
Plasma kisspeptin is raised in patients with gestational trophoblastic neoplasia and falls during...
36
1 Plasma kisspeptin is raised in patients with gestational trophoblastic neoplasia and falls during treatment Running title: Kisspeptin is raised in trophoblastic neoplasia Waljit S. Dhillo 1 , Philip Savage 2 , Kevin G. Murphy 1 , Owais B. Chaudhri 1 , Michael Patterson 1 , Gurjinder M. Nijher 1 , Vanessa M. Foggo 2 , Garin S. Dancey 2 , Hugh Mitchell 2 , Michael J. Seckl 2 , Mohammad A. Ghatei 1 & Stephen R. Bloom 1 1 Department of Metabolic Medicine, Hammersmith Hospital, Imperial College London, UK & 2 Department of Medical Oncology, Charing Cross Hospital, Imperial College London, UK. Corresponding author: Prof SR Bloom, Department of Metabolic Medicine, Hammersmith Hospital, Imperial College London, 6 th Floor Commonwealth Building, Du Cane Road, London, W12 ONN, UK. Tel: +44 208 383 3242. Fax: +44 208 383 3142. E-mail: [email protected] . Page 1 of 36 Articles in PresS. Am J Physiol Endocrinol Metab (June 6, 2006). doi:10.1152/ajpendo.00555.2005 Copyright © 2006 by the American Physiological Society.
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Plasma kisspeptin is raised in patients with gestational trophoblastic neoplasia and falls during...

1
Plasma kisspeptin is raised in patients with gestational trophoblastic neoplasia and
falls during treatment
Running title: Kisspeptin is raised in trophoblastic neoplasia
Waljit S. Dhillo1, Philip Savage2, Kevin G. Murphy1, Owais B. Chaudhri1, Michael
Patterson1, Gurjinder M. Nijher1, Vanessa M. Foggo2, Garin S. Dancey2, Hugh Mitchell2,
Michael J. Seckl2, Mohammad A. Ghatei1 & Stephen R. Bloom1
1Department of Metabolic Medicine, Hammersmith Hospital, Imperial College London,
UK & 2Department of Medical Oncology, Charing Cross Hospital, Imperial College
London, UK.
Corresponding author: Prof SR Bloom, Department of Metabolic Medicine,
Hammersmith Hospital, Imperial College London, 6th Floor Commonwealth Building,
Du Cane Road, London, W12 ONN, UK. Tel: +44 208 383 3242. Fax: +44 208 383
3142. E-mail: [email protected].
Page 1 of 36Articles in PresS. Am J Physiol Endocrinol Metab (June 6, 2006). doi:10.1152/ajpendo.00555.2005
Copyright © 2006 by the American Physiological Society.

2
Abstract Kisspeptin is a 54 amino acid peptide, encoded by the anti-metastasis gene
KiSS-1, that activates the G-protein-coupled receptor, GPR54. The kisspeptin/GPR54
system is critical to normal reproductive development. KiSS-1 gene expression is
increased in the human placenta in normal and molar pregnancies. Circulating kisspeptin
is dramatically increased in normal pregnancy but levels in gestational trophoblastic
neoplasia (GTN) have not previously been reported. The present study was designed to
determine if plasma kisspeptin levels are altered in patients with malignant GTN. Thirty
nine blood samples were taken from 11 patients with malignant GTN at presentation,
during and following chemotherapy. Blood was also sampled from non-pregnant and
pregnant volunteers. Plasma kisspeptin immunoreactivity (-IR) and human chorionic
gonadotrophin (hCG) concentrations were measured. Plasma kisspeptin-IR concentration
in non-pregnant (n=16) females <2 pmol/L. Plasma kisspeptin-IR in females in the first
trimester of pregnancy (n=13) was 803 ± 125 pmol/L, in the third trimester of pregnancy
(n=7) was 2483 ± 302 pmol/L and day 15 post partum (n=7) was <2 pmol/L. Plasma
kisspeptin-IR and hCG concentrations in patients with malignant GTN were elevated at
presentation and fell during and following treatment with chemotherapy in each patient
(mean plasma kisspeptin-IR: pre-chemotherapy 1363 ± 1076 pmol/L vs. post-
chemotherapy <2 pmol/L, p<0.0001. Mean plasma hCG: pre-chemotherapy 227191 ±
152354 U/L vs. post-chemotherapy 2 U/L, p<0.0001). Plasma kisspeptin-IR strongly
positively correlated with plasma hCG levels (r2=0.99, p<0.0001). Our results suggest
that measurement of plasma kisspeptin-IR may be a novel tumor marker in patients with
malignant GTN.
Keywords: kisspeptin, metastin, hCG, GPR54, gestational trophoblastic neoplasia.
Page 2 of 36
3
Introduction
Kisspeptin is a 54 amino acid peptide, encoded by the KiSS-1 gene (20, 21, 32) which
activates the previously orphan G-protein-coupled receptor, GPR54 (20). The
kisspeptin/GPR54 system has recently been shown to be critical to normal reproductive
development in rodents and humans. GPR54 deficient (GPR54-/-) mice have abnormal
sexual development, low circulating gonadotrophin concentrations and are infertile (12,
39). GPR54 mutations have been shown to cause hypogonadotrophic hypogonadism in
humans (7, 39, 40). Kisspeptin potently stimulates the hypothalamo-pituitary-gonadal
(HPG) axis in rodents, primates and human males (9, 13, 25, 28, 29, 30, 41, 46). The
stimulatory effects of kisspeptin on the HPG axis appear to be mediated via the
hypothalamic gonadotrophin releasing hormone (GnRH) system (13, 17, 25, 26).
Hypothalamic KiSS-1 expression is regulated by circulating sex steroids in rodents and
primates, suggesting that kisspeptin is involved in the HPG negative feedback cycle (17,
28, 41, 43, 44).
KiSS-1 and GPR54 genes are highly expressed in the placenta (1, 21, 32) and endogenous
forms of kisspeptin 54, 14 and 13 amino acids in length have been isolated from human
placenta. The common C terminal decapeptide shared by these forms, kisspeptin-10, is
the minimum sequence necessary for receptor activation (20, 27, 32) and is secreted from
cultured human trophoblasts (1). All these kisspeptin fragments, including kisspeptin-10,
have a similar affinity and efficacy in vitro at the GPR54 (20). KiSS-1 and GPR54 gene
expression are highly expressed in the placenta of normal pregnant humans (1, 18, 35).
Circulating kisspeptin is low in healthy men and non-pregnant women, but dramatically
Page 3 of 36

