
Physical activity, ethnicity and cardio-metabolic health: Does one size fit all?
15
Review Physical activity, ethnicity and cardio-metabolic health: Does one size fit all? Jason M.R. Gill a, * , Carlos A. Celis-Morales b , Nazim Ghouri a a Institute of Cardiovascular and Medical Sciences, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK b Human Nutrition Research Centre, Institute for Ageing and Health, Newcastle University, Newcastle on Tyne, UK article info Article history: Received 1 August 2013 Received in revised form 7 November 2013 Accepted 8 November 2013 Available online 23 November 2013 Keywords: Cardiovascular disease Diabetes Ethnicity Race Physical activity Fitness Exercise abstract A large and consistent body of epidemiological evidence indicates that low levels of physical activity, low levels of cardiorespiratory fitness and high levels of sedentary behaviour are associated with increased risk of cardio-metabolic diseases. However, most such studies have been undertaken in populations of White European descent. The available data from non-White populations suggests that physical activity is also protective in these groups, but the threshold level of activity needed to confer low risk, partic- ularly for type 2 diabetes, may not be the same across all ethnic groups. In patients with impaired glucose regulation, lifestyle interventions, including physical activity as a component (often in combination with weight loss), are effective at reducing risk of incident diabetes across a range of ethnic groups. However, the optimal levels of physical activity for prevention of diabetes and cardiovascular disease amongst the general populations of different ethnic groups have not been firmly established. Emerging data suggest that innate differences in cardiorespiratory fitness levels and capacity for fat oxidation potentially contribute to ethnic differences in the cardio-metabolic risk profile and that ethnicityespecific physical activity guidelines may be conceptually warranted. More study is needed to understand how and why the doseeresponse relationship between physical activity and cardio-metabolic risk differs according to ethnicity and to determine the best approaches to promote physical activity in non-White ethnic groups. Ó 2013 Elsevier Ireland Ltd. All rights reserved. Contents 1. Physical activity, cardiorespiratory fitness and sedentary behaviour: three related factors influencing cardio-metabolic disease risk ................1 2. Physical activity guidelines and population attributable risk associated with inactivity ............................. ..........................8 3. Physical activity and cardio-metabolic disease risk in non-White populations ................................................................9 4. Lifestyle intervention trials for cardiovascular disease prevention ......................................................................... 10 5. Lifestyle intervention trials for diabetes prevention ...................................................................................... 11 6. Ethnicityeenvironment interactions and diabetes risk ................................................................................... 12 7. Can physiological differences between ethnic groups explain the ethnic differences in diabetes risk? .......................................... 13 8. Can ethnicespecific physical activity recommendations help to overcome innate differences in diabetes risk between ethnic groups? ...... ...... 14 9. Conclusions ........................................................................................................................ 15 References ......................................................................................................................... 15 1. Physical activity, cardiorespiratory fitness and sedentary behaviour: three related factors influencing cardio-metabolic disease risk A large and consistent body of prospective epidemiological data (>1.5 million participants) has firmly established that a low level of physical activity is an important modifiable risk factor for all-cause mortality, cardiovascular disease and type 2 diabetes [1e5]. The * Corresponding author. BHF Glasgow Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow G12 8TA, UK. Tel.: þ44 (0) 141 3302916; fax: þ44 (0) 141 3305481. E-mail address: [email protected] (J.M.R. Gill). Contents lists available at ScienceDirect Atherosclerosis journal homepage: www.elsevier.com/locate/atherosclerosis 0021-9150/$ e see front matter Ó 2013 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.atherosclerosis.2013.11.039 Atherosclerosis 232 (2014) 319e333
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Physical activity, ethnicity and cardio-metabolic health: Does one size fit all?

lable at ScienceDirect
Atherosclerosis 232 (2014) 319e333
Contents lists avai
Atherosclerosis
journal homepage: www.elsevier .com/locate/atherosclerosis
Review
Physical activity, ethnicity and cardio-metabolic health: Does one sizefit all?
Jason M.R. Gill a,*, Carlos A. Celis-Morales b, Nazim Ghouri a
a Institute of Cardiovascular and Medical Sciences, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UKbHuman Nutrition Research Centre, Institute for Ageing and Health, Newcastle University, Newcastle on Tyne, UK
a r t i c l e i n f o
Article history:Received 1 August 2013Received in revised form7 November 2013Accepted 8 November 2013Available online 23 November 2013
Keywords:Cardiovascular diseaseDiabetesEthnicityRacePhysical activityFitnessExercise
* Corresponding author. BHF Glasgow Cardiovascuof Cardiovascular and Medical Sciences, College ofSciences, University of Glasgow, Glasgow G12 8TA, Ufax: þ44 (0) 141 3305481.
E-mail address: [email protected] (J.M.R. Gi
0021-9150/$ e see front matter � 2013 Elsevier Irelahttp://dx.doi.org/10.1016/j.atherosclerosis.2013.11.039
a b s t r a c t
A large and consistent body of epidemiological evidence indicates that low levels of physical activity, lowlevels of cardiorespiratory fitness and high levels of sedentary behaviour are associated with increasedrisk of cardio-metabolic diseases. However, most such studies have been undertaken in populations ofWhite European descent. The available data from non-White populations suggests that physical activityis also protective in these groups, but the threshold level of activity needed to confer low risk, partic-ularly for type 2 diabetes, may not be the same across all ethnic groups. In patients with impaired glucoseregulation, lifestyle interventions, including physical activity as a component (often in combination withweight loss), are effective at reducing risk of incident diabetes across a range of ethnic groups. However,the optimal levels of physical activity for prevention of diabetes and cardiovascular disease amongst thegeneral populations of different ethnic groups have not been firmly established. Emerging data suggestthat innate differences in cardiorespiratory fitness levels and capacity for fat oxidation potentiallycontribute to ethnic differences in the cardio-metabolic risk profile and that ethnicityespecific physicalactivity guidelines may be conceptually warranted. More study is needed to understand how and whythe doseeresponse relationship between physical activity and cardio-metabolic risk differs according toethnicity and to determine the best approaches to promote physical activity in non-White ethnic groups.
� 2013 Elsevier Ireland Ltd. All rights reserved.
Contents
1. Physical activity, cardiorespiratory fitness and sedentary behaviour: three related factors influencing cardio-metabolic disease risk . . . . . . . . . . . . . . . .12. Physical activity guidelines and population attributable risk associated with inactivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .83. Physical activity and cardio-metabolic disease risk in non-White populations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .94. Lifestyle intervention trials for cardiovascular disease prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .105. Lifestyle intervention trials for diabetes prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .116. Ethnicityeenvironment interactions and diabetes risk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .127. Can physiological differences between ethnic groups explain the ethnic differences in diabetes risk? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .138. Can ethnicespecific physical activity recommendations help to overcome innate differences in diabetes risk between ethnic groups? . . . . . . . . . . . .149. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
lar Research Centre, InstituteMedical, Veterinary and LifeK. Tel.: þ44 (0) 141 3302916;
ll).
nd Ltd. All rights reserved.
1. Physical activity, cardiorespiratory fitness and sedentarybehaviour: three related factors influencing cardio-metabolicdisease risk
A large and consistent body of prospective epidemiological data(>1.5 million participants) has firmly established that a low level ofphysical activity is an important modifiable risk factor for all-causemortality, cardiovascular disease and type 2 diabetes [1e5]. The

J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333320
most active individuals experience about a 30% reduction in car-diovascular disease, diabetes all-cause mortality risk compared tothe least active [1,3e5], although themagnitude of the diabetes riskreduction reduces by about half after adjustment for BMI [2,4].These risk reduction values are likely to be underestimates becausethe studies generally assessed physical activity by self-reportquestionnaire which can attenuate the true relationship betweenactivity and health outcome measures, due to regression dilutionbias errors due to mis-reporting of activity levels [6,7] and(particularly for all-cause mortality and cardiovascular disease)because many studies adjusted for factors that are likely to mediatesome of the beneficial effects of physical activity (e.g. blood pres-sure, diabetes) [1,3,5]. Studies of the association of cardiorespira-tory fitness (i.e. a physiological trait defined as the ability of thecardiovascular and respiratory systems to supply oxygen to work-ing muscles during sustained physical activity, which is typicallyassessed by measuring maximal oxygen uptake (VO2max) during anincremental exercise test) and health outcomes generally reportlarger effects than studies of physical activity (i.e. a behaviourdefined as bodily movement produced by skeletal muscles thatresults in energy expenditure, which can be assessed by self-reportquestionnaire or objective (e.g. accelerometers) methods). A highlevel of fitness is typically associated with a reductions in all-causemortality risk of w40e45% [1,3], cardiovascular disease risk byw50e60% [1,3] and type 2 diabetes risk ofw50e70% [1], comparedto a low level of fitness, in prospective cohort studies. Limited datasuggest that there may be an interaction between physical activitylevel, cardiorespiratory fitness and cardiovascular disease risk, withthe benefits of a high level of physical activity in reducing riskappearing to be most pronounced in individuals with low innatecardiorespiratory fitness levels and those with innately high fitnesslevels appear to be at relatively low risk cardiovascular disease riskirrespective of their physical activity level [8]. In recent years, it hasemerged that time spent engaged in sedentary behaviours e
defined as non-sleeping activities in a sitting or reclining posturewith energy expenditure�1.5METS (where 1MET is resting energyexpenditure) [9] e is associated with increased risk of cardiovas-cular disease, diabetes, metabolic syndrome, obesity and deathfrom any cause, with this effect often being independent of timespent engaged in moderate-to-vigorous physical activity (i.e. ac-tivities at an intensity >3 METS) [10e12].
2. Physical activity guidelines and population attributablerisk associated with inactivity
Underpinned by this substantial and consistent evidence base,many national and international bodies have made guideline rec-ommendations that all adults should engage in at least 150 min ofmoderate intensity (3e6 METS), or 75 min of vigorous intensity(>6 METS), physical activity per week [13e15]. This is equivalent toexpendingw1000 kcal/week (w4.2 MJ/week) in physical activity ofat least moderate intensity, a level of activity shown to substantially(although not maximally e higher levels of activity reduce riskfurther) reduce risk of mortality and cardio-metabolic disease [1].Recent UK physical activity guidelines have also recommended thatindividuals should limit extended periods of sedentary time [13],although there are currently insufficient data available to provide aspecific target to aim for.
The number of people worldwide not achieving these physicalactivity levels, and the consequent public health implications, aresubstantial. It has recently been estimated that about 35% of theadults worldwide do not meet these physical activity targets and,accordingly, that inactivity is responsible for 9% of prematuremortality worldwide, equating to 5.3 million deaths annually e
more than is attributable to smoking [16]. In a study of American
adults, it was estimated 16% of mortality could be attributed to lowcardiorespiratory fitness; more than smoking, obesity and hyper-cholesterolaemia combined [17].
3. Physical activity and cardio-metabolic disease risk in non-White populations
However, it is important to note that the majority of studiesprospectively investigating the effect of physical activity dose oncardio-metabolic disease and mortality risk have been performedin people of white European ethnicity, with a relatively smallnumber of studies including groups of non-white origin. This is keylimitation to the evidence base that has been highlighted in sys-tematic reviews of the literature [1] and physical activity guidelinestatements [14]. Prospective cohort studies which have evaluatedthe effects of physical activity on cardio-metabolic disease ormortality risk in non-White populations are summarised in Table 1.There is evidence of a protective effect of physical activity in Chi-nese and Japanese populations. A study from the National HealthInterview Survey (NHIS) in Taiwan reported a dose-dependent in-verse relationship between level of physical activity and mortalityrisk in Taiwanese adults aged over 65 years [18]. Data from theShanghai women’s health study indicated that high levels ofphysical activity were protective against cardiovascular and all-cause mortality [19], and incident type 2 diabetes [20] in middle-aged Chinese women. A recent report from the Shanghai Men’sHealth Study showed that regular participation in walking, joggingand Tai Chi was associated with reduced risk of CVD and all-causemortality [21]. A series of publications from the Honolulu HeartProgram have reported inverse associations between physical ac-tivity level and risk of coronary heart disease [22e24], stroke[25,26], diabetes [27], and mortality [28] in middle-aged to elderlyJapanese-American men. The protective effect of physical activityagainst incident diabetes has been confirmed in Japanesemen [29e31], and against CHD, stroke and total CVD, and all-cause mortalityin has been confirmed in Japanese men and women [32,33] in re-ports from a number of other cohorts. There is also evidence thathigh physical activity reduces incidence of all-cause mortality inelderly Mexican-Americans [34]. However, while these studiesdemonstrated a protective effect of physical activity in Chinese,Japanese andMexican-American populations, none of these reportsprovide a head-to-head comparison of the doseeresponse rela-tionship between physical activity and disease risk betweendifferent ethnic groups. Because of differences in the quantificationof physical activity between the various questionnaire-basedphysical activity instruments used in different studies, such head-to-head comparisons within a single study are needed to deter-mine whether the doses of physical activity required for benefit aresimilar across ethnic groups. Cohort studies including more thanone ethnic group provide data that suggest that the doseeresponserelationship between physical activity level and cardio-metabolicdisease or mortality risk may not be identical across all ethnic-ities. An early report (after 4e7 years follow-up) from the Athero-sclerosis Risk in Communities (ARIC) study in the US found thatincreasing levels physical activity attenuated risk of incident cor-onary heart disease (CHD) events in non-Black (who were 99%White), but not in Black adults [35]. The authors could not provide adefinitive explanation for this differential effect of physical activitybetween the Black and non-Black groups, but suggested that thesmall number of Black participants engaging in vigorous exercise,lower reliability of the physical activity questionnaire in Blacks, andthe small number of CHD events in the Black cohort, may havecontributed to this null effect in this early report [35]. This inter-pretation is borne out by a more recent analysis from ARIC cohort(after 19e21 years follow-up), which reported similar associations
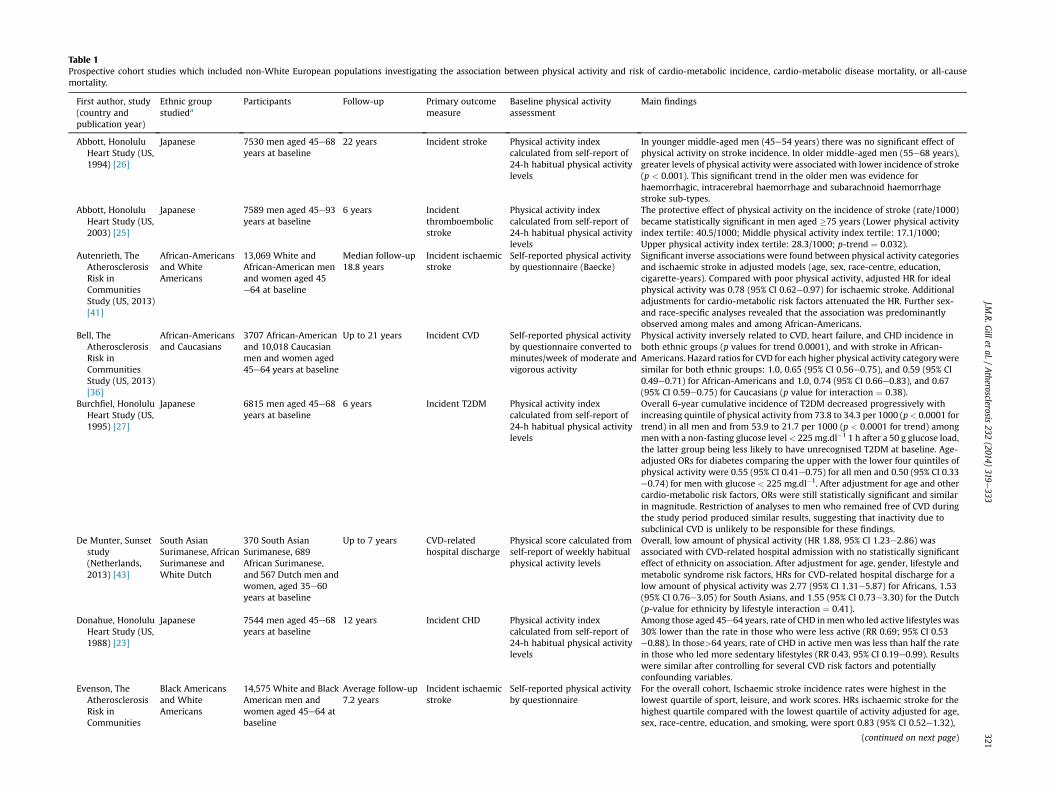
Table 1Prospective cohort studies which included non-White European populations investigating the association between physical activity and risk of cardio-metabolic incidence, cardio-metabolic disease mortality, or all-causemortality.
