
Oxfam India
103
Oxfam India Section-wise comments on the proposed draft of Right to Health Act of Rajasthan State We welcome the introduction of the Right to Health Bill by the Government of Rajasthan. This holds the potential for protecting the lives of millions of people in the State, particularly those from marginalized communities. Oxfam India would like to leverage the space provided for making suggestions for the text to make a few recommendations. The lens for the submission is from the perspective of the experience of marginalized communities. It draws on Oxfam India‘s over a decade of experience of working on healthcare in India from a rights-based lens. Through our recommendations, we seek to make the Act more comprehensive, legally viable, and people-centred. We recommend the addition of the following clauses in- Rights of Residents Chapter II under the „Right of Residents‟ section could be expanded to include additional clauses that are part of the patient‟s rights charter 1 Right to get basic emergency medical care irrespective of paying capacity of patient or attendant in all health care establishments be it public or private Right to receive treatment in public or private without any discrimination based on his or her illnesses or conditions, including HIV status or other health condition, religion, caste, ethnicity, gender, age, sexual orientation, linguistic or geographical /social origins. Right to choose between alternative treatment/management options, if these are available, after considering all aspects of the situation. Right to affordable surgeries could be rephrased to right to care according to prescribed rates as a whole. At the same time, the right to choose a source of obtaining medicines or tests could be recognized. Clause (h) in chapter II under the „Right of Residents‟ section - Right to confidentiality, human dignity and privacy at all health care establishments as may be defined by rules made under this act Right of Health Care Provider clause (c) given in chapter II under Right of Health Care Provider- decent remuneration, working condition and training. Duties of Health Care Provider Chapter II under the „Duties of Health Care provider‟ section needs to be expanded to include- Providing protection to participants involved in Clinical Trials, biomedical and health research Obligations of the Government Chapter III- Obligation of the Government needs to be broken down to spell out the roles of individual tiers of the government – viz state, district, block and Panchayati raj levels. This would be critical to fix the responsibility and accountability of these individual structures who have different roles with respect to the delivery of the right to health. It would also be important to define the role of the existing structures and bodies with a role for the delivery of healthcare in the state such as PRIs, VHNSCs, district and state Authority Body under CEA, etc. which are constituted under the constitution, health policy or part of existing health programme interventions. The proposed structures/bodies under this act would need to be linked to existing constitutional structures/bodies. The RtH would need to eventually help to identify the accountabilities of the concerned officials with a role in public health including frontline health workers, medical staff, and health 1 http://www.clinicalestablishments.gov.in/WriteReadData/3181.pdf
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Oxfam India

Oxfam India
Section-wise comments on the proposed draft of Right to Health Act of Rajasthan State
We welcome the introduction of the Right to Health Bill by the Government of Rajasthan. This
holds the potential for protecting the lives of millions of people in the State, particularly those from
marginalized communities.
Oxfam India would like to leverage the space provided for making suggestions for the text to make
a few recommendations. The lens for the submission is from the perspective of the experience of
marginalized communities. It draws on Oxfam India‘s over a decade of experience of working on
healthcare in India from a rights-based lens. Through our recommendations, we seek to make the
Act more comprehensive, legally viable, and people-centred.
We recommend the addition of the following clauses in-
Rights of Residents
Chapter II under the „Right of Residents‟ section could be expanded to include additional
clauses that are part of the patient‟s rights charter1
Right to get basic emergency medical care irrespective of paying capacity of patient or
attendant in all health care establishments be it public or private
Right to receive treatment in public or private without any discrimination based on his or her
illnesses or conditions, including HIV status or other health condition, religion, caste,
ethnicity, gender, age, sexual orientation, linguistic or geographical /social origins.
Right to choose between alternative treatment/management options, if these are available,
after considering all aspects of the situation.
Right to affordable surgeries could be rephrased to right to care according to prescribed rates
as a whole. At the same time, the right to choose a source of obtaining medicines or tests
could be recognized.
Clause (h) in chapter II under the „Right of Residents‟ section - Right to confidentiality,
human dignity and privacy at all health care establishments as may be defined by rules made
under this act
Right of Health Care Provider
clause (c) given in chapter II under Right of Health Care Provider- decent
remuneration, working condition and training.
Duties of Health Care Provider
Chapter II under the „Duties of Health Care provider‟ section needs to be expanded
to include- Providing protection to participants involved in Clinical Trials, biomedical and
health research
Obligations of the Government
Chapter III- Obligation of the Government needs to be broken down to spell out the roles of
individual tiers of the government – viz state, district, block and Panchayati raj levels. This would
be critical to fix the responsibility and accountability of these individual structures who have
different roles with respect to the delivery of the right to health.
It would also be important to define the role of the existing structures and bodies with a role
for the delivery of healthcare in the state such as PRIs, VHNSCs, district and state Authority
Body under CEA, etc. which are constituted under the constitution, health policy or part of existing
health programme interventions. The proposed structures/bodies under this act would need to be
linked to existing constitutional structures/bodies.
The RtH would need to eventually help to identify the accountabilities of the concerned
officials with a role in public health including frontline health workers, medical staff, and health
1 http://www.clinicalestablishments.gov.in/WriteReadData/3181.pdf

officials working at each level i.e. from village to state. Defining the responsibility of each service
provider will help to fix accountability and improve the implementation of the proposed act.
Hence, more specifically, the RtH Act needs to not only spell out the broad responsibilities of the
Rajasthan government and the rights of its citizens but also help to fix appropriate accountability
and delineate the mechanisms/processes to be taken to ensure the same.
Clause (c) given chapter III- Obligation of the Government. We recommend the following
change in the text “Within one year, lay down and notify standards for quality (IPHS standards)
and safety of all levels of health care as notified under the rules‖. It would be desirable to notify a
set of existing public health standards as the standards of quality. The IPHS standards could form
the basis for the laying down of the standards for the state.
It would be critical to add the following clause in chapter III- Obligation of the Government.
Within one year, set up the mechanism for regulation of private health care establishment as
notified in the rules under the Act.
In order to not only provide more clarity but also avoid misinterpretation of the following key
terms, there is need to specify or elaborate on the following terms used in the given draft-
- Appropriate state budget
- Notify standard for quality and safety of all levels of health care
- Co-ordination mechanisms among the relevant government departments
Chapter- VI Penalties and Procedures- The suggested punishable fine in Rupees needs to be
linked with inflation.
We are looking forward to considering and including the above recommendations in the act by the
state government of Rajasthan. Along with asking for recommendations, the state government
should conduct a consultation with various stakeholders including CSOs working on Health Rights
at pan India. The proposed consultation/meeting will provide space for dialogue for sharing the
views on the drafted act and will enable the state government in finalizing the drafted act in
consultation with various stakeholders.
For further communication -
Dr. Nitin Jadhav, Program Coordinator-Health, Oxfam India, New Delhi
Contact details- [email protected]; 9923107623

AMITY INSTITUTE OF BIOTECHNOLOGY 1. Till date treatment of rare diseases are not covered by Govt of Rajasthan like Wilson's Disease. The disease is rare, earlier patients were dying undetected but now health care professionals are sensitive/intelligent enough to detect the disease. Even medicines for patients of Wilson are not available in Govt supply, how is this Act going to protect the rights of the residents of the state? The treatment of rare disease being costly, the Act must clearly state that the cost of such treatment will be taken care of by the state. 2. Treatment for rare diseases are not covered under the CM Chiranjeevi Scheme. The scheme (CM Chiranjeevi Scheme) should also be mentioned in the act as a financial source to support health care of the residents of the state. 3. Similar to this Celiac disease patients are also increasing in the state, the state should promote gluten free products and provide gluten free food material at subsidised rates. 4. Grievance redressal system is literally poor. Rajsampark portal is useless. If you make a complaint, you will receive irrelevant responses. If twice you are not satisfied the complaint file will be closed. It seems by providing such a portal the Government wants to complete formalities. There must be a separate online complaint system for health care related issues and responsibilities may be fixed for certain officers to respond. 5. Hygiene and cleanliness maintenance in Govt Hospitals may also be ascertained by this Act. The penalty provisions may be added if there is any negligence in maintenance of hygiene or cleanliness in any Govt or Private hospital. (Till date public toilets are in horrible situations) 6. To facilitate the patients in overloaded hospitals proper provisions may be mentioned. Otherwise you will find long queues in hospitals at various windows of OPD/ Labs etc.

Lt. idrees khan bagaria
1. ऩहऱा सुझाव यह है कि राजस्थान िे प्रत्येि जजऱे में स्थापऩत RTPCR Lab में ऱगे सभी ऱैब technician िार्मििों िो स्थायी किया जाए और RTPCR Lab िो ऩूर्ित् जजऱा अस्ऩताऱ से पवऱय िर सुचारू रूऩ से संचाऱन किया जाए ताकि भपवष्य में आने वाऱी अनेि महामारी से असानी से ननऩटा जा सिे। और राजस्थान िे प्रत्येि नागररि िो RTPCR से संबंधधत सभी जांचों (Covid
gene detect , TB, HIV, HBV, HCV, Leprosy gene Real time pcr, VDRL Gene detection, etc) िा ऱाभ तुरंत प्रभाव से मुफ्त र्मऱ सिे।
2. दसूरा सुझाव यह है कि आऩिो पवददत है कि किसी ना किसी ददन प्राय यह देखने िो र्मऱता है कि िोई ना िोई संघठन वेतन पवसंगनत िो ऱेिर हड़ताऱ िरते रहत ेहैं जजसिे चऱते आम जनता िो ऩरेशानी िा सामना िरना ऩड़ता है और एि गंभीर यथाजस्थनत िा खर्मयाजा भी जानता िो भुगतना ऩड़ता है तो आऩसे अनुरोध िरते हैं कि RTPCR में िायिरत सभी Lab
Technicians िार्मििों िा मानदेय NRHM िे तहत हुई घोषर्ा िे अनुरूऩ मानदेय में 20% िी वदृ्धध िर 20350 से बढािर 24420 ₹ किया जाए।
3. तीसरा सुझाव यह है कि जजस प्रिार RTPCR िार्मििों िा अनुमोदन सीधा NRHM directorate
से होता है उसी प्रिार हमारा वेतन सीधे खाते में Transfer किया जाए ताकि हमारे मानदेय िी ऩारदर्शिता यथावत बनी रहे और हमारे वेतन में से िोई भी किसी भी प्रिार िी िटौती नहीं िर ऩाएगा।

Dr. Nitin Jadhav, Program Coordinator-Health, Oxfam India, New Delhi
Contact details- [email protected]; 9923107623
Section-wise comments on the proposed draft of Right to Health Act of Rajasthan State
We welcome the introduction of the Right to Health Bill by the Government of Rajasthan. This
holds the potential for protecting the lives of millions of people in the State, particularly those from
marginalized communities.
Oxfam India would like to leverage the space provided for making suggestions for the text to make
a few recommendations. The lens for the submission is from the perspective of the experience of
marginalized communities. It draws on Oxfam India‘s over a decade of experience of working on
healthcare in India from a rights-based lens. Through our recommendations, we seek to make the
Act more comprehensive, legally viable, and people-centred.
We recommend the addition of the following clauses in-
Rights of Residents
Chapter II under the „Right of Residents‟ section could be expanded to include additional
clauses that are part of the patient‟s rights charter2
Right to get basic emergency medical care irrespective of paying capacity of patient or
attendant in all health care establishments be it public or private
Right to receive treatment in public or private without any discrimination based on his or her
illnesses or conditions, including HIV status or other health condition, religion, caste,
ethnicity, gender, age, sexual orientation, linguistic or geographical /social origins.
Right to choose between alternative treatment/management options, if these are available,
after considering all aspects of the situation.
Right to affordable surgeries could be rephrased to right to care according to prescribed rates
as a whole. At the same time, the right to choose a source of obtaining medicines or tests
could be recognized.
Clause (h) in chapter II under the „Right of Residents‟ section - Right to confidentiality,
human dignity and privacy at all health care establishments as may be defined by rules made
under this act
Right of Health Care Provider
clause (c) given in chapter II under Right of Health Care Provider- decent
remuneration, working condition and training.
Duties of Health Care Provider
Chapter II under the „Duties of Health Care provider‟ section needs to be expanded
to include- Providing protection to participants involved in Clinical Trials, biomedical and
health research
Obligations of the Government
Chapter III- Obligation of the Government needs to be broken down to spell out the roles of
individual tiers of the government – viz state, district, block and Panchayati raj levels. This would
be critical to fix the responsibility and accountability of these individual structures who have
different roles with respect to the delivery of the right to health.
It would also be important to define the role of the existing structures and bodies with a role
for the delivery of healthcare in the state such as PRIs, VHNSCs, district and state Authority
Body under CEA, etc. which are constituted under the constitution, health policy or part of existing
2 http://www.clinicalestablishments.gov.in/WriteReadData/3181.pdf

health programme interventions. The proposed structures/bodies under this act would need to be
linked to existing constitutional structures/bodies.
The RtH would need to eventually help to identify the accountabilities of the concerned
officials with a role in public health including frontline health workers, medical staff, and health
officials working at each level i.e. from village to state. Defining the responsibility of each service
provider will help to fix accountability and improve the implementation of the proposed act.
Hence, more specifically, the RtH Act needs to not only spell out the broad responsibilities of the
Rajasthan government and the rights of its citizens but also help to fix appropriate accountability
and delineate the mechanisms/processes to be taken to ensure the same.
Clause (c) given chapter III- Obligation of the Government. We recommend the following
change in the text “Within one year, lay down and notify standards for quality (IPHS standards)
and safety of all levels of health care as notified under the rules‖. It would be desirable to notify a
set of existing public health standards as the standards of quality. The IPHS standards could form
the basis for the laying down of the standards for the state.
It would be critical to add the following clause in chapter III- Obligation of the Government.
Within one year, set up the mechanism for regulation of private health care establishment as
notified in the rules under the Act.
In order to not only provide more clarity but also avoid misinterpretation of the following key
terms, there is need to specify or elaborate on the following terms used in the given draft-
- Appropriate state budget
- Notify standard for quality and safety of all levels of health care
- Co-ordination mechanisms among the relevant government departments
Chapter- VI Penalties and Procedures- The suggested punishable fine in Rupees needs to be
linked with inflation.
We are looking forward to considering and including the above recommendations in the act by the
state government of Rajasthan. Along with asking for recommendations, the state government
should conduct a consultation with various stakeholders including CSOs working on Health Rights
at pan India. The proposed consultation/meeting will provide space for dialogue for sharing the
views on the drafted act and will enable the state government in finalizing the drafted act in
consultation with various stakeholders.
For further communication -
Dr. Nitin Jadhav, Program Coordinator-Health, Oxfam India, New Delhi
Contact details- [email protected]; 9923107623

1. Edify Group 2. Arun Soni 390207 3. Dr Naresh Somani 4. vishnu bhutia 5.Marudhar Hospital 5. Dr. Bharat Rajpurohit HCG Hospital Mansrovar 6. Asopa Hospital, 7. Indus Jaipur Hospital, 8. Jain ENT Hospital lalkothi, 9. Dr Shivraj Sigh Rathor AHPI 10. Dr. Ashok Sharda IMA
Grievances and Suggestions for Rajasthan Right to
Health Care Act 2022
CHAPTER-I
Section 2(t)- The definition of Healthcare provider is not exhaustive. Must include the
qualifications and relevant licenses required to be obtained by them.
Section 2- Define ―Quackery‖
CHAPTER-II Section 3(c)- Replace all public hospitals to public health institutions as defined.
Section 3(j)- Proper referral transport includes the cost incurred in acquiring the vehicle, equipment, medicines, trained staff etc., which should be clearly mentioned. Healthcare facilities, especially private hospitals, cannot bear the cost of such services by themselves.
Section 3(l)- Define Redressal Mechanism
Section 3(m)- Unfavorable for the Private Healthcare Facilities as the Provision allows patients to not pay their dues for an indefinite period. Should only be allowed to take the body
of the deceased after providing an assurance/bond to pay the dues within a specific period of time and within the limits of capping of dues on total bill.
Section 4- Should include duty of patients to pay the all the bills and dues for services rendenered before discharge to private healthcare establishments.
Section 4(f)- Include punishment under The Rajasthan Medicare Service Persons
and Medicare Service Institutions (Prevention of Violence and Damage to Property) Act, 2008.
Section 4(h)- Specify the Prescribed Authority to which such acts should be reported.
Section 5- Include right to:
- practice profession without undue pressure, distress and harassment - refuse treatment to patients indulging in disruptive and violent behavior - refuse treatment to patients if required services are not available - report unruly patients and attendants - receive timely payments for services

Section 5(a)- no criminal proceedings against healthcare providers such as FIR/arrest
should be initiated without obtaining a report from district level committee of
subject specialists
Section 5(d)- Right to have physical safety and security at the workplace , through proper safety
measures by government. CHAPTER-III
Section 7- Include:
- Ensure proper safety and prevention of violence against health care workers and
establishments. Enact proper rules and stringent laws against physical violence, verbal abuse, mob lynching harassment etc. for the same and direct all concerned
authorities to implement them.
- Make provisions to prevent quackery and crosspathy by unqualified persons in health care. Respective authorities like CMHO, District Collector or SDM of the
concerned territory must be made liable and accountable to prevent quackery. CHAPTER-IV
Section 8 (b) VII 2. - Specify representatives of health associations: must be from office bearers of
Indian Medical Association and Private Hospital association. Chairperson should
not appoint any representative by ―Pick & Choose‖ method. Exclusive power to the Chairperson to appoint the representatives can create a bias.
Section 9(b)VI2. - Specify representatives of health associations: must be from office bearers of
Indian Medical Association and Private Hospital association. Chairperson should not appoint any representative by ―Pick & Choose‖ method. Exclusive power to the
Chairperson to appoint the representatives can create a bias.
Section 11(b)(VI)- Representatives of health associations should be their concerned executives or
office bearers. Should also include President/Secretary of Indian Medical Association (IMA),
representatives of Private Hospital associations. Exclusive power to the Chairperson to appoint the
representatives can create a bias. Section 12(b) – IPC section 176 and 177 should not be applicable. Required information must be
defined properly.
Section 12 (c) – Totally unconstitutional provisions. Any authority or officer should not be given rights for a search and seize operation. Only related documents and records can be asked to produce according to section 91 of CrPC.
Section 12 (d) – Unconstitutional provision of fixing responsibility and accountability of private institutions for services. Clear Contraventions of Article 19 1(g) of constitution of India. State Health Authority and District Health Authority can have only supervision and advisory rights. Not acceptable to extent of deciding the prices for private hospitals as the services provided at each establishment are diverse.
The government shall have powers to regulate prices for the packages of
government schemes only. Private institutions should not have any bindings for
participation and empanelment of such government schemes. State Health Authority
and District Health Authority committee may have powers to send
recommendations to revise the rates of packages of government schemes to
concerned departments to encourage participation of more and more private
institutions.

CHAPTER-V
Section 13 (a) – Complaint forums and Grievance redressal must be at three levels:
1. Institutional Level 2. District Level: Must have members from representative of local
medical association, subject medical specialist and CMHO
3. State Level: Must have members from representative of state medical association, subject medical specialist from Medical College
Section 13 (b) – No grievance, complaint and investigation summary should not be shared on public domain. Goodwill and reputation of health care providers and institutions must be properly preserved and maintained.
Section 13 – Include following provisions:
- Burden of proof must be on complainant
- Must have penalty provisions for frivolous and misleading complaints. - Health care providers and institutions should be allowed to lodge complaints
against any person, groups and authorities against infringement of their rights.
CHAPTER-VI
Section 16 – Totally unconstitutional provision, legal remedies and appeals are constitutional
rights and principal of natural justice. Should be deleted. We believe that the said act should be beneficial to public and health care providers. No
adverse relationship between public and health care providers] should develop in the society
due to vague provisions of the act.

Nitin Pandey
Humble submission for Grievances and Suggestions for Rajasthan Right to Health Care
Act 2022
CHAPTER-I
Section 2(t)- The definition of Healthcare provider is not exhaustive. Must include the
qualifications and relevant licenses required to be obtained by them. Section 2- Define
“Quackery”
CHAPTER-II
Section 3(c)- Replace all public hospitals to public health institutions as defined.
Section 3(j)- Proper referral transport includes the cost incurred in acquiring the vehicle,
equipment, medicines, trained staff etc., which should be clearly mentioned. Healthcare
facilities, especially private hospitals, cannot bear the cost of such services by
themselves.
Section 3(l)- Define Redressal Mechanism
Section 3(m)- Unfavorable for the Private Healthcare Facilities as the Provision allows
patients to not pay their dues for an indefinite period. Should only be allowed to take the
body of the deceased after providing an assurance/bond to pay the dues within a specific
period of time and within the limits of capping of dues on total bill.
Section 4- Should include duty of patients to pay the all the bills and dues for services
rendenered before discharge to private healthcare establishments.
Section 4(h)- Specify the Prescribed Authority to which such acts should be reported.
Section 4(f)- Include punishment under The Rajasthan Medicare Service Persons
and Medicare Service Institutions (Prevention of Violence and Damage to Property) Act,
2008.
Section 5-
Include right to:
- practice profession without undue pressure, distress and harassment
- refuse treatment to patients indulging in disruptive and violent behavior
- refuse treatment to patients if required services are not available
- report unruly patients and attendants
- receive timely payments for services
Section 5(a)- no criminal proceedings against healthcare providers such as FIR/arrest
should be initiated without obtaining a report from district level committee of subject
specialists
Section 5(d)- Right to have physical safety and security at the workplace , through proper
safety measures by government.
CHAPTER-III Section 7- Include:
- Ensure proper safety and prevention of violence against health care workers and
establishments. Enact proper rules and stringent laws against physical violence, verbal
abuse, mob lynching harassment etc. for the same and direct all concerned authorities to
implement them.
- Make provisions to prevent quackery and crosspathy by unqualified persons in health
care. Respective authorities like CMHO, District Collector or SDM of the concerned
territory must be made liable and accountable to prevent quackery.

CHAPTER-IV
Section 8 (b) VII 2. - Specify representatives of health associations: must be from office
bearers of Indian Medical Association and Private Hospital association. Chairperson
should not appoint any representative by “Pick & Choose” method. Exclusive power to the
Chairperson to appoint the representatives can create a bias.
Section 9(b)VI2. - Specify representatives of health associations: must be from office
bearers of Indian Medical Association and Private Hospital association. Chairperson
should not appoint any representative by “Pick & Choose” method. Exclusive power to the
Chairperson to appoint the representatives can create a bias.
Section 11(b)(VI)- Representatives of health associations should be their concerned
executives or office bearers. Should also include President/Secretary of Indian Medical
Association (IMA), representatives of Private Hospital associations. Exclusive power to
the Chairperson to appoint
the representatives can create a bias.
Section 12(b) – IPC section 176 and 177 should not be applicable. Required information
must be defined properly.
Section 12 (c) – Totally unconstitutional provisions. Any authority or officer should not be
given rights for a search and seize operation. Only related documents and records can be
asked to produce according to section 91 of CrPC.
Section 12 (d) – Unconstitutional provision of fixing responsibility and accountability of
private institutions for services. Clear Contraventions of Article 19 1(g) of
constitution of India. State Health Authority and District Health Authority can have only
supervision and advisory rights. Not acceptable to extent of deciding the prices for private
hospitals as the services provided at each establishment are diverse.
The government shall have powers to regulate prices for the packages of government
schemes only. Private institutions should not have any bindings for participation and
empanelment of such government schemes. State Health Authority and District Health
Authority committee may have powers to send recommendations to revise the rates of
packages of government schemes to concerned departments to encourage participation
of more and more private institutions.
CHAPTER-V
Section 13 (a) – Complaint forums and Grievance redressal must be at three levels:
1. Institutional Level
2. District Level: Must have members from representative of local medical association,
subject medical specialist and CMHO
3. State Level: Must have members from representative of state medical association,
subject medical specialist from Medical College
Section 13 (b) – No grievance, complaint and investigation summary should not be
shared on public domain. Goodwill and reputation of health care providers and
institutions must be properly preserved and maintained. Section 13 – Include following
provisions:
- Burden of proof must be on complainant
- Must have penalty provisions for frivolous and misleading complaints.
- Health care providers and institutions should be allowed to lodge
complaints against any person, groups and authorities against infringement of their rights.

