
pnw347.pdf - IUPUI ScholarWorks
12
INTEGRATIVE MEDICINE SECTION Original Research Article Real-World Massage Therapy Produces Meaningful Effectiveness Signal for Primary Care Patients with Chronic Low Back Pain: Results of a Repeated Measures Cohort Study William G. Elder, PhD,* Niki Munk, PhD, LMT, † Margaret M. Love, PhD,* Geza G. Bruckner, PhD, ‡ Kathryn E. Stewart, BS, LMT,* and Kevin Pearce, MD, MPH* Departments of *Family and Community Medicine and ‡ Clinical Sciences, University of Kentucky, Lexington, Kentucky; † Department of Health Sciences, Indiana University–Purdue University Indianapolis, Indianapolis, Indiana, USA Correspondence to: William G. Elder, PhD, Family and Community Medicine, University of Kentucky, The Department of Family and Community Medicine, 2195 Harrodsburg Rd., Suite 125, Lexington, KY 40504- 3504, USA. E-mail: [email protected]. Funding sources: The Kentucky Pain Research and Outcomes Study received the following funding: National Center for Complementary and Integrative Health – National Institutes of Health (NIH) grant #R21AT004544 and National Center for Advancing Translational Sciences - National Institutes of Health (NIH) grant #UL1 TR000117. Conflicts of interest: There are no conflicts of interest to report. Authors William G. Elder and Niki Munk are co-first authors. Abstract Objective. While efficacy of massage and other non- pharmacological treatments for chronic low back pain is established, stakeholders have called for pragmatic studies of effectiveness in “real-world” primary health care. The Kentucky Pain Research and Outcomes Study evaluated massage impact on pain, disability, and health-related quality of life for primary care patients with chronic low back pain. We report effectiveness and feasibility results, and make comparisons with established minimal clini- cally important differences. Methods. Primary care providers referred eligible patients for 10 massage sessions with community practicing licensed massage therapists. Oswestry Disability Index and SF-36v2 measures obtained at baseline and postintervention at 12 and 24 weeks were analyzed with mixed linear models and Tukey’s tests. Additional analyses examined clinically significant improvement and predictive patient characteristics. Results. Of 104 enrolled patients, 85 and 76 com- pleted 12 and 24 weeks of data collection, respec- tively. Group means improved at 12 weeks for all outcomes and at 24 weeks for SF-36v2’s Physical Component Summary and Bodily Pain Domain. Of those with clinically improved disability at 12 weeks, 75% were still clinically improved at 24 weeks (P < 0.01). For SF-36v2 Physical and Mental Component Summaries, 55.4% and 43.4%, respec- tively, showed clinically meaningful improvement at 12 weeks, 46.1% and 30.3% at 24 weeks. For Bodily Pain Domain, 49.4% were clinically improved at 12 weeks, 40% at 24 weeks. Adults older than age 49 years had better pain and disability outcomes than younger adults. Conclusions. Results provide a meaningful signal of massage effect for primary care patients with chronic low back pain and call for further research in practice settings using pragmatic designs with control groups. Key Words. Massage Therapy; Health-Related Outcomes; Primary Care; Practice-Based Research; Pragmatic Research; Complementary Therapies; Rural Population V C 2017 American Academy of Pain Medicine. All rights reserved. For permissions, please e-mail: [email protected] 1394 Pain Medicine 2017; 18: 1394–1405 doi: 10.1093/pm/pnw347
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of pnw347.pdf - IUPUI ScholarWorks
INTEGRATIVE MEDICINE SECTION
Original Research Article
Real-World Massage Therapy ProducesMeaningful Effectiveness Signal for PrimaryCare Patients with Chronic Low Back PainResults of a Repeated Measures Cohort Study
William G Elder PhD Niki Munk PhD LMTdagger
Margaret M Love PhD Geza G Bruckner PhDDagger
Kathryn E Stewart BS LMT and Kevin PearceMD MPH
Departments of Family and Community Medicine andDaggerClinical Sciences University of Kentucky Lexington
Kentucky daggerDepartment of Health Sciences Indiana
UniversityndashPurdue University Indianapolis
Indianapolis Indiana USA
Correspondence to William G Elder PhD Family and
Community Medicine University of Kentucky The
Department of Family and Community Medicine 2195
Harrodsburg Rd Suite 125 Lexington KY 40504-
3504 USA E-mail welderukyedu
Funding sources The Kentucky Pain Research and
Outcomes Study received the following funding
National Center for Complementary and Integrative
Health ndash National Institutes of Health (NIH) grant
R21AT004544 and National Center for Advancing
Translational Sciences - National Institutes of Health
(NIH) grant UL1 TR000117
Conflicts of interest There are no conflicts of interest
to report
Authors William G Elder and Niki Munk are co-firstauthors
Abstract
Objective While efficacy of massage and other non-pharmacological treatments for chronic low backpain is established stakeholders have called forpragmatic studies of effectiveness in ldquoreal-worldrdquoprimary health care The Kentucky Pain Researchand Outcomes Study evaluated massage impact onpain disability and health-related quality of life for
primary care patients with chronic low back painWe report effectiveness and feasibility results andmake comparisons with established minimal clini-cally important differences
Methods Primary care providers referred eligiblepatients for 10 massage sessions with communitypracticing licensed massage therapists OswestryDisability Index and SF-36v2 measures obtainedat baseline and postintervention at 12 and 24 weekswere analyzed with mixed linear models and Tukeyrsquostests Additional analyses examined clinicallysignificant improvement and predictive patientcharacteristics
Results Of 104 enrolled patients 85 and 76 com-pleted 12 and 24 weeks of data collection respec-tively Group means improved at 12 weeks for alloutcomes and at 24 weeks for SF-36v2rsquos PhysicalComponent Summary and Bodily Pain DomainOf those with clinically improved disability at 12weeks 75 were still clinically improved at 24weeks (P lt 001) For SF-36v2 Physical and MentalComponent Summaries 554 and 434 respec-tively showed clinically meaningful improvement at12 weeks 461 and 303 at 24 weeks For BodilyPain Domain 494 were clinically improved at 12weeks 40 at 24 weeks Adults older than age 49years had better pain and disability outcomes thanyounger adults
Conclusions Results provide a meaningful signalof massage effect for primary care patients withchronic low back pain and call for further researchin practice settings using pragmatic designs withcontrol groups
Key Words Massage Therapy Health-RelatedOutcomes Primary Care Practice-Based ResearchPragmatic Research Complementary TherapiesRural Population
VC 2017 American Academy of Pain Medicine All rights reserved For permissions please e-mail journalspermissionsoupcom 1394
Pain Medicine 2017 18 1394ndash1405doi 101093pmpnw347
Introduction
Low back pain is a prevalent health condition that leadsall disorders in years lost to disability in the United States[1] While most patients improve rapidly [2] one-third re-port persistent back pain [3] and 15 develop chroniclow back pain (CLBP) with significant physical limitations[4] Randomized controlled trials meta-analyses and sys-tematic reviews have found clinical massage therapy tohave efficacy for CLBP [5ndash10] Clinical massage therapyrefers to massage applied and practiced by trained mas-sage professionals and delivered within a professionaland therapeutic setting to support optimal health andfunctioning The most recent and comprehensive lowback pain treatment guidelines (2007) recommend mas-sage specifically for CLBP [1112] noting its ldquoproven ben-efitsrdquo [12] However a recent meta-analysis [13] highlightsmethodological weaknesses in massage research andCLBP treatment guideline authors [1112] and others [14]have expressed concern that massage effectiveness hasnot been evaluated in primary care For example mas-sage is rarely integrated into primary care limiting thepotential for interdisciplinary awareness knowledge orcommunication between the fields In the event thathealth care providers recommend patients to massagethe likelihood of them knowing the massage therapist orpractice-specific patients accessed would be low The ex-tent to which massage treatments applied in real-worldsettings replicates those examined in controlled researchsettings would also be reasonably unknown to health careproviders Research designs reflective of real-world prac-tice situations (of both primary care and massage applica-tion) are needed for CLBP stakeholders to understand theextent to which patients will benefit from massage if rec-ommended by their primary care provider (PCP)
This report details outcomes of the Kentucky PainResearch and Outcomes Study (KYPROS) KYPROSwas selected by a National Institutes of Health (NIH)funding opportunity specifically designated for pragmaticstudies using practice-based research networks(PBRNs) [15] With a focus on pilot and pragmatic re-search the funding opportunity announcement consid-ered applications with control groups as nonresponsive[15] Thus this study does not employ a control groupAs a pilot and feasibility study KYPROS was designedand powered to detect and descriptively compare out-comes to established minimal clinically important differ-ences as a means to determine if real-world massagecould produce a meaningful benefit signal for CLBP pa-tients referred by their PCP A secondary aim ofKYPROS was to examine study design feasibilityKYPROS provided participants with cost-free access to10 massage treatments provided by licensed massagetherapists practicing in their community with five ormore years of experience We expected KYPROSparticipants would be satisfied with massage for theirCLBP and report benefit from provided treatment Ourprimary aim was to evaluate health-related outcomesof real-world massage for CLBP compared with
established minimal clinically important differences forour measures of interest pain with disability and health-related quality of life
Methods
The University of Kentuckyrsquos Office of Research Integrityprovided ethical review and approval (09-0687-FIV) forKYPROS Written informed consent was collected fromall participants
Study Design
KYPROS was a repeated measures cohort study (clini-caltrialsgov registration NCT01147120) It had nocomparison group focused on feasibility and outcomes(Figure 1) in urban and rural central Kentucky counties ofthe Kentucky Ambulatory Network a large statewidepractice-based research network Evaluation of out-comes was based on statistically significant change frombaseline and recommended methodology [16] applyingnonstatistical comparisons of outcomes for achievementof identified clinically meaningful changes We report pa-tient data from three data collection time points Visit 1(V1) at baseline Visit 2 (V2) at 12 weeks (immediately fol-lowing course of treatment) and Visit 3 (V3) at 24 weeks(12-week follow-up from course of treatment)
Study Participants
All CLBP patients enrolled in KYPROS were referred bytheir PCP which ultimately led to two study participantgroups referring PCPs and CLBP patients
Referring Primary Care Providers
We randomly selected from Kentucky Ambulatory Networkpractice locations then serially invited PCPs from 18 prac-tices (14 being group practices) to refer patients into ourstudy Practice locations included four rural sites (all grouppractices) and one major academic medical facility Thestudy team visited each practice to orient the PCPs andstaff including a 20-minute discussion of massage alongwith risks and benefits PCPs who consented to participatewere asked to 1) complete and return a point-of-carepocket card for each patient with CLBP they saw in theirpractice for any reason during their study participation win-dow and 2) refer eligible patients to the study if they thoughtthe study intervention would be of benefit PCPs were in-structed to document their referral on the pocket card addpatient contact information if the patient agreed and returnpocket cards to study personnel weekly Study personnelcontacted patients to explain the study confirm eligibilityanswer questions and schedule an informed consentbaseline study visit
