Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents
11
Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents Jonatan R. Ruiz, PhD, Francisco B. Ortega, PhD, Ruth Castillo, BSc, Miguel Martı´n-Matillas, PhD, Lydia Kwak, PhD, German Vicente-Rodrı´guez, PhD, Jose Noriega, PhD, Pablo Tercedor, PhD, Michael Sjo ¨ stro ¨ m, MD, PhD, and Luis A. Moreno, MD, PhD , on behalf of the AVENA Study Group* Objective To examine the association of participation in physical sports activity during leisure time, sedentary be- haviors, cardiorespiratory and muscular fitness, and weight status with cognitive performance in Spanish adoles- cents. Study design This cross-sectional study comprised a total of 1820 adolescents (958 female) aged 13.0 to 18.5 years. Cognitive performance (verbal, numeric and reasoning abilities, and an overall score) was measured with the ‘‘SRA-Test of Educational Ability.’’ Participation in physical sports activity during leisure time (yes/no) and time de- voted to study, television viewing, and playing video games were self-reported and categorized as #3 hours/day and >3 hours/day. We assessed cardiorespiratory and muscular fitness with field-based tests. Adolescents were classified as underweight, normal weight, overweight, and obese. Results Participation in physical sports activities during leisure time was associated with better cognitive perfor- mance study variables (all P < .001), independent of potential confounders including cardiorespiratory fitness and body mass index. We did not observe an association of time devoted to study, television viewing, or playing video- games with cognitive performance. Likewise, cognitive performance was similar across cardiorespiratory and mus- cular fitness levels and body weight categories. Conclusion Participation in physical sports activity during leisure time may positively influence cognitive perfor- mance in adolescents. (J Pediatr 2010;157:917-22). T here is increasing evidence that regular physical activity has positive effects on brain health and that it delays cognitive decline in adults. 1 Whether this effect also apply to young people is not clear. Results from cross-sectional studies in- dicate a positive association between physical activity and academic performance in children. 2,3 Findings from interven- tional studies also show that children in the physical activity intervention group have at least similar academic performance compared with children in the control group, despite a substantial reduction in time devoted to academics. 2,3 Less is known, however, about the association between physical activity and specific cognitive abilities during adolescence, a period of life when the brain has profound plasticity. 4 The effect that sedentary behaviors have on cognitive performance is of concern. Increased television viewing time is associ- ated with worse academic performance in children 5-7 and adolescents, 8 yet play- ing action video games seems to improve cognitive performance in adults. 9-11 Both cardiorespiratory fitness and fatness are considered important health markers already in both children and adolescents. 12,13 The association between physical fitness and cognitive performance in adolescents is contradictory. 3 Et- nier et al 14 concluded from a meta-analysis that there is no evidence for an as- sociation between cardiorespiratory fitness and cognitive performance in adults, whereas Hillman et al 2 provided evidence that cardiorespiratory fitness can have a positive effect on cognitive performance, at least in pre-pubertal children. The association between overweight or obesity and cognitive performance in youth is also inconclusive. 15-19 From the Department of Medical Physiology, School of Medicine, University of Granada, Granada, Spain (J.R., F.O.); Unit for Preventive Nutrition, Department of Biosciences and Nutrition at NOVUM, Karolinska Institutet, Huddinge, Sweden (J.R., F.O, L.K., M.S.); Department of Basic Psychology, School of Psychology, University of Malaga, Malaga, Spain (R.C.); Department of Physical Education and Sport, School of Sport Sciences, University of Granada, Granada, Spain (M.M-M., P.T.); Department of Physiotherapy and Nursing, School of Health and Sport Sciences, University of Zaragoza, Huesca, Spain (G.V-R.); Department of Pediatrics, University of Cantabria, Santander, Spain (J.N.); and Department of Physiotherapy and Nursing, School of Health Sciences, University of Zaragoza, Zaragoza, Spain (L.M.) *List of members of the AVENA Study Group available at www.jpeds.com (Appendix). Supported by the Spanish Ministry of Health (FIS no 00/ 0015), the Spanish Ministry of Education (grants EX- 2007-1124 and EX-2008-0641), Panrico S.A., Madaus S.A., Procter and Gamble S.A, the Swedish Council for Working Life and Social Research (F.S.), the Swedish Heart-Lung Foundation (20090635), and the Spanish Ministry of Health: Maternal, Child Health and Develop- ment Network (RD08/0072). The authors declare no conflicts of interest. 0022-3476/$ - see front matter. Copyright Ó 2010 Mosby Inc. All rights reserved. 10.1016/j.jpeds.2010.06.026 ANCOVA One-way analysis of covariance AVENA [Alimentacio ´ n y Valoracio ´ n del Estado Nutricional de los Adolescentes Espan ˜ oles] Food and Assessment of the Nutritional Status of Spanish Adolescents study BMI Body mass index CI Confidence interval OR Odds ratio SD Standard deviation TEA Test of Educational Ability VO 2max Maximum oxygen consumption 917
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents

Physical Activity, Fitness, Weight Status, and Cognitive Performancein Adolescents
Jonatan R. Ruiz, PhD, Francisco B. Ortega, PhD, Ruth Castillo, BSc, Miguel Martın-Matillas, PhD, Lydia Kwak, PhD,
German Vicente-Rodrıguez, PhD, Jose Noriega, PhD, Pablo Tercedor, PhD, Michael Sjostrom, MD, PhD,
and Luis A. Moreno, MD, PhD , on behalf of the AVENA Study Group*
Objective To examine the association of participation in physical sports activity during leisure time, sedentary be-haviors, cardiorespiratory and muscular fitness, and weight status with cognitive performance in Spanish adoles-cents.Study design This cross-sectional study comprised a total of 1820 adolescents (958 female) aged 13.0 to 18.5years. Cognitive performance (verbal, numeric and reasoning abilities, and an overall score) was measured with the‘‘SRA-Test of Educational Ability.’’ Participation in physical sports activity during leisure time (yes/no) and time de-voted to study, television viewing, and playing video games were self-reported and categorized as #3 hours/dayand >3 hours/day. We assessed cardiorespiratory and muscular fitness with field-based tests. Adolescents wereclassified as underweight, normal weight, overweight, and obese.Results Participation in physical sports activities during leisure time was associated with better cognitive perfor-mance study variables (all P < .001), independent of potential confounders including cardiorespiratory fitness andbody mass index. We did not observe an association of time devoted to study, television viewing, or playing video-games with cognitive performance. Likewise, cognitive performance was similar across cardiorespiratory and mus-cular fitness levels and body weight categories.Conclusion Participation in physical sports activity during leisure time may positively influence cognitive perfor-mance in adolescents. (J Pediatr 2010;157:917-22).
