
Nutraceuticals: do they represent a new era in the management of osteoarthritis? – a narrative...
21
Review Nutraceuticals: do they represent a new era in the management of osteoarthritis? e a narrative review from the lessons taken with five products Y. Henrotin y * , C. Lambert y, D. Couchourel z, C. Ripoll x, E. Chiotelli z y Bone and Cartilage Research Unit, Institute of Pathology, level 5, CHU Sart-Tilman, 4000 Liège, Belgium z Danone Research, avenue de la Vauve, F-91767 Palaiseau cedex, France x Naturalpha SAS, 85 rue Nelson Mandela, 59120 Loos, France article info Article history: Received 11 May 2010 Accepted 17 October 2010 Keywords: Osteoarthritis Nutraceuticals summary Objectives: The aim of this first global systematic review on selected nutraceuticals was to synthesize and evaluate scientific relevant data available in the literature. Evidences that can support health, physio- logical or functional benefit on osteoarthritis (OA) were gathered and the level of evidence relative to each of these ingredients was highlighted. Methodology: Relevant scientific data (positive or not) regarding OA were searched for five groups of compounds (avocado/soybean unsaponifiables (ASU), n-3 polyunsaturated fatty acids, collagen hydro- sylates (CHs), vitamin D, polyphenols) within preclinical (in vitro and in vivo), epidemiological, and clinical studies. The following criteria were evaluated to assess the methodology quality of each study: (1) study question; (2) study population; (3) primary endpoint; (4) study design (randomization, control, blinding, duration of follow up); (5) data analysis and interpretation. A scientific consensus was deter- mined for all studied nutraceuticals to evaluate their efficacy in OA. Results: The studied compounds demonstrated different potencies in preclinical studies. Most of them have demonstrated anti-catabolic and anti-inflammatory effects by various inhibitory activities on different mediators. Vitamin D showed a pro-catabolic effect in vitro and the polyphenol, Genistein, had only anti-inflammatory potency. The evaluation of the clinical data showed that ASU was the only one of the studied ingredients to present a good evidence of efficacy, but the efficient formulation was considered as a drug in some countries. Pycnogenol showed moderate evidence of efficacy, and vitamin D and collagen hydrolysate demonstrated a suggestive evidence of efficacy, whereas curcumin, epi- gallocatechin-3-gallate (EGCG) and resveratrol had only preclinical evidence of efficacy due to the lack of clinical data. The literature gathered for n-3 PUFA, nobiletin and genistein was insufficient to conclude for their efficacy in OA. Conclusion: Additional data are needed for most of the studied nutraceuticals. Studies of good quality are needed to draw solid conclusions regarding their efficacy but nutraceuticals could represent good alternates for OA management. Their use should be driven by any recommendations. Ó 2010 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved. Introduction Osteoarthritis (OA) is the most prevalent joint disease. It causes pain and disability in a large proportion of the population world- wide. It is considered as the most consequential rheumatic condi- tion in terms of social-economic impacts. The incidence of the disease increases with age. The disease evolves over decades to end by the loss of joint function. In addition, aging patients present various co-morbid conditions that add to the complexity of the treatment of OA patients. To date, there is no cure for OA. The only available treatments aim at reducing symptoms, as pain and inflammation, maintain joint mobility and limit the loss of function. The main goals that the ideal OA treatment has to achieve are symptom-modifying effect, reducing pain and inflammation, and structure-modifying effect, sparing joint structure and preventing joint degradation in order to maintain articular function. Several guidelines, as the European League Against Rheumatism (EULAR), the American College of Rheumatology (ACR) or the * Address correspondence and reprint requests to: Y. Henrotin, Bone and carti- lage Research Unit, Institute of Pathology, level 5, CHU Sart-Tilman, 4000 Liège, Belgium. Tel: 32-4-3662516. E-mail address: [email protected] (Y. Henrotin). URL: http://www.bcru.be 1063-4584/$ e see front matter Ó 2010 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.joca.2010.10.017 Osteoarthritis and Cartilage 19 (2011) 1e21
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Nutraceuticals: do they represent a new era in the management of osteoarthritis? – a narrative...

Osteoarthritis and Cartilage 19 (2011) 1e21
Review
Nutraceuticals: do they represent a new era in the management ofosteoarthritis? e a narrative review from the lessons taken withfive products
Y. Henrotin y*, C. Lambert y, D. Couchourel z, C. Ripoll x, E. Chiotelli zyBone and Cartilage Research Unit, Institute of Pathology, level 5, CHU Sart-Tilman, 4000 Liège, BelgiumzDanone Research, avenue de la Vauve, F-91767 Palaiseau cedex, FrancexNaturalpha SAS, 85 rue Nelson Mandela, 59120 Loos, France
a r t i c l e i n f o
Article history:Received 11 May 2010Accepted 17 October 2010
Keywords:OsteoarthritisNutraceuticals
* Address correspondence and reprint requests to:lage Research Unit, Institute of Pathology, level 5, CBelgium. Tel: 32-4-3662516.
E-mail address: [email protected] (Y. Henrotin)URL: http://www.bcru.be
1063-4584/$ e see front matter � 2010 Osteoarthritidoi:10.1016/j.joca.2010.10.017
s u m m a r y
Objectives: The aim of this first global systematic review on selected nutraceuticals was to synthesize andevaluate scientific relevant data available in the literature. Evidences that can support health, physio-logical or functional benefit on osteoarthritis (OA) were gathered and the level of evidence relative toeach of these ingredients was highlighted.Methodology: Relevant scientific data (positive or not) regarding OA were searched for five groups ofcompounds (avocado/soybean unsaponifiables (ASU), n-3 polyunsaturated fatty acids, collagen hydro-sylates (CHs), vitamin D, polyphenols) within preclinical (in vitro and in vivo), epidemiological, andclinical studies. The following criteria were evaluated to assess the methodology quality of each study:(1) study question; (2) study population; (3) primary endpoint; (4) study design (randomization, control,blinding, duration of follow up); (5) data analysis and interpretation. A scientific consensus was deter-mined for all studied nutraceuticals to evaluate their efficacy in OA.Results: The studied compounds demonstrated different potencies in preclinical studies. Most of themhave demonstrated anti-catabolic and anti-inflammatory effects by various inhibitory activities ondifferent mediators. Vitamin D showed a pro-catabolic effect in vitro and the polyphenol, Genistein, hadonly anti-inflammatory potency. The evaluation of the clinical data showed that ASU was the only one ofthe studied ingredients to present a good evidence of efficacy, but the efficient formulation wasconsidered as a drug in some countries. Pycnogenol showed moderate evidence of efficacy, and vitaminD and collagen hydrolysate demonstrated a suggestive evidence of efficacy, whereas curcumin, epi-gallocatechin-3-gallate (EGCG) and resveratrol had only preclinical evidence of efficacy due to the lack ofclinical data. The literature gathered for n-3 PUFA, nobiletin and genisteinwas insufficient to conclude fortheir efficacy in OA.Conclusion: Additional data are needed for most of the studied nutraceuticals. Studies of good quality areneeded to draw solid conclusions regarding their efficacy but nutraceuticals could represent goodalternates for OA management. Their use should be driven by any recommendations.
� 2010 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Introduction
Osteoarthritis (OA) is the most prevalent joint disease. It causespain and disability in a large proportion of the population world-wide. It is considered as the most consequential rheumatic condi-tion in terms of social-economic impacts. The incidence of thedisease increases with age. The disease evolves over decades to end
Y. Henrotin, Bone and carti-HU Sart-Tilman, 4000 Liège,
.
s Research Society International. P
by the loss of joint function. In addition, aging patients presentvarious co-morbid conditions that add to the complexity of thetreatment of OA patients.
To date, there is no cure for OA. The only available treatmentsaim at reducing symptoms, as pain and inflammation, maintainjoint mobility and limit the loss of function. The main goals that theideal OA treatment has to achieve are symptom-modifying effect,reducing pain and inflammation, and structure-modifying effect,sparing joint structure and preventing joint degradation in order tomaintain articular function.
Several guidelines, as the European League Against Rheumatism(EULAR), the American College of Rheumatology (ACR) or the
ublished by Elsevier Ltd. All rights reserved.

Table IStudied compounds
- n-3 PUFAs
B EPAB DHAB ALA
- ASU- CHs- Vitamin D- Polyphenols
Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e212
Osteoarthritis Research Society International (OARSI) recommen-dations for the management of knee OA1e4 have been published forOA management. They all recommend both non-pharmacologicaland pharmacological approaches. The non-pharmacological inter-ventions include education and self-management, regular tele-phone contact, referral to a physical therapist, aerobic, musclestrengthening and water-based exercises, weight reduction,walking aids, knee braces, footwear and insoles, thermal modali-ties, transcutaneous electrical nerve stimulation and acupuncture.The pharmacological treatments consist of acetaminophen, cyclo-oxygenase-2 (COX-2) non-selective and selective oral non-steroidalanti-inflammatory drugs (NSAIDs), topical NSAIDs and capsaicin,intra-articular injections of corticosteroids and hyaluronates,glucosamine and/or chondroitin sulphate, and avocado/soybeanunsaponifiables (ASU) for symptom relief; glucosamine sulphate,chondroitin sulphate and diacerein for possible structure-modi-fying effects and the use of opioid analgesics for the treatment ofrefractory pain1,5. Most of the pharmacological treatments availableto relieve OA symptoms present serious adverse events, as the riskof gastro-intestinal or cardiovascular adverse events with NSAIDs.
Moreover, this disease implies treatment or drug intake fordecades, increasing the risk of serious adverse events and theincidence of co-morbidity factors.
Many efforts have been developed to find a cure to OA that cansatisfy all the above-mentioned goals. The perfect drug would benot only able to relieve inflammation and pain but also to slowdown, stop or even better prevent disease progression. This wouldresult in the maintenance of joint function, sparing joint structuresinvolved in OA, meaning cartilage, synovial membrane and sub-chondral bone.
From the molecular point of view, OA joints are the site ofinflammation and catabolism. Many key mediators have beenidentified in cartilage for both pathways. Inflammation is linked tointerleukin (IL)-1b, COX-2 expression and prostaglandin E2 (PGE2)and nitric oxide (NO) production. Catabolism results from animbalance with anabolism. The synthesis of catabolic enzymes asdifferent matrix metalloproteinases (MMP-1, 3 or -13) or the dis-integrin and metalloprotease with thrombospondine motifs(ADAMTS)-4 and -5 (also known as aggrecanases) is increasedresulting in the degradation of the main cartilage matrix compo-nents (proteoglycan (PG) and type II collagen). In parallel, thesynthesis of the matrix components is decreased. Synovialinflammation is directly linked to cartilage degradation. In addition,subchondral bone is the site of strong remodeling processesresulting in bone sclerosis. All these factors produce the loss of thearticular integrity and the loss of joint function.
Indeed, there is a strong necessity for prevention of OA. The firststep passes by healthy lifestyle, weight loss and nutrition, withspecific nutrients that could help to achieve this goal. Nutraceut-icals are good candidates to help patient preventing OA ormanaging their disease using them as treatment adjuvant.
Nutraceutical comes from the combination of the words nutri-tion and pharmaceutical. It corresponds to food or food productthat provide health and medical benefits, including prevention andtreatment6,7. By definition and regulatory laws they are devoid ofadverse effects.
Nutraceuticals are good candidates for long-term prevention ofchronic disease, such as OA. Many compounds have already beenstudied and a review by Ameye and Chee6 has gathered all thescientific data available at that time. There are several emergingalternatives. It is more and more recognized that nutraceuticalscould help to maintain bone and joint health. However this isparamount to give a critical point of view to judge the quality of thestudies. Nutraceuticals are under minimal and vague regulation.Dietary supplements do not have to be approved by the US Food
and Drug Administration (FDA). Nutraceuticals are monitored asdietary supplement within the US and the definition for functionalfoods varies depending on countries. In Europe the situation isdifferent with an ongoing regulatory reform tightening the existingregulatory framework. Indeed, European Food Safety Authority(EFSA) adopted Regulation 1924/2006 on the use of nutrition andhealth claims for food in December 2006. This regulationharmonised rules across the European Union (EU) for the use ofhealth or nutritional claims on foodstuffs, which are based onnutrient profiles. One of its key objectives is to ensure that allclaims made on food labels in the EU are “clear and substantiatedby scientific evidence”. EFSA is responsible for verifying the scien-tific substantiation of the submitted claims, some of which arecurrently in use, some of which are proposed by applicants. Thisinformation serves as a basis for the European Commission andMember States, which will decide whether to authorize eachindividual product claim. EFSA started to release opinions inOctober 2009 on health claims submitted under Article 13 of theregulation, covering so-called generic health claims.
The aim of this first global systematic review on selectednutraceuticals was to synthesize and evaluate scientific relevantdata available in the literature. Evidences that can support health,physiological or functional benefit on OA were gathered and thelevel of evidence relative to each of these ingredients washighlighted.
Methodology
Relevant scientific data (positive or not) regarding OA weresearched for five groups of compounds (Table I) within in vitro(Table III), in vivo (Table IV), epidemiological (Table V), and clinicalstudies (Table VI). The selection of compounds discussed in thispaper is arbitrary and was based mainly on the following criteria:amount of emerging science, safety of use, regulatory constrains(Novel Food), natural presence in food. The objective was in the endto identify ingredients that could support joint health, but also thatcould be authorized in food and would be relevant to be deliveredthrough a food matrix.
We have voluntary eliminated glucosamine sulphate, glucos-amine-HCl, and chondroitin sulphate because these naturalcompounds are considered as drugs in some countries, and thatthey have been the main topic of numerous systematic review andmeta-analysis5,8e13. The search was performed according to thefollowing criteria: (1) only scientific data with a direct link to OAwere selected; (2) only orally administered treatments wereselected for in vivo studies and clinical trials (CTs); (3) only publi-cations in English were considered (4) only scientific data allowingto evaluate the effect of the compound alone were considered.Articles describing the results of a study previously published wereexcluded. The search was performed in Pubmed/Medline databasebetween January 1990 and 2010.
This search was performed using the combination of termsrelated to OA (arthrosis or osteoarthr* OR gonarthro* OR coxarthro*OR “joint pain” OR “joint comfort” or chondro* or fibroblast* OR

