PEPFAR Country/Regional Operational Planning (COP/ROP ...
106
January 20, 2022 PEPFAR Country/Regional Operational Planning (COP/ROP) 2022 Overview Webinar for PEPFAR/USG Teams
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PEPFAR Country/Regional Operational Planning (COP/ROP ...

January 20, 2022
PEPFAR Country/Regional Operational Planning (COP/ROP) 2022 Overview
Webinar for PEPFAR/USG Teams

2
Agenda
Welcome and Introduction
1. PEPFAR’s Contributions to Global and Country Goals
2. Strategic Direction for COP/ROP22
3. Targets and Budgets
4. Tools Overview
5. COP/ROP22 Process, Timelines and Stakeholder Engagement
*Throughout the presentation, COP refers to Country Operational Plans and Regional Operational Plans, including Plans by Country Pairs.

3
Unwavering Bipartisan Congressional and Presidential Leadership of PEPFAR
• Emergency response to save lives• Rapid delivering prevention, care, and
treatment services• Focus on individuals with late-stage AIDS
defining illness
• Shared responsibility & country-driven programs • Ensuring an AIDS Free generation• Building & strengthening health systems to
deliver HIV services• Scaling up of prevention, care, and treatment
services for people without AIDS defining illness
• Granular data, transparency & accountability for impact and increasing efficiency
• Accelerating core interventions for epidemic control with equitable access of all vulnerable and marginalized populations
• Treatment of all HIV positive individuals and stop transmissions
• Sustainability based on data, actual costs and local partner delivery
• Robust community engagement• Resilient systems and sustainable capacity in the
context of COVID-19

4
Summary of PEPFAR’s Latest Global Results - Announced by President Biden December 1, 2021
PEPFAR has supported:
At least 20 countries achieved epidemic control of HIV or reached the 90-90-90 HIV treatment targets
18.96 million women, men, and children on life-saving treatment – 17.2 million last year
63.4 million people received HIV testing services in FY 2021– 50 million last year
27.7 million voluntary medical male circumcisions to prevent HIV infections in men and boys – 25.3 million last year
7.1 million orphans, vulnerable children, and their caregivers provided with critical care – 6.7 million last year
2.9 million adolescent girls and young women reached with comprehensive HIV prevention services in FY 2021
Nearly 300,000 new health workers trained

5
PEPFAR has been adapting its program
and leveraging its platform to protect HIV gains and respond to
COVID-19
COVID-19 continues to affect PEPFAR
programs in COP21 and in planning for
COP22

PEPFAR Country/Regional Operational Planning (COP/ROP22) planning represents a momentous and pivotal twentieth year for PEPFAR implementation in FY 2023.
In COP20 into COP21, with PEPFAR’s data-driven approach, laser focus on core policies that were essential to support clients, and commitment to developing local partners, PEPFAR and countries continued to be better positioned to protect and sustain our collective gains through COVID-19.

7

8
PEPFAR’s Ongoing Response to HIV and COVID-19

9
PEPFAR’s Guiding Pillars for Success

10
Core Operating Principles and Values Highlighted in COP/ROP 22
1. Local Ownership
2. Person-Centered
3. Evidence-Based
4. Data-Driven
5. Diversity, Equity, Inclusion, and
Accessibility (DEIA)
6. Gender-Responsive
7. Collaboration and Partnership
8. Agility and Adaptability
9. Resilience
10. Linkage and Integration

11
Maintaining Gains and Evolving Programs During COVID-19
• In countries striving to reach epidemic control and address programmatic gaps, resilient, dedicated teams continue to protect gains and address safety during COVID-19
• review granular program and financial data to understand what is working and allocate resources effectively
• proactively adapt programs to achieve results in changing conditions
• In countries reaching epidemic control, our work is not done• teams have achieved remarkable success driving down new
infections and mortality among people living with HIV• epidemic control is a dynamic state and sustained impact is a long-
term, gradual process tailored to country context• programs will begin planning to evolve and sustain impact while
preventing a resurgence of HIV with a country-led public health response

Sustaining Impact in the HIV Epidemic: Equitable Access, Everyone’s Voice
• Community-led Monitoring• Empowering local, key population and
women-led organizations• Continuous quality improvement and people-
centered design• Peer led prevention and treatment service
delivery• Comprehensive domestic response with
increasing local responsibility• Enabling environments, policies and ensuring
systems and capacities

13
Vision and Implementation Themes for PEPFAR COP/ROP22
Goal 1 is to Accomplish the MissionAchieve and sustain epidemic control using Evidence-based, Equitable, People-Centered HIV Prevention and Treatment Services.
Goal 2 is to Build Enduring CapabilitiesResilient and Capacitated Country Health Systems, Communities, Enabling Environments, and Local Partners.
Goal 3 is to Build Lasting CollaborationsStrengthen Cooperation and Coordination for Greater Impact, Responsibility Sharing, and Sustainability.
The COP/ROP22 Vision: to advance sustained epidemic control of HIV by supporting equitable health services and solutions, enduring national health systems and capabilities, and lasting collaborations

14
1PEPFAR’s Contributions to Global and Country Goals

15
Epidemiologic Impact – Particularly in Africa

16
General Population and HIV Population Pyramids

17
Progress Towards 95/95/95 across select countries in Southern, East and West Africa (PHIAs)

18
Progress Towards 95/95/95 among 15- to 24-year-olds across select countries in Southern, East and West Africa (PHIAs)
Progress Towards 95/95/95 tables, including 15–24-year-olds and adult males and females; Source: PEPFAR PHIA; Note: Those treated are shown as a percent of those aware of their HIV status; those virally suppressed are shown as a percent of those treated

19
New Infections among Females 15- to 24-years-old in Countries at Epidemic Control vs Select Countries not at Epidemic Control

20
New Infections among Males 15- to 24-years-old in Countries at Epidemic Control vs Select Countries not at Epidemic Control

21
PEPFAR-funded PHIAs – Countries Showing Achievements towards the Global HIV SDG 90/90/90 Goals
Trends by Region and Age Distribution of Pediatric HIV Infections

