
On the relationship between tibia torsional deformation and regional muscle contractions in habitual...
9
On the relationship between tibia torsional deformation and regional muscle contractions in habitual human exercises in vivo Peng-Fei Yang a,b,c,n , Andreas Kriechbaumer b , Kirsten Albracht c , Maximilian Sanno c , Bergita Ganse b , Timmo Koy d , Peng Shang a , Gert-Peter Brüggemann c , Lars Peter Müller d , Jörn Rittweger b a Key Laboratory for Space Bioscience and Biotechnology, Institute of Special Environment Biophysics, School of Life Sciences, Northwestern Polytechnical University, Xi'an, China b Institute of Aerospace Medicine, German Aerospace Center, Cologne, Germany c Institute of Biomechanics and Orthopaedics, German Sport University Cologne, Germany d Department of Orthopaedic and Trauma Surgery, University of Cologne, Germany article info Article history: Accepted 5 December 2014 Keywords: Bone–muscle interactions Tibia deformation Torsion Optical approach In vivo abstract The mechanical relationship between bone and muscle has been long recognized. However, it still remains unclear how muscles exactly load on bone. In this study, utilizing an optical segment tracking technique, the in vivo tibia loading regimes in terms of tibia segment deformation in humans were investigated during walking, forefoot and rear foot stair ascent and running and isometric plantar flexion. Results suggested that the proximal tibia primarily bends to the posterior aspect and twists to the external aspect with respect to the distal tibia. During walking, peak posterior bending and peak torsion occurred in the first half (22%) and second half (76%) of the stance phase, respectively. During stair ascent, two noticeable peaks of torsion were found with forefoot strike (38% and 82% of stance phase), but only one peak of torsion was found with rear foot strike (78% of stance phase). The torsional deformation angle during both stair ascent and running was larger with forefoot strike than rear foot strike. During isometric plantar flexion, the tibia deformation regimes were characterized more by torsion (maximum 1.351) than bending (maximum 0.521). To conclude, bending and torsion predominated the tibia loading regimes during the investigated activities. Tibia torsional deformation is closely related to calf muscle contractions, which further confirm the notion of the muscle– bone mechanical link and shift the focus from loading magnitude to loading regimes in bone mechan- obiology. It thus is speculated that torsion is another, yet under-rated factor, besides the compression and tension, to drive long bone mechano-adaptation. & 2014 Elsevier Ltd. All rights reserved. 1. Introduction Mechanical loading is a key determinant for bone adaptions. Locomotor activities evoke various types of bone deformation that differ in terms of type, amplitude, rate and frequency (Turner et al., 1995; Warden and Turner, 2004). It follows from beam theory that the hollow cylindrical geometry of the limb long bones is well designed to resist bending and torsion. Evidence also suggested that bending and torsion primarily constitute the human tibia loading regimes during walking and running (Yang et al., 2014b). However, in contrast to the amount of attention that compression, tension and thus loading has received in literature, the occurrence of torsional loading on bone has mostly been neglected—an omission that is probably owed to the technical difficulties of assessing torsion with conventional approaches. Ample evidence demonstrates that muscles are closely related to bone adaptation (Kohrt et al., 2009; Rittweger, 2008; Rittweger et al., 2000; Sharir et al., 2011; Zanchetta et al., 1995). As muscles generally work against short levers, there is a good mechanical reason to hold that muscle contractions are responsible for the largest forces experienced by bone and would cause considerable bone bending. However, the near cylindrical structure of long bones does not only resist harness against unidirectional bending. Rather, it is speculated that torsion plays an important role in maintaining the near cylindrical structure of long bones, e.g. the distal tibia. And further suppose that muscle contractions may greatly contribute to the torsional loading. Nevertheless, to date, it remains unclear which loading regimes on bone are primarily produced by muscle contrac- tions—another apparent omission in literature. The aim of the present paper is to examine the hypotheses that regional muscle contractions would be temporarily related to bone Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/jbiomech www.JBiomech.com Journal of Biomechanics http://dx.doi.org/10.1016/j.jbiomech.2014.12.031 0021-9290/& 2014 Elsevier Ltd. All rights reserved. n Corresponding author at: Key Laboratory for Space Bioscience and Biotechnol- ogy, School of Life Sciences, Northwestern Polytechnical University, Xi'an, China. Tel.: þ86 29 88491613 (Lab); fax: þ86 29 88491671. E-mail address: [email protected] (P.-F. Yang). Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions in habitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of On the relationship between tibia torsional deformation and regional muscle contractions in habitual...