Table IIResults of Pubmed data search performance
Compound Total number ofpublicationsretrieved
Total number ofpublicationsselected
Nb of in vitrostudies
Nb of in vivostudies
Nb ofobservational CTs
Nb ofinterventional CTs
n-3 PUFAs 1508 9 4 2 1 2ASU 59 17 9 4 0 4CHs 51 7 2 1 0 4Vitamin D 2249 9 3 1 5 0Pine bark extract 13 4 0 0 0 4Prodelphinidins 1 1 1 0 0 0Nobiletin 10 3 3 0 0 0Genistein 571 3 2 1 0 0EGCG 81 7 7 0 0 0Resveratrol 146 6 5 1 0 0Curcumin 231 12 12 0 0 0Ventol 2 1 1 0 0 0Quercetin 210 1 1 0 0 0
Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 3
synov* OR subchond* OR cartilage OR collagen) and each studiedcompound name (or abbreviation).
The methodological quality of each CT supporting functionalingredient efficacy was determined according to an assessmentmodel adapted from EFSA and FDA recommendations (EFSA, 2007;FDA, 2003), AFSSA (“Agence Française de Sécurité Sanitaire desAliments”) guidelines (AFSSA, 2007) and other relevant refer-ences6,14,15 (ANAES “Agence Nationale d’Accréditation et d’Evaluationen Santé”, 2000). The quality is scored according to a set of 14criteria. One point is marked for each criterion presented in thedescription of the CT. The points are then summed and the finalscore allow classifying the CT quality in four different categories:a score below six represents a poor methodological quality, from 7to 9 represents a medium methodological quality, from 10 to 11represents a good methodological quality and finally a score from12 to 14 represents a very good methodological quality.
A scientific consensus was reached between the two evaluators(YH and CL) by considering different points: the total number of CTs(showing or not a beneficial effect), the quality of these CTs, thenumber of epidemiological studies showingor not a relationship, theheterogeneity in the body of evidence, the presence of preclinicalbasis and the presence of ongoing CTs. The studies were then clas-sified as good evidence of efficacy, moderate evidence of efficacy,limited evidence of efficacy but suggestive, preclinical evidence ofefficacy, lack of evidence of efficacy, some evidence of inefficacy.Scientific consensus for each ingredient is summarized in Table VII.
Furthermore, a search of ongoing CTs (Table VIII) was carried outon the clinicaltrials.gov database using the term “osteoarthritis” andeach studied compound’s name, in order to complete existingpublished data and give an overview of current research interest onthe selected ingredients.
Results
Bibliographic search results
The results of the search performed on Pubmed/Medline data-base are described in Table II.
N-3 polyunsaturated fatty acids (n-3 PUFAs)
n-3 PUFAs (linolenic acid and eicosapentenoic acid (EPA)) areessential fatty acids. These compounds are candidate for thereduction of inflammation as they can substitute arachidonic acid(main precursor of prostaglandins) in the synthetic pathway ofinflammatory mediators. The reduction of inflammation can alsohave an impacton the catabolic pathwaysandby thatwayondiseaseprogression. They have been widely studied in cardiovascular and
inflammatory diseases as rheumatoid arthritis16,17. These studiesdemonstrated the beneficial effects of a higher n-3 intake. It isimportant to note that Western diet is richer in n-6 PUFAs (linoleicacid and arachidonic acid) rather than in n-3 PUFAs6.
In vitro and preclinical datan-3 PUFAs have been extensively studied in various cell types,
but only few studies have assessed their anti-inflammatory or anti-OA effects in joint cell models. Three in vitro studies have beenidentified using bovine chondrocytes or human and bovine carti-lage explants. These studies used n-3 PUFAs alpha-linolenic acid(ALA), EPA and docohexanoic acid (DHA)18e20. These studiesdemonstrated the potency of n-3 PUFAs at reducing inflammatorymediators (IL-1a, COX-2, 5-lipoxygenase (LOX) and its activatorFLAP) and also catabolic factors (MMPs or ADAMTS). Furthermore,recent published data have also shown that n-3 PUFAs reducedIL-1b-induced ADAMTS-4, -5, MMP-3, -13 and COX-2 mRNA inbovine chondrocytes culture21.
Similarly, only one animal study on n-3 PUFAs and OA has beenidentified in the literature22. This study investigated the effect ofn-3 PUFAs on rats with a marginally deficient essential fatty acidstate. n-3 PUFA produced a 70% maximum decrease in the linoleicand arachidonic acid content of articular cartilage. n-3 PUFA alsoproduced a 30e40% decrease in the cartilage hexosamine contentand a 32% inhibition of PG synthesis. This is important to keep inmind that this study demonstrated that a too low n-6/n-3 ratio canbe negative, as a diet with very low n-6 PUFAs intake inducedsurface irregularities and PG depletion in cartilage of rats6,22.
Finally, the only one in vivo study testing n-3 PUFAs in client-owned OA dogs was just published23. The results are in favor of thebeneficial effect of n-3 PUFAs on OA dogs.
Epidemiological dataOne observational study was identified. This study investigated
using Magnetic resonance Imaging (MRI), the association ofdifferent fatty acids consumptionwith cartilage structure and bonemarrow lesions (which have been shown to be associatedwith kneepain and predictive of cartilage loss in knee OA)24. The main obser-vation of this study showed that high intakes of monounsaturated,total and n-6 PUFAs are associated with increased risks of bonemarrowlesions. The resultsmadeno associationbetweenn-3 PUFAsand either bone marrow lesions or cartilage volume or defects.
Clinical dataThe clinical data on n-3 PUFAs are limited. Two studies that
investigated the effect of natural extract or oil with high content ofn-3 PUFAs on OA symptoms were identified. One study of mediumquality (score: 7)25 showed that a daily intake of 10 ml of cod liver

Table IIISummary of the in vitro effects of the studied products on OA
Reference Product Dose and incubationduration (ID)
In vitro model Results
n-3 PUFAsCurtis et al. 200018 EPA, DHA or ALA 10e100 mg/ml
ID: 8 hBovine chondrocytes Dose-dependent reducti of IL-1a induced-aggrecanase expression and activity
Reduction of IL-1a, TNF- nd COX-2 (with ALA) expressionCurtis et al. 200219 ALA or EPA 10e100 mg/ml
ID: 24 hHuman OA cartilage explants Reduction of endogenou nd IL-1-induced release of PG
metabolites in a dose-de ndant manner by n-3 PUFA but not by n-6 PUFASuppression of the endo ous proteolytic activity of aggrecanaseand collagenase by n-3 P AsSuppression of the mRN xpression of ADAMTS, MMP-3 andMMP-13 by n-3 PUFANo effect of n-3 PUFA on MP-1, -2 and -3
Curtis et al. 200220 EPA or ALA 10e300 mg/ml24 h pre-treatment with EPA or ALAand 4 days ncubation with IL-1b
Normal bovine orosteoarthritic human cartilageexplants stimulated with IL-1b
Reduction of IL-1-induce nflammation and catabolism(reduction of GAG releas nd of aggrecanase activity, loss ofCOX-2 and 5-LOX expres n) by n-3 PUFANo effect of n-3 PUFA on rmal tissue homeostasis
Zainal et al. 200921 EPA, DHA or ALA 2.5e30 mg/ml8 h pre-treatment and 4 daysincubation with IL-1b
Normal bovine articularchondrocytes stimulated withIL-1b
Demonstration of the ch drocyte ability to incorporate exogenous PUFAsReduction of IL-1b-induc production of cartilage degradatingenzyme (agrecanases, M s) and inflammatory cytokinesInhibition of COX-2 by n PUFAs but not COX-1
ASUMauviel et al. 198933 ASU 0.1e10 mg/ml
ID: 24 h and 8e14 daysSynoviocytesRabbit articular chondrocytes
No impact of ASU alone collagen synthesis in synoviocytes andchondrocytes after 24 hI ibition of IL-1b-induced collagen synthesis decreasein synoviocytes after 24 imulation of collagen synthesis on articularchondrocytes after 8e14 ys
Mauviel et al. 199134 ASU Piascledine� 10 mg/mlID: 48 h
Rabbit articular chondrocytesHuman rheumatoidsynovial cells
Slight increase of collage roduction in both cell typesPartial inhibition of IL-1b duced release of collagen in synovialcells and total suppressi in chondrocytes
Henrotin et al. 199835 ASU mixed inthree ratios1:2 (A1S2)2:1 (A2S1)1:1 (A2S2)
10 mg/mlID: 72 h
Human chondrocytes Reduction of the strome in (MMP-3), IL-6, IL-8 and PGE2 spontaneousproductionDecrease of th collagenase activity in unstimulated and stimulatedchondrocytes by A1S2Pa l inhibition of IL-1 effects
Boumediene et al. 199939 ASU 10e25 mg/ml Bovine articular chondrocytes Stimulation of the expre n of TGFb1, TGFb2, plasminogenactivating inhibitor-1 (PA )
Henrotin et al. 200336 ASU (A1S2) 0.625e40 mg/mlID: 12 days
Human OA chondrocytesstimulated or not with IL-1b
Stimulation of aggrecan duction and restoration of aggrecanproduction after IL-1b st ulationDecrease of basal and IL- -stimulated MMP-3 productionWeak inhibition of IL-1b nduced TIMP reductionInhibition of basal produ on of MIP-1b, IL-6, IL-8, NO and PGE2Stimulation of TIMP-1 p uction
Henrotin et al. 2006(abstract)40
ASU 10 mg/mlID: 72 h
Human OA chondrocytesco-cultured or not withosteoblasts (obtained fromsclerotic (SC) or non-sclerotic(NSC) zones of OAsubchondral plate
Prevention of the inhibit effects of SC osteoblasts on matrixcomponents by pre-trea ent of SC osteoblasts with ASUIncrease of type II collag mRNA level in co-culture withASU-pretreated SC osteo stsNo modification of MMP IMP-1, TGF-b1, TGF-b3 or iNOSexpression and COX-2 m A levels in chondrocytes whenco-cultured with ASU-pr eated SC osteoblasts
Au et al. 200738 ASU 25 mg/mlID: 72 h
ChondrocytesTHP-1 monocytes/macrophages
Reduction of TNF-a, IL-1 OX-2 and iNOS expression in LPS-stimulatedchondrocytes to non-act ted control levelsReduction of PGE2 produ on and COX-2 and iNOS expressionReduction of TNF-a in LP timulated monocyte/macrophage
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
4
ona as apegenUFA e
TId ie, asionoonedMP-3
onnhhStdan p-in
onlysertia
ssioI-1proim1beictirodorytmenbla, TRNetrb, CivactiS-s

Lippiello et al. 200832 Sterols extracted fromthree ASU preparations
1e10 mg/ml (sterols)ID: 48 h
Bovine chondrocytes Upregulation of non-collagenous protein and collagen synthesis as wellas of labelled sulphate uptakeInhibition of IL-1-induced MMP-3 activity, PGE2 synthesis andsulphate release
Gabay et al. 200837 ASU 10 mg/ml Mouse or humanchondrocytes stimulatedwith IL-1bCartilage submitted to acompressive mechanicalstress (MS)
Decrease of MMP-3 and -13 expression and PGE2 synthesisInhibition of the degradation of IkBa and suppression of NF-kB translocationInhibition of Erk 1/2 but no effect on the other IL-1b-induced MAPK
CHOesser and Seifert, 200350 CH 0.5 mg/ml
ID: 48 hBovine chondrocytes Dose-dependant increase of type II collagen secretion
No increase in type II collagen secretion by native collagens andcollagen-free hydrosylate of wheat proteins (used as control)No effect on the expression of proteases
Schunck et al. 200651 CHGlucosamine
Not provided (NP) Porcine articular chondrocytesHuman femoral head chondrocytes
Increase of PG synthesis, aggrecan expression and type II collagen biosynthesiswith CHNo effect of glucosamine on extracellular matrix macromolecules(glucosamine sulphate and hydrochloride)
Vitamin DTetlow and Woolley, 199966 1,25-dihydroxy-
vitamine D310�8 MID: 48 h
Rheumatoid synovialfibroblasts (RSF)stimulated or not with IL-1bHuman articular chondrocytesstimulated or not with IL-1b
No effect on spontaneous MMP and PGE2 production by RSFReduction of IL-1b-induced MMP and PGE2 production (up to 50%) by RSFSlight reduction of spontaneous MMP-1 and -3 production by chondrocytesNo effect on IL-1b-induced MMP and PGE2 production and stimulation ofIL-1b-induced MMP-3 production by chondrocytes
Cantatore et al. 200460 1,25-dihydroxy-vitamine D3
10�8 MID: 48 h
Osteoblasts from OA subchondralbone samples
Increased stimulation of osteoclacin production by maximally damagedOsteoblasts compared to minimally damaged ones
Tetlow and Woolley, 200165 1,25-dihydroxy-vitamine D3
10�8 MID: 48 h
Human articular chondrocytesstimulated with TNF-a orphorbol myristate acetate (PMA)
No effect on MMP-1, -9 and PGE2 productionUpregulation of MMP-3 with or without stimulation with TNF-a or PMA
PolyphenolsIshiwa et al. 200078 Nobiletin NP
ID: NPRabbit synovial fibroblastsRabbit articular chondrocytes
Suppression of IL-1-induced MMP-9 mRNA expression and productionReduction of IL-1-induced PGE2 productionNo modification of the synthesis of total protein
Imada et al. 200877 Nobiletin 16e24 mMID: 24 h
Normal human synovialfibroblasts
Suppression of IL-1b-induced ADAMTS-4 and -5 mRNA expression
Lin et al. 200379 Nobiletin 6e64 mMID: 24 h
Normal human synovialfibroblasts
Suppression of IL-1b-induced productionof PGE2 in a dose-dependant mannerSelective downregulation of COX-2 but notCOX-1 mRNA expressionDownregulation of IL-1b-induced geneexpression and production of pro-MMP-1and pro-MMP-3Increased production of the endogenousMMP inhibitor, TIMP-1
Williamson et al. 2006(abstract)86
Resveratrol and/or Curcumin
2.5 mMID: 5 days
LPS-stimulated caninecartilage explants
Decrease of GAG release by curcuminalone and in combination with resveratrol
Lev-Ari et al. 200692 Curcumin 0e20 mMID: 72 h
OA synovial adherent cells Increased inhibitory effect of celecoxib on COX-2 activityStimulation of the growth-inhibitory and anti-apoptotic effects of celecoxib
Schulze-Tanzil et al. 200482 Curcumin 50 mMID: 12e48 h
Human chondrocytesstimulated with IL-1b
Prevention of IL-1b-induced MMP-3 upregulationInhibition of IL-1b-induced-type II collagen synthesis suppressionPrevention of NF-kB translocation
Shakibaei et al. 200584 Curcumin 50 mMID: 5e30 min
Human articular chondrocytes Anti-apoptotic and anti-catabolic effects on IL-1b-stimulated chondrocytes
(continued on next page)
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
5