4
increased in normal pregnancy, reaching a concentration approximately 7000 fold higher
in the third trimester compared to non-pregnant controls (14).
The kisspeptin/GPR54 system is also important in tumor biology. KiSS-1 was first
discovered as an anti-metastasis gene (21, 32). KiSS-1 suppresses metastasis in human
breast carcinomas (22), and KiSS-1 expression inversely correlates with increased
metastasis and/or cancer progression in gastric, esophageal and pancreatic cancer,
phaeochromocytoma, bladder cancer, melanoma and breast cancer (8, 15, 24, 31, 37, 42,
45). KiSS-1 therefore represents a potential marker to distinguish metastatic from non-
metastatic forms of specific cancers.
Placental KiSS-1 gene expression has also recently been shown to inversely correlate
with cancer progression in gestational trophoblastic disease (GTD) or neoplasia (GTN)
(18, 35). GTN comprises a number of disorders characterized by an abnormal
proliferation of placental tissue. Complete (CHM) and partial hydatidiform moles (PHM)
are the commonest form of the disease, occurring in 1-3 of every 1000 pregnancies. They
are best regarded as premalignant, as 16% of CHM and 0.5% of PHM transform with
time into the malignant conditions of invasive mole, choriocarcinoma (CC) or placental
site trophoblastic tumor (PSTT) (33, 38). The latter three diseases are often referred to as
malignant GTN or as gestational trophoblastic tumors.
All forms of GTN secrete human chorionic gonadotrophin (hCG) and serum
measurement of this hormone is extremely helpful in the diagnosis, staging and
subsequent assessment of the therapeutic response of malignant GTN. Following uterine
evacuation of a molar pregnancy, the serum hCG in most women returns to normal.
However, in those developing malignant change, the hCG plateaus and/or starts rising
Page 4 of 36

5
and requires urgent chemotherapy which is curative in virtually 100% of cases. The
onset of malignant change following a molar pregnancy can take some months to occur
and women on hCG surveillance have to avoid becoming pregnant. Clearly, earlier
detection of this malignant change would be helpful, as it would enable rapid selection of
patients for additional therapy. Consequently, the development of new markers for GTN
may provide better predictive models of trophoblastic behavior. Moreover, many existing
commercial assays for hCG detection are troubled by false positives (3), usually induced
by heterophile antibodies. Heterophile antibodies are IgG immunoglobulins raised against
poorly defined antigens from other species and can be found in 3–15% of healthy people.
Furthermore, these assays usually do not detect all the forms of circulating hCG produced
in GTN (5, 19). New markers might also help to reduce these problems.
We hypothesized that plasma kisspeptin-IR may be altered in patients with malignant
GTN since placental KiSS-1 gene expression is increased in normal and molar
pregnancies (18, 35) and circulating kisspeptin is dramatically increased in normal
pregnancy (14).
In the present study we used a specific radioimmunoassay (RIA) for human kisspeptin
and investigated kisspeptin-IR in human plasma in pregnant and non-pregnant volunteers
and in patients with malignant GTN at presentation, during and following chemotherapy.
Kisspeptin-IR in plasma was characterized using reverse phase fast protein liquid
chromatography (FPLC). We found that kisspeptin-IR was elevated in patients with
malignant GTN compared to controls and positively correlated with plasma hCG levels.
Chemotherapy treatment reduced kisspeptin-IR and hCG levels in each patient.
Page 5 of 36
6
Methods
Subjects
Eleven healthy females who had never been pregnant with normal menstrual cycles
(mean age 26.1 ± 2.2 years), five healthy females who had previously been pregnant with
normal menstrual cycles (mean age 29.1 ± 3.1 years), thirteen healthy women in the first
trimester (10.4 ± 0.5 weeks) of a normal pregnancy (mean age 30.7 ± 1.7 years), seven
healthy women at 38 weeks of a normal pregnancy and the same women 15 days post
partum (mean age 34.4 ± 1.1 years) and eleven female subjects diagnosed with invasive
mole (mean age 27.2 ± 3.4 years) participated in the study. Patients were diagnosed with
molar pregnancy if they had amenorrhea with a raised plasma hCG and an ultrasound
confirming a molar pregnancy. Patients were diagnosed with an invasive mole if they had
a persistently elevated or rising serum and urine hCG following evacuation of their molar
pregnancy. Blood was collected at first presentation (between 1 to 6 months after removal
of their molar pregnancy) and then during and following chemotherapy as their serum
hCG levels fell. Patients with malignant GTN had their disease risk assessed according to
the FIGO scoring system for GTN (16). Women scoring six or less (low risk) received
intramuscular methotrexate on alternate days for eight days, followed by six rest days,
with each course consisting of four injections (36). Women scoring seven or more (high
risk) received combination therapy with intravenous etoposide, methotrexate, dactomycin
for two days followed by vincristine and cyclophosphamide (EMA-CO) one week later.
The course was then repeated after six days. Treatment was continued, in all cases, until
the hCG level had returned to normal and then for a further six consecutive weeks (36).
Page 6 of 36
7
Subjects gave written informed consent and ethical approval was obtained from the
Hammersmith and Queen Charlotte’s & Chelsea Hospitals Research Ethics Committee
(number 04/Q0406/80). Studies were performed in accordance with the Declaration of
Helsinki. Blood was taken from all subjects between 9am and noon.
(i) Determination of plasma kisspeptin-IR in healthy female volunteers
Eleven healthy females with regular menstrual cycles, not taking any oral contraception
had blood sampled during the follicular and luteal phases of their menstrual cycle. Five
healthy females who had previously been pregnant (mean 2.9 ± 2.4 years post partum)
with normal menstrual cycles also had blood sampled in the follicular phase of their
menstrual cycle. Thirteen healthy pregnant women had blood sampled during the first
trimester (10.4 ± 0.5 weeks) of their pregnancy. Blood was also sampled from seven
healthy pregnant females at both 38 ± 0.8 weeks gestation of normal pregnancy and day
15 ± 6 post partum. Ten ml of blood was taken and collected into lithium-heparin tubes
(LIP Ltd., Cambridge, UK) containing 5000 kallikrein inhibitor units (0.2 ml) aprotinin
(Trasylol, Bayer, Newbury, UK) and stored on ice. After centrifugation, plasma was
immediately separated and stored at -20oC until measurement of kisspeptin-IR in all
subjects and hCG in the pregnant subjects.
(ii) Determination of plasma hormones in patients at diagnosis of malignant GTN,
during treatment and post chemotherapy
Blood was sampled from patients with malignant GTN at first presentation, during
chemotherapy and following chemotherapy once the patient’s plasma hCG had fallen
Page 7 of 36

