ParPadox of the Lebanese Health care System and the Role of the NSSF
203
Lebanese University Faculty of Economics and Business Administration First branch Paradox of the Lebanese Health care System and the Role of the NSSF A research submitted for the fulfillment of the requirements for the Degree of Master Research in Business Administration (Finance and Banking) Prepared by Lama Ali Danash Debate Committee Dr. Hussein Badran .......................................................................... Chairman Dr. Rita Naimeh ............................................................................... Supervisor Dr. Mohammad Wehbi............................................................. Co-supervisor Academic Year 2012-2013
Transcript of ParPadox of the Lebanese Health care System and the Role of the NSSF

Lebanese University
Faculty of Economics and
Business Administration
First branch
Paradox of the Lebanese Health care System and
the Role of the NSSF
A research submitted for the fulfillment of the requirements for the Degree of
Master Research in Business Administration
(Finance and Banking)
Prepared by
Lama Ali Danash
Debate Committee
Dr. Hussein Badran .......................................................................... Chairman
Dr. Rita Naimeh ............................................................................... Supervisor
Dr. Mohammad Wehbi ............................................................. Co-supervisor
Academic Year 2012-2013

To the souls of those who died deprived from the health care

Acknowledgments
Many people contributed to this project and my entire graduate experience. I
owe a debt of gratitude to my thesis committee. Each member inspired me in a
different and important way. The chair of the committee, Dr. Hussein Badran,
pushed me to improve as a student and as a professional and always took time
to teach me something new. The supervisor, Dr. Rita Naimeh, provided me
with advice and comments to end with this valuable project. The co-supervisor,
Dr. Mohammad Wehbe, provided us with a beneficial lecture ―Financial
Information System‖ which facilities many things in this project.
Thanks for the continuous support and kind communication which had a
great effect regarding to feel interesting about what I was working on. Finally
yet importantly, I wish to extend my gratitude to my family and supportive
friends for their encouragements to complete this academic year.

خالصة
. في اآلونةالتي تمس حياة الماليين من المبنانيين في كل لحظة ةالضروري الخدمات منالرعاية الصحية تعتبر . الصحيةالرعاية امكانية تحسين طريقة تقديمالصيدالنية ، والمعرفة االدوية،اظير تطور التكنولوجيا األخيرة
القضايا من الرعاية الصحية وسيولة الحصول عمىعمى الرغم من ىذه اإلنجازات ، أصبحت التكمفة، والجودة ، قد حممت تكمفة الرعاية الصحية ىذا وان الزيادة الممحوظة في المبناني. التي تشغل بال التشريعية والسياسية الرئيسية
فضال التغطية الصحية. المبنانيين يفتقرون الى العديد منكما ان . عبء كبيرا األسرو التأمين الصحي انظمة الحكومة ، مي الرعاية الصحية والمستيمكين .تكاليف تقديم الرعاية المجانية ىي عبء كبير لمقدعن ان
سوق . انيا تعرض اإلدارية و المالية ةيالناحوتيدف ىذه األطروحة إلى دراسة نظام الرعاية الصحية المبناني من راضا تطمب ىذه الدراسة استعتابل العام. مب ، القطاع الخاص مقزوايا مختمفة: العرض مقابل الط منالخدمات الصحية
دور الصندوق ىذا وانيا تعرضالخاصة والعامة. الييئاتجميع ستطالعات سابقة إضافة لجمع البيانات منااللجميع م مناقشتيا منذ فترة طويمة .تي تفي التصدي ليذه التحديات ، وىي الفكرة الت الوطني لمضمان االجتماعي
التأمين تقديم الصحية المتعددة في مييئاتأساسيين . أوال، ما ىو الدور الحالي ل اشكاليتينطروحة ألىذه ا تتناول ، وكيف يمكن تحسين ىذه الرعاية بشكل يؤمن كفاية المواطن من التغطية المنخفض الجودة والعالي التكمفةالصحي
لمصندوق الوطني لمضمان االجتماعي تضييق فجوة يمكن ثانيا، كيف الصحية ويحافظ عمى ربحية الييئات الصحية؟ ؟ خدمات التي يقدميا وتوسيع دائرة االنتسابفي اطار ال في تقديم الرعاية الصحية الالمساواة
الخاصةالرعاية مع عمى حد سواء قطاع الخاص ىو المزود الرئيسي لالستشفاءاألطروحة أنو بالرغم من أن ال تبين من قبل خارج المستشفيات ل رعاية مرضى يتمو يتم المال العام ، بينما حساب اصة تزدىر عمىالمستشفيات الخفان
األسر .
ضوح أن اإلنفاق عمى الصحة يدد استدامة النظام . كما أنو يظير بو فان الزيادة المستمرة في التكمفة تومع ذلك ، مضمان الوطني ل دور صندوق اظيارإلى مستوى ينذر بالخطر من حصة الناتج المحمي اإلجمالي. ىدفنا ىو قد وصل
تطبيقو لصالح إصالح النظام الصحي .دائرة اإلجتماعي من خالل توسيع
Abstract
Health care is an essential service that daily touches the lives of millions of Lebanese at
major and weak times. Recently, technology, pharmaceuticals, and knowledge have
considerably improved how care is delivered and the prospects for recovery.
Despite these unusual accomplishments, the cost, quality, and accessibility of Lebanese
health care have become main legislative and policy issues. Considerable increases in the
cost of health care have placed significant stress on government, households’ health
insurance system. Many Lebanese lack health coverage. The costs of providing
uncompensated care are a large load for health care providers and consumers.
This thesis aims to examine the Lebanese health care system from the managerial and
financial points of view. It allows for an over viewing of the health services' market by
undertaking it from different angles: supply versus demand, private versus public sectors.
This study requires a review of all previous surveys additional to the collection of related
data with all private and public agencies. It also examines the role of NSSF in addressing
these challenges, an idea that has long been debated.
The thesis addresses two basic questions. First, what is the current role of multi-
insurance health providers in low quality health care versus high cost, and how can it be
enhanced to increase consumer welfare in parallel with the providers return? Second, how
has, and how should, the National Social Security Fund work to narrow the gap of the
Lebanese health inequality regarding services and expansion in application?
The thesis reveals that, although the private sector is the main provider of both hospital
and ambulatory care, private hospitals are booming on public money, whereas outpatients
care is mainly financed by the households.
However, at the price of an ever increased cost, threatening the sustainability of the
system. This is what is achieved in this thesis, as it shows obviously that expenditures on
health have reached an alarming level of the GDP share. Our purpose is clearing the role of
the NSSF by expanding its application in favor of reforming the health system.
Résumé
La santé est un service essentiel qui touche quotidiennement la vie de millions de
Libanais à des moments importants et faibles. Récemment, la technologie, les produits
pharmaceutiques et les connaissances ont considérablement amélioré la prestation des soins
et les perspectives de reprise.
En dépit de ces réalisations exceptionnelles, le coût, la qualité et l'accessibilité des soins
de santé libanais sont devenus des principales questions d'ordre législatif et politique.
L'augmentation considérable du coût des soins de santé a mis un accent important sur le
gouvernement, le système d'assurance- santé des ménages ». Beaucoup de Libanais ont un
manque de couverture sanitaire. Le coût des soins non compensés est une charge importante
pour les fournisseurs de soins de santé et les consommateurs.
Cette thèse vise à examiner le système de soins de santé libanais à partir d’un point de
vue managérial et financier. Il permet une visualisation du marché des services de santé en
procédant à des angles différents : l'offre face à la demande, le secteur privé et le secteur
public. Cette étude nécessite un examen de toutes les enquêtes précédentes supplémentaires
pour la collecte des données relatives à tous les organismes publics et privés. Il examine
également le rôle de la CNSS à relever ces défis, une idée qui a été longuement débattue.
La thèse aborde deux questions fondamentales. Tout d'abord, quel est le rôle actuel des
prestataires de santé multi- assurance dans les soins de santé de qualité inférieure et du coût
élevé, et comment peut-il être amélioré pour augmenter le bien-être des consommateurs et le
gain des fournisseurs ? Deuxièmement, comment, la CNSS devrait elle travailler pour
réduire la lacune des inégalités de prestation de service concernant la protection sanitaire et
l’expansion de son accès.
La thèse montre que, bien que le secteur privé est a la fois le principal fournisseur les
soins hospitaliers, les hôpitaux privés se prospèrent au détriment de l’argent public, alors
que les soins en ambulatoire est essentiellement financé par les ménages.
Cependant, l’augmentation continuelle des coûts, menace la pérennité du système. Ce
qui est réalisé dans cette thèse, montre évidemment que les dépenses de santé ont atteint un

niveau alarmant de la part du PIB. Notre but est de compenser le rôle de la CNSS en
élargissant son application en faveur de la réforme du système de santé.

(Article 22, UDHR)

Table of Contents
Introduction .................................................................................................. 1
Part One: Lebanese Health System Profile ............................................... 6
Chapter I: Background on Lebanon ............................................................... 6
A. Macro picture ..............................................................................................................6
1. Geographic and administrative profile ..........................................................................6
2. Demographic and social profile ....................................................................................7
3. Economic profile ...........................................................................................................8
B. History of Lebanon .....................................................................................................10
1. Ottoman period .............................................................................................................10
2. French intervention .......................................................................................................10
3. Lebanon after independence ........................................................................................ 11
4. Civil war .......................................................................................................................11
5. Lebanon today ..............................................................................................................12
Chapter II: Lebanese Health System ............................................................ 15
A. History of health system .............................................................................................15
1. Pre-independence phase (1864-1943) ......................................................................... 15
2. Independence phase (1943-1960) .................................................................................15
3. Reforms (1960-1975) .................................................................................................. 16
4. Civil war (1975-1992) ................................................................................................ 16
5. Current health system ................................................................................................. 18
6. Millennium Declaration goals for Lebanon .................................................................19
B. Determinants of health ...............................................................................................23
1. Poverty ......................................................................................................................... 23
2. Employment .................................................................................................................26
3. Environment .................................................................................................................27
C. Health status indicators .............................................................................................28
1. Mortality in Lebanon ....................................................................................................28

2. Morbidity in Lebanon ...................................................................................................30
3. Risk factors (Intentional and non-intentional) .............................................................37
4. Special groups .............................................................................................................39
Part Two: Lebanese Health Sub-system Profile ...................................... 44
Chapter I: Health system indicators .............................................................. 44
A. Health system Infrastructure ..................................................................................44
1. Ambulatory care ..........................................................................................................44
2. The hospital sector .......................................................................................................45
3. Technology and heavy equipment in hospitals ............................................................51
4. Pharmacies and laboratories .........................................................................................53
5. Dialysis, physiotherapy and radiology centers ............................................................54
6. Insurance companies ...................................................................................................55
B. Human Resources .......................................................................................................55
1. Orders and Syndicates ..................................................................................................57
C. Health care financing in Lebanon ............................................................................59
1. National Social Security Fund (NSSF) ........................................................................59
2. Security forces coverage ..............................................................................................60
3. Cooperative of the Civil Servants ................................................................................60
4. Ministry of Public Health – insurer of last resort .........................................................61
5. Mutual funds .................................................................................................................61
6. Private insurance ......................................................................................................... 61
7. Other health insurance funding resources ....................................................................62
Chapter II: Lebanese Health care System Financial Analysis ...................... 67
A. Lebanese health expenditure .....................................................................................67
1. External resources for health (% of total expenditure on health) .................................67
2. Health expenditure, private (% of GDP) ..................................................................... 67
3. Health expenditure, public (% of total health expenditure) .........................................68
4. Health expenditure, public (% of government expenditure) ....................................... 69
5. Health expenditure, public (% of GDP) ..................................................................... 69
6. Health expenditure, total (% of GDP) ..........................................................................70
7.Health expenditure per capita (current US$) ................................................................ 71
8. Health expenditure per capita, PPP (constant 2005 international $) .......................... 71
9. Out-of-pocket health expenditure (% of private expenditure on health) .................... 72
B. Data analysis of the Lebanese health quality versus cost .......................................73
1. Population and Sample Selection ................................................................................ 73
2. Instrumentation .............................................................................................................73
3. Questionnaire construction & Conceptual Framework for Data Analysis ...................74
4. Results ..........................................................................................................................74
C. Financial analysis of Lebanese Health expenditures ..............................................77
1. Pharmaceutical sector ...................................................................................................77
2. Hospitals .......................................................................................................................79
3. Ministry of health .........................................................................................................81
4. Expenditure by public financing agents .......................................................................82
5. Private insurance market ..............................................................................................83
6. Analysis of sources and uses of funds ..........................................................................85
7. Choice of providers by type of service ........................................................................ 87
Chapter III: Cross Country Comparison ....................................................... 90
A. International comparison of health expenditure .....................................................90
B. Assessment of the Lebanese Health Care System Performance ............................92
1. Sustainability ................................................................................................................92
2. Cost containment .........................................................................................................92
3. Rationalizing capacity in the hospital sector ................................................................93
4. Reallocating expenditure from curative to primary health care ...................................93
5. Controlling capital investment in medical technology .................................................93
6. Rationalizing expenditure on pharmaceuticals .............................................................93
7. Expanding health insurance coverage, limiting multiple coverage ..............................93
8. Equity ...........................................................................................................................94
Chapter IV: The Singapore Healthcare System ............................................ 95
A. Overview ......................................................................................................................95
1. Political Unity and Constancy of Purpose ....................................................................96
2. Establishing Priorities ...................................................................................................96
3. Promoting a way of Collective Well-Being and Social Harmony ...............................97
4. Respect and Education for Women ..............................................................................98
5. Building the Foundation ...............................................................................................98
6. Ensure Good and Affordable Basic Medical Services for All Singaporeans .............100
7. Engage Competition to Improve Service and Raise Efficiency ..................................100
8. Interfere Directly in the Healthcare Sector ..................................................................100
B. Demographics ............................................................................................................101
C. Health system Indicators ..........................................................................................102
1. Hospital beds ..............................................................................................................102
2. Physicians ...................................................................................................................103
D. Health care Expenditures .........................................................................................103
E. Lessons to learn .........................................................................................................105
1. Price and Outcome Transparency ................................................................................105
2. Higher Co-Pays ..........................................................................................................106
3. Payment by Capitation and Outcome, not Fee for Service .........................................106
4. Differentiated Service .................................................................................................107
5. Catastrophic Health Insurance .....................................................................................107
6. Transition from Hospital to Home and Community Care ...........................................107
Part Three: Lebanese National Social Security Fund ............................ 108
Chapter I: Applied Branches and Categories subject to NSSF ................... 108
A. Establishment of the National Social Security Fund ..............................................108
B. The Gradient in the application of social security in Lebanon ............................108
C. Branches of social security and their submissions .................................................110
1. Branch of sickness and maternity ................................................................................111
2. Branch of emergency work and occupational diseases ...............................................112
3. The branch of family allowances ................................................................................112
4. Branch for end of service ...........................................................................................113
D. People subject to all branches of social security .....................................................114
E. People subject to certain branches ...........................................................................116
Chapter II: Expansion in the application of NSSF ...................................... 119
1. The branches and submissions under study ...........................................................119
1. Dental care ...................................................................................................................121
2. Branch of emergency work and occupational diseases ...............................................122
3. The pension and social protection system ..................................................................125
2. The reasons for increasing the categories covered by Social Security .................128
1. Tobacco farmers ..........................................................................................................129
2. Writers and artists ........................................................................................................130
3. Municipal workers .......................................................................................................131
C. Data analysis about NSSF’s beneficiary health care satisfaction .........................132
1. Population and Sample Selection ................................................................................132
2. Instrumentation ............................................................................................................132
3. Questionnaire construction & Conceptual Framework for Data Analysis ..................133
4. Results .........................................................................................................................134
Chapter III: The financial situation of the NSSF ......................................... 137
A. Funding National Social Security Fund currently in Lebanon ...........................137
1. Finance by professional Subscriptions .......................................................................137
2. Financing by tax ..........................................................................................................138
3. Finance by a dual system .............................................................................................139
4. Funding of the Lebanese social security system .........................................................140
B. Financial situation ....................................................................................................145
1. The current financial situation of the National Social Security Fund .........................146
2. Financial results of the National Social Security Fund 2000 - 2009 ..........................148
3. The reasons for the accumulated deficit for both branches the sickness and maternity and
that of family allowances .................................................................................................152
C. Proposals to restore fiscal balance and cover the costs of expansion ..................156
1. Reduce expenses ..........................................................................................................156
2. Increase revenues ........................................................................................................157
3. Invest Social Security funds reserves .........................................................................159
Conclusion ......................................................................................................................161
Recommendations ..........................................................................................................166
References .......................................................................................................................170
Illustrations
List of Tables
Table (1): Demographic indicators in Lebanon .................................................................... 7
Table (2): Social Indicators in Lebanon ............................................................................... 8
Table (3): Economic indicators in Lebanon ......................................................................... 9
Table (4): Progress in MDG 4 – Reduce under-five mortality in Lebanon .........................20
Table (5): Maternal and reproductive health statistics in Lebanon .....................................21
Table (6): National Statistics for Tuberculosis in Lebanon (2009) .....................................23
Table (7): Average per capita and per governorate consumption (1000 LBP) ....................24
Table (8): Poverty measures per Mohafazat (2004-2005) ..................................................25
Table (9): Mortality in Lebanon (2011) ..............................................................................28
Table (10): Distribution of hospitals per size ......................................................................47
Table (11): Distribution of technology by region (2010) ....................................................52
Table (12): Geographic distribution of pharmacies and labs (2011) ...................................54
Table (13): distribution of dialysis, physiotherapy and radiology centers by region ......... 54

Table (14): percentage of population covered by various financing agencies ....................63
Table (15): Tutelage, entitlement, coverage and sources of financing of funding agencies 64
Table (16): Benefits under Various Public Financing Schemes ..........................................66
Table (17): frequency results of Q‖0‖ of the questionnaire .................................................75
Table (18): Distribution of hospital expenditures (%) .........................................................80
Table (19): Distribution of hospital reimbursement by type of service (%) .......................81
Table (20): Budgetary resources in the public health sector ...............................................82
Table (21): break-down of public expenditure on health services provided by the private
sector .....................................................................................................................................83
Table (22): Distribution of Private Insurance Expenditures ................................................84
Table (23): Private insurance account ($) ............................................................................84
Table (26): Distribution of health care expenditure ............................................................85
Table (27): Percentage of distribution of Out-of-Pocket Expenditures by Sector ...............85
Table (28): sources of funds to health providers (million LL) ...........................................86
Table (29): Choice of providers ...........................................................................................88
Table (30): International Comparison of Health Expenditures ............................................91
Table (31): Most efficient health care systems within the world .......................................95
Table (32): Singaporean demographic indicators .............................................................102
Table (33): number of secured subject to all branches 2012 .............................................116
Table (34): number of secured people subject to some branches 2012 .............................117
Table (35): number of foreigners registered in Fund and non-beneficiaries ....................118

Table (36): frequency results of Q‖0‖ of the questionnaire ..............................................134
Table (37): annual financial result for each branch 2000 (Amounts in billion LBP.) .......148
Table (38): annual financial result for each branch 2001(Amounts in billion LBP.) ........149
Table (39): annual financial result for each branch 2002 (Amounts in billion LBP.) .......149
Table (40): annual financial result for each branch 2003 (Amounts in billion LBP.) .......149
Table (41): annual financial result for each branch 2004 (Amounts in billion LBP.) .......149
Table (42): annual financial result for each branch 2005 (Amounts in billion LBP.) .......150
Table (43): annual financial result for each branch 2006 (Amounts in billion LBP.) .......150
Table (44): annual financial result for each branch 2007 (Amounts in billion LBP.) .......150
Table (45): annual financial result for each branch 2008 (Amounts in billion LBP.) .......151
Table (46): annual financial result for each branch 2009 (Amounts in billion LBP.) .......151
Table (47): Debt owed for the National Social Security Fund (Amounts in billions LBP)
.............................................................................................................................................153
Table (48): Interest on treasury bonds 2000-2009 (Amounts in billions of LBP.) ........... 154
List of Figures
Figure (1): Distribution of children by reason given for not-immunizing them ..................20
Figure (2): Distribution of the population by poor and non-poor categories (2004-2005)..23
Figure (3): Employment rate in Lebanon by gender (2009) ...............................................27
Figure (4): Mortality in Lebanon by age (2011) (rate/1000) ..............................................29
Figure (5): Mortality in Lebanon by region (2011) (rate/1000) .........................................29
Figure (6): Evolution of death rate between 2004 and 2011 ...............................................29
Figure (7): Mortality by causes in Lebanon (2011) ............................................................30
Figure (8): Number of patients suffering from infectious diseases by region (2011) ........31
Figure (9): Cases of tuberculosis in Lebanon (2011) ..........................................................32
Figure (10): Distributions of patients suffering from cancer (2011) ...................................32
Figure (11): % of declared cases of HIV/AIDS (2011) .......................................................33
Figure (12): Distribution of the population at the "Hopital de la Croix" (2010) ................34
Figure (13): Data on Burn cases in Lebanon (2010) ..........................................................35
Figure (14): Road accident cases in Lebanon (2011) .........................................................36
Figure (15): Age of initiation of drug consumption (2011) .................................................37
Figure (16): % of risk factors by age and gender in Lebanon (2009) ..................................38
Figure (17): distribution of elderly population by age, gender and region (2011) .............39
Figure (18): Institutions that provide elderly care (2010)....................................................40
Figure (19): Distribution of disability according to gender, age and region (2009) ............41
Figure (20): Distribution of diseases by type in prisons (2011) .........................................43
Figure (21): Distribution of number of beds by region ......................................................47
Figure (22): Number of hospitals having contracts with the MOPH by type and Mohafaza
49
Figure (23): Percentage of hospitals in public and private sectors distribution per
Mohafaza...............................................................................................................................49
Figure (24): Percentage of hospitals distribution per Mohafaza ..........................................50
Figure (25): Number of admission by type of hospital and geographic location (2011) .....50
Figure (26): The evolution of MOPH subsidized admissions in public and private hospitals
between 2005 and 2011 ........................................................................................................51

Figure (27): statistics of professional orders........................................................................58
Figure (28): External resources for health (% of total expenditure on health) ...................67
Figure (29): Health expenditure, private (% of GDP) .........................................................68
Figure (30): Health expenditure, public (% of total health expenditure).............................68
Figure (31): Health expenditure, public (% of government expenditure) ...........................69
Figure (32): Health expenditure, public (% of GDP) ..........................................................70
Figure (33): Health expenditure, total (% of GDP) .............................................................70
Figure (34): Health expenditure per capita (current US$) .................................................71
Figure (35): Health expenditure per capita, PPP ($) ............................................................72
Figure (36): Out-of-pocket health expenditure (% of total expenditure on health) .............72
Figure (37): pie chart frequency result of the questionnaire ................................................75
Figure (38): Health expenditure by source of financing ......................................................86
Figure (39): Treasury sources of health financing ...............................................................87
Figure (40): Sources of private health financing ................................................................87
Figure (41): Total population in Singapore ......................................................................101
Figure (42): number of beds in Singapore ........................................................................102
Figure (43): Number of physicians in Singapore ..............................................................103
Figure (44): Total expenditure on health as % of gross domestic product ........................103
Figure (45): GGE vs. PE as % of total health expenditure ...............................................104
Figure (46): out-of-pocket expenditure vs. private prepaid plans as % of PE ..................104
Figure (47): per capita GHE vs. per capita THE ...............................................................105
Figure (48): pie chart frequency result of the questionnaire ..............................................134

Figure (49): Accumulated debt of the state (2000-2009) ..................................................154

Introduction
Good health is, by definition, an integral part of sustainable human development. Good
health as a right and as a responsibility is covered by the concept of health security and
health accountability. Health security demands equity and health accountability implies the
obligation on the part of state and health professionals as well as a wider societal
responsibility to take account of the impact of development and other policies on health. To
fully achieve the dimension of health in social and economic development, it is essential to
invest in health as economic growth is based on a productive work force. It is also essential
to realize more equitable access to the benefits of development, as inequities have severe
health consequences and cause an unacceptable threat to human well-being and security.
Health indicators are among the major measurements used to assess the socio-economic
standing of the population, as well as to determine the position of a country with respect to
the development and sustainability processes. Among the major criteria adopted in this
context, are the health demographic indicators (mortality, morbidity, diseases,). However,
another factor that is also playing an integral role in evaluating health status is the existence
of the suitable policies, calling for equitable supply of health services at a reasonable and
bearable cost. The role of the government is essential in this regard not only as a provider
and producer, but also as a regulator, promoter and supervisor of these services. Most
societies are currently going into the process of minimizing the role of governments as a
direct actor in different fields, however, social services are still being handled by
governments, either directly through the provision of the primary health care, or indirectly
through setting up the suitable environment, to avoid monopolies and insure fair coverage.
Lebanon’s spending on health, as a percentage of the national income, is currently the
highest in the Middle East and North Africa (US$ 872 per capita, and 7.4% of the national
product in 2011).1
1 WHO Department of Health Statistics and Informatics (May 16, 2012). "World Health Statistics
2012
In Lebanon, the situation is relatively complicated, mainly as to the wide variety of
players (financing, providers and even regulators) and the lack of communication among
these different players. The long period of civil war has contributed to intensifying and
widening the problems facing the health sector in Lebanon, the fact that was mainly
reflected in the relatively huge size of the "health care bill", measured as a percentage of
gross domestic product, coupled with an apparent inequitable access to health care services
for the different regions and social segments. It is needless to say that the role of the private
sector grew dramatically during the war period, with the persistence of out-dated policies
governing the performance of the sector. This fact was illustrated through the regional
imbalances in the distribution of hospitals, medical and par-medical staffs, in addition to the
ascending trend in the health care prices, mainly relative to the consumer prices.
Six government health funds cover around 38% of the population, while 8% are covered
by private insurance companies. As for the remaining 54% of the population, it is the MOH
that covers their high-cost hospital and pharmaceutical services.2 Scattered funding and the
lack of control over the private market seriously impede MOH and public insurance funds
from purchasing health services at a good price from the public sector. Only 5% of the
public health sector expenditure is allocated to primary health care services. Actually, the
use of the primary health care network is extremely low, and it seems to be motivated by the
availability of free medications.
In Lebanon, there are social expenditures on health, education, and others. But those are
not performed within the framework of a social vision having well determined objectives,
programs and institutions. When some officials justify the social aids, presenting the annual
budgets figures in the fields of education, health and social assistance, they tend to neglect
the social policy and programs. One of the French companies that elaborated the orientation
plan for the Social Security showed the first defect represented by the absence of a clear
vision regarding the social security; the same thing applies to health and education. It is
therefore our right to ask: Is there a health policy? How can we allow the multiplication of
health orientations such as social security, Health Ministry, the cooperative of civil servants,
internal security service and cooperative, mutual, assistance funds?
2 National Health Accounts, 2008

The body in which influential people in government have interest, is the first to be
supported, whereas the bodies in which they have no interests is marginalized, neglected
and deprived form the state’s assistance even if the law clearly stipulates the state’s
obligations towards it.
These obvious imbalances call for an elaboration on the structure of the existing health
system, and tracing the different schemas relating the different components of this system to
come out with a set of policies to enhance the overall performance of the sector.
This inefficiency in the health care system, the neglect of the environment and the
adoption of unhealthy lifestyles by a significant number of citizens, have been the target of
every public health intervention in the country, as well as other donors, and agencies’
interventions. However, till now the health body system in Lebanon is still suffering from a
lot of diseases the most prevalent is the fiscal deficit.
In the passionate debates over healthcare, one fact is often lost—Lebanese people pay
more but get less for their health care than inhabitants of other countries. However, efforts
must be done to change the fact. How can we improve the quality of care and reduce our
expenses, saving a millions by making our health care system more efficient?
The thesis addresses two basic questions. First, what is the current role of multi-
insurance health providers in low quality health care versus high cost, and how can it be
enhanced to increase consumer welfare in parallel with the providers return? Second, how
has, and how should, the National Social Security Fund work to narrow the gap of the
Lebanese health inequality regarding services and expansion in application?
In order to tackle these two problematic questions and analyze them, the thesis followed
an analytical methodology contains a data analysis of a study done about the Lebanese
health quality satisfaction compared with the cost they pay. This thesis depends to a large
extent on previous studies in the same sector done by many organizations mentioning WHO,
World Bank, Lebanese National Health Account and others. Also it studies the role of the
NSSF in health services. This study was built on questionnaire filled by Lebanese people
from the society. Its purpose was to investigate the issue of the health care quality they
receive via the multi-insurance scheme in Lebanon and the cost they bear. Also we focus on
the financial situation of the NSSF and the success of the new suggestions of expanding the
field of application as one of the everyday concern of the Lebanese people since its
application cover the largest number of Lebanese citizens and cover the most
comprehensive of the risks.
I have faced a lot of problems during the thesis beginning with collecting information on
the distribution of expenditures by function, and linking expenditures to utilization. The
information on private sector expenditures was not easily available Even when data was
available its quality, validity, and reliability remained a matter of concern. Reliable data on
the number of beneficiaries and dependents by type of social insurance scheme is difficult.
Additional to that the different agencies classify expenditures differently, and do not have
the same definitions for functions and services.
This thesis is carried out with the aim of highlighting how the current structure of the
health system is affecting the health care bill, and consequently the right of citizens, from
the different regions and income levels, to equitably access health services. This issue is
raised in light of the sensitive situation the country is currently going through, recording
notably slow rate of economic growth and apparent recession, uncontrollable and
continuous levels of budget deficits, and growing public debt exceeding the gross domestic
product. One of the major consequences of the fiscal and monetary policies adopted in the
recent years was widening the gap among the different social classes, creating further
imbalances in income distribution, consequently adding more burdens to the low and middle
income groups that were, severely affected during the civil strife, and limiting thus their
access to the basic social services (health, education,..).
The first part of the study presents a quick review of the main demographic and health
indicators recorded in the country. The second part illustrates the different sources of health
financing and their contributions to the overall health care bill and analyses the flow of
funds between financing agents and health service providers. The third part elaborates on
the role of the national social security fund in the Lebanese social health policy. And finally
ends with a conclusion and some policy recommendations.

Part One: Lebanese Health System Profile

Chapter I: Background on Lebanon
A. Macro picture
1. Geographic and administrative profile
The Republic of Lebanon is a democratic, parliamentary state sited within the Near East.
It is a country of 10452 sq. km. on the Mediterranean Sea. It is composed of six
administrative provinces (or Mohafaza) divided into twenty-six districts (or Qada), counting
the district of Beirut.
The natural resources of the country include limestone, iron ore and salt, but, maybe
the most precious resource of Lebanon is water which is not well managed where huge
quantities of water are lost annually.
Environmental concerns include deforestation (forest covers less than 6% of Lebanon),
soil erosion and desertification. Lebanon also suffers from significant traffic, burning of
industrial wastes and pollution of coastal waters from raw sewage and oil spills. Medical
waste management has been a main issue in the past few years with still no accord reached
concerning the appropriate methodology to the arrangement of hospital waste. 3
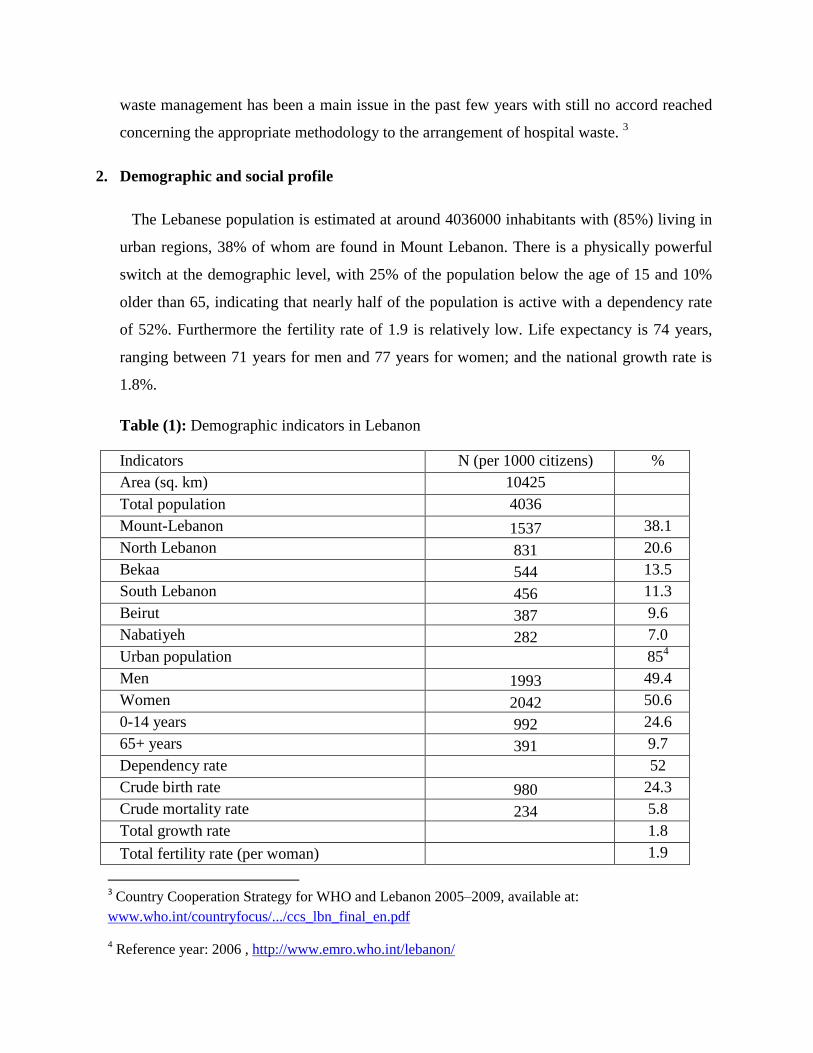
2. Demographic and social profile
The Lebanese population is estimated at around 4036000 inhabitants with (85%) living in
urban regions, 38% of whom are found in Mount Lebanon. There is a physically powerful
switch at the demographic level, with 25% of the population below the age of 15 and 10%
older than 65, indicating that nearly half of the population is active with a dependency rate
of 52%. Furthermore the fertility rate of 1.9 is relatively low. Life expectancy is 74 years,
ranging between 71 years for men and 77 years for women; and the national growth rate is
1.8%.
Table (1): Demographic indicators in Lebanon
Indicators N (per 1000 citizens) %
Area (sq. km) 10425
Total population 4036
Mount-Lebanon 1537 38.1
North Lebanon 831 20.6
Bekaa 544 13.5
South Lebanon 456 11.3
Beirut 387 9.6
Nabatiyeh 282 7.0
Urban population 854
Men 1993 49.4
Women 2042 50.6
0-14 years 992 24.6
65+ years 391 9.7
Dependency rate 52
Crude birth rate 980 24.3
Crude mortality rate 234 5.8
Total growth rate 1.8
Total fertility rate (per woman) 1.9
3 Country Cooperation Strategy for WHO and Lebanon 2005–2009, available at:
www.who.int/countryfocus/.../ccs_lbn_final_en.pdf
4 Reference year: 2006 , http://www.emro.who.int/lebanon/
Source: MOPH, 2011, Statistics Bulletin, available at:
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx
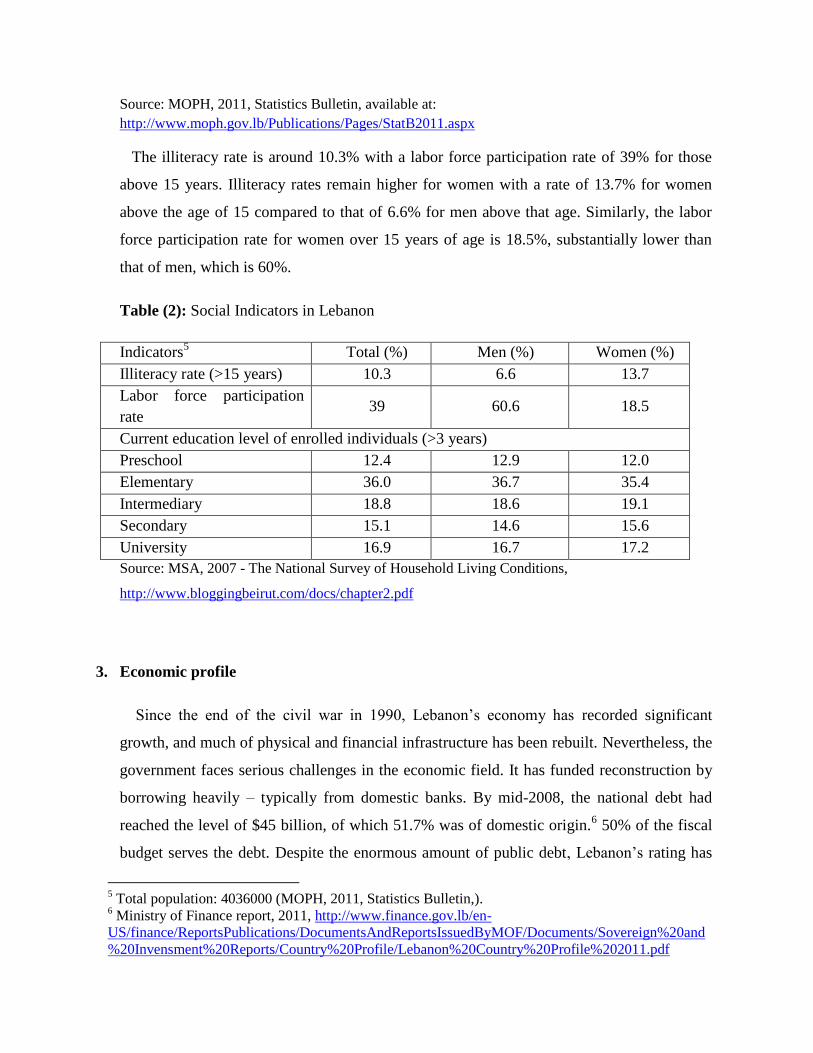
The illiteracy rate is around 10.3% with a labor force participation rate of 39% for those
above 15 years. Illiteracy rates remain higher for women with a rate of 13.7% for women
above the age of 15 compared to that of 6.6% for men above that age. Similarly, the labor
force participation rate for women over 15 years of age is 18.5%, substantially lower than
that of men, which is 60%.
Table (2): Social Indicators in Lebanon
Indicators5 Total (%) Men (%) Women (%)
Illiteracy rate (>15 years) 10.3 6.6 13.7
Labor force participation
rate 39 60.6 18.5
Current education level of enrolled individuals (>3 years)
Preschool 12.4 12.9 12.0
Elementary 36.0 36.7 35.4
Intermediary 18.8 18.6 19.1
Secondary 15.1 14.6 15.6
University 16.9 16.7 17.2
Source: MSA, 2007 - The National Survey of Household Living Conditions,
http://www.bloggingbeirut.com/docs/chapter2.pdf
3. Economic profile
Since the end of the civil war in 1990, Lebanon’s economy has recorded significant
growth, and much of physical and financial infrastructure has been rebuilt. Nevertheless, the
government faces serious challenges in the economic field. It has funded reconstruction by
borrowing heavily – typically from domestic banks. By mid-2008, the national debt had
reached the level of $45 billion, of which 51.7% was of domestic origin.6 50% of the fiscal
budget serves the debt. Despite the enormous amount of public debt, Lebanon’s rating has
5 Total population: 4036000 (MOPH, 2011, Statistics Bulletin,).
6 Ministry of Finance report, 2011, http://www.finance.gov.lb/en-
US/finance/ReportsPublications/DocumentsAndReportsIssuedByMOF/Documents/Sovereign%20and
%20Invensment%20Reports/Country%20Profile/Lebanon%20Country%20Profile%202011.pdf

remained acceptable. The National debt in Lebanon7 by the end of June 2012 rated the
following:
the gross public debt reached LL 67 060 billion (US$ 44.5 billion), a 5.83% increase over
the end of December 2011 level
net public debt stood at LL 60 909 billion (US$ 40.4 billion), registering an increase of LL
2072 billion over the end of December 2011 level
domestic currency debt registered LL 34 672 billion, higher than the end of December 2011
level by 10.52%
Foreign currency debt totaled LL 32 388 billion, 1.24% higher than the end of December
2011 level.
GDP growth has slowed notably in the past few years. Rising oil prices, the economic
hold back, and payments of debts have all weakened public finances. Consequently the
government debt has risen to 175% of GDP. The trade balance showed a deficit of US$
8999 million in 2011.8
Sensible progress has been made on the structural financial reform agenda. Most public
sector reforms have been of an administrative nature, with a number of legislative proposals
awaiting in parliament, together with those on revenue administration and debt
management, laws to order capital markets and bank mergers, as well as competition and
domestic market reform.
Table (3): Economic indicators in Lebanon
Indicators Value
GDP (billions L.P.) 62224
GDP annual growth (%) 3
Annual inflation rate (%) 4
Unemployment rate (%)9 9.2
7 Ibid.
8 Central Bank annual report, 2011, http://www.bdl.gov.lb/webroot/statistics/
9 CAS annual report 2011, http://www.cas.gov.lb/images/Mics3/CAS_MICS3_survey_2011.pdf

Source: Lebanese Republic, President of the Council of Ministers, October 2012, Economic
Accounts, http://www.ilo.org/dyn/travail/docs/721/
B. History of Lebanon
1. Ottoman period
The Ottoman (modern-day Turkish) Empire rose between 1512 and 1520.10
In World War
I, the Ottoman Empire joined forces with Germany and Austria-Hungary in battling the
Allied Forces of England, France and later, the United States. When the war ended, the
Ottoman Empire was no more. The Allies put Lebanon under French control. The first
Lebanese constitution went into effect in 1926.11
2. French intervention
At the end of World War I, the Allied forces put Lebanon under French military
occupation. In 1923, the League of Nations (forerunner to the United Nations) formally
gave Lebanon and Syria to France.12
Under French rule, education, public utilities and
communication improved. Beirut prospered as a trade center. As the middle class of Beirut
grew, so did a frail sense of common national interest and a desire for more independence.13
But France was having troubles at home. Its neighbor Germany had slipped into the rule
of the Nazis. When France fell to Germany in 1940 during World War II, British and Free
10
The Massacres of 1840-1860, http://www.geocities.com/CapitolHill/Parliament/2587/1860.html
11 Daily Star, http://www.dailystar.com.lb
12 The Maronites and Lebanon (2003),
http://www.geocities.com/CapitolHill/Parliament/2587/maronite.html
13 Lebanon History (2003), http://workmall.com/wfb2001/lebanon/lebanon_history_index.html

French troops occupied Lebanon. These troops proclaimed Lebanon and Syria independent,
but because their own status was so precarious, the Free French continued to occupy
Lebanon.
In 1943, they allowed elections to take place. Under the new president, the legislature
adopted changes in the constitution that did away with French influence. The French
objected. On Nov. 11, 1943, the French arrested almost the entire Lebanese government,
leading to war. The British intervened, and the French restored the government and
transferred power to it.14
In 1945, after more insurrection and as World War II reached its climax, the British and
French began withdrawing from Lebanon. By 1946, the withdrawal was complete, and
Lebanon became officially independent.
3. Lebanon after independence
Lebanon's history from independence can be defined largely in terms of its presidents,
each of whom shaped Lebanon by a personal brand of politics.
In 1958, during the last months of President Chamoun's term, an insurrection broke out,
aggravated by external factors. In July 1958, in response to an appeal by the Lebanese
Government, U.S. forces were sent to Lebanon. They were withdrawn in October 1958,
after the inauguration of President Shihab and a general improvement in the internal and
international aspects of the situation.
President Franjiyah's term saw the outbreak of full-scale civil conflict in 1975. Prior to
1975, difficulties had arisen over the large number of Palestinian refugees in Lebanon and
the presence of Palestinian fedayeen (commandos). Frequent clashes involving Israeli forces
and the fedayeen endangered civilians in south Lebanon and unsettled the country.
Following minor skirmishes in the late 1960s and early 1970s, serious clashes erupted
between the fedayeen and Lebanese Government forces in May 1973.
14
Encyclopedia of the orient (July 27, 2002), http://i-cias.com/e.o/lebanon_5.htm