There is increasing evidence that regular physical activity has positive effects on brain health and that it delays cognitivedecline in adults.1 Whether this effect also apply to young people is not clear. Results from cross-sectional studies in-dicate a positive association between physical activity and academic performance in children.2,3 Findings from interven-
tional studies also show that children in the physical activity intervention group have at least similar academic performancecompared with children in the control group, despite a substantial reduction in time devoted to academics.2,3 Less is known,however, about the association between physical activity and specific cognitive abilities during adolescence, a period of lifewhen the brain has profound plasticity.4
The effect that sedentary behaviors have on cognitive performance is of concern. Increased television viewing time is associ-
From the Department of Medical Physiology, School ofMedicine, University of Granada, Granada, Spain (J.R.,F.O.); Unit for Preventive Nutrition, Department ofBiosciences and Nutrition at NOVUM, KarolinskaInstitutet, Huddinge, Sweden (J.R., F.O, L.K., M.S.);Department of Basic Psychology, School of Psychology,University of Malaga, Malaga, Spain (R.C.); Departmentof Physical Education and Sport, School of SportSciences, University of Granada, Granada, Spain(M.M-M., P.T.); Department of Physiotherapy andNursing, School of Health and Sport Sciences, Universityof Zaragoza, Huesca, Spain (G.V-R.); Department ofPediatrics, University of Cantabria, Santander, Spain(J.N.); and Department of Physiotherapy and Nursing,
ated with worse academic performance in children5-7 and adolescents,8 yet play-ing action video games seems to improve cognitive performance in adults.9-11
Both cardiorespiratory fitness and fatness are considered important healthmarkers already in both children and adolescents.12,13 The association betweenphysical fitness and cognitive performance in adolescents is contradictory.3 Et-nier et al 14 concluded from a meta-analysis that there is no evidence for an as-sociation between cardiorespiratory fitness and cognitive performance in adults,whereas Hillman et al2 provided evidence that cardiorespiratory fitness can havea positive effect on cognitive performance, at least in pre-pubertal children. Theassociation between overweight or obesity and cognitive performance in youth isalso inconclusive.15-19
School of Health Sciences, University of Zaragoza,Zaragoza, Spain (L.M.)
*List of members of the AVENA Study Group available atwww.jpeds.com (Appendix).
Supported by the Spanish Ministry of Health (FIS no 00/0015), the Spanish Ministry of Education (grants EX-2007-1124 and EX-2008-0641), Panrico S.A., MadausS.A., Procter and Gamble S.A, the Swedish Council forWorking Life and Social Research (F.S.), the SwedishHeart-Lung Foundation (20090635), and the SpanishMinistry of Health: Maternal, Child Health and Develop-ment Network (RD08/0072). The authors declare noconflicts of interest.
0022-3476/$ - see front matter. Copyright � 2010 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2010.06.026
ANCOVA One-way analysis of covariance
AVENA [Alimentacion y Valoracion del Estado Nutricional de los Adolescentes Espanoles]
Food and Assessment of the Nutritional Status of Spanish Adolescents study
BMI Body mass index
CI Confidence interval
OR Odds ratio
SD Standard deviation
TEA Test of Educational Ability
VO2max Maximum oxygen consumption
917

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 157, No. 6
Most of the aforementioned studies rely on self-reporteddata of academic performance, and did not control for po-tential confounders such as socioeconomic status and familystructure.20,21 In this study, we examined the association ofparticipation in physical sports activity during leisure time,sedentary behaviors (time devoted to study, television view-ing, and playing videogames), cardiorespiratory and muscu-lar fitness, and weight status with cognitive performance(including verbal, numeric and reasoning abilities, and anoverall score) in Spanish adolescents. We also examined therelationships in the studied lifestyle-related factors and howthese contribute to better understand the lifestyle-cognitiveperformance associations in adolescents.
Methods
Participants were recruited from the AVENA (Alimentaciony Valoracion del Estado Nutricional de los Adolescentes Es-panoles [Food and Assessment of the Nutritional Status ofSpanish Adolescents]) study. The AVENA study is a cross-sectional study that was primarily designed to assess the nu-tritional status of a representative sample of Spanish adoles-cents aged 13.0 to 18.5 years. Data collection took place from2000 to 2002 in 5 Spanish cities (Madrid, Murcia, Granada,Santander, and Zaragoza). The complete methodology ofthe AVENA study has been detailed.22,23 This study includedadolescents with complete data on cognitive performance (n= 1820; 958 female). The study sample did not differ from thecomplete AVENA sample (n = 2894) in any of the demo-graphic variables (all P > .1).
A comprehensive verbal description of the nature and pur-pose of the study was given to the parents, school supervisors,and adolescents. Written consent to participate was re-quested from both parents and adolescents. Adolescentswith a personal history of cardiovascular disease or cognitivedysfunction, who were taking medication at the time of thestudy, or who were pregnant, were excluded. The study pro-tocol was performed in accordance with the ethical standardslaid down in the 1961 Declaration of Helsinki (as revised in2000), and approved by the Review Committee for ResearchInvolving Human Subjects of the Hospital UniversitarioMarques de Valdecilla (Santander, Spain).
We used the Spanish version of the ‘‘SRA Test of Educa-tional Ability’’ (TEA) to assess cognitive performance.24
This questionaire assesses intelligence with 3 basics schoolskills: verbal, numeric, and reasoning. The TEA test batteryprovides 3 complexity levels: level 1 for children aged 8 to12 years, level 2 for children aged 11 to 14 years, and level3 for adolescents aged 14 to 18 years. On the basis of theage range of our sample, we used levels 2 and 3. The psycho-metric properties of level 2 TEA test battery showed an inter-nal consistency reliability of a = 0.78 for the verbalcomponent, a = 0.83 for the numeric component, a = 0.88for the reasoning component, and a = 0.92 for overall cogni-tive performance. For level 3, internal consistency reliabilitywas a = 0.74 for the verbal component, a = 0.87 for the nu-
918
meric component, a = 0.77 for the reasoning component,and a = 0.89 for overall cognitive performance. The TEA bat-tery administration is collective and requires 42 and 27 min-utes for level 2 and 3, respectively.
Verbal ability assesses command of language, verbal iden-tification, and vocabulary; numeric ability assesses speed andprecision in performing operations with numbers and quan-titative concepts; and reasoning ability assesses logical ordi-nation criteria in sets of figures, numbers, or letters. Directscores (range, 0-33) were obtained for each of these variables,and we also computed an overall cognitive performance vari-able by summing the individual scores of the 3 items (range,0-99).
The adolescents answered the following question: ‘‘Do youpractice any type of physical sports activity outside the schooltime?’’ The possible answers were yes (coded as 1) or no(coded as 0).
We obtained the information about time devoted to studyand time spent in television viewing and playing video gamesfrom the following questions: ‘‘How many hours a day doyou do homework or study?’’ ‘‘How many hours a day doyou watch television?’’ and ‘‘How many hours a day do youplay videogames?’’ Possible answers were 0 = none, 1 = <30minutes, 2 = <1 hour, 3 = 1 to 3 hours, 4 = >3 to 4 hours,5 = >4 hours. Because of the relatively small sample size ineach single category, we re-coded the variables in two cate-gories: 0 when #3 hours/day and 1 when >3 hours/day.25
We assessed cardiorespiratory fitness with the 20-minuteshuttle run test. The score was considered as the number ofstages completed (precision of 0.5 stage). We estimated max-imal oxygen consumption (VO2max) (mLO2/kg/min) withthe equation reported by Leger.26 Adolescents were classifiedin two levels (ie, meeting/not meeting the cardiorespiratoryfitness standards) on the basis of the FITNESSGRAM stan-dards for Healthy Fitness Zone.27 The FITNESSGRAM stan-dards are associated with cardiovascular disease risk factorsin children and adolescents,28,29 and it would be of clinicaland public health importance to understand whether theyare also associated with cognitive performance. This test isvalid and reliable in young people.30,31
Upper body muscular strength was assessed by means ofthe handgrip strength test. The test was performed on bothhands with a hand dynamometer (Takei TKK 5101 Grip-D;Takey, Tokyo, Japan), standing and with the arm completelyextended. The test was performed twice, and the best scorewas retained (in kg). The sum of the right and left handwas used in the analysis.
