manipulation.

5
(1) Classical conditioning One of the psychological mechanisms underlying placebo effects is considered to be classical conditioning (also known as ‘Pavlovian conditioning’). Classical conditioning is a technique used in behavioral training that involves learning by association. Basically, an unconditioned stimulus is paired with a neutral stimulus. Initially, the unconditioned stimulus is a type of stimulus (something causing a response) that naturally and automatically triggers a response from an organism, while a neutral stimulus does not cause an observable response (apart from focusing attention). When the pairing is repeated many times, the unconditioned stimulus and the neutral stimulus will eventually result in the same response. In other words, classical conditioning is the repeated association between an unconditioned stimulus and neutral stimulus which can result in the ability of the neutral stimulus to evoke a response characteristic of the unconditioned stimulus.
Figure 2 on the left shows the classical conditioning of the eye blink reflex in three stages (before, during and after conditioning). As soon as the flash bulb, which is the UCS (unconditioned stimulus) in this situation, is turned towards the eye, a response is evoked (‘Anna blinks’). The UCS automatically produces UCR (unconditioned response). The camera is the neutral stimulus in this situation; it does not cause a response (‘Anna does not blink’). When the UCS is repeatedly paired with the neutral stimulus, the neutral stimulus produces a CR (conditioned response), which is like the UCR produced by the flashbulb.
The UCR and the CR have essentially become the same thing.
Classical conditioning mechanisms have been observed in both animal and human studies. In human beings, conditioning mechanisms are substantiated by the fact that the magnitudes of placebo effects are higher after a conditioning protocol. In other words, placebo responses depend on previous experiences. For example, a young woman who was treated with chemotherapy for breast cancer in a certain hospital always used to experience nausea as a side effect of the treatment. Years later, whenever she would drive past that same hospital, she’d start to feel extremely nauseous again. In this case, sight of the hospital had become the conditioned stimulus which caused a conditioned response (nausea).5 (2) Expectancies Studies have shown that in human beings conditioned placebo responses are mostly, if not completely, mediated by expectancy. This means that when a person expects something to happen, it will. The difference between the expectancy-mechanism and the conditioning-mechanism is that expectancy is always a conscious process. Expectancies help to prepare body and mind for what is going to happen. The open/hidden paradigm has been used in many studies to investigate the impact of patient’s expectancies on placebo responses. The open/hidden paradigm is a model wherein a patient either fully views a treatment (e.g. an injection is administered by a nurse) or receives it in a ‘hidden’ manner (e.g. medication is administered via a computer-operated
Figure 2 – Classical conditioning of the eye blink reflex

6
pump so that patients are unaware when the medication starts or stops). This paradigm has been used in many different studies, including investigations on pain analgesia, Parkinson, addiction, anxiety and Alzheimer’s. An example of a study that used the open/hidden paradigm was a study conducted in 2006.6 The study investigated the contribution of the placebo effect in the use of morphine. Figure 3 shows the results of this study. It was consistently found that the open administration was significantly more effective than the hidden administration. Open and hidden interruptions during interventions were also investigated. Relapse of pain occurred faster and the pain intensity was greater when the patient saw the open interruption compared with the hidden one. It appeared that a patient’s negative expectation of pain relapse would activate a nocebo-like response (antipode of the placebo effect).
(3) Affect manipulation The effectiveness of a placebo doesn’t only depend on a conditioned response and expectancy: it is also influenced by the way it is administered. Therefore the third psychological mechanism that the placebo effect can be attributed to is considered to be affect manipulation. For example, in the case of illness, many people experience stress and fear when they need to go see a physician. If the physician treats the patient with empathy and support, there’s a good chance those negative feelings might decrease, which can lead to a positive outcome of the illness. On the other hand, if the physician treats the patient in a cold manner or the patient feels misunderstood by the physician, this may result in a negative outcome of the illness. So in other words, the resulting change in affect can lead to placebo effects in different ways, which eventually plays a crucial role in the outcome of an illness. Placebo studies have shown that physician variables influence placebo responsiveness. Placebos administered with greater confidence and concern produce stronger positive responses.7 Also, placebos administered by high status physicians appear to have greater effects than those administered by those of lowlier status.8 Another study also found that certain personality characteristics of the patients themselves play an important role in the placebo responsiveness. The study found that extraversion, openness to experience,
Figure 3 – Results of open/hidden administration and interruption of morphine
7
agreeableness and female gender were strongly associated with a positive placebo response. However, these personality traits only influenced the outcome if there was a patient-practitioner interaction involved.9 Interestingly, another study found evidence that the influence of the doctor's expectations on the patient's response to a treatment may even bypass the expected limits of the double-blind control procedure.10 (In a double-blind experiment, neither the subjects of the experiment nor the researchers know who belongs to the control group and the experimental group.) In 1985, the study was conducted to investigate the influence of physicians’ expectations in placebo analgesia. The researchers found that even though the experiment was performed under double-blind conditions, the expectations of the physician influenced the outcome of the patient’s response to injections of fentanyl, naloxone, or placebo. From this it can be concluded that the behaviour of a physician has a subtle yet powerful influence on the placebo response of a patient. 1.2.2 – Neurobiological mechanisms
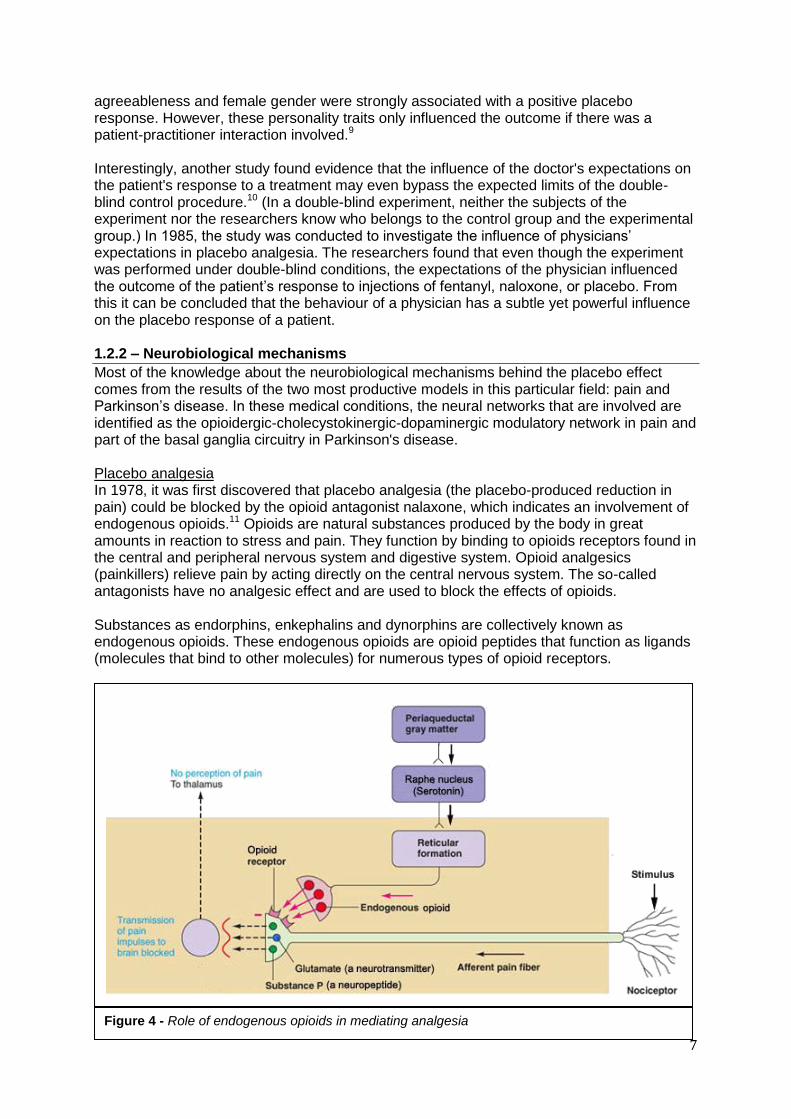
Most of the knowledge about the neurobiological mechanisms behind the placebo effect comes from the results of the two most productive models in this particular field: pain and Parkinson’s disease. In these medical conditions, the neural networks that are involved are identified as the opioidergic-cholecystokinergic-dopaminergic modulatory network in pain and part of the basal ganglia circuitry in Parkinson's disease. Placebo analgesia In 1978, it was first discovered that placebo analgesia (the placebo-produced reduction in pain) could be blocked by the opioid antagonist nalaxone, which indicates an involvement of endogenous opioids.11 Opioids are natural substances produced by the body in great amounts in reaction to stress and pain. They function by binding to opioids receptors found in the central and peripheral nervous system and digestive system. Opioid analgesics (painkillers) relieve pain by acting directly on the central nervous system. The so-called antagonists have no analgesic effect and are used to block the effects of opioids. Substances as endorphins, enkephalins and dynorphins are collectively known as endogenous opioids. These endogenous opioids are opioid peptides that function as ligands (molecules that bind to other molecules) for numerous types of opioid receptors.
Figure 4 - Role of endogenous opioids in mediating analgesia