On the relationship between tibia torsional deformation and regionalmuscle contractions in habitual human exercises in vivo
Peng-Fei Yang a,b,c,n, Andreas Kriechbaumer b, Kirsten Albracht c, Maximilian Sanno c,Bergita Ganse b, Timmo Koy d, Peng Shang a, Gert-Peter Brüggemann c, Lars Peter Müller d,Jörn Rittweger b
a Key Laboratory for Space Bioscience and Biotechnology, Institute of Special Environment Biophysics, School of Life Sciences,Northwestern Polytechnical University, Xi'an, Chinab Institute of Aerospace Medicine, German Aerospace Center, Cologne, Germanyc Institute of Biomechanics and Orthopaedics, German Sport University Cologne, Germanyd Department of Orthopaedic and Trauma Surgery, University of Cologne, Germany
a r t i c l e i n f o
Article history:Accepted 5 December 2014
Keywords:Bone–muscle interactionsTibia deformationTorsionOptical approachIn vivo
a b s t r a c t
The mechanical relationship between bone and muscle has been long recognized. However, it still remainsunclear how muscles exactly load on bone. In this study, utilizing an optical segment tracking technique, thein vivo tibia loading regimes in terms of tibia segment deformation in humans were investigated duringwalking, forefoot and rear foot stair ascent and running and isometric plantar flexion. Results suggested thatthe proximal tibia primarily bends to the posterior aspect and twists to the external aspect with respect tothe distal tibia. During walking, peak posterior bending and peak torsion occurred in the first half (22%) andsecond half (76%) of the stance phase, respectively. During stair ascent, two noticeable peaks of torsion werefound with forefoot strike (38% and 82% of stance phase), but only one peak of torsion was found with rearfoot strike (78% of stance phase). The torsional deformation angle during both stair ascent and running waslarger with forefoot strike than rear foot strike. During isometric plantar flexion, the tibia deformationregimes were characterized more by torsion (maximum 1.351) than bending (maximum 0.521). To conclude,bending and torsion predominated the tibia loading regimes during the investigated activities. Tibia torsionaldeformation is closely related to calf muscle contractions, which further confirm the notion of the muscle–bone mechanical link and shift the focus from loading magnitude to loading regimes in bone mechan-obiology. It thus is speculated that torsion is another, yet under-rated factor, besides the compression andtension, to drive long bone mechano-adaptation.
& 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Mechanical loading is a key determinant for bone adaptions.Locomotor activities evoke various types of bone deformation thatdiffer in terms of type, amplitude, rate and frequency (Turner et al.,1995; Warden and Turner, 2004). It follows from beam theory thatthe hollow cylindrical geometry of the limb long bones is welldesigned to resist bending and torsion. Evidence also suggested thatbending and torsion primarily constitute the human tibia loadingregimes during walking and running (Yang et al., 2014b). However, incontrast to the amount of attention that compression, tension andthus loading has received in literature, the occurrence of torsionalloading on bone has mostly been neglected—an omission that is
probably owed to the technical difficulties of assessing torsion withconventional approaches.
Ample evidence demonstrates that muscles are closely related tobone adaptation (Kohrt et al., 2009; Rittweger, 2008; Rittweger et al.,2000; Sharir et al., 2011; Zanchetta et al., 1995). As muscles generallywork against short levers, there is a good mechanical reason to holdthat muscle contractions are responsible for the largest forcesexperienced by bone and would cause considerable bone bending.However, the near cylindrical structure of long bones does not onlyresist harness against unidirectional bending. Rather, it is speculatedthat torsion plays an important role in maintaining the nearcylindrical structure of long bones, e.g. the distal tibia. And furthersuppose that muscle contractions may greatly contribute to thetorsional loading. Nevertheless, to date, it remains unclear whichloading regimes on bone are primarily produced by muscle contrac-tions—another apparent omission in literature.
The aim of the present paper is to examine the hypotheses thatregional muscle contractions would be temporarily related to bone
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jbiomechwww.JBiomech.com
Journal of Biomechanics
http://dx.doi.org/10.1016/j.jbiomech.2014.12.0310021-9290/& 2014 Elsevier Ltd. All rights reserved.
n Corresponding author at: Key Laboratory for Space Bioscience and Biotechnol-ogy, School of Life Sciences, Northwestern Polytechnical University, Xi'an, China.Tel.: þ86 29 88491613 (Lab); fax: þ86 29 88491671.
E-mail address: [email protected] (P.-F. Yang).
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i
Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎

deformations (hypothesis 1), and that these contractions wouldengender specific deformation regimens, e.g. antero-posterior (AP)and medio-lateral (ML) bending, internal–external (IE) torsion(hypothesis 2). For this purpose, an optical segment tracking (OST)approach previously described (Ganse et al., 2014; Yang et al., 2014a)was utilized to assess tibia deformation regimes in a set of char-acteristic habitual exercises, namely during walking, stair ascent andrunning with forefoot and rear foot strike, and isometric plantarflexion. The character of calf muscular contractions in tibia loadingregimes was examined by analyzing the phase constitution ofthe tibia deformation regimes, assessing phase relationship betweenpeak muscle activities and peak tibia deformation, comparingthe tibia deformation between forefoot and rear foot exercises,respectively.
2. Materials and methods
2.1. Test subjects
Five healthy male participants (Table 1) were recruited in this study. They werefree of any muscle or joint injury and have not had orthopedic surgery in the lowerextremities within the last 12 months prior to the study (Ganse et al., 2014). Ethicalapproval was obtained from both the ethical committee of the North-Rhine MedicalBoard in Düsseldorf and the ethical committee of the Faculty of Medicine in theUniversity of Cologne. All subjects provided written informed consent. The studyconformed to the standards set by the latest modified Declaration of Helsinki. Theoperation and the experiments were performed at the Department of Orthopedicand Trauma Surgery of the University Hospital of Cologne.
2.2. The OST approach for tibia deformation recording
2.2.1. Dynamic trials for tibia deformation recordingBone screws were partially implanted uni-cortically into the antero-medial
cortex of the tibia. A marker cluster, with a set of three non-collinear retro-reflective markers (∅5 mm, Géodésie Maintenance Services, Nort Sur Erdre,France), was then mounted onto the bone screw (Fig. 1A). A specifically configuredmotion capture system with 8 F40 cameras (Vicon Motion System Ltd., LA, USA)was used to capture the marker trajectories at 300 Hz (Fig. 1B) with optimizedperformance (Yang et al., 2012).