Lower body muscular strength was assessed by means of thestanding long jump test. The participants were instructed topush off vigorously and jump as far forward as possible, tryingto land on both feet. The distance from the takeoff line to thepoint where the back of the heel closest to the take-off linelanded on the floor was scored. The result was recorded incentimeters. The test was performed twice, and the best scorewas retained. Adolescents were classified in two levels accord-ing to their upper and lower body muscular strength levels asbelow (low) and above (high) the median. The handgrip
Ruiz et al
December 2010 ORIGINAL ARTICLES
strength and stranding long jump tests are valid and reliablefield-based tests in children and adolescents.30-32
Weight and height were measured following standardizedprocedures, and body mass index (BMI) was calculated asweight in kilograms divided by square of height in meters(kg/m2). BMI was used as a surrogate marker of total bodyfat. Adolescents were classified according to the BMI interna-tional cutoff values as underweight, normal weight, over-weight, and obese.33,34
Parents completed a questionnaire that addressed the ad-olescents’ earlier and current health status and socioeco-nomic status defined as the educational level andoccupation of the father. According to this information,and following the recommendation of the Spanish Societyfor Epidemiology, the adolescents were classified in 5 cate-gories of socioeconomic status: low (I), medium-low (II),medium (III), medium-high (IV), and high (V). We also ob-tained information on maternal education level (primary,secondary, or university). There is evidence indicating thatsocioeconomic status is one of the most important determi-nants of childhood cognitive performance.20
We obtained information about family structure throughthe aforementioned questionnaire. Family structure was de-fined as living with parents or any other arrangement (onlymother, only father, grandparents, others). Family structuremay positively influence adolescents’ cognitive perfor-mance.21
We assessed pubertal development according to Tannerand Whitehouse.35 Self-reported breast development in girlsand genital development in boys was used for pubertal stageclassification.
Statistical AnalysisData are presented as means and SDs, unless otherwise indi-cated. Analyses were performed with the Statistical Packagefor Social Sciences software version 16.0 for Windows(SPSS, Chicago, Illinois) and the level of significance wasset to 0.05.
We analyzed the differences in cognitive performance (in-cluding verbal, numeric, and reasoning abilities and an over-all score) between adolescents who participated in physicalsports activity and adolescents who did not with one-wayanalysis of covariance (ANCOVA) after adjusting for ageand pubertal status (model 1). We performed a second model
Table I. Cognitive performance by participation in physical s
Model 1
Yes (n = 1053) No (n = 506) P Cohen’s d
Overall cognitiveperformance (0-99)
54.7 (13.0) 50.1 (13.5) <.001 0.32 (0.22
Verbal ability (0-33) 21.4 (6.5) 19.8 (6.7) <.001 0.25 (0.15Numeric ability (0-33) 14.6 (3.2) 13.1 (4.5) <.001 0.29 (0.19Reasoning ability (0-33) 18.6 (6.5) 17.2 (6.7) <.001 0.26 (0.16
Values are means (SD).Covariates model 1: sex, age, and pubertal status.Covariates model 2: model 1 plus socioeconomic status and family structure.
Physical Activity, Fitness, Weight Status, and Cognitive Performa
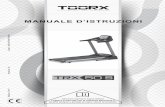
further including socioeconomic status and family structureas co-variates (model 2). We repeated the same model for theother exposures (ie, watching television, playing videogames,and time devoted to study #3 hours/day versus >3 hours/day), cardiorespiratory and muscular fitness (low versushigh), and weigh status (underweight, normal weight, over-weight, and obese). Because we did not observe an interac-tion effect between sex * exposure variables and cognitiveperformance (all P > .2), all the analyses were performedwith boys and girls together and sex was included in the anal-yses as a co-variate. We performed separate models for eachmain exposure, and sex, age and pubertal status were alwaysretained as co-variates (in model 1), whereas socioeconomicstatus and family structure were additionally included as co-variates in model 2.
We also analyzed the associations in exposures with binarylogistic regression analysis. Further, we determined the dif-ferences in cardiorespiratory fitness, muscular strength, andBMI among adolescents who participated in physical sportsactivity, those who did not, and those spending >3 hours/day watching television or playing videogames with AN-COVA. All the models included sex, age, and pubertal statusas co-variates.
We calculated the effect size statistics as Cohen d (stan-dardized mean differences) and 95% CI.36 Values of d equalto 0.2, 0.5, and 0.8 are considered small, medium, and largeeffects, respectively.
Results
Adolescents engaged in physical sports activities during leisuretime had significantly better cognitive performance that thosewho were not (Table I, model 1). The effect size, as determinedwith Cohen d, ranged from 0.25 (verbal ability) to 0.32 (overallcognitive performance). The results did not change whensocioeconomic status and family structure were entered inthe model (Table I, model 2). Further adjustments forcardiorespiratory fitness, BMI, and television viewing (orvideo games or time devoted to study) did not materiallymodify the results (data not shown). Similarly, whenmaternal educational status was used instead ofsocioeconomic status, the findings remained unaltered.