8
back into the normal range for non-pregnant females. The average length of time between
the collection of the second blood sample and the initiation of chemotherapy was 21.1 ±
2.8 days. The average time post chemotherapy at which a blood sample was taken was
14.3 ± 1.4 days. Blood was collected into lithium-heparin tubes (LIP Ltd., Cambridge,
UK) containing 5000 kallikrein inhibitor units (0.2 ml) aprotinin (Trasylol, Bayer,
Newbury, UK) and stored on ice. After centrifugation, plasma was immediately separated
and stored at -20oC until measurement of kisspeptin-IR, hCG, progesterone and
oestradiol.
(iii) Characterization of kisspeptin-IR in human plasma
Kisspeptin-IR was characterized in human plasma from patients with malignant GTN
(n=4).
Peptide extraction procedure
Peptide was extracted from plasma using Sep-Pak C18 cartridges (Waters Ltd.,
Hertfordshire, UK) as previously described (34). Briefly, Sep-Pak C-18 cartridges were
activated using 10 ml of 100% methanol and then 20 ml water. Plasma (2ml) from
patients with malignant GTN was mixed with 2 ml of 0.1M HCl and loaded onto the
cartridge. The cartridge was then washed with 10 ml of 4% acetic acid (vol/vol). The Sep-
Pak bound sample was eluted in 1.5 ml methanol and this eluant dried in a Savant
vacuum centrifuge and reconstituted in water plus 0.05% trifluoroacetic acid (TFA)
(vol/vol) for FPLC.
Page 8 of 36
9
Reverse phase FPLC
Peptide extracts from plasma were dissolved in 0.6 ml distilled water plus TFA 0.05%
(vol/vol). Of this volume, 0.5 ml was fractionated by FPLC on a high-resolution reverse-
phase (Pep RPC 1 ml HR) C-18 column (Pharmacia, Uppsala, Sweden) as previously
described (1). The column was eluted with a 24.5–29.5% gradient of acetonitrile
(AcN)/water containing 0.05% (vol/vol) TFA over 40 min and fractions collected at 1
min intervals. The kisspeptin-IR in all fractions was determined by radioimmunoassay.
The remaining 0.1 ml of sample was used to calculate the percentage recovery. Recovery
was calculated as kisspeptin-IR (pmol) recovered from each sample, compared with
kisspeptin-IR loaded on to the FPLC column (pmol), multiplied by 100 and expressed as
a percentage. Prolactin releasing peptide was also run on this column to determine its
elution position.
Analytical methods
(i) Human chorionic gonadotrophin, progesterone and oestradiol measurement
Human chorionic gondotrophin was measured by the Endocrine Laboratory at Charing
Cross Hospital (London, UK) using the UK RIA (radioimmunoassay) (6). Progesterone
and oestradiol were measured using commercially available Chemiluminescent
Microparticle Immunoassays (ARCHITECT progesterone and ARCHITECT oestradiol,
Abbott Laboratories, Abbott Park, Illinois, USA).
(ii) Kisspeptin radioimmunoassay (RIA)
Page 9 of 36
10
Plasma kisspeptin was measured using an established RIA (9). Briefly, antibody GQ2
was raised in a sheep immunized with synthetic human kisspeptin-54 (Bachem, UK Ltd.),
conjugated to BSA by glutaraldehyde and used at a final dilution of 1: 3,500,000. The
antibody cross reacted 100% with human kisspeptin-54, kisspeptin-14, and kisspeptin-10
and less than 0.01% with any other related human RFamide (arginine phenylalanine
amide) peptide, including prolactin releasing peptide, RF amide related peptide (RFRP1),
RFRP2, RFRP 3 neuropeptide FF and neuropeptide AF. The 125I-kisspeptin-54 label was
prepared using the iodogen method and purified by reverse phase high pressure liquid
chromatography on a C18 column (Waters, Milford, USA) over a 15-45% 90 minute
gradient of AcN / water 0.1% (vol/vol) TFA. The specific activity of the kisspeptin label
was 56 Bq/fmol. The assay was performed in duplicate using dilutions of neat plasma in
0.7 ml of 0.06 M phosphate buffer pH 7.2 containing 0.3% bovine serum albumin and
incubated for 3 days at 4oC. Free and antibody bound label were then separated by
charcoal adsorption. The assay detected changes of 2 pmol/L of plasma kisspeptin-IR
with a 95% confidence limit. The intra- and inter-assay coefficients of variation were
8.3% and 10.2% respectively.
Statistical analysis
All results are presented as mean (± SEM). The differences between plasma kisspeptin-
IR pre chemotherapy and post chemotherapy and hCG pre chemotherapy and post
chemotherapy were calculated by a Mann Whitney Rank Sum test. Correlations were
estimated using Pearson Product Moment analysis. In all cases p < 0.05 was considered
to be statistically significant.
Page 10 of 36

