
The Kinetics of Liberatory Pedagogy: An Exploratory Narrative ...
Upload
independentCategory
view
5download
0
IntroductionTwo of the greatest problems encountered in
acupuncture research relate to difficulties choosing
appropriate controls, and uncertainties about the
stimulation strength of different acupuncture
techniques. ‘Sham’ points or minimally invasive
techniques are often used as controls in randomised
controlled trials (RCTs), yet it is accepted that both
suffer inherent problems, not the least of which
being the assumption that they have no, or at least
minimal, effect. It is recognised that sham points
may have a physiological effect, may induce the
subjective needling sensation (de qi), and may
produce an overt clinical outcome. Araujo concludes
that ‘sham’ acupuncture appears almost as active
as ‘real’ acupuncture.1 This conclusion is
strengthened by functional magnetic resonance
(fMRI) studies, such as that by Wu et al.2 While
some researchers have found substantial effects
from sham acupuncture, other studies have found no
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.166 www.acupunctureinmedicine.org.uk/volindex.php
Papers
Point injection as an alternative acupuncturetechnique – an exploratory study of responses in healthy subjectsMark W Strudwick, Roderick C Hinks, S T Boris Choy
Mark W Strudwickresearch officerCentre for MagneticResonanceUniversity ofQueenslandSt Lucia Brisbane,Australia
Roderick C Hinkshead of faculty(acupuncture)Australian College ofNatural MedicineFortitude ValleyBrisbane, Australia
S T Boris ChoylecturerDepartment ofMathematical SciencesUniversity ofTechnology SydneySydney, Australia
Correspondence:Mark W Strudwick
AbstractIntroduction Point injection as a therapeutic technique is well documented, but its physiological effects
have not been formally compared with traditional acupuncture. One aim of this study was to compare the effects
of the two techniques at one acupuncture point, as a step towards understanding the mode of action of point
injection and validating its clinical use. A second aim was to explore whether repeated point injection at the
same site might provide a way of increasing the dose of stimulation, in the hope of identifying a dose response
curve which could be an alternative strategy to placebo control in demonstrating the biological effects of
acupuncture.
Methods Sixty nine healthy subjects (age range 18-56 years, mean 29.9; 48 females) completed the study, which
employed a counterbalanced experimental design with two stimulation sessions of LI4 approximately one week
apart. One half of the participants received point injection first, and the other half received traditional
acupuncture first. Baseline physiological data were recorded, then measurements were made before, during
and after stimulation; each subject also reported needle sensation (de qi). The measures were heart rate,
derived pressure rate product and mean arterial pressure.
Results Although stronger sensations of de qi were reported with point injection, no significant differences
were found for mean heart rate (HR), pressure rate product (PRP) and mean arterial pressure (MAP) before
and after stimulation by the two techniques. No subject gender or age bias was encountered and previous
exposure to acupuncture had no effect on outcome. Power spectral analysis of heart rate variability (HRV) made
on data from a small subset (n=10) of this cohort also showed no significant differences in autonomic
response.
Conclusion Point injection and traditional acupuncture seem to provoke similar physiological responses,
although the greater needle sensation seen with point injection might indicate it could have more powerful
clinical effects. Further studies of repeated point injection are necessary to indicate whether this technique may
provide a method of increased strength of point stimulation, as an alternative to traditional needling in
acupuncture research.
KeywordsAcupuncture, point injection, physiology, heart rate, mean arterial pressure, de qi.
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 166
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from

effects.3 Vincent concludes that the results of RCTs
using sham points as controls only show the
difference between sham and real acupuncture, not
the real effect of acupuncture.4 In light of this, the
conclusion reached by Ryan that acupuncture
researchers should cease using sham acupuncture
as a control in trials seems valid.5 Even the newer
Streitberger placebo needle has been demonstrated
to have shortcomings.6 Minimal acupuncture is
designed to produce just that – minimal effect. Yet,
this method may also produce distinct subjective
and objective effects, as noted by White et al.7
Marcus postulates that the effect of acupuncture is
the result of several factors that are operative during,
and very shortly after, the initial skin penetration:8
1) manipulation for longer than five seconds does
not appear to increase stimulus strength since the
initial tissue damage caused by skin penetration
leads to the release of inflammatory mediators that
sensitise local nerve endings; 2) the acupuncture
effect is a direct result of a cone of tissue damage
proportional to the depth of needling and the
diameter of the needle, this damage regulating the
dose of inflammatory mediators released; 3) the
needle may also cause direct nerve and muscle
stimulation. Skin penetration also induces
microcurrents that may have a local effect. 9 These
latter two mechanisms occur during the initial
penetration and settle quickly thereafter.
Acupuncture point injection (PI) of a small
amount of a drug, vitamin, saline, or plant extract is
a recent innovation of traditional acupuncture that
aims to enhance and prolong the effect of stimulation
of acupuncture points.10 One suggested advantage
of this technique is that it offers the opportunity to
standardise and replicate treatment, which is difficult
to achieve with classic acupuncture. PI is well
documented, and many standard texts contain
references to the use of PI.11-14 A PubMed search of
<acupuncture AND point injection> produced more
than 100 references, the earliest (reporting the
treatment of acute appendicitis by distilled water
injection to an acupuncture point) having been
published in Chinese in 1960.15 Belitskaia et al
concluded that the clinical response to PI was due
to the specificity of acupuncture stimulation by the
introduction of fluid, and not the composition of the
fluid itself.16 Yang and colleagues demonstrated that
PI to PC6 (Neiguan) controlled post surgical
vomiting, and thus lent support to the suggestion
that PI is simple, convenient, timesaving and
effective.17 We suggest that PI offers the opportunity
to titrate the dose of saline injected into an
acupuncture point, thus increasing the stimulus in a
controlled and measurable manner. Identifying a
dose response curve for acupuncture could be an
alternative strategy to comparing acupuncture with
‘placebo’ in the demonstration of biological effects of
acupuncture. One aim of this study, therefore, was to
explore the effects of titrated injections.