22
PEPFAR-funded PHIAs – Countries Showing Achievements towards the Global HIV SDG 90/90/90 Goals
Distribution of New HIV Infections, 2021
23
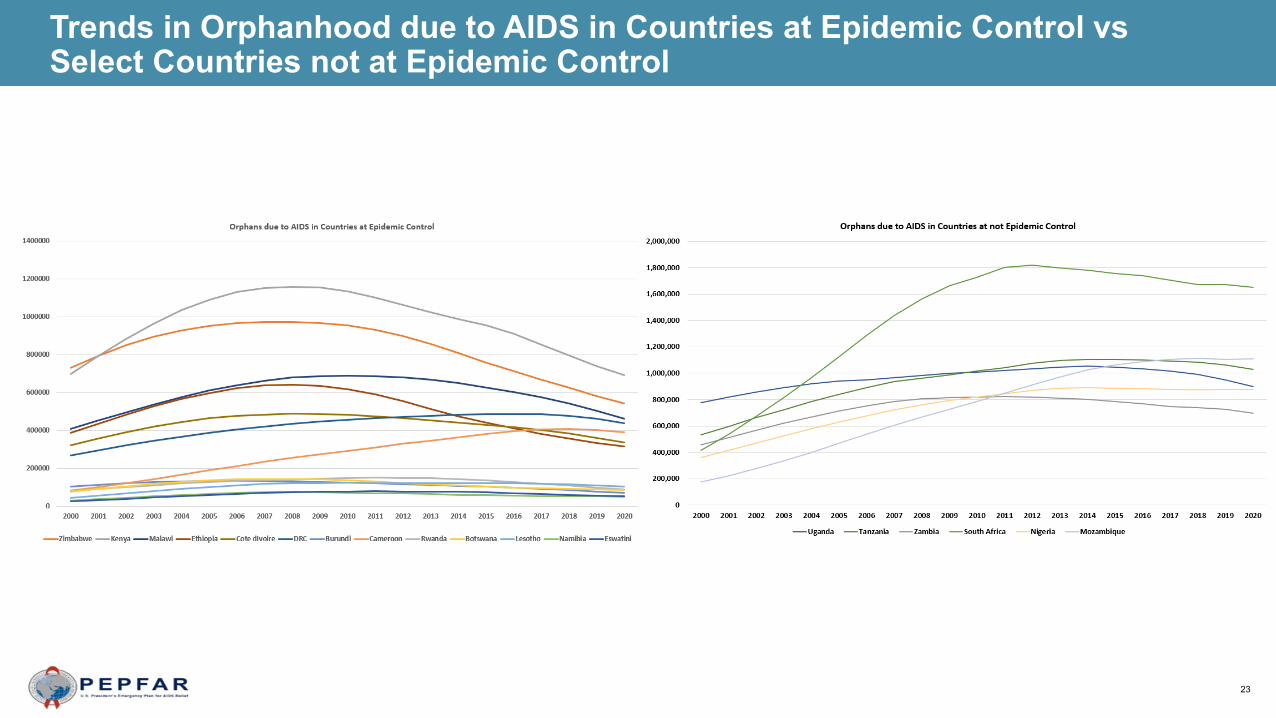
Trends in Orphanhood due to AIDS in Countries at Epidemic Control vs Select Countries not at Epidemic Control

24
Trends in New Infections and All-Cause Mortality

25
Trends in New Infections and All-Cause Mortality

26
Trends in New Infections and All-Cause Mortality

27
Trends in New Infections and All-Cause Mortality

28
Trends in New Infections and All-Cause Mortality

29
Trends in New Infections and All-Cause Mortality

30
Trends in New Infections and All-Cause Mortality

31
Trends in New Infections and All-Cause Mortality

32
2Strategic Direction
for COP/ROP22

33
Path to Epidemic Control – COP22 Vision
COP/ROP15Geographic andPopulation Pivot
COP/ROP16Efficiencies for Key Policies
COP/ROP17Above Service Delivery and
Scaling Districts
COP/ROP18Programmatic Solutions and
Cost
COP/ROP 19 PEPFAR
Minimum ProgramRequirements
COP/ROP20Quality client-
centered Servicesand Retention
COP/ROP21Client-centered services, community engagement,
resilient systems and sustainable capacity
COP/ROP22
Sustaining Epidemic Control:Equitable Services & Solutions
Enduring CapabilitiesLasting Collaborations
34
What’s New in COP22
• COP22 guidance emphasizes themes of Completing the Mission (95/95/95), Building Enduring Capabilities, and Building Lasting Collaborations.
• COP22 begins to shift language from “client-centered” to “person-centered.”
• Equity has been added to Accountability, Transparency, and Impact as a guiding pillar for PEPFAR and a key theme for COP22.
• Minimum Program Requirements are updated to demonstrate progress in equity, stigma, discrimination, and human rights, to add KP-led and women-led organizations among local partners, and to include infection prevention and control activities with quality assurance and continuous quality improvement functions and increase flexibility for targeted assessments.
• Quality Assurance standards supported by SIMS will be updated to better translate Minimum Program Requirements into site standards and increase flexibility for targeted assessments. (Section 3).

35
What’s New in COP22
• Testing guidance is updated, highlighting the need for a strategic mix of testing modalities that adapts as countries approach treatment saturation and takes into account positivity rate, cost, number of positives, and epidemiologic impact. Safe, ethical index testing should be offered to all who are eligible, including newly diagnosed PLHIV.
• Case finding for undiagnosed children living with HIV is a high priority requiring specific planning and investment.
• Sustainability Guidance is updated as more countries are at or near 95/95/95 benchmarks, underscoring PEPFAR’s need to move toward a vision for sustained epidemic control. Sensible adaptations moving toward sustainability will be incorporated into COP22 planning.
• Technical Considerations have been updated, and highlights of “What’s New” are included at the beginning of each section.

36
• Attaining Epidemic Control: Approaching 95/95/95• Assess gaps and address equity• Adaptations and changes should be anticipated, planned and programmed.• Stakeholders should begin discussing and anticipating program shifts well in
advance of achieving 95/95/95, so that adaptation to a program reaching treatment saturation may be tailored to the country context.
• Sustaining Epidemic Control: Building Blocks of Sustainability
• Over time, PEPFAR’s role will transform from a direct funder of services, to an accountability partner, helping governments and communities sustain services.
• Sustaining impact in this context requires countries have functional and financial capacity to maintain key programs at scale.
• COP22 SDS includes an appendix: Assessing Progress towards Sustainable Control of the HIV/AIDS Epidemic where OUs address sustainability questions
Attaining and Sustaining Epidemic Control
37
Equity in COP22: As we approach 95/95/95, who is left behind?
Equity• Absence of unfair and avoidable or remediable differences in health among population
groups defined socially, economically, demographically, or geographically
Equity Lens• Approach that prioritizes actions that reduce inequalities and advance equity• Includes actions to address the underlying social determinants of inequality.
Global Priority Populations to Advance Equity in COP/ROP22• Children• Adolescent Girls and Young Women• Key Populations
Approach to equity• Focused efforts and tailored services• Promoting an enabling environment addressing stigma, discrimination, and human rights

38
Closing Equity Gaps for Pediatrics and PMTCT
• Goals: to eliminate vertical transmission of HIV and close the treatment gap for children and adolescents.
• Seven PEPFAR-supported countries have the largest gaps per UNAIDS 2020 estimates triangulated with PEPFAR data/footprint:
• Nigeria• Mozambique• Zambia• South Africa• Tanzania• Uganda• DRC
• Plan, resources, and accountability scheme should be part of COP22

