Parents' and Teachers' Concordance with Children's Self-Ratings of Suicidality: Findings from a...
15
167 Suicide and Life-Threatening Behavior 36(2) April 2006 2006 The American Association of Suicidology Parents’ and Teachers’ Concordance with Children’s Self-Ratings of Suicidality: Findings from a High-Risk Sample Richard Thompson, PhD, Howard Dubowitz, MD, MS, Diana J. English, PhD, Kate B. Nooner, MS, Traci Wike, MSW, Shrikant I. Bangdiwala, PhD, Desmond K. Runyan, MD, DrPH, and Ernestine C. Briggs, PhD This study examined concordance between adult and child reports of child suicidality using a sample of 1,046 8-year-old children at risk for, or having experi- enced, maltreatment. Concordance was low with both caregivers and teachers. For children reporting no suicidality, caregiver-child agreement was associated with few transitions in caregiver and low social withdrawal and aggression, and teacher-child agreement was associated with non-White ethnicity, good academic performance, and low thought problems. For children reporting suicidality, care- giver-child agreement was associated with perceptions of child mental health needs, aggression, and somatic complaints, and teacher-child agreement was asso- ciated with thought problems. Although the problem of youth suicide is whom completed suicide is relatively rare, such ideation may still be important, particu- widely acknowledged (U.S. Public Health Service [USPHS], 2000), there continue to larly as an indicator of risk for ongoing men- tal health problems throughout childhood, be barriers to suicidal children receiving nec- essary care. Most children who commit sui- and for later completed suicide. From this perspective, identification and early interven- cide have never received mental health care (Brent & Perper, 1995). Furthermore, al- tion are very important. An important barrier to treatment of suicidality in children may be though only a minority of children with sui- cidal ideation commit suicide (Anderson, failure of parents and teachers, the traditional gatekeepers to child mental health care, to 2002), such ideation often marks unmet men- tal health needs. In younger children, for recognize child suicidality. Parents have the Richard Thompson is with the Juvenile Runyan is with the Injury Prevention Research Center at the University of North Carolina, Protective Association, and the University of Illi- nois at Chicago; Howard Dubowitz is with the Chapel Hill; Ernestine Briggs is with the Center for Child and Family Health at Duke University Department of Pediatrics at the University of Maryland School of Medicine; Diana English is Medical Center. This research was supported by grants from with the Office of Children’s Administration Re- search in Seattle, WA; Kate Nooner is with the the Office of Child Abuse and Neglect to the Con- sortium of Longitudinal Studies on Child Abuse Department of Psychology at San Diego State University; Traci Wike is with the School of and Neglect (LONGSCAN). Address correspondence to R. Thompson, Public Health at the University of North Caro- lina, Chapel Hill; Shrikant Bangdiwala is with Juvenile Protective Association, 1333 N. Kingsbury, Suite 306, Chicago, IL 60622; E-mail: rthompson the Department of Biostatistics at the University of North Carolina, Chapel Hill; Desmond @juvenile.org
Transcript of Parents' and Teachers' Concordance with Children's Self-Ratings of Suicidality: Findings from a...

167Suicide and Life-Threatening Behavior 36(2) April 2006 2006 The American Association of Suicidology
Parents’ and Teachers’ Concordancewith Children’s Self-Ratings of Suicidality:Findings from a High-Risk SampleRichard Thompson, PhD, Howard Dubowitz, MD, MS, Diana J. English, PhD,Kate B. Nooner, MS, Traci Wike, MSW, Shrikant I. Bangdiwala, PhD,Desmond K. Runyan, MD, DrPH, and Ernestine C. Briggs, PhD
This study examined concordance between adult and child reports of childsuicidality using a sample of 1,046 8-year-old children at risk for, or having experi-enced, maltreatment. Concordance was low with both caregivers and teachers.For children reporting no suicidality, caregiver-child agreement was associatedwith few transitions in caregiver and low social withdrawal and aggression, andteacher-child agreement was associated with non-White ethnicity, good academicperformance, and low thought problems. For children reporting suicidality, care-giver-child agreement was associated with perceptions of child mental healthneeds, aggression, and somatic complaints, and teacher-child agreement was asso-ciated with thought problems.
Although the problem of youth suicide is whom completed suicide is relatively rare,such ideation may still be important, particu-widely acknowledged (U.S. Public Health
Service [USPHS], 2000), there continue to larly as an indicator of risk for ongoing men-tal health problems throughout childhood,be barriers to suicidal children receiving nec-
essary care. Most children who commit sui- and for later completed suicide. From thisperspective, identification and early interven-cide have never received mental health care
(Brent & Perper, 1995). Furthermore, al- tion are very important. An important barrierto treatment of suicidality in children may bethough only a minority of children with sui-
cidal ideation commit suicide (Anderson, failure of parents and teachers, the traditionalgatekeepers to child mental health care, to2002), such ideation often marks unmet men-
tal health needs. In younger children, for recognize child suicidality. Parents have the
Richard Thompson is with the Juvenile Runyan is with the Injury Prevention ResearchCenter at the University of North Carolina,Protective Association, and the University of Illi-
nois at Chicago; Howard Dubowitz is with the Chapel Hill; Ernestine Briggs is with the Centerfor Child and Family Health at Duke UniversityDepartment of Pediatrics at the University of
Maryland School of Medicine; Diana English is Medical Center.This research was supported by grants fromwith the Office of Children’s Administration Re-
search in Seattle, WA; Kate Nooner is with the the Office of Child Abuse and Neglect to the Con-sortium of Longitudinal Studies on Child AbuseDepartment of Psychology at San Diego State
University; Traci Wike is with the School of and Neglect (LONGSCAN).Address correspondence to R. Thompson,Public Health at the University of North Caro-
lina, Chapel Hill; Shrikant Bangdiwala is with Juvenile Protective Association, 1333 N. Kingsbury,Suite 306, Chicago, IL 60622; E-mail: rthompsonthe Department of Biostatistics at the University
of North Carolina, Chapel Hill; Desmond @juvenile.org

168 Concordance with Self-Ratings of Suicidality
most contact with their children, and are most porting suicidal ideation (Prinstein, Nock,Spirito, & Grapentine, 2001).likely to be aware of problems they are experi-
encing; this is especially true of young chil- What is it that determines whetherparents and children agree about child sui-dren. Most suicide prevention programs for
youth are based in schools and depend on cidality? There are two broad spheres thathave been examined: parental or family func-teacher detection of child suicidality (Gould,
Greenberg, Veltin, & Shaffer, 2003). Thus, tioning, and child functioning. Both parentalbipolar disorder and major depressive disor-adult detection of child suicidality is a critical
first step in the process that leads to suicidal der are associated with less accuracy in re-porting child suicidality. Bipolar parents tendchildren getting the help they need. Little is
understood about this first step, however. How to overreport ideation, relative to their chil-dren, whereas clinically depressed parentsaware are these key adults of child suicidality?