8
Figure 4 shows the role of endogenous opioids in mediating analgesia. Pain impulses generated in the nociceptors are transmitted via the afferent pain fiber. Endogenous opioids bind to the opioid receptors, thereby inhibiting the transmission of pain to the brain. There is no perception of pain in the thalamus. As mentioned earlier, not only opioidergic, but also dopaminergic and cholecystokinergic networks have been found to be involved in placebo analgesia. Dopaminergic neurons form a neurotransmitter system. Dopamine is commonly associated with the reward system of the brain, providing feelings of enjoyment and reinforcement. Cholecystokinin (CCK) is a neuropeptide with anti-opioid properties found in high concentrations throughout the central nervous system. Increased CCK has been associated with motivational loss, anxiety and panic attacks. CCK is considered to be at the basis of nocebo hyperalgesia, the phenomenon that is opposite to placebo analgesia.
Figure 5 on the left shows a clear overview of the opioidergic-cholecystokinergic-dopaminergic modulatory network in placebo analgesia and nocebo hyperalgesia.
A descending pain inhibitory opioidergic system starts from the cerebral cortex (the layer of brain known as grey matter) and goes down to the hypothalamus (HYPO), periaqueductal gray (PAG), rostroventromedial medulla (RVM), and spinal cord. The dopaminergic neurons in the ventral tegmental area (VTA) go down to the nucleus accumbens (NAcc). These opioidergic and dopaminergic networks are antagonized by the cholecystokininergic network (CCKergic). The CKK antagonizes the opioidergic circuit at different levels, for example, in the rostroventromedial medulla (RVM).
Thus, the placebo analgesic response seems to result from a balance between endogenous opioids, dopaminergic neurons and CCK. Placebo-activated opioids do not only act on pain mechanisms; they also act on the respiratory centres. They have been found to produce
Figure 5 – Neural network involved in placebo analgesia and nocebo hyperalgesia
9
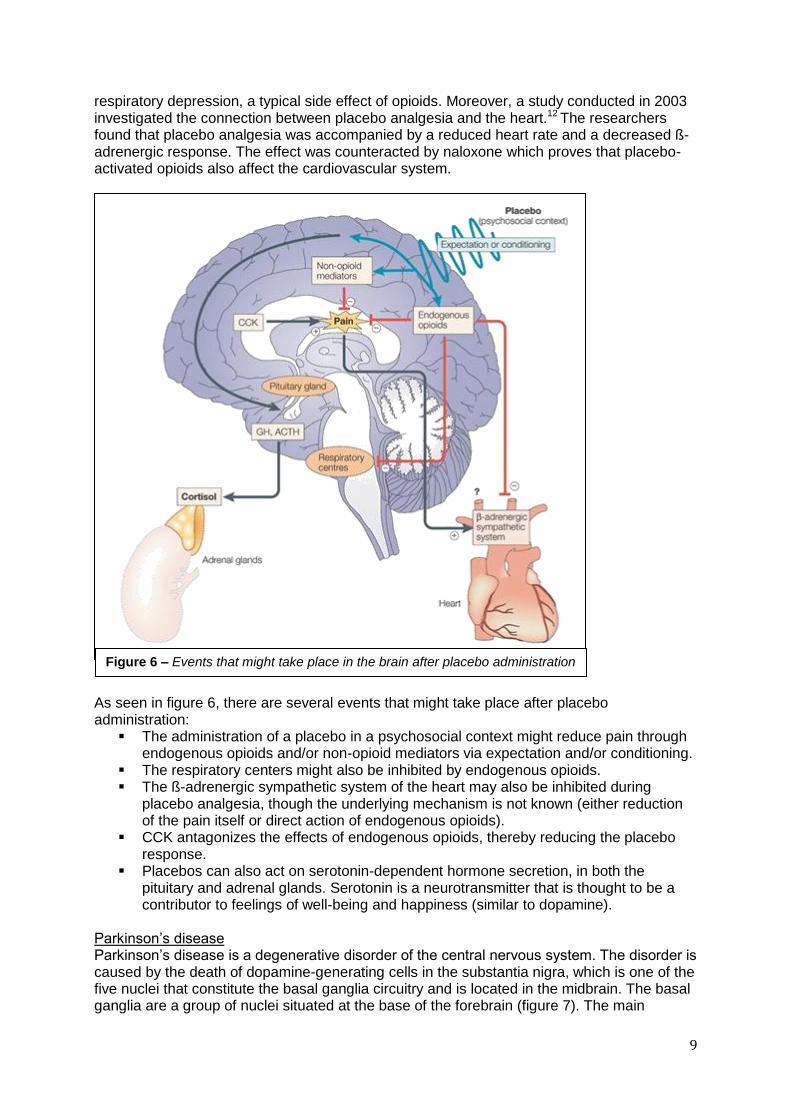
respiratory depression, a typical side effect of opioids. Moreover, a study conducted in 2003 investigated the connection between placebo analgesia and the heart.12 The researchers found that placebo analgesia was accompanied by a reduced heart rate and a decreased ß-adrenergic response. The effect was counteracted by naloxone which proves that placebo-activated opioids also affect the cardiovascular system.
As seen in figure 6, there are several events that might take place after placebo administration:
The administration of a placebo in a psychosocial context might reduce pain through endogenous opioids and/or non-opioid mediators via expectation and/or conditioning.
The respiratory centers might also be inhibited by endogenous opioids. The ß-adrenergic sympathetic system of the heart may also be inhibited during
placebo analgesia, though the underlying mechanism is not known (either reduction of the pain itself or direct action of endogenous opioids).
CCK antagonizes the effects of endogenous opioids, thereby reducing the placebo response.
Placebos can also act on serotonin-dependent hormone secretion, in both the pituitary and adrenal glands. Serotonin is a neurotransmitter that is thought to be a contributor to feelings of well-being and happiness (similar to dopamine).
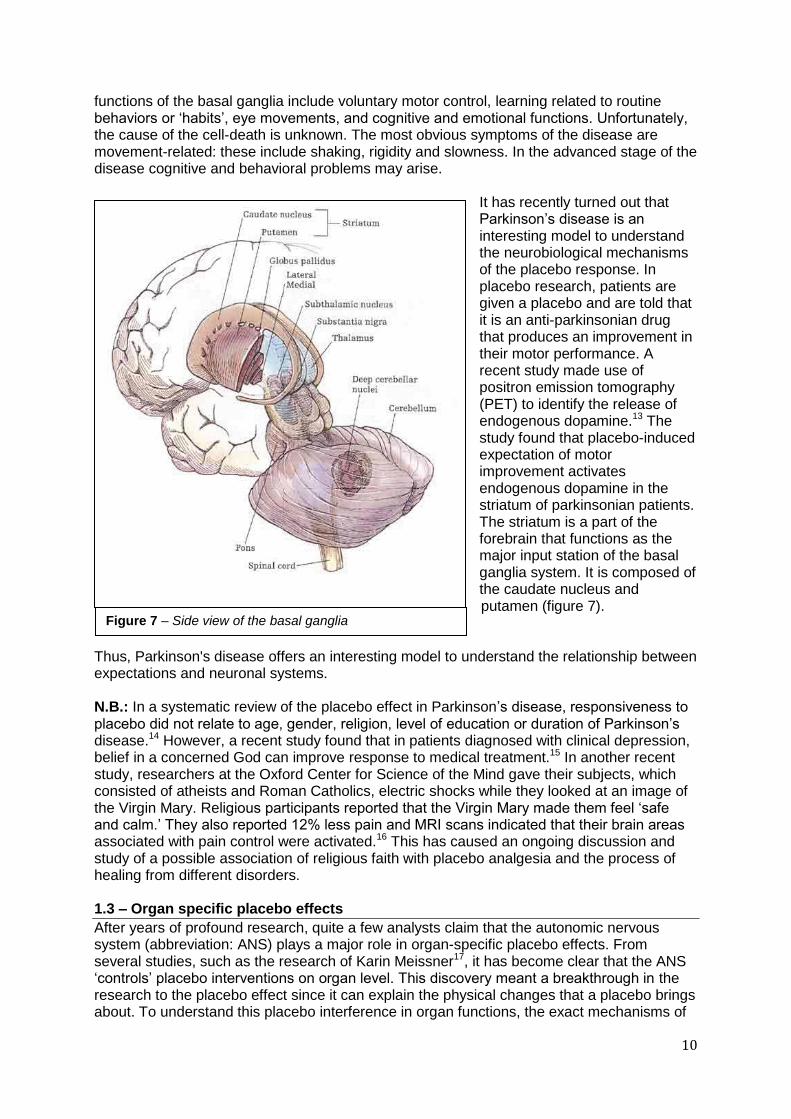
Parkinson’s disease Parkinson’s disease is a degenerative disorder of the central nervous system. The disorder is caused by the death of dopamine-generating cells in the substantia nigra, which is one of the five nuclei that constitute the basal ganglia circuitry and is located in the midbrain. The basal ganglia are a group of nuclei situated at the base of the forebrain (figure 7). The main
Figure 6 – Events that might take place in the brain after placebo administration
10
functions of the basal ganglia include voluntary motor control, learning related to routine behaviors or ‘habits’, eye movements, and cognitive and emotional functions. Unfortunately, the cause of the cell-death is unknown. The most obvious symptoms of the disease are movement-related: these include shaking, rigidity and slowness. In the advanced stage of the disease cognitive and behavioral problems may arise.
It has recently turned out that Parkinson’s disease is an interesting model to understand the neurobiological mechanisms of the placebo response. In placebo research, patients are given a placebo and are told that it is an anti-parkinsonian drug that produces an improvement in their motor performance. A recent study made use of positron emission tomography (PET) to identify the release of endogenous dopamine.13 The study found that placebo-induced expectation of motor improvement activates endogenous dopamine in the striatum of parkinsonian patients. The striatum is a part of the forebrain that functions as the major input station of the basal ganglia system. It is composed of the caudate nucleus and putamen (figure 7).
Thus, Parkinson's disease offers an interesting model to understand the relationship between expectations and neuronal systems. N.B.: In a systematic review of the placebo effect in Parkinson’s disease, responsiveness to placebo did not relate to age, gender, religion, level of education or duration of Parkinson’s disease.14 However, a recent study found that in patients diagnosed with clinical depression, belief in a concerned God can improve response to medical treatment.15 In another recent study, researchers at the Oxford Center for Science of the Mind gave their subjects, which consisted of atheists and Roman Catholics, electric shocks while they looked at an image of the Virgin Mary. Religious participants reported that the Virgin Mary made them feel ‘safe and calm.’ They also reported 12% less pain and MRI scans indicated that their brain areas associated with pain control were activated.16 This has caused an ongoing discussion and study of a possible association of religious faith with placebo analgesia and the process of healing from different disorders. 1.3 – Organ specific placebo effects
After years of profound research, quite a few analysts claim that the autonomic nervous system (abbreviation: ANS) plays a major role in organ-specific placebo effects. From several studies, such as the research of Karin Meissner17, it has become clear that the ANS ‘controls’ placebo interventions on organ level. This discovery meant a breakthrough in the research to the placebo effect since it can explain the physical changes that a placebo brings about. To understand this placebo interference in organ functions, the exact mechanisms of
Figure 7 – Side view of the basal ganglia
11
the central nervous system have to be clear. Therefore, a detailed overview on the processes which are involved in the central nervous system is given in the paragraphs below.
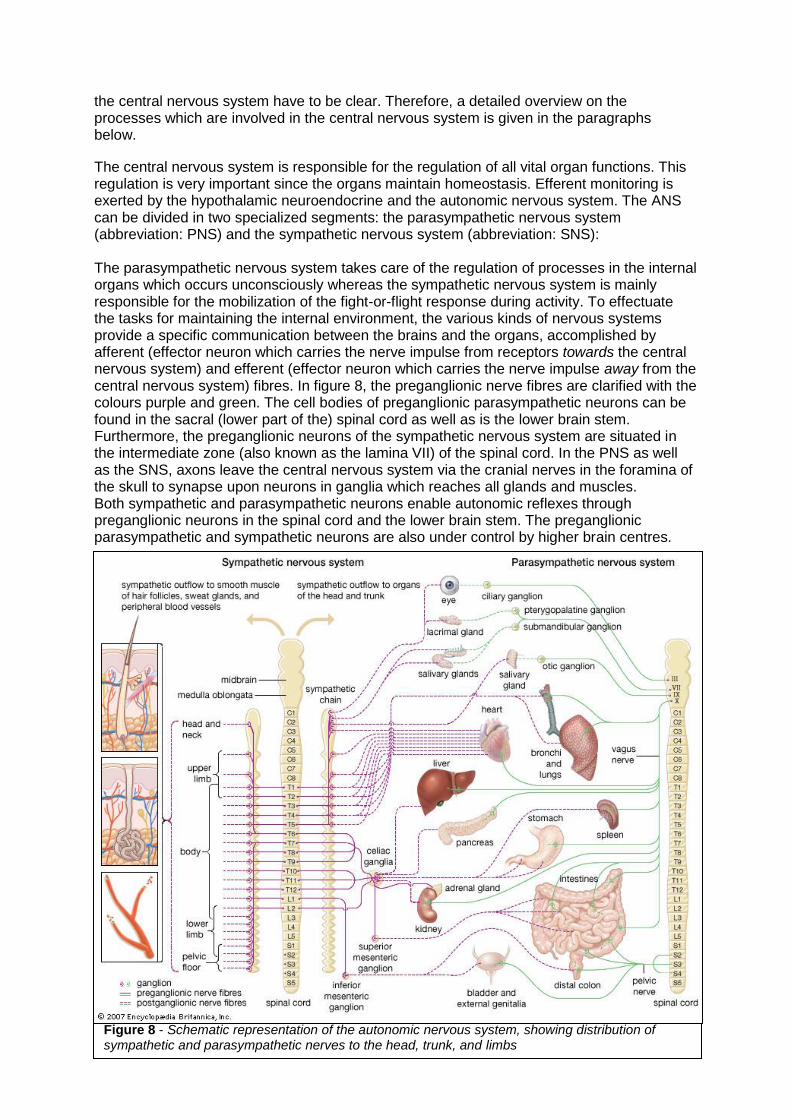
The central nervous system is responsible for the regulation of all vital organ functions. This regulation is very important since the organs maintain homeostasis. Efferent monitoring is exerted by the hypothalamic neuroendocrine and the autonomic nervous system. The ANS can be divided in two specialized segments: the parasympathetic nervous system (abbreviation: PNS) and the sympathetic nervous system (abbreviation: SNS): The parasympathetic nervous system takes care of the regulation of processes in the internal organs which occurs unconsciously whereas the sympathetic nervous system is mainly responsible for the mobilization of the fight-or-flight response during activity. To effectuate the tasks for maintaining the internal environment, the various kinds of nervous systems provide a specific communication between the brains and the organs, accomplished by afferent (effector neuron which carries the nerve impulse from receptors towards the central nervous system) and efferent (effector neuron which carries the nerve impulse away from the central nervous system) fibres. In figure 8, the preganglionic nerve fibres are clarified with the colours purple and green. The cell bodies of preganglionic parasympathetic neurons can be found in the sacral (lower part of the) spinal cord as well as is the lower brain stem. Furthermore, the preganglionic neurons of the sympathetic nervous system are situated in the intermediate zone (also known as the lamina VII) of the spinal cord. In the PNS as well as the SNS, axons leave the central nervous system via the cranial nerves in the foramina of the skull to synapse upon neurons in ganglia which reaches all glands and muscles. Both sympathetic and parasympathetic neurons enable autonomic reflexes through preganglionic neurons in the spinal cord and the lower brain stem. The preganglionic parasympathetic and sympathetic neurons are also under control by higher brain centres.
Figure 8 - Schematic representation of the autonomic nervous system, showing distribution of sympathetic and parasympathetic nerves to the head, trunk, and limbs

