TILAPIA FARMING A Manual for Commercial Tilapia Production in Trinidad and Tobago

Phylogeographical and molecular characterization of an emerging Mycobacteriumtuberculosis clone in Trinidad and Tobago
Julie Millet a, Shirematee Baboolal b,c, Patrick Eberechi Akpaka b, Dottin Ramoutar d, Nalin Rastogi a,*a Unite de la Tuberculose et des Mycobacteries, Institut Pasteur de Guadeloupe, Abymes, Guadeloupeb Department of Para-Clinical Sciences, Faculty of Medical Sciences, The University of the West Indies, St. Augustine, Trinidad and Tobagoc Caribbean Epidemiology Centre, Jamaica Boulevard, Port of Spain, Trinidad and Tobagod Caura Chest Hospital, Caura, Trinidad and Tobago
1. Introduction
Despite improvements in diagnosis, treatment and livingconditions, tuberculosis (TB) continues to be one of the most
important infectious diseases in the world; in 2007 it accounted for9 million new cases and 1.75 million deaths (http://www.who.int/tb/publications/global_report/2009/pdf/full_report.pdf). If currenttools for TB diagnosis, treatment and prevention are not improved,an additional 1 billion persons will become infected withMycobacterium tuberculosis between 2000 and 2020; among these200 million will develop active disease and 35 million will die fromTB (http://www.theglobalfund.org/en/about/tuberculosis). In thiscontext, a precise description of epidemiologically important
Infection, Genetics and Evolution 9 (2009) 1336–1344
A R T I C L E I N F O
Article history:
Received 26 June 2009
Received in revised form 7 September 2009
Accepted 14 September 2009
Available online 22 September 2009
Keywords:
Tuberculosis
Mycobacterium
Spoligotyping
Minisatellites
MIRU-VNTR
Epidemiology
Phylogeny
Trinidad and Tobago
A B S T R A C T
We report on a fine molecular and phylogenetical characterization of circulating Mycobacterium
tuberculosis strains isolated from patients during a 1-year period in Trinidad and Tobago (T&T). The
spoligotyping data coupled to minisatellite typing and available epidemiological data showed that a
single major clone of ‘‘evolutionary modern’’ tubercle bacilli (SIT566) was responsible for more than half
of the tuberculosis (TB) cases. It preferentially infected younger age groups (mean 39.1 years versus 47.7
years for other genotypes, p < 0.0005), and was overrepresented in Port-of-Spain (1 out of 3 patients). A
comparison of genotyping results to data gathered for 6 Caribbean countries (n = 2653 clinical isolates)
showed that the overall lineage distribution in T&T was completely different from its neighbors, e.g., T&T
was the only country harboring a unique sublineage of the Latin American & Mediterranean (LAM)
family, designated LAM-10CAM with phylogeographical specificity for Cameroon and neighboring
countries in West Africa; interestingly 3/4 of the patients within this group in T&T were African
descendants. Similarly, strains belonging to East African Indian (EAI) lineage with phylogeographical
specificity for the Indian subcontinent, were found in T&T (13% of all strains), but were absent among the
neighboring countries. Although the predominant SIT566 was not yet detected elsewhere in the
Caribbean, available information underlined that this genotype was already present in the United States
as imported cases of disease among T&T-born patients. Characterization of SIT566 strains using 12-, 15-
and 24-loci MIRU typing, and comparison of results to international databases showed that these isolates
were characterized by a common 12-loci MIRU pattern 224315153324 corresponding to MIRU
International Type—MIT633 in 21/25 strains tested, as well as its 4 variants; an orphan pattern
, MIT27— , MIT117— , and MIT1158—
. Extended 24-loci MIRU typing led to a predominant pattern
224315153324323483334323 in a total of 16/21 MIT633 isolates, as well as identification of 3
supplemental patterns. Comparison of 24-loci MIRU data with the international database MIRU-
VNTRplus showed the unique nature of the patterns obtained in T&T. Further analysis using the
Levenshtein algorithm showed that the first 2 closest matches with the SIT566/MIT633 clone belonged
to the X lineage strains in MIRU-VNTRplus. This observation corroborates our preliminary spoligotyping-
based analysis using minimum spanning and neighbor-joining trees, which suggested a phylogenetical
relatedness of the SIT566 clone with SIT119, which represents X1 lineage prototype in SpolDB4 database.
We hypothesize that the predominant SIT566 clone might have evolved from a pool of X lineage M.
tuberculosis strains with phylogeographical affinity for Anglo-Saxon descendants.
� 2009 Elsevier B.V. All rights reserved.
* Corresponding author at: Unite de la Tuberculose et des Mycobacteries, WHO
Supranational TB Reference Laboratory, Institut Pasteur de Guadeloupe, 97183
Abymes Cedex, Guadeloupe. Tel.: +590 590 897661; fax: +590 590 896941.
E-mail address: [email protected] (N. Rastogi).
Contents lists available at ScienceDirect
Infection, Genetics and Evolution
journal homepage: www.elsev ier .com/ locate /meegid
1567-1348/$ – see front matter � 2009 Elsevier B.V. All rights reserved.
doi:10.1016/j.meegid.2009.09.006

clones of tubercle bacilli, their geographical distribution anddynamics of their dissemination, are useful parameters to identifythe populations at risk and factors associated with TB transmissionin a community, a goal made attainable today thanks to DNAfingerprinting techniques (Bennett et al., 2002; Ellis et al., 2002;Rastogi and Sola, 2007; Small et al., 1994).
Among various genetic markers used, the IS6110-restrictionfragment length polymorphism (RFLP) considered a gold standardfor M. tuberculosis genotyping in early nineties (van Embden et al.,1993), was too cumbersome, time consuming, and required largeamounts of highly purified DNA. Subsequently, it was replaced byspoligotyping a PCR-based method targeting the direct repeat (DR)locus which is well conserved and stable enough in tubercle bacilli,making it possible to discriminate various members of the M.
tuberculosis complex (Kamerbeek et al., 1997). Simple andeconomical, spoligotyping has shown its usefulness for strainidentification, to correctly identify ‘‘outbreak’’ episodes, as well asthe spread of the disease due to human migratory movements(Bauer et al., 1999; Brudey et al., 2006a,b; Candia et al., 2007;Kamerbeek et al., 1997; Kibiki et al., 2007; Streicher et al., 2004). Itis significantly more discriminative than IS6110-RFLP for M.
tuberculosis clinical isolates containing few copies of IS6110 (Baueret al., 1999; Kremer et al., 1999), and results obtained are easilyconverted in a numerical format (binary or octal codes) facilitatingglobal database construction and exchange of results betweenlaboratories (Brudey et al., 2006a; Filliol et al., 2003). Today, thespoligotyping method in conjunction with variable-numbertandem repeats of mycobacterial interspersed repetitive units(MIRU-VNTRs) has been adopted as a new gold-standard for TBmolecular epidemiology as well as precise phylogeographicalcharacterization of emerging clones (Rastogi and Sola, 2007). Thenumber of MIRU-VNTR loci analyzed was limited initially to 12-loci (Supply et al., 2001; Sola et al., 2003), but recently extended to15-loci for epidemiological studies (Alonso-Rodrıguez et al., 2008),and to 24-loci for an extended phylogenetical analysis (Supplyet al., 2006).
In this study, we present a fine molecular characterization ofcirculating M. tuberculosis strains in the twin island Republic ofTrinidad and Tobago (T&T) using spoligotyping and MIRU-VNTRs.Human immunodeficiency virus (HIV) infection is one of the mainfactors fuelling the TB epidemic in T&T (HIV prevalence of 3.2%among adults in 2003; https://www.cia.gov/library/publications/the-world-factbook/geos/td.html), characterized by an annual TBincidence rate of 17 cases/100,000 population with a high male tofemale sex ratio of 4, and a HIV/TB co-infection rate of 30%(Baboolal et al., 2009). We present novel evidence showing theemergence of a new clone in this island, yet not detected elsewherein the Caribbean but already present in United States as importedcases of disease among T&T-born patients.
