Pediatric Palliative Care in Bangladesh- an overview
44
Pediatric Palliative Care in Bangladesh- an overview Dr. Zohora Jameela Khan, MD, DCH Assistant Professor Dhaka Medical College Hospital Dr. Zafor Md. Masud, FCPS, MPhil Dr. Shahinur Kabir, Dip Pall Med
Transcript of Pediatric Palliative Care in Bangladesh- an overview

Pediatric Palliative Care in Bangladesh-an overview
Dr. Zohora Jameela Khan, MD, DCHAssistant Professor
Dhaka Medical College Hospital
Dr. Zafor Md. Masud, FCPS, MPhil
Dr. Shahinur Kabir, Dip Pall Med

Pediatric palliative care
The American Academy of Pediatrics set the following as a minimum standard for pediatric palliative care:
“Excellence in pediatric palliative care is essential for hospitals and other facilities caring for children. Program development in pediatric palliative care, along with community outreach & public education, must be a priority of tertiary care centers serving children.”

Palliative care in children with cancer: which child and when?
• Approximately 40-50% of children who have the need of palliative care have malignancy.
Relapse cases of Leukemia(Marrow, CNS and Testicular relapse),metastatic solid tumor, ICSOL.
• Parents refused treatment when there is chance of cure.
(3)

Appropriate care near the end of life.
Murray S A et al. BMJ 2005;330:1007-1011
©2005 by British Medical Journal Publishing Group

Need of Pediatric Palliative Care in Bangladesh
•WPCA categorization : Bangladesh is in group 3a.
•Actual children cancer burden: Not known?
•New children cancer diagnosed in 2013 in different hospitals of Dhaka:
a)Dhaka Medical College Hospital- 171
b)National Institute of Cancer Research & Hospital-302
c)BSMMU- 455
•Poor referral

Palliative and Supportive Care Networks
Bangladesh
Centre for Palliative Care(CPC), BSMMU
National Institute of Cancer Research and Hospital.
ASHIC Palliative Care Unit
Shanti Oncology and Palliative Care Unit
Bangladesh Palliative and Supportive Care Foundation
Afzalunnessa Foundation(6)

ASHIC Palliative Care Unit
• Non-profit charity organization.
• Started in May 2006 with funding from UICC under its My Child Matters campaign.
• It is the first and only facility in Bangladesh to offer palliative care to the terminally ill children.
• Capacity-9 bed.
• Mission: To ensure that every child affected with cancer should get proper tender loving care, treatment and quality of life.

Mrs Choudhury started the ASHIC Foundation in 1994 after the loss of her son Ashiq due to cancer when he was just 3 years old. During Ashiq’s yearlong treatment in a hospital in London, she experienced medical and community support to help the cancer-affected children and their families. Deeply inspired by these charities, Mrs Choudhury wanted to make a difference in the field of childhood cancer in Bangladesh. In 2006, it started ASHIC Palliative Care Unit.

Staff flow chart of ASHIC Palliative Care Unit
Chairperson
4 Medical Officers
Manager
Medical Social Worker
Ward Boy
Aya5 Stuff Nurses
3 (Three) Consultant
Pediatric Oncologist
Medical Oncologist
Palliative specialist

ASHIC PCU Team

Palliative care is often said “low tech & high touch”
(11)

Relieve of Suffering
(12)

Methodology
• Study design: Retrospective type of observational study
• Duration of the study: May 2006 to August 2013
• Place of the study: ASHIC palliative care unit,
Dhaka.
• Study population: Cancer Patient less than18 years of age attending in palliative care unit

Methodology……..
• Sample size: All the patient age less then 18 years attending in PCU during the study period. That is 540 patients.
• Sampling Technique: Purposive sampling technique was adapted.
Selection criteria:
-Less than18 years of both sexes.
-Children with cancer of palliative stage.

Methodology………..
• Data Collection Tool: Data collected from patient’s register book and bed head tickets by a checklist
• Data Analysis: Data were checked cleaned and edited properly before analysis. Data analysis was done through Micro soft EXCEL and was evaluated by frequency, percentage, table and figure.

Methodology………
• Ethical Consideration: . Written consent was taken from the concerned authority.

Aim of this study
•To assess demographic profile
•To observe type of cancer & clinical profile
•To observe treatment modalities needed for symptom management in pediatric palliative patients.