12
Together, these series of brain centres form the central autonomic network (abbreviation: CAN). All mechanisms covered by the central autonomic network contribute to physical parameters such as gastric cramps and lung illnesses. Research has shown that the physical state of placebo-treated patients who suffer from these physical parameters undergoes an improvement18 when compared to untreated patients. This is an example of organ specific placebo effects and the possible presence of a relationship between the CAN and a placebo19. Karin Meissner has done further research in the field of organ specific placebo effects and all the mechanisms that are involved. She has especially focussed on the influence of a placebo on hypertension20 (high blood pressure). Hypertension is a chronic disease caused by errors (deregulations) in the ANS or vascular or renal defects. Meissner’s study has shown that placebo therapy is effective in reducing blood pressure. In her research she randomly assigned 45 healthy volunteers into three groups: a placebo group, a homeopathic group and a no treatment group. The research was done double-blind and the placebo as well as the homeopathic medicine were given to the participants with the verbal suggestion that it would lower their blood pressure. Thirty minutes before and after the intervention, several autonomic parameters were measured. In this way, the effect of a placebo could be measured. The result was rather surprising: volunteers from the placebo group showed a reduction of systolic blood pressure whereas the no treatment group showed a slight increase in the systolic blood pressure. In both groups, no effect was found on the diastolic blood pressure or on the heart rate. Based on these compelling results, K. Meissner drew the following conclusion: ‘Thus, the fall of systolic blood pressure induced by verbal suggestions appeared to be mediated specifically by ANS efferents involved in blood pressure regulation.’17
However, she couldn’t fully explain the processes that eventually led to the reduction in the systolic blood pressure by the placebo-treated participants. Therefore Meissner added this note to her conclusion: ‘However, how this is achieved, that is, how cortical processing of the placebo suggestion modulated the activity of preganglionic neurons so specifically, is far from clear.’17
1.4 – Usage of the placebo effect
The placebo effect is a classic example of the mind-body relationship since it can affect the psychophysiological state of a person. These mechanisms can be very useful and effective in regular health care. But how can the placebo effect be implemented in our health care system?21 First of all, the diseases which can be cured by a placebo have to be selected. Research has shown that placebo’s have most impact in pain and disorders in the autonomic nervous system22, such as psychoneuroses, nausea, phobias, hypertension (neurohumoral control), depression and bronchial airflow illnesses (neurohumoral control). There are two situations in which a placebo will definitely not work: when a disease is hyperacute (e.g. a cardiac arrest) or when vital functions are degenerating (e.g. severe metabolic acidosis). Utilising the placebo effect in our modern health care system is possible. With the exception of the two situations mentioned above of course. However, in our current health care system placebos are rarely used. The possible association with quackery and the openness that patients expect from a doctor, restrain many physicians from prescribing placebos. A law on the medicinal treatment of patients commits practitioners to inform the patients extensively about their prescribed medicine. This law is also called the ‘informed consent’ and the effect of the legal rule is that the use of placebos in our health care system is forced back even

13
more. Nevertheless, in practice, there are several options to apply the placebo effect. Two examples of these options are mentioned here:
Patient centred behaviour of the doctor can increase the effect of medicines5. When prescribing certain pharmacological effective medicines the doctor has to give clear instructions accompanied with the suggestion that the medicine will bring about beneficial effects.
Placebo’s (in different forms) can also be used in the treatment of drug-addicted patients. The ‘fake’ medicines can be prescribed in the context of a drug reduction program.
The essential meaning of ‘placebo effect’ and ‘placebo’ is that it demonstrates the power of the doctor to make the patient feel better23. In order to achieve a favourable treatment outcome, a good doctor-patient relationship is of great importance. For this reason quite a few scientists prefer the term ‘knowledge framing’24 instead of ‘placebo effect’ for describing this non-pharmacological effect. This effect is considered to be an important component of any doctor-patient encounter. ‘Knowledge framing’ provides a positive outlook and therefore induces hope. This is exactly what desperate patients expect to receive from their physician. The shown importance of the doctor’s role in the usage of the placebo effect is captured in a slogan of the English psychiatrist Balint: ‘the doctor as a drug’. A more specified version of this motto is: ‘communication as medicine’25. Conditioning processes, manipulating expectancies and the reduction of negative feeling can bring about the placebo effect. The doctor-patient communication offers ample possibilities to influence these mechanisms (two examples are mentioned above). It is important that physicians are aware of these mechanisms and that they try to assess the effect of it for effectiveness of the treatment26. They can use targeted communication as an instrument to help the patient in different ways. When the treatment fails due to conditioning effects, the physician should explain these conditioning processes. Purposefully creating positive expectancies of a treatment can also have a positive effect on the course of the disease. By creating positive expectancies, the physician too helps the patient to overcome painful or difficult medical interventions. These positive effects are a result of the patient gaining more confidence in his own competence to deal with the situation. Obviously, there are certain ‘ethical borders’ in this kind of ‘placebo treatment’ as the close doctor-patient relationship should not be put at risk. Equally important is reducing the negative feelings of the patient by communicating in a warm and empathic way. 1.5 – Disadvantages of the placebo effect
If applied properly, a placebo can cause many beneficial results for the patient’s health. This is what we positively call the placebo effect. Nevertheless, there are also some negative sides to the placebo effect. Two ways in which the placebo effect has a negative effect can be distinguished. First of all, the placebo effect can distort the results of medical research if not properly accounted for. When the placebo effect interferes in a placebo-controlled clinical trial, the outcome of the trial gives a distorted view on how effective a medicine really is. The goal of a placebo-controlled clinical trial is, namely, to find out whether a medicine works or not. To find this out, part of the participants is given an inert dummy drug and the other ones are given the real medicine. Researchers assume that when the medicine is effective, only the real medicine can bring about profound changes in the well-being of a patient. In this case you would expect to see a clear difference in the effect of a placebo on someone’s health and the effect of the real medicine on someone else’s state. However, in this theory, the possible occurrence of the placebo effect is not taken into account. When a patient’s condition does improve due to a placebo, researchers can’t compare the effectiveness of the placebo and the real medicine in the clinical trial anymore.

14
Secondly, the placebo effect does not only have the competence to improve the condition of a patient, but it can also worsen the physical state of a person. This phenomenon is often referred to as the ‘negative placebo effect’ or the ‘opposite of the placebo effect. However, its most well-known synonym is the nocebo effect27. The nocebo effect occurs when a patient is warned of fictional side-effects of an inert or real medicine. When a patient is convinced that those side-effects belong to the medicine he is taking, the patient is very likely to suffer from these side-effects even though they are fictional. An extreme example of the nocebo effect is the death of a man in 1973. The Southern Medical Journal reported in 1992 the case of a man who had been diagnosed with widespread cancer in 197328. The man died and he and his family and physicians believed that he died of metastatic carcinoma of the esophagus. However, after his death, at autopsy, only a 2 centimetre tumour of cancer in his liver was found. The intern doctor Clifton Meador is convinced that the man didn’t die of cancer. He stated: ‘I do not know the pathologic cause of his death.’ Nowadays, the conclusion that the man was ‘killed’ by his expectation of death instead of the cancer seems plausible. There hasn’t yet been done much research to how the nocebo effect exactly works, but a number of scientists are very busy with the subject. At Oxford’s University, Professor Irene Tracy has published a study29 showing that when a person feels so-called nocebo pain, the corresponding brain activity can be detected in an MRI scanner. Her conclusion is that the volunteers are responding to actual, non-imaginary pain at the neurological level. Another important study30 on the nocebo effect is done by Fabrizio Benedetti, from the University of Turin. He and his teams have discovered that when cholecystokinin (CCK) is blocked with the help of drugs, a person feels no nocebo pain except for being anxious. Tracey and Benedetti are pioneers in the research field of the nocebo effect. In the future, the findings of Benedetti can help to invent a technique to remove nocebo outcomes from medical procedures. Hopefully this new knowledge will help doctors to become aware of the fact that they can negatively influence the result of a treatment when they stress too much on the side-effects of a drug. It must be avoided that a patient’s negative expectations undermine the effectiveness of a treatment. 1.6 – Research field
Dysmenorrhoea (menstrual pain) is a fairly common medical condition; more than 50% of post pubescent menstruating women are affected by dysmenorrhoea. 31 There are two types of dysmenorrhoea: primary and secondary dysmenorrhoea. Primary dysmenorrhoea can be defined as common menstrual cramps felt in the lower abdomen or back. Common menstrual cramps usually become less painful as a woman ages, and may stop completely if the woman has already given birth. Secondary dysmenorrhoea is pain that is caused by a disorder in the woman's reproductive organs. Compelling evidence from various studies confirms the hypothesis that the pathogenesis of primary dysmenorrhoea is due to an increased production and release of endometrial prostaglandins F2alpha (PGF2alpha) and E2 (PGE2). 32 A prostaglandin is a natural chemical compound derived from fatty acids that is present in most tissue and organs. Its function is quite similar to that of a hormone in the sense that it affects other cells. However, a prostaglandin is not classified as a hormone because it doesn’t travel. Instead, it is immediately active at the site of its production. Prostaglandins are responsible for a broad range of physiological impacts in the human body. Prostaglandins are produced when tissue is injured. Their main function is to activate an inflammatory response, which is the body’s way of neutralizing an infection. They also increase the sensitivity of nerve endings to pain.

15
Excess release of these prostaglandins during menstrual shedding of the endometrium (the inner lining of the uterus) causes an increased muscle contraction of the uterus. This is what women experience as a cramp-like pain. Most of the women who experience such pain reach for pain relievers such as ibuprofen, naproxen and paracetamol. The figure below (figure 9) shows the mechanisms involved in the generation of pain in primary dysmenorrhoea.
(1) Progesterone thickens and prepares the endometrium for implantation of the fertilized egg. (2) Prostaglandins are released during menstruation. These prostaglandins sensitize pain fibers in the pelvis and uterus. (3) Release of prostaglandins in the uterus causes the uterus to contract and gives rise to increased abnormal uterine activity (dysrhythmia). (4) When the uterine muscles contract they constrict the blood flow to the tissue of the endometrium (uterine ischemia), which causes a temporary oxygen deprivation to surrounding tissue. (5) These contractions, the resulting uterine ischemia and the sensitization of pain fibers are responsible for primary dysmenorrhoea.
In patients with primary dysmenorrhoea, nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (e.g. Advil) and naproxen (e.g. Aleve Feminax) have been shown to reduce high levels of prostaglandin in the menstrual fluid and to reduce the frequency of uterine contractions. NSAIDs relieve primary dysmenorrhoea by inhibiting prostaglandin synthethase (an enzyme that catalyzes the linking together of two molecules); and also appear to have direct analgesic properties at the central nervous system. Some NSAIDs have been found to act through the activation of endogenous opioids and serotionergic mechanisms (see ‘1.2.2 – Neurobiological mechanisms’ for the definition of serotonin). 33 Furthermore, according to the results of a systematic review reported online in 2010, NSAIDs may be more effective than paracetamol for menstrual pain. 34 Research question In this paper, the effectiveness of a placebo on women who suffer from primary dysmenorrhoea will be investigated. The focus will mainly be on the effect of a placebo pill. Therefore, the research question is:
Figure 9 – Mechanisms involved in the generation of pain in primary dysmenorrhoea (pelvic structure)
What is the effectiveness of a placebo pill in the reduction of menstrual pain?

