Policy Management of Adult Nasogastric/Orogastric Feeding ...
42
Reference Number: CPIC006 Version Number: V1.1 Date of issue 06/02/2018 Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes What is this document for? The purpose of this policy is to ensure that all patients requiring nasogastric/orogastric feeding/drainage receive a safe quality service and that risks are minimised. Who needs to know? All medical, nursing and support staff that care for patients who require enteral feeding/drainage via a nasogastric route. Community based staff with a clinical responsibility for patients with a nasogastric/orogastric feeding tube Related PAHNT Documents: Consent to Examination of Treatment EDQ002 ANTT Policy EDN035 Hand Hygiene Policy EDC004 Procedures Relating to the Supply of Enteral Feeding Products for Adults (NCPDI002) Waste Management Policy EDE023 Clinical Record Keeping Policy EDN004 Policy for Management and Use of Medical Devices (EDE019) Policy for Training and Assessment for Safe Use of Medical Devices and Equipment (EDE020) Standard for Patient Observation Practice (CPDI044) Adult Restraint Policy (EDN049) Mental capacity Act Policies and Procedures (EDQ029) Related Legislation/ Obligations: National Institute Clinical Excellence (NICE) CG32 Nutritional Support for adults: oral nutritional support enteral tube feeding and parenteral nutrition (February, 2006). CQC Standards Outcome 5 (Regulation 14) – “Meeting Nutritional Needs” 3 . NPSA Alert (NHS/PSA/RE/2016/006) – “Nasogastric tube misplacement, continuing risk of death and severe harm” (July, 2016) Accountable Executive: Group Chief Nursing Officer Elaine Inglesby-Burke Document Author(s): Artificial Nutritional Steering Group (ANSG) & Acting Chair (Consultant Gastroenterologist) Dr Xola Mcfarlane Developed with: Consultant Gastroenterologist, Dietetics, Pharmacy, Learning and Organisational Development, Infection Prevention Team, Safeguarding Team & Radiology
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Policy Management of Adult Nasogastric/Orogastric Feeding ...

Reference Number: CPIC006 Version Number: V1.1 Date of issue 06/02/2018
Policy
Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes
What is this document for?
The purpose of this policy is to ensure that all patients requiring nasogastric/orogastric feeding/drainage receive a safe quality service and that risks are minimised.
Who needs to know? All medical, nursing and support staff that care for patients who require enteral feeding/drainage via a nasogastric route. Community based staff with a clinical responsibility for patients with a nasogastric/orogastric feeding tube
Related PAHNT Documents:
Consent to Examination of Treatment EDQ002 ANTT Policy EDN035 Hand Hygiene Policy EDC004 Procedures Relating to the Supply of Enteral Feeding Products for Adults (NCPDI002) Waste Management Policy EDE023 Clinical Record Keeping Policy EDN004 Policy for Management and Use of Medical Devices (EDE019) Policy for Training and Assessment for Safe Use of Medical Devices and Equipment (EDE020) Standard for Patient Observation Practice (CPDI044) Adult Restraint Policy (EDN049) Mental capacity Act Policies and Procedures (EDQ029)
Related Legislation/ Obligations:
National Institute Clinical Excellence (NICE) CG32 Nutritional Support for adults: oral nutritional support enteral tube feeding and parenteral nutrition (February, 2006). CQC Standards Outcome 5 (Regulation 14) – “Meeting Nutritional Needs”3. NPSA Alert (NHS/PSA/RE/2016/006) – “Nasogastric tube misplacement, continuing risk of death and severe harm” (July, 2016)
Accountable Executive: Group Chief Nursing Officer Elaine Inglesby-Burke
Document Author(s):
Artificial Nutritional Steering Group (ANSG) & Acting Chair (Consultant Gastroenterologist) Dr Xola Mcfarlane
Developed with: Consultant Gastroenterologist, Dietetics, Pharmacy, Learning and Organisational Development, Infection Prevention Team, Safeguarding Team & Radiology
Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 2 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Ratified by: Group Chief Nursing Officer on behalf of Executive Quality and Patient Experience
Date Ratified: 5th February 2018
Replaces:
This policy has been devised ensuring that management of nasogastric tube information is within a standalone document. Any information in relation to nasogastric tubes has now been removed from the Nutrition Support in Adult: Guidelines for Enteral Tube Feeding CPDI148 (Part 3) Version 2.2. Also replaces V1 of this policy
How is this different from the previous document?
3.1.2 Title added feeding/medication tubes 3.1.4 Title added drainage tube and sticker completion advice 3.2 Feeding title only 3.3 New paragraph added for drainage tubes 3.7.3 Wording added for altered anatomy 3.8.2 Additional sentence added 3.9.1 Additional sentence added 3.9.6 Additional sentence added Added Appendix 9 for inclusion of any differentiation to the policy for community services
What dissemination & training arrangements have been made?
This Policy will be available via the Document Management System. This policy and its contents will also be disseminated within the Nasogastric Insertion and Verification training delivered by the Clinical Skills Team in Learning and Organisational Development. This will be delivered to staff groups that have been identified who insert and verify nasogastric and orogastric tubes. See chapter 3.15.1
Review arrangements: Review every 3 years or earlier should a change in legislation best practice or other circumstance dictate
Safety Arrangements: Compliance & effectiveness of this policy will be via accident, incident & complaints monitoring, in addition to compliance audits, Enteral Tube Feeding annual audit (monitored via ANSG action plan). Staff experiencing difficulties with implementing this policy should contact their line manager.
Addendum Section 3: Following recommendation from a coroner’s report, changes to this policy were required in order to acknowledge that in a relatively small group of patients who have altered upper gastrointestinal anatomy a naso-intestinal tube must be placed gastroscopically or fluoroscopically to ensure correct and verified positioning. Differentiation throughout this guideline was required to separate advice for feeding tubes and for drainage tubes to ensure clarification and safe practice. Section 3.8.2 As a recommendation following an RCA of a patient case, an additional sentence has been added to advise that the patient is positioned at an angle, even when the feed is temporarily off, to ensure reduced risk of aspiration of feed. Appendix 9: This was added to ensure any variations to practice around naso/orogastric feeding for patients in the community setting were indicated. These agreed changes were approved by Dr Macfarlane (Gastroenterologist) January 2018.

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 3 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 4 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Priority Level: 1 Impact Level: Trustwide Keywords: Nasogastric, Orogastric, nasal bridle, Feeding tube, Guidewire, insertion,
verification,
Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 5 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Contents Page 1. What is this policy for? 4
2. Why do I need to know? 4
3. What is the policy? 4
Nasogastric tube description and tube selection 5
Indications and contraindications 6
Nasogastric placement 7
Fine bore nasogastric feeding tube insertion 8
Verification of nasogastric tube placement 13
Second line test method x-ray 14
Initiating feeding 15
Positional checks 16
Fixation device 16
Skin care 16
Mouth care 16
Enteral feeding 17
Tube flushing 17
Medication 17
Other areas of care 18
Ancillary items 18
Troubleshooting 19
Preparing for discharge 22
Nasal Bridle 22
4. What do I need to do? 24
5. List of Abbreviations & Terms used 25
6. References 25
7. Appendices
Appendix 1 – Equality Impact Assessment 27 Appendix 2 – Common indications for enteral tube feeding 28 Appendix 3 – Nasogastric or Orogastric Tube Checklist 29

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 6 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix 4 – Nasogastric/Orogastric Tube Care Plan 30-31 Appendix 5 – Procedural Guidelines: Insertion and management of AMT Bridle™ System 32-34 Appendix 6 – Medicines Advice 35 Appendix 7 – BAPEN Medications Poster 36
Appendix 8 - Nasogastric/Nasojejunal Tube Feeding - Discharge Checklist for Ward Staff 37-38 Appendix 9 – Community Management of Adult Nasogastric/Orogastric Feeding Tubes 39-40

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 7 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
1. What is this Policy for? 1.1 The purpose of this policy is to ensure that all patients requiring nasogastric/ orogastric feeding/drainage receive a safe quality service and that risks are
minimised. All nasogastric feeding/drainage in adult patients within Pennine Acute NHS Trust will be initiated and monitored in compliance with the National Patient Safety Agency (NPSA) guidelines and this policy.
2. Why do I need to know? 2.1 To prevent patient death and never events from happening by ensuring best practice
is implemented:
In February 2005, following reports of patient death and harm caused by misplaced nasogastric feeding tubes, the NPSA issued a Patient Safety Alert.
Between September 2005 and March 2010 nationally there were further 21 deaths and 79 cases of harm related to feeding through misplaced nasogastric tubes reported to the National Reporting Learning System (NRLS).
In 2009 feeding into the lung from a misplaced nasogastric tube became a Never Event in England.
During 2009/10 there were 41 Never Events reported to the NPSA where a misplaced nasogastric or orogastric tube was not detected prior to use.
The NPSA issued a further Patient Safety Alert in March 2011 and March 2012 (which does not change the advice provided in Patient Safety Alert 05) documenting actions required by the NHS Trust to reduce the harm caused by misplaced nasogastic feeding tubes.
The NPSA Alert in 2007 advised healthcare organisations on how to design medical devices and the correct methods required to measure and administer oral liquid medicines via tubes which support improved patient safety.
A review of the data from the NPSA’s National Reporting and Learning System (NRLS) showed 33 patient safety incidents involving intravenous administration or oral liquid medicines between 1st January 2005 and 31st May 2006. In correct intravenous administration of oral liquid medicines resulted in 3 reported deaths between 2001 and 2004.
NHS Improvement issued a further Patient Safety Alert July 2016 “Nasogastric tube misplacement: continuing risk of death and severe harm” which documented actions required by NHS Trusts to reduce the harm caused by misplaced nasogastic feeding tubes.
3. What is the policy
Nasogastric (NG)/Orogastric tube (OG) feeding is the choice for patients who require short term enteral feeding i.e. 4-6 weeks. Nasogastric drainage tubes are also included within this policy but are not to be used for feeding.
3.1 Nasogastric tube description and tube selection 3.1.1 NG tubes are temporary enteral feeding tubes placed trans-nasally into the Stomach. They are used mainly for short-term support in patients who require feeding access but do not have problems such as vomiting, gastro-oesophageal