CHAPTER-VI
Section 16 – Totally unconstitutional provision, legal remedies and appeals are
constitutional
rights and principal of natural justice. Should be deleted.
We believe that the said act should be beneficial to public and health care providers. No
adverse relationship between public and health care providers] should develop in the
society due to vague provisions of the act.

Pallavi Gupta
Comments on the draft Rajasthan Right to Health Care Bill, 2022
Submitted by: Health Systems Transformation Platform*, New Delhi on 24 March 2022
We would like to congratulate the Government of Rajasthan for recognising health care as a right and being the first state in the country to introduce a legislation in this regard. It is commendable that the draft Bill lays down the rights and duties of the care users and the care providers (both in the public and in the private sectors), along with the obligations of the state government. However, there are certain issues which we would like to bring to your kind attention and suggest ways to further strengthen the Bill. Hope you will find our suggestions useful and consider them while finalising the draft. Chapter, Section,
Clause of the draft
Bill
Problem/issue
with the
concerned clause Proposed change
Reason for proposing
the change
Chapter I, Section 2 Definitions e) "capacity to consent" means ability of an individual, including a minor or mentally
challenged person, assessed by the relevant health service provider on an objective basis…”
It is incorrect to use the term “mentally challenged person” in the present context.
Replace, “mentally challenged person” with “a person with mental illness/ disability”.
The proposed change is in accordance with the terminology used in Central legislations, i.e., Mental Healthcare Act, 2017 and Rights of Persons with Disabilities Act, 2016.
Chapter I, Section 2 Definitions (v) Health impact assessment
The draft Bill defines health impact assessment but there is no further mention of how it would be put into practice.
Consider adding a clause in Chapter III- Obligation of the Government that health impact assessment of new projects, programmes, technology etc. would be conducted.
As a preventive measure, it is important to ensure that no harm is done to people’s health, even if unintended, in undertaking any new initiative.
Chapter I, Section 2 Definitions (tt) “Resident”: Person who is a bonafide resident of the state or is currently residing in the state.
The definition of ‘resident’ as given in the draft Bill does not cover persons who may be visiting or travelling through the state.
Replace ‘Resident’ with ‘People’, defined as “all those persons who may need health care while they are in the state of Rajasthan”.
Since need for health care may arise at any moment, the term ‘resident’ may be replaced with ‘people’ to provide a more comprehensive coverage under the legislation.
Chapter II, Section 3 Right of Residents
Certain crucial Rights are excluded in Section 3.
May please include the following Rights: Right to seek services such as laboratory investigations, purchase of medicines and other
There are several instances when patients suffer because service providers do not follow these practices. Enshrining these in the

consumables from vendors of their choice. Right to be given an estimate of cost of health care before initiating treatment. Right to be provided itemised bill with break up of costs before making the payment. Right to be provided emergency health care in case of a serious/life threatening situation irrespective of the ability to pay. Right to be provided health care without having to necessarily make advance payment. Right against discrimination: No person shall be subject to any discrimination in any form or manner, by the Government or any other person or body of persons, whether public or private, in access to health care services and health care establishments, on one or more of the grounds of sex, class, monetary or other economic status, place of birth, age, marital status, actual or perceived health status, sexual orientation, physical or mental disability, occupation, religion, language, political or other opinions, caste, civil, political, social or other status or affiliation, race, or any
legislation would help in more ethical delivery of health care services. An example: https://timesofindia.indi atimes.com/india/private -hospitals-making-over- 1700-profit-on-drugs consumables-and diagnostics study/articleshow/62997 879.cms In accordance with Article 14 of the Constitution of India, it is important to ensure people’s right to equality in accessing health care without any discrimination

other ground. Right to be treated with dignity and to be free from any inhuman, cruel or degrading treatment, at the hands of Government or any other person or body of persons, whether public or private, in the matter of health rights.
Chapter IV Section 9: Constitution and Duties of State Executive Committee Section 11: Constitution and Duties of District Health Authority.
While the composition of the State Health Authority includes representatives of patients’ groups, the same are missing from the other two bodies that the Bill proposes.
Representatives of patients’ groups may be included in the State Executive Committee and District Health Authority as they are the implementing bodies.
Patients’/Users’ voices need to be heard both in policy formulation and implementation as they are the ones who are directly impacted by such measures. Therefore, their inclusion in the implementing bodies is equally important.
Chapter IV, Section 12 (d)
With respect to fixing the cost of health care at private health care facilities and displaying rates in public domain, reference may be given to the Clinical Establishments Act, 2010 which has similar provisions and has been adopted by the state of Rajasthan.
To Section 12, clause (d) add “as also prescribed under the Clinical Establishments (Registration and Regulation) Act, 2010 which has been adopted by the Government of Rajasthan”.
This would help in laying emphasis on the importance of fixing costs and displaying them publicly.
Chapter VI, Section 16: Bar of jurisdiction.
This Section restricts people’s access to judicial recourse.
The Section may be deleted.
It would be unconstitutional to hamper people’s right to seek legal remedy if the grievance redressal mechanism provided for in the legislation does not resolve a dispute satisfactorily.
Note: We would be happy to provide any further information/clarification.
Contact Person: Ms. Pallavi Gupta, Specialist, Health Systems Governance, Health Systems
Transformation Platform, New Delhi. [email protected]; 9560080907.

* About Health Systems Transformation Platform (HSTP) (hstp.org.in)
Health Systems Transformation Platform (HSTP) was conceptualised as a Centre of Excellence under
the guidance of Prof. (Late) Maharaj Kishan Bhan, renowned scientist and visionary in 2017 with a
grant from Sir Ratan Tata Trusts. In May 2018, HSTP was incubated within the Tata Trusts family and
registered as Forum for Health Systems Design and Transformation, a not for profit company (section
8) under the Indian Companies Act 2013. Our mission is to enable Indian health systems to respond
to people’s needs. We do this in collaboration with Indian and Global expertise through research for
health systems design, enhancing stakeholders’ capabilities and fostering policy dialogue. Our
multidisciplinary team with expertise in health financing, service delivery, governance and health policy
and
systems research works under the able guidance of the Chief Executive Officer, Mr. Rajeev
Sadanandan, former Additional Chief Secretary, Government of Kerala.
As part of the Health Systems Governance work, we conducted a study, ‘Regulation of Health Care
Delivery in India – A Landscape Study’ to review health legislations with a focus on health care delivery
in India and document the strengths, gaps, and challenges. The study report is available here.

Dr. Dhavani Mehta 1 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
2. Introduction
o On 8 March, 2022, the Rajasthan State Government released a draft of the Rajasthan Right to Healthcare
Bill, 2022 (―Bill‖) and invited public comments on the same.
o The Vidhi Centre for Legal Policy (―Vidhi‖) is submitting this Note in response to this call.
o This Note is divided into two parts: I.
II. Comments on Drafting and Definitions
Comments on Substantive Aspects of the Bill A. The Need for a distinction between Public Health & Healthcare, and addition of a separate
chapter on Public Health Emergencies
B. Interface of the Bill with existing laws
C. Rights & Duties of stakeholders
D. Obligations of the State Government
E. Regulatory Architecture and Administration
F. Grievance Redressal Mechanisms
III. Details that Require Clarity through Rules 3
PART I: COMMENTS ON DRAFTING AND DEFINITIONS This Part examines whether the language of the Bill lends itself to clear and unambiguous implementation and
enforceability. Specific instances of drafting errors have been enlisted and explained below.
o Preliminarily, it may be noted that the section on definitions is traditionally not seen as a substantive
provision of a law. Unless the defined term has been used in a substantive provision, it has no
enforceability. This is the case with several terms defined in Clause 2 of this Bill.
o As such, these terms may be linked to substantive provisions to ensure that they can be enforced.
o For example, the term ‗capacity to consent‘ has been defined in Clause 2(e) of the Bill, but has not been
employed anywhere else in the Bill. To ensure that its intended implication is realised and its significance is
clearly understood, this term may be linked to the provision which gives persons the right to informed
consent (Clause 3 of the Bill).
A. Drafting errors Provision Error Long title Long title of the Bill is absent. Enacting formula Enacting formula of the Bill is absent.
Preamble
The Preamble seems incomplete and ends abruptly. The
last sentence is ―The
Constitution of India incorporates provisions Article 21 of
the constitution
guarantees protection of life and personal liberty to every
citizen‖ – This is
incomplete.
Clause 1(c) - Short Title,
extent and
commencement
This clause states that the Act ―shall come into force on
such date as the
government may, by notification in the official Gazette.‖
There seems to be a
missing word here, leading to the lack of clarity. As per
the general norm, this
clause should read as follows: ―It shall come into force on
such date as the
government may, by notification in the official Gazette
appoint.‖
Clause 2 - Definitions
The numbering format (alphabets) used for the sub-
clauses under this clause
hampers the readability of the text. Instead, a numerical
pattern should be used. Clauses 2(o)(I) and 2(o)(II) A mistaken repetition of the same clause.
Clause 8(b)(VI) -
Constitution and Duties
of State Health Authority
The clause does not mention the procedure for the
appointment of the three
persons from the Government Medical Teachers of the
state. Adding the phrase
―nominated by the state government‖ or any other
qualification would address
this.

Clause 11(c)(III) -
Constitution and Duties
of District Health
Authority
There is no clarity with respect to the way in which the
quotation marks have
been placed when mentioning a potential outbreak. It
seems as though the
intention was to put the phrase ‗potential outbreak‘ in
quotes, which suggests
that the drafters meant to use it in a specific sense. If this
is the case, ‗potential
outbreak‘ should be explicitly defined in Clause 2 of the
Bill. B. Ambiguous Drafting Provision Issue
Clause 2(a) - Definition of
„affordable‟
This clause defines ‗catastrophic household healthcare
expenditure‘ as
health expenditure exceeding 10% of its total monthly
consumption
expenditure or 40% of its monthly non-food consumption
expenditure.
This may be reconsidered as the WHO defines
expenditure as being
catastrophic if a household‘s financial contributions to the
health system 4 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan Provision Issue exceed 40% of income remaining after subsistence needs
(not just food)
have been met.
Clauses 2(b) and 2(d) – Definition
of „basic primary healthcare
services‟ and „comprehensive
primary healthcare services‟
These clauses provide the definitions for the phrases
‗Basic Primary
Healthcare Services‘ and ‗Comprehensive Primary
Healthcare Services‘.
In defining these terms, the wording used is ‗as defined
from time to
time‘. However, the Bill does not state how specific
services that fall
under either of these definitions will be defined or who
will define them.
Clause 2(e) - Definition of
„capacity to consent‟
Uses archaic language such as the phrase ―mentally
challenged‖. Instead,
it is advised to either try and list out the specific
disabilities that are
intended to be covered, or provide a more acceptable
phrasing. For
guidance, the UK government‘s guide on inclusive
language (here) can
be referred to.
This term should be linked to the right to informed
consent in Clause 3
of the Bill.
Clause 2(jj) - Definition of „public
health‟
The draft defines public health as the health of the
population, as a
whole, specially as monitored, regulated and promoted by
the
Government.
This definition is at odds with the generally accepted,
more
comprehensive definition of public health - Public health
is defined as
―the art and science of preventing disease, prolonging life
and promoting
health through the organized efforts of society‖ (Acheson,
1988; WHO). Clause 2(k) - Definition of primary The word ‗disaster‘ is loosely defined, and seems to be an

healthcare services‟ incomplete
version of the definition provided in Clause 2(d) of the
National Disaster
Management Act.
The complete definition from the National Disaster
Management Act
should be adopted.
Clauses 2(i), (j), and 2(l) -
Definition of „decontamination‟,
„deratting‟, and „disinfection‟
These terms do not find further mention in the Bill,
although these are
important public health functions.
In defining ‗Decontamination‘ and ‗Disinfection‘‘, the
Bill mentions
‗health measures‘ without defining the same. Considering
the broad
scope of this phrase, a clear outline of what such measures
can include
should be provided.
Clause 2(o) - Definition of
„essential public health functions‟
This clause specifies that monitoring and evaluating health
status to
identify community health problems and taking measures
to solve them
are one of the essential public health functions. However,
the procedure
for this should be outlined in the chapter which lays out
the obligations
of the relevant authorities under the Bill.
The various sub-clauses under this provision seem to use
the phrases
‗health problems‘ and ‗health issues‘ interchangeably,
without outlining
the scope of either of these.
Clause 2(t) - Definition of
„healthcare provider‟
The definition of ‗healthcare provider‘ is vague. In the
interest of clarity,
an illustrative and inclusive list of healthcare providers
should be set out
in this provision (for e.g., registered medical practitioners,
nurses, ANMs,
ASHA workers etc.).
Clauses 2(w) - Identifiable health
information; and 2(dd) - non
identifiable health information
While the intent behind this provision is commendable,
the terms have
not been employed in any of the substantive provisions of
the Bill.
Clause 2(y) - Definition of
„Informed consent‟
Suggestion to use gender-neutral language instead of
phrases like
‗himself/herself‘.
Clause 2(kk) - Definition of „public
health institution‟
The term ‗health services‘ should be defined with
reference to the
definition of ‗health care‘ set out in Clause 2(r) of the Bill.
Clause 2(ll)(II) – Definition of
„public health emergency‟
Given that the definition uses broad phrases like ‗large
number‘ and
‗widespread exposure‘ which are subjective, the
substantive provisions
of the Bill must provide a more detailed method for
determining these
thresholds.

5 Provision Issue
Clause 2(oo) – Definition of
„public health surveillance‟
Surveillance powers granted in respect of collecting
‗health-related‘
data. To ensure that the broad phrasing carries does not
give rise to the
possibility of potential misuse, reasonable safeguards
should be
introduced in the substantive provision, i.e., Clause
8(d)(IX). Clause 2(ww) - Definition of
„Secondary Health Care Services‟
and 2(xx) - Definition of „Tertiary
Health Care Services‟
Including some examples or illustrations may be useful
here, to make the
definitions more holistic/ comprehensive.
Clause 3 (Rights of Residents) and
Clause 5 (Rights of Health Care
provider)
There should be a uniformity in the drafting language. For
instance, some
of the sub-clauses of Clause 3, relating to rights of
residents start with
‗Residents will have a Right to‘, whereas some start with
‗Right to—‘
Clause 3(a)
‗Residents have the right to collect information to make
themselves
healthy‘ - This is drafted in a vague manner and would be
difficult to
operationalise.
Clauses 3(g), 3(h), 3(j) and 3(m)
These clauses use the term ‗health care establishment‘ in
different ways.
For instance, while in some sub-clauses it is used in
conjunction with the
terms like ‗be it public or private‘, in other ones it is used
broadly (‗every
health care establishment‘). This creates an unexplained
inconsistency.
The terms ‗be it public or private‘ need not be used if
health care
establishment itself has been defined in the Definitions
section to
include both public and private establishments.
Clause 3(k)
‗Right to take treatment summary in case of patient,
leaving against the
medical advice‘ - The language used to draft this is
unclear and the
meaning, responsibility, and implication are vague.
Instead, this should be broadened to provide a general
right of patients
to access medical records at all times, irrespective of
whether they are
discharged against medical advice.
Clause 2 (e) - Capacity to consent,
Clause 3 (dd) - non-identifiable
health information
The terms defined here do not find specific references in
the act. The
act does not utilize the terms defined in these clauses later
in the draft,
making the implications of such definitions ambiguous.
Clause 7(a) under Obligations of
the government
Vague mention of ‗appropriate state budget‘ without
outlining what is
intended by the use of the word ‗appropriate‘ or which
body will
determine whether it is appropriate or not.
Clause 7(i)
It should be made clear that the standard to be followed in
determining
the threshold of ‗nutritionally adequate and safe food‘
should be clarified
in the rules framed under the Bill. Clause 7(j) Broad phrasing like ‗effective measures‘ used which can

potentially vest
excess power in the government to impose restrictions in
this regard. A
clearer outline of the kind of measures that can be taken
under the
mandate of the Bill should be provided.
The Bill should contain a distinct chapter on public health
emergencies,
given that they will require special measures over and
above the
performance of essential public health functions and the
delivery of
health care services.
Clause 9(d)(V) under Constitution
and Duties of State Executive
Committee
The acceptable procedures that can be used to monitor
health status
should be outlined to avoid the risk of legitimizing
excessive surveillance.
Moreover, a definition of what parameters fall within the
umbrella of
‗health status‘ should be provided.
Clause 11(b)(IV) under
Constitution and Duties of
District Health Authority
The number of senior-most officers that the Bill seeks to
include in the
District Health Authority from each of the 7 departments
mentioned
must be clarified.
Clause 11(c)(VI)
This clause discusses the creation of tools for monitoring
as one of the
functions of the District Health Authority. It also
discusses the collection
of data. It must be clarified what the extent and scope of
the usage of
these tools would be. Additionally, clear rules must be
laid down for
what kind of data will be collected, whether it will be
stored or not, etc.
6 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan Provision Issue
Clause 12 - Powers of the State
Health Authority and District
Health Authority
In this clause, there is an absence of proportionality
requirements that
would be in keeping with the rights-based nature of the
Bill. For
instance, the references to carrying out inquiries (Clause
12(a)), entering
a building (Clause 12(c)), etc. should all reflect the
principle that only
such measures should be taken as are necessary,
proportionate and least
restrictive of the rights of those concerned.

7
PART II: COMMENTS ON SUBSTANTIVE ASPECTS OF THE
BILL
A. The Need for a distinction between Public
Health & Healthcare, and addition of a separate
chapter on Public Health Emergencies 1. Current Position under the Bill
Although the instant Bill is titled as the ‗Right to Healthcare Bill‘ (emphasis supplied), it regulates both public
health as well as healthcare without any clear demarcation between the two. For example, it includes prevention,
treatment, and control of epidemics as an obligation of the government [Clause 7(j)]. However, the rights and
duties of stakeholders, obligations of the Government, regulatory architecture, grievance redressal mechanisms
etc. are have not been separated from each other, thus creating scope for confusion.1 At the same time, the
public health aspects of the bill are inadequate and require more careful articulation and implementation
mechanisms.
2. Vidhi’s Comments
The field of health law has traditionally recognised a distinction between public health and healthcare. This
distinction is generally captured in the following terms:
―[public health] is a collective (―public‖) responsibility, geared toward improving the health and well-being of
an entire community—or state, or country—as opposed to diagnosing or treating particular individuals. In
addition, public health addresses the ―conditions to be healthy,‖ meaning that it is focused on ―the prevention
of disease and the promotion of health‖ … as opposed to medical care for those who are already ill…Public
health studies the causes and distribution of disease and injury in populations. This is one of the defining
differences between public health and healthcare.‖2
Further, the World Health Organisation has defined ‗public health law‘ in the following terms:
―Public health law refers to the formal set of laws – and to the legal processes for implementing and enforcing
them – that seek to ensure the conditions for people to live healthy lives. Apart from laws pertaining directly
and palpably to health infrastructure and health regulation, a robust public health system uses a combination
of laws, regulations, public awareness, public trust, and public participation mechanisms – under an umbrella
of recognized human/ health rights – to promote community and individual health (physical, mental, social,
etc.) in the society. Such mechanisms include focus on larger social, economic, and political factors that
promote or discourage health behaviours.‖3
Thus, laws relating to public health generally aim to prevent the potential outbreak of diseases, tackle public
health emergencies, and generally ensure the overall health and well-being of a population. On the other hand,
laws relating to healthcare aim to provide citizens with the best possible standards of medical diagnosis and
treatment by, inter alia, regulating clinical establishments. 1 See comments on Chapters II & III of the Bill. 8 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
The aims being distinct, the rights and duties as well as regulatory approach which is adopted to secure them are
also different. As such, India (as well as other jurisdictions) has traditionally enacted separate legislations to
address each aspect. For example, the state of Rajasthan itself addresses public health through third-tier
legislations such as the Rajasthan Municipalities Act, 2009 and the Rajasthan Panchayati Raj Act, 1994, or
through specific laws such as the Rajasthan Vaccination Act, 1957, while healthcare is addressed through laws
such as the Rajasthan Medical Act, 1952 and the Clinical Establishments Act, 2010.
In the interests of clarity, ease and efficiency of administration, and enforceability of the rights and duties, the
Bill should be divided into two clear Parts. The Part which addresses public health may contain, inter alia,
provisions relating to the public health functions of the State Government and third tier bodies, rights and duties
of citizens, etc. while the Part relating to healthcare may contain, inter alia, provisions relating to the rights of
patients, duties of clinical establishments etc. A common authority with oversight over both may be retained,
provided that its functions and powers in relation to public health and healthcare are clearly delineated. The Part
dealing with public health should have a chapter solely dedicated to public health emergencies, given the powers
required to be exercised in order to tackle them, and the special duties and responsibilities which arise in such
conditions. 2 Scott Burris et al, 'The New Public Health Law: A Transdisciplinary Approach to Practice and Advocacy' (Oxford University Press, 2018),
pp.4-5. 3 WHO, ‗Advancing the right to health: The Vital Role of Law‘, 2017.

