Orthodontic Management of Occlusal Prematurity in Early Mixed Dentition
Upload
independentCategory
view
1download
0
Population pharmacokinetics of intravenous caffeine in neonates with apnea of prematurity
Objwtive: To study the population pharmacokinetics of caEeine after intravenous administration to pre- mature infants with apnea. Met&oh: A prospective, blinded parallel study in which daily caffeine citrate doses of 30,15, and 3 mg/kg were administered over 7 days by intermittent intravenous infusion. Arterial blood samples (three to six per patient) were assayed for caffeine content by means of HPLC. Population pharmawkinetic modeling was performed with NONMEM. Resulfs: Clearance (L/hr) = (0.00000399 * current weight [grams]) + (0.000128 * postnatal age [days]). For gestational age >28 weeks, volume of distribution (L) = (0.000764 l weight [grams]) + (0.0468 * postnatal age [days]); for gestational age ~28 weeks, volume of distribution (L) = (0.000755 * weight [grams]) + (0.0224 * postnatal age [days]). Interpatient variability (coefficient of variation, in percent) was -25% for &arance and -11% for volume of distribution. Intrapatient error (standard deviation) was 3.9 mg/L. There was hu@ificaut bias between observed and model-predicted serum caffeine concentrations in a separate group of 30 infants. Cu~~~~tts: Caffeine was well tolerated at all doses. Clearance was markedly lower and volume of distri- bution was higher than the values reported previously for term infants and adults. Both parameters were signi8cantly infhtenced by postnatal age and current body weight, whereas volume of distribution in infants >28 weeks’ gestational age was higher than that in more premature babies. The predictive performance and the clinical application of the derived population models was satisfactorily shown. (Clin Pharmawl Ther 1997;61:628-40.)
Toong Chow Lee, BPharm (Hons), Bruce Charles, PhD, Peter Steer, PRACP, Vi&i Flenady, RM, and Andrew Shearman, BTC St. Lucia and South Brisbane, @eensland, Amtralia
Recurrent apnea of prematurity is a potentially serious neonatal disorder, especially in very low- birth-weight infants. Although this condition occurs in about one quarter of babies weighing less than 2500 gm at birth, its incidence in those weighing less than 1000 gm approaches 9O%.l Inadequate man- agement of apnea exposes these infants to signifi- cantly increased risk of hearing loss, hypoxemia, hypotension, brain damage, and death.24 Treatment
From the School of Pharmacy, University of Queensland, St. Lucia, and the Department of Neonatology, Mater Mothers’ Hospital, South Brisbane.
Supported by the Mayne Bequest Fund (University of Queens- land) and by the National Health and Medical Research Coun- cil.
Received for publication July 30, 1996; accepted Jan. 9, 1997. Reprint requests: Bruce Charles, PhD, School of Pharmacy, Uni-
versity of Queensland, St. Lucia 4072, Queensland, Australia. E-mail: [email protected]
Copyright Q 1997 by Mosby-Year Book, Inc. 0009-9236/97/$5.00 + 0 13/l/80325
includes modification of the feeding regime, oxygen therapy, peripheral stimulation, continuous positive airway pressure, or intermittent mandatory ventila- tion after endotracheal intubation. However, a phar- macologic approach that involves administration of intravenous or oral theophylline has been a main- stay for the treatment and prevention of apnea,’ particularly for infants being weaned off mechanical ventilation.6 Caffeine is a potentially useful altema- tive to theophylline because of its decreased propen- sity for toxicity and because of its longer terminal half-life, which permits dosing either once a day or every other day.7-9 Furthermore, caffeine can be effective in infants who are refractory to standard theophylline treatment. lo Caffeine and theophylline are thought to act by increasing central respiratory drive and by lowering the threshold of response to hypercarbia, as well as by stimulating contractility in the diaphragm and preventing diaphragmatic fa- tigue.5,9*10
628

CLINICAL PHARMACOLDGY &THERAPEUTICS VOLUME 61, NUMBER 6 Lee et al. 629
The lack of pharmacokinetic data on caffeine in very premature infants is largely attributable to the fact that such studies are difficult to perform in these patients. Ethical and logistic factors severely hinder the collection of data required by most traditional pharmacokinetic protocols; however, population- based approaches offer a powerful and convenient means of studying the disposition of drugs in pre- term infants for which severe restrictions apply on the rate and extent of blood sampling.” Except for one very recent but smaller study that used trough concentration data,12 there have been no reports of the population pharmacokinetics of caffeine, despite a steady increase in the use of this drug for apnea. In this article, we report the pharmacokinetics of caf- feine after intravenous administration of widely dif- fering doses of caffeine citrate to 119 premature infants soon after birth. The validity of the derived population models was confirmed in a subgroup of randomly selected infants whose data had not been used to develop the models.
METHODS Ethics. The protocol was approved by the Medical
Research Ethics Committees of the Mater Hospital and The University of Queensland, and the study was conducted according to the National Health and Medical Research Council (Australia) Statement on Human Experimentation. Written and verbal in- structions on the efficacy and possible adverse ef- fects of caffeine were provided to the parent(s) be- fore written consent to participate was obtained.
Patients. All preterm infants younger than 32 weeks’ gestational age whose lungs were ventilated for >48 hours were eligible for entry. Any congen- ital chromosomal abnormality, infection (sepsis con- firmed by blood culture), or neurologic condition were grounds for exclusion. Infants with grade 3 or 4 intraventricular hemorrhage and those whose lungs were ventilated for ~28 days were also ineli- gible. Characteristics of the study patients are pre- sented in Table I.
Caffeine administration. The study was conducted as a parallel dosing design to which the investigators and all clinical, nursing, and laboratory personnel were blinded. Patients were assigned randomly to one of three dosage regimens of caffeine. These consisted of unit dose ampoules that contained 60 mg/2 ml, 30 mg/2 ml, and 6 mg/2 ml of caffeine citrate in Water for Injection B.P., manufactured under contract by Ophthalmic Laboratories Pty. Ltd. (Sydney, New South Wales, Australia) accord-
ing to the Code of Good Manufacturing Practice. A loading dose of 60,30, or 6 mglkg was administered over 20 minutes by intravenous infusion, either 24 hours before a planned extubation or within 6 hours of an unanticipated extubation. A maintenance dose of 30, 15, or 3 mg/kg was begun 24 hours after the loading dose and continued at 24-hour intervals for 6 days. Overall, 38 infants received 3 mg/kg, 39 received 15 mg/kg, and 42 received 30 mg/kg main- tenance doses of caffeine citrate.
