
Period Medicine - SMS Research Foundation
102
Czasopismo indeksowane w MEDLINE/PUBMED, SCOPUS, Index Copernicus, EBSCO, BioMedLib, Research Gate, MNiSW (7 pkt) i Polskiej Bibliografii Lekarskiej Number 2 April-June Vol. XIX 2015 Warsaw ISSN 1428-345X Instytut Matki i Dziecka Smith-mageniS Syndrome and itS circadian influence on development, behavior, and obeSity Sleep and gaStrointeStinal diSturbanceS in autiSm Spectrum diSorder in children coeliac diSeaSe not reSponding to a gluten-free diet in children fecal pyruvate kinaSe iS not Suitable for diScrimination between inflammatory bowel diSeaSe exacerbation and acute gaStroenteritiS hemodiafiltration efficacy in treatment of methanol and ethylene glycol poiSoning in a 2-year-old girl wielokomorowy guz krezki i przeStrzeni zaotrzewnowej ceftriaxone-aSSociated acute gallbladder enlargement – an unexpected diagnoSiS in the child with urinary tract infection rare renal ectopia in children – intrathoracic ectopic kidney central giant cell granuloma located in the maxilla in a 8-year old boy habitual eating of breakfaSt, conSumption frequency of Selected food and overweight prevalence in adoleScentS from variouS age groupS teenagerS’ perception of being an active patient and putting the concept into practice evaluation of changeS in the width of gingiva in children and youth ocena tolerowania preparatu żelaza actiferol fe ® u dzieci z niedokrwiStością z niedoboru żelaza profilaktyka zakażeń Szpitalnych w oddziale pediatrycznym Period Medicine Medycyna Wieku Rozwojowego DEVELOPMENTAL
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Period Medicine - SMS Research Foundation
Czasopismo indeksowane w MEDLINE/PUBMED, SCOPUS, Index Copernicus,EBSCO, BioMedLib, Research Gate, MNiSW (7 pkt) i Polskiej Bibliografii Lekarskiej
Number 2 April-June vol. XIX 2015 Warsaw ISSN 1428-345X
InstytutMatki i Dziecka
Smith-mageniS Syndrome and itS circadian influence on development, behavior, and obeSity
Sleep and gaStrointeStinal diSturbanceS in autiSm Spectrum diSorder in children
coeliac diSeaSe not reSponding to a gluten-free diet in children
fecal pyruvate kinaSe iS not Suitable for diScrimination between inflammatory bowel diSeaSe exacerbation and acute gaStroenteritiS
hemodiafiltration efficacy in treatment of methanol and ethylene glycol poiSoning in a 2-year-old girl
wielokomorowy guz krezki i przeStrzeni zaotrzewnowej
ceftriaxone-aSSociated acute gallbladder enlargement – an unexpected diagnoSiS
in the child with urinary tract infection
rare renal ectopia in children – intrathoracic ectopic kidney
central giant cell granuloma located in the maxilla in a 8-year old boy
habitual eating of breakfaSt, conSumption frequency of Selected food and overweight prevalence
in adoleScentS from variouS age groupS
teenagerS’ perception of being an active patient and putting the concept into practice
evaluation of changeS in the width of gingiva in children and youth
ocena tolerowania preparatu żelaza actiferol fe® u dzieci z niedokrwiStością z niedoboru żelaza
profilaktyka zakażeń Szpitalnych w oddziale pediatrycznym
Period MedicineMedycyna Wieku Rozwojowego
Developmental


141Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
InstytutMatki i Dziecka
P e r i o d M e d i c i n eMedycyna Wieku Rozwojowego
Developmental

142Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Developmental perioD meDicine
Quarterly/KwartalniK
Number 2 (April-June), Volume 19, 2015 Nr 2 (Kwiecień-Czerwiec), tom 19, 2015
© Copyright by National Research Institute of Mother and Child and Aluna Publishing, Warsaw, Poland 2015
Wydanie czasopisma Developmental Period Medicine w formie papierowej jest wersją pierwotną (referencyjną). Redakcja wdraża procedurę zabezpieczającą oryginalność publikacji naukowych
oraz przestrzega zasad recenzowania prac zgodnie z wytycznymi Ministerstwa Nauki i Szkolnictwa Wyższego.
edited by: National Research Institute of Mother and Child and Aluna Publishingwydawca: Instytut Matki i Dziecka oraz Wydawnictwo Aluna
wydawca:Wydawnictwo Aluna 05-510 Konstancin Jeziorna ul. Przesmyckiego 29Joanna Grocholskae-mail: [email protected] reklama: Agnieszka Rosatel. kom. 600-600-938, e-mail: [email protected]
Adres Redakcji/Editorial Office AddressInstytut Matki i Dzieckaul. Kasprzaka 17a , 01-211 Warszawatel. (+48 22) 327-71-97; fax (+48 22) 327-73-72e-mail: [email protected]
Medycyna Wieku Rozwojowego jest indeksowanaw MEDLINE/PUBMED, SCOPUS oraz INDEX COPERNICUS, EBSCO, BioMedLib,
Research Gate, MNiSW i Polskiej Bibliografii Lekarskiej
Punktacja Ministerstwa Nauki i Szkolnictwa Wyższego – 7 pkt
Developmental Period Medicinecited by MEDLINE/PUBMED, SCOPUS, INDEX COPERNICUS, EBSCO, BioMedLib,
Research Gate, MNiSW and Polish Medical Bibliography
The preferred language of submission is English. To facilitate the processof publication, it is advised that all non-English speaking authors enlist the aid
of a native-English speaking colleague to correct English language usage before submission.

143Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
national research institute of mother anD chilD/instytut matKi i DziecKaDirector/Dyrektor: dr n. med. Tomasz M. Maciejewski
eDitorial BoarD/Komitet reDaKcyjnyeditor in chief/redaktor naczelny – Prof. zw. dr hab. n. med. Krystyna Bożkowa
associate editor/z-ca redaktora naczelnego – Prof. dr hab. n. med. Maciej Jóźwikassociate editor/z-ca redaktora naczelnego – Prof. dr hab. n. med. Barbara Woynarowska
Członkowie Komitetu Redakcyjnego:editorial secretary/sekretarz redakcji – Dr n. med. Ilona Szilágyi-Pągowska
editorial aid – mgr Grzegorz Święćkowski
topic eDitors/reDaKtorzy tematyczniProf. zw. dr hab. n. med. Ewa Helwich – neonatologia
Prof. zw. dr hab. n. med. Michał Jóźwik – ginekologia i położnictwoProf. zw. dr hab. n. farm. Maciej Małecki – terapia genowa i farmakogenomika
Prof. zw. dr hab. n. med. Teresa Matthews-Brzozowska – stomatologiaProf. nadzw. n. med. Ewa Pańkowska – pediatria i endokrynologiaProf. nadzw. n. med. Dorota Sands – pulmonologia i alergologia
Prof. nadzw. n. med. Ewa Sawicka – chirurgia dziecięcaProf. dr hab. n. med. Tomasz Szczepański – onkologia
Prof. nadzw. n. med. Halina Weker – żywienieProf. zw. dr hab. n. med. Barbara Woynarowska – zdrowie publiczne
lanGuaGe eDitor/REdAKtOR języKOwyDoc. dr hab. n. med. Aldona Sito
Mgr Agnieszka Rosa
linGuistic supervisorOsazee Ewemade Okungbowa, MD, PhD, London, UK
statistical eDitor/reDaKtor statystyczny dr hab. n. med. Joanna Mazur, prof. nadzw.
honorary scientific BoarD/honorowy Komitet nauKowyProf. zw. dr hab. n. med. Anna Balcerska Prof. zw. dr hab. med. Tadeusz MazurczakProf. zw. dr hab. n. med. Krzysztof Drews Prof. nadzw. med. Krystyna Mikiel-KostyraProf. zw. dr hab. n. med. Wanda Kawalec Prof. zw. dr hab. n. med. Michał TroszyńskiProf. zw. dr hab. n. med. Barbara Kowalewska-Kantecka
INtERNAtIONAL SCIENtIFIC BOARd/MIędzyNAROdOwy KOMItEt NAUKOwyProf. Vladimir Alminderov (Russia) Dr Mercedes de Onis (WHO – Genewa)Assoc. Prof. Sa’eed Halilu Bawa (Rep. of Trinidad and Tobago) Prof. Leonardo Pinelli (Italy)Dr Mark Klukowski (Canada/Poland) Prof. Kairolla Rakhimov (Kazakhstan)Prof. Berthold Koletzko (Germany) Prof. Timothy R.H. Regnault (Canada)Prof. Olga Kordonouri (Germany) Prof. Michael P. Sherman (USA)Prof. Gunta Lazdane (WHO – Kopenhaga) Prof. Paweł Stankiewicz (USA)Prof. James R. Lupski (USA) Prof. Anatol Svintsitskyi (Ukraine)Dr Lieuwe J. Melchers (The Netherlands) Prof. András Szatmári (Hungary)Prof. Olga G. Morozowa (Ukraine) Prof. Sergo I. Tabagari (Georgia) Smeeta Sardesai, MD, MS Ed Ass. Prof. (USA)
scientific BoarD/Komitet nauKowyProf. nadzw. n. med. Monika Bekiesińska-Figatowska Prof. zw. dr hab. n. med. Andrzej MilanowskiProf. zw. dr hab. n. med. Ewa Bocian Prof. zw. dr hab. n. med. Jacek J. PietrzykProf. zw. dr hab. n. med. Maria Katarzyna Borszewska-Kornacka Prof. nadzw. n. med. Magdalena RutkowskaProf. zw. dr hab. n. med. Andrzej Habior Prof. zw. dr hab. n. med. Janusz SiedleckiProf. nadzw. n. med. Teresa Jackowska Prof. zw. dr hab. n. med. Marek SpaczyńskiProf. nadzw. n. med. Alicja Krzyżaniak Prof. nadzw. n. med. Elżbieta SzczepanikProf. zw. dr hab. n. med. Janusz Książyk Prof. dr hab. n. med. Jarosław WalkowiakProf. zw. dr hab. n. med. Ryszard Lauterbach

144Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Developmental Period Medicine – informacje ogólne
Czasopismo jest kwartalnikiem. Indeksowane jest w MeDlIne/PubMeD, Scopus, Index Copernicus, ebSCO, bioMedlib, Research Gate, MniSW (7 pkt) i Polskiej bibliografii lekarskiej.
W Developmental Period Medicine publikowane są prace oryginalne o charakterze podstawowym i kli-nicznym, prace poglądowe oraz prace związane ze zdrowiem publicznym, zdrowiem prokreacyjnym, oceną stanu zdrowia populacji w wieku rozwojowym i programami mającymi na celu poprawę istniejącej sytuacji zdrowotnej. Wszystkie prace są recenzowane.
Prace publikowane są w języku polskim i angielskim, ze streszczeniami oraz słowami kluczowymi w języku polskim i angielskim. Tablice i ryciny mają również objaśnienia w obu językach.
Zasady prenumeraty
Wpłaty na prenumeratę przyjmuje Wydawnictwo Aluna:− telefonicznie: (22) 754-60-79− e-mail: [email protected]− wpłaty na numer rachunku: 82 1940 1076 3010 7407 0000 0000− listownie na adres: Wydawnictwo Aluna
ul. Z.M. Przesmyckiego 29, 05-510 Konstancin-Jeziorna
Cena prenumeraty:− prenumeratorzy indywidualni – 105 zł/rok (w tym 5% vat)− biblioteki i inne instytucje – 147 zł/rok (w tym 5% vat)− prenumerata zagraniczna – 100 euro− cena pojedynczego numeru – 31,50 zł (w tym 5% vat)− cena numeru złożonego z dwóch zeszytów – 42 zł (w tym 5% vat)− cena jednego zeszytu – 21 zł (w tym 5% vat)
www.devperiodmed.pl

145Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
contents
157
162
167
174
182
186
149
invitation review
Li Chen, Sureni V. Mullegama, Joseph T. Alaimo, Sarah H. ElseaSmith-Magenis syndrome and its circadian influence on development, behavior, and obesity – own experience ............................................................................................................................................................................
Mark Klukowski, Jolanta Wasilewska, Dariusz LebensztejnSleep and gastrointestinal disturbances in autism spectrum disorder in children......................................................
oriGinaL artiCLeS
Wojciech Jańczyk, J.H.C. de Roo, Joachim Schweizer, Jerzy Socha, Piotr Socha, M. Luisa MearinCoeliac disease not responding to a gluten-free diet in children: case studies and literature review .................
Elżbieta Czub, Jan K. Nowak, Jerzy Moczko, Przemysław Mankowski, Aleksandra Lisowska, Aleksandra Banaszkiewicz, Tomasz Banasiewicz, Jarosław WalkowiakFecal pyruvate kinase is not suitable for discrimination between inflammatory bowel disease exacerbation and acute gastroenteritis ...............................................................................................................................................................
Agnieszka Szmigielska, Hanna Szymanik-Grzelak, Elżbieta Kuźma-Mroczkowska, Maria Roszkowska-BlaimHemodiafiltration efficacy in treatment of methanol and ethylene glycol poisoning in a 2-year-old girl.........
Anna Obuchowicz, Magdalena Łoboda, Wojciech Madziara, Małgorzata Krzywiecka, Beata JareckaMultiloculated mesenteric and retroperitoneal tumour – lymphatic malformation – in a 4-year-old girl .......
Grażyna Krzemień, Tomasz Książczyk, Agnieszka Szmigielska, Przemysław Bombiński, Maria Roszkowska-Blaim, Bożena Werner, Michał BrzewskiCeftriaxone-associated acute gallbladder enlargement − an unexpected diagnosis in the child with urinary tract infection ...................................................................................................................................
Agnieszka Szmigielska, Aleksandra Księżopolska, Maria Roszkowska-Blaim, Michał Brzewski, Grażyna KrzemieńRare renal ectopia in children – intrathoracic ectopic kidney .........................................................................................
Anna Janas, Piotr OsicaCentral giant cell granuloma located in the maxilla in a 8-year old boy .....................................................................
178
189

146 Contents
217
225
202
212
Justyna Weronika Wüenstel, Joanna Kowalkowska, Lidia Wądołowska, Małgorzata Anna Słowińska, Ewa Niedźwiedzka, Lidia KurpHabitual eating of breakfast, consumption frequency of selected food and overweight prevalence in adolescents from various age groups...................................................................................................................................
Magdalena Woynarowska-Sołdan, Izabela Tabak, Antonina Doroszewska, Karolina Jabłkowska-GóreckaTeenagers’ perception of being an active patient and putting the concept into practice .........................................
Beata Wyrębek, Agata Orzechowska, Dorota Cudziło, Paweł PlakwiczEvaluation of changes in the width of gingiva in children and youth. Review of literature .................................
MiSCeLLanea
Teresa Jackowska, Alicja Sapała-Smoczyńska, Ewa KamińskaTolerability of iron preparation Actiferol Fe® in children treated for iron deficiency anemia ..........................
Teresa Jackowska, Katarzyna PawlikPrevention of nosocomial infections in the pediatric ward – own experiences ........................................................
Instructions for Authors in Developmental Period Medicine........................................................................................... 235
193

147Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
SPIS tREŚCI
invitation review
Li Chen, Sureni V. Mullegama, Joseph T. Alaimo, Sarah H. ElseaSmith-Magenis syndrome and its circadian influence on development, behavior, and obesity – own experience ............................................................................................................................................................................
Mark Klukowski, Jolanta Wasilewska, Dariusz LebensztejnSleep and gastrointestinal disturbances in autism spectrum disorder in children......................................................
praCe oryGinaLne
Wojciech Jańczyk, J.H.C. de Roo, Joachim Schweizer, Jerzy Socha, Piotr Socha, M. Luisa MearinCeliakia oporna na leczenie dietą bezglutenową: opis przypadków oraz przegląd literatury ..............................
Elżbieta Czub, Jan K. Nowak, Jerzy Moczko, Przemysław Mankowski, Aleksandra Lisowska, Aleksandra Banaszkiewicz, Tomasz Banasiewicz, Jarosław WalkowiakPomiar stężenia kinazy pirogronianowej w kale nie pozwala na rozróżnienie między zaostrzeniem nieswoistego zapalenia jelit a ostrym nieżytem żołądkowo-jelitowym .......................................................................
Agnieszka Szmigielska, Hanna Szymanik-Grzelak, Elżbieta Kuźma-Mroczkowska, Maria Roszkowska-BlaimSkuteczność hemodiafiltracji w leczeniu zatrucia metanolem i glikolem u 2-letniej dziewczynki ..................
Anna Obuchowicz, Magdalena Łoboda, Wojciech Madziara, Małgorzata Krzywiecka, Beata JareckaWielokomorowy guz krezki i przestrzeni zaotrzewnowej – malformacja chłonna u czteroletniej dziewczynki ........................................................................................................................................................
Grażyna Krzemień, Tomasz Książczyk, Agnieszka Szmigielska, Przemysław Bombiński, Maria Roszkowska-Blaim, Bożena Werner, Michał BrzewskiOstre powiększenie pęcherzyka żółciowego związane z leczeniem ceftriaksonem − niespodziewane rozpoznanie u dziecka z zakażeniem układu moczowego............................................................
Agnieszka Szmigielska, Aleksandra Księżopolska, Maria Roszkowska-Blaim, Michał Brzewski, Grażyna KrzemieńRzadki przypadek ektopii nerek u dzieci – nerka w klatce piersiowej ........................................................................
Anna Janas, Piotr OsicaCentralny ziarniniak olbrzymiokomórkowy zlokalizowany w szczęce u 8-letniego chłopca ..............................
157
162
167
174
182
186
149
178
189

148 Spis treści
Justyna Weronika Wüenstel, Joanna Kowalkowska, Lidia Wądołowska, Małgorzata Anna Słowińska, Ewa Niedźwiedzka, Lidia KurpZwyczajowe spożycie śniadania a częstość spożycia wybranej żywności i występowania nadwagi u młodzieży z różnych grup wiekowych ................................................................................................................................
Magdalena Woynarowska-Sołdan, Izabela Tabak, Antonina Doroszewska, Karolina Jabłkowska-GóreckaPostrzeganie i podejmowanie przez nastolatki zachowań aktywnego pacjenta ...................................................
Beata Wyrębek, Agata Orzechowska, Dorota Cudziło, Paweł PlakwiczOcena zmiany szerokości dziąsła u dzieci i młodzieży. Przegląd literatury ..............................................................
MiSCeLLanea
Teresa Jackowska, Alicja Sapała-Smoczyńska, Ewa KamińskaOcena tolerowania preparatu żelaza Actiferol Fe® u dzieci z niedokrwistością z niedoboru żelaza ..................
Teresa Jackowska, Katarzyna PawlikProfilaktyka zakażeń szpitalnych w oddziale pediatrycznym – doświadczenia własne ........................................
Zasady przyjmowania i ogłaszania prac w Developmental Period Medicine...........................................................
217
225
202
212
237
193

149Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
i n v i tat i o n r e v i e w
Li Chen1, Sureni V. Mullegama2, Joseph T. Alaimo2, Sarah H. Elsea2
Smith-mageniS Syndrome and itS circadian influence on development,
behavior, and obeSity – own experience*
1Department of Cellular and Genetic Medicine, School of basic Medical Sciences, Fudan university, Shanghai 200032, China
2Department of Molecular and Human Genetics, baylor College of Medicine, Houston, TX, uSA
AbstractSmith-Magenis syndrome (SMS) is a complex genetic disorder characterized by sleep disturbance, multiple developmental anomalies, psychiatric behavior, and obesity. It is caused by a heterozygous 17p11.2 microdeletion containing the retinoic acid-induced 1 (RAI1) gene or mutation within RAI1. Sleep disorder is one of the most penetrant features of SMS. Molecular genetic studies indicate that RAI1 regulates circadian rhythm genes and when haploinsufficient, causes a distorted molecular circadian network that may be the cause of the sleep disturbance and the inverted rhythm of melatonin present in most individuals with SMS. RAI1 also regulates genes involved in development, neurobehavior, and lipid metabolism. Sleep debt, daytime melatonin secretion, and environmental stress often contribute to negative behavior in persons with SMS, and food entrained circadian rhythm also influences food intake behavior and humoral signals, which also affect development and neurobehavior. The cross-talk between circadian rhythm, development, metabolism and behaviors affect the multiple phenotypic outcomes in Smith-Magenis syndrome. These findings shed light on possible effective and personalized drug treatments for SMS patients in the future.
Key words: melatonin, RAI1, CLOCK, BDNF, intellectual disability, 17p11.2 deletion
DEV pErioD mED. 2015;XiX,2:149-156
*This work was supported by Smith-Magenis Syndrome Research Foundation (SHE, SVM), National Science Foundation-China (NSFC) grant 31200937 (LC), and Shanghai Health and Family Planning Commission grant 20144Y0106 (LC).
1. PhenotyPIc FeAtures AnD MoleculAr GenetIcs oF sMsSmith-Magenis syndrome (SMS) is a complex
neurobehavioral disorder with an estimated prevalence of 1:15,000 to 1:25,000 live births [1]. Characteristic SMS features include sleep abnormalities (Figure 1A), craniofacial (Figure 1b) and skeletal anomalies, intellectual disability, self-injurious behaviors (Figure 1C), stereotypical behavior (Figure 1D), metabolic problems and obesity (Figure 1e) [2]. A more detailed clinical phenotypic spectrum of SMS catalog in sleeping disorder, developmental anomalies, neurological and behavior problems, and obesity is listed in Table I.
Molecular cytogenetic analyses of SMS patients show a common deletion in ~70% of individuals that spans ~3.8 Mb and contains 76 genes in chromosome band 17p11.2 [1, 3]. Within this region lies RAI1, the primary
causative gene [4]. RAI1 spans ~130 kb and contains six exons, including 4 coding exons which encode a 1906 amino acid protein. Rai1 was first identified as a gene (designated Gt1) induced by retinoic acid in P19 mouse embryonic carcinoma cells [5]. It is localized in the nucleus and is expressed in migrating neural crest cells and the nervous system early in development, and also, at lower levels, in adult brain [6]. It functions as a transcriptional regulator with a PHD (plant homeodomain) motif [7] and acts as a “histone reader,” bridging specific histone modifications and other transcription factors [8].
About 90% of SMS patients carry a 17p11.2 deletion containing RAI1 [3], with the remaining 10% of individuals harboring mutations within the gene, including insertions or deletions within the coding region that result in frameshifts and truncated proteins, as well as missense and nonsense mutations [7, 9-11]. All reported mutations to date lie within the coding region of exon 3, which represents

150 Li Chen et al.
Fig. 1. Phenotypic features of smith-Magenis syndrome. A. SmS patient with sleep disturbance, illustrating commonly observed “sleep attacks”; B. Craniofacial anomalies can include midface hypoplasia and tented upper lip in SmS; C. Self-injurious behaviors like pulling out of fingernails and/or toenails are unique to SmS; D. Stereotypical behavior like self-hugging in SmS patient, typically observed during times of excitement or happiness; E. obesity is frequently observed in persons with sMs.
approximately 95% of the coding sequence of this gene. A mutation hotspot region in exon 3 has been identified for causing frameshifts within RAI1 [10].
Studies have shown that variability and severity in SMS are modified by other genes in the common deletion region [3, 12, 13]. For example, indirect evidence links subunit 3 of the COP9 complex (COPS3) with melatonin metabolism. The COP9 complex encoded by COPS3 is related to 26S proteasome regulatory complex, which has been associated with control of the rate-limiting step in melatonin metabolism by n-acetyltransferase [14]. Also, TnFRSF13b is associated with IgA deficiency [15], FlCn is associated with renal disorder, pneumothoraces, and birt-Hogge-Dube syndrome [16], and mutations in MYO15A cause sensorineural hearing loss (MYO15A) [17]. These genes further complicating the SMS phenotypic spectrum. Data show that phenotypes like short stature, hearing loss, speech and motor delay, hypotonia and cardiovascular anomalies are more associated with 17p11.2 deletion rather than with RAI1 mutation [3]. This suggests the presence of other genetic contributors to SMS phenotype spectrum in addition to RAI1. However, sleep disturbance, intellectual disability, and neurobehavioral features are consistent in all SMS patients, including both individuals with17p11.2 deletion and those with RAI1 mutations, indicating that RAI1 is the key gene accounting for these major phenotypes [3].
2. cIrcADIAn DeFect In Persons WIth sMs
Sleep disorder is one of the most penetrant features of SMS [18] and includes difficulties in falling asleep at night, reduced or absent rapid eye movement (ReM) sleep, early waking, frequent night-time arousals, and daytime napping [18-21].
The pineal gland in human brain suprachiasmatic
nucleus (SCn) controls the central circadian rhythm and melatonin secretion through light stimulation in day-night cycles. Several studies have implicated an inverted rhythm of melatonin secretion in SMS patients as the underlying cause of the sleep disturbance [19, 22]. Individuals with SMS typically have elevated melatonin secretion from the pineal gland in the daytime in contrast to very low excretion at nighttime [21-23] (Figure 2A). Studies have shown that β1-adrenergic antagonist (acetbutolol) treatment during the day may alleviate daytime melatonin peaks and improve behavior, but melatonin levels at night are not improved with acetbutolol alone [24] (Figure 2b). However, the addition of a low dose of melatonin (<3 mg) before bedtime improves the sleep time duration of SMS patients [25] (Figure 2C). Combined treatment with β-blocker (acetbutolol) to block endogenous melatonin production during the day plus exogenous melatonin administration in the evening improved the overall sleep disturbance of SMS patients and resulted in fewer daytime naps and fewer awakenings throughout the night [26-28] (Figure 2D).
The inverted secretion of melatonin, while a common finding in SMS, is not present in 100% of patients. Recent studies reported two individuals with atypical 17p11.2 deletions having normal melatonin secretion but still have sleep disturbance, included a 5 year-old female carrying a ~5 Mb deletion that extended beyond the distal SMS-ReP region and a 18 year-old female carrying a ~5.8 Mb deletion that extended beyond the proximal SMS-ReP region detected by high resolution CGH and FISH [14, 19]. Given that melatonin is secreted during daylight hours, its secretion is not suppressed by light in most persons with SMS. However, a pulse of bright light temporarily inhibited melatonin secretion at night for the 18 year-old female SMS patient [14], suggesting that the sleep disturbances in SMS cannot be solely attributed to the abnormal diurnal melatonin secretion versus the normal nocturnal pattern. Additionally, while Rai1+/- mice do not have melatonin, they do have circadian abnormalities [29, 30], supporting a key role for Rai1 in circadian regulation without significant melatonin impact. These facts indicate that the dysregulation of sleep is not solely due to an altered circadian secretion of melatonin. Instead, the inverted melatonin maybe a secondary effect of a dysregulated molecular circadian network, thus, influencing sleeping patterns [22].
Circadian disturbances in SMS are likely due to abnormal functioning of RAI1, as SMS patients with point mutations in this gene have been reported with both sleep disturbance and altered melatonin rhythms [9]. Recent studies have shown that RAI1 is a critical player in maintaining the molecular clock system, both in the hypothalamus, where the suprachiasmatic nucleus (SCn) lies and is responsible for controlling the central circadian rhythm, and also within the peripheral circadian oscillators, including the liver, heart and kidney. Haploinsufficiency of RAI1 in SMS fibroblasts and Rai1+/- mice hypothalamus results in the dysregulation of critical genes involved in circadian biology, such as circadian locomotor output cycles kaput (ClOCK),

151Smith-Magenis syndrome and its circadian influence on development, behavior, and obesity
Smith-magenis Syndrome clinical findings
Sleep disturbance reduced total sleep, difficulty falling asleep, diminished rapid eye movement sleep, fragmented and shortened sleep cycles, early-morning awakenings
Developmental anomalies
craniofacial anomalies
mid-face hypoplasia, brachycephaly, tented upper lip, micrognathia and prognathism
q Skeletal anomalies Brachydactyly, short stature, scoliosis, vertebral anomalies
q otolaryngological anomalies
Hearing loss, chronic ear infections, deep hoarse voice
q ophthalmologic anomalies
myopia, strabismus, microcornea, Wolfflin-Kruckman spots
q other anomalies
Cardiovascular defects (VSD, ASD, tetralogy of Fallot), enlarged and ectopic kidneys,
immunological abnormalities, failure to thrive
neurological and behavioral features Motor aspect infantile hypotonia, hyporeflexia, delayed fine motor skills,
sensory integration problems
q Cognitive aspect
mild to moderate intellectual disability, delayed speech, short-term memory impairment
q Gait aspect Seizures, an abnormal gait, toe walking, balance problems
q Central nervous system defects
Decreased gray matter in the insula and lenticular nucleolus, underdeveloped cerebellar vermis,
malformed brain stem, enlarged ventricles
q self-injurious behaviors
Skin picking, wrist biting, head banging, pulling out of nails,
and insertion of objects into bodily orifices, insensitivity to pain
q maladaptive behaviors
Frequent outbursts, temper tantrums, attention seeking,
impulsivity, aggression, disobedience, hyperactivity, attention deficits
q stereotypical behaviors
Spasmodic upper body squeeze, self-hugging with excitement, autistic-like behaviors,
mouthing of objects, bruxism, spinning or twirling objects
metabolic problems Feeding difficulties, hypercholesterolemia, early on-set obesity, impaired satiety
Table i. Clinical features of Smith-magenis syndrome. Features are variable across the SmS population, with consistent neurobehavioral findings in all individuals.
brain and muscle Arnt-like protein-1 (bMAl1), period circadian protein homolog genes (PeR1, PeR2, PeR3), cryptochrome gene (CRY1, CRY2) , nuclear receptor subfamily 1 group D (nR1D1, nR1D2), and RAR-related orphan receptor A genes (RORA, RORC). Functional studies have shown that RAI1 siRnA knockdown in a transgenic cell line that carries the firefly luciferase gene under the control of the bMAl1 gene promoter
results in a shortened period and reduced amplitude of bMAl1 expression [32]. Furthermore, ChIP-Chip and luciferase data showed that RAI1 also binds to the first intron of ClOCK and positively regulate its transcriptional activity in vitro, suggesting that RAI1 acts as an enhancer to bind, directly or in a complex, to the ClOCK gene, and plays an important role in the circadian loop of transcription [31].

152
3. sMs cIrcADIAn DeFect InFluences DEVElopmEnT, BEHAVior,
AnD mETABoliSmThe outputs of endogenous circadian oscillator
and melatonin secretion rhythm influence a series of physiology and development event, neurological behavior and metabolism, in response to environmental changes and physiological homeostasis [32]. besides synthesis and release of melatonin by the pineal gland abnormally, the circadian defect in SMS might also affect the entrainment pathway (retinohypothalamic tract) and pacemaker functions (suprachiasmatic nucleus), thus further contributing the physiological processes and metabolic disturbances observed in SMS patients [28].
Many psychiatric disorders are known to involve sleep disturbance, such as autism spectrum disorder (ASD)[33], brachydactyly mental retardation syndrome (bDMR) [34], PTlS [35], Rett syndrome (RTT) [36], 2q23.1 deletion syndrome [37], fragile X syndrome [38], and Prader-Willi syndrome [39]. Several studies have shown that the severity of sleep disturbances and degree of developmental delay are proportionate to the behavior and learning problems [40-42]. evaluation of a child with developmental delays or cognitive disability usually includes questions about sleep and napping [43]. And adverse sleep patterns often correlated to higher
levels of depression and anxiety [44]. For SMS children, sleep debt, daytime melatonin secretion, and expectations from school, society and family often make them even more irritable. Stereotypical behaviors including body squeeze, self-hugging with excitement, autistic-like behaviors, and maladaptive behaviors including temper tantrums, attention seeking, aggression, and self-injurious behaviors are unique in SMS patients. Response to anxiety, in addition to insensitivity to pain, which is a consistent finding in persons with SMS, are thought to be the major contributors to the observed self-injurious behaviors [45]. Improvement of sleep quality and quantity have a direct positive effect on behavioral adherences in persons with SMS [45]. Resetting the molecular circadian network by a combined treatment with β-blocker (acetbutolol) to block endogenous melatonin production during the day plus exogenous melatonin administration in the evening improved school performance and behaviors of SMS children [24]. However, this approach has not been successful or adequate for all individuals [46], so additional treatment approaches are necessary.
Food entrained circadian rhythm also reinforces the humoral signals, such as hormones and blood glucose, and forms a feedback loop between circadian, development, metabolism, and behaviors [47]. brain-derived neurotrophic factor (bDnF) is a growth
Fig. 2. inverted circadian rhythm of melatonin in SmS. A. The green line refers to the normal rhythm of melatonin in control individuals who have a normal sleep and awake pattern (green arrow). The red line refers to inverted rhy-thm of melatonin in SmS patients, who have more daytime napping and night awakening (red arrow). B. The blue dotted line represents the change in melatonin in SmS patients treated with β1-adrenergic antagonist acetbutolol during the day. β-blocker blockade significantly alleviates daytime melatonin peaks, but melatonin levels at night are not improved. C. The yellow dotted line refers to the change in melatonin in SmS patients with exogenous melatonin administration before bedtime, indicating the melatonin levels at night are elevated. D. purple dotted line represents the change in melatonin in SmS patients with combined treatment with β-blocker (acetbutolol) to block endogenous melatonin production during the day plus exogenous melatonin administration in the evening, resulting suppressed melatonin level in the daytime and increased melatonin level at night.
Li Chen et al.

153
factor crucial for the growth of striatal neurons and is involved in several neuropsychiatric disorders like depression, schizophrenia, and obsessive-compulsive disorder. bDnF is also known to be involved in energy metabolism pathways and satiety signals [48] and is reported to be downregulated in the hypothalamus of Rai1+/- mice, which are hyperphagic, have an impaired satiety response, develop adult onset obesity, and consume more food during light phase. Rai1+/- mice also have altered fat distribution, with increased abdominal fat deposition and a reduced proportion of subcutaneous fat in females [49]. luciferase reporter studies also showed that RAI1 regulates bDnF expression, via intronic enhancer elements. In vitro, RAI1 isoform 1 (RAI1a, long form, localized to nucleus) increased bDnF expression ~2-fold, while RAI1 isoform 4 (RAI1c, not localized to nucleus) does not enhance transcription [49]. Also, a study has shown that SMS mice fed a high carbohydrate or a high fat diet gained weight at a significantly faster rate than wild type mice and exhibited an altered fat distribution pattern. This finding suggested that mice that are haploinsufficient for Rai1 are more susceptible to diet induced obesity, and that a high fat or high carbohydrate diet may exacerbate early onset obesity outcomes in SMS patients [50]. Individuals with RAI1 mutations are more likely to exhibit obesity and somatic overgrowth compared to those with 17p11.2 deletions [51]. These data provide evidence that RAI1 is likely involved in the regulation of brain development and probably contributes to behavior, growth, and developmental problems in SMS patients.
Complicated cross-talk and feedback loops exists across circadian, behavioral, developmental and metabolic processes. For example, Rai1+/- mice exhibit altered circadian rhythm, including a shorter period and disrupted circadian rhythm, and abnormal neurological responses, such as pain insensitivity, gating problems, muscle weakness, and seizures. Df11(17)/+ mice, with a SMS-equivalent deletion that includes Rai1, exhibit a shorter period and a dysregulated rhythm in the dark phase, similar to what was found in Rai1+/- mice [52]. Reduced expression of bDnF has been associated with obesity, hyperphagia, and behavioral abnormalities in mice and human [53, 54], similar to the phenotypes of Rai1+/- mice. Furthermore, Clock mutant mice also develop obesity [55], indicating there might be a complex feedback loop within RAI1, ClOCK and bDnF, and that they may share common regulatory and downstream pathways. Among SMS patients, obesity is prevalent, starting in early adolescence and throughout adulthood; this may be due to a combination of the disrupted function of RAI1 and its impact on both ClOCK and bDnF.
A recent study also demonstrated that RAI1, as a histone reader, recognizes a set of histone modification marks and binds histones and the nucleosome core through C-terminus PHD domain in vitro [8]. Acting as a chromatin remodeling factor, RAI1 may mediate interactions between chromatin, chromatin modulators, and transcriptional regulators, and regulate its downstream genes epigenetically [56]. Furthermore, histone deacetylase 4 (HDAC4) and methyl-CpG binding domain protein 5
(MbD5) are reported to indirectly regulate RAI1 expression [57]. HDAC4, a histone deacetylase, acts as an eraser in histone modification, while MbD5 is a methyl-CpG binding protein and acts as a reader in DnA methylation [58]. RAI1 expression is reduced in cells from individuals with HDAC4 deletion or mutation [34]. Haploinsufficiency of MbD5 in both 2q23.1 deletion patient cell lines and SH-SY5Y cells causes a decrease in RAI1 and alters circadian gene expression, including ClOCK, PeR1, PeR2, PeR3, nR1D2, CRY1, CRY2, RORb [37]. These data suggested RAI1 may have direct or indirect effects on these pathways or have multiple targets in these pathways, and likely further modulates the phenotypic spectrum of SMS through multiple genetic networks.
Gene expression microarray and pathway studies also showed that RAI1 acts as a transcription factor to regulate its downstream genes in several phenotype-specific biological pathways that are dysregulated in SMS. RAI1 gene dosage is crucial not only for normal regulation of circadian rhythm but also for neurotransmitter function and lipid metabolism, as well. Haploinsufficiency of RAI1 expression results in dysregulation of its downstream genes and pathways, including growth signaling and insulin sensitivity, neuronal differentiation, lipid biosynthesis and fat mobilization, circadian activity, behavior, renal, cardiovascular and skeletal development, gene expression, and cell-cycle regulation and recombination, all reflecting the spectrum of clinical features observed in SMS [59]. These dysregulated genes have been confirmed in the SMS mouse models and/or SMS patient cell lines and are potential drug targets in SMS treatments.
Since RAI1 is a dosage sensitive gene, and thought to function as a transcription factor and histone reader, these data imply that RAI1 serves as a master switch for multiple genes involved in development, neurobehavior and metabolic regulation, explaining the diverse range of symptoms seen in SMS. (Figure 3).
4. Future reseArch AnD treAtMent oF sMs
Given the broad phenotypic spectrum of SMS, future research may identify additional genetic and environmental modifiers. Molecular cytogenetic analysis suggests that other genes in the SMS common deletion region need further investigation and may play a role in modifying circadian rhythm, cognitive development, neurobehavior, and obesity [12, 13]. As a possible contributor to neuropsychiatric disorders, RAI1 function in specific brain regions or different developing stages of the brain needs to be investigated. The promoter region of RAI1 and its regulatory sequences are not well defined; thus, elucidating its transcriptional regulators and regulatory mechanisms will help to screen drug targets for SMS. Restoring expression of both RAI1 and its downstream genes could rescue some of SMS phenotypes, such as sleep disturbance, cognitive function, behavioral problems, and obesity.
Smith-Magenis syndrome and its circadian influence on development, behavior, and obesity
154
early accurate diagnose is essential for patients, families, and the society as a whole. Some SMS phenotypic features are subtle in infancy and early childhood and overlap with many other neurodevelopmental disorders like Down syndrome, Prader-Willi syndrome, Williams syndrome, Sotos syndrome, 9q34 deletion syndrome, 2q37 deletion syndrome, and bardet-biedl syndromes [60]. Some of the core and early onset SMS features such as craniofacial anomalies, sleep disturbance, and self-injury may help to diagnose SMS distinct from other disease. early intervention to address developmental delays, such as speech, motor function, and behavior and sleep management, will improve quality of life for the patient and family. Further, evaluations to assess other medical complications often associated with SMS can be targeted and addressed early before negative consequences occur.
So far, most pharmacological interventions used to alleviate the multisystem impact of SMS are not consistently effective, or many are effective only for a limited period. elucidating pathophysiological mechanisms of this complex genetic disorder will help to provide evidence for molecular targets for pharmaceutical intervention and personalized therapeutic approaches for SMS patients.
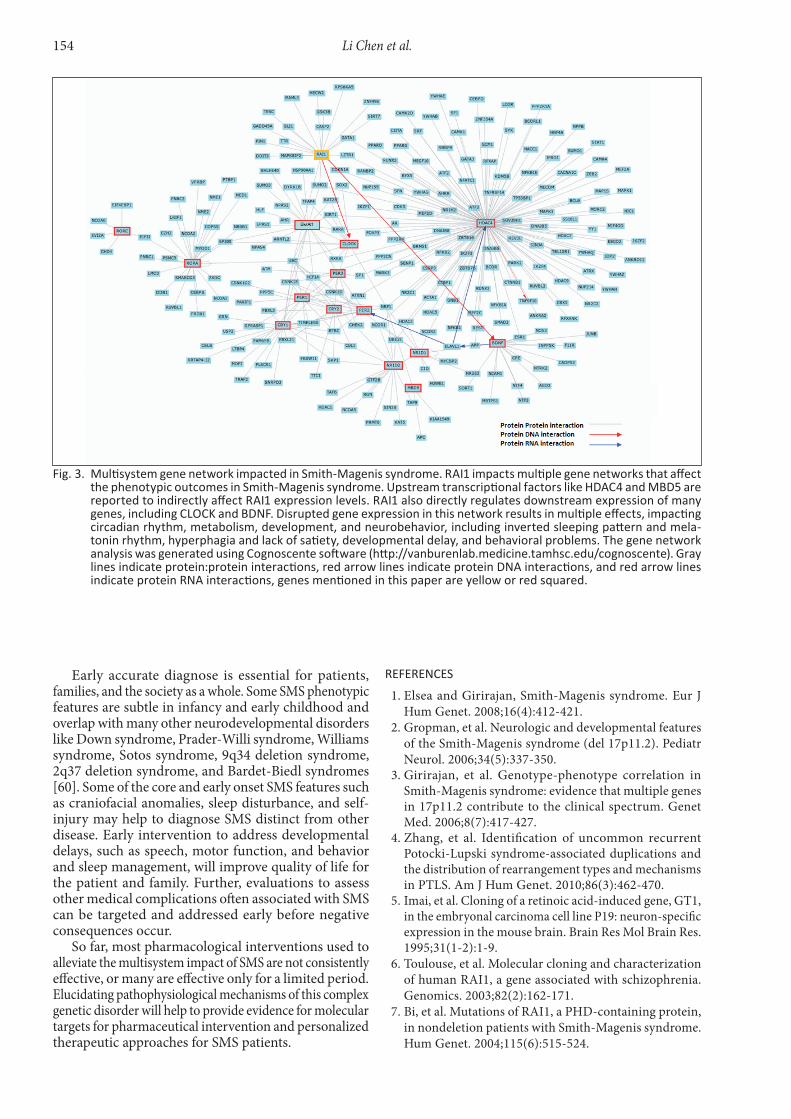
Fig. 3. multisystem gene network impacted in Smith-magenis syndrome. rAi1 impacts multiple gene networks that affect the phenotypic outcomes in Smith-magenis syndrome. Upstream transcriptional factors like HDAC4 and mBD5 are reported to indirectly affect rAi1 expression levels. rAi1 also directly regulates downstream expression of many genes, including CloCK and BDnF. Disrupted gene expression in this network results in multiple effects, impacting circadian rhythm, metabolism, development, and neurobehavior, including inverted sleeping pattern and mela-tonin rhythm, hyperphagia and lack of satiety, developmental delay, and behavioral problems. The gene network analysis was generated using Cognoscente software (http://vanburenlab.medicine.tamhsc.edu/cognoscente). Gray lines indicate protein:protein interactions, red arrow lines indicate protein DnA interactions, and red arrow lines indicate protein rnA interactions, genes mentioned in this paper are yellow or red squared.
reFerences
1. elsea and Girirajan, Smith-Magenis syndrome. eur J Hum Genet. 2008;16(4):412-421.
2. Gropman, et al. neurologic and developmental features of the Smith-Magenis syndrome (del 17p11.2). Pediatr neurol. 2006;34(5):337-350.
3. Girirajan, et al. Genotype-phenotype correlation in Smith-Magenis syndrome: evidence that multiple genes in 17p11.2 contribute to the clinical spectrum. Genet Med. 2006;8(7):417-427.
4. Zhang, et al. Identification of uncommon recurrent Potocki-lupski syndrome-associated duplications and the distribution of rearrangement types and mechanisms in PTlS. Am J Hum Genet. 2010;86(3):462-470.
5. Imai, et al. Cloning of a retinoic acid-induced gene, GT1, in the embryonal carcinoma cell line P19: neuron-specific expression in the mouse brain. brain Res Mol brain Res. 1995;31(1-2):1-9.
6. Toulouse, et al. Molecular cloning and characterization of human RAI1, a gene associated with schizophrenia. Genomics. 2003;82(2):162-171.
7. bi, et al. Mutations of RAI1, a PHD-containing protein, in nondeletion patients with Smith-Magenis syndrome. Hum Genet. 2004;115(6):515-524.
Li Chen et al.

