From strategy to action – overcoming barriers to change ... - Deloitte
Upload
independentCategory
view
3download
0
Overcoming Barriers to Cancer Pain Management: An InstitutionalChange Model
Virginia Chih-Yi Sun, RN, MSN, ANP1, Tami Borneman, RN, MSN, CNS1, Betty Ferrell, RN,PhD, FAAN1, Barbara Piper, DNSc, RN, AOCN, FAAN3, Marianna Koczywas, MD2, and KyongChoi, MA41 Department of Nursing Research & Education, Division of Population Sciences, BeckmanResearch Institute2 Department of Medical Oncology and Therapeutics Research, City of Hope National MedicalCenter, Duarte, California3 Adult Health and Illness Department, College of Nursing, University of Nebraska Medical Center,Omaha, Nebraska4 Vital Research, Los Angeles, California, USA
AbstractThe Agency for Health Care Policy and Research (AHCPR) Pain Guidelines of 1994 recognizedpain as a critical symptom that impacts quality of life (QOL). The barriers to optimum pain reliefwere classified into three categories: patient, professional and system barriers. A prospective,longitudinal clinical trial is underway to test the effects of the “Passport to Comfort” innovativeintervention on pain and fatigue management. This paper reports on pre-intervention findings relatedto barriers to pain management. Cancer patients with a diagnosis of breast, lung, colon, or prostatecancer who reported a pain rating of ≥ 4 were accrued. Subjects completed questionnaires to assesssubjective ratings of overall QOL, barriers to pain management, and pain knowledge at baseline andat one- and three-month evaluations. A chart audit was conducted at one month to document objectivedata related to pain management. The majority of subjects had moderate (4–6 on a zero to ten numericrating scale) pain at the time of accrual. Patient barriers to pain management existed in attitudes andknowledge regarding addiction, tolerance, and not being able to control pain. Subjects who werecurrently receiving chemotherapy were reluctant to communicate their pain with health careprofessionals. Professional and system barriers were focused around screening, documentation, re-assessment, and follow-up of pain. Lack of referrals to supportive care services for patients was alsonoted. Several well-described patient, professional, and system barriers continue to hinder efforts toprovide optimal pain relief. Phase II of this initiative will attempt to eliminate these barriers usingthe “Passport” intervention to manage cancer pain.
KeywordsPain; barriers; quality of life; QOL
Address reprint requests to: Virginia Chih-Yi Sun, RN, ANP, Nursing Research and Education, City of Hope National Medical Center,1500 East Duarte Road, Duarte, CA 91010, E-mail: [email protected]'s Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resultingproof before it is published in its final citable form. Please note that during the production process errors may be discovered which couldaffect the content, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptJ Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
Published in final edited form as:J Pain Symptom Manage. 2007 October ; 34(4): 359–369. doi:10.1016/j.jpainsymman.2006.12.011.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

IntroductionMajor deficiencies in the treatment of cancer symptoms such as pain have been documentedover the past two decades. Pain is recognized as impacting all dimensions of patient’s qualityof life (QOL).1 One framework often applied to understanding the reasons for unrelievedsymptoms is to examine the barriers to their relief. The barriers to optimum pain relief werecaptured during the development of the first national clinical practice guidelines on cancer painpublished by the Agency for Health Care Policy and Research in 1994. 2 These barriers wereclassified into three categories: patient, professional and system barriers.
The literature has consistently documented that patients play a key role in the undertreatmentof pain.3,4 Patients are reluctant to report their pain for reasons including fear of side effects,fatalism about the possibility of achieving pain control, fear of distracting physicians fromtreating cancer, and belief that pain is indicative of progressive disease.4–9 There are alsosignificant health care professional barriers to adequate pain relief. Physicians, nurses, andother members of the interdisciplinary team often fail to adequately assess the patient’s painor to recognize patient barriers.10–12 Professionals lack knowledge of the principles of painrelief, side effect management, or understanding of key concepts like addiction, tolerance,dosing, and communication.13–15
System barriers include legal and regulatory structures that interfere with the provision ofoptimal care as well, as inadequate reimbursement for pain services. System barriers can beinternal, such as low referrals to supportive care services, or external, such as reimbursementand regulatory constraints.2 Synthesis of pain literature by the Institute of Medicine and theNational Cancer Policy Board have continued to document the importance of these systembarriers on the ultimate outcomes of patient care. 1,16,17
In response to overwhelming evidence of the impact of these barriers on symptom management,the United States National Cancer Institute (NCI) issued a call for proposals with the intent ofmoving beyond descriptive studies to test innovative models that would eliminate thesebarriers. This paper reports on Phase I results from one of the projects supported by this NCIinitiative and conducted at a NCI-designated comprehensive cancer center to test the effectsof an intervention on pain and fatigue management.
