
The spatial arrangement of blastomeres at the 4-cell stage and IVF outcome

RBMOnline - Vol 15 No 5. 2007 539-546 Reproductive BioMedicine Online; www.rbmonline.com/Article/2938 on web 25 September 2007
539
© 2007 Published by Reproductive Healthcare Ltd, Duck End Farm, Dry Drayton, Cambridge CB3 8DB, UK
Mr Yakoub Khalaf is a Consultant Gynaecologist and a Sub-specialist in Reproductive Medicine and Surgery at Guy’s and St Thomas’ Hospital, London. He is the Clinical Director for the assisted conception unit, Guy’s and St Thomas’ Hospital. He is an Honorary Senior Lecturer at Kings College, London. His area of interest is management of uterine fibroids and ovarian reserve. He has published widely on these topics and other areas relating to infertility.
Dr Yakoub Khalaf
Sesh Kamal Sunkara1, Josephine Tuthill1, Mohammed Khairy1, Tarek El-Toukhy1, Arri Coomarasamy1,2,3, Yakoub Khalaf1, Peter Braude1
1Assisted Conception Unit, 4th Floor, Thomas Guy House, Guy’s Hospital, St Thomas Street, London, SE1 9RT; 2University of Birmingham Department of Public Health and Epidemiology, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK3Correspondence: Tel: +44 207 1880496; Fax: +44 207 1880490; e-mail: [email protected]
Abstract
Many randomized trials have evaluated the use of various pituitary suppression regimens to improve outcome of poor responders undergoing IVF treatment. A systematic review was conducted of the trials of gonadotrophin-releasing hormone (GnRH) agonist long regimen, GnRH agonist short regimen, GnRH antagonist regimen, as well as other pituitary suppression regimens in poor responders undergoing IVF/intracytoplasmic sperm injection (ICSI) treatment. The search included MEDLINE, EMBASE, Cochrane Library, National Research Register and ISI proceedings, and all randomized controlled trials comparing the various pituitary suppression regimens in poor responders were included. Study selection, quality appraisal and data extraction were performed independently and in duplicate. The main outcome measures were number of oocytes retrieved, cycles cancelled before oocyte retrieval and pregnancy rates. A total of 680 women considered as poor responders undergoing IVF/ICSI treatment were included in nine randomized controlled trials. The quality of these studies was variable: for example, only three of the studies had clear evidence of allocation concealment. Meta-analyses of the results of the studies did not show a consistent benefit for any one pituitary suppression regimen over the other regimens in improving outcome measures. Currently available evidence does not favour any one pituitary suppression regimen for women with poor ovarian response undergoing IVF/ICSI treatment.
Keywords: GnRH agonist long regimen, GnRH agonist short regimen, GnRH antagonist regimen, meta-analysis, randomized trials, systematic review
Poor ovarian response, defined as failure of the development of sufficient number of mature follicles to proceed to oocyte retrieval or yielding only a few oocytes following gonadotrophin stimulation in women undergoing IVF treatment, occurs in 5–25% of women (Keay et al., 1997). Poor ovarian response is likely to be an increasing problem with women delaying childbearing and presenting for treatment later in their reproductive life. In comparison with normal responders, these patients have impaired fertilization rates, lower embryo quality and decreased pregnancy rates (Mahutte and Arici, 2002). Poor responders often have their treatment cycle cancelled because of expected poor outcome (Lashen and Ledger, 1999). This
causes emotional distress for the couple, as well as increasing the financial burden on the couple or the service provider.
Treatment of poor responders who are undergoing IVF treatment remains a challenge. Various treatment regimens and interventions have been proposed in an effort to improve ovarian response and IVF outcome in this group of patients. These include different regimens for pituitary suppression and ovarian stimulation, as well as adjuvant therapies (Shanbhag et al., 2007). Currently, the choice of pituitary suppression regimens proposed for the management of poor responders is based mainly on the preferences of individual centres or clinicians,
Article
Pituitary suppression regimens in poor responders undergoing IVF treatment: a systematic review and meta-analysis
Introduction

Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
with no single protocol considered to be superior over others. The reasons for this variation in practice are likely to include paucity of published evidence and heterogeneity in the trials with regards to issues such as the definition for poor response and clinical protocols used in individual studies. In an attempt to summarize the existing evidence on the various regimens for pituitary suppression, a systematic review was conducted.