9
B. Interface of the Bill with Existing Laws 1. Current Position under the Bill
The Bill attempts to harmonise its provisions with existing laws relating to healthcare and public health in
Rajasthan.4 This is sought to be achieved in the following manner:
o Generally speaking, the Bill is to be applied in uniformity with, and not in derogation of, any other laws
in force in Rajasthan which deal with the same subject matter.5
o However, in the event of a conflict between this Bill and other laws, the provisions of this Bill are to
prevail over the other laws to the limited extent of the conflict.6
Notwithstanding these precepts, the Bill enjoins the State Government to undertake comprehensive reviews of
the existing laws on health within one year of this Bill coming into force, in order to ensure the compatibility of
those other laws with this Bill.
2. Vidhi’s Comments
Instead of laying down a set of general rules governing the interaction between existing laws and the Bill, the
potentially conflicting laws should first be identified. The conflicts should then be explicitly addressed in the text
of the Bill.
The Rajasthan State Government has already enacted the following legislations which touch upon various
aspects of public health and healthcare:
o Clinical Establishments (Registration and Regulation) Act, 2010: this Act enables the registration and
provides for the regulation of clinical establishments.
o The Rajasthan Para-Medical Council Act, 2008: this Act provides for the constitution of a Para-Medical
Council, regulation of Para-Medical profession, and recognition of institutions imparting education or
training in Para-Medical subjects in the State and for matters connected therewith or incidental thereto.
o The Rajasthan Medical Act, 1952: this Act provides for the registration of Medical Practitioners in
Rajasthan.
o The Rajasthan Vaccination Act, 1957: this Act makes the vaccination of children compulsory.
o The Rajasthan Panchayati Raj Act, 1994: this Act obligates the Panchayati Raj institutions to perform
certain public health functions.
o The Rajasthan Municipalities Act, 2009: this Act obligates the urban local bodies to perform certain
public health functions.
o A careful mapping of the provisions of these laws must first be undertaken and potential conflicts must
be identified. After decisions have been made on how these conflicts are to be addressed, appropriate
provisions may be placed in the body of the Bill explaining its interface with these existing laws. For
instance, there must be clarity on the mechanisms that will be used to fix prices for healthcare services
at healthcare establishments. Currently, the Central Government exercises this power under the
Clinical Establishments Act, 2010. The power of price fixation for services in clinical establishments in
the state of Rajasthan already exists under rule 9(ii) of the Clinical Establishments Rules, 2012, read
with section 52 of the Clinical Establishments Act, 2010. This power is currently exercised by the
Central Government in consultation with the concerned State Government. If this power is now
proposed to be exercised under the proposed law, any overlap with the Clinical Establishments Act
must be appropriately clarified. In the same vein, the Clinical Establishments Act, under which
standards for healthcare establishments are set must also ensure that such standards meet the rights 4 Rajasthan Right to Health Care Bill, 2022, s.18. 5 Rajasthan Right to Health Care Bill, 2022, s.18(b)
6 Rajasthan Right to Health Care Bill, 2022, s.18(c). 10 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
of accessibility, affordability, and quality guaranteed under the proposed law. For all future
laws/rules/regulations/notifications/other instruments dealing with public health or healthcare, the
State Government should ensure that these are fully compatible with the provisions of the Bill. 11
C. Rights and Duties of Stakeholders 1. Current position under the Bill
Chapter-II of the Bill provides for the rights and duties of residents and health care providers.
Residents have been defined as persons who are bona fide residents of Rajasthan or are currently residing in
Rajasthan. These residents have been given a range of rights and duties only in the domain of healthcare.
Rights of Residents
According to Clause 3, Residents have the right to:
o collect information to make themselves healthy
o free consultation, drugs, diagnostics, emergency transport and emergency care at all public health
institutions
o free/affordable care for surgeries at all public hospitals
o avail free services the empaneled hospitals, if they are covered under insurance scheme through

o avail free services from the private hospitals established through land allocation on concession rates as
per the terms and conditions mentioned at the time of the allotment of the land
o receive information, records and reports of self from the health care establishment, be it public or
private
o informed consent at all health care establishments, be it public or private
o confidentiality at all health care establishments
o safe and quality care according to standards prescribed for different levels of health care
establishments run or managed by Government or private institutions.
o proper referral transport by all health care establishments be it public or private
o take treatment summary in case of patient, leaving against the medical advice
o be heard and seek redressal from health care establishment if any grievance occurred after availing
services
o receive the dead body of the deceased person, to be exercised by the family member/authorized person,
irrespective of payment due status from every health care establishment
Duties of Residents
According to Clause 4, Residents must:
o Avail of tertiary healthcare services only after following referral from primary or secondary level institutions
or service providers
o Provide healthcare providers with relevant and accurate information 12 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
o Comply with the prescribed healthcare
o Sign a discharge certificate or release of liability if they refuse to accept or continue the recommended
treatment
o Not pollute the premises where the treatment is being provided
o Refrain from misconduct and misbehaviour with healthcare providers, and treat them with respect and
dignity
o Refrain from physical assault on healthcare personnel or damage to property
o Report illegal or unethical behaviour
o Permit post-mortem to be done in case of unnatural death
Healthcare providers (―HCP‖s) have been defined as persons who are authorised by the Government to engage
in identifying, preventing, and/or treatment of illness and/or disability.
Rights of healthcare provider
According to Clause 5, healthcare providers have the right to:
o protection from complaints relating to adverse consequences on providing services of any kind as long as
the provider has acted bonafide to the best of their professional capability through application of standard
treatment procedure and judgment, and in the best interests of the residents and exercised all reasonable
care
o be treated with respect and dignity by the patients and attendants.
o decent working conditions and training.
o right of physical safety and security at the workplace. o
availability of protective measures for any accidental exposure to harm.
Duties of healthcare provider According to Clause 6, healthcare providers must:
o Follow the standard treatment guidelines and protocols as notified from time to time, and using the
clinical judgement in the best interest of the resident.
o Maintain confidentiality, privacy, dignity of residents, and treat them with respect.
o Respect the rights of residents to take a decision to get a lab investigation or to purchase medicines from
a vendor of their choice.
o Ensure informed consent is taken before every procedure.
o Regularly explain and inform either patient or relatives regarding the severity of the disease, progression,
treatment and prognosis. 13
2. Vidhi’s Comments
Rights of residents
o It is commendable that ‗residents‘ has not been defined in a restrictive way that requires proof of
domicile, citizenship, etc. However, there should be a differentiation between rights of residents and
users. While certain rights like state health insurance may be reserved for residents of the state, certain
rights such as emergency health care, information, quality of care, etc. should be applicable to any user
or patient.
o The chapter mentions ‗Collective‘ rights, but most of these rights are individual rights, and community
health rights have been left out of the draft. There is scope here for the inclusion of rights of marginalised

communities, rights of participation in decision-making and representation, articulation of broader public
health rights, etc.
o In the same vein, some rights such as right to confidentiality, treatment summary, receive dead body,
etc. should be part of ‗user rights‘ as opposed to ‗rights of residents‘.
o In 2018, the Ministry of Health and Family Welfare (―MoHFW‖), Government of India, adopted a Charter
of Patient Rights, on the basis of a list prepared by the National Human Rights Commission. It has since
been updated and approved by the National Council for Clinical Establishments.7 As per this charter, a
patient/ user and their representative has the following rights with respect to a clinical establishment:
o To adequate relevant information about the nature, cause of illness, proposed investigations and care,
expected results of treatment, possible complications and expected costs
o To information on the Rates charged for each type of service provided and facilities available. Clinical
Establishment shall display the same at a conspicuous place in the local as well as in English language.
o To access a copy of the case papers, patient records, investigation reports and detailed bill (itemized).
o To informed consent prior to specific tests/treatment (e.g. surgery, chemotherapy etc.)
o To seek second opinion from an appropriate clinician of patients' choice, with records and information
being provided by the treating hospital.
o To confidentiality, human dignity and privacy during treatment.
o To have ensured presence of a female person, during physical examination of a female patient by a
male practitioner.
o To non-discrimination about treatment and behaviour on the basis of HIV status
o To choose alternative treatment if options are available
o Release of dead body of a patient cannot be denied for any reason by the hospitals.
o It was recommended that patient seeking transfer to another hospital/discharge from a hospital will
have the responsibility to "settle the agreed upon payment".
7 ‗Charter of Patients‘ Rights and Responsibilities‘, <http://clinicalestablishments.gov.in/WriteReadData/3181.pdf>. 14 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
o It may be specified in the charter that no discrimination in treatment based upon his or his illness or
conditions, including HIV status or other health condition, religion ethnicity, gender (including
transgender), age, sexual orientation, linguistic or geographical/social origins.
o Informed consent of patient should be taken before digitization of medical records Right to care
according to prescribed rates wherever relevant.
o Right to choose source for obtaining medicines or tests
o Right to protection and compensation for patients involved in clinical trials, as per Drugs and
Cosmetics Act and other Government Guidelines.
o Right to protection and compensation for participants involved in biomedical and health research as
per ICMR and other Government Guidelines.
o Right to Patient Education
o Right to be heard and seek redressal: Every Hospital shall have/establish a time bound Grievance
redressal mechanism to address the grievances of the patients. A Grievance redressal officer will be
identified by the hospital and his name and contact details will be displayed at a conspicuous place in
local language and in English. The records of grievances received and remedial action taken will be
maintained. The name and contact details of the district registering authority will also be displayed
who may be contacted in case of non-redressal of the grievance of patients to their satisfaction
o Right to proper referral and transfer, which is free from perverse commercial influences
▪ In case of referral by the hospital, the referring hospital will provide proper referral transport
facility in the most appropriate vehicle/ambulance for transfer of patient to the nearest
possible hospital where facilities for appropriate and timely management of the condition of
the patient, are available.
▪ Such transfer of patient will not be refused even if not referred by the treating hospital and
even if the patient is leaving against medical advice (LAMA). The applicable reasonable
charges may be levied by the Clinical Establishments for such transfers. However, in case of
an emergency situation, such referral transport will be provided free of cost as far as possible
and will not be refused for want of any payment.
▪ State/UT Government may consider to define various charges for different types of
ambulance for compliance by the hospitals and other clinical establishments. The Clinical
Establishments will be required to display the rates of charges of ambulance(s)

▪ The referring hospital shall provide a qualified and trained person to monitor and manage the
condition of the patient enroute till the patient is received by the referee hospital
Since the state government is empowered by the Constitution to implement such rights through statelevel laws,
MoHFW had written to the states to do the same in 2019. Although the draft of this Bill
mentions some of these rights under Clause 3, a more comprehensive articulation of all the rights
articulated in the Charter of Patient Rights is crucial under ‗user rights‘ in healthcare establishments.
o The ‗right to collect information to make themselves healthy‘ is vaguely worded and therefore difficult
to operationalise. A more detailed public awareness and information right, with specific allocation of
duties, would be more useful here. 15
o Although the title of the Act mentions that it is a Right to Health Care Bill and not a public health law,
certain public health provisions (such as inclusion of public health emergencies) have been included in
the draft. In that context, public health rights should be included in the bill, and there should be separate
sections/ clauses dealing with public health and healthcare rights. Separate sections on these two
categories of rights would help in appropriate allocation of responsibilities for their implementation.
o There is no mention of allied rights which pertain to underlying determinants of health – such as food,
water, sanitation, housing, etc.
o While availability, accessibility, and quality of health care services have been guaranteed, there has been
no mention of acceptability (which refers to cultural suitability and approachability of the health system).
Rights of Health Care Providers
o There should be a section on rights of HCP vis-à-vis the government, and appropriate modifications may
be made in other health-related laws in the state (which currently lack a rights-based approach for HCP).
Apart from registered medical practitioners, other healthcare workers and frontline workers involved in
public health functions (ASHA workers, sanitation workers, ANMs, etc.) should be included within the
ambit of such rights. Apart from working conditions, safety, pay, dignity, etc. health insurance
mechanisms (especially in situations of public health emergencies) may be envisaged here.
o The right to be treated with respect and dignity by patients and attendants is vague. Since the violation
of any right under this law is a ground for grievance redressal (as per Clause 13), the rights should be
worded more carefully and specifically.
o Rights to decent working conditions, physical safety, security, etc. should be drafted in clearer and more
detailed ways. There are two ways of doing this – (a) Mention the components of these rights in the
body of the Bill, (b) Refer to appropriate labour or service laws.
Duties of residents and HCP
Ideally, duties of residents and HCP should not be part of state-level legislation. By not only including duties in
the legislation but also placing rights and duties in the same chapter, the draft fails to highlight the justiciability
of rights over duties.
o Some of these provisions (such as providing accurate information to HCPs, complying with prescribed
healthcare, etc.) are better suited to be part of service rules, patient charters, HCP training programmes,
public awareness programmes, etc. – as opposed to being legislated. Imposing legally enforceable duties
on all residents and HCPs will make them susceptible to disproportionate and unfair legal claims/
procedure under this Bill, and infringement of their other rights.
o More appropriate and efficient alternative mechanisms are already in use in case of some of these duties.
For grave violations such as physical assault of HCPs by residents and medical negligence by HCPs,
criminal law provisions and criminal court procedure are used. In case of littering or pollution of premises,
fines may be imposed at the institutional level.
o Some of these duties (e.g. availing tertiary healthcare only after obtaining referral, signing a discharge
certificate or release of liability if they refuse to accept or continue recommended treatment, etc.) are
excessive and restrictive. Legislating them within this Bill is likely to result in harassment of users and
infringements of their rights to healthcare and health services. The practise of ‗discharge against medical
advice‘ is often a result of a breakdown of trust between HCPs and patients/relatives/next friends. To
address this, more emphasis is needed on training HCPs in a process of shared decision-making, rather
than on imposing a potentially legally enforceable duty on patients. 16 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
o Some of the duties, such as the duty to report illegal or unethical behaviour, refrain from misconduct or
misbehaviour, etc. are worded in vague and undefined terms. Since the grievance redressal mechanisms
do not clarify grounds for complaint or appeal, and any violation pertaining to the Bill may be brought

within the ambit of a grievance, such vague articulation is likely to be harmful to users. Instead, there
should be an easily accessible mechanism that allows users to report grievances against HCPs or
healthcare establishments.
o Duties of HCPs pertaining to obtaining informed consent, maintaining confidentiality, respecting the
right to take a decision to get a lab investigation or to purchase medicines from a vendor of their choice,
informing patients regarding severity of the disease, progression, treatment and prognosis, etc. would
be better framed under ‗rights of users‘.
Some specific comments on Clauses 4 and 6
o Traditional public health duties, such as duty to self-report symptoms of a contagious disease, or
operating an established community reporting or surveillance system for the same, are missing from this
draft. These may be included in the proposed chapter on Public Health Emergencies, with specific
reference to the contours and limits of the duties, the powers of the government vis-à-vis the
enforcement of such duties, and their overall implications.
o It is not clear as to what an HCP should do if a user does not possess the capacity to consent under this
law. The capacity to consent has been defined in Clause 2 of the Bill, but does not find any use in the
rest of the Bill.
o The duty to inform patients or relatives – there should be careful consideration of the patient‘s right to
privacy and confidentiality when informing relatives. 17
D. Obligations of the State Government 1. Position under the Bill
Chapter-III of the Bill (Section 7) lays down the general obligations of the government under this law. It includes
obligations ranging from resource optimization and budgetary allocation, alignment of services and schemes
towards a robust health system in the state, notification of safety and quality standards, setting up coordination
mechanisms, and education and empowerment of people regarding health issues.
2. Vidhi’s Comments
o ‗Appropriate state budget should be provided‘ is a vague obligation that cannot be operationalized in the
absence of clearly laid down procedural, output-based, and/ or impact-based obligations
o The chapter mentions arbitrary timelines for implementing and developing a Human Resource Policy,
without describing the vision, components, or intended impact of the same.
o Six months have been provided for setting up social audit and grievance redressal mechanisms under
this Bill. Please refer to Chapter II. E of this document for more details on the issues with the mechanisms
envisaged therein.
o Clause 7(d) mentions that the state government should ‗align all health services and schemes‘ within one
year of enactment of this Bill. Please refer to Chapter II. B of this document for more details regarding
this.
o Safety and quality standards are better suited to the Clinical Establishments Act of respective states.
Therefore, such functions should be performed under the suitable legislation instead of creating multiple
overlapping laws, while ensuring that such standards meet the rights-based guarantees under this Bill.
o Certain provisions, such as consideration of criteria such as distance, geographical area, population
density, etc. for allocation of health services – are better dealt with by existing programmes under the
National Health Mission (―NHM‖) or existing standards such as the Indian Public Health Standards
(―IPHS‖). Partial duplication of the same in this Bill may cause unnecessary confusion.
o The chapter includes the obligation to set up coordination mechanisms among relevant government
departments to facilitate other determinants of health such as food, drinking water, and sanitation. The
mechanism envisaged under this Bill in Chapter IV (the State and District Health Authority), which
includes representation from diverse departments pertaining to various components of public health, is
better suited for such coordination function, rather than the governance, executive, and grievance
redressal functions assigned to these authorities under this Bill. 18 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
E.Regulatory Architecture/Administration 1. Current Position under the Bill
The Bill sets up regulators at two tiers: state (State Health Authority and State Executive Committee) and district

(District Health Authorities).
State-level: State Health Authority & State Executive Committee
The State Health Authority (‗SHA‘) is the primary regulator/administrator under the Bill.
The composition of the SHA is as follows:8
o Chief Secretary of the State Government of Rajasthan – Chairperson.
o Secretary in charge of the Medical, Health and Family Welfare Department – Co-Chairperson.
o Director of Health Services (Public Health) – Member-Secretary.
o Secretaries in charge of a range of relevant departments:
1. Medical Education
2. Public Health Engineering
3. Women & Child Development
4. Panchayati Raj and Rural Development
5. Social Justice and Empowerment
6. Tribal Area Development
7. Urban Development
8. Finance
9. Information and Public Relations
10. Revenue
11. Ayurveda, Yoga, Naturopathy, Unnai, Siddha, and Homeopathy
12. Education
13. Relief
14. Rehabilitation
o Three members of the Legislative Assembly to be nominated by the State Government.
o Three persons from the Government Medical Teachers, especially from clinical specialties.
o Four non-official persons from the following classes:
1. Public health experts to be nominated by the Chairperson.
2. Representatives of health associations to be nominated by the Chairperson.
3. Civil society organisations to be nominated by the Chairperson.
4. One member from a reputed NGO, preferably working in Rajasthan, to be nominated by the Chairperson.
o A Representative of the Chairman of the State Pollution Control Board.
o Three representatives from patient groups, to be nominated by the Chairperson.
The SHA is expected to perform 5 broad kinds of functions:
1. Advise the Government on all matters concerning public health.9
2. Formulate the health goals of the State and get these included in the mandate of the Panchayati Raj
institutions and urban local bodies,10 formulate the state-level strategic plans for implementation of
8 Rajasthan Right to Health Care Bill, 2022, s.8(b).
9 Rajasthan Right to Health Care Bill, 2022, s.8(d)(I).
10 Rajasthan Right to Health Care Bill, 2022, s.8(d)(II). 19
the Act including action on the determinants of health, viz., food, water, and sanitation,11 and
formulate a comprehensive policy/plan to prevent, track, mitigate, and control a public health
emergency.12
3. Monitor the preparedness of the State to manage public health emergencies,13 and develop
mechanisms for regular medical, clinical, and social audits to ensure quality healthcare at all levels.14
4. Involve the community as active co-facilitators, help them in identifying key indicators, and create
tools for monitoring, providing feedback, and validating any data that is collected as a result of such
feedback or monitoring.15
5. Delegate its functions by constituting committees/scientific panels/technical panels,16 and associate
with institutions, experts, NGOs etc. to ensure that its functions are efficiently discharged.17
To enable efficient discharge of functions, SHA has been given the following powers:
o It may require any person to furnish information by resorting to sections 176 and 177 of the Indian
Penal Code, 1860 (‗IPC‘).18
o It may enter any building or place if they have reason to believe that any document relating to the
subject matter of an enquiry may be found there. It may proceed to seize such documents, subject to
section 100 of the IPC.19
o It may fix responsibilities and hold to account private institutions, facilities, buildings or places, which

provide inpatient or outpatient services.20
o The Government may regulate prices for packages and ensure that rates for the packages are
displayed in the public domain.21
o During a pandemic or during any other public health emergency, the Government may take-over
buildings, facilities, services, and duties of human resources from private institutions, and also
prescribe rates for treatment provided by private institutions.22
State Executive Committee
The State Executive Committee (‗SEC‘) is an independent body under the Bill, to be set up by the SHA.23 It
essentially appears to be the executive arm of the SHA, as its functions are to implement the
plans/policies/strategies formulated by the SHA.
The composition of the SEC is as follows:
o Secretary in charge of Medical, Health, and Family Welfare Department – Chairperson.
o Secretaries in charge of a range of relevant departments:
1. Medical Education
2. Women & Child Development
3. Panchayati Raj and Rural Development
11 Rajasthan Right to Health Care Bill, 2022, s.8(d)(III).
12 Rajasthan Right to Health Care Bill, 2022, s.8(d)(IV).
13 Rajasthan Right to Health Care Bill, 2022, s.8(d)(V).
14 Rajasthan Right to Health Care Bill, 2022, s.8(d)(VI).
15 Rajasthan Right to Health Care Bill, 2022, s.8(d)(IX).
16 Rajasthan Right to Health Care Bill, 2022, s.8(d)(VII).
17 Rajasthan Right to Health Care Bill, 2022, s.8(d)(VIII).
18 Rajasthan Right to Health Care Bill, 2022, s.12(b).
19 Rajasthan Right to Health Care Bill, 2022, s.12(c).
20 Rajasthan Right to Health Care Bill, 2022, s.12(c).
21 Rajasthan Right to Health Care Bill, 2022, s.12(d).
22 Rajasthan Right to Health Care Bill, 2022, s.12(d)(I).
23 Rajasthan Right to Health Care Bill, 2022, s.9(a). 20 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
4. Ayurveda, Yoga, Naturopathy, Unnai, Siddha, and Homeopathy
5. Elementary education
o Mission Director (National Health Mission), Rajasthan.
o Director of Medical and Health Services (Public Health).
o Additional Director (Hospital/Administrator), Rajasthan.
o Nodal officer (under this Act), Rajasthan.
o Three persons from the Government Medical Teachers, especially from clinical specialties.
o Four non-official persons from the following classes:
1. Public health experts to be nominated by the Chairperson.
2. Representatives of health associations to be nominated by the Chairperson.
3. Civil society organisations to be nominated by the Chairperson.
4. One member from a reputed NGO, preferably working in Rajasthan, to be nominated by the Chairperson.
o A Representative of the Chairman of the State Pollution Control Board.
The SEC is expected to perform 5 broad kinds of functions:
1. Implement the state-level strategic plans formulated by the SHA for implementation of the Act
including action on the determinants of health, viz., food, water, and sanitation,24 implement the
comprehensive policy/plan formulated by the SHA to prevent, track, mitigate, and control a public
health emergency, as well as situations of outbreaks or potential outbreaks in the state.25
2. Ensure that the State Government is prepared for the management of public health emergencies.26
3. Ensure that there are mechanisms for regular medical, clinical, and social audits to ensure quality
healthcare at all levels.27
4. Monitor the health status of the population to identify and solve community health problems.28
District-level: District Health Authority
The District Health Authorities (‗DHAs‘) are the federated units of the SHA at the district level. Their primary
function is to implement the plans/policies/strategies of the SHA and coordinate between departments and
agencies of the State Government to ensure that the interests of the districts are adequately safeguarded.
The composition of the DHAs is as follows:
o District Collector – Chairperson

o CEO of the Zila Parishad – Co-chairperson
o Chief Medical & Health Officer (CMHO) – Member Secretary
o Senior most officers from the following departments in the district:
1. Public Health Engineering
2. Social Justice and Empowerment
3. Integrated Child Development Services (ICDS)
4. Women Empowerment
5. Local Body
6. Education
7. Ayurveda, Yoga, Naturopathy, Unnai, Siddha, and Homeopathy
24 Rajasthan Right to Health Care Bill, 2022, s.9(d)(I).
25 Rajasthan Right to Health Care Bill, 2022, s.9(d)(II).
26 Rajasthan Right to Health Care Bill, 2022, s.9(d)(III): it may be noted that this is Vidhi‘s understanding of the clause. The text itself reads:
―to ensure the State for management of public health emergencies‖.
27 Rajasthan Right to Health Care Bill, 2022, s.8(d)(IV).
28 Rajasthan Right to Health Care Bill, 2022, s.8(d)(V). 21
o Pramukh, Zila Parishad of the district and three Pradhans‘ of the Panchayat Samitis in rotation.
o Four non-official members:
1. Public health experts to be nominated by the Chairperson.
2. Representatives of health associations to be nominated by the Chairperson.
3. Civil society organisations to be nominated by the Chairperson.
4. One member from a reputed NGO, preferably working in Rajasthan, to be nominated by the
Chairperson.
The DHA is expected to perform the following broad kinds of functions:
o Implement the policies, recommendations, and directions of the SHA.29
o Formulate and implement strategies and plans of action for the determinants of health, viz., food, water,
sanitation, and environment.30
o Formulate a comprehensive policy/plan to prevent, track, mitigate, and control a public health emergency,
as well as situations of outbreak or potential outbreak based on the state plan.31
o Coordinate with government departments and agencies to ensure availability of and access to safe food,
water and sanitation throughout the district.32
o Organise hearings for beneficiaries coming to hospitals to improve healthcare services.33
o Involve the community as active co-facilitators, help them in identifying key indicators, and create tools for
monitoring, providing feedback, and validating any data that is collected as a result of such feedback or
monitoring.34
2. Vidhi’s Comments
The composition of the SHA and the DHAs should include full-time executive members
o Every member of the SHA and DHAs are ex-officio appointees. As a result, they are all ‗multi-hatting‘,
i.e., their regular occupation is entirely different, and they are administering these authorities only as
an additional obligation. In order for a body of this nature to function effectively and efficiently, it
requires a class of full-time executive functionaries (a CEO, a CFO, directors, and officers, and
employees.) as is the case with a majority of statutory regulators. In its present form, the SHA and
DHAs are functionally not regulators or authorities, but mere platforms for coordination.
o The following regulators at the central level have full-time executive members:
▪ Agricultural and Processed Food Products Export Development Authority: Consists of a fulltime Chairman shall be
appointed by the Central Government and is to be the CEO of the
Authority.
▪ Airports Authority of India: Consists of a full-time Chairperson who is to be appointed by the
Central Government. The other members of the Authority may be appointed as full-time or
part-time members as the Central Government may think fit.
▪ Airports Economic Regulatory Authority of India: All three members of the Authority are to be
full-time members. These are the Chairperson (who is also the CEO of the Authority) and two
other members.
▪ Atomic Energy Regulatory Board: Currently, the Board consists of a full-time Chairman, an exofficio Member, four
part-time Members and a Secretary.
▪ Central Electricity Regulatory Commission: Consists of a full-time Chairperson who is also to