MethodsDesign
Figure 1 presents the overall “Passport” model of care. Barriers to the management of pain areidentified in the three categories of patient, professional, and system. This five-year study isdesigned in three phases. Phase I, from which data on pain is presented in this paper, assessedUsual Care in order to describe the current status of pain and fatigue management in thispopulation and setting. Phase II will be a High Intensity Intervention in which patient andprofessional education, as well as peer audit and feedback will be implemented in order toaddress the barriers. Phase III will be a Low Intensity Support Intervention, during which theintervention will be moved to a more realistic model of care in clinical settings so that it canbe replicated and maintained at after the project concludes.
This project demonstrates innovation by translating the evidence-based guidelines for pain asdeveloped by the National Comprehensive Cancer Network (NCCN).18 The symptom of painwas selected because it is consistently cited to be common and distressing for cancer patients.The NCCN Pain Guidelines have not been evaluated clinically to test feasibility inimplementation. This study will provide insight into the use of NCCN guidelines and serve as
Sun et al. Page 2
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

a model for extending these and other guidelines into practice to eliminate barriers. The studydesign was reviewed and approved by the Institutional Review Board.
SampleStudy participants were recruited from the Medical Oncology Adult Ambulatory Care Clinicat an NCI-designated comprehensive cancer center. Eligibility criteria included a diagnosis ofbreast, colon, lung, or prostate cancer, time since diagnosis of at least one month, an expectedprognosis of six months or greater, and subjective pain rating of ≥ 4 (moderate to severe pain)on a numeric scale of 0–10 (0=no pain; 10=worst pain imaginable). The criteria were intendedto target patients with moderate to severe symptom intensity who would serve as an appropriatecomparison for the intervention phase and to decrease the heterogeneity of the population byfocusing on patients with solid tumors who have some degree of common treatment regimens.Eligible patients were recruited to assess Usual Care in Phase I of this three-phase clinical trial.Stratification was conducted to reflect a sample of the four diagnoses that were proportionalto the cancer center population.
ProcedureResearch nurses approached all individuals meeting eligibility criteria during a regularlyscheduled clinic visit. Written informed consent was obtained from all participants prior toparticipation in this study. Participants provided demographic and disease data at baselinealong with other outcome measures to assess overall QOL, barriers to pain management, andpain knowledge. All outcome measures were repeated later at one month and three months. Achart audit was conducted at the one-month evaluation to assess potential system barriers topain assessment and management.
Outcome MeasuresThe Demographic and Treatment Data Tool was designed to capture key disease and treatmentvariables of importance in describing the population and for analysis of influencing variables.Basic demographic data, such as age, gender, disease type, stage of disease, and treatmentsreceived, were collected at baseline. Other variables, such as current medications, co-morbidities, and Karnofsky Performance Scale (KPS), were obtained at baseline and duringfollow-up evaluations. A detailed medication list was also obtained at all follow-up evaluationsto capture types of pain medications provided for patients.
The City of Hope Quality of Life–Patient Tool (COH QOL) is a 45-item multidimensional toolencompassing four domains of Physical, Psychological, Social, and Spiritual Well-Being basedon the QOL conceptual model developed by the investigators.19,20 Internal consistencyreliability is 0.77–0.89 for the four subscales and .93 overall. Measures of validity of the genericpatient version include content validity with the FACT instrument (r = 0.78), and factoranalysis.
The Barriers Questionnaire-II (BQ-II) AU: CHANGE OKAY? was developed by Ward andcolleagues8 to measure patient-reported barriers to pain management. Significant (t=−2.16,P<0.05) construct validity and a factor analysis revealed four factors: 1) physiologic effects,2) fatalism, 3) communication, and 4) harmful effects. The BQ-II total has an internalconsistency reliability coefficient alpha of 0.89 (n=134), and a range of 0.75–0.85 for thesubscales. The mean score for the total scale was 1.53 (SD=0.73).
The Patient Pain Knowledge Tool was drafted by the investigators based on the NCCN PainGuidelines.18 This 15-item questionnaire was used as an assessment of patient’s knowledgeand beliefs. The questions asked subjects to identify whether each statement regarding pain istrue or false. This tool was written at a low literacy level and to be less burdensome for subjects
Sun et al. Page 3
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

to complete. Internal consistency reliability analysis was performed on these subjects’ scoresfor the QOL, BQ-II, and knowledge tests using Cronbach’s alpha. Internal consistencyreliability of the instrument was 0.67.
The Pain Chart Audit Tool compared the recommendations of the NCCN Pain Guidelines withthe actual care provided and served as the primary measure to identify professional and systembarriers to pain management. The audit tool was pilot-tested and refined prior to subject accrual.The audits were conducted by research nurses during the one-month evaluation.