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 8 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
reflux, delayed gastric emptying, ileus or intestinal obstruction. They can also be used for long term support where other enteral access is not possible or carries a risk. NG tubes are potentially dangerous in patients with an unsafe swallow and those who need to be nursed prone or flat. A risk/benefit assessment should be carried out by the nurse and documented before placement. 3.1.2 Feeding/Medication tubes: At Pennine Acute NHS Trust (PAHT), two types of adult nasogastric enteral feeding tube are available as part of the enteral feeding contract. The Nutricia range are polyurethane tubes with a guide wire licensed for up to 8 weeks. They are radio-opaque throughout the length of the tube and have externally visible length markings, as advocated by the NPSA/2011/PSA00214. The fine bore (CH/FR 8) feeding tubes are recommended as the best option in terms of patient comfort and prevention of nasopharyngeal erosions. CH/FR 10 tubes are available for patients on multiple medications to reduce the risk of tube blockage. Alternatively a Fresenius Freka NG tube can be used for feeding via wide bore tubes (12 CH/FG or more) in some specialised areas following area-specific guidance.
3.1.3 The Orogastric technique is used if the patient has facial base of skull fractures.
The technique and precautions taken are the same as those for the passage of a nasogastric tube, except that the tube is passed directly through the mouth. The length of the tube must be adjusted appropriately, the measurement being taken from the xiphisternum to the lips. The tube should, if possible, be secured to the chin using a suitable hypoallergenic tape. Care should be taken not to damage the lips or gums. Testing and documentation of the tube are the same as the nasogastric tube.
3.1.4 Drainage tubes: Wider bore Ryles tubes, often made from PVC are not to be inserted for
enteral tube feeding. These tubes are designed and intended to be used to allow rapid gastric decompression for example after surgery. When placed for decompression they should not be left in place longer than 14 days without being changed, because over time they can harden and become brittle. This then may lead to ulceration and erosions of the nasal passage with the soft mucosa and increase the risk of gastric reflux and aspiration. They can also impair normal swallowing. Ensure that the NG risk assessment sticker is ticked “for drainage” as indicated on the sticker.
3. 2 Indications and contraindications for feeding
3.2.1 Healthcare professionals should consider nasogastric/orogastric insertion for people who are malnourished or at risk of malnutrition and have:
Inadequate or unsafe oral intake and
A functional, accessible gastrointestinal tract
Absolute contraindications:

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 9 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Obstructive pathology in oropharynx or oesophagus preventing passage of the
tube
Persistent large gastric aspirates with high risk of aspiration
Intractable vomiting that cannot be controlled by anti-emetics
Other relative contraindications: In some circumstances patients may require referral to a specialist team (i.e. ENT,
Endoscopy, Radiography) for advice/tube insertion. These are:
Maxillo-facial disorders, surgery or trauma
Patients who have had oropharyngeal tumours or oropharyngeal surgery
Laryngectomy
Oesophageal varices
Skull fractures (basal skull fractures – orogastric feeding tube)
Unstable cervical spinal injuries.
Altered abdominal anatomy
Common indications for placement of a nasogastric/orogastric tubes can be found
appendix 2
3. 3 Indications and contraindications for drainage Healthcare professionals should consider a naso drainage tube insertion for people
who have:
Gastrointestinal obstruction i.e. volvulus, tumour, stenosis, gastroparesis
Other relative contraindications:
In some circumstances patients may require referral to a specialist team (i.e. ENT,
Endoscopy, Radiography) for advice/tube insertion. These are:
Maxillo-facial disorders, surgery or trauma
Patients who have had oropharyngeal tumours or oropharyngeal surgery
Laryngectomy
Oesophageal varices
Gastric surgery such as partial, total or extended gastrectomy, bariatric surgery and gastric bypass surgery.
Skull fractures (basal skull fractures – orogastric feeding tube)
Unstable cervical spinal injuries
Altered abdominal anatomy

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 10 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
3.4 Nasogastric Placement
3.4.1 Before any nasogastric tube is inserted a risk assessment should be carried out to identify if it is in the best interests of the patient balancing the potential risks with the need to feed, is clinically urgent and to ensure that verification expertise is available (NPSA/2011/PSA002). The decision to pass an NG tube and to
artificially feed is a multi-disciplinary team decision which is in the best interest of the patient. The appropriateness of tube feeding, the route of feeding, the risks benefits and impact on quality of life should be discussed. Trust patient information leaflets for the most common feeding routes are available.
3.4.2 Informed consent must be obtained according to the guidance in the Trust’s ‘Policy on Consent to Examination and Treatment’ (EDQ002). If feeding via nasogastric/orogastric tube is unsafe, not possible (e.g. inaccessible GI tract) or not successful (e.g. severe malabsorption, excessive gastrointestinal losses) parenteral nutrition should be considered. 3.4.3 Patients who are comatose or semi-conscious, have swallowing dysfunction or recurrent retching or vomiting have a higher risk of placement error or migration of the tube, whereas patients on antacid medication are more likely to have gastric pH levels of 6 and above making bedside verification of NG tube position difficult. Actions to reduce the risks and the rationale behind the actions should be documented in the patient’s medical notes prior to tube insertion Patient Safety Alert 05 NPSA, February 200511 and NPSA/2011/PSA002. This risk assessment
should be documented by using a purple ‘NGT Risk Assessment Sticker’ (3.3.4), placed in the patient’s medical note by the person completing the
assessment. This may be a medical doctor or competent nurse. 3.4.4 Nasogastric Risk Assessment Sticker
3.4.5 Placement should be delayed if there is not sufficient experienced support
available to accurately confirm nasogastric tube placement e.g. at night, unless clinically urgent, and the rationale for any decisions made should be recorded in the patient’s medical notes. Any individual involved with nasogastric position checks should be assessed as competent through theoretical and practical learning NPSA/2011/PSA002.
3.4.6 Any practitioner should not make more than two attempts to insert a tube. Should

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 11 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
the tube meet resistance / obstruction and cannot be advanced or tube insertion is unsuccessful for whatever reason, then the practitioner should reassure the patient and escalate accordingly to a more experienced practitioner.
3.5 Fine bore nasogastric feeding tube insertion:
3.5.1 Infection control Any handling of the nasogastric tube should be kept to a minimum and should be carried out utilising ANTT aseptic non-touch technique (Rowley, 2001). All items should be single use.
Equipment:
1 Tube of choice – size 8 or 10 CH/FR is usually sufficient (10 better if giving multiple medications)
2 Clinically clean tray or trolley 3 Fixation device – e.g. Nasofix 4 Water-based lubricant (single use) 5 Sterile Gauze swabs 6 50ml purple ENfit enteral syringe – sterile/single use 7 pH indicator strips – CE marked 8 Sterile spigot (or drainage bag if required) 9 Glass of water (if patient safe to swallow)
10 Tissues 11 Disposable apron 12 Non sterile disposable gloves 13 Indelible pen.
The tube will be inserted using the following procedure adapted from the Royal Marsden Manual (Mallet J and Doherty L, 2015) and the NPSA Safety alert (2005 and 2011). 3.5.2
Action Rationale
1 Explain the procedure to the patient and obtain his / her consent. Explain the importance of not tilting the head backwards Agree on a signal by which the patient can communicate if s/he wants to stop the procedure e.g. raising of the hand
To ensure full informed consent To help reduce any anxieties the patient may have and enable him / her to co-operate To ensure co-operation and promote confidence.
2 Prepare the environment If the patient’s condition allows, help into a semi-upright position, and support the head and back with pillows
To maintain privacy, confidentiality and dignity To facilitate easy passage of the tube. This position enables easy swallowing and ensures that the epiglottis is not obstructing the oesophagus
3 Place required equipment within a clean To facilitate the procedure and reduce the risk of

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 12 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
tray or trolley that has been wiped clean with a 2%CHG/70% IPA wipe and allow to dry for 30 secs
cross infection following ANTT
4 Decontaminate hands using seven step hand cleansing technique as per trust policy and don a disposable apron
To minimise the risk of infection
5 Open and prepare equipment onto aseptic field, using NTT
The equipment is ready for use and maintain asepsis
6 The length of tube required is determined by measurement of the distance between the bridge of the patient’s nose and ear lobe plus the length measured between the ear lobe and the xiphisternum
This measurement is called the NEX measurement
The measurement length will act as a guide that the tube when passed will have reached the stomach This should be documented on the ‘Nasogastric or Orogastric Tube Checklist’ see appendix 3
7 Give the patient the opportunity to blow his / her nose with tissues, place an apron on the patient and ensure a vomit bowl is at hand
To clear the patient’s nostrils and ensuring the patient is comfortably prepared.
8 Decontaminate hands again using seven step technique and apply non sterile gloves as per trust policy Do NOT flush the tube with water before insertion
Flushing with any substance may result in false positives when verifying position using pH paper (NPSA/2012/RRR001 22.03.12)
9 Lubricate about 15-20cm of the tube with a thin coat of lubricating jelly that has been placed on a sterile gauze swab
To reduce the friction between the mucous membranes and the tube and assist its passage
10 Gently pass the tube into the clearest nostril and slide it backwards and inwards along the floor of the nose to the nasopharynx. If an obstruction is felt, withdraw the tube and try again in a slightly different direction or use the other nostril.
To facilitate the passage of the tube by following the natural anatomy of the nose and to avoid trauma to the nasal mucosa