39
Gender & AGYW
Gender Equality (Section 6.6.2)• New section on Gender Equality, stressing the importance of gender norms change
activities across PEPFAR programming• Focuses on gender transformative activities within HIV prevention, testing, and treatment
services; in HRH programs; and within health information systems
GBV (Section 6.6.2.1)• Updated to better reflect GBV prevention, case identification, and response across the HIV
clinical cascade• Includes new language on safeguarding against violence within PEPFAR programming• Key GBV considerations have been integrated throughout the full COP Guidance
AGYW/DREAMS (Section 6.6.2.2)• Updated to include psychosocial support, STIs, short-term program adaptations to fill gaps,
and expanded mentoring guidance (see DREAMS slide in Goal 1 section for more details)

40
Gaps in the Global HIV Response for Key Populations
• Globally, KP and their sexual partners represent a large and growing percentage of new infections (estimated 65% globally).
• There is a lack of systematic, quality data about key populations
• High levels of stigma, discrimination, violence, marginalization and criminalization.
Across the PEPFAR program:• PrEP has room for further expansion
• Need to ensure we are reaching high risk networks
• Viral load testing coverage rates are sub-optimal (both reporting and service access issues)
41
Key Populations: Areas of Emphasis for COP 22 (6.5)
• Build on what has worked well: KPIF, PrEP scale-up, KP differentiated service delivery
• Continue to improve KP data and promote regular KP size estimation efforts & bio-behavioral surveys
• Expand community-led monitoring specific to KP
• Promote enabling environments and address structural barriers that impede the scale-up of KP-led and KP–competent services
• Mitigate harmful policy and social norms that fuel stigma, discrimination and violence faced by key populations
– promote funding, capacity building and other support to KP-led organizations
– strengthen the KP-competency of HIV service providers.
– coordinate strategically with relevant State and U.S. government units (e.g. DRL), partner governments, multilateral and other donor funding streams and institutions
• Specific program expectations detailed in Section 6.5

42
Human Rights: PEPFAR countries must support a sustainable, non-discriminating, enabling environment
• Work with IPs to maintain a posted “Patients’ Bill of Rights”
• Designate an in-country, interagency POC to coordinate human rights-centered programming
• Maintain an in-country, interagency POC to oversee PEPFAR USG staff Gender and Sexual Diversity (GSD) Training and ensure a system tracks compliance at the OU level.
• At the headquarters level, each PEPFAR implementing agency must also identify a POC to carry out the same functions.
• Detail how OU will meet requirements during COP22 planning meetings with specific activities and budgets.
• Develop a plan, timeline, and resource allocations to measure, document, and mitigate HIV-related stigma, discrimination, and violence.
• Include non-discrimination in design and administration of programs in PEPFAR trainings
• Reinforce PEPFAR-funded IPs have zero-tolerance policies to protect participants from all forms of abuse, unethical behavior, and misconduct.

43
Goal 1Accomplish the Mission
Achieve Sustained Epidemic Control of HIV through Evidence-based, Equitable, People-Centered HIV
Prevention and Treatment Services

44
• Section 7 (COP Planning Steps) recommends OUs begin analysis with population viral load suppression and has analytic recommendations and examples for programs that are approaching epidemic control.
Begin With the End in Mind...

45
HIV Testing Services

46
HIV Positive Test Results by Modality for Males and Females

47
Testing Guidance Updates
• Safe, ethical index testing should be offered to all who are eligible, including newly diagnosed people living with HIV.
• Strategic mix of testing modalities that adapts as countries approach treatment saturation
• Plan considers positivity rate, cost, number of positive results, and epidemiologic impact.
• Case finding for undiagnosed children living with HIV is a high priority requiring specific planning and investment.

49
Anticipated evolution of HIV testing modalities
HIV testing modalities should evolve as countries approach and achieve equitable epidemic control across subpopulation groups

50
Person-CenteredPrevention Services

51
Trends in PrEP Scale Up Among Key Populations

52
Average Percent Decline of New Diagnoses in DREAMS Geographic Areas 2015-2020Q2

53
Prevention Themes: Scaling PrEP, Person-Centered Engagement.
Myers JE, et al. Open Forum Infect Dis. 2018 May 2;5(6): https://doi.org/10.1093/ofid/ofy097
Source:NYCDOH

54
Continuity of ART

55
COVID Adaptation and Progress of Multi-Month Dispensing in FY21

56
Viral Load Coverage by Country
57
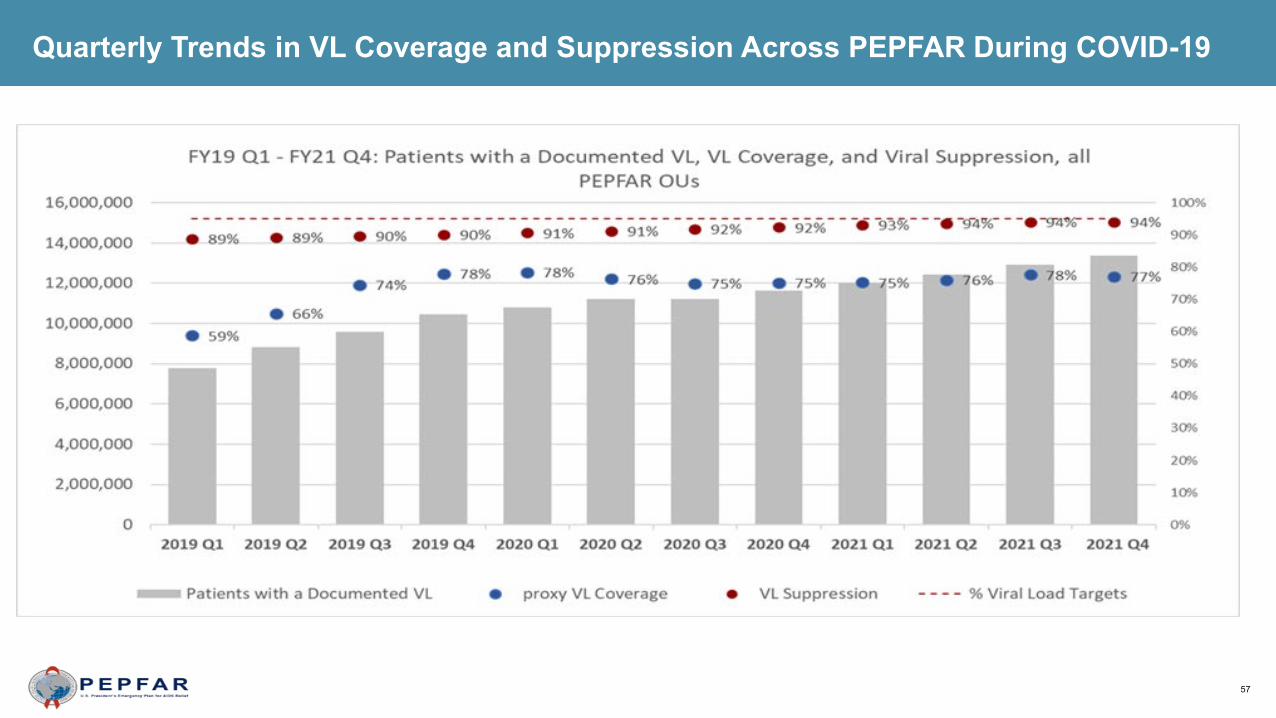
Quarterly Trends in VL Coverage and Suppression Across PEPFAR During COVID-19