2. Materials and methods
2.1. Genotyping
The study included all the TB patients presenting with a positiveM. tuberculosis culture over a 1-year period in T&T (n = 132,October 2006–September 2007). Patients were recruited in thevarious chest clinics and the Caura Chest Hospital, followed byculture, identification, drug susceptibility testing and DNApreparation at the Caribbean Epidemiology Centre (T&T) asreported in a previous study (Baboolal et al., 2009). The DNAsshipped to the Pasteur Institute of Guadeloupe were submitted tospoligotyping (Kamerbeek et al., 1997), classical 12-loci MIRU-typing (Supply et al., 2001), as well as recently-proposed 15-lociformat ideal for epidemiological investigations (Alonso-Rodrıguezet al., 2008), and extended 24-loci MIRU typing (Supply et al., 2006)
using published protocols. Results for MIRU typing performedmanually (Millet et al., 2007) were independently confirmed for aset of DNAs using automated high-throughput genotypingavailable commercially (Genoscreen, Lille, France).
2.2. Database comparison
Spoligotypes in binary format and 12-digit MIRU patterns wereentered in the SITVIT2 proprietary database of the Pasteur Instituteof Guadeloupe, which is an updated version of the previouslyreleased SpolDB4 database (Brudey et al., 2006a; available onlinehttp://www.pasteur-guadeloupe.fr:8081/SITVITDemo). At thetime of the present study, SITVIT2 contained genotyping informa-tion on more than 70,000 M. tuberculosis clinical isolates from 160countries of origin. In this database, spoligotype international type(SIT) designates spoligotyping shared by 2 or more patient isolates,whereas MIRU international type (MIT) designates 12-locus MIRUpatterns shared by 2 or more patient isolates as opposed to‘‘orphan’’ which designates patterns reported for a single isolate.
The 24-loci MIRU patterns were compared with the patternsfrom the MIRU-VNTRplus Database (http://www.miru-vntrplu-s.org) by using the Levenshtein algorithm (also called Edit-Distance) which permits to calculate the least number of editoperations that are necessary to modify one string to obtainanother string, where an operation is an insertion, deletion orsubstitution of a single character (http://www.levenshtein.net). Inour case, the distance was calculated between each of our 24-locipattern with all the patterns available online (n = 186) in theMIRU-VNTRplus database. A dynamic programming algorithm wasimplemented in-house using the perl programming language(http://www.cpan.org). The perl implementation is available uponrequest from Thomas Burguiere ([email protected]).
Major spoligotyping-based phylogenetic clades were assignedaccording to signatures provided in SpolDB4, which defines 62genetic lineages/sub-lineages (Brudey et al., 2006a). These includespecific signatures for M. tuberculosis complex members, as well asrules defining major lineages/sub-lineages for M. tuberculosis sensustricto, i.e., Central-Asian (CAS) clade and its 2 sublineages, theEast-African-Indian (EAI) clade with its 9 sublineages, the Haarlem(H) clade and its 4 sublineages, the Latin-American-Mediterranean(LAM) clade and its 12 sublineages, the ‘‘Manu’’ family and its 3sublineages, the IS6110-low banding X clade and its 3 sublineages,and an ill-defined T clade and their 13 sublineages.
2.3. Geographical distribution and phylogenetical analysis
The spoligotyping patterns observed in T&T strains (n = 132)were correlated to the patterns extracted from the SITIVIT2database for TB clinical isolates from 6 surrounding Caribbeanneighbors (n = 2653; Cuba n = 256, Haiti n = 404, Guadeloupen = 342, Martinique n = 158, Venezuela n = 927, French Guianan = 566). Major lineages were designated following SpolDB4 rules,and a map was drawn to compare the geographical distribution ofcirculating lineages. The evolutionary relationships between allthe spoligotype patterns in our sample from T&T were alsoinvestigated by drawing a minimum spanning tree (MST) usingBionumerics software (Version 3.5, Applied Maths, Sint-Marteen-Latem, Belgium). MST is an undirected network in which all thesamples are linked together with the smallest possible linkagesbetween nearest neighbors. In this approach, one considers that allintermediate stages are present within the sample analyzed, byincluding first the individual that shows most possible linkages toother individuals within the population studied. It summarizes thephylogenetic links between two spoligotypes differing by geneticchanges; the length of the branches indicates the level of changes
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–1344 1337

induced by loss or gain of spoligotype spacers in the 43-oligonucleotide format to induce a shift from one allele to another.Solid lines show a single spacer change, while dotted lines show 2or more spacer changes.
3. Results and discussion
3.1. Spoligotyping
Spoligotyping of the 132 isolates resulted in 12 clusters(n = 119, 2–74 strains per cluster), and 13 single patterns. Thepresence of a single large cluster (SIT566, n = 74) as opposed to 11
other smaller clusters (n = 45, 2–7 isolates per cluster) wasnoteworthy (Table 1). The available epidemiological data com-bined with spoligotypes data is provided as supplemental Table S1.The spoligotype-based lineage determination (Table 1) showedthat 57/132 or 43.2% of the clinical isolates were correctlyclassified among one of the lineages (including the single orphanpattern which was classified as AFRI-2 lineage). The highproportion of undetermined lineage attribution in T&T wasessentially due to the single largest cluster belonging to SIT566(n = 74) with an undefined lineage attribution. In addition, a singleunclustered strain corresponding to SIT450 was also labeled as‘‘undefined’’. Thus the major lineages observed ranked in the
Table 1Description of the spoligotypes (n = 132), and classical 12-loci and new 15-loci MIRU profiles for all strains other than SIT566 in Trinidad and Tobago (n = 58).
aClades were assigned following SpolDB4 rules; Unk: unknown patterns within any of the major clades described in SITVIT2.bNew SITs created after a match within this study (SIT2934) or with an orphan strain in SITVIT2 (SIT2935).cNew 12-loci MITs created after a match within this study (MIT1154, 1155, 1156) or with an orphan strain in SITVIT2 (MIT1157).dNA, Not applicable since a complete 12-loci MIRU pattern was not obtained for this isolate.
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–13441338

following order: LAM, 20/132 (15.2%), EAI, 17/132 (12.9%), X, 8/132(6.1%), Beijing, 6/132 (4.5%), ill-defined T, 2/132 (1.5%), Haarlem, 2/132 (1.5%), CAS, 1/132 (0.8%) and AFRI, 1/132 (0.8%). Detailedepidemiological data for strains classified within the 6 prevalentgenotypic groups (Beijing, EAI, LAM, LAM10-CAM, X, SIT566 clone)versus ‘‘other’’ strains (which grouped minor numbers of strainsbelonging to Harlem, Africanum, CAS, T, and undefined SIT450lineage) is provided as supplemental Table S2.
The important rate of clustered isolates (90.2%) in our studysuggests a high level of active TB transmission in T&T, and might belinked to the high HIV/TB coinfection rate observed (over 30%,results not shown). Similar clustering was seen in North Tanzaniawhere a high clustering rate was seen in a population with a highHIV/AIDS prevalence (Kibiki et al., 2007); indeed, the highprevalence of HIV infection is known to increase the risk ofdeveloping TB in a community (Odhiambo et al., 1999). Further-more, our study significantly led to the identification of a highlypredominant clone (SIT566) infecting more than half of thepatients that unexpectedly emerged as the major contributor tothe TB epidemic in T&T. The very high rate of clustering obtainedthrough genotyping (90.2% or 119/132) was mainly due to theover-representation of SIT566 in our setting. A search in theSITVIT2 database revealed the rare nature of this spoligotype,which was present only among 11 TB patients in USA, out of whichthe patient origin was known for 6 cases, all being originated fromT&T (J. Driscoll, personal communication).