2.2.2. Static trials for reference segment coordinate system determinationFour generic retro-reflective markers (∅16 mm, Vicon Motion System Ltd., LA,
USA) were attached onto the skin at the tip of medial and lateral malleolus, tip oftibia tuberosity and the head of fibula. While dangling the lower leg, skin-attachedand tibia-affixed markers were simultaneously captured for 1–2 s before each testtrial for generating a Shank Anatomical Coordinate System (SACS) and determiningthe relative position of tibia-affixed markers in the SACS.
2.3. Surgical technique
Prior to the operation, Ibuprofen (600 mg) and Cefuroxime (1500 mg) wereadministered for analgesia and to reduce the risk of infection. Under localanesthesia injected to the skin and periosteum with Xylocain 1% and Carbostesin0.5%, skin incisions of approximately 1 cm length were made at the midsite of thetibia, approximately 10 cm below the tibia plateau and above the tibia medialmalleolus. Bone screws (Asnis Micro, ∅3 mm, 24/6 mm, Stryker Leibinger GmbH &Co. KG, Germany) were implanted into the tibia cortex perpendicular to the bonesurface with a depth of 3–4 mm and removed at the end of the experiment,typically 6–8 h later. All procedures were well tolerated by the subjects (Ganseet al., 2014). No exercise abnormalities were observed and the bone screws werestill firmly implanted at termination of the experiments (Yang et al., 2014a).
2.4. Investigated locomotor activities
All subjects wore gymnastic shoes during the experimental procedures. Tibiadeformationwas investigated during the following locomotor activities: (1) walkingon a walkway at self-selected speed; (2) stair ascent with forefoot strike (Fig. 1C)and rear foot strike at self-selected comfort speed; (3) two subjects participated inthe running test at 5.5 and 9 km/h with forefoot and rear foot strike on a treadmill,respectively; (4) 100% and 50% maximum isometric voluntary plantar flexion(Fig. 1D). Rear foot strike refers to the situation when the subjects' foot land onthe heel and rolls to the toes during the exercises. At least three repetitions wereperformed during walking, stair ascent and plantar flexion, and a minimum of16 complete running cycles were recorded.
2.5. Assessment of ground reaction force (GRF) and muscle electromyography (EMG)
GRF during walking and stair ascent was recorded at 1000 Hz using a forceplate system (AMTI OR6-5, Watertown, MA, USA). After skin preparation, thesurface electrodes were then attached above the belly of the targeted muscles withthe long axis of electrodes parallel to muscle fibers. Surface EMG of soleus,gastrocnemius medialis (GM), tibialis anterior (TA) and vastus medialis (VM)muscles was sampled at 4000 Hz using a Trigno wireless EMG system (DelsysInc., Boston, USA).
2.6. Implementation of isometric contractions
Isometric plantar flexion was conducted using a custom-made dynamometerplaced on the force plate (Fig. 1D). The GRF during isometric contractions wasdocumented when the subject was in the sitting position with the knee joint angleof approximate 901 and foot on the force plate. A trigger from the EMG systemsynchronized EMG system, motion capturing system and force plate.
2.7. Data analysis
Marker trajectory data, EMG and GRF were processed with custom-writtenMATLAB routines (The MathWorks, Inc., Version 7.9.0 R2009b). The markertrajectories were filtered using a low pass moving average filter with a span of10 samples. GRF was filtered using a 2nd order, zero lag, and low-pass Butterworthfilter with cut-off frequency at 15 Hz. The result graphs were generated usingGraphpad Prism statistical software (version 5.00, GraphPad software, Inc., LaJolla, CA).
2.7.1. Determination of SACS and tibia deformation angles in SACSA randomly selected frame of the skin-attached marks' coordinate from the
static trial was used to determine a Cartesian SACS (Grood and Suntay, 1983). TheCardan rotation angles between the proximal and distal tibia-affixed markerclusters in the SACS were calculated by matrix transformation (Lafortune et al.,1992; Soderkvist and Wedin, 1993) to represent the tibia deformation regimes(Fig. 2). The tibia AP bending angle, IE torsion angle and ML bending angle referredto the Cardan rotation angles around the Z, Y and X axes. Peak-to-peak (p2p)deformation angles during the exercises were computed. The phase of the peaktibia deformations (%) was computed during the stance phase of walking.
2.7.2. Calculation of GRF during locomotor activitiesVertical GRF during walking was derived from the filtered GRF data and
normalized to body weight. The peak vertical GRF during plantar flexion wasidentified to represent the level of isometric force.
2.7.3. EMG analysisThe raw EMG signal was band pass filtered with the pass frequency of
20–500 Hz and then rectified. EMG linear envelope was constructed using a 2ndorder, zero lag Butterworth filter with low pass frequency at 10 Hz. Soleus, GM andTA EMG were normalized to the maximal EMG during maximum volunteercontractions (MVC). The peak amplitude of the VM EMG during general squatswas taken to normalize the VM EMG.
2.7.4. Phase analysis of the peak EMG and peak tibia deformationThe locations of the linear envelope peak of the soleus and GM EMG and the
peak tibia torsional deformation were calculated, and expressed as the percentageof the stance phase during gait cycle. The phase location was used to assess thephase relationship between muscle activities and tibia torsional deformation.
2.8. Statistics
Statistical analyses were performed using R statistic software (version 2.15.1,R Development Core Team, 2012). Two different one-way ANOVA linear models
Table 1Test subject information.