Statistical MethodsSPSS Sample Power and the PASS power calculation software were used to estimate samplesize for this study based on findings of the PI’s previous pain intervention studies. A sampleof 50 patients provided 80% power to detect significance in the interaction effect of thisstatistical design, with a two-tailed alpha of 0.05.
Analyses included tabulation of standard summary statistics of demographic characteristics,disease/treatment characteristics, and all scores at each time period. In addition to demographicand clinical characteristics, descriptive statistics were computed for QOL items, subscalescores and total score, as well as the Karnofsky performance scale score. Using Pain ChartAudit data, the frequencies of NCCN Guideline pain assessment and management providerbehaviors were calculated. Multiple response frequencies were calculated on support servicesordered, co morbidities, and medications.
BQ-II subscale scores and total score, and knowledge test score were compared across selecteddemographics (race/ethnicity, education, religious preference, marital status, cancer diagnosis,and chemotherapy status) using Multivariate Analysis of Variance (MANOVA) for subscales,and ANOVA for total BQ-II score and knowledge test score.
Subjects with missing scale or subscale scores were compared with subjects having non-missing scores to determine any bias underlying the missing data. For data that are missingcompletely at random (MCAR) or missing at random (MAR), the EM (estimation-maximization) method of imputation was used to replace missing values.
ResultsA total of 100 subjects were accrued for Phase I. Of the 100 subjects, 83 had complete datathat was evaluable. Of the 83 subjects with evaluable data, 38 of these met the criterion forhaving moderate to severe pain (≥ 4) at the time of accrual. This paper reports on findings forthe 38 evaluable subjects with pain. The mean age of these subjects was 57 and 76% werefemale. This sample included 55% Caucasian, 18% African American, 23% Hispanic and 3%Asian subjects. The majority of subjects (52.6%) had a college degree or graduate degree, while44.8% had an education level of high school or less. Most subjects (34%) were retired while26% were currently unemployed secondary to their cancer.
In terms of disease-specific variables, the sample included 57% breast, 24% colon, 16% lung,and 8% prostate cancer patients. The majority of subjects had Stage III or IV disease at thetime of accrual. They were diagnosed at a mean of 3.9 years ago and had received multimodalitytreatments including surgery (63%), chemotherapy (82%) and radiation (42%). The majorityof subjects (73%) were currently receiving chemotherapy. Forty-five percent of subjectsreported a baseline KPS of 90. The majority of subjects (76.2%) reported having moderatepain (4–6) based on a 0–10 scale, and the mean pain score was 5. Complete demographic datais provided in Table 1.
Sun et al. Page 4
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

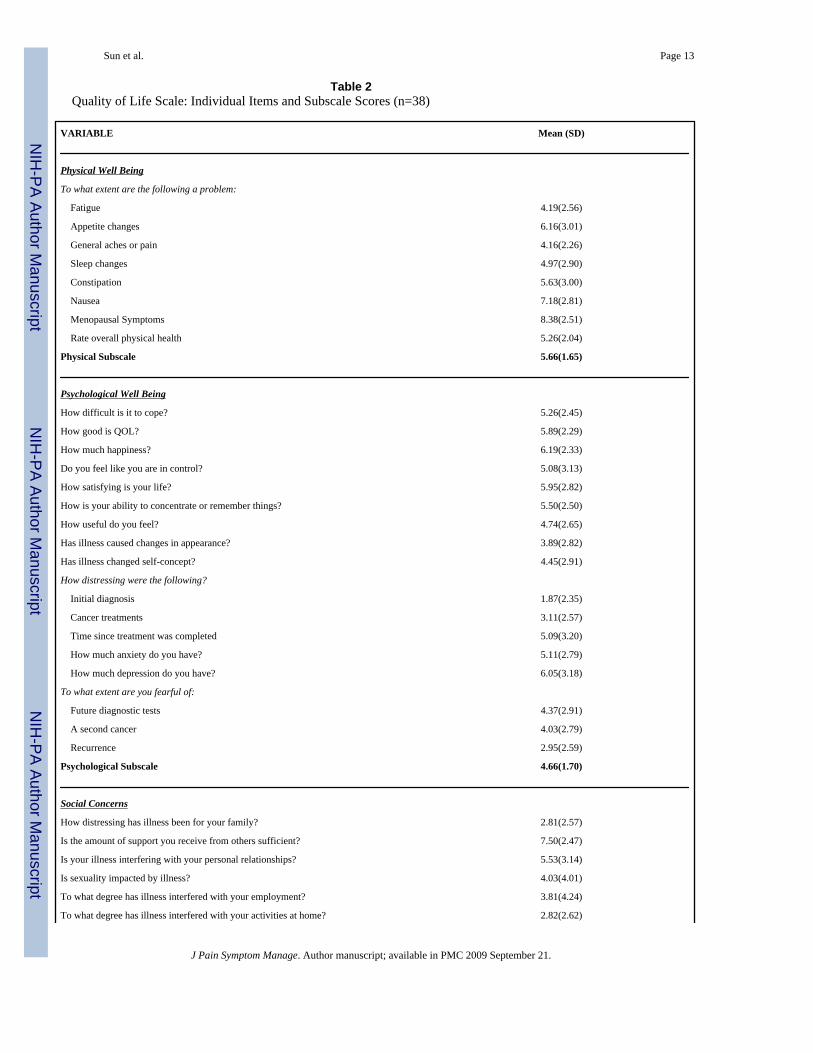
Overall QOLBaseline QOL data revealed low scores for all four subscales of the COH QOL tool. As onewould expect for this sample with primarily advanced disease, overall QOL was decreased.The overall QOL score was only 5.11(SD 1.46) on a scale where 0 = worst outcome to 10 =best outcome. All domains, including physical, psychological, social, and spiritual well-being,had moderately low scores. In the area of physical well-being, patients experienced fewproblems with symptoms such as nausea but had trouble with pain, sleep changes, and fatigue.Subject’s scores in the psychological domain were particularly low. These results reflect severedistress at initial diagnosis, fear of recurrence, distress with cancer treatments, and fear of asecond cancer. In the domain of social well-being, subjects reported receiving support, butreported severe family distress. Spiritually, subjects sensed a purpose or mission in their livesand were hopeful, but felt tremendous uncertainty for their futures. Overall QOL score,individual item scores, and subscale scores by QOL domain are provided in Table 2.