3.2. Geographical distribution of genotypic lineages
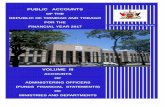
Regarding the geographic distribution of genotypic lineages inT&T (Fig. 1A), except for the SIT566 clone that mostly originated fromcentral St. George County (31.4% of all SIT566 patients, p < 0.05), andthe X lineage which was more often found in the East St Georgecounty as compared to other lineages (3/7 or 42.9% vs. 13/116 or11.2%; p < 0.05), no significant differences in the distribution forother lineages were observed. Beijing strains were limited to thethree counties of St. George West, St George Central, and St. Andrew/St. David, while the 2 isolates of the Haarlem lineage were limited tothe central county of Caroni. However, the number of patients fromindividual counties was too small to be statistically significant.Particular attention was therefore given to investigate the pre-dominant genotype SIT566 that represented 74/132 (56.1%) of all TBcases in T&T. With respect to its geographical distribution, 31.4% ofall SIT566 patients in T&T were from St George Central, the capitalcity of Port-of-Spain as compared to 15.1% of the patients harboring‘‘other genotypes’’ in T&T (p < 0.05).
The overall lineage distribution in T&T was completely differentfrom other Caribbean neighbors (Fig. 1B). First of all, thepredominant SIT566 clade from T&T was completely absentamong all the 2653 strains from 6 neighboring countries forwhich spoligotyping information was available in SITVIT2 data-base. Many of the strains belonging to EAI and CAS lineages foundin T&T were totally absent among the neighboring Caribbeancountries, and showed phylogeographical specificity for the Indiansubcontinent (ISC for India, Nepal, Pakistan, Bangladesh, Sri Lanka)in the SITVIT2 database, e.g., SIT126 (n = 90, ISC 44.5%), SIT138(n = 95, ISC 50.5%), SIT288 (n = 86 ISC 51.2%). Interestingly, thedistribution of remaining strains within these same shared-typeswas essentially limited to the countries with high proportion ofEast-Indian immigrants known to harbor EAI and CAS lineages inSITVIT2 database (UK, USA, Saudi Arabia), and represented 32.2%for SIT126, 27.4% for SIT138, and 33.7% for SIT288. In our setting,the strains corresponding to SIT126 (EAI) and SIT288 (CAS) wereisolated from East-Indian males aged 32 and 67 years (both HIV-negative). The EAI strains are highly prevalent in Far-East Asia,Middle East, Central Asia and Oceania (Brudey et al., 2006a). There
is a substantial amount of travel between Trinidad and Tobago andmany of the Asian countries especially India and Pakistan as almostone half of the population in Trinidad and Tobago is composed ofdescendants from these countries. When compared with othercountries of the Caribbean and South America, a similar proportionof EAI strains is only found in Guyana (our ongoing study, resultsnot shown).
As respect to LAM lineage, it is highly prevalent in Latin Americaand the Caribbean (Brudey et al., 2006a,b), nonetheless thedistribution of specific LAM lineage strains found in T&T ismarkedly different: it is the only country showing African LAM-10CAM lineage (present with its prototype SIT61; n = 6/132 and avariant SIT2550; n = 7/132), and LAM strains commonly foundelsewhere are absent from T&T (SIT17, SIT20, SIT93; Fig. 1B). Onthe contrary, T&T shares with its French-speaking Caribbeanneighbors (Haiti, Guadeloupe, and Martinique) the specificpresence of the X lineage (Fig. 1B) known to have phylogeogra-phical specificity for Anglo-Saxon descendants (Brudey et al.,2006a; Filliol et al., 2003; Rastogi and Sola, 2007). This lineage ispresent in Guadeloupe for decades, and could represent discontin-uous periods of English colonization during 1691–1816 (http://www.in-west-indies.com/guadeloupe/discover/history.htm).Among various sublineages, X1 is found in Haiti, Martinique andT&T, X2 in T&T alone, and X3 is absent from T&T but present inGuadeloupe and Haiti (Fig. 1B).
We found 6 strains of the Beijing family, majority being isolatedfrom patients below 45 years of age. Beijing strains werepreviously associated with mostly younger persons in Vietnam,thought to be an indicator of recent and ongoing transmission (Anhet al., 2000). Beijing isolates were also considered as hypervirulent(van Soolingen et al., 1995), however, contrary to MDRTB Beijinggenotypes observed in Vietnam, Korea, Hong-Kong, Russia, andother East-European countries (Anh et al., 2000; Bifani et al., 1999;European concerted action, 2006; Glynn et al., 2002), all our strainswere pansusceptible. This absence of drug resistance in T&T issurprising especially with the high levels of TB/HIV co-infection(30.6% of the TB-positive cases) and the high defaulter rate (22.7%of the TB-positive cases).
Lastly, we also observed a relatively small number of strains ofthe Haarlem lineage (1.5%) and the ill-defined T super family (1.6%)in T&T, although they represented around 25% and 20%,respectively, of the strains found in Guadeloupe, Martinique andFrench Guiana (Fig. 1B) (Brudey et al., 2006b). The Haarlemlineages H1 (SIT47) and H3 (SIT50) are prevalent in Europe and H2(SIT2) is mainly found into the Caribbean and Latin Americaprobably due to previous colonization by Europeans. Contrarily, inVenezuela and T&T the proportion of clones of the Haarlem lineageonly represented 4.5% (42/927) and 1.5% (2/132), respectively, ofthe patterns identified in those countries. The Haarlem clade is ofEuropean origin and is highly prevalent in Northern Europe(Brudey et al., 2006a; Filliol et al., 2003), and has been reported tobe highly present in the Caribbean where European colonizationwas evident (Brudey et al., 2006b). This result could underline acommon past history between T&T and Venezuela with limitedactual links with Europe. Lastly, the low proportion of T lineagestrains in T&T is noteworthy. This lineage was defined ‘‘by default’’to regroup ill-defined spoligotype patterns. It essentially includesubiquitous spoligotypes; e.g., SIT53 the prototype pattern of the Tlineage which is widely spread in the world (Brudey et al., 2006a;Filliol et al., 2003).
3.3. Evolutionary relationships among spoligotypes and lineages
The evolutionary relationships between all the spoligotypepatterns in our sample from T&T were investigated using aminimum spanning tree (MST) illustrated in Fig. 1C. Based on the
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–1344 1339

suggestion by van Embden et al. (2000) that the evolution of the DRlocus proceed by deletion of single or adjacent direct variablerepeats (DVRs), we drew a MST that was set to integrate data basedboth on single or multiple DVR deletions. The central node of thisunrooted tree is represented by SIT53, which is the prototype of theT1 lineage. It allowed the identification of 4 groups of strains thatcould easily shift from one state to another by a single or doublespacer changes, tentatively referred to as group A (SIT2934 and2935 of EAI2-Manilla lineage), B (SIT17, 42, 60, 64,93,1710 of
various LAM sublineages), C (SIT61, 2550 of LAM10-CAM), and D(SIT50, 53, 73, 119, 1823 of various lineages—X, T and H). Wefurther investigated if there was a link between availabledemographic and epidemiological data (sex-ratio, HIV serologyand ethnicity) and these closely related groups of spoligotypes,which showed the following distribution patterns: group A (sex-ratio 3.3, HIV serology and ethnicity known for 11/13 patients, 6/11 or 55% HIV-positive, 9/11 or 82% African descendants), group B(sex-ratio 6.0, none HIV-positive, 5/7 or 71% African descendants),
Fig. 1. Geographical distribution and evolutionary relationships among spoligotypes and genotypic lineages observed. (A) Origin of patients and distribution of genotypic
lineages in Trinidad and Tobago. (B) Distribution of genotypic lineages in surrounding Caribbean neighbors (representing 2653 clinical isolates in the SITVIT2 database; Cuba
n = 256, Haiti n = 404, Guadeloupe n = 342, Martinique n = 158, Venezuela n = 927, French Guiana n = 566). (C) Minimum spanning tree showing evolutionary relationships
among spoligotypes and lineages observed in Trinidad & Tobago. The length of the branches indicates the level of changes induced by loss or gain of spoligotype spacers to
induce a shift from one allele to another (solid lines, single spacer change; dotted lines, 2 or more spacer changes; color of circles shows number of isolates: sky-blue, 1 to 2
isolates; marine blue, 3 to 5 isolates; deep blue, 6–8 strains; and red, >8 strains). Clades were assigned following SpolDB4 rules; CAS (Central-Asian), EAI (East-African-
Indian), H (Haarlem), LAM (Latin-American-Mediterranean), X (the IS6110-low banding X clade), T (ill-defined T clade), Unk, unknown patterns within any of the major clades
described. Lastly, 4 closely related groups of strains are tentatively labeled as groups A–D (see text for details). (For interpretation of the references to color in this figure
legend, the reader is referred to the web version of the article.)