4. Civil war
In 1970, Jordan expelled the PLO from its territories sending many civilian refugees and
armed guerillas into Lebanon. Meanwhile, the communist countries were having economic
problems.
Armies and funding were flowing to Lebanon and many political parties were turned into
armed forces while the Lebanese army was getting weaker and unable to take control. In
April 13, 1975, a brutal fight broke up the war in Lebanon. In 1976, the Syrian army
invaded the Lebanese northern region of Akkar, and advanced into the Bekaa valley east of
Lebanon.
The League of Arab Countries tried to send peace-keeping troops to Lebanon, but they
were forced to leave the country for the Syrian army later. Palestinian militiamen kept
launching attacks from the areas they controlled in South Lebanon against Northern Israel.
The Israeli response was more severe and often impacted Lebanese civilians.
The attacks developed into an Israeli invasion of Southern Lebanon in March 1978. The
United Nation Interim Forces were deployed in South Lebanon to reduce the tension and the
Israeli forces pulled back later.
In the early eighties, Lebanon was being destroyed with contentious fighting, while PLO
militias occupied most of Beirut and kept launching attacks against Northern Israel.
5. Lebanon today
In 1982, Israel invaded the southern half of Lebanon up to and including Beirut. In
October 1989, the Taif Accords were signed and, in November of the same year, Elias
Hrawi was elected President. 15
A new Government, known as the national reconciliation
Government, was formed and began implementation of the Taif Accords.
In October 1990, the fighting came to an end, and, in 1991, most of the militias were
disbanded by the Lebanese Army. On 2 September 2004, the U.N. Security Council adopted
15
―Risk Factors—Risks Relating to the Government—Uncertainties Regarding Formation and Policies
of the New Government‖, available at: http://www.ccfr.org.cn/cicf2012/papers/20120201114734.pdf

Resolution 1559, which was co‐sponsored by the United States and France. 16
Among other
matters, Resolution 1559 declared support for a free and fair electoral process in the
Republic without foreign interference or influence, for the restoration of the territorial
integrity, full sovereignty and political independence of the Republic, the withdrawal of
foreign troops from the territory of the Republic and the disarming of Lebanese and non‐
Lebanese militia.
On 14 February 2005, the former Prime Minister, Mr. Rafik Hariri, together with a
number of his bodyguards and assistants, was assassinated in Beirut.17
Between 1992‐2004,
Mr. Hariri served as Prime Minister for a total of approximately ten years. He was
instrumental in the economic revival and reconstruction of the Republic following the 1975‐
1990 conflict and was the principal architect of the Paris II Conference.18
On 1 December 2006, the opposition commenced a sit‐in in downtown Beirut, as well as
a number of large demonstrations and a general strike, which the opposition sought to
enforce by blocking public roads, which lasted until the conclusion of the Doha
Agreement.19
On 5 May 2008, the Council of Ministers adopted a series of resolutions, including: (i)
increasing the minimum wage from LL 300,000 per month to LL 500,000 per month; (ii)
reassigning the Chief of Security of the Rafic Hariri International Airport to another
position; and (iii) declaring that the telecommunications network operated by Hizbollah on
the territory of the Republic is illegal and unconstitutional.20
In January 2012, Decree № 7426 was adopted (i) increasing the monthly minimum wage
for private sector employees from LL 500,000 to LL 675,000 and (ii) providing for a cost‐
of‐living increase up to a maximum of LL 299,000 per month, both effective 1 February
16
―Conflicts With Israel,The July 2006 War‖, available at: http://smallwarsjournal.com/jrnl/art/the-
2006-lebanon-war-a-short-history 17
The Special Tribunal for Lebanon, available at: http://www.stl-tsl.org/en/ 18
―The Economy—Economic History—Fiscal Reform and the Paris II Conference‖, available at:
http://www.institutdesfinances.gov.lb/english/loadFile.aspx?pageid=838&phname=FileEN 19
―History, Recent Developments, The Doha Agreement‖, available at:
http://www.mof.go.jp/english/customs_tariff/wto/n05.pdf 20
―Recent Developments, Doha Agreement‖, available at:
http://en.wikipedia.org/wiki/Doha_Development_Round

2012. Although Decree № 7426 applies to private sector employees, similar increases have
been proposed in favor of public sector employees. Such increases in the minimum wage
and other salaries could have an inflationary impact on prices. In addition, in September
2012 cost of living payments for public sector employees were increased with retroactive
effect from 1 February 2012. The Ministry of Finance disbursed LL 632 billion (U.S.$419
million) in 2012 to cover this increase. The annual expenditure for this cost of living
increase is estimated at approximately LL 851 billion (U.S.$564 million). In addition, the
Council of Ministers approved the transmittal to Parliament of a new salary scale for public
sector employees, which may be retroactive. Ongoing demonstrations and strikes in support
of this measure, including by members of labor unions and public sector employees, have
been occurring in Beirut, and there have been calls for public sector strikes and further
demonstrations if the measure is not referred to Parliament. The Prime Minister and the
Minister of Finance have stated that this measure will not be implemented until new revenue
sources are identified to cover the new expenditures.21
21
―Risk Factors, Risks Relating to the Republic, Fiscal Deficit‖ and ―Risk Factors, Risks Relating to
the Republic, Prices and Inflation‖, available at:
http://www.un.org/en/development/desa/policy/wesp/wesp2013/wesp13update.pdf

Chapter II: Lebanese Health System
A. History of health system22
1. Pre-independence phase (1864-1943)
Around the middle of the 19th century, the medical field became known in Lebanon. It
was a characteristic of huge cities and included a few qualified doctors or surgeons.
Throughout this era, health care was carried out in medical units belonging to charitable
institutions. The government’s main concern was to protect the people from infectious
diseases and environmental risks.
After World War I, under the French mandate, a number of institutions were established
including the first Health Department which was found within the Ministry of the Interior.
All the public administrations that were set up at that time in addition to the few small
22
Extracts Ammar, M. (2011), Inter-professional collaboration, Paediatric unit case in a university
hospital in Lebanon (PhD thesis).

private hospitals that were established were highly influenced by the French especially in
terms of inspection, control and centralization.
2. Independence phase (1943-1960)
Lebanon’s independence was declared in 1943. Health-related problems became the only
responsibility of the Ministry of Health and Social Affairs whose main role was the
oversight, coordination, and legislation of these matters additionally to the protection of the
surrounding and the observation of transmissible diseases. During the 1950s, this Ministry
began developing a public health system thus establishing the interior structures and a
network of hospitals and primary health care centers where the poor may get care. In spite of
these initiatives, a huge part of the country remained deprived of these services thus limiting
the accessibility of the population to healthcare. Private hospitals started to grow and offered
better quality services. Efforts were carried out to strengthen the ties between the private and
public sectors.
3. Reforms (1960-1975)
Starting in 1958, the Lebanese government undertook a series of reforms within the
health field namely:
The 1961 decree that stipulated that additionally to its restrictive role in the health field,
the Ministry of Health was in charge for the public health of the population and the health of
the disadvantaged. Therefore, principles of primary health care, likewise a regional private
and public network were developed to confirm the healthcare of the population.
The creation in 1963 of the National Social Security Fund (NSSF) by decree number
13955 and the Cooperative of Civil Servants (CSC) by virtue of the law issued by decree
number 14273. The NSSF is a semi-public, autonomous, social institution with a legal
personality and financial and administrative autonomy. It was based, once again, on the
European model of social security. The CSC is a public organization under the authority of
the Council of Ministers.
Even though these reforms were essential, they did not have the required positive impact.
On the contrary, they weakened the role of the Ministry of Health in the public sector and
formed duplications in terms of services settled and health coverage. The result was obvious
in terms of:
The appearance of new modes of compensation, such as fee for service which had
considerable consequences including the abuse of medical consultations, laboratory tests, x-
rays and medication prescriptions.
An increase of publicly managed social insurance funds (a total of 6) ending with
competition and political fights, instead of cooperation and coordination.
4. Civil war (1975-1992)
With the start of the Civil War in 1975, the services of the Ministry of Public Health
(MOPH) declined and with time, the Ministry became dysfunctional. The demand for aid
and healthcare increased and in parallel, the public sector collapsed leaving the private
hospitals as the only practical source for healthcare. The Ministry found itself beneath the
requirement of contracting to these hospitals in order to provide care for war victims as well
as the general population.
As a result, the MOPH became the major funder of these hospitals and its role shifted to
that of a contracting agent. Health expenses increased swiftly. They represented 80% of the
Ministry’s budget and covered mainly secondary and tertiary healthcare services. The
MOPH also had to distribute expensive medication free of charge. By the end of the war, the
MOPH was taking care of the health of the population with no social coverage as the NSSF
seemed unable to cover healthcare expenses due to the rapid increase in their cost as well as
the existing economic situation. The only remaining ray of hope lied in private insurances
which unfortunately were only available to a specific socio-economic class and could not,
alone, cover the needs of the entire population.
War had a negative impact and harmful consequences. Its influence was catastrophic on
infrastructure, human resources and the economy of the country, in both the private and
public sectors.

At the end of the war in 1990, the Lebanese health system was at its worst. The war had
damaged the health sector, as well as several other sectors in the country. Although most of
the issues of the healthcare system stemmed immediately from the war, some were inherent
to the conception of the system itself (The World Bank 2000). Regardless the causes, the
main outcomes are summarized below:
• In terms of governance the country found itself with a MOPH that was unable to play its
role as a health system regulator due to weak institutional, financial and managerial
capacities. The whole public hospital network had started to collapse and consequently the
public hospital sector was paralyzed, and became dependent on the private hospital sector
that now existed, a predominant place in the Lebanese health field.
This sector continued to grow but in a very messy way leading to an increasing trend
towards highly technological curative care at the expense of preventive care and primary
healthcare.
• In terms of equity and efficiency the health coverage of the population was inadequate.
There was a considerable gap between the quality and the quantity of services provided, as
well as inequalities in their geographic distribution, therefore reducing their accessibility.
• In terms of human resources qualified personnel were attracted by job opportunities
elsewhere leading to the migration of health professionals.
• In terms of financing regime and healthcare expenses the existing fragmentation and
compartmentalization between numerous public, semi-public and private funds
(approximately 100) (Kronfol, 2006), as well as the absence of efficient controlling
mechanisms led to weakened purchasing power and expensive administrative costs as well
as perverse behaviors aiming at increasing income (Ammar, 2003). In addition, the
continuous upsurge in costs placed the country at a level close to that of industrialized
countries with a very heavy financial burden on household expenses.
5. Current health system
The present health system is described by several authors as being fragmented and
pluralistic. The public sector has been absent for a long time because of the civil war. Since
then, the MOPH realized a number of achievements. The health reform that started more
than 15 years ago has achieved the aims that are recognized by worldwide experts, such as
those described in the WHO 2010 World Report on Health.
―Lebanon’s reforms: improving health system efficiency, increasing coverage and
lowering out-of-pocket spending‖. The key components of these reforms have been: a
restoring of the public-sector primary-care network; improving quality in public hospitals;
and improving the rational use of medical technologies and medicines. The latter has
included increasing the use of quality-assured generic medicines.
The Ministry of Health has also sought to strengthen its leadership and governance
functions through a national regulatory authority for health and biomedical technology, a
certification system for all hospitals, and contracting with private hospitals for specific
inpatient services at specified prices. Improved quality of services in the public sector, at
both the primary and tertiary levels, has resulted in increased utilization, particularly among
the poor.
Utilization of preventive, primitive and curative services, particularly among the poor,
has improved since 1998, as have health outcomes. Reduced spending on medicines
combined with other efficiency gains, means that health spending as a share of GDP has
fallen from 12.4% to 8.4%. Out of- pocket spending as a share of total health spending fell
from 60% to 44%, increasing the levels of financial risk protection.
6. Millennium Declaration goals for Lebanon
The Millennium Declaration adopted in September 2000 by the UN General Assembly
has been ratified by 189 member states. It includes eight goals, twenty-one targets and fifty-
eight indicators.
The eight goals are:
1. Eradicate extreme poverty and hunger

2. Achieve universal primary education
3. Promote gender equality and empowerment of women
4. Reduce under-five child mortality
5. Improve maternal health
6. Combat HIV/AIDS, malaria and other diseases
7. Ensure environmental sustainability
8. Develop a global partnership for development.
These goals are interdependent and influence each other. Three goals (goals 4, 5 and 6)
out of the eight are focused on health. Today, 13 years later, results are encouraging,
especially with respect to child and maternal health. However, additional efforts are still
required for combating AIDS, malaria and tuberculosis.
Target: Reduce the under-five child mortality rate by two-third by the year 2015
Lebanon has made important efforts towards achieving MDG 4, especially in reducing
infant mortality. The gap is observed across the country especially in disadvantaged regions
where mortality and morbidity rates are higher and vaccination rates are lower.
Table (4): Progress in MDG 4 – Reduce under-five mortality in Lebanon
Indicators 1996 2000 2007 2015
Under-five mortality rate (per 1,000) * 32 33 18.3 12
Under-five mortality rate (per 1,000) * 28 26 16.1 10
Proportion of children under-one year immunized
against DPT (%) ** 94.2 93.6 57 95
Proportion of children under-two years immunized 88 79.2 56 90

against MMR (measles, mumps, rubella) (%) **
Source: * CAS and League of Arab countries, 2006, Lebanon Family Health Survey (PAPFAM)
2004, Principal Report
** Based on vaccination carried out by the public sector (excluding the contribution of the private
sector which varies between 10 and 85% according to regions).
The MOPH, in cooperation with the private sector, has revised the national vaccination
calendar in order to gradually introduce new vaccines that will supported common
vaccination.
Figure (1): Distribution of children by reason given for not-immunizing them
Source: MOPH-WHO (joint report), 2009, Study on the measles coverage in Lebanon
However, there seems to be a problem with awareness about availability of some
vaccines and vaccination campaigns especially in regions mostly at need of vaccination
(Bekaa and South).
According to data available from the MOPH, neonatal causes (64.9%), injuries (11.1%),
pneumonia (1.1%) and diarrhea (1%) are the main causes of mortality among children
below five years of age. Twenty-two percent (22%) of deaths result from unknown causes.
MDG 5 – Improve maternal health
05
1015202530354045
Previouslyvaccinated
Doctor'sadvice
Unaware ofthe campaign
Refusal ofschool
Obstacles orlack of
information/motivation
reason for not immunizing the children
Beirut
Mount-Lebanon
Bekaa
North
South

Target: Reduce the maternal mortality rate by three-quarters and achieve universal
access to reproductive health by the year 2015,
Maternal mortality rate was estimated at 86.3 per 100000 live births (PAPFAM 2004) in
2008. Since then however, considerable efforts have been exerted to improve maternal
health in general.
Table (5): Maternal and reproductive health statistics in Lebanon
Indicators 1990
* 1996* 2000* 2004**
2009
*
Maternal mortality rate (per
100000 live births) 140 107 - 86.3 23
Proportion of births carried out
by qualified professionals (%) N/A N/A 96 98
Modern and traditional
contraceptive prevalence rate
(%)
53 61 63 74.2
Antenatal Care coverage (at least
one visit) (%) 87.1 87 93.9 95.6
Source: * CAS and League of Arab countries, 2006, Lebanon Family Health Survey (PAPFAM)
2004, Principal Report.
** WHO-MOPH, 2009, Reproductive Age Mortality Survey, (RAMOS).
The RAMOS study (2009) showed a maternal mortality rate of 23 per 100,000 live births
(with an uncertainty margin of 15.3 to 30.6). The prevalence of maternal death varied from
one region to another with a rate in the Bekaa and the North that are two and 1.5 times
higher respectively than the national average (21.3% and 16.1 against 10.7%),. The South
presented the lowest rate. The main causes for mortality were bleeding and asepsis
(Maternal Morbidity and Case Fatality Rate Study, MOPH, 2009, Unpublished)
MDG 6 – Combat HIV/AIDS, malaria and other diseases
Target: Have halted by 2015 and begun to reverse the spread of HIV/AIDS; Ensure,
by 2010, to all those in need, access to HIV/AIDS treatment

HIV/AIDS
Lebanon is still considered a country with a low prevalence of HIV. The potential risks
associated with the population’s high mobility, migration and relative sexual permissive
behavior require immediate and intensive interventions.
The total cumulative number of cases reported by the national program on combating
HIV/AIDS since 1989 was by the end of 2011, 1455, with an average of 85 new cases per
year.
Target: Have halted, by 2015, and begun to reverse the spread of malaria and other
major diseases.
Malaria
The disease has been eradicated in Lebanon since the 1950’s. Sporadic cases are rarely
reported among Lebanese living in endemic areas.
Tuberculosis
The joint MOPH and WHO National TB control program adopted the DOTS program in
1998, to combat tuberculosis, and has achieved encouraging results with a 100% coverage
rate by the end of 2009, as compared to 92% in 2005.
The Lebanese Government, through the MOPH has been providing treatment and care
for all Lebanese citizens suffering from tuberculosis and HIV/AIDS.
Table (6): National Statistics for Tuberculosis in Lebanon (2009)
Year 2002 2003 2004 2005 2006 2007 2008 2009
National 378 330 330 331 311 357 378 368
Non- 48 50 63 60 64 119 145 133

national
total 426 380 393 391 375 476 523 501
Source: WHO-MOPH, 2009, National Report on Tuberculosis
B. Determinants of health
1. Poverty23
The study carried out on poverty, growth and revenue distribution in Lebanon showed
that 21% of the Lebanese population was classified as poor while 8% (300,000 individuals)
were considered extremely poor. Moreover, the study highlighted the existence of regional
disparities: these are insignificant in Beirut whereas they are significantly higher in Akkar,
North Lebanon. Poverty levels are highest in South Lebanon.
Figure (2): Distribution of the population by poor and non-poor categories (2004-2005)
Source: Laithy, H. ; Abu-Ismail, K., ; Hamdan, K.; 2008, Poverty, growth and income distribution in
Lebanon, Country study, International Poverty centre, number 13. http://www.eldis.org/go/country-
profiles&id=35243&type=Document
Expenditure level and inequality
23
Laithy, H. ; Abu-Ismail, K., ; Hamdan, K.; 2008, Poverty, growth and income distribution in
Lebanon,Country study, International Poverty centre, number 13. http://www.eldis.org/go/country-
profiles&id=35243&type=Document
0
20
40
60
80
Extremly Poor Poor Non-Poor
Distribution of the population by poor and non-poor categories (2004-2005)

• Mean per capita consumption was highest in Beirut (6,514,000 LBP) (more than one and
one-half times the national average) and lowest in the North (3,975,000 LBP) (three-
quarters of the national average).
• The distribution of expenditure among the population was relatively uneven. The bottom
20% of the population accounted for only 7% of all consumption in Lebanon while the
wealthiest 20% accounted for 43% (over six times higher).
• Inequality within-Mohafazats accounted for most of the inequality in Lebanon (about 92%
of aggregate inequality in consumption can be attributed to within-Mohafazats inequality).
Table (7): Average per capita and per governorate consumption (1000 LBP) (2004-2005)
Mohafazats Mean nominal per capita consumption
Beirut 6514
Mount-Lebanon 4512
Nabatieh 3924
Bekaa 3385
South 3007
North 2532
All Lebanon 3975
Source: Laithy, H. ; Abu-Ismail, K., ; Hamdan, K.; 2008, Poverty, growth and income distribution in
Lebanon, Country study, International Poverty centre, number 13. http://www.eldis.org/go/country-
profiles&id=35243&type=Document
Regional disparities
Poverty measures indicated:
• A low prevalence of extreme poverty (<1%) and overall poverty (<6%) in Beirut.
• A low prevalence of extreme poverty (2-4%) and a below-average prevalence of overall
poverty (close to 20%) in Nabatieh and Mount-Lebanon;
• A higher-than-average prevalence of extreme poverty in Bekaa and the South, an average
prevalence of overall poverty in Bekaa (29%) and a higher-than-average prevalence of
overall poverty in the South (42%).

• A high prevalence of extreme and overall poverty in the North (18% and 53%,
respectively).
Table (8): Poverty measures per Mohafazat (2004-2005)
Mohafazats Extremely poor Poverty in the entire population
Bierut 0.67 5.85
Nabatieh 2.18 19.19
Mount-Lebanon 3.79 19.56
Bekaa 10.81 29.36
South 11.64 42.21
North 17.75 52.57
Total 7.97 28.55
Source: Laithy, H. ; Abu-Ismail, K., ; Hamdan, K.; 2008, Poverty, growth and income distribution in
Lebanon, Country study, International Poverty centre, number 13. http://www.eldis.org/go/country-
profiles&id=35243&type=Document
The North consisted of 20.7% of Lebanon’s population as well as 46% of the extremely
poor population and 38% of the entire poor population. The extremely poor households
were also predominant in the South and Bekaa governorates. The moderately poor
households were also over-represented in the South.
There were considerable differences in poverty within the North governorate with Tripoli
and the Akkar/Minieh-Dennieh regions presenting the highest percentages of overall
poverty. In contrast, the Koura Zgharta/Batroun/Bsharre areas had relatively low poverty
rates.
With respect to poverty, it is important to note that:
• Unemployment rates in Lebanon were high among the poor.
• Youth unemployment was aggravated by poverty.
• Households exposed to a combination of adverse factors faced the highest risk of poverty.

• Households headed by individuals with less than elementary education constituted 45% of
all the poor.
• Poverty was closely associated with school participation. There was a lower likelihood of
school enrolment, attendance and retention for poor children
• Widowed heads of households with children were more likely to be poor
• Poverty was affected by place of residence. Households in the North were four times more
likely to be poor compared to households in Beirut.
2. Employment
In general, the private sector absorbed a larger share of the employment. A quarter of
the labor force is relatively unskilled while another quarter was highly qualified. Salaries
differed by gender with the women’s average salary lower than the men’s. Highly qualified
individuals suffered more from unemployment. Foreign labor contributed to the economy as
145,684 (11% of the labor force) work permits were delivered in 2009, 80% of which were
given to domestic workers.
The economic activity rate of the population aged 15 years and above, reached 48% in
2009. In other words approximately half of the population was working or available for
work.
Clearly services had the biggest share of the economy (39%), followed by trade (27%)
and manufacturing (12%). Half (50%) of those in employment were employees paid on a
monthly basis and 31% were self-employed.
Unemployment is defined according to ILO as ―all individuals aged between 15 and 64
years who were not working one week before the study but were actively seeking
employment and were available for work‖. Considering this definition, the national
unemployment rate in 2009 was 6% with a higher for women (10%) compared to men (5%).

Figure (3): Employment rate in Lebanon by gender (2009)
Source: CAS, 2011, the labor market in Lebanon, Statistics in Focus, issue 01.
The highest unemployment rates were recorded among young people, particularly
women below the age of 30 years. Beirut and the North recorded higher levels of
unemployment rates (around 8%). Lower unemployment rates were found in the South
(5%), Baalbek and Hermel (4%). Unemployment rates were high among highly skilled
persons, 9% for those people who had already obtained a university degree and 8% for
individuals with a secondary level of education. The unemployment rate was higher for
women except among the uneducated.
3. Environment
Major environmental degradation in Lebanon has resulted from the years of war
including: air pollution, inadequate solid waste management, water pollution in some
remote places, and uncontrolled use of pesticides for agriculture and public health. There are
various institutions and sectors involved in environmental management Country
Cooperation Strategy for WHO and Lebanon Country Cooperation Strategy for WHO and
Lebanon but with unclear responsibilities and no coordination of activities. Medical waste
management has been a major issue of debate in recent years with no clear consensus on
how this problem should be tackled; hospitals continue to dispose of their waste in an
unorganized way and the relevant law passed by the Ministry of Environment is not
enforced.
Employment rates by gender (%)
Male
Female

The sanitary engineering department of the MOPH is responsible for assessing water
supply and sanitation projects, and quality control of air, water and soil. However, it is
unable to fulfill its mandate and implement legislation due to lack of qualified personnel,
staff and allocated budget. There is no national centre for poison information and control
although the WHO office in Beirut and the Faculty of Pharmacy at the Lebanese University
are working jointly on creating a collaborative anti-poison centre in Lebanon.
C. Health status indicators
1. Mortality in Lebanon
In 2011, the mortality rate was 5.4/1000. This rate has been rather stable since 2006. The
declared and registered deaths reached 21 012 in 2011. The highest death rate is found in
Beirut, followed by Nabatiyeh; whereas Mount Lebanon has the lowest rate. Life
expectancy at birth was 74 years (77 years for women and 71 years for men).
The maternal death rate is 23/100000 live births. Cardiac arrests were the most frequent
causes of death cited by physicians or Ministry of the Interior employees on death
certificates. The main cause of death was linked to circulatory system diseases (22%),
followed by neoplasm (19%) and cardiac arrests (17%). No death due to eye and related
diseases, ear and skin mastoid or subcutaneous tissue, or pregnancy, childbirth were
registered in this hospital based mortality survey. Also, there were no deaths due to mental
or behavioral disorders in the hospital survey.
Table (9): Mortality in Lebanon (2011)
Gender n
Male 10055
Female 7994
Total 21012
Life expectancy at birth (years) 73.6
Source: MOPH, 2011, Statistics Bulletin,
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx

Figure (4): Mortality in Lebanon by age (2011) (rate/1000)
Source: MOPH, 2011, Statistics Bulletin,
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx
Figure (5): Mortality in Lebanon by region (2011) (rate/1000)
Source: MOPH, 2011, Statistics Bulletin,
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx
Figure (6): Evolution of death rate between 2004 and 2011
0
5
10
15
20
0-1
1..
5
5..
10
10
..15
15
-20
20
-25
25
-30
30
-35
35
-40
40
-45
45
-50
50
-55
55
-60
60
-65
65
-70
70
-75
75
-80
80
-85
85
-90
90
+
Mortality in Lebanon by age (2011)
Mortality in Lebanonby age (2010)
02468
10 Mortality in Lebanon by region (2011)
Mortality in Lebanon byregion (2011)
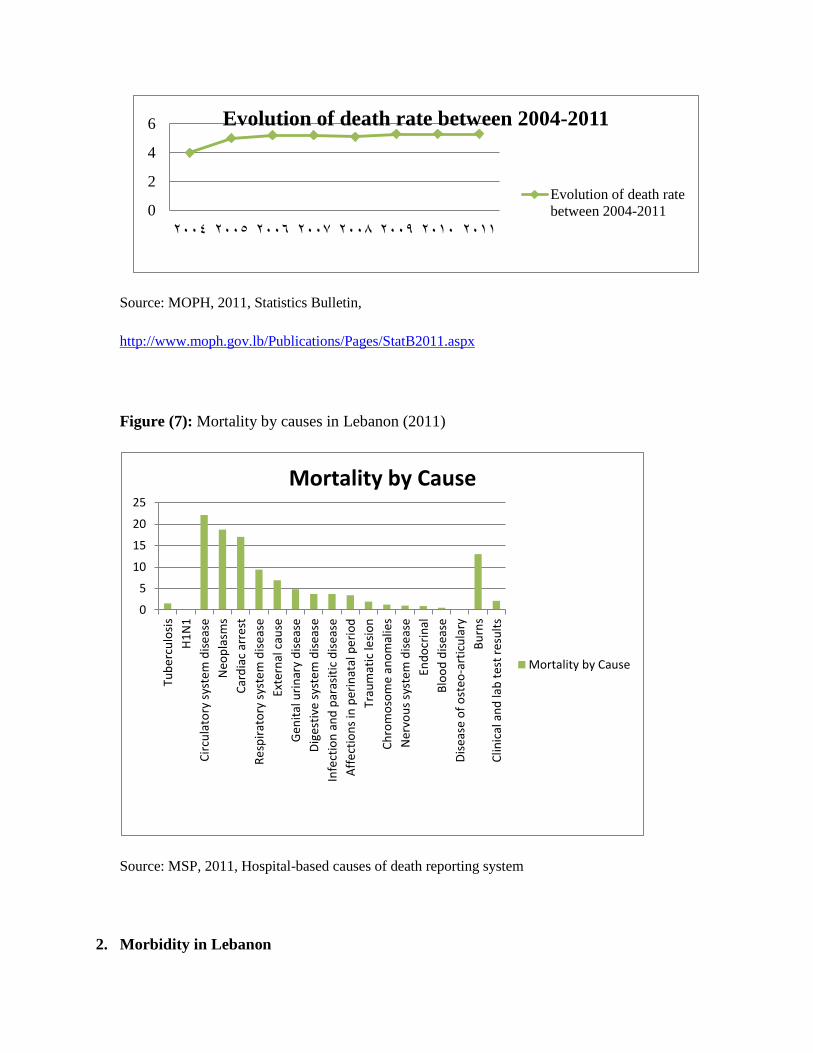
Source: MOPH, 2011, Statistics Bulletin,
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx
Figure (7): Mortality by causes in Lebanon (2011)
Source: MSP, 2011, Hospital-based causes of death reporting system
2. Morbidity in Lebanon
0
2
4
6
2004 2005 2006 2007 2008 2009 2010 2011
Evolution of death rate between 2004-2011
Evolution of death rate
between 2004-2011
0
5
10
15
20
25
Tub
erc
ulo
sis
H1
N1
Cir
cula
tory
sys
tem
dis
eas
e
Neo
pla
sms
Car
dia
c ar
rest
Re
spir
ato
ry s
yste
m d
isea
se
Exte
rnal
cau
se
Gen
ital
uri
nar
y d
isea
se
Dig
esti
ve s
yste
m d
isea
se
Infe
ctio
n a
nd
par
asit
ic d
isea
se
Aff
ect
ion
s in
per
inat
al p
eri
od
Trau
mat
ic le
sio
n
Ch
rom
oso
me
ano
mal
ies
Ner
vou
s sy
stem
dis
eas
e
End
ocr
inal
Blo
od
dis
ease
Dis
ease
of
ost
eo-a
rtic
ula
ry
Bu
rns
Clin
ical
an
d la
b t
est
resu
lts
Mortality by Cause
Mortality by Cause
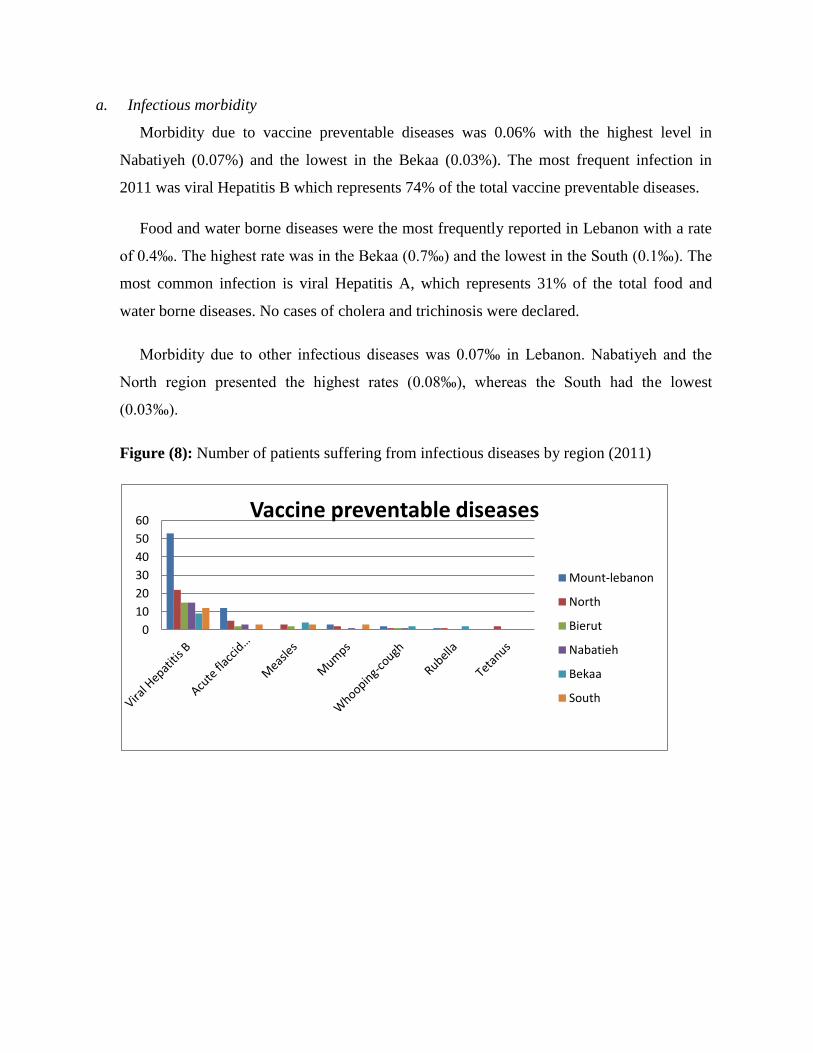
a. Infectious morbidity
Morbidity due to vaccine preventable diseases was 0.06% with the highest level in
Nabatiyeh (0.07%) and the lowest in the Bekaa (0.03%). The most frequent infection in
2011 was viral Hepatitis B which represents 74% of the total vaccine preventable diseases.
Food and water borne diseases were the most frequently reported in Lebanon with a rate
of 0.4‰. The highest rate was in the Bekaa (0.7‰) and the lowest in the South (0.1‰). The
most common infection is viral Hepatitis A, which represents 31% of the total food and
water borne diseases. No cases of cholera and trichinosis were declared.
Morbidity due to other infectious diseases was 0.07‰ in Lebanon. Nabatiyeh and the
North region presented the highest rates (0.08‰), whereas the South had the lowest
(0.03‰).
Figure (8): Number of patients suffering from infectious diseases by region (2011)
0
10
20
30
40
50
60Vaccine preventable diseases
Mount-lebanon
North
Bierut
Nabatieh
Bekaa
South

Source: MOPH, Data 2011, http://www.moph.gov.lb
b. Tuberculosis
The declared prevalence in Lebanon was estimated at 12/100000 inhabitants in 2009.
Beirut and Tripoli account for the highest number of patients suffering from tuberculosis,
107 and 40 respectively, with the highest incidence rate in Beirut district and Hermel
district.
Figure (9): Cases of tuberculosis in Lebanon (2011)
0
50
100
150
200Food and Water borne disease
Mount-Lebanon
North
Bierut
Nabatieh
Bekaa
South
05
101520253035404550
Other Diseases
Mount-Lebanon
North
Bierut
Nabatieh
Bekaa
South
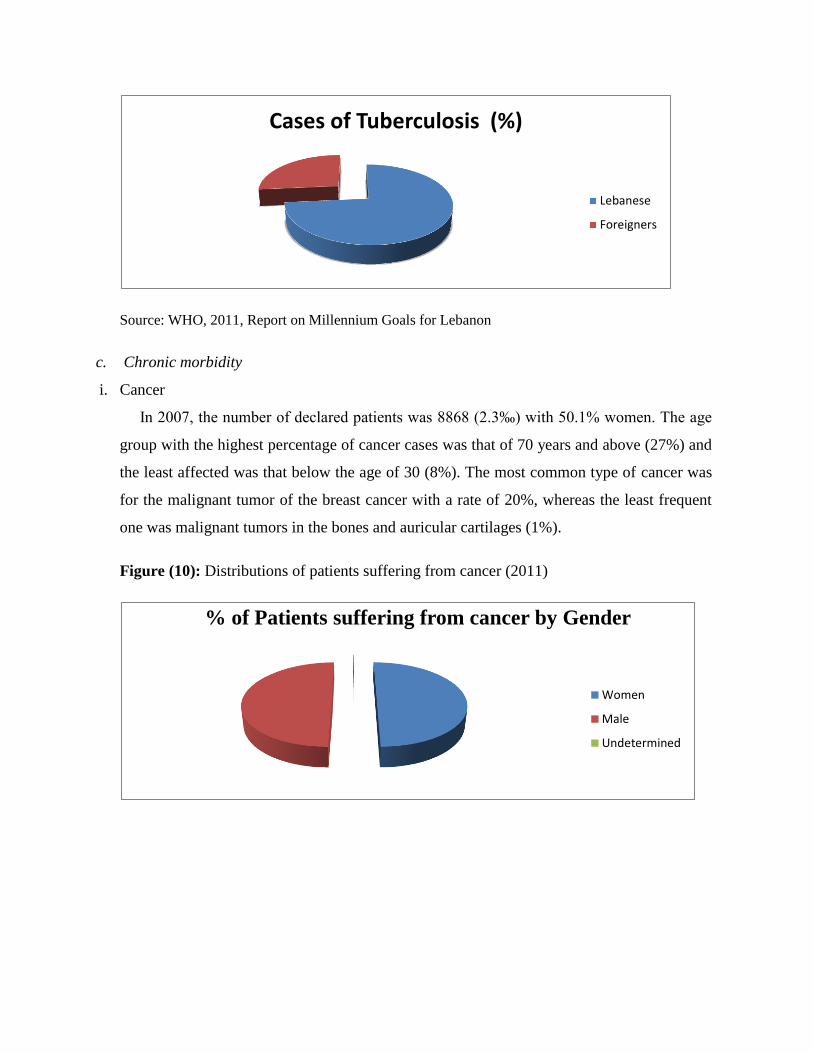
Source: WHO, 2011, Report on Millennium Goals for Lebanon
c. Chronic morbidity
i. Cancer
In 2007, the number of declared patients was 8868 (2.3‰) with 50.1% women. The age
group with the highest percentage of cancer cases was that of 70 years and above (27%) and
the least affected was that below the age of 30 (8%). The most common type of cancer was
for the malignant tumor of the breast cancer with a rate of 20%, whereas the least frequent
one was malignant tumors in the bones and auricular cartilages (1%). T
Figure (10): Distributions of patients suffering from cancer (2011)
Cases of Tuberculosis (%)
Lebanese
Foreigners
% of Patients suffering from cancer by Gender
Women
Male
Undetermined
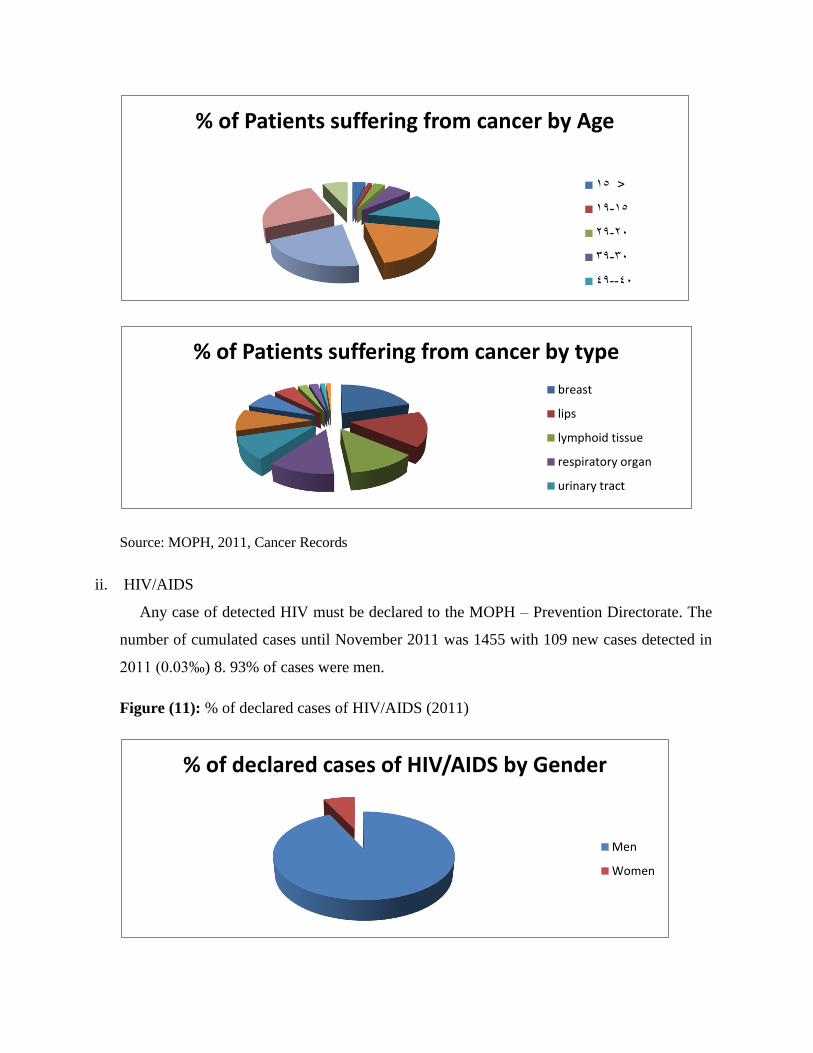
Source: MOPH, 2011, Cancer Records
ii. HIV/AIDS
Any case of detected HIV must be declared to the MOPH – Prevention Directorate. The
number of cumulated cases until November 2011 was 1455 with 109 new cases detected in
2011 (0.03‰) 8. 93% of cases were men.
Figure (11): % of declared cases of HIV/AIDS (2011)
% of Patients suffering from cancer by Age
<15
15-19
20-29
30-39
40--49
% of Patients suffering from cancer by type
breast
lips
lymphoid tissue
respiratory organ
urinary tract
% of declared cases of HIV/AIDS by Gender
Men
Women
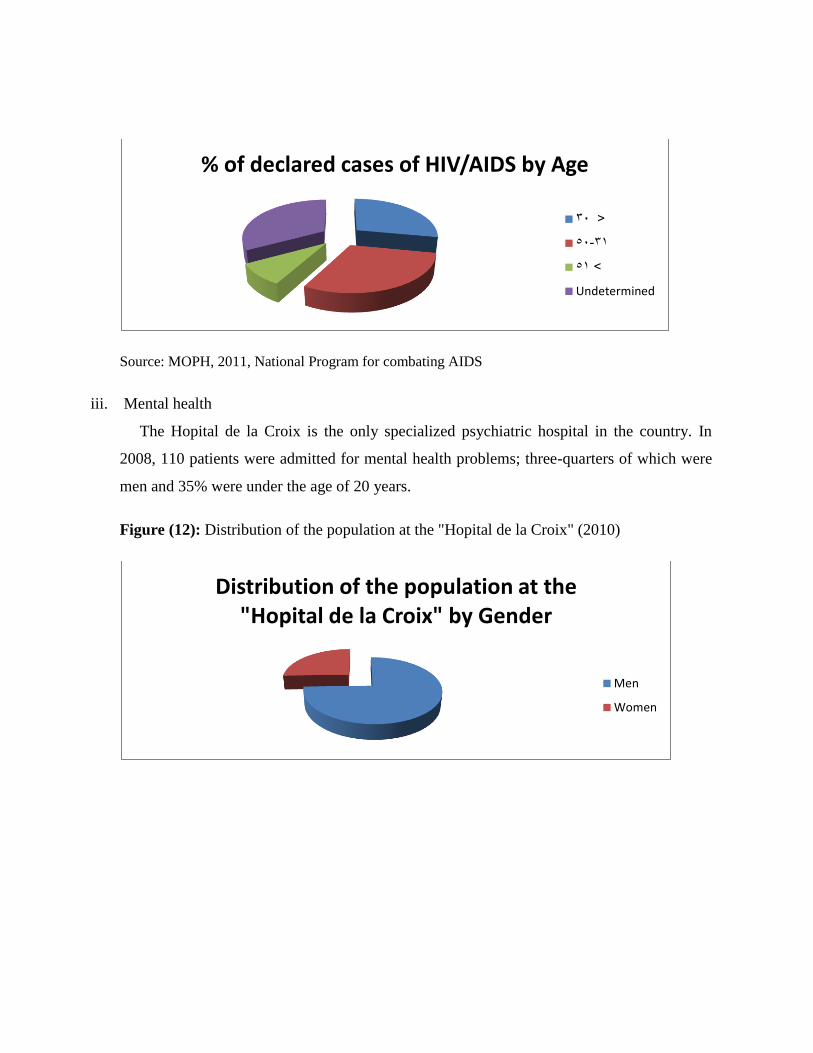
Source: MOPH, 2011, National Program for combating AIDS
iii. Mental health
The Hopital de la Croix is the only specialized psychiatric hospital in the country. In
2008, 110 patients were admitted for mental health problems; three-quarters of which were
men and 35% were under the age of 20 years.
Figure (12): Distribution of the population at the "Hopital de la Croix" (2010)
% of declared cases of HIV/AIDS by Age
<30
31-50
>51
Undetermined
Distribution of the population at the "Hopital de la Croix" by Gender
Men
Women
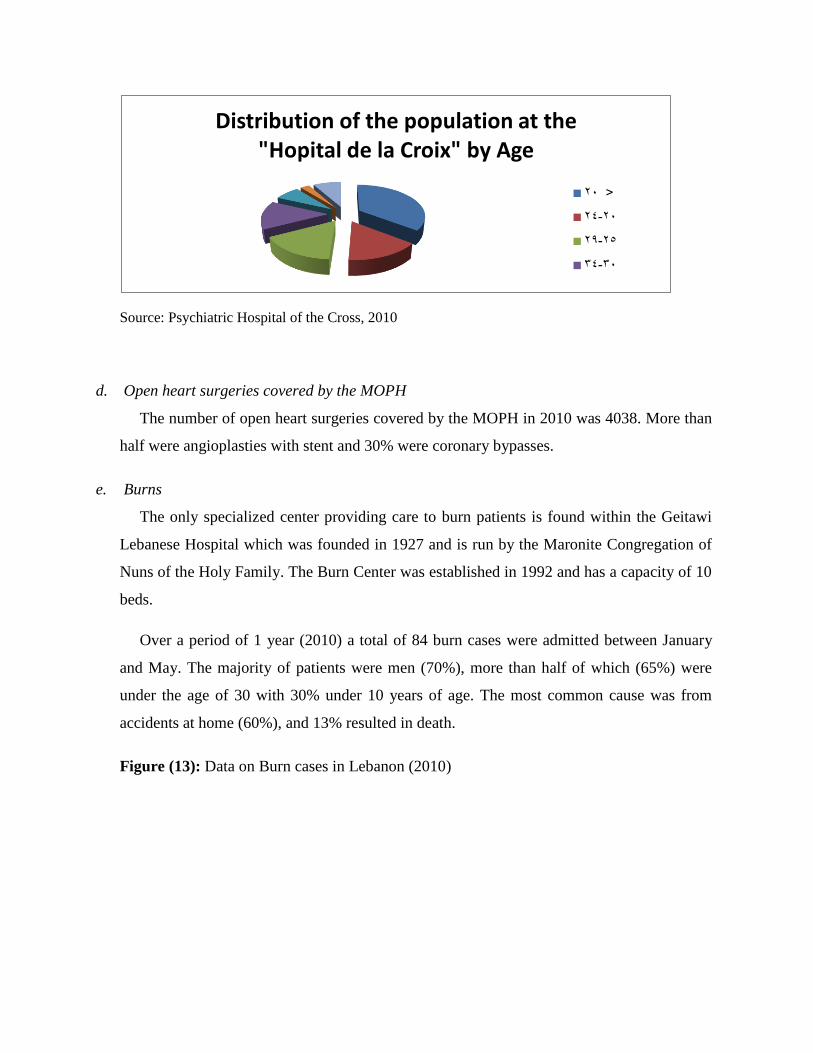
Source: Psychiatric Hospital of the Cross, 2010
d. Open heart surgeries covered by the MOPH
The number of open heart surgeries covered by the MOPH in 2010 was 4038. More than
half were angioplasties with stent and 30% were coronary bypasses.
e. Burns
The only specialized center providing care to burn patients is found within the Geitawi
Lebanese Hospital which was founded in 1927 and is run by the Maronite Congregation of
Nuns of the Holy Family. The Burn Center was established in 1992 and has a capacity of 10
beds.
Over a period of 1 year (2010) a total of 84 burn cases were admitted between January
and May. The majority of patients were men (70%), more than half of which (65%) were
under the age of 30 with 30% under 10 years of age. The most common cause was from
accidents at home (60%), and 13% resulted in death.
Figure (13): Data on Burn cases in Lebanon (2010)
Distribution of the population at the "Hopital de la Croix" by Age
<20
20-24
25-29
30-34