be the CEO of the Commission, and three other full-time members.
▪ Central Pollution Control Board: Consists of a full-time Chairman and a full-time member
secretary.
29 Rajasthan Right to Health Care Bill, 2022, s.11(c)(I).
30 Rajasthan Right to Health Care Bill, 2022, s.11(c)(II).
31 Rajasthan Right to Health Care Bill, 2022, s.11(c)(III).
32 Rajasthan Right to Health Care Bill, 2022, s.11(c)(IV).
33 Rajasthan Right to Health Care Bill, 2022, s.11(c)(V).
34 Rajasthan Right to Health Care Bill, 2022, s.11(c)(VI). 22 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
▪ Coal Regulatory Authority of India: Consists of a full-time Chairperson and four other full-time
members with expertise in legal, financial, technical and consumer interest.
▪ Coffee Board: consists of full-time executive functionaries (a CEO, a CFO, directors, and
officers, and employees.)
▪ Competition Commission of India: The Chairperson and all other members of the CCI are
whole-time members.
▪ Food Safety and Standards Authority of India: Full-time Chairperson and other part-time
members.
▪ Inland Waterways Authority of India: Consists of a Chairman, a Vice-Chairman, not more than
three full-time members and not more than three part-time members.
▪ Insurance Regulatory and Development Authority of India: Consists of a full-time Chairperson,
not more than five whole-time members and not more than four part-time members.
▪ Pension Fund Regulatory and Development Authority: Consists of a full-time Chairperson,
three whole-time members and three part-time members.
▪ Petroleum and Natural Gas Regulatory Board: Consists of the following full-time members:
Chairperson, a Member (Legal) and three other members to be appointed by the Central
Government.
▪ Reserve Bank of India: Full-time Governor and Deputy Governors.
▪ Rubber Board: consists of full-time executive functionaries (a CEO, a CFO, directors, and
officers, and employees.)
▪ Securities and Exchange Board of India: Currently, it consists of a full-time Chairperson, two
full-time members and four part-time members.
▪ Spices Board: consists of full-time executive functionaries (a CEO, a CFO, directors, and
officers, and employees.)
▪ Tea Board: consists of full-time executive functionaries (a CEO, a CFO, directors, and officers,
and employees.)
▪ Telecom Regulatory Authority of India: Consists of a Chairperson (full-time), not more than
two full-time members, and not more than two part-time members to be appointed by the
Central Government.
▪ Tobacco Board: consists of full-time executive functionaries (a CEO, a CFO, directors, and
officers, and employees.)
o At the state-level in Rajasthan, the Rajasthan Electricity Regulatory Commission consists of a full-time
Chairperson who is also to be the CEO of the Commission, and three other full-time members.
o Specifically, in relation to regulators in the field of health, the Governing Board of the National Health
Authority consists of one full-time member, that is the CEO of the NHA.
The composition of the SHA should include representation from third-tier bodies
o The SHA has no members from Urban Local Bodies or Panchayati Raj institutions. This may pose a
problem with coordination and overlap in jurisdiction/functions, as it is these entities which are
obligated to perform public health actions at the granular level under the third-tier laws.
o If the concern is that owing to the large number of these bodies, it may be difficult to distribute
membership in an equitable manner, representatives from these bodies can be made rotating members
with fixed metrics for rotation (for e.g., at least one representative from municipalities which have
consistently performed poorly in public health metrics).
The composition of the SHA & DHAs should be stratified, with a clear delineation of functions
o Although both the SHA and the DHAs are composed of different classes of members (for e.g.,
secretaries of government departments, MLAs, representatives of patient groups, etc.) there is no
stratification of these classes. As a result, the functions of each class have not been separately

identified and delineated. This reduces clarity in the roles to be played by each member, leading to a
potential loss of efficiency. 23
o The SHA and DHAs may consist of three distinct classes of members: non-executive supervisory
members such as the Chairperson and Vice-Chairperson (MLAs, Chief Secretary etc.), an advisory
board (directors of relevant departments of the State Government, public health and healthcare
professionals etc.) and the full-time executive members (CEO & CFO of the SHA, officers, directors,
and employees).
o For an example of this kind of structure, one may refer to the National Institute for Health and Care
Excellence, United Kingdom (‗NICE‘) is an independent, standard-setting body constituted under the
Health and Social Care Act, 2012, which is responsible for providing National Health Service staff with
clear and robust advice on quality of care. The composition of NICE is stratified in nature. It is
composed of the Board and the Senior Management. The former sets out strategic priorities and
policies, and determines the broad framework, while the latter is responsible for day-to-day decisionmaking and
implementation in general. The organization is further split into six directorates for
performance of its functions. The CEO of the Senior Management team is also a member of NICE‘s
Board. The Board is composed of experienced health and social care professionals with wide
experience in management, trusteeship and administration. The Senior Management is composed of
technical experts from the areas of medicine, health technology, health policy etc. and is responsible
for NICE‘s day to day functioning.
The number of members of the SHA should be reduced
o The 31-member SHA is large and unwieldy, and is required to meet only twice a year. Decisionmaking is likely to be
a laborious process, with the SHA being unable to fulfil all its functions through
bi-annual meetings.
o While all the members may be obligated to convene on a bi-annual basis, the full-time executive
members should dedicate the entirety of their time to the administration of the SHA or the DHAs, as
the case may be.
The powers of the SHA should not be conflated with those of the State Government & reasonable safeguards
should be introduced to prevent potential abuse/misuse of powers
o The provision which deals with general powers of the Authorities is not the ideal place to house the
power of the Government to regulate prices for healthcare in private institutions. The power may
either be transferred to the SHA, or a separate section may be framed to enable the Government to
exercise this power.
o It may be noted that as it stands, the power of price fixation for services in clinical establishments in
the state of Rajasthan already exists under rule 9(ii) of the Clinical Establishments Rules, 2012, read
with section 52 of the Clinical Establishments Act, 2010. This power is currently exercised by the
Central Government in consultation with the concerned State Government. If a new power to fix
prices is to be given under the Bill, a rigorous compatibility review will thus be necessary.
o The provision which deals with general powers of the Authorities is not the ideal place to house the
power of the Government during a pandemic or a public health emergency. A separate Chapter should
be framed for this purpose. Further, given the extraordinary nature of the powers which have been
granted to the Government, certain minimum safeguards should be put in place to prevent the
possibility of misuse or regulatory overreach.
The SEC should not be a separate body
o Having an executive arm for the SHA is a sound proposition. However, no purpose is served by making
this an independent body, as its sole function is to execute the plans/strategies prepared by the SHA.
There is no scope for disagreement/difference in opinion. 24 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
o In any case, there is significant overlap between both the composition and the functions of the SHA
and the SEC which leads to redundancy and may present problems with coordination.
o Moreover, representatives from the CSOs and NGOs should ideally be members of the supervisory
body, and not the executive arm, as they cannot be expected to dedicate all their time to undertaking
the activities of the SHA.
o The aim of creating a separate executive arm can be better achieved by designating certain members
of the SHA as full-time executive members. This is the standard model followed by the majority of
statutory regulators in India, as has been explained in the comments above.

25
F. Grievance Redressal Mechanisms 1. Current Position under the Bill
The Rajasthan Right to Health Care Act 2022 (The Healthcare Act) has laid down a provision for setting up a
grievance redressal mechanism through its Clause 13. The said act, has laid down time-sensitive obligations for
the state to set up a complaint forum. The Healthcare Act:
o Obligates the Government to frame rules on issues pertaining to denial of services and infringement of
rights under the Healthcare Act
o Envisages setting up of a web-portal and a user-friendly helpline
o Lays down specific timelines within which the concerned officers should resolve the complaint
o Lays down timeframes for each level of grievance redressal to redress the complaint within a stipulated
timeframe. Its failure to do so will result in escalation of the complaint to a higher authority.
2. Vidhi’s Comments
Lack of mechanisms to ensure accountability of the State Government and the authorities set up under the
Bill
There are several issues in the manner with which the Healthcare Act approaches grievance redressal. Firstly,
the act only considers the need for grievance redressal when a service is denied or rights under the healthcare
act are infringed upon. While it has not been specifically mentioned, it may be presumed that only complaints
against healthcare providers are being considered under the ambit of Chapter V. The larger question regarding
the accountability of the State Health Authority and District Health Authorities set up under the act should be
considered while drafting the chapter on grievance redressal.
In addition to setting up a grievance redressal mechanism to redress complaints against healthcare
establishments, a distinct and independent monitoring mechanism for ensuring accountability of the State
Government and the authorities should be established. This body should ideally consist of sectoral experts that
will specifically consider the performance of obligations by the State Government set out in Clause 7 of the Bill.
For instance, The National Health Bill, 2009 imagines a monitoring and accountability mechanism that comprises
the establishment of a health information system, governmental mechanisms through establishment of
committees, and community-based monitoring framework. Further, the National Rural Health Mission envisaged
an accountability framework through the following mechanisms: community-based monitoring, external
surveys, and stringent internal monitoring. Rogi Kalyan Samitis are facility-level community-based committees to
monitor the performance of health facilities and health outcomes at such facilities.35 These may be considered
in devising an independent monitoring mechanism under the proposed law.
Obligations pertaining to Web based portal/user-friendly helpline
According to the Act, a resident can file a complaint at a specified web-portal or a customer friendly helpline
number. The accessibility of these measures to the common user should be considered while designing them.
35Guidelines for establishing grievance redressal and health helpline, National Health Mission,
<http://nhm.gov.in/images/pdf/programmes/Grievance_Redressal_System/Guidelines_for_Establishing_Grievance_Redressal_and%20_He
alth_Helpline.pdf>. 26 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
Further, the reader of the act faces an ambiguity in terms of understanding where such mechanisms are
stationed, and who has the obligation of maintaining them.
The Healthcare Act should clearly mention the body/institution/establishment in charge of setting up of the
web-based portal/ user-helpline and the kinds of complaints or grievances that may be lodged.
Accountability of Grievance Redressal Bodies
Under Clause 13 of the Bill, if the concerned officer does not respond to a complaint within 30 days, the
complaint may be forwarded to the District Health Authority and then elevated to the State Health Authority if
required. However, it is not clear under the Act whether there will be any legal consequences, in the nature of
penalties, for the failure of the concerned officers or authorities to resolve the complaint.
Non-performance of duties to redress complaints within the timeframe stipulated in the act should have a
performance-related disincentive for the concerned officer.
Lack of Appellate Mechanisms to redress grievances
Even as the failure of the concerned officer to redress a complaint escalates it to the higher authority, nothing
in the act provides for the right of a complainant to appeal in cases where they do not find the redressal
satisfactory. This is especially problematic, as the act further bars the jurisdiction of civil courts in matters
pertaining to this act.

A provision which allows the complainant to appeal to the higher authority should be included within the ambit
of the proposed law.
Lack of independence of the grievance redressal bodies
Under the Healthcare Act, District Health Authority and State Health Authority, both of which are functionaries
under this act, have been recognized as grievance redressal bodies. From a reading of this act, the relationship
between the proposed in-house complaints‘ redressal forum that the government is required to constitute under
Clause 13, and the District Health Authority, and the State Health Authority is unclear.
Conflicts of interest would arise if District Health Authorities and the State Health Authority play the role of
administrators and adjudicators at the same time. We suggest that instead of making District Health Authorities
and State Health Authorities function as grievance redressal mechanisms, independent ombudsperson offices
be set up at various levels, through this Bill.
The concept of an ombudsperson in facilitating healthcare delivery, and as a means to resolve grievances in
healthcare delivery, is not new. In Brazil, Municipal Health Ombudspersons are appointed. For instance; in the
State of Minas Girais, the Municipal Health Ombudsperson was observed to have been acting as an ―instrument
of power and access to the rights of ‗Brazilian Unified Health System users.'36 'The Role of such an ombudsperson
is said to have been to listen and to clarify issues regarding Brazilian Unified Health Systems Operations and
procedure, and to support resolution of health problems.
In the UK, the Health Service Ombudsperson for England draws his powers almost wholly from the Health
Service Commissioners Act 1993.37 The general remit of the powers of such an ombudsperson is to act on
36 Rita de Cássia Costa da Silva et al, ‗Ombudsmen in health care: case study of a municipal health ombudsman‘, 48 (1) Rev Saude Publica
2014, available at <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4206117/#fn03>.
37 Health Service Commissioners Act, 1993. 27
complaints made in relation to failure in a service by a service provider, failure of a body to provide a service,
and maladministration in provision of services.
In Rajasthan, we can look at ombudsperson as a body that either facilitates resolution of grievances at the local
level, or resolves them in a more formalistic manner, if resolution at the local level is not possible. Here, there is
a possibility of gradation in the kind of disputes, infringement of rights, non-fulfilment of obligations etc.
regarding which a local ombudsperson at the block level can be approached, and grievances for which the
complainant may have to go to ombudspersons at a higher level (i.e., at the district and then the state level), were
such resolution at local level unsuccessful or dissatisfactory.
The Bill also must provide examples of the kinds of grievances or complaints that can be brought to local
ombudspersons. For instance, these will broadly include the denial of healthcare services and the infringement
of user rights. Whether these occur at private or public healthcare establishments, the ombudsperson will have
the power to take action to resolve them. On the other hand, the Bill must also clarify the kinds of issues that
the ombudsperson will not be able to adjudicate on, i.e. awarding damages or compensation, or cancelling the
licence of healthcare establishments. Their role should largely deal with investigation of grievances, ordering
inquiries, directing healthcare establishments to issue apologies or conduct internal audits to prevent such
complaints from recurring, etc.
Bar of jurisdiction of civil courts
Ombudspersons (or other grievance redressal mechanisms envisaged under this Bill) would not possess the
ability, resources, or authority to adjudicate on legal claims that may result in awarding damages or
compensation, or cancelling the license of healthcare establishments. Given that it will not be practicable or
appropriate for them to adequately address all infarctions, infringements, disputes, claims etc., jurisdiction of civil
courts should not be barred through a blanket provision such as Clause 16. In any case, it may be noted that
owing to the current position of law, writ petitions before the jurisdictional High Court or the Supreme Court
cannot be barred. 28 Comments on the Rajasthan Right to Health Care Bill, 2022: Submissions to the Government of Rajasthan
PART III: DETAILS THAT REQUIRE CLARITY
THROUGH RULES Implementation of any law requires delegated legislation or rules that clarify components, constituents, and
procedure under the umbrella of the parent law. In order to reduce ambiguity and ensure that the vision of the
law is realised to the fullest extent, careful and detailed drafting of rules – with adequate scope for flexibility and
modification where necessary – is important.

In particular, the following aspects of the Bill require clarity through rules:
o Detailed components of each right (of residents, users, and HCPs) envisaged in Chapter II of the Bill.
This could be in the form followed by the general comments on the Articles of the International
Covenant on Economic, Social and Cultural Rights (ICESCR).
o The following provisions under Clause 7 of the Bill (Obligations of the Government) require clarity
through Rules:
o The process and timelines for budget allocation for health in the state, through a
comprehensive analysis of various funds (under the NHM, state‘s own funds, funds under
diverse schemes, state health insurance, corporate social responsibility or CSR plans, etc.).
Appropriate flexibilities for decentralised fund planning and use at the district and lower
levels, as well as during emergent situations, should be provided here.
o Details of the Human Resource Policy envisaged here should be thoroughly planned and in
line with diverse schemes and programmes pertaining to the same. A common portal which
takes into account district and institutional flexibilities, and details of deputation, may be
created.
o The availability, quality, and affordability norms provided here should be details in line with
existing standards under the Clinical Establishments Acts and Rules at the central and state
levels, NHM, IPHS, etc.
o Composition, powers, functions, accountability structures, and procedure pertaining to the
coordination mechanism envisaged under Clause 7 (i)
o Components, procedure, timelines, and circumstances pertaining to health impact assessment [Clause
2(v)] and social audit [Clauses 2(vv) and 7(c)] - as well as the details and limits of powers, duties, and
functions of the authorities assigned to plan and implement the same.
o Components, procedure, timelines, and circumstances pertaining to the proposed chapter on public
health emergencies - as well as the details and limits of powers, duties, and functions of the
authorities assigned to plan and implement the same.
o Apart from incorporating recommendations provided in Chapter II. E of this document, details of the
composition, appointment/ transfer/ resignation/ termination/ dismissal of functionaries, procedural
norms, etc. pertaining to regulatory architecture and administration.
o Apart from incorporating recommendations provided in Chapter II. F of this document, details of the
composition, appointment/ transfer/ resignation/ termination/ dismissal of functionaries, procedural
norms, formats for complaint and appeal, etc. pertaining to grievance redressal mechanisms.
o Contours, process, responsibility, and accountability pertaining to compatibility review and other
processes envisaged under Clause 18.
___________ 20 The Legal Framework for Public Health in West Bengal – Vidhi Centre for Legal Policy
www.vidhilegalpolicy.in
Vidhi Centre for Legal Policy
D-359, Defence Colony
New Delhi – 110024
011-43102767/43831699

Jan Swasthya Abhiyan Rajasthan
Government of Rajasthan‟s Draft of “Rajasthan Right to Heath Care Act 2022”
Government of Rajasthan
Department- of Medical, Health and Family Welfare
Rajasthan Right to Heath Care Act 2022
Clause
no.
Clause in Govt. Draft Suggested Changes Justification for
the suggested
change/clause
PREAMBLE
To provide protection and
fulfilment of rights, equity in
relation to health and well-
being for achieving the goal of
health care for all through
guaranteed access to quality
health care to all the residents of
the State, without any
catastrophic out-of-pocket
expenditure.
And whereas the persisting
inequitable accessibility and
denials in the matter of health
care in the State are a concern to
all.
The Government of
Rajasthan is committed to ensure
that people's right to health care
is realized. The most important
stakeholders in realization of
right to health care are the people
themselves. Therefore, people's
participation is crucial and
critical for realization of people's
right to health care services.
The constitution of India
incorporates provisions
Article 21 of the constitution
guarantees protection of life and
personal liberty to every-citizen.
21 of the constitution guarantees protection of life and personal liberty to every-citizen.
To provide for protection and
fulfilment of rights and equity in
relation to health and well-being
under Article 47 of the Indian
constitution to accomplish the goal of
health care for all through guaranteed
access to quality health care to all the
residents of the State, without any
medical out of pocket expenditure.
And whereas every resident
of the state of Rajasthan is entitled to
enjoyment of the highest attainable
standard of physical, mental,
intellectual and social well-being and
health, conducive to living a life in
dignity;
And whereas the right to
health care is an inclusive right
extending not only to timely health
care but also to the underlying socio-
economic, cultural and
environmental determinants of
health;
And whereas to address the
persisting iniquitous accessibility
and denials in the matter of health
care in the State;
And whereas the
Government of Rajasthan is
committed to ensure that
people's right to health care is
realized. The most important
stakeholders in realization of
right to health care are the people
themselves. Therefore, people's
The Preamble
ought to exhibit
a clear intent of
the Act in
symmetry with
the rights laid
down in the
constitution and
those stipulated
in different
covenants.

participation is crucial and
critical for realization of people's
right to health care services.
And whereas there is also a
need to set a broad legal framework
to ensure availability, accessibility,
acceptability and quality (AAAQ)
comprehensive health care services
and functions including powers to
respond to public health
emergencies.
It is hereby enacted in the
Seventy second Year of the
Republic of India as follows:-
Chapter-I: Short title, Extent and Commencement-Definitions
2(a) Affordable
It should be removed. It is absolutely
difficult to
measure the
affordability
(food or non-
food
expenditure) of
individual
families because
of the wide
variations even
within the same
economic
cohort.
2(tt) Resident
To be modified that no proof of
residence would be asked for.
It could be a
barrier if proof
of residence is
dended as many
patients may not
have it or not
readily
available.
Suggest
ed new
definiti
on 1
Accessible
(This term is being used in the
draft but not defined)
Basic primary care within half an hour
of walking distance, comprehensive
primary care within 12 kms, secondary
level care within an hours distance by
motorized vehicle and tertiary care
within 150 kms.
Parameters of
accessibility are
paramount as
this only
ensures
realization of
the obligations
under the Act.
Suggest
ed new
definiti
on 2
Out of pocket expenditure.
(This term is being used in the
draft but not defined)
Medical expenditure –Drugs,
diagnostics, consultation, ambulance
services, surgical procedures, charges
of blood
Non-medical: Transport, lodging,
food, attendant charges.
Out of pocket is
measurable.