Blood collection. Arterial blood (0.25 ml) was col- lected by means of a heel prick or umbilical catheter before caffeine administration; preallocated random samples were then drawn between 20 minutes and 23 hours after the loading dose. When possible, further samples were taken immediately before the second and fourth maintenance dose, as well as 24 hours after the sixth maintenance dose. Serum sam- ples were collected and stored at less than -75” C before analysis by HPLC.
HPLC analysis. Serum concentrations of caf- feine, theobromine, paraxanthine, and theophyl- line were determined by HPLC according to the following procedure. Serum (100 pl) was pipetted into a 12 ml glass tube to which was added 50 ~1 of 1 mol/L sodium hydroxide. Caffeine was ex- tracted into 1 ml of 10% isopropanol (vol/vol) in chloroform that contained the internal standard, B-hydroxyethyltheophylline (1.5 mg/L). After cen- trifugation at -2000g for 1 minute, the organic layer was carefully decanted into a second similar tube and dried under a gentle air flow at 60” C. The residue was dissolved in 0.2 ml of the mobile phase of which 50 l.~l was injected into the HPLC. The mobile phase comprised methanol-tetrahydrofuran- ammonium acetate buffer (0.05 mol/L, pH 4.7) 20:15:965 parts by volume, respectively, and was pumped at 1 ml/min through a Cis Nova Pak column (150 mm X 3.9 mm internal diameter, Waters Aus- tralia Pty. Ltd., Sydney, New South Wales, Austra- lia). The maximum wavelength of detection for caf- feine and other methylxanthines was 273 nm. Calibration curves were linear (r > 0.999) from 0.2 to 80 mg/L. The within-day and between-day impre- cision (CV%) across this range was 1.4% to 6.8% and 1.5% to 5.2%, respectively. Absolute recoveries were >75%, and the limit of quantitation was 0.2 mgn*
Population modeling. Population pharmacokinetic modeling was performed in double precision by use of NONMEM (version 4.2)13 with MS-DOS (ver- sion 6.2) on a 486 DX2-66 computer equipped with

630 Lee et al. CLINICAL PHAIWACOMGY & THEIUF’EWl-ICS
JUNE 1997
Table I. Characteristics of study infants Characteristic Model development Predictive performance
Patients Female Male Race
White Aboriginal Asian Other
Birth weight (gm) All infants* <loo0 gin
Gestational age (wk)* Gestational age 528 wk Length (cm)* Head circumference (cm)* Entry age (day)* Route of delivery
Cesarean Vaginal
Current pregnancy Single Multiple
Apgar score (1 min)* Apgar score (5 min)* Birth asphyxia Respiratory distress syndrome Patent ductus arteriosus Feed intolerance Total blood samples Samples per infant* Serum caffeine cont. (mgL)*t
3Owk 15Wk 3mgflrg
52
30 16 14
82 2 2 3
26 1
ii
1167(571-2307) 1158(597-2154)
287;(24-31) 27&i-31)
3&30.5-43.5) 3&29.7-47.0) 26.3 (21.5-31.2) 26.0 (21.3-30.9)
4.0(2-15) 3.7(2-8)
62 22 27 8
57
&l-9) 8.2 (l-10) 19 84 17 22
430 4.8 (3-6)
60.7 (29.7-93.3) 31.1(14.8-49.9)
6.8 (2.5-10.9)
18 12
4.6 (O-9) 7.4 (l-lb) 12 28
2 10
144 4.8 (3-6)
59.8 (31.9-81.3) 32.5 (22.1-44.8) 5.9 (4.0-7.9)
*Mean, with range given in parentheses; otherwise, data are expressed as the number of patients. tAverage of all serum caffeine concentrations at each dose.
16 MB of random access memory. Compilations were achieved using the Microsoft PowerStation Fortran 77 compiler (version 1.00). A one- compartment model (ADVANl TRANM) and a two-compartment model (ADVAN TRANS4) were employed with use of the library subroutines in PREDPP. Initial parameter estimates were ob- tained from the results of a previous pharmacoki- netic study conducted by a nonpopulation approach in a smaller but clinically and demographically sim- ilar group of neonates to those in this study.’
Eighty-nine infants (430 serum caffeine concen- trations) were randomly allocated to the test data set for population modeling, whereas 30 infants (147 caffeine concentrations) were allocated to assess the predictive performance (Table I). An initial analysis was conducted by permitting NONMEM to estimate
the base parameters (i.e., no covariates) of the one- and two-compartment models. Next, the influence of individual candidate covariates was assessed by adding these to the base model, in turn, and noting the change in the objective function and the distri- bution of residuals and observed serum caffeine con- centration plotted against predicted concentration. The following neonatal covariates were screened: current weight, birth weight, body length, head cir- cumference, gestational age, postnatal age, route of delivery, day of caffeine treatment, gender, race, Apgar score at 1 minute, Apgar score at 5 minutes, birth asphyxia (defined as an Apgar score at 1 minute of ~3), feed intolerance, presence of respi- ratory distress syndrome, a patent ductus arteriosus, respiratory support, period of intubation before study entry, surfactant therapy, and starting age on

CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME 61. NUMBER 6 Lee et al. 631
breast milk. The effects of concomitant administra- tion of medication were also screened, but only when a drug was prescribed in more than 15% of the infants in the study. Maternal covariates screened encompassed prenatal smoking history, current mul- tiple pregnancy, antepartum hemorrhage, chorio- amnionitis, preeclampsia, and premature rupture of the membranes.