To date, the physiological effects of PI have not
been compared with those of traditional acupuncture
(TA). A comparison of the effects of two methods
applied at the same acupuncture point is a first step
in investigating PI and validating the technique for
clinical use. Previous studies of the physiological
response to acupuncture have used, in part, heart rate
(HR) and non-invasive (measurement of) blood
pressure (NIBP).18-21 Others have used invasive
measures such as microelectrode implant in muscle
or repeated blood sampling. Ballegaard also used
the derived pressure rate product (PRP) as an
outcome measure of cardiac workload, which Wright
et al had demonstrated to be a sensitive assessment
for even small cardiac workloads.22 The main aim
of this study, therefore, was to compare the
physiological responses to PI and TA, using non-
invasive measures (HR, MAP, and PRP) along with
self reported sensation of de qi, to facilitate a
comparison with published data.
MethodsVolunteers
An initial sample size calculation determined that
we would need a minimum of 63 subjects (assuming
a 50% difference between groups, with a power of
0.8, and 95% confidence level). With the approval of
the Human Research Ethics Committees of the
University of Queensland (UQ) and Australian
College of Natural Medicine (ACNM), 75 healthy
subjects were initially recruited. Healthy subjects
were chosen, as this was a laboratory study and not
a clinical trial. All gave written informed consent.
None had a history of psychiatric or neurological
disorders or head trauma with loss of consciousness.
Sixty nine (48 female) aged between 18 and 56 (mean
29.9) completed the study. Of these, 59 had
experienced acupuncture previously (they were either
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.www.acupunctureinmedicine.org.uk/volindex.php 167
Papers
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 167
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from

students or faculty in acupuncture school) and 10
were naïve to acupuncture.
Procedure
A counterbalanced experimental design was
employed to avoid order effects. Volunteers were
randomly assigned to one of two groups, the first
group received TA in the first session and PI in the
second, this being reversed for the second group.
Sessions were scheduled one week apart to allow
for washout of any effects. Prior to enrolment in the
study, personal details were collected. Physiologic
data (resting HR, NIBP, and respiration rate) were
obtained before entering the laboratory. These
parameters, as well as peripheral oxygen saturation
(SpO2) were then measured 10 minutes before and 10
minutes after point stimulation. During the
intervention, these parameters were measured
continuously at 2.5 second intervals. After each
session, volunteers scored their experience of the
stimulation (pain on insertion, pain at needle site, de
qi, and any unpleasant feeling) on an 11-point
numerical scale, where 0 signified no noticeable
sensation and 10 signified maximum tolerable
sensation. De qi was defined as any one of numbness,
heaviness, distension, soreness at the point, spreading
away from the point with time, or other sensation
that the subject may have related to the acupuncture
point stimulation.23
The laboratory was controlled for temperature
and humidity and each session was conducted at
approximately the same time of day and week for
each volunteer. During each session, the volunteer
rested comfortably on a standard treatment couch
facing away from the investigator and monitoring
apparatus.
Stimulation
The acupuncture point LI4 (Hegu), situated on the
dorsum of the left hand between the first and second
metacarpals at the midpoint of the second metacarpal
bone close to its radial border, was chosen for this
study. Being easy to identify and having only
pregnancy or possible pregnancy as its only described
traditional contraindication, it is one of the most
commonly studied points.12 As this study was
intended to compare two methods of acupuncture
point stimulation, it was appropriate to use only one
acupuncture point and not use a control point. An