Massage Produces Meaningful Effectiveness Signal
1395
Patient Participants
CLBP patients were eligible for referral if having a PCPvisit for any reason during their PCPrsquos participation win-dow CLBP was defined as pain in the lumbar or sacralregions persisting for three months or longer Table 1outlines full exclusioninclusion criteria Participants re-ceived a $25 gift card after each data collection pointwas completed
Massage Intervention and Providers
Participants referred and enrolled into the study wereeach assigned to a KYPROS-affiliated massage therapistKYPROS protocol stipulated that study massage thera-pists schedule develop treatment plans and apply 10massage treatments during the 12 weeks between studyV1 and V2 for study participants Study therapists pro-vided treatments at no cost to study participants and
Table 1 Study patient criteria
Inclusion criteria Exclusion criteria
Currently have chronic low back pain Pregnant at point of referral
Patient in referring practice for 3thorn mo Currentpast history of psychosis
Has visit with participating primary care provider
during study referral window (visit for any reason)
Presence of nonconsolidated fracture deep vein thrombosis
or advanced osteoporosis
21thorn years old with life expectancy of 6thorn mo Course of massage in the past six mo for any reason
(spa visits andor an occasional massage were acceptable)
Massage contraindications ndash presence of skin wounds or infections
eczema active cancer tumor or advanced kidney disease
Figure 1 Flow diagram of study activities
Elder et al
1396
were compensated $25 per completed massage sessionDetails of KYPROS massage therapists are describedelsewhere [17] but briefly assignment was informed byparticipant convenience to therapist practice location anddistribution All KYPROS-affiliated massage therapistswere licensed in Kentucky had to have at least five yearsof professional experience provide treatment space andsupplies complete study personnel training and com-plete and submit treatment documentation forms specificto KYPROS Study massage therapists scheduled visitsprovided treatments in their usual treatment setting andutilized any massage technique within the purview of theirtraining experience Techniques included Swedish mas-sage active isolated stretching myofascial techniqueslymphatic drainage movement trigger point therapyneuromuscular therapy cranialsacral therapy reflexologyReiki acupressure and positional release Included tech-niques represent those typically taught in foundation mas-sage education (ie Swedish massage the United Stateshas no consistent massage training parameters with re-gards to duration of training or necessary content taughtalthough efforts to establish such parameters exist amongprofessional organizations) as well as those inconsistentlytaught in foundation massage education but taught incontinuing education (most professional massage certifi-cations and licensures maintain continuing education re-quirements for renewal) or advancedspecialized trainingsettings (eg cranialsacral therapy lymphatic drainageReiki trigger point)
Measures
Patient Descriptors
Patient descriptors were collected from both PCPs (viapocket cards) and patients (via self-report) Descriptorvariables included PCP reportedperceived health painseverity function ability and pain-related medications(categorized as pain-specific muscle relaxers andmood-specific) patient age gender race body massindex (BMI) CLBP duration education and means ofhealth care payment Three medication-related variableswere created from PCP-provided medication lists 1)total number of pain-related medications reported(continuous) 2) dichotomous US Drug EnforcementAdministration (DEA) scheduled medications usage (ie
opioids benzodiazepines and Tramadol) and 3) totalnumber of reported scheduled medications (continuous)A dichotomous age variable was created to better con-sider age-related differences between younger and olderstudy participants We rounded the average sample ageto determine the dichotomous cut-point (50 years)which also happened to neatly divide the sample be-tween the established Baby Boomer and X generations
Outcomes
Primary outcome measures were the Oswestry DisabilityIndex (ODI) [18] and the Medical Outcomes Study 36-Item Short Form version 2 (SF-36v2) [19] The ODI is afrequently used condition-specific measure for pain withdisability [20] Examination of internal consistency yieldsCronbachrsquos alphas between 071 and 087 [21]Researchers have found that ODI scores of 12 andhigher indicate pain with disability in the Japanese pop-ulation (a country with a higher population age lowerobesity rates and better population health than theUnited States) [22] and changes of six points or moreare clinically meaningful (group means and for individ-uals) [2123] Sample size was sufficient to detect suchchange with greater than 90 power The SF-36v2 is awidely used and validated 36-item patient questionnaireto assess health-related quality of life It includes eighthealth domains and yields two summary scalesDimensions of interest from the SF-36v2 were thePhysical Component Summary the Mental ComponentSummary and the Bodily Pain Domain
Table 2 displays specific point change thresholds showingclinically meaningful improvement for the ODI and SF-36v2 Physical Component Summary Mental ComponentSummary and Bodily Pain Domain when consideringgroup means and individual change scores [19] Basedon V1V2 and V1V3 change scores dichotomoussuccess variables were calculated for each participant tosignify whether clinically meaningful change occurred ineach of the measures [1923]
Participant satisfaction and perceived treatment effectscan be used to judge whether delivery of the interventionis complete and acceptable [24] thus they are important
Table 2 Comparison points clinically meaningful threshold changes for groups and individuals
Domain
Mean point change
threshold for group
clinical significance
Point change threshold
for individual clinical
significance
Oswestry Disability Index (ODI) NA Change of 6 Change of6
SF-36v2dagger Physical Component Summary Change of 3 Change of38
Mental Component Summary Change of 3 Change of46
Bodily Pain Domain Change of 2 Change of55
ODI clinical significance parameters [2124]daggerSF-36v2 clinical significance parameters [19]
Massage Produces Meaningful Effectiveness Signal
1397
low back pain measure domains [25] KYPROS measuredperceived treatment effects and satisfaction in two waysAt V2 and V3 an 11-point numeric scale was used forthe question ldquoHow helpful do you believe this therapy wasfor your chronic low back painrdquo with 0frac14 ldquonot at all help-fulrdquo and 10frac14 ldquoextremely helpfulrdquo This variable was treatedas continuous At V2 participants completed a satisfactionsurvey that used a seven-point Likert scale for the extentto which participants agreed with statements such asldquoThis therapy relieved my painrdquo Dichotomous positive sat-isfaction and perceived effectiveness variables were cre-ated for each question that combined responses ofldquostrongly agreerdquo and ldquovery strongly agreerdquo as recom-mended by Ostelo and de Vet [25]
Data Collection Management and Analysis
Data were collected at V1 V2 and V3 with paper andpencil surveys either on the University of Kentucky cam-pus or in a neutral participant-convenient place whererelative privacy could be provided (most often a public li-brary) Study data were double-entered by research as-sistants into and managed using Research ElectronicData Capture (REDCap) [26] a secure web-based ap-plication designed to support data capture for researchstudies providing an intuitive interface for data entryaudit trails for tracking data manipulation and exportand automated export procedures Participants did notinteract with REDCap in any way nor were the com-pleted surveys printed from REDCap
Statistical analyses used SAS 93 (SAS Institute CaryNC USA) Comparisons of baseline variables weremade for loss to follow-up status at V2 and V3 usingchi-square tests for categorical variables and t tests forcontinuous variables This study was powered to detecta six-point change in mean ODI which constitutesmeaningful clinical change [2127] Our main analyseswere completed in two steps Step 1 Mean changeswere examined for each primary outcome (ODI and per-tinent SF-36v2 componentsdomains) using repeatedmeasures (time V1 V2 V3) mixed linear models andTukeyrsquos post hoc tests Step 2 Where Step 1 analysisindicated that significant outcomes changes occurreddescriptive analyses examined the extent of clinicallysignificant improvement and exploratory Spearman cor-relations chi-square odds ratio and logistical regres-sion analyses identified predictive patient characteristicsLarge numbers of PCPs (Nfrac14 67) and practices (Nfrac14 18)relative to number of referred patients (Nfrac14 177) obvi-ated the use of practice as a variable in analyses
Results
Sixty-seven urban and rural (Nfrac14 14) PCPs from 18 providersites (ruralfrac144) consented to participate in the study withone to 25 PCPs participating from each site (medianfrac14 2)Forty-eight PCPs returned pocket cards for 177 recommen-dations to massage Of the recommended 177 CLBPpatients 151 (81) were interested in being contacted by
study personnel One-hundred four (69) patients enrolledand completed baseline measures (Nfrac14 104)
Sixty percent of participants completed all 10 massagetreatments and 75 received at least five treatmentsNo adverse events were attributed to the study Threecomplaints about massage therapists were recorded(personalitybelief conflicts) Two participants were reas-signed to a different massage therapist and the third is-sue was resolved by notifying the massage therapist ofpatient concerns [17]
Baseline Measures and Attrition
To limit rates of participants lost to follow-up data col-lection at V2 and V3 was vigorously pursued for allstudy participants regardless of the extent to whichtreatments were accessed Of the 104 participants 85completed V2 (18 attrition) and 76 completed V3(27 attrition) Baseline measures for study participantsare reported in Table 3 Those lost to follow-up at V2had a higher mean number of PCP-reported pain-re-lated prescriptions (29 617 vs 21 6 14 Pfrac14003)had a lower mean age (38 years 6 99 vs 511 years 6
127 Plt 00001) and were more likely to be under age50 years (v2frac1476) those who reported current smokingbehavior were more likely to be lost to follow-up at V2(v2frac1458) Study participants lost to follow-up at V3 (in-cludes V2 attrition) had lower mean age (404 years 6
114 vs 518 years 6 125 Plt00001) and were morelikely to be younger than age 50 years (v2frac1481)
Intervention Effectiveness
Step 1 Analysis ndash Group Means
Mixed model linear regressions were used to examinechange in scores across time points for each of the four mainoutcomes Significant improvements were demonstratedfor the ODI (Ffrac142272 Plt 00001) SF-36v2 PhysicalComponent Summary (Physical Ffrac14 198 Plt 00001)and Mental Component Summary (Ffrac14 977 Pfrac14 00001)and SF-36v2 Bodily Pain Domain (Ffrac14 244 Plt00001)Figure 2 graphs the pattern of mean score improvementfrom V1 to V2 and subsequent decrement from V2 to V3for each outcome Significant improvements in meanscores for all measures were evident from V1 to V2 andsignificant improvements in disability functioning and painwere retained at V3 for the ODI Physical ComponentSummary and Bodily Pain Domain