Next, significant covariates were cumulatively added to the model in a forward stepwise manner in order of their contribution to the reduction in the objective function in the initial analysis until there was no further reduction in the objective function. Finally, a backward elimination step was performed in which the influence of each covariate was re- moved from the model by setting the appropriate coefficient to zero and reestimating the remaining parameters. This procedure was performed in de- scending order of the contribution to the change in the objective function by each covariate, as deter- mined in the initial analysis. The difference in the objective function before and after nullifying the coefficient of a given covariate approximates the x2 distribution with 1 degree of freedom. The level of significance (01) chosen was 0.01, which corresponds to a required change in the objective function value of 6.6.13
Pharmucostat&ic maieling. Deviations of caffeine clearance (CLj) and volume of distribution (Vj) of the jth individual from the true (but unknown) pop- ulation mean values were estimated according to the following interpatient error models13,14:
Additive model:
CLj = TVCL + qcL
vi = Tvv + q”
Proportional model:
cLj = TVCL- (1 + v$&
vj = Tvv * (1 + q”)
Exponential model:
CLj = TVCL - EXP(T&
Vj = Tw. ExP(rlj,v)
in which qj,cr and qj,v are random variables distrib- uted with zero means and respective variances of w?.. and 4, and TVCL and TVV are the population mean values for CL and V, respectively.
NONMEM also estimates residual variability be-
tween the observed response (i.e., serum caffeine concentrations) and those predicted by the mod- el(s). These differences (Eij) are attributable to in- trapatient pharmacokinetic variability, such as those in the timing of blood collections, dosing times, drug assay, and by misspecification of the pharmacoki- netic model (e.g., one-compartment instead of two- compartment). The following intrapatient error models were evaluated:
Additive model:
cij = cpred.ij + %j
Proportional model:
cij = Cpred,ij ’ t1 + $j)
Exponential model:
Cij = Cp~d,ij . EXP(E~~)
in which Cij is the ith observed concentration for the jth individual, Cpred,ij is the serum caffeine concen- tration predicted by the pharmacokinetic model, and Eij (difference between C, and Cpred,ij) is a ran- domly distributed variable with zero mean and vari- ance of 02.13*14
Predictive pe@wmance. Postanalysis bayesian pre- dictions of serum caffeine concentrations were performed in an independent cohort of 30 infants by setting the fixed-effects and random-effects parameters to the values estimated in the final model with use of the POSTHOC argument in the $ESTIMATION command in NONMEM. Residu- als (predicted minus observed concentrations) were calculated, and the absolute predictive performance in terms of precision and bias was assessed as de- scribed previously.15p16
RESULTS The clinical and demographic characteristics of
the patients are shown in Table I. A frequency histogram that shows the distribution of sampling times in relation to dosing times appears in Fig. 1. Mean serum caffeine concentrations 24 hours after the final dose (day 8) were 7.4,35.8, and 69.0 mg/L, respectively, whereas concentrations of three me- tabolites (theobromine, paraxanthine, and theoph- ylline) ranged from 0 to 3.4 mg/L.
In the preliminary screening phase, several covari- ates reduced the objective function by the required a priori cutoff value of 6.6. For clearance, these were weight, birth weight, respiratory support, head cir- cumference, body length, gestational age, route of

632 Lee et al. CLINICAL PHAlWACOLOGY &THERAPEUTICS
JUNE 1997
o-4. 4-6. ai2. 12-w. ia20. 20-24. 224
lime (h)
Fig. 1. Frequency histograms of blood sampling times in relation to dosing times.
delivery, patent ductus arteriosus, and postnatal age. For volume of distribution, these covariates were weight, birth weight, head circumference, body length, gestational age, and postnatal age. In the forward stepwise model building, the cumulative inclusion of weight and postnatal age in clearance and of weight, postnatal age and gestational age in volume of distribution reduced the objective func- tion by more than 12.6 at each addition. In the backward elimination phase both weight and post- natal age were identified as essential covariates modifying clearance, whereas weight, postnatal age, and gestational age were significant covariates for volume of distribution, as shown by an increase of >6.6 in the objective function when any of these were deleted from the model (Table II).
Gestational age and birth weight were analyzed both as dichotomized variables (gestational age >28 weeks; 128 weeks, birth weight >lOOO gm; 51000 gm, respectively) and as continuous variables. The cutoff age of 28 weeks was chosen because that age is used widely by neonatologists as an ad hoc index of the degree of immaturity (e.g., gestational age of 528 weeks denotes extreme prematurity). However, lower objective functions and better precision of estimation was obtained when modeling was per- formed with gestational age as a dichotomized vari- able. Other dichotomized variables screened were birth asphyxia (Apgar score at 1 minute 53; Apgar score at 1 minute >3), respiratory distress syndrome (present; absent), patent ductus arteriosus (present; absent), feed intolerance (present; absent), route of delivery (cesarean; vaginal), current pregnancy (sin- gle; multiple), antepartum hemorrhage (present; ab- sent), chorioamnionitis (present; absent), pre-
eclampsia (present; absent), premature rupture of membranes (present; absent), and gender. All other potential covariates were evaluated as continuous variables.
Summary results of the final fixed-effects and random-effects models are presented in Table III. Both the interpatient and intrapatient variability were best described by an additive error model. Although a mixed (additive plus proportional) in- trapatient error model gave the lowest objective function value, the predictive performance and the standard errors associated with the parameter esti- mation were inferior to those obtained with an ad- ditive error model. The scatterplots of Fig. 2 show that deviations among pairs of predicted and ob- served caffeine concentrations in the model devel- opment data set of 89 infants (430 concentrations) was small and distributed randomly about the refer- ence lines.
