º. 4 - eScholarship.org
300
THE INFLUENCE OF HEALTH STATUS, GENDER, AND ANXIETY ON THE STRESS AND COPING PROCESSES OF HOSPITALIZED SCHOOL-AGE CHILDREN by Elizabeth Anne Bossert DISSERTATION Submitted in partial satisfaction of the requirements for the degree of DOCTOR OF NURSING SCIENCE in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA San Francisco ~ C■ gº klº - - - - ■º. 4 -º- Committee in Charge Deposited in the Library, University of California, San Francisco Date Degree Conferred: . ///?o. - - - University Librarian
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of º. 4 - eScholarship.org

THE INFLUENCE OF HEALTH STATUS, GENDER, AND ANXIETYON THE STRESS AND COPING PROCESSES OF
HOSPITALIZED SCHOOL-AGE CHILDREN
by
Elizabeth Anne Bossert
DISSERTATION
Submitted in partial satisfaction of the requirements for the degree of
DOCTOR OF NURSING SCIENCE
in the
GRADUATE DIVISION
of the
UNIVERSITY OF CALIFORNIA
San Francisco
~ C■ gº klº- - - -
■ º. 4 -º-
Committee in Charge
Deposited in the Library, University of California, San Francisco
Date
Degree Conferred: . ///?o.- - -
University Librarian

The Influence of Health Status, Gender, and Anxiety
on the Stress and Coping Processes of
Hospitalized School-Age Children
Elizabeth Anne Bossert
University of California, San Francisco
School of Nursing
December 20, 1990

copyright 1990
by
Elizabeth A. Bossert
ii

DEDICATION
To my parents,
Robert and Lois Bossert
iii

ACKNOWLEDGMENTS
During the process of preparing for, planning, and executing this
research, I have been blessed by the support and guidance of a number of
persons who have been instrumental in helping me achieve this milestone.
To these people, I want to express my appreciation.
Throughout my life, two people have consistently listened to my plans
and concerns, shared my highs and lows, and encouraged, supported, and
prayed for me. Thank-you, Mom and Dad.
While at UCSF, I have the privilege of studying with many excellent
faculty and appreciate the role of each in contributing to my education.
However, there are four faculty who have had major roles in helping me
develop the skills of a nurse researcher to whom I would like to express
individual thanks.
Bonnie Holaday has served as my advisor throughout the program, has
chaired both the preliminary examination and the dissertation committee,
and has been my sponsor for the NRSA proposal. Through her guidance I
have learned what is needed to develop a sound research plan, a fundable
proposal, a publishable paper, and so much more. Her ability to stimulate
thought, critique written work, her willingness to share knowledge and
resources, and her advocacy has been greatly appreciated. Thank-you,
Bonnie.
Lynn Savedra was the first faculty member with whom I discussed the
possibility of pursuing doctoral education at UCSF and greatly facilitated
my investigation of the program. She consistently has been supportive of
my work as evidenced by her willingness to participate in the preliminary,
qualifying, and dissertation committees, but most importantly, she has
iv.
helped me integrate a Christian viewpoint into secular education. Thank
you, Lynn.
Ida Martinson has also served on all my committees throughout my
course of study and chaired the qualifying examination. In addition, she
has promoted my professional growth by providing the opportunity for
participation in data analysis, publication, and presentation at a
professional meeting. I have appreciated her willingness to listen and to
give suggestions for successfully integrating research into a faculty
role. Thank-you, Ida.
Steve Paul has served as my guide into the world of statistics. His
sense of humor and willingness to answer endless questions has been
greatly appreciated. Thank-you, Steve.
In addition to the faculty at UCSF, I want to extend my appreciation
to my friends among the students and staff. Without your encouragement
and facilitation, this project would not have been completed.
I would also like to express my appreciation to my friends at Loma
Linda University School of Nursing for their encouragement to explore the
possibility of doctoral education and to persevere during the process.
Grateful appreciation is also extended to the persons who facilitated
the process of obtaining access to children at the facilities used for
data collection and also to those who participated in the actual process
of data collection: Debbie Trevithick, Inez Wieging, and Lael Lambert at
the University of California, San Francisco Medical Center; Cheryl
Montague, Paul Maxwell, Nan Ground, Andrea McClean, and Louanne La Fosse
of Shriner's Hospital for Crippled Children, San Francisco; Gene
O'Connell, Artie Glickman, and Barbara Martin of San Francisco General
Hospital and Medical Center; Carolyn Dare, Laurel Kersten, Celia Buckley,
and Margie Crandall of University of California, Davis, Medical Center;
V

Joann Konkel, Debbie Echtenkamp, and Martin Goldsmith of Valley Children's
Hospital; Pat Frost-Hartzer, Nancy Dinsmore, and Cheri Plungy of
Children's Hospital Stanford; and Linda Johnson, Helen Staples, Vera
Durrant, Audrey Burgess, Dee Hart, and Dorthy Neufeld of Loma Linda
University. Appreciation is also extended to the many nurses and staff
personnel who took the time to assist in the process of identifying
potential subjects. Without the support and encouragement of each of
these persons, the process of data collection would have been difficult,
if not impossible.
I also would like to thank the parents who gave me permission to talk
with their children and the children who were willing to talk with me and
share their experiences. I greatly appreciate each one of you.
Appreciation is also extended to the organizations contributing to the
financing of my doctoral education: Loma Linda University, the National
Center for Nursing Research at NIH, University of California, San
Francisco Graduate Division and School of Nursing Century Club Funds, and
the Northern California Affiliate of the Association for Care of
Children's Health.
vi

THE INFLUENCE OF HEALTH STATUS, GENDER, AND ANXIETYON THE STRESS AND COPING PROCESSES OF
HOSPITALIZED SCHOOL-AGE CHILDREN
Elizabeth Anne Bossert
University of California, San Francisco, 1990
ABSTRACT
This study investigated the influence of health status (acutely or
chronically ill), gender, and trait anxiety on the stress and coping
process of hospitalized children, ages 8 through 11. Two aspects were
examined: 1) the specific events appraised as stressful and the coping
behaviors used in response to the events, and 2) the appraised
stressfulness of the global event of hospitalization and the perceived
effectiveness of the coping process. Conceptualization of the study was
guided by Lazarus' theory of stress and coping and Piaget's theory of the
cognitive development of children.
The design was nonexperimental and cross-sectional. The convenience
sample was comprised of 82 children admitted to a pediatric unit in one of
six California hospitals. The children completed six self-report
instruments.
Through content analysis, six categories of stressful events were
identified: intrusive events, physical symptoms, therapeutic
interventions, restricted activity, separation, and environment.
Synthesis of prior research resulted in six categories of coping behaviors
used by hospitalized children: cognitive processing, cognitive
restructuring, cooperation, countermeasures, control, and seeking support.
Based on these categories, analysis of the interviews indicated that of
the six possible relationships between the dependent variables of health
status, gender, and trait anxiety and the independent variables of stress
vii

appraisal and coping behaviors, only the relationship between health
status and stress appraisal was statistically significant; chronically ill
children identified more intrusive events and acutely ill children
identified more physical symptoms as stressful.
Data pertaining to the global hospital experience were examined using
path analysis. As a set, health status, gender, and trait anxiety
accounted for 14% of the variance in the children's stress appraisal;
trait anxiety alone contributed significantly to the model. Trait anxiety
is positively related to appraisal of hospitalization as stressful. As a
set, health status, gender, and trait anxiety accounted for 12% of the
variance in perception of coping effectiveness; both health status and
trait anxiety contributed significantly to the model. Acutely ill
children perceive their coping as more effective than chronically ill
children, and trait anxiety is inversely related to perception of coping
effectiveness. Gender did not have a significant influence in any of the
analyses.
2-2. f 2.z -->(O cºvvv^^{- 4-º'-- 4. /. Z. ~~ º
Bonnie Holaday, Chair 2. Elizabeth Anne Bossert
viii
TABLE OF CONTENTS
CHAPTER ONE: INTRODUCTION
PurposeSignificance
CHAPTER TWO : CONCEPTUAL FRAMEWORK AND LITERATURE REVIEWThe Conceptual Frameworks
The Lazarus Paradigm of Stress and CopingStress
AppraisalThe Coping ProcessAdaptational Outcomes of the Stress and
Coping ProcessPiaget's Theory of Cognitive Development
The Process of Cognitive DevelopmentStages of Cognitive Development
Application of Lazarus' Theory to ChildrenLiterature Review
Research on Sources of Stress during HospitalizationSources of Children's Stress during
Hospitalization Identified by AdultsSources of Stress during Hospitalization
Identified by ChildrenCritique of the Studies of Sources of StressComparison of Adult and Child Identification
of Sources of StressResearch on Coping during Hospitalization
Coping Strategies Reported in the LiteratureSummary of Coping StudiesCritique of the Coping StudiesVariables Influencing Coping as Reported
in the Literature
Conceptual ModelHealth Status
AnxietyGender
Stress AppraisalHypothesesDefinition of Terms
CHAPTER THREE: METHODOLOGYDesign
Strengths and Weaknesses of the DesignResearch SettingsHuman Subject's AssuranceSample
Sample Selection Constraints due to Variablesof Interest
38
4145
4646646974
78798081818284
86868790959697
ix

Page
Inclusion/Exclusion Criteria 99Rationale for Inclusion Criteria 100Rationale for Exclusion Criteria 104
Potential Sources of Uncontrolled Variance 106
Population to Whom Results May Be Generalized 108Sample Size 108Sample Selection 109
Data Collection Methods 110
State-Trait Anxiety Inventory for Children (STAIC) 111Hospital Stress Scale (HSS) and Hospital Coping 114
Scale (HCS)Child Medical Fear Scale (CMFS) 117Coping Response Inventory (CRI) 122Hospital Stress and Coping Interview 125
Data Collection 128The Phases of Data Collection 128The Protocol for Data Collection 130
Description of Data Collectors and Training Process 133Data Analysis 135
CHAPTER FOUR : RESULTS 138
Characteristics of the Sample 138Preliminary Analyses 144
Site of Data Collection 145
Age Differences 145Prior Out-Patient Experience 14.6Prehospitalization Programs 146Parental Rooming-in 147
Analysis of Hypotheses 148Analysis of the Interview Data 148
Stress Categories 148Coping Categories 150Quantification of Interview Data 150Restatement of Theoretical Model 154
Hypothesis 1 155Hypothesis 2 158Hypothesis 3 161Hypothesis 4 164Hypothesis 5 167Hypothesis 6 168Summary of Interview Data Analysis 169
Analysis of the Stress and Coping Word Graphic Scales 170Concurrent validity 171Preliminary Information Regarding Analysis 172Hypothesis 7 172Hypothesis 8 176Revision of Model 180
Summary of Word Graphic Scale Analyses 184Summary of Findings 186

CHAPTER FIVE: DISCUSSIONRevision of the Model
Relation of Results to HypothesesDiscussion of Results Relating to Stress Appraisal
Health Status and Stress AppraisalGender and Stress AppraisalAnxiety and Stress Appraisal
Discussion of Results Relating to CopingHealth Status and Coping BehaviorsGender and Coping BehaviorTrait Anxiety and Coping Behavior
Limitations
Limitations Related to the SampleLimitations Related to Instrumentation
Implications for NursingPersonHealthEnvironment
NursingImplications for Future ResearchConclusion
BIBLIOGRAPHY
APPENDICESA
:
Human Subjects Committee ApprovalUniversity of California, San FranciscoThe State-Trait Anxiety Inventory for ChildrenHospital Stress ScaleHospital Coping ScalePractice ScaleChild Medical Fear Scale
Coping Response InventoryHospital Stress/Coping InterviewUniversity of California, San FranciscoPermission for Child to Be a Research SubjectExperimental Subjects Bill of RightsGeneral Data Form
Summary of Research ResultsConsent to be a Research SubjectChild Assent Form
191191192192196200202204208212213214215217219219221222224227229
232
255255
257258260262264266268270
274276279281
xi
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
Table
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
LIST OF TABLES
Coping Strategies of Children
Synthesis of Reported Coping BehaviorsItem Contents of Four Fear Scales
Gender and Age of Subjects (in years)
Family Income
Health Status and Condition of Subjects
Description of Subjects by Site
Categories of Stressful Events During Hospital
Categories of Coping Behaviors Used DuringHospital
Events Appraised as Stressful by HospitalizedChildren
Coping Behaviors Used by Hospitalized Children
Interrater Reliability for Content Analysis
Frequency of Stressful Events by Health Status
Frequency of First Stressful Event by Health Status
Frequency of All Coping Behaviors by Health Status
1st Coping Behavior used in Response to IntrusiveEvent by Health Status
Frequency of Stressful Events by Gender
Frequency of First Stressful Event by Gender
Frequency of Coping Behaviors by Gender
1st Coping Behavior used in Response to IntrusiveEvent by Health StatusMean Trait Anxiety Score by Stressful Event Category
Mean Trait Anxiety Score by Coping Behavior Categories
Results of Interview Data Analyses
The Effects of Independent Variables on DependentVariable of Stress
Effects of Independent Variables on DependentVariable of Coping
Revised Effects of Independent Variables on DependentVariable of Coping
Summary of the Effects of Independent Variables onDependent Variables
47
65
121
139
140
141
143
149
151
152
152
153
156
157
159
161
162
163
165
166
167
169
170
173
177
18i
185
xii

Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
LIST OF FIGURES
Diagram of the Lazarus Stress and Coping Process
Model of the Relationship Between Three ModifyingVariables and the Stress and Coping Process
Theoretical Model of Relationships Between Variables
Model of Statistical Relationships Between Variables
Theoretical Model of Variables InfluencingStress Appraisal
Theoretical Model of Factors Influencing CopingAppraisal
Theoretical Model of Factors Influencing CopingAppraisal
Theoretical Model of Relationships Between Variables
155
170
174
178
182
184
xiii

CHAPTER ONE
INTRODUCTION
In the hospital you get used to lots of things.
You get used to staying in bed when you don't want to.
And feeling your back itch when you can't scratch it.
You get used to having your bath in bed and even going to thetoilet in a bed pan.
You get used to missing your dog and missing your friends.
Your get used to listening to babies cry, and seeing yourmommy and daddy just when they want to come to visit you.
That's quite a lot of getting used to.
(Shore, 1965, p. 62)
The hospitalized child unquestionably has a lot to "get used to".
Very few of the child's daily routines are conducted in the same manner as
at home. Additionally, many events and situations are encountered that
are unlikely to occur at home. The child may find some of these changes
to be relatively unimportant and ignore the situation or event. Other
changes may cause considerable distress for the child resulting in various
behaviors designed to reduce the stress of the situation or event. While
it is generally accepted that certain common experiences encountered
during hospitalization are stressful for children and that children will
attempt to cope with the situation, little is known about factors that may
influence the individual child's stress and coping responses during
hospitalization.

Purpose
The purpose of this study was to examine the influence of three
selected factors on, first, the child's global reaction to
hospitalization, and second, the child's reaction to specific events
encountered during hospitalization. The specific questions asked were:
1. What is the affect of health status, gender, and trait anxiety
on the school-age hospitalized child's appraisal of the event
of hospitalization as stressful and the resulting perception
of the effectiveness of coping behaviors?
2. What is the relationship of health status, gender, and trait
anxiety on the school-age hospitalized child's appraisal of
events during hospitalization as stressful and on the coping
behaviors used during hospitalization?
Significance
Although numerous researchers have investigated the phenomenon of
children's reactions to hospitalization, as evidenced by the research
literature reviews by Vernon, Foley, Sipowicz, and Schulman (1965), and by
Thompson (1985), there remains a paucity of information available
concerning factors that may be responsible for differences in the
reactions of children. Some previous studies have assumed that all
hospitalized children have similar reactions (Adams & Bergman, 1965;
Gofman, Buckman, & Schade, 1957; Holt, 1968; May & Sparks, 1983). Other
studies have limited the investigation to the reactions of children
admitted for medical reasons (Prugh, Staub, Sands, Kirschbaum, & Lenihan,
1953; Neff, 1978) or more often for surgical procedures (Blom, 1958;

Reissland, 1983; Rose, 1972; Savedra & Tesler, 1981; Timmerman, 1983).
While these studies have provided information that is important in the
quest to understand the hospitalized child, other equally important
variables have not yet been fully explored.
One variable that has received little attention is that of the
child's health status as either acutely or chronically ill. Currently, it
is uncertain if chronically ill children have similar or dissimilar
patterns of stress and coping in response to the experiences of
hospitalization as do acutely ill peers. Although chronically ill
children are a subgroup of the total population of children, and therefore
might be expected to have similar reactions to the event of
hospitalization, it is possible that the prior experiences of this group
with hospitalization may alter their reactions during subsequent
admissions. Considering that between 10 to 15 percent of children are
chronically ill (Perrin, 1985), with 1 to 2 percent severely affected
(Hobbs, Perrin, & Ireys, 1975), and that approximately 36 percent of the
total number of pediatric hospital days are used by chronically ill
children (Butler, Budetti, McManus, Stenmark, & Newacheck, 1985), it is
evident that chronically ill children are hospitalized more frequently
than are healthy children with an acute illness. Thus, it is important to
identify what this group of children perceives as stressful during
hospitalization and how they cope with it. Without this information it is
difficult to plan programs or individualize care that will meet the needs
of these children. The commonalities of chronically ill children's
hospital experiences, despite the precise diagnosis involved, support the
importance of using the noncategorical approach (Pless & Perrin, 1985;
Stein & Jessop, 1982, 1984, 1989) rather than a diagnostic oriented

scheme. Currently, only one research team has published the results of a
comparison between the reactions of acutely ill and chronically ill
children during hospitalization reporting that in preschool children there
are few differences in the number of coping behaviors used by the two
groups, but that chronically ill children do use more coping behaviors
than do acutely ill children (Ritchie, Caty, & Ellerton, 1987; 1988).
A second area of study, investigation of the relationship between
personality variables and the child's stress and coping during
hospitalization, has only begun to be explored. The two factors that have
been examined are locus of control (LaMontagne, 1984, 1987; Rothbaum,
Wolfer, & Visintainer, 1979), and state anxiety (Burstein & Meichenbaum,
1979; Field, Alpert, Vega-Lahr, Goldstein, & Perry, 1988). The
relationship between trait anxiety and the child's reactions to
hospitalization, has not yet been reported in the scientific literature,
although trait anxiety is an easily identifiable and fundamental
personality characteristic.
A third variable needing further study is gender. It is uncertain
whether the gender of the child has a relationship to the appraisal of
stress and resulting coping behaviors during hospitalization. Brown,
O'Keefe, Sander, and Baker (1986), studying the cognitive reactions of
healthy children to stressful situations, found no difference related to
gender, a finding paralleled by a recent study of hospitalized children
(Field et al., 1988). In contrast, other studies (Savedra & Tesler, 1981;
Tesler, Wegner, Savedra, Gibbons, & Ward, 1981; Aisenberg, Wolff,
Rosenthal, & Nadas, 1973) found that gender was a significant factor in .
the type of coping strategy used by school-age hospitalized children.
Further investigation in this area is needed.

Finally, although a few researchers have focused specifically on
school-age children (LaMontagne, 1984; Savedra & Tesler, 1981; Timmerman,
1983; Youssef, 1981), much of the research involving school-age children
has failed to limit the age of the subjects to a recognized developmental
level (Burstein & Meichenbaum, 1979; LaMontagne, 1987; May & Sparks, 1982;
Neff, 1978; Peterson & Toler, 1986; Reissland, 1983; Rose, 1972; Rothbaum,
Wolfer, & Visintainer, 1979), possibly clouding interpretation and
generalization of the results.
It was evident that a study investigating the stress and coping
process of hospitalized school-age children in relation to the variables
of health status, gender, and anxiety would provide a unique contribution
to the knowledge base of pediatric nursing. By filling this gap in the
theoretical base of nursing science, the information generated by the
proposed study will increase the nurse clinician's understanding of the
reactions and behaviors of school-age, acutely ill versus chronically ill
children, boys versus girls, and children with high anxiety versus those
with low anxiety during hospitalization. Rather than assuming that all
hospitalized children have the same concerns and needs, the professional's
awareness of possible differences will be increased, resulting in an
increased ability to design care to meet the needs of specific
populations. Through this awareness, unnecessary stressful situations may
be avoided and support provided to assist the child's coping processes
during the necessary stressful events.
To accomplish the purpose of studying the affect of health status,
gender, and trait anxiety on the stress and coping process of school-age
children during hospitalization, a nonexperimental, cross-sectional design
was used. Qualitative data was collected through an interview with the

child focusing on the events appraised as stressful during hospitalization
and the coping behaviors used in response to that event. Quantitative
data involved administration of standardized instruments to determine the
child's trait anxiety level, medical fears, and coping responses, and word
graphic scales developed for this study to assess the child's stress and
coping responses in relation to the event of hospitalization.
CHAPTER TWO
CONCEPTUAL FRAMEWORK AND LITERATURE REVIEW
Two theoretical frameworks were used to guide the investigation of
factors influencing the school-age child's stress and coping processes
during hospitalization. The first framework was the Lazarus paradigm of
stress and coping. This approach focuses on the cognitive aspects of
stress and coping, rendering it an appropriate framework for studying
psychological reactions to the hospital experience, as contrasted with
either a physiological model, such as that begun by Selye (Mason, 1975a,
1975b ; Selye, 1980), or a sociological model such as proposed by Pearlin
(Pearlin, Lieberman, Menaghan, & Mullan, 1981; Pearlin & Schooler, 1978).
Although the Lazarus model was developed based on research involving
adults, the key concept of individual appraisal of the stressfulness of
events allows appropriate extension to children. Because children's
thought processes differ from that of adults, it was also necessary to
base the research on a theoretical model that considers the mental
development of the school-age child. Piaget's theory of cognitive
development was used for this purpose because of the emphasis on the
cognitive development and functioning of the child. This chapter will
examine these theories, review the literature relevant to the constructs
of stress and coping in child, with emphasis primarily on studies relating
to the hospitalized child, and will describe the model used for this
study.

The Conceptual Frameworks
The Lazarus paradigm of stress and coping will be presented first,
detailing the key points of the theory. Following this will be a
discussion of the elements of Piaget's theory of cognitive development
relevant to this study.
The Lazarus Paradigm of Stress and Coping
The model of stress and coping developed by Richard Lazarus uses a
cognitive phenomenological approach based on three key components: stress,
appraisal, and coping. Each of these constructs will be described as used
in the Lazarus model. A diagram of this process is presented in Figure 1.
Stress
Lazarus defines the concept of psychological stress as "a particular
relationship between the person and the environment that is appraised by
the person as taxing or exceeding his or her resources and endangering his
or her well-being" (Lazarus & Folkman, 1984a, pp. 19). Unlike other
perspectives, stress is not due to interaction with noxious stimuli in the
environment (Selye, 1980; Pearlin et al., 1981), but rather is due to a
transactional process between the person and the environment which results
in stress (Lazarus & Folkman, 1984a). In other words, stress only exists
if that person interprets the environmental events as stressful. As
implied in the above definition, a key element in the Lazarus model of
stress and coping is the process of appraisal.

Personal EnvironmentalVariables Variables
`s _TEvent
|Cognitive Appraisal:
_T Primary SecondaryN ... /Irrelevant Stress
Benign |Harm/Threat/Challenge
|Coping:
Problem EmotionFocused Focused
Reappraisal
Adaptation
Figure 1. Diagram of the Lazarus stress and coping process.

10
Appraisal
Appraisal is defined as, "an evaluative process that determines why
and to what extent a particular transaction or series of transactions
between the person and the environment is stressful" (Lazarus & Folkman,
1984a, pp. 19). Simply, appraisal is the process of assessing whether or
not an event is stressful.
As the definitions of stress and appraisal indicate, the process of
appraisal is dependent on both personal and environmental variables.
Lazarus has identified three general categories of personal factors that
may influence the appraisal process: 1) commitments or motivational
characteristics, 2) belief systems regarding personal control, and 3)
intellectual resources and skills (Cohen & Lazarus, 1983; Lazarus &
Folkman, 1984b). Based on these categories, the personal variables likely
to influence the appraisal process of the hospitalized child would include
the child's commitment to and need for his or her parents, personality
characteristics, and developmental level. Additionally, the child's
appraisal of the situation may be affected by the nature of the child's
illness and type and severity of symptoms, as the physical condition is
likely to impact the child's motivation, perception of control, and
cognitive functioning.
When identifying environmental factors that may affect the appraisal
process, Lazarus focuses on the properties of situations, rather than on
the situation itself, as no one event is appraised as equally stressful by
all persons. Common properties of situations that influence an appraisal
of stress are, 1) the novelty or the extent of prior experience with the
event, 2) event uncertainty or the likelihood an event will occur, 3) the
imminence or period of anticipation of the event, 4) the duration of the

11
event, 5) temporal uncertainty or not knowing when the event will occur,
and 6) ambiguity or a lack of clear environmental clues to the nature of
the situation (Lazarus & Folkman, 1984a). For the hospitalized child, the
novelty of the situation will depend on prior knowledge of the event
through personal experience or vicarious experience such as a family
member, friend, television, books, or preadmission teaching or
preprocedural preparation. Event uncertainty and the temporal elements of
imminence, duration, and uncertainty regarding the timing of the event are
a constant problem during hospitalization since protocols and hospital
policies make it difficult for medical personnel, much less the pediatric
patient, to predict with certainty if and when an event will occur.
Additionally, the child may not be able to interpret the clues that are
available from the environment, resulting in a state of ambiguity.
The relationship of the person and environment in the Lazarus model
is not merely an interaction of the two elements in which the effect of
each separate factor may be determined, but rather it is a two-way
interchange, or transaction. The person acts on and is acted on by the
environment. Both factors, person and environment, merge in the
transaction to form a new entity, different from the original separate
elements (Lazarus & Folkman, 1984 a ; Lazarus & Launier, 1978). As quoted
by Lazarus, "the whole is different from the sum of the parts" (1981, pp.
184). Thus, an event is appraised as stressful, or not stressful, based
on the merging of the unique characteristics of the person and situation
at that specific time.
Cognitive appraisal occurs when the transactional process is
evaluated for relevance to the person. It consists of three components:
primary appraisal, secondary appraisal, and reappraisal. Primary and

12
secondary appraisal take place simultaneously, despite the implied
hierarchy in the names (Lazarus & Folkman, 1984a). Reappraisal follows an
irnitial appraisal process.
Primary appraisal. Primary appraisal is "the process of evaluating
the significance of a transaction for one's wellbeing" (Lazarus, 1981, pp.
192) . The questions are asked, "Am I in trouble or being benefited, now
or in the future, and in what way?" (Lazarus & Folkman, 1984 a, pp. 31).
In other words, the person is determining how and when the situation will
be helpful or harmful.
During primary appraisal it is determined if the event is
irrelevant, benign-positive, or stressful for the individual. An event is
appraised as irrelevant if the person has determined that it has no impact
for their well-being, either positive or negative. A benign- positive
appraisal is one in which the event appears to maintain or increase the
individual's well-being, generally resulting in a feeling of joy, pleasure
or relief. If the event is appraised as stressful, the person perceives
his personal resources as inadequate to deal with the situation. (Cohen
& Lazarus, 1983; Lazarus, 1981; Lazarus & Folkman, 1984a, 1984b.)
An appraisal of stress is further classified as one of harm 'or loss,
threat, or challenge. Harm or loss indicates that the injury, physical,
psychological, or social, has already occurred. Threat indicates a future
occurrence of harm, and is likely to occur when the person perceives the
environment as dangerous and does not believe he is able to master the
situation. Challenge indicates the person believes he may be successful
in dealing with the situation regardless of the problems associated with
it. Whereas with an appraisal of harm or loss the person must cope with
the damage that has happened, an appraisal of threat or challenge allows

13
the person to use anticipatory coping strategies. (Cohen & Lazarus, 1983;
Lazarus, 1981; Lazarus & Folkman, 1984a and 1984b. )
Secondary appraisal. Whereas in primary appraisal the focus is
individual appraisal of personal well-being, in secondary appraisal the
focus is on the appraisal of the resources available for coping (Lazarus
& Launier, 1978). The question being asked is, "What can I do?" (Folkman,
1984, pp. 842). Through an evaluative process that may range from
conscious thought to unconscious reaction (Cohen & Lazarus, 1979), the
person evaluates the potential effectiveness of available resources and
options. Resources would include the individual's physical health and
capabilities; psychological characteristics and functioning; social
support systems; and material assets (Folkman, 1984). Options would
involve behaviors such as information seeking, acceptance, restraint, or
acting to change the situation (Folkman, Lazarus, Dunkel-Schetter,
DeLongis, & Gruen, 1986). The probable effectiveness of the identified
available resources or options in helping the person deal with the threat
to personal well-being will influence the appraisal of the situation as
harmful or challenging. A situation in which the person has a sense of
control is more likely to be appraised as challenging than will
circumstances beyond the control of the person (Lazarus & Folkman, 1984a).
Thus, the processes of primary and secondary appraisal interact and are
highly interdependent (Folkman et al., 1986; Lazarus, 1981).
Reappraisal. Lazarus defines reappraisal as an, "appraisal that
follows an earlier appraisal in the same encounter and modifies it"
(Lazarus & Folkman, 1984a, pp. 38). The transaction between the person
and environment is a dynamic process, subject to change due to feedback
from within the system or from new information outside the system.

14
Whenever a change of this nature occurs, reappraisal of the event is
rhe cessary, essentially beginning a new cycle in the process of appraisal
of stress and coping. (Lazarus, 1981; Lazarus & Folkman, 1984 a ; Lazarus
& Laurier, 1978).
The Coping Process
In this section, four aspects of coping will be discussed. First
the definition of coping as used by Lazarus will be given and analyzed.
Second, the functions of coping will be presented. Third, modes of coping
will be discussed. Finally, the outcome of the coping process will be
briefly addressed.
Definition of coping. Lazarus defines coping as, "constantly
changing cognitive and behavioral efforts to manage specific external
and/or internal demands that are appraised as taxing or exceeding the
resources of the person" (Lazarus & Folkman, 1984a, pp. 141). This
definition encompasses several elements that are essential to
understanding the Lazarus perspective of coping. The first element is
that coping is a process. It involves all that a person actually does to
deal with the situations appraised as stressful. This perspective differs
from coping research that focuses on what the person is likely to do: the
coping style, disposition, or trait (Lazarus & Launier, 1978). The
typical coping style of a person and the coping behaviors actually used
in a situation may differ greatly, due to the transactional nature of
stress appraisal. An a priori determination of coping behaviors cannot be
completely accurate as the unique person-environment situation has not yet
occurred. Because of this, Lazarus encourages naturalistic research,studying coping reactions to stress as it occurs in the person's real
world (Lazarus, 1981).

15
A second important element of the definition is that coping is
dependent on the psychological mediation that occurs during the appraisal
process (Cohen & Lazarus, 1983; Lazarus & Folkman, 1984b). Thus, coping
is contextual, conditional upon the person's appraisal of the demands of
the situation and available resources (Folkman et al., 1986). Only if the
situation has been appraised as stressful and the resources available are
insufficient to meet the demand of the situation will coping occur.
A third element of the above definition is that coping is
differentiated from automatized reactions (Lazarus & Folkman, 1984).
Coping requires effort. Automatized reactions occur without effort.
Therefore, a situation managed by an automatic reaction or reflex has not
required the use of coping. Interestingly, due to a changes in appraisal,
a situation may require coping at one time, and at another time the
response may be automatic. For example, while driving in a new city a
high level of cognitive and behavioral effort or coping is required, but
after a becoming familiar with the area and traffic patterns, driving
becomes routine or automatized. This automatic behavior will continue
unless a new demand develops, such as road construction, that requires
effort and resumption of coping behaviors. Children's responses to
situations may also fluctuate between automatized reactions and coping
behaviors. For example, beginning school may be a stressful situation for
many children, requiring coping to deal with the unknown routines and
expectations. After a period of time the child becomes familiar with the
experience and automatically reacts according to the immediate situation.
However, a change in the routine, such as moving to a new school or
entering the less structured environment of junior high, places new
demands on the child that cannot be adequately met with former automatic

16
reactions, necessitating the use of coping behaviors until the situation
is no longer appraised as stressful. In sum, situations that can be
managed by routine behaviors do not require coping. It is only when the
situation is appraised as taxing or exceeding the person's resources that
the effort of coping is required.
A fourth element in the definition is that any effort to manage the
situation is considered to be coping, regardless of whether or not the
behavior is effective. A value judgement of "good" or "bad" coping is not
made (Folkman et al., 1986), because it is difficult to accurately assess
the person-environment transaction to determine if the choice of coping
behavior is appropriate.
A fifth point derived from the definition is that emphasis is placed
on the attempt to manage, not master, the situation. Mastery implies that
the person has changed the situation or gained control of it. This
perspective often is not realistic because many situations in life cannot
be changed or mastered, such as illness, injury, and hospitalization.
Instead of mastery, the person does have the option of attempting to
manage the situation by controlling his or her personal response to the
situation through coping behaviors such as minimization, avoidance,
tolerance, or acceptance (Cohen & Lazarus, 1983; Lazarus & Folkman,
1984a).
The final point to be drawn from the definition is the distinction
between coping and adaptation. Coping is the process of dealing with a
situation appraised as stressful. Adaptation is the outcome of this
process. Unlike coping, adaptation may be evaluated as either beneficial
or detrimental to the person. This distinction prevents the confounding

17
of the concept of coping with the outcomes it is used to explain (Lazarus
& Folkman, 1984a; Folkman et al., 1986).
Functions of coping. Lazarus has identified two principal purposes
or functions of coping, problem-focused coping and emotion-focused coping.
Problem-focused coping involves attempts to change the demand that has
resulted in the appraisal of stress. The source of the demand may be
either external, such as a challenging event, or internal, such as
personal expectations. Emotion-focused coping is directed toward managing
the emotional reaction, physical or behavioral, to the stress. Generally,
both modes are used to deal with a stressful situation. A study of
middle-age adults reported using both problem-focused and emotion-focused
coping in 98% of stressful transactions (Folkman & Lazarus, 1980), and a
study of college students facing examinations indicated that both forms of
coping were used 96% of the time (Folkman & Lazarus, 1985). The inter
action of these two functions of coping may be either positive, enhancing
the person's coping process, or negative, counteracting each other and
interfering with optimal usefulness (Cohen & Lazarus, 1983).
Modes of coping. Lazarus and colleagues have theoretically
identified five modes, or categories, of coping that are used in response
to a stressful situation. Information seeking is used to gather
information about the situation and to try to determine appropriate
methods of dealing with it. Direct action includes any behavioral act
directed toward dealing with either the problem or the emotional reaction
to the stress. Inhibition of action is refraining from action. Intra
psychic processes are cognitive activities that may occur consciously or
unconsciously. Turning to others involves seeking support from other
individuals. Early descriptions of the modes of coping include only the

18
first four categories. The need to include the final mode was recognized
in about 1979. (Cohen & Lazarus, 1979; Cohen & Lazarus, 1983; Lazarus &
Launier, 1978. )
Adaptational Outcomes of the Stress and Coping Process
The purpose of examining the process of stress, appraisal, and
coping is to understand the relationship of these elements to the person's
adaptation. Lazarus and colleagues have identified three classes of
adaptational outcomes: physiological, psychological, and social (Cohen &
Lazarus, 1983; Lazarus & Folkman, 1984a).
Lazarus postulates that coping may influence the physiological
status of a person through three pathways: 1) the neurochemical system, 2)
increased involvement with dangerous substances or behaviors, and 3) by
delaying or avoidance of health-care behaviors (Lazarus & Folkman, 1984a).
Similarly, the coping process may affect the psychological well-being of
an individual by: 1) influencing the current emotional status of the
person experiencing a stressful situation (Folkman & Lazarus, 1988), and
by 2) the outcome of the specific stressful transaction on the
psychological well-being person over time (Lazarus & Folkman, 1984a).
Finally, coping processes may influence the social well-being of the
person through the appropriateness of the fit between 1) the person's
primary appraisal of stress and the actual event taking place, and 2) the
person's secondary appraisal of coping resources and the actual demands of
the situation (Cohen & Lazarus, 1983; Lazarus & Folkman, 1984a).
In summary, stress results from a transactional process between the
person and the environment. Appraisal is the cognitive process ofevaluating an environmental situation to determine if it is personally
threatening, a process influenced by variables related to both the person

19
and environment. Coping is the process of dealing with the situation that
has been evaluated as stressful. Two purposes of coping have been
identified: problem solving and emotion-regulation, functions that often
occur simultaneously when dealing with stress. In order to accomplish
these purposes, five types, or modes, of coping may be used: information
seeking, direct action, inhibition of action, intrapsychic process, and
seeking support from others. The outcomes of coping may be determined by
assessing the effect on the psychological, physiological, or social
aspects of the person.
Having carefully examined the major components of the Lazarus
paradigm of stress, appraisal and coping, it is necessary to recognize
that the theory was not developed for the explicit purpose of studying
children. Therefore the child's cognitive functioning must be understood
to determine how the child's cognitive processes of stress and coping
might function. To meet this need, Piaget's theory of cognitive
development will be examined.
Piaget's Theory of Cognitive Development
Jean Piaget's (1896-1980) theory of cognitive development describes
the process of intellectual maturation as evidenced by the child's
understanding of his or her world. Rather than focusing on quantitative
aspects of intelligence, such as measurement and stability of IQ, Piaget
chose to study qualitative characteristics of the child's thinking, such
as common characteristics in the thought processes of children and the
differences between the thinking of children from birth throughadolescence (Brainerd, 1978). Two key concepts of Piaget's theory are the

20
process through which cognitive development occurs and the stages of
cognitive development.
The Process of Cognitive Development
Piaget believed that intellectual development occurs through the
process of growth and change in cognitive structures (Brainerd, 1978);
structures being the internalized, mental operations that constitute the
process of thinking and understanding (Piaget, 1983). Developmental
changes in these structures occur through a process of self-regulation or
equilibration (Piaget & Inhelder, 1969), defined as, "a set of active
reactions of the subject to external disturbances" (Piaget, 1983, pp.
122). As the child becomes aware of external elements in the world that
cannot be understood according to his or her current cognitive structures,
a disequilibrium occurs. Because the basic functions of cognition are
organization and adaption (Brainerd, 1978), the disturbance must be
addressed and equilibrium reestablished.-
The processes through which equilibrium is reestablished are
assimilation and accommodation. Piaget (1983, pp. 106) defines
assimilation as, "the integration of external elements into evolving or
completed structures of an organism." Practically, this means that the
reality of the situation is altered to fit the child's current patterns of
understanding. For example, when a hot water bottle is first encountered,
the child may think it is a type of pillow. However, as the child
observes how the hot water bottle is used by adults, it becomes evident
that the object is different from a pillow, resulting in the need for the
child to change the existing mental structures to incorporate the new
object. This portion of the process, accommodation, is defined by Piaget
(1983, pp. 107) as, ". . . any modification of assimilatory scheme or

21
structure by the elements it assimilates." In essence, the child's
thought patterns have been changed to fit the reality of the situation.
Assimilation and accommodation are considered by Piaget (1952, 1954,
1983) to be complimentary aspects of adaptation, always occurring
together, yet the two processes are in opposition. Assimilation attempts
to maintain the status quo of the child's thinking, whereas accommodation
changes the child's cognitive structures to correspond more directly
reality (Piaget, 1954). As equilibration is achieved through assimilation
and accommodation, the child's cognitive structures are gradually modified
and broadened, resulting in an advancement of the child's cognitive
development (Brainerd, 1978).
As the child develops, the invariant functions of organization and
adaptation remain stable. However, the child's cognitive structures
change due to the adaptive processes of assimilation and accommodation.
Piaget observed that these structural changes occurred in a similar
sequence in different children, an observation that lead to the
formulation of a model of developmental stages of cognitive maturation.
Stages of Cognitive Development
From his observations, Piaget identified distinctive stages in a
child's cognitive development, consisting of behaviors indicative of
differences in the cognitive structure of the child. Basic principles of
this portion of the theory are that the stages are qualitatively
different, that they occur in an universally invariant sequence, that each
stage incorporates and builds on the preceding stage, and that successful
achievement of each stage requires integration of the structures into s
functional whole (Brainerd, 1978). Although support for some of these

22
principles is more theoretical than empirical, Piaget's stages of
development have been widely accepted.
Piaget (1957) identified four stages of a child's cognitive
development: 1) sensorimotor, 2) preoperational, 3) concrete operations,
and 4) formal operations, although at times he combined the second and
third stages under the heading of representative intelligence (Piaget,
1983). For the purposes of this overview, the four stage approach will be
used. It should be noted that the age range provided for each stage is an
approximation. Piaget believed that the actual emergence of the stage
would depend on the child's individual characteristics and environment
(Brainerd, 1978; Ginsburg & Opper, 1988). Although the current study
focuses on children within the age range of concrete-operations, an
understanding of the other stages provides a necessary framework for
understanding the discussion of the findings.
Sensorimotor intelligence. The first stage, sensorimotor, extends
from birth to approximately eighteen months or two years of age. From his
observations, Piaget believed that infants are not capable of internalized
representation (thought), but rather that their behavior indicated a
sequential developmental pattern of motoric schemes or action sequences;
precursors to the development of cognitive structures by older children
(Brainerd, 1978; Piaget, 1957). Two subperiods occur. The first extends
from birth until 7 or 9 months; a period of concentration on the child's
own body. During this time, the child progresses through the first three
substages, moving from simple reflex schemes to a beginning awareness of
the external world. The second subperiod involves objectivization and
spatialization of the child's schemes. During the corresponding last
three substages, the child learns to coordinate schemes, experiment with

23
the schemes to observe differing results, and shows evidence of the
beginning of internalized cognitive functioning (Beilin, 1989; Piaget,
1983). The primary evidence of the precursors of cognitive structure
during this stage is the development of object permanence, the awareness
that an object continues to exist after it is no longer visible (Ginsburg
& Opper, 1988; Crain, 1985; Piaget, 1957).
Preoperational thought. The second stage, pre-operational thought,
extends from approximately two until seven years. During these years the
child develops the cognitive ability of mental representation, "the
internalization of actions into thoughts" (Piaget, 1957, pp. 11). Mental
representation is accomplished through the child's acquisition of semiotic
function, or the ability to use mental symbols to represent a personal,
knowledge of something (Ginsburg & Opper, 1988; Piaget, 1983). Because of
the individualization of the symbols, the child's mental representations
often are somewhat idiosyncratic and may be quite different from that of
the adult, or even of another child the same age.
Although Piaget tended to emphasize what the child in this stage of
development could not yet do, the preoperational child does acquire
several important abilities that give evidence of development of the
cognitive structures. First, Piaget believed that true language, as
semiotic function, emerges during the preoperational period. Earlier
vocalizations of infants do not involve mental representation, and
therefore are not language (Brainerd, 1978; Ginsburg & Opper, 1988).
Second, an understanding of unidirectional functions develops (Beilin,
1989; Piaget, 1983), the ability to understand that if a specific event
occurs, another will follow it, or y - f(x) (Piaget, 1983, pp. 110),

24
an important step in the development of mental functioning. Third, the
child develops the ability to understand correspondences (comparisons)
between objects and event, a necessary precursor to the concept of
conservation, classification, and relations (Beilin, 1989; Ginsburg &
Opper, 1988).
Several characteristics of the preoperational child distinguish this
stage from the next and must undergo gradual restructuring. First,
centration or egocentrism, a difficulty in considering two differing
viewpoints or aspects of a situation at a time, is a typical
characteristic of the preoperational child (Brainerd, 1978). Because of
this, the child's language and play occurs in a parallel, rather than
interactive, pattern. Centration also interferes with the child's
achievement of conservation tasks because the child is able to focus on
only one dimension at a time (Crain, 1985; Ginsburg & Opper, 1988). A
second factor interfering with conservation is the lack of reversibility
(Piaget, 1957). Although the development of the unidirectional function
is fundamental, the child cannot yet mentally reverse the action and
understand that an object or situation may return to its original state,
hindering an understanding of the real world.
Concrete operational thought. The third stage, concrete operations,
begins to emerge about age seven and extends until approximately age
eleven. Operations are reversible mental representations of actions that
are organized into larger systems (Piaget & Inhelder, 1969; Siegler,
1986). The operations are concrete in that the child's thinking is
limited to tangible objects or situations (Ginsburg & Opper, 1988; Piaget,
1957; Piaget & Inhelder, 1969).

25
During the concrete operational stage, the cognitive structure
undergoes a number of important changes. First, the child moves from
centration to decentration, acquiring the ability to think about two or
more aspects of a situation simultaneously (Ginsburg & Opper, 1988).
Second, the child develops reversibility, the ability to mentally reverse
a situation without seeing it done physically. The two key aspects of
reversibility are inversion and reciprocity. Inversion, also called
negation, is the ability to invert an operation, to think through a
situation in one direction and then reverse the thinking process to return
the situation to the original state (Brainerd, 1978; Piaget & Inhelder,
1969). Reciprocity, also called compensation, results in reversibility in
a different manner. This principle is based on the law that for every
action there is a reciprocal action that will compensate or nullify the
first action (Brainerd, 1978; Piaget & Inhelder, 1969). The difference
between these types of reversibility is that inversion reverses the
original process, whereas reciprocity achieves reversibility through a
different process.
The development of decentration and reversibility allows the
concrete operational child to achieve a number of cognitive abilities that
were not present in the preoperational stage including conservation,
classification, and relations. Conservation is the understanding that the
quantitative quality of a substance does not change when the form of the
substance is changed (Brainerd, 1978). Acquisition of this concept begins
around 7 or 8 years with the conservation of substance, illustrated by the
classical liquid or clay experiments, conservation of weight occurs at
nine or ten years, and conservation of volume at eleven or twelve (Piaget,
1957; Piaget & Inhelder, 1969), an example of horizontal decalage

26
(Ginsburg & Opper, 1988). Classification is the grouping of things that
share a similar property accompanied by an understanding of class
boundaries (intension) and membership (extension) (Ginsburg & Opper,
1988). The preoperational child forms graphic collections, a grouping of
objects forming a pattern rather than a class. As the child moves toward
concrete operations, non-graphic collections are made, grouping of objects
according to one or two properties. It is not until 8 years or later that
the child acquires the hierarchial concept of the relationship of a
subclass to its general class (Ginsburg & Opper, 1988; Inhelder & Piaget,
1964; Piaget & Inhelder, 1969). Relations or seriation is the arrangement
of objects according to increase or decrease of a property such as size or
color (Piaget & Inhelder, 1969). Given a set of objects to arrangeserially, the preoperational child may determine the relationship of pairs
of items, but not the whole set simultaneously. Around age seven the
child is able to create a hierarchial arrangement of all the items without
using a trial and error process, evidence that the child is using mental
representation of the objects to determine the serial relationships.
Formal operational thinking. The fourth stage, formal operations,
begins to develop at 11 or 12 years of age and, when achieved at about age
15 (Brainerd, 1978; Piaget, 1957), forms the basis for adult thinking.
Formal operations differs from concrete operations in that the child
develops the ability to think about things beyond his or her own
experience and to formulate alternative options through manipulation of
these mental representations, a process called hypothetico-deductive, or
propositional, thinking (Beilin, 1989; Brainerd, 1978).
The thinking that takes place during the stage of formal operations
is made possible by the combination of the inversion and reciprocity of
S
3.