Table III (continued)
Reference Product Dose and incubationduration (ID)
In vitro model Results
Liacini et al. 200381 Curcumin 10e15 mMID: 24 h
Human OA chondrocytes Inhibition of TNF-a-induced MMP-13 gene expression
Shakibaei et al. 200783 Curcumin 50 mMID: 72 h
Human articular chondrocytesstimulated with IL-1b
Suppression of NF-kB mediated IL-1b or TNF-a catabolic signalling pathways
resulting in COX-2 and MMP-9 downregulation and type II collagen upregulationToegel et al. 200885 Curcumin 5e50 mM
ID: 24e48 hImmortalized human chondrocytes(C-28/I2) stimulated with IL-1b
No effect on aggrecan and type I and II collagen gene expression, proliferationand morphology at low concentrationsCell damages at high concentrations (reduction of cell viability)Increase of type II collagen, MMP-3 and ADAMTS-4expression and decrease of type I collagen expression with high concentrations
Clutterbuck et al. 2008 (abstract)89 Curcumin 25e100 mMID: 5 days
Equine cartilage explantsstimulated with IL-1b
Reduction of IL-1b-induced GAG release (50e100 mM)Decrease of PGE2 release (25e100 mM)
Clutterbuck et al. 200987 Curcumin 0.1e100 mMID: 5 days
Equine cartilage explantsstimulated with IL-1b
Suppression of IL-1b-induced GAG release
Mathy et al. 2007 (abstract)88 Curcumin 1e30 mMID: 24 h
Primary bovine chondrocytesstimulated with IL-1b
No effect on cell viabilityDose-dependant inhibition of IL-1b-induced COX-2, iNOS, IL-6 and IL-8 geneexpression, PGE2 and NO production
Chowdhury et al. 200891 Curcumin 0.01e1000 ng/mlID: 48 h
Bovine chondrocytes culturedin agarose
Inhibition of IL-1b-induced NO and PGE2 releaseInhibition of 35SO4 incorporation
Mathy-Hartert et al. 200990 Curcumin 5e20 mMID: 12 days
Human articular chondrocytesin alginate beads andhuman cartilage explantsstimulated with IL-1b
No effect on cell viabilityDose-dependent reduction of the synthesis of inflammatory mediators(NO, PGE2, IL-6, IL-8) and catabolic factor (MMP-3)
Claassen et al. 200894 Genistein 10�11e10�4 MID: 24 h(for incubation orpreincubation)
Foetal bovine articular chondrocytes No effect on GAG release within the physiological range of concentrationsDecrease of GAG release with high doses (10�5e10�4 M)No effect on sulphate incorporation by chondrocytesPreincubation with 10�9e10�5 M enhanced the stimulatory effect of insulinon sulphate incorporation by chondrocytes
Hooshmand et al. 200795 Genistein 50e100 mMID: 1 hpreincubationþ24 h
Human chondrocytes stimulatedby LPS
Reduction of pro-inflammatory molecules (COX-2 and NO)No effect of YKL-40 (marker of cartilage metabolism) or IL-1b levels
Singh et al. 200298 EGCG 1e100 mMID: 30 minpreincubationþ24 h
Human OA chondrocytesstimulated with IL-1b
Inhibition of IL-1b-induced NO production by interfering with NF-kB activation
Ahmed et al. 200297 EGCG 100e200 mMID: 2 hpreincubationþ24 hor 24 h withoutpreincubation
Human OA chondrocytesstimulated with IL-1b
Dose-dependant inhibition of NO and PGE2, iNOS and COX-2 expression
Singh et al. 200399 EGCG 5e200 mMID: 24e48 h
Human OA chondrocytes stimulatedwith IL-1b
Suppression of IL-1b-induced upregulation of catabolic mediators dependanton the activation of c-jun N-terminal kinase (JNK) activation
Rasheed et al. 2009102 EGCG 25-200 mMID: 1e2 h pre-treatmentwith EGCGþ4 days treatmentwith AGE
Human OA chondrocytes stimulatedwith AGE
Inhibition of AGE-induced expression of TNF-a and MMP-13Attenuation of the AGE-induced MAP kinase signalling pathwaysInhibition of NF-kB activation
Ahmed et al. 2004 103 EGCG 1e200 mMID: 72 h
Human cartilage explants andchondrocytes
Inhibition of IL-1b-induced GAG release from human cartilage explantsDose-dependant inhibition of MMP-1 and MMP-13 IL-1b-induced mRNA andprotein expression in human chondrocytesDose-dependant inhibition of transcription activity of NF-kB and AP-1
Tokuda et al. 2008 (abstract)100 EGCG NP Osteoblast-like MC3T3-E1 cells Inhibition of the fibroblast growth factor (FGF)-2-stimulated synthesis of IL-6at least in part through the suppression of p44/p42 and the p38Map kinase pathways
Huang et al. 2009101 EGCG 10e50 mMID: 12 h
Human synovial fibroblasts stimulatedwith IL-1b
Inhibition of IL-1b-induced COX-2 expression and synthesisInhibition of IL-1b-induced PGE2 and IL-8 secretion
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
6
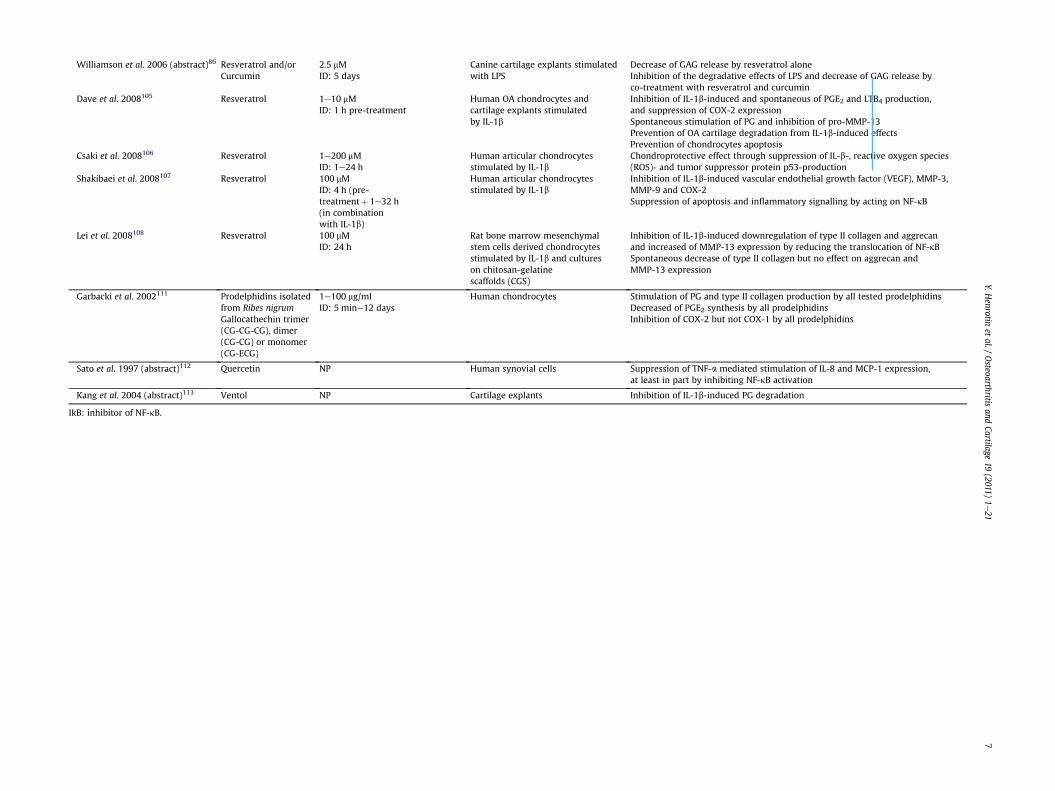
Williamson et al. 2006 (abstract)86 Resveratrol and/orCurcumin
2.5 mMID: 5 days
Canine cartilage explants stimulatedwith LPS
Decrease of GAG release by resveratrol aloneInhibition of the degradative effects of LPS and decrease of GAG release byco-treatment with resveratrol and curcumin
Dave et al. 2008105 Resveratrol 1e10 mMID: 1 h pre-treatment
Human OA chondrocytes andcartilage explants stimulatedby IL-1b
Inhibition of IL-1b-induced and spontaneous of PGE2 and LTB4 production,and suppression of COX-2 expressionSpontaneous stimulation of PG and inhibition of pro-MMP-13Prevention of OA cartilage degradation from IL-1b-induced effectsPrevention of chondrocytes apoptosis
Csaki et al. 2008106 Resveratrol 1e200 mMID: 1e24 h
Human articular chondrocytesstimulated by IL-1b
Chondroprotective effect through suppression of IL-b-, reactive oxygen species(ROS)- and tumor suppressor protein p53-production
Shakibaei et al. 2008107 Resveratrol 100 mMID: 4 h (pre-treatmentþ 1e32 h(in combinationwith IL-1b)
Human articular chondrocytesstimulated by IL-1b
Inhibition of IL-1b-induced vascular endothelial growth factor (VEGF), MMP-3,MMP-9 and COX-2Suppression of apoptosis and inflammatory signalling by acting on NF-kB
Lei et al. 2008108 Resveratrol 100 mMID: 24 h
Rat bone marrow mesenchymalstem cells derived chondrocytesstimulated by IL-1b and cultureson chitosan-gelatinescaffolds (CGS)
Inhibition of IL-1b-induced downregulation of type II collagen and aggrecanand increased of MMP-13 expression by reducing the translocation of NF-kBSpontaneous decrease of type II collagen but no effect on aggrecan andMMP-13 expression
Garbacki et al. 2002111 Prodelphidins isolatedfrom Ribes nigrumGallocathechin trimer(CG-CG-CG), dimer(CG-CG) or monomer(CG-ECG)
1e100 mg/mlID: 5 mine12 days
Human chondrocytes Stimulation of PG and type II collagen production by all tested prodelphidinsDecreased of PGE2 synthesis by all prodelphidinsInhibition of COX-2 but not COX-1 by all prodelphidins
Sato et al. 1997 (abstract)112 Quercetin NP Human synovial cells Suppression of TNF-a mediated stimulation of IL-8 and MCP-1 expression,at least in part by inhibiting NF-kB activation
Kang et al. 2004 (abstract)113 Ventol NP Cartilage explants Inhibition of IL-1b-induced PG degradation
IkB: inhibitor of NF-kB.
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
7

Table IVSummary of the in vivo effects of the studied products on OA
Reference Product Dose and ID In vivo model Results
n-3 PUFAsLippiello et al., 1990 (abstract)22 n-3 PUFA
(menhaden fish oil)Diet with 10% menhaden fish oilID: NP
Male SpragueeDawley with a “marginallydeficient” essential fatty acid state
70% maximum decrease in articular cartilage content of thelinoleic and arachidonic acid in the fish oil treated group30e40% decrease in cartilage hexosamine content and 32%inhibition of PG synthesis
Roush et al., 201023 n-3 PUFA Diet with 31-fold increase of thetotal omego-3 fatty acidsID: 24 weeks
Client-owned dogs with OAN¼ 127
Significant improvement of dog conditions
ASUCake et al., 200028 ASU 900 mg/weekday vs placebo
ID: 6 monthsOvine model of knee OA (bilateral lateralmeniscectomy)N¼ 32
Reduction of subchondral bone sclerosis and increase of PGcontent and of articular knee joint thickness
Altinel et al., 200742 ASU 300 mg every day or every 3 daysID: 3 months
SheepdogsControl: normal dietN¼ 24
Increase of both TGF-b1 and TGF-b2 levels in knee joint fluid
Kawcak et al., 2007 41 ASU (A1:S2) NPID: 70 days
Experimentally induced OA in horsesN¼ 16
No effect on pain and lamenessReduction of the severity of cartilage erosion and synovialhaemorrhageIncrease of articular cartilage GAG synthesis
Boileau et al., 200929 ASU 10 mg/kg/dayID: 8 weeks
Experimental knee dog model Decrease of the size of the macroscopic lesions (tibialplateaus) compared to controlDecrease in the severity of cartilage lesions (tibial plateausand femoral condyles)Decrease in the scores of all histological parameters(structural changes, cellularity, Safranin-O staining andpannus invasion on the femoral condyles)No difference on the tibial plateaus for Safranin-O andpannus invasionReduction of iNOS production in cartilageReduction of the total histological changes and cellularinfiltration in synovium
CHOesser et al., 2008 (abstract)52 CH (Fortigel, Gelita AG) 0.15 mg/g of body weight daily
ID: 4 monthsMale STR/ort (model of naturally occurring OA)Control: albumin
Decrease of cartilage tissue degeneration in knee jointsDecrease of the incidence of severe joint degradation and inthe determinate grade of OA in comparison to the untreatedcontrol
Vitamin DJefferies et al., 200267 25-hydroxyvitamin D3
supplement0.1 mg/kg/dayID: 21 weeks
PigsN¼ 200Control: commercial diet
No effect on the incidence or severity of OA lesions, articularPG or collagen contents
PolyphenolsHam et al., 200496 Genistein
Soy phytoestrogenEquivalent of 129 mg/dayfor womenID: 3 years
Monkey model of naturally occurring OAafter ovariectomy
No effect on insulin-like growth factor binding protein(IGFBP)-2 and IGFBP-3, total protein, PG or collagen levels incartilage tissue
Elmali et al., 2005110 Resveratrol 10 mmol/kgIntra-articular
Rabbit model of OA by transaction of theanterior cruciate ligament
Protection against cartilage degradation (histologicalevaluation)
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
8

Table VSummary of the epidemiological data for the studied products on OA
Reference Product Population Design Results
n-3 PUFAsWang et al., 200824 Different types of
fatty acidAustralian healthymiddle-aged subjectswithout clinical knee OAMean y: 58N¼ 297
CohortY: 10
Higher intakes of monounsaturated fattyacids, total and n-6 PUFAs associated withincreased risk of bone marrow lesionsNo association of n-3 PUFA intake andbone marrow lesionsNo association of fatty acid intakewith cartilage volume of defects
Vitamin DMcAlindon et al., 199658 Vitamin dietary intake
and serum levels of 25-hydroxyvitamin D
English patientsMean y: 70.3N¼ 556
CohortY: 9e10
Modest correlation between serumvitamin D and vitamin D intakeIncreased risk of knee OA progression(global score including joint spacenarrowing, osteophytosis and sclerosis)for low levels of vitamin D andvitamin D intakeAssociation between low vitamin D serumlevels and knee loss of cartilage as assessedby joint space and osteophyte growth(disease progression)No association between vitamin D intakeand serum level of vitamin D andknee OA incidence
Lane et al., 199968 Serum levels of 25-hydroxyvitamin Dand 1,25-dihydroxyvitamin D
American elderly whitewomenY� 65N¼ 237
CohortY: 8
Association between low serum levelsof 25-hydroxyvitamin D and radiographicchanges for hip OA characterized byjoint space narrowing but not osteophyteNo association between serum 1,25-dihydroxyvitamin D and incidentchanges of radiographic hip OA
Felson et al., 200769 Serum levels of 25-hydroxyvitamin D
English adultsMean y: 53.1N¼ 715
Cohort Y: 9 No association between vitamin Dlevels and structural joint degradation(disease incidence) defined as jointspace loss on radiography
Felson et al., 200769 Serum level of 25-hydroxyvitamin D
American adults withknee OAMean y: 66.2N¼ 388
Cohort Y: 9 No association between vitamin Dlevels and structural disease worsening(disease progression) defined as joint spaceloss on radiography and as cartilage loss on MRI
Breijawi et al., 200964 Serum levels of 25-hydroxyvitamin D
Patients undergoingtotal hip or kneereplacementMean y: 69e70N¼ 117
Cross-section High prevalence of low vitamin D status inpatients with knee OA
Bergink et al., 200963 Serum levels of 25-hydroxyvitamin D
Knee OA patientsN¼ 1248
Cohort Y: 6.5(mean follow up time)
Low dietary vitamin D intake the risk ofprogression of knee OAVitamin D influences the incidence andprogression of knee OA more particularlyin low BMD patients
Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 9
oil (equivalent to 786 mg EPA) by OA patients as an adjunct toNSAIDmedicationwas not effective to improve pain and ability. Theuse of olive oil as placebo control may have introduced a bias in theresult of this study. On the contrary, the second study of lowmethodological quality (score: 4)26 showed that the consumptionof an extract of New-Zealand green-lippedmussel rich in n-3 PUFAsimproved OA symptoms, including pain and joint function inKorean OA patients.
ASU
ASU are derived from unsaponifiable residues of avocado andsoybean oils, generally mixed in the ratio one-thirdetwo-thirdsrespectively27e30. The large majority of the in vitro and in vivodata have been obtained with ASU found in Piascledine�300(Laboratoires Expanscience, France). The ASU contained inPiascledine�300 are extracted according to a patented processgiving them a particular formulation30. This formulation isconsidered as a drug in France and some of the observed beneficialeffects seem to be related to this particular formulation. In other
countries, ASU mixtures are delivered as over-the-counter prod-ucts. Therefore, extrapolation of the data obtained withPiascledine�300 to other ASU mixtures must be done with anextreme caution. The main components of ASU are the phytosterolsb-sitosterol, campesterol and stigmasterol31.
In vitro and preclinical dataOver the last 20 years, ASU have raised a great research interest.
In vitro data are abundant. Most of in vitro studies were performedwith normal or OA chondrocytes stimulated or not with IL-1b, thekey pro-inflammatory cytokine in OA physiopathology. Thesestudies demonstrated that ASU contained in Piascledine�300exerted positive effects on human chondrocytes by stimulating thesynthesis of aggrecan and extracellular matrix component as type IIcollagen31e33 and by reducing the production of catabolic (MMP-3)and pro-inflammatory (IL-8 and IL-6) mediators34. These anabolicand anti-catabolic effects were also observed in human OAchondrocytes35. What is more, this ASU mixture was able tocounteract IL-1b-induced deleterious effects on cartilage in normaland OA chondrocytes31e36. It reversed IL-1b-induced collagen