16
Hypothesis It is expected that a placebo pill can reduce menstrual pain. However, the magnitude of the placebo effect will depend on three factors: whether the women regularly use medication to relieve their menstrual pain or not, the expectations of the women and of course the way it is administered (affect manipulation). If the women do happen to regularly take pain relievers for their menstrual pain it means they already have a positive experience with taking medication, and probably have developed a certain conditioning mechanism over a length of time which may trigger a placebo conditioned response. After all, the magnitude of a placebo effect is higher after a conditioning protocol. However, this will most likely not take place if the women do not expect the pill to work. This of course has to do with previous experience, but may also be influenced by the appearance (size, shape, color) and the taste of the pill. Those who for example take medicines that are not identical in appearance to the placebo pill will probably be more skeptical about its effectiveness than those who take medication that does look like the placebo pill (or those who do not take any medication at all). Also, it is expected that those who have ever tried an alternative pain relief remedy to relieve pain and have found it to be successful, might have a more positive expectation of the placebo pill than those who have not tried alternative pain relief remedies. Finally, the way the placebo pill is administered affects the outcome of the response. The placebo response can for example be enhanced by certain verbal suggestions made about the pill by the researchers. It has been proven that even in a double-blind experiment, the expectations of the physician can still influence the outcome of the patient’s response. In this case, the experiment won’t be performed under double-blind conditions, which makes it even more likely that the women will be affected by comments made by the researchers. Furthermore, it is not expected that age, level of education and duration of primary dysmenorrhoea will influence the outcome of the placebo response. Religion could influence the magnitude of the placebo effect, but since the women are not exposed to a religious image and do not suffer from clinical depression (see ‘1.2.2 – Neurobiological mechanisms’ – N.B.), it is expected that religion will not play a significant role in the outcome. So, if the women do believe in the effectiveness of the pill, it is expected that they will be relieved from their pain due to a reduction of menstrual prostaglandin and/or the activation of endogenous opioids and serotionergic mechanisms. (The level of prostaglandin and the activation of endogenous opioids and serotionergic mechanisms can however not be measured in this investigation).
17
2. Method and material 2.1 – Method
The purpose of the following experiment is to investigate the effectiveness of a placebo pill in the reduction of menstrual pain. Three psychological factors that could influence the effectiveness (conditioning, expectancy and affect manipulation) are also taken into account during the experiment. This experiment is a single-blind trial, which means that the individual subjects do not know whether they belong to the control group or the test group. The experimenters are the only ones who are in full possession of the facts. The participants can be divided into two groups: the control group and the test group. The control group consists of women who suffer from menstrual pain, but are not given a placebo pill during the investigation. They are only asked to fill in a questionnaire regarding their menstrual pain. The test group consists of women who suffer from menstrual pain and are all given a placebo pill. However, there is a catch. The women in the test group are told that they either belong to the control group (the group that receives a placebo pill) or the test group (the group that receives an actual medicine). They do not know which group they supposedly belong to. In fact, all the women in the test group are given a placebo pill, but they do not know that! (No one receives an actual medicine). It is extremely important that the women in the test group do not find out about the existence of the actual control group; otherwise the experiment will fail. Therefore the women must be carefully selected; in this case, most of the participants will be students from different schools. The advantage of the single-blind trial is that the experimenters can consciously and/or subconsciously affect the subject’s response. Most of the time this is seen as a disadvantage, but in this case affect manipulation (e.g. comments made by the experimenters about the pill) is one of the factors that can have a significant impact on the magnitude of the placebo effect. (It goes hand in hand with the expectations that the participants have about the pill.) Therefore, half of the participants will be personally approached by the experimenters; while the other half will not be personally approached by the experimenters (these women will only receive a letter). In this way, it can be determined whether affect manipulation has an influence on the effectiveness of a placebo pill in the reduction of menstrual pain or not. The participants are asked to fill in a questionnaire which consists of three parts: general information concerning their menstrual pain, specific questions on their menstrual pain and questions about the effectiveness of the pill. The control group, of course, does not receive the questions about the effectiveness of the pill. The participants in the test group will also all receive a letter in which the experiment is explained to them. The letter and the questionnaire are both in Dutch. In the letter, the participants are assured that the pills they are about to take are completely safe and can be taken in combination with other medication. The letter also contains instructions on how the pills should be taken. The minimum dosing interval is 4 hours. In the case of the participants who are personally approached by the experimenters, the experimenters will put emphasis on the fact that the participants must be extremely careful not to take an overdose. This emphasis will hopefully create certain expectations about the pills (that they are probably the actual medicine) and will hopefully enhance the placebo response. Attached to the letter is a package that contains five placebo pills. The pills are manufactured by Spruyt Hillen BV. The pills are white, odourless tablets with a diameter of 7 mm. They are

18
in appearance very similar to paracetamol tablets – they even have the same line running down the middle (figure 10, 11 and 12 below). They are also soluble in water, just like paracetamol tablets. They taste slightly less bitter and a little drier than paracetamol tablets. In order to prevent any suspicion, the participants in the test group are asked to swallow the pills with a glass of water. The only feature that could cause suspicion is the size of the pills; they are quite smaller than paracetamol tablets. However, it is expected that this won’t influence the placebo response significantly, since the letter already says there is no difference in appearance between the placebo and the medicine. Furthermore, the letter says that the packages of the pills are numbered and randomized. This increases the credibility of the experiment. (For the experimenters, these numbers do not serve any purpose).
Figure 11 – Placebo pills
Figure 12 – Paracetamol tablets
Figure 10 – Placebo pills
19
Further explanation on the questionnaire Part 1: This part consists of 10 general questions concerning the menstrual pain of the control group and the test group. First of all, the participants are asked how old they are, whether they’re religious or not and what their highest level of education is. Later on, when the results are compared with each other, it is important to see if there is any association between these factors and the placebo response. Question 4 until 8 focuses on the menstrual pain. Only those who often suffer from menstrual pain during their periods (1 out of 3 periods or more) are qualified for the experiment. It has to be certain that the participants who are given pills will indeed use them. Also, the participants are asked whether they regularly use medication to relieve the pain. When comparing the results later on, it’s important to know who might have had a placebo conditioned response and who not. Moreover, in question 9, the participants are asked if they have ever tried an alternative pain relief remedy to relieve the pain, and if so, whether it helped or not. And finally, in question 10, they are asked if, and if so, what king of drugs, pills, hormones or other supplements they use on a regular basis. Question 9 and 10 are closely related to expectancies that the participants might have about the placebo pill, and are therefore important for the outcome. Part 2: This part consists of 3 specific questions regarding the menstrual pain of the control group and the test group. First of all, the participants are asked where their pain usually is located and what kind of pain they usually experience. If the placebo pill does appear to work, it is important to know where the pain was located in order to explain the neurobiological mechanisms involved in this particular placebo effect. They are also asked to rate the pain they usually experience per day during a ‘normal’ period by making use of the pain scale of Andrea Mankoski. Andrea Mankoski devised this pain scale in 1995 so she could objectively communicate her pain in concrete terms to her doctors and family. Though it was initially designed to describe menstrual pain, it has been used to quantify other kinds of pain as well over the years. The results of the test group are compared to the results of the control group to determine whether the women in the test group really do have a ‘normal’ period or not. If the periods of some women in the test group appear to deviate from the ‘normal standard’, this could indicate secondary dysmenorrhoea or other complications. Though this chance is very small, it is important that erratic results are as much excluded from the experiment as possible. Part 3: This part consists of 6 questions regarding the effectiveness of the pill. The participants are first asked what the number is on their packages of pills. They are then asked if they felt any pain relief within 4 hours of taking a pill. Then the participants are asked to fill in two tables. The first one is a table regarding the amount of pills they have taken on each day of their period. The second table is again the pain scale of Andrea Mankoski, but this time the participants have to fill it in before taking any pills and 4 hours after taking a pill to see whether their pain level has remained the same or has changed. In the final question the participants are asked whether they believe they were given the medicine or a placebo pill.
Each question in the questionnaire serves a specific purpose. In part 1 of the questionnaire, some questions are related to one of the three psychological mechanisms involved in the placebo effect. When the results are compared to each other in the end and a conclusion has to be drawn, the experimenters will be able to easily see which psychological mechanism(s) were involved in the response. So, for example, if it turns out the women who regularly take drugs that look like the placebo pill all experienced pain relief, it can be presumed that a placebo conditioned response and/or certain expectancies about the pills may have caused the positive outcome. Table 1 shows the connection between the questions in part 1 of the questionnaire (only those believed to be related to the psychological mechanisms) and the three psychological mechanisms (classical conditioning, expectancies and affect manipulation). Though age, education and religiosity are not expected to influence the