Table 4 provides the mean point change scores fromV1 to V2 V2 to V3 and V1 to V3 as well as whetherreported change is clinically significant according to es-tablished guidelines Clinically meaningful improvementsin group mean scores were evident from V1 to V2 for alloutcomes and from V1 to V3 for the PhysicalComponent Summary and Bodily Pain Domain of theSF-36v2 Decrements in mean scores were clinically
Elder et al
1398
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

Introduction
Low back pain is a prevalent health condition that leadsall disorders in years lost to disability in the United States[1] While most patients improve rapidly [2] one-third re-port persistent back pain [3] and 15 develop chroniclow back pain (CLBP) with significant physical limitations[4] Randomized controlled trials meta-analyses and sys-tematic reviews have found clinical massage therapy tohave efficacy for CLBP [5ndash10] Clinical massage therapyrefers to massage applied and practiced by trained mas-sage professionals and delivered within a professionaland therapeutic setting to support optimal health andfunctioning The most recent and comprehensive lowback pain treatment guidelines (2007) recommend mas-sage specifically for CLBP [1112] noting its ldquoproven ben-efitsrdquo [12] However a recent meta-analysis [13] highlightsmethodological weaknesses in massage research andCLBP treatment guideline authors [1112] and others [14]have expressed concern that massage effectiveness hasnot been evaluated in primary care For example mas-sage is rarely integrated into primary care limiting thepotential for interdisciplinary awareness knowledge orcommunication between the fields In the event thathealth care providers recommend patients to massagethe likelihood of them knowing the massage therapist orpractice-specific patients accessed would be low The ex-tent to which massage treatments applied in real-worldsettings replicates those examined in controlled researchsettings would also be reasonably unknown to health careproviders Research designs reflective of real-world prac-tice situations (of both primary care and massage applica-tion) are needed for CLBP stakeholders to understand theextent to which patients will benefit from massage if rec-ommended by their primary care provider (PCP)
This report details outcomes of the Kentucky PainResearch and Outcomes Study (KYPROS) KYPROSwas selected by a National Institutes of Health (NIH)funding opportunity specifically designated for pragmaticstudies using practice-based research networks(PBRNs) [15] With a focus on pilot and pragmatic re-search the funding opportunity announcement consid-ered applications with control groups as nonresponsive[15] Thus this study does not employ a control groupAs a pilot and feasibility study KYPROS was designedand powered to detect and descriptively compare out-comes to established minimal clinically important differ-ences as a means to determine if real-world massagecould produce a meaningful benefit signal for CLBP pa-tients referred by their PCP A secondary aim ofKYPROS was to examine study design feasibilityKYPROS provided participants with cost-free access to10 massage treatments provided by licensed massagetherapists practicing in their community with five ormore years of experience We expected KYPROSparticipants would be satisfied with massage for theirCLBP and report benefit from provided treatment Ourprimary aim was to evaluate health-related outcomesof real-world massage for CLBP compared with
established minimal clinically important differences forour measures of interest pain with disability and health-related quality of life
Methods
The University of Kentuckyrsquos Office of Research Integrityprovided ethical review and approval (09-0687-FIV) forKYPROS Written informed consent was collected fromall participants
Study Design
KYPROS was a repeated measures cohort study (clini-caltrialsgov registration NCT01147120) It had nocomparison group focused on feasibility and outcomes(Figure 1) in urban and rural central Kentucky counties ofthe Kentucky Ambulatory Network a large statewidepractice-based research network Evaluation of out-comes was based on statistically significant change frombaseline and recommended methodology [16] applyingnonstatistical comparisons of outcomes for achievementof identified clinically meaningful changes We report pa-tient data from three data collection time points Visit 1(V1) at baseline Visit 2 (V2) at 12 weeks (immediately fol-lowing course of treatment) and Visit 3 (V3) at 24 weeks(12-week follow-up from course of treatment)
Study Participants
All CLBP patients enrolled in KYPROS were referred bytheir PCP which ultimately led to two study participantgroups referring PCPs and CLBP patients
Referring Primary Care Providers
We randomly selected from Kentucky Ambulatory Networkpractice locations then serially invited PCPs from 18 prac-tices (14 being group practices) to refer patients into ourstudy Practice locations included four rural sites (all grouppractices) and one major academic medical facility Thestudy team visited each practice to orient the PCPs andstaff including a 20-minute discussion of massage alongwith risks and benefits PCPs who consented to participatewere asked to 1) complete and return a point-of-carepocket card for each patient with CLBP they saw in theirpractice for any reason during their study participation win-dow and 2) refer eligible patients to the study if they thoughtthe study intervention would be of benefit PCPs were in-structed to document their referral on the pocket card addpatient contact information if the patient agreed and returnpocket cards to study personnel weekly Study personnelcontacted patients to explain the study confirm eligibilityanswer questions and schedule an informed consentbaseline study visit
Massage Produces Meaningful Effectiveness Signal
1395
Patient Participants
CLBP patients were eligible for referral if having a PCPvisit for any reason during their PCPrsquos participation win-dow CLBP was defined as pain in the lumbar or sacralregions persisting for three months or longer Table 1outlines full exclusioninclusion criteria Participants re-ceived a $25 gift card after each data collection pointwas completed
Massage Intervention and Providers
Participants referred and enrolled into the study wereeach assigned to a KYPROS-affiliated massage therapistKYPROS protocol stipulated that study massage thera-pists schedule develop treatment plans and apply 10massage treatments during the 12 weeks between studyV1 and V2 for study participants Study therapists pro-vided treatments at no cost to study participants and
Table 1 Study patient criteria
Inclusion criteria Exclusion criteria
Currently have chronic low back pain Pregnant at point of referral
Patient in referring practice for 3thorn mo Currentpast history of psychosis
Has visit with participating primary care provider
during study referral window (visit for any reason)
Presence of nonconsolidated fracture deep vein thrombosis
or advanced osteoporosis
21thorn years old with life expectancy of 6thorn mo Course of massage in the past six mo for any reason
(spa visits andor an occasional massage were acceptable)
Massage contraindications ndash presence of skin wounds or infections
eczema active cancer tumor or advanced kidney disease
Figure 1 Flow diagram of study activities
Elder et al
1396
were compensated $25 per completed massage sessionDetails of KYPROS massage therapists are describedelsewhere [17] but briefly assignment was informed byparticipant convenience to therapist practice location anddistribution All KYPROS-affiliated massage therapistswere licensed in Kentucky had to have at least five yearsof professional experience provide treatment space andsupplies complete study personnel training and com-plete and submit treatment documentation forms specificto KYPROS Study massage therapists scheduled visitsprovided treatments in their usual treatment setting andutilized any massage technique within the purview of theirtraining experience Techniques included Swedish mas-sage active isolated stretching myofascial techniqueslymphatic drainage movement trigger point therapyneuromuscular therapy cranialsacral therapy reflexologyReiki acupressure and positional release Included tech-niques represent those typically taught in foundation mas-sage education (ie Swedish massage the United Stateshas no consistent massage training parameters with re-gards to duration of training or necessary content taughtalthough efforts to establish such parameters exist amongprofessional organizations) as well as those inconsistentlytaught in foundation massage education but taught incontinuing education (most professional massage certifi-cations and licensures maintain continuing education re-quirements for renewal) or advancedspecialized trainingsettings (eg cranialsacral therapy lymphatic drainageReiki trigger point)
Measures
Patient Descriptors
Patient descriptors were collected from both PCPs (viapocket cards) and patients (via self-report) Descriptorvariables included PCP reportedperceived health painseverity function ability and pain-related medications(categorized as pain-specific muscle relaxers andmood-specific) patient age gender race body massindex (BMI) CLBP duration education and means ofhealth care payment Three medication-related variableswere created from PCP-provided medication lists 1)total number of pain-related medications reported(continuous) 2) dichotomous US Drug EnforcementAdministration (DEA) scheduled medications usage (ie
opioids benzodiazepines and Tramadol) and 3) totalnumber of reported scheduled medications (continuous)A dichotomous age variable was created to better con-sider age-related differences between younger and olderstudy participants We rounded the average sample ageto determine the dichotomous cut-point (50 years)which also happened to neatly divide the sample be-tween the established Baby Boomer and X generations
Outcomes
Primary outcome measures were the Oswestry DisabilityIndex (ODI) [18] and the Medical Outcomes Study 36-Item Short Form version 2 (SF-36v2) [19] The ODI is afrequently used condition-specific measure for pain withdisability [20] Examination of internal consistency yieldsCronbachrsquos alphas between 071 and 087 [21]Researchers have found that ODI scores of 12 andhigher indicate pain with disability in the Japanese pop-ulation (a country with a higher population age lowerobesity rates and better population health than theUnited States) [22] and changes of six points or moreare clinically meaningful (group means and for individ-uals) [2123] Sample size was sufficient to detect suchchange with greater than 90 power The SF-36v2 is awidely used and validated 36-item patient questionnaireto assess health-related quality of life It includes eighthealth domains and yields two summary scalesDimensions of interest from the SF-36v2 were thePhysical Component Summary the Mental ComponentSummary and the Bodily Pain Domain
Table 2 displays specific point change thresholds showingclinically meaningful improvement for the ODI and SF-36v2 Physical Component Summary Mental ComponentSummary and Bodily Pain Domain when consideringgroup means and individual change scores [19] Basedon V1V2 and V1V3 change scores dichotomoussuccess variables were calculated for each participant tosignify whether clinically meaningful change occurred ineach of the measures [1923]
Participant satisfaction and perceived treatment effectscan be used to judge whether delivery of the interventionis complete and acceptable [24] thus they are important
Table 2 Comparison points clinically meaningful threshold changes for groups and individuals
Domain
Mean point change
threshold for group
clinical significance
Point change threshold
for individual clinical
significance
Oswestry Disability Index (ODI) NA Change of 6 Change of6
SF-36v2dagger Physical Component Summary Change of 3 Change of38
Mental Component Summary Change of 3 Change of46
Bodily Pain Domain Change of 2 Change of55
ODI clinical significance parameters [2124]daggerSF-36v2 clinical significance parameters [19]