Patient Barriers to Pain ManagementThe BQ-II captured patient-related barriers regarding pain management. The lowest scoreswere found in the subscales of harmful effects and physiological effects of pain medications(Table 3). Subjects believed that pain cannot be relieved, and thought that pain medicine is notan effective way to control pain. There was a strong belief that pain medicines are addictive,and that cancer patients are at high risk of developing addiction. Subjects also believed thattheir body becomes tolerant to the effects of pain medicine and the medications would notprovide pain relief in the future. Additionally, there was a fear that pain medicine will maskhealth changes. Additional item scores are provided in Table 3.
The overall score for the Patient Pain Knowledge Tool was 73% correct, which was fairly high.Subjects had the most knowledge in items such as methods to prevent constipation, the use ofa pain scale, the two types of pain, and other common side effects of pain medication. However,important knowledge deficits existed in the cause of pain, addiction with opioids, stoppingpain medicine suddenly, and the need to increase pain medicine as being a sign of addiction.Table 4 provides overall scores and individual item scores for this tool.
Mean comparisons between selected demographic variables and the BQ-II and Patient PainKnowledge Tool were undertaken. Results indicate that subjects’ ethnicity, education level,religious preference, marital status, and cancer diagnosis did not affect barriers to painmanagement for this sample. However, subjects who are currently receiving chemotherapytreatments were more likely to believe that communication of pain might distract physiciansfrom treatment of underlying disease (0.98 vs. 1.97; P=0.024). Subjects with pain who arereceiving chemotherapy were also more likely to believe that “good patients” do not complainabout pain.
Professional and System Barriers to Pain ManagementThe Pain Chart Audit Tool captured barriers to pain management that were related toprofessional practice and system outcomes. Items in the audit tool assessed documentation andassessment of pain, as well as treatment and referrals to supportive care services. Overall, only7.8% of subjects were screened for pain at each clinic visit. There was no correlation with painrating documentation and re-assessment at subsequent follow-up visits. Only 2.6% of subjectshad the quality of their pain documented. Seventy-six percent of patients had pain ratings ofmoderate severity (4–6) and 24% had severe pain (7–10). The patient’s pain management asdocumented in the medical record was compared to the recommendations in the NCCN painguidelines (Table 5). There was very limited (7.9%) documented pain screening, nodocumentation of numerical pain ratings or evidence of reassessment.
Sun et al. Page 5
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

In terms of pharmacologic management, 5.2% of subjects received nonsteroidal anti-inflammatory drugs. Sixty percent of patients were on short acting opioids and 26% were givenlong-acting opioids. Similarly, only 26% of patients had a bowel regimen prescribed. Nopatients had documented pain reassessment after opioids were initiated. Only 45% of patientswere receiving an adjuvant medication such as antidepressants or anticonvulsants. Finally, only5.2% of subjects received a social work consult and there were no other psychosocial supportconsults. No patients in this sample received a consult to a pain specialist and there was nodocumented pain education. Table 6 provides audited chart items as compared torecommendations in the NCCN pain guidelines.