First author, study(country andpublication year)
Ethnic groupstudieda
Participants Follow-up Primary outcomemeasure
Baseline physical activityassessment
Main findings
Abbott, HonoluluHeart Study (US,1994) [26]
Japanese 7530 men aged 45e68years at baseline
22 years Incident stroke Physical activity indexcalculated from self-report of24-h habitual physical activitylevels
In younger middle-aged men (45e54 years) there was no significant effect ofphysical activity on stroke incidence. In older middle-aged men (55e68 years),greater levels of physical activity were associated with lower incidence of stroke(p < 0.001). This significant trend in the older men was evidence forhaemorrhagic, intracerebral haemorrhage and subarachnoid haemorrhagestroke sub-types.
Abbott, HonoluluHeart Study (US,2003) [25]
Japanese 7589 men aged 45e93years at baseline
6 years Incidentthromboembolicstroke
Physical activity indexcalculated from self-report of24-h habitual physical activitylevels
The protective effect of physical activity on the incidence of stroke (rate/1000)became statistically significant in men aged �75 years (Lower physical activityindex tertile: 40.5/1000; Middle physical activity index tertile: 17.1/1000;Upper physical activity index tertile: 28.3/1000; p-trend ¼ 0.032).
Autenrieth, TheAtherosclerosisRisk inCommunitiesStudy (US, 2013)[41]
African-Americansand WhiteAmericans
13,069 White andAfrican-American menand women aged 45e64 at baseline
Median follow-up18.8 years
Incident ischaemicstroke
Self-reported physical activityby questionnaire (Baecke)
Significant inverse associations were found between physical activity categoriesand ischaemic stroke in adjusted models (age, sex, race-centre, education,cigarette-years). Compared with poor physical activity, adjusted HR for idealphysical activity was 0.78 (95% CI 0.62e0.97) for ischaemic stroke. Additionaladjustments for cardio-metabolic risk factors attenuated the HR. Further sex-and race-specific analyses revealed that the association was predominantlyobserved among males and among African-Americans.
Bell, TheAtherosclerosisRisk inCommunitiesStudy (US, 2013)[36]
African-Americansand Caucasians
3707 African-Americanand 10,018 Caucasianmen and women aged45e64 years at baseline
Up to 21 years Incident CVD Self-reported physical activityby questionnaire converted tominutes/week of moderate andvigorous activity
Physical activity inversely related to CVD, heart failure, and CHD incidence inboth ethnic groups (p values for trend 0.0001), and with stroke in African-Americans. Hazard ratios for CVD for each higher physical activity category weresimilar for both ethnic groups: 1.0, 0.65 (95% CI 0.56e0.75), and 0.59 (95% CI0.49e0.71) for African-Americans and 1.0, 0.74 (95% CI 0.66e0.83), and 0.67(95% CI 0.59e0.75) for Caucasians (p value for interaction ¼ 0.38).
Burchfiel, HonoluluHeart Study (US,1995) [27]
Japanese 6815 men aged 45e68years at baseline
6 years Incident T2DM Physical activity indexcalculated from self-report of24-h habitual physical activitylevels
Overall 6-year cumulative incidence of T2DM decreased progressively withincreasing quintile of physical activity from 73.8 to 34.3 per 1000 (p< 0.0001 fortrend) in all men and from 53.9 to 21.7 per 1000 (p < 0.0001 for trend) amongmenwith a non-fasting glucose level< 225mg.dl�1 1 h after a 50 g glucose load,the latter group being less likely to have unrecognised T2DM at baseline. Age-adjusted ORs for diabetes comparing the upper with the lower four quintiles ofphysical activity were 0.55 (95% CI 0.41e0.75) for all men and 0.50 (95% CI 0.33e0.74) for men with glucose < 225 mg.dl�1. After adjustment for age and othercardio-metabolic risk factors, ORs were still statistically significant and similarin magnitude. Restriction of analyses to men who remained free of CVD duringthe study period produced similar results, suggesting that inactivity due tosubclinical CVD is unlikely to be responsible for these findings.
De Munter, Sunsetstudy(Netherlands,2013) [43]
South AsianSurimanese, AfricanSurimanese andWhite Dutch
370 South AsianSurimanese, 689African Surimanese,and 567 Dutch men andwomen, aged 35e60years at baseline
Up to 7 years CVD-relatedhospital discharge
Physical score calculated fromself-report of weekly habitualphysical activity levels
Overall, low amount of physical activity (HR 1.88, 95% CI 1.23e2.86) wasassociated with CVD-related hospital admission with no statistically significanteffect of ethnicity on association. After adjustment for age, gender, lifestyle andmetabolic syndrome risk factors, HRs for CVD-related hospital discharge for alow amount of physical activity was 2.77 (95% CI 1.31e5.87) for Africans, 1.53(95% CI 0.76e3.05) for South Asians, and 1.55 (95% CI 0.73e3.30) for the Dutch(p-value for ethnicity by lifestyle interaction ¼ 0.41).
Donahue, HonoluluHeart Study (US,1988) [23]
Japanese 7544 men aged 45e68years at baseline
12 years Incident CHD Physical activity indexcalculated from self-report of24-h habitual physical activitylevels
Among those aged 45e64 years, rate of CHD inmenwho led active lifestyles was30% lower than the rate in those who were less active (RR 0.69; 95% CI 0.53e0.88). In those>64 years, rate of CHD in active men was less than half the ratein those who led more sedentary lifestyles (RR 0.43, 95% CI 0.19e0.99). Resultswere similar after controlling for several CVD risk factors and potentiallyconfounding variables.
Evenson, TheAtherosclerosisRisk inCommunities
Black Americansand WhiteAmericans
14,575 White and BlackAmerican men andwomen aged 45e64 atbaseline
Average follow-up7.2 years
Incident ischaemicstroke
Self-reported physical activityby questionnaire
For the overall cohort, Ischaemic stroke incidence rates were highest in thelowest quartile of sport, leisure, and work scores. HRs ischaemic stroke for thehighest quartile compared with the lowest quartile of activity adjusted for age,sex, race-centre, education, and smoking, were sport 0.83 (95% CI 0.52e1.32),
(continued on next page)
J.M.R.G
illet
al./Atherosclerosis
232(2014)
319e333
321

Table 1 (continued )
First author, study(country andpublication year)
Ethnic groupstudieda
Participants Follow-up Primary outcomemeasure
Baseline physical activityassessment
Main findings
Study (US, 1999)[40]
leisure 0.89 (95% CI 0.57e1.37), and work 0.69 (95% CI 0.47e1.00). Furtheradjustment for factors that likely were intermediate variables (hypertension,diabetes, fibrinogen, and BMI) between physical activity and stroke attenuatedthe associations. No ethnicity interaction given. Ischaemic stroke incidencedeclined with increasing physical activity score for Black Americans, whileamong White Americans the pattern was less consistent (numerical data notreported).
Fretts, The StrongHeart Study (US,2009) [47]
American Indians 1651 men and women,aged 45e74 years atbaseline
10 years Incident T2DM Self-reported physical activityquestionnaire over the pastyear
Compared with participants who reported no physical activity, those whoreported any physical activity had a lower risk of diabetes: ORs were 0.67 (95%CI 0.46e0.99), 0.67 (95% CI 0.45e0.99), and 0.67 (95% CI 0.45e0.99) forincreasing tertile of physical activity, after adjustment for age, sex, study site,education, smoking, alcohol use, and family history of diabetes. Furtheradjustment for body mass index and other potential mediators attenuated therisk estimates.
Folsom, TheAtherosclerosisRisk inCommunitiesStudy (US, 1997)[35]
Black and non-Black Americans
14,040 Black and non-Black men and women(non-Black participantswere 99% White), aged45e64 at baseline
Up to 4e7 years Incident CHD Self-reported physical activityby questionnaire converted tosport, leisure and work indices
Age-, race-, and field centre-adjusted RR of CHD was 0.73 in women and 0.82 inmen per each SD increment in the sports index (P < 0.05). For the leisure index,these relative risks were 0.78 for both sexes (p < 0.05). The work index was notassociated with CHD. Associations held for non-blacks, but there was noassociation between the sport or leisure indices and CHD among blacks(numerical data not reported).
Gregg, NationalHealth InterviewSurvey (US,2003) [42]
Non-Hispanicwhites, non-Hispanic blacks,Hispanic and ‘other’
2896 men and womenwith diabetes (73.8%Non-Hispanic whites,16.6% non-Hispanicblacks, 7.9% Hispanicand 2.7% ‘other’) aged18e95 years at baseline
8 years All-cause mortalityand CVD mortality
Self-reported physical activityand time spent walking inpreceding 2 weeks byquestionnaire
Compared with inactive individuals, those whowalked at least 2 h per week hada 39% lower all-cause mortality rate (HR 0.61, 95% CI 0.48e0.78) and a 34% lowerCVD mortality rate (HR 0.66, 95% CI 0.45e0.96), controlling for sex, age, race,body mass index smoking, and comorbid conditions. Mortality rates werelowest for persons who reported that their walking involved moderateincreases in heart and breathing rates (all-cause mortality HR 0.57, 95% CI 0.41e0.80; CVD mortality HR 0.69, 95% CI 0.43e1.09). Ethnicity interaction was notsignificant.
Gillum, NHANES 1(US, 1996) [39]
Black Americansand WhiteAmericans
771 Black and 5058white men and womenaged 45e74 at baseline
Mean follow-up11.6 years
Incident stroke Recreational and habitualphysical activitycharacterisation byquestionnaire
In White women aged 65e74 years, low non-recreational activity wasassociated with an increased risk of stroke (RR 1.82, 95% CI 1.10e3.02) afteradjusting for the baseline risk factors of age, smoking, history of diabetes,history of heart disease, education, systolic blood pressure, serum totalcholesterol, body mass index, and haemoglobin concentration. Similarassociations were seen for men and for Blacks (numerical data not reported).
Hakim, HonoluluHeart Study (US,1998) [28]
Japanese 707 non-smokingretired men aged 81e61 years at baseline
12 years All-cause mortality Self-reported distance walkedper day
Mortality rate among men who walked less than 1 mile per day was nearlytwice that among those who walkedmore than 2 miles per day (40.5% vs. 23.8%,p ¼ 0.001). The cumulative incidence of death after 12 years for the most activewalkers was reached in less than 7 years among the men who were least active.
Hakim, HonoluluHeart Study (US,1999) [24]
Japanese 2678 men aged 71e93years at baseline
2e4 years Incident CHD Self-reported distance walkedper day
Men who walked 0.25 miles per day had a 2-fold increased risk of coronaryheart disease versus those who walked 1.5 mile/d (5.1% versus 2.5%; p <0.01).Men who walked 0.25 to 1.5 mile per day were also at a significantly higher riskof coronary heart disease than men who walked longer distances (4.5% versus2.5%; p< 0.05). Adjustment for age and other risk factors failed to alter findings.
Hsia, Women’sHealth InitiativeObservationalStudy (US, 2005)[45]
Caucasian, African-American, Hispanic,American Indiansand Asian/PacificIslander
74,240 Caucasianwomen, 6465 African-American women, 3231Hispanic women, 327American Indianwomen, and 2445Asians/Pacific Islanderwomen, aged 50e79years at baseline
5.1 years Incident T2DM Self-reported physical activityby questionnaire
Among Caucasian women, walking (multivariate-adjusted HRs 1.00, 0.85, 0.87,0.75, 0.74; p < 0.001 for trend across exercise quintiles) and total physicalactivity score (hazard ratios 1.00, 0.88, 0.74, 0.80, 0.67; p¼ 0.002) demonstrateda strong inverse relationship with diabetes risk. In BMI-adjusted models,African-American women in higher physical activity categories were less likelyto develop diabetes than women in the lowest physical activity category. Afteradjusting for age and multiple risk factors, however, no significant associationbetween physical activity and diabetes risk was apparent for African-American,Hispanic, or Asian women.
J.M.R.G
illet
al./Atherosclerosis
232(2014)
319e333
322
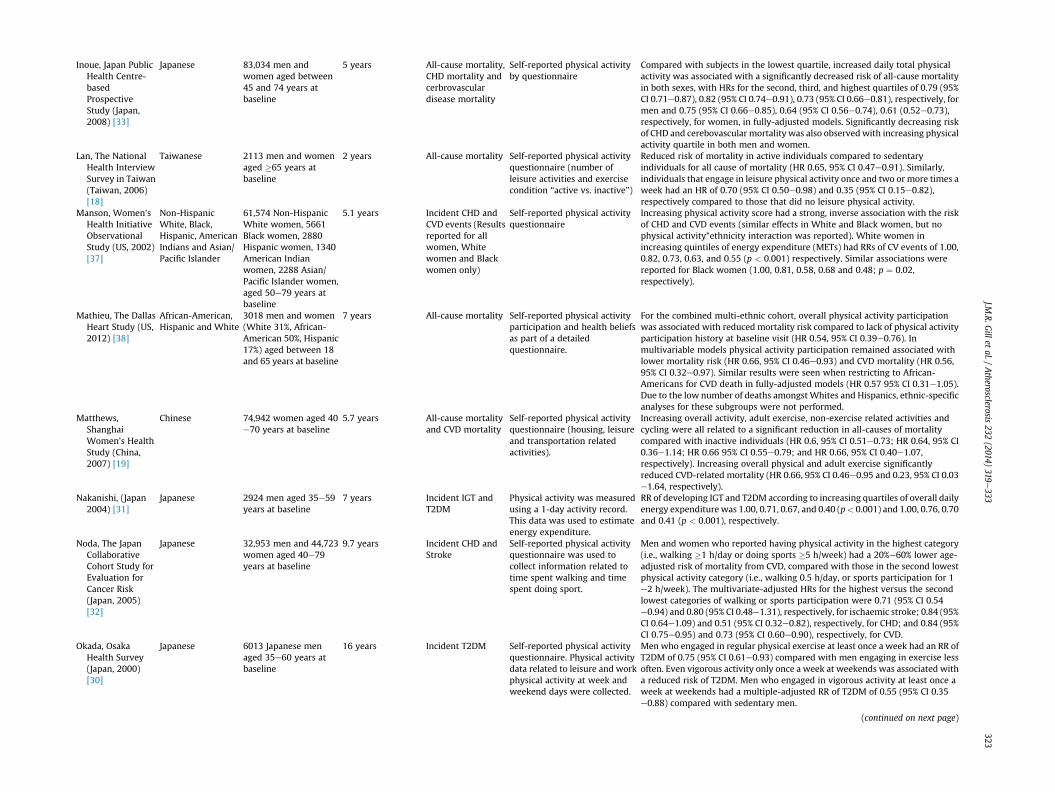
Inoue, Japan PublicHealth Centre-basedProspectiveStudy (Japan,2008) [33]
Japanese 83,034 men andwomen aged between45 and 74 years atbaseline
5 years All-cause mortality,CHD mortality andcerbrovasculardisease mortality
Self-reported physical activityby questionnaire
Compared with subjects in the lowest quartile, increased daily total physicalactivity was associated with a significantly decreased risk of all-cause mortalityin both sexes, with HRs for the second, third, and highest quartiles of 0.79 (95%CI 0.71e0.87), 0.82 (95% CI 0.74e0.91), 0.73 (95% CI 0.66e0.81), respectively, formen and 0.75 (95% CI 0.66e0.85), 0.64 (95% CI 0.56e0.74), 0.61 (0.52e0.73),respectively, for women, in fully-adjusted models. Significantly decreasing riskof CHD and cerebovascular mortality was also observedwith increasing physicalactivity quartile in both men and women.