Table VISummary of the clinical data of the studied products on OA
Reference Product Dose and interventionduration (ID)
Population Design Results Score(1e14)
n-3 PUFAsStammerset al.,199225
Cod liver oil(EPA)
10 ml (786 mg EPA)/dayID: 24 weeks
English middle-ages andold patients with OAY: 49e87N¼ 86
Double-blind, placebo-controlled trial
No effect on pain and ability compared to oliveoil(Cod liver oil was used as an adjunct to NSAIDs)
7
Cho et al.,200326
Lyprinol� extract fromNew-Zealand green-lipped mussel rich inn-3 PUFAs (EDA, DHA, DPA)
four capsules/dayID: 8 weeks
Korean patients with hip orknee OAY: 40e75N¼ 60
Multicenter open trial Improvement of OA signs and symptoms (painVAS, joint function LFI)
4
ASULequesneet al.,200243
Piascledine� 300 mg (capsule)ID: 2 years
French patients withregular pain due to primaryhip OAY: 50e80N¼ 108
Prospective, multicenter,randomized, parallel group,double-blind, placebo-controlled trial
No structural effect (joint space width) (primaryoutcome)Reduction of the progression of joint space lossin the subgroup with advanced spacenarrowing (post-hoc analysis)No difference for clinical parameters (secondaryoutcomes) between ASU and placebo groups(LFI, global pain on VAS, NSAID use and patient’sglobal assessment) over the first year follow up
11.5
Appelboomet al.,200144
Piascledine� 300 or 600 mgID: 3 months
Belgian patients withprimary knee OA underanalgesics and/or NSAIDsY:45e80
Prospective multicenter,double-blind, randomized,parallel group, placebo-controlled trial
Decrease of NSAID and analgesic intake(primary outcome), compared to placebo fromthe first monthNo difference between 300 mg and 600 mgDecrease of LFI (improvement noticed from thesecond month) and pain by VAS
11
Maheuet al.,199845
Piascledine� 300 mg (capsule)ID: 6 monthsþ 2 monthpost)treatment follow up
French patients withsymptomatic primary hipor knee OAY: 45e75N¼ 164
Prospective, randomized,double-blind, placebo-controlled multicenter trial
Decrease of LFI scores (primary outcome) after 6months, compared to baseline and placebogroupsReduction of pain by VAS, overall functionaldisability and patient’s overall assessmentefficacyMore important improvement in hip OApatientsNo difference in NSAID consumption except forthe period ranging from 6 to 8 monthsBeneficial effects measured by LFI, pain by VASand functional disability started after 2 months(delayed action)Prolonged effect of ASU, persisting 2 monthsafter treatment discontinuation
14
Blotman etal., 1997(abstract)46
Piascledine� 300 mgID: 3 months
French patients withsymptomatic knee or hipOA requiring NSAIDtherapyMean y: 62.9N¼ 163
Prospective, randomized,double-blind, placebo-controlled, parallel-grouptrial
Reduction of NSAID consumption(primary outcome)Improvement of LFI compared to placeboNo difference in pain score between ASU andplacebo
CHClark et al.,200854
CH(liquid formulation)
10 g/dayID: 24 weeks
American physically activehealthy adults withoutdegenerative joint diseasebut with joint painMean y: 20.1N¼ 97
Prospective, randomized-placebo-controlled, double-blind trialControl: xanthan
Improvement of joint pain, increase of mobilityand reduction of dependency to analgesics inpatients consuming CH dietary supplement
8
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
10
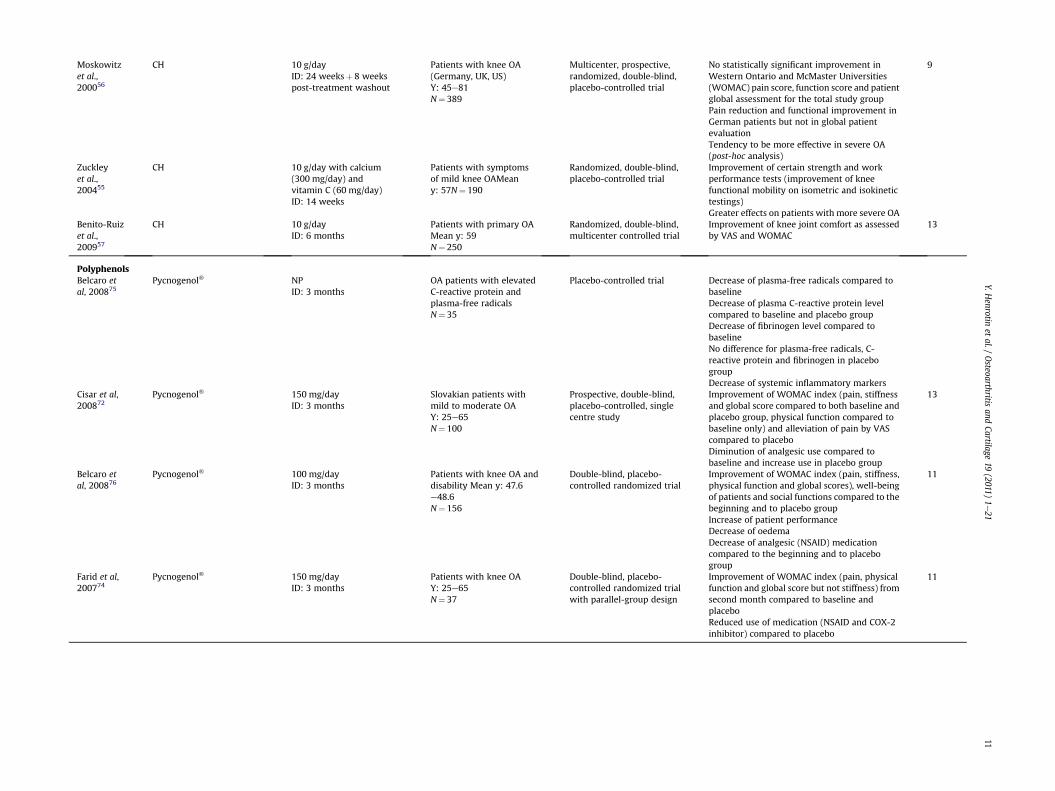
Moskowitzet al.,200056
CH 10 g/dayID: 24 weeksþ 8 weekspost-treatment washout
Patients with knee OA(Germany, UK, US)Y: 45e81N¼ 389
Multicenter, prospective,randomized, double-blind,placebo-controlled trial
No statistically significant improvement inWestern Ontario and McMaster Universities(WOMAC) pain score, function score and patientglobal assessment for the total study groupPain reduction and functional improvement inGerman patients but not in global patientevaluationTendency to be more effective in severe OA(post-hoc analysis)
9
Zuckleyet al.,200455
CH 10 g/day with calcium(300 mg/day) andvitamin C (60 mg/day)ID: 14 weeks
Patients with symptomsof mild knee OAMeany: 57N¼ 190
Randomized, double-blind,placebo-controlled trial
Improvement of certain strength and workperformance tests (improvement of kneefunctional mobility on isometric and isokinetictestings)Greater effects on patients with more severe OA
Benito-Ruizet al.,200957
CH 10 g/dayID: 6 months
Patients with primary OAMean y: 59N¼ 250
Randomized, double-blind,multicenter controlled trial
Improvement of knee joint comfort as assessedby VAS and WOMAC
13
PolyphenolsBelcaro etal, 200875
Pycnogenol� NPID: 3 months
OA patients with elevatedC-reactive protein andplasma-free radicalsN¼ 35
Placebo-controlled trial Decrease of plasma-free radicals compared tobaselineDecrease of plasma C-reactive protein levelcompared to baseline and placebo groupDecrease of fibrinogen level compared tobaselineNo difference for plasma-free radicals, C-reactive protein and fibrinogen in placebogroupDecrease of systemic inflammatory markers
Cisar et al,200872
Pycnogenol� 150 mg/dayID: 3 months
Slovakian patients withmild to moderate OAY: 25e65N¼ 100
Prospective, double-blind,placebo-controlled, singlecentre study
Improvement of WOMAC index (pain, stiffnessand global score compared to both baseline andplacebo group, physical function compared tobaseline only) and alleviation of pain by VAScompared to placeboDiminution of analgesic use compared tobaseline and increase use in placebo group
13
Belcaro etal, 200876
Pycnogenol� 100 mg/dayID: 3 months
Patients with knee OA anddisability Mean y: 47.6e48.6N¼ 156
Double-blind, placebo-controlled randomized trial
Improvement of WOMAC index (pain, stiffness,physical function and global scores), well-beingof patients and social functions compared to thebeginning and to placebo groupIncrease of patient performanceDecrease of oedemaDecrease of analgesic (NSAID) medicationcompared to the beginning and to placebogroup
11
Farid et al,200774
Pycnogenol� 150 mg/dayID: 3 months
Patients with knee OAY: 25e65N¼ 37
Double-blind, placebo-controlled randomized trialwith parallel-group design
Improvement of WOMAC index (pain, physicalfunction and global score but not stiffness) fromsecond month compared to baseline andplaceboReduced use of medication (NSAID and COX-2inhibitor) compared to placebo
11
Y.Henrotin
etal./
Osteoarthritis
andCartilage
19(2011)
1e21
11

Table VIISummary of scientific consensus on the reviewed ingredients
Ingredient Scientific consensus
n-3 PUFA Lack of evidence of efficacyASU Good evidence of efficacyCH Limited evidence of efficacy but suggestiveVitamin D Limited evidence of efficacy but suggestiveNobiletin Lack of evidence of efficacyCurcumin Preclinical evidence of efficacyGenistein Lack of evidence of efficacyEGCG Preclinical evidence of efficacyResveratrol Preclinical evidence of efficacyPycnogenol Moderate evidence of efficacyProbiotics Lack of evidence of efficacy
Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e2112
release, MMP-3, MMP-13, and PGE2 production in normal chon-drocytes31,33,34,36. It was also shown that ASU mixture contained inPiascledine�300 restored aggrecan production and inhibited MMP-3 synthesis in OA chondrocytes stimulated with IL-1b35. Other ASU
Table VIIISummary of the ongoing CTs for the studied products on OA
Product Population Design
ASU(Piascledin� 300)
Patients with hip OAAge: 45e75 yearsEnrollement: NP
Multicenter, randomized,double-blind, placebo-controlled trialDuration: 3 yearsTreatment: Piascledine�
300
CH solution10 g/day
Patients with knee OAAge: 49e90 yearsEnrollement: 30
Treatment, randomized,double-blind(subject, caregiver, investigator,outcome assessors),placebo-controlled,parallel assignment,safety-efficacy study
Vitamin D(cholecalciferol)2 000 UI/day(capsule)
Patients withsymptomatic knee OAAge: 45e90 yearsEnrollement: 146
Treatment, randomized,double-blind(subject, caregiver, investigator,outcomes assessor), parallelassignment, efficacy studyDuration: 2 yearsTreatments: vitamin D32 000 UI daily or placebo
Vitamin D(cholecalciferol)2 000 UI/day(capsule)
Patients undergoinguni-lateral total kneereplacementdue to sever OAAge: 60 yearsEnrollement: 80
Treatment, randomized,double-blind(subject, caregiver, investigator,outcomes assessor),dose comparison,parallel assignment, efficacy studyDuration: 2 yearsTreatments: vitamin D32 000 UI or 800 UI daily
Curcuma domestica1 500 mg/day (oral)divided into 3 timesfor 28 days
Patients with knee OAAge: 50e75 yearsEnrollement: 396
Treatment, randomized,double-blind(subject, outcomes assessor),active control,parallel assignment,safety/efficacy studyDuration: 28 daysTreatments: curcuma domestica oribuprofen (1 200 mg/day)
Highly bioavailableturmeric extract(Arantal�)four capsules/day
Patients with knee OAAge: 40e80 yearsEnrollement: 280
Treatment, randomized, placebo-controlled, double-blind, parallelassignment, efficacy/tolerance studyDuration: 15 daysTreatment: turmeric extract(Arantal�) or placebo
formulations produced similar effect on IL-1b, COX-2 and iNOS inLPS-stimulated chondrocytes37 and were also shown to enhancetransforming growth factor (TGF)-b production in bovine articularchondrocytes38. The ASU contained in Piascledine�300 were alsoshown to have beneficial effects on osteoblasts and synoviocytes.Indeed, this compound prevented inhibitory effect of osteoblasts onchondrocyte matrix component synthesis39 and reversed IL-1b-induced collagenase production by synoviocytes33.
Four in vivo studies with ASU were identified. They were per-formed in four different animal models of OA and they all supportthe beneficial effect of Piascledine�300 in OA. Piascledine�300treatment prevents cartilage degradation (decrease in cartilagelesion severity, increase in cartilage thickness) by stimulatingmatrix component production as glycosaminoglycans (GAG) andPGs content in experimental models27,28,40. In addition, one in vivostudy in dogs without any diagnosed joint disease suggests aneffect of ASU by increasing growth factors (TGF-b1 and 2) involvedin extracellular matrix synthesis41. All these preclinical studiesstrongly support anti-OA properties for ASU mixtures.
Primary outcome measure Sponsor Stage
Effect of treatment on jointspace narrowingevaluated on X-ray
Laboratoires Expanscience Completed
Effect of collagen hydrolysison knee cartilage measuredby MRI
GELITA Completed
Cartilage volume loss (MRI)Knee symptoms (WOMAC)
National Institute of Arthritisand Musculoskeletal and SkinDiseases (NIAMS)Office of Dietary Supplement(ODS)
Ongoing,notrecruiting
Pain and function of theoperated and non-operatedkneeRate of falls
University of ZurichHarvard School of PublicHealthTufts UniversityBoston University
Recruiting
Change in mean WOMACpain scale
Mahidol UniversityNational research Council ofThailand
Not yetopen forpatientrecruitment
Pain assessment using VAS Bioxtract S.A.NuKleus
Recruiting