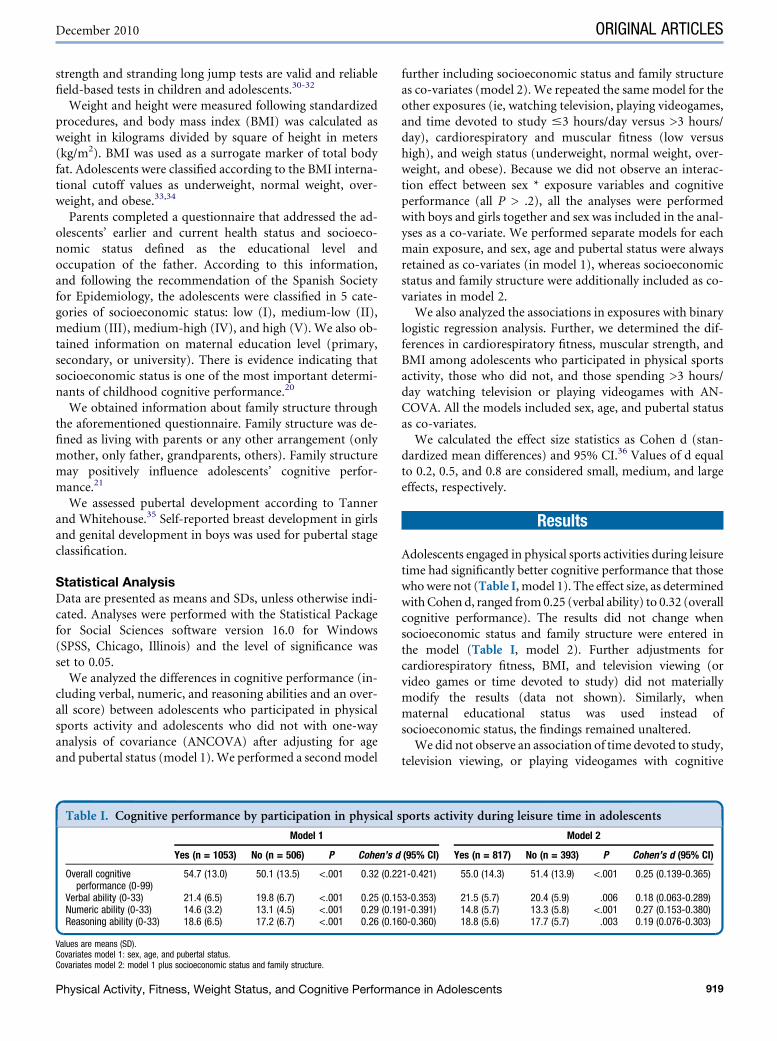
We did not observe an association of time devoted to study,television viewing, or playing videogames with cognitive
ports activity during leisure time in adolescents
Model 2
(95% CI) Yes (n = 817) No (n = 393) P Cohen’s d (95% CI)
1-0.421) 55.0 (14.3) 51.4 (13.9) <.001 0.25 (0.139-0.365)
3-0.353) 21.5 (5.7) 20.4 (5.9) .006 0.18 (0.063-0.289)1-0.391) 14.8 (5.7) 13.3 (5.8) <.001 0.27 (0.153-0.380)0-0.360) 18.8 (5.6) 17.7 (5.7) .003 0.19 (0.076-0.303)
nce in Adolescents 919
Table II. Cognitive performance and sedentary behaviors in adolescents
Model 1 Model 2
£3 hours/day >3 hours/day P £ 3 hours/day <3 hours/day P
Study (n = 1207) (n = 353) (n = 928) (n = 290)Overall cognitive performance (0-99) 53.3 (13.9) 53.3 (14.3) .969 54.1 (13.7) 53.6 (13.8) .599
Verbal ability (0-33) 20.8 (6.3) 21.2 (6.2) .325 21.1 (6.1) 21.2 (6.1) .711Numeric ability (0-33) 14.1 (4.9) 14.0 (5.1) .568 14.3 (4.9) 14.1 (4.9) .441Reasoning ability (0-33) 18.3 (5.6) 18.1 (5.6) .632 18.6 (5.5) 18.2 (5.6) .307
Television viewing (n = 1392) (n = 177) (n = 1096) (n = 125)Overall cognitive performance 53.3 (13.8) 52.1 (13.3) .255 53.8 (13.6) 54.7 (13.8) .510
Verbal ability 20.9 (6.0) 20.5 (6.3) .341 21.1 (6.0) 21.4 (6.1) .643Numeric ability 14.1 (4.9) 13.8 (4.9) .484 14.2 (4.6) 14.6 (4.9) .457Reasoning ability 18.3 (5.6) 17.8 (5.7) .244 18.5 (5.6) 18.7 (5.6) .651
Playing videogames (n = 1483) (n = 85) (n = 1161) (n = 61)Overall cognitive performance 53.4 (13.9) 51.3 (14.2) .194 53.9 (13.6) 54.7 (13.9) .648
Verbal ability 20.9 (6.2) 20.1 (6.3) .218 21.1 (6.1) 21.0 (6.2) .856Numeric ability 14.1 (5.0) 13.4 (5.0) .208 14.3 (4.8) 14.7 (4.9) .534Reasoning ability 18.3 (5.4) 17.8 (5.7) .447 18.5 (5.5) 19.1 (5.6) .439
Covariates model 1: sex, age and pubertal status.Covariates model 2: model 1 plus socioeconomic status and family structure.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 157, No. 6
performance (Table II). Likewise, cardiorespiratory fitnesswas not associated with cognitive performance (Figure 1;available at www.jpeds.com). The results did not materiallychange when we used a different equation to estimatecardiorespiratory fitness (VO2max).37 Neither upper bodynor lower body muscular strength were associated withcognitive performance (Figures 2 and 3; available at www.jpeds.com), and the results persisted after we repeated theanalysis comparing the upper and lower sex- and age-specific quintiles (data not shown). Cognitive performancewas similar across weight status categories (Figure 4;available at www.jpeds.com).
We did not observe an association between physical sportsactivity and time devoted to study (odds ratio [OR], 0.818;95% CI, 0.630-1.064). Participation in physical sports activityduring leisure time was associated with a lower OR of watch-ing television for >3 hours/day (0.631; 95% CI, 0.445-0.894)and playing videogames for >3 hours/day (0.533; 95% CI,0.320-0.887). Adolescents participating in physical sports ac-tivity had better cardiorespiratory and muscular fitness levelscompared with those who did not for cardiorespiratory fit-ness (5.9 � 2.0 versus 4.9 � 1.9 stages, respectively; P <.001), standing long jump (177 � 31 versus 154 � 28 cm, re-spectively; P < .001), and handgrip strength (61.1 � 0.4 ver-sus 59.6 � 0.5 cm, respectively; P = .023). BMI did not differin physical sports activity categories (P = .606).
Adolescents who spent >3 hours/day watching televisiontended to have a lower OR of spending >3 hours/day study-ing (0.629; 95% CI, 0.384-1.029). Adolescents who spent <3hours/day playing video games had a significantly lower ORof spending >3 hours/day studying (0.375; 95% CI, 0.147-0.959).
Levels of cardiorespiratory fitness were lower in adoles-cents who spent >3 hours/day watching television comparedwith adolescents who spent #3 hours/day watching televi-sion (4.9 � 1.3 versus 5.6 � 2.1 stages, respectively; P <.001) and so were standing long jump levels (162� 31 versus169 � 32 cm, respectively; P = .019). BMI was higher in ad-
920
olescents who spent >3 hours/day watching television com-pared with those who spent #3 hours/day (22.4 � 3.4versus 21.5 � 3.2 kg/m2, respectively; P = .002), regardlessof sex, age, and puberty stage.
Adolescents who played videogames for >3 hours/day hadlower cardiorespiratory fitness compared with their peerswho spent #3 hours/day (4.5 � 1.0 versus 5.6 � 2.2 stages,respectively; P < .001). The results were similar when we re-peated all the analyses in boys and girls separately.
Discussion
Although no conclusion can be drawn from this cross-sectionalstudy about whether participation in physical sports activityduring leisure time leads to improvements in cognitive perfor-mance in adolescents, these findings are of public health andclinical interest and extend earlier results that suggested the po-tential benefit of physical activity on cognitive performance al-ready in youth.2,3 Adolescence is a period of life when the brainhas profound plasticity because of changes in both structureand function.4 Therefore, the pubertal period offers high pos-sibilities of stimulating cognitive function.4
The relationship between participation in physical sportsactivity and cognitive performance has been a subject of dis-cussion between advocates and skeptics of physical sports ac-tivity, and especially in parents concerned about decreases instudy and homework time. The assumption is based on theparticipation in physical sports activity may ‘‘displace’’ timethat would normally be spent doing schoolwork, readingfor pleasure, or engaging in other educational activities. Inthis study, we observed that participation in physical sportsactivity is not associated with lower time devoted to study.This concurs with intervention studies that indicated thatchildren enrolled in more physical sports activity do nothave poorer academic performance, despite a reduction intime in the so-called ‘‘academic subjects.’’3 Furthermore,we also observed that participation in physical sports activitywas associated with lower television viewing and time
Ruiz et al

December 2010 ORIGINAL ARTICLES
devoted to play video games and with higher levels of cardio-respiratory and muscular fitness. This suggest that physicalsports activity may indirectly prevent the deleterious effectsascribed to sedentary behaviors39, 40 and may have an indirectpositive effect on health through its effect on fitness. Findingsfrom intervention studies also reported a positive effect onfitness besides the aforementioned effects on academic per-formance.3 Even single bouts of physical activity (20 minutesof aerobic exercise at 60% of estimated maximum heart rate)may improve cognitive control and attention in children.41
Collectively, these findings are particularly important be-cause of the existing pressure on children and adolescents,parents, and schools to maximize academic performance.We do not know whether sports participation is a markerof adolescents who are high achievers and who do better inthis type of cognitive tests. Moreover, whether adolescentswho persist in sports activity have other characteristics thatallow them to perform well on cognitive tests remains to beelucidated.