Chapter-II: Collective and Individual Rights in Relation to Health Care
3. Rights of residents 3(a) Residents will have the right to
collect information to make
themselves healthy.
Residents will have the right to the
following information communicated
to them in a manner most appropriate to their capacity with due respect and
minimum use of unfamiliar or
complicated technical terminologies:
i) rights and entitlements
stipulated under this Act, and any other statutes, rules, policies or regulations which directly or indirectly concern right to health or health care.
ii) health care goods, facilities, services, schemes, programmes, technologies available at all health care establishments, their costs and how, where and when to access them
iii) health concerns prevalent in the community, including methods of prevention, control, treatment and counselling to lead a healthy and active life;
iv) provisions, procedures and processes to seek redressal for any violation of their rights under this Act
The modified
clause explicitly
outlines the kind
of health
information the
residents would
be entitled to
receive.
3 (b) Residents will have the right to free
consultation, drugs, diagnostics,
emergency transport and emergency
care at all public health institutions
as may be prescribed
by rules made under this Act;
Residents will have the right to free
and dignified consultation, drugs,
diagnostics, emergency
transport, emergency care and
counselling at all public health
institutions as may be prescribed by
rules made under this Act
To signify access
to ―dignified‖
health care and
the component of
―counselling‖.
3 (c) Residents will have the right to
free/affordable care for surgeries at all
public
hospitals as may be notified by rules
made under this Act;
Residents will have the right to free,
dignified, SOP care for surgeries at all
public hospitals as may be notified by
rules made under this Act;
Removed word
―affordable‖. All
the services at
public health
facilities must be
free for everyone.
3(d) Residents covered under insurance
scheme will have the right to avail free
services
under the insurance scheme through the
empanelled Hospitals as notified in
terms
and conditions of the insurance scheme
when in force and as modified from time
to
time;
Residents covered under health
insurance scheme will have the right to
avail all the health care services, except
those which are excluded, without
bearing any out of pocket payment from
an empanelled private hospital under the
scheme only on being referred from a
public health care establishment or in
the case of emergency;
In fact, there is no
need of any health
insurance scheme
unless it is
universal because it
adds to miseries of
patients rather than
any relief. Public
health facilities
ought to be kept out

of the insurance
schemes.
3 (e) Residents will have the right to free
services from the private hospitals
established through the land allocation
on concession rates as per the terms and
conditions mentioned at the time of the
allotment of the land;
Residents will have the right to free,
ethical, safe and as per SOP services
from the private hospitals established
through the land allocation on
concession rates as per the terms and
conditions mentioned at the time of the
allotment of the land;
Ideally no private
institution should
be provided land on
concessional rates
and other subsidies
because it is very
difficult to get and
monitor free
services from them
3 (f) Right to receive information, records
and reports of self from the health care
establishment be it public or private;
Every user shall have the right to be informed about the following by relevant and qualified healthcare workers at all health care establishments in a manner most appropriate to the capacity of the user with due respect and minimum use of unfamiliar or complicated technical terminology : i) identity and professional status of
the health care providers providing
him/her services and of any rules
and routines of the establishment
which would bear on his/her care.
ii) his/her health status including the
medical facts about his/her health
condition, required health care,
together with the potential risks and
benefits, costs and consequences
generally associated with each
option of health care
iii) alternatives to the proposed health
care, including the implications,
risks and effects of refusal of health
care;
iv) the diagnosis, prognosis and
progress of health care;
v) and any other information that may
be pertinent to the user in taking a
decision, providing consent or to
understand his/her current and
possible future health status.
Every user shall also have the right to:
i) his/her medical files and technical
records and to any other files and
records pertaining to his/her
diagnosis, treatment and care
(including X-ray, laboratory reports
and other investigation reports)
and to receive a copy of own files
and records or parts thereof; and
ii) request for and to be given a
written summary of his/her
diagnosis, treatment and care and in
case of an inpatient, the complete
discharge report at the time of
The modified clause explicitly outlines the kind of medical information and records the patients or their families would be entitled to receive.

discharge, which must also include
the advised, follow-up actions to be
taken by the user.
3 (g) Right to informed consent at all
health care establishments be it public
or private;
Every user shall have the right to informed consent before accessing any health care intervention proposed for him at all health care establishments be it public or private. In the case of emergency or when the user is unable to express his/her consent due to medical reasons, his/her authorised representative, close relative or caregiver’s consent shall be taken and in the absence of all when the medical intervention is urgently needed to save user’s life, the consent of the user may be presumed. When the user lacks full capacity to give
consent, due to his/her being a minor or
due to any proven mental disability,
temporary or permanent, shall to the
extent of incapacity, have the right to be
supported or substituted only where
absolutely necessary by a decision-
making on his/her behalf, through a de
jure or de facto guardian, next friend or
personal representative, whose
credentials are clear to the service
provider;
The modified clause explicitly outlines “consent” under different circumstances.
3 (h) Right to confidentiality through all
health care establishments as may be
defined by rules made under this Act.
Every user has the right that all
information about his/her health status,
medical condition, diagnosis;
prognosis and health care and all other
information of a personal kind
(identified or identifiable to him/her)
must be kept confidential by all health
care establishments, even after his/her
death, and such confidential
information can only be disclosed if
the user gives explicit consent or any
law expressly provides for this; it may
be used for study, teaching or research
only with the authorization of the user,
the head of the health care
establishment concerned and the
institutional ethics committee of the
establishment.
The modified
clause explicitly
explains what
confidentiality
signifies.
3 (i) Right to safe and quality care

according to standards prescribed for
different levels of health care
establishments run or managed by
Government or private institutions.
3 (j) Right to proper referral transport by
all health- care establishments be it-
public or
private as per the procedures detailed
in the rules made under the act.
Every user has the right to be
provided with proper referral
transport from the health care
establishment be it public or
private as per the procedures detailed
in the rules made under the act.
Referrals will be considered valid
only on the following grounds :
(i) the referring healthcare establishment does not have the capacity, resources or expertise to fulfil the healthcare user’s right to healthcare;
(ii) the transfer is in the best interest of the user, and is unlikely to cause any injury or death;
(iii) the referring healthcare establishment has provided the user or their caregiver with a written explanation for referral and transfer;
(iv) the referring healthcare establishment has arranged, in a timely manner, free or affordable and quality transportation to the healthcare user. Provided that until the user is transported to and received by the receiving healthcare establishment, the referring healthcare establishment shall bear the sole responsibility for the health, safety and wellbeing of the healthcare user.
The modified
clause details out
referrals.
3 (k) Right to take treatment summary in
case of patient, leaving against the
medical
advice.
Every user will have the right to take
treatment summary in case of patient,
leaving against the medical advice.
3 (l) Right to be heard and seek redressal
from health care establishment in
case of any
grievance occurred after availing
services.
Every user will have the right to be
heard and seek redressal from
health care establishment or
through the state established
grievance redressal mechanism or
through legal intervention in case of
any grievance which occur during or
after availing services.
The right to seek
legal
intervention in
case not satisfied
with
departmental
grievance
redressal is
crucial.
3 (m) Right to the family
member/authorized person of the
Family member/authorized person of the deceased user will have the
The modified clause details

deceased to receive dead body
irrespective of payment due status-
from every health-care establishment.
right to receive the dead body, medical records, sensitive information and all the belongings of the deceased irrespective of the payment due status from every health care establishment be it public or private, other than for necessary medical reasons, to comply with legal obligations or in case of a public health emergency.
out what all information etc of the deceased the family would be entitled to receive.
Suggest
ed
clause 1
Right to outreach services Residents will have the right to free,
dignified and SOP compliant
outreach health care services in both
rural and urban areas through public
health care establishments as per the
services mandated to be delivered as
outreach under various government
schemes and programs.
Access to
outreach health
care services is
crucial and must
be stipulated in
the Act.
Suggest
ed
clause 2
Right to not be discriminated Residents shall have the right to receive
health and healthcare information and
services from all health care
establishments be it public or private
without any kind of direct or indirect
discrimination, including but not limited
to, discrimination on the basis of their
age, caste, criminal antecedents,
disability, financial status, gender
identity or gender expression,
geographical location or residence,
health status or condition, language,
level of education, marital status,
nationality or citizenship, occupation,
place of birth, race, religion, sexual
orientation, sex characteristics and/or
any other social, economic, cultural or
political characteristics.
It is an important
right to receive
health care services
without any
discrimination and
must be stipulated
in the Act.
Suggest
ed
clause 3
Right to not be coerced Residents shall have the right to not be
subjected to any kind of direct or
indirect coercion, force, threat or denial
of his/her fundamental rights by the state
or health care providers, public or
private, in the absence of their explicit,
autonomous and informed consent to
receive a health care procedure or
medical intervention.
Coercion of any
kind in accessing
health care must
not be tolerated
and this needs to be
outlined in the Act
explicitly.
Suggest
ed
clause 4
Right to second opinion Residents will have the right to obtain a
second or more opinion from another
health service provider and choose to
seek health care, medicines, diagnostics,
vaccines, devices or implants from a
source most suitable to them.
Every user must be
entitled to right to
seek second
opinion if they wish
to and the Act must
have a clause on
the same.
Suggest
ed
clause 5
Right to refuse or halt medical
intervention
Every user shall have the right to
refuse or to halt a medical intervention
at any health care establishment be it
public or private and on his/her
exercising such right, the implications
This clause lays
down a crucial
right of the
patient to refuse
or halt treatment

of 'refusing or halting such an
intervention must be carefully
explained by the service provider to the
user, provided that the refusal or
halting comes to the knowledge of the
provider;
if not satisfied
with the services.
Suggest
ed
clause 6
Right to attendant Every user whether in-patient or out-patient shall have the right to be accompanied by or have access to at least one attendant/caregiver of their choice. In the absence of an attendant/ caregiver, a qualified healthcare worker shall be provided by the healthcare establishment to deliver caregiving services either within the healthcare establishment or elsewhere.
Every patient has the right to be accompanied by an attendant and this must be stated in the Act.
Suggest
ed
clause 7
Right to protection of persons/patients
under clinical trial
Right to protection for persons/patients
involved in clinical trials, biomedical
and health research as defined by
concerned clause in the rules;
The right of
persons/patients
under clinical trial
to be protected
must be stipulated
in the Act.
4. Duties of Residents 4 (a) Tertiary health care services can be
availed by following referral from
primary and
secondary level institution or a service
provider.
Remove
4 (b) Provide health care providers with
the relevant and accurate
information for health
care, subject to the user's right to
confidentiality and privacy.
Remove
4 (c) Comply with the prescribed health
care. Remove
4 (d) Sign a discharge certificate or
release of liability if he or she
refuses to accept
recommended treatment.
Remove
4 (e) Ensure that the premises occupied
by the residents are kept clean and
indulge in no
activity that pollutes the atmosphere
physically or otherwise.
Remove
4 (f) Refrain from misconduct and
misbehavior with any health care
providers, and treat
them with respect and dignity.
Retain
4 (g) Refrain from physical assault on any
healthcare personnel or damage to
property.
Retain
4 (h) Report illegal or unethical behavior. Retain

4 (i) Permit post-mortem to be done in
case of unnatural death. Retain
5. Rights of Health Care Provider
5 (a) Protection from complaints relating
to adverse consequences on
providing his/her services of any
kind as long as the provider has
acted bonafide to the best if his/her
professional capability through
application of standard treatment
procedure and judgment, and in the
best interests of the residents and
exercised all reasonable care;
5(b) Be treated with respect and dignity by
the patient and attendants.
5 (c) Decent working conditions and
training.
Enunciate a policy on living and
working conditions, training and
accreditation for health care
providers especially in the primary
health care for their continued
nursing and medical education and
career advancement.
The modified
clause details
out the right to
decent
working
conditions and
training to
make it more
explicit.
5 (d) Right of physical safety and security
at the workplace.
5 (e) Availability of protective measures
for any accidental exposure to harm.
6. Duties of Health Care Provider
6 (a) Follow the standard treatment
guidelines, protocols as notified
time to time under the rules made
under this Act, and using the clinical
judgement in the best interest of
resident.
6(b) Maintain confidentially, privacy,
dignity of residents, and treat them
with respect.
6 (c) Respect the rights of residents to take a
decision for getting either a lab
investigation or medicines be purchased
from the vendor of his/her choice.
6 (d) Ensure informed consent is taken before
every procedure
6(e) Explain and inform either patient or
relatives regarding the diseases severity,
progression, treatment and prognosis
regularly.

Chapter-III: Obligations of the Government
7 Government has the following general
obligations at all times, by enhancing the
quantum of the resources towards the
time bound realization of health and
wellbeing of every resident in the state;
7(a) Appropriate State budget would be
provided.
Incrementally enhance state health
budget to 10% of the state budget in
next five years or 3% of the GSDP
whichever is more, to satisfy the
obligations and rights set out herein,
for ensuring planning and rational
allocation and attributions of resources
for various health care related issues
and concerns ;
The Act should
clearly state in
the Act itself what
it is committing in
terms of financing
the health care
how the State
aims to increase
its health budget
to meet the
obligations
stipulated in the
Act.
7 (b) Within six months of the enactment,
develop and institutionalise a Human
Resource
Policy for Health to ensure
availability and equitable distribution
of doctors, nurses
and other ancillary health
professionals and workers at all
levels of healthcare as
notified in the rules under the act.
Within six months of the enactment,
develop and institutionalise a Human
Resource
Policy for Health stipulating norms
for transfers and promotions to
ensure availability and equitable
distribution of doctors, nurses
and other ancillary health
professionals and workers at all
levels of healthcare as
notified in the rules under the act.
7 (c) Within six months, set up the social
audit and grievance redressal
mechanisms as notified under the rules
under this Act.
Within six months, set up mechanisms
for social audit of public health care
services, public dialogues at PHC, block
and district levels, and grievance
redressal processes as notified under this
Act.
Social Audits and
Public Dialogues
are as crucial as
grievance redressal
and the
mechanisms for the
same must also be
devised at the
earliest as the Act
is legislated.
7(d) Within one year, align all health
services and schemes to strengthen
a system of
health services to empower and make
residents aware for preventive,
promotive and protective health care,
not merely an absence of disease.
7 (e) Within one year, lay down and
notify standards for quality and
safety of all levels
of health care as notified under the
Within one year, lay down and notify
specific standards and norms for safety
and quality assurance of all aspects of
health care including health care
IPHS/NABH
should be the
standards the
government
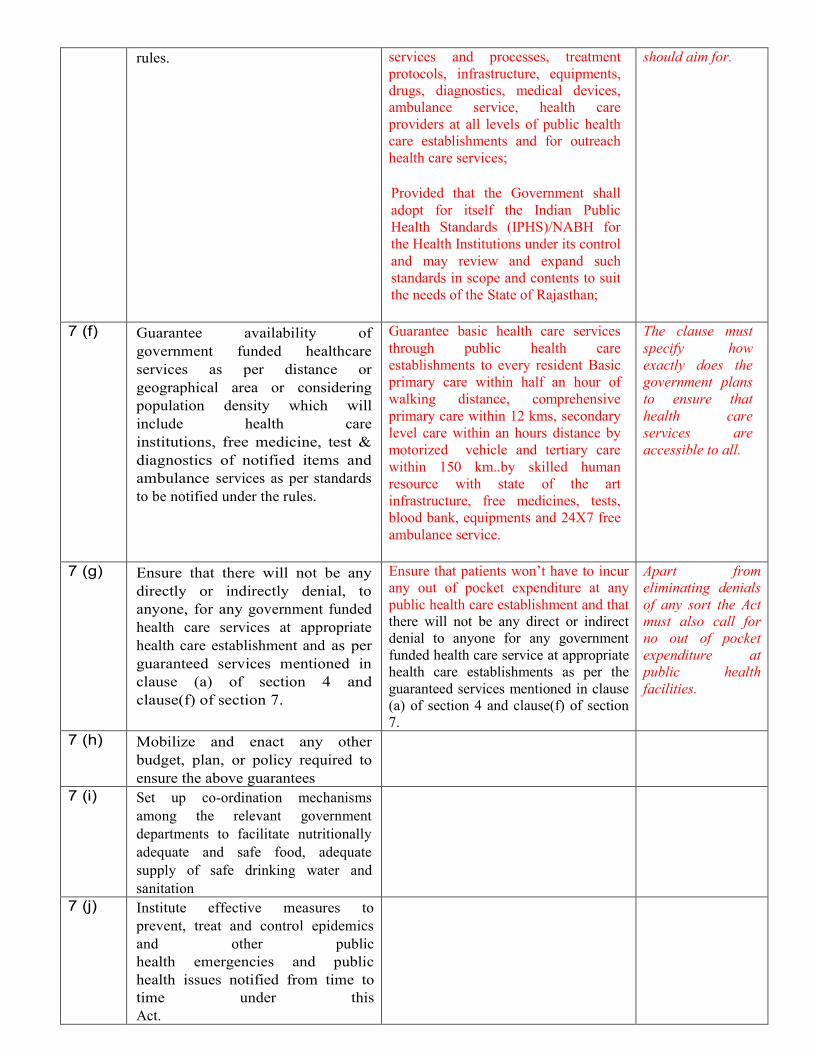
rules. services and processes, treatment
protocols, infrastructure, equipments,
drugs, diagnostics, medical devices,
ambulance service, health care
providers at all levels of public health
care establishments and for outreach
health care services;
Provided that the Government shall
adopt for itself the Indian Public
Health Standards (IPHS)/NABH for
the Health Institutions under its control
and may review and expand such
standards in scope and contents to suit
the needs of the State of Rajasthan;
should aim for.
7 (f) Guarantee availability of
government funded healthcare
services as per distance or
geographical area or considering
population density which will
include health care
institutions, free medicine, test &
diagnostics of notified items and
ambulance services as per standards
to be notified under the rules.
Guarantee basic health care services
through public health care
establishments to every resident Basic
primary care within half an hour of
walking distance, comprehensive
primary care within 12 kms, secondary
level care within an hours distance by
motorized vehicle and tertiary care
within 150 km..by skilled human
resource with state of the art
infrastructure, free medicines, tests,
blood bank, equipments and 24X7 free
ambulance service.
The clause must
specify how
exactly does the
government plans
to ensure that
health care
services are
accessible to all.
7 (g) Ensure that there will not be any
directly or indirectly denial, to
anyone, for any government funded
health care services at appropriate
health care establishment and as per
guaranteed services mentioned in
clause (a) of section 4 and
clause(f) of section 7.
Ensure that patients won‘t have to incur
any out of pocket expenditure at any
public health care establishment and that
there will not be any direct or indirect
denial to anyone for any government
funded health care service at appropriate
health care establishments as per the
guaranteed services mentioned in clause
(a) of section 4 and clause(f) of section
7.
Apart from
eliminating denials
of any sort the Act
must also call for
no out of pocket
expenditure at
public health
facilities.
7 (h) Mobilize and enact any other
budget, plan, or policy required to
ensure the above guarantees
7 (i) Set up co-ordination mechanisms
among the relevant government
departments to facilitate nutritionally
adequate and safe food, adequate
supply of safe drinking water and
sanitation
7 (j) Institute effective measures to
prevent, treat and control epidemics
and other public
health emergencies and public
health issues notified from time to
time under this
Act.

7 (k) Take appropriate measures to
inform, educate - and empower
people about health
issues.
Take appropriate measures to
inform, educate and empower
people about health
issues through sustained and regularly
updated state and local level IEC
programme which reflect the latest
developments in the
laws/policies/schemes/programs and the
best available scientific knowledge.
The modified
clause highlights
the significance
of regularly
updating and
evolving IEC
tools and
mechanisms.
Suggested
clause 1
Obligation to safeguard rights Take effective measures to safeguard
all the rights related to health and
health care as laid down under Chapter
II
Suggested
clause 2
Obligation to devise a system for
referrals to tertiary hospitals
Devise a robust system of referral
to ensure that there‘s no
unnecessary crowding at Tertiary
health care services. Ensure that
Tertiary care can be availed by
following referral from primary and
secondary level institution or a
service provider or in the case of
emergency.
Ensure that every resident family is
provided with the health card and
assigned to a designated primary health
care provider who would be the first
port of call for health problems not
warranting emergency hospitalisation.
Persons travelling could locate and
access nearest Health and Wellness
Centre through mobile phone.
Suggested
clause 3
Obligation to provide alternate
measure in case the required
health care service could not be
delivered
Fix alternate measures in case a patient
fails to receive due medical attention or
health service, drugs or diagnostics
because of absence of the doctors or
any other medical staff or due to lack
of essential equipments or supplies in a
public health care establishment or a
private health care establishment
empanelled to deliver public funded
health care services
Suggested
clause 4
Obligation to ensure transparency
at the health care establishment
Ensure that all health care
establishments be it public or private
maintain transparency by explicitly
displaying the following information
within their premises at a place where
it is clearly visible and in a language
easily understood by majority of the
local population :
- List of services available along
with their costs or if free it
being clearly specified
- List of free drugs, diagnostics
available
- List of packages covered under

public funded health insurance
scheme available.
- Schedule/timings when the
available services can be
accessed
- List of serving doctors and
other health care staff with
their names and designations
and if they are entitled to Non
Practicing Allowance (NPA) if
serving in public health
establishments.
- Name and contact details of
the in house
complaints/grievance redressal
officer as well as the details of
government portal or helpline
number where the grievance
could be registered in case the
user is not satisfied by the in
house response to his/her
complaint.
- Accreditations if any
- Patients‘ rights charter
Awareness materials on major health
care schemes/programs/entitlements or
information on prevention of diseases,
healthy lifestyle etc.
Suggested
clause 5
Obligation to monitor health care
establishments and prescription
practices
Devise and implement structure and
plans for the following :
i)routine inspection of all health care
establishments be it public or private.
ii) routine prescription audits at all
public health care establishments.
iii) Formation of drugs
formular and creation
of drugs and
therapeutic committees
in each institution .
Suggested
clause 6
Obligation to regulate private
health care establishments
Implement Clinical Establishments Act
2010 and devise and execute rules and
plans for the regulation of all health
care establishments be it public or
private.
Suggested
clause 7
Obligation to regulate government
doctors also practicing from homes
Ensure that doctors from public health
establishments who also practice from
home after duty hours only prescribe
medicines and diagnostics which are
under the free medicines and free
diagnostic lists devised and updated by
the State from time to time and that
patients are able to avail them from
public health care establishments for
free. Such doctors should only be
allowed to charge consultation fee
from the patients as per the rates fixed
by the State.

Suggested
clause 8
Obligation to regularly devise and
review policies, budgets, plans etc
Promote health research and devise,
adopt, implement and regularly review
health policies, strategies and plans of
action on the basis of epidemiological,
sociological, anthropological,
economic and environmental evidence
to address the health concerns of
various population of the state;
Suggested
clause 9
Obligation to ensure transparency
in budget, policy etc formulations
Ensure transparency in the
formulation, amendments and
implementation of health care budgets,
policies, programs and schemes and
involve participation of different
stakeholders including community
members and civil society
representatives in their development
processes.
Suggested
clause 10
Obligation to strengthen
community action for health
Constitute, orient and empower
Village, Health, Sanitation and
Nutrition Committees (VHSNCs) in
every village of the state as outlined in
the MoHFW guidelines, provide them
with the annual untied fund that they
are entitled for and engage them in
community-based and decentralised
health monitoring, evaluation,
governance and planning.
Suggested
clause 11
Obligation to ensure access to
health care services for the
specially abled
Devise policy and ensure that all health care establishments be it public or private have the required orientation, arrangements and infrastructure to make healthcare facilities and services easily and in a sensitive manner accessible to persons who are specially abled.
Suggested
clause 12
Obligation to ensure access to
health care services for persons
with rare diseases
Ensure that every resident has access to latest facilities and technologies for the timely diagnosis and prognosis of rare diseases and that persons with rare diseases have access to the latest and scientifically sound information, required resources and services for leading a life with dignity and for timely treatment and care.
Suggested
clause 13
Obligation to ensure proper waste
management at health care
establishments
Ensure sanitation and environmental
hygiene, including waste management
for every kind of waste in all health
care establishments.
Suggested
clause 14
Obligation to ensure quality meals
for the inpatients
Ensure availability of safe and quality
food for the inpatients at all public
health care establishments.
Suggested
Obligation to ensure safe drinking
water at health care establishments
Ensure regular water supply and
availability of safe potable water for

clause 15
the users as well as health care
providers at all public health care
establishments.
Suggested
clause 16
Obligation to ensure power supply
at health care establishments
Ensure regular power supply and
arrangements for power back up at all
public health care establishments.
Suggested
clause 17
Obligation to provide protective
gears to health care workers
Ensure that doctors and healthcare workers at the all levels have timely and adequate access to standardised safety and protective gears/equipments and are well oriented on their usage.
Suggested
clause 18
Obligation to promote other
codified systems of medicines
Promote different codified systems of
medicines and ensure adequate
financial allocations for them;
Suggested
clause 19
Obligation to carry out Health
Impact Assessments
Devise and implement plans for Health
Impact Assessment (HIA) of all new
development projects;
Chapter-IV: Constitution, Power and Duties of State Health Authority, State Executive Committee and District Health Authority
8. Constitution and Duties of State Health Authority
8 (a) The Government shall, by notification in the official gazette, constitute an independent 'body as State Health Authority, to exercise powers conferred on, and perform the functions assigned to that Authority under this Act;
The authority
should be the
apex body for
execution of the
obligations of the
State under the
Right to Health
Care Act.
8 (b) The State Health Authority shall consist
of the following members, namely:-
I. The Chief Secretary,
Government of Rajasthan, -Chairperson,
II. Secretary in-charge of Medical,
Health and Family Welfare Department-
Co-Chairperson,
III. The Director of Health Services
(Public Health), Rajasthan,
- Member-
Secretary
IV. Secretary in-charge of the following
departments shall be members, namely
1. Medical Education Department,
2. Public Health Engineering,
The State Health Authority shall consist
of the following members, namely:-
I. The Chief Secretary, Government of
Rajasthan, -Chairperson,
II. An independent person with at least
30 years experience of public health
in the state- Co-Chairperson
III. Secretary in-charge of Medical,
Health and Family Welfare
Department- Executive Chairperson,
IV. The Director of Health Services
(Public Health), Rajasthan,
- Member Secretary
V. Secretary in-charge of the following
departments shall be members,
namely:
1. Medical Education Department,
It is to be an
independent body
therefore it ought
to be headed by
an independent
person with 30
years experience
of public health in
the state.
Representation by
non government
members must be
increased.