Materials and methods
Literature searches
MEDLINE (1966-January 2007), EMBASE (1974-January 2007), Cochrane Library and the National Research Register were searched for relevant studies. The search also included ISI Conference Proceedings, which cover over 4.1 million abstracts from over 60,000 conferences since 1990, as well as databases for registration of ongoing and archived randomized controlled trials (RCT) namely ISRCTN register and meta-register for RCT (mRCT). A combination of Medical Subject Headings (MeSH) and text words were used to generate two subsets of citations, one including studies of poor ovarian response (‘poor response’, ‘low response’, ‘non response’, ‘weak response’, ‘failed response’) and the other, studies of IVF and intracytoplasmic sperm injection (‘in-vitro fertilization’, ‘fertilization in vitro’, ‘intracytoplasmic sperm injection’, ‘sperm injections intracytoplasmic’, ‘reproductive techniques assisted’, ‘embryo transfer’ and ‘embryo implantation’). These subsets were combined using ‘AND’ to generate a subset of citations relevant to the research question. The reference lists of all known primary and review articles were examined to identify cited articles not captured by electronic searches. Articles frequently cited were used in the Science Citation Index to identify additional citations. Enquiries were also made about unpublished studies from researchers investigating in this field. No language restrictions were placed in any of the searches.
Study selection and data extraction
Studies were selected if the target population were women with a history of poor ovarian response undergoing IVF or ICSI treatment and the therapeutic interventions were the gonadotrophin-releasing hormone (GnRH) agonist long regimen (A), the GnRH agonist short regimen (B), the GnRH antagonist regimen (C), or other pituitary suppression regimens. Studies were included if they were of randomized design. The primary outcomes were number of oocytes retrieved and cycles cancelled and the secondary outcomes were clinical and ongoing pregnancies. Data were also obtained on duration of gonadotrophin use as a surrogate outcome.
Studies were selected in a two-stage process. Firstly, two reviewers scrutinized the titles and abstracts from the electronic searches independently (SKS and JT), and full manuscripts of all citations that definitely or possibly met the predefined selection criteria were obtained. Secondly, final inclusion or exclusion decisions were made on examination of the full manuscripts. In cases of duplicate publication, the most recent and complete versions were selected. The assessment of manuscripts was performed independently by two reviewers (SKS and JT) and any disagreements about inclusion were resolved by consensus or arbitration by a third reviewer (MK).
The selected studies were assessed for methodological quality by using the components of study design that are related to internal validity (CRD Report Number 4, 2001). Information on the adequacy of randomization, allocation concealment, blinding, intention to treat analysis and follow-up rates was sought by examining the full text articles and by contacting the authors if necessary. Study characteristics such as population features and interventions were extracted from each study.
Regimens for pituitary suppression
Ovarian stimulation is performed in order to increase the number of available oocytes for assisted reproductive technologies. Premature surges of LH can disrupt oocyte maturation, thereby affecting oocyte quality, fertilization rates, endometrial receptivity and pregnancy rates (Griesinger et al., 2004). Pituitary suppression prevents these LH surges and can be achieved either by using GnRH agonists or GnRH antagonists.
GnRH agonist long regimen
With the long regimen, pituitary desensitization with the GnRH agonist is commenced in the mid-luteal phase of the previous cycle. After confirmation of ovarian quiescence, gonadotrophins for ovarian stimulation are commenced and continued with a reduced dose of GnRH agonist until the administration of human chorionic gonadotrophin (HCG).
GnRH agonist short regimen
In the short regimen, the GnRH agonist is commenced in the early follicular phase of the cycle (day 2 or day 3) followed by gonadotrophin (which is usually commenced a day later). Both the GnRH agonist and the gonadotrophin are continued until the administration of HCG.
GnRH antagonist regimen
The GnRH antagonists competitively block the pituitary receptors and thereby cause immediate suppression of LH (Klingmuller et al., 1993). In the antagonist regimen, ovarian stimulation with gonadotrophins is commenced in the early follicular phase. The GnRH antagonist is commenced either on day 5 or 6 of stimulation or when the leading follicle is ≥14 mm. Both the gonadotrophins and the GnRH antagonist are continued until the day of HCG.
Long GnRH agonist stop regimen
With this regimen pituitary desensitization with the GnRH agonist is commenced in the mid-luteal phase of the previous cycle. The GnRH agonist administration is discontinued on the commencement of gonadotrophin administration. The GnRH agonist stop regimen is thought to improve ovarian responsiveness based on a hypothetical effect on the ovary, via GnRH receptor or indirectly the vascular network within the ovary (Garcia-Velasco et al., 2000).
Statistical analysis
From each study, outcome data were extracted in 2 × 2 tables 540
RBMOnline®

(for discrete variables) or as means or medians with a measure of variance (such as standard deviation) for continuous variables. For discrete variables, relative risks were pooled using fixed and random effects models, if significant heterogeneity could be excluded. Weighted mean difference (WMD) was calculated for continuous variables using means and standard deviations (SD) from individual studies. As the GnRH agonist long regimen, the GnRH agonist short regimen and the GnRH antagonist regimen are the commonly used regimens, these formed the focus of the analysis.