11
Results
(i) Determination of plasma kisspeptin-IR in healthy female volunteers
Plasma kisspeptin-IR concentration in all non-pregnant females investigated was below
the detection limit of the assay (<2 pmol/L). The plasma kisspeptin in pregnant females
in the first trimester of normal pregnancy (n=13) was 803 ± 125 pmol/L and plasma hCG
was 72,053 ± 10, 936 U/L. The plasma kisspeptin in pregnant females third trimestser of
normal pregnancy (n=7) was 2483 ± 302 pmol/L and plasma hCG was 28,818 ± 11, 348
U/L. By day 15 post partum plasma (n=7), plasma kisspeptin was below the detection
limit of the assay (<2 pmol/L) (Figure 1).
(ii) Determination of plasma hormones in patients at diagnosis of malignant GTN,
during treatment and post chemotherapy
Plasma kisspeptin-IR in patients with malignant GTN were elevated at presentation and
fell during and following treatment with chemotherapy in each patient (plasma
kisspeptin-IR: pre chemotherapy 1363 ± 1076 pmol/L vs. post chemotherapy <2 pmol/L,
n=11, p<0.0001) (Figure 2a, supplementary information Table 1). As expected plasma
hCG levels also showed a similar pattern (plasma hCG: pre-chemotherapy 227191 ±
152354 U/L vs. post chemotherapy 2 U/L, n=11, p<0.0001) (Figure 2b, supplementary
information Table 1). Plasma kisspeptin-IR strongly positively correlated with plasma
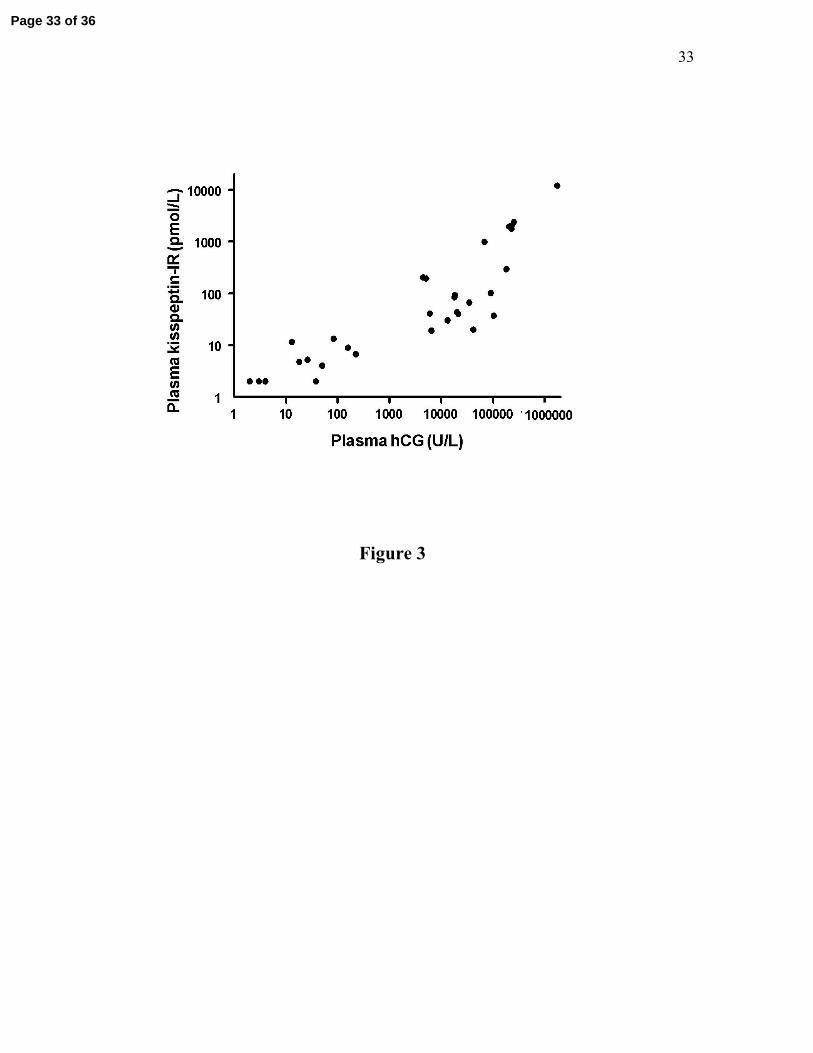
hCG levels (r2= 0.99, n=39, p<0.0001, Figure 3). Plasma kisspeptin-IR showed
significant positive correlations with circulating levels of progesterone (r2 = 0.92, n=39,
p<0.0001) and oestradiol (r2 = 0.70, n=39, p<0.0001) as did hCG (r2 = 0.89, n=39,
p<0.0001 for progesterone and r2 = 0.64, n=39, p<0.0001 for oestradiol).
Page 11 of 36

12
(iii) Analysis of kisspeptin-IR in human plasma
Reverse-phase FPLC was used to further analyze kisspeptin-IR extracted from plasma by
Sep-Pak cartridge. All columns had a recovery greater than 60%. In each plasma extract
the kisspeptin-IR eluted in a single peak corresponding to the elution position of synthetic
kisspeptin-54 (fractions 14-17). Synthetic prolactin releasing peptide eluted at an earlier
fraction compared to kisspeptin-54 (fraction 10). A representative profile from a patient
with malignant GTN is shown in Figure 4.
Page 12 of 36

13
Discussion
Plasma kisspeptin has been proposed as a novel tumor marker indicating the metastatic
potential of specific tumors (14). However, to date no reports have investigated this
possibility by examining the correlation between circulating kisspeptin concentrations
and malignancy. The data described in this paper demonstrate that plasma kisspeptin-IR
is raised in patients with malignant GTN, and falls during treatment. Our results suggest
that plasma kisspeptin-IR may be a novel tumor marker in patients with this disease.
To ensure that the elevated kisspeptin-IR levels observed were not due to levels of
circulating kisspeptin persisting after pregnancy, we compared plasma kisspeptin levels
from malignant GTN patients to those of normal post-partum women. Blood was
collected from GTN patients at first presentation between 1 and 6 months after removal
of their molar pregnancy. Plasma kisspeptin levels in normal women were below the
detection limit of the assay (<2 pmol/L) as early as day 15 post partum, suggesting that
the elevated kisspeptin levels observed in GTN patients were not due to normal post-
partum processes.
Though the kisspeptin/GPR54 system has recently been shown to be critical to normal
reproductive development in rodents and man (7, 12, 39, 40), the role of circulating
kisspeptin is currently unclear. Kisspeptin circulates in non-pregnant females at
concentrations lower than 2pmol/L (14). However, high levels of plasma kisspeptin-IR
are seen in normal pregnancy. The plasma kisspeptin-IR in pregnant females measured
using our single site radioimmunoassay are lower than previously published plasma
kisspeptin levels using a two site enzyme immunoassay (14). However, in accord with
previously published results, plasma kisspeptin was found to be greatly increased in
Page 13 of 36

14
pregnancy, and to rise between the first and third trimesters. Further experiments are
needed to determine whether the differences in absolute concentrations detected are due
to, for example, the different assay methods used, the subtle differences in subject
populations, or the slightly different protocols used for blood sampling and storage. There
is currently no international standard protocol for measuring plasma kisspeptin, and it
would be interesting to directly compare the kisspeptin assays currently available.
The source of circulating kisspeptin in pregnant women is assumed to be the placenta,
where the KiSS-1 gene is highly expressed (14, 18). The role of elevated plasma
kisspeptin-IR in pregnancy and malignant GTN is currently unclear, and the release of
kisspeptin may be regulated by different mechanisms in these conditions. Kisspeptin
mediates its effects on the HPG axis via an increase in GnRH. It is therefore possible that
elevated plasma kisspeptin levels in pregnancy chronically increase GnRH release,
leading to a downregulation of the HPG axis, as is seen following the administration of
synthetic GnRH agonists (11). The KiSS-1 gene is an anti-metastasis gene, and
transfection of melanoma cells with KiSS-1 cDNA expression-dependently suppresses
metastasis (21, 23). Kisspeptin-10 has been shown to inhibit trophoblast migration
without affecting proliferation in vitro (1). Interestingly, placental KiSS-1 gene
expression has been shown to inversely correlate with the metastatic potential of patients
with GTN. Placental KiSS-1 gene expression in molar pregnancy is elevated to a similar
degree to that seen in normal pregnancy, but is undetectable in choriocarcinoma (18, 35).
Plasma kisspeptin-IR may therefore be elevated in patients with an invasive mole to
inhibit tumor metastasis and the development of choriocarcinoma (18, 35). Further
studies are required to determine whether plasma kisspeptin-IR is significantly lower in
Page 14 of 36