3. Women & Child Development,
4. Panchayati Raj and Rural
Development,
5. Social Justice and Empowerment,
6. Tribal Area Development,
7. Urban Development,
8. Finance,
9. Information and Public Relations,
10. Revenue,
11.Ayurveda, Yoga, Naturopathy,
Unani, Siddha, and Homoeopathy,
12. Education department,
13. Relief and
14. Rehabilitation
V. Three members of the Rajasthan
Legislative Assembly as nominated by
the State Government,
VI. Three persons from the
Government Medical Teachers of the
State especially from clinical specialties,
VII. Four non-official persons,
1. Public health experts to be nominated
by the Chairperson,
2.Representatives of health associations
to be nominated by the Chairperson,
3.Civil society organizations to be
nominated by the Chairperson,
4. One member from an NGO of repute,
preferably working in the state
to be nominated by the Chairperson.
VIII. Representative of Chairman, State
Pollution Control Board, and
IX. Three representatives of patient
groups - nominated by the Chairperson.
2. Public Health Engineering,
3. Women & Child Development,
4. Panchayati Raj and Rural
Development,
5. Social Justice and Empowerment,
6. Tribal Area Development,
7. Urban Development,
8. Finance,
9. Information and Public Relations,
10. Revenue,
11.Ayurveda, Yoga, Naturopathy,
Unani, Siddha, and Homoeopathy,
12. Education department,
13. Relief and Rehabilitation
VI. Three members of the Rajasthan
Legislative Assembly as nominated by
the State Government,
VII. Two persons from the Government
Medical Teachers of the State
especially from clinical specialties,
VIII. Representative of Chairman,
State Pollution Control Board, and
IX. Two representatives of
government medical officers from
PHCs/CHCs (On rotation)
X. Two representatives of nursing
staff (On rotation)
XI. Two representatives of ASHAs
(On rotation)
XII. Four PRI representatives (On
rotation):
1- zila pramukh
1 – pradhan
2- sarpanch
XIII. Eight non-official persons,
1. Public health experts to be nominated
by the Chairperson,
2.Representatives of health associations
to be nominated by the Chairperson,
3.Civil society organizations to be
nominated by the Chairperson,
4. One member from an NGO of repute,
preferably working in the state to be
nominated by the Chairperson.
5. Four representatives of patients
groups (On rotation).
Of the non-official or nominated

members at least 50% should be
women and 50% S.C., S.T. and BPL
8 (c) I. The appointment of each member of
the State Health. Authority, except the
ex-officio appointees, shall be for three
years.
II. The State Health Authority shall meet
at least once in six months; and
8 (d) The State Health Authority shall carry
out the following functions:-
I. To advise the Government on any
matter concerning public health,
including preventive, promotive,
curative. and rehabilitative aspects of
health and occupational, environmental,
and social determinants of health;
II. Formulate State's health goals and get
these included in the mandate of
Panchayati Raj Institutions and urban
local bodies;
III. Formulate state level strategic plans
for implementation of Right to Health
Care Act provisions, including action on
the determinants of health - food,
water and sanitation:
IV. Formulate a comprehensive written
State Public Health Policy/plan for
prevention, tracking, mitigation, and
control of a "public health emergency",
as well as situations of "outbreak" or
"potential outbreak "in the State;
V. To monitor the preparedness of the
State for management of public health
emergencies;
VI. To develop mechanisms and systems
for regular medical, clinical, and social
audits for good quality of health care at
all levels;
VII. The State Health Authority may, as
and when it considers necessary,
constitute one or more
committees/scientific panels/technical
panels for the
efficient discharge of its functions;
VIII. The State Health Authority may,
as and when it considers necessary,
associate with institutions, experts, Non-
Government organizations for the
efficient discharge of its functions;
IX. The State Health Authority through
the community-based monitoring
methods, as may be prescribed by rules
made under this Act, shall involve
the communities as active co-facilitators
articulating their needs, helping in
identification of key indicators and
creation of tools for monitoring,
ADDITIONAL FUNCTIONS TO BE
ADDED :
i) Overseeing the functioning of Block
and District Health Authorities;
ii) Establishing specific, time-bound
and verifiable benchmarks, and
indicators for each of the obligations
under the Act;
iii) Formulating human resource
development plans/policies for
health to ensure availability,
efficiency and regular capacity
building of healthcare workers
iv) Overseeing the functioning of
grievance redressal mechanisms and
ensure effective investigation and
redressal of grievances in a time
bound manner as and when
complaints are escalated for its
consideration to the State Health
Authority or suo moto in case of
grave violation of health/patient‘s
right as and when it comes to its
notice.

providing feedback as well as validating
the data collected by these methods; and
X. Carry out other functions as may be
defined by rules made under this Act.
9. Constitution and Duties of State Executive Committee 9 (a) The State Health Authority shall,
by notification in the official
gazette, constitute an independent
body as State Executive
Committee, to exercise powers
conferred on and perform the
functions assigned under this Act;
The State Executive Committee
shall consist of the following
members, namely: -
I. Secretary in-charge of Medical,
Health and Family Welfare
Department -
Chairperson,
II. Secretary in-charge of the
following departments shall be
members, namely
1. Medical Education
Department,
2. Women & Child Development,
3. Panchayati Raj and Rural
Development
4. Ayurveda, Yoga, Naturopath,
Unani, Siddha, and
Homoeopathy,
and
5. Elementary Education
department
III. Mission Director (National
Health Mission), Rajasthan -
Member,
IV. The Director Medical
Health
Services (Public
Health),Rajasthan - Member,
V.Additional Director (Hospital
Administrator), Rajasthan-
Member,
VI. Nodal officer (Right to
Health Care Act), Rajasthan-
Member Secretary,
VII. Three persons from the
Government Medical Teachers of
the State especially from clinical
specialties, to be nominated by
the Chairperson.
VIII. Four non-official persons,
1. Public health experts to be
nominated by the Chairperson,

2. Representatives of health
associations to be nominated by
the Chairperson
3. Civil society organizations to be
nominated by the Chairperson,
4. One member from an NGO of
repute, preferably working in
the state
to be nominated by the
Chairperson.
IX. Representative of Chairman, State
Pollution Control Board
9(c) I. The appointment of each
member of the State Executive
Committee, except
the ex-officio appointees, shall be
for three years.
II. The State Executive
Committee shall meet at least
once in three months; and
9(d) The State Executive Committee
shall carry out the following
functions: -
I. Implement state level strategic
plans for implementation of Right
to Health
Care Act provisions, including
action on the determinants of
health - food,
water and sanitation;
II. Implement a State Public
Health Policy/plan for prevention,
tracking,
mitigation, and control of a
"public health emergency", as
well as situations
of "outbreak" or "potential
outbreak "in the State.
III. To ensure the State for
management of public health
emergencies;
IV. To ensure mechanisms and
systems for regular medical,
clinical, and social
audits for good quality of health
care at all levels,
V. To monitor population health
status to identify and solve
community health
problems,
VI. Carry out, other functions as
given by Chairperson from time
to time.
ADDITIONAL FUNCTIONS TO BE
ADDED:
i) Facilitating and organising periodic
public dialogues to ensure and
strengthen direct accountability of
the health system to the community
and beneficiaries
ii) Ensure that the standards,
benchmarks and targets formulated
by the State Health Authority for
health care improvement in the state
are met.
iii) Ensure effective functioning of
grievance redressal mechanisms as
suggested in the Act
iv) Ensure effective execution of
community-based monitoring
methods through active participation
of community members, especially
via VHSNCs.
10. Meeting of State Health Authority 10(a) The State Health Authority shall

meet at least two times in a year,
by giving such
reasonable advance notice to its
members and shall observe such
rules of procedure regarding the
transaction of business at its
meetings as may be prescribed by
rules
made under this Act.
Provided that if, in the opinion of
the Chairperson, any business of
an urgent nature is to be
transacted, he/she may convene a
meeting of the authority at such
time as he/she thinks fit for the
aforesaid purpose.
10 (b) The meetings of the Authority
and the mode of transaction of
business at such meetings,
including quorum etc., shall be
governed by such regulations as
may be prescribed by rules made
under this Act.
11. Constitution and Duties of District Health Authority 11 (a) The Government shall constitute an
independent body as District Health
Authority within one month from the
date of constitution of State Health
Authority;
11 (b) The District Health Authority shall
consist of the following members,
namely:-
I. The District Collector -
Chairperson,
II. Chief Executive Officer, Zila
Parishad - Co-Chairperson
III. The CM&HO - Member
Secretary,
IV. Senior most officers of the
district from the departments shall be
members, namely .
1. Public Health Engineering,
2. Social Justice and Empowerment,
3. ICDS,
4. Women Empowerment,
5. Local Body,
6. Education, and
7. Ayurveda, Yoga, Naturopathy,
Unani, Siddha, and Homoeopathy
V. Pramukh, Zila Parishad of the
district and three Pradhans' of the
Panchayat
The District Health Authority shall
consist of the following members,
namely:-
I. The District Collector -
Chairperson,
II. A person with at least 20 years of
public health experience and preferably
belonging to the district – Co-
Chairperson
III. Chief Executive Officer, Zila
Parishad – Executive Chairperson
IV. The CM&HO - Member
Secretary,
IV. Senior most officers of the
district from the departments shall be
members, namely .
1. Public Health Engineering,
2. Social Justice and Empowerment,
3. ICDS,
4. Women Empowerment,
5. Local Body,
6. Education, and
7.Ayurveda, Yoga, Naturopathy,

Samitis in rotation, as may be
prescribed by rules made under this
Act.
VI. Four non-official members,
namely
1. Public health experts, to be
nominated by the Chairperson,
2. Representatives of health
associations, to be nominated by the
Chairperson,
3. Civil society organizations
preferably working in health sector,
to be nominated by the Chairperson,
4. One member from an NGO of
repute, preferably working in the
district in the health sector, to be
nominated by the Chairperson,
Unani, Siddha, and Homoeopathy
V. Two representatives of medical
teachers if there are any.
VI. Two representatives of
government
medical officers from PHCs/CHCs
VII. Two representatives of nursing
staff.
VIII. Two representatives of ASHAs
IX. Pramukh, Zila Parishad of the
district and two Pradhans of the
Panchayat
Samitis and two sarpanchs in
rotation, as may be prescribed by
rules made under this Act.
IX. Six non-official members,
namely
1. Public health experts, to be
nominated by the Chairperson,
2. Representatives of health
associations, to be nominated by the
Chairperson,
3. Civil society organizations
preferably working in health sector,
to be nominated by the Chairperson,
4. One member from an NGO of
repute, preferably working in the
district in the health sector, to be
nominated by the Chairperson,
5. Two representatives of patients
groups.
Of the non official or nominated
members at least 50% members should
be women and 50% S.C. , S.T. and BPL
(c) The District Health Authority shall
carry out the following functions:-
I. Ensure implementation of the
policies, recommendations, and
directions of
State Health Authority;
II. Formulate and implement
strategies and plans of action for the
determinants
of health, especially food, water,
sanitation, and environment.
III. Formulate a comprehensive
written plan for prevention,
tracking, mitigation, and control of a
"public health emergency", as well as
situations of "outbreak" or "potential
outbreak "in the district based on
State Plan.
IV. Coordinate- with the relevant
ADDITIONAL FUNCTIONS TO BE
ADDED:
i) Ensure that the standards,
benchmarks and targets formulated
by the State Health Authority for
health care improvement in the state
are met.
ii) Ensure effective functioning of
grievance redressal mechanisms in
the district as suggested in the Act

Government departments and
agencies to
ensure availability and access to
adequate and safe food, water and
sanitation throughout the district.
V. Organize hearing of the
beneficiaries coming to the hospital
once in three
months with a view to improve the
health care services; and
VI. District Health Authority
through the community-based
monitoring
methods, as may be prescribed by
rules made under this Act, shall
involve
the communities as active co-
facilitators articulating their needs,
helping in
identification of key indicators and
creation of tools for monitoring,
providing feedback as well as
validating the data collected by these
methods.
VII. Carry out other functions as may
be defined by rules made under this
Act.
12. Powers of the State Health Authority and District Health Authority 12 (a) For purposes of carrying out the
inquiry under this Act, the authority
shall nominate
one or more persons / committees for
the efficient discharge of its
functions, as may
be prescribed by rules made under this
Act.
12 (b) The authority shall have the power of
only official purpose to require any
person, to
furnish information on such points or
matters as may the subject matter of
the
inquiry and any person so required
shall be deemed to be legally
bound to furnish such
information within the meaning of
sections 176 and 177 of the Indian
Penal
Code (45 of 1860).
12 (c) The authority or any other officer
authorized on this behalf by the State
Health
Authority and District Health
Authority may enter in any building

or place where
the authority has reason to believe
any document relating to the subject
matter of an
inquiry may be found, and may seize
any such document or take extracts or
copies
therefrom subject to the provisions of
section 100 of the code of Criminal
Procedure,1973, in so far may be
appliable.
12 (d) Fixing responsibility and
accountability of private institutions,
facilities, buildings,
or places, whether for profit or not,
operated to provide inpatient and/or
outpatient
services. The government shall have
the power to regulate prices for the
packages
and ensure display of rates for each
of the packages in public domain, as
may be
notified by rules made under this Act.
I. In case of a pandemic, or any other
public health emergency the
government
shall have the right; -'
1. to takeover building of private
institutions;
2.to takeover facilities of private
institutions;
3. to takeover services of private
institutions;
4. to takeover duties of human
resources working in private
institutions; and
5. to prescribe treatment rate of
services provided by private
institutions during the pandemic, as
may be specified in the
government notification issued under
this Act.
12 (e) Other powers as defined under the
rules of the act.
Suggested
Clause 1
Constitution of Block Health Authority
The Block Health Authority shall
consist of the following members,
namely:-
I. Pradhan, Panchayat Samiti,
Chairperson
II. A person with at least 10 years
of public health experience and
preferably belonging to the Block – Co-
Chairperson
Block Health
Authorities must
be formed to
ensure
decentralised
planning and for
gathering regular
grassroots
feedback on

III. The Block CM&HO - Member
Secretary,
IV. Senior most officers of the block
from the departments shall be
members, namely .
1. Social Justice and Empowerment,
2. ICDS,
3. Education, V.Two representatives of government
medical officers from PHCs/CHCs
VI. Two representatives of nursing
staff.
VII. Two representatives of ASHAs
VIII. Block Development Officer
(BDO)
IX..Four sarpanchs in rotation, as
may be prescribed by rules made
under this Act.
X. Eight non-official members,
namely
1. Four representatives of CBOs to be
nominated by the
Chairperson,
2. Two members from an NGO of
repute, preferably working in the
block in the health sector, to be
nominated by the Chairperson,
3. Two representatives of patients
groups.
Of the non official or nominated
members at least 50% members should
be women and 50% S.C. , S.T. and BPL
delivery of health
care services and
health care needs.
Suggested
Clause 2
Duties of Block Health Authority I. Review, plan and execute
preventive, curative, palliative and
health promotion activities and
programmes in the overall guidance of
State and District Health Authorities.
II. Formulate and implement
strategies and plans of action for the
determinants
of health, especially food, water,
sanitation, and environment.
III. Formulate a comprehensive
written plan for prevention,
tracking, mitigation, and control of a
"public health emergency", as well as
situations of "outbreak" or "potential
outbreak in the block based on
District and State plans.
IV. Coordinate- with the relevant
Government departments and
agencies to
ensure availability and access to
adequate and safe food, water and
II.

sanitation throughout the block.
V. Organize hearing of the
beneficiaries coming to the hospital
once in three
months with a view to improve the
health care services; and
VI. Block Health Authority
through the community-based
monitoring
methods, as may be prescribed by
rules made under this Act, shall
involve
the communities as active co-
facilitators articulating their needs,
helping in
identification of key indicators and
creation of tools for monitoring,
providing feedback as well as
validating the data collected by these
methods.
VII. Carry out other functions as may
be defined by rules made under this
Act.
Suggested
Clause 3
Meetings of Block Health Authority Block Health Authority will hold
meeting every month.
Suggested
Clause 3
Meetings of District Health Authority
District Health Authority will hold
meeting every two months.
Chapter-V: Grievance Redressal and Social Accountability Mechanism
13. Grievance Redressal Mechanism
13 (a) The Government shall constitute in-
house complaints forum at an
appropriate level
within one year from the date of
notification of the provisions of this
Act,
13 (b) The Government shall define rules,
within six months from the date of
notification
of the provisions of this Act, which
may include,-
I. On denial of services and
infringement of rights provided by
the right to
health care Act, residents can lodge
the grievances for redressal -at a
specified web-portal and helpline
banda,
II. On denial of services and
The Government shall define rules,
within six months from the date of
notification
of the provisions of this Act, which
may include,-
I. Every health institution would have
designated complaint officer like a
public authority who would receive
complaint related to the health
facility and address it within 10
days to the satisfaction of the
complainant.
The component of
having a
designated
Complaints
Officer at the
health institution
level is crucial to
streamline
grievance
redressal process.
The stipulated
time period for

infringement of rights provided by
the right to
health care Act, residents can lodge
the grievances for redressal at a
specified web-portal and a user-
friendly helpline center. The web-
portal/
helpline centre will forward the
grievances received to the concerned
officer
and his/her immediate supervisors
within 24 hours,
III. The concerned officer must
respond to the complainant within 30
days. The
grievances and their redressals will
be noted in the personnel file of the
respective staff member,
IV. If the complaint is not resolved
by concerned officer within 30
days the
complaint will be forwarded to
District Health Authority, as the case
may be,
V. District Health Authority will
investigate the grievance/complaint
and share
the summary of the investigation
with the complainant and in public
domain, within 60 days. District
Health Authority will invite the
complainant and try to resolve and
close the grievance within 30 days.
VI. If the grievance is still not
resolved within 30 days by the
district health authority, then the
complainant will be escalated to the
State Health Authority within 30
days.
II. On denial of services and
infringement of rights provided
by the right to
health care Act, residents can
lodge the grievances for redressal
at a
specified web-portal or a user
friendly helpline centre or in
writing to the Complaint Officer
of the concerned health facility.
The web-portal/helpline centre
must forward the grievances
received to the concerned
Complaint Officer within 24
hours. The concerned officer
must respond to the complainant
within 15 days. The
grievances and their redressals
will be noted in the personnel file
of the
respective staff member,
III. If the complaint is not resolved by
concerned officer within 15 days
the complaint will be forwarded
to Block Health Authority, as the
case may be,
IV. The Block Health Authority will
investigate the
grievance/complaint and share the
summary of the investigation in
speaking order with the
complainant and in public
domain, within 15 days. Block
Health Authority will invite the
complainant and try to resolve
and close the grievance within 30
days of receiving the complaint.
The travel cost borne by the
complainant during such visits
will be reimbursed by the state.
V. If the grievance is still not
resolved within 30 days by the
Block health authority, then the
complainant will be escalated to
the District Health Authority
within 15 days.
VI. The District Health Authority will
investigate the
grievance/complaint and share the
summary of the investigation in
speaking order with the
complainant and in public
domain, within 15 days. District
Health Authority will invite the
complainant and try to resolve
and close the grievance within 30
days of receiving the complaint.
The travel cost borne by the
resolving
complaints must
be reduced.

complainant during such visits
will be reimbursed by the state.
VII. If the grievance is still not
resolved within 30 days by the
District health authority, then the
complainant will be escalated to
the State Executive Committee
within 15 days.
VIII. The State Executive
Committee will investigate the
grievance/complaint and share the
summary of the investigation in
speaking order with the
complainant and in public
domain, within 30 days. State
Health Authority will invite the
complainant and try to resolve
and close the grievance within 60
days of receiving the complaint.
The travel cost borne by the
complainant during such visits
will be reimbursed by the state.
Chapter-VI: Penalties and Procedures
14. Penalties
14 (a) Any contravention due to negligence as defined in detail in rules of any provisions of this Act or any Rule or Order made or issued there under shall be punishable with a fine not exceeding Rupees ten thousand for the first contravention and not exceeding Rupees twenty-five thousand for the repeat contravention.
Any contravention due to negligence as defined in detail in rules of any provisions of this Act or any Rule or Order made or issued thereunder shall be punishable with a fine not exceeding Rupees twenty five thousand for the first contravention and not exceeding Rupees one lakh for repeat contraventions.
The range of penalty amount has been increased in the modified clause to consider violations of all kinds of gravity into account.
15. Appeals
15 (a) Any person or body aggrieved by
order of the District Health
Authority passed under the
provision of this Act can appeal
against the said order to the State
Executive Committee within 30
days as per the detailed procedure
notified under the rules
The complainant would have the right to
appeal to the Block Health Authority
within 15 days if not satisfied with the
decision of the concerned institution
who would have powers to impose fine
on the erring official which would not be
more than Rs. 10,000.00 and also call
for a departmental enquiry in case of
gross negligence.
The complainant may appeal to the
District Health Authority within 15 days
if not satisfied by the decision of the
Block Health Authority who would have
The right to appeal
to a higher
Authority if not
satisfied with the
decision cannot be
denied to the
aggrieved.
The provision of
departmental
inquire against an
official if found
guilty must also be
there.

powers to impose fine on the erring
official which would not be more than
Rs. 25,000.00 and also call for a
departmental enquiry in case of gross
negligence.
Any person or body aggrieved by
order of the District Health
Authority passed under the
provision of this Act can appeal
against the said order to the State
Executive Committee within 30
days as per the detailed procedure
notified under the rules. State
Executive Committee who would have
powers to impose fine on the erring
official and also call for a departmental
enquiry in case of gross negligence.
16. Bar of Jurisdiction
No civil court shall have
jurisdiction to entertain any suit
or proceeding in respect of any
matter which an Appellate
Authority constituted under this
Act is empowered by or under
this Act to determine, and no
injunction shall be granted by any
court or other authority in respect
of any action taken or to be taken
in pursuance of any power
conferred by or under this Act.
This clause must be removed To deny an
aggrieved the
right to seek legal
course of action if
not satisfied with
the departmental
inquiry and
decision goes
against the
principle of
natural justice
and curtails
constitutional
rights. This clause
therefore must be
removed entirely.

Naina Seth
Suggestions on the Draft Rajasthan Right to Health Care Act, 2022
Submission to the Department of Medical, Health & Family
Welfare, Government of Rajasthan
At the outset, and as articulated in a previous letter to the Secretary of Department of Medical,
Health & Family Welfare, Government of Rajasthan, we desperately urge the Department to
extend the date of submitting suggestions/comments/objections to the draft of the proposed
Rajasthan Right to Health Care Act, 2022 and to hold statewide consultations. We are willing to
facilitate these consultations and present the findings to the government at a state-level
consultation. This will enable the Department to include views and suggestions of those who can
otherwise contribute to the framing of this important legislation but are being left out because a
wider set of consultations are not being held, and in this way, prepare a more comprehensive and
enforceable law. Due to the limitations of the current deadline in place (which we could not
adhere to due to the consultative nature of our exercise), however, we, the listed members from
civil society groups working in public health and human rights in Rajasthan and
other parts of the country, want to bring the following suggestions to the Department‘s notice.
Broad set of suggestions and objections to the draft Act:
1. Unclear vision and attendant incoherence in the drafting of the Act. The vision and
framework of the right to health care legislation must be clear from the Preamble itself,
which it currently lacks. Therefore, we have provided an alternative to the currently
drafted Preamble, with a short statement setting out the aim of the Act, viz. ―to provide
for free, accessible and quality health care to all the residents of the State‖. Similarly,
the draft Act does not emphasise on issues of equity in health care access. In this way,
it completely misses provisioning for non- discrimination in seeking, accessing, and
receiving health care services.
2. Quality, safety, and accessibility standards. The specific standards for quality, safety,
and accessibility of health care services must be clearly spelled out in the text of the Act,
and not be left for notification in the rules.
3. The private health care sector. The draft Act seems to be silent on the dominance of
private sector providers in healthcare, including their presence in financing in health
care financing and service delivery. It, therefore, does not set out any provisions for
regulating the private health care sector, the absence of which will keep the state short of
achieving the goal of universal health coverage, in an equitable manner.
4. State funding. The Act must state the commitment of the State of Rajasthan by
outlining the share of the state budget that would be allocated to the health care sector,
and in this way towards realising the rights and obligations set out in the Act.