Heterogeneity of treatment effects was evaluated graphically
using forest plot and statistically using chi-squared test. Exploration of clinical heterogeneity was planned using variation in features of the population, intervention, outcome and study quality. All statistical analyses were performed using RevMan 4.2 (The Cochrane Collaboration).
Results
The process of literature identification and selection is summarized in Figure 1. Of the 1154 citations identified, 92 were selected during the initial screening, and on examination
541
Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
RBMOnline®
Figure 1. Study selection process for the systematic review of pituitary suppression regimens in patients with poor ovarian response undergoing IVF/ICSI treatment.

Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
of manuscripts, nine articles that included a total of 680 women were identified that satisfied the selection criteria for the review. The literature search found one randomized controlled trial comparing the GnRH agonist long regimen (A) with the GnRH agonist short regimen (B) (Weissman et al., 2003), two randomized controlled trials comparing the GnRH agonist long regimen (A) with the GnRH antagonist regimen (C) (Cheung et al., 2005; Marci et al., 2005) and four randomized controlled trials comparing the GnRH agonist short regimen (B) with the GnRH antagonist regimen (C) (Akman et al., 2001; Malmusi et al., 2005; Schmidt et al., 2005; De Placido et al., 2006). It also identified one randomized controlled trial comparing the GnRH agonist long regimen with the long GnRH agonist stop regimen (Garcia-Velasco et al., 2000), and one randomized controlled trial comparing the GnRH antagonist regimen with IVF cycles not having pituitary suppression with either the GnRH agonist or antagonist (Akman et al., 2000). Two randomized trials were excluded (Dirnfeld et al., 1999; Morgia et al., 2004), as a proportion of participants in these trials contributed more than one cycle to research, making the observations not completely independent from each other. The quality of the nine included trials was generally poor (for example, there was no evidence of allocation concealment in six of the nine studies). These trials were also generally small, leading to imprecision in their findings, even when combined in meta-analyses. Furthermore, there was substantial clinical and statistical heterogeneity amongst the trials, weakening any inferences that could be drawn from these studies. The quality and the main characteristics of the included studies are presented in Tables 1 and 2.
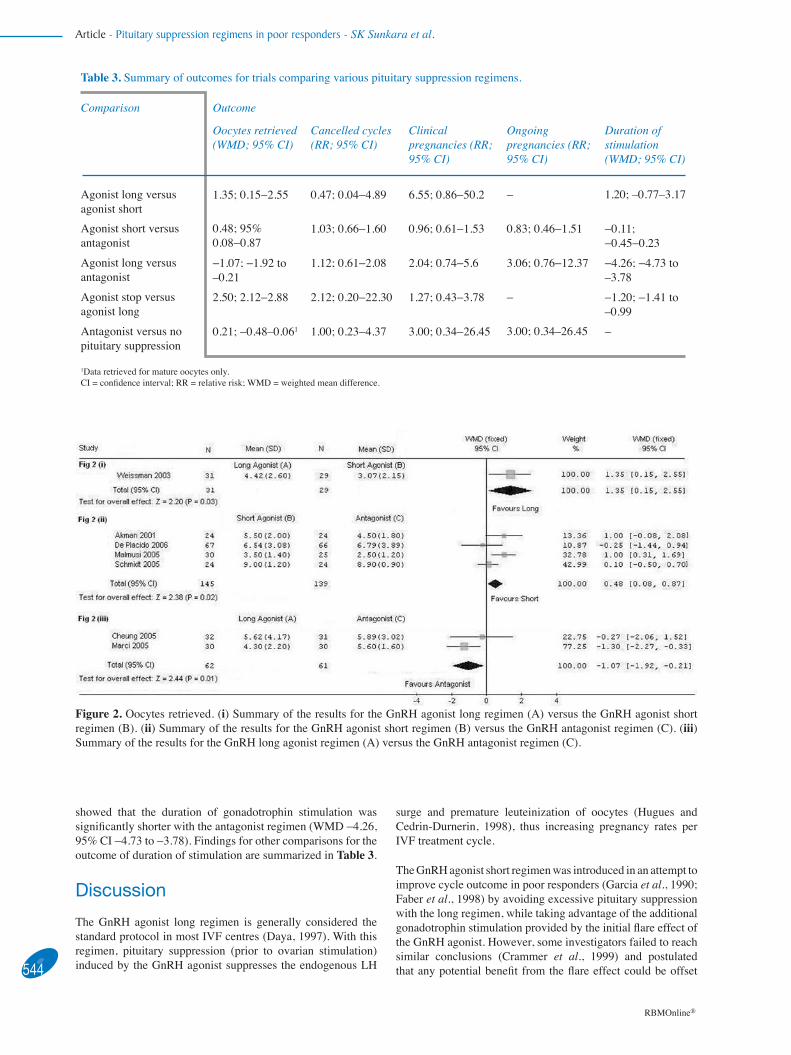
Number of oocytes retrieved
Results for the number of oocytes retrieved are summarized in Figure 2. In the trial comparing the GnRH agonist long regimen (A) with the GnRH agonist short regimen (B), a significantly greater number of oocytes were retrieved with the long regimen [WMD 1.35, 95% confidence interval (CI) 0.15−2.55; Figure 2(i)]. Meta-analysis of the four randomized controlled trials comparing the GnRH agonist short regimen (B) with the GnRH antagonist regimen (C) showed a significant benefit with the short regimen [WMD 0.48, 95% CI 0.08−0.87; Figure 2(ii)]. However, meta-analysis of the two trials comparing the GnRH