Subject Age (year) Body mass (kg) Height (cm) Tibia length (mm)
A 50 72.5 177 357B 26 80.2 178 379C 30 79.5 185 392D 39 89.9 188 384E 43 72.6 179 382
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎2
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i
were employed to assess the effects of foot strike pattern during stair ascent andrunning on the tibia deformation angles and muscle EMG RMS (Supplementarymaterials). For each test subject, minimum 3 repetitions of every locomotiveactivity were included into the statistics. The results of the tibia deformationangles were expressed as mean7standard deviation. Po0.05 was considered to besignificant.
3. Results
3.1. Phase of the peak tibia deformation during walking
Peak posterior bending was recorded at 2276% of the stancephase, but peak external torsion occurred at 7673% of the stancephase (Fig. 3A). The noticeable peaks of the EMG linear envelopes
from soleus and GM were found at 6478% and 61710% ofthe stance phase (Fig. 3B and C). The peak VM EMG typicallydistributed in the initial stance phase of the gait cycle (Fig. 3D).The time delay between peak muscle activities and peak tibiatorsion angles was nearly constant, typically 12% of the stancephase for soleus and 15% for GM.
3.2. Tibia deformation during stair ascent
3.2.1. Stair ascent with rear foot strikePosterior bending (p2p AP bending angle: between 0.9070.071
and 1.4870.101) and external axial torsion (p2p torsion angle:between 0.6870.021 and 1.0870.061) of the proximal tibia withrespect to the distal tibia were found. By contrast, the p2p ML
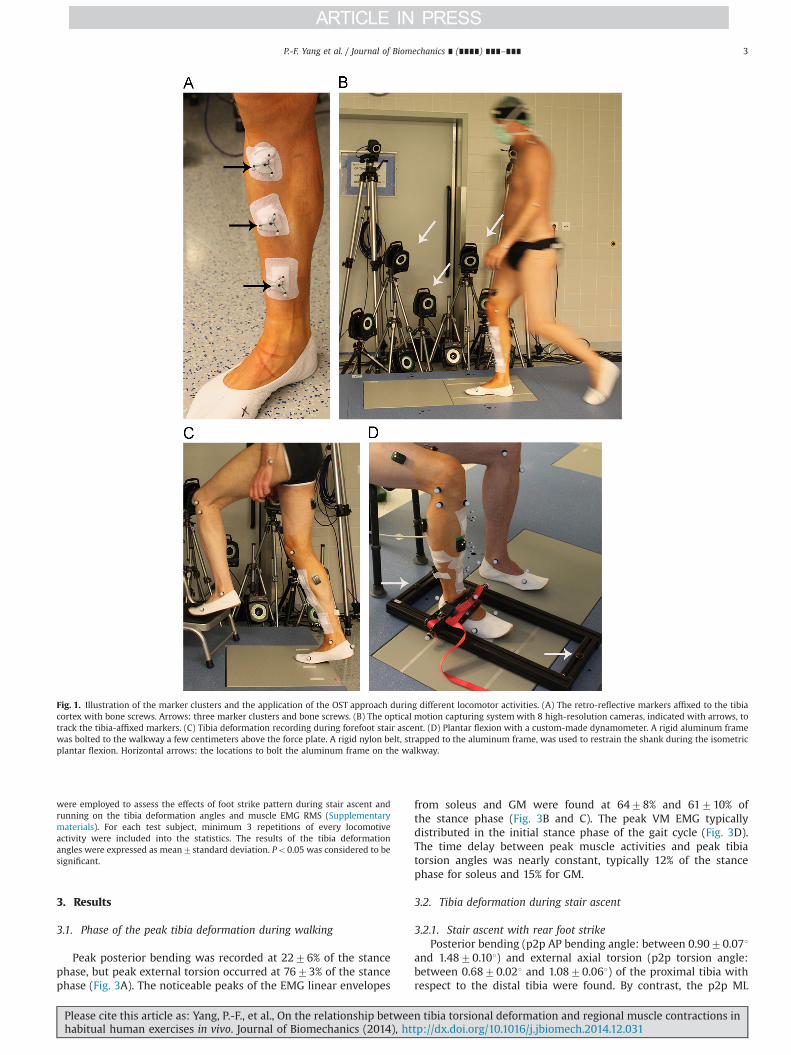
Fig. 1. Illustration of the marker clusters and the application of the OST approach during different locomotor activities. (A) The retro-reflective markers affixed to the tibiacortex with bone screws. Arrows: three marker clusters and bone screws. (B) The optical motion capturing system with 8 high-resolution cameras, indicated with arrows, totrack the tibia-affixed markers. (C) Tibia deformation recording during forefoot stair ascent. (D) Plantar flexion with a custom-made dynamometer. A rigid aluminum framewas bolted to the walkway a few centimeters above the force plate. A rigid nylon belt, strapped to the aluminum frame, was used to restrain the shank during the isometricplantar flexion. Horizontal arrows: the locations to bolt the aluminum frame on the walkway.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 3
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i

bending angle was rather small, maximally 0.7770.151. The mostnoticeable peaks in the posterior bending angle and externaltorsion angle occurred at 2973% and 7879% of the stance phase,respectively (Fig. 4A).
3.2.2. Stair ascent with forefoot strikePosterior bending (p2p AP bending angle: 0.7470.241–1.757
0.081) and external axial torsion (p2p torsion angle: 0.9070.091–1.3970.261) were observed as well. The ML bending angleremained relatively small. A major noticeable peak and a secondrelatively small peak in the posterior bending angle were found at2874% and at 8676% of the stance phase. Two noticeable peaksof the torsion angle with almost equal amplitudes were found at3879% and 8272% of the stance phase (Fig. 4B).
Statistical results suggested that torsion angle was largerduring forefoot stair ascent than rear foot stair ascent (Table 2),both during the first (p¼0.009) and the second half of the stancephase (p¼0.002).