The limited research available suggests tend to underreport child suicidal ideation(Klimes-Dougan, 1998). Thus, parental men-that agreement between parent and child
reports of child suicidality is, at best, modest tal illness, rather than sensitizing parents topossible problems with children, appears to(Breton, Tousignant, Bergeron, & Berthi-
aume, 2002; Edelbrock, Costello, Dulcan, often have the opposite effect. Less is knownabout the effect of family functioning on par-Conover, & Kalas, 1986; Kashani, Goddard,
& Reid, 1989). Estimates of agreement on ent recognition of child suicidality. Presum-ably, a good relationship between parents andsuicidal ideation vary greatly, depending on
the means of assessment and age of children, children would be associated with more par-ent recognition of child problems, but thisbut are consistently low, with kappa statistics
ranging from .10 ( Joffe, Offord, & Boyle, remains largely untested. At the other extreme,one might expect that parents who maltreat1988) to .33 (Herjanic & Reich, 1982). Agree-
ment tends to be somewhat higher between their children would be especially insensitiveto their children’s needs, including mentalparents and children on reporting of child sui-
cide attempts, but this too is still modest (Her- health needs. Indicators of child functioninghave been more frequently studied. Psycho-janic & Reich, 1982; Walker, Moreau, &
Weissman, 1990). The literature consistently logical distress in children is associated withhigher agreement between parents and chil-shows that parents report much less child sui-
cidality than do children (Dhossche, Ferdi- dren (Klimes-Dougan, 1998), and the greaterlikelihood that the child will receive mentalnand, van der Ende, Hofstra, & Verhulst,
2002; Joffe et al., 1988; Klimes-Dougan, health services (Breton et al., 2002; Mokros,Poznanski, Grossman, & Freeman, 1987).1998; Velez & Cohen, 1988). This may be
part of a general trend of parents reporting One relatively large study found that parentreports of child suicidal ideation were unre-fewer internalizing symptoms than children
(Bird, Gould, & Staghezzo, 1992; Stanger & lated to their reports of child internalizing orexternalizing disorders (Breton et al., 2002).Lewis, 1993). Parental underreporting is not
the only source of disagreement; the majority Demographic factors also may be important;parents are more likely to perceive problemsof parents who report child suicidal ideation
do so when their children do not (Breton et in older children (Edelbrock et al., 1986;Klimes-Dougan, 1998) and in girls (Klimes-al., 2002; Dhossche et al., 2002). Whether
this discrepancy is the result of children de- Dougan, 1998; Walker et al., 1990).There is also a dearth of research onnying problems of which parents are aware
or parents misattributing child problems re- teacher detection of child mental healthproblems in general, and child suicidality inmains unclear. Even in extremely high risk
children, such as psychiatric patients, where particular. This is especially problematicgiven that school-based suicide preventionreports from both children and parents indi-
cate high rates of suicidal ideation, there is programs rely heavily on teacher detection ofstudents’ suicidality and mental health prob-very limited overlap between the two in re-

Thompson et al. 169
lems (Gould et al., 2003). The limited re- Herjanic & Reich, 1982; Mokros et al.,1987). More recent research has focused spe-search available on teacher assessments of
child mental health problems in general sug- cifically on parent knowledge of suicide ide-ation or attempts, either in its own rightgests that teachers underreport symptoms,
especially internalizing symptoms, even more (Velez & Cohen, 1988), or as part of abroader survey of child suicidality ( Joffe etso than parents (Stanger & Lewis, 1993).
Much of the research on teacher detection of al., 1988; Kashani et al., 1989). Most of thisresearch, however, has been conducted onchild problems has focused on ADHD and
other externalizing problems (e.g., Wolraich adolescent children, and it is unclear how thisapplies to pre-adolescent children. The stud-et al., 2004). On the other hand, most of the
research on teacher knowledge of child sui- ies that have included younger children haveused small, high risk, or clinical samples (e.g.,cidality has relied on teachers’ reports of their
confidence in dealing with the issue (e.g., Klimes-Dougan, 1998). The current samplecan be considered high risk, given that theKing, Price, Telljohann, & Wahl, 1999), or
assessments of teachers’ general knowledge sampling frame focused on maltreated chil-dren and those at risk of suffering maltreat-about suicide (e.g., Scouller & Smith, 2002).
Less than 10% of teachers feel confident in ment. Maltreatment is a well-established riskfactor for suicidality, but appears to influencetheir ability to identify students at risk of sui-
cide (King et al., 1999), and teacher knowl- risk primarily through its impact on child de-velopment and psychopathology (Goldsmithedge about suicide is very low (Scouller &
Smith, 2002). Large class size and minimal et al., 2002; Thompson et al., 2005).Our research seeks to address two im-direct contact with children may contribute
to this, as well as a tendency to interpret portant questions pertaining to pre-adoles-cent children, in a high-risk sample:quiet behavior as “good behavior.” In gen-
eral, schools have been expected to broaden1. What is the level of agreement amongthe scope of their involvement in children’schildren, caregivers, and teacherslives, often without the necessary trainingregarding child suicidality?and resources (USPHS, 2000). Thus, from
2. What contextual and child function-both parents or teachers, we know very littleing factors are associated with agree-about what aspects of children or the adultsment among children and caregiversin their lives predict child-adult discrepancyand teachers regarding child suicid-in identifying suicidality. Only a handful ofality?studies have examined this issue at all, and
most have been limited to demographic pre-dictors of agreement (for an important ex-
METHODSception see Klimes-Dougan, 1998), or havelooked, more generally, at adult-child agree- The data presented here were col-ment in reports of child psychopathology. In lected as part of the Longitudinal Studies onother words, a basic, unanswered question is: Child Abuse and Neglect (LONGSCAN). AUnder what conditions do adult reports of detailed description of the methods used inchild suicidality disagree with child self- LONGSCAN and of the sample has beenreports? presented elsewhere (Runyan et al., 1998).
Aside from this largely unanswered With the exceptions of elements unique toquestion, there are a number of limitations to the current analyses, only a brief descriptionthe extant knowledge about adults’ recogni- of the sample and methods is given.tion of child suicidality. Early research exam-ined parent recognition of child suicidal ide- Sample, Design, and Proceduresation as part of more general research onparent recognition of child psychopathology LONGSCAN is a consortium of stud-
ies operating under common protocols, basedand/or depression (Edelbrock et al., 1986;

170 Concordance with Self-Ratings of Suicidality
at five sites in different regions of the United pleted age 8 interviews) and on 683 teacher-child dyads (60.1% of those who completedStates: the South, the East, the Midwest, the
Northwest, and the Southwest. The current age 8 interviews).In terms of demographic factors, 52.4%analysis is based on pooled data from these
five studies. At each site, a sample of children of the sample were male; 55.1% of the sam-ple were White, 26.2% were African Ameri-who had been maltreated or were at risk of
maltreatment was recruited when children can, and 18.7% were of another ethnicity;41.5% of the caregivers had never been mar-were 4 years old or younger. Risk of mal-
treatment was defined in a variety of ways, ried, 34.3% were married, and 23.6% wereformerly married; 6.1% of the sample werevarying by site, including demographic risk
factors such as extreme poverty and very currently in a foster home; and 57.4% of thesample had experienced documented mal-young mother age at birth. Each site fol-
lowed informed consent procedures ap- treatment.proved by institutional or local Human Sub-jects Review committees. Assessments of Measures of Child Suicidalitychildren and caregivers were conducted atages 4, 6, and 8; assessments of children and Child Suicidal Ideation. Suicidal ide-caregivers at ages 12, 14, 16, and 18 are on- ation was defined as endorsement of the itemgoing. At each data collection point, children “Wanting to kill yourself,” from the Traumaand caregivers participated separately in in- Symptom Checklist for Children (TSCC;terviews administered by trained interviewers Briere, 1996), which was completed by thethat included measures of demographics, pa- child. The response set on the TSCC is pre-rental and family functioning, life events and sented as a 4-point Likert-scale, but for theseother contextual variables, and child func- analyses, this item was scored dichotomouslytioning. Families were compensated finan- as either Absent (never) or Present (sometimes,cially for their participation. Brief question- lots of time, almost all the time).naire packets were also mailed to children’s Caregiver-Reported Child Suicidality.teachers to assess functioning in multiple do- Two items from the Child Behavior Checklistmains. (CBCL; Achenbach, 1991a), a well-knownThe analyses reported here focus on scale assessing caregiver-report of child be-data collected at age 8. Because of a large havior problems, elicited caregiver reports ofwindow to allow for as complete data collec- child suicidality, broadly defined. One itemtion as possible, children’s ages at the age 8 dealt with reported child verbalizations ofinterview ranged from 7 to 9, with a mean of suicidal intent (“talks about killing self ”), and8.2 years. A total of 1,354 child-caregiver dy- one dealt with reported child self-harm (“de-ads comprised the baseline age 4 sample, and liberately harms self or attempts suicide”).at age 8, 1,136 were interviewed, a retention Endorsement of either item was interpretedrate of 83.9%. Retention was not associated as caregiver-reported child suicidality.1with demographic, maltreatment, or child orparent functioning.