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–13441340

group C (sex-ratio 3.3, HIV serology and ethnicity known for 12/13patients, 3/12 or 25% HIV-positive, 9/12 or 75% African descen-dants), and group D (sex-ratio 2.0, 1/9 or 11% HIV-positive, 5/9 or56% East-Indians). Apparently, the 2 newly described shared-typesin T&T (group A, SIT2934 and 2935) are mostly isolated from HIV-positive males of African descent, an observation whose sig-nificance could not be evaluated statistically because of the smallnumbers of patients analyzed in each group.
The group A strains (n = 13 for 2 patterns) are linked to other EAIstrains in this tree via SIT126, but intermediate stages of evolutionare missing in our setting. A search in the database suggested that arare SIT342 (n = 15) present in former French and British coloniescould be this hypothetical missing link (results not shown). Thegroup B strains (n = 7 for 6 patterns) were made up of various LAMsublineages that differed only by a single spacer change suggestingan ongoing transmission and evolution of these strains. The groupC strains (n = 13 for 2 patterns) belonged to the LAM10-CAMsublineage with phylogeographical specificity for Cameroon andneighboring countries in West Africa (Brudey et al., 2006a,b;Niobe-Eyangoh et al., 2004). Interestingly, 75% of the patients inthe LAM10-CAM sublineage group in our study were Africandescendants. Finally, the group D (n = 9 for 5 patterns) was mostphylogenetically diversified as it contained spoligotypes aroundthe central node made up of SIT53 (T1 prototype), which had as itsnearest neighbors SIT50 (Haarlem3 prototype) on one end, andSIT119 (X1 prototype) with a single spacer change and SIT73 (ill-defined T lineage) with a 2 spacer change on the other end.
Regarding the predominant SIT566 (Fig. 1C), it was situatedclose to the group D strains, in particular to the X1 prototypeSIT119, with which it varied with more than 4 changes (see thebinary patterns shown in Table 1). A parallel neighbor-joining (NJ)tree suggested that the undefined SIT566 is closer to strains of theX lineage than to other lineages such as the T (results not shown).Lastly, Fig. 1C grouped distinctly the strains belonging to theprincipal genetic group 1 (PGG1, ancestral and/or evolutionaryolder) and PGG2/3 (modern tubercle bacilli, easily characterized inspoligotyping by the lack of spacers 33–36), as defined previouslyusing KatG463-gyrA95 polymorphism (Brudey et al., 2006a; Rastogiand Sola, 2007; Singh et al., 2007; Sreevatsan et al., 1997). In total,only 25/132 (18.9%) of the strains from T&T belonged to the PGG1(such as EAI, Beijing, CAS, and AFRI), as opposed to nearly 90% of theclustered isolates in India (Singh et al., 2007).
3.4. MIRU typing
The classical 12-loci and the new 15-loci MIRU-typing wereinitially performed on a panel of 58 isolates (11 spoligotyping-defined clusters containing 45 strains and 13 singletons) otherthan the predominant SIT566 spoligotype. The 12-loci patternssplit this panel in a total of 31 SIT-MIT combinations (Table 1),among which 8 profiles preexisted in the SITVIT2 database (SIT1-MIT84, SIT50-MIT33, SIT53-MIT770, SIT60-MIT25, SIT93-MIT25,SIT42-MIT25, SIT119-MIT34, and SIT478-MIT34); interestingly, 4/8 were identified in surrounding countries such as Guadeloupe,Martinique, French Guiana, and Haiti (results not shown). Thissuggests the specificity of SIT-MIT combinations found in T&T, aswell as a relative affinity for the Caribbean neighbors.
As illustrated in Table 1, a total of 8 clusters remained aftercombined spoligotyping + 12-loci MIRUs (SIT2934-MIT1154,SIT2935-MIT1154, SIT61-MIT1155, SIT61-MIT1156, SIT2550-MIT263, SIT478-MIT34, SIT1-MIT491, SIT50-MIT33), and com-prised a total of 32 strains. Additional typing using 15-loci MIRU-VNTR led to 7 clusters comprising 27 strains (Table 1); theseincluded 4 previously defined clusters (SIT61-MIT1155, SIT478-MIT34, SIT2550-MIT263, SIT2934-MIT1154) that remainedunsplitted. Out of 27 clustered cases, ethnicity, gender, and HIV
serology information was available for 24, 26, and 24 patients,respectively. Clustered strains involved African descendants(n = 20/24 patients), of male gender (n = 21/26 patients), reflectingthe overall population structure of the patients since these valueswere not statistically significant as compared to the unclusteredgroup for which this information was available (African descen-dants 16/19, male gender 16/20). Nonetheless, the proportion ofHIV positive patients in the clustered group (10/24) wassignificantly higher that the unclustered group (3/22, p < 0.05).
Regarding the predominant SIT566 (T&T clone), a set repre-senting 1/3rd of all strains (25/74 of SIT566 isolates) was selectedfor detailed molecular characterization using all the 3 sets of MIRUloci, i.e., the classical 12-loci, the new 15-loci MIRU-typing recentlyproposed to be ideal for epidemiological investigations (Alonso-Rodrıguez et al., 2008), as well as the extended 24-loci forphylogenetical characterization (Supply et al., 2006). The resultsobtained are summarized in Tables 1–3. The classical 12-locityping (Table 2) provided following patterns: 224315153324(MIT633, n = 21), 224315153323 (MIT27, n = 1), 224325143324(MIT117, n = 1), 224215153324 (MIT1158, n = 1), and224315153424 (orphan). A search into the database showed thatthese MITs were differently represented worldwide: MIT1158 waslimited to USA (1 strain), MIT27 and MIT117 were shared by 15 and70 strains from 7 and 9 countries, respectively (Belgium, Croatia,Spain, Great Britain, Senegal, Sweden, and USA for MIT27; andBelgium, Canada, Croatia, Germany, Great Britain, French Guiana,USA and South Africa for MIT117). Except MIT117 found for 2clinical isolates in French Guyana, none of those MITs haspreviously been identified in the Caribbean, Central or SouthAmerica.
MIT633 was the most predominant pattern in our study. It wasfound in 21/25 of SIT566 strains (Table 2), as well as 3 other SITs,namely SIT70, SIT450, and SIT1823 (Table 1). SIT70 belonged toX3_var, SIT1823 to X1, whereas SIT450 belonged to a yet undefinedsignature, but shared the absence of spacer 18 with the X-lineagestrains. In the SITVIT2 database, MIT633 was rarely reported forcountries other than T&T with only 12 strains in 3 countries (Spain,n = 1, origin Peru; Great Britain, n = 2, origin unknown; USA, n = 9,origin unknown n = 6, origin T&T, n = 3). Spoligotyping data wereavailable in parallel for 10/12 MIT633 strains, 5 out of which werestrictly identical to SIT566 (absence of spacers 14–18, 33–36, and40). All these 5 strains were isolated in USA, and 3 corresponded toT&T-born patients, which constitutes an evidence for the spread ofthis T&T-specific clone of M. tuberculosis to the United States.