15
patients with choriocarcinoma compared to plasma kisspeptin-IR in patients with molar
pregnancy. It would be of particular interest to investigate whether patients with molar
pregnancy who go on to develop choriocarcinoma have different circulating kisspeptin
levels to those who do not.
Measurement of placental KiSS-1 gene expression requires a placental biopsy, which is
impractical in clinical practice. If plasma kisspeptin acts as a marker of tumor activity, its
measurement would be more clinically applicable. We found large variations in
circulating hCG and kisspeptin concentrations between GTN patients before treatment.
However, plasma hCG and kisspeptin levels showed a strong correlation, and each
patient with a plasma hCG level above the normal range (>5U/L), suggesting disease
activity, also had an elevated plasma kisspeptin. As plasma hCG is one of the factors
used to score disease severity in patients with GTN by the FIGO scoring system (16), this
variation in pre-chemotherapy plasma kisspeptin levels may also reflect differences in
disease activity between subjects.
GTN is currently diagnosed by measuring hCG. Circulating levels of hCG were higher
than those of kisspeptin in the GTN patients in this study. Further work using a larger
group of GTN patients would be required to confirm the sensitivity of hCG compared to
kisspeptin. However, there are problems with using hCG as a diagnostic tool. Though
hCG is a sensitive diagnostic tumor marker, in addition to regular hCG, at least five
major variants of hCG are present in serum samples. In patients with GTN, these variants
of hCG can be the principal circulating form of hCG (4, 5). Some hCG assays do not
detect these hCG variants which can result in a failure to diagnose GTN (5, 19). In
addition, false positive hCG-IR (phantom hCG) results can also occur with hCG assays
Page 15 of 36
16
due to proteolytic enzymes that mimic hCG or heterophile antibodies in the serum that
interfere with the hCG assay (3). This can lead to an incorrect diagnosis of GTN and
unnecessary testing and treatment (10). New tumor markers may help to reduce these
problems. Interestingly, though endogenous forms of kisspeptin 54, 14 and 13 amino
acids in length have been isolated from human placenta (20), chromatographic
characterization of the circulating kisspeptin-IR in GTN patients detected only a single
form eluting at an identical position to synthetic kisspeptin-54. Analysis of plasma from
women with a normal pregnancy also shows only a single peak in the same position (data
not shown). Our results suggest that measurement of plasma kisspeptin-IR might be
useful as a novel alternative or complementary tumor marker in patients with malignant
GTN. Further work is required to determine if measurement of plasma kisspeptin-IR
correlates with disease activity in patients with GTN in whom a variant of hCG is the
major circulating form, or in patients with phantom hCG-IR.
The high plasma kisspeptin-IR concentrations in our patients with malignant GTN may
simply reflect the mass of material of placental origin. Kisspeptin is expressed in
trophoblasts, which are known to secrete hCG, oestradiol and progesterone (2, 14).
Circulating concentrations of both kisspeptin-IR and hCG were positively correlated with
circulating oestradiol and progesterone in patients with malignant GTN. There is also a
positive correlation between progesterone and oestradiol levels with kisspeptin levels in
normal pregnancy (14). This might suggest that the release of kisspeptin is related to the
number or mass of trophoblasts (14). However, there is evidence to suggest that
circulating kisspeptin concentrations are not directly correlated to KiSS-1 expression in
the placenta. Although plasma kisspeptin concentration rises throughout pregnancy and
Page 16 of 36

17
peaks at term (14), placental KiSS-1 gene expression is not significantly different
between early and term placentas (18). In rats, KiSS-1 gene expression has been found to
decrease in trophoblasts during placental maturation and gestation (1, 47).
Interestingly, although our results suggest that plasma kisspeptin-IR correlates strongly
and significantly with hCG in patients with malignant GTN, there is no significant
correlation between plasma hCG and plasma kisspeptin concentration in pregnancy (14).
Plasma hCG is markedly elevated in the first trimester of pregnancy, but lower levels are
found in the second and third trimester. In contrast, plasma kisspeptin concentrations are
elevated in the first trimester of pregnancy, and continue to increase to a maximum of
approximately 7000-fold basal levels in the third trimester of pregnancy (14).
In conclusion, we have demonstrated that plasma kisspeptin-IR is raised in patients with
malignant GTN and falls during and following treatment. Kisspeptin-IR strongly and
significantly correlated with plasma hCG levels in these patients. Our results suggest that
plasma kisspeptin-IR may be a novel tumor marker in patients with malignant GTN.
Page 17 of 36

18
Acknowledgements
We are very grateful to Becky Maddison and Mandy Donaldson for their technical
assistance with the progesterone and oestradiol measurements. The authors would also
like to thank the Department of Health for their continued support of the Charing Cross
Gestational Trophoblastic Disease Centre.
Grants
W.S.D. is funded by a Department of Health Clinician Scientist Fellowship. K.G.M. is
supported by a Biotechnology and Biological Sciences Research Council New
Investigator Award. O.B.C. is funded by a Wellcome Trust Clinical Training Fellowship.
M.P is supported by the Biotechnology and Biological Sciences Research Council. The
Department of Metabolic Medicine is funded by a Medical Research Council programme
grant.
Page 18 of 36

19
References
1. Bilban M, Ghaffari-Tabrizi N, Hintermann E, Bauer S, Molzer S, Zoratti C,
Malli R, Sharabi A, Hiden U, Graier W, Knofler M, Andreae F, Wagner O,
Quaranta V and Desoye G. Kisspeptin-10, a KiSS-1/metastin-derived
decapeptide, is a physiological invasion inhibitor of primary human trophoblasts.
J Cell Sci 117: 1319-1328, 2004.
2. Clayton LA, Tyrey L, Weed JC, Jr. and Hammond CB. Endocrine aspects of
trophoblastic neoplasia. J Reprod Med 26: 192-199, 1981.
3. Cole LA. Phantom hCG and phantom choriocarcinoma. Gynecol Oncol 71: 325-
329, 1998.
4. Cole LA and Butler S. Detection of hCG in trophoblastic disease. The USA hCG
reference service experience. J Reprod Med 47: 433-444, 2002.
5. Cole LA, Shahabi S, Butler SA, Mitchell H, Newlands ES, Behrman HR and
Verrill HL. Utility of commonly used commercial human chorionic gonadotropin
immunoassays in the diagnosis and management of trophoblastic diseases. Clin
Chem 47: 308-315, 2001.
6. Cole LA and Sutton JM. Selecting an appropriate hCG test for managing
gestational trophoblastic disease and cancer. J Reprod Med 49: 545-553, 2004.
Page 19 of 36