Residence of the patients’
Outside the Dhaka 82% Within Dhaka
18%

Distribution of the patients by age group
0
50
100
150
200
250
0 to <5 >5 to 10 >10 to 15
226, 41.85%
17031.48% 144
26.67

Distribution of patients by gender
349, 65%
191, 35%
Boys Girls

63%15%
22%
Government Hospital)BSMMU (Bangabandhu Shiekh Mujib Medical University)Private Hospital
Source of PCU patient referral
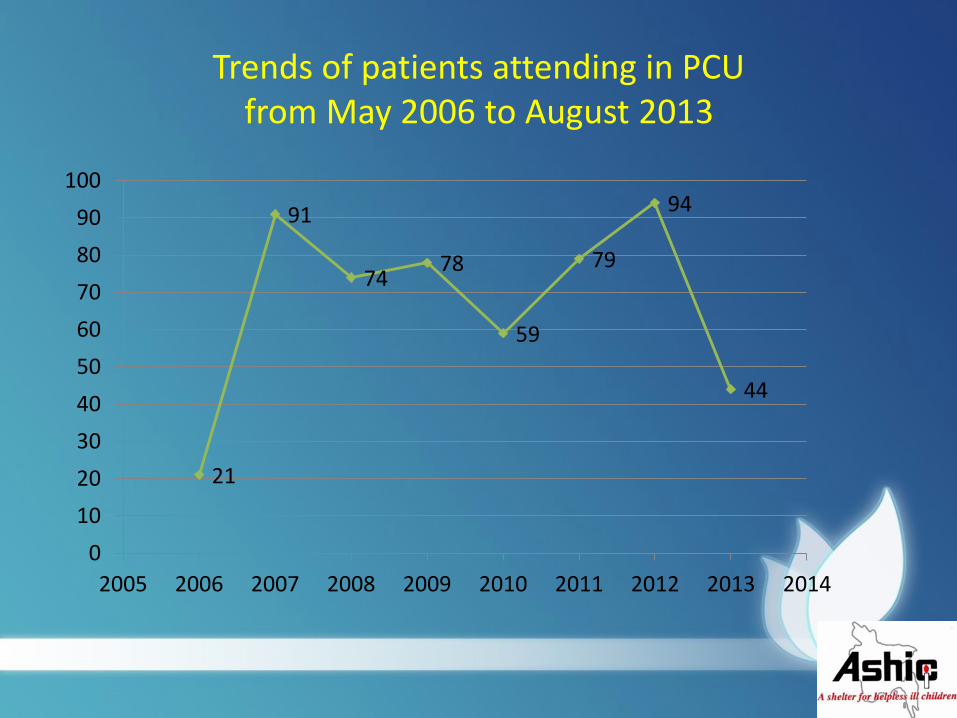
Trends of patients attending in PCU from May 2006 to August 2013
21
91
7478
59
79
94
44
0
10
20
30
40
50
60
70
80
90
100
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014

0
20
40
60
80
100
120
140138
82
62
34 32
22 22 20 19 18
91
Retinoblastoma
ALL
NHL
Ewing’s Sarcoma
AML
Rhabdomyo Sarcoma
HD
Neuroblastoma
Wilms’ Tumour
Osteosarcoma
Others
Disease profile

Distribution of PCU patients by type of malignancy
342, 63%
198, 37%
Solid tumour Hematological

Solid Tumour
Metastatic/locally advanced retinoblastoma 26.73%
Metastatic Ewing sarcoma 6.37%
Recurrence Rhabdomyosarcoma 3.89%
Metastatic Nephroblastoma 3.54%
Neuroblastoma 3.72%
Germ cell tumor 3.02%
Osteosarcoma with pulmonary mets 3.19%
Miscellaneous malignancies 16.99%

Clinical presentation
Moderate to severe pain, fever, pallor and bleeding manifestation
75%
Respiratory distress 46%
Skin sore (Infection/extravasation of chemo drug)
35%
Bowel/bladder incontinence 11%
Diarrhea 0.86%
Convulsion 1.9%

‘quality of life is what a person says it is’
It relates to individual’s subjective satisfactionwith life
(27)
Quality of life

Pain
• Assessment• Monitoring• Analgesics• Management should include reducing
stress/anxiety as far as possible as well as analgesic measures
(28)

Management needed for pain
• Morphine(oral/injectable): 48.70%
• Paracetamol ± NSAID: 20.9%
• Steroid: 8.6%
• Gabapentin: 0.86%• Palliative chemotherapy: 19.39%• Palliative radiotherapy: 6.8%• Acupressure: 0.37%

Acupressure

Commonly Used Medicine

Pain assessment
(32)

Other supportive care given
• Oxygen inhalation• Nebulization• Transfusion of blood component• Antibiotics• Antiulcerant• Anticonvulsant• Pleural fluid aspiration• Ascitic fluid aspiration• Ryles tube feeding