58
Viral Suppression Trends by Age

59
Age Distribution of People on Treatment
Number of PEPFAR Clients on Treatment by Fine Age Band in Q4 2021
Treatment Current by Age Group at Q4 2021

60
Clinical Cascade and ART Scale Up for Key Populations Through FY21 Q4
Trends in ART Scale Up Among FSW and PWID
Trends in ART Scale Up Among MSM and Transgender
61
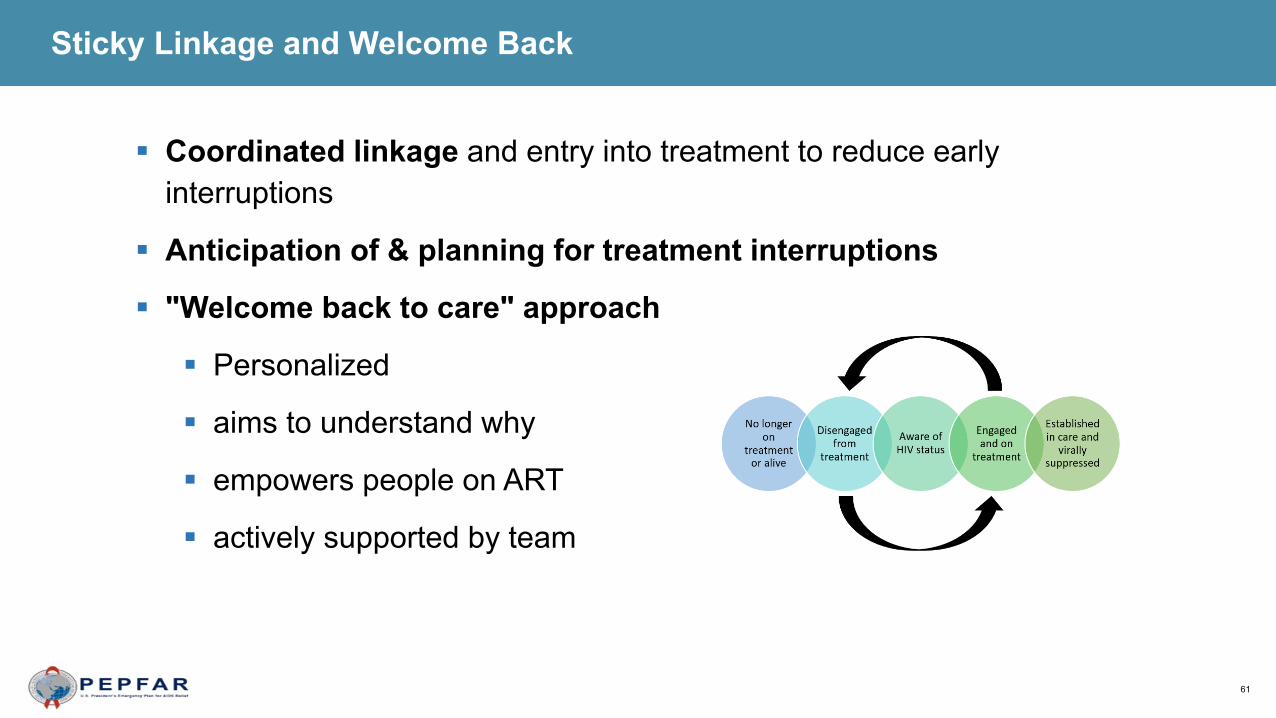
Coordinated linkage and entry into treatment to reduce early interruptions
Anticipation of & planning for treatment interruptions
"Welcome back to care" approach
Personalized
aims to understand why
empowers people on ART
actively supported by team
Sticky Linkage and Welcome Back
62
Other Considerations for Quality, Person-Centered HIV Treatment
Approach to CD4 testing revised to allow identification and improve management of advanced HIV disease
Updated TB case finding among PLHIV: 2021 WHO updated guidelines
Updated cervical cancer screening and treatment guidelines and algorithm
New section on psychosocial support

63
Goal 2Build Enduring Capabilities

64
Theory of Change for Countries at Epidemic Control – Ensuring a Sustainable Response

65
Integrated Analytics for Sustainability PlanningUnderstanding Functional Responsibility from Responsibility Matrix and Resource Alignment

66
Critical Public Health Capabilities to Sustain HIV Program Impact
Critical public health capabilities that must be addressed for long-term HIV epidemic control include:
Ensuring Availability of Critical Strategic Epidemiologic Information
Strengthening Key Public Health Institutions and Infrastructure
Establishing Strong Public Health Laboratory Networks
Building a Skilled and Capable Workforce
Implementing Data Driven Public Health Programs
Supporting Critical Operational/Applied Research

67
Impact Driven, Interoperable Health Information Systems for Person-Centric Care, Surveillance, and Program Monitoring and Evaluation

68
• Recency surveillance provides • information about new and chronic infection
patterns • insights on where recent infections may be
diagnosed, and • demographic patterns
• Recency data are even more needed in light of COVID-19 to identify pattens in recent infections
• Other patient level data should be incorporated into case surveillance systems, to understand the current dynamics of the HIV epidemic, populations at risk and intervention targeting
Recency and Broader Surveillance

69
Leadership Capacity: • The lynchpin to success is a laser focus on leadership, people who can not
only manage a process but ensure the informal systems, internal culture, and behaviors of actors within the system change and that program direction and adaptation respond to evolving challenges.
Functional Systems: • The most important basis for all change is engaging in proper and
continuous problem diagnosis. Start with a framework of an ideal system to sustain epidemic control that must be adapted to realities on the ground.
Person Centered Supply Chain Modernization• Maximize product availability, quality, and affordability as well as
convenience for the individual
Other Enduring Capabilities
70
Ensuring continuity of HIV treatment and prevention services
Leveraging the country health systems and infrastructure supported by PEPFAR to strengthen country COVID-19 response
The safety of PEPFAR-supported clients and health care workers is of critical importance
Extending flexibility to the PEPFAR country teams within the PEPFAR’s mandates and authorities to the extent possible to take into account COVID-19 related needs
Principles of PEPFAR’s COVID-19 Response Extending into COP22

71
Sustaining Delivery of HIV Services by Local Partners
• Significant progress has been made toward the FY20 goal, with the overall number of partners that are local surpassing 70% in FY20.
• Currently, at the start of FY22, the 70% benchmark has still not been achieved for the total amount of funding that is going to local partners.
• In OUs that have not met the 70% target, capacity-building and mentorship efforts for local partners should be prioritized in COP22 planning, with funding set aside and specific, measurable and time-bound benchmarks identified for capacity-building efforts.