Lan, The NationalHealth InterviewSurvey in Taiwan(Taiwan, 2006)[18]
Taiwanese 2113 men and womenaged �65 years atbaseline
2 years All-cause mortality Self-reported physical activityquestionnaire (number ofleisure activities and exercisecondition “active vs. inactive”)
Reduced risk of mortality in active individuals compared to sedentaryindividuals for all cause of mortality (HR 0.65, 95% CI 0.47e0.91). Similarly,individuals that engage in leisure physical activity once and two or more times aweek had an HR of 0.70 (95% CI 0.50e0.98) and 0.35 (95% CI 0.15e0.82),respectively compared to those that did no leisure physical activity.
Manson, Women’sHealth InitiativeObservationalStudy (US, 2002)[37]
Non-HispanicWhite, Black,Hispanic, AmericanIndians and Asian/Pacific Islander
61,574 Non-HispanicWhite women, 5661Black women, 2880Hispanic women, 1340American Indianwomen, 2288 Asian/Pacific Islander women,aged 50e79 years atbaseline
5.1 years Incident CHD andCVD events (Resultsreported for allwomen, Whitewomen and Blackwomen only)
Self-reported physical activityquestionnaire
Increasing physical activity score had a strong, inverse association with the riskof CHD and CVD events (similar effects in White and Black women, but nophysical activity*ethnicity interaction was reported). White women inincreasing quintiles of energy expenditure (METs) had RRs of CV events of 1.00,0.82, 0.73, 0.63, and 0.55 (p < 0.001) respectively. Similar associations werereported for Black women (1.00, 0.81, 0.58, 0.68 and 0.48; p ¼ 0.02,respectively).
Mathieu, The DallasHeart Study (US,2012) [38]
African-American,Hispanic and White
3018 men and women(White 31%, African-American 50%, Hispanic17%) aged between 18and 65 years at baseline
7 years All-cause mortality Self-reported physical activityparticipation and health beliefsas part of a detailedquestionnaire.
For the combined multi-ethnic cohort, overall physical activity participationwas associated with reduced mortality risk compared to lack of physical activityparticipation history at baseline visit (HR 0.54, 95% CI 0.39e0.76). Inmultivariable models physical activity participation remained associated withlower mortality risk (HR 0.66, 95% CI 0.46e0.93) and CVD mortality (HR 0.56,95% CI 0.32e0.97). Similar results were seen when restricting to African-Americans for CVD death in fully-adjusted models (HR 0.57 95% CI 0.31e1.05).Due to the low number of deaths amongstWhites and Hispanics, ethnic-specificanalyses for these subgroups were not performed.
Matthews,ShanghaiWomen’s HealthStudy (China,2007) [19]
Chinese 74,942 women aged 40e70 years at baseline
5.7 years All-cause mortalityand CVD mortality
Self-reported physical activityquestionnaire (housing, leisureand transportation relatedactivities).
Increasing overall activity, adult exercise, non-exercise related activities andcycling were all related to a significant reduction in all-causes of mortalitycompared with inactive individuals (HR 0.6, 95% CI 0.51e0.73; HR 0.64, 95% CI0.36e1.14; HR 0.66 95% CI 0.55e0.79; and HR 0.66, 95% CI 0.40e1.07,respectively). Increasing overall physical and adult exercise significantlyreduced CVD-related mortality (HR 0.66, 95% CI 0.46e0.95 and 0.23, 95% CI 0.03e1.64, respectively).
Nakanishi, (Japan2004) [31]
Japanese 2924 men aged 35e59years at baseline
7 years Incident IGT andT2DM
Physical activity was measuredusing a 1-day activity record.This data was used to estimateenergy expenditure.
RR of developing IGT and T2DM according to increasing quartiles of overall dailyenergy expenditure was 1.00, 0.71, 0.67, and 0.40 (p< 0.001) and 1.00, 0.76, 0.70and 0.41 (p < 0.001), respectively.
Noda, The JapanCollaborativeCohort Study forEvaluation forCancer Risk(Japan, 2005)[32]
Japanese 32,953 men and 44,723women aged 40e79years at baseline
9.7 years Incident CHD andStroke
Self-reported physical activityquestionnaire was used tocollect information related totime spent walking and timespent doing sport.
Men and women who reported having physical activity in the highest category(i.e., walking �1 h/day or doing sports �5 h/week) had a 20%e60% lower age-adjusted risk of mortality from CVD, compared with those in the second lowestphysical activity category (i.e., walking 0.5 h/day, or sports participation for 1e2 h/week). The multivariate-adjusted HRs for the highest versus the secondlowest categories of walking or sports participation were 0.71 (95% CI 0.54e0.94) and 0.80 (95% CI 0.48e1.31), respectively, for ischaemic stroke; 0.84 (95%CI 0.64e1.09) and 0.51 (95% CI 0.32e0.82), respectively, for CHD; and 0.84 (95%CI 0.75e0.95) and 0.73 (95% CI 0.60e0.90), respectively, for CVD.
Okada, OsakaHealth Survey(Japan, 2000)[30]
Japanese 6013 Japanese menaged 35e60 years atbaseline
16 years Incident T2DM Self-reported physical activityquestionnaire. Physical activitydata related to leisure and workphysical activity at week andweekend days were collected.
Men who engaged in regular physical exercise at least once a week had an RR ofT2DM of 0.75 (95% CI 0.61e0.93) compared with men engaging in exercise lessoften. Even vigorous activity only once a week at weekends was associated witha reduced risk of T2DM. Men who engaged in vigorous activity at least once aweek at weekends had a multiple-adjusted RR of T2DM of 0.55 (95% CI 0.35e0.88) compared with sedentary men.
(continued on next page)
J.M.R.G
illet
al./Atherosclerosis
232(2014)
319e333
323
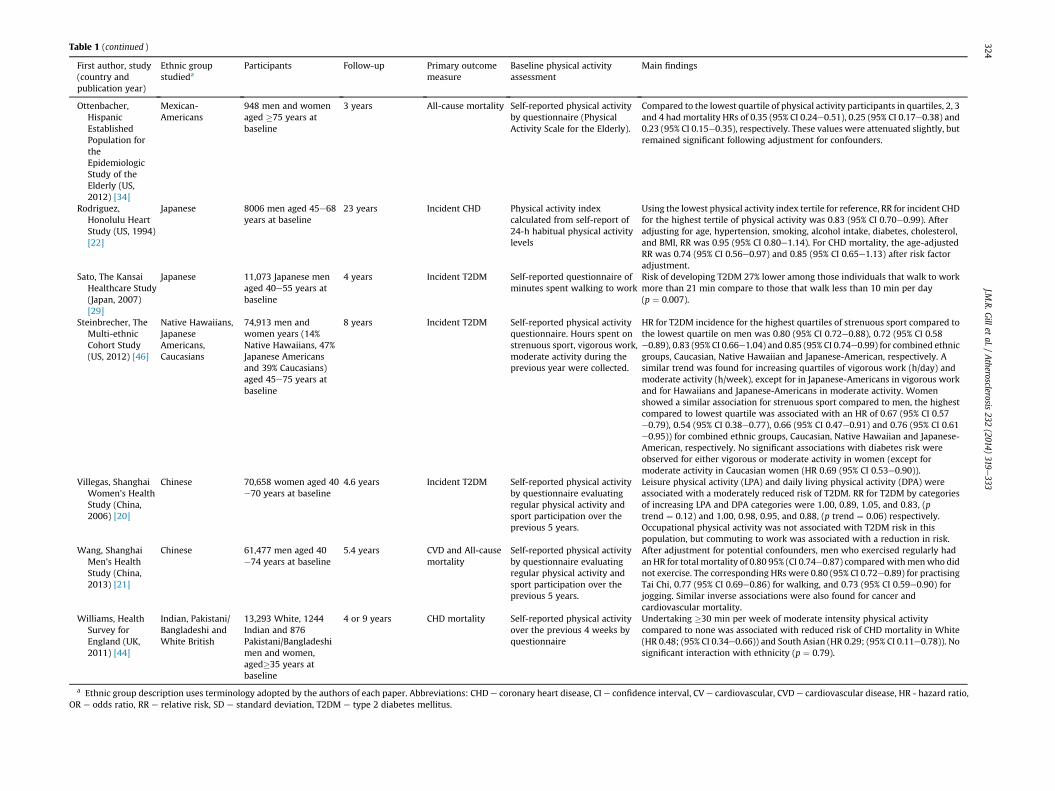
Table 1 (continued )
First author, study(country andpublication year)
Ethnic groupstudieda
Participants Follow-up Primary outcomemeasure
Baseline physical activityassessment
Main findings
Ottenbacher,HispanicEstablishedPopulation fortheEpidemiologicStudy of theElderly (US,2012) [34]
Mexican-Americans
948 men and womenaged �75 years atbaseline
3 years All-cause mortality Self-reported physical activityby questionnaire (PhysicalActivity Scale for the Elderly).
Compared to the lowest quartile of physical activity participants in quartiles, 2, 3and 4 had mortality HRs of 0.35 (95% CI 0.24e0.51), 0.25 (95% CI 0.17e0.38) and0.23 (95% CI 0.15e0.35), respectively. These values were attenuated slightly, butremained significant following adjustment for confounders.
Rodriguez,Honolulu HeartStudy (US, 1994)[22]
Japanese 8006 men aged 45e68years at baseline
23 years Incident CHD Physical activity indexcalculated from self-report of24-h habitual physical activitylevels
Using the lowest physical activity index tertile for reference, RR for incident CHDfor the highest tertile of physical activity was 0.83 (95% CI 0.70e0.99). Afteradjusting for age, hypertension, smoking, alcohol intake, diabetes, cholesterol,and BMI, RR was 0.95 (95% CI 0.80e1.14). For CHD mortality, the age-adjustedRR was 0.74 (95% CI 0.56e0.97) and 0.85 (95% CI 0.65e1.13) after risk factoradjustment.
Sato, The KansaiHealthcare Study(Japan, 2007)[29]
Japanese 11,073 Japanese menaged 40e55 years atbaseline
4 years Incident T2DM Self-reported questionnaire ofminutes spent walking to work
Risk of developing T2DM 27% lower among those individuals that walk to workmore than 21 min compare to those that walk less than 10 min per day(p ¼ 0.007).
Steinbrecher, TheMulti-ethnicCohort Study(US, 2012) [46]
Native Hawaiians,JapaneseAmericans,Caucasians
74,913 men andwomen years (14%Native Hawaiians, 47%Japanese Americansand 39% Caucasians)aged 45e75 years atbaseline
8 years Incident T2DM Self-reported physical activityquestionnaire. Hours spent onstrenuous sport, vigorous work,moderate activity during theprevious year were collected.
HR for T2DM incidence for the highest quartiles of strenuous sport compared tothe lowest quartile on men was 0.80 (95% CI 0.72e0.88), 0.72 (95% CI 0.58e0.89), 0.83 (95% CI 0.66e1.04) and 0.85 (95% CI 0.74e0.99) for combined ethnicgroups, Caucasian, Native Hawaiian and Japanese-American, respectively. Asimilar trend was found for increasing quartiles of vigorous work (h/day) andmoderate activity (h/week), except for in Japanese-Americans in vigorous workand for Hawaiians and Japanese-Americans in moderate activity. Womenshowed a similar association for strenuous sport compared to men, the highestcompared to lowest quartile was associated with an HR of 0.67 (95% CI 0.57e0.79), 0.54 (95% CI 0.38e0.77), 0.66 (95% CI 0.47e0.91) and 0.76 (95% CI 0.61e0.95)) for combined ethnic groups, Caucasian, Native Hawaiian and Japanese-American, respectively. No significant associations with diabetes risk wereobserved for either vigorous or moderate activity in women (except formoderate activity in Caucasian women (HR 0.69 (95% CI 0.53e0.90)).
Villegas, ShanghaiWomen’s HealthStudy (China,2006) [20]
Chinese 70,658 women aged 40e70 years at baseline
4.6 years Incident T2DM Self-reported physical activityby questionnaire evaluatingregular physical activity andsport participation over theprevious 5 years.
Leisure physical activity (LPA) and daily living physical activity (DPA) wereassociated with a moderately reduced risk of T2DM. RR for T2DM by categoriesof increasing LPA and DPA categories were 1.00, 0.89, 1.05, and 0.83, (ptrend ¼ 0.12) and 1.00, 0.98, 0.95, and 0.88, (p trend ¼ 0.06) respectively.Occupational physical activity was not associated with T2DM risk in thispopulation, but commuting to work was associated with a reduction in risk.
Wang, ShanghaiMen’s HealthStudy (China,2013) [21]
Chinese 61,477 men aged 40e74 years at baseline
5.4 years CVD and All-causemortality
Self-reported physical activityby questionnaire evaluatingregular physical activity andsport participation over theprevious 5 years.
After adjustment for potential confounders, men who exercised regularly hadan HR for total mortality of 0.80 95% (CI 0.74e0.87) compared withmenwho didnot exercise. The corresponding HRs were 0.80 (95% CI 0.72e0.89) for practisingTai Chi, 0.77 (95% CI 0.69e0.86) for walking, and 0.73 (95% CI 0.59e0.90) forjogging. Similar inverse associations were also found for cancer andcardiovascular mortality.