155
8. Darvekar, et al. A phylogenetic study of SPbP and RAI1: evolutionary conservation of chromatin binding modules. PloS One. 2013;8(10):e78907.
9. Girirajan, et al. RAI1 variations in Smith-Magenis syndrome patients without 17p11.2 deletions. J Med Genet. 2005;42(11):820-828.
10. Truong, et al. Frameshift mutation hotspot identified in Smith-Magenis syndrome: case report and review of literature. bMC Med Genet. 2010;11:142.
11. bi, et al. RAI1 point mutations, CAG repeat variation, and SnP analysis in non-deletion Smith-Magenis syndrome. Am J Med Genet A. 2006;140(22):2454-2463.
12. lucas, et al. Genomic organisation of the approximately 1.5 Mb Smith-Magenis syndrome critical interval: transcription map, genomic contig, and candidate gene analysis. eur J Hum Genet. 2001;9(12):892-902.
13. Vlangos, et al. Refinement of the Smith-Magenis syndrome critical region to approximately 950kb and assessment of 17p11.2 deletions. Are all deletions created equally? Mol Genet Metab, 2003;79(2):134-141.
14. boudreau, et al. Review of disrupted sleep patterns in Smith-Magenis syndrome and normal melatonin secretion in a patient with an atypical interstitial 17p11.2 deletion. Am J Med Genet A. 2009;149A(7):1382-1391.
15. Castigli, et al. TACI is mutant in common variable immunodeficiency and IgA deficiency. nat Genet. 2005;37(8):829-834.
16. Khoo, et al. Clinical and genetic studies of birt-Hogg-Dube syndrome. J Med Genet. 2002;39(12):906-912.
17. Friedman, et al. A gene for congenital, recessive deafness DFnb3 maps to the pericentromeric region of chromosome 17. nat Genet. 1995;9(1):86-91.
18. Smith, et al. Sleep disturbance in Smith-Magenis syndrome (del 17 p11.2). Am J Med Genet. 1998;81(2):186-191.
19. Potocki, et al. Circadian rhythm abnormalities of melatonin in Smith-Magenis syndrome. J Med Genet. 2000;37(6):428-433.
20. De leersnyder, et al. Inversion of the circadian melatonin rhythm in Smith-Magenis syndrome. Rev neurol (Paris). 2003;159(11 Suppl):6S21-26.
21. De leersnyder, et al. Circadian rhythm disorder in a rare disease: Smith-Magenis syndrome. Mol Cell endocrinol. 2006;252(1-2):88-91.
22. De leersnyder, et al. Inversion of the circadian rhythm of melatonin in the Smith-Magenis syndrome. J Pediatr. 2001;139(1):111-116.
23. boone, et al. Abnormal circadian rhythm of melatonin in Smith-Magenis syndrome patients with RAI1 point mutations. Am J Med Genet A. 2011;155A(8):2024-2027.
24. De leersnyder, et al. beta(1)-adrenergic antagonists improve sleep and behavioural disturbances in a circadian disorder, Smith-Magenis syndrome. J Med Genet. 2001;38(9):586-590.
25. Smith, et al. Smith-Magenis Syndrome, in GeneReviews(R), R.A. Pagon, et al., editors: Seattle (WA), 1993.
26. Carpizo, et al. Smith-Magenis syndrome: a case report of improved sleep after treatment with beta1-adrenergic antagonists and melatonin. J Pediatr. 2006;149(3):409-411.
27. Van Thillo, et al. Sleep disturbances in Smith-Magenis syndrome: treatment with melatonin and beta-adrenergic antagonists. Tijdschr Psychiatr. 2010;52(10):719-723.
28. De leersnyder. Smith-Magenis syndrome. Handb Clin neurol. 2013;111:295-296.
29. bi, et al. Inactivation of Rai1 in mice recapitulates phenotypes observed in chromosome engineered mouse models for Smith-Magenis syndrome. Hum Mol Genet. 2005;14(8):983-995.
30. Kasahara, et al. Genetic variation of melatonin productivity in laboratory mice under domestication. Proc natl Acad Sci uSA. 2010;107(14):6412-6417.
31. Williams, et al. Smith-Magenis syndrome results in disruption of ClOCK gene transcription and reveals an integral role for RAI1 in the maintenance of circadian rhythmicity. Am J Hum Genet. 2012;90(6):941-949.
32. Kohyama. Circadian rhythm disruption and human development. nihon Rinsho. 2013;71(12):2082-2088.
33. Kotagal and broomall. Sleep in children with autism spectrum disorder. Pediatr neurol, 2012;47(4):242-251.
34. Williams, et al. Haploinsufficiency of HDAC4 causes brachydactyly mental retardation syndrome, with brachydactyly type e, developmental delays, and behavioral problems. Am J Hum Genet, 2010;87(2):219-228.
35. lacaria, et al. Circadian abnormalities in mouse models of Smith-Magenis syndrome: evidence for involvement of RAI1. Am J Med Genet A. 2013;161A(7):1561-1568.
36. Smeets, et al. Rett Syndrome. Mol Syndromol. 2012;2(3-5):113-127.
37. Mullegama, et al. MbD5 haploinsufficiency is associated with sleep disturbance and disrupts circadian pathways common to Smith-Magenis and fragile X syndromes. eur J Hum Genet. 2014.
38. Weiskop, et al. behavioural treatment to reduce sleep problems in children with autism or fragile X syndrome. Dev Med Child neurol. 2005;47(2):94-104.
39. Cassidy, et al. Prader-Willi and Angelman syndromes: sister imprinted disorders. Am J Med Genet. 2000;97(2):136-146.
40. Krakowiak, et al. Sleep problems in children with autism spectrum disorders, developmental delays, and typical development: a population-based study. J Sleep Res. 2008;17(2):197-206.
41. Cortesi, et al. Sleep in children with autistic spectrum disorder. Sleep Med. 2010;11(7):659-664.
42. Wiggs. Sleep problems in children with developmental disorders. J R Soc Med. 2001;94(4):177-179.
43. Steinsbekk and Wichstrom, Stability of Sleep Disorders From Preschool to First Grade and Their bidirectional Relationship With Psychiatric Symptoms. J Dev behav Pediatr. 2015.
44. Sutton. Psychiatric disorders and sleep issues. Med Clin north Am. 2014;98(5):1123-1143.
45. Gropman, et al. new developments in Smith-Magenis syndrome (del 17p11.2). Curr Opin neurol. 2007;20(2):125-134.
46. laje, et al. Pharmacological treatment of disruptive behavior in Smith-Magenis syndrome. Am J Med Genet C Semin Med Genet. 2010;154C(4):463-468.
47. Carneiro and Araujo. The food-entrainable oscillator: a network of interconnected brain structures entrained
Smith-Magenis syndrome and its circadian influence on development, behavior, and obesity

156
by humoral signals? Chronobiol Int. 2009;26(7):1273-1289.
48. noble, et al. The lighter side of bDnF. Am J Physiol Regul Integr Comp Physiol. 2011;300(5):R1053-1069.
49. burns, et al. Rai1 haploinsufficiency causes reduced bdnf expression resulting in hyperphagia, obesity and altered fat distribution in mice and humans with no evidence of metabolic syndrome. Hum Mol Genet. 2010;19(20):4026-4042.
50. Alaimo, et al. Dietary regimens modify early onset of obesity in mice haploinsufficient for Rai1. PloS One. 2014;9(8):e105077.
51. Haas-Givler. Smith-Magenis Syndrome: Genetic basis and Clinical Implications. Journal of Mental Health Research in Intellectual Disabilities. 2009;2(2):5.
52. Walz, et al. behavioral characterization of mouse models for Smith-Magenis syndrome and dup(17)(p11.2p11.2). Hum Mol Genet. 2004;13(4):367-378.
53. Coppola and Tessarollo, Control of hyperphagia prevents obesity in bDnF heterozygous mice. neuroreport, 2004;15(17):2665-2668.
54. Gray, et al. Hyperphagia, severe obesity, impaired cognitive function, and hyperactivity associated with functional loss of one copy of the brain-derived neurotrophic factor (bDnF) gene. Diabetes. 2006;55(12):3366-3371.
55. Turek, et al. Obesity and metabolic syndrome in circadian Clock mutant mice. Science. 2005;308(5724):1043-1045.
Li Chen et al.
56. Tahir, et al. Retinoic acid induced-1 (Rai1) regulates craniofacial and brain development in Xenopus. Mech Dev. 2014;133:91-104.
57. Morris, et al. Dose dependent expression of HDAC4 causes variable expressivity in a novel inherited case of brachydactyly mental retardation syndrome. Am J Med Genet A. 2012;158A(8):2015-2020.
58. Fahrner and bjornsson. Mendelian disorders of the epigenetic machinery: tipping the balance of chromatin states. Annu Rev Genomics Hum Genet. 2014;15:269-293.
59. Girirajan, et al. A functional network module for Smith-Magenis syndrome. Clin Genet. 2009;75(4):364-374.
60. Smith, et al. Overview of Smith-Magenis syndrome. J Assoc Genet Technol. 2005;31(4):163-167.
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 02.03.2015 r.Accepted/Zaakceptowano: 10.03.2015 r.
Published online/Dostępne online
Address for correspondence:Sarah H. Elsea, Ph.D, FACMG
Department of Molecular and Human Genetics One baylor Plaza, nAb2015baylor College of Medicine
Houston, TX 77030 uSAPhone: 713-798-5484
Fax: 832-825-1269e-mail: [email protected]

157Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
i n v i t e d r e v i e w
Mark Klukowski, MD, Jolanta Wasilewska, MD, PhD and Dariusz Lebensztejn, MD, PhD
Sleep and gaStrointeStinal diSturbanceS in autiSm Spectrum diSorder in children
Department of Pediatrics, Gastroenterology and Allergology Medical university of białystok,
białystok, Poland
Abstract Autism spectrum disorder (ASD), a neurodevelopmental disorder with a prevalence of 1 in 68 children, commonly presents with comorbid conditions which include sleep disorders. Sleep disorders reported in ASD include, among others, increased bedtime resistance, insomnia, parasomnia, sleep disordered breathing, morning rise problems, and daytime sleepiness. Polysomnography studies show that children with ASD have altered sleep architecture including shorter total sleep time and longer sleep latency than typically developing peers. Sleep-related problems have been shown to affect overall autism scores, social skills deficits, stereotypic behavior, and cognitive performance. Additionally, problematic sleep in children with ASD has been associated with higher levels of parental stress. Underlying causes specifically related to sleep disorders are not fully known. Gastrointestinal (GI) disorders are commonly associated with sleep problems in these patients. Children with ASD and GI symptoms have been found to have a higher prevalence of sleep disturbances compared with typically developing peers who do not have GI symptoms. Treatment approaches to children with sleep disorders are varied and range from lifestyle modifications and behavioral interventions to drug therapies and surgical interventions. Physicians should take into account GI disorders as possible underlying causes of sleep-related problems in children with ASD. Therapeutic interventions should begin with less invasive methods before progressing to more invasive options such as pharmacotherapy and should be based on medical indications in order to provide effective care while minimizing potential adverse health effects. Evidence-based studies concerning GI and sleep disorders in children with ASD are limited and further studies are warranted.
Key words: autism spectrum disorder, gastroesophageal reflux, gastrointestinal diseases, insomnia, pharmacotherapy, sleep disorders
DEV pErioD mED. 2015;XiX,2:157-161
IntroDuctIon Autism spectrum disorder (ASD) is a neurodevelopmental
disorder that is characterized by persistent deficits in social communication, social interaction and restricted repetitive and stereotyped behavior, interests, and activities [1]. Attention on ASD has been rapidly increasing due to the fact that for the past 40 years its prevalence has been steadily rising worldwide with about 1 in 68 children being identified with ASD in the united States according to estimates from the CDC’s Autism and Developmental Disabilities Monitoring network [2]. This rise in incidence is not fully understood and may be the result of several factors including an increased awareness of the condition by both parents and professionals, better diagnostic and assessment methods and/or screening tests, modifications to previous definitions and criteria of diagnosis, and a possible increase in the condition itself.
sleeP DIsorDers In AutIsM Sleep disorders are among the many comorbid
conditions present in ASDs [3]. Sleep problems in children with ASD are commonly reported. Fifty-three percent of young children with ASD may have at least one sleep problem [4]. Self-administered child sleep questionnaires completed by parents show that possibly even up to 86% of these children have at least one sleep problem almost every day [5]. A study by liu et al. on sleep problems in children with ASD showed that 54% had problems with bedtime resistance, 56% with insomnia, 53% with parasomnias, 25% with sleep disordered breathing, 45% with morning rise problems, and 31% with daytime sleepiness [5]. Krakowiak et al. found that the most common sleep complaints among children with ASDs were related to shortened sleep time, nighttime awakening, bedtime resistance, and sleep initiation [4]. In addition, Miano

158
et al. showed that parents of children with ASD reported a higher prevalence of disorders of maintaining sleep, enuresis, and repetitive behavior when falling asleep. Moreover, the authors observed altered sleep architecture and cyclic alternating patterns in polysomnography studies [6]. A recent meta-analysis by elrod and Hood found that children with ASD in general had shorter total sleep time, longer sleep latency, and lower sleep efficiency than typically developing peers [7].
Sleep is an essential part of a healthy lifestyle being linked with many physiological processes such as wound healing, immune system functioning, metabolite clearance of the brain, ontogenesis, memory processes, and others [8-11]. The importance of sleep is especially highlighted by the lack or impairment thereof. A lack of sleep or decreased quality of sleep have been reported in numerous studies to be associated with multiple adverse health effects such as arterial hypertension, diabetes/impaired glucose metabolism, obesity, depression, as well as impaired neurobehavioral performance [12, 13].
Studies on abnormal sleep in pediatric populations have shown that children differ from adults in their response to restrictions in sleep. Acute sleep restrictions have been found to cause decreases in all stages of sleep (except slow-wave sleep), reductions in sleep-onset latency and rapid eye movement (ReM) latency, and reductions of wakefulness during the sleep period. Significant increases in daytime sleepiness following sleep restriction seem to persist into the morning. Children seem to be more severely affected by sleep restriction than adults. Results of polysomnography studies are comparable to adults, but children do not show recovery rebound of slow-wave sleep and ReM sleep [13]. Sleep problems or restriction in pediatric populations have been associated with emotions, impulsivity, school performance, and executive functioning tasks, among others [14].
Sleep problems may significantly influence the cause and/or exacerbate the core disease of ASD if left untreated. A study by Schreck et al. found that fewer hours of sleep per night predicted overall autism scores and social skills deficits. Similarly, stereotypic behavior was predicted by fewer hours of sleep per night and screaming during the night. Increased sensitivity to environmental stimuli in the bedroom and screaming at night predicted communication problems [15]. Most recently, a study by Tessier et al. noted that children with ASD had lower sleep spindle density which had a significant correlation with cognitive performance [16]. Sleep problems not only affect the child’s health and behavior but as well as the parent’s (and quite possibly other family members). Problematic sleep in children with ASD has been associated with higher levels of parental stress which in turn may have an effect on subsequent care of the child [17, 18].
unfortunately, sleep problems are commonly underdiagnosed, underappreciated, undertreated. The road to diagnosing sleep problems is equally problematic and filled with roadblocks. For one, the very nature of ASD greatly increases the difficulty of a diagnostic approach. Verbal communication with children affected by ASD can range from difficult to nearly impossible. unlike normally developing children, they cannot simply state what they
are feeling or going through. because of this, clinicians as well as parents have to be aware of other clues that may point to underlying causes of these sleep problems.
SlEEp proBlEmS AnD AlimEnTArY trAct AIlMents In AsD
An important point to consider is that sleep problems may be exacerbated by, or even be the result of, other comorbid conditions. Other comorbid disorders in children with ASD are quite prevalent. In a population of over 160 children with ASD, liu et al. observed attention deficit hyperactivity disorder (31%), epilepsy (11%), asthma (17%), allergies (50%), and gastrointestinal (GI) symptoms (21% with vomiting, reflux, spit-ups, 17% with chronic diarrhea, 18% with chronic constipation, 18% with abdominal pain, and 14% with intestinal bloating) [5].
Alimentary tract symptoms and disorders have been progressively taking the spotlight in terms of comorbid conditions in patients with ASDs in recent years. As we proposed in our recent paper, GI disorders and ASD co-incidence may be an example of an overlap syndrome [19]. A common pathogenic background of both disorders may be composed of many pathways including genetic factors, immune abnormalities, enzyme insufficiencies, and genetic and metabolic activity of the microbiome and dietary metabolites which may contribute to brain dysfunction and neuroinflammation [20, 21]. Although the mechanism of these sleep disturbances is difficult to ascertain, nighttime awakening with pain or abdominal discomfort is common with gastroesophageal reflux and reflux esophagitis in children. Autistic children with GI symptoms have been found to have a higher prevalence of sleep disturbances, compared with those in the general population who do not have GI symptoms and with their siblings [22-24]. Furthermore, GI symptoms have been significantly correlated with insomnia and parasomnias [5]. More recently, a prospective study by Geier et al. showed that even up to 48% of children with ASD may present with GI disturbances [25]. Interestingly, individuals with comorbid psychiatric disorders, which are also common in individuals with ASD, had poorer rated health, as well as more frequent GI problems and sleep problems [26]. However, certain studies show that children with ASDs may not necessarily differ from typically developing children in sleep disturbances. Schreck and Mulick found that overall sleep duration was similar between ASD and normal children in a population of 5-12 year-olds and Polimeni et al. noted that hours of sleep per night were likewise similar between ASD and normal children [27, 28].
poSSiBlE THErApEUTiC ApproACHES Treatment approaches to children with sleep disorders
are varied and range from behavioral interventions to drug therapies. Parent-based education and behavioral interventions are usually the first-line therapy unless symptoms are severe [29]. behavioral parent training has been shown to significantly improve sleep problems versus comparison groups based on primary sleep outcomes of parental reports [30]. A study by Malow et al. showed that
Mark Klukowski et al.

159
parent-based education was beneficial in reducing sleep problems associated with mean sleep onset latency and sleep onset delay [31]. Decreasing bedroom media access may also prove to be very beneficial. bedroom access to a television or a computer was more strongly associated with reduced sleep among boys with ASD compared with typically developing children. In addition to bedroom access, the amount of time spent playing video games was associated with less sleep also among boys with ASD [32].
Table I presents specific drug therapies [33-40]. They include melatonin (which has hypnotic and chronobiotic properties) and its derivatives as candidates for physiological sleep induction in disorders of insomnia and circadian rhythm sleep. Melatonin and its agonists are potentially effective and safe drugs in the treatment of comorbid insomnia with accompanying beneficial effects in a variety of neurological, psychiatric, cardiovascular and metabolic disorders [33, 34]. ubiquinol supportive therapy has been shown in a study by Gvozdjakova et al. to improve sleep symptoms in 34% of children with ASD, but also improved communication with parents (in 12%), verbal communication (in 21%), playing games (in 42%), and food rejection (in 17%) [35]. Other pharmacological approaches include α2-adrenergic receptor agonists, such as clonidine, selective norepinephrine reuptake inhibitors, such as atomoxetine, selective serotonin reuptake inhibitors, such as fluoxetine, or neuroleptics, such as aripiprazole and risperidone [36-40]. Although these therapeutic choices have been shown to have positive results, these treatments may also bring with them adverse effects including weight gain, sedation, symptoms of restless legs, sleepiness, or even insomnia itself.
Taking into account that GI problems may be responsible for a great deal of sleep problems, one should consider that treatment focused on these conditions may bring relief or at least improvement in sleep problems symptoms [41]. lifestyle modifications, including smaller but more frequent meals or elevated head position during sleep should be considered as possible first-line treatments. Other approaches that should be taken into account
whenever a child with ASD presents with sleep problems include, but are not limited to, proton pump inhibitors for gastroesophageal reflux or diet elimination/substitution therapies in food allergy such as cow milk protein allergy, lactose intolerance or celiac disease [41, 42]. naturally, of paramount importance is adhering to medical indications for introducing these treatments by way of proper diagnostic tests.
conclusIons Concisely, neurodevelopmental disorders such as ASD
commonly present with comorbid disorders including sleep-related problems. underlying causes specifically related to sleep disorders are not fully known. Furthermore, GI disorders are commonly associated with sleep problems and a patient history and physical examination should always include a GI aspect. Treatment approaches should begin with less invasive methods before progressing to options such as pharmacological interventions. lastly, physicians should be open to discuss all available approaches in order to provide maximal care, as well as to minimize potential adverse health effects.
reFerences
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
2. Centers for Disease Control and Prevention. Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, united States, 2010. MMWR Surveill Summ, 2014;63:1-21.
3. lai MC, lombardo MV, baron-Cohen S. Autism. lancet, 2014;383:896-910.
4. Krakowiak P, Goodlin-Jones b, Hertz-Picciotto I, Croen lA, Hansen Rl. Sleep problems in children with autism spectrum disorders, developmental delays, and typical development: A population-based study. J Sleep Res, 2008;17:197-206.
example drug drug class principal role reference(s)
Melatonin indoleamine derivative improvement of sleep-wake rhythm and sleep latency [33, 34]
Ubiquinol coenzyme Q10 derivative
modulation of neuronal activity through decreasing oxidative stress [35]
clonidine α2-Adrenergic receptor agonist
improvement of sleep initiation latency and nighttime awakening [37]
Atomoxetine norepinephrine reuptake inhibitor
Symptom reduction in hyperactivity, self-stimulation [38]
Fluoxetine Selective serotonin reuptake inhibitor
reduction of repetitive behaviors and irritability [39]
Aripiprazole risperidone neuroleptic reduction of challenging
and repetitive behaviors [36, 40]
Table i. possible pharmacological interventions in children with autism spectrum disorder and sleep disorders.
Sleep and gastrointestinal disturbances in autism spectrum disorder in children

160
5. liu X, Hubbard JA, Fabes RA, Adam Jb. Sleep disturbances and correlates of children with autism spectrum disorders. Child Psychiatry Hum Dev, 2006;37:179-191.
6. Miano S, bruni O, elia M, Trovato A, Smerieri A, Verrillo e, Roccella M, Terzano MG, Ferri R. Sleep in children with autistic spectrum disorder: A questionnaire and polysomnographic study. Sleep Med, 2007;9:64-70.
7. elrod MG, Hood bS. Sleep differences among children with autism spectrum disorders and typically developing peers: A meta-analysis. J Dev behav Pediatr, 2015;36:166-177.
8. Xie l, Kang H, Xu Q, Chen MJ, liao Y, Thiyagarajan M, O’Donnell J, Christensen DJ, nicholson C, Iliff JJ, Takano T, Deane R, nedergaard M. Sleep drives metabolite clearance from the adult brain. Science, 2013;342:373-377.
9. Morrissey MJ, Duntley SP, Anch AM, nonneman R. Active sleep and its role in the prevention of apoptosis in the developing brain. Med Hypotheses, 2004;62:876-879.
10. Turner TH, Drummond SP, Salamat JS, brown GG. effects of 42 hr of total sleep deprivation on component processes of verbal working memory. neuropsychology, 2007;21:787-795.
11. Zager A, Andersen Ml, Ruiz FS, Antunes Ib, Tufik S. effects of acute and chronic sleep loss on immune modulation of rats. Am J Physiol Regul Integr Comp Physiol, 2007;293:R504-R509.
12. buysse DJ. Sleep health: Can we define it? Does it matter? Sleep, 2014;37:9-17.
13. Sheldon SH, Ferber R, Kryger MH, Gozal D. Principles and practice of pediatric sleep medicine. 2nd ed. Philadelphia: elsevier Saunders; 2014.
14. Maski KP, Kothare SV. Sleep deprivation and neurobehavioral functioning in children. Int J Psychophysiol, 2013; 89:259-264.
15. Schreck KA, Mulick JA, Smith AF. Sleep problems as possible predictors of intensified symptoms of autism. Res Dev Disabil, 2004;25:57-66.
16. Tessier S, lambert A, Chicoine M, Scherzer P, Soulières I, Godbout R. Intelligence measures and stage 2 sleep in typically-developing and autistic children. Int J Psychophysiol, 2015;97:58-65.
17. Doo S, Wing YK. Sleep problems of children with pervasive developmental disorders: Correlation with parental stress. Dev Med Child neurol, 2006;48:650-655.
18. Patzold lM, Richdale Al, Tonge bJ. An investigation into sleep characteristics of children with autism and Asperger’s disorder. J Paediatr Child Health, 1998;34:528-533.
19. Wasilewska J, Klukowski M. Gastrointestinal symptoms and autism spectrum disorder: links and risks. Pediatr Health Med Ther, 2015;6: in press.
20. Wasilewska J, Kaczmarski M, Stasiak-barmuta A, Tobolczyk J, Kowalewska e. low serum IgA and increased expression of CD23 on b lymphocytes in peripheral blood in children with regressive autism aged 3-6 years old. Arch Med Sci, 2012;8:324-331.
21. Cieślińska A, Sienkiewicz-Szłapka e, Wasilewska J, Fiedorowicz e, Chwała b, Moszyńska-Dumara M, Cieśliński T, bukało M, Kostyra e. Influence of candidate polymorphisms on the dipeptidyl peptidase IV and μ-opioid receptor genes expression in aspect of the β-casomorphin-7 modulation functions in autism. Peptides, 2015;65:6-11.
22. Horvath K, Perman JA. Autism and gastrointestinal symptoms. Curr Gastroenterol Rep, 2002;4:251-258.
23. Molloy CA, Manning-Courtney P. Prevalence of chronic gastrointestinal symptoms in children with autism and autistic spectrum disorders. Autism, 2003;7:165-171.
24. Valicenti-McDermott M, McVicar K, Rapin I, Wershil bK, Cohen H, Shinnar S. Frequency of gastrointestinal symptoms in children with autistic spectrum disorders and association with family history of autoimmune disease. J Dev behav Pediatr, 2006;27:S128-S136.
25. Geier DA, Kern JK, Geier MR. A prospective cross-sectional cohort assessment of health, physical, and behavioral problems in autism spectrum disorders. Maedica (buchar), 2012;7:193-200.
26. Kring SR, Greenberg JS, Seltzer MM. Adolescents and adults with autism with and without co-morbid psychiatric disorders: Differences in maternal well-being. J Ment Health Res Intellect Disabil, 2008;1:53-74.
27. Schreck KA, Mulick JA. Parental report of sleep problems in children with autism. J Autism Dev Disord, 2000;30:127-135.
28. Polimeni MA, Richdale Al, Francis AJ. A survey of sleep problems in autism, Asperger’s disorder and typically developing children. J Intellect Disabil Res, 2005;49:260-268.
29. Grigg-Damberger M, Ralls F. Treatment strategies for complex behavioral insomnia in children with neurodevelopmental disorders. Curr Opin Pulm Med, 2013;19:616-625.
30. Johnson CR, Turner KS, Foldes e, brooks MM, Kronk R, Wiggs l. behavioral parent training to address sleep disturbances in young children with autism spectrum disorder: A pilot trial. Sleep Med, 2013;14:995-1004.
31. Malow bA, Adkins KW, Reynolds A, Weiss SK, loh A, Fawkes D, Katz T, Goldman Se, Madduri n, Hundley R, Clemons T. Parent-based sleep education for children with autism spectrum disorders. J Autism Dev Disord, 2014;44:216-228.
32. engelhardt CR, Mazurek MO, Sohl K. Media use and sleep among boys with autism spectrum disorder, ADHD, or typical development. Pediatrics, 2013;132:1081-1089.
33. laudon M, Frydman-Marom A. Therapeutic effects of melatonin receptor agonists on sleep and comorbid disorders. Int J Mol Sci, 2014;15:15924-15950.
34. bruni O, Alonso-Alconada D, besag F, biran V, braam W, Cortese S, Moavero R, Parisi P, Smits M, Van der Heijden K, Curatolo P. Current role of melatonin in pediatric neurology: Clinical recommendations. eur J Paediatr neurol, 2015;19:122-133.
35. Gvozdjakova A, Kucharska J, Ostatnikova D, babinska K, nakladal D, Crane Fl. ubiquinol improves symptoms in children with autism. Oxid Med Cell longev, 2014;2014:798957.
36. Owen R, Sikich l, Marcus Rn, Corey-lisle P, Manos G, McQuade RD, Carson WH, Findling Rl. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics, 2009;124:1533-1540.
37. Ming X, Gordon e, Kang n, Wagner GC. use of clonidine in children with autism spectrum disorders. brain Dev, 2008;30:454-460.
38. Arnold le, Aman MG, Cook AM, Witwer An, Hall Kl, Thompson S, Ramadan Y. Atomoxetine for hyperactivity
Mark Klukowski et al.

161
in autism spectrum disorders: Placebo-controlled crossover pilot trial. J Am Acad Child Adolesc Psychiatry, 2006;45:1196-1205.
39. Hollander e, Phillips A, Chaplin W, Zagursky K, novotny S, Wasserman S, Iyengar R. A placebo controlled crossover trial of liquid fluoxetine on repetitive behaviors in childhood and adolescent autism. neuropsychopharmacology, 2005;30:582-589.
40. lemmon Me, Gregas M, Jeste SS. Risperidone use in autism spectrum disorders: A retrospective review of a clinic-referred patient population. J Child neurol, 2011;26:428-432.
41. Wasilewska J, Semeniuk J, Cudowska b, Klukowski M, Dębkowska K, Kaczmarski M. Respiratory response to
Sleep and gastrointestinal disturbances in autism spectrum disorder in children
proton pump inhibitor treatment in children with obstructive sleep apnea syndrome and gastroesophageal reflux disease. Sleep Med, 2012;13:824-830.
42. Veatch OJ, Maxwell-Horn AC, Malow bA. Sleep in autism spectrum disorders. Curr Sleep Med Rep, 2015;1:131-140.
Conflicts of interestThe Authors declare no conflict of interest.
Received: June 19, 2015Accepted: June 30, 2015
Published online
Address for correspondence: Mark Klukowski, MD
Department of Pediatrics, Gastroenterology and Allergology
Medical university of białystok Children’s Clinical Hospital of l. Zamenhof
ul. Waszyngtona 17, 15-274 białystok, Poland tel.: +48 85 745 0703 fax: +48 85 742 3841
e-mail: [email protected]

162Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Wojciech Jańczyk1, J.H.C. de Roo2, Joachim Schweizer2, Jerzy Socha1, Piotr Socha1, M. Luisa Mearin2
coeliac diSeaSe not reSponding to a gluten-free diet in children:
caSe StudieS and literature review
celiakia oporna na leczenie dietą bezglutenową: opiS przypadków oraz przegląd literatury
1Department of Gastroenterology, Hepatology and eating Disorders, The Children’s Memorial Health Institute, Warsaw, Poland
2Department of Pediatrics leiden university Medical Center, The netherlands
AbstractWe presented the cases of three children with coeliac disease who despite good adherence to a gluten-free diet remained non-responsive to treatment. Two patients, one of them with IgA deficiency, were successfully treated by complete gluten exclusion with enteral nutrition. However the third child with a severe coeliac disease did not achieve clinical and histologic improvement, even on immunosuppressive treatment. If no hidden sources of gluten can be identified, other causes of persistent villous atrophy, different from coeliac disease, have to be considered. They include e.g. inflammatory, immune and endocrine diseases of the digestive tract. In severe cases of childhood coeliac disease not responding to a gluten free diet, autoimmune enteropathy and refractory coeliac disease must be taken into account.
Key words: coeliac disease, enteropathy, gluten-free diet, enteral nutrition, refractory coeliac disease, children
StreszczeniePrzedstawiamy trzy przypadki dzieci z celiakią oporną na leczenie pomimo przestrzegania diety bezglutenowej. Dwóch pacjentów, w tym jeden z niedoborem IgA, było skutecznie leczonych żywieniem dojelitowym z wyłączeniem glutenu. Trzeci pacjent z ciężką postacią choroby trzewnej nie uzyskał poprawy klinicznej ani histologicznej mimo zastosowania leczenia immunosupresyjnego. Wśród przyczyn braku odpowiedzi na leczenie celiakii należy rozważyć przede wszystkim ekspozycję na gluten w diecie. Do innych przyczyn przewlekłego zaniku kosmków jelitowych należą m.in. choroby zapalne przewodu pokarmowego, niedobory immunologiczne oraz zaburzenia hormonalne. W celiakii o ciężkim przebiegu, niereagującej na leczenie dietą bezglutenową jako przyczynę należy rozważyć celiakię oporną na leczenie oraz enteropatię o podłożu autoimmunologicznym.
Slowa kluczowe: celiakia, enteropatia, dieta bezglutenowa, żywienie dojelitowe, celiakia oporna na leczenie, dzieci
DEV pErioD mED. 2015;XiX,2:162-166
oriGinaL artiCLeS/praCe oryGinaLne

163Coeliac disease not responding to a gluten-free diet in children
IntroDuctIonCoeliac disease (CD) is an immune-mediated systemic
disorder elicited by gluten and related prolamines in genetically susceptible individuals and is characterized by the presence of a variable combination of gluten-dependent clinical manifestations, CD-specific antibodies, HlA-DQ2 or HlA-DQ8 haplotypes, and enteropathy. CD-specific antibodies comprise autoantibodies against tissue transglutaminase (TG2), anti-endomysial antibodies (eMA), and antibodies against deamidated forms of gliadin peptides (DGP) [1].
After the elimination of gluten from the diet, patients usually demonstrate clinical improvement and restoration of the intestinal architecture. However, sometimes clinical and histologic response to a gluten-free diet (GFD) cannot be achieved. In these circumstances first of all gluten contamination should be considered. If this can be ruled out, further investigations towards any concomitant pathologies that could mimic CD have to be done. They include food allergy, inflammatory bowel disease, microscopic colitis, autoimmune enteropathy, exocrine pancreatic insufficiency, bacterial overgrowth, endocrine and immune deficiency etc. In severe cases of true non-responsiveness to a GFD, refractory CD (RCD) should be considered [2-4].
In the following section we present three patients with CD, who were initially non-responsive to a GFD.
The presentations of patients
Patient 1A 7-year-old boy was referred to our clinic for a second
opinion because of CD which was not responsive to treatment with a GFD. The clinical history comprised of cerebral palsy, hemiplegia and epilepsy from the age of 13 months, caused by multiple thrombotic infarctions in the brain of an unknown origin. At the age of 16 months he presented with abdominal pain. IgA class anti-endomysial antibodies (eMA) were strongly positive and histologic examination of the duodenum showed subtotal villous atrophy, classified as Marsh class 3b. CD was diagnosed and he was treated with a GFD. However, during the 5-year follow-up, the complaints persisted and eMA remained elevated. Repeated duodenal biopsies, reviewed by two pathologists experienced in CD, revealed Marsh class 3 lesions.
On admission to our clinic the patient was in a good clinical condition, but eMA remained strongly positive (TG2 antibodies were unavailable at that time in our centre). His HlA typing was DR3-DQ2/DR7-DQ2. The GFD was re-evaluated several times by a registered dietician, but no gluten contamination could be identified. His anti-epileptic drugs were tested by the Dutch Food and Consumer Product Safety Authority for gluten, but they were found to be gluten-free (<200 ppm). To be certain that gluten was completely excluded from his diet, he was treated with exclusive enteral feeding for three months. Afterwards we repeated the duodenal biopsies. The histology showed some improvement, described as Marsh class 3a. The CD3 staining showed no refractory CD (confirmed by laboratories in Rijnstate Ziekenhuis
Hospital, Arnhem, the netherlands and l’Hospital necker-enfantes Malades, Paris, France). High intraepithelial lymphocytosis on biopsy and absence of anti-enterocyte antibodies were against the diagnosis of autoimmune enteropathy. The boy was further treated with an oral GFD and during the follow-up his abdominal pain resolved, the eMA and TG2 antibodies disappeared. At the age of 9 years and 4 months, after 8 years on a GFD, duodenal histology was normal, consistent with a good response to the GFD.
Patient 2A 7-year-old girl with an unremarkable medical history
presented with abdominal pain and constipation that was not responsive to treatment with macrogol. Among other causes, CD was suspected. examinations revealed a selective IgA-deficiency (IgA <0.05 g/l), strongly positive IgG class eMA, and markedly increased IgG-class TG2 antibodies (2510 u/ml). Duodenal biopsies showed subtotal villous atrophy consistent with Marsh class 3b. CD was diagnosed and she was treated with a GFD. The clinical symptoms resolved soon but, despite thorough dietary evaluation, after 19 months of follow-up, the IgG class eMA and IgG class TG2 antibodies remained strongly positive.
At the age of 8 years and 8 months, the girl was referred to our clinic. Repeated CD serology continued to show highly positive IgG eMA and slowly decreasing IgG TG2 antibodies. no overt sources of gluten intake were identified. Duodenal biopsies were repeated and showed Marsh-class 3a lesions in the duodenal bulbus and normal mucosa (Marsh 0) in the descending duodenum. CD3 staining did not reveal abnormalities seen in the refractory CD. T-cell flow cytometry performed on Iels isolated form duodenal biopsies showed 22% aberrant T cells (CD52+, sCDR-, cytCD3+). To guarantee complete gluten avoidance the patient was treated with exclusive enteral feeding for three months. After this period, the eMA and the IgG TG2 antibodies remained elevated, but repeated duodenal biopsies showed an almost complete restoration of the bulbus mucosa (Marsh 1) and normal mucosa in the descending duodenum. T-cell flow cytometry showed 23% Iel of aberrant phenotype (CD52+, sCDR-, cytCD3+). At present, after nearly 5 years of follow-up on a GFD, she reports no complaints. Although the levels of IgG eMA in serum are still elevated, the titers of IgG TG2 antibodies have gradually decreased and are now almost normal.
Patient 3A male infant with provisional diagnosis of CD was
referred to our clinic at the age of 12 months. His past medical record included poor weight and prolonged diarrhea that started after introduction of gluten in the 4th month of life. On admission he had positive serum IgA eMA, TG2, IgA and IgG anti-gliadin (AGA) and anti-reticulin (ARA) antibodies. Duodenal biopsy showed villous atrophy grade Marsh 3c. His HlA typing was DQ2 homozygous. Diagnosis of CD was confirmed. However, treatment with a GFD was not successful and diarrhea and malnutrition persisted throughout the 20 years of

164 Wojciech Jańczyk et al.
clinical follow-up. In the meantime, the patient developed osteopenia, anemia, hypoalbuminemia, hypokalemia, and hyponatremia. Several duodenal biopsies revealed persistent villous atrophy grade Marsh 3c accompanied by crypt hyperplasia, high intraepithelial lymphocytosis (>50 Iel/100e) and lymphoplasmocytosis of lamina propria, although he strictly adhered to the GFD. Autoimmune enteropathy was ruled out based on duodenal histology suggestive for CD (as described above), absence of other autoimmune diseases, lack of anti-enterocyte and other auto-antibodies. Repeated gastroscopies and coloscopies were consistent with histology and showed lesions limited only to the duodenum. Thorough investigations made the following unlikely: food allergy, inflammatory bowel diseases, microscopic colitis, pancreatic insufficiency, bacterial overgrowth, cystic fibrosis, rheumatoid and collagen diseases, tuberculosis, endocrine disorders and immune deficiency. At the age of 4 years eMA, AGA and TG2 antibodies became negative.
GFD was maintained for over 20 years with good compliance, verified by negative TG2, eMA antibodies and evaluated by an experienced dietician and gastroenterologist. because constant adherence to a GFD did not significantly improve either the patient’s clinical condition or his severe duodenal villous atrophy, we considered the possibility of refractory CD.
At the age of 16 years, we started therapy with prednisone (2mg/kg) and within a month we observed a major clinical improvement. The patient eventually reported well being and gained weight (about 2 kg per month). After twelve months of corticosteroid treatment villous atrophy improved to Marsh 2. However, on a tapering dose of prednisone, the patient’s condition deteriorated again. He also suffered from corticosteroid-related severe osteopenia. Azathioprine (2mg/kg) was started in order to withdraw prednisone but subsequent duodenal biopsy revealed reoccurrence of villous atrophy Marsh 3c. elemental diet (amino acid-based formula) was maintained for 5 months without improvement. The patient was switched to cyclosporine, which had to be withdrawn after 4 months, because of the lack of efficacy and side effects (thrombocytopenia and musculoskeletal pain). At the age of 20, apparently after a dietetic error, the patient was urgently admitted to our unit presenting with severe diarrhea, significant weight loss (2.5kg within 3 days), muscle cramps, pruritus, urticaria and electrolytic and biochemical disturbances. He was treated with hydrocortisone, antibiotics i.v. and total parenteral nutrition (TPn). A few years after being discharged from our health centre, he remains in a stable condition, but still requires TPn.
DIscussIonOur paper describes three cases of children with
symptomatic, non-responsive CD, who strictly adhered to GFD for a long period of time (5-20 years). In all the patients the diagnosis of CD was confirmed by duodenal histology and the presence of eMA and TG2 antibodies that are considered highly sensitive and specific for CD. In addition, patients 1 and 3 had HlA typing highly predisposing to CD.
non-responsive CD should first of all raise questions over the strict gluten avoidance. As shown previously, exposure to even a small amount of gluten (for example nutritional preservatives) might be sufficient to maintain intestinal damage in exceptionally gluten-sensitive individuals [5,6]. Therefore, deliberate or covert gluten contamination should always be taken into account. To provide appropriate surveillance of a gluten-free diet our patients were closely monitored by experienced dieticians. Where available, food was tested for possible gluten content in specialized laboratories.
Patients 1 and 2 eventually reacted to complete gluten exclusion on enteral nutrition. As reported earlier, patients with CD not responding to a GFD may benefit from further dietary restrictions, such as elemental diet or parenteral nutrition [7, 8]. However, to the best of our knowledge, improvement of a GFD applied via enteral nutrition has not previously been described in these patients. We speculate that the use of gluten-free enteral formulas may prevent accidental gluten contamination or ingestion.
Patient 2 presented with CD and concomitant IgA deficiency. Interestingly, in this case the serologic markers of CD (eMA) remained elevated after clinical improvement and histologic restoration of the duodenal mucosa. However, it is known that in IgA-deficient patients, the IgG CD serology may be persistently elevated, despite histologic recovery [9]. Specific antibody production is dependent on T helper lymphocyte function, T cell priming and cytokine profiles and b cell responsiveness shows alterations in IgA deficiency. Therefore, the slow disappearance of IgG coeliac antibodies may be part of the immunoregulatory defect seen in IgA deficiency [10].
Patient 3 did not achieve clinical and histologic improvement, even on immunosuppressive treatment. He presented with a clinical picture of severe CD which was confirmed by duodenal histology, HlA typing and the presence of eMA and TG2 antibodies on several occasions. In addition, extensive differential diagnosis excluded potential causes of coeliac-like enteropathy, such as food allergy, inflammatory bowel disease, microscopic colitis, exocrine pancreatic insufficiency, bacterial overgrowth, endocrine and immune deficiency etc. [2-4]
The early onset of symptoms, no response to GFD, persistent villous atrophy and improvement on immunosuppressive therapy could be indicative of autoimmune enteropathy (AIe), an immune-mediated disease that may cause protracted diarrhea and malabsorption, usually with onset in infants and young children. The endoscopic and histologic lesions in AIe show similarities to these found in untreated CD. Moreover, AIe is linked to other autoimmune disorders and may present with circulating anti-enterocyte antibodies or other autoantibodies, however their pathogenic role is not clear [11]. On the contrary to the findings in our patient, villous atrophy in AIe is characterized by reduced intraepithelial lymphocytosis and AIe patients do not present with CD-specific antibodies, such as eMA and TG2 [12]. Anti-enterocyte antibodies were never found. neither were there any coexisting autoimmune disorders or immune deficits. The family record was

165Coeliac disease not responding to a gluten-free diet in children
negative for autoimmune disease. AIe is considered a generalized autoimmune disorder of the gastrointestinal tract [13], but in our patient repeated upper and lower GI endoscopies showed lesions limited only to the duodenum. Furthermore, our patient achieved long-term improvement on total parenteral nutrition, while patients with AIe usually do not improve on any diet restriction therapy. Immunosuppressive treatment, which is claimed beneficial for patients with AIe [14-17], was not successful in our patient in the long-term. All these facts made the diagnosis of AIe unlikely in patient 3.
In patients with non-responsive CD, after exclusion of other CD-mimicking disorders, refractory CD should be taken into account [4]. We speculate that, based on the course of the disease and no response to dietary intervention and pharmacotherapy, RCD could be the most probable diagnosis in patient 3, although specific immunochemical testing for RCD was not available at that time in our centre.
Refractory coeliac disease (RCD) should be suspected in CD patients with persistent enteropathy in spite of good adherence to treatment with a gluten-free diet for at least 12 months [2-4]. The definition of RCD also includes the occurrence of severe clinical deterioration in diagnosed CD, which requires rapid intervention independent of the duration of the GFD. RCD accounts for 7-15% of all adult-onset CD and predominantly concerns HlA-DQ2 homozygous individuals [18,19]. Two types of RCD have been recognized on the basis of immunophenotyping of intraepithelial lymphocytes: type I - without or with less that 20% aberrant CD3- CD4- T-cells and type II - with over 20% aberrant T-cells in the intestinal mucosa [20]. RCD type II is usually resistant to any conventional treatment and has a higher risk of transition into malignancies, particularly enteropathy associated T-cell lymphoma (eATl) [21].
RCD has been seen almost only in adult-onset CD, while in children it is a rare condition. Only incidental cases of RCD in the pediatric population have been described so far. Recently, Mubarak et al. reported a single case of a child with RCD type I, in whom the GFD was sufficient to achieve a good clinical but not a histologic response. Complete resolution of duodenal lesions was eventually seen after a 1-year-long treatment with azathioprine [22].
Current therapeutic guidelines in RCD include both nutritional and pharmacological therapy. The maintenance of GFD and enteral nutrition should be the primary approach in these patients. A further dietary regime, such as an elemental diet, proved to be successful in several studies [7]. Corticosteroids are the first-line pharmacological option to induce remission followed by azathioprine [21, 23, 24]. Cyclosporine was also claimed beneficial in some studies [25]. There have been reports that budesonide may reverse the clinical symptoms of RCD without the side effects associated with systemic corticosteroids, however no improvement on mucosal histology was seen in these patients [26, 27]. There is growing evidence that infliximab may induce remission in RCD patients resistant to conventional treatment (favorably RCD type I). The initial results are encouraging but the safety and efficacy of this therapy has
to be proven in longitudinal, large cohorts studies [28-30]. Interleukin 10 is generally not successful in adults with RCD and the effects of alemtuzumab are uncertain [31, 32]. Cladribine (2-chlorodeoxyadenosine), a cytotoxic purine nucleoside effective in hairy cell leukemia, showed some promising results in recent open-label studies in RCD II, as it potentially decreases the number of aberrant T-cells and may reduce transition into eATl [33]. Autologous stem cell transplantation (ASCT) remains the ultimate treatment for carefully selected patients who did not respond to any pharmacotherapy including cladribine, however its results are not satisfactory at the moment [34]. As the interleukin 15 overexpression is supposed to be responsible for intraepithelial lymphocytic expansion, Il-15 blocker-drugs may be useful in the management of clonal refractory coeliac disease in future research [35].
In conclusion, the medical records of our patients show that childhood CD which is not responsive to GFD may be managed by complete gluten exclusion with enteral nutrition. However, in the case of failure after total gluten exclusion, other diagnoses, such as autoimmune enteropathy or refractory CD should be considered. These patients may benefit from immunosuppressive treatment or total parenteral nutrition.
reFerences
1. Husby S, Koletzko S, Korponay-Szabó IR, Mearin Ml, Phillips A, Shamir R et al. european Society for Pediatric Gastroenterology, Hepatology, and nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol nutr. 2012;54(1):136-160.
2. biagi F, Corazza GR. Defining gluten refractory enteropathy. eur J Gastroenterol Hepatol. 2001;13:561-565.
3. O’Mahony S, Howdle PD, losowsky MS. Review article: management of patients with non-responsive celiac disease. Aliment Pharmacol Ther. 1996;10:671-678.
4. Mooney PD, evans Ke, Singh S, Sanders DS. Treatment failure in coeliac disease: a practical guide to investigation and treatment of non-responsive and refractory coeliac disease. J Gastrointestin liver Dis. 2012;21(2):197-203.
5. biagi F, Campanella J, Martucci S, Pezzimenti D, Ciclitira PJ, ellis HJ, Corazza GR. A milligram of gluten a day keeps the mucosal recovery away: a case report. nutrition Reviews. 2004;62(9):360-363.
6. Hollon JR, Cureton PA, Martin Ml, Puppa el, Fasano A. Trace gluten contamination may play a role in mucosal and clinical recovery in a subgroup of diet-adherent non-responsive celiac disease patients. bMC Gastroenterology. 2013;13:40.
7. Olaussen RW, lovik A, Tollefsen S, Andresen PA, Vatn MH, De lange T, et al. effect of elemental diet on mucosal immunopathology and clinical symptoms in type 1 refractory celiac disease. Clin Gastroenterol Hepatol. 2005;3(9):875-885.
8. Mandal A, Mayberry J. elemental diet in the treatment of refractory coeliac disease. eur J Gastroenterol Hepatol. 2001;13(1):79-80.
9. Chow MA, lebwohl b, Reilly nR, Green PH. Immunoglobulin A Deficiency in Celiac Disease. J Clin Gastroenterol. 2012;46(10):850-854

166
10. Korponay-Szabo IR, Dahlbom I, laurila K, Koskinen S, Woolley n, Partanen J et al. elevation of IgG antibodies against tissue transglutaminase as a diagnostic tool for coeliac disease in selective IgA deficiency. Gut. 2003;52:1567-1571.
11. unsworth DJ, Walker-Smith JA. Autoimmunity in diarrhoeal disease. J Pediatr Gastroenterol nutr. 1985;4(3):375-380.
12. Mirakian R, Hill S, Richardson A, Milla PJ, Walker-Smith JA, bottazzo GF. HlA product expression and lymphocyte subpopulations in jejunum biopsies of children with idiopathic protracted diarrhoea and enterocyte autoantibodies. J Autoimmun. 1988;1(3):263-277.
13. Hill SM, Milla PJ, bottazzo GF, Mirakian R. Autoimmune enteropathy and colitis: is there a generalised autoimmune gut disorder? Gut. 1991;32(1):36-42.
14. Sanderson IR, Phillips AS, Spencer J, Walker-Smith JA. Response to autoimmune enteropathy to cyclosporin A therapy. Gut 1991;32:1421-1425.
15. Seidman eG, lacaille F, Russo P, Galeano n, Murphy G, Roy CC. Successful treatment of autoimmune enteropathy with cyclosporin. J Pediatr 1990;117:929-932.
16. Quiros-Tejeira R, Ament Me, Vargas JH. Induction of remission in a child with autoimmune enteropathy using mycophenolate mofetil. J Pediatr Gastroenterol nutr 2003;36:482-485.
17. Vanderhoof JA, Young RJ. Autoimmune enteropathy in a child: response to infliximab therapy. J Pediatr Gastroenterol nutr 2002;34:312-316.
18. Al-Toma A, Verbeek WHM, Mulder CJJ. update on the management of refractory celiac disease. J Gastrointestin liver Dis. 2007;16:57-63.
19. Al-Toma A, Goerres MS, Meijer JW, Peña AS, Crusius Jb, Mulder CJ. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin Gastroenterol Hepatol. 2006;4(3):315-319.
20. Cellier C, Patey n, Mauvieux l, Jabri b, Delabesse e, Cervoni JP et al. Abnormal intestinal intraepithelial lymphocytes in refractory sprue. Gastroenterology. 1998;114(3):471-481.
21. Cellier C, Delabesse e, Helmer C, Patey n, Matuchansky C, Jabri b et al. Refractory sprue, coeliac disease, and enteropathy-associated T-cell lymphoma. lancet. 2000;356:203-208.
22. Mubarak A, Oudshoorn JH, Kneepkens CM, butler JC, Schreurs MW, Mulder CJ. A child with refractory coeliac disease. J Pediatr Gastroenterol nutr. 2011;53(2):216-218.
23. Goerres MS, Meijer JW, Wahab PJ, Kerckhaert JA, Groenen PJ, Van Krieken JH et al. Azathioprine and prednisone combination therapy in refractory coeliac disease. Aliment Pharmacol Ther. 2003;18(5):487-494.
24. Maurino e, niveloni S, Chernavsky A, Pedreira S, Mazure R, Vazquez H et al. Azathioprine in refractory sprue: results from a prospective, open-label study. Am J Gastroenterol. 2002;97(10):2595-2602.
25. Wahab PJ, Crusius Jb, Meijer JW, uil JJ, Mulder CJ. Cyclosporin in the treatment of adults with refractory coeliac disease - an open pilot study. Aliment Pharmacol Ther. 2000;14(6):767-774.
26. brar P, lee S, lewis S, egbuna I, bhagat G, Green PH. budesonide in the treatment of refractory celiac disease. Am J Gastroenterol. 2007;102(10):2265-2269.
27. Daum S, Ipczynski R, Heine b, Schulzke JD, Zeitz M, ullrich R. Therapy with budesonide in patients with refractory sprue. Digestion. 2006;73(1):60-68.
28. Gillett HR, Arnott ID, McIntyre M, Campbell S, Dahele A, Priest M et al. Successful infliximab treatment for steroid-refractory celiac disease: a case report. Gastroenterology. 2002;122(3):800-805.
29. Turner SM, Moorghen M, Probert CS. Refractory coeliac disease: remission with infliximab and immunomodulators. eur J Gastroenterol Hepatol. 2005;17(6):667-669.
30. Costantino G, della Torre A, lo Presti MA, Caruso R, Mazzon e, Fries W. Treatment of life-threatening type I refractory coeliac disease with long-term infliximab. Dig liver Dis. 2008;40(1):74-77.
31. Mulder CJ, Wahab PJ, Meijer JW, Metselaar e. A pilot study of recombinant human interleukin-10 in adults with refractory coeliac disease. eur J Gastroenterol Hepatol. 2001;13(10):1183-1188.
32. Vivas S, Ruiz de Morales JM, Ramos F, Suárez-Vilela D. Alemtuzumab for refractory celiac disease in a patient at risk for enteropathy-associated T-cell lymphoma. n engl J Med. 2006;354(23):2514-2415.
33. Tack GJ, Verbeek WH, Al-Toma A, Kuik DJ, Schreurs MW, Visser O et al. evaluation of Cladribine treatment in refractory celiac disease type II. World J Gastroenterol. 2011;28;17(4):506-513.
34. Tack GJ, Wondergem MJ, Al-Toma A, Verbeek WH, Schmittel A, Machado MV et al. Auto-SCT in refractory celiac disease type II patients unresponsive to cladribine therapy. bone Marrow Transplant 2011;46:840-846.
35. Di Sabatino A, Ciccocioppo R, Cupelli F, Cinque b, Millimaggi D, Clarkson MM et al. epithelium derived interleukin 15 regulates intraepithelial lymphocyte Th1 cytokine production, cytotoxicity, and survival in coeliac disease. Gut. 2006;55(4):469-477.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 21.01.2015 r.Accepted/Zaakceptowano: 09.03.2015 r.
Published online/Dostępne online
Address for correspondence:Wojciech Jańczyk
Department Gastroenterology, Hepatology and eating Disorders, The Children’s Memorial Health Institute
Al. Dzieci Polskich 20, 04-730 Warsaw, Polandfax: (+48 22) 815-73-82
e-mail: [email protected])
Wojciech Jańczyk et al.

167Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
Elżbieta Czub1, Jan K. Nowak2, Jerzy Moczko3, Przemysław Mankowski4, Aleksandra Lisowska2, Aleksandra Banaszkiewicz5, Tomasz Banasiewicz6, Jarosław Walkowiak2
fecal pyruvate kinaSe iS not Suitable for diScrimination between inflammatory
bowel diSeaSe exacerbation and acute gaStroenteritiS*
pomiar Stężenia kinazy pirogronianowej w kale nie pozwala na rozróżnienie między zaoStrzeniem
nieSwoiStego zapalenia jelit a oStrym nieżytem żołądkowo-jelitowym
1Child and Mother Specialist Hospital in Poznan, Poland2Department of Pediatric Gastroenterology and Metabolic Diseases,
Poznan university of Medical Sciences, Poznan, Poland3Department of Informatics and Statistics, Poznan university of Medical Sciences, Poznan, Poland
4Department of Pediatric Surgery, Poznan university of Medical Sciences, Poznan, Poland5Department of Pediatric Gastroenterology and nutrition, Medical university of Warsaw, Warsaw, Poland
6Department of General, Gastroenterological and endocrinological Surgery, Poznan university of Medical Sciences, Poznan, Poland
AbstractIntroduction: In inflammatory bowel diseases (IBD) diarrhea can be caused by exacerbation and/or infectious agents. Fecal calprotectin (FC) is a well-established biomarker of intestinal inflammation in IBD. However, its usefulness in depiction of IBD exacerbation from infectious diarrhea is limited. The value of fecal pyruvate kinase isoenzyme type 2 (M2-PK) in this application remains unknown. Aim: To compare the performance of M2-PK and FC in discriminating between diarrhea caused by IBD and infectious agents.Materials and methods: One hundred three patients were enrolled for the study, including 32 with ulcerative colitis (UC), 21 with Crohn’s disease (CD), 29 with acute diarrhea caused by rotavirus (AD-RV), and 21 with acute diarrhea caused by Salmonella enteritidis (AD-SE). M2-PK and FC were measured using ELISA. Areas under receiver operating characteristic curves (AUCs), sensitivities and specificities for both tests in distinguishing between patient subgroups with moderate to severe UC and CD from AD-RV and AD-SE were calculated.Results: Differences in AUCs between M2-PK and FC for distinguishing UC [CD] from AD-RV were -0.06 (p < 0.028) [-0.10 (p < 0.0018)] and for differentiating UC [CD] from AD-SE were 0.03 (NS) [-0.19 (p < 0.0011)].M2-PK sensitivities and specificities in distinguishing UC [CD] from AD-RV were 75.0% [71.4%] and 89.7% [89.7%] and for differentiation of UC [CD] from AD-SE were 56.3% [71.4%] and 95.2 [57.1%].Conclusions: The performance of M2-PK in distinguishing between children with moderate-to-severe IBD and patients with infectious gastroenteritis was inferior to FC. Neither test had sensitivity and specificity sufficient for everyday clinical application.
Key words: ulcerative colitis, Crohn’s disease, calprotectin, fecal biomarker, rotavirus, Salmonella
*The study was supported by a grant (number 502-01-01103115-07588) from Poznan university of Medical Sciences.

168 Elzbieta Czub et al.
StreszczenieWstęp: Ostra biegunka jest objawem występującym zarówno w nieswoistych zapaleniach jelit, jak i w ostrym nieżycie żołądkowo-jelitowym. Oznaczenie stężenia kalprotektyny w kale służy jako biomarker procesów zapalnych toczących się w obrębie jelita. Wykazano, że podobne zastosowanie może mieć izoenzym 2 kinazy pirogronianowej.Cel: Porównanie wartości oznaczenia stężeń izoenzymu 2 kinazy pirogronianowej i kalprotektyny w kale w różnicowaniu autoimmunologicznej i zakaźnej etiologii ostrej biegunki.Materiał i metody: W badaniu wzięły udział 103 osoby w wieku do 19 lat, w tym: 32 z wrzodziejącym zapaleniem jelita grubego, 21 z chorobą Leśniowskiego-Crohna (aktywność umiarkowana lub znaczna), 29 z ostrym nieżytem żołądkowo-jelitowym o etiologii rotawirusowej i 21 z ostrym nieżytem żołądkowo- -jelitowym wywołanym przez Salmonella enteritidis. Stężenia izoenzymu 2 kinazy pirogronianowej i kalprotektyny w stolcu oznaczano metodą ELISA.Wyniki: Porównanie pól pod krzywymi ROC (Receiver Operating Characteristic) wykazało mniejszą wartość izoenzymu 2 kinazy pirogronianowej w porównaniu z kalprotektyną w rozróżnianiu między ostrą biegunką wywołaną nieswoistymi zapaleniami jelit a nieżytem żołądkowo-jelitowym o etiologii rotawirusowej (wrzodziejące zapalenie jelita grubego: -0,06 [p<0,028; w chorobie Leśniowskiego- -Crohna -0,10 (p<0,0018)], a także między ostrą biegunką w przebiegu choroby Leśniowskiego-Crohna a wynikającą z zakażenia Salmonella enteritidis [-0,19 (p<0,0011)]. Czułości (swoistości – podane w nawiasach) w rozróżnianiu między osobami z wrzodziejącym zapaleniem jelita grubego a biegunką o etiologii rotawirusowej i Salmonella enteritidis były równe odpowiednio 75,0% (89,7%) i 56,3% (95,2%). Czułości (swoistości) dla rozróżniania między uczestnikami badania z chorobą Leśniowskiego-Crohna a biegunką o etiologii rotawirusowej i Salmonella enteritidis były równe odpowiednio 71,4% (89,7%) i 71,4% (57,1%).Wnioski: W rozróżnianiu między ostrą biegunką, u podłoża której było nieswoiste zapalenie jelit lub infekcja rotawirusowa albo Salmonella enteritidis badane testy nie cechowały się czułością i swoistością wystarczającymi dla codziennego zastosowania w praktyce lekarskiej.
Słowa kluczowe: wrzodziejące zapalenie jelita grubego, choroba Leśniowskiego-Crohna, kalprotektyna, biomarkery kałowe, rotawirus, Salmonella
DEV pErioD mED. 2015;XiX,2:167-173
IntroDuctIonDiarrhea is one of the main symptoms of inflammatory
bowel disease (IbD) exacerbation [1, 2]. However, it can also be caused by viral or bacterial gastroenteritis. Differentiating diagnosis between these two main causes of diarrhea in IbD patients often presents difficulty and may require extensive laboratory work-up [3]. So far, it was shown that distinguishing between IbD and noninflammatory diarrhea could be achieved using blood gene expression profiling [4]. However, as oligonucleotide arrays technology is still too expensive to be widely used in clinical setting, a fast, reliable and inexpensive test that would enhance differential diagnostics in IbD patients with diarrhea is needed.
Pyruvate kinase isoenzyme type M2 (M2-PK) is a protein expressed in proliferating cells of many tissues, including leukocytes and tumour cells [5]. It takes part in glycolysis by facilitating a phosphate group transfer [6]. Destruction of cells containing M2-PK that are present in the gastrointestinal tract leads to release of the enzyme to the fecal stream, where it remains stable [7]. M2-PK was investigated as a marker in colorectal cancer [8]. We proposed that M2-PK could serve as a biomarker of IbD activity and severity [7].
Calprotectin is a low molecular weight calcium-binding protein that is also one of at least twenty-one S100 family proteins [9]. It is present in neutrophils and exerts bacteriostatic action [10]. Fecal calprotectin (FC) concentration measurement can be used to assess the severity of IbD [11, 12] and to predict its course [13, 14]. It was shown that FC has sensitivity of 87% and specificity of 83% in identifying patients with bacterial acute diarrhea among patients with acute diarrhea [15]. The study was carried out in a group of 2383 adults with acute diarrhea. In a similar study that included 66 children with acute gastroenteritis FC’s sensitivity and specificity were 93% and 88% [16].
So far, comparison of clinical utility of M2-PK and FC in patients with IbD was the subject of two studies. In 2008 Shastri et al. demonstrated lower specificity of M2-PK in a population of 276 patients with Crohn’s disease (CD) and ulcerative colitis (uC) [17]. In 2010 Turner et al. described the use of M2-PK, FC, lactoferrin and S100A12 for outcome prediction and response monitoring in 101 children with uC [18]. Although the performance of M2-PK was similar to that of other fecal markers, it differed from them in that it had construct and predictive validity.
FC is a well-established biomarker of intestinal inflammation, However, its usefulness in depiction of

169Fecal pyruvate kinase is not suitable for discrimination between inflammatory bowel disease exacerbation
IbD exacerbation from infectious diarrhea is limited. The value of pyruvate kinase isoenzyme type 2 (M2-PK) in this application remains unknown. The aim of the study was to determine whether M2-PK could be superior to FC in differentiating between underlying disease exacerbation and infective causes of diarrhea in children with IbD.
MAterIAls AnD MethoDsOne hundred three subjects were enrolled for the
study, including 32 with uC (age range 2-19 years), 21 with CD (age range 9-19 years), 29 with acute diarrhea caused by rotavirus (AD-RV; age range 1-7 years) and 21 with acute diarrhea caused by Salmonella enteritidis (AD-Se; age range 1-12 years).
uC and CD were diagnosed according to Porto criteria using a combination of information coming from the physical examination, endoscopy, radiologic investigations, histologic analysis and supplementary laboratory tests [19-21]. The severity of uC was assessed using the pediatric ulcerative colitis activity index (PuCAI) [20, 22]. The severity of CD was described using The Pediatric Crohn’s Disease Activity Index (PCDAI) [1]. PuCAI value greater than 34 and PCDAI value greater than 29 were considered as indicators of moderate-to-severe disease [23].
AD was diagnosed on basis of clinical criteria [24]. Rotaviral infection was diagnosed when typical symptoms were present and a latex agglutination test gave positive result. S. enteritidis presence in stools was determined by stool cultures.
The median patients’ age (interquartile range [IQR]) was: 14.0 (11.7-15.0) in uC, 14.0 (12.0-15.0) in CD, 2.0 (1.3-3.0) in AD-RV, and 3.5 (2.6-8.0) in AD-Se. Median PuCAI score was 42.5 (IQR: 35-55), and median PCDAI score was 60 (42.5-62.5).
The study took place in four tertiary hospitals and one secondary care centre. Fresh stool specimens were obtained from hospitalized patients and stored in 4 degrees Celsius initially and in -70 degrees Celsius in the laboratory. The concentration of dimeric M2-PK was determined using a commercially available sandwich elISA (Schebo biotech, Giesen, Germany). The cut-off value was 4 u/g. The concentration of FC was measured employing PhiCal elISA Test (Calpro, lysaker, norway).
The cut-off concentration was 15 μg/ml. Analyses were carried out by the same laboratory technician unaware of diagnosis, in the same stool samples for M2-PK and FC.
Statistical analyses were carried out in STATISTICA data analysis software system v. 10 (Statsoft Inc., Tulsa, united States of America) and Analyse-it v. 2.30 (Analyse-it Software, leeds, united Kingdom). Sensitivities, specificities and areas under (AuC) receiver operating characteristic curves were calculated. The AuCs for M2-PK and FC were then compared after equaling M2-PK specificity to FC specificity at 15 μg/ml. The level of significance was set at p<0.05.
Parents of all patients and patients at least 16 years old have expressed their written, informed consent to participation in the study after receiving full information on its scope and purpose. The study plan was approved by the bioethical Committee at Poznan university of Medical Sciences (decision 1740/04). The study adhered to the tenets of the Declaration of Helsinki.
results The median concentrations of M2-PK and FC in
all four groups are shown in Table I. The sensitivities, specificities, and AuCs for M2-PK and FC in distinguishing children with IbD from children with AD-RV are shown in Tables II and III. The performance of FC was superior in uC and CD when AuCs were compared. Although the performance of both tests was good, it was still insufficient when analyzed in the context of the needs of clinical practice.
The sensitivities, specificities, and AuCs for M2-PK and FC in discriminating between children with IbD and children with AD-Se are shown in Tables IV and V. The AuCs plotted for FC in this application were greater than for M2-PK in CD, but not in uC. However, none of the two tests was sensitive and specific enough to have practical value in differentiating between patients with IbD exacerbation and S. enteritidis infection.
DIscussIonThis is the first study to investigate the potential value of
M2-PK and FC in identifying causes of diarrhea in children with IbD. AD-RV served as a model of viral gastroenteritis,
uc cd ad-Se ad-rv
m2-pK, U/g 152.9 (26.6-408.3) 96.3 (20.8-130.7) 22.3 (16.3-113.0) 8.7 (2.8-18.8)
FC, μg/ml 187.5 (52.7-334.2) 167.0 (78.0-256.0) 55.0 (22.0-62.5) 20.0 (4.0-40.0)
Table i. median concentrations (interquartile range) of fecal pyruvate kinase isoenzyme m2 (m2-pK) and fecal calprotectin (FC) in children with moderate-to-severe ulcerative colitis (UC), moderate-to-severe Crohn’s disease (CD), acute diarrhea caused by Salmonella enteritidis (AD-SE), and rotaviral acute diarrhea (AD-rV).
Tabela I. Mediany stężeń (w nawiasach podano rozstępy międzykwartylowe) izoenzymu M2 kinazy pirogronianowej (M2-PK) i kalprotektyny (FC) w kale dzieci z wrzodziejącym zapaleniem jelita grubego o umiarkowanej lub znacznej aktywności (UC), chorobie Leśniowskiego-Crohna o umiarkowanej lub znacznej aktywności (CD), ostrej biegunce wywołanej przez Salmonella enteritidis (AD-SE) lub rotawirus (AD-RV).

170 Elzbieta Czub et al.
M2-pK fc
uc SensitivityCzułość 93.8% [79.2-99.2%] 95.3% [81.5-99.6%]
SpecificitySwoistość 25.6% [11.6-45.6%] 44.8% [26.4-64.3%]
Auc, p 0.82 [0.71-0.94], p < 0.0001 0.89 [0.81-0.97], p < 0.0001
AUC difference, pRóżnica AUC, p -0.06 [-0.12-(-0.01)], p < 0.028
cD SensitivityCzułość 100% [83.9-100%] 97.6% [76.2-99.9%]
SpecificitySwoistość 26.7% [11.9-46.1%] 44.8% [26.4-64.3%]
Auc, p 0.82 [0.70-0.94], p < 0.0001 0.92 [0.84-0.99], p < 0.0001
AUC difference, pRóżnica AUC, p -0.10 [-0.16-(-0.04)], p < 0.0018
M2-pK fc
uc Cut-off Próg odcięcia 28.2 U/g 42.0 μg/ml
SensitivityCzułość 75.0% [56.6-88.5%] 81.3% [63.6-92.8%]
SpecificitySwoistość 89.7% [72.6-97.8%] 79.3% [60.3-92.0%]
cD Cut-offPróg odcięcia 38.0 U/g 78.0 μg/ml
SensitivityCzułość 71.4% [47.8-88.7%] 81.0% [58.1-94.6%]
SpecificitySwoistość 89.7% [72.6-97.8%] 93.1% [77.2-99.2%]
Table ii. The sensitivities*, specificities*, and the areas under receiver operating curves (AUC) for fecal pyruvate kinase isoenzyme m2 (m2-pK) and fecal calprotectin (FC) in distinguishing children with moderate-to-se-vere inflammatory bowel diseases from children with rotaviral acute diarrhea; 95% confidence intervals for all data are shown.
Tabela II. Czułości i swoistości* oraz pola pod krzywymi ROC (Receiver Operating Characteristic) (AUC) oznaczenia stężenia izoenzymu M2 kinazy pirogronianowej (M2-PK) i kalprotektyny (FC) w kale w diagnostyce różnicowej dzieci z nieswoistymi zapaleniami jelit o umiarkowanej lub znacznej aktywności i ostrą biegunką o etiologii rotawirusowej; w nawiasach kwadratowych podano przedziały 95% ufności.
CD – Crohn’s disease/choroba Leśniowskiego-Crohna, UC – ulcerative colitis/wrzodziejące zapalenie jelita grubego.*According to manufacturers’ cut-off levels./Stosując próg odcięcia zalecony przez producentów.
Table iii. The sensitivities and specificities of fecal pyruvate kinase isoenzyme m2 (m2-pK) and fecal calprotectin (FC) in distinguishing children with moderate-to-severe inflammatory bowel diseases from children with rotaviral acute diarrhea at optimal cut-off values. ninety-five percent confidence intervals are shown for all data.
Tabela III. Czułości i swoistości oznaczenia stężenia izoenzymu M2 kinazy pirogronianowej (M2-PK) i kalprotektyny (FC) w kale w diagnostyce różnicowej dzieci z nieswoistymi zapaleniami jelit o umiarkowanej lub znacznej aktywności i ostrą biegunką o etiologii rotawirusowej przy zastosowaniu optymalnych progów odcięcia; w nawiasach kwadratowych podano przedziały 95% ufności.
CD – Crohn’s disease/choroba Leśniowskiego-Crohna, UC – ulcerative colitis/wrzodziejące zapalenie jelita grubego.

171Fecal pyruvate kinase is not suitable for discrimination between inflammatory bowel disease exacerbation
M2-pK fc
uc SensitivityCzułość 94.7% [80.6-99.4%] 93.8% [79.2-99.2%]
SpecificitySwoistość 0% [0-16.1%] 0% [0-16.1%]
Auc, p 0.69 [0.55-0.84], p < 0.0046 0.72 [0.58-0.87], p < 0.0013
AUC difference, pRóżnica AUC, p -0.03 [-0.10-0.04], p = 0.4192
cD SensitivityCzułość 100% [83.9-100%] 95.2% [83.9-100%]
SpecificitySwoistość 0% [0-16.1%] 0% [0-16.1%]
Auc, p 0.59 [0.41-0.77], p = 0.1536 0.78 [0.62-0.94], p = 0.0003
AUC difference, pRóżnica AUC, p -0.19 [-0.30-(-0.08)], p < 0.0011
M2-pK fc
uc Cut-offpróg odcięcia 146.8 U/g 112.0 μg/ml
SensitivityCzułość 56.3% [37.7-73.6%] 65.6% [46.8-81.4%]
SpecificitySwoistość 95.2% [76.2-99.9%] 90.5% [69.6-98.8%]
cD Cut-offpróg odcięcia 38.0 U/g 78.0 μg/ml
SensitivityCzułość 71.4% [47.8-88.7%] 81.0% [58.1-94.6%]
SpecificitySwoistość 57.1% [34.0-78.2%] 90.5% [69.6-98.8%]
Table V. The sensitivities and specificities of fecal pyruvate kinase isoenzyme m2 (m2-pK) and fecal calprotectin (FC) in distinguishing children with moderate-to-severe inflammatory bowel diseases from children with acute diarrhea caused by Salmonella enteritidis at optimal cut-off values. ninety-five percent confidence intervals are shown for all data.
Tabela V. Czułości i swoistości oznaczenia stężenia izoenzymu M2 kinazy pirogronianowej (M2-PK) i kalprotektyny (FC) w kale w diagnostyce różnicowej dzieci z nieswoistymi zapaleniami jelit o umiarkowanej lub znacznej aktywności i ostrą biegunką wywołaną przez Salmonella enteritidis przy zastosowaniu optymalnych progów odcięcia; w nawiasach kwadratowych podano przedziały 95% ufności.
Table iV. The sensitivities*, specificities*, and the areas under receiver operating curves (AUC) for fecal pyruvate kinase isoenzyme m2 (m2-pK) and fecal calprotectin (FC) in distinguishing children with moderate-to- -severe inflammatory bowel diseases from children with acute diarrhea caused by Salmonella enteritidis; 95% confidence intervals for all data are shown.
Tabela IV. Czułości i swoistości* oraz pola pod krzywymi ROC (Receiver Operating Characteristic) (AUC) oznaczenia stężenia izoenzymu M2 kinazy pirogronianowej (M2-PK) i kalprotektyny (FC) w diagnostyce różnicowej dzieci z nieswoistymi zapaleniami jelit o umiarkowanej lub znacznej aktywności i ostrą biegunką wywołaną przez Salmonella enteritidis; w nawiasach kwadratowych podano przedziały 95% ufności.
CD – Crohn’s disease/choroba Leśniowskiego-Crohna, UC – ulcerative colitis/wrzodziejące zapalenie jelita grubego.*According to manufacturers’ cut-off levels./Stosując próg odcięcia zalecony przez producentów.
CD – Crohn’s disease/choroba Leśniowskiego-Crohna, UC – ulcerative colitis/wrzodziejące zapalenie jelita grubego.

172 Elzbieta Czub et al.
and AD-Se represented bacterial gastrointestinal inflammation. Here, as in previous research, M2-PK and FC levels in moderate-to-severe IbD were markedly elevated [25, 26]. M2-PK and FC concentrations in AD-RV were lower than in AD-Se, as in a study by Shastri et al. [15]. Therefore, the potential value of both markers in distinguishing between exacerbation and infectious diarrhea in IbD patients would be greater in case of viral than bacterial origin. We conclude that M2-PK and FC served as markers of intestinal inflammation, and this was comparable in IbD exacerbation and gastroenteritis caused by S. enteritidis [27].
because of the relatively low number of patients in whom IbD and acute gastroenteritis co-occured we decided not to enroll them in the study. However, it must be underscored that although the numbers of such patients are small, bacterial and viral infections need to be excluded in almost all IbD patients with diarrhea because of the differences in treatment. It is known that infectious gastroenteritis may cause exacerbations of IbD [28]. However, the causes of IbD relapses are varied, including chronic and acute stress, infections in sites other than the gastrointestinal tract and exposure to allergens [29].
conclusIonThe study showed that the performance of M2-PK in
distinguishing between children with moderate-to-severe IbD and patients with infectious gastroenteritis was inferior to FC. neither test had sensitivity and specificity sufficient for everyday clinical application.
reFerences
1. Hyams JS, Ferry GD, Mandel FS, et al. Development and validation of a pediatric Crohn’s disease activity index. J Pediatr Gastroenterol nutr. 1991;12:439-447.
2. Mahadevan u, loftus eV Jr, Tremaine WJ, et al. Azathioprine or 6-mercaptopurine before colectomy for ulcerative colitis is not associated with increased postoperative complications. Inflamm bowel Dis. 2002;8:311-316.
3. Thielman nM, Guerrant Rl. Clinical practice. Acute infectious diarrhea. n engl J Med. 2004;350:38-47.
4. burakoff R, Chao S, Perencevich M, et al. blood-based biomarkers can differentiate ulcerative colitis from Crohn’s disease and noninflammatory diarrhea. Inflamm bowel Dis. 2011;17:1719-1725.
5. Tonus C, Sellinger M, Koss K, neupert G. Faecal pyruvate kinase isoenzyme type M2 for colorectal cancer screening: a meta-analysis. World J Gastroenterol WJG. 2012;18:4004-4011.
6. Walkowiak J, banasiewicz T, Krokowicz P, Hansdorfer-Korzon R, Drews M, Herzig KH. Fecal pyruvate kinase (M2-PK): a new predictor for inflammation and severity of pouchitis. Scand J Gastroenterol. 2005;40:1493-1494.
7. Czub e, Herzig K-H, Szaflarska-Popawska A, et al. Fecal pyruvate kinase: a potential new marker for intestinal inflammation in children with inflammatory bowel disease. Scand J Gastroenterol. 2007;42:1147-1150.
8. Gupta V, bamezai RnK. Human pyruvate kinase M2: a multifunctional protein. Protein Sci Publ Protein Soc. 2010;19:2031-2044.
9. Marenholz I, Heizmann CW, Fritz G. S100 proteins in mouse and man: from evolution to function and pathology (including an update of the nomenclature). biochem biophys Res Commun. 2004;322:1111-1122.
10. Yui S, nakatani Y, Mikami M. Calprotectin (S100A8/S100A9), an inflammatory protein complex from neutrophils with a broad apoptosis-inducing activity. biol Pharm bull. 2003;26:753-760.
11. Aomatsu T, Yoden A, Matsumoto K, et al. Fecal calprotectin is a useful marker for disease activity in pediatric patients with inflammatory bowel disease. Dig Dis Sci. 2011; 56:2372-2377.
12. Önal İK, beyazit Y, Şener b, et al. The value of fecal calprotectin as a marker of intestinal inflammation in patients with ulcerative colitis. Turk J Gastroenterol. 2012;23:509-514.
13. Mao R, Xiao Y, Gao X, et al. Fecal calprotectin in predicting relapse of inflammatory bowel diseases: a meta-analysis of prospective studies. Inflamm bowel Dis. 2012;18:1894-1899.
14. lasson A, Simrén M, Stotzer P-O, Isaksson S, Ohman l, Strid H. Fecal calprotectin levels predict the clinical course in patients with new onset of ulcerative colitis. Inflamm bowel Dis. 2013;19:576-581.
15. Shastri YM, bergis D, Povse n, et al. Prospective multicenter study evaluating fecal calprotectin in adult acute bacterial diarrhea. Am J Med. 2008;121:1099-1106.
16. Sýkora J, Siala K, Huml M, Varvařovská J, Schwarz J, Pomahačová R. evaluation of faecal calprotectin as a valuable non-invasive marker in distinguishing gut pathogens in young children with acute gastroenteritis. Acta Paediatr Oslo nor. 2010;99:1389-1395.
17. Shastri YM, Povse n, Schröder O, Stein J. Comparison of a novel fecal marker--fecal tumor pyruvate kinase type M2 (M2-PK) with fecal calprotectin in patients with inflammatory bowel disease: a prospective study. Clin lab. 2008;54:389-390.
18. Turner D, leach ST, Mack D, et al. Faecal calprotectin, lactoferrin, M2-pyruvate kinase and S100A12 in severe ulcerative colitis: a prospective multicentre comparison of predicting outcomes and monitoring response. Gut. 2010;59:1207-1212.
19. Kornbluth A, Sachar Db, Practice Parameters Committee of the American College of Gastroenterology. ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2004;99:1371-1385.
20. Turner D, Otley AR, Mack D, et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: a prospective multicenter study. Gastroenterology. 2007;133:423-432.
21. Van Assche G, Dignass A, Panes J, et al. The second european evidence-based Consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J Crohns Colitis. 2010;4:7-27.
22. Turner D, levine A, escher JC, et al. Management of pediatric ulcerative colitis: joint eCCO and eSPGHAn evidence-based consensus guidelines. J Pediatr Gastroenterol nutr. 2012;55:340-361.
23. Hyams J, Markowitz J, Otley A, et al. evaluation of the pediatric crohn disease activity index: a prospective multicenter experience. J Pediatr Gastroenterol nutr. 2005;41:416-421.

173
24. King CK, Glass R, bresee JS, Duggan C, Centers for Disease Control and Prevention. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep Morb Mortal Wkly Rep Recomm Rep Cent Dis Control. 2003;52:1-16.
25. D’Haens G, Ferrante M, Vermeire S, et al. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm bowel Dis. 2012;18:2218-2224.
26. Kolho K-l, Sipponen T, Valtonen e, Savilahti e. Fecal calprotectin, MMP-9, and human beta-defensin-2 levels in pediatric inflammatory bowel disease. Int J Colorectal Dis. 2013;29:43-50.
27. licata A, Randazzo C, Cappello M, et al. Fecal calprotectin in clinical practice: a noninvasive screening tool for patients with chronic diarrhea. J Clin Gastroenterol. 2012;46:504-508.
28. Friswell M, Campbell b, Rhodes J. The role of bacteria in the pathogenesis of inflammatory bowel disease. Gut liver. 2010;4:295-306.
29. levenstein S, Prantera C, Varvo V, et al. Stress and exacerbation in ulcerative colitis: a prospective study of patients enrolled in remission. Am J Gastroenterol. 2000;95:1213-1220.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 12.08.2014 r.Accepted/Zaakceptowano: 13.01.2015 r.
Published online/Dostępne online
Address for correspondence:Jarosław Walkowiak
Poznan university of Medical Sciences, Department of Pediatric
Gastroenterology & Metabolic DiseasesSzpitalna 27/33, 60-572 Poznań, Poland
tel. (+48 61) 84-91-432fax (+48 61) 84-7-685
e-mail: [email protected]
Fecal pyruvate kinase is not suitable for discrimination between inflammatory bowel disease exacerbation

174Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Agnieszka Szmigielska1, Hanna Szymanik-Grzelak1, Elżbieta Kuźma-Mroczkowska1, Maria Roszkowska-Blaim1
hemodiafiltration efficacy in treatment of methanol and ethylene glycol poiSoning
in a 2-year-old girl
Skuteczność hemodiafiltracji w leczeniu zatrucia metanolem i glikolem u 2-letniej dziewczynki
1Department of Pediatric nephrology, The Medical university of Warsaw, Poland
AbstractIntroduction: Every year about 2.4 million people in USA are exposed to toxic substances. Many of them are children below 6 years of age. Majority of poisonings in children are incidental and related to household products including for example drugs, cleaning products or antifreeze products. Antifreeze solutions contain ethylene glycol and methanol. Treatment of these toxic substances involves ethanol administration, fomepizole, hemodialysis and correction of metabolic acidosis.Purpose: The aim of the study was to check the efficacy of continuous venovenous hemodiagiltration in intoxication with ethylene glycol and methanol.Material and methods: One year and 7 months old girl after intoxication with ethylene glycol and methanol was treated with continuous venovenous hemodiafiltration instead of hemodialysis because of technical problems (circulatory instability).Results: Intravenous ethanol infusion with hemodiafiltration resulted in rapid elimination of methanol from the body and significantly reduced blood ethylene glycol level.Conclusions: Continuous venovenous hemodiafiltration can be helpful in treatment of ethylene glycol and methanol intoxication.
Key words: continuous venovenous hemodiafiltration, methanol, glycol, intoxication, fomepizol
StreszczenieWstęp: Każdego roku około 2,4 mln ludzi w Stanach Zjednoczonych ma kontakt z toksycznymi substancjami. Wielu z nich stanowią dzieci poniżej 6. roku życia. Większość zatruć u dzieci ma charakter przypadkowy, spowodowany środkami przechowywanymi w domu, np. lekami, środkami czyszczącymi lub odmrażaczami. Odmrażacze zawierają metanol i glikol etylenowy. Leczenie zatrucia tymi toksycznymi środkami obejmuje: podawanie etanolu, fomepizolu, dializoterapię i wyrównywanie kwasicy metabolicznej.Cel pracy: Ocena skuteczności ciągłej żolno-żylnej hemodiafiltracji w zatruciu metanolem i glikolem etylenowym.Materiał i metody: Dziewczynka w wieku 1 rok i 7 miesięcy po spożyciu metanolu i glikolu etylenowego, u której z powodu trudności technicznych w prowadzeniu hemodializy (niestabilność krążenia) zastosowano ciągłą żylno-żylną hemodiafiltrację.Wyniki: Zastosowanie dożylnej podaży etanolu i hemodiafiltracji spowodowały szybką eliminację metanolu oraz glikolu etylenowego z krwi.Wnioski: Ciągła żylno-żylna hemodiafiltracja może być skuteczną metodą leczenia zatrucia metanolem i glikolu etylenowego.
Słowa kluczowe: ciągła żylno-żylna hemodiafiltracja, metanol, glikol, zatrucie, fomepizol
DEV pErioD mED. 2015;XiX,2:174-177

175Hemodiafiltration efficacy in treatment of methanol and ethylene glycol poisoning in a 2-year-old girl
IntroDuctIonAccording to the American Academy of Pediatrics,
about 2.4 million people including 50% of children <6 years of age are exposed to/or ingest toxic substances [1]. Most poisonings are incidental and related to household products. The most toxic substances include drugs, cleaning products, antifreeze, petroleum-based products, and alcohols. Among alcohols, the most dangerous are methanol and ethylene glycol poisonings [2].
Methanol is an alcohol used mostly in industry, but it may also be found in small amounts in cleaning products, antifreeze, solvents, and coolants. Methanol is slowly metabolized to formic acid and formaldehyde, which results in the development of clinical symptoms within 8-24 hours from ingestion. Severe manifestations of toxicity include severe metabolic acidosis and optic nerve damage [3]. Management of methanol poisoning includes administration of bicarbonates, ethanol, folic acid, and fomepizole, and hemodialysis [3-7].
ethylene glycol, used as a component of coolants, brake fluids and solvents, is also very toxic. Due to its sweet taste and an odour resembling ethanol, it is sometimes inadvertently consumed. ethylene glycol is metabolized by alcohol dehydrogenase to glycoaldehyde, glycolic acid, glyoxylic acid, and oxalic acid. It induces severe metabolic acidosis, hypocalcemia, central nervous system symptoms, gastrointestinal symptoms, and acute tubular necrosis. Management of ethylene glycol poisoning includes administration of fomepizole and bicarbonates along with hemodialysis [7-10].
AIMThe aim of the study was to check the efficacy of
continuous venovenous hemodiafiltration in intoxication with ethylene glycol and methanol.
MAterIAl AnD MethoDsA girl aged one year and 7 months was admitted after
inadvertent consumption of windshield washer fluid during playing with an “empty” 5-liter container. It was not possible to determine the amount of ingested fluid that contained ethanol (25-35%), isopropanol (1-5%), methanol (2.5%), and ethylene glycol (0.5%). before hospital admission, parents of the child gave her 30 ml of sunflower oil to provoke vomiting, 20 ml of milk, and about 20 ml of 40% ethanol solution. On admission, the child was in good overall condition, with normal vital signs (heart rate 99 per minute, blood pressure 100/70 mm Hg, oxygen saturation 99%). laboratory tests performed 2 hours after ingestion of windshield washer fluid showed moderate metabolic acidosis (pH of 7.32, bicarbonate level of 15.5 mmol/l, base excess (be) of -10.6 mmol/l), normal kidney function, ethanol level of 0‰, methanol level of 50 mg/dl, and ethylene glycol level of 125 mg/dl (Table I). Intravenous infusion of 5% ethanol solution was started, aiming for blood ethanol level of about 1‰. A decision was made to proceed with hemodialysis (HD). under general anesthesia, an
8F Mahurkar catheter was introduced into the right jugular vein and HD was initiated using AK 96 machine (Gambro) and 0.4 m2 hemofilter, with blood flow rate (Qb) of 50 ml/min, and dialysate fluid flow rate (QD) of 500 ml/min. After 2 hours of HD, methanol was no longer detectable in blood. In contrast, blood ethylene glycol level remained high and HD was continued, complicated by blood pressure falls to 78/28 mm Hg, two episodes of dialyzer thrombosis, and an episode of supraventricular tachycardia which resulted in termination of HD. Due to poor tolerance of HD and technical problems, continuous venovenous hemodiafiltration (CVVHDF) was started using a Prismaflex machine (Gambro), 0.6 m2 Prismaflex ST 60 filter, and An69ST membrane, with Ob of 50 ml/min, QD of 15 ml/min/m2 (500 ml/h), and supplement flow rate of 300 ml/h. CVVHDF was performed for 18 hours. During both HD and CVVHDF, intravenous infusion of 5% ethanol solution was continued with monitoring of serum ethanol level. The patient also required transfusion of 2 units of packed red blood cells, and intravenous potassium and calcium supplementation.
resultsFollow-up of laboratory tests at 18 hours showed no
ethylene glycol in blood, with kidney and liver function parameters, arterial blood gases, and blood glucose level all within normal limits (Table I). blood ethylene glycol and methanol levels during renal replacement therapy are shown in Figure 1. Ophthalmological and neurological examination showed no abnormalities.
DIscussIonClinical symptoms of ethylene glycol and methanol
intoxication depend on the amount of ingested substance and duration of intoxication [7]. Parents of this 1-year and 7 months old girl presented to the hospital immediately after ingestion of windshield washer fluid by the patient. It was difficult to determine the ingested amount of fluid, as it was not known how much of it was left in a 5-liter container. Time from ingestion to initial blood collection for laboratory tests was about 2 hours. laboratory findings indicated moderate metabolic acidosis with no hypoglycemia and no hypocalcemia. Methanol elimination depends on the ingested amount [3, 7]. With blood methanol level of 10 mg/dl, elimination half-time is 2.5-3 hours, and with levels of 200-300 mg/dl, methanol is eliminated at a rate of 8.5-9 mg/dl/kg per hour [3]. If ethanol is administered, duration of methanol elimination may be increased to 30.3-52 hours [3]. Due to toxic effects of ethanol administered in the management of methanol intoxication, hemodialysis should be considered [4-5]. elimination of ethylene glycol depends on patient renal function. With normal renal function, blood ethylene glycol is reduced by 50% after 8.6 hours, but with renal failure this elimination half-time may extend to 49 hours [6]. In recent years, alcohol dehydrogenase inhibitor fomepizole has been introduced to clinical practice [6, 7, 9, 10]. Administration of fomepizole prolongs methanol elimination half-time

176 Agnieszka Szmigielska et al.
evaluated parameterOceniane parametry
2 hours after ingestion2 godziny po zatruciu
after 10 hrs of hd10 godz. HD
after 10 hrs of cvvhd10 godz. CVVHD
after 18 hrs of cvvhd18 godz. CVVHD
Urea (mg/dl) 20 12 5 15Creatinine (mg/dl) 0.3 0.2 0.2 0.2
GoT (U/l) 51 46 41 42GpT (U/l) 26 39 26 24
GGTp (U/l) <10 <10Bilirubin (mg/dl) 0.3 0.3
Albumin (g/l) 3.6 3.1 3.1Ph 7.32 7.37 7.46 7.46
BE (mmol/l) -10.6 -10.8 -1.0 -0.3hco3 (mmol/l) 15.5 14.5 22.8 22.8
Glucose (mg/dl) 66 95 80 80Calcium (mmol/l) 5.0 4.5 4.7 4.9
magnesium (mg/dl) 1.8 1.6 1.6Chloride (mg/dl) 108 108
potassium (mmol/l) 4.9 4.1 4.7 3.8Sodium (mmol/l) 142 145 142 141WBC (x 103/mm3) 17.9 13.8 15.9 20.1rBC (x 106/mm3) 4.44 4.26 3.79 4.21Hematocrit (%) 36.3 36.1 32.1 36.7
platelets (x 103/mm3) 381 205 155 107Hemoglobin (g/dl) 12 11.5 11.4 11.0
Table i. Biochemical parameters during treatment. Tabela I. Badania laboratoryjne w trakcie leczenia.
HD – hemodialysis/hemodializa; CVVHDF − continuous venovenous hemodiafiltration/ciągła żylno-żylna hemodiafiltracja; BE − base excess/niedobór zasad, hco3 – bicarbonates/dwuwęglany.
Fig. 1. Blood methanol and ethylene glycol levels during renal replacement therapy with hemodialysis (HD) and continuous venovenous hemodiafiltration (CVVHDF).
Ryc. 1. Stężenie metanolu i glikolu we krwi w czasie stosowania terapii nerkozastępczej: hemodializy (HD) i ciągłej żylno- -żylnej hemodiafiltracji (CVVHDF).
concentration of methanol (mg/dl)/stężenie metanolu
concentration of ethylene glycol (mg/dl)/stężenie glikolu etylenowego

177
to about 54 hours, and glycol elimination half-time to 14-17 hours. We did not use fomepizole in our patient as the drug was not immediately available and could not be provided in a reasonable time. Instead, combination therapy including ethanol administration and HD was used. Hemodialysis is the best method of rapid elimination of methanol and its metabolites from blood, and it should be considered treatment of choice [4, 5]. This approach resulted in rapid lowering of blood methanol level in our patient. However, HD is not always feasible and may be associated with various complications. Hemodynamic instability and technical problems during dialysis necessitated change of the renal replacement modality from HD to CVVHDF. During this switch, a rebound increase of blood ethylene glycol level was observed. Although methanol elimination during HD is 5-fold faster compared to CVVHDF, methanol clearance during CVVHDF is still threefold higher compared to non-dialyzed subjects [5]. Similar observations were made in regard to ethylene glycol poisonings. Management of methanol and ethylene glycol intoxication should be continued until normalization of pH and lowering of blood methanol and glycol levels below 10-15 mg/dl or to undetectable values. In addition, CVVHDF allowed rapid elimination of ethanol given for therapeutic purposes in the management of intoxication. Rapid initiation of therapy after inadvertent consumption of a toxic substance by a child allowed avoiding multiple organ toxicities including vision and kidney damage. Intravenous ethanol infusion together with hemodialysis resulted in rapid elimination of methanol from the body and significantly reduced blood ethylene glycol level. CVVHDF allowed effective elimination of glycol and ethanol, reducing the risk of central nervous system toxicity.
conclusIonsContinuous venovenous hemodiafiltration can be
helpful in treatment of ethylene glycol and methanol intoxication.
reFerences
1. American Academy of Pediatrics (AAP). Poison Prevention and Treatment Tips: national Poison Prevention Week, March 18-24, 2012 www.aap.org.
2. Sein Anand J, Swiderska A, Pach J, burda P. Selected data of acute intoxications with glycol and methanol in Poland in the year 2009. Przegl lek. 2011;68(8):453-458.
3. Coulter CV, Isbister GK, Duffull Sb. The pharmacokinetics of methanol in the presence of ethanol: a case study. Clin Pharmacol. 2011;50(4):245-251.
4. Hirsch DJ, Jindal KK, Wong P, Fraser AD. A simple method to estimate the required dialysis time for cases of alcohol poisoning. Kidney Int. 2001;60(5):2021-2024.
5. Kan G, Jenkins I, Rangan G, Woodroffe A, Rhodes H, Joyce D. Continuous haemodiafiltration compared with intermittent haemodialysis in the treatment of methanol poisoning. nephrol Dial Transplant. 2003:18(12):2665-2667.
6. Mégarbane b, Houzé P, baud FJ. Oral fomepizole administration to treat ethylene glycol and methanol poisonings: advantages and limitations. Clin Toxicol (Phila). 2008;46(10):1097.
7. lepik KJ, levy AR, Sobolev bG, Purssell RA, DeWitt CR, erhardt GD, et al. Adverse drug events associated with the antidotes for methanol and ethylene glycol poisoning: a comparison of ethanol and fomepizole. Ann emerg Med. 2009;53(4):439-450.
8. boyer eW, Mejia M, Woolf A, Shannon M. Severe ethylene glycol ingestion treated without hemodialysis. Pediatrics. 2001;1:172-173.
9. Hovda Ke, Andersson KS, urdal P, Jacobsen D. Methanol and formate kinetics during treatment with fomepizole. Clin Toxicol (Phila). 2005;43(4):221-227.
10. brent J. Fomepizole for the treatment of pediatric ethylene and diethylene glycol, butoxyethanol, and methanol poisonings. Clin Toxicol (Phila). 2010;48(5):401-406.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 21.10.2014 r.Accepted/Zaakceptowano: 16.12.2014 r.
Published online/Dostępne online
Address for correspondence:Agnieszka Szmigielska
Department of Pediatric nephrology, The Medical university of Warsaw, Warsaw, Poland
Marszałkowska 24, 00-576 Warsaw, Poland tel. (+48-22) 522-74-96
fax: (+48-22) 771-48-26e-mail: [email protected]
Hemodiafiltration efficacy in treatment of methanol and ethylene glycol poisoning in a 2-year-old girl

178Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Anna Obuchowicz1, Magdalena Łoboda1, Wojciech Madziara2, Małgorzata Krzywiecka1, Beata Jarecka1
wielokomorowy guz krezki i przeStrzeni zaotrzewnowej – malformacja chłonna
u czteroletniej dziewczynki
multiloculated meSenteric and retroperitoneal tumour – lymphatic malformation – in a 4-year-old girl
1Wydział nauk o Zdrowiu w Katowicach, Śląskiego uniwersytetu Medycznego Katedra Pediatrii, Oddział Kliniczny Pediatrii
2Oddział Chirurgii i urologii, Górnośląskie Centrum Zdrowia Dziecka im. Jana Pawła II, Samodzielny Publiczny Szpital Kliniczny nr 6,
Śląskiego uniwersytetu Medycznego w Katowicach
StreszczenieTorbiele krezki należą do rzadko występujących, zwykle łagodnych guzów brzucha u dzieci. Najczęściej mają charakter torbielowatego naczyniaka chłonnego (malformacji chłonnej). Przedstawiamy przypadek 4-letniej dziewczynki, u której rozpoznano wielokomorową, rozległą torbiel krezki i przestrzeni zaotrzewnowej, z nasilonym stanem zapalnym. Leczenie operacyjne było w pełni skuteczne.
Słowa kluczowe: guz torbielowaty, malformacja chłonna, krezka, przestrzeń zaotrzewnowa, dziecko
AbstractMesenteric cysts are rare and mostly benign abdominal tumours in children. Majority of them are lymphangiomas (lymphatic malformations). We diagnosed a broad, multiloculated mesenteric and retroperitoneal cyst, associated with intensive inflammation, in a 4-year-old girl. Surgical therapy was fully successful.
Key words: cystoid tumour, lymphatic malformation, mesentery, retroperitoneal space, child
DEV pErioD mED. 2015;XiX,2:178-181
WSTępGuzy torbielowate mogą występować w każdym miej-
scu przewodu pokarmowego, najczęściej w krezce jelita cienkiego (ok.60%) [1, 2]. etiologia ich jest niepewna. Wśród możliwych przyczyn, najczęściej wymieniana jest proliferacja tkanki limfatycznej, niepozostającej w łączności z układem chłonnym. Pozostałe hipotezy obejmują związek z embrionalnym wadliwym połączeniem pomiędzy układem chłonnym i żylnym, z urazem, nowotworem, zmianami degeneracyjnymi w obrębie układu chłonnego [3].
Torbiele krezki i sieci występują rzadko. Po raz pierwszy torbiel krezki opisana została u 8-letniego dziecka przez Antonio benevieniego (1443-1502) na podstawie materiału autopsyjnego [1, 4]. Zapadalność wynosi około 1 na 105 000 [3, 5] do 1 na 140 000 [2] wszystkich hospitalizacji i około 1 na 20 000 hospitalizacji u dzieci. Około jedna trzecia przypadków diagnozowana jest u dzieci poniżej 15 roku życia, z czego 60% rozpoznawana jest poniżej 5 roku życia. Przedoperacyjne, szczegółowe określenie lokalizacji torbieli, jest – zdaniem niektórych autorów – trudne [6].