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 13 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Gentle rotation of the tube can be helpful at this stage. If unable to place the tube, seek advice from a senior colleague.
11 As the tube passes down into the nasopharynx, ask the patient to start swallowing tilting the chin down slightly at the same time. If the patient’s condition allows he/she may swallow or sip water to help the procedure. If patient is Nil by Mouth then mouth care may be used to stimulate swallow with water damped gauze.
The swallowing action closes the glottis, enabling the tube to pass into the oesophagus and avoid entering the trachea. Only use water so as not to alter the pH of gastric fluid
12 Advance the tube through the pharynx as the patient swallows (maintaining a calm manner and encourage the patient to take slow even breaths) until the required length of the tube has been passed If the patient shows any signs of distress e.g. gasping, coughing or cyanosis, remove the tube immediately. Recommence after giving the patient time to compose him/herself
Assists relaxation and avoids laryngeal spasm Distress may indicate that the tube is in the bronchus
13 Check the position of the tube to confirm it is in the stomach: With the guide wire still in the tube Using a 50 ml purple ENFit enteral syringe aspirate a small amount (0.5-1ml) of stomach contents and test with pH indicator paper that is CE marked to test human gastric aspirate. If you are unable to aspirate try doing the following:-
- If possible turn the patient onto their left side
- Inject 10-20ml air into the tube - Advance or withdraw tube 10-
20cm
To ensure that the tube is in the stomach Verifies the position of the tube See chapter 3.10.1 page 19 This will allow the tip of the tube to enter the gastric fluid pool To clear the tube/exit port and push the tip away from the mucosal folds of the stomach. If there is no aspirate or the patient belches immediately on injection of air then the tube is probably in the oesophagus. Advancing the tube may allow it to pass into the stomach

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 14 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
- Give mouth care to patients who are nil by mouth
- Wait for 15-30 minutes before aspirating again
- Do not flush with water until the placement of the tube has been verified
The pH should be 5.5 or below
Where pH reading are between 5 and 6 a second competent person should check the reading or retest the aspirate If the pH is 6 or above :
- If patient’s swallow is intact and not NBM give acidic drink e.g. pineapple, blackcurrant or orange juice
- Leave for up to one hour - Consider withdrawing and/or
repositioning the tube - Try aspirating again - Consider replacement of the
tube and/or checking position by x-ray Ensure reason for x-ray clearly documented on form
In patients with altered anatomy, dysphagia, altered GCS or in whom insertion was difficult it may be preferable to leave the guide wire in position until the tube position has been confirmed by x-ray
Stimulates gastric secretion of acid If the tube is in the lungs this could be fatal A pH of between 1 and 5.5 is reliable confirmation that the tube is not in the lung (NPSA/2011/PSA002) A pH of 5.5 or below indicates gastric placement Note: the pH of some drinks will vary – check the pH beforehand to ensure accuracy of verification A pH of 6 or above may indicate that the tube is in the intestine or bronchial tree or that acid-inhibiting medications are affecting the pH – waiting will allow time for the stomach to empty and the pH to fall To confirm placement of radio-opaque NG tube NPSA/2011/PSA002 guidelines Leaving the guide wire in makes the tube much easier to see on x-ray
14 Competent clinician must document confirmation of nasogastric tube position in stomach either by pH testing or x-ray Secure the tube to the patients nose using a suitable fixation device
NPSA/2011/PSA002 guidelines To ensure the tube remains in situ and to maintain patient comfort
15 Mark the tube where it leaves the patients nose with an indelible pen and document on the ‘Nasogastric or Orogastric Tube Checklist’ see appendix 3
To enable easy observation of tube position change
16 Once the position of the tube has been Water, feed or medication should only be

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 15 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
confirmed, flush the tube with 10ml of sterile water and remove the guide wire and close the access port This should come out easily with gentle traction. If there is any resistance try flushing the tube with water. If there is still resistance or the wire is ‘uncoiling’, remove the whole tube and repeat the procedure from the start Under no circumstances the guide wire nor any other wire should ever be re-introduced when the tube is in place in the patient (National Nurses Nutritional Group, 2012)
administered down the tube once the position of the tube has been confirmed. Flushing the tube with water activates the internal lubricant in the tube assisting in the removal of the guide wire. Any resistance may mean that the guide wire is stuck and it can uncoil if too much traction is used The guide wire could perforate the tube and cause harm to internal organs.
17
If the tube is not going to be used straight away for feed / drugs then flush with 30ml sterile water every 4 hours in conjunction with the ANTT policy
To maintain tube patency
18 Dispose of all used equipment safely and appropriately, remove PPE and decontaminate hands using seven step technique
To maintain a safe environment and to prevent cross infection
19 Document the procedure on the NG tube placement bedside checklist and the technique used to confirm the position of the tube in the nursing notes. Record the tube make, CH/FR size and length of time the tube can remain in situ. If placement of the tube is verified by x-ray a purple verification sticker will need to be completed by the competent practitioner who undertakes this procedure and be placed into the medical notes.
To ensure accurate documentation. For audit results and in the event of a query.
3.6 Verification of NG Tube placement 3.6.1 Follow NPSA Guidance: First line test method: pH paper
Using a 50ml ENFit enteral syringe a minimum of 0.5ml-1ml should be withdrawn from the NG tube as this will cover an adequate area on the reagent panels of the pH testing strips.
The NG aspirate must be checked using pH indicator paper which has 0.5

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 16 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
increments, is CE marked and manufactured to test human gastric aspirate. Allow 10 seconds for any colour change to occur.
The pH reading must be between 1 and 5.5 to confirm placement.
A second competent person must check any reading that falls within the pH range of 5.0-6.0.
Please Note: The feed itself can increase the pH in the stomach, so aspiration should take place at least 1 hour after the feed has been stopped. 3.6.2 Results of the initial check post-insertion (and re-insertion) should be recorded on the Nasogastric or Orogastric Tube Checklist under Nasogastric/orogastric tube verification and each subsequent pH test result should be documented on the same document under pH Monitoring (Appendix 3). A record of pH at different
times of the day helps establish what is normal for the patient and provides a baseline for future readings. The patient should then be cared for according to the correct care plan once the placement has been verified as correct (appendix 4).
3.6.3 As it is possible for the distal tip to migrate back into the stomach, once initial position verification has taken place, the tube should be marked where it exits the nose with an indelible pen at the length of the tube at the patient’s nostril. On initial placement and prior to use of the tube the position should be checked and documented on both the placement bedside checklist and the Aspirates pH monitoring chart. If the tube has moved the external length will be either longer or shorter than expected. If this occurs the pH testing method should be used to re check position. 3.6.4 If aspirate cannot be obtained or the pH is greater than 5.5, feeding should not commence. The NG tube should be left in place, the patient’s position changed and
the aspirate re-tested in one hour. Difficulty in obtaining aspirate may arise because the exit holes are blocked by secretions, the tube is kinked, the exit holes are lying against the folds of the stomach or the exit holes are not under fluid level. See 3.10 troubleshooting unable to obtain a gastric aspirate to check
position of the tube. 3.7 Second line test method: X-ray 3.7.1 X-ray is used only as second line test method when no aspirate could be obtained
or pH >5.5 and troubleshooting has been followed. Confirmation of tube position by radiography (a chest x-ray) is not recommended routinely. It is important that the number of x-rays is minimised to avoid undue exposure to radiation, loss of feeding time and increased handling of seriously ill patients. Staff should be aware that radiology only confirms a tube’s position at the time the x-ray is taken.
3.7.2 Radiological confirmation should only be considered for high risk groups i.e. patient with altered anatomy, dysphagia, altered GCS or in whom insertion was difficult and as a second line test when no aspirate can be obtained or pH indicator paper has failed to confirm the position of the NG tube. 3.7.3 To assist Radiology it is important that the referral contains the reason why a tube’s position needs radiological confirmation, which may include head and neck surgery, dysphagia, altered anatomy and whether or not attempts to confirm position by aspiration have been successful, appropriate or not. Insufficient clinical information

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 17 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
may result in the x-ray being delayed.
3.7.4 Follow NPSA Guidance:
X-ray request forms should clearly state that the purpose of the x-ray is to establish the position of the nasogastric/drainage tube for the purpose of feeding, administration of medication or drainage.
The radiographer takes responsibility to ensure that the nasogastric tube can be clearly seen on the x-ray to be used to confirm tube position
Documentation of the tube placement checking process includes confirmation that any x-ray viewed was the most current x-ray for the correct patient, how placement was interpreted and clear instructions as to required actions. Verification of nasogastric tube placement should be undertaken by a competent healthcare professional and a purple ‘NGTube Verification Sticker’ should be placed in the patient’s medical notes (3.6.5). In addition this is documented on the ‘Nasogastric or Orogastric Tube Checklist’, Appendix 3.
Any tubes identified to be in the lung should be removed immediately. (At PAHT this should be done by nursing staff on return to the ward).
3.7.5 Nasogastric Tube Verification Sticker:
3.7.6 Staff experiencing problems interpreting an x-ray to confirm tube position, should contact Radiology for assistance, before ordering further x-rays. If a competent clinician (with evidence of training) is unable to confirm nasogastric tube position in the stomach the tube should not be used. The tube should be re-sited or senior advice sought.
3.7.7 Please Note: The use of litmus paper, auscultation of air, observation of respiratory distress, the presence of air bubbles from the proximal tube and visual inspection of tube aspirate are unreliable methods of confirming tube position and should never be used. See NPSA Patient Safety Alert 05, February 200511 3.7.8 NG tubes should not be flushed, nor have any liquid or feed introduced through the