agonist long regimen (A) with the GnRH antagonist regimen (C) showed significantly fewer oocytes retrieved with the long regimen [WMD −1.07, 95% CI −1.92 to –0.21; Figure 2(iii)]. Findings for other comparisons for the outcome of oocytes retrieved are summarized in Table 3.
Cancelled cycles
Results for the cancellation rate are summarized in Figure 3 and Table 3. No statistically significant differences were identified in any of the five comparisons.
Clinical and ongoing pregnancy rates
In the trial comparing the GnRH agonist long regimen (A) with the GnRH agonist short regimen (B) there was a higher clinical pregnancy rate with the long regimen, although this effect was not statistically significant (RR 6.55, 95% CI 0.86−50.02).
A meta-analysis of the trials comparing the GnRH agonist short regimen (B) with the GnRH antagonist regimen (C) showed no significant difference with clinical pregnancy rates (RR 0.96, 95% CI 0.61−1.53) and ongoing pregnancy rates (RR 0.83, 95% CI 0.46−1.51). In the trials comparing the GnRH agonist long regimen (A) with the GnRH antagonist regimen (C), there was a trend of benefit with the antagonist regimen for clinical pregnancy rates (RR 2.04, 95% CI 0.74−5.6) and ongoing pregnancy rates (RR 3.06. 95% CI 0.76−12.37), but the results were not statistically significant. Findings for other comparisons for the outcomes of clinical and ongoing pregnancy rates are summarized in Table 3.
Surrogate outcome
There was no significant difference in the duration of stimulation between the long GnRH agonist regimen (A) versus the short GnRH agonist regimen (B) (WMD 1.20, 95% CI −0.77−3.17) and the short GnRH agonist regimen (B) versus the GnRH antagonist regimen (C) (WMD −0.11, 95% CI −0.45−0.23). Meta-analysis of the trials comparing the long GnRH agonist regimen (A) with the GnRH antagonist regimen (C), however,
542
RBMOnline®
Table 1. Quality of studies included in the review of pituitary suppression regimens in poor responders.
Study Method of randomization Method of allocationconcealment
Intention to treat analysis
Follow-up rate
Clinical pregnancy
Ongoing pregnancy
Akman et al., 2000 Consecutive number method Unreported Yes >95% >95%Garcia-Velasco et al., 2000 Computer-generated list Opaque sealed envelopes Yes >95% No dataAkman et al., 2001 Unclear Unreported Yes >95% >95%Weissman et al., 2003 Computer-generated list Unreported Yes >95% No dataCheung et al., 2005 Computer-generated list Opaque envelopes No >95% >95%Schmidt et al., 2005 Computer-generated list Sealed envelopes No >95% >95%Malmusi et al., 2005 Unclear Unreported No >95% No dataMarci et al., 2005 Randomization list Unreported Yes >95% >95%De Placido et al., 2006 Computer-generated list Unreported No >95% >95%
543
Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
RBMOnline®
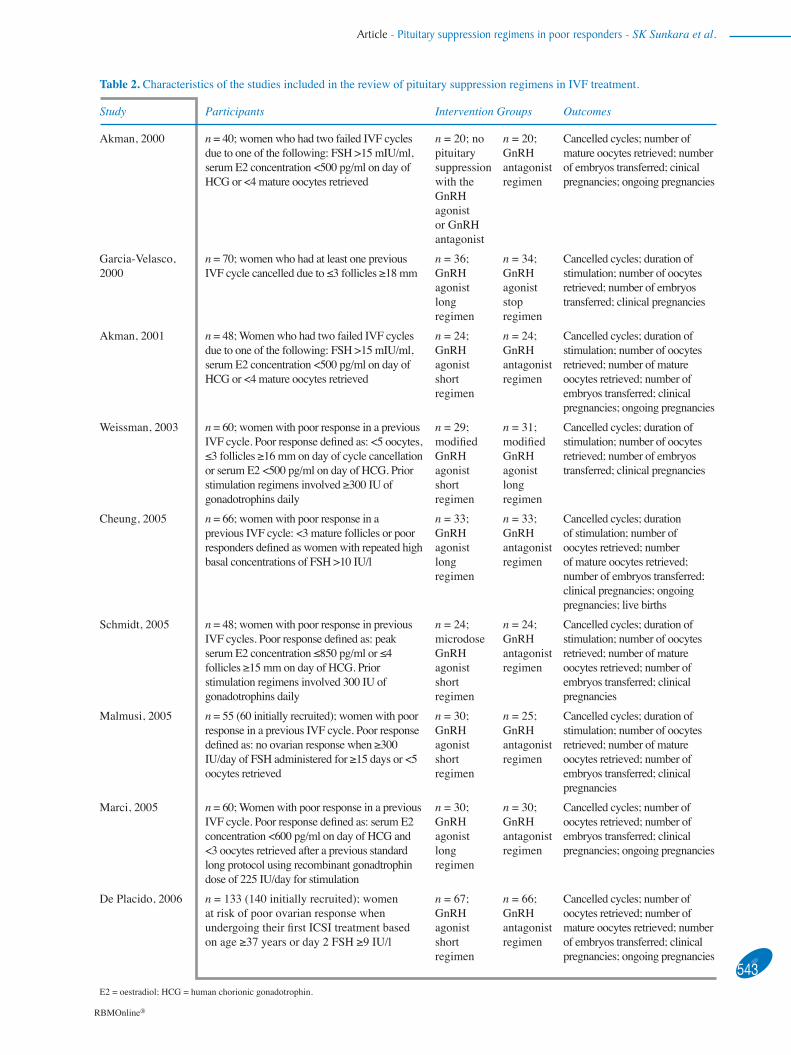
Table 2. Characteristics of the studies included in the review of pituitary suppression regimens in IVF treatment.
Study Participants Intervention Groups Outcomes
Akman, 2000 n = 40; women who had two failed IVF cycles due to one of the following: FSH >15 mIU/ml, serum E2 concentration <500 pg/ml on day of HCG or <4 mature oocytes retrieved