179Wielokomorowy guz krezki i przestrzeni zaotrzewnowej – malformacja chłonna u czteroletniej dziewczynki
Wśród zmian torbielowatych krezki najczęstszy jest torbielowaty naczyniak chłonny (obecnie określany jako malformacja chłonna). Guz ten najczęściej występuje u dzieci przed 10. rokiem życia, około 3 razy częściej u chłopców. Rzadziej występującą zmianą torbielowatą jest torbiel nabłonka mezotelialnego, która w 60-70% przypadków lokalizuje się w krezce jelita cienkiego [1, 2]. Pierwotne guzy lite o tej lokalizacji występują znacznie rzadziej. Wśród nich najczęstszy jest międzybłoniak, pozostałe to chłoniaki, guzy włókniste, tłuszczaki i tłusz-czakomięsaki, guzy pochodzenia naczyniowego (najczę-ściej naczyniakośródbłoniaki) oraz guzy podścieliskowe przewodu pokarmowego (GIST) [5].
Przedstawiamy przypadek torbieli wielokomoro-wej wychodzącej z korzenia krezki, z towarzyszącymi nasilonymi zmianami zapalnymi wewnątrz torbieli, w przestrzeni zaotrzewnowej oraz w jamie brzusznej u czteroletniej dziewczynki.
opiS przYpADKU4-letnia dziewczynka została skierowana do Kliniki
z powodu występującej od dwóch tygodni gorączki, utrzymującej się pomimo stosowanej antybiotykote-rapii oraz powiększenia obwodu brzucha, rozpozna-wanego początkowo jako wzdęcie. Matka podała, że od dłuższego czasu dziecko miało „większy brzuszek”, mimo to badań diagnostycznych nie wykonywano. Przy przyjęciu do Kliniki stan ogólny dziecka był średni. W badaniu fizykalnym z odchyleń od stanu prawidłowego stwierdzono: nieprawidłowy rozwój somatyczny (wysokość ciała <3c, masa ciała = 3c), duszność wdechowo-wydechową bez zmian osłucho-wych, cechy odwodnienia, bladość powłok skórnych, zez zbieżny oka prawego, opadanie prawej powieki, tachykardię ok. 160/min., nadmierne uniesienie powłok brzusznych i ich znaczne napięcie. Wyczuwalny był opór w śródbrzuszu i podbrzuszu po stronie lewej. ultrasonograficznie stwierdzono obecność masy guza w obrębie jamy brzusznej, o charakterze torbielowa-tym (wielkości około 10x8,2x7,5 cm) –sięgającej od wnęki wątroby po lewe śródbrzusze. Po stronie lewej, poniżej zmiany, widoczny był wyraźnie oddzielony lity guz, wielkości około 5,7 x 5,9 x 4,8 cm. W dia-gnostyce różnicowej uwzględniono: torbielowato-lity guz jajnika, wady rozwojowe przewodu pokarmowego (m. in. zdwojenie, jelit, torbiele krezki), wady układu moczowego, a także guzy przestrzeni zaotrzewno-wej. Wobec charakteru stwierdzonych zmian dziecko przekazano do Kliniki Chirurgii Dziecięcej GCZD w Katowicach w trybie pilnym, z rozpoznaniem roz-ległego, torbielowatego guza jamy brzusznej. Po przy-jęciu do wymienionej Kliniki powtórzono badanie uSG jamy brzusznej, a następnie wykonano tomogra-fię komputerową (TK). Rozległość uwidocznionych w TK zmian torbielowatych była znacząco większa od opisywanej w badaniach uSG, przy czym wszystkie badania obrazowe wskazywały na obecność zmian w obrębie krezki i lewego śródbrzusza. W badaniu tomograficznym uwidoczniono w jamie brzusznej: do przodu od aorty i dolnych części nerek aż do poziomu
naczyń biodrowych w miednicy, masę policykliczną o gęstości płynowej niewzmacniającej się po podaniu kontrastu, ze wzmacniającymi się torebkami zmian. Wielkość zmiany: 16x10x9,4 cm, największa z torbieli po stronie lewej o średnicy 72 mm. naczynia krezko-we przemieszczone były do przodu, pętle jelitowe do przodu, w dół i na stronę prawą. nie uwidoczniono zwapnień i obszarów litych.
Z uwagi na stan ogólny i utrzymującą się gorączkę oraz wysokie wartości wskaźników laboratoryjnych świadczących o stanie zapalnym, dziewczynka wymagała intensywnego leczenia (nawodnienie i.v., antybiotyko-terapia, wyrównanie niedoborów elektrolitowych, leki przeciwbólowe i przeciwgorączkowe). Po uzyskaniu poprawy, w 5. dobie pobytu została zakwalifikowana do laparotomii zwiadowczej. Zabieg przeprowadzono w znie-czuleniu ogólnym. Z dostępu poprzecznego w górnym śródbrzuszu otwarto jamę otrzewnową, potwierdzono obecność rozległego torbielowatego guza wychodzącego z korzenia krezki i przechodzącego rozlegle na stronę lewą. Guzowi towarzyszyły liczne, masywne zrosty pętli jelita cienkiego tak z guzem, jak i międzypętlowo. Po uwolnieniu zrostów uzyskano dostęp do korzenia krezki. Otwarto przestrzeń zaotrzewnową, wyłuszczono przednią i lewoboczną część zmiany. Odsłonięto pra-wą okolicę przykręgosłupową, stwierdzając masywne płaszczyznowe nacieki zapalne. W trakcie uwalniania doszło do przypadkowego pęknięcia torbieli położonej przykręgosłupowo – zawierała treść ropno-płynną. Dopiero wówczas można było stwierdzić obecność rozległej przestrzeni płynowej w prawej przestrzeni zaotrzewnowej, której dno sięgało wysokości wnęki wątroby. Guzowi w tym odcinku towarzyszyły nasilone zmiany zapalne. Preparując dogłowowo patologicznie zmienione tkanki odsłonięto kolejną przestrzeń zawie-rającą treść płynną. Po jej otwarciu i odessaniu ropnej treści, stwierdzono obecność martwiczych mas tkan-kowych. Zawartość ropnia ewakuowano, lożę ropnia zdrenowano. Końcowa rewizja narządów przestrzeni zaotrzewnowej, otrzewnej i miednicy małej nie wyka-zała dalszych patologii.
na podstawie oceny histopatologicznej posłanego do badania materiału, rozpoznano: lymphangioma cy-sticum. Ponadto stwierdzono: w świetle części torbieli ropny wysięk zapalny, w ścianach guza skupiska tkan-ki chłonnej oraz ropne nacieki zapalne o przewlekłym charakterze.
W okresie pooperacyjnym rozszerzono antybiotyko-terapię (dziecko otrzymywało początkowo amoksycylinę z kwasem klawulanowym i metronidazol, a po operacji otrzymało piperacylinę z tazobaktamem). Dren z loży po ropniu usunięto w 3 dobie po operacji.
W kontrolnym uSG w 5. dobie po operacji nie stwier-dzono obecności płynu w przestrzeni zaotrzewnowej, a badania laboratoryjne wykazały normalizację wskaźni-ków stanu zapalnego. Dziewczynkę wypisano do domu w 7. dobie po operacji, w stanie bardzo dobrym, z raną wygojoną rychłozrostem. Dalszą obserwację prowadzono w Poradni Chirurgii Onkologicznej. Kolejne badania obrazowe nie wykazywały nawrotu procesu chorobo-wego. Obserwacja trwa 22 miesiące.

180 Anna Obuchowicz et al.
oMóWIenIeTorbiele krezki mają prawie zawsze charakter łagod-
ny. Torbiele o charakterze złośliwym opisywane były u około 3% osób dorosłych. nigdy nie opisano przypad-ków złośliwych torbieli u dzieci [1]. Torbiele mogą być pojedyncze lub mnogie, jedno- lub, jak u opisywanego dziecka, wielokomorowe (ok. 20%). Mogą zawierać krew, chłonkę lub płyn ropny. Wielkość opisanych torbieli sięga od kilku milimetrów do 40 centymetrów, a masa usuniętej torbieli może wynosić 2000 g [1, 2].
Torbiele krezkowe mogą rozciągać się do przestrzeni zaotrzewnowej, co miało miejsce u naszej pacjentki. Sieciowe ograniczają się do sieci mniejszej i większej [1]. Torbiele krezki najczęściej nie powodują objawów lub dają niecharakterystyczne dolegliwości brzuszne na przykład: ból brzucha o różnym umiejscowieniu (65-75%), wzdęcie brzucha (35%), nudności i wymioty. napadowe bóle brzucha mogą pojawić się w procesach rozległych, które powodują upośledzenie czynności i/lub drożności przewodu pokarmowego. u 10% chorych mogą być przyczyną objawów „ostrego brzucha” [1, 5]. Opisywane dziecko nie skarżyło się na dolegliwości bólo-we, ale powiększenie obwodu brzucha oraz pogarszanie się stanu odżywienia obserwowano od dłuższego czasu. Przedmiotowo można stwierdzić prawidłowy obraz po-włok brzusznych oraz brak zmian patologicznych w ba-daniu palpacyjnym. Może jednak wystąpić uniesienie powłok brzusznych oraz tkliwość palpacyjna brzucha. Sam guz nie zawsze jest dostępny badaniu palpacyjnym. W postaciach zaawansowanych dochodzi do znacznego powiększenia obwodu brzucha [7].
Podobny obraz kliniczny, zazwyczaj utrudniający ustalenie właściwego rozpoznania przed operacją, dają guzy torbielowate sieci, które występują 3-4 razy rza-dziej niż torbiele krezki [2, 5]. W 20% przypadków guzy torbielowate są stwierdzane przypadkowo, gdyż są bez-objawowe. Jeżeli dolegliwości występują, to wymagają różnicowania z ostrym zapaleniem wyrostka robaczko-wego, skrętem jajnika i jajowodu, zapaleniem uchyłków jelita grubego (raczej u osób dorosłych), niedrożnością przewodu pokarmowego.
Powikłaniami torbieli krezki mogą być: niedrożność jelit, zastój w obrębie dróg moczowych, dysfunkcja ze-wnętrznych dróg żółciowych, skręt torbieli, krwawie-nie do jej światła lub zakażenie treści torbieli, co miało miejsce u opisywanej dziewczynki. Opisano także jeden przypadek pseudohipoaldosteronizmu typu 1, będącego skutkiem uropatii zaporowej spowodowanej torbielą krezki u noworodka [8].
Diagnostyka laboratoryjna nie wnosi istotnych danych rozpoznawczych. Przeglądowe zdjęcie rentgenowskie jamy brzusznej (w pozycji stojącej) może uwidocznić mode-lowanie jelit przez masę guza oraz – rzadko występujące – zwapnienia w ścianie torbieli. uSG jamy brzusznej jest podstawową metodą diagnostyczną. Pozwala określić rozmiary, umiejscowienie i położenie guza, uwidacznia przestrzenie płynowe. W nielicznych przypadkach obser-wowano powiększenie węzłów chłonnych krezkowych i zaotrzewnowych. Opisywano także przypadki ultraso-nograficznego wykrycia torbieli w okresie prenatalnym
[3, 6]. TK jamy brzusznej z podwójnym kontrastem pozwala zwykle na dokładne określenie miejsca wyjścia torbieli, a angio-TK uwidacznia ewentualne pochodzenie unaczynienia guza [1, 4]. Istnieją doniesienia o znaczeniu diagnostycznym wielorzędowej spiralnej TK w różni-cowaniu torbielowatych i litych guzów przewodu po-karmowego i określaniu ich lokalizacji [9]. W badaniu histopatologicznym, torbiele krezkowe mają najczęściej ścianę zbudowaną z tkanki włóknistej, której towarzyszyć może komponenta mięśniowa lub nabłonkowa a wyście-lone są nabłonkiem sześciennym [1].
Podstawowym sposobem leczenia jest radykalna resek-cja torbieli. Zwykle guz może być wyłuszczony. W około 50-60% przypadków konieczna jest jednak resekcja jelita, z następowym zespoleniem koniec do końca. Ma to miejsce głównie w przypadku torbieli krezki, z uwagi na niemożliwe do rozdzielenia, wspólne unaczynienie [1, 6, 10]. Jeżeli niemożliwe jest całkowite usunięcie torbieli, wykonywana jest resekcja częściowa z marsupializacją do jamy otrzewnej.
Innym sposobem jest wszycie brzegów ściany torbieli w ścianę jelita cienkiego, co zapobiega jej zamknięciu i pozwala na stały odpływ jej zawartości. Zabiegu tego może wymagać około 10% operowanych pacjentów [1, 2]. Wskazaniami do wykonania zespolenia torbieli z je-litem cienkim są zmiany nawrotowe o dużej dynamice wzrostu, a także wyjściowa lokalizacja uniemożliwiająca radykalny zabieg operacyjny (np. okolice wnęk narządów miąższowych). Zespolenia można wykonać dwojako: jako proste zespolenie torbieli ze ścianą przeciwkrezkową jelita lub zespolenie z wyłączoną pętlą jelitową sposobem Roux-en-Y. Resekcja torbieli dokonywana jest metodą laparotomii lub laparoskopii. Dostępna literatura porów-nująca obie metody operacyjne wykazuje, że laparoskopia jest metodą bezpieczną, efektywną i opłacalną, może być wykorzystywana w leczeniu torbieli krezki i sieci także u małych dzieci [3, 7, 11].
Powikłania leczenia chirurgicznego występują rzad-ko. Do najczęstszych należą objawy zespołu krótkiego jelita, związane z koniecznością rozległej resekcji jelita u niektórych pacjentów. nawroty choroby dotyczą do 13% pacjentów. Gorsze wyniki leczenia obserwowano w przypadkach torbieli położonych zaotrzewnowo i po resekcjach częściowych – wskaźnik nawrotów w tej grupie jest znacząco wyższy [1, 2].
u opisywanego przez nas dziecka mimo, wyjściowo złych czynników rokowniczych takich jak: rozległość zmian torbielowatych, zajęcia przestrzeni zaotrzewnowej, nasilonych zmian zapalnych wewnątrz torbieli i w jamie brzusznej, złego stanu odżywienia, przebieg pooperacyjny był niepowikłany. niemal dwuletni okres obserwacji bez nawrotu objawów chorobowych pozwala optymistycznie rokować na przyszłość.
Prezentowany przypadek potwierdza dobitnie koniecz-ność wykonywania badania usg jamy brzusznej u każdego dziecka z powiększonym obwodem brzucha lub wystę-pującymi dolegliwościami brzusznymi. To nieinwazyjne badanie, może być wykonane w trybie natychmiastowym. należy zatem podkreślić, że każda nieuzasadniona zwłoka, naraża pacjenta na opóźnienie rozpoznania ze wszystkimi możliwymi konsekwencjami.

181
piśmiEnniCTWo
1. Saxena A: Mesenteric and omental cysts. [http://emedicine.medscape.com/article/938463-overview#showall].
2. Chang TS, Ricketts R, Abramowksy CR, Cotter bD, Steelman ChK, Husain A, Shehata bM. Mesenteric cystic masses: A series of 21 pediatric cases and review of the literature. Fetal and Pediatric Pathology. 2011;40-44.
3. Pampal A, Yagmurlu A. Successful laparoscopic removal of mesenteric and omental cysts in toddlers: 3 cases with a literature revive. J Pediatr Surg. 2012;47(8):e5-8.
4. Punguyire D, Iserson KV. Mesenteric dermoid cyst in a child. Pan Afr Med J. 2011;10:1-6.
5. Szmidt J, Kurdżala J. [w]: Podstawy chirurgii. 2003;1109-1111.
6. nam SH, Kim DY, Kim SC, Kim IK. The surgical experience for retroperitoneal, mesenteric and omental cyst in children. J Korean Surg Soc. 2012;83(2):102-106.
7. Makni A, Chebbi F, Fetirich F, Ksantini R, bedioui H, Jouini M, et al. Surgical management of intra-abdominal cystic lymphangioma. Report of 20 cases. World J Surg. 2012;36 (5):1037-1043.
8. Zaki SA, Shenoy P, Shanbag P, Mondkar J, Kalgutkar A. Mesenteric cyst in a neonate causing obstructive uropathy and secondary type 1 pseudohypoaldosteronism – a case report. J Paediatr Child Health. 2011;47(7):486-488.
9. liu Y, Peng Y, Jianying li J, Zeng J, Suna G, Gao P. MSCT manifestations with pathologic correlation of abdominal gastrointestinal tract and mesenteric tumor and tumor-like lesions in children: A single center experience. eur J Radiol. 2010;75:293-300.
10. Chen H-P, liu W-Y, Tang Y-M, Ma b-Y, Xu b, Yang G, Wang X-J. Chylous Mesenteric Cysts in Children. Surgery today, 2011;358-362.
11. Tran nS, nguyen Tl. laparoscopic management of abdominal lymphatic cyst in children. J laparoendosc Adv Surg Tech. 2012;22 (5):505-507.
Wkład Autorów/Authors’ contributionsWedług kolejności/According to the order of the Authorship
Konflikt interesu/Conflicts of interestAutorzy pracy nie zgłaszają konfliktu interesów.The Authors declare no conflict of interest.
Nadesłano/Received: 08.10.2014 r.Zaakceptowano/Accepted: 16.12.2014 r.
Published online/Dostępne online
Adres do korespondencji:Anna Obuchowicz
Katedra i Oddział Kliniczny Pediatriiul. batorego 15, 41-902 bytom
tel./fax (+48 32) 78-61-498e-mail: [email protected]
Wielokomorowy guz krezki i przestrzeni zaotrzewnowej – malformacja chłonna u czteroletniej dziewczynki
182Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Grażyna Krzemień1, Tomasz Książczyk2, Agnieszka Szmigielska1, Przemysław Bombiński3, Maria Roszkowska-Blaim1, Bożena Werner2, Michał Brzewski3
ceftriaxone-aSSociated acute gallbladder enlargement − an unexpected diagnoSiS
in the child with urinary tract infection
oStre powiękSzenie pęcherzyka żółciowego związane z leczeniem ceftriakSonem − nieSpodziewane rozpoznanie u dziecka z zakażeniem układu
MoCzoweGo
1Department of Pediatrics and nephrology, The Medical university of Warsaw, Poland2Department of Pediatrics and Cardiology, The Medical university of Warsaw, Poland
3Department of Pediatrics Radiology, The Medical university of Warsaw, Poland
AbstractBiliary sludge and/or biliary pseudolithiasis occur in patients treated with ceftriaxone with prevalence of 3-57%. Biliary obstruction can be the cause of the acute gallbladder enlargement. It is a minor complication, that usually does not give clinical symptoms and resolves once the drug is discontinued. The authors present a case of a 5-month old boy treated for the acute pyelonephritis. Routine ultrasound, performed on the 5th day of treatment with ceftriaxone, showed gallbladder enlargement. In the consecutive studies small gallblader sludge was visible. Patient had no symptoms related to the gallbladder enlargement. Ultrasound performed 6 weeks from the drug discontinuation was completely normal. Conclusions: Patients treated with ceftroiaxone should be monitored for biliary sludge and pseudolithiasis.
Key words: biliary sludge, biliary pseudolithiasis, ceftriaxone, children, gallbladder
StreszczenieZagęszczenie żółci i/lub rzekoma kamica pęcherzyka żółciowego rozpoznawana jest u pacjentów leczonych ceftriaksonem z częstością od 3 do 57%. Utrudnienie odpływu żółci może być przyczyną ostrego powiększenia pęcherzyka żółciowego. Jest to łagodne powikłanie, które na ogół nie daje objawów klinicznych i ustępuje po odstawieniu antybiotyku.Opisano 5-miesięcznego chłopca przyjętego do szpitala z powodu ostrego odmiedniczkowego zapalenia nerek. Rutynowe badanie USG jamy brzusznej wykonane w 5 dobie leczenia ceftriaxonem wykazało powiększenie pęcherzyka żółciowego. W kolejnym badaniu uwidoczniono niewielką ilość zagęszczonej żółci w postaci poziomu osadu w świetle pęcherzyka. Dziecko nie demonstrowało żadnych objawów klinicznych związanych z powiększeniem pęcherzyka żółciowego. Kontrolne badanie USG wykonane po 6 tygodniach od odstawienia antybiotyku było prawidłowe.Wnioski: Pacjenci leczeni ceftriaksonem powinni być monitorowani w kierunku zagęszczenia żółci i rzekomej kamicy pęcherzyka żółciowego.
Słowa kluczowe: zagęszczenie żółci, rzekoma kamica żółciowa, ceftriaxon, dzieci, pęcherzyk żółciowy
DEV pErioD mED. 2015;XiX,2:182-185

183Ceftriaxone-associated acute gallbladder enlargement − an unexpected diagnosis
IntroDuctIonCeftriaxone – the 3rd generation cephalosporin
antibiotic for its broad spectrum, long halftime period and convenient once-a-day dosing is widely used for treating infections in pediatric patients [1, 2]. In circulation the drug combines with albumins in about 85-95%, in 60% it is eliminated unchanged by kidneys and in 40% by biliary route [3, 4, 5]. Concentration of ceftriaxone in bile can be 100-200 times greater than in the blood serum [4, 6, 7, 8]. liver eliminates high proportion of the drug in the form of water soluble salts. When there is a high concentration of ceftriaxone in the bile, it can react with calcium ions and form insoluble substances, which precipitate and lead to biliary sludge and/or cholelithiasis [1, 2, 5, 7]. Obstruction of the bile outflow can be the cause of acute gallbladder enlargement. biliary sludge and/or pseudolithiasis (name underlines its reversible character) is a known side effect of ceftriaxone, and was reported for the first time in 1986 (9). biliary sludge and pseudolithiasis occurs shortly after the introduction of the treatment with ceftriaxone and resolves soon after its discontinuation (3, 10). Insoluble compounds of ceftriaxone and calcium can precipitate also in urine and lead to urinary lithiasis. (3, 7)
cAse rePortThe patient was a boy, born from the 3rd pregnancy,
41 weeks of gestation, body weight at birth 3880 g, Apgar score 10. Postnatal period was uneventful and abdomen ultrasound was normal. At the age of 5 months he was admitted to our hospital because of high fever 39˚C, malaise and lack of appetite. laboratory blood tests showed: elevated inflammation markers: WbC 20,1 G/l, CRP 18,6 mg/dl (norm <1.0 mg/dl), prokalcytonin 2.68 ng/ml (norm <0.05 ng/ml), urinalysis showed leukocyturia 15-20 (HPF), urine culture was positive for Escherichia coli >105. Other blood tests including: aminotransferases, gamma-glutamyl transferase, AlP, bun and serum creatinine
were normal. Treatment with IV ceftriaxone 100 mg/kg/24 h was introduced. ultrasound performed in the 5th day of treatment revealed gallblader enlargement (61 x 30mm), with no signs of biliary sludge nor gallbladder wall thickening. (Figure 1). Follow up examination was done after 6 days and showed similar result, in the consecutive study performed after 22 days some biliary sludge was found (Figure 2). Antibiotic therapy was continued for 10 days with clinical status improvement and normalization of the laboratory tests. ultrasound examination performed after 6 weeks from drug discontinuation showed normal size gallbladder (Figure 3).
DIsscusIonPrevalence of biliary sludge and/or pseudolithiasis
in patients treated with ceftriaxone is reported in 3-57% of cases [1, 3, 4, 10, 11]. low prevalence of
Fig. 1. Gallblader enlargement 61 x 30 mm.Ryc. 1. Powiększenie pęcherzyka żółciowego do wymiarów
61 x 30 mm.
Fig. 2. Gallbladder enargement 40 x 10 mm, some biliary sludge.
Ryc. 2. Powiększenie pęcherzyka żółciowego do wymiarów 40 x 10 mm, niewielka ilość zagęszczonej żółci w postaci poziomu osadu w świetle pęcherzyka.
Fig. 3. normal gallbladder.Ryc. 3. Prawidłowy pęcherzyk żółciowy.

184 Grażyna Krzemień et al.
these complications in part of the reports is probably due to the fact that ultrasound was performed late in the course of treatment, and some cases might be missed [8]. ultrasound changes occur in 2-7 days after the introduction of ceftriaxone [1, 3]. In about 90% of cases in the first 5 days of treatment [10]. biliary sludge or stones within the gallbladder are the most common findings in ultrasound examination. In most cases the size of the gallstones is below 3 mm [2, 10]. ultrasound changes resolve in 2-150 days, but usually in the first days, after discontinuation of the treatment [1, 2, 3, 4, 8, 10].
There are many factors predisposing to biliary sludge and gallstones formation in children. The most common are: hemolysis in sickle cell anemia, congenital defects of the biliary routs, bone marrow disorders, diseases of the bowels, as well as the biliary tract and liver, mucoviscidosis, malabsorption, abdominal surgeries, solid organs transplant, prolonged total parenteral nutrition, obesity and drugs [1, 4, 5, 12]. Ceftriaxone and octreotide are most commonly responsible for biliary sludge and pseudolithiasis [4, 12]. Meng compared the prevalence of pseudolithiasis in children treated with ceftriaxone and ceftazidime. It was present in 43.1% of patients treated with ceftriaxone and only in 2% in ceftazidime group. Ceftriaxone is widely used in patients treated for hepatitis and biliary tract infections. However, pseudolithiasis occurs in this group of patients significantly more often than in those who receive it for other reasons (68.6% vs 11.5%). because of that, Meng postulates that ceftriaxone should be avoided in patients treated for hepatitis and biliary tract infections [1].
There are many reports of studies considering ceftriaxone side effects. no statistically significant differences have been found in prevalence of ultrasound changes in patients treated with ceftriaxone depending on: age, sex, body weight, time of year, dose, time of treatment, use of calcium supplements, parenteral nutrition nor fasting for surgeries [8, 10, 11]. However, ceftriaxone related biliary sludge and pseudolithiasis occurs slightly more often in children. Possible causes are: 1) non effective bile secretion due to long and narrow biliary tracts in children; 2) weaker contraction of gall bladder due to relatively lower concentration of cholecystokinin; 3) common febrile illnesses and dehydration which may contribute to bile congestion [1].
biliary sludge and pseudolithiasis are minor complications, and usually do not give clinical symptoms. nausea, vomiting, abdominal pain, jaundice, cholecystitis, biochemical sings of cholestasis occur in 2.6-43% of cases. [1, 3, 4, 8, 10]. ultrasound examination should be performed in all children presenting with symptoms of cholelithiasis. In case of ceftriaxone related pseudolithiasis, discontinuation of the drug is the only recommended intervention. All the symptoms resolve once the drug is withdrawn [1, 2, 3, 5]. need for the surgical intervention is very rare [8]. Precipitation of the compounds of ceftriaxone and calcium in urine can lead to urinary lithiasis in 6.3% of children [3, 7]. Asymptomatic urinary lithiasis
most commonly occurs in 2-7 days of treatment with ceftriaxone [7].
In the presented case the gall bladder enlargement was found in the 5th day of the treatment with ceftriaxone. It was a routine abdominal ultrasound, performed in a child with acute pyelonephritis. The patient had no symptoms related to the gall bladder enlargement. In the consecutive ultrasound examination done after 22 days of treatment some biliary sludge was detected. Ceftriaxone is a broad spectrum antibiotic used for treating the most severe bacterial infections in children [2, 4, 5, 12], and it is rarely required for uncomplicated urinary tract infections. When deciding on the use of ceftriaxone, one has to keep in mind possible side effects.
conclusIonPatients treated with ceftriaxone should be monitored
for possible biliary sludge, biliary pseudolithiasis and urinary lithiasis.
reFerences
1. Meng D, Cao Y, Fu J, Chen R, lu l, Tu Y. Sonographic Assessment of Ceftriaxone-Associated biliary Pseudolithiasis in Chinese Children. J Int Med Res. 2010;38:2004-2010.
2. Araz n, Okan V, Demirici M, Araz M. Pseudolithiasis due to Ceftriaxone Treatment fo Meningitis in Children: Report of 8 Cases. Tohoku J ex Med. 2007;211:285-290.
3. biner b, Öner n, Celtic C, bostancioğlu M, Tuncbilek n, Güzel A., Karasalihoğlu S. Ceftriaxone-Associated biliary Pseudolithiasis in Children. J Clin ultrasound. 2006;34:217-222.
4. bor O, Dinleyici eC, Kebabci M, Aydogdu SD. Ceftriaxone-associated biliary sludge and pseudocholelithiasis during childhood: A prospective study. Pediatr Int. 2004;46:322-324.
5. von Martels JZH, Van de Meeberg eK, Holman M, ligtenberg JJM, ter Maaten JC. Pseudolithiasis after recent use of ceftriaxone: an unexpected diagnosis in a child with abdominal pain. Am J emerg Med. 2013;31:1294.e5-1294.e6.
6. lee SM, benjamin Al, Teefey SA. Gallbladder sludge and antibiotics. Pediatr Infect Dis J. 1990;9:422-423.
7. Fesharakinia A, ehsanbakhsh A-R, Ghorashadizadeh n. Ceftriaxone-Associated nephrolithiasis in Children. Iran J Pediatr. 2013;23 (6):643-647.
8. Alemayehu H, Desai A, Thomas P, Sharp SW, St. Peter SD. Ceftriaxone-induced pseudolithiasis in children treated for perforated appendicitis. Pediatr Surg Int. 2014;30:323-326.
9. Schaad ub, Tschappeler H, lentze MJ. Transient formation of precipitations in the gallbladder associated with ceftriaxone therapy. Pediatr Infect Dis. 1986;5:708-710.
10. Rangel DAR, Orejaarena APP, Diaz Mb, Garcia lH, Cadena Al, Camargo RM, Moreno lA. Gallstones in association with the use of ceftriaxone in children. An Pediatr (barc). 2014;80 (2):77-80.

185
11. Ceran C, Oztoprak I, Cankorkmaz l, Gumuş C, Yildiz T, Koyluoglu G. Ceftriaxone-associated biliary pseudolithiasis in paediatric surgical patients. Int J Antimicrob Agents. 2005;25:256-259.
12. Ko CW, Sekijima JH, lee SP. biliary sludge. Ann Intern Med. 1999;130:301-311.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 04.05.2015 r.Accepted/Zaakceptowano: 11.05.2015 r.
Published online/Dostępne online
Address for correspondence:Grażyna Krzemień
Department of Pediatric nephrology,The Medical university of Warsaw, PolandMarszałkowska 24, 00-576 Warsaw, Poland
tel. (+48-22) 52-27-388fax (+48-22) 621-98-63
e-mail: [email protected]
Ceftriaxone-associated acute gallbladder enlargement − an unexpected diagnosis

186Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Agnieszka Szmigielska1, Aleksandra Księżopolska2, Maria Roszkowska-Blaim1, Michał Brzewski3, Grażyna Krzemień1
rare renal ectopia in children – intrathoracic ectopic kidney
rzadki przypadek ektopii nerek u dzieci – nerka w klatce pierSiowej
1Department of Pediatric nephrology, The Medical university of Warsaw, Poland2Student’s Scientific Group, Department of Pediatric nephrology,
The Medical university of Warsaw, Poland3Department of Pediatric Radiology, The Medical university of Warsaw, Poland
AbstractRenal ectopia occurs in 1:3000-1:7000 children. Simple ectopia refers to the abnormal kidney location on the same side; in crossed ectopia the ureter crosses the midline of the body. In most cases ectopic kidney is found in the pelvis minor, in 5% of cases in the thoracic cavity. Kidney displacement does not give any clinical symptoms in the majority of patients, sometimes it may cause abdominal pain, urinary tract infection, chest pain or promote nephrolithiasis. Renal ectopia is usually discovered during routine abdominal ultrasound. We describe a boy with prenatal ultrasound diagnosis of left kidney agenesis. Right normal kidney and displaced to the thoracic cavity, smaller, with normal echostructure left kidney were found in postnatal ultrasound. Left kidney ectopia was confirmed in renal scinthigraphy, radiography and computed tomography of the chest. Voiding cystourethrography (VCUG) excluded vesicoureteral reflux. Conclusions: In case of kidney’s absence in typical localization in the abdominal ultrasonography, the ectopic kidney should be suspected. Diagnosis of ectopic kidney requires further additional imaging examination to check renal function and other urinary tract anomalies.
Keywords: renal ectopia, crossed renal ectopia, thoracic kidney, scintigraphy, CAKUT
StreszczenieEktopia nerek występuje z częstością 1:3000-1:7000 dzieci. Ektopia prosta dotyczy nieprawidłowego położenia nerki po tej samej stronie; w ektopii skrzyżowanej moczowód przecina linię pośrodkową ciała. Nerka ektopowa położona jest najczęściej w miednicy małej, w 5% przypadków leży w klatce piersiowej. Przemieszczenie nerki u większości dzieci nie daje objawów klinicznych, czasami nerka ektopowa może powodować bóle brzucha, zakażenia układu moczowego lub sprzyjać wystąpieniu kamicy. Ektopia nerki wykrywana jest najczęściej w rutynowych badaniach ultrasonograficznych jamy brzusznej. Przedstawiamy przypadek chłopca, u którego na podstawie prenatalnych badań ultrasonograficznych rozpoznano agenezję nerki lewej. W badaniach ultrasonograficznych jamy brzusznej wykonanych po urodzeniu stwierdzono prawidłową nerkę prawą i przemieszczoną do klatki piersiowej nerkę lewą, mniejszą od prawej, o prawidłowej echostrukturze. Ektopię potwierdzono scyntygrafią nerek, badaniem radiologicznym klatki piersiowej i tomografią komputerową klatki piersiowej. W cystografii mikcyjnej wykluczono odpływy pęcherzowo-moczowodowe. Wnioski: W przypadku braku nerki w miejscu typowym w badaniu ultrasonograficznym należy poszukiwać nerki ektopowej. Obecność nerki ektopowej wymaga wykonania dodatkowych badań obrazowych w celu oceny jej funkcji i towarzyszących wad układu moczowego.
Słowa kluczowe: ektopia nerki, skrzyżowana ektopia nerki, nerka w klatce piersiowej, scyntygrafia, CAKUT
DEV pErioD mED. 2015;XiX,2:186-188

187Rare renal ectopia in children - intrathoracic ectopic kidney
BACKGroUnDAnatomically, human kidneys are located in abdomen,
retroperitoneal, on the level of two last thoracic vertebrae (Th11-Th12) and first three lumbar vertebrae (l1-l3). left kidney is generally placed higher than the right one. It measures about 10-12 cm in adults, average weight is 120-200 g [1]. Kidneys exhibit respiratory mobility. Renal ectopia means the displacement of kidney from its normal lumbar location. It is connected with the abnormal prenatal kidneys migration from sacral spine to the lumbar region, which appears about 5-9 week of gestation. ectopia may touch one or both kidneys. In the simple ectopia, kidney is placed on the same side of body in the pelvis minor or in the chest. In crossed ectopia, kidney is placed on the opposite side of the body and the ureter crosses the midline of the body and reaches bladder in the normal place. In 90% of crossed renal ectopia kidneys are fused. About 60% of ectopic kidneys are placed in pelvis minor, 35% paravertebrally, 5% in thoracic cavity [2]. The incidence of ectopic kidney in pelvis minor is 1:3000, crossed renal ectopia 1:7000, the solitary kidney in pelvis minor 1:22 000 births [3]. In most cases of ectopic kidney does not give any clinical symptoms. However, the abnormal position of kidney and ureters can cause urinary tract infection, nephrolithiasis, abdominal pain, chest pain, tachypnoe or hypertension [4, 5]. Renal ectopia may appear in children with trisomy of 21 or 18 chromosome, Turner syndrome, beckwith-Wiedemann syndrome, be part of VACTeRl or CHARGe sequence [6].
cAse rePortThe boy was born at term, with birth weight 3340g,
in good general condition. Agenesis of left kidney was diagnosed in prenatal ultrasonography. Postnatal abdominal ultrasound showed correctly placed right kidney (55 mm) and displaced to the chest left kidney (35 mm), both with normal echostructure. The control abdominal and chest ultrasound performed at the age of three years showed the normal right kidney of 76mm and hypoplastic left kidney in the thoracic cavity, which measured 57 mm (Figure 1). Renal scinthigraphy DMSA described physiologically placed right kidney and intrathoracic left kidney. Static scintigraphy (DMSA) revealed normal function of right kidney (58%), and decreased function of the left kidney (42%). Voiding cystourethrography (VCuG) excluded vesicoureteral reflux. Four years later the chest radiography was done, because of the suspicion of pneumonia. It showed a shadow of 70x30 mm placed over the diaphragm, which could correspond to the left ectopic kidney (Figure 2). because of this suspicious mass in the chest, the computed tomography was performed and it confirmed the ectopia of left kidney located in the thoracic cavity (Figure 3). During the seven-year follow-up arterial blood pressure, kidney function and urinalysis are normal.
DIscussIonCongenital abnormalities of kidney and urinary tract
(CAKuT) are one of the most common malformations in
Fig. 1. ultrasonography of the chest; arrows shows thoracic ectopic kidney.
Ryc. 1. Badanie ultrasonograficzne klatki piersiowej; strzałka wskazuje nerkę ektopową w klatce piersiowej.
Fig. 2. X-ray of the chest in patient with intrathoracic ectopic kidney.
Ryc. 2. Zdjęcie radiologiczne klatki piersiowej u pacjenta z ektopią nerki w klatce piersiowej.
Fig. 3. CT of the chest, arrows shows ectopic kidney.Ryc. 3. Tomografia komputerowa; strzałka wskazuje nerkę
ektopową w klatce piersiowej.

188 Agnieszka Szmigielska et al.
children. Kidneys reach the final correct position in the early stages of embryogenesis, by the 9th week of gestation. Prenatally, there are a lot of risk factors such as genetic, teratogenic which may disturb the physiological development of kidneys and lead to congenital defects. Absence of kidney in its typical location in the ultrasound may be associated with agenesis or ectopia in a different location, most often in pelvis minor. Intrathoracic ectopic kidney is a rare kidney abnormality. The incidence of intrathoracic ectopic kidney in autopsies was rated 1:13 000 (Campbell, 1930). It occurs more often in males and on the left side of the body. Renal function is usually correct, proportional to the kidney’s size. ectopic kidney is generally discovered accidentally during routine abdominal ultrasounds [7]. In the literature, one can find descriptions of patients with ectopic intrathoracic kidney diagnosed in the adulthood [8]. In every case, when the kidney cannot be found in its typical location in ultrasound, it is necessary to look for it outside the lumbar area. Most commonly, ectopic kidney is placed in pelvis minor, but it is highly recommended to always consider the thoracic location during the diagnosis. On the other hand, seeing the mass in the chest, the ectopic kidney should be taken in account in the differential diagnosis. not only ultrasound may be useful in the diagnosis of renal ectopia, but also renal scintigraphy and voiding cystourethrography may apply. In case of absence of kidney in its typical location, renal scintigraphy can detect the ectopic kidney. Scintigraphy does not measure accurately the share in filtration of ectopic and normal kidney. The reason of this difficulty is the difference in distance kidneys from gamma camera. ectopic kidney is usually rotated and placed deeper than the normal one, so it may understate its share in filtration [9]. In some cases computed tomography is performed to confirm the diagnosis. In this case, the ultrasound was repeated after birth because of the prenatal suspicion of renal agenesis and it showed the left kidney’s displacement to the thoracic cavity. Renal scinthigraphy and computed tomography confirmed this ectopia. In the ultrasound examination, the ectopic kidney was smaller than the normal one, but its functioning was correct and proportional to size. Voiding cystourethrography excluded the presence of vesicoureteral reflux. Routine chest radiography proceed because of the pneumonia exposed suspicious mass in chest, which proved to be the ectopic kidney. During the long observation, the boy did not report any complaints and his psychomotor development is correct.
conclusIons1. In case of kidney’s absence in its typical location in the
ultrasonography, an ectopic kidney should be sought. 2. ectopic kidney needs further additional imaging exa-
mination to check the renal function and other urinary tract abnormalities.
reFerences
1. Dudek RW. High-Yield Kidney. lWW 2007, Chapter 2. 2. Jhun bW, lee K-J. A right thoracic kidney with a pulmonary
vascular malformation in an adult. Respirol Case Rep. 2013;1(2):55-57.
3. Cinman nM, Okeke Z, Smith AD. Pelvic kidney: associated disease and treatment. J endourol. 2007;21 (8):836-842.
4. Fadaii A, Rezaian S, Tojari F. Intrathoracic kidney presented with chest pain. Iran J Kidney Dis. 2008;2(3):160-162.
5. Sesia Sb, Haecker FM. late-presenting diaphragmatic hernia associated with intrathoracic kidney: tachypnoea as unique clinical sign. bMJ Case Rep. 2012 Apr 23;2012.
6. Stein JP, Kurzrock eA, Freeman JA, esrig D, Ginsberg DA, Grossfeld GD, Hardy be. Right intrathoracic renal ectopia: a case report and review of the literature. Tech urol. 1999 Sep;5(3):166-168.
7. Sumner Te, Volberg FM, Smolen PM. Intrathoracic kidney − diagnosis by ultrasound. Pediatr Radiol. 1982;12(2):78-80.
8. liddell R, Rosenbaum D, blumhagen J. Delayed radiologic appearance of bilateral thoracic ectopic kidneys, AJR 1989;152:120-122.
9. Allen D, bultitude MF, nunan T, Glass JM. Misinterpretation of radioisotope imaging in pelvic kidneys. Int J Clin Pract Suppl. 2005 Apr;(147):111-112.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 21.04.2015 r. Accepted/Zaakceptowano: 12.05.2015 r.
Published online/Dostępne online
Address for correspondence:Agnieszka Szmigielska
Department of Pediatric nephrology, The Medical university of Warsaw, Warsaw, Poland
Marszałkowska 24, 00-576 Warsaw, Poland tel. (+48 22) 522-74-96
fax: (+48 22)-771-48-26e-mail: [email protected]

189Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
Anna Janas1, Piotr Osica2
central giant cell granuloma located in the maxilla in a 8-year old boy*
centralny ziarniniak olbrzymiokomórkowy zlokalizowany w Szczęce u 8-letniego chłopca
1Department of General Dentistry, Medical university of lodz, Poland2Department of Oral Surgery, Medical university of lodz, Poland
AbstractCentral giant cell granuloma is a rare occurring tumor-like lesion of the facial part of the skull, located more often in mandible (from 2:1 to 3:1), than in the maxilla. It accounts for 7% of all benign tumors of the jaws, whereas the brown tumor is a complication of a primary hyperparathyroidism and occurs in approximately 4.5%, or in 1.5%, when the tumor is a complication of secondary hyperparathyroidism. However, the brown tumor is significantly less often observed than the presented lesion. The authors describe a case of central giant cell granuloma of the maxilla, located in the area of premolar teeth. Pantomograhic x ray showed unilocular osteolytic bone loss of the maxilla with ectopic teeth. As a part of the One Day surgery procedures, the tumor has been removed with the margin and embedded teeth, and oroantral communication closure performed. In follow-up examination after 10 months and 2 years from the surgery, no recurrence of the tumor has been observed.Conclusion: In differential diagnosis of tumors of face and skull, it is needed to consider the giant cell granuloma and also the brown bone tumor.
Key words: tumor-like lesion, central giant cell granuloma, maxilla, treatment
StreszczenieCentralny ziarniniak olbrzymiokomórkowy to rzadko występująca zmiana guzopodobna w części twarzowej czaszki, zlokalizowana częściej w żuchwie od 2:1 do 3:1 niż w szczęce. Stanowi 7% wszystkich guzów łagodnych. Natomiast guz brunatny występuje w ok. 4,5%, jako powikłanie pierwotnej nadczynności przytarczyc, zaś we wtórnej nadczynności przytarczyc stwierdzany jest w 1,5%.W pracy przedstawiono przypadek centralnego ziarniniaka olbrzymiokomórkowego szczęki w okolicy zębów przedtrzonowych. Na zdjęciu pantomograficznym widoczny był jednokomorowy ubytek osteolityczny kości szczękowej z przemieszczonymi zębami. W procedurach chirurgii jednego dnia usunięto guz z marginesem tkanek zdrowych i zębami tkwiącymi w jego masie. Wykonano plastykę połączenia ustno-zatokowego. W badaniach kontrolnych wykonanych po 10 miesiącach i 2 latach od zabiegu nie stwierdzono nawrotu choroby.Wniosek: W różnicowaniu guzów twarzoczaszki należy brać pod uwagę ziarniniaka olbrzymio- -komórkowego, a także guz brunatny kości.
Słowa kluczowe: zmiana guzopodobna, centralny ziarniniak olbrzymiokomórkowy, szczęka, leczenie
DEV pErioD mED. 2015;XiX,2:189-192
*The study is financed by the Medical university of lodz, as a part of it’s statutory activity number 503/2-163-01/503-21-001.

190 Anna Janas, Piotr Osica
Central giant cell granuloma was first described by Jaffe in 1953. It is a rarely occurring tumor-like lesion of the facial part of the skull, located more often in mandible (from 2:1 to 3:1), than in the maxilla. Its incidence is approximately 7% of all benign tumors of the jaws. Central giant cell granuloma can also occur in fingers and toes, cranial vault, collar and scapular bone. The lesion can develop at any age, though it is more common in patient’s second and third decade of life (74%), and shows a slight female predilection (65%). It may also occur in children. Inflammatory or injury background, reparative bone reaction and also a possibility of a hemorrhagic bone cyst transformation, where osteoclasts appear in the areas formed out of fibroblasts, are being considered [1, 2].
Aim of the study: To present a rarely occurring lesion, so that it can be taken into consideration in differential diagnosis.
cAse rePort8-year old boy has been referred to our hospital by
an orthodontist, for a consultation, due to an existing lump of hard palate. The interview revealed a sustained trauma, 6 months before, during biking. because of no visible injuries, the patient has not been consulted by a physician. After 2 months from the trauma, the parents decided to seek general dental practitioner help, who in local anesthesia incised the hard palate and administered antibiotics. no improvement in patient’s condition encouraged the parents to seek further help. General condition of the patient was good, no pain reported.
extra oral examination showed no changes from the normal state (Figure 1). Intraoral examination revealed persistent teeth in the right side of the maxilla (52, 53, 54) and painless, medium-hard lump on hard palate, covered with normal mucous membrane (Figure 2).
Pantomographic image revealed unilocular osteolytic loss of maxillary bone on the right side with ectopic teeth (Figure 3).
Fine needle aspiration biopsy (bAC) has been performed as an outpatient procedure, and showed numerous multinucleated giant cells, whereas laboratory investigations of calcium (2.3 mmol/l), phosphate (3.5 mmol/l), alkaline phosphatase (40 mmol/l) and parathormone (1.2 pmol/l) were normal. Hence the decision of a surgical procedure.
The parents were presented with the preliminary diagnosis and treatment plan, consisting of a surgery performed as a part of One-Day Surgery procedures. After obtaining written consent, the appointment has been set.
In general anesthesia, persistent teeth 52, 53 and 54 were extracted; the mucoperiosteal flap has been cut and prepared. The tumor-like lesion has been removed as a whole, with the embedded tooth 14 and a margin of healthy tissue. (Figure 4 and 5). The material has been sent
Fig. 1. in extraoral examination of a 8-year old boy no changes have been noted.
Ryc. 1. W badaniu zewnątrzustnym nie stwierdzono odchyleń od stanu prawidłowego u 8- letniego chłopca.
Fig. 2. intraoral examination showed persistent teeth 52,53,54 and not painful lump on the right side of the hard palate.
Ryc. 2. W badaniu zewnątrzustnym obserwowano przetrwałe zęby 52, 53 i 54 oraz niebolesne wygórowanie na podniebieniu twardym po stronie prawej.
Fig. 3. panotomograhic x ray showed unilocular osteolytic bone loss of the maxilla with ectopic teeth.
Ryc. 3. Na zdjęciu pantomograficznym widoczny był jednokomorowy ubytek osteolityczny kości szczękowej po stronie prawej z przemieszczonymi zębami.

191Central giant cell granuloma located in the maxilla in a 8-year old boy
for histopathological examination. Postoperative wound has been rinsed and closure of oro-antral communication performed. The intra- and postoperative course was uneventful.
After the procedure, the boy has been referred to the postoperative care ward, where his general condition has been controlled by specialists. Critical concerns were airway clearance, pain control, mental status, double vision, nausea and vomiting. examination eliminating such symptoms, allowed the discharge of the patient.
Follow up examination one day after the surgery showed oedema of the operated area (Figure 6). Post-operative wound has been rinsed with antiseptic and further follow up ordered. On the 3rd day, the reduction of oedema has been observed, which subsided completely on the 5th day after the surgery. On the 12th day the sutures have been removed and the wound’s healing was uneventful.
Despite long standing observations, no clear-cut etiopathogenesis of central giant cell granuloma has been determined hitherto.
Results of histopathological verification confirmed the initial diagnosis of central giant cell granuloma.
The boy still stays under clinical observation, and after 10 months and 2 years of follow up, no sign of recurrence was observed.
DIscussIonCentral Giant Cell Granuloma (CGCG) is found in
75% in the mandible, usually near the mental foramen and often crossing the midline, also in the region of molar teeth [3, 4]. In presented case, the tumor affected premolar teeth and maxillary sinus.
Clinical picture of the CGCG varies. From slow and asymptomatic growth, associated with non-aggressive form, which applies to 60-80% of cases, that stay unnoticed for a long time, because of their growth inside of the trabecular bone and no pain or neurological disorders. However migration of teeth can be observed. To the rarely occurring aggressive type, usually found in 19 to 40% of all CGCG cases, which causes bone mutilation, migration and loss of teeth, root resorption and infiltration of the soft tissues. Frequent symptoms are pain and paresthesia, pathological fractures and recurrences. ultrastructural and immunohistochemical examinations performed to estimate the type of the tumour, showed no difference between aggressive an non-aggressive types. Whereas in patient with aggressive type tumor, high level of proliferation marker − Ki 67 was observed [5].
Macroscopically, CGCG is built of fibrous tissue with typical fibroblasts. basically CGCG is composed of many multinucleated cells of osteoclast type, that lie individually or in small aggregations (6) (Figure 7).
Fig. 4 and 5. The whole tumour-like lesion has been removed, together with embedded teeth.Ryc. 4 i 5. Usunięto w całości zmianę guzopodobną z tkwiącym w niej zębem.
45
Fig. 6. in the first day after the surgery, the postoperative oedema is observed.
Ryc. 6. W 1. dobie po zabiegu stwierdzono obrzęk okolicy operowanej.