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 18 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
tube following initial placement until the tube tip is confirmed by pH testing or x-ray to be in the stomach and this verification should be documented as correct NPSA/2011/ and NPSA/2012/RRR001.
3.8 Initiating feeding
3.8.1 Unless speciality-specific guidelines exist, feeding via a newly placed NG tube should start as soon as position is confirmed according to NPSA/2011/PSA00214 guidelines. 3.8.2 All patients with a nasogastric/orogastric tube must be referred to the dietitian using the Dietetic Online Referral form. Feeding should be commenced according to the dietetic feeding regimen. If the dietitian is not available, start feeding according to the Enteral Feeding Starter Regimen. The patient should be nursed at 30° angle or higher if not contra-indicated by their medical condition because of the risk of
pulmonary aspiration when feeding (DeLegge, 2016). The patient should remain elevated at this angle when providing any other nursing care with the feeding pump on hold.
3.9 Continuous Care 3.9.1 Positional checks of the Nasogastric Tube The most common risk associated with the insertion of an NG tube is misplacement of the tube into the bronchus and subsequent pulmonary aspiration when enteral feeding is in progress. Patients with oral or tracheal intubations and those with reduced level of consciousness, impaired swallow or decreased gag reflex are at higher risk of tube misplacement. The tube can be misplaced at insertion or dislodged at a later stage19. Therefore continued checks of position should be carried out:
Before administering each feed
Before administering medication – if on rest period
At least once daily during continuous feeds
Following episodes of vomiting, retching or coughing spasms
When there is suggestion of tube displacement
When there are any new or unexplained respiratory symptoms or if oxygen saturations decrease
For naso drainage tubes check the external length of the tube from exit of the nose daily.
3.9.2 Each time the checks are performed utilising ANTT including failure to obtain aspirate should be documented on the Nasogastric or Orogastric tube checklist (Appendix 3). 3.9.3 Some drugs increase gastric pH which may make pH testing for verification of NG tube position invalid. These include Antacids, H2 Antagonists, Proton Pump Inhibitors and some antibiotics. Clinical judgment needs to be exercised. Consideration should be given to stopping PPIs as soon as the decision is made to start nasogastric feeding and using Gaviscon or an H2 Receptor Antagonists instead but if in any doubt pharmacy should be contacted for advice. The ward pharmacist can be the first port

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 19 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
of call, but otherwise Medicines Information will be more than willing to assist.
3.9.4 The fixation device This needs checking daily to ensure it is intact and should be changed if loose or soiled and replaced when required. If there are any concerns over tube displacement during changes then follow 3.10.5 within this document. Additional dressings may be used to secure the tube onto the patient’s cheek to keep the tube away from the patient’s mouth.
3.9.5 Skin care Cleansing of the face should be carried out as per individual routine; gentleman Should be kept clean shaven (if they are normally), also barrier cream may be used for skin protection / comfort. The position of the enteral tube within the nostril should be checked at least once daily and kept clean to prevent necrosis/debris build up. In specialised areas care of the patients skin is documented within a skin bundle.
3.9.6 Mouth care Mouth care should be maintained 2-4 hourly and teeth should be cleaned as individual routine and followed with mouthwash if required. If the patient wears dentures these should be cleaned as normal, to prevent any infection or sores forming. If patient is suffering from a dry mouth oral lubricant may be used and lip
balm can be used on dry lips to aid patient comfort. During routine mouth care it is an opportunity to visually check the tube is not coiled at the back of the throat.
3.9.7 Enteral Feeding The ENFit giving set must be changed every 24 hours and any remaining feed discarded (NICE, 2017). Document input and output accurately on a fluid balance chart.
3.9.8 Tube flushing Utilising the principles of ANTT, decontaminating hands as per trust policy and donning appropriate PPE the tube should be flushed to maintain patency. The tube should be flushed with at least 30mls of sterile water unless stated otherwise by the dietitian, on the patient’s feeding regimen or the doctor specifies. Additional water may be required short term due to warm weather, pyrexia, diarrhoea or for some patients water may be more closely monitored due to them being fluid restricted. The tube should be flushed:
After each gastric aspiration for pH check
Before and after the administration of feed
Before/after the administration of each medication and 10mls between administration of each medicines via the feeding tube. Guidance on the recommended fluid volume to give with medication is outlined in Medicines Advice (Appendix 6). Extra care is needed when patients are on a fluid restriction.
At each bottle change
Every 4 hours when the tube is not in use.

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 20 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
3.9.9 Tubes which are not flushed immediately before and after feed and or medications have a much higher risk of blocking. Flushes should be administered using a ‘push- pause’ technique as this causes turbulence within the tube and reduces the risk of tube blockage. Any water flushes that are administered should be recorded on the patient’s fluid balance chart. 3.9.10 Any syringes should be purple enteral syringes (NPSA/2007/19) and 50ml in size, as smaller syringes may produce too much pressure and split the tube (BAPEN, 2003). If the tube becomes blocked refer to chapter 3.10.2 within this policy 3.9.11 Sterile water should be used for all patients in the hospital setting. It should be at room temperature when administered. Sterile water containers opened for flushing should be clearly labelled with the patient’s name, hospital number and the date and time it was opened. Any water remaining after 24 hours should be discarded and a new bottle opened. The bottle top must be firmly attached between each use. 3.9.12 ANTT should be utilised when decanting sterile water to reservoir sets to prevent contamination for patients requiring water via a feeding pump.
3.9.13 Medication Administering drugs via feeding tubes increases the risk of tube blockage. Before administering medication, the feed should be stopped. The tube should be flushed with at least 30ml sterile water before and after administration of medication to prevent interaction between the drug and feed. If more than one drug is required they should be given separately with a different syringe used for 10ml flushes between to prevent interactions between the drugs. 3.9.13 Administration of medications via a feeding tube and especially the flushes required may be difficult in patients whose fluid intake is restricted. Ward staff should liaise with the ward pharmacist and dietitian to ensure optimum care. Information on administration of medicines (appendix 6 and 7).
Other areas of care 3.9.14 Bowel care should be monitored and maintained to prevent patients becoming either constipated or having diarrhoea. All bowel activity should be recorded on a stool
chart. 3.9.15 Blood sugars should be monitored regularly as feed can cause them to fluctuate and they may require treatment for this. These should be recorded on a blood glucose chart. 3.9.16 Bloods should be checked regularly to monitor electrolytes, hydration status, magnesium and phosphate levels.
3.9.17 Patients should be weighed weekly or more often if clinically indicated.

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 21 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
3.10 Ancillary items 3.10.1 Supplies of items available via the enteral feeding contract should be ordered by wards directly using the ‘Ward Order Form’ on the Intranet (Nutrition and Dietetics webpage). Other items should be sourced via pharmacy ‘stock’ or ‘non stock’ order routes as appropriate 3.10.2 Giving sets are ‘single patient use’. If attached directly to ready-to-hang sterile feed packs they can be used for 24 hours. 3.10.3 Flexitainers (for decanted feed): 1000ml reservoirs should be changed every 4 hours when used for decanted and reconstituted feed. 3.10.4 Flexitainers (water): 1000ml reservoirs are used for patients with high fluid requirements. They should be changed daily.
3.10.5 Syringes: ENFit oral/enteral syringes (Purple plunger) should be used when flushing
tubes and administering feed or medication via an enteral feeding tube (NPSA/2007/19). 3.10.6 Enteral feed pumps: PAHT has a contract with an enteral feeding company which includes provision of enteral feed pumps and stands. All Nursing staff that use or provide information in relation to the feeding pump must ensure they adhere to the medical devices polices: Policy for the Management and Use of Medical Devices’ (EDE019) and ‘Policy for Training and Assessment for Safe Use of Medical Devices and Equipment’ (EDE020). Service users and carers also need to receive appropriate training as per manufacturer’s recommendations for use at home prior to discharge. Guidance on using the feeding pump should be located either within the ward nutritional folder or on the medical devices intranet webpage. For indemnity reasons, only hospital loan pumps should be used on hospital premises. Patients’ own pumps, provided on home loan schemes, should not be used on wards.
3.11 Troubleshooting
3.11.1 (a). Unable to obtain a gastric aspirate to check position of tube
Problem Solution
1 Air but no aspirate
Check the length of the tube inserted. Advance the tube by 10-20cm for adults then re-aspirate Advancing the tube may allow it to pass into the stomach if it is in the oesophagus

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 22 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
2 No air or aspirate
Check the length of the tube inserted. Consider withdrawing the tube then aspirate
3 Not much fluid in the stomach
Check the length of the tube. Place the patient in the left lateral position then aspirate. Ask patient to take a drink of acidic fluid (orange juice) if not NBM or swallowing problem
4 Tube occluded on mucosa
Check the length of the tube. Inject 10 – 20 mls of air using a 20ml or 50ml syringe. Wait for 15-30 minutes and try again Please Note: This is not a testing procedure: Do not carry out auscultation of air (‘whoosh’ test) to test tube position Injecting air through the tube will dispel any residual fluid (feed, water or medicine) and may also dislodge the exit-port of the nasogastric feeding tube from the gastric mucosa.
Consider x-ray All radiographs should be read by appropriately trained staff and verification of the correct position should be clearly documented in the patient’s notes using the purple ‘NGT Verification Sticker’
The radiographer will need to know that aspiration of gastric fluid has been unsuccessful. If x-ray verification is used the tip of the tube should be seen in the stomach not just ‘below the diaphragm’.
3.11.2 Tube blockage A common problem associated with enteral feeding tubes is that they may become partially or completely blocked. Occlusions or blockages are often caused by the feed or medication (Smith R; Myers SA, 2005). Therefore to prevent these blockages occurring regular flushing of the