n = 20; no pituitary suppression with the GnRH agonist or GnRH antagonist
n = 20; GnRH antagonist regimen
Cancelled cycles; number of mature oocytes retrieved; number of embryos transferred; cinical pregnancies; ongoing pregnancies
Garcia-Velasco, 2000
n = 70; women who had at least one previous IVF cycle cancelled due to ≤3 follicles ≥18 mm
n = 36; GnRH agonist long regimen
n = 34; GnRH agonist stop regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of embryos transferred; clinical pregnancies
Akman, 2001 n = 48; Women who had two failed IVF cycles due to one of the following: FSH >15 mIU/ml, serum E2 concentration <500 pg/ml on day of HCG or <4 mature oocytes retrieved
n = 24; GnRH agonist short regimen
n = 24; GnRH antagonist regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of mature oocytes retrieved; number of embryos transferred; clinical pregnancies; ongoing pregnancies
Weissman, 2003 n = 60; women with poor response in a previous IVF cycle. Poor response defined as: <5 oocytes, ≤3 follicles ≥16 mm on day of cycle cancellation or serum E2 <500 pg/ml on day of HCG. Prior stimulation regimens involved ≥300 IU of gonadotrophins daily
n = 29; modified GnRH agonist short regimen
n = 31; modified GnRH agonist long regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of embryos transferred; clinical pregnancies
Cheung, 2005 n = 66; women with poor response in a previous IVF cycle: <3 mature follicles or poor responders defined as women with repeated high basal concentrations of FSH >10 IU/l
n = 33; GnRH agonist long regimen
n = 33; GnRH antagonist regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of mature oocytes retrieved; number of embryos transferred; clinical pregnancies; ongoing pregnancies; live births
Schmidt, 2005 n = 48; women with poor response in previous IVF cycles. Poor response defined as: peak serum E2 concentration ≤850 pg/ml or ≤4 follicles ≥15 mm on day of HCG. Prior stimulation regimens involved 300 IU of gonadotrophins daily
n = 24; microdose GnRH agonist short regimen
n = 24; GnRH antagonist regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of mature oocytes retrieved; number of embryos transferred; clinical pregnancies
Malmusi, 2005 n = 55 (60 initially recruited); women with poor response in a previous IVF cycle. Poor response defined as: no ovarian response when ≥300 IU/day of FSH administered for ≥15 days or <5 oocytes retrieved
n = 30; GnRH agonist short regimen
n = 25; GnRH antagonist regimen
Cancelled cycles; duration of stimulation; number of oocytes retrieved; number of mature oocytes retrieved; number of embryos transferred; clinical pregnancies
Marci, 2005 n = 60; Women with poor response in a previous IVF cycle. Poor response defined as: serum E2 concentration <600 pg/ml on day of HCG and <3 oocytes retrieved after a previous standard long protocol using recombinant gonadtrophin dose of 225 IU/day for stimulation
n = 30; GnRH agonist long regimen
n = 30; GnRH antagonist regimen
Cancelled cycles; number of oocytes retrieved; number of embryos transferred; clinical pregnancies; ongoing pregnancies
De Placido, 2006 n = 133 (140 initially recruited); women at risk of poor ovarian response when undergoing their first ICSI treatment based on age ≥37 years or day 2 FSH ≥9 IU/l