Williams, HealthSurvey forEngland (UK,2011) [44]
Indian, Pakistani/Bangladeshi andWhite British
13,293 White, 1244Indian and 876Pakistani/Bangladeshimen and women,aged�35 years atbaseline
4 or 9 years CHD mortality Self-reported physical activityover the previous 4 weeks byquestionnaire
Undertaking �30 min per week of moderate intensity physical activitycompared to none was associated with reduced risk of CHD mortality in White(HR 0.48; (95% CI 0.34e0.66)) and South Asian (HR 0.29; (95% CI 0.11e0.78)). Nosignificant interaction with ethnicity (p ¼ 0.79).
a Ethnic group description uses terminology adopted by the authors of each paper. Abbreviations: CHD e coronary heart disease, CI e confidence interval, CV e cardiovascular, CVD e cardiovascular disease, HR - hazard ratio,OR e odds ratio, RR e relative risk, SD e standard deviation, T2DM e type 2 diabetes mellitus.
J.M.R.G
illet
al./Atherosclerosis
232(2014)
319e333
324

J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333 325
between physical activity category (poor, intermediate or recom-mended level) and incidence of CVD, CHD and heart failure be-tween Black and White groups [36]. In both White and Blackgroups, intermediate levels of physical activity (i.e. more than zero,but less than recommended levels) were associatedwith significantreductions in risk compared to no physical activity. Interestingly,however, when physical activity level was categorised into quar-tiles, significant physical activity by ethnicity interactions wereobserved for CHD and CVD in women, and for CHD in both sexescombined, with a greater protective effect observed in the Blackgroup [36]. Furthermore, a report from the Women’s HealthInitiative Observational Study (WHIOS) indicated that the doseeresponse relationship for reduction in cardiovascular events withincreasing physical activity was similar amongst White and BlackAmerican postmenopausal women [37] and data from the DallasHeart Study indicated that risk of CVD mortality decreased withincreasing physical activity in African-American adults [38]. Anal-ysis of data from different cohorts has revealed contrasting effectsof ethnicity on the relationship between physical activity andstroke. In the NHANES I Epidemiologic Follow-up Study, the sig-nificant reduction in stroke risk with increasing levels of physicalactivity observed in White adults was not seen in Black adults,which may be a consequence of insufficient statistical power todetect the effect due to smaller number of Black participants withinthe cohort [39]. However in the ARIC cohort, in analyses under-taken at multiple follow-up time-points, the protective effect ofphysical activity against stroke incidence was more consistent inBlacks than Whites [36,40,41]. Interestingly, the greater protectiveeffect of physical activity on ischaemic stroke in Blacks in the ARICcohort persisted in models adjusted for smoking, blood pressure,anti-hypertensive medication use, left ventricular hypertrophy,diabetes, lipids, fibrinogen, van Willebrand factor, white blood cellcount, waist-to-hip ratio, as well as demographic factors, suggest-ing that the greater benefit of physical activity for ischaemic strokeprotection in Blacks was largely independent of effects on theseconventional risk factors [41]. Data from the US National HealthInterview Survey, found that themortality risk reduction associatedwith walking at least 2 h per week in adults with type 2 diabeteswas similar for White and non-White subgroups [42]. Prospectivedata on physical activity and cardio-metabolic disease or mortalityrisk in populations of South Asian origin are particularly limited. Areport from the Dutch SUNSET study investigated the effect ofbaseline physical activity level on risk of subsequent for CVD-related hospital discharge in middle-aged South Asian Sur-imamese, African Surimansese, and Dutch European adults over a5.5-year follow-up period [43]. While an overall benefit of physicalactivity was observed in the group as a whole, the relatively smallsample size (n ¼ 1626 in total) and low event rate (178 total cases),meant that when ethnicity-stratified analyses were undertaken,the protective effect of physical activity against CVD-related hos-pital discharge was not statistically significant for either the DutchEuropean or South Asian Surimamese groups (but was for the Af-rican Surimansese group), and no significant ethnicityephysicalactivity interactionwas observed [43]. A longitudinal analysis of the1999 and 2004 Health Survey for England datasets (with 9 or 4years of follow-up) found that undertaking at least 30 min.week�1
of moderate intensity activity was associated with reduced risk ofCHD mortality in both White and South Asian adults, with no sig-nificant interaction with ethnicity [44]. However, the dichotomousnature of physical activity classification in this analysis means thatpotential for interpretation of any ethnic differences in doseeresponse relationship between physical activity and CHD in thisstudy is limited [44].
The most consistent evidence for differential effects of physicalactivity on health outcomes between ethnic groups is for type 2
diabetes. Data from theWHIOS revealed that whilst higher levels ofphysical activity were significantly associated with reduced risk ofincident diabetes in White post-menopausal women, these find-ings were not replicated in other ethnic groups, with no significantassociation being observed between physical activity level anddiabetes risk in African-American, Hispanic or Asian/PacificIslander women in multivariate-adjusted analysis [45]. This mayreflect lack of statistical power to detect a relationship in the non-White groups, in which the cohort sizes were more than 10-foldsmaller than the White group; ethnic differences in the self-reporting of actual physical activity levels and/or incident dia-betes; and/or real ethnic differences in the doseeresponse rela-tionship between physical activity and diabetes risk. Data from TheMultiethnic Cohort was also suggestive of ethnic differences in thedoseeresponse relationship between physical activity and type 2diabetes risk. In both men and women, there was a significant in-verse association between increasing levels of moderate activityand diabetes risk in Caucasians (Whites), but not in Native Ha-waiians or Japanese-Americans, with significant ethnic interactioneffects [46]. Whilst engaging in strenuous sports was inverselyassociated with diabetes risk in men and women from all threeethnic groups, there was a tendency for the protective effect ofstrenuous sports to be greater in Caucasian men, than in men fromthe other two ethnicities (p ¼ 0.07 for ethnicity interaction) [46]. Inaddition, data from the Strong Heart Study show higher levels ofphysical activity are associated with reduced risk of incident dia-betes in American Indians [47], but there was no direct comparisonwith other ethnic groups in this cohort. Thus, there is emergingevidence from the limited data available, that the doseeresponserelationship between physical activity and risk of type 2 diabetesmay not be the same across all ethnic groups, with the level ofphysical activity needed to gain benefit potentially being higher innon-white populations. One clear limitation to the available evi-dence, is the lack of data comparing the doseeresponse relation-ship for physical activity and diabetes risk between Europeans andSouth Asians. Interestingly, diabetes risk is elevated compared towhite European groups, in most non-White ethnic groups, partic-ularly when they adopt Westernised or urbanised lifestyles (seesection 6 below), and it may be that a higher threshold for physicalactivity level is needed in these groups to obtain a low level ofabsolute diabetes risk. Thus, currently recommended levels ofphysical activity, based on the available epidemiological evidencebase of largely White European ethnicity cohorts, may not neces-sarily be appropriate for all ethnic groups.
4. Lifestyle intervention trials for cardiovascular diseaseprevention
The randomised controlled trial (RCT) represents the goldstandard for evaluating the efficacy and effectiveness of an inter-vention on a health outcome. Given the low CVD event rate in thegeneral population, it is not feasible to perform RCTs to evaluate theeffectiveness of physical activity (either alone or in the context of awider ‘lifestyle’ intervention trial) for the primary prevention ofCVD events in the general population (in order to have sufficientpower such a trial would need to be too large and too long to belogistically viable). Patients with type 2 diabetes have increasedrisk of CVD compared to the general population [48], so form agroup in which a lifestyle intervention RCT could conceivablydemonstrate benefit in terms of reduced cardiovascular event rate.However, the recent Look AHEAD trial in which 5145 overweight orobese patient with type 2 diabetes were randomised to intensivelifestyle intervention (physical activity, dietary modification andweight loss) or diabetes support education (control), was stoppedearly (after 9.6 years of the planned 13.5-year follow-up period)
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333326
after an interim analysis revealed that it was unlikely for a signif-icant difference between groups in the primary endpoint (com-posite of death from CVD, non-fatal myocardial infarction, non-fatalstroke and hospitalisation for angina) to be seen by the plannedend-date [49]. Potential reasons for this include a lower than ex-pected CVD event rate reducing power to detect any differencesbetween groups; the relatively intensive intervention in the controlgroup (which was comparable in intensity the intervention groupin many lifestyle intervention trials) [50] that would act to atten-uate any potential differences between groups; diminishingcompliance to the intervention over time in the intervention groupe differences in fitness and weight between the intervention andcontrol groups decreased steadily from a peak difference at 1-yearas the trial progressed; and the greater use of diabetes, anti-hypertensive and lipid-lowering drugs over the course of the trialin the control group [49]. At the time the trial was stopped, thehazard ratio for a CVD event in the intervention compared tocontrol group was 0.95 (95%CI 0.83e1.09) overall, 0.94 (0.80e1.11)in Whites, 1.34 (0.91e1.96) in Blacks, 0.71 (0.06e8.28) in Asians orPacific Islanders, 0.66 (0.41e1.05) in Hispanics and 0.74 (0.21e1.76)in Native Americans. There was no significant interaction withethnicity (p¼ 0.17), but power to detect any ethnicityeinterventioninteraction effect, would have been particularly limited given theabsence of a significant effect of the intervention overall. Althoughthe Look AHEAD intervention did not significantly impact on CVDevents, rates of full (reversion to normoglycaemia without diabetesmedication) and partial (reversion to pre-diabetes glycaemia levelswithout diabetes medication) remission of type 2 diabetes were 3e6 fold greater over the course of the trial in the interventioncompared with the control group [51]. In addition, the interventionreduced HbA1c concentrations and improved cardiorespiratoryfitness levels [51], with the change in fitness level at 4-years beingassociated with change in HbA1c, independent of a range of con-founders including change in weight [52]. A study 20-year follow-up data (i.e. continuing for 14 years after completion of the 6-yeartrial) from the Da Qing Study, a diabetes-prevention lifestyleintervention trial in Chinese adults with impaired glucose toler-ance, reported 20-year hazard rate ratio for CVD death of 0.83 in theintervention compared to the control group, although the 95% CIincluded 1 (0.48e1.40) [53]. However, it is important to note thatthe Da Qing Study was a diabetes prevention trial, rather than aCVD mortality prevention trial, and thus was not designed to havesufficient power to detect an intervention effect for this outcome.Interestingly, separation of CVD death rates between control andintervention groups did not start to become apparent until 10-yearsof follow-up, (indeed reduction in hazard rate ratio for CVD deathnumerically larger at 0.73 (95% CI 0.42e1.26) when only the 14-yearpost-trial period was considered), which raises the possibility thatthe Look AHEAD trial, which was stopped after 9.6 years of follow-up, may have been too short for a clear effect of lifestyle inter-vention on CVD event rates to have become evident. Event rates aremuch higher in secondary CVD prevention settings, making RCTsevaluating the effects of physical activity on hard CVD endpointsmore feasible. Meta-analyses of RCTs of exercise-based cardiacrehabilitation programmes in patients post-myocardial infarctionindicate significant reductions in all-cause, CHD and CVD mortalityin patients in the exercise intervention groups [54,55]. Thus, insecondary prevention settings, where CVD event rates are highenough for clear intervention effects to be seen, RCTs reveal clearbenefits of exercise in reducing CVD mortality risk.
It is, however, important to note that despite the equivocal na-ture of the end-point trial evidence to date, there is clear andconsistent experimental evidence to demonstrate that increasingphysical activity positively influences a number of mechanisticpathways and bio-markers known to play a causal role in the
atherosclerotic andmetabolic disease process, including favourablealterations to the lipid and lipoprotein profile [56e58], improve-ments in insulin sensitivity [59,60], improvements in endothelialfunction [61e63], reductions in blood pressure [64e66], and re-ductions in systemic inflammation [67,68], which supports thelarge body of observational epidemiological evidence indicatingthat high levels of physical activity are associated with reducedlevels of cardio-metabolic disease risk. Nevertheless, given theexperiences with the Look AHEAD trial, which had estimated costsof over a quarter billion US Dollars [69], it seems unlikely that adefinitive RCT to determine the effects increasing physical activityon prevention of hard CVD outcomes in a primary preventionsetting will ever be successfully completed.
5. Lifestyle intervention trials for diabetes prevention
Unlike CVD, where progression rate to events is relatively low inprimary prevention settings, even in groups regarded as havingelevated risk (for example, a 20% 10-year risk of a CVD event, putssomeone in a high-risk category [70]), it is possible to easily identifyindividuals with the pre-diabetic conditions of impaired glucosetolerance (IGT) and impaired fasting glucose (IFG), where pro-gression rates to diabetes are high (w3e18% per year [2]). Thishigher event rate and faster disease progression means that un-dertaking RCTs with sufficient power to evaluate the effects oflifestyle intervention on diabetes incidence are much more feasiblethan undertaking lifestyle intervention RCTs evaluating CVD out-comes. Consequentially, over the last two decades, there have beena substantial number of major RCTs which have demonstrated thatlifestyle intervention (increased physical activity and dietarychange, usually coupled with weight loss) is effective at reducingincidence of diabetes in individuals with IFG/IGT (reviewed in Ref.[2]). Recently published reports of long-term follow-up data fromthe Chinese Da Qing study [53], the Finnish Diabetes PreventionStudy (DPS) [71] and the US Diabetes Prevention Program Out-comes Study [72], have shown that the protective effect of lifestyleintervention in reducing incident diabetes persists for at least 10e20 years, indicating clear long-term benefit. Importantly, there isevidence that lifestyle intervention is effective at preventingmicrovascular complications of diabetes as well as onset of thedisease. Data published from the Da Qing study showed a 47%reduction in incidence of diabetic retinopathy in the lifestyleintervention compared to control group over 20 years of follow-up[73].
The protective effect of lifestyle intervention against incidentdiabetes has been demonstrated in a number of different ethnicgroups including Chinese [53,74], Japanese [75] and Indians [76] intrials containing single ethnic groups; inWhite Europeans, African-Americans, Hispanics, American Indians, and Asians/Pacific Is-landers within the multi-ethnic US Diabetes Prevention Program(DPP) [77]; and in White Europeans in a number of trials [2,78].Although differences in the protocols for lifestyle intervention andcompliance of participants to the interventions makes directcomparison of intervention effect sizes between studies difficult,the magnitude of diabetes risk reduction, at w28e67% has beenbroadly comparable between trials. Risk reduction in the IndianDiabetes Prevention Programme (IDPP), at 28% [76], was at thelower end of this range. Potential explanations for this smallerrelative reduction in risk include the fact that this was one of thefew trials in which participants did not lose weight on the inter-vention and the fact that the absolute rate of progression to dia-betes, at 18.3% per year in the Control group, was approximatelytwice as high in this study than the othermajor diabetes preventiontrials (e.g.11.0% per year in the DPP [77] and 7.8% per year in the DPS[79]). The latter point is an important, but subtle, one: the

J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333 327
reduction in absolute rates of progression to diabetes with lifestyleintervention in the IDPP (reduction of 52 cases per 1000 person-years) [76] was comparable with reductions seen in the DPS(reduction of 46 cases per 1000 person-years [79]) and DPP(reduction of 62 cases per 1000 person-years [77]). In the DPP,which was the one trial which had large enough numbers of par-ticipants from different ethnic groups to allow the effects of life-style intervention to be separately evaluated, the reduction indiabetes incidence rates were comparable between White (reduc-tion of 51%; 51 cases per 1000 person-years), African-American(reduction of 61%; 73 cases per 1000 person-years), Hispanic(reduction of 66%; 75 cases per 1000 person-years), American In-dian (reduction of 65%, 82 cases per 1000 person-years) and Asians/Pacific Islander (reduction of 71%, 83 cases per 1000 person-years)ethnic groups [77].