72
Goal 3Build Lasting Partnerships

73
Strengthening Coordination and Cooperation
• For COP22, teams are expected to actively engage stakeholders in all aspects of strategic planning.
• Each PEPFAR OU team is required to conduct a country-centered strategic planning consultation (retreat) with local stakeholders by the end of January 2022/early February 2022.
• The consultation/retreat will introduce and discuss all COP22 tools, guidance, results, and targets, as well as the proposed trajectory and strategy for COP22.
• Following COP22 submission, teams should continue engagement with external stakeholders through routine sharing of data on at least a quarterly basis from the PEPFAR Oversight and Accountability Response Team (POART).

74
Working with Partner Country Governments and Multilateral and Private Sector Partners
• Partner Governments: Collaborative with partner-country governments is critical to ensuring that prioritized interventions are scaled, geographic priorities are shared, and that all available resources for HIV/AIDS in the country are optimally utilized
• Multilateral partners (GF, UNAIDS, UNICEF, etc.) often complement PEPFAR competencies and can play a significant role influencing partner government policy and program decisions, addressing implementation challenges, and coordinating and aligning efforts across partners.
• Private Sector: Scalability and sustainability of programs is more likely with support of and collaboration with the private sector, and partnership with private sector can help foster innovation that can be replicated .

75
Global Fund Collaboration
It remains critical that PEPFAR and the Global Fund use the same information for COP planning and Global Fund proposals
Portfolio optimization offers an opportunity to recipient countries to access additional Global Fund resources to further support the national response.
The Global Fund C19RM financed interventions in countries receiving Global Fund investments to mitigate the effects of COVID-19
• Countries may request C19RM funds through March 31, 2022. PEPFAR teams work with CCMs to ensure complementarity
• For all resources, jointly identify unmet need based on the same data• Jointly put forth proposed resources to address unmet gaps• Joint dialogue with Host Government to reach Goals for impact• Engage UNAIDS and other multilateral partners on policy advocacy

76
Global Fund Collaboration
Trends in Total HIV Investments by Funder, 2018-2022

77
Minimum Program Requirements

78
COP22 Minimum Program Requirements
Care and Treatment• Adoption and implementation of Test and Start, with demonstrable access across all age, sex, and risk
groups, and with direct and immediate (>95%) linkage of clients from testing to uninterrupted treatment across age, sex, and risk groups.
• Rapid optimization of ART by offering TLD to all PLHIV weighing >30 kg (including adolescents and women of childbearing potential), transition to other DTG-based regimens for children who are >4 weeks of age and weigh >3 kg, and removal of all NVP- and EFV-based ART regimens.
• Adoption and implementation of differentiated service delivery models for all clients with HIV, including six-month multi-month dispensing (MMD), decentralized drug distribution (DDD), and services designed to improve identification and ART coverage and continuity for different demographic and risk groups.
• All eligible PLHIV, including children and adolescents, should complete TB preventive treatment (TPT), and cotrimoxazole, where indicated, must be fully integrated into the HIV clinical care package at no cost to the patient.
• Completion of Diagnostic Network Optimization activities for VL/EID, TB, and other coinfections, and ongoing monitoring to ensure reductions in morbidity and mortality across age, sex, and risk groups, including 100% access to EID and annual viral load testing and results delivered to caregiver within 4 weeks.

79
COP22 Minimum Program Requirements
Case Finding• Scale-up of index testing and self-testing, ensuring consent procedures and confidentiality are
protected and assessment of intimate partner violence (IPV) is established. All children under age 19 with an HIV positive biological parent should be offered testing for HIV.
Prevention and OVC• Direct and immediate assessment for and offer of prevention services, including pre-exposure
prophylaxis (PrEP), to HIV-negative clients found through testing in populations at elevated risk of HIV acquisition (PBFW and AGYW in high HIV-burden areas, high-risk HIV-negative partners of index cases, key populations and adult men engaged in high-risk sex practices)
• Alignment of OVC packages of services and enrollment to provide comprehensive prevention and treatment services to OVC ages 0-17, with particular focus on 1) actively facilitating testing for all children at risk of HIV infection, 2) facilitating linkage to treatment and providing support and case management for vulnerable children and adolescents living with HIV, 3) reducing risk for adolescent girls in high HIV-burden areas and for 10-14 year-old girls and boys in regard to primary prevention of sexual violence and HIV.

80
COP22 Minimum Program RequirementsPolicy & Public Health Systems Support
• In support of the targets set forth in the Global AIDS strategy and the commitments expressed in the 2021 political declaration, OUs demonstrate evidence of progress toward advancement of equity, reduction of stigma and discrimination, and promotion of human rights to improve HIV prevention and treatment outcomes for key populations, adolescent girls and young women, and other vulnerable groups.
• Elimination of all formal and informal user fees in the public sector for access to all direct HIV services and medications, and related services, such as ANC, TB, cervical cancer, PrEP and routine clinical services affecting access to HIV testing and treatment and prevention.
• OUs assure program and site standards, including infection prevention & control interventions and site safety standards, are met by integrating effective Quality Assurance (QA) and Continuous Quality Improvement (CQI) practices into site and program management. QA/CQI is supported by IP work plans, Agency agreements, and national policy.
• Evidence of treatment literacy and viral load literacy activities supported by Ministries of Health, National AIDS Councils and other partner country leadership offices with the general population and health care providers regarding U=U and other updated HIV messaging to reduce stigma and encourage HIV treatment and prevention.
• Clear evidence of agency progress toward local partner direct funding, including increased funding to key populations-led and women-led organizations in support of Global AIDS Strategy targets related to community-, KP- and women-led responses
• Evidence of partner government assuming greater responsibility of the HIV response including demonstrable evidence of year after year increased resources expended
• Monitoring and reporting of morbidity and mortality outcomes including infectious and non-infectious morbidity.• Scale-up of case surveillance and unique identifiers for patients across all sites.