An interesting information concerned the incomplete MIRUpattern 2243*5153324 (a SIT119 strain belonging to the X lineage;Table 1). Except for the single missing value for MIRU-20, it isidentical to MIT633 ( ), the predominant 12-lociMIRU pattern of SIT566 clone in T&T as well as MIT34( ) in our study (Table 1). The SITVIT2 databasecontained a total of 146 MIT34 isolates, with spoligotypes beingavailable for 72/146 strains, and as high as 87.5% belonged to the Xlineage. This data not only permits to label MIT34 as specific to theX lineage, but further argues in favor of the phylogenetical link ofMIT633 to the X lineage. This assumption is further strengthenedby the fact that in the present study, we also found MIT633among strains other than SIT566 (Table 1), often classified intothe X lineage, i.e., SIT70 (X3-var), SIT1823 (X1 var), SIT450(undefined). Interestingly, the 15-loci MIRU patterns obtained forthe SIT566 strains (Table 2; a total of 8 individual patternsfor 25 strains), revealed a high similarity to the SIT1823-MIT633pattern corresponding to the X1 lineage (Table 1, pattern243534334833323). Indeed, 6 of the 8 patterns were single locusvariant (SLV) of the SIT1823-MIT633 strain.
Addition of 12-loci of the 24-loci MIRU typing scheme allowedidentification of 3 supplemental patterns but globally, strains with
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–1344 1341

SIT566 remained remarkably clustered. A comparison of the 24-loci MIRU patters obtained with the international MIRU-VNTRplusdatabase (http://www.miru-vntrplus.org) revealed that none ofthe strains out of the 186 present in this database matched ourprofiles. Consequently, we decided to compare our patterns withthe MIRU-VNTRplus database by using the Levenshtein algorithm(http://www.levenshtein.net) which permits to calculate the leastnumber of edit operations that are necessary to modify one stringto obtain another string. For example, the Levenshtein distancebetween the word ‘‘kitten’’ and ‘‘sitting’’ is 3, since the followingthree edits change one into the other, and there is no way to do itwith fewer than three edits: kitten! sitten (substitution of ‘s’ for‘k’); sitten! sittin (substitution of ‘i’ for ‘e’); sittin! sitting (insert‘g’ at the end). We calculated the distance between each of our 24-loci MIRU patterns with all the 186 patterns available online in theMIRU-VNTRplus database, and the first 5 closest matches, as wellas our predominant pattern ‘‘224315153324323483334323’’ (16/
21 MIT633 isolates), are shown in Table 3. Regarding the changesobserved between patterns, MIRU 2, 4, 23, 24, 27, 39, ETR-A, B, C,QUB 4156, Mtub 29, and 34 were entirely invariable. Among the 5strains identified, the first 2 matches belonged to the X lineage(SIT119) and 3 following ones to the Haarlem clade (Table 3).Independently of their clade attribution, all these 5 strains werepansusceptible to antituberculous drugs, and belonged to theEuro-American lineage according to the classification proposed byGagneux and Small (2007). Thus the suggestion made earlier aboutthe probable relationship of the SIT566 to the X1 prototype SIT119using spoligotyping-based analysis (Fig. 1C) is further corrobo-rated using 24-loci MIRU typing. We hypothesize that thepredominant SIT566 clone might have evolved locally in T&Tfrom a pool of X lineage M. tuberculosis strains with phylogeo-graphical affinity for Anglo-Saxon descendants.
Last but not least, it is worth mentioning that the bulk ofdiscrimination obtained within the 25 strains of the SIT566 clone
Table 2Classical 12-loci MIRU patterns and associated MIT designations as compared to extended MIRU typing using 12-additional loci for a selected panel of 25 strains belonging to
SIT566.
aMIRU international type (MIT) designates 12-loci MIRU patterns shared by 2 or more patient isolates in the SITVIT2 database.bNew 15-loci format ideal for epidemiological investigations (Alonso-Rodrıguez et al., 2008) corresponds to 6-loci in the classical 12-loci MIRU format (column A), and 9-loci
out of the additional 12-loci (column B); it is highlighted in blue color for easy identification.cOrphan designates patterns reported for a single isolate in the SITVIT2 database.
Table 3Comparison of 24-loci MIRU patterns for MIT633 strains and its variants shown in Table 2 with the 24-loci patterns reported in the MIRU-VNTRplus database. Only the first
five closest matches based on the Levenshtein edit distances between each of our patterns and every pattern of VNTRplus are shown.
aCorresponding 12-loci MIRU international type in SITVIT2 database.bIdentification number in MIRU-VNTRplus database.cCorresponding spoligotype international type in SITVIT2 database.dClades were assigned following SpolDB4 rules.eLarge sequence polymorphism (LSP)-based lineages according to Gagneux and Small (2007).
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–13441342

was achieved by the 15-loci MIRU typing, and the only exceptionconcerned a variation for MIRU-20 loci in a MIT117 strain (Table 2).This observation indirectly suggests that we are in the presence ofa highly conserved clone of M. tuberculosis (SIT566) that hasprobably only recently evolved and expanded in T&T.
3.5. Conclusion
In summary, available information underlines that we are inthe presence of a highly conserved clone of M. tuberculosis(SIT566) that has probably only recently evolved and expandedin T&T. Indeed, the spoligotyping data coupled to MIRU typing,and available epidemiological data suggests that the ongoingtransmission in T&T is essentially due to a single major clone of‘‘evolutionary modern’’ (PGG2/3) tubercle bacilli, apparentlyresponsible for more than half of the TB cases. This clone (SIT566)preferentially infects younger age groups (mean 39.1 years vs.47.7 years for other genotypes, p < 0.0005), and is overrepre-sented in St George Central, the capital city of Port-of-Spain (1out of 3 patients). This clone is highly conserved withphylogeographically specific to T&T, yet without any transmis-sion to the neighboring Caribbean islands. The only exception forthe time being is limited to 11 TB cases observed in USA, out ofwhich the patient origin was known for 6 cases, all beingoriginated from T&T (J. Driscoll, personal communication). Asexplained previously, the longer a clone takes to evolve, the moreextensive will be the observed genetic diversity (Rastogi andSola, 2007), hence the exceptionally limited 24-loci MIRU-basedpolymorphism of the SIT566 clone argues in favor of its relativelyrecent, and endemic emergence in T&T. Whether the high affinityof SIT566 to T&T is linked to the possibility of a stable associationbetween M. tuberculosis strains and their human host popula-tions (Hirsh et al., 2004), or due to another selection pressure, hasto be further studied. This clone will now be investigated usingSNPs and LSPs-based characterization to see its localizationwithin evolutionary-recent TB lineages (Filliol et al., 2006;Gagneux and Small, 2007).
Acknowledgments
JM was awarded a Ph.D. fellowship by the European SocialFunds through the Regional Council of Guadeloupe. The work doneat the Pasteur Institute of Guadeloupe was financed by theRegional Council of Guadeloupe (CR/08-1612: Biodiversite etRisque Infectieux dans les modeles insulaires). SB is grateful to theUniversity of West Indies for financial support, to L. Francis fortechnical assistance, and to Dr. A. Rattan, and Dr. J. Campione-Piccardo, Caribbean Epidemiology Center, Trinidad & Tobago, fortheir help. The authors thank Dr. A. Cumberbatch, Chief MedicalOfficer, Trinidad & Tobago for granting permission to use M.
tuberculosis isolates in this study. We also acknowledge theassistance of the staff of the Chest Clinics at the Eric WilliamsMedical Sciences Complex, the San Fernando General Hospital, andTrinidad Public Health Laboratory for data collection, and to T.Burguiere, Bioinformatics engineer at Institut Pasteur de laGuadeloupe for in-house implementation of the Levenshteinalgorithm using the perl programming language. NR and JM thankDr. J. Driscoll for providing information regarding the SIT566 clonein USA.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.meegid.2009.09.006.
References
Alonso-Rodrıguez, N., Martınez-Lirola, M., Herranz, M., Sanchez-Benitez, M., Bar-roso, P., group, INDAL-TB., Bouza, E., Garcıa de Viedma, D., 2008. Evaluation ofthe new advanced 15-loci MIRU-VNTR genotyping tool in Mycobacteriumtuberculosis molecular epidemiology studies. BMC Microbiol. 8, 34.