Massage Produces Meaningful Effectiveness Signal
1397
low back pain measure domains [25] KYPROS measuredperceived treatment effects and satisfaction in two waysAt V2 and V3 an 11-point numeric scale was used forthe question ldquoHow helpful do you believe this therapy wasfor your chronic low back painrdquo with 0frac14 ldquonot at all help-fulrdquo and 10frac14 ldquoextremely helpfulrdquo This variable was treatedas continuous At V2 participants completed a satisfactionsurvey that used a seven-point Likert scale for the extentto which participants agreed with statements such asldquoThis therapy relieved my painrdquo Dichotomous positive sat-isfaction and perceived effectiveness variables were cre-ated for each question that combined responses ofldquostrongly agreerdquo and ldquovery strongly agreerdquo as recom-mended by Ostelo and de Vet [25]
Data Collection Management and Analysis
Data were collected at V1 V2 and V3 with paper andpencil surveys either on the University of Kentucky cam-pus or in a neutral participant-convenient place whererelative privacy could be provided (most often a public li-brary) Study data were double-entered by research as-sistants into and managed using Research ElectronicData Capture (REDCap) [26] a secure web-based ap-plication designed to support data capture for researchstudies providing an intuitive interface for data entryaudit trails for tracking data manipulation and exportand automated export procedures Participants did notinteract with REDCap in any way nor were the com-pleted surveys printed from REDCap
Statistical analyses used SAS 93 (SAS Institute CaryNC USA) Comparisons of baseline variables weremade for loss to follow-up status at V2 and V3 usingchi-square tests for categorical variables and t tests forcontinuous variables This study was powered to detecta six-point change in mean ODI which constitutesmeaningful clinical change [2127] Our main analyseswere completed in two steps Step 1 Mean changeswere examined for each primary outcome (ODI and per-tinent SF-36v2 componentsdomains) using repeatedmeasures (time V1 V2 V3) mixed linear models andTukeyrsquos post hoc tests Step 2 Where Step 1 analysisindicated that significant outcomes changes occurreddescriptive analyses examined the extent of clinicallysignificant improvement and exploratory Spearman cor-relations chi-square odds ratio and logistical regres-sion analyses identified predictive patient characteristicsLarge numbers of PCPs (Nfrac14 67) and practices (Nfrac14 18)relative to number of referred patients (Nfrac14 177) obvi-ated the use of practice as a variable in analyses
Results
Sixty-seven urban and rural (Nfrac14 14) PCPs from 18 providersites (ruralfrac144) consented to participate in the study withone to 25 PCPs participating from each site (medianfrac14 2)Forty-eight PCPs returned pocket cards for 177 recommen-dations to massage Of the recommended 177 CLBPpatients 151 (81) were interested in being contacted by
study personnel One-hundred four (69) patients enrolledand completed baseline measures (Nfrac14 104)
Sixty percent of participants completed all 10 massagetreatments and 75 received at least five treatmentsNo adverse events were attributed to the study Threecomplaints about massage therapists were recorded(personalitybelief conflicts) Two participants were reas-signed to a different massage therapist and the third is-sue was resolved by notifying the massage therapist ofpatient concerns [17]
Baseline Measures and Attrition
To limit rates of participants lost to follow-up data col-lection at V2 and V3 was vigorously pursued for allstudy participants regardless of the extent to whichtreatments were accessed Of the 104 participants 85completed V2 (18 attrition) and 76 completed V3(27 attrition) Baseline measures for study participantsare reported in Table 3 Those lost to follow-up at V2had a higher mean number of PCP-reported pain-re-lated prescriptions (29 617 vs 21 6 14 Pfrac14003)had a lower mean age (38 years 6 99 vs 511 years 6
127 Plt 00001) and were more likely to be under age50 years (v2frac1476) those who reported current smokingbehavior were more likely to be lost to follow-up at V2(v2frac1458) Study participants lost to follow-up at V3 (in-cludes V2 attrition) had lower mean age (404 years 6
114 vs 518 years 6 125 Plt00001) and were morelikely to be younger than age 50 years (v2frac1481)
Intervention Effectiveness
Step 1 Analysis ndash Group Means
Mixed model linear regressions were used to examinechange in scores across time points for each of the four mainoutcomes Significant improvements were demonstratedfor the ODI (Ffrac142272 Plt 00001) SF-36v2 PhysicalComponent Summary (Physical Ffrac14 198 Plt 00001)and Mental Component Summary (Ffrac14 977 Pfrac14 00001)and SF-36v2 Bodily Pain Domain (Ffrac14 244 Plt00001)Figure 2 graphs the pattern of mean score improvementfrom V1 to V2 and subsequent decrement from V2 to V3for each outcome Significant improvements in meanscores for all measures were evident from V1 to V2 andsignificant improvements in disability functioning and painwere retained at V3 for the ODI Physical ComponentSummary and Bodily Pain Domain
Table 4 provides the mean point change scores fromV1 to V2 V2 to V3 and V1 to V3 as well as whetherreported change is clinically significant according to es-tablished guidelines Clinically meaningful improvementsin group mean scores were evident from V1 to V2 for alloutcomes and from V1 to V3 for the PhysicalComponent Summary and Bodily Pain Domain of theSF-36v2 Decrements in mean scores were clinically
Elder et al
1398
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

Patient Participants
CLBP patients were eligible for referral if having a PCPvisit for any reason during their PCPrsquos participation win-dow CLBP was defined as pain in the lumbar or sacralregions persisting for three months or longer Table 1outlines full exclusioninclusion criteria Participants re-ceived a $25 gift card after each data collection pointwas completed
Massage Intervention and Providers
Participants referred and enrolled into the study wereeach assigned to a KYPROS-affiliated massage therapistKYPROS protocol stipulated that study massage thera-pists schedule develop treatment plans and apply 10massage treatments during the 12 weeks between studyV1 and V2 for study participants Study therapists pro-vided treatments at no cost to study participants and
Table 1 Study patient criteria
Inclusion criteria Exclusion criteria
Currently have chronic low back pain Pregnant at point of referral
Patient in referring practice for 3thorn mo Currentpast history of psychosis
Has visit with participating primary care provider
during study referral window (visit for any reason)
Presence of nonconsolidated fracture deep vein thrombosis
or advanced osteoporosis
21thorn years old with life expectancy of 6thorn mo Course of massage in the past six mo for any reason
(spa visits andor an occasional massage were acceptable)
Massage contraindications ndash presence of skin wounds or infections
eczema active cancer tumor or advanced kidney disease
Figure 1 Flow diagram of study activities
Elder et al
1396
were compensated $25 per completed massage sessionDetails of KYPROS massage therapists are describedelsewhere [17] but briefly assignment was informed byparticipant convenience to therapist practice location anddistribution All KYPROS-affiliated massage therapistswere licensed in Kentucky had to have at least five yearsof professional experience provide treatment space andsupplies complete study personnel training and com-plete and submit treatment documentation forms specificto KYPROS Study massage therapists scheduled visitsprovided treatments in their usual treatment setting andutilized any massage technique within the purview of theirtraining experience Techniques included Swedish mas-sage active isolated stretching myofascial techniqueslymphatic drainage movement trigger point therapyneuromuscular therapy cranialsacral therapy reflexologyReiki acupressure and positional release Included tech-niques represent those typically taught in foundation mas-sage education (ie Swedish massage the United Stateshas no consistent massage training parameters with re-gards to duration of training or necessary content taughtalthough efforts to establish such parameters exist amongprofessional organizations) as well as those inconsistentlytaught in foundation massage education but taught incontinuing education (most professional massage certifi-cations and licensures maintain continuing education re-quirements for renewal) or advancedspecialized trainingsettings (eg cranialsacral therapy lymphatic drainageReiki trigger point)
Measures
Patient Descriptors
Patient descriptors were collected from both PCPs (viapocket cards) and patients (via self-report) Descriptorvariables included PCP reportedperceived health painseverity function ability and pain-related medications(categorized as pain-specific muscle relaxers andmood-specific) patient age gender race body massindex (BMI) CLBP duration education and means ofhealth care payment Three medication-related variableswere created from PCP-provided medication lists 1)total number of pain-related medications reported(continuous) 2) dichotomous US Drug EnforcementAdministration (DEA) scheduled medications usage (ie
opioids benzodiazepines and Tramadol) and 3) totalnumber of reported scheduled medications (continuous)A dichotomous age variable was created to better con-sider age-related differences between younger and olderstudy participants We rounded the average sample ageto determine the dichotomous cut-point (50 years)which also happened to neatly divide the sample be-tween the established Baby Boomer and X generations
Outcomes
Primary outcome measures were the Oswestry DisabilityIndex (ODI) [18] and the Medical Outcomes Study 36-Item Short Form version 2 (SF-36v2) [19] The ODI is afrequently used condition-specific measure for pain withdisability [20] Examination of internal consistency yieldsCronbachrsquos alphas between 071 and 087 [21]Researchers have found that ODI scores of 12 andhigher indicate pain with disability in the Japanese pop-ulation (a country with a higher population age lowerobesity rates and better population health than theUnited States) [22] and changes of six points or moreare clinically meaningful (group means and for individ-uals) [2123] Sample size was sufficient to detect suchchange with greater than 90 power The SF-36v2 is awidely used and validated 36-item patient questionnaireto assess health-related quality of life It includes eighthealth domains and yields two summary scalesDimensions of interest from the SF-36v2 were thePhysical Component Summary the Mental ComponentSummary and the Bodily Pain Domain
Table 2 displays specific point change thresholds showingclinically meaningful improvement for the ODI and SF-36v2 Physical Component Summary Mental ComponentSummary and Bodily Pain Domain when consideringgroup means and individual change scores [19] Basedon V1V2 and V1V3 change scores dichotomoussuccess variables were calculated for each participant tosignify whether clinically meaningful change occurred ineach of the measures [1923]
Participant satisfaction and perceived treatment effectscan be used to judge whether delivery of the interventionis complete and acceptable [24] thus they are important
Table 2 Comparison points clinically meaningful threshold changes for groups and individuals
Domain
Mean point change
threshold for group
clinical significance
Point change threshold
for individual clinical
significance
Oswestry Disability Index (ODI) NA Change of 6 Change of6
SF-36v2dagger Physical Component Summary Change of 3 Change of38
Mental Component Summary Change of 3 Change of46
Bodily Pain Domain Change of 2 Change of55
ODI clinical significance parameters [2124]daggerSF-36v2 clinical significance parameters [19]
Massage Produces Meaningful Effectiveness Signal
1397