acupuncturist with 30 years’ experience in traditional
needling techniques and four years’ experience in
PI (MWS) performed all stimulations. The selected
needle – either a solid 0.35 x 13mm sterile, single
use needle (Cathay Herbal Laboratories, Sydney,
2010, Australia) for TA or a hollow 0.50 x 16mm
sterile, single use hypodermic needle (Terumo Corp,
Elkton, MD, 21921, USA) for PI – was inserted to a
depth of 13mm.
At 30 seconds after needle insertion, LI4 was
stimulated for one second by needle rotation at 3Hz
(TA intervention) or by infusion of 0.5ml normal
physiological saline (PI intervention) repeated at 30
second intervals for five stimulation periods, a total
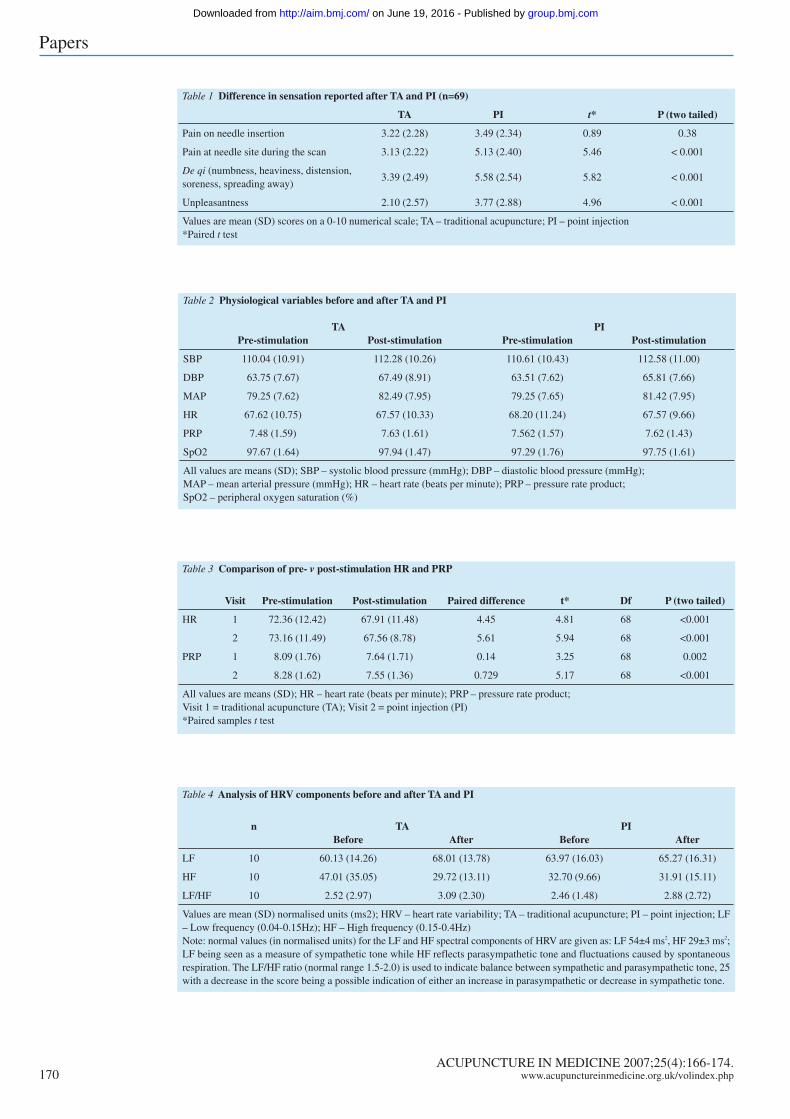
intervention time of 180 seconds (see Figure 1). A
purpose built, computer controlled syringe driver
(Figure 2) was used to perform precise saline
infusion; the fluid delivery line was connected by 3
way tap to a Baxter Uniflow pressure transducer
(Baxter Healthcare Corp, Irvine, CA) allowing
measurement and recording of intra acupuncture
point pressure at 2.5 second intervals, simultaneously
with the HR and SpO2 recordings. The
instrumentation has been previously reported.24
Heart rate variability (HRV)
Towards the end of the study, a recording
electrocardiograph (PowerLab 5, ADInstruments Pty
Ltd) became available. During both intervention
sessions, a subset (n=10) of the enrolled cohort
underwent continuous electrocardiograph (ECG)
recording from limb leads (I, II, or III) for later
analysis of HRV, with the aim of monitoring any
modulation of the autonomic nervous system (ANS)
activity resulting from acupuncture stimulation.25
Statistical analysis
Data were analysed with SPSS (Macintosh Version
11.0.4, SPSS Inc). Using paired samples t tests at a
significance level of 0.05 to determine any significant
differences between the baseline and endpoint of the
experiment, comparative analyses were made of self
reported de qi sensation, MAP, HR, and derived PRP,
all measured before and after stimulation. Repeated
measures ANOVA of peak pressure recordings was
made to determine any differences in acupuncture
point pressure from injection to injection. ECG
recordings were analysed in Chart 5 with HRV
extension (ADInstruments Pty Ltd) and the computed
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.168 www.acupunctureinmedicine.org.uk/volindex.php
Papers
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 168
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
low frequency (LF) and high frequency (HF)
components (expressed in normalised units) and
LF/HF ratio were imported to SPSS for analysis of
any differences of the mean by paired samples t test.
Results
Of the original 75 volunteers enrolled, five were
unable to complete the second session within the
one week timeframe and a sixth experienced anxiety
during the first session and withdrew, leaving 69 to
complete the study. Separate analysis of the
acupuncture naïve group demonstrated no differences
when compared with the group that had prior
acupuncture experience. In addition, there were no
significant differences between the male and female
subjects, nor were there any age related differences.
Therefore data from all participants were analysed
together. Data are presented as means and standard
deviations, and P values of the paired samples t tests
are reported, where appropriate.
Table 1 presents the results of self reported
subjective data. In general, there were significant
differences in the in situ needle sensation (P<0.001),
de qi (P<0.001) and unpleasantness during
experiment (P<0.001) with subjects reporting that
TA provided a lower intensity in all three sensations.
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.www.acupunctureinmedicine.org.uk/volindex.php 169
Papers
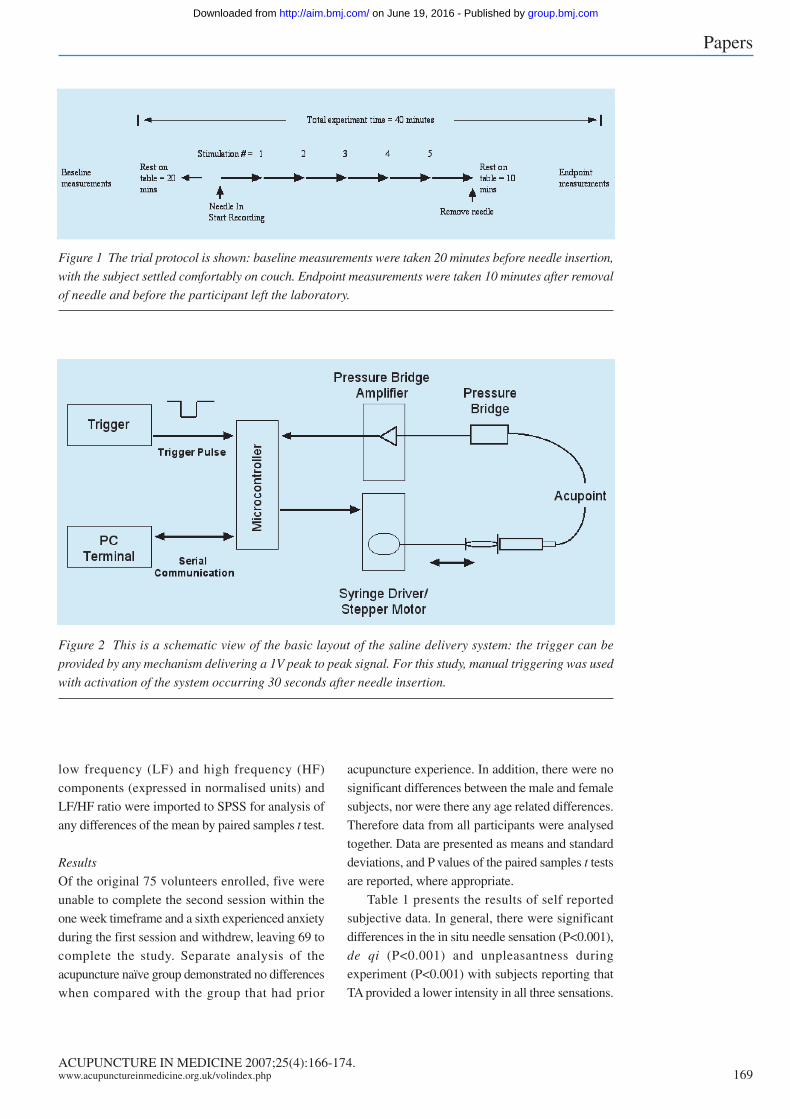
Figure 1 The trial protocol is shown: baseline measurements were taken 20 minutes before needle insertion,
with the subject settled comfortably on couch. Endpoint measurements were taken 10 minutes after removal
of needle and before the participant left the laboratory.