81
COP22 Minimum Program Requirements
PEPFAR country programs must address quality management practices
Quality Assurance (QA) for site standards
Continuous Quality Improvement (CQI)
Community-Led Monitoring (CLM)
SIMS Update 4.2
Alignment of CEEs with MPRs to aid in documenting MPRs at the site level (where applicable).
Increase flexibility for targeted assessments

82
Language Updates to Note in COP22
Language: From ‘client-centered’ toward ‘person-centered’ or ‘people-centered’
• Aligns with the UNAIDS Global AIDS Strategy• People are more than HIV clients• People make their own decisions, we respect their rights and
preferences• Differentiated services adapted to their life course and social context

84
Part 3:Targets and Budgets

85
Targets and Budgets for COP22
• Budgets are largely based on a flatline from COP21 levels, less ARPA funding, which was a one-time infusion. There are modest decreases in some countries based on overall funding constraints and specific country circumstances. Budgets include specific directives for PrEP (AGYW), PrEP (KP), and OVC (non-DREAMS) in addition to standard initiative and earmark controls from the last COP.
• Increased budgets for PrEP(KP) should not come at the expense of existing KP programming.
• Budget and targets should build on ARPA and other COVID mitigation efforts in COP21 to continue program recovery in areas disrupted during the COVID-19 pandemic in COP22.
• For local partner funding, in OUs that have not met the 70% target, capacity-building and mentorship efforts for local partners should be prioritized in COP22 planning, with funding set aside to support this work.

86
Targets and Budgets for COP22
• All OUs should budget to implement community-led monitoring
• As in COP21, COP22 targets and the subsequent approved budget should reflect the level of ambition the PEPFAR team in collaboration with the Government and civil society believes is critical for the country’s progress towards achieving and maintaining HIV epidemic control.
• Country teams and agencies should propose to S/GAC the targets they believe are achievable and feasible and hold their partners accountable to that achievement.
• Country teams are expected to make trade offs wherever possible to meet the various earmark, initiative, and programmatic control directives within their topline levels. The control change request process from last year remains in place in cases where, despite best efforts, not all controls can be met (including in cases where the presence of significant applied pipeline impacts ability to meet controls). Teams should describe trade offs made or considered before seeking relief from a given control.

87
Part 4:COP22 ToolsFAST, Datapack, Supply Planning Tool, Resource Alignment, Table 6 and SRE

88
COP22 Updates to the FAST
• Mechs List-R will automatically update with web-based connection to FACTS Info• SGAC will insert controls, no longer requiring manual data entry• “Not Specified: Not Specified-NSD” Program Area available for State/SGAC TBDs only• State/SGAC TBDs available for programming in unusual circumstances–Budgets require
prior approval from M&B• Users can manually add additional rows to Initiative-E tab without requiring update from
SGAC• Initiative-E metadata shortcuts available to reduce manual data entry• Earmarks calculations shown on Initiative-E tab, increasing earmark calculation
transparency• Quality Assurance and In-Country Logistics entered as overhead lump dollar sums rather
than percentages on Commodities-E tab• Standard COP Matrix-R tab will update automatically without requiring power query or data
tables• Approval Memo Tables will be made available to teams and HQ agency users early in the
COP process, on an ongoing basis

89
COP22 Updates to the Supply Plan Tool
• The Commodities Supply Plan Tool underwent numerous changes in COP21 that facilitate its completion and will carry through into COP22.
• New in COP22, the tool includes a Gap Analysis tab that will enable greater integration with program targets and will allow teams to identify commodities gaps and risks that are anticipated for COP22.
• The Gap Analysis tab consists of four data entry sections: ARVs, RTKs, EID and Viral Load, and PrEP. The data needed to complete the tab is largely from the SDS and represents a merger of the SDS data, PEPFAR targets, and the commodity quantification.
• Each section outputs visualizations that can and should be incorporated into OU COP presentations and discussions, especially where a “high risk” is determined.

90
COP22 Updates to the Datapack
● Reorienting of the Cascade Tab around PVLS, rather than ART Coverage, although both are taken into account.
● More tools to understand each element contributing to PVLS, and how these translate to PEPFAR MER targets.
● Changes in line with MER 2.6:
○ 50+ finer age bands across the clinical cascade. These will be aggregated to 50+ upon DATIM import for all but TX_CURR.
○ Use of PrEP_CT in lieu of PrEP_CURR.
○ Integration of the new SNS modality.
WHAT HAS CHANGED?
● Overall structure that begins with Spectrum Data and a Cascade tab that flows throughout the rest of the DataPack.
● PSNUxIM tab structure that will handle de-duplication and IM allocation.
● Use of the DataPack Self-Service App for tool validation.
● Availability of Zendesk Chat for rapid support, and ZoomGov for real-time troubleshooting.
● Integration with PAW for near real-time visualization of Data Pack targets alongside FAST budgets and historic trends.
WHAT IS THE SAME?
91
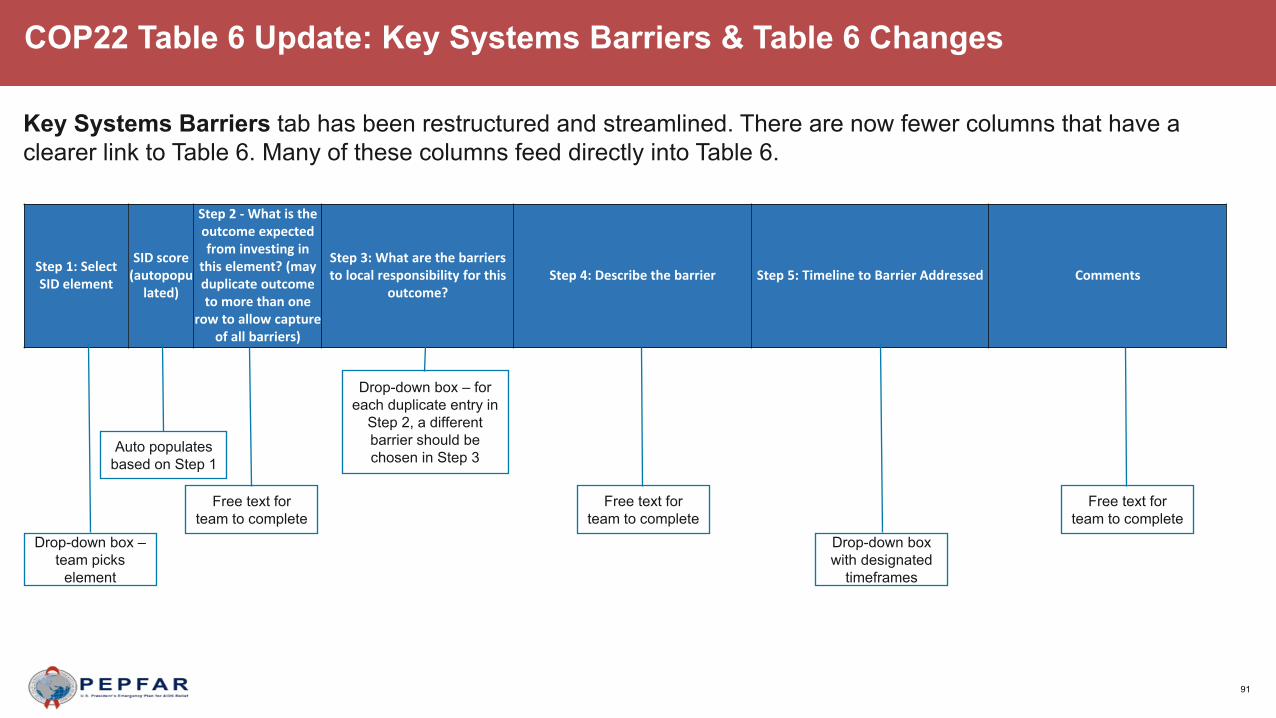
COP22 Table 6 Update: Key Systems Barriers & Table 6 Changes
Key Systems Barriers tab has been restructured and streamlined. There are now fewer columns that have a clearer link to Table 6. Many of these columns feed directly into Table 6.
Step 1: Select SID element
SID score (autopopu
lated)
Step 2 - What is the outcome expected from investing in
this element? (may duplicate outcome to more than one
row to allow capture of all barriers)
Step 3: What are the barriers to local responsibility for this
outcome? Step 4: Describe the barrier Step 5: Timeline to Barrier Addressed Comments
Drop-down box –team picks
element
Auto populates based on Step 1
Free text for team to complete
Drop-down box – for each duplicate entry in
Step 2, a different barrier should be chosen in Step 3
Free text for team to complete
Drop-down box with designated
timeframes
Free text for team to complete