Keeping Charcoal beside patient’s bed side to minimize foul smell
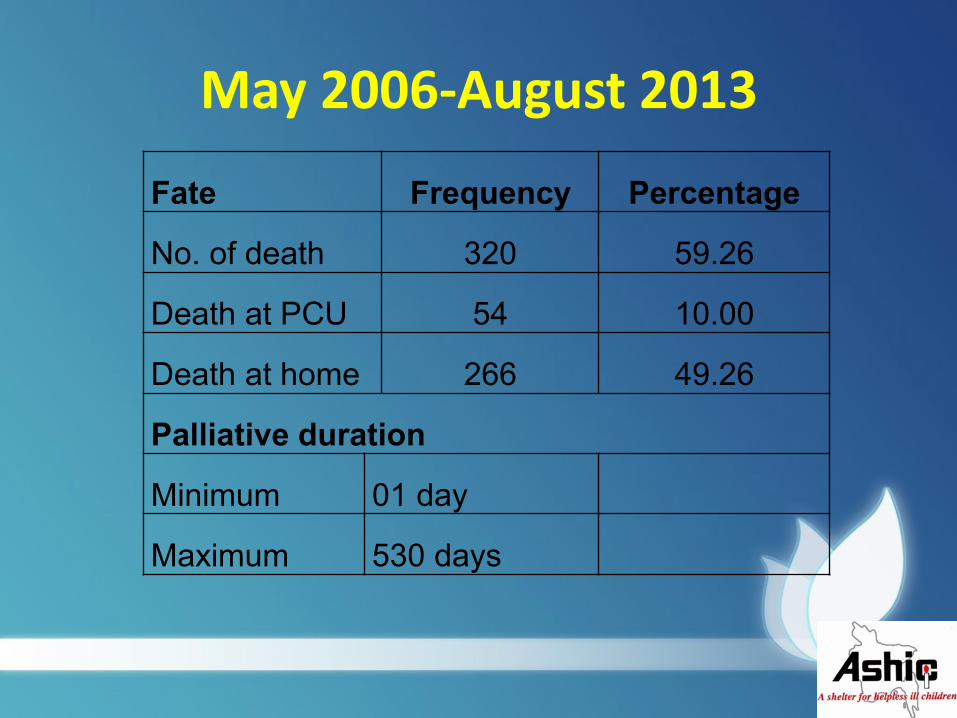
May 2006-August 2013
Fate Frequency Percentage
No. of death 320 59.26
Death at PCU 54 10.00
Death at home 266 49.26
Palliative duration
Minimum 01 day
Maximum 530 days

Discussion• A total number of 540 children aged below 18 years
of both sexes were included in the study. Of the total 540 patients, majority(41%) were <5 years,31% were between 5-10 years and the rest (26%) were >10-15 years and only 2 cases were >15 years. A male preponderance was noted (64%).
• Majority(82%) of patients residence are outside Dhaka.
• Most of the patients presented with pain,fever,pallorand bleeding manifestation. The next common presentation was respiratory distress. Different type of skin manifestation was present in 35% patients.

Cont.
• Out of 540 patients solid tumour was
observed in 63% cases and the rest (37%)
had Hematological malignancies.

Cont.
• Pain assessment in younger children done
by observing signs & facial expression
and by visual analog scale in older child.
Majority(48%) of children needed
Morphine to control pain. Paracetamol ±
NSAID were needed in 20%.Steroid
reduce pain in 9% cases. Palliative
chemotherapy got 19% children and 7%
children received palliative radiotherapy.

Conclusion
•Out of total 540 patients majority were <5 years.
•Male preponderance was noted.
•Majority of patients came from outside the Dhaka.
•Solid tumor is more common.
•Common symptoms were pain, fever, pallor & bleeding.
•Morphine was needed for effective pain control in maximum patients.

Recommendation
Considering all above findings it may beconcluded that skill medical attention torelieve symptoms of children with palliativestage is essential. But the pediatric palliativecare service in Bangladesh is limited. Soestablishment of pediatric palliative care unitin government hospitals as well as in privatesector will reduce sufferings of dying childrenwith cancer and their parents.

Challenges
Lack of awareness about palliative care among health professionals.
Scarcity of trained professionals.
Psychological aspect of children often ignored by physicians.
Intention of treatment almost always to cure rather than palliation.

Contd.
Clinical guidelines of palliative care written in text book but rarely practiced.
Philanthropic support is not satisfactory.
No fund for research.
Erratic supply of opioids.
Conflicts.

“ Go around and see what is being done and then see how your own circumstances can produce another version; there is need for diversity in this field.”
Dame Cicely Saunders, Founder St. Christopher’s Hospice
(43)

To correspondence:
Dr. Zohora Jameela Khan
Assistant Professor
Paediatric Hematoma-Oncology Department
Dhaka Medical College Hospital, Bangladesh
Consultant
ASHIC Paediatric Palliative Care Unit
Dhaka, Bangladesh
Mobile: +88-01716616499
Email: [email protected]