20
outcome, these three factors must also be taken into consideration. There is one question from part 3 which may be related to the expectancy mechanism, i.e. the number of placebo pills taken during the period. (Someone who takes several pills will most likely have better expectancies than someone who takes just one pill).
Table 1 Classical conditioning Expectancies Affect manipulation Par
t 1 Question 1 (age) x Question 2 (religiosity)
x Question 3 (education)
x Question 8 (medication for menstrual pain)
x x
Question 9 (alternative pain remedy)
x
Question 10 (other medication)
x x
Part 3
Question 5 (number of pills taken)
x
N.B.: Affect manipulation can only be involved if the participants are indeed personally approached. Furthermore, affect manipulation does not depend on any of the factors above; it mainly depends on whether the participant is open to the experiment or not. 2.2 – Material
The materials that are needed in this experiment are the following: Placebo pills (the total amount depends on the number of participants in the test
group) Packages for the placebo pills Letter to test group (see 6. Appendix) Questionnaires for the control group and the test group (see 6. Appendix for the
English translation of the questionnaire) Computer for research paper
o Microsoft Word o Microsoft Excel
21
3. Results In this chapter, the results of the research on the effectiveness of a placebo against primary dysmenorrhoea will be revealed. All data given here can be found in the questionnaires filled in by the participants. Two research groups are distinguished:
The test group Women in this group were given 5 placebo pills to take in when they experienced menstrual pain. They had to give detailed information about their regular menstrual pain and their menstrual pain during the trial (before and after taking a placebo pill).
The control group The participants in this group are only asked to give detailed information about their regular menstrual pain.
Each completed questionnaire (15 of the test group and 10 of the control group) is given a number since the questionnaires were filled in anonymously. 3.1.1 – Profiles of the participants: test group
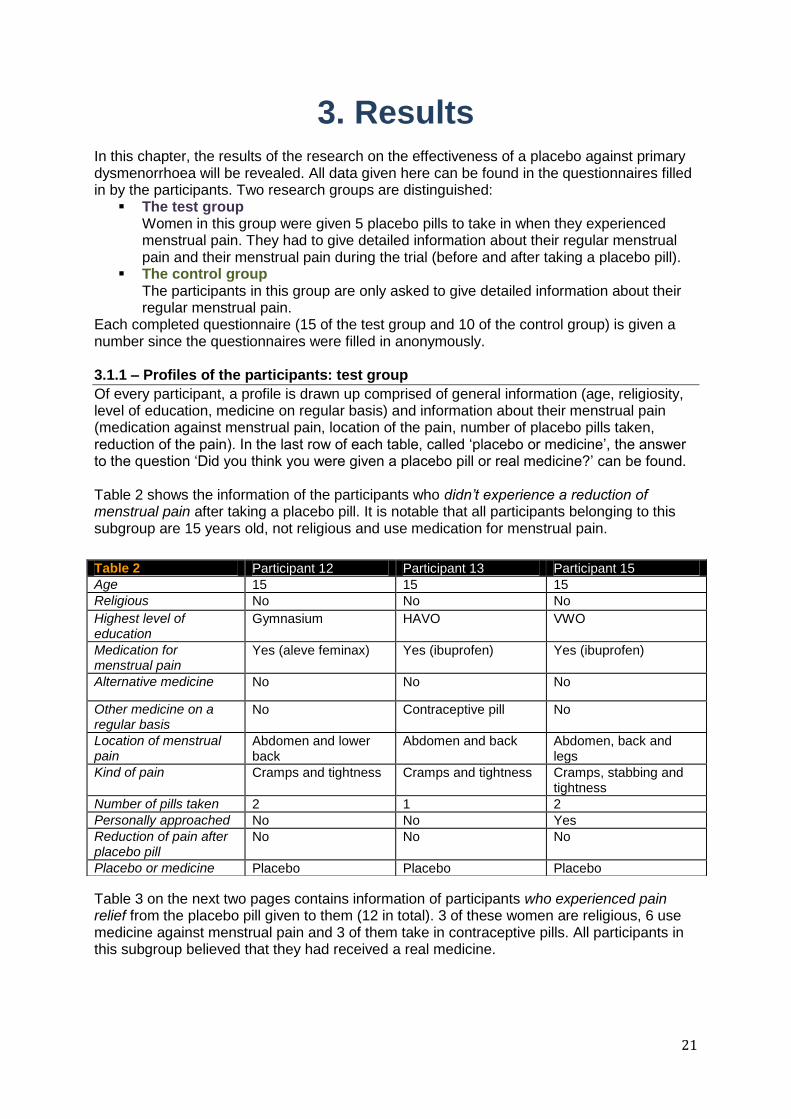
Of every participant, a profile is drawn up comprised of general information (age, religiosity, level of education, medicine on regular basis) and information about their menstrual pain (medication against menstrual pain, location of the pain, number of placebo pills taken, reduction of the pain). In the last row of each table, called ‘placebo or medicine’, the answer to the question ‘Did you think you were given a placebo pill or real medicine?’ can be found. Table 2 shows the information of the participants who didn’t experience a reduction of menstrual pain after taking a placebo pill. It is notable that all participants belonging to this subgroup are 15 years old, not religious and use medication for menstrual pain.
Table 3 on the next two pages contains information of participants who experienced pain relief from the placebo pill given to them (12 in total). 3 of these women are religious, 6 use medicine against menstrual pain and 3 of them take in contraceptive pills. All participants in this subgroup believed that they had received a real medicine.
Table 2 Participant 12 Participant 13 Participant 15
Age 15 15 15
Religious No No No
Highest level of education
Gymnasium HAVO VWO
Medication for menstrual pain
Yes (aleve feminax) Yes (ibuprofen) Yes (ibuprofen)
Alternative medicine No No No
Other medicine on a regular basis
No Contraceptive pill No
Location of menstrual pain
Abdomen and lower back
Abdomen and back Abdomen, back and legs
Kind of pain Cramps and tightness Cramps and tightness Cramps, stabbing and tightness
Number of pills taken 2 1 2
Personally approached No No Yes
Reduction of pain after placebo pill
No No No
Placebo or medicine Placebo Placebo Placebo

22
Table 3 Participant 1 Participant 2 Participant 3
Age 16 16 15
Religious No Yes No
Highest level of education
VWO VWO HAVO
Medication for menstrual pain
No Yes (aleve feminax) No
Alternative medicine No No No
Other medicine on a regular basis
No No Contraceptive pill
Location of menstrual pain
Abdomen Abdomen Legs and abdomen
Kind of pain Cramps and stabbing Tightness Stabbing
Number of pills taken 3 1 2
Approached personally No Yes Yes
Reduction of pain after placebo pill
Yes Yes Yes
Placebo or medicine Medicine Medicine Medicine
Participant 4 Participant 5 Participant 6
Age 15 19 15
Religious No Yes No
Highest level of education
VWO MBO VWO
Medication for menstrual pain
Yes (ibuprofen, aleve feminax, paracetamol)
Yes (paracetamol) No
Alternative medicine No No No
Other medicine on a regular basis
No Contraceptive pill No
Location of menstrual pain
Abdomen, lower back and cervix
Abdomen and back Abdomen
Kind of pain Cramps and tightness Cramps, tightness and stabbing
Cramps
Number of pills taken 2 3 3
Approached personally Yes No No
Reduction of pain after placebo pill
Yes Yes Yes
Placebo or medicine Medicine Medicine Medicine
Participant 7 Participant 8 Participant 9
Age 24 15 15
Religious No No No
Highest level of education
HBO VWO TVWO
Medication for menstrual pain
Yes (advil) No No
Alternative medicine No No No
Other medicine on a regular basis
Contraceptive pill, Euthyrox
No No
Location of menstrual pain
Abdomen Abdomen Abdomen and back
Kind of pain Cramps and tightness
Number of pills taken 3 2 5
Approached personally No Yes Yes
Reduction of pain after placebo pill
Yes Yes Yes
Placebo or medicine Medicine Medicine Medicine

23
3.1.2 – Summary of the participants’ profiles – test group
By summarizing all information received from the participants, a clearer view on the research is created. Per subject the numbers and possibly percentages are stated. (1) Age: EXPECTANCIES The ages of the participants range from 15 years to 24 years. The average age of the participants is 16,3 years. (2) Religiosity: EXPECTANCIES None of the participants of the ‘no pain reduction group’ is religious. In the ‘pain relief group’ 3 women are religious. (3) Highest level of education: EXPECTANCIES The highest level of education of women who participated in the research is either MBO, HBO, HAVO, (T)VWO or Gymnasium. (4) Medication for menstrual pain: CLASSICAL CONDITIONING AND/OR EXPECTANCIES 10 out of the 15 participants use medication for menstrual pain (66,7%). This medication includes paracetamol, aleve feminax (dysmenorrhoea-specific medicine) and ibuprofen. 3 women take in contraceptive pills (20%). No one in this group has used alternative medicine. Notable: all participants of the ‘no pain reduction group’ use medication for menstrual pain. (5) Menstrual pain Where most participants experience menstrual pain: abdomen (lower stomach) and back. The kind of pain experienced: tightness, cramps and stabbing. (6) Placebo pills taken: EXPECTANCIESI
In total 39 pills have been taken. » 34 of these pills did help against menstrual pain. This means that 87,2% of the pills were effective.
Every participant took an average of 2,6 pills. » The average amount of pills taken of the ‘no pain reduction group’ is 1,7. » The average amount of pills taken of the ‘pain reduction group’ is 2,8.
(7) Approach: AFFECT MANIPULATION 8 of the 15 participants were approached personally for this research (53,3%). Only 1 woman of the ‘personally approached group’ didn’t experience pain relief after taking a placebo pill (12,5%).
Participant 10 Participant 11 Participant 14
Age 17 17 15
Religious No Yes No
Highest level of education VWO VWO HAVO
Medication for menstrual pain
Yes (paracetamol) Yes (aleve feminax, paracetamol)
Yes (paracetamol, aleve feminax, ibuprofen)
Alternative medicine No No No
Other medicine on a regular basis
Contraceptive pill No No
Location of menstrual pain
Abdomen and back Abdomen and back Abdomen and lower back
Kind of pain Cramps, stabbing and tightness
Stabbing and tightness Cramps, tightness and stabbing
Number of pills taken 3 4 3
Personally approached No Yes Yes
Reduction of pain after placebo pill
Yes Yes Yes
Placebo or medicine Medicine Medicine Medicine

24
(8) Pain relief: PLACEBO RESPONSE 80% of the participants have experienced a reduction of menstrual pain after taking a placebo pill. 3.2.1 – Profiles of the participants: control group
The questionnaires of the control group were very similar to the ones given to the participants of the test group. Therefore the tables which can be find below have almost the same composition as the tables of the test group. The only difference between the tables of the test group and the control group is the information about the placebo pill and the possible pain reduction. In table 4 general information about the participants’ menstrual pain is given.
Table 4 Participant 1 Participant 2 Participant 3
Age 18 18 17
Religious No No Yes
Highest level of education
VWO VWO VWO
Medication for menstrual pain
Yes (paracetamol) Yes (paracetamol) Yes (paracetamol)
Alternative medicine No No No
Other medicine on a regular basis
Contraceptive pill No No
Location of menstrual pain
Womb and abdomen Abdomen Back, abdomen and legs
Kind of pain Cramps Cramps, stabbing Cramps, stabbing and tightness
Participant 4 Participant 5 Participant 6
Age 16 17 18
Religious No No No
Highest level of education
VWO VWO VWO
Medication for menstrual pain
Yes (aleve feminax and fiminal)
Yes (paracetamol and ibuprofen)
Yes (paracetamol)
Alternative medicine No No No
Other medicine on a regular basis
Yasmin pill No Insuline, novarapid and levimir
Location of menstrual pain
Back and abdomen Abdomen Abdomen and the sides of the womb
Kind of pain Cramps and stabbing Cramps, stabbing and tightness
Cramps and stabbing
Participant 7 Participant 8 Participant 9 Participant 10
Age 17 18 18 14
Religious No No No No
Highest level of education VWO VWO VWO VWO
Medication for menstrual pain
Yes (paracetamol and ibuprofen)
Yes (finimal) No No
Alternative medicine No No No No
Other medicine on a regular basis
Contraceptive pill Contraceptive pill Contraceptive pill L-lysine
Location of menstrual pain Abdomen, lower back
Abdomen Abdomen, back Abdomen
Kind of pain Stabbing, tightness Cramps Cramps, stabbing Cramps

25
3.2.2 – Summary of the participants’ profiles: control group
(1) Age The ages of the participants from the control group range from 14 years to 18 years. The average age of the participants is 17.1 years. (2) Religiosity 1 out of the 10 participants from this group is religious. (3) Medication for menstrual pain 8 control group participants use drugs against their menstrual pain which is equal to 80% of the participants. Most used medicines are paracetamol, aleve feminax, finimal and ibuprofen). No one in this group has used alternative medicine. 4 women take in contraceptive pills (40%). There are also 3 participants who use complementary medication for different diseases such as diabetes. (4) Menstrual pain Location of the menstrual pain: abdomen, (lower) back, womb and legs. Kind of pain: Cramps, stabbing and tightness. 3.3 – Regular menstrual pain: test group
The participants of the test group had to fill in the pain scale of Andrea Mankoski for each day of a regular menstruation. The pain scale ranges from 0 (no pain) to 10 (unbearable pain). The data collected in the questionnaire about the participants’ regular menstruation is processed into one table. In table 5 you can see the pain intensity per day of the women. On the horizontal cells of the table the numbers of the participants are given (these numbers correspond with the numbers of paragraph 3.1.1) and in the vertical cells the days of the menstruation are indicated. Per day and per participant the amount of pain is indicated by a number from the pain scale of Andrea Mankoski. In the upper right column, the average ‘amount’ of menstrual pain is given.
With the data from table 5 the graph, figure 13, on the following page is drawn up. In this graph, the course of the pain intensity during the menstruation per participant is clearly indicated. The caption on the right indicates the participant-number corresponding to table 4. Some obvious peaks are visible in this graph, especially of participant 10.
Table 5
Participants
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Average
Da
ys
1 2 2 3 1 3 1 3 2 6 7 6 6 4 4 6 3,538462
2 3 0 3 6 2 1 4 1 4 8 6 1 6 5 5 3,461538
3 1 0 4 2 0 8 4 3 2 7 7 2 6 6 5 3,538462
4 0 1 1 0 0 1 0 1 0 6 4 1 4 3 3 1,461538
5 0 0 0 0 0 0 0 0 1 6 0 1 0 0 1 0,615385
6 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0