Thus, there is good evidence that lifestyle intervention iscomparably effective at preventing diabetes in individuals with IFG/IGT across a range of ethnic groups. However, it is important torecognise that individuals with IFG/IGT are at high risk of diabetesirrespective of ethnic group. They progress to frank diabetes at therate of w3e18% per year without intervention, and even withintensive lifestyle intervention progress to diabetes at the rate ofw2e13% per year [2]. Thus, an argument can be made that it maybe too late to primarily focus on individuals with IFG/IGT in effortsfor diabetes prevention and earlier intervention with lifestyleintervention for diabetes prevention in groups at increased dia-betes risk, but who are still normoglycaemic, is warranted. It is alsoimportant to recognise that, with the exception of the IDPP inwhich rates of progression to diabetes were higher [76], rates ofprogression to diabetes in the control arms of the various diabetesprevention trials of patients with IFG/IGT were broadly similaracross the different ethnic groups [74,77]. Thus, when an individualprogresses to IFG/IGT, they are at high risk of diabetes, irrespectiveof ethnic group. This, however, is not reflective of the pattern ofdiabetes risk amongst the general populationwhere there are largedifferences in risk between different ethnic groups, for examplediabetes risk for South Asians living in the UK is three to fivefoldhigher than the background White European population [80,81](see Section 6 below). Thus to develop IFG/IGT a European hasprogressed further along the diabetes risk continuum compared tothe average European in the population, than a South Asian withIFG/IGT has progressed compared to the average South Asian in thepopulation. Accordingly, findings from studies of patients with IFG/IGT from different ethnic groups cannot necessarily be extrapolatedto guidelines for diabetes prevention for different ethnic groupswithin the normoglycaemic general population. The optimal levelof physical activity for diabetes prevention may differ betweenethnic groups with widely varying levels of diabetes risk.
6. Ethnicityeenvironment interactions and diabetes risk
There are clear differences in risk of type 2 diabetes betweenethnic groups and while prevalence of diabetes is increasingworldwide, the rate of differs widely between regions [82]. This canbe partly attributed to differences in urbanisation and obesity [83],but differences in environment alone do not appear to tell thewhole story, particularly in elucidating why certain populationsand ethnic groups experience a disproportionately higher preva-lence of type 2 diabetes when they adopt urbanised lifestyles withgreater energy-dense food availability and low levels of physicalactivity. There is a growing body of evidence that the adverse ef-fects of urbanisation on diabetes risk are substantially larger innon-White populations than in populations of White Europeandescent. For example, diabetes prevalence in South Asian adultsliving in the United Kingdom and North America is 12e26% [81,84e
86] compared to 4e8% amongst the UK and US populations ofwhite European descent [82,85,87]. However, diabetes prevalencein rural India is low, at w3% (0.7% in active rural dwellers withoutabdominal obesity) [88], rising to 7e18% in the cities [88,89]. Thus,when lean and active and living in rural environments, SouthAsians have low diabetes risk but adoption of an urban or Wes-ternised lifestyle appears to have a disproportionately large influ-ence on diabetes risk in South Asians, compared to those of WhiteEuropean descent. A similar pattern is observed when comparingWhite populations to populations of Black African descent. Dia-betes prevalence amongst African-Americans is about twice as highas forWhite Americans for a given BMI [87], and similarly in the UKdiabetes prevalence is more than twice as high amongst the Blackpopulation compared to the background White population [81]. Incontrast diabetes prevalence in African countries e where there islimited urbanisation e is low [82]. In the Multiethnic Cohort Studyof residents of California and Hawaii in the US (i.e. different ethnicgroups sharing a similar Westernised environment) the prevalenceodds ratio for diabetes, in age, sex and BMI-adjusted models wasgreater than two for all non-White ethnic groups (Native Hawai-ians, Latinos, African-Americans, Japanese) compared to WhiteEuropeans [90].
This disproportionately large adverse effect of urbanisation ondiabetes risk is also observed in a number of indigenous pop-ulations throughout the Americas and Australasia [91]. The classicexample is the Pima Indians, who have relatively low diabetesprevalence at 6.9% when living rurally in Mexico (which was notsignificantly different from the rate in non-Pima Mexicans), whichrises more than fivefold to 38% amongst Pima Indians living in theUS [92,93]. It is of particular note that reported energy intake didnot differ significantly between the Mexican and US Pimas, butMexican Pima men and women reported w2.5-fold and w7-foldhigher physical activity levels than the US Pima counterparts[92,93]. This large difference in physical activity level was verifiedby using doubly-labelled water measurement in a sub-group of theMexican and US Pima cohorts. Activity energy expenditure levels inMexican Pimas were over 500 kcal/day higher than their US Pimacounterparts [94]. Thus, Pima Indians appear to be able to over-come their clear genetic susceptibility to diabetes [95] by engagingin very high levels of physical activity e levels of activity muchhigher than are needed to confer low diabetes risk in populations ofWhite European descent.
We have recently reported similar observations for the Mapu-ches, an indigenous American-Indian group living in Chile whohave low levels of diabetes when they live in traditional rural en-vironments, which rises substantially when they adopt an urban-ised lifestyle [96e99]. We made detailed phenotypicmeasurements (including a cardiorespiratory fitness test, objectiveassessment of physical activity by accelerometer, dietary assess-ment, body composition measurement, and assessment of a rangeof cardio-metabolic risk biomarkers) in 123 Mapuche adults livingin traditional rural environments, 124 Mapuche adults living in anurban environment, 91 Chileans of European descent living rurallyand 134 Chileans of European descent living in an urban setting[100]. Our principal findings were twofold. Firstly, there was asignificant ethnicityeenvironment interaction for insulin resis-tance (as estimated by HOMAIR [101]) (p ¼ 0.0003): the adverseeffect of urbanisation on this biomarker of cardio-metabolic riskwas over fourfold greater inMapuches than in Chileans of Europeanorigin [100]. Secondly, the adverse effects of low levels of physicalactivity and high levels of time spent sedentary were substantiallygreater in Mapuches than European Chileans (p ¼ 0.0001 for bothfor ethnicity interactions), an observation that persisted afteradjustment for several potential confounders (see Fig. 1). Thus, itappears that Mapuches are protected from insulin resistance when

0
2
4
6
8
Lower Middle Upper
HO
MA I
R
Tertiles of Sedentary Time
EuropeansMapuches
0
2
4
6
8
Lower Middle Upper
HO
MA I
R
Tertiles of Physical Activity
p(interaction) = 0.0001
p(interaction) = 0.0001
Fig. 1. Homoeostasis model assessment-estimated insulin resistance (HOMAIR) inChilean adults of Mapuche or European ethnic origin according to level of sedentarytime (top panel) and level of physical activity (bottom panel). Bars show mean � SEM.p(interaction) describes the ‘ethnicity � physical activity/sedentary time’ interaction forHOMAIR after adjustment for potential confounding covariates (i.e. age, sex, environ-ment (rural or urban), socio-economic level, education level, smoking status, BMI,waist, body fat, accelerometer wear time, fitness, energy intake, and physical activity(for sedentary time relationship) or sedentary time (for physical activity relationship)).Modified from Ref. [100].
55
65
in-1
)
South AsiansEuropeans
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333328
they are very active, but the consequences of low levels of physicalactivity and high levels of sedentary behaviour for them areparticularly large. In other words, they need to undertake greaterlevels of physical activity than their counterparts of Europeanorigin to maintain a favourable metabolic risk profile.
Thus, the interaction between innate susceptibility and envi-ronmental influence on diabetes risk and insulin resistance appearsto be much steeper most non-White compared with White Euro-pean populations. Accordingly, it could be argued that people ofWhite European descent (w15% of the world’s population) are infact the outliers with respect to the role of environmental in-fluences on diabetes and metabolic risk. Given the fact that theglobal burden of diabetes is increasingly falling on non-Whitepopulations, understanding of how environmental factors, suchas physical activity, modulate diabetes risk in non-White ethnicgroups is of pressing global public health concern.
15
25
35
45
0 20 40 60 80 100 120
VO2m
ax (m
l kg-
1 m
Moderate-to-vigorous physical activity (min.day-1)
Fig. 2. Relationship between cardiorespiratory fitness (as assessed by maximal oxygenuptake; VO2max) and objectively-measured physical activity in South Asian and Euro-pean men. Dotted regression line describes the relationship in European men; solidregression line describes the relationship in South Asian men. For all levels of physicalactivity, VO2max was significantly lower in South Asians. Modified from Ref. [118].
7. Can physiological differences between ethnic groupsexplain the ethnic differences in diabetes risk?
Of themajor worldwide ethnic groups, South Asians, comprisingw20% of the world’s population, are amongst those with thehighest susceptibility to type 2 diabetes, particularly when theymigrate to Westernised countries [81,84e86]. When living in theUK, South Asians tend to develop diabetes about a decade earlier inlife at lower levels of BMI than White Europeans [80,81] and non-diabetic South Asians in the general UK or US population havehigher glucose levels and aremore insulin resistant than Europeans[102e105]. A number of hypotheses have been proposed to explainSouth Asians’ increased insulin resistance and diabetes risk(reviewed in detail here [106]), including greater adiposity for agiven BMI, with more central fat distribution [84,104,107], andpotentially greater liver fat accumulation [108]; early origins/thriftyphenotype effects [109e111]; genetic factors including potential
differences in the prevalence and effects of diabetes risk alleles inSouth Asian compared to other populations [112,113]; differences inlifestyle characteristics, particularly lower physical activity level[114e117]; and differences in cardiorespiratory fitness and skeletalmuscle metabolism [105,118]. South Asians increased adiposity hasreceived considerable focus as a potential explanatory factor fortheir increased insulin resistance and diabetes risk. However, SouthAsians remain more insulin resistant than Europeans after match-ing or adjustment for a range of adiposity markers [105,119], indi-cating other factors also contribute to the South Asian insulinresistance phenotype. A number of studies have reported thatSouth Asians living in Western countries are less physically activethan Europeans. This has been observed in studies using bothobjective [118,120,121] and self-report [114e117] measures ofphysical activity and is evident throughout the lifecourse, startingin childhood [121] and continuing throughout adulthood intomiddle-age and older [114e118], and has even been observed astudy that objectively measured physical activity levels duringpregnancy [120]. Furthermore, while these lower levels of physicalactivity are likely to contribute to the greater insulin resistance anddiabetes risk in South Asians, this does not explain the whole story,South Asians remain more insulin resistant than Europeans evenafter adjustment for differences in physical activity level [105,118].One particularly interesting observation is that cardiorespiratoryfitness levels are lower in South Asians than comparable groups ofEuropeans [105,118,122,123]. This is a consistent finding that is notexplained by South Asians’ lower levels of physical activity. Whilefitness increases with increasing levels of physical activity in bothEuropeans and South Asians, cardiorespiratory fitness levels arelower in South Asians than Europeans for any given level ofobjectivelymeasured physical activity (Fig. 2). This finding of innateethnic differences in fitness levels is supported by recent data fromthe US NHANES study, which showed systematic differences infitness levels between Mexican Americans (highest), non-Hispanicwhites and non-Hispanic blacks (lowest) groups in the US, inde-pendent of the level of (self-reported) physical activity and de-mographic factors [124]. The heritable contribution tocardiorespiratory fitness has been estimated to be up to 50%[125,126] and thus, it seems likely that there will be a genetic (and/or early origins) contribution to the lower fitness levels observed in
0
2
4
6
8
45 50 55 60 65
Fat o
xida
tion
(mg.
kg-1
.min
-1)
Exercise intensity (%VO2max)
EuropeanSouth Asian
p(ethnicity) = 0.001
0
2
4
6
8
10
12
1 2 3 4 5Fa
t oxi
datio
n @
55%
VO
2max
(mg.
kg-1
.min
-1)
Square-root insulin sensitivity index
r = 0.423p = 0.011
0
2
4
6
8
10
12
0.5 1 1.5 2 2.5
Fat o
xida
tion
@ 5
5% V
O2m
ax(m
g.kg
-1.m
in-1
)
Log PKB Ser473 phosphoryation
r = 0.475p = 0.025
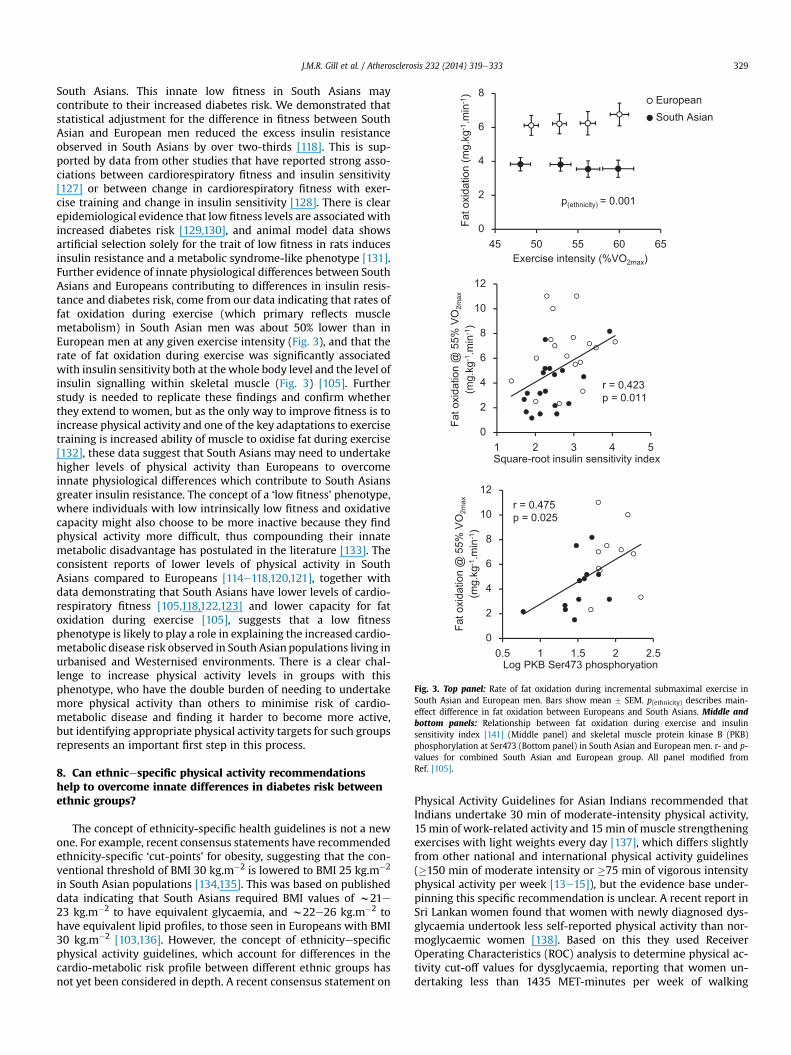
Fig. 3. Top panel: Rate of fat oxidation during incremental submaximal exercise inSouth Asian and European men. Bars show mean � SEM. p(ethnicity) describes main-effect difference in fat oxidation between Europeans and South Asians. Middle andbottom panels: Relationship between fat oxidation during exercise and insulinsensitivity index [141] (Middle panel) and skeletal muscle protein kinase B (PKB)phosphorylation at Ser473 (Bottom panel) in South Asian and European men. r- and p-values for combined South Asian and European group. All panel modified fromRef. [105].