Source: Getawi Hospital 2010, Traumatology Unit, http://www.hopital-libanais.com
Data on Burn cases by Gender
Male
Female
Data on Burn cases by Age
0-10
11..20
21-30
31-40
41-50
Death data on Burn cases
Yes
No
Data on Burn Cause cases
Accidents at home
Accidents at work
Leisure activities

f. Road accidents
The Lebanese Red Cross and Kunhadi, a local NGO, estimate the number of road
accidents in 2011 at approximately 11161 cases.
Figure (14): Road accident cases in Lebanon (2011)
Source: Yasa, http://www.yasa.org ,data of the Internal Security Forces, 2011.
3. Risk factors (Intentional and non-intentional)
a. Drug Use
The number of individuals admitted to the rehabilitation program of Oum El Nour
between 2003 and 2011 seems stable, with an average of nearly 85 admissions per year. The
age at first consumption is in more than half of the cases between 14 and 19 years (58%)
with slightly less than 25% initiating their consumption between 20 and 24 years.24
24
http://www.skoun.org
0
10
20
30
40
50
Accidents Injured Killed
% of Road accident cases by region
Mount-Lebanon
Beirut
North
Bekaa
South
0
50
100
Male Female
% of Road accident cases by Gender
Injured
Killed

Figure (15): Age of initiation of drug consumption (2011)
Source: http://www.oum-el-nour.org/factsstat10.php?i=3010.2
7
b. Cigarette Use and other Risk Factors
Thirty-nine percent (39%) of adults were current smokers, whereas 57% claimed to have
never smoked. Half of the individuals between the ages of 45 to 54 were current smokers,
whereas 70% of individuals aged between 25 and 34 never smoked. The current smoking
rate was higher among men (47% vs. 32%).
Twenty-one percent (21%) of adults currently consumed alcohol with 32% for the men
and 11% for the women. It is noteworthy to mention that 43% of those between 25 and-34
years are former drinkers.
Physical activity was measured on a scale varying between high and low activity. Almost
half of the individuals (46%) showed low physical activity, with the highest percentage
(54%) being for those aged between 25 and 34 years; 52% of the men and 40% of the
women report low physical activity.
Age of initiation of drug consumption (2011)
14-19
20-24
25-29
30-34
35-39
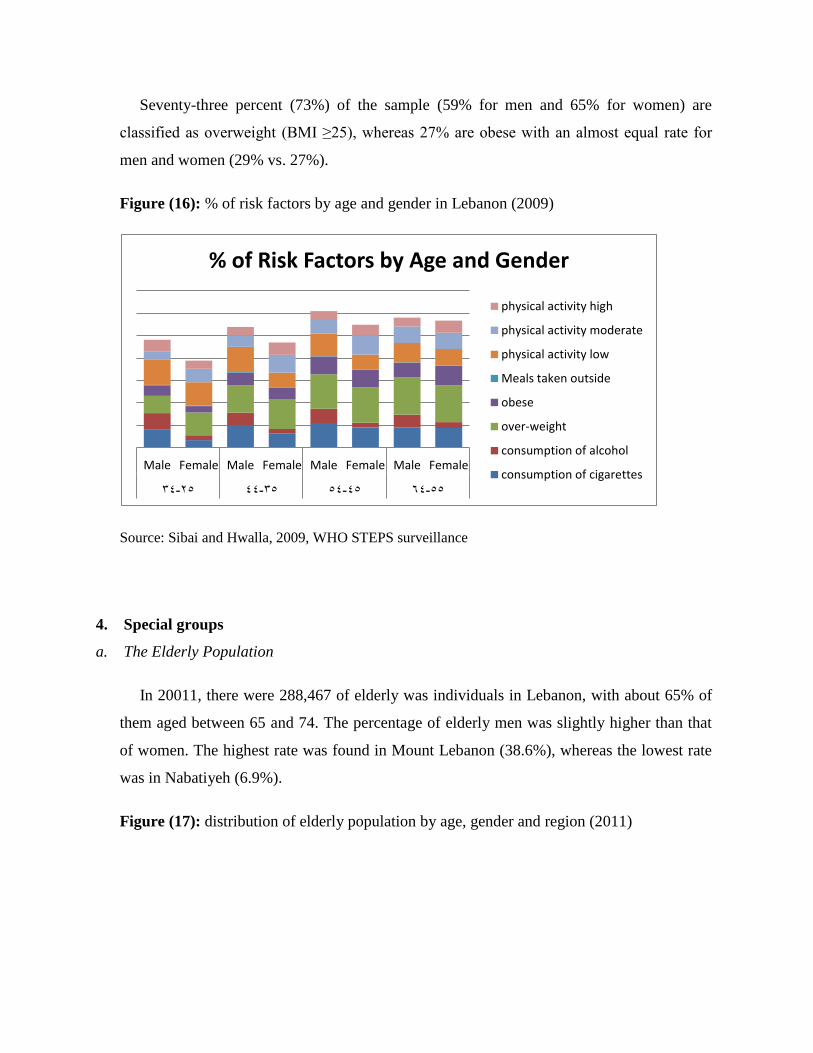
Seventy-three percent (73%) of the sample (59% for men and 65% for women) are
classified as overweight (BMI ≥25), whereas 27% are obese with an almost equal rate for
men and women (29% vs. 27%).
Figure (16): % of risk factors by age and gender in Lebanon (2009)
Source: Sibai and Hwalla, 2009, WHO STEPS surveillance28
4. Special groups
a. The Elderly Population
In 20011, there were 288,467 of elderly was individuals in Lebanon, with about 65% of
them aged between 65 and 74. The percentage of elderly men was slightly higher than that
of women. The highest rate was found in Mount Lebanon (38.6%), whereas the lowest rate
was in Nabatiyeh (6.9%).
Figure (17): distribution of elderly population by age, gender and region (2011)
Male Female Male Female Male Female Male Female
25-34 35-44 45-54 55-64
% of Risk Factors by Age and Gender
physical activity high
physical activity moderate
physical activity low
Meals taken outside
obese
over-weight
consumption of alcohol
consumption of cigarettes

Source MOPH, 2011, Statistics Bulletin,
http://www.moph.gov.lb/Publications/Pages/StatB2011.aspx
Figure (18): Institutions that provide elderly care (2010)
Distribution of elderly of population by Age
65-69
70-74
75-79
80-84
85 +
Distribution of elderly population by Gender
Men
Female
Distribution of elderly population by age
Mount-Lebanon
North
Bekaa
South
Beirut
Nabatieh
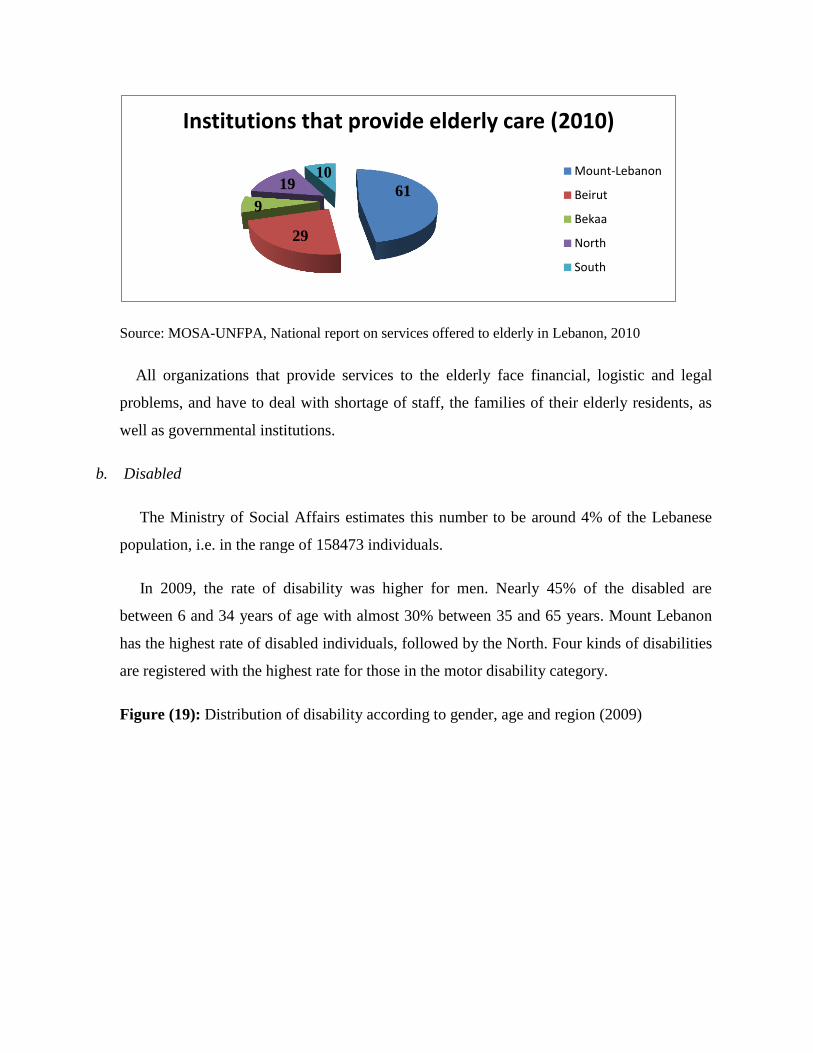
Source: MOSA-UNFPA, National report on services offered to elderly in Lebanon, 2010
All organizations that provide services to the elderly face financial, logistic and legal
problems, and have to deal with shortage of staff, the families of their elderly residents, as
well as governmental institutions.
b. Disabled
The Ministry of Social Affairs estimates this number to be around 4% of the Lebanese
population, i.e. in the range of 158473 individuals.
In 2009, the rate of disability was higher for men. Nearly 45% of the disabled are
between 6 and 34 years of age with almost 30% between 35 and 65 years. Mount Lebanon
has the highest rate of disabled individuals, followed by the North. Four kinds of disabilities
are registered with the highest rate for those in the motor disability category.
Figure (19): Distribution of disability according to gender, age and region (2009)
61
29
9
19 10
Institutions that provide elderly care (2010)
Mount-Lebanon
Beirut
Bekaa
North
South

Source: MOSA, 2009, Access and Right Program.
c. Prisoners
Distribution of disability according to Gender
Men
Female
Distribution of disability according to Age
0-5
6..18
19-34
35-65
Distribution of disability according to Region
Mount-Lebanon
North
South
Bekaa
Nabatieh

Lebanon has 21 prisons distributed all over the Lebanese territory. The majority of these
prisons serve adult males. There are three prisons for women only one specialized for
minors. Some minors are also kept in the Roumieh prison in a special department.
Many recommendations were proposed during the first congress on the health in
prisons that took place in Lebanon in 2008. These recommendations included:
1. Elaborating a specific health system for prisoners
2. Developing the current medical structure
3. Increasing the number of hospitalization beds in hospitals; especially beds in the intensive
care unit
4. Reinforcing mental health
5. Developing an individual medical file for every sick prisoner
6. Providing the medication required for treatment
7. Developing a declaration system for emergencies
8. Establishing an efficient transport system for sick prisoners
9. Ensuring the presence in the prisons of a permanent medical team
10. Developing a prevention policy
11. Improving incarceration conditions
12. Guaranteeing the rights of prisoners.
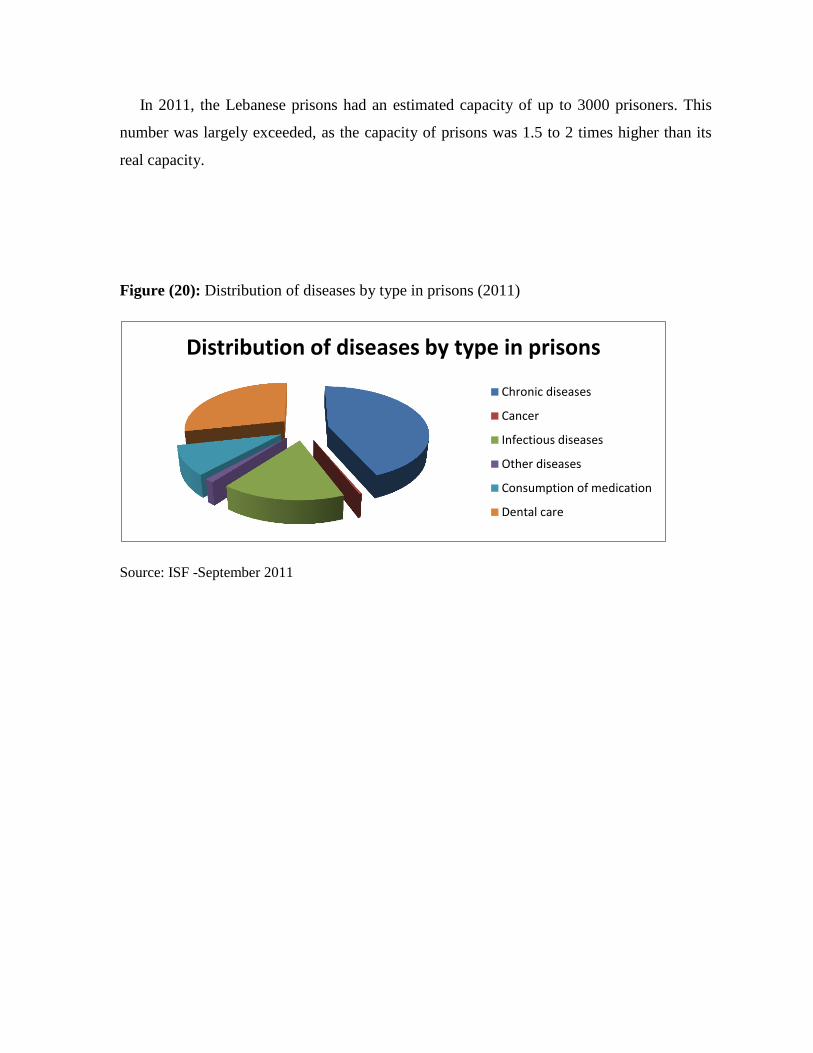
In 2011, the Lebanese prisons had an estimated capacity of up to 3000 prisoners. This
number was largely exceeded, as the capacity of prisons was 1.5 to 2 times higher than its
real capacity.
Figure (20): Distribution of diseases by type in prisons (2011)
Source: ISF -September 2011ble 50
Distribution of diseases by type in prisons
Chronic diseases
Cancer
Infectious diseases
Other diseases
Consumption of medication
Dental care

Part Two: Lebanese Health Sub-system Profile
Chapter I: Health system indicators
The concept of health for all, to which Lebanon has subscribed, places equal access to
quality health care at the center of health development. This goal can best be achieved
through sustained services that provide better care, use resources more efficiently and
facilitate regular access to basic care. The strength of the health care system rests on the
quality and quantity of resources available such as hospital capacity, advanced technology
and medical expertise.
These resources have made possible the observed overall high level of accessibility to
health care services. However, the health sector in Lebanon appears to have an inverted
structure whereby resources are essentially concentrated in tertiary care rather than in
secondary and primary health care levels.
Also, the impact of such resources on improving the health situation remains questionable
in the absence of clear policies for the development of needed human resources, including
those needed in support of sophisticated technology, and the absence of adapted regulatory
mechanisms for control of costs and ensuring the quality of care.
A. Health system Infrastructure
1. Ambulatory care

The country has 950 dispensaries and primary healthcare centers operating with minimal
human and physical capacities and offer limited services. Primary healthcare centers are in
constant evolution and offer a multitude of services including prevention programs,
reproductive health programs, family planning and prenatal care. They also develop training
programs and offer logistic support, via a wide network, in buying and distributing essential
medication. In spite of this, the public primary healthcare system remains weak. The number
of individuals making use of these centers remains limited (estimated at a maximum of 20%
of the population) and the quality of services varies by region and provider.
The MOPH has chosen 130 centers among all the primary healthcare centers operating in
the country to establish a primary healthcare network distributed as follow:
Seventy-one % (71%) of the 130 primary healthcare centers (PHC) of the national PHC
network of the country belong to NGOs. Of the 130 PHCs, 21 are under a trial period, 14
belong to the public sector (10 belong to and are managed by the MOPH, and 4 belong to
and are managed by the MOSA), 29 belong to the MOPH and are managed by NGOs or
local authorities and 106 are managed and belong to NGOs and/or municipalities.25
The private sector is the main source of ambulatory medical care in the country. This
phenomenon is facilitated by the large supply of physicians. NGOs play a critical role in the
success of programs of vaccination, AIDS control, iodine deficiency, diarrheal disease
control and to a lesser extent in health education and school health. The set up of these
health centers is varied. Some have lots of staff, various specializations and extensive
equipment; others are poorly equipped in terms of facilities and staff.
All ambulatory care, including that provided at the level of NGOs centers, is structured
to respond to emergency and acute demands but lacks in comprehensiveness and continuity.
The function of these centers is to provide a balanced and good quality care, including both
curative and preventive care.
Disease prevention is an integral part of any effort to improve the health situation of the
population. Some national health promotion and disease prevention programs have been
25
WHO EMRO, 2011, Health System Profile, Lebanon

successfully introduced with the help of UN organizations. Still, the priority given to kidney
dialysis contrasts with the absence of hypertension and diabetes national prevention
programs; diabetes being the underlying cause in over one-fifth of kidney failures; and the
priority given to open heart surgery contrasts with the lack of a national primary prevention
initiative for the control of smoking.
2. The hospital sector
The hospital sector has witnessed very rapid expansion. This has occurred concurrently
with the development of sophisticated medical technologies in the world. It has been
observed globally that the introduction of advanced technologies usually influences the
hospitalization capacity. In Lebanon there has been a concomitant use of both heavy
technology and bed capacity. This has undoubtedly fueled the escalating costs of health care
in the country.
In the absence of any regulating mechanism, and encouraged by the government policy
to subsidize sophisticated medical interventions, the private sector has been encouraged to
invest in such technologies. These are now spread in all regions in contrast to the persistent
lack of some basic medical disciplines and hospital services, in such areas as medical
emergency care and prenatal services.
Also, the small number of sophisticated medical technology procedures handled by each
of the health facilities do not allow for an adequate accumulation of expertise in the field.
Besides, it is commonly observed that acquisition of sophisticated equipment is not always
coupled with training or opportunities for the development of human resources in the field.
Another important weakness of the health care system is observed in pre-hospital care
such as in emergency care. The existing services are rudimentary and concerned with
transportation and transfer of patients. The services are diffused and their management is
uncoordinated. They are completely dependent on voluntary staff which are often
inadequately trained and equipped.
The public hospitals were until recently under-equipped, offered bad quality services and
lacked qualified professionals. These hospitals provided free general care, were managed

like administrative units of the MOPH and did not benefit from financial autonomy. Their
management was centralized and the budget allocation was based on estimations rather than
studies of actual need.
The hospital sector in Lebanon suffers from the inefficiency at more than one level, first
being the size.
Hospitals in Lebanon are generally small (less than 70 beds); this delayed the appropriate
management of quality of acute care. About 70% of hospitals in public sectors have 70 beds
or less, 30% have between 71 and 200 beds, with 0% having over 200 beds.
Table (10): Distribution of hospitals per size
Beds Public hospitals Private hospitals
Up to 70 beds 14 96
71 to 200 beds 6 43
Over 200 beds 0 4
Source: MOPH, Statistics bulletin, 2011
There is a different classification of hospital size where 67% of private hospitals in
Lebanon have less than 70 beds, i.e. classified as small. Lebanon has only 43 private
hospitals with 71 to 200 beds, and only 4 with 200 beds or more; these are located in Beirut
and its suburbs. Besides, the size of a hospital correlates not only with efficiency, but also
with the cost and quality of medical care provided.
The private hospital sector is the main component and backbone of the Lebanese
healthcare system. Highly developed both in number and capacity, it includes 135 long and
short stay hospitals, with a total of 12648 beds (Private Hospitals Syndicate, 2009) which
account for 82% of the country’s total capacity. They are mainly general multidisciplinary
hospitals with 80 to 400 beds per hospital.
Figure (21): Distribution of number of beds by region

Source: Syndicate of Private Hospitals, 2011; MOPH, 2011; Ministry of Defence, 2010.
The supply of beds in Lebanon has been balanced since 2005; the number of beds
available per 1000 individuals was maintained between 3.43 and 3.60. Currently, the
number of hospital beds available in Lebanon s estimated around 14864 beds, i.e. a ratio of
3.5 beds per 1000 individuals.
Among 181 Countries surveyed by index-mundi website, Japan has the highest hospital
beds density, 13.75 beds/1000 populations while Ethiopia and Cambodia have the lowest
rate at 0.18 and 0.1 beds/1000 population. Lebanon is ranked 59th in total, however, as
compared to the Arab World, Lebanon is ranked the 1st.26
Occupancy is the other efficiency reason. This could be attributed to one (or both) of the
following two reasons:
a. There are some public hospitals that have been equipped and ready to function, but not
operational yet due to administrative reasons. The inefficiency lies in the fact that nothing is
being done to operate these hospitals so as to cover the huge investment costs pertaining to
building, equipping and most importantly financing these hospitals.
b. Many groups find it easier and more profitable to construct and run new tailor-made
hospitals rather than operate existing ones. These groups usually develop private or
religious-institutions hospitals.
26
Index-mundi website http://www.indexmundi.com/facts/lebanon
3350
4686
665 782 1701 2027 1766
365
010002000300040005000
Distribution of number of beds by region
Number of beds

There is a total of 163 Hospitals contracting with the MOPH, 84.66% of the Hospitals are
private Hospitals while 15% are public hospitals. The highest concentration of hospitals is
attributed to Mount-Lebanon with 37.40% of the total number of hospitals while the lowest
number of hospitals available is in Nabatiyeh at 675%.
Amongst private hospitals, Mount Lebanon holds the highest number of hospitals
(40.58%) followed by North Lebanon (18.84%) with the lowest number existing in
Nabatiyeh (3.62%). Between public hospitals, the highest number of hospitals available is in
North Lebanon and Nabatiyeh (24%) with the lowest number in Beirut and South Lebanon
(8%).
The Ministry of Public Health contracts with both the public and the private hospitals for
the services it pays for with the aim of ensuring universal accessibility to services in an
equitable distribution. Accordingly, the MOPH issues contracts with 138 private hospitals
where the patient share is 15% of the hospital bill, and 25 public hospitals where the patient
pays only 5% of the bill.
Figure (22): Number of hospitals having contracts with the MOPH by type and Mohafazat
Source: MOPH, Statistics bulletin, 2011
Figure (23): Percentage of hospitals in public and private sectors distribution per Mohafaza
2 5 6 4 2 6 11
56
26 23 17
5
0102030405060
Number of hospitals having contracts with the MOPH
by type and Mohafazat (2011)
Public
Private

Source: MOPH, Statistics bulletin, 2011
Figure (24): Percentage of hospitals distribution per Mohafaza
Source: MOPH, Statistics bulletin, 2011
05
1015202530354045
Beirut MountLebanon
North bekaa South Nabatiyeh
Private
Public
8
37
20
16
12 7
Total distribution of hospitals among Mohafaza
Beirut
Mount Lebanon
North
bekaa
South
Nabatiyeh

There were 236,643 MOPH subsidized admissions to hospitals during 2011. The share of
the private hospital is estimate around 69.41% compared to 30.59% of the total number of
admissions. Mount Lebanon has the highest rate of admissions (23.28%) followed by North
Lebanon (21.28%) while the lowest admission rate is in Beirut (9.82%).
Among private hospitals there were 164,244 admissions, where, Mount Lebanon holds
the highest share of admission (27.48%) followed by Bekaa (23.4%) with the lowest number
existing in Beirut (5.37%).
Figure (25): Number of admission by type of hospital and geographic location (2011)
Source: MOPH, Statistics bulletin, 2011
However the number of admissions in the public hospitals reached 72,399. Amongst
public hospitals, the highest number of admission is in Nabatiyeh (21.64%) followed by
North Lebanon (21.37%) with the lowest number in South Lebanon (8.27%).
As expected, in areas where there are active and contracted public hospitals, the number
of admissions in public hospital exceeds that in contracted private hospitals.
Figure (26): The evolution of MOPH subsidized admissions in public and private hospitals
between 2005 and 2011
14408 9962
15475 10900
5989
15665 8828
45134
34879 38439
27830
9134
0
10000
20000
30000
40000
50000
Public
Private
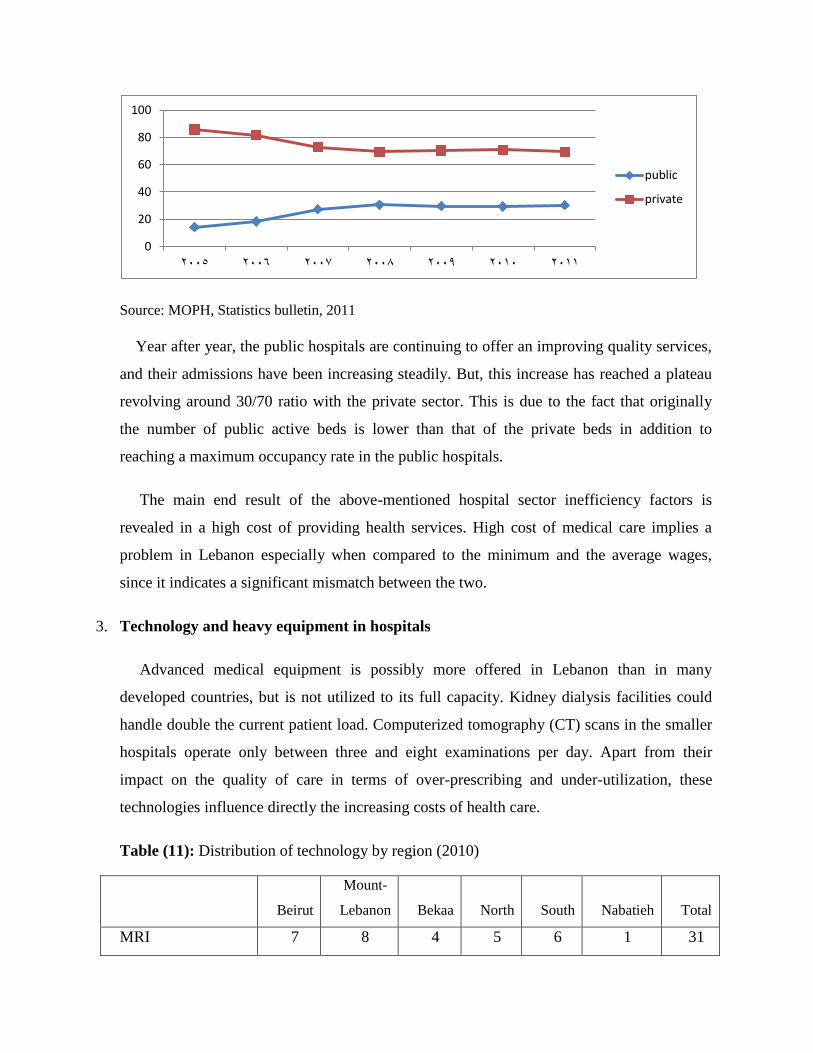
Source: MOPH, Statistics bulletin, 2011
Year after year, the public hospitals are continuing to offer an improving quality services,
and their admissions have been increasing steadily. But, this increase has reached a plateau
revolving around 30/70 ratio with the private sector. This is due to the fact that originally
the number of public active beds is lower than that of the private beds in addition to
reaching a maximum occupancy rate in the public hospitals.
The main end result of the above-mentioned hospital sector inefficiency factors is
revealed in a high cost of providing health services. High cost of medical care implies a
problem in Lebanon especially when compared to the minimum and the average wages,
since it indicates a significant mismatch between the two.
3. Technology and heavy equipment in hospitals
Advanced medical equipment is possibly more offered in Lebanon than in many
developed countries, but is not utilized to its full capacity. Kidney dialysis facilities could
handle double the current patient load. Computerized tomography (CT) scans in the smaller
hospitals operate only between three and eight examinations per day. Apart from their
impact on the quality of care in terms of over-prescribing and under-utilization, these
technologies influence directly the increasing costs of health care.
Table (11): Distribution of technology by region (2010)
Beirut
Mount-
Lebanon Bekaa North South Nabatieh Total
MRI 7 8 4 5 6 1 31
0
20
40
60
80
100
2005 2006 2007 2008 2009 2010 2011
public
private
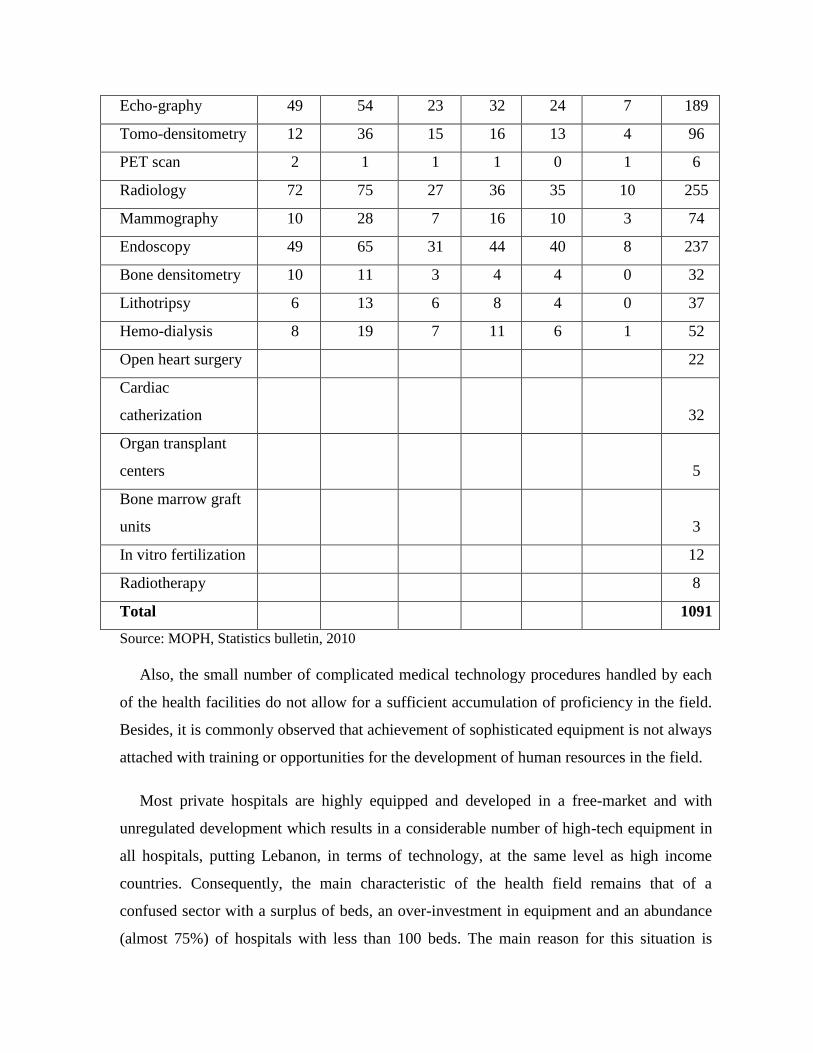
Echo-graphy 49 54 23 32 24 7 189
Tomo-densitometry 12 36 15 16 13 4 96
PET scan 2 1 1 1 0 1 6
Radiology 72 75 27 36 35 10 255
Mammography 10 28 7 16 10 3 74
Endoscopy 49 65 31 44 40 8 237
Bone densitometry 10 11 3 4 4 0 32
Lithotripsy 6 13 6 8 4 0 37
Hemo-dialysis 8 19 7 11 6 1 52
Open heart surgery 22
Cardiac
catherization 32
Organ transplant
centers 5
Bone marrow graft
units 3
In vitro fertilization 12
Radiotherapy 8
Total 1091
Source: MOPH, Statistics bulletin, 201062
Also, the small number of complicated medical technology procedures handled by each
of the health facilities do not allow for a sufficient accumulation of proficiency in the field.
Besides, it is commonly observed that achievement of sophisticated equipment is not always
attached with training or opportunities for the development of human resources in the field.
Most private hospitals are highly equipped and developed in a free-market and with
unregulated development which results in a considerable number of high-tech equipment in
all hospitals, putting Lebanon, in terms of technology, at the same level as high income
countries. Consequently, the main characteristic of the health field remains that of a
confused sector with a surplus of beds, an over-investment in equipment and an abundance
(almost 75%) of hospitals with less than 100 beds. The main reason for this situation is
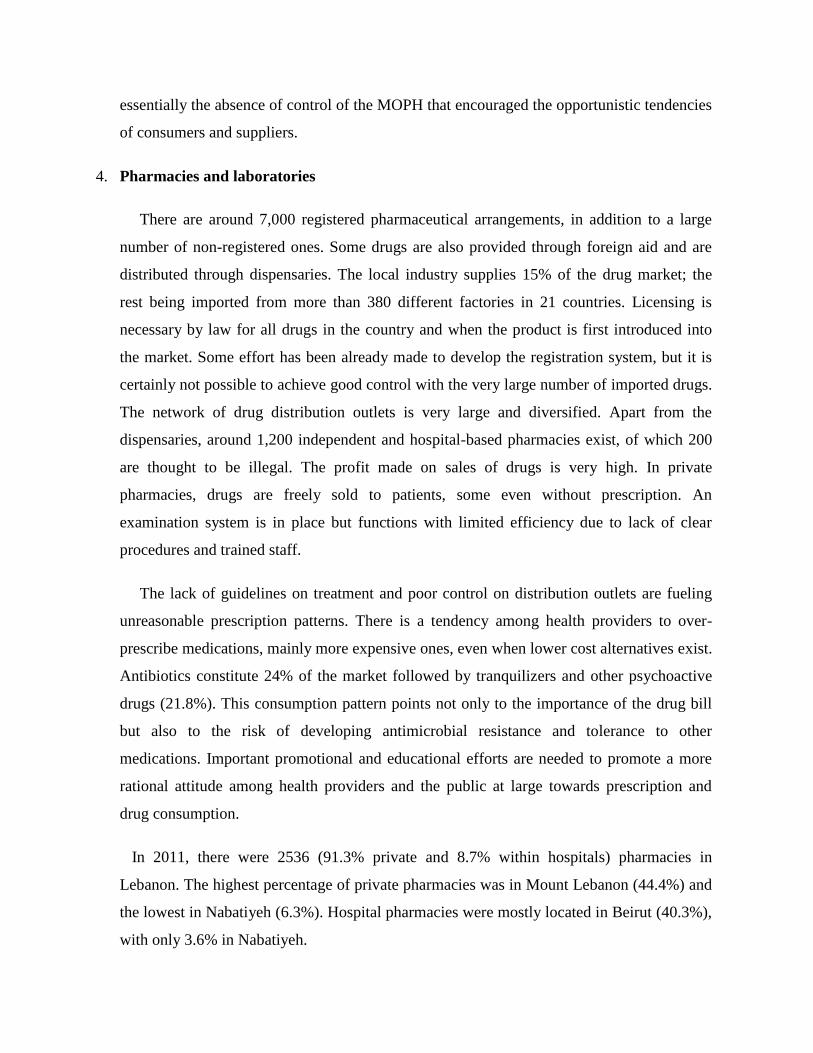
essentially the absence of control of the MOPH that encouraged the opportunistic tendencies
of consumers and suppliers.
4. Pharmacies and laboratories
There are around 7,000 registered pharmaceutical arrangements, in addition to a large
number of non-registered ones. Some drugs are also provided through foreign aid and are
distributed through dispensaries. The local industry supplies 15% of the drug market; the
rest being imported from more than 380 different factories in 21 countries. Licensing is
necessary by law for all drugs in the country and when the product is first introduced into
the market. Some effort has been already made to develop the registration system, but it is
certainly not possible to achieve good control with the very large number of imported drugs.
The network of drug distribution outlets is very large and diversified. Apart from the
dispensaries, around 1,200 independent and hospital-based pharmacies exist, of which 200
are thought to be illegal. The profit made on sales of drugs is very high. In private
pharmacies, drugs are freely sold to patients, some even without prescription. An
examination system is in place but functions with limited efficiency due to lack of clear
procedures and trained staff.
The lack of guidelines on treatment and poor control on distribution outlets are fueling
unreasonable prescription patterns. There is a tendency among health providers to over-
prescribe medications, mainly more expensive ones, even when lower cost alternatives exist.
Antibiotics constitute 24% of the market followed by tranquilizers and other psychoactive
drugs (21.8%). This consumption pattern points not only to the importance of the drug bill
but also to the risk of developing antimicrobial resistance and tolerance to other
medications. Important promotional and educational efforts are needed to promote a more
rational attitude among health providers and the public at large towards prescription and
drug consumption.
In 2011, there were 2536 (91.3% private and 8.7% within hospitals) pharmacies in
Lebanon. The highest percentage of private pharmacies was in Mount Lebanon (44.4%) and
the lowest in Nabatiyeh (6.3%). Hospital pharmacies were mostly located in Beirut (40.3%),
with only 3.6% in Nabatiyeh.