Detailed suggestions on the draft Act:
Serial No.
Section and Clause No.
Suggestions (Addition/ Modification/ Deletion/ Others)
Details of the suggestion or exact wording of the proposed addition/ modification/ deletion/ others
Remarks
1 Preamble Modification and Addition
Preamble to be read as: "To provide for free, accessible, and quality health care to all the residents of the State, and with a progressive reduction in out-of-pocket expenditure and removal of any catastrophic expenditure in seeking, accessing or receiving health care. Whereas, the State is to provide for improving the level of nutrition, the standard of living, and public health as per Article 47 of the Constitution of India, and secure the right to health as per the expanded definition of Article 21 of the Constitution of India. And whereas every resident of the state of Rajasthan is entitled to enjoying the highest attainable standard of physical, mental, intellectual, and social well-being and health, conducive to living a life with dignity; And whereas the right to health care is an inclusive right extending not only to timely health care but also to the underlying socio-economic, cultural, and environmental determinants of health; And whereas to address the persisting iniquitous accessibility and denials in the matter of health care in the State; And whereas the Government of Rajasthan is

committed to ensuring that people's right to health care is realized. The most important stakeholders in the realization of the right to health care are the people themselves. Therefore, people's participation, and transparency and accountability to the people themselves, is crucial and critical for realization of peoples right to health care services."
2 Section 2(a) Others Section 2(a) on the definition of affordability to be revisited conceptually and modified.
There is variation in the definition of catastrophic household healthcare expenditure, especially depending on the income level of the household, and it needs to be clarified why this particular threshold in monthly consumption and non-food consumption expenditures is being used.
Further, how will it be verified that health care expenditure exceeds 10% of total monthly consumption expenditure and/or 40% of monthly non-food consumption expenditure?
Sections 2(b) Addition Curative, rehabilitative and palliative care to be added to the definition of basic primary healthcare services.
Therefore, Section 2(b) to be read as “”Basic Primary Healthcare Services” means preventive, promotive, curative, rehabilitative and palliative care, as defined from time to time for health & wellness centers at sub-centers. They include consultation, drugs and diagnostics, among other services.”

Section 2(e) Modification and Addition
Section 2(e) to be read as “”Capacity to consent” means the ability of an individual, including a minor or a person with mental illness, assessed by a healthcare provider on an objective basis, to understand and appreciate the nature and consequences of proposed healthcare or of a proposed disclosure of health-related information, and to make an informed decision in relation to such health care or disclosure. In order to ensure that the person concerned makes an 'informed decision', it will be the duty of the State to ensure that: 1. All information is made available to the user in simple language, which such user understands or in sign language or visual aids or any other means to enable him to understand the information. 2. Pro-active facilitation is provided to enable the person to access the information and use it."
Note that "mentally challenged" is a term whose usage has been discontinued post the enactment of the Rights of Persons with Disabilities Act, 2016. It should also be noted that Section 4 of the Mental Healthcare Act, 2017 which deals with people’s capacity to mental healthcare and treatment decisions states the following: 4. (1) Every person, including a person with mental illness shall be deemed to have capacity to make decisions regarding his mental healthcare or treatment if such person has ability to— (a) understand the information that is relevant to take a decision on the treatment or admission or personal assistance; or (b) appreciate any reasonably foreseeable consequence of a decision or lack of decision on the treatment or admission or personal assistance; or (c) communicate the decision under sub- clause (a) by means of speech, expression, gesture or any other means. (2) The information referred to in sub- section (1) shall be given to a person using simple language, which such person understands or in sign language or visual aids or any other means to enable him to understand the information. Therefore, the proviso on how an informed decision can be made needs to be outlined.

Section 2(o)(IV) Modification Section 2(o)(IV) to be read as “inform, educate, and empower people about health issues by enabling their access to information on an individual and collective basis and through ensuring community-based monitoring (CBM) and social audits on a regular basis.”
The modification helps provide the conditions under which it would be possible to inform, educate and empower people on health issues in an effective manner.
Section(o)(VII) Modification Section 2(o)(VII) to be read as "enforce laws and regulations that protect and ensure public health and safety, including the regulation of private sector health care providers"
While the section on essential public health functions is a progressive addition to the draft Act, the provisions do not clearly specific the regulatory role of the government.
Section 2(o)(X) Addition The function may also include affordability, i.e. Section 2(o)(X) should be read as "evaluate effectiveness, accessibility, quality, and affordability of personal and population-based health services,"
Section(o)(XII) Addition Section(o)(XII) to be read as "efficient and equitable health care financing"
Section 2(o)(XIII) Addition Section 2(o)(XIII) to read as "health protection, including management of environmental, food, toxicological and occupational safety"
Health protection, particularly in Rajasthan's context, where for instance pneumoconiosis is a significant occupational disease among mining workers in the state, should be a critical component of essential public health functions.
Section 2(t) Addition The term ‘health care worker’ or 'frontline health worker' could be defined to include a wider set of workers in health care, such as ASHAs, ANMs, etc. who are involved in health prevention and promotion, as well as identification and treatment of illness and/or disability.

Section 2(v) Modification Section 2(v) to be read as "“Health impact assessment” means a combination of procedures, methods, and tools, including mandatory participatory planning, CBM and social audit, for identifying, predicting, evaluating, and mitigating potential effects of a proposed law, policy, program, project, technology, or a potentially damaging activity, in relation health prior to taking decisions thereon and making commitments thereunder, on the health of the population, and other relevant effects, and the distribution of those effects within the population, and any reference to health impact assessment shall mean the same;"
Section 2(w) Modification Instead of the phrase “relates to” use the phrase “allows specific identification of an individual’s past. Present, future….”
which implies, Section 2(w) should be read as "“Identifiable health information” means any information, whether oral, written, electronic, visual, pictorial, physical or any other form, that allows specific identification of an individual's past, present or future physical or mental health status, condition, treatment, service, products, purchased or provision of care, and reveals that identity of the individual or that of a group of people, whose health care is the subject of the information, or there is a reasonable basis to believe the information could be utilized (either alone or with other information) to reveal the identity of the individual"

Section 2(x) Addition Add the following: Information disseminated will include the use of platforms such as Jan Soochna Portal where information not exempt under Section 8 of the RTI Act will be made openly available on a transaction basis so that people do not have to resort to using of the RTI to obtain information related tot he public health sector.
Section 2(kk) Addition Add the following after the phrase “governmental organizations and private institutions"...
Section 2(nn) Addition Add the following after the phrase “part or whole of” infrastructure, operations and/or costs of care.
Section 2(oo) Addition Add the following: Provided that such surveillance while ensuring the privacy of the individual is protected will be governed by transparent and participatory norms.
1. State must provide reasoned explanations for how the parameter of information collected will contribute to meeting the objectives of this Act 2. The process of arriving at the list of parameters of information that will be collected and analysed must be in a participatory and transparent manner.
Section 2(vv) Modification Replace with "Social audit to be conducted as per the Auditing Standards of Social Audit as laid down by the C&AG."
Section 2(yy) Addition Need to include family members/support system of patients.

Section 2(zz) Addition Add the following definitions after 2(zz) Complaint: "complaint" means a complaint lodged under Section (13) in relation to,-
a. any failure in the functioning of a public health institution or violation of any law, rules, or schemes currently in force; b. any grievance relating to, or arising out of, a failure in the delivery of goods or provision of services notified by the State Government under this Act; or c. any violation of duties and obligations upon public officials responsible for delivery of goods or rendering of services under this Act; Explanation.- For removal of doubts, a complaint does not include grievance relating to the service matters of a public servant whether serving or retired. Grievance Redress Officer: Every public authority shall, within one-twenty days from the date of commencement, designate as many officers as the Grievance Redress Officer in all administrative units or offices under it may be necessary to receive complaints and provide redressal of grievances in accordance with this Act: Provided that the Grievance Redress Officer so designated is at least one level superior to the official in charge of delivery of service and shall be deemed to have administrative control over the concerned official delivering the service

Section 2(aaa) Addition and Others The additional sub-section should mention how the State is defining out-of-pocket expenditure on health care. For instance, as per one source, OOPE on health care could include payments made towards health care provider’s fees, medicine, diagnostics, any surgical procedure, charges for blood, ambulance services, other in-patient and outpatient charges, etc., while non-medical expenditure includes money spent towards traveling expenses, shelter and food charges of self and escort, attendant charges, etc.
Section 3(a) Modification Section 3(a) to be read as "Residents will have the right to receive health interventions (information, services and products) in a manner most appropriate to them for promotion, prevention, and management of health at home, community and at health facilities to lead a healthy and active life, and/or access any rights under this Law."
Section 3(b) Modification Section 3(b) to be read as "Residents will have the right to free, timely and quality consultation, drugs, diagnostics, vaccination, emergency transport and emergency care, and rehabilitation and palliative care, at all public health institutions as may be prescribed by rules made under this Act."
Section 3(c) Modification Section 3(c) to be read as "Residents will have the right to free/affordable and quality inpatient care, surgeries and post-surgical care at all public hospitals as may be notified by rules made under this Act."
Section 3(d) Others It must be clear that all residents will
have the right to be covered under
government- funded insurance scheme,
and once
insured, they will have the right to avail

free services under the insurance scheme through the empanelled healthcare facilities. At the same time, it must be ensured that no one who is uninsured should be denied health care services, including emergency health care services at any health care establishment.
Section 3(e) Modification and Others To be read as “Residents will have the right to free, timely, and quality services from the private hospitals established through the land allocation on concession rates”
At the same time, it should be mentioned that we object to the proviso that says that “terms and conditions mentioned at the time of the allotment of the land” would govern the enforcement of Section 3(e). The Act should be laying the terms of individual contracts and not be governed by them.
Section 3(f) Modification Section 3(f) to be replaced with: Right to receive all information, records, and reports of self, including through authorized persons from the health care establishment be in public or private
Section 3(h) Addition Add the following Provided: All residents shall have a right to all information about the institutions and its funds, functioning, and functionaries as long as it does not violate the right to privacy of any individual user.
Section 3(i) Modification Section 3(i) to be read as "Right to safe and quality care according to standards prescribed for different levels of health care establishments run or managed by government or private institutions, including provisioning barrier-free access and reasonable accommodation."

Section 3(j) Modification Right to free and proper referral transport by all health care establishments, public or private (within 30 minutes from home to facility; and between health care establishments), as per the procedures detailed in the rules made under the act.
Section 3(k) Modification Section 3(k) to be replaced with: Right to details of treatment provided including treatment summaries and all costs incurred, even in cases of patients leaving against the medical advice.
Section 3(l) Modification Section 3(l) to be replaced with: Right to be heard, duly acknowledged, and seek time-bound redressal from health care establishments or through the state established grievance redressal mechanism or through legal intervention in case of any grievances occurring before, during, and after availing services
Section 3(m) Modification Section 3(a) to be read as "Right of family member/authorized person of the deceased user to receive the dead body, medical records, sensitive information and all the belongings of the deceased irrespective of the payment due status from every health care establishment."

Section 3(n) Addition Right to not be discriminated: Residents shall have the right to receive health and healthcare information and services from all health care establishments be it public or private without any kind of direct or indirect discrimination, including but not limited to, discrimination on the basis of their age, caste, criminal antecedents, disability, financial status, gender identity or gender expression, geographical location or residence, health status or condition, language, level of education, marital status, nationality or citizenship, occupation, place of birth, race, religion, sexual orientation, sex characteristics and/or any other social, economic, cultural or political characteristics.
Section 3(o) Addition Right to not be coerced: Residents shall have the right to not be subjected to any kind of direct or indirect coercion, force, threat or denial of his/her fundamental rights by the state or health care providers, public or private, in the absence of their explicit, autonomous and informed consent to receive a health care procedure or medical intervention.
Section 3(p) Addition Residents will have the right to obtain a second or more opinion from another health service provider and choose to seek health care, medicines, diagnostics, vaccines, devices or implants from a source most suitable to them.
Sections 4, 5 and 6 Others Instead of three different sections, there must be one section titled “Model Code of Conduct of Public Health Institutions and Users”. The existing provisions under Sections 4, 5, and 6 can be brought under one section.
Section 4 Modification Section 4 to be read as "Every resident has duties as may be prescribed by rules under this Act as follows, but which shall not constraint the residents' rights under this Act:"

Section 4(a) Others Tertiary health care services can be availed by following referral from primary and secondary level institution or a service provider.
While this is an important inclusion in the draft Act, it would be important to spell out how people would be encouraged to follow this path of seeking healthcare.
Section 4(c) Deletion Section 4(c) to be deleted. While engaging with health care advice is important, complying should not be a necessary condition in all cases.
Section 5(c) Modification Section 5(c) to be read as "Enunciate a policy on living and working conditions, remuneration, training and accreditation for health care providers and workers, especially at the primary health care level for their continued education and career advancement."
The policy must also be inclusive of health workers such as ASHAs, ANMs, health volunteers, etc.
Section 6(b) Modification Section 6(b) to be read as "Maintain confidentiality, privacy dignity of residents, and treat them with respect, including providing reasonable accommodation wherever required."
Section 7(a) Addition and Others Appropriate State budget should be provided so that rights under this law can be realized for all residents of the State. To this extent, the following must be included as part of Section 7(a):
"The state health budget would be progressively enhanced, at least to the extent of 10 per cent of the total state budget by the year 2028, two- thirds or more of which must be allocated to primary healthcare followed by secondary and tertiary care. Further, greater budgetary allocations must be made to desert and tribal districts to facilitate the provisioning of quality health care."
It is to be noted that the National Health Policy, 2017 recommends that a major proportion (up to two-thirds or more) of resources be allocated to primary care followed by secondary and tertiary care (Item 12 on financing of health care).

Section 7(b) Modification Add after the phrase “Human Resources Policy for Health”
including a fair and transparent recruitment, appointment, and transfer policy
Section 7(c) Modification Replace set up with “put in place”
Section 7(e) Modification Section 7(e) to be read as "Within one year lay down, notify and publicize standards for quality and safety of all levels and aspects of health care including job charts of all functionaries in public health institutions, provided that the Government shall: (1) adopt the Indian Public Health Standards (IPHS)/NABH for the health Institutions under its control and may review and expand such standards in scope and contents to suit the needs of the State of Rajasthan; (2) Set up a quality assurance institution that monitors the quality of health care establishments, reviews the evidence and revises standards accordingly from time to time, (3) Put in place a mechanism for quality and safety standards audit which includes community representatives"
Standards outlined in Sections 7(e) and 7(f) should be notified in a Schedule to the Act
Section 7(f) Modification Section 7(f) to be read as "Guarantee basic health care services through public health care establishments to every resident within 3 km (or 30 minutes of walking distance), comprehensive primary health care within 12 km, secondary health care same within 50 km (one hour by transport) and access to tertiary care (including treatment of critical illnesses) within 150 km by
Standards outlined in Sections 7(e) and 7(f) should be notified in a Schedule to the Act

fully skilled human resource with state of the art infrastructure, free medicines, tests, blood bank,
equipment, and 24X7 free ambulance service.
Section 7 Addition After sub-section 7(k), add the following
l. Ensure that a real-time transaction-based information system guides the implementation of this Act. Information from the portal will be shared with the JSP on a continuous basis subject to Section 8 of the RTI Act m. Ensure six-monthly review of the implementation of the Law n. Ensure that the annual report on implementation is laid in the Assembly o. Implement the Clinical Establishments Act 2010 and devise and execute rules and plans for the regulation of all health care establishments be it public or private.
Section 8(IV)(14) and 9(b)(II) and 11(b)(IV)
Addition Add the following after: Any other Department as needed
Section 8(VII) and 9(b)(VIII) and 11(b)(VI)
Modification Replace “Four non official persons” with the following
At least four non official persons with atleast one representative of each of the 4 categories below

Section 8(d)(IX) Modification Replace with: The State Health Authority should build and update a citizens charter which will involve the communities in articulating their needs and the Department in indicating the best ways possible to fulfil those needs. Community participation and monitoring shall be undertaken through concurrent and annual social audit processes as prescribed under this Act. A mandatory planning exercise will be conducted through community- based institutions at each level such as VHSNC etc.
Section 8(d)(X) Addition Add the following after:
XI. Review social audit findings and action taken on the same XII. Prepare the annual report that should be submitted in the Legislative Assembly XIII. Review grievances registered and the action taken thereunder. The Authority shall advise the Government on policy reforms that should be taken
Section 9(d)(VI) Addition Add the following after:
VII. There should be a dedicated secretariat to assist the functioning of the State Executive Committee in ensuring the implementation of the Act.
VIII. The State Executive Committee shall report to the State Health Authority.

Section 11(c)(V) Modification Replace with Organize a quarterly dialogue (samwaad) between the implementing agencies, public and CSOs with a view to improving the health care services.
Section 11(c)(VI) Modification Replace with To ensure that social audits carried out are independent and effective, it will be the responsibility of the District Health Authority to a. ensure that records are provided to the social audit teams 15 days prior to the audit b. ensure participation of concerned implementing agencies in the social audit public hearing c. Review action taken on social audit findings.
Section 12 Others There is no clarity on who is responsible for executing the orders issued by the Authorities. Further, it is not clear on what legal grounds the authorities are being given the powers under IPC.
In the current formulation, the State Health Authority is a collective body. It currently does not have an investigation/inquiry wing. It cannot fulfil the functions defined under this section

Section 12(d) Others and Modification In the current formulation, the State and District Health Authorities are given functions of a monitoring body. Section 12(d) describes the functioning of a regulatory authority. If Section 12(d) is to be actually implemented, a regulatory authority needs to be set up under this Law.
Section 12(d)(5) to be read as "to prescribe treatment rate of services provided by private institutes during the pandemic or any other public health emergency."
Section 13 Modification Replace with
a. Any person who is aggrieved by a denial of any goods and services of the medical establishment, including standards and services laid under this Act shall be entitled to file a complaint.
b. Complaints may be filed through multiple modes including in writing, through existing and specially created helplines, web portals etc
c. All complaints should be duly acknowledged by a dated receipt d. At the time of filing of the complaint, the complainant will be asked whether they would like the proceedings and ATR to be in the public domain. In case privacy and confidentiality are specifically requested by the complainant, personally identifiable information shall be redacted. The rest shall be in the public domain. e. All complaints will be forwarded to the concerned Grievance Redress Officer (GRO)
The time duration of responding to a complainant could be shortened from the 30-day period in the case of an exigency/emergency situation, similar to the RTI Act where the information sought will be supplied in 48 hours if it concerns the life and liberty of a person.

f. The following shall be the duties of the GRO - Inquire into the facts of the case, including a
physical visit to the site of the complaint - Give a hearing to the complainant within 15 days of registration of complaint as prescribed under the rules. The complainant may request that the hearing and the subsequent process of redressal of his/her grievance be held in camera in order to maintain privacy. The complainant may also present witnesses and others to be a part of the proceedings of the hearing. - Submit an action taken report within 30 days to the complainant. ATR will contain steps taken to resolve the grievance and will be furnished as per rules prescribed.
g. If the complainant is dissatisfied with the ATR, he /she has a right to file a first appeal with an Ombudsperson, at the district or state level, as the case may be
h. Failure of submission of an ATR within 30 days aby the concerned GRO will result in the automatic escalation of the complaint as a first appeal with a with an Ombudsperson, at the district or state level, as the case may be
i. Social Audits should be conducted by the independent social audit unit of the State as per the Auditing Standards of Social Audit laid out in the C&AG. j. the Social Audit Unit shall frame a calendar such that 100% of the institutions and their functions undergo a social audit once a year. The same shall be in the public domain k. All social audit Reports shall be in the

public domain l. All social audit findings should be responded to and resolved within 60 days
m. All Action Taken Reports of social audits conducted shall be in public domain
n. Requisite funds as per auditing standards shall be provided to the independent social audit unit which will carry out social audits as per Auditing Standards of Social Audit of the C&AG appropriately modified for the public health sector.
Section 14(a) Modification and Addition
Retitle Section 14 as Penalties and Compensation and add the following
b. The GRO or the Ombudsperson in addition to the penalty prescribed above may upon finding of serious contravention require the initiation of department proceedings, filing of an FIR in case of criminal violation has been found.
c. The GRO or the Ombudsperson may prescribe awarding of compensation to aggrieved persons
Individuals and organisations involved in the discussions (in alphabetical order):
1. Chhaya Pachauli, Prayas
2. Kavita Srivastava, People‘s Union for Civil Liberties (PUCL)
3. Naina Seth
4. Narendra Gupta, Jan Swasthya Abhiyan (JSA)
5. Nikhil Dey, Mazdoor Kisan Shakti Sangathan (MKSS)
6. Pavitra Mohan, Basic Healthcare Services (BHS)
7. Prakash Tyagi, Gramin Vikas Vigyan Samiti (GRAVIS)
8. Rakshita Swamy
9. Sharad Iyengar, Action Research and Training for Health (ARTH) Society
10. Vandana Prasad, Public Health Resource Network (PHRN)