3.3. Muscle activities during stair ascent
3.3.1. Stair ascent with rear foot strikeThe EMG linear envelope peaks of soleus muscle (Fig. 4C) and
GM (Fig. 4E) were found at 75715% and 8073% of the stancephase, respectively.
3.3.2. Stair ascent with forefoot strikeTwo apparent activity bursts of soleus (32711% and 8077% of
stance phase, Fig. 4D) and GM (36710% and 8075% of stancephase, Fig. 4F) were distinguished. The peaks of EMG linearenvelopes of TA (Fig. 4G and H) and VM EMG (Fig. 4I and J) weregenerally distributed in the initial stance phase for both foot strikepatterns.
3.4. Tibia deformation during running
Posterior bending and external axial torsion of the proximaltibia with respect to the distal tibia were found (Fig. 5A and B). Theactive duration of soleus and GM generally tended to be longerduring forefoot running than rear foot running (Fig. 5C–F).Statistical analysis yielded significant effects of forefoot vs. rearfoot strike on the both bending and torsion angles (po0.001),although the bending angle responded differently between thesubjects. For one subject, the torsion angle during forefoot runningwas 55.7% (1.7970.011 vs. 1.1570.091) larger than rear footrunning, while it was 21.2% (1.7070.041 vs. 1.4070.141) largerin the other subject (Table 3).
3.5. Tibia deformation during isometric plantar flexion
Compared to the other exercises, both AP and ML bendingangles during MVCs remained on a low level and were in oppositedirections. Nevertheless, p2p IE torsion did occur with dramati-cally noticeable magnitude, with the maximum torsion angle of0.7470.121 during the 50% MVC and 1.3570.071 during 100%MVC (Table 4).
4. Discussion
In this paper, the in vivo human tibia loading regimes, in termsof segment deformation, and its relationship to calf muscleactivities were investigated with an OST approach during locomo-tor activities. It was found that bending and torsion are regularconstituents of human tibia deformation in vivo. In agreementwith hypothesis 1, the calf muscle contractions were in close
Fig. 2. Tibia bending and torsion angles as measured in the study.
Fig. 3. Illustration of tibia deformation angles and muscle EMG during the stancephase of the gait cycle from test subject B. (A) tibia deformation angles (solid line:antero-posterior (AP) bending angle, dashed line: internal–external (IE) torsionangle, dotted line: medio-lateral (ML) bending angle) and vertical ground reactionforce (dash-dotted line). (B) EMG of soleus muscle; (C) EMG of GM muscle;(D) EMG of VM muscle. Deg: degree, GM: gastrocnemius medialis muscle, VM:vastus medialis muscle, and %MVC: normalized to the corresponding value duringmaximum volunteer contractions.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎4
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i

temporal relation to bone deformation in all trial conditions.In particular, torsional deformation of the tibia was invariantlylinked to calf muscle contractions, while bending deformationpartly varied between different trial conditions (hypothesis 2). Thepresent findings therefore provide new insights on the mechanicallink between regional muscles and tibia loading.
4.1. The constitution analysis of tibia deformation during walking
During the initial stance phase of gait, the center of mass and thequadriceps muscle force result considerable flexion moment in theknee joint (Fig. 6A), which explains the posterior bending of the tibiaobserved in the present study. The tibia is near vertically oriented andprojects through the center of mass during the mid-stance phase
(Fig. 6B), which lead a small bending moment to the tibia (Wehner etal., 2009). Although large posterior bending moment on the tibiaplateau was detected during push off phase (Heinlein et al., 2009;Kutzner et al., 2010), the moment acting on tibia plateau may notreflect the true loading pattern across the tibia segment. One of thereasons is that the posterior bending moment acting on the tibiaplateau might be compensated by the soleus muscle contraction(Fig. 6C), as its origin inserts in the middle third posterior margin ofthe tibia. It therefore may explain why posterior tibia bending wasbarely observed during the push off phase. Muscle forces aregenerally transmitted through aponeurosis and tendons to bone.The lag between muscle activities and force development has beenwell documented as the electromechanical delay (EMD) (Cavanaghand Komi, 1979). Interestingly, the present results also suggested that
Fig. 4. Illustration of tibia deformation angles and the EMG of soleus, GM from test subjects C during the stance phase of rear foot (A, C, E, G and I) and forefoot (B, D, F, H andJ) stair ascent. (A, B) Solid line: antero-posterior (AP) bending angle, dashed line: internal–external (IE) torsion angle, dotted line: medio-lateral (ML) bending angle.Torsionp2p: the p2p torsion angle, Posp2p: the p2p AP bending angle, Medp2p: the p2p ML bending angle. Torsionp2p-1: the peak torsion angle during the first half of thestance phase, Torsionp2p-2: the peak torsion angle during the second half of the stance phase. (C–J) Dashed line: the rectified raw muscle EMG signal, solid line: the muscleEMG linear envelope. Deg: degree, GM: gastrocnemius medialis muscle, TA: tibialis anterior muscle, VM: vastus medialis muscle, and %MVC: normalized to thecorresponding value during maximum volunteer contractions.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 5
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i

the peak tibia torsional deformation and peak muscle EMG are closetiming with near consistent lag of 12–15% of the stance phase. It wastypically 80–90ms (details of calculation were not shown), whichwas congruent with the order of EMD reported previously(80720 ms) (Inman et al., 1952). Therefore, the present consistentlag was likely caused by EMD.