low back pain measure domains [25] KYPROS measuredperceived treatment effects and satisfaction in two waysAt V2 and V3 an 11-point numeric scale was used forthe question ldquoHow helpful do you believe this therapy wasfor your chronic low back painrdquo with 0frac14 ldquonot at all help-fulrdquo and 10frac14 ldquoextremely helpfulrdquo This variable was treatedas continuous At V2 participants completed a satisfactionsurvey that used a seven-point Likert scale for the extentto which participants agreed with statements such asldquoThis therapy relieved my painrdquo Dichotomous positive sat-isfaction and perceived effectiveness variables were cre-ated for each question that combined responses ofldquostrongly agreerdquo and ldquovery strongly agreerdquo as recom-mended by Ostelo and de Vet [25]
Data Collection Management and Analysis
Data were collected at V1 V2 and V3 with paper andpencil surveys either on the University of Kentucky cam-pus or in a neutral participant-convenient place whererelative privacy could be provided (most often a public li-brary) Study data were double-entered by research as-sistants into and managed using Research ElectronicData Capture (REDCap) [26] a secure web-based ap-plication designed to support data capture for researchstudies providing an intuitive interface for data entryaudit trails for tracking data manipulation and exportand automated export procedures Participants did notinteract with REDCap in any way nor were the com-pleted surveys printed from REDCap
Statistical analyses used SAS 93 (SAS Institute CaryNC USA) Comparisons of baseline variables weremade for loss to follow-up status at V2 and V3 usingchi-square tests for categorical variables and t tests forcontinuous variables This study was powered to detecta six-point change in mean ODI which constitutesmeaningful clinical change [2127] Our main analyseswere completed in two steps Step 1 Mean changeswere examined for each primary outcome (ODI and per-tinent SF-36v2 componentsdomains) using repeatedmeasures (time V1 V2 V3) mixed linear models andTukeyrsquos post hoc tests Step 2 Where Step 1 analysisindicated that significant outcomes changes occurreddescriptive analyses examined the extent of clinicallysignificant improvement and exploratory Spearman cor-relations chi-square odds ratio and logistical regres-sion analyses identified predictive patient characteristicsLarge numbers of PCPs (Nfrac14 67) and practices (Nfrac14 18)relative to number of referred patients (Nfrac14 177) obvi-ated the use of practice as a variable in analyses
Results
Sixty-seven urban and rural (Nfrac14 14) PCPs from 18 providersites (ruralfrac144) consented to participate in the study withone to 25 PCPs participating from each site (medianfrac14 2)Forty-eight PCPs returned pocket cards for 177 recommen-dations to massage Of the recommended 177 CLBPpatients 151 (81) were interested in being contacted by
study personnel One-hundred four (69) patients enrolledand completed baseline measures (Nfrac14 104)
Sixty percent of participants completed all 10 massagetreatments and 75 received at least five treatmentsNo adverse events were attributed to the study Threecomplaints about massage therapists were recorded(personalitybelief conflicts) Two participants were reas-signed to a different massage therapist and the third is-sue was resolved by notifying the massage therapist ofpatient concerns [17]
Baseline Measures and Attrition
To limit rates of participants lost to follow-up data col-lection at V2 and V3 was vigorously pursued for allstudy participants regardless of the extent to whichtreatments were accessed Of the 104 participants 85completed V2 (18 attrition) and 76 completed V3(27 attrition) Baseline measures for study participantsare reported in Table 3 Those lost to follow-up at V2had a higher mean number of PCP-reported pain-re-lated prescriptions (29 617 vs 21 6 14 Pfrac14003)had a lower mean age (38 years 6 99 vs 511 years 6
127 Plt 00001) and were more likely to be under age50 years (v2frac1476) those who reported current smokingbehavior were more likely to be lost to follow-up at V2(v2frac1458) Study participants lost to follow-up at V3 (in-cludes V2 attrition) had lower mean age (404 years 6
114 vs 518 years 6 125 Plt00001) and were morelikely to be younger than age 50 years (v2frac1481)
Intervention Effectiveness
Step 1 Analysis ndash Group Means
Mixed model linear regressions were used to examinechange in scores across time points for each of the four mainoutcomes Significant improvements were demonstratedfor the ODI (Ffrac142272 Plt 00001) SF-36v2 PhysicalComponent Summary (Physical Ffrac14 198 Plt 00001)and Mental Component Summary (Ffrac14 977 Pfrac14 00001)and SF-36v2 Bodily Pain Domain (Ffrac14 244 Plt00001)Figure 2 graphs the pattern of mean score improvementfrom V1 to V2 and subsequent decrement from V2 to V3for each outcome Significant improvements in meanscores for all measures were evident from V1 to V2 andsignificant improvements in disability functioning and painwere retained at V3 for the ODI Physical ComponentSummary and Bodily Pain Domain
Table 4 provides the mean point change scores fromV1 to V2 V2 to V3 and V1 to V3 as well as whetherreported change is clinically significant according to es-tablished guidelines Clinically meaningful improvementsin group mean scores were evident from V1 to V2 for alloutcomes and from V1 to V3 for the PhysicalComponent Summary and Bodily Pain Domain of theSF-36v2 Decrements in mean scores were clinically
Elder et al
1398
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

were compensated $25 per completed massage sessionDetails of KYPROS massage therapists are describedelsewhere [17] but briefly assignment was informed byparticipant convenience to therapist practice location anddistribution All KYPROS-affiliated massage therapistswere licensed in Kentucky had to have at least five yearsof professional experience provide treatment space andsupplies complete study personnel training and com-plete and submit treatment documentation forms specificto KYPROS Study massage therapists scheduled visitsprovided treatments in their usual treatment setting andutilized any massage technique within the purview of theirtraining experience Techniques included Swedish mas-sage active isolated stretching myofascial techniqueslymphatic drainage movement trigger point therapyneuromuscular therapy cranialsacral therapy reflexologyReiki acupressure and positional release Included tech-niques represent those typically taught in foundation mas-sage education (ie Swedish massage the United Stateshas no consistent massage training parameters with re-gards to duration of training or necessary content taughtalthough efforts to establish such parameters exist amongprofessional organizations) as well as those inconsistentlytaught in foundation massage education but taught incontinuing education (most professional massage certifi-cations and licensures maintain continuing education re-quirements for renewal) or advancedspecialized trainingsettings (eg cranialsacral therapy lymphatic drainageReiki trigger point)
Measures
Patient Descriptors
Patient descriptors were collected from both PCPs (viapocket cards) and patients (via self-report) Descriptorvariables included PCP reportedperceived health painseverity function ability and pain-related medications(categorized as pain-specific muscle relaxers andmood-specific) patient age gender race body massindex (BMI) CLBP duration education and means ofhealth care payment Three medication-related variableswere created from PCP-provided medication lists 1)total number of pain-related medications reported(continuous) 2) dichotomous US Drug EnforcementAdministration (DEA) scheduled medications usage (ie
opioids benzodiazepines and Tramadol) and 3) totalnumber of reported scheduled medications (continuous)A dichotomous age variable was created to better con-sider age-related differences between younger and olderstudy participants We rounded the average sample ageto determine the dichotomous cut-point (50 years)which also happened to neatly divide the sample be-tween the established Baby Boomer and X generations
Outcomes
Primary outcome measures were the Oswestry DisabilityIndex (ODI) [18] and the Medical Outcomes Study 36-Item Short Form version 2 (SF-36v2) [19] The ODI is afrequently used condition-specific measure for pain withdisability [20] Examination of internal consistency yieldsCronbachrsquos alphas between 071 and 087 [21]Researchers have found that ODI scores of 12 andhigher indicate pain with disability in the Japanese pop-ulation (a country with a higher population age lowerobesity rates and better population health than theUnited States) [22] and changes of six points or moreare clinically meaningful (group means and for individ-uals) [2123] Sample size was sufficient to detect suchchange with greater than 90 power The SF-36v2 is awidely used and validated 36-item patient questionnaireto assess health-related quality of life It includes eighthealth domains and yields two summary scalesDimensions of interest from the SF-36v2 were thePhysical Component Summary the Mental ComponentSummary and the Bodily Pain Domain
Table 2 displays specific point change thresholds showingclinically meaningful improvement for the ODI and SF-36v2 Physical Component Summary Mental ComponentSummary and Bodily Pain Domain when consideringgroup means and individual change scores [19] Basedon V1V2 and V1V3 change scores dichotomoussuccess variables were calculated for each participant tosignify whether clinically meaningful change occurred ineach of the measures [1923]
Participant satisfaction and perceived treatment effectscan be used to judge whether delivery of the interventionis complete and acceptable [24] thus they are important
Table 2 Comparison points clinically meaningful threshold changes for groups and individuals
Domain
Mean point change
threshold for group
clinical significance
Point change threshold
for individual clinical
significance
Oswestry Disability Index (ODI) NA Change of 6 Change of6
SF-36v2dagger Physical Component Summary Change of 3 Change of38
Mental Component Summary Change of 3 Change of46
Bodily Pain Domain Change of 2 Change of55
ODI clinical significance parameters [2124]daggerSF-36v2 clinical significance parameters [19]
Massage Produces Meaningful Effectiveness Signal
1397
low back pain measure domains [25] KYPROS measuredperceived treatment effects and satisfaction in two waysAt V2 and V3 an 11-point numeric scale was used forthe question ldquoHow helpful do you believe this therapy wasfor your chronic low back painrdquo with 0frac14 ldquonot at all help-fulrdquo and 10frac14 ldquoextremely helpfulrdquo This variable was treatedas continuous At V2 participants completed a satisfactionsurvey that used a seven-point Likert scale for the extentto which participants agreed with statements such asldquoThis therapy relieved my painrdquo Dichotomous positive sat-isfaction and perceived effectiveness variables were cre-ated for each question that combined responses ofldquostrongly agreerdquo and ldquovery strongly agreerdquo as recom-mended by Ostelo and de Vet [25]
Data Collection Management and Analysis
Data were collected at V1 V2 and V3 with paper andpencil surveys either on the University of Kentucky cam-pus or in a neutral participant-convenient place whererelative privacy could be provided (most often a public li-brary) Study data were double-entered by research as-sistants into and managed using Research ElectronicData Capture (REDCap) [26] a secure web-based ap-plication designed to support data capture for researchstudies providing an intuitive interface for data entryaudit trails for tracking data manipulation and exportand automated export procedures Participants did notinteract with REDCap in any way nor were the com-pleted surveys printed from REDCap