jktLFkku ukxfjd eap
*jktLFkku LokLF; dk vf/kdkj Mªk¶V dkuwu 2022
& lq>ko vkSj vkifÙk;ka*
ge jktLFkku ukxfjd eap dh vksj ls loZçFke Jh v'kksd xgyksr] eq[;ea=h]
jktLFkku ljdkj dk lknj vfHkuanu djrs gSa] ftUgksaus tuLokLF; ij xEHkhjrk fn[kkrs gq,
^LokLF; vf/kdkj dkuwu^ ykus dh ea'kk trkbZ gSA
gekjh fpark ;g gS fd lkoZtfud LokLF; lsokvksa dks çkFkfedrk fn;s fcuk vkSj
i;kZIr ctVh; vkoaVu ds vHkko esa ;g egRoiw.kZ tu vf/kdkj dsoy dkxth cu dj u
jg tk,A blfy, ;fn ljdkj okLro esa xEHkhj gS rks mls esfMDyse vkfn futhdj.koknh
rkSj&rjhdksa ls LokLF; lsokvksa dks c<+kok nsus dh ctk, jktdh; LokLF; lsokvksa ds i;kZIr
ctVh; vkoaVu ds tfj, xzkeh.k {ks=ksa esa gj iapk;r Lrj ij vkSj 'kgj ds gj okMZ esa
ljdkjh LokLF; dsaæ ftldh lsok,a 24 ?k.Vs lqyHk gks] LFkkfir fd, tkus vkSj mUgsa çksUur
fd;s tkus dh igyh t:jr gSA
jktLFkku ukxfjd eap ,oa LokLF; vf/kdkj eap tuLokLF; ds eqís ij çns'k ,oa jk"Vªh;
Lrj ij ejhtksa ds bykt] nok] tkap] 'kks/k o nok ijh{k.k ,oa muds çHkko dks ysdj lnSo
lpsr ,oa lfØ; jgs gSa vkSj le; le; ij jkT; ,oa dsaæ ljdkj ds v/khu LokLF;
lEcaf/kr eqíksa ij vius lq>ko ds tfj;s /;kukd"kZ.k djrs jgs gSa] mlh Øe esa jkT; ljdkj
}kjk çLrqr Mªk¶V jktLFkku LokLF; dk vf/kdkj dkuwu 2022 jkT; dh turk ds LokLF;
dh ns[kHkky lsok,¡ nsus dh ckr djrk gSa] ijarq jktLFkku ljdkj }kjk çLrqr bl Mªk¶V esa
dbZ fo"k;ksa esa Li"Vrk dk lh/kk lh/kk vHkko gSa] ;k dgsa fd yksxksa dks ;g lsok,¡ dSls
feysxh bl ckjs esa iwjs Mªk¶V esa dgha ij Hkh bl lanHkZ esa ppkZ ugha dh xbZ gSaA ;|fi
çLrkfor Mªk¶V ls ,slk vo’; çrhr gksrk gSa fd jkT; ljdkj jkT; ds ukxfjdksa dks muds
fudV] xq.koÙkkiw.kZ vkSj fu'kqYd lkoZHkkSfed LokLF; lsok,¡ çnku djus ds fy, fdlh Hkh
çdkj ls ck/; gSA lEiw.kZ nLrkost esa flQZ ;gh dgk x;k gS fd tc fu;e cusaxs rks mleas
foLr̀r fooj.k gksxk] ysfdu fu;e fuekZ.k ds fy;s izLrkfor le; lhek 6 ekg cgqr vf/kd
gSA
jktLFkku ljdkj }kjk çLrkfor Mªk¶V jktLFkku LokLF; dk vf/kdkj dkuwu 2022 dks
v/;;u djus ij ge bl çLrfor Mªk¶V dkuwu esa fuEu la’kks/kuksa gsrq lq>ko izLrqr djrs
gSaA
çLrqr Mªk¶V jktLFkku LokLF; dk dkuwu vf/kdkj ds lEiw.kZ nLrkost esa ge fcanqokj
viuh vkifÙk;ka ,oa lq>ko vkids le{k is'k dj jgs gSa%&
1- ljdkj ls gekjh ;g ekax gS fd dkuwu ds rgr fu;e Hkh dkuwu fuekZ.k ds lkFk gh
vFkok vf/kdre ,d ekg dh vof/k esa izdkf’kr dj fn;s tkus dk izko/kku fd;k tkosA
2- çLrkfor dkuwu esa jkT; dh turk dks LokLF; ns[kHkky lsok,a nsus dk oknk fd;k x;k
gSa ijarq turk ds fy, lHkh LokLF; lqfo/kk;sa dSls lqyHk miyC/k gksxh] bl lanHkZ esa dqN
ugha dgk x;k gSaA jkT; ljdkj dks pkfg, fd izfr 3 fdeh ds Hkhrj cqfu;knh lsok,a] izfr
12 fdeh ds Hkhrj iw.kZ çkFkfed ns[kHkky] izfr 50 fdeh ¼,d ?kaVs dh ;k=k½ ds Hkhrj xaHkhj
chekfj;ksa dk bykt vkSj 150 fdeh ds Hkhrj iwjh rjg ls dq'ky fo'ks"kKksa ds lkFk xaHkhj
chekfj;ksa ds bykt dh O;oLFkk bl dkuwu ds tfj;s lqfuf'pr gksA
3- ejhtksa dks bu lHkh lsokvksa ls tksM+us ds fy, 24x7 ,Ecqysal dh miyC/krk gksA
4- çLrkfor dkuwu esa ljdkj yksxksa dks LokLF; lsok,¡ fu'kqYd vkSj lLrh ¼Affordable½ lsokvksa dk ftØ fd;k x;k gSa ijarq lLrh lsokvksa dks ifjHkkf"kr djrs gq, dgk x;k gS fd
O;fä dh ekfld vk; dk 10% r; fd;k x;k gSa tcfd jkT; ds e/;e] xjhc vkSj
vfrxjhc yksxksa ds fy, ;g Ikzko/kku lgh ugh gSa A ljdkj bl çko/kku esa la'kks/ku djs
vkSj ;g lqfuf'pr djs fd fcuk tsc [kpZ ds mi;qä LokLF; ns[kHkky vkSj lacaf/kr
dk;kZRed midj.k ,oa vU; cqfu;knh <kaps] ,Ecqysal lsok,¡] çf'kf{kr fpfdRlk&dehZ rFkk
midj.kksa o Mk;XuksfLVDl lfgr vko';d nok,sa lHkh fu’kqYd ikus dk vf/kdkj lHkh dks
feysA
5- çLrkfor dkuwu esa LokLF; laLFkkuksa esa cqfu;knh lqfo/kkvksa ds ckjs esa fdlh çdkj dk
ftØ ugh gSA tSls i;kZIr is;ty dh vkiwfrZ] LoPNrk] Hkou] fctyh] lM+d] LokLF;

laLFkku rd igq¡p vkfn A lkFk gh çLrkfor dkuwu esa efgykvksa] yM+fd;ksa ,oa LGBTQ leqnk; ds lnL;ksa ds fy, fdlh çdkj ds dksbZ fo'ks"k çko/kku ugha fd, x, gSa] buds
fy, çLrkfor dkuwu esa fo'ks"k /;ku ds lkFk çtuu LokLF; lsokvksa vkSj ;kSu LokLF;
ns[kHkky ds fy, çko/kku fd, tk,¡ A
6- lHkh vko';d vkSj thou j{kd nokvksa] midj.kksa vkSj Mk;XuksfLVDl dh miyC/krk vkSj
igqap] nokvksa dk rdZlaxr mi;ksx vkSj nok çfrjks/k vkSj çfrdwy çHkkoksa dh fuxjkuh dh
ckr bl dkuwu esa ugha gSa A blls 'kkfey fd;k tk,A
7- ljdkj çLrkfor Mªk¶V dkuwu esa ,d rjQ jkT; dh turk dks eq¶r vkSj lLrh LokLF;
lsok;s¡ nsus dh ckr dj jgh gSa] ogh nwljh vkSj bl dkuwu esa chek vk/kkfjr ;kstukvksa dh
Hkh iSjoh djrh utj vk jgh gSaA gekjh ekax gSa fd ,d dY;k.kdkjh jkT; gksus ds ukrs
ljdkj dh ;g uSfrd ftEesnkjh gSa fd og jkT; dh turk dks eq¶r LokLF; ns[kHkky
lsok;s¡ miyC/k djk;sA chek vk/kkfjr ;kstukvksa dks ljdkj foÙkiksf"kr u djs ] bUgsa iwjh
rjg ls can fd;k tk,A fo’ks"k:Ik ls chek vk/kkfjr ;kstukvksa ds tfj;s futh vLirkyksa ds
fy;s vuki ’kuki iSlk olwyh dk tks }kj [kksy fn;k x;k gS mls iw.kZr% cUn fd;k tkosA
8- çLrkfor Mªk¶V dkuwu esa dgk x;k gS fd jkT; ds mUgh futh LokLF; laLFkkuksa esa
ukxfjdksa dks eq¶r lsok;s¡ feysaxh ftUgsa fdQk;rh nj tehu vkoafVr dh xbZ gS A gekjh
ekax gS fd jkT; ds lHkh futh LokLF; laLFkkuks esa nq?kZVuk] vkdfLed thouj{kd ekeyksa
esa eq¶r bykt dh O;oLFkk gksuh pkfg,A
9 -ljdkj }kjk cuk;s x;s ijUrq ckn esa lapkyu gsrq ihihih ekWMy ij futh dkWjiksjsV ds
gkFk esa ns fn;s x;s vLirkyksa dk ljdkj iqu% vf/kxzg.k dj [kqn lapkyu djsA crkSj
mngkj.k t;iqj ds ekuljksoj ds ekul vkjksX; vLirky dks esVªks dks ns fn;k x;k Fkk
vkSj lhdj jksM+ ds Vªksek vLirky ftls lksuh vLirky dks ns fn;k x;k Fkk] us ckn esa
efuiky vLirky dks csp fn;k] dks iqu% ljdkj vius fu;a=.k esa ysdj [kqn lapkfyr
djsA
10 - xzkeh.k {ks=ksa esa vLirkyksa esa fpfdRldksa dks tkus ds fy, rS;kj djus o muds Bgjko
dks lqfuf'pr djus ds fy, muds vkokl dh lqfo/kk,a lqyHk djokus ds lkFk lkFk muds
cPpksa dh f'k{kk ds fy, ogka dsaæh; fo|ky; ds cjkcj Lrj ds ekWMy Ldwy Hkh [kksyus
t:jh gSA bu lqfo/kkvksa ds lkFk gh ,d le;kof/k rd MkDVjksa dk xzkeh.k {ks=ksa esa jksLVj
ds tfj, Bgjko laHko gSA
11 - ;g egRoiw.kZ gS fd jktLFkku ukxfjd eap ds lq>ko dks vaxhdkj dj nw/k o [kk|
inkFkksaZ dh 'kq)rk dh tkap&ij[k ds fy, vkius gky gh çns'k esa eksckby yscksjsVªh pykus
dk QSlyk fd;k gS] ftldk ge gkfnZd Lokxr djrs gSaA blds lkFk gh mldh lqpk:
ikyuk dh ftEesnkjh vkSj fu;e dk;ns cukus Hkh mrus gh t:jh gSaA [kksyh xbZ eksckby
rFkk LFkk;h tkap yscksjsVªh ds ckjs esa tkudkjh o tupsruk txkus ds fy, vko';d çpkj
çlkj Hkh t:jh gSA
blds lkFk gh nw/k dh ek=k c<+kus ds fy, xk; HkSal dks fn;s tkus okys batsD'ku vkSj Qy
lfCt;ksa dks tYn idkus ds fy, fn;s tkus okys batsD'ku Hkh iwjh rjg ls çfrcaf/kr gksA
12 - vLirky rd igqapkus ls igys vkikrdkyhu LokLF; lsokvksa ds eísutj ^^LokLF;
fe=^^ tks thou j{kkFkZ vko';d bykt ds ckjs esa foK cukus gsrq de vof/k ds ØS'k dkslZ
ds çf'k{k.k dsaæ [kksydj mUgsa t:jh bykt o nok ds çf'k{k.k fn;s tkus pkfg,A bu
dkslsZt ds tfj;s Ik;kZIr la[;k esa nok forj.k gsrq QkesZflLV ,oa gksfe;ksiSFkh fpfdRld
rS;kj fd;s tk ldrs gSaA ;s fpfdRld tgka lkekU; lnhZ tqdke tSlh ekSleh leL;kvksa
dh fLFkfr esa xzkeh.k turk dks Rofjr lsok miyC/k djok ldrs gSa ogha mUgs csjkstxkjh ls
Hkh dqN futkr feysxhA QkesZflLVksa ds ykbZlsal fdjk;s ij fy;k tkdj nok fodzsrkvksa }kjk
QSyk;k tk jgk Hkz"Vkpkj jksdus gsrq Ik;kZIr la[;k esa QkesZflLV bl rjhds ls miyC/k fd;s
tk ldrs gaSA
13- dkuwu esa LokLF; ns[kHkky lsokvksa ds ekudksa ds ckjs esa Hkh Li"Vrk ugha gSa] çLrkfor
Mªk¶V dkuwu esa dgk x;k gS fd dkuwu ds rgr tks fu;e cusxs mlh ds vuqlkj ekud
r; gksaxsA tcfd gekjs ns'k esa Hkkjrh; lkoZtfud LokLF; ekud ¼IPHS) vkSj us'kuy
,ØhfMVs'ku cksMZ Q‚j g‚fLiVYl ,aM gsYFkds;j çksokbMlZ ¼NABH) igys ls ekStwn gSa A
blfy, dkuwu esa IPHS vkSj NABH dks vk/kkj ekudj] buds vuqlkj LokLF; ns[kHkky
lsokvksa vkSj lqfo/kkvksa dks lqfuf'pr djuk pkfg,A

14- LokLF; vkSj ifjokj dY;k.k ea=ky;] Hkkjr ljdkj vkSj jk"Vªh; ekuokf/kdkj vk;ksx
¼NHRC½ rS;kj fd, x, jksxh ds vf/kdkjksa ds ?kks"k.kki= dks ykxw djukA¼—i;k
NHRC }kjk viuk, x, pkVZj v‚Q is'ksaV~l jkbV~l dks ns[ksa½A
çLrkfor dkuwu esa bldk dksbZ ftØ ugh gSa A
bl v/;k; ds fcUnw Øekad 14 ¼a½ esa çLrkfor dkuwu ds fdlh Hkh çko/kku ds igyh ckj
mYya?ku ij ek= 10000@& ¼nl gtkj½ #i, vkSj nksgjko ij vf/kdre tqekZuk
25000@& ¼iPphl gtkj ek=½ çLrkfor fd;k x;k gS A ;g tqekZuk çko/kkuksa ds igyh
ckj mYya?ku ij 25000@& ¼iPphl gtkj ek=½ rFkk nksgjko ij de ls de 50000@&
¼ipkl gtkj #i,½ fd;k tkuk pkfg,A
bl v/;k; ds fcUnq Øekad 16 esa bl dkuwu ds vuxZr xfBr vihyh; çkf/kdj.k ds
fdlh Hkh vkns'k ;k xfrfrof/k ds fo#) U;k;ky; es tkus ls jksdrk gSa] tks xyr gS vkSj
turk dks LokLF; vf/kdkj nsus dh jkg esa eqf'dy iSnk djsxk] blfy, bl çko/kku dks
gVk;k tkuk pkfg,A
15- bl dkuwu ds varxZr jkT; ljdkj ds ikl fuxjkuh ds fy, ,d fuxjkuh ç.kkyh vkSj
lR;kiu ds fy, ,d lkekftd ys[kk ijh{kk ra= vfuok;Z :i ls gksuk pkfg, A ,d
çHkkoh] vktek, gq, vkSj ijh{k.k fd, x, fu;ked <kaps esa] ftlesa Lora= fuxjkuh]
okLrfod lkoZtfud Hkkxhnkjh vkSj xSj&vuqikyu ds fy, naM 'kkfey gSa] jkT; ljdkj dks
lkoZtfud LokLF; laLFkkuksa dks rhljs i{kksa ds çca/ku vkSj pykus dh ftEesnkfj;ksa dks
lkSaius esa vR;f/kd lko/kkuh cjruh pkfg,A ljdkj dks futh fgr/kkjdksa dks çkFkfed]
ek/;fed vkSj r`rh;d lkoZtfud LokLF; ns[kHkky dh ftEesnkjh ugha lkSaiuh pkfg,] blds
ctk; jkT; vkSj lkoZtfud /ku dk mi;ksx djds lkoZtfud ç.kkfy;ksa dks etcwr djuk
pkfg,A çca/ku ij dlkoV ds fy, tulgHkkfxrk dh Hkwfedk lqfuf'pr dh tkuh pkfg,A
16- lHkh Lrjksa ij LokLF; ns[kHkky vf/kdkjksa ds fy, ukxfjdksa ls mRiUu gksus okyh lHkh
f'kdk;rksa vkSj fooknksa dks laHkkyus ds fy, ,d çHkkoh vkSj Rofjr f'kdk;r fuokj.k ç.kkyh
dh vko';drk gSA f'kdk;rksa ds fuokj.k ds fy, f'kdk;r ra= lHkh laLFkkxr Lrjksa ij
LFkkfir dh tkuh pkfg,A ukxfjdksa dh f'kdk;rksa dks rqjar lacksf/kr djus vkSj can djus ds
vykok] ;g ftyk vnkyrksa vkSj vU; mPprj eapksa ij fooknksa dh la[;k dks Hkh de
djsxkA f'kdk;r fuokj.k dk tks <kapk bl çk:i esa n'kkZ;k gS og tehuh Lrj ij dSls
fØ;kfUor gksxk\ bldk mYys[k fd;k tkuk pkfg,] çLrkfor <kaps esa ejht vkSj LokLF;
lsok çnkrk ds chp fdlh çdkj ds laokn dh ckr ugh dgh xbZ gS mls lqfuf'pr djokus
ds çko/kku fd, tk,A
17- nok fodzsrkvksa vkSj futh fpfdRldksa }kjk tSufjd nokvksa ds ek/;e ls dh tk jgh
turk dh ywV dks iw.kZr% jksds tkus gsrq izHkkoh dne mBk;s tkosaA
18- lHkh QSfDVª;ksa] dk;Z’kkykvksa vkfn esa Jfedksa ds fy;s LokLF;dkjh O;oLFkk,sa dh tkosaA
vukSipkfjd vkSj vkSipkfjd {ks=ksa esa Jfedksa ds fy, jk"Vªh; O;kolkf;d lqj{kk fn'kk
funsZ'kksa ds vuqlkj fofHkUu LokLF; vf/kdkfj;ksa }kjk ljdkjh o futh LokLF; laLFkkuksa dk
O;kolkf;d LokLF; lqj{kk ds –f"Vdks.k ls fujh{k.k dh vuqlwph r; djuk vkSj
O;kolkf;d LokLF; ds fofHkUu eqíksa dks çLrkfoÙk dkuwu esa 'kkfey djuk vko';d gS A
bl fo"k; ij fo’ks"k ppkZ gsrq gekjh Vhe lnSo rRij gSA
ldkjkRed ifj.kke dh vis{kkvksa ds lkFkA
jktLFkku ukxfjd eap

1. Mr. Sandeep Vijay 2. Dr gulam Ali Kamdar 3. Mr. Rajkumar
Sharma, 4. Dr. Mayank Agarwal
Rajasthan Right to Healthcare Act 2022
The broader notion of the ‗right to health‘ emphasizes its interlinkages with rights and
regulations relating to the protection of life and liberty, privacy, education, housing, transport,
environmental protection and labour standards among others.
The traditional notion of healthcare has tended to be individual-centric and has focused on
aspects such as access to medical treatment, medicines and procedures. The field of professional
ethics in the medical profession has accordingly dealt with the doctor-patient relationship and the
expansion of facilities for curative treatment. In such a context, healthcare at the collective level
was largely identified with statistical determinants such as life-expectancy, mortality rates and
access to modern pharmaceuticals and procedures. It is evident that such a conception does not
convey a wholesome picture of all aspects of the protection and promotion of health in society.
There is an obvious intersection between healthcare at the individual as well as societal level and
the provision of nutrition, clothing and shelter.
Furthermore, the term ‗public health‘ has a distinct collective dimension and has an inter-
relationship with aspects such as the provision of a clean living environment, protections against
hazardous working conditions, education about disease-prevention and social security measures
in respect of disability, unemployment, sickness and injury. Special emphasis is laid on elements
such as women‘s reproductive health and the healthcare of children.
The incorporation of health concerns in the ‗rights‘ discourse, the onus on governmental
agencies goes beyond aspects like the regulation of the medical profession and support for
research and development (R&D) in the medical field. It also includes policy-choices pertaining
to education, housing, environmental protection, labour laws, social security provisions and the
protection of intellectual property among others.
CHAPTER-I
Section 2(t)- The definition of Healthcare provider is not exhaustive. Must include the
qualifications and relevant licenses required to be obtained by them.
Section 2- Define ―Quackery‖
CHAPTER-II
Section 3(c)- Replace all public hospitals to public health institutions as defined.
Section 3(j)- Proper referral transport includes the cost incurred in acquiring the vehicle,
equipment, medicines, trained staff etc., which should be clearly mentioned.
Healthcare facilities, especially private hospitals, cannot bear the cost of such
services by themselves.
Section 3(l)- Define Redressal Mechanism

Section 3(m)- Unfavorable for the Private Healthcare Facilities as the Provision allows patients
to not pay their dues for an indefinite period. Should only be allowed to take the
body of the deceased after providing an assurance/bond to pay the dues within a
specific period of time and within the limits of capping of dues on total bill.
Section 4- Should include duty of patients to pay the all the bills and dues for services rendered
to private healthcare establishments before discharge.
Section 4(f)- Include punishment under The Rajasthan Medicare Service Persons
and Medicare Service Institutions (Prevention of Violence and Damage to
Property) Act, 2008.
Section 4(h)- Specify the Prescribed Authority to which such acts should be reported.
Section 5- Include right to:
- practice profession without undue pressure, distress and harassment
- refuse treatment to patients indulging in disruptive and violent behavior
- refuse treatment to patients if required services are not available
- report unruly patients and attendants
- receive timely payments for services
Section 5(a)- no criminal proceedings against healthcare providers such as FIR/arrest should be
initiated without obtaining a report from district level committee of subject
specialists.
Section 5(d)- Right to have physical safety and security at the workplace , through proper safety
measures by government.
CHAPTER-III
Section 7- Include:
- Ensure proper safety and prevention of violence against health care workers
and establishments. Enact proper rules and stringent laws against physical
violence, verbal abuse, mob lynching harassment etc. for the same and direct
all concerned authorities to implement them.
- Make provisions to prevent quackery and crosspathy by unqualified persons in
health care. Respective authorities like CMHO, District Collector or SDM of
the concerned territory must be made liable and accountable to prevent
quackery.
CHAPTER-IV
Section 8(b)VII 2. - Specify representatives of health associations: must be from office bearers
of Indian Medical Association and Private Hospital association. Chairperson
should not appoint any representative by ―Pick & Choose‖ method. Exclusive
power to the Chairperson to appoint the representatives can create a bias.
Section 9(b)VI 2. - Specify representatives of health associations: must be from office bearers of
Indian Medical Association and Private Hospital association. Chairperson should
not appoint any representative by ―Pick & Choose‖ method. Exclusive power to
the Chairperson to appoint the representatives can create a bias.
Section 11(b)(VI)- Should also include President/Secretary of Indian Medical Association
(IMA), representatives of Private Hospital associations. Exclusive power
to the Chairperson to appoint the representatives can create a bias.
Section 12(b) – IPC section 176 and 177 should not be applicable. Required information must be
defined properly.
Section 12 (c) – Totally unconstitutional provisions. Any authority or officer should not be given
rights for a search and seize operation. Only related documents and records can be
asked to produce according to section 91 of CrPC.
Section 12 (d) – Unconstitutional provision of fixing responsibility and accountability of private
institutions for services. Clear Contraventions of Article 19 1(g) of constitution of
India. State Health Authority and District Health Authority can have only
supervision and advisory rights. Not acceptable to extent of deciding the prices for
private hospitals as the services provided at each establishment are diverse.
The government shall have powers to regulate prices for the packages of
government schemes only. Private institutions should not have any bindings for
participation and empanelment of such government schemes. State Health
Authority and District Health Authority committee may have powers to send
recommendations to revise the rates of packages of government schemes to
concerned departments to encourage participation of more and more private
institutions.
CHAPTER-V
Section 13 (a) – Complaint forums and Grievance redressal must be at three levels:

1. Institutional Level
2. District Level: Must have members from representative of local
medical association, subject medical specialist and CMHO
3. State Level: Must have members from representative of state
medical association, subject medical specialist from Medical
College
Section 13 (b) – No grievance, complaint and investigation summary should not be shared on
public domain. Goodwill and reputation of health care providers and
institutions must be properly preserved and maintained.
Section 13 – Include following provisions:
- Burden of proof must be on complainant
- Must have penalty provisions for frivolous and misleading complaints.
- Health care providers and institutions should be allowed to lodge complaints
against any person, groups and authorities against infringement of their rights.
CHAPTER-VI
Section 16 – Totally unconstitutional provision, legal remedies and appeals are constitutional
rights and principal of natural justice. Should be deleted.
We believe that the said act should be beneficial to public and health care providers. No
adverse relationship between public and health care providers] should develop in the
society due to vague provisions of the act.

Mr. Ganesh Sharma, IMA Jaipur Branch

