The imprecision (coefficient of variation, in per- cent) in estimating the parameters of the models was calculated by dividing the standard error of estima- tion of each parameter by its value and expressing the result as a percentage.13*i4 Table III shows that the coefficients for weight in the clearance model (0,) and for weight in the volume of distribution model (t3,, 0,) were estimated more precisely (coef- ficient of variation, 5.9% to 16.5%) than for postna- tal age in clearance (O,,) and in volume of distribu- tion (e,, 0,) in which the coefficient of variation was 29.5% to 57.9%. Population variability in clearance and volume of distribution was calculated by taking the square root of the individual elements of the OMEGA matrix and expressing the result as a per- centage of the population mean values for clearance and volume of distribution, respectively.13*14 Ac- cordingly, the coefficient of variation in clearance for infants at entry to and exit from the study was 26% and 24%, respectively. Similarly, the interpa- tient coefficient of variation for volume of distribu- tion at entry and exit was 13% and 9%, respectively. Intrapatient variability was estimated by taking the square root of the single element of the SIGMA matrix (i.e., error variance, cr2) and expressing this value (standard deviation of 3.9 mg/L) as a percent- age of the mean caffeine concentration.13”4 Thus the random error (coefficient of variation, in per- cent) associated with the mean trough caffeine con- centration of 6.8 mg/L produced by the lowest (3 mg/kg/day) dose was 57%, compared with a coeffi- cient of variation of 6% for a mean concentration of 69 mg/L. produced by the highest (30 mg/kg/day)

CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME 61, NUMBER 6 Lee et al. 633
Table II, Model development Model AOF* P Inteq2retation
CL = f (WT, PNA) V = f (GA, WT, PNA)
CL = f (PNA) V = f (GA, WT, PNA)
CL=f(wT) V = f (GA, WI-, PNA)
CL = f (WT, PNA) V = f (WT, PNA)
CL = f (WT, PNA) V = f (GA, PNA)
CL = f (WT, PNA) V=f(GA,WT)
0
t 18.5
t 8.2
1‘ 12.6
t 181
t 21.3
<0.01t
<0.01-t
<0.01t
<0.01t
<0.01+
Full model
WT influences clearance
PNA influences clearance
GA influences volume of distribution
WT influences volume of distribution
PNA affects volume of distribution
PNA, Postnatal age (days); WI, current body weight (gm); GA, gestational age (weeks); CL, total clearance (I.&r); V, volume of distribution (L); AOF, change in objective function value of fuII model.
*Change in obpctive function caused by deletion of individual covariates from the full population model. tSignificant (x i, c.ci > 6.6).
Table III. Parameters of final fixed-effects and random-effects population models for caffeine in preterm infants
Variability in estimation Parameter Meaning Estimated value SE cv (%)
Coefficient for WT in CL o.OOOOO399 O.OOOOOO658 16.5 Coefficient for PNA in CL 0.000128 0.0000741 57.9 Coefficient for WT in V, for GA >28 wk 0.000764 0.0000584 7.6 Coefficient for PNA in V, for GA >28 wk 0.0468 0.0138 29.5 Coefficient for WT in V, for GA ~28 wk 0.000755 0.0000444 5.9 Coefficient for PNA in V, for GA 5 wk 0.0224 0.00780 34.8 Interpatient variance in CL O.OOOOO176 o.OOOOOO47 26.7 Interpatient variance in V 0.0109 0.00517 47.4 Intrapatient variance 15.4 2.88 18.7
Fired-&crs mod& TVCL = Cil * WI’ + 13, .PNA;IfGA>28weeks;TW=8,.WT+8,.PNA;IfGAS28weeks:TW=6,.WT+8,.PNA. Random-fleets mod& CL = TVCL + na; V = TW + qr; C,, = C,, + c. PNA, Postnatal age (days); WI, current body weight (gm); GA, gestational age (weeks); CL, total clearance (I&); V, volume of distribution (L); TVCL,
population mean value for CL; TVV, population mean value for V; SE, standard error; CV(%), coefficient of variation of estimate = SE + Value . 100%; Cobs and CRedt observed and predicted serum caffeine concentrations, respectively.
dose. First-order conditional estimates of clearance for each of the 89 patients at entry to and exit from the study are plotted against dose in Fig. 3, A, and the corresponding plots of the volume of distribu- tion values are in Fig. 3, B. Mean clearances were similar after administration of the low, medium, and high doses either at entry to (0.0044, 0.0043, 0.0047 IJkg/hr, respectively) or exit from the study (0.0051, 0.0050, 0.0056 L/kg/hr, respectively). Likewise, the average volumes of distribution also were similar with respect to dose either at entry (0.858, 0.851, 0.896 I&g, respectively) or exit (1.037, 1.053, 1.114 I&g, respectively).
The predictive performance of the derived popu- lation models is shown in Table IV. There was sta- tistically insignificant bias between measured and predicted serum caffeine concentrations. Scatter- plots of observed versus predicted concentration (Fig. 4, A) and weighted residuals versus predicted serum caffeine concentration (Fig. 4, B) showed that differences between pairs of observed and predicted values were small, whereas a frequency histogram (Fig. 4, C) confirmed that these differences approx- imated a normal distribution. Examples of the sat- isfactory longitudinal predictive capability of the NONMEM-derived models are shown for three in-
634 Lee et al. CLINICAL PHARMACOLOGY & THERAF’EUTICS
TUNE 1997
100 e90 g 60 g 70 .- $ 60
E $ 50 g 40
:: E
30
20
d 0
10
0 0 IO 20 30 40 50 60 70 60 90 100
A Predicted concentration (mgll)
-6 ’ t 0 IO 20 30 40 50 60 70 60 90 100
B Predicted concentration (mgll)
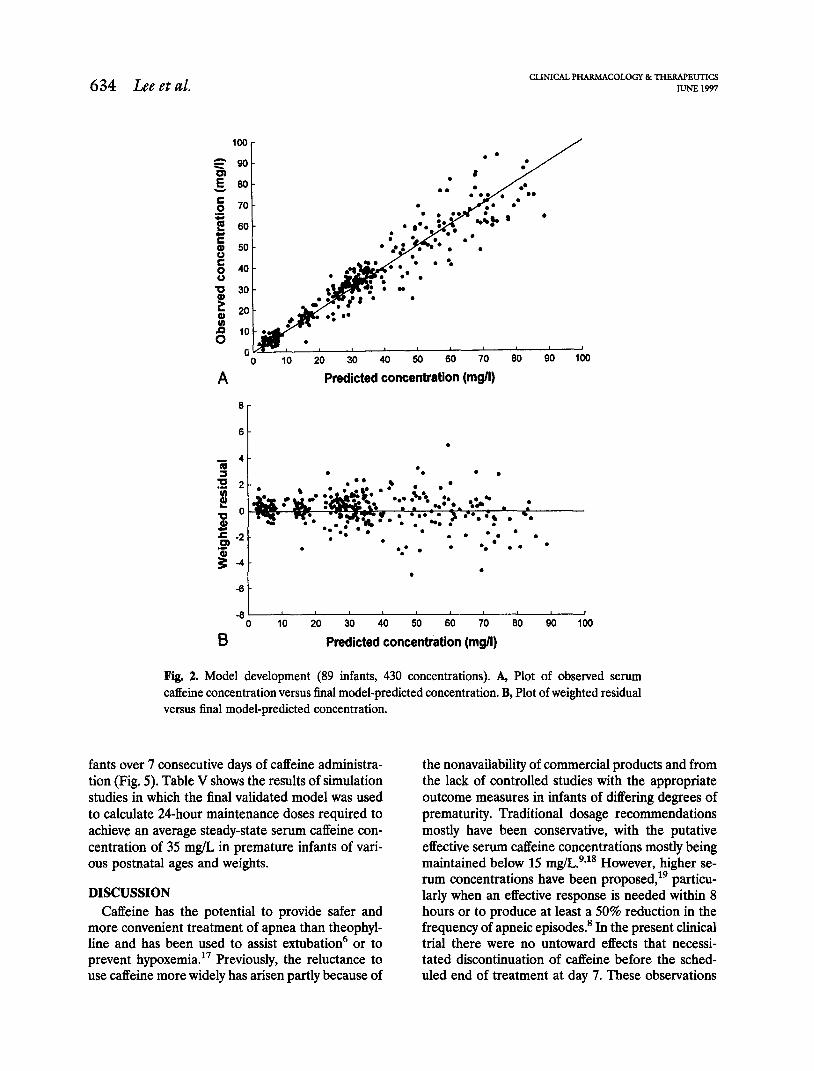
Fig. 2. Model development (89 infants, 430 concentrations). A, Plot of observed serum caffeine concentration versus final model-predicted concentration. B, Plot of weighted residual versus final model-predicted concentration.