20
7. de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL and Milgrom E.
Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived
peptide receptor GPR54. Proc Natl Acad Sci U S A 100: 10972-10976, 2003.
8. Dhar DK, Naora H, Kubota H, Maruyama R, Yoshimura H, Tonomoto Y,
Tachibana M, Ono T, Otani H and Nagasue N. Downregulation of KiSS-1
expression is responsible for tumor invasion and worse prognosis in gastric
carcinoma. Int J Cancer 111: 868-872, 2004.
9. Dhillo WS, Chaudhri OB, Patterson M, Thompson EL, Murphy KG,
Badman MK, McGowan BM, Amber V, Patel S, Ghatei MA and Bloom SR.
Kisspeptin-54 stimulates the hypothalamic-pituitary gonadal axis in human males.
J Clin Endocrinol Metab September 20, 2005: 10.1210/jc.2005-1468.
10. Esfandiari N and Goldberg JM. Heterophile antibody blocking agent to confirm
false positive serum human chorionic gonadotropin assay. Obstet Gynecol 101:
1144-1146, 2003.
11. Faure N and Lemay A. Inhibition of testicular androgen biosynthesis by chronic
administration of a potent LHRH agonist in adult men. Arch Androl 14: 95-106,
1985.
12. Funes S, Hedrick JA, Vassileva G, Markowitz L, Abbondanzo S, Golovko A,
Yang S, Monsma FJ and Gustafson EL. The KiSS-1 receptor GPR54 is
Page 20 of 36

21
essential for the development of the murine reproductive system. Biochem
Biophys Res Commun 312: 1357-1363, 2003.
13. Gottsch ML, Cunningham MJ, Smith JT, Popa SM, Acohido BV, Crowley
WF, Seminara S, Clifton DK and Steiner RA. A Role for Kisspeptins in the
Regulation of Gonadotropin Secretion in the Mouse. Endocrinology 145: 4073-
4077, 2004.
14. Horikoshi Y, Matsumoto H, Takatsu Y, Ohtaki T, Kitada C, Usuki S and
Fujino M. Dramatic elevation of plasma metastin concentrations in human
pregnancy: metastin as a novel placenta-derived hormone in humans. J Clin
Endocrinol Metab 88: 914-919, 2003.
15. Ikeguchi M, Yamaguchi K and Kaibara N. Clinical significance of the loss of
KiSS-1 and orphan G-protein-coupled receptor (hOT7T175) gene expression in
esophageal squamous cell carcinoma. Clin Cancer Res 10: 1379-1383, 2004.
16. International Federation of Obstetrics and Gynaecology Oncology Committee
Report. FIGO staging for gestational trophoblastic neoplasia. Int J Gynecol Obstet
77, 285-287. 2002.
17. Irwig MS, Fraley GS, Smith JT, Acohido BV, Popa SM, Cunningham MJ,
Gottsch ML, Clifton DK and Steiner RA. Kisspeptin activation of gonadotropin
Page 21 of 36

22
releasing hormone neurons and regulation of KiSS-1 mRNA in the male rat.
Neuroendocrinology 80: 264-272, 2004.
18. Janneau JL, Maldonado-Estrada J, Tachdjian G, Miran I, Motte N, Saulnier
P, Sabourin JC, Cote JF, Simon B, Frydman R, Chaouat G and Bellet D.
Transcriptional expression of genes involved in cell invasion and migration by
normal and tumoral trophoblast cells. J Clin Endocrinol Metab 87: 5336-5339,
2002.
19. Kohorn EI and Cole L. Nicked human chorionic gonadotropin in trophoblastic
disease. Int J Gynecol Cancer 10: 330-335, 2000.
20. Kotani M, Detheux M, Vandenbogaerde A, Communi D, Vanderwinden JM,
Le PE, Brezillon S, Tyldesley R, Suarez-Huerta N, Vandeput F, Blanpain C,
Schiffmann SN, Vassart G and Parmentier M. The metastasis suppressor gene
KiSS-1 encodes kisspeptins, the natural ligands of the orphan G protein-coupled
receptor GPR54. J Biol Chem 276: 34631-34636, 2001.
21. Lee JH, Miele ME, Hicks DJ, Phillips KK, Trent JM, Weissman BE and
Welch DR. KiSS-1, a novel human malignant melanoma metastasis-suppressor
gene. J Natl Cancer Inst 88: 1731-1737, 1996.
Page 22 of 36

23
22. Lee JH and Welch DR. Suppression of metastasis in human breast carcinoma
MDA-MB-435 cells after transfection with the metastasis suppressor gene, KiSS-
1. Cancer Res 57: 2384-2387, 1997.
23. Lee JH and Welch DR. Identification of highly expressed genes in metastasis-
suppressed chromosome 6/human malignant melanoma hybrid cells using
subtractive hybridization and differential display. Int J Cancer 71: 1035-1044,
1997.
24. Masui T, Doi R, Mori T, Toyoda E, Koizumi M, Kami K, Ito D, Peiper SC,
Broach JR, Oishi S, Niida A, Fujii N and Imamura M. Metastin and its variant
forms suppress migration of pancreatic cancer cells. Biochem Biophys Res
Commun 315: 85-92, 2004.
25. Matsui H, Takatsu Y, Kumano S, Matsumoto H and Ohtaki T. Peripheral
administration of metastin induces marked gonadotropin release and ovulation in
the rat. Biochem Biophys Res Commun 320: 383-388, 2004.
26. Messager S, Chatzidaki EE, Ma D, Hendrick AG, Zahn D, Dixon J, Thresher
RR, Malinge I, Lomet D, Carlton MB, Colledge WH, Caraty A and Aparicio
SA. Kisspeptin directly stimulates gonadotropin-releasing hormone release via G
protein-coupled receptor 54. Proc Natl Acad Sci U S A 102: 1761-1766, 2005.
Page 23 of 36