92
COP22 Table 6 Update: Key Systems Barriers & Table 6 Changes Cont’d
This is a drop-down list that links the activity to the SID question/componentSID component the activity is expected to impact
Expected Outcome This pulls from the key systems barrier tab which is free text
Primary Barrier to Local Responsibility this activity addresses
This is the same drop-down list from the key systems barrier tab
Barrier to Local Responsibility this activity addresses-2 (optional)
This is the same drop-down list from the key systems barrier tab
Barrier to Local Responsibility this activity addresses-3 (optional)
This is the same drop-down list from the key systems barrier tab
If ongoing from a previous year, please provide rationale for continued spending
This is free text providing space for explanation for ongoing activity
Table 6 has been reorganized and several new columns have been added. This is in an effort to better link the above site activities with the SID and sustainable outcomes. Listing of the new columns are below.

93
Surveillance, Surveys, Research and Evaluation Tool (SRE)• The SRE Tool provides an overview of all surveys-surveillance, research, and evaluation activities that are planned to be
implemented during the COP22 period within an OU.
• All SREs expected to receive a COP22 budget should be included in the SRE Tool (and Table 6 and FAST).
• Previously there was one SRE Tool-E tab. For COP22, this is broken out into two tabs for evaluations (Eval E-tab) and then surveillance, surveys, and research (SaSR E-tab).
• Additionally, new columns have been added to the Eval and SaSR tabs to better align with the data entry fields from DATIM enrollment forms.
• Lastly, the instructions within each SRE tab have been expanded to provide additional direction, and an open entry column titled ‘additional comments/notes’ has been added to the end of the SRE tabs.
• Please find below a high-level outline of the SRE data submission process:
Review status of activities and identify relevant program gaps, if any, in January/February.
Submit SRE Tool to SGAC with proposed SREs in February/March prior to Planning Meeting.
At COP22 meetings in February/March, OUs receive feedback on approval of proposed SREs.
Once feedback is addressed and final approval has been received, SRE tools should be included in the OU’s final COP22 submissions.

94
Resource Alignment Funding Landscape Table
OUTPUT• Verified and updated information will allow
production of RA Country Profiles (illustrative screenshot below)
• RA Country Profiles will be available to teams for C/ROP planning
• Populated tables will be readily available for teams to include in their SDS investment profile section 2.3
USE• Harmonized financial data across
funding sources, in particular, across two large HIV donors and partner country govt
• Strengthens joint collaboration and improves efficiency in resource allocation
• Supports achieving strategic alignment and complementarity across all available HIV and broader health resources to maximize impact and value of PEPFAR, Global Fund, and partner country investments
• Informs evolution of greater responsibility for and control of, the HIV response to partner country governments and communities to support sustained control of the HIV epidemic
INPUT• HIV Resource Alignment provides routine
harmonized financial data across all funding sources
• Annual C/ROP process provides opportunity to verify and update Domestic Govt and Other Funder contributions
• Request from Country Teams: Pre-populated* RA Funding Landscape Table (illustrative screenshot below) will be sent to country teams to verify/update only Domestic Govt and Other Funders data where applicable
• PEPFAR and Global Fund data sourced from HQ systems * Where data is available

95
COP22 Elements and Supplemental Document Checklist

96
COP22 Elements and Supplemental Document Checklist

97
Part 5:External stakeholder engagement, timeline for COP22virtual COP meetings

98
Planning, Implementation and Management for Program Impact
Implementation/ POART Cycle(COP20 Q4 POART included agency
strategic recommendations and country presentations with Country
Accountability and Support Teams (CASTs)
• COP Cycle• Plan and budget to achieve program goals, along with program
quality and sustainability
• OU-level strategy translated into actionable IM work plans
• COP22 will continue to focus on translating solutions, adaptive practices, and innovations into full-scale implementation in a rapid and efficient manner
• Quarterly POART Discussions• COVID-19 updates and impact on PEPFAR programs
• Financial & program performance
• Partner management• Results (current challenges include over-testing and
treatment continuity)• Risk mitigation (fraud, underperformance, capacity of sub
awardees)
• Real time adjustments
• Q4 closes the previous FY and checks trajectory for current FY

99
COP22 Virtual Planning Timeline – Three Tracks
• Bilateral programs (Single OUs) will participate in 1 of 3 groups
• Regional Platforms will have a longer timeframe to finalize planning and tools
• Sustaining HIV Impact OUs have additional engagement and longer timeline to finalize planning and tools

100
COP22 Virtual Planning Considerations
• The same as in COP21, country teams should plan for best use of time before and after the in-country (hybrid, in-person or virtual) retreat / stakeholder meeting to advance planning before the formal COP Planning Meeting.
• Continue meaningful engagement with external stakeholders throughout the development and implementation of COP22.
• The same as in COP21, teams create a country-specific calendar of events that details when documents will be shared and when meetings will be conducted so CSOs can plan and effectively support COP development.
101
Recommendations for strengthened CSO engagement for COP/ROP 22 Meetings: SGAC Chairs & PPMs
• Create multiple spaces in the agenda for CSO representatives to offer priorities, with ample notification to be prepared for such input. Consider adding a component for a 5 min summary statement for any stakeholders (e.g., CSO representatives, government officials, multilateral colleagues) at the end of sessions to offer concerns.
• Make good use of the comments section in the virtual meeting. Set ground rules for open and professional engagement. Do not mute comments and be diligent in answering questions and concerns as appropriate.
• Consider hosting a check-in with stakeholders prior about a week prior to the beginning of the meeting to understand any higher-level concerns or points of contention.
• Cultivate informal communication channels (e.g., side bar conversations)• Be aware of when CSO representatives are less engaged. Be sure to actively seek their input.• Recognize the role of Global and Regional CSO partners present in the meetings, who have
affiliations to local CSO representatives. Their advocacy efforts are informed by their relationships and collaboration with local CSOs, and often reflect global trends that assist in the success of PEPFAR.