There is increasing concern about the amount of time thatyouth spend watching television or playing video games be-cause of the potential effect they may have on health. Indeed,we observed that both television viewing and playing videogames had a negative effect on cardiorespiratory fitness, lowerbody muscular strength, and BMI. Several studies reported anassociation between increased television viewing and decreasedtime spent reading and doing homework,42,43 which inturn may affect academic performance. Results from cross-sectional and longitudinal studies reported that increasedtelevision time had a detrimental impact on academic perfor-mance in children5-7 and self-reported academic performancein adolescents.8 We observed that adolescents who spent moretime watching television or playing video games devoted lesstime to study, which concurs with the so called ‘‘displacementhypothesis.’’44 However, despite this observation, we did notobserve an association between television time and cognitiveperformance. Our data do not concur with experimental stud-ies showing that playing action video games improve cognitiveperformance in young adults.9,10 Differences in the outcomevariable, the participants’ age, and the study design make com-parisons between studies difficult.
Cardiorespiratory fitness is strongly linked to cardiovascu-lar disease risk factors in youth.12,13 Whether it is also associ-ated with cognitive performance is, however, debated. Theconclusion from a meta-regression analysis was that cardio-respiratory fitness was not associated with cognitive perfor-mance in adults,14 which concur with our results, whereasother studies suggested the opposite in children.2 Hillmanand co-workers showed in a series of studies that high cardio-respiratory fitness was associated with better cognition inpre-adolescent children.19,45,46 Several studies hypothesizedthat aerobic fitness may mediate the relationship betweenphysical activity and cognitive performance,47 whereas otherstudies argued that cardiorespiratory fitness is a ‘‘‘gross’’measure of the physiological status and therefore might notbe sensitive enough for one to see any association with cog-nitive performance.14 The association between physical
Physical Activity, Fitness, Weight Status, and Cognitive Performa
sports activity and cognitive performance observed in thisstudy persisted after further adjusting for either cardiorespi-ratory or muscular fitness. Whether more precise measure-ments of both cardiorespiratory fitness (ie, directlymeasured maximum oxygen consumption) and cognitivefunction (eg, electroencephalogram, neuroelectric activity)would yield to a different results in adolescents remains tobe investigated.45 We did not observe an association betweenmuscular fitness and cognitive performance, which concurwith the results observed by other authors.19
A limited number of studies have examined whether in-creased body weight per se is associated with poorer cognitiveperformance.15-19 We did not observe an association betweenweight status and cognitive performance, which concurs withother studies.17,18 Overweight children and adolescents havelower cognitive performance than normal-weight ones afteradjusting for a number of potential confounders.16 Mo-suwan et al17 observed an association between overweightstatus and poor academic performance in children, but notin adolescents. Severely obese Chinese children had signifi-cantly lower intelligence quotient than the control subjects.15
Children with higher cognitive function in early life can be atdecreased risk of overweight years later.48
Limitations of this study include its cross-sectional design,which precludes drawing conclusions on the direction of theassociations. A second limitation relies on the use of a self-reported measure of physical sports activity. Moreover, thisstudy focused only on sports-related activity, and therefore,the duration of the participation and other leisure time phys-ical activity was not recorded. Further research should usephysical activity assessed with objective measures such as ac-celerometry. We did not have data on watching televisionduring weekends, which limited the analysis. We also didnot ask what kinds of video games adolescents play. Strengthsof this study include the use of a relatively large national sam-ple, the inclusion of several potential confounders, and theuse of an objective and standardized measure of cognitiveperformance.
Because cognitive performance is potentially modifiableduring the pubertal phase,4 it would be of interest to investi-gate whether targeted physical activity interventions espe-cially on individuals with cognitive impairment mightinfluence cognitive performance during adolescence andlater in life. n
Submitted for publication Feb 16, 2010; last revision received Apr 30, 2010;
accepted Jun 16, 2010.
Reprint requests: Jonatan R. Ruiz, PhD. Department of Biosciences and
Nutrition, Unit for Preventive Nutrition, Karolinska Institutet, Stockholm,
Sweden, Halsovagen 7-9, SE-141 57 Huddinge, Sweden. E-mail: [email protected].
References
1. Dishman RK, Berthoud HR, Booth FW, Cotman CW, Edgerton VR,
Fleshner MR, et al. Neurobiology of exercise. Obesity (Silver Spring)
2006;14:345-56.
2. Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart:
exercise effects on brain and cognition. Nat Rev Neurosci 2008;9:58-65.
nce in Adolescents 921
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 157, No. 6
3. Trudeau F, Shephard RJ. Physical education, school physical activity,
school sports and academic performance. Int J Behav Nutr Phys Act
2008;5:10.
4. Romeo RD, McEwen BS. Stress and the adolescent brain. Ann N Y Acad
Sci 2006;1094:202-14.
5. Borzekowski DL, Robinson TN. The remote, the mouse, and the no 2
pencil: the household media environment and academic achievement
among third grade students. Arch Pediatr Adolesc Med 2005;159:607-13.
6. Zimmerman FJ, Christakis DA. Children’s television viewing and cogni-
tive outcomes: a longitudinal analysis of national data. Arch Pediatr
Adolesc Med 2005;159:619-25.
7. Hancox RJ, Milne BJ, Poulton R. Association of television viewing dur-
ing childhood with poor educational achievement. Arch Pediatr Adolesc
Med 2005;159:614-8.
8. Sharif I, Sargent JD. Association between television, movie, and video
game exposure and school performance. Pediatrics 2006;118:e1061-70.
9. Green CS, Bavelier D. Action video game modifies visual selective atten-
tion. Nature 2003;423:534-7.
10. Boot WR, Kramer AF, Simons DJ, Fabiani M, Gratton G. The effects of
video game playing on attention, memory, and executive control. Acta
Psychol (Amst) 2008;129:387-98.
11. Owen AM, Hampshire A, Grahn JA, Stenton R, Dajani S, Burns AS, et al.
Putting brain training to the test. Nature 2010;465:775-8.
12. Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M. Physical fitness in child-
hood and adolescence: a powerful marker of health. Int J Obes (Lond)
2008;32:1-11.
13. Ruiz JR, Castro-Pinero J, Artero EG, Ortega FB, Sjostrom M, Suni J, et al.
Predictive validity of health-related fitness in youth: a systematic review.
Br J Sports Med 2009;43:909-23.