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 13
Clinical dataThe results of four CTs, all double-blind placebo-controlled and
randomized, were published and identified in the literature.All of these studies used the same pharmaceutical product,Piascledine�300, which is under drug authorization (AMM). All ofthem investigated the beneficial effects of Piascledine�300 onpatients with symptomatic OA. All of them were conducted inpatients with primary knee or hip OA and were by the way focusingon OA treatment. OA outcomes were NSAID/analgesics medicationreplacement, pain, function and structural changes (joint space nar-rowing). They studied the potential of symptom-modifying effect ofPiascledine�300 and one of them was interested in the structure-modifying effect of ASU. Three out of the four evaluated studies wereof good methodological quality (Lequesne et al, 200242, score: 11.5;Appelboom et al, 200143, score: 11; Maheu et al, 199844, score: 14).
The only one study assessing efficacy of Piascledine�300 inmodifying articular structure failed to show any structural effect inpatientswithhipOA in spite of its longduration (2 years)42. However,a subgroup analysis suggested an effect in patients with the mostsevere hip OA, supporting further studies in this population group.
Data suggested that Piascledine�300 decreased NSAID/anal-gesic intake in the medium term (3e6 months) for patients withhip or knee OA43e45. However, the only long-term study (2 years)did not show any effect of Piascledine�300 on the NSAIDconsumption in patients with hip OA42. Nevertheless, the later wasdesigned to detect radiographic changes more than to study thechanges in symptoms. This could explain the fact that no differencewas observed on clinical parameters (function, pain and NSAIDsconsumption). In contrast, data regarding pain and patient’s globalassessment are more conflicting42e45. Piascledine�300 treatmentseemed to improve patient’s function assessed by LFI (LequesneFunctional Index) or VAS (Visual Analog Scale)43e45.
A recent meta-analysis evaluating these four clinical studiesconcluded Piascledine�300 was efficient for reducing pain andimproving function in OA46.
Collagen hydrosylates (CHs)
CH is obtained by the enzymatic hydrolysis of collagenoustissues (bone, hide or hide split) form mammals. The main char-acteristic of CH is its amino acid composition, which is identical totype II collagen, thus providing high levels of glycine and proline,two amino acids essential for the stability and regeneration ofcartilage47. This product is generally recognized as a safe foodingredient by regulatory agencies. CH is well digested and is pref-erentially accumulated in cartilage48. Although clinical use of CH isassociated with minimal adverse effects, some gastro-intestinalside effects, as fullness and unpleasant taste, have been described.
In most studies, CH was administered alone in a water solution.However, it seems that CH is well absorbed and digested in otherfood matrix, such as fermented milk47.
In vitro and preclinical dataFew preclinical data on the effect of CH on OAwere identified in
the literature. The search retrieved only one in vitro study assessingthe stimulation of articular cartilage matrix by CH in culturedbovine chondrocytes49. This study demonstrated the stimulatorypotency of CH on type II collagen and PG synthesis, as well asaggrecan expression by chondrocytes. This result was also reportedin a scientific communication on CH effect in porcine chon-drocytes50. In addition, an in vivo study with STR/ort mice whichspontaneously developed OA51 has shown that long-term CHsupplementation may decrease OA cartilage degeneration anddelay the progression of OA. These results are in favor of a disease-modifying effect of CH and its potential efficacy in OA. The
chondroprotective effect of CH was also confirmed in an otherstudy investigating both in vitro and in vivo effect in mice52. CH wasdemonstrated to protect cartilage against degradation induced byphosphorus injection. The same study showed that CH preventedchondrocyte differentiation into mineralized chondrocytes.
Clinical dataOnly three relevant CTs were identified in the literature. The first
study investigated the effect of CH supplementation in healthyadult without degenerative joint disease but with joint pain. Thisstudy of medium methodological quality (score: 8)53 showed thatCH dietary supplement can improve joint pain, mobility and reduceanalgesic medication in healthy active adults without degenerativejoint disease. The CH supplementation can then improve kneefunction during joint-stressing activities. These observations werealso reported in a scientific communication54 in patients withsymptomatic mild OA patients. The second report of mediummethodological quality (score: 9)55 mentioned a better effect of CHcompared to placebo in severe OA patients than in the overallstudied population. More recently, in another relevant CT of verygood methodological quality (score: 13), the joint functionimprovement after CH treatment was shown in patients withprimary OA56.
Vitamin D
OA was traditionally considered as a cartilage disease, charac-terized by cartilage degeneration. But many evidences, as osteo-phytosis, subchondral bone sclerosis and cyst formation havegrown up and demonstrated the prominent role played by sub-chondral bone in OA pathophysiology57. Some studies even indicatethat bone alteration could precede cartilage changes58. But whetherbone abnormalities, such as bone sclerosis, initiate or are simplyinvolved in the progression of cartilage degradation is underdiscussion59e61.
Normal bonemetabolism depends on the presence of vitamin D,a compound derived mostly from cutaneous exposure to ultravioletand from the diet in a lesser extent. Suboptimal levels of vitamin Dmay have adverse effects on calcium metabolism, osteoblasticactivity, matrix ossification and bone density. Low serum levels ofvitamin D may increase the progression of knee OA62 and mayimpair the ability of bone to respond optimally to OA pathophysi-ologic processes and may predispose patients to joint degrada-tion57. High prevalence of low vitamin D status has beendemonstrated in persons with knee OA63. Moreover, in low bonemineral density (BMD) patient, the level of vitamin D seemed toinfluence the incidence and progression of the disease62. Somestudies have consequently investigated the relationship betweenvitamin D and OA. The main drawback is that they are all obser-vational. Most of them have looked at the association of vitamin Dserum level rather than vitamin D intake with OA.
In vitro and preclinical dataThree in vitro studies investigating the role of 1,25-dihydroxy-
vitamin D3 in the pathophysiology of OA are available59,64,65. Thesestudies used different cell models: synovial fibroblasts, chon-drocytes or osteoblasts. Data showed that 1,25-dihydroxyvitaminD3 had no inhibitory effect on articular catabolic enzymes and ona potent pro-inflammatory mediators but rather upregulatedcatabolic enzymes (MMP-1 and -3) in human articular chon-drocytes64, 65. Interestingly, 1,25-dihydroxyvitamin D3 exertsa positive effect on rheumatoid synovial fibroblasts by reducingMMP and PGE2 production65. In addition, 1,25-dihydroxyvitaminD3-induced osteocalcin production appears to be increased in OAosteoblasts compared to healthy one, which can cause an increase

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e2114
in bone metabolism resulting in bone sclerosis and osteophyteformation59.
Only one in vivo study was identified. This study evaluated theimpact of a supplementation of vitamin D3 (25-hydroxyvitaminD3) on OA in pigs66. The supplementation revealed no effect on theincidence or the severity of OA lesions, articular PG and collagencontent.
Clinical dataThemajority of available evidence on the efficacy of vitamin D in
the treatment or in the prevention of OA comes from epidemio-logical data. Most of them investigated the relationship betweenvitamin D serum levels and joint structure parameters (joint spacenarrowing, osteophytes, cartilage loss and volume). A total of fourstudies have assessed this relationship57,67,68 and only one hasinvestigated the association of vitamin D intake and OA57. Thisstudy revealed that low levels of vitamin D intake are related to anincreased risk of OA progression but no correlation was made withOA incidence. Interestingly, in this study, vitamin D intakemodestlycorrelatedwith vitamin D serum levels. In addition, one other studywas found to evaluate the prevalence of vitamin D deficiency inindividuals with OA63. This study revealed a high prevalence of lowvitamin D status in patients with knee OA. The other studiesinvestigating the association between vitamin D serum level (25-vitamin D) and joint structure parameters gave inconsistent data.Two of them showed a relationship between vitamin D serum leveland OA parameters such as joint space narrowing and/or cartilagevolume in the knee or hip joint67,69. An other study did not showany association between vitamin D serum level and joint space lossin hip OA patients68. This difference could be explained by the factthat the population of this study was younger than the populationof the other two. However no linear associationwas foundwhen OAwas assessed with a structural global score57,70. These studiessuggested a U-shaped relationship. Serum Vitamin D level isreported to be predictive of knee OA, when measured by quartileswith the lowest risk in the middle quartile70.
Polyphenols
Research on the effect of dietary polyphenols on human healthhas developed considerably in the past 10 years. The resultsstrongly support the role of polyphenols in the prevention ofdegenerative diseases. The anti-oxidant properties of polyphenolshave been widely studied, but it has become clear that the mech-anisms of action go beyond the modulation of oxidative stress.Some researchers have investigated the potential effect of somepolyphenols in OA. Only pine bark extract-Pycnogenol� has beentested in CTs.
Pine bark extract-Pycnogenol�
Pycnogenol� is a special standardized extract from the bark ofthe French maritime pine (Pinus pinaster). This extract representsa concentrate of polyphenols, containing several phenolic acids,catechin, taxifolin and procyanidins with various biological andclinical effects71. No-preclinical or in vitro data were found forPycnogenol� and OA. However, the anti-oxidant and anti-inflam-matory profile of Pycnogenol� and its inhibitory effect on MMPsand iNOS are well documented in conditions other than OA72,73.
The symptom-modifying effect of Pycnogenol� has been rela-tively well documented in OA patients. The search retrieved fourCTs 71,73e75. They assessed the impact of Pycnogenol� in patientswith knee OA in a medium term (3 months). These studies indicatethat the daily intake of 150 mg of Pycnogenol� alleviated OAsymptoms. All studies showed that Pycnogenol� was effective in
reducing NSAIDs or COX-2 inhibitor medication, suggesting thatPycnogenol� could be used as an effective adjuvant treatment. Datastrongly support the pain-alleviating effect of Pycnogenol�. Despitesome discordant results, physical function and stiffness seem to beimproved by intake of Pycnogenol� in OA subjects. All these studiesare of good to very good quality (Farid et al, 200773 and Belcaro et al,200875, score: 11; Cisar et al, 200871, score: 13).
Nobiletin
Nobiletin is a citrus polymethoxyflavone which was proven tohave pharmacological actions as anti-inflammatory, anti-tumorproliferation and anti-tumor invasion and metastasis in vitro and invivo76. This product has been exclusively studied in vitro in synovialfibroblasts and in articular chondrocytes. Nobiletin was able toinhibit the production of catabolic factors (MMP-3 and -9,ADAMTS-4 and 5) and of mediators of inflammation (PGE2) inrabbit and human synovial fibroblasts76e78. Nobiletin was alsoshowed to activate the MMP inhibitor (TIMP-1)78. This inhibitorypotential was also demonstrated in rabbit articular chondrocytes77.Nobiletin demonstrated a potential to inhibit cartilage degradation.This chondroprotective potency should be further documented.
Curcumin
Curcumin (diferuloylmethane) is the major component ofturmeric, a yellow spice derived from the plant Curcuma longa anda potent anti-oxidant. It has been extensively investigated due to itsanti-tumor, anti-oxidant and anti-inflammatory and analgesicproperties. We have recently reviewed the biological activities ofcurcumin79. The anti-OA potential of curcumin has been widelystudied in vitro. Twelve studies were found. Theywere all carried outin chondrocytes or on articular cartilage explants. Curcuminwas ableto downregulate catabolic and degradative effect observed in carti-lage explants or chondrocytes stimulated with IL-1b, LPS or tumornecrosis factor (TNF). Curcumin inhibited the production of MMP-3,-9 and -1380e82 and restored type II collagen andGAG synthesis81e85.Curcuminpositive effectonGAGreleasewasconfirmed86. Inaddition,curcumin demonstrated potent anti-inflammatory properties byinhibiting key inflammatory mediators (IL-6, IL-8, PGE2, NO) andenzymes (COX-2 and iNOS)87e90 and anti-catabolic properties byinhibitingMMP-3 synthesis89. Curcumin has also demonstrated anti-apoptotic activity on chondrocytes83 and growth-inhibitory and pro-apoptotic effects on synovial adherent cells, which are the mainsource of inflammatory mediators and other mediators of cartilagedegradation, all of them playing key role in the pathogenesis ofarthritis91. This is important to note that one study has reporteda toxic effect of curcumin used at high dosage (50 mM) without anybeneficial effect in cartilage matrix84. This study was performed ina novel immortalized human OA chondrocytes model, which canexplain the discordance with previous studies.
No clinical data are available for the effect of curcumin in OA.However, one study tested the clinical efficacy of a herbomineralformulation containing a component rich in curcumin in subjectswith OA in a randomized, double-blind, placebo-controlled, cross-over study92. Positive results in pain management and mobilitywere obtained in the treated group. Curcumin in OA is a currentresearch interest.
Genistein
Genistein is one of the several known isoflavones and is found insoybeans and soy products. Genistein is considered as a phytoes-trogen. Clinical observations have suggested a relationshipbetween OA and a changed estrogen metabolism in menopausal