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 23 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
enteral tube, especially before and after medications have been administered must be completed and documented. Carbonated drinks should never be used for unblocking of Nasogastric tubes. The potential problem is that the acidic contents precipitate a protein build up,
therefore increasing the risk of occlusion in the feeding tube (Shipley et al 2016)
Suggested techniques
Try to remove as much of the contents in the tube as possible by attaching the purple enteral syringe and using a push-pull technique try to release any obstruction.
With gloved hands, manipulate the feeding tube by rolling and squeezing the feeding tube in-between two fingers to try to un-block any debris stuck inside the feeding tube.
Use a disposable warm cloth to run up and down the external part of the tube to try to loosen / un-block any debris inside the feeding tube.
Fill a 50ml purple ENfit enteral syringe with 10mls of sterile water. Pull back the plunger to create a vacuum in the feeding tube. Invert the syringe pointing downwards and push the water into the tube to try and move the blockage.
If the above steps fail, consider sodium bicarbonate which will be available from pharmacy. Mix 1/2 teaspoon sodium bicarbonate with 50mls of sterile water and use vacuum technique (as above) to try and loosen the blockage.
If all of the above fail, an enzymatic substance e.g. Clog Zapper should be considered. This product contains enzymes that are designed to dissolve blockages. Clog Zapper is only kept in certain hospital areas i.e. Endoscopy Units. It is not available via Pharmacy, but can be ordered via the NHS Supply Chain. Clog Zapper is very expensive and should only be used if it is possible to syringe liquid down the tube. Follow the enclosed instructions carefully.
3.11.3 Aspiration of feed To reduce the risk and recognise the signs of aspiration:
During feeding (and for 1 hour post feed) the patient’s head and shoulders should be elevated by at least 30° (DeLegge, 2016), if not contraindicated by their medical condition. Extra care should be taken when feed is in progress overnight or the patient is immobile.
All routine nursing observations should be undertaken in accordance with the ‘Standard for Patient Observation Practice’ (CPDI044) policy. Key symptoms of aspiration i.e. pyrexia and tachycardia associated with wheezing should be observed for.
If aspiration is suspected ward staff should stop the feed, ensure that the patient’s airway is clear, monitor patient’s condition and report situation to medical staff.

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 24 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
3.11.4 Ulceration/Erosions of the nasal passage and other soft mucosa The patient’s oral cavity should be observed for dryness, soreness, tongue coating and discomfort, particularly if the tube feed is the patient’s only source of nutrition. Regular oral hygiene should be provided using the ‘Oral Assessment Tool’ and ‘Core Care Plan for Mouth Care’. Nostrils should be kept clean, crustations removed with mild soap and water and the nasal area observed for any sores or erosions caused by the tube. If these are severe it may mean the tube should be removed and re-inserted into the other nostril. The tape securing the tube should be changed as required, e.g. when the dressing is dirty or lifting off. However, changing the dressing too frequently may lead to skin excoriation and blister formation and increase the risk of tube displacement. When applying a new fixation dressing, the nose should be washed with mild soap and water and dried thoroughly, to remove excess grease and maximise dressing adherence. Advice can be sought via Tissue Viability for additional advice on choice of dressings if a patient has skin excoriation or if concerns are documented within the skin bundle.
3.11.5 Tube displacement Displaced NG tubes should be replaced promptly if nasogastric feeding is to continue, using a new sterile tube. Once a guide wire has been removed it should never be re-inserted into a tube due to the risk of perforating the tube. The tube replacer should document the replacement on the Nasogastric or Orogastric Tube Checklist within a new column under the nasogastric/ orogastric tube verification (see appendix 3).
3.12 Preparing for Discharge with an Enteral feed Planning for discharge should start as soon as possible, in order to ensure that patients are discharged from hospital into the community safely and with adequate support. Ward staff should give the Dietitian at least 48hrs in order to prevent a delay. Nurses should provide training to the patient and / or carer and encourage them to maintain competency in all aspects of tube feeding, tube care and the administration of medication via the feeding tube to promote early self-care. Patients and carers should be trained so they are able to recognise potential problems and know the route to solving them. From the time of tube placement, the care provided to patients should involve and educate them and / or their carers as much as possible to be as independent as possible. The Home Enteral Tube Feeding Discharge Checklist for Ward Nurses’ (Appendix 8), should be used to identify what training is required and indicate how training is progressing. Ward staff should check that nursing home staff are familiar with management of the tube. The Trust contracted feeding company will attend the ward to provide training to patients and carers when requested by the ward staff. The ward staff should also inform the dietitian if the nursing home staff require training.
3.13 Tube removal
The tube should remain in place until the dietitians have assessed oral intake as adequate. During any periods when the tube is not being used for feeding but is still in place the tube should be kept patent by flushing with 30mls of sterile water 4

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 25 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
times a day. Standard ANTT should be used throughout the procedure when removing the Nasogastric tube. The tube should be removed with gentle traction and documented in the patient’s notes.
3.14 Nasal Bridle An AMT nasal bridle is a nasogastric tube retaining device designed for use in patients who inadvertently and / or repeatedly pull out their nasogastric tubes. It is a soft piece of ribbon gauze passed round the nasal septum to which the nasogastric tube can be secured. If the patient pulls on the nasogastric tube when a bridle is in situ they pull the tape down on their nasal septum causing themselves pain. Its use has been successfully introduced into practice in UK hospitals (Anderson et al, 2004) with few associated complications and minimal discomfort for the patient (Johnson et al, 2008). Using a nasal bridle avoids feeding delays and can be used to avoid gastrostomy insertion in some patients.
(See Appendix 5 for Procedural Guidelines for Insertion)
3.15 Restraint/Capacity
The use of an AMT bridle is considered a form of restraint. When the use of a bridle is being considered there needs to be a discussion with the responsible consultant/registrar which should include a risk assessment and consideration of mental capacity of the patient. A proforma document must be completed before
bridle insertion can be completed (see appendix 5). Further discussion with the Trust Safeguarding team may be required for those patients lacking capacity as
Deprivation of Liberty Safeguards (DOLS) may also need to be considered. Please refer to Trust Adult Restraint policy (EDN049) and Trust Mental Capacity Act Policies and Procedures (EDQ029) for further information.
3.15.1 Criteria for use of nasal bridle
The patient has pulled out or displaced at least two nasogastric tubes
Other tube securing methods have been optimised
The patient has had mittens tried and monitored feeding.
The patient is unable to receive their nutritional requirements without an NG tube
The patient has a size 8, 10 or 12 CH/FR NG tube in situ
Any agitation, confusion or restlessness should have been investigated and treated accordingly
The feeding tube was extremely difficult to place requiring endoscopic or radiological guidance.
3.15.2 Exclusion criteria
The patient has capacity and has refused bridle insertion
Basal skull fracture
Patients with structural deformity of the nose or nasopharynx
Patients who are so agitated that they may pull on the bridle to such a degree
as to cause serious injury.
Advice should be sought from the medical team in patients on regular

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 26 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Anticoagulant medication or with a known clotting abnormality/disorder.
3.15.3 Insertion The placement of a nasal bridle must only be undertaken by registered practitioners who are experienced in their insertion. The main areas where this expertise may be found are acute stroke, critical care and gastroenterology wards. The bridle should be inserted after the nasogastric tube has been verified in the correct place. Bridles are available in different sizes (8, 10 or 12 CH/FR) and the bridle size should match the nasogastric tube size.
3.15.4 Care of a patient with a nasal bridle
Clean and dry the nasal bridle tape at least daily with soap and water/disposable wipes. This may need to be done more frequently if there are excessive secretions from the nose. Any tape securing the NG tube and/or tape should be replaced as required. The nasal mucosa should be frequently observed for signs of irritation or bleeding. Oral hygiene should be provided as required.
3.15.5 Removal of the bridle
The bridle can remain in place for the entire duration of the feeding tube When removal is required, simply cut one side of the tape (between the nose and the clip) and gently pull the bridle through the nose taking great care not to remove the feeding tube. More often both the feeding tube and the bridle are removed at
the same time.
3.16 Training and Competency 3.16.1 All healthcare professionals must ensure that, if involved with a nasogastric tube for insertion and positional verification, they have been assessed via both theoretical and practical training. 3.16.2 All staff (medical and nursing) must complete the essential job related NG competency package; this requires attendance at an NG insertion and verification training workshop (includes a presentation, practical demonstration followed by a practical assessment NPSA/2011/PSA002) where they will be instructed in the documentation and the assessment process and the need to maintain their own knowledge base. The session is facilitated by the Learning and Organisational department and can be booked by trust staff via the training bulletin. 3.16.3 For the foundation trainees the nasogastric training is embedded into their training programme and records of completion are held within the foundation office, PGME Department. They must also complete a nasogastric e-learning package “Reducing the risk of feeding through a misplaced nasogastric tube”. This can be accessed via the trusts intranet or via the e-learning department. A copy of completion of this must be provided to the programme lead within PGME. 3.16.4 The competency log must be signed as completed by the designated assessor/facilitator and attendance of the workshop will be maintained within the Electronic Staff Records (ESR). It is the individual practitioners’ responsibility to ensure that they are trained and assessed and this will be monitored via the