192
Martins et alia [7] believe that this lesion should be differentiated with brown tumor in association with hyperthyroidism. because both diseases have identical clinical and histopathological picture, PTH levels should be examined, hence performing such an investigation in our patient. no deviation from normal state in received results, encouraged us to determine the diagnosis of CGCG.
Radiographically CGCG may appear as a unilocular or multilocular radiolucency, with well-defined or ill-defined margins and varying degrees of expansion of the cortical plates, with no osteolytic areola and periosteal reaction. Migration of teeth and teeth’ germs is also observed (8). In treated patient, the tumor was unilocular with migrated teeth.
Treatment of CGCG depends on a particular case, patient’s age an general condition, state of tumor’s development, its localization, clinical type and infiltration of soft tissue. Apart from the surgical treatment, which was performed in our case, many authors [5, 9] suggest daily systemic doses of calcitonin, because osteoclasts have calcitonin receptors, thus it may suppress their activity. Others [10] show that the process of osteoclastogenesis influences the osteoprotegerin (OPG), which in turn suppresses resorption through RAnK (Receptor Activator of nuclear Factor) and RAnKl, which is a mediator of osteoclasts’ activity and also plays a role in bone resorption. OPG neutralizes its effect and causes a suppression of osteoclasts formation.
conclusIonsIn differential diagnosis of tumors of face and skull,
it is needed to consider the giant cell granuloma and also the brown bone tumor.
reFerences
1. Chiba I, Teh Gb, Irzyka T, Fukada H. Conversion of a traumatic bone cyst into central mcell gigant granuloma.
Implication for pathogenesis – a case report. J Oral Maxillofac Surg. 2002;60:222-225.
2. Janas A. Ziarniniak olbrzymiokomórkowy. Dental Forum. 2007;35:69-73.
3. batained Ab, Al.-Khateeb T, Rawashdeb MA. The surgical treatment of central giant cell granuloma of the mandible. J Oral Maxillofac Surg. 2002;60:756-761.
4. nowak R, Pawlak W, Kaczkowski H. Centralny ziarniniak olbrzymiokomórkowy żuchwy u 16-letniego pacjenta – opis przypadku. Dent Med Prob. 2004;41,4:803-806.
5. Carlos R, Sedano H. Intralesional corticosteroids as an alternative treatment for central giant cell granuloma. Oral Surg Oral Med Oral Pathol. 2002;93:161-166.
6. Abu-el-naaj I, Ardekian I, liberman R, Pelled M. Central giant cell granuloma of the mandibular condyle: a rare presentation. J Oral Maxillofac Surg. 2002;60:939-841.
7. Martins WD., Ribas M, braosi AP. Multiple giant cell lesions of the maxillofacial skeleton. J Oral Maxillofac Surg. 2007;65:1250-1253.
8. Stavropoulos F, Katz I. Central giant cell granuloma: a systematic review of the radiographic characteristics with addition of 20 new cases. Dentomaxillofac. Radiol, 2002;31:213-217.
9. Vered M, buchner A, Dayan D. Immunohistochemical expression of glucocorticoid and calcitonin receptors as a tool for selecting therapeutic in central giant cell granuloma of the jaw bones. Int J Maxillofac Surg, 2006;35:756-760.
10. Tay JY, bay bH, Yeo JF, Harris M, Meghij S, Dheen ST. Identification of RAnKl in osteolityc lesions of the facial skeleton. J Dent Res. 2004;83:349-353.
Author’s contributions/Wkład AutorówDr hab. n. med. Prof. nadzw. Anna Janas – koncepcja i pro-Prof. nadzw. Anna Janas – koncepcja i pro-jekt pracy, zbieranie danych, napisanie artykułu, krytyczna recenzjaDr n. med. Piotr Osica – koncepcja i projekt pracy, zbiera-nie danych, ryciny, krytyczna recenzja
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 31.03.2015 r.Accepted/Zaakceptowano: 19.05.2015 r.
Published online/Dostępne online
Address for correspondence:Piotr Osica
Zakład Chirurgii Stomatologicznej uM w Łodziul. Pomorska 251, 92-213 Łódź
e-mail: [email protected].: (42) 67-57-529, 692-607-174
Fig. 7. Micrograph of a central giant cell granuloma- h+e stain.200x
Ryc. 7. Ziarniniak olbrzymiokomórkowy − obraz mikroskopowy. Preparat barwiony H+E, pow. 200x.
Anna Janas, Piotr Osica

193Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
Justyna Weronika Wüenstel, Joanna Kowalkowska, Lidia Wądołowska, Małgorzata Anna Słowińska, Ewa Niedźwiedzka, Lidia Kurp
habitual eating of breakfaSt, conSumption frequency of Selected food
and overweight prevalence in adoleScentS from variouS age groupS
zwyczajowe Spożycie śniadania a częStość Spożycia wybranej żywności i wyStępowania nadwagi
u młodzieży z różnych grup wiekowych
Department of Human nutrition, university of Warmia and Mazury, Olsztyn, Poland
AbstractAim: To assess the influence of eating breakfast on the consumption of selected food and overweight prevalence among adolescents from different age groups.Material and methods: The study group consisted of students aged 13-18.9 (n=1700). Their height and weight measurements were used to calculate their body mass index and interpreted according to international standards for adolescents. Food consumption was assessed via the frequency method and involved the consumption of breakfast, dietary fibre and sweetened beverages. We used Block’s validated questionnaire to assess the intake of dietary fibre and its sources. Analysis of the results was carried out in three age groups: 13-14.9, 15-16.9 and 17-18.9 years old. We used one-factor logistic regression adjusted by gender. Results: The percentage of adolescents with a regular habit of eating breakfast dropped by 5.7 percentage points when compared to adolescents aged 13-14.9 and 17-18.9 (from 54.2% to 48.5%), which was a phenomenon accompanied by an increase in the percentage of adolescents who ate breakfast irregularly or hardly ever (by 3.7 and 1.9 percentage points, respectively). Eating breakfast infrequently was related to a more frequent consumption of sweetened beverages (the odds ratio: from 2.32 to 2.67 depending on the age group) and a higher prevalence of a fibre-poor diet (from 1.49 to 2.23). Among adolescents aged 13-14.9 who hardly ever ate breakfast, the chance of being overweight increased by 83% in comparison to adolescents with regular habits of eating breakfast. Conclusions: The frequency of eating breakfast decreased with the adolescents’ age, especially among girls. Eating breakfast infrequently was associated with unhealthy nutrition, typical examples of which are lower intake of dietary fibre and more frequent consumption of sweetened beverages, and in the youngest group of adolescents caused a higher prevalence of overweight.
Key words: overweight, adolescents, dietary habits, consumption of breakfast
StreszczenieCel pracy: Ocena wpływu zwyczajowego spożycia śniadania na częstość spożycia wybranych grup żywności oraz występowania nadwagi u młodzieży w różnych grupach wiekowych.Materiał i metody: Badaną grupę stanowiła młodzież szkolna w wieku 13-18.9 lat (n=1700). Na podstawie pomiarów wysokości i masy ciała obliczono wskaźnik względnej masy ciała, który interpretowano według międzynarodowych standardów dla młodzieży. Ocena sposobu żywienia była przeprowadzona metodą częstości spożycia i objęła spożycie śniadań, błonnika pokarmowego oraz słodzonych napojów. W badaniach użyto zwalidowany kwestionariusz Block’a do oceny spożycia błonnika i jego źródeł. Analizę wyników przeprowadzono w 3 grupach wiekowych: 13-14,9 lat, 15-16,9 lat i 17-18,9 lat. Do analizy statystycznej użyto jednoczynnikowej regresji logistycznej, adjustowanej na płeć.

194 Justyna Weronika Wüenstel et al.
Wyniki: Procent młodzieży regularnie spożywającej śniadania był mniejszy o 5,7 punktów procentowych pomiędzy młodzieżą w wieku 13-14,9 lat i 17-18,9 lat, podczas gdy procent młodzieży nieregularnie spożywającej śniadanie i prawie nigdy niespożywających śniadania był większy o odpowiednio: 3,7 p.p. i 1,9 p.p. Rzadsze spożycie śniadań sprzyjało częstszemu spożyciu słodzonych napojów (iloraz szans: od 2,32 do 2,67 w zależności od grupy wiekowej) oraz mniejszemu spożyciu błonnika pokarmowego (od 1,49 do 2,23). Wśród młodzieży prawie nigdy nie spożywającej śniadania w wieku 13-14,9 lat odnotowano wzrost szansy wystąpienia nadwagi o 83% w porównaniu do młodzieży regularnie spożywającej śniadania.Wnioski: Procent młodzieży spożywającej regularnie śniadania zmniejszał się wraz z wiekiem, w szczególności wśród dziewcząt. Rzadsze spożycie śniadania sprzyjało nieprawidłowym nawykom żywieniowym, takim jak mniejsze spożycie błonnika oraz częstsze spożycie słodzonych napojów oraz w najmłodszej grupie młodzieży zwiększało szansę wystąpienia nadwagi.
Słowa kluczowe: nadwaga, młodzież, zwyczaje żywieniowe, spożycie śniadań
DEV pErioD mED. 2015;XiX,2:193-201
IntroDuctIonbreakfast is commonly called “the most important
meal of the day” [1, 2]. The regular eating of breakfast improves mental performance, psychosocial functioning, school attendance rates, mood and cognition among children and adolescents [1, 2]. Daily eaters of breakfast have a higher energy, macro- and micronutrient intake and overall a better quality of diet [1, 2]. Furthermore, the regular consumption of breakfast is part of a healthy lifestyle among adolescents and adults. Overweight or obese adolescents who usually skipped breakfast, were more often inactive, smoked, dieted and consumed more fast food and alcohol [1, 3, 4]. However, the influence of the habitual eating of breakfast on their body mass and the prevalence of overweight and obesity remains unclear [1]. Most studies indicate that eating breakfast regularly reduces the risk of being overweight or obese among children, adolescents and adults, however some of them confirmed these results only among boys [2, 5]. The results referred to are inconsistent with two experimental studies and an analysis of the epidemiological data from the uSA which support the belief that the “consumption of breakfast daily is essential for good health and weight management” [6]. “Skipping breakfast does not result in accurate energy compensation at subsequent meals and suggests that skipping breakfast may be an effective means to reduce daily energy intake in some adults” and “occasionally skipping breakfast may be an effective strategy to reduce total daily energy intake” [6]. On the other hand, there is evidence that adolescents skipping breakfast might have a higher risk of larger waist circumference, higher fasting insulin levels and insulin resistance [7].
Skipping breakfast concerns about 10-30% of european and uS adolescents, despite positive evidence of the regular eating of breakfast on the health and well-being of adolescents [1]. The adolescent’s age plays an important role in the frequency of eating breakfast. Generally, teenagers eat breakfast less frequently with increasing age [1]. The percentage of breakfast skippers rose by 22 percent points from childhood (1-7 years) to adolescence (15-18
years) (from 8% to 30%) [1]. During adolescence the consumption of sweetened beverages increases. Quite often they replace other liquid sources, like water, milk and 100% fruit juice and moreover increase the risk of being overweight [8]. Another health risk factor which appears during adolescence is connected with the declining consumption of fruit and vegetables [9]. Most adolescents have an insufficient amount of dietary fibre, whose high intake is a good indicator of a pro-healthy dietary pattern, which consists mostly of a high amount of fresh vegetables, fruit and whole grains [10, 11]. The high consumption of sweetened beverages, low intake of dietary fibre and skipping breakfast are representative of unhealthy nutritional behaviour. However, there is a lack of information about the connection between these risk factors among adolescents in the literature. Thus, the aim of the study was to assess the connection of the habitual eating of breakfast with the consumption of sweetened beverages and dietary fibre, as well as overweight prevalence among adolescents from various age groups.
MAterIAl AnD MethoDsSample collection
The study was conducted in 2010-2011 among a convenience sample of middle and high school students, following the consent of school principals and parents for the children to participate in our research. We carried out an observational study, where the population was purposefully selected. The sample was taken in such a way as to ensure adequate numbers of persons in every age subgroup (quota sampling). The study was carried out in different areas of northern, eastern and central Poland and the precise conditions regarding the inclusion or exclusion of adolescents in our study group were described earlier and published in another paper we authored [8]. We finally classified 1700 pupils aged 13-18.9 as suitable for our study. We divided them into three age groups: (i) 13-14.9 years, (ii) 15.0-16.9 years and (iii) 17-18.9 years. According to the initial quota sampling, the percentages of boys and girls in the three

195Habitual eating of breakfast, consumption frequency of selected food
age subgroups were similar. The distribution of boys and girls in various age groups was as follows: 37.9% of the boys and 38.7% of the girls were aged 13-14.9, 30.3% and 30.3% respectively were 15.0-16.9 years old and 31.9% and 31.0% respectively 17.0-18.9. We obtained the ethical approval of the Commission of bioethics at the Faculty of Medical Sciences in Olsztyn (Resolution no. 20/2010 of 17.06.2010) to carry out the study.
Assessment of body mass and food consumptionThe assessment of the body mass of adolescents was
carried out by using bMI, which was calculated on the basis of measurements of body mass and height. The measurements were carried out by trained interviewers. The bMI was calculated and interpreted for each person according to the international standards for adolescents developed by Cole [12, 13].
Information on the intake of dietary fibre was collected by means of the validated block questionnaire [14]. It includes questions on the consumption frequency of the following food groups and dishes: fruit juices, fruit, fresh vegetables, beans, potatoes, other vegetables, white bread and rolls, brown bread and rolls, high-fibre or bran cereals. The frequency of consumption was expressed in five categories, which were assigned points: less often than once a week (0 points), once a week (1 point), 2-3 times per week (2 pts.), 4-6 times per week (3 pts.) and every day (4 pts.). On the basis of the total points obtained, adolescents with a fibre-average diet (≥20 pts.) and with a fibre-poor diet (<20 pts.) can be distinguished. The consumption frequency of breakfast and sweetened beverages (Sb) was expressed in the same category as the consumption of dietary fibre sources. The categories of frequency were aggregated into three groups: (i) regular consumption (every day), (ii) irregular consumption (1-6 times per week) and (iii) consumption hardly ever (less than once a week). Such layouts of food consumption frequency are widely used in scientific research [15].
Statistical analysislogistic regression analysis was used to assess
the influence of the eating frequency of breakfast on dietary fibre intake, the consumption frequency of sweetened beverages and overweight prevalence. We used univariate logistic regression adjusted by gender and stratified by age. The reference group (OR=1.00) were adolescents with regular habits of eating breakfast. We used the Wald statistics in the estimation. Our distribution analysis was checked via the Pearson Chi2 test, with the Yates correction for dichotomic values. Statistical analysis was carried out using STATISTICA StatSoft 10.0 Pl.
resultsDietary fibre intake and breakfast consumption
An analysis of the relation between the frequency of eating breakfast and dietary fibre intake was carried out among adolescents from various age groups, as shown in table I. The percentage of adolescents regularly eating breakfast decreased by 5.7 percent points (pp.) with age,
whereas the percentages of adolescents eating breakfast irregularly or hardly ever increased by 3.7 pp. and 1.9 pp., respectively. We also noticed an increase of adolescents having a fibre-poor diet with age. The intake of dietary fibre was related to the habitual eating of breakfast in all age groups. The skipping of breakfast was an additional factor increasing the chance of having a fibre-poor diet. Adolescents who ate breakfast irregularly or hardly ever had a higher chance (from 1.49 to 2.23 pp depending on age) to have a fibre-poor diet in comparison to adolescents who regularly ate breakfast.
Sweetened beverages and breakfast consumption
The relation between the consumption frequency of sweetened beverages and habitual eating of breakfast is shown in table II. From 12% to 31.4% of adolescents (depending on age) consumed sweetened beverages every day. The lowest percentage of regular consumers was observed in the oldest group (17-18.9 years). The consumption frequency of sweetened beverages was related to habitual eating of breakfast regardless of age. Overall, breakfast skippers drank sweetened beverages more often in comparison to regular eaters. Consuming breakfast hardly ever or irregularly increased the chance of consuming sweetened beverages by ~2-times and for regular consumption by ~2.5-times.
overweight and breakfast consumptionThe influence of habitual eating of breakfast on body
mass is presented in table III. The percentage of adolescents with overweight was from 13.1% to 26.8%, depending on age. Overall, the prevalence of overweight dropped with age. A significant difference in weight according to breakfast consumption was confirmed only in the youngest group. Adolescents aged 13-14.9 who hardly ever consumed breakfast had a 1.8-times higher chance of being overweight in comparison to regular consumers of breakfast.
Gender is an additional differential factor in overweight prevalence and consumption of breakfast, dietary fibre and sweetened beverages.
Our analysis of the cumulative influence of age and gender on chosen eating habits and body mass is shown in table IV. Girls over 15 years old skipped breakfast almost twice as often as boys. boys and girls under 15 years had a similar frequency of breakfast consumption. boys who hardly ever ate breakfast drank sweetened beverages more often regardless of age. Girls more often had a normal weight than boys, independent of age or how frequently they had breakfast.
DIscussIonThe percentage of adolescents from our study who
regularly eat breakfast was a little lower than the results of the WHO data for Poland obtained for school-days (mean percentage: 51.5% vs. 55.6%, respectively) [16]. The percentage of regular consumption at weekends in comparison to school-days was much higher and equalled about 86%. The percentage of adolescents eating

196 Justyna Weronika Wüenstel et al.
inta
ke
of d
ieta
ry fi
bre
Spoż
ycie
bło
nnik
a po
karm
oweg
o
eati
ng fr
eque
ncy
of b
reak
fast
in a
ge g
roup
sSp
ożyc
ie ś
niad
ania
w r
óżny
ch g
rupa
ch w
ieko
wyc
h
13.0
-14.
9 ye
ars/
lat
15.0
-16.
9 ye
ars/
lat
17.0
-18.
9 ye
ars/
lat
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dyre
gula
rly
Regu
larn
ieir
regu
larl
yN
iere
gula
rnie
Har
dly
ever
Praw
ie n
igdy
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dy
sam
ple
size
Li
czeb
ność
pró
by
%54
.233
.212
.751
.731
.716
.648
.536
.914
.6
n35
121
582
268
164
8625
919
778
Fibr
e-av
erag
e di
etPr
zeci
ętne
%54
.440
.542
.749
.638
.432
.641
.732
.526
.9
or
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
Fibr
e-po
or d
iet
Die
ta u
boga
w b
łonn
ik
%45
.659
.557
.350
.461
.667
.458
.367
.573
.1
or
(95%
Ci)
1.00
1.80
***
(1
.27,
2.5
5)1.
60
(0.9
8, 2
.61)
1.00
1.64
*
(1.1
0, 2
.44)
2.23
**
(1.3
2, 3
.77)
1.00
1.49
*
(1.0
1, 2
.19)
1.89
*
(1.0
8, 3
.32)
Tabl
e i.
Eatin
g fr
eque
ncy
of b
reak
fast
with
ref
eren
ce to
the
inta
ke o
f die
tary
fibr
e in
ado
lesc
ents
from
var
ious
age
gro
ups.
Tabe
la I.
Czę
stoś
ć sp
ożyc
ia ś
niad
ania
w z
ależ
nośc
i od
spoż
ycia
bło
nnik
a w
śród
mło
dzie
ży z
różn
ych
grup
wie
kow
ych.
Cons
umpti
on fr
eque
ncy:
reg
ular
ly −
eve
ry d
ay, i
rreg
ular
ly −
1-6
tim
es p
er w
eek,
har
dly
ever
− le
ss th
an o
nce
a w
eek;
fibr
e-av
erag
e di
et (�
20 p
ts.),
fi br
e-po
or d
iet (
<20
pts.
); o
r −
odds
rati
o, C
i − c
onfi -
(�20
pts
.), fi
bre-
poor
die
t (<2
0 pt
s.);
or
− od
ds r
ati o
, Ci −
con
fi -; o
r −
odds
rati
o, C
i − c
onfi-
denc
e in
terv
als,
***
p<0.
001,
**p
<0.0
1, *
p<0.
05.
Częs
tość
spo
życi
a: r
egul
arni
e −
codz
ienn
ie, n
iere
gula
rnie
− 1
-6 r
azy
na t
ydzi
eń, p
raw
ie n
igdy
− r
zadz
iej n
iż r
az n
a ty
dzie
ń; S
poży
cie
błon
nika
: prz
ecię
tne
(≥20
pkt
), di
eta
ubog
a w
bło
nnik
(<20
pkt
); O
R −
ilora
z sz
ans,
CI −
prz
edzi
ały
ufno
ści,
***p
<0,0
01, *
*p<0
,01,
*p<
0,05
.

197
cons
umpti
on fr
eque
ncy
of s
wee
tene
d be
vera
ges
Częs
tość
spo
życi
a sł
odzo
nych
nap
ojów
eati
ng fr
eque
ncy
of b
reak
fast
in a
ge g
roup
sSp
ożyc
ie ś
niad
ania
w r
óżny
ch g
rupa
ch w
ieko
wyc
h
13.0
-14.
9 ye
ars/
lat
15.0
-16.
9 ye
ars/
lat
17.0
-18.
9 ye
ars/
lat
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dyre
gula
rly
Regu
larn
ieir
regu
larl
yN
iere
gula
rnie
Har
dly
ever
Praw
ie n
igdy
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dy
sam
ple
size
Li
czeb
ność
pró
by
%54
.233
.212
.751
.731
.716
.648
.536
.914
.6
n35
121
582
268
164
8625
919
778
Har
dly
ever
(ref
. gro
up)
Praw
ie n
igdy
(gru
pa re
f.)
%24
.514
.914
.618
.715
.917
.424
.713
.715
.4
or
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
Irre
gula
rly
Nie
regu
larn
ie
%58
.469
.859
.862
.767
.751
.263
.371
.671
.8
or
(95%
Ci)
1.00
2.10
**
(1.3
2, 3
.35)
1.73
(0
.87,
3.4
4)1.
001.
36
(0.7
9, 2
.34)
1.13
(0
.57,
2.2
7)1.
002.
05**
(1
.23,
3.4
3)2.
02*
(1
.00,
4.0
7)
regu
larl
yRe
gula
rnie
%17
.115
.325
.618
.716
.531
.412
.014
.712
.8
or
(95%
Ci)
1.00
1.63
(0
.89,
3.0
0)2.
38*
(1
.08,
5.2
7)1.
001.
04
(0.5
1, 2
.14)
2.32
*
(1.0
2, 5
.28)
1.00
2.67
*
(1.2
5, 5
.68)
2.53
(0
.88,
7.2
7)
Tabl
e ii.
Con
sum
ption
freq
uenc
y of
sw
eete
ned
beve
rage
s w
ith r
efer
ence
to th
e ha
bitu
al c
onsu
mpti
on o
f bre
akfa
st in
ado
lesc
ents
from
var
ious
age
gro
ups.
Ta
bela
II. C
zęst
ość
spoż
ycia
śni
adan
ia w
zal
eżno
ści o
d cz
ęsto
ści s
poży
cia
słod
zony
ch n
apoj
ów w
śród
mło
dzie
ży z
różn
ych
grup
wie
kow
ych.
Cons
umpti
on fr
eque
ncy:
reg
ular
ly −
eve
ry d
ay, i
rreg
ular
ly −
1-6
tim
es p
er w
eek,
har
dly
ever
− le
ss th
an o
nce
a w
eek;
or
− od
ds r
atio,
Ci −
con
fiden
ce in
terv
als,
**p
<0.0
1, *
p<0.
05.
Częs
tość
spo
życi
a: re
gula
rnie
− c
odzi
enni
e, n
iere
gula
rnie
− 1
-6 ra
zy n
a ty
dzie
ń, p
raw
ie n
igdy
− r
zadz
iej n
iż ra
z na
tyd
zień
; OR
− ilo
raz
szan
s, C
I − p
rzed
ział
y uf
nośc
i, **
p<0,
01, *
p<0,
05.
Habitual eating of breakfast, consumption frequency of selected food

198 Justyna Weronika Wüenstel et al.
cate
gori
es o
f bod
y m
ass
Ka
tego
rie
mas
y ci
ała
eati
ng fr
eque
ncy
of b
reak
fast
in a
ge g
roup
sSp
ożyc
ie ś
niad
ania
w r
óżny
ch g
rupa
ch w
ieko
wyc
h
13.0
-14.
9 ye
ars/
lat
15.0
-16.
9 ye
ars/
lat
17.0
-18.
9 ye
ars/
lat
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dyre
gula
rly
Regu
larn
ieir
regu
larl
yN
iere
gula
rnie
Har
dly
ever
Praw
ie n
igdy
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dy
sam
ple
size
Li
czeb
ność
pró
by
%40
.637
.933
.830
.328
.834
.229
.233
.332
.0
n33
120
976
247
159
7723
818
472
nor
mal
wei
ght (
ref.
grou
p)Pr
awid
łow
a m
.c. (
grup
a re
f.)
%81
.678
.571
.184
.678
.084
.485
.784
.283
.3
or
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
1.00
ove
rwei
ght
Nad
wag
a
%18
.421
.528
.915
.422
.015
.614
.315
.816
.7
or
(95%
Ci)
1.00
1.28
(0
.82,
1.9
8)1.
83*
(1
.03,
3.2
6)1.
001.
65
(0.9
8, 2
.77)
1.20
(0
.58,
2.4
9)1.
001.
11
(0.6
4, 1
.91)
1.33
(0
.64,
2.7
8)
Tabl
e iii
. Eati
ng fr
eque
ncy
of b
reak
fast
with
ref
eren
ce to
ove
rwei
ght p
reva
lenc
e in
ado
lesc
ents
from
var
ious
age
gro
ups.
Tabe
la II
I. Cz
ęsto
ść s
poży
cia
śnia
dani
a w
zal
eżno
ści o
d w
ystę
pow
ania
nad
wag
i wśr
ód m
łodz
ieży
z ró
żnyc
h gr
up w
ieko
wyc
h.
Cons
umpti
on fr
eque
ncy:
reg
ular
ly −
eve
ry d
ay, i
rreg
ular
ly −
1-6
tim
es p
er w
eek,
har
dly
ever
− le
ss th
an o
nce
a w
eek;
or
− od
ds r
atio,
Ci −
con
fiden
ce in
terv
als,
**p
<0.0
1, *
p<0.
05.
Częs
tość
spo
życi
a: re
gula
rnie
− c
odzi
enni
e, n
iere
gula
rnie
− 1
-6 ra
zy n
a ty
dzie
ń, p
raw
ie n
igdy
− r
zadz
iej n
iż ra
z na
tyd
zień
; OR
− ilo
raz
szan
s, C
I − p
rzed
ział
y uf
nośc
i, **
p<0,
01, *
p<0,
05.

199
ana
lyze
d pa
ram
eter
Bada
ny p
aram
etr
eati
ng fr
eque
ncy
of b
reak
fast
in a
ge g
roup
sSp
ożyc
ie ś
niad
ania
w r
óżny
ch g
rupa
ch w
ieko
wyc
h
13.0
-14.
9 ye
ars/
lat
15.0
-16.
9 ye
ars/
lat
17.0
-18.
9 ye
ars/
lat
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dyre
gula
rly
Regu
larn
ieir
regu
larl
yN
iere
gula
rnie
Har
dly
ever
Praw
ie n
igdy
regu
larl
yRe
gula
rnie
irre
gula
rly
Nie
regu
larn
ieH
ardl
y ev
erPr
awie
nig
dy
Sam
ple
size
(n)
Licz
ebno
ść p
róby
(n)
♂♀
♂♀
♂♀
♂♀
♂♀
♂♀
♂♀
♂♀
♂♀
165
166
9011
938
3813
411
373
8625
5211
911
995
8928
44
Fibr
e-po
or d
iet
Die
ta u
boga
w b
łonn
ik67
.654
.168
.5*
53.8
49.7
45.6
76.0
68.6
69.9
55.3
55.4
48.2
64.3
77.3
73.4
65.2
56.8
61.3
Fibr
e-av
erag
e di
etPr
zeci
ętne
sp
ożyc
ie b
łonn
ika
32.4
45.9
31.5
46.2
50.3
54.4
24.0
31.4
30.1
44.7
44.6
51.8
35.7
22.7
26.6
34.8
43.2
38.7
SB −
Har
dly
ever
S
− Pr
awie
nig
dy
13.5
16.2
9.0
17.9
17.0
**32
.54.
0**
25.5
9.6
18.8
10.0
***
28.2
7.1
15.9
5.3*
*22
.514
.4**
*37
.0
SB −
irre
gula
rly
SN −
Nie
regu
larn
ie56
.864
.975
.368
.462
.952
.540
.052
.967
.169
.466
.958
.278
.670
.576
.667
.466
.956
.3
SB −
reg
ular
lySN
− R
egul
arni
e29
.718
.915
.713
.720
.115
.056
.021
.623
.311
.823
.113
.614
.313
.618
.110
.118
.66.
7
nor
mal
wei
ght
Praw
idło
wa
m.c
. 57
.9*
84.2
71.1
*84
.077
.0*
86.1
64.0
**94
.268
.5*
86.0
82.8
86.7
75.0
88.6
78.9
89.9
80.7
*90
.8
ove
rwei
ght
Nad
wag
a42
.115
.828
.916
.023
.013
.936
.05.
831
.514
.017
.213
.325
.011
.421
.110
.119
.39.
2
SB −
sw
eete
ned
beve
rage
s. C
onsu
mpti
on fr
eque
ncy:
reg
ular
ly −
eve
ry d
ay, i
rreg
ular
ly −
1-6
tim
es/w
eek,
har
dly
ever
− <
1/w
eek;
***
p<0.
001,
**p
<0.0
1, *
p<0.
05.
SN −
sło
dzon
e na
poje
. Czę
stoś
ć sp
ożyc
ia: r
egul
arni
e −
codz
ienn
ie, n
iere
gula
rnie
− 1
-6 ra
zy/t
ydz.
, pra
wie
nig
dy −
<1/
tydz
.; **
*p<0
,001
, **p
<0,0
1, *
p<0,
05.
Tabl
e iV
. ove
rwei
ght p
reva
lenc
e an
d co
nsum
ption
of b
reak
fast
, die
tary
fibr
e an
d sw
eete
ned
beve
rage
s w
ith r
efer
ence
to a
ge a
nd g
ende
r.Ta
bela
iV. W
ystę
pow
anie
nad
wag
i i s
poży
cie
śnia
dań,
bło
nnik
a po
karm
oweg
o or
az s
łodz
onyc
h na
pojó
w w
zal
eżno
ści o
d w
ieku
i pł
ci.
Habitual eating of breakfast, consumption frequency of selected food

200 Justyna Weronika Wüenstel et al.
breakfast every day was much lower in Poland (51.5%) in comparison to other countries, like Sweden (82%), or Denmark (81%) [18, 19]. Despite the difficulty to establish a geographic pattern of eating breakfast among adolescents, skipping breakfast usually happens less frequently in northern and western european countries than in eastern countries [17]. According to the WHO, eating breakfast on every school day was observed among 35-75% of the adolescents from eastern europe aged 11-15 years (depending on country and age) [17]. usually skipping breakfast is more frequent among children and adolescents with lower socio-economic backgrounds, which could explain our results and those of the WHO [16, 17]. On the other hand, there are countries with a high socio-economic status, where the frequency of eating breakfast was quite low. One example would be the uSA, where only ~47% of adolescents consumed breakfast on every school day [16]. Our study is consentaneous with other studies indicating the fact, that as the adolescents get older, the frequency of breakfast eating drops [1, 16, 17, 18, 19, 20, 21]. However, the decrease of the percentage of adolescents regularly eating breakfast between the age groups was lower in our study than in others (6% vs 11-21%, self checked − according to particular age group) [19, 20]. The decrease in the frequency of eating breakfast in adolescence is alarming, since habits of breakfast eating usually do not change during the transition from adolescence to adulthood [22].
The intake of dietary fibre declined with age regardless of breakfast eating habits. However, a higher intake of fibre was noticed in adolescents regularly eating breakfast, compared to adolescents eating breakfast irregularly or hardly ever, which was consistent with other authors’ results [10,12]. Adolescents who usually ate cereals for breakfast had 2.4 g/day more dietary fibre in their diet compared to adolescents frequently omitting breakfast [10]. Furthermore, the consumption of high-insoluble-fibre cereals for breakfast caused a cumulative reduction of energy intake during breakfast and lunch and “led to a lower glycemic response before and immediately after lunch” [23]].
eating breakfast rarely was related to a higher frequency of the consumption of sweetened beverages in adolescence. Postpartum teens eating breakfast on 6-7 days/week on average consumed 1,337 kilocalories less per week from sweetened drinks, but also 1,197 kilocalories less per week from sweet and salty snacks [24]. Among adolescents, caffeinated soda was more often drunk by breakfast skippers than by daily breakfast consumers (OR=1.78) [15]. Furthermore, the level of added sugar in the adolescents’ diet in the uSA was on average 13 g/day (~3% of eI) higher among breakfast skippers than among regular consumers of breakfast [10]. However, regular eaters of breakfast usually take in more overall energy than breakfast skippers [1, 10]. Abdominal obesity and an overall prevalence of obesity was more common among breakfast skippers than among breakfast consumers, despite the fact that a breakfast consumer’s energy intake was on average 375 kcal/day higher than a breakfast skipper’s [10]. Skipping meals is a cause of the decrease of the basal metabolic rate, which
can paradoxically lead to a higher incidence of obesity, despite the reduction of energy intake [25].
In the youngest group (13-14.9 years), we noticed a higher chance of being overweight among adolescents less frequently eating breakfast than among adolescents regularly consuming breakfast. Our results were consistent with the cross-national OlAF study, which also indicated a higher prevalence of overweight in breakfast skippers aged 13-15 [26]. In the older group of adolescents (≥15 years), we did not confirm these results. The increase of skipping breakfast with a simultaneous decrease of overweight prevalence could be explained by a higher interest in the body image and a higher dieting rate among older adolescents. This hypothesis is supported via results: a) older girls (≥15 years) skipped breakfast more often than boys, b) the prevalence of overweight was higher among boys than girls. A literature review showed that one of the most common reasons for skipping breakfast is weight concern among adolescents [21]. However, it should be emphasized that breakfast skipping is usually associated with lower socio-economic status, which is strongly connected to obesity prevalence as well [1]. It might be that low socio-economic status contributes to high body mass “mediated by the low nutritional quality of breakfast” or lack of this meal [27]. Additionally, breakfast skipping could be part of a dietary pattern rich in unhealthy products (including sweetened beverages) [26]. Furthermore, overall low intake of some macro- and micronutrients (like calcium and dietary fibre) is related to both: low socio-economic status and skipping breakfast [10, 27]. It is difficult to decide to what extent skipping breakfast is a contributing factor to obesity prevalence.
conclusIonsThe number of breakfast skippers rises with age,
especially among girls. Independently of age, eating breakfast was rarely associated with unhealthy nutrition, e.g. lower intake of dietary fibre and more frequent consumption of sweetened beverages. Moreover, male breakfast skippers had a higher tendency to a more frequent consumption of sweetened beverages compared to female ones. Overweight was more common among the youngest adolescents (13-14.9 years), who skipped breakfast more often in comparison to regular consumers. The habitual consumption of breakfast is an important factor in pro-healthy dietary habits among adolescents.
reFerences
1. Rampersaud GC, Pereira MA, Girard bl, Adams J, Metzl JD. breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J Am Diet Assoc. 2005;105(5):743-760.
2. Affenito SG. breakfast: a missed opportunity. J Am Diet Assoc. 2007;107(4):565-569.
3. niemeier HM, Raynor HA, lloyd-Richardson ee, Rogers Ml, Wing RR. Fast food consumption and breakfast skipping: predictors of weight gain from adolescence to adulthood in a nationally representative sample. J Adolescent Health. 2006;39(6):842-849.

201
4. Croezen S, Visscher TlS, Ter bogt nCW, Veling Ml, Haveman-nies A. Skipping breakfast, alcohol consumption and physical inactivity as risk factors for overweight and obesity in adolescents: results of the e-MOVO project. eur J Clin nutr. 2009;63(3):405-412.
5. Szajewska H, Ruszczyński M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in europe. Crc Cr Rev Food Sci. 2010;50(2):113-119.
6. levitsky DA, Pacanowski CR. effect of skipping breakfast on subsequent energy intake. Physiol behav. 2013;119:9-16.
7. Karatzi K, Moschonis G, barouti AA, lionis C, Chrousos GP, Manios Y. Dietary patterns and breakfast consumption in relation to insulin resistance in children. The Healthy Growth Study. Public. Health nutr. 2014;15(1):1-8.
8. Wuenstel JW., Wądołowska l, Słowińska MA, niedźwiedzka e, Kowalkowska J, Antoniak l. Consumption Frequency of Fruit Juices and Sweetened beverages: Differences Related to Age, Gender and the Prevalence of Overweight among Polish Adolescents. Pol J Food nutr Sci. 2015;65(3), DOI: 10.2478/pjfns-2013-0013.
9. larson nI, neumark-Sztainer D, Hannan PJ, Story M. Trends in Adolescent Fruit and Vegetables Consumption, 1999-2004 Project eAT. Am J Prev Med. 2007;32(2):147-150.
10. Deshmukh-Taskar PR, nicklas TA, O’neil Ce, Keast DR, Radcliffe JD, Cho S. The relationship of breakfast skipping and type of breakfast consumption with nutrient intake and weight status in children and adolescents: the national Health and nutrition examination Survey 1999-2006. J Am Diet Assoc, 2010;110 (6):869-878.
11. Reicks M, Jonnalagadda S, Albertson AM, Joshi n. Total dietary fiber intakes in the uS population are related to whole grain consumption: Results from the national Health and nutrition examination Survey (nHAneS) 2009-10. nutr Res, 2014;34(3):226-234.
12. Cole TJ, bellizzi MC, Flegal KM, Dietz WH. establishing a standard definition for child overweight and obesity worldwide, international survey. bMJ. 2000;320:1240-1243.
13. Cole TJ, Flegal KM, nicholls D, Jackson AA. body mass index cut offs to define thinness in children and adolescents, international survey. bMJ. 2007;335(7612):194-197.
14. Thompson Fe, byers T. Dietary Assessment Resource Manual. J nutr. 1994;124:2245-2317.
15. Keski-Rahkonen A, Kaprio J, Rissanen A, Virkkunen M, Rose RJ. breakfast skipping and health-compromising behaviors in adolescents and adults. eur J Clin nutr. 2003;57(7):842-853.
16. Health behaviour in School-aged Children (HbSC) study. WHO Collaborative Cross national Study, Poland, Instytut Matki i Dziecka, Warszawa 2011.
17. Health behaviour In School-Aged Children International Report From The 2005/2006 Survey. Health Policy For Children And Adolescents, no. 5, WHO 2008.
18. Sjöberg A, Hallberg l, Höglund D, Hulthén l. Meal pattern, food choice, nutrient intake and lifestyle factors in The Göteborg Adolescence Study. eur J Clin nutr. 2003;57(12):1569-1578.
19. Pedersen TP, Meilstrup C, Holstein be, Rasmussen M. Fruit and vegetable intake is associated with frequency of breakfast, lunch and evening meal: cross-sectional
study of 11-, 13-, and 15-year-olds. Int J behav nutr Phy. 2012;9(9):1-10.
20. Affenito SG, Thompson DR, barton bA, Franko Dl, Daniels SR, Obarzanek e, et al. breakfast consumption by African-American and white adolescent girls correlates positively with calcium and fiber intake and negatively with body mass index. J Am Diet Assoc. 2005;105(6):938-945.
21. bruening M, larson n, Story M, neumark-Sztainer D, Hannan P. Predictors of adolescent breakfast consumption: longitudinal findings from Project eAT. J nutr educ behav. 2011;43 (5):390-395.
22. Von Post-Skagegård M, Samuelson G, Karlström b, Mohsen R, berglund l, bratteby le. Changes in food habits in healthy Swedish adolescents during the transition from adolescence to adulthood. eur J Clin nutr, 2002;56 (6):532-538.
23. Hamedani A, Akhavan T, Samra RA, Anderson GH. Reduced energy intake at breakfast is not compensated for at lunch if a high-insoluble-fiber cereal replaces a low-fiber cereal. Am J Clin nutr. 2009;89(5):1343-1349.
24. Haire-Joshu D, Schwarz C, budd e, Yount bW, lapka C. Postpartum teens’ breakfast consumption is associated with snack and beverage intake and body mass index. J Am Diet Assoc. 2011;111(1):124-130.
25. McCarter RJ, McGee JR. Transient reduction of metabolic rate by food restriction. Am J Physiol-endoc M. 1989;257(2):175-179.
26 Jodkowska M, Oblacińska A, Tabak I, Radiukiewicz, K. Differences in dietary patterns between overweight and normal-weight adolescents. Med Wieku Rozwoj. 2010;15(3):266-273.
27. O’Dea JA, Wilson R. Socio-cognitive and nutritional factors associated with body mass index in children and adolescents: possibilities for childhood obesity prevention. Health educ Res. 2006;21(6):796-805.
28. Darmon n, Drewnowski A. Does social class predict diet quality? Am J Clin nutr. 2008;87(5):1107-1117.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 01.10.2014 r.Accepted/Zaakceptowano: 24.02.2015 r.
Published online/Dostępne online
Address for correspondence:Justyna Weronika Wüenstel
Department of Human nutritionuniversity of Warmia and Mazuryul. Słoneczna 44a, 10-718 Olsztyn
e-mail: [email protected]
Habitual eating of breakfast, consumption frequency of selected food

202Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Magdalena Woynarowska-Sołdan1, Izabela Tabak2, Antonina Doroszewska3, Karolina Jabłkowska-Górecka1
teenagerS’ perception of being an active patient and putting the concept into practice
poStrzeganie i podejmowanie przez naStolatki zachowaŃ aktywnego pacjenta
1Public Health Division, Faculty of Health Sciences, the Medical university of Warsaw, Poland
2Department of Child and Adolescent Health, Institute of Mother and Child in Warsaw, Poland
3Department of Didactics in Gynaecology and Obstetrics, Faculty of Health Sciences, the Medical university of Warsaw, Poland
AbstractAim: To analyse the results of research on how adolescents understand the “active patient” concept, how often they undertake that role depending on gender and on whether they are suffering from a chronic disease. Material and methods: The research was conducted in a group of 14-15 year-olds. It comprised qualitative research (focus groups, N=24) concerning the way the concept of an “active patient” is understood and quantitative research (questionnaire study, N=716). The research tool was an anonymous authored questionnaire with questions concerning the role of the active patient and chronic illnesses. Results: The idea of the “active patient” was not understandable to the teenagers, but they were able to enumerate many kinds of behaviours which are typical for such a patient. Among the 7 kinds of such behaviours, only two (presenting their ailments to the doctor and following the doctor’s recommendations) were always or almost always followed by over half the respondents. The frequencies of undertaking behaviours typical for an active patient by girls and boys were similar. Teenagers with chronic diseases more often behaved actively during their visit to the doctor, but less frequently followed the doctor’s recommendations. Conclusions: Few adolescents actively participate in the process of diagnosis and treatment. There is a need for early education of children and young people to become active patients, since such an attitude promotes health throughout one’s lifetime. Such education is first of all the task of doctors and nurses, and it can be effective only if the intercommunication skills with patients are improved. It is a necessity to support young people with chronic diseases in their treatment and in coping with their disease.
Key words: adolescents, active patient, chronic disease
StreszczenieCel: Analiza wyników badań dotyczących rozumienia przez nastolatki pojęcia „aktywny pacjent” i częstości podejmowania przez nie zachowań aktywnego pacjenta w zależności od płci oraz występowania choroby przewlekłej.Materiał i metody: Badania przeprowadzono w grupie 14-15-latków. Obejmowały one badanie jakościowe (wywiady grupowe, N=24) dotyczące rozumienia pojęcia „aktywny pacjent” oraz badanie ilościowe (ankieta, N=716). Narzędziem badawczym był anonimowy autorski kwestionariusz zawierający pytania dotyczące częstości podejmowania zachowań aktywnego pacjenta oraz występowania chorób przewlekłych.

203Teenagers’ perception of being an active patient and putting the concept into practice
Wyniki: Pojęcie „aktywny pacjent” nie było dla nastolatków zrozumiałe, ale potrafiły one wymienić wiele zachowań charakterystycznych dla takiego pacjenta. Wśród 7 analizowanych zachowań aktywnego pacjenta tylko dwa (przedstawianie lekarzowi dolegliwości i przestrzeganie jego zaleceń) podejmowane były zawsze lub prawie zawsze przez nieco ponad połowę badanych. Częstość podejmowania zachowań aktywnego pacjenta przez dziewczęta i chłopców była podobna. Nastolatki z chorobami przewlekłymi częściej niż te bez chorób przewlekłych zachowywały się aktywnie w czasie wizyty u lekarza, ale rzadziej przestrzegały jego zaleceń. Wnioski: Niewielu nastolatków aktywnie uczestniczy w procesie diagnozy i leczenia. Istnieje potrzeba wczesnej edukacji dzieci i młodzieży na rzecz stawania się aktywnym pacjentem, gdyż taka postawa sprzyja zdrowiu człowieka w każdym okresie jego życia. Edukacja ta jest przede wszystkim zadaniem lekarzy i pielęgniarek, a warunkiem jej skuteczności jest doskonalenie ich umiejętności komunikacji interpersonalnej z młodymi pacjentami. Niezbędne jest wsparcie młodzieży z chorobami przewlekłymi w leczeniu i radzeniu sobie z chorobą.
Słowa kluczowe: nastolatki, aktywny pacjent, choroba przewlekła
DEV pErioD mED. 2015;XiX,2:202-211
IntroDuctIonPublications devoted to the communication of health
professionals with patients underline the importance of active participation on the part of the patient in the process of prophylaxis, diagnosis, treatment and rehabilitation [1, 2, 3, 4]. The pro-active involvement of patients in these areas increases the effectiveness of their efforts to improve prevention, and either preserve or recover good health and strengthen it. For this reason many authors point out how necessary it is for patients to cooperate with health professionals. The scope of such a cooperation depends on many factors, such as the condition of the patient, his/her age and individual character features, as well as the patient’s competences and expectations [5, 6, 7].
Currently, some authors point out that patients seek partnership and empowerment in their contacts with doctors, full access to medical records regarding their own health and want to take part in decisions which take into account not only medical recommendations but also such circumstances of their lives as work or family. There are many factors that promote the development of such a trend, i.e. the growing level of education and access to medical information, increasing life expectancy, the rising number of chronic diseases, or the patient’s using fee-paying medical services. The granting of Patient’s Rights was a milestone in improving patient empowerment [8].
The concept of patient involvement is not unambiguous. Qualitative research done among health care providers and adult patients as part of eurobarometer 2012 shows that the term “patient involvement” can be differently understood by health professionals and by patients; each of these groups can perceive the active role of the patient in health care differently [9]. An attempt to specify the term “active patient” was undertaken by b. Woynarowska, who isolated the features and kinds of behaviour of an active patient [10]:
• inthecaseof illness(e.g. lookingforinformationabout one’s disease, its causes and treatment; asking the doctor questions; recognising the symptoms of the disease, its exacerbation; taking medication exactly as prescribed, and observing the doctor’s recommenda-tions; developing the skills to cope with one’s disease, as well as with negative emotions and tension),
• withreferencetoprophylacticexamination(e.g.apositiveattitude to tests and procedures, preparing one’s medical history; considering what questions to ask the doctor; asking questions, requesting information about one’s health condition, the need to undertake extra tests or procedures, explaining the terms one does not understand, obtaining lifestyle recommendations, implementing the recommendations following test results).
The process of teaching/learning the active patient role is long and starts in one’s childhood. According to I. Obuchowska [11] from the point of view of the child, evaluation of a his/her role as a patient constitutes one of the factors with a real significance in the course of his/her disease – one that needs to be strengthened. One of the factors that are conducive to such a development is allowing the child to make decisions on some aspects of treatment. For the child who suffers from disease, making decisions is important for developing his/her feeling of self-esteem and helps to form an active attitude in the role of a patient as a grown-up.
From the point of view of teaching/learning the role of an active patient, it is particularly important to focus on adolescents. This is a time of a growing need for independence and self-reliance in taking different kinds of decisions, including those connected with one’s health [12]. Although this period of human life is considered “the healthiest”:• a�o�t������ofteenagerss��erfromchronic�ise�about 20-25% of teenagers suffer from chronic dise-
ases or disabilities [13, 14],• they frequently suffer from many ailments and negative
emotional states connected with different biological and psychological changes [15],

204 Magdalena Woynarowska-Sołdan et al.
• they undertake many kinds of behaviour which pose risks to their health [16].
All of those are connected with frequent contacts with health care providers, using medical services, i.e. taking the role of the patient.
According to current regulations [8], a child who reached the age of 16 is called an underage patient and can take decisions regarding his/her health. Such a patient can agree to have medical tests done and undergo other kinds of medical examinations performed by the doctor. He/she can also disagree with the opinion of their parents or legal guardian. Moreover, patients over the age of 16 have a right to obtain information about the state of their health from the doctor, find out the diagnosis and seek recommendations regarding possible diagnostic and treatment procedures, learn about the effects of implementing these or not, find out the results of their health tests, or procedures and prognosis. nurses should give them information how to look after themselves and take care of the disease. It is important that young people should know their patient’s rights, learn how to take the role of an active patient and understand the benefits resulting from this [10]. The active role of the patient promotes his/her health throughout his/her life.
AIM The aim of the paper is to analyse the results of research
conducted among 14-15-year olds regarding:1. Their understanding of the “active patient”
concept.2. The frequency of their undertaking the role of an active
patient depending on gender and on whether they suffer from a chronic disease, suffer from a disability or other serious health conditions diagnosed by a doctor.
MethoDA triangulation of methods was used: both qualitative
and quantitative research was conducted:1. Qualitative research involved group interviews focusing
on the way teenagers understand the “active patient” concept. The main question was formulated, i.e.: What does it mean to be an active patient? Then an additional questions were asked: What does it mean to “cooperate with the doctor?” What does it mean to “cooperate in treatment?” What kinds of behaviour before and after the medical appointment support treatment? Interviews were conducted in January 2013 and took place in 4-5- person groups attending one lower secondary school.
2. Qualitative research used the technique of an anonymous questionnaire. The research tool was an authored questionnaire including such questions as:• The frequency of taking the ”active patient” role.
A scale of active patient behaviours was used. This scale was developed based on the character features of an active patient specified by b. Woynarowska [10]. It consisted of 7 statements (enumerated in Table II) describing features of desirable patient behaviour connected with medical appointments
and treatment. The adolescents surveyed specified how often they behaved in the ways described in the statements using a 4-point scale: always or almost always (3), often (2), sometimes (1), never or almost never (0). The total indicator accepted values from 0 (lack of listed behaviours) up to 21 (the highest frequency of all the kinds of listed behaviours).
• The existence of chronic health conditions: Do you have a chronic (long-term) disease (e.g. diabetes, allergy) or do you suffer from any form of disabi-lity or other major health problems which were diagnosed by a doctor? Categories of answer: yes, no. A question from the international standard HbSC (Health behaviour in School-aged Chil-dren. A WHO Cross-national Collaborative Study) questionnaire [17] was used in the survey.
The qualitative survey was conducted in April and May 2013 after obtaining the consent of the head teachers of the schools and the children’s parents. The anonymous survey was conducted using the auditorium test method, and was administered by the children’s teachers according to detailed instructions. The survey was preceded by a pilot study performed in February 2013 in two groups of 14-15-year-olds (second year of lower secondary school, n=36).
The groups surveyed The qualitative survey was conducted in a group of
24 teenagers (11 girls, 13 boys) aged 14-15 years. They were students of the second year of a lower secondary school in a small town (of about 20 thousand inhabitants) in the Warmian-Masurian Voivodship.
In the quantitative survey analysed data from 716 teenagers (365 girls and 350 boys) aged 14-15 years. These were students of the second year of seven lower secondary schools located in five voivodships (provinces), i.e. łódzkie, mazowieckie, pomorskie, warmińsko-mazurskie, wielkopolskie, in places of different sizes (villages: 2 schools; towns of under 100 thousand inhabitants: 4 schools; city over 500 thousand inhabitants: 1 school). The surveys were filled out by 84.9% of the second-year students attending those schools.
About 24% of the respondents said they suffered from some kind of a chronic disease, a disability or other serious health conditions diagnosed by a doctor. The percentage of girls providing such an answer (25.9%) was slightly higher than that of boys (21.6%), however the difference between the genders was not statistically significant. later in the paper, members of this group are referred to as respondents with chronic diseases.
Statistical analysis of the resultsThe statistical analysis of the results was performed
using the SPSS v.14.0 programme. It took into account the gender of the respondents, as well as the presence of a chronic disease, a disability of some kind, or other major health conditions diagnosed by a doctor. The significance of the difference was examined by chi-square and t-Student methods for independent samples; differences were considered statistically significant if p<0.05.