27
the concrete operational stage into a structural whole (Beilin, 1989;
Piaget & Inhelder, 1969). This new structure is known as the INRC group;
I representing the identity of the group in question, N representing the
inverse operation, R representing the reciprocal operation, and C
representing the correlative operation (Brainerd, 1978; Piaget & Inhelder,
1969). Through the use of these operations the adolescent or adult is
able to consider any possible combination of transformations pertaining to
either a concrete or hypothetical situation.
Because of the emergence of propositional thinking, the adolescent
develops new mental schemes not possible during the concrete stage of
thinking. These include an understanding of 1) proportions: the
equivalence of ratios between quantities; 2) probability: the occurrence
of events by change; 3) double systems of references: the positive or
negative influence of one factor on another, the classical example being
the motion of a snail on a movable board; and 4) mechanical or hydrostatic
equilibrium: Newton's physical principle of action and reaction (Brainerd,
1978; Piaget & Inhelder, 1969).
In summary, Piaget's theory focuses on the process of cognitive
development from infancy through adolescence when patterns of adult
thinking are achieved. The cognitive structures undergo continual change
as the child gradually becomes aware of the real world and adapts his or
her thought processes to it. Adaption is achieved as assimilation and
accommodation act to maintain or reestablish equilibrium. Four
qualitatively distinctive stages of cognitive development were identified
by Piaget: 1) sensorimotor, 2) preoperational, 3) concrete operations, and
4) formal operations. The cognitive structure of the child at each stage
determines the cognitive abilities, such as object permanence during the

28
first stage, uni-directional functions during the second stage,
conservation and classification during the third stage, and propositional
thinking during the fourth stage.
Clearly, children's thinking, as described by Piaget, differs from
that of adults. When proposing the use of the Lazarus paradigm of stress
and coping to study children's reactions during hospitalization, the
question must be asked: May the theory be appropriately applied to
children? This concern will be discussed in the following section.
Application of Lazarus' Theory to Children
Because the basis of Lazarus's stress and coping theory is cognitive
appraisal, and because children's cognitive functioning differs from that
of adults, it was necessary to examine the key elements of the stress and
coping theory to determine if it could be used appropriately to study the
stress and coping of children. Factors considered were the child's
ability to engage in appraisal, the child's ability to determine personal
irrelevance of a situation, and the child's use of problem solving
techniques as a resource for coping.
The first issue addressed was the child's ability to engage in the
process of appraisal. At what age are children able to appraise an event
and is there a relation between appraisal and Piaget's concept of
classification? The question of classification arose because to appraise
an event as benign-positive, irrelevant, or stressful some type of
classificatory function must occur. As noted previously, formal
classificatory ability, involving class inclusion, intension, and
extension, is achieved during the stage of concrete operations (Brainerd,
1978; Ginsburg & Opper, 1988). However, precursors to classification do
29
occur during the sensorimotor and preoperational stages (Piaget &
Inhelder, 1969). In a summary of research concerning classification,
Gelman and Baillargeon (1983) discussed the indications that children as
young as 12 months appear to perceive and classify objects as similar or
different. Therefore it is reasonable to assume that from a very early
age, children are able to classify an object or event, although not
according to the formal properties of the concept.
The process of appraisal, however, is not identical with that of
classification. While general classification of the object or event is
necessary for appraisal, it is not sufficient. The child must also
determine the implications of the event for personal well-being, a element
not involved in classification. A study by Levy (1960) illustrates the
interaction of the classification and appraisal concepts. Observing the
reactions of children receiving injections, Levy noted that children as
young as six months of age who had received previous shots reacted
negatively to the appearance of a needle and syringe. This gives evidence
that the child recognized and classified the object based on prior
experience and then appraised the situation as having personal
implications for well-being. To continue this example, the same six month
old child would likely have reacted positively to the sight of a bottle,
additional confirmation that the very young child is able to appraise the
personal implications of an event for well-being. Although a young child
may not have achieved an understanding of class inclusion properties, he
or she does appear to appraise an event based on the current level of
cognitive functioning. In this manner, appraisal may be considered to be
an age independent function; whether or not an adult would consider a

30
child's appraisal as accurate, if the child appraises an event as
stressful, it is stressful for that child.
A second issue concerning application of the Lazarus theory of
stress and coping to children centers on the child's ability to appraise
of an event as irrelevant to personal well-being. Although children of
all ages have some form of egocentric thought (Inhelder & Piaget, 1958),
it is the child less than 7 years of age, not yet in the stage of concrete
operations, who is incapable of taking another's role or viewpoint
(Piaget, 1959). A child who is unable to take the viewpoint of another
thinks that all events (of which he or she is aware) occur because of him
or for his benefit and therefore will assume that all events have
implications for his personal well-being, either beneficial or stressful.
Therefore, it is likely that the child in the sensorimotor or
preoperational stages is incapable of appraising an event as irrelevant to
their well-being. In contrast, the child who has experienced decentration
in the process of cognitive restructuring will understand that not all
events are personally relevant, and will be more likely to judge some
events as irrelevant to personal well-being. Thus, the appropriateness of
the concept of irrelevant appraisal will depend on the age of the children
being studied.
A third issue when using the Lazarus paradigm to study the process
of stress and coping in children is related to secondary appraisal of
coping resources and the individual's problem solving ability. In
Piaget's research, the process of children's thinking was studied by
observing the child in problem solving activities such as finding hidden
objects, conservation tasks, or establishing equilibrium on a balance
scale. In general, children tended to use trial and error to deal with a
º

31
novel situation until they discovered the principles needed for that
activity. Once the principles were grasped, the child quickly achieved
mastery of the problem, the age of mastery varying with the specific
problem. The trial and error process does require the child to think of
alternative solutions to the problem, but the total range of alternative
actions and the potential effectiveness of one solution as compared to
another is not considered a priori. It is only in the stage of formal
operations that the adolescent becomes able to engage in hypothetico
deductive reasoning, developing propositions and systematically testing
the results of alternative solutions (Inhelder & Piaget, 1958).
Although Piaget's research using problem solving situations did not
involve events likely to result in an appraisal of stress by the child,
the child's process of using the personal resource of problem solving when
dealing with a stressful event would be similar. When confronted with a
stressful event, the child will act according to the most apparent, method
of dealing with the event, rather than selecting the method most likely to
produce the desired outcome as would the adolescent or adult. If the
first method is not successful, an alternative will be used, until either
a successful mode is discovered or the event is over. From experience,
observation of other children, or guidance from an adult, the child may
learn what behaviors are most likely to be effective in coping with a
stressful situation and will selectively use these behaviors in the
problem solving process of secondary appraisal.
In summary, examination of these key elements has demonstrated
several important points. First, the child is able to engage in the
process of appraisal from a very early age, although the result of the
appraisal may differ from that of an adult in the same situation. Because
s

32
appraisal is based on a individual interpretation of the transaction
between the person and environment, if the individual, in this case a
child, appraises as event as stressful, it is stressful to that child,
whether or not an adult, or even another child, would agree. Second, the
ability of the child to appraise an event as irrelevant to personal well
being will be dependent on the child's current thinking in terms of the
concept of centration/decentration. If the child has developed the
understanding that all events do not have implications for personal well
being, then that child will be able to appraise an event as irrelevant.
Acquisition of this cognitive process generally occurs during the
transition period between the preoperational and concrete operational
stages. Finally, from an early age the child is able to use problem
solving techniques to cope with perplexing or stressful events. However,
it is not until the child is able to use propositional thinking that
problem solving is used in a systematic manner. Until that time, coping
behaviors may occur in a haphazard manner or may reflect prior experience
despite the potentially greater efficacy of untried coping behaviors. In
conclusion, because the Lazarus paradigm considers stress to be a personal
phenomenon based on individual's thinking about the event and because
coping is based on the individual's personal resources, such as the
current cognitive approach to problem solving, this theory permits
examination of the unique individual and developmental differences in
stress and coping process, rendering it an appropriate model for use in
studying the stress and coping of children.
ºs*

33
Literature Review
In developing this study, literature pertaining to the constructs of
children's stress and coping was reviewed with an emphasis on research
directly relating to hospitalized school-age children, although other
studies dealing with stress and coping of non-hospitalized child or other
age groups were included as appropriate. The questions guiding this
literature review were, 1) What events during hospitalization do school
age children appraise as stressful?, 2) What coping behaviors do school
age children use during hospitalization, dental care, or other health
related situations?, 3) What variables have been studied in relation to
the child's stress and coping process during hospitalization?
Accordingly, the first section will analyze the information available
pertaining to events or situations children appraise as stressful while
hospitalized. The second section will review studies focusing on the
coping behaviors used by school-age children to deal with stress during
hospitalization or other health care situations. The final section will
examine research relating to the variables responsible for differences in
children's appraisal of stress and the resulting coping behaviors.
Research on Sources of Stress during Hospitalization
A basic premise of this study was that the experience of
hospitalization is psychologically upsetting for a child. Numerous
authors have referred to the disturbing effect of hospitalization on
children. In their classic work on children's emotional reactions to
hospitalization, Prugh, Staub, Sands, Kirschbaum, & Lenihan (1953)
concluded that all the subjects showed some reaction to the event of

34
hospitalization as distinct from the reaction to illness. Later Prugh
(1965) generalized this conclusion to include all hospitalized children.
Sipowicz and Vernon (1965), following a comparison of hospitalized and
nonhospitalized twins, concluded that even a brief hospitalization is
psychologically upsetting to children. Oremland and Oremland (1973) and
Goslin (1978) both describe the event of hospitalization as a life crisis
for a child. Adams (1965) and Illingworth (1958) discuss the trauma
associated with hospitalization, and Erickson (1963) states, "Illness and
hospitalization are traumatic at every stage and age of development" (pp.
47). Erickson also unequivocally identified hospitalization as stressful
for children by entitling a paper discussing anxiety of the pediatric
patient, Stress in the Pediatric Ward (1972), a view that is supported by
both Belmont (1970) and Langford (1961). Finally, in the extensive
literature reviews by Vernon, Foley, Sipowicz, and Schulman (1965) and by
Thompson (1985), the conclusion was reached that research indicates
hospitalization is upsetting to a child."
As the importance of this body of work has been recognized, the
focus of research has shifted toward events thought to be responsible for
the child's psychological upset. Empirical knowledge of the types of
events hospitalized children are likely to appraise as stressful comes
from two sources; indirectly through the observation and interaction with
children and directly from interviewing the child. The majority of
* The concept of psychological upset was defined, based on the workof Gellert (1958) and Chapman, Loeb, and Gibbons (1956), as a situation inwhich the child manifests behaviors such as crying of varying intensities,clinging to parents, eating problems, sleep disturbances, lack of controlof elimination processes, regression, withdrawal, restlessness, anxiety,fear of medical procedures, personnel and hospitals, death fears, tics,excessive concern with bodily functions, and destructive behavior (Vernonet al., 1965, pp. 5, 6).
;º

35
theoretical articles and research reports have been based on the indirect
knowledge, assuming that adults are able to correctly determine which
events will be stressful for the hospitalized child and then proceeding
with guidelines for preprocedural preparation or experimental testing of
various forms of intervention. Only a small portion of the literature
reports what the child actually appraised as stressful during
hospitalization. The sources of stress identified in these two bodies of
literature will be presented and commonalities discussed.
Sources of Children's Stress during Hospitalization Identified by Adults
Studies of children's stress during hospitalization generally have
proceeded on the basis that adults know what events are stressful for the
child. In the literature over three dozen sources of stress for the
hospitalized child have been identified. To analyze this information
common themes will be identified using the five categories of threats
identified by Visintainer and Wolfer (1975) and Wolfer and Visintainer
(1975): 1) physical harm or bodily injury, 2) separation, 3) the strange
or unknown, 4) uncertainty about limits, and 5) loss of control.
The category, physical harm or bodily injury, is perhaps the most
recognized and discussed area of threat and stress for the hospitalized
child. Children fear intrusion into their body (Ritchie, Caty, &
Bllerton, 1984; Ellerton, Caty, & Ritchie 1985) which may occur in the
Process of routine procedures such a temperature measurement and
*dministration of an oral medication (Erickson, 1958a, 1958b), in any
Procedure associated with needles, such as injections, I. V.'s. and
Venipuncture (Eiser & Patterson, 1984; Erickson, 1958a, 1958b, 1972;
Langford 1961), or in any of the multitude of diagnostic or therapeuticProcedures such as surgery, cardiac catheterization, cystoscoP+* *
º
º

36
bronchoscopic exams, paracentesis, or lumbar puncture (Langford, 1961;
Prugh et al., 1953). They fear mutilation during cast removal (Johnson,
Kirchhoff, & Endress, 1975) and during procedures or surgery (Barowsky,
1978; Erickson, 1972; Heavenrich, 1963; Hughes, 1967; Hughes 1982;
Jessner, Blom, & Waldfogel, 1952; Langford 1961; Prugh et al., 1953;
Vernon et al., 1965). They fear pain (Eiser & Patterson, 1984; Gofman,
Buckman, & Schade, 1957; Langford, 1961; May & Sparks, 1983; Rankin, 1988;
Stevens, 1986). They fear death by specific means such as suffocation,
drowning, starvation (Erickson, 1972), drugs (Astin 1977), being crushed
by radiological equipment (Fischman & Friedland, 1986), or death in
general (Erickson, 1972; Hughes, 1967; Prugh et al., 1953; Rankin, 1988;
Vernon et al., 1965).
The second category of threat, separation and abandonment, has been
well documented as a source of stress to the hospitalized child (Bowlby,
1973; Jessner, Blom, & Waldfogel, 1952; Robertson, 1970; Vernon et al.,
1965). Although children between the ages of 6 months and 3 to 4 years
demonstrate the most pronounced effects of separation (Prugh et al., 1953;
Vernon et al., 1965), older children also find separation from parents to
be a difficult experience (Erickson, 1965; May & Sparks, 1983; Prugh et
al., 1965).
The third category of threat or stress for the child is the strange
and the unknown. Heavenrich (1963), Lambert (1984), Meeks (1970), and
Thompson and Stanford (1981), as well as Visintainer and Wolfer (1975),
identify unfamiliarity with the hospital as a source of stress for
children.
The fourth category of potential stress for the child is uncertainty
**&arding limits and unacceptable behavior. Limit setting is a basic
s
º

37
principle of child discipline (Wise, 1986). However, it was mentioned by
only two authors (Lambert, 1984; Visintainer & Wolfer, 1975) in relation
to the hospitalized child. Perhaps uncertainty regarding behavioral
expectations is not as obvious a source of stress for the child as
intrusive procedures or separation from parents, but without such
structure, the child cannot know how to adapt his or her routine actions
to fit the hospital situation. To decrease stress, the child needs to be
told what behavior is acceptable and the reasons for the expectations.
The fifth category that may cause stress in the hospitalized child
is loss of control, both of the environment and of self (Heavenrich, 1963;
Lambert, 1984; Visintainer & Wolfer, 1975). The physical restrictions of
immobilization (Blom, 1958; Erickson, 1965, 1972; Freud, 1952; Thompson,
1985) or confinement, such as isolation (Kueffner, 1975; McGuire,
Shepherd, & Greco, 1978; Powazek, Goff, Schyving, & Paulson, 1978;
Thompson, 1985) are particularly stressful to the child due to hinderingthe child's normal activities and preventing release of stress and tension
through action. Another source of stress related to loss of control is
anesthesia and loss of consciousness (Blom, 1958; Erickson, 1965; Hughes,
1967; Thompson & Stanford, 1981). Children often fear what might happen
to them while under anesthesia, and also what they might do when not in
full control of their impulses (Jessner, Blom, & Waldfogel 1952). This
fear is more prevalent in the late school-age years (Erickson, 1965;
Hughes, 1967).
While the impressions of adults, based on observation and
interaction with hospitalized children, regarding the events children find
**ressful during hospitalization are likely to be accurate, it is possible
that not all possible sources of stress may be identified in this manner.
º,
º
r*
i
º

38
It is important to find out directly from the child what aspects of
hospitalization are stressful.
Sources of Stress during Hospitalization Identified by Children
An extensive literature search resulted in only five studies in
which the school-age child's identification of stressful events during
hospitalization was assessed. The most comprehensive of these was done by
Menke (1972). For the purpose of identifying the stimuli that
hospitalized children perceive as stressful and the relationship between
these stimuli and the variables of age, gender, medical or surgical
diagnosis, length of admission, preparation for hospitalization, and prior
separation from family, the author used a self-developed instrument, based
on projective assessment techniques, to ascertain sources of stress for
hospitalized children, ages 4 to 12 years. One hundred and four children
were asked to respond to a set of 19 cards with pictures of stressful and
nonstressful stimuli relating to hospital procedures (a nurse, doctor.thermometer, hospital gown, hospital bed, medications, syringe, and
stethoscope) or relating to stimuli not normally associated with the
hospital (a man, woman, boy, girl, baby, dog, cat, food, toys, house, and
school). The stressful stimuli were selected based on the researcher's
experience with children, the literature, and a group of expert judges.
The child was asked to pick a card and tell what he or she thought about
the pictured item, a procedure that was repeated until all the cards were
used or the child declined to continue. Following the cards, the children
Were asked open-ended questions about their reaction to being in the
hospital. The children's responses were coded as stressful, nonstressful,* no reaction. All but one of the cards, the picture of toys, "**
identified as stressful by one or more children, and 18 additional
s
.
º
39 º,
stressful stimuli were mentioned during the interview. Analysis of the
data indicated that injections, hospital gowns, thermometers, pain,
confinement in bed, and separation from mother were the most frequently
cited sources of stress for the children. Of the variables examined, only
two factors, length of hospitalization and preparation for
hospitalization, had a significant relationship with the children's
perception of stressful stimuli during hospitalization.
In a partial replication of this study with a sample of 50 children,
ages 6 to 12 years, Menke (1981) focused on the two significant variables
in the previous study, preadmission preparation and length of admission as
related to the hospitalized child's perception of stressful stimuli.
Analysis of the data indicated that 86% of the children considered the
syringe to be stressful, 38% perceived the dog to be stressful, 36%
identified the doctor and food as stressful, and 32% indicated that the
Picture of the hospital gown was stressful. The rest of the pictures were
perceived as stressful by less than 32% of the subjects. The open-ended
questions yielded twenty-three additional sources of stress, such as
confinement to bed, having to remain indoors, pain, absence of parents,
and operations. In this replication the relationship between the
independent variables of preadmission preparation or length of admission
and the dependent variable of perception of stressful stimuli was not
supported.
Similar results were reported by Reissland (1983) in a study of the
relationship between cognitive maturity and the 4 to 13 year old child's
Perception of the hospital experience. Data was collected through an
interview, one segment of which assessed the child's hospital related
fears. Although analysis of these responses was not fully presented, it
s
º
s

40
was mentioned that the children's fears included specific events related
to surgery such as x-rays, injections, anaesthetic mask, and the
operation, as well as general concerns such as sleeping away from home and
branches rubbing on the windows at night.
The remaining two studies identified sources of children's stress in
conceptual categories rather than as specific events. As a measure of the
effectiveness of an inservice education program focused on increasing
awareness of children's needs, May and Sparks (1983) used a self-developed
questi ornnaire to assess the fears and concerns of 36 hospitalized children
between the ages of 7 to 12 years. Concerns identified by the children
included pain, permanence of condition, confinement, the unfamiliar,
**rtainty, socialization, and separation. Similar categories were
*Pºrted by Timmerman (1983) in a study of the preoperative fears of 10 to
12 year old children. Analysis of interviews conducted with 16 subjects
**sulted in nine categories of fears: loss of control, the unknown,in i -"Je stions, pain or discomfort, lagging school achievement, destruction of
body i - - - - -mage, separation, disruption of peer relationships, and death.
Although the categorization scheme used by Timmerman (1983) and Mayand S
- - - - - - -Parks (1983) does not permit direct comparison with the specific
events- - -identified by Menke (1981) and Reissland (1983), several similar
theme- - -5 of stressful events are evident. The most evident theme is that of
fearS f intrusive procedures, primarily in the form of injections or
*Y. A second theme, pain, could be associated with the intrusiveP+ 9 se ea
- - -ures, or may be associated with other aspects of the illness. Thethira
- - - - -theme is that of separation from family, peers, and familiaract i
-*Yities, and the final common theme is confinement to bed or indoors.

41
Critique of the Studies of Sources of Stress
The critique of these studies of sources of children's stress during
hospitalization will be discussed according to the four categories of
threats to validity discussed by Cook and Campbell (1979). These
categories are threats to : construct validity, statistical validity,
internal validity, and external validity.
Threats to construct validity. The primary threat to construct
validity of this group of studies was related to the theoretical framework
and subsequent definition of the construct being studied, that is stress,
fear, needs, or concerns. Of the five studies, only the first of the
Menke (1972) investigations stated a theoretical basis for the study, an
integration of several theories of perception and stress, and provided a
definition of the target construct. Her subsequent work (1981) did not
discuss the framework but did give the same definition of stress. None of
the other authors indicated use of a theoretical framework to guide the
investigation of the children's perception of stress or identification of
fears and concerns or provided a definition of the target construct,
resulting in a possible lack of clarity of the construct and uncertainty
regarding the validity of the information.
An additional threat to construct validity present in all the
studies, although most identifiable in Menke's (1972, 1981) research due
to the inclusion of the "no reaction" coding, was the assumption that the
subjects would identify the major sources of stress or fear. This may be
*n inaccurate assumption as it is possible that some children may have
Perceived selected stimuli as so stressful that they avoided talking about
that situation, possibly resulting in an inaccuracy in identify the
*ources of stress. Although it would be difficult to design a study to
C
y
º

42
circumvent this problem, it should be recognized as a limitation of the
studies.
Threats to statistical validity. The primary threat to statistical
validity was the low power of the most of the studies due to small sample
sizes - None of the studies provided information on statistical power, but
assuming the standard alpha of .05 and a medium effect size coupled with
the sample size of each study, the power of the studies were .21
(Timmerman, 1983), .44 (May & Sparks, 1983), . 57 (Menke, 1981), .64
(Reiss land, 1983), and . 86 (Menke, 1972). Only the original Menke (1972)
study achieved a power above the generally acceptable .80 level (Munro,
Visintainer, & Page, 1986). Interpreted, this means that most of the
***dies had a very low probability of rejecting a false null hypothesis
****1 tirig in a failure to recognize a difference existed if it existed.
Thus, some sources of stress for hospitalized children may not have been
identified.
4A second threat to statistical validity is the use of researcherd *Yeloped instruments. Use of self-developed tools in these studies wasn **essar due to the lack of standardized instruments to examine they
constr- - - - - -Victs; however, the result is a deficit of information regarding
Validi- - - - - -ty and reliability. Of the five studies, all used semi-structured
int **Views, permitting the child to individually identify sources ofstres
- -5 or fear, an approach that is appropriate for exploratory studies.In a cl -cli tion, the Menke (1972, 1981) studies used pictures of predeterminedsti *Ali. somewhat circumscribing the child's report of stressful events,but
**is was balanced by the open-ended questioning regarding additionalSOvl *ses of stress. Ideally, these studies should be replicated and the

43 º,
interview questions refined as needed to develop an interview schedule
that may be tested for validity and reliability.
Threats to internal validity. The internal validity of a study is
of concern in experimental and quasi-experimental research when events
occurring between the pretest and posttest may influence the performance
on the latter (Phillips, 1986). Of the five studies reviewed in this
section, all were descriptive in nature; none examined change in response
over time due to experimental intervention or nature events. Therefore,
no threats to internal validity, such as history, maturation, or repeated
testing occurred.
Threats to external validity. External validity is threatened due
to the failure to control variance of extraneous factors sufficiently
through randomization or the inclusion/exclusion criteria of the samples,
resulting in difficulty generalizing the results to other populations. In
this group of studies, none of the studies were randomized and only Menke
(1972, 1981) stated inclusion/exclusion criteria that attempted to control
extraneous variables. The only control identified by two other
researchers was limiting the investigation to surgical patients
(Reissland, 1983; Timmerman, 1983). The final study (May & Sparks, 1983)
included all children of the designated age admitted to the pediatric
unit. While these approaches have provided necessary basic information
and may have been appropriate for the purposes of the studies, they do not
Provide sufficient basis for generalization to specific subgroups of
*ubjects, such as children with chronic or acute illnesses, males versus
females, or subjects with varying levels of trait anxiety.
A second factor preventing appropriate generalization of the
ºnformation is the broad age range of subjects, 4 through 13 years. None
*

44
of the studies provided rational for the target age group and none focused
on children within one cognitive developmental stage. Menke (1972) did
subdivide the children into two groups, 4 to 7 years and 7 to 12 years
based on Piaget's stages, but did not state which group the 7 year-olds
were assigned to, and did not test for evidence of concrete operational
thinking in these children or for formal operational thinking in the older
subjects. Although Reissland (1983) stated a purpose of examining the
child's reactions to hospitalization according to cognitive maturity, and
her cluster analysis indicated that the subjects under 7 years 3 months
did differ in their responses from subject over 7 years 4 months, this was
not linked to any developmental theory, such as Piaget's cognitive
developmental stages. The assumption that the level of cognitive
development does not influence appraisal of stressful events should not be
made, but rather should be carefully investigated to determine possible
differences in appraisal due to cognitive functioning.-
In general, because research regarding events children appraise as
stressful during hospitalization is in an early stage, the descriptive,
exploratory design of the individual studies appears to be appropriate for
the question. Although the theoretical basis of the studies was weak, the
methodology generally is congruent with the Lazarus concept of individual
*PPraisal of stress as in each study the child was asked what he or she
Perceived to be stressful. The use of interview to obtain baseline
information was appropriate for the age of the subjects (with the possible
exception of Menke's [1972) and Reissland's [1983) inclusion of four year
old children in the general interview process). The generally low
statistical power, and the potential difficulties generalizing the results
emphasize the need for further research in this area. Despite these
■
º
X
** ** -

45
limitations, the studies do provide important information about what
school-age children are likely to appraise as stressful during
hospitalization.
Comparison of Adult and Child Identification of Sources of Stress
Comparison of what children appraise as stressful during
hospitalization and what adults think is likely to be stressful to the
hospitalized child demonstrates striking similarities. Both children and
adults identify intrusive procedures as a source of stress, the child
interpreting these events as a threat to physical well-being, one of the
sub-classifications of stress (Lazarus & Folkman, 1984a). Separation is
identified as a source of stress by both the children and adults.
According to the stress and coping framework, this could result in stress
due to the alteration in the child's resources for coping with altered
person-environment situation (Lazarus & Folkman, 1984a). Similarly, both
groups identify the unknown, uncertainty and loss of control as stressful.
According to Lazarus and Folkman (1984a), these are not direct sources of
stress, but rather are factors that will determine if the person is able
to consider a stressful encounter as a threat or a challenge. Finally,
adults generally assume that hospitalization will be stressful for all, an
assumption that may not be accurate. Because appraisal of stress is an
individual process, it is possible that not all children will consider
hospitalization to be stressful, a possibility that is supported by the
9°casional child who prefers to remain in the hospital rather than face a
*ifficult family or peer situation. In sum, while adults are generally
able to identify the events a hospitalized child will find to be
stressful, only the child can identify the event that he or she has
personally appraised as stressful. Both perspectives are needed to
º
º
º

46
providesupporttothechildduringhospitalization.Ageneralawareness
oftheeventslikelytobeappraisedasstressfulwillhelpthe
professionalsdevelopaphilosophyofpediatriccarethatislikelyto
meettheneedsofmostchildren,whileknowledgeoftheindividualchild's
appraisalofstresswillpermittheprofessionaltoadapttheplanofcare
tomeetthatchild'sneeds.
ResearchonCopingduringHospitalization
Theconstructofcopinghasreceivedattentionfromresearchers
focusingonboththehospitalizedchildandonchildrenexperiencingother
typesofstressfulevents.Theprimaryfocusofthisportionofthe
literaturereviewwillbeonresearchrelevanttopatternsofcopingused
bytheschool-age,hospitalizedchild,withinclusionofotherselected
studiesrelatingtohealthcaresituationsand/orschool-agechildrenasappropriate.First,thecopingstrategiesofchildren,asreport.inthe
literature,willbeexamined(SeeTable1)andthemajorfindingsofthe
studiesgiven.Second,variablesthathavebeennotedtoinfluencethe
typeofcopingbehaviorusedwillbediscussed.
CopingStrategiesReportedintheLiterature
Examinationoftheresearchindicatesthatseveraldistinctive
approacheshavebeenusedtoclassifyoridentifythecopingbehaviors
usedbychildren.Theseare1)Murphy'scategoriesofcoping
(Murphy,1962;Murphy&Moriarty,1976),2)Lazarus'modesofcoping(Cohen
&Lazarus,1979,1983;Lazarus&Launier,1978),3)uni-dimensional
assessmentofcopingbehavior,4)useofcontentanalysistoidentify

47
Table 1
Coping Strategies of Children
Investigator Subjects
Murphy's Categories of Coping:
Murphy, L. B. N: 32(1962) and Age: PreschoolMurphy, L. B., Healthy
& Moriarty, A. E.(1976)
Rose, M. H. N: 14(1972a, 1972b) Age: 18 m to 7 y
Hospitalized forelective surgery orcardiac catheterization
Savedra, M. N: 33& Tesler, M. Age: 6 to 12 years(1981) Hospitalized for
elective surgery
Lazarus Modes of Coping:
Caty, s., N: 39 case studiesEllerton, M. , Age: 20 months to& Ritchie, S. 10 years(1984) Hospitalized
Ritchie, J. A., N: 208Caty, S., Age: 2 to 5 years& Ellerton, M. Hospitalized(1987, 1988)
Coping Strategies
Preparatory steps towardcoping
Active copingPassive coping
Precoping/OrientingActive Copingattempting to controlresistingcooperating or complying
Inactive
Pre-coping or OrientingActive Coping
attempts to controlcooperation
-
resistance
suspendsignoresnegatesattacksmixed
Information-ExchangeAction/InactionIntrapsychic
Information seekingDirect ActionInhibition of action
Seeking or acceptinghelp or comfort from others
IntrapsychicMovement toward independence
or growth
º,

48
Hamner, S. B. ,& Miles, M. S.(1988)
Wertlieb, D.,Weigel, C.,& Feldstein, M.(1987)
N: 15
Age: 4 to 18 yearsBone Marrow Aspiration
N: 176Age: 6 to 9 yearsHealthy
Unidimensional Coping Constructs:
LaMontagne, L.(1984)
LaMontagne, L.(1987)
Field, T.,Alpert, B.,Vega-Lahr, N.,Goldstein, S.,& Perry, s.(1988)
Altshuler, J. L.,Ruble, D. N.(1989)
Burstein, S. ,& Meichenbaum, D.(1979)
Peterson, L.,& Toler, S. M.(1986)
N: 51
Age: 8 to 12 yearsHospitalized for minorsurgery
N: 42
Age: 8 to 18 yearsHospitalized for minorsurgery
N: 56Age: 4-10Hospitalized for minorsurgery
N: 72 (24 per group)Age: 5 to 6 years
7 to 8 years10 to 11 years
Healthy children
N: 20Age: 4.8-8.6 yearsHospitalized fortonsillectomy,adenoidectomy, ormyringotomy
N: 59 children
Age: 5 to 11 yearsHospitalized for minorelective surgery
Action/InactionIntrapsychicInformation-Exchange
Focus : SelfEnvironmentOther
Function: Problem SolvingEmotion-Management
Mode: Information SeekingSupport seekingDirect ActionInhibition of action
Intrapsychic
Avoidant-Active Dimension
Avoidant-Active Dimension
Sensitizer/Repressor
Approach-Avoidant strategiesDirect Emotional Manipulation/tension reduction
Maladaptive strategies
Low defensive/High defensiveWork of worrying/Avoidance
Information-seekingdisposition
Avoidance disposition
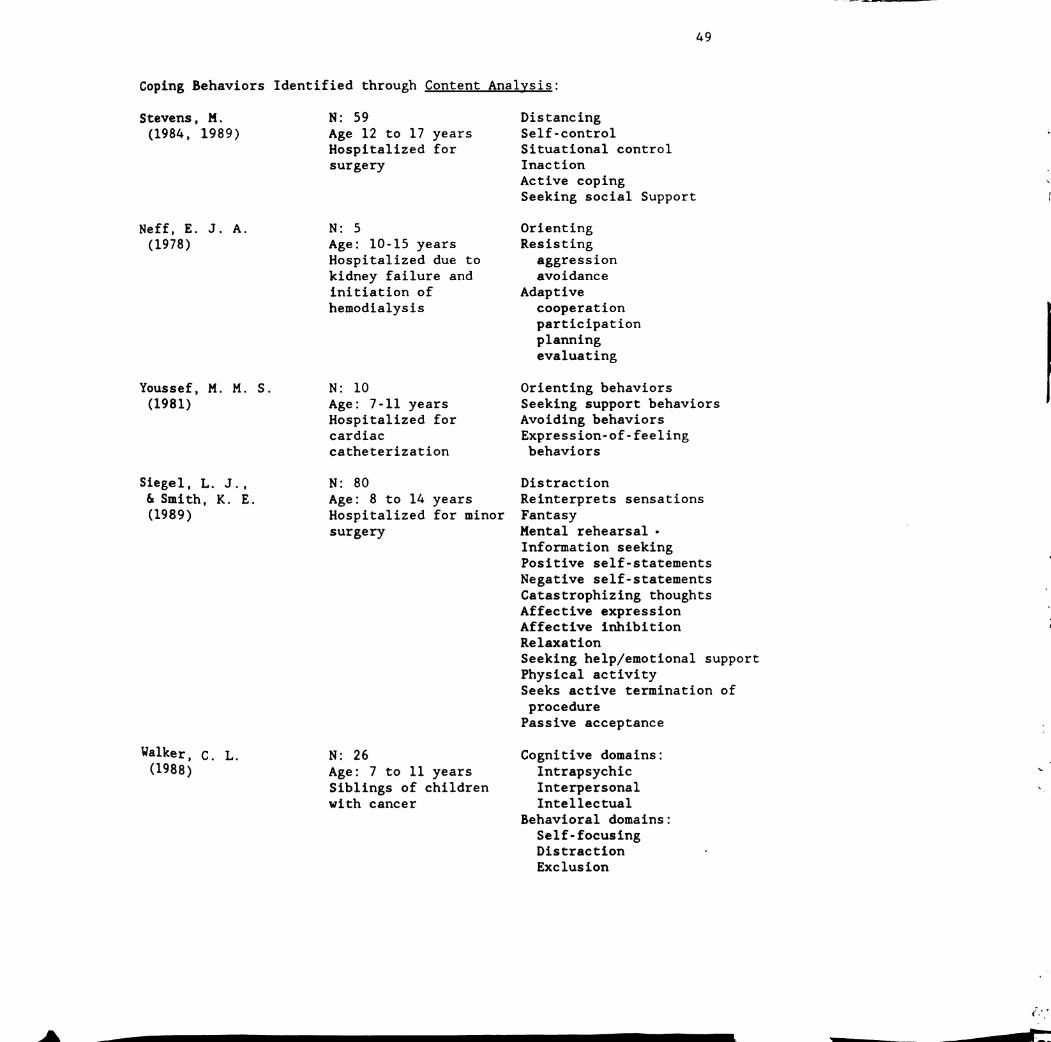
49
Coping Behaviors Identified through Content Analysis:
Stevens, M.(1984, 1989)
Neff, E. J. A.(1978)
Youssef, M. M. S.(1981)
Siegel, L. J.,& Smith, K. E.(1989)
Walker, C. L.(1988)
N: 59
Age 12 to 17 yearsHospitalized forsurgery
N: 5
Age: 10-15 yearsHospitalized due tokidney failure andinitiation ofhemodialysis
N: 10Age: 7-11 yearsHospitalized forcardiaccatheterization
N: 80
Age: 8 to 14 yearsHospitalized for minorsurgery
N: 26
Age: 7 to 11 yearsSiblings of childrenwith cancer
DistancingSelf-controlSituational controlInaction
Active copingSeeking social Support
OrientingResisting
aggressionavoidance
Adaptivecooperationparticipationplanningevaluating
Orienting behaviorsSeeking support behaviorsAvoiding behaviorsExpression-of-feelingbehaviors
Distraction
Reinterprets sensationsFantasyMental rehearsal -
Information seekingPositive self-statements
Negative self-statementsCatastrophizing thoughtsAffective expressionAffective inhibitionRelaxation
Seeking help/emotional supportPhysical activitySeeks active termination of
procedurePassive acceptance
Cognitive domains:IntrapsychicInterpersonalIntellectual
Behavioral domains:
Self-focusingDistractionExclusion
K

50
Ryan, N. M. N: 103(1989) Age: 8 to 12 years
Healthy children
Sorensen, E. S. N: 32(1990) Age: 8 to 11 years
Healthy children
Social supportAvoidant activitiesEmotional behaviorsDistracting activitiesCognitive activitiesPhysical exerciseAggressive motor activitiesAggressive verbal activitiesIsolating activitiesHabitual activitiesSpiritual activitiesRelaxation activities
Cognitive-intrapsychicEmotional/sensoryAnalyzing/intellectualizingThought reframingEmotional/external focus
Cognitive-behavioralSubmission/enduranceEmotional expressionsTaking responsibilityRebellion
Behavioral
Problem solvingDistraction
Behavioral reframingAvoidance/flightAggression
-
Manipulation/deceptionImmobilizationSelf-effacing behaviors
IntrapersonalMom and DadOthersPeers
Coping Strategies Identified through other methods:
Curry, S. L., N: 48& Russ, S. W. Age: 8 to 10 years(1985) Well children having
dental work
Categories basedon cognitivebehavioralliterature
Behavioral Coping StrategiesInformation-seekingSupport-seekingDirect efforts to maintaincontrol
Cognitive Coping StrategiesReality-oriented working
throughPositive cognitiverestructuring
Defensive reappraisalEmotion-regulationBehavior-regulationDiversionary thinking

51
patterns of coping behavior, 5) other approaches. The coping research
will be discussed according to these groups.
Murphy's categories of coping. The pioneer researcher in the study
of children's coping was Lois Murphy. In 1953, while working at the
Menninger Foundation, Murphy began a longitudinal study of the ways
normal, healthy children cope with the stresses of life (Murphy &
Moriarty, 1976). Both naturalistic and experimental settings were used to
observe thirty children in a variety of situations over an eighteen year
period. In Murphy's early work, three categories of coping were
identified: 1) preparatory steps toward coping, 2) coping acts, and 3)
secondary efforts needed to manage the results of the precoping or coping
acts (Murphy, 1962), and later she also referred to "passive coping
devices" (Murphy & Moriarty, 1976). In Murphy's later work two global
categories of coping were identified: Coping I and Coping II. Coping I
involves the child's "capacity to cope with opportunities, challenges,
frustrations, threats in the environment; and Coping II, maintenance of
internal integration--that is, capacity to manage one's relation to the
environment so as to maintain integrated functioning" (Murphy & Moriarty,
1976, pp. 117). Examination of these concepts demonstrates a close fit
with Lazarus' concepts of problem focused and emotion focused coping
(Lazarus & Folkman, 1984a), providing additional support that the Lazarus
Paradigm may be appropriately used when studying children.
The earliest study on the coping of hospitalized children was
conducted by Rose (1972a, 1972b). Using Murphy's (1962) work as a
theoretical framework, Rose investigated the coping behaviors of fourteen
children, ages eighteen months to seven years of age, hospitalized for
surgery or cardiac catheterization. The children were observed at home
2
s

52
twice prior to admission, twice after discharge, and one or two times a
day while admitted (range of 5 to 27 in-hospital observations).
Additionally, the mothers were interviewed prior to the child's
hospitalization and after discharge. Analysis of the observations and
interviews indicated that during hospitalization the children used pre
coping or orienting behaviors, defined as, "the process by which the child
familiarizes himself with the environment" (Rose, 1972a, pp. 18), and
active coping, defined as, "the process by which a person deals with
threatening, frustrating, or challenging situations" (Rose, 1972a, pp.
19). Active coping was further subdivided into attempts to control,
resistance, and cooperation or compliance. Using these categories, the
results showed that during hospitalization the children demonstrated an
increase in precoping or orienting behaviors and a decrease in active
coping as compared with prehospitalization behavior. Following discharge
the children's behaviors returned to prehospitalization patterns.”
These findings were partially confirmed by Savedra and Tesler (1981)
(also Tesler and Savedra, 1981). Using a direct coding adaptation of
Rose's protocol”, the subjects, 33 children ages 6 through 12 admitted for
elective surgery, were observed during key stress points of
hospitalization (Wolfer & Visintainer, 1975) for a total of 1,093 five
"inute intervals. The intervals were categorized as inactive, precoping,
°º active coping (subcategorized as attempts to control, cooperative,
resistive, suspends [defined as avoidance), ignores, negates, attacks, and
mixed) according to the frequency of the behaviors. Analysis of the data
*This direct coding adaptation of Rose's coping categories was doneby Bishop (1976) and later used by Stewart (1978). These reports are notincluded in this literature review as the focus was limited to preschoolchildren and does not directly contribute to the foundation of knowledgefor the current study.

53
indicated that preoperatively the children were more likely to use
precoping or orienting behaviors and active-controlling behaviors. Post
operatively the children primarily used controlling behaviors. It was
also noted that multiple forms of coping were used within a short time
frame, emphasizing the dynamic nature of the coping process.
In sum, the studies using Murphy's work on children's coping have
identified two primary categories of coping. Pre-coping or orientating
behaviors are used to gain information about the environment. Active
behaviors are used to deal with a threatening or challenging situation and
have been subcategorized as attempts to control, resistance, cooperation,
suspends, ignore, negatation, and attack.
Lazarus' modes of coping. As an alternate to using Murphy'scategories of coping, a number of researcher's have used Lazarus' modes of
coping to study children's methods of dealing with the stress. In an
early exploration to determine if the Lazarus model could be applied to
children's coping, Caty, Ellerton, and Ritchie (1984) reviewed 39 case
studies of the coping behaviors of hospitalized children, ages 20 months
through 10 years. Through content analysis it was determined that the
reported behaviors of the children could be categorized systematically
using a modified version of the Lazarus modes of coping: 1) information
exchange, 2) action/inaction, and 3) intra-psychic. Reflecting on theprocess of this analysis and a theoretical discussion with Lazarus, it was
recommended that the first category be limited and the second expanded in
future investigations of child's coping behaviors. Accordingly, in
subsequent work by the same group (Ritchie, Caty, & Ellerton, 1987;
Ritchie, Caty, & Ellerton, 1988), the categories used more directly
reflected Lazarus' original five modes of coping: 1) information seeking,

54
2) direct action, 3) inhibition of action, 4) seeking or accepting help or
comfort from others, and 5) intrapsychic, with one additional category,
6) movement toward independence or growth. In this study, the coping of
208 hospitalized children, age 2 to 5 years was observed during low stress
(routine activities of daily living taking place in an unfamiliar
environment such as meals, play, and hygiene) and high stress situations
(illness related activities such as physical assessment, intrusive
procedures, and treatments). Analysis indicated that children use fewer
coping behaviors during high stress situations than in low, and that
chronically ill children with prior experience use more coping behaviors
than do acutely ill children who have had limited prior hospital
experience. This study used the six modes of coping as a vehicle for
examining differences in the responses of children to stress; no further
recommendations for changes in the categorization were given.
Hamner and Miles (1988) used the three category modification (Caty,
Ellerton, & Ritchie, 1984) of Lazarus' modes of coping to study the coping
strategies of fifteen 4 to 18 year old children during bone marrow
aspiration as a part of a cancer protocol. They found the largest
percentage of coping strategies reported by the children were action
inaction behaviors; intrapsychic strategies were reported second most
frequently; and information-exchange was reported least frequently. This
latter finding differs from the high occurrence of information seeking in
the studies based on Murphy's coping concepts. While the children stated
that they wanted the doctors to describe what was being done, the children
seldom reported asking for information. A possible explanation for this
is that all had been in treatment for the disease for over a year and were
familiar with the procedure.
-

55
Another study strongly based on the Lazarus paradigm was conducted
by Wertlieb, Weigel, and Feldstein (1987) to develop a taxonomy of the
coping processes used by children in everyday activities. A semi
structured interview was used to obtain a self-report of stressful events
and the resulting coping behaviors from 176 children ages 6 to 9 years,
the sample obtained from the cliental of a health maintenance
organization. The results were coded according to 1) a focus of self,
environment, or other; 2) a function of problem-solving or emotion
management coping; and 3) a mode of information seeking, support seeking,
direct action, inhibition of action, or intrapsychic. Analysis indicated
that this taxonomy did provide an effective method of categorizing
children's coping behaviors. However, it should be noted that the probes
used during the interview (D. Wertlieb, personal communication, July 7,
1989) were strongly biased toward eliciting responses that would be
congruent with the proposed taxonomy, compounding the methodology with the
OutCOme .
In sum, Lazarus' five modes of coping have been used directly as
delineated by those developing the theory and also have been modified to
a three mode and a six mode version to attempt a better fit with
children's coping behaviors. It appears that the five modes, direct
action, inhibition of action, intrapsychic, information seeking, and
support seeking, represent categories of coping behaviors that are used by
children. Additionally, identification of other modes of coping such as
movement toward independence or growth may be necessary when studying
children's coping behaviors.
Uni-dimensional coping constructs. A third method of categorizing
child's coping behaviors has followed a uni-dimensional assessment of
-
56
coping, focusing on the broad range of one behavior, rather than a multi
dimensional approach such as used by Murphy and Lazarus. This approach
was used by LaMontagne (1984, 1987) in a series of studies examining the
relationship between an avoidant/active coping dimension and the child's
locus of control”. The children's preoperative mode of coping was
determined by interviewing the child and rating the data on a 1 to 10
scale with avoidant coping (little knowledge of the impending surgery and
little tendency to seek such knowledge) at the low end, and active coping
(detailed knowledge of the reason for and procedure of surgery and
willingness to discuss the event) at the high end. As hypothesized,
children who used active modes of coping preoperatively were more likely
to have an internal locus of control than were children who used avoidant
or a combination of avoidant/active coping.
A similar, if not identical, uni-dimensional construct was studied
by Field, Alpert, Vega-Lahr, Goldstein, and Perry (1988). In this study
the dimension was labeled as sensitizer/repressor, sensitizers being those
children whose normal behavior was to actively seek information about a
stressful event, and repressors being those who avoided such information
or used defenses such as denial. Using mother-report, the coping style of
56 children, 4 to 10 years of age, during hospitalization for minor
surgery was determined and compared to their responses to stressful
hospital experiences. Analysis of the data indicated that children rated
as being sensitizers showed more activity, more information seeking, were
*This study was based on the approach-avoidance coping behaviors ofadults (Cohen and Lazarus, 1973; Cohen, 1975). In investigatingchildren's coping, LaMontagne (1984) believed the term active coping moreaccurately reflected the process of a child's coping than the termvigilant coping used by Cohen.

57
more distressed by intrusive procedures, and had shorter ICU admissions
than did children rated as repressors.
Altshuler and Ruble (1989) also used the approach-avoidance
dimension in a study of developmental changes in child's coping with an
unavoidable stressor, incorporating a distinction between complete and
partial avoidance. Seventy-two healthy children were studied, 24 in each
age group of 5 to 6 years, 7 to 8 years, and 10 to 11 years. The children
were told four stories, two depicting positive stress and two negative
stress, and were asked questions pertaining to how they thought the child
in the story might cope with the situation. In the analysis of the data,
two categories were added to the approach-avoidance scheme: direct emotion
manipulation/tension reduction, and maladaptive strategies. Statistical
analysis indicated that the strongly dominant coping strategy of choice
for children of all ages was avoidance, the younger children being more
likely to suggest escape strategies and the older children more likely to
identify methods of decreasing emotional distress through cognitive
distraction. Behavioral distraction, the coping strategy most frequently
reported, was mentioned by children at all ages. Although the sample was
healthy children, because the focus was on children's coping with
uncontrollable situations, the results may have important implications for
the study of the coping behaviors of the hospitalized child.
Burstein and Meichenbaum (1979) studied the dimension of a child's
defensiveness, as well as the characteristic of anxiety, prior to surgery
in relation to coping behaviors. The play of 20 children, ages 4.8
through 8.6 years was observed before and following surgery. The children
were presented with two sets of toys, each set consisting of one toy
relevant to the hospital and one toy of equal interest. Analysis of the

58
play sessions indicated that the children who played with the hospital
related toys prior to surgery, a behavior designated as low defensiveness,
had less post-operative anxiety than did those children demonstrating high
defensiveness by avoiding the stress related toys. The researchers
believed this was indication of coping behaviors similar to the "work of
worrying" and avoidance seen in adults.
Peterson and Toler (1986) examined a narrower segment of the
approach-avoidance dimension of coping in a study focusing on the presence
of an information seeking versus avoidance disposition in children. Data
were collected from 59 children admitted for minor surgery using a variety
of researcher developed tools. The major results indicated that children
do have an information seeking dimension; that children with high
information seeking behaviors are more adaptive during anesthesia, less
distressed following surgery than are children with avoidant behaviors;
and that age and information seeking are positively related.
In sum, five researchers have used a unidimensional approach to
studying children's coping behaviors. Although the labeling differs, it
appears that the same dimension has been examined in all of the studies:
avoidant, repressor, or high defensive behaviors as compared to active,
sensitizer, low defensive, or information seeking behaviors. That these
behaviors occur is evident. Perhaps the primary question is the optimal
method of identifying coping categories: should these behaviors should be
considered as the extremes of one dimension of coping or should they be
considered to represent two or more distinctive modes of coping.
Content analysis. Rather than imposing a predetermined scheme of
coping on the data, a number of researchers chose to use the process of
content analysis to identify categories of children's coping. In one of

59
these studies the category derivation was strongly linked, although not
identical to, a theoretical base, while other researchers developed an
atheoretical categorization scheme.
The study by Stevens (1984, 1989) illustrates the use of content
analysis while retaining a definite link between a conceptual framework
and the identified categories of coping. The coping strategies of 59
adolescents hospitalized for surgery were examined by talking to the
subjects prior to and following surgery using a semistructured interview
based on Lazarus' theory of stress and coping. Content analysis of the
data resulted in six categories of coping: distancing, self-control,
situational control, inaction, active coping, and seeking social support.
While the first three categories are distinct from the modes proposed by
Lazarus, the last three categories reflect the researchers familiarity
with the Lazarus modes of coping, a correspondence that is appropriate
when supported by the data.-
Atheoretical content analysis was used by the remaining researchers
in this category. In two methodologically similar studies conducted by
doctoral students at the University of Pittsburgh, the purpose was to
investigate how children manage and adapt to (Neff, 1978), or their
behavioral responses to (Youssef, 1981), a stressful hospital experience.
Although the term coping was not used, the authors' operationalization of
manage and behavioral responses are congruent with the definition of
coping used in this paper. Neff (1978) examined the adjustment of 5
children, ages 10 to 15 years, to shunt insertion and hemodialysis and
observed three responses used by the children to manage the physical
changes associated with their treatment: orientation, resistive, and
adaptive responses. It was noted that the child's behaviors changed as

60
experience was gained with the procedure with orientation behaviors
decreasing and adaptive behaviors increasing. In the study by Youssef
(1981), observations were made of the behavioral responses of 10 children,
ages 7 to 11 years, undergoing echocardiography and cardiac
catheterization. The four categories of self control identified during
content analysis of the data were orienting, seeking support, avoiding,
and expression-of-feeling. Orienting behaviors, the most frequently
observed behavior, occurred significantly more often during the
echocardiogram than during the catheterization, whereas seeking support,
the second most frequent behavior, occurred significantly more often
during the catheterization than during the echocardiogram. The remaining
two categories were infrequently used and did not have a significant
relationship with any of the variables.
Siegel (Siegel, 1983; Siegel & Smith, 1989) investigated the
relationship between the coping strategies used by hospitalized children
in response to painful and stressful procedures and the child's adjustment
to the hospital. Using a structured interview format, data were collected
from 80 children, 8 to 14 years of age, hospitalized for minor surgery.
Analysis of the responses resulted in fifteen categories of coping: 1)
distraction, 2) reinterprets sensations, 3) fantasy, 4) mental rehearsal,
5) information seeking, 6) positive self-statements, 7) negative self
statements, 8) catastrophizing thoughts, 9) affective expression, 10)
affective inhibition, 11) relaxation, 12) seeking help/emotional support,
13) physical activity, 14) seeks active termination of procedure, and 15)
passive acceptance. It was noted that children who were successful copers
(defined as being cooperative, showing low anxiety, and having high
thresholds for physical discomfort) were more likely to ask questions and

61
used a greater number of coping strategies than did the unsuccessful
copiers. As noted above in the presentation of Lazarus' theory, labeling
coping as good or bad is not appropriate as it is difficult to determine
the effectiveness of the coping and because it confounds coping with
outcome. From the reports of this study it is difficult to determine if
the researcher actually was focusing on the child's adaptation to the
hospital and confused the process of coping with the outcome of
adaptation, or if the purpose was to actually evaluate effectiveness of
the coping behaviors.
The final three studies in this category focus on the coping of
healthy, rather than hospitalized, school-age children, and are included
to provide a broad understanding of children's coping behaviors. In a
study of the coping behaviors of 26 siblings, ages 7 to 11 years, of
childhood cancer patients, Walker (1988) used parent interview, sibling
interview, and a variety of projective tools to develop a taxonomy of
sibling coping. The cognitive domains identified were intrapsychic,
interpersonal, and intellectual, and the behavioral domains were self
focusing, distraction, and exclusion. Thirty-three separate categories
corresponding to the domains were listed. The author reported difficulty
in determining whether a behavior was primarily a cognitive or behavioral
strategy, supporting the findings of Lazarus and colleagues (cited above)
that emotion and problem focused coping generally occur simultaneously and
that one coping behavior may serve both functions. It was also noted that
there was a 44% disagreement in the parent's and child's reports of the
child's coping strategies indicating that the child, rather than the
parent, is the most accurate source of data for this type of study.