Additional inclusion criteria for these1. It could be argued that including theanalyses were: the child and either the care-
item on self-harming behaviors in the adult reportgiver and/or teacher having completed thedefinition of suicidality would decrease concor-assessment of child suicidality at age 8. This dance with child reports, as it may reflect self-
resulted in a sample size of 1,051 (92.5%) of harming behaviors that do not emerge from sui-cidal ideation (e.g., self-mutilation or risk-taking).those who had completed the age 8 interview.However, similar analyses conducted eliminatingThere were no significant differences in de-this item resulted in slightly lower, rather thanmographic variables between those who methigher, concordance. This suggests that the lowthese inclusion criteria and those who did concordance is not due to the inclusion of this
not. Data were available on 1,046 caregiver- item. In fact, inclusion of this item may have in-flated concordance.child dyads (92.1% of those who had com-

Thompson et al. 171
Teacher-Reported Child Suicidality. Two (twice a month or less, 3 to 5 times a month,more than 5 times a month, or daily) theyitems from the Teacher’s Report Form (TRF;
Achenbach, 1991b), a well-known scale as- used illegal drugs, as well as alcohol and ciga-rettes. “Substance use problems” was definedsessing teacher-report of child behavior prob-
lems, elicited teachers’ reports of child sui- as: currently using illegal drugs, or using al-cohol at least daily. This summary of care-cidality, broadly defined. One item dealt with
reported child verbalizations of suicidal in- giver substance use problems has been usedin other research on this sample (e.g., Thomp-tent (“talks about killing self ”), and one dealt
with reported child self-harm (“deliberately son et al., 2005).Caregiver Mental Health Needs. Asharms self or attempts suicide”). Endorse-
ment of either item was interpreted as part of a broader assessment of their needsand service utilization (Hunter et al., 2003),teacher-rated child suicidality.caregivers were asked the dichotomous ques-tion, “Do you feel you needed counseling orContextual/Family and Parent
Functioning Measures therapy for any reason during the past year?”Affirmative responses were coded as indicat-ing mental health needs. This item has beenDemographic Factors. The caregiver
interview included child gender, child ethnic- used in other research to indicate adults’ feltneed for mental health services (e.g., Thomp-ity, caregiver marital status, number of other
children in the home, and whether children son et al., 2005).Domestic Violence. Domestic violencewere in foster care.
Transitions in Residence and Caregiver. was assessed using the Conflict Tactics Scale(CTS; Straus & Gelles, 1986) for partnersA structured life events scale, based on Cod-
dington’s work (1972), was used to assess, (Couple Form R), which was administered tocaregivers. Two scales of the CTS were used,through caregiver report, significant events
in the child’s life in the past year. The life assessing the degree to which the caregiver’spartner used mild or severe physical violenceevents scale included several items related to
transitions in the child’s living situation (sep- in dealing with conflict. These scales haveadequate internal consistency, and have beenarations from or transitions in primary care-
giver, and changes in residence). These items extensively validated (Straus, 1990).Family Cohesion and Conflict. Familywere extracted from the larger scale and
summed to produce counts of transitions in cohesion and conflict were assessed using theSelf-Report Family Inventory (SFI; Beavers,caregiver and residence, respectively. The se-
lection of these subsets of items to represent Hampson, & Hulgus, 1990), which was ad-ministered to caregivers. The SFI is a 36-important transitions in a child’s living situa-
tion has been used in other work using this item measure that assesses family functioningin five domains, and has demonstrated ade-sample (e.g., Thompson et al., 2005).
Caregiver Psychological Distress. Care- quate reliability and validity (Beavers et al.,1990). The present study included two sub-giver psychological distress was assessed us-
ing the global severity index of the Brief scales, family conflict and cohesion. Thescores used in these analyses are item meansSymptom Inventory (BSI; Derogatis & Spen-
cer, 1982), a 53-item scale assessing psycho- for both subscales.Child Exposure to Violence. An ex-logical symptomatology, which was adminis-
tered to caregivers. The global severity index panded version of the Things I Have Seenand Heard Questionnaire (Richters & Marti-of the BSI has a reliability of .90 (Derogatis
& Spencer, 1982). The total raw score on the nez, 1992) was administered to children toassess exposure to violence and feelings ofBSI was used in all analyses.
Caregiver Substance Use Problems. As safety at home, at school, and in the commu-nity. It has high test-retest reliability, andpart of a broader assessment of health-related
behavior (Hunter et al., 2003), caregivers correlates highly with indices of communityand home violence (Richters & Martinez,were asked whether and how frequently

172 Concordance with Self-Ratings of Suicidality
1992). The LONGSCAN version used in the sion, and social withdrawal. The suicidalityitems described previously were taken frompresent study added five items to include vio-
lence witnessed in the home. Children were the scale assessing depression/anxiety. Forthe depression/anxiety scale, these items wereasked to endorse each item using a 5-point
Likert scale (0–no times to 4–many times). subtracted from the total score. For each ofthe other scales, the sum of items comprisingMaltreatment. Investigators at the five
sites reviewed Child Protective Services data the scale was calculated. The CBCL is oneof the most widely used and extensively vali-to determine the presence and nature of alle-
gations of maltreatment on children in their dated caregiver reports of child behaviorproblems (Achenbach & Rescorla, 2001).samples. For the current analyses, maltreat-
ment allegations were limited to those that Caregiver-Reported Child Mental HealthNeeds. As part of a broader assessment ofoccurred before the target child was 8 years
old. Children were assigned a dichotomous child needs and service utilization (Hunter etal., 2003), caregivers were asked, “Do youcode, based on whether maltreatment allega-
tions had occurred. This dichotomous cod- feel (target child) needed counseling or ther-apy for any reason during the past year?” Af-ing has been used in many other studies us-
ing LONGSCAN data (e.g., Black et al., firmative responses were coded as indicatingchild mental health needs, regardless of2002)whether the child actually received treatmentor not. This summary of child mental healthChild Functioning Variablesneeds has been used in other research on thissample (e.g., Thompson, 2005).Child Self-Reported Psychological Func-
tioning. The TSCC includes subscales that Teacher-Rated Child Behavior Problemsand Academic Performance. The Teacher Re-assess symptoms of depressed mood, anger,
anxiety, dissociation, and posttraumatic stress. port Form (TRF; Achenbach, 1991b) was ad-ministered to assess teacher ratings of childThe suicidal ideation item described above
was taken from the scale assessing depressed behavior problems in a variety of domains.The domains assessed, and items comprisingmood, and thus was not used in calculating
the total score for the depressed mood scale. each domain, are identical to those in theCBCL; in addition, one item elicited theThe TSCC is a valid, reliable measure of
symptoms of psychological distress in chil- teacher’s overall rating of the child’s academicperformance. As was done with the CBCL,dren (Briere, 1996).