Anh, D.D., Borgdorff, M.W., Van, L.N., Lan, N.T., van Gorkom, T., Kremer, K., vanSoolingen, D., 2000. Mycobacterium tuberculosis Beijing genotype emerging inVietnam. Emerg. Infect. Dis. 6, 302–305.
Baboolal, S., Millet, J., Akpaka, P.E., Ramoutar, D., Rastogi, N., 2009. First Insight intoMycobacterium tuberculosis epidemiology and genetic diversity in Trinidad andTobago. J. Clin. Microbiol. 47, 1911–1914.
Bauer, J., Anderson, A.B., Kremer, K., Miorner, H., 1999. Usefulness of spoligotypingto discriminate IS6110 low copy number Mycobacterium tuberculosis complexstrains cultured in Denmark. J. Clin. Microbiol. 37, 2602–2606.
Bennett, D.E., Onorato, I.M., Ellis, B.A., Crawford, J.T., Schable, B., Byers, R., Kam-merer, J.S., Braden, C.R., 2002. DNA fingerprinting of Mycobacterium tuberculosisisolates from epidemiologically linked case pairs. Emerg. Infect. Dis. 8, 1224–1229.
Bifani, P.J., Mathema, B., Liu, Z., Moghazeh, S.L., Shopsin, B., Tempalski, B., Driscol, J.,Frothingham, R., Musser, J.M., Alcabes, P., Kreiswirth, B.N., 1999. Identificationof a W-variant outbreak of Mycobacterium tuberculosis via population-basedmolecular epidemiology. JAMA 282, 2321–2327.
Brudey, K., Driscoll, J.R., Rigouts, L., Prodinger, W.M., Gori, A., Al-Hajoj, S.A., Allix, C.,Aristimuno, L., Arora, J., Baumanis, V., Binder, L., Cafrune, P., Cataldi, A., Cheong,S., Diel, R., Ellermeier, C., Evans, J.T., Fauville-Dufaux, M., Ferdinand, S., Garcia deViedma, D., Garzelli, C., Gazzola, L., Gomes, H.M., Gutierrez, M.C., Hawkey, P.M.,van Helden, P.D., Kadival, G.V., Kreiswirth, B.N., Kremer, K., Kubin, M., Kulkarni,S.P., Liens, B., Lillebaek, T., Ly, H.M., Martin, C., Mokrousov, I., Narvskaia, O.,Ngeow, Y.F., Naumann, L., Niemann, S., Parwati, I., Rahim, M.Z., Rasolofo-Razanamparany, V., Rasolonavalona, T., Rossetti, M.L., Rusch-Gerdes, S., Saj-duda, A., Samper, S., Shemyakin, I., Singh, U.B., Somoskovi, A., Skuce, R., vanSoolingen, D., Streicher, E.M., Suffys, P.N., Tortoli, E., Tracevska, T., Vincent, V.,Victor, T.C., Warren, R., Yap, S.F., Zaman, K., Portaels, F., Rastogi, N., Sola, C.,2006a. Mycobacterium tuberculosis complex genetic diversity: mining the fourthinternational spoligotyping database (SpolDB4) for classification, populationgenetics and epidemiology. BMC Microbiol. 6, 23.
Brudey, K., Filliol, I., Ferdinand, S., Guernier, V., Duval, P., Maubert, B., Sola, C.,Rastogi, N., 2006b. Long-term population-based genotyping study of Mycobac-terium tuberculosis complex isolates in the French departments of the Americas.J. Clin. Microbiol. 44, 83–191.
Candia, N., Lopez, B., Zozio, T., Carrivale, M., Diaz, C., Russomando, G., de Romero,N.J., Jara, J.C., Barrera, L., Rastogi, N., Ritacco, V., 2007. First insight intoMycobacterium tuberculosis genetic diversity in Paraguay. BMC Microbiol. 7, 75.
Ellis, B.A., Crawford, J.T., Braden, C.R., McNabb, S.J., Moore, M., Kammerer, S., 2002.Molecular epidemiology of tuberculosis in a sentinel surveillance population.Emerg. Infect. Dis. 8, 1197–1209.
European concerted action on new generation genetic markers and techniques forthe epidemiology control of tuberculosis, 2006. Beijing/W genotype Mycobac-terium tuberculosis and drug resistance. Emerg. Infect. Dis. 12, 736–743.
Filliol, I., Driscoll, J.R., van Soolingen, D., Kreiswirth, B.N., Kremer, K., Valetudie, G.,Dang, R., Barlow, D.A., Banerjee, D., Bifani, P.J., Brudey, K., Cataldi, A., Cooksey,R.C., Cousins, D.V., Dale, J.W., Dellagostin, O.A., Drobniewski, F., Engelmann, G.,Ferdinand, S., Gascoyne-Binzi, D., Gordon, M., Gutierrez, M.C., Haas, W.H.,Heersma, H., Kassa-Kelembho, E., Ho, M.L., Makristathis, A., Mammina, C.,Martin, G., Mostrom, P., Mokrousov, I., Narbonne, V., Narvskaya, O., Nastasi,A., Niobe-Eyangoh, S.N., Pape, J.W., Rasolofo-Razanamparany, V., Ridell, M.,Rossetti, M.L., Stauffer, F., Suffys, P.N., Takiff, H., Texier-Maugein, J., Vincent, V.,de Waard, J.H., Sola, C., Rastogi, N., 2003. Snapshot of moving and expandingclones of Mycobacterium tuberculosis and their global distribution assessed byspoligotyping in an international study. J. Clin. Microbiol. 41, 1963–1970.
Filliol, I., Motiwala, A.S., Cavatore, M., Qi, W., Hazbon, M.H., Bobadilla del Valle, M.,Fyfe, J., Garcıa-Garcıa, L., Rastogi, N., Sola, C., Zozio, T., Guerrero, M.I., Leon, C.I.,Crabtree, J., Angiuoli, S., Eisenach, K.D., Durmaz, R., Joloba, M.L., Rendon, A.,Sifuentes-Osornio, J., Ponce de Leon, A., Cave, M.D., Fleischmann, R., Whittam,T.S., Alland, D., 2006. Global phylogeny of Mycobacterium tuberculosis based onsingle nucleotide polymorphism (SNP) analysis: insights into tuberculosisevolution, phylogenetic accuracy of other DNA fingerprinting systems, andrecommendations for a minimal standard SNP set. J. Bacteriol. 188, 759–772(Erratum in: J. Bacteriol., 188 (2006) 3162–3163).
Gagneux, S., Small, P.M., 2007. Global phylogeography of Mycobacterium tubercu-losis and implications for tuberculosis product development. Lancet Infect. Dis.7, 328–337.
Glynn, J.R., Whiteley, J., Bifani, P.J., Kremer, K., van Soolingen, D., 2002. Worldwideoccurrence of Beijing/W strains of Mycobacterium tuberculosis: a systematicreview. Emerg. Infect. Dis. 8, 843–849.
Hirsh, A.E., Tsolaki, A.G., DeRiemer, K., Feldman, M.W., Small, P.M., 2004. Stableassociation between strains of Mycobacterium tuberculosis and their human hostpopulations. Proc. Natl. Acad. Sci. U.S.A. 101, 4871–4876.
Kamerbeek, J., Schouls, L., Kolk, A., van Agterveld, M., van Soolingen, D., Kuijper, S.,Bunschoten, A., Molhuizen, H., Shaw, R., Goyal, M., van Embden, J., 1997.Simultaneous detection and strain differentiation of Mycobacterium tuberculosisfor diagnosis and epidemiology. J. Clin. Microbiol. 35, 907–914.
Kibiki, G.S., Mulder, B., Dolmans, W.M.V., de Beer, J.L., Boeree, M., Sam, N., vanSoolingen, D., Sola, C., van der Zanden, A.G.M., 2007. Mycobacterium tuberculosis
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–1344 1343

genotypic diversity and drug susceptibility pattern in HIV-infected and non-HIV-infected patients in Northern Tanzania. BMC Microbiol. 7, 51.