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 15
women. Moreover phytoestrogens have been shown to amelioratevarious menopausal symptoms93. The effect of phytoestrogens,including genistein, has been studied on articular cartilage matrixmetabolism and inflammation. Nevertheless, the data for genisteinand OA are limited. The in vitro and preclinical data are notconsistent to support a beneficial effect of genistein on articularcartilage. Genistein does not affect cartilage metabolism93,94 butcould have an anti-inflammatory effect by suppressing COX-2 butnot NO production94. In addition, the consumption of an extract ofsoy phytoestrogen in animal failed to modify cartilage metabolismin ovariectomised monkey95. Additional experiments are needed toclarify the potential benefit of genistein in articular cartilagemetabolism.
Epigallocatechin-3-Gallate (EGCG)
EGCG is amajor component of the polyphenolic fraction of greentea and exhibits anti-oxidant, anti-tumor and anti-mutagenicactivities. The in vitro effect of EGCG iswell documented.Most of theavailabledata onEGCGandOAcome fromexperimentsperformed invitro in human chondrocytes looking at the anti-inflammatoryeffectof EGCG. Data suggest that EGCG exerts an anti-inflammatory effecton OA chondrocytes by inhibiting the production of key inflamma-tory mediators (NO, PGE2, COX-2 and iNOS)96e98. This anti-inflam-matory effect has also been observed in osteoblasts by the inhibitionof IL-699 and synovial fibroblasts by the inhibition of COX-2expression and synthesis and by the inhibition of PGE2 and IL-8secretion100. Additional anti-inflammatory and anti-cataboliceffects have been demonstrated for EGCG in human chondrocytes.Indeed, EGCG can inhibit the TNF-a and MMP-13 productioninduced by advanced glycation end products (AGEs) which areresponsible for cartilage mechanical properties loss101. This effectcould happen through the attenuation ofMAP kinase activation andinhibition of nuclear factor kB (NF-kB) activation. This is supportedby the previous report of anti-catabolic activity and inhibitory effectonNF-kBandAP-1 signalling102. Finally, this is of interest tonote thatthe polyphenolic fraction of green tea can prevent the onset ofarthritis and the severity of the disease in mice collagen-inducedarthritis103. Complementary experiments are necessary in order toconfirm the anti-inflammatory effect of EGCG on OA in vivo.
Resveratrol
Resveratrol is a stilbene that is naturally present at highconcentration in grape skin and red wine. It has significant anti-inflammatory and anti-oxidant properties which could be benefi-cial in OA104. Only in vitro studies were identified for thiscompound. A total of five studies were performed in cartilageexplants and chondrocytes85,104e107. These studies indicated thatresveratrol can have beneficial effects. It has demonstrated anti-inflammatory and anti-apoptotic properties104,106. Resveratrolinhibited catabolic factors as MMPs and pro-inflammatory media-tors as PGE2 and COX-2, and stimulated the synthesis of matrixcomponents (PG, GAG, type II collagen)104,106,107. These effects couldprevent cartilage degradation. In addition, cartilage protection maybe achieved with intra-articular injection of resveratrol. This wasobserved both in anterior cruciate ligament transaction OA modeland LPS-induced arthritis model in rabbit108,109. These preclinicalevaluations indicate an interesting potential of resveratrol in OAbut additional in vivo studies are needed.
Prodelphinidins
Prodelphinidins are a type of condensed tannins and arecomposed of gallocatechin and epigallocathechin110. Only one in
vitro study has investigated the effect of prodelphinidins. This studyshowed potential in vitro effects on human chondrocytes. Prodel-phinidins seemed to increase PG and type II collagen and inhibitedPGE2 synthesis by acting on COX-2110. These data are in favor ofadditional preclinical evaluations.
Quercetin
Quercetin is a plant-derived flavonoid. Anti-inflammatory andanti-oxidant properties have been suggested for this nutraceutical.Only one in vitro study in human synovial cells has been identi-fied111. This study demonstrated potential anti-inflammatory effectby the inhibition of TNF-a mediated-IL-8 and monocyte chemo-attractant protein-1 (MCP-1) expression. This suggested a potentialanti-arthritic effect but further preclinical investigations areneeded especially in OA.
Ventol
Ventol is a phlorotannin-rich natural agent derived from Eck-lonia cava with anti-oxidant and anti-inflammatory activities112.One in vitro study on cartilage explants has shown the inhibition ofPG degradation after IL-1a stimulation. This should be furtherstudied to confirm the anti-OA potential of this compound.
Discussion
OA is a debiliting chronic disease with a serious need of alter-native treatments that could help patients to preserve their jointfunction and therefore maintain a certain quality of life. We havehere summarized most of the published effects of some nutra-ceuticals. Many results have been highlighted and the quality of thestudies addressed.
Globally, we can conclude to a lack of evidence for most of thestudied compounds. The review by Ameye and Chee6 has alsoanalyzed the available studies at that time for ASU, n-3 PUFAs andCH. The same conclusions as ours were made, meaning that thereare no strong clinical data available. So, there is a need for addi-tional preclinical studies and CTs of good quality. In addition, this isimportant to note that the potencies demonstrated in preclinicalstudies for most compounds are not concordant with their clinicalefficacy. This could be explained by the doses used in vitro and inanimal models that are most of the time higher that the ones usedin CTs. An other explanation could come from the fact thatpreclinical studies deal most of the time with early stages of thedisease whereas CTs involve patients at later stages. This can justifythe discordance between preclinical data and clinical and epide-miological observations.
Many efforts have been carried out to find a cure for OA. OAmanagement is a challenge for physicians and rheumatologists.Many alternatives are now available but recommendations have tobe done. Nutraceuticals is one of these alternatives. They have greatpotential in OA but there is a need of strongly substantiated data.
Many questions still remain to be addressed. Where should bethe line between food and drugs drawn? This issue is well illus-trated by ASU mixture. ASU are considered as prescribed drugs inFrance, but as food supplement in other countries. The prescribeddrug, Piascledine�300, is now recommended for the treatment ofOA symptoms. These recommendations are based on strong clinicalevidence. However, in vitro studies have demonstrated that some ofthe beneficial effects of Piascledine�300 were related to itsparticular formulation resulting of a patented extraction process,and were not observed with other formulation (personal commu-nication). This extraction process is responsible for specific changesin the unsaponifiable fractions of avocado and soybean that could

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e2116
explain their particular effects. This means that the natural foodingredient has underwent some modifications that are related toparticular biological effects. Therefore, ASU should be chemicallyanalyzed before to be considered as a food supplement or a nutra-ceutical. Nutraceutical is a broad term to qualify any productderived from food source that provides extra health benefits. Thisdefinition fails to precise whether a modified product derived fromfood source can be considered as a nutraceutical. The line betweena nutraceutical and a drug is thin. Other criterion that can help todistinguish between a drug, food supplement, and nutraceuticalsare the oral dose administrated and the bioavailability. Foodsupplement should be administrated at concentration found in thenormal diet. Bioavailability would be a great criterion to demon-strate the potent efficacy of a product. For example, the pharma-cokinetic of curcumin has been studied113 and many parametersthat are opposed to curcumin efficacy have been described. Inhuman, the serum concentrations of curcumin after an oral massivedose of 4, 6 or 8 g/day reach 0.5, 0.6 and 1.8 mM respectively. Theseconcentrations are below the concentration showing a biologicalactivity in vitro. However, new formulation of curcumin114 hasenhanced cellular uptake, increased bioactivity in vitro andimproved bioavailability in vivo. This is in favor of a better efficacy,meaning that the anti-inflammatory and other potencies of cur-cumin could be even more effective. Curcumin would become bythe way a potent anti-inflammatory agent. For this reason, a clinicalstudy has been initiated with complexed curcumin in patients withknee OA. This complexed curcumin (Arantal�) showed a 7000times increased solubility. Can it be considered as a food supple-ment any longer? This critical point can also be illustrated byresveratrol. The pharmacokinetic of resveratrol can be modified bythe addition of glycosyl groups that improved its absorption115. Thisprocess could be applied to other polyphenols to increase theirbioavailability.
Can nutraceuticals still be considered as food supplement whenused under drug formulation? These modifications should also becontrolled and regulated. Moreover, food nutrients can targetmultiple pathways compared to monomodal mode of action ofdrugs. For example, some natural anti-oxidant peptides have alsobeen identified in porcine CH116. CH has hypotensive potential117,118.This is an additional advantage for the use of CH. Moreover, it hasrecently been demonstrated that some nutraceuticals are evenmore effective when used in combination. It has been shown forEGCG and ASU119 and resveratrol and curcumin120. Safety andtoxicity of nutraceuticals added alone or in combination should alsobe addressed, especially if bioavailability and biological activity areincreased. Pharmacokinetic of all these compounds should bedescribed and safety monitoring should be done.
For these reasons, the safety and effectiveness of these productsare under strict regulation in Europe. The problem is that thecriterion of evaluation for clinical studies are defined as for phar-maceutic standards and this penalizes foods in terms of effect sizeand also of absence of acute effect. OA as a chronic disease hasa long time window for intervention and should benefit fromfunctional food alternatives to pharmacological interventions toimprove subjects’ quality of life day after day.
We have also searched for the ongoing CTs with nutraceuticals.They are all summarized on Table VIII and given an overview of thecurrent research interest on the selected ingredients. The numberof ongoing trials supports the growing interest to identify their rolein OA treatment. Two CTs are ongoing in order to evaluate theefficacy of vitamin D supplementation on pain, mobility and jointstructure in OA patients. Because of their high quality (long dura-tion and strong study design) these results will be valuable for thedetermination of the role that could play vitamin D supplementa-tion in OA. More evidences are needed regarding the role that it
could play in the prevention of OA. Two CTs are ongoing on cur-cumin to determine whether the consumption of a plant extractwith high curcumin content alleviates pain in subjects with OA.Furthermore, one CT was just completed with CH. It was the firstone interested in the structure-modifying effect of the studiedcompound. The results are not yet available. Additional CTs shouldassess the potential of nutraceuticals in a long-term use in OA andshould also be interested in their structure-modifying effect whichis the great challenge in seeking new OA treatment.
We have shown here that most of the studied compounds couldhave beneficial effects in the treatment of OA, even if we still needmore evidence. They could represent great alternatives for OAmanagement. We have only detailed here the information for a fewcompounds but others can also represent great potential. Indeed,other lipids, vitamins, minerals or plant extracts have also beendemonstrated to be effective in OA. Probiotics could also beconsidered for the treatment of OA. Several studies havehighlighted the importance of intestinal flora in inflammatoryauto-immune diseases, such as rheumatoid arthritis. Beneficialanti-inflammatory properties and modulatory effect of immuneresponse of probiotics on rheumatoid arthritis were demonstratedin animals121e123. In addition, the consumption of lactobacilli con-tained in a yogurt demonstrated the preventive and curative effectson T-cell-dependent experimental arthritis by reducing theintensity of inflammation and joint destruction in animals124. In thesame way, CTs have evaluated the effects of probiotics on theactivity and on the symptoms of rheumatoid arthritis125,126. Thepositive findings of these studies suggested the need of comple-mentary studies on the effects on probiotic bacteria in rheumatoidarthritis. There is a lack of data on the effect of probiotics on OA inthe literature. The potential effect of probiotics on OA has not beenextensively studied but the data on their effect in arthritis suggestthat they could have a potential interest in OA.
Conclusion
We have gathered here all the studies and CTs about somenutraceuticals. Some results are really promising and encouraging.The main concern remains the quality of studies. There is a need ofserious and well designed studies that could answer most of thequestions regarding the safety and efficacy of such compounds. Thiscould help their recommendation for OA treatment.
Many studies have been carried out in order to highlight thepotency of several nutraceuticals for the treatment of OA. Nutra-ceuticals offer a large variety of products with a wide range ofeffects. They open new and large horizons for the treatment ofchronic disease as OA. Clinical endpoints for foods should bereconsidered. Further investigations are needed but nutraceuticalsare not negligible for OA management. They should be consideredas potent adjuvant treatments with NSAIDs for example. Earlymarkers development would also enable to build preventionstrategies for food, in absence of cure treatment for OA.
Author contributions
Conception and design of the study: YH, EC.Acquisition of data: CL, DC, CR.Analysis and interpretation of data: YH, EC, CL, DC, CR.Preparation of manuscript: YH, EC, DC.Final approval of manuscript: YH, CL, DC, CR, EC.
Conflict of interestYH is a consultant for BioXtract and Danone. He is also the coor-dinator of the CTs on curcuma operated by BioXtract. (Arantal�;NCT00992004). Naturalpha was financed by Danone to set-up

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 17
scoring methodology, perform the identification, selection andscoring of relevant studies for the review. Other authors declare noconflict of interest.
Acknowledgments
The authors would like to thank Eric Chappuis and AdelinePierre for their active role in the quality assessment methodologyset-up and for performing the literature search.
References
1. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD,Arden N, et al. OARSI recommendations for the managementof hip and knee osteoarthritis, Part II: OARSI evidence-based,expert consensus guidelines. Osteoarthritis Cartilage2008;16:137e62.
2. Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW,Dieppe P, et al. EULAR Recommendations 2003: an evidencebased approach to the management of knee osteoarthritis:report of a Task Force of the Standing Committee for Inter-national Clinical Studies Including Therapeutic Trials (ESCI-SIT). Ann Rheum Dis 2003;62:1145e55.
3. Zhang W, Doherty M, Arden N, Bannwarth B, Bijlsma J,Gunther KP, et al. EULAR evidence based recommendationsfor the management of hip osteoarthritis: report of a taskforce of the EULAR Standing Committee for InternationalClinical Studies Including Therapeutics (ESCISIT). Ann RheumDis 2005;64:669e81.
4. American College of Rheumatology Subcommittee on Oste-oarthritis G. Recommendations for the medical managementof osteoarthritis of the hip and knee: 2000 update. ArthritisRheum 2000;43:1905e15.
5. Zhang W, Nuki G, Moskowitz RW, Abramson S, Altman RD,Arden NK, et al. OARSI recommendations for the managementof hip and knee osteoarthritis Part III: changes in evidencefollowing systematic cumulative update of research publishedthrough. Osteoarthritis Cartilage 2010;18(4):476e99.
6. Ameye LG, Chee WS. Osteoarthritis and nutrition. Fromnutraceuticals to functional foods: a systematic review of thescientific evidence. Arthritis Res Ther 2006;8. R127.
7. Kalra EK. Nutraceuticaledefinition and introduction. AAPSPharmSci 2003;5. E25.
8. Hochberg MC, Clegg DO. Potential effects of chondroitinsulfate on joint swelling: a GAIT report. Osteoarthritis Carti-lage 2008;16(Suppl 3):S22e4.
9. Lee YH, Woo JH, Choi SJ, Ji JD, Song GG. Effect of glucosamineor chondroitin sulfate on the osteoarthritis progression:a meta-analysis. Rheumatol Int 2010;30:357e63.
10. Vangsness Jr CT, Spiker W, Erickson J. A review of evidence-based medicine for glucosamine and chondroitin sulfate usein knee osteoarthritis. Arthroscopy 2009;25:86e94.
11. Huskisson EC. Glucosamine and chondroitin for osteoar-thritis. J Int Med Res 2008;36:1161e79.
12. Scarpellini M, Lurati A, Vignati G, Marrazza MG, Telese F,Re K, et al. Biomarkers, type II collagen, glucosamine andchondroitin sulfate in osteoarthritis follow-up: the “Magentaosteoarthritis study”. J Orthop Traumatol 2008;9:81e7.
13. Sawitzke AD, Shi H, Finco MF, Dunlop DD, Bingham 3rd CO,Harris CL, et al. The effect of glucosamine and/or chondroitinsulfate on the progression of knee osteoarthritis: a reportfrom the glucosamine/chondroitin arthritis intervention trial.Arthritis Rheum 2008;58:3183e91.
14. Bornhoft G, Maxion-Bergemann S, Wolf U, Kienle GS,Michalsen A, Vollmar HC, et al. Checklist for the qualitative
evaluation of clinical studies with particular focus on externalvalidity and model validity. BMC Med Res Methodol2006;6:56.
15. Schneeman B. FDA’s review of scientific evidence for healthclaims. J Nutr 2007;137:493e4.
16. Calder PC, Yaqoob P. Omega-3 polyunsaturated fatty acidsand human health outcomes. Biofactors 2009;35:266e72.
17. Darlington LG, Stone TW. Antioxidants and fatty acids in theamelioration of rheumatoid arthritis and related disorders.Br J Nutr 2001;85:251e69.
18. Curtis CL, Hughes CE, Flannery CR, Little CB, Harwood JL,Caterson B. n-3 fatty acids specifically modulate catabolicfactors involved in articular cartilage degradation. J BiolChem 2000;275:721e4.
19. Curtis CL, Rees SG, Cramp J, Flannery CR, Hughes CE, Little CB,et al. Effects of n-3 fatty acids on cartilage metabolism. ProcNutr Soc 2002;61:381e9.
20. Curtis CL, Rees SG, Little CB, Flannery CR, Hughes CE,Wilson C, et al. Pathologic indicators of degradation andinflammation in human osteoarthritic cartilage are abrogatedby exposure to n-3 fatty acids. Arthritis Rheum2002;46:1544e53.
21. Zainal Z, Longman AJ, Hurst S, Duggan K, Caterson B,Hughes CE, et al. Relative efficacies of omega-3 poly-unsaturated fatty acids in reducing expression of key proteinsin a model system for studying osteoarthritis. OsteoarthritisCartilage 2009;17:896e905.
22. Lippiello L, Fienhold M, Grandjean C. Metabolic and ultra-structural changes in articular cartilage of rats fed dietarysupplements of omega-3 fatty acids. Arthritis Rheum1990;33:1029e36.
23. Roush JK, Dodd CE, Fritsch DA, Allen TA, Jewell DE,Schoenherr WD, et al. Multicenter veterinary practiceassessment of the effects of omega-3 fatty acids on osteoar-thritis in dogs. J Am Vet Med Assoc 2010;236:59e66.
24. Wang Y, Wluka AE, Hodge AM, English DR, Giles GG,O’Sullivan R, et al. Effect of fatty acids on bone marrowlesions and knee cartilage in healthy, middle-aged subjectswithout clinical knee osteoarthritis. Osteoarthritis Cartilage2008;16:579e83.
25. Stammers T, Sibbald B, Freeling P. Efficacy of cod liver oil asan adjunct to non-steroidal anti-inflammatory drug treat-ment in the management of osteoarthritis in general practice.Ann Rheum Dis 1992;51:128e9.
26. Cho SH, Jung YB, Seong SC, Park HB, Byun KY, Lee DC, et al.Clinical efficacy and safety of Lyprinol, a patented extractfrom New Zealand green-lipped mussel (Perna Canaliculus) inpatients with osteoarthritis of the hip and knee: a multi-center 2-month clinical trial. Eur Ann Allergy Clin Immunol2003;35:212e6.
27. Cake MA, Read RA, Guillou B, Ghosh P. Modification ofarticular cartilage and subchondral bone pathology in anovine meniscectomy model of osteoarthritis by avocado andsoya unsaponifiables (ASU). Osteoarthritis Cartilage 2000;8:404e11.
28. Boileau C, Martel-Pelletier J, Caron C, Cheng S, Msika P,Guillou GB, et al. Protective effects of total fraction ofavocado/soybean unsaponifiables (ASU) on the structuralchanges in experimental dog osteoarthritis: inhibition ofnitric oxide synthase and MMP-13. Arthritis Res Ther2009;11. R41 doi10.1186/ar2649.
29. Msika P, Baudouin C, Saunois A, Bauer T. Avocado/soybeanunsaponifiables, ASU EXPANSCIENCEtrade mark, are strictlydifferent from the nutraceutical products claiming ASUappellation. Osteoarthritis Cartilage 2008;16(10):1275e6.