Table (12): Geographic distribution of pharmacies and labs (2011)
pharmacies labs
Hospital Private Hospital Private
Bierut 89 223 20 41
Mount-Lebanon 57 1027 38 67
North 24 349 22 29
South 23 343 23 31
Nabatieh 8 145
Bekaa 20 328 18 13
Source: Order of Pharmacists, 2011; Syndicate of Biologists, May 2011.
5. Dialysis, physiotherapy and radiology centers
In 2011, the largest concentration of dialysis (23) physiotherapy (171) and radiology (78)
centers was found in Mount Lebanon, and the lowest in Nabatiyeh.
Table (13): distribution of dialysis, physiotherapy and radiology centers by region (2011)
Dialysis Physiotherapy Radiology center
Beirut 8 59 22
Bekaa 9 26 24
North 12 79 35
Mount-Lebanon 23 171 78
South 7 34 20
Nabatieh 3 12 6
Source: MOPH, Statistics bulletin, 2011
6. Insurance companies
The number of active insurance companies decreased by 15% from 2001 (61 companies)
to 2011 (52 companies). The total gross premiums on the Lebanese market were estimated
at 1.2 billion dollars in 2010.27
27
Ministry of Economy and Trade, 2010, Annual report

This represented an increase of 12.5% from 2009. Since 2001, the premium yearly
turnover was multiplied by 2.8, the profits by 4.5, assets by 3.9, equities by 3.3 and reserves
by 6.3. The fire, accidents and miscellaneous risks branch has dominated the market with a
market share estimated at 70%. The progression of these branches in 2011 is of 12%. The
life insurance branch represented 30% of the overall turnover, with a progression of 15% in
2011.28
Between 2007 and 2011, the medical insurance branch evolved by 16.1% per year for all
categories, except for the claims paid which increased by 13.7% per year for the same
period. The market is heavily concentrated as the first 10 companies capture 80% of the
market.
B. Human Resources
There is evidently a surplus of physicians. The total number of medical doctors is
currently estimated to be between 7,900 and 9,500 physicians, including those practicing but
not legally registered. The physician - population ratio is presently estimated to be between
one doctor for every 330 persons and 392 persons. This is higher than in most parts of the
world, having 1 to 446 reported for the United States of America.29
The majority of doctors are graduates of medical schools abroad with widely different
training backgrounds and of variable quality. Only 37.8 % of doctors received their basic
medical education in Lebanon. The rest have been trained in 66 different countries, mainly
Arab and Eastern European countries. As a result, many of these doctors are not equipped to
meet the country’s health needs.
The medical work force operates in an environment which is largely unregulated and
dominated by the private sector. National protocols for disease management and treatment,
and continuing medical education and quality assessment schemes, are lacking. Highly
specialized medical categories such as surgery are in surplus; whereas there is scarcity of
28
Ibid. 29
WHO website http://www.who.int/gho/countries/lbn/en/
well-trained primary care and family medicine practitioners. Some regional imbalances also
exist with physicians concentrated mainly in urban areas.
While there is a surplus of medical personnel, except for primary care practitioners,
family doctors and other public health related specializations, there is a critical lack of other
categories of health workers, particularly nurses and midwives. The imbalance in health
manpower resources becomes even more glaring when relating the number of existing
physicians to that of nurses.
Other health care workers and technical paramedical staff categories such as health
inspectors, laboratory and X-ray technicians are also in short supply. This is a cause of
concern, especially with the development and implementation of national strategies for
primary health care and reactivation of national specific- disease control programs.
The launching of the school for training health inspectors as a joint venture of the
Ministry of Public Health and the Ministry of Vocational Training is an attempt to overcome
the shortage in this field. On the other hand, an important gap is noted between the rapid
rate of acquiring advanced medical technology in the country, and the preparation of skilled
technicians for its operation. Training programs for medical equipment engineers and
maintenance technicians are very scarce.
Health professionals today include physicians, pharmacists, dentists, nurses, as well as
other paramedical professionals such as physiotherapists, psychologists, speech therapists,
psychomotor therapists, and others. These professionals are educated and trained in
Lebanon or abroad (France, Europe, Latin America, Eastern Europe, North America).
Health professionals are granted a working permit from the Ministry of Public Health
and must register in their Order or professional Syndicate to obtain the authorization to work
in Lebanon.
1. Orders and Syndicates
a. Physicians

In 2010, around 11782 physicians 70% of which were specialists were registered in the
two Orders of Physicians in the country (Beirut and North Lebanon)30
. Approximately, 10-
15% of registered physicians did not practice in Lebanon. The rate of doctors in Lebanon
was on the average 2 per 1000 inhabitants but was unevenly distributed among regions, with
a large concentration in the capital.
b. Pharmacists
There were 5457 pharmacists.31
c. Dentists
Dentists, like physicians, were in surplus in Lebanon. In 2008, they reached 5116, with
the highest concentration in Beirut and Mount Lebanon. Only 3795 dentists were practicing
at the time32
.
d. Nurses
The number of nurses registered at the Order of Nurses in Lebanon as of April 30, 2011
was 9460. Nearly 72% were active. Among the active nurse population, 81% are women
and 19% men. Approximately 68.51% were between 26 and 40 years old, and 46.41% had a
university degree. Almost 71.92% worked in Lebanon, whereas 10.68% did not work or had
retired. Five thousand nine hundred and sixty-five nurses (87.6%) worked in hospitals,
80.3% in private and 19.70% in public hospitals. The ratio of qualified nurses/population is
3/10000. This ratio is one of the lowest in the world. The nurse/physician ratio is 1/2.5; this
ratio is generally reversed in most countries33
.
e. Physiotherapists
The number of physiotherapists registered at the Order as of April 2010 was of 1431,
among which 780 are women. The majority (731) live in the Mount Lebanon region 34
.
f. Other health professionals
30
Order of Physicians in Beirut and North Lebanon, 2010 31
Order of Pharmacists in Lebanon, 2009 32
Order of Dentists in Beirut and the North, 2008 33
Order of Nurses in Lebanon, 2011 34
Order of Physiotherapists in Lebanon, 2010
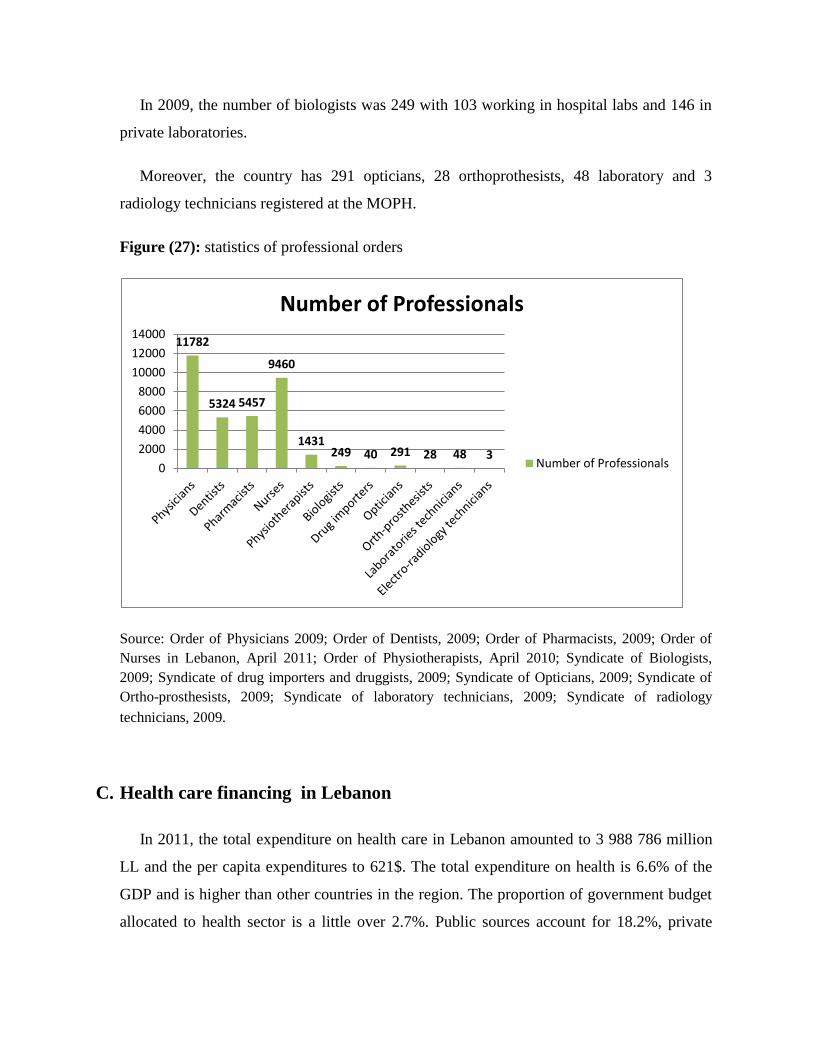
In 2009, the number of biologists was 249 with 103 working in hospital labs and 146 in
private laboratories.
Moreover, the country has 291 opticians, 28 orthoprothesists, 48 laboratory and 3
radiology technicians registered at the MOPH.
Figure (27): statistics of professional orders
Source: Order of Physicians 2009; Order of Dentists, 2009; Order of Pharmacists, 2009; Order of
Nurses in Lebanon, April 2011; Order of Physiotherapists, April 2010; Syndicate of Biologists,
2009; Syndicate of drug importers and druggists, 2009; Syndicate of Opticians, 2009; Syndicate of
Ortho-prosthesists, 2009; Syndicate of laboratory technicians, 2009; Syndicate of radiology
technicians, 2009.74
C. Health care financing in Lebanon
In 2011, the total expenditure on health care in Lebanon amounted to 3 988 786 million
LL and the per capita expenditures to 621$. The total expenditure on health is 6.6% of the
GDP and is higher than other countries in the region. The proportion of government budget
allocated to health sector is a little over 2.7%. Public sources account for 18.2%, private
11782
5324 5457
9460
1431 249 40 291 28 48 3
0
2000
4000
6000
8000
10000
12000
14000
Number of Professionals
Number of Professionals

sources for 79.8% of health care financing and international donors for the remaining 2%.
The single largest source of financing comes from households which represents 69.7% of
total expenditures. In terms of expenditures, public sector providers accounted for 1.7%,
private sector providers for 89.2%, and others accounted for the remaining 9.1%. This
pattern of expenditures reflects the fact that Lebanon relies largely on the private sector in
the health services.35
There are six employment based social insurance funds publicly managed in Lebanon,
the largest one is the National Social Security Fund (NSSF) meant to cover all employees in
the formal sector (private sector and government-owned corporations, in addition to
contractual and wage earners of the public administration). The Civil Servants Cooperative
(CSC) covers the regular government staff. The remaining four funds cover the Military and
Security Forces. CSC is under the tutelage of the presidency of the Council of Ministers and
the others are overseen by three separate ministries other than MOH.
1. National Social Security Fund (NSSF)
The NSSF was established in 1964 and is similar to the French model of social security.
As essentially a service for workers, the NSSF comes under the Ministry of Labor. The
MOPH has little input into its operations or decisions. The NSSF is the most important
source of public health insurance in Lebanon. It covers, in principle, Lebanese citizens who
are: workers and employees in the private, non-agricultural sector; permanent employees in
agriculture, employees of public institutions and independent offices who are not subject to
civil service; teachers in public schools; taxi drivers; newspaper sellers; and university
students.
Health coverage includes sickness and maternity allowances amounting to 90% of
hospitalization costs and 80% of medical consultations and medication excluding dental
care.36
Thus to a large extent, the Fund is financed from private sources yet it is a public
institution. The household survey revealed that only 26.1% of the Lebanese population was
covered by the NSSF.
35
WHO website http://www.who.int/gho/countries/lbn/en/ 36
National Social Security Fund- A brief review, August 2005

2. Security forces coverage
Insurance for the security forces is organized through several funds. The Military are
covered by the Ministry of Defense. The Internal Security Forces have their own plan, under
the Ministry of Interior. The staffs of Public Security, Customs employees and those of State
Security are covered through 2 different funds, under the Office of the Prime Minister. All
uniformed staff members are covered with their dependents and their parents. Together,
these funds constitute the second most important source of public health insurance.
Coverage here is the most generous: 100% of hospitalization and medical expenses for
the member, 75% for spouse and children and 50% for dependent parents.
3. Cooperative of the Civil Servants
The Cooperative of the Civil Servants (CCS) is the third most important source of public
health insurance which was instituted in 1964. The CCS insures all employees of the public
sector who are subject to the laws of the Civil Service.
Health insurance covers 90% of hospitalization costs and 75% of consultations,
medication and dental treatment for the employee (up to a ceiling, beyond which the CCS
covers all). The CCS is operated by the Office of the Prime Minister and is financed from a
1% deduction off the payroll of the individual; the balance is covered by the Government.
4. Ministry of Public Health – insurer of last resort
The MOPH funds the hospitalization costs for any citizen who is not covered under a
public insurance plan. This coverage is independent of the income and assets of the
individual. In addition, the MOPH covers the cost of some interventions such as
chemotherapy, open heart surgery, dialysis and renal transplant, and drugs for chronic
diseases. This coverage engulfs some 40%– 45% of the Ministry’s budget for contracted
services. As such, the Ministry has the largest share of the total cost of public expenditure,
including insurance, on health services in the country.
The MOPH covers 85% of hospital care: the incumbent is expected to pay 15% of the
hospital bill. However, even this co-payment is frequently waived altogether, on account of
need. Recently, the Ministry has taken steps to introduce ―flat rate‖ payments in its contracts
with private hospitals.
5. Mutual funds
There are a growing number of mutual funds covering health expenses in the context of
syndicates, associations and other groups. This sector comes under the Ministry of Housing
and Cooperatives. The law governing mutual funds allows any group of 50 persons (or
above) to form a mutual fund.
The linkage could be professional, religious or community-based. Tax laws that provide
tax breaks to not-for-profit groups have led to a proliferation of mutual funds that offer
health insurance coverage to those enrolled in the fund. Mutual funds do not pay taxes on
the premium, unlike the private insurance companies.
6. Private insurance
Private health insurance is well established in Lebanon. According to the Ministry of
Economy, approximately 70 private insurance companies provide both complementary and
comprehensive health insurance policies. The former are to complement and fill gaps in the
benefits provided by NSSF, CCS, and health insurance arrangements for the army and
police. The latter refer to stand alone health insurance policies that can cover a range of
benefits, including inpatient and outpatient care, and coverage for pharmaceutical expenses.
Nearly 85% of the policies are purchased by employers as an employee benefit or to fill
gaps in NSSF coverage. The private insurance market is not well regulated. Consequently,
insurers indulge in ―cream skimming‖, selecting only good risks and either denying
coverage or setting very high premiums for individuals with pre-existing conditions.
Private insurance companies are taking full advantage of the system by selecting younger
and better-off clientele. Expensive interventions are usually excluded and the burden of this
is being shifted onto the MOPH. According to the National Household Expenditure and
Utilization Survey, 8.3% of residents adhered only to private insurance; of that 0.7% held
more than one policy, and 2.5% had private insurance as complementary to the NSSF
coverage.37
7. Other health insurance funding resources
7.1. Local and foreign not-for-profit organizations
There is a relatively small proportion of the total health bill that is covered by local and
foreign not-for-profit organizations and NGOs operating generally at the local level in
poorer urban districts and underprivileged rural areas. Medical care offered through NGOs
increased during the war but this has waned somewhat since 1990. However, the
involvement of the community in the provision of medical care did offer some innovative
models for the financing, governance and management of health services.
7.2. Donor assistance
The sharpest decline in donor assistance has been to immunization and control of
diseases and there has been a significant increase in support for family planning activities.
The MOPH and other government agencies are the primary beneficiaries of donor
assistance.
7.3. Large companies
Major firms such as banks and large manufacturers often offer employees health
insurance. The majority of this health expenditure represents reimbursements for services in
private clinics. Survey results show that 78% of companies have private insurance for their
employees, which is complementary to the NSSF in 75% of the cases: 20% of these
companies provide extra health services that may not be covered by NSSF or the private
health insurance.38
7.4. Out-of-pocket payments
The most important item in the total health bill is the out-of-pocket payments, which is
the health expenditure borne directly by individuals, covering supplementary payments by
those who are covered by insurance or the MOPH as well as full payment by those who are
not covered by any insurance or are not beneficiaries of MOPH assistance. Household
37
National Household Expenditure and Utilization Survey, 2008 38
Households Living Conditions, Central Administration of Statistics, 2011

expenditure accounts for 69.7% of total health expenditure. Of this, 97% is spent in the
private sector, 2% in the NGO sector, and just 1% in the public sector.
On average, households spend a little over 14% of their household expenditure on health
services. However, the burden of out-of-pocket expenditure, measured as a proportion of
household expenditure, is not equitably distributed. Nearly a fifth of expenditure in
households in the lowest income category goes to health. The amount spent on health
decreases with income where households of highest income spend only 8% on health care.
Spending on health by households (14.1%) ranks second after food (31.4%). The average
out-of-pocket health expenditure in 2008 amounted to US$ 343.14 15.2% of household
spending on health goes for purchasing pharmaceuticals. If the proportion of hospital bills
for drugs is included, that share rises to 21.5% of household health expenditure.
Table (14): percentage of population covered by various financing agencies
Financing agency % of population covered
NSSF 26.1
Civil service cooperative 4.4
Army 8.8
Internal security 1.9
GS+ SS 0.4
Private insurance 8.0 (complete coverage)
4.6 (gap coverage)
Mutual funds 1.6
MOPH 42.7
Source: national health accounts, 2011
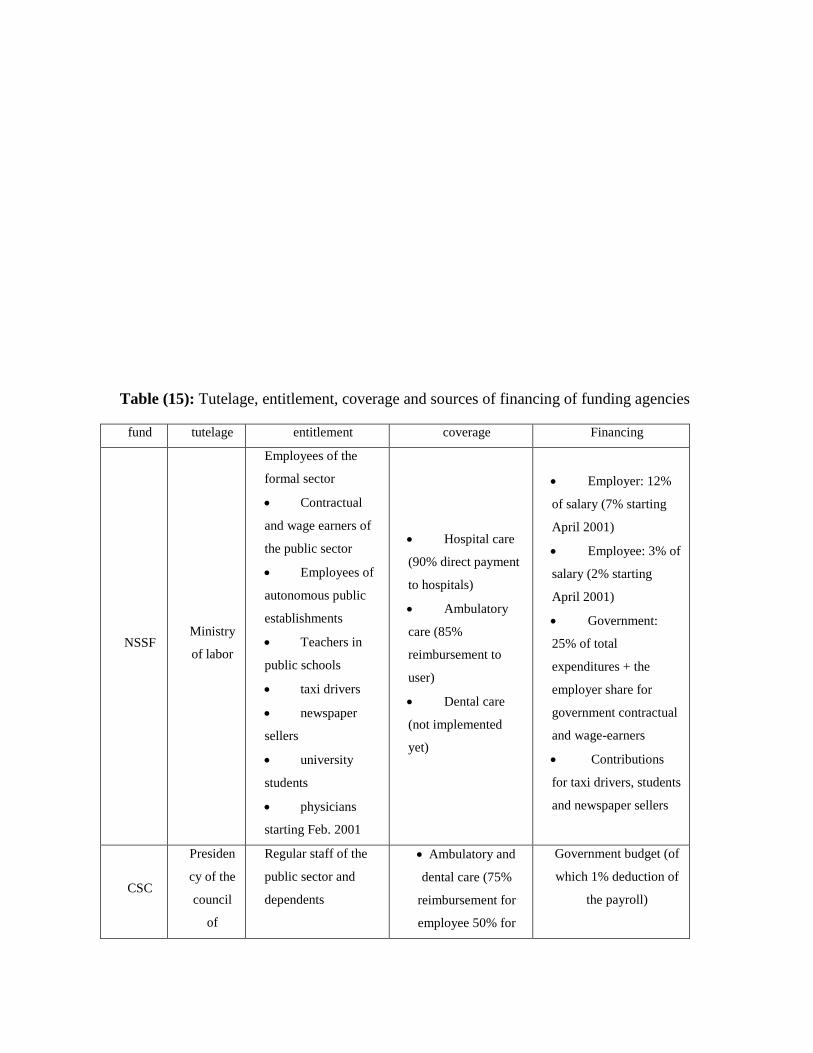
Table (15): Tutelage, entitlement, coverage and sources of financing of funding agencies
fund tutelage entitlement coverage Financing
NSSF Ministry
of labor
Employees of the
formal sector
Contractual
and wage earners of
the public sector
Employees of
autonomous public
establishments
Teachers in
public schools
taxi drivers
newspaper
sellers
university
students
physicians
starting Feb. 2001
Hospital care
(90% direct payment
to hospitals)
Ambulatory
care (85%
reimbursement to
user)
Dental care
(not implemented
yet)
Employer: 12%
of salary (7% starting
April 2001)
Employee: 3% of
salary (2% starting
April 2001)
Government:
25% of total
expenditures + the
employer share for
government contractual
and wage-earners
Contributions
for taxi drivers, students
and newspaper sellers
CSC
Presiden
cy of the
council
of
Regular staff of the
public sector and
dependents
Ambulatory and
dental care (75%
reimbursement for
employee 50% for
Government budget (of
which 1% deduction of
the payroll)
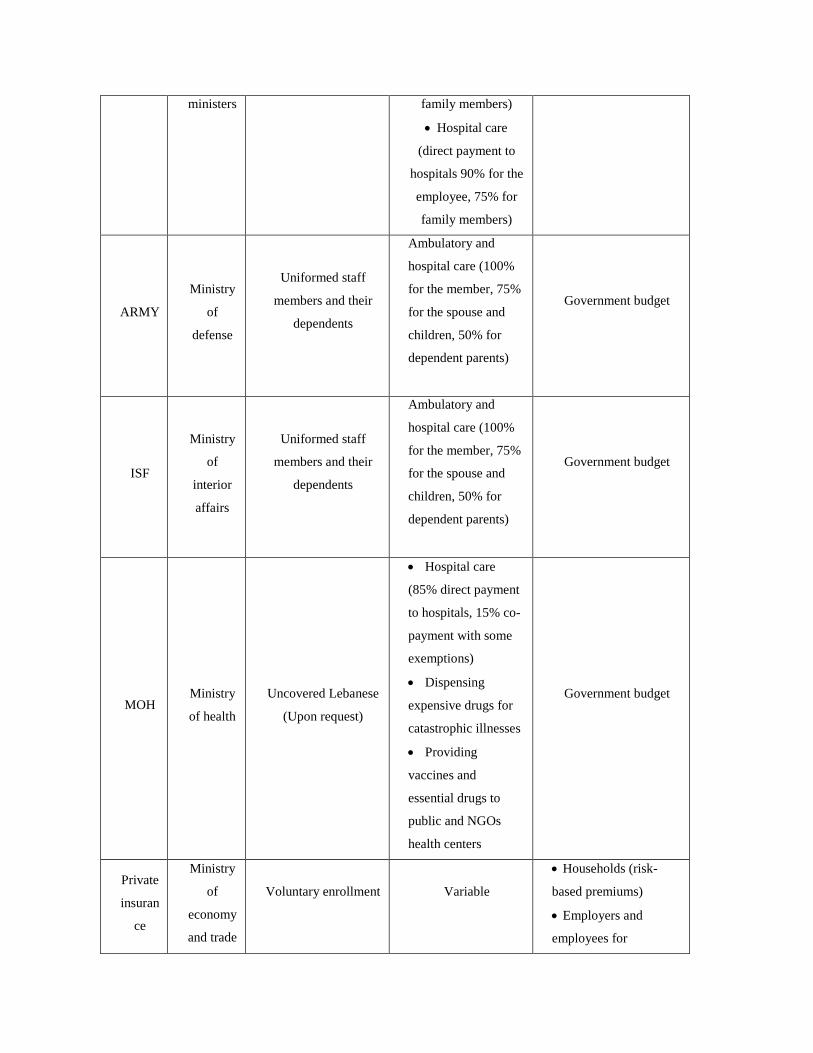
ministers family members)
Hospital care
(direct payment to
hospitals 90% for the
employee, 75% for
family members)
ARMY
Ministry
of
defense
Uniformed staff
members and their
dependents
Ambulatory and
hospital care (100%
for the member, 75%
for the spouse and
children, 50% for
dependent parents)
Government budget
ISF
Ministry
of
interior
affairs
Uniformed staff
members and their
dependents
Ambulatory and
hospital care (100%
for the member, 75%
for the spouse and
children, 50% for
dependent parents)
Government budget
MOH Ministry
of health
Uncovered Lebanese
(Upon request)
Hospital care
(85% direct payment
to hospitals, 15% co-
payment with some
exemptions)
Dispensing
expensive drugs for
catastrophic illnesses
Providing
vaccines and
essential drugs to
public and NGOs
health centers
Government budget
Private
insuran
ce
Ministry
of
economy
and trade
Voluntary enrollment
Variable
Households (risk-
based premiums)
Employers and
employees for

complementary
insurance
Mutual
fund
Ministry
of
agricultu
re
Voluntary enrollment
Variable
Households
Government
subsidies; ear-marked
taxes for the judges
mutual fund
Source: regional national health account
Table (16): Benefits under Various Public Financing Schemes
Type of
Services
MOH NSSF CSC Armed Forces
Hospitalization 85% 90% 90% 100%
Physician No Up to 13000LL 75% up to
12000 LL
Up to 20000 LL
Specialists No Up 18000 LL 75% up to
12000 LL
Up to 30000 LL
Ambulatory No Yes 90% 100%
Drugs No yes yes Yes
Emergency
clinics
No As physicians
and specialists
As physicians
and specialists
As physicians and
specialists
Emergency
hospitals
Hospital As
hospitalization
As
hospitalization
As hospitalization
Dental
coverage
No No 75 %of tariff 100%

Ophthalmology No No 75% up to
35000 LL
60000/80000/1000
00LLL
Immunization Yes at
health
centers
No No no
Treatment
abroad
No No 90% pre
admission
10000$ pre
admission
Open heart 8000000
LL
90% As MOPH 100%
Kidney
treatment
19000000
LL
90% As MOPH 100%
dialysis 135000
LL/session
100% 100% 100%
Source: regional national health account
Chapter II: Lebanese Health care System Financial Analysis
A. Lebanese health expenditure
1. External resources for health (% of total expenditure on health)
External resources for health care funds or services in kind that are provided by entities
not part of the country in question. The resources may come from international
organizations, other countries through bilateral arrangements, or foreign nongovernmental
organizations. These resources are part of total health expenditure.
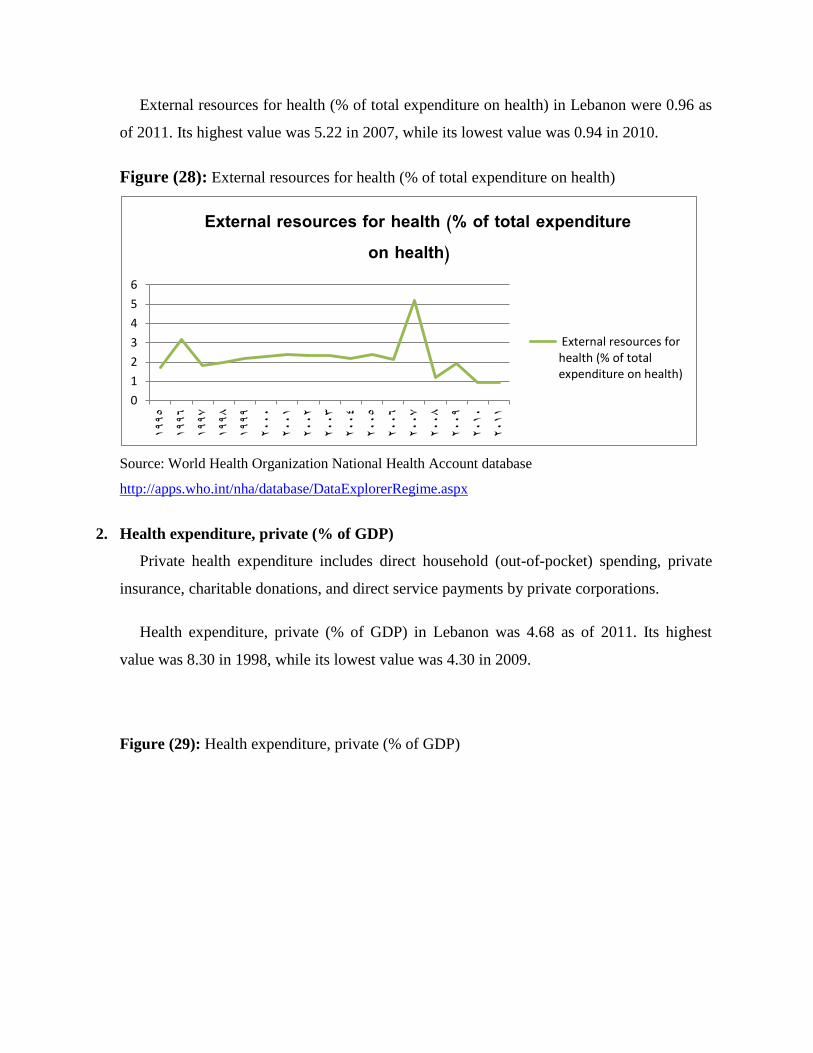
External resources for health (% of total expenditure on health) in Lebanon were 0.96 as
of 2011. Its highest value was 5.22 in 2007, while its lowest value was 0.94 in 2010.
Figure (28): External resources for health (% of total expenditure on health)
Source: World Health Organization National Health Account database
http://apps.who.int/nha/database/DataExplorerRegime.aspx
2. Health expenditure, private (% of GDP)
Private health expenditure includes direct household (out-of-pocket) spending, private
insurance, charitable donations, and direct service payments by private corporations.
Health expenditure, private (% of GDP) in Lebanon was 4.68 as of 2011. Its highest
value was 8.30 in 1998, while its lowest value was 4.30 in 2009.
Figure (29): Health expenditure, private (% of GDP)
0
1
2
3
4
5
6
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
External resources for health (% of total expenditure on health)
External resources forhealth (% of totalexpenditure on health)

Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
3. Health expenditure, public (% of total health expenditure)
Public health expenditure consists of recurrent and capital spending from government
(central and local) budgets, external borrowings and grants (including donations from
international agencies and nongovernmental organizations), and social (or compulsory)
health insurance funds. Total health expenditure is the sum of public and private health
expenditure. It covers the provision of health services (preventive and curative), family
planning activities, nutrition activities, and emergency aid designated for health but does not
include provision of water and sanitation.
Figure (30): Health expenditure, public (% of total health expenditure)
0
2
4
6
8
101995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure, private (% of GDP)
Health expenditure, private(% of GDP)
0
10
20
30
40
50
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure, public (% of total health expenditure)
Health expenditure, public(% of total healthexpenditure)

Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
The value for Health expenditure, public (% of total health expenditure) in Lebanon was
25.50 as of 2011. As the figure below shows, this indicator reached a maximum value of
45.63 in 2005 and a minimum value of 25.50 in 2011.
4. Health expenditure, public (% of government expenditure)
Public health expenditure consists of recurrent and capital spending from government
(central and local) budgets, external borrowings and grants (including donations from
international agencies and nongovernmental organizations), and social (or compulsory)
health insurance funds.
Health expenditure, public (% of government expenditure) in Lebanon was 5.79 as of
2011. Its highest value was 11.87 in 2005, while its lowest value was 5.79 in 2010.
Figure (31): Health expenditure, public (% of government expenditure)
Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
5. Health expenditure, public (% of GDP)
0
5
10
15
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure, public (% of government expenditure)
Health expenditure, public(% of governmentexpenditure)

Public health expenditure consists of recurrent and capital spending from government
(central and local) budgets, external borrowings and grants (including donations from
international agencies and nongovernmental organizations), and social (or compulsory)
health insurance funds.
Health expenditure, public (% of GDP) in Lebanon was 1.60 as of 2011. Its highest value
over the past 16 years was 3.75 in 2002, while its lowest value was 1.60 in 2011.
Figure (32): Health expenditure, public (% of GDP)
Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
6. Health expenditure, total (% of GDP)
Total health expenditure is the sum of public and private health expenditure. It covers the
provision of health services (preventive and curative), family planning activities, nutrition
activities, and emergency aid designated for health but does not include provision of water
and sanitation.
Figure (33): Health expenditure, total (% of GDP)
0
1
2
3
4
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure, public (% of GDP)
Health expenditure, public(% of GDP)
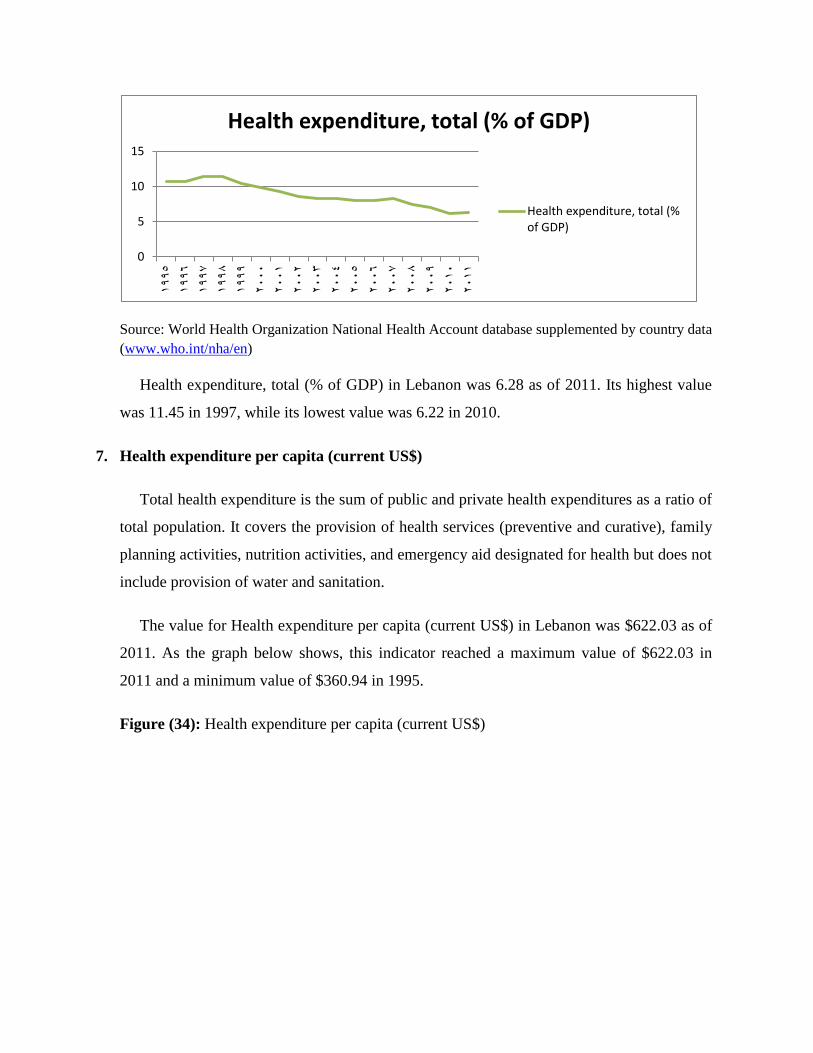
Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
Health expenditure, total (% of GDP) in Lebanon was 6.28 as of 2011. Its highest value
was 11.45 in 1997, while its lowest value was 6.22 in 2010.
7. Health expenditure per capita (current US$)
Total health expenditure is the sum of public and private health expenditures as a ratio of
total population. It covers the provision of health services (preventive and curative), family
planning activities, nutrition activities, and emergency aid designated for health but does not
include provision of water and sanitation.
The value for Health expenditure per capita (current US$) in Lebanon was $622.03 as of
2011. As the graph below shows, this indicator reached a maximum value of $622.03 in
2011 and a minimum value of $360.94 in 1995.
Figure (34): Health expenditure per capita (current US$)
0
5
10
151995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure, total (% of GDP)
Health expenditure, total (%of GDP)

Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
8. Health expenditure per capita, PPP (constant 2005 international $)
Total health expenditure is the sum of public and private health expenditures as a ratio of
total population. It covers the provision of health services (preventive and curative), family
planning activities, nutrition activities, and emergency aid designated for health but does not
include provision of water and sanitation.
The latest value for Health expenditure per capita, PPP (constant 2005 international $) in
Lebanon was 923.79 as of 2011. The value for this indicator has fluctuated between 923.79
in 2011 and 704.99 in 2003.
Figure (35): Health expenditure per capita, PPP ($)
$0.00
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
$700.00
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure per capita (current US$)
Health expenditure percapita (current US$)
0
200
400
600
800
1000
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Health expenditure per capita, PPP ($)
Health expenditure percapita, PPP ($)

Source: World Health Organization National Health Account database supplemented by country data
(www.who.int/nha/en)
9. Out-of-pocket health expenditure (% of private expenditure on health)
Figure (36): Out-of-pocket health expenditure (% of total expenditure on health)
Source: World Health Organization National Health Account database supplemented by country
data (www.who.int/nha/en)
Out of pocket, expenditure is any direct outlay by households, including gratuities and
in-kind payments, to health practitioners and suppliers of pharmaceuticals, therapeutic
appliances, and other goods and services whose primary intent is to contribute to the
restoration or enhancement of the health status of individuals or population groups. It is a
part of private health expenditure.
Out-of-pocket health expenditure (% of total expenditure on health) in Lebanon was
56.47 in 2011. Its highest value was 59.61 in 1998, while its lowest value was 39.40 in
2005.
B. Data analysis of the Lebanese health quality versus cost
1. Population and Sample Selection:
The population of the study was selected randomly from whole Lebanese people in the
society without a previous knowledge about their demographic indicators or social level
they refer. Respondents had to be affective members whom are financially responsible about
the health expenditures.
0
20
40
60
80
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Out-of-pocket health expenditure (% of total expenditure on health)
Out-of-pocket healthexpenditure (% of totalexpenditure on health)

2. Instrumentation:
The instrument of the study is a questionnaire made up of nineteen questions to be filled
on the preference of respondent and a question to give a comment about the social
insurance, it is arranged to collect Data that helped the study to make findings that will be
included in this thesis.
The questionnaire is divided into three sections:
a. Introduction:
In its first part, the questionnaire informed respondents about its purpose which was to
investigate the issue of their satisfaction within the health quality they receive compared to
the high cost they bear.
It also assured that the participation in this questionnaire was voluntary and the collected
information will only be used for educational purposes.
b. Identification Variables:
In this part, the questionnaire asked about the respondents’ general information about
them including gender, age, and status, number of dependents, employment, education and
monthly income.
There is a Q‖0‖ of the study which determined whether the respondents feel that the
health services’ fees they pay is reasonable to the service they are provided with.
c. Dependent Variables:
In this section, there were 11 questions about the health insurance and the share the
respondents pay additional to their satisfaction with the quality of service they provide.
3. Questionnaire construction & Conceptual Framework for Data Analysis:
Based on the review of literature and previous studies and Data stated in the chapters
above, this questionnaire was developed on variables determine the higher cost of the health
service in Lebanon regardless the variety of the insurance providers available.
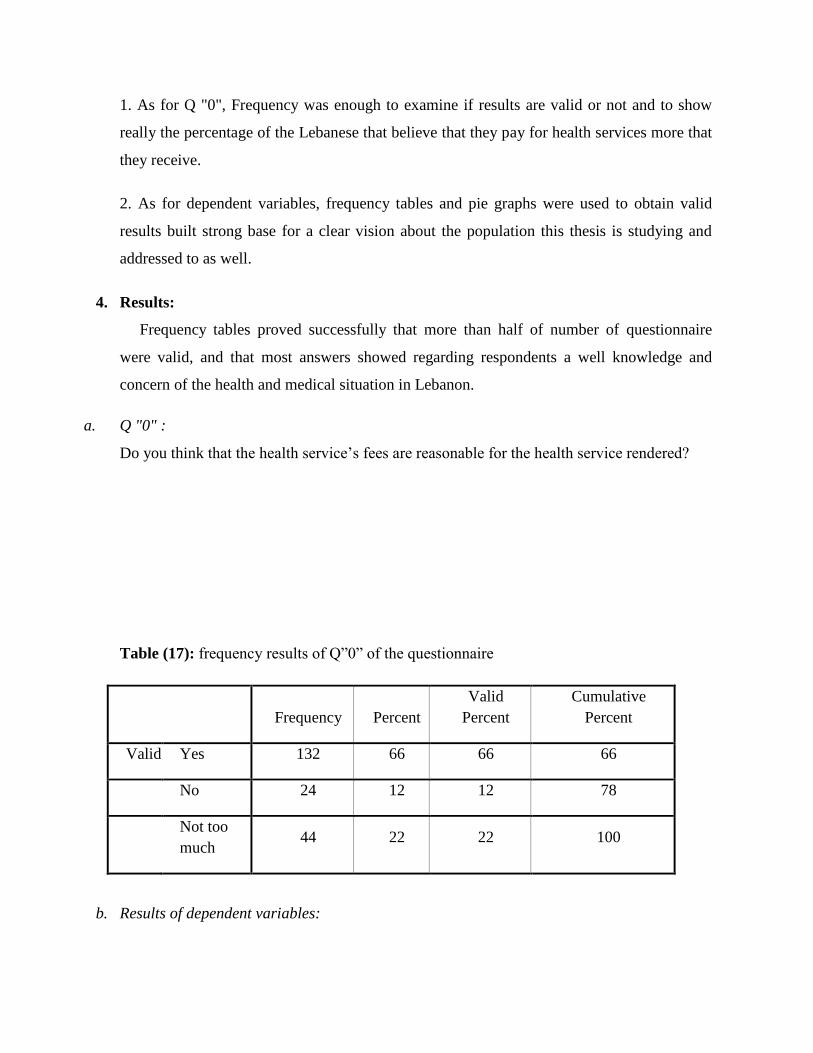
1. As for Q "0", Frequency was enough to examine if results are valid or not and to show
really the percentage of the Lebanese that believe that they pay for health services more that
they receive.
2. As for dependent variables, frequency tables and pie graphs were used to obtain valid
results built strong base for a clear vision about the population this thesis is studying and
addressed to as well.
4. Results:
Frequency tables proved successfully that more than half of number of questionnaire
were valid, and that most answers showed regarding respondents a well knowledge and
concern of the health and medical situation in Lebanon.
a. Q "0" :
Do you think that the health service’s fees are reasonable for the health service rendered?
Table (17): frequency results of Q‖0‖ of the questionnaire
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid Yes 132 66 66 66
No 24 12 12 78
Not too
much 44 22 22 100
b. Results of dependent variables:
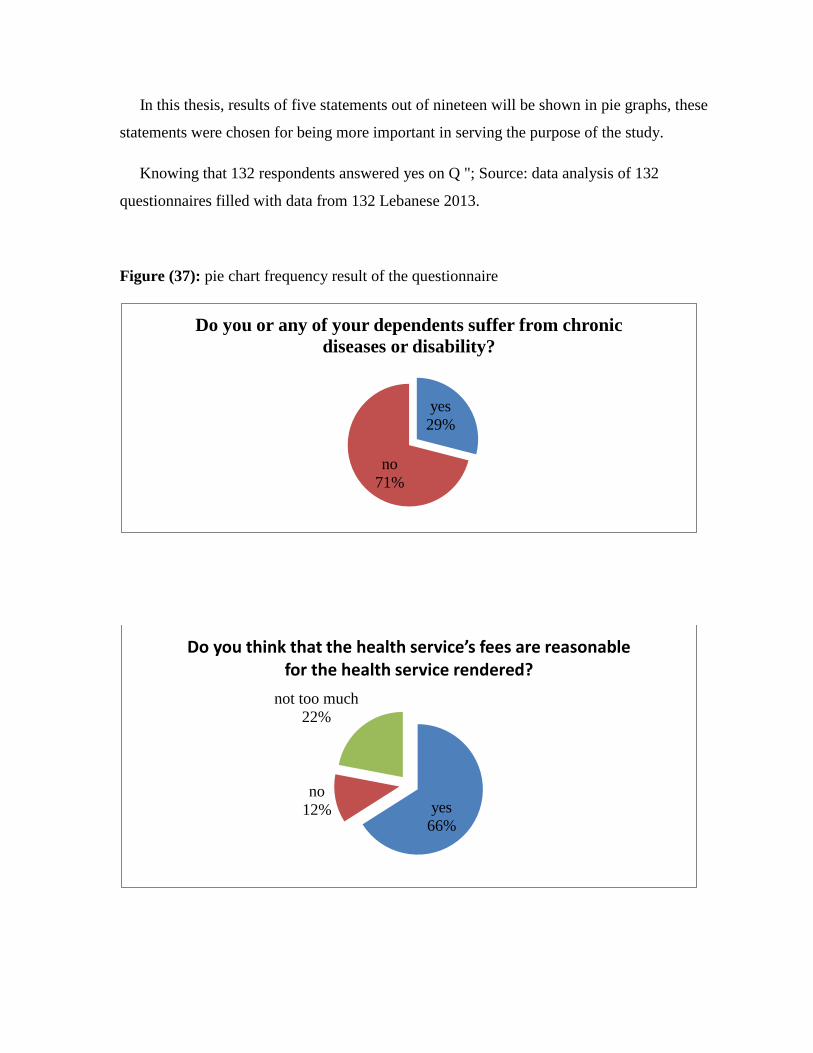
In this thesis, results of five statements out of nineteen will be shown in pie graphs, these
statements were chosen for being more important in serving the purpose of the study.
Knowing that 132 respondents answered yes on Q "; Source: data analysis of 132
questionnaires filled with data from 132 Lebanese 2013.
Figure (37): pie chart frequency result of the questionnaire
yes
29%
no
71%
Do you or any of your dependents suffer from chronic
diseases or disability?
yes
66%
no
12%
not too much
22%
Do you think that the health service’s fees are reasonable for the health service rendered?

c. Our assessment:
37%
48%
8% 7%
On which health service do you spend more expense
hospitalization medication examination service laboratories
64% 20%
16%
Do you face some problems to cover your share of cost of
the medical care
yes no not too much
47%
23%
30%
Do you think that doctors and hospitals are satisfied with
everything they need to provide a sufficient medical care
yes no not too much

In our 200 interviews, the questionnaire examined how the Lebanese people suffer from
the health service cost and the quality they receive. We can also recognize the weak role the
health providers are playing.
The questionnaire results push us to analyze the cost of the health services and the
coverage of the different providers in Lebanon so that to end up by a choice which providers
is the lower in cost with better quality.
C. Financial analysis of Lebanese Health expenditures
1. Pharmaceutical sector39
The pharmaceutical sector in Lebanon forms a significant part of the health services bill;
where it covers about 26 % of total household health care expenditures. 85% of drug
consumed are imported, with only 15% being manufactured locally.
a. High Levels of Profit Margins
The high health expenditure recorded refers to the high proportions of consuming trade
names and imported drugs, where the prices of the imported drugs are significantly higher
than that of the local by a multiple of 1.69 the locally manufactured prices. This obvious
difference in the prices refers to different margins added to the original price at the
following levels:
· Freight (7.5%)
· Clearance (10%)
· Agent’s Margin (10%)
· Pharmacist’s Margin (30%)
However, efforts are being done by MOH to reduce the drugs prices, by moderating the
margins received at the levels listed above. The solutions were applying different lower
margins to different categories of drugs depending on their selling prices. ―A‖ lies in the
39
Lebanon National Health Accounts 2009, December 2009
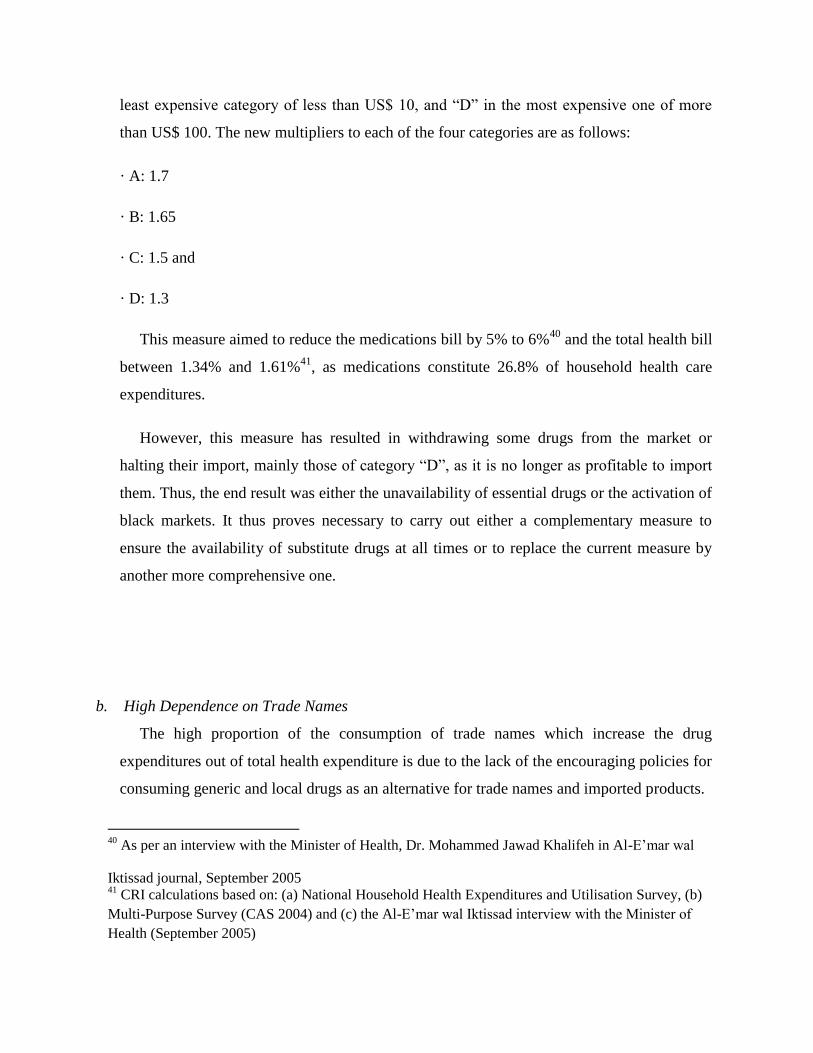
least expensive category of less than US$ 10, and ―D‖ in the most expensive one of more
than US$ 100. The new multipliers to each of the four categories are as follows:
· A: 1.7
· B: 1.65
· C: 1.5 and
· D: 1.3
This measure aimed to reduce the medications bill by 5% to 6%40
and the total health bill
between 1.34% and 1.61%41
, as medications constitute 26.8% of household health care
expenditures.
However, this measure has resulted in withdrawing some drugs from the market or
halting their import, mainly those of category ―D‖, as it is no longer as profitable to import
them. Thus, the end result was either the unavailability of essential drugs or the activation of
black markets. It thus proves necessary to carry out either a complementary measure to
ensure the availability of substitute drugs at all times or to replace the current measure by
another more comprehensive one.
b. High Dependence on Trade Names
The high proportion of the consumption of trade names which increase the drug
expenditures out of total health expenditure is due to the lack of the encouraging policies for
consuming generic and local drugs as an alternative for trade names and imported products.
40
As per an interview with the Minister of Health, Dr. Mohammed Jawad Khalifeh in Al-E’mar wal
Iktissad journal, September 2005 41
CRI calculations based on: (a) National Household Health Expenditures and Utilisation Survey, (b)
Multi-Purpose Survey (CAS 2004) and (c) the Al-E’mar wal Iktissad interview with the Minister of
Health (September 2005)

Imported drugs market is controlled by a group of importers and distributors who work
interdependently and dominate the market. They follow an aggressive marketing leading to
increased consumption of imported drugs, and disregard of locally produced ones,
especially with the lack of awareness campaigns that encourage people to use local drugs. It
should be also mentioned, that many doctors play a vital role in this marketing, seeking
extra profits through special deals provided by the distributors.
c. Rise in the Number of Pharmacies and Pharmacists
The large number of pharmacies in the Lebanese market is also a reason for the relatively
high prices of drugs. In order to be gain profits, these pharmacies keep their high selling
prices in such a way as to compensate for the low number of customers.
2. Hospitals
a. NSSF and the Increasing Hospitalization Rates
NSSF in-hospital services can be classified into three different types: delivery, surgery
and in hospital medication. In this respect, the cases of the NSSF in-hospital medication out
of the total number of in-hospitals cases is quite significant so as it record an average of
60% overall the Lebanese regions.
This high contribution of the NSSF in the in-hospital medication reflect the curative
nature of health care in Lebanon, however it hint at some irregular practices taking place
reflects the tight economic and social conditions of people (demand side) and low hospital
occupancy rates (supply side).
On the demand side, the patient seeks a medical consultation upon which he pays the
fees to doctor, drugs and medical tests. If these paid fees are equivalent to those set by
NSSF for the required services, the patient will receive 80% of the total amount paid, but
not before five or six months later. However, patients pay for the medical services received
much more than the NSSF set prices, leading to a total compensation received much less
than the set 80%. This procedure involves of high costs, low return rate and long delays
represents an unfair practice especially against the poor.