205Teenagers’ perception of being an active patient and putting the concept into practice
In order to check the psychometric features on the scale of active patient behaviours, an analysis of its reliability was performed (Cronbach’s α coefficient) and its construct validity (factor analysis). Cronbach’s α for the whole scale was 0.706, which can be considered a satisfactory result, on the basis of which the scale can be considered reliable. Factor analysis showed that the statements included in the scale depend on two factors, and not on one, as it had been assumed. It was decided that the first one includes statements no. 3, 4, 5 and 6, and the second one statements 1, 2 and 7 (factor loadings from 0.505 to 0.781). Statement no. 4 had similar factor loadings in both factors but on the basis of content analysis it was placed in the first factor (Table II). Two subscales were identified, which were given the name of:•� es��scaleof��ehavio�rsconnecte�withtheme�i�The subscale of “behaviours connected with the medi-
cal appointment” (statements 3, 4, 5, 6); Cronbach’s α coefficient: 0.620. The total indicator accepted values from 0 (lack of listed behaviours) up to 12 (the highest frequency of all the kinds of listed behaviour).
•� es��scaleof��ehavio�rs�eforean�a�ertheappo�The subscale of “behaviours before and after the appo-intment” (statements 1, 2, 7); Cronbach’s α coefficent: 0.628. The total indicator accepted values from 0 (lack of listed behaviours) up to 9 (the highest frequency of all the kinds of listed behaviours).
Due to the unexpected structure of the factors and the rather low values of Cronbach’s α coefficients in the two sub-scales, the research tool requires further development and verification in future research.
resultsAdolescents’ perception of the “active patient” concept
Adolescents’ answers in group interviews concerning their understanding of the active patient role were analysed. It was found that the term “active patient” was not clear to the young people. This is why additional questions were used. The adolescents’ answers were divided into two categories called “polite patient” and “active patient” (Table I).
CategoryKategoria
examples of authentic teenagers’ expressionPrzykłady autentycznych wypowiedzi nastolatków
number of responses
Liczba wskazań
polite patientKulturalny pacjent
Have a positive attitudeMieć pozytywne nastawienie Be polite, niceByć kulturalnym, miłym Be calm, not get annoyedByć spokojnym, nie wkurzać sięBe tolerant, patient, patiently wait in the queue, not push through the queueByć tolerancyjnym, cierpliwym, cierpliwie czekać w kolejce, nie wpychać się w kolejkęBe punctualByć punktualnym Thank after the appointmentPo wizycie: podziękować
13
Active patientsAktywny pacjent
should cooperate with a doctorPacjent powinien współpracować z lekarzem Be talkative, get into a conversation with the doctorByć rozmownym, wdać się w rozmowę z lekarzemHonestly talk about the condition of their health, openly say what is wrongSzczerze rozmawiać o stanie swego zdrowia, otwarcie mówić, co mu dolegaHonestly answer questions about their healthSzczerze odpowiadać na pytania dotyczące zdrowiaAsk questions (about the possible further health complication and ways of solving them), seek information on their health, talk the doctor about everything that worries them regarding healthDopytywać (o możliwe komplikacje naszego stanu zdrowia i ich rozwiązania),szukać informacji na temat własnego zdrowia,pytać lekarza o wszystko, co go trapi w sprawach zdrowiaFollow the doctor’s instructions during an appointmentWykonywać polecenia lekarza w trakcie wizytyAfter an appointment: follow the doctor’s recommendations, buy the prescribed medicationPo wizycie: dostosować się do zaleceń lekarza, wykupić receptę
10
Table i. The way adolescents understand the term “active patient”.
Tabela I. Rozumienie przez nastolatki pojęcia „aktywny pacjent”.

206 Magdalena Woynarowska-Sołdan et al.
Undertaking the role of the active patientAmong the seven kinds of behavior of an active
patient that were analysed, only two were undertaken always or almost always by over half of the adolescent respondents. These were: giving a detailed description of one’s symptoms to the doctor (52.9%) and following the doctor’s recommendations (55.7%). The other kinds of behavior were undertaken by the respondents less frequently, in particular when considering before the appointment what one would like to ask (8.5%), asking the doctor questions during the appointment if the need arises (20.9%), and asking for clarification if something was unclear (22%).
There was no statistically significant difference in undertaking active patient roles between girls and
boys. Those adolescents who suffered from chronic diseases asked the doctor questions more frequently than their peers who did not have such ailments, but less frequently followed the doctor’s recommendations (in both cases p<0,05).
The analysis of differences between mean results in the total scale of active patient behavior conducted by the t-Student test did not reveal statistically significant differences depending on gender, or the presence of a chronic disease (Table III). The test was repeated for the two subscales revealed on the basis of factor and content analysis. no statistically significant difference between girls and boys was found in either of the subscales analysed. On the other hand, adolescents with chronic diseases undertook selected kinds of active patient
StatementsStwierdzenia to
tal
Ogó
łem
Gir
lsD
ziew
częt
a
Boys
Chło
pcy
pers
ons
wit
h ch
roni
c di
seas
esO
soby
z c
horo
bam
i pr
zew
lekł
ymi
pers
ons
wit
hout
ch
roni
c di
seas
esO
soby
bez
cho
rób
prze
wle
kłyc
h
1. When i notice disease symptoms and i feel bad, i ask grown-ups 1. for help (e.g. my parents, teachers, the school nurse)1. Kiedy zauważam objawy choroby, źle się czuję, proszę o pomoc 1. dorosłych (np. rodziców, nauczycieli, pielęgniarkę szkolną)
40.8 42.2 39.4 40.2 41.0
2. When i have to see the doctor, i do not object or procrastinate1. Kiedy muszę iść do lekarza, robię to bez sprzeciwu, bez ociągania 43.3 42.5 44.1 41.1 44.2
3. Before my medical appointment i think about what questions 1. to ask1. Przed wizytą u lekarza zastanawiam się, o co chcę go zapytać
8.5 6.9 10.2 8.4 8.5
4. During the medical appointment i describe my symptoms 1. in detail1. W czasie wizyty u lekarza dokładnie przedstawiam mu moje 1. dolegliwości
52.9 53.8 52.6 53.8 52.6
5. During the medical appointment i ask the doctor questions, e.g. 1. about my health, how to look after it, how to treat my disease 1. if the need arises1. W czasie wizyty u lekarza, jeśli mam taką potrzebę, 1. zadaję mu pytania, np. na temat mojego zdrowia, dbałości o nie, 1. leczenia choroby
20.9 19.5 22.4 26.6* 18.9
6. During the medical appointment i ask for clarification 1. if I do not understand something1. W czasie wizyty u lekarza, jeśli czegoś nie rozumiem, 1. proszę o wyjaśnienie
22.0 21.6 22.3 21.3 22.2
7. i follow the doctor’s recommendations regarding e.g. 1. taking medication, nourishment, physical activity1. Stosuję się do zaleceń lekarza dotyczących 1. np. stosowania leków, sposobu odżywiania, 1. aktywności fizycznej
55.7 56.4 54.9 49.1* 57.8
Table ii. Adolescents who always or almost always undertook active patient roles according to gender sex and the presence of a chronic disease (percentage of respondents).
Tabela II. Nastolatki, które zawsze lub prawie zawsze podejmowały zachowania aktywnego pacjenta według płci i występowania choroby przewlekłej (odsetek badanych).
*Difference between persons with and without chronic diseases p<0,05/Różnice między osobami z chorobami przewlekłymi i bez tych chorób p<0,05.

207Teenagers’ perception of being an active patient and putting the concept into practice
behavior connected with medical appointments (the mean result in the scale “behaviours connected with the medical appointment” in this group was 6.37 vs. 5.88, p<0.05) (Table III).
DIscussIonThe article presents the results of research regarding
the way how 14-15-year-olds understand the “active patient” concept and the frequency of their undertaking such a role depending on gender and on whether they suffer from a chronic disease, a disability or other serious health conditions diagnosed by a doctor. In the group analysed, 24% of the respondents stated that they do suffer from the above-mentioned health conditions. A similar result (20.3%) was obtained in a representative sample of Polish youth aged 11-15 in international HbSC surveys conducted in 2010 [14, 18].
The “active patient” concept turned out to be unclear for many of the respondents. It was necessary to use additional questions to guide them. An analysis of answers to these questions shows that the respondents usually associated this concept with being polite during their medical appointment, e.g. displaying a positive attitude to the visit and coping with negative emotions. It was slightly less frequently that they enumerated behaviour which is typical of the active patient role, such as two-way communication with the doctor or following the doctor’s recommendations. The results can, however, be a good starting point for developing the competences of an active patient.
The research assumed that there are seven kinds of behaviour, which, if undertaken always or almost
always demonstrate that the active patient role has been implemented. These have been assigned to two groups:
1. behaviours before and after the medical appointment: seeing the doctor without objections or procrastination, following the doctor’s recommendations. It can be assumed that such behaviour reflects the patient’s discipline. Such behaviour was displayed by only about half of the respondents (40.8–55.7%).
2. behaviours connected with the medical appointment: considering before the appointment what one would like to ask, giving a detailed description of one’s symptoms to the doctor, asking questions, asking for clarification if something was unclear. Such behavior can be considered a reflection of a conscientious attitude to the medical appointment. It was undertaken with a desirable frequency (almost or almost always) by 8.5 to 52.9% of the respondents.
Such results must be considered unfavourable. They show that a large number of our adolescents do not display an active attitude to their medical appointment. The passive attitude of patients at this age can remain the same when they grow up.
It seems that two groups of reasons for the passivity of adolescent patients can be isolated:
1. Reasons connected with the adolescents: • Teenagers are young people who:
– usually enjoy good health. HbSC research conducted in 2010 on a representative sample of 15-year-olds showed that 76% said that their health is good or excellent [19];
– live “here and now” and do not realise the consequences of insufficiently looking after their health [20],
Table iii. mean results (with standard deviation) obtained by the respondents in the full scale of active patient be-havior and in both of its subscales according to gender and the presence of a chronic disease (percentage of respondents).
Tabela III. Średnie wyniki (z odchyleniem standardowym) uzyskane przez badanych w pełnej skali zachowań aktywnego pacjenta i w obu jej podskalach według płci i występowania choroby przewlekłej (odsetek badanych).
Scale/subscalesSkala/podskale po
ints
:Pu
nkta
cja:
min
. – m
ax.
tota
lO
gółe
m
Gir
lsD
ziew
częt
a
Boys
Chło
pcy
pers
ons
wit
h ch
roni
c di
seas
esO
soby
z c
horo
bam
i pr
zew
lekł
ymi
pers
ons
wit
hout
ch
roni
c di
seas
esO
soby
bez
cho
rób
prze
wle
kłyc
h
Full aggregate scale of active patient behaviourPełna sumaryczna skala zachowań aktywnego pacjenta 0-21 12.45
(4.05)12.34(3.91)
12.57 (4.20)
12.69 (4.15)
12.37 (3.97)
Subscale “behaviours connected with the medical appointment” (statements 3, 4, 5, 6)Podskala „Zachowania związane z wizytą”
0-12 6.00(2.82)
5.91(2.72)
6.11(2.93)
6.37 (2.84)*
5.88 (2.77)
Subscale “behaviours before and after the appointment” (statements 1, 2, 7)Podskala „Zachowania przed i po wizycie”
0-9 6.44(2.00)
6.42(2.01)
6.45(2.00)
6.33(2.00)
6.48(1.99)
*Difference between persons with and without chronic diseases p<0.05/Różnice między osobami z chorobami przewlekłymi i bez tych chorób p<0,05.

208 Magdalena Woynarowska-Sołdan et al.
– Make a medical appointment usually in the event of an acute disease or injury [21],
– Many of them do not treat a medical appointment as a situation which is something important and difficult [22];
• Health usually has low priority in the hierarchy of young people’s values [23];
• Adolescents may still have a limited understanding of some health issues [24, 25].
2. Reasons connected with the behaviour of grown-ups:• During their medical appointment teenagers are
accompanied by their parents, who usually take initiative in contacts with the doctor. Such beha-vior can be illustrated with the statements made by girls who took part in the pilot study that was used for the present paper: It does not make any sense to answer questions about the behaviour of an active patient. When I’m at the doctor’s, my parents do everything for me and I have to say no whatsoever.
• The existence of barriers in the doctor – adolescent patient relation. These can be e.g.:– A patronizing attitude of the doctor to the patient,
which is expressed in behaviour that gives the impression that the teenager’s feelings, sensations and views are unimportant, trivial, funny and not worthy of the doctor’s attention [25],
– A communication model of asking and examining the teenager and giving results or recommendations to his/her parents [24].
In the case of underage patients, a three-way communication and relationship model is established during the appointment. The parties involved are the doctor, the child and the parent [25]. The parent is a source of information, supports the child, reduces the feeling of threat, and takes decisions in the name of the child [26], but should not talk to the doctor instead of the child. P.D. Sloane said that there should be no doubt that it is the maturing human being and not his/her parents who is the patient [21]. According to A. Jakubowska-Winiecka, if the doctor discusses important matters not with the teenager but with his/her parents, then in the eyes of the teenager the patient’s autonomy is not respected. This can be a source of conflicts and lack of cooperation in the treatment, and moreover increase the dependence of the teenager on grown-ups [27].
e. Pyörälä [28] is of the opinion that the more adults there are in the surgery, the more marginalised is the role of the child-patient. In research devoted to the relationship between 13-15 year-olds with dieticians, it was found that teenage patients were most active in direct contacts with their dietician, even in conversations concerning sensitive issues, or in the course of time-consuming tests. In situations when a parent acted on behalf of the adolescent, the teenager took the role of a withdrawn, reticent, passive witness of the grown-ups conversation. Also A. van Staa [29] underlines that communication in a triad is not conducive to promoting the active role of a teenager in his/her contacts with the
doctor. The teenagers with chronic diseases that took part in her research wanted to be treated as partners during their hospital consultation, but the level of their participation in the interaction with doctors was low: they were not the main partners in the presence of their parents. According to this author, teenagers with chronic diseases should be prepared for playing the active patient role in their adulthood. Health care professionals should encourage them to be active in communication with doctors, to make their medical appointments themselves, and to influence changes in the behaviour of their parents. According to R. lopez, [30], starting from the age of 13-14, children should be given the possibility of having face-to-face contacts with the doctor. This can be done gradually, e.g. parents can leave the doctor’s office for the duration of the examination and ask to be called in when the examination is over. Parents should respect the child’s increasing need for privacy and at the same time be ready to accompany the growing child, when he/she wants they stay with him/her in the surgery.
The literature focuses on the principles of building proper relations between medical personnel and underage patients and overcoming communication barriers between them [12, 24, 25, 30]. Young people are very sensitive to various forms of patronising treatment and it is particularly important not to do this, and express a sincere interest in whatever concerns them and be ready to listen. Conversations with an underage patient is really a mutual solving of a problem and not “doing something” for the teenager or instead of him [12]. The underage patient is the first source of information about himself and can not be ignored in the course of speaking about his health or illness [25]. The teenager should be treated like a patient with full rights. During the appointment, health care professionals should speak directly to the adolescent using his/her name. Their comments and questions should not be addressed to the parent [27]. In the case of talking to the teenager without the presence of the parents, the young person should have a maximum feeling of confidentiality (if the doctor thinks the parents should know about something, he should inform the teenager about it and discuss with him what and how he is going to say it). Respecting such principles makes it possible to form a bond with the patient, to find out his opinions about his condition, health problems, and to build the kind of trust that lies at the foundation of good cooperation. The observations of doctors in Great britain show that most teenagers are willing to share their problems with the doctor and treat him as a grown-up they trust [12].
Research results show that there are no statistically significant differences in the frequency of undertaking active patient roles between girls and boys, although HbSC survey results regarding 15-year-olds point out what follows [19]:•Girls think their health condition is worse than boys
do (69% girls and 83% boys evaluated their health as good or excellent),
• �irlsreportvario�ssomatican�mentalhealth�isor�Girls report various somatic and mental health disor-ders more often that boys (e.g. frequent headaches are

209Teenagers’ perception of being an active patient and putting the concept into practice
reported by 31% girls and 13% boys, while anxiety is reported by 42% and 29% respectively).
It was found that adolescents with chronic diseases more frequently undertook the roles of an active patient than their peers without such diseases (above all, they more frequently asked questions about their condition and treatment). It can be assumed that such adolescents have more frequent contacts with the doctor, and therefore are more confident and relaxed in this relationship, in addition to which they have more knowledge and their own experiences concerning their disease and treatment.
Teenagers with chronic diseases less often followed doctor’s recommendations (the differences were statistically significant). A chronic disease is a mental burden and can lead to such disorders as fear, feeling of discomfort; it can restrict their life activities and force them to submit to a regimen connected with the disease (such as observing a certain diet) [11, 26, 31]. One of the defense mechanisms used in the situation of a chronic disease is denying its existence, which manifests itself e.g. in not observing the doctor’s recommendations. Teenagers without chronic diseases usually undergo acute forms of disease, which are quickly treated and less burdensome.
The literature points out that children with different kinds of chronic diseases have problems particularly during puberty [32-36]. They become more aware of the nature of their disease and the resulting limitations and often do not want to accept these. They want to be perfect, while the illness makes them feel different, inferior; they fear rejection. This is why rebellion can appear, a negative attitude to the disease and treatment, manifesting itself e.g. to being reluctant to take medication and follow other recommendations given by the doctor, as these make them different from their peers. This can lead to the worsening of treatment results, and their condition. In this situation, it is particularly important for the adolescents to obtain help from grown-up, especially their parents, doctor and teachers in the treatment process and in coping with the disease.
The results of the research presented show that there is a need for the education of teenagers in becoming an active patient. It is thought that patients can learn how to be active and take more responsibility for their health. encouraging them to do so is first of all the task of medical professionals. Developing interpersonal communication competences on the part of health care personnel is a precondition to achieving this task [1, 29].
In educating adolescents to become active patients, a significant role has to be fulfilled by: •General practitioners who have many contacts with
the child throughout his illness and during the me-dical check-ups and when they examine them before vaccination [37],
• Schooln�rseswhomst��entsseewitho�ttheirpar-ents. These are adolescents’ first independent contacts with health care professionals. The role of the nurse in health education was emphasised in formulating the standards of preventive health care performed
by the school nurse and hygienist and the GP. These early experiences can play later a decisive role in the attitudes of adolescents as patients [38].
It is worth mentioning that in some countries, e.g. Canada, efforts have been undertaken to develop communication competences between teenagers and health care professionals as part of the school health education [39]. In Poland the current core curriculum for upper lower secondary schools states that when finishing the school “the student should be able to explain the concept of an active patient and know the basic patient rights.” [40]. This makes it possible to have an additional influence on promoting an active patient attitude among young people as part of school health education.
The present paper is limited due to the non-representative group of young people surveyed, as only one age group was researched and it was not possible to compare the results with those of other authors. no other research projects devoted to the perception of the active patient role and undertaking such a role by teenagers have been found.
conclusIons1. Teenagers are not able to make a definition of the
active patient concept, but they enumerate behaviours which characterise such a patient. This can form the grounds for their developing their active patient competences.
2. In practice, the frequency of undertaking active patient behaviours is unsatisfactory in a significant percentage of young people. There is a need to start educating children in the active patient role early in their lives. Such an approach is particularly important with reference to adolescents, because the active patient attitude is conducive to health at any stage of human life.
3. encouraging young people to be an active patient is the first of all the task of health care professionals, particularly doctors and nurses. In order to cope with this, they need to develop their competences of interpersonal communication with young people.
4. Teenagers with chronic diseases more frequently displayed active behaviour in their contacts with their doctor during the appointment that their peers without such disorders, but they observed doctor’s recommendations less frequently. not following the doctor’s recommendations is detrimental to the course of their treatment. It is necessary to support young people in their treating and coping with a chronic disease.
reFerences
1. Gordon T, edwards WS. Rozmawiać z pacjentem. Podręcznik doskonalenia umiejętności komunikacyjnych i budowania partnerskich relacji, Warszawa, Wydawnictwo SWPS „Academica”, 2009.
2. Siejka D. Relacja lekarz-pacjent – istotny element specjalizacji nie tylko lekarza rodzinnego, w: Porozumiewanie się lekarza z pacjentem i jego rodziną. Wybrane zagadnienia, Steciwko

210 Magdalena Woynarowska-Sołdan et al.
A, barański J (red), Wrocław, elsevier urban&Partner, 2012;69-79.
3. Rollnick S, Miller WR, butler ChC. Wywiad motywujący w opiece zdrowotnej, Warszawa: Wydawnictwo SWPS “Academica”, 2010.
4. Makara-Studzińska M. Komunikacja z pacjentem, lublin: Wydawnictwo Czelej, 2012.
5. Heszen I, Sęk H. Psychologia zdrowia, Warszawa: Wydawnictwo naukowe PWn, 2007.
6. Salmon P. Psychologia w medycynie wspomaga współpracę z pacjentem i proces leczenia, Gdańsk, GWP, 2002.
7. Porozumiewanie się lekarza z pacjentem i jego rodziną. Wybrane zagadnienia, Steciwko A, barański J (red), Wrocław, elsevier urban&Partner, 2012.
8. ustawa z dnia 6 listopada 2008 r. o prawach pacjenta i Rzeczniku Praw Pacjenta, Dz.u. 2009 nr 52 poz. 417 z późn. zmian.
9. eurobarometer Qualitative Study. Patient involvement. Aggregate Report (2012) Conducted by TnS Qual+ at the request of the european Commission, Survey co-ordinated by the european Commission, Directorate-General for Communication: http://ec.europa.eu/public_opinion/archives/quali/ql_5937_patient_en.pdf (dostęp: 7.11.2014).
10. Woynarowska b. Aktywny pacjent. Prawa pacjenta, w: edukacja zdrowotna. Poradnik dla nauczycieli wychowania fizycznego w gimnazjach i szkołach ponadgimnazjalnych, Woynarowska b (red), Wydawnictwo Pedagogiczne ZnP, Kielce, 2012;166-170.
11. Obuchowska I. Rodzice i chore dziecko, w: Obuchowska I, Krawczyński M, Chore dziecko, Warszawa: nasza Księgarnia, 1991.
12. Wrate RM. Rozmawianie z nastolatkami, w: Jak rozmawiać z pacjentem, Mayerscough PR, Ford M (red), Gdańsk: GWP, 2001;185-203.
13. Woynarowska b, Oblacińska A. Stan zdrowia dzieci i młodzieży w Polsce. najważniejsze problemy zdrowotne, w: Zdrowie dzieci i młodzieży. Wybrane zagadnienia, Szymańczak J (red), Studia biura Analiz Sejmowych Kancelarii Sejmu, 2(38) 2014;41-64.
14. Małkowska-Szkutnik A. Choroby przewlekłe u dzieci i młodzieży jako narastający problem społeczny, w: Zdrowie dzieci i młodzieży. Wybrane zagadnienia, Szymańczak J (red), Studia biura Analiz Sejmowych Kancelarii Sejmu, 2(38) 2014;89-112.
15. Mazur J. Subiektywne dolegliwości somatyczne i psychiczne, w: Tendencje zmian zachowań zdrowotnych i wybranych wskaźników zdrowia młodzieży szkolnej w latach 1990-2010, Woynarowska b, Mazur J (red), Warszawa: Instytut Matki i Dziecka, Wydział Pedagogiczny uW, 2012;151-178.
16. Dzielska A, Kowalewska A. Zachowania ryzykowne młodzieży – współczesne podejście do problemu, w: Zdrowie dzieci i młodzieży. Wybrane zagadnienia, Szymańczak J (red), Studia biura Analiz Sejmowych Kancelarii Sejmu, 2(38) 2014;139-168.
17. Mazur J, Woynarowska b, Kołoło H. Zdrowie subiektywne, styl życia i środowisko psychospołeczne młodzieży szkolnej w Polsce. Warszawa: Instytut Matki i Dziecka, 2007.
18. Mazur J, Sentenac M, brooks F, Małkowska-Szkutnik A, Gajewski J, Gavin A. burden of chronic health conditions in
adolescence measured by schools surveys, Developmental Period Medicine, 2013;XVII,2:157-164.
19. Mazur J, Małkowska-Szkutnik A (red). Wyniki badań HbSC 2010. Raport techniczny 1, Warszawa: Instytut Matki i Dziecka, 2011.
20. Wistoft K. Health strategies and reservoirs of knowledge among adolescents in Denmark, Global Health Promotion, 2010;17(2):16-24.
21. Sloane PD. Opieka nad pacjentem w okresie dorastania, w: PD Sloane, lM Slatt, P Curtis P. Medycyna rodzinna, red. wyd. I pol. A Steciwko, Wrocław: urban&Partner, 1998;71-78.
22. Woynarowska-Sołdan M, Tabak I. Doroszewska A. The feelings of adolescents connected with medical visits and their perception of the physicians’ behavoiur, Dev Period Med, 2014;XVIII,3:331-342.
23. Woynarowska b. edukacja zdrowotna. Podręcznik akademicki, Warszawa, Wydawnictwo naukowe PWn, 2012.
24. Woynarowska b. edukacja zdrowotna dzieci, młodzieży i rodziców, w: b. Woynarowska (red). Profilaktyka w pediatrii, Warszawa: Wydawnictwo lekarskie PZWl, 2008;94-102.
25. Jankowska AK. Postepowanie z dzieckiem i jego opiekunami, w: Porozumiewanie się lekarza z pacjentem i jego rodziną (poz. 6), 83-93.
26. Góralczyk e. Choroba dziecka w twoim życiu, Warszawa: CMPPP Men, 1996.
27. Jakubowska-Winiecka A. Rozwój psychiczny dziecka, w: W Kawalec, R Grenda, H Ziółkowska (red). Pediatria, Warszawa: Wydawnictwo lekarskie PZWl, 2013;29-36.
28. Pyörälä e. The participation roles of children and adolescents in the dietary counseling of diabetics, „Patient educ Couns.” 2004;55:385-395.
29. van Staa A. unraveling triadic communication in hospital consultations with adolescents with chronic conditions: The added value of mixed methods research, Patient education and Counseling, 2011.
30. lopez RI. Twój nastolatek. Zdrowie i dobre samopoczucie, Warszawa: Wydawnictwo lekarskie PZWl, 2004.
31. Woynarowska b. Wpływ chorób przewlekłych na rozwój, zachowania i sytuację szkolną dzieci i młodzieży, w: uczniowie z chorobami przewlekłymi. Jak wspierać ich rozwój, zdrowie i edukację, Woynarowska b. (red. nauk.) Wydawnictwo naukowe PWn, Warszawa, 2010;19-41.
32. Kmieć T. Padaczka, w: uczniowie z chorobami przewlekłymi (poz. 31), 194-209.
33. Korycińska-Chaaban D. Fenyloketonuria, w: uczniowie z chorobami przewlekłymi (poz. 31), 100-111.
34. Marczyńska M, Szczepańska-Putz M. Zakażenie HIV, w: uczniowie z chorobami przewlekłymi (poz. 31), 210-221.
35. Woynarowski M. Przewlekłe choroby układu pokarmowego i wątroby, w: uczniowie z chorobami przewlekłymi (poz. 31), 260-283.
36. Kawalec W, Turska-Kmieć A, Kowalczyk M. Choroby układu sercowo-naczyniowego, w: uczniowie z chorobami przewlekłymi (poz. 31), 222-243.
37. Rozporządzenie Ministra Zdrowia z 28 sierpnia 2009 w sprawie organizacji profilaktycznej opieki zdrowotnej nad dziećmi i młodzieżą, Dz.u. nr 139 poz. 1133.

211
38. Woynarowska b, Oblacińska A, Jodkowska M, Ostręga W. Standardy w profilaktycznej opiece zdrowotnej nad uczniami sprawowanej przez pielęgniarkę lub higienistkę szkolną i lekarza podstawowej opieki zdrowotnej, Warszawa: Instytut Matki i Dziecka, 2003.
39. Towle A, Godolphin W, Van Staalduinen S. enhancing the relationship and improving communication between adolescents and their health care providers: a school based intervention by medical students, Patient education and Counseling, 2006;62:189-192.
40. Rozporządzenie Ministra edukacji narodowej z dnia 23 grudnia 2008 w sprawie podstawy programowej wychowania przedszkolnego oraz kształcenia ogólnego w poszczególnych typach szkół, Dz.u. 2009 nr 4 poz. 17 z późn. zmian.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest. Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 16.12.2014 r.Accepted/Zaakceptowano: 10.02.2015 r.
Published online/Dostępne online
Adres do korespondencji:Magdalena Woynarowska-Sołdan
Public Health Division, Faculty of Health Sciences, Medical university of Warsaw, Poland
ul. banacha 1A, blok F, 02-097 Warsaw, Polandtel. 668-128-137
e-mail: [email protected]
Teenagers’ perception of being an active patient and putting the concept into practice

212Developmental Period Medicine, 2015;XIX,2 © IMiD, Wydawnictwo Aluna
Beata Wyrębek1, Agata Orzechowska1, Dorota Cudziło2, Paweł Plakwicz1
evaluation of changeS in the width of gingiva in children and youth. review of literature
ocena zmiany Szerokości dziąSła u dzieci i młodzieży. przegląd literatury
1Department of Periodontology, Medical university of Warsaw, Poland2Orthodontic Department for Children, Institute of Mother and Child
AbstractComprehensive health care in children and youth includes periodic oral examinations. The mucogingival complex undergoes significant changes during development. The factors that impact the width of attached and keratinized gingiva during this period of life are: tooth eruption phase, the position in the arch, the type of frena attachment and oral hygiene. Along with the child’s development the width of attached and keratinized gingiva increases, except for the period of tooth replacement, when a temporary narrowing of attached gingiva of erupting permanent teeth is observed. The understanding of physiological processes of the mucogingival complex is prerequisite for diagnostics and treatment of gingival abnormalities in children and youth. Therefore close cooperation between paediatrician and dental specialists: paedodontist, orthodontist and periodontologist is essential.
Key words: gingival recession, mucogingival surgery, tooth position, width of attached gingiva
StreszczenieKompleksowa opieka medyczna nad dziećmi i młodzieżą obejmuje również opiekę nad prawidłowym stanem jamy ustnej. Kompleks śluzówkowo-dziąsłowy ulega u pacjentów w wieku rozwojowym istotnej przebudowie. Do czynników, które w okresie rozwojowym wpływają na zmiany szerokości dziąsła przyczepionego i skeratynizowanego należą: etap wyrzynania zęba, pozycja w łuku, rodzaj przyczepów wędzidełek i poziom higieny jamy ustnej. Szerokość dziąsła przyczepionego i skeratynizowanego rośnie wraz z wiekiem dziecka, z wyjątkiem okresu wymiany uzębienia, kiedy obserwowane jest zwężenie dziąsła przyczepionego przy wyrzynających się zębach stałych. Znajomość fizjologicznych procesów zachodzących w kompleksie śluzówkowo-dziąsłowym jest podstawą diagnostyki i leczenia nieprawidłowości dziąsłowych u pacjentów w okresie wzrastania wymaga ścisłej współpracy lekarza pediatry ze specjalistami z dziedzin stomatologii: pedodonty, ortodonty i periodontologa.
Słowa kluczowe: chirurgia śluzówkowo-dziąsłowa, dziąsło przyczepione, dziąsło skeratynizowane, recesje dziąsłowe
DEV pErioD mED. 2015;XiX,2:212-216
IntroDuctIonHolistic treatment of children and youth provided by a
multidisciplinary team allows more effective patient care [1]. There is a proven association between periodontal status and occurrence of systemic diseases [2, 3]. Healthy oral cavity of a child is an important element of general health prophylaxis. Significant changes occur in morphological structure of periodontal tissues in primary, mixed and
permanent dentition [4]. The awareness of those differences allows initiation of prophylaxis and optimal treatment selection if any pathology occurs [5].
Mucogingival defects may occur even in early childhood. They are caused by alterations of teeth development and eruption, malformations of mandible or maxilla, poor oral hygiene or bacterial and viral infections. Changes in the width of attached and keratinized gingiva at various stages of dentition development are still under investigation. A

213evaluation of changes in the width of gingiva in children and youth. Review of literature
close relationship between the process of tooth eruption and the width of keratinized and attached gingiva has been proven [6, 7, 8, 9].
The width of keratinized gingiva is measured as the distance from the free gingival margin to the mucogingival junction. The width of attached gingiva is calculated by subtracting the depth of gingival sulcus from the measurement of keratinized gingiva [10]. (Figure 1). The attached gingiva is wider in the maxilla than in the mandible, both in deciduous and permanent dentition [11, 12]. Previously it was believed that a wide zone of attached and keratinized gingiva (at least 1 mm and 2 mm respectively) constitutes a protective barrier against inflammation and forces operating during mastication, tooth brushing and orthodontic treatment [9, 13, 14]. Subsequent studies have shown, however, that with the attached gingiva lesser than 1 mm, healthy periodontal tissues can be preserved if proper oral hygiene is maintained [15, 16, 17].
During the development of the jaws and dentition, the morphology of the mucogingival complex undergoes certain changes. These changes are associated also with the position of teeth in alveolus. Rose and App [8] as well as bowers [9] observed that the position of the tooth in the arch impacts the width of attached gingiva. The movement of both deciduous and permanent teeth during growth
in the lingual or vestibular direction causes changes in the width of attached gingiva [6]. A tooth which is positioned lingualy after eruption has a wider gingiva on the vestibular side, whereas a tooth in a vestibular position has a narrower gingiva than normally positioned teeth [6, 7, 8, 9. 17, 18].
Malformations of the mucogingival complex at anterior teeth in children are most commonly associated with a narrow zone of attached gingiva, abnormal frena attachments, occurrence of pull syndrome and, less frequently, gingival recessions. The width of attached gingiva can be reduced and the oral vestibule can be shallower congenitally, as a result of teeth malposition or abnormal attachment of labial and lingual frena. Gingival problems in children are most commonly detected while planning of orthodontic treatment. It is important that paediatrician pay close attention to gingiva and frena condition during patient’s examination, and refer patient to a specialist in case of malformations.
If lack of attached gingiva and/or presence of recession occur, following aspects should be considered before planning the surgery stage of dentition development, type of defect and position of teeth in the arch, intended direction of teeth movements during orthodontic treatment [10, 17].
Fig. 1. Schematic drawing of hard and soft periodontal tissues (Author: maryla Siwiec).Ryc. 1. Schemat obrazujący elementy tkanek zębowych wraz z przyzębiem (Autor: Maryla Siwiec).

214 Beata Wyrębek et al.
Changes in the width of gingiva in children and youth
Additionally to age, the degree of tooth eruption, the position in the arch and the presence of inflammation are factors which impact dimensions of gingiva [8, 9, 10, 17]. Recent study compared the width of gingiva during and after active tooth eruption phase. Some authors referred only to teeth properly aligned in the arch, while others studied children with diagnosed malocclusions. Due to the different criteria of patient selection, different results were obtained [8, 9, 11, 17, 19].
Rose and App [8] as well as bowers [9] found that the attached gingiva is wider in permanent than in deciduous teeth. Other authors however, did not observe this association [11]. It is proven that the width of gingiva increases with age, both in deciduous and permanent dentition [11, 19]. In permanent dentition, the increase of the width of attached gingiva is associated with gradual reduction of the sulcus depth, while the width of keratinized gingiva remains the same. In deciduous dentition, however, it is not correlated with a reduction in the depth of the sulcus, for it remains constant [11]. Thus initially the sulcus of erupting permanent teeth is deeper than that of corresponding deciduous teeth, but later it becomes shallower [8, 19, 20]. These differences may result from initially weaker periodontal attachment, which is less resistant to probing [13] as well as from the occurrence of false pockets and temporary inflammation during gingival phase of teeth eruption. These two factors cause higher probing depth recordings [19, 21]. The width of the attached gingiva of newly erupted permanent teeth is therefore smaller than in the case of deciduous teeth. However, the width of attached gingiva increases while permanent teeth erupt [19]. Similar findings were described by Sayrafi et al [12] and Srivastawa et al [22], who conducted their study at deciduous, mixed and permanent dentition. Sarrio et al [23, 24] used radiographs to measure the width of gingiva in deciduous and permanent teeth. In both groups, the width of the attached gingiva increased during eruption of teeth. This can be explained by the fact that the mucogingival junction remains stable and the erupting teeth “pull” the surrounding tissues [24].
To evaluate the sulcus depth and the width of attached and keratinized gingiva of anterior teeth, Andlin-Sobocki [17] took into account only the teeth properly aligned in the arch, without orthodontic treatment before or during the study. The results indicated that the width of attached and keratinized gingiva increased with age both in deciduous and permanent teeth. The increase in the erupted permanent teeth was reversely proportional to the initial value [17]. Ochsenbein and Maynard [13] and Hall [25] however, noted that there is no increase in the width of attached gingiva with age, i.e. when eruption is complete the width does not change any more.
influence of position of the tooth in the arch on width of attached gingiva and risk of recession in children and youth
Gingival recessions in adults are caused by many factors. In children, however, the most important factor in the etiology of recessions is abnormal position of teeth
[6, 18, 26, 27]. The presence of gingival recession during development concerns mostly permanent lower central incisors and is observed in 8.3% of cases [11]. It was observed that absence or limited attached gingiva (less than 1 mm) on the vestibular side does not always cause recession [15]. The width of the attached gingiva is less critical for the development of recession than the position of the tooth, if proper oral hygiene is maintained [15, 16]. Proper alignment of teeth is necessary to maintain healthy periodontal tissues [28]. Crowded, rotated, protruded and tilted anterior teeth are recognised aetiological factors of recessions. buccal bone and gingiva on the vestibular side are thin and less resistant to mechanical injuries in teeth in vestibular position [29]. bone dehiscence and fenestrations may also occur in such cases. It was noted, however, that gingival recessions in children may decrease or disappear without surgical treatment, as a result of normal position of teeth after eruption or orthodontic treatment [6, 27, 29, 30] (Figure 2a and Figure 2b).
Fig. 2a. 11-year-old-patient presenting lack of keratinized gingiva at toot 41.
Ryc. 2a. Pacjent lat 11 – brak skeratynizowanego dziąsła przy zębie 41.
Fig. 2b. The same patient at age of 19 presenting normal width of keratinized gingiva at tooth 41.
Ryc. 2b. Ten sam pacjent w wieku 19 lat w trakcie leczenia ortodontycznego – prawidłowa szerokość dziąsła skeratynizowanego przy zębie 41.

215evaluation of changes in the width of gingiva in children and youth. Review of literature
During orthodontic treatment the mucogingival complex undergoes various changes. They depend on the initial width and thickness of attached gingiva and on the direction of tooth movement [31]. lingual tooth movement increases the thickness of gingiva on the vestibular side. As a consequence, it causes coronary migration of the gingival margin, reduction of the length of clinical crowns and an increase of the width of attached gingiva [26, 31]. This results in decrease of existing recessions. Vestibular tooth movement decreases thickness of the gingiva and the width of attached gingiva[7, 31]. If this movement does not exceed the alveolar bone, then the orthodontic treatment will not cause or increase existing recession [31]. The above-mentioned changes in mucogingival parameters occur both as a result of orthodontic movements and spontaneously due to eruption of teeth.
mucogingival surgical procedures in children and youth
Maynard and Ochsenbein [7] claimed that greater risk of gingival recession exists in newly erupted permanent teeth with a narrow gingival zone. According to the authors it was the indication for gingival grafting, especially before orthodontic treatment. Formerly some mucogingival surgical procedures were performed routinely because it was believed that the lack of correction of a narrow gingival zone in childhood may cause mucogingival defects in adults [13]. Considering a surgical procedure one should take into account the fact that during the mixed dentition the width of attached gingiva decreases only temporarily [11, 20, 32]. When permanent teeth erupted completely, a gradual increase in the width of gingiva occurs [33]. A decrease in the width of gingiva in mixed dentition may be caused by greater sulcus depth and by vestibular movement of newly erupted teeth [20, 34]. In this period an increased accumulation of bacterial plaque resulting in gingivitis may also occur [11]. If oral hygiene is maintained the risk of recession is significantly limited [35]. Absence of gingival margin inflammation is the most important, in reducing, or eliminating gingival recessions.
The recessions in children decreased with age despite the fact that at the baseline a narrow zone of attached gingiva or no attached gingiva was observed [29]. The thickness of gingiva is more important than its width. Therefore the thickness of gingiva should be examined prior to orthodontic treatment, especially when vestibular movement is planned [36]. Gingival graft should be considered only in cases of limited gingival thickness.
non-surgical treatment should be considered first [37]. Observation is recommended in malpositioned teeth as well as in normally positioned teeth with a narrow attached gingiva. normal teeth eruption or orthodontic alignment may result in changes of dimensions of keratinized and attached gingiva [6, 17]. These changes should be considered before planning a surgical procedure in the mandibular incisors region. The area may be affected with high attachments of frena and muscles, often coexisting with a shallow vestibule of the oral cavity. This may cause pull syndrome of the gingival margin, which favours accumulation of plaque
and development gingivitis. In such situations frenectomy alone or deepening oral vestibule procedures may be performed in order to remove abnormal frena. These are alternative methods to gingival grafting performed to cover recessions. Kazanijan vestibuloplasty, may be performed in children since it does not prevent gingiva grafting in the future.
suMMAryComprehensive care ensures proper development of
child since the earliest years. During the child’s development essential changes occur in morphology of mucogingival complex such as: bone growth, changes in the width of attached and keratinized gingiva. Additionally, changes in the alignment and position of teeth are observed. Physiological changes that occur during development should be identified before carrying out the mucogingival surgery in children [31]. Surgical treatment of recessions including gingival grafting should be preceded by observation and postponed until final teeth alignment which may enable increase of gingiva and spontaneous reduction of recessions. Close cooperation between medical and dental specialists is crucial for proper diagnostics and treatment of mucogingival defects in children and youth.
reFerences
1. Matthews-Kozanecka M. Holistic approach to treatment in the context of bioethics. Dev Period Med. 2014;1:13-15.
2. Górska R. Relationship between Periodontitis and Systemic Disorders. Dent Med Probl. 2009;46,4:379-383.
3. Pawlaczyk-Kamieńska T, Pawlaczyk-Wróblewska e. niedoceniany problem choroby odogniskowej u dzieci. Dev Period Med., 2014:2:228-232.
4. Karłowska I. Podręcznik dla studentów i lekarzy stomatologów. Wydawnictwo lekarskie PZWl, Warszawa 2005.
5. bednarz W, Sokołowski b. Kompleks śluzówkowo-dziąsłowy w wieku rozwojowym. e-Dentico, 2007;1:59-64.
6. Andlin-Sobocki A, bodin l. Dimensional alterations of the gingiva related to changes of facial/lingual tooth position in permanent anterior teeth of children. A 2-year longitudinal study. J Clin Periodonto 1993;20:219-224.
7. Maynard JG Jr, Ochsenbein C. Mucogingival problems, prevalence and therapy in children. J Periodontol. 1975;46:543-552.
8. Rose ST, App GR. A clinical study of the development of the attached gingiva along the facial aspect of the maxillary and mandibular anterior teeth in the deciduous transitional and permanent dentition. J Periodontol. 1973;44:131-149.
9. bowers GM. A study of the width of attached gingiva. J Periodontol. 1963;34:201-209.
10. Hall Wb. The current status of mucogingival problems and their therapy. J Periodontol. 1981;52,5:69-75.
11. Tenenbaum H, Tenenbaum M. A clinical study of the width of the attached gingiva in the deciduous, transitional and permanent dentitions. J Clin Periodontol. 1986;13:270-275.
12. Sayrafi M, Sadeghi n, Haghighat M. A clinical study of the width of attached gingiva and depth of gingival sulcus in the primary, mixed and permanent dentition. Journal of Islamic Dental Association 1999;11:9-19.

216
13. Ochsenbein C, Maynard JG. The problem of attached gingiva in children. ASDC J Dent Child. 1974;41,4:263-272.
14. lang nP, loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol. 1972;43,10:623-627.
15. Wennström Jl. lack of association between width of attached gingiva and.development of soft tissue recession. A 5-year longitudinal study. J Clin Periodontol. 1987;14:181-184.
16. Kennedy J, bird WC, Palcanis KG, Dorfman HS. A longitudinal evaluation of varying widths of attached gingiva. J Clin Periodontol. 1985;12:667-675.
17. Andlin-Sobocki A. Changes of facial gingival dimensions in children. J Clin Periodontol. 1993;20:212-218.
18. Geiger AM. Mucogingival problems and the movement of mandibular incisors: a clinical review. Am J Orthod. 1980;78:511-527.
19. bimstein e. eidelman e. Morphological changes in the attached and keratinized gingiva and gingival sulcus in the mixed dentition period. A five-year longitudinal study. J Clin Periodontol. 1988;15:175-179.
20. bimstein e, eidelman e. Dimensional difference in the attached and gingival sulcus in the mixed dentition. ASDC J Dent Child. 1983;50:264-267.
21. Van der Velden u. Probing force and the relationship of the probe tip to the periodontal tissues. J Clin Periodontol. 1979;6:106-114.
22. Srivastava b, Chandra S, Jaiswal Jn, Saimbi CS, Srivastava D. Cross-sectional study to evaluate variations in attached gingiva and gingival sulcus in the three periods of dentition. J Clin Pediatr Dent. 1990;15:17-24.
23. Saario M, Ainamo A, Mattila K, Suomalainen K, Ainamo J. The width of radiologically-defined attached gingiva over deciduous teeth. J Clin Periodontol. 1995;22:895-898.
24. Saario M, Ainamo A, Mattila K, Ainamo J. The width of radiologically-defined attached gingiva over permanent teeth in children. J Clin Periodontol. 1994;21,10:666-669.
25. Hall Wb. Present status of soft tissue grafting. J Periodontol. 1977;148:587-597.
26. Karring T, nyman S, Thilander b, Magnusson I. bone regeneration in orthodontically produced alveolar bone dehiscences. J Periodontal Res. 1982; May, 17(3):309-315
27. Steiner GG, Pearson JK, Ainamo J. Changes of the marginal periodontium as a result of labial tooth movement in
monkeys. J Periodontol. 1981;52:314-320.28. Joss-Vassalli I, Grebenstein C, Topouzelis n, Sculean A, Katsaros
C. Orthodontic therapy and gingival recession: a systematic review. Orthod Craniofac Res. 2010;13:127-141.
29. Andlin-Sobocki A, Marcusson A, Persson M. 3-year observations on gingival recession in mandibular incisors in children. J Clin Periodontol. 1991;18,3:155-159.
30. Persson M, lennartsson b. Improvement potential of isolated gingival recession in children. Swed Dent J. 1986;10:45-51.
31. Wennström J.l. Mucogingival considerations in orthodontic treatment. Semin Orthod. 1996;2,1:46-54.
32. bimstein e, Machtei e, eidelman e. Dimensional differences in the attached and keratinized gingiva and gingival sulcus in the early permanent dentition: a longitudinal study. J Pedod. 198; Spring, 10(3):247-253.
33. Vincent JW, Machen Jb, levin MP. Assessment of attached gingiva using tension test and clinical measurements. J Periodontol. 1976;47:412-414.
34. Abrishami MR, Akbarzadeh A. Attached gingival width and gingival sulcus depth in three dentition systems. Journal Dental School 2013;31:142-149.
35. Powell Rn, Mcemery TM. A longitudinal study of isolated gingival recession in the mandibular central incisor region of children aged 6-8 years. J Clin Periodontol. 1982;9:357-364.
36. Wennström Jl. The significance of the width and thickness of the gingiva in orthodontic treatment. Dtsch Zahnarztl Z. 1990;45,3:136-141.
37. bimstein e, Machtei e, becker A. The attached gingiva in children: diagnostic, developmental and orthodontic considerations for its treatment. ASDC J Dent Child. 1988;55:351-356.
Authors’ contributions/Wkład AutorówAccording to the order of the Authorship/Według kolejności
Conflicts of interest/Konflikt interesuThe Authors declare no conflict of interest.Autorzy pracy nie zgłaszają konfliktu interesów.
Received/Nadesłano: 21.04.2015 r.Accepted/Zaakceptowano: 19.05.2015 r.
Published online/Dostępne online
Address for correspondence:Dorota Cudziło
Orthodontic Department for Children, Institute of Mother and Child,
Kasprzaka 17a, 01-211 Warsaw, Polandtel. (+48 22) 32-77-128
e-mail: [email protected]
Beata Wyrębek et al.

217Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
Teresa Jackowska1,2, Alicja Sapała-Smoczyńska1,2, Ewa Kamińska3
ocena tolerowania preparatu żelaza actiferol fe® u dzieci z niedokrwiStością
z niedoboru żelaza*
tolerability of iron preparation actiferol fe® in children treated for iron deficiency anemia
1Klinika Pediatrii, Centrum Medyczne Kształcenia Podyplomowego, Warszawa2Kliniczny Oddział Pediatryczny, Szpital bielański, Warszawa
3Zakład Farmakologii, Instytut Matki i Dziecka
Streszczenie Wstęp: Niedokrwistość spowodowana niedoborem żelaza jest najczęściej występującą niedokrwistością wieku dziecięcego. Podstawową metodą profilaktyki i leczenia jest suplementacja preparatem żelaza w odpowiedniej dawce. Dostępnych jest wiele preparatów żelaza, charakteryzujących się różnym stopniem tolerowania przez pacjentów. Actiferol Fe® jest produktem zawierającym pirofosforan żelaza w postaci zmikronizowanej, co pozwala na całkowitą dyspersję jego cząsteczek w roztworze, a tym samym zwiększa rozpuszczalność i biodostępność żelaza. Cel badania: Ocena tolerowania preparatu Actiferol Fe® u dzieci, u których zastosowano go w celu leczenia lub zapobiegania niedokrwistości z niedoboru żelaza. Poddano analizie sposoby podawania oraz częstość występowania działań niepożądanych. Materiał i metody: Do badania włączono 80 dzieci (64 chłopców i 16 dziewczynek) w wieku od 1. miesiąca do 6. roku życia, u których występowały wskazania do włączenia żelaza. Do oceny badanych parametrów posłużyła ankieta, zawierająca pytania dotyczące tolerowania preparatu przez dziecko, sposobu podania, wygody stosowania oraz występowania działań niepożądanych. Ankietę samodzielnie wypełniali rodzice (najczęściej matka).Wyniki: Actiferol Fe® został oceniony przez 87,5% (70/80) uczestników badania jako preparat bardzo dobrze lub dobrze tolerowany przez pacjentów (odpowiednio: 46,3%, tj. 37/80, i 41,2%, tj. 33/80 dzieci). Najczęściej preparat podawano w postaci płynnej po dodaniu do wody − 31,3% (25/80), soku pomarańczowego – 18,8% (15/80) lub mleka modyfikowanego – 17,5% (14/80). W 84% (67/80) ankiet oceniono sposób podawania preparatu jako wygodny lub bardzo wygodny. Odnotowano działania niepożądane, takie jak zmiana konsystencji stolca na twardszy, bóle brzucha i zaparcie – częstość ich występowania wynosiła odpowiednio: 20% (16/80), 11,25% (9/80) i 10% (8/80) pacjentów. Sporadycznie występowały: biegunka, bolesność przy oddawaniu stolca. Ciemne zabarwienie stolca odnotowano u 55% (44/80) pacjentów. Tylko w jednym przypadku (1,25%) rodzice odstąpili od podawania preparatu Actiferol Fe®, zmieniając go na inny, przy czym nie miało to związku z wystąpieniem działań niepożądanych. Wnioski: Actiferol Fe® jest preparatem dobrze tolerowanym, wygodnym w stosowaniu i wykazującym jedynie nieznaczne działania niepożądane.
Słowa kluczowe: niedokrwistość z niedoboru żelaza, Actiferol Fe®
AbstractIntroduction: Iron deficiency anemia is the most frequently occurring anemia during the childhood period. Supplementation with adequate doses of iron remains a basic method of prevention and
*Praca wykonana w ramach grantu CMKP 501-1-20-19-14.
MiSCeLLanea

218 Teresa Jackowska i wsp.
treatment. The various available products containing iron are characterized by a different degree of patient tolerability. Actiferol Fe® is a micronized, dispersible ferric pyrophosphate which improves its water solubility, and therefore it has better absorption and bioavailability. Aim of the study: The assessment of tolerability of Actiferol Fe® in children who were administered this product to treat or prevent of iron deficiency anemia. The methods of administration and the incidence of adverse effects were analyzed.Materials and methods: Eighty children (64 boys and 16 girls) aged from one month to 6 years who met the criteria of an indication to be treated with iron were included into the study. The assessment of selected parameters was based on the questionnaire which included questions about tolerability, method of administration, convenience of usage and adverse effects. The questionnaire was filled in by parents (usually by the mother).Results: The study indicated that Actiferol Fe® has very good or good tolerability in 87.5% (70/80) of patients − 46.3% (37/80) and 41.2% (33/80), respectively. The most frequent method of administration was in liquid form after dissolving: in water − 31,3% (25/80), in orange juice − 18.8% (15/80) or in milk formulas – in 17.5% (14/80) of patients. The method of administration was assessed as convenient or very convenient by 84% (67/80) of participants. Out of the adverse effects reported, the most frequent were change in the stool consistency into harder, abdominal pain and constipation – in 20% (16/80), 11.25% (9/80), 10% (8/80) cases, respectively. Diarrhea, pain during defecation occurred occasionally. A dark color of the stool was reported by 55% (44/80) of patients. In only one case (1.25%) the parents resigned from the product administration and replaced it with another iron product (no connection with tolerability of the formulation). Conclusion: Actiferol Fe® is a product characterized by good tolerability, convenient usage and mild adverse effects.
Key words: iron deficiency anemia, Actiferol Fe®
DEV pErioD mED. 2015;XiX,2:217-224
WSTęp
zapotrzebowanie na żelazo, jego rola w organizmie i stany niedoboru
Żelazo jest mikroelementem, którego główne funkcje − jako składnika hemoglobiny i mioglobiny − są związane z transportem tlenu z płuc do wszystkich komórek orga-nizmu. Jest też kofaktorem licznych enzymów, biorących udział w różnorodnych procesach biologicznych, w tym wpływających na odporność immunologiczną, proces wytwarzania krwinek, syntezę neuroprzekaźników od-powiadających za sprawność intelektualną [1].
Dzienne zapotrzebowanie na żelazo jest uwarunkowane wielkością strat, utrzymaniem odpowiedniego stężenia hemoglobiny we krwi i zwiększonymi potrzebami roz-wijającego się organizmu. u dzieci zapotrzebowanie na żelazo zwiększa się proporcjonalnie do przyrostu masy ciała, objętości krwi i masy erytrocytarnej. najnowsze (2012 r.) normy dla populacji Polski [2], dotyczące śred-niego zapotrzebowania (eAR) oraz zalecanego dziennego zapotrzebowania (RDA) na żelazo u dzieci i młodzieży przedstawiono w tabeli I.
niedobór żelaza może być spowodowany jego niedo-stateczną podażą z dietą (np. u niemowląt lub wegetarian) [3], nieprawidłowym wchłanianiem (np. w celiakii, nieto-lerancji mleka krowiego, chorobie leśniowskiego-Crohna) [4], obecnością pasożytów w przewodzie pokarmowym, krwotokiem, zwiększonym zapotrzebowaniem organi-zmu w okresie intensywnego wzrostu [5]. u młodych
dziewcząt i kobiet w wieku rozrodczym istotne znacze-nie mają także straty żelaza związane z krwawieniem miesiączkowym, ciążą i karmieniem piersią.
niedobór żelaza rozwija się w trzech fazach (tab. II), z których pierwsze dwie są niekiedy trudne do wykrycia. W fazie pierwszej dochodzi do zmniejszenia zapasów żelaza w organizmie, ale bez zaburzeń czynnościowych organizmu i z utrzymaną prawidłową syntezą hemoglo-biny. W fazie drugiej stężenie hemoglobiny we krwi jest nadal prawidłowe, ale erytropoeza wykazuje znamiona niedoboru żelaza (zwiększone stężenie protoporfiryny w krwinkach czerwonych), zaś w fazie trzeciej rozwija się jawna niedokrwistość [1, 6].
Charakterystycznym objawem niedoboru żelaza, wy-nikającym z niedotlenienia tkanek, jest przemęczenie, osłabienie siły mięśniowej i ogólnej kondycji fizycz-nej. Zmniejsza się także − zwłaszcza u dzieci w wieku szkolnym − zdolność koncentracji i zapamiętywania oraz zaburzona zostaje koordynacja psychomotoryczna. u niemowląt w wieku 6 mż. występuje związek między niedoborem żelaza, a zaburzonym metabolizmem w neu-ronach i mielinizacją [7]. niedobór żelaza w okresie niemowlęcym odpowiada za opóźnienie wzrostu dziecka i wpływa negatywnie na jego późniejszy rozwój emo-cjonalny i zdolności poznawcze [8, 9]. Znaczny i długo utrzymujący się niedobór żelaza powoduje bowiem trwałe zmiany emocjonalne w wyniku wpływu na czynności mózgu, gdyż zaburza uwalnianie z neuronów kwasu gamma-aminomasłowego (GAbA) i syntezę neuroprze-kaźników. W niedoborze żelaza zmniejszone jest także

219Ocena tolerowania preparatu żelaza Actiferol Fe® u dzieci z niedokrwistością z niedoboru żelaza
wytwarzanie krwinek, w tym limfocytów T, co prowadzi do osłabienia odpowiedzi komórkowej i zwiększonej zapadalności na infekcje.
niedokrwistość z niedoboru żelazaniedokrwistość wciąż pozostaje jednym z najczęściej
występujących schorzeń zarówno u dorosłych jak i dzieci. Szacuje się, że na świecie choruje na nią blisko 1,62 mld ludzi, co stanowi około 25% populacji [5]. Wśród różnych przyczyn prowadzących do powstania niedokrwistości najczęstszą jest niedobór żelaza, dotykający około 500 mln ludzi [10].
na rozwój niedokrwistości z niedoboru żelaza (Iron Deficiency Anemia − IDA) szczególnie narażone są nie-mowlęta i małe dzieci (6-24 miesięcy), u których dzienne spożycie żelaza jest mniejsze niż w innych grupach wie-kowych [11, 12]. niemowlęta urodzone przedwcześnie oraz z małą masą urodzeniową są bardziej podatne na
faza niedoboru żelazaIron deficiency phase
objawySymptoms
1. Faza wstępnaInitial phase
Wyczerpywanie się tkankowych zapasów żelazaIron depletion due to reduced storage pools
2. Faza fizjologicznaPhysiological phase
zmniejszenie transportu żelaza i upośledzenie erytropoezyDecreased iron transport and impaired erythropoiesis
3. Faza klinicznaClinical phase
Jawna niedokrwistość z niedoboru żelazaIron-deficiency anaemia
Tabela i. normy dla populacji polski, dotyczące średniego zapotrzebowania (EAr) oraz zalecanego dziennego zapo-trzebowania (rDA) na żelazo u dzieci i młodzieży wg norm Żywienia instytutu Żywności i Żywienia [2].
Table I. Iron requirements in children and adolescents expressed as average requirement (EAR) and recommended dietary allowances (RDA), according to Dietary Reference Values for Polish population elaborated by Instytut Żywności i Żywienia [2].
wiek/płećAge/sex ear (mg fe) rda (mg fe)
6-12 mż.6-12 months 7 11
1-3 lata1-3 years 3 7
4-9 lat4-9 years 4 10
chłopcy 10-12 latboys 10-12 years 7 10
dziewczęta 10-12 latgirls 10-12 lat 7 (8)* 10 (15)*
chłopcy 13-18 latboys 13-18 years 8 12
dziewczęta 13-18 latgirls 13-18 years 8 15
*po wystąpieniu miesiączki*after menarche
Tabela ii. Fazy niedoboru żelaza w organizmie.Table II. Phases of iron deficiency.
rozwinięcie się stanu niedoboru żelaza, bowiem zapasy żelaza są zmniejszone, a zapotrzebowanie zwiększone. na rozwój niedokrwistości w tej grupie dzieci ma tak-że wpływ zwiększona hemoliza, krótszy czas przeżycia krwinek czerwonych, małe stężenie krążącej erytropo-etyny [13, 14].
Podstawowym kryterium rozpoznania niedokrwistości jest stężenie hemoglobiny we krwi poniżej normy dla danego wieku, natomiast zmniejszenie zapasów żelaza w organizmie jest przeważnie definiowane jako zmniej-szenie stężenia ferrytyny i stopnia wysycenia transferyny oraz zwiększenie całkowitej zdolności wiązania żelaza (TIbC) [15].
Do objawów niedokrwistości z niedoboru żelaza na-leżą: ogólne osłabienie, duszność, ból i zawroty głowy, kołatanie serca, upośledzenie zdolności poznawczych [15]. Przedmiotowo stwierdza się zazwyczaj bladość skóry i błon śluzowych, a w bardziej zaawansowanej niedokrwistości

220 Teresa Jackowska i wsp.
również tachykardię, czynnościowy szmer skurczowy nad zastawką dwudzielną, łamliwość, matowość i wypadanie włosów, zmiany troficzne paznokci (blade, kruche paznokcie z podłużnym prążkowaniem, paznokcie łyżeczkowate), zapalenie jamy ustnej i języka [16-18].
leczenie pacjentów z niedokrwistością z niedoboru żelaza polega przede wszystkim na wyeliminowaniu jej przyczyny, zastosowaniu odpowiedniej diety oraz poda-waniu preparatu żelaza [15]. W leczeniu IDA optymalna dawka dobowa żelaza elementarnego wynosi 4-6 mg/kg mc.; należy ją podawać w dwóch − trzech dawkach po-dzielonych. Powszechnie stosowane są doustne preparaty żelaza, jedynie w wyjątkowych przypadkach żelazo jest podawane domięśniowo lub dożylnie. niezależnie od sposobu podawania preparaty żelaza mogą wywoływać działania niepożądane, takie jak nudności i dyskomfort w nadbrzuszu, wymioty, zaparcie, biegunkę, bóle brzucha i bóle głowy. Może wystąpić zmiana zabarwienia stolca, a po podaniu niektórych preparatów − przebarwienie zębów. uważa się, że żołądkowo-jelitowe działania nie-pożądane mają związek z podrażnieniem błony śluzowej i upośledzeniem perystaltyki. Ich występowanie i nasilenie zależy od stężenia żelaza w świetle przewodu pokarmo-wego oraz zastosowanej dawki [11, 15].
Wchłanianie żelaza Szacuje się, że wchłanianie żelaza z przewodu pokar-
mowego wynosi 5-15% [19]. Jest ono większe w przy-padku żelaza hemowego, tj. pochodzenia zwierzęcego (około 25%), natomiast w znacznie mniejszym stopniu wchłania się żelazo niehemowe (5-10%) [20]. Wchłanianie żelaza zależy również od jego zawartości w organizmie i jest odwrotnie skorelowane ze stężeniem ferrytyny w surowicy [11].
Po podaniu doustnym żelazo niehemowe ulega w kwa-śnym środowisku żołądka redukcji z Fe (III) do Fe (II) przy udziale reduktazy żelaza [21]. Wchłanianie żelaza zachodzi w dwunastnicy i początkowym odcinku jelita czczego przy udziale białka nośnikowego DMT-1, które dostarcza je do enterocytów [22]. Proces ten przebiega nieregularnie, gdyż wpływają na niego także w istotnym stopniu składniki posiłku.
Do składników ułatwiających wchłanianie żelaza należą: kwas askorbowy i inne kwasy organiczne (cytrynowy, jabłkowy, winowy itp.), niektóre białka (kazeina) i ami-nokwasy (np. cysteina, lizyna, histydyna), cukry (laktoza, fruktoza, sorbitol). Zmniejszają natomiast wchłania-nie żelaza: fityniany zawarte w roślinach strączkowych i zbożach, polifenole, taniny i metyloksantyny (obecne np. w kawie i herbacie), wapń, fosforany, niektóre leki (inhibitory pompy protonowej, antagoniści receptora H2, fluorochinolony, tetracykliny), achlorhydria [17, 19, 23]. Szczególnie niekorzystnie na biodostępność żelaza wpływa zawartość w diecie fitynianów i polifenoli.
Po wchłonięciu żelazo jest wiązane przez białko transportowe − transferynę − i dostarczane do szpiku kostnego, w którym zostaje wykorzystane do syntezy hemoglobiny, a jego nadmiar gromadzony w szpiku, wą-trobie i śledzionie w postaci żelaza zapasowego (ferrytyna i hemosyderyna), które jest wykorzystywane, gdy podaż z dietą nie wystarcza na pokrycie jego bieżących strat.
Mikronizowany pirofosforan żelaza (Actiferol Fe®) a inne preparaty żelaza
Dostępnych jest wiele doustnych preparatów żelaza charakteryzujących się różną biodostępnością, właści-wościami organoleptycznymi oraz różnym stopniem tolerowania przez pacjentów. Od kilku dekad najczęściej stosowanymi w suplementacji związkami żelaza są trzy sole o porównywalnej biodostępności, tj. siarczan, glu-konian i fumaran [19].
Za preparat z wyboru w stanach niedoboru żela-za przyjmuje się dobrze rozpuszczalny w wodzie siar-czan żelaza (II), którego biodostępność jest punktem odniesienia w badaniach oceniających biodostępność innych związków żelaza (tzw. biodostępność względ-na, relative biological value, RbV). Wprawdzie siarczan oraz inne rozpuszczalne sole żelaza (II) mają większą biodostępność, jednak mogą reagować ze składnikami pokarmu, powodując istotną zmianę jego smaku lub koloru. Z tego powodu nie nadają się do wzbogacania pokarmów (fortyfikacji) w żelazo. Ponadto siarczan żelaza może wywoływać zaburzenia żołądkowo-jelitowe, co jest przyczyną gorszego tolerowania przez niektórych pacjentów i niekiedy zmusza do jego odstawienia.
nierozpuszczalne w wodzie związki żelaza nie po-wodują takich reakcji, a więc nie zmieniają właściwości organoleptycznych pokarmu. Ich biodostępność jest jednak mniejsza wskutek częściowego wytrącania się nierozpuszczalnego osadu, przez co nie mogą być po-dawane w płynnych pokarmach lub płynnych lekach [24]. Do związków tych należy m.in. nierozpuszczalny w wodzie pirofosforan żelaza, który jest stosowany do wzbogacania w żelazo produktów o stałej konsystencji, np. płatków śniadaniowych. biodostępność pirofosforanu żelaza u ludzi po podaniu doustnym wynosi 30-50% w porównaniu do siarczanu żelaza [25].
Zastosowanie odpowiedniej technologii, polegającej na mikronizacji w połączeniu z emulgacją, która umoż-liwiła dyspersję (rozproszenie) mikrocząsteczek związku w wodzie, pozwoliło na otrzymanie zmikronizowanej postaci pirofosforanu żelaza (micronized dispersible ferric pyrophosphate − MDFP), którego cząsteczki mają wielkość około 0,3 µm i są ok. 20 razy mniejsze niż cząsteczki nierozpuszczalnego pirofosforanu żelaza. Dzięki temu preparat Actiferol Fe®, zawierający MDFP, charakteryzuje się dobrą rozpuszczalnością (zawieszeniem cząsteczek) w wodzie oraz wchłanianiem i biodostępnością porówny-walnymi do siarczanu żelaza. Korzystną cechą MDFP jest także długotrwała stabilność jego cząsteczek, uzyskana przez dodanie emulgatorów, dzięki czemu nie ulegają one agregacji [24].
badania na zwierzętach wykazały, że wchłanianie i biodostępność MDFP są porównywalne do siarczanu żelaza, oraz potwierdziły jego skuteczność w norma-lizacji stężenia hemoglobiny [24, 26, 27]. Wykazano, że biodostępność względna pirofosforanu żelaza jest odwrotnie proporcjonalna do wielkości jego cząsteczek. W randomizowanych badaniach kontrolowanych prze-prowadzonych na szczurach RbV wynosiła odpowiednio 59, 69 i 95% dla cząsteczek o wielkości 21 µm, 2,5 µm i 0,5 µm [26] oraz 120% dla MDFP o wielkości cząsteczek 0,3 µm [24] − w tym ostatnim badaniu była większa niż

221Ocena tolerowania preparatu żelaza Actiferol Fe® u dzieci z niedokrwistością z niedoboru żelaza
siarczanu. Po podaniu MDFP stężenie maksymalne żelaza we krwi występowało po 2 h i było większe niż po poda-niu siarczanu, cytrynianu lub pirofosforanu o klasycznej wielkości cząsteczek. Także znaczące stężenia żelaza we krwi utrzymywały się dłużej (do 12 h) po podaniu MDFP niż innych soli żelaza (8 h) [24].
u ludzi wchłanianie żelaza z MSDF i siarczanu było porównywalne zarówno po ich podaniu w postaci płatków śniadaniowych, jak i jogurtu [23]. Także biodostępność względna żelaza podanego w postaci MDFP była duża i w zależności od rodzaju pokarmu wynosiła: jogurt − 92% [23] i 95% [28]; płatki śniadaniowe 82% [23] i 95% [28]; sok jabłkowy − 60% [10]. najmniejszą wartość RbV odnotowano po podaniu MDFP z ryżem − 15-25% [28], podczas gdy po podaniu klasycznego pirofosforanu żelaza wynosiła ona 8,3-12,8% [29].
cel PrAcyCelem pracy jest ocena tolerowania przez niemow-
lęta i małe dzieci preparatu Actiferol Fe® zastosowanego
w profilaktyce i leczeniu niedoboru żelaza.
mATEriAłY i mEToDYDo badania, prowadzonego w latach 2012-2013
w trzech poradniach hematologicznych w Warszawie, zakwalifikowano 80 dzieci (64 chłopców i 16 dziewczy-nek) w wieku od 1. miesiąca do 6. roku życia (średnia wieku 14 miesięcy).
Kryteria włączenia:1. rozpoznanie niedoboru żelaza lub niedokrwisto-
ści z niedoboru żelaza (definiowanej jako zmniejszenie stężenia hemoglobiny poniżej 11 mg/dl, zmniejszenie stężenia żelaza i/lub ferrytyny poniżej normy dla danego wieku)
2. bezwzględna konieczność profilaktycznego zasto-sowania preparatów żelaza zgodnie z przyjętymi zale-ceniami (dzieci matek z niedokrwistością w przebiegu ciąży, urodzone przedwcześnie, urodzone o czasie z małą urodzeniową masą ciała, z ciąż mnogich, ze zmniejszo-nym stężeniem hemoglobiny w okresie noworodkowym) [14].
Do leczenia dzieci włączono preparat żelaza Actiferol Fe® w dawce 4-6 mg/kg mc./24 h w dwóch dawkach podzielonych, stosowany przez co najmniej 6 tygodni. W czasie wizyt kontrolnych w poradni rodzice (naj-częściej matka) wypełniali ankiety zawierające pytania, dotyczące tolerowania preparatu przez dziecko, sposobu podania (rodzaj pokarmu, w którym podawano preparat), wygody jego stosowania oraz występowania ewentual-nych działań niepożądanych (ból brzucha, nudności, wymioty, biegunka, zaparcie, bolesność przy oddawaniu stolca, ciemne zabarwienie zębów). Rodzice samodzielnie wypełniali ankietę, aby uniknąć ewentualnego wpły-wu badacza na odpowiedzi. badanie przeprowadzono w zakresie rutynowej praktyki klinicznej, zgodnie z mię-dzynarodowymi wytycznymi i zasadami określonymi w Deklaracji Helsińskiej, w związku z czym nie było konieczne uzyskanie pozwolenia od komisji etycznej na przeprowadzenie badania.
WYniKiActiferol Fe® został oceniony jako preparat o bardzo
dobrej lub dobrej tolerancji przez 87,5% (70/80) badanych; odpowiednio 46,3% (37/80) i 41,2% (33/80). najczęściej był on podawany w postaci płynnej po rozpuszczeniu w wodzie − u 31,3% (25/80) pacjentów, w soku poma-rańczowym – 18,8% (15/80) oraz w mleku modyfiko-wanym – 17,5% (14/80). Sposób podawania preparatu określono w 84% (67/80) odpowiedzi jako wygodny lub bardzo wygodny w stosowaniu (ryc. 1).
Na podstawie subiektywnej oceny rodziców odno-towano podczas leczenia zmianę konsystencji stolca na twardszy, bóle brzucha i zaparcie; działania te występo-wały odpowiednio u 20% (16/80), 11,25% (9/80) i 10% (8/80) pacjentów (ryc. 2). Objawy te oceniane były w sposób niemedyczny, a ich występowanie nie wiązało się z przerwaniem leczenia ani gorszym tolerowaniem preparatu. Sporadycznie występowały takie działania niepożądane, jak biegunka, bolesność przy oddawaniu stolca lub ciemne zabarwienie zębów, chociaż wiadomo, że ta postać żelaza nie daje zmian w zabarwieniu zębów. Ciemne zabarwienie stolca zgłaszano w przypadku 55% (44/80) pacjentów. U 40% (32/80) pacjentów odnoto-wano wystąpienie co najmniej jednego działania niepo-żądanego. Spośród włączonych do badania pacjentów tylko w jednym przypadku (1,25%) rodzice odstąpili od podawania preparatu Actiferol Fe®, zmieniając go na inny preparat, wygodniejszy do stosowania w podróży. Nie miało to związku z tolerowaniem preparatu przez dziecko.
DYSKUSJA Zapobieganie i leczenie niedokrwistości z niedoboru
żelaza jest istotnym problemem w codziennej praktyce pediatrycznej, szczególnie u dzieci młodszych. W raporcie WHO, dotyczącym niedokrwistości na świecie, częstość jej występowania w grupie dzieci przedszkolnych (do 5. roku życia) w Polsce oszacowano na 22,7%, co jest po-równywalne ze średnią europejską, wynoszącą 21,7% [5]. W skali światowej częstość występowania IDA u dzieci w wieku przedszkolnym jest znacznie większa - szacuje się ją na 47,4% [5].
niedobór żelaza może upośledzać prawidłowy roz-wój dziecka wskutek zaburzenia funkcji poznawczych i zdolności psychomotorycznych [5, 8, 9]. Zaburzenia te wiążą się z upośledzoną mielinizacją w ośrodkowym układzie nerwowym, a także z zaburzeniem metabolizmu neuronów i neuroprzekaźników, gdyż do jego prawidło-wego przebiegu niezbędne jest odpowiednie wysycenie organizmu żelazem [11, 14]. Z tego powodu niezwykle istotne jest zarówno zapobieganie, jak i wyrównywanie niedoborów żelaza poprzez prawidłowe podawanie jego odpowiednich preparatów.
Dostępnych jest wiele preparatów żelaza, różniących się stopniem tolerowania przez pacjentów i częstością występowania działań niepożądanych. Preparat Actiferol Fe®, zawierający zmikronizowaną postać pirofosforanu żelaza, jest dobrze rozpuszczalny w płynach, dzięki czemu charakteryzuje się dobrą rozpuszczalnością i biodostęp-

222 Teresa Jackowska i wsp.
ryc. 2. Częstość zgłaszanych działań niepożądanych (%).Fig. 2. Frequency of side effects (%).
ryc. 1. przedstawienie wyników badania dotyczących oceny stopnia tolerancji, wygody stosowania oraz sposobu poda-wania preparatu Actiferol Fe®.
Fig. 1. Results of Actiferol Fe® tolerance, convenience of use, and way of administration.
1. zaparcia, 2. zmiana konsystencji stolca na twardszą, 3. Bolesność przy oddawaniu stolca, 4. Biegunka, 5. nudności, 6. Wymioty, 7. Ból brzucha, 8. Ciemne zabarwienie zębów.1. Constipation, 2. Hardened of the stool, 3. Pain during defecation, 4. Diarrhea, 5. Nausea, 6. Vomiting, 7. Stomach ache, 8. Dark tint of teeth.
Lek przyjmowany jest chętnieProduct is taken willinglynie
no13%
Wygoda stosowaniaConvenience of usage
niewygodnyinconvenient
3%
Sposób podawaniaWay of administration
dodat. dopożywienia
food additive3%
innyother2%
Stopień tolerancjiTolerance
z mlekiem matkiwith breast milk
15%
z mlekiemmodyf.
with infantformula
21%
z sokiempomar.
with orange j22%
średnimoderate
9%
b. słabyv. poor
1%

223Ocena tolerowania preparatu żelaza Actiferol Fe® u dzieci z niedokrwistością z niedoboru żelaza
nością oraz neutralnym smakiem. Jest skuteczny zarówno w zapobieganiu, jak i leczeniu IDA [10, 23, 30, 31], także u dzieci. W randomizowanym badaniu z podwójnie ślepą próbą z udziałem 458 dzieci w wieku szkolnym zastosowanie MDFP jako dodatku do soli kuchennej zmniejszyło odsetek przypadków niedokrwistości z 16,8% do 7,7% [31].
Przeprowadzone przez nas badanie wykazało, że MDFP jest dobrze tolerowany i wygodny w stosowa-niu. W ocenie rodziców, podczas stosowania preparatu występowały nieliczne działania niepożądane, jednak ich nasilenie było niewielkie i nie powodowało konieczności przerwania leczenia ani zmiany preparatu żelaza. Jest to zgodne z wynikami badań innych autorów, którzy wykazali, że preparaty żelaza (III) są lepiej tolerowane niż zawierające żelazo (II), a ich biodostępność jest po-równywalna [32-34].
WnioSKiPreparat Actiferol Fe® jest dobrze tolerowany, o czym
świadczy występowanie jedynie nieznacznych działań niepożądanych związanych z przewodem pokarmowym. Mimo stosunkowo dużego (40%) odsetka pacjentów, u których wystąpił choć jeden rodzaj działań niepożą-danych, nie zachodziła konieczność jego odstawienia, a objawy niepożądane miały mierne nasilenie. W opinii rodziców preparat jest wygodny w podawaniu.
Zarówno fakt dobrego tolerowania przez dzieci, zwią-zany z neutralnym smakiem preparatu, jak i wygoda jego podawania − dzięki możliwości rozpuszczenia preparatu w napoju lub jedzeniu, bez zmiany smaku pokarmu − są istotne z punktu widzenia stosowania preparatu u nie-mowląt i małych dzieci.
piśmiEnniCTWo
1. Zaim M, Piselli l, Fioravanti P, Kanony-Truc C. efficacy and tolerability of a prolonged release ferrous sulphate formulation in iron deficiency anaemia: a non-inferiority controlled trial. eur J nutr. 2012;51(2):221-229.
2. Jarosz M (red.). normy Żywienia dla Populacji Polskiej – nowelizacja. Instytut Żywności i Żywienia, Warszawa, 2012.
3. Gorczyca D, Prescha A, Szeremeta K, Jankowski A. Iron status and dietary iron intake of vegetarian children from Poland. Ann nutr Metab. 2013;62:291-297.
4. De Vizia b, Poggi V, Conenna R, et al. Iron absorption and iron deficiency In infants and children with gastrointestinal diseases. J Pediatr Gastroenterol nutr. 1992;14(1):21-26.
5. De benoist b, Mclean e, egli I, Cogswell M (eds). Worldwide prevalence of anemia 1993-2005: WHO Global Database. Geneva: World Health Organization, 2008.
6. Panczenko-Kresowska b, Ziemlański Ś. Składniki mineralne – ich znaczenie w żywieniu człowieka. W: Ziemlański Ś (red). normy Żywienia Człowieka. Fizjologiczne Podstawy. Wydawnictwo lekarskie PZWl, Warszawa, 2001;pp. 379-398.
7. lozoff b, De Andraca I, Castillo M, et al. behavioral and developmental effects of preventing iron-deficiency anemia in healthy full-term infants. Pediatrics. 2003;112:846-854.
8. beard Jl. Recent evidence from human and animal studies regarding iron status and infant development. J nutr. 2007;137:524S-530S.
9. Congdon el, Westerlund A, Algarin CR, et al. Iron deficiency in infancy is associated with altered neural correlates of recognition memory at 10 years. J Pediatr. 2012;160:1027-1033.
10. Roe MA, Collings R, Hoogewerff J, Fairweather-Tait SJ. Relative bioavailability of micronized, dispersible ferric pyrophosphate added to an apple juice drink. eur J nutr. 2009;48(2):115-119.
11. Schümann K, ettle T, Szegner b, elsenhans b, Solomons nW. On risks and benefits of iron supplementation recommendations for iron intake revisited. J Trace elem Med biol. 2007;21(3):147-168.
12. eden An. Iron deficiency and impaired cognition in toddlers: an underestimated and undertreated problem. Paediatr Drugs. 2005;7(6):347-52.
13. long H, Yi JM, Hu Pl, et al. benefits of iron supplementation for low birth weight infants: a systematic review. bMC Pediatr. 2012;12:99.
14. baker RD, Greer FR. Committee on nutrition American Academy of Pediatrics. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics. 2010;126(5):1040-1050.
15. lyseng-Williamson KA, Keating GM. Ferric carboxymaltose: a review of its use in iron-deficiency anaemia. Drugs. 2009;69(6):739-756.
16. borgna-Pignatti C, Marsella M. Iron deficiency in infancy and childhood. Pediatr Ann. 2008;37(5):329-337.
17. Orlicz-Szczęsna G, Żelazowska-Posiej J, Kucharska K. niedokrwistość z niedoboru żelaza. Curr Probl Psychiatry. 2011;12(4):590-594.
18. Pleskaczyńska A, Dobrzańska A. Profilaktyka niedoboru żelaza u dzieci – standard postępowania. Standardy Medyczne/Pediatria. 2011;8:100-106.
19. Martindale. The Complete Drug Reference (38th ed.). brayfield A (red.). Pharmaceutical Press, london 2014.
20. Anderson GJ, Frazer DM, Mickie AT, et al. Mechanisms of haem and non-haem iron absorption: lessons from inherited disorders of iron metabolism. biometals. 2005;18:339-348.
21. barrand MA, Hider RC, Callingham bA. The importance of reductive mechanisms for intestinal uptake of iron from iron ferric maltol and ferric nitriloacetic acid (nTA). J Pharm Pharmacol. 1990;42:279-282.
22. Aggett PJ, Agostini C, Axelsson I, et al. Iron metabolism and requirements in early childhood: Do we know enough?: A commentary by the eSPGHAn Committee on nutrition. J Ped Gastroenterol. 2002;34:337-345.
23. Fidler MC, Walczyk T, Davidsson l, et al. A micronised, dispersible ferric pyrophosphate with high relative bioavailability in man. br J nutr. 2004;91(1):107-112.
24. Sakaguchi n, Rao TP, nakata K, et al. Iron absorption and bioavailability in rats of micronized dispersible ferric pyrophosphate. Int J Vitam nutr Res. 2004;74(1):3-9.
25. Hurrell RF. How to ensure adequate iron absorption from iron-fortified food. nutr Rev. 2002;132:60:S7-S15.
26. Wegmuller R, Zimmermann Mb, Moretti D, et al. Particle size reduction and encapsulation affect the bioavailability of ferric pyrophosphate in rats. J nutr. 2004;134:3301-3304.

224
27. Haro-Vicente JF, Perez-Conesa D, Rincon F, et al. Does ascorbic acid supplementation affect iron bioavailability in rats fed micronized dispersible ferric pyrophosphate fortified fruit juice? eur J nutr. 2008;47:470-478.
28. Moretti D, Zimmermann Mb, Wegmuller R, et al. Iron status and food matrix strongly affect the relative bioavailability of ferric pyrophosphate in humans. Am J Clin nutr. 2006;83:632-638.
29. Zimmerman Mb, biebinger R, egli I, et al. Iron deficiency up-regulates iron absorption from ferrous sulphate but not ferric pyrophosphate and consequently food fortification with ferrous sulphate has relatively greater efficacy in iron-deficient individuals. br J nutr. 2011;105:1245-1250.
30. nambu H, nakata K, Sakaguchi n, Yamazaki Y (2000) Inventors; Taiyo Kagaku ltd, assignee. Mineral composition. uS patent 6074675. June 13
31. Andersson M, Thankachan P, Muthayya S, et al. Dual fortification of salt with iodine and iron: a randomized, double-blind, controlled trial of micronized ferric pyrophosphate and encapsulated ferrous fumarate in southern India. Am J Clin nutr. 2008;88(5):1378-1387.
32. naude S, Clijsen S, naulaers H, et al. Iron supplementation in preterm infants: A study comparing the effect and tolerance
of a Fe2+ and a nonionic Fe III compound. J Clin Pharmacol. 2000;40:1447-1451.
33. Maxton DG, Thompson RP, Hider RC. Absorption of iron from ferric hydroxypyranone complexes. br J nutr. 1994;71:203-207.
34. ehrenkranz RA: Iron requirements of preterm infants. nutrition. 1994;10:77-78.
35. Sas G, nemeszansky e, brauer H, Scheffer K. On the therapeutic effect of trivalent and divalent iron in iron deficiency anaemia. Arzneimittel-Forsch 1984;34:1575-1579.
Wkład Autorów/Authors’ contributionsWedług kolejności/According to the order of the Authorship
Konflikt interesu/Conflicts of interestAutorzy pracy nie zgłaszają konfliktu interesów.The Authors declare no conflict of interest.
Nadesłano/Received: 21.01.2015 r.Zaakceptowano/Accepted: 24.03.2015 r.
Published online/Dostępne online
Adres do korespondencji:Teresa Jackowska Klinika Pediatrii,
Centrum Medyczne Kształcenia Podyplomowego ul. Marymoncka 99/103, 01-813 Warszawa
tel. (+22) 864-11-67e-mail: [email protected]
Teresa Jackowska i wsp.

225Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
Teresa Jackowska1,2, Katarzyna Pawlik1,2
profilaktyka zakażeŃ Szpitalnych w oddziale pediatrycznym – doświadczenia właSne*
prevention of noSocomial infectionS in the pediatric ward – own experienceS
1Klinika Pediatrii, Centrum Medyczne Kształcenia Podyplomowego, Warszawa, Polska2Kliniczny Oddział Pediatryczny Szpitala bielańskiego, Warszawa, Polska
StreszczenieWprowadzenie: Pacjenci oddziałów pediatrycznych są szczególnie narażeni na zakażenia szpitalne. Dlatego też powinny być wdrażane i systematycznie monitorowane zasady profilaktyki zakażeń.Cel pracy: 1) określenie częstości występowania, etiologii i postaci klinicznych zakażeń szpitalnych u pacjentów hospitalizowanych; 2) ocena skuteczności procedur zapobiegania szpitalnym zakażeniom rotawirusowym i odcewnikowym zakażeniom krwi; 3) analiza zapadalności na grypę wśród personelu w dwóch kolejnych sezonach epidemicznych grypy A/H1N1v (2009/2010 i 2010/2011); 4) realizacja szczepień ochronnych u personelu medycznego. Materiał i metody: Badaniem objęto 4432 hospitalizowanych dzieci od października 2007 do grudnia 2009 roku i 57 osób personelu medycznego (lekarze, pielęgniarki, salowe). Poddano ocenie skuteczność procedur profilaktyki zakażeń szpitalnych, oraz zachorowalność i wyszczepialność przeciwko grypie wśród personelu zgodnie z Ustawą o zapobieganiu i zwalczaniu zakażeń oraz chorób zakaźnych u ludzi oraz kryteriami opracowanymi przez Centrum ds. Zapobiegania i Kontroli Chorób.Wyniki: Zakażenia szpitalne rozpoznano u 2,2% hospitalizowanych dzieci, w tym 96% stanowiły ostre nieżyty żołądkowo-jelitowe, 3% zakażenia krwi, które były związane z obwodowymi cewnikami naczyniowymi. W 1% występowały zakażenia dróg oddechowych. Szpitalne nieżyty żołądkowo-jelitowe były spowodowane przez rotawirusy (78%), norowirusy (13%) i adenowirusy (0,9%). U 1,1% nie ustalono etiologii. Uzyskano znamienną statystycznie redukcję częstości występowania szpitalnych zakażeń rotawirusowych poprzez aktywne działania profilaktyczne (z 7,1 do 1,5%). Całkowicie wyeliminowano występowanie odcewnikowych zakażeń krwi. Grypę i zachorowania grypopodobne stwierdzono u 7% personelu medycznego w sezonie 2009/2010 i 5% w sezonie 2010/2011. Przeciwko grypie zaszczepiło się 42% personelu (92% lekarzy, 7% pielęgniarek, 0% salowych). Wnioski: Najczęstszą przyczyną zakażeń szpitalnych na oddziale ogólnopediatrycznym są rotawirusy. Zakażeniom rotawirusowym i odcewnikowym zakażeniom krwi można skutecznie zapobiegać poprzez systematyczne, aktywne działania profilaktyczne. Szczepienia personelu medycznego przeciwko grypie nadal wymagają wdrożenia działań promujących i edukacyjnych.
Słowa kluczowe: zakażenia szpitalne, nieżyty żołądkowo-jelitowe, odcewnikowe zakażenia krwi, grypa
AbstractIntroduction: Patients pediatric wards are particularly at risk of nosocomial infections. Therefore, the newest principles of prevention of infections should be implemented and monitored.Aim: 1) to determine the prevalence, etiology and clinical manifestations of nosocomial infections in hospitalized patients; 2) to evaluate the effectiveness of procedures that aim at preventing hospital rotavirus infections and catheter-related bloodstream infections; 3) to analyse the incidence of flu among staff in two consecutive seasons of the epidemic influenza H1N1 (2009/2010 and 2010/2011); 4) to promote vaccinations of the medical staff.
*Praca wykonana w ramach grantu CMKP 501-1-20-19-14.

226 Teresa Jackowska, Katarzyna Pawlik
Material and methods: The study involved 4432 children hospitalized from October 2007 to December 2009 and 57 medical staff (doctors, nurses, orderlies). The effectiveness was assessed of prevention procedures for nosocomial infections and morbidity, and of vaccination against influenza among the staff, as defined by the Act on the prevention and suppression of infection and infectious diseases human and the criteria developed by the Centers for Disease Control and Prevention.Results: Nosocomial infections were diagnosed in 2.2% of hospitalized children, where 96% were of acute gastroenteritis; 3% were bloodstream infections associated with peripheral vascular catheter. The 1% had respiratory infections (influenza). Hospital gastrointestinal infections were caused by the rotavirus (78%), norovirus (13%) and adenovirus (0.9%). In 1.1% of cases the etiology had not been determined. As a result of implementing prophylactic activities, a statistically significant reduction of the incidence of nosocomial infections by the rotavirus was achieved (from 7.1 to 1.5%). The occurrence catheter-related bloodstream infections was entirely eliminated. Influenza and influenza-like infections were reported in 7% of the medical staff in the season of 2009/2010 and 5% in the season of 2010/2011. 42% of the medical staff was immunized against the influenza (92% of doctors, 7% nurses, 0% orderlies).Conclusions: The most common cause of nosocomial infections in the pediatric ward are rotaviruses. Rotavirus infections and catheter-related bloodstream infections are possible to be effectively prevented through regular, proactive preventive measures. Vaccinations of the medical staff against influenza medical staff against influenza still require implementing measures of a promotional and educational character.
Key words: nosocomial infections, acute gastroenterititis, catheter-related bloodstream infections, influenza
DEV pErioD mED. 2015;XiX,2:225-234
WSTępWedług raportu europejskiego Centrum ds. Zapobiegania
i Kontroli Chorób (European Centre for Disease Prevention and Control; eCDC) z 2013 roku rocznie w europie na zakażenie szpitalne zapada ponad 4 miliony pacjentów, co stanowi główny problem zdrowia publicznego. Średnia częstość występowania zakażeń szpitalnych wśród pacjentów hospitalizowanych w europejskich szpitalach pracujących w trybie ostrodyżurowym wynosi 5,7% (95%CI: 4,5-7,4%) [1]. W wielu krajach programy profilaktyki zakażeń szpitalnych są priorytetowymi działaniami mającymi na celu poprawę jakości usług medycznych i zwiększenie bezpieczeństwa pacjentów [2, 3]. Analizy badań interwencyjnych wykazały, że około 20-30% zakażeniom można zapobiec [4, 5, 6, 7]. Do najczęstszych postaci zakażeń szpitalnych według badań punktowych eCDC (2011-2012) należą: zakażenia krwi (19,7%) i miejsca operowanego (19,6%), zakażenia dolnych dróg oddechowych (zapalenie płuc – 19,4%, inne zakażenia dolnych dróg oddechowych – 4,1%), układu moczowego (19%) oraz przewodu pokarmowego (7,7%) w tym najczęściej o etiologii Clostridium difficile (48%) [1].
Według Centrum ds. Zapobiegania i Kontroli Chorób (Centre for Disease Prevention and Control; CDC) zastosowanie kryteriów rozpoznania zakażenia szpitalnego, zwłaszcza u najmłodszych dzieci, często sprawia trudność pomimo uwzględnienia w 2008 roku w rekomendacjach objawów charakterystycznych dla dzieci poniżej 1. roku życia [8]. Jeszcze trudniejsze wydaje się rozpoznanie zakażeń wirusowych, które dominują w tej grupie wiekowej, bowiem nie ma powszechnie zaakceptowanych kryteriów rozpoznania zakażenia wirusowego. Wielu
autorów podkreśla konieczność wykonania badania w dniu przyjęcia dziecka aby móc później potwierdzić zakażenie szpitalne. Jednak zrealizowanie takiej procedury w rutynowym postępowaniu jest zbyt kosztowne [9].
Częstość występowania zakażeń szpitalnych na oddziałach pediatrycznych w krajach rozwijających się wynosi od 0,9 do 17,7%, a w szpitalach dziecięcych od 2,7 do 26,9% [10]. Zakażenia szpitalne u dzieci występują z częstością odwrotnie proporcjonalną do ich wieku. na oddziałach ogólnopediatrycznych dominują zakażenia wirusowe dróg oddechowych i przewodu pokarmowego. natomiast na oddziałach noworodkowych oraz intensywnej terapii zakażenia związane ze stosowanymi procedurami inwazyjnymi (kaniulacja naczyń krwionośnych, wentylacja mechaniczna, cewnikowanie pęcherza moczowego) [12, 13]. Specyfika oddziałów/szpitali dziecięcych tzn. stała obecność rodzica/opiekuna podczas hospitalizacji, duża liczba osób odwiedzających, którzy często nie przestrzegają zasad higieny rąk, samodzielne przygotowywanie pokarmu na sali chorych, przynoszenie zabawek, których nie można dezynfekować, bardzo bliski kontakt z innymi dziećmi, hospitalizowanie na tej samej sali dzieci z zakażeniami o innej etiologii – to wszystko stanowi dodatkowe ryzyko transmisji zakażeń szpitalnych [9, 11].
cel PrAcy1. Określenie częstości występowania, etiologii i postaci
zakażeń szpitalnych u pacjentów hospitalizowanych. 2. Ocena skuteczności wdrożonych na podstawie
aktualnej sytuacji epidemiologicznej procedur zapobiegania szpitalnym zakażeniom rotawirusowym i odcewnikowym zakażeniom krwi.