62
Ryan (1989) used content analysis to examine the data collected from
103 healthy children, ages 8 to 12 years of age, regarding the strategies
they used to help themselves deal with stressors encountered in daily
living. Group discussion and individual questionnaires were used to
obtain the children's responses to questions designed to tap the process
of coping and the efficacy of the coping. The resulting categories of
coping were: 1) social support, 2) avoidant activities, 3) emotional
behaviors, 4) distracting activities, 5) cognitive activities, 6) physical
exercise, 7) aggressive motor activities, 8) aggressive verbal activities,
9) isolating activities, 10) habitual activities, 11) spiritual
activities, and 12) relaxation activities. Statistical analysis indicated
that the first five categories accounted for two-thirds of the coping
behaviors, that different coping behaviors were used before, during, and
after the stressful event, and that children are able to evaluate the
effectiveness of the coping strategy in helping deal with the stressful
situation.
Finally, Sorensen (1990) used content analysis to examine the daily
coping responses of 32 healthy children ages 8 through 11 years. The
children were interviewed using a sentence completion list adapted from
Walker (1986) and were asked to keep a record of daily stress and coping
responses in a semistructured journal for a period of six weeks. Analysis
of the data resulted in identification of 21 categories (See Table 1)
grouped according to four major themes: cognitive-intrapsychic, cognitive
behavioral, behavioral, and interpersonal. Statistical analyses were
limited to frequency of category occurrence. It was noted that submission
or endurance was the most common response to daily stressors, and that

63
boys were more likely to use physical aggression whereas girls more
frequently reported using emotional forms of coping.
It is more difficult to summarize the categories of coping
identified though content analysis due to the lack of uniformity in
definition of a category, but certain behaviors do appear in most of the
lists. The coping behaviors repeatedly identified through content
analysis are: orienting or information seeking; active coping such as
cooperation or avoidance by attempting to escape the situation either
physically or psychologically; efforts to control the event; and seeking
social support.
Other approaches to categorizing coping behaviors. The remaining
study does not follow any of the previous methods of categorizing coping
behaviors, but it is useful in understanding children's coping behaviors.
Curry and Russ (1985) investigated the coping strategies of 8 to 10 year
old children during dental treatment. A total of forty-eight children,
(Phase I, N-18; Phase II, N-30) were observed during dental treatment and
interviewed following the procedure. Prior to data collection, the work
of major coping theoreticians was examined and synthesized into seven
categories of coping. During the process of data analysis these were
expanded to nine coping categories: 1) information-seeking, 2) support
seeking, 3) direct efforts to maintain control, 4) reality-oriented
working through, 5) positive cognitive restructuring, 6) defensive
reappraisal, 7) behavior-regulating coping cognitions, 8) emotion
regulating coping cognitions, and 9) diversionary thinking. The first
three were considered to be behavioral coping strategies and the last were
classified as cognitive coping strategies. It should be noted that in a
later article (Curry, Fuss [sic], Johnsen, & DiSantis, 1988) applying this

64
categorization to clinical work, defensive reappraisal was not included.
While impressive in the much needed attempt to synthesize the multitude of
coping categorizations, a major difficulty in this taxonomy is the failure
to consider that differences in the conceptual basis may render it
inappropriate to merge the categories from diverse theories, demonstrated
by the authors' inclusion of Lazarus' key construct of appraisal as a form
of coping equivalent to Murphy's (1962) cognitive mastery or Janis' (1958,
1965) work of worrying.
Summary of Coping Studies
The construct of coping has received considerable consideration from
researchers in the recent years. The primary difficulty in synthesizing
this information is the semantical, and sometimes theoretical, differences
in the labeling of coping behaviors and categories. Despite this problem,
several dominant themes repeatedly occur in the reports of children's
coping behaviors (See Table 2). One of the most frequently identified
categories describes the child's behavior when actively taking in the
environment to clarify and understand a situation. This category is
variously labeled precoping (Rose, 1972a, 1972b; Savedra & Tesler, 1981),
orienting (Neff, 1978; Youssef, 1981), information-exchange (Ritchie,
Caty, & Ellerton, 1987, 1988), information seeking (Peterson & Toler,
1986; Siegel & Smith, 1989), approach (Altshuler & Ruble, 1989),
sensitizers (Field et al., 1988) low defensive or the work of worrying
(Burstein & Meichenbaum, 1979), and analyzing/intellectualizing (Sorensen,
1990). A second recurring category is the child's physical or mentalattempts to remove self from the stressful situation identified as
avoidance (Altshuler & Ruble 1989; Burstein & Meichenbaum 1979;
LaMontagne, 1984, 1987; Neff, 1978; Peterson & Toler, 1986; Ryan, 1989;

65
Table 2
Synthesis of Reported Coping Behaviors
Category
Actively takingin theenvironment to
clarify andunderstand asituation
Physical ormental attemptsto remove selffrom thestressfulsituation
Label
Precoping
Orienting
Information-exchange
Information seeking
Approach
Sensitizer
Low defensiveness or
the work of worrying
Analyzing/intellectualizing
Avoidance
Resistance
Suspends
Ignores
Source
Rose, 1972; Savedra &Tesler, 1981
Neff, 1978; Youssef,1981
Ritchie, Caty, andEllerton 1987, 1988
Peterson and Toler,1986; Siegel andSmith, 1989
Altshuler and Ruble,1989
Field et al., 1988
Burstein andMeichenbaum, 1979
Sorensen, 1990
Altshuler and Ruble1989; Burstein andMeichenbaum 1979;LaMontagne, 1984,1987; Neff, 1978;Peterson and Toler,1986; Ryan, 1989;Sorensen, 1990Youssef, 1981
Rose, 1972a, 1972b;Savedra and Tesler,1981
Savedra and Tesler,1981
Savedra and Tesler,1981

66
Behaviorsintended tobring thechild's personalresponse to thestressfulsituation inline withreality
Attempts to dealwith thestressfulsituation bychangingthinking aboutthe situation
Distancing
Distraction
Seeks activetermination of
procedure
Diversionary thinking
Adaptation
Cooperation
Compliance
Reality-orientedworking through
Submission/endurance
Intrapsychic
Direct emotionalmanipulation
Reinterpretation ofsensations
Cognitive activities
Defensive reappraisalEmotion-regulatingcognitions
Positive cognitiverestructuring
Stevens, 1984, 1989
Siegel and Smith,1989; Ryan, 1989;Sorensen, 1990 Walker,1988
Siegel and Smith, 1989
Curry and Russ, 1985
Neff, 1978
Neff, 1978; Rose,1972a, 1972b; Savedraand Tesler, 1981
Rose, 1972a, 1972b
Curry and Russ, 1985
Sorensen, 1990
Caty, Ellerton, andRitchie, 1984; Hamnerand Miles, 1988;Ritchie, Caty andEllerton, 1987, 1988;Walker, 1988;Wertlieb, Weigel andFeldstein, 1987
Altshuler, and Ruble,1989
Siegel and Smith, 1989
Ryan, 1989
Curry and Russ, 1985
Curry and Russ, 1985
Curry and Russ, 1985

67
Control
Turning toothers for helpin coping
Coping throughexpression offeeling
Thought reframing
Control of thesituation
Control of others
Control of self
Control (unspecified)
Seeking social support
Expression of feeling
Affective expression
Emotional expression
Sorensen, 1990
Stevens, 1989
Ritchie et al., 1986;Savedra and Tesler,1981
Ritchie et al., 1986;Stevens, 1989;Youssef, 1981
Curry and Russ, 1985;Rose, 1972a, 1972b;Savedra and Tesler,1981
Curry and Russ, 1985;Ritchie, Caty, andEllerton, 1987, 1988;Ryan, 1989; Siegel andSmith, 1989; Sorensen,1990; Stevens, 1984,1989; Wertlieb,Weigel, and Feldstein,1987; Youssef, 1981
Youssef, 1981
Siegel and Smith, 1989
Sorensen, 1990
º
º
&

68
Sorensen, 1990; Youssef, 1981), resistive behaviors (Rose, 1972a, 1972b;
Savedra & Tesler, 1981); attacks (Savedra & Tesler, 1981) suspends
(Savedra & Tesler, 1981); ignores (Savedra & Tesler, 1981), distancing
(Stevens, 1984, 1989), distraction (Ryan, 1989; Siegel & Smith, 1989;
Sorensen, 1990; Walker, 1988), seeks active termination of procedure
(Siegel & Smith, 1989), rebellion (Sorensen, 1990) and diversionary
thinking (Curry & Russ, 1985). A third category is comprised of behaviors
intended to bring the child's personal response to the stressful situation
in line with reality. These were labeled adaptation (Neff, 1978),
cooperation (Neff, 1978; Rose, 1972a, 1972b; Savedra & Tesler, 1981),
compliance (Rose, 1972a, 1972b), submission/endurance (Sorensen, 1990) and
reality-oriented working through (Curry & Russ, 1985). A fourth category
frequently listed as a coping behavior is the child's attempts to deal
with the stressful situation by changing how he or she thinks about the
situation, identified as intrapsychic (Caty, Ellerton, & Ritchie, 1984;
Ritchie, Caty, & Ellerton, 1987, 1988; Hamner & Miles, 1988; Walker, 1988;
Wertlieb, Weigel, & Feldstein, 1987); direct emotional manipulation
(Altshuler & Ruble, 1989), reinterpretation of sensations (Siegel & Smith,
1989), cognitive activities (Ryan, 1989), though reframing (Sorensen,
1990), and defensive reappraisal, emotion-regulating cognitions and
positive cognitive restructuring (Curry & Russ, 1985). A fifth category
involves control and includes control of the situation (Stevens, 1989),
control of others (Ritchie et al., 1986; Savedra & Tesler, 1981), and
control of self (Ritchie et al., 1986; Stevens, 1989; Youssef, 1981), or
unspecified attempts to control (Curry & Russ, 1985; Rose, 1972a, 1972b;
Savedra & Tesler, 1981). The sixth category of coping used by children is
seeking social support (Curry & Russ, 1985; Ritchie, Caty, & Ellerton,

69
1987, 1988; Ryan, 1989; Siegel & Smith, 1989; Sorensen, 1990; Stevens,
1984, 1989; Wertlieb, Weigel, & Feldstein, 1987; Youssef, 1981). A final
category is coping through expression of feeling (Youssef, 1981) also
labeled affective expression (Siegel & Smith, 1989), and emotional
expression (Sorensen, 1990). Although active coping or direct action are
mentioned a number of times (Caty, Ellerton, & Ritchie, 1984; Hamner &
Miles, 1988; LaMontagne, 1984, 1987; Murphy, 1962; Ritchie, Caty, &
Ellerton, 1987, 1988; Rose 1972a, 1972b; Savedra & Tesler, 1981; Stevens,
1984, 1989; Wertlieb, Weigel, & Feldstein, 1987) as is inhibition of
action (Ritchie, Caty, & Ellerton, 1987, 1988; Wertlieb, Weigel, &
Feldstein, 1987), the coping behaviors that could be classified under
these headings have been included under the more specific categories
listed above such as the second and third categories. Taken as a whole,
these studies provide a good basis for understanding the range of coping
behaviors likely to be used by hospitalized school-age children.
Critique of the Coping Studies
As with the critique of research pertaining to sources of children's
stress during hospitalization, the studies relating to children's coping
will be discussed according to the four categories of threats to validity
discussed by Cook and Campbell (1979). These categories are threats to:
construct validity, statistical validity, internal validity, and external
validity.
Threats to construct validity. Threats to construct validity were
minimal in this group of reports. In contrast to the stress studies, the
use of a theoretical framework was a strength in the coping studies. Of
the 20 studies, 16 were based more or less firmly on a specific
theoretical framework, one could be considered to be a theory generating

70
study, one attempted to synthesize categories of behaviors from a number
coping theories, and only two failed to base the research on a theory of
coping. Thus a consistent theme generally was evident, flowing from the
initial construct of coping to the interpretation of the data.
The design of the studies were non-experimental or quasi
experimental, research. For the questions being examined this was
appropriate. At the time many of these studies were conducted, research
concerning children's coping was still in the early stages and exploratory
studies were needed to determine the broad spectrum of coping used by
children. Data was obtained primarily through observation and/or
interview. Many studies used both approaches, decreasing the chance of
bias due to use of only one method. It should be noted that the
observations were often conducted during an event believed by the
researcher to be stressful to the child, such as Visintainer and Wolfer's
(1975) six stress points" or a cardiac catheterization, dialysis, bone
marrow aspiration, etc., rather than allowing the child to identify events
personally appraised as stressful. Although this approach is not
congruent with Lazarus' construct of appraisal, it is representative of
the alternate view of stress as a generally noxious event, and therefore
did not constitute a threat to the construct validity.
Threats to statistical validity. The major threat to statistical
validity was the low power of the studies. Although none of the studies
stated a power analysis, a rough estimate of the power (based on an alpha
of . 05, a medium effect size, and the individual sample size of the study)
“The six stress points identified by Visintainer and Wolfer (1975, pp.189) are 1) admission, 2) blood test, 3) the afternoon of the day beforesurgery, 4) preoperative medications, 5) before and during transport tothe operating room, and 6) return from the recovery room.

71
ranged from less than . 19 (the lowest value given on the chart [Cohen &
Cohen, 1983]) to .99. Only three studies (Ritchie, Caty, & Ellerton,
1987, 1988; Wertlieb, Weigel, & Feldstein, 1987; Ryan, 1989) were above
the generally acceptable .80 level (Munro, Visintainer, & Page, 1986).
Two additional studies (Altshuler & Ruble, 1989; Siegel & Smith, 1989)
were above .70 and may have been higher if more specific information had
been provided in the study. The generally low power accepted by the
authors threatens the validity of the study as it is possible that the
sampling was not sufficient to determine the actual characteristics of the
group studied.
A second threat to statistical validity is the use of researcher
developed instruments. Because the study of coping in hospitalized
children is still relatively new, no standardized instruments or interview
formats are available, with the exception of the Children's Coping
Strategies Checklist currently being developed for use in observing
hospitalized preschool children (Ritchie, Caty, & Ellerton, 1988).
Therefore, the interviews and observational guides were self-developed by
the researchers. Unfortunately no information regarding pilot testing of
the instruments was given, possibly jeopardizing the reliability of the
data. Of the four studies that did use standardized instruments in
addition to interview and/or observation, only two presented information
concerning the validity and reliability of the tool. While the numerous
similarities in the categories of coping emerging from the data imply that
the instruments are targeting the child's coping behaviors, the study of
children's stress and coping would be strengthened by the development and
use of standardized instruments.
mº-T-
72
Techniques used for data analysis ranged from content analysis and
descriptive statistics through parametric tests such as Pearson's product
moment correlation, independent t-tests, paired t-tests, ANOVA, MANOVA,
and multiple regression; and nonparametric tests such as chi-square and
Spearman rank-order correlation coefficient. Because of the descriptive
nature of the work, the dominant mode of analysis was content analysis and
descriptive statistics. For the studies using inferential statistics it
appeared that the tests were used appropriately, although the information
needed for this determination was at times minimal. Several authors did
mention details such as using multiple regression rather than ANOVA to
take full advantage of the continuous nature of the data, or rationale for
using a .01 or .05 alpha level. In general it appeared that the use of
statistical tests did not threaten the validity of the studies.
Threats to internal validity. Of the studies considered in this
section, only three (Burstein & Meichenbaum, 1979; Rose, 1972; Stevens,
1984, 1989) were of a quasi-experimental nature; examining the coping
behaviors of children before and after hospitalization for surgery.
Because the purpose was to determine the affect of experience on coping,
changes due to maturation of the child was the dependent variable and not
a threat to internal validity. As the studies used observation or
interview, potential enhancement of performance due to repeated testing
was not a threat. However, observer drift in the scoring of the child's
behavior was a possibility. To avoid this threat, Rose (1972a) used
intermittent inter-observer reliability checks during data collection.
Burstein and Meichenbaum (1979) did not mention using such a system. It
is possible that the internal validity of the studies may have been
affected by an extraneous event that took place between the first and last

73
session of data collection, but no mention of this type of historical
affect was noted.
Threats to external validity. Similar to the stress studies, a
major limitation in generalization of the coping research is the age range
considered in the individual studies. Only five studies (Ritchie, Caty,
& Ellerton, 1987, 1988; Stevens, 1984, 1989; Youssef, 1981; Walker, 1988;
Curry & Russ, 1985) limited the subjects to one cognitive developmental
stage, and in several of these it was probable that the some of the
children were in a transitional phase between stages. Additionally, one
study (Altshuler & Ruble, 1989) purposely studied the developmental
differences in the children's coping. The assumption should not be made
that children of various ages use the same coping behaviors, but rather
should be carefully investigated.
A second limitation in generalizing the findings is that fourteen of
the twenty studies specifically focused on focused on coping in response
to intrusive procedures such as surgery, hemodialysis, cardiac
catheterization, injections, or dental work. Thus, while good progress
has been made in understanding how school-age children cope with intrusive
procedures, it is remains uncertain what coping behaviors children are
likely to use in response to non-intrusive situations that have been
appraised as stressful.
In summary, while a variety of methodological problems are present
in the cited research, a critique of the studies indicates that the
theoretical basis and design of the research generally is appropriate for
the state of knowledge in this area. Although the power of the studies,
age factor, and predetermination of a stressful event limit
generalization, the evident similarity in the coping behaviors identified

=m-
74
suggests that synthesis of these studies is likely to provide a reasonably
accurate picture of the coping behaviors used by hospitalized, school-age
children.
Variables Influencing Coping as Reported in the Literature
Although the primary purpose of the studies cited above was to
identify coping behaviors used by children rather than to identify factors
influencing the coping process, occasionally such information was included
as a portion of the demographic analysis. The variables which have been
addressed in this manner are : gender, age, race, diagnosis, and prior
experience. In addition, the personality trait of locus of control (LOC)
has been the variable of interest in several studies, and the relationship
between anxiety and the child's behavior was considered in two studies.
The findings from the previously reviewed studies and other relevant work
relating to these variables will be summarized and discussed.
Of the nine studies reporting the analysis of the correlation
between the gender of the child and the coping behaviors, five reported no
significant relationship (Altshuler & Ruble, 1989; Curry & Russ, 1985;
Hamner & Miles, 1988; LaMontagne, 1984, 1987). The remaining four studies
reported a significant difference between the coping behaviors used by
boys as compared to girls. These studies indicated that boys tend to use
more active coping, including physical activity (Murphy, 1976; Ryan,
1989); use more self-focused coping (Wertlieb et al., 1987); use more
attempts to control (Savedra & Tesler, 1981), and are more likely to be
unable to identify any form of helpful coping (Wertlieb et al., 1987) as
compared to girls. In contrast, girls are more likely to use
environmentally focused coping (Wertlieb et al., 1987); to use emotional
coping strategies (Ryan, 1989); to use pre-coping behaviors (Savedra &

75
Tesler, 1981) and to seek social support as a form of coping (Ryan, 1989),
a trend also noted in Hamner and Miles (1988) study although not
statistically significant. It is difficult to explain the discrepancies
between these results. All the studies were of a descriptive nature and
variety of categorization schemes were represented in both the "not
significant" and in the "significant" findings groups. Clearly more study
is needed in this area.
Eight studies reported on relationship between age and coping
behaviors. Two studies found no significant difference in the coping of
children at different ages (Field et al., 1988; Hamner & Miles, 1988).
Each of these studies included children from two or more stages of
cognitive development. In contrast, six studies found a significant
relationship between age and coping. The relationship most frequently
noted was a positive correlation between age and intrapsychic or cognitive
coping strategies (Altshuler & Ruble, 1989; Curry & Russ, 1985; Ryan,
1989; Wertlieb et al., 1987); as the child ages, and presumably matures
intellectually, there is an increase in cognitive forms of coping. It was
also noted that with increased age there is an increase of emotion focused
coping, seeking support, and inhibition of action (Wertlieb et al., 1987),
and a trend to focus on the positive aspects of the situation (Curry &
Russ, 1985; Brown, O'Keefe, Sanders, & Baker, 1986). Considering the
dimension of active-avoidant coping, it was noted that older children tend
to use more active modes of coping (LaMontagne, 1987). The relationship
between age and information seeking is unclear; Peterson and Toler (1986)
found a positive correlation between these factors, while Curry and Russ
(1985) found a negative relationship. While these results are
inconclusive, it is probable that as the child's cognitive processes

76
change, his or her knowledge of how to cope with a stressful situation
will change. The discrepancies in the findings may be due to the
difficulty in assessing children's coping. Standardized tools are not
available, observational techniques cannot identify the cognitive coping
processes, and, due to the school-age child's difficulty thinking about an
abstract concept such as his own thinking, interviewing also may not
identify the child's coping behaviors fully. Again, further study is
needed in this area.
The remaining demographic variables have only been mentioned by a
few researchers. No significant relationship between race and coping
behaviors has been noted (Curry & Russ, 1985; Knight et al., 1979;
LaMontagne, 1984). Generally, no significant difference between prior
exposure to the stressful situation and coping behavior has been noted
(Curry & Russ, 1985; Field et al., 1988; Knight et al., 1979; LaMontagne,
1984), although one study did indicate that children with prior
experience, in this case chronically ill children, tended to use a greater
number of coping behaviors than did acutely ill children without
experience (Ritchie, Caty, & Ellerton, 1988). Finally, the type of
surgery was not found to have significant relationship to the child's
coping (Knight et al., 1979).
Only two personality characteristics, locus of control (LOC) and
anxiety, have been studied in relation to the coping behaviors of
children. Regarding LOC, research has indicated that an external LOC is
related to avoidant or inward coping behaviors and that and internal LOC
is correlated with active or outward coping behaviors (LaMontagne, 1984,
1987; Rothbaum, Wolfer, & Visintainer, 1979). State anxiety has been
included as an independent variable in two unidimensional studies

77
(Burstein & Meichenbaum, 1979; Field et al., 1988). State anxiety refers
to the situational anxiety as compared to the trait anxiety, the
relatively stable, dispositional aspect of anxiety. Neither study found
a significant relationship between the child's state anxiety and the
coping dimension. Trait anxiety has not been studied in relation to the
child's coping behaviors.
In summary, the reports of the relationship between demographic
variables and children's coping have generally been incidental to the main
purpose of the study. The findings pertaining to the relationship between
gender and coping are inconclusive, although it is possible that there is
a tendency for boys and girls to use different types of coping behaviors.
Regarding the variable of age, it appears probable that coping changes as
the child matures intellectually, evidenced by an increase in cognitive
forms of coping and in self-control. The available research is
insufficient to establish a pattern between ethnicity and coping or prior
experience and coping. Study of the relationship between personality
characteristics and coping has been limited to locus of control and state
anxiety. It appears that an internal locus of control is related to
active coping, and that there is no relationship between state anxiety
levels and coping behaviors. Further research is needed to clarify these
relationships.
As is evident from the literature reviewed, the current knowledge
base concerning sources of stress and the coping of school-age,
hospitalized children provides a basic understanding of these processes.
However, it is evident that little is known about factors that may
influence the differences in appraisal of stress and coping behaviors. If
the available knowledge base is to be of practical use in assisting the

78
child to cope with stressful events, more must be known about the
variables affecting the individual child's responses. Therefore, it is
necessary to carefully select factors to be analyzed in subsequent studies
that will add to the knowledge base in a substantive manner.
Conceptual Model
In the Lazarus paradigm, the appraisal of an event as stressful and
the resulting coping behaviors are dependent on the modifying influence of
personal and environmental variables (Lazarus & Folkman, 1984a). Because
little research has been conducted concerning the influence of such
antecedent variables on the stress and coping process, it was decided to
examine factors that were of a fundamental nature so that the findings
would be of practical use to the nurse clinician. Additionally, the study
of the antecedent variables relevant to the appraisal of stress limits the
problem of circularity that occurs when using a relational definition of
stress (Lazarus & Folkman, 1984a: Lazarus, DeLongis, Folkman, & Gruen,
1985). While there are many variables that may influence the stress and
coping process of the hospitalized school-age child, three personal
variables were selected for investigation in this study: health status as
either acutely or chronically ill, trait anxiety, and gender (See Figure
2).

79
Health Status
Anxiety =~ Nº.
Stress - Coping
_-tº Tº behaviorsGender ~
Figure 2. Model of the relationship between three modifying variables andthe stress and coping process
Health Status
Health status as acutely or chronically ill was postulated to have
an influence on the child's appraisal of stress and coping behaviors due
to the differences in prior experience with hospitalization. The process
of stress appraisal is influenced by prior experience according to the
extent that the situation is novel or familiar to the person (Lazarus &
Folkman, 1984a). Although few situations are completely novel, the child
who has had prior experience as a patient in the hospital will be likely
to have a different knowledge of the meaning of events for his or her
well-being than will the child who's knowledge is derived from the stories
of family members, friends, television or other vicarious sources. A
differing understanding of the hospital experience may result in a
differing appraisal of stress. Similarly, prior experience affects the
coping process by increasing the child's awareness of the extent of
controllability of the event, modifying his or her beliefs in the ability

80
to cope with the current situation (Melamed, Siegel, & Ridley-Johnson,
1988), and through enhancing the child's repertoire of problem solving
skills (Lazarus & Folkman, 1984a). As noted earlier, chronically ill
children are hospitalized more frequently than are healthy children with
an acute illness (Perrin, 1985; Butler et al., 1985). Therefore, it was
thought possible that the stress and coping processes of the chronically
ill child would be different than that of the acutely ill child. As
evident from the above literature review, minimal attention has been given
to this variable in research. Thus, the extent of influence of health
status on the child's reactions and behavior is unknown.
Anxiety
The child's characteristic level of anxiety was postulated to have
an influence on the stress and coping processes. Anxiety has been
conceptualized as having two distinct aspects: trait and state (Endler &
Edwards, 1982). Trait anxiety, the person's predisposition toward
anxiety, is a relatively stable personality characteristic. In contrast,
state or situational anxiety, the transient reaction to an event, follows
the person's appraisal of the stress in a specific situation (Endler &
Edwards, 1982; Folkman & Lazarus, 1988). Therefore, it is the trait
anxiety that may influence the person's appraisal of stress (Klein, 1988)
whereas state anxiety would act as a mediating factor in the coping
process. Trait anxiety would appear to affect stress directly by
influencing the level of threat the individual perceives in the
environment. The level of perceived threat would then result in anxietyindirectly influencing coping by affecting cognitive functioning and the
resulting use of problem-focused coping, such as occurs when high trait

81
anxiety interferes with optimum thinking and problem solving (Lazarus &
Folkman, 1984a, pp. 167). It is also possible that trait anxiety may have
an undetermined direct affect on the child's coping responses.
Gender
Gender also was postulated to have an influence on the stress and
coping processes under consideration. The process of secondary appraisal
of stress may be influenced by gender related personality characteristics,
such as the learned helplessness of girls, and the mastery-orientation
seen more often in boys (Dweck & Wortman, 1982), by determining whether or
not the child believes that resources are available to deal with the
stressful event. Additionally, gender may affect the type of coping
behaviors used by children. Although a portion of the literature found no
gender related difference in coping behaviors (Altshuler & Ruble, 1989;
Curry & Russ, 1985; Hamner & Miles 1988; LaMontagne, 1984, 1987), several
studies did identify important differences in the strategies used by boys
as compared to girls (Murphy, 1976; Ryan, 1989; Savedra & Tesler, 1981;
Wertlieb et al., 1987). Further investigation is needed to gain a better
understanding of this fundamental variable.
Stress Appraisal
The individual's appraisal of stress affects coping behavior.
According to Lazarus (Lazarus & Folkman, 1984a) the type of appraisal
occurring in a situation will influence the resulting coping behaviors.
If the situation cannot be changed or is not controllable, emotion focused
coping is more often used, whereas if the person believes that they may

82
alter the situation, problem-focused modes of coping are more likely to be
used.
It is recognized that many other person and environmental variables
may influence the child's appraisal of stress and resulting coping
behaviors. However; it is believed that these selected variables
represent fundamental and easily identifiable characteristics, and thus
will contribute practical information to the knowledge base.
Hypotheses
Based on the theoretical frameworks of Lazarus and Piaget, on the
current status of knowledge concerning stress and coping of the
hospitalized school-age child, and on the proposed conceptual model, the
hypotheses for this study were:
1. There will be a relationship between health status and the type of
event appraised as stressful during hospitalization.
2. There will be a relationship between health status and the type of
coping behavior used during a stressful hospital event.
3. There will be a relationship between gender and the type of event
appraised as stressful during hospitalization.
4. There will be a relationship between gender and the type of coping
behavior used during a stressful hospital event.
5. There will be a relationship between trait anxiety and the type of
event appraised as stressful during hospitalization.
6. There will be a relationship between trait anxiety and the type of
coping behavior used during a stressful hospital event.-
7. Health status, gender, and trait anxiety will affect the appraisal
of hospitalization as stressful.

83
a . acutely ill children will appraise the event of
hospitalization as more stressful than will chronically ill,
children
b. girls will appraise the event of hospitalization as more
stressful than will boys
C. children with high levels of trait anxiety will appraise the
event of hospitalization as more stressful than will children
with low levels of trait anxiety
8. Health status, gender, trait anxiety, and stress appraisal will
affect the perception of effectiveness of the coping behavior.
a . chronically ill children will perceive their coping behaviors
during hospitalization as more effective than will acutely
ill, children
girls will perceive their coping behaviors during
hospitalization as more effective than will boys
children with low levels of trait anxiety will perceive their
coping behaviors during hospitalization as more effective than
will children with high levels of trait anxiety
children who appraise hospitalization as of low stressfulness
will perceive their coping behaviors during hospitalization as
more effective than will children who appraise the event of
hospitalization as highly stressful.

84
Definition of Terms
In this study key terms will be defined as follows:
Stress: ". . . a particular relationship between the person and the
environment that is appraised by the person as taxing or exceeding
his or her resources and endangering his or her well-being" (Lazarus
& Folkman, 1984a, pp. 19).
Appraisal: ". . . an evaluative process that determines why and to what
extent a particular transaction or series of transactions between
the person and the environment is stressful" (Lazarus & Folkman,
1984a, pp. 19).
Coping: ". . . the process through which the individual manages the demands
of the person-environment relationship that are appraised as
stressful and the emotions they generate" (Lazarus & Folkman, 1984a,
pp. 19).
Health Status: the general state of a person's physical condition, for
this study, specifically either chronically or acutely ill.
Chronic Illness: ". . . a physical . . . condition lasting longer than
three months or necessitating a period of continuous hospitalization
of more than one month" (Pless & Pinkerton, 1975, pp. 90, 91).
Acute Illness: a physical condition that has been present less than three
months, has not necessitated a hospitalization of more than one
month, and that is not normally considered to be a chronic illness.
Trait Anxiety: the "relatively stable individual differences in anxiety
proneness, i.e. to differences among people in the disposition or
tendency to perceive a wide range of situation as threatening..."(Spielberger, 1975, pp. 137)
Gender: The child's sex as male or female.

85
School-age child: a child between the ages of 8 to 11 years of age.
Non-categorical: An approach to studying health related problems that
"focuses on dimensions that vary across disease categories rather
than on disease-specific differences." (Stein & Jessop, 1982, pp.
355)

86
CHAPTER THREE
METHODOLOGY
In the following section the methodology of this study will be
described. This will include the design, description of the research
settings, human subjects assurance, the sample, instrumentation, process
of data collection, and data analysis.
Design
The design selected for this study was nonexperimental and cross
sectional using a nonprobability sample. Nonexperimental is defined as a
"systematic empirical inquiry in which the scientist does not have direct
control of independent variables because their manifestations have already
occurred or because they are inherently not manipulable" (Kerlinger, 1986,
pp. 348). In nonexperimental research, direct control through treatment
or randomization is not attempted, rather the affect of the theoretically
identified independent variable on the dependent variable is inferred from
the observation that the two vary together. Cross-sectional is defined as
a "design that involves selecting a representative sample from the
population of interest and observing all the phenomena . . . of interest
at the same point in time" (Woods & Catanzaro, 1988, pp. 554). In cross
sectional research the variables of interest are assessed once, at a time
determined by the purpose of the study. Nonprobability sampling is a
sampling technique that does not use random sampling (Kerlinger, 1986, pp.119). In nonprobability sampling each potential subject does not have an
equal chance of being in the sample, but rather eligibility is determined

87
through purposive, quota, or convenience sampling. Accordingly, in this
study a convenience sample of subjects were each tested once in the
naturally occurring environment of the hospital; no manipulation of the
setting, subjects, or intervention was involved. This is in keeping with
the purpose of the study to determine the relationship between the
selected independent variables of health status, gender, and trait anxiety
and the naturally occurring dependent variables of stress appraisal and
coping behavior.
Strengths and Weaknesses of the Design
The use of a non-experimental design in the study of stress and
coping has increasingly been recognized as the preferable method of
inquiry (Lazarus, 1981; Lazarus & Folkman, 1984a). Naturalistic research,
rather than experimental investigations, permits the study of the coping
processes that are used in response to actual experiences appraised as
stressful. Use of a non-experimental design in the present study
therefore allows examination of the naturally occurring stress appraisal
and coping processes of hospitalized children. A weakness of using a non
experimental model is the inability to randomly assign subjects to
treatment groups (Kerlinger, 1986). Although less than ideal, this is the
only acceptable alternative when studying the reactions of children to
hospitalization and events occurring while hospitalized. Because the
therapeutic interventions are determined by the child's physiological
needs, it is not possible to randomly assign a subject to a group
receiving a specific, potentially stressful experience such as anintrusive procedure or immobilization. Similarly, use of a model that
would expose a hospitalized child to experimentally induced stressful

88
stimuli would not be ethically acceptable. An alternative, presenting
stressful stimuli to the subjects in story form and asking for their
stress and coping response, would only examine the child's general style
of stress and coping, not his or her actual responses to a real situation.
Thus, use of the non-experimental model to assess the hospitalized child's
appraisal of actual stressful event and their resultant coping behavior
most fully met the purpose of this study.
Use of the cross-sectional design is common in naturalistic research
(Woods & Catanzaro, 1988). One strength of cross-sectional design is that
it permits collection of the independent and dependent variable data at
the same point in time. This characteristic is of great importance when
dealing with a population that is highly transient, such as hospitalized
children. A second advantage of this design is that is allows inter
individual comparison of the variables of interest. Thus, comparisons in
stress and coping may be made across health status groups, gender, and
anxiety. A weakness of the cross-sectional design is the inability to
examine change in behavior over time. Lazarus (Lazarus & Folkman, 1984a)
emphasizes the need to study both the changes in intraindividual stress
and coping behavior through longitudinal designs and the interindividual
differences obtainable through cross-sectional studies. Although
investigating the changes in hospitalized children's stress and coping
over time would contribute valuable information to nursing practice,
inclusion of a longitudinal component in this study was not possible.
Children's admission to the hospital is usually sporadic and
unpredictable. Collection of intraindividual data either would have
necessitated limiting the subjects to children admitted frequently, such
as those on a chemotherapy protocol or would have involved following a

89
large sample of children over a period of years to obtain a sample of
subjects hospitalized several times during childhood. Neither option fit
the purposes of the present study. Therefore, while a design permitting
both interindividual and intraindividual examination would have been
ideal, the use of a cross-sectional design was appropriate to answer the
questions of this study.
It is possible that selection of subjects though convenience
sampling, rather than using randomized selection, may have affected the
generalization of the results of the study. While randomization would
have decreased the possibility of consistent extraneous variables
influencing the data, it was not thought to be a realistic alternative for
this study, as the population of school-aged children admitted to the
hospital is limited. As an alternate method of controlling for variance
in subjects, stringent inclusion/exclusion criteria were developed and
followed (see discussion below).
One additional potential weakness of the design was the exclusion of
a control group. Control groups are a characteristic of experimental or
quasi-experimental research. It would have been possible to design the
current study as quasi-experimental, using children who had not been
hospitalized as the control group, as the presumed intervention is the
experience of hospitalization. However, as discussed above, asking
subjects who had not experienced hospitalization what they thought would
be stressful and how they would cope with it would be assessing the
child's coping trait or style, that is what he or she would be likely to
do. It could not determine the child's coping process or state, what he
or she would actually do when hospitalized, a distinction deemed crucial
to study of stress and coping behaviors (Lazarus & Folkman, 1984b).

90
Additionally, the inclusion of a control group would have asked the
question, is there difference in non-hospitalized and hospitalized
children's interpretation of stress associated with hospitalization and
resulting coping patterns. This would not have allowed examination of the
variables thought to influence the child's stress and coping behaviors
during hospitalization. For these reasons, a control group was not
included in this study.
In summary, a nonexperimental design was used to study the naturally
occurring processes of stress appraisal and coping of hospitalized
children. The cross-sectional aspect of the design was necessary to
gather sufficient data to conduct interindividual comparisons of the
variables in question. Finally, convenience sampling was used due to the
scarcity of the population, but was balanced by inclusion/exclusion
designed to control for variance in the sample. This design provided the
needed structure to investigate factors influencing the stress appraisal
and coping processes of hospitalized school-age children.
Research Settings
Data collection for this study was conducted at seven facilities.
Four of these were large medical centers affiliated with a university and
three were children's hospitals. It was determined that multiple sites
were necessary for the following reasons: 1) use of multiple facilities
would increase the likelihood of obtaining a sample representative of the
target population, thus avoiding an artificial imbalance in chronic versus
acutely ill children and avoiding testing of the subject's reactions tothe milieu of one specific facility; 2) the benefits and burdens of
participation in research would be equitably distributed among

91
hospitalized children in California, rather than limited to a sometimes
overused subgroup in the Bay area; 3) additional sites for data collection
would obviate the potential difficulty obtaining the needed sample size
due to the limited number of children likely to be admitted during the
school year who would meet the selection criteria. To control the
variance in the sample responses, all sites used were designated pediatric
units or hospitals, all allowed rooming-in of the parents according to the
parents availability, and all had a play room available to the children
that was staffed by Child Life Specialists or other trained personnel.
Children admitted to an adult, rather than the pediatric unit, at the
facilities, were not included in the study.
The first setting was the pediatric units of the University of
California, San Francisco, Medical Center (UCSFMC), a teaching hospital
affiliated with a university health science campus. The sixth floor of
the Moffit and Long Hospitals is a designated pediatric hospital within
the medical center and serves as a tertiary referral center for northern
and central California and southern Oregon. There are a total of 75
pediatric beds, including the ambulatory medical and surgical care units,
the PICU, the Pediatric Clinical Research Center (PCRC), and the Pediatric
Transplant unit. The age range admitted to the units extends from infants
through adolescents. For this study, only patients on the ambulatory
medical and surgical pediatric units, and the PCRC were used as subjects.
The medical unit has a high census of children with cancer and as well as
other problems, and has 24 beds, configured as two 4-bed rooms (primarily
used for infants and toddlers), eight 2-bed rooms, and eight private rooms
(often used for immunosuppressed patients). The surgical unit accepts
children with diagnoses ranging from ruptured appendicitis to
º
s

92
neurosurgical and cardiac problems, and also has 24 beds, configured as
two 4-bed rooms (used for the younger patients), eight 2-bed rooms, and
two private rooms. The PCRC has 6 beds and houses children involved as
subjects in medical research who would otherwise be admitted to the
ambulatory medical or surgical units. Primary nursing care is given by
registered nurses. Occasionally student nurses are present on the units.
The playroom is open at designated hours, and a school room and teacher
are located on the floor to work with children experiencing a lengthy
admission.
The second setting is the Shriner's Hospital for Crippled Children,
San Francisco (SHCC). This facility is one of 19 Shriner's Hospitals
providing a philanthropical service for children with orthopedic problems
needing either medical or surgical treatment, for children with spinal
cord injuries, or for children with burn scars needing surgical revision.
The San Francisco unit has three basic units, the spinal cord injury unit,
a boys unit, and a girls unit, with a total capacity of 48 beds. The
patients' ages range from infancy through adolescence. Nursing staff is
composed of approximately 50% registered nurses and 50% nursing
assistants. A team nursing approach is used. A large recreation room is
open at designated hours and provides a variety of activities and crafts.
A school room large enough to provide easy access by wheelchair and gurney
is staffed by teachers and the children are encouraged to attend class on
a regular basis.
The third facility is the pediatric unit of San Francisco General
Hospital Medical Center (SFGHMC). This is a 444 bed facility serving the
lower income residents of the city. The pediatric unit has a capacity of
24 beds, although it is currently budgeted for only 14 beds, and serves
º
º

93
children between the ages of newborn through 17 years having medical,
emergency surgical, or trauma related problems. Most of the rooms have
two beds, although there is a large room with four or more cribs for
infants and toddlers. Primary nursing care is provided by staff comprised
of 75% registered nurses and 25% licensed vocational nurses. Student
nurses are also are involved in care giving several days a week. The
playroom is open at designated hours. Teachers from the school system are
available for children having a lengthy admission, but this is uncommon.
The fourth setting was Children's Hospital at Stanford (CHGS). This
is a 56 bed, non-profit, teaching hospital serving children from infancy
through adolescence. It is located near Stanford University Hospital
(SUH) and interfaces with SUH in coordinating services for children. For
example, CH@S primarily provides services for the children with chronic
physical or psychological problems, while SUH focuses more on the
intensive care and acute care needs. Services such as medical staff and
institutional review board are shared. Three of the four patient care
units at CH@S were used for data collection: the 15 bed Babcock Unit
caring for children of school-age or younger with illnesses such as
gastrointestinal, pulmonary, orthopedic, rehabilitation, and overflow
oncology; the 14 bed McElroy Unit caring for older children with pulmonary
problems, cystic fibrosis patients from early childhood through adults,
orthopedic, and arthritis; and the 13 bed Auxiliary Unit caring for
hematology/oncology patients. The 14 bed Roth Unit, caring for children
with psychosomatic problems, was not used. Each unit has a variety of
single, double, or four-bed rooms. Primary nursing care is provided by
staff consisting of 90 % registered nurses and 10 % nursing assistants.
A recreation department and occupational therapy department are available
Tº- *
/ 7.