Child Substance Use. As part of a suicidality items described previously weretaken from the scale assessing depression/broader assessment of health behavior (Hunter
et al., 2003), children were asked whether anxiety, and were not included in the calcula-tion of the total score for this scale. Thethey had ever used tobacco, alcohol, or a list
of illegal drugs. The results of these ques- TRF is one of the most widely used and ex-tensively validated teacher reports of childtions were coded dichotomously; an endorse-
ment of having tried any of these substances behavior problems (Achenbach & Rescorla,2001).was coded as indicating child substance use.
This summary of child substance use has Days Suspended from School. As part ofa broader assessment of children’s school be-been used in other research on this sample
(e.g., Thompson et al., 2005). havior (Hunter et al., 2003), teachers re-ported the number of days the child had beenCaregiver-Rated Child Behavior Prob-
lems. The CBCL (Achenbach, 1991a) was suspended from school during the past year.Child’s Peer Status. Teachers ratedadministered to assess caregiver ratings of
child behavior problems in a variety of do- child’s peer status using the Teacher’s Estima-tion of Child’s Peer Status measure, devel-mains, including: aggressiveness, delinquency,
social problems, thought problems, attention oped by Lemerise and Dodge (1990). Thismeasure elicits teacher ratings about theproblems, somatic problems, anxiety/depres-

Thompson et al. 173
child’s popularity and social standing with analyses involved a two-step procedure. Inthe first step, the relationships of all possibleclassmates. It correlates well with peer rat-
ings of child popularity (Lemerise & Dodge, predictors to child-adult agreement were ex-amined. The complete list of predictor vari-1990).ables examined is presented in Table 1. In thesecond step, those predictors that were sig-nificant univariate predictors of child-adultRESULTSagreement entered simultaneously into amultivariate logistic regression predictingPrevalence of Suicidality and Agreement
Between Children and Adults group membership. Subsequent tables (Ta-bles 2 through 4) present the group meansor proportions for these variables only, alongFrom the child report, the prevalence
of suicidality was 9.8%. According to care- with the multivariate statistics for them.For caregiver-child concordance, thegiver reports, the prevalence was 5.4%. Ac-
cording to teacher report, the prevalence was relevant comparisons are presented in Table2 (Group 1 vs. Group 2) and Table 3 (Group2.9%. The association between child and
caregiver reports of suicidality was signifi- 3 vs. Group 4). Many factors were associatedwith caregiver-child disagreement wherecant, χ2(1) = 31.07, p < .001, but with low
concordance, κ = .171. Limiting this analysis children did not report suicidality, while theircaregivers reported suicidality (Table 2).to caregiver-child dyads that included a natu-
ral or adoptive mother did not change this These factors included: male gender, Whiteethnicity, caregiver-reported elevations onassociation. The association between child
and teacher reports of child suicidality was every domain of behavioral problems, care-giver-reported need for mental health ser-only marginally significant, χ2(1) = 3.24, p =
.07, and the concordance was very low, κ = vices for the child, caregiver psychologicaldistress and need for mental health services,.067.high number of transitions in identified care-giver, low family cohesion and high familyFactors Associated with Agreement
Between Children and Caregivers conflict, and child self-reported elevated de-pressive symptoms and anger. These signifi-cant univariate predictors were entered si-In examining the factors associated
with adult-child concordance on reports of multaneously into a multivariate logisticregression predicting group membership. Insuicidality, four groups were generated: (1)
child-adult agreement that there was no sui- the multivariate regression, three factors re-mained significant: more caregiver transi-cidality; (2) adult reports of suicidality, but
not child reports of suicidality; (3) child re- tions, caregiver-rated child aggressiveness,and caregiver-rated child social withdrawal.ports of suicidality but no adult reports of
suicidality; and (4) adult-child agreement that Far fewer factors were associated withcaregiver-child disagreement among childrenthere was suicidality. For both caregivers and
teachers, there were two essential compari- who did report suicidal suicidality (Table 3):lower caregiver-rated child aggression andsons: Group 1 vs. Group 2, and Group 3 vs.
Group 4. Thus, we were interested, among child somatic symptoms, and a lower likeli-hood that caregivers felt their children neededchildren who reported no suicidality, in dif-
ferences in terms of who was labeled as sui- mental health care. No child-reported or de-mographic information predicted caregiver-cidal by the relevant adult (Group 1 vs.
Group 2). Similarly, among children who re- child agreement among children reportingsuicidality. When the significant univariateported suicidality, we were interested in dif-
ferences in terms of who was labeled as sui- predictors were entered simultaneously intoa multivariate logistic regression predictingcidal by the relevant adult group (Group 3
vs. Group 4). In each case, the exploratory group membership, only greater caregiver-

174 Concordance with Self-Ratings of Suicidality
TABLE 1Possible Predictors of Child-Adult Agreement on ChildSuicidality Examined
Administration
CONTEXTUAL/FAMILY FACTORSChild GenderEthnicityCaregiver Marital StatusChild Placement CNumber of other Children CTransitions in CaregiverTransitions in ResidenceCaregiver Psychological Distress (BSI) CCaregiver Substance Use Problem CCaregiver Mental Health Needs CMild Domestic Violence (CTS) CSevere Domestic Violence (CTS) CFamily Cohesion (SFI) CFamily Conflict (SFI) CExposure to ViolenceDocumented Maltreatment C
CHILD FUNCTIONING FACTORSChild ReportsDepressive Symptoms (TSCC)Anxiety (TSCC)Posttraumatic Symptoms (TSCC)Dissociative Symptoms (TSCC)Anger (TSCC)Child Substance Use
Caregiver or Teacher ReportsChild Aggressiveness (CBCL or TRF) SChild Delinquency (CBCL or TRF) SChild Social Problems (CBCL or TRF) SChild Thought Problems (CBCL or TRF) SChild Attention Problems (CBCL or TRF) SChild Somatic Problems (CBCL or TRF) SChild Anxiety/Depression (CBCL or TRF) SChild Social Withdrawal (CBCL or TRF) S
Caregiver ReportsChild Had Mental Health Needs C
Teacher ReportsDays Suspended from School TAcademic Performance (TRF) TChild Peer Relations T
Note. BSI = Brief Symptom Inventory, CTS = ConflictTactics Scale, SFI = Self-Report Family Inventory, TSCC =Trauma Symptom Checklist, CBCL = Child Behavior Check-list, TRF = Teacher Report Form, C = Only examined as a pre-dictor of caregiver-child agreement, T = Only examined as apredictor of teacher-child agreement, S = similar scales adminis-tered to caregivers and teachers.