As for the supply side, some hospitals respond to their low occupancy rates by setting
attracting arrangements with patients, as a result of the availability of beds and consequently
low revenues. Hospitals would admit patients (even if their condition does not require
hospital admission) and provide them with consultations, drugs and medical tests that they
would have otherwise required outside. In these cases, patients will be exempted from
paying their due fees where the bill will be compensated by the NSSF. In this respect, the
patient would have avoided the high costs and the hospital would have benefited from
employing its empty beds, and thus receiving revenues.
b. Public Investment in Hospitals
Table (18) shows that 73% of the amount Ministry of Health’s reimbursements for
hospital care was on surgical care and the remaining 23% were for non-surgical care. The
CSC spent 59% of its hospital reimbursements for surgical care, the ISF 53%, the Army
51%, and the NSSF 60%.
This distribution probably reflects the fact that the Ministry of Health is the insurer of
last resort and hence tends to pay more for inpatient admissions. With regard to the other
agencies hospitalization costs are part of the benefits available to their beneficiaries.
Table (18): Distribution of hospital expenditures (%)
category MOPH Armed
forces
CSC NSSF
Non-surgical
costs
27 49 41 40
Surgical costs 73 53 59 60
Source: Lebanese National Health Accounts
Table (19): Distribution of hospital reimbursement by type of service (%)

category MOPH Army forces NSSF CSC Weighted
average
Surgery 16.7 11.1 13.1 16.1 14.3
Doctor fees 8.6 11.8 11.1 11.4 10.7
Anesthesia 4.8 2.3 4.7 4.9 4.2
Room and board 15.6 16 17 12.8 15.4
Operation room 12.6 9 18.2 10.3 12.5
Lab tests 12.2 13.1 10.5 9.2 11.3
Radiology 7 6 6.9 4.6 6.1
MRI 0.5 0.8 0.8 0.2 0.6
CT Scan 2.4 1.9 0.6 1.1 1.5
Drugs 15.7 16.7 11.9 19.3 15.9
Medical
supplies
2.8 7.5 4.5 3.7
4.7
Others 1.1 3.8 0.7 6.4 3.0
Source: Lebanese National Health Accounts
3. Ministry of health
In Lebanon the Ministry of Health is the insurer of last resort. The Ministry of Health
funds the hospitalization costs for any citizen who is not covered under an insurance plan
(social or private). This coverage is independent of the income and asset status of the
individual. In addition the Ministry of Health also covers the cost of some narrow specialties
such as chemotherapy, open heart surgery, dialysis and renal transplant, and drugs for
chronic diseases.
Table (20): Budgetary resources in the public health sector

2009 2010 2011
MOPH allocated budget (as % of total government budget) 2.7 2.5 2.7
Public expenditure on health (as % of GDP) 439.7 486.7 527.9
Annual MOPH budget (USD per capita 73.3 82 87
Source: MOPH 2011, Statistical bulletin
With a modest allocation of 2.7% of the total government budget, the MOPH has to
cover the hospitalization cost of uninsured patients and provide them with expensive
treatments that cannot be afforded by some households
A proportion of the MOPH’s annual budget is allocated for covering uninsured
patients, with the aim of ensuring universal accessibility to health services. These
allocations have been growing over years with the development of the Ministry’s
financing function, leaving scarce resources to prevention, public health and regulation
functions.
4. Expenditure by public financing agents:
Among the six social providers in Lebanon, NSSF comes in the second rate after
MOPH in the number of beneficiaries with 1293220. With reference to the total cost
spend, NSSF come in the first rate with 575899104 LL. However, the spending per
beneficiary accounts 534386 LL for NSSF being in the third rate having the lowest
amount after the MOPH and army with 221854 LL and 372013 LL respectively. This
break down can end up with a conclusion that NSSF turns first as an efficient health
provider either from number of beneficiaries or with the costs spent.

Table (21): break-down of public expenditure on health services provided by the private
sector (thousand LPB)
NSSF GSF Army SSF ISF CSC MOH
Number of
beneficiaries 1293220 17172 270300 6774 93131 236870 1954818
Number of
adherents 590502 6360 102000 1736 32114 75197 1954818
Number of
hospital
admissions 253840 2160 61996 1463 32062 29714 220038
Cost of
hospital
admission 334 4855 68304 1936 29610 50056 293714
Cost of
ambulatory
care 241185 6359 15491 2842 14755 54969 54308
Total cost 575899 11215 83796 4779 44365 105025 361402
Spending/
beneficiary 534 783 372 846 571 532 221
Source: Walid Ammar, 2009, health beyond politics
5. Private insurance market
The private insurance market is growing rapidly in Lebanon. According to the Ministry
of Economy sources approximately 70 private insurance companies provide health
insurance. They provide both complementary and comprehensive health insurance
policies. The former is to complement and fill gaps in the benefits provided by NSSF,
CSC, and health insurance arrangements for the Army and Police. The latter refer to stand
alone health insurance policies that can cover a range of benefits including inpatient and
outpatient care, and coverage for pharmaceutical expenses. It is estimated that 8% of the
population has comprehensive coverage and 4.6% gap insurance.
Compared to other countries in the region, Lebanon has a fairly well developed private
insurance sector. Private insurance is licensed by the Ministry of Economy. Insurance
companies are required by law to set aside 40% of premiums as reserves.
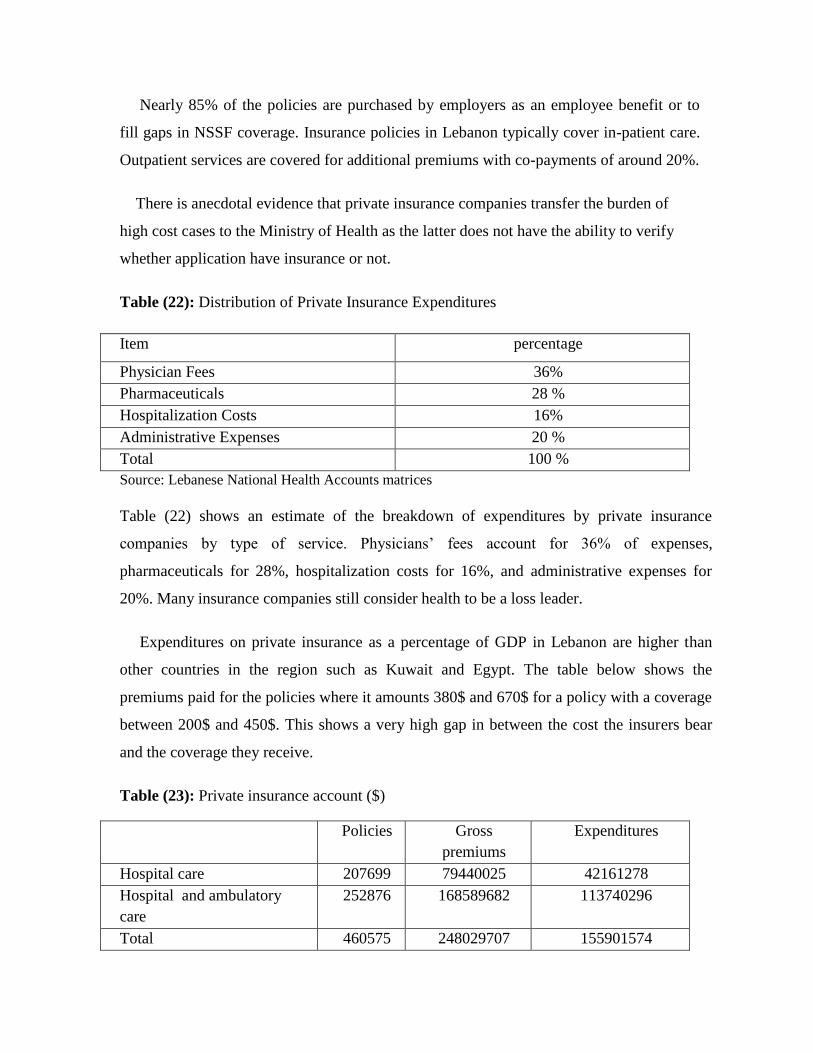
Nearly 85% of the policies are purchased by employers as an employee benefit or to
fill gaps in NSSF coverage. Insurance policies in Lebanon typically cover in-patient care.
Outpatient services are covered for additional premiums with co-payments of around 20%.
There is anecdotal evidence that private insurance companies transfer the burden of
high cost cases to the Ministry of Health as the latter does not have the ability to verify
whether application have insurance or not.
Table (22): Distribution of Private Insurance Expenditures
Item percentage
Physician Fees 36%
Pharmaceuticals 28 %
Hospitalization Costs 16%
Administrative Expenses 20 %
Total 100 %
Source: Lebanese National Health Accounts matrices
Table (22) shows an estimate of the breakdown of expenditures by private insurance
companies by type of service. Physicians’ fees account for 36% of expenses,
pharmaceuticals for 28%, hospitalization costs for 16%, and administrative expenses for
20%. Many insurance companies still consider health to be a loss leader.
Expenditures on private insurance as a percentage of GDP in Lebanon are higher than
other countries in the region such as Kuwait and Egypt. The table below shows the
premiums paid for the policies where it amounts 380$ and 670$ for a policy with a coverage
between 200$ and 450$. This shows a very high gap in between the cost the insurers bear
and the coverage they receive.
Table (23): Private insurance account ($)
Policies Gross
premiums
Expenditures
Hospital care 207699 79440025 42161278
Hospital and ambulatory
care
252876 168589682 113740296
Total 460575 248029707 155901574

Source: MedNet Liban Health Insurance Portfolio, 2011
6. Analysis of sources and uses of funds:
Households spent 69 % of total health expenditures. Of this 97% was spent in the private
sector, 2% in the NGO sector, and just 1% in the Public Sector. However these expenditures
are distributed with 41% on private providers with 25.4% on drugs and only 24.5% for
hospitalization.
Table (26): Distribution of health care expenditure
Public hospitals 1.7%
Private hospitals 22.8%
Private providers 41.0%
Pharmaceuticals 25.4%
Others 9.1%
Source: national health accounts, 2008
Table (27): Percentage of distribution of Out-of-Pocket Expenditures by Sector
Sector %
Public 2
Private 93
donors 5
Source: national health accounts, 2008
Public sources account for 19 % and private sources for 79 % of health care financing.
International donors account for the remaining 2 %. The treasury funds the five public
insurance providers with the highest amount for the MOPH with 339663 million LL.

However the households’ payments are all directed towards the private insurance with a
percentage of 98% where the remaining 2% are for the mutual funds and NSSF.
Table (28): sources of funds to health providers (million LL)
Health
provider
treasur
y
Private sector dono
rs
total % of
health
financing
employ
ers
household
s
MOPH 339663 0 0
6453
1 404193 10%
Armed
forces 192345 0 0 0 192345 5%
CSC 58666 0 0 0 58666 2%
NSSF 103134 225464 56365 0 384964 10%
Mutual
funds 21411 0 22594 0 44005 1%
Private
sector 0 176290 2593240 0
276953
0 72%
Total 715220 401755 2672199
6453
1
385370
4 100%
% of health
financing 19% 10% 69% 2% 100% 10%
Source: Regional National Health Accounts
Figure (38): Health expenditure by source of financing

Source: Regional National Health Accounts
Figure (39): Treasury sources of health financing
Source: Regional National Health Accounts
18%
80%
2%
Health expenditures by source of financing
public source
private source
donations andloans
47%
3%
15% 10%
25%
Treasury sources of health financing
MOPH Mutual Funds NSSF CSC Armed forces
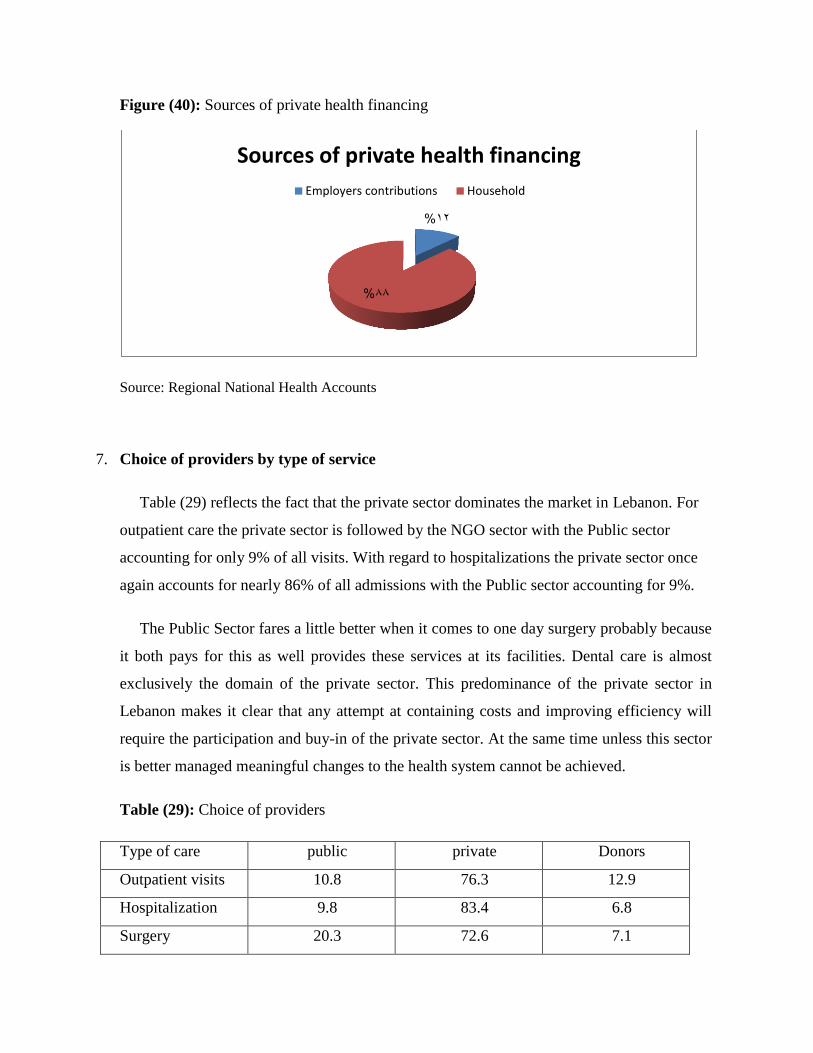
Figure (40): Sources of private health financing
Source: Regional National Health Accounts
7. Choice of providers by type of service
Table (29) reflects the fact that the private sector dominates the market in Lebanon. For
outpatient care the private sector is followed by the NGO sector with the Public sector
accounting for only 9% of all visits. With regard to hospitalizations the private sector once
again accounts for nearly 86% of all admissions with the Public sector accounting for 9%.
The Public Sector fares a little better when it comes to one day surgery probably because
it both pays for this as well provides these services at its facilities. Dental care is almost
exclusively the domain of the private sector. This predominance of the private sector in
Lebanon makes it clear that any attempt at containing costs and improving efficiency will
require the participation and buy-in of the private sector. At the same time unless this sector
is better managed meaningful changes to the health system cannot be achieved.
Table (29): Choice of providers
Type of care public private Donors
Outpatient visits 10.8 76.3 12.9
Hospitalization 9.8 83.4 6.8
Surgery 20.3 72.6 7.1
12%
88%
Sources of private health financing
Employers contributions Household

Dental care 2.1 83.9 14.0
Source: These data are based on ―National Household Health Expenditure and Utilization Survey‖,
2011

In summary:
The health system is very costly with a very expensive health bill accounting for 7.4% of
gross domestic product.
Equity is not well protected, despite the fact that the MOPH has provided a coverage safety
net; this inequity is well documented by the high cost incurred by households. The
percentage of income spent on health by households is higher in the poor population.
The heath system is inefficient with an oversupply of medical technologies and regional
disparities in their distribution.
Main Findings
The main findings inferred from the analysis and the survey done is summarized below:
Summary Statistics
Total Population: 4,800,000
Per Capita Expenditure: 622 USD
Health Expenditure as % GDP: 7.4 %
% GOL budget allocated to health: 2.7%
Sources of Funds:
Public: 19 %

Private:
Households 69 %
Employers 10%
Donors: 2%
Distribution of Health Care Expenditures:
Public Hospitals 1.7%
Private Hospitals 22.8%
Private Non-Institutional Providers 41%
Pharmaceuticals 25.4%
Others 9.1%
Chapter III: Cross Country Comparison
A. International comparison of health expenditure
Historically, health care
spending among developed nations has grown considerably each year. However, beginning
in 2010, spending has flattened. As of 2011, health care cost $1017per person in the world.
As for Asia, Pakistan records 28$ as health expenditure per capita totaling 2.2% of GDP.
India being an over populated country as China, they spend 126$ and 373$ per capita
accounting 4.2% and 5.1% of GDP relatively.

The spending per capita reaches 1039$ in turkey, 2592$ in Singapore and 3120$ in
Japan, noting that Singapore and Japan are of the first five countries having better health
quality at lower cost.
As for the European countries, the spending per capita approximates between 881$ for
Romania and 6612$ for Luxemburg. Here it is must be noted that from the first ten countries
having the highest health expenditure in the world, Europe contain eight of them beginning
with France rating tenth with 3997$, then Germany rating ninth for 4342$, Denmark rating
eighth with 4467$, Austria rating sixth with 4398$, Luxemburg rating fifth with 6712$,
Netherlands rating fourth with 5112$, Switzerland rating third with 5297$ and Norway
rating the second with 5391$ totaling as percentage of GDP between 7.9 in Luxemburg and
11.9 in France.
For Africa, the spending per capita on health accounts 17$ in Eritrea being the lowest
amount around the world. As for South Africa the amount is high reaching 915$ per capita
accounting 9.2% of GDP.
By comparing the Arab countries, it is noted that Yemen, Sudan, republic of Syria,
Egypt, Iraq and Jordan spend below 500$ for health expenditure per capita accounting
between 3.5% and 9.6% of GDP. As for Lebanon, it is classified in the category which
involve Saudi Arabia, United Arab Emirates and Qatar spending between 872$ and 1621$
per capita totaling 2.6% and 7.4% of GDP being the latest for Lebanon.
The United States of America rates at the first being the country with the highest health
expenditure in the world with 8233$ per capita totaling 17.6 of GDP. As for Canada, it rates
the seventh in the countries having the highest cost spending 4443$ per capita and
accounting 11.4% of GDP.
Table (30): International Comparison of Health Expenditures
Location Total Health
Expenditure
Per Capita
Total Health
Expenditure Per
Capita, PPP ($)
Total Health
Expenditure % of
GDP
Asian counties
Pakistan $28 57 2.2

Afghanistan $52 46 7.6 Bangladesh $61 53 3.4 India $126 124 4.2 China $373 347 5.1 Malaysia $645 629 4.6 Iran (Islamic Republic of) $797 728 5.7 Turkey $1,039 957 6.7 Singapore $2,592 2111 4.1 Japan $3,120 3045 9.5
European countries
Romania $881 818 5.6 Italy $3,046 3071 9.4 Spain $3,057 3067 9.6 Greece $3,069 3054 10.6 France $3,997 3969 11.9 Germany $4,342 4219 11.7 Austria $4,398 4288 11 Denmark $4,467 4345 11.5 Netherlands $5,112 4881 12 Switzerland $5,297 5105 11.4 Norway $5,391 5353 9.7 Monaco $5,915 5932 4.2 Luxembourg $6,712 6592 7.9
African countries
Eritrea $17 16 2.8 Central African Republic $30 30 4 South Africa $915 930 9.2
Arab countries
Yemen $155 139 5.5 Sudan $162 159 7.3 Syrian Arab Republic $175 182 3.5 Egypt $293 286 4.8 Iraq $346 342 8.4 Jordan $493 493 9.6 Tunisia $544 479 6.4 Libyan Arab Jamahiriya $573 722 3.9 Oman $591 826 3 Lebanon $872 965 7.4 Saudi Arabia $914 964 4.4 Bahrain $937 1083 4.7 Kuwait $1,133 1671 3.8 United Arab Emirates $1,562 1956 4.4 Qatar $1,621 1965 2.6
American countries
Haiti $76 71 6.1 Canada $4,443 4314 11.4
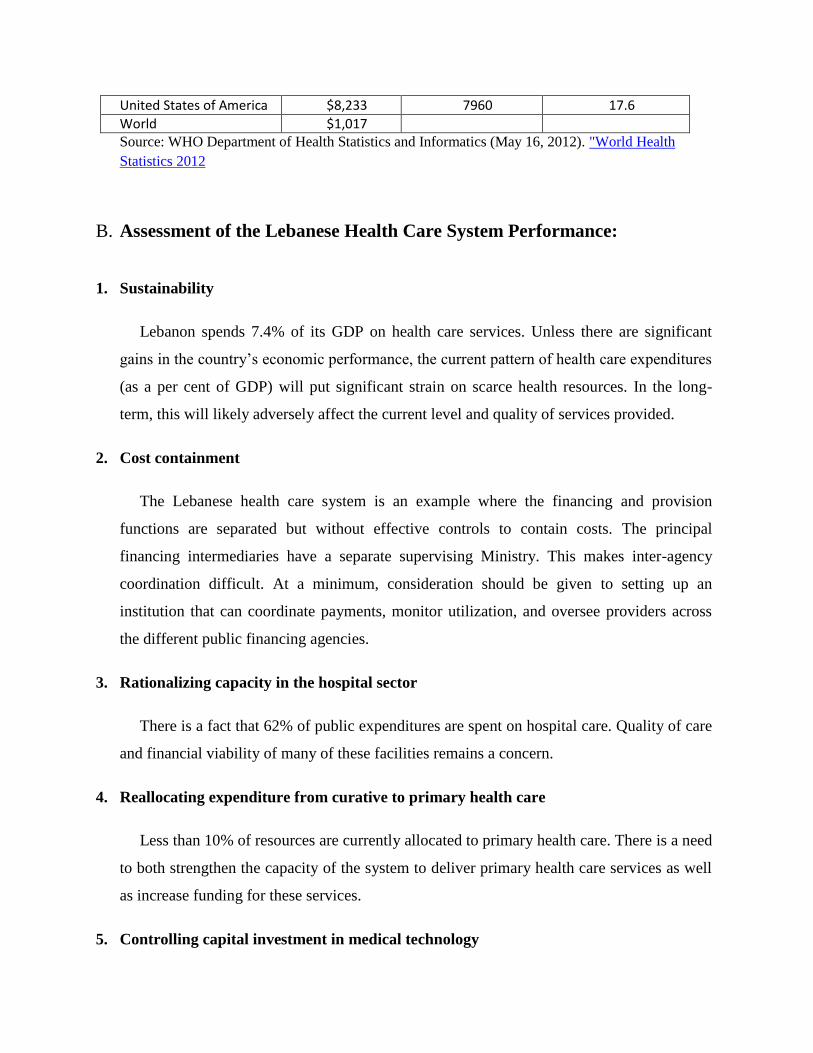
United States of America $8,233 7960 17.6 World $1,017 Source: WHO Department of Health Statistics and Informatics (May 16, 2012). "World Health
Statistics 2012
B. Assessment of the Lebanese Health Care System Performance:
1. Sustainability
Lebanon spends 7.4% of its GDP on health care services. Unless there are significant
gains in the country’s economic performance, the current pattern of health care expenditures
(as a per cent of GDP) will put significant strain on scarce health resources. In the long-
term, this will likely adversely affect the current level and quality of services provided.
2. Cost containment
The Lebanese health care system is an example where the financing and provision
functions are separated but without effective controls to contain costs. The principal
financing intermediaries have a separate supervising Ministry. This makes inter-agency
coordination difficult. At a minimum, consideration should be given to setting up an
institution that can coordinate payments, monitor utilization, and oversee providers across
the different public financing agencies.
3. Rationalizing capacity in the hospital sector
There is a fact that 62% of public expenditures are spent on hospital care. Quality of care
and financial viability of many of these facilities remains a concern.
4. Reallocating expenditure from curative to primary health care
Less than 10% of resources are currently allocated to primary health care. There is a need
to both strengthen the capacity of the system to deliver primary health care services as well
as increase funding for these services.
5. Controlling capital investment in medical technology
The government reimbursements for high cost services have resulted in a rapid growth of
high technology centre. This in turn has contributed to cost escalation. For efforts at cost
containment to be effective, policies need to be developed that will control investments in
medical technology.
6. Rationalizing expenditure on pharmaceuticals
Lebanon has not only a high per capita expenditure on pharmaceuticals (US$ 120) but
almost all of the drugs are imported proprietary products. To effectively contain overall
health care expenditures, the Government should initiate policies for improving the
efficiency by which pharmaceuticals are imported, distributed and sold in the country and
improve its management and overseeing of this sector.
7. Expanding health insurance coverage, limiting multiple coverage
In Lebanon health insurance is tied with employment and those in low income
households are less likely to be employed in the formal sector. Further, the presence of
multi-insurance coverage allows for inefficiencies and cost escalation. The Government
needs to improve its management of the private insurance market and reduce multi-
insurance coverage.
8. Equity
Household out-of-pocket expenditure accounts for 69% of the health expenditure in
Lebanon. The burden of out-of-pocket expenditure appears to be inequitably distributed,
with lower income households spending a much greater proportion of their income on health
than higher income households.
Even though the MOPH as the insurer of last resort pays for hospitalization costs for all
(including those with low incomes) there is no formal financing mechanism for primary and
preventive health services. The government should consider designing a targeted program to
provide good quality basic health services for those with low incomes.

Chapter IV: The Singapore Healthcare System:
A. Overview
Table (31): Most efficient health care systems within the world
Efficiency
score
Life
expectancy
Healthcare cost
(% GDP per
capita)
Healthcare
cost (per
capita)
Sweden 62.6 81.8 9.6% 5331$
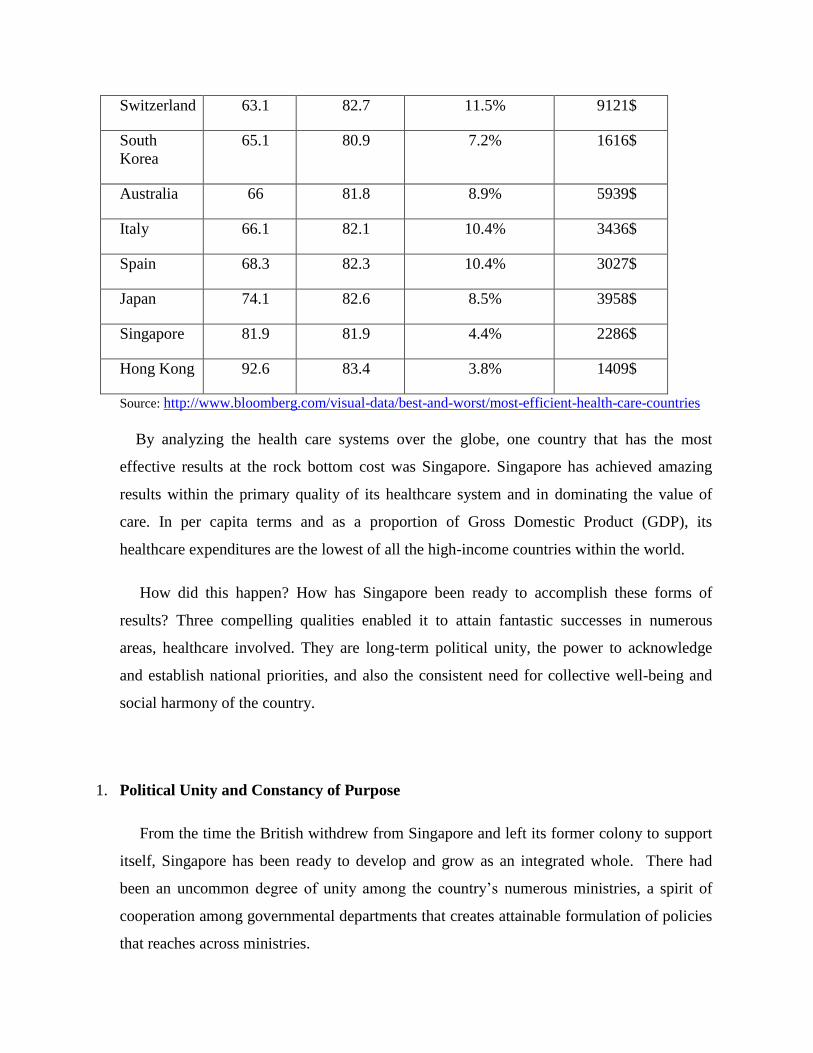
Switzerland 63.1 82.7 11.5% 9121$
South
Korea
65.1 80.9 7.2% 1616$
Australia 66 81.8 8.9% 5939$
Italy 66.1 82.1 10.4% 3436$
Spain 68.3 82.3 10.4% 3027$
Japan 74.1 82.6 8.5% 3958$
Singapore 81.9 81.9 4.4% 2286$
Hong Kong 92.6 83.4 3.8% 1409$
Source: http://www.bloomberg.com/visual-data/best-and-worst/most-efficient-health-care-countries
By analyzing the health care systems over the globe, one country that has the most
effective results at the rock bottom cost was Singapore. Singapore has achieved amazing
results within the primary quality of its healthcare system and in dominating the value of
care. In per capita terms and as a proportion of Gross Domestic Product (GDP), its
healthcare expenditures are the lowest of all the high-income countries within the world.
How did this happen? How has Singapore been ready to accomplish these forms of
results? Three compelling qualities enabled it to attain fantastic successes in numerous
areas, healthcare involved. They are long-term political unity, the power to acknowledge
and establish national priorities, and also the consistent need for collective well-being and
social harmony of the country.
1. Political Unity and Constancy of Purpose
From the time the British withdrew from Singapore and left its former colony to support
itself, Singapore has been ready to develop and grow as an integrated whole. There had
been an uncommon degree of unity among the country’s numerous ministries, a spirit of
cooperation among governmental departments that creates attainable formulation of policies
that reaches across ministries.
The government realized early that improvement in health conditions and care had to be
approached as an inseparable part of the overall development planning for the country.42
As
a heavily urban city-state, caring for the health of the individuals meant quite simply
building hospitals and clinics. Health would be affected by life style: housing, water supply,
food provide, air quality, waste disposal, and more.
Ensuring the health of the Singaporeans had to be designed into each side of urban
planning, requiring a comprehensive approach and also the cooperation of various ministries
over all the varied sectors of presidency. There have been additionally issues that the
government was not doing enough for the elderly whose families were suffering severe
financial strain for older family members’ care.
The government responded with a new program of inflated outlays to handle citizens’
issues. It pronounced enlarged financial supports for lasting care, even for patients being
cared for in the house, giving middle-income families some financial relief.
2. Establishing Priorities
The health of the public was not a prime priority for the government at the start of
independence, where the fundamentals of public health, healthcare planning and
development would need to wait till the state achieved a level of military and economic
stability.
This ordering of priorities was apt for the time, as it was vitally important first to set up
the defense of this small nation, so to draw in investors to set in motion economic progress,
and tackle problems of unemployment, housing, and education. After these essential issues
had been addressed, others, including healthcare, could be taken on.
42 Ministry of Social and Family Development. ―Ministerial Committee to Spearhead Successful Ageing for
Singapore,‖ 4 Mar. 2007. Available at
http://app.msf.gov.sg/PressRoom/MinisterialCommitteeToSpearheadSuccessfulAgei.aspx.
Wisely, the initial focus in Singapore was on public health: putting right sanitation
procedures in site, dominating infectious diseases, all flourishing efforts.
In time, the priorities set by the government verified to be effective. The security
situation stabilized and also the economy grew to the advantage of all. The GDP grew from
just below $8.5 billion in 1964, to over $50 billion in 1983, to nearly $300 billion in 2011.43
3. Promoting a way of Collective Well-Being and Social Harmony
One among the most vital tenets of Singaporean governance is that a powerful society
requires social harmony. If tensions between social teams and races are to be avoided, all
teams ought to be enclosed in the life of the country and should benefit, to some extent,
from its successes.
To even out the intense results of free-market competition, we tend to redistribute the
national income through subsidies on things that improved the earning power of citizens,
like education. Housing and public health were also clearly desirable. However finding the
proper solutions for private medical aid, pensions, or retirement benefits was not simple.
The solution was a policy where people set five percent of their wages into the fund and
their employers matched it. The accumulated cash may be withdrawn at age 55. The
government had a long-range vision to extend the investment of the fund over time and
broaden it to permit people to save for and pay for education and healthcare similarly as
retirement and home-buying.44
In the long run, however, the government recognized that the health savings program
would not be enough to support care, and alternative systems were placed, including a
medical insurance program and a social safety web.
4. Respect and Education for Women
43 Singapore Department of Statistics. Yearbook of Statistics Singapore, 2011. Singapore: Singapore
Department of Statistics, 2011.
44 Chong, S.A., Mythily et al. ―Performance Measures for Mental Healthcare in Singapore.‖ Ann Acad Med
Singapore 37, 9 (2008): 791–6.
Singapore recognized early on the importance of respect and education for women, as
well as seeing to their health needs. The government accomplished a great deal well before
the women’s movement began in several countries.
Specifically, women’s health education was considered as an important to the long run of
the country. The Education Ministry took the lead in educating young women regarding
vital health topics.
5. Building the Foundation
a. Bringing Care to the People
An early move was to bring medical aid services nearer to the individuals by developing
a network of satellite outpatient dispensaries and maternal and child health clinics. They
presented a one-stop center for immunization, health promotion, health screening, well-
women programs, family planning services, nutritional recommendation, psychiatric
counseling, dental care, pharmaceutical, x-ray, clinical laboratory, and even home-nursing
and rehabilitative services for non-ambulatory patients.45
b. Introduction of User Fees at Public Clinics
Services at the outpatient clinics had been free-of-charge; however the government
quickly modified that. The principles of free medical services run over the fact of human
behavior, definitely in Singapore.
Once doctors given free antibiotics, patients took their pills or capsules for some days,
did not get better, and threw away the balance.46
They then seek advice from private
doctors, bought their antibiotics, completed the course, and recovered. This daring move
45 Central Provident Fund, ―My CPF—Having Children: Providing for Your Precious Ones. Life Events:
Having Children: Immediate Concerns 2011.‖ Available at http://mycpf.cpf.gov.sg/CPF/my-cpf/have-
child/HC2.htm. Ministry of Health, ―Marriage and Parenthood Schemes. Costs and Financing: Schemes and
Subsidies 2011.‖ Available at
http://www.moh.gov.sg/content/moh_web/home/costs_and_financing/schemes_subsidies/Marriage_and_Pa
renthood_Schemes.html
46 ―Grow and Share’ Package Overview,‖ 2011. Available at http://www.growandshare.gov.sg/Overview.htm
reminded Singaporeans that healthcare is not free, for which the state would not be building
a welfare system. People would be expected to a large degree to pay their own manner.
c. Early Human Resources/Manpower Designing
Before 1960, there have been fewer than 50 medical specialists in Singapore to serve
Singapore’s two million residents. To boost their numbers, the government sent its brightest
doctors within the public sector to the best medical institutions around the world for
training. This action raises a new generation of extremely experienced specialists and set the
stage for developing Singapore’s current world class capability in highly-specialized,
advanced medicine.
Over the years, Singapore has continued to form strategic partnerships with healthcare
organizations all around the world and continues to send doctors for training at world-class
medical facilities. In 2009, 1,750 doctors practicing in Singapore were foreign-trained.
d. Healthcare Infrastructure enhancements
Early on, the government began advancing the infrastructure at public hospitals. One at a
time, services were improved, investments were made in modern equipment, and difficult
specialties were developed. Motivated hospital construction and enlargement programs have
been undertaken to encourage community participation and initiative in providing
healthcare.
e. Housing
Although not a section of the healthcare system, the country’s early housing initiative has
contributed immeasurably to the health of Singaporeans. Several Singaporeans were living
in ―unhealthy slums and crowded unlawful resident settlements.‖ At the time, the
government started investing in good, clean cheap housing that greatly improved living
conditions and health conditions. The government did not stop at providing housing. Over
the years, alternative investments were created in clean water, proper sanitation services,
clean atmosphere, good nutrition, and health education. All these actions completed a vital
in improving the health status of Singaporeans.