Statistical analyses used SAS 93 (SAS Institute CaryNC USA) Comparisons of baseline variables weremade for loss to follow-up status at V2 and V3 usingchi-square tests for categorical variables and t tests forcontinuous variables This study was powered to detecta six-point change in mean ODI which constitutesmeaningful clinical change [2127] Our main analyseswere completed in two steps Step 1 Mean changeswere examined for each primary outcome (ODI and per-tinent SF-36v2 componentsdomains) using repeatedmeasures (time V1 V2 V3) mixed linear models andTukeyrsquos post hoc tests Step 2 Where Step 1 analysisindicated that significant outcomes changes occurreddescriptive analyses examined the extent of clinicallysignificant improvement and exploratory Spearman cor-relations chi-square odds ratio and logistical regres-sion analyses identified predictive patient characteristicsLarge numbers of PCPs (Nfrac14 67) and practices (Nfrac14 18)relative to number of referred patients (Nfrac14 177) obvi-ated the use of practice as a variable in analyses
Results
Sixty-seven urban and rural (Nfrac14 14) PCPs from 18 providersites (ruralfrac144) consented to participate in the study withone to 25 PCPs participating from each site (medianfrac14 2)Forty-eight PCPs returned pocket cards for 177 recommen-dations to massage Of the recommended 177 CLBPpatients 151 (81) were interested in being contacted by
study personnel One-hundred four (69) patients enrolledand completed baseline measures (Nfrac14 104)
Sixty percent of participants completed all 10 massagetreatments and 75 received at least five treatmentsNo adverse events were attributed to the study Threecomplaints about massage therapists were recorded(personalitybelief conflicts) Two participants were reas-signed to a different massage therapist and the third is-sue was resolved by notifying the massage therapist ofpatient concerns [17]
Baseline Measures and Attrition
To limit rates of participants lost to follow-up data col-lection at V2 and V3 was vigorously pursued for allstudy participants regardless of the extent to whichtreatments were accessed Of the 104 participants 85completed V2 (18 attrition) and 76 completed V3(27 attrition) Baseline measures for study participantsare reported in Table 3 Those lost to follow-up at V2had a higher mean number of PCP-reported pain-re-lated prescriptions (29 617 vs 21 6 14 Pfrac14003)had a lower mean age (38 years 6 99 vs 511 years 6
127 Plt 00001) and were more likely to be under age50 years (v2frac1476) those who reported current smokingbehavior were more likely to be lost to follow-up at V2(v2frac1458) Study participants lost to follow-up at V3 (in-cludes V2 attrition) had lower mean age (404 years 6
114 vs 518 years 6 125 Plt00001) and were morelikely to be younger than age 50 years (v2frac1481)
Intervention Effectiveness
Step 1 Analysis ndash Group Means
Mixed model linear regressions were used to examinechange in scores across time points for each of the four mainoutcomes Significant improvements were demonstratedfor the ODI (Ffrac142272 Plt 00001) SF-36v2 PhysicalComponent Summary (Physical Ffrac14 198 Plt 00001)and Mental Component Summary (Ffrac14 977 Pfrac14 00001)and SF-36v2 Bodily Pain Domain (Ffrac14 244 Plt00001)Figure 2 graphs the pattern of mean score improvementfrom V1 to V2 and subsequent decrement from V2 to V3for each outcome Significant improvements in meanscores for all measures were evident from V1 to V2 andsignificant improvements in disability functioning and painwere retained at V3 for the ODI Physical ComponentSummary and Bodily Pain Domain
Table 4 provides the mean point change scores fromV1 to V2 V2 to V3 and V1 to V3 as well as whetherreported change is clinically significant according to es-tablished guidelines Clinically meaningful improvementsin group mean scores were evident from V1 to V2 for alloutcomes and from V1 to V3 for the PhysicalComponent Summary and Bodily Pain Domain of theSF-36v2 Decrements in mean scores were clinically
Elder et al
1398
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

low back pain measure domains [25] KYPROS measuredperceived treatment effects and satisfaction in two waysAt V2 and V3 an 11-point numeric scale was used forthe question ldquoHow helpful do you believe this therapy wasfor your chronic low back painrdquo with 0frac14 ldquonot at all help-fulrdquo and 10frac14 ldquoextremely helpfulrdquo This variable was treatedas continuous At V2 participants completed a satisfactionsurvey that used a seven-point Likert scale for the extentto which participants agreed with statements such asldquoThis therapy relieved my painrdquo Dichotomous positive sat-isfaction and perceived effectiveness variables were cre-ated for each question that combined responses ofldquostrongly agreerdquo and ldquovery strongly agreerdquo as recom-mended by Ostelo and de Vet [25]
Data Collection Management and Analysis
Data were collected at V1 V2 and V3 with paper andpencil surveys either on the University of Kentucky cam-pus or in a neutral participant-convenient place whererelative privacy could be provided (most often a public li-brary) Study data were double-entered by research as-sistants into and managed using Research ElectronicData Capture (REDCap) [26] a secure web-based ap-plication designed to support data capture for researchstudies providing an intuitive interface for data entryaudit trails for tracking data manipulation and exportand automated export procedures Participants did notinteract with REDCap in any way nor were the com-pleted surveys printed from REDCap
Statistical analyses used SAS 93 (SAS Institute CaryNC USA) Comparisons of baseline variables weremade for loss to follow-up status at V2 and V3 usingchi-square tests for categorical variables and t tests forcontinuous variables This study was powered to detecta six-point change in mean ODI which constitutesmeaningful clinical change [2127] Our main analyseswere completed in two steps Step 1 Mean changeswere examined for each primary outcome (ODI and per-tinent SF-36v2 componentsdomains) using repeatedmeasures (time V1 V2 V3) mixed linear models andTukeyrsquos post hoc tests Step 2 Where Step 1 analysisindicated that significant outcomes changes occurreddescriptive analyses examined the extent of clinicallysignificant improvement and exploratory Spearman cor-relations chi-square odds ratio and logistical regres-sion analyses identified predictive patient characteristicsLarge numbers of PCPs (Nfrac14 67) and practices (Nfrac14 18)relative to number of referred patients (Nfrac14 177) obvi-ated the use of practice as a variable in analyses
Results
Sixty-seven urban and rural (Nfrac14 14) PCPs from 18 providersites (ruralfrac144) consented to participate in the study withone to 25 PCPs participating from each site (medianfrac14 2)Forty-eight PCPs returned pocket cards for 177 recommen-dations to massage Of the recommended 177 CLBPpatients 151 (81) were interested in being contacted by
study personnel One-hundred four (69) patients enrolledand completed baseline measures (Nfrac14 104)
Sixty percent of participants completed all 10 massagetreatments and 75 received at least five treatmentsNo adverse events were attributed to the study Threecomplaints about massage therapists were recorded(personalitybelief conflicts) Two participants were reas-signed to a different massage therapist and the third is-sue was resolved by notifying the massage therapist ofpatient concerns [17]
Baseline Measures and Attrition
To limit rates of participants lost to follow-up data col-lection at V2 and V3 was vigorously pursued for allstudy participants regardless of the extent to whichtreatments were accessed Of the 104 participants 85completed V2 (18 attrition) and 76 completed V3(27 attrition) Baseline measures for study participantsare reported in Table 3 Those lost to follow-up at V2had a higher mean number of PCP-reported pain-re-lated prescriptions (29 617 vs 21 6 14 Pfrac14003)had a lower mean age (38 years 6 99 vs 511 years 6
127 Plt 00001) and were more likely to be under age50 years (v2frac1476) those who reported current smokingbehavior were more likely to be lost to follow-up at V2(v2frac1458) Study participants lost to follow-up at V3 (in-cludes V2 attrition) had lower mean age (404 years 6
114 vs 518 years 6 125 Plt00001) and were morelikely to be younger than age 50 years (v2frac1481)
Intervention Effectiveness
Step 1 Analysis ndash Group Means
Mixed model linear regressions were used to examinechange in scores across time points for each of the four mainoutcomes Significant improvements were demonstratedfor the ODI (Ffrac142272 Plt 00001) SF-36v2 PhysicalComponent Summary (Physical Ffrac14 198 Plt 00001)and Mental Component Summary (Ffrac14 977 Pfrac14 00001)and SF-36v2 Bodily Pain Domain (Ffrac14 244 Plt00001)Figure 2 graphs the pattern of mean score improvementfrom V1 to V2 and subsequent decrement from V2 to V3for each outcome Significant improvements in meanscores for all measures were evident from V1 to V2 andsignificant improvements in disability functioning and painwere retained at V3 for the ODI Physical ComponentSummary and Bodily Pain Domain
Table 4 provides the mean point change scores fromV1 to V2 V2 to V3 and V1 to V3 as well as whetherreported change is clinically significant according to es-tablished guidelines Clinically meaningful improvementsin group mean scores were evident from V1 to V2 for alloutcomes and from V1 to V3 for the PhysicalComponent Summary and Bodily Pain Domain of theSF-36v2 Decrements in mean scores were clinically
Elder et al
1398
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-
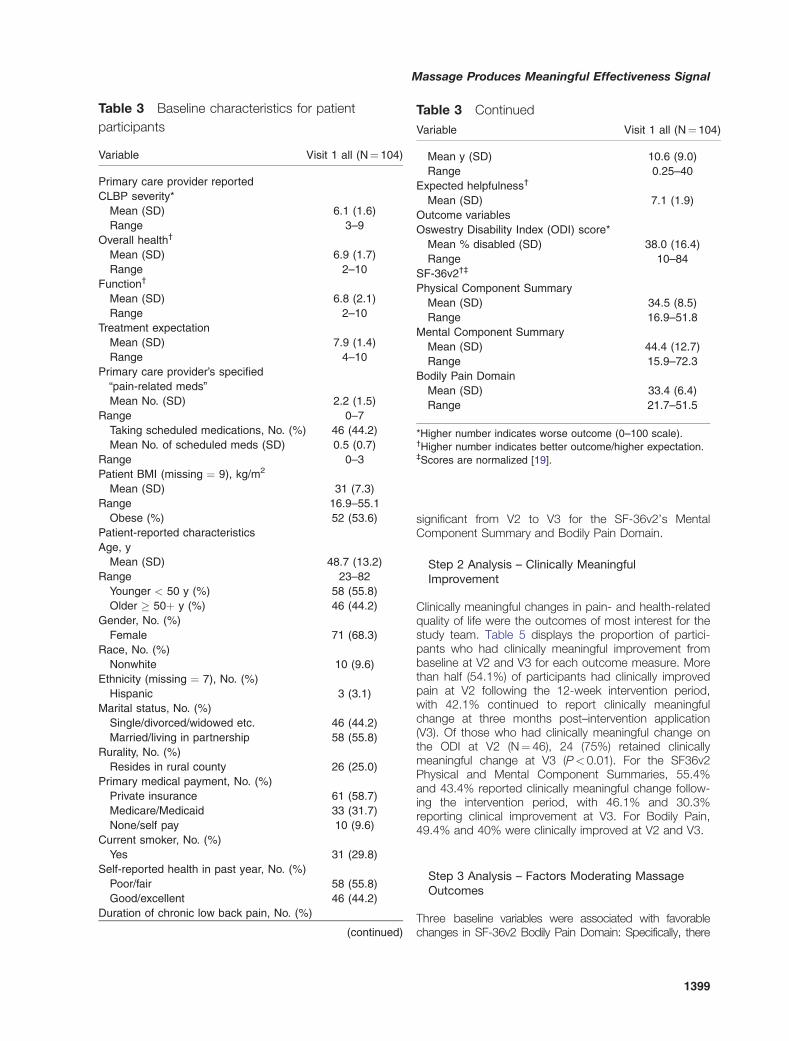
significant from V2 to V3 for the SF-36v2rsquos MentalComponent Summary and Bodily Pain Domain
Step 2 Analysis ndash Clinically MeaningfulImprovement
Clinically meaningful changes in pain- and health-relatedquality of life were the outcomes of most interest for thestudy team Table 5 displays the proportion of partici-pants who had clinically meaningful improvement frombaseline at V2 and V3 for each outcome measure Morethan half (541) of participants had clinically improvedpain at V2 following the 12-week intervention periodwith 421 continued to report clinically meaningfulchange at three months postndashintervention application(V3) Of those who had clinically meaningful change onthe ODI at V2 (Nfrac14 46) 24 (75) retained clinicallymeaningful change at V3 (Plt 001) For the SF36v2Physical and Mental Component Summaries 554and 434 reported clinically meaningful change follow-ing the intervention period with 461 and 303reporting clinical improvement at V3 For Bodily Pain494 and 40 were clinically improved at V2 and V3
Step 3 Analysis ndash Factors Moderating MassageOutcomes
Three baseline variables were associated with favorablechanges in SF-36v2 Bodily Pain Domain Specifically there
Table 3 Baseline characteristics for patient
participants
Variable Visit 1 all (Nfrac14104)
Primary care provider reported
CLBP severity
Mean (SD) 61 (16)
Range 3ndash9
Overall healthdagger
Mean (SD) 69 (17)
Range 2ndash10
Functiondagger
Mean (SD) 68 (21)
Range 2ndash10
Treatment expectation
Mean (SD) 79 (14)
Range 4ndash10
Primary care providerrsquos specified
ldquopain-related medsrdquo
Mean No (SD) 22 (15)
Range 0ndash7
Taking scheduled medications No () 46 (442)
Mean No of scheduled meds (SD) 05 (07)
Range 0ndash3
Patient BMI (missing frac14 9) kgm2
Mean (SD) 31 (73)
Range 169ndash551
Obese () 52 (536)
Patient-reported characteristics
Age y
Mean (SD) 487 (132)
Range 23ndash82
Younger lt 50 y () 58 (558)
Older 50thorn y () 46 (442)
Gender No ()
Female 71 (683)
Race No ()
Nonwhite 10 (96)
Ethnicity (missing frac14 7) No ()
Hispanic 3 (31)
Marital status No ()
Singledivorcedwidowed etc 46 (442)
Marriedliving in partnership 58 (558)
Rurality No ()
Resides in rural county 26 (250)
Primary medical payment No ()
Private insurance 61 (587)
MedicareMedicaid 33 (317)
Noneself pay 10 (96)
Current smoker No ()
Yes 31 (298)
Self-reported health in past year No ()
Poorfair 58 (558)