Thompson et al. 175
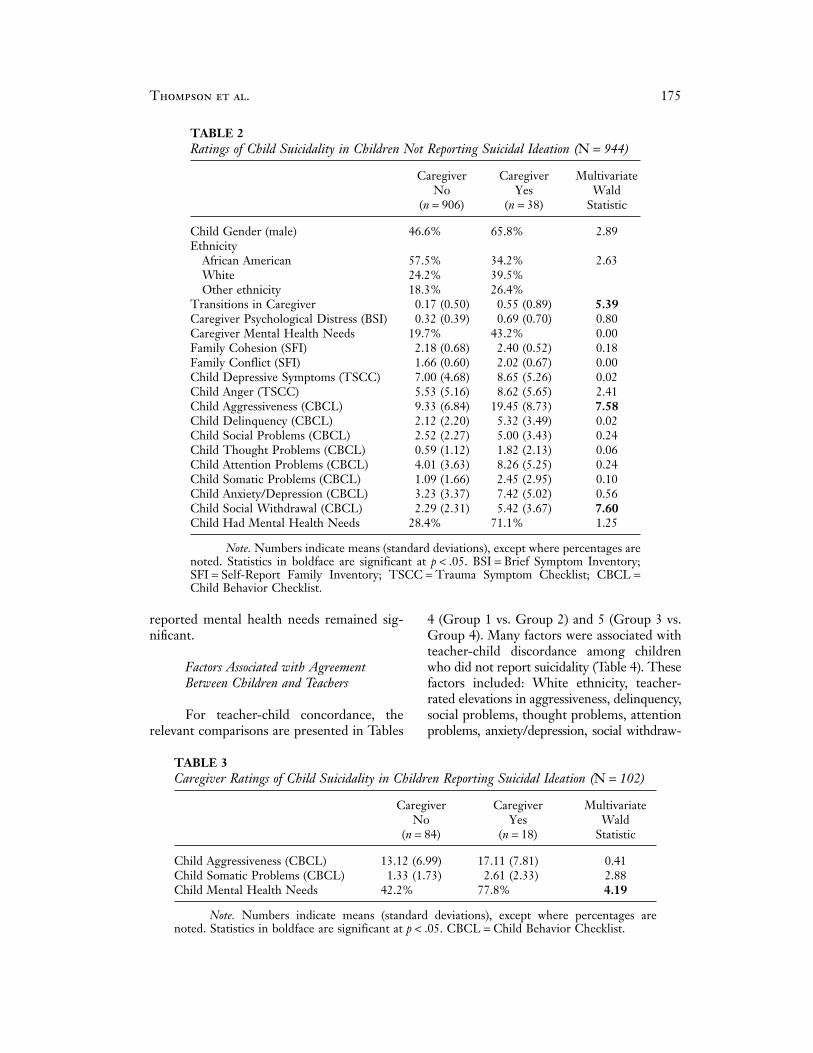
TABLE 2Ratings of Child Suicidality in Children Not Reporting Suicidal Ideation (N = 944)
Caregiver Caregiver MultivariateNo Yes Wald
(n = 906) (n = 38) Statistic
Child Gender (male) 46.6% 65.8% 2.89EthnicityAfrican American 57.5% 34.2% 2.63White 24.2% 39.5%Other ethnicity 18.3% 26.4%
Transitions in Caregiver 0.17 (0.50) 0.55 (0.89) 5.39Caregiver Psychological Distress (BSI) 0.32 (0.39) 0.69 (0.70) 0.80Caregiver Mental Health Needs 19.7% 43.2% 0.00Family Cohesion (SFI) 2.18 (0.68) 2.40 (0.52) 0.18Family Conflict (SFI) 1.66 (0.60) 2.02 (0.67) 0.00Child Depressive Symptoms (TSCC) 7.00 (4.68) 8.65 (5.26) 0.02Child Anger (TSCC) 5.53 (5.16) 8.62 (5.65) 2.41Child Aggressiveness (CBCL) 9.33 (6.84) 19.45 (8.73) 7.58Child Delinquency (CBCL) 2.12 (2.20) 5.32 (3.49) 0.02Child Social Problems (CBCL) 2.52 (2.27) 5.00 (3.43) 0.24Child Thought Problems (CBCL) 0.59 (1.12) 1.82 (2.13) 0.06Child Attention Problems (CBCL) 4.01 (3.63) 8.26 (5.25) 0.24Child Somatic Problems (CBCL) 1.09 (1.66) 2.45 (2.95) 0.10Child Anxiety/Depression (CBCL) 3.23 (3.37) 7.42 (5.02) 0.56Child Social Withdrawal (CBCL) 2.29 (2.31) 5.42 (3.67) 7.60Child Had Mental Health Needs 28.4% 71.1% 1.25
Note. Numbers indicate means (standard deviations), except where percentages arenoted. Statistics in boldface are significant at p < .05. BSI = Brief Symptom Inventory;SFI = Self-Report Family Inventory; TSCC = Trauma Symptom Checklist; CBCL =Child Behavior Checklist.
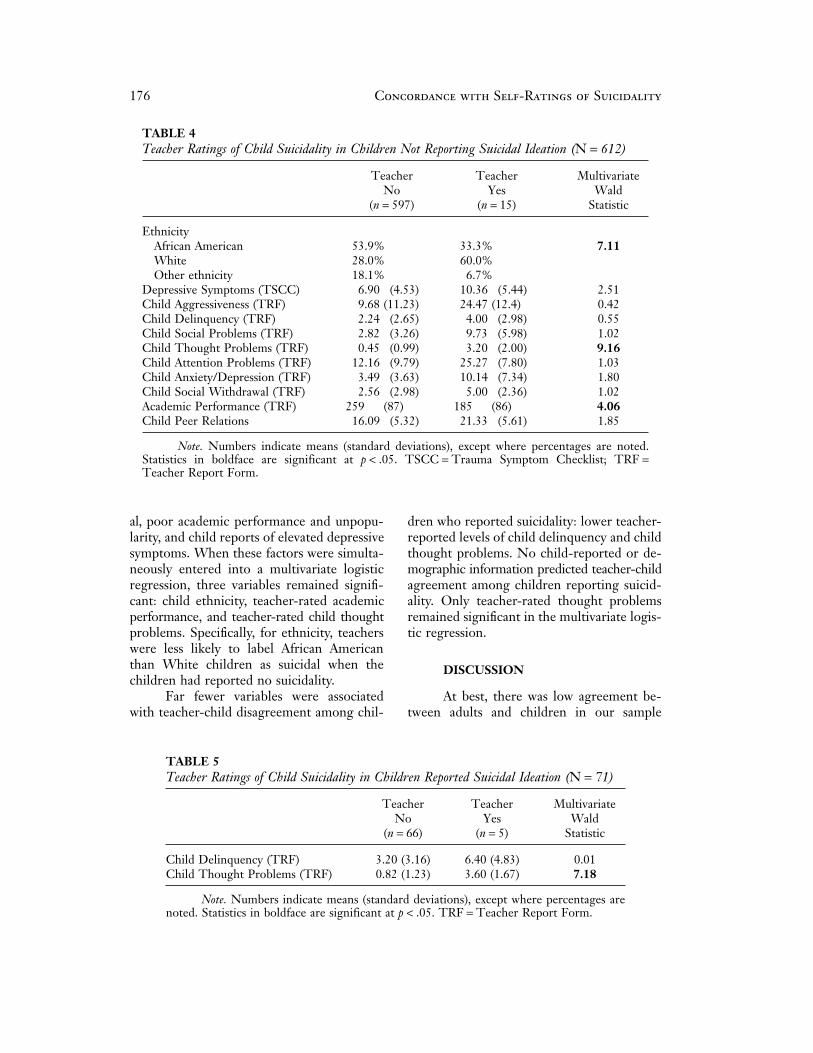
reported mental health needs remained sig- 4 (Group 1 vs. Group 2) and 5 (Group 3 vs.Group 4). Many factors were associated withnificant.teacher-child discordance among childrenwho did not report suicidality (Table 4). TheseFactors Associated with Agreement
Between Children and Teachers factors included: White ethnicity, teacher-rated elevations in aggressiveness, delinquency,social problems, thought problems, attentionFor teacher-child concordance, the
relevant comparisons are presented in Tables problems, anxiety/depression, social withdraw-
TABLE 3Caregiver Ratings of Child Suicidality in Children Reporting Suicidal Ideation (N = 102)
Caregiver Caregiver MultivariateNo Yes Wald
(n = 84) (n = 18) Statistic
Child Aggressiveness (CBCL) 13.12 (6.99) 17.11 (7.81) 0.41Child Somatic Problems (CBCL) 1.33 (1.73) 2.61 (2.33) 2.88Child Mental Health Needs 42.2% 77.8% 4.19
Note. Numbers indicate means (standard deviations), except where percentages arenoted. Statistics in boldface are significant at p < .05. CBCL = Child Behavior Checklist.