24
27. Muir AI, Chamberlain L, Elshourbagy NA, Michalovich D, Moore DJ,
Calamari A, Szekeres PG, Sarau HM, Chambers JK, Murdock P, Steplewski
K, Shabon U, Miller JE, Middleton SE, Darker JG, Larminie CG, Wilson S,
Bergsma DJ, Emson P, Faull R, Philpott KL and Harrison DC. AXOR12, a
novel human G protein-coupled receptor, activated by the peptide KiSS-1. J Biol
Chem 276: 28969-28975, 2001.
28. Navarro VM, Castellano JM, Fernandez-Fernandez R, Barreiro ML, Roa J,
Sanchez-Criado JE, Aguilar E, Dieguez C, Pinilla L and Tena-Sempere M.
Developmental and hormonally regulated messenger ribonucleic acid expression
of KiSS-1 and its putative receptor, GPR54, in rat hypothalamus and potent
luteinizing hormone-releasing activity of KiSS-1 peptide. Endocrinology 145:
4565-4574, 2004.
29. Navarro VM, Castellano JM, Fernandez-Fernandez R, Tovar S, Roa J,
Mayen A, Barreiro ML, Casanueva FF, Aguilar E, Dieguez C, Pinilla L and
Tena-Sempere M. Effects of KiSS-1 peptide, the natural ligand of GPR54, on
follicle-stimulating hormone secretion in the rat. Endocrinology 146: 1689-1697,
2005.
30. Navarro VM, Castellano JM, Fernandez-Fernandez R, Tovar S, Roa J,
Mayen A, Nogueiras R, Vazquez MJ, Barreiro ML, Magni P, Aguilar E,
Dieguez C, Pinilla L and Tena-Sempere M. Characterization of the potent
Page 24 of 36
25
luteinizing hormone-releasing activity of KiSS-1 peptide, the natural ligand of
GPR54. Endocrinology 146: 156-163, 2005.
31. Ohta S, Lai EW, Pang AL, Brouwers FM, Chan WY, Eisenhofer G, de KR,
Ksinantova L, Breza J, Blazicek P, Kvetnansky R, Wesley RA and Pacak K.
Downregulation of metastasis suppressor genes in malignant pheochromocytoma.
Int J Cancer 114: 139-143, 2005.
32. Ohtaki T, Shintani Y, Honda S, Matsumoto H, Hori A, Kanehashi K, Terao
Y, Kumano S, Takatsu Y, Masuda Y, Ishibashi Y, Watanabe T, Asada M,
Yamada T, Suenaga M, Kitada C, Usuki S, Kurokawa T, Onda H,
Nishimura O and Fujino M. Metastasis suppressor gene KiSS-1 encodes peptide
ligand of a G-protein-coupled receptor. Nature 411: 613-617, 2001.
33. Palmieri C, Fisher RA, Sebire NJ, Lindsay I, Smith JR, McCluggage WG,
Savage P and Seckl MJ. Placental site trophoblastic tumour arising from a
partial hydatidiform mole. Lancet 366: 688, 2005.
34. Patterson M, Murphy KG, le Roux CW, Ghatei MA and Bloom SR.
Characterization of ghrelin-like immunoreactivity in human plasma. J Clin
Endocrinol Metab 90: 2205-2211, 2005.
Page 25 of 36

26
35. Qiao C, Cheng DL, Zhang SL, Wang CH and Lin QD. [The role of KiSS-1
and matrix metalloproteinase-9 in regulation of invasion of trophoblasts].
Zhonghua Yi Xue Za Zhi 85: 839-842, 2005.
36. Royal College of Obstetricians and Gynaecologists. The management of
gestational trophoblastic neoplasia : Guideline number 38. 1-7. 2004.
37. Sanchez-Carbayo M, Capodieci P and Cordon-Cardo C. Tumor suppressor
role of KiSS-1 in bladder cancer: loss of KiSS-1 expression is associated with
bladder cancer progression and clinical outcome. Am J Pathol 162: 609-617,
2003.
38. Seckl MJ, Fisher RA, Salerno G, Rees H, Paradinas FJ, Foskett M and
Newlands ES. Choriocarcinoma and partial hydatidiform moles. Lancet 356: 36-
39, 2000.
39. Seminara SB, Messager S, Chatzidaki EE, Thresher RR, Acierno JS, Jr.,
Shagoury JK, Bo-Abbas Y, Kuohung W, Schwinof KM, Hendrick AG, Zahn
D, Dixon J, Kaiser UB, Slaugenhaupt SA, Gusella JF, O'Rahilly S, Carlton
MB, Crowley WF, Jr., Aparicio SA and Colledge WH. The GPR54 gene as a
regulator of puberty. N Engl J Med 349: 1614-1627, 2003.
Page 26 of 36

27
40. Semple RK, Achermann JC, Ellery J, Farooqi IS, Karet FE, Stanhope RG,
O'Rahilly S and Aparicio SA. Two novel missense mutations in g protein-
coupled receptor 54 in a patient with hypogonadotropic hypogonadism. J Clin
Endocrinol Metab 90: 1849-1855, 2005.
41. Shahab M, Mastronardi C, Seminara SB, Crowley WF, Ojeda SR and Plant
TM. Increased hypothalamic GPR54 signaling: a potential mechanism for
initiation of puberty in primates. Proc Natl Acad Sci U S A 102: 2129-2134, 2005.
42. Shirasaki F, Takata M, Hatta N and Takehara K. Loss of expression of the
metastasis suppressor gene KiSS1 during melanoma progression and its
association with LOH of chromosome 6q16.3-q23. Cancer Res 61: 7422-7425,
2001.
43. Smith JT, Cunningham MJ, Rissman EF, Clifton DK and Steiner RA.
Regulation of Kiss1 Gene Expression in the Brain of the Female Mouse.
Endocrinology 146: 3686-3692, 2005.
44. Smith JT, Dungan HM, Stoll EA, Gottsch ML, Braun RE, Eacker SM,
Clifton DK and Steiner RA. Differential Regulation of KiSS-1 Gene Expression
by Sex Steroids in the Brain of the Male Mouse. Endocrinology 146: 2976-2984,
2005.
Page 27 of 36

28
45. Stark AM, Tongers K, Maass N, Mehdorn HM and Held-Feindt J. Reduced
metastasis-suppressor gene mRNA-expression in breast cancer brain metastases. J
Cancer Res Clin Oncol 131: 191-198, 2005.
46. Thompson EL, Patterson M, Murphy KG, Smith KL, Dhillo WS, Todd JF,
Ghatei MA and Bloom SR. Central and peripheral administration of kisspeptin-
10 stimulates the hypothalamic-pituitary-gonadal axis. J Neuroendocrinol 16:
850-858, 2004.
47. Terao Y, Kumano S, Takatsu Y, Hattori M, Nishimura A, Ohtaki T, Shintani
Y. Expression of KiSS-1, a metastasis suppressor gene, in trophoblast giant cells
of the rat placenta. Biochim Biophys Acta 1678:102-10, 2004.
Page 28 of 36
29
Figure Legends
Figure 1: Plasma kisspeptin-IR in normal females.
Non-preg = non-pregnant. This included healthy females who had never previously had a
pregnancy in the follicular and luteal phases of their menstrual cycle (n=11) and also
healthy females who had previous pregnancies in the follicular phase of their menstrual
cycles (n=5). First trim = pregnant females in the first trimester of normal pregnancy
(n=13). Third trim = pregnant females at 38 ± 0.8 weeks gestation of normal pregnancy
(n=7). 15d post = females who were day 15 ± 6 post partum (n=7). Values are mean ±sem except for plasma kisspeptin in non-preg and 15d post females which was below the
detection limit of the assay (<2pmol/L).
Figure 2: Plasma kisspeptin-IR (a) and hCG (b) in patients with malignant gestational
trophoblastic neoplasia at presentation (pre chemotherapy) and following chemotherapy
(post chemotherapy).
The thick black line on each graph represents the mean values. n=11. Plasma kisspeptin-
IR in patients with malignant GTN were elevated at presentation and fell during and
following treatment with chemotherapy in each patient (plasma kisspeptin-IR: pre
chemotherapy 1363 ± 1076 pmol/L vs. post chemotherapy <2 pmol/L, n=11, p<0.0001).
Plasma hCG levels also showed a similar pattern (plasma hCG: pre-chemotherapy
227191 ± 152354 U/L vs. post chemotherapy 2 U/L, n=11, p<0.0001).
Page 29 of 36