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 27 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
ward/unit manager and the ward based nutritional link nurses. Staff that have reduced exposure to NG insertion and management or require a refresher to reassure competencies should book onto one of the available nasogastric tube workshops as required.
3.17 Accreditation of Prior Experience Learning (RPEL) Staff new to the organisation that feel competent to complete this clinical skill based upon training and experience gained in a different Trust, must discuss this with the work based assessor from their area and contact the L&OD programme coordinator to discuss APEL to agree how this learning will be recorded within Electronic Staff Records (ESR). This may include completing the Trust under pinning knowledge booklet, a summative workplace assessment or attending the course.
4. What do I need to do?
As a clinician managing nasogastric/orogastric feeding tubes you must read and follow this policy. You must attend training every two years on insertion and verification on Nasogastric/orogastric tubes.
4.1 The Artificial Nutritional Steering Group is responsible for:
Updating this policy
Auditing the policy standards
Educating staff with respect to this policy via nasogastric insertion and verification sessions and e learning.
Liaising with the ward nutritional link nurses
Training at ward level if requested 4.1.2 Dissemination of the updated policy to all Trust staff will be via the Care
organisations.The Clinical Skills Trainer (L&OD) will provide training and training statistics regarding attendance and completion records etc. Ward managers will identify training needs with regards to the insertion and post insertion care of a nasogastric tube for staff in their clinical areas via the appraisal process identified through the essential job related pathway.
4.1.3 Pennine Acute NHS Trust is committed to ensuring that the practitioner is supported in this learning process though teaching and assessment to meet NPSA recommendations.
4.1.4 It is the responsibility of all staff and carers involved in the insertion and post insertion care of nasogastric tubes to ensure they are able to maintain the practice of insertion and management of the Nasogastric tube.

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 28 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
5. Abbreviations & Definitions of terms used
AMT Applied Medical Technology
ANTT Aseptic Non Touch Technique
BAPEN British Association for Enteral and Parenteral Nutrition
BMI Body Mass Index
EBME Electro Bio-Medical Engineering
ETF Enteral Tube Feeding
FR French Gauge
GI Gastro Intestinal
HEF Home Enteral Feeding
HETF Home Enteral Tube Feeding
NEX Nose Earlobe Xiphisternum
NG Nasogastric
NICE National Institute for Health and Clinical Excellence
NJ Nasojejunal
NPSA National Patient Safety Agency
OG Orogastric
pH Potential or Power of Hydrogen
PPE Personal Protective Equipment
PPI Proton Pump Inhibitor
6. References and Bibliography
1.1 Supporting References
Anderson MR, O’Connor M, Mayer P, Mahoney D et al (2004). The nasal loop provides an alternative to Percutaneous Endoscopic Gastrostomy in high-risk dysphagia stroke patients. Clinical Nutrition; 23(4): 501-506.
British Association for Parenteral and Enteral Nutrition. (2003) Administering drugs via enteral feeding tubes – a practical guide. London: BAPEN
DeLegge M H (2016) Gastrostomy tubes: Uses, patient selection and efficacy in adults. www.uptodate.com
Johnston RD, O’Dell L, Patrick M et al (2008). Outcome of patients fed via a nasogastric tube retained with a bridle loop: do bridle loops reduce the requirement for percutaneous endoscopic gastrostomy and 30-day mortality. Proceedings ofthe Nutrition Society; 67: E116

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes CPIC006 Version V1.1
Page 29 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Mallett J, Doherty L (2015) The Royal Marsden Hospital Manual of Clinical Nursing Procedures (9th Edition). Blackwell Science. National Nurses Nutritional Group (2012) Good Practice Guideline – Safe Insertion of Nasogastric (NG) Feeding Tubes in Adults: www.nnng.org.uk National Patient Safety Agency (2005) and (2011) Reducing the harm caused by misplaced nasogastric tubes. Department of Health, London. National Institute for Clinical Excellence. (2017) Healthcare associated infections prevention and control in primary and community care, CG139 www.nice.org.uk Rowley S (2001) Aseptic Non Touch Technique, Nursing Times 97 (7) (Infection Control Supplement) 6-8 Shipley K, Gallo M-A, Fields W (2006) Is your Feeding Tube Clogged? Maintenance of Gastrostomy and Gastrojejunostomy Tubes. Medsurg Nursing; Pitman 25.4 p.224-228.
Smith R; Myers SA (2005) Devices that unclog feeding tubes. RN, Jan 2005; vol.68 (no.1); p.36-43

Pennine Acute Hospitals NHS Trust Policy Management of Adult Nasogastric/Orogastric Feeding and Drainage Tubes
Page 30 of 42 It is your responsibility to check that this print out is the most up-to-date version of this document
Check on the Document Management System available via the Trust Intranet
Appendix 1 – Equality Impact Assessment
To be completed by the Lead Author (or a delegated staff member)
For each of the Protected Characteristics & equality & diversity streams listed answer the questions below using
Y to indicate yes and
N to indicate no:
Ag
e
Dis
ab
ilit
y
Eth
nic
ity
/
Ra
ce
Ge
nd
er
Ge
nd
er
Re
as
sig
nm
en
t
Ma
rria
ge
&
Civ
il
Pa
rtn
ers
hip
Pre
gn
an
cy &
Ma
tern
ity
Re
lig
ion
/belief
S
exu
al
ori
en
tati
on
Hu
ma
n R
igh
ts
Ca
rers
Please explain your justification
1. Does the practice covered have the potential to affect individuals or communities differently or disproportionately, either positively or negatively (including discrimination)?
N N N N N N N N N N N This policy is for adult patients only and currently does not cover Neonates or Paediatric patients.
2. Is there potential for, or evidence that, the proposed practice will promote equality of opportunity for all and promote good relations with different groups?
Y Y Y Y Y Y Y Y Y Y Y This policy is for adult patients only and currently does not cover Neonates or Paediatric patients.
3. Is there public concern (including media, academic, voluntary or sector specific interest) in the document about actual, perceived or potential discrimination about a particular community?
N N N N N N N N N N N
Your Name: Dr Howard J Klass
Your Designation: Consultant Gastroenterologist
Signed*:
Date: 12.05.2017
To be completed by the relevant Equality Champion following satisfactory completion & discussion of answers above with author
Equality Champion: Naheed Nazir
Directorate: Workforce &OD
Signed*:
Date: 12th may 2017
*Please scan or insert electronic signature

Pennine Acute Hospitals NHS Trust
Page 31 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix -2- Common Indications
Common indications for enteral tube feeding
Indication for enteral tube feeding
Example
Unconscious patient
Head injury, ventilated patient
Neurological swallowing disorder
Post-CVA, multiple sclerosis, motor neurone disease, Parkinson’s disease
Physiological anorexia
Cancer, sepsis, liver disease, HIV
Upper GI obstruction Oro-pharyngeal or oesophageal stricture or tumour
GI dysfunction or malabsorption
Dysmotility, inflammatory bowel disease, reduced bowel length (although PN may also be needed)
Increased nutritional requirement
Cystic fibrosis, burns
Psychological problems
Severe depression or anorexia nervosa
Specific treatment Inflammatory bowel disease, for short term enteral access during surgery i.e. head and neck cancer
Dementia Usually not appropriate but each case should be considered on its merits.

Pennine Acute Hospitals NHS Trust
Page 32 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix -3- Nasogastric or Orogastric Tube Checklist Patient name: ................................. Hospital number: ........................... Ward: ................ Site: ..........................
Nasogastric/orogastric tube verification - complete each column for each insertion/reinsertion
Date
Time
NEX measurement - place exit port of tube at tip of nose. Extend tube to earlobe, and then to xiphisternum
External length once secured
Nostril used on insertion/reinsertion Left / Right Left / Right Left / Right Left / Right Left / Right
Aspirate obtained? Yes / No Yes / No Yes / No Yes / No Yes / No
pH of aspirate on insertion
X-ray required - sticker should be completed in notes
Yes / No Yes / No Yes / No Yes / No Yes / No
Signature
Print name
Gastric acid inhibitor prescribed: Yes / No Type: ..................................
Times of administration: ..................................................................................
pH Monitoring
Date
Time aspirate checked
Time feeding stopped before aspirate check
pH of aspirate
External tube length
Signature
Print name
Complete a NG Tube Insertion Risk Assessment and place this sticker in the medical notes. Do not use the nasogastric tube until the position has been confirmed. The position should be checked: Following initial insertion
When there is a suspicion of tube displacement
Following episodes of vomiting, retching or coughing spasms
Before administering each feed/medication and at least once daily during continuous feed
When there are any new or unexplained respiratory symptoms or if oxygen saturations decrease
When checking tube position, pH indicator strips must be CE marked. pH should be 5.5 or less. If the pH is 5.5 it should be re-checked by another nurse
If you are unable to obtain aspirate, follow actions in the Nasogastric Tube Policy – chapter 3.10.1 Troubleshooting. Do not start feed until the position of the tube has been confirmed and documented on a NG Tube Verification sticker