176 Concordance with Self-Ratings of Suicidality
TABLE 4Teacher Ratings of Child Suicidality in Children Not Reporting Suicidal Ideation (N = 612)
Teacher Teacher MultivariateNo Yes Wald
(n = 597) (n = 15) Statistic
EthnicityAfrican American 53.9% 33.3% 7.11White 28.0% 60.0%Other ethnicity 18.1% 6.7%
Depressive Symptoms (TSCC) 6.90 (4.53) 10.36 (5.44) 2.51Child Aggressiveness (TRF) 9.68 (11.23) 24.47 (12.4) 0.42Child Delinquency (TRF) 2.24 (2.65) 4.00 (2.98) 0.55Child Social Problems (TRF) 2.82 (3.26) 9.73 (5.98) 1.02Child Thought Problems (TRF) 0.45 (0.99) 3.20 (2.00) 9.16Child Attention Problems (TRF) 12.16 (9.79) 25.27 (7.80) 1.03Child Anxiety/Depression (TRF) 3.49 (3.63) 10.14 (7.34) 1.80Child Social Withdrawal (TRF) 2.56 (2.98) 5.00 (2.36) 1.02Academic Performance (TRF) 259 (87) 185 (86) 4.06Child Peer Relations 16.09 (5.32) 21.33 (5.61) 1.85
Note. Numbers indicate means (standard deviations), except where percentages are noted.Statistics in boldface are significant at p < .05. TSCC = Trauma Symptom Checklist; TRF =Teacher Report Form.
al, poor academic performance and unpopu- dren who reported suicidality: lower teacher-reported levels of child delinquency and childlarity, and child reports of elevated depressive
symptoms. When these factors were simulta- thought problems. No child-reported or de-mographic information predicted teacher-childneously entered into a multivariate logistic
regression, three variables remained signifi- agreement among children reporting suicid-ality. Only teacher-rated thought problemscant: child ethnicity, teacher-rated academic
performance, and teacher-rated child thought remained significant in the multivariate logis-tic regression.problems. Specifically, for ethnicity, teachers
were less likely to label African Americanthan White children as suicidal when the DISCUSSIONchildren had reported no suicidality.
Far fewer variables were associated At best, there was low agreement be-tween adults and children in our samplewith teacher-child disagreement among chil-
TABLE 5Teacher Ratings of Child Suicidality in Children Reported Suicidal Ideation (N = 71)
Teacher Teacher MultivariateNo Yes Wald
(n = 66) (n = 5) Statistic
Child Delinquency (TRF) 3.20 (3.16) 6.40 (4.83) 0.01Child Thought Problems (TRF) 0.82 (1.23) 3.60 (1.67) 7.18
Note. Numbers indicate means (standard deviations), except where percentages arenoted. Statistics in boldface are significant at p < .05. TRF = Teacher Report Form.

Thompson et al. 177
about the presence of child suicidality, with their interpretation. First, the data analyzedhere provide no guidance in determiningadults consistently underestimating child sui-
cidality, relative to child reports. Among other who is the “better” reporter on child suicidal-ity—caregivers, teachers, or children them-things, this suggests that estimates of the
prevalence of child suicidality are likely to be selves. It is certainly likely that some of thechildren who failed to report suicidal ide-heavily influenced by the source of the data.
In our sample, estimates of the prevalence of ation were in fact experiencing such ideation.Similarly, it is very possible that caregivers orchild suicidality based on child reports were
about twice as high as those based on care- teachers missed some suicidality that childrenwere experiencing. It is also possible thatgiver reports and more than three times as
high as those based on teacher reports. This some children who were identified (or self-identified) as suicidal were in fact not suicidal.is consistent with past research demonstrat-
ing that children typically report higher lev- More research is clearly needed in determin-ing the optimal reporter (or combination ofels of internalizing problems in general (e.g.,
Bird et al, 1992) and suicidality in particular reporters) for child suicidality. In the mean-time, reports from any source should not be(e.g., Breton et al., 2002), relative to parents.
In other words, in our sample of maltreated ignored. Furthermore, parents and teachersneed education about signs of suicidality and,and at-risk 8-year-olds, parents of more than
three-quarters of children reporting suicidal more generally, depression and internalizingproblems in children. Finally, routine screen-ideation were not aware of this problem. If,
as is usually the case (Gould et al., 2003), it ing is likely justified, at least in high-risk pop-ulations.is the responsibility of caregivers to identify
and seek help for children who have suicidal Another important issue to keep inmind when interpreting these findings is thatthoughts or behaviors, this suggests a large
number of suicidal children are likely to go the questions asked of adults and childrenwere not identical. Children were asked aboutuntreated. Teachers, often the gatekeepers of
suicide prevention efforts in schools (Gould suicidal thoughts (“wanting to kill yourself ”),whereas adults were asked about suicidalet al., 2003), fared even worse in this study,
“missing” more than 9 out of 10 children speech (“talks about killing self ”) and behav-ior (“deliberately harms self or attempts sui-who reported suicidality. Thus it appears that
reports of suicidality in young children are cide”). Thus, some of the discrepancy be-tween adults and children may be due to theno more likely than those of adolescents to
be concordant with reports by adults. The different questions asked. The findings shouldbe taken as an initial impression of the degreediscrepancy between children and the adults
in their lives is not solely due to adult under- to which adults are aware that suicidality isan issue for children, and preliminary explo-estimation relative to children. Instead, some
children who do not report suicidality are la- ration of factors that might explain discrep-ancy between adult and child reports. A re-beled as suicidal by parents or teachers. It is
possible that some children who are experi- lated concern is the brevity of the assessmentsof child suicidiality—consisting of one itemencing suicidality fail to disclose this to the
interviewer, but have either disclosed it to for child report and two items for adult re-port. Finally, several of the other measurescaregivers or teachers, or had caregivers or
teachers recognize such problems. These used for these analyses have not been widelyused in other studies and may have limitedchildren may have failed to understand the
question regarding suicidality, or may not validity or reliability.There were many more children whohave been comfortable disclosing to a stranger.