fants over 7 consecutive days of caffeine administra- tion (Fig. 5). Table V shows the results of simulation studies in which the final validated model was used to calculate 24-hour maintenance doses required to achieve an average steady-state serum caffeine con- centration of 35 mg/L in premature infants of vari- ous postnatal ages and weights.
DISCUSSION Caffeine has the potential to provide safer and
more convenient treatment of apnea than theophyl- line and has been used to assist extubation6 or to prevent hypoxemia. l7 Previously, the reluctance to use caffeine more widely has arisen partly because of
the nonavailability of commercial products and from the lack of controlled studies with the appropriate outcome measures in infants of differing degrees of prematurity. Traditional dosage recommendations mostly have been conservative, with the putative effective serum caffeine concentrations mostly being maintained below 15 mgLgS1* However, higher se- rum concentrations have been proposed,lg particu- larly when an effective response is needed within 8 hours or to produce at least a 50% reduction in the frequency of apneic episodes.8 In the present clinical trial there were no untoward effects that necessi- tated discontinuation of caffeine before the sched- uled end of treatment at day 7. These observations

CLINICAL l’HARMACOLOGY &THERAPEUTICS VOLUME 61. NUMBER 6 Lee et al. 635
0.01 -
0.008 -
Gl ti 0.006 -
< = J 0.004 - 0
0.002 -
. . . I .
.
A
0 ’ Low Low Med Med High High Ent. Exit Ent. Exit Ent. Exit
Treatment
1.6 -
1.4 -
1.2 - %I < 1.0 - r; >
0.8 -
0.6 -
0.4 ’ Low Low Med Med High High Ent. Exit Ent. Exit Ent. Exit
B Treatment
Fig. 3. NONMEM-generated conditional pharmacokinetic parameter estimates from the final population model. Clearance (CL; A) and volume of distribution (V; B) for individual infants (n = 89) in the model development data set at entry to (Ent) and exit from the study for caffeine citrate maintenance doses of 3 mg/kg/day (Low), 15 mgkg/day (Med), and 30 mgIkg/day (High).

636 Lee et al. CLINICAL PHARhlACOLOGY &THERAPEUTICS
JUNE 1997
Table IV. Predictive performance of caffeine population pharmacokinetic models in an independent group of premature neonates (n = 30)
value SD 95% Cl (wfU
Precision 3.62 7.83 1.43 0.79 to 6.45 (RMSE)
Bias (ME) 0.034 1.66 0.303 -0.057 to 0.633
RMSE, Root mean square error; ME, mean error.
confirmed previous findings that preterm infants tol- erate caffeine very well, even at serum concentra- tions of 70 mg/L or above.7,8
This study differed in several important respects from a previous one published during preparation of the manuscript.” First, there were more patients (89 versus 60) who were more premature (gestation- al age, 28 versus 31 weeks) and from whom consid- erably more serum samples (430 versus 263) con- taining a much wider distribution of caffeine concentrations were obtained (range, 2 to 93 versus 5 to 19 mg/L). Second, in addition to predose (trough) sampling, at least two samples per patient were drawn at random intervals after the loading dose to obtain reasonable estimates of the volume of distribution. Third, an assessment of the predictive performance of the models was made with the use of a confidence limit approach, which indicated that the currently derived population models were valid and robust.
A two-compartment model offered no improve- ment over a single-compartment model in fitting the data. Preliminary experiments showed that caffeine is very rapidly distributed, with a half-life of <lo minutes, which is negligible compared with the mean estimated terminal half-life of 144 hours. In- formation on volume of distribution was facilitated by obtaining at least two serum caffeine concentra- tions at randomly allocated times over the 24-hour interval after the loading dose. However, more than half the samples were drawn close to the trough, as reflected by the better precision associated with the estimation of clearance than with volume of distri- bution. In the final fixed-effects model the popula- tion clearance could be described as a simple func- tion of current body weight and postnatal age. Using routine monitoring data, we previously reported a similar result when estimating theophylline clear- ance in patients similar to those in the present
study.16 The reasonably large coefficient of variation (30% to 58%) associated with estimating the coef- ficient for postnatal age in clearance probably re- flects the fact that >90% of the patients were younger than 6 days of age, whereas only 2% were older than 10 days at time of entry to the study. The influence of weight and postnatal age as significant influences on caffeine clearance agreed with previ- ous data conducted with noncompartmental methods2’-” and in a population study,12 in which higher clearances were recorded in infants of greater weight and postnatal age. Collectively, these findings were not altogether surprising because both weight and postnatal age are known to be correlated to varying degrees with renal and hepatic develop- ment.21
An additive intrapatient random error model was superior to a proportional model, even though se- rum caffeine concentrations ranged from 2.5 to 93.3 mg/L. Random error, expressed as a standard devi- ation of 3.9 mg/L, from drug assay sources and timing of drug administration and blood sampling may have been exacerbated by the contribution of exogenous caffeine in the mothers’ breast milk. Al- most 80% of infants had detectable predose caffeine concentrations that ranged from 0.2 to 5.1 mg/L (mean, 1.2 mg/L), which agrees with a previous report. 23 In addition, the hepatic methylation of theophylline, a known caffeine metabolite,24 back to caffeine may have contributed to the error at low serum caffeine concentrations.