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333 329
South Asians. This innate low fitness in South Asians maycontribute to their increased diabetes risk. We demonstrated thatstatistical adjustment for the difference in fitness between SouthAsian and European men reduced the excess insulin resistanceobserved in South Asians by over two-thirds [118]. This is sup-ported by data from other studies that have reported strong asso-ciations between cardiorespiratory fitness and insulin sensitivity[127] or between change in cardiorespiratory fitness with exer-cise training and change in insulin sensitivity [128]. There is clearepidemiological evidence that low fitness levels are associated withincreased diabetes risk [129,130], and animal model data showsartificial selection solely for the trait of low fitness in rats inducesinsulin resistance and a metabolic syndrome-like phenotype [131].Further evidence of innate physiological differences between SouthAsians and Europeans contributing to differences in insulin resis-tance and diabetes risk, come from our data indicating that rates offat oxidation during exercise (which primary reflects musclemetabolism) in South Asian men was about 50% lower than inEuropean men at any given exercise intensity (Fig. 3), and that therate of fat oxidation during exercise was significantly associatedwith insulin sensitivity both at thewhole body level and the level ofinsulin signalling within skeletal muscle (Fig. 3) [105]. Furtherstudy is needed to replicate these findings and confirm whetherthey extend to women, but as the only way to improve fitness is toincrease physical activity and one of the key adaptations to exercisetraining is increased ability of muscle to oxidise fat during exercise[132], these data suggest that South Asians may need to undertakehigher levels of physical activity than Europeans to overcomeinnate physiological differences which contribute to South Asiansgreater insulin resistance. The concept of a ‘low fitness’ phenotype,where individuals with low intrinsically low fitness and oxidativecapacity might also choose to be more inactive because they findphysical activity more difficult, thus compounding their innatemetabolic disadvantage has postulated in the literature [133]. Theconsistent reports of lower levels of physical activity in SouthAsians compared to Europeans [114e118,120,121], together withdata demonstrating that South Asians have lower levels of cardio-respiratory fitness [105,118,122,123] and lower capacity for fatoxidation during exercise [105], suggests that a low fitnessphenotype is likely to play a role in explaining the increased cardio-metabolic disease risk observed in South Asian populations living inurbanised and Westernised environments. There is a clear chal-lenge to increase physical activity levels in groups with thisphenotype, who have the double burden of needing to undertakemore physical activity than others to minimise risk of cardio-metabolic disease and finding it harder to become more active,but identifying appropriate physical activity targets for such groupsrepresents an important first step in this process.
8. Can ethnicespecific physical activity recommendationshelp to overcome innate differences in diabetes risk betweenethnic groups?
The concept of ethnicity-specific health guidelines is not a newone. For example, recent consensus statements have recommendedethnicity-specific ‘cut-points’ for obesity, suggesting that the con-ventional threshold of BMI 30 kg.m�2 is lowered to BMI 25 kg.m�2
in South Asian populations [134,135]. This was based on publisheddata indicating that South Asians required BMI values of w21e23 kg.m�2 to have equivalent glycaemia, and w22e26 kg.m�2 tohave equivalent lipid profiles, to those seen in Europeans with BMI30 kg.m�2 [103,136]. However, the concept of ethnicityespecificphysical activity guidelines, which account for differences in thecardio-metabolic risk profile between different ethnic groups hasnot yet been considered in depth. A recent consensus statement on
Physical Activity Guidelines for Asian Indians recommended thatIndians undertake 30 min of moderate-intensity physical activity,15 min of work-related activity and 15min of muscle strengtheningexercises with light weights every day [137], which differs slightlyfrom other national and international physical activity guidelines(�150 min of moderate intensity or �75 min of vigorous intensityphysical activity per week [13e15]), but the evidence base under-pinning this specific recommendation is unclear. A recent report inSri Lankan women found that women with newly diagnosed dys-glycaemia undertook less self-reported physical activity than nor-moglycaemic women [138]. Based on this they used ReceiverOperating Characteristics (ROC) analysis to determine physical ac-tivity cut-off values for dysglycaemia, reporting that women un-dertaking less than 1435 MET-minutes per week of walking
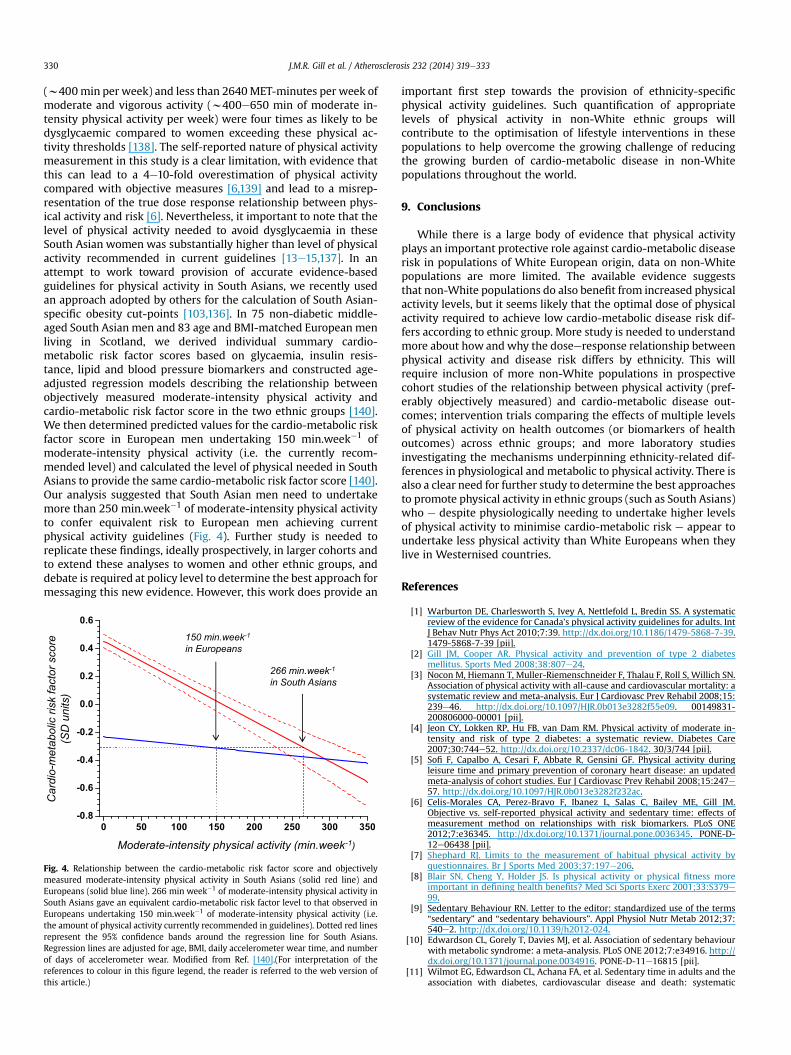
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333330
(w400min per week) and less than 2640MET-minutes per week ofmoderate and vigorous activity (w400e650 min of moderate in-tensity physical activity per week) were four times as likely to bedysglycaemic compared to women exceeding these physical ac-tivity thresholds [138]. The self-reported nature of physical activitymeasurement in this study is a clear limitation, with evidence thatthis can lead to a 4e10-fold overestimation of physical activitycompared with objective measures [6,139] and lead to a misrep-resentation of the true dose response relationship between phys-ical activity and risk [6]. Nevertheless, it important to note that thelevel of physical activity needed to avoid dysglycaemia in theseSouth Asian women was substantially higher than level of physicalactivity recommended in current guidelines [13e15,137]. In anattempt to work toward provision of accurate evidence-basedguidelines for physical activity in South Asians, we recently usedan approach adopted by others for the calculation of South Asian-specific obesity cut-points [103,136]. In 75 non-diabetic middle-aged South Asian men and 83 age and BMI-matched European menliving in Scotland, we derived individual summary cardio-metabolic risk factor scores based on glycaemia, insulin resis-tance, lipid and blood pressure biomarkers and constructed age-adjusted regression models describing the relationship betweenobjectively measured moderate-intensity physical activity andcardio-metabolic risk factor score in the two ethnic groups [140].We then determined predicted values for the cardio-metabolic riskfactor score in European men undertaking 150 min.week�1 ofmoderate-intensity physical activity (i.e. the currently recom-mended level) and calculated the level of physical needed in SouthAsians to provide the same cardio-metabolic risk factor score [140].Our analysis suggested that South Asian men need to undertakemore than 250 min.week�1 of moderate-intensity physical activityto confer equivalent risk to European men achieving currentphysical activity guidelines (Fig. 4). Further study is needed toreplicate these findings, ideally prospectively, in larger cohorts andto extend these analyses to women and other ethnic groups, anddebate is required at policy level to determine the best approach formessaging this new evidence. However, this work does provide an
0 50 100 150 200 250 300 350
-0.8
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
150 min.week-1
in Europeans
266 min.week-1
in South Asians
Ca
rd
io-m
eta
bo
lic r
isk fa
cto
r s
co
re
(S
D u
nits)
Moderate-intensity physical activity (min.week-1
)
Fig. 4. Relationship between the cardio-metabolic risk factor score and objectivelymeasured moderate-intensity physical activity in South Asians (solid red line) andEuropeans (solid blue line). 266 min week�1 of moderate-intensity physical activity inSouth Asians gave an equivalent cardio-metabolic risk factor level to that observed inEuropeans undertaking 150 min.week�1 of moderate-intensity physical activity (i.e.the amount of physical activity currently recommended in guidelines). Dotted red linesrepresent the 95% confidence bands around the regression line for South Asians.Regression lines are adjusted for age, BMI, daily accelerometer wear time, and numberof days of accelerometer wear. Modified from Ref. [140].(For interpretation of thereferences to colour in this figure legend, the reader is referred to the web version ofthis article.)
important first step towards the provision of ethnicity-specificphysical activity guidelines. Such quantification of appropriatelevels of physical activity in non-White ethnic groups willcontribute to the optimisation of lifestyle interventions in thesepopulations to help overcome the growing challenge of reducingthe growing burden of cardio-metabolic disease in non-Whitepopulations throughout the world.
9. Conclusions
While there is a large body of evidence that physical activityplays an important protective role against cardio-metabolic diseaserisk in populations of White European origin, data on non-Whitepopulations are more limited. The available evidence suggeststhat non-White populations do also benefit from increased physicalactivity levels, but it seems likely that the optimal dose of physicalactivity required to achieve low cardio-metabolic disease risk dif-fers according to ethnic group. More study is needed to understandmore about how and why the doseeresponse relationship betweenphysical activity and disease risk differs by ethnicity. This willrequire inclusion of more non-White populations in prospectivecohort studies of the relationship between physical activity (pref-erably objectively measured) and cardio-metabolic disease out-comes; intervention trials comparing the effects of multiple levelsof physical activity on health outcomes (or biomarkers of healthoutcomes) across ethnic groups; and more laboratory studiesinvestigating the mechanisms underpinning ethnicity-related dif-ferences in physiological and metabolic to physical activity. There isalso a clear need for further study to determine the best approachesto promote physical activity in ethnic groups (such as South Asians)who e despite physiologically needing to undertake higher levelsof physical activity to minimise cardio-metabolic risk e appear toundertake less physical activity than White Europeans when theylive in Westernised countries.
References
[1] Warburton DE, Charlesworth S, Ivey A, Nettlefold L, Bredin SS. A systematicreview of the evidence for Canada’s physical activity guidelines for adults. IntJ Behav Nutr Phys Act 2010;7:39. http://dx.doi.org/10.1186/1479-5868-7-39.1479-5868-7-39 [pii].
[2] Gill JM, Cooper AR. Physical activity and prevention of type 2 diabetesmellitus. Sports Med 2008;38:807e24.
[3] Nocon M, Hiemann T, Muller-Riemenschneider F, Thalau F, Roll S, Willich SN.Association of physical activity with all-cause and cardiovascular mortality: asystematic review and meta-analysis. Eur J Cardiovasc Prev Rehabil 2008;15:239e46. http://dx.doi.org/10.1097/HJR.0b013e3282f55e09. 00149831-200806000-00001 [pii].
[4] Jeon CY, Lokken RP, Hu FB, van Dam RM. Physical activity of moderate in-tensity and risk of type 2 diabetes: a systematic review. Diabetes Care2007;30:744e52. http://dx.doi.org/10.2337/dc06-1842. 30/3/744 [pii].
[5] Sofi F, Capalbo A, Cesari F, Abbate R, Gensini GF. Physical activity duringleisure time and primary prevention of coronary heart disease: an updatedmeta-analysis of cohort studies. Eur J Cardiovasc Prev Rehabil 2008;15:247e57. http://dx.doi.org/10.1097/HJR.0b013e3282f232ac.
[6] Celis-Morales CA, Perez-Bravo F, Ibanez L, Salas C, Bailey ME, Gill JM.Objective vs. self-reported physical activity and sedentary time: effects ofmeasurement method on relationships with risk biomarkers. PLoS ONE2012;7:e36345. http://dx.doi.org/10.1371/journal.pone.0036345. PONE-D-12e06438 [pii].
[7] Shephard RJ. Limits to the measurement of habitual physical activity byquestionnaires. Br J Sports Med 2003;37:197e206.
[8] Blair SN, Cheng Y, Holder JS. Is physical activity or physical fitness moreimportant in defining health benefits? Med Sci Sports Exerc 2001;33:S379e99.
[9] Sedentary Behaviour RN. Letter to the editor: standardized use of the terms“sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab 2012;37:540e2. http://dx.doi.org/10.1139/h2012-024.
[10] Edwardson CL, Gorely T, Davies MJ, et al. Association of sedentary behaviourwith metabolic syndrome: a meta-analysis. PLoS ONE 2012;7:e34916. http://dx.doi.org/10.1371/journal.pone.0034916. PONE-D-11e16815 [pii].
[11] Wilmot EG, Edwardson CL, Achana FA, et al. Sedentary time in adults and theassociation with diabetes, cardiovascular disease and death: systematic
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333 331
review and meta-analysis. Diabetologia 2012;55:2895e905. http://dx.doi.org/10.1007/s00125-012-2677-z.
[12] Thorp AA, Owen N, Neuhaus M, Dunstan DW. Sedentary behaviors andsubsequent health outcomes in adults a systematic review of longitudinalstudies, 1996e2011. Am J Prev Med 2011;41:207e15. http://dx.doi.org/10.1016/j.amepre.2011.05.004. S0749e3797(11)00312-6 [pii].
[13] Department of Health. Start active, stay active: a report on physical activityfor health from the four home countries’ Chief Medical Officers; 2011. pp. 1e59.
[14] U.S.Department of Health and Human Services. 2008 physical activityguidelines for Americans; 2008.
[15] World Health Organisation. Global recommendations on physical activity forhealth; 2010. pp. 1e58.