DiscussionIn this study, we identified a cancer population with mainly advanced disease, which is typicalfor a tertiary cancer center. The majority of subjects was Caucasian, had a breast cancerdiagnosis, and are currently receiving chemotherapy. Subjects primarily reported experiencingmoderate (4–6 on a zero to ten numeric rating scale) pain. Baseline overall QOL, as expected,was fairly low. Predictably, subjects had many QOL concerns. Physically, our sample reportedproblems with pain, sleep changes, and fatigue, symptoms described in the literature asdistressing for cancer patients.21,22 Severe problems in this sample in the psychological domainunderscores the need for psychosocial health care professionals. Subjects in this study alsoreported severe family distress. This is consistent with previous studies conducted by this teamrelated to understanding the family perspective of cancer pain management.23–28
The patient-related barriers to pain management obtained from this study confirm data reportedin the literature,29,30 as well as underscores the importance of addressing these barriers.Overall, subjects in this study believed that addiction and tolerance to pain medication iscommon in cancer patients. Furthermore, there was a strong belief in the masking of healthchanges if pain medication is used. Numerous studies have documented the very significantpatient barrier of fears of addiction. 3,4,31 Overall, subjects in this study scored fairly high onpain knowledge, but knowledge deficits continue to exist in areas related to addiction andproper utilization of pain medications. Model programs have emphasized patient teachinginterventions including the use of pain assessment tools, strategies to dispel misconceptions,and patient coaching regarding the reporting and documenting of their symptoms. 32–34 Thefindings from our study support this hypothesis.
Previous studies have found that patients are reluctant to communicate information about theirpain or its relief to health care professionals. 4,8,10 In this study, we found that subjects whoare currently receiving active treatment with chemotherapy were more reluctant tocommunicate their pain experience to their health care professionals. Future pain interventionswith cancer patients, particularly those in active treatment, should address and facilitate thecommunication of symptoms between patient and health care professionals.
Results related to professional and system barriers indicate that much improvement is neededin the screening, re-assessment, and follow-up evaluations of pain. More importantly, properutilization of long- vs. short-acting opioid analgesics and aggressive bowel regimen to preventopioid-related constipation is needed for optimal pain relief. Finally, internal system barrierssuch as a lack of referral to supportive care services should be addressed. The investigatorsrealize that some interventions, including consultations or pain reassessment, may haveoccurred but simply were not documented. One overall observation was that patients seen inthe outpatient clinic setting had much less supportive care available as compared to the inpatientsetting.
Sun et al. Page 6
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Following Phase I, Phase II (High Intensity Intervention) began with the two intensiveeducation sessions of medical oncology staff on assessment and management of pain andfatigue. The sessions were taught by two nationally recognized physicians in palliative care.Patients in Phase II receive four individual education sessions on the assessment andmanagement of pain and fatigue. An education packet containing information on pain andfatigue is provided to subjects and are based on NCCN Guidelines. Follow-up and datacollection time points are identical to those in Phase I. Peer feedback is provided to physicianson a monthly basis. Large posters available throughout the clinic serve as a reminder for bothpatient and provider of the importance to assess for pain and fatigue.
In conclusion, this Phase I (Usual Care) study identified several patient, professional, andsystem related barriers to pain management that continues to hinder our efforts to provideoptimal pain relief. Phase II (High Intensity Intervention) for this five-year, NCI-fundedclinical trial will attempt to eliminate these barriers through intensive patient education andprofessional interaction using the innovative “Passport to Comfort” model.
AcknowledgmentsThis research was supported by a grant from the National Cancer Institute (R-01 CA115323).
References1. National Institutes of Health State-of-the-Science Statement. Symptom management in cancer: Pain,
depression and fatigue. 2002. Available at: http://consensus.nih.gov/ta/022/022_statement.htm2. Agency for Health Care Policy and Research: Clinical practice guideline cancer pain management.
Rockville, MD: US Department of Health and Human Services; 1994.3. Cleeland C. The impact of pain on the patient with cancer. Cancer 1984;58:2635–2641. [PubMed:
6498754]4. Miaskowski C, Dibble SL. The problem of pain in outpatients with breast cancer. Oncol Nurs Forum
1995;22:791–797. [PubMed: 7675686]5. Ward S, Hughes S, Donovan H, et al. Patient education in pain control. Supp Care Cancer 2001;9:148–
155.6. Ward S, Donovan HS, Owen B, et al. An individualized intervention to overcome patient-related
barriers to pain management in women with gynecological cancers. Res Nurs Health 2000;23:393–405. [PubMed: 11052393]
7. Pargeon KL, Hailey BJ. Barriers to effective cancer pain management: a review of the literature. J PainSymptom Manage 1999;18:358–368. [PubMed: 10584460]
8. Ward SE, Goldberg N, Miller-McCauley V, et al. Patient-related barriers to management of cancerpain. Pain 1993;52:319–324. [PubMed: 7681557]
9. Potter VT, Wiseman CE, Dunn SM, et al. Patient barriers to optimal cancer pain control.Psychooncology 2003;12:153–160. [PubMed: 12619147]
10. McCaffery M, Ferrell BR, O’Neil-Page E, et al. Nurses knowledge of opioid analgesic drugs andpsychological dependence. Cancer Nurs 1990;13(1):21–27. [PubMed: 2306717]
11. Ferrell BR, Grant M, Ritchey KJ, et al. The pain resource nurse training program: a unique approachto pain management. J Pain Symptom Manage 1993;8(8):549–556. [PubMed: 7525784]
12. McCaffery M, Ferrell BR, Pasero C. Nurses’ personal opinions about patients’ pain and their effecton recorded assessments and titration of opioid doses. Pain Manage Nurs 2000;1(3):79–87.