Figure 2 This is a schematic view of the basic layout of the saline delivery system: the trigger can be
provided by any mechanism delivering a 1V peak to peak signal. For this study, manual triggering was used
with activation of the system occurring 30 seconds after needle insertion.
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 169
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.170 www.acupunctureinmedicine.org.uk/volindex.php
Papers
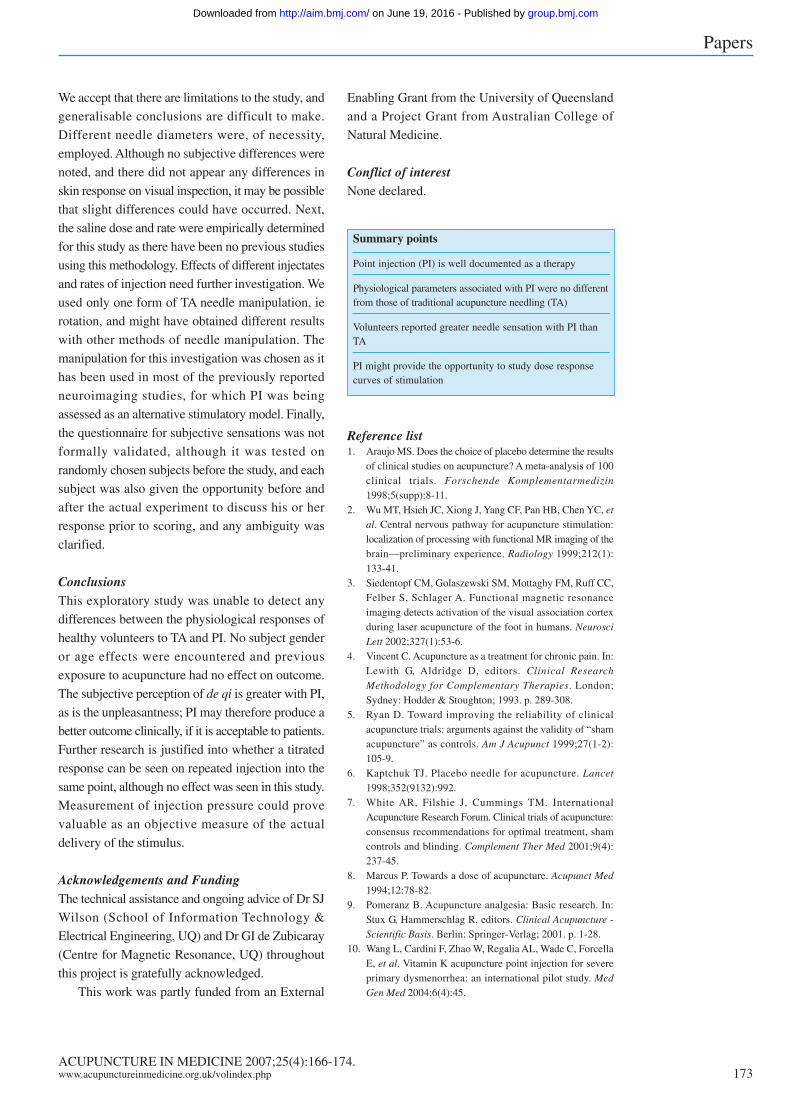
Table 1 Difference in sensation reported after TA and PI (n=69)
TA PI t* P (two tailed)
Pain on needle insertion 3.22 (2.28) 3.49 (2.34) 0.89 0.38
Pain at needle site during the scan 3.13 (2.22) 5.13 (2.40) 5.46 < 0.001
De qi (numbness, heaviness, distension,soreness, spreading away)
3.39 (2.49) 5.58 (2.54) 5.82 < 0.001
Unpleasantness 2.10 (2.57) 3.77 (2.88) 4.96 < 0.001
Values are mean (SD) scores on a 0-10 numerical scale; TA – traditional acupuncture; PI – point injection*Paired t test
Table 2 Physiological variables before and after TA and PI
TA PIPre-stimulation Post-stimulation Pre-stimulation Post-stimulation
SBP 110.04 (10.91) 112.28 (10.26) 110.61 (10.43) 112.58 (11.00)
DBP 63.75 (7.67) 67.49 (8.91) 63.51 (7.62) 65.81 (7.66)
MAP 79.25 (7.62) 82.49 (7.95) 79.25 (7.65) 81.42 (7.95)
HR 67.62 (10.75) 67.57 (10.33) 68.20 (11.24) 67.57 (9.66)
PRP 7.48 (1.59) 7.63 (1.61) 7.562 (1.57) 7.62 (1.43)
SpO2 97.67 (1.64) 97.94 (1.47) 97.29 (1.76) 97.75 (1.61)
All values are means (SD); SBP – systolic blood pressure (mmHg); DBP – diastolic blood pressure (mmHg);MAP – mean arterial pressure (mmHg); HR – heart rate (beats per minute); PRP – pressure rate product;SpO2 – peripheral oxygen saturation (%)
Table 3 Comparison of pre- v post-stimulation HR and PRP
Visit Pre-stimulation Post-stimulation Paired difference t* Df P (two tailed)
HR 1 72.36 (12.42) 67.91 (11.48) 4.45 4.81 68 <0.001
2 73.16 (11.49) 67.56 (8.78) 5.61 5.94 68 <0.001
PRP 1 8.09 (1.76) 7.64 (1.71) 0.14 3.25 68 0.002
2 8.28 (1.62) 7.55 (1.36) 0.729 5.17 68 <0.001