26
3.4 – Regular menstruation pain: control group
Just as with the test group, a table is made that shows the pain intensity (according to the pain scale of Andrea Mankoski) per day of a regular menstruation of every participant. Table 6 shows the exact number on the pain scale indicating the intensity of menstrual pain per day. Horizontally the participants are numbered and vertically the days. The upper right column gives the average amount of pain per day of the control group.
To make the information given in table 6 more clear, a graph with these data is drawn up and can be seen in figure 14. On the x-axis the day during the menstruation is given and the y-axis indicates the pain intensity according to the pain scale of Andrea Mankoski.
Table 6
Participants
1 2 3 4 5 6 7 8 9 10 Average
Da
ys
1 4 8 0 1 7 0 5 6 6 8 4,5
2 6 2 3 5 7 6 4 4 5 7 4,9
3 5 1 4 6 6 4 4 3 3 5 4,1
4 5 0 4 6 4 3 1 1 1 1 2,6
5 1 0 3 7 0 1 1 1 0 1 1,5
6 0 0 2 6 0 1 0 0 0 0 0,9
7 0 0 0 0 0 0 0 0 0 0 0
Figure 13 – The course of the pain intensity per participant of the test group during a regular menstruation
Figure 14 - The course of the pain intensity per participant of the control group during of a regular menstruation

27
3.5 – Regular menstrual pain test group vs. regular menstrual pain control group
To compare the course of the regular menstrual pain of the test group with the menstrual pain of the control group, the average amount of pain per day must be used. The data from the last column of table 5, the average amount of pain per day, is processed in the graph of figure 15. The graph indicates the average course of the intensity of pain during a menstruation. The peak of the pain intensity lies obviously on the second day of the menstruation.
The data of the average amount of pain per day from table 6 (upper right column) is used to draw up an overview on the average amount of menstrual pain per day. The result is the graph in figure 16.
Figure 15 – The average pain experienced per day by the test group
Figure 16 – The average pain experienced per day by the control group

28
The two diagrams from figure 15 and 16 show a very similar course of menstrual pain although the peak in pain intensity of the control group lies higher (4,9) than the peak of the test group (3,5). Most probably this higher peak is a result of some participants (especially participants 4 and 10) with and exceptional amount of menstrual pain. The peak of the average amount of menstruation pain of the test group is situated on the third day of the menstruation. The peak of the control group can be found on the second day of the menstruation. 3.6 – Menstrual pain during the trial: test group
During the trial/experiment, the individual subjects of the test group had to fill in how much pain they experienced before taking a pill and 4 hours after taking a pill. In this way the possible placebo response can be determined from the number on the pain scale indicated. Table 7 shows the menstrual pain intensity of every participant before they took the dummy drug. Again, in the upper right column the average amount of pain per day is given.
The next table (8) shows the fierceness of menstrual pain per day after taking a placebo. If on one day a woman didn’t take a placebo pill, the number of the pain scale stays the same. The light red column indicates the average amount of pain per day after taking a placebo.
In the diagram on the next page (figure 17) the tables 7 and 8 are combined and processed into one graph. The blue line represents the pain before taking a placebo pill and the red line after taking a dummy drug. In this diagram it becomes visible that the placebo pills were effective in reducing menstrual pain. Especially on the first four days of the menstruation, the pain intensity was reduced significantly by the placebo pill.
Table 7
Participants
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Average
Da
ys
1 2 2 3 1 3 1 2 2 6 6 6 6 4 5 5 3,090909
2 3 0 3 4 1 1 1 1 4 6 5 1 6 7 5 2,636364
3 1 0 2 2 0 0 1 1 2 5 3 2 6 5 4 1,545455
4 0 0 1 0 0 8 0 1 0 5 3 1 4 1 6 1,636364
5 0 0 0 0 0 0 0 0 0 2 0 1 0 0 2 0,181818
6 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Pain intensity per day before taking in a placebo pill.
Table 8
Participants
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Average
Da
ys
1 1 0 3 1 2 0 1 2 5 5 5 6 4 4 5 2,272727
2 1 0 3 1 0 0 0 1 1 5 4 1 6 5 5 1,454545
3 1 0 1 2 0 0 1 1 0 3 3 2 6 4 4 1,090909
4 0 0 0 0 0 1 0 1 0 4 3 1 4 1 6 0,818182
5 0 0 0 0 0 0 0 0 0 2 0 1 0 0 2 0,181818
6 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Pain intensity per day after taking in a placebo pill.

29
In table 9, the average pain level per day before and after taking a placebo pill are once again given. In the last column (light red) the average change in pain level after taking a placebo per day is stated. These numbers are obtained by subtracting the average pain level after taking a placebo off the average pain level before taking a placebo.
» The average pain reduction due to the placebo pill expressed in pain levels is 0,8182. 3.7 – Brief summary results
To give a clearer view on the results of the research, the most important data obtained from the research is given here.
80% of the participants from the test group felt pain relief after taking a placebo pill. 66,7% of the participants from the test group uses medication against menstrual pain.
» This medication includes: paracetamol, aleve feminax and ibuprofen. » All women from the ‘no pain relief group’ use either aleve feminax or ibuprofen.
The course of the regular menstruation pain of the test- and control group are very similar.
Every participant took an average of 2,6 pills. » The average amount of pills taken of the ‘no pain reduction group’ is 1,7. » The average amount of pills taken of the ‘pain reduction group’ is 2,8.
3 participants from the test group are religious and all of them experienced pain relief after taking a placebo pill.
Most participants experience menstrual pain in their abdomen (lower stomach) and back. The pain they experience: tightness, cramps and stabbing.
Table 9
Average pain level before taking a placebo pill
Average pain level after taking a placebo pill
Average change in pain level
Da
ys
1 3,090909 2,272727 0,818182
2 2,636364 1,454545 1,181819
3 1,545455 1,090909 0,454546
4 1,636364 0,818182 0,818182
5 0,181818 0,181818 0
6 0 0 0
0
0,5
1
1,5
2
2,5
3
3,5
0 1 2 3 4 5 6 7 8
Pain
inte
nsity
Day during the menstruation
Average amount of pain per day during the trial
Before taking aplacebo
After taking aplacebo
Figure 17 – Comparison between menstrual pain before and after taking a placebo pill

30
4. Conclusion To find out whether a placebo pill can reduce the intensity of menstrual pain, twenty-five women in total were investigated. These women were to give very detailed information on the pain they experienced during their menstruation. Fifteen participants were asked to take in placebo pill(s) if they suffered from menstrual pain. This experiment has resulted in profound information on how women experience menstruation and the associated dysmenorrhoea. By combining different data obtained from the participants, the answer to the research question ‘What is the effectiveness of a placebo pill in the reduction of menstrual pain?’ can be formulated. Before conclusions can be drawn from the outcome of this experiment, it should be checked whether the regular menstrual pain of the participants can be considered as ‘normal’. Therefore, the control group consisting of 10 women had to fill in the pain scale of Andrea Mankoski for each day of the menstruation. Although the average highest level of pain during the menstruation differs, the average course of the pain intensity during the menstruation of the test group is very similar to the average course of the control group. This can be seen in figures 15 and 16. Because of the clear similarities between the test group and the control group it can be presumed that the menstrual pain of the test group is not exceptional and that the results of the experiment are therefore representative.
As expected (see 1.6 - hypothesis) age did not influence the outcome of the placebo response in the research. The average age of the test group is 16,3: the oldest participant is 24 years old and the youngest 14 years old. No significant difference in their placebo response could be spotted. All three women who did not experience reduction in menstrual pain after taking a placebo are 15 years old, but this is to be most likely coincidental since 8 out of the 15 participants is 15 years old. Women who suffer from primary dysmenorrhoea usually suffer from menstrual cramps felt in the lower abdomen and back. This too was the case with the participants in the test group. The menstrual cramps in the abdomen are caused by an increased production and release of prostaglandins (which causes an increased muscle contraction of the uterus). The placebo pills were clearly effective in the reduction of menstrual cramps, and therefore it can be presumed that the pill caused a reduction of menstrual prostaglandin, most likely by inhibiting prostaglandin synthethase. The reduction of back pain is presumably due to the descending pain inhibitory opioidergic system that starts from the cerebral cortex and goes all the way down to the spine (see figure
Figure 15 – The average pain experienced per day by the test group
Figure 16 – The average pain experienced per day by the control group

31
5). It should be noted that NSAIDs are prostaglandin synthetase inhibitors, while paracetamol is an analgesic medicine that acts on the opioidergic system. Therefore it can be presumed that the placebo pills triggered the same response as NSAIDs and/or paracetamol; so a placebo conditioned response. In the case with the participants who do not use NSAIDs and/or paracetamol, and are therefore not influenced by a conditioning protocol, the placebo responses were probably due to positive expectations about the pill, and perhaps even affect manipulation in the case of the five participants who were personally approached. However, the three participants who did not experience pain relief all use NSAIDs (ibuprofen and aleve feminax). This probably means that their expectations of the placebo pill (based on a few plausible factors) outweighed the conditioning protocol. These factors could have been the appearance of the pill or a bad experience with paracetamol. These factors however are not certain. And even though one of these participants was personally approached by the experimenters, the affect manipulation apparently didn’t enhance the placebo response since she already had negative expectations of the pill. Three religious women participated in the experiment and they all experienced pain relief after taking a placebo pill. However, it can’t be stated for sure that the menstrual pain reduction is due to the fact that they are religious. These participants, namely, were not confronted with religious images during the trial and therefore the placebo response is not expected to be conditioned. Nevertheless, the fact that these women are religious could have contributed to the placebo response in a way that is not yet discovered. It seems plausible, for example, that religious people are less suspicious than atheists and that they are more convinced that what the distributors say about the pills is true. Their belief (since they have believe in God) in the pill may be stronger and therefore the placebo response greater. Surprisingly, when studying the results it can be presumed that the number of pills taken plays a role in the effect of the placebo pill. The average amount of pills taken during the trial of the ‘no pain reduction group’ is 1,7 and the average amount of pills taken of the ‘pain reduction group’ is 2,8. The average amount of pills taken in the ‘pain reduction group’ is significantly higher than in the ‘no pain reduction group’ which suggests that the placebo effect is stronger when the participant takes more pills (the expectancies of the pills are enhanced). A possible explanation for this phenomenon is that the participants of the ‘no pain relief group’ were already reluctant about the effectiveness of the pill before they even took one. Therefore they took fewer pills than the personal subjects of the ‘pain relief group’. As it can be presumed that the pill can cause a reduction of menstrual prostaglandin (by inhibiting prostaglandin synthethase) it would be convincing that the placebo response of participants who take more pills is stronger than the placebo response of a woman who takes less. This leads to the conclusion that a placebo pill is effective in reducing menstrual pain, just as expected in the hypothesis. The ultimate evidence for this statement can be found in figure 17. This graph shows the average pain relief participants experienced per day (expressed in pain levels).
0
0,5
1
1,5
2
2,5
3
3,5
0 1 2 3 4 5 6 7 8
Pain
inte
nsity
Day during the menstruation
Average amount of pain per day during the trial
Beforetaking aplacebo