13. Rabow MW, Hardie GE, Fair JM, et al. End-of-life care content in 50 textbooks from multiplespecialties. JAMA 2000;283:771–778. [PubMed: 10683056]
14. Ferrell B, Virani R, Grant M. Analysis of pain content in nursing textbooks. J Pain Symptom Manage2000;19(3):216–228. [PubMed: 10760627]
Sun et al. Page 7
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

15. Elliot TE, Murray DM, Elliot BA, et al. Physician knowledge and attitudes about cancer painmanagement: a survey from the Minnesota Cancer Pain Project. J Pain Symptom Manage1995;10:494–504. [PubMed: 8537691]
16. Institute of Medicine. Approaching death: Improving care at the end of life. Washington, DC: NationalAcademy Press; 1997.
17. Gee RE, Fins JJ. Barriers to pain and symptom management, opioids, health policy, and drug benefits.J Pain Symptom Manage 2003;25:101–103. [PubMed: 12590024]
18. NCCN Practice Guidelines in Oncology: Cancer-related pain version 1. 2004. Available at:http://nccn.org
19. Ferrell BR, Dow KH, Grant M. Measurement of the quality of life in cancer survivors. Qual Life Res1995;4:523–531. [PubMed: 8556012]
20. Ferrell BR, Hassey-Dow K, Leigh S, et al. Measurement of the QOL in cancer survivors. Qual LifeRes 1995;4:523–531. [PubMed: 8556012]
21. Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status ofpatients with cancer. Oncol Nurs Forum 2001;28:465–470. [PubMed: 11338755]
22. Gift AG, Jablonski A, Stommel M, Given CW, et al. Symptom clusters in elderly patients with lungcancer. Oncol Nurs Forum 2004;31:202–212. [PubMed: 15017438]
23. Ferrell BR, Grant M, Chan J, Ahn C, Ferrell BA. The impact of cancer pain education on familycaregivers of elderly patients. Oncol Nurs Forum 1995;22:1211–1218. [PubMed: 8532545]
24. Ferrell BR, Rhiner M, Cohen M, Grant M. Pain as a metaphor for illness. Part I: impact of cancerpain on family caregivers. Oncol Nurs Forum 1991;18:1303–1309. [PubMed: 1762971]
25. Ferrell BR, Cohen M, Rhiner M, Rozek A. Pain as a metaphor for illness. Part II: family caregivers’management of pain. Oncol Nurs Forum 1991;18:1315–1321. [PubMed: 1762972]
26. Ferrell BR, Rhiner M, Rivera LM. Development and evaluation of the family pain questionnaire. JPsych Oncol 1993;10:21–35.
27. Johnston-Taylor E, Ferrell BR, Grant M, Cheyney L. Managing cancer pain at home: The decisionsand ethical conflicts of patients, family caregivers, and homecare nurses. Oncol Nurs Forum1993;20:919–927. [PubMed: 8367345]
28. Ferrell B, Taylor E, Sattler G, Fowler M, Cheyney L. Searching for the meaning of pain. Cancer Pract1993;1:185–194.
29. Ferrell BR, Grant M, Borneman T, Juarez G, Veer A. Family caregiving in cancer pain management.J Palliat Med 1999;2:185–195. [PubMed: 15859815]
30. Randall-David E, Wright J, Porterfield DS, Lesser G. Barriers to cancer pain management: homehealth and hospice nurses and patients. Supp Care Cancer 2003;11:660–665.
31. Paice JA, Toy C, Shott S. Barriers to cancer pain relief: fear of tolerance and addiction. J Pain SymptomManage 1998;16:1–9. [PubMed: 9707652]
32. Ward S, Donovan HS, Owen B, et al. An individualized intervention to overcome patient-relatedbarriers to pain management in women with gynecological cancers. Res Nurs Health 2000;23:393–405. [PubMed: 11052393]
33. Miaskowski C, Dodd M, West C, et al. Randomized clinical trial of the effectiveness of a self-careintervention to improve cancer pain management. J Clin Oncol 2004;22:1713–1720. [PubMed:15117994]
34. Ferrell BR, Rhiner M, Ferrell BA. Development and implementation of a pain education program.Cancer 1993;72:3426–3432. [PubMed: 8242574]
Sun et al. Page 8
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Study model.