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e2118
30. Henrotin Y. Avocado/soybean unsaponifiable (ASU) to treatosteoarthritis: a clarification. Osteoarthritis Cartilage2008;16:1118e9. author reply 1120.
31. Lippiello L, Nardo JV, Harlan R, Chiou T. Metabolic effects ofavocado/soy unsaponifiables on articular chondrocytes. EvidBased Complement Alternat Med 2008;5:191e7.
32. Mauviel A, Daireaux M, Hartmann DJ, Galera P, Loyau G,Pujol JP. Effects of unsaponifiable extracts of avocado/soybeans (PIAS) on the production of collagen by cultures ofsynoviocytes, articular chondrocytes and skin fibroblasts. RevRhum Mal Osteoartic 1989;56:207e11.
33. Mauviel A, Loyau G, Pujol JP. Effect of unsaponifiable extractsof avocado and soybean (Piascledine) on the collagenolyticaction of cultures of human rheumatoid synoviocytes andrabbit articular chondrocytes treated with interleukin-1. RevRhum Mal Osteoartic 1991;58:241e5.
34. Henrotin Y, Labasse A, Jaspar JM, De Groote D, Zheng SX,Guillou B, et al. Effects of three avocado/soybean unsaponi-fiable mixtures on metalloproteinases, cytokines and pros-taglandin E2 production by human articular chondrocytes.Clin Rheumatol 1998;17:31e9.
35. Henrotin YE, Sanchez C, Deberg MA, Piccardi N, Guillou GB,Msika P, et al. Avocado/soybean unsaponifiables increaseaggrecan synthesis and reduce catabolic and proin-flammatory mediator production by human osteoarthriticchondrocytes. J Rheumatol 2003;30:1825e34.
36. Gabay O, Gosset M, Levy A, Salvat C, Sanchez C, Pigenet A,et al. Stress-induced signaling pathways in hyalin chon-drocytes: inhibition by Avocado-Soybean Unsaponifiables(ASU). Osteoarthritis Cartilage 2008;16:373e84.
37. Au RY, Al-Talib TK, Au AY, Phan PV, Frondoza CG. Avocadosoybean unsaponifiables (ASU) suppress TNF-alpha, IL-1beta, COX-2, iNOS gene expression, and prostaglandin E2and nitric oxide production in articular chondrocytesand monocyte/macrophages. Osteoarthritis Cartilage2007;15:1249e55.
38. Boumediene K, Felisaz N, Bogdanowicz P, Galera P,Guillou GB, Pujol JP. Avocado/soya unsaponifiables enhancethe expression of transforming growth factor beta1 andbeta2 in cultured articular chondrocytes. Arthritis Rheum1999;42:148e56.
39. Henrotin YE, Deberg MA, Crielaard JM, Piccardi N, Msika P,Sanchez C. Avocado/soybean unsaponifiables prevent theinhibitory effect of osteoarthritic subchondral osteoblasts onaggrecan and type II collagen synthesis by chondrocytes.J Rheumatol 2006;33:1668e778.
40. Kawcak CE, Frisbie DD, McIlwraith CW, Werpy NM, Park RD.Evaluation of avocado and soybean unsaponifiable extractsfor treatment of horses with experimentally induced osteo-arthritis. Am J Vet Res 2007;68:598e604.
41. Altinel L, Saritas ZK, Kose KC, Pamuk K, Aksoy Y, Serteser M.Treatment with unsaponifiable extracts of avocado andsoybean increases TGF-beta1 and TGF-beta2 levels in caninejoint fluid. Tohoku J Exp Med 2007;211:181e6.
42. Lequesne M, Maheu E, Cadet C, Dreiser RL. Structural effect ofavocado/soybean unsaponifiables on joint space loss inosteoarthritis of the hip. Arthritis Rheum 2002;47:50e8.
43. Appelboom T, Schuermans J, Verbruggen G, Henrotin Y,Reginster JY. Symptoms modifying effect of avocado/soybeanunsaponifiables (ASU) in knee osteoarthritis. A double blind,prospective, placebo-controlled study. Scand J Rheumatol2001;30:242e7.
44. Maheu E, Mazieres B, Valat JP, Loyau G, Le Loet X, Bourgeois P,et al. Symptomatic efficacy of avocado/soybean unsaponifi-ables in the treatment of osteoarthritis of the knee and hip:
a prospective, randomized, double-blind, placebo-controlled,multicenter clinical trial with a six-month treatment periodand a two-month followup demonstrating a persistent effect.Arthritis Rheum 1998;41:81e91.
45. Blotman F,MaheuE,WulwikA, CaspardH, Lopez A. Efficacy andsafety of avocado/soybean unsaponifiables in the treatment ofsymptomatic osteoarthritis of the knee and hip. A prospective,multicenter, three-month, randomized, double-blind, placebo-controlled trial. Rev Rhum Engl Ed 1997;64:825e34.
46. Christensen R, Bartels EM, Astrup A, Bliddal H. Symptomaticefficacy of avocado-soybean unsaponifiables (ASU) in osteo-arthritis (OA) patients: a meta-analysis of randomizedcontrolled trials. Osteoarthritis Cartilage 2008;16:399e408.
47. Walrand S, Chiotelli E, Noirt F, Mwewa S, Lassel T.Consumption of a functional fermented milk containingcollagen hydrolysate improves the concentration of collagen-specific amino acids in plasma. J Agric Food Chem2008;56:7790e5.
48. Bello AE, Oesser S. Collagen hydrolysate for the treatment ofosteoarthritis and other joint disorders: a review of theliterature. Curr Med Res Opin 2006;22:2221e32.
49. Oesser S, Seifert J. Stimulation of type II collagen biosynthesisand secretion in bovine chondrocytes cultured with degradedcollagen. Cell Tissue Res 2003;311:393e9.
50. Schunck M, Schulze CH, Oesser S. disparate efficacy ofcollagen hydrolysate and glucosamine on the extracellularmatrix metabolism of articular chondrocytes. OA and Carti-lage 2006;14:S114 (Abstract).
51. Oesser S, Proksch E, Schunck M. prophylactic treatmentwith a special collagen hydrosylate decreases cartilage tissuedegeneration in the knee joints. OA and Cartilage2008;16:S45 (Abstract).
52. Nakatani S, Mano H, Sampei C, Shimizu J, Wada M.Chondroprotective effect of the bioactive peptide prolyl-hydroxyproline in mouse articular cartilage in vitro and invivo. Osteoarthritis Cartilage 2009;17:1620e7.
53. Clark KL, Sebastianelli W, Flechsenhar KR, Aukermann DF,Meza F, Millard RL, et al. 24-week study on the use of collagenhydrolysate as a dietary supplement in athletes with activity-related joint pain. Curr Med Res Opin 2008;24:1485e96.
54. Zuckley L, Angelopoulou K, Carpenter MSS, Meredith BA,Kline G, Rowinski M, et al. Collagen hydrosylate improvesjoint function in adults with mild symptoms of osteoarthritisof the knee. Medecine & Science in Sports & Excercise2004;36:S153e4.
55. Moskowitz RW. Role of collagen hydrolysate in bone andjoint disease. Semin Arthritis Rheum 2000;30:87e99.
56. Benito-Ruiz P, Camacho-Zambrano MM, Carrillo-Arcentales JN, Mestanza-Peralta MA, Vallejo-Flores CA,Vargas-Lopez SV, et al. A randomized controlled trial on theefficacy and safety of a food ingredient, collagen hydrolysate,for improving joint comfort. Int J Food Sci Nutr 2009;60(Suppl 2):99e113.
57. McAlindon TE, Felson DT, Zhang Y, Hannan MT, Aliabadi P,Weissman B, et al. Relation of dietary intake and serum levelsof vitamin D to progression of osteoarthritis of the kneeamong participants in the Framingham Study. Ann InternMed 1996;125:353e9.
58. Radin EL, Rose RM. Role of subchondral bone in the initiationand progression of cartilage damage. Clin Orthop Relat Res1986;213:34e40.
59. Cantatore FP, Corrado A, Grano M, Quarta L, Colucci S,Melillo N. Osteocalcin synthesis by human osteoblasts fromnormal and osteoarthritic bone after vitamin D3 stimulation.Clin Rheumatol 2004;23:490e5.