Kremer, K., van Soolingen, D., Frothingham, R., Haas, W.H., Hermans, P.W., Martin,C., Palittapongampim, P., Plikaytis, B., Riley, L.W., Yakrus, M.A., Musser, J.M., vanEmbden, J.D., 1999. Comparison of methods based on different molecularepidemiological markers for typing of Mycobacterium tuberculosis complexstrains: interlaboratory study of discriminatory power and reproducibility. J.Clin. Microbiol. 37, 2607–2618.
Millet, J., Miyagi-Shiohira, C., Yamane, N., Sola, C., Rastogi, N., 2007. Assessment ofmycobacterial interspersed repetitive unit-QUB markers to further discrimi-nate the Beijing genotype in a population-based study of the genetic diversity ofMycobacterium tuberculosis clinical isolates from Okinawa, Ryukyu Islands,Japan. J. Clin. Microbiol. 45, 3606–3615.
Niobe-Eyangoh, S.N., Kuaban, C., Sorlin, P., Thonnon, J., Vincent, V., Gutierrez, M.C.,2004. Molecular characteristics of strains of the Cameroon family, the majorgroup of Mycobacterium tuberculosis in a country with a high prevalence oftuberculosis. J. Clin. Microbiol. 42, 5029–5035.
Odhiambo, J.A., Borgdorff, M.W., Kiambih, F.M., Kibuga, D.K., Kwamanga, D.O.,Ng’ang’a, L., Agwanda, R., Kalisvaart, N.A., Misljenovic, O., Nagelkerke, N.J.,Bosman, M., 1999. Tuberculosis and HIV the epidemic: increasing annual riskof infection in Kenya. 1986–1996. Am. J. Public Health 89, 1078–1082.
Rastogi, N., Sola, C., 2007. Molecular evolution of the Mycobacterium tuberculosiscomplex. In: Palomino, J.C., Leao, S., Ritacco, V. (Eds.), Tuberculosis 2007.Amedeo Online Textbooks, pp. 53–91., http://www.tuberculosistextbook.com/index.htm.
Singh, U.B., Arora, J., Suresh, N., Pant, H., Rana, T., Sola, C., Rastogi, N., Pande, J.N.,2007. Genetic biodiversity of Mycobacterium tuberculosis isolates from patientswith pulmonary tuberculosis in India. Infect. Genet. Evol. 7, 441–448.
Small, P.M., Hopewell, P.C., Singh, S.P., Paz, A., Parsonnet, J., Ruston, D.C., Schecter,G.F., Daley, C.L., Schoolnik, G.K., 1994. The epidemiology of tuberculosis in SanFrancisco. A population-based study using conventional and molecular meth-ods. N. Engl. J. Med. 330, 1703–1709.
Sola, C., Filliol, I., Legrand, E., Lesjean, S., Locht, C., Supply, P., Rastogi, N., 2003.Genotyping of the Mycobacterium tuberculosis complex using MIRUs: associa-
tion with VNTR and spoligotyping for molecular epidemiology and evolutionarygenetics. Infect. Genet. Evol. 3, 125–133.
Sreevatsan, S., Pan, X., Stockbauer, K.E., Connell, N.D., Kreiswirth, B.N., Whittam, T.S.,Musser, J.M., 1997. Restricted structural gene polymorphism in the Mycobac-terium tuberculosis complex indicates evolutionarily recent global dissemina-tion. Proc. Natl. Acad. Sci. U.S.A. 94, 9869–9874.
Streicher, E.M., Warren, R.M., Kewlwy, C., Simpson, J., Rastogi, N., Sola, C., van derSpuy, G.D., van Helden, P.D., Victor, T.C., 2004. Genotypic and phenotypiccharacterization of drug resistant Mycobacterium tuberculosis isolates from ruraldistricts of Western Cape Province of South Africa. J. Clin. Microbiol. 42, 891–894.
Supply, P., Lesjean, S., Savine, E., Kremer, K., van Soolingen, D., Locht, C., 2001.Automated high-throughput genotyping for study of global epidemiology ofMycobacterium tuberculosis based on mycobacterial interspersed repetitiveunits. J. Clin. Microbiol. 39, 3563–3571.
Supply, P., Allix, C., Lesjean, S., Cardoso-Oelemann, M., Rusch-Gerdes, S., Willery, E.,Savine, E., de Haas, P., van Deutekom, H., Roring, S., Bifani, P., Kurepina, N.,Kreiswirth, B., Sola, C., Rastogi, N., Vatin, V., Gutierrez, M.C., Fauville, M.,Niemann, S., Skuce, R., Kremer, K., Locht, C., van Soolingen, D., 2006. Proposalfor standardization of optimized mycobacterial interspersed repetitive unit-variable-number tandem repeat typing of Mycobacterium tuberculosis. J. Clin.Microbiol. 44, 4498–4510.
van Embden, J.D., Cave, M.D., Crawford, J.T., Dale, J.W., Eisenach, K.D., Gicquel, B.,Hermans, P., Martin, C., McAdam, R., Shinnick, T.M., Small, P., 1993. Strainidentification of Mycobacterium tuberculosis by DNA fingerprinting: recommen-dations for a standardized methodology. J. Clin. Microbiol. 31, 406–409.
van Embden, J.D., van Gorkom, T., Kremer, K., Jansen, R., van Der Zeijst, B.A., Schouls,L.M., 2000. Genetic variation and evolutionary origin of the direct repeat locusof Mycobacterium tuberculosis complex bacteria. J. Bacteriol. 182, 2393–2401.
van Soolingen, D., Qian, L., de Haas, P.E.W., Douglas, J.T., Traore, H., Portaels, F., Qing,D., Enkhsaikan, H.Z., Nymadawa, P., van Embden, J.D.A., 1995. Predominance ofa single genotype of Mycobacterium tuberculosis in countries of East Asia. J. Clin.Microbiol. 33, 3234–3238.
J. Millet et al. / Infection, Genetics and Evolution 9 (2009) 1336–13441344

Infection, Genetics & Evolution
Phylogeographical and molecular characterization of an emerging Mycobacterium tuberculosis clone in Trinidad and Tobago Julie Millet, Shirematee Baboolal, Patrick Eberechi Akpaka, Dottin Ramoutar, and Nalin Rastogi*
Supplemental Table S1: Epidemiological data available for the 132 patients combined with spoligotypes data of the corresponding M. tuberculosis complex clinical isolates.