Sun et al. Page 9
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 10
Table 1Subject Demographic and Treatment Variables
VARIABLE COUNT PERCENTAGE (%)
Ethnicity
Caucasian 21 55.3
African American 7 18.4
Hispanic 9 23.7
Asian 2.6 2.6
Education
No high school 2 5.3
High school only 15 39.5
College 17 44.7
Graduate/Professional 3 7.9
Marital Status
Never married 4 10.5
Married 18 47.4
Living with partner 2 5.3
Divorced 8 21.1
Widowed 6 15.8
Living Arrangements
Spouse 18 47.4
Parents 3 7.9
Children 19 50.0
Friends/signif. other 1 2.6
Other 3 7.9
Live alone 4 10.5
Employment status
Full time 6 15.8
Part time 4 10.5
Retired 13 34.2
Retired b/c of cancer 3 7.9
Homemaker 2 5.3
Unemployed on disability 10 26.3
Cancer Diagnosis
Breast 20 52.9
Colon 9 23.7
Lung 6 15.8
Prostate 3 7.9
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 11
VARIABLE COUNT PERCENTAGE (%)
Stage of disease
I 2 5.2
II 6 15.8
III 11 29
IV 18 47.4
Current status of disease
Newly diagnosed, under tx 10 26.3
Completed tx, CA free 2 5.3
Recurrent, under tx 20 52.6
Other 5 13.2
Current and Previous Tx
Surgery
Yes 24 63.2
No 13 34.2
Chemotherapy
Yes 31 81.6
No 7 18.4
Currently receiving chemo
Yes 28 73.7
No 10 26.3
Radiation
Yes 16 42.1
No 22 57.9
Currently receiving radiation
Yes 1 2.6
No 37 97.4
KPS
100 3 7.9
90 17 44.7
80 9 23.7
70 4 10.5
60 4 10.5
Pain rating
4 11 28.9
5 11 28.9
6 7 18.4
7 4 10.5
8 4 10.5
9 1 2.6
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 12
Tx = treatment; CA = cancer; KPS = Karnofsky Performance Status.
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 13
Table 2Quality of Life Scale: Individual Items and Subscale Scores (n=38)
VARIABLE Mean (SD)
Physical Well Being
To what extent are the following a problem:
Fatigue 4.19(2.56)
Appetite changes 6.16(3.01)
General aches or pain 4.16(2.26)
Sleep changes 4.97(2.90)
Constipation 5.63(3.00)
Nausea 7.18(2.81)
Menopausal Symptoms 8.38(2.51)
Rate overall physical health 5.26(2.04)
Physical Subscale 5.66(1.65)
Psychological Well Being
How difficult is it to cope? 5.26(2.45)
How good is QOL? 5.89(2.29)
How much happiness? 6.19(2.33)
Do you feel like you are in control? 5.08(3.13)
How satisfying is your life? 5.95(2.82)
How is your ability to concentrate or remember things? 5.50(2.50)
How useful do you feel? 4.74(2.65)
Has illness caused changes in appearance? 3.89(2.82)
Has illness changed self-concept? 4.45(2.91)
How distressing were the following?
Initial diagnosis 1.87(2.35)
Cancer treatments 3.11(2.57)
Time since treatment was completed 5.09(3.20)
How much anxiety do you have? 5.11(2.79)
How much depression do you have? 6.05(3.18)
To what extent are you fearful of:
Future diagnostic tests 4.37(2.91)
A second cancer 4.03(2.79)
Recurrence 2.95(2.59)
Psychological Subscale 4.66(1.70)
Social Concerns
How distressing has illness been for your family? 2.81(2.57)
Is the amount of support you receive from others sufficient? 7.50(2.47)
Is your illness interfering with your personal relationships? 5.53(3.14)
Is sexuality impacted by illness? 4.03(4.01)
To what degree has illness interfered with your employment? 3.81(4.24)
To what degree has illness interfered with your activities at home? 2.82(2.62)
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 14
VARIABLE Mean (SD)
How much isolation do you feel? 4.24(2.89)
How much financial burden have you incurred as a result of illness? 3.16(3.21)
Social Subscale 4.21(2.13)
Spiritual Well Being
How important are religious activities such as praying, going to church? 7.50(3.25)
How important are spiritual activities such as meditation? 6.68(3.76)
How much has your spiritual life changed as a result of cancer diagnosis? 7.61(2.98)
How much uncertainty do you feel about your future? 3.37(3.11)
To what extent has illness made positive changes in your life? 5.50(3.62)
Do you sense a purpose/mission in life or a reason for being alive? 7.68(2.96)
How hopeful do you feel? 7.58(2.49)
Spiritual Subscale 6.56(2.32)
OVERALL QOL SCALE SCORE 5.11 (1.46)
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 15
Table 3Barriers Questionnaire-II (BQ-II)
Variable Mean (SD)
Subscale
Physiological Effects 2.29 (0.83)
Fatalism 1.36 (0.94)
Communication 1.24 (1.20)
Harmful Effects 2.5 (1.13)
Items with Greatest Barriers to Pain Management
Reports of pain could distract a doctor from curing the cancer 0.84 (1.19)
If doctors have to deal with pain they won’t concentrate on curing the disease 0.87 (1.21)
Doctors might find it annoying to be told about pain 1.08 (1.50)
Cancer pain can be relieved 1.18 (1.18)
It is important for the doctor to focus on curing illness, and not waste time controllingpain
1.19 (1.16)
Medicine can relieve cancer pain 1.32 (1.12)
It is important to be strong by not talking about pain 1.47 (1.70)
Pain medicine can hurt your immune system 1.58 (1.55)
Pain medicine can effectively control cancer pain 1.58 (1.08)
Constipation from pain medicine cannot be relieved 1.62 (1.48)
Pain medicine makes you say or do embarrassing things 1.68 (1.58)
It is easier to put up with the pain than with the side effects that come from painmedicine
1.81 (1.53)
AU: CHANGE IN TITLE OKAY WITH YOU?