n = 67; GnRH agonist short regimen
n = 66; GnRH antagonist regimen
Cancelled cycles; number of oocytes retrieved; number of mature oocytes retrieved; number of embryos transferred; clinical pregnancies; ongoing pregnancies
E2 = oestradiol; HCG = human chorionic gonadotrophin.
showed that the duration of gonadotrophin stimulation was significantly shorter with the antagonist regimen (WMD −4.26, 95% CI −4.73 to −3.78). Findings for other comparisons for the outcome of duration of stimulation are summarized in Table 3.
Discussion
The GnRH agonist long regimen is generally considered the standard protocol in most IVF centres (Daya, 1997). With this regimen, pituitary suppression (prior to ovarian stimulation) induced by the GnRH agonist suppresses the endogenous LH
Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
544
RBMOnline®
Table 3. Summary of outcomes for trials comparing various pituitary suppression regimens.
Comparison Outcome
Oocytes retrieved (WMD; 95% CI)
Cancelled cycles (RR; 95% CI)
Clinical pregnancies (RR; 95% CI)
Ongoing pregnancies (RR; 95% CI)
Duration of stimulation (WMD; 95% CI)
Agonist long versus agonist short
1.35; 0.15−2.55 0.47; 0.04−4.89 6.55; 0.86−50.2 − 1.20; –0.77–3.17
Agonist short versus antagonist
0.48; 95% 0.08−0.87
1.03; 0.66−1.60 0.96; 0.61−1.53 0.83; 0.46−1.51 −0.11; −0.45−0.23
Agonist long versus antagonist
−1.07; −1.92 to –0.21
1.12; 0.61−2.08 2.04; 0.74−5.6 3.06; 0.76−12.37 −4.26; −4.73 to –3.78
Agonist stop versus agonist long
2.50; 2.12−2.88 2.12; 0.20−22.30 1.27; 0.43−3.78 − −1.20; −1.41 to –0.99
Antagonist versus no pituitary suppression
0.21; −0.48–0.061 1.00; 0.23−4.37 3.00; 0.34−26.45 3.00; 0.34–26.45 −
1Data retrieved for mature oocytes only. CI = confidence interval; RR = relative risk; WMD = weighted mean difference.
Figure 2. Oocytes retrieved. (i) Summary of the results for the GnRH agonist long regimen (A) versus the GnRH agonist short regimen (B). (ii) Summary of the results for the GnRH agonist short regimen (B) versus the GnRH antagonist regimen (C). (iii) Summary of the results for the GnRH long agonist regimen (A) versus the GnRH antagonist regimen (C).
surge and premature leuteinization of oocytes (Hugues and Cedrin-Durnerin, 1998), thus increasing pregnancy rates per IVF treatment cycle.
The GnRH agonist short regimen was introduced in an attempt to improve cycle outcome in poor responders (Garcia et al., 1990; Faber et al., 1998) by avoiding excessive pituitary suppression with the long regimen, while taking advantage of the additional gonadotrophin stimulation provided by the initial flare effect of the GnRH agonist. However, some investigators failed to reach similar conclusions (Crammer et al., 1999) and postulated that any potential benefit from the flare effect could be offset

by the GnRH agonist-induced LH rise in the early follicular phase. The GnRH antagonist regimen also avoids profound suppression of the endogenous FSH and LH concentrations in the early follicular phase at the stage of follicular recruitment (Kenigsberg et al., 1984). It was postulated the combination of exogenous and endogenous FSH enables recruitment of more follicles in poor responders.