Goodexcellent 46 (442)
Duration of chronic low back pain No ()
(continued)
Table 3 Continued
Variable Visit 1 all (Nfrac14104)
Mean y (SD) 106 (90)
Range 025ndash40
Expected helpfulnessdagger
Mean (SD) 71 (19)
Outcome variables
Oswestry Disability Index (ODI) score
Mean disabled (SD) 380 (164)
Range 10ndash84
SF-36v2daggerDagger
Physical Component Summary
Mean (SD) 345 (85)
Range 169ndash518
Mental Component Summary
Mean (SD) 444 (127)
Range 159ndash723
Bodily Pain Domain
Mean (SD) 334 (64)
Range 217ndash515
Higher number indicates worse outcome (0ndash100 scale)daggerHigher number indicates better outcomehigher expectationDaggerScores are normalized [19]
Massage Produces Meaningful Effectiveness Signal
1399
was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

was a positive correlation between the measure and PCPrsquosperception of health (Pfrac14004) but inverse correlations of themeasure with PCP perception of pain (Plt001) and numberof pain-related medications (Pfrac14005) Regression analysisshowed that participants age 50 years and older had higherODI change scores from baseline to 12 weeks (46 6 97 vs103 6 108 Pfrac14 001) and ODI change scores increased asnumber of scheduled medications decreased (r2frac14007
Pfrac14 002) The negative influence of the number of scheduledmedications on ODI change scores remained when control-ling for baseline ODI score gender and duration of CLBP(model Plt001 number of scheduled medicationsPlt 001) Participants prescribed at least one scheduledmedication were 246 times more likely to not achieve clini-cally significant improvement in SF-36v2 physical functionalhealth (95 confidence interval [CI]frac14101ndash599) The
Figure 2 Group means of primary outcomes ODI frac14 Oswestry Disability IndexCompared to Baseline p6 001
Compared to 12-weeks p6 001
Table 4 Mean point change scores for primary outcomes
Outcome variables
Mean point change
score V1ndashV2
Mean point change
score V1ndashV3
Mean point change
score V2ndashV3
Oswestry Disability Index (ODI)
Mean (SD) 75 (106) 42 (121) 38 (109)
SF-36v2daggerDagger
Physical Component Summary
(missing frac14 2 TD2) mean (SD) 47 (70) 35 (81) 16 (64)
Mental Component Summary
(missing frac14 2 TD2) mean (SD) 31 (87) 08 (93) 30 (76)
Bodily Pain Domain
Mean (SD) 64 (86) 41 (89) 26 (76)
Determines group mean change is clinical significant improvement (see Table 2)daggerHigher number indicates better outcomehigher expectationDaggerSF-36v2 scores are T-scores with meanfrac1450 and SDfrac1410
Elder et al
1400
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-
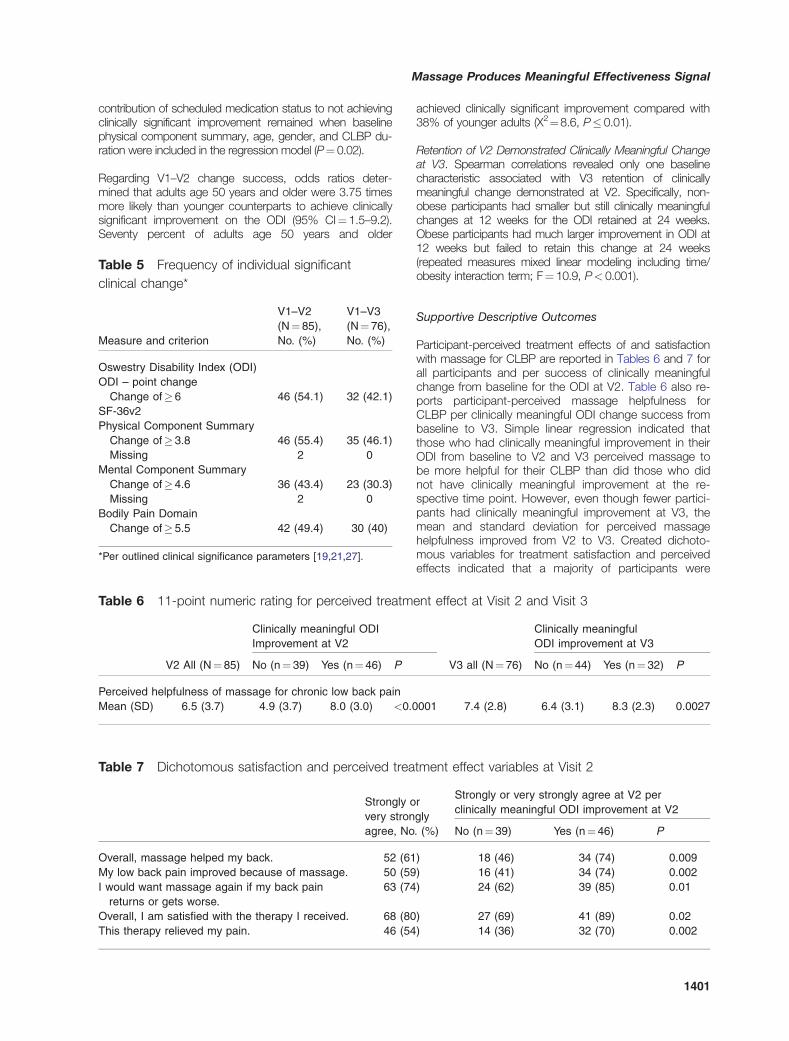
contribution of scheduled medication status to not achievingclinically significant improvement remained when baselinephysical component summary age gender and CLBP du-ration were included in the regression model (Pfrac14 002)
Regarding V1ndashV2 change success odds ratios deter-mined that adults age 50 years and older were 375 timesmore likely than younger counterparts to achieve clinicallysignificant improvement on the ODI (95 CIfrac1415ndash92)Seventy percent of adults age 50 years and older
achieved clinically significant improvement compared with38 of younger adults (X2frac1486 P 001)
Retention of V2 Demonstrated Clinically Meaningful Changeat V3 Spearman correlations revealed only one baselinecharacteristic associated with V3 retention of clinicallymeaningful change demonstrated at V2 Specifically non-obese participants had smaller but still clinically meaningfulchanges at 12 weeks for the ODI retained at 24 weeksObese participants had much larger improvement in ODI at12 weeks but failed to retain this change at 24 weeks(repeated measures mixed linear modeling including timeobesity interaction term Ffrac14 109 Plt 0001)
Supportive Descriptive Outcomes
Participant-perceived treatment effects of and satisfactionwith massage for CLBP are reported in Tables 6 and 7 forall participants and per success of clinically meaningfulchange from baseline for the ODI at V2 Table 6 also re-ports participant-perceived massage helpfulness forCLBP per clinically meaningful ODI change success frombaseline to V3 Simple linear regression indicated thatthose who had clinically meaningful improvement in theirODI from baseline to V2 and V3 perceived massage tobe more helpful for their CLBP than did those who didnot have clinically meaningful improvement at the re-spective time point However even though fewer partici-pants had clinically meaningful improvement at V3 themean and standard deviation for perceived massagehelpfulness improved from V2 to V3 Created dichoto-mous variables for treatment satisfaction and perceivedeffects indicated that a majority of participants were
Table 5 Frequency of individual significant
clinical change
Measure and criterion
V1ndashV2
(Nfrac1485)
No ()
V1ndashV3
(Nfrac14 76)
No ()
Oswestry Disability Index (ODI)
ODI ndash point change
Change of 6 46 (541) 32 (421)
SF-36v2
Physical Component Summary
Change of 38 46 (554) 35 (461)
Missing 2 0
Mental Component Summary
Change of 46 36 (434) 23 (303)
Missing 2 0
Bodily Pain Domain
Change of 55 42 (494) 30 (40)
Per outlined clinical significance parameters [192127]
Table 6 11-point numeric rating for perceived treatment effect at Visit 2 and Visit 3
V2 All (Nfrac1485)
Clinically meaningful ODI
Improvement at V2
V3 all (Nfrac1476)
Clinically meaningful
ODI improvement at V3
No (nfrac14 39) Yes (nfrac14 46) P No (nfrac1444) Yes (nfrac14 32) P
Perceived helpfulness of massage for chronic low back pain
Mean (SD) 65 (37) 49 (37) 80 (30) lt00001 74 (28) 64 (31) 83 (23) 00027
Table 7 Dichotomous satisfaction and perceived treatment effect variables at Visit 2
Strongly or
very strongly
agree No ()
Strongly or very strongly agree at V2 per
clinically meaningful ODI improvement at V2
No (nfrac14 39) Yes (nfrac1446) P
Overall massage helped my back 52 (61) 18 (46) 34 (74) 0009
My low back pain improved because of massage 50 (59) 16 (41) 34 (74) 0002
I would want massage again if my back pain
returns or gets worse
63 (74) 24 (62) 39 (85) 001
Overall I am satisfied with the therapy I received 68 (80) 27 (69) 41 (89) 002
This therapy relieved my pain 46 (54) 14 (36) 32 (70) 0002
Massage Produces Meaningful Effectiveness Signal
1401
satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

satisfied with and perceived benefit from massage fortheir CLBP although a higher proportion of participantswith clinically meaningful ODI improvement at V2 stronglyor very strongly agreed with each measurement statement
Discussion
Treatment options for CLBP are numerous with care of-ten discordant with clinical guidelines [28] While com-peting demands patient preferences and costsinfluence treatment decisions clinician perception ofwhether a treatment works for patients in their practicelikely plays a critical role in the selection of treatments[2930] Our findings of statistically and clinically mean-ingful benefit to CLBP after a course of real-world mas-sage therapy suggest the need for further study ofmassage when recommended by PCPs
We sought to address concerns that massage is insuffi-ciently studied in primary care and embraced a pragmaticapproach [31] Briefly PCPs made the decision as towhich patients to recommend to massage Patients werenot excluded due to comorbidities The broad inclusioncriteria permitted a wider range of patient characteristicsincluding age and obesity that proved to be significantfactors The ability of study massage therapists to developand apply individualized specific treatment plans informedby their unique training and continuing education experi-ences enhances confidence that specific massage inter-ventions need not be selected by the PCP but left up tothe clinical decision-making of massage therapists Theseare marked differences from methods of more controlledstudies and are reflective of how a course of massagetherapy would typically be applied and accessed in theUnited States
Patient-Related Factors Uncovered
Not limiting advanced age allowed for a broad agerange (23ndash82 years) in KYPROS This contributed to ourfinding that CLBP patients 50 years of age and oldermay have a greater probability of receiving clinicallymeaningful benefit from massage This is an importantfinding considering that CLBP prevalence is high in theBaby Boomer cohort (born 1946ndash1964) [32] and our di-chotomous age variable categorized this cohort in ourolder age category (50thorn years)
Another novel methodology aspect of KYPROS permit-ted inclusion of patients on DEA scheduled medicationsWhile the number of scheduled medications was nega-tively associated with ODI improvement the fact thatparticipants were on scheduled medications at all wasnot associated with the likelihood of clinically meaningfulbenefit in pain and disability It may be the quantity ofsuch medications that affects massage benefit ratherthan whether the patient is simply on scheduled medi-cations However we are unsure of the extent to whichour study sample is representative of those on sched-uled medications for CLBP First there were differences
in total number of pain-related medications betweenthose who were lost to follow-up or completed V2those with higher pharmacological burden were lesslikely to complete data collection at 12 weeks Inaddition patients who were prescribed at least onescheduled medication made up a larger proportion(70) of those for whom PCPs completed pocket cardsbut did not refer into the study or specifically recom-mend massage (Plt001) Of those who were referredto the study from PCPs and agreed to be contactedCLBP patients prescribed at least one scheduled medi-cation had a lower proportion of enrollment (63) thanthose not reported as being on a scheduled medication(73 nonsignificant P values) Understanding the extentto which massage is beneficial for those on scheduledmedications is important especially in light of efforts toreduce the use of opioids and other scheduled medica-tions in pain populations [3334] Accordingly targetedmethods to recruit and retain more pharmacologicallyburdened (and specifically opioid-using) CLBP patientsshould be incorporated in future studies
Brief Feasibility Findings
KYPROS incorporated novel design features the feasibil-ity of which had not been examined previously Novel de-sign features of note included the use of communitypracticing massage therapists for intervention deliveryand research participants accessing real-world massageas they would in a nonresearch setting While a singlemassage therapist was assigned to each participant alltherapistparticipant communication and contact were ini-tiated and maintained by study therapists and partici-pants Research study personnel were not involved withthe scheduling or management of treatments accessed orapplied By taking these key elements out of the hands ofthe researchers a less controlled and more pragmatic ap-proach was employed Ultimately we did not know theextent to which study participants would access andschedule the stipulated 10 massage sessions on theirown We found that 90 of patients initiated at least onemassage treatment and 60 received all 10 treatmentsThe extent to which our CLBP participants accessed andcompleted the course of massage treatments allowed inthis protocol gives us confidence that adequate treatmentexposure can be delivered with our study design
We also found age differences in attrition at V2 and V3 withthose younger than age 50 years more likely to drop out ofthe study Younger people may have more obligationsmaking the extra care visits required for massage treatmentto address their CLBP harder This finding is important lowadherence rates in younger patients may make these treat-ments less advisable from a clinical perspective and from aresearch perspective design considerations to support ac-cessibility may be needed for younger patients
The proportion of completed massage treatments was alsoconsidered in regards to feasibility of KYPROSrsquos novel studydesign Adherence to protocols of similar massage dosage(10 sessions over 10ndash12 weeks) for CLBP was considered