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 16
Table 4Patient Pain Knowledge Tool
Knowledge Item Mean (SD)
Pain can be divided into two types: acute and chronic 0.87 (0.34)
The most common cause of pain is cancer 0.45 (0.50)
Taking opioids will always leads to addiction 0.53 (0.51)
The side effects that pain medications cause can be prevented or treated 0.66 (0.48)
It is not important for doctors and nurses to know about your pain 0.79 (0.41)
A pain scale is used to describe how much pain you are feeling 0.95 (0.27)
Cancer pain can be treated only with medicines and not by using other treatments such as chemotherapy, radiation, surgery 0.68 (0.47)
Non-opioid medicines such as Tylenol and ibuprofen are used for severe pain only 0.79 (0.41)
Opioid medicines are divided by how quickly they begin to work and how long they work 0.76 (0.43)
One of the most common side effect of taking morphine is constipation 0.68 (0.47)
Drinking more fluids, eating more fiber foods, and some mild exercise along with some laxatives are the best ways to prevent constipation 1.0 (0.00)
Other common side effects of pain medicine include nausea and some confusion 0.84 (0.37)
A need to increase the dose of your pain medicine is a sign of addiction 0.61 (0.50)
You can stop your pain medications suddenly without worries about side effects 0.63 (0.49)
Around-the-clock dosing of pain medicine means that the medicine will be given on a regular basis, whether you are in pain or not 0.74 (0.45)
OVERALL SCORE 0.73 (0.13)
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 17
Table 5Pain Chart Audit Results Compared to NCCN Pain Guideline Recommendations
NCCN Recommendations AUDIT RESULTS (% Yes)
Screening of pain at all visits 7.9
Pain rating documented in transcriptions 0
Pain rating documented consistently 0
Quality of pain documented 2.63
Reassessment at each visit 0
Pain Management Recommendations
NSAID 5.2
Short-acting opioids 60
Long-acting opioids initiated 26
Bowel regimen 26
Education 2.63
Psychosocial support 0
Pain specialty consults 0
Reassessment after initiation of opioids 0
Adjuvant Medications 45
Other Supportive Care Services Referrals
Rehabilitation/PT 0
Psychology/Psychiatry 0
Social Work 5.26
Pastoral Care 0
Transitions Program (Hospice/Palliative Care) 0
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Sun et al. Page 18
Table 6Pain Chart Audit Items Based on NCCN Pain Guideline Recommendations
NCCN Recommendations Chart Audit Items
Quantify pain intensity • Was screening for pain documented routinely at visit?
Pain intensity rating • Was pain rating documented?
Characterize quality of pain • Was the quality of the pain documented (i.e. sharp, stabbing, dull)?
Management of patients with no pain • Was re-assessment documented at subsequent visits?
Managing mild to moderate (1–6)pain
• Was NSAIDs used?
• Were opioids initiated?
• Was re-assessment documented after initial dosing?
Management of severe (7–10) pain • Rapid titration initiated?
• Was continuation of long-acting plus short-acting opioids documented?
• Was re-assessment documented at the subsequent visits?
• Was the use of adjuvant analgesics documented?
Managing side effects of opioids • Was a bowel regimen documented?
• Was bowel status documented?
Patient and family education • Was a list of potential side effects of pain medication given to patient and family?
• Was patient and family educated and counseled on managing side effects of pain medications?
Supportive care consultations • Were consultations to supportive care services (pain specialist, physical therapy, psychology/psychiatry,social work, pastoral care) initiated?
J Pain Symptom Manage. Author manuscript; available in PMC 2009 September 21.
Copyright © 2022 FDOKUMEN