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 19
60. Goldring MB, Goldring SR. Articular cartilage and sub-chondral bone in the pathogenesis of osteoarthritis. Ann N YAcad Sci 2010;1192:230e7.
61. Martel-Pelletier J, Pelletier JP. Is osteoarthritis a diseaseinvolving only cartilage or other articular tissues? EklemHastalik Cerrahisi 2010;21:2e14.
62. Bergink AP, Uitterlinden AG, Van Leeuwen JP, Buurman CJ,Hofman A, Verhaar JA, et al. Vitamin D status, bone mineraldensity, and the development of radiographic osteoarthritis ofthe knee: the Rotterdam Study. J Clin Rheumatol2009;15:230e7.
63. Breijawi N, Eckardt A, Pitton MB, Hoelzl AJ, Giesa M, vonStechow D, et al. Bone mineral density and vitamin D statusin female and male patients with osteoarthritis of the knee orhip. Eur Surg Res 2009;42:1e10.
64. Tetlow LC, Woolley DE. Expression of vitamin D receptorsand matrix metalloproteinases in osteoarthritic cartilage andhuman articular chondrocytes in vitro. Osteoarthritis Carti-lage 2001;9:423e31.
65. Tetlow LC, Woolley DE. The effects of 1 alpha,25-dihydroxy-vitaminD(3) onmatrixmetalloproteinase and prostaglandin E(2) production by cells of the rheumatoid lesion. Arthritis Res1999;1:63e70.
66. Jefferies D, Farquharson C, Thomson J, Smith W,Seawright E, McCormack H, et al. Differences in metabolicparameters and gene expression related to osteochond-rosis/osteoarthrosis in pigs fed 25-hydroxyvitamin D3. VetRes 2002;33:383e96.
67. Lane NE, Gore LR, Cummings SR, Hochberg MC, Scott JC,Williams EN, et al. Serum vitamin D levels and incidentchanges of radiographic hip osteoarthritis: a longitudinalstudy. Study of Osteoporotic Fractures Research Group.Arthritis Rheum 1999;42:854e60.
68. Felson DT, Niu J, Clancy M, Aliabadi P, Sack B, Guermazi A,et al. Low levels of vitamin D and worsening of knee osteo-arthritis: results of two longitudinal studies. Arthritis Rheum2007;56:129e36.
69. Ding C, Parameswaran V, Burgess J, Cicuttini F, Jones G. Serumlevel of vitamin d, winter sun exposure knee radiographicosteoarthritis and knee cartilage loss in older adults: theTasmania Older Adult Cohort (TASOAC) Study. OA andCartilage 2008;16:S147 (Abstract).
70. Javaid M, Tolskykh I, Neogi T, Guermazi A, Curtis J, Torner J,et al. Non-linear association between baseline serum 25(OH)vitamin d concentration and incident radiographic knee OA:the MOST Study. OA and Cartilage 2008;16:S150 (Abstract).
71. Cisar P, Jany R, Waczulikova I, Sumegova K, Muchova J,Vojtassak J, et al. Effect of pine bark extract (Pycnogenol) onsymptoms of knee osteoarthritis. Phytother Res2008;22:1087e92.
72. Grimm T, Schafer A, Hogger P. Antioxidant activity andinhibition of matrix metalloproteinases by metabolites ofmaritime pine bark extract (pycnogenol). Free Radic Biol Med2004;36:811e22.
73. Farid R, Mirfeizi Z, Mirheidari M, Rezaieyazdi Z, Mansouri H,Esmaelli H, et al. Pycnogenol supplementation reduces painand stiffness and improves physical function in adults withknee osteoarthritis. Nutrition Research 2007;27:692e7.
74. Belcaro G, Cesarone MR, Errichi S, Zulli C, Errichi BM,Vinciguerra G, et al. Variations in C-reactive protein, plasmafree radicals and fibrinogen values in patients with osteoar-thritis treated with Pycnogenol. Redox Rep 2008;13:271e6.
75. Belcaro G, Cesarone MR, Errichi S, Zulli C, Errichi BM,Vinciguerra G, et al. Treatment of osteoarthritis with Pycno-genol. The SVOS (San Valentino Osteo-arthrosis Study).
Evaluation of signs, symptoms, physical performance andvascular aspects. Phytother Res 2008;22:518e23.
76. Imada K, Lin N, Liu C, Lu A, Chen W, Yano M, et al. Nobiletin,a citrus polymethoxy flavonoid, suppresses gene expressionand production of aggrecanases-1 and -2 in collagen-induced arthritic mice. Biochem Biophys Res Commun2008;373:181e5.
77. Ishiwa J, Sato T, Mimaki Y, Sashida Y, Yano M, Ito A. A citrusflavonoid, nobiletin, suppresses production and geneexpression of matrix metalloproteinase 9/gelatinase B inrabbit synovial fibroblasts. J Rheumatol 2000;27:20e5.
78. Lin N, Sato T, Takayama Y, Mimaki Y, Sashida Y, Yano M, et al.Novel anti-inflammatory actions of nobiletin, a citrus poly-methoxy flavonoid, on human synovial fibroblasts and mousemacrophages. Biochem Pharmacol 2003;65:2065e71.
79. Henrotin Y, Clutterbuck AL, Allaway D, Lodwig EM, Harris P,Mathy-Hartert M, et al. Biological actions of curcuminon articular chondrocytes. Osteoarthritis Cartilage2010;18:141e9.
80. Liacini A, Sylvester J, Li WQ, Huang W, Dehnade F, Ahmad M,et al. Induction of matrix metalloproteinase-13 geneexpression by TNF-alpha is mediated by MAP kinases, AP-1,and NF-kappaB transcription factors in articular chon-drocytes. Exp Cell Res 2003;288:208e17.
81. Schulze-Tanzil G, Mobasheri A, Sendzik J, John T, Shakibaei M.Effects of curcumin (diferuloylmethane) on nuclear factorkappaB signaling in interleukin-1beta-stimulated chon-drocytes. Ann N Y Acad Sci 2004;1030:578e86.
82. Shakibaei M, John T, Schulze-Tanzil G, Lehmann I,Mobasheri A. Suppression of NF-kappaB activation by cur-cumin leads to inhibition of expression of cyclo-oxygenase-2and matrix metalloproteinase-9 in human articular chon-drocytes: implications for the treatment of osteoarthritis.Biochem Pharmacol 2007;73:1434e45.
83. Shakibaei M, Schulze-Tanzil G, John T, Mobasheri A. Curcu-min protects human chondrocytes from IL-l1beta-inducedinhibition of collagen type II and beta1-integrin expressionand activation of caspase-3: an immunomorphological study.Ann Anat 2005;187:487e97.
84. Toegel S, Wu SQ, Piana C, Unger FM, Wirth M, Goldring MB,et al. Comparison between chondroprotective effectsof glucosamine, curcumin, and diacerein in IL-1beta-stimu-lated C-28/I2 chondrocytes. Osteoarthritis Cartilage 2008;16:1205e12.
85. Williamson SM, Mobasheri A, Vaughan-Thomas A,Thompson NJ, Shakibaei M. Curcumin and resveratrol reducelipopolysaccharide mediated glycosaminoglycan release inan explant model of canine articular cartilage. OA andCartilage 2006;14:S102 (Abstract).
86. Clutterbuck AL, Mobasheri A, Shakibaei M, Allaway D,Harris P. Interleukin-1beta-induced extracellular matrixdegradation and glycosaminoglycan release is inhibited bycurcumin in an explant model of cartilage inflammation. AnnN Y Acad Sci 2009;1171:428e35.
87. Mathy M, Sanchez C, Priem F, Henrotin Y. Curcumin inhibitsinterleukin-6, -8, nitric oxide and prostaglandin E2 synthesisby bovine chondrocytes. OA and Cartilage 2007;15:C115(Abstract).
88. Clutterbuck AL, Mobasheri A, Rogers TC, Wiseman J,Allaway D, Harris P. Curcumin (diferuloylmethane) blocks il-1 beta stimulated glycosaminoglycan and prostaglandin e2release from cartilage explants in an in vitro model of oste-oarthritis. OA and Cartilage 2008;16:S221 (Abstract).
89. Mathy-Hartert M, Jacquemond-Collet I, Priem F, Sanchez C,Lambert C, Henrotin Y. Curcumin inhibits pro-inflammatory
Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e2120
mediators and metalloproteinase-3 production by chon-drocytes. Inflamm Res 2009;58:899e908.
90. Chowdhury TT, Salter DM, Bader DL, Lee DA. Signal trans-duction pathways involving p38 MAPK, JNK, NFkappaB andAP-1 influences the response of chondrocytes cultured inagarose constructs to IL-1beta and dynamic compression.Inflamm Res 2008;57:306e13.
91. Lev-Ari S, Strier L, Kazanov D, Elkayam O, Lichtenberg D,Caspi D, et al. Curcumin synergistically potentiates thegrowth-inhibitory and pro-apoptotic effects of celecoxib inosteoarthritis synovial adherent cells. Rheumatology(Oxford) 2006;45:171e7.
92. Kulkarni RR, Patki PS, Jog VP, Gandage SG, Patwardhan B.Treatment of osteoarthritis with a herbomineral formulation:a double-blind, placebo-controlled, cross-over study. J Eth-nopharmacol 1991;33:91e5.
93. Claassen H, Briese V, Manapov F, Nebe B, Schunke M, Kurz B.The phytoestrogens daidzein and genistein enhance theinsulin-stimulated sulfate uptake in articular chondrocytes.Cell Tissue Res 2008;333:71e9.
94. Hooshmand S, Soung do Y, Lucas EA, Madihally SV,Levenson CW, Arjmandi BH. Genistein reduces the produc-tion of proinflammatory molecules in human chondrocytes.J Nutr Biochem 2007;18:609e14.
95. Ham KD, Oegema TR, Loeser RF, Carlson CS. Effects of long-term estrogen replacement therapy on articular cartilageIGFBP-2, IGFBP-3, collagen and proteoglycan levels in ovari-ectomized cynomolgus monkeys. Osteoarthritis Cartilage2004;12:160e8.
96. Ahmed S, Rahman A, Hasnain A, Lalonde M, Goldberg VM,Haqqi TM. Green tea polyphenol epigallocatechin-3-gallateinhibits the IL-1 beta-induced activity and expression ofcyclooxygenase-2 and nitric oxide synthase-2 in humanchondrocytes. Free Radic Biol Med 2002;33:1097e105.
97. Singh R, Ahmed S, Islam N, Goldberg VM, Haqqi TM. Epi-gallocatechin-3-gallate inhibits interleukin-1beta-inducedexpression of nitric oxide synthase and production of nitricoxide in human chondrocytes: suppression of nuclear factorkappaB activation by degradation of the inhibitor of nuclearfactor kappaB. Arthritis Rheum 2002;46:2079e86.
98. Singh R, Ahmed S, Malemud CJ, Goldberg VM, Haqqi TM.Epigallocatechin-3-gallate selectively inhibits interleukin-1beta-induced activation of mitogen activated protein kinasesubgroup c-Jun N-terminal kinase in human osteoarthritischondrocytes. J Orthop Res 2003;21:102e9.
99. Tokuda H, Takai S, Hanai Y, Matsushima-Nishiwaki R,Yamauchi J, Harada A, et al. (�)-Epigallocatechin gallateinhibits basic fibroblast growth factor-stimulated inter-leukin-6 synthesis in osteoblasts. Horm Metab Res2008;40:674e8.
100. Huang GS, Tseng CY, Lee CH, Su SL, Lee HS. Effects of(�)-epigallocatechin-3-gallate on cyclooxygenase 2, PGE(2),and IL-8 expression induced by IL-1beta in human synovialfibroblasts. Rheumatol Int 2010;30(9):1197e203.
101. Rasheed Z, Anbazhagan AN, Akhtar N, Ramamurthy S,Voss FR, Haqqi TM. Green tea polyphenol epigallocatechin-3-gallate inhibits advanced glycation end product-inducedexpression of tumor necrosis factor-alpha and matrix met-alloproteinase-13 in human chondrocytes. Arthritis Res Ther2009;11. R71.
102. Ahmed S, Wang N, Lalonde M, Goldberg VM, Haqqi TM.Green tea polyphenol epigallocatechin-3-gallate (EGCG)differentially inhibits interleukin-1 beta-induced expressionof matrix metalloproteinase-1 and -13 in human chon-drocytes. J Pharmacol Exp Ther 2004;308:767e73.
103. Haqqi TM, Anthony DD, Gupta S, Ahmad N, Lee MS,Kumar GK, et al. Prevention of collagen-induced arthritis inmice by a polyphenolic fraction from green tea. Proc NatlAcad Sci U S A 1999;96:4524e9.
104. Dave M, Attur M, Palmer G, Al-Mussawir HE, Kennish L,Patel J, et al. The antioxidant resveratrol protects againstchondrocyte apoptosis via effects on mitochondrial polari-zation and ATP production. Arthritis Rheum2008;58:2786e97.
105. Csaki C, Keshishzadeh N, Fischer K, Shakibaei M. Regulationof inflammation signalling by resveratrol in human chon-drocytes in vitro. Biochem Pharmacol 2008;75:677e87.
106. Shakibaei M, Csaki C, Nebrich S, Mobasheri A. Resveratrolsuppresses interleukin-1beta-induced inflammatory signalingand apoptosis in human articular chondrocytes: potential foruse as a novel nutraceutical for the treatment of osteoarthritis.Biochem Pharmacol 2008;76:1426e39.
107. Lei M, Liu SQ, Liu YL. Resveratrol protects bone marrowmesenchymal stem cell derived chondrocytes cultured onchitosan-gelatin scaffolds from the inhibitory effect of inter-leukin-1beta. Acta Pharmacol Sin 2008;29:1350e6.
108. Elmali N, Baysal O, Harma A, Esenkaya I, Mizrak B. Effects ofresveratrol in inflammatory arthritis. Inflammation2007;30:1e6.
109. Elmali N, Esenkaya I, Harma A, Ertem K, Turkoz Y, Mizrak B.Effect of resveratrol in experimental osteoarthritis in rabbits.Inflamm Res 2005;54:158e62.
110. Garbacki N, Angenot L, Bassleer C, Damas J, Tits M. Effects ofprodelphinidins isolated from Ribes nigrum on chondrocytemetabolism and COX activity. Naunyn Schmiedebergs ArchPharmacol 2002;365:434e41.
111. Sato M, Miyazaki T, Kambe F, Maeda K, Seo H. Quercetin,a bioflavonoid, inhibits the induction of interleukin 8 andmonocyte chemoattractant protein-1 expression by tumornecrosis factor-alpha in cultured human synovial cells.J Rheumatol 1997;24:1680e4.
112. Kang K, Hwang HJ, Hong DH, Park Y, Kim SH, Lee BH, et al.Antioxidant and antiinflammatory activities of ventol,a phlorotannin-rich natural agent derived from Ecklonia cava,and its effect on proteoglycan degradation in cartilageexplant culture. Res Commun Mol Pathol Pharmacol2004;115e116:77e95.
113. Anand P, Kunnumakkara AB, Newman RA, Aggarwal BB.Bioavailability of curcumin: problems and promises. MolPharm 2007;4:807e18.
114. Anand P, Nair HB, Sung B, Kunnumakkara AB, Yadav VR,Tekmal RR, et al. Design of curcumin-loaded PLGA nano-particles formulation with enhanced cellular uptake, andincreased bioactivity in vitro and superior bioavailability invivo. Biochem Pharmacol 2010;79:330e8.
115. Biasutto L, Marotta E, Bradaschia A, Fallica M, Mattarei A,Garbisa S, et al. Soluble polyphenols: synthesis and bioavail-ability of 3,40,5-tri(alpha-D-glucose-3-O-succinyl) resveratrol.Bioorg Med Chem Lett 2009;19:6721e4.
116. Li B, Chen F, Wang X, Ji B, Wu Y. Isolation and identification ofantioxidative peptides from porcine collagen hydrolysate byconsecutive chromatography and electrospray ionization-mass spectrometry. Food Chemistry 2007;102:1135e43.
117. Zhang Y, Kouguchi T, Shimizu M, Ohmori T, Takahata Y,Morimatsu F. chicken collagen hydrolysate protects ratsfrom hypertension and cardiovascular damage. J Med Food2010;56(3):208e10.
118. Faria M, da Costa EL, Gontijo JA, Netto FM. Evaluation of thehypotensive potential of bovine and porcine collagenhydrolysates. J Med Food 2008;11:560e7.

Y. Henrotin et al. / Osteoarthritis and Cartilage 19 (2011) 1e21 21
119. Heinecke LF, Grzanna MW, Au AY, Mochal CA, Rashmir-Raven A, Frondoza CG. Inhibition of cyclooxygenase-2expression and prostaglandin E2 production in chondrocytesby avocado soybean unsaponifiables and epigallocatechingallate. Osteoarthritis Cartilage 2010;18:220e7.
120. Csaki C, Mobasheri A, Shakibaei M. Synergistic chon-droprotective effects of curcumin and resveratrol in humanarticular chondrocytes: inhibition of IL-1beta-induced NF-kappaB-mediated inflammation and apoptosis. Arthritis ResTher 2009;11. R165.
121. Cobelens PM, Heijnen CJ, Nieuwenhuis EE, Kramer PP, vander Zee R, van Eden W, et al. Treatment of adjuvant-inducedarthritis by oral administration of mycobacterial Hsp65during disease. Arthritis Rheum 2000;43:2694e702.
122. So JS, Kwon HK, Lee CG, Yi HJ, Park JA, Lim SY, et al. Lacto-bacillus casei suppresses experimental arthritis by down-
regulating T helper 1 effector functions. Mol Immunol2008;45:2690e9.
123. So JS, Lee CG, Kwon HK, Yi HJ, Chae CS, Park JA, et al.Lactobacillus casei potentiates induction of oral toler-ance in experimental arthritis. Mol Immunol2008;46:172e80.
124. Baharav E, Mor F, Halpern M, Weinberger A. Lactobacillus GGbacteria ameliorate arthritis in Lewis rats. J Nutr2004;134:1964e9.
125. Hatakka K, Martio J, Korpela M, Herranen M, Poussa T,Laasanen T, et al. Effects of probiotic therapy on the activityand activation of mild rheumatoid arthritisea pilot study.Scand J Rheumatol 2003;32:211e5.
126. Nenonen MT, Helve TA, Rauma AL, Hanninen OO. Uncooked,lactobacilli-rich, vegan food and rheumatoid arthritis. Br JRheumatol 1998;37:274e81.




