Pennine Acute Hospitals NHS Trust
Page 33 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix -4- Care Plan for NG/OG tubes
NAME HOSPITAL No WARD
SITE CONSULTANT
CARE PLAN - NASOGASTRIC OR OROGASTRIC TUBE
ALL ENTRIES MADE BY UNQUALIFIED STAFF MUST BE CHECKED AND COUNTERSIGNED BY A QUALIFIED NURSE
DATE / TIME NEEDS / GOALS ACTIONS SIGNATURE REVIEW DATE
NEED: The patient requires a nasogastric or orogastric tube for feeding GOAL: To ensure safe administration of enteral feed via a nasogastric or orogastric tube
Initial care:
A) Follow nursing procedure for placing a nasogastric tube and complete Nasogastric or Orogastric Tube Checklist (including use of Nasogastric Tube Risk Assessment and NG Tube Verification stickers)
B) Commence feeding following the regimen provided by the dietitian
C) If the patient is not known to the dietitian, complete an online referral. Date referred: .....................................
If the dietitian is not available, use the Out of Hours Enteral Feeding Starter Regimen (http://nww.pat.nhs.uk/clinical-departments/Nursing-Documentation/nutrition---ward-documents.htm)
Ongoing care:
D) Check gastric aspirates at the frequency recommended on the Nasogastric or Orogastric Tube Checklist and record the pH and external tube length on the checklist
E) Use ANTT procedures when setting up feed. Use sterile water for all flushes
F) Ensure the patient is not lying flat. The patient’s head and shoulders should be elevated to at least 30
o during feeding
and for at least one hour after the feed has been discontinued
G) Flush the tube with 50mls sterile water using a 50 ml purple oral/enteral syringe - after aspiration of the tube, before starting feed, at each bag change, at the end of the feed and before and after medication
H) Additional water may be required due to warm weather, pyrexia or diarrhoea. Discuss how much with medical staff and dietitian. Administer this as regular boluses throughout the day
I) Discard any unused feed. Change giving sets with each bag change or if the patient is disconnected from the feed
J) Consult the ward pharmacist regarding suitability and method of administering medication via a nasogastric tube
K) Stop the feed if any clinical signs of reflux, vomiting or aspiration. Consult with doctor
Monitoring:
L) Document all feed and fluid given on a Fluid Balance Chart
M) Complete a Stool Chart
N) If the patient is eating and drinking, complete the Food and Drink Record Chart
O) If the patient has diabetes, monitor blood glucose on the Blood Glucose Monitoring - Best Practice Document

Pennine Acute Hospitals NHS Trust
Page 34 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
P) Weigh the patient at least once a week. Document on the Weight Record Chart and/or MUST as appropriate

Pennine Acute Hospitals NHS Trust
Page 35 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix -5- Procedure: Insertion and management of AMT Bridle™ System
(Nasal bridal from Applied Medical Technology)
Equipment 1 AMT nasal bridle of appropriate size
2 Water-based lubricant gel (single use sachet)
3 Scissors
4 Clean trolley or tray
5 Disposable apron and gloves (ANTT - assess for sterile / non sterile gloves, if the `key parts` need to be touched need sterile gloves)
6 Indelible pen.
Procedure (Note: the product literature includes pictures to aid this procedure)
Action Rationale
1 Explain the procedure to the patient and obtain his / her consent (where capacity exists)
To help reduce anxieties and enable the patient to cooperate
2 Prepare the environment
To maintain privacy and dignity
3 Wash and dry hands using seven step hand cleansing technique and put on disposable apron and gloves
To minimise the risk of infection
4 Prepare the required equipment and place within easy reach
To facilitate the procedure
5 Position the patient in the supine position if possible
To facilitate easy insertion
6 Generously lubricate both ends of the insertion probes
To ensure smooth insertion into nasal passages
7 Insert the retrieving probe (blue) into one nostril until the first rib is at the bottom of the nostril (2/3 rds of the way in). Insert the bridle catheter (white with a guide wire) into the opposite nostril. An audible click signifies contact between the magnets which may or may not be tactilely felt. If necessary gently move the retrieving probe from side to side and/or up and down to encourage contact between the magnets. If no contact has occurred, then advance both the bridle catheter and the retrieving probe to the second (paired) rib
To ensure contact between two magnetic probes
8 Once contact has occurred, remove the stylet/ guide wire from the bridle catheter. Slowly withdraw the retrieving probe while allowing the bridle tape to advance in to the nose - continue until only the tape is in the nose.
To enable nasal tape to be brought through both nostrils

Pennine Acute Hospitals NHS Trust
Page 36 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
If the tape does not come out of the opposite nostril, start over at step 7 after reinserting the guide wire
9 Using scissors cut the bridle insertion catheter off the tape, leaving only the tape in the nose. Dispose of both catheter tube and probe. If the feeding tube has not already been inserted it should be inserted and its position verified now
To prepare tape to be secured to feeding tube
10 Select the correct size retaining clip for the feeding tube. Lay both ends of the tape in the clip’s deep channel near the tip of the nose Note: Both ends of the tape must be placed in the clip prior to the feeding tube Snap the feeding tube into the deep channel on top of the tape. The clip should be positioned just beyond the tip of the nose, so that it will rest on the upper lip when released
To ensure the tape and feeding tube are placed inside the clip
11 Fold the two halves of the clip together and press tightly until the clip snaps shut Note: the clip cannot reopen after closing so ensure proper position of the tape and feeding tube prior to closure Also some feeding tubes are more rigid than others so a higher force may be required to close the clip
To ensure NG tube, tape and clamp are all secure
12 Ensure the clip is fully closed by gently pulling both ends of the tape away from the feeding tube – if the clip reopens go back to step 10 and repeat
To test the security of the clip
13 After the clip has been fully closed, tie the two tape ends together underneath the tube in a simple knot. The excess length of the tape may then be trimmed as desired using the scissors
To ensure excess tape is secure
14 Mark the feeding tube (with the indelible pen) where it enters the nose so that any change in its position can be noted
To monitor tube position
15 Dispose of used equipment appropriately and decontaminate hands using seven stage method
To maintain the safety of all staff and patients and to reduce infection risks
16 Document the procedure in the patient’s careplan.
To ensure accurate documentation.
Note: if the available clip/bridle is not the right size for the feeding tube that is already in situ it is still possible to use the bridle – simply ignore steps 10 – 12 and tie the tape underneath the nasal septum leaving a small gap to prevent nasal erosion. Tie the excess tape onto the feeding tube and use hypoallergenic tape to secure it to the tube.

Pennine Acute Hospitals NHS Trust
Page 37 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix - 5-
Proforma for Insertion and management of AMT Bridle™ System This form must be completed for all patients BEFORE the bridle is inserted
Patient Name
Ward
Hospital Number
Site
Responsible Consultant
Consideration of need for NGT/bridle YES NO
Is the NGT essential for this patient’s treatment?
Has NGT insertion risk assessment ‘sticker’ been completed?
Has the patient pulled out/removed at least two tubes? How many times?
Have other attempts to secure the tube been attempted/optimised? Eg. mittens and patient watch been adhered to
Has any agitation/confusion/restlessness been investigated and treated accordingly?
Was the NGT difficult to place - requiring endoscopic or radiological guidance?
Is there the possibility of a basal skull fracture or are there any structural deformities of the nose/nasopharynx?
Does the patient have capacity to consent to this treatment?
Is the patient able to understand information relevant to the decision?
Is the patient able to retain the information?
Is the patient able to use the information as part of the process of making a decision
Has the patient been given the best possible opportunity of making their own decisions?
Is the patient able to communicate their decision
If patient has capacity - do they consent to insertion of bridle?
If patient does NOT have capacity, does the responsible consultant/registrar believe it is in the patient’s best interests to have a nasal bridle inserted?
Has the Trust Safeguarding team been informed? (May need to consider best interests meeting/IMCA) and seek a DOL’s authorisation.
Has the next of kin been informed – if so who?
Responsible Consultant/Registrar name/signature
Nurse in charge name / signature
Date/time
Date/time when bridle removed