94
for the children. There are three school rooms, one each for primary,
intermediate, and high school classes. Teachers also work with children
at the bedside as needed.
The fifth setting was the University of California, Davis, Medical
Center (UCDMC), a 378 bed facility located in south Sacramento. Pediatric
facilities include an ICU, a special care unit, and a 27 bed basic unit.
The rooms on the basic unit house either two or three beds, with the
exception of two infant rooms having room for four or five cribs each.
The hospital is known for its trauma facilities, but also provides
services for chronically ill children. The pediatric nursing staff is
approximately 85% registered nurses and 15% licensed vocational nurses.
The method of care is total care nursing. The playroom is open at
designated hours and a teacher from the school district comes to the unit
as needed.
The sixth setting was Valley Children's Hospital (VCH), located in
Fresno, California. This is a 148 bed facility providing tertiary care to
children in central California from birth through adolescence. In
addition to the usual ethnic mix of California, the Fresno area has a
large population of Southeast Asian refugees, a fact reflected in the
admissions to VCH. Eligible subjects are usually admitted to either the
medical unit or the adolescent unit which takes overflow of older children
from other units as needed. Most patient rooms on the basic units have
two beds. Nursing care is provided by a staff comprised of 86% registered
nurses, 12% licensed vocational nurses, 2% certified nursing assistants,
and periodic rotations of student nurses. The playroom is open at
designated hours, and a school room is located within the facility.
-
2
º
95
The seventh setting was Loma Linda University Medical Center
(LLUMC), a 627 bed, tertiary care facility located in southern California,
approximately 60 miles east of Los Angeles. This is a private, non
profit, teaching hospital affiliated with a health science university.
There are three basic pediatric units, in addition to a pediatric
intensive care unit and a neonatal intensive care unit. Unit 5100 has 26
beds and primarily cares for hematology/oncology patients. Primary
nursing care is given by registered nurses. Unit 5200 has 7 beds for
ambulatory care patients and an 8 bed stepdown unit for patients from
PICU. Team nursing is used to provide care for the ambulatory patients
with a nursing ratio of approximately five registered nurses to one or two
licensed vocational nurses or nursing assistants. The rooms on both units
are semi-private two bed rooms, with each unit also having one or two
three-bed rooms. Unit 5300 has 32 beds and primarily serves NICU
graduates, infants and toddlers and has an all RN staff. Most of the
acutely ill children receive care in a local community hospital. Student
nurses also are involved in the children's care. The playroom is open at
designated hours and arrangements may be made for a teacher to come to the
child's room.
Human Subject's Assurance
Application for Human Subject's approval was made according to the
protocol for each facility and approval obtained. (See Appendix A for a
sample of letter of approval.) Listed below are the institutional review
boards granting approval and the facilities accepting that approval:
1. Committee on Human Research, University of California, San
Francisco, # H1777-05091-01. This approval was accepted by
s
96
University of California, San Francisco, Medical Center; San
Francisco General Hospital and Medical Center; and Shiner's
Hospital for Crippled Children, San Francisco.
2. University of California, Davis, Human Subjects Review
Committee, # 90-309. This approval was accepted by the
University of California, Davis, Medical Center.
3. Stanford University Hospital, Medical Committee for the Use of
Human Subjects in Research, # M1272. This approval was
accepted by Children's Hospital at Stanford.
4). Valley Children's Hospital Human Subject's Committee, (no
number assigned). This approval was accepted by Valley
Children's Hospital.
5. Loma Linda University, Institutional Review Board, (no number
assigned). This approval was accepted by Loma Linda
University Medical Center.
Sample
The following section will discuss the criteria guiding the
selection of the sample for this study. First, the characteristics of
interest will be reviewed and the constraints placed on sample selection
due to the variables will be identified. Second, the specific
inclusion/exclusion criteria used for control of variance in this study
will be delineated. Third, rationale for the criteria will be provided.
Fourth, major potential sources of variance that were not controlled will
be identified and discussed. Fifth, the population to which the results
of this study may be generalized will be described. Sixth, the method of
s

97
determining the sample size will be stated. Seventh, the process of
sample selection will be discussed.
Sample Selection Constraints due to Variables of Interest
The characteristics that were of specific interest in this study
were the child's health status as acutely or chronically ill, the child's
gender, the child's trait anxiety level, and the child's identification of
the stress and coping processes used in relation to hospitalization. The
influence of each of these variables on the sample selection will be
discussed.
The variable of health status was examined by using the
noncategorical approach rather than a diagnostic specific approach. Stein
and Jessop (1982, pp. 355) define this as an method that "focuses on
dimensions that vary across disease categories rather than on disease
specific differences." The argument for using this strategy was that when
working with the psychosocial needs of chronically ill children, there is
more variance within the specific diagnostic groups than between them
(Stein, 1983; Stein & Jessop, 1982, 1984, 1989; Pless & Pinkerton, 1975;
Pless & Perrin, 1985). For the purposes of this study, this principle was
applied to the psychosocial needs of not only the chronically ill child in
the hospital, but also the acutely ill hospitalized child. Regardless of
the diagnosis and specific therapeutic treatment, all children admitted to
the hospital will have similar experiences, such as intrusive procedures,
separation from the familiar home environment, separation from parents
either for brief or lengthy periods of time, realization that parents are
not all-powerful, and loss of personal privacy. Using a noncategorical
approach, rather than the traditional disease specific approach, the
º
-
s

98
commonalities in the stress and coping of hospitalized children may be
examined and variables possibly influencing these reactions may be more
easily studied. As all children admitted to the hospital have either an
acute or chronic condition, inclusion of this variable did not eliminate
any categories of potential subjects from the study.
Similarly, the inclusion of gender as a variable of interest did not
limit the sample of children selected for the study. All hospitalized
children would be either male or female. Therefore, no potential subjects
were excluded due to lack of fit with one of the subcategories of this
variable.
The constraints imposed by the measurement of the variable of trait
anxiety was partially responsible for determining the age of the subjects
in this study. Theoretically, all children would have a typical level of
trait anxiety. However, psychometrically strong instruments to measure
this variable are available only for children from first grade and above
(Reynolds & Richmond, 1978; Spielberger, 1973). Therefore, because the
characteristic of trait anxiety was to be examined, the subjects selected
for inclusion in this study needed to be within the school-age years.
To determine what the child personally appraised as stressful and
the coping behaviors used to deal with the stress, it was necessary to
work directly with the child. Prior research has shown that the agreement
between childrens' and adults' ratings of the stressfulness of childhood
experiences is moderate. Yamamoto and Felsenthal (1982) found a .68
correlation between the adult ratings and the child ratings of the
stressfulness of life events. Lapouse and Monk (1959) found that mothers
underreported the number of their child's fears and worries by 41%.
Similarly, parental identification of coping behaviors used by children
º

99
also fails to identify many of the strategies the child reports using by
about 44 X (Walker, 1988). Based on these studies, it was believed that
the child, rather than the parent or another adult, would be able to
provide the most accurate data regarding the child's appraisal of stress
and coping responses during hospitalization. Therefore, it was decided
that data collection would only involve the child, rather than including
adults familiar with the hospitalized child's experiences such as the
parents, nurse, or child life specialist.
Inclusion/Exclusion Criteria
Because a convenience, rather than random, sample was used,
stringent inclusion/exclusion criteria were developed to control for
variance that could occur due to extraneous factors. Using these criteria
as a control, it was believed a representative sample of hospitalized
school-age children would be obtained. General inclusion criteria for the
subjects in this study were an age range of 8 to 11 years, normal
cognitive ability as determined by age appropriate grade, and minimum
length of admission of 2 to 3 days. Additionally, the chronically ill
children needed to have at least one previous hospitalization, including
overnight stay, in the prior three years, and the acutely ill children
could not have had a hospital admission since two years of age. General
exclusion criteria for the study were an inability of the child to speak
sufficient English to participate in testing, any intensive care
experience during the current hospitalization prior to the time of data
collection, an admission associated with child abuse, any major perceptual
deficits, and terminal phase of the illness.
º
* }
100
Rationale for Inclusion Criteria
The purpose of the inclusion criteria was to control for possible
extraneous factors that might influence the dependent variable: the
child's report of stress appraisal and coping behaviors. The major factor
that was believed to have a possible affect on the responses was the
child's thinking, which is dependent on age and cognitive maturity. In
order to obtain a sample of children with similar thinking processes, it
was decided to use only children likely to be in Piaget's stage of
concrete operational thinking, ages 8 through 11 years. As noted earlier,
the concrete operational stage begins to emerge at about 7 years of age
(Piaget & Inhelder, 1969), but a period of transition occurs as the child
acquires the ability to mentally manipulate the internal representations
of the external, observable world. Therefore, 8 years of age was selected
as the youngest age for potential subjects to increase the likelihood that
the child was indeed using concrete operational thinking. The option of
including some 7 year olds by administering Piage tian tests to determine
the stage of thinking was not used as it would have increased the length
of the testing session, an alternative not feasible when working with sick
children who may become fatigued easily. Eleven years of age was selected
as the upper extreme of age for the subjects. The earliest evidence of
the development of Piaget's stage of formal operations may occur toward
the end of 11th year or during the 12th year (Brainerd, 1978; Ginsburg &
Opper, 1988) and is not well established until the middle of the teen
years. Because a common reaction of children exposed to stressful
situations, such as hospitalization, is regression, it was thought to be
unlikely that 11 year old hospitalized child would use the early
beginnings of hypothetico-deductive reasoning in discussing his or her
! }

101
stress and coping reactions during hospitalization. For these reasons, it
was decided that the subjects would be within the ages of 8 to 11 years of
age. This decision provided more control over possible variance than
would have the broader categorization of "school-age", generally
considered to be ages 6 through 12 years, which would have included
children likely to be in the transitional phases of cognitive functioning.
Because cognitive functioning may not correspond directly with
chronological age, it was also necessary to determine that the subjects be
of normal cognitive ability. This was determined by asking if the child
was in an age appropriate grade in school and by asking if the child
attended any special educational classes. Age appropriate grade was
identified as :
8 years of age -- grade 2 or higher
9 years of age -- grade 3 or higher
10 years of age -- grade 4 or higher
11 years of age -- grade 5 or higher
If the child attended a special education class the reason for this
placement was requested. If it was due to physical limitations, a
learning disability such as dyslexia, or some minor difficulty in a basic
skill, such as needing extra practice and help with reading or math, the
child was considered a potential subject. If the parents response
indicated that the child was receiving remedial help in all academic
areas, the child was not considered a potential subject. Through these
criteria, age of 8 to 11 years and age appropriate grade, it was likely
that the subjects would have similar thinking processes and that possible
variance due to inclusion of children within earlier or later stages of
cognitive development would be limited.
7.

102
A second factor that could be expected to influence the children's
responses and introduce undesirable variance into the results was the
extent of exposure to the hospital environment. It was believed that the
responses of children regarding appraisal of stress and coping behaviors
might be affected by the length of time they had been exposed to the
hospital environment. A child who had been admitted for only a few hours
might have a very different impression than would the child who had been
hospitalized for several weeks, the former having had fewer experiences
and less time to differentiate the potentially harmful events from those
that are personally irrelevant or benign, the latter having had many
experiences and the opportunity to distinguish between personally
stressful and innocuous situations. Therefore it was decided that to
control for this possible source of variance, data collection would need
to be conducted within a set time frame. As all subjects would need
sufficient time to be exposed to a variety of potentially stressful
situations and to use coping behaviors, and because insurance regulations
dictate that the length of hospital admission is kept as short as
possible, it was decided that data collection would occur on the second or
third day of the child's hospital admission. One exception was made to
this criteria, if the child had surgery on the second day of admission,
the period for data collection was extended to the fourth day, as on the
third day the child generally was not alert enough to participate in the
testing. For these children, the fourth day of admission was the third
day in which they were awake and aware of the hospital experience,
rendering it likely that the data from these children would not be
significantly different than that of children tested on the second or
third day. It was believed that this criteria would provide sufficient
º

103
time for all children to experience a variety of potentially stressful
events and use coping behaviors, while controlling for differences that
might occur if comparing children who had been admitted only briefly with
those who had been on the unit for a lengthy period.
An issue related to control of experience during the present
admission is control of prior hospitalization experience. As discussed
earlier, a basic premise of this study was that chronically ill children
are hospitalized more frequently than are healthy children with an acute
illness, and that due to prior experience the chronically ill child may
have different patterns of stress and coping than does the acutely ill
child not having such past experience. It was recognized however that
some chronically ill children, such as a diabetic in good control of his
or her condition, may have only been admitted at the time of diagnosis,
whereas an acutely ill child may have been admitted several times for
unrelated conditions. Essentially then, there were four possible groups
of subjects:
1. chronically ill children with minimal prior hospitalizations
2. chronically ill children with several prior hospitalizations
3. acutely ill children with minimal prior hospitalizations
4. acutely ill children with several prior hospitalizations
Because the number of children in groups one and four were likely to be
limited and inclusion of these children would not provide a clear answer
to the question of the affect of health status on the stress and coping
response of hospitalized children, it was decided that only children in
groups 2 and 3 would be included in the study. No attempt was made to
balance the number of children from the two groups.
-
º

104
Another possible source of variance in the study was the child's
memory of prior hospitalizations. Because the purpose was to examine the
differences between acutely ill children who were unfamiliar with the
hospital environment and chronically ill children who were accustomed to
hospital routines and events, it was decided that the acutely ill subjects
would not have been admitted to a hospital since two years of age and the
chronically ill subjects would have had one or more hospitalizations
within the last three years. This would ensure a comparison between
chronically ill children who know what to expect during hospitalization
and acutely ill children who have no concrete memory of hospitalization,
and thus control for possible variance within groups due to prior
experience in the hospital.
Rationale for Exclusion Criteria
To provide further control for possible extraneous variables, five
exclusion criteria were delimited. Because it was necessary that the
subjects be able to give assent, participate in an interview, and respond
to standardized instruments written in English, it was necessary to
exclude any child with limited communication skills in English. This was
determined by talking with the primary nurse about the child's
communication skills and/or attempting to engage the child is a simple
conversation. If the child was not able to understand and respond to
basic questions relating to age and favorite activities, the child was
excluded from the study.
Similarly, because the study was dependent on the child's ability to
respond to verbal and written questions, children with any major
perceptual deficits were not considered potential subjects. This was
determined by talking with the child's nurse and/or attempting to engage
º

105
the child in a simple conversation or determine the extent of visual or
hearing impairment. If the child's deficit was such that it would hinder
his or her ability to participate fully in the data collection, the child
was not considered to be a potential subject.
Three additional groups of children were excluded from the study due
to experiences that could potentially increase the child's appraisal of
stress during hospitalization and alter the coping behaviors. The first
of these was the exclusion of children who had been admitted to the
intensive care unit during the current hospitalization. Because the child
admitted to the intensive care unit is likely to experience and observe
many more stressful events and because the physical condition of the child
would decrease the options available for coping, it was believed the
experiences of this child would be sufficiently different from that of the
child admitted to a general medical or surgical unit to result in
undesirable variance in the responses of the child. Therefore, children
having been admitted to ICU during the current hospitalization prior to
data collection were excluded from the study.
The second group having an experience that could potentially
introduce extraneous variance into the study was children admitted for a
diagnosis related to child abuse. It was thought possible that an abused
child might appraise events differently than an child that had not been
abused. Additionally, it is possible that the child who has been abused
has learned to use different coping behaviors in response to a stressful
situation. Therefore, to control for this possible source of variance,
children admitted to the hospital due to abuse were not included in the
study.
º

106
Similarly, children who were considered to be in the terminal phase
of their illness were not considered potential subjects. Because the
dying child is generally aware that the end of life is nearing, the
relative importance of events may be altered, resulting in differences in
the appraisal of stressful events. To control this source of extraneous
variance, the chart was read and the nurse consulted to determine the
child's condition. If a "do not resuscitate" order was written or it was
apparent that vigorous curative treatment had been stopped and palliative
care was being provided, the child was excluded from the study.
The above inclusion and exclusion criteria were developed to
reduce the variance in the subject's responses that may have occurred due
to use of a convenience, rather than random, sampling. Despite these
rigorous criteria, several relevant extraneous variables were not
controllable and may have increased the source of error variance.
Potential Sources of Uncontrolled Variance
Although many potential sources of uncontrolled variance could be
identified, four dominant factors should be recognized. The first of
these would be the multitude of specific diagnostic or therapeutic
experiences that might be encountered by an individual subject.
Obviously, only a child who had experienced a bone marrow aspiration or a
bronchoscopy would be likely to identify that event as stressful.
Therefore, despite the similarities in the experiences of all hospitalized
children, individual events uncommon to the population will occur and may
act as a source of uncontrollable variance. A second extraneous variable
would be the child's knowledge about the hospital acquired through
indirect, rather than direct, experience. Possible sources for such
-

107
information would include books, television, family or friends, and pre
hospitalization programs. This knowledge could function to either
increase or decrease the child's appraisal of events as stressful, and
thus would contribute to uncontrollable variance in the child's responses.
A third source of variance would be the child's prior positive or negative
experiences in a medical office, clinic, or emergency room. Although
these events would be of limited length, the child may have developed an
opinion about the stressfulness of a physical exam, of the measurement of
the blood pressure, or of intrusive procedures such as injections. These
previous experiences would be likely to influence the child's reactions to
similar events during hospitalization. A fourth major source of variance
would be the ability of the parents to provide reassurance and support to
the child during hospitalization through their presence. While it is
likely that most parents will attempt to spend time with the child during
hospitalization, the actual number of hours the parent is able to be
present would vary greatly. It is possible that children appraise the
stressfulness of an event differently according to whether the parents are
available or unavailable. Thus, the child's responses may vary depending
on the presence or absence of the parents during potentially stressful
events.
While it would have been ideal to control for all possible sources
of extraneous variance, such an option is not possible in nonexperimental
research. It is recognized that the inability to control all extraneous
independent variables that may influence the dependent variables could
pose a threat to the internal validity of the study. The affect of the
uncontrolled extraneous variables may mask the true affect of the
independent variables on the dependent variable. Accordingly, while the
*
108
results of this study should provide a reasonable representation of the
influence of health status, gender, and trait anxiety on the stress and
coping of hospitalized, school-age children, the results are study
specific. It is probable that a replication would yield somewhat
differing results due to fluctuations in the influence of the uncontrolled
variables.
Population to Whom Results may be Generalized
Because randomization and a sampling framework was not used in this
study, the external validity of the study may have been threatened and it
should not be assumed that the findings are representative of all
hospitalized children. Rather, generalization must be made only to
children similar to the sample obtained for the study. However, due to
the use of a noncatagorical approach and the use of clinical facilities
throughout California the ability to generalize the results is broad.
Succinctly, the findings may be generalized to English speaking, 8-11 year
old children of normal cognitive and sensory functioning, living in
California, hospitalized for any condition other than child abuse, or a
critical or terminal illness.
Sample Size
Sample size was determined through a power analysis based on an
alpha of . 05, power of .80, and an estimated medium effect size. The
standard alpha and power were used as this was a descriptive psychosocial
study and more stringent parameters were not needed as might have been the
situation if the study had been testing differences in new, and possibly

109
costly, interventions. The medium effect size was based on clinical
intuition that the variables have a moderate influence on the child's
stress and coping behaviors during hospitalization. No previous research
was available on which to base this judgement. Using these parameters,
the necessary sample size for a regression analysis involving the maximum
of four independent variables influencing one dependent variable was 82
subjects (Cohen, 1988).
Sample Selection
As stated above, convenience sampling was used to obtain the
subjects for this study. Each child meeting the inclusion criteria and
admitted to the participating facilities was considered a potential
subject. At all facilities except one”, the admission list or Kardex was
checked daily or every other day by the data collector to determine if any
children between the ages of 8 to 11 years had been admitted to the unit.
If so, the chart was checked to determine if the child met the
inclusion/exclusion criteria. The data collector then spoke with the head
nurse, charge nurse, or primary nurse to verify the information and to
determine the child's current physical and psychosocial status and the
appropriateness of approaching the parents and child regarding the study.
Occasionally, the nurses would suggest or request that the data collector
wait a few hours as the child had just been medicated or was very tired.
*At Shriner's Hospital for Crippled Children, the Head Nursespreferred to screen for potential subjects as children were preadmitted tothe hospital. The researcher contacted the nurses several times a weekregarding subject availability and the nurses would provide names andsuggest the best time to contact the parent and approach the child fordata collection. Eligibility was verified by the researcher by readingthe child's chart and talking with the nurses and parents.
~"
ºº

110
Following this preliminary determination of eligibility, at three
facilities* the physician was then contacted for permission to approach
the parents and child about the study. Finally, if any questions
regarding eligibility remained, such as the child's grade in school, the
parents were contacted, a brief overview of the study given and the
additional information obtained. If the child met all the
inclusion/exclusion criteria the process of obtaining informed consent
(described below) from the parent and child was begun.
Data Collection Methods
Data collection consisted of a combination of standardized
instruments, graphic rating scales, and semi-structured interview.
Six instruments were used. To measure the independent variable of trait
anxiety, Spielberger's State-Trait Anxiety Inventory for Children, A-Trait
scale was used. To measure the dependent variables of a child's appraisal
of the event of hospitalization as stressful and the accompanying
perception of the effectiveness of the coping behaviors, the Hospital
Stress Scale and the Hospital Coping Scale were used. Because these are
new measures, concurrent validity was assessed using the Child Medical
Fear Scale and the Coping Response Inventory, instruments measuring
similar, but not identical, constructs. Finally, the Hospital Stress and
Coping Interview was used to assess the dependent variables of the child's
*Individual physician consent was required by the PCRC at theUniversity of California, San Francisco Medical Center, due to possibleconflicts with other ongoing research; by two of the five services atChildren's Hospital at Stanford, the orthopedic service and thehematology/oncology service; and by the private physicians admittingchildren to Valley Children's Hospital. At all other facilities, generalpermission was given for data collection by the chief of pediatrics, thechief of the service, or the medical director of the unit.
*** *---as

111
sal of events during hospitalization as stressful and the coping
.ors used in response to these events. Each of these instruments
ye described.
State-Trait Anxiety Inventory for Children (STAIC)
The purpose of the STAIC, or the "How I Feel Questionnaire", is to
le a measure of the state and trait anxiety of children. State
y is defined as the , "subjective, consciously perceived feelings of
ºn, apprehension, and nervousness . . . that may vary in intensity
uctuate over time as a function of the stresses that impinge on the
sm (Spielberger, 1975, pp. 137). Trait anxiety, "refers to
vely stable individual differences in anxiety proneness . . . the
;ition or tendency to perceive a wide range of situations as
:ening and to respond to these situations with differential
ions in state anxiety (Spielberger, 1975, pp. 137). For the
es of the present study only trait anxiety, as a measure of the
indent variable, was assessed, as trait anxiety would be an
dent to appraisal of stress, modifying the transaction between the
and situation, whereas state anxiety would be a mediating variable
incing the child's reactions during the event.
The STAIC form C-2 or A-Trait scale was developed to measure the
anxiety of children between the ages of 9 through 12 years
berger, 1973), although the author reports that it may be used
riately with children as young as 6 years of age if the items are
o the child (Spielberger, 1989). The self-report scale consists of
items scored on a three point Likert scale of 1 - hardly-ever, 2 -
mes, 3 - often. The child is asked to choose the response that
º
112
ibes how he or she usually feels. The scores are added, resulting in
jective determination of interval data.
The items for the STAIC were developed based on examination of other
ty inventories for children and on the previously developed State
Anxiety Inventory (STAI) for adults and adolescents. Criterion for
tion of items were concurrent validity with the Children's Manifest
ty Scale (CMAS) (Castaneda, McCandless, & Palermo, 1956) and the
al Anxiety Scale for Children (GASC) (Sarason, Davidson, Lighthall,
, & Ruebush, 1960) and internal consistency based on item-remainder
lations, therefore, although additional details regarding the
ptual development of the tool would be helpful, it appears likely
the content and construct validity of the STAIC are good.
Normative data was based on testing of population of over 1500
n, fifth, and sixth grade children from 5 counties in Florida during
arly 1970s. Approximately 35 to 40 percent of the children tested
Black; the ethnicity of the remainder of the sample was not given.
1thor reports that concurrent validity has been established through
risons with other measures of anxiety: in a sample of 75 children,
»rrelation of the STAIC A-Trait with the Children's Manifest Anxiety
(Castaneda et al., 1956) and the General Anxiety Scale for Children
son et al., 1960) were .75 and .63 respectively (Spielberger, 1973).
retest reliability over an eight week period, estimated on a 246
5up of the original sample, was moderate, .65 for boys and . 71 for
The internal consistency for the scale, based on Cronbach's alpha,
78 for boys and .81 for girls. In sum, the both the validity and
>ility of the A-Trait scale appear to range from moderate to good.
Appendix B for a copy of the instrument.)
º
º
º

113
The STAIC was selected for use in this study because the
psychometric properties appear to be equal to or better than those of
other anxiety inventories for children and because the length of the STAIC
was shorter than the other tools, an advantage when working with ill
children who may have limited energy and a short attention span. Of the
other instruments that appear to measure the child's trait anxiety, the
Child's Manifest Anxiety Scale, developed in the early 1950s, consists of
53 items and had a .90 test-retest reliability over a one-week period
(Castaneda et al., 1956). The Revised Children's Manifest Anxiety Scale
has 37 items, an KR-20 reliability of .85 (Reynolds & Richmond, 1978), and
test-retest correlation of . 68 over nine months (Reynolds, 1981). The
construct validity of two other instruments is uncertain. The Child
Anxiety Scale by Gillis is a 20 item, self report inventory with a KR-20
reliability of .73, and a one-week test-retest coefficient of .81.
However, construct and concurrent validity have not been established for
the tool, and reviewers do not recommend the use of the instrument at this
time (Maxwell, 1985; Sterling 1985). The Junior Manifest Anxiety Scale by
Joshi (1974) is a 40 item inventory with a reported test-retest two week
reliability of .86 based on 200 children. Content validity as judged by
two experts was . 88, and concurrent validity believed to be good as
determined by comparing the scale with the theoretically opposite trait of
neuroticism (Johnson, 1976). Further validity and reliability studies are
needed prior to using this instrument. One final instrument, the Observer
Rating Scale of Anxiety by Melamed and Lumley (1988) states a purpose of
measuring overt state anxiety, rather than trait anxiety. Because of the
length of the potentially appropriate instruments or the weaknesses of the

114
available short inventories, the STAIC presented the best combination of
properties for use in the current study.
Hospital Stress Scale (HSS) and Hospital Coping Scale (HCS)
The purpose of the Hospital Stress Scale was to provide a measure of
the degree of stress the child perceived in relation to being
hospitalized. Stress, as discussed earlier, occurs as a result of a
person-environment transaction that is appraised as threatening the well
being of the person. Because no instrument was available to measure the
child's stress in relation to the hospital environment, the Hospital
Stress Scale was devised by the researcher based on Savedra and colleagues
(Tesler, Savedra, Wilkie, Holzemer, Ward, & Paul, 1989) findings in
developing a tool for assessing children's pain (see discussion below).
The HSS is a word graphic rating scale consisting of a 10 centimeter line
with five verbal descriptors in order of ascending degree of stress at
equal intervals along the line. Because prior work by Elwood (1987)
indicated that fourth grade children generally use the term "upsetting"
rather than stress or stressful, and because Menke (1981) found that
school-age children used "upset" as a synonym for stress, the word "upset"
was used on the scale. Accordingly, the verbal descriptors were: not
upset, little upset, medium upset, large upset, and worst possible upset.
The child was asked to place a single, vertical mark on the scale to
indicate how upsetting the event of hospitalization was . The point at
which the mark intersected the line was measured in millimeters from the
left side of the scale and used as continuous data. (See Appendix C for
a copy of the instrument.)

115
Similarly, the purpose of the Hospital Coping Scale was to provide
sure of the child's perception of the effectiveness of the coping
iors used in response to the event of hospitalization. Coping, as
in this study, is the process of attempting to manage a situation
has been appraised as stressful. Again, because no instrument was
able to measure the child's perception of the effectiveness of his or
oping with the stress of hospitalization, the Hospital Coping Scale
evised by the researcher based on the work of Savedra and colleagues
discussion below). The HCS is a word graphic rating scale consisting
10 centimeter line with five verbal descriptors in order of ascending
e of perceived effectiveness at equal intervals along the line. The
1 descriptors were: no help, little help, medium help, large help,
est possible help. The child was asked to place a mark on the scale
dicate how much the things they did to take care of the upset really
d. The point at which the mark intersected the line was measured in
meters from the left side of the scale and used as continuous data.
Appendix D for a copy of the instrument.)
Because the subjects were not likely to be familiar with the use of
d graphic scale, a practice word graphic scale was used prior to the
istration of the HSS and HCS. The practice scale asked the child to
ify his or her favorite class in school, least favorite class, and
ther class. The verbal descriptors on the ten centimeter line were:
like class at all, like the class a little, like the class a medium
t, like the class a lot, and like the class best of all. The concept
class in school was chosen as it represented an activity with which
:hild would be familiar, but something that was not physically
ete such as favorite food or game would have been. In this way the
:
c
* * *-

116
child was encouraged to think about rating an intangible event as would be
necessary with the HSS and HCS scales. The purpose of asking the child to
indicate three classes ranging from the class liked best to the class
liked least was to demonstrate that the mark could be placed anywhere on
the 10 centimeter line. (See Appendix E for a copy of the instrument.)
Because these instruments are researcher developed, there is no data
available on the reliability and validity of the scales. Concurrent
validity was determined through correlation with scales measuring similar
constructs; the results of the HSS being correlated with the Child Medical
Fear Scale, and the HCS correlated with the Coping Response Inventory (see
discussion below). The objectivity of the scoring of these instruments
was likely to be good, as it only required the measurement of the
placement of the child's mark on the 10 centimeter line. The same
measuring device was used to determine the placement of the marks for all
subjects.
The word graphic scale has been used in other research with children
with good results. It has been reported that children as young as five
years of age have used the graphic rating scale effectively (Ross & Ross,
1988). Additionally, the responses of school-age children to self-report
rating scales have been carefully analyzed in the development of a tool
for pain assessment in children (Tesler, Savedra, Wilkie, Holzemer, Ward,
& Paul, 1989). Comparing five types of scales, it was found that
hospitalized children preferred the word graphic rating scale to a color
scale, visual analogue scale, graded graphic rating scale, or magnitude
estimation scale. Test-retest reliability for the pain assessment word
graphic rating scale, determined by having the subjects mark identical
scales at separate intervals of one testing session, was .91, indicating
R
117
strong reliability in this use of the scale. Construct validity was
demonstrated by the decrease in children's markings of pain intensity over
a five day post-operative period. Correlations between the five scales,
ranging from .68 to .97, demonstrate concurrent validity for the pain
scale. It was evident that the word graphic rating scale has been shown
to be reliable and valid when used to assess self-reports of school-age
children's pain intensity. Therefore, it was reasonable to believe that
a word graphic scale used to assess other situations of self-report in
school-age children might also have similar potential for reliability and
validity, such as in the measurement of the target constructs of stress
and coping during hospitalization.
Child Medical Fear Scale (CMFS)
The purpose of including the Child Medical Fear Scale (Broome,
Hellier, Wilson, Dale, & Glanville, 1988) in the current study was to
provide a test of concurrent validity for the Hospital Stress Scale. Fear
was conceptualized by the authors of the CMFS as, "a temporary reaction
and an emotional response to specific real or unreal danger" (Broom et
al., 1988, pp. 203), whereas the construct of stress, as identified in
this study, occurs as the result of a person-environment transaction that
is appraised as threatening the well-being of the person. Appraisal of an
event as stressful precedes the emotional reaction of fear to the event.
While these constructs are not identical, because the appraisal of stress
must be made before fear is experienced, the determination of a child's
fear in relation to medical events should provide a measure of the degree
of stress the child perceives in the situation.

118
The CMFS was developed to provide a measure of children's
fearfulness of medical experiences. The original 29 item self-report
scale used a three point, forced choice format. The responses are scored
not at all - 1 point, a little = 2 points, and a lot - 3 points, for a
possible total score ranging from 17 to 51, the low scores reflecting low
fearfulness and the high scores indicating high fearfulness. Because the
scoring only involves a simple calculation of the child's responses, the
objectivity of the scoring process is good. The items for the
instrument were developed by interviewing 146 children, ages 6 to 11
years, about medically related concerns and fears. The sample consisted
of 48% males and 52% females, and 71% were white. The ethnicity of the
remaining 29% was not stated. From this data the items for the instrument
were developed, resulting in probable good content validity of the
measure. Three child health experts were asked to rate the relevance of
the items, resulting in a content validity index of .78%. Criterion
validity was established by a .71 correlation with the Medical Fear
Subscale of the Fear Survey Schedule for Children (Scherer & Nakamura,
1968). However, an expected relationship between the child's age and
score on the CMFS was not demonstrated (Broome et al., 1988).
Reliability testing was conducted using a separate group of healthy
84 children, ages 5 to 11 years. The sample was 38% male and 62% female;
88% Caucasian and 11% Black. Internal consistency was demonstrated by a
Cronbach's alpha of .93; a test-retest coefficient of . 84 over a two week
period; and an intercorrelation of the theoretical subscales of . 69,
indicating that the test measures one factor: children's fears of medical
experiences. Following additional testing it was decided to revise the
CMFS to eliminate items that showed little variability and to combine

119
similar or redundant items. The revised version consists of 17 items,
scored as described above for the original version. Preliminary testing
of the revised CMFS is currently in process. Data is available for a
sample of 12 well children, ages 5-12 years, and their parents, and 23
sick children and their parents. Internal consistency estimates were: for
the mothers of well children, .75; for the well children, .82; for the
mothers of ill children, .90; and for the ill children, . 83. Correlation
between the ratings of the well child and parent was .67, and between the
ill child and parent was .46. The test-retest validity for well children
over a two week period was .81. The total scores for the well children
and ill children were not significantly different (M. E. Broome, personal
communication, November, 27, 1989).
Although psychometric testing of the revised CMFS is still in
process, the validity of the instrument should not have been affected by
the changes and the early estimates of reliability remain good. Because
less time is needed to complete the revised version, thus reducing the
length of the data collection session and decreasing the possibility of
causing unnecessary fatigue for the hospitalized children, the 17 item
revision of the CMFS was used in this study. (See Appendix F for a copy
of instrument.)
Four alternate medical fear scales were considered for use in this
study. The first was the medical fear subscale of the Fear Survey
Schedule for Children by Scherer and Nakamura (1968). Using factor
analysis, 11 of 80 items were assigned to the medical fear subscale (See
Table 3). Six items were possibly relevant to medical fears and five were
In Ot. An internal consistency of .94 was reported for the totalinstrument. A second scale was a revision of Sherer and Nakamura's tool:

120
the medical fear subscale of the Revised Fear Survey Schedule for Children
by Ollendick (1983). Again, using factor analysis, a medical fear scale
was identified, consisting of seven items (See Table 3), five possibly
related to medical situations and two unrelated. For the total instrument
validity was claimed because girls indicated a greater number of fears
than did boys, a positive correlation with trait anxiety was noted, and an
inverse relation with self-concept and locus of control was identified.
Reliability was established by an internal consistency of .94 and a test
retest of .55 over a 3 month period. The third scale was the Hospital
Fears Rating Scale by Melamed. This twenty-five item tool consists of the
first eight fears for the Scherer and Nakamura (1968) medical fears
subscale, eight additional items considered by the author to have face
validity as hospital fears, and nine other nonmedical fear items (See
Table 3). Additional support for validity is stated to be the change in
children's scores on the scale following hospital experience or structured
hospital preparation programs. One study showed a test-retest reliability
of .75 as determined immediately before and after viewing a hospital
related slide tape (Melamed, Dearborn, & Hermecz, 1983). The fourth
scale, the Hospital Fear Questionnaire, was developed by Roberts, Wurtele,
Boone, Ginther, and Elkins (1981) and consisted of five items considered
to have face validity for child's fears during hospitalization (See Table
3). Although used in three studies to evaluate the effectiveness of
prehospitalization programs (Roberts et al., 1983; Elkins & Roberts, 1984,
1985), no information was given regarding any additional determination of
validity or reliability of the instrument.
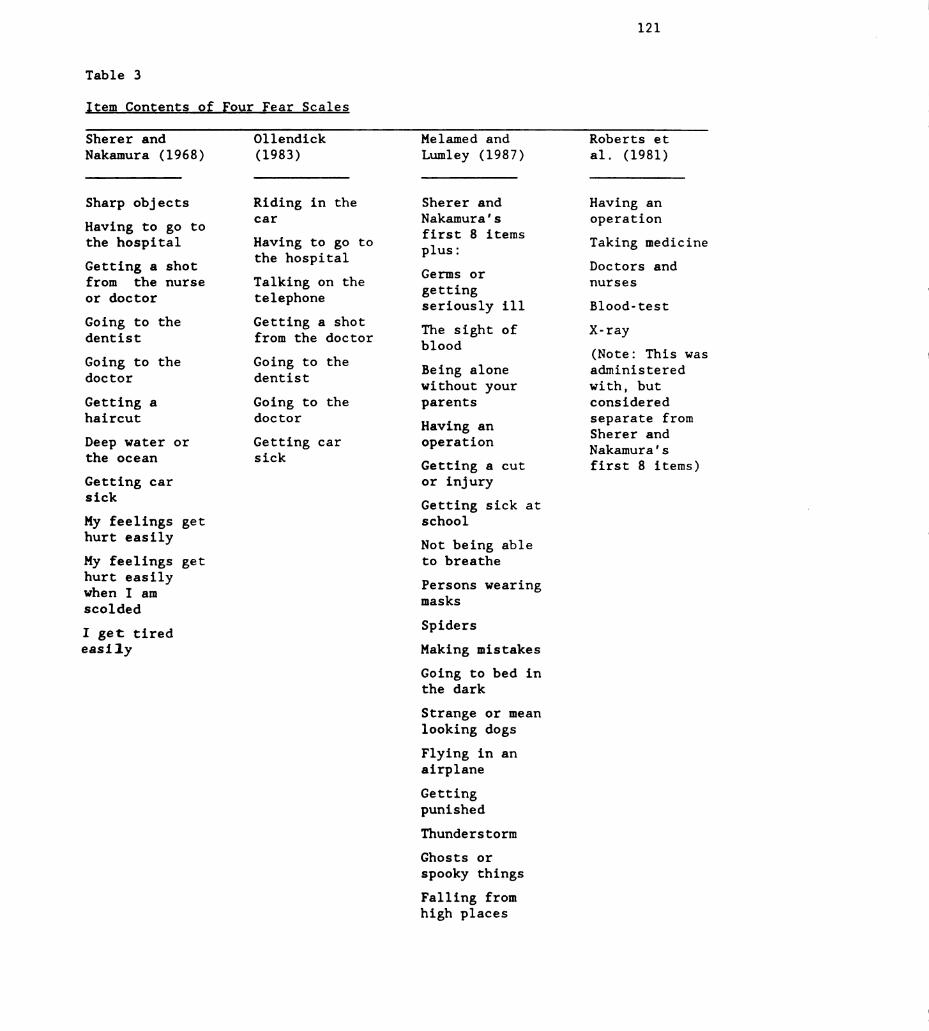
121
Table 3
Item Contents of Four Fear Scales
Sherer andNakamura (1968)
Sharp objects
Having to go tothe hospital
Getting a shotfrom the nurseor doctor
Going to thedentist
Going to thedoctor
Getting ahaircut
Deep water orthe ocean
Getting carsick
My feelings gethurt easily
My feelings gethurt easilywhen I amscolded
I get tiredeasily
Ollendick
(1983)
Riding in theCar
Having to go tothe hospital
Talking on thetelephone
Getting a shotfrom the doctor
Going to thedentist
Going to thedoctor
Getting carsick
Melamed and
Lumley (1987)
Sherer andNakamura'sfirst 8 items
plus:Germs or
gettingseriously ill
The sight ofblood
Being alonewithout yourparents
Having anoperation
Getting a cutor injury
Getting sick atschool
Not being ableto breathe
Persons wearingmasks
Spiders
Making mistakes
Going to bed inthe dark
Strange or meanlooking dogs
Flying in anairplane
GettingpunishedThunderstorm
Ghosts or
spooky things
Falling fromhigh places
Roberts etal. (1981)
Having anoperation
Taking medicineDoctors andnurses
Blood-test
X-ray
(Note: This wasadministered
with, butconsidered
separate fromSherer andNakamura'sfirst 8 items)

122
These instruments for measuring children's fears related to
hospitalization have four major weaknesses. First, the items for the
scales were identified theoretically by adults. Children were not asked
to identify sources of fear during hospitalization. Second, with the
exception of the Hospital Fear Scale by Melamed, the instruments are
relatively short, indicating a strong probability that they do not
adequately sample the range of children's fears during hospitalization.
Third, the scales borrowing items from the Scherer and Nakamura (1968)
medical fear subscale included items that do not have a logical
relationship, or face validity, for the hospital experience. Therefore,
the validity of the instruments for measuring what children actually fear
is jeopardized. Finally, the reliability estimates for the instruments
has remained inadequate. For these reasons, and because the Children's
Medical Fear Scale by Broom et al. (1988) has strong evidence of validity
and reasonable early reliability estimation, the CMFS was selected for use
as a measure of concurrent validity in the present study of children's
stress and coping during hospitalization.
Coping Response Inventor CRI
The purpose of the Coping Response Inventory was to provide a test
of concurrent validity for the Hospital Coping Scale. The construct of
coping, as used in this study, is the process of attempting to manage a
situation that has been appraised as stressful. The question asked by
both the HCS and CRI is how effective has the coping been in helping
manage the stressful event. Because the CRI is not specific for use with
hospitalized children, it could not be used as a direct measure of this

123
iable, but rather was used to estimate the validity of the newly
sloped HCS.
The CRI was developed by Elwood (1987) to provide a measure of the
activeness of children's coping responses to situations they have
raised as stressful. The author interviewed children both singly and
groups to determine what types of events were perceived as stressful
typical coping behaviors. Children from five fourth grade classes and
n five seventh grade classes representing a cross-section of
ioeconomic levels were interviewed. The total number in these groups
not given, nor was the geographic or ethnic mix of the subjects
ted. Based on the children's discussion, three inventories were
*loped for each age group: a major event inventory, a daily has sle
2ntory and a coping response inventory. These inventories were then
ted for reliability by administering the tools to a group of 156 fourth
le children and 147 seventh grade children. It was not stated if these
* the same children initially interviewed, and again geographic
ation and ethnicity were not given.
For the purposes of the present study to determine the concurrent
idity of the HCS, the coping response inventory for grade four children
used, as more subjects would be likely to be in or near this grade
, the seventh grade. The fourth grade CRI is a 14 item, self-report
ºntory. The child is asked to read the item and decide if he or she
I that behavior when an upsetting situation occurred. If the answer is
the child indicates on a four point Likert scale how much the
lvior helped solve the situation, the responses being: 1 - made it
;e, 2 – no change, 3 – helpful, and four - very helpful. The children
instructed to skip any items they did not use. The scores are summed
-*

124
and divided by the total possible for the number of items answered,
yielding a percentile indicating the child's perception of the
effectiveness of their coping response. Calculation of the score in this
manner will result in a high degree of evaluator objectivity.
The content validity of the instrument appears to be strong as it
was based on what children have identified as coping behaviors rather than
on what adults assume children do to cope with a stressful situation.
Additionally, the content validity was further strengthened by
administering early versions of the inventory to a grade-appropriate group
of children, revising the tool based on the subject's responses, and
readministering the inventory until the CRI results strongly reflected the
children's comments during an interview. Construct validity was
established by comparing the fourth grade inventory to the seventh grade
inventory and examining the responses to determine that the developmental
changes expected between the two groups were reflected in the instruments.
Test-retest reliability on a subgroup of 17 fourth grade children showed
no significant change across a two week period although the upsetting
event to which the child was referring may not have been the same (Elwood,
1987). No additional reliability scores were given for the CRI. (See
Appendix G for a copy of instrument.)
Although the CRI is new and is still in the process of being tested,
it was the best instrument available for use in the present study. Two
other instruments were considered. The Coping Inventory, by Zeitlin
(1980, 1985) is an observational instrument designed for use in
educational and therapeutic planning. The author states the tool is based
on the work of Murphy's study of children's coping, Lewin's Field Theory,
Piaget's model of cognitive development, a transactional model of child

125
development, Chess and Thomas's study of temperament, Burton White's study
of competency, and Coelho's and Haan's model of coping. In short, because
of theoretical differences in the conceptualization of the coping process,
such as a confounding of coping with adaptation and the assumption that
coping behaviors may be categorized as adaptive or maladaptive, the
Zeitlin tool not appropriate for use in a study based on the Lazarus
theory of stress and coping. The second available coping tool is the
Assessment of Coping Style, by Boyd and Johnson (1981). This is a
revision of the earlier School Picture - Story test and uses a projective
approach to assess coping styles used in interpersonal interactions with
peers and authority. The author has developed the instrument based on six
coping styles: externalized attack, avoidance, and denial, and
internalized attack, avoidance, and denial (Stone, 1985; Zarske, 1985).
Again, the theoretical basis is not congruent with the Lazarus model and
therefore is not appropriate for use in this study. In sum, the Coping
Response Inventory by Elwood (1987) is the only instrument available for
use in assessing children's coping behaviors that is congruent with the
Lazarus conceptualization of coping. Therefore, the CRI was selected for
use in estimating the concurrent of the Hospital Coping Scale.
Hospital Stress and Coping Interview
The purpose of the Hospital Stress and Coping Interview was to
identify the events occurring during hospitalization that school-age
children appraise as stressful and the resulting coping behaviors. The
*evel of the data obtained with this instrument is categorical. The
format developed by Wertlieb, Weigel, and Feldstein (1987) to assess the
*tress and coping of nonhospitalized school-age children was adapted for
126
use with the hospitalized child resulting in an interview consisting of a
series of open ended questions designed to elicit the events the child has
appraised as stressful during hospitalization and the actual coping
behaviors used in response to that event. Following assurance that there
were no right or wrong answers, and a reminder that the interview would be
tape recorded (previously discussed with the child in the assent process),
the child first was asked a non-threatening question about the positive
aspects of being in the hospital to decrease the child's anxiety and
facilitate the child's responsiveness. The child then was asked what has
happened in the hospital that has been upsetting (see above for discussion
of the term "upsetting"), followed by a question designed to elicit the
coping process, what the child did or thought when the upsetting event
Oc curred. In the event the child had difficulty understanding the
questions on stress and coping, follow-up probes were included to help the
child answer the questions without providing suggestions for specific
answers (Holaday & Turner-Henson, 1989; Woods & Catanzaro, 1988). To
Provide a therapeutic closure to the interview, the child was asked what
could be done by the nurses or doctors to make it easier to manage the
*Pse tting things. (See Appendix H for copy of instrument.)
The interview has been identified as the optimal method of studying
the school-age child's world (Deatrick & Faux, 1989) and it is generally
*&ree d that school-age children are able to provide reliable information
through interviewing (Faux, Walsh, & Deatrick, 1988; Gorman, 1980; Yarrow,
1999) , but careful planning is needed to obtain reliable and valid data.
* enhance the validity of the interview data the following elements were
**t into the interview process: 1) privacy during the interview (Holaday
& *rner-Henson, 1989; Faux et al., 1988; Rich, 1968), 2) focus on recent

127
events (Faux et al., 1988), 3) questions structured to move from the easy,
positive, or nonthreatening to potentially stressful concepts (Faux et
al., 1988; Holaday & Turner-Henson, 1989; Rich, 1968; Sattler, 1988;
Yarrow, 1960), 4) use of age appropriate words and concepts (Faux et al.,
1988; Holaday & Turner-Henson, 1989; Rich, 1968; Sattler, 1988; Yarrow,
1960), 5) use of action oriented words rather than abstract words, such as
"what did you do" rather than "what did you feel" (Faux et al., 1988;
Rich, 1968), 6) provision of periodic reassurance that the interview is
proceeding satisfactorily (Amato & Ochiltree, 1987; Sattler, 1988), 7)
minimization of socially desirable responses by acknowledging that
everyone finds something in the hospital upsetting (Faux, 1988; Rich,
1968; Yarrow, 1960), 8) audio recording of the interview to avoid
interruptions for transcription that may cause the child to loose interest
(Amato & Ochiltree, 1987) (Note: audio recording is considered to be a
nonreactive technique due to children's familiarity with such equipment
[Faux et al., 1988; Webb et al., 1981]), and 9) limiting the length of the
interview to avoid fatigue which may result in less than optimal answers
(Faux et al., 1988; Yarrow 1960). Additionally, content validity was
established by basing the interview on the work of Wertlieb et al. (1987)
and through comparison with other stress and coping interviews in the
current literature. Consensual validity was determined through a review
of the instrument by three pediatric nursing experts. Construct validity
was assessed through a pilot test of the instrument with five subjects
meeting the inclusion-exclusion criteria. The children's responses were
analyzed and revisions made as necessary to enhance their understanding of
the questions. Interrater reliability for the categories developed from

128
the content analysis portion of the data analysis will be reported in the
next chapter.
Data Collection
The process of data collection, including the preliminary trial, the
pilot study, and the final protocol used for data collection, including
obtaining informed consent, will be detailed in this section. A
description of the persons participating in data collection will also be
given.
The Phases of Data Collection
Two preparatory phases, the preliminary trial and the pilot study,
preceded data collection. A separate group of children was used in each
of these phases, so that data were collected from each subject only once.
Data from the preliminary trial and pilot study were not included in the
final data analysis.
Following the selection of instruments needed to obtain information
regarding the variables of the investigation and development of the
interview, a preliminary trial of the instruments was conducted during
November 1989. The purpose of this trial was to gain a sense of the
responses of the children to the instruments and estimation of the length
of time needed to complete the process. Three children, ages eight, ten,
and eleven years, who had experienced a medical or dental procedure within
the last year were interviewed in their homes. The parents, friends of
the investigator, were given a copy of the consent form, both to obtain
appropriate consent and to gain feedback regarding the clarity of the
129
consent. All parents stated that the consent form was clear and easily
understood. The children responded well to the interview and answered the
questionnaires easily within about a thirty minute session.
While the preliminary trial indicated that the protocol was
appropriate for use with eight to eleven year old children who were
currently healthy, it was necessary to determine if it would be reasonable
for use with hospitalized children of the same age. Therefore, following
approval of the Committee on Human Research at the University of
California, San Francisco and the Nursing Research Committee of the same
facility, a pilot study was conducted during January 1990. Parental and
child consent was obtained, and five children meeting the
inclusion/exclusion criteria were interviewed and completed the
questionnaires and scales. While the children were able to complete the
interview and questionnaires without difficulty, it was evident that minor
modifications were needed. First, the wording of the interview was
awkward. Accordingly, the questions were restructured to create a more
natural flow to the process. Second, use of both direct questioning to
determine the children's stress and coping processes and indirect
questioning to verify the responses appeared to be confusing or irritating
to the children. After being asked what they found upsetting and what
they did to take make it less upsetting, an indirect probe was asked
regarding what they would tell a friend about upsetting things in the
hospital and how to manage them. The subjects repeated the answers given
in direct questioning and gave nonverbal messages of impatience in
repeating the answers. Because of this, and because the ill children
tended to tire toward the end of the session, the interview was shortened
to four questions with suggested probes (See Appendix H). The third

130
phase of data collection, the actual study, was conducted from February
through August 1990. During this time data were collected from 82
subjects meeting the inclusion/exclusion criteria following the protocol
described below.
The Protocol for Data Collection
Following the identification of potential subjects, the parent (s) of
the child were approached, given a brief explanation of the study, the
reason their child had been selected, and asked if they would be willing
to listen to more information about the study. If so, the parents'
consent form and the Experimental Subject's Bill of Rights (See Appendix
I and J for copies of the University of California, San Francisco consent
form. Consents for other facilities contained the same information, but
in the format required by that facility. ) was given to the parent(s) and
each step of the protocol explained. The parent(s) were asked if they
would like time to consider the information before signing. If so, the
consent was left with them and the researcher returned in approximately
one-half hour to ask for their decision. Generally, however, the parents
stated they did not need any additional time and were willing to give
permission immediately. An attempt was made to discuss the study away
from the child's hearing, but this was not always possible. Parental
consent was obtained whenever it was possible to contact the parents
following admission of the child to the facility. At the time of consent
the parents were requested to complete a demographic form pertaining to
the child (See Appendix K) and given the opportunity to request a summary
of the research results, if so desired (See Appendix L).