14. Etnier JL, Nowell PM, Landers DM, Sibley BA. A meta-regression to ex-
amine the relationship between aerobic fitness and cognitive perfor-
mance. Brain Res Rev 2006;52:119-30.
15. Li X. A study of intelligence and personality in children with simple obe-
sity. Int J Obes Relat Metab Disord 1995;19:355-7.
16. Li Y, Dai Q, Jackson JC, Zhang J. Overweight is associated with decreased
cognitive functioning among school-age children and adolescents. Obe-
sity (Silver Spring) 2008;16:1809-15.
17. Mo-suwan L, Lebel L, Puetpaiboon A, Junjana C. School performance
and weight status of children and young adolescents in a transitional so-
ciety in Thailand. Int J Obes Relat Metab Disord 1999;23:272-7.
18. Datar A, Sturm R, Magnabosco JL. Childhood overweight and academic
performance: national study of kindergartners and first-graders. Obes
Res 2004;12:58-68.
19. Castelli DM, Hillman CH, Buck SM, Erwin HE. Physical fitness and ac-
ademic achievement in third- and fifth-grade students. J Sport Exerc
Psychol 2007;29:239-52.
20. Lawlor DA, Najman JM, Batty GD, O’Callaghan MJ, Williams GM,
Bor W. Early life predictors of childhood intelligence: findings from
the Mater-University study of pregnancy and its outcomes. Paediatr
Perinat Epidemiol 2006;20:148-62.
21. Riesch SK, Anderson LS, Krueger HA. Parent-child communication pro-
cesses: preventing children’s health-risk behavior. J Spec Pediatr Nurs
2006;11:41-56.
22. Gonzalez-Gross M, Castillo MJ, Moreno L, Nova E, Gonzalez-
Lamuno D, Perez-Llamas F, et al. Alimentacion y valoracion del estado
nutricional de los adolescentes espanoles (estudio AVENA). Evaluacion
de riesgos y propuesta de intervencion. I. descripcion metodologica del
proyecto. Nutricion Hospitalaria 2003;18:15-28.
23. Ortega FB, Ruiz JR, Castillo MJ, Moreno LA, Gonzalez-Gross M,
Warnberg J, et al. [Low level of physical fitness in Spanish adolescents.
Relevance for future cardiovascular health (AVENA study)]. Rev Esp
Cardiol 2005;58:898-909.
24. Thurstone L, Thurtone T. SRA Test of Educational Ability. Chicago: Sci-
ence Research Associates; 1958.
25. Pate RR, Wang CY, Dowda M, Farrell SW, O’Neill JR. Cardiorespiratory
fitness levels among US youth 12 to 19 years of age: findings from the
1999-2002 National Health and Nutrition Examination Survey. Arch Pe-
diatr Adolesc Med 2006;160:1005-12.
922
26. Leger LA, Mercier D, Gadoury C, Lambert J. The multistage 20 metre
shuttle run test for aerobic fitness. J Sports Sci 1988;6:93-101.
27. Cureton KJ, Warren GL. Criterion-referenced standards for youth
health-related fitness tests: a tutorial. Res Q Exerc Sport 1990;61:7-19.
28. Ruiz JR, Ortega FB, Rizzo NS, Villa I, Hurtig-Wennlof A, Oja L, et al. High
cardiovascular fitness is associated with low metabolic risk score in chil-
dren: the European Youth Heart Study. Pediatr Res 2007;61:350-5.
29. Lobelo F, Pate RR, Dowda M, Liese AD, Ruiz JR. Validity of cardiorespi-
ratory fitness criterion-referenced standards for adolescents. Med Sci
Sports Exerc 2009;41:1222-9.
30. Ortega FB, Artero EG, Ruiz JR, Vicente-Rodriguez G, Bergman P,
Hagstromer M, et al. Reliability of health-related physical fitness tests
in European adolescents. The HELENA Study. Int J Obes (Lond)
2008;32 Suppl. 5:S49–S57.
31. Castro-Pinero J, Artero EG, Espana-Romero V, Ortega FB, Sjostrom M,
Suni J, et al. Criterion-related validity of field-based fitness tests in youth:
a systematic review. Br J Sports Med 2009 [Epub ahead of print].
32. Espana-Romero V, Ortega FB, Vicente-Rodriguez G, Artero EG, Rey JP,
Ruiz JR. Elbow position affects handgrip strength in adolescents: validity
and reliability of Jamar, DynEx, and TKK dynamometers. J Strength
Cond Res 2010;24:272-7.
33. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard def-
inition for child overweight and obesity worldwide: international survey.
BMJ 2000;320:1240-3.
34. Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to
define thinness in children and adolescents: international survey. BMJ
2007;335:194.
35. Tanner JM, Whitehouse RH. Clinical longitudinal standards for height,
weight, height velocity, weight velocity, and stages of puberty. Arch Dis
Child 1976;51:170-9.
36. Nakagawa S, Cuthill IC. Effect size, confidence interval and statistical sig-
nificance: a practical guide for biologists. Biol Rev Camb Philos Soc 2007;
82:591-605.
37. Ruiz JR, Ramirez-Lechuga J, Ortega FB, Castro-Pinero J, Benitez JM,
Arauzo-Azofra A, et al. Artificial neural network-based equation for es-
timating VO(2max) from the 20m shuttle run test in adolescents. Artif
Intell Med 2008;44:233-45.
38. Cotman CW, Berchtold NC. Exercise: a behavioral intervention to en-
hance brain health and plasticity. Trends Neurosci 2002;25:295-301.
39. Ekelund U, Brage S, Froberg K, Harro M, Anderssen SA, Sardinha LB,
et al. TV viewing and physical activity are independently associated
with metabolic risk in children: the European Youth Heart Study.
PLoS Med 2006;3:e488.
40. Rey-Lopez JP, Vicente-Rodriguez G, Biosca M, Moreno LA. Sedentary
behaviour and obesity development in children and adolescents. Nutr
Metab Cardiovasc Dis 2008;18:242-51.
41. Hillman CH, Pontifex MB, Raine LB, Castelli DM, Hall EE, Kramer AF.
The effect of acute treadmill walking on cognitive control and academic
achievement in preadolescent children. Neuroscience 2009;159:1044-54.
42. Wiecha JL, Sobol AM, Peterson KE, Gortmaker SL. Household television
access: associations with screen time, reading, and homework among
youth. Ambul Pediatr 2001;1:244-51.
43. Wolfe DA, Mendes MG, Factor D. A parent-administered program to re-
duce children’s television viewing. J Appl Behav Anal 1984;17:267-72.
44. Anderson DR, Huston AC, Schmitt KL, Linebarger DL, Wright JC. Early
childhood television viewing and adolescent behavior: the recontact
study. Monogr Soc Res Child Dev 2001;66. I-VIII, 1–147.
45. Hillman CH, Castelli DM, Buck SM. Aerobic fitness and neurocognitive
function in healthy preadolescent children. Med Sci Sports Exerc 2005;
37:1967-74.
46. Buck SM, Hillman CH, Castelli DM. The relation of aerobic fitness to
stroop task performance in preadolescent children. Med Sci Sports Exerc
2008;40:166-72.
47. North TC, McCullagh P, Tran ZV. Effect of exercise on depression. Exerc
Sport Sci Rev 1990;18:379-415.