Pennine Acute Hospitals NHS Trust
Page 38 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix - 6- Medicines Advice (to be read in conjunction with the Trusts Medicine Policy EDC018)
Administering drugs via feeding tubes increases the risk of tube blockage. Before administering medication, the feed should be stopped. The tube should be flushed with at least 30ml sterile water before and after administration of medication to prevent interaction between the drug and feed.
If more than one drug is required they should be given separately with 10ml flushes between to prevent interactions between the drugs.
Administration of medications via a feeding tube and especially the flushes required may be difficult in patients whose fluid intake is restricted. Ward staff should liaise with the ward pharmacist and dietitian to ensure optimum care. Crushing tablets/Opening capsule: This practice is almost always outside the product licence. This means that the manufacturer will not take any responsibility for any adverse effects that may occur as a result. For this reason, tablets should be crushed/capsules opened only when there is no suitable liquid or dispersible alternative available, and only if it is pharmaceutically appropriate to do so. Prescribers must be made aware that the drug is being administered in an off-license manner, as they will take responsibility for its use. If tablets are to be crushed then they should be crushed to a fine powder using a tablet crusher and then dissolved in a suitable liquid (pharmacy should advise). Ensuring no sedimentation is present and well enough to prevent clogging of the tube. It is also important to ensure that the whole dose is delivered, i.e. by flushing the tablet crusher of any residual powder. An example of when it is not appropriate is when the tablets are modified release (MR/SR/LA/XL). Such products are designed to release the drug over a controlled period of time. Crushing them could therefore risk too much drug being released at once, which could lead to adverse drug reactions. Conversion to a standard release product is usually necessary, and this will often involve an alteration in dose, therefore the doctors would need to review the prescription before anything is administered. Enteric coated tablets are also usually unsuitable for administration via enteral feeding tube as the coating is designed to prevent stomach irritation and improve absorption. The coating may also block enteral tubes
Some tablets are film or sugar coated. These can usually be crushed, but the coating may make this difficult. It is important to ensure the coating is well broken up and the tube is flushed well after use to prevent the coating blocking the tube.
Buccal/sublingual tablets should NOT be crushed and given via enteral tube. The bioavailability of drugs given buccally/sublingually is different from when they are given orally/enterally, therefore the doses are NOT the same and under treatment will occur if given by the enteral tube.
Cytotoxic tablets should be handled with great care. If any of the patient’s medications are cytotoxic, the nurse must contact pharmacy for advice (Risk of exposure from the powered drug).
If there is ever any doubt as to whether a drug is suitable for tube administration, the nurse should contact pharmacy for advice. The ward pharmacist is the first port of call, but otherwise Medicines Information will be more than willing to assist.
Mixing crushed tablets: This must NOT occur. Drugs are more likely to interact with each other if mixed together directly, particularly after tablet crushing. Also, if the tube becomes blocked it may be difficult to determine how much of each dose has been given. All drugs should be administered separately, and the tube flushed in between each one. Some liquid medications (elixirs, emulsions and suspensions) are viscous and can increase the risk of tube blockage. (Pharmacy should advise on dilution with a suitable liquid)
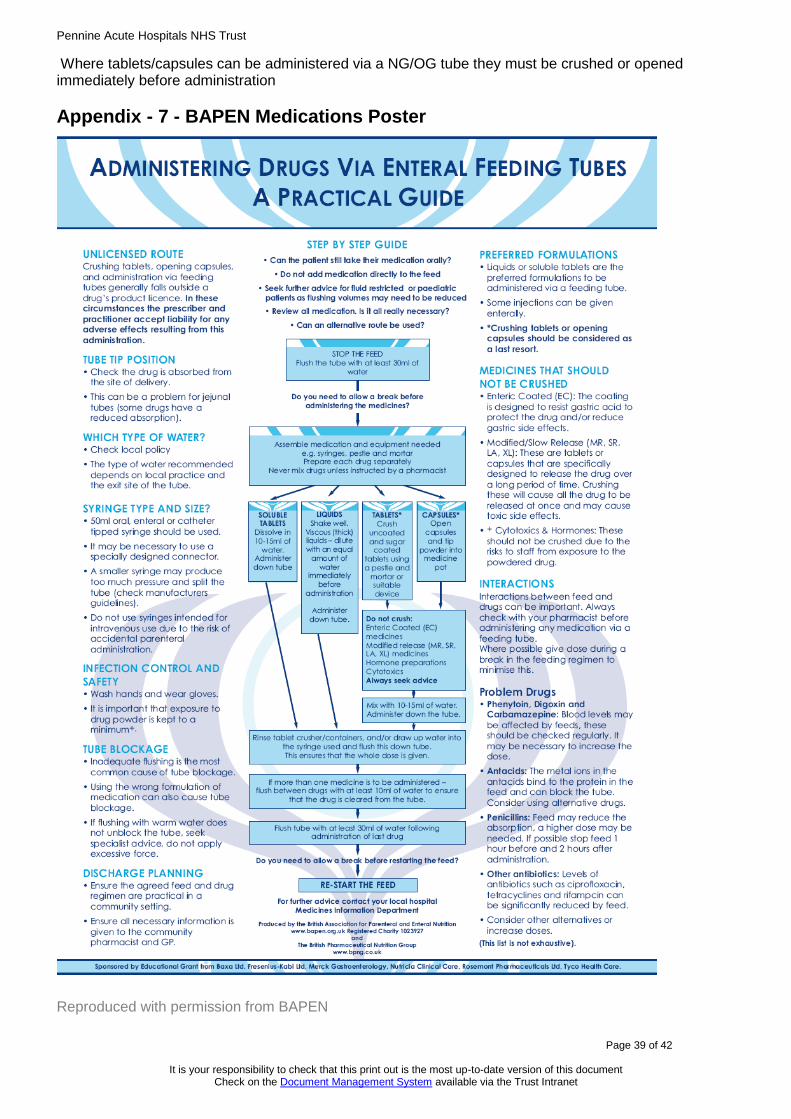
Pennine Acute Hospitals NHS Trust
Page 39 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Where tablets/capsules can be administered via a NG/OG tube they must be crushed or opened immediately before administration
Appendix - 7 - BAPEN Medications Poster
Reproduced with permission from BAPEN

Pennine Acute Hospitals NHS Trust
Page 40 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix -8-Nasogastric/Nasojejunal Tube Feeding - Discharge Checklist for Ward Staff
Patient’s name: ............................................ Hospital No: ........................... Date of birth: ....................
EDD: .................................. Type of tube: ................................
1. For patient going to own/carer’s home requiring district nurse input: Nurse has contacted district nurse regarding feed start and finish times, medication administration via feeding tube and for Rochdale discharges only - provision of syringes. Yes N/A
For patient going to nursing home: Nurse has checked that nursing home staff are familiar with the tube feeding procedures required for this patient. Nurse has informed dietitian if nursing home require training.
Yes N/A Date ...………………..
Patient’s name: ……………………… Hospital No:……..……… Date of birth:………………..
2. For patient/carers who will be self-caring with tube feed at home: Training should be provided by nursing staff as early as possible.
Looking after the feeding tube Training
date
Signature of ward nurse
Securing the tube, skincare Check daily, change fixation device if loose or soiled
Confirming tube position (Nasogastric tube only) Tube length, gastric aspirate pH and when to check. If unable to obtain gastric aspirate or gastric aspirate is 5.5. or above - phone emergency number in Home Enteral Feeding discharge pack provided by dietitian
Flushing the tube At least 30ml water before and after feed, using 50ml purple enteral syringe
Unblocking the tube Push-pull water flushing technique, gently massage the tube with a warm cloth, if the blockage is seen
Preparing to feed
Correct positioning for feeding Head and shoulders elevated to at least 30 degrees
Hand washing and clean handling of feed and equipment
Storing feed safely, checking expiry date, shaking bottle gently prior to use
Feeding via the pump and by bolus
Attaching the pump to the stand
Setting the feed rate/dose
Pump features and cleaning
Connecting and disconnecting the feed to the giving set, and the giving set to the pump
Hanging feed no longer than 24 hours, changing giving set at least 24 hours
Administering a bolus feed

Pennine Acute Hospitals NHS Trust
Page 41 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
General care Training
date
Signature of ward nurse
Administering medication via the tube. Each medication prepared and given separately. At least 30ml water flush at start and finish, 10ml flush in between each medication, using 50ml purple enteral syringe
Mouth care / nasal care
Recognising potential problems and actions required e.g. nausea, vomiting, abdominal pain, chest pain, breathing difficulties
Signature of patient / carer to confirm competency:
Carers name:
Date: .................................................
3. For all patients - the items listed below should be supplied at discharge
Supplies required at home Ward to provide Dietitian to provide
7* day supply of feed Yes / No Yes / No
7* day supply of giving sets Yes / No Yes / No
7* day supply of 50ml purple enteral feeding syringes (compatible with tube)
Yes (1 per bolus feed) -
pH indicator strips Yes / N/A -
Feeding pump - Yes / N/A
Pump stand - Yes / N/A
Home Enteral Feeding discharge pack with feeding regimen, contact numbers for tube emergencies etc
No Yes
* provide 10 day supply if close to a Bank Holiday.
Name Signature Designation

Pennine Acute Hospitals NHS Trust
Page 42 of 42
It is your responsibility to check that this print out is the most up-to-date version of this document Check on the Document Management System available via the Trust Intranet
Appendix - 9 Community Management of Adult Nasogastric/Orogastric Feeding Tubes. This appendix highlights areas of practice with NG/OG feeding which may differ in the PAT community setting, and should be read in conjunction with the full body of the policy. With reference to section:
3.4.1 Infection Control Any handling of the nasogastric tube should be kept to a minimum and should be carried out utilising ANTT (Aseptic Non-Touch Technique) (Rowley, 2001). In the community a sterile dressings pack maybe used rather than an ANTT pack. Not all feeding equipment in the community will be single-use, for example some enteral syringes will be multiuse. For all community feeding equipment you should refer to the manufacturer’s guidance as to their usage and how to clean and decontaminate correctly. Current guidance (BDA, NICE, PENG) does not endorse the practice of putting blended diet or beverages down artificial feeding tubes as this practice carries a number of infection control risks. Where patients/carers choose to use a blended diet, either with or without commercial tube formulations, a risk assessment should be completed by the multidisciplinary team to aid safe practice guidance and indicate points of risk to consider. Please refer to the community policy “Blended food down feeding tubes” currently in development.
3.7 Initiating Feeding All patients with a nasogastric/orogastric tube must be referred to the community dietitian for ongoing monitoring and management of artificial feeding. An enteral feeding regimen will be provided by the hospital dietitian on discharge, this should be used to continue feeding until the first community dietitian review.
3.8.8 Tube Flushing The tube should be flushed with at least 30mls of water - ‘cool boiled’ water rather than sterile water is recommended in the community setting.
3.9 Ancillary items If a patient is admitted to hospital with their own supply of ancillary items ie: non-single use syringes, these should not be used within the hospital setting. On discharge a patient will be provided with 7 days’ supply of feed and ancillary items for use before the first homecare delivery of equipment (over longer public holidays such as Christmas a larger supply maybe agreed). After this, on-going supplies of items for tube feeding will be ordered through the Homecare company and delivered directly to the patients home or via the patient’s local pharmacy - the homecare set up will be arranged by the community dietitian services. In some community areas the only ancillary items provided by the homecare company will be the giving sets and feed, other equipment (for example spare tubes, pH testing strips or syringes) will be supplied by the district nursing services (this will depend on local agreements).