131
Following parental consent, the study was be explained to the child
and assent for participation requested. The child's assent form (See
Appendix M) was given to the child. For most children it was read to or
with the child, but a few older children purposely held the form away from
the researcher's view and read it independently. All children were
reassured that there were no right or wrong answers to the questions and
the rights of privacy, with the exception that the parent might request to
see the child's answers, and withdrawal of assent were reinforced before
asking if the child was willing to participate. The child's consent was
obtained immediately before proceeding with the data collection on the
second or third day of admission.
Data collection was conducted in the child's hospital room or
another nearby quiet location. During the consent process it was
explained to the parents that children tend to expect parents to answer
questions for them, so it would be helpful if the parent would leave the
room during the data collection. If the parent was hesitant to do so, or
if the child wanted the parent to stay, the parent was asked not to coach
the child's answers, and the data collector attempted to position herself
so that the child was not looking directly at the parent during the data
collection.
The instruments were grouped and administered as follows:
1. Hospital Stress and Coping Interview
2. in random order:
STAIC A-Trait scale
As a set: the Practice Scale, Hospital Fear Scale, and
Hospital Coping Scale
Coping Response Inventory

132
3. Child Medical Fear Scale
The rationale for administering the interview first was to provide the
necessary frame of reference for the child to understand the concepts
being tapped in the Hospital Fear and Coping Scales and Coping Response
Inventory, moving from the concrete to the abstract, a principle of
interview development (Faux et al., 1988) that was reasonable to apply to
the general data collection process. The rationale for administering the
Practice Scale, Hospital Fear Scale, and Coping Scale as a set was the
similarity of format and logical flow of questioning. The Hospital Fear
and Coping Scales, the STAIC A-Trait Scale, and the Coping Response
Inventory were administered in random order to correct for unrecognized
interaction between the tests. The Child Medical Fear Scale was
administered last to avoid suggesting possible sources of stress to the
children.
The interview was recorded on audio tape, transcribed, and the tapes
permanently erased at the completion of the study. To control for
probable variations in reading level, an attempt was made to read the
instruments aloud to the subjects, however, some older children were
resistive to this, and read the instruments independently. All children
did respond independently in answering the items. The total testing time
ranged from twenty minutes to one and one-half hours, depending on how
talkative the child was and how many interruptions occurred.
Interruptions occurred for a variety of reasons. The most common
was the entrance of hospital personnel for necessary assessment or
treatment. These episodes included the nurse taking the child's vital
signs, giving medicine, resetting the I. V., the physician checking the
child, or the physical therapist repositioning the child. Occasionally,

133
the parent arrived during the session, and a break was taken so the child
could greet and talk with the parent. Finally, on a few occasions, the
child tired during the session and was given a chance to rest before
continuing.
Description of Data Collectors and Training Process
Because of the geographical distance between the participating
facilities, research assistants collected the data at several of the
facilities. All of the data collectors were female, registered nurses and
had a minimum of one year experience working with hospitalized children.
Of the six research assistants, four had an earned Master's degree in
Nursing one of whom was working toward a doctorate in public health; one
was working on her Master's degree; and one was in the process of applying
for admission to a Master's program. These persons conducted the data
collection at UC Davis Medical Center, Children's Hospital at Stanford,
Valley Children's Hospital, and Loma Linda University Medical Center. The
primary investigator collected the data at UC San Francisco Medical
Center, Shriner's Hospital for Crippled Children, and San Francisco
General Hospital Medical Center.
To ensure that all data was collected using the same procedure, and
thus minimize the potential variance that could occur due to having the
data collected by seven individuals, the primary investigator developed a
manual entitled, Instructions for Data Collection. The following areas
were discussed in this manual: background and purpose of the research,
definition of key terms, responsibilities of the data collectors, the
materials needed for each session, identification of potential subjects,
the process of informed consent, a description of each instrument with

134
guidelines for proper administration, guidelines for interviewing
children, and answers to common questions that could occur. Each data
collector received and read a copy of the manual and a sample packet of
consent forms and instruments before the researcher came to the facility
to conduct a training session.
Training sessions were held at each facility where research
assistants would be collecting the data. During the session, an overview
of the Lazarus theory of stress and coping was presented to give the
nurses a better understanding of the theoretical basis of the study to
enable them to participate intelligently in the data collection and
understand the importance of allowing the child to independently identify
sources of stress during hospitalization. The process of identifying
potential subjects was reviewed and the importance of following the
inclusion/exclusion criteria was emphasized. Examples were given of types
of patients that would or would not be eligible. Because all data
collectors were pediatric nurses familiar with the purpose and process of
obtaining consent it was not necessary to explain the legal necessity of
obtaining consent from parents; rather the emphasis in the training
session was placed on the initial approach to the parent, how to describe
the protocol in lay terms, and answers to common questions that might be
asked. Each instrument was reviewed with the data collectors and
suggestions given for facilitating the child's participation, such as
during the interview jotting notes of the "upsetting" things identified by
the child to guide the next question on coping. Each nurse was asked to
use the sample packet of instruments on a non-hospitalized child by
focusing on an experience in the doctor's or dentist's office or emergency
room, and then report back to the researcher. At that time any questions
135
were clarified and suggestions given as needed. Following the first data
collection session, the primary investigator again talked with the data
collector and provided feedback on the session. This procedure was
repeated intermittently throughout the process of data collection.
To further control the variance that could occur when data is
collected by multiple persons, data collection packets consisting of all
forms needed were precollated and numbered. Numbered cassette tapes were
provided corresponding to the numbers of the data collection packets. A
ruler-shaped piece of poster board was provided to help the children track
the line for the items and responses on the various instruments. Tape
recorders and batteries were provided. Finally, a supply of colorful
"thank-you" stickers were given to each data collector.
Periodic telephone calls and on-site visits indicated that the data
collectors followed the protocol for subject identification and data
collection very carefully. All data collected by the assistants was
reviewed by the primary investigator before inclusion in the study. Data
collected by the assistants from eight subjects were eliminated from the
final analysis due to questionable eligibility for the study.
Data Analysis
The plan for data analysis is presented below. Descriptive
statistics were used for preliminary examination of the data, and
inferential statistics for testing the hypotheses and drawing conclusions
from the data.
Descriptive statistics were used to determine the measures of
central tendency and variation for the variables of gender, health status
group, trait anxiety, stress appraisal associated with the event of

136
hospitalization, perceived satisfaction with coping behaviors during
hospitalization, and for the categories of stress and coping used during
hospitalization. In addition, the demographic data of age, ethnicity,
prior experience with hospitalization, prior experience as an out-patient,
participation in a prehospitalization program, and extent of parental
rooming-in during hospitalization were examined by the same procedures to
determine any unexpected variations in the sample.
Hypotheses 1, 2, 3, 4, 5, and 6, examining the relationship between
health status and the child's identification of stressful events and
coping behaviors; between gender and the stressful events and coping
behaviors; and between trait anxiety and the stressful events and coping
behaviors, were analyzed using a two part process. First, the data
obtained during the interview with the child was examined through the
process of content analysis (Asher, 1983), reducing the qualitative data
to mutually exclusive categories. For the purpose of statistical
analysis, only the child's first response to the stress probe and the
coping probe was included in this portion of the statistical analysis.
Second, Chi square analysis, or analysis of variance, as appropriate, was
used to determine the relationship between each independent variable and
the categories, resulting in three analyses for each set of categories:
health status by stress categories, gender by stress categories, trait
anxiety by stress categories, health status by coping categories, gender
by coping categories, and trait anxiety by coping categories.
Hypothesis 7, the affect of health status, gender, and trait anxiety
on the child's appraisal of hospitalization as stressful, and Hypothesis
8, the affect of health status, gender, trait anxiety, and stress
appraisal on the child's perception of effectiveness of the coping

137
behavior, were analyzed using the statistical technique of path analysis
because of the fit between the proposed question and this technique.
Theoretically, the purpose of path analysis is to calculate the direct and
indirect influences of the independent variables on the dependent variable
(Kerlinger, 1986). In this study, as in most nonexperimental research, it
was probable that the independent variables were related, requiring use of
multiple regression techniques (Kerlinger, 1986). Additionally, use of
multiple regression techniques made full use of the continuous nature of
the data.
At each stage of the model, multiple regression was used to evaluate
the effect of the independent variables on the dependent variable. The
categorical variables of health status and gender were dummy coded for
quantitative analysis. For the analysis of Stage I, the relative effects
of health status, gender, and trait anxiety on stress appraisal were
determined. Stage II examined the relative effects of health status,
gender, trait anxiety, and stress appraisal on coping behavior.
The Pearson product moment correlation coefficient was calculated
for the necessary tests of concurrent validity. The results of the
Hospital Stress Scale were correlated with the results of the Child
Medical Fear Scale, and the results of the Hospital Coping Scale were
correlated with the results of the Coping Response Inventory.

138
CHAPTER FOUR
RESULTS
In this chapter, the results of the data analysis will be presented.
First, the demographic characteristics of the sample will be described,
providing information regarding the age of the subjects, ethnicity,
residence in an urban or rural setting, family income, health status and
diagnostic groupings, any ongoing therapeutic interventions, prior
hospitalization, and description of subjects by site of data collection.
Additionally, the subjects that refused to participate in the study will
be described. Second, the preliminary analyses of the data to determine
unexpected differences in characteristics will be described. Factors to
be considered are site of data collection, age, prior out-patient
experiences, prehospitalization teaching programs, and parental rooming
in. Third, the hypotheses will be discussed in numerical order, according
to two naturally occurring subgroups: Hypotheses 1 through 6, addressing
the analysis of the interview data in relation to health status, gender,
and trait anxiety; and Hypotheses 7 and 8, addressing the analysis of the
stress and coping word graphic scales in relation to health status,
gender, and trait anxiety. The results of each subgroup of hypotheses
will be summarized and schematically portrayed using the theoretical model
described in Chapter 2.
Characteristics of the Sample
Data were collected from 82 children, the sample size needed to
achieve the desired power of . 80. The convenience sample was comprised of

139
41 (50%) males and 41 (50%) females. The average age was 9.6 (s.d. l. 2)
years; 9.63 (s.d. l. 2) for males and 9.65 (s.d. l. 2) for females. Table
4 provides the number of subjects by age and gender.
Table 4
Gender and Age of Subiects (in years)
8 9 10 11
Gender n (%) n (%) n (%) n (%) Total
Males 11 (13.4) 7 ( 8.5) 9 (11.0) 14 (17.1) 41 ( 50%)
Females 9 (11.0) 9 (11.0) 10 (12.2) 13 (15.6) 41 ( 50%)
Total 20 (24.4%) 16 (19.5%) 19 (23.2%) 27 (32.9%) 82 (100%)
The ethnicity of the subjects was : 52 (63.41%) Caucasian, 13
(15.85%) Hispanic, 10 (12.2%) Black, 2 (3.66%) Asian, and 4 (4.88%)
"Other" consisting of two Portuguese and two of mixed heritage, as
indicated by the parent on the demographic data sheet. Thus, all major
ethnic groups were represented in the sample. Seventy-one percent of the
children resided in an urban area (within the city limits), and 29 percent
in a rural location (outside the city limits). Family income is
summarized in Table 5.
Regarding the health status of the children, 21 (25.6%) were
admitted to the hospital for an acute illness and 61 (74.4%) for a chronic
illness, as defined previously. Table 6 provides information regarding

140
Table 5
Family Income
Range N Percent
less than $ 9,999 15 19.2%
$ 10,000 to $ 19,999 12 15.4%
$ 20,000 to $ 29,999 15 19.2%
$ 30,000 to $ 39,999 14 18.0%
$ 40,000 and higher 22 28.2%
the subjects's health status by condition requiring hospitalization. The
use of the non-categorical approach provided a wide range of diagnostic
conditions. Included in the category of cardiac disorders were diagnoses
of congestive heart disease and pending surgical correction of cardiac
defects. The category of gastrointestinal disorders included children
with appendicitis, gastric or intestinal surgery, ulcerative colitis,
Crohn's disease, and pancreatitis. Hemopoietic disorders included
diagnoses of idiopathic thrombocytopenia, sickle cell anemia, neutropenia,
and aplastic anemia. Neurological disorders included children with spina
bifida admitted for surgery to release a tethered spinal cord.
Oncological disorders included leukemias, lymphomas, and a variety of
solid tumors. Orthopedic disorders included open reduction of fractures,
surgical intervention for non-union of fractures, osteomyelitis,
corrective surgery for orthopedic anomalies, osteogenesis imperfecta, and
Legg's Perthes Disease. The category of reconstructive surgery included

141
Table 6
Health Status and Condition of Subiects
Acute Chronic
Condition N (%) N (%)
Cardiac Disorder 0 (0%) 2 (2.4%)
Gastrointestinal Disorder 9 (11.0%) 6 (7.3%)
Hemopoietic Disorder 1 (1.2%) 9 (11.0%)
Neurological Disorder 0 (0%) 2 (2.4%)
Oncology 0 (0%) 13 (15.9%)
Orthopedic Disorder 7 (8.5%) 9 (11.0%)
Reconstructive Surgery 0 (0%) 7 (8.5%)
Renal Disorder 0 (0%) 5 (6.1%)
Respiratory Disorder 0 (0%) 6 (7.3%)
Other 4 (4.8%) 2 (2.4%)
Total: 21 (25.6%) 61 (74.4%)
children admitted for burn scar revision and correction of congenital
structural
diagnoses
correction
transplant
fibrosis.
defects, such as malformed ears. Renal disorders included
of nephrotic syndrome, ureter reimplantation, surgical
of congenital abnormalities, and evaluation of possible renal
rejection. Respiratory disorders included asthma and cystic
Conditions not directly related to the above categories were
grouped under the label of "other" and included trauma not involving

142
orthopedic injuries, arterio-venous malformation, systemic lupus
erythematosus, and children admitted for rehabilitation training.
During data collection, 61 (74.4%) of the children were experiencing
some sort of mechanical device used for ongoing assessment or
intervention. Forty-four children (53.7%) had an IV or heparin lock.
Eleven children (13.4%) had a cast. Five (6.1%) had a central line. Five
(6.1%) had a naso-gastric tube. Four (4.9%) were receiving oxygen by mask
or nasal cannula. Two (2.4%) had a urinary catheter. Two (2.4%) were on
cardiac monitoring. One child (1.2%) was in traction.
Considering prior experience with hospitalization, of the acutely
ill children, only 2 of the 21 subjects (9.5%) had been previously
admitted to the hospital. As stipulated in the eligibility criteria,
these admissions occurred when the child was less than two years of age.
For the chronically ill children, the number of prior hospitalizations
ranged from 1 to 100, with a mean admission rate of 9.8 (s.d. - 15.9). It
is possible that this range is skewed toward the high side, as the
parental response to number of admissions appeared to be rounded to a
convenient estimate after 16 admissions. It was not possible to verify
this information as old charts were not readily available and the children
had often been admitted to more than one facility.
Of the seven clinical facilities described in chapter 3, data were
collected at only six of the hospitals. No subjects were obtained from
Children's Hospital at Stanford. This was due to an unusually low
admission of children between eight and eleven years of age that met the
inclusion/exclusion criteria at that facility during the period of data
collection. The research assistant reported that during the entire period
of data collection, only three potential subjects were identified, and all

143
were unwilling to participate in the study. Therefore, all analyses will
be based on the remaining six facilities. The total number, age in years,
gender, and health status of the subjects obtained from each facility is
reported in Table 7.
Table 7
Description of Subjects by Site
UCSF" SHCC” UCDMC" VCH* LLUMC" SFGH"
Variable N N N N N N
Total N 42 14 7 6 8 5
Age in years
8 10 3 2 1 2 2
9 9 2 O 3 2 O
10 11 2 2 1 2 1
11 12 7 2 1 2 2
Gender
Male 20 8 2 3 5 3
Female 22 6 5 3 3 2
Health Status
Acute 7 l 5 5 O 3
Chronic 35 13 2 1 8 2
"UCSF - University of California, San Francisco Medical Center;SHCC - Shriner's Hospital for Crippled Children;UCDMC - University of California, Davis Medical Center;VCH - Valley Children's Hospital;LLUMC - Loma Linda University Medical Center;SFGH = San Francisco General Hospital and Medical Center

144
Information on potential subjects that refused to be in the study,
was kept by the data collectors at all of the seven facilities. During
the period of data collection, 18 potential subjects declined to
participate in the study. This group was comprised of 13 (72.2%) males
and five (27.8%) females, 11 (61.1%) chronically ill and 7 (38.9%) acutely
ill, with an average age of 9.4 years. In nine cases the parent refused
permission, in seven the child was not interested in participating, and in
one the physician denied permission as the child was exhibiting behavioral
problems. Reasons for not participating were that the child was too
tired, was grouchy, was nauseated, that the child didn't want to talk
about the hospital experience, hoarseness due to surgery, imminent
discharge, and in two cases no reason was given. Three of the children
were reapproached during a subsequent admission when feeling better and
were then willing and even eager to participate.
At each facility, periods of time elapsed during which no data were
collected, due to illness, vacation, or work schedule of the data
collector. Due to the difficulty of gathering post hoc data to determine
if children admitted during these periods met the eligibility criteria,
the number and characteristics of missed potential subjects is not known.
Preliminary Analyses
It was possible that subgroups of the total sample may have had
subtle differences in factors that could influence the results of the
study. In order to determine if the subjects could be treated as a total
sample, preliminary analyses were conducted to examine the data for
possible differences due to site of data collection, age, prior out

145
patient experiences, prehospitalization teaching programs, and parental
rooming-in.
Site of Data Collection
Although each site used for data collection met the stipulations of
being a pediatric unit, allowing rooming-in of parents, and having a
staffed playroom, it was possible that differences existed in the
psychosocial support provided for the children that could result in
differences in the degree of stressfulness experienced by the children and
the perceived effectiveness of the coping behaviors. To examine for this
possibility, one-way analysis of variance was run on site by Hospital
Stress Scale scores and on site by Hospital Coping Scale scores. The
results indicated no significant differences in the dependent variables
between the six different sites. Therefore, it was appropriate to combine
the subjects from the six facilities as a total sample for data analysis.
Age Differences
In order to obtain a fairly homogenous group of children with
similar thought processes, the age range of 8 to 11 years, was used.
However, it was possible that even within the stage of concrete
operations, children's appraisal of stress and perception of their coping
could differ due to cognitive level. To check for this possibility, a
one-way analysis of variance was run comparing the subjects's age in years
with their responses to the dependent variables of the Hospital Stress
Scale score and the Hospital Coping Scale score. There was no significant
difference in the children's responses to these scales when examined by

146
age in years. Therefore it was not necessary to examine these groups
separately.
Prior Out - Patient Experience
Prior experience in a clinic or medical office with in the last year
ranged from 0 visits to 1000. Eliminating the subject on whom the parent
indicated 1000 visits, assuming that this was an overstatement as that
number of appointments within a 365 day period is highly unlikely, the
number of clinic or office visits ranged from 0 to 104, with a mean rate
of 10.4 (s. d. 15. 7). As would be expected, the parents of the chronically
ill children reported a significantly greater number of clinic and office
visits, with a range from 0 to 104, a mean of 13.3 (s. d. 17.4) than did
the acutely ill children. The acutely ill children had a range of 0 to 10
clinic appointments, with a mean of 2.3 (s. d 2.35). Therefore, the
chronically ill child was much more likely to have gained some knowledge
of health care procedures through office or clinic appointments than was
the acutely ill child. Although prior out-patient experience was not
included as a independent variable in this study, this preliminary finding
supports the assumption that the health care experiences of chronically
ill children differ from that of acutely ill children.
Prehospitalization Programs
Another source of prior experience with hospital situations might be
gained through prehospitalization teaching programs. Of the total sample,
only 16 (19.5%) had participated in such a program, 57 (69.5%) had not
had such an experience, and the parents of 9 children (11%) were uncertain

147
if their child had this type of an opportunity. Interestingly, all of the
children who had participated in a prehospitalization program were
chronically ill; none of the acutely ill children had been exposed to this
source of knowledge. A comparison of the scores on the Hospital Stress
Scale of children having participated in such as program as compared to
those who had not was statistically not significant. Therefore it was not
necessary to examine these two groups separately.
Parental Rooming-in
The number of hours per day in which the parent was able to stay
with the child ranged from 0 to 24 with a mean of 17.5 hours. The mean
for the acutely ill children was 18.3 hours (s. d - 6.1), and for the
chronically ill group was 17. 1 hours (s. d - 8.6), a difference that was
statistically not significant. Therefore it was not necessary to examine
these two groups separately.
In sum, five extraneous factors that could have potentially
influenced the children's stress appraisal and coping behaviors were
assessed. These factors were: site of data collection, age, out-patient
experience, prehospitalization programs, and parental rooming-in. None of
these caused a significant difference in the children's perception of the
stressfulness of the hospital or their perception of the effectiveness of
their coping behaviors. Therefore, it was appropriate to consider the
sample to be a homogenous group for the statistical analysis of the
hypotheses.

148
Analysis of Hypotheses
Discussion of the analytical strategies used for data analysis will
be presented in two sections. First, the approach used to analyze the
interview data in relation to the independent variables will be discussed
and the results presented. Second, the results of analyzing the data
obtained from the stress and coping word graphic scales will be described.
Within these two groups, the hypotheses will be examined in numerical
order.
Analysis of the Interview Data
The children's responses to the interview were examined using the
process of content analysis to develop categories of stressful events and
coping behaviors. This was followed by statistical analysis of the
quantification of these categories.
Stress Categories
Content analysis has been defined as, "a research methodology that
utilizes a set of procedures to make valid inferences from text" (Weber,
1985, pp. 9). For this study, the set of procedures used to analyze
stressful events was: 1) careful analysis of the interview data to
identify stressful events according to the definition of this concept used
in this study (see chapter 2); 2) identification of specific events stated
by more that one subject; 3) grouping of the specific events into a
conceptually similar categories; 4) development of an operational
definition for each category; 5) selection of a label representative of
the events included in the category; and 6) identification of events
representative of the category. Table 8 lists the stressful event

149
Table 8
Categories of Stressful Events During Hospital
Label Operational Definition Examples
Intrusive Any event involving entry Injections, blood workeVents into the body through the Intravenous insertion,
skin or a natural body surgery, pills,orifice nasogastric tubes,
suppositories
Physical Any physical symptom or Pain, nausea, sidesymptoms sensation relating to the effects of medications
illness or treatment such as blurry eyes,dizziness, burning ofintravenous medication
Therapeutic Any activity relating to Physical exam by doctor,intervention treating or assessing the palpation of abdomen,
physical status of the walking after surgery,patients vital signs taken at
night, dressing andremoval of stitches
Restricted Limitation of normal or Bed rest, holding stillactivity desired activity due to during x-rays,
illness or hospital rules not allowed to leaveunit, can't go outside
Separation Any expression of concern Parent's leaving,due to separation from miss friends, pets, etc.family, friends, pets, etc.,due to hospitalization
Environment Any physical or interpersonal Cords and wires onaspect of the child'senvironment
walls look like monstersat night, changingrooms, unpleasant ornoisy roommates;impatient or "mad"doctors and nurses
categories and operational definitions developed during the process of
content analysis and provides examples of the event.

150
Coping Categories
Content analysis was also employed to identify the coping behaviors
the children reported using during hospitalization. However, the
development of the categories differed somewhat from that of the stress
categories. The procedure used to analyze the coping behavior data was:
1) careful analysis of the interview data to identify coping behaviors
according to the definition of this concept used in this study (see
chapter 2); 2) identification of specific behaviors stated by more that
one subject; 3) assignment of the specific behaviors into one of the
coping categories derived from the synthesis of prior research relating to
coping of hospitalized children (see chapter 2); 4) selection of a label
representative of the category; and 5) identification of events
representative of the category. Table 9 lists the coping behavior
categories and operational definitions and provides examples of the event.
Quantification of Interview Data
A total of 337 stressful events were identified, with a mean of 4.1
(s.d. - 2.6), and a range of 0 to 16. Three children could identify no
stressful events. A total of 347 coping behaviors were identified, with
a mean of 4.2 (s. d - 3.2), and a range of 0 to 18 behaviors. Four
children did not identify any coping behaviors, the three who were unable
to state any stressful events and one additional child. Table 10 lists
the frequency with which a stress category was mentioned and the
percentage relative to the total number of stressful events. As is
evident from this table, the most frequently occurring category was that
of intrusive events, named more than twice as often as the next most
frequent category. Table 11 provides the frequency with which a coping
category was mentioned and the percentage relative to the total number of

151
Table 9
Categories of Coping Behaviors Used During Hospital
Label Operational Definition Examples
Cognitive Actively taking in or seeking Thinking about theprocessing information to clarify and situation, asking
understand a situation questions aboutthe event
Cognitive Any attempt to deal with the The shot will feelrestructuring stressful situation by like a mosquito
changing thinking about the bite, the surgerysituation was good because I
will get well
Cooperation Any behavior intended to bring I let them do it,the child's personal response I held still, Iin line with reality drank so I
wouldn't have to
get an IV
Countermeasure Any physical or cognitive Don't let them doattempts to remove self from it, ignoreor mitigate the effect of the doctors, sleep,stressful situation don’t think about
it, watchtelevision
Control Any attempt to influence the Relaxationsituation to control the techniques such asstressful event tapes or deep
breathing
Seeking Turning to others for help Wanting parentssupport in coping present, holding
someone's hand,calling friends onphone, talkingwith roommate

152
Table 10
Events Appraised as Stressful by Hospitalized Children
Categories Frequency (N–337) Percentage
Intrusive events 131 38.9
Physical Symptoms 56 16.6
Therapeutic Interventions 39 11.6
Restricted Activity 40 11.9
Separation 24 7.1
Environment 47 13.9
Table 11
Coping Behaviors Used by Hospitalized Children
Categories Frequency (N-347) % of subjects
Cognitive Processing 15 4.3
Cognitive Restructuring 34 9.8
Cooperation 32 9.2
Countermeasure 117 33.7
Control 76 21.9
Seeking Support 72 21.0

153
coping behaviors. The three most commonly mentioned categories were, in
decreasing rank order, countermeasures, control, and seeking support; the
remaining categories occurred with far less frequency.
Interrater reliability was determined by comparing the above
categorizations with those of two pediatric nurse researchers who
separately reviewed 10% of the interviews, randomly selected. The
correlation in the number of identified stressful events, the number of
identified coping behaviors, the percentage of agreement in the
categorization of the items, as determined by Cohen's Kappa, and the
number of significant findings in the comparison of assignment to the six
categories is presented in Table 12.
Table 12
Interrater Reliability for Content Analysis
P.I./1st" P.I/2nd” 1st/2nd”
Stress
r for number of events .9842 .9845 . 99.35
mean Ž of category agreement 62.5% 70.8% 68.75%
# of significant comparisons 2 of 6 2 of 6 4 of 6
Coping
r for number of behaviors . 9928 . 9772 . 98.91
mean X of category agreement 56.25% 66.67% 70.8%
# of significant comparisons 1 of 6 6 of 6 4 of 6
ºr - - - - -Comparison of primary investigator and first reviewerºr ºr - - -Comparison of primary investigator and second reviewerºr ºr - - -
ºr Comparison of first and second reviewers

154
The correlation between raters for the identification of stress
items and coping items was very high, all above .97. The mean percentage
of agreement in assignment to categories was determined by calculating the
average percent of agreement between each pair of raters for the six
stress categories and then for the six coping categories. For the stress
categories the mean percent of agreement was moderate, ranging between
62.5% to 70.8%, the individual comparisons ranging from 62.5% to 100%.
The number of significant comparisons between the raters ranged from two
to four of the six possible results. The mean rate of agreement in
assignment to the categories among all raters was : Separation, 100%;
Restricted activities, 70.85; Physical symptoms, 62.5%; Environment,
62.5%; Intrusive events, 54.2%; and Therapeutic interventions, 54.2%. For
the coping categories the mean percent of agreement also was moderate,
ranging between 56.25% and 70.8%, the individual comparisons ranging from
37.5% to 87.5%. The number of significant comparisons between the raters
ranged from one to six of the six possible results. The mean rate of
agreement in assignment to the categories among all raters was: Cognitive
processing, 75%; Seeking Support, 75%; Cooperation, 70.8%; Cognitive
restructuring, 62.5%; Countermeasure, 58.3%; Control, 45.8%.
Restatement of Theoretical Model
Before beginning analysis of the individual hypotheses, the
theoretical model (first introduced in Chapter 2) will be briefly reviewed
to regain an overall perspective of the study. To reiterate, the model
schematically illustrates the proposal that health status, anxiety, and
gender influence stress appraisal, and that all four factors are related
to coping behaviors. For ease of referral, the entire model is reproduced
below (Figure 3).

155
Health Status
Anxiety -~ Nº.Stress T* Coping
- mº- -appraisal Tº behaviors
Gender ~.
Figure 3. Theoretical model of relationships between variables.
Hypothesis 1
The first hypothesis postulated that there would be a relationship
between health status and the type of event appraised as stressful during
hospitalization. The descriptive statistics for this question were
examined by determining the frequency and percentage of each category of
stressful event by health status (see Table 13). These statistics were
based on N - 78, one acutely ill child and two chronically ill children
did not identify any stressful events associated with hospitalization.
Acutely ill children identified a total of 81 stressful events, with a
mean of 3.9 per child (s.d.- 3.0), and a range of 0 to 14 events.
Chronically ill children identified a total of 256 stressful events, with
a mean of 4.2 per child (s.d.- 2.4), and a range of 0 to 16 events. The
difference in the mean number of stressful events of the two groups was
not statistically significant at a .05 level. A comparison of the
percentage for each category between groups demonstrate that there is
little difference except in two categories: intrusive events in which the
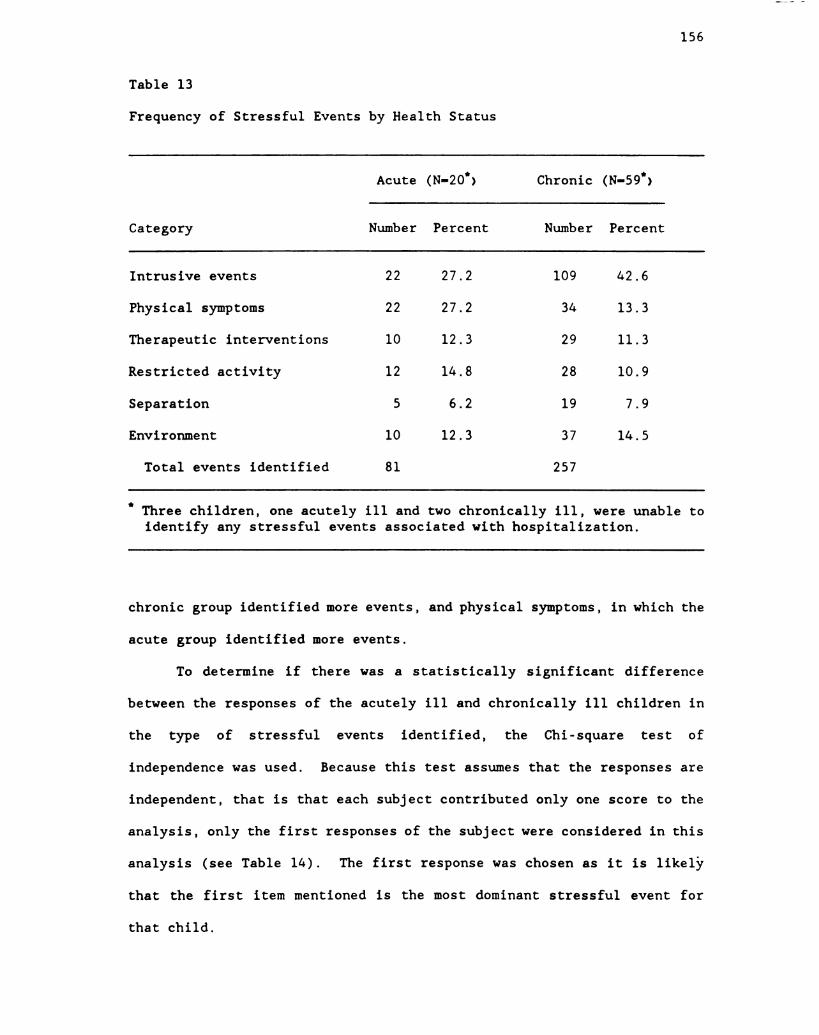
156
Table 13
Frequency of Stressful Events by Health Status
Acute (N-20") Chronic (N-59")
Category Number Percent Number Percent
Intrusive events 22 27.2 109 42.6
Physical symptoms 22 27.2 34 13.3
Therapeutic interventions 10 12.3 29 11.3
Restricted activity 12 14.8 28 10. 9
Separation 5 6.2 19 7. 9
Environment 10 12. 3 37 14.5
Total events identified 81 257
" Three children, one acutely ill and two chronically ill, were unable toidentify any stressful events associated with hospitalization.
chronic group identified more events, and physical symptoms, in which the
acute group identified more events.
To determine if there was a statistically significant difference
between the responses of the acutely ill and chronically ill children in
the type of stressful events identified, the Chi-square test of
independence was used. Because this test assumes that the responses are
independent, that is that each subject contributed only one score to the
analysis, only the first responses of the subject were considered in this
analysis (see Table 14). The first response was chosen as it is likely
that the first item mentioned is the most dominant stressful event for
that child.

157
Table 14
Frequency of First Stressful Event by Health Status
Acute (N–20") Chronic (N-59")
Category Number Percent Number Percent
Intrusive events 8 40.0 39 66.1
Physical symptoms 9 45. 0 5 8.5
Therapeutic interventions O 0.0 6 10. 2
Restricted activity 1 5. 0 3 5.1
Separation O 0.0 4 6.8
Environment 2 10. 0 2 3.4
Total stressful events 20 59
" Three children, one acutely ill and two chronically ill, were unable toidentify any stressful events associated with hospitalization.
For the test of the relationship between health status and the type
of events appraised as stressful, the value of the Chi Square statistic
was 17.6342, d.f. - 5, p < 0.01, statistically significant. It should be
noted that 9 of the cell expected frequencies were less 5, resulting in a
possible inaccuracy of the statistic. To determine if the small cell
frequencies influenced the significance of this finding, similar
categories were collapsed, such as combining therapeutic intervention with
restricted activity and merging separation and environment. reexaminationof the Chi-square statistic indicated that the findings remained
significant at the .01 significance level. Therefore, it is reasonable to

158
conclude that, despite the less than ideal cell frequencies, the
relationship between health status and the categories of stressful events
is significant.
To determine in which categories there was a significant difference
between acutely and chronically ill children's responses, the test of
differences of proportion was used. Based on an alpha of .05, the
percentage of acutely ill children citing an intrusive response was
significantly lower than was that of chronically ill children. Also, the
percentage of acutely ill children citing a physical symptom was
significantly higher than that of chronically ill children. The remaining
four categories were not examined due to possible instability related to
low cell frequency.
Hypothesis 2
The second hypothesis postulated that there would be a relationship
between health status and the type of coping behavior used during
hospitalization. The descriptive statistics for this question were
examined by determining the frequency and percentage of each category of
coping behavior by health status (see Table 15). These statistics were
based on N - 77; the three children who could not identify a stressful
event were not questioned regarding coping behaviors and one additional
chronically ill child was unable to identify any coping behaviors used in
response to stressful events associated with hospitalization. Acutely ill
children identified a total of 69 coping behaviors, with a mean of 3.3 per
child (s.d.- 2.6), and a range of 0 to 11 events. Chronically ill
children identified a total of 278 stressful events, with a mean of 4.6
per child (s.d.- 3.3), and a range of 0 to 18 events. The difference in
the mean number of coping behaviors of the two groups was not

159
Table 15
Frequency of All Coping Behaviors by Health Status
Acute (N-20)." Chronic (N-58)"
Category Number Ž Number 7.
Cognitive Processing 3 4.3 12 4.3
Cognitive Restructuring 12 17.4 22 7. 9
Cooperation 4 5.8 28 10.1
Countermeasure 22 31.9 95 37.1
Control 18 26.1 58 22.7
Seeking Support 10 14.5 63 24.6
Total 69 278
* One acutely ill child and three chronically ill children were unable toidentify any coping behaviors used during hospitalization.
statistically significant at a .05 level. A comparison of the percentage
for each category between groups demonstrated that there is little
difference except in two categories: cognitive restructuring in which the
acute group reported more behaviors, and seeking support, in which the
chronic group reported more behaviors.
To determine if there was a statistically significant difference
between the responses of the acutely ill and chronically ill children in
the type of coping behavior identified, the Chi-square test of
independence was used. Because the concept of coping must always be

160
considered in relation to a specific stressful event, it was believed that
the theoretical basis for analyzing the coping behavior would be strongest
if the response to a specific category of stress was analyzed. As the
category of intrusive events received the largest number of first
responses, this category was selected for analysis of the child's coping
response. This technique avoids comparison of coping behaviors elicited
by diverse stressful situations such as intrusive events, restricted
activity, and separation, that logically could produce very different
coping behaviors. Again, only the first coping behavior stated in
response to the intrusive event was used to maintain the Chi Square
assumption of independence. Although the category of intrusive events was
the most frequently cited stressful category only 16 acutely ill children
and 48 chronically ill children were able to identify a coping behavior
used in response to an intrusive event, thus the total N for this analysis
was 64. (See Table 16 for descriptive statistics on the first response
data).
For the test of the relationship between health status and the type
of coping behavior used in response to an intrusive event, the value of
the Chi Square statistic was 5. 3484, d.f. - 5, p > 0.5, statistically not
significant. The expected frequencies of 7 cells in the 2 x 6 table were
less than 5, therefore the data were further examined by collapsing
conceptually similar categories, such as combining cognitive processing
and cognitive restructuring, both a form of cognitive coping, and
counteraction and control, both behavioral coping. Although the results
of these Chi-square analyses moved toward the .05 level, the results
remained not significant. Therefore, despite the difficulty with cell
size, it is clear that in this sample there was no significant

161
Table 16
1st Coping Behavior used in Response to Intrusive Event by Health Status
Acute (N-16)." Chronic (N-48)"
Category Number Ž Number Ž
Cognitive Processing l 6.5 3 6.3
Cognitive Restructuring 3 18.8 4 8. 3
Cooperation 1 6. 3 7 14.6
Countermeasure 4. 25. 0 15 31. 3
Control 4 25. 0 4 8.3
Seeking Support 3 18.8 15 31. 3
" The N's for this table represent only the children who identified anintrusive event as stressful and who verbalized a coping behavior usedin response to the intrusive event.
relationship between health status and the type of coping behavior used by
school-age children during hospitalization.
Hypothesis 3
The third hypothesis postulated that there would be a relationship
between gender and the type of event appraised as stressful during
hospitalization. The descriptive statistics for this question were
examined by determining the frequency and percentage of each category of
stressful event by gender (see Table 17). These statistics were based on
N - 78, one male and two females did not identify any stressful events
associated with hospitalization. Males identified a total of 155

162
Table 17
Frequency of Stressful Events by Gender
Male (N-40") Female (N-39")
Category Number 7. Number 7.
Intrusive events 57 36.8 74 40.7
Physical symptoms 28 18.1 28 15.4
Therapeutic interventions 16 10.3 23 12.6
Restricted activity 27 17.4 13 7.1
Separation 8 5.2 16 8.8
Environment 19 12.3 28 15.4
Total N 155 182
* One male and two females did not identify any stressful events associatedwith hospitalization.
stressful events, with a mean of 3.7 per boy (s.d.- 2.4), and a range of
0 to 14 events. Females identified a total of 182 stressful events, with
a mean of 4.4 per girl (s.d.- 2.7), and a range of 0 to 16 events. The
difference in the mean number of stressful events between the two groups
was not statistically significant at a .05 level. A comparison of the
percentage for each category between groups demonstrated that there is
little difference except in the category of restricted activity that the
boys reported more frequently.
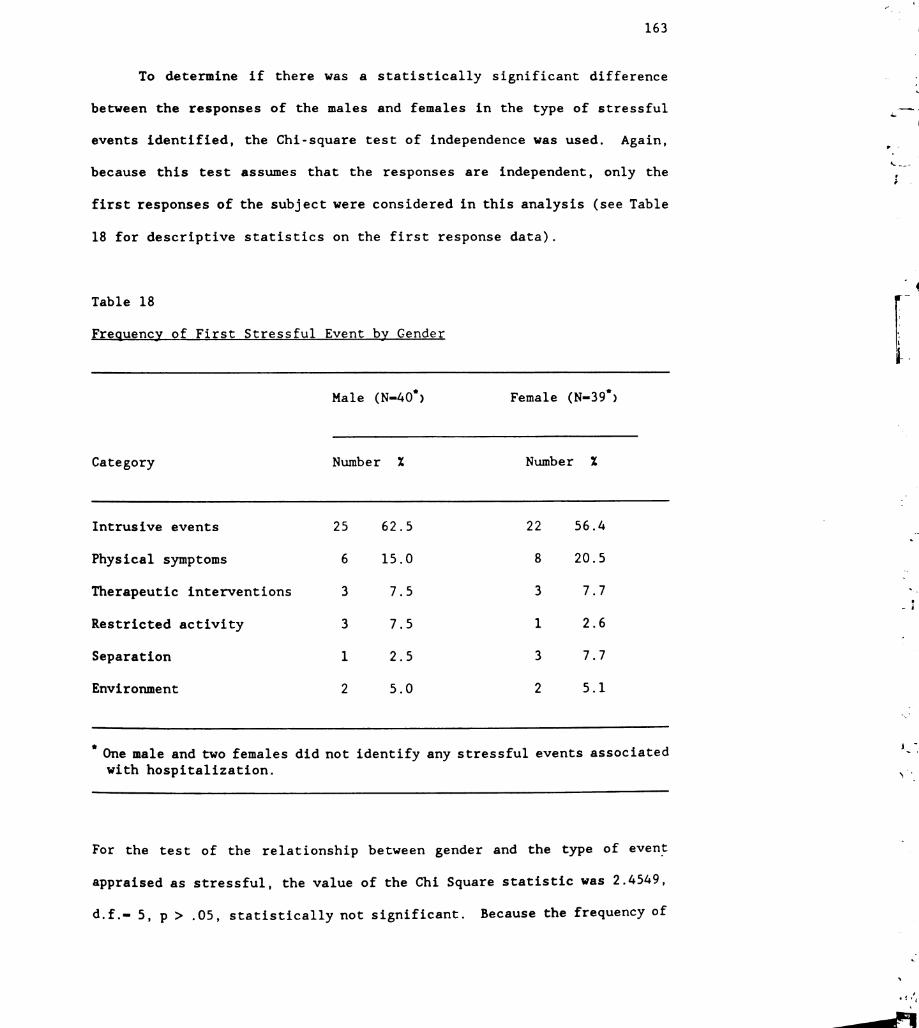
163
To determine if there was a statistically significant difference
between the responses of the males and females in the type of stressful
events identified, the Chi-square test of independence was used. Again,
because this test assumes that the responses are independent, only the
first responses of the subject were considered in this analysis (see Table
18 for descriptive statistics on the first response data).
Table 18
Frequency of First Stressful Event by Gender
Male (N-40") Female (N-39")
Category Number 7. Number 7.
Intrusive events 25 62.5 22 56.4
Physical symptoms 6 15. 0 8 20.5
Therapeutic interventions 3 7.5 3 7.7
Restricted activity 3 7.5 1 2.6
Separation 1 2.5 3 7.7
Environment 2 5.0 2 5.1
* One male and two females did not identify any stressful events associatedwith hospitalization.
For the test of the relationship between gender and the type of event
appraised as stressful, the value of the Chi Square statistic was 2.4549,
d. f. - 5, p > . 05, statistically not significant. Because the frequency of

164
eight of the cells was lower than the expected frequency of 5, the
statistic was reexamined by collapsing conceptually similar categories,
such as therapeutic interventions and restricted activity, and separation
and environment. Although these measures moved the p-value toward the .05
level, statistical significance was not achieved. Therefore, it is
evident that in this sample there was no significant relationship between
the gender of the child and the type of stressful event first mentioned in
relation to hospitalization.
Hypothesis 4
The fourth hypothesis postulated that there would be a relationship
between gender and the type of coping behavior used during
hospitalization. The descriptive statistics for this question were
examined by determining the frequency and percentage of each category of
coping behavior by health status (see Table 19). These statistics were
based on N = 77; the three children who could not identify any stressful
events were not questioned regarding coping behaviors and one additional
male was unable to identify any coping behaviors used in response to
stressful events associated with hospitalization. The males identified a
total of 151 coping behaviors, with a mean of 3.7 per child (s.d.- 2.4),
and a range of 0 to 11 events. The females identified a total of 196
stressful events, with a mean of 4.7 per child (s.d.- 3.7), and a range of
0 to 18 events. The difference in the mean number of coping behaviors of
the two groups was not statistically significant at a .05 level. A
Comparison of the percentage for each category between groups demonstrated
that there is little difference except in one category, countermeasure,
reported more frequently by the boys than by the girls.
-
Z.º.
-

165
Table 19
Frequency of Coping Behaviors by Gender
Male (N–39)." Female (N–39)."
Category Number 2. Number 7.
Cognitive Processing 5 3.3 10 5. 1
Cognitive Restructuring 15 9.9 19 9.7
Cooperation 15 9.9 17 8.7
Countermeasure 60 40.4 57 29.1
Control 27 17. 9 49 25. 0
Seeking Support 29 19.2 44 22.4
Total 151 196
* Two males and two females were unable to identify any coping behaviorsused during hospitalization.
To determine if there was a statistically significant difference
between the responses of the males and females in the type of coping
behavior identified, the Chi-square test of independence was used. Again,
because the concept of coping must always be considered in relation to a
specific stressful event, the category of intrusive events was selected
for analysis of the child's coping response. Only the first coping
behavior stated in response to the intrusive event was used to maintain
the Chi Square assumption of independence. Although the category of
intrusive events was the most frequently cited stressful category only 29

166
males and 35 females were able to identify a coping behavior used in
response to an intrusive event, thus the total N for this analysis was 64.
(See Table 20 for the descriptive statistics on the first response data.)
Table 20
1st Coping Behavior used in Response to Intrusive Event by Health Status
Male (N-29)." Female (N–35)."
Category Number 7. Number 7.
Cognitive Processing 1 3.4 3 8.6
Cognitive Restructuring 2 6.9 5 14.3
Cooperation 4 13.79 4 11.4
Countermeasure 12 41.4 7 20. 0
Control 4 13.8 4 11.4
Seeking Support 8 29.0 12 34.3
* Twelve males (29.27%) and six females (14.63%) did not state any copingbehaviors used in conjunction with an intrusive event.
For the test of the relationship between gender and the type of
coping behavior used in response to an intrusive event, the value of the
Chi Square statistic was 5.0837, d.f. - 5, p >.05, statistically not
significant. Because the frequency of eight of the cells was lower than
the expected frequency of 5, the statistic was reexamined by collapsing
conceptually similar categories, such as cognitive processing and

167
cognitive restructuring and counteraction and control. Although these
measures moved the p-value toward the .05 level, statistical significance
was not achieved. Therefore, it is evident that in this sample there was
no significant relationship between the gender of the child and the type
of coping behavior first described in connection with an intrusive event.
Hypothesis 3
The fifth hypothesis postulated that there would be a relationship
between trait anxiety and the type of event appraised as stressful during
hospitalization. Because the trait anxiety score provided interval data,
the descriptive statistics examined were the mean and the standard
deviation (see Table 21).
Table 21
ean Trait Anxiety Score by Stressful Event Category
Category N Mean StandardDeviation
Intrusive events 47 39.1 6.6
Physical symptoms 14 37.3 6.9
Therapeutic interventions 6 33. O 5.9
Restricted activity 4. 34.5 8.6
Separation 4. 36.7 4.1
Environment 4 38.8 5. 7
Total 79
s
º
>

168
To determine if there was a relationship between the trait anxiety
scores and the number of stressful events identified by the children, the
correlation between the variables was determined. The test was not
significant at the .05 level.
To determine if there was significant difference in the trait
anxiety scores between the six stress categories, the one-way analysis of
variance was used. As an assumption of this test is that the groups are
mutually exclusive, only the first responses of the subjects were
considered in this analysis. The total N was 79, because three subjects
were unable to identify any stressful events associated with
hospitalization. The one-way analysis of variance was not significant at
dif = 5, 73, F = 1. 231.
Hypothesis 6
The sixth hypothesis postulated that there would be a relationship
between trait anxiety and the type of coping behavior used during
hospitalization. The descriptive statistics for this question were
examined by determining the mean and standard deviation of trait anxiety
for each category of coping behavior (see Table 22).
To determine if there was a relationship between the trait anxiety
scores and the number of coping behaviors reported by the children, the
correlation between the variables was determined. The test was not
significant at the .05 level.
To determine if there was significant difference in the trait
anxiety scores between the six coping categories, the one-way analysis of
variance was used. Again, because the concept of coping must always be
considered in relation to a specific stressful event, the category of
7...",^--
-

169
Table 22
Mean Trait Anxiety Score by Coping Behavior Categories
Category N Mean Standard Deviation
Cognitive Processing 4 41.2 9.7
Cognitive Restructuring 7 39.9 4.9
Cooperation 8 38.2 6.9
Countermeasure 19 38.9 8.0
Control 8 37.2 7.3
Seeking Support 18 37.2 5.9
Total 64
intrusive events was selected for analysis of the child's coping response,
and only the first coping behavior stated in response to the intrusive
event was used to maintain the assumption of independence. Because 18
subjects did not identify any coping behaviors used in relation to
intrusive events, the total N for this portion of the analysis was 64.
The one-way analysis of variance was not statistically significant at d■
- 5, 58, F - 0.356 at dif - 5, 58.
Summary of Interview Data Analysis
Analysis of the data for Hypotheses 1 through 6 demonstrated one
significant relationship and five non-significant relationships. Table 23
summarizes these findings. Figure 4 schematically illustrates these
relationships.