Before examining the theoretical im- reported no suicidal ideation than childrenwho did, which reduced the power for detect-plications of these findings, it is important to
point out some methodological issues which ing differences among children who reportedsuicidality, relative to differences among chil-may help explain the findings and temper

178 Concordance with Self-Ratings of Suicidality
dren who did not. This might explain the fact In general, it appeared that, for bothparents and teachers, contextual and childthat a large number of factors were found to
distinguish adult ratings of nonsuicidal chil- functioning factors both predicted adult-child agreement, as did demographic factors.dren, but relatively few to distinguish adult
ratings of suicidal children. To some degree, When children did not report suicidality, anumber of demographic and contextual fac-the multivariate follow-up analyses compen-
sate for this discrepancy, but the results tors were important predictors of adult rat-ings of suicidality. Boys, White children, andshould be considered tentative, and factors
that failed to distinguish between adult rat- children who had experienced transitions incaregiver were all more likely to be reportedings of suicidal children should not be ruled
out as having influence. In the univariate as suicidal by caregivers, and race also pre-dicted teacher ratings. These all likely reflectanalyses, a very large number of analyses
were conducted, raising the possibility that increased adult vigilance about the mentalhealth needs of these children, as there is evi-some null hypotheses were incorrectly re-
jected. Although the multivariate follow-up dence that adults are more sensitive to themental health needs of boys and White chil-analyses largely addressed this issue, it is im-
portant, again, to keep in mind the tentative dren (Thompson, 2005). Recent transitionsin caregiver may also result in increased adultand exploratory nature of the analyses pre-
sented here. vigilance. Caregivers who reported their chil-dren as suicidal (absent child reports of sui-Finally, an important factor to keep in
mind in interpreting the results presented cidality) tended to be experiencing high levelsof psychological distress and saw themselveshere is the fact that this sample was predomi-
nantly children who either had a history of as needing mental health care. There is a largebody of work examining whether parentalmaltreatment or were at risk for maltreat-
ment. In this sample, maltreatment was asso- depression affects ratings of child behavior,with some indication that depressed parentsciated with child suicidal ideation, but this
association disappeared once child function- may be accurate reporters of their children’sfeelings (Richters, 1992), and some that theying was taken into account (Thompson et al.,
2005). This is consistent with much of the are biased to overreport problems (Brody &Forehand, 1986). In this sample, at least rel-established literature on the link between
maltreatment and suicidality (Goldsmith et ative to children, there is some support forthe latter hypothesis, although suicidal chil-al., 2002), and suggests that the presence of
maltreatment does not influence the relation- dren with psychologically distressed parentsmay learn to deny their own problems as aship between other risk factors and child sui-
cidality. More importantly, maltreatment was means of coping. Several studies have docu-mented the negative impact of parent depres-not associated with parent-child agreement
in the current analyses; however, caution sion on child functioning (Cicchetti, Ro-gosch, Toth, & Spagnola, 1997; Downey &should be exercised in generalizing from this
sample to children who are not at significant Coyne, 1990).Most child functioning indicatorsrisk for maltreatment. It is important to
highlight that the data presented here were rated by adults strongly predicted ratings ofsuicidality in children who did not report sui-collected as part of LONGSCAN, a consor-
tium of longitudinal studies on child mal- cidal ideation. Social withdrawal and aggres-sion were especially salient for caregivers andtreatment. As data continue to accrue, it will
be important to examine the longer-term im- academic problems and thought problemswere most salient for teachers. This is proba-plications of child-adult agreement on suicid-
ality. In any case, this study illustrates some bly in part a halo effect (Stevens, Quittner, &Abikoff, 1998), where children rated poorlyof the benefits of applying existing longitudi-
nal data to questions of concern to suicidolo- in one area are also rated poorly in other ar-eas. In particular, social behavior of childrengists.

Thompson et al. 179
appears especially important for caregiver by adults more often than it is recognized.This at least suggests that public health ini-ratings, whereas for teachers, the most rele-
vant aspect of perceived child behavior was tiatives targeting child suicidality will have toeither rethink the focus on adults as gate-odd or bizarre behavior (reflected in the
“thought problems” category of the CBCL keepers, or involve more education for theseadults about child mental health. In particu-and TRF) and low achievement. The chil-
dren who did not report suicidal ideation, but lar, teachers, as professionals, have great po-tential as gatekeepers in a position to identifywere reported to be suicidal by caregivers, re-
ported more feelings of depression them- child needs, since children detected by teach-ers as needing mental health treatment areselves (and more anger). Thus it is not neces-
sarily that these children were denying any especially likely to receive it (Angold, Messer,Stangl, & Burns, 1998). In this sample, how-depressive symptomatology; it certainly re-
mains possible that they were experiencing ever, teachers were less likely than caregiversto perceive suicidality in children, suggestingsuicidality that they failed to report.
Among children who reported suicidal the need for improving teacher educationabout child suicidality (Scouller & Smith,ideation, contextual and demographic factors
were far less important to adult recognition, 2002). In general, it appears that in assessingchild suicidality, caregivers and teachers re-and adult-rated child functioning were the only
predictors of adult-child agreement. Gener- spond to child behavior in other domains ascues for determining whether children areally, child disruptive behavior, low achieve-
ment, and the general sense that children had suicidal. Given that children with suicidalideation are likely to have poor relationshipsmental health needs were all associated with
adult-child agreement, where children reported with the adults in their lives (Thompson etal., 2005), and often fail to express the emo-suicidality. Children who are experiencing
suicidality but do not exhibit aggressive or tional disturbances they are experiencing,adult reliance on such cues is likely to leaveinappropriate behavior are unlikely to be rec-
ognized as such by the adults in their lives. many suicidal children undetected. System-atic screening in high risk children may beAs mentioned earlier, these findings
should be seen as tentative, and replication is warranted as well, but it would be importantthat treatment resources be available to meetneeded. Nevertheless, it appears that, among
high risk children, suicidality goes unnoticed identified needs.
REFERENCES
Achenbach, T. M. (1991a). Manual for gus, Y. F. (1990). Beavers systems model manual:1990 edition. Dallas, TX: Southwest Family Insti-child behavior checklist/4–18 and 1991 profile. Burl-
ington, VT: University of Vermont. tute.Bird, H. R., Gould, M. S., & Staghezza,Achenbach, T. M. (1991b). Manual for
teacher’s report form and 1991 profile. Burlington, B. (1992). Aggregating data from multiple infor-mants in child psychiatry epidemiological re-VT: University of VT, Department of Psychiatry.
Achenbach, T. M., & Rescorla, L. A. search. Journal of the American Academy of Childand Adolescent Psychiatry, 31, 78–85.(2001). Manual for the ASEBA school-age forms and
profiles. Burlington, VT: University of Vermont, Black, M. M., Papas, M. A., Hussey,J. M., Hunter,W., Dubowitz, H., Kotch, J., etResearch Center for Children, Youth and Families.
Anderson R. N. (2002). Deaths: Leading al. (2002). Behavior and development of pre-school children born to adolescent mothers: Riskcauses for 2000. National Vital Statistics Report, 50,
16. and 3-generation households. Pediatrics, 109, 573–580.Angold, A., Messer, S. C., Stangl, D., &
Burns, E. J. (1998). Perceived parental burden Brent, D.A., & Perper, J. A. (1995). Re-search in adolescent suicide: Implications forand service use for child and adolescent disorders.