The mean elimination half-life (144 hours) was longer, the clearance (0.0049 L/h&g) was smaller, and the volume of distribution (0.97 L/kg) was larger than the values reported in infants from 1 to 2% months old2’ and in adults.25326 In particular, the slow elimination of this drug in our patients was exemplified by the very long half-life of 86 to 277 hours, compared with 5 hours in adults.z,26 Other caffeine pharmacokinetic studies conducted on pre- term infants with use of nonpopulation modeling found the half-life, clearance, and volume of distri- bution values of 41 to 231 hours, 0.003 to 0.017 I&/kg, and 0.78 to 0.92 Likg, respectively?Y’9 Despite the very wide range of doses, there was no evidence of dose-dependent pharmacokinetics, a different result from that reported in two previous studies in adults.27,28 The linear disposition at high doses prob- ably reflects the fact that the metabolism of caffeine in the newborn is deficienp9: the large majority of the drug is cleared by the kidneys, thereby avoiding poten- tial saturation of metabolic pathways in the liver. Urine

CLINICAL P HARMACOLOGY & THERAPEUTICS VOLUME 61, NUMBER 6 Lee et al. 637
A Predicted concentration (me/l)
6
4 1 . 3 . . s2 . . 0. . l .
. -
t .* e
l . .” .*
l t
B 0 -5
& . . . l ,&.- _ l 4 r,‘. l . .
8.. l c . . - l , : * . i - . .
4s . l 9.
. .
. . 2 -2 - l . *
e l 0.
. -4
6~ 0 10 20 30 40 50 60 70 80 90
B Predicted concentration (mg/l)
3 30
s 25
f 3 20 u g! 15
L 10
0 -4.5 -4 -3.5 -3 -2.5 -2 -1.5 -1 -0.5 0 0.5 1 1.5 2 2.5 3 3.5
C Weighted residual
Fig. 4. Posthoc assessment of predictive performance (30 infants, 144 concentrations). A, Plot of observed serum caffeine concentration versus final model-predicted concentration. B, Plot of weighted residual versus final model-predicted concentration. C, Superimposed histogram and fitted normal curve plots of frequency of occurrence versus weighted residual interval.
from term neonates up to 1 month old contains X35% of the caffeine dose2’; the fraction of the dose renally excreted in preterm infants is likely to be even higher in view of their very immature hepatic function, Unfortunately, it was not possible to esti- mate the renal clearance of caffeine in our patients because of logistic factors and the risk of infection from indwelling urinary catheters.
Compared with adult values, the larger volume of distribution could reflect a partitioning of caffeine into the relatively larger extracellular fluid volume of the newbom,3’ especially in skeletal muscle.31 The binding to serum albumin is reasonably low (-35%) for caffeine concentrations up to 20 mgiL.32 Indeed, it is likely that the protein binding of caf- feine in premature neonates is linear to at least 70 mg/L, because even the highest caffeine dose did not significantly affect volume of distribution. In con- trast to the data of Pons et a1.,22 the final population
model indicated that volume of distribution was significantly influenced by gestational age, as well as by postnatal age up to 20 days. Infants of gestational age >28 weeks had a slightly higher but statistically significant volume of distribution and therefore had increased loading dose requirements compared with those of gestational age 528 weeks. It was interest- ing to note that a previous study found no modifying developmental influences on volume of distribution, even though postnatal age and weight ranged from 1 to 100 days and 0.6 to 2.9 kg, respectively.12 This result could be attributed to the lack of blood sam- ples from the distribution phase because the inter- patient variability in volume of distribution (coeffi- cient of variation, -24%) was considerably greater than the 9% to 13% calculated in the present study; unfortunately, no data on the standard errors asso- ciated with estimating clearance and volume of dis- tribution were provided by those authors.
638 Lee et al. CLINICAL PHARMACOLOGY & THER4F’EUTICS
IUNE 1997
75 . 0
. 0
0
.