170
Table 23
ult terview ta Analyses
Hypothesis Statistical Result Significance
1 (health status by stress) X* - 17. 6342, d.f. - 5 p < 0.01
2 (health status by coping) X* - 5.3484, d.f.- 5 N. S.
3 (gender by stress) X* - 2.4549, d.f. - 5 N. S.
4 (gender by coping) X* - 5.0837, d.f.- 5 N. S.
5 (anxiety by stress) F - 1.241, d. f. - 5, 73 N. S.
6 (anxiety by coping) F - 0.356, d. f. - 5, 58 N. S.
Health Status
NS>.O1
Anxiety -
NS Stress Tº Copingappraisal _- behaviors_º-
Gender ~. NS
Figure 4. Model of statistical relationships between variables.
Analysis of the Stress and Coping Word Graphic Scales
Analysis of the data provided by the word graphic scales proceeded
in two phases. First, concurrent validity of the word graphic rating
scales was determined. Second, the examination of Hypotheses 7 and 8 was
conducted using multiple regression and path analysis.

171
Concurrent validity
Because the Hospital Stress Scale and the Hospital Coping Scale were
new instruments developed for use in this study, it was necessary to
examine the validity of the instruments. As described in Chapter 3, the
Child Medical Fear Scale (Broome et al., 1988) was selected to examine the
validity of the Hospital Stress Scale, and the Coping Response Inventory
(Elwood, 1987) was selected to examine the validity of the Hospital Coping
Scale. These instruments purport to measure similar, although not
identical, constructs. Because all four tools provide interval level
data, the Pearson Product Moment Correlation Coefficient was used to
determine the relationship.
Based on the sample of 82 subjects, the correlation between the
Hospital Stress Scale and the Child Medical Fear Scale was .3388, The
statistical significance of this correlation is low positive. This
indicates that the instruments do measure similar constructs, but that the
overall relationship between the instruments is not strong. Although a
stronger relationship would have been preferred, the low correlation may
be acceptable in this case as the tool used for concurrent validity is
newly developed and is still, itself, in the process of having validity
examined. Additionally, the Children's Medical Fear Scale measures the
emotion of fear, rather than stress itself. Fear may be generated in a
stressful situation, but not all stressful situations result in fear.
Therefore, achievement of a positive correlation, although it may have
been low, may be interpreted as evidence that the Hospital Stress Scale
does appear to assess children's appraisal of the stressfulness of the
hospital experience.
172
The correlation between the Hospital Coping Scale and the Coping
Response Inventory was .3448. Again, the statistical significance of this
correlation is low positive. The two instruments do appear to measure
similar constructs, but the relationship is not strong. The construct of
coping as used in the Coping Response Inventory appears to be congruent
with that of the current study, but the instrument was developed for use
with healthy, rather than ill, children and may not have adequately
represented coping behaviors used by the hospitalized child. Again, the
positive, although low correlation, may be interpreted as evidence that
the Hospital Coping Scale does appear to assess children's perception of
the effectiveness of their coping behaviors during hospitalization.
Preliminary Information Regarding Analysis
In determining the path coefficients through multiple regression,
several methods may be used to enter the data into the equation. It was
of interest to know how much variance was contributed to the model by each
variable, regardless of the significance of the factor. Additionally,
there was no theoretical basis for examining the independent variables
separately. Accordingly, for this investigation, the method used was
simultaneous regression analysis. It is also important to note that a
residual analysis was performed to check for evidence of deviations such
as curvilinearity, outliers, and homogenous variance that would violate
the assumptions of the regression procedure. Examination of the residuals
indicated that all assumptions were met.
Hypothesis 7
Hypothesis 7 postulated that health status, gender, and trait
anxiety would affect the appraisal of hospitalization as stressful in that

173
a) acutely ill children would appraise the event of hospitalization as
more stressful than would chronically ill children; b) girls would
appraise the event of hospitalization as more stressful than would boys;
and c) children with high levels of trait anxiety would appraise the event
of hospitalization as more stressful than would children with low levels
of trait anxiety. This hypothesis comprised the first stage of the
theoretical model.
Simultaneous regression analysis was used to test this first portion
of the model, with all three variables being entered in one step. The
results of this analysis are presented in Table 24. The cumulative R* of
. 14, due to the three independent variables, indicates that together they
explain a significant (<.01) proportion of the variance in Stress
appraisal. Examination of the unique contribution attributable to each
variable indicates that only trait anxiety had a significant (<.001)
influence on stress appraisal.
Table 24
The Effects of Independent Variables on Dependent Variable of Stress
Variable df Cumulative R* Unique R* F p-value
Independent variables 3 0.1426 4.323 <. 01
Health status 1 . 0104 0.948 N. S.
Gender 1 .0002 0.015 N. S.
Trait anxiety 1 . 1310 11. 919 <. 001
Residual 78

174
Before addressing the subhypotheses of Hypothesis 7, it is necessary
to determine the nature of the relationship between the independent
variables and the dependent variable. This information is provided by the
standardized beta weights, and is graphically shown in Figure 5, the
portion of the theoretical model relevant to this hypothesis.
Health Status
. 104
Anxiety → * >_*—
Stressappraisal
Gender
Figure 5. Theoretical model of variables influencing stress appraisal.
The first subhypothesis proposed that acutely ill children would
appraise the event of hospitalization as more stressful than would
chronically ill children. To interpret the above data it is necessary to
note that the coding for health status was as follows: 1 - acute
condition, 2 - chronic condition. It is also necessary to recall that the
higher the score on the Hospital Stress Scale, that is the closer to 100
on a scale of 0 to 100, the greater the degree stressfulness appraised by
the child. The standardized beta of . 104 indicated that the relationship
was in a positive direction. This implies that a child who was assigned
a higher score on the variable of health status (chronic condition) had a
tendency to score higher on the variable of stress appraisal, although the
strength of the association was not strong. In sum, the chronically ill
child was somewhat more likely to appraise the event of hospitalization as

175
stressful than was the acutely ill child. However, the unique portion of
variance attributable to this variable was not statistically significant.
Therefore, Hypothesis 7. a. was not supported.
The second subhypothesis proposed that girls would appraise the
event of hospitalization as more stressful than would boys. To interpret
the above data it is necessary to note that the coding for gender was as
follows: 1 - male, 2 - female. Again, it is necessary to recall that the
higher the score on the Hospital Stress Scale, the greater the degree of
stressfulness appraised by the child. The standardized beta of . 013,
indicated that the relationship was in a positive direction. However,
this result was so close to zero that it cannot be stated that a trend was
evident. As would be expected, the unique portion of variance
attributable to this variable was not statistically significant.
Therefore, Hypothesis 7.b. was not supported.
The third subhypothesis proposed that children with high levels of
trait anxiety would appraise the event of hospitalization as more
stressful than would children with low levels of trait anxiety. To
interpret the above data it is again necessary to note that the trait
anxiety scale of the State-Trait Anxiety Inventory for Children is scored
so that the higher the score, the greater the degree of trait anxiety.
The scoring of the Hospital Stress Scale follows the same pattern, the
higher the score, the greater the degree of stressfulness appraised by the
child. The standardized beta was . 378, indicating that the relationship
was in a positive direction. The child who was assigned a higher score on
the variable of trait anxiety was more likely to score higher on the
variable of stress appraisal. In sum, the child who scored high in the
personality characteristic of trait anxiety was more likely to appraise
176
the event of hospitalization as highly stressful than was the child who
scored low in trait anxiety. The unique portion of variance attributable
to this variable was statistically significant at the .001 level.
Therefore, for this sample, Hypothesis 7. c. was supported.
Hypothesis 8
Hypothesis 8 postulated that health status, gender, and trait
anxiety would affect the perception of effectiveness of the coping
behavior in that a) chronically ill children would perceive their coping
behaviors during hospitalization as more effective than would acutely ill
children; b) girls would perceive their coping behaviors during
hospitalization as more effective than would boys; c) children with low
levels of trait anxiety would perceive their coping behaviors during
hospitalization as more effective than would children with high levels of
trait anxiety; d) children who appraise hospitalization as of low
stressfulness would perceive their coping behaviors during hospitalization
as more effective than would children who appraise the event of
hospitalization as highly stressful. This hypothesis comprised the second
stage of the theoretical model. It is important to note that stress
appraisal is treated as an independent variable in this phase of the
model, rather than as a dependent variable as in the first phase.
Simultaneous regression analysis was used to test this second
portion of the model, with all four variables being entered in one step.
The results of this analysis are presented in Table 25. The cumulative R2
of . 14, due to the set of four independent variables, indicated that
together they explain a significant (<.05) proportion of the variance inperceived coping effectiveness. Interestingly, an examination of the
unique contribution to the variance in coping of any one characteristic,

177
Table 25
Effects of Independent Variables on Dependent Variable of Coping
Variable df Cumulative R* Unique * F p-value
Characteristics 4 0.1437 3. 230 <. 05
Health status 1 . 0.391 3.513 N. S.
Gender 1 . 0.063 0. 564 N. S.
Trait anxiety 1 . 0334 3.007 N. S.
Stress appraisal 1 . 0240 2. 157 N. S.
Residual 77
after the contribution of the remaining three characteristics was held
constant, indicated that no one variable accounted for a unique
contribution above and beyond that which it shared with the other
characteristics.
Before addressing the subhypotheses of Hypothesis 8, it is necessary
to examine the nature of the relationship between the independent
variables and the dependent variable. This information is provided by the
standardized beta weights, and is graphically shown in Figure 6, the
portion of the theoretical model relevant to this hypothesis.
The first subhypothesis proposed that chronically ill children would
perceive their coping behaviors during hospitalization as more effective
than would acutely ill children. To interpret the above data it is again
necessary to recall that the coding for health status was as follows: 1 -
acute condition, 2 - chronic condition. It is also necessary to recall

178
Health Status
Anxiety -
StreSS -. 167 - CopingO8 appraisal Tº behaviors-.O8 1
Gender -
Figure 6: Theoretical model of factors influencing coping appraisal
that the higher the score on the Hospital Coping Scale, that is the closer
to 100 on a scale of 0 to 100, the greater the perceived effectiveness of
the child's coping behaviors. The standardized beta of -. 203 indicated
that ine relationship was inverse. This implies that a child who was
assigned a lower score on the variable of health status (acute condition)
had a tendency to score higher on the variable of perception of coping
effectiveness. In sum, the acutely ill child was more likely to perceive
his or her coping as effective than was the chronically ill child.
However, the unique portion of variance attributable to this variable was
not statistically significant. Thus, Hypothesis 8. a. was not supported.
The second subhypothesis proposed that girls would perceive their
coping behaviors during hospitalization as more effective than would boys.
To interpret the findings it is again necessary to note that the coding
for gender was as follows: 1 - male, 2 - female. It is also necessary to
recall that the higher the score on the Hospital Coping Scale, the greater
the perceived effectiveness of the child's coping behaviors. The

179
standardized beta was - .081, indicating that the relationship was inverse.
This result was so close to zero, that it cannot be stated that a trend
was evident. As would be expected, the unique portion of variance
attributable to this variable was not statistically significant.
Therefore, Hypothesis 8.b. was not supported.
The third subhypothesis proposed that children with low levels of
trait anxiety would perceive their coping behaviors during hospitalization
as more effective than would children with high levels of trait anxiety.
To interpret the above data, it is necessary to recall that the trait
anxiety scale of the State-Trait Anxiety Inventory for Children is scored
so that the higher the score, the greater the degree of trait anxiety.
The scoring of the Hospital Coping Scale follows the same pattern, the
higher the score, the greater the perceived effectiveness of the coping.
The standardized beta was - .205, indicating that the relationship was
inverse. This implies that the child who scored lower on the variable of
trait anxiety was more likely to score higher on the perceived coping
effectiveness. In sum, the child who has a low level of trait anxiety was
more likely to perceive his or her coping behaviors as being effective
than was the child who scored high in trait anxiety. However, the unique
portion of variance attributable to this variable was not statistically
significant. Therefore, Hypothesis 8. c. was not supported.
The fourth subhypothesis proposed that children who appraise
hospitalization as lowly stressful would perceive their coping behaviors
during hospitalization as more effective than would children who appraise
the event of hospitalization as highly stressful. To interpret the data
relevant to this proposition, it is necessary to recall that the Hospital
Stress Scale is scored so that the higher the score, the greater the

18O
appraisal of stress related to hospitalization. The scoring of the
Hospital Coping Scale follows the same pattern, the higher the score, the
greater the perceived effectiveness of the coping. The standardized beta
was - . 167, indicating that the relationship was inverse. The child who
scored lower on the variable of stress appraisal had a tendency to score
higher on the perceived coping effectiveness. In sum, the child who
appraised the degree of stress during hospitalization as low was more
likely to perceive his or her coping behaviors as being effective than was
the child who appraised the degree of stress associated with hospitali
zation as high. However, the unique portion of variance attributable to
this variable was not statistically significant. Therefore, for this
sample, Hypothesis 8...d. was not supported.
Revision of Model
Consideration of the preceding results raised the question of the
relevance of the variable, stress appraisal, in the second portion of the
model. Because 1) the set of four variables, health status, gender, trait
anxiety, and stress appraisal, had a significant influence on the
perceived coping effectiveness, yet individually no one variable
contributed significantly to the model (Table 25), and because 2) the
correlation between stress appraisal and coping effectiveness (the
Hospital Stress Scale and the Hospital Coping Scale respectively) was - .26
(p< 0.05), yet when the effects of health status, gender, and trait
anxiety were partialed out, the unique variance contributed to coping
effectiveness by stress appraisal was only 0.02 (p = 0.146), and because
3) in the first portion of the model the influence of trait anxiety onstress appraisal was highly significant (Table 24), it appeared probable
that the influence of stress appraisal on perception of coping

181
effectiveness was highly dependent on the moderating characteristics of
the person. Therefore it was decided to revise the second portion of the
model, eliminating the path between stress and coping, and reexamine the
statistics.
As before, simultaneous regression analysis was used to test the
revised second portion of the model, with all three variables being
entered in one step. The results of this analysis are presented in Table
26 and illustrated graphically by Figure 7. The cumulative R* of . 12 due
to the set of three independent variables, indicated that together they
explain a significant (<.05) proportion of the variance in perceived
coping effectiveness. Examination of the unique contribution attributable
to each variable indicates that both health status and trait anxiety had
a significant influence on perceived coping effectiveness, but that the
relationship between gender and coping was not significant.
Table 26
Revised Effects of Independent Variables on Dependent Variable of Coping
Variable df Cumulative R* Unique R* F p-value
Characteristics 3 0.1197 3.536 <. 05
Health status 1 . 0466 4. 131 <. 05
Gender 1 . 0.066 0. 587 N. S.
Trait anxiety 1 . 0660 5. 847 <. 05.
Residual 78
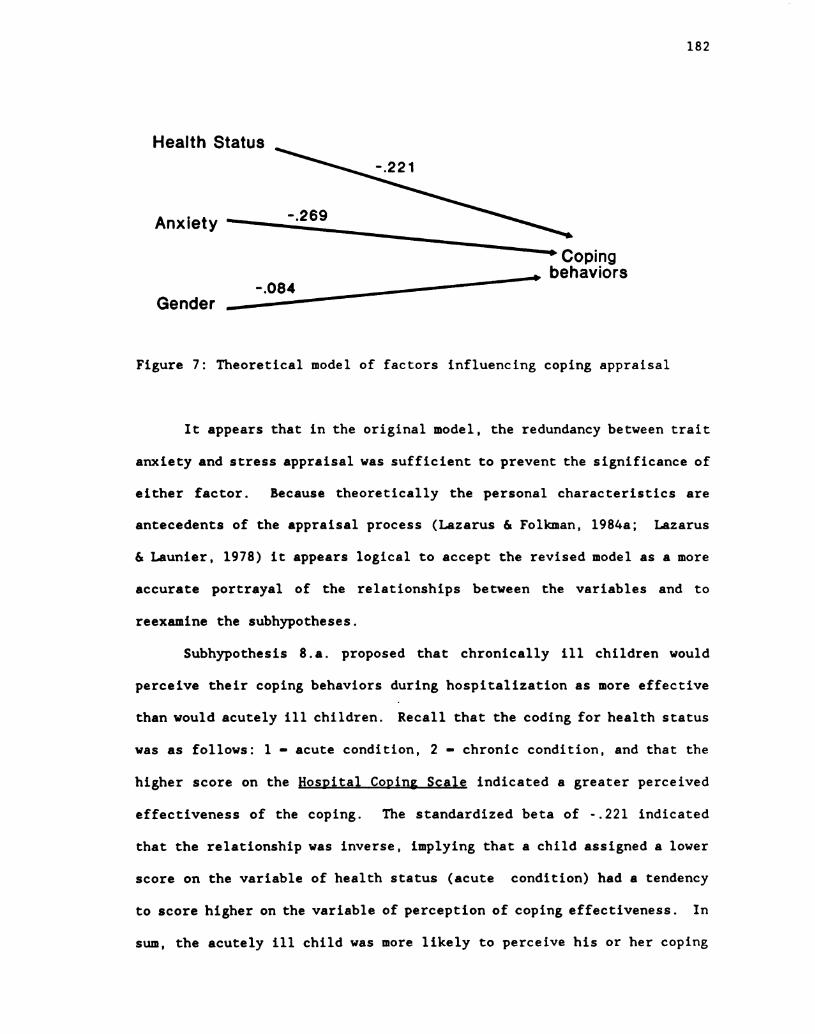
182
Health Status
Anxiety -
Tº Coping_- behaviors
-.084Gender —
Figure 7: Theoretical model of factors influencing coping appraisal
It appears that in the original model, the redundancy between trait
anxiety and stress appraisal was sufficient to prevent the significance of
either factor. Because theoretically the personal characteristics are
antecedents of the appraisal process (Lazarus & Folkman, 1984a; Lazarus
& Launier, 1978) it appears logical to accept the revised model as a more
accurate portrayal of the relationships between the variables and to
reexamine the subhypotheses.
Subhypothesis 8. a. proposed that chronically ill children would
perceive their coping behaviors during hospitalization as more effective
than would acutely ill children. Recall that the coding for health status
was as follows: 1 - acute condition, 2 - chronic condition, and that the
higher score on the Hospital Coping Scale indicated a greater perceived
effectiveness of the coping. The standardized beta of - .221 indicated
that the relationship was inverse, implying that a child assigned a lower
score on the variable of health status (acute condition) had a tendency
to score higher on the variable of perception of coping effectiveness. In
sum, the acutely ill child was more likely to perceive his or her coping
183
as effective than was the chronically ill child. The unique portion of
variance attributable to this variable was statistically significant at
the .05 level. However, the relationship was not in the direction
predicted in the hypothesis, therefore, Hypothesis 8. a. was not supported.
Subhypothesis 8. b. proposed that girls would perceive their coping
behaviors during hospitalization as more effective than would boys.
Recall that the coding for gender was as follows: 1 - male, 2 - female,
and that the higher score on the Hospital Coping Scale indicated a greater
perceived effectiveness of coping. The standardized beta was - .084,
indicating that the relationship was inverse. Although slightly
increased, this result remains so close to zero that the previous
conclusion stands. No trend was evident due to gender, and the unique
portion of variance attributable to this variable was not statistically
significant. Therefore, Hypothesis 8. b. was not supported.
Subhypothesis 8... c. proposed that children with low levels of trait
anxiety would perceive their coping behaviors during hospitalization as
more effective than would children with high levels of trait anxiety.
Again recall that the trait anxiety scale of the State-Trait Anxiety
Inventory for Children is scored so that the higher score indicates a
greater degree of trait anxiety. The scoring of the Hospital Coping Scale
is similar, the higher score indicates a greater perceived effectiveness
of the coping. The standardized beta was - .269, indicating that the
relationship was inverse. This implies that the child who scored lower on
the variable of trait anxiety was more likely to score higher on the
perceived coping effectiveness. In sum, the child who has a low level of
trait anxiety was more likely to perceive his or her coping behaviors as
being effective than was the child who scored high in trait anxiety. The

184
unique portion of variance attributable to this variable was statistically
significant at the .05 level. Therefore, for this sample, Hypothesis 8. c.
was supported.
At this point is must be noted that elimination of the path between
stress appraisal and coping behavior in the model, eliminated
Subhypothesis 8...d. Therefore, analysis of this hypothesis was not
conducted for the revised model.
Summary of Word Graphic Scale Analyses
Figure 8 shows the entire revised theoretical model with
standardized beta weights illustrating the relationships between the
variables. For comparison, the beta weights from the original second
portion of the model are included in parentheses.
Health Status
... 104
-.221 (-.2O3)
Anxiety - -.269 (-,205)Nº.
.378 Stress (.-.167) T* Coping
*—- appraisal Tº behaviorsGender ~. -.O84 (-.081)
Figure 8. Theoretical model of relationships between variables
Note: Beta weights in () are from original model
Table 27 presents a decomposition of the relationships between the
independent and dependent variables in the original and in the revised
models. In examining the table, note that in the original model there are
both indirect and direct relationships necessitating a separate

185
Table 27
Summary of the Effects of Independent Variables on Dependent Variables
Original Model Revised Model
Bivariate Relationship Direct Indirect Total Direct/Total
Health status/Stress appraisal . 104 none . 104 ... 104
Anxiety/Stress appraisal . 378 none . 378 . 378
Gender/Stress appraisal . 013 none . 013 . 013
Health status/Coping effectiveness - .203 - . 017 - .220 - .221
Anxiety/Coping effectiveness - . 205 - . 063 - .268 - .269
Gender/Coping effectiveness - . 082 - . 002 - . 084 - .084
Stress appraisal/Coping effectiveness - . 167 none - . 167 none
calculation of the total relationship. In the revised model, however,
only direct relationships exist, so the direct relationship is also the
total relationship.
A comparison of the standardized beta weights in the decomposition
table (Table 26) provides further support for the revised theoretical
model. The first portion of the model was not effected by the revision,
so the relationship between the independent variables, health status,
anxiety and gender, and the dependent variable, stress appraisal, remained
the same. The revision of the second portion did increase the effect of
the independent variables of health status and anxiety on the dependentvariable of coping effectiveness through elimination of redundancy
resulting in a difference in the original and revised total effects of

186
only .001 for both variables. This small difference further demonstrates
the very limited contribution of stress appraisal to the original model.
The relationship between gender and coping effectiveness was not changed
by the revision. Because the path between stress appraisal and coping
effectiveness was not eliminated from the model, this relationship was not
examined in the revised calculations.
Summary of Findings
Eighty-two, children, ages 8 through 11 years, meeting the
inclusion-exclusion criteria, completed the protocol for this study. This
sample was comprised of 41 males and 41 females; 21 acutely ill children
and 61 chronically ill children; 20 eight year olds, 16 nine year olds, 19
ten year olds, and 27 eleven year olds; 52 Caucasian children, 13
Hispanic children, 10 African American children, 2 Asian children, and 4
of other ethnicity.
Analysis of potential confounding factors indicated no differences
in stress appraisal and perception of coping behavior effectiveness due to
site of data collection, age, prior out-patient experiences,
prehospitalization teaching programs, and parental rooming-in. Therefore
all analyses were conducted on the total sample.
Content analysis was used to examine the interview data. Six
categories of stressful events were derived from the data: intrusive
events, physical symptoms, therapeutic intervention, restricted activity,
separation, and environment. The individual events identified in the
interviews were assigned to one of these categories and quantified bycounting the responses in each category. These data then were used to
examine the first six hypotheses of the study, Chi square being used to
187
examine Hypotheses 1 through 4, and one-way analysis of variance being
used to examine Hypotheses 5 and 6. Of the first six hypotheses, only
Hypothesis 1 was significant indicating that there is a relationship
between health status and the type of event appraised as stressful by the
subjects. Specifically, chronically ill children were significantly more
likely to identify intrusive events as stressful than were acutely ill
children, and acutely ill children were significantly more likely to
identify physical symptoms as stressful than were chronically ill
children. No significant relationship was found between Hypothesis 2:
health status and coping behavior; Hypothesis 3: gender and the appraisal
of an event as stressful; Hypothesis 4: gender and coping behavior;
Hypothesis 5: trait anxiety and the appraisal of an event as stressful; or
Hypothesis 6: trait anxiety and coping behavior.
Multiple regression and path analysis, used in this study for the
purpose of description, was employed to examine the data obtained from the
Hospital Stress Scale and the Hospital Coping Scale. The theoretical
model was tested in two phases corresponding with Hypotheses 7 and 8.
First, the relation between the independent variables of health status,
gender, trait anxiety and the dependent variable of stress appraisal was
examined. Simultaneous regression analysis was used to test this portion
of the model, with the three independent variables being entered as a set
in the first step and the dependent variable of stress appraisal in the
second step. The overall significance of this portion of the model was <
.01. Further examination indicated that only trait anxiety contributed
significantly (<.001) to the model. Therefore, Hypothesis 7. c. , proposing
that a high level of trait anxiety would be related to a high level of
stress appraisal was supported. However, Hypothesis 7. a. , proposing that

188
acutely ill children would appraise hospitalization as more stressful than
would chronically ill children was not supported because the contribution
of health status to the model was not significant and because the trend of
the data indicated that chronically ill children appraise hospitalization
as more stressful than do acutely ill children. Similarly, Hypothesis
7.b., proposing that girls would appraise hospitalization as more
stressful than boys, was not supported because the contribution of gender
to the model was not significant, and because the standardized beta weight
was very near zero.
The second portion of the model was tested using the same procedure.
Simultaneous regression analysis again was used, with the four independent
variables, health status, gender, trait anxiety, and stress appraisal,
being entered as a set in the first step and the dependent variable of
coping entered in the second step. The overall significance of this step
was < .05. Further examination indicated that individually none of the
independent variables contributed significantly to the model. Therefore,
while Hypothesis 8 was supported, the subhypotheses were not supported.
Hypothesis 8...a., proposing that chronically ill children would perceive
their coping as more effective than would acutely ill children was not
supported because the contribution of health status to the model was not
significant and because the trend of the data indicated that acutely ill
children appeared to perceive their coping as more effective than did
chronically ill children. Hypothesis 8.b., proposing that girls would
perceive their coping behaviors as more effective than would boys, was not
supported because the contribution of gender to the model was not
significant, and because the standardized beta weight was very near zero.
Hypothesis 8. c. proposing that children with a low trait anxiety level
189
would perceive their coping as more effective than would children with a
high trait anxiety level, was not supported because the contribution of
trait anxiety to the model was not significant, although the trend of the
data did show this proposal to be accurate. Hypothesis 8. d. , proposing
that children who appraise hospitalization as lowly stressful perceive
their coping behaviors during hospitalization as more effective than
children who appraise the event of hospitalization as highly stressful,
was not supported because the contribution of stress appraisal to the
model was not significant, although again the trend of the data did show
this proposal to be accurate.
Consideration of the statistical results relating to Hypothesis 8
indicated that the variable of stress appraisal contributed little to the
model. Therefore the model was revised, eliminating the path between
stress appraisal and coping effectiveness, and the multiple regression
analysis recalculated entering the independent variables of health status,
gender, and trait anxiety as a set in the first step and the dependent
variable of coping in the second step. The overall significance of the
set was ‘ .05. Examination of the data pertaining to Subhypothesis 8. a.
indicated that health status contributed significantly to the model at 3
.05 level, however, the results were not in the direction of the
hypothesis. Therefore, the proposal that chronically ill children would
perceive their coping as more effective than would acutely ill children
was not supported as the results indicated that the reverse relationship
was true for this sample. The acutely ill children perceived their coping
as more effective than did chronically ill children. The findings
pertaining to Hypothesis 8.b. were not altered by the revision of the
model. As stated before, the proposal that girls would perceive their
*.
s

190
coping behaviors as more effective than would boys, was not supported
because the contribution of gender to the model was not significant.
Additionally, because the standardized beta weight was very near zero a
trend cannot be assumed from the data. Examination of Hypothesis 8. c.
indicated that the results were significant at the 3.05 level and that the
direct of the hypothesis was correct. The proposal that children with a
low trait anxiety level would perceive their coping as more effective than
would children with a high trait anxiety level, was supported for this
sample.

191
CHAPTER FIVE
DISCUSSION
In this chapter the results of the study will be discussed.
First, the theoretical rationale for revision of the model will be
detailed. Second, the meaning of the results will be examined in view of
the theoretical basis of the study and prior relevant research. Third,
limitations of the present research related to the sample and
instrumentation will be identified. Fourth, implications for nursing
practice and education will be presented. Last, suggestions for future
research in the area will be offered.
Revision of the Model
While examining the statistical results relevant to hypotheses 7 and
8, the portion of the data analyzed by multiple regression and path
analysis, it became evident that the discussion pertaining to the relation
between stress appraisal and coping effectiveness (8. d.) was a repetition
of the discussion pertaining to the relation between trait anxiety and
stress appraisal (8.c.). To try to understand this situation, the
theoretical basis of the study was reexamined. Briefly, coping may be
examined either in relation to the type of stress appraisal made, harmful,
threatening, or challenging, or according to the coping resources and
constraints relevant to the individual (Lazarus & Folkman, 1984a). If the
current research study had been examining the relationship between an
appraisal of harm, threat, or challenge and the type of coping behavior
192
appraisal of harm, threat, or challenge and the type of coping behavior
used, then inclusion of the path between stress appraisal and coping
behavior would have been appropriate. However, the purpose of the study
was to examine the relationship between personal characteristics of the
child and the appraisal process and between those same characteristics and
coping behaviors. Therefore, inclusion of the path between stress
appraisal and coping behaviors was unnecessary. Furthermore, because
there is some overlap between the person and situation factors influencing
appraisal and the resources and constraints that influence coping, such as
experience and beliefs (Lazarus & Folkman, 1984a), inclusion of the
pathway in question was redundant. For these reasons the theoretical
model for this study was modified by removing the path between stress
appraisal and coping behavior. As described in Chapter 4, the statistics
relevant to these variables supported this decision, as did the results of
the regression analysis based on the revised model. Revision of the model
did not affect the analysis of the interview data, hypotheses 1 through 6.
Relation of Results to Hypotheses
The results of the study will be discussed according to the two
primary concepts of the study, stress and coping. First, the findings
relating to the appraisal of stress will be discussed, followed by the
findings relating to coping.
Discussion of Results Relating to Stress Appraisal
There is no question that hospitalized school-age children are
capable of appraising events as stressful. As "stress is in the eye of

193
the beholder" (McGrath, 1977), whatever the child believes to have
personal implications for well-being involving harm, threat, or challenge
is stressful. When asked what were the upsetting things that happen in
the hospital, most of the children responded easily, without need for the
prompts provided with the interview. Only three children were unable to
identify any stressful events associated with hospitalization. One child,
who appeared tense and restrained while answering, denied the occurrence
of any stressful events. Interestingly, this child's score on the
Hospital Stress Scale was quite high, implying that hospitalization indeed
was appraised as stressful. The remaining two children seemed somewhat
surprised to think that anything associated with hospitalization would be
upsetting, possibly indicating use of defensive reappraisal (Lazarus &
Folkman, 1984a) as a coping mechanism. As would be expected if this
explanation was correct, the Hospital Stress Scale scores for these two
children were very low. In general, the other children easily identified
stressful events that had occurred while they were hospitalized.
Similarly, most of the children did not seem to have difficulty
switching from thinking about the specific stressful events to considering
the global stressfulness of the event when asked to respond to the
Hospital Stress Scale. Occasionally, a child would begin to mark the
scale for separate events, but when redirected to think about "everything
that had happened all together" would erase the first marks and place a
new line on the scale. This would indicate that the subjects for this
study had moved beyond the earlier thought processes of syncreatism and
juxtaposition typical of the pre-operational stage and were able to
consider the relationship of the parts to the whole (Ginsburg & Opper,
1988).

194 º
Of the six categories of stressful events identified through content
analysis of the interviews with the children, all were identified in the
literature, but with varying frequency. Four categories of stressful
events were well represented: intrusive events, physical symptoms,
restricted activity, and separation. The types of intrusive events
mentioned by the children and in the literature were similar, primarily
procedures involving needles (Eiser & Patterson, 1984; Erickson, 1958a,
1958b, 1972; Langford, 1961; Menke, 1972; Reissland, 1983; Timmerman,
1983). The physical symptom of pain was named frequently in the
literature (Eiser & Patterson, 1984; Gofman, Buckman, & Schade, 1957;
Langford, 1961; May & Sparks, 1983; Menke, 1972; Stevens, 1986; Timmerman,1983) and by the children, but the children also identified a number of
other symptoms, often side effects of medication, such as nausea, blurry
eyes, and dizziness. Regarding restricted activity, the literature
mentioned immobilization (Blom, 1968; Erickson, 1965, 1972; Freud, 1952)
and confinement (Kueffner, 1975; May & Sparks, 1983; McGuire, Shepherd, &
Greco, 1978; Menke, 1972; Powazek, Goff, Schyving, & Paulson, 1978), but
the children seemed to be more bothered by not being allowed to leave the
unit to go out to eat, shopping, or participate in sports. Separation was
mentioned by only a small number of the children, in contrast to frequent
identification in the literature (Bowlby, 1973; Erickson, 1965; May &
Sparks, 1983; Menke, 1972; Prugh, et al., 1953; Reissland, 1983;
Robertson, 1970; Timmerman, 1983), the probable explanation being that the
literature often did not distinguish between age groups. The two
categories infrequently mentioned in the literature were therapeutic
interventions and environment. Regarding therapeutic interventions, the
primary area of agreement was measurement of vital signs (Erickson, 1958a,
º

195
1958b; Menke, 1972), but the children also identified aspects of the
physical exam, dressing removal, and walking after surgery as stressful.
Stressful aspects of the environment were seldom mentioned in the
literature (Reissland, 1983), but frequently identified by the children,
ranging from nightmares caused by the equipment on the walls to
interpersonal problems with roommates and staff. In general, although
little research has been focused on what children perceive as stressful
during hospitalization, the major stresses have been accurately identified
in the literature. However, there are events that children appraise as
stressful that the adult health care provider may tend to overlook,
underscoring the importance of gaining input directly from the children
regarding events encountered during hospitalization that are likely to be
appraised as stressful.
Examination of the events identified by the total groups of children
as stressful has several interesting parallels with developmental
research. First, the most frequently named category of stressful
situations, intrusive events, was identified twice as often as the next
most frequent event. This finding is paralleled by Miller's (1979)
conclusion, following a review of eleven studies examining the fears of
school-age children, that fear of bodily injury increases in the 7 to 12
year old age group. The current study demonstrates that school-age
children continue to appraise bodily injury as a major source of concern
while in the hospital, just as they do when healthy.
Second, separation was identified as stressful less frequently than
any other category. Separation from parents is less difficult for the
child of school-age, than it was during the toddler or preschool years
(Prugh, 1965). Although hospitalized school-age children tend to want

196
parents to be present, the child does not appear to appraise separation as
a major source of stress. Factors contributing to the decreased appraisal
of separation as stressful would be acquisition of a sense of time and
knowledge that parents will return, familiarity with being separated from
parents during the school hours, and rooming-in by parents when possible.
Thus, the frequencies with which the children reported intrusive events
and separation as stressful during hospitalization is in accordance with
the developmental changes of this age group.
Beyond these initial observations, the question remains, given the
statistical results of the data analysis, what do the numbers mean? This
will be addressed by discussing the relationship of the three factors,
health status, gender, and trait anxiety, to stress appraisal, considering
the theoretical basis of the study and prior research.
Health Status and Stress Appraisal
The results of the data analysis indicated that health status does
have an affect on the type of event appraised as stressful by the child
during hospitalization with acutely ill children more likely to identify
physical symptoms as stressful and chronically ill children more likely to
identify intrusive procedures as stressful. A careful review of the
literature located only one prior study examining these same
relationships. Ritchie, Caty, and Ellerton (1984), studying preschool
children, also noted that chronically ill children demonstrated more
concern with intrusive events than did acutely ill children. Key elements
of the Lazarus theory that explain these findings are the process of
primary appraisal and the affect of novelty on the appraisal process.
Primary appraisal involves determining whether the situation is harmful or
º

*.197
helpful to personal well-being, a decision that is based partially on the
novelty or familiarity of the situation for the person (Lazarus & Folkman,
1984a). This premise is supported by McGrath (1977), in a review of
literature concerning the role of prior experience in stress appraisal,
concluding that the type of experience, as positive or negative, will
influence stress appraisal. For the chronically ill children in the
study, the intrusive events associated with hospitalization were not
novel, and prior experience likely had taught them that the procedures
were painful and unpleasant. Therefore, when asked what events were
stressful during hospitalization, the chronically ill children identified
intrusive events significantly more often than did the acutely ill
children. This did not appear to be due to a greater knowledge of
possible types of intrusive procedures. The majority of the items named
were common events experienced by both acutely and chronically ill,
hospitalized children, such as shots, intravenous needles, blood work, and
surgery. Only occasionally were more uncommon procedures such as lumbar
punctures or bone marrow taps mentioned. Similarly, it is not likely that
the result was due to differences in the extent of experience during the
current hospitalization, as all subjects were interviewed on the second or
third day of admission as stipulated in the inclusion criteria.
A reason that the acutely ill children did not appraise intrusive
events as stressful as frequently as did the chronically ill children may
be related to the influence of a sense of personal control on stress
appraisal (Lazarus & Folkman, 1984a). As was seen in the coping responses
of the children, the acutely ill group tended to report behaviors that
would provide a measure of personal control over the situation more than
did the chronically ill group. Lazarus has hypothesized that a sense of
3.
º
2
s
>

198
control of a situation may influence the process of stress appraisal
(Lazarus & Folkman, 1984a). If the acutely ill children thought that
relaxing or holding still would provide a measure of control over
harmfulness of the intrusive event, they would be less likely to appraise
it as stressful than would the chronically ill child who may have learned
that it will be uncomfortable, painful, or unpleasant regardless of what
behaviors are used to deal with the situation.
The element of novelty and the process of primary appraisal (Lazarus
& Folkman, 1984) may also explain the finding that acutely ill children
were significantly more likely to report physical symptoms as stressful
than were chronically ill children. Prior to admission to the hospital,
the acutely ill group were basically healthy children. The experience of
physical symptoms related to the illness, injury, or treatment was new.
But rather than being neutral, these symptoms were appraised as posing a
threat or harm to personal well-being of the child, emphasized by the
concern of parents and health care personnel. Simply, the child had not
experienced these exact physical symptoms before and had good cause to
believe that the symptoms would result in some type of personal jeopardy.
However, for the chronically ill children, the physical symptoms were not
novel. Having had the problem for a minimum of three months, or for some,
since birth, the children were apparently accustomed to the symptoms and
were not as likely to consider physical symptoms to be threatening as were
the acutely ill children.
In contrast to the above findings regarding the stressfulness of
specific events during hospitalization, health status was not
significantly related to the child's appraisal of the stressfulness of the
hospital experience as a whole, although there was a tendency for

199
chronically ill children to appraise the event as more stressful than
acutely ill children. There are several possible explanations for this
finding. First, it may be correct. It is possible that the emphasis on
creating a non-threatening environment (Mott, Fazekas, & James, 1985;
Petrillo & Sanger, 1980; Waechter, Phillips, & Holaday, 1985) that may be
individualized to meet the needs of a specific child has been successful,
resulting in similar appraisals of the global stressfulness of
hospitalization by acutely and chronically ill children. Another possible
reason for this finding may be the use of defensive reappraisal by the
children. Defensive reappraisal is the positive reinterpretation of the
past so that it is viewed in a less threatening or harmful light (Lazarus
& Folkman, 1984a). Ascertaining the child's appraisal of the
stressfulness of hospitalization requires a retrospective analysis of the
eVent. It is possible that in this process the child reframes the
hospital experience so that it does not seem so stressful, thereby
eliminating differences in the appraisal of the two groups.
It is also possible that this finding was not accurate, that a
difference actually exists in the appraisal of hospitalization as
stressful by acutely and chronically ill children. The rationale for this
possibility lies in the power analysis of the study. In planning the
investigation, it was decided to assign a medium effect size to the
variable of health status, as this would be the conservative approach when
beginning research in an unexplored area. However, the results of this
study indicate that relationship between health status and stress is of a
small magnitude. Therefore, with the current sample size, the probability
of finding an actual difference, if it existed, was greatly reduced. It
may be that the present finding of no difference between the two groups is
--
s
sº
º,) º

200
true, or it may be that the trend of chronically ill children to appraise
the event of hospitalization as more stressful than acutely ill children
is accurate. If the latter is true, the influence of novelty, event
uncertainty, and temporal uncertainty (Lazarus & Folkman, 1984a) on the
primary appraisal process may explain the difference. The chronically ill
hospitalized child knows from prior experience that specific events are
likely to occur during each hospitalization, such as insertion of an
intravenous needle and administration of chemotherapy for the child with
cancer. This child also knows that new procedures may occur unexpectedly.
Thus, due to uncertainty of when expected events will occur and if a new
and possibly threatening event will occur, the chronically ill child may
perceive hospitalization as more stressful than the acutely ill child who,
due to the relative novelty of the situation, does not have these
expectations. For these reasons, it does appear that health status is
likely to have an influence on the process of stress appraisal of
hospitalized school-age children.
Gender and Stress Appraisal
The results of the data analysis indicated that gender does not have
an affect on the type of event appraised as stressful by the child during
hospitalization or on the child's appraisal of the global event of
hospitalization as stressful. Lazarus and colleagues have identified
three characteristics of the person that will influence the appraisal
process: 1) intellectual resources and skills, 2) belief systems, and 3)
commitments or motivational characteristics (Cohen & Lazarus, 1983;
Lazarus & Folkman, 1984a). The question is whether or not these factors,
all dependent on cognitive functioning, may be influenced by the gender of
■

201
the child. Studies comparing the intellectual abilities of boys and girls
are mixed. Although, in a review of research, Maccoby and Jacklin (1974)
concluded that girls have better verbal skills and that boys perform
better in math and spatial skills, other research has demonstrated such
findings may be culturally specific (Lesser, Fifer, & Clark, 1965; Nash,
1979; Schratz, 1978), implying that the gender difference may be due to
environmental, rather than genetic, factors. Some motivational
characteristics of the child also appear to be gender specific due to
disparate treatment, such as the lower achievement expectations of girls
(Dweck & Elliot, 1983), the learned helplessness seen more commonly in
girls, and the mastery-orientation more common in boys (Dweck & Wortman,
1982). In contrast, children's beliefs about personal control do not
appear to be gender related, as indicated in a review by Nowicki (1986) of
35 studies of children's locus of control beliefs.
Regardless of whether such characteristics are inherent or learned,
the differences in the resources and motivations of girls and boys would
be expected to influence the appraisal process, particularly secondary
appraisal, the process of evaluating the resources available for coping
(Lazarus & Folkman, 1984a). However, this was not the finding in the
current study or in the study by Menke (1972). Other researchers (May &
Sparks, 1983; Reissland, 1983; Timmerman, 1983) examining children's
concerns or fears during hospitalization have not commented on the gender
stress relationship. It is difficult to explain the difference between
the expected results and the actual findings. One possible explanation
may be that the hospital environment tends to encourage passivity in
patients, negating any possible difference in motivation or achievement
due to gender. A second possibility is that the results of the two
g º
**
S. s
sº
W.

202
studies finding no difference are sample specific and not representative
of the actual relationship between gender and stress appraisal of
hospitalized children. Further research is needed to clarify this
relationship.
Anxiety and Stress Appraisal
The results of the data analysis indicated that trait anxiety does
not have an affect on the type of event appraised as stressful by the
child during hospitalization, but that it does have a significant affect
on the child's appraisal of the global event of hospitalization as
stressful. As a personality characteristic, trait anxiety is a factor
likely to influence the transaction between the person and environment,
resulting in an appraisal of stress (Lazarus, 1981; Lazarus & Launier,
1978). Unlike situational anxiety that occurs in response to a specific
event, trait anxiety is the child's "tendency to perceive a wide range of
situations as threatening..." (Spielberger, 1975, pp. 137). Trait anxiety
is the person's global tendency toward being anxious. However, as it
influences global, rather than specific, reactions, it is not surprising
that there was no relationship between a specific category of stressful
events and the level of trait anxiety. Rather, it would be expected that
a relationship would exist between the trait anxiety score and the global
appraisal of the stressfulness of hospitalization, which was found. It is
logical that the highly anxious child would have a greater tendency to
perceive the hospital environment as threatening than would the child with
a lower trait anxiety level, and would therefore appraise the event as
more stressful.

203
Surprisingly, a careful review of Spielberger's (1989) comprehensive
bibliography of over 3000 studies using either the adult or child form of
the State-Trait Anxiety Inventory and a computer search of the literature
since that publication failed to locate any other study assessing the
relationship between trait anxiety and either the specific or global
stress appraisal of hospitalized children. Rather, the emphasis in the
health related studies has seemed to be on the relationship between
physical illness and state-trait anxiety (e.g., Kellerman et al., 1980;
Sides, 1977), or between emotional illness and state-trait anxiety (e.g.,
Bedell & Roitzsch, 1976; Ollendick, Finch, & Nelson, 1976). Because no
prior reports are available to support or refute the result of the current
study, the findings that trait anxiety was not related to appraisal of
specific events as stressful, but that it did appear to be related to the
global appraisal of hospitalization as stressful, should be considered to
be possible, but not definite, evidence of the influence of the modifying
influence of trait anxiety on the stress appraisal process of hospitalized
children.
In summary, the results of the current study appear to indicate that
the appraisal of specific events as stressful during hospitalization may
be influenced by the health status of the child as acutely or chronically
ill, but that it is uncertain if either gender or trait anxiety influence
this process. It also appears possible that the stress appraisal of the
global event of hospitalization may be influenced by the child's trait
anxiety, but it is uncertain if either health status or gender have a
modifying influence on this relationship.
y ‘.*-

204
Discussion of Results Relating to Coping
Unlike the inquiry regarding stressful events, some of the subjects
seemed to have difficulty answering the interview question about coping
behaviors used in response to stressful events. This was not unexpected
as asking the child to relate how they coped with the stressful event (in
the language of the interview, what did you do or think about to help
yourself take care of the upsetting thing) required a form of thinking
beyond the basic concrete thought process. Rather than simply asking for
identification of things that upset them, as with the stress question, the
coping question asked them to think about and relate what they did or
thought. While thinking about what you did is still clearly concrete
thinking, thinking about your thinking moves toward the abstract thought
patterns of the formal operational stage (Siegler, 1986), although it does
not require hypothesis formulation or testing. Accordingly, the probes
for the coping question were used fairly often in the interviews to help
the children understand the question. With the use of the probes, the
children seemed to understand what was being asked and replied
appropriately.
Four children did not answer the coping question. Three of these
were the children who were unable to identify any stressful events, and
therefore could not be questioned regarding subsequent coping behaviors.
The fourth child did identify two stressful events, both intrusive, but
even with the probes was unable to identify any coping behaviors. Review
of the interview seemed to indicate that rather than being unable to
cognitively process the information needed to answer the question, the
child was overwhelmed by the illness and hospitalization, supported by the

205
fact that this was one of the few children unable to respond to the first
interview question regarding good things that happen during
hospitalization.
The frequency of the responses in each of the coping categories also
raises the question of children's use of cognitive coping behaviors. The
two categories requiring primarily cognitive coping, cognitive processing
and cognitive restructuring, occurred with low frequency in the current
study. In particular, cognitive processing behaviors were mentioned by
only 4.3% of the children, nearly one-half less frequently than the next
lowest category. It is possible that, as discussed above, relating
cognitive coping techniques is more difficult for concrete operational
children than is relating behavioral coping techniques. It is also
possible that the concrete thinker uses proportionately less cognitive
than behavioral coping as a function of the developmental level. This
latter proposition appears to be refuted by Savedra and Tesler's (1981)
findings that hospitalized school-age children used this type of behavior
frequently, particularly in the anticipatory phase of coping before a
procedure, as evidenced by the questions the children asked and their
looking at or taking in of the situation. The disparity in these results
may be partially due to the method of data collection, the current study
being based on interview and the Savedra and Tesler (1981) study based on
observation. It is possible that both propositions are correct, children
use less cognitive than behavioral coping and have difficulty recalling
this more abstract behavior. Further work is needed to clarify this
issue.
In contrast, the most frequently reported categories were those
requiring behavioral coping; countermeasure, control, and seeking support.
206
These involved recalling something that the child had done, not just
thought. Countermeasures were identified by 33.7% of the children, a
higher frequency than any of the other coping categories. Most of the
countermeasure behaviors involved avoiding the stressful situation by
ignoring it, such as watching television, playing video games, or
sleeping; or by refusing to participate, for example by not eating. These
same behaviors have been described by other researchers under the labels
of suspends, ignores, negates (Savedra & Tesler, 1981), avoidance (Neff,
1978; Ryan, 1989; Youssef, 1981), and distracting activities (Ryan, 1989).
Very seldom did the children describe trying to physically escape the
stressful event. Whether this did not happen or whether the child did not
recall or choose to report it is uncertain. Other researchers have
identified school-age children's attempts to physically escape a stressful
event as a coping behavior (Neff, 1978; Rose, 1972a, 1972b; Savedra &
Tesler, 1981; Siegel & Smith, 1989), but none have commented on the
frequency with which this occurs. Atshuler and Ruble (1989), presenting
a hypothetical negative (stressful) situation to healthy 5 to 12 year old
children, noted that use of escape strategies decreased significantly with
age. Given sufficiently threatening circumstances, the school-age child
may attempt to escape or resist, as would the adult under comparable
circumstances (Schuster & Ashburn, 1986), but it appears that at this age
the child has developed the self-control to attempt to cope with most
stressful events by using coping behaviors other than escape.
Developmentally, an interesting facet of this study is the use of
cognitive restructuring and countermeasures by the subjects. Cognitive
restructuring acts to mentally reverse the meaning of the situation and
countermeasures act to nullify or negate the stressful situation.
2O7
Acquisition of the operations of negation and reversibility are
characteristics of the concrete-operational child (Ginsburg & Opper,
1988). It is unlikely that the younger child would spontaneously use
these coping behaviors, a premise supported by the noticeable absence of
such behaviors in research describing the behaviors of the hospitalized
preoperational child (Ritchie, Caty, & Ellerton, 1988; Rose, 1972a,
1972b).
Concerning the utility of the six categories of coping behaviors
that were derived from the literature (see Chapter 2), each category was
represented by the coping behaviors described by the children, however the
frequency of use was quite uneven. To an extent this should be expected;
some behaviors may be more developmentally appropriate than other
behaviors. As discussed above, the categories of cognitive processing and
restructuring were mentioned infrequently. In contrast, coping responses
belonging to the more behaviorally oriented categories of countermeasures,
control, and seeking support were mentioned frequently. Interestingly,
the category of cooperation, a behavioral oriented response, was seldom
identified in the children's responses. A possible explanation for this
is the difficulty in determining the purpose of some coping behaviors due
to the highly contextual nature of coping, a phenomenon also noted by
Walker (1988). For example, if a restricted activity such as staying on
the unit is stressful to a child and the reported coping behavior is
watching television or playing a video game, is that an attempt to remove
the self mentally from the stressful situation, a countermeasure, or is it
an attempt to cooperate with the restriction? Because the interview was
not structured to clarify the purpose of the coping, a question that would
have been difficult for the concrete - operational child to answer, it was
208
at times difficult to determine the purpose of the coping behavior,
possibly resulting in underrepresentation of the cooperation category and
overrepresentation in other categories.
Although these insights are important, the primary issue remains the
interpretation of the statistical analysis. This will be addressed by
discussing the relationship of the four factors, health status, gender,
trait anxiety, and stress appraisal to coping behaviors, considering the
theoretical basis of the study and prior research.
Health Status and Coping Behaviors
The results of the data analysis indicated that health status does
not have a significant influence on the type of coping behavior used by
the child in response to an intrusive event during hospitalization. This
pattern was also noted by Ritchie, Caty, and Ellerton (1988), although it
must be noted that study focused on preschool rather than school-age
children and the findings may not be generalizable to a different age
group. If the results of the current study are accurate, the most
probable explanation would be the dynamic nature of the coping process.
During the transaction between person and environment, the appraisal and
reappraisal process are continuous, possibly resulting in changes in
coping behavior that may occur very quickly (Lazarus, 1981; Lazarus &
Folkman, 1984a). This dynamic nature of coping has been observed in
hospitalized children (Savedra & Tesler, 1981). Thus, the ongoing
appraisal process may result in use of a wide spectrum of coping behaviors
determined primarily by the immediate situation rather than in a narrow
range of behaviors the child is familiar with due to prior experience.
s
**
º

209
However, it is possible that the initial hypothesis may have been
correct, that a relationship between health status and coping behaviors
does exist. Examination of the frequency data (Table 16) indicated that
in three categories, cognitive restructuring, control, and seeking
support, there was a trend (greater than 10%) toward a difference between
the groups. The acutely ill children reported using cognitive
restructuring 10.5% more frequently and control 16.7% more frequently than
did the chronically ill group. The chronically ill children reported
using seeking support 12.5% more frequently than did the acutely ill
children.
It is possible that these trends may reflect the true relationship
between health status and coping, but that this was not evident due to the
low cell frequency for the less common coping behaviors. The possibility
that there is a relationship is supported by Lazarus' (Lazarus & Folkman,
1984a) proposal that problem solving skills, dependent on prior experience
and knowledge, influence coping behaviors. Acutely ill children are
relatively unfamiliar with the stressful events that occur during
hospitalization. They may be able to convince themselves that a shot does
feel like a mosquito bite. They also may believe that they have some
degree of control over the situation as they do at home, bargaining to
delay an event or trying to control how the event takes place, and so
attempt to use these behaviors in the hospital. Although chronically ill
children do use control and cognitive restructuring, it is not to the
extent of the acutely ill group, the chronically ill children know better.
Due to past experience they know the shot will hurt more than a mosquito
bite, and they know that they have very little actual control over the
procedures that are imposed upon them. They may have learned that the
—-
c
º&
*
* * *

210
benefit gained from these techniques is not sufficient to compensate for
the energy expended in using them. The chronically ill children, however,
do tend to use seeking support behaviors more than do the acutely ill
children. Perhaps this form of coping requires less expenditure of effort
by transferring some of the burden to someone else. Although this trend
to use different coping behaviors cannot be supported statistically at
this time, the information is of clinical interest and may be useful when
planning methods of supporting children's coping during hospitalization.
The position that different coping behaviors may be emphasized by
acutely ill and chronically ill children is not in conflict with the
preceding argument regarding the dynamic nature of coping. Both groups
did report a wide range of behaviors. However, it is possible, that due
to differences in prior experience, the repertoire of behaviors used by
the two groups is somewhat different, yet remains dynamic, responsive to
a change in the appraisal of the situation.
The hypothesis that health status affects the perception of
effectiveness of coping behavior was supported in the revised model,
although not in the direction predicted. The analysis indicated that
acutely ill children perceive their coping behaviors to be more effective
than do chronically ill children. It seems strange that the group with
less experience in coping with the stresses of hospitalization should
perceive their coping to be more effective. Logically, it would seem that
through experience the chronically ill group would learn which behaviors
are more helpful, would use those behaviors, and would therefore be more
likely to rate their coping as effective. A possible explanation for this
unexpected finding may be the concept of learned helplessness.

211
Learned helplessness occurs when an organism learns that its
responses do not influence the outcome of a situation (Seligman, 1975).
Applied to humans, the model proposes that the greater the belief that
control is possible, the longer the period needed to realize the outcome
is independent of control efforts, but that when this belief is destroyed,
repeated exposure to uncontrollable situations is likely to result in
lowered motivation and passivity (Dweck & Wortman, 1982). This perception
of noncontingency is probably influenced by prior experience (Fincham &
Cain, 1986). Applying this concept to the findings of this study, the
acutely ill child may believe that he or she will be able to control the
occurrence of negative events in the hospital by his or her behavior in
much the same manner as negative events are avoided at home or school. In
contrast, the chronically ill child, due to prior experience, will likely
have learned that in the hospital negative events cannot always be
controlled, regardless of personal efforts to cooperate or to find
alternate solutions. If this premise is true, the chronically ill child
may exhibit characteristics of learned helplessness, such as passivity,
low motivation, and depression (Dweck & Wortman, 1982), resulting in
decreased effort and less effective coping (Compas, 1987). Thus, the
phenomenon of learned helplessness may explain the finding that
chronically ill children perceive their coping to be less effective than
do acutely ill children. Further examination of this possibility by
including learned helplessness in the stress and coping model is
warranted.

212
Gender and Coping Behavior
The results of the data analysis indicated that gender does not have
an affect on the type of coping behavior used in response to an intrusive
procedure or on the child's perception of the effectiveness of the coping
behavior. In the Lazarus theory (Lazarus & Folkman, 1984a) it is proposed
that coping behavior is dependent on available coping resources, such as
health and energy, positive beliefs, problem solving, social skills,
social support, and material resources; and on constraints against using
these resources, such as personal or cultural beliefs, the environment,
and the level of threat. Most of these resources and constraints are
unlikely to have an influence during childhood. For example, for the
hospitalized child, health and energy is dependent on the acuity of the
illness, not on gender; children's belief system is not likely to differ
due to gender as discussed earlier regarding locus of control and gender
(Nowicki, 1986); and the material status of the family is not dependent of
the gender of the child. However, it is possible that the social support
given to children and behavioral expectations of children may differ
according to gender. In the classic examination of sexual differences by
Maccoby and Jacklin (1974) it was note that there were many differences in
parental treatment of boys and girls, such as encouraging more physical
activity in boys and perceiving girls as more fragile, yet it was
concluded that young children are treated quite similarly by parents
regardless of gender. In a more recent review, Huston (1983) concluded
that there is more support for differences in treatment according to
gender than was originally thought, such as permitting school-age boys
more independence than same age girls (Newson & Newson, 1976), and
assigning failure of boys to lack of motivation and failure of girls to
* ** ~ *

213 *--
lack of ability (Dweck, Davidson, Nelson & Enna, 1978). Accordingly, it
could be expected that if coping behavior is dependent in part on social
support, the coping used by boys and girls during hospitalization would
differ. This premise is supported by the work of Savedra and Tesler
(1981), who found that hospitalized boys are more likely to use control
and girls are more likely to use pre-coping (cognitive processing). In
the current study, however, gender did not influence the coping behavior,
a finding supported by other research of children in health care
situations (Curry & Russ, 1985; Hamner & Miles, 1988; LaMontagne, 1984,
1987). It is difficult to explain this discrepancy. Perhaps further
refinement of instruments and methodology will provide additional insights
in this area.
Trait Anxiety and Coping Behavior
The results of the data analysis indicated that trait anxiety does
not have a significant influence on the type of coping behaviors used by
the child during hospitalization. Examination of the relationship between
trait anxiety and the types of coping behaviors used by hospitalized
children was exploratory, no prior research had been reported in this
area. As shown in Table 22, there was only a four point difference in the
means of the trait anxiety score between the coping categories and the Chi
square statistic was not significant. Regardless of the category of
coping behavior used in response to an intrusive event, there was very
little difference in the trait anxiety scores of the children. Although
personal characteristics influence the coping process (Lazarus & Folkman,
1984b), it does not appear that the characteristic of trait anxiety
influences the type of coping behavior used by a hospitalized child.

214
In contrast, data analysis of the revised model indicated that trait
anxiety does have a significant influence on the child's perception of the
effectiveness of the coping behaviors used during hospitalization.
Theoretical support for this relationship comes from the coping
constraints detailed above (Lazarus & Folkman, 1984a), specifically the
level of threat. A child with a higher level of trait anxiety approaches
a situation with increased apprehension and fear. This increases the
perceived level of threat regarding the situation, in turn interfering
with problem solving, resulting in decreased effectiveness of coping
(Lazarus & Folkman, 1984a). Although no other research examining this
relationship was found, the finding is logical, providing one more piece
of information that will help health care professionals understand
children's reactions during hospitalization.
In summary, the results of the current study appear to indicate that
the coping behaviors used during hospitalization in response to an
intrusive event may possibly be related to health status, although this
relationship is tenuous, but that it is less likely that either gender or
trait anxiety influence the coping process. It also appears possible that
the perceived effectiveness of coping may be influenced by the child's
health status and trait anxiety, but it is uncertain if gender has a
modifying influence on this relationship.
Limitations
All research is limited in generalizability due to decisions that
must be made in the development and implementation of the research
.

215
protocol. The limitations of this study will be discussed according to
those pertaining to the sample and those relevant to data collection.
Limitations Related to the Sample
The primary limitation due to sampling was the decision to use a
convenience, rather than random, sample. While use of a probability
sample would have increased the generalizability of the findings, for the
purposes of this study, a convenience sample was necessary due to
limitation of time and resources. An advantage of the convenience sample
was the ability to specify inclusion-exclusion criteria that resulted in
a fairly homogenous group of children in respect to cognitive functioning
and extraneous factors. These same criteria define the population to
which the results may be generalized: English speaking children between
the ages of 8 through 11 years of normal cognitive and sensory
functioning, who have been hospitalized for two to three days, but have
not been in the intensive care unit during the current admission, were not
admitted due to child abuse, and were not in the terminal phase of
illness.
An additional limitation was the underrepresentation of acutely ill
children in the sample. Had a quota sample been obtained, resulting in
equal numbers in the acute and chronic groups, it is possible that the
results of the data analysis may have been different, particularly the Chi
square analysis due to a probably increased frequency of cell size.
Several, factors may have contributed to the low number of acutely ill
children in the study. First, during the school-age years, acute
illnesses of sufficient severity to require hospitalization appear to be

216
less common than chronic illness resulting in admission. The most common
diagnoses of the acutely ill children were appendectomy and fracture.
Other acute illnesses such as pneumonia, croup, meningitis, and
gastroenteritis occur more commonly in younger children. In contrast,
many chronic illnesses persist throughout childhood, resulting in
hospitalization during the school-age years, although diagnosis may have
been made quite early in life. Therefore, it seemed that the number of
potential subjects that were acutely ill was less than that of chronically
ill children. Second, two of the six facilities used for data collection
were tertiary hospitals likely to draw a population of chronically ill
children and one of the six facilities specialized in orthopedic problems
primarily of a chronic nature. While the remaining three facilities
accepted both chronic and acute illnesses, it is possible that, as a total
group, chronically ill children comprised a greater percentage of the
potential subjects than did acutely ill children. Third, as noted in
description of the sample (see Chapter 4) of the potential subjects who
were approached about the study but declined to participate, 39% were
acutely ill children, a number considerably higher than the 25.6% of
acutely ill children that participated in the study. This further
contributed to the low number of acutely ill subjects. Finally, at each
facility there were periods of time when no data collection was attempted
due to the unavailability of the data collector. Due to the difficulty of
gathering post hoc data to determine if children admitted during these
periods met the eligibility criteria, it is not known whether the
proportion of acutely ill to chronically ill children during these periods
was the same or different from that of the sample.

217
Limitations Related to Instrumentation
The results of a study, and thereby the generalization of the
findings, are always affected by the instruments used to collect the data.
In this study, a major portion of the findings were dependent on
assumptions related to the stress and coping interview. First, it was
assumed that the interview would provide an accurate sampling of the
stressful events and coping behaviors used by the children. Consideration
of the data implies, however, that the coping behaviors identified in this
study are representative only of those the children are aware of using,
and may not adequately represent the behaviors that are actually used, as
evident by the difference in frequency of cognitive processing in this
study and orienting behaviors in the study by Savedra and Tesler (1981)
that used observation rather than interview. Second, as addressed above
in the section, Discussion of Results Relating to Coping, thinking about
cognitive coping behaviors was difficult for the some of the children.
Although it is necessary to ask the child about these behaviors as
cognitive coping cannot be observed, the results must be interpreted
recognizing that such an inquiry is pushing the child toward a higher
level of thinking than he or she may use on a routine basis, possibly
influencing the types of responses given by the subjects.
Another limitation of the study, relating to the interview data,
centers on the categories of stress and coping developed for use in this
study. This was the first study to use these stress and coping
categories. Although the validity of the categories is likely to have
be en good, due to the method of developing the categories (see chapters 2
and 4), it is possible the categories did not fully represent the range of

218
stressful events and coping behaviors characteristic of hospitalized
school-age children. For example, the researchers who participated in the
interrater reliability estimate suggested adding a coping category of
emotional behaviors. The reliability of the categories was also a
limitation. As detailed in chapter 4, the mean rate of interrater
reliability for assignment of stressful events to categories ranged
between 62.5 % to 70.8%, and for coping categories the mean rate ranged
between 56.25% and 70.8%. Although the moderate rate of agreement is
partially due to the process of the rating (the items were first
identified by the raters, and then categorized, causing the accuracy of
the Cohen's kappa to be dependent on the accuracy of the recognition of
items), it may also be due to the structure and definition of the
categories. Comments by the raters indicated that some categories
appeared to overlap, such as intrusive events and therapeutic
interventions, and control and cooperation. Further refinement of the
definitions of the categories may be helpful in increasing the reliability
of the coding scheme.
An additional limitation of the study is the low correlation between
the word graphic scales and the instruments used to determine concurrent
validity. As discussed in chapter 4, this finding may be acceptable as
the validity of the Child Medical Fear Scale and the Coping Response
Inventory are still being determined as both are fairly new instruments.
However, further psychometric testing of the Hospital Stress Scale and the
H ospital Coping Scale is needed to establish the reliability and validity
of the instruments.
219
Implications for Nursing
The fundamental concepts of the discipline of nursing have been
identified as person, environment, health, and nursing (Chinn & Jacobs,
1987; Flaskerud & Halloran, 1980; Fawcett, 1978; Fawcett, 1984; Yura &
Torres, 1975), although some nurse theoreticians have proposed a condensed
(Kim, 1983) or expanded (Meleis, 1985) version of the concepts. These
four basic concepts will be used to discuss the implications for nursing
derived from the current study.
Person
The concept of person has been defined for the nursing paradigm as
"the individual, family, community, society, or any other entity that is
the identified recipient of nursing" (Fawcett, 1984). For the purpose of
this study, the focus was placed on the individual, specifically, the 8 to
11 year old child receiving nursing care while hospitalized.
Three aspects related to the concept of person were examined in this
study. The first was the child's psychological reaction to
hospitalization with a particular focus on the appraisal of stress and
coping, the primary concepts of Lazarus' theory (Lazarus & Folkman,
1984 a). Analysis of the data indicated that children within the generally
accepted age range of concrete operational development (Brainerd, 1978;
Crain, 1985; Siegler, 1986) did have definite opinions on what events were
stressful during hospitalization, and were able to describe the things
they did to deal with the stressful events, more often describingbe havioral than cognitive coping activities. The second aspect of the
Person examined in the study was gender. With this sample, gender was not

220
found to be related to the stress and coping process in relation to
specific events occurring during hospitalization or the global event of
hospitalization. The third aspect of the person examined in this study
was trait anxiety. This relatively stable aspect of the personality of
was not found to be related to the appraisal of specific events as
stressful or the resulting coping behaviors, but it was related to the
child's perception of the stressfulness of the global event of
hospitalization and the effectiveness of the coping behaviors.
Several implications for nursing practice are evident in these
findings. First, children between the ages of 8 to 11 years are not
merely passive recipients of care and treatment while hospitalized.
Rather, they are actively engaged in an ongoing appraisal of the meaning
of the environment for their well-being. Second, when an appraisal of
stress is made, the child uses coping behaviors to reduce the
stressfulness of the situation. Thus, as Piaget (1983) noted children are
active participants in structuring and modifying their world, even when in
the hospital. Third, expectations regarding the behavior of hospitalized
children should not be based on gender. There is insufficient evidence to
support the common assumption that boys and girls appraise different
events as stressful or use different forms of coping. Finally, because of
the possible relationship between trait anxiety and the child's reaction
to the global event of hospitalization, the nurse should be aware that the
highly anxious child may need more preparation and support to deal with a
stressful event than will the child with a low level of anxiety.

221
Health
The concept of health has been defined for the nursing paradigm as
"wellness and/or illness" (Fawcett, 1984). All of the children in this
study were experiencing sufficient physical problems to warrant
hospitalization, and therefore would be considered to be ill. However,
the severity of the illness was limited to children not considered to have
a critical or terminal condition.
The concept of health also determined two key aspects of the study
design. First, the noncategorical approach to illness (Stein & Jessop,
1982, 1989), focusing on the commonalities of experience and needs rather
than on disease specific treatment, was used as this approach is more
congruent with a nursing, rather than medical, model. Second, health
status as acutely or chronically ill was selected for examination as a
moderating variable. Study of the Lazarus theory (Lazarus & Folkman,
1984a) indicated the extent of a child's prior experience with
hospitalization is likely to be a strong determinate of the stress and
coping process. The factor most likely to result in a difference in
experience would be the health status of the child as acutely or
chronically ill. In addition to the potential theoretical importance of
this factor, understanding the relationship between health status and the
stress and coping process also was thought to be of practical important as
chronically ill children are hospitalized more frequently and/or for long
periods than are acutely ill children (Butler et al., 1985; Perrin, 1985).
As discussed above, the findings of this study did support the inclusion
of the health status variable as a contributing factor in model of stress
and coping.
222
Several implications for nursing practice are evident relating to
the concept of health as used in this study. First, use of the
noncategorical approach promotes transference of nursing knowledge to new
situations by emphasizing the commonalities of children's experiences,
rather than the diagnostic and treatment related differences. Second, it
should not be assumed that chronically ill children eventually get used to
the stressful events occurring during hospitalization and develop methods
of coping effectively. Rather, dealing with stressful events,
particularly intrusive procedures, is an ongoing challenge for chronically
ill children. Nurses need to place a high priority on avoiding or
minimizing intrusive events and on supporting the child when the events
are inevitable. Additionally, because chronically ill children seem to
perceive their coping as less effective, possibly due to learned
helplessness (Fincham & Cain, 1986), effort needs to be made to provide
appropriate opportunities for control, adequate explanation of essential
events that are uncontrollable, support for the child's coping behaviors
with supplementation as needed by teaching additional coping techniques,
and confirmation that the effort to cope was helpful.
Environment
The concept of environment has been defined for the nursing paradigm
as encompassing "relevant animate and inanimate surroundings" (Fawcett,
1984). For the purposes of this study the environment was considered to
be the structural and interpersonal aspects of the hospital encountered by
the child while a patient.

223
Although the environment was not one of the independent variables of
the study, it was a primary determinant of the dependent variable of
stress appraisal. By definition, stress is the result of a transaction
between the person and environment (Lazarus & Folkman, 1984a, pp. 19).
Therefore, when the children were asked to identify upsetting things that
happen in the hospital, the answers were reflective of the immediate
environment. Inanimate aspects of the environment that resulted in an
appraisal of stress ranged from medical equipment mounted on the walls
causing nightmares to a variety of intrusive events and therapeutic
interventions. Interpersonal aspects of the environment resulting in
stress included separation from family, incompatibility of roommates, and
impatient nurses and doctors.
The primary implication for nursing practice related to the concept
of environment, as used in this study, is the modification of the hospital
environment to reduce elements that are likely to be stressful to the
child, whenever this is possible. Ask the children to tell you what is
upsetting to them about being in the hospital. If the child's concern
centers on the physical environment, redecorate the room with personal art
work or posters from the child, cover or remove unnecessary equipment, or
avoid unnecessary noise, such as flushing the toilet at night. If the
child's concern centers on aspects of the health care regimen, reduce the
frequency of the stressful event if possible, such as limiting the number
of persons conducting a physical assessment during a shift, or if the
event is necessary, provide information and support. If the source of the
child's stress is interpersonal, attempt to find compatible roommates,
follow hospital regulations reasonably rather than rigidly, and do not
allow irritation or frustration due to work related problems to spill over

224
into interaction with the child. Obviously in a hospital situation not
all sources of stress can be eliminated. However, those that can be
removed or modified should be .
Nursing
The concept of nursing has been defined for the nursing paradigm as
"the totality of activities of members of the discipline" (Fawcett, 1984).
For the clinician caring for hospitalized children, one facet of these
nursing activities involves caring for the psychological needs of the
child, of which stress and coping is a part.
This study was a descriptive examination of selected factors
influencing the stress and coping process of hospitalized children,
therefore nursing actions were not directly assessed. Rather, the purpose
was to further develop the foundation of nursing knowledge relating to
children's reactions during hospitalization, enabling the nurse working
with children to provide care based on scientific knowledge.
The specific implications of the study for nursing care have been
discussed under the headings of person, health, and environment. A more
general implication for nursing would be the inclusion of the knowledge
relating to the stress and coping of hospitalized children in the nursing
process. Pediatric nurses are generally quite aware that children find
intrusive events and separation to be stressful. It may be less well
recognized, however, that therapeutic interventions, restricted activity,
physical symptoms, and environmental factors may also be stressful for the
child. Knowledge of these potential sources of stress and the unique
reactions of chronically ill and acutely ill children will guide the nurse

225
in the assessment process. Similarly, knowledge of the types of coping
behaviors used by children in response to stressful hospital events may
provide an additional tool for the pediatric nurse to use in assessment of
the psychosocial status of the hospitalized child. Awareness of the
categories of coping behaviors typically used by hospitalized school-age
children and the possible differences in coping behaviors related to
health status and anxiety, will guide the assessment process as the nurse
talks with and observes the child.
In the current taxonomy of nursing diagnoses, the category most
closely related to stress appraisal is that of Fear, defined as, "a state
in which the individual experiences a feeling of physiological or
emotional disruption related to an identifiable source which the person
perceives as dangerous" (Carpenito, 1987, pp. 242). Although this
diagnosis places more emphasis on the emotional reaction to the event than
does Lazarus' definition of stress cited in chapter 2 (Lazarus & Folkman,
1984a, pp. 19), the focus on perception of personal danger is closely
aligned to the appraisal of harm and threat in the stress concept.
Therefore, this diagnosis could be used appropriately to represent actual
or potential appraisals of stress that may occur.
The diagnosis most closely pertaining to the child's coping process
is Ineffective Individual Coping, defined as "a state in which the
individual experiences or is at risk of experiencing an inability to
manage internal or environmental stressors adequately due to inadequate
resources (physical, psychological, or behavioral)" (Carpenito, 1987, pp.
202). Because this diagnosis assumes that the person is having or will
have ineffective coping, careful assessment of the individual child's
coping behaviors must occur before listing this diagnosis as a nursing

226
problem. The child's repertoire of coping behaviors may be sufficient to
deal with the stresses encountered during hospitalization, removing the
need for this diagnosis.
If the child has successfully coped with the stress previously, the
most effective nursing plan and intervention may be to support the child
in that coping behavior. For example, if separation from parents at night
is difficult, but manageable, as long as the child has a favorite security
object and is allowed to call home at bedtime, then incorporate these
elements into the plan of care. Be aware, however, that the appraisal of
stress may change due to changes in the the person and environment.
Therefore, due to excessive fatigue or additional stresses, the situation
may be appraised differently and the usual coping behaviors may be
insufficient. In this case, the nurse may need to help the child find
alternative methods of dealing with the situation, such as distraction by
reading a bedtime story or social support in the form of a hug or holding
the child's hand until sleep occurs.
If the diagnosis of Ineffective Individual Coping is appropriate, a
more structured approach may be needed to help the child cope with the
event. In recent years a number of methods of helping children cope with
stressful health care situations have been developed and studied, such as
preprocedural teaching (Ferguson, 1979; Peterson & Shigetomi, 1981;
Visintainer, 1977), relaxation (LaMontagne, Mason, & Hepworth, 1985;
Zastowny, Kirschenbaum, & Meng, 1986; Peterson & Shigetomi, 1981),
modeling (Ferguson, 1979; Melamed & Siegel, 1975; Peterson & Shigetomi,
1981), mental imagery (Johnson, Whitt, & Martin, 1987; Kuttner, Bowman, &
Teasdale, 1988; Peterson & Shigetomi, 1981), and self-talk (Peterson &
Shigetomi, 1981; Ross, 1984). Selection of a particular approach will be

227
dependent on the child's personality, needs, and the characteristics of
the stressful event. Implementation requires careful planning and
possibly specialized training of the clinical nurse specialist or other
health care professional who will guide the child in the use of these
coping techniques.
Finally, it should be remembered that the appraisal of stress is an
ongoing process, constantly changing and shifting in response to changes
in the person or environment (Lazarus & Folkman, 1984a). Because of this,
the plan of care must be frequently reevaluated to ensure that the child's
ever changing needs are being met.
In sum, the nursing process may be used to apply the knowledge
gained through this study to the clinical practice of nursing. Through
this approach the fundamental goal of this research, the promotion of the
psychological well-being of the hospitalized child by the professional
nurse, will be met.
Implications for Future Research
Pediatric nurse researchers responsible for the basic foundation of
knowledge pertaining to the coping behaviors of hospitalized children have
made a valuable contribution to nursing knowledge (Caty, Ellerton, &
Ritchie, 1984; LaMontagne, 1984, 1987; Ritchie, Caty, & Ellerton, 1988;
Rose, 1972a, 1972b; Savedra & Tesler, 1981; Stevens, 1984, 1989). This
study has added to the building of this base of knowledge. Clinical
interaction with sick children demonstrates that not all children appraise
the same events as stressful or use the same coping behaviors, yet very
little is known about the factors contributing to these differences.

228
While this study has contributed much needed information about three
fundamental characteristics of the child to the knowledge base, the
factors studied account for only 14% of the variance in children's
appraisal of the stressfulness of hospitalization and only 12% of the
variance in children's perception of coping effectiveness. More research
is needed before a clear understanding of hospitalized children's stress
and coping will emerge.
In order to proceed with research in this area, the first step
needed is a reexamination of the representativeness of the categories of
stress and coping used in this study, further refinement of the
operational definitions, and testing of the taxonomy. Based on the
taxonomy, an instrument then could be developed that will facilitate
assessment of children's stress and coping during hospitalization. Given
a standardized method of assessing these concepts, examination of factors
influencing stress and coping will be facilitated. More information is
needed regarding the personal and environmental factors that influence the
child's stress and coping process. Factors needing examination include
temperament, ethnicity, self-concept, and locus of control. It may also
be beneficial to further examine the concept of health status and tease
out possible differences in the reactions of children with a chronic
condition versus those with a chronic illness. Research is also needed
that will examine the nature of a child's stress appraisal and coping
behavior over time to determine if the processes are a relatively stable
characteristic of the person or if the behaviors change as the child
develops cognitively.
A second line of needed research is the development of intervention
studies that will assess the efficacy of teaching coping strategies to
229
children experiencing specific stressful events during hospitalization.
We need to know if teaching specific techniques such as relaxation or
imagery are helpful to hospitalized children and if so, is promotion of
these techniques more effective than support of the child's own coping
behaviors. We also need to understand the relationship between various
personality styles and the use of coping techniques. Such information
will enhance the nurse's ability to plan psychosocial interventions that
will best meet the needs of the child. In this manner, nursing research
will contribute directly to the nursing practice of those working with
children.
Conclusion
The two-fold purpose of this study was to examine the influence of
health status, gender, and trait anxiety, on 1) the specific events
school-age children perceive as stressful during hospitalization and the
coping behaviors used in response to the events, and on 2) school-age
children's appraisal of stressfulness of the global event of
hospitalization and their perception of the effectiveness of their coping
behaviors. Conceptualization of the problem and development of the
protocol were guided by Lazarus' cognitive theory of stress and coping and
Piaget's theory of the cognitive development of children.
Eighty-two children meeting the inclusion-exclusion criteria
comprised the sample. Data were collected on the second or third day of
the child's hospitalization. All instruments required self-report from
the children and included an interview, two word graphic scales, and three
inventories using Likert-type responses.

230
Analysis of the interview data indicated that of the six possible
relationships between the independent variables of health status, gender,
and trait anxiety and the dependent variables of stress appraisal and
coping behaviors, only the relationship between health status and stress
appraisal was statistically significant. Analysis of the data pertaining
to the global stressfulness of the hospital experience and the perceived
effectiveness of coping indicated that the health status, gender, and
trait anxiety, as a set, accounted for 14% of the variance in the
children's stress appraisal, with trait anxiety alone contributing
significantly to the model; and that health status, gender, trait anxiety,
and stress appraisal, as a set, accounted for 14% of the variance in the
children's perception of coping effectiveness, with none of the variables
contributing significantly to the model. Due to redundancy, stress
appraisal was eliminated from the second portion of the model, and the
relationship reexamined. In the revised model, health status, gender, and
trait anxiety, as a set, accounted for 12% of the variance in perception
of coping effectiveness, with both health status and trait anxiety
contributing significantly to the model.
These findings indicate that both health status and trait anxiety
are important variables to take into consideration when trying to
understand the stress and coping process of hospitalized school-age
children, but that gender does not appear to have any affect on the
process. Although the contribution of these factors is small, the
knowledge generated through this study provides needed information
concerning the stress and coping of hospitalized children that will
enhance the understanding of the professional nurse and other health care
providers. Additional research that will identify other personal and

231
environmental variables affecting the model is needed to further advance
the development of knowledge concerning the stress and coping process of
hospitalized school-age children. r_< *
a

232
BIBLIOGRAPHY
Adams, M. L., & Bergman, D. C. (1965). The hospital through a child's
eyes. Children, 12, 102-104.
Aisenberg, R. B., Wolff, P., H., Rosenthal, A., & Nadas, A. S. (1973).
Psychological impact of cardiac catheterization. Pediatrics, 51,
1051 - 1059.
Altshuler, J. L., & Ruble, D. N. (1989). Developmental changes in
children's awareness of strategies for coping with uncontrollable
stress. Child Development, 60, 1337-1349.
Amato, P. R., & Ochiltree, G. (1987). Interviewing children about their
families: A note on data quality. Journal of Marriage and the
Family, 49, 669-675.
Asher, N. B. (1983). Causal Modeling. Newbury Park: Sage.
Astin, E. W. (1977). Self reported fears of hospitalized and non
hospitalized children aged ten to twelve. Maternal-Child Nursing
Journal, 6, 17-24.
Barowsky, E. I. (1978). Young children's perceptions and reactions to
hospitalization. In E. Gellert (Ed.), Psychosocial issues of
pediatric care (pp. 37-49). New York: Grune & Stratton.
Bedell, J. R. , & Roitzsch, J. (1976). The effects of stress on state and
trait anxiety in emotionally disturbed, normal, and delinquent
children. Journal of Abnormal Child Psychology, 4(2), 173-177.
Beilin, H. (1989). Piagetian theory. In R. Vasta (Ed.), Annals of Child
Development: Vol. 6. Six theories of child development: Revised
formulations and current issues (PP. 85-131). Greenwich,
Connecticut: Jai Press.
4
T
º

233
Belmont, H. S. (1970). Hospitalization and its effects upon the total
child. Clinical Pediatrics, 2, 472-483.
Bishop, M. (1976). Coping behaviors of children born with a cleft lip and
palate. Unpublished master's thesis, Arizona State University,
Tempe, Arizona.
Blom, G. E. (1958). The reactions of hospitalized children to illness.
Pediatrics, 22, 590-600.
Bowlby, J. (1973). Attachment and loss; Separation, anxiety and anger.
Vol. 2. New York: Basic Books.
Boyd, H. F., & Johnson, G. O. (1981). Analysis of Coping Style. Charles
E. Merrill Publishing Company.
Brainerd, C. J. (1978). Piaget's theory of intelligence. New Jersey:
Prentice Hall.
Broome, M. E., Hellier, A., Wilson, T., Dale, S., & Glanville, C. (1988).
Measuring children's fears of medical experiences. In C. F. Waltz,
& O. L. Strickland (Eds.), Measurement of nursing outcomes: Vol. 1.
Measuring client outcomes (pp. 201-214). New York: Springer.
Brown, J. M., O'Keefe, J., Sander, S. H., Baker, B. (1986). Developmental
changes in children's cognition to stressful and painful situations.
Journal of Pediatric Psychology, 3, 343-357).
Burstein, S., & Meichenbaum, D. (1979). The work of worrying in children
undergoing surgery. Journal of Abnormal Child Psychology, 7, 121
132.
Butler, J. A., Budetti, P., McManus, M. A., Stenmark, S., & Newacheck, P.
W. (1985). Health care expenditures for children with chronic
illness. In Hobbs, N., & Perrin, J. M. (Eds.), Issues in the care

234
of children with chronic illness (pp. 827-863). San Francisco:
Jossey-Bass.
Carpenito, L. J. (1987). Nursing diagnosis: Application to clinical
practice (2nd ed.). Philadelphia: J. B. Lippincott.
Castaneda, A., McCandless, B. R. , & Palermo, D. S. (1956). The children's
form of the manifest anxiety scale. Child Development, 27, 317-326.
Caty, S., Ellerton, M. L., Ritchie, J. A. (1984). Coping in hospitalized
children: An analysis of published case studies. Nursing Research,
33, 277-282.
Chinn, P. L., & Jacobs, M. K. (1987). Theory and nursing: A systematic
approach. S. Louis: C. V. Mosby.
Cohen, F., & Lazarus, R. S. (1979). Coping with the stresses of illness.
In G. C. Stone, F. Cohen, N. E. Adler & associates (Eds.), Health
Psychology--A Handbook (pp. 217-254). San Francisco: Jossey-Bass.
Cohen, F., & Lazarus, R. S. (1983). Coping and adaptation in health and
illness. In D. Mechanic (Ed.), Handbook of health, health care, and
the health professions (pp. 608-635). New York: Free Press.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences.
(2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.
Cohen, J., & Cohen, P. (1983). Applied multiple regression/correlation
analysis for the behavioral sciences. New Jersey: Lawrence Erlbaum.
Compas, B. E. (1987). Coping with stress during childhood and
adolescence. Psychological Bulletin, 101, 393-403.
Cook, T. D. & Campbell, D. T., (1979). Quasi- Experimentation: Design &
analysis issues for field settings. Boston: Houghton Mifflin.
Crain, W. C. (1985). Theories of development: Concepts and applications.
2nd ed. New Jersey, Prentice-Hall.
235
Curry, S. L., & Russ, S. W. (1985). Identifying coping strategies in
children. Journal of Clinical Child Psychology, 14., 61-69.
Curry, S. L., Fuss, S. W., Johnsen, D. C., DiSantis, T. A., (1988). The
role of coping in children's adjustment to the dental visit.
Journal of Dentistry for Children, 55, 231-236.
Deatrick, J. A., & Faux, S. A. (1989). Conducting qualitative studies
with children and adolescents. In J. M. Morse (Ed.), Qualitative
nursing research: A contemporary dialogue (pp. 185-203). Rockville,
MA: Aspen.
Dweck, C. S. Davidson, W., Nelson, S., & Enna, B. (1978). Sex differences
in learned helplessness: II. The contingencies of evaluative
feedback in the classroom; and III. An experimental analysis.
Developmental Psychology, 14, 268-276.
Dweck, C. S. & Elliot, E. S. (1983). Achievement motivation. In P. H.
Mussen (Ed.), Handbook of child psychology. Vol. IV. Socialization.
personality, and social development. (pp. 644-691). New York: John
Wiley & Sons.
Dweck, C. S. & Wortman, C. B. (1982). Learned helplessness, anxiety, and
achievement motivation. In H. W. Krohne & L. Laux (Eds),
Achievement, stress, and anxiety (93-125), Washington: Hemisphere.
Eiser, C., and Patterson, D. (1984). Children's perceptions of hospital:
a preliminary study. International Journal of Nursing Studies, 21,
45-50.
Elkins, P. D., & Roberts, M. C. (1984). A preliminary evaluation of
hospital preparation for nonpatient children: Primary prevention in
a "Let's pretend hospital". Children's Health Care, 13(1), 31-36.

236
Elkins, P. D. , & Roberts, . M. C. (1985). Reducing medical fears in a
general population of children: A comparison of three audiovisual
modeling procedures. Journal of Pediatric Psychology, 10, 65-75.
Elwood, S. W. (1987). Stressor and coping response inventories for
children. Psychological Reports, 60, 931-947.
Ellerton, M. L., Caty, S., Ritchie, J. A. (1985). Helping young children
master intrusive procedures through play. Children's Health Care,
13, 167-173.
Endler, N. S., & Edwards, J. (1982). Stress and personality. In L.
Goldberger & S. Breznitz (Eds.), Handbook of stress: Theoretical and
clinical aspects (pp. 36-48). NY: Free Press.
Erickson, F. H. (1958a). Play interviews for four-year-old hospitalized
children. Monographs of the Society for Research in Child
Development, 23 (3, Serial No. 69), 1-77.
Erickson, F. (1958b). Reactions of children to hospital experience.
Nursing Outlook, 6, 501-504.
Erickson, F. (1963). Viewpoints on children in hospitals. Hospitals, 37,
47-48.
Erickson, F. (1965). When 6- to 12-year olds are ill. Nursing Outlook,
13 (7), 48-50.
Erickson, F. (1972). Stress in the pediatric ward. Maternal - Child
Nursing Journal, 1, 113-116.
Faux, S. A., Walsh, M., Deatrick, J. A. (1988). Intensive interviewing
with children and adolescents. Western Journal of Nursing Research,
10, 180-194.

237
Fawcett, J. (1978). The "what" of theory development. In Theory
development: What, why, how? (pp. 17-33). New York: National League
for Nursing.
Fawcett, J. (1984). Analysis and evaluation of conceptual models of
nursing. Philadelphia: F. A. Davis.
Ferguson, B. F. (1979). Preparing young children for hospitalization: A
comparison of two methods. Pediatrics, 64, 656-664.
Field, T., Alpert, B., Vega-Lahr, N., Goldstein, S., Perry, S. (1988).
Hospitalization stress in children: Sensitizer and repressor coping
styles. Health Psychology, 6, 433-445.
Fincham, F. D., & Cain, K. M. (1986). Learned helplessness in humans: A
developmental analysis. Developmental Review, 6, 301-333.
Fischman, S. E., & Friedland, G. W. (1986). Psychologic aspects of
dealing with children in uroradiology. Urology, 27, 478-481.
Flaskerud, J. H. & Halloran, E. J. (1980). Areas of agreement in nursing
theory development. Advances in Nursing Science, 3, 1-7.
Folkman, S. (1984). Personal control and stress and coping processes: A
theoretical analysis. Journal of Personality and Social Psychology,
46, 839-852.
Folkman, S., & Lazarus, R. S. (1980). An analysis of coping in a middle
aged community sample. Journal of Health and Social Behavior, 21,
219 - 239.
Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process:
Study of emotion and coping during three stages of a college
examination. Journal of Personality and Social Psychology, 48, 150
170.

238
Folkman, S., & Lazarus, R. S. (1988). Coping as a mediator of emotion.
Journal of personality and social psychology, 54, 466-475.
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLongis, A., Gruen, R.
J. (1986). Dynamics of a stressful encounter: Cognitive appraisal,
coping, and encounter outcomes. Journal of Personality and Social
Psychology, 50, 992-1003.
Freud, A. (1952). The role of bodily illness in the mental life of
children. The Psychoanalytic Study of the Child, 7, 69-81.
Gelman, R. & Baillargeon, R. (1983). A review of some Piagetian concepts.
In P. H. Mussen (Ed.), Handbook of child psychology: Volume III:
Cognitive Development (pp. 167-230). 4th ed. New York: John Wiley.
Ginsburg, H. P., & Opper, S. (1988). Piaget's theory of intellectual
development (3rd ed.). New Jersey: Prentice Hall.
Gofman, H., Buckman, W., Schade, G. H. (1957). The child's emotional
response to hospitalization. American Medical Association Journal
of Disease of Children, 93, 157-163.
Gorman, G. (1980). The school-age child as historian. Pediatric Nursing,
5 (1), 39-40.
Goslin, E. R. (1978). Hospitalization as a life crisis for the preschool
child: A critical review. Journal of Community Health, 3, 321-346.
Hamner, S. B., & Miles, M. S., (1988). Coping strategies in children with
cancer undergoing bone marrow aspirations. Journal of the
Association of Pediatric Oncology Nurses, 5 (3), 11-15.
Heavenrich, R. M. (1963). Viewpoints on children in hospitals.
Hospitals, 37, 40-46.
Hobbs, N., Perrin, J. M., & Ireys, H. T. (1975). Chronically ill
children and their families. San Francisco: Jossey-Bass.

239
Holaday, B., & Turner-Henson, A. (1989). Response effects in surveys with
school-age children. Nursing Research, 38, 248-250.
Holt, J. L. (1968). Discussion of the method and the clinical
implications from the study "children's recall of a preschool age
hospital experience after an interval of five years". In M. V. Batey
(Ed.), Communicating nursing research (PP. 56-84). Boulder,
Colorado: Western Interstate Commission for Higher Eduction.
Hughes, M. C. (1982). Chronically ill children in groups: Recurrent
issues and adaptations. American Journal of Orthopsychiatry, 52,
704 - 711.
Hughes, R. B. (1967). Children's fears of surgery. Hospital Topics,
45 (9), 116-117.
Huston, A. C. (1983). Sex- typing. In P. H. Mussen (Ed.), Handbook of
child psychology. Vol. IV. Socialization, personality, and social
development. (pp. 387-467). New York: John Wiley & Sons.
Illingworth, R. S (1958). Children in hospital. The Lancet, 2, 165-171.
Inhelder, B. & Piaget, J. (1958). The growth of logical thinking from
childhood to adolescence. New York: Basic Books.
Inhelder, B. & Piaget, J. (1964). The early growth of logic in the child:
Classification and seriation. New York: Harper & Row.
Janis, I. (1958). Psychological stress. New York: Wiley.
Janis, I. (1965). Psychodynamic aspects of stress tolerance. In S. F.
Klausner (Ed.), The quest for self-control (pp. 213-246). New York:
Free Press.
Jessner, L., Blom, G. E., & Waldfogel, S. (1952). Emotional implications
of tonsillectomy and adenoidectomy on children. The Psychoanalytic
Study of the Child, 7, 126-169.

240
Johnson, J. E., Kirchhoff, K. T., & Endress, M. P. (1975). Altering
children's distress behavior during orthopedic cast removal.
Nursing Research, 24, 404-410.
Johnson, M. R., Whitt, J. K., & Martin, B. (1987). The effect of fantasy
facilitation of anxiety in chronically ill and healthy children.
Journal of Pediatric Psychology, 12, 273-283.
Johnson, R. T. (1976). Tests and measurements in child development:
Handbook II. San Francisco: Jossey Bass.
Joshi, R. T. (1974). Field-dependence, anxiety and personality.
Perceptual and Motor Skills, 38, 1328.
Kellerman, J., Zeltzer, L., Ellenberg, L., Dash, J., & Rigler, D. (1980).
Psychological effects of illness in adolescence. I. Anxiety, self
esteem, and perception of control. The Journal of Pediatrics, 97,
126-131.
Kerlinger, F. N. (1986). Foundations of behavioral research. New York:
Holt, Rinehart, & Winston.
Kim, H. S. (1983). The nature of theoretical thinking in nursing.
Norwalk, CN: Appleton-Century-Crofts.
Klein, R. G. (1988). Childhood anxiety disorders. In C. J. Kestenbaum &
D. T. Williams (Eds.), Handbook of clinical assessment of children
and adolescents (pp. 722-742). NY: New York University.
Knight, R. B., Atkins, A., Eagle, C. J., Evans, N., Finkelstein, J. W.,
Fukushima, D., Katz, J., & Weiner, H. (1979). Physiological
stress, ego defenses, and cortisol production in children
hospitalized for elective surgery. Psychosomatic Medicine, 41, 40
49.
-7 ■ º*-I7, º
º
-

241
Kueffner, M. (1975). Passage through hospitalization of severely burned,
isolated school-age children. Communicating Nursing Research, 7,
181-197.
Kuttner, L., Bowman, M., Teasdale, M. (1988). Psychological treatment of
distress, pain, and anxiety for young children with cancer.
Developmental and Behavioral Pediatrics, 2, 374-381.
Lambert, S. A. (1984). Variable that affect the school-age child's
reaction to hospitalization and surgery: A review of the literature.
Maternal-Child Nursing Journal, 13, 1-18.
LaMontagne, L. L. (1984). Children's locus of control beliefs as
predictors of preoperative coping behavior. Nursing Research, 33,
76 - 85.
LaMontagne, L. L. (1987). Children's preoperative coping: Replication and
extension. Nursing Research, 36, 163-167.
LaMontagne, L. L., Mason, K. R., & Hepworth, J. T. (1985). Effects of
relaxation on anxiety in children: Implications for coping with
stress. Nursing Research, 34, 289-292.
Langford, W. S. (1961). The child in the pediatric hospital: Adaptation
to illness and hospitalization. American Journal of
Orthopsychiatry, 31, 667-684.
Lapouse, R., & Monk, M. A. (1959). Fears and worries in a representative
sample of children. American Journal of Orthopsychiatry, 29, 223
248.
Lazarus, R. S. (1981). The stress and coping paradigm. In E. Eisdorfer,
E. Cohen, A. Kleinman, & P. Maxim (Eds.), Models for clinical
psychopathology (pp. 175-214). New York: SP Medical & Scientific
Books.
- |

242
Lazarus, R. S., DeLongis, A., Folkman, S., & Gruen, R. (1985). Stress
and adaptational outcomes: The problem of confounded measures.
American Psychologist, 40, 770-779.
Lazarus, R. S., & Folkman, S. (1984a). Stress, appraisal, and coping.
New York: Springer.
Lazarus, R. S., & Folkman, S. (1984b). Coping and adaptation. In W. P.
Gentry (Ed.), The handbook of behavioral medicine (pp. 282-325).
New York: Guilford.
Lazarus, R. S. , & Launier, R. (1978). In L. A. Pervin & M. Lewis, (Eds.),
Perspectives in interactional psychology (pp. 287-327). New York:
Plenum Press.
Lesser, G. S., Fifer, G. , & Clark, D. H., (1965). Mental abilities of
children from different social-class and cultural groups. Monograph
of the Society for Research in Child Development, 30 (4, Serial No.
102).
Levy, D. M. (1960). The infant's earliest memory of inoculation: A
contribution to public health procedures. Journal of Genetic
Psychology, 96, 3-46.
Maccoby, E. E., & Jacklin, C. N. (1974). The psychology of sex
differences. Stanford, CA: Stanford University Press.
Mason, J. W. (1975a). A historical view of the stress field, part I.
Journal of Human Stress, 1, (1), 6-12.
Mason, J. W. (1975b). A historical view of the stress field, part II.
Journal of Human Stress, 1, (2), 22-36.
Maxwell, S. (1985). Review of Child Anxiety Scale. In J. V. Mitchell
(Ed.), The ninth mental measurements yearbook: Vol. 1. (pp. 297
298). Lincoln, NE: University of Nebraska Press.

243
May, B. K., & Sparks, M. (1983). School age children: Are their needs
recognized and met in the hospital setting? Children's Health Care,
11, 118-121.
McGrath, J. E. (1977). Settings, measures, and themes: An integrative
review of some research on social-psychology factors in stress. In
A. Monat and R. S. Lazarus, (Eds.), Stress and coping : An anthology.
(pp. 67-76). New York: Columbia University.
McGuire, M., Shepherd, R., & Greco, A. (1978). Hospitalized children in
confinement. Pediatric Nursing, 4 (6), 31-35.
Meeks, J. E. (1970). Dispelling fears of the hospitalized child.
Hospital Medicine, 6 (10), 77-81.
Melamed, B. G., Dearborn, M., & Hermecz, D. A. (1983). Necessary
considerations for surgery preparation: Age and experience.
Psychosomatic Medicine, 45, 5117-525.
Melamed, B. G., & Lumley, M. A. (1988). Observer rating scale of anxiety.
In M. Hersen, & A. S. Bellack (Eds.), Dictionary of behavioral
assessment techniques (pp. 319-320). New York: Pergamon.
Melamed, B. G., & Siegel, L. J. (1975). Reduction of anxiety in children
facing hospitalization and surgery by use of filmed modeling.
Journal of Consulting and Clinical Psychology, 43, 511-521.
Melamed, B. G., Siegel, L. J., Ridley-Johnson, R. (1988). Coping
behaviors in children facing medical stress. In T. Field, P. M.
McCabe, & Schneiderman, N. (Eds.), Stress and coping across
development (pp. 109-137). New Jersey: Lawrence Erlbaum
Meleis, A. I. (1985). Theoretical nursing: Development and progress.
Philadelphia: J. B. Lippincott.

244
Menke, E. M. (1972). Factors related to children's perception of stress
in the hospital. Unpublished doctoral dissertation, Ohio State
University.
Menke, E. M. (1981). School-aged children's perception of stress in the
hospital. Journal of the Association for the Care of Children's
Health, 9, 80-86.
Miller, S. R. (1979). Children's fears: A review of the literature with
implications for nursing research and practice. Nursing Research,
28, 217-223.
Mott, S. R., Fazekas, N., R., & James, S. R. (1985). Nursing Care of
Children and Families: A holistic approach. Menlo Park, CA:
Addison-Wesley.
Munro, B. H., Visintainer, M. A., Page, E. B. (1986). Statistical methods
for health care research. Philadelphia: J. B. Lippincott.
Murphy, L. B. (1962). The widening world of childhood. New York: Basic
Books.
Murphy, L. B., & Moriarty, A. E. (1976). Vulnerability, coping, and
growth from infancy to adolescence. New Haven: Yale Press.
Nash, S. C. (1979). Sex role as a mediator of intellectual functioning.
In M. A. Wittig & A. C. Petersen (Eds.), Sex related differences in
cognitive functioning (pp. 263-302). New York: Academic Press.
Neff, E. J. A. (1978). Orienting, resistive and adaptive responses of
children undergoing hemodialysis for kidney failure. Maternal-Child
Nursing Journal, 7, 195-254.
Newson, J. & Newson, E. (1976) Seven years old in the home environment.
London: Allen & Unwin.

245
Nowicki, S. (1986). A manual for the children's Nowicki-Strickland
internal - external control scale. Emery University: Atlanta,
Georgia.
Ollendick, T. H. (1983). Reliability and validity of the revised fear
survey schedule for children (FSSC-R). Behaviour Research Therapy,
21, 685 - 692.
Ollendick, T. H., Finch, A. J., Nelson, W. M. (1976). Correlates of
question- asking by emotionally disturbed and normal children.
Psychological reports, 38, 923-929.
Oremland, E. K., & Oremland, J. D. (1973). The effects of hospitalization
on children. Springfield: Charles C. Thomas.
Pearlin, L. I., Lieberman, M. A., Menaghan, E. G., & Mullan, J. T.,
(1981). The stress process. Journal of Health and Social Behavior,
22, 337-356.
Pearlin, L. I., & Schooler, C. (1978). The structure of coping. Journal
of Health and Social Behavior, 19, 2-21.
Perrin, J. M. (1985). Introduction. In N. Hobbs & J. M. Perrin (Eds.),
Issues in the care of children with chronic illness (pp. 1-10). San
Francisco: Jossey-Bass.
Peterson, L., & Shigetomi, C. (1981). The use of coping techniques to
minimize anxiety in hospitalized children. Behavior Therapy, 12, 1
14.
Peterson, L., & Toler, S. M. (1986). An information seeking disposition
in child surgery patients. Health Psychology, 5 (4), 343-358.
Petrillo, M. & Sanger, S. (1980). Emotional care of hospitalized
children: An environmental approach (2nd ed.). Philadelphia: J. B.
Lippincott.
*
*. º

246
Phillips, L. R. F. (1986). A clinician's guide to the critique and
utilization of nursing research. Norwalk, CT: Appleton-Century
Crofts.
Piaget, J. (1952). The origins of intelligence in children. New York: W.
W. Norton.
Piaget, J. (1954). The construction of reality in the child. New York:
Ballantine Books.
Piaget, J. (1957). Logic and psychology. New York: Basic Books.
Piaget, J. (1959). The language and thought of the child. New York:
Meridian.
Piaget, J. (1983). Piaget's Theory. In P. H. Mussen (Ed.), Handbook of
child psychology: Vol. I. History, theory, and methods (PP. 103
128). New York: John Wiley & Sons.
Piaget, J., & Inhelder, B. (1969). The psychology of the child. New
York: Basic Books.
Pless, I. B., & Perrin, J. M. (1985). Issues common to a variety of
illnesses. In Hobbs, N., & Perrin, J. M. (Eds.), Issues in the care
of children with chronic illness (PP. 41-60). San Francisco :
Jossey-Bass.
Pless, I. B., and Pinkerton, P. (1975). Chronic childhood disorder:
Promoting patterns of adiustment. Chicago: Year Book Medical
Publishers.
Powazek, M., Goff, J. R., Schyving, J., & Paulson, M. A. (1978).
Emotional reactions of children to isolation in a cancer hospital.
The Journal of Pediatrics, 92, 834 - 837.
aw
\ º, sº a

247
Prugh, D. G. (1965). Emotional aspects of the hospitalization of
children. In M. F. Shore (Ed.), "Red is the color of hurting" (pp.
17-34). Bethesda, Maryland: National Institutes of Health.
Prugh, D. G., Staub, E. M., Sands, H. H., Kirschbaum, R. M., & Lenihan, E.
A. (1953). A study of the emotional reactions of children and
families to hospitalization and illness. American Journal of
Orthopsychiatry, 23, 70-106.
Rankin, W. W. (1988). Fear and courage. Journal of Pediatric Nursing, 3,
46-47.
Reissland, N. (1983). Cognitive maturity and the experience of fear and
pain in hospital. Social Science Medicine, 17, 1389–1395.
Reynolds, C. R. (1981). Long-term stability of scores on the revised
children's manifest anxiety scale. Perceptual and Motor Skills, 53,
702.
Reynolds, C. R., & Richmond, B. O. (1978). What I think and feel: A
revised measure of children's manifest anxiety. Journal of Abnormal
Child Psychology, 6, 271-280.
Rich, J. (1968). Interviewing children and adolescents. London:
Macmillan.
Ritchie, J. A., Caty, S. & Ellerton, M. L. (1984). Concerns of acutely
ill, chronically ill, and healthy preschool children. Research in
Nursing and Health, 7, 265-274.
Ritchie, J. A., Caty, S., Ellerton, M. L., (1987). Coping in preschool
hospitalized children: Are there differences between chronically ill
and acutely ill children? 1987 International Nursing Research
Conference abstract (pp. 374), American Nurses' Association.
º
* * *'i ( , ,

248
Ritchie, J. A., Caty, S., Ellerton, M. L. (1988). Coping behaviors of
hospitalized preschool children. Maternal-Child Nursing Journal,
17, 153-171.
Ritchie, J. A., Ellerton, M., Caty, S. (1986, May). Children’s coping:
Innovative methods in research design. Paper presented at
International Nursing Research Conference, Edmonton, Alberta.
Roberts, M. C., Wurtele, S. K. , Boone, R. R. (1981). Reduction of
medical fears by use of modeling: A preventive application in a
general population of children. Journal of Pediatric Psychology, 6.
293-300.
Robertson, J. (1970). Young children in hospital. 2nd ed. London:
Tavistock.
Rose, M. H. (1972a) The effects of hospitalization on the coping
behaviors of children. Unpublished doctoral dissertation, The
University of Chicago, Chicago, Illinois.
Rose, M. H., (1972b). The effects of hospitalization on the coping
behaviors of children. In M. V. Batey (Ed.), Communicating nursing
research: The many sources of nursing knowledge: Vol. 5 (Pp. 115
126). Boulder, Colorado : WICHE.
Ross, D. M. (1984). Thought-stopping: A coping strategy for impending
feared events. Issues in Comprehensive Pediatric Nursing, 7, 83-89.
Ross, D. M., & Ross, S. A. (1988). Childhood pain: Current issues,
research, and management. Baltimore : Urban & Schwarzenberg.
Rothbaum, R., Wolfer, J., Visintainer, M., (1979). Coping behavior and
locus of control in children. Journal of Personality, 47, 118-135.* --- ?

249
Ryan, N. M., (1989). Stress-coping strategies identified from school age
children's perspective. Research in Nursing and Health, 12, 111
122.
Sarason, S. B., Davidson, K. S., Lighthall, F. F. Waite, R. R. & Ruebush,
B. K., (1960). Anxiety in elementary school children. New York:
Wiley.
Sattler, J. M. (1988). Assessment of children (3rd ed.). San Diego:
Jerome M. Sattler, Pub.
Savedra, M., & Tesler, M. (1981). Coping strategies of hospitalized
school-age children. Western Journal of Nursing Research, 3(4),
371-384.
Scherer, M. W., & Nakamura, C. Y. (1968). A fear survey schedule for
children (FSS-FC): A factor analytic comparison with manifest
anxiety (CMAS). Behaviour Research and Therapy, 6, 173-182.
Schuster, C. S., & Ashburn, S. S. (1986). The process of human
development: A holistic life-span approach. Boston: Little, Brown,
and Company.
Schratz, M. (1978). A developmental investigation of sex differences in
spatial (visual-analytic) and mathematical skills in three ethnic
groups. Developmental Psychology, 14, 263-267.
Seligman, M. E. P. (1975). Helplessness. San Francisco: Freeman.
Selye, H. (1980). The stress concept today. In I. L. Kutash, & L. B.
Schlesinger (Eds.), Handbook on stress and anxiety (pp. 127-143).
San Francisco: Jossey-Bass.
Sherer, M. W., & Nakamura, C. Y. (1968). A fear survey schedule for
children (FSS-FC): A factor analytic comparison with manifest
anxiety (CMAS). Behaviour Research and Therapy, 6, 173-182.
º

250
Shore, M. F. (Ed.). (1965). "Red is the color of hurting". Bethesda,
Maryland: National Institutes of Health.
Sides, J. P. (1977). Emotional responses of children to physical illness
and hospitalization. Dissertation Abstract International, 38, 917
B.
Siegel, L. J. (1983). Hospitalization and medical care of children. In
C. E. Walker & M. C. Roberts (Eds.) Handbook of child psychology
(1089-1108). New York: John Wiley.
Siegel, L. J., & Smith, K. E. (1989). Children's strategies for coping
with pain. Pediatrician, 16, 110-118.
Siegler, R. S. (1986). Children's thinking. New Jersey: Prentice-Hall.
Sipowicz, R. R., & Vernon, D. T. A. (1965). Psychological responses of
children to hospitalization. American Journal of Diseases of
Children, 109, 228-231.
Sorensen, E. S. (1990). Children's coping responses. Journal of
Pediatric Nursing, 5, 259-267.
Spielberger, C. D. (1973). State-Trait Anxiety Inventory for Children.
Palo Alto, CA: Consulting Psychologists Press.
Spielberger, C. D. (1975). Anxiety: State-trait process. In C. D.
Spielberger & I. G. Sarason (Eds.), Stress and anxiety, Vol. 1, New
York: Wiley.
Spielberger, C. D. (1989). State- trait anxiety inventory: A comprehensive
bibliography (2nd ed. ). Palo Alto, CA: Consulting Psychologists
Press.
Stein, R. (1983). Growing up with a physical difference. Children's
Health Care, 12, 53-61.
-z&
s
º
251
Stein, R. E. K., & Jessop, D. J. (1982). A noncategorical approach to
chronic childhood illness. Public Health Reports, 97, 354-362.
Stein, R. E. K., & Jessop, D. J. (1984) General issues in the care of
children with chronic physical conditions. Pediatric Clinics of
North America, 31, 189-198.
Stein, R. E. K., & Jessop, D. J. (1989). What diagnosis does not tell:
The case for a noncategorical approach to chronic illness in
childhood. Social Science Medicine, 29, 769-778.
Sterling, F. E. (1985). Review of Child Anxiety Scale. In J. V. Mitchell
(Ed.), The ninth mental measurements yearbook: Vol. 1. (PP. 298
300). Lincoln, NE: University of Nebraska Press.
Stewart, C. (1978). A study of coping behaviors of hospitalized children
as affected by environmental factors. Unpublished master's thesis,
University of Washington, Seattle, Washington.
Stevens, M. (1984). Adolescents coping with hospitalization for surgery.
Unpublished doctoral dissertation, University of California, San
Francisco, San Francisco, CA.
Stevens, M. (1986). Adolescents' perception of stressful events during
hospitalization. Journal of Pediatric Nursing, 1, 303-313.
Stevens, M. (1989). Coping strategies of hospitalized adolescents.
Children's Health Care, 18, 163-169.
Stone, G. L. (1985). Review of Assessment of Coping Style. In J. V.
Mitchell (Ed.) The ninth mental measurements yearbook: Vol I (pp.
95-96). Lincoln, NE: The University of Nebraska Press.
Tesler, M., & Savedra, M. (1981). Coping with hospitalization: A study of
school-age children. Pediatric Nursing, 7(2), 35-38.

252
Tesler, M. D., Savedra, M. C., Wilkie, D. J., Holzemer, W. L., Ward, J.
A., & Paul, S. (1989). The word- graphic rating scale as a measure
of children's and adolescents' pain intensity. Manuscript submitted
for publication.
Tesler, M. D., Wegner, C., Savedra, M., Gibbons, P. T., Ward, J. A.
(1981). Coping strategies of children in pain. Issues in
Comprehensive Pediatric Nursing, 5, 351-359.
Thompson, R. H. (1985). Psychosocial research on pediatric
hospitalization and health care. Springfield: Charles C. Thomas.
Thompson, R. H., & Stanford, Gene . (1981). Child life in hospitals.
Springfield: Charles C. Thomas.
Timmerman, R. R. (1983). Preoperative fears of older children. AORN
Journal, 38, 827-834.
Vernon, D. T. A., Foley, J. M., Sipowicz, R. R., & Schulman, J. L. (1965).
The psychological responses of children to hospitalization and
illness : A review of the literature. Springfield: Charles C.
Thomas.
Visintainer, M. (1977). The effects of pre-admission psychological
preparation on children's stress responses and adjustment during and
following hospitalization for minor surgery. Nursing Research
Report, 12(2), 3-5.
Visintainer, M. A., & Wolfer, J. A. (1975). Psychological preparation for
surgical pediatric patient: The effect on children's and parents'
stress responses and adjustment. Pediatrics, 56, 187-202.
Walker, C. L. (1988). Stress and coping in siblings of childhood cancer
patients. Nursing Research, 37, 208-212.

253
Waechter, E. H., Phillips, J., & Holaday, B. (1985). Nursing Care of
Children. Philadelphia: J. B. Lippincott.
Webb, E. T., Campbell, D. T., Schwartz, R. D., Sechrest, L., & Grove, J.
B. (1981). Nonreactive measures in the social sciences, 2nd ed.
Boston: Houghton Mifflin.
Weber, R. P. (1985). Basic content analysis. Beverly Hills: Sage
Publications.
Wertlieb, D., Weigel, C., Feldstein, M. (1987). Measuring children's
coping. American Journal of Orthopsychiatry, 56, 548-560.
Wolfer, J. A. & Visintainer, M. A. (1975). Pediatric surgical patients'
and parents' stress responses and adjustment. Nursing Research, 24.
244-255.
Woods, N. F., & Catanzaro, M. (1988). Nursing research: Theory and
practice. St. Louis: C. V. Mosby.
Wise, F. F. (1986). Development of self-discipline. In C. S. Schuster,
& S.S. Ashburn (Eds.), The process of human development: A holistic
life - span approach (357-379). Boston: Little, Brown.
Yarrow, L. J. (1960). Interviewing children. In P. H. Mussen (Ed.),
Handbook of research methods in child development (561-602). New
York: John Wiley.
Yamamoto, K, & Felsenthal, H. M. (1982). Stressful experiences of
children: Professional judgments. Psychological Reports, 50, 1087
1093.
Youssef, M. M. S. (1981). Self control behaviors of school-age children
who are hospitalized for cardiac diagnostic procedures. Maternal
Child Nursing Journal, 10, 219-284.

254
Yura, H., & Torres, G. (1975). Today's conceptual frameworks within
baccalaureate nursing programs. In Faculty-curriculum development.
Part III. Conceptual framework-- its meaning and function (PP. 17
25). New York: National League for Nursing.
Zarske, J. A. (1985). Review of Assessment of Coping Style. In J. V.
Mitchell (Ed.) The ninth mental measurements yearbook: Vol I (pp.
96-97). Lincoln, NE: The University of Nebraska Press.
Zastowny, T. R., Kirschenbaum, D. S., & Meng. A. L. (1986). Coping skills
training for children: Effects on distress before, during, and after
hospitalization for surgery. Health Psychology, 5, 231-247.
Zeitlin, S. (1980). Assessing coping behavior. American Journal of
Orthopsychiatry, 50, 139-144.
Zeitlin, S. (1985). Coping Inventory: A measure of adaptive behavior.
Bensenville, IL: Scholastic Testing Service.
-*tº~º*
>
AT:
0 ºl

255
APPENDIX A
Human Subjects Committee Approval
University of California, San Francisco
º

CCMMITTEE ON HUMAN RESEARCH 2560. FICE OF RESEARCH AFFAIRS, Box O616UNIVERSITY OF CALIFORNLA, SAN FRANCISCO
TO: Bonnie Holaday, RN, DNS Elizabeth Bossert, RN, MSBox 0606 480 Warren Dr., &430
San Francisco, CA 94131
RE: The Influence of Health Status, Gender, and Anxiety on the Stress and CopingProcess of Hospitalized School Age Children
The UCSF Committee on Human Research (an Institutional Review Board holdingDepartment of Health and Human Services assurance #M-1169) has approved the aboverequest to involve humans as research subjects, with the following
CONDITION: First, because Bonnie Holaday is the Principal Investigator, her name andphone number should be included in the Questions section of the consent form. Second, themembers wished to compliment you on the excellent Child Assent Form. Once these havebeen received, the status of this protocol will automatically be changed from ConditionalApproval to Approval.
.*PPROVAL NUMBER: H1777-05091-01. This number is a UCSF CHR number whichshould be used on all consent forms, correspondence and patient charts.
APPROVAL DATE: November 30, 1989. Expedited Review
LXPIRATION DATE: November 15, 1990. If the project is to continue, it must be renewedby the expiration date. See reverse side for details.
ADVERSE REACTIONS/COMPLICATIONS: All problems having to do with subjectsafety must be reported to the CHR within ten working days.
MODIFICATIONS: All protocol changes involving subjects must have prior CHRapproval.LEGAL NOTICE: The University will defend and indemnify a principal investigator inlegal actions arising from research activities involving humans only if the activities hadcurrent CHR approval.
QUESTIONS: Please contact the office of the Committee on Human Research at(415) 476-1814 or campus mail stop, Box 0616.
\}ood luck on your project.
ChairmanCommittee of Human Research
HEPC Project ºf 89005091
-** * * *

257 º
APPENDIX B
The State-Trait Anxiety Inventory for Children
by C. D. Spielberger
is a copyrighted instrument
for information regarding this tool contact:
Consulting Psychologists Press
3803 East Bayshore Road S.Palo Alto, CA 94.303 *-*

258 º,
APPENDIX C
Hospital Stress Scale
C

259
Code #:
Hospital Stress Scale
Everybody in the hospital has things happen that are upsettingor that bother them. Some children in the hospital get alittle upset and some get very upset.
When you think about everything that has happened to you sinceyou have been in the hospital, how upset has it made you?
On the line below put a mark at the place that shows how upsetyou have been. You may put your mark any place on the line.
| |not little medium large Worst
upset upset upset upset possibleupset

260
APPENDIX D
Hospital Coping Scale

261
Code #:
ospital C cal
When you think about everything you have done to take care ofor manage the upsetting things that happen in the hospital, howmuch has it really helped with the upset?
On the line below put a mark at the place that shows how muchwhat you did or thought really helped you with the upsettingthings.
You may put your mark any place on the line.
l |no little medium large best
help help help help possiblehelp
yº,*~
L; ;

262 º
APPENDIX E
Practice Scale

263
Code #:
actice ale
Everybody likes some classes in school more than other classes.
The scale below is a way of showing how much you like, or don'tlike, some of your classes.
What class do you like best of all?Put a straight mark on the line near the right end of the line toshow how much you like the class.
What class don't you like at all?Put a straight mark on the line near the left end of the line toshow how much you don't like the class.
What is another class you have in school?How much do you like that class? Put a mark on the line to showhow much you like that class. You may put your mark any place onthe line.
|don't like the like the like the like thelike class a class a class class
class little medium a lot best ofat all amount all

264 º
APPENDIX F
Child Medical Fear Scale

265
Listed below are things that children are sometimes afraid of when they aresick or need to go to the hospital. Beside each item please circle whetheryou are: not at all afraid, a little afraid, a lot afraid
1.
2.
10.
11.
12.
13.
14.
15.
16.
17.
I am afraid
I am afraidoffice
I am afraid
I am afraidout of me
I am afraid
I am afraidstuck
I am afraidnot tell meto me
I am afraid
I am afraidI'm sick
I am afraidhurt
I am afraidI'd have to
I am afraid
Child Medical Fear Scale
of hurting myself
of going to the doctor's
of getting a shot
of seeing blood come
of going to the hospital
of having my finger
the doctor and nurse willwhat they are going to do
to throw up
of missing school if
I will cry when I get
if I went to the hospitalstay a long time
my friends/family willcatch something I have if I'm sickand play with them
I am afraid I might die if I goto the hospital
I am afraid of having the doctoror nurse look down my throat
I am afraid the nurse or doctor will
tell me something is wrong with me
I am afraidfamily if I
I am afraid
of being away from mygo to the hospital
of the doctor puttinga tongue blade in my mouth
not
not
not
not
In Ot
not
not
In Ot
not
not
not
not
not
not
not
not
not
at
at
at
at
at
at
at
at
at
at
at
at
at
at
at
at
at
all
all
all
all
all
all
all
all
all
all
all
all
all
all
all
all
all
Code #:
little
little
little
little
little
little
little
little
little
little
little
little
little
little
little
little
little
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot
lot

266
APPENDIX G
Coping Response Inventory

267
Code #:O esdo VentO
Listed below are different ways other children your age behave when they are in asituation that they find upsetting or stressful. Read through all the behaviors listedbelow.
Now think about the situation of being in the hospital. What have you done to takecare of the upsetting things that have happened? Beside each of the behaviors below,circle the answer that tells how much that way helped you. If you didn't use that way atall, skip that line.
made it worse no change helpful very helpful
1. I talked to someone else about l 2 3 4
what happened.
2. I tried to ignore it. 1 2 3 4
3. I went away and did something l 2 3 4else with a friend.
4. I went away and did something 1 2 3 4else by myself.
5. I went off by myself but did l 2 3 4did nothing.
6. I was mean to the person that l 2 3 4was bothering me.
7. I hit or messed up something l 2 3 4else. (punch pillow, kick bed)
8. I misbehaved or acted "weird". l 2 3 4
9. I asked for help. 1 2 3 4
10. I tried to do the thing or to l 2 3 4do something about the thing thatwas bothering me.
ll. I worried or got mad but kept l 2 3 4it inside.
12. I cried or yelled. 1 2 3 4
13. I planned what I should do 1 2 3 4the next time.
14. I kept on doing what I was 1 2 3 4already doing.

268
APPENDIX H
Hospital Stress/Coping Interview
º*
:

269
O tal Stress/Copi Inte w Code #
First, I want to talk with you about what it is like to be in the hospital.Remember, there are no right or wrong answers, anything you say is O.K.Would you like to turn the tape recorder on for me?
Code Number
l. (Name), lots of different kinds of things happen in the hospital.What are some of the good things that have happened while you have been in
the hospital?(Anything else?)Those are good answers :
Besides all the good things, everybody in the hospital has somethinghappen that is upsetting or that bothers them.
What kind of upsetting things have happened to you here in the hospital?(Anything else?)
(Suggested probes if needed:Have you had to do something you don't want to do?Have the nurses done anything to help you get well that is upsetting?Have the doctors done anything to help you get well that is upsetting?Is there something that you usually do at home that might not be
allowed in the hospital?)
Those do sound like really upsetting things.
When the upsetting things happen, different kids try to take care of ordeal with them in different ways.
Think real hard and try to remember what it was like whenhappened.
What things did you do or say to yourself to help you deal with7
(Repeat for each upsetting event identified in # 2)
(Suggested probe if needed:When some kids are upset they will try to think about something else, or
ask questions about it, or try to stop it from happening, or asksomeone to help them, or just try to get it over fast. Sometimessomething else might help.
What did you do or say to yourself to help you deal with 2)
Those sound like good ways of trying to deal with the upsetting things.
Is there anything you wish the nurses or doctors would do to help you whenthe upsetting things happen?
Those are good ideas. Thank-you!
Would you like to turn the tape recorder off?

270
APPENDIX I
University of California, San Francisco
Permission for Child to Be a Research Subject

271
Code Number :
UNIVERSITY OF CALIFORNIA, SAN FRANCISCOPERMISSION FOR CHILD TO BE A RESEARCH SUBJECT
A. PURPOSE AND BACKGROUND
Bonnie Holaday, R.N., D. N. S., Associate Professor, and Elizabeth Bossert,R.N., M. S., doctoral candidate, School of Nursing, University of California,San Francisco, are conducting a study of the school age child's stress andcoping during hospitalization. My child is being asked to participate in thisstudy.
B. PROCEDURES
If I agree that my child may be in this study, the following will happen:
1. I will be asked to provide some general information about my child, suchas age, grade, number of previous hospital admissions, and health status.
2. My child will receive a simplified version of this consent form and willbe asked if he/she is willing to be a part of the study. If so,
3. My child will be interviewed about what is stressful duringhospitalization and how he/she copes with the stress. The interview will beaudio tape recorded, and the tape destroyed after the study is completed.
4. My child will also be given three short questionnaires on anxiety,hospital fears, and coping, and two scales on stress and coping.
5. Because children sometimes expect their parents to answer questions forthem, I will be asked to step out of the room while my child answers thequestions. If I want to know what my child said, the answers will be sharedwith me at the end of the session.
These procedures will be done in my child's hospital room or another nearbyquiet room in the hospital. The time needed for the session will be aboutthirty to forty-five minutes.
C. RISKS/DISCOMFORTS
1. During the interview or while filling out the questionnaires, my child maybe reminded of unpleasant events during hospitalization. He/she will be freeto stop answering questions at any time if it becomes too upsetting. If mychild becomes upset, the nurse research will attempt to comfort him/her andwill call me or my child's nurse to further reassure my child.
2. While responding to the interview and questionnaires, it is possible thatmy child may become tired, if so he/she may stop participating at any time.

272
3. All study records will be kept as confidential as is possible. No namesor information that would permit identification of my child by the public willbe given in any report or publications resulting from the study. Studyinformation will be coded by number, not name, and kept in a locked locationat all times. Only study personnel will have access to the files and theaudiotapes. After the study has been completed and all data has beentranscribed from the tapes, the tapes will be permanently erased.
D. BENEFITS
There will be no direct benefit for my child from participation in this study.The anticipated benefit is a better understanding of school age children'sreactions to hospitalization, which may lead to better understanding of how toprovide emotional support for children during hospitalization.
E. ALTERNATIVES
I am free to choose not to allow my child to participate in this study.
F. COSTS
There will be no costs to me as a result of my child taking part in this study
G. REIMBURSEMENT
There will be no financial reimbursement for my child participating in thisstudy. However, with my approval, if my child participates partially or fullyin the study he/she will be offered a small token of appreciation, such as astrip of colorful stickers, costing less than $1.00. I will not tell my childof the possibility of receiving the stickers so that his/her decision toparticipate in the study will not be influenced.
H. QUESTIONS
I have talked to Bonnie Holaday, (415) 476-4663, Elizabeth Bossert, (415) 753 -6215, or , phone number , about this study,and have had my questions answered. If I have any further questions aboutthis study, I may call either person at the numbers provided above.
If I have any questions or comments about my child participating in thisstudy, I should first talk with the investigator. If for some reason, I donot wish to do this, I may contact the Committee on Human Research, which isconcerned with protection of volunteers in research projects. I may reach theCommittee office between 8:00 AM and 5:00 PM, Monday to Friday, by calling(415) 476-1814, or by writing to the Committee on Human Research, Suite 11,Laurel Heights Campus, Box 0616, University of California, San Francisco, CA94143.

273
I. CONSENT
I have been given a copy of this consent form to keep.
PARTICIPATION IN RESEARCH IS VOLUNTARY. I am free to decline permission formy child to be in this study and may withdraw my child from the study at anypoint. My decision as to whether or not to permit my child to participate inthis study will have no influence on the present or future status of myself ormy child as a patient, student, or employee at the University of California,San Francisco, or as a patient or employee of the hospital where my child is apatient.
If I wish for my child to participate, I should sign below.
Date Legally Authorized Representative
Person Obtaining Consent
H1777 - 05091 - 01 11 - 30 - 89

274
APPENDIX J
Experimental Subjects Bill of Rights

UNIVERSITY OF CALIFORNIA, SAN FRANCISCO 275
EXPERIMENTAL SUBJECT'SBILL OF RIGHTS
The rights below are the rights of every person who is asked to be in a researchstudy. As an experimental subject I have the following rights:
1)
2)
3)
4)
5)
6)
7)
8)
9)
10)
To be told what the study is trying to find out,
To be told what will happen to me and whether any of the proce.dures, drugs, or devices is different from what would be used instandard practice,
To be told about the frequent and/or important risks, side effectsor discomforts of the things that will happen to me for researchpurposes,
To be told if I can expect any benefit from participating, and, if so,what the benefit might be,
To be told the other choices I have and how they may be better orworse than being in the study,
To be allowed to ask any questions concerning the study both be.fore agreeing to be involved and during the course of the study,
To be told what sort of medical treatment is available if any compli.cations arise,
To refuse to participate at all or to change my mind about partici.pation after the study is started. This decision will not affect myright to receive the care I would receive if I were not in the study.
To receive a copy of the signed and dated consent form,
To be free of pressure when considering whether I wish to agree tobe in the study.
—%—
If I have other questions I should ask the researcher or the research assistant. Inaddition, I may contact the Committee on Human Research, which is concernedwith protection of volunteers in research projects. I may reach the committeeoffice by calling; (415) 476-1814 from 8:00 AM to 5:00 PM, Monday to Friday,or by writing to the Committee on Human Research, University of California, SanFrancisco, CA 94143.
Call X1814 for information on translations.

276
APPENDIX K
General Data Form

277
Code #
GENERAL DATA FORM
Child's gender:
1) Male2) Female
Birth date : Month Day Year
Age:1) 8 years2) 9 years3) 10 years4) 11 years
Child's ethnic group:
1) African American2) Asian3) Hispanic4) White5) Other
Grade in school:
1) First grade2) Second grade3) Third grade4) Fourth grade5) Fifth grade6) Sixth grade7) Seventh grade8) Not enrolled in school
Is your child in a special education classroom?
1) Yes2) No
If yes, has this placement been made because of your child's :
1) physical problems2) learning difficulties3) other

278
10.
11.
12.
Does your child have any chronic health problems?
1) Yes2) No
If yes, what is the condition and when it was first diagnosed?
How many times before this admission has your child been a patient in ahospital?
If your child has been in the hospital before, when was the most recentadmission?
In the last year, about how many times has your child been seen as apatient in a clinic or doctor's office?
Has your child ever attended a program at a hospital designed to helpthem understand the hospital and be less afraid of being a patient?
1) Yes2) No3) Uncertain
While your child has been in the hospital, how many hours a day have youstayed with him/her?
Does your family live in:
1) a rural area (country)2) an urban area (city)?
Approximately, how much was the total income for your family last year,before taxes?
1) less than $ 5,000 6) $ 25,000 to $ 29,9992) $ 5,000 to $ 9,999 7) $ 30,000 to $ 34,9993) $ 10,000 to $ 14,999 8) $ 35,000 to $ 39,9994) $ 15,000 to $ 19,999 9) $ 40,000 and higher5) $ 20,000 to $ 24,999

279
APPENDIX L
Summary of Research Results

280
SUMMARY OF RESEARCH RESULTS
When this research study is completed, do you want a brief summary of theresults sent to you?
1) Yes--please complete the rest of this form2) No -- leave this form blank
If yes, please print your name and address below:
Name
Street Address or P.O. Box
City State Zip Code

281
APPENDIX M
Consent to be a Research Subject
Child Assent Form

282
Code Number:
UNIVERSITY OF CALIFORNIA, SAN FRANCISCO
CONSENT TO BE A RESEARCH SUBJECT
CHILD ASSENT FORM
I have been asked to be part of a project that will find out
what children my age think are the upsetting parts of being in
the hospital and what they do when the upsetting things happen.
This project is being done by Elizabeth Bossert, a nurse at the
School of Nursing, University of California, San Francisco.
All I will need to do is to talk with someone who will ask
me questions about what it is like to be in the hospital and to
answer some written questions. There are no right or wrong
answers to any of the questions. The questions and answers will
be tape recorded. While I am answering the questions my parents
will leave the room for a little while. When they come back, if
they want to know how I answered the questions they will be told.
It will take about thirty to forty-five minutes for me to do
everything in the project.
If I get tired or upset and want to quit answering
questions, I can stop any time I want.
No one except the people doing the study and my parents will
know what I say or write.
Answering these questions will not help me right now while I
am in the hospital, but it may someday help other kids my age.

283
I have had a chance to ask questions and Elizabeth Bossert
Or has answered them for me.
By signing my name below, I am giving my permission to be a
part of the study. I don't have to be in the study if I don't
want to do it. If I decide to be in the study and later change
my mind and want to quit, that is O.K., I can stop anytime I
want. If I do stop, no one will be unhappy with me.
I give my permission to be a part of this study. I will be
given a copy of this form to keep.
(put today's date here) (sign your name here)
(nurses name)
H1777-05091-01 11-3 0-89
-— º ■ ºlº Li B RARY sº L- º Z/~ º ■ º LIBRARY sº----
º,- º --- º, - r- º O- ■ º º –– *o --- º L. º- -
| * *-
^, - + | |& ºvº º 17 º sº a- ■ / º *… " -- " --> ºf vº; G | T ºr s cº- / /*J.- º
- -
--" º, sº * | *- %, sº º, º ºf C.- º - » fºr * -º º, ºr **** * **** 2-1 : ~ º º
-
dº?!/? º/?-
Q.º --- - - - *.N. dº/*. '4, \
- - - : - -º sº cº■ º º
ºº sº, cºyºcº*. º - -- - -->
- * -
º 0) º º º º -- - º ))) º º) ''', *** - sº ■ - º, Li º RARY | || º t * Sº ■ º º, L■ B R A R Y-
(). º — -- º º) c ---º, y r º - º > *-
º r- ºº C,º – sº ~ : * > * - | º - º º, —l & ~1 v. N. ■ ºº L. s
* º'-' ºuti º Tº .." -- s ºvº. 9 in º. º--" º, * 1. s t C
- - º, ~ * º, º... -- , - - -- - - -" -- -
º º gº.) º/º © V, , 7......, * - Cºolº■ MºC 2.5 .- * * * * * ***** - ------ - --- - -- - - -ºf tºº -S ºr-- 4- ... *. * * * º/7º º ºs A- .Nº º, *-
* > º - -- * , *- wº- *.*, * - -º- "…
- º _O)
-- • *. .* ** y) -º- ‘’’,* R Y sº [-r-, *, J/1 sº- lip RARY ºr -º L// -5. Nº ■ º-º-, *º---
sº /- t ■ - *** - f º - )*- r o .* - -- - - -- ~ – - *
- -ºf º, *—
- - : S. 0. - -
_l ~ * *T/C º T. * M ºf J 17 º-
tº- º - C º T s Aºvº; J in- * *
- * *
º_s * …" - º - - º, sº
~. _ * > nº . . . º, sº ~ **, * - **, ºr º º º __
-- º - ----- 1. Cºyº / º \- - -- - ???, ºf ■ º, ". *.* (7.7).
- - -
2 Sººn, ■ º sº %- - -
º º *. º 7 .” (75. º s & º→
º- * - ~ * ,
- - *- L■ B RARY ". O).- º º n L■ tº RARY sº- ”, O■ lº
Q- To |* --Co
** - -
- º-
- *sº
-
->
- o [-r] … r-º-, -º-
* L. ~º | || § i. T º Cº. v. M■ J 17 º º- C - - - C* Q 17 4,-º, º º
-- º
º ~ ! . . . * * * , - - - - - - ->- ! -" -A■ ºº ºs S. -*.*.*, *- * > (1.7% º/ºº *.s .." ºf #1-7/7, -º- º i.
-
º sº % C 17//, .*. ºt () º º- - *- º * <- º / .7/7 ºt () º º
-- - *- * * */ --º- º º º
7 * º º º * - ) jº wº- º º *- - - * "-- n - * -– * ,
~ is T- º, L■ 6 RARY º |-* º, a '' –" sº ■ º º, L■ ■ º RARY sº | º,
-
º —l %) --- sº * - - * º - * - so -r- º |**- & ~ : * > * º L. º - º t º, ■ º º - N. *… L. ** c- y
& A Nºv. M G | T º - Sº - // º' sº A-Tºv M. J . T º -> (■º º, - * ! - - -- **, *
--> * --> *Y.-
...º º 1, Nº
-tº ■ /º (C. z - -\ * * * *- : * ~ * * > tº yº/º *.* º --- ºr ~, --
• *,- *- _º º, º º } it?'t ■ º Al º º, 4- & º, º & 7 *** * * * * *
º * º º *-- * * * O- -S ºr* * Y --- - !” º ( * *
--
º, ...) n 2 º ■ º ”, L. B R A R Y sº -- º, " - sº ■ º º, LIBRARYº sº - * – - ( –
z * , -* - º-
*. […] -> sº - ºr-- ºtº- |- -
f ~ * * r | | ~y - - ºz. L l º r º ~ -- º **/ * - / Sº ºvºi g ■ º, º –– º º■■ % ----' sº ºf a 1-1 %, ºº -- -
º º º º º -->- † - sº- - ~ ". sº -
; , ºr ■ º Q ■ º vº-
12. - º -- w - - - - ^4 º tº 71/11/ º// - º º,gº - * * ~ *- 7 º º tº 7/11/ 7/?' - º .."
". .”: º 1) Q & -" 4– .Nº * * * * º 7.7/7. ■ º t º &-
º º º, *-- - ** - ** &- --
-n sº C.Ole sºº º O) n º º In 15 ºvº Lºº º-' s ■ ºlº tºº Lº […] …
c -----' --C º 0. &
~ º | | ~-s — (C * -- ºg in
- -º ^ º ~ º ºr--ºc º Tº sººn tº L ºy ** º
- *-
º º- * * * - *- º, S. º *** { º ~, º º
- - * -- º, sº dº / º* , CYº! / i■■ i■■ ºt * 2 --~ :-
-
Sº sº 17//, 7.1//cºld sº % -º-, *-* * -- * - \!.- gº !, º º
-º *- º º * *~/
º*z.
*A.
-º* } º ** º o C * +
º L■ ■ º & – ’ o - -> S. º O º- ºl. ! {} RA R_Y º L- º tº ' --> sº T º, L■ ■ º RA R_* º º, / —"* - º —- - so o
º - A- -
º, —r-- º º º ■ º ~ *-
f | ] sº "c T- wººglu º TAC * - sº ºvºgº º * - (C *… 1–1 &~, 1. Sº -* '?... -- º
2- . 12 º' !, N* -s tº ^. Sº■ º ºf Sº, Zºº, º cºlº/” 2s 20-–4 º, Cº■ º sº, ^ "lº “Yº sº. CY.7/7-i■ ºciº- - -
*- - º- -º - .** º - -
º
* – is […] tº B RARY _º [...] *. 2. le s º L■ B RARY sº -- "º-
& º º º * •o ---- sº
ºuri º Lºlº - C º■ lºs ºvºgri º Lºlº - C-> * - -*
-- ~, ■ º º º sº--" - -- º - - -
º º }//?! / º º º- - -
º, º º , ºf º -N" -y -
- . -- *-* - * * * º 1. ("Yº, ■ º ºn-
~ *-* - ºf 'V' ºr - - ºr fºr--, -, ---º: § 2, * Jº'■ tº i■ ºut .Nº º A- º 'º, O.7'■ ■ º--- *-
- A- ~ -
*Oyn *, ) -* -
O º * ,*.. º º :- Tº ■ º. A nº- * * ** / .* -| º, º' ' --" sº ■ º * L ■ º ºv : R^. º L_ º, * * º * sº ■ º º Li ■ º R_* Qº■ º [ ] sº º _º - - - - - - -- * : ~ * º ...Sº -* - - -7 * - º º-
º, L l º* / Q. vºj J in º. º “Tº ■ º º' -- sº ºvºi gin º. º
- - ~
*** * * * ºgº ºf '''''', e.
// º I º, w
* * -- º, º-
º tº /■ º o os -\

*_*
_y sº […]” Li B RA R_Y sº L_ º , V/ 4– º […] ”, L! B RA R_Y s' L– º, º
º-
*o sº C. •o ~ *-
|ºv’■ gº º, L– sº ~/C *-s ºvºgº º LC s - C -
ºf, ºr º º, sº-ºut■ º 5 * *
*º, sº º/* 5 °2's Sººncº
- - , Sº, 17//, nºnci■ co * 64*
sº *, 77/7-incºro-
sº "… º () cº, Ole sº tierº sº. On sº tie Rºss' s
º, * - _º […] 4- L. °o. 4. * T- J -|*
ºx C c ~&w so , -
[…] sº ºvº gº * -- cº
*
º
.** *
sº […] –-
~ * * rº
% CT s ºvº an º-'º [[C *, 's (º - ~ --- * º 72 S
12 Nº º 42, sº º, Nº nº 91 º' ■ ■ º 12 S-" ºf ~ 71/?? / / / /* º
º * -- ºf . Cºl/?'—■ ■ (2/??(J- -
tº sº, anyºl, º/?Sº is *. & frºncºco sº ºº
sº º º** cº º
- º º * * *-
c O º, º ** -tº sº I jº, Ole s -- tº Luº O■ lº st- tº*- -C - * *
_2 º […] & T o, | __ -> º, […] sº º |s - (C %2 -a- sº Jºvºi g in º, º “I■ C ”, –– º Aºvº g : T *,º,
z º º, S.-
-> '4. se 4./... .º. º * ~,º º ºr a * ºff 2 * 7. - * º 0.0 putº■ º
*cºncººr &, cºin '■ º º & cº ºf Cºco sº &
~
\*~ cº º n ºlº tºº sº º 0/] sºº < º, º, º - & ºº, tº Lº 07 s Tºº, "ºº" […]” . s’ ■,” I sº * [Tº sº. […] sº º, [T] sº,
1-1 % º sº % - sº ºvºi gin º. º (C * -- s ºr* - *... sº * >º
* a *. º dº? !/?? Z/º Q 2.S. C■ .- -: *- º dº 1/
! C ºnciº -S º* *- sº (7//7.1/■ ci■■ o SS º
* **, sº º * * º & a'
- sº º, L16 RARY sº —r- º, O/ le .* T- º, L■ B RARY sº [T º, * ,º L. CA --- *o L.
7, ºf -> 74, sº-
12 N. 2. Nº 2 -º *
* , º/” O % . - - - - - *S ºut■ º cºncº* !S 3 * C■ º it/?c■ . To sº °, sº º, & 777/7c, ■ co*
! *-
-~ º * 1. 0) º, O *
º º, () *- ar +, º Sº
º, 0) sº º, L. BRARY is ■ ºlº, , /2 s ■ ºlº tºc → - w
L. C * 2.*
•º r- &&Lºl * -
() —r- sº […] cº º Qºvariº, Lºls * I■ c º'-'º ºvº an *. L. Jºs - C *-
!sº
O. ■ º-* º --- º 2. [T]
~ -- ~ -f ~, o sº- -
º,* !--- sº ºvº gº º, -- - C - ºgº º2 º º, &
*s ºr ”, sº * ºnº ”, sºº
* - ..)- f * º - * - - - - * : * * * * - /?” * -
C■ .^{(0 is 2, cºyotº º is *. Sºft. 1//c■ . To § 4,
-
Sº sº º, *- º/S 4. p ~ *k, º “º <- {) º
Y sº | º, 4. / le sº […] º, L■ B RARY sº L. J º, O) le º […] ”, L; Gsº Oe T- sº – 29 L. J sº 9. ■ º- sº –– º, |º o
- ºf sº * _j &- -
ºIIC *-- ºgº ºs - C º'-'º ºvugin º.º º, sº ºn ■ ººn ºs' º, sº ºut ■ ºro
C º/rºne (VC)-
3. *: ony, !/?-
7// \- sº cºnciº s % *- º // S.*~ -- %. <-A- º *. A- º
* - C-
sº º c º,-
º"º tº 2- tº tºº ■ º. Oley cy- ---- --- º o c
-
º L., - C | | º o, | sº º | | o”* - -11 * is cº-º/* *2 L_1 | Sº cºvº, c. - %. & * L__j & Cº.
J. ~ L * ,-
r º sºº, º cºC
() c’7, º A º, S- * ~º º, sº FO R REF ERENCE º, sº* * * % º dº
*sº, •)º, * * 17///7-incºco sº º
* **, T ~ & 4, ºf "º5 s ■ º L■ B s […] °, L18 RARY sº —r-
º,* .
&--
a OM THE ROOM-
Vo --- S- - º -z ■º
- -º | NOT TO BE TAKEN FR ****o *z, L. J sº º
*ºuri º º ºgº º- ºC º,º % car. Ma. as ovº
-~7. sº º - - -
* ºf 77.1 / / /* - a º, S 757.01/11/ / ///#! 2 - C■ . --~~~~~■ º jº 1/?? / º s' * c).7/■ . 7-incºco º & () nº !/?º sº * 11/7, 11/7( ■ º º*S* * f. * -
%. º 9. -*
o / º º º ■ º Dyn * -- ", Lip RARY sº º º, Li P RARY S –– º cº'' 4–2 Nº […] º ~~~ 1 º' ■A- ** […] o Cº 'o. º ~ • X * l>
-Vo rº- &
* (C * [I] ºvº G 11 %. | || º c-
* º-- T - -
"e […] sº –– 'o -- r-
&-Yº- -
º *
% -- sº ºvº■ q ■ º * -- ~ *y A. -º, s-- -
!-- ~~- -
* → ºf ■ ºvo 2.S. -C.º, 2
º, º ~- -… ** dº ■ ºno ºs C.