6. Ensure Good and Affordable Basic Medical Services for All Singaporeans
The government declared the necessity to form a good, basic medical package available
to all people, no matter their means. The essential package had to be cheap and be provided
by hospitals receiving government subsidies. The package should be reviewed frequently to
reflect, among other things, the purchasing power of Singaporeans and productivity
increases in medical science.
7. Engage Competition to Improve Service and Raise Efficiency
The resources available for healthcare were restricted and should be placed for
economical use. Market forces should be used to encourage efficiency, improve quality of
services, develop additional elections for patients, and make sure patients are getting good
value for their money. The healthcare providers were in a very distinctive position to
regulate the demand for their services as patients rely on doctors for recommendations since
they were unaware of better or competing alternatives.47
Yet, too much competition and too
several providers would possibly drive up the demand for medical services, since patients
would naturally want to try new treatments or technologies or popular doctors. Oversupply
or overabundance of choices would successively drive healthcare costs up instead of
keeping them under control and defeat the aim of encouraging competition.
8. Interfere Directly in the Healthcare Sector
Singapore’s chosen approach to the healthcare market as a form of highly-calibrated
capitalism. Government intervention is permitted in certain conditions to redirect the
market. This approach is clearly recognized by funding public hospitals and other care
facilities but also encourages the participation of private hospitals and clinics.
Situations which may demand government action included preventing an oversupply of
healthcare services, moderating demand, and making reasons to keep costs down. The
interference has included creating and adjusting medical savings programs, sponsoring
47 M.D. Barr, ―Medical Savings Accounts in Singapore: A Critical Inquiry,‖ J Health Polit Policy Law 26, 4
(2001): 709–26.

insurance programs, providing subsidies to hospitals and polyclinics, determining the
number of beds and their distribution in public hospitals, funding new medical faculties,
controlling the number and type of doctors who can practice in the country, and regulating
and limiting the kind and range of private insurance programs available to Singaporeans.
B. Demographics
The Republic of Singapore consists of the main island of Singapore, off the southern tip
of the Malay Peninsula between the South China Sea and the Indian Ocean, and 58 close
islands.
As of 2012, the population of Singapore is 5.312 million people, of whom 3.285 million
(62%) are citizens while the rest (38%) are permanent residents or foreign workers/students.
The median age of Singaporeans is 37 years old. The life expectancy at birth is 81.9 years
old.
Figure (41): Total population in Singapore
Source: WHO National Health Accounts, 2013
The total fertility rate is estimated to be 0.79 children per woman in 2013, the lowest in
the world and well below the 2.1 needed to replace the population. The literacy rate among
adult of age 15 and above rated 95.86% which indicates the importance of education in the
governmental calendar. The Singaporean unemployment rate has not exceeded 4% in the
0
1000
2000
3000
4000
5000
6000
Population (in thousands) total
Population (in thousands)total

past decade, hitting a high of 3% during the 2009 global financial crisis and falling to 1.9%
in 2011. The gross national income per capita reaches 59380 $.
Table (32): Singaporean demographic indicators
Indicator
mortality rate (per 100 000 population) 326
Annual population growth rate (%) -2.1
Crude birth rate (per 1000 population) 9.91
Crude death rate (per 1000 population) 4.3
Gross national income per capita (PPP int. $) 59380
Literacy rate among adults aged >= 15 years (%) 95.86
Life expectancy at birth 81.9
Source: WHO National Health Accounts, 2013
C. Health system Indicators
1. Hospital beds
Hospital beds include inpatient beds available in public and private hospitals and
rehabilitation centers. Hospital beds (per 1,000 people) in Singapore were 2.71 as of 2011.
Its highest value over the past 51 years was 4.39 in 1960, while its lowest value was 2.71 in
2011.
Figure (42): number of beds in Singapore
Source: WHO National Health Accounts, 2013
2. Physicians
0
1
2
3
4
1994 2001 2003 2005 2006 2007 2008 2011
Number of beds
number of beds
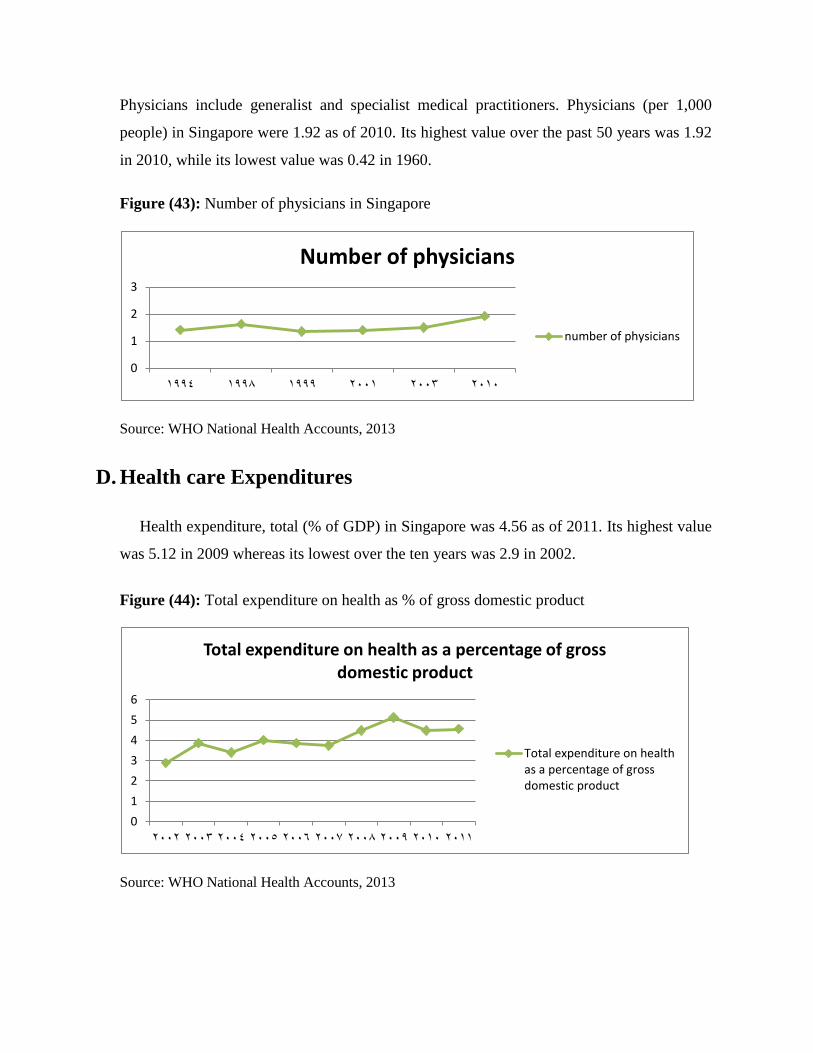
Physicians include generalist and specialist medical practitioners. Physicians (per 1,000
people) in Singapore were 1.92 as of 2010. Its highest value over the past 50 years was 1.92
in 2010, while its lowest value was 0.42 in 1960.
Figure (43): Number of physicians in Singapore
Source: WHO National Health Accounts, 2013
D. Health care Expenditures
Health expenditure, total (% of GDP) in Singapore was 4.56 as of 2011. Its highest value
was 5.12 in 2009 whereas its lowest over the ten years was 2.9 in 2002.
Figure (44): Total expenditure on health as % of gross domestic product
Source: WHO National Health Accounts, 2013
0
1
2
3
1994 1998 1999 2001 2003 2010
Number of physicians
number of physicians
0
1
2
3
4
5
6
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Total expenditure on health as a percentage of gross domestic product
Total expenditure on healthas a percentage of grossdomestic product
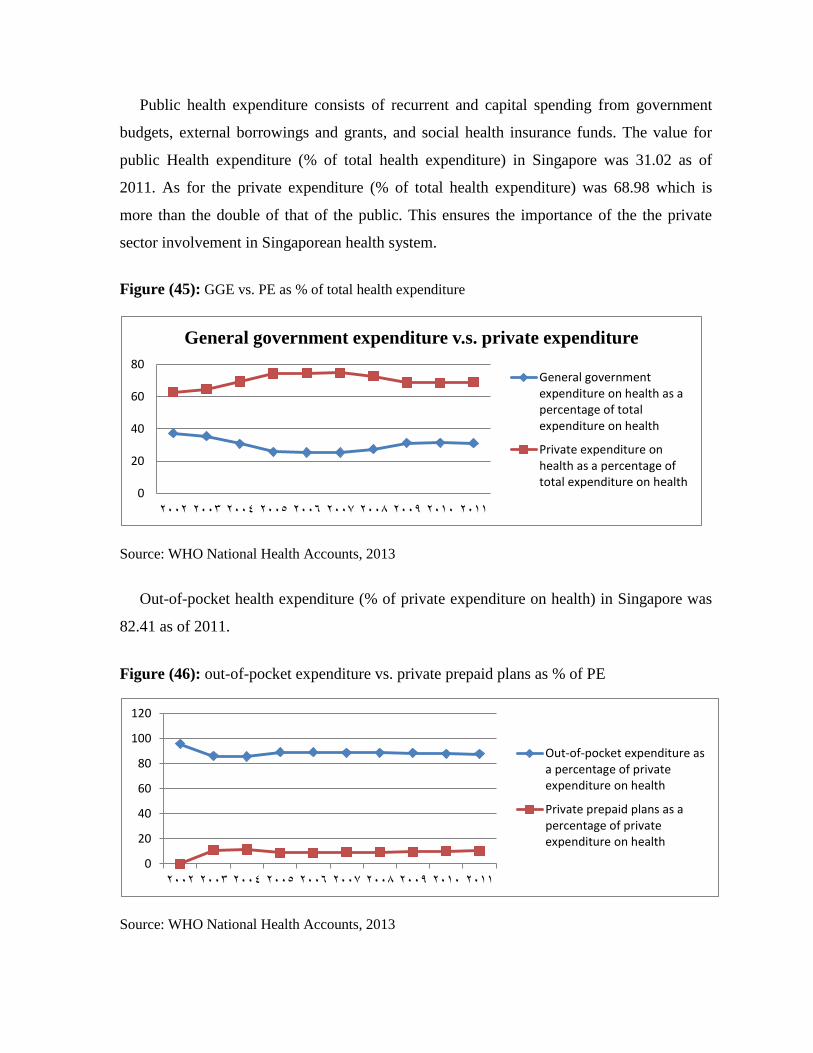
Public health expenditure consists of recurrent and capital spending from government
budgets, external borrowings and grants, and social health insurance funds. The value for
public Health expenditure (% of total health expenditure) in Singapore was 31.02 as of
2011. As for the private expenditure (% of total health expenditure) was 68.98 which is
more than the double of that of the public. This ensures the importance of the the private
sector involvement in Singaporean health system.
Figure (45): GGE vs. PE as % of total health expenditure
Source: WHO National Health Accounts, 2013
Out-of-pocket health expenditure (% of private expenditure on health) in Singapore was
82.41 as of 2011.
Figure (46): out-of-pocket expenditure vs. private prepaid plans as % of PE
Source: WHO National Health Accounts, 2013
0
20
40
60
80
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
General government expenditure v.s. private expenditure
General governmentexpenditure on health as apercentage of totalexpenditure on health
Private expenditure onhealth as a percentage oftotal expenditure on health
0
20
40
60
80
100
120
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Out-of-pocket expenditure asa percentage of privateexpenditure on health
Private prepaid plans as apercentage of privateexpenditure on health

Total health expenditure is the sum of public and private health expenditures as a ratio of
total population. The value for Health expenditure per capita (current US$) in Singapore
was $2,286.38 as of 2011. This indicator reached a maximum value of $2,286.38 in 2011.
The latest value for Health expenditure per capita, PPP (constant 2005 international $) in
Singapore was 2,786.96 as of 2011.
Figure (47): per capita GHE vs. per capita THE
Source: WHO National Health Accounts, 2013
E. Lessons to learn
Singapore has developed the most efficient, high-quality health care system within the
world, and one that provides us with vital lessons. While Lebanon is not near to adopt
another country’s health system entirely, we can learn from the best. How can we tend to
make this happen? At this point are some lessons from Singapore experience.
1. Price and Outcome Transparency: Singapore obliges that all prices for doctors and
hospitals are publicly available. This permits the patient and payers to shop for the best
price. In contrast, pricing in Lebanon is not clear, with the costs of pharmaceuticals,
0
500
1000
1500
2000
2500
3000
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Per capita governmentexpenditure on health (PPPint. $)
Per capita totalexpenditure on health (PPPint. $)

services, and procedures differ from one supplier to another.48
Similarly, information
concerning medical outcomes is not clear. Price and outcomes transparency will eliminate
arbitrary pricing, allow customers to chose the best services at the best price, and
considerably lower health care costs.
2. Higher Co-Pays: They are the fees we pay each time we tend to visit a doctor, have a
treatment, or go to the hospital. Higher co-payments are essential to Singapore’s system.
Knowing that they must pay a sizable portion of their medical bills, people are extremely
wary in using health services. However Singapore also makes it attainable for its citizens to
pay by commanding an individual saving program. Such a program is not advantageous in
Lebanon, instead, co-payments should be indexed to income—the higher the income the
higher the co-payment.
3. Payment by Capitation and Outcome, not Fee for Service: Today most doctors and
hospitals are paid for each diagnostic or medical procedure performed. The result has been
huge numbers of tests and procedures and greater costs. The solution may be by a mixed
payment plan. Singapore's health care system is basically funded by individual
contributions. However, the system is supported by the public sector: individuals are needed
to contribute a percentage of their monthly salary based on age to a personal fund to obtain
treatments and hospital expenditures. Additionally, the government provides a safety net to
cover expenses for which these personal savings are insufficient. Private health care still
plays an important role in Singapore's system, but takes a backseat to public contributions,
which boast the best part of doctors, nurses, and procedures performed. Such a hybrid
system would allow hospitals and doctors some measure of predictable income while
48 National Coalition on Health Care, ―Health Care Spending as Percentage of GDP Reaches All-Time
High,‖ 12 Sept. 2011. Available at http://nchc.org/node/1171
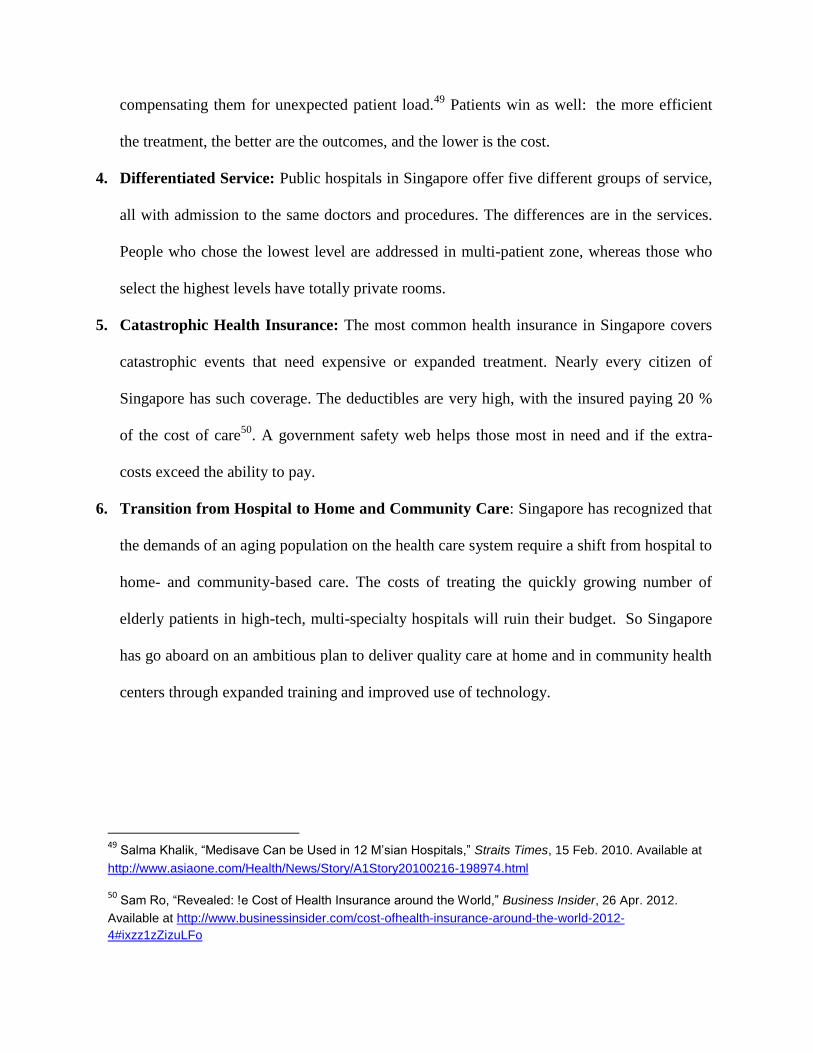
compensating them for unexpected patient load.49
Patients win as well: the more efficient
the treatment, the better are the outcomes, and the lower is the cost.
4. Differentiated Service: Public hospitals in Singapore offer five different groups of service,
all with admission to the same doctors and procedures. The differences are in the services.
People who chose the lowest level are addressed in multi-patient zone, whereas those who
select the highest levels have totally private rooms.
5. Catastrophic Health Insurance: The most common health insurance in Singapore covers
catastrophic events that need expensive or expanded treatment. Nearly every citizen of
Singapore has such coverage. The deductibles are very high, with the insured paying 20 %
of the cost of care50
. A government safety web helps those most in need and if the extra-
costs exceed the ability to pay.
6. Transition from Hospital to Home and Community Care: Singapore has recognized that
the demands of an aging population on the health care system require a shift from hospital to
home- and community-based care. The costs of treating the quickly growing number of
elderly patients in high-tech, multi-specialty hospitals will ruin their budget. So Singapore
has go aboard on an ambitious plan to deliver quality care at home and in community health
centers through expanded training and improved use of technology.
49 Salma Khalik, ―Medisave Can be Used in 12 M’sian Hospitals,‖ Straits Times, 15 Feb. 2010. Available at
http://www.asiaone.com/Health/News/Story/A1Story20100216-198974.html
50 Sam Ro, ―Revealed: !e Cost of Health Insurance around the World,‖ Business Insider, 26 Apr. 2012.
Available at http://www.businessinsider.com/cost-ofhealth-insurance-around-the-world-2012-
4#ixzz1zZizuLFo
Part Three: Lebanese National Social Security Fund
Chapter I: Applied Branches and Categories subject to NSSF
A. Establishment of the National Social Security Fund
Since the downfall of the Berlin Wall in 1989, the world is governed by one bloc. At the
economic level, there is hegemony toward globalization, privatization, market economy
technology development, and the formation of large economic coalitions; whereas on the
social level there is hindrance in role of the welfare state. The absence of such role led to
many perils threatening the social protection systems and workers’ rights such as the
maintenance of jobs, health insurance, free education, and social security.51
Lebanon is part of this changing world, as it is affected and influenced by the prevalent
economic orientations: Liberalizing economy, adopting open-space and open-market
policies, and resorting – in theory – to privatizations. All this is occurring in the shadow of
the increase in the mass of public debt and its price volume, economic stagnation, the
closing of many productive institutions and the great dangers affecting the workers and the
persons with limited revenue. This in turn led to the intensification of the social crisis
affecting mostly the social security issue. One cannot tackle the social security outside the
framework of the social situation, and its effect outside the social policy. Indeed security
forms part of a whole and this whole is the adopted social policy.
B. The Gradient in the application of social security in Lebanon
―Everyone, as a member of society, has the right in social security, the right to provide it,
through national effort and international cooperation, and consistent with the structure of
51 Makhzoumi,fouad, The National Dialogue Party Political Program, available at:
www.alhiwar.info/Political_Program_English.p
each country and its resources, economic and social rights and cultural rights indispensable
for his dignity and development of his personality in freedom.‖52
Note that the Universal Declaration of Human Rights of 1948 (i.e. since 63 years) gave
each person in the community the right in social protection.
"To enact legislation for social security, the employer must pay the employee for the
expense of service for any reason ..." 53
, we conclude from this article cited by the legislator
in the Lebanese labor law in 1946 that he was thinking since that time about the
development of legislation for social security. Indeed, this social security saw the light after
seventeen years of hint to it, and thirteen years of its plan in 195054
, under the Social
Security Law Decree port 13955 Date 26/9/1963.
The legislature put the plan to be applied over the three phases; by its completeness, the
social security includes, as a whole or some of its branches, all the Lebanese. Thus, the
Lebanese legislature has adopted the main lines of policy of the modern social security, in
terms of either totalitarianism or the terms of the mandatory nature of its provisions.55
The actual application of the law of security began after the set of the first section, a
branch of the compensation system of the service end, in place in 1/5/1965. However, we
can ask after more than 46 years on this date, is this law applied as a whole to all the groups
mentioned in it? Are all branches declared in the Code of Social Security applied? Is three-
phase plan that was originally developed for the application of the Social Security Law
carried out? Alternatively, have it been modified? Are all the presentations mentioned in the
sections already set in place applied? Who is subject to the guarantee under the provisions
of the general text? In addition, who are the people held under the special provisions? What
are the applicable sections? Who is subject to all branches of social security? In addition,
who are those subject to part of them? What are the benefits they provide?
52
22انادة – 10/12/1948 –اإلػال انؼان نحقىق االسا 53
54انادة – 23/9/1946قاى انؼم انهبا تارخ 54
Durand Paul – La politique contemporaine de sécurité sociale – Paris – Dalloz – 1953 – P157
55
13ص – 1987 – 2ط – 1ج –انستفذو ي انضا االجتاػ انهبا –د. اج شىفا
The Lebanese legislature followed the legislators in other states that have systems to
ensure a social gradient in the application of this guarantee in the terms of the sections
included either in the social security system or in terms of people whom are applied to them.
The articles 8, 9, 10, 11 and 12 of the Social Security Law set the stages of application.
1 - First stage: This stage begins after the expiration of 18 months from the date of
publication of the Social Security Law in the official gazette (published on 09/30/63). This
phase began with the implementation of the branch system of compensation at the end of
service 1/5/65 and include all categories of employees who work in the non-agricultural
enterprises.
2 - The second phase starts after two years at most from the date of implementation of the
first phase, and include all categories of wage earners working in agricultural institutions.
3 - Third stage: This stage begins after at least two years from the date of implementation of
the second phase, including the categories of persons who are not covered by the first and
second phases like employers and independent workers.
However, this plan for the implementation of social security have been exposed to
significant modification, in particular, under Law No. 16/75 Date 11 April,1975 which
amended Article 9 of the Social Security Act which specifies the persons subject to social
security since the first phase. the government became able to decide whether to subject one
or more of the categories of drivers of public vehicles, craftsmen, and other categories of
Lebanese persons who were in need to be subject since the first phase even if they are
employers and independent workers, through decrees taken in the Council of Ministers upon
the proposal of the Minister of Labor and end of the Board of management of the Fund.56
C. Branches of social security and their submissions
Social Security includes the following sections:
a. sickness and maternity branch
b. work injury and professional disease
56
انقطغ – 1انبذ –انفقزة أوال – 9 انادة – 26/9/1963تارخ 13955قاى انضا االجتاػ انفذ بانزسىو

c. family allowances
d. end of service indemnity
And it is implemented in three phases:57
It was supposed that the application of the branch of sickness and maternity to begin
before the other branches, although the Social Security law did not specify the branch that
should be applied first, but there are reasons to give this branch a priority over the other
branches, in addition of its citation at the head of branches enumerated in Article 7 of the
Social Security Law mentioned above, it is the only branch which was not regulated by the
laws or the private provisions. The Labor Law includes provisions dealing with the old age
and compensations at the retirement. Moreover, Legislative Decree No. 25 issued on May 4,
1943 forms a sort of protection to the employees in relation to work emergencies. Lebanon
was one of the thirtieth countries in the world which recognized in 1947, the importance of
paying compensation of family allowances branch and the first country in the Middle East at
this level, the imposition of legislative decree No. 29 issued on May 12, 1943 had given to
each employer or worker and all working widow and every working woman married from a
disabled husband family allowance compensation.58
As a whole it had not been taken into account the priority of branches and the
implementation of the branches started in the following order:
1. Branch of sickness and maternity:
The date of implementation of this branch was defined as follows: As of 11/01/1970 to
Subscriptions maturity, as of 1/2/1971 for entitlement to benefits under Decree 14035 Date
16/3/1970 amended by Decree No. 456 Date 27/1/1971.59
57
7انادة – 26/9/1963تارخ 13955قاى انضا االجتاػ انفذ بانزسىو
58
20 -19ص – 1987 – 2ط – 1ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا 59
265ص –يذكىر سابقا –غ وانفق واالجتهاد انضا االجتاػ ف انتشز –د. ػايز ػبذ انهك

The submissions of sickness and maternity branch as specified in paragraph 1 of Article
15 of the Social Security Law include the following:
a. Preventive medical care and treatment.
b. In case of maternity testing and prenatal care and care necessary during and after childbirth.
c. In the case of temporary inability of work resulting from illness or maternity, sickness and
maternity compensation. However, this part of the guarantee of the disease and motherhood
has not been implemented so far are applied, in this case in respect of disability from work
because of illness, the provisions of Article 39 of the labor law relating to sick leave; With
regard to disability from work because of maternity provisions of Article 28 of the Labor
Law on maternity leave.
d. In case of death, compensation of burial expenses.
It is noted that the Lebanese legislature leave the choice to the guaranteed to choose his
doctor and the institution which he wants from the hospitals between institutions and
physicians accepted by the Fund.
2. Branch of emergency work and occupational diseases:
Not implemented so far, it applies to emergency work that affects employees provisions of
Legislative Decree No. 136 Date 09/16/1983, and apply the provisions of the Code of
Obligations and Contracts on occupational diseases. As for the benefits of the branch of
emergency work and occupational diseases were announced in Article 32 of the Social
Security Law amended by Decree-Law No. 116 Date 6/30/1977 as follows:
a. Medical care.
b. Compensation for temporary inability of work.
c. Disability pension compensation in case of permanent disability, total or partial.
d. Pension of holders of the right and compensation of burial expenses in the case of the death
of the guaranteed.
Finally, it should be noted that all of these submissions have not been applied so far.
3. The branch of family allowances:
This branch was placed in force on November 1, 1965, and it provides payments of sum of
money for married employees in the form of family allowances for spouse and children up
to 5 children maximum in accordance with the provisions of Articles 46 and 47 of the Social
Security Law. He does not believe any educational benefits contrary to the name.
4. Branch for end of service:
this branch has been developed and place in force in 1/5/1965, under the Decree 1519 Date
24/4/1965; and therefore become mandatory to associate this branch, each employee hired
after that date, where it was left for the employee already hired either to remain subject to
the provisions of labor law or to choose the branch of end of service (retirement) in
accordance with the provisions of Article 49 of the Social Security law.
So the retirement system had partially substitute the layoff compensation system, which
was in force under the labor law; Article 49 of the Social Security Law stipulates in its first
paragraph as follows: ―until the legislation of the aging security60
, a fund is established to
compensate the retirees ... ―; So that it can be said that this section is temporary and is a
transitional stage to reach old age security.
In general the system provides for wage earners secured mandatory or optional end of
service compensation when there is a one of the following conditions: the total years of
work at least 20 years or to be suffering from a disability of at least 50% or that the
guaranteed has reached sixty years old, or in the case of marriage of women from the
employee and she left work during the twelve months following the date of her marriage or
in the case of the death of the employee in accordance with the provisions of Article 50 of
the Social Security Law. The subjection of the guaranteed to this branch ends at the age of
sixty-fourth in accordance to the provisions. Finally it should be noted that the employee is
given reduced compensation if he left his work and the amount of compensation 50% of the
original value if he is engaged 5 years at most, 65% of the original value If more than five
years and ten years most, 75% of the original value If more than ten years and 15 years at
most, 85% of the original value If more than 15 years and less than 20.
60
389ص – 2005 –بزوث –صادر –انضا االجتاػ ف انتشزغ وانفق واالجتهاد –د. ػايز ػبذ انهك
D. People subject to all branches of social security
The people who are subject to all branches of social security are:
a. permanent employees: the permanent employee is the employee associated with the
institution with a working relationship in accordance with the operative part of Article 624
of the Code of Obligations and contracts under the employment contract of indefinite
duration, subject to the Social Security Law, whatever the duration or the type or nature,
shape, or validity of the contract which he links to his employer and whatever the nature of
wages or earns in accordance with the provisions of Article IX, Section 1, first paragraph
section A of the Social Security Law.
b. Temporary employees: those whom their work nature requires their use temporary and
associated with their employers under the written contracts, as defined by paragraph 1 of
Article II of Registration and registration. They are subject to Social Security Law, in
accordance with the provisions of Article IX, paragraph, first item 1 section A.
c. Probationer employees: they are associated with the employer by an employment contract
on a trial basis. They are subject to Social Security Law, in accordance with the provisions
of Article IX, Section 1, first paragraph a section.
d. Seasonal employees: Having decided that the seasonal employee who does seasonal work
for a period not exceeding eight months, they work in the activity associated with certain
seasons. They are subject to the Social Security Law and in accordance with the provisions
of Article IX, paragraph, first item 1 section A.
e. Trainees: it was defined in Article III of the Labor Law as workers under preparation who
have not yet acquired their craft in the authentic experience of the employee. They are
subject to Social Security Law, in accordance with the provisions of Article IX, Section 1,
first paragraph a section.
f. Lebanese employees non-associated with a particular employer: people working for more
than one employer at one time, so difficult to determine their association with any of them
permanently. The Article ninth paragraph, first item 1 section b of the Social Security Law
on the subordination of Lebanese employees non-associated to specific employer, who are

working in the sectors of the sea and harbors, construction, loading and unloading of all
branches of social security.
g. Members of the teaching staff in institutions of higher education and technical institutes:
They are subject to Social Security Law, in accordance with the provisions of Article IX,
Section 1, first paragraph c section.
h. People working in the public sector: The text of the law announced their subjection in
Article IX, paragraph, first item 1 section d: "People Lebanese working for the state or
municipalities, or any department or public institution or independent systems, whatever the
duration, or type, or the nature of, or shape, or their appointment, or contracted with,
including clients of the Ministry of Information .... Where the permanent state employees
are accepted from the subjection to security. "
i. Sellers of newspapers and magazines: Full-time for the sale of newspapers and magazines as
independent workers, who are a class of non-traders, have been subjected by Decree No.
4885 Date 18/2/1982 amended by Decree No. 265 Date 24/2/1983.
j. Drivers of public vehicles: Owners and non-owners of their cars (non-associated with a
work contract with the owner of the car are not any of the action.) Has been subjected by
Decree No. 4886 Date 18/2/1982 amended by Decree No. 265 Date 24/2/1983.
k. Permanent employees working in an agricultural institution: Article X of the Social Security
Law stated the subordination of all Lebanese employees’ workers and users, trainees and
interns, working on Lebanese territory for an employer and one or more of the Lebanese or
foreign, during the second stage of the application of social security.
l. Journalists: They are those who just do not get a legal subordinate relationship with the
employer, because of who possess this relationship have been subjected since the beginning
of the first phase of employees, while the subject of those under the Law No. 16/75 Date
11.04.1975 from the date of 8/5/1975, and journalist is taken from the profession of
journalism and his basic means of livelihood, as defined by Article 10 of the Law
publications.
m. Foreign employees: for the foreigners, they are subject to and benefit from all the branches
when the State to which they belong, recognizes the Lebanese principle of equal treatment
with nationals as regards social security, and who possess a work permission, and these

countries are France, Italy, Belgium, Britain . The rest are subject only to sickness and
maternity and family allowances branches but do not benefit.
And the following table shows the number of secured subject to all the branches in the
year 2012
Table (33): number of secured subject to all branches 2012
Job description secured in 31/12/2012
Employees 439747
Employees in the marine sector 91
Drivers of public vehicles 40679
Sellers of news papers and magazines 46
Total 480563
Source: statistics center in NSSF
E. People subject to certain branches
They are of two types:
1 - Persons subject to the benefits of medical care in cases of sickness and maternity and
emergency work and occupational diseases:
a. Permanent government employees: they are defined in paragraph 2 of Article I of the
Legislative Decree No. 112 Date 06/12/1959, and they were subject under the provisions of
Article 9, first paragraph item 2 a section of the Code of Social Security.
b. Members of the teaching staff in private schools entering into owners and non-entrants in
the owners and it means those carrying out the functions of teaching or educational
administration, and are subject by Law No. 20/72 Date 23/12/1972 as of 1/10/1971.
2 - Persons subject to the benefits of medical care in cases of sickness and maternity:
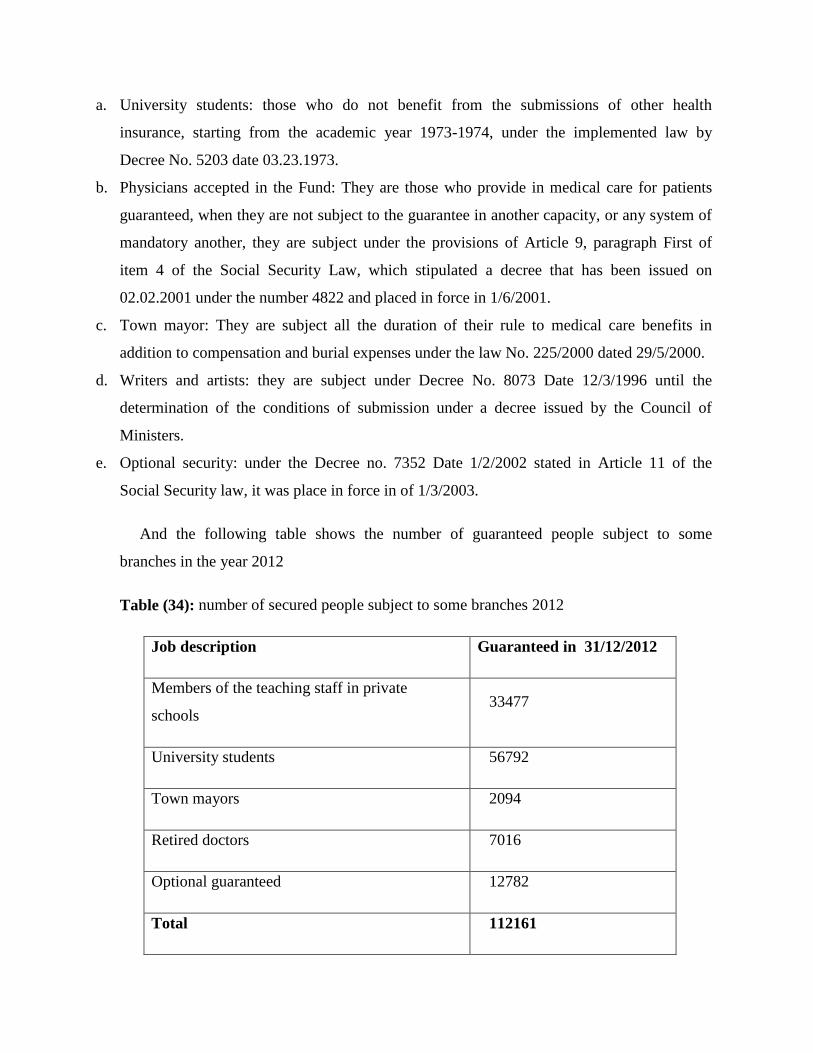
a. University students: those who do not benefit from the submissions of other health
insurance, starting from the academic year 1973-1974, under the implemented law by
Decree No. 5203 date 03.23.1973.
b. Physicians accepted in the Fund: They are those who provide in medical care for patients
guaranteed, when they are not subject to the guarantee in another capacity, or any system of
mandatory another, they are subject under the provisions of Article 9, paragraph First of
item 4 of the Social Security Law, which stipulated a decree that has been issued on
02.02.2001 under the number 4822 and placed in force in 1/6/2001.
c. Town mayor: They are subject all the duration of their rule to medical care benefits in
addition to compensation and burial expenses under the law No. 225/2000 dated 29/5/2000.
d. Writers and artists: they are subject under Decree No. 8073 Date 12/3/1996 until the
determination of the conditions of submission under a decree issued by the Council of
Ministers.
e. Optional security: under the Decree no. 7352 Date 1/2/2002 stated in Article 11 of the
Social Security law, it was place in force in of 1/3/2003.
And the following table shows the number of guaranteed people subject to some
branches in the year 2012
Table (34): number of secured people subject to some branches 2012
Job description in 31/12/2012 Guaranteed
Members of the teaching staff in private
schools 33477
University students 56792
Town mayors 2094
Retired doctors 7016
Optional guaranteed 12782
Total 112161

Source: statistics center in NSSF
As for foreigners who do not belong to one of the countries that recognize the Lebanese
principle of equal treatment with nationals as regards to social security they are subject to
both sickness and maternity branch and family allowances but do not benefit from the
submissions of these two branches.
The following table shows the number of foreigners registered in the Fund and non-
beneficiaries up to 31/12/2012:
Table (35): number of foreigners registered in Fund and non-beneficiaries
Tot
al
docto
rs
studen
ts Oven workers
teache
rs
employee
s Job description
032
02 1 2 62 401 22561 Number
Source: statistics center in NSSF
Chapter II: Expansion in the application of NSSF
A. The branches and submissions under study
There is no doubt that the number of branches currently applied in Lebanon and the
amount of benefits provided by NSSF are very few, if compared with its launch in the mid-
sixties. We can obviously notice that the last branch applied was sickness and maternity
branch since 01.11.1970, noting that it haven’t been completely applied yet.
There had been many reasons, most notably the outbreak of the Lebanese civil war 1975
- 1990 , the NSSF who began the implementation of its branches in the 01/05/1965 with the
end of service indemnity branch , had carried out three out of the four branches provided
for in this law until the date of the outbreak of this war . This war led to the dismantling of
the society and the state and the deterioration of the standard of living and the destruction of
infrastructure. People were obliged to adapt to the new situation, which was the declining
role of the public sector and the growth of the role of non-governmental sector in the areas
of health and financial aids, so the familiar and religious institutions played an integral role ,
and political parties established their own institutions to provide aids , declining role of the
government and public institutions in this area , including the NSSF. There are also other
reasons for this decline such as the deteriorating economic and political situations in
Lebanon and its surroundings since the end of the civil war.

But all that has to motivate the management of the NSSF and the government to develop
the social security, and expand its services, since historical indications show that poverty
and lack of insurance and security are the most important factors of the outbreak of many
crises. In periods of crisis, governments must give citizens a sense of protection from risk.
With reference to the national conciliation document in Taif has focused on social justice
and balanced development and financial, economic and social reforms.
However, legally there are many legal provisions that call for increased benefits, where
there are many benefits stipulated by the Lebanese Social Security Law issued on
26.09.1963 have not yet been implemented; These submissions and branches can be
summarized in the following form:
1 - Branch to of work emergency and professional diseases, which are stipulated in articles
28 to 45 of the Nations Social Security law.
2 - Disease compensation provided by the National Social Security Law as part of the
sickness and maternity branch in articles 23 to 25.
3 - Maternity compensation stipulated in the National Social Security Law as part of the
sickness and maternity branch in Article 26.
4 – Aging insurance hinted by the National Social Security Law in paragraph 1 of Article
49.
5 - Retirement System, hinted by the National Social Security Law in paragraph 5 of Article
54.
At the level of international and regional standards, Convention No. 102 Date June 4, 1952
issued by the International Labor Conference concerning minimum standards of social
security stipulates that each government member in the convention shall cover three risk of
at least the following risks: medical care, subsidy disease, unemployment benefit , old age
benefit , employment injury benefits , family allowance , maternity allowance , disability
benefits, noting that Lebanon has not ratified this convention.

The Arab Convention No. 3 about the minimum level of social insurance, date
27/03/1971 in Article VII has recommended that social security shall includes at least two
branches of the following sections: work injury insurance, health insurance ( against the
disease ) , maternity insurance ( pregnancy and childbirth ), disability insurance , old-age
insurance , death insurance , unemployment insurance, family allowances .61
In fact, Lebanon had provided a large part of these minimum standards, but these
standards are no longer sufficient at the present time. The Social Fund is now suffering from
a fiscal deficit, and the government suffers too from a large deficit in its budget, and
employers and employees are unable to pay a high proportion of subscriptions due to the
current economic situation. The management of the Social Fund is currently working on
expanding the field of services, where they were preparing a series of studies and laws for
this purpose.
1. Dental care
Paragraph 2 of Article 17 of the National Social Security Act Decree 13955 Date
26.09.1963 listed the medical care benefits of the sickness and maternity branch ,as stated in
item A section III of this paragraph that the dental care should be applied after the issuance
of the decree by the Council of Ministers on the proposal of the Minister of Labor and
Social Affairs and the end of the Governing Council.
And so after, the sickness and maternity branch had been applied without the dental care
since the decree hadn’t been issued until this date. In 15 March, 2001, the board of directors
in the NSSF adopted Resolution No. 182 aimed at licensing for the National Social Security
Fund to provide dental cares.
After 38 years of the issuance of the law, and after the issuance of the opinion of the
Council of State of approval No. 158 Date 03.22.2001 .On 24 March 2001, Decree 5104
about licensing for the National Social Security Fund to provide dental care was issued
identifying in its first article the benefits covered by the dental care.
61
35ص – 1987 – 2ط – 1ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا
In 1/7/2001 was the default date for the application of the dental care benefits. Since
dental care health implementation requires accuracy in logistics, administrative and financial
procedures, the Board of Directors has asked to postpone the implementation of the project
until November 2001, so the Council of Ministers issued Decree 6516, dated 11/10/2001,
which amended the text of Article III of the former Decree No. 5104 mentioned that the
default date of the implementation became in 1/11/2001. The Fund issued a medical system
special for dental care, in addition to the agenda and pricing of medicines and coding and
tables of drugs and laboratory tests and radiographs.
In August 2001, a contest was made to select dentist’s observers and they accepted 20
dentist. National Social Security Fund Administration began to make tenders for the
preparation of the reception centers.
In the 2002 budget, Board of Directors approved amount 34 billion pounds to cover the
cost of dental treatment, including processing centers and crew observer. Since that date,
and until now, the dental care hadn’t been applied. knowing that the World Health
Organization ( WHO ) ranked Lebanon worst in the region in terms of oral health and its
impact on public health , where the index of number of brackish teeth , lost ,or stuffed rated
5.7 % among children aged between zero and twelve years old, compared with 3.3 % to
neighboring countries.
It is proposed to start the implementation of these submissions, by starting working out
basic treatments gradually, so as not to be a high cost to the Fund, also the percentage of the
Fund’s contribution can be decreased in the beginning to 40 %,62
for example, and the
insured bear the remaining 60 %, knowing that the other official health institutions cover the
dental care.
2. Branch of emergency work and occupational diseases
62
سؤال يىج ي انائب حىري إنى انحكىيت ػ – 10ص – 2005تشز األول 18انثالثاء – 2073انؼذد –صحفت انستقبم
يصز ضا طب األسا

The branch of emergency work and occupational diseases is the only branch texted in the
Lebanese National Social Security Law and haven’t been implemented until now, even
though it has passed so far about 50 years of the issuance of this law.
And thus the provisions of Legislative Decree No. 136 dated 09/16/1983 are applied on
emergency work and the provisions of the Code of Obligations and Contracts is applied on
occupational diseases.
We can summarize the reasons that requires the development of this branch as follows:
The system of employer's responsibility currently in force , despite the developments that
have passed it , it was not optimal system to meet the occupational hazards , it had many
disadvantages, most notably is that the employer bears the compensation for damages
resulting from these risks , and he tries to evade from it in multiple ways , so that the
employee will be obliged to resort to the law in order to get his right.63
So it was normal that
all the society should bear the risk that face the employee, so the employer will not any
more compensate on the damages that face the employee, however he will contribute in the
compensation by paying a subscription of a certain percentage of the wage of each worker ,
through National Social Security.
And the risks covered by the emergency work and occupational diseases branch in
accordance with the provisions of Articles 28 and 29 of the National Social Security Act
are:
a. Emergency which affects the insured during or on the occasion of doing his job.
b. Emergency faced by insured during the period he is going from his home to the workplace
or returning from it , with a condition that the way should be without interruption or
deviation from the natural way for a reason independent of his work
c. Emergency which affects the insured during or on the occasion of the ongoing rescue
operations in the institution where he work.
d. Emergency which affects the insured outside Lebanese territory during or on the occasion of
doing his job.
e. Occupational diseases.
63
756ص –يذكىر سابقا –انضا االجتاػ ف انتشزغ وانفق واالجتهاد –د. ػايز ػبذ انهك

It is important to differentiate between work emergency and occupational disease
because conditions for the worker to take the compensation from the fund vary according to
its source. With regard to work emergencies, the emergency that satisfies the standards
stated in the law, is considered a work emergency, and covered by work emergency branch.
64The occupational disease is not covered by the fund unless it is recorded in the list of
occupational diseases as set by Article 29 of the Social Security Act.
Emergency can be defined as: ―any act affecting human body as long as it is surprising
and caused by an external cause."65
The disease can be defined as any slow and gradual contact by the human body as a result
of an internal factor.
The Submissions of work emergency and occupational diseases branch are the following:
a. medical care Submissions: all the submissions listed in the provisions of Article 33 of the
National Social Security Act.
b. Work emergency compensation: paid in case of temporary disability beginning of the
eleventh day of the date of work stoppage. The compensation range between three-quarters
of daily average earning and half of that gain in case the insured is in the hospital, according
to the provisions of Article 34 of the Social Security Act.
c. Disability pension : stipulated in Articles 35 to 38 of the Social Security Act , which is paid
in case of total or partial permanent disability:
In the case of total and permanent disability: the insured receive a disability pension for
whole life equal to two-thirds of the annual value of his earnings.
In the case of partial permanent disability: in case of disability of at least 30 %, the insured
shall receive a disability pension determined, according to the degree of disability. In case of
disability less than 30%, the insured shall receive a compensation paid at once, and be
equivalent to three annual payments of partial disability pension that is worth to him.
d. Right owners’ pensions after the death of insured: This amount is equal to two-thirds of
annual earnings, or 50 % of this gain according to the provisions of Article 40 of the
64
760-759ص –يذكىر سابقا –اػ ف انتشزغ وانفق واالجتهاد انضا اإلجت –د. ػايز ػبذ انهك 65
635-3 –فزح أبى راشذ – 20/12/1950تارخ –و.ع.ث. جبم نبا

Insurance Law. It is paid to the right owners under Decree 4896 Date 08/02/1974 ,
according to the order of priority, and in accordance with the provisions of Article 39 of the
Law social Security. And right owners are the spouse, children, father and mother (required
for the insured to be the only supporter for his parents in Lebanon and their wage shall be
less than the minimum wage rate);66
in the absence of a husband and children, the pension is
taken by his siblings or grandparents.
e. Burial expenses compensation: is a constant amount determined by the decree issued by the
Council of Ministers, paid for the right owners in case of the death of the insured, according
to the provisions of Article 45 of the Law of National Social Security Fund.
It should be noted that before placing this section in to implementation, some amendments
should be done to the law, particularly in terms of imposing some conditions on the right
owners who receive the disability pension after the death of insured and in terms of
reducing the beneficiaries , so that not to charge on the fund very high amounts .
According to our opinion, provisions must be adopted to the right owners similar to the
beneficiaries of the submissions of the sickness and maternity branch set them in Article 14
of the National Social Security Law. It also important to pay attention to the application of
the provisions of Article 59 of the Social Security Law relating to taking the necessary
measures to provide safety and health conditions in order to prevent work emergency and
diseases, which would reduce the injuries and therefore the costs to the National Social
Security Fund.
3. The pension and social protection system
It was Supposed that this system will replace the end of service indemnity branch since
this branch doesn’t provide an income to the insured for life time after his retirement, while
the insured get a compensation once after his retirement, but this compensation it not
enough especially in these economic situations from inflation and declined purchasing
66
207ص – 1985 –بزوث – 1ط – 2ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا

power.67
the pension and social protection system includes the submissions of security and
maternity for retirees.
The Lebanese legislator has hinted from the beginning to his desire to apply this system,
we conclude that from the text of Article 49, paragraph 1: " until the issuance of the elderly
insurance, the end of service and indemnity branch is established ... " As in the text of
Article 54, paragraph 5: "You can convert indemnity for the benefit of the employee who
has completed sixty years of age to a pension for life ... ―.
The end of service and indemnity system is the only way for the elderly to complete their
lives secured after they spent their lives working and producing.
There are two basic ways to retire:
Capitalization method, a system based on taking savings from the income during the
period of work to invest them and benefit from the profits. So there is a direct relationship
between savings of each person during his productivity period and the pension which he
gets during his retirement. Capitalization has disadvantages that are the risk of volatility in
the market.
Retirement based on a system of distribution. An obligatory monthly subscription should
be paid from the wages. These subscriptions are distributed on the employees after their
retirement. There is a relationship between the duration of contributions, its amount, and the
amount of pension which the insured will have.
Some countries, especially in Western Europe, adopted important systems for Social
Security to give specific submissions based on distribution system funding , while others
adopted specific retirement programs managed either by the state (as in Singapore and
Malaysia) or regulations within the framework of the state (Chile and Argentina ).68
67
345ص – 1985 –بزوث – 1ط – 2ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا
68
480ص –يذكىر سابقا –انضا اإلجتاػ ف انتشزغ وانفق واالجتهاد –د. ػايز ػبذ انهك
In Lebanon, it has developed several draft laws to the pension system. With respect to
retirement pension, legislator tries to merge between capitalization and distribution. It is
based on the capitalization because the pension depends on the elements of age, number of
years of participation and individual account of the insured of which consists of
contributions paid and owed and portion of this account from the investment of funds,
according to the provisions of Articles 50-1 and 50-6 of the bill. It is also based on
distribution through guaranteeing minimum pension of LBP 180,000 from those who
participated in this system for a period of twenty years and the amount increase by 3000
LBP for each additional year of subscription, until it reaches 240,000 LBP, in accordance to
the provisions of paragraph 3 of Article 50-7 of the project.
In relation to pension, it is pension allocated to the insured, who suffer from permanent
disability, physical or mental, as the result of a work emergency or occupational disease,
which reduces his ability to work or to earn income by two-thirds at least, and prevents him
from performing any work, according the provisions of Article 51-1 of the proposed project.
As for the pension of the right owners , it regulates the transmission of the pension upon
the death of the insured who benefits from the pension system , or meets the conditions to
benefit from this pension , or disability pension , to his right owners whom are his legal wife
who doesn’t practice any profession or dependent and independent paid work, and the
husband of the insured and the legitimate or adopted children , and Father and Mother, in
accordance with the provisions of Article 52-1 of the proposed project. Article 52-2 of the
same project Has distributed pension according to the following: 40% for the surviving
partner and this percentage is reduced to 30% of pension in the case of his/her parents or
one of them alive; and 40% for children; and 10% for the parents or one of them surviving
this ratio becomes 30% in the absence of any of the other beneficiaries.
As for the submissions of sickness and maternity for retirees, Article 53 of this project, had
subjected pensioner who completed the age of sixty-fourth or reached the retirement age and
the owner of a disability pension and pension owners from the right owners to the sickness
and maternity branch in the National Social Security Fund, and they benefit from the
medical care submissions as well as the burial cost compensation.
Finally, we can list some notes about this project:
The project must be based on facts and figures relating to the labor market and the number
of employees and the number of public and private institutions and the average age and the
average number of families and the average income ... In order not to be threatened by
failure
Ensure the government’s ability to pay its portion in order to prevent any deficit that
threatens the whole system.
The project requires in Article 49-1 the creation a new public institution with legal
personality and financial and administrative independency for the management of the
pension social security fund.
B. The reasons for increasing the categories covered by Social Security
The number of people subject to National Social Security at the end of the year 2012
reached about 393523, the beneficiaries on their responsibility reached more than
1,200,000 citizens.
The aim of Lebanese legislator target upon the issuance of the National Social Security
Law in 1963 is to cover all the Lebanese at the end of the third and final phase. Article 12 of
the law text as follow: "In the third phase, special law defines the conditions of the
application of the social security system, or some of its branches, to people whom are not
submitted yet to its provisions in the first and second phases.
And so far, many years have passed and the goal hadn’t been reached yet. Perhaps one of
the most important reasons for the delay is the Lebanese war and the economic and social
conditions.