In this review, it was demonstrated that there is insufficient evidence to suggest any one pituitary suppression regimen is associated with improved cycle outcomes, including number of oocytes retrieved, cycle cancellation rate, and clinical and ongoing pregnancy rates. The validity of this finding depends on the methodological rigour of the review and the component primary studies. A prospective protocol was used, and a concerted effort made to find all the evidence. Two independent reviewers assessed study quality and extracted data and the agreement between the two reviewers was high.
One major problem usually encountered when synthesizing the evidence in meta-analyses is clinical and methodological heterogeneity between the studies, namely the differences between the studies in the populations they evaluated (definition of poor ovarian response), the dosages of the GnRH agonist and antagonist used, times of commencement and duration of treatment, differences in the way outcomes were defined and reported, as well as important differences in the quality features between the studies. Although these factors were encountered during the analysis, a rigorous exploration of their effect on the study conclusion using techniques such as meta-regression was not feasible due to the limited number of studies identified. In addition, the wide confidence intervals around the relative risks for the outcome measures suggest imprecise results, which
could be directly attributed to the relatively small sample sizes of the studies in this review.
Furthermore, the results show inconsistency in trial outcomes. For example, the agonist long regimen (A) was shown to be superior to the agonist short regimen (B), whilst the agonist short regimen (B) was superior to the antagonist regimen (C). Even though it would be logical to predict the agonist long regimen (A) would be superior to the antagonist regimen (C), the opposite result was found as the antagonist regimen (C) yielded a significantly greater number of oocytes and higher clinical and ongoing pregnancy rates in comparison to the long GnRH agonist regimen (A) (Figure 2). This inconsistency limits the reliability of existing evidence in informing clinical decision-making while treating poor responders.
Finally, it is important to highlight that existing studies were not powered to assess differences in pregnancy rates, rendering their use in counselling patients regarding treatment success rates uninformative. None of the differences observed in the included trials reached statistical significance with regard to clinical or ongoing pregnancy rates. This methodological shortcoming is most probably due to the expected low pregnancy rates in poor responders (Surrey and Schoolcraft, 2000), such that sample sizes with enough power to detect differences in pregnancy rate would be prohibitive for a single centre trial. Recently, a Cochrane Review has examined the various interventions in poor responders, including some of the comparisons made in the present review (Shanbhag et al., 2007). There were important differences in the inclusion and exclusion criteria between this review and the Cochrane Review, resulting in a difference in the selection of studies. However, the inferences were broadly 545
Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
RBMOnline®
Figure 3. Cancelled cycles. (i) Summary of the results for the GnRH agonist long regimen (A) versus the GnRH agonist short regimen (B). (ii) Summary of the results for the GnRH agonist short regimen (B) versus the GnRH antagonist regimen (C). (iii) Summary of the results for the GnRH agonist long regimen (A) versus the GnRH antagonist regimen (C).

Article - Pituitary suppression regimens in poor responders - SK Sunkara et al.
similar, thus confirming the present findings.
Because of these inconsistent findings, a well designed, adequately powered, multi centre three arm trial comparing the long GnRH agonist regime versus the short GnRH agonist regime versus the GnRH antagonist regime is needed.
References
Akman MA, Erden HF, Tosun SB et al. 2001 Comparison of agonistic flare-up-protocol and antagonistic multiple dose protocol in ovarian stimulation of poor responders: results of a prospective randomized trial. Human Reproduction 16, 868–870.
Akman MA, Erden HF, Tosun SB et al. 2000 Addition of GnRH antagonist in cycles of poor responders undergoing IVF. Human Reproduction 15, 2145–2147.
Cheung LP, Lam PM, Lok IH et al. 2005 GnRH antagonist versus long GnRH agonist protocol in poor responders undergoing IVF: a randomized controlled trial. Human Reproduction 20, 616–621.
Crammer DW, Powers DR, Oskowitz SP et al. 1999 Gonadotrophin-releasing hormone agonist use in assisted reproduction cycles: the influence of long and short regimens on pregnancy rates. Fertility and Sterility 72, 83−89.
CRD 2001 CRD Report Number 4, 2nd Edition. Undertaking Systematic Reviews of Research on Effectiveness. CRD’s Guidance For Carrying Out of Commissioning Reviews. NHS Center for Reviews and Dissemination, University of York.
Daya S 1997 Optimal protocol for gonadotrophin-releasing hormone agonist use in ovarian stimulation. In: Gomel V, Cheung PCK (eds) In Vitro Fertilization and Assisted Reproduction. Monduzzi Editore, Bologna, pp. 405−415.