4.2. Torsional deformation during stair ascent and running
The foot strike pattern during locomotion activities representsthe active level of the plantar flexors. Larger plantar flexionmoments are required to keep the heel lifted during forefootrunning (Perl et al., 2012) and the initial stance phase of forefootstair ascent (Riener et al., 2002), which coincide with the presentsoleus and GM EMG results (Supplementary materials).
Interestingly, compared to the single torsion angle peak duringrear foot stair ascent, two peaks of the torsion angle during forefootstair ascent again spoke for muscle contractions contributing to thetibia torsion (Fig. 4). This notion was further supported by thestatistical results (Table 2). By contrast, the bending angle remainedunchanged between two different types of foot strike.
Table 2Peak-to-peak tibia deformation angles during 0–60% and 60–100% stance phase offorefoot and rear foot stair ascent.
Subject Deformation regime 0–60% stance phase(deg.)
60–100% stance phase(deg.)
Forefoot Rear foot Forefoot Rear foot
A AP bending 0.7370.24 1.0970.04 0.1870.07 0.2470.13IE torsion 0.6070.18** 0.2770.08 0.9070.09** 0.6870.02ML bending 0.2570.10 0.4570.06 0.6170.07 0.4670.01
B AP bending 1.0270.08 1.0870.03 0.5870.09 0.6370.05IE torsion 0.8870.27** 0.6370.23 0.9370.23** 0.8170.15ML bending 0.6370.09 0.5570.04 0.7470.03 0.6770.08
C AP bending 1.0870.05 0.9170.07 0.4570.08 0.3170.05IE torsion 0.8870.04** 0.3370.08 1.0070.14** 0.9270.05ML bending 0.2270.11 0.1770.05 0.3870.15 0.4370.11
E AP bending 1.7470.08 1.4870.10 1.0870.07 0.8770.15IE torsion 1.3570.29** 0.4870.20 1.3970.26** 1.0870.06ML bending 0.3970.02 0.4570.12 0.4770.04 0.7870.15
Values are mean7standard deviation; AP bending: antero-posterior bending angle, IEtorsion: internal–external torsion angle, ML bending: medio-lateral bending angle.
nn po0.01, indicating the differences between forefoot and rear foot.
Fig. 5. Illustration of tibia deformation angles and the EMG of soleus, GM muscles during one trial of rear foot (A, C, E and G) and forefoot (B, D, F and H) running cycle fromsubject E at 9 km/h. (A, B) solid line: antero-posterior (AP) bending angle, dashed line: internal–external (IE) torsion angle, dotted line: medio-lateral (ML) bending angle.Torsionp2p: p2p torsion angle, Posp2p: p2p AP bending angle, Medp2p: p2p ML bending angle. (C–H) Dashed line: the rectified raw muscle EMG signal, the solid line: themuscle EMG linear envelope. Deg: degree, GM: gastrocnemius medialis muscle, VM: vastus medialis muscle, and %MVC: normalized to the corresponding value duringmaximum volunteer contractions.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎6

No apparent difference in the profile of the tibia deformationregimes was observed between two types of running (Fig. 5). Of note,larger torsion indeed was generated during the forefoot running thanrear foot running. Although the sample size was limited and inter-individual differences possibly induced by the variance of the tibialength existed, it still can be deduced that greater torsion iscontributed by the active plantar flexor contractions during forefootrunning.
4.3. Findings during isometric contractions
In the absence of axial loading on the tibia from body weight,isometric plantar flexion derived loading on tibia solely withmuscles. Since the quadriceps and hamstring muscles wereintentionally not active (unpublished data), the anterior tibiabending was probably caused by the passive force pointinganteriorly on the knee joint (Fig. 7, Fpas). Most notably, it isapparent that torsion, rather than bending, prevails in the tibiadeformation regimes (Table 4), which again supported that plantarflexors considerably contribute to the tibia torsional deformation.
Table 3Peak-to-peak tibia deformation angles during the stance phase of forefoot and rearfoot running.
Subject Speed (km/h) Deformation regime Forefoot (deg.) Rear foot (deg.)
D 5.5 AP bending 1.5870.19 1.6370.22IE torsion 1.7870.15*** 1.0970.14ML bending 0.8570.20 0.4470.13
D 9 AP bending 1.7270.08 1.9270.11IE torsion 1.8070.18*** 1.2170.14ML bending 0.8670.07 0.6470.11
E 5.5 AP bending 1.8670.13 1.1470.12IE torsion 1.7270.19*** 1.5070.18ML bending 0.4070.11 0.7470.13
E 9 AP bending 2.2570.21 2.1570.27IE torsion 1.6770.15*** 1.3070.20ML bending 0.3370.13 0.8570.18
Values are mean7standard deviation; AP bending: antero-posterior bendingangle, IE torsion: internal–external torsion angle, ML bending: medio-lateralbending angle.
nnn po0.001, indicating the differences between forefoot and rear foot.
Table 4Peak-to-peak tibia deformation angles during the 50% and 100% maximumisometric voluntary plantar flexion.
Subject Tibia deformation Plantar flexion (deg.)
50% MVC 100% MVC
A AP bending �0.1470.03 �0.3870.03IE torsion 0.5070.05 0.8970.07ML bending �0.1070.02 �0.3170.04
B AP bending �0.2170.03 �0.2670.02IE torsion 0.4070.09 0.7270.15ML bending �0.2770.05 �0.4070.06
C AP bending �0.1770.01 �0.2270.03IE torsion 0.7470.12 0.8770.03ML bending �0.1370.01 �0.2270.06
D AP bending �0.1570.03 �0.2370.02IE torsion 0.7470.02 1.3570.07ML bending �0.1670.06 �0.3870.07
E AP bending �0.1170.03 �0.1870.04IE torsion 0.3570.00 0.6270.16ML bending �0.2970.03 �0.5270.07
Values are mean7standard deviation; AP bending: antero-posterior bendingangle, IE torsion: internal–external torsion angle, ML bending: medio-lateralbending angle. Negative values referred to the tibia bending situations of anterioror lateral bending of the proximal tibia with respect to the distal tibia. MVC:maximum voluntary contraction.