American Journal of Public Health, 88, 75–80. training, service delivery, and public policy. Suicideand Life-Threatening Behavior, 25, 222–230.Beavers, W. R., Hampson, R. B., & Hul-

180 Concordance with Self-Ratings of Suicidality
Breton, J.-J., Tousignant,M., Bergeron, outcomes in longitudinal research on child abuse. Vol-L., & Berthiaume, C. (2002). Informant-specific ume 2: Middle childhood. Retrieved from the LON-correlates of suicidal behavior in a community GSCAN Web site: http://www.sph.unc.edu/iprc/sample of 12- to 14-year-olds. Journal of the Amer- longscan/Measures%20Manual/Ages5to11/index.ican Academy of Child and Adolescent Psychiatry, 41, html.723–730. Joffe, R. T., Offord, D. R., & Boyle,
Briere, J. (1996). Trauma symptom checklist M. H. (1988). Ontario child health study: Suicidalfor children: Professional manual. Odessa, FL: Psy- behavior in youth age 12–16 years. American Jour-chological Assessment Resources. nal of Psychiatry, 146, 1420–1423.
Brody, G. H., & Forehand, R. (1986). Kashani, J. H., Goddard, P., & Reid,Maternal perception of child maladjustment as a J. C. (1989). Correlates of suicidal ideation in afunction of combined influence of child behavior community sample of children and adolescents.and maternal depression. Journal of Consulting and Journal of the American Academy of Child and Ado-Clinical Psychology, 54, 237–240. lescent Psychiatry, 28, 912–917.
Cicchetti, D., Rogosch, F. A., Toth, King, K. A., Price, J. H., Telljohann,S. L., & Spagnola, M. (1997). Affect, cognition, S. K., & Wahl, J. (1999). High school healthand the emergence of self-knowledge in the tod- teachers’ perceived self-efficacy in identifying stu-dler offspring of depressed mothers. Journal of Ex- dents at risk for suicide. Journal of School Health,perimental Child Psychology, 67, 338–362. 69, 202–207.
Coddington, R. D. (1972). The signifi- Klimes-Dougan, B. (1998). Screening forcance of life events as etiologic factors in the dis- suicidal ideation in children and adolescents: Meth-eases of children—II: A study of a normal popula- odological considerations. Journal of Adolescence,tion. Journal of Psychosomatic Research, 16, 205–213. 21, 435–444.
Derogatis, L. R., & Spencer P.M. (1982). Lemerise, E., & Dodge, K. A. (1990).The brief symptom inventory (BSI): Administration, Teacher simulation of peer sociometric status. Unpub-and procedures manual-I. Baltimore, MD: Clinical lished instrument, Vanderbilt University, Nash-Psychometric Research. ville, TN.
Dhossche, D., Ferdinand, R., van der Mokros, H. B., Poznanski, E., Grossman,Ende, J.,Hofstra,M. B., & Verhulst, F. (2002). J. A., & Freeman, L. N. (1987). A comparison ofDiagnostic outcome of adolescent self-reported child and parent ratings of depression for normalsuicidal ideation at 8-year follow-up. Journal of Af- and clinically referred children. Journal of Childfective Disorders, 72, 273–279. Psychology and Psychiatry, 28, 613–627.Downey, G., & Coyne, J. C. (1990). Chil- Prinstein, M. J., Nock, M. K., Spirito,dren of depressed parents: An integrative review. A., & Grapentine, W. L. (2001). MultimethodPsychological Bulletin, 108, 50–76. assessment of suicidality in adolescent psychiatricEdelbrock, C., Costello, A., Dulcan, inpatients: Preliminary results. Journal of theM. K., Conover, N. C., & Kalas, R. (1986). Par- American Academy of Child and Adolescent Psychia-ent-child agreement on child psychiatric symp-
try, 40, 1053–1061.toms assessed via structured interview. Journal ofRichters, J. E. (1992). Depressed mothersChild Psychology and Psychiatry, 27, 181–190.
as informants about their children: A critical re-Goldsmith, S. K., Pellmar, T. C., Klein-view of the evidence for distortion. Psychologicalman, A. M., Bunney, W. E., & Committee onBulletin, 112, 485–499.Pathophysiology and Prevention of Adoles-
Richters, J. E., & Martinez, P. (1992).cent and Adult Suicide, Board of NeuroscienceThings I have seen and heard: A structured interviewand Behavioral Health, Institute of Medi-for assessing young children’s violence exposure. Wash-cine. (2002). Reducing suicide: A national imperative.ington, DC: National Institute of Mental Health.Washington, DC: The National Academies Press.
Runyan, D. K., Curtis, P., Hunter, W.Gould, M. S., Greenberg, T., Velting,M., Black, M. M., Kotch, J. K., Bangdiwala, S.D. M., & Shaffer, D. (2003). Youth suicide risket al. (1998). LONGSCAN: A consortium forand preventive interventions: A review of the pastlongitudinal studies of maltreatment and the life10 years. Journal of the American Academy of Childcourse of children. Aggression and Violent Behavior,and Adolescent Psychiatry, 42, 386–405.3, 275–285.Herjanic, B., & Reich, W. (1982). Devel-
Scouller, K. M., & Smith, D. I. (2002).opment of a structured psychiatric interview forPrevention of youth suicide: How well informedchildren: Agreement between parent and child onare the potential gatekeepers of adolescents in dis-individual symptoms. Journal of Abnormal Childtress? Suicide and Life-Threatening Behavior, 32,Psychology, 10, 307–324.67–79.Hunter, W. M., Cox, C. E., Teagle, S.,
Stanger, C., & Lewis, M. (1993). Agree-Johnson, R. M., Mathew, R., Knight, E. D., etal. (2003).Measures for assessment of functioning and ment among parents, teachers, and children in in-

Thompson et al. 181
ternalizing and externalizing behavior problems. Findings from a multi-site study. Child Maltreat-ment, 10, 26–36.Journal of Clinical Child Psychology, 33, 107–115.
U.S. Public Health Service. (2000). Re-Stevens, J., Quittner, A. L., & Abikoff,port of the surgeon general’s conference on children’sH. (1998). Factors influencing elementary schoolmental health: A national action agenda. Washing-teachers’ ratings of ADHD and ODD behaviors.ton, DC: Department of Health and Human Ser-Journal of Clinical Child Psychology, 27, 406–414.vices.Straus, M. A. (1990). The conflict tactics
Velez, C. N., & Cohen, P. (1988). Sui-scales and its critics: An evaluation and new datacidal behavior and ideation in a community sam-on validity and reliability. In M. A. Straus & R. J.ple of children: Maternal and youth reports. Jour-Gelles (Eds.), Physical violence in American families:nal of the American Academy of Child and AdolescentRisk factors and adaptations to violence in 8,145 fami-Psychiatry, 27, 349–356.lies (pp. 49–73). New Brunswick, NJ: Transaction.
Walker, M., Moreau, D., & Weissman,Straus, M. A., & Gelles, R. J. (1986). So-M.M. (1990). Parents’ awareness of children’s sui-cietal change and change in family violence fromcide attempts. American Journal of Psychiatry, 147,1975 to 1985 as revealed by two national surveys.1364–1366.Journal of Marriage and the Family, 48, 465–479. Wolraich, M. L., Lambert, E. W., Bick-Thompson, R. (2005). The course and cor- man, L., Simmons, T., Doffing, M. A., & Wor-relates of mental health care received by young ley, K. A. (2004). Assessing the impact of parentchildren: Descriptive data from a longitudinal ur- and teacher agreement on diagnosing attention-
ban high-risk sample. Children and Youth Services deficit hyperactivity disorder. Journal of Develop-Review, 27, 39–50. mental and Behavioral Pediatrics, 25, 41–47.
Thompson, R., Briggs, E. C., English,D. J., Dubowitz, H., Lee, L.-C., Brody, K., et Manuscript Received: December 14, 2004
Revision Accepted: August 25, 2005al. (2005). Suicidal ideation among 8-year-olds: