On Models of Hospital Chaplaincies: Which One Works Best for the Muslim Community?
16
This article was downloaded by:[Hamza, Doha Raik] [Hamza, Doha Raik] On: 20 April 2007 Access Details: [subscription number 777068931] Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Muslim Mental Health Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t716100768 On Models of Hospital Chaplaincies: Which One Works Best for the Muslim Community? To cite this Article: , 'On Models of Hospital Chaplaincies: Which One Works Best for the Muslim Community?', Journal of Muslim Mental Health, 2:1, 65 - 79 To link to this article: DOI: 10.1080/15564900701238591 URL: http://dx.doi.org/10.1080/15564900701238591 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material. © Taylor and Francis 2007
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of On Models of Hospital Chaplaincies: Which One Works Best for the Muslim Community?

This article was downloaded by:[Hamza, Doha Raik][Hamza, Doha Raik]
On: 20 April 2007Access Details: [subscription number 777068931]Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Muslim Mental HealthPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t716100768
On Models of Hospital Chaplaincies: Which One WorksBest for the Muslim Community?
To cite this Article: , 'On Models of Hospital Chaplaincies: Which One Works Best forthe Muslim Community?', Journal of Muslim Mental Health, 2:1, 65 - 79To link to this article: DOI: 10.1080/15564900701238591URL: http://dx.doi.org/10.1080/15564900701238591
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will becomplete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should beindependently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with orarising out of the use of this material.
© Taylor and Francis 2007

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
Journal of Muslim Mental Health, 2:65–79, 2007Copyright © Taylor & Francis Group, LLCISSN: 1556-4908 print / 1556-5009 onlineDOI: 10.1080/15564900701238591
Faith-Based PracticeOn Models of Hospital Chaplaincies: WhichOne Works Best for the Muslim Community?
DOHA RAIK HAMZAStanford Hospital & Clinics, Stanford, California, USA
The Muslim community and professional chaplains associationsare realizing the need for Muslim chaplains to get involved in themany institutions that require their services, such as universities,hospitals, prisons, and the military. Having observed different mod-els by which hospital chaplaincies operate, the research presented inthis article seeks to outline and examine three models of operatingchaplaincy service: the chaplain-only model, the volunteer model,and the volunteer-chaplain model. While the models outlined hereare restricted to hospital ministry, they might be beneficial, withvarying degrees, to people engaged in other areas of chaplaincyservices. This article investigates the model that might work best forthe Muslim community, and ends with a summary of future stepsfor the proper implementation of this health care chaplaincy model.
Keywords health care chaplaincy models, Muslim chaplains,Muslim volunteers, spiritual care
INTRODUCTION
The media and the Muslim community are becoming aware of the urgentneed for more Muslims to join the area of chaplaincy work1 (Kaske, 2006;Mulford, 2005; Rossi, 2002). In August 2005, the Islamic Society of North
The author thanks Dr. George Fitzgerald, Dr. Kamyar Hedayat, Rev. John Hester, KathrynStucki, and Ahmed Kamal Sultan Salem for reviewing the structure of this article and providingvaluable insights that helped clarify the concepts presented here. The author also thanks themany Muslim patients who inspired the ideas and examples in this article.
Doha Raik Hamza was formerly Muslim Volunteer Coordinator in the Spiritual CareService, Stanford Hospital & Clinics, Stanford, CA, USA.
Address correspondence to Doha Hamza, 26B Khalil El Khayyat Street, Apartment 15,Moustafa Kamel, Alexandria, Egypt. E-mail: [email protected]
65

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
66 D. R. Hamza
America’s Leadership Development Center organized the first conference forMuslim chaplains from all chaplaincy disciplines. (For a summary report onthe conference, see Kowalski, 2005.) The Muslim chaplains conference is be-coming a tradition to provide networking and educational opportunities. Fur-thermore, the professional chaplains associations are reaching out to Muslimorganizations to recruit more students. In fall 2004, the Association of ClinicalPastoral Education (ACPE), one of the largest health care chaplaincy organi-zations in North America (VandeCreek & Burton, 2001), assigned a task forceto recruit more Muslim students to join the Clinical Pastoral Education (CPE)program. ACPE planned its first pre-ACPE conference program in Florida inNovember 2006 to “foster dialogue between ACPE and the Islamic commu-nity and to engage more Muslim chaplains in CPE” (Fitzgerald, 2006, p. 7).
Amid the flurry of action taken by all of these organizations, it is usefulto pause and examine the modus operandi of chaplaincy service that wouldbest serve the needs of the Muslim community. The efforts to establishMuslim chaplaincy services need not stumble on the same pitfalls as didchaplaincies of other faith traditions when they started. Instead, Muslimchaplainey services can benefit from the accumulated and rich experiencesof the chaplaincies other faiths.
Based on the author’s observations, there are three models governingthe functioning of chaplaincy work in hospitals: the chaplain-only model, thevolunteer model, and the volunteer-chaplain model (VCM). It is importantto note that these models do not follow the conventional historical ortheoretical models found in chaplaincy literature (e.g., see Fichtner &McKenny, 1991; South Yorkshire Strategic Health Authority, 2006). In fact,in relation to the discussion that follows, those models in the literaturecan be considered variations of the first chaplain-only model. Rather,the classification in this article is based on assessing the efficacy of thethree models described in: (1) meeting patients’ spiritual needs despitespiritual, cultural, and language barriers; and (2) the ability of the healthcare chaplaincy model to foster links with the community that cultivateunderstanding, a spirit of volunteerism, and partnership.
In order to understand the reasoning beyond the criteria of thisclassification, we need to look at the specificity of the Muslim chaplaincycase within the health care setting. This is discussed below following adescription of the three models.
THE CHAPLAIN-ONLY MODEL
The chaplian-only model is implemented in most hospitals where certifiedchaplains of various faith traditions, who usually have completed four units inClinical Pastoral Education (CPE), provide “a transcendent dimension to thehuman dilemmas of illness, suffering and death” (South Yorkshire Strategic

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 67
Health Authority, 2006, p. 6) by offering spiritual support to all in needand mobilizing appropriate spiritual resources for effective patient coping,while being sensitive to “multi-cultural and multi-faith realities”(VandeCreek& Burton, 2001, p. 85). Having been established for years, this model is wellstructured, and apparently one to which the Muslim community and the pro-fessional chaplaincy associations are directing their efforts. Like any structure,there are strengths and weaknesses associated with a chaplain-only model.2
On the strengths side, there are several benefits gained from having aprofessional approach to chaplaincy work. These benefits are not restrictedsimply to the patients, but encompass the staff, the organization, and thecommunity within which the chaplains operate (Vandecreek & Burton,2001). By virtue of their training, chaplains can address the theologicaland ontological questions that people facing trauma or the crisis of illnessmay have. In addition, chaplains are a part of interdisciplinary health careteams that “draw on the expertise of specialists in each of these separatedomains—biological/medical, psychological, and social—to diagnose andtreat the whole person in the context of the illness” (Connor, Egan, Kwilosz,Larson, & Reese, 2002, p. 343). It is not uncommon to find notes in apatient’s chart about the patient’s spiritual belief alongside notes abouttheir psychosocial support network and their current physical status, therebyunderscoring the centrality of the patient’s spiritual beliefs to his or heroverall well-being.
The chaplain, being a recognized health care provider with direct accessto a patient’s health care information and other providers, ensures that thespiritual and cultural needs of his or her patients are fulfilled and actedon. In this model, a Muslim chaplain ministering to Muslim patients wouldhave the added benefit of being able to perform faith-specific rituals forhis or her patients, such as reciting the Qur’an in Arabic to a dying patientand performing appropriate supplications. In short, the chaplain connectstogether the patient, family, staff, hospital, and faith community.
However, with the mean number of full time-equivalent chaplainsemployed per 100 inpatients ranging from 1.20 to 1.66 and reaching 2.9in religiously affiliated hospitals (VandeCreek, Siegel, Gorey, Brown, &Toperzer, 2001; see also Flannelly, Handzo, & Weaver, 2004), it becomesclear that this model lacks enough personnel power to meet, let aloneminister, to all patients and to fulfill the chaplains’ pivotal community roles.It is estimated that chaplains visit only 10% to 30% of patients who arehospitalized (Flannelly, Galek, & Handzo, 2005).
A chaplain who comes from an ethnic background similar to his or herpatients may be better able to build trust with the patient and her familywho are likely to identify with the chaplain and look upon him or her as anadvocate (Siriwardena & Clark, 2004; for a case study, see also Connor et al.,2002). Conversely, a difference between the chaplain and the patient’s andfamily’s ethnic background can pose barriers to the care provided and its

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
68 D. R. Hamza
acceptability by the patient and family (Tripp-Reimer, Choi, Kelley, & Enslein,2001). It is difficult for a chaplain who does not share the same faith traditionas his or her patients to minister to those patients’ faith-specific spiritual needsand rituals as is typical in beginning-of-life and end-of-life spiritual care. (Foran interesting discussion of the possibilities and limitations of interreligiouspastoral care to Muslim patients by Protestant chaplains, see Schmidt &Egler, 1998.) After all, would a Muslim chaplain be comfortable performingbaptisms? And, would a Muslim family and a non-Muslim chaplain both becomfortable with the non-Muslim chaplain giving the Adhan to a newbornMuslim infant?
Even if the chaplain shares the same faith tradition as his or her patient,there may be existing language and cultural barriers that can seriously affectthe spiritual assessment and care of the patient given, for instance, the hugediversity within the Muslim community (Haniff, 2003). Although probablyperceived as an “expert” on Islam and Muslims, there is little left for anon-Iranian Muslim chaplain to share with his or her Muslim Farsi-speakingpatient beyond a good smile, Assalamu alaikom, and a heavy-accentedHalet chetore? and Khuda Hafiz. The diversity of cultures presents differentexperiences and consequently differing challenges for Muslims in America,such as those of immigrant Muslims versus their indigenous American cohorts(Altareb, 1996). As a result, a Muslim chaplain runs the risk of being culturallyinsensitive to his or her Muslim patients.
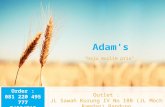
Figure 1 illustrates and summarizes the mechanism by which thechaplain-only model works, and its strengths and weaknesses. Havingrealized its limitations and owing to the hospitals’ professional commitment
Figure 1 In the chaplain-only model, the chaplain has the benefit of being connected withthe medical team, but due to spiritual, cultural, or language barriers, may not have access tothe family. Also, although having some ties to the community, the chaplain may not have thetime to get involved and provide some proactive measures to educate the community aboutthe health care setting.

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 69
not to displace local religious leaders, but rather to complement their services(Vandecreek & Burton, 2001), many hospitals moved into the direction ofenlisting the help of their neighboring faith communities. This discussionwill begin with an elaboration.
THE VOLUNTEER MODEL
The volunteer model involves (1) chaplaincies exclusively run by clergy orvolunteers (e.g., some chaplaincies in rural areas), and (2) volunteer groupsthat specifically provide spiritual care to patients from ethnic minority groups(e.g., Buddhists, Hindus, Jews, Muslims, and Sikhs), while having no chaplainof that same ethnic group, albeit under the supervision of the staff chaplains.The Muslim Spiritual Care Service at Stanford Hospital is one example of thismodel because it is currently run by volunteers without a Muslim chaplain.
Stanford Hospital provides an interesting historical example regardingthe volunteer model. In 1959, a group of community volunteers went to eachpatient in the hospital to ascertain if they would like a member of their faithtradition to visit them. The volunteers then telephoned local clergy to comein and visit the patients who responded affirmatively. In this case, there wasno “in-house” chaplain until 1976 when Stanford Hospital hired its first staffchaplain (J. P. Hester, personal communication, July 21, 2006). Concerningthe relation of volunteer model to population density effects, Flannelly et al.(2004) found that:
Population density effects were generally related to increased relianceon community clergy and volunteers to meet the spiritual needs ofpatients in suburban and, especially, rural facilities in all settings, 57.9%of rural facilities relied solely on clergy and/or volunteers, with 9.8% ofthem saying they relied solely on volunteers. In contrast, only 14.2% ofurban facilities and 31.3% of suburban facilities said they relied solely onvolunteers and/or local clergy, with less than 3.5% of each saying theyrelied exclusively on volunteers. (p. 129)
This model exists to some degree or another in most health carefacilities. Chaplaincies either rely on frequently updated lists of emergencycontacts of faith communities within the immediate vicinity of the healthcare facility, or more formally establish a volunteer program supplementalto the services provided by staff chaplains. In the latter case, which is ourconcern here, a volunteer program is deemed desirable or even necessaryby the hospital when the percentage of the patient population of one faithis significant, or there are particular challenges in providing quality spiritualcare support, or the patient population is so large to the extent that a singlestaff chaplain is not sufficient to meet the various spiritual needs of thepatients. The available data suggest that volunteers provide between 10%and 20% of hospital ministry (VandeCreek et al., 2001).

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
70 D. R. Hamza
In the volunteer model, the volunteers usually receive some formof training from the chaplaincy staff. The training ordinarily centers ontechniques for initiating conversations with patients, assessing their spiritualneeds, and praying for them. It usually entails familiarization with somehospital policy guidelines and mandates such as lectures on infectiousdisease in the hospital, tuberculosis clearance, developing appropriatepatient-volunteer boundaries, and confidentiality compliance in accordancewith the Health Insurance Portability and Accountability Act. The volunteersthen complete their training by going on rounds with staff chaplains orexperienced volunteers to put their theoretical training into practice. Havingcompleted their training, the volunteers—mostly regular attendants of theirfaith congregations, and sometimes referred to as “volunteer chaplains” or“pastoral visitors”—begin visiting patients to provide spiritual support tothem.
On the positive side, the volunteer model, if designed properly with afocus on needed volunteer diversity, offers a rich array of cultures, faiths, andlanguages that provides access to patients of different backgrounds, therebyenhancing the spiritual support and services provided to them (Payne, 2001).When it became known in 2005 that the number of Muslim patients whosecountry of origin was either Iran or Afghanistan exceeded 60% of the totalMuslim patient visits (close to half of those patients [47%], spoke only Farsi),the Muslim Spiritual Care Service at Stanford Hospital took measures torecruit more volunteers who could better serve this patient population. Todate, roughly 55% of the Muslim volunteers at the Spiritual Care Service atStanford Hospital speak Farsi, in addition to Arabic-, French-, Hindi-, Malay-,Pashto-, Tagalog-, Turkish-, and Urdu-speaking volunteers. Diversity, andthe consequent capacity for wide effective communications, constitutes animportant advantage for the volunteer model. For example, the wish of aPashto-only speaking patient to not have her stillborn baby photographedbecause it is not customary in her culture can be readily ascertained byan Afghan volunteer and then communicated to the staff chaplain. Thiscommunication can help the patient mentally and spiritually rather thandistressing her by a well-meaning procedure that contravenes her culture;more importantly, it eliminates the feelings of helplessness and frustrationcreated by the inability to communicate her simple needs and concerns tothe hospital staff.
This model has the potential of providing total patient and familycoverage, because volunteers, as a group, have the time to visit all patients.Coming from diverse life experiences and community backgrounds, andoften being active in those communities, the volunteers provide insightson many community resources that can assist patients. An Urdu-speakingvolunteer, for example, might know a friend of a friend who has undergonea colostomy and is willing to share his experience with an Urdu-speakingpatient who is worried about his impending colostomy. A volunteer who is

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 71
employed as a graphic designer might find designing the Du’a pamphlet forpatients a simple and fun activity. Having navigated the health care system,the volunteers, are better informed about its increasing complexity than theaverage person, and potentially can educate their own communities aboutit. (For an effective faith-based community and health care partnership, seeSutherland, Hale, & Harris, 1995.) What might be an important added benefitfrom this model, especially for Muslims, is that it strengthens a much-neededculture of volunteerism and community involvement. Volunteers in general,and especially spiritual care volunteers (“A Growing Connection,” 2003),have reported a sense of fulfillment and joy in volunteering (Payne, 2001;Zweigenhaft, Armstrong, Quintis, & Riddick, 1996).
On the negative side, there is a risk, when volunteers are not mindful ofor comfortable with the concept of spiritual care, of having a casual attitudethat makes patients’ visits void of meaning and purpose with little or norelevance to a patient’s spiritual well-being. Without a rigorous volunteerscreening process prior to training, as that which is usual for chaplains, thevolunteer model risks the admission of people ill-suited for the job, withchronic evangelism, who might exploit access to patients as a means forsome proselytizing ambitions with little regard for the patients’ vulnerabilityand right to respect of their faith preferences. Health care facilities dependentsolely on volunteers to meet the requirement of the Joint Commission forAccreditation of Healthcare Organizations to secure respect for the spiritualvalues of patients could then find their credentials in peril. Furthermore, thevolunteers may not have adequate training to respond to the deep theologicalquestions that patients devastated by serious illnesses might posit. As withany volunteer activity, the services rendered by the volunteers might not beconsistent or reliable due to conflicting work schedules or a low level ofcommitment. A volunteer commitment is by definition a contract “at will” onthe part of the volunteer, and can be terminated at any time. In addition,sometimes tension, issues of boundaries, and lack of acknowledgment ofvolunteer skills arise between the paid staff and volunteers (Payne, 2001),which could hinder the volunteering activity and the effectiveness of servicesprovided.
Finally, without proper training and constant reporting to their assignedsupervisors, volunteers may pose potential legal and ethical hazards totheir institutions in issues like developing inappropriate patient-volunteerrelationships, breaching patient confidentiality, giving inappropriate adviceregarding medical treatment or decisions, and offering services not withinthe capacity of the volunteer to fulfill such as “counseling.” Much time andeffort must be invested in the overall supervision of this model if it is tobe effective. Figure 2 illustrates the way in which a volunteer model works,highlighting its positives and negatives.
What then is the solution? The answer is a merge between the twomodels yielding the VCM.

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
72 D. R. Hamza
Figure 2 The volunteer model can provide access to the patient’s and family’s world. Also adiverse group of volunteers can enhance ties to different communities to educate them aboutthe health care setting. The volunteers may not be able to communicate reliably, effectively,and consistently with the medical team.
THE VOLUNTEER-CHAPLAIN MODEL
The VCM combines the expertise, professionalism, and leadership capabili-ties of a chaplain from a particular faith tradition with the time and language,cultural, life experience diversity of volunteers. In the case of the SpiritualCare Service at Stanford Hospital, that means the Catholic, Jewish, andMormon chaplaincies. It makes sense to present the VCM as the model thatpossibly could overcome the limitations and weaknesses of the previouslydiscussed structures.
With little time on his or her hands, the chaplain can make the spiritualassessment and devise the spiritual care plan for follow up by the volunteersfor patients on regular units, while personally coordinating spiritual supportto those patients who are in the critical care units and also responding toemergencies and end-of-life care. The volunteers’ diversity brings in richexperiences that are likely to enhance not just the interaction with patientsand their families, but also the chaplaincy’s and the health care facility’s staffexperience and culturally competent care for patients. An Iranian volunteermight note to the Muslim chaplain that his or her sincere suggestion forreading short suras, including al-Fatiha, to patients would not be appreciatedby Iranian patients for whom al-Fatiha is read only when people are dying!
The presence of the chaplain and his or her continued monitoringensures that the chaplaincy maintains a minimal level of spiritual care

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 73
provision for its respective patients. The chaplain, the brainpower, recruitsa number of volunteers consistent with the patients’ demands, and providesadequate initial and ongoing training for them. The volunteers in this modelalso make appropriate referrals to the chaplain for follow-up, such as withpatients requiring a professional level of spiritual care.
With the many roles that a chaplain can perform in the health caresetting (Flannelly, Galek, Bucchino, Handzo, & Tannenbaum, 2005), andespecially a Muslim chaplain as will be explained below, the volunteers couldprove invaluable in carrying out activities that otherwise would be deemeddifficult to initiate and maintain single-handedly despite their importance topatient, family, and community well-being. Celebrating religious holidays,helping with clerical and administrative work, organizing health fairs at localcongregations are but a few examples. Similar to the volunteer model, albeitsuperior to it with its added benefits, this model of team ministry requiressupervision and the investment of time by the chaplain for it to be effective.In order to demand the commitment of volunteers, the chaplain must bewilling to show it first.
Figure 3 further illustrates how the VCM works. As mentioned through-out this article, cultural and language barriers isolate the patient (and, in somecases, the family) from the medical team, including the chaplain. Withoutappropriate access, tapping into a patient’s feelings toward their experiencewith illness, and appreciating how spiritual and cultural values are shapingthis experience becomes a dangerous second-guessing game among health
Figure 3 The volunteer-chaplain model combines the language and cultural strengths of thevolunteers with the health care access of the chaplain. It enhances and supports the chaplain’spivotal role in the community.

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
74 D. R. Hamza
care providers (Ho, 2006). A trained volunteer who shares a similar culturaland language background can provide the staff with access to the patient andidentify pressing needs as well as make appropriate referrals to the staff andchaplain. Having interacted with the health care system and appreciated theimpact of spiritual support, volunteers can support the chaplain’s access andprovision of community services.
Despite its seeming superiority from both empirical observation and thetheoretical discussion above, the VCM seems to receive some resistance inthe areas of professional chaplaincy work. The main arguments are usuallydirected against the endorsement of, and investment in, the “V” in VCM;that is, the volunteer component of it. These might be along the linesthat volunteers waste the time of the chaplains without a significant returnon investment, or that the volunteers might take away from the chaplains’positions when hospitals realize they can get the work done for free ratherthan paying for it. Such arguments are myopic at best. They reflect thetension, ambivalence, and perceived threat documented elsewhere in thehealth care setting on volunteerism versus professionalism (Payne, 2002).
As for the criticism that volunteers waste the chaplain’s time, case studieshave demonstrated the opposite (Payne, 2001). For example, in 2005, theMuslim volunteers at the Spiritual Care Service at Stanford Hospital donatedapproximately 1,280 hours and visited about 85% of Muslim inpatients (thepercentage calculated as the quotient of dividing patient visits conductedby Muslim volunteers by the total number of Muslim patients’ days). Theyalso organized Ramadan and Eid events and, as of July 2006, 10 culturalcompetency events about Muslim patients and their spiritual and culturalneeds as well as participating in the “health care awareness month” event attheir local mosque. This means that with proper investment, volunteers canand do contribute. As for the “jeopardy” argument, In their questionnairesurvey, VandeCreek et al. (2001) observed that, “volunteer chaplains aresignificantly associated with a smaller number of employed chaplains per100 inpatients” (p. 297). This might at a glance seem to validate the notionthat volunteers take away from chaplains’ positions. However, VandeCreek etal. were quick to point out the limitations of their study and to suggest futureresearch to clarify the issue of paid chaplains versus volunteer chaplains:
Would further research results reveal that volunteer chaplains take theplace of employed chaplains? If so, at least two further importantquestions emerge. First, is the quality of ministry and the circumstanceswithin which it is delivered, equivalent for employed chaplains andvolunteers? Second, assuming some differences between employed andvolunteer chaplains can be established, in what circumstances are thesedifferences appropriate and acceptable? If a difference between thequality and content of pastoral care provided by employed staff andvolunteers remains unclear, then it must seem logical to at least some

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 75
health care administrators to conclude that there is no need to spendmoney by employing chaplains to carry out pastoral care functions.(p. 300)
Until further research is conducted to clarify this point, perhaps it canbe said from the above that the issue here is not that of volunteers takingaway the chaplains’ positions. Rather, the issue is lack of clarity on the part ofsome health care administrators concerning the significantly different roles ofchaplains and spiritual care volunteers. Perhaps the solution then lies in somecreative measures by the chaplains’ representative bodies in educating thehealth care setting about the indispensability of the chaplain and the pivotalrole of both the chaplain and the volunteers. Simply put, a chaplain is achaplain, and a volunteer is a volunteer. “The task of the chaplain is to offerpastoral care to people in situations of ultimate concern. For this the chaplainneeds to acquire skills in counseling and inter-personal relationships to placealongside their ministerial formation and religious tradition” (South YorkshireStrategic Health Authority, 2006, p. 8). These are clearly beyond what avolunteer can offer. The volunteer is not expected to attend multi-disciplinarymeetings. It also is not conceivable that a volunteer would have access to apatient’s chart or the accumulated time to do what a professional chaplaincan. In short, the chaplain and the volunteers complement each other’s workto provide the best care possible to patients and their families.
THE SPECIFICITY OF THE MUSLIM CHAPLAINCY CASE
In this section, several points are investigated with regard to the Muslimchaplaincy in the context of the Muslim community. First, the Muslimcommunity, generally speaking, lacks adequate knowledge of the role ofa chaplain and the concept of spiritual care. This may be the consequenceof the near absence of chaplaincy services in Muslim countries which resultsin the immigrant Muslims, who constitute 64% of Muslims living in the UnitedStates (Haniff, 2003), not knowing who a chaplain is and what he or shedoes. In fact, for some Muslims, the word “chaplain” itself may be associatedwith Christian proselytization. It has been our empirical observation fromvisiting Muslim patients and their families at the hospital that on numerousoccasions, despite the patients and their families being very appreciative ofthe visits, they appear to be oblivious of the role of a Muslim spiritual carevolunteer and similarly that of a Muslim chaplain. Muslim chaplaincy workneeds to gain publicity and recognition within the Muslim community ifefforts to increase the number of chaplains and better influence the lives ofMuslims are to be fruitful. The volunteer component of the VCM could proveto be a bridge or a gate for the Muslim chaplaincy in practically educatingthe Muslim community about the art and science of spiritual care.

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
76 D. R. Hamza
Second, in a presentation to the first annual Muslim chaplains con-ference, the author argued that the roles and challenges faced by Muslimchaplains are many, especially in relation to providing spiritual support forMuslim patients and their families, which is naturally expected of them.These roles include, but are not limited to being:
Ĺ a bridge between the medical team and the patient and their family,explaining treatment plans and the roles of health care providers, andrelaying any spiritual and cultural issues to the medical team that is guidingthe patients and family’s health care decisions,
Ĺ a researcher documenting their experience since there is a paucity ofresources on spirituality and spiritual support according to the Islamicweltanschauung, and
Ĺ a problem solver trying to find answers to pressing and emergentquestions.
In an area as dynamic as a health care setting, the Muslim chaplain needsto find and maintain connections to Islamic scholarship that will provideinstantaneous, reliable, and accurate information regarding the permissibilityof withdrawal of life support, abortion, organ donation, and declaring a donot resuscitate (DNR) status, to name a few challenging examples. He or shemust be:
Ĺ a leader in his or her community, for example in promoting healthand wellness, initiating and maintaining support groups, and providingbereavement care; and
Ĺ sufficiently flexible to meet the various spiritual needs of the diverseMuslim population: the very devout, the moderate, and the nonpracticingor secular Muslim.
With the language and cultural diversity of Muslims, and the Muslimchaplain’s need to fulfill all his or her other roles, most notably that of theclinical interaction with all patients not just Muslims, the task of the Muslimchaplain could be anything but easy. The VCM could be very effective insupporting the chaplain’s effort to fulfill all those roles.
CONCLUSION
The Muslim community and the professional chaplaincy associations aretaking practical measures to involve more Muslims in the areas of chaplaincywork. This article is an attempt to investigate the best model of operationof a health care chaplaincy that meets the current needs of the Muslimcommunity. Three models by which health care chaplaincies operate were

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 77
discussed: the chaplain-only model, the volunteer model, and the VCM.The article highlighted the pros and cons of the first two models and thenpresented the VCM as the model that possibly could combine the positives,and overcome the negatives of the other two by synergizing the expertise ofthe chaplain with the support of the volunteers.
Then the article discussed some issues pertaining to the specificcircumstances of the nascent field of Muslim chaplaincy that make theVCM even more fitting. These include: (1) the lack of adequate knowledgeabout the role of a Muslim chaplain within the Muslim community, (2) thepossibility of the existence of cultural and language barriers owing to thediversity of Muslims that could hinder the Muslim chaplain’s interaction withMuslim patients, and (3) the many roles a Muslim chaplain in particular isasked to take and the lack of time to fulfill them.
More work is needed to determine how to best apply the VCM forthe Muslim chaplaincy. As a beginning, the author suggests a survey ofhospitals within the United States and an assessment of the number of Muslimpatients they have. This strategic information can be used to deploy theVCM where it is needed most. Where funding or lack of Muslim chaplainsis a challenge, perhaps a volunteer model could be a short-term goal. Sucha model however, could possibly be supported by a parent VCM in thevicinity that provides guidance, resources, and emergency support whereneeded.
Notwithstanding the many challenges that lie ahead of it, the Muslimchaplaincy has the potential to transform the health of the Muslimcommunity, define a distinct mode of Muslim spirituality, revive religiousmandates such as the obligation of visiting the sick and volunteerism, andcraft a position for Muslims in a crucial area of public involvement.
We conclude by the story, or the plight, of Mohammad Kochi, an olderAfghan patient, which was the focus of the Hold Your Breath documentary(see Program in Bioethics and Film, n.d.).
When the oncologist encourages chemotherapy, Mr. Kochi rejects atreatment he feels will interfere with his daily prayer ritual. Instead,he undertakes a visit to Mecca, which he hopes will cure his dis-ease. . . . Meanwhile, the medical staff worry that the family interpretersare not telling Mr. Kochi the whole truth about his disease. (Hold YourBreath, n.d.)
This documentary makes a compelling, albeit at times disturbing, case for theimpact of cultural and spiritual beliefs on health care. We are left wonderingabout all the other half-informed “Kochis” out there, and what role theauthentic community represented in the chaplain and the volunteers couldplay in their care.

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
78 D. R. Hamza
NOTES
1. Similar to other research trends (see VandeCreek and Burton, 2001, p. 81), “spirituality” in thisarticle includes “religion,” and “spiritual care” includes “pastoral care.” In addition, for the scope of thisarticle, the terms “chaplaincy” and “spiritual care” will be used interchangeably.
2. It can be argued from reviewing The Functions and Activities of Healthcare Chaplains as outlinedby Vandecreek and Burton (2001), that one of those activities is “[t]raining and supervising volunteersfrom religious communities who can provide spiritual care to the sick” (p. 87), The author here is referringto the fact that some chaplaincies do not find it necessary to enlist help from a faith community outsidethe hospital; hence, the classification of the chaplain-only model.
REFERENCES
A growing connection: A pastoral care volunteer program and the community(2003, Spring). The Beacon, 28(1). Retrieved July 30, 2006, from the Health-Care Chaplaincy Web site: http://www.healthcarechaplaincy.org/publications/Beacon/2003/Beacon spring 2003.pdf
Altareb, B. Y. (1996). Islamic spirituality in America: A middle path to unity.Counseling and Values, 41, 29–38.
Connor, S. R., Egan, K. A., Kwilosz, D. M., Larson, D. G., & Reese, D. J. (2002).Interdisciplinary approaches to assisting with end-of-life care and decisionmaking. American Behavioral Scientist, 46, 340–356.
Fichtner, C. G. & McKenny, G. P. (1991). Values interpretation: A new model forhospital ministry. Journal of Religion and Health, 30, 109–118.
Fitzgerald, C. G. (2006, Spring). Islam: The next wave. ACPE News, 7–8Flannelly, K. J., Galek, K., Bucchino, J., Handzo, G. F., & Tannenbaum, H. P.
(2005). Department directors’ perceptions of the roles and functions of hospitalchaplains: A national survey. Hospital Topics, 83, 19–27.
Flannelly, K. J., Galek, K., & Handzo, G. F. (2005). To what extent are the spiritualneeds of hospital patients being met? International Journal of Psychiatry inMedicine, 35, 319–323.
Flannelly, K. J., Handzo, G. F., & Weaver, A. J. (2004). Factors affecting healthcarechaplaincy and the provision of pastoral care in the United States. Journal ofPastoral Care & Counseling, 58 (1–2), 127–130.
Haniff, G. M. (2003). The Muslim community in America: A brief profile. Journal ofMuslim Minority Affairs, 23, 303–311.
Ho, A. (2006). Family and informed consent in multicultural setting. AmericanJournal of Bioethics, 6, 26–28.
Hold your breath. (n. d.). Retrieved July 30, 2006, from http://medethicsfilms.stanford.edu/film/hyp onesheet.pdf
Kaske, M. (2006, April). Help wanted: Hospitals need Muslim chaplains. ColumbiaNews Service. Retrieved July 31, 2006, from http://jscms.jrn.columbia.edu/cns/2006-04-04/kaske-muslimchaplains
Kowalski, M. (2005, September 11). Muslim chaplains determined to join hands inserving community and nation. ISNA Leadership Development Center. RetrievedJuly 27, 2006, from http://www.ildc.net/ildc-news/2005/9/11/muslim-chaplains-determined-to-join-hands-in-serving-community-and-nation.html

Dow
nloa
ded
By: [
Ham
za, D
oha
Rai
k] A
t: 20
:04
20 A
pril
2007
On Models of Hospital Chaplaincies 79
Mulford, K. (2005, April 16). Need increasing for Muslim chaplains. CourierPost Online. Retrieved July 31, 2006, from http://www.courierpostonline.com/columnists/ cxmu041605 a.htm
Payne, S. (2001). The role of volunteers in hospice bereavement support in NewZealand. Palliative Medicine, 15, 107–115.
Payne, S. (2002). Dilemmas in the use of volunteers to provide hospice bereavementsupport: Evidence from New Zealand. Mortality, 7, 139–154.
Program in Bioethics and Film, Stanford Center for Biomedical Ethics (Producer),& Grainger-Monsen, M. (Director). (n. d.). Hold your breath [Motion picture].(Available from Transit Media, P.O. Box 1084, 190 Route 17M, Harriman, NY10926)
Rossi, H. L. (2002, May 16). Muslim chaplains a new priority for colleges.Religion News Service. Retrieved July 31, 2006, from http://pewforum.org/news/display.php? NewsID = 1203
Schmidt, K. W., & Egler, G. (1998). A Christian for the Christians, a Muslim forthe Muslims? Reflections on a Protestant view of pastoral care for all religions.Christian Bioethics, 4, 239–256.
Siriwardena, A. N., & Clark, D. H. (2004). End-of-life care for ethnic minority groups.Clinical Cornerstone, 6, 43–49.
South Yorkshire Strategic Health Authority. (2006, May). A review of some theoreticalmodels of healthcare chaplaincy service and practice. In Caring for the SpiritNHS Project. Retrieved July 31, 2006, from http://www.southyorkshire.nhs.uk/chaplaincy/documents/chapservicepracticemodels.pdf
Sutherland, M., Hale, C. D., & Harris, G. J. (1995). Community health promotion: thechurch as partner. Journal of Primary Prevention, 16, 201–216.
Tripp-Reimer, T., Choi, E., Kelley, L. S., & Enslein, J. C. (2001). Cultural barriers tocare: Inverting the problem. Diabetes Spectrum, 14, 13–22.
VandeCreek, L. & Burton, L. (2001). Professional chaplaincy: Its role and importancein healthcare. Journal of Pastoral Care, 55, 81–97.
VandeCreek, L., Siegel, K., Gorey, E., Brown, S., & Toperzer, R. (2001). Howmany chaplains per 100 inpatients? Benchmarks of health care chaplaincydepartments. Journal of Pastoral Care, 55, 289–301.
Zweigenhaft, R. L., Armstrong, J., Quintis, F., & Riddick, A. (1996). The motivationsand effectiveness of hospital volunteers. Journal of Social Psychology, 136, 25–34.