48. Guxens M, Mendez MA, Julvez J, Plana E, Forns J, Basagana X, et al. Cog-
nitive function and overweight in preschool children. Am J Epidemiol
2009;170:438-46.
Ruiz et al

Appendix
Members of the AVENA Study Group: Coordinator: A.Marcos, Madrid; principal researchers: M.J. Castillo, Gran-ada; A. Marcos, Madrid; S. Zamora, Murcia; M. GarcıaFuentes, Santander; M Bueno, Zaragoza.
Granada: M.J. Castillo, M.D. Cano, R. Sola (biochemistry),A. Gutierrez, J.L. Mesa, J. Ruiz (physical fitness), M. Delgado,P. Tercedor, P. Chillon (physical activity), F.B. Ortega, M.Martın, F. Carreno, G.V. Rodrıguez, R. Castillo and F.Arellano (collaborators), Dpto Fisiologıa, Universidad deGranada, E-18071 Granada; Madrid: A. Marcos, M. Gonza-lez-Gross, J. Warnberg, S. Medina, F. Sanchez Muniz, E.Nova, A. Montero, B. de la Rosa, S. Gomez, S. Samartın, J.Romeo, R. Alvarez (coordination, immunology), A. Alvarez(cytometric analysis), L. Barrios (statistical analysis), A.Leyva, B. Paya (psychological assessment), L. Martınez, E.Ramos, R. Ortiz and A. Urzanqui (collaborators), Institutode Nutricion y Bromatologıa, Consejo Superior de Investiga-ciones Cientıficas (CSIC), E-28040 Madrid; Murcia: S. Za-mora, M. Garaulet, F. Perez-Llamas, J.C. Baraza, J.F.Marın, F. Perez de Heredia, M.A. Fernandez, C. Gonzalez,R. Garcıa, C. Torralba, E. Donat, E. Morales, M.D. Garcıa,J.A. Martınez, J.J. Hernandez, A. Asensio, F.J. Plaza andM.J. Lopez (diet analysis), Dpto Fisiologıa, Universidad deMurcia, E-30100 Murcia; Santander: M. Garcıa Fuentes, D.Gonzalez-Lamuno, P. de Rufino, R. Perez-Prieto, D. Fernan-dez and T. Amigo (genetic study), Dpto Pediatrıa, Universi-dad de Cantabria, E- 19003 Santander; Zaragoza: M. Bueno,L.A. Moreno, A .Sarria, J. Fleta, G. Rodrıguez, C.M. Gil, M.I.Mesana, J.A. Casajus, V. Blay and M.G. Blay (anthropometricassessment), Escuela Universitaria de Ciencias de la Salud,Universidad de Zaragoza, E-50009 Zaragoza.
December 2010 ORIGINAL ARTICLES
Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents 922.e1
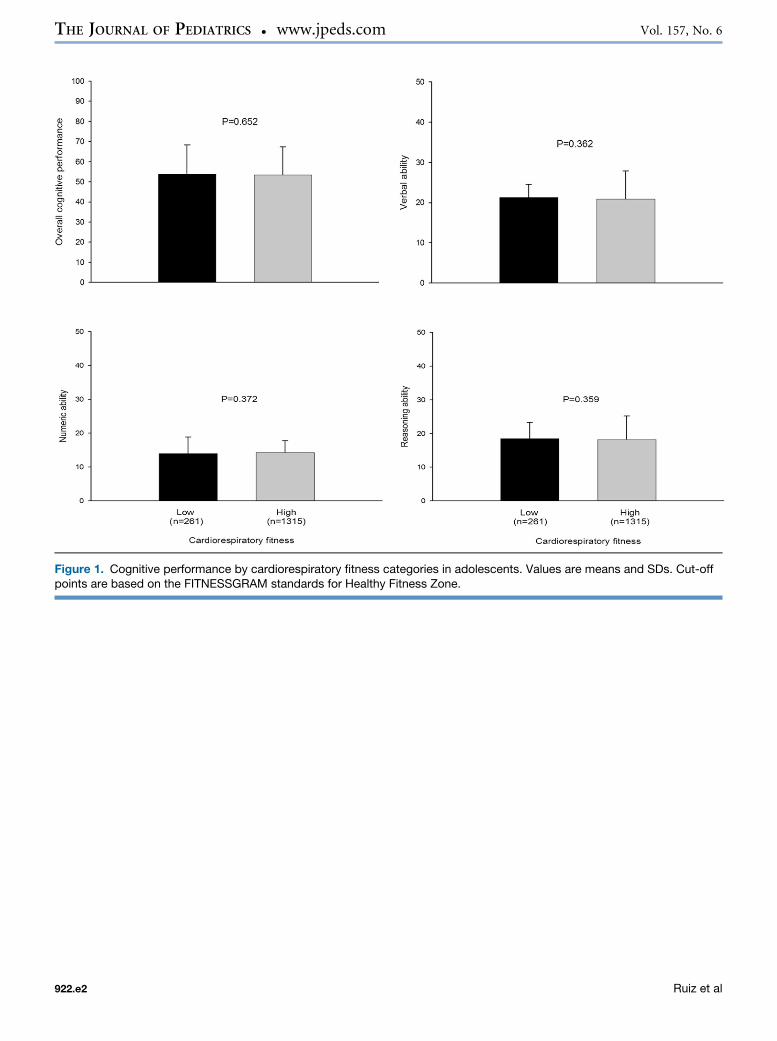
Figure 1. Cognitive performance by cardiorespiratory fitness categories in adolescents. Values are means and SDs. Cut-offpoints are based on the FITNESSGRAM standards for Healthy Fitness Zone.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 157, No. 6
922.e2 Ruiz et al
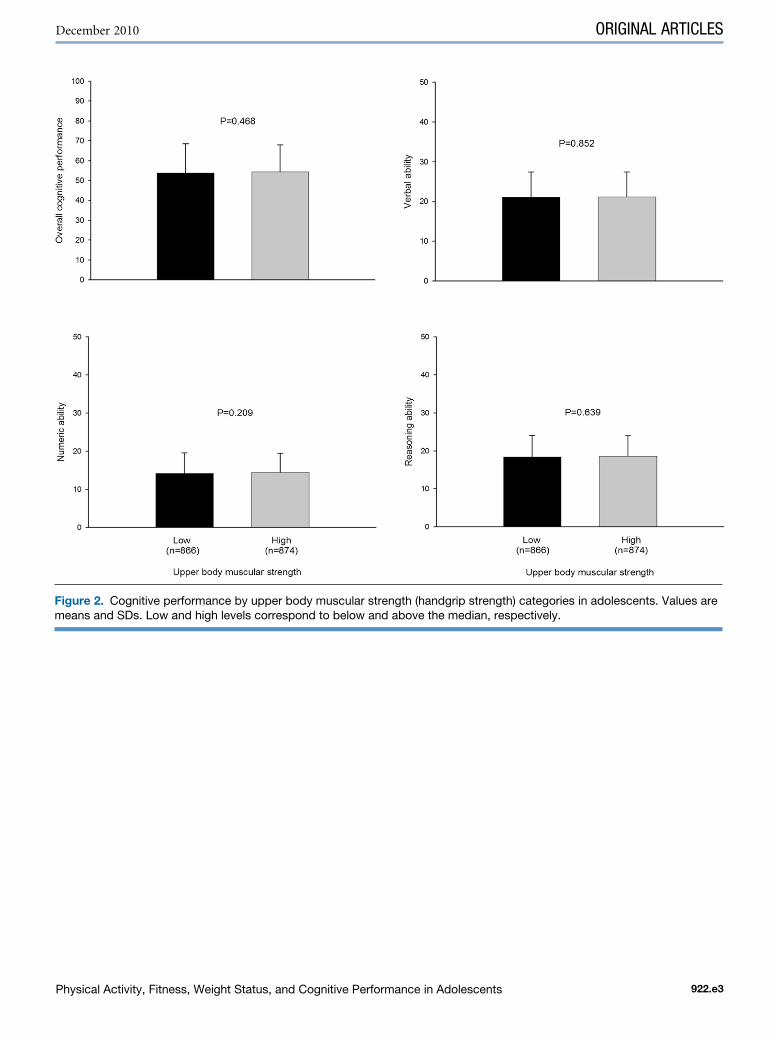
Figure 2. Cognitive performance by upper body muscular strength (handgrip strength) categories in adolescents. Values aremeans and SDs. Low and high levels correspond to below and above the median, respectively.