Fig. 6. Illustration of primary forces and moments acting on the tibia during the initial (A), mid- (B) and push-off (C) stance phase. Fmass: the force induced by gravity. FQua:the force generated by the quadriceps contractions. Msum: the moment generated by both the body weight and the quadriceps contraction. Fcalf: the force generated by thecalf muscle contractions.
Fig. 7. Illustration of primary forces acting on the lower leg during the voluntaryisometric plantar flexion using the custom-made dynamometer. FPas: the passiveforce acting on the proximal tibia generated by the voluntary muscle contractions.Flim: the limitation force from the dynamometer to avoid the movement of the footduring the isometric plantar flexion. Fground: the ground reaction force producedduring the plantar flexion. Fmus: the force generated by the plantar flexorscontractions.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 7
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i

4.4. Possible mechanism behind tibia torsion and regional musclecontractions
The question arises how plantar flexors, in particular the soleusand GM, can be associated with the external torsional deformationof the tibia. In theory, the soleus muscle is capable of generating aconsiderable horizontal external torque on the tibia, due to themisalignment of the line of action of the soleus muscle and theaxial orientation of the tibia (Loram et al., 2006) and largepennation angle of the soleus muscle (Agur et al., 2003).
Moreover, the potential transverse angular momentum from theadjacent segments may also load tibia in torsion. However, firstly, inthe present study, the contribution of the transverse angularmomentum from the adjacent segments, if there is any, on tibiatorsion can be excluded by comparing tibia deformation betweenforefoot and rear foot exercises with similar locomotion pattern.Secondly, the transverse momentum from the adjacent segmentsshould be transmitted through the ligaments and, in essence, stilloriginally from the muscles. Evidence indicated that muscle forcesare the primary contributors of the joint loading (Herzog et al.,2003). In particular, the second peak of the knee joint loading duringgait is mostly contributed by calf muscle (Sasaki and Neptune, 2010),or through dynamic coupling, e.g. ground reaction forces (Schacheet al., 2007). However, to our knowledge, it is still remain unexploredabout the transverse moment level of calf muscle. Future studies areneeded to further clarify the remained above concerns.
4.5. Limitations
Some open questions remain to be addressed with the OSTapproach and the present study. Firstly, the local tibia strain canonly be estimated indirectly from the deformation angles. Theestimated average tibia strains were nearly consistent with pre-vious reported strain levels using strain gauge approaches, typi-cally �1000 με for peak bending strain and 1033–2845 με forpeak torsional strain (Supplementary materials). Admittedly, thepresent estimation of the bone strains includes several simplifica-tions and still lacks accuracy. A high-fidelity tibia strain calculationshould rely on an inversely driven Finite Element Model with theanatomical tibia data—an approach that is by no means trivial.Secondly, the comparatively small sample size in the present studymay attenuate the statistical power of the analysis. However, noessential difference between parametric and nonparametric sta-tistical analysis results was found, which indicated that the samplesize does not likely influence the statistical results (Supplementarymaterials). Thirdly, the present study only included male testsubjects with widely ranged age. The extent to expand the presentconclusions to broader population might be limited. Larger samplesizes, age-appropriate and female test subjects would still befavored in future studies.
5. Conclusions
In summary, the tibia torsional deformation follows the calfmuscle contractions with near constant lag during walking. Forefootstrike caused an ‘extra’ noticeable peak of tibia torsion than rear footstrike during stair ascent. Larger tibia torsional deformation wasinduced with forefoot strike than rear foot strike during stair ascentand running. Torsion rather than bending prevailed in the tibiadeformation regimes during isometric plantar flexion. Therefore, itis reasonable to conclude that calf muscle contractions are closelyrelated to tibia torsional deformation in humans during locomotoractivities. These new findings confirm the notion of the mechanicallink between muscle and bone and also shift the focus from loadingmagnitude to loading patterns in bone mechanobiology.
Conflict of interest statement
All authors state that they have no conflicts of interest. Thisresearch itself received no specific grant from any funding agency.
Acknowledgments
Great thanks to Peter Gauger, Wolfram Sies, Tobias Weber, JakobKümmel, Hans-Martin Küsel-Feldker and Jürgen Geiermannat fortheir help during the study. Peng-Fei Yang acknowledges his scholar-ship by the China Scholarship Council (CSC no.: 2009629013).
Appendix A. Supporting information
Supplementary data associated with this article can be found inthe online version at http://dx.doi.org/10.1016/j.jbiomech.2014.12.031.
References
Agur, A.M., Ng-Thow-Hing, V., Ball, K.A., Fiume, E., McKee, N.H., 2003. Documenta-tion and three-dimensional modelling of human soleus muscle architecture.Clin. Anat. 16, 285–293.
Cavanagh, P.R., Komi, P.V., 1979. Electromechanical delay in human skeletal muscleunder concentric and eccentric contractions. Eur. J. Appl. Physiol. Occup.Physiol. 42, 159–163.