All values are means (SD); HR – heart rate (beats per minute); PRP – pressure rate product;Visit 1 = traditional acupuncture (TA); Visit 2 = point injection (PI)*Paired samples t test
Table 4 Analysis of HRV components before and after TA and PI
n TA PIBefore After Before After
LF 10 60.13 (14.26) 68.01 (13.78) 63.97 (16.03) 65.27 (16.31)
HF 10 47.01 (35.05) 29.72 (13.11) 32.70 (9.66) 31.91 (15.11)
LF/HF 10 2.52 (2.97) 3.09 (2.30) 2.46 (1.48) 2.88 (2.72)
Values are mean (SD) normalised units (ms2); HRV – heart rate variability; TA – traditional acupuncture; PI – point injection; LF– Low frequency (0.04-0.15Hz); HF – High frequency (0.15-0.4Hz)Note: normal values (in normalised units) for the LF and HF spectral components of HRV are given as: LF 54±4 ms2, HF 29±3 ms2;LF being seen as a measure of sympathetic tone while HF reflects parasympathetic tone and fluctuations caused by spontaneousrespiration. The LF/HF ratio (normal range 1.5-2.0) is used to indicate balance between sympathetic and parasympathetic tone, 25with a decrease in the score being a possible indication of either an increase in parasympathetic or decrease in sympathetic tone.
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 170
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
There was no significant difference between TA and
PI (P=0.38) for the sensation associated with needle
insertion.
Results for the physiological variables are
presented in Table 2. No significant differences that
could be related to the method of acupuncture
stimulation were demonstrated. Although SpO2 was
measured throughout, there was no change from
measurement to measurement.
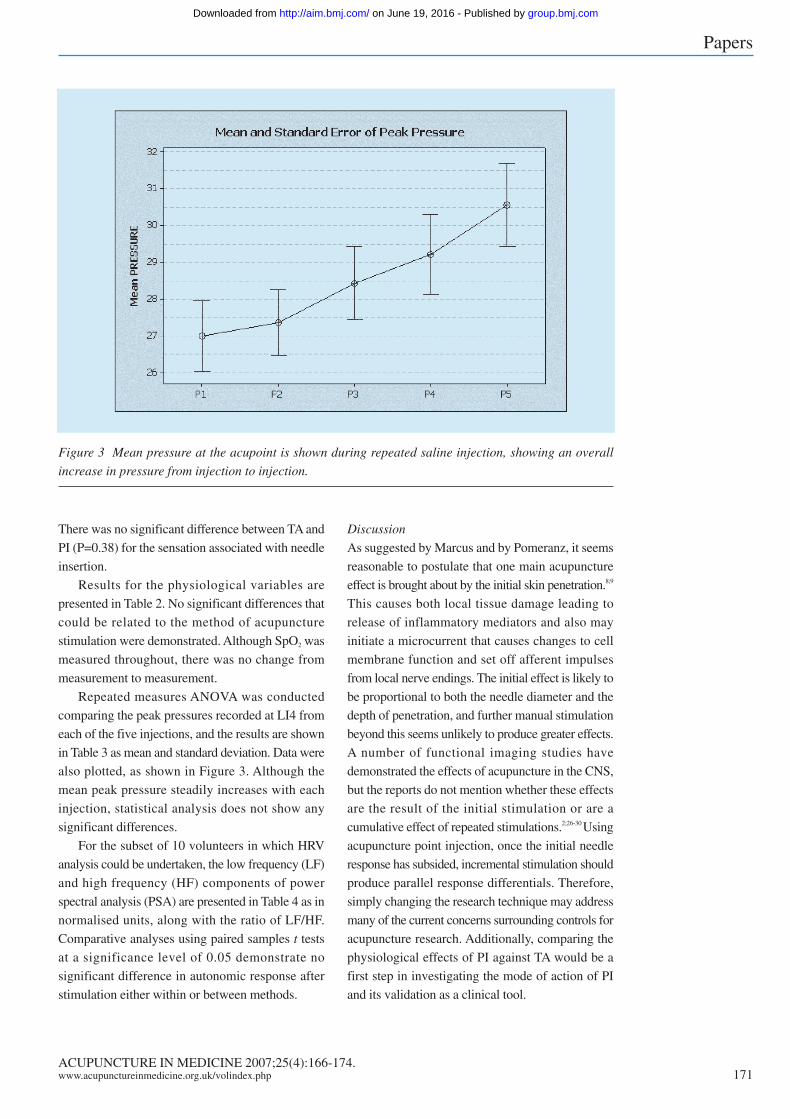
Repeated measures ANOVA was conducted
comparing the peak pressures recorded at LI4 from
each of the five injections, and the results are shown
in Table 3 as mean and standard deviation. Data were
also plotted, as shown in Figure 3. Although the
mean peak pressure steadily increases with each
injection, statistical analysis does not show any
significant differences.