32
5. Discussion A critical look at the research
The conclusion drawn from the experiment and the research done on the subject is that a placebo pill can positively influence menstrual pain in a way that it actually reduces the menstrual pain experienced. However, as often is the case in an experiment, the trial contains quite a few flaws which will be discussed here. Firstly, the test group and control group altogether included only 25 women. More participants would be desirable, because only then certain patterns can be distinguished from the results. Secondly, it would have been interesting to have more religious participants in the test group in order to really find out about the influence of religiosity on the placebo effect. In that case, more research should be done on the relationship between religion and psychological mechanisms such as conditioning, expectancy and affect manipulation. Moreover, the experimenters should have asked in the questionnaire what the expectancies of the participants in the test group were before taking a pill. Now it can only be presumed whether the expectancies were positive or negative. Furthermore, although it was done purposefully to only approach part of the test group personally and give detailed information on the procedure, the questionnaires would probably have been filled in clearer when given more directions. Also, the participants who were personally approached by the experimenters were all told the same thing, but the way in which the message was communicated by the experimenters was not always the same. (The participants were not all approached at the same time). Since the experimenters are only human, their mood and emotions were different in every situation. Therefore it would have been best if the participants were all approached at the same time. Finally, it is known that middle-aged women suffer less from menstrual pain than post pubescent women, but nevertheless it would have given a broader view if there had been some participants in the test group older than 25 years. Problems faced by the experimenters
One of the problems faced by the experimenters was the fact that some of the women suddenly decided to withdraw themselves from the experiment. In most of the cases, this happened too late to find new replacements for these women. The experimenters should have taken into account that not all the women who are given a package of placebo pills will actually use the pills. Furthermore, since menstruation only occurs about once in four weeks and especially younger girls still have an irregular menstrual cycle, the experimenters should probably have started a lot earlier with recruiting participants for the experiment. Most of the results were received at the last minute, which caused a lot of stress. Follow-up study
This research focused on the effectiveness of a placebo pill in the reduction of menstrual pain. Because of the limited amount of material available to the experimenters, some interesting factors could unfortunately not be investigated. For a follow-up study it would be interesting to investigate the difference in effectiveness of different placebo pills. You could alternate and combine different variables such as size, color, shape, smell and taste to see if any of these factors, or combinations of these factors, influence the magnitude of the response. Another interesting factor to investigate is the relationship between the use of alternative medicine and the response to a placebo pill. Unfortunately, none of the fifteen

33
participants in the test group had ever tried an alternative pain relief remedy. For a follow-up study, it would be an idea to select the participants on this, though this is only feasible if there is a large group of participants available. Furthermore, if available, a PET (positron emission tomography) scan could be used to identify the activation of endogenous opioids and serotionergic mechanisms after the administration of a placebo pill. Moreover, the menstrual prostaglandin level could be measured by radioimmunoassay.35 Radioimmunoassay (RIA) is an in vitro assay technique used to measure concentrations of antigens (for example, hormone levels in the blood; in this case the PGF2alpha level) by use of antibodies (immune system-related proteins). A known amount of antigens is first made radioactive and then mixed with a known amount of the antibody. Then a sample of the serum of the patient containing PGF2alpha is added. This causes the antigens of the patient’s serum (‘unlabeled substances’) to compete with the radioactive antigens (‘labeled substances’) for antibody binding sites. As the concentration of the ‘unlabeled substance’ increases, they displace the ‘labeled substances’, thus ‘freeing’ the radioactive antigens. The bound antibodies are then separated from the unbound ones and the radioactivity of the free radioactive antigens that have remained behind is then measured. Finally, a so-called binding curve can then be drawn up to determine to amount of PGF2alpha in the patient's serum. This technique would be perfect for a follow-up study because of its great sensitivity, but this could then only be done in a clinical laboratory. Also, now that it has been proven that a placebo pill is effective in reducing menstrual pain, it would be interesting to find out if medicines really are as effective as they are claimed to be. This experiment could again be performed, but this time under double-blind conditions and with a real medicine that is identical in appearance to the placebo pill. The same experiment could even be performed under single-blind conditions to see if there is a significant difference. As mentioned earlier, the placebo effect truly is a puzzle – but with experiments like these, the puzzle is nearing its completion.

34
6. Appendix
Letter to the test group (in Dutch)
Muiden, 20 november, 2011
Geachte deelneemster, Ontzettend fijn dat u mee wilt werken aan ons onderzoek. In deze brief zullen wij uitleggen wat het onderzoek precies inhoudt en welk doel het heeft, zodat u weet wat er van u verwacht wordt. We zullen ons eerst voorstellen: wij zijn Naomi Lagerweij en Nienke Schalij en wij zitten in de zesde klas van het tweetalig VWO op het Vechtstede College te Weesp. Dit jaar moeten we een profielwerkstuk maken en aangezien we allebei geneeskunde willen gaan studeren, hebben we gekozen voor het onderwerp ‘placebo effect’. Hiervoor gaan wij zelf een onderzoek uitvoeren naar het effect van een placebo op menstruatiepijn. We hebben dit besproken met Dr. Prof. Jozien Bensing (zij heeft veel onderzoek gedaan naar het placebo effect) en zij heeft het onderzoek goedgekeurd. Menstruatiepijn is namelijk een 'onschuldige' klacht (niet levensbedreigend) en komt veel voor. Om het placebo effect te onderzoeken, krijgt de helft van de deelneemsters met menstruatiepijn een werkzaam medicijn en de andere helft een placebo. Dit medicijn is alom bekend en het is wetenschappelijk bewezen dat het werkzaam is. Het gebruik hiervan wordt aanbevolen door artsen. Ook zijn er geen bijwerkingen van bekend en het kan geslikt worden in combinatie met andere medicijnen. Omwille van het onderzoek kunnen wij u echter niet de naam van het medicijn geven. Gebruiksaanwijzing: In deze enveloppe zit een zakje met pilletjes en het is de bedoeling dat u er één inneemt zodra u last begint te krijgen van menstruatiepijn. De pilletjes mogen één voor één met water geslikt worden met een minimaal tussenliggend tijdsbestek van vier uur. Neem alstublieft geen andere medicijnen tegen menstruatiepijn in ten tijde van het onderzoek. Bijgevoegd is tevens een vragenlijst waarin u kunt aangeven wat voor pijn u ervaart en of het pilletje verlichting heeft geboden. Wij vragen u deze zo nauwkeurig mogelijk in te vullen. NB: Aan de vorm van het pilletje is niet af te zien of het om het werkend medicijn gaat of om de placebo, want deze zien er namelijk exact hetzelfde uit. Ook de nummers op het zakje geven geen aanduiding om welk soort pil het gaan aangezien ze gerandomiseerd zijn. Alvast hartelijk dank voor uw medewerking. Met vriendelijke groet, Naomi Lagerweij en Nienke Schalij

35
Questionnaire for the control group (excl. part 3) and the test group
Part 1: General information menstrual pain
1. What is your age?
______
2. Are you religious?
□ Yes
□ No
3. What is your highest level of education?
4. What date did your last period start and how long did it last?
Starting date: _____________ Duration: ______________ days
5. Do you often suffer from menstrual pain during your period? (1 out of 3 periods or more)
□ Yes
□ No
›› If your answer is yes, please proceed to question 6. If your answer is no, then you have finished the questionnaire.
6. Did you suffer from menstrual pain during your most recent period?
□ Yes
□ No
›› If no, when was the last time you suffered from it? ______ months ago
7. Does the pain affect your daily life?
□ Yes
□ No
›› If yes, how does it affect your daily life?
8. Do you usually take medication to relieve the pain?

36
□ Yes
□ No
›› If yes, what kind of medication?
›› If no, what measures do you then take to relieve the pain?
9. Have you ever tried an alternative pain relief remedy, such as herbs, acupuncture or chiropractic, to relieve pain (not necessarily menstrual pain)?
□ Yes
□ No
›› If yes, did it help to relieve the pain?
□ Yes
□ No
10. What kind of drugs, pills, hormones and / or supplements do you use on a regular
basis? (including the contraceptive pill)

37
Part 2: Specific questions about your menstrual pain
1. Where is the pain usually located?
2. What kind of pain do you usually experience? (cramps, stabs, etc.)
3. Making use of the pain scale of Andrea Mankoski (see below), could you rate the pain
you usually experience per day during a ‘normal’ period?
Pain scale of Andrea Mankoski Day 1 2 3 4 5 6 7 8
0 You are pain free and there is no need for medication.
1 The pain is a very minor annoyance with occasional minor twinges.
2 The pain is a minor annoyance with occasional strong twinges.
3 The pain is annoying enough to be distracted by it.
4 The pain can be ignored if you are really involved in your work, but it is still distracting.
5 The pain can’t be ignored for more than 30 minutes.
6 The pain can't be ignored for any length of time, but you can still go to work and participate in social activities.
7 The pain makes it difficult to concentrate and it interferes with sleep. You can still function with effort.
8 Physical activity is severely limited. You can read and converse with effort. Nausea and dizziness set in as factors of pain.
9 You are unable to speak. You can’t stop crying out or moaning uncontrollably.
10 The pain makes you pass out.

38
Part 3: Questions about the effectiveness of the pill
1. What is the number on your package of pills?
2. Has your pain decreased within 4 hours of taking a pill?
□ Yes
□ No
3. How many pills have you taken on each day of your period? Please fill in the table
below.
4. Step 1: For each day of your period, check a box with a cross (x) to rate the pain that
you experience before taking any pills. See the table below. Step 2: In the same table, use a circle (O) to rate the pain you experience 4 hours after taking a pill. If your pain level has remained the same, put a circle around the cross.
Day 1 2 3 4 5 6 7 8
Numbers of pills taken
Pain scale of Andrea Mankoski Day 1 2 3 4 5 6 7 8
0 You are pain free and there is no need for medication.
1 The pain is a very minor annoyance with occasional minor twinges.
2 The pain is a minor annoyance with occasional strong twinges.
3 The pain is annoying enough to be distracted by it.
4 The pain can be ignored if you are really involved in your work, but it is still distracting.
5 The pain can’t be ignored for more than 30 minutes.
6 The pain can't be ignored for any length of time, but you can still go to work and participate in social activities.
7 The pain makes it difficult to concentrate and it interferes with sleep. You can still function with effort.
8 Physical activity is severely limited. You can read and converse with effort. Nausea and dizziness set in as factors of pain.

39
5. How many pills have you taken in total during this period?
_______ pills
6. Do you believe you were given the medicine or a placebo pill?
9 You are unable to speak. You can’t stop crying out or moaning uncontrollably.
10 The pain makes you pass out.