De Placido G, Mollo A, Clarizia R et al. 2006 Gonadotropin-releasing hormone (GnRH) antagonist plus recombinant luteinizing hormone vs. a standard GnRH agonist short protocol in patients at risk for poor ovarian response. Fertility and Sterility 85, 247–250.
Dirnfeld M, Fruchter O, Yshai D et al. 1999 Cessation of gonadotrophin-releasing hormone analogue (GnRH-a) upon down-regulation versus conventional long GnRH-a protocol in poor responders undergoing in vitro fertilization. Fertility and Sterility 72, 406–411.
Faber BM, Mayer J, Cox B et al. 1998 Cessation of gonadotropin-releasing hormone agonist therapy combined with high-dose gonadotropin stimulation yields favorable pregnancy results in low responders. Fertility and Sterility 69, 826-830.
Garcia J, Padilla S, Bayati J, Baramki T 1990 Follicular phase gonadotrophin releasing hormone agonist and human gonadotrophins: a better alternative for in vitro fertilization. Fertility and Sterility 53, 302- 305.
Garcia-Velasco JA, Isaza V, Requena A et al. 2000 High doses of gonadotrophins combined with stop versus non-stop protocol of GnRH analogue administration in low responder IVF patients: a prospective, randomized controlled trial. Human Reproduction 15, 2292−2296.
Griesinger G, Felberbaum RE, Schultze-Mosgau A, Diedrich K 2004 Gonadotropin-releasing hormone antagonists for assisted reproductive techniques. Are there clinical differences between agents? Drugs 64, 563–575.
Hugues J, Cedrin-Durnerin I 1998 Revisiting gonadotrophin-releasing hormone agonist protocols and management of poor ovarian responses to gonadotrophins. Human Reproduction Update 4, 83–101.
Keay SD, Liversedge NH, Mathur RS, Jenkins JM 1997 Assisted conception following poor ovarian reponse to gonadotrophin stimulation. British Journal of Obstetrics and Gynaecology 104, 521–527.
Kenigsberg D, Littman BA, Hodgen GD 1984 Medical hypophysectomy: 1. Dose-response using a gonadotrophin-releasing hormone antagonist ganirelix for in vitro fertilization cycles in which the lead follicle is >14 mm. Fertility and Sterility 42, 112−115.
Klingmuller D, Schepke M, Enzweiler C, Bidlingmaier F 1993 Hormonal responses to new potent GnRH antagonist cetrorelix. Acta Endocrinologica 128, 15−18.
Lashen H, Ledger W 1999 Management of poor responders. Human Reproduction 14, 1919–1921.
Marci R, Caserta D, Dolo V, Tatone C et al. 2005 GnRH antagonist in IVF poor-responder patients: results of a randomized trial. Reproductive BioMedicine Online 11, 189–193.
Mahutte NG, Arici A 2002 Poor responders: does the protocol make a difference? Current Opinion in Obstetrics and Gynaecology 14, 275–281.
Malmusi S, La Marca A, Giulini S et al. 2005 Comparison of a gonadotropin-releasing hormone (GnRH) antagonist and GnRH agonist flare-up regimen in poor responders undergoing ovarian stimulation. Fertility and Sterility 84, 402–406.
Morgia F, Sbracia M, Schimberni M et al. 2004 A controlled trial of natural cycle versus microdose gonadotrophin-releasing hormone analog flare cycles in poor responders undergoing in vitro fertilization. Fertility and Sterility 81, 1542–1547.
Schmidt DW, Bremner T, Orris JJ et al. 2005 A randomized prospective study of microdose leuprolide versus ganirelix in in vitro fertilization cycles for poor responders. Fertility and Sterility 83, 1568–1571.
Shanbhag S, Aucott L, Bhattacharya S et al. 2007 Interventions for ‘poor responders’ to controlled ovarian hyperstimulation (COH) in in-vitro fertilisation (IVF). Cochrane Database of Systematic Reviews. Issue1: Art No.: CD004379. DOI:10.1002/14651858.CD004379.pub2.
Surrey ES, Schoolcraft WB 2003 Evaluating strategies for improving ovarian response of the poor responder undergoing assisted reproductive techniques. Fertility and Sterility 73, 667–676.
Weissman A, Farhi J, Royburt M et al. 2003 Prospective evaluation of two stimulation protocols for low responders who were undergoing in vitro fertilization-embryo transfer. Fertility and Sterility 79, 886–892.
Declaration: The authors report no financial or commercial conflicts of interest.
Received 16 May 2007; refereed 27 June 2007; accepted 7 August 2007.
546
RBMOnline®
Copyright © 2022 FDOKUMEN




