For the subset of 10 volunteers in which HRV
analysis could be undertaken, the low frequency (LF)
and high frequency (HF) components of power
spectral analysis (PSA) are presented in Table 4 as in
normalised units, along with the ratio of LF/HF.
Comparative analyses using paired samples t tests
at a significance level of 0.05 demonstrate no
significant difference in autonomic response after
stimulation either within or between methods.
Discussion
As suggested by Marcus and by Pomeranz, it seems
reasonable to postulate that one main acupuncture
effect is brought about by the initial skin penetration.8;9
This causes both local tissue damage leading to
release of inflammatory mediators and also may
initiate a microcurrent that causes changes to cell
membrane function and set off afferent impulses
from local nerve endings. The initial effect is likely to
be proportional to both the needle diameter and the
depth of penetration, and further manual stimulation
beyond this seems unlikely to produce greater effects.
A number of functional imaging studies have
demonstrated the effects of acupuncture in the CNS,
but the reports do not mention whether these effects
are the result of the initial stimulation or are a
cumulative effect of repeated stimulations.2;26-30 Using
acupuncture point injection, once the initial needle
response has subsided, incremental stimulation should
produce parallel response differentials. Therefore,
simply changing the research technique may address
many of the current concerns surrounding controls for
acupuncture research. Additionally, comparing the
physiological effects of PI against TA would be a
first step in investigating the mode of action of PI
and its validation as a clinical tool.
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.www.acupunctureinmedicine.org.uk/volindex.php 171
Papers
Figure 3 Mean pressure at the acupoint is shown during repeated saline injection, showing an overall
increase in pressure from injection to injection.
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 171
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from

For this correlational study of differing acupuncture
methods, a single point (LI4, Hegu) was chosen for
several reasons: 1) point location is easy and
reproducible; 2) Hegu has an excellent research track
record; and 3) it is relatively safe to use. Healthy
subjects were chosen in line with previously reported
research protocols.18;31;32
Although there were some differences between
needles used – Terumo hypodermic needles having
a low friction coating not obtainable with similar
sized acupuncture needles – we considered this might
have little effect on de qi. As no difference in skin
erythema was observed between sessions, our
conclusion appeared to be supported. However, the
needles were also of slightly differing diameters
(Terumo: 0.5mm, Cathay: 0.35mm), since needles
of comparable size were not commercially available.
Therefore the decision was taken to examine
subjective reports of any differences in needling
sensations as part of the study. It was noted that
sensations of de qi and unpleasantness were greater
with the hypodermic needle, an outcome that might
be related to the larger diameter or the cutting edge.
To test this relationship further would require the
manufacture of 0.5mm diameter acupuncture needles
at a cost beyond the scope of this study.
HR and NIBP are two of the most commonly
used physiological markers of acupuncture effect;
although we considered derived PRP a more sensitive
measure of physiological response.18;33;22 A comparison
of these data provided no significant differences that
could be related to the differing methods of acupoint
stimulation. Examining changes in autonomic
response with power spectral analysis of HRV or
non-linear measures (such as Poincaré plots) may
improve the statistical value of the physiologic
data.34;35 Although apparatus for measuring HRV only
became available towards the end of the data
collecting period, we used HRV to examine whether
this would provide further data to address our
hypotheses. Analysis of HRV in a small cohort of
volunteers likewise provided no demonstrable
difference in autonomic response, although this must
be interpreted with considerable caution as the sample
size was small and the time between final stimulation
and final ECG recording was only 10 minutes.
Interestingly, the stress induced increase in ANS
activity that may have been anticipated was not noted.
A previous study has considered the usefulness and
limitations of HRV analysis in neuroimaging using PI
as the method of acupuncture point stimulation.36
The one significant difference between PI and
TA appeared in the subjective response, de qi. De qi
is typically described as a response to insertion and
manipulation of a filiform acupuncture needle,
although it has also been described in connection
with electroacupuncture (EA).9;23;37-39 As there is a lack
of consensus on whether de qi is necessary to produce
clinical effects,7 it was deemed reasonable to accept
de qi as an outcome measure of subjective response.
Most subjects reported a more powerful stimulation
response with PI. This may be an anticipatory
response even though a counterbalanced design was
used and every effort was made to provide exactly the
same environment and stimulation at every
encounter.38 Since de qi is claimed to relate to clinical
outcome,14;23;40 these subjective differences may
indicate that PI provides a more powerful clinical
outcome; with stronger sensations being translated
into a stronger clinical response, as outlined by Wang
et al10 and Luo and Chen.41 Not all subjects adequately
reported the quality of de qi experienced; therefore
analysis of the qualitative results was not formally
undertaken. The increased sensation of unpleasantness
needs further exploration, as it was not adequately
defined in this study. ‘Unpleasantness’ is a very broad
term that includes responses to experiences or events
that are not pleasing or a situation that is not pleasing.
It was noted that a number of subjects had formed
preconceptions of the needlestick experience that
might have biased the results of this study.
Although the measured pressure at LI4
demonstrated a trend to increase from injection to
injection, these changes were not statistically
significant; therefore, this trend must be regarded as
inconclusive and worthy of further investigation.
Pressure measurement is mathematically one step
removed from actual compliance; although pressure
and volume were measurable, it does not follow that
compliance has been measured. When interstitial
fluid volume increases above control volume, the
interstitial volume pressure curve levels off; above
150-200% of the control volume, the interstitial
compliance is virtually infinite.42 Therefore it is
possible that an incremental response occurred but
could not be observed. This measure was still
valuable as it can be used as an objective measure of
stimulus delivery.
Papers
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.172 www.acupunctureinmedicine.org.uk/volindex.php
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 172
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
We accept that there are limitations to the study, and
generalisable conclusions are difficult to make.