102
Recommendations for strengthened CSO engagement for COP/ROP 22 Meetings: PEPFAR Coordinators
• COP/ROP Meeting delegation guidance prescribes participation of diverse constituencies, with specific requirement related to PLHIV, KP, AGYW and faith communities. Ensure meeting delegations include CSO representatives from a variety of communities, with emphasis placed on PLWHAs, KPs, and Youth/AGYW. Seek to engage CSO representatives who are knowledgeable about PEPFAR processes and represent entire communities vs. specific implementing partners.
• Create or update a contact list of national/regional civil society leaders and organizations. Update and circulate the USG/PEPFAR contact list among CSOs.
• Email all contacts on the civil society list to provide an open door for communication and describe the R/COP22 Process.
• Consider a meeting in mid-January to solicit preliminary questions or suggestions for R/COP22, both technical and logistical.

103
Recommendations for strengthened CSO engagement for COP/ROP 22 Meetings: PEPFAR Coordinators
• Provide notice as early as possible of the schedule for strategic retreats and other meetings and provide time on the agenda for CSOs to raise concerns.
• Engage CSOs in validating CLM data.
• Ensure quarterly meetings with CSOs throughout the year to provide opportunities for input outside of the R/COP process during which there is usually limited time/bandwidth
• Cultivate informal communication channels (e.g., side bar conversations) during the COP/ROP meeting
• Ensure CSO feedback is documented throughout the process, and specifically during the approval meeting, with PEPFAR’s team response, and rationale.

104
COP22 Virtual Planning Groups
Initial Tools Submission for HQ Review (at least 7 days prior to Planning Meetings)
• Group 1: February 28, 2022
• Group 2: March 7, 2022
• Group 3: March 14, 2022
Virtual COP Planning Meeting Dates● Group 1: Week of March 7, 2022
o Single OUs▪ Nigeria, Rwanda, Cameroon, Mozambique, Ukraine, South
Sudan, South Africao Sustaining HIV Impact OUs
▪ Lesotho● Group 2: Week of March 14, 2022
o Single OUs▪ Burundi, Dominican Republic, Zimbabwe, Tanzania, Côte
d’Ivoire, Ethiopia, DRC, Angola, Malawio Sustaining HIV Impact OUs
▪ Ugandao Regional Platforms
▪ West Africa Region● Group 3: Week of March 21, 2022
o Single OUs▪ Vietnam, Zambia, Haiti
o Sustaining HIV Impact OUs▪ Kenya, Botswana, Eswatini, Namibia
o Regional Platforms ▪ Western Hemisphere Region, Asia Region
COP22 Submission Dates• Group 1: April 19, 2022
• Group 2: April 22, 2022
• Group 3: April 29, 2022
All COP22 Approval Meetings should take place betweenApril 25 – May 13, 2022

105
COP22 Stakeholder Townhalls and Planning Meeting Delegation Information
Cross-cutting virtual webinars as part of COP/ROP22 Planning meetings.
Pre-retreat Leadership Meeting for the six ‘Sustaining Impact’ OUs(Botswana, Eswatini, Kenya, Lesotho, Namibia, Uganda)
Thursday, January 27, 2022time 7-8:30 am EST
COP22 Live Virtual Stakeholder & Civil Society Webinar
Thursday, February 24, 20227-8 am EST
COP22 Live Virtual Opening Plenary Monday, February 28, 20227-8 am EST
COP22 Live Virtual Government Partner Meetings Thursday, March 10, 2022 & Wednesday, March 23, 20227-8 am EST
COP22 Live Virtual Stakeholder & Civil Society Townhalls
Thursday, March 10, 2022 &Wednesday, March 23, 20228-9 am EST
COP22 Live Virtual Closing Plenary Monday, March 28, 20227-8 am EST

106
Field TeamFor Regional OUs: Regional programs (Asia, West Africa, and Western Hemisphere) should broadly follow the below guidance. However, field teams, S/GAC Chairs, and PEPFAR Program Managers should work together to determine optimal representation balanced with prudent meeting management.Each team should ensure there are individuals identified to attend in the following roles.
Front Office Representative (Chief of Mission or Deputy Chief of Mission only)Required USG PEPFAR interagencyparticipants:• Front Office Representative (1)• USAID Mission Director (1)• CDC Country Director (1)• PEPFAR Coordinator or individual in
that capacity (1)• Interagency SI Lead (up to 2)• Agency Lead (1 person per
agency implementing in country)• USAID Budget Lead (1)• HHS/CDC Budget Lead (1)• USG Technical experts (up to 14)• Interpreter (if needed)
Required Field Stakeholder participants: (to be invited by the Field team)• MOH/MOF and other government representatives (up to 4)• Civil Society representatives (up to 7)• Must represent multiple and diverse constituencies• For all countries: 1 delegate must be a representative of people living with HIV, 1
delegate must represent key populations (where safe to do so), 1 delegate must represent faith communities; and in countries with DREAMS/other AGYW programming: 1 representative must represent AGYW
• Regional programs and country pairs should work with their chairs and PPMs to determine the optimal number of representatives.
• Global Fund Portfolio Manager (1)• Global Fund Principal Recipient (1)• UNAIDS representative (1)• WHO representative (1)
COP22 Virtual Planning Meeting Delegation Guidance

107
COP22 Virtual Planning Meeting Delegation Guidance
Headquarters
The USG headquarters delegation must includeCountry-Specific USG HQ Team:• SGAC Chair (1 per country)• PEPFAR Program Manager (1 per country)• CAST Members (1 per agency per country, as
allocated to POART calls)• SGAC Support Liaison (up to 3)
• DUIT• PET• M&B
At-large headquarters members:• Deputy Principals• HQ Financial Points of Contact• Technical Experts on the ISME list (prioritized
technical areas to be determined by Chairs/PPMs and CAST)
Headquarters Stakeholder Delegation• Global Civil Society and Community Organizations: Each invited organization will select up to 4 representatives
per week for single country OUs and 1 per organization for regions.• Multilateral Organizations (WHO, UNAIDS, Global Fund): Up to two (2 total) staff members from Headquarters
per organization will be invited per week.• Other Global Stakeholders: Up to two representatives from other key stakeholder organizations will be invited per
week.

"The United States reaffirms our steadfast commitment to partnering with countries and communities to help end the HIV epidemic, support resilient
and responsive health systems, and create a healthier, more equitable, and more secure world."
U.S. Secretary of State Antony J. Blinken, World AIDS Day December 1, 2021
THANK YOU!
18