December 2010 ORIGINAL ARTICLES
Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents 922.e3
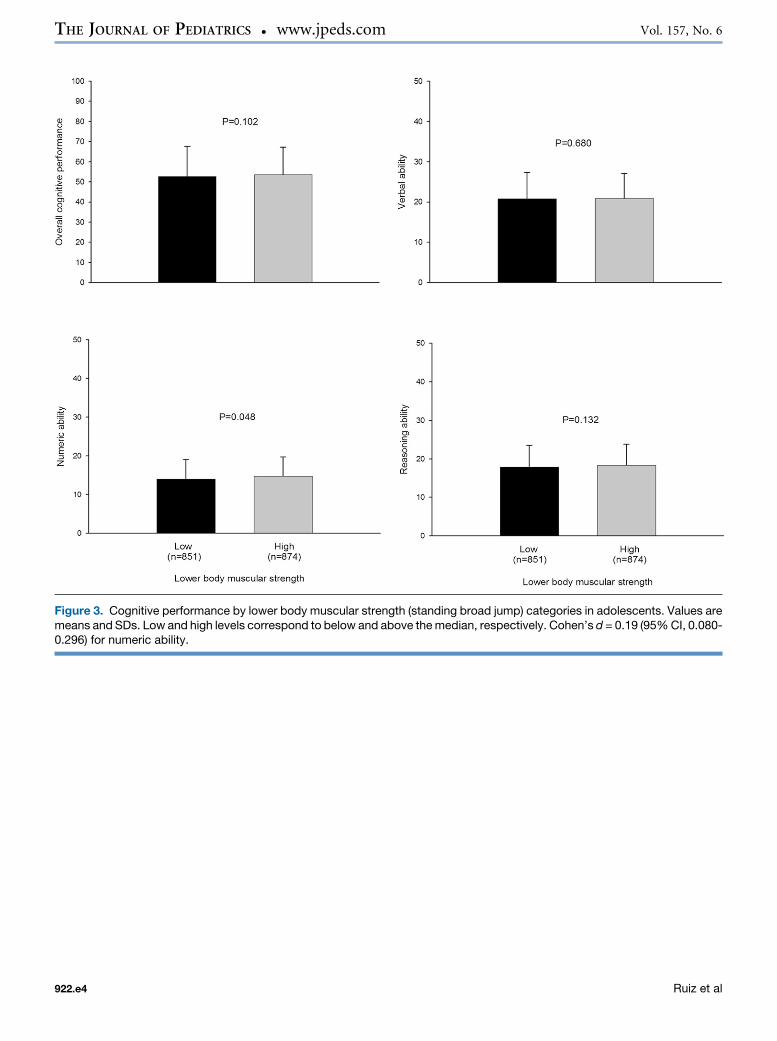
Figure 3. Cognitive performance by lower body muscular strength (standing broad jump) categories in adolescents. Values aremeans and SDs. Low and high levels correspond to below and above the median, respectively. Cohen’s d = 0.19 (95% CI, 0.080-0.296) for numeric ability.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 157, No. 6
922.e4 Ruiz et al
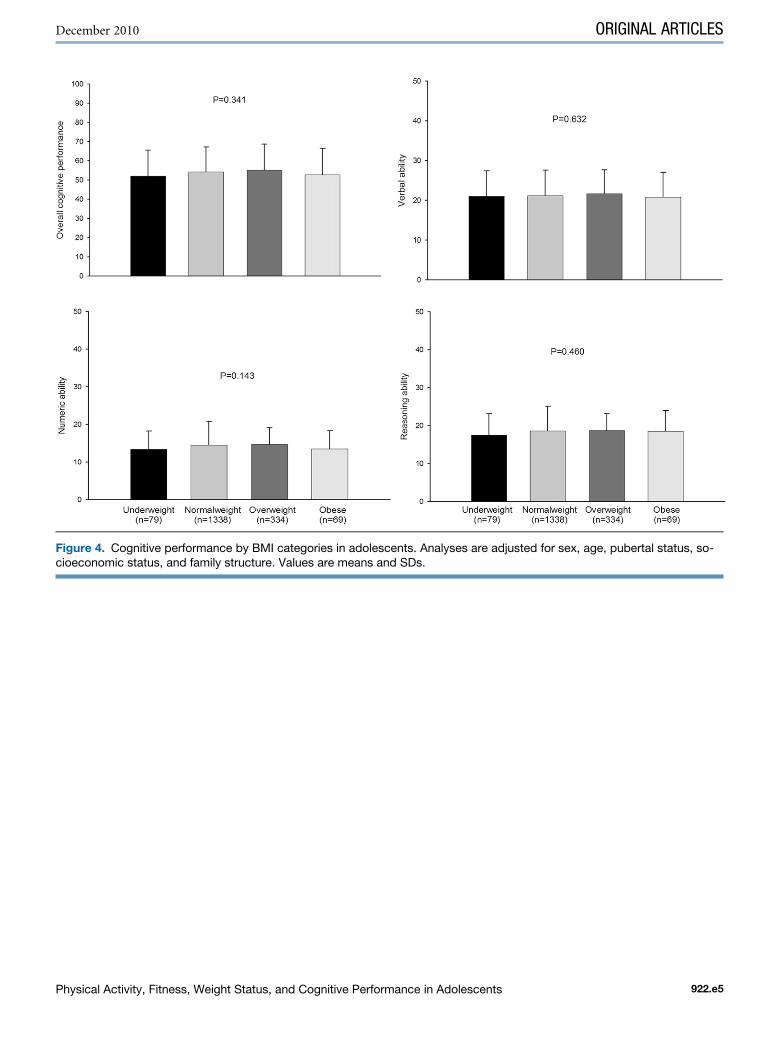
Figure 4. Cognitive performance by BMI categories in adolescents. Analyses are adjusted for sex, age, pubertal status, so-cioeconomic status, and family structure. Values are means and SDs.
December 2010 ORIGINAL ARTICLES
Physical Activity, Fitness, Weight Status, and Cognitive Performance in Adolescents 922.e5




