Different needle diameters were, of necessity,
employed. Although no subjective differences were
noted, and there did not appear any differences in
skin response on visual inspection, it may be possible
that slight differences could have occurred. Next,
the saline dose and rate were empirically determined
for this study as there have been no previous studies
using this methodology. Effects of different injectates
and rates of injection need further investigation. We
used only one form of TA needle manipulation, ie
rotation, and might have obtained different results
with other methods of needle manipulation. The
manipulation for this investigation was chosen as it
has been used in most of the previously reported
neuroimaging studies, for which PI was being
assessed as an alternative stimulatory model. Finally,
the questionnaire for subjective sensations was not
formally validated, although it was tested on
randomly chosen subjects before the study, and each
subject was also given the opportunity before and
after the actual experiment to discuss his or her
response prior to scoring, and any ambiguity was
clarified.
ConclusionsThis exploratory study was unable to detect any
differences between the physiological responses of
healthy volunteers to TA and PI. No subject gender
or age effects were encountered and previous
exposure to acupuncture had no effect on outcome.
The subjective perception of de qi is greater with PI,
as is the unpleasantness; PI may therefore produce a
better outcome clinically, if it is acceptable to patients.
Further research is justified into whether a titrated
response can be seen on repeated injection into the
same point, although no effect was seen in this study.
Measurement of injection pressure could prove
valuable as an objective measure of the actual
delivery of the stimulus.
Acknowledgements and FundingThe technical assistance and ongoing advice of Dr SJ
Wilson (School of Information Technology &
Electrical Engineering, UQ) and Dr GI de Zubicaray
(Centre for Magnetic Resonance, UQ) throughout
this project is gratefully acknowledged.
This work was partly funded from an External
Enabling Grant from the University of Queensland
and a Project Grant from Australian College of
Natural Medicine.
Conflict of interestNone declared.
Reference list1. Araujo MS. Does the choice of placebo determine the results
of clinical studies on acupuncture? A meta-analysis of 100clinical trials. Forschende Komplementarmedizin1998;5(supp):8-11.
2. Wu MT, Hsieh JC, Xiong J, Yang CF, Pan HB, Chen YC, etal. Central nervous pathway for acupuncture stimulation:localization of processing with functional MR imaging of thebrain—preliminary experience. Radiology 1999;212(1):133-41.
3. Siedentopf CM, Golaszewski SM, Mottaghy FM, Ruff CC,Felber S, Schlager A. Functional magnetic resonanceimaging detects activation of the visual association cortexduring laser acupuncture of the foot in humans. NeurosciLett 2002;327(1):53-6.
4. Vincent C. Acupuncture as a treatment for chronic pain. In:Lewith G, Aldridge D, editors. Clinical ResearchMethodology for Complementary Therapies. London;Sydney: Hodder & Stoughton; 1993. p. 289-308.
5. Ryan D. Toward improving the reliability of clinicalacupuncture trials: arguments against the validity of “shamacupuncture” as controls. Am J Acupunct 1999;27(1-2):105-9.
6. Kaptchuk TJ. Placebo needle for acupuncture. Lancet1998;352(9132):992.
7. White AR, Filshie J, Cummings TM. InternationalAcupuncture Research Forum. Clinical trials of acupuncture:consensus recommendations for optimal treatment, shamcontrols and blinding. Complement Ther Med 2001;9(4):237-45.
8. Marcus P. Towards a dose of acupuncture. Acupunct Med1994;12:78-82.
9. Pomeranz B. Acupuncture analgesia: Basic research. In:Stux G, Hammerschlag R, editors. Clinical Acupuncture -Scientific Basis. Berlin: Springer-Verlag; 2001. p. 1-28.
10. Wang L, Cardini F, Zhao W, Regalia AL, Wade C, ForcellaE, et al. Vitamin K acupuncture point injection for severeprimary dysmenorrhea: an international pilot study. MedGen Med 2004;6(4):45.
Papers
Summary points
Point injection (PI) is well documented as a therapy
Physiological parameters associated with PI were no differentfrom those of traditional acupuncture needling (TA)
Volunteers reported greater needle sensation with PI thanTA
PI might provide the opportunity to study dose responsecurves of stimulation
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.www.acupunctureinmedicine.org.uk/volindex.php 173
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 173
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
11. Yanjiuyan Z. An Outline of Chinese Acupuncture. Peking:Foreign Languages Press; 1975.
12. Deadman P, Al-Khafaji M, Baker K. A Manual ofAcupuncture. Hove, East Sussex: Journal of ChineseMedicine Publications; 1998.
13. The Treatment of 100 Common Diseases by NewAcupuncture. Hong Kong: Medicine & Health PublishingCompany; 1977.
14. O’Connor J, Bensky D, Shanghai College of TraditionalMedicine. Acupuncture: A comprehensive text. Chicago:Eastland Press; 1981.
15. Tsung JL. [Injection of distilled water at acupuncturing pointin the treatment of acute appendicitis.]. Zhonghua Wai Ke ZaZhi 1960;8:62-4.
16. Belitskaia RA, Vasilenko GF, Krasnova LB, Popkova EV,Chuzavkova EA, Agasarov LG. [The effect ofpharmacopuncture on the blood biochemical indices ofpatients with tunnel syndromes of the hands]. Vopr KurortolFizioter Lech Fiz Kult 1999(5):14-7.
17. Yang LC, Jawan B, Chen CN, Ho RT, Chang KA, Lee JH.Comparison of P6 acupoint injection with 50% glucose inwater and intravenous droperidol for prevention of vomitingafter gynecological laparoscopy. Acta Anaesthesiol Scand1993;37(2):192-4.
18. Ballegaard S, Muteki T, Harada H, Ueda N, Tsuda H,Tayama F, et al. Modulatory effect of acupuncture on thecardiovascular system: a cross-over study. AcupunctElectrother Res 1993;18(2):103-15.