[16] Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect ofphysical inactivity on major non-communicable diseases worldwide: ananalysis of burden of disease and life expectancy. Lancet 2012;380:219e29.http://dx.doi.org/10.1016/S0140-6736(12)61031-9. S0140e6736(12)61031-9 [pii].
[17] Blair SN. Physical inactivity: the biggest public health problem of the 21stcentury. Br J Sports Med 2009;43:1e2. 43/1/1 [pii].
[18] Lan TY, Chang HY, Tai TY. Relationship between components of leisurephysical activity and mortality in Taiwanese older adults. Prev Med 2006;43:36e41. http://dx.doi.org/10.1016/j.ypmed.2006.03.016. S0091e7435(06)00137-X [pii].
[19] Matthews CE, Jurj AL, Shu XO, et al. Influence of exercise, walking, cycling,and overall nonexercise physical activity on mortality in Chinese women.Am J Epidemiol 2007;165:1343e50. http://dx.doi.org/10.1093/aje/kwm088.kwm088 [pii].
[20] Villegas R, Shu XO, Li H, et al. Physical activity and the incidence of type 2diabetes in the Shanghai women’s health study. Int J Epidemiol 2006;35:1553e62.
[21] Wang N, Zhang X, Xiang YB, et al. Associations of Tai Chi, walking, andjogging with mortality in Chinese men. Am J Epidemiol 2013. http://dx.doi.org/10.1093/aje/kwt050. kwt050 [pii].
[22] Rodriguez BL, Curb JD, Burchfiel CM, et al. Physical activity and 23-yearincidence of coronary heart disease morbidity and mortality amongmiddle-aged men. The Honolulu Heart Program. Circulation 1994;89:2540e4.
[23] Donahue RP, Abbott RD, Reed DM, Yano K. Physical activity and coronaryheart disease in middle-aged and elderly men: the Honolulu Heart Program.Am J Public Health 1988;78:683e5.
[24] Hakim AA, Curb JD, Petrovitch H, et al. Effects of walking on coronary heartdisease in elderly men: the Honolulu Heart Program. Circulation 1999;100:9e13.
[25] Abbott RD, Curb JD, Rodriguez BL, et al. Age-related changes in risk factoreffects on the incidence of thromboembolic and hemorrhagic stroke. J ClinEpidemiol 2003;56:479e86. S089543560200611X [pii].
[26] Abbott RD, Rodriguez BL, Burchfiel CM, Curb JD. Physical activity in oldermiddle-aged men and reduced risk of stroke: the Honolulu Heart Program.Am J Epidemiol 1994;139:881e93.
[27] Burchfiel CM, Sharp DS, Curb JD, et al. Physical activity and incidence ofdiabetes: the Honolulu Heart Program. Am J Epidemiol 1995;141:360e8.
[28] Hakim AA, Petrovitch H, Burchfiel CM, et al. Effects of walking on mortalityamong nonsmoking retired men. N Engl J Med 1998;338:94e9. http://dx.doi.org/10.1056/NEJM199801083380204.
[29] Sato KK, Hayashi T, Kambe H, et al. Walking to work is an independentpredictor of incidence of type 2 diabetes in Japanese men: the KansaiHealthcare Study. Diabetes Care 2007;30:2296e8. http://dx.doi.org/10.2337/dc07-0090. dc07-0090 [pii].
[30] Okada K, Hayashi T, Tsumura K, Suematsu C, Endo G, Fujii S. Leisure-timephysical activity at weekends and the risk of type 2 diabetes mellitus inJapanese men: the Osaka Health Survey. Diabet Med 2000;17:53e8.
[31] Nakanishi N, Takatorige T, Suzuki K. Daily life activity and risk of developingimpaired fasting glucose or type 2 diabetes in middle-aged Japanese men.Diabetologia 2004;47:1768e75.
[32] Noda H, Iso H, Toyoshima H, et al. Walking and sports participation andmortality from coronary heart disease and stroke. J Am Coll Cardiol 2005;46:1761e7. http://dx.doi.org/10.1016/j.jacc.2005.07.038. S0735e1097(05)01782-1 [pii].
[33] Inoue M, Iso H, Yamamoto S, et al. Daily total physical activity level andpremature death in men and women: results from a large-scale population-based cohort study in Japan (JPHC study). Ann Epidemiol 2008;18:522e30.http://dx.doi.org/10.1016/j.annepidem.2008.03.008. S1047e2797(08)00063-X [pii].
[34] Ottenbacher AJ, Snih SA, Karmarkar A, et al. Routine physical activity andmortality in Mexican Americans aged 75 and older. J Am Geriatr Soc2012;60:1085e91. http://dx.doi.org/10.1111/j.1532-5415.2012.03995.x.
[35] Folsom AR, Arnett DK, Hutchinson RG, Liao F, Clegg LX, Cooper LS. Physicalactivity and incidence of coronary heart disease in middle-aged women andmen. Med Sci Sports Exerc 1997;29:901e9.
[36] Bell EJ, Lutsey PL, Windham BG, Folsom AR. Physical activity and cardio-vascular disease in African Americans in atherosclerosis risk in communities.Med Sci Sports Exerc 2013;45:901e7. http://dx.doi.org/10.1249/MSS.0b013e31827d87ec.
[37] Manson JE, Greenland P, LaCroix AZ, et al. Walking compared with vigorousexercise for the prevention of cardiovascular events in women. N Engl J Med2002;347:716e25.
[38] Mathieu RA, Powell-Wiley TM, Ayers CR, et al. Physical activity participation,health perceptions, and cardiovascular disease mortality in a multiethnicpopulation: the Dallas Heart Study. Am Heart J 2012;163:1037e40. http://dx.doi.org/10.1016/j.ahj.2012.03.005. S0002e8703(12)00170-6 [pii].
[39] Gillum RF, Mussolino ME, Ingram DD. Physical activity and stroke incidencein women and men. The NHANES I Epidemiologic Follow-up Study. Am JEpidemiol 1996;143:860e9.
[40] Evenson KR, Rosamond WD, Cai J, et al. Physical activity and ischemic strokerisk. The atherosclerosis risk in communities study. Stroke 1999;30:1333e9.
[41] Autenrieth CS, Evenson KR, Yatsuya H, Shahar E, Baggett C, Rosamond WD.Association between physical activity and risk of stroke subtypes: theatherosclerosis risk in communities study. Neuroepidemiology 2013;40:109e16. http://dx.doi.org/10.1159/000342151. 000342151 [pii].
[42] Gregg EW, Gerzoff RB, Caspersen CJ, Williamson DF, Narayan KM. Relation-ship of walking to mortality among US adults with diabetes. Arch Intern Med2003;163:1440e7. http://dx.doi.org/10.1001/archinte.163.12.1440. 163/12/1440 [pii].
[43] de Munter JS, Agyemang C, Stronks K, van Valkengoed IG. Association ofphysical activity, smoking, and alcohol intake with CVD-related hospitaldischarge in people of European, South Asian, or African descent. Eur J PrevCardiol 2013;20:80e8. http://dx.doi.org/10.1177/2047487311434232.2047487311434232 [pii].
[44] Williams ED, Stamatakis E, Chandola T, Hamer M. Physical activity behaviourand coronary heart disease mortality among South Asian people in the UK:an observational longitudinal study. Heart 2011;97:655e9. http://dx.doi.org/10.1136/hrt.2010.201012. hrt.2010.201012 [pii].
[45] Hsia J, Wu L, Allen C, et al. Physical activity and diabetes risk in post-menopausal women. Am J Prev Med 2005;28:19e25.
[46] Steinbrecher A, Erber E, Grandinetti A, Nigg C, Kolonel LN, Maskarinec G.Physical activity and risk of type 2 diabetes among Native Hawaiians, Japa-nese Americans, and Caucasians: the Multiethnic Cohort. J Phys Act Health2012;9:634e41. 2010e0209 [pii].
[47] Fretts AM, Howard BV, Kriska AM, et al. Physical activity and incident dia-betes in American Indians: the Strong Heart Study. Am J Epidemiol2009;170:632e9. http://dx.doi.org/10.1093/aje/kwp181. kwp181 [pii].
[48] Sattar N. Revisiting the links between glycaemia, diabetes and cardiovasculardisease. Diabetologia 2013;56:686e95. http://dx.doi.org/10.1007/s00125-012-2817-5.
[49] Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive life-style intervention in type 2 diabetes. N Engl J Med 2013;369:145e54. http://dx.doi.org/10.1056/NEJMoa1212914.
[50] Wesche-Thobaben JA. The development and description of the comparisongroup in the Look AHEAD trial. Clin Trials 2011;8:320e9. http://dx.doi.org/10.1177/1740774511405858. 8/3/320 [pii].
[51] Gregg EW, Chen H, Wagenknecht LE, et al. Association of an intensive life-style intervention with remission of type 2 diabetes. J Am Med Assoc2012;308:2489e96. http://dx.doi.org/10.1001/jama.2012.67929. 1486829[pii].
[52] Jakicic JM, Egan CM, Fabricatore AN, et al. Four-year change in cardiorespi-ratory fitness and influence on glycemic control in adults with type 2 dia-betes in a randomized trial: the Look AHEAD Trial. Diabetes Care 2013;36:1297e303. http://dx.doi.org/10.2337/dc12-0712. dc12-0712 [pii].
[53] Li G, Zhang P, Wang J, et al. The long-term effect of lifestyle interventions toprevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-yearfollow-up study. Lancet 2008;371:1783e9. http://dx.doi.org/10.1016/S0140-6736(08)60766-7. S0140e6736(08)60766-7 [pii].
[54] Heran BS, Chen JM, Ebrahim S, et al. Exercise-based cardiac rehabilitation forcoronary heart disease. Cochrane Database Syst Rev 2011:CD001800. http://dx.doi.org/10.1002/14651858.CD001800.pub2.
[55] Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac reha-bilitation post-myocardial infarction: a systematic review and meta-analysisof randomized controlled trials. Am Heart J 2011;162:571e84. http://dx.doi.org/10.1016/j.ahj.2011.07.017. S0002e8703(11)00559-X [pii].
[56] Durstine JL, Grandjean PW, Davis PG, Ferguson MA, Alderson NL, DuBose KD.Blood lipid and lipoprotein adaptations to exercise: a quantitative analysis.Sports Med 2001;31:1033e62.
[57] Malkova D, Gill JMR. Effects of exercise on postprandial lipoprotein meta-bolism. Future Lipidol 2006;1:743e55.
[58] Al-Shayji IA, Caslake MJ, Gill JM. Effects of moderate exercise on VLDL andintralipid kinetics in overweight/obese middle-aged men. Am J PhysiolEndocrinol Metab 2012;302:E349e55. http://dx.doi.org/10.1152/ajpendo.00498.2011. ajpendo.00498.2011 [pii].
[59] Maarbjerg SJ, Sylow L, Richter EA. Current understanding of increased insulinsensitivity after exercise - emerging candidates. Acta Physiol (Oxf) 2011;202:323e35. http://dx.doi.org/10.1111/j.1748-1716.2011.02267.x.
[60] Turcotte LP, Fisher JS. Skeletal muscle insulin resistance: roles of fatty acidmetabolism and exercise. Phys Ther 2008;88:1279e96. http://dx.doi.org/10.2522/ptj.20080018. ptj.20080018 [pii].
[61] Green DJ, Maiorana A, O’Driscoll G, Taylor R. Effect of exercise training onendothelium-derivednitric oxide function inhumans. J Physiol 2004;561:1e25.http://dx.doi.org/10.1113/jphysiol.2004.068197. jphysiol.2004.068197 [pii].

J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333332
[62] Szostak J, Laurant P. The forgotten face of regular physical exercise: a ‘nat-ural’ anti-atherogenic activity. Clin Sci (Lond) 2011;121:91e106. http://dx.doi.org/10.1042/CS20100520. CS20100520 [pii].
[63] Padilla J, Simmons GH, Bender SB, Arce-Esquivel AA, Whyte JJ, Laughlin MH.Vascular effects of exercise: endothelial adaptations beyond active musclebeds. Physiology (Bethesda) 2011;26:132e45. http://dx.doi.org/10.1152/physiol.00052.2010. 26/3/132 [pii].
[64] Whelton SP, Chin A, Xin X, He J. Effect of aerobic exercise on blood pressure:a meta-analysis of randomized, controlled trials. Ann Intern Med 2002;136:493e503.
[65] Cornelissen VA, Buys R, Smart NA. Endurance exercise beneficially affectsambulatorybloodpressure:a systematic reviewandmeta-analysis. JHypertens2013;31:639e48. http://dx.doi.org/10.1097/HJH.0b013e32835ca964.
[66] Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematicreview and meta-analysis. J Am Heart Assoc 2013;2:e004473. http://dx.doi.org/10.1161/JAHA.112.004473. 2/1/e004473 [pii].
[67] Mathur N, Pedersen BK. Exercise as a mean to control low-grade systemicinflammation. Mediators Inflamm 2008;2008:109502. http://dx.doi.org/10.1155/2008/109502.
[68] You T, Arsenis NC, Disanzo BL, LaMonte MJ. Effects of exercise training onchronic inflammation in obesity: current evidence and potential mecha-nisms. Sports Med 2013;43:243e56. http://dx.doi.org/10.1007/s40279-013-0023-3.
[69] Ryan D. Risks and benefits of weight loss: challenges to obesity research. EurHeart J Suppl 2005;7:L27e31.
[70] Collins GS, Altman DG. Predicting the 10 year risk of cardiovascular diseasein the United Kingdom: independent and external validation of an updatedversion of QRISK2. BMJ 2012;344:e4181.
[71] Lindstrom J, Peltonen M, Eriksson JG, et al. Improved lifestyle and decreaseddiabetes risk over 13 years: long-term follow-up of the randomised FinnishDiabetes Prevention Study (DPS). Diabetologia 2013;56:284e93. http://dx.doi.org/10.1007/s00125-012-2752-5.
[72] Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetesincidence and weight loss in the Diabetes Prevention Program OutcomesStudy. Lancet 2009;374:1677e86. http://dx.doi.org/10.1016/S0140-6736(09)61457-4. S0140e6736(09)61457-4 [pii].
[73] Gong Q, Gregg EW, Wang J, et al. Long-term effects of a randomised trial of a6-year lifestyle intervention in impaired glucose tolerance on diabetes-related microvascular complications: the China Da Qing Diabetes Preven-tion Outcome Study. Diabetologia 2011;54:300e7. http://dx.doi.org/10.1007/s00125-010-1948-9.
[74] Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDMin people with impaired glucose tolerance. The Da Qing IGT and DiabetesStudy. Diabetes Care 1997;20:537e44.
[75] Kosaka K, Noda M, Kuzuya T. Prevention of type 2 diabetes by lifestyleintervention: a Japanese trial in IGT males. Diabetes Res Clin Pract 2005;67:152e62. http://dx.doi.org/10.1016/j.diabres.2004.06.010. S0168e8227(04)00178-0 [pii].
[76] Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V. TheIndian Diabetes Prevention Programme shows that lifestyle modification andmetformin prevent type 2 diabetes in Asian Indian subjects with impairedglucose tolerance (IDPP-1). Diabetologia 2006;49:289e97.
[77] Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence oftype 2 diabetes with lifestyle intervention or metformin. N Engl J Med2002;346:393e403.