0 1 2 3 4 5 6 7
Time (d)
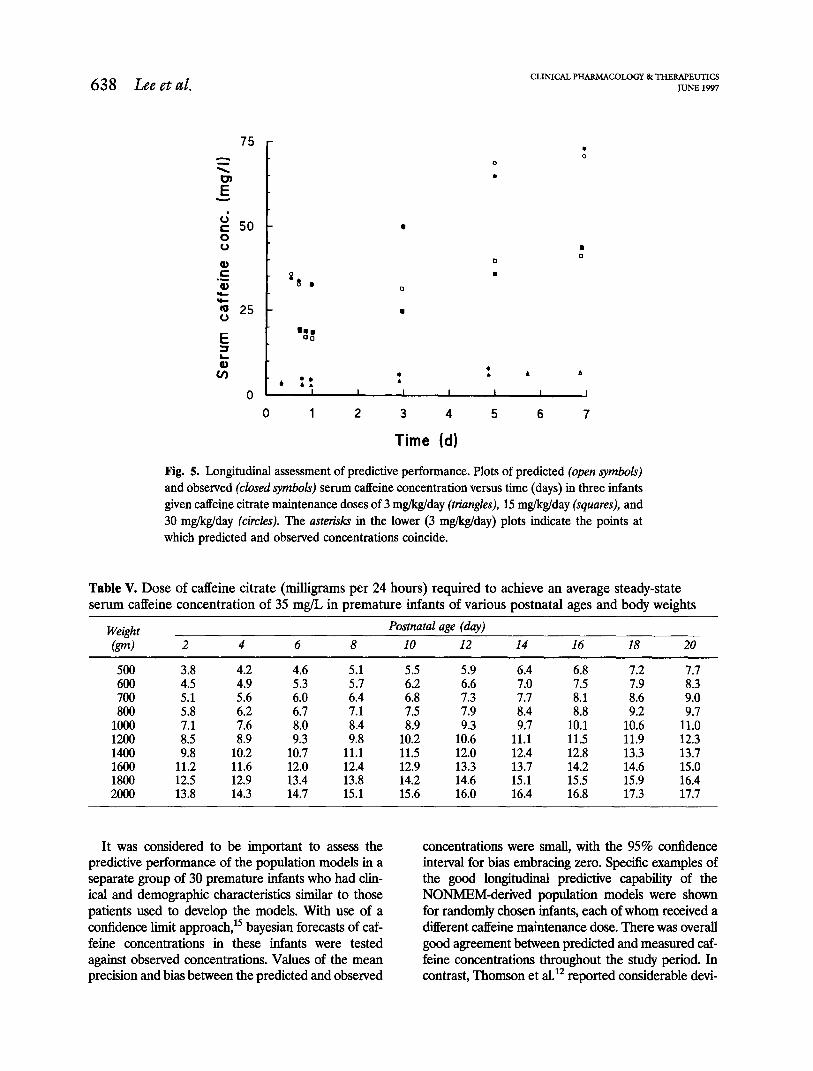
Fig. 5. Longitudinal assessment of predictive performance. Plots of predicted (open symbols) and observed (closed symbols) serum caffeine concentration versus time (days) in three infants given caffeine citrate maintenance doses of 3 mg/kg/day (triangles), 15 mgikglday (squares), and 30 mgikg/day (circles). The asferisks in the lower (3 m&g/day) plots indicate the points at which predicted and observed concentrations coincide.
Table V. Dose of caffeine citrate (milligrams per 24 hours) required to achieve an average steady-state serum caffeine concentration of 35 mg/L in premature infants of various postnatal ages and body weights
Weight @d 2 4 6 8
Postnatal age (day) 10 12 14 16 18 20
500 3.8 4.2 4.6 5.5 5.9 6.4 6.8 7.2 7.7 600 4.5 4.9 5.3 8 6.2 6.6 7.0 7.5 7.9 8.3 700 5.1 5.6 6.0 6:4 6.8 7.3 7.7 8.1 8.6 9.0 800 5.8 6.2 6.7 7.1 7.5 7.9 8.4 8.8 9.2 9.7
1000 7.1 7.6 8.0 8.4 8.9 9.3 9.7 10.1 10.6 11.0 1200 8.5 8.9 9.3 9.8 10.2 10.6 11.1 11.5 11.9 12.3 1400 9.8 10.2 10.7 11.1 11.5 12.0 12.4 12.8 13.3 13.7 1600 11.2 11.6 12.0 12.4 12.9 13.3 13.7 14.2 14.6 15.0 1800 12.5 12.9 13.4 13.8 14.2 14.6 15.1 15.5 15.9 16.4 2000 13.8 14.3 14.7 15.1 15.6 16.0 16.4 16.8 17.3 17.7
It was considered to be important to assess the concentrations were small, with the 95% confidence predictive performance of the population models in a interval for bias embracing zero. Specific examples of separate group of 30 premature infants who had chn- the good longitudinal predictive capability of the icaI and demographic characteristics simiIar to those NONMEM-derived population models were shown patients used to develop the models. With use of a for randomly chosen infants, each of whom received a confidence limit approach,” bayesian forecasts of caf- different caffeine maintenance dose. There was over-ah feine concentrations in these infants were tested good agreement between predicted and measured caf- against observed concentrations. Values of the mean feine concentrations throughout the study period. In precision and bias between the predicted and observed contrast, Thomson et aI.12 reported considerable devi-
CLINICAL PHARMACOLOGY&THERAPEUTICS VOLUME 61, NUMBER 6
ation among pairs of predicted and measured caffeine concentrations during validation, particularly with re- spect to dexamethasone treatment. Among other fac- tors, variability may have been introduced in that study by fixing the bioavailability of caffeine to lOO%, an assumption that is yet to be proved for premature infants and that is the focus of a current investigation in our unit.
A major aim of the study was to develop a nomo- gram that would have the potential for providing more effective treatment of apnea. The parameters of the derived fixed-effects models can be used either directly to guide dosing strategies or as initial estimates for bayesian forecasting in which the population pharma- cokinetic responses (and therefore dosing require- ments) are refined for individual infants as further drug level data are accumulated through routine monitoring. Furthermore, estimates of the population variability required by the bayesian analysis can be supplied directly from the parameters of the random- effects models estimated by NONMEM. Until now, most other sources have recommended caffeine doses based only on current body weight, but in this study caffeine clearance was influenced by body weight and postnatal age. Published results on the incidence of apneic attacks’ and preliminary pharmacodynamic data from our laboratory on oxygen desaturation read- ings indicated that very premature infants require se- rum caffeine concentrations of -35 mgiL for effective prophylaxis against apnea after extubation. Simula- tions with the final population model indicated that a 2-day-old infant that weighed 1000 gm would require a maintenance intravenous caffeine citrate dose of 7.1 mg every 24 hours to achieve this average concentra- tion at steady state (Table V). However, 10 days later a 31% increase in dose (to 9.3 mg) would be required to maintain levels at 35 mg/L if body weight had not changed during the intervening period, a common situation with very sick preterm babies.
In conclusion, the population pharmacokinetics of caffeine are reported after intravenous adminis- tration of a wide range of doses of caffeine citrate to 119 premature infants with apnea. Further studies are now underway to investigate the pharmacokinet- its and pharmacodynamics of oral and intravenous caffeine in extremely low-birth-weight infants (~12.50 gm), including long-term treatment.
We thank Dr. D. Tudehope (Director of Neonatology, Mater Mothers’ Hospital), Sr. T. Grant, and Sr. T. Walters (Mater Mothers’ Hospital) for their assistance in the study.