30
Figure 3: Correlation between plasma kisspeptin-IR and hCG in patients with malignant
gestational trophoblastic neoplasia at presentation, during and following chemotherapy.
Correlation was calculated using Pearson’s Product Moment analysis. r2 = 0.99, n=39, p
< 0.0001.
Figure 4: Representative elution profile of kisspeptin-IR extracted from 2 ml plasma by
Sep-Pak cartridge and fractionated by reverse-phase FPLC from a patient with malignant
gestational trophoblastic neoplasia.
Dotted line indicates % AcN = percentage acetonitrile; the elution position of synthetic
kisspeptin-54 was identical to that of plasma kisspeptin-IR from patients with malignant
GTN (fractions 14-17). Synthetic prolactin releasing peptide eluted as fraction 10.
Page 30 of 36

31
Figure 1
Page 31 of 36

32
Figure 2 a
Figure 2 b
Page 32 of 36
33
Figure 3
Page 33 of 36

34
Figure 4
Page 34 of 36
35
Patientno
Time Kiss (pmol/L)
hCG (U/L)
Prog (ng/mL)
E2 (pg/mL)
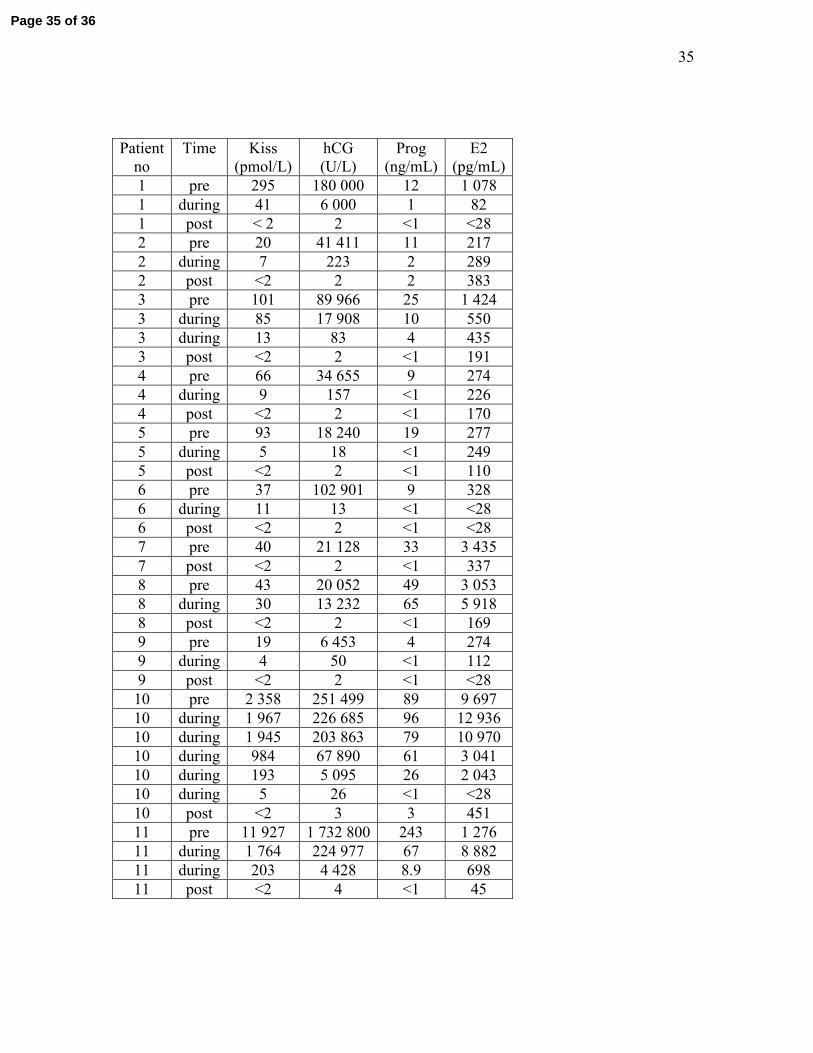
1 pre 295 180 000 12 1 078 1 during 41 6 000 1 82 1 post < 2 2 <1 <28 2 pre 20 41 411 11 217 2 during 7 223 2 289 2 post <2 2 2 383 3 pre 101 89 966 25 1 424 3 during 85 17 908 10 550 3 during 13 83 4 435 3 post <2 2 <1 191 4 pre 66 34 655 9 274 4 during 9 157 <1 226 4 post <2 2 <1 170 5 pre 93 18 240 19 277 5 during 5 18 <1 249 5 post <2 2 <1 110 6 pre 37 102 901 9 328 6 during 11 13 <1 <28 6 post <2 2 <1 <28 7 pre 40 21 128 33 3 435 7 post <2 2 <1 337 8 pre 43 20 052 49 3 053 8 during 30 13 232 65 5 918 8 post <2 2 <1 169 9 pre 19 6 453 4 274 9 during 4 50 <1 112 9 post <2 2 <1 <28 10 pre 2 358 251 499 89 9 697 10 during 1 967 226 685 96 12 93610 during 1 945 203 863 79 10 97010 during 984 67 890 61 3 041 10 during 193 5 095 26 2 043 10 during 5 26 <1 <28 10 post <2 3 3 451 11 pre 11 927 1 732 800 243 1 276 11 during 1 764 224 977 67 8 88211 during 203 4 428 8.9 698 11 post <2 4 <1 45
Page 35 of 36

36
Supplementary information Table 1: Results of plasma kisspeptin-IR concentration
(Kiss), hCG, progesterone (Prog) and oestradiol (E2) in patients with malignant
gestational trophoblastic neoplasia at presentation (pre), during chemotherapy
(during) and following chemotherapy (post).
Page 36 of 36





![UNARY NEGATION 1. Introduction Vardi [46] raised the ... - arXiv](https://static.fdokumen.com/doc/165x107/63175313f68b807f8803968f/unary-negation-1-introduction-vardi-46-raised-the-arxiv.jpg)