[78] Penn L, White M, Lindstrom J, et al. Importance of weight loss maintenanceand risk prediction in the prevention of type 2 diabetes: analysis of EuropeanDiabetes Prevention Study RCT. PLoS ONE 2013;8:e57143. http://dx.doi.org/10.1371/journal.pone.0057143. PONE-D-12e30924 [pii].
[79] Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetesmellitus by changes in lifestyle among subjects with impaired glucosetolerance. N Engl J Med 2001;344:1343e50.
[80] Mukhopadhyay B, Forouhi NG, Fisher BM, Kesson CM, Sattar N. A comparisonof glycaemic and metabolic control over time among South Asian and Eu-ropean patients with type 2 diabetes: results from follow-up in a routinediabetes clinic. Diabet Med 2006;23:94e8.
[81] Sproston K, Mindell J. The health of minority ethnic groups, vol. 1; 2006.[82] International Diabetes Federation. IDF diabetes atlas. Brussels: International
Diabetes Federation; 2009.[83] Zimmet P. Globalization, coca-colonization and the chronic disease
epidemic: can the Doomsday scenario be averted? J Intern Med 2000;247:301e10. jim625 [pii].
[84] McKeigue PM, Shah B, Marmot MG. Relation of central obesity and insulinresistance with high diabetes prevalence and cardiovascular risk in SouthAsians. Lancet 1991;337:382e6.
[85] Venkataraman R, Nanda NC, Baweja G, Parikh N, Bhatia V. Prevalence ofdiabetes mellitus and related conditions in Asian Indians living in the UnitedStates. Am J Cardiol 2004;94:977e80. http://dx.doi.org/10.1016/j.amj-card.2004.06.048. S0002e9149(04)00976-2 [pii].
[86] Kanaya AM, Wassel CL, Mathur D, et al. Prevalence and correlates of diabetesin South Asian Indians in the United States: findings from the metabolicsyndrome and atherosclerosis in South Asians living in America study andthe multi-ethnic study of atherosclerosis. Metab Syndr Relat Disord 2010;8:157e64. http://dx.doi.org/10.1089/met.2009.0062.
[87] Zhang Q, Wang Y, Huang ES. Changes in racial/ethnic disparities in theprevalence of type 2 diabetes by obesity level among US adults. Ethn Health2009;14:439e57. http://dx.doi.org/10.1080/13557850802699155.910365654 [pii].
[88] Mohan V, Mathur P, Deepa R, et al. Urban rural differences in prevalence ofself-reported diabetes in Indiaethe WHO-ICMR Indian NCD risk factor sur-veillance. Diabetes Res Clin Pract 2008;80:159e68.
[89] Ramachandran A, Mary S, Yamuna A, Murugesan N, Snehalatha C. Highprevalence of diabetes and cardiovascular risk factors associated with ur-banization in India. Diabetes Care 2008;31:893e8. http://dx.doi.org/10.2337/dc07-1207. dc07-1207 [pii].
[90] Maskarinec G, Grandinetti A, Matsuura G, et al. Diabetes prevalence andbody mass index differ by ethnicity: the Multiethnic Cohort. Ethn Dis2009;19:49e55.
[91] Yu CH, Zinman B. Type 2 diabetes and impaired glucose tolerance inaboriginal populations: a global perspective. Diabetes Res Clin Pract2007;78:159e70. http://dx.doi.org/10.1016/j.diabres.2007.03.022. S0168e8227(07)00249-5 [pii].
[92] Valencia ME, Bennett PH, Ravussin E, Esparza J, Fox C, Schulz LO. The PimaIndians in Sonora, Mexico. Nutr Rev 1999;57:S55e7.
[93] Schulz LO, Bennett PH, Ravussin E, et al. Effects of traditional and westernenvironments on prevalence of type 2 diabetes in Pima Indians in Mexicoand the U.S. Diabetes Care 2006;29:1866e71. http://dx.doi.org/10.2337/dc06-0138. 29/8/1866 [pii].
[94] Esparza J, Fox C, Harper IT, et al. Daily energy expenditure in Mexican andUSA Pima indians: low physical activity as a possible cause of obesity. Int JObes Relat Metab Disord 2000;24:55e9.
[95] Baier LJ, Hanson RL. Genetic studies of the etiology of type 2 diabetes in PimaIndians: hunting for pieces to a complicated puzzle. Diabetes 2004;53:1181e6.
[96] Perez-Bravo F, Carrasco E, Santos JL, Calvillan M, Larenas G, Albala C. Prev-alence of type 2 diabetes and obesity in rural Mapuche population fromChile. Nutrition 2001;17:236e8. S0899900700005505 [pii].
[97] Perez-Bravo F, Fuentes M, Angel B, et al. Lack of association between the fattyacid binding protein 2 (FABP2) polymorphism with obesity and insulinresistance in two aboriginal populations from Chile. Acta Diabetol 2006;43:93e8. http://dx.doi.org/10.1007/s00592-006-0221-7.
[98] Larenas G, Arias G, Espinoza O, et al. Prevalence of diabetes mellitus in aMapuche community of Region IX, Chile. Rev Med Chil 1985;113:1121e5.
[99] Carrasco EP, Perez FB, Angel BB, et al. Prevalence of type 2 diabetes andobesity in two Chilean aboriginal populations living in urban zones. Rev MedChil 2004;132:1189e97.
[100] Celis-Morales CA, Perez-Bravo F, Ibanes L, et al. Insulin resistance in Chileansof European and Indigenous descent: evidence for an ethnicity x environ-ment interaction. PLoS ONE 2011;6:e24690.
[101] Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC.Homeostasis model assessment: insulin resistance and beta-cell functionfrom fasting plasma glucose and insulin concentrations in man. Diabetologia1985;28:412e9.
[102] Forouhi NG, Sattar N, Tillin T, McKeigue PM, Chaturvedi N. Do known riskfactors explain the higher coronary heart disease mortality in South Asiancompared with European men? Prospective follow-up of the Southall andBrent studies, UK. Diabetologia 2006;49:2580e8.
[103] Gray LJ, Yates T, Davies MJ, et al. Defining obesity cut-off points for migrantSouth Asians. PLoS ONE 2011;6:e26464. http://dx.doi.org/10.1371/journal.-pone.0026464. PONE-D-11e06667 [pii].
[104] Chandalia M, Lin P, Seenivasan T, et al. Insulin resistance and body fat dis-tribution in South Asian men compared to Caucasian men. PLoS ONE 2007;2:e812.
[105] Hall LM, Moran CN, Milne GR, et al. Fat oxidation, fitness and skeletal muscleexpression of oxidative/lipid metabolism genes in South Asians: implicationsfor insulin resistance? PLoS ONE 2010;5:e14197. http://dx.doi.org/10.1371/journal.pone.0014197.
[106] Hall LML, Sattar N, Gill JMR. Risk of metabolic and vascular disease in SouthAsians: potential mechanisms for increased insulin resistance. Future Lip-idology 2008;3:411e24.
[107] Misra A, Vikram NK. Insulin resistance syndrome (metabolic syndrome) andobesity in Asian Indians: evidence and implications. Nutrition 2004;20:482e91.
[108] Petersen KF, Dufour S, Feng J, et al. Increased prevalence of insulin resistanceand nonalcoholic fatty liver disease in Asian-Indian men. Proc Natl Acad SciU S A 2006;103:18273e7.
[109] Yajnik CS. Early life origins of insulin resistance and type 2 diabetes in Indiaand other Asian countries. J Nutr 2004;134:205e10.
[110] Yajnik CS, Lubree HG, Rege SS, et al. Adiposity and hyperinsulinemia in In-dians are present at birth. J Clin Endocrinol Metab 2002;87:5575e80.
[111] Yajnik CS, Fall CH, Coyaji KJ, et al. Neonatal anthropometry: the thin-fatIndian baby. The Pune Maternal Nutrition Study. Int J Obes Relat MetabDisord 2003;27:173e80.
[112] Ramachandran A, Ma RC, Snehalatha C. Diabetes in Asia. Lancet 2010;375:408e18. http://dx.doi.org/10.1016/S0140-6736(09)60937-5. S0140e6736(09)60937-5 [pii].
[113] Gujral UP, Pradeepa R, Weber MB, Narayan KM, Mohan V. Type 2 diabetes inSouth Asians: similarities and differences with white Caucasian and other
J.M.R. Gill et al. / Atherosclerosis 232 (2014) 319e333 333
populations. Ann N Y Acad Sci 2013;1281:51e63. http://dx.doi.org/10.1111/j.1749-6632.2012.06838.x.
[114] Fischbacher CM, Hunt S, Alexander L. How physically active are South Asiansin the United Kingdom? A literature review. J Public Health (Oxf) 2004;26:250e8. http://dx.doi.org/10.1093/pubmed/fdh158. 26/3/250 [pii].
[115] Hayes L, White M, Unwin N, et al. Patterns of physical activity and rela-tionship with risk markers for cardiovascular disease and diabetes in Indian,Pakistani, Bangladeshi and European adults in a UK population. J PublicHealth Med 2002;24:170e8.
[116] Yates T, Davies MJ, Gray LJ, et al. Levels of physical activity and relationshipwith markers of diabetes and cardiovascular disease risk in 5474 whiteEuropean and South Asian adults screened for type 2 diabetes. Prev Med2010. http://dx.doi.org/10.1016/j.ypmed.2010.06.011. S0091e7435(10)00238-0 [pii].
[117] Williams ED, Stamatakis E, Chandola T, Hamer M. Assessment of physicalactivity levels in South Asians in the UK: findings from the Health Survey forEngland. J Epidemiol Community Health 2011;65:517e21. http://dx.doi.org/10.1136/jech.2009.102509. jech.2009.102509 [pii].
[118] Ghouri N, Purves D, McConnachie A, Wilson J, Gill JMR, Sattar N. Lowercardiorespiratory fitness contributes to increased insulin resistance andfasting glycaemia in middle-aged South Asian compared to European menliving in the UK. Diabetologia 2013. http://dx.doi.org/10.1007/s00125-013-2969-y.
[119] Forouhi NG, Jenkinson G, Thomas EL, et al. Relation of triglyceride stores inskeletal muscle cells to central obesity and insulin sensitivity in Europeanand South Asian men. Diabetologia 1999;42:932e5.
[120] Berntsen S, Richardsen KR, Morkrid K, Sletner L, Birkeland KI, Jenum AK.Objectively recorded physical activity in early pregnancy: a multiethnicpopulation-based study. Scand J Med Sci Sports 2012. http://dx.doi.org/10.1111/sms.12034.
[121] Duncan MJ, Birch S, Al-Nakeeb Y, Nevill AM. Ambulatory physical activitylevels of white and South Asian children in Central England. Acta Paediatr2012;101:e156e62. http://dx.doi.org/10.1111/j.1651-2227.2011.02566.x.
[122] Davey GJG, Roberts JD, Patel S, et al. Effects of exercise on insulin resistancein South Asians and Europeans. Journal of Exercise Physiology 2000;3:6e11.
[123] Hardy CP, Eston RG. Aerobic fitness of Anglo-Saxon and Indian students. Br JSports Med 1985;19:217e8.
[124] Ceaser TG, Fitzhugh EC, Thompson DL, Bassett Jr DR. Association of physicalactivity, fitness, and race: NHANES 1999e2004. Med Sci Sports Exerc2013;45:286e93. http://dx.doi.org/10.1249/MSS.0b013e318271689e.
[125] Bouchard C, Daw EW, Rice T, et al. Familial resemblance for VO2max in thesedentary state: the HERITAGE family study. Med Sci Sports Exerc 1998;30:252e8.
[126] Bouchard C, Lesage R, Lortie G, et al. Aerobic performance in brothers,dizygotic and monozygotic twins. Med Sci Sports Exerc 1986;18:639e46.
[127] Larsen FJ, Anderson M, Ekblom B, Nystrom T. Cardiorespiratory fitness pre-dicts insulin action and secretion in healthy individuals. Metabolism
2012;61:12e6. http://dx.doi.org/10.1016/j.metabol.2011.05.010. S0026e0495(11)00139-9 [pii].
[128] Gan SK, Kriketos AD, Ellis BA, Thompson CH, Kraegen EW, Chisholm DJ.Changes in aerobic capacity and visceral fat but not myocyte lipid levelspredict increased insulin action after exercise in overweight and obese men.Diabetes Care 2003;26:1706e13.
[129] Lynch J, Helmrich SP, Lakka TA, et al. Moderately intense physical activitiesand high levels of cardiorespiratory fitness reduce the risk of non-insulin-dependent diabetes mellitus in middle-aged men. Arch Intern Med1996;156:1307e14.
[130] Wei M, Gibbons LW, Mitchell TL, Kampert JB, Lee CD, Blair SN. The associ-ation between cardiorespiratory fitness and impaired fasting glucose andtype 2 diabetes mellitus in men. Ann Intern Med 1999;130:89e96.
[131] Wisloff U, Najjar SM, Ellingsen O, et al. Cardiovascular risk factors emergeafter artificial selection for low aerobic capacity. Science 2005;307:418e20.
[132] Holloszy JO, Coyle EF. Adaptations of skeletal muscle to endurance exerciseand their metabolic consequences. J Appl Physiol 1984;56:831e8.
[133] Church T. The low-fitness phenotype as a risk factor: more than just beingsedentary? Obesity (Silver Spring) 2009;17(Suppl. 3):S39e42. http://dx.doi.org/10.1038/oby.2009.387. oby2009387 [pii].
[134] Misra A, Chowbey P, Makkar BM, et al. Consensus statement for diagnosis ofobesity, abdominal obesity and the metabolic syndrome for Asian Indiansand recommendations for physical activity, medical and surgical manage-ment. J Assoc Physicians India 2009;57:163e70.
[135] Kumar S, Hanif W, Zaman MJ, Sattar N, Patel K, Khunti K. Lower thresholdsfor diagnosis and management of obesity in British South Asians. Int J ClinPract 2011;65:375e85.
[136] Razak F, Anand SS, Shannon H, et al. Defining obesity cut points in amultiethnic population. Circulation 2007;115:2111e8.
[137] Misra A, Nigam P, Hills AP, et al. Consensus physical activity guidelines forAsian Indians. Diabetes Technol Ther 2012;14:83e98. http://dx.doi.org/10.1089/dia.2011.0111.
[138] Waidyatilaka I, Lanerolle P, Wickremasinghe R, Atukorala S,Somasundaram N, de SA. Sedentary behaviour and physical activity in SouthAsian women: time to review current recommendations? PLoS ONE 2013;8:e58328. http://dx.doi.org/10.1371/journal.pone.0058328. PONE-D-12e33340 [pii].
[139] Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physicalactivity in the United States measured by accelerometer. Med Sci SportsExerc 2008;40:181e8. http://dx.doi.org/10.1249/mss.0b013e31815a51b3.
[140] Celis-Morales CA, Ghouri N, Bailey MES, Sattar N, Gill JMR. Should physicalactivity recommendations be ethnicity-specific? Evidence from a cross-sectional study of South Asian and European men. PLoS ONE 2013;8:e82568. http://dx.doi.org/10.1371/journal.pone.0082568.
[141] Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oralglucose tolerance testing: comparison with the euglycemic insulin clamp.Diabetes Care 1999;22:1462e70.




