Lee et al. 639
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
Alden ER, Mandelkom T, Woodrum DE, Wennberg RP, Parks CR, Hodson WA. Morbidity and mortality of infants weighing less than 1000 grams in an inten- sive care nursery. Pediatrics 1972;50:40-8. Henderson-Smart DJ. The effect of gestational age on the incidence and duration of recurrent apnoea in newborn babies. Aust Paediatr J 1981;17:273-6. Poets CF, Samuels MP, Southall DP. Epidemiology and pathophysiology of apnoea of prematurity. Biol Neonate 1994;65:211-9. Tudehope DI, Rogers YM, Bums YR, Mohay H, O’Callaghan MJ. Apnoea in very low birth weight infants: outcome at 2 years. Aust Paediatr J 1986;22: 131-4. Aranda JV, Turmen T. Methylxanthines in apnea of prematurity. Clin Perinatal 1979;6:87-108. Sims ME, Rangasamy R, Lee S, Chung H, Cohen J, Walther FJ. Comparative evaluation of caffeine and theophylline for weaning premature infants from the ventilator. Am J Perinatol 1989;6:72-5. Aranda JV, Cook CE, Gorman W, Collinge JM, Loughnan PM, Outerbridge EW, et al. Pharmacoki- netic profile of caffeine in the premature newborn infant with apnea. J Pediatr 1979;94:664-8. Scanlon JEM, Chin KC, Morgan MEI, Durbin GM, Hale KA, Brown SS. Caffeine or theophylline for neonatal apnoea? Arch Dis Child 1992;67:425-8. Aranda JV, Gorman W, Bergsteinsson H, Gunn T. Efficacy of caffeine in treatment of apnea in the low- birth-weight infant. J Pediatr 1977;90:467-72. Davis JM, Spitzer AR, Stefano JL, Bhutani V, Fox WW. Use of caffeine in infants unresponsive to the- ophylline in apnoea of prematurity. Pediatr Pulmonol 1987;3:90-3. Collart L, Blaschke TF, Boucher F, Prober CG. Po- tential of population pharmacokinetics to reduce the frequency of blood sampling required for estimating kinetic parameters in neonates. Dev Pharmacol Ther 1992;18:71-80. Thomson AH, Kerr S, Wright S. Population pharma- cokinetics of caffeine in neonates and young infants. Ther Drug Monit 1996;18:245-53. Boeckmann A, Sheiner L, Beal S. NONMEM users’ guide. San Francisco: NONMEM Project Group, 1992. Grasela TI-I, Sheiner LB. Pharmacostatistical model- ing for observational data. J Pharmacokinet Bio- pharm 1991;19:25S-368. Sheiner LB, Beal SL. Some suggestions for measuring predictive performance. J Pharmacokinet Biopharm 1981;9:503-12. Lee TC, Charles BG, Steer PA, Flenady VJ, Grant TC. Theophylline population pharmacokinetics from routine monitoring data in very premature infants with apnoea. Br J Clin Pharmacol 1996;41:191-200. Bucher HU, Due G. Does caffeine prevent hypox-

640 Lee et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
JUNE 1997
aemic episodes in premature infants? Eur J Pediatr 1988;147:288-91.
18. Pearhnan SA, Duran C, Wood MA, Maisels MJ, Berlin CM. Caffeine pharmacokinetics in preterm infants older than 2 weeks. Dev Pharmacol Ther 198%12:65-g.
19. Gorodischer R, Karplus M. Pharmacokinetic aspects of caffeine in premature infants with apnoea. Eur J Clin Pharmacol 1982;22:47-52.
20. Aranda JV, Collinge JM, Zinman R, Watters G. Mat- uration of caffeine elimination in infancy. Arch Dis Child 1979;54:946-9.
21. Morselli PL, France-Morselli R, Bossi L. Clinical pharmacokinetics in newborns and infants: age- related differences and therapeutic implications. Clin Pharmacokinet 1980;5:485-527.
22. Pons G, Carrier 0, Richard MO, Rey E, d’Athis P, Moran C, et al. Developmental changes of caffeine elim- ination in infancy. Dev Pharmacol Ther 1988;11:258-64.
23. Stavric B. Methylxanthines-toxicity to humans; II: caffeine. Food Chem Toxic01 1988;26:645-62.
24. Bory C, Baltassat P, Porthault M, Bethenod M, Fred- erich A. Metabolism of theophylhne to caffeine in pre- mature newborn infants. J Pediatr 1979;94:988-93.
25. Bonati M, Latini R, Galletti F, Young JF, Tognoni G, Garattini S. Caffeine disposition after oral doses. Clin Pharmacol Ther 1982;32:98-106.
26. Kennedy JS, Leduc BW, Scavone JM, Harmatz JS, Shader RI, Greenblatt DJ. Pharmacokinetics of intra- venous caffeine: comparison of high-performance liq- uid chromatographic and gas chromatographic meth- ods. J Chromatogr 1987;422:274-80.
27. Cheng WSC, Murphy TL, Smith MT, Cooksley WGE, Halliday JW, Powell LW. Dose-dependent pharmaco- kinetics of caffeine in humans: relevance as a test of quantitative liver function. Clin Pharmacol Ther 1990; 47:516-24.
28. Denaro CP, Brown CR, Wilson M, Jacob P, Benowitz NL. Dose-dependency of caffeine metabolism with repeated dosing. Clin Pharmacol Ther 1990;48:277- 85.
29. Aldridge A, Aranda JV, Neims AH. Caffeine me- tabolism in the newborn. Clin Pharmacol Ther 1979;25:447-53.
30. Heimler R, Nemeth P, Yassin M, Jendrzejczak B, Doumas B. Total body water and extracellular water of premature infants during the first week of life [abstract]. Clin Res 1990;38:825a.
31. Warszawsiki D, Gorodischer R. Tissue distribution of caffeine in premature infants and in newborn and adult dogs. Pediatr Pharmacol 1981;1:341-6.
32. Blanchard J. Protein binding of caffeine in young and elderly males. J Pharm Sci 1982;71:1415-8.
Copyright © 2022 FDOKUMEN