19. Sugiyama Y, Xue YX, Mano T. Transient increase in humanmuscle sympathetic nerve activity during manualacupuncture. Jpn J Physiol 1995;45(2):337-45.
20. Nishijo K, Mori H, Yosikawa K, Yazawa K. Decreased heartrate by acupuncture stimulation in humans via facilitation ofcardiac vagal activity and suppression of cardiac sympatheticnerve. Neurosci Lett 1997;227(3):165-8.
21. Backer M, Hammes MG, Valet M, Deppe M, Conrad B,Tolle TR, et al. Different modes of manual acupuncturestimulation differentially modulate cerebral blood flowvelocity, arterial blood pressure and heart rate in humansubjects. Neurosci Lett 2002;333(3):203-6.
22. Wright RA, Contrada RJ, Patane MJ. Task difficulty,cardiovascular response, and the magnitude of goal valence.J Pers Soc Psychol 1986;51(4):837-43.
23. Park H, Park J, Lee H, Lee H. Does Deqi (needle sensation)exist? Am J Chin Med 2002;30(1):45-50.
24. Strudwick MW, Wilson SJ. Automated Syringe Driver forAcupoint Injection in fMRI Studies: a case for quantifiedpoint injection in neuroimaging studies of acupuncture.Expert Rev Med Devices 2007;4(6):In Press.
25. Task Force of the European Society of Cardiology and theNorth American Society of Pacing and Electrophysiology.Heart rate variability: standards of measurement,physiological interpretation and clinical use. Circulation1996;93(5):1043-65.
26. Biella G, Sotgiu ML, Pellegata G, Paulesu E, Castiglioni I,Fazio F. Acupuncture produces central activations in painregions. Neuroimage 2001;14(1 Pt 1):60-6.
27. Hui KK, Liu J, Makris N, Gollub RL, CHen AJ, Moore CI,et al. Acupuncture modulates the limbic system andsubcortical gray structures of the human brain: evidencefrom fMRI studies in normal subjects. Hum Brain Mapp2000;9(1):13-25.
28. Kong J, Ma L, Gollub RL, Wei J, Yang X, Li D, et al. Apilot study of functional magnetic resonance imaging of thebrain during manual and electroacupuncture stimulation ofacupuncture point (LI-4 Hegu) in normal subjects revealsdifferential brain activation between methods. J AlternComplement Med 2002;8(4):411-9.
29. Pariente J, White P, Frackowiak RS, Lewith G. Expectancyand belief modulate the neuronal substrates of pain treatedby acupuncture. Neuroimage 2005;25(4):1161-7.
30. Yoo SS, Teh EK, Blinder RA, Jolesz FA. Modulation ofcerebellar activities by acupuncture stimulation: evidencefrom fMRI study. Neuroimage 2004;22(2):932-40.
31. Hui KK, Liu J, Marina O, Napadow V, Haselgrove C,Kwong KK, et al. The integrated response of the humancerebro-cerebellar and limbic systems to acupuncturestimulation at ST 36 as evidenced by fMRI. Neuroimage2005;27(3):479-96.
32. Vincent C, Lewith G. Placebo controls for acupuncturestudies. J R Soc Med 1995;88(4):199-202.
33. Li P, Ayannusi O, Reid C, Longhurst JC. Inhibitory effect ofelectroacupuncture (EA) on the pressor response inducedby exercise stress. Clin Auton Res 2004;14(3):182-8.
34. Haker E, Egekvist H, Bjerring P. Effect of sensorystimulation (acupuncture) on sympathetic andparasympathetic activities in healthy subjects. J Auton NervSyst 2000;79(1):52-9.
35. Sayers BM. Analysis of heart rate variability. Ergonomics1973;16(1):17-32.
36. Strudwick MW, McMahon KL, Choy STB. Rapid responseof autonomic nervous system to acupuncture in subjectsunder stress. Aust J Acupunct Chin Med 2007;2(1):9-15.
37. Kong J, Fufa DT, Gerber AJ, Rosman IS, Vangel MG,Gracely RH, et al. Psychophysical outcomes from arandomized pilot study of manual, electro, and shamacupuncture treatment on experimentally induced thermalpain. J Pain 2005;6(1):55-64.
38. Park J, Park H, Lee H, Lim S, Ahn K, Lee H. Deqisensation between the acupuncture-experienced andthe naive: a Korean study II. Am J Chin Med 2005;33(2):329-37.
39. Pomeranz B. Electroacupuncture and transcutaneouselectrical nerve stimulation. In: Stux G, Berman BM,Pomeranz B, editors. Basics of acupuncture. 5th rev ed.Berlin: Springer-Verlag; 2003. p. 315-25.
40. Vincent CA, Richardson PH, Black JJ, Pither CE. Thesignificance of needle placement site in acupuncture. JPsychosom Res 1989;33(4):489-96.
41. Luo L, Chen WJ. Development of acu-injection treatment.J Clin Acupunct Moxibust 2001;17:53-6.
42. Reed RK, Woie K, Rubin K. Integrins and controlof interstitial fluid pressure. News Physiol Sci 1997;12(1):42-9.
Papers
ACUPUNCTURE IN MEDICINE 2007;25(4):166-174.174 www.acupunctureinmedicine.org.uk/volindex.php
AIM December 2007 Text.qxd 21/12/2007 06:38 Page 174
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
responses in healthy subjects an exploratory study of−technique
Point injection as an alternative acupuncture
Mark W Strudwick, Roderick C Hinks and S T Boris Choy
doi: 10.1136/aim.25.4.1662007 25: 166-174 Acupunct Med
http://aim.bmj.com/content/25/4/166Updated information and services can be found at:
These include:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on June 19, 2016 - Published by http://aim.bmj.com/Downloaded from
Copyright © 2022 FDOKUMEN




