There are many factors that impose the coverage of the social security on various
members:
Achieve equality among the Lebanese of different categories according to the Lebanese
constitution.
Economic factors: In the absence of social security coverage to all categories of citizens,
the only solution for them is the traditional way to handle with the consequences of the risks
that threaten their economic status and their future which is savings. However, this method
has several disadvantages, since it is linked to a large extent with the level of income. The
holders of small incomes cannot save, but they spend all their income on essential needs.
Accordingly, the ability to retain certain amounts saved is limited to those of large incomes.
Also, the money loses its purchasing power because its value diminishes over time.69
social factors : the need to Social Security , arise due to the evolution of modern life and
its requirements , the high cost of living and disintegration and decline in family ties, and
thus difficult to handle with the consequences of the social risks .70
There are many categories that are in need to be covered by Social Security benefits,
however the most essential to be covered are:
tobacco farmers
writers and artists
municipal workers
1. Tobacco farmers
countries Usually tries to encourage the rural population to stay in the villages through the
support of farmers , and there is no doubt that Lebanon is among the countries most in need
to follow this policy due to large- displacement movements that empty countryside led to
overcrowding in cities , especially the capital Beirut and its suburbs .
69
30-29ص – 1987 –بزوث – 1ج – 2ط –انستفذو ي انضا االجتاػ انهبا –د. اج شىفا 70
31ص – 1987 –بزوث – 2ط – 1ج –انستفذو ي انضا االجتاػ انهبا –د. اج شىفا

The best way to encourage the farmers to stay in their villages is to help them in providing
the protection from risks through including them in the Social Security System.
For the agricultural sector, the legislator had included permanent workers in agricultural
institution for all branches of social security under the law No. 8 / 74 date 03/25/1974 and
Decree No. 7757 dated 07.05.1974, while it excluded the farmers and the independent
agricultural workers.
The selection of tobacco farmers group among other farmers refers to several factors:
They can be easily subjected to social security, because their numbers are known and can
be easily identified.
Their ability to pay their subscriptions especially that tobacco is one of the plants that the
Lebanese government to encourages its marketing.
Tobacco cultivation is concentrated in the south and the Bekaa and Akkar, which is the
most deprived areas and must remain under the government’s sponsorship and interest. The
distribution of areas planted with tobacco in Lebanon is as follows: 76 % in the South, 17 %
in the North, 4.6 % in Mount Lebanon, and 2.4 % in the Bekaa.
Its contribution in reducing the prohibited plants, and in the development of the rural
economy, and also contribute in providing jobs for thousands of people, farmers, employees
and workers.
Importance of tobacco farming, where tobacco is one of the main agricultural crops in
Lebanon, comes in fourth place after the production of lemon, banana and olive.
The Tobacco and Cigarettes Company estimates the numbers of tobacco farmers by about
30 thousand families ( about 16,000 families in the south) , which means about 150,000
citizen benefit from Social Security in case of including this category for all branches of this
security.

The National Social Security Fund must work on the necessary studies to determine the
best way to include this category in the social security system, and the preparation of
necessary laws and decrees.
2. Writers and artists
For the category of writers and artists, the situation is different for that of tobacco farmers,
since there is a decree for their including but they are still waiting the issuance of the decree.
Legislator has amended Article 9 of the Social Security Law under the law No. 16 / 75
Date 04/11/1975 , so the first paragraph item 1 H section became as follows: " under decree
issued in the Council of Ministers, and the proposal of the Minister of Labor , and ending of
the Board of directors , and under the conditions specified , categories of public-drives and
artisans , and other categories of non- Lebanese persons mentioned in this article who
should be included since the first phase , for some or all branches of social security , are
specified. "
Under the provisions of this section, the government issued Decree No. 8073 dated 12
March 1996, based on ending the temporary Committee to carry out the management of the
National Social Security Fund r by Resolution No. 212 adopted at the session number 124 /
A / Z Date 11.08.1995 and after consulting the Government Consultative Council based on
the opinion 39 / 96 date of 11/30/1995.
The decree in its first article mandated the subjection of Lebanese writers and artists to
sickness and maternity branch stipulated in the Social Security Law. But the same decree
suspended its implementation till the issuance of a new decree by the Council of Ministers
upon the proposal of the Minister of Labor and ends the Board of Directors of the National
Social Security Fund.
From here, the need to give priority to this category in the subject of their including to the
branches of the Social Security National Fund is for the following reasons:
Issuance of an earlier decree that subject this category to the NSSF, and suspending its
implementation until setting a new decree.

This category represents a civilized picture of Lebanon; however, the state is still absent
from their health insurance, where there are many artists and writers whom are unable to
pay the expenses of their medication.
The addition of this category contribute to achieving the primary objective of the
Lebanese lawmaker and management of the National Fund for Social Security by adding
new segments secured to the base on the road to coverage of all the Lebanese .
3. Municipal workers
The situation of this category is quite similar to the situation of writers and artists, as there
is a law for their subjection, but they are still waiting for determining the date of its
implementation.
The municipal workers are included in the social security system under section d of item 1
of the first paragraph of Article 9 , as amended by Law 16 /75, and under the law 3 / 82 Date
01/28/1982 .
The law No. 10 / 84 Date of 12/18/1984 amended the date of including the municipal
workers However; this decree has not been issued yet, leaving the Lebanese people working
in municipalities outside the circle of submission.
But now the government should as soon as possible issue the decree which requires
subjecting municipal workers to the provisions of the Social Security Law for the following
reasons:
The rate of contributions and earnings, which will be taken as the basis for calculating
these contributions specified in paragraph 4 of Article 68: ―Subscriptions for Lebanese
municipal workers calculated on the basis of earnings texted in the preceding paragraphs
The contributions are easily collected by municipalities or by the Ministry of Internal
Affairs. Paragraph IV of Article 68 provides as follows: " ... and if the contributions of the
municipalities are not paid, they are taken from the Independent Municipal Fund,
C. Data analysis about NSSF’s beneficiary health care satisfaction
i. Population and Sample Selection:
The population of the study was selected at random from Lebanese people in the society
whom they are subjected to the National Social Security Fund without a previous
knowledge about their demographic indicators or social level they refer. Respondents had to
be affective members whom are financially responsible about the health expenditures.
1. Instrumentation:
The instrument of the study is a questionnaire made up of twelve questions to be filled on
the preference of respondent, it is arranged to collect Data that helped the study to make
findings that will be included in this thesis.
The questionnaire is divided into three sections:
9. Introduction:
In its first part, the questionnaire informed respondents about its purpose which was to
investigate the issue of the importance and the impact of the NSSF’s proposal on the
Lebanese health system on both levels of expense and quality
It also assured that the participation in this questionnaire was voluntary and the collected
information will only be used for educational purposes.
10. Identification Variables:
In this part, the questionnaire asked about the respondents’ general information including
gender, age, and status, number of dependents, employment, education and monthly income.
There is a Q‖0‖ of the study which determined whether the respondents feel financially
and qualitatively satisfied with the NSSF’s services.
11. Dependent Variables:
In this section, there were five questions about the NSSF’s services and the impact of the
new proposal on the health sector.

2. Questionnaire construction & Conceptual Framework for Data Analysis:
Based on the review of literature and previous studies and Data stated in the chapters
above, this questionnaire was developed on variables determine the ability of applying the
new NSSF’s proposal and its role in developing the Lebanese health sector even if it will be
a tiny push forward.
1. As for Q "0", Frequency was enough to examine if results are valid or not and to show
really the percentage of the Lebanese that believe that the new proposal can be a step for
better health security in Lebanon.
2. As for dependent variables, frequency tables and pie graphs were used to obtain valid
results built strong base for a clear vision about the population this thesis is studying and
addressed to as well.
3. Results:
Frequency tables proved successfully that less than half of number of questionnaire were
valid, and that answers showed regarding respondents a well knowledge and concern of the
health and medical situation in Lebanon due to the sufferings they face..
a. Q "0" :
Do you feel that you are financially and qualitatively insured within the NSSF’s services?
Table (36): frequency results of Q‖0‖ of the questionnaire
Frequenc
y
Percen
t
Valid
Percent
Cumulative
Percent
Val
id
Yes 236 47.2 47 47
No 178 35.6 36 83
Not too
much 86 17.2 17 100

f. Results of dependent variables:
In this thesis, results of five statements out of twelve will be shown in pie graphs, these
statements were chosen for being more important in serving the purpose of the study.
Knowing that 236 respondents answered yes on Q "; Source: data analysis of 236
questionnaires filled with data from 236 Lebanese 2013.
Figure (48): pie chart frequency result of the questionnaire
yes
63%
no
37%
Do you feel that the coverage of the NSSF is fair within
the economic situation?
yes
56% no
24%
sometimes
20%
Do you face any problem while receiving any
service as a beneficiary of the NSSF?

d. Our assessment:
74%
15%
9% 2%
Do you expect a progress in the services of the NSSF in
the field of expanding the application to cover more
categories?
Yes No Maybe Not interested
59% 16%
18%
7%
Do you think that this expansion will affect the
rate of contributions?
Yes No Maybe Not interested
64%
36%
Do you feel that the NSSF coverage is enough and you
are not obliged to have a complementary insurance?
Yes No

In our 500 interviews, the questionnaire examined how the Lebanese people suffer in
benefiting from the health care that it had to be a right for them. We can also recognize the
role of the NSSF that it plays in the Lebanese health system.
Although the results showed a weak validity where there was less that the half suffering
from the NSSF’s service. However, this questionnaire can be studied neglecting 86
respondents with the answer ―Not too much‖ which reflects the weak knowledge of the
Lebanese people with the services that are from their rights and paying for. So, and starting
with 414 respondents, we can notice that 57% are satisfied with the NSSF’s service.
From the above start, our recognitions continue to find that the beneficiaries are not
complaining about the rate of contributions, however they fear from the rise of this rate as
the new proposal of expansion is applied.
Also there is a high percentage of those who believe that the application of the NSSF’s
proposal can be a positive turn-over for the health system where most of them feel satisfied
with the services provides even though the dental care and pension and social protection are
not involved yet.
The questionnaire results push us to analyze the ability of the National Social Security
Fund to apply this proposal within the financial deficit in its balance.
Chapter III: The financial situation of the NSSF
A. Funding National Social Security Fund currently in Lebanon
Whatever the projects vary, they all need funding to grow and continue since finance is
the backbone of any project. Funding is to provide the cash necessary for the development
of the project, whether it is private or public.
Supplying the Institutions with the necessary funds for their establishment or expansion is
one of the most complex problems that may be encountered, how are the social security
systems funded?
What are the methods of funding the social security adopted in various countries around
the world? Which method is the best and what are the advantages and disadvantages of each
method? Is it possible to combine these methods? What is the method adopted in Lebanon?
There are two methods adopted by countries around the world to finance the social
security systems: funding by professional subscriptions and financing by public taxes.
1. Finance by professional Subscriptions
Subscriptions constitute the main source of financing many systems, including the
systems of the Lebanese and French, where the social security system is funded through the
subscriptions of employers and employees or through subscriptions of the guarantees when
they belong to the categories of non-wage earners; also the government contributes by a
portion of these subscriptions, especially when it comes to the categories of non-wage-
earners, who are unable to pay their subscriptions.
The advantage of funding by professional Subscriptions:
g. Subscriptions entitle the one who pay to participate in the Social Security Administration:
The payment of the employer and employees of the subscriptions gives them the right to
participate in the management of social security and decision-making relating to the conduct
of this system. It also gives them the right to view the methods of investing the funds of the
system.71
The best confirmation that the administrative organization of the National Social
Security Fund in Lebanon, is that the Board of Directors of the National Social Security
Fund consist of 26 delegates, including ten delegates representing employers and ten
delegates representing employees which represent a proportion of three-quarters of the
members of the Council.
h. Subscriptions are a reflection of the principle of solidarity: the payment by employers of
their share of the subscriptions is a reflection of the principle of social solidarity on which it
is the Social Security. Also this principle is shown clearly through family allowances branch
where subscriptions are paid for employees, whether they are married or single men.
71
M.R. Jambu Merlin, cours de sécurité sociale, Paris ,les cours de droit 1968-1969 P 112
i. Subscriptions release the employer from liability: the subscriptions paid by employers
liberate them from liability in respect of certain risks.72
The disadvantages of the method of financing by professional Subscriptions are:
a. The difficulty of determining earnings subject to the subscriptions and the resort of some to
evade the payment of subscriptions owed to them by the avoidance of the announcement of
the numbers of employees or the full wage.
b. Payment based on a percentage of profits does not take into account some of the institutions
because this way this account does not fully take into account the profits of these
institutions. This burden maybe more visible as far as labor is used, which makes some
institutions considering the adoption of the reduction in the number of employees.73
2. Financing by tax
Taxes are the most important source of financing security systems in many countries,
particularly in New Zealand and some Scandinavian countries. Instead of a system based in
its funding on professional subscriptions and dedicated primarily to protect the working
class, it can be adopted the financing of social security by the tax where the State allocate in
its public budget the amounts needed for the social security to provide the benefits to the
beneficiaries, or it imposes a special tax collected for Social Security.74
The advantage of the method of financing by tax is simply the collection, which is at the
same time taxes are collected.75
The funding by taxes leads to a fair distribution of the
burden of Social Security.
The main disadvantages of the method of financing by tax is not the possibility of
evasion of paying these taxes, nor do they provide a link between the stakeholders whom
employers and employees and the social security because they do not pay subscriptions, and
thus do not provide a direct sacrifice of the social security.
3. Finance by a dual system
72
20ص – 1991 –بزوث – 3ج –جتاػ انهبا انستفذو ي انضا اإل –د. اج شىفا 73
Durand Paul – la politique contemporaine de sécurité sociale – Dalloz – 1953 – P 331 74
26ص – 1991 –بزوث – 3ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا 75
M.R. Jambu Merlin, cours de sécurité sociale, Paris ,les cours de droit 1968-1969 P 114
According to the traditional model of financing, the distribution of financial
responsibilities relate to the development of branches, where there are equality in the
contribution between workers and employers in the framework of social insurance. With the
modern theory of social security, and expanding the field of protection that started in the
social insurance to reach Social Security, methods of funding has developed, and the
traditional balance of the distribution of burdens had been developed too.76
Has also stated in paragraph 1 of Article 71 of Convention No. 102 Date June 4, 1952
issued by the International Labor Conference, concerning Minimum Standards of Social
Security stated as follows: "financing the costs of benefits provided pursuant to this
Agreement and the costs of management, total funding, from insurance subscriptions or
taxes, or both, in a manner ensuring the absence of heavy burdens on people with small
incomes, and takes into account the economic situation of the Member State and the
categories of protected persons. "
On the Arab level, the Arab document about Social Security issued in 2003 in Article VII
recommended as follows: "The fund of Social Security is through: Subscriptions that are
identified by the system in each country and the amounts allocated by the State in the public
budget for social security as permanent resources and invest the proceeds of social security
fund and reserves and property and other income that accrue to the Social Security Fund.‖77
Currently, we find that many countries that rely in financing social security system
through subscriptions have started to resort to the adoption of double-funding through taxes
and contributions.
Germany, for example, that rely on the system of financing social security through
subscriptions and taxes began to seek to reduce the share of subscriptions from the cost of
public funding, may now have reached to 66% (was 72% in 1990), where Government of
Angela Merkel raised the proportion of value added tax from 16 % to 19% in the January 1,
2007 to finance part of the cost of Social Security.
76
627ص –يذكىر سابقا –انضا اإلجتاػ ف انتشزغ وانفق واالجتهاد –د.ػايز ػبذ انهك 77
5ص –2005 –انتظى انان نهضا اإلجتاػ ف نبا واقؼا وتصىراث –دراست –د. ػايز ػبذ انهك

4. Funding of the Lebanese social security system
Lebanese social security system mainly funded by subscriptions of people subject to this
system, the employers and employees, and the owners themselves, for non-wage earners
category, however the state contributes a portion of this funding.
It is noted that the bulk of subscriptions borne by employers, where employees
contribute only by very low portion (2% vs. 21.5% borne by the employers).
With regard to the majority of employees, the subscriptions are calculated based on a
percentage of the total wages they are paid, not to exceed a certain level of wages (max).
Also the earning subject to the subscriptions should not be below the minimum wage.78
Article 64 of the Social Security Law in its first paragraph stated as follows: "Every
branch of social security announced in Article 7 of this law, enjoy financial independence,
and act with its own resources to cover its performance." So as to determine the rate of
subscriptions for each branch separately, and every branch that provide the balance between
expenditure and revenues.
Article 71 of the Social Security Law stated the following: "the subscription rates are
identified by decree of the Council of Ministers upon the proposal of the Minister of Labor
and Social Affairs and end of the Board of Directors, which are set as a percentage of
earnings subjected to the discounts, so as to enable its revenues to cover benefits and
expenses of administration and composition of the permanent capital of the reserve stated in
Article 66 of this Law. " these subscription rates were adjusted, and are currently distributed
as follows:
a. Branch of retirement compensation: Select the subscription rate of for this section eight and
a half percent (8.5%) of earnings subject to subscription under Article I of Decree No. 2951
Date of 20/10/1965, with no limit to this gain, and it is still in force until now, and this rate
is distributed as follows: eight percent (8%) for the employees guaranteed and half percent
78
31ص – 1991 –بزوث – 3ج –انستفذو ي انضا اإلجتاػ انهبا –شىفا د. اج
(0.5%) to cover administrative costs and burden; and eight percent (8%) of earnings subject
to subscriptions under Article II of the same decree for craft institutions (one of its
conditions that the capital does not exceed twenty thousand LBP.); added to that the
settlement amounts paid by the employer upon the liquidation of the employees
compensation as announced in paragraph 4 of Article 54 of the Social Security law.
b. Branch of family allowances: the subscription rate for this branch has been adjusted and is
currently identified for the non-craft institutions by six percent (6%) of subject earnings
starting in 04.01.2001 under Article II of the 5102 Decree No. 24 / 3 / 2001. As for craft
institutions it have been identified ten percent (10%) of the official minimum wage for the
employee and three percent (3%) of the official minimum wage for trainee starting in
1/3/1992 under Decree No. 2181 Date 29 / 1 / 1992.
c. Branch of sickness and maternity: the subscriptions rate of this branch has been adjusted
and is currently identified for the non-craft institutions by nine percent (9%) of subject
earnings starting in 01.04.2001 under Article II of the 5101 Decree No. 24 / 3 / 2001. As for
craft institutions it has been identified by seven percent (7%) of the official minimum wage
starting in 1/7/1993 under Decree No. 3684 date 22/6/1993
d. Branch of emergency of work and occupational diseases: the rate of subscription of this
branch is not yet identified, because it has not been realized so far.
As for the earning subject to the subscriptions it was defined in paragraph 1 of Article 68
of the Social Security Law, as follows: "The earnings taken for subscription include a total
income from work, including all components and accessories, especially the overtime paid,
and the amounts paid to third parties are usually from people (gratuities), as well as benefits
provided to the worker.79
One can say that all compensation, bonuses and grants given to the employee because of
his membership of the institution or the project is one of the complements of payment unless
officially excluded by a paragraph, whether the professional expenses, or malfunction or
damage. The complementary Elements of the wage are as follows:
79
641ص –يذكىر سابقا –انضا اإلجتاػ ف انتشزغ وانفق واالجتهاد –د. ػايز ػبذ انهك
a. Grants and awards: They are paid extra when they have a relationship with the organization
and conditions of employment and as overtime, granting holidays, end of the year award,
grant budgets, grants production and other. In order to regard the bonus as part of the wage,
it shall meet the elements of the public, and remain permanent and stable.80
b. Overtime Compensation: You must be characterized by the nature of continuity and
stability, and to be paid for periods of special work outside working hours applicable in the
organization.81
c. Compensation of transportation and representation: all the expenses the employee incurred
because of his work are not part of his wages.82
d. Housing allowance: it has been identified in paragraph 2 of Article II as follows: "the
estimated value of the benefit in kind for accommodation per month is 20% of the official
minimum wage if the house is within the scope of the work place.83
If the house is owned by
employer and outside the scope of the work place, the estimated value of benefits in kind is
identified according to the rental value specified by the Ministry of Finance. The amount of
housing allowance cash is one of the appendages of the pay and included in the
subscriptions‖.
e. Food and clothing: paragraph 1 of Article II of the assessment system stated as follows: ―the
subscriptions include the excess of the limit value of the food subsidy specified in the law
No. 137 of 28/10/1999 which is five thousand LBP. per employee and per working day
actually in the form of a meal. Also it includes the excess of the annual value of the clothing
specified in the law No. 137. "
f. Compensation and grant of a personal and social nature: the subscriptions include the excess
of the legal family allowances paid by the Fund. The granting of marriage, birth, death and
school grants are not included in the calculation of earnings subject to subscriptions.84
With regard to the maximum earning subject to subscriptions, it was specified in the
Social Security Law in paragraph 2 of Article 68; by one million five hundred thousand
LBP for both sickness and maternity branch and that of family allowances.
80
245ص – 1ج –انىسظ ف قاى انؼم –انشخب – 8/7/1997تارخ 273و.ع.ث. رقى 81
21ص – 1971 –يجىػت أبى اضز وبشز – 4/2/1971تارخ 165رقى –و.ع.ث. بزوث 82
19ص 1971يجىػت أبى اضز وبشز – 12/2/71تارخ 188-181،ورقى 20/1/1968و.ع.ث. تارخ 83
Encyclopedie Dalloz – Soc. salaire n 95 84
644ص –يذكىر سابقا –انتشزغ وانفق واالجتهاد انضا اإلجتاػ ف –د. ػايز ػبذ انهك

For the amounts approved for the subscriptions of some categories of non-wage earners
are defined as follows: 200% of the official minimum wage as stated in 01/07/93 Decree
No. 3683 date 22.06.1993 and with respect to the sellers of newspapers, magazines, and
drivers non-owners of public vehicles; and by 200% of the official minimum wage for both
sickness and maternity branch and that of family allowances.
As for the distribution of subscriptions in funding branches are defined as follows:
a. Branch of retirement compensation: employer and employees of non-wage earners category
bear Subscriptions belonging to this section.
b. Branch of family allowances: the employer bears the subscriptions of his employees for this
branch. Also the sellers of newspapers, magazines, and drivers non-owners of public
vehicles pay subscriptions to this section. The drivers’ owners of public vehicles pay 5.5%
of the official minimum wage and the state treasury bears the amount remaining.
c. Branch of sickness and maternity: for employees in the non-craft institutions, the
proportions of subscriptions belonging to this section are distributed as follows: 7%
employer and 2% on the employee; and for employees in the craft institutions as follows:
5% employer and 2% on employee guaranteed. Also the sellers of newspapers, magazines,
and drivers non-owners of public vehicles pay subscriptions to this branch. The drivers’
owners of public vehicles pay 5.5% of the official minimum wage and the state treasury
bears the amount remaining.
There are also some groups that are not subject only to the branch of sickness and
maternity; like town mayors where their rate of subscription to fund this branch has been
identified by 9% of twice the minimum wage, distributed as follows: 1/5 borne by mayor
and 4/5 on the responsibility of the State Treasury in accordance to The provisions of
paragraph 2 of Article I of the Law No. 225 dated 29/5/2000. As well as the where their
rate of subscriptions to fund this section have been identified by 9% on the basis of defined
monthly earning sum of one million one hundred thousand LBP., under the provisions of
Article II of the Decree No. 12374 Date of April 30, 2004. As well as for university students
whom their rate of their contributions to the branch have been identified by 30% of the
official minimum wage, per year, for the student and for each beneficiary with him
(husband, children).
With regard to the subscriptions of the State in funding the social security, there are
many reasons that brought the state to contribute to this most notably: the inadequacy of
resources provided by subscriptions, the inability of some economically vulnerable to pay
full subscriptions, achieving greater solidarity among all segments of society.
The most prominent forms of the state's subscription in financing the security is its
contribution by 25% of the value of benefits relating to branch of sickness and maternity as
announced in paragraph 2 of Article 73 of the Social Security law. The state also bears the
proportion of the subscriptions of town mayors and drivers who own public vehicles as
mentioned above.
In addition, the state gave the National Social Security Fund some privileges, even if it is
not sufficient: it relieved the Fund to pay all taxes and fees, including stamp fees and legal
fees, real estate and taxes due on real estate that can be owned by the Fund, in addition to
the mailing exemptions and the possibility of exemption from customs fees when importing
pharmaceuticals and machinery protease according to the text of Article 67 of the Social
Security law. The state can also, in accordance to the provisions of paragraphs 3 and 4 of
Article 66 of the Social Security law to provide money on account to the Fund in the case of
loss of balance in its budget or to grant him exceptional assistance in the case of a national
disaster.
The social security fund include also the value of delays increases, half per thousand for
each day of delay in accordance to the provisions of paragraph 1 of Article 79 of the Social
Security Law, and the value of the fines stated in Articles 75 and 80 and 81 of the same law.
Finally, it can be regarded that the revenues invested of the Fund are important source of
funding, especially with a surplus of funds in the retirement fund, the social security law has
established for this purpose, a financial committee tasked to invest the fund and identify its
powers and functions in paragraph 2 of Article 64. Also the same law gave the social

security fund the right to build and fund the establishment and investment institutions,
clinics and medical or pharmacy and that in paragraphs 1 and 2 of Article 22.
B. Financial situation:
The National Social Security Fund is a safety net for many Lebanese as the only sector
that give social and human services through the implementation of the policy of the
Lebanese state in the context of the social field. For that we must maintain the integrity of
its financial position in light of the current trend to expand the field of application of social
security coverage through the new categories of the Lebanese, and secure additional
benefits. What is the financial situation of the Fund now?
The figures we will focus on in this chapter refer to the Fund's results in fiscal years 2000
through 2009, the numbers that we could get them from the accounting department in the
National Social Security Fund.
1. The current financial situation of the National Social Security Fund:
The financial results until the end of the year 2009 and projected for future years for the
status of the National Fund for Social Security in the three branches and their submissions
(sickness and maternity insurance, family allowances, and compensation for the end of the
service), worth an analysis from the economical, social and Financial points since it is an
indicator for many primary issues and one of the basics of living burdens of interest to more
than 500 thousand guaranteed benefit on their responsibility more than one million and 200
thousand Lebanese citizen.85
In the fiscal subject, the permanent deficits in both the health insurance and family
allowances need a radical and rapid solution on the levels of administrative, political and
living conditions, especially as the size of the accumulated deficit of the branch of health
85
ػذا انحاج –انصفحت اإلقتصادت – 4/10/2010ػذد –صحفت انسفز
insurance exceeded 316 billion pounds until the end of 2009 despite the savings achieved by
the branch at the end of the latter year the by the State's contributions which exceeded the
210 billion pounds of which about 191 billion pounds of the branch above, in addition to
raising the minimum wage 200,000, which contributed in the increase in subscriptions.
But more important is that the money taken to cover the deficit is from the branch of old
age which represent the compensations of the beneficiaries, and this is contrary to law,
because of the independence of the financial and administrative branches. With this in mind
that the revenues of health insurance during the year 2009 amounted to 627.9 billion
pounds, up about 44.42 percent, however, the balance is still missing on the short and
medium term if the issue of contributions and of tax and installment accumulated debt by
the public and private sectors is not solved.
So is the branch of family allowances, which its accumulated deficits reached about 307
billion pounds, making the total deficit in the branch of the service end about 623 billion
pounds. 86
The most serious of all, the Social Security Law imposes composition of reservations and
savings for these two branches, according to the provisions of Article 66 of the Social
Security Law, that the reserve constitute the sixth with regard to sickness and maternity fund
and family allowances; also the same article in the second paragraph announced that if
capital reserve didn’t reach the minimum previously mentioned at the end of fiscal year
certain, the government on the proposal of the Minister of Labor and an end to the
Governing Council may decide to raise the contribution rate starting in July of the year
following the fiscal year that are complaining about the deficit, so that the subscriptions
become sufficient to restore financial balance and achieve the minimum capital reserve
required in the period of three years at most, i.e., that this paragraph has given six months to
increase the contribution rate which is not received after almost 10 years, what constitutes a
contravention of the provisions of the Social Security Law. This requires further treatment at
the legal level, either to amend the law, or to reconsider immediately in the rates of
contribution.
86
ػذا انحاج –انصفحت اإلقتصادت – 4/10/2010ػذد –صحفت انسفز
The most important point in all of these things is that financial outlooks that show the
results refer to something like a lack of growth in the people associated to insurance, where
it was expected that the employees working in institutions to increase until 2011 by about
1.5 percent, and this means that the association to the Fund is still in its weakest level, an
indicator of more high unemployment on the one hand, the high frequency of workers'
silence on the other hand. This is with reference to the fact that Lebanon needs to create
between 25 to 30 thousand jobs per year, while what the Social Security Fund estimated in
regard with the new members associated does not exceed 5400 guaranteed.87
Searching in the same subject, the end of service branch can be considered as a full
branch since it is based at a rate of 8.5% on the whole wage in its subscriptions, and that its
submissions are limited in cases of resignation or liquidation, making its contributions larger
than its provisions, in particular that the amount of the settlement between the contributions
paid from the employers for employees and the compensation the employee bears. noting
that during the years of inflation and the deterioration of the LBP. and the melting of the
value of compensation of employees after their wages, the percentage of the settlement
amounts reached more than 60 percent of the value of compensation, which made employers
before workers seek to apply the system of old age, retirement and social protection, rather
than the branch end of the service so as to avoid of the value of the settlement amounts
equal to multiple of times the value of compensation and assets of the end of service branch.
88
The most important point is that the assets of the branch of end of the service at the end
of 2009 and the beginning of 2010 was more than 6400 billion LBP., and that the bulk of
this money goes back to the investment of the money of the Branch in Treasury bonds since
the eighties. The end of service branch has achieved a surplus in 2009 reached about 884
billion pounds, with revenue of about 1137.3 billion pounds, an increase of 49.9 per cent,
while the value of submissions reached about 424.9 billion, meaning that the savings
achieved equivalent to twice the benefits and compensation paid by the Fund, this without
87
ػذا انحاج –انصفحت اإلقتصادت – 4/10/2010ػذد –صحفت انسفز 88
ػذا انحاج –انصفحت اإلقتصادت – 4/10/2010ػذد –صحفت انسفز
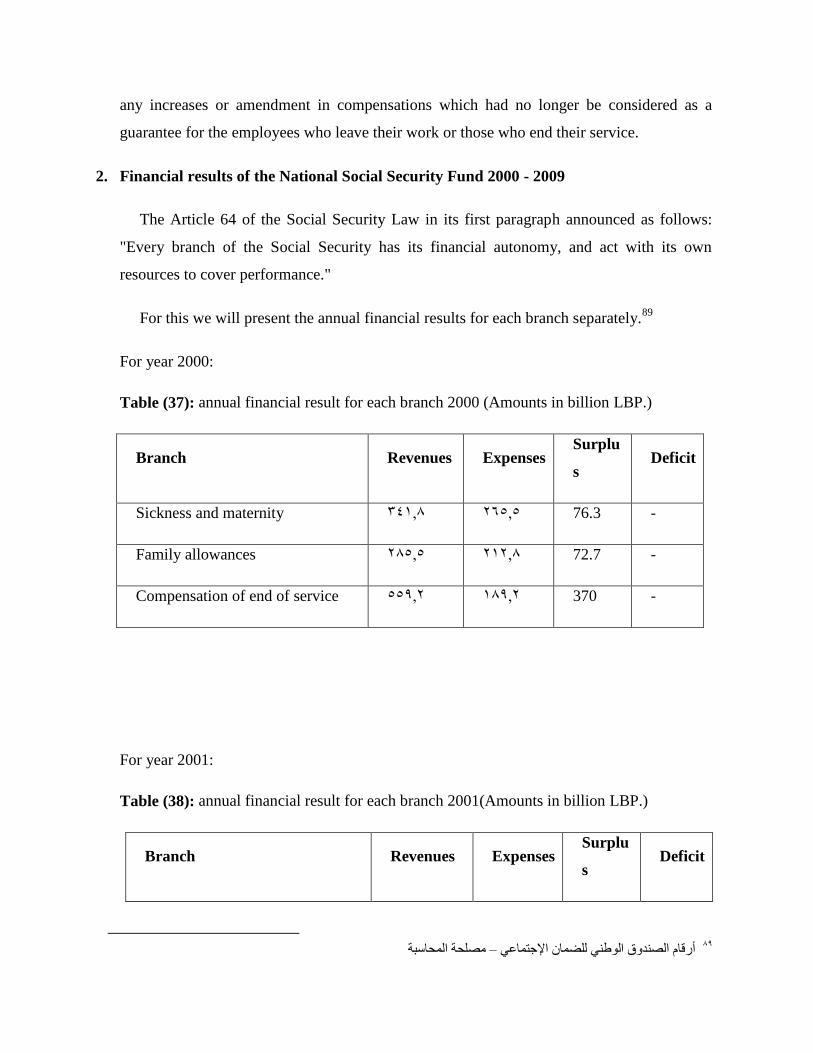
any increases or amendment in compensations which had no longer be considered as a
guarantee for the employees who leave their work or those who end their service.
2. Financial results of the National Social Security Fund 2000 - 2009
The Article 64 of the Social Security Law in its first paragraph announced as follows:
"Every branch of the Social Security has its financial autonomy, and act with its own
resources to cover performance."
For this we will present the annual financial results for each branch separately.89
For year 2000:
Table (37): annual financial result for each branch 2000 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
- 76.3 26565 34168 Sickness and maternity
- 72.7 21268 28565 Family allowances
- 370 18962 55962 Compensation of end of service
For year 2001:
Table (38): annual financial result for each branch 2001(Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
89
يصهحت انحاسبت –أرقاو انصذوق انىط نهضا اإلجتاػ
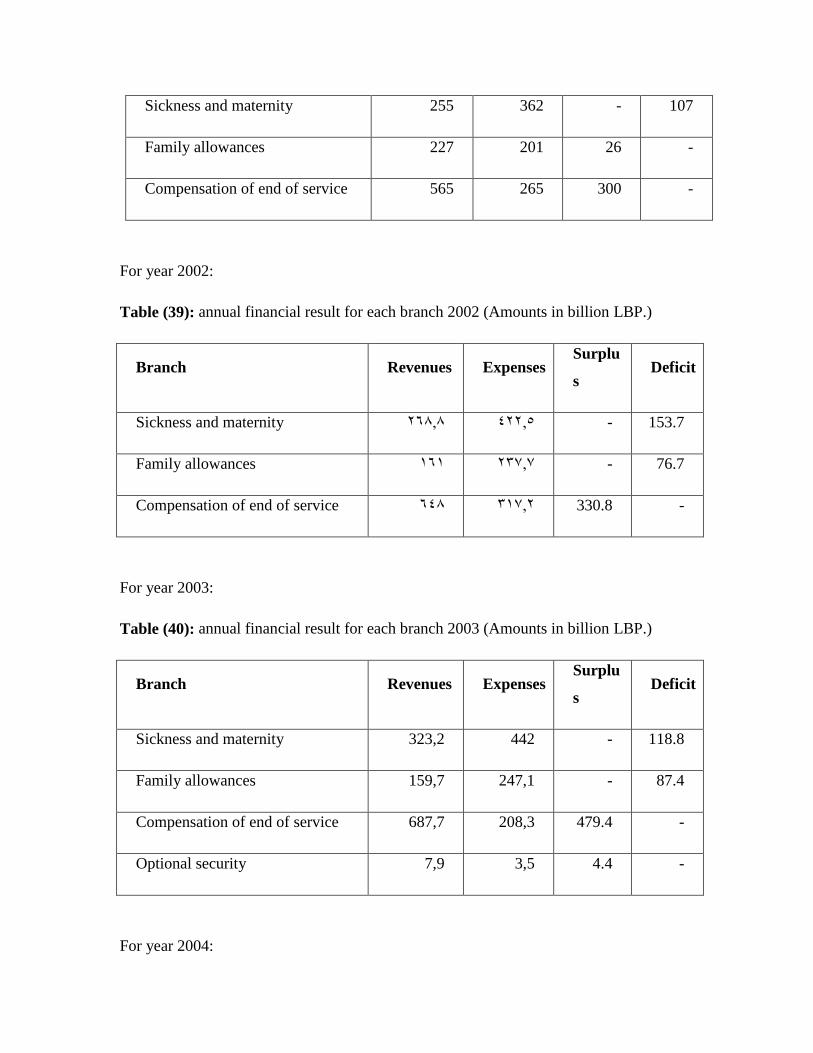
107 - 362 255 Sickness and maternity
- 26 201 227 Family allowances
- 300 265 565 Compensation of end of service
For year 2002:
Table (39): annual financial result for each branch 2002 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
153.7 - 42265 26868 Sickness and maternity
76.7 - 23767 161 Family allowances
- 330.8 31762 648 Compensation of end of service
For year 2003:
Table (40): annual financial result for each branch 2003 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
118.8 - 442 323,2 Sickness and maternity
87.4 - 247,1 159,7 Family allowances
- 479.4 208,3 687,7 Compensation of end of service
- 4.4 3,5 7,9 Optional security
For year 2004:
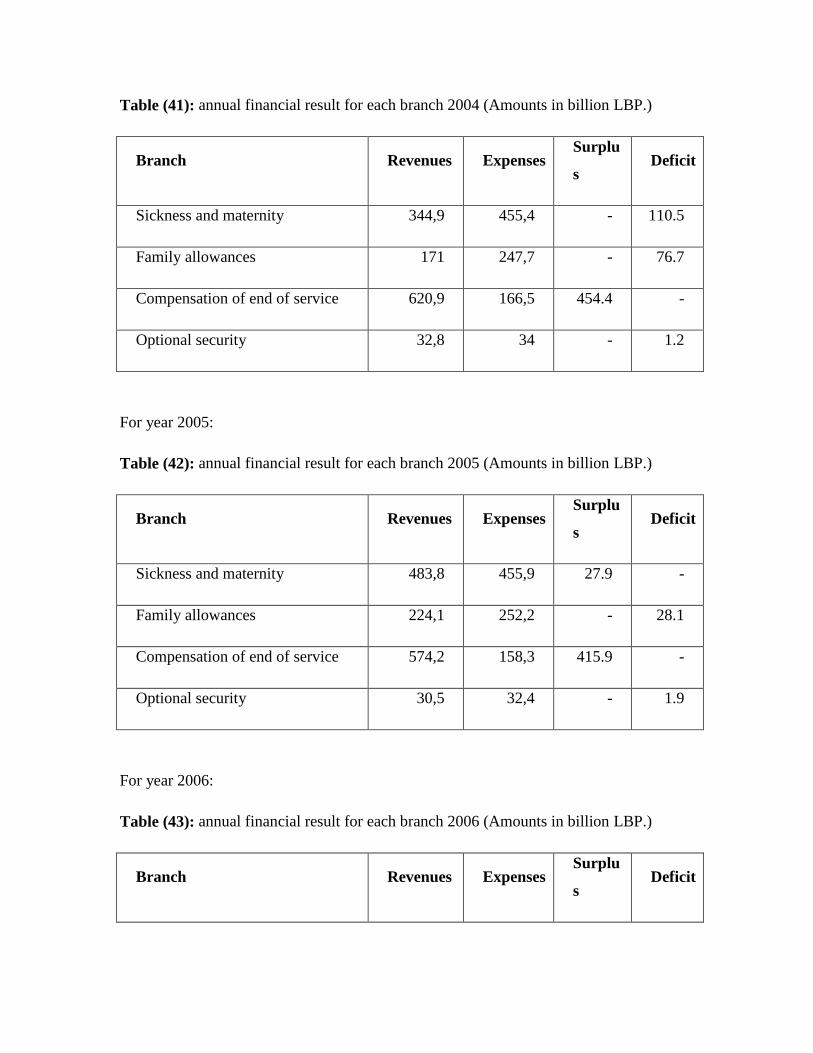
Table (41): annual financial result for each branch 2004 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
110.5 - 455,4 344,9 Sickness and maternity
76.7 - 247,7 171 Family allowances
- 454.4 166,5 620,9 Compensation of end of service
1.2 - 34 32,8 Optional security
For year 2005:
Table (42): annual financial result for each branch 2005 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
- 27.9 455,9 483,8 Sickness and maternity
28.1 - 252,2 224,1 Family allowances
- 415.9 158,3 574,2 Compensation of end of service
1.9 - 32,4 30,5 Optional security
For year 2006:
Table (43): annual financial result for each branch 2006 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
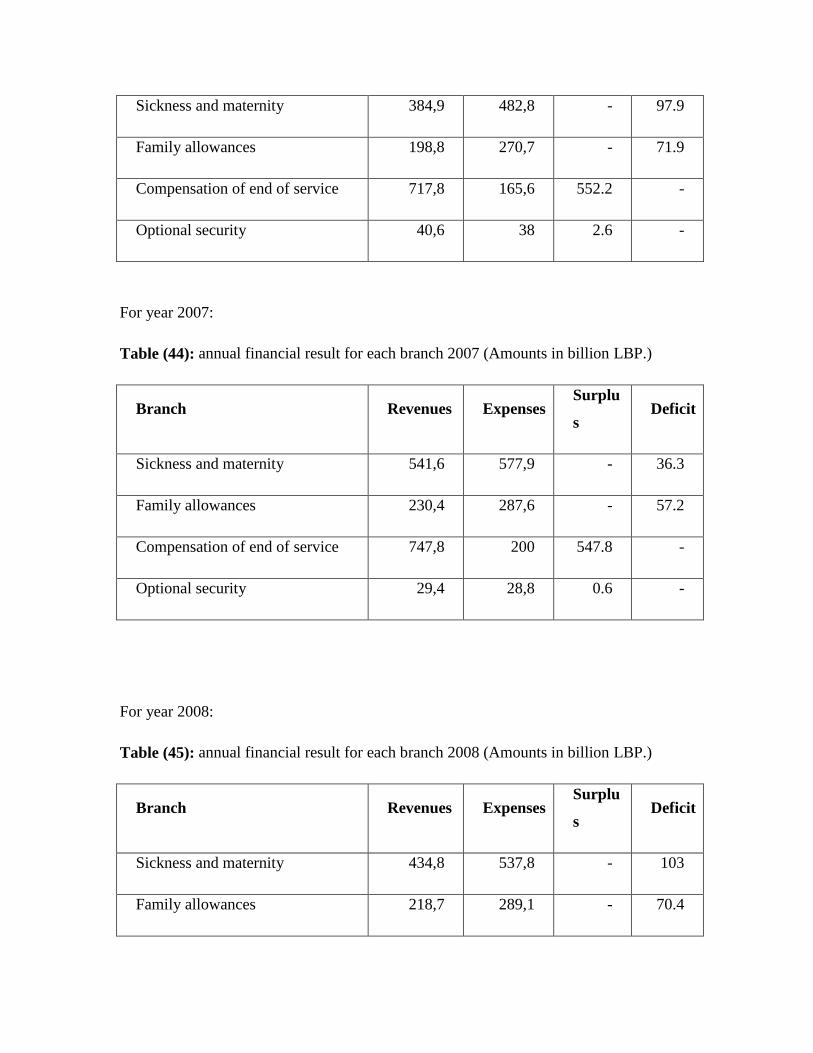
97.9 - 482,8 384,9 Sickness and maternity
71.9 - 270,7 198,8 Family allowances
- 552.2 165,6 717,8 Compensation of end of service
- 2.6 38 40,6 Optional security
For year 2007:
Table (44): annual financial result for each branch 2007 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
36.3 - 577,9 541,6 Sickness and maternity
57.2 - 287,6 230,4 Family allowances
- 547.8 200 747,8 Compensation of end of service
- 0.6 28,8 29,4 Optional security
For year 2008:
Table (45): annual financial result for each branch 2008 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
103 - 537,8 434,8 Sickness and maternity
70.4 - 289,1 218,7 Family allowances
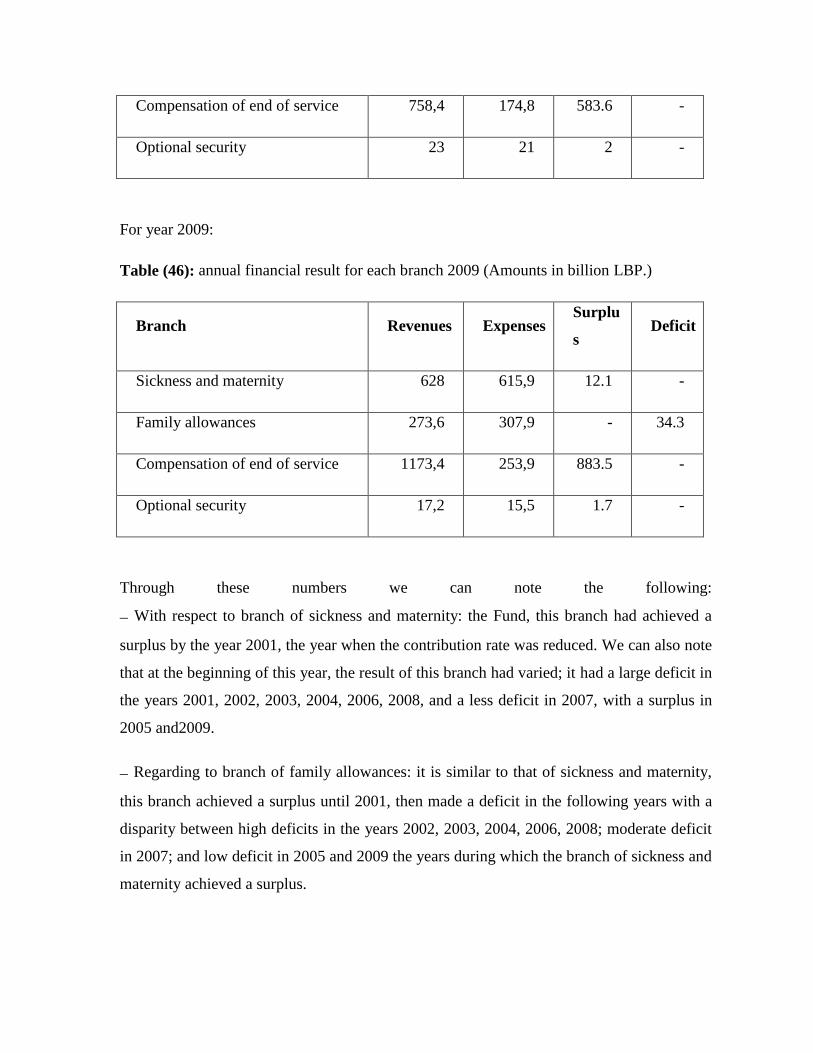
- 583.6 174,8 758,4 Compensation of end of service
- 2 21 23 Optional security
For year 2009:
Table (46): annual financial result for each branch 2009 (Amounts in billion LBP.)
Deficit Surplu
s Expenses Revenues Branch
- 12.1 615,9 628 Sickness and maternity
34.3 - 307,9 273,6 Family allowances
- 883.5 253,9 1173,4 Compensation of end of service
- 1.7 15,5 17,2 Optional security
Through these numbers we can note the following:
With respect to branch of sickness and maternity: the Fund, this branch had achieved a
surplus by the year 2001, the year when the contribution rate was reduced. We can also note
that at the beginning of this year, the result of this branch had varied; it had a large deficit in
the years 2001, 2002, 2003, 2004, 2006, 2008, and a less deficit in 2007, with a surplus in
2005 and2009.
Regarding to branch of family allowances: it is similar to that of sickness and maternity,
this branch achieved a surplus until 2001, then made a deficit in the following years with a
disparity between high deficits in the years 2002, 2003, 2004, 2006, 2008; moderate deficit
in 2007; and low deficit in 2005 and 2009 the years during which the branch of sickness and
maternity achieved a surplus.
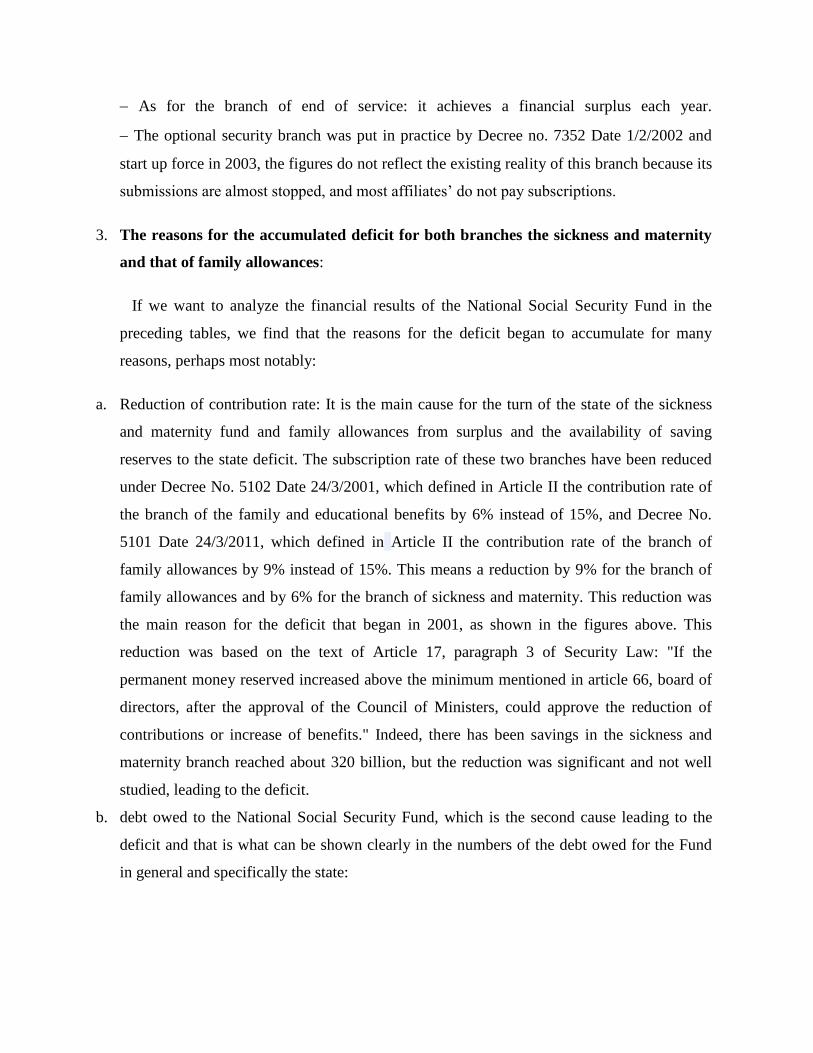
As for the branch of end of service: it achieves a financial surplus each year.
The optional security branch was put in practice by Decree no. 7352 Date 1/2/2002 and
start up force in 2003, the figures do not reflect the existing reality of this branch because its
submissions are almost stopped, and most affiliates’ do not pay subscriptions.
3. The reasons for the accumulated deficit for both branches the sickness and maternity
and that of family allowances:
If we want to analyze the financial results of the National Social Security Fund in the
preceding tables, we find that the reasons for the deficit began to accumulate for many
reasons, perhaps most notably:
a. Reduction of contribution rate: It is the main cause for the turn of the state of the sickness
and maternity fund and family allowances from surplus and the availability of saving
reserves to the state deficit. The subscription rate of these two branches have been reduced
under Decree No. 5102 Date 24/3/2001, which defined in Article II the contribution rate of
the branch of the family and educational benefits by 6% instead of 15%, and Decree No.
5101 Date 24/3/2011, which defined in Article II the contribution rate of the branch of
family allowances by 9% instead of 15%. This means a reduction by 9% for the branch of
family allowances and by 6% for the branch of sickness and maternity. This reduction was
the main reason for the deficit that began in 2001, as shown in the figures above. This
reduction was based on the text of Article 17, paragraph 3 of Security Law: "If the
permanent money reserved increased above the minimum mentioned in article 66, board of
directors, after the approval of the Council of Ministers, could approve the reduction of
contributions or increase of benefits." Indeed, there has been savings in the sickness and
maternity branch reached about 320 billion, but the reduction was significant and not well
studied, leading to the deficit.
b. debt owed to the National Social Security Fund, which is the second cause leading to the
deficit and that is what can be shown clearly in the numbers of the debt owed for the Fund
in general and specifically the state:

Table (47): Debt owed for the National Social Security Fund (Amounts in billions LBP.)90
Government Debt Total Debt Year
16361 31761 2000
24465 47364 2001
33867 613 2002
43762 74465 2003
48365 82668 2004
44069 71569 2005
47865 72462 2006
44565 63568 2007
50364 69762 2008
47769 64365 2009
Source: accounting branch in the NSSF
We can note that the debt of the state constitute more than half of the total debt owed,
and debt to be levied on the state as an employer and shareholder by 25% of the value of
sickness and maternity benefits, and as a shareholder in the contributions of the owner
drivers. If the numbers of the above debt is analyzed, we can explain the reduction in the
deficit in the years 2005, 2007 and 2009. The state's debt in 2005 decreased by 42.6 billion,
which means that the State has paid the amounts due by it for that year and paid a sum of the
accumulated debt and this situation was repeated the same in 2007, when the value of the
accumulated debt dropped by 33 billion, and in the year 2009 dropped by 25.5 billion.
90
يصهحت انحاسبت –أرقاو انصذوق انىط نهضا اإلجتاػ
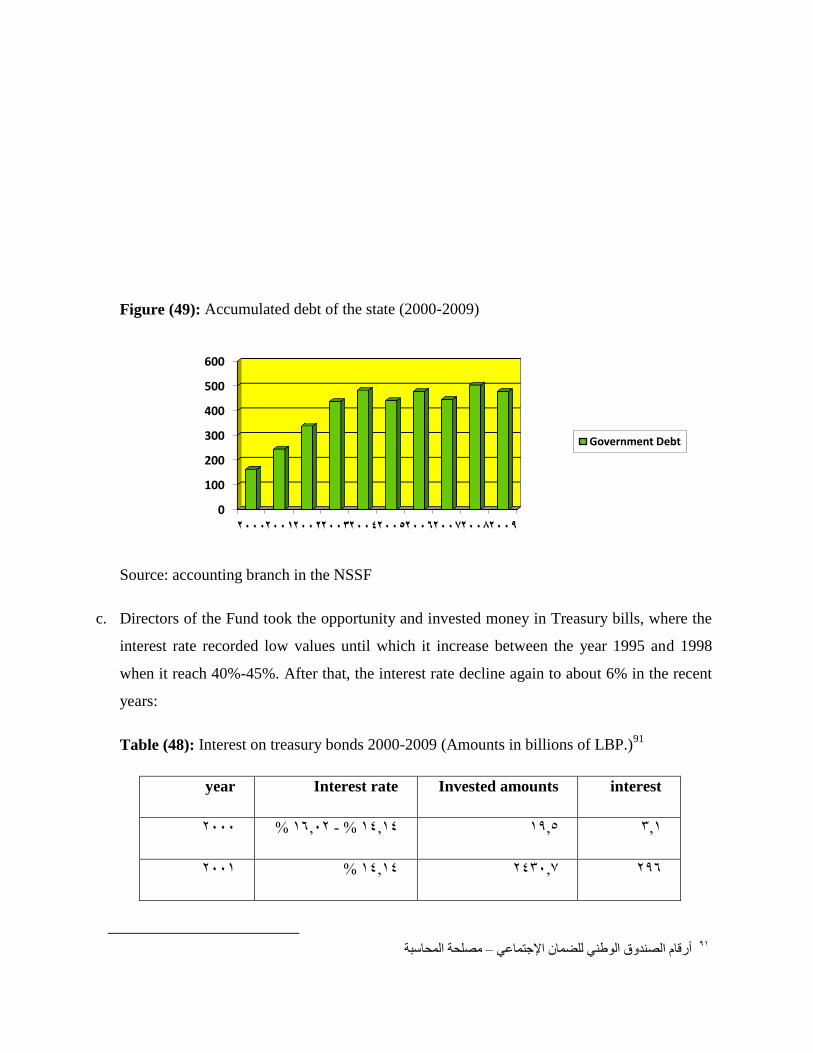
Figure (49): Accumulated debt of the state (2000-2009)
Source: accounting branch in the NSSF
c. Directors of the Fund took the opportunity and invested money in Treasury bills, where the
interest rate recorded low values until which it increase between the year 1995 and 1998
when it reach 40%-45%. After that, the interest rate decline again to about 6% in the recent
years:
Table (48): Interest on treasury bonds 2000-2009 (Amounts in billions of LBP.)91
interest Invested amounts Interest rate year
361 1965 14614 %- 16602 % 2000
296 243067 14614 % 2001
91
يصهحت انحاسبت –أرقاو انصذوق انىط نهضا اإلجتاػ
0
100
200
300
400
500
600
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Government Debt

31263 250862 10688 %- 14614 % 2002
35165 176967 6638 %- 14614 % 2003
20161 135866 5615 %- 6627 % 2004
6363 150766 6627 %- 7619 % 2005
171691 221164 7619 %- 9634 % 2006
20863 343664 7619 %- 9632 % 2007
22162 356861 865 %- 9632 % 2008
43867 4465 6620 %- 9632 % 2009
Source: accounting branch in the NSSF
d. Employers evade the payment of contributions, and authorizing their employees and real
wages.
e. Increase in the international price in medicine
f. Increase of benefits for example, Decree 8641 Date 12/9/2002, and Law No. 220 of 29 / 5 /
2000.
4. expected additional expenditure for the future
In addition to the accumulated deficit in both the sickness and maternity branch and the
family allowances, is expected that these two branches in particular and the other branches
will suffer from additional expenses , that result from the expected expansion in the field of
application and from economic and social factors :
family allowances and education branch : workers ' claims began long ago about raising
the value of family allowances , that are defined under Decree No. 1348 dated 13.06.1991
and the applicable as of 07/01/1991 75% of the official minimum wage for wife and five
children . Has been amended by Decree 5103 dated 24/3/2001 and applied on 1/4/2001,
where the maximum become 225,000 for wife and five children, who means it remained
constitute 75 % of the minimum wage of the time 300000. In the year 2008 the minimum
wage was raise to 500,000 without an increase in the value of family allowances.
Sickness and maternity branch: hospitals and doctors should be asked about a new rate
that will undoubtedly increase the expenses of this branch , in addition to the continuous rise
in the prices of medicines . This is with reference to the completion in applying the
submissions relating to health insurance owed to insured and paying the amounts owed to
hospitals will increase the value of the deficit.
Branches and new submissions that we proposed in this research: For work emergency
branch and occupational diseases branch, it would impose high expenditures on the fund in
the absence of security and the necessary equipment for prevention in the workplace in most
of the Lebanese factories. This will impose variable rates of subscriptions according to the
kinds of professional activities with of extra addition to the contributions of institutions with
equipment not in conformity. For dental care, it will increase the expenses of the sickness
and maternity branch under a large deficit where the studies indicate that the expenses of
dental care could constitute between 10 to 20% of the costs of the branch’s current
expenses. As for the pension and social security system, it is similar to the end - of - service
and indemnity and it is supposed that it is totally funded.
New categories that are proposed to be subjected : for tobacco farmers , their high number
will impose additional expenses on both sickness and maternity branch and family
allowances because their numbers are large (about 30,000 ) in addition of being of rural
place of living, where the percentage of births is high and hence beneficiaries. As well as for
municipal workers, artists and writers who represent a model from all segments of the
Lebanese society and therefore the expenses of branches that they will be subject to and so
the revenue will increase at approximately the same proportions which means increasing the
expected deficit in the two branches. Finally, the attempt to find a solution to the
accumulated deficit and the expected additional expenses has become a matter of urgency.
C. Proposals to restore fiscal balance and cover the costs of expansion
There is no doubt that the social security of Lebanon, has become in need to a modern
comprehensive reconsideration, and for that we should wary about the agreements and
recommendations of the International Labour Organization, and refer to studies and
comprehensive research , organized by international experts , and give necessary
recommendations in the matter . The difficulties facing social security systems in Lebanon
and the world, make it necessary to go to the reform , and in this regard it highlights the
special importance of the reform of financial regulation of these systems , and reconsider the
traditional means of funding.
1. Reduce expenses
National Fund for Social Security, in the context of trying to restore fiscal balance, and
achieve desired reform, Must seeks to reduce expenses , particularly in funds of the
branches that suffer from continues deficit over years, with reference to the need for
attention not to diminish the submissions ; reducing the expenses can be achieved by
reducing administrative and social expenditure :
a. reducing social expenditure:
Adoption of a family doctor as an intermediary between the patient and the specialist doctor
or the hospital ,
Find alternatives to hospitalization (One day Clinic) adopted and developed by many
countries including the United States and most European countries, where it became the
policy of credit that led to a cost reduction by about 30 %.
Activating medical and administrative control devices in hospitals in order to adjust the
hospital bill.
Activating the role of the Directorate of inspection and control, so as to adjust unrealistic
earners who benefit from the submissions with no right for them.
Create , build and invest clinics and medical and pharmaceutical institutions , according to
the provisions of paragraph 1 of Article 22 of the Social Security Law , which relieves the
medical bill ;
Import of medicines and pharmaceuticals and other medical and surgical directly from
abroad, according to the provisions of paragraph 2 of Article 22 of the Social Security Law;

and benefit from the provisions of paragraph 2 of Article 67 of the same Law which
provides exemption from customs tariffs.
Put a (Flat rate) for surgical interventions as happening in many countries.
b. reduction of administrative expenses , by: activating the role of the administrative inspection
of the Fund, as though the administrative costs of the Fund is the lowest percentage among
the all guarantors systems in Lebanon, the current administration is serious about mitigation
(incentives, monitoring productivity, ...).
2. Increase revenues
The funding of the National social Security Fund is based on the contributions of employers
and insured; the success of the process of financial reform of the social Security requires
undoubtedly the increase in the revenue, which requires the government's contribution
through taxes specialized for this funding, even if this is on more than one stage due to the
current economic situation the country passing through.
Here are some suggestions to increase the revenues of the National Social Security Fund,
taking into consideration the financial difficulties facing employers and insured and the
government:
a. Increase the contribution rate: The contribution rate reduction in 2001 was not logically or
based on studies, where the total rate of subscriptions of both the sickness and maternity and
family allowances branch has been reduced from 30% (15% sickness and maternity and
15% family allowances) to 15 % (9 % sickness and maternity and 6% family allowances),
which led to a deficit in both branches since that date. And therefore contribution rates re-
raise of the two branches mentioned, need to take into account not to overburden employers
with very high rates in order to protect national institutions and labor. Raising contribution
rates without any study would have a negative impact more than those resulted from the
reduction, which happened in 2001. the high increase in these rates will increase the
financial burden on institutions which would make it unable to face international
competition also will lead to reduction in the volume of employment to reduce their
burdens. However we can suggest to raise the rate of subscriptions of the family allowances

branch one point so that it becomes 7% instead of 6 %, and raise the rate of subscriptions of
the sickness and maternity branch three points (two points on the responsibility of
employers and point the responsibility of the procedure) so that it becomes 12 % instead of
9 %, which could contribute in funding dental care.
b. Raise the maximum value for Subscriptions: The maximum value of the earnings subject to
subscriptions identified in 2001, by 1,500,000 LP for sickness and maternity branch and
family allowances which was equivalent to five times the minimum wage (the minimum
wage was three hundred thousand pounds). In 2008, the adjustment of the minimum wage ,
which became five hundred thousand LP , without modifying the maximum earning subject
to Subscriptions which became equivalent to three times the minimum wage only. Not so
far, the minimum wages had been modified to become 675,000 LBP .this situation requires
the issuance of a decree to raise the maximum earnings subject to subscriptions to stay at the
same proportion five times the minimum wage, which provides funds to sickness and
maternity and family allowances branches. however the maximum subjected earning policy
should be canceled because its abolishment helps in achieving the redistribution of income
by Social Security, also contributes to the achievement of equality between employees ;
Under the current policy , the employee , who receive a salary of one million LBP. ,pays 2%
of his income as a subscription in sickness and maternity branch ; while the employee , who
receive a salary of three million LBP. contribute by only 1% of his earnings .
c. Activating the role of the Directorate of inspection and control, making it possible to declare
about hidden institutions and employees, and to ensure coordination between the Fund and
the Ministry of Finance monitors, including identifying real wages. also it is working on a
regular and periodic control for all institutions registered with the fund once every five years
as stipulated in item (a) of paragraph 3 of Article 11 of the system of inspection and
monitoring of employers, and to conduct the survey for the hidden institutions once every
ten years at least to declare them and settle their financial positions towards the Fund as
provided in clause (b) of paragraph 3 of Article 11 of the same system; especially since a
large proportion of hidden employees are foreigners , the fact that this category of wage
earners do not benefit from social Security benefits (except for wage earners who belong to
one of the following countries: France, Belgium, Britain , Italy) and therefore those earners

ar not interested to claim their employers about the security , while declaring those earners
provide a high earn for the fund, where subscriptions are paid without the benefit from
submissions.
d. The government and public sector organizations pay the accumulated debt, allowing the
Fund to benefit from these funds through investment.
e. Encourage private sector institutions to repay debts owed them
f. Diversify the sources of funding for social security where the government can impose taxes
and fees specialized for this aim, where to impose such taxes and duties on goods and
sectors that will increase the expenses of medical care, like the taxes levied on alcohol and
alcoholic beverages or smoke.
And as an example is the French experience, where they were supporting social security by
imposing fees on vehicle registration and insurance, and fees on alcohol and pharmaceutical
advertising.
3. Invest Social Security funds reserves
This reserve is a surplus in the money after the benefits and administrative expenses, and
whenever possible, increase the rate of the proceeds of this investment whenever possible
diminish the Subscriptions or increase benefits both quantitatively and qualitatively, in
addition to that, following an investment plan lead to control inflation factors and their
impact on the submissions and on social security funds, so as to maintain the continuity of
the real value of these funds. In Lebanon it was previously limited to investments in banks
and loans to some academic educational and humanity institutions,. Currently investments
are focused on Treasury bonds, which were achieving a high rate of revenues between 1995
and 1998, where the interest rates on Treasury bonds were between 40 and 45%, but now it
is no longer feasible dropping these benefits to between 6 and 9 % in recent years (2004
until now).

Conclusion
The health sector contributes to the development of national wealth, through the terms of
health care services and creation of employment chances. On the other hand, improvements
in income and living conditions have a positive impact on the state of health, as shown in
the case of Lebanon by the reduction in mortality, increases in life expectancy and changes
in epidemiological and demographic profiles. Economic growth also allows for the
development of the health infrastructure and technological innovation.
Unsatisfactory health conditions add to the cost of development through unhealthy
lifestyles, and losses due to morbidity, mortality and disability; and through the burden of
disease and high cost of treatment and hospitalization.
The health-care system displays a number of weaknesses that affect adversely the overall
process of sustainable human development. The public financial resources allocated to
health go mostly to cover increasing spending on reimbursement of hospital care provided
predominantly by the private sector. These have a tendency to over-prescribe expensive
medical technology and high cost drugs in a largely unregulated environment. As a result,
total health expenditures, both in absolute terms and as a percentage of GDP, have risen

sharply (the former doubling in less than three years) to levels comparable to those
prevailing in the industrialized countries, and higher than in most of the rest of the world.
The bulk of health expenditures are paid by households’ out-of pocket; thus affecting
disproportionately the less affluent and the poorer segments of the population.
Little resources are available to primary health care including preventive care. National
health policy is based on health being the right of every citizen. Health policy also
emphasizes increasingly that prevention should take precedence over cure within the context
of primary health and through providing a degree of autonomy to regional and sub-regional
units. The policy also stresses pooling of publicly financed resources to achieve maximum
coordination, effectiveness and efficiency, while at the same time promoting partnership
with the private sector, professional associations and community representatives.
The main problem in the health sector, specifically at the household level, is access to
quality care due to lack of health insurance coverage, low income levels and rigid patterns
of household expenditures, which are devoted to essential items that cannot be reduced or
replaced. Available information indicates that spending by the poor is directed first to food
needs, then to housing, education and transport, in that order. Health care is postponed until
the need for treatment becomes acute and cannot be delayed further. This, in the end, will
raise treatment costs.
This paper addressed basic problem on which the Lebanese suffer from high cost
health insurance for low quality service. The financial analysis shows that the health care
system in Lebanon is suffering from structural problems that are directly affecting the cost
and hence the equal accessibility by all citizens to this service. Among the major
predicaments and constraints contributing to the high cost and inequity features are:
1. The inequity in accessing both protective and healing health care among the different
Lebanese regions which was clearly illustrated through the huge disparities in child and
reproductive health indicators.
2. The relatively huge amount paid as out-of-pocket reflects, to large extent, many constraints
facing the health system in Lebanon. Out-of-pocket spending on drugs is clearly
unmanageable resulting from two major facts: first, the lack of control at the drug market
level. The second fact lying behind the huge drug bill is directly related to the lack of
control on physicians and pharmacists.
3. The pluralistic nature of the health care system and the consequent incoherent and
inconsistent flow of both financial resources and regulations through the chain of players
involved in the health system.
4. The multiplicity of the system results in a redundancy in the administrative staffs
responsible for the health care system. Specifically, the problem arises in the health care
financing agencies, having a notable proportion of expenditures allocated for the
administration and staffing.
5. The health care market ceased, to large extent, to be a social basic service with every citizen
owning the right to have access to. However, it is currently driven by the forces of supply
and demand, mainly in terms of pricing the health services against the quality of services
provided. The problem is further accentuated by the relative weakness of the preventive
health care which is attributing to raising demand for health services, and hence affecting
the trend of pricing of these services.
6. The role of the government in this messy environment is not clearly identified. On the one
hand, the Ministry of Health- being the main government representative in this regard- is
tending to invest in health market by providing additional hospital beds and health centers,
meanwhile the statistics reveal that the market is almost over-saturated, except for some
specific geographic areas. On the other hand, the regulatory role of the government is still
lacking efficiency mainly as to controlling the private sector in terms of pricing of health
services and insuring equitable access to these services.
Also, an international comparison of the health expenditure push us to highlight on the
Singaporean health system which teaches us that patients must understand that health
services cost money and that they should pay a portion of those costs. It teaches us that
hospital and doctor incentives must encourage them to provide the best service at the best
price. Government can create a framework of rules that does that. And it does not have to be
a cold-hearted solution. The framework must also assure that people have the ability to pay,
and it must provide a safety net for those who cannot. Lastly, all health costs and outcomes
should be transparent to the patient and the payer.

The third part was about studying the role of the National Social Security Fund in
developing the health system by applying a proposal that aim for the expansion of its
application by including new categories. Moreover, the proposal also includes the expansion
in the services by covering new services like dental care and pension and social security.
Also it is discussed in this chapter the current financial situation of the National Social
Security Fund and the reasons for the accumulated deficit.
We have come to the following conclusions:
1. The need of social security to cover all risks and should include all the Lebanese people to
achieve equality and the principle of national solidarity and social solidarity.
2. Accelerate the application of the branches and submissions provided for in the Social
Security Law and not applicable till this date (emergency work and occupational diseases
and dental cares).
3. Adoption of the pension system and social protection which embodies the hopes of the
workers and other persons secured in achieving security for them after their retirement, and
after conducting the necessary studies to ensure its continuation.
4. Both branches sickness and maternity and family allowances suffer from accumulated
deficits since 2001, and the reasons for this inability to reduce the subscriptions rates of
branches mentioned, and not to raise the maximum of the gain subject to membership fees
and delay by the State for payment of debts owed to the National Social Security Fund.
5. The need to reduce the expenses of the Fund's administrative and social, without affecting
the submissions.
6. Increase revenues by raising subscriptions rates and raise the minimum and activating the
role of inspection and control and debt collection.
7. The need to increase the state's subscriptions, with the imposition of new taxes and fees
specialized to return the proceeds to fund the National Fund Social Security.
8. Improve the methods of the investment of fund reserve.
I hope that this thesis have successful achieved its objective through giving an overview
of the current situation of social security, methods of funding it, and proposals to restore
fiscal balance. I hoped to find more statistics on the labor market and the number of

employees and the number of public and private institutions and the average age and
average number and average family income, but there were very few statistics.
In the end, some questions that concern the Lebanese public opinions are asked:
When can the National Social Security Fund submissions include all the Lebanese?
When can the Lebanese social security cover all the risks? What is the possibility of
establishing a fund for unemployment which records high rates in Lebanon?
Generally speaking, there is a need to define roles and improve activities on the different
levels of health systems in order to prevent wasting resources, set health standards and
improve the quality of health services. Concerning health reform, the self-evident question
is: will the current health expenditure remain the same?
Recommendations
Health sector reform has been described as a sustained purposeful attempt to improve the
performance of the health sector. It is motivated by the need to address fundamental
deficiencies in health care systems. It is an inherently political process, and it is often
implemented on a sector-wide level.
Countries undertake health reforms when there is evidence of poor performance, when
public expenditure neglects the poor, when resources are scarce and demands are increasing
forcing governments to reconsider the situation, when consumers are unhappy about poor
treatment and when there are concerns about sustainability.
There is an immediate need to introduce fundamental reforms in order to establish a
sound basis for an equitable, efficient and financially sustainable health care system. These
reforms must address the points of weaknesses encountered in the health system in Lebanon
from different perspectives.
1. Recommendations regarding the Lebanese health system
a. Developing National Health Accounts: The introduction of a new national health strategy
cannot take place in the absence of relevant data for appropriate analysis and decision
making. The high complexity of the health care system in Lebanon, coupled with the lack of
reliable data on the structure and functioning of this system, has weakened the performance

of policy-makers as well as the financing agents. The introduction of national health
accounts, which quantify patterns of data on health spending by sources of revenues and
types of services purchased, would significantly contribute to improving the ability of
decision-makers to identify problems and opportunities for change, and to develop and
monitor reform strategies.
b. Regulating the private sector: The uncontrollable growth of the private sector burdens the
ministry of health and hinders the effective operation of the health care market in Lebanon.
In this regard, it is strongly recommended that the ministry of health regain its role as a
regulator of the health care market, rather than as a financing agent. There is a need to
license and monitor the health care market, regulate and control the delivery of health care
services, improve the quality of care, contain health care cost and improve the management
of the heath care sector. In addition, the ministry of health needs to get a better
understanding of the size, composition, and characteristics of the private sector, in order to
be able to contain costs, unify prices, ensure quality of care and build a public-private
partnership (Public hospital autonomy).
c. Unifying Coverage schemes and prices among different Financing agents and
providers: there is a discrepancy in the coverage schemes adopted by the different
financing agents, as well as in the prices charged by the different providers. The major
reason behind these discrepancies is the diversity of the supervisory ministries in the health
care market. It is recommended to have one health financing agent (as the National Social
Security Fund), under the supervision of one regulatory ministry (as the Ministry of Health),
and to establish a high level committee at the Ministry of Health that will coordinate and
supervise this effort.
d. Regulating the pharmaceutical sector: The drug bill has dramatically increased in the last
few years. The proliferation of drug types, coupled with the over-use and the inappropriate
use of these drugs, is significantly contributing to the magnification of the annual health bill
in Lebanon. In this context, it is recommended to undertake some reforms including:
limiting the number of drugs that can be imported by adopting essential drugs lis
Controlling and monitoring the quality, specifications and prices of all imported drugs.
Encouraging domestic drug production within an effective regulatory framework.
e. Ministry of Health efforts on Flat Rate payments and Clinical protocols: The Ministry
of Health is burdened by high health expenditures. The first priority of the MOH is to cover
the bill of private hospitals. The MOH is troubled with this bill and its complexity and the
way of reimbursing private hospitals, setting tariffs and trying to bear cost. One decision
was to change the way MOH reimburses hospitals by using the flat rate payment by
diagnosis or surgical procedures (DRG Diagnosis Related Group) instead of the Fee for
Service (FFS) following the American or the Canadian system. The flat rate system is
attempted to solve the MOH problem with the bill control, the money spent on
administration and using the physician control at the private hospital to control the billing.
But this strategy will create another problem for other financing agents that have no problem
in control. The DRG doesn't fit in Lebanon especially that cheating will affect the quality of
service delivered and so clinical protocol is necessary. What the MOH will face is the
application of the system with the other financing agents. Another problem is highlighted in
this context which is that every decision taken by the MOH should be applicable country-
wide and compatible with the other financing agents.
f. Hospital Classification and pricing: The Private Providers are paid against their
classification. Classification decision results from the committee and is declared and signed
by the Minister. The upgrade of any Hospital classification will automatically affect the
price system of the hospital. The MOH will follow this classification, while other financing
agents will stick to the old classification (e. g., NSSF), resulting in discrepancies among the
different financing agents. One other point to be raised is the specialization of the public and
private hospitals creating redundancy in high-cost technological equipment. The trend in the
advanced countries is toward establishing specialized centers for specific diseases (heart,
cancer, fertility,). Taking into consideration the size of the country and the improving
conditions of the communication means, the establishment of such center seems viable and
will increase the efficiency of the service, and at the same time reduce the cost. The role of
the government should be the formulation of strategies to expand coverage in under-served
areas, develop protocols for specializing the existing hospital and establishing new facilities
and investments by the private sector in new technologies.
2. Recommendations regarding the National Social Security fund

a. Government is called to reconsider the level of spending on social issues, so that the credit
allocated to these expenditures are not used in disseminated projects that are not in relation
to one another. It should adopt a policy according to which expenditures are included within
the framework of a well defined social plan.
b. Contract the squandering and the social expenditures stemming from political, family, and
sectarian considerations, let alone corruption prevalent in public administration. All this
diverts the social spending from its target.
c. The state should have a clear vision about the Social Security Fund in which it defines the
kind of social security it wants, the social categories, which should benefit from such a fund,
and what kind of administrative structure should be adopted in order to ensure all these
contributions, the means of financing, the states part in financing. This vision is important to
adopt following years of lack of trust between state and the Social Security. This is due to
the spoils distribution system, which should be dealt with: such a policy leads to the
designation of according, not to their qualification, but to their political and social positions
as well as their degree of influence.
d. Activate the role of the Social Security by pumping new blood in the administrative body.
The average age of the personnel is 53 years old. A system of incentives should be adopted
to substitute the old sick elements with young ones as these would accompany the evolution
and modernization of the Social Security system and rationalize the health expenditures and
above all nominate new doctors to activate proper supervision and prevent them from being
submerged to sectarian blackmail.
e. Not to submit to political or sectarian pressures. This is what happened when the
administrative board decided to designate new doctors.
f. Strengthening the health system, including improving governance, health financing,
institutional capacity and service delivery, human resources development, medical
technologies and an integrated health information system.
g. Improving partnership for health development, including educating/ informing people,
orienting and involving parliamentarians and national decision makers, enhancing public–

private sector collaboration, collaborating with UN agencies, development banks and
donors, and helping in coordination of external support for health.
References
Books:
English:
1. Central Provident Fund, ―My CPF—Having Children: Providing for Your Precious
Ones. Life Events: Having Children: Immediate Concerns 2011.‖ Available at
http://mycpf.cpf.gov.sg/CPF/my-cpf/have-child/HC2.htm. Ministry of Health, ―Marriage
and Parenthood Schemes. Costs and Financing: Schemes and Subsidies 2011.‖ Available at
http://www.moh.gov.sg/content/moh_web/home/costs_and_financing/schemes_subsidies/M
arriage_and_Parenthood_Schemes.html
2. Chong, S.A., Mythily et al. ―Performance Measures for Mental Healthcare in
Singapore.‖ Ann Acad Med Singapore 37, 9 (2008): 791–6.
3. ―Grow and Share’ Package Overview,‖ 2011. Available at
http://www.growandshare.gov.sg/Overview.htmM.D. Barr, ―Medical Savings Accounts in
Singapore: A Critical Inquiry,‖ J Health Polit Policy Law 26, 4 (2001): 709–26.
4. National Coalition on Health Care, ―Health Care Spending as Percentage of GDP
Reaches All-Time High,‖ 12 Sept. 2011. Available at http://nchc.org/node/1171
5. Salma Khalik, ―Medisave Can be Used in 12 M’sian Hospitals,‖ Straits Times, 15 Feb.
2010. Available at http://www.asiaone.com/Health/News/Story/A1Story20100216-
198974.html

6. Sam Ro, ―Revealed: !e Cost of Health Insurance around the World,‖ Business Insider,
26 Apr. 2012. Available at http://www.businessinsider.com/cost-ofhealth-insurance-around-
the-world-2012-4#ixzz1zZizuLFo
7. ―Risk Factors—Risks Relating to the Government—Uncertainties Regarding Formation
and Policies of the New Government‖, available at:
http://www.ccfr.org.cn/cicf2012/papers/20120201114734.pdf
8. ―Conflicts With Israel,The July 2006 War‖, available at:
http://smallwarsjournal.com/jrnl/art/the-2006-lebanon-war-a-short-history
9. The Special Tribunal for Lebanon, available at: http://www.stl-tsl.org/en/
10. ―The Economy—Economic History—Fiscal Reform and the Paris II Conference‖,
available at:
http://www.institutdesfinances.gov.lb/english/loadFile.aspx?pageid=838&phname=FileEN
11. ―History, Recent Developments, The Doha Agreement‖, available at:
http://www.mof.go.jp/english/customs_tariff/wto/n05.pdf
12. ―Recent Developments, Doha Agreement‖, available at:
http://en.wikipedia.org/wiki/Doha_Development_Round
13. ―Risk Factors, Risks Relating to the Republic, Fiscal Deficit‖ and ―Risk Factors, Risks
Relating to the Republic, Prices and Inflation‖, available at:
http://www.un.org/en/development/desa/policy/wesp/wesp2013/wesp13update.pdf
14. Extracts Ammar, M. (2011), Inter-professional collaboration, Paediatric unit case in a
university hospital in Lebanon (PhD thesis).
15. Laithy, H. ; Abu-Ismail, K., ; Hamdan, K.; 2008, Poverty, growth and income
distribution in Lebanon,Country study, International Poverty centre, number 13.
http://www.eldis.org/go/country-profiles&id=35243&type=Document
16. Ministry of Social and Family Development. ―Ministerial Committee to Spearhead
Successful Ageing for Singapore,‖ 4 Mar. 2007. Available at
http://app.msf.gov.sg/PressRoom/MinisterialCommitteeToSpearheadSuccessfulAgei.aspx.
French:
1. Durand Paul – la politique contemporaine de sécurité sociale – Dalloz

2. Encyclopedie Dalloz – Soc. salaire n 95
3. M.R. Jambu Merlin – cours de sécurité sociale – Paris – les cours de droit 1968-1969
Arabic:
2005 –بزوث –صادر –انضا اإلجتاػ ف انتشزغ وانفق واالجتهاد –د. ػايز ػبذ انهك .1
1987 – 2ط – 1ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا .2
1985 –بزوث – 1ط – 2ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا .3
1991 –بزوث – 3ج –انستفذو ي انضا اإلجتاػ انهبا –د. اج شىفا .4
Studies:
English:
1. Country Cooperation Strategy for WHO and Lebanon 2005–2009, available at:
www.who.int/countryfocus/.../ccs_lbn_final_en.pdf
2. Makhzoumi,fouad, The National Dialogue Party Political Program, available at:
www.alhiwar.info/Political_Program_English.p
Arabic:
2005 –انتظى انان نهضا اإلجتاػ ف نبا واقؼا وتصىراث –د. ػايز ػبذ انهك .1
Jurisprudence and laws:
10/12/1948 –اإلػال انؼان نحقىق االسا .1
23/9/1946قاى انؼم انهبا تارخ .2
26/9/1963تارخ 13955قاى انضا االجتاػ انفذ بانزسىو .3
–يجىػت أبى اضز وبشز – 4/2/1971تارخ 165رقى –بزوث قزار صادر ػ يجهس انؼم انتحك .4
1971

يجىػت أبى – 12/2/71تارخ 188-181، ورقى 20/1/1968تارخ قزار صادر ػ يجهس انؼم انتحك ، .5
1971اضز وبشز
1ج –انىسظ ف قاى انؼم–ب انشخ – 8/7/1997تارخ 273رقى قزار صادر ػ يجهس انؼم انتحك .6
Patrols:
English:
1. Central Bank annual report, 2011, http://www.bdl.gov.lb/webroot/statistics/
2. CAS annual report 2011,
http://www.cas.gov.lb/images/Mics3/CAS_MICS3_survey_2011.pdf
3. Daily Star, http://www.dailystar.com.lb
4. Encyclopedia of the orient (July 27, 2002), http://i-cias.com/e.o/lebanon_5.htm
5. Households Living Conditions, Central Administration of Statistics, 2011
6. Index-mundi website http://www.indexmundi.com/facts/lebanon
7. Lebanon History (2003),
http://workmall.com/wfb2001/lebanon/lebanon_history_index.html
8. Lebanon National Health Accounts 2009, December 2009
9. MOPH, 2011, Statistics Bulletin,
10. Ministry of Finance report, 2011, http://www.finance.gov.lb/en-
US/finance/ReportsPublications/DocumentsAndReportsIssuedByMOF/Documents/Sovereig
n%20and%20Invensment%20Reports/Country%20Profile/Lebanon%20Country%20Profile
%202011.pdf
11. Ministry of Economy and Trade, 2010, Annual report
12. National Health Accounts, 2008
13. National Social Security Fund- A brief review, August 2005
14. National Household Expenditure and Utilization Survey, 2008
15. Order of Physicians in Beirut and North Lebanon, 2010
16. Order of Pharmacists in Lebanon, 2009
17. Order of Dentists in Beirut and the North, 2008
18. Order of Nurses in Lebanon, 2011
19. Order of Physiotherapists in Lebanon, 2010
20. Singapore Department of Statistics. Yearbook of Statistics Singapore, 2011.
Singapore: Singapore Department of Statistics, 2011.
21. The Massacres of 1840-1860,
http://www.geocities.com/CapitolHill/Parliament/2587/1860.html
22. The Maronites and Lebanon (2003),
http://www.geocities.com/CapitolHill/Parliament/2587/maronite.html
23. WHO EMRO, 2011, Health System Profile, Lebanon
24. WHO website http://www.who.int/gho/countries/lbn/en/
25. WHO Department of Health Statistics and Informatics (May 16, 2012). "World Health
Statistics 2012
Arabic:
ػذا انحاج –انصفحت اإلقتصادت – 4/10/2010 –انسفز صحفت .1
سؤال يىج ي انائب حىري إنى – 10ص – 2005تشز األول 18انثالثاء – 2073انؼذد –صحفت انستقبم .2
انحكىيت ػ يصز ضا طب األسا
يصهحت انحاسبت –أرقاو انصذوق انىط نهضا اإلجتاػ .3