227Profilaktyka zakażeń szpitalnych w oddziale pediatrycznym – doświadczenia własne
3. Ocena obowiązujących procedur profilaktyki zakażeń rozprzestrzeniających się drogą powietrzno-kropelkową oraz zapadalności na grypę,
4. Analiza wyszczepialności przeciwko grypie wśród personelu medycznego.
mATEriAł i mEToDYbadaniem objęto 4432 hospitalizowanych dzie-
ci w Klinicznym Oddziale Pediatrycznym Szpitala bielańskiego od października 2007 do grudnia 2009 roku i 57 osób personelu medycznego (lekarze, pie- i 57 osób personelu medycznego (lekarze, pie-lęgniarki, salowe). Oceniano częstość występowania zakażeń szpitalnych rozpoznawanych zgodnie z ich definicją, określoną ustawą o zapobieganiu oraz zwalczaniu zakażeń i chorób zakaźnych u ludzi [14] oraz zgodnie z kryteriami CDC [8]. Podstawowym kryterium rozpoznania zakażenia szpitalnego była ustawowa definicja [14], która określa zakażenie szpi-talne jako „zakażenie związane z udzielaniem świadczeń zdrowotnych w przypadku, gdy: nie pozostawało ono w okresie wylęgania w momencie udzielania świadczeń zdrowotnych, albo wystąpiło po udzieleniu świadczeń zdrowotnych, w okresie nie dłuższym niż najdłuższy okres jego wylęgania”.
Przeanalizowano zapadalność na zakażenia szpi-talne wywołane rotawirusami, które rozpoznawano na podstawie kryteriów klinicznych i laboratoryjnych CDC [8], z uwzględnieniem średniego okresu wylęgania – 48 godz. Oceniono również skuteczność wdrożenia aktywnej strategii zapobiegania szpitalnym nieżytom żołądkowo-jelitowym oraz wpływ poprawy warunków sanitarnych oddziału po remoncie (z sal 4-5-łóżkowych na sale 1-3-łóżkowe z węzłem sanitarnym) na ilość szpitalnych zakażeń rotawirusowych. Aktywna strategia polegała na: opracowaniu i wdrożeniu szczegółowego planu higieny (opisanego poniżej), systematycznego szkolenia personelu medycznego z zakresu higieny rąk i procedur profilaktyki zakażeń rozprzestrzenia-jących się drogą kontaktową, wprowadzeniu ulotek informacyjnych dla rodziców/opiekunów wszystkich hospitalizowanych pacjentów, z którymi zapoznawano w momencie przyjmowania do oddziału.
W przypadku stwierdzenia odcewnikowego zaka-żenia krwi prowadzono dochodzenie epidemiczne, szczegółową kontrolę oddziału z uwzględnieniem oceny procedur postępowania aseptycznego oraz szkolenia personelu z zakresu procedur zapobiegania zakażeniom krwi związanych z kaniulacją naczyń.
W okresie pandemicznym grypy A/H1n1v (2009/2010) oceniano istniejące procedury zapobiegania rozprzestrzeniania się zakażeń w oparciu o tymczaso-we wytyczne CDC, które pojawiały się sukcesywnie w czasie trwania pandemii (http://www.cdc.gov/h1n1flu/guidance/). Określono częstość zachorowań na grypę i zakażeń grypopodobnych u personelu medyczne-go oraz wyszczepienie przeciwko grypie personelu medycznego. Grypę rozpoznawano na podstawie objawów klinicznych w oparciu o rekomendacje CDC, z uwzględnieniem średniego czasu wylęgania od 48 godz. do 7 dni.
WYniKiZakażenia szpitalne rozpoznano u 2,2% (99/4432)
hospitalizowanych dzieci. najczęstszą przyczyną były ostre nieżyty żołądkowo-jelitowe (nŻJ), które rozpozna-no u 96% (95/99) pacjentów. najczęściej występowały zakażenia rotawirusowe, które potwierdzono u 77,9% (74/95) pacjentów, co dało zapadalność 16,7/1000. następnie norowirusy − 12,6% (12/95) i adenowirusy − 4,2% (4/95), a u pięciorga – 5,3% (5/95) nie ustalono etiologii zakażenia (ryc. 1). najwyższa zapadalność na szpitalne zakażenia rotawirusowe była od paździer-nika do grudnia 2007 roku (71/1000 hospitalizacji), co skłoniło Zespół ds. Kontroli Zakażeń Szpitalnych (ZKZS) do wdrożenia odpowiednich działań napraw-czych. W kolejnych roku stwierdzono znamienny spa-dek szpitalnych zakażeń rotawirusowych z 7,1% do 1,5% (p<0,05), pomimo utrzymującego się wysokiego odsetka zewnątrzszpitalnych zakażeń rotawirusowych (od października do grudnia 2007 roku 8,1%, a w 2008 roku 6,4%).
W 2009 roku pomimo poprawy warunków lokalo-wych oddziału (mniejsze sale, łazienki w salach cho-rych) nie zaobserwowano znamiennego zmniejszenia liczby szpitalnych zakażeń rotawirusowych (n=15; 0,7%) w porównaniu z rokiem poprzednim (p>0,05) (tab. I, ryc. 2.)
W 2008 roku stwierdzono trzy przypadki odcew-nikowych zakażeń krwi, związanych z obwodowymi wkłuciami naczyniowymi. We wszystkich przypadkach czynnikiem etiologicznym zakażenia był Staphylococcus aureus metycylino-wrażliwy (MSSA) o tym samym profilu lekowrażliwości. Do rozwoju zakażenia doszło u trójki dzieci poniżej 1 roku życia, które były hospitali-zowane z powodu ostrego nieżytu żołądkowo-jelitowego. Objawy zakażenia pojawiły się w 4-6 dobie hospitalizacji. Rozpoznano ognisko epidemiczne, które wywołane było zakażeniem gronkowcowym (Staphylococcus aureus mety-cylino-wrażliwy) wkłucia obwodowego, u 9-miesięcznego chłopca z atopowym zapaleniem skóry.
W analizowanym okresie stwierdzono jedno szpitalne zakażenie górnych dróg oddechowych wywołane wiru-sem grypy A/H1n1v u 37/12-letniego chłopca w 8 dobie hospitalizacji (sezon pandemiczny grypy 2009/2010).
W sezonie epidemicznym 2009/2010 zachorowało na grypę lub infekcje grypopodobne troje (3/24) lekarzy (12,5%) i jedna (1/27) pielęgniarka (3,7%). ZKZS stwierdził gorsze przestrzeganie przez lekarzy procedur ochrony dróg oddechowych (maseczki ochronne) niż u pielęgniarek. W kolejnym sezonie epidemicznym (2010/2011) po raz pierwszy wprowadzono szczepienia przeciwko grypie dla personelu szpitala. Przed sezonem zachorowań na grypę prowadzono szkolenia pracowników szpitala na temat przestrzegania procedur profilaktyk zakażeń wi-rusem grypy i roli szczepeń ochronnych w profilaktyce zakażeń. W oddziale pediatrycznym zaszczepiło się 91,7% (22/24) lekarzy, dwie (2/27) pielęgniarki (7,4%) i żadna salowa. na grypę lub infekcje grypopodobne zachorował jeden (1/24) lekarz (4,2%), dwie pielęgniarki (7,4%), nikt z personelu salowego. Żadna z tych osób nie była szczepiona przeciwko grypie.

228 Teresa Jackowska, Katarzyna Pawlik
ryc. 1. rozkład przyczyn zakażeń szpitalnych (n=99).Fig. 1. Distribution of causes of hospital-acquired infections.
Tabela i. zakażenia rotawirusowe zewnątrzszpitalne i szpitalne u dzieci hospitalizowanych.Table I. Rotavirus out-of-hospital and nosocomial infections in children hospitalized.
1różnica istotna statystycznie pomiędzy okresem i/ii (p<0,05)/statistically significant difference between the time I/II (p<0.05)2różnica istotna statystycznie pomiędzy okresem i/iii (p<0,05)/statistically significant difference between the time I / III (p <0.05)3brak różnicy istotnej statystycznie pomiędzy okresem ii/iii (p>0,05)/no statistically significant difference between the period II / III (p> 0.05)
okresPeriod
liczba hospitalizacjiHospitalization
(N)
zewnątrzszpitalne zakażenia rotawirusowe
Out-of-hospital rotavirus infection
wewnątrzszpitalne zakażenia rotawirusowe
Nosocomial rotavirus infection
(n) (%) (n) (%)
I X-XII 2007 481 39 8,1 34 7,11,2
II 2008 1647 106 6,4 25 1,51, 3
III 2009 2304 36 1,6 15 0,72,3
razeMTOTAL 4432 181 4,1 74 1,7

229Profilaktyka zakażeń szpitalnych w oddziale pediatrycznym – doświadczenia własne
ryc. 2. zakażenia rotawirusowe zewnątrzszpitalne (CA-rVi) i wewnątrzszpitalne (HA-rVi) u dzieci hospitalizowanych.Fig. 2. Rotavirus out-of-hospital (CA-RVI) and nosocomial (HA-RVI) infections in children hospitalized.
ryc. 3. Ulotka informacyjna dla rodziców/opiekunów.Fig. 3. Information leaflet for parents/carers.

230 Teresa Jackowska, Katarzyna Pawlik
DYSKUSJAustawa o zapobieganiu oraz zwalczaniu zakażeń i chorób
zakaźnych u ludzi nakazuje zakładom opieki zdrowotnej zapobieganie zakażeniom szpitalnym [14].
Do najważniejszych zadań w tym zakresie należą: 1. ocena ryzyka wystąpienia zakażenia szpitalnego, 2. monitorowanie czynników alarmowych i zaka-
żeń związanych z udzielaniem świadczeń zdrowotnych w zakresie ich wykonywania,
3. opracowanie, wdrożenie i nadzór nad procedurami zapobiegającymi zakażeniom i chorobom zakaźnym związanym z udzielaniem świadczeń zdrowotnych,
4. stosowanie środków ochrony indywidualnej i zbio-rowej w celu zapobieżenia przeniesienia zakażenia na inne osoby,
5. wykonywanie badań laboratoryjnych oraz analiza lokalnej sytuacji epidemiologicznej w celu optymalizacji profilaktyki i terapii antybiotykowej,
6. prowadzenie kontroli wewnętrznej w zakresie re-alizacji podjętych działań [14].
W celu realizacji powyższych zadań powoływany jest Zespół i Komitet ds. Kontroli Zakażeń Szpitalnych, który aktywnie monitoruje i rejestruje zakażenia, we współpracy z personelem oddziałów. Zespół wprowa-dza procedury profilaktyki zakażeń i kontroluje ich przestrzeganie.
W Szpitalu bielańskim profilaktyka zakażeń szpi-talnych od 2006 roku jest procesem zidentyfikowanym w ramach funkcjonującego zgodnie z normą ISO 9001 Zintegrowanego Systemu Zarządzania. Dzięki temu proces profilaktyki i realizacja jego celów są usystematyzowane i doskonalone od wielu lat, a ich wyniki podlegają co roku audytowi. Systemowe podejście do profilaktyki zakażeń wymusiło opracowanie procedury zarządzania ryzykiem zakażeń szpitalnych jeszcze przed wejściem w życie ustawy, która taki obowiązek narzucała (14). Program profilaktyki zakażeń szpitalnych opracowa-no w oparciu o wytyczne Międzynarodowej Federacji Kontroli Zakażeń (International Federation of Infection Control – IFIC) i CDC [8, 15]. Sukces profilaktyki za-każeń szpitalnych zależy od ścisłej współpracy ZKZS z personelem medycznym. efektem takiej współpracy są wyniki uzyskane w Klinicznym Oddziale Pediatrycznym Szpitala bielańskiego, które dowodzą, że można skutecznie zapobiegać rozprzestrzenianiu się zakażeń rotawiruso-wych i odcewnikowych zakażeń krwi.
Doniesień na temat kompleksowych badań z zakresu zakażeń szpitalnych na oddziałach pediatrycznych jest niewiele. Przeprowadzona przez Allegranzi i wsp. [10] metaanaliza wyników badań z zakresu zakażeń szpitalnych na oddziałach pediatrycznych w latach 1995-2008 w więk-szości dotyczyła pediatrycznych oddziałów intensywnej terapii. Wykazano, że częstość zakażeń szpitalnych wynosi 0,9-17,7%. W naszym oddziale ogólnopediatrycznym było to 2,2% zakażeń i dominowały zakażenia przewodu pokarmowego (96%). Rzadziej występowały odcewnikowe zakażenia krwi, związane z cewnikami obwodowymi (3%) oraz zakażenia dróg oddechowych (1%).
Szpitalne zakażenia przewodu pokarmowego wy-wołane przez rotawirusy są bardzo rozpowszechnione.
W krajach europejskich ich częstość wynosi od 0,3% (Anglia) do 27,7% (Włochy) [16]. Źródłem zakażeń szpitalnych są pacjenci przyjmowani do szpitala z zaka-żeniem o tej samej etiologii, dlatego ważne jest bardzo wczesne wykrywanie zakażenia i izolacja pacjentów [17]. badania Gaggero i wsp. [18] wykazały, że 81% przypadków zakażeń szpitalnych było wywołanych tym samym typem wirusa jaki wykryto w obrębie sali, a 92% przypadków w obrębie oddziału. nasze badania również wykazały, że rotawirusy są najczęstszym czynnikiem etiologicznym szpitalnych zakażeń przewodu pokarmo-wego. W 77,9% były przyczyną wszystkich szpitalnych nieżytów żołądkowo-jelitowych. Trudność w ograniczaniu rozprzestrzeniania się zakażeń rotawirusowych związana jest z długim okresem wydalania zarazka z organizmu, średnio 10-12 dni od zachorowania, zdolnością przeżycia wirusów w środowisku szpitalnym, małą dawką zakaźną i opornością na preparaty dezynfekcyjne. Wirus rota jest zdolny przetrwać na powierzchniach przez 7 miesięcy, w wodzie tydzień, a na rękach 4 godziny [14]. badania Gallimore i wsp. [19, 20] wykazały obecność wirusów rota na bateriach w toalecie personelu oddziału i rodziców, telefonie dla pacjentów i personelu, kuchence mikro-falowej, klamkach do pokoju i toalet rodziców, do sal chorych, pompie infuzyjnej, konsoli do gier, włączniku światła w sali chorych. W związku z wysoką częstością występowania zakażeń rotawirusowych od końca 2007 roku zostały wdrożone aktywne działania profilaktyczne, polegające przede wszystkim na higienie rąk zarówno personelu, pacjentów i ich opiekunów, izolacji kon-taktowej i dekontaminacji środowiska. Po wdrożeniu działań profilaktycznych uzyskano znamienny spadek częstości szpitalnych zakażeń rotawirusowych z 7,1% do 1,5%, pomimo nadal wysokiego odsetka zakażeń zewnątrzszpitalnych (stosunek zakażeń wewnątrzsz-pitalnych do zewnątrzszpitalnych w latach 2007 i 2008 wynosił odpowiednio 0,87 i 0,24). Podobne wyniki uzy-skała Zerr i wsp. [21], przy czym interwencja polegała jedynie na szkoleniu z zakresu higieny rąk personelu i rodziców/opiekunów, oraz obserwacjach przestrzegania obowiązku dezynfekcji rąk. Rodzice/opiekunowie byli szkoleni w pierwszej dobie hospitalizacji dziecka przez personel pielęgniarski i równocześnie otrzymywali ulotki z instrukcją dezynfekcji rąk wraz z prośbą o zwracanie uwagi i przypominaniu personelowi medycznemu o ko-nieczności higieny rąk. Częstość zakażeń zmniejszyła się znamiennie z 5,9 do 2,2/1000 pacjentów, przy nadal utrzymującej się wysokiej chorobowości zewnątrzszpital-nej. Znaczenie dezynfekcji rąk w rozprzestrzenianiu się zakażeń rotawirusowych potwierdziło również badanie obserwacyjne Waisbourd-Zinman i wsp. [22].
Drugim pod względem częstości występowania czyn-nikiem etiologicznym nieżytów żołądkowo-jelitowych u dzieci są norowirusy (23, 24, 25). Odpowiadały one za 13% zakażeń szpitalnych przewodu pokarmowego. Zakażenia szpitalne o etiologii norowirusów wymagają ścisłej kontroli ze względu na łatwość rozprzestrzeniania się tych zakażeń, która związana jest z małą dawką zakaźną, możliwością rozprzestrzeniania się drogą kropelkową (szczególnie podczas wymiotów), ich stabilnością w śro-dowisku (wykrywano je na wyposażeniu medycznym,

231Profilaktyka zakażeń szpitalnych w oddziale pediatrycznym – doświadczenia własne
salach pacjenta, urządzeniach sanitarnych, klawiaturach komputera), oraz zdolnością wywoływania zakażeń bez-objawowych [26]. Po zakażeniu wirus wydalany jest przez dzieci średnio do 22 dni, a przez pacjentów dorosłych przez około 2 tygodnie od zachorowania [27].
Po remoncie oddziału (2008/2009) nie uzyskano dal-szego zmniejszenia szpitalnych zakażeń rotawirusowych (0,7%), tym samym nie potwierdzając doniesień innych autorów [10, 11] o znaczeniu warunków sanitarnych oddziału/szpitala pediatrycznego na ograniczanie roz-przestrzeniania się zakażeń szpitalnych rotawirusowych. Tłumaczymy to tym, że nadal pozostały 4 sale niemow-lęce 3-osobowe, bez łazienek dla rodziców/opiekunów, ze wspólną toaletą i kuchnią z lodówką, gdzie na tych salach hospitalizowane są małe dzieci z nieżytami żołąd-kowo-jelitowymi. Wprawdzie sale zostały wyposażone w śluzy fartuchowo-umywalkowe i w punkt do mycia i pielęgnacji niemowlęcia oraz zwiększono odległości pomiędzy łóżkami to uważamy, że jest to nadal niewy-starczające do całkowitego wyeliminowania szpitalnych zakażeń rota- jak i norowirusowych.
W 2008 roku rozpoznaliśmy jedno ognisko epi-demiczne zakażenia krwi o etiologii Staphylococcus aureus metycylino-wrażliwy (MSSA − methicillin-sen-sitive Staphylococcus aureus), związane z obwodowymi wkłuciami naczyniowymi (PVC – peripheral venous catheter). W okresie kolejnych trzech miesięcy zdia-gnozowano trzy zakażenia. Wprawdzie dochodzenie epidemiczne nie wykazało źródła epidemii, jednak przypuszczamy, że mógł nim być pierwszy pacjent, którego zakażenie było pochodzenia endogennego. Pozostałe dwa przypadki zakażeń były spowodowane gronkowcem złocistym o tym samym fenotypie opor-ności. nie wyhodowano drobnoustroju w wymazach pobranych ze środowiska oddziału. Ognisko epide-miczne zostało wygaszone. Działania profilaktyczne ZKZS we współpracy z personelem oddziału, głównie pielęgniarskim spowodowały brak występowania tego typu zakażeń w kolejnych latach.
Zingg i wsp. [28] na podstawie dwóch badań oszacowali częstość występowania zakażeń związanych z PVC od 0,2 do 0,7 przypadków na 1000 cewniko-dni, co równa się występowaniu 0,08% zakażeń związanych z cewnikami. lee i wsp. [29, 30] wskazali, że niezależnymi czynnikami ryzyka zakażenia miejsca wkłucia są: doświadczenie osoby zakładającej cewnik, używanie cewnika dłużej niż 96 godzin do czasu utrzymywania się jego drożno-ści, a dłużej niż 24 godziny, przy stosowanym wlewie ciągłym, założenie cewnika na kończynie dolnej, stoso-wanie pompy infuzyjnej, hospitalizacja na oddziałach neurologicznych i neurochirurgicznych. Pujol i wsp. [31] porównali zakażenia krwi związane z cewnikami centralnymi (n=73) z cewnikami obwodowymi (n=77), wykazując, że cewniki obwodowe były częściej zakładane na oddziałach ratunkowych, do zakażeń dochodziło wcześniej niż w przypadkach cewników centralnych, a gronkowiec złocisty był częstszym czynnikiem etiolo-gicznym zakażenia (33 v. 53%). Ponadto stwierdzili, że w przypadkach zakażeń krwi związanych z cewnikiem obwodowym o etiologii Staphylococcus aureus czę-ściej występowały powikłania pod postacią bakteriemii
i była wyższa śmiertelność. Według bruno i wsp. [32] w Irlandii bakteriemia o etiologii Staphylococcus aureus była związana z centralnymi liniami naczyniowymi w 26%, a z PVC w 4-6% i występowały w większości przypadków na oddziale ratunkowym, do 96. godzin od ich założenia.
Profilaktyka zakażeń związanych z PVC wymaga kompleksowego podejścia, obejmującego zarówno ocenę konieczności zakładania PVC, kontrolę przestrzega-nia procedur (postępowanie aseptyczne, pielęgnacja miejsca wkłucia, postępowania z pacjentem z dojściem naczyniowym), monitorowania powikłań, planowania i weryfikacji procedur pod kątem aktualnych wytycznych i wyników badań klinicznych. boyd i wsp. [33] ujęli działania profilaktyczne w proces: planuj, monitoruj, analizuj, działaj, co pozwoliło im skuteczne ograniczyć liczbę powikłań związanych z PVC. Podobnie bruno i wsp. [32] oraz Couzigou i wsp. [34] wykazali, że kompleksowa implementacja standardów postępowania z cewnikami obwodowymi znamiennie zmniejsza ryzyko wystąpienia powikłań.
Zakażenia szpitalne wirusowe dróg oddechowych dominują na oddziałach pediatrycznych. Około 20% szpitalnych zapaleń płuc spowodowanych jest etiologią wirusową (w 70% to adenowirusy, wirus grypy, para-grypy, RSV) [35].
W latach 2007-2009 nie stwierdziliśmy szpitalnych zakażeń o etiologii RSV, co może być spowodowane fak-tem, że dopiero w 2009 roku wdrożono do diagnostyki zakażeń RSV szybkie testy, a diagnostyka poza szpitalem ze względu na koszt była wykonywana rzadziej. należy jednak pamiętać, że RSV może także powodować zaka-żenia szpitalne, włącznie z ogniskami epidemicznymi, a w szczególności na oddziałach pediatrycznych i neo-natologicznych [36, 37].
Ogłoszona w 2009 roku pandemia grypy zweryfi-kowała przygotowanie zakładów opieki zdrowotnej do wzrostu zachorowań na grypę. na szczególną uwagę w tym okresie zasługuje fakt szybkiego rozwoju i upo-wszechnienia diagnostyki molekularnej grypy, oraz poprawy skuteczności wymiany informacji w zakresie epidemiologii zakażeń [38, 39].
W 2009 roku hospitowaliśmy sześcioro dzieci z po-twierdzonym zakażeniem wirusem grypy A/H1n1v. u jednego z nich rozpoznano zakażenie szpitalne, co daje częstość 16,7%. W innych ośrodkach odsetek zakażeń szpitalnych spowodowanych wirusem grypy wynosił od 4,4 do 10% hospitalizowanych dzieci z grypą [39, 40].
W czerwcu 2009 roku przez CDC zostały opubliko-wane wytyczne postępowania z pacjentami zakażonymi nowym typem wirusa grypy A/H1n1v w placówkach opieki zdrowotnej. Oprócz standardowej procedury pro-filaktyki rozprzestrzeniania się zakażeń z włączeniem drogi kontaktowej i kropelkowej zaleciło stosowanie przez personel medyczny ochrony oczu oraz dróg oddecho-wych przy użyciu maseczek o poziomie bezpieczeństwa n95 [41]. ZKZS zweryfikował procedury zapobiegania zakażeniom rozprzestrzeniającym się drogą kropelkową i powietrzno-pyłową. Opracował nowe instrukcje postę-powania w przypadku grypy i zaplanował postępowanie w przypadkach wzrostu liczby zachorowań w okresie

232 Teresa Jackowska, Katarzyna Pawlik
pandemii, wymagających hospitalizacji. ZKZS po prze-analizowaniu wyników badań skuteczności stosowania zwykłych maseczek i n95 zalecił stosowanie maseczek o zwiększonym poziomie bezpieczeństwa jedynie pod-czas wykonywania procedur o podwyższonym ryzyku powstania aerozolu (bronchoskopia, inhalacja, odsysanie wydzieliny z drzewa oskrzelowego).
W naszym oddziale napotkaliśmy problem stosowania maseczek ochronnych przez lekarzy. Pediatrzy to grupa zawodowa mająca kontakt z chorobami zakaźnymi na co dzień i dość trudno było nakłonić do zakładania mase-czek, co miało swoje odzwierciedlenie w odsetku lekarzy chorujących na grypę lub zachorowania grypopodobne (13%) w sezonie 2009/2010. u pielęgniarek, które lepiej zastosowały się do tych zaleceń, a nawet je nadużywały, stwierdzono zachorowanie u 4%. Zastanawiające jest, że nie odnotowano zachorowań wśród personelu salowego, może to wynikać z luźniejszego kontaktu z osobami chorymi. na trzykrotnie częstsze zachorowania wśród lekarzy mogły mieć wpływ też inne czynniki, których nie monitorowaliśmy, jak praca w pierwszych dniach infekcji, zagęszczenie gabinetów lekarski, większa liczba godzin pracy w miesiącu (dyżury). laVela i wsp. [42] wykazali, że 36% personelu oddziału choruje w sezonie grypy, a 86% z nich przychodzi do pracy z objawami choroby. Wyniki obserwacji Choi i wsp. [43] wskazały na możliwość zwiększonego ryzyka przeniesienia za-każenia zarówno z personelu na domowników jak i na pacjentów.
Ważnym elementem profilaktyki rozprzestrzeniania się wirusa grypy w środowisku szpitalnym są szczepienia ochronne. Wyszczepialność personelu w sezonie 2010/2011 w naszym oddziale wynosiła 42%. Szczepili się najczęściej lekarze (92%), przy bardzo niskim odsetku zaszczepionych pielęgniarek (7%) i całkowitym braku szczepień u salowych. Chen SC i wsp. [44] na oddziale pediatrycznym w Anglii, gdzie zaszczepiło się przeciw grypie 52% personelu, także potwierdzili największą wyszczepialność u lekarzy. Zwiększenie liczby szczepień u personelu medycznego powinno być prio-rytetowym działaniem dla zapobiegania grypie, ponieważ poziom zaszczepienia personelu medycznego jest istotnym, niezależnym predykatorem śmiertelności pacjentów (OR 0,8; 95% CI, 0,67-0,97) [36].
Profilaktyka zakażeń szpitalnych w ostatnim dziesię-cioleciu, w Polsce stała się wielospecjalistyczną dziedziną o ogromnym znaczeniu dla bezpieczeństwa pacjentów i personelu medycznego. Sprawnie działający proces profilaktyki zakażeń jest potwierdzeniem kompeten-cji zakładów opieki zdrowotnej i przynosi wymierne korzyści finansowe. Oddziały pediatryczne wymagają wdrożenia wszelkich możliwych metod profilaktyki, aby w myśl najważniejszej zasady w medycynie pacjentom pomagać, a nie szkodzić.
postępowanie zespołu ds. Kontroli zakażeń Szpitalnych Szpitala Bielańskiego
Celem zapobiegania zakażeniom jelitowym określono szczegółowy plan higieny z uwzględnieniem najbliższego otoczenia pacjenta i stref dotykowych. ustalono szcze-gółowy plan postępowania na oddziale, przy aktywnym wsparciu ordynatora i pielęgniarki oddziałowej.
1. Zalecono: a) przynajmniej raz dziennie dezynfekcję stolików
przyłóżkowych, ram łóżek, powierzchni dotyko-wych, koszy na odpady, zlewów, blatów, krzesełek w salach pacjentów i zabawek w świetlicy;
b) dwa razy dziennie dezynfekcji klamek i powierzch-ni drzwi w miejscach dotykowych, łokciowych pojemników na mydło i stosowanie środków de-zynfekcyjnych w miejscach dotykowych (włączniki światła, toalety, powierzchnie dotykowe w kuchni oddziałowej);
c) po każdym użyciu dezynfekowanie stetoskopu, inhalatora, wagi, przewijaka, wanienki do kąpieli dzieci;
d) mycie wszystkich podłóg oddziału preparatem my-jąco-dezynfekującym co najmniej raz dziennie, a na salach „biegunkowych” dwa razy dziennie,
2. Prowadzone są ustawiczne szkolenia personelu medycznego z zakresu higieny rąk i procedur profilaktyki zakażeń szpitalnych. Określono szczegółowo dla każdej z grup zawodowych sytuacje, w których konieczna jest dezynfekcja rąk.
3. Wprowadzono bezwzględną izolację/kohortację pacjentów zakażonych.
4. Stosowany jest stały nadzór nad przestrzeganiem procedur i zasad higieny rąk poprzez częste kontrole oddziału przez członków ZKZS w trakcie pracy pielęgniarek, lekarzy, salowych. Wyniki kontroli są omawiane na szkoleniach z zakresu profilaktyki zakażeń,
5. Przygotowana została ulotka informacyjna dla wszystkich rodziców/opiekunów pacjentów bez względu na przyczynę hospitalizacji. W ulotce zawarto informację o etiologii zakażeń jelitowych, w jakich sytuacjach można się zarazić, jak dbać o bezpieczeństwo dziecka podczas hospitalizacji oraz instrukcję dezynfekcji rąk, z określeniem sytuacji w jakich jest ona konieczna (przed karmieniem dziecka, przed i po myciu/kąpieli dziecka, po zmianie pieluszki, po skorzystaniu przy przyjęciu do oddziału (ryc. 3).
PoDsuMoWAnIe1. W KOP zakażenia szpitalne rozpoznano u 2,2% hospi-
talizowanych dzieci, w tym 96% stanowiły ostre nieżyty żołądkowo-jelitowe, 3% to zakażenia krwi związane z obwodowymi cewnikami naczyniowymi, a w 1% były to zakażenia dróg oddechowych (grypa).
2. Szpitalne nieżyty żołądkowo-jelitowe spowodowane były w 78% przez rotawirusy, w 13% przez norowirusy, a w 0,9% przez adenowirusy. u 1,1% dzieci nie ustalono etiologii.
3. Zakażenia odcewnikowe krwi dotyczyły obwodowych cewników naczyniowych, występowały sporadycznie i wywołane były metycylinowrażliwym gronkowcem złocistym.
4. Zakażenia szpitalne u personelu spowodowane były przez grypę i zachorowania grypopodobne. najczęściej chorowali lekarze, którzy rzadko używali maseczek ochronnych na drogi oddechowe.
5. Przeciwko grypie zaszczepiło się 92% lekarzy, 7% pie-lęgniarek, 0% salowych.

233Profilaktyka zakażeń szpitalnych w oddziale pediatrycznym – doświadczenia własne
WnioSKi1. Profilaktyka występowania zakażeń szpitalnych u per-
sonelu medycznego opiera się na trzech elementach: higiena rąk, prawidłowe stosowanie środków ochrony indywidualnej i szczepieniach ochronnych.
2. Profilaktyka zakażeń szpitalnych wymaga ustalenia szeregu procedur, które muszą być stale monitorowane pod względem skuteczności i uaktualniane.
piśmiEnniCTWo
1. http://www.ecdc.europa.eu/en/publications/Publications/annual-epidemiological-report-2013.pdf
2. Fukuda H, lee J, Imanaka Y. Variations In analytical methodology for estimating costs of hospital-acquired infections: a systematic review. J Hosp Infect. 2011;77:93-105.
3. Yokoe DS, Classen D. Improving patient safety trough infection control: A new healthcare imperative. Infect Control Hosp epidemiol. 2008;29 (Supl 1):3-11.
4. Harbarth S, Sax H, Gastmeier P. The preventable proportion of nosocomial infections: an overview of published reports. J Hosp Infect. 2003;54: 258-266.
5. Gastmeier P, Geffers C. Prevention of catheter-related bloodstream infections: analysis of studies published between 2002 and 2005. J Hosp Infect. 2006;64:3263-35.
6. Pronovost P, needham D, berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICu. n engl J Med. 2006;28;355(26):2725-2732.
7. Gastmeier P, Geffers C. Prevention of ventilator-associated pneumonia: analysis of studies published since 2004. J Hosp Infect. 2007;67:1-8.
8. Horan TC, Andrus M, Dudeck MA. CDC/nHSn surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309-332.
9. Posfay-barbe KM, Zerr DM, Pittet D. Infection control in paediatrics. lancet Infect Dis. 2008;8:19-31.
10. Allegranzi b, nejad Sb, Combescure C, Graafmans W, Attar H, Donaldson l, Pittet D. burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. lancet. 2011;377:228-241.
11. Richards MJ, edwards JR, Culver DH, Gaynes RP, nnISS. nosocomial infections in pediatric intensive care units in the unated States. Pediatrics. 1999;103:1-7.
12. elward AM, McGann KA. Steps to reduce nosocomial infection in children. Infect Med. 2002;19:414-424.
13. Cavalcante SS, Mota e, Rodrigues e, Rodrigues Silva l, Teixeira F, Cavalcante lb. Risk factors for developing nosocomial infections among pediatric patients. Pediatr Infect Dis J. 2006;25:438-445.
14. ustawa z dnia 5 grudnia 2008 roku o zapobieganiu oraz zwalczaniu zakażeń i chorób zakaźnych u ludzi. Dz. u. z 2008 r., nr 234, poz. 1570.
15. International Federation of Infection Control: basic Concepts of Infection Control. ed: Fridman C, newsom W; IFIC 2007.
16. Gleizes O, Desselberger u, Tatochenko V, Rodrigo C, Salman n, Mezner Z, et al. nosocomial rotavirus infection in european countries. Pediatr Infect Dis J. 2006;25 (1 suppl.):12-21.
17. Smith MJ, Clark HF, lawley D, bell lM, Hodinka Rl, DiStefano DJ, et al. The clinical and molecular epidemiology of community - and healthcare-acquired rotavirus gastroenteritis. Pediatr Infect Dis J. 2008;27:54-58.
18. Gaggero A, Avendano lF, Fernandez J, Spencer e. nosocomial transmission of rotavirus from patients admitted width diarrhea. J Clin Microbiol. 1992;30:3294-3297.
19. Gallimore CI, Taylor C, Gennery AR, Cant AJ, Galloway A, Xerry J, et al. Contamination of the hospital environment with gastroenteric viruses: comparision of two pediatric wards over winter season. J Clin Microbiol. 2008;46:3112-3115.
20. Gallimore CI, Taylor C, Gennery AR, Cant AJ, Galloway A, Iturriza-Gomara M, Gray JJ. enviromental monitoring for gastroenteric viruses in a pediatric primary immunodeficiency unit. J Clin Microbiol. 2006;44:395-399.
21. Zerr DM, Allpress Al, Heath J, bornemann R, bennet e. Decreasing hospital-associated rotavirus infection. Pediatr Infect Dis J. 2005;24:397-403.
22. Waisbourd-Zinamn O, ben-Ziony S, Solter e, Chodick G, Ashkenazi S, livini G. The percentage of nosocomial-related out of total hospitalizations for rotavirus gastroenteritis and its association with hand hygiene compliance. Am J Infect Control. 2011;39:166-168.
23. Sulik A, Pogorzelska e, Wojtkowska M, Rożkiewicz D, Ołdak e. Zakażenia norowirusowe u dzieci hospitalizowanych z ostrą biegunką w północno-wschodniej Polsce. Przegl epidemiol. 2007;61:477-482.
24. Weigering V, Kaiser J, Tappe D, Weißbrich b, Morbach H, Grischick HJ. Gastroenteritis in childhood: a retrospective study of 650 hospitalized pediatric patients. Int J Infect Dis. 2011;15:401-407.
25. lopman bA, Reacher MH, Vipond Ib, Hill D, Perry C, Halladay T, et al. epidemiology and cost of nosocomial gastroenteritis, Avon, england, 2003-2003. em Infect Dis. 2004;10:1827-1834.
26. Morter S, bennet G, Fish J, Richards J, Allen DJ, nawaz S, et al. norovirus in the hospital setting: virus introduction and spread within the hospital environment. J Hosp Infect 2011;77:106-112.
27. Murata T, Katsuhima n, Mizuta K, Muraki Y, Hongo Y, Matsuzaki Y. Prolonged norovirus shedding in infants ≤6 months of age with gastroenteritis. Pediatr Infect Dis J. 2007;26:46-49.
28. Zingg W, Pittet D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents. 2009;345:38-42.
29. lee Wl, Chen Hl, Tsai TY, lai I, Chang WC, Huang CH, Fang CT. Risk factors for peripheral intravenous catheter infection in hospitalized patients: A prospective study of 3165 patients. Am J Infect Control. 2009;37:683-686.
30. lee Wl, liao SF, lee WC, Huang CH, Fang CT. Soft tissue infections related to peripheral intravenous catheters in hospitalized patients: a case-control study. J Hosp Infect. 2010;76:124-129.
31. Pujol M, Hornero A, Saballs M, Argerich MJ, Verduger R, Cisnal M, et al. Clinical epidemiology and outcomes of peripheral venous catheter-related bloodstream infections at a university-affiliated hospital. J Hosp Infect. 2007;67:22-29.

234
32. bruno M, brennan D, Redpath Mb, bowens G, Murphy J, love b, et al. Peripheral-venous-catheter-related Staphylococcus aureus bacteraemia: a multi-factorial approach to reducing incidence. J Hosp Infect. 2011;Jul 6. (epub ahead of print).
33. boyd S, Aggarwal I, Davey P, logan M, nathwani D. Peripheral intravenous catheters: the road to quality improvement and safer patient care. J Hosp Infect. 2011;77:37-41.
34. Couzigou C, lamory J, Salmon-Ceron D, Figard J, Vidal-Trecan GM. Short peripheral venous catheters: effect of evidence-based guidelines on insertion, maintenance and outcomes in a university hospital. J Hosp Infect. 2005;59:197-204.
35. Tablan OC, Anderson lJ, besser R, bridges C, Hajjeh R. CDC, Healthcare Infection Control Practices Advisory Committee: Guidelines for preventing health-care--associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep. 2004;26: 53(RR-3):1-36.
36. Goins WP, Talbot HK, Talbot TR. Helath care-acquired viral respiratory diseases. Infect Dis Clin n Am. 2011;25:227-44.
37. Hall Cb, Douglas RG, Geiman JM. Possible transmission by fomites of respiratory syncytial virus. J Infect Dis. 1980;141:98-102.
38. Pada S, Tambyah PA. Overview/reflections on the 2009 H1n1 pandemic. Microb Infect. 2011;13:470-478.
39. lunay e, Ovetchkine P, Saint-Jean M, Coic l, Ducruet T, Charest H, et al. novel influenza A(H1n1): clinical features of pediatric hospitalizations. Int J Infect Dis. 2011;15:122-130.
40. Fanella ST, Pinto MA, bridger nA, bullard JMP, Coombs JMl, Crockett Me, et al. Pandemic (H1n1) 2009 influenza in
hospitalized children in Manitoba: nosocomial transmission and lessons learned from first wave. Infect Control Hosp epidemiol. 2011;32:435-443.
41. CDC: Interim guidance for infection control for care of patients with confirmed or suspected novel influenza A (H1n1) virus infection in healthcare setting. http:www.cdc.gov/h1n1flu/guidelines_infection_control.htm. 2009.
42. laVela S, Goldstein b, Smith b, Weaver FM. Working with symptoms of a respiratory infection: staff who care for high-risk individuals. Am J Infect Control. 2007;35:558-54.
43. Choi SH, Chung JW, Jeon MH, lee MS. Risk factors for pandemic H1n1 2009 infection in healthcare personnel of four general hospitals. J Infect. 2011;doi10.1016./j.jonf.2011.04.009.
44. Chen SC, Hawkins G, Aspinall e, Patel n. Factros influencing uptake of influenza A (H1n1) vaccine amongst healthcare workers in regional pediatric centre: lessons for improving vaccination rates. Vaccine 2011; doi:10.1016/j/vaccine.2011.04.032.
Wkład Autorów/Authors’ contributionsWedług kolejności/According to the order of the Authorship
Konflikt interesu/Conflicts of interestAutorzy pracy nie zgłaszają konfliktu interesów.The Authors declare no conflict of interest.
Nadesłano/Received: 12.01.2015 r.Zaakceptowano/Accepted: 21.01.2015 r.
Published online/Dostępne online
Adres do korespondencji:Teresa Jackowska Klinika Pediatrii,
Centrum Medyczne Kształcenia Podyplomowego ul. Marymoncka 99/103, 01-813 Warszawa
tel. (22) 864-11-67e-mail: [email protected]
Teresa Jackowska, Katarzyna Pawlik

235Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
instructions for authors in Developmental perioD meDicine
1. Developmental period medicine is a journal published by the Institute of Mother and Child in Warsaw. It
is indexed in MEDLINE/PUBMED. The journal publishes original research studies, reviews, clinical case studies, public health studies and communications, both in Polish and in English. It is preferable for the texts to be submitted in English.
2. Manuscripts should be sent to the editors’ address in two copies of single-sided computer printouts, on A4 format paper with a margin of 4 cm on the left side and double space between the lines. Authors are asked to make the text available on electronic media and specify the word processor used, preferably be Word for Windows. Texts can be sent by e-mail.
3. Original articles, together with tables, figures and references should not exceed 21 600 characters (12 pages), reviews 36 000 characters (20 pages).
4. The front page of the manuscript should contain:– the title of the article in English and Polish– the author(s)’ forename(s) and surname(s)– the authors’ affiliation– their scientific titles– the first letter of the first name and the surname of the head of the institution.
5. The text of original research studies must have the following structure: introduction, aim, materials and methods, results, discussion, conclusions (which cannot be a summary of the paper). Abbreviations must be preceded by the full text when first used. In research studies in which investigations were carried out on human beings or animals, as well as in clinical studies, approval of the Bioethics Committee must be obtained and relevant information be included in the manuscript.
6. An abstract of 200-250 words should precede the main article. Abstracts in English and in Polish should contain the following structure: aim, material and methods, results, conclusions. Abbreviations should not be used in the title or the abstract.
7. Key words (3-6) will be printed both in English and in Polish, according to the Medical Subject Heading Index Medicus Catalogue (MeSH) website http://www.nim.nih.gov.mesh/MBrower.html). Key words should not be a repetition of the title.
8. Illustrative material may include clear black and white or colour photographs on glossy paper, or clearly contrasting, carefully executed technical drawings on white paper. Photographs must be scanned on CD-ROM. On the back of each figure, please mark the top, and write the name of the author, title of the article and number of the figure. Captions for the figures should also be provided on a separate page in Polish and English. The text in the figures should also be both in Polish and in English.
9. Tables, their titles and content should be written both in English and Polish in Word for Windows in A4 format, with double spacing. All the footnotes referring to each table should be placed underneath the text of the table. Please mark on the margin of the text where the table or figure should be inserted.
10. References should be given in the order of citation and should be limited to those quoted in the text. In original articles, the number of references should not exceed 30, while in review papers 40. Each reference should include the surname(s) of the author(s) and the first letter of their first name(s), the title of the article, the abbreviated title of the journal (according to Index Medicus), the year, and number of the first and last page. When quoting book references, give the surname of the author(s), the first letter of the first name, the title of the chapter, the title of the book, the publisher, the place and year of publication. It is allowed to cite Internet references with the URL, with the date when the article was used and, if possible, the names of the authors.
11. After the references, the surname and first name, correspondence address, telephone number and e-mail address of the first author should be given.

236 Instruction for Authors
12. The submitted manuscript must include a statement signed by all the authors describing the impact of each individual in preparing the article (concept and plan of the work, data collection and analysis, responsibility for statistical analysis, writing the article, critical review, etc.) including a declaration they take full responsibility for its contents. The statement must also include the assurance that the contents have not been published or sent for publication in other journals.
13. The authors also state that there is no conflict of interests at the time of submission, such as:– financial (employment, counseling, paid reviews, stock ownership, remuneration, etc.)– personal links– academic competition or other competition that can have an influence on the content of the paper– sponsoring of research or other studies involved in the submitted paper at the stage of designing research, collecting and interpreting data, or writing a report.A conflict of interests takes place when one or more authors has links of financial dependence with industry (through investment, employment, owning stocks or remuneration), directly or through the immediate family. If the work concerns products sponsored by a firm, the authors must include this information.
14. Submitted papers are peer-reviewed by two independent reviewers and are then qualified for publication by the Editor in Chief. Reviews are anonymous. The authors receive each reviewer’s comments concerning corrections or disqualification. The review procedure follows the recommendations of the Ministry of Science and Higher Education published as “Good Practice in Review Procedures in Science” (Warsaw 2012) and was described in detail on the www.medwiekurozwoj.pl website.
15. The editing board reserves the right to make relevant editing corrections.16. Accepting the article for publication means that the copyright of the papers belongs to the editors of Developmental
Period Medicine.17. The authors receive one copy of the journal free of charge. On request, access to the PDF file containing
their article is available.18. Manuscripts not concordant with the above instructions will be returned to be corrected.19. The editors do not return papers which have not been commissioned.20. The editors take no responsibility for the contents of the advertisements.
Please submit your manuscript and their electronic version to:Prof. Krystyna BożkowaEditor in Chief Developmental Period MedicineInstitute of Mother and ChildKasprzaka 17a, 01-211 Warsaw, PolandTel. (22) 32-77-197e-mail: [email protected]

237Developmental Period Medicine, 2015;XIX,2© IMiD, Wydawnictwo Aluna
zASAdy PRzyjMOwANIA I OGŁASzANIA PRAC w Developmental perioD meDicine
1. Kwartalnik Developmental Period Medicine jest pismem wydawanym przez Instytut Matki i Dziecka i in-deksowanym w MEDLINE/PUBMED. Zamieszczane są prace oryginalne, kliniczne i doświadczalne oraz poglądowe w języku angielskim lub polskim. Preferowane są prace w języku angielskim.
2. Prace powinny być nadesłane pod adresem Redakcji w 2 egz., w formie jednostronnego wydruku kompu-terowego, na arkuszach formatu A4, z marginesem 4 cm od lewej strony, z podwójnymi odstępami między wierszami. Prace należy nadsyłać łącznie z nośnikiem elektronicznym – z zaznaczeniem użytego edytora, najlepiej Word for Windows. Prace mogą być przesyłane droga mailową.
3. Objętość prac oryginalnych – łącznie z rycinami i piśmiennictwem – nie może przekraczać 21 600 znaków (12 stron maszynopisu), prac poglądowych do 36 000 znaków (20 stron).
4. Strona tytułowa powinna zawierać: – tytuł w języku angielskim i polskim, – pełne imiona i nazwiska autorów, – afiliację autorów, – stopień/tytuł naukowy, pierwsza litera imienia i nazwisko kierownika.5. Praca oryginalna powinna mieć następującą strukturę: wstęp, cel pracy, materiał i metody, wyniki, dysku-
sja i wnioski, które nie mogą być streszczeniem pracy. Przy zastosowaniu skrótów konieczne jest podanie pełnego brzmienia przy pierwszym użyciu. W pracach doświadczalnych, w których wykonano badania na ludziach lub zwierzętach, a także w badaniach klinicznych, należy umieścić informację o uzyskaniu zgody komisji etyki badań naukowych.
6. Streszczenia zarówno w języku polskim jak i angielskim powinny zawierać 200-250 słów. Streszczenia prac oryginalnych, klinicznych i doświadczalnych powinny posiadać następującą strukturę: cel, materiał i metody, wyniki wnioski. Nie należy używać skrótów w tytule ani w streszczeniu.
7. Słowa kluczowe (3-6) należy podawać w języku angielskim i polskim, zgodnie z katalogami MeSH (Medical Subject Headings Index Medicus http://www.nim.nih.gov.mesh/MBrower.html). Słowa kluczowe nie mogą być powtórzeniem tytułu pracy.
8. Materiał ilustracyjny mogą stanowić fotografie czarno-białe lub kolorowe, na błyszczącym papierze, wyraźnie kontrastowe lub rysunki wykonane starannie na białym papierze. Fotografie powinny być zeskanowane na CD-ROM. Na odwrocie każdej ryciny należy podać (zaznaczając górę): nazwisko autora, tytuł pracy i kolejny numer. Podpisy pod rycinami powinny być napisane na oddzielnej kartce w języku polskim i angielskim. Treść rycin powinna być również podana w języku polskim i angielskim.
9. Tabele – ich tytuły i treść powinny być pisane w edytorze tekstu w formacie A4 z podwójnym odstępem w języku angielskim i polskim (dwujęzyczne). Wszystkie stopki dotyczące tabeli powinny znajdować się poniżej tekstu tabeli. W tekście pracy na marginesie należy zaznaczyć, gdzie powinna być zamieszczona rycina i tabela.
10. W wykazie piśmiennictwa ułożonym według kolejności cytowania należy uwzględnić wyłącznie te prace, na które autor powołuje się w tekście. W pracach oryginalnych nie powinno być więcej niż 30 pozycji, a w poglądowych nie więcej niż 40 pozycji. Każda pozycja powinna zawierać: nazwiska wszystkich autorów, pierwsze litery imion, tytuł pracy, skrót tytułu czasopisma (wg Index Medicus), rok, numer, stronę począt-kową i końcową. Przy pozycjach książkowych należy podać: nazwisko autora (autorów), pierwszą literę imienia, tytuł rozdziału, tytuł książki, wydawnictwo, miejsce i rok wydania. Dopuszcza się cytowanie stron internetowych z podaniem adresu URL i daty użycia artykułu oraz o ile to możliwe nazwisk autorów.
11. Po piśmiennictwie należy podać adres do korespondencji, nazwisko i imię pierwszego autora, adres, numer telefonu oraz adres e-mail.
12. Do maszynopisu należy dołączyć oświadczenie podpisane przez wszystkich autorów określające udział po-szczególnych autorów w przygotowaniu pracy (np. koncepcja i projekt pracy, zbieranie danych i ich analiza, odpowiedzialność za analizę statystyczną, napisanie artykułu, krytyczna recenzja itd.), a także oświadcza że biorą oni odpowiedzialność za treść. Ponad to należy zaznaczyć, że praca nie była publikowana ani zgłaszana do druku w innym czasopiśmie.

238 Zasady przyjmowania i ogłaszania prac
13. Jednocześnie autorzy powinni podać do wiadomości wszelkie inne informacje mogące wskazywać na istnienie konfliktu interesów, takie jak:
– zależności finansowe (zatrudnienie, płatna ekspertyza, doradztwo, posiadanie akcji, honoraria), – zależności osobiste, – współzawodnictwo akademickie i inne mogące mieć wpływ na stronę merytoryczną pracy, – sponsorowanie całości lub części badań na etapie projektowania, zbierania, analizy i interpretacji danych
lub pisanie raportu. Konflikt interesów ma miejsce wtedy, gdy przynajmniej jeden z autorów ma powiązania lub zależności finan-
sowe z przemysłem (poprzez inwestycje, zatrudnienie, doradztwo, posiadanie akcji, honoraria) bezpośrednie lub za pośrednictwem najbliższej rodziny. Jeśli praca dotyczy badań nad produktami częściowo lub całkowicie sponsorowanymi przez firmy, autorzy mają obowiązek ujawnić ten fakt w załączonym oświadczeniu.
14. Nadesłane prace są oceniane przez dwóch niezależnych recenzentów a następnie kwalifikowane do druku przez Redaktora Naczelnego. Recenzje mają charakter anonimowy. Krytyczne recenzje autorzy otrzymują wraz z prośbą o poprawienie pracy lub z decyzją o niezakwalifikowaniu jej do druku. Procedura recenzowania artykułów jest zgodna z zaleceniami Ministerstwa Nauki i Szkolnictwa Wyższego zawartymi w opracowaniu „Dobre parktyki w procedurach recenzyjnych w nauce” (Warszawa 2012) i szczegółowo została opisana na stronie www.medwiekurozwoj.pl
15. Redakcja zastrzega sobie prawo redagowania nadesłanych tekstów. 16. Przyjęcie pracy do druku oznacza przejęcie praw autorskich przez Redakcję Developmental Period
Medicine. 17. Autorzy otrzymują nieodpłatnie 1 egz. czasopisma i dostęp na życzenie do pliku PDF swojej pracy. 18. Prace przygotowane niezgodnie z regulaminem zostaną zwrócone autorom do poprawienia. 19. Redakcja nie zwraca materiałów niezamówionych.20. Redakcja nie odpowiada za treść zamieszczanych reklam.
Prace należy nadsyłać na adres Redakcji: Prof. dr hab. med. Krystyna BożkowaRedaktor NaczelnyDevelopmental Period MedicineInstytut Matki i Dzieckaul. Kasprzaka 17 A, 01-211 Warszawatel. (22) 32 77 197e-mail: [email protected]






