40
7. Sources References
1. Harrington, A., ‘The placebo effect: an interdisciplinary exploration’, Harvard
University Press, 1997 2. Shapiro, A., Shapiro, E., ‘The powerful placebo: from ancient priest to modern
physician’, Johns Hopkins University Press, 1997 3. Carruthers, Hoffman, Melmon & Nierenberg, ‘Melmon and Morrelli's Clinical
Pharmacology’, 2000, p.1268 4. Beecher, H.K., ‘The powerful placebo’, J Am Med Assoc, 1955 December 24 5. Bensing, J.M., Verheul, W., ‘The silent healer: The role of communication in placebo
effects’, Patient Education and Counseling, 2010 6. Benedetti, F. et al., ‘Open versus hidden medical treatments: The patient's knowledge
about a therapy affects the therapy outcome’, Prevention & Treatment, Vol 6(1), 2003 7. Grevert, P., Albert, L.H., Goldstein, A., ‘Partial antagonism of placebo analgesia by
naloxone’, 1983 8. Shapiro, A., Morris, L., ‘The placebo effect in medical and psychological therapies’,
1978 9. Kelley, J.M. et al., ‘Patient and Practitioner Influences on the Placebo Effect in
Irritable Bowel Syndrome’, Psychosom Med. 2009 September 10. Gracely, R.H. et al., 'Clinical expectations influence placebo analgesia’, 1985 11. Levine, J.D., Gordon, N.C., Fields, H.L., ‘The mechanisms of placebo analgesia’,
1978 12. Pollo, A., Vighetti, S., Rainero, I., Benedetti, F., ‘Placebo analgesia and the heart’,
2003 13. De la Fuente-Fernandez, R. et al., ‘Expectation and dopamine release: mechanism of
the placebo effect in Parkinson's disease’, 2001 14. Shetty, N. et al., ‘The placebo response in Parkinson's disease. Parkinson Study
Group.’, Source Department of Clinical Neurosciences, Brown University School of Medicine, Providence, Rhode Island, USA, 1999
15. Murphy, P., Fitchett, G., ‘Belief in a concerned god predicts response to treatment for adults with clinical depression’, Journal of Clinical Psychology, 2009
16. Wiech, K. et al., ‘An fMRI study measuring analgesia enhanced by religion as a belief system’, 2008
17. Meissner, K. ‘The placebo effect and the autonomic nervous system: evidence for an intimate relationship’, The Royal Department, 2011
18. Benedetti, F. et al., Neurobiological Mechanisms of the Placebo Effect’, The Journal of Neuroscience, November 9, 2005
19. Jubb, J., ‘The neuroscience underlying the placebo effect’, Literature Dissertation in Fulfilment of Criteria for Master’s Degree in Biomedical Science (Advanced Neuroscience), 2010
20. Meissner, K., ‘Organ specificity of placebo effects on blood pressure’, Elsevier, 2011 21. Crow, H., ‘The role of expectancies in the placebo effect and their use in the delivery
of health care: a systematic review’, Health Technology Assessment, 1999 22. Blasi, Di, Zelda, ‘Influence of context effects on health outcomes: a systematic
review’, The Lancet, 2001 23. Verheul, W., ‘The effects of physicians' affect-oriented communication style and
raising expectations on analogue patients' anxiety, affect and expectancies’, Elsevier, 2009
24. Meulen, ter, R., ‘Evidence-based Practice in Medicine & Health Care’, publishing company ‘Springer’, 2005

41
25. Vernon, S.O., ‘The placebo effect: can we use it better?’, British Medical Journal, July 9 2011
26. Long, M.D., ‘Expectation and outcome’, Catalina Medical Centre, August 14 2010 27. Sarchet, P., ‘The nocebo effect: Wellcome Trust science writing prize’, November 13,
2011 28. Meador, C.K., ‘Hex death: Voodoo Magic or Persusion?’, Southern Medical Journal,
Volume 85: Issue 3, March 1992 29. Tracey, I., ‘Getting the pain you expect: mechanisms of placebo, nocebo and
reappraisal effects in humans’, Nature Medicine, October 2010 30. Benedetti, F. et al, ‘The Biochemical and Neuroendocrine bases of the Hyperalgesic
Nocebo Effect’, Society for Neuroscience, November 2006 31. Dawood, M.Y., ‘Dysmenorrhea’, J Reprod Med 30: 154, 1985 32. Willman, E.A., Collins, W.P., Clayton, S.G., ‘Studies in the involvement of
prostaglandins in uterine symptomatology and pathology’, Br J Obstet Gynaecol, May 1976
33. Hanna, M.H. et al., ‘Comparative study of analgesic efficacy and morphine-sparing effect of intramuscular dexketoprofen trometamol with ketoprofen or placebo after major orthopaedic surgery’, Br J Clin Pharmacol, 2003
34. Marjoribanks, J. et al., ‘Nonsteroidal anti-inflammatory drugs for dysmenorrhoea’, Cochrane Database of Systematic Reviews, January 20, 2010
35. http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/R/Radioimmunoassay.html Figures
Fig 1. Finniss, D.G., Kaptchuk, T.D., Miller, F., Benedetti, F., ‘Biological, clinical, and
ethical advances of placebo effects’, Lancet 2010; 375: 686–95 Fig 2. Papalia 7e, ‘Human Development’,1998, McGraw-Hill Companies, Inc Fig 3. Benedetti, F. et al., ‘Open versus hidden medical treatments: The patient's
knowledge about a therapy affects the therapy outcome’, Prevention & Treatment, Vol 6(1), 2003
Fig 4. ‘Human psychology (IPHY 3430)’, University of Colorado, Lecture Outline chapter 10, II-D
Fig 5. Benedetti, F. et al., ‘How placebos change the brain’, neuropsychopharmacology advance online publication, 30 June 2010
Fig 6. Benedetti, F. et al., ‘Neurobiological mechanisms of the placebo effect’, 2005, J Neurosci 25: 10390–10402.
Fig 7. St Clair, R., Rodriguez, W.E., Joshua, I., ‘The Basal Ganglia and the Serial Order of Communicative Signs’, University of Louisville
Fig 8. Encyclopaedia Britannica, 2007 Fig 9. Dawood, M.Y. [ed],’ Dysmenorrhea’, Baltimore: Williams & Wilkins, 1981 Fig 12. 'Paracetamol beter bij lage rugpijn', de Gelderlander, February 2010
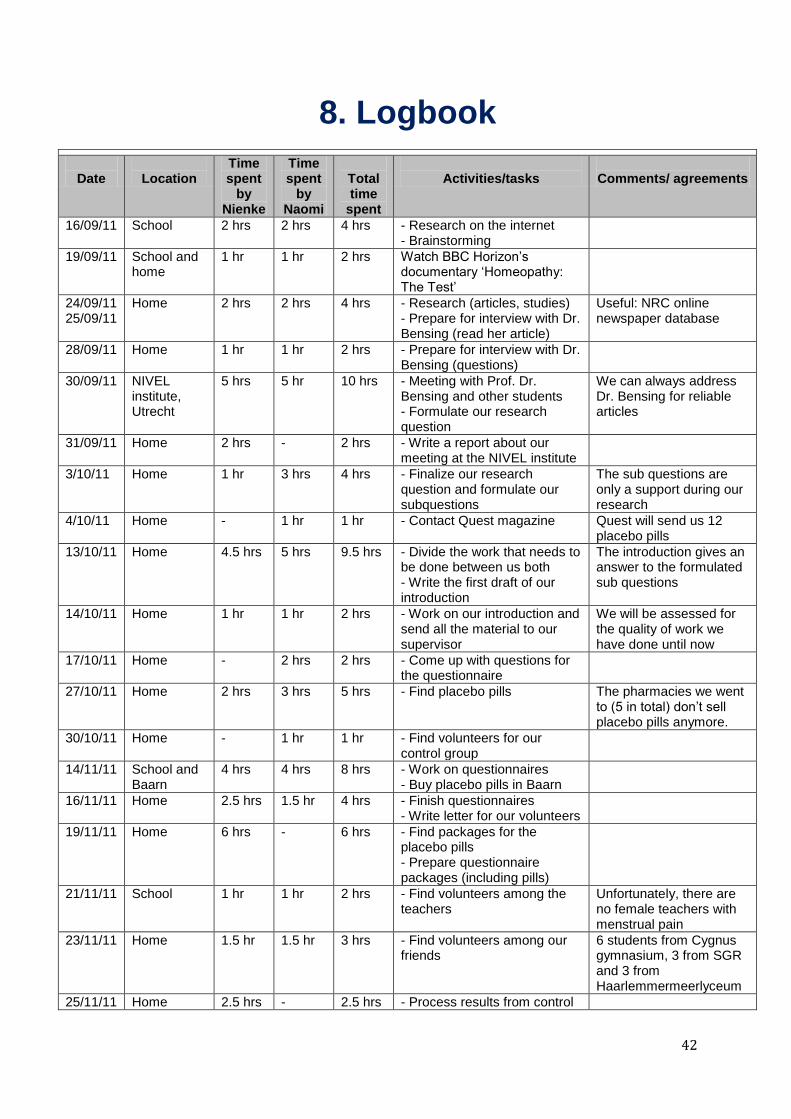
42
8. Logbook
Date
Location
Time spent
by Nienke
Time spent
by Naomi
Total time
spent
Activities/tasks
Comments/ agreements
16/09/11 School 2 hrs 2 hrs 4 hrs - Research on the internet - Brainstorming
19/09/11 School and home
1 hr 1 hr 2 hrs Watch BBC Horizon’s documentary ‘Homeopathy: The Test’
24/09/11 25/09/11
Home 2 hrs 2 hrs 4 hrs - Research (articles, studies) - Prepare for interview with Dr. Bensing (read her article)
Useful: NRC online newspaper database
28/09/11 Home 1 hr 1 hr 2 hrs - Prepare for interview with Dr. Bensing (questions)
30/09/11 NIVEL institute, Utrecht
5 hrs 5 hr 10 hrs - Meeting with Prof. Dr. Bensing and other students - Formulate our research question
We can always address Dr. Bensing for reliable articles
31/09/11 Home 2 hrs - 2 hrs - Write a report about our meeting at the NIVEL institute
3/10/11 Home 1 hr 3 hrs 4 hrs - Finalize our research question and formulate our subquestions
The sub questions are only a support during our research
4/10/11 Home - 1 hr 1 hr - Contact Quest magazine Quest will send us 12 placebo pills
13/10/11 Home 4.5 hrs 5 hrs 9.5 hrs - Divide the work that needs to be done between us both - Write the first draft of our introduction
The introduction gives an answer to the formulated sub questions
14/10/11 Home 1 hr 1 hr 2 hrs - Work on our introduction and send all the material to our supervisor
We will be assessed for the quality of work we have done until now
17/10/11 Home - 2 hrs 2 hrs - Come up with questions for the questionnaire
27/10/11 Home 2 hrs 3 hrs 5 hrs - Find placebo pills The pharmacies we went to (5 in total) don’t sell placebo pills anymore.
30/10/11 Home - 1 hr 1 hr - Find volunteers for our control group
14/11/11 School and Baarn
4 hrs 4 hrs 8 hrs - Work on questionnaires - Buy placebo pills in Baarn
16/11/11 Home 2.5 hrs 1.5 hr 4 hrs - Finish questionnaires - Write letter for our volunteers
19/11/11 Home 6 hrs - 6 hrs - Find packages for the placebo pills - Prepare questionnaire packages (including pills)
21/11/11 School 1 hr 1 hr 2 hrs - Find volunteers among the teachers
Unfortunately, there are no female teachers with menstrual pain
23/11/11 Home 1.5 hr 1.5 hr 3 hrs - Find volunteers among our friends
6 students from Cygnus gymnasium, 3 from SGR and 3 from Haarlemmermeerlyceum
25/11/11 Home 2.5 hrs - 2.5 hrs - Process results from control

43
group
29/11/11 School 3 hrs 3 hrs 6 hrs - Work on introduction and method
30/11/11 School 1.5 hr 1.5 hr 3 hrs - Find volunteers at school 2 girls from havo 4 and 3 girls from tvwo 4
02/12/11 School and home
3 hrs 3 hrs 6 hrs - Find volunteers at school - Work on introduction
2 girls from tvwo 3, 2 other girls
08/12/11 Home - 1.5 hr 1.5 hr - Work on method
11/12/11 Home 2 hrs 1 hr 3 hrs - Work on introduction - Process results from control group
17/12/11 Home 3 hrs 5 hrs 8 hrs - Finish introduction 6 paragraphs, incl. research question and hypothesis
23/12/11 School 1 hr 1 hr 2 hrs - Collect questionnaires
27/12/11 Home 4 hrs 4 hrs 8 hrs - Work on method
29/12/11 Home 3 hrs 2.5 hrs 5.5 hrs - Finish method - Finish results from the control group
02/01/12 Home 7 hrs 7 hrs 14 hrs - Collect final questionnaires - Process the results from the placebo group
Unfortunately, we didn’t receive the results from 6 girls due to withdrawal and other personal reasons.
03/01/12 Home 1.5 hrs 4.5 hrs 6 hrs - Work on results
04/01/12 Home 6 hrs 5 hrs 11 hrs - Finish results - Write the conclusion
05/01/12 Home 4 hrs 3 hrs 7 hrs - Write the conclusion - Write the discussion
06/01/12 Home 6 hrs 6 hrs 12 hrs - Finish the conclusion - Finish the discussion
07/01/12 Home 2 hrs 1.5 hrs 3.5 hrs - Sources and final touches
Total: 86 hrs 84.5 hrs
170.5 hrs