Elder et al
1402
as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

as completing eight treatments in prior research with88ndash93 of participants meeting adherence [35] By com-parison our study found that approximately 78 of thosewho completed data collection at 12 weeks (Nfrac14 85) hadaccessed at least eight sessions and so could be consid-ered compliant to treatment utilization We recognize thatour numbers are lower than those of other studies butKYPROS is the only study to our knowledge in which re-search study personnel were in no way responsible for inter-vention scheduling and follow-up All responsibility forscheduling and access fell to study participants and mas-sage therapists again reflecting real-world massage ac-cessutilization for most in the United States To this endour finding suggests that CLBP patients will access real-world massage treatment if recommended to do so by theirPCP at least under the conditions studied here in whichfee barriers were alleviated
Limitations and Future Directions
Several limitations of KYPROS could be addressed by alarger more comprehensive study As a pilot study de-veloping methods to examine massage in real-worldpractice KYPROS made no comparison to usual careTo elucidate the extent to which benefits experiencedby KYPROS participants were specifically attributable tomassage a no-treatment control or placebo comparisongroup is needed [36] However changes reported herewere sufficient to be clinically meaningful specificallypsychometric research has determined a six-pointchange as representing meaningful differences in lowback pain with disability for the ODI [212327] While a10-point change has been suggested as the minimallyclinically important change for the ODI Ostelo and deVet also state the 10-point threshold is not set and de-pending on aims ldquoshould be used as an indicationrdquo[25] For our pilot and feasibility purposes and consider-ing that many participants not meeting the six-pointchange threshold in KYPROS still reported treatmentsatisfaction (69) pain improvement (41) pain relief(36) and the desire to have massage again if the painwere to return or get worse (62) we are confident inour use of the validated ODI six-point change thresholdas indicative of meaningful change in low back pain anddisability Without a control group we cannot unequivo-cally determine that massage was efficacious howeverKYPROS results serve as a signal of real-world massageeffect for CLBP and further study using our pilotedtreatment application methods is needed Finally thisstudy was conducted exclusively with Kentucky PCPsand patients attitudes toward and availability of thetreatments may differ elsewhere [37] HoweverKYPROS results do speak to a region where massageis more novel [38] and not covered by health plans
Conclusion
KYPROS results provide a meaningful signal of massageeffect and call for further research in practice settingsemploying pragmatic designs with control groups to ex-amine real-world massage effectiveness for primary care
patients with CLBP Our exploratory findings about therole of age medications and obesity on clinically mean-ing benefit and retention of benefit from massage forCLBP patients are promising Increased study breadthwill allow further examination of these variables includ-ing physician perceptions by treatment effects as wellas other patient-oriented variables in relation to healthoutcomes Ultimately our results and efforts may moveus closer to giving PCPs comprehensive multiple optionstrategies for select patient characteristics
Authorsrsquo Contributions
Authors William G Elder and Niki Munk contributedequally to this work and are co-first authors
Acknowledgments
In alphabetical order Heather M Bush PhD consulted onstatistical analyses Honey V Elder assisted with projectdesign and grant writing Maureen A Flannery MD MPHand David A Greene MD primary care physicians cham-pioned project and consulted on methods pertaining toprovider practices Steve Kramen MD contributed to(and member of) studyrsquos Data Safety Monitoring BoardLaura Lee Johnson PhD NIH statistician providingexplanations for using historical data in place of controlgroups medical students Jennifer France Jake ByrneCandace McKee and Nishi Patel assisted in preparing thePCP survey instruments literature review andor recruit-ing the PCPs and LMTs Trish Rippetoe Freeman RPhPhD consulted on the coding and categorization of medi-cations Laura Lyons MPH conducted extensive datacollection and data entry Marta Mendiondo PhD pro-vided substantive contribution to the study design and sta-tistical analysis plan Karen Roper PhD providedmanuscript editing formatting proofing and submissionsupport Stephen Wells MPH served as original ProjectManager massage therapists enthusiastic contributiondelivering massage therapy and providing data primarycare clinicians for their participation and their staff supportfor facilitating patient recruitment
References1 US Burden of Disease Collaborators The state of
US health 1990-2010 Burden of diseases injuriesand risk factors JAMA 2013310(6)591ndash608
2 Pengel LH Herbert RD Maher CG Refshauge KMAcute low back pain Systematic review of its prog-nosis BMJ 2003327(7410)323
3 Von Korff M Saunders K The course of back painin primary care Spine 199621(24)2833ndash7
4 Gore M Sadosky A Stacey BR Tai KS Leslie D Theburden of chronic low back pain Clinical comorbidities
Massage Produces Meaningful Effectiveness Signal
1403
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-
treatment patterns and health care costs in usual caresettings Spine 201237(11)E668ndash77
5 Astin JA Shapiro SL Eisenberg DM Forys KLMind-body medicine State of the science implica-tions for practice JABFM 200316(2)131ndash47
6 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Intern Med 2011155(1)1ndash9
7 Chou R Huffman LH Medications for acute andchronic low back pain A review of the evidence foran American Pain SocietyAmerican College ofPhysicians clinical practice guideline Ann InternMed 2007147(7)505ndash14
8 Chou R Huffman LH Nonpharmacologic therapiesfor acute and chronic low back pain A review of theevidence for an American Pain SocietyAmericanCollege of Physicians clinical practice guideline AnnIntern Med 2007147(7)492ndash504
9 Furlan AD Yazdi F Tsertsvadze A et alComplementary and Alternative Therapies for BackPain II Evidence ReportsTechnology AssessmentsNo 194 Rockville MD Agency for HealthcareResearch and Quality 20101941ndash764
10 Richmond J Berman B Docherty J et alIntegration of behavioral and relaxation approachesinto the treatment of chronic pain and insomniaJAMA 1996276(4)313ndash8
11 Chou R Huffman LH Guideline for the Evaluationand Management of Low Back Pain EvidenceReview Glenview IL American Pain Society 2009
12 Chou R Qaseem A Snow V et al Diagnosis andtreatment of low back pain A joint clinical practiceguideline from the American College of Physiciansand the American Pain Society Ann Intern Med2007147(7)478ndash91
13 Furlan AD Giraldo M Baskwill A Irvin E ImamuraM Massage for low-back pain Cochrane DatabaseSyst Rev 2015(9)CD001929
14 Elder WG Jr King M Dassow P Macy B Managinglower back pain You may be doing too much JFam Pract 200958(4)180ndash6
15 National Center for Complementary and AlternativeMedicine (NCCAM) National Cancer Institute (NCI)Outcomes and cost-effectiveness studies of CAMusing existing practice-based research networks2007 Available at httpgrantsnihgovgrantsfundingr21htm (accessed November 2015)
16 Farb A Center for Devices and Radiological Health(CDRH) Center for Devices and Radiological Health(CDRH) Food and Drug Administration (FDA) PublicworkshopmdashOptimizing clinical trial design for the de-velopment of pediatric cardiovascular devices Whenis a randomized clinical trial appropriate vs a histori-cal control vs a performance goal 2014 Availableat httpwwwfdagovdownloadsmedicaldevicesnewseventsworkshopsconferencesucm240786pdf(accessed November 2015)
17 Munk N Stewart K Love MM Carter E Elder WGThe intersection of massage practice and researchCommunity massage therapists as research person-nel on an NIH-funded effectiveness study Int J TherMassage Bodywork 20147(2)10ndash9
18 Fairbank JC Pynsent PB The Oswestry DisabilityIndex Spine 200025(22)2940ndash52
19 Maruish ME ed Userrsquos Manual for the SF-36v23rd edition Lincoln RI Quality Metric Incorporated2011
20 Holm I Friis A Storheim K Brox JI Measuring self-reported functional status and pain in patients withchronic low back pain by postal questionnaires Areliability study Spine 200328(8)828ndash33
21 Roland M Fairbank J The Roland-Morris DisabilityQuestionnaire and the Oswestry DisabilityQuestionnaire Spine 200025(24)3115ndash24
22 Tonosu J Takeshita K Hara N et al The normativescore and the cut-off value of the Oswestry DisabilityIndex (ODI) Eur Spine J 201221(8)1596ndash602
23 Muller U Duetz MS Roeder C Greenough CGCondition-specific outcome measures for low backpain Part I Validation Eur Spine J 200413(4)301ndash13
24 Saunders RP Evans MH Joshi P Developing aprocess-evaluation plan for assessing health promo-tion program implementation A how-to guideHealth Promot Pract 20056(2)134ndash47
25 Ostelo RW de Vet HC Clinically important out-comes in low back pain Best Pract Res ClinRheumatol 200519(4)593ndash607
26 Harris PA Taylor R Thielke R et al Research elec-tronic data capture (REDCap)-A metadata-drivenmethodology and workflow process for providingtranslational research informatics support J BiomedInform 200942(2)377ndash81
27 Muller U Roeder C Dubs L Duetz MS GreenoughCG Condition-specific outcome measures for low
Elder et al
1404
back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-

back pain Part II Scale construction Eur Spine J200413(4)314ndash24
28 Mafi JN McCarthy EP Davis RB Landon BEWorsening trends in the management and treatment ofback pain JAMA Intern Med 2013173(17)1573ndash81
29 Hsu C Cherkin DC Hoffmeyer S Sherman KJPhillips WR Patient and clinician openness to in-cluding a broader range of healing options in pri-mary care Ann Fam Med 20119(5)447ndash53
30 Patient-Centered Outcomes Research InstituteTreatment options for back pain 2013 Available athttpwwwpcoriorgtreatment-options-back-pain(accessed November 2015)
31 Elder WG Munk N Using the Pragmatic-Explanatory Continuum Indicator Summary (PRECIS)model in clinical research Application to refine apractice-based research network (PBRN) studyJABFM 201427(6)846ndash54
32 Smith M Davis MA Stano M Whedon JM Agingbaby boomers and the rising cost of chronic backpain Secular trend analysis of longitudinal MedicalExpenditures Panel Survey data for years 2000 to2007 J Manipulative Physiol Ther 201336(1)2ndash11
33 Franklin GM Fulton-Kehoe D Turner JA SullivanMD Wickizer TM Changes in opioid prescribing forchronic pain in Washington State J Am Board FamMed 201326(4)394ndash400
34 Westanmo A Marshall P Jones E Burns K KrebsEE Opioid dose reduction in a VA Health CareSystemmdashImplementation of a primary care popula-tion-level initiative Pain Med 2015161019ndash26
35 Cherkin DC Sherman KJ Kahn J et al A compari-son of the effects of 2 types of massage and usualcare on chronic low back pain A randomized con-trolled trial Ann Int Med 2011155(1)1ndash9
36 de Vet HC Beckerman H Terwee CB Terluin BBouter LM Definition of clinical differences JRheumatol 200633(2)434
37 Barnes PM Bloom B Nahin RL Complementaryand Alternative Medicine Use Among Adults andChildren United States 2007 Hyattsville MDNational Center for Health Statistics 2008
38 Flannery MA Love MM Pearce KA Luan JJ ElderWG Communication about complementary and al-ternative medicine Perspectives of primary care cli-nicians Altern Ther Health Med 200612(1)56ndash63
Massage Produces Meaningful Effectiveness Signal
1405
- pnw347-TF1
- pnw347-TF2
- pnw347-TF3
- pnw347-TF4
- pnw347-TF5
- pnw347-TF6
- pnw347-TF7
- pnw347-TF8
- pnw347-TF9
-




