Ganse, B., Yang, P.F., Bruggemann, G.P., Muller, L.P., Rittweger, J., Koy, T., 2014. In vivomeasurements of human bone deformation using optical segment tracking:surgical approach and validation in a three-point bending test. J. Musculoskelet.Neuronal Interact. 14, 95–103.
Grood, E.S., Suntay, W.J., 1983. A joint coordinate system for the clinical descriptionof three-dimensional motions: application to the knee. J. Biomech. Eng. 105,136–144.
Heinlein, B., Kutzner, I., Graichen, F., Bender, A., Rohlmann, A., Halder, A.M., Beier,A., Bergmann, G., 2009. ESB clinical biomechanics award 2008: complete dataof total knee replacement loading for level walking and stair climbingmeasured in vivo with a follow-up of 6–10 months. Clin. Biomech. 24,315–326.
Herzog, W., Longino, D., Clark, A., 2003. The role of muscles in joint adaptation anddegeneration. Langenbeck's Arch. Surg./Dtsch. Ges. Chir. 388, 305–315.
Inman, V.T., Ralston, H.J., Saunders, J.B., Feinstein, B., Wright Jr., E.W., 1952. Relationof human electromyogram to muscular tension. Electroencephalogr. Clin.Neurophysiol. 4, 187–194.
Kohrt, W.M., Barry, D.W., Schwartz, R.S., 2009. Muscle forces or gravity: whatpredominates mechanical loading on bone? Med. Sci. Sports Exerc. 41,2050–2055.
Kutzner, I., Heinlein, B., Graichen, F., Bender, A., Rohlmann, A., Halder, A., Beier, A.,Bergmann, G., 2010. Loading of the knee joint during activities of daily livingmeasured in vivo in five subjects. J. Biomech. 43, 2164–2173.
Lafortune, M.A., Cavanagh, P.R., Sommer 3rd, H.J., Kalenak, A., 1992. Three-dimensional kinematics of the human knee during walking. J. Biomech. 25,347–357.
Loram, I.D., Maganaris, C.N., Lakie, M., 2006. Use of ultrasound to make noninvasivein vivo measurement of continuous changes in human muscle contractilelength. J. Appl. Physiol. 100, 1311–1323.
Perl, D.P., Daoud, A.I., Lieberman, D.E., 2012. Effects of footwear and strike type onrunning economy. Med. Sci. Sports Exerc. 44, 1335–1343.
Riener, R., Rabuffetti, M., Frigo, C., 2002. Stair ascent and descent at differentinclinations. Gait Posture 15, 32–44.
Rittweger, J., 2008. Ten years muscle-bone hypothesis: what have we learned sofar?—almost a festschrift. J. Musculoskelet. Neuronal Interact. 8, 174–178.
Rittweger, J., Beller, G., Ehrig, J., Jung, C., Koch, U., Ramolla, J., Schmidt, F., Newitt, D.,Majumdar, S., Schiessl, H., Felsenberg, D., 2000. Bone-muscle strength indicesfor the human lower leg. Bone 27, 319–326.
Sasaki, K., Neptune, R.R., 2010. Individual muscle contributions to the axial kneejoint contact force during normal walking. J. Biomech. 43, 2780–2784.
Schache, A.G., Baker, R., Vaughan, C.L., 2007. Differences in lower limb transverseplane joint moments during gait when expressed in two alternative referenceframes. J. Biomech. 40, 9–19.
Sharir, A., Stern, T., Rot, C., Shahar, R., Zelzer, E., 2011. Muscle force regulates boneshaping for optimal load-bearing capacity during embryogenesis. Development138, 3247–3259.
Soderkvist, I., Wedin, P.A., 1993. Determining the movements of the skeleton usingwell-configured markers. J. Biomech. 26, 1473–1477.
Turner, C.H., Owan, I., Takano, Y., 1995. Mechanotransduction in bone: role of strainrate. Am. J. Physiol. 269, E438–442.
Warden, S.J., Turner, C.H., 2004. Mechanotransduction in the cortical bone is mostefficient at loading frequencies of 5–10 Hz. Bone 34, 261–270.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎8
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i

Wehner, T., Claes, L., Simon, U., 2009. Internal loads in the human tibia during gait.Clin. Biomech. 24, 299–302.
Yang, P.F., Sanno, M., Ganse, B., Koy, T., Brüggemann, G.P., Müller, L.P., Rittweger, J.,2014a. In vivo application of an optical segment tracking approach for boneloading regimes recording in humans: a reliability study. Med. Eng. Phys. 36,1041–1046.
Yang, P.F., Sanno, M., Ganse, B., Koy, T., Brüggemann, G.-P., Müller, L.P., Rittweger, J.,2014b. Torsion and antero-posterior bending in the in vivo human tibia loadingregimes during walking and running. PLoS One 9, e94525.
Yang, P.F., Sanno, M., Bruggemann, G.P., Rittweger, J., 2012. Evaluation of theperformance of a motion capture system for small displacement recordingand a discussion for its application potential in bone deformation in vivomeasurements. Proc. Inst. Mech. Eng. H: J. Eng. Med. 226, 838–847.
Zanchetta, J.R., Plotkin, H., Filgueira, M.L.A., 1995. Bone mass in children—normativevalues for the 2–20-year-old population. Bone 16, S393–S399.
P.-F. Yang et al. / Journal of Biomechanics ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 9
Please cite this article as: Yang, P.-F., et al., On the relationship between tibia torsional deformation and regional muscle contractions inhabitual human exercises in vivo. Journal of Biomechanics (2014), http://dx.doi.org/10.1016/j.jbiomech.2014.12.031i




