Genotypic lineages
Genotypic lineage SIT Year of
isolation Age Sex HIV
Geographical
origin of patients(a)
Ethnicity
(b) Status
(c)
Beijing Beijing 1 2007 40 M - SGW AD D
Beijing 1 2007 63 M - SASD EI N
Beijing 1 2007 43 M + SGC AD D
Beijing 1 2007 29 F - SGW AD N
Beijing 1 2007 30 F + SGW AD N
Beijing 1 2007
EAI EAI 126 2007 32 M - SGW EI N
EAI 138 2007 30 F - SGE M N
EAI1-SOM var 958 2006 50 M - SGC AD TF
EAI1-SOM var 958 2007 25 M - SGW AD N
EAI2-Manilla var 2935 2007 54 M + SGC AD RT
EAI2-Manilla var 2934 2007 57 M + SGE AD RT
EAI2-Manilla var 2934 2007 32 F - C AD N
EAI2-Manilla var 2934 2007 62 M - SGC AD N
EAI2-Manilla var 2935 2007 60 M + SP AD N
EAI2-Manilla var 2935 2007 38 M + V AD N
EAI2-Manilla var 2934 2007 62 F - C AD N
EAI2-Manilla var 2935 2007 25 M - SP AD N
EAI2-Manilla var 2935 2007 35 M - T AD N
EAI2-Manilla var 2934 2006 42 M + V EI N
EAI2-Manilla var 2934 2007 39 F + SGC EI N
EAI2-Manilla var 2934 2007 M
EAI2-Manilla var 2934 2007 M
LAM LAM 1710 2007 78 M - V AD N
LAM2 17 2007 49 M - SP AD N
LAM4 60 2007 45 M - SGC EI
LAM5 93 2007 42 F - T M N
LAM6 64 2006 45 M - SGC AD N
LAM9 42 2007 33 M - SGE AD N
LAM9 42 2006 60 M - SP AD N
LAM10-CAM 61 2007 54 M - SGE AD N
LAM10-CAM 61 2007 58 F - V EI N
LAM10-CAM 61 2007 56 M - C EI
LAM10-CAM 61 2007 45 M - SGW AD N
LAM10-CAM 61 2007 59 M - SGW AD N
LAM10-CAM 61 2007 62 F - SGE AD N
LAM10-CAM var 2550 2007 28 F + V AD N
LAM10-CAM var 2550 2006 45 M - SGW AD N
LAM10-CAM var 2550 2007 23 M - C AD N
LAM10-CAM var 2550 2007 46 M + V AD D
LAM10-CAM var 2550 2007 60 M + SP AD N
LAM10-CAM var 2550 2007 56 M - SGC M N
LAM10-CAM var 2550 2007 50 M
X X1 Family 119 2007 64 M - SGE AD N
X1 Family 119 2007 64 F - V EI RT
X1 Family 119 2007 M
X1 Family var 1823 2007 44 M - V EI N
X1 Family var 1823 2007 51 M - SASD AD N
X2 Family var 478 2007 41 M + SGE AD N
X2 Family var 478 2007 47 M - SGE AD N
X3 Family var 70 2007 48 M - SGW AD N

T&T clone Unknown 566 2007 43 M + SP AD D
Unknown 566 2006 50 F - C AD N
Unknown 566 2007 43 M + SGC AD N
Unknown 566 2007 55 M + SGC AD N
Unknown 566 2007 22 M - V M N
Unknown 566 2007 40 M + SGW AD D
Unknown 566 2007 64 M - SGC AD N
Unknown 566 2007 52 M - SGW AD N
Unknown 566 2007 29 F + SGC AD
Unknown 566 2007 27 M - V AD N
Unknown 566 2006 65 M - SGE M D
Unknown 566 2007 63 M - SGC AD N
Unknown 566 2007 24 M + SGC AD N
Unknown 566 2007 31 M + SGW AD N
Unknown 566 2006 32 M - V AD N
Unknown 566 2007 29 M + C AD RT
Unknown 566 2007 41 M - SGW M TF
Unknown 566 2007 58 M - C EI N
Unknown 566 2007 27 F - SGC EI N
Unknown 566 2007 49 M + SGC EI N
Unknown 566 2007 25 F - SGE EI N
Unknown 566 2007 56 M - V EI N
Unknown 566 2007 56 M - C EI RT
Unknown 566 2007 37 M - SP AD N
Unknown 566 2007 39 M - SGW AD D
Unknown 566 2007 54 M - SGW EI D
Unknown 566 2007 37 M + C EI N
Unknown 566 2007 47 M - SGE EI N
Unknown 566 2007 42 M - SGC AD RT
Unknown 566 2007 37 M - SGC AD D
Unknown 566 2007 31 M + SGC AD N
Unknown 566 2007 18 F + SGC AD D
Unknown 566 2007 37 M + SP AD N
Unknown 566 2007 48 M - SGW M N
Unknown 566 2007 45 M - V EI N
Unknown 566 2006 22 F - C AD N
Unknown 566 2007 17 M - SGW M N
Unknown 566 2006 45 M - SGW AD D
Unknown 566 2007 25 M + SGC AD D
Unknown 566 2007 45 M - SGC AD D
Unknown 566 2006 18 M - SGE EI D
Unknown 566 2007 18 F - SGC AD N
Unknown 566 2007 58 F - SGC AD N
Unknown 566 2007 64 M SGW EI N
Unknown 566 2007 48 M - C AD N
Unknown 566 2007 31 F - SGC AD N
Unknown 566 2007 27 M - SGE AD N
Unknown 566 2007 52 M - SGW AD N
Unknown 566 2007 33 M - SGW AD N
Unknown 566 2006 48 M - V AD N
Unknown 566 2007 25 F + V AD N
Unknown 566 2007 39 M - V AD N
Unknown 566 2007 27 M + SGC M N
Unknown 566 2007 40 M - SASD AD D
Unknown 566 2007 46 M + SGC AD D
Unknown 566 2007 32 F + SGW AD D
Unknown 566 2006 40 M - T M D
Unknown 566 2006 48 M + SGC AD N
Unknown 566 2006 32 M + SGE AD N
Unknown 566 2007 19 M - SGW AD N
Unknown 566 2007 22 M - SGW AD N
Unknown 566 2007 39 F - T AD N
Unknown 566 2007 55 M - T AD N

Unknown 566 2007 39 M - C EI N
Unknown 566 2007 27 M + SGC AD N
Unknown 566 2007 40 M - SP AD N
Unknown 566 2007 21 M + T AD N
Unknown 566 2007 58 M - C EI N
Unknown 566 2007 63 M - SGC AD RT
Unknown 566 2007 33 M M
Unknown 566 2007 F
Unknown 566 2007 27 M +
Unknown 566 2007 M
Unknown 566 2007 M
Other AFR-2 var Orphan 2007 30 M - SGW AD N
CAS2 288 2006 67 M - V EI N
Haarlem 3 50 2007 70 M - C EI N
Haarlem 3 50 2007 38 M - N EI N
T 73 2007 69 F - SGE AD N
T1 53 2007 56 F + C AD N
Unknown 450 2007 47 M + SGE M N
(a)
Abbreviations for Geographical origin of patients: C, Caroni; M, Mayaro; N, Nariva; V, Victoria; SASD, St Andrew/St David; SGC, St George Central; SGE, St George East; SGW, St George West; SP, St Patrick; T, Tobago
(b) Abbreviations for ethnicity: AD, African Descendant; EI, East Indian; M, Mixed populations.
(c) Abbreviations for Status: D, Defaulters; N, Newly treated; RT, Retreatment; TF, Treatment Failure

Infection, Genetics & Evolution
Phylogeographical and molecular characterization of an emerging Mycobacterium tuberculosis clone in Trinidad and Tobago Julie Millet, Shirematee Baboolal, Patrick Eberechi Akpaka, Dottin Ramoutar, and Nalin Rastogi*
Supplemental Table S2: Detailed epidemiological data for strains classified within the 6 prevalent genotypic groups (Beijing, EAI, LAM, LAM10-CAM, X, SIT566 clone) versus “other” strains (which grouped minor numbers of strains belonging to Harlem, Africanum, CAS, T, and undefined SIT450 lineage) from Trinidad and Tobago.
Geographical origin of
patients(a)
Ethnicity
(b) Status
(c)
Genotypic lineages No. of strains
Age Sex (M/F) HIV (+/-)
SGC SGE SGW O EI AD O N O
Beijing 6 41,0 3/2 2/3 1 0 3 1 1 4 0 3 2
EAI 17 42,9 13/4 6/9 4 2 2 7 3 11 1 12 3
LAM 7 50,3 6/1 0/7 2 1 0 4 1 5 1 6 0
LAM10-CAM 13 49,4 10/3 3/9 1 2 3 6 2 9 1 10 1
X 8 51,3 7/1 1/6 0 3 1 3 2 5 0 6 1
Other 7 53,9 5/2 2/5 0 2 1 3 3 3 1 7 0
T&T clone 74 39,1 61/13 23/46 22 6 15 26 14 48 7 48 20
All 132 42,8 105/26 37/85 30 16 25 50 26 85 11 92 27
(a)
Abbreviations for Geographical origin of patients: SGC, St George Central; SGE, St George East; SGW, St George West; O, Other (b)
Abbreviations for ethnicity: EI, East Indian; AD, African Descendant; O, Other (c)
Abbreviations for Status: N, Newly treated; O, Other status (retreatment, treatment failure)
Copyright © 2022